User login
Biosimilars and sources show mostly parallel safety profiles
Biosimilars are primarily as safe as their originators, based on data from a review of current European regulatory documents. The findings were published online in the British Journal of Clinical Pharmacology.
“Biosimilars are officially approved as similar products to a biopharmaceutical originator, which often share the same International Nonproprietary Name,” wrote L.R.A. Lepelaars, MD, of Utrecht University, the Netherlands, and colleagues. However, many clinicians remain cautious about using biosimilars, particularly those in the United States, they noted. The European Medicines Agency (EMA) has filed safety data on biosimilars, but comparative effectiveness studies often are lacking, they wrote.
In this study, the researchers compared data on 25 biologic medicinal products (19 biosimilars and 6 originators). The biosimilars were authorized by the EMA between Jan. 1, 2005 and Oct. 30, 2015 (Br. J. Clin. Pharmacol. 2017 Nov 22; doi: 10.1111/bcp.13454).
Overall, the researchers found 55 general safety concerns, including 22 that were deemed highly clinically relevant. Another 21 were defined as medium, while 12 had low levels of clinical relevance.
Infliximab was the only active substance with more than one difference in safety concerns between the biosimilar and originator; three more general safety concerns (all of medium clinical relevance) were noted for infliximab biosimilars compared with the originator (bowel obstruction, hematologic reactions, and lack of efficacy).
For all other active substances included in the study, one difference or no difference was found in the general safety concerns between the biosimilars and originators, and none of the differences was related to immunogenicity
The researchers assessed the safety of biosimilars by comparing them with European Risk Management Plan or Summary of Product Characteristics.
The findings support the value of biosimilars based on comparable safety profiles, the researchers noted. However, “a direct comparison between biosimilars and related originators through formal postmarketing studies (observational or clinical trials) is mandatory for specific safety and effectiveness issues emerging during the products’ life cycle,” they said.
The researchers had no financial conflicts to disclose.
Biosimilars are primarily as safe as their originators, based on data from a review of current European regulatory documents. The findings were published online in the British Journal of Clinical Pharmacology.
“Biosimilars are officially approved as similar products to a biopharmaceutical originator, which often share the same International Nonproprietary Name,” wrote L.R.A. Lepelaars, MD, of Utrecht University, the Netherlands, and colleagues. However, many clinicians remain cautious about using biosimilars, particularly those in the United States, they noted. The European Medicines Agency (EMA) has filed safety data on biosimilars, but comparative effectiveness studies often are lacking, they wrote.
In this study, the researchers compared data on 25 biologic medicinal products (19 biosimilars and 6 originators). The biosimilars were authorized by the EMA between Jan. 1, 2005 and Oct. 30, 2015 (Br. J. Clin. Pharmacol. 2017 Nov 22; doi: 10.1111/bcp.13454).
Overall, the researchers found 55 general safety concerns, including 22 that were deemed highly clinically relevant. Another 21 were defined as medium, while 12 had low levels of clinical relevance.
Infliximab was the only active substance with more than one difference in safety concerns between the biosimilar and originator; three more general safety concerns (all of medium clinical relevance) were noted for infliximab biosimilars compared with the originator (bowel obstruction, hematologic reactions, and lack of efficacy).
For all other active substances included in the study, one difference or no difference was found in the general safety concerns between the biosimilars and originators, and none of the differences was related to immunogenicity
The researchers assessed the safety of biosimilars by comparing them with European Risk Management Plan or Summary of Product Characteristics.
The findings support the value of biosimilars based on comparable safety profiles, the researchers noted. However, “a direct comparison between biosimilars and related originators through formal postmarketing studies (observational or clinical trials) is mandatory for specific safety and effectiveness issues emerging during the products’ life cycle,” they said.
The researchers had no financial conflicts to disclose.
Biosimilars are primarily as safe as their originators, based on data from a review of current European regulatory documents. The findings were published online in the British Journal of Clinical Pharmacology.
“Biosimilars are officially approved as similar products to a biopharmaceutical originator, which often share the same International Nonproprietary Name,” wrote L.R.A. Lepelaars, MD, of Utrecht University, the Netherlands, and colleagues. However, many clinicians remain cautious about using biosimilars, particularly those in the United States, they noted. The European Medicines Agency (EMA) has filed safety data on biosimilars, but comparative effectiveness studies often are lacking, they wrote.
In this study, the researchers compared data on 25 biologic medicinal products (19 biosimilars and 6 originators). The biosimilars were authorized by the EMA between Jan. 1, 2005 and Oct. 30, 2015 (Br. J. Clin. Pharmacol. 2017 Nov 22; doi: 10.1111/bcp.13454).
Overall, the researchers found 55 general safety concerns, including 22 that were deemed highly clinically relevant. Another 21 were defined as medium, while 12 had low levels of clinical relevance.
Infliximab was the only active substance with more than one difference in safety concerns between the biosimilar and originator; three more general safety concerns (all of medium clinical relevance) were noted for infliximab biosimilars compared with the originator (bowel obstruction, hematologic reactions, and lack of efficacy).
For all other active substances included in the study, one difference or no difference was found in the general safety concerns between the biosimilars and originators, and none of the differences was related to immunogenicity
The researchers assessed the safety of biosimilars by comparing them with European Risk Management Plan or Summary of Product Characteristics.
The findings support the value of biosimilars based on comparable safety profiles, the researchers noted. However, “a direct comparison between biosimilars and related originators through formal postmarketing studies (observational or clinical trials) is mandatory for specific safety and effectiveness issues emerging during the products’ life cycle,” they said.
The researchers had no financial conflicts to disclose.
FROM THE BRITISH JOURNAL OF CLINICAL PHARMACOLOGY
Key clinical point: Most biosimilars show safety profiles comparable to their originators.
Major finding: Infliximab biosimilars demonstrated three more general safety concerns than the originator.
Data source: The data come from a cross-sectional analysis 19 biosimilars and 6 originators.
Disclosures: The researchers had no financial conflicts to disclose.
Expert discusses risks of biosimilars in rheumatology
SAN DIEGO – If you perceive that the use of biosimilars for rheumatic diseases hasn’t gained the traction one would expect, you’re not alone. In the opinion of J. Eugene Huffstutter, MD, the expected risks of biosimilar products have clinicians concerned, especially when it comes to immunologic characteristics.
“We’ve all had patients on biologics for years: Everything’s fine, but then the patient has an infusion reaction,” Dr. Huffstutter said at the annual meeting of the American College of Rheumatology. “I’ve had it happen with the first infusion of a biologic and I’ve had it with the 20th infusion of that same biologic product. It’s impossible to predict.”

Other unforeseen risks of biosimilars include the impact on pharmacovigilance, manufacturing, and politics. “What if our government says we want to use this agent or that agent? Or, what if it advises everyone to use the bio-originator? Then there are coverage challenges,” he said. “How are the insurance companies going to look at this? Then there are corporate impacts. The companies that make biosimilars have invested a tremendous amount of resources to bring these to market. We have a huge market in the U.S., but the uptake has been very slow. So are they going to say, ‘We’re going to take our resources and do something else?’ ”
Practice protocols for using biosimilars vary depending on your practice environment. For example, if biosimilars are administered by a freestanding practice, “you have to depend a lot on your state laws in terms of what the pharmacist is able to do,” said Dr. Huffstutter, who is also the past president of the Tennessee Rheumatology Society. “What are the patient support programs available for that biosimilar compared with bio-originator? What do the insurance contracts say in terms of can you get this filled or not? What’s the formulary status? How well do physicians in your community accept biosimilars? More importantly, how do your patients feel about biosimilars? I think they’ve been left out of this whole discussion.”
Dr. Huffstutter disclosed that he has received research support from GlaxoSmithKline, Pfizer, and UCB. He is also a member of the speakers bureau and/or is an adviser to Janssen, Lilly, Pfizer, Genentech, Novartis, Regeneron, and UCB.
SAN DIEGO – If you perceive that the use of biosimilars for rheumatic diseases hasn’t gained the traction one would expect, you’re not alone. In the opinion of J. Eugene Huffstutter, MD, the expected risks of biosimilar products have clinicians concerned, especially when it comes to immunologic characteristics.
“We’ve all had patients on biologics for years: Everything’s fine, but then the patient has an infusion reaction,” Dr. Huffstutter said at the annual meeting of the American College of Rheumatology. “I’ve had it happen with the first infusion of a biologic and I’ve had it with the 20th infusion of that same biologic product. It’s impossible to predict.”
Other unforeseen risks of biosimilars include the impact on pharmacovigilance, manufacturing, and politics. “What if our government says we want to use this agent or that agent? Or, what if it advises everyone to use the bio-originator? Then there are coverage challenges,” he said. “How are the insurance companies going to look at this? Then there are corporate impacts. The companies that make biosimilars have invested a tremendous amount of resources to bring these to market. We have a huge market in the U.S., but the uptake has been very slow. So are they going to say, ‘We’re going to take our resources and do something else?’ ”
Practice protocols for using biosimilars vary depending on your practice environment. For example, if biosimilars are administered by a freestanding practice, “you have to depend a lot on your state laws in terms of what the pharmacist is able to do,” said Dr. Huffstutter, who is also the past president of the Tennessee Rheumatology Society. “What are the patient support programs available for that biosimilar compared with bio-originator? What do the insurance contracts say in terms of can you get this filled or not? What’s the formulary status? How well do physicians in your community accept biosimilars? More importantly, how do your patients feel about biosimilars? I think they’ve been left out of this whole discussion.”
Dr. Huffstutter disclosed that he has received research support from GlaxoSmithKline, Pfizer, and UCB. He is also a member of the speakers bureau and/or is an adviser to Janssen, Lilly, Pfizer, Genentech, Novartis, Regeneron, and UCB.
SAN DIEGO – If you perceive that the use of biosimilars for rheumatic diseases hasn’t gained the traction one would expect, you’re not alone. In the opinion of J. Eugene Huffstutter, MD, the expected risks of biosimilar products have clinicians concerned, especially when it comes to immunologic characteristics.
“We’ve all had patients on biologics for years: Everything’s fine, but then the patient has an infusion reaction,” Dr. Huffstutter said at the annual meeting of the American College of Rheumatology. “I’ve had it happen with the first infusion of a biologic and I’ve had it with the 20th infusion of that same biologic product. It’s impossible to predict.”
Other unforeseen risks of biosimilars include the impact on pharmacovigilance, manufacturing, and politics. “What if our government says we want to use this agent or that agent? Or, what if it advises everyone to use the bio-originator? Then there are coverage challenges,” he said. “How are the insurance companies going to look at this? Then there are corporate impacts. The companies that make biosimilars have invested a tremendous amount of resources to bring these to market. We have a huge market in the U.S., but the uptake has been very slow. So are they going to say, ‘We’re going to take our resources and do something else?’ ”
Practice protocols for using biosimilars vary depending on your practice environment. For example, if biosimilars are administered by a freestanding practice, “you have to depend a lot on your state laws in terms of what the pharmacist is able to do,” said Dr. Huffstutter, who is also the past president of the Tennessee Rheumatology Society. “What are the patient support programs available for that biosimilar compared with bio-originator? What do the insurance contracts say in terms of can you get this filled or not? What’s the formulary status? How well do physicians in your community accept biosimilars? More importantly, how do your patients feel about biosimilars? I think they’ve been left out of this whole discussion.”
Dr. Huffstutter disclosed that he has received research support from GlaxoSmithKline, Pfizer, and UCB. He is also a member of the speakers bureau and/or is an adviser to Janssen, Lilly, Pfizer, Genentech, Novartis, Regeneron, and UCB.
EXPERT ANALYSIS FROM ACR 2017
Study explores why RA patients discontinue methotrexate
SAN DIEGO – Despite the well-recognized role of methotrexate in the management of rheumatoid arthritis, about 30% of patients with RA discontinue treatment with methotrexate 1-2 years after starting it, according to results from a registry study.
“We know that methotrexate is an acceptable and certainly well-characterized treatment for RA,” study author Jeffrey R. Curtis, MD, said at the annual meeting of the American College of Rheumatology. “Despite, this, though, patterns of persistence, intolerance, and inadequate response with methotrexate [MTX] are not well characterized in real-world settings. We all get the sense that there are patients who greatly dislike it.”

The researchers analyzed patients not previously treated with a biologic DMARD (bDMARD) or a targeted synthetic DMARD (tsDMARD). They compared 1,488 patients who initiated MTX monotherapy with 656 patients who initiated MTX in combination with csDMARDs during October 2001 through February 2017 and had at least one follow-up visit after treatment initiation.
The mean age of patients was 57 years, 75% were female, and 84% were white. Patients in the MTX combination therapy group were more likely to be white, better educated, and employed, but were slightly less likely to have active disease. Dr. Curtis reported that the proportion of MTX monotherapy patients who discontinued MTX was 24% at 1 year, 37% at 2 years, and 46% at 3 years, and was not significantly different from the figures for the combination MTX therapy group (P = .99). “The survival curve was overlapping and nonsignificant,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham. “For example, at 12 months, 24.4% of people stopped methotrexate if they had started it alone, but it was 26% if they were on combination therapy. Flipping that around, 75% stayed on MTX at 1 year’s time.”
