User login
Hand Sanitizers and Alcohol Abuse: A Dangerous Cocktail
Since the COVID-19 pandemic, alcoholic hand sanitizers have become widely accessible nationwide. They can pose a problem, especially for emergency departments, when alcohol-dependent patients start drinking them. One example that demonstrates the challenge of diagnosing alcohol abuse is the medical history of a young man, as reported by Mahmoud El Hussein, MD, and colleagues from Hôpital Lariboisière in Paris, France.
Presentation and History
A 26-year-old man presented with severe abdominal pain at the emergency department. Upon arrival, he was hemodynamically stable but nervous and verbally aggressive at times. The patient reported no relevant preexisting conditions and was not taking any medications.
Findings
Upon initial physical examination, the patient had a soft, diffusely tender abdomen; tachycardia; and notably poor hygiene. The patient was afebrile. An ECG confirmed the tachycardia but showed no signs of ischemia. Blood work, except for slightly elevated liver values, did not reveal any abnormalities, particularly ruling out bleeding or kidney disease.
A urease rapid test to rule out kidney stones also showed no pathologic findings. In consultation with the surgical department, a CT scan of the abdomen was performed to rule out organ perforation, volvulus, or mesenteric ischemia. Only signs of fatty liver were found.
A Neighbor’s Tip
During all examinations, the patient’s abdomen was repeatedly palpated to promptly detect signs of an acute abdomen. However, there was never any defense tension at any point.
Intravenous analgesics and proton pump inhibitors (ie, paracetamol, phloroglucin, and pantoprazole) did not relieve the patient’s symptoms. Morphine was administered intravenously for sedation.
Only after a frustrating diagnostic process did a neighbor of the patient inform a nurse that he suspected the patient of stealing and consuming hand sanitizer. With the patient’s consent, a blood alcohol test was performed, revealing a blood alcohol concentration of 0.2% (2 g/L). A urine test, also conducted with the patient’s consent, tested positive for tetrahydrocannabinol. Additional tests showed the following results:
- Venous pH: 7.29 (normal, 7.32-7.38)
- Anion gap (mEq/L): 14 (normal, 3-9)
- Ketone bodies (mmol/L): 0.2 (normal, < 0.6)
- Calculated serum osmolality (mOsm/kg): 292 (normal, 285-295)
- Measured serum osmolality (mOsm/kg): 320 (normal, 285-295)
- Osmolality gap (mOsm/kg): 2 (normal, < 10)
The patient was informed of the test results and confessed to feigning abdominal pain. He was dependent on alcohol and experiencing withdrawal symptoms. The patient had stolen seven 475-mL bottles of hand sanitizer and consumed one and a half in the past 4-6 hours. According to the authors, the sanitizer consisted of 80% ethanol, 1.45% glycerol, and 0.13% hydrogen peroxide.
Discussion
In Germany, alcohol consumption results in approximately €57 billion in direct economic costs annually, according to data from the Federal Ministry of Health. In 2021, about 7.9 million people aged 18-64 years consumed alcohol in a risky manner (approximately 9.6% of the German population). About 9 million people (approximately 11%) were classified as alcoholics.
Therefore, staff in emergency departments, where potential abusers encounter a wide range of potential abuse items, should exercise caution.
Although hand sanitizers are mainly composed of ethanol, they may also contain isopropanol, methanol, or acetone. Methanol poisoning can cause abdominal pain, visual disturbances, central nervous system damage, and death. Other alcohols such as ethylene glycol, commonly found in antifreeze, can distort blood values (lactate) and complicate a correct diagnosis.
Physicians working in emergency departments should proceed with caution when suspecting alcohol abuse. Questioning the patient’s environment and determining additional laboratory parameters (such as osmolality gap in the case report) can help unmask substance abuse if it is in doubt.
This story was translated from Univadis Germany, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Since the COVID-19 pandemic, alcoholic hand sanitizers have become widely accessible nationwide. They can pose a problem, especially for emergency departments, when alcohol-dependent patients start drinking them. One example that demonstrates the challenge of diagnosing alcohol abuse is the medical history of a young man, as reported by Mahmoud El Hussein, MD, and colleagues from Hôpital Lariboisière in Paris, France.
Presentation and History
A 26-year-old man presented with severe abdominal pain at the emergency department. Upon arrival, he was hemodynamically stable but nervous and verbally aggressive at times. The patient reported no relevant preexisting conditions and was not taking any medications.
Findings
Upon initial physical examination, the patient had a soft, diffusely tender abdomen; tachycardia; and notably poor hygiene. The patient was afebrile. An ECG confirmed the tachycardia but showed no signs of ischemia. Blood work, except for slightly elevated liver values, did not reveal any abnormalities, particularly ruling out bleeding or kidney disease.
A urease rapid test to rule out kidney stones also showed no pathologic findings. In consultation with the surgical department, a CT scan of the abdomen was performed to rule out organ perforation, volvulus, or mesenteric ischemia. Only signs of fatty liver were found.
A Neighbor’s Tip
During all examinations, the patient’s abdomen was repeatedly palpated to promptly detect signs of an acute abdomen. However, there was never any defense tension at any point.
Intravenous analgesics and proton pump inhibitors (ie, paracetamol, phloroglucin, and pantoprazole) did not relieve the patient’s symptoms. Morphine was administered intravenously for sedation.
Only after a frustrating diagnostic process did a neighbor of the patient inform a nurse that he suspected the patient of stealing and consuming hand sanitizer. With the patient’s consent, a blood alcohol test was performed, revealing a blood alcohol concentration of 0.2% (2 g/L). A urine test, also conducted with the patient’s consent, tested positive for tetrahydrocannabinol. Additional tests showed the following results:
- Venous pH: 7.29 (normal, 7.32-7.38)
- Anion gap (mEq/L): 14 (normal, 3-9)
- Ketone bodies (mmol/L): 0.2 (normal, < 0.6)
- Calculated serum osmolality (mOsm/kg): 292 (normal, 285-295)
- Measured serum osmolality (mOsm/kg): 320 (normal, 285-295)
- Osmolality gap (mOsm/kg): 2 (normal, < 10)
The patient was informed of the test results and confessed to feigning abdominal pain. He was dependent on alcohol and experiencing withdrawal symptoms. The patient had stolen seven 475-mL bottles of hand sanitizer and consumed one and a half in the past 4-6 hours. According to the authors, the sanitizer consisted of 80% ethanol, 1.45% glycerol, and 0.13% hydrogen peroxide.
Discussion
In Germany, alcohol consumption results in approximately €57 billion in direct economic costs annually, according to data from the Federal Ministry of Health. In 2021, about 7.9 million people aged 18-64 years consumed alcohol in a risky manner (approximately 9.6% of the German population). About 9 million people (approximately 11%) were classified as alcoholics.
