User login
Chikungunya virus goes undetected despite chronic arthritis in 25% of patients after 20 months
Up to a quarter of patients infected with chikungunya virus who reported joint pain as one of their initial symptoms continue to have joint pain after 20 months of follow-up, and evidence suggests that the persistent joint symptoms are not related to the continued presence of the virus in synovial fluid, according to two studies of patients infected during the 2014-2015 Colombian epidemic.
In the first large-scale, cross-sectional follow-up of a prospective cohort from the Colombian epidemic, Aileen Chang, MD, of George Washington University, Washington, and her colleagues at multiple other institutions reported persistent joint pain and multiple swollen and/or tender joints after 20 months in 123 of 485 Colombian patients who initially had joint pain with their Chikungunya virus infection (CHIKV) diagnosis. In their report in Arthritis & Rheumatology, they said that increased initial viral load and severe initial joint pain were predictors of persistent arthritis, which is consistent with the work of other researchers.
Dr. Chang worked with a variety of coinvestigators, some of whom were also involved in the larger symptom follow-up study, to conduct this Study of Chikungunya Arthritis Mechanisms in the Americas (CAMA). They collected synovial fluid and blood plasma from these 38 patients as well as 10 healthy controls who were serologically negative for CHIKV and never had arthritis, and analyzed the fluid and plasma for signs of CHIKV. They assessed viral RNA via quantitative reverse transcription polymerase chain reaction (qRT-PCR) testing, looked at viral proteins via mass spectrometry, and did viral cultures.
All samples from the 38 patients in the study were negative for CHIKV in two separate qRT-PCR assays. To determine if low-level viremia was present in synovial fluid samples, the samples were added to cell cultures to expand viral replication. No viral growth was found after three attempts and 10 days of culture. Conversely, controls with low quantities of virus (about 1 plaque-forming unit per well) yielded growth and detection of the virus.
Patients with CHIKV-associated arthritis also had no significant increase in rheumatoid arthritis markers or C-reactive protein. In fact, plasma markers for rheumatoid arthritis were found in only a fraction of patients with CHIKV arthritis: rheumatoid factor (RF) IgM antibody in 9%, RF IgG antibody in 12%, and anti–cyclic citrullinated peptide in 0%.
The more probable potential mechanisms through which CHIKV could cause persistent arthritis symptoms is through the presence of persistent CHIKV or viral antigens at low enough levels in the synovial tissue that it is undetectable in the synovial fluid, Dr. Chang and her associates suggested. There is also a possibility of epigenetic changes to the host DNA, altering host gene transcription. Other epigenetic changes, like epigenetic imprinting, could be possible in macrophages, leading to more aggressive cell behavior, they said. Unlikelier scenarios would be the presence of seronegative RA in these patients or, alternatively, the presence of seronegative RA indicating prior infection with CHIKV or other arthritogenic viruses.
Whatever mechanisms are causing CHIKV-associated arthritis, “these study findings may have important clinical relevance for CHIKV in the Americas. Since there is no current standard of care guidance for the treatment of CHIKV arthritis, some patients are currently being treated with immunosuppressant medications such as methotrexate, hydroxychloroquine, etanercept, adalimumab, sulfasalazine, fingolimod, abatacept, and tofacitinib,” Dr. Chang and her colleagues wrote. “This practice could be potentially harmful in the setting of replicating virus in the synovium as it could permit reemergence of a systemic viral infection.”
The CAMA study has several important limitations , the investigators said, the first being that during collection of synovial fluid, 0-20 mL of saline solution were used to flush the joints, which could have affected the ability to detect virus in the samples. In an attempt to mitigate this, the researchers cultured 0.5-1.5 mL of sampled synovial fluid to expand any replication-competent virus present in the sample, used two complementary PCR assays to detect nucleic acids, and a proteomic approach to look for viral proteins.
The researchers acknowledged that despite these measures, “proving the absence of a target is difficult, and we recognize that it is possible that our approach failed to detect low-level viral antigen; however, our orthogonal approach clearly demonstrates that if viral antigen exists in the synovial fluid, it is at extremely low levels.” They advised that future studies may want to use synovial biopsies rather than extracted fluid.
The investigators also did not include patients who had previously been infected by CHIKV without chronic arthritis. This issue was compounded by the lack of age- and sex-matched healthy controls.
All researchers involved in the studies reported no financial conflicts of interest. The studies were supported by various grants from the National Institutes of Health and the Rheumatology Research Foundation.
SOURCE: Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40383 and Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40384
Up to a quarter of patients infected with chikungunya virus who reported joint pain as one of their initial symptoms continue to have joint pain after 20 months of follow-up, and evidence suggests that the persistent joint symptoms are not related to the continued presence of the virus in synovial fluid, according to two studies of patients infected during the 2014-2015 Colombian epidemic.
In the first large-scale, cross-sectional follow-up of a prospective cohort from the Colombian epidemic, Aileen Chang, MD, of George Washington University, Washington, and her colleagues at multiple other institutions reported persistent joint pain and multiple swollen and/or tender joints after 20 months in 123 of 485 Colombian patients who initially had joint pain with their Chikungunya virus infection (CHIKV) diagnosis. In their report in Arthritis & Rheumatology, they said that increased initial viral load and severe initial joint pain were predictors of persistent arthritis, which is consistent with the work of other researchers.
Dr. Chang worked with a variety of coinvestigators, some of whom were also involved in the larger symptom follow-up study, to conduct this Study of Chikungunya Arthritis Mechanisms in the Americas (CAMA). They collected synovial fluid and blood plasma from these 38 patients as well as 10 healthy controls who were serologically negative for CHIKV and never had arthritis, and analyzed the fluid and plasma for signs of CHIKV. They assessed viral RNA via quantitative reverse transcription polymerase chain reaction (qRT-PCR) testing, looked at viral proteins via mass spectrometry, and did viral cultures.
All samples from the 38 patients in the study were negative for CHIKV in two separate qRT-PCR assays. To determine if low-level viremia was present in synovial fluid samples, the samples were added to cell cultures to expand viral replication. No viral growth was found after three attempts and 10 days of culture. Conversely, controls with low quantities of virus (about 1 plaque-forming unit per well) yielded growth and detection of the virus.
Patients with CHIKV-associated arthritis also had no significant increase in rheumatoid arthritis markers or C-reactive protein. In fact, plasma markers for rheumatoid arthritis were found in only a fraction of patients with CHIKV arthritis: rheumatoid factor (RF) IgM antibody in 9%, RF IgG antibody in 12%, and anti–cyclic citrullinated peptide in 0%.
The more probable potential mechanisms through which CHIKV could cause persistent arthritis symptoms is through the presence of persistent CHIKV or viral antigens at low enough levels in the synovial tissue that it is undetectable in the synovial fluid, Dr. Chang and her associates suggested. There is also a possibility of epigenetic changes to the host DNA, altering host gene transcription. Other epigenetic changes, like epigenetic imprinting, could be possible in macrophages, leading to more aggressive cell behavior, they said. Unlikelier scenarios would be the presence of seronegative RA in these patients or, alternatively, the presence of seronegative RA indicating prior infection with CHIKV or other arthritogenic viruses.
Whatever mechanisms are causing CHIKV-associated arthritis, “these study findings may have important clinical relevance for CHIKV in the Americas. Since there is no current standard of care guidance for the treatment of CHIKV arthritis, some patients are currently being treated with immunosuppressant medications such as methotrexate, hydroxychloroquine, etanercept, adalimumab, sulfasalazine, fingolimod, abatacept, and tofacitinib,” Dr. Chang and her colleagues wrote. “This practice could be potentially harmful in the setting of replicating virus in the synovium as it could permit reemergence of a systemic viral infection.”
The CAMA study has several important limitations , the investigators said, the first being that during collection of synovial fluid, 0-20 mL of saline solution were used to flush the joints, which could have affected the ability to detect virus in the samples. In an attempt to mitigate this, the researchers cultured 0.5-1.5 mL of sampled synovial fluid to expand any replication-competent virus present in the sample, used two complementary PCR assays to detect nucleic acids, and a proteomic approach to look for viral proteins.
The researchers acknowledged that despite these measures, “proving the absence of a target is difficult, and we recognize that it is possible that our approach failed to detect low-level viral antigen; however, our orthogonal approach clearly demonstrates that if viral antigen exists in the synovial fluid, it is at extremely low levels.” They advised that future studies may want to use synovial biopsies rather than extracted fluid.
The investigators also did not include patients who had previously been infected by CHIKV without chronic arthritis. This issue was compounded by the lack of age- and sex-matched healthy controls.
All researchers involved in the studies reported no financial conflicts of interest. The studies were supported by various grants from the National Institutes of Health and the Rheumatology Research Foundation.
SOURCE: Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40383 and Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40384
Up to a quarter of patients infected with chikungunya virus who reported joint pain as one of their initial symptoms continue to have joint pain after 20 months of follow-up, and evidence suggests that the persistent joint symptoms are not related to the continued presence of the virus in synovial fluid, according to two studies of patients infected during the 2014-2015 Colombian epidemic.
In the first large-scale, cross-sectional follow-up of a prospective cohort from the Colombian epidemic, Aileen Chang, MD, of George Washington University, Washington, and her colleagues at multiple other institutions reported persistent joint pain and multiple swollen and/or tender joints after 20 months in 123 of 485 Colombian patients who initially had joint pain with their Chikungunya virus infection (CHIKV) diagnosis. In their report in Arthritis & Rheumatology, they said that increased initial viral load and severe initial joint pain were predictors of persistent arthritis, which is consistent with the work of other researchers.
Dr. Chang worked with a variety of coinvestigators, some of whom were also involved in the larger symptom follow-up study, to conduct this Study of Chikungunya Arthritis Mechanisms in the Americas (CAMA). They collected synovial fluid and blood plasma from these 38 patients as well as 10 healthy controls who were serologically negative for CHIKV and never had arthritis, and analyzed the fluid and plasma for signs of CHIKV. They assessed viral RNA via quantitative reverse transcription polymerase chain reaction (qRT-PCR) testing, looked at viral proteins via mass spectrometry, and did viral cultures.