In contrast, the researchers also found that patients in the MTX monotherapy group were significantly more likely to start a bDMARD or a tsDMARD earlier than patients in the MTX combination therapy group (P less than .001). In an adjusted Cox proportional hazards model, higher risk for MTX discontinuation was associated with being disabled (hazard ratio, 1.33), being retired (HR, 1.37), or using alcohol regularly (the HR ranged from 1.22 to 2.03 depending on the mean units consumed per day). MTX discontinuation was less likely in patients with older age (HR, 0.94), longer duration of RA (HR, 0.92), or higher baseline Clinical Disease Activity Index score (HR, 0.96).
About 20% of physicians in the registry provided reasons for discontinuation of MTX. The top reasons they gave were the presence of infection and cancer (about 85% and 15%, respectively). The reasons patients gave for discontinuation of MTX were wide ranging and included unusual fatigue (about 67%), followed by stomach problems (48%), hair loss (about 36%), mental fog (about 29%), sores in the mouth (about 25%), nausea (about 19%), and diarrhea (about 19%). “Patients are telling us very different things about why this drug is being stopped,” Dr. Curtis said. “Doctors in this registry could specify a reason for stopping that would map to these reasons, and yet they didn’t.”
He acknowledged certain limitations of the study, including the potential for missing data and the possibility that some of the patients may have reinitiated MTX. “We know from other data that people may stop MTX for a period of time but then may resume it,” Dr. Curtis said. Going forward, he called for strategies “to better identify patients with suboptimal persistence to MTX and predict those most likely to not tolerate MTX, to optimize overall RA treatment.”
The study was supported by Corrona, and the analysis was funded by Pfizer. Dr. Curtis reported that he has received research grants from Amgen, Corrona, Crescendo Bioscience, and Pfizer, and consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Myriad, Pfizer, Roche/Genentech, and UCB.
SAN DIEGO – Despite the well-recognized role of methotrexate in the management of rheumatoid arthritis, about 30% of patients with RA discontinue treatment with methotrexate 1-2 years after starting it, according to results from a registry study.
“We know that methotrexate is an acceptable and certainly well-characterized treatment for RA,” study author Jeffrey R. Curtis, MD, said at the annual meeting of the American College of Rheumatology. “Despite, this, though, patterns of persistence, intolerance, and inadequate response with methotrexate [MTX] are not well characterized in real-world settings. We all get the sense that there are patients who greatly dislike it.”
The researchers analyzed patients not previously treated with a biologic DMARD (bDMARD) or a targeted synthetic DMARD (tsDMARD). They compared 1,488 patients who initiated MTX monotherapy with 656 patients who initiated MTX in combination with csDMARDs during October 2001 through February 2017 and had at least one follow-up visit after treatment initiation.
The mean age of patients was 57 years, 75% were female, and 84% were white. Patients in the MTX combination therapy group were more likely to be white, better educated, and employed, but were slightly less likely to have active disease. Dr. Curtis reported that the proportion of MTX monotherapy patients who discontinued MTX was 24% at 1 year, 37% at 2 years, and 46% at 3 years, and was not significantly different from the figures for the combination MTX therapy group (P = .99). “The survival curve was overlapping and nonsignificant,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham. “For example, at 12 months, 24.4% of people stopped methotrexate if they had started it alone, but it was 26% if they were on combination therapy. Flipping that around, 75% stayed on MTX at 1 year’s time.”
In contrast, the researchers also found that patients in the MTX monotherapy group were significantly more likely to start a bDMARD or a tsDMARD earlier than patients in the MTX combination therapy group (P less than .001). In an adjusted Cox proportional hazards model, higher risk for MTX discontinuation was associated with being disabled (hazard ratio, 1.33), being retired (HR, 1.37), or using alcohol regularly (the HR ranged from 1.22 to 2.03 depending on the mean units consumed per day). MTX discontinuation was less likely in patients with older age (HR, 0.94), longer duration of RA (HR, 0.92), or higher baseline Clinical Disease Activity Index score (HR, 0.96).
About 20% of physicians in the registry provided reasons for discontinuation of MTX. The top reasons they gave were the presence of infection and cancer (about 85% and 15%, respectively). The reasons patients gave for discontinuation of MTX were wide ranging and included unusual fatigue (about 67%), followed by stomach problems (48%), hair loss (about 36%), mental fog (about 29%), sores in the mouth (about 25%), nausea (about 19%), and diarrhea (about 19%). “Patients are telling us very different things about why this drug is being stopped,” Dr. Curtis said. “Doctors in this registry could specify a reason for stopping that would map to these reasons, and yet they didn’t.”
He acknowledged certain limitations of the study, including the potential for missing data and the possibility that some of the patients may have reinitiated MTX. “We know from other data that people may stop MTX for a period of time but then may resume it,” Dr. Curtis said. Going forward, he called for strategies “to better identify patients with suboptimal persistence to MTX and predict those most likely to not tolerate MTX, to optimize overall RA treatment.”
The study was supported by Corrona, and the analysis was funded by Pfizer. Dr. Curtis reported that he has received research grants from Amgen, Corrona, Crescendo Bioscience, and Pfizer, and consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Myriad, Pfizer, Roche/Genentech, and UCB.
SAN DIEGO – Despite the well-recognized role of methotrexate in the management of rheumatoid arthritis, about 30% of patients with RA discontinue treatment with methotrexate 1-2 years after starting it, according to results from a registry study.
“We know that methotrexate is an acceptable and certainly well-characterized treatment for RA,” study author Jeffrey R. Curtis, MD, said at the annual meeting of the American College of Rheumatology. “Despite, this, though, patterns of persistence, intolerance, and inadequate response with methotrexate [MTX] are not well characterized in real-world settings. We all get the sense that there are patients who greatly dislike it.”
The researchers analyzed patients not previously treated with a biologic DMARD (bDMARD) or a targeted synthetic DMARD (tsDMARD). They compared 1,488 patients who initiated MTX monotherapy with 656 patients who initiated MTX in combination with csDMARDs during October 2001 through February 2017 and had at least one follow-up visit after treatment initiation.
The mean age of patients was 57 years, 75% were female, and 84% were white. Patients in the MTX combination therapy group were more likely to be white, better educated, and employed, but were slightly less likely to have active disease. Dr. Curtis reported that the proportion of MTX monotherapy patients who discontinued MTX was 24% at 1 year, 37% at 2 years, and 46% at 3 years, and was not significantly different from the figures for the combination MTX therapy group (P = .99). “The survival curve was overlapping and nonsignificant,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham. “For example, at 12 months, 24.4% of people stopped methotrexate if they had started it alone, but it was 26% if they were on combination therapy. Flipping that around, 75% stayed on MTX at 1 year’s time.”
In contrast, the researchers also found that patients in the MTX monotherapy group were significantly more likely to start a bDMARD or a tsDMARD earlier than patients in the MTX combination therapy group (P less than .001). In an adjusted Cox proportional hazards model, higher risk for MTX discontinuation was associated with being disabled (hazard ratio, 1.33), being retired (HR, 1.37), or using alcohol regularly (the HR ranged from 1.22 to 2.03 depending on the mean units consumed per day). MTX discontinuation was less likely in patients with older age (HR, 0.94), longer duration of RA (HR, 0.92), or higher baseline Clinical Disease Activity Index score (HR, 0.96).
About 20% of physicians in the registry provided reasons for discontinuation of MTX. The top reasons they gave were the presence of infection and cancer (about 85% and 15%, respectively). The reasons patients gave for discontinuation of MTX were wide ranging and included unusual fatigue (about 67%), followed by stomach problems (48%), hair loss (about 36%), mental fog (about 29%), sores in the mouth (about 25%), nausea (about 19%), and diarrhea (about 19%). “Patients are telling us very different things about why this drug is being stopped,” Dr. Curtis said. “Doctors in this registry could specify a reason for stopping that would map to these reasons, and yet they didn’t.”
He acknowledged certain limitations of the study, including the potential for missing data and the possibility that some of the patients may have reinitiated MTX. “We know from other data that people may stop MTX for a period of time but then may resume it,” Dr. Curtis said. Going forward, he called for strategies “to better identify patients with suboptimal persistence to MTX and predict those most likely to not tolerate MTX, to optimize overall RA treatment.”
The study was supported by Corrona, and the analysis was funded by Pfizer. Dr. Curtis reported that he has received research grants from Amgen, Corrona, Crescendo Bioscience, and Pfizer, and consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Myriad, Pfizer, Roche/Genentech, and UCB.
AT ACR 2017
Key clinical point: Nearly one-third of patients with RA discontinue methotrexate 1–2 years after initiation.
Major finding: The proportion of MTX monotherapy patients who discontinued MTX was 24% at 1 year, 37% at 2 years, and 46% at 3 years, and was not significantly different from the combination MTX therapy group (P = .99).
Study details: A registry study that compared 1,488 patients who initiated MTX monotherapy with 656 patients who initiated MTX in combination with conventional synthetic DMARDs.
Disclosures: The study was supported by Corrona, and the analysis was funded by Pfizer. Dr. Curtis reported that he has received research grants from Amgen, Corrona, Crescendo Bioscience, and Pfizer, and consulting fees from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Myriad, Pfizer, Roche/Genentech, and UCB.
For women with RA, small-joint surgery rate nearly twice that of men
SAN DIEGO – but the rate of small-joint procedures is declining for both sexes. However, no differences in rates of large-joint procedures between sexes were observed during the same time period.
Those are key findings from a retrospective study which set out to determine if there are sex differences in the incidence and trends of large- versus small-joint surgery rates in rheumatoid arthritis over time. “Why is orthopedic surgery important to rheumatology? The main reason is because it’s a surrogate for failed medical management,” lead study author Michael D. Richter, MD, said at the annual meeting of the American College of Rheumatology.

Dr. Richter, an internal medicine resident at Mayo Clinic, Rochester, Minn., said that women with RA generally present with more severe symptoms and higher rates of disability, while men have a better treatment response and a higher remission rate. For example, results from the multinational Quantitative Standard Monitoring of Patients with RA study found that remission rates were around 30% in men and 17% in women (Arthritis Res Ther. 2009;11[1]:R7). “However, a lot of these studies are criticized because it’s thought that gender can play a role in the disease measures,” he said. “By looking at joint surgery we have an objective outcome, and we can look at differences in treatment efficacy.”
Dr. Richter and his associates drew from the Rochester Epidemiology Project to identify 1,077 patients from Olmstead County, Minn., who fulfilled ACR criteria for RA between 1980 and 2013, and who were followed up until death, migration, or July 1, 2016. They classified surgeries as small joint (wrist, hand, or foot) or large joint (shoulder, elbow, hip, knee, or ankle). A majority of the patients (70%) were women. Compared with women, men were slightly older at diagnosis (a mean of 58 years vs. 55 years, respectively), were more likely to have a history of smoking (67% vs. 46%), and were more likely to have large-joint swelling upon initial presentation (49% vs. 42%). The mean follow-up was 12 years. No differences between men and women were noted in obesity, inflammatory biomarkers, or seropositivity.
During the study period, 112 patients underwent at least one small-joint surgery, 90 of whom were women (80%). The cumulative incidence of small-joint surgery at 15 years was nearly double that of men: 14.4% vs. 7.6%, respectively (P = .008). “Prior to the year 2000 there were no significant trends in the rate of small-joint surgery but it was more common in women,” he said. “After 2000 there was a significant decline for men and women (P = .002), but no significant difference between sexes.”
At the same time, 204 patients underwent at least one large-joint surgery during the time period, 141 of whom were women (69%). The cumulative incidence of large-joint surgery at 15 years was 20.2% for women and 18.8% for men, which was statistically similar (P = .55). “We saw no significant change over time in the rate of large-joint surgery from 1980 to 2016,” Dr. Richter said. “This is in contrast to what we see in the general population, where orthopedic procedures for osteoarthritis are more common.”
He acknowledged certain limitations of the study, including its retrospective design and the fact that the researchers were unable to include specific surgical indications in the analysis. “This becomes particularly important for the large-joint procedures,” he said. “We don’t know if osteoarthritis or chronic inflammatory arthritis is leading to the large-joint procedure.”
The National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute on Aging funded the study. Dr. Richter reported having no financial disclosures.
SAN DIEGO – but the rate of small-joint procedures is declining for both sexes. However, no differences in rates of large-joint procedures between sexes were observed during the same time period.
Those are key findings from a retrospective study which set out to determine if there are sex differences in the incidence and trends of large- versus small-joint surgery rates in rheumatoid arthritis over time. “Why is orthopedic surgery important to rheumatology? The main reason is because it’s a surrogate for failed medical management,” lead study author Michael D. Richter, MD, said at the annual meeting of the American College of Rheumatology.