Therefore, staff in emergency departments, where potential abusers encounter a wide range of potential abuse items, should exercise caution.
Although hand sanitizers are mainly composed of ethanol, they may also contain isopropanol, methanol, or acetone. Methanol poisoning can cause abdominal pain, visual disturbances, central nervous system damage, and death. Other alcohols such as ethylene glycol, commonly found in antifreeze, can distort blood values (lactate) and complicate a correct diagnosis.
Physicians working in emergency departments should proceed with caution when suspecting alcohol abuse. Questioning the patient’s environment and determining additional laboratory parameters (such as osmolality gap in the case report) can help unmask substance abuse if it is in doubt.
This story was translated from Univadis Germany, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Since the COVID-19 pandemic, alcoholic hand sanitizers have become widely accessible nationwide. They can pose a problem, especially for emergency departments, when alcohol-dependent patients start drinking them. One example that demonstrates the challenge of diagnosing alcohol abuse is the medical history of a young man, as reported by Mahmoud El Hussein, MD, and colleagues from Hôpital Lariboisière in Paris, France.
Presentation and History
A 26-year-old man presented with severe abdominal pain at the emergency department. Upon arrival, he was hemodynamically stable but nervous and verbally aggressive at times. The patient reported no relevant preexisting conditions and was not taking any medications.
Findings
Upon initial physical examination, the patient had a soft, diffusely tender abdomen; tachycardia; and notably poor hygiene. The patient was afebrile. An ECG confirmed the tachycardia but showed no signs of ischemia. Blood work, except for slightly elevated liver values, did not reveal any abnormalities, particularly ruling out bleeding or kidney disease.
A urease rapid test to rule out kidney stones also showed no pathologic findings. In consultation with the surgical department, a CT scan of the abdomen was performed to rule out organ perforation, volvulus, or mesenteric ischemia. Only signs of fatty liver were found.
A Neighbor’s Tip
During all examinations, the patient’s abdomen was repeatedly palpated to promptly detect signs of an acute abdomen. However, there was never any defense tension at any point.
Intravenous analgesics and proton pump inhibitors (ie, paracetamol, phloroglucin, and pantoprazole) did not relieve the patient’s symptoms. Morphine was administered intravenously for sedation.
Only after a frustrating diagnostic process did a neighbor of the patient inform a nurse that he suspected the patient of stealing and consuming hand sanitizer. With the patient’s consent, a blood alcohol test was performed, revealing a blood alcohol concentration of 0.2% (2 g/L). A urine test, also conducted with the patient’s consent, tested positive for tetrahydrocannabinol. Additional tests showed the following results:
- Venous pH: 7.29 (normal, 7.32-7.38)
- Anion gap (mEq/L): 14 (normal, 3-9)
- Ketone bodies (mmol/L): 0.2 (normal, < 0.6)
- Calculated serum osmolality (mOsm/kg): 292 (normal, 285-295)
- Measured serum osmolality (mOsm/kg): 320 (normal, 285-295)
- Osmolality gap (mOsm/kg): 2 (normal, < 10)
The patient was informed of the test results and confessed to feigning abdominal pain. He was dependent on alcohol and experiencing withdrawal symptoms. The patient had stolen seven 475-mL bottles of hand sanitizer and consumed one and a half in the past 4-6 hours. According to the authors, the sanitizer consisted of 80% ethanol, 1.45% glycerol, and 0.13% hydrogen peroxide.
Discussion
In Germany, alcohol consumption results in approximately €57 billion in direct economic costs annually, according to data from the Federal Ministry of Health. In 2021, about 7.9 million people aged 18-64 years consumed alcohol in a risky manner (approximately 9.6% of the German population). About 9 million people (approximately 11%) were classified as alcoholics.
Therefore, staff in emergency departments, where potential abusers encounter a wide range of potential abuse items, should exercise caution.
Although hand sanitizers are mainly composed of ethanol, they may also contain isopropanol, methanol, or acetone. Methanol poisoning can cause abdominal pain, visual disturbances, central nervous system damage, and death. Other alcohols such as ethylene glycol, commonly found in antifreeze, can distort blood values (lactate) and complicate a correct diagnosis.
Physicians working in emergency departments should proceed with caution when suspecting alcohol abuse. Questioning the patient’s environment and determining additional laboratory parameters (such as osmolality gap in the case report) can help unmask substance abuse if it is in doubt.
This story was translated from Univadis Germany, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Storybooks Can Help Children Deal with Skin Conditions
TORONTO —
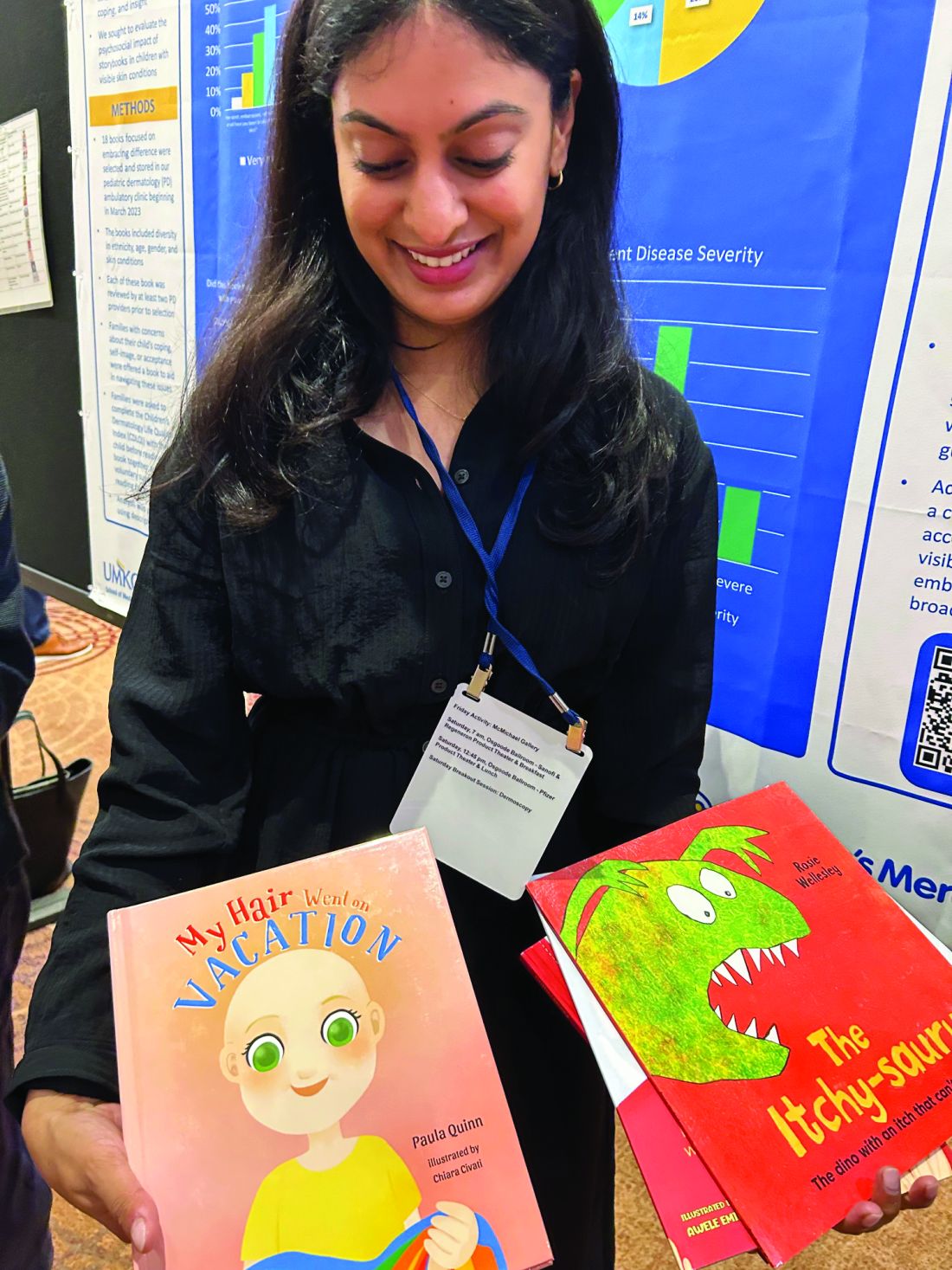
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
TORONTO —
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
TORONTO —
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SPD 2024
CBD Use in Pregnant People Double That of Nonpregnant Counterparts
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
FROM OBSTETRICS & GYNECOLOGY
PTSD Needs a New Name, Experts Say — Here’s Why