All samples from the 38 patients in the study were negative for CHIKV in two separate qRT-PCR assays. To determine if low-level viremia was present in synovial fluid samples, the samples were added to cell cultures to expand viral replication. No viral growth was found after three attempts and 10 days of culture. Conversely, controls with low quantities of virus (about 1 plaque-forming unit per well) yielded growth and detection of the virus.
Patients with CHIKV-associated arthritis also had no significant increase in rheumatoid arthritis markers or C-reactive protein. In fact, plasma markers for rheumatoid arthritis were found in only a fraction of patients with CHIKV arthritis: rheumatoid factor (RF) IgM antibody in 9%, RF IgG antibody in 12%, and anti–cyclic citrullinated peptide in 0%.
The more probable potential mechanisms through which CHIKV could cause persistent arthritis symptoms is through the presence of persistent CHIKV or viral antigens at low enough levels in the synovial tissue that it is undetectable in the synovial fluid, Dr. Chang and her associates suggested. There is also a possibility of epigenetic changes to the host DNA, altering host gene transcription. Other epigenetic changes, like epigenetic imprinting, could be possible in macrophages, leading to more aggressive cell behavior, they said. Unlikelier scenarios would be the presence of seronegative RA in these patients or, alternatively, the presence of seronegative RA indicating prior infection with CHIKV or other arthritogenic viruses.
Whatever mechanisms are causing CHIKV-associated arthritis, “these study findings may have important clinical relevance for CHIKV in the Americas. Since there is no current standard of care guidance for the treatment of CHIKV arthritis, some patients are currently being treated with immunosuppressant medications such as methotrexate, hydroxychloroquine, etanercept, adalimumab, sulfasalazine, fingolimod, abatacept, and tofacitinib,” Dr. Chang and her colleagues wrote. “This practice could be potentially harmful in the setting of replicating virus in the synovium as it could permit reemergence of a systemic viral infection.”
The CAMA study has several important limitations , the investigators said, the first being that during collection of synovial fluid, 0-20 mL of saline solution were used to flush the joints, which could have affected the ability to detect virus in the samples. In an attempt to mitigate this, the researchers cultured 0.5-1.5 mL of sampled synovial fluid to expand any replication-competent virus present in the sample, used two complementary PCR assays to detect nucleic acids, and a proteomic approach to look for viral proteins.
The researchers acknowledged that despite these measures, “proving the absence of a target is difficult, and we recognize that it is possible that our approach failed to detect low-level viral antigen; however, our orthogonal approach clearly demonstrates that if viral antigen exists in the synovial fluid, it is at extremely low levels.” They advised that future studies may want to use synovial biopsies rather than extracted fluid.
The investigators also did not include patients who had previously been infected by CHIKV without chronic arthritis. This issue was compounded by the lack of age- and sex-matched healthy controls.
All researchers involved in the studies reported no financial conflicts of interest. The studies were supported by various grants from the National Institutes of Health and the Rheumatology Research Foundation.
SOURCE: Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40383 and Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40384
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: No signs of persistent CHIKV infection can be found in synovial fluid or blood plasma from patients with chronic arthritis after CHIKV.
Study details: Cross-sectional studies of 485 Colombian patients who had clinical CHIKV and associated arthritis symptoms in 2014-2015 and another 38 patients who underwent further synovial fluid and blood plasma testing after a median of 22 months.
Disclosures: All researchers involved in the studies reported no financial conflicts of interest. The studies were supported by various grants from the National Institutes of Health and the Rheumatology Research Foundation.
Source: Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40383 and Chang A et al. Arthritis Rheumatol. 2017 Dec 20. doi: 10.1002/art.40384.
Children of moms with RA have higher risk of RA, too
The prevalence of rheumatoid arthritis, as well as thyroid disease and epilepsy, was significantly higher in children whose mothers had RA, according to data from a nationwide cohort study in Denmark.
RA runs in families, and many women with RA are concerned about the possible impact of their disease on a developing fetus, wrote Line R. Jølving of Odense (Denmark) University Hospital and the University of Southern Denmark in Odense and her colleagues in Arthritis Care & Research. “However, we do not have sufficient knowledge on the association between maternal RA and long-term chronic childhood outcomes, and still we do not know which specific chronic diseases to be especially aware of in children of women with RA,” they said.

Overall, the risk of RA was almost three times as high for the children of mothers with RA (hazard ratio, 2.89) as it was for the children of women without RA. In addition, the risk of thyroid disease was more than twice as high (HR, 2.19), and the risk of epilepsy was more than 50% higher (HR, 1.61). Maternal RA during pregnancy had no significant impact on children’s anxiety and personality disorders or on the presence of chronic lung disease.
Mothers with RA were generally older than were those without the condition. The children of mothers with RA were significantly more likely to be born via cesarean section, preterm, and small for gestational age, the researchers said.
The results were limited by the potential inclusion of misclassified diagnoses of child outcomes and by the lack of data on medication use. In addition, the study was not designed to determine the effect of biologic mechanisms or genes, the researchers said. Despite these limitations, “the findings in this study are relevant for pediatricians, rheumatologists, and general practitioners in order to have special awareness of early symptoms of RA, thyroid disease, and epilepsy in offspring of mothers with RA,” they said.
The researchers had no financial conflicts to disclose. The study was funded by several sources, including the Region of Southern Denmark, the University of Southern Denmark in Odense, the Center for Clinical Epidemiology, Odense University Hospital, and the Colitis-Crohn Association in Denmark.
SOURCE: Jølving L et al. Arthritis Care Res. 2017 Dec 11. doi: 10.1002/acr.23461.
The prevalence of rheumatoid arthritis, as well as thyroid disease and epilepsy, was significantly higher in children whose mothers had RA, according to data from a nationwide cohort study in Denmark.
RA runs in families, and many women with RA are concerned about the possible impact of their disease on a developing fetus, wrote Line R. Jølving of Odense (Denmark) University Hospital and the University of Southern Denmark in Odense and her colleagues in Arthritis Care & Research. “However, we do not have sufficient knowledge on the association between maternal RA and long-term chronic childhood outcomes, and still we do not know which specific chronic diseases to be especially aware of in children of women with RA,” they said.
Overall, the risk of RA was almost three times as high for the children of mothers with RA (hazard ratio, 2.89) as it was for the children of women without RA. In addition, the risk of thyroid disease was more than twice as high (HR, 2.19), and the risk of epilepsy was more than 50% higher (HR, 1.61). Maternal RA during pregnancy had no significant impact on children’s anxiety and personality disorders or on the presence of chronic lung disease.
Mothers with RA were generally older than were those without the condition. The children of mothers with RA were significantly more likely to be born via cesarean section, preterm, and small for gestational age, the researchers said.
The results were limited by the potential inclusion of misclassified diagnoses of child outcomes and by the lack of data on medication use. In addition, the study was not designed to determine the effect of biologic mechanisms or genes, the researchers said. Despite these limitations, “the findings in this study are relevant for pediatricians, rheumatologists, and general practitioners in order to have special awareness of early symptoms of RA, thyroid disease, and epilepsy in offspring of mothers with RA,” they said.
The researchers had no financial conflicts to disclose. The study was funded by several sources, including the Region of Southern Denmark, the University of Southern Denmark in Odense, the Center for Clinical Epidemiology, Odense University Hospital, and the Colitis-Crohn Association in Denmark.
SOURCE: Jølving L et al. Arthritis Care Res. 2017 Dec 11. doi: 10.1002/acr.23461.
The prevalence of rheumatoid arthritis, as well as thyroid disease and epilepsy, was significantly higher in children whose mothers had RA, according to data from a nationwide cohort study in Denmark.
RA runs in families, and many women with RA are concerned about the possible impact of their disease on a developing fetus, wrote Line R. Jølving of Odense (Denmark) University Hospital and the University of Southern Denmark in Odense and her colleagues in Arthritis Care & Research. “However, we do not have sufficient knowledge on the association between maternal RA and long-term chronic childhood outcomes, and still we do not know which specific chronic diseases to be especially aware of in children of women with RA,” they said.
Overall, the risk of RA was almost three times as high for the children of mothers with RA (hazard ratio, 2.89) as it was for the children of women without RA. In addition, the risk of thyroid disease was more than twice as high (HR, 2.19), and the risk of epilepsy was more than 50% higher (HR, 1.61). Maternal RA during pregnancy had no significant impact on children’s anxiety and personality disorders or on the presence of chronic lung disease.
Mothers with RA were generally older than were those without the condition. The children of mothers with RA were significantly more likely to be born via cesarean section, preterm, and small for gestational age, the researchers said.
The results were limited by the potential inclusion of misclassified diagnoses of child outcomes and by the lack of data on medication use. In addition, the study was not designed to determine the effect of biologic mechanisms or genes, the researchers said. Despite these limitations, “the findings in this study are relevant for pediatricians, rheumatologists, and general practitioners in order to have special awareness of early symptoms of RA, thyroid disease, and epilepsy in offspring of mothers with RA,” they said.
The researchers had no financial conflicts to disclose. The study was funded by several sources, including the Region of Southern Denmark, the University of Southern Denmark in Odense, the Center for Clinical Epidemiology, Odense University Hospital, and the Colitis-Crohn Association in Denmark.
SOURCE: Jølving L et al. Arthritis Care Res. 2017 Dec 11. doi: 10.1002/acr.23461.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point: Children whose mothers had RA were significantly more likely to have RA, epilepsy, and thyroid problems than children born to mothers without RA.
Major finding: Children of mothers with RA were almost three times as likely to have RA (hazard ratio, 2.89).
Data source: A nationwide cohort study of live births in Denmark that included 2,106 children born to women with RA and 1,378,539 children born to women without RA.
Disclosures: The researchers had no financial conflicts to disclose. The study was funded by several sources, including the Region of Southern Denmark, the University of Southern Denmark in Odense, the Center for Clinical Epidemiology, Odense University Hospital, and the Colitis-Crohn Association in Denmark.
Source: Jølving L et al. Arthritis Care Res. 2017 Dec 11. doi: 10.1002/acr.23461.
Leflunomide use in pregnancy shows little impact on newborns
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point: Exposure to leflunomide during pregnancy was not associated with significantly increased risk of major congenital malformations, low birth weight, premature birth, or spontaneous abortions.
Major finding: No significant association was seen between leflunomide use in the first trimester and an increased risk of major congenital malformations based on five cases (adjusted odds ratio, 0.97).