Dr. Richter, an internal medicine resident at Mayo Clinic, Rochester, Minn., said that women with RA generally present with more severe symptoms and higher rates of disability, while men have a better treatment response and a higher remission rate. For example, results from the multinational Quantitative Standard Monitoring of Patients with RA study found that remission rates were around 30% in men and 17% in women (Arthritis Res Ther. 2009;11[1]:R7). “However, a lot of these studies are criticized because it’s thought that gender can play a role in the disease measures,” he said. “By looking at joint surgery we have an objective outcome, and we can look at differences in treatment efficacy.”
Dr. Richter and his associates drew from the Rochester Epidemiology Project to identify 1,077 patients from Olmstead County, Minn., who fulfilled ACR criteria for RA between 1980 and 2013, and who were followed up until death, migration, or July 1, 2016. They classified surgeries as small joint (wrist, hand, or foot) or large joint (shoulder, elbow, hip, knee, or ankle). A majority of the patients (70%) were women. Compared with women, men were slightly older at diagnosis (a mean of 58 years vs. 55 years, respectively), were more likely to have a history of smoking (67% vs. 46%), and were more likely to have large-joint swelling upon initial presentation (49% vs. 42%). The mean follow-up was 12 years. No differences between men and women were noted in obesity, inflammatory biomarkers, or seropositivity.
During the study period, 112 patients underwent at least one small-joint surgery, 90 of whom were women (80%). The cumulative incidence of small-joint surgery at 15 years was nearly double that of men: 14.4% vs. 7.6%, respectively (P = .008). “Prior to the year 2000 there were no significant trends in the rate of small-joint surgery but it was more common in women,” he said. “After 2000 there was a significant decline for men and women (P = .002), but no significant difference between sexes.”
At the same time, 204 patients underwent at least one large-joint surgery during the time period, 141 of whom were women (69%). The cumulative incidence of large-joint surgery at 15 years was 20.2% for women and 18.8% for men, which was statistically similar (P = .55). “We saw no significant change over time in the rate of large-joint surgery from 1980 to 2016,” Dr. Richter said. “This is in contrast to what we see in the general population, where orthopedic procedures for osteoarthritis are more common.”
He acknowledged certain limitations of the study, including its retrospective design and the fact that the researchers were unable to include specific surgical indications in the analysis. “This becomes particularly important for the large-joint procedures,” he said. “We don’t know if osteoarthritis or chronic inflammatory arthritis is leading to the large-joint procedure.”
The National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute on Aging funded the study. Dr. Richter reported having no financial disclosures.
SAN DIEGO – but the rate of small-joint procedures is declining for both sexes. However, no differences in rates of large-joint procedures between sexes were observed during the same time period.
Those are key findings from a retrospective study which set out to determine if there are sex differences in the incidence and trends of large- versus small-joint surgery rates in rheumatoid arthritis over time. “Why is orthopedic surgery important to rheumatology? The main reason is because it’s a surrogate for failed medical management,” lead study author Michael D. Richter, MD, said at the annual meeting of the American College of Rheumatology.
Dr. Richter, an internal medicine resident at Mayo Clinic, Rochester, Minn., said that women with RA generally present with more severe symptoms and higher rates of disability, while men have a better treatment response and a higher remission rate. For example, results from the multinational Quantitative Standard Monitoring of Patients with RA study found that remission rates were around 30% in men and 17% in women (Arthritis Res Ther. 2009;11[1]:R7). “However, a lot of these studies are criticized because it’s thought that gender can play a role in the disease measures,” he said. “By looking at joint surgery we have an objective outcome, and we can look at differences in treatment efficacy.”
Dr. Richter and his associates drew from the Rochester Epidemiology Project to identify 1,077 patients from Olmstead County, Minn., who fulfilled ACR criteria for RA between 1980 and 2013, and who were followed up until death, migration, or July 1, 2016. They classified surgeries as small joint (wrist, hand, or foot) or large joint (shoulder, elbow, hip, knee, or ankle). A majority of the patients (70%) were women. Compared with women, men were slightly older at diagnosis (a mean of 58 years vs. 55 years, respectively), were more likely to have a history of smoking (67% vs. 46%), and were more likely to have large-joint swelling upon initial presentation (49% vs. 42%). The mean follow-up was 12 years. No differences between men and women were noted in obesity, inflammatory biomarkers, or seropositivity.
During the study period, 112 patients underwent at least one small-joint surgery, 90 of whom were women (80%). The cumulative incidence of small-joint surgery at 15 years was nearly double that of men: 14.4% vs. 7.6%, respectively (P = .008). “Prior to the year 2000 there were no significant trends in the rate of small-joint surgery but it was more common in women,” he said. “After 2000 there was a significant decline for men and women (P = .002), but no significant difference between sexes.”
At the same time, 204 patients underwent at least one large-joint surgery during the time period, 141 of whom were women (69%). The cumulative incidence of large-joint surgery at 15 years was 20.2% for women and 18.8% for men, which was statistically similar (P = .55). “We saw no significant change over time in the rate of large-joint surgery from 1980 to 2016,” Dr. Richter said. “This is in contrast to what we see in the general population, where orthopedic procedures for osteoarthritis are more common.”
He acknowledged certain limitations of the study, including its retrospective design and the fact that the researchers were unable to include specific surgical indications in the analysis. “This becomes particularly important for the large-joint procedures,” he said. “We don’t know if osteoarthritis or chronic inflammatory arthritis is leading to the large-joint procedure.”
The National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute on Aging funded the study. Dr. Richter reported having no financial disclosures.
AT ACR 2017
Key clinical point: Women with RA had a higher rate of small-joint surgery, compared with men.
Major finding: The cumulative incidence of small-joint surgery was significantly higher among women, compared with men (14.4% vs. 7.6%, respectively), but there were no differences between sexes in the rates of large-joint surgery.
Study details: A retrospective, population-based study of 1,077 patients with RA.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute on Aging funded the study. Dr. Richter reported having no financial disclosures.
VIDEO: Advanced alternative payment model for RA set to undergo testing
SAN DIEGO – for evaluation, in order to provide rheumatologists with another payment pathway under Medicare’s new Quality Payment Program.
The draft version of the rheumatoid arthritis advanced alternative payment model (APM), prepared by the American College of Rheumatology and unveiled at its annual meeting, aims to give rheumatologists a more focused opportunity to participate in value-based care and potentially earn greater incentive payments. The model is geared not only to private practice rheumatologists, but also to those in academia.
The Quality Payment Program, including its advanced APM track, was established by the Medicare and CHIP Reauthorization Act of 2015 (MACRA).

Other societies are working on or have submitted APMs for approval, Timothy Laing, MD, a member of the RA APM working group and also the ACR representative to the American Medical Association’s Relative Value Scale Update Committee and CPT Advisory Committee, said at the ACR meeting.
After presenting a draft of the RA APM at an AMA workshop in October, Dr. Laing came away encouraged by the attendees’ response to the usefulness and flexibility of the model to pay for services that rheumatologists are currently frustrated by in a fee-for-services system. “It’s a big if, but I think if we can make the money work, this will be a shift and it will have a lot of impact on how we practice, and I think it will be generalizable to more than one condition.”
The cochair of the RA APM working group, Kwas Huston, MD, presented the draft at the meeting. He noted that advanced APMs could be developed just for specific diseases, for all inflammatory arthritis, all types of vasculitis, or for all rheumatic diseases. RA was chosen first because the ACR is new to the development of APMs and “needed to start somewhere.”
“This model allows us to improve our ability to care for patients and is more sustainable over time for rheumatologists from a revenue standpoint,” Dr. Huston, a rheumatologist with Kansas City (Mo.) Physician Partners, said in an interview.
The RA APM helps to reduce barriers to good care by providing adequate reimbursement for cognitive services through monthly payments rather than relying on payment for separate office visits, Dr. Huston said. The model allows for more time spent in shared decision making, educational activities, and improving treatment adherence. It also builds in payment for non–face-to-face communication between rheumatologists, primary care physicians, and other specialists; interaction with patients via phone calls, email, and telemedicine; and using nurses or other staff to help with chronic disease management. It’s meant to be flexible for use in diverse settings by allowing comanagement of patients in rural areas and places where there is a shortage of rheumatologists or travel is difficult.
Why join an advanced APM?
Rheumatologists may want to join an advanced APM because of the potentially unsustainable, “zero-sum” nature of MACRA’s Merit-based Incentive Payment System (MIPS), in which the losers pay for the winners, said Angus Worthing, MD, chair of the ACR’s Government Affairs Committee and a member of the RA APM working group. In MIPS, there are expected over time to be fewer and fewer “losers” in the program, either because participants perform better or the losers drop out. In addition, advanced APM participants will receive a 5% bonus in 2019-2024 and Medicare payment updates will be higher for advanced APMs in 2026 and beyond than for MIPS (0.75% vs. 0.25%).
Beyond the financial practicalities of MACRA, it’s beneficial for rheumatologists to have their own advanced APM because it’s better than being stuck in one that’s “written by the government and doesn’t cater to other specialties; it’s specific to rheumatology, our patients, our work flow, and what we think is valuable,” said Dr. Worthing, a practicing rheumatologist in the Washington area.

To participate in an advanced APM, clinicians will need to have 25% of payments for Part B fall under professional services in the advanced APM or have 20% of their patients receive Part B professional services through the advanced APM. However, Dr. Worthing advised keeping an eye out for new thresholds for participating in the APM track because “it will probably be hard to get 25% of your Medicare reimbursements or 20% of your patients in the first year you’re in it.”
The RA APM’s treatment pathway
Undergirding the whole model is a treatment pathway that takes a standardized approach to RA care, based on ACR 2015 guidelines, and will be updated regularly by the ACR, Dr. Huston said. Following the guidelines gives an opportunity to lower spending but increase the percentage that’s going to rheumatologists by reducing the variability in initiation of expensive medications. “Currently, we get about 2.5 cents on the dollar for every dollar that’s spent on rheumatoid arthritis care, and we want to increase the part that’s going to the rheumatologist to provide more services but decrease total spending,” he said.
The pathway requires the use of methotrexate and/or another disease-modifying antirheumatic drug (DMARD) before targeted therapy. However, the model also allows for treating unique patients by requiring only 75% adherence to the guidelines. Deviation from the guidelines is allowed if a patient has a contraindication, intolerance, or inadequate response to a DMARD, or if there are barriers outside of the rheumatologist’s control, such as insurance coverage. The ACR guidelines also specify the frequency and type of monitoring that’s needed for treatment.
Because the ACR guidelines will be followed, the model asks that payers make patients eligible for lower out-of-pocket costs for medications. Following the guidelines should also reduce the need for prior authorizations. Providers in the advanced APM would attest to 75% adherence to the pathway, which would be subject to audit. “We want to reduce the reporting burden. In MIPS, it’s very complicated. It’s hard to know how to report all of this. In the APM pathway, we’re trying to simplify reporting. You only have to report two things; one of them is following the treatment pathway 75% of the time” and the other is an outcome measure, he said.
The payments made under this RA treatment pathway are divided into four areas: diagnosis and treatment planning, support for primary care physicians in diagnosing joint symptoms, the initial treatment of RA patients, and continued care for RA.
Diagnosis and treatment planning
This step offers a one-time payment to support all the costs of evaluation, testing, diagnosis, and treatment planning for a patient who has symptoms that potentially indicate RA, has not been previously treated or diagnosed with RA, or has been treated unsuccessfully for RA by other physicians. It is not dependent on the number of visits.
This phase also covers basic lab testing and imaging, which if not done by the rheumatology practice, would then have a standardized amount deducted from the payment and be paid separately. Lab tests and imaging performed for other conditions would be paid separately as well.
The payment covers communication with other physicians, spending more time with patients in a shared decision-making process regarding treatment options, and developing a RA treatment plan.
“If you don’t end up diagnosing RA, you still get the payment. But there will be two different payments; one is a little lower if they don’t have RA. If they do have RA, then you spend more time with them developing this treatment plan, so that would be a higher payment,” Dr. Huston said.
Support for primary care physicians in diagnosing joint symptoms
This payment goes to a rheumatologist or a nurse practitioner or physician assistant who is working under the supervision of a rheumatologist for a patient who is under the care of a primary care physician who has an agreement to work collaboratively with the rheumatology practice. The payment, which is limited to one bill for one patient in a 1-year period, is for communication between the rheumatologist and the primary care physician about patients with symptoms that might indicate RA to determine the need for referral.
“This communication could be a phone call, an email, face-to-face, or some other form of communication ... to discuss how fast the patient may need to be seen or if there are other tests that need to be done before expediting referrals for patients who are higher risk,” Dr. Huston explained.
The payment would still be made if the patient does not require referral to a rheumatologist.
Initial treatment of RA patients
Payment for initial treatment can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or a team comprising the rheumatologist and a primary care physician who have a formal arrangement to support the early treatment of RA.