In a bid to reduce stigma and improve treatment rates, for inclusion in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). The APA’s policy is that a rolling name change is available if the current term is determined to be harmful.
Currently led by anesthesiologist Eugene Lipov, MD, clinical assistant professor, University of Illinois Chicago, and chief medical officer of Stella Center, also in Chicago, the formal request for the proposed name change to the APA’s DSM-5-TR Steering Committee in August 2023.
The APA Steering Committee rejected the proposed name change in November 2023, citing a “lack of convincing evidence.” However, Dr. Lipov and colleagues remain undeterred and continue to advocate for the change.
“The word ‘disorder’ is both imprecise and stigmatizing,” Dr. Lipov said. “Because of stigma, many people with PTSD — especially those in the military — don’t get help, which my research has demonstrated.”
Patients are more likely to seek help if their symptoms are framed as manifestations of an injury that is diagnosable and treatable, like a broken leg, Dr. Lipov said. “Stigma can kill in very real ways, since delayed care or lack of care can directly lead to suicides, thus satisfying the reduce harm requirement for the name change.”
Neurobiology of Trauma
Dr. Lipov grew up with a veteran father affected by PTSD and a mother with debilitating depression who eventually took her life. “I understand the impact of trauma very well,” he said.
Although not a psychiatrist, Dr. Lipov pioneered a highly successful treatment for PTSD by adapting an anesthetic technique — the stellate ganglion block (SGB) — to reverse many trauma symptoms through the process of “rebooting.”
This involves reversing the activity of the sympathetic nervous system — the fight-or-flight response — to the pretrauma state by anesthetizing the sympathetic ganglion in the neck. Investigating how SGB can help ameliorate the symptoms of PTSD led him to investigate and describe the neurobiology of PTSD and the mechanism of action of SGB.
The impact of SGD on PTSD was supported by a small neuroimaging study demonstrating that the right amygdala — the area of the brain associated with the fear response — was overactivated in patients with PTSD but that this region was deactivated after the administration of SGB, Dr. Lipov said.
“I believe that psychiatric conditions are actually physiologic brain changes that can be measured by advanced neuroimaging technologies and then physiologically treated,” he stated.
He noted that a growing body of literature suggests that use of the SGB for PTSD can be effective “because PTSD has a neurobiological basis and is essentially caused by an actual injury to the brain.”
A Natural Response, Not a Disorder
Dr. Lipov’s clinical work treating PTSD as a brain injury led him to connect with Frank Ochberg, MD, a founding board member of the International Society for Traumatic Stress Studies, former associate director of the National Institute of Mental Health, and former director of the Michigan Department of Mental Health.
In 2012, Dr. Ochberg teamed up with retired Army General Peter Chiarelli and Jonathan Shay, MD, PhD, author of Achilles in Vietnam: Combat Trauma and the Undoing of Character, to petition the DSM-5 Steering Committee to change the name of PTSD to PTSI in the upcoming DSM-5.
Dr. Ochberg explained that Gen. Chiarelli believed the term “disorder” suggests a preexisting issue prior to enlistment, potentially making an individual appear “weak.” He noted that this stigma is particularly troubling for military personnel, who often avoid seeking so they are not perceived as vulnerable, which can lead to potentially dire consequences, including suicide.
“We received endorsements from many quarters, not only advocates for service members or veterans,” Dr. Ochberg said.
This included feminists like Gloria Steinem, who championed the rights of women who had survived rape, incest, and domestic violence. As one advocate put it: “The natural human reaction to a life-threatening event should not be labeled a disorder.”
The DSM-5 Steering Committee declined to change the name. “Their feeling was that if we change the word ‘disorder’ to something else, we’d have to change every condition in the DSM that’s called a ‘disorder’. And they felt there really was nothing wrong with the word,” said Dr. Ochberg.
However, Dr. Lipov noted that other diagnoses have undergone name changes in the DSM for the sake of accuracy or stigma reduction. For example, the term mental retardation (DSM-IV) was changed to intellectual disability in DSM-5, and gender identity disorder was changed to gender dysphoria.
A decade later, Dr. Lipov decided to try again. To bolster his contention, he conducted a telephone survey of 1025 individuals. Of these, about 50% had a PTSD diagnosis.
Approximately two thirds of respondents agreed that a name change to PTSI would reduce the stigma associated with the term “PTSD.” Over half said it would increase the likelihood they would seek medical help. Those diagnosed with PTSD were most likely to endorse the name change.
Dr. Lipov conducts an ongoing survey of psychiatrists to ascertain their views on the potential name change and hopes to include findings in future research and communication with the DSM-5 Steering Committee. In addition, he has developed a new survey that expands upon his original survey, which specifically looked at individuals with PTSD.