Data source: A population-based cohort study of 289,688 pregnancies in Canada between 1998 and 2015.
Disclosures: The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
Source: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
FDA approves infliximab biosimilar Ixifi for all of Remicade’s indications
The Food and Drug Administration has approved Ixifi (infliximab-qbtx), a biosimilar of Remicade, the original infliximab product. Ixifi is the third infliximab biosimilar to be approved by the FDA, and it is approved for all the same indications as Remicade, according to an announcement from its manufacturer, Pfizer.
Ixifi and Remicade are approved for the treatment of rheumatoid arthritis in combination with methotrexate, Crohn’s disease, pediatric Crohn’s disease, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis.![]()
The most common adverse events associated with Ixifi are upper respiratory infections, sinusitis, pharyngitis, infusion-related reactions, headache, and abdominal pain.
The Food and Drug Administration has approved Ixifi (infliximab-qbtx), a biosimilar of Remicade, the original infliximab product. Ixifi is the third infliximab biosimilar to be approved by the FDA, and it is approved for all the same indications as Remicade, according to an announcement from its manufacturer, Pfizer.
Ixifi and Remicade are approved for the treatment of rheumatoid arthritis in combination with methotrexate, Crohn’s disease, pediatric Crohn’s disease, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis.![]()
The most common adverse events associated with Ixifi are upper respiratory infections, sinusitis, pharyngitis, infusion-related reactions, headache, and abdominal pain.
The Food and Drug Administration has approved Ixifi (infliximab-qbtx), a biosimilar of Remicade, the original infliximab product. Ixifi is the third infliximab biosimilar to be approved by the FDA, and it is approved for all the same indications as Remicade, according to an announcement from its manufacturer, Pfizer.
Ixifi and Remicade are approved for the treatment of rheumatoid arthritis in combination with methotrexate, Crohn’s disease, pediatric Crohn’s disease, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis.![]()
The most common adverse events associated with Ixifi are upper respiratory infections, sinusitis, pharyngitis, infusion-related reactions, headache, and abdominal pain.
Testing for latent tuberculosis infection
While cases of active tuberculosis are relatively rare in the United States, TB is a major cause of morbidity and mortality worldwide. In the United States, there are an estimated 11 million individuals who have latent TB infection (LTBI). Without prophylactic treatment, somewhere between 4%-6% of individuals with LTBI will develop active disease during their lifetimes; roughly half of these cases will occur within a few years of the initial infection. Treatment of LTBI reduces – but does not eliminate – the risk for active disease, decreasing the consequences of active disease for the patient and the risk of transmitting infection to others.

Diagnostic tests for LTBI
The tuberculin skin test (TST) has been the standard method of diagnosing LTBI. It involves measuring induration caused by a delayed-type hypersensitivity reaction to Mycobacterium tuberculosis (Mtb) 2 or 3 days after injecting the reagent into the skin. The TST can result in false positives when detecting antibodies to BCG and nontuberculous mycobacteria, and false negatives when the patient does not demonstrate a robust immune response. A newer testing method is the Interferon Gamma Release Assay (IGRA), which involves phlebotomy, followed by a series of laboratory procedures that measure IFN-gamma release by T cells that have been sensitized to Mtb. The sensitivity of IGRA is similar to the TST, but it has better specificity; it is much less likely to react to antigens from BCG or nontuberculous mycobacteria. As detailed below, this guideline suggests a significantly more prominent role for IGRA, compared with previous recommendations.
Recommendation 1. Perform an IGRA, rather than a TST, in individuals 5 years or older who meet the following criteria: 1) are likely to be infected with Mtb; 2) have a low or intermediate risk of disease progression; 3) in whom it has been decided that testing for LTBI is warranted. A TST is an acceptable alternative, particularly if an IGRA is not available, is too costly, or is too burdensome. If an individual either has a history of BCG vaccination or is unlikely to return to have their TST read, then it is strongly recommended to use the IGRA as the test of choice.
Recommendation 2. There are insufficient data to recommend a preference for either a TST or an IGRA as the first-line diagnostic test in individuals 5 years or older who are likely to be infected with Mtb, who have a high risk of progression to active disease, and in whom it has been determined that diagnostic testing for LTBI infection is warranted; either test would be acceptable. In very high-risk patients, consider dual testing, with a positive result from either test (TST or IGRA) being considered positive.
Recommendation 3. Guidelines do not recommend testing for persons at low risk for Mtb infection. However, the authors recognize that testing in such persons may nevertheless be mandated in certain situations (for example in some school or child care settings). In these cases, the authors recommend performing an IGRA instead of a TST, to minimize the chance of a false-positive result, although a TST is an acceptable alternative. Furthermore, if the initial test is positive, they suggest performing a confirmatory test (either an IGRA or TST) and considering the person infected only if both tests are positive.
Recommendation 4. The authors suggest performing a TST rather than an IGRA in healthy children less than 5 years of age for whom it has been decided that diagnostic testing for LTBI is warranted. This recommendation reflects the limited body of evidence regarding IGRA testing in young children and the apparent decreased sensitivity (i.e. more false negatives) in this population, compared with TST use.
In the area of serial testing for TB infection, often done in health care and institutional settings, the guideline points out areas of uncertainty with IGRA testing. Specifically, the IGRA test is subject to variability in readings and boosting with antigen exposure that can complicate interpretation of apparent conversion on repeat testing. One longitudinal study showed conversion rates with IGRA to be six to nine times higher than that seen for the TST, and those conversions were thought to represent false positive tests. The guideline concludes that, “There is insufficient information available to guide the establishment of definitive criteria for the conversion.” The committee thought that a positive test in a low-risk individual was likely to be a false-positive result and recommended repeat testing. Because of the possibility of boosting with antigen exposure in situations where dual testing is anticipated, it may be preferable to obtain a specimen for IGRA prior to, or concurrently with TST placement.
Bottom line
Current guidelines suggest a more prominent role for IGRA in testing for LTBI, particularly when the likelihood of exposure is low and in situations where a person may have received BCG vaccination, or would be unlikely to return for TST reading.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
Reference
Lewisohn DM et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Inf Dis. 2017;64(2):111-5.
While cases of active tuberculosis are relatively rare in the United States, TB is a major cause of morbidity and mortality worldwide. In the United States, there are an estimated 11 million individuals who have latent TB infection (LTBI). Without prophylactic treatment, somewhere between 4%-6% of individuals with LTBI will develop active disease during their lifetimes; roughly half of these cases will occur within a few years of the initial infection. Treatment of LTBI reduces – but does not eliminate – the risk for active disease, decreasing the consequences of active disease for the patient and the risk of transmitting infection to others.
Diagnostic tests for LTBI
The tuberculin skin test (TST) has been the standard method of diagnosing LTBI. It involves measuring induration caused by a delayed-type hypersensitivity reaction to Mycobacterium tuberculosis (Mtb) 2 or 3 days after injecting the reagent into the skin. The TST can result in false positives when detecting antibodies to BCG and nontuberculous mycobacteria, and false negatives when the patient does not demonstrate a robust immune response. A newer testing method is the Interferon Gamma Release Assay (IGRA), which involves phlebotomy, followed by a series of laboratory procedures that measure IFN-gamma release by T cells that have been sensitized to Mtb. The sensitivity of IGRA is similar to the TST, but it has better specificity; it is much less likely to react to antigens from BCG or nontuberculous mycobacteria. As detailed below, this guideline suggests a significantly more prominent role for IGRA, compared with previous recommendations.
Recommendation 1. Perform an IGRA, rather than a TST, in individuals 5 years or older who meet the following criteria: 1) are likely to be infected with Mtb; 2) have a low or intermediate risk of disease progression; 3) in whom it has been decided that testing for LTBI is warranted. A TST is an acceptable alternative, particularly if an IGRA is not available, is too costly, or is too burdensome. If an individual either has a history of BCG vaccination or is unlikely to return to have their TST read, then it is strongly recommended to use the IGRA as the test of choice.
Recommendation 2. There are insufficient data to recommend a preference for either a TST or an IGRA as the first-line diagnostic test in individuals 5 years or older who are likely to be infected with Mtb, who have a high risk of progression to active disease, and in whom it has been determined that diagnostic testing for LTBI infection is warranted; either test would be acceptable. In very high-risk patients, consider dual testing, with a positive result from either test (TST or IGRA) being considered positive.
Recommendation 3. Guidelines do not recommend testing for persons at low risk for Mtb infection. However, the authors recognize that testing in such persons may nevertheless be mandated in certain situations (for example in some school or child care settings). In these cases, the authors recommend performing an IGRA instead of a TST, to minimize the chance of a false-positive result, although a TST is an acceptable alternative. Furthermore, if the initial test is positive, they suggest performing a confirmatory test (either an IGRA or TST) and considering the person infected only if both tests are positive.
Recommendation 4. The authors suggest performing a TST rather than an IGRA in healthy children less than 5 years of age for whom it has been decided that diagnostic testing for LTBI is warranted. This recommendation reflects the limited body of evidence regarding IGRA testing in young children and the apparent decreased sensitivity (i.e. more false negatives) in this population, compared with TST use.
In the area of serial testing for TB infection, often done in health care and institutional settings, the guideline points out areas of uncertainty with IGRA testing. Specifically, the IGRA test is subject to variability in readings and boosting with antigen exposure that can complicate interpretation of apparent conversion on repeat testing. One longitudinal study showed conversion rates with IGRA to be six to nine times higher than that seen for the TST, and those conversions were thought to represent false positive tests. The guideline concludes that, “There is insufficient information available to guide the establishment of definitive criteria for the conversion.” The committee thought that a positive test in a low-risk individual was likely to be a false-positive result and recommended repeat testing. Because of the possibility of boosting with antigen exposure in situations where dual testing is anticipated, it may be preferable to obtain a specimen for IGRA prior to, or concurrently with TST placement.
Bottom line
Current guidelines suggest a more prominent role for IGRA in testing for LTBI, particularly when the likelihood of exposure is low and in situations where a person may have received BCG vaccination, or would be unlikely to return for TST reading.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
Reference
Lewisohn DM et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Inf Dis. 2017;64(2):111-5.