The latter scenario is intended for rural areas and other areas where there is a shortage of rheumatologists. The formal arrangement would specify how payments are shared and who is responsible for each of the accountability requirements and for treatment pathway, “but there is a lot of flexibility, and this can vary quite a bit, so what happens in rural Alaska where the primary care doctors might be more involved is not going to be the same as in a big city where the primary care doctors may not want to be involved at all. So there is no requirement for primary care doctors to be involved, but it just provides the resources in areas where that might make sense,” Dr. Huston noted.
The initial treatment payment would be made monthly for 6 months, replacing evaluation and management billing for office visits related to RA. It pays for typical lab tests and imaging and allows flexibility for non–face-to-face communications, and enhanced services to patients who need them. This payment is also stratified to adjust for sicker patients who have more comorbidities, he said.
Continued care for RA
This component of the payment structure also can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or the rheumatologist–primary care physician team. Continued care payments are made monthly and, just as with initial treatment payments, they are meant to replace E&M billing for office visits and pay for the same kinds of resources used in initial treatment, including stratified payments to adjust for patient characteristics.
Patients who come to a rheumatologist with established RA would enter this treatment pathway under this kind of payment.
RA APM’s accountability requirements
Participants in this model would be required to see a patient face-to-face at least every 6 months and to document their disease activity using a validated scale approved by the ACR for use in the RA APM, such as the RAPID-3 (Routine Assessment of Patient Index Data–3), the CDAI (Clinical Disease Activity Index), the SDAI (Simple Disease Activity Index), or the DAS28 (28-joint Disease Activity Score). Payment would also require keeping a written treatment plan that’s consistent with the ACR’s approved treatment pathway.
Changes in medication require communication with the patient within 2 weeks to help improve treatment adherence. Quality measures will still need to be recorded, such as a functional assessment, tuberculosis screening prior to starting biologics, and having a plan for steroid use, but they are not required to be reported. “You attest to that,” he said.
However, participants will need to report that they are following the treatment pathway for patients and an outcome measure for continued care of RA. These are necessary, Dr. Huston said, because “we are asking that we increase the money that’s going to the rheumatologist for managing patients with RA, so we have to show that we’re accountable and doing good with that money and that we’re taking care of our patients. ... and if we have an outcome measure, then we don’t have to report all those process measures that we do in MIPS.”
The outcome measure would be reporting:
• At least (some %) of patients with low disease activity remained in low disease activity.
• At least (some %) of patients with moderate disease activity stayed in the same or a lower disease activity category.
• At least (some %) of patients with a high disease activity had a lower disease activity category.
It’s unknown yet what the threshold percentage for each disease activity level would be, but it will be obtained from the ACR’s Rheumatology Informatics System for Effectiveness (RISE) Registry and will be refined over time from there. The outcome measure is not validated yet – none exists for RA for use in clinical practice – because it’s not yet known how to risk stratify patients in these disease activity levels for their comorbidities and socioeconomic factors. “Those are all things we need to learn over time,” Dr. Huston said, “but this is our good-faith effort at developing an outcome measure which we think will become more robust as we gather more and more data.”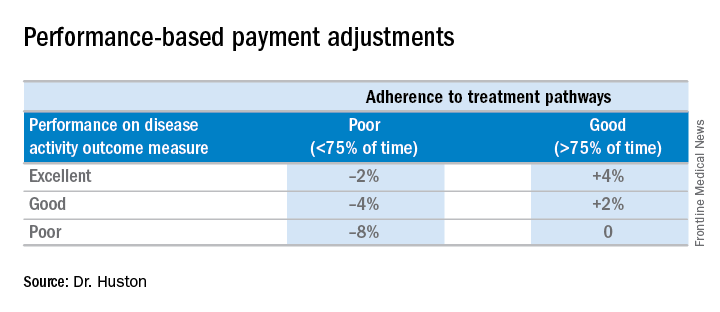
Performing all of these requirements would likely require more staff, and so the model will be built to account for these higher costs, Dr. Huston said.
Advantages of the RA APM
The RA APM’s advantages, according to Dr. Huston, stem from its payment for high-value services; the avoidance of the penalties and reporting burdens imposed by MIPS; a reduction in documentation requirements, allowing clinicians to take notes on history of present illness and review of systems however they want; a reduction in prior authorizations; and more control over performance measures.
Another big advantage of the RA APM is that participants “are not responsible for the price of drugs, whereas in MIPS you are responsible. When [the Centers for Medicare & Medicaid Services] calculates your cost category [in MIPS], that includes Part B drugs, and when the MIPS adjustment factor is applied to your revenue, that includes revenue from Part B drugs,” Dr. Huston said.
In addition, he noted that it will be possible for a rheumatologist to be a participant in just one or two APMs and still have the benefit of being out of MIPS.
Next steps
The next steps for the development of the RA APM include refining the treatment pathway, analyzing RISE data outcome thresholds, and modeling the financial impact on practices by running data from three to five practices across the country through the model to determine what the payment levels should be. Once those steps are completed, the RA APM can be submitted to the Physician-Focused Payment Model Technical Advisory Committee for approval, which will then send it to the CMS to run it through its Innovation Center to test the model in several practices to gather more data and refine the payment rates until it is ready to be expanded and implemented.
Dr. Huston, Dr. Worthing, and Dr. Laing had no relevant conflicts of interest to disclose.
SAN DIEGO – for evaluation, in order to provide rheumatologists with another payment pathway under Medicare’s new Quality Payment Program.
The draft version of the rheumatoid arthritis advanced alternative payment model (APM), prepared by the American College of Rheumatology and unveiled at its annual meeting, aims to give rheumatologists a more focused opportunity to participate in value-based care and potentially earn greater incentive payments. The model is geared not only to private practice rheumatologists, but also to those in academia.
The Quality Payment Program, including its advanced APM track, was established by the Medicare and CHIP Reauthorization Act of 2015 (MACRA).
Other societies are working on or have submitted APMs for approval, Timothy Laing, MD, a member of the RA APM working group and also the ACR representative to the American Medical Association’s Relative Value Scale Update Committee and CPT Advisory Committee, said at the ACR meeting.
After presenting a draft of the RA APM at an AMA workshop in October, Dr. Laing came away encouraged by the attendees’ response to the usefulness and flexibility of the model to pay for services that rheumatologists are currently frustrated by in a fee-for-services system. “It’s a big if, but I think if we can make the money work, this will be a shift and it will have a lot of impact on how we practice, and I think it will be generalizable to more than one condition.”
The cochair of the RA APM working group, Kwas Huston, MD, presented the draft at the meeting. He noted that advanced APMs could be developed just for specific diseases, for all inflammatory arthritis, all types of vasculitis, or for all rheumatic diseases. RA was chosen first because the ACR is new to the development of APMs and “needed to start somewhere.”
“This model allows us to improve our ability to care for patients and is more sustainable over time for rheumatologists from a revenue standpoint,” Dr. Huston, a rheumatologist with Kansas City (Mo.) Physician Partners, said in an interview.
The RA APM helps to reduce barriers to good care by providing adequate reimbursement for cognitive services through monthly payments rather than relying on payment for separate office visits, Dr. Huston said. The model allows for more time spent in shared decision making, educational activities, and improving treatment adherence. It also builds in payment for non–face-to-face communication between rheumatologists, primary care physicians, and other specialists; interaction with patients via phone calls, email, and telemedicine; and using nurses or other staff to help with chronic disease management. It’s meant to be flexible for use in diverse settings by allowing comanagement of patients in rural areas and places where there is a shortage of rheumatologists or travel is difficult.
Why join an advanced APM?
Rheumatologists may want to join an advanced APM because of the potentially unsustainable, “zero-sum” nature of MACRA’s Merit-based Incentive Payment System (MIPS), in which the losers pay for the winners, said Angus Worthing, MD, chair of the ACR’s Government Affairs Committee and a member of the RA APM working group. In MIPS, there are expected over time to be fewer and fewer “losers” in the program, either because participants perform better or the losers drop out. In addition, advanced APM participants will receive a 5% bonus in 2019-2024 and Medicare payment updates will be higher for advanced APMs in 2026 and beyond than for MIPS (0.75% vs. 0.25%).
Beyond the financial practicalities of MACRA, it’s beneficial for rheumatologists to have their own advanced APM because it’s better than being stuck in one that’s “written by the government and doesn’t cater to other specialties; it’s specific to rheumatology, our patients, our work flow, and what we think is valuable,” said Dr. Worthing, a practicing rheumatologist in the Washington area.
To participate in an advanced APM, clinicians will need to have 25% of payments for Part B fall under professional services in the advanced APM or have 20% of their patients receive Part B professional services through the advanced APM. However, Dr. Worthing advised keeping an eye out for new thresholds for participating in the APM track because “it will probably be hard to get 25% of your Medicare reimbursements or 20% of your patients in the first year you’re in it.”
The RA APM’s treatment pathway
Undergirding the whole model is a treatment pathway that takes a standardized approach to RA care, based on ACR 2015 guidelines, and will be updated regularly by the ACR, Dr. Huston said. Following the guidelines gives an opportunity to lower spending but increase the percentage that’s going to rheumatologists by reducing the variability in initiation of expensive medications. “Currently, we get about 2.5 cents on the dollar for every dollar that’s spent on rheumatoid arthritis care, and we want to increase the part that’s going to the rheumatologist to provide more services but decrease total spending,” he said.
The pathway requires the use of methotrexate and/or another disease-modifying antirheumatic drug (DMARD) before targeted therapy. However, the model also allows for treating unique patients by requiring only 75% adherence to the guidelines. Deviation from the guidelines is allowed if a patient has a contraindication, intolerance, or inadequate response to a DMARD, or if there are barriers outside of the rheumatologist’s control, such as insurance coverage. The ACR guidelines also specify the frequency and type of monitoring that’s needed for treatment.
Because the ACR guidelines will be followed, the model asks that payers make patients eligible for lower out-of-pocket costs for medications. Following the guidelines should also reduce the need for prior authorizations. Providers in the advanced APM would attest to 75% adherence to the pathway, which would be subject to audit. “We want to reduce the reporting burden. In MIPS, it’s very complicated. It’s hard to know how to report all of this. In the APM pathway, we’re trying to simplify reporting. You only have to report two things; one of them is following the treatment pathway 75% of the time” and the other is an outcome measure, he said.
The payments made under this RA treatment pathway are divided into four areas: diagnosis and treatment planning, support for primary care physicians in diagnosing joint symptoms, the initial treatment of RA patients, and continued care for RA.
Diagnosis and treatment planning
This step offers a one-time payment to support all the costs of evaluation, testing, diagnosis, and treatment planning for a patient who has symptoms that potentially indicate RA, has not been previously treated or diagnosed with RA, or has been treated unsuccessfully for RA by other physicians. It is not dependent on the number of visits.
This phase also covers basic lab testing and imaging, which if not done by the rheumatology practice, would then have a standardized amount deducted from the payment and be paid separately. Lab tests and imaging performed for other conditions would be paid separately as well.
The payment covers communication with other physicians, spending more time with patients in a shared decision-making process regarding treatment options, and developing a RA treatment plan.
“If you don’t end up diagnosing RA, you still get the payment. But there will be two different payments; one is a little lower if they don’t have RA. If they do have RA, then you spend more time with them developing this treatment plan, so that would be a higher payment,” Dr. Huston said.
Support for primary care physicians in diagnosing joint symptoms
This payment goes to a rheumatologist or a nurse practitioner or physician assistant who is working under the supervision of a rheumatologist for a patient who is under the care of a primary care physician who has an agreement to work collaboratively with the rheumatology practice. The payment, which is limited to one bill for one patient in a 1-year period, is for communication between the rheumatologist and the primary care physician about patients with symptoms that might indicate RA to determine the need for referral.
“This communication could be a phone call, an email, face-to-face, or some other form of communication ... to discuss how fast the patient may need to be seen or if there are other tests that need to be done before expediting referrals for patients who are higher risk,” Dr. Huston explained.
The payment would still be made if the patient does not require referral to a rheumatologist.
Initial treatment of RA patients
Payment for initial treatment can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or a team comprising the rheumatologist and a primary care physician who have a formal arrangement to support the early treatment of RA.
The latter scenario is intended for rural areas and other areas where there is a shortage of rheumatologists. The formal arrangement would specify how payments are shared and who is responsible for each of the accountability requirements and for treatment pathway, “but there is a lot of flexibility, and this can vary quite a bit, so what happens in rural Alaska where the primary care doctors might be more involved is not going to be the same as in a big city where the primary care doctors may not want to be involved at all. So there is no requirement for primary care doctors to be involved, but it just provides the resources in areas where that might make sense,” Dr. Huston noted.
The initial treatment payment would be made monthly for 6 months, replacing evaluation and management billing for office visits related to RA. It pays for typical lab tests and imaging and allows flexibility for non–face-to-face communications, and enhanced services to patients who need them. This payment is also stratified to adjust for sicker patients who have more comorbidities, he said.