“The new survey includes a wide range of people, many of whom have never been diagnosed. One of the questions we ask is whether they’ve ever heard of PTSD, and then we ask them about their reaction to the term,” he said.
A Barrier to Care
Psychiatrist Marcel Green, MD, director of Hudson Mind in New York City, refers to himself as an “interventional psychiatrist,” as he employs a comprehensive approach that includes not only medication and psychotherapy but also specialized techniques like SBG for severe anxiety-related physical symptoms and certain pain conditions.
Dr. Green, who is not involved in the name change initiative, agrees that the term “disorder” carries more stigma than “injury” for many groups, including those who have experienced childhood trauma, those struggling with substance abuse, or who are from backgrounds or peer groups where seeking mental health care is stigmatized.
Patients like these “are looking to me to give them a language to frame what they’re going through, and I tell them their symptoms are consistent with PTSD,” he said. “But they tell me don’t see themselves as having a disorder, which hinders their pursuit of care.”
Framing the condition as an “injury” also aligns with the approach of using biologic interventions to address the injury. Dr. Green has found SGB helpful in treating substance abuse disorder too, “which is a form of escape from the hyperactivation that accompanies PTSD.” And after the procedure, “they’re more receptive to therapy.”
Unfortunately, said Dr. Lipov, the DSM Steering Committee rejected his proposed name change, stating that the “concept of disorder as a dividing line from, eg, normal reactions to stress, is a core concept in the DSM, and the term has only rarely been removed.”
Moreover, the committee “did not see sufficient evidence ... that the name PTSD is stigmatizing and actually deters people with the disorder from seeking treatment who would not be deterred from doing so by PTSI.”
‘An Avenue for Dignity’
Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness (NAMI), noted that the organization does not have an official position on this issue. However, he shared his own personal perspective.
There may be merit in the proposed name change, said Dr. Duckworth, but more evidence is needed. “If it’s clear, after rigorous studies have been performed and there’s compelling data, that calling it a ‘disorder’ rather than an ‘injury’ is actually preventing people from getting the care they need, then it merits serious attention.”
If so, Dr. Duckworth would be “interested in having a conversation with the policy team at NAMI to start to see if we could activate the DSM Committee.”
Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto in Ontario, Canada, and head of the Mood Disorders Psychopharmacology Unit, said the name change initiative is a “really interesting proposal.”
Dr. McIntyre, chairman and executive director of the Brain and Cognition Discovery Foundation, also in Toronto, who is not involved in the initiative, has also heard “many people say that the term ‘disorder’ is stigmatizing and might even come across as pejorative in some ways.”
By contrast, “the word ‘injury’ parallels physical injury, and what we currently call ‘PTSD’ is a psychological or emotional injury no less devastating than torn tissue or broken bones,” added Dr. McIntyre, who is also the chairman of the board of the Depression and Bipolar Support Alliance.
Dr. Ochberg agreed. “In the military, ‘injury’ opens up an avenue for dignity, for a medal. Being injured and learning how to deal with an injury is part of having yet another honorable task that comes from being an honorable person who did an honorable thing.”
While disappointed, Dr. Lipov does not plan to give up on his vision. “I will continue to amass evidence that the word ‘PTSD’ is stigmatizing and indeed does prevent people from seeking care and will resubmit the proposal to the DSM Steering Committee when I have gathered a larger body of compelling evidence.”
Currently, Dr. Lipov is in active discussions with the special operations force of the US Army to obtain more evidence. “This will be the follow-up to bolster the opinion of Peter Chiarelli,” he said. “It is known that suicide and PTSD are highly related. This is especially urgent and relevant because recent data suggest suicide rate of military personnel in the VA may be as high as 44 per day,” Dr. Lipov said.
Dr. Lipov is the chief medical officer and an investor in the Stella Center. Dr. Green performs SGBs as part of his psychiatric practice. Drs. Ochberg, McIntyre, and Duckworth reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
In a bid to reduce stigma and improve treatment rates, for inclusion in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). The APA’s policy is that a rolling name change is available if the current term is determined to be harmful.
Currently led by anesthesiologist Eugene Lipov, MD, clinical assistant professor, University of Illinois Chicago, and chief medical officer of Stella Center, also in Chicago, the formal request for the proposed name change to the APA’s DSM-5-TR Steering Committee in August 2023.
The APA Steering Committee rejected the proposed name change in November 2023, citing a “lack of convincing evidence.” However, Dr. Lipov and colleagues remain undeterred and continue to advocate for the change.
“The word ‘disorder’ is both imprecise and stigmatizing,” Dr. Lipov said. “Because of stigma, many people with PTSD — especially those in the military — don’t get help, which my research has demonstrated.”
Patients are more likely to seek help if their symptoms are framed as manifestations of an injury that is diagnosable and treatable, like a broken leg, Dr. Lipov said. “Stigma can kill in very real ways, since delayed care or lack of care can directly lead to suicides, thus satisfying the reduce harm requirement for the name change.”
Neurobiology of Trauma
Dr. Lipov grew up with a veteran father affected by PTSD and a mother with debilitating depression who eventually took her life. “I understand the impact of trauma very well,” he said.
Although not a psychiatrist, Dr. Lipov pioneered a highly successful treatment for PTSD by adapting an anesthetic technique — the stellate ganglion block (SGB) — to reverse many trauma symptoms through the process of “rebooting.”
This involves reversing the activity of the sympathetic nervous system — the fight-or-flight response — to the pretrauma state by anesthetizing the sympathetic ganglion in the neck. Investigating how SGB can help ameliorate the symptoms of PTSD led him to investigate and describe the neurobiology of PTSD and the mechanism of action of SGB.
The impact of SGD on PTSD was supported by a small neuroimaging study demonstrating that the right amygdala — the area of the brain associated with the fear response — was overactivated in patients with PTSD but that this region was deactivated after the administration of SGB, Dr. Lipov said.
“I believe that psychiatric conditions are actually physiologic brain changes that can be measured by advanced neuroimaging technologies and then physiologically treated,” he stated.
He noted that a growing body of literature suggests that use of the SGB for PTSD can be effective “because PTSD has a neurobiological basis and is essentially caused by an actual injury to the brain.”
A Natural Response, Not a Disorder
Dr. Lipov’s clinical work treating PTSD as a brain injury led him to connect with Frank Ochberg, MD, a founding board member of the International Society for Traumatic Stress Studies, former associate director of the National Institute of Mental Health, and former director of the Michigan Department of Mental Health.
In 2012, Dr. Ochberg teamed up with retired Army General Peter Chiarelli and Jonathan Shay, MD, PhD, author of Achilles in Vietnam: Combat Trauma and the Undoing of Character, to petition the DSM-5 Steering Committee to change the name of PTSD to PTSI in the upcoming DSM-5.