While cases of active tuberculosis are relatively rare in the United States, TB is a major cause of morbidity and mortality worldwide. In the United States, there are an estimated 11 million individuals who have latent TB infection (LTBI). Without prophylactic treatment, somewhere between 4%-6% of individuals with LTBI will develop active disease during their lifetimes; roughly half of these cases will occur within a few years of the initial infection. Treatment of LTBI reduces – but does not eliminate – the risk for active disease, decreasing the consequences of active disease for the patient and the risk of transmitting infection to others.
Diagnostic tests for LTBI
The tuberculin skin test (TST) has been the standard method of diagnosing LTBI. It involves measuring induration caused by a delayed-type hypersensitivity reaction to Mycobacterium tuberculosis (Mtb) 2 or 3 days after injecting the reagent into the skin. The TST can result in false positives when detecting antibodies to BCG and nontuberculous mycobacteria, and false negatives when the patient does not demonstrate a robust immune response. A newer testing method is the Interferon Gamma Release Assay (IGRA), which involves phlebotomy, followed by a series of laboratory procedures that measure IFN-gamma release by T cells that have been sensitized to Mtb. The sensitivity of IGRA is similar to the TST, but it has better specificity; it is much less likely to react to antigens from BCG or nontuberculous mycobacteria. As detailed below, this guideline suggests a significantly more prominent role for IGRA, compared with previous recommendations.
Recommendation 1. Perform an IGRA, rather than a TST, in individuals 5 years or older who meet the following criteria: 1) are likely to be infected with Mtb; 2) have a low or intermediate risk of disease progression; 3) in whom it has been decided that testing for LTBI is warranted. A TST is an acceptable alternative, particularly if an IGRA is not available, is too costly, or is too burdensome. If an individual either has a history of BCG vaccination or is unlikely to return to have their TST read, then it is strongly recommended to use the IGRA as the test of choice.
Recommendation 2. There are insufficient data to recommend a preference for either a TST or an IGRA as the first-line diagnostic test in individuals 5 years or older who are likely to be infected with Mtb, who have a high risk of progression to active disease, and in whom it has been determined that diagnostic testing for LTBI infection is warranted; either test would be acceptable. In very high-risk patients, consider dual testing, with a positive result from either test (TST or IGRA) being considered positive.
Recommendation 3. Guidelines do not recommend testing for persons at low risk for Mtb infection. However, the authors recognize that testing in such persons may nevertheless be mandated in certain situations (for example in some school or child care settings). In these cases, the authors recommend performing an IGRA instead of a TST, to minimize the chance of a false-positive result, although a TST is an acceptable alternative. Furthermore, if the initial test is positive, they suggest performing a confirmatory test (either an IGRA or TST) and considering the person infected only if both tests are positive.
Recommendation 4. The authors suggest performing a TST rather than an IGRA in healthy children less than 5 years of age for whom it has been decided that diagnostic testing for LTBI is warranted. This recommendation reflects the limited body of evidence regarding IGRA testing in young children and the apparent decreased sensitivity (i.e. more false negatives) in this population, compared with TST use.
In the area of serial testing for TB infection, often done in health care and institutional settings, the guideline points out areas of uncertainty with IGRA testing. Specifically, the IGRA test is subject to variability in readings and boosting with antigen exposure that can complicate interpretation of apparent conversion on repeat testing. One longitudinal study showed conversion rates with IGRA to be six to nine times higher than that seen for the TST, and those conversions were thought to represent false positive tests. The guideline concludes that, “There is insufficient information available to guide the establishment of definitive criteria for the conversion.” The committee thought that a positive test in a low-risk individual was likely to be a false-positive result and recommended repeat testing. Because of the possibility of boosting with antigen exposure in situations where dual testing is anticipated, it may be preferable to obtain a specimen for IGRA prior to, or concurrently with TST placement.
Bottom line
Current guidelines suggest a more prominent role for IGRA in testing for LTBI, particularly when the likelihood of exposure is low and in situations where a person may have received BCG vaccination, or would be unlikely to return for TST reading.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
Reference
Lewisohn DM et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Inf Dis. 2017;64(2):111-5.
Study supports methotrexate monotherapy with TNF inhibitor rescue for early RA treatment
For patients with early rheumatoid arthritis, starting with methotrexate and adding adalimumab after 26 weeks if needed led to clinical and functional outcomes similar to those of starting with a dual adalimumab-methotrexate regimen, according to a study published in Annals of the Rheumatic Diseases.
Although upfront adalimumab-methotrexate led to about a 14% decrease in the likelihood of radiographic progression, nearly one in four patients did well over more than a year of follow-up without ever needing to add a biologic disease-modifying antirheumatic drug (DMARD), said Arthur Kavanaugh, MD, of the University of California at San Diego, La Jolla, Calif., and his associates.

At week 26, patients who had achieved stable low disease activity (LDA; 28-joint modified Disease Activity Score of less than 3.2, based on C-reactive protein) on dual therapy were re-randomized to either stay on or withdraw from adalimumab. Patients who achieved stable LDA on methotrexate alone stayed on it. Patients who did not achieve stable LDA by week 26 either stayed on methotrexate-adalimumab or received adalimumab rescue. For the current post hoc study, Dr. Kavanaugh and his associates compared longer-term outcomes between patients who received adalimumab-methotrexate at baseline and patients who started with methotrexate only. In addition to stable LDA, the investigators assessed normal function (Health Assessment Questionnaire Disability Index less than 0.5) and radiographic nonprogression (no more than 0.5 change in modified total Sharp score).
Patients who started on adalimumab-methotrexate instead of methotrexate monotherapy were significantly more likely to achieve stable LDA (53% vs. 30%), good function (45% vs. 33%), and radiographic nonprogression (87% vs. 72%) at week 26 (Ann Rheum Dis. 2013;72:64-71). However, as-needed rescue treatment with adalimumab at week 26 achieved very similar clinical and functional outcomes compared with initial treatment with methotrexate-adalimumab. At week 52, 62% and 65% of patients in these two groups had stable LDA, and 44% and 47% had normal function, respectively. At week 78, 65% of patients in both groups had stable LDA and 45% and 48% had normal function, respectively. However, initial therapy with adalimumab-methotrexate was associated with lower chances of radiographic progression compared with methotrexate monotherapy (86% and 72% at both time points, respectively).
This is the first study to assess whether rapidly adding a TNFi improves disease outcomes compared with starting treatment with both adalimumab and methotrexate in patients with early RA, the researchers said. Importantly, 24% of patients who started on methotrexate alone never needed to add a biological DMARD, experiencing “little to no radiographic progression and mostly good physical function thereafter,” they reported. The study supports current guidelines and a stepwise treat-to-target strategy can prevent overtreatment in about one in four patients with early RA, they concluded.
AbbVie makes adalimumab, sponsored the study, and was involved in its design, analysis, writeup, and review. Dr. Kavanaugh disclosed ties to AbbVie through his institution. Nine coinvestigators disclosed ties to AbbVie; five of the nine reported current or former employment with the company.
SOURCE: Ann Rheum Dis. 2017 Nov 16. doi: 10.1136/annrheumdis-2017-211871
This study is of general interest and its design is complex, with double-blind, open re-randomization, and open-label extension arms.
There are a number of points to highlight:
1. Both methotrexate-adalimumab arms eventuate in a small advantage with respect to radiographs, with less accrued damage than with methotrexate alone. As in multiple other studies, the radiographic differences, although statistically significant, are not clinically important during this short study. However, if extended over a number of years, they could become clinically important, and that should not be ignored.
2. The authors state that methotrexate monotherapy patients who later added adalimumab achieved symptomatic and functional relief equivalent to starting on methotrexate-adalimumab – which I fully agree with – but the authors pointed out that there may well be some bias in that conclusion because the “add-on” patients did so during an open-label phase of the study. The complex design of the study makes this a bit hard to dissect.

4. Also, this study design did not allow corticosteroids. While I am a staunch advocate of minimizing steroids, some clinicians would have used steroids early on to improve early response, thus mitigating the early differential effect of methotrexate monotherapy.
So what is the bottom line? In my mind, this study supports that methotrexate-adalimumab decreases the rate of bony damage (not a new finding among biologics plus methotrexate in RA) and gently advocates that using methotrexate alone as the first DMARD is appropriate.
The data actually do not clarify the potentially important symptomatic/functional differences during the early months between the group that went from methotrexate monotherapy to methotrexate-adalimumab vs. the group that received immediate methotrexate-adalimumab, where the “immediate” methotrexate-adalimumab patients probably felt better faster. Still, one needs to consider potential toxicity and cost of the immediate methotrexate-adalimumab group, and that is not well addressed here.
When faced with a patient, I always ask how bad are the symptoms (worse leaning me toward immediate methotrexate-adalimumab) vs. how frail is the patient (more frail leaning me toward first using methotrexate) and how good is their insurance (sadly a consideration in the United States, with better insurance leaning me toward the “immediate” combo because I think other data show this yields a faster response).
Daniel E. Furst, MD, is professor of rheumatology at the University of California, Los Angeles (emeritus), at the University of Washington, Seattle, and at the University of Florence (Italy). He reported receiving grant/research support from Bristol-Myers-Squibb, Pfizer, and Roche/Genentech. He is also a consultant to AbbVie, Novartis, Pfizer, and Roche/Genentech.
This study is of general interest and its design is complex, with double-blind, open re-randomization, and open-label extension arms.
There are a number of points to highlight:
1. Both methotrexate-adalimumab arms eventuate in a small advantage with respect to radiographs, with less accrued damage than with methotrexate alone. As in multiple other studies, the radiographic differences, although statistically significant, are not clinically important during this short study. However, if extended over a number of years, they could become clinically important, and that should not be ignored.
2. The authors state that methotrexate monotherapy patients who later added adalimumab achieved symptomatic and functional relief equivalent to starting on methotrexate-adalimumab – which I fully agree with – but the authors pointed out that there may well be some bias in that conclusion because the “add-on” patients did so during an open-label phase of the study. The complex design of the study makes this a bit hard to dissect.
4. Also, this study design did not allow corticosteroids. While I am a staunch advocate of minimizing steroids, some clinicians would have used steroids early on to improve early response, thus mitigating the early differential effect of methotrexate monotherapy.