Continued care for RA
This component of the payment structure also can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or the rheumatologist–primary care physician team. Continued care payments are made monthly and, just as with initial treatment payments, they are meant to replace E&M billing for office visits and pay for the same kinds of resources used in initial treatment, including stratified payments to adjust for patient characteristics.
Patients who come to a rheumatologist with established RA would enter this treatment pathway under this kind of payment.
RA APM’s accountability requirements
Participants in this model would be required to see a patient face-to-face at least every 6 months and to document their disease activity using a validated scale approved by the ACR for use in the RA APM, such as the RAPID-3 (Routine Assessment of Patient Index Data–3), the CDAI (Clinical Disease Activity Index), the SDAI (Simple Disease Activity Index), or the DAS28 (28-joint Disease Activity Score). Payment would also require keeping a written treatment plan that’s consistent with the ACR’s approved treatment pathway.
Changes in medication require communication with the patient within 2 weeks to help improve treatment adherence. Quality measures will still need to be recorded, such as a functional assessment, tuberculosis screening prior to starting biologics, and having a plan for steroid use, but they are not required to be reported. “You attest to that,” he said.
However, participants will need to report that they are following the treatment pathway for patients and an outcome measure for continued care of RA. These are necessary, Dr. Huston said, because “we are asking that we increase the money that’s going to the rheumatologist for managing patients with RA, so we have to show that we’re accountable and doing good with that money and that we’re taking care of our patients. ... and if we have an outcome measure, then we don’t have to report all those process measures that we do in MIPS.”
The outcome measure would be reporting:
• At least (some %) of patients with low disease activity remained in low disease activity.
• At least (some %) of patients with moderate disease activity stayed in the same or a lower disease activity category.
• At least (some %) of patients with a high disease activity had a lower disease activity category.
It’s unknown yet what the threshold percentage for each disease activity level would be, but it will be obtained from the ACR’s Rheumatology Informatics System for Effectiveness (RISE) Registry and will be refined over time from there. The outcome measure is not validated yet – none exists for RA for use in clinical practice – because it’s not yet known how to risk stratify patients in these disease activity levels for their comorbidities and socioeconomic factors. “Those are all things we need to learn over time,” Dr. Huston said, “but this is our good-faith effort at developing an outcome measure which we think will become more robust as we gather more and more data.”
Performing all of these requirements would likely require more staff, and so the model will be built to account for these higher costs, Dr. Huston said.
Advantages of the RA APM
The RA APM’s advantages, according to Dr. Huston, stem from its payment for high-value services; the avoidance of the penalties and reporting burdens imposed by MIPS; a reduction in documentation requirements, allowing clinicians to take notes on history of present illness and review of systems however they want; a reduction in prior authorizations; and more control over performance measures.
Another big advantage of the RA APM is that participants “are not responsible for the price of drugs, whereas in MIPS you are responsible. When [the Centers for Medicare & Medicaid Services] calculates your cost category [in MIPS], that includes Part B drugs, and when the MIPS adjustment factor is applied to your revenue, that includes revenue from Part B drugs,” Dr. Huston said.
In addition, he noted that it will be possible for a rheumatologist to be a participant in just one or two APMs and still have the benefit of being out of MIPS.
Next steps
The next steps for the development of the RA APM include refining the treatment pathway, analyzing RISE data outcome thresholds, and modeling the financial impact on practices by running data from three to five practices across the country through the model to determine what the payment levels should be. Once those steps are completed, the RA APM can be submitted to the Physician-Focused Payment Model Technical Advisory Committee for approval, which will then send it to the CMS to run it through its Innovation Center to test the model in several practices to gather more data and refine the payment rates until it is ready to be expanded and implemented.
Dr. Huston, Dr. Worthing, and Dr. Laing had no relevant conflicts of interest to disclose.
SAN DIEGO – for evaluation, in order to provide rheumatologists with another payment pathway under Medicare’s new Quality Payment Program.
The draft version of the rheumatoid arthritis advanced alternative payment model (APM), prepared by the American College of Rheumatology and unveiled at its annual meeting, aims to give rheumatologists a more focused opportunity to participate in value-based care and potentially earn greater incentive payments. The model is geared not only to private practice rheumatologists, but also to those in academia.
The Quality Payment Program, including its advanced APM track, was established by the Medicare and CHIP Reauthorization Act of 2015 (MACRA).
Other societies are working on or have submitted APMs for approval, Timothy Laing, MD, a member of the RA APM working group and also the ACR representative to the American Medical Association’s Relative Value Scale Update Committee and CPT Advisory Committee, said at the ACR meeting.
After presenting a draft of the RA APM at an AMA workshop in October, Dr. Laing came away encouraged by the attendees’ response to the usefulness and flexibility of the model to pay for services that rheumatologists are currently frustrated by in a fee-for-services system. “It’s a big if, but I think if we can make the money work, this will be a shift and it will have a lot of impact on how we practice, and I think it will be generalizable to more than one condition.”
The cochair of the RA APM working group, Kwas Huston, MD, presented the draft at the meeting. He noted that advanced APMs could be developed just for specific diseases, for all inflammatory arthritis, all types of vasculitis, or for all rheumatic diseases. RA was chosen first because the ACR is new to the development of APMs and “needed to start somewhere.”
“This model allows us to improve our ability to care for patients and is more sustainable over time for rheumatologists from a revenue standpoint,” Dr. Huston, a rheumatologist with Kansas City (Mo.) Physician Partners, said in an interview.
The RA APM helps to reduce barriers to good care by providing adequate reimbursement for cognitive services through monthly payments rather than relying on payment for separate office visits, Dr. Huston said. The model allows for more time spent in shared decision making, educational activities, and improving treatment adherence. It also builds in payment for non–face-to-face communication between rheumatologists, primary care physicians, and other specialists; interaction with patients via phone calls, email, and telemedicine; and using nurses or other staff to help with chronic disease management. It’s meant to be flexible for use in diverse settings by allowing comanagement of patients in rural areas and places where there is a shortage of rheumatologists or travel is difficult.
Why join an advanced APM?
Rheumatologists may want to join an advanced APM because of the potentially unsustainable, “zero-sum” nature of MACRA’s Merit-based Incentive Payment System (MIPS), in which the losers pay for the winners, said Angus Worthing, MD, chair of the ACR’s Government Affairs Committee and a member of the RA APM working group. In MIPS, there are expected over time to be fewer and fewer “losers” in the program, either because participants perform better or the losers drop out. In addition, advanced APM participants will receive a 5% bonus in 2019-2024 and Medicare payment updates will be higher for advanced APMs in 2026 and beyond than for MIPS (0.75% vs. 0.25%).
Beyond the financial practicalities of MACRA, it’s beneficial for rheumatologists to have their own advanced APM because it’s better than being stuck in one that’s “written by the government and doesn’t cater to other specialties; it’s specific to rheumatology, our patients, our work flow, and what we think is valuable,” said Dr. Worthing, a practicing rheumatologist in the Washington area.
To participate in an advanced APM, clinicians will need to have 25% of payments for Part B fall under professional services in the advanced APM or have 20% of their patients receive Part B professional services through the advanced APM. However, Dr. Worthing advised keeping an eye out for new thresholds for participating in the APM track because “it will probably be hard to get 25% of your Medicare reimbursements or 20% of your patients in the first year you’re in it.”
The RA APM’s treatment pathway
Undergirding the whole model is a treatment pathway that takes a standardized approach to RA care, based on ACR 2015 guidelines, and will be updated regularly by the ACR, Dr. Huston said. Following the guidelines gives an opportunity to lower spending but increase the percentage that’s going to rheumatologists by reducing the variability in initiation of expensive medications. “Currently, we get about 2.5 cents on the dollar for every dollar that’s spent on rheumatoid arthritis care, and we want to increase the part that’s going to the rheumatologist to provide more services but decrease total spending,” he said.
The pathway requires the use of methotrexate and/or another disease-modifying antirheumatic drug (DMARD) before targeted therapy. However, the model also allows for treating unique patients by requiring only 75% adherence to the guidelines. Deviation from the guidelines is allowed if a patient has a contraindication, intolerance, or inadequate response to a DMARD, or if there are barriers outside of the rheumatologist’s control, such as insurance coverage. The ACR guidelines also specify the frequency and type of monitoring that’s needed for treatment.
Because the ACR guidelines will be followed, the model asks that payers make patients eligible for lower out-of-pocket costs for medications. Following the guidelines should also reduce the need for prior authorizations. Providers in the advanced APM would attest to 75% adherence to the pathway, which would be subject to audit. “We want to reduce the reporting burden. In MIPS, it’s very complicated. It’s hard to know how to report all of this. In the APM pathway, we’re trying to simplify reporting. You only have to report two things; one of them is following the treatment pathway 75% of the time” and the other is an outcome measure, he said.
The payments made under this RA treatment pathway are divided into four areas: diagnosis and treatment planning, support for primary care physicians in diagnosing joint symptoms, the initial treatment of RA patients, and continued care for RA.
Diagnosis and treatment planning
This step offers a one-time payment to support all the costs of evaluation, testing, diagnosis, and treatment planning for a patient who has symptoms that potentially indicate RA, has not been previously treated or diagnosed with RA, or has been treated unsuccessfully for RA by other physicians. It is not dependent on the number of visits.
This phase also covers basic lab testing and imaging, which if not done by the rheumatology practice, would then have a standardized amount deducted from the payment and be paid separately. Lab tests and imaging performed for other conditions would be paid separately as well.
The payment covers communication with other physicians, spending more time with patients in a shared decision-making process regarding treatment options, and developing a RA treatment plan.
“If you don’t end up diagnosing RA, you still get the payment. But there will be two different payments; one is a little lower if they don’t have RA. If they do have RA, then you spend more time with them developing this treatment plan, so that would be a higher payment,” Dr. Huston said.
Support for primary care physicians in diagnosing joint symptoms
This payment goes to a rheumatologist or a nurse practitioner or physician assistant who is working under the supervision of a rheumatologist for a patient who is under the care of a primary care physician who has an agreement to work collaboratively with the rheumatology practice. The payment, which is limited to one bill for one patient in a 1-year period, is for communication between the rheumatologist and the primary care physician about patients with symptoms that might indicate RA to determine the need for referral.
“This communication could be a phone call, an email, face-to-face, or some other form of communication ... to discuss how fast the patient may need to be seen or if there are other tests that need to be done before expediting referrals for patients who are higher risk,” Dr. Huston explained.
The payment would still be made if the patient does not require referral to a rheumatologist.
Initial treatment of RA patients
Payment for initial treatment can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or a team comprising the rheumatologist and a primary care physician who have a formal arrangement to support the early treatment of RA.
The latter scenario is intended for rural areas and other areas where there is a shortage of rheumatologists. The formal arrangement would specify how payments are shared and who is responsible for each of the accountability requirements and for treatment pathway, “but there is a lot of flexibility, and this can vary quite a bit, so what happens in rural Alaska where the primary care doctors might be more involved is not going to be the same as in a big city where the primary care doctors may not want to be involved at all. So there is no requirement for primary care doctors to be involved, but it just provides the resources in areas where that might make sense,” Dr. Huston noted.
The initial treatment payment would be made monthly for 6 months, replacing evaluation and management billing for office visits related to RA. It pays for typical lab tests and imaging and allows flexibility for non–face-to-face communications, and enhanced services to patients who need them. This payment is also stratified to adjust for sicker patients who have more comorbidities, he said.
Continued care for RA
This component of the payment structure also can be made to a rheumatologist, a nurse practitioner or physician assistant under the supervision of a rheumatologist, or the rheumatologist–primary care physician team. Continued care payments are made monthly and, just as with initial treatment payments, they are meant to replace E&M billing for office visits and pay for the same kinds of resources used in initial treatment, including stratified payments to adjust for patient characteristics.
Patients who come to a rheumatologist with established RA would enter this treatment pathway under this kind of payment.
RA APM’s accountability requirements
Participants in this model would be required to see a patient face-to-face at least every 6 months and to document their disease activity using a validated scale approved by the ACR for use in the RA APM, such as the RAPID-3 (Routine Assessment of Patient Index Data–3), the CDAI (Clinical Disease Activity Index), the SDAI (Simple Disease Activity Index), or the DAS28 (28-joint Disease Activity Score). Payment would also require keeping a written treatment plan that’s consistent with the ACR’s approved treatment pathway.
Changes in medication require communication with the patient within 2 weeks to help improve treatment adherence. Quality measures will still need to be recorded, such as a functional assessment, tuberculosis screening prior to starting biologics, and having a plan for steroid use, but they are not required to be reported. “You attest to that,” he said.
However, participants will need to report that they are following the treatment pathway for patients and an outcome measure for continued care of RA. These are necessary, Dr. Huston said, because “we are asking that we increase the money that’s going to the rheumatologist for managing patients with RA, so we have to show that we’re accountable and doing good with that money and that we’re taking care of our patients. ... and if we have an outcome measure, then we don’t have to report all those process measures that we do in MIPS.”
The outcome measure would be reporting:
• At least (some %) of patients with low disease activity remained in low disease activity.