Dr. Ochberg explained that Gen. Chiarelli believed the term “disorder” suggests a preexisting issue prior to enlistment, potentially making an individual appear “weak.” He noted that this stigma is particularly troubling for military personnel, who often avoid seeking so they are not perceived as vulnerable, which can lead to potentially dire consequences, including suicide.
“We received endorsements from many quarters, not only advocates for service members or veterans,” Dr. Ochberg said.
This included feminists like Gloria Steinem, who championed the rights of women who had survived rape, incest, and domestic violence. As one advocate put it: “The natural human reaction to a life-threatening event should not be labeled a disorder.”
The DSM-5 Steering Committee declined to change the name. “Their feeling was that if we change the word ‘disorder’ to something else, we’d have to change every condition in the DSM that’s called a ‘disorder’. And they felt there really was nothing wrong with the word,” said Dr. Ochberg.
However, Dr. Lipov noted that other diagnoses have undergone name changes in the DSM for the sake of accuracy or stigma reduction. For example, the term mental retardation (DSM-IV) was changed to intellectual disability in DSM-5, and gender identity disorder was changed to gender dysphoria.
A decade later, Dr. Lipov decided to try again. To bolster his contention, he conducted a telephone survey of 1025 individuals. Of these, about 50% had a PTSD diagnosis.
Approximately two thirds of respondents agreed that a name change to PTSI would reduce the stigma associated with the term “PTSD.” Over half said it would increase the likelihood they would seek medical help. Those diagnosed with PTSD were most likely to endorse the name change.
Dr. Lipov conducts an ongoing survey of psychiatrists to ascertain their views on the potential name change and hopes to include findings in future research and communication with the DSM-5 Steering Committee. In addition, he has developed a new survey that expands upon his original survey, which specifically looked at individuals with PTSD.
“The new survey includes a wide range of people, many of whom have never been diagnosed. One of the questions we ask is whether they’ve ever heard of PTSD, and then we ask them about their reaction to the term,” he said.
A Barrier to Care
Psychiatrist Marcel Green, MD, director of Hudson Mind in New York City, refers to himself as an “interventional psychiatrist,” as he employs a comprehensive approach that includes not only medication and psychotherapy but also specialized techniques like SBG for severe anxiety-related physical symptoms and certain pain conditions.
Dr. Green, who is not involved in the name change initiative, agrees that the term “disorder” carries more stigma than “injury” for many groups, including those who have experienced childhood trauma, those struggling with substance abuse, or who are from backgrounds or peer groups where seeking mental health care is stigmatized.
Patients like these “are looking to me to give them a language to frame what they’re going through, and I tell them their symptoms are consistent with PTSD,” he said. “But they tell me don’t see themselves as having a disorder, which hinders their pursuit of care.”
Framing the condition as an “injury” also aligns with the approach of using biologic interventions to address the injury. Dr. Green has found SGB helpful in treating substance abuse disorder too, “which is a form of escape from the hyperactivation that accompanies PTSD.” And after the procedure, “they’re more receptive to therapy.”
Unfortunately, said Dr. Lipov, the DSM Steering Committee rejected his proposed name change, stating that the “concept of disorder as a dividing line from, eg, normal reactions to stress, is a core concept in the DSM, and the term has only rarely been removed.”
Moreover, the committee “did not see sufficient evidence ... that the name PTSD is stigmatizing and actually deters people with the disorder from seeking treatment who would not be deterred from doing so by PTSI.”
‘An Avenue for Dignity’
Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness (NAMI), noted that the organization does not have an official position on this issue. However, he shared his own personal perspective.
There may be merit in the proposed name change, said Dr. Duckworth, but more evidence is needed. “If it’s clear, after rigorous studies have been performed and there’s compelling data, that calling it a ‘disorder’ rather than an ‘injury’ is actually preventing people from getting the care they need, then it merits serious attention.”
If so, Dr. Duckworth would be “interested in having a conversation with the policy team at NAMI to start to see if we could activate the DSM Committee.”
Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto in Ontario, Canada, and head of the Mood Disorders Psychopharmacology Unit, said the name change initiative is a “really interesting proposal.”
Dr. McIntyre, chairman and executive director of the Brain and Cognition Discovery Foundation, also in Toronto, who is not involved in the initiative, has also heard “many people say that the term ‘disorder’ is stigmatizing and might even come across as pejorative in some ways.”
By contrast, “the word ‘injury’ parallels physical injury, and what we currently call ‘PTSD’ is a psychological or emotional injury no less devastating than torn tissue or broken bones,” added Dr. McIntyre, who is also the chairman of the board of the Depression and Bipolar Support Alliance.
Dr. Ochberg agreed. “In the military, ‘injury’ opens up an avenue for dignity, for a medal. Being injured and learning how to deal with an injury is part of having yet another honorable task that comes from being an honorable person who did an honorable thing.”
While disappointed, Dr. Lipov does not plan to give up on his vision. “I will continue to amass evidence that the word ‘PTSD’ is stigmatizing and indeed does prevent people from seeking care and will resubmit the proposal to the DSM Steering Committee when I have gathered a larger body of compelling evidence.”
Currently, Dr. Lipov is in active discussions with the special operations force of the US Army to obtain more evidence. “This will be the follow-up to bolster the opinion of Peter Chiarelli,” he said. “It is known that suicide and PTSD are highly related. This is especially urgent and relevant because recent data suggest suicide rate of military personnel in the VA may be as high as 44 per day,” Dr. Lipov said.
Dr. Lipov is the chief medical officer and an investor in the Stella Center. Dr. Green performs SGBs as part of his psychiatric practice. Drs. Ochberg, McIntyre, and Duckworth reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
In a bid to reduce stigma and improve treatment rates, for inclusion in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). The APA’s policy is that a rolling name change is available if the current term is determined to be harmful.
Currently led by anesthesiologist Eugene Lipov, MD, clinical assistant professor, University of Illinois Chicago, and chief medical officer of Stella Center, also in Chicago, the formal request for the proposed name change to the APA’s DSM-5-TR Steering Committee in August 2023.
The APA Steering Committee rejected the proposed name change in November 2023, citing a “lack of convincing evidence.” However, Dr. Lipov and colleagues remain undeterred and continue to advocate for the change.
“The word ‘disorder’ is both imprecise and stigmatizing,” Dr. Lipov said. “Because of stigma, many people with PTSD — especially those in the military — don’t get help, which my research has demonstrated.”
Patients are more likely to seek help if their symptoms are framed as manifestations of an injury that is diagnosable and treatable, like a broken leg, Dr. Lipov said. “Stigma can kill in very real ways, since delayed care or lack of care can directly lead to suicides, thus satisfying the reduce harm requirement for the name change.”