So what is the bottom line? In my mind, this study supports that methotrexate-adalimumab decreases the rate of bony damage (not a new finding among biologics plus methotrexate in RA) and gently advocates that using methotrexate alone as the first DMARD is appropriate.
The data actually do not clarify the potentially important symptomatic/functional differences during the early months between the group that went from methotrexate monotherapy to methotrexate-adalimumab vs. the group that received immediate methotrexate-adalimumab, where the “immediate” methotrexate-adalimumab patients probably felt better faster. Still, one needs to consider potential toxicity and cost of the immediate methotrexate-adalimumab group, and that is not well addressed here.
When faced with a patient, I always ask how bad are the symptoms (worse leaning me toward immediate methotrexate-adalimumab) vs. how frail is the patient (more frail leaning me toward first using methotrexate) and how good is their insurance (sadly a consideration in the United States, with better insurance leaning me toward the “immediate” combo because I think other data show this yields a faster response).
Daniel E. Furst, MD, is professor of rheumatology at the University of California, Los Angeles (emeritus), at the University of Washington, Seattle, and at the University of Florence (Italy). He reported receiving grant/research support from Bristol-Myers-Squibb, Pfizer, and Roche/Genentech. He is also a consultant to AbbVie, Novartis, Pfizer, and Roche/Genentech.
This study is of general interest and its design is complex, with double-blind, open re-randomization, and open-label extension arms.
There are a number of points to highlight:
1. Both methotrexate-adalimumab arms eventuate in a small advantage with respect to radiographs, with less accrued damage than with methotrexate alone. As in multiple other studies, the radiographic differences, although statistically significant, are not clinically important during this short study. However, if extended over a number of years, they could become clinically important, and that should not be ignored.
2. The authors state that methotrexate monotherapy patients who later added adalimumab achieved symptomatic and functional relief equivalent to starting on methotrexate-adalimumab – which I fully agree with – but the authors pointed out that there may well be some bias in that conclusion because the “add-on” patients did so during an open-label phase of the study. The complex design of the study makes this a bit hard to dissect.
4. Also, this study design did not allow corticosteroids. While I am a staunch advocate of minimizing steroids, some clinicians would have used steroids early on to improve early response, thus mitigating the early differential effect of methotrexate monotherapy.
So what is the bottom line? In my mind, this study supports that methotrexate-adalimumab decreases the rate of bony damage (not a new finding among biologics plus methotrexate in RA) and gently advocates that using methotrexate alone as the first DMARD is appropriate.
The data actually do not clarify the potentially important symptomatic/functional differences during the early months between the group that went from methotrexate monotherapy to methotrexate-adalimumab vs. the group that received immediate methotrexate-adalimumab, where the “immediate” methotrexate-adalimumab patients probably felt better faster. Still, one needs to consider potential toxicity and cost of the immediate methotrexate-adalimumab group, and that is not well addressed here.
When faced with a patient, I always ask how bad are the symptoms (worse leaning me toward immediate methotrexate-adalimumab) vs. how frail is the patient (more frail leaning me toward first using methotrexate) and how good is their insurance (sadly a consideration in the United States, with better insurance leaning me toward the “immediate” combo because I think other data show this yields a faster response).
Daniel E. Furst, MD, is professor of rheumatology at the University of California, Los Angeles (emeritus), at the University of Washington, Seattle, and at the University of Florence (Italy). He reported receiving grant/research support from Bristol-Myers-Squibb, Pfizer, and Roche/Genentech. He is also a consultant to AbbVie, Novartis, Pfizer, and Roche/Genentech.
For patients with early rheumatoid arthritis, starting with methotrexate and adding adalimumab after 26 weeks if needed led to clinical and functional outcomes similar to those of starting with a dual adalimumab-methotrexate regimen, according to a study published in Annals of the Rheumatic Diseases.
Although upfront adalimumab-methotrexate led to about a 14% decrease in the likelihood of radiographic progression, nearly one in four patients did well over more than a year of follow-up without ever needing to add a biologic disease-modifying antirheumatic drug (DMARD), said Arthur Kavanaugh, MD, of the University of California at San Diego, La Jolla, Calif., and his associates.
At week 26, patients who had achieved stable low disease activity (LDA; 28-joint modified Disease Activity Score of less than 3.2, based on C-reactive protein) on dual therapy were re-randomized to either stay on or withdraw from adalimumab. Patients who achieved stable LDA on methotrexate alone stayed on it. Patients who did not achieve stable LDA by week 26 either stayed on methotrexate-adalimumab or received adalimumab rescue. For the current post hoc study, Dr. Kavanaugh and his associates compared longer-term outcomes between patients who received adalimumab-methotrexate at baseline and patients who started with methotrexate only. In addition to stable LDA, the investigators assessed normal function (Health Assessment Questionnaire Disability Index less than 0.5) and radiographic nonprogression (no more than 0.5 change in modified total Sharp score).
Patients who started on adalimumab-methotrexate instead of methotrexate monotherapy were significantly more likely to achieve stable LDA (53% vs. 30%), good function (45% vs. 33%), and radiographic nonprogression (87% vs. 72%) at week 26 (Ann Rheum Dis. 2013;72:64-71). However, as-needed rescue treatment with adalimumab at week 26 achieved very similar clinical and functional outcomes compared with initial treatment with methotrexate-adalimumab. At week 52, 62% and 65% of patients in these two groups had stable LDA, and 44% and 47% had normal function, respectively. At week 78, 65% of patients in both groups had stable LDA and 45% and 48% had normal function, respectively. However, initial therapy with adalimumab-methotrexate was associated with lower chances of radiographic progression compared with methotrexate monotherapy (86% and 72% at both time points, respectively).
This is the first study to assess whether rapidly adding a TNFi improves disease outcomes compared with starting treatment with both adalimumab and methotrexate in patients with early RA, the researchers said. Importantly, 24% of patients who started on methotrexate alone never needed to add a biological DMARD, experiencing “little to no radiographic progression and mostly good physical function thereafter,” they reported. The study supports current guidelines and a stepwise treat-to-target strategy can prevent overtreatment in about one in four patients with early RA, they concluded.
AbbVie makes adalimumab, sponsored the study, and was involved in its design, analysis, writeup, and review. Dr. Kavanaugh disclosed ties to AbbVie through his institution. Nine coinvestigators disclosed ties to AbbVie; five of the nine reported current or former employment with the company.
SOURCE: Ann Rheum Dis. 2017 Nov 16. doi: 10.1136/annrheumdis-2017-211871
For patients with early rheumatoid arthritis, starting with methotrexate and adding adalimumab after 26 weeks if needed led to clinical and functional outcomes similar to those of starting with a dual adalimumab-methotrexate regimen, according to a study published in Annals of the Rheumatic Diseases.
Although upfront adalimumab-methotrexate led to about a 14% decrease in the likelihood of radiographic progression, nearly one in four patients did well over more than a year of follow-up without ever needing to add a biologic disease-modifying antirheumatic drug (DMARD), said Arthur Kavanaugh, MD, of the University of California at San Diego, La Jolla, Calif., and his associates.
At week 26, patients who had achieved stable low disease activity (LDA; 28-joint modified Disease Activity Score of less than 3.2, based on C-reactive protein) on dual therapy were re-randomized to either stay on or withdraw from adalimumab. Patients who achieved stable LDA on methotrexate alone stayed on it. Patients who did not achieve stable LDA by week 26 either stayed on methotrexate-adalimumab or received adalimumab rescue. For the current post hoc study, Dr. Kavanaugh and his associates compared longer-term outcomes between patients who received adalimumab-methotrexate at baseline and patients who started with methotrexate only. In addition to stable LDA, the investigators assessed normal function (Health Assessment Questionnaire Disability Index less than 0.5) and radiographic nonprogression (no more than 0.5 change in modified total Sharp score).
Patients who started on adalimumab-methotrexate instead of methotrexate monotherapy were significantly more likely to achieve stable LDA (53% vs. 30%), good function (45% vs. 33%), and radiographic nonprogression (87% vs. 72%) at week 26 (Ann Rheum Dis. 2013;72:64-71). However, as-needed rescue treatment with adalimumab at week 26 achieved very similar clinical and functional outcomes compared with initial treatment with methotrexate-adalimumab. At week 52, 62% and 65% of patients in these two groups had stable LDA, and 44% and 47% had normal function, respectively. At week 78, 65% of patients in both groups had stable LDA and 45% and 48% had normal function, respectively. However, initial therapy with adalimumab-methotrexate was associated with lower chances of radiographic progression compared with methotrexate monotherapy (86% and 72% at both time points, respectively).
This is the first study to assess whether rapidly adding a TNFi improves disease outcomes compared with starting treatment with both adalimumab and methotrexate in patients with early RA, the researchers said. Importantly, 24% of patients who started on methotrexate alone never needed to add a biological DMARD, experiencing “little to no radiographic progression and mostly good physical function thereafter,” they reported. The study supports current guidelines and a stepwise treat-to-target strategy can prevent overtreatment in about one in four patients with early RA, they concluded.
AbbVie makes adalimumab, sponsored the study, and was involved in its design, analysis, writeup, and review. Dr. Kavanaugh disclosed ties to AbbVie through his institution. Nine coinvestigators disclosed ties to AbbVie; five of the nine reported current or former employment with the company.
SOURCE: Ann Rheum Dis. 2017 Nov 16. doi: 10.1136/annrheumdis-2017-211871
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point:
Major finding: Adding adalimumab as rescue therapy at 26 weeks achieved outcomes at 78 weeks similar to those of starting treatment with adalimumab-methotrexate.
Data source: A post hoc analysis of a 78-week, randomized, double-blind, phase 4 study of 926 methotrexate-naive patients with a less than 1-year history of active RA.
Disclosures: AbbVie makes adalimumab, sponsored the study, and was involved in its design, analysis, writeup, and review. Dr. Kavanaugh disclosed ties to AbbVie through his institution. Nine coinvestigators disclosed ties to AbbVie; five of the nine reported current or former employment with the company.
Source: Ann Rheum Dis. 2017 Nov 16. doi: 10.1136/annrheumdis-2017-211871
Early weight change has no special effect on mortality in RA
Weight loss at the time of rheumatoid arthritis diagnosis had the same impact on mortality in patients with and without RA, according to research trying to solve the so-called obesity paradox in RA, which has been related to prior observations of a protective effect of obesity on mortality in RA patients.