• At least (some %) of patients with moderate disease activity stayed in the same or a lower disease activity category.
• At least (some %) of patients with a high disease activity had a lower disease activity category.
It’s unknown yet what the threshold percentage for each disease activity level would be, but it will be obtained from the ACR’s Rheumatology Informatics System for Effectiveness (RISE) Registry and will be refined over time from there. The outcome measure is not validated yet – none exists for RA for use in clinical practice – because it’s not yet known how to risk stratify patients in these disease activity levels for their comorbidities and socioeconomic factors. “Those are all things we need to learn over time,” Dr. Huston said, “but this is our good-faith effort at developing an outcome measure which we think will become more robust as we gather more and more data.”
Performing all of these requirements would likely require more staff, and so the model will be built to account for these higher costs, Dr. Huston said.
Advantages of the RA APM
The RA APM’s advantages, according to Dr. Huston, stem from its payment for high-value services; the avoidance of the penalties and reporting burdens imposed by MIPS; a reduction in documentation requirements, allowing clinicians to take notes on history of present illness and review of systems however they want; a reduction in prior authorizations; and more control over performance measures.
Another big advantage of the RA APM is that participants “are not responsible for the price of drugs, whereas in MIPS you are responsible. When [the Centers for Medicare & Medicaid Services] calculates your cost category [in MIPS], that includes Part B drugs, and when the MIPS adjustment factor is applied to your revenue, that includes revenue from Part B drugs,” Dr. Huston said.
In addition, he noted that it will be possible for a rheumatologist to be a participant in just one or two APMs and still have the benefit of being out of MIPS.
Next steps
The next steps for the development of the RA APM include refining the treatment pathway, analyzing RISE data outcome thresholds, and modeling the financial impact on practices by running data from three to five practices across the country through the model to determine what the payment levels should be. Once those steps are completed, the RA APM can be submitted to the Physician-Focused Payment Model Technical Advisory Committee for approval, which will then send it to the CMS to run it through its Innovation Center to test the model in several practices to gather more data and refine the payment rates until it is ready to be expanded and implemented.
Dr. Huston, Dr. Worthing, and Dr. Laing had no relevant conflicts of interest to disclose.
AT ACR 2017
Blindness linked to HCQ use rare in rheumatic patients
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
dbrunk@frontlinemedcom.com
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
dbrunk@frontlinemedcom.com
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
dbrunk@frontlinemedcom.com
AT ACR 2017
Key clinical point: The incidence of blindness due to hydroxychloroquine toxicity is very low.
Major finding: No patients developed blindness attributable to toxic maculopathy from using hydroxychloroquine.
Study details: A single-center retrospective study of 2,898 rheumatic patients.
Disclosures: Dr. Singh reported having no disclosures.
Use of opioids, SSRIs linked to increased fracture risk in RA
SAN DIEGO – The use of selective serotonin reuptake inhibitors and opioids was associated with an increased osteoporotic fracture risk in patients with rheumatoid arthritis, results from an analysis of national data showed.
“Osteoporotic fractures are one of the important causes of disability, health-related costs, and mortality in RA, with substantially higher complication and mortality rates than the general population,” study author Gulsen Ozen, MD, said in an interview prior to the annual meeting of the American College of Rheumatology. “Given the burden of osteoporotic fractures and the suboptimal osteoporosis care, identifying the factors associated with fracture risk in RA patients is of paramount importance.”

During a median follow-up of nearly 6 years, 863 patients (7.8%) sustained osteoporotic fractures. Compared with patients who did not develop fractures, those who did were significantly older, had higher disease duration and activity, glucocorticoid use, comorbidity and FRAX, a fracture risk assessment tool, scores at baseline. After adjusting for sociodemographics, comorbidities, body mass index, fracture risk by FRAX, and RA severity measures, the researchers found a significant risk of osteoporotic fractures with use of opioids of any strength (weak agents, hazard ratio, 1.45; strong agents, HR, 1.79; P less than .001 for both), SSRI use (HR, 1.35; P = .003), and glucocorticoid use of 3 months or longer at a dose of at least 7.5 mg per day (HR, 1.74; P less than .05). Osteoporotic fracture risk increase started even after 1-30 days of opioid use (HR, 1.96; P less than .001), whereas SSRI-associated risk increase started after 3 months of use (HR, 1.42; P = .054). No significant association with fracture risk was observed with the use of other disease-modifying antirheumatic drugs, statins, antidepressants, proton pump inhibitors, NSAIDs, anticonvulsants, and antipsychotics.
“One of the first surprising findings was that almost 40% of the RA patients older than 40 years of age were at least once exposed to opioid analgesics,” said Dr. Ozen, who is a research fellow in the division of immunology and rheumatology at the medical center. “Another surprising finding was that even very short-term (1-30 days) use of opioids was associated with increased fracture risk.” She went on to note that careful and regular reviewing of patient medications “is an essential part of the RA patient care, as the use of medications not indicated anymore brings harm rather than a benefit. The most well-known example for this is glucocorticoid use. This is valid for all medications, too. Therefore, we hope that our findings provide more awareness about osteoporotic fractures and associated risk factors in RA patients.”
She acknowledged certain limitations of the study, including its observational design. “Additionally, fracture and the level of the trauma in our cohort were reported by patients,” she said. “Therefore, there might be some misclassification of fractures as osteoporotic fractures. Lastly, we did not have detailed data regarding fall risk, which might explain the associations we observed with opioids and potentially, SSRIs.”
Dr. Ozen reported having no disclosures.
SAN DIEGO – The use of selective serotonin reuptake inhibitors and opioids was associated with an increased osteoporotic fracture risk in patients with rheumatoid arthritis, results from an analysis of national data showed.
“Osteoporotic fractures are one of the important causes of disability, health-related costs, and mortality in RA, with substantially higher complication and mortality rates than the general population,” study author Gulsen Ozen, MD, said in an interview prior to the annual meeting of the American College of Rheumatology. “Given the burden of osteoporotic fractures and the suboptimal osteoporosis care, identifying the factors associated with fracture risk in RA patients is of paramount importance.”
During a median follow-up of nearly 6 years, 863 patients (7.8%) sustained osteoporotic fractures. Compared with patients who did not develop fractures, those who did were significantly older, had higher disease duration and activity, glucocorticoid use, comorbidity and FRAX, a fracture risk assessment tool, scores at baseline. After adjusting for sociodemographics, comorbidities, body mass index, fracture risk by FRAX, and RA severity measures, the researchers found a significant risk of osteoporotic fractures with use of opioids of any strength (weak agents, hazard ratio, 1.45; strong agents, HR, 1.79; P less than .001 for both), SSRI use (HR, 1.35; P = .003), and glucocorticoid use of 3 months or longer at a dose of at least 7.5 mg per day (HR, 1.74; P less than .05). Osteoporotic fracture risk increase started even after 1-30 days of opioid use (HR, 1.96; P less than .001), whereas SSRI-associated risk increase started after 3 months of use (HR, 1.42; P = .054). No significant association with fracture risk was observed with the use of other disease-modifying antirheumatic drugs, statins, antidepressants, proton pump inhibitors, NSAIDs, anticonvulsants, and antipsychotics.
“One of the first surprising findings was that almost 40% of the RA patients older than 40 years of age were at least once exposed to opioid analgesics,” said Dr. Ozen, who is a research fellow in the division of immunology and rheumatology at the medical center. “Another surprising finding was that even very short-term (1-30 days) use of opioids was associated with increased fracture risk.” She went on to note that careful and regular reviewing of patient medications “is an essential part of the RA patient care, as the use of medications not indicated anymore brings harm rather than a benefit. The most well-known example for this is glucocorticoid use. This is valid for all medications, too. Therefore, we hope that our findings provide more awareness about osteoporotic fractures and associated risk factors in RA patients.”
She acknowledged certain limitations of the study, including its observational design. “Additionally, fracture and the level of the trauma in our cohort were reported by patients,” she said. “Therefore, there might be some misclassification of fractures as osteoporotic fractures. Lastly, we did not have detailed data regarding fall risk, which might explain the associations we observed with opioids and potentially, SSRIs.”
Dr. Ozen reported having no disclosures.
SAN DIEGO – The use of selective serotonin reuptake inhibitors and opioids was associated with an increased osteoporotic fracture risk in patients with rheumatoid arthritis, results from an analysis of national data showed.
“Osteoporotic fractures are one of the important causes of disability, health-related costs, and mortality in RA, with substantially higher complication and mortality rates than the general population,” study author Gulsen Ozen, MD, said in an interview prior to the annual meeting of the American College of Rheumatology. “Given the burden of osteoporotic fractures and the suboptimal osteoporosis care, identifying the factors associated with fracture risk in RA patients is of paramount importance.”
During a median follow-up of nearly 6 years, 863 patients (7.8%) sustained osteoporotic fractures. Compared with patients who did not develop fractures, those who did were significantly older, had higher disease duration and activity, glucocorticoid use, comorbidity and FRAX, a fracture risk assessment tool, scores at baseline. After adjusting for sociodemographics, comorbidities, body mass index, fracture risk by FRAX, and RA severity measures, the researchers found a significant risk of osteoporotic fractures with use of opioids of any strength (weak agents, hazard ratio, 1.45; strong agents, HR, 1.79; P less than .001 for both), SSRI use (HR, 1.35; P = .003), and glucocorticoid use of 3 months or longer at a dose of at least 7.5 mg per day (HR, 1.74; P less than .05). Osteoporotic fracture risk increase started even after 1-30 days of opioid use (HR, 1.96; P less than .001), whereas SSRI-associated risk increase started after 3 months of use (HR, 1.42; P = .054). No significant association with fracture risk was observed with the use of other disease-modifying antirheumatic drugs, statins, antidepressants, proton pump inhibitors, NSAIDs, anticonvulsants, and antipsychotics.
“One of the first surprising findings was that almost 40% of the RA patients older than 40 years of age were at least once exposed to opioid analgesics,” said Dr. Ozen, who is a research fellow in the division of immunology and rheumatology at the medical center. “Another surprising finding was that even very short-term (1-30 days) use of opioids was associated with increased fracture risk.” She went on to note that careful and regular reviewing of patient medications “is an essential part of the RA patient care, as the use of medications not indicated anymore brings harm rather than a benefit. The most well-known example for this is glucocorticoid use. This is valid for all medications, too. Therefore, we hope that our findings provide more awareness about osteoporotic fractures and associated risk factors in RA patients.”
She acknowledged certain limitations of the study, including its observational design. “Additionally, fracture and the level of the trauma in our cohort were reported by patients,” she said. “Therefore, there might be some misclassification of fractures as osteoporotic fractures. Lastly, we did not have detailed data regarding fall risk, which might explain the associations we observed with opioids and potentially, SSRIs.”
Dr. Ozen reported having no disclosures.
AT ACR 2017
Key clinical point: When managing with opioids, even in the short-term, clinicians should be aware of the fracture risk.
Major finding: In patients with RA, concomitant use of selective serotonin reuptake inhibitors was associated with an increased risk of osteoporotic fracture (HR, 1.35; P = .003), as was opioid use (HR, 1.45 and HR, 1.79) for weak and strong agents, respectively; P less than .001 for both).
Study details: An observational study of 11,049 patients from the National Data Bank for Rheumatic Diseases.
Disclosures: Dr. Ozen reported having no disclosures.
Obesity linked to RA disease activity, disability
SAN DIEGO – In what may be the largest study of its kind, British researchers have linked obesity to significantly higher odds of rheumatoid arthritis disease activity and disability.
“This study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis,” says Elena Nikiphorou, MD, of King’s College London, who presented the study findings at the annual meeting of the American College of Rheumatology. “Obesity reduced the odds of achieving remission or low disease activity by around 30%. And the odds of having disability were increased by 63%. This confirms what’s been shown in other, smaller studies.”

Despite obesity having been tied to decreased joint damage in established RA, Eric L. Matteson, MD, noted in an interview, that“the biomechanical effect of [being] overweight, especially on the weight-bearing joints” is one of the two “especially important” mechanisms explaining the link between RA and obesity. “The other is that fat cells produce inflammatory proteins, which contribute to the disease process and make it more difficult to treat,” said Dr. Matteson, a rheumatologist at the Mayo Clinic, Rochester, Minn.
“In my view the mechanical risk to the joint outweighs any possible ‘protective’ effect of RA,” Dr. Matteson added in an interview.
For the new study, Dr. Nikiphorou and colleagues compiled statistics from two consecutive United Kingdom RA inception cohorts. One tracked 1,465 patients for up to 25 years (median follow-up, 10 years), and the other tracked 1,236 patients for as many as 10 years (median follow-up, 6 years).
At baseline, 37.2% of 2,420 patients (90% of total) were overweight, and 21.3% were obese. Average body mass index (BMI) rose between the two consecutive studies from 25.5 to 27.6.