Neurobiology of Trauma
Dr. Lipov grew up with a veteran father affected by PTSD and a mother with debilitating depression who eventually took her life. “I understand the impact of trauma very well,” he said.
Although not a psychiatrist, Dr. Lipov pioneered a highly successful treatment for PTSD by adapting an anesthetic technique — the stellate ganglion block (SGB) — to reverse many trauma symptoms through the process of “rebooting.”
This involves reversing the activity of the sympathetic nervous system — the fight-or-flight response — to the pretrauma state by anesthetizing the sympathetic ganglion in the neck. Investigating how SGB can help ameliorate the symptoms of PTSD led him to investigate and describe the neurobiology of PTSD and the mechanism of action of SGB.
The impact of SGD on PTSD was supported by a small neuroimaging study demonstrating that the right amygdala — the area of the brain associated with the fear response — was overactivated in patients with PTSD but that this region was deactivated after the administration of SGB, Dr. Lipov said.
“I believe that psychiatric conditions are actually physiologic brain changes that can be measured by advanced neuroimaging technologies and then physiologically treated,” he stated.
He noted that a growing body of literature suggests that use of the SGB for PTSD can be effective “because PTSD has a neurobiological basis and is essentially caused by an actual injury to the brain.”
A Natural Response, Not a Disorder
Dr. Lipov’s clinical work treating PTSD as a brain injury led him to connect with Frank Ochberg, MD, a founding board member of the International Society for Traumatic Stress Studies, former associate director of the National Institute of Mental Health, and former director of the Michigan Department of Mental Health.
In 2012, Dr. Ochberg teamed up with retired Army General Peter Chiarelli and Jonathan Shay, MD, PhD, author of Achilles in Vietnam: Combat Trauma and the Undoing of Character, to petition the DSM-5 Steering Committee to change the name of PTSD to PTSI in the upcoming DSM-5.
Dr. Ochberg explained that Gen. Chiarelli believed the term “disorder” suggests a preexisting issue prior to enlistment, potentially making an individual appear “weak.” He noted that this stigma is particularly troubling for military personnel, who often avoid seeking so they are not perceived as vulnerable, which can lead to potentially dire consequences, including suicide.
“We received endorsements from many quarters, not only advocates for service members or veterans,” Dr. Ochberg said.
This included feminists like Gloria Steinem, who championed the rights of women who had survived rape, incest, and domestic violence. As one advocate put it: “The natural human reaction to a life-threatening event should not be labeled a disorder.”
The DSM-5 Steering Committee declined to change the name. “Their feeling was that if we change the word ‘disorder’ to something else, we’d have to change every condition in the DSM that’s called a ‘disorder’. And they felt there really was nothing wrong with the word,” said Dr. Ochberg.
However, Dr. Lipov noted that other diagnoses have undergone name changes in the DSM for the sake of accuracy or stigma reduction. For example, the term mental retardation (DSM-IV) was changed to intellectual disability in DSM-5, and gender identity disorder was changed to gender dysphoria.
A decade later, Dr. Lipov decided to try again. To bolster his contention, he conducted a telephone survey of 1025 individuals. Of these, about 50% had a PTSD diagnosis.
Approximately two thirds of respondents agreed that a name change to PTSI would reduce the stigma associated with the term “PTSD.” Over half said it would increase the likelihood they would seek medical help. Those diagnosed with PTSD were most likely to endorse the name change.
Dr. Lipov conducts an ongoing survey of psychiatrists to ascertain their views on the potential name change and hopes to include findings in future research and communication with the DSM-5 Steering Committee. In addition, he has developed a new survey that expands upon his original survey, which specifically looked at individuals with PTSD.
“The new survey includes a wide range of people, many of whom have never been diagnosed. One of the questions we ask is whether they’ve ever heard of PTSD, and then we ask them about their reaction to the term,” he said.
A Barrier to Care
Psychiatrist Marcel Green, MD, director of Hudson Mind in New York City, refers to himself as an “interventional psychiatrist,” as he employs a comprehensive approach that includes not only medication and psychotherapy but also specialized techniques like SBG for severe anxiety-related physical symptoms and certain pain conditions.
Dr. Green, who is not involved in the name change initiative, agrees that the term “disorder” carries more stigma than “injury” for many groups, including those who have experienced childhood trauma, those struggling with substance abuse, or who are from backgrounds or peer groups where seeking mental health care is stigmatized.
Patients like these “are looking to me to give them a language to frame what they’re going through, and I tell them their symptoms are consistent with PTSD,” he said. “But they tell me don’t see themselves as having a disorder, which hinders their pursuit of care.”
Framing the condition as an “injury” also aligns with the approach of using biologic interventions to address the injury. Dr. Green has found SGB helpful in treating substance abuse disorder too, “which is a form of escape from the hyperactivation that accompanies PTSD.” And after the procedure, “they’re more receptive to therapy.”
Unfortunately, said Dr. Lipov, the DSM Steering Committee rejected his proposed name change, stating that the “concept of disorder as a dividing line from, eg, normal reactions to stress, is a core concept in the DSM, and the term has only rarely been removed.”
Moreover, the committee “did not see sufficient evidence ... that the name PTSD is stigmatizing and actually deters people with the disorder from seeking treatment who would not be deterred from doing so by PTSI.”
‘An Avenue for Dignity’
Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness (NAMI), noted that the organization does not have an official position on this issue. However, he shared his own personal perspective.
There may be merit in the proposed name change, said Dr. Duckworth, but more evidence is needed. “If it’s clear, after rigorous studies have been performed and there’s compelling data, that calling it a ‘disorder’ rather than an ‘injury’ is actually preventing people from getting the care they need, then it merits serious attention.”
If so, Dr. Duckworth would be “interested in having a conversation with the policy team at NAMI to start to see if we could activate the DSM Committee.”
Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto in Ontario, Canada, and head of the Mood Disorders Psychopharmacology Unit, said the name change initiative is a “really interesting proposal.”
Dr. McIntyre, chairman and executive director of the Brain and Cognition Discovery Foundation, also in Toronto, who is not involved in the initiative, has also heard “many people say that the term ‘disorder’ is stigmatizing and might even come across as pejorative in some ways.”
By contrast, “the word ‘injury’ parallels physical injury, and what we currently call ‘PTSD’ is a psychological or emotional injury no less devastating than torn tissue or broken bones,” added Dr. McIntyre, who is also the chairman of the board of the Depression and Bipolar Support Alliance.
Dr. Ochberg agreed. “In the military, ‘injury’ opens up an avenue for dignity, for a medal. Being injured and learning how to deal with an injury is part of having yet another honorable task that comes from being an honorable person who did an honorable thing.”