The finding indicates that clinicians can continue to encourage patients with rheumatoid arthritis to follow healthy weight-loss strategies, according to first author of the study, Jeffrey Sparks, MD, of Brigham and Women’s Hospital in Boston.
Dr. Sparks and his colleagues examined the impact of weight change and mortality in RA patients based on data from the Nurses’ Health Study.

“Our study is the first to focus on weight change around RA diagnosis and risk of death, rather than weight change in patients who had RA for many years,” Dr. Sparks noted.
By examining changes in weight near the time of RA diagnosis, Dr. Sparks and his colleagues said that they hoped to extract information about RA-specific processes rather than the underlying pathologies that might cause weight changes near the end of life.
In the study published in Arthritis & Rheumatology, the researchers compared women diagnosed with RA during follow-up to women without RA during the same index time period of 1976-2016. The study population included 121,701 women. Of these, 902 developed incident RA and were matched with 7,884 non-RA controls.
During an average of 18 years of follow-up, 41% of the RA cohort and 29% of the controls died. The risk of death was approximately twice as high (hazard ratio, 2.78; 95% confidence interval, 1.58-4.89) among those with weight loss greater than 30 pounds at the time of RA diagnosis, compared with those whose weight remained stable. However, the risk for mortality was similarly increased (HR, 2.16; 95% CI, 1.61-2.88) among the controls with weight loss greater than 30 pounds, compared with those with stable weight. No association with mortality was noted in either group among women who gained more than 30 pounds at the time of RA diagnosis.
Dr. Sparks said he was somewhat surprised by the findings.
“We expected severe, pathologic weight loss to be associated with increased risk of death among patients with RA and comparators. It was somewhat surprising that the risks in both groups were similar,” he said. “Conversely, prior studies suggested that weight gain might have been associated with increased risk of death. However, we found no association of weight gain with risk of death,” he noted.
In addition, “Our findings argue that there is not an RA-specific mortality risk based on either weight loss or gain,” he said. “While we found that weight loss was associated with increased mortality, this was most pronounced in the severe weight loss group, so was likely due to unintentional weight loss.”
Joshua F. Baker, MD, of the University of Pennsylvania, Philadelphia, and his colleagues identified an association between weight change and risk of death in RA patients in a study first published online in Arthritis & Rheumatology in 2015 (Arthritis Rheumatol. 2015 Jul;67[7]:1711-17). That study addressed the so-called obesity paradox in RA, and Dr. Baker and his colleagues noted that weight loss associated with the development of chronic illness is a significant confounder that may explain the observed protective effect of obesity on mortality.

“It is not clear how best to monitor changes in weight, when exactly to become concerned, and what to do when changes are observed,” Dr. Baker noted. “RA patients may lose weight for a number of reasons, not all related to their arthritis, and it is unlikely that there is a ‘one size fits all’ approach,” he said.
The study was limited in part by the women-only study population, so the results might not be generalizable to men, Dr. Sparks said. “The reason for weight change was unavailable,” he added. Directions for further research include investigation of how factors such as physical activity, diet, and weight loss may affect the risk of death among individuals with and without RA, he said.
Dr. Sparks had no financial conflicts to disclose. The study was supported in part by the National Institutes of Health and the Rheumatology Research Foundation’s Disease-Targeted Innovative Award and Scientist Development Awards.
SOURCE: Sparks J et al. Arthritis Rheumatol. 2017 Nov 30. doi: 10.1002/art.40346.
Weight loss at the time of rheumatoid arthritis diagnosis had the same impact on mortality in patients with and without RA, according to research trying to solve the so-called obesity paradox in RA, which has been related to prior observations of a protective effect of obesity on mortality in RA patients.
The finding indicates that clinicians can continue to encourage patients with rheumatoid arthritis to follow healthy weight-loss strategies, according to first author of the study, Jeffrey Sparks, MD, of Brigham and Women’s Hospital in Boston.
Dr. Sparks and his colleagues examined the impact of weight change and mortality in RA patients based on data from the Nurses’ Health Study.
“Our study is the first to focus on weight change around RA diagnosis and risk of death, rather than weight change in patients who had RA for many years,” Dr. Sparks noted.
By examining changes in weight near the time of RA diagnosis, Dr. Sparks and his colleagues said that they hoped to extract information about RA-specific processes rather than the underlying pathologies that might cause weight changes near the end of life.
In the study published in Arthritis & Rheumatology, the researchers compared women diagnosed with RA during follow-up to women without RA during the same index time period of 1976-2016. The study population included 121,701 women. Of these, 902 developed incident RA and were matched with 7,884 non-RA controls.
During an average of 18 years of follow-up, 41% of the RA cohort and 29% of the controls died. The risk of death was approximately twice as high (hazard ratio, 2.78; 95% confidence interval, 1.58-4.89) among those with weight loss greater than 30 pounds at the time of RA diagnosis, compared with those whose weight remained stable. However, the risk for mortality was similarly increased (HR, 2.16; 95% CI, 1.61-2.88) among the controls with weight loss greater than 30 pounds, compared with those with stable weight. No association with mortality was noted in either group among women who gained more than 30 pounds at the time of RA diagnosis.
Dr. Sparks said he was somewhat surprised by the findings.
“We expected severe, pathologic weight loss to be associated with increased risk of death among patients with RA and comparators. It was somewhat surprising that the risks in both groups were similar,” he said. “Conversely, prior studies suggested that weight gain might have been associated with increased risk of death. However, we found no association of weight gain with risk of death,” he noted.
In addition, “Our findings argue that there is not an RA-specific mortality risk based on either weight loss or gain,” he said. “While we found that weight loss was associated with increased mortality, this was most pronounced in the severe weight loss group, so was likely due to unintentional weight loss.”
Joshua F. Baker, MD, of the University of Pennsylvania, Philadelphia, and his colleagues identified an association between weight change and risk of death in RA patients in a study first published online in Arthritis & Rheumatology in 2015 (Arthritis Rheumatol. 2015 Jul;67[7]:1711-17). That study addressed the so-called obesity paradox in RA, and Dr. Baker and his colleagues noted that weight loss associated with the development of chronic illness is a significant confounder that may explain the observed protective effect of obesity on mortality.
“It is not clear how best to monitor changes in weight, when exactly to become concerned, and what to do when changes are observed,” Dr. Baker noted. “RA patients may lose weight for a number of reasons, not all related to their arthritis, and it is unlikely that there is a ‘one size fits all’ approach,” he said.
The study was limited in part by the women-only study population, so the results might not be generalizable to men, Dr. Sparks said. “The reason for weight change was unavailable,” he added. Directions for further research include investigation of how factors such as physical activity, diet, and weight loss may affect the risk of death among individuals with and without RA, he said.
Dr. Sparks had no financial conflicts to disclose. The study was supported in part by the National Institutes of Health and the Rheumatology Research Foundation’s Disease-Targeted Innovative Award and Scientist Development Awards.
SOURCE: Sparks J et al. Arthritis Rheumatol. 2017 Nov 30. doi: 10.1002/art.40346.
Weight loss at the time of rheumatoid arthritis diagnosis had the same impact on mortality in patients with and without RA, according to research trying to solve the so-called obesity paradox in RA, which has been related to prior observations of a protective effect of obesity on mortality in RA patients.
The finding indicates that clinicians can continue to encourage patients with rheumatoid arthritis to follow healthy weight-loss strategies, according to first author of the study, Jeffrey Sparks, MD, of Brigham and Women’s Hospital in Boston.
Dr. Sparks and his colleagues examined the impact of weight change and mortality in RA patients based on data from the Nurses’ Health Study.
“Our study is the first to focus on weight change around RA diagnosis and risk of death, rather than weight change in patients who had RA for many years,” Dr. Sparks noted.
By examining changes in weight near the time of RA diagnosis, Dr. Sparks and his colleagues said that they hoped to extract information about RA-specific processes rather than the underlying pathologies that might cause weight changes near the end of life.
In the study published in Arthritis & Rheumatology, the researchers compared women diagnosed with RA during follow-up to women without RA during the same index time period of 1976-2016. The study population included 121,701 women. Of these, 902 developed incident RA and were matched with 7,884 non-RA controls.
During an average of 18 years of follow-up, 41% of the RA cohort and 29% of the controls died. The risk of death was approximately twice as high (hazard ratio, 2.78; 95% confidence interval, 1.58-4.89) among those with weight loss greater than 30 pounds at the time of RA diagnosis, compared with those whose weight remained stable. However, the risk for mortality was similarly increased (HR, 2.16; 95% CI, 1.61-2.88) among the controls with weight loss greater than 30 pounds, compared with those with stable weight. No association with mortality was noted in either group among women who gained more than 30 pounds at the time of RA diagnosis.
Dr. Sparks said he was somewhat surprised by the findings.
“We expected severe, pathologic weight loss to be associated with increased risk of death among patients with RA and comparators. It was somewhat surprising that the risks in both groups were similar,” he said. “Conversely, prior studies suggested that weight gain might have been associated with increased risk of death. However, we found no association of weight gain with risk of death,” he noted.
In addition, “Our findings argue that there is not an RA-specific mortality risk based on either weight loss or gain,” he said. “While we found that weight loss was associated with increased mortality, this was most pronounced in the severe weight loss group, so was likely due to unintentional weight loss.”
Joshua F. Baker, MD, of the University of Pennsylvania, Philadelphia, and his colleagues identified an association between weight change and risk of death in RA patients in a study first published online in Arthritis & Rheumatology in 2015 (Arthritis Rheumatol. 2015 Jul;67[7]:1711-17). That study addressed the so-called obesity paradox in RA, and Dr. Baker and his colleagues noted that weight loss associated with the development of chronic illness is a significant confounder that may explain the observed protective effect of obesity on mortality.
“It is not clear how best to monitor changes in weight, when exactly to become concerned, and what to do when changes are observed,” Dr. Baker noted. “RA patients may lose weight for a number of reasons, not all related to their arthritis, and it is unlikely that there is a ‘one size fits all’ approach,” he said.