The researchers found that obesity was linked to lower likelihoods of remission and low disease activity status (odds ratio, 0.71; 95% confidence interval, 0.55-0.93 and OR, 0.69; 95% CI, 0.55-0.87, respectively.) After controlling for factors such as age and gender, they also saw slightly lower odds of remission in those with higher BMI (OR, 0.97; 95% CI, 0.95-0.99). But there was no statistically significant link between higher BMI and low disease activity status.
The study also connected obesity to higher odds of disability (OR, 1.63; 95% CI, 1.20-2.23). Furthermore, higher BMI was linked to higher odds of disability (OR, 1.04; 95% CI, 1.01-1.06).
Study lead author Dr. Nikiphorou, who spoke in an interview and in comments at an ACR press conference, said “this study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis. It creates a strong case for addressing BMI and addressing obesity, flagging it up to primary care.”
She added that rheumatologists too often focus on only rheumatoid conditions. “We place so much evidence on disease activity scores,” she said. “How often do we really address the patient in terms of other things going on, including obesity? What we can do is include discussion of BMI, exercise, nutrition.”
Dr. Nikiphorou and Dr. Matteson report no relevant disclosures. No specific study funding is reported.
This article was updated 11/10/17.
SAN DIEGO – In what may be the largest study of its kind, British researchers have linked obesity to significantly higher odds of rheumatoid arthritis disease activity and disability.
“This study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis,” says Elena Nikiphorou, MD, of King’s College London, who presented the study findings at the annual meeting of the American College of Rheumatology. “Obesity reduced the odds of achieving remission or low disease activity by around 30%. And the odds of having disability were increased by 63%. This confirms what’s been shown in other, smaller studies.”
Despite obesity having been tied to decreased joint damage in established RA, Eric L. Matteson, MD, noted in an interview, that“the biomechanical effect of [being] overweight, especially on the weight-bearing joints” is one of the two “especially important” mechanisms explaining the link between RA and obesity. “The other is that fat cells produce inflammatory proteins, which contribute to the disease process and make it more difficult to treat,” said Dr. Matteson, a rheumatologist at the Mayo Clinic, Rochester, Minn.
“In my view the mechanical risk to the joint outweighs any possible ‘protective’ effect of RA,” Dr. Matteson added in an interview.
For the new study, Dr. Nikiphorou and colleagues compiled statistics from two consecutive United Kingdom RA inception cohorts. One tracked 1,465 patients for up to 25 years (median follow-up, 10 years), and the other tracked 1,236 patients for as many as 10 years (median follow-up, 6 years).
At baseline, 37.2% of 2,420 patients (90% of total) were overweight, and 21.3% were obese. Average body mass index (BMI) rose between the two consecutive studies from 25.5 to 27.6.
The researchers found that obesity was linked to lower likelihoods of remission and low disease activity status (odds ratio, 0.71; 95% confidence interval, 0.55-0.93 and OR, 0.69; 95% CI, 0.55-0.87, respectively.) After controlling for factors such as age and gender, they also saw slightly lower odds of remission in those with higher BMI (OR, 0.97; 95% CI, 0.95-0.99). But there was no statistically significant link between higher BMI and low disease activity status.
The study also connected obesity to higher odds of disability (OR, 1.63; 95% CI, 1.20-2.23). Furthermore, higher BMI was linked to higher odds of disability (OR, 1.04; 95% CI, 1.01-1.06).
Study lead author Dr. Nikiphorou, who spoke in an interview and in comments at an ACR press conference, said “this study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis. It creates a strong case for addressing BMI and addressing obesity, flagging it up to primary care.”
She added that rheumatologists too often focus on only rheumatoid conditions. “We place so much evidence on disease activity scores,” she said. “How often do we really address the patient in terms of other things going on, including obesity? What we can do is include discussion of BMI, exercise, nutrition.”
Dr. Nikiphorou and Dr. Matteson report no relevant disclosures. No specific study funding is reported.
This article was updated 11/10/17.
SAN DIEGO – In what may be the largest study of its kind, British researchers have linked obesity to significantly higher odds of rheumatoid arthritis disease activity and disability.
“This study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis,” says Elena Nikiphorou, MD, of King’s College London, who presented the study findings at the annual meeting of the American College of Rheumatology. “Obesity reduced the odds of achieving remission or low disease activity by around 30%. And the odds of having disability were increased by 63%. This confirms what’s been shown in other, smaller studies.”
Despite obesity having been tied to decreased joint damage in established RA, Eric L. Matteson, MD, noted in an interview, that“the biomechanical effect of [being] overweight, especially on the weight-bearing joints” is one of the two “especially important” mechanisms explaining the link between RA and obesity. “The other is that fat cells produce inflammatory proteins, which contribute to the disease process and make it more difficult to treat,” said Dr. Matteson, a rheumatologist at the Mayo Clinic, Rochester, Minn.
“In my view the mechanical risk to the joint outweighs any possible ‘protective’ effect of RA,” Dr. Matteson added in an interview.
For the new study, Dr. Nikiphorou and colleagues compiled statistics from two consecutive United Kingdom RA inception cohorts. One tracked 1,465 patients for up to 25 years (median follow-up, 10 years), and the other tracked 1,236 patients for as many as 10 years (median follow-up, 6 years).
At baseline, 37.2% of 2,420 patients (90% of total) were overweight, and 21.3% were obese. Average body mass index (BMI) rose between the two consecutive studies from 25.5 to 27.6.
The researchers found that obesity was linked to lower likelihoods of remission and low disease activity status (odds ratio, 0.71; 95% confidence interval, 0.55-0.93 and OR, 0.69; 95% CI, 0.55-0.87, respectively.) After controlling for factors such as age and gender, they also saw slightly lower odds of remission in those with higher BMI (OR, 0.97; 95% CI, 0.95-0.99). But there was no statistically significant link between higher BMI and low disease activity status.
The study also connected obesity to higher odds of disability (OR, 1.63; 95% CI, 1.20-2.23). Furthermore, higher BMI was linked to higher odds of disability (OR, 1.04; 95% CI, 1.01-1.06).
Study lead author Dr. Nikiphorou, who spoke in an interview and in comments at an ACR press conference, said “this study emphasizes that obesity can have a profound effect on treatment goals in rheumatoid arthritis. It creates a strong case for addressing BMI and addressing obesity, flagging it up to primary care.”
She added that rheumatologists too often focus on only rheumatoid conditions. “We place so much evidence on disease activity scores,” she said. “How often do we really address the patient in terms of other things going on, including obesity? What we can do is include discussion of BMI, exercise, nutrition.”
Dr. Nikiphorou and Dr. Matteson report no relevant disclosures. No specific study funding is reported.
This article was updated 11/10/17.
AT ACR 2017
Key clinical point: Obesity may worsen the risk of disease activity and disability in rheumatoid arthritis.
Major finding: In an adjusted analysis, obese patients with RA were less likely to reach remission and low disease activity status (OR, 0.71; 95% CI, 0.55-0.93 and OR, 0.69; 95% CI, 0.55-0.87, respectively).
Data source: Two consecutive inception cohorts with a total of 1,236 RA patients followed for up to 25 years.
Disclosures: The lead study author reports no disclosures, and no other disclosures are reported. No specific study funding is reported.
Methotrexate holiday linked to better flu vaccine immunogenicity
SAN DIEGO – Patients with well-controlled rheumatoid arthritis (RA) fared well during a 2-week holiday from methotrexate after flu vaccination and later showed signs of boosted immunity against the flu in comparison with patients who had not stopped the drug, according to results from a randomized controlled trial.
The research doesn’t confirm that vaccinated patients who take a break from methotrexate actually have lower rates of flu. Still, the findings suggest that brief holidays from methotrexate could be feasible in a variety of situations, such as after vaccinations and prior to surgery, said Jin Kyun Park, MD, of Seoul (South Korea) National University Hospital, lead author of the study presented at the annual meeting of the American College of Rheumatology.
The study notes that RA patients are especially prone to infections for two reasons: dysfunctional immune systems and immunity-weakening treatments. According to Dr. Park, methotrexate reduces the effectiveness of flu vaccines by 15%-20%.
In a previous study, Dr. Park and his colleagues found no statistically significant sign of increased flares in patients who went without methotrexate for 2 weeks before and 2 weeks after vaccination, 4 weeks after vaccination, and 4 weeks before vaccination (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
The earlier findings also suggested that flu vaccine uptake is highest in those who stop methotrexate after vaccination.
For the new study, a randomized controlled trial, researchers recruited patients with well-controlled RA. They assigned 159 to continue weekly doses of methotrexate after flu vaccination and 161 to stop it for 2 weeks.
The groups in the final analysis (156 and 160 subjects, respectively) were similar – about 85% women, average age of 52-53 years, and about half took glucocorticoids. Their methotrexate dose per week was about 13 mg.
At 4 weeks, just over three-quarters of the patients who had briefly stopped methotrexate showed at least a fourfold increase in hemagglutination inhibition antibody titer against two or more vaccine strains. Of those who continued the medication, just 54.5% showed this level of response, which the researchers considered to be satisfactory.
The researchers reported that there was no appreciable increase in RA disease activity.
Dr. Park cautioned that vaccine titers don’t directly reflect immunoprotection levels. Patients who took a break from methotrexate were less likely to develop a flulike illness, but the difference wasn’t statistically significant.
The research raises questions about whether methotrexate could be stopped a week or two before surgery to lower the risk of infections, Dr. Park said.
Dr. Park said that future research should focus on whether stopping methotrexate briefly affects whether patients go on to develop the flu. He would also like to look at whether a break from the medication will boost the immune response in RA patients who get herpes zoster (shingles) vaccines.
Paul Sufka, MD, of HealthPartners and Regions Hospital in St. Paul, Minn., praised the research. The 2-week break from methotrexate is “a fairly pragmatic approach,” said Dr. Sufka, who moderated a press conference where Dr. Park presented his research.
“You can actually pull this off,” he said, versus telling patients to stop the medication for the 2 weeks before they get vaccinated. He cautioned, however, that “these people have a fairly low disease activity. You may not be able to pull this off with those who have high disease activity.”
Dr. Park and Dr. Sufka reported no relevant disclosures. A study author reported consulting for Pfizer and receiving research grants from Green Cross Corp. and Hanmi Pharmaceutical. The study was funded by Green Cross.
SAN DIEGO – Patients with well-controlled rheumatoid arthritis (RA) fared well during a 2-week holiday from methotrexate after flu vaccination and later showed signs of boosted immunity against the flu in comparison with patients who had not stopped the drug, according to results from a randomized controlled trial.
The research doesn’t confirm that vaccinated patients who take a break from methotrexate actually have lower rates of flu. Still, the findings suggest that brief holidays from methotrexate could be feasible in a variety of situations, such as after vaccinations and prior to surgery, said Jin Kyun Park, MD, of Seoul (South Korea) National University Hospital, lead author of the study presented at the annual meeting of the American College of Rheumatology.
The study notes that RA patients are especially prone to infections for two reasons: dysfunctional immune systems and immunity-weakening treatments. According to Dr. Park, methotrexate reduces the effectiveness of flu vaccines by 15%-20%.
In a previous study, Dr. Park and his colleagues found no statistically significant sign of increased flares in patients who went without methotrexate for 2 weeks before and 2 weeks after vaccination, 4 weeks after vaccination, and 4 weeks before vaccination (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
The earlier findings also suggested that flu vaccine uptake is highest in those who stop methotrexate after vaccination.
For the new study, a randomized controlled trial, researchers recruited patients with well-controlled RA. They assigned 159 to continue weekly doses of methotrexate after flu vaccination and 161 to stop it for 2 weeks.
The groups in the final analysis (156 and 160 subjects, respectively) were similar – about 85% women, average age of 52-53 years, and about half took glucocorticoids. Their methotrexate dose per week was about 13 mg.
At 4 weeks, just over three-quarters of the patients who had briefly stopped methotrexate showed at least a fourfold increase in hemagglutination inhibition antibody titer against two or more vaccine strains. Of those who continued the medication, just 54.5% showed this level of response, which the researchers considered to be satisfactory.
The researchers reported that there was no appreciable increase in RA disease activity.
Dr. Park cautioned that vaccine titers don’t directly reflect immunoprotection levels. Patients who took a break from methotrexate were less likely to develop a flulike illness, but the difference wasn’t statistically significant.
The research raises questions about whether methotrexate could be stopped a week or two before surgery to lower the risk of infections, Dr. Park said.
Dr. Park said that future research should focus on whether stopping methotrexate briefly affects whether patients go on to develop the flu. He would also like to look at whether a break from the medication will boost the immune response in RA patients who get herpes zoster (shingles) vaccines.
Paul Sufka, MD, of HealthPartners and Regions Hospital in St. Paul, Minn., praised the research. The 2-week break from methotrexate is “a fairly pragmatic approach,” said Dr. Sufka, who moderated a press conference where Dr. Park presented his research.
“You can actually pull this off,” he said, versus telling patients to stop the medication for the 2 weeks before they get vaccinated. He cautioned, however, that “these people have a fairly low disease activity. You may not be able to pull this off with those who have high disease activity.”