While disappointed, Dr. Lipov does not plan to give up on his vision. “I will continue to amass evidence that the word ‘PTSD’ is stigmatizing and indeed does prevent people from seeking care and will resubmit the proposal to the DSM Steering Committee when I have gathered a larger body of compelling evidence.”
Currently, Dr. Lipov is in active discussions with the special operations force of the US Army to obtain more evidence. “This will be the follow-up to bolster the opinion of Peter Chiarelli,” he said. “It is known that suicide and PTSD are highly related. This is especially urgent and relevant because recent data suggest suicide rate of military personnel in the VA may be as high as 44 per day,” Dr. Lipov said.
Dr. Lipov is the chief medical officer and an investor in the Stella Center. Dr. Green performs SGBs as part of his psychiatric practice. Drs. Ochberg, McIntyre, and Duckworth reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Family Not Flourishing? The Hidden Issue of Food Insecurity and How We Can Help
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.

Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.
Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.
Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Data Trends 2024: Depression and PTSD
- Inoue C, Shawler E, Jordan CH, Moore MJ, Jackson CA. Veteran and military mental health issues. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing. Updated August 17, 2023. Accessed April 1, 2024. https://www.ncbi.nlm.nih.gov/books/NBK572092/
- Panaite V, Cohen NJ, Luter SL, et al. Mental health treatment utilization patterns among 108,457 Afghanistan and Iraq veterans with depression. Psychol Serv. 2024 Feb 1. doi:10.1037/ser0000819
- Holder N, Holliday R, Ranney RM, et al. Relationship of social determinants of health with symptom severity among veterans and non-veterans with probable posttraumatic stress disorder or depression. Soc Psychiatry Psychiatr Epidemiol. 2023;58(10):1523-1534. doi:10.1007/s00127-023-02478-0
- Merians AN, Gross G, Spoont MR, Bellamy CD, Harpaz-Rotem I, Pietrzak RH. Racial and ethnic mental health disparities in U.S. military veterans: results from the National Health and Resilience in Veterans Study. J Psychiatr Res. 2023;161:71-76. doi:10.1016/j.jpsychires.2023.03.005
- Fischer IC, Schnurr PP, Pietrzak RH. Employment status among US military veterans with a history of posttraumatic stress disorder: results from the National Health and Resilience in Veterans Study. J Trauma Stress. 2023;36(6):1167-1175. doi:10.1002/jts.22977
- Portnoy GA, Relyea MR, Presseau C, et al. Screening for intimate partner violence experience and use in the Veterans Health Administration. JAMA Netw Open. 2023;6(10):e2337685. doi:10.1001/jamanetworkopen.2023.37685
- Cowlishaw S, Freijah I, Kartal D, et al. Intimate Partner Violence (IPV) in Military and Veteran Populations: A Systematic Review of Population-Based Surveys and Population Screening Studies. Int J Environ Res Public Health. 2022;19(14):8853. Published 2022 Jul 21. doi:10.3390/ijerph19148853
- Ranney RM, Maguen S, Bernhard PA, et al. Treatment utilization for posttraumatic stress disorder in a national sample of veterans and nonveterans. Med Care. 2023;61(2):87-94. doi:10.1097/MLR.0000000000001793
- Inoue C, Shawler E, Jordan CH, Moore MJ, Jackson CA. Veteran and military mental health issues. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing. Updated August 17, 2023. Accessed April 1, 2024. https://www.ncbi.nlm.nih.gov/books/NBK572092/
- Panaite V, Cohen NJ, Luter SL, et al. Mental health treatment utilization patterns among 108,457 Afghanistan and Iraq veterans with depression. Psychol Serv. 2024 Feb 1. doi:10.1037/ser0000819