The study was limited in part by the women-only study population, so the results might not be generalizable to men, Dr. Sparks said. “The reason for weight change was unavailable,” he added. Directions for further research include investigation of how factors such as physical activity, diet, and weight loss may affect the risk of death among individuals with and without RA, he said.
Dr. Sparks had no financial conflicts to disclose. The study was supported in part by the National Institutes of Health and the Rheumatology Research Foundation’s Disease-Targeted Innovative Award and Scientist Development Awards.
SOURCE: Sparks J et al. Arthritis Rheumatol. 2017 Nov 30. doi: 10.1002/art.40346.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: The risk of death was approximately twice as high among women with weight loss greater than 30 pounds both for those diagnosed around the same time with RA (hazard ratio, 2.78) and for controls (HR, 2.16), compared with those whose weight remained stable.
Study details: A case-control study of 8,786 participants in the Nurses’ Health Study during 1976-2016.
Disclosures: Dr. Sparks had no financial conflicts to disclose. The study was supported in part by the National Institutes of Health and the Rheumatology Research Foundation’s Disease-Targeted Innovative Award and Scientist Development Awards.
Source: Sparks J et al. Arthritis Rheumatol. 2017 Nov 30. doi: 10.1002/art.40346.
Health disparities in rural America: Chronic conditions
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
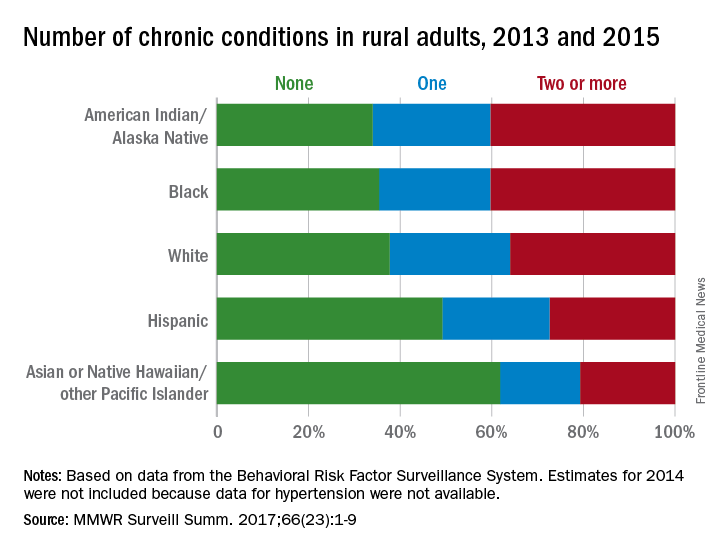
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
FROM MMWR SURVEILLANCE SUMMARIES
Novel oral orphan drug tames pemphigus
GENEVA – An oral reversible Bruton tyrosine kinase inhibitor known as PRN1008 showed promising efficacy and safety for the treatment of pemphigus vulgaris in an interim analysis of an ongoing small-to-date, open-label phase 2 study, according to DeDee Murrell, MD.
PRN1008 is a designer drug intended as an alternative to the long-standing standard therapy for pemphigus, months to years of moderate- or high-dose systemic corticosteroids, with all the debilitating side effects that sledgehammer approach often brings, she said at the annual congress of the European Academy of Dermatology and Venereology.

Thus, PRN1008 inhibits a range of inflammatory cellular activities in mast cells, neutrophils, and other cells activated in autoimmune diseases, without killing those cells or directly affecting T cells. And – like corticosteroids – it works quickly, according to Dr. Murrell, professor of dermatology at the University of New South Wales in Sydney.
“The development of an oral, fast-acting treatment that could safely and effectively modulate B-cell function without depleting B cells would be a major advance in treating autoimmune diseases like pemphigus, vasculitis, immune thrombocytopenic purpura, multiple sclerosis, and rheumatoid arthritis,” she said.
Also, PRN1008 was designed to provide durable inhibition of BTK, coupled with rapid systemic clearance of the drug in order to minimize side effects.
The ongoing phase 2 multicenter international study, known as Believe-PV, to date includes 12 patients with biopsy-proven mild to moderate pemphigus vulgaris. Five patients were newly diagnosed and treatment naive, while seven had relapsing disease. All were placed on fixed-dose PRN1008 at 400 mg b.i.d. for 12 weeks with low-dose prednisone as needed, then followed for an additional 12 weeks off PRN1008 to evaluate the durability of responses.
The primary study endpoint was control of disease activity by week 4 on a background of little or no prednisone, which 5 of 12 patients achieved. The secondary endpoint of complete clinical remission at 12 weeks was achieved in half of patients. Total pemphigus disease activity index (PDAI) scores dropped throughout the study period, reaching a mean 70% reduction at 12 weeks from a baseline of 20 points. Scores on the autoimmune bullous quality of life metric improved by 43%.
Eight of the 11 individuals who completed the study had control of disease activity by week 4 and/or complete clinical remission at 12 weeks. Those results are comparable with those typically seen with high-dose steroids at 12 weeks, the dermatologist noted.
Levels of anti–desmoglein-1 and/or -3 autoantibodies, which were elevated at baseline in 10 of 12 subjects, decreased during treatment with PRN1008.
Seventy-five percent of Bruton tyrosine kinase receptors were occupied by PRN1008 by day 2 of the study, confirming earlier studies in canine models of pemphigus. It turns out that pemphigus foliaceus is as common in dogs as atopic dermatitis is in humans, according to Dr. Murrell.
Side effects were limited to mild headache in two patients. One patient developed serious grade 3 cellulitis. She was taken off the study medication, although it was deemed unlikely that the infection was treatment related because she had had a recent history of multiple episodes of cellulitis.
During the second 12-week phase of the trial, after discontinuation of PRN1008, most patients retained their on-treatment reduction in total PDAI scores.
Dr. Murrell noted that the gradient of improvement in PDAI scores seen with PRN1008 in the Believe-PV study was quite similar to that seen in a recent 90-patient French randomized trial of rituximab (Rituxan) for the treatment of pemphigus. That’s of considerable interest, she said, because rituximab is a much more powerful drug, which drastically depletes the B-cell population. Moreover, the gradient of improvement in the rituximab-treated patients in the French trial was achieved with the aid of moderate-dose prednisone at 1 or 1.5 mg/kg per day, while PRN1008-treated patients in Believe-PV were taking on average only 0.2 mg/kg per day.
Asked if she thinks PRN1008 has a future as a stand-alone treatment for pemphigus or is better suited as an adjunct to systemic corticosteroids, Dr. Murrell said she believes the drug can be used effectively without steroids. However, since it’s recommended that patients be screened for tuberculosis before going on rituximab, and PRN1008 also targets B cells, she and her coinvestigators followed the same practice in Believe-PV. And because it takes a couple of weeks for the results of the Quantiferon-TB Gold In-Tube test to come back, it would be unethical for patients newly diagnosed with pemphigus to go untreated and in pain during that period, they get corticosteroids, at least initially.
Dr. Murrell reported serving as a paid consultant to Principia Biopharma, which is developing PRN1008.
GENEVA – An oral reversible Bruton tyrosine kinase inhibitor known as PRN1008 showed promising efficacy and safety for the treatment of pemphigus vulgaris in an interim analysis of an ongoing small-to-date, open-label phase 2 study, according to DeDee Murrell, MD.
PRN1008 is a designer drug intended as an alternative to the long-standing standard therapy for pemphigus, months to years of moderate- or high-dose systemic corticosteroids, with all the debilitating side effects that sledgehammer approach often brings, she said at the annual congress of the European Academy of Dermatology and Venereology.
Thus, PRN1008 inhibits a range of inflammatory cellular activities in mast cells, neutrophils, and other cells activated in autoimmune diseases, without killing those cells or directly affecting T cells. And – like corticosteroids – it works quickly, according to Dr. Murrell, professor of dermatology at the University of New South Wales in Sydney.
“The development of an oral, fast-acting treatment that could safely and effectively modulate B-cell function without depleting B cells would be a major advance in treating autoimmune diseases like pemphigus, vasculitis, immune thrombocytopenic purpura, multiple sclerosis, and rheumatoid arthritis,” she said.
Also, PRN1008 was designed to provide durable inhibition of BTK, coupled with rapid systemic clearance of the drug in order to minimize side effects.
The ongoing phase 2 multicenter international study, known as Believe-PV, to date includes 12 patients with biopsy-proven mild to moderate pemphigus vulgaris. Five patients were newly diagnosed and treatment naive, while seven had relapsing disease. All were placed on fixed-dose PRN1008 at 400 mg b.i.d. for 12 weeks with low-dose prednisone as needed, then followed for an additional 12 weeks off PRN1008 to evaluate the durability of responses.
The primary study endpoint was control of disease activity by week 4 on a background of little or no prednisone, which 5 of 12 patients achieved. The secondary endpoint of complete clinical remission at 12 weeks was achieved in half of patients. Total pemphigus disease activity index (PDAI) scores dropped throughout the study period, reaching a mean 70% reduction at 12 weeks from a baseline of 20 points. Scores on the autoimmune bullous quality of life metric improved by 43%.
Eight of the 11 individuals who completed the study had control of disease activity by week 4 and/or complete clinical remission at 12 weeks. Those results are comparable with those typically seen with high-dose steroids at 12 weeks, the dermatologist noted.
Levels of anti–desmoglein-1 and/or -3 autoantibodies, which were elevated at baseline in 10 of 12 subjects, decreased during treatment with PRN1008.
Seventy-five percent of Bruton tyrosine kinase receptors were occupied by PRN1008 by day 2 of the study, confirming earlier studies in canine models of pemphigus. It turns out that pemphigus foliaceus is as common in dogs as atopic dermatitis is in humans, according to Dr. Murrell.
Side effects were limited to mild headache in two patients. One patient developed serious grade 3 cellulitis. She was taken off the study medication, although it was deemed unlikely that the infection was treatment related because she had had a recent history of multiple episodes of cellulitis.
During the second 12-week phase of the trial, after discontinuation of PRN1008, most patients retained their on-treatment reduction in total PDAI scores.