Dr. Park and Dr. Sufka reported no relevant disclosures. A study author reported consulting for Pfizer and receiving research grants from Green Cross Corp. and Hanmi Pharmaceutical. The study was funded by Green Cross.
SAN DIEGO – Patients with well-controlled rheumatoid arthritis (RA) fared well during a 2-week holiday from methotrexate after flu vaccination and later showed signs of boosted immunity against the flu in comparison with patients who had not stopped the drug, according to results from a randomized controlled trial.
The research doesn’t confirm that vaccinated patients who take a break from methotrexate actually have lower rates of flu. Still, the findings suggest that brief holidays from methotrexate could be feasible in a variety of situations, such as after vaccinations and prior to surgery, said Jin Kyun Park, MD, of Seoul (South Korea) National University Hospital, lead author of the study presented at the annual meeting of the American College of Rheumatology.
The study notes that RA patients are especially prone to infections for two reasons: dysfunctional immune systems and immunity-weakening treatments. According to Dr. Park, methotrexate reduces the effectiveness of flu vaccines by 15%-20%.
In a previous study, Dr. Park and his colleagues found no statistically significant sign of increased flares in patients who went without methotrexate for 2 weeks before and 2 weeks after vaccination, 4 weeks after vaccination, and 4 weeks before vaccination (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
The earlier findings also suggested that flu vaccine uptake is highest in those who stop methotrexate after vaccination.
For the new study, a randomized controlled trial, researchers recruited patients with well-controlled RA. They assigned 159 to continue weekly doses of methotrexate after flu vaccination and 161 to stop it for 2 weeks.
The groups in the final analysis (156 and 160 subjects, respectively) were similar – about 85% women, average age of 52-53 years, and about half took glucocorticoids. Their methotrexate dose per week was about 13 mg.
At 4 weeks, just over three-quarters of the patients who had briefly stopped methotrexate showed at least a fourfold increase in hemagglutination inhibition antibody titer against two or more vaccine strains. Of those who continued the medication, just 54.5% showed this level of response, which the researchers considered to be satisfactory.
The researchers reported that there was no appreciable increase in RA disease activity.
Dr. Park cautioned that vaccine titers don’t directly reflect immunoprotection levels. Patients who took a break from methotrexate were less likely to develop a flulike illness, but the difference wasn’t statistically significant.
The research raises questions about whether methotrexate could be stopped a week or two before surgery to lower the risk of infections, Dr. Park said.
Dr. Park said that future research should focus on whether stopping methotrexate briefly affects whether patients go on to develop the flu. He would also like to look at whether a break from the medication will boost the immune response in RA patients who get herpes zoster (shingles) vaccines.
Paul Sufka, MD, of HealthPartners and Regions Hospital in St. Paul, Minn., praised the research. The 2-week break from methotrexate is “a fairly pragmatic approach,” said Dr. Sufka, who moderated a press conference where Dr. Park presented his research.
“You can actually pull this off,” he said, versus telling patients to stop the medication for the 2 weeks before they get vaccinated. He cautioned, however, that “these people have a fairly low disease activity. You may not be able to pull this off with those who have high disease activity.”
Dr. Park and Dr. Sufka reported no relevant disclosures. A study author reported consulting for Pfizer and receiving research grants from Green Cross Corp. and Hanmi Pharmaceutical. The study was funded by Green Cross.
AT ACR 2017
Key clinical point:
Major finding: More than three-quarters of patients who had briefly stopped methotrexate and 54.5% of patients who kept using methotrexate showed at least a fourfold increase in hemagglutination inhibition antibody titer against two or more vaccine strains at 4 weeks.
Data source: A randomized controlled trial of 320 patients with RA who were taking methotrexate.
Disclosures: The study was funded by Green Cross Corp. The presenter reported no relevant disclosures. A study author reported consulting for Pfizer and receiving research grants from Green Cross and Hanmi Pharmaceutical.
VIDEO: Biologic use during pregnancy had no impact on serious infection risks in infants
SAN DIEGO – Researchers found no evidence of increased risk of serious or opportunistic infections in infants born to pregnant women who were treated with biologic medication for their rheumatoid arthritis, according to a cohort study.
“These data add to what we’re beginning to learn about these medications that are so commonly used in women of reproductive age, and who have concerns about whether they can use them safely or not during pregnancy,” lead study author Christina D. Chambers, PhD, MPH, said during a press briefing at the annual meeting of the American College of Rheumatology. To date, theoretical concern exists that the use of biologics could interfere with postnatal immune function in the infant, said Dr. Chambers, a perinatal epidemiologist and teratologist at the University of California, San Diego. “The theory has been that because of the size of the molecule, little placental transfer is thought to take place early in pregnancy, but later in pregnancy, more placental transfer may be possible,” she said.
In an effort to investigate the risk of serious or opportunistic infections for infants whose mothers used biologics during pregnancy, the researchers conducted an observational cohort study from pregnant women participating in the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Project from 2004 through 2016. Mothers fell into one of three groups: 502 pregnancies where the mother with RA was treated with a biologic with or without other disease modifying anti-rheumatic medications during her pregnancy (group A); 231 pregnancies where the mother had RA but did not use any biologics during pregnancy (group B), and 423 pregnancies where the mother had no chronic diseases at all (group C). The investigators defined the serious or opportunistic infections as a list of 16 infections that included X-ray proven pneumonia, septic arthritis, osteomyelitis, tuberculosis, herpes, listeria, legionella, mycobacteria, systemic cytomegalovirus and abscess. The one-year follow-up data was collected from medical records and corroborated with maternal reports.
Among the pregnant mothers in group A, 43% took their last dose in the first or second trimester, and 57% percent took their last dose in the third trimester. Dr. Chambers reported that 20 of the 502 infants in group A developed at least one serious or opportunistic infection, for a rate of 4%, while the rates among infants in groups B and C were 2.6% and 2.1%, respectively. The most common infections seen were X-ray proven pneumonia, sepsis, bacteremia, meningitis, and abscess. Between 11% and 19% of infants had more than one infection over the one-year period.
In a subset analysis of 285 women in group A who had third trimester exposure to one of the biologics, 10 infants had at least one serious or opportunistic infection, for a rate of 3.5%, which was statistically similar to that of groups B and C (2.6% and 2.1%, respectively).
“These data provide some reassurance for clinicians who are concerned that their patients need to be treated with a biologic late in pregnancy rather than take them off the drug during that period of time,” Dr. Chambers said. She acknowledged certain limitations of the study, including the fact that the researchers did not examine risk of less serious infections, such as more frequent colds or ear infections in the infants, and they did not have any direct measure of their immune function.
Dr. Chambers disclosed having received research support from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Janssen Pharmaceutica Products, L.P., Pfizer Inc, Roche Pharmaceuticals, Seqirus, GSK, UCB, and Sanofi-Aventis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Researchers found no evidence of increased risk of serious or opportunistic infections in infants born to pregnant women who were treated with biologic medication for their rheumatoid arthritis, according to a cohort study.
“These data add to what we’re beginning to learn about these medications that are so commonly used in women of reproductive age, and who have concerns about whether they can use them safely or not during pregnancy,” lead study author Christina D. Chambers, PhD, MPH, said during a press briefing at the annual meeting of the American College of Rheumatology. To date, theoretical concern exists that the use of biologics could interfere with postnatal immune function in the infant, said Dr. Chambers, a perinatal epidemiologist and teratologist at the University of California, San Diego. “The theory has been that because of the size of the molecule, little placental transfer is thought to take place early in pregnancy, but later in pregnancy, more placental transfer may be possible,” she said.
In an effort to investigate the risk of serious or opportunistic infections for infants whose mothers used biologics during pregnancy, the researchers conducted an observational cohort study from pregnant women participating in the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Project from 2004 through 2016. Mothers fell into one of three groups: 502 pregnancies where the mother with RA was treated with a biologic with or without other disease modifying anti-rheumatic medications during her pregnancy (group A); 231 pregnancies where the mother had RA but did not use any biologics during pregnancy (group B), and 423 pregnancies where the mother had no chronic diseases at all (group C). The investigators defined the serious or opportunistic infections as a list of 16 infections that included X-ray proven pneumonia, septic arthritis, osteomyelitis, tuberculosis, herpes, listeria, legionella, mycobacteria, systemic cytomegalovirus and abscess. The one-year follow-up data was collected from medical records and corroborated with maternal reports.
Among the pregnant mothers in group A, 43% took their last dose in the first or second trimester, and 57% percent took their last dose in the third trimester. Dr. Chambers reported that 20 of the 502 infants in group A developed at least one serious or opportunistic infection, for a rate of 4%, while the rates among infants in groups B and C were 2.6% and 2.1%, respectively. The most common infections seen were X-ray proven pneumonia, sepsis, bacteremia, meningitis, and abscess. Between 11% and 19% of infants had more than one infection over the one-year period.
In a subset analysis of 285 women in group A who had third trimester exposure to one of the biologics, 10 infants had at least one serious or opportunistic infection, for a rate of 3.5%, which was statistically similar to that of groups B and C (2.6% and 2.1%, respectively).
“These data provide some reassurance for clinicians who are concerned that their patients need to be treated with a biologic late in pregnancy rather than take them off the drug during that period of time,” Dr. Chambers said. She acknowledged certain limitations of the study, including the fact that the researchers did not examine risk of less serious infections, such as more frequent colds or ear infections in the infants, and they did not have any direct measure of their immune function.
Dr. Chambers disclosed having received research support from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Janssen Pharmaceutica Products, L.P., Pfizer Inc, Roche Pharmaceuticals, Seqirus, GSK, UCB, and Sanofi-Aventis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Researchers found no evidence of increased risk of serious or opportunistic infections in infants born to pregnant women who were treated with biologic medication for their rheumatoid arthritis, according to a cohort study.
“These data add to what we’re beginning to learn about these medications that are so commonly used in women of reproductive age, and who have concerns about whether they can use them safely or not during pregnancy,” lead study author Christina D. Chambers, PhD, MPH, said during a press briefing at the annual meeting of the American College of Rheumatology. To date, theoretical concern exists that the use of biologics could interfere with postnatal immune function in the infant, said Dr. Chambers, a perinatal epidemiologist and teratologist at the University of California, San Diego. “The theory has been that because of the size of the molecule, little placental transfer is thought to take place early in pregnancy, but later in pregnancy, more placental transfer may be possible,” she said.
In an effort to investigate the risk of serious or opportunistic infections for infants whose mothers used biologics during pregnancy, the researchers conducted an observational cohort study from pregnant women participating in the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Project from 2004 through 2016. Mothers fell into one of three groups: 502 pregnancies where the mother with RA was treated with a biologic with or without other disease modifying anti-rheumatic medications during her pregnancy (group A); 231 pregnancies where the mother had RA but did not use any biologics during pregnancy (group B), and 423 pregnancies where the mother had no chronic diseases at all (group C). The investigators defined the serious or opportunistic infections as a list of 16 infections that included X-ray proven pneumonia, septic arthritis, osteomyelitis, tuberculosis, herpes, listeria, legionella, mycobacteria, systemic cytomegalovirus and abscess. The one-year follow-up data was collected from medical records and corroborated with maternal reports.
Among the pregnant mothers in group A, 43% took their last dose in the first or second trimester, and 57% percent took their last dose in the third trimester. Dr. Chambers reported that 20 of the 502 infants in group A developed at least one serious or opportunistic infection, for a rate of 4%, while the rates among infants in groups B and C were 2.6% and 2.1%, respectively. The most common infections seen were X-ray proven pneumonia, sepsis, bacteremia, meningitis, and abscess. Between 11% and 19% of infants had more than one infection over the one-year period.
In a subset analysis of 285 women in group A who had third trimester exposure to one of the biologics, 10 infants had at least one serious or opportunistic infection, for a rate of 3.5%, which was statistically similar to that of groups B and C (2.6% and 2.1%, respectively).
“These data provide some reassurance for clinicians who are concerned that their patients need to be treated with a biologic late in pregnancy rather than take them off the drug during that period of time,” Dr. Chambers said. She acknowledged certain limitations of the study, including the fact that the researchers did not examine risk of less serious infections, such as more frequent colds or ear infections in the infants, and they did not have any direct measure of their immune function.
Dr. Chambers disclosed having received research support from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Janssen Pharmaceutica Products, L.P., Pfizer Inc, Roche Pharmaceuticals, Seqirus, GSK, UCB, and Sanofi-Aventis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ACR 2017
Key clinical point:
Major finding: Infections occurred in 4% of infants born to mothers with RA treated with a biologic with or without other disease modifying anti-rheumatic medications during her pregnancy.
Study details: An observational cohort study of 1,156 pregnant women with RA.
Disclosures: Dr. Chambers disclosed having received research support from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Janssen Pharmaceutica Products, L.P., Pfizer Inc, Roche Pharmaceuticals, Seqirus, GSK, UCB, and Sanofi-Aventis.