- Holder N, Holliday R, Ranney RM, et al. Relationship of social determinants of health with symptom severity among veterans and non-veterans with probable posttraumatic stress disorder or depression. Soc Psychiatry Psychiatr Epidemiol. 2023;58(10):1523-1534. doi:10.1007/s00127-023-02478-0
- Merians AN, Gross G, Spoont MR, Bellamy CD, Harpaz-Rotem I, Pietrzak RH. Racial and ethnic mental health disparities in U.S. military veterans: results from the National Health and Resilience in Veterans Study. J Psychiatr Res. 2023;161:71-76. doi:10.1016/j.jpsychires.2023.03.005
- Fischer IC, Schnurr PP, Pietrzak RH. Employment status among US military veterans with a history of posttraumatic stress disorder: results from the National Health and Resilience in Veterans Study. J Trauma Stress. 2023;36(6):1167-1175. doi:10.1002/jts.22977
- Portnoy GA, Relyea MR, Presseau C, et al. Screening for intimate partner violence experience and use in the Veterans Health Administration. JAMA Netw Open. 2023;6(10):e2337685. doi:10.1001/jamanetworkopen.2023.37685
- Cowlishaw S, Freijah I, Kartal D, et al. Intimate Partner Violence (IPV) in Military and Veteran Populations: A Systematic Review of Population-Based Surveys and Population Screening Studies. Int J Environ Res Public Health. 2022;19(14):8853. Published 2022 Jul 21. doi:10.3390/ijerph19148853
- Ranney RM, Maguen S, Bernhard PA, et al. Treatment utilization for posttraumatic stress disorder in a national sample of veterans and nonveterans. Med Care. 2023;61(2):87-94. doi:10.1097/MLR.0000000000001793
- Inoue C, Shawler E, Jordan CH, Moore MJ, Jackson CA. Veteran and military mental health issues. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing. Updated August 17, 2023. Accessed April 1, 2024. https://www.ncbi.nlm.nih.gov/books/NBK572092/
- Panaite V, Cohen NJ, Luter SL, et al. Mental health treatment utilization patterns among 108,457 Afghanistan and Iraq veterans with depression. Psychol Serv. 2024 Feb 1. doi:10.1037/ser0000819
- Holder N, Holliday R, Ranney RM, et al. Relationship of social determinants of health with symptom severity among veterans and non-veterans with probable posttraumatic stress disorder or depression. Soc Psychiatry Psychiatr Epidemiol. 2023;58(10):1523-1534. doi:10.1007/s00127-023-02478-0
- Merians AN, Gross G, Spoont MR, Bellamy CD, Harpaz-Rotem I, Pietrzak RH. Racial and ethnic mental health disparities in U.S. military veterans: results from the National Health and Resilience in Veterans Study. J Psychiatr Res. 2023;161:71-76. doi:10.1016/j.jpsychires.2023.03.005
- Fischer IC, Schnurr PP, Pietrzak RH. Employment status among US military veterans with a history of posttraumatic stress disorder: results from the National Health and Resilience in Veterans Study. J Trauma Stress. 2023;36(6):1167-1175. doi:10.1002/jts.22977
- Portnoy GA, Relyea MR, Presseau C, et al. Screening for intimate partner violence experience and use in the Veterans Health Administration. JAMA Netw Open. 2023;6(10):e2337685. doi:10.1001/jamanetworkopen.2023.37685
- Cowlishaw S, Freijah I, Kartal D, et al. Intimate Partner Violence (IPV) in Military and Veteran Populations: A Systematic Review of Population-Based Surveys and Population Screening Studies. Int J Environ Res Public Health. 2022;19(14):8853. Published 2022 Jul 21. doi:10.3390/ijerph19148853
- Ranney RM, Maguen S, Bernhard PA, et al. Treatment utilization for posttraumatic stress disorder in a national sample of veterans and nonveterans. Med Care. 2023;61(2):87-94. doi:10.1097/MLR.0000000000001793
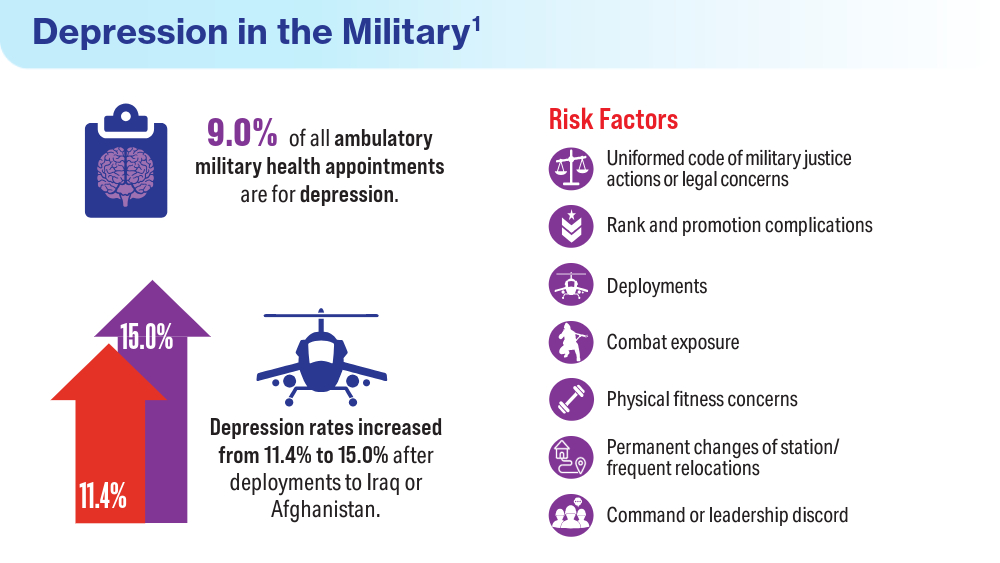
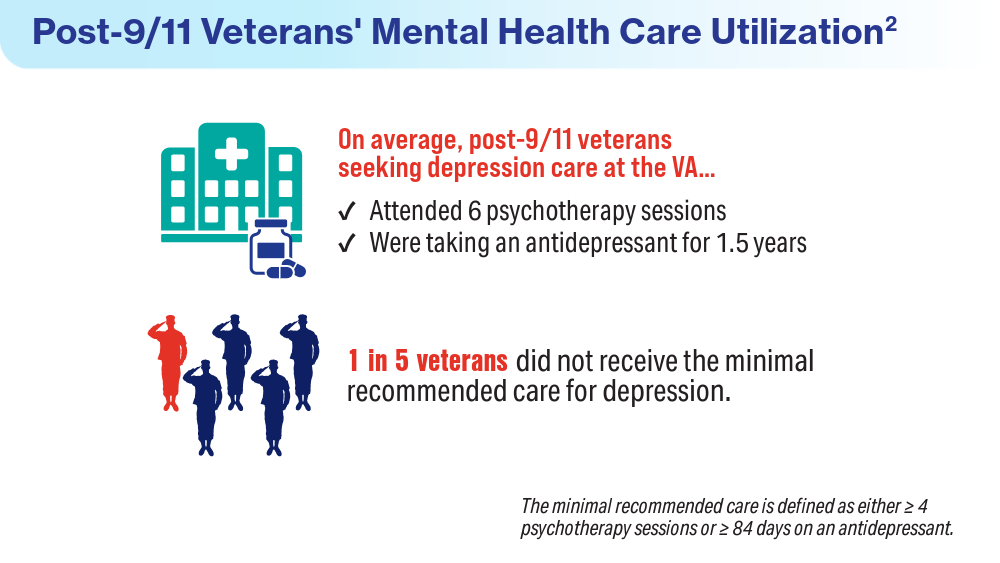
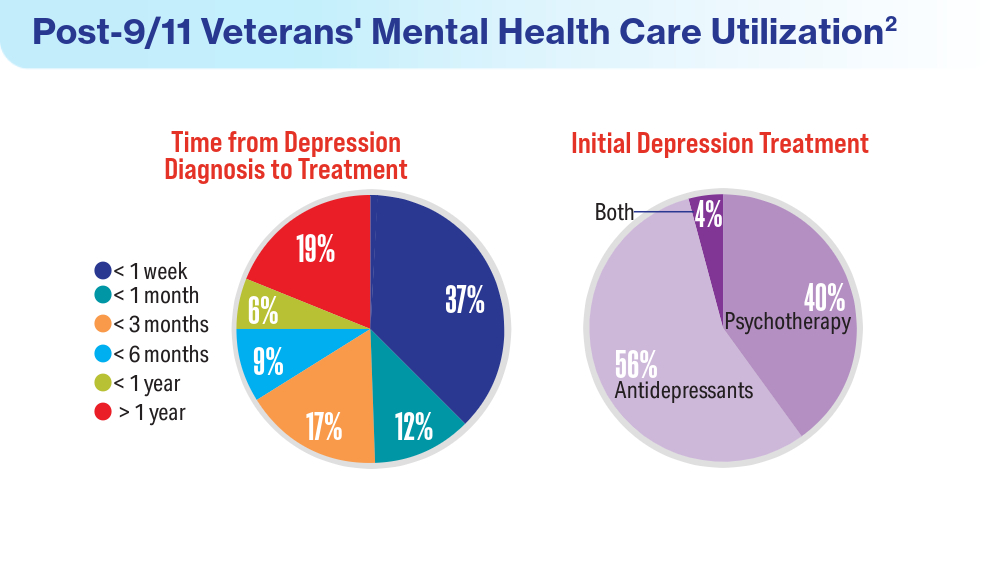