Dr. Murrell noted that the gradient of improvement in PDAI scores seen with PRN1008 in the Believe-PV study was quite similar to that seen in a recent 90-patient French randomized trial of rituximab (Rituxan) for the treatment of pemphigus. That’s of considerable interest, she said, because rituximab is a much more powerful drug, which drastically depletes the B-cell population. Moreover, the gradient of improvement in the rituximab-treated patients in the French trial was achieved with the aid of moderate-dose prednisone at 1 or 1.5 mg/kg per day, while PRN1008-treated patients in Believe-PV were taking on average only 0.2 mg/kg per day.
Asked if she thinks PRN1008 has a future as a stand-alone treatment for pemphigus or is better suited as an adjunct to systemic corticosteroids, Dr. Murrell said she believes the drug can be used effectively without steroids. However, since it’s recommended that patients be screened for tuberculosis before going on rituximab, and PRN1008 also targets B cells, she and her coinvestigators followed the same practice in Believe-PV. And because it takes a couple of weeks for the results of the Quantiferon-TB Gold In-Tube test to come back, it would be unethical for patients newly diagnosed with pemphigus to go untreated and in pain during that period, they get corticosteroids, at least initially.
Dr. Murrell reported serving as a paid consultant to Principia Biopharma, which is developing PRN1008.
GENEVA – An oral reversible Bruton tyrosine kinase inhibitor known as PRN1008 showed promising efficacy and safety for the treatment of pemphigus vulgaris in an interim analysis of an ongoing small-to-date, open-label phase 2 study, according to DeDee Murrell, MD.
PRN1008 is a designer drug intended as an alternative to the long-standing standard therapy for pemphigus, months to years of moderate- or high-dose systemic corticosteroids, with all the debilitating side effects that sledgehammer approach often brings, she said at the annual congress of the European Academy of Dermatology and Venereology.
Thus, PRN1008 inhibits a range of inflammatory cellular activities in mast cells, neutrophils, and other cells activated in autoimmune diseases, without killing those cells or directly affecting T cells. And – like corticosteroids – it works quickly, according to Dr. Murrell, professor of dermatology at the University of New South Wales in Sydney.
“The development of an oral, fast-acting treatment that could safely and effectively modulate B-cell function without depleting B cells would be a major advance in treating autoimmune diseases like pemphigus, vasculitis, immune thrombocytopenic purpura, multiple sclerosis, and rheumatoid arthritis,” she said.
Also, PRN1008 was designed to provide durable inhibition of BTK, coupled with rapid systemic clearance of the drug in order to minimize side effects.
The ongoing phase 2 multicenter international study, known as Believe-PV, to date includes 12 patients with biopsy-proven mild to moderate pemphigus vulgaris. Five patients were newly diagnosed and treatment naive, while seven had relapsing disease. All were placed on fixed-dose PRN1008 at 400 mg b.i.d. for 12 weeks with low-dose prednisone as needed, then followed for an additional 12 weeks off PRN1008 to evaluate the durability of responses.
The primary study endpoint was control of disease activity by week 4 on a background of little or no prednisone, which 5 of 12 patients achieved. The secondary endpoint of complete clinical remission at 12 weeks was achieved in half of patients. Total pemphigus disease activity index (PDAI) scores dropped throughout the study period, reaching a mean 70% reduction at 12 weeks from a baseline of 20 points. Scores on the autoimmune bullous quality of life metric improved by 43%.
Eight of the 11 individuals who completed the study had control of disease activity by week 4 and/or complete clinical remission at 12 weeks. Those results are comparable with those typically seen with high-dose steroids at 12 weeks, the dermatologist noted.
Levels of anti–desmoglein-1 and/or -3 autoantibodies, which were elevated at baseline in 10 of 12 subjects, decreased during treatment with PRN1008.
Seventy-five percent of Bruton tyrosine kinase receptors were occupied by PRN1008 by day 2 of the study, confirming earlier studies in canine models of pemphigus. It turns out that pemphigus foliaceus is as common in dogs as atopic dermatitis is in humans, according to Dr. Murrell.
Side effects were limited to mild headache in two patients. One patient developed serious grade 3 cellulitis. She was taken off the study medication, although it was deemed unlikely that the infection was treatment related because she had had a recent history of multiple episodes of cellulitis.
During the second 12-week phase of the trial, after discontinuation of PRN1008, most patients retained their on-treatment reduction in total PDAI scores.
Dr. Murrell noted that the gradient of improvement in PDAI scores seen with PRN1008 in the Believe-PV study was quite similar to that seen in a recent 90-patient French randomized trial of rituximab (Rituxan) for the treatment of pemphigus. That’s of considerable interest, she said, because rituximab is a much more powerful drug, which drastically depletes the B-cell population. Moreover, the gradient of improvement in the rituximab-treated patients in the French trial was achieved with the aid of moderate-dose prednisone at 1 or 1.5 mg/kg per day, while PRN1008-treated patients in Believe-PV were taking on average only 0.2 mg/kg per day.
Asked if she thinks PRN1008 has a future as a stand-alone treatment for pemphigus or is better suited as an adjunct to systemic corticosteroids, Dr. Murrell said she believes the drug can be used effectively without steroids. However, since it’s recommended that patients be screened for tuberculosis before going on rituximab, and PRN1008 also targets B cells, she and her coinvestigators followed the same practice in Believe-PV. And because it takes a couple of weeks for the results of the Quantiferon-TB Gold In-Tube test to come back, it would be unethical for patients newly diagnosed with pemphigus to go untreated and in pain during that period, they get corticosteroids, at least initially.
Dr. Murrell reported serving as a paid consultant to Principia Biopharma, which is developing PRN1008.
AT THE EADV CONGRESS
Key clinical point:
Major finding: Five of 12 pemphigus vulgaris patients achieved control of disease activity within the first 4 weeks on the investigational oral Bruton tyrosine kinase inhibitor PRN1008.
Data source: An interim analysis of the first 12 patients with pemphigus vulgaris in an ongoing multicenter, international open-label, phase 2 clinical trial.
Disclosures: The study presenter reported serving as a paid consultant to Principia Biopharma, which is developing PRN1008 and sponsored the Believe-PV trial.
Arthritis prevalence higher than previously thought, especially in adults under 65
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).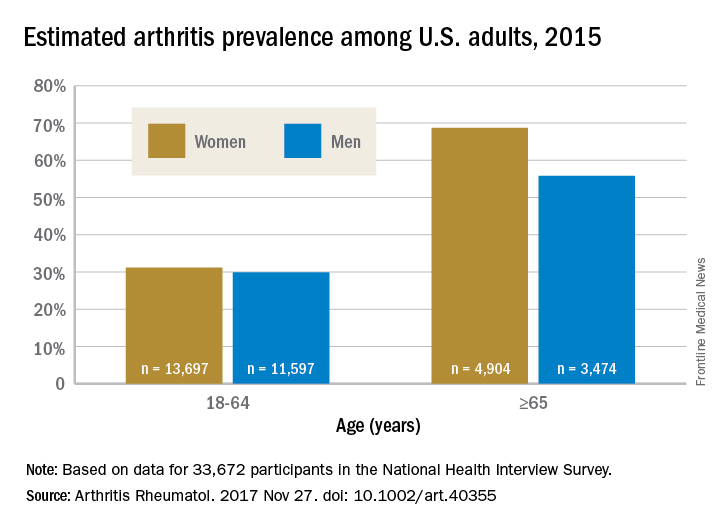
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
By including two additional survey criteria in their study of arthritis prevalence, Dr. Jafarzadeh and Dr. Felson introduced a method that “may be considerably more accurate than prior estimates that use the single NHIS [National Health Interview Survey] item on doctor-diagnosed arthritis,” said Jeffrey N. Katz, MD, in an editorial accompanying the study.
The study raises important questions about how “arthritis” is defined, as well as how prevalence estimates could affect policy agendas, and could potentially have “far-reaching consequences” related to investment in research, prevention, and treatment, he added.
Dr. Katz is with the Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40357). No conflicts of interest were disclosed.
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
The prevalence of arthritis in the United States is much higher than current estimates indicate, especially among adults under 65 years of age, a study showed.
The higher prevalence can be largely attributed to “the previous underestimate of arthritis in adults between 18-64 years of age,” according to S. Reza Jafarzadeh, PhD, and David T. Felson , MD, both of Boston University. Using a new surveillance model, they estimated that 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%). Of these, 61.1 million were between 18 and 64 years of age (Arthritis Rheumatol. 2017 Nov 27. doi: 10.1002/art.40355).
Arthritis prevalence was 29.9% in men aged 18-64 years (95% probability interval, 23.4-42.3), 31.2% in women aged 18-64 years (95% PI, 25.8-44.1), 55.8% in men aged 65 years and older (95% PI, 49.9-70.4), and 68.7% in women aged 65 years and older (95% PI, 62.1-79.9), the authors reported.
Among respondents aged 18-64 years, 19.3% of men and 16.7% of women reported that they had chronic joint symptoms but no physician-diagnosed arthritis. Among those 65 years of age or older, 15.7% of men and 13.5% of women responded that they had chronic joint symptoms without physician-diagnosed arthritis.
Current methodology for estimating arthritis prevalence is based on a single survey question asking whether a health care provider has ever told the patient that he or she has arthritis, a method that has previously been shown to have a sensitivity of 68.8% in adults 65 years of age and older and 52.5% for those aged 45-64 years, Dr. Jafarzadeh and Dr. Felson reported. “Such a low sensitivity, especially in a younger population, where almost half of true arthritis cases are missed, results in substantial misclassification and underestimation of prevalence and would have a detrimental effect for planning and needs assessment,” the authors wrote.
The two additional questions on joint pain, aching, and stiffness that the investigators included in the study captured “a substantial (i.e., 65%-80%) fraction of the population with arthritis, who are between 18-64 years of age, but are misclassified as healthy by the doctor-diagnosed arthritis criterion due to low sensitivity,” they said.
The study authors also speculated that younger patients might be more likely to ignore symptoms or visit a doctor less often.
“Further studies are needed to evaluate potential changes in the specific causes of arthritis, especially among adults below the age of 65,” they concluded.
The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: An estimated 91.2 million adults in the United States (36.8%) had arthritis in 2015, compared with a previously reported national estimate of 54.4 million adults (22.7%).
Data source: Data from 33,672 respondents to the 2015 National Health Interview Survey.
Disclosures: The study was supported by a grant from the National Institutes of Health. The investigators did not disclose any other conflicts of interest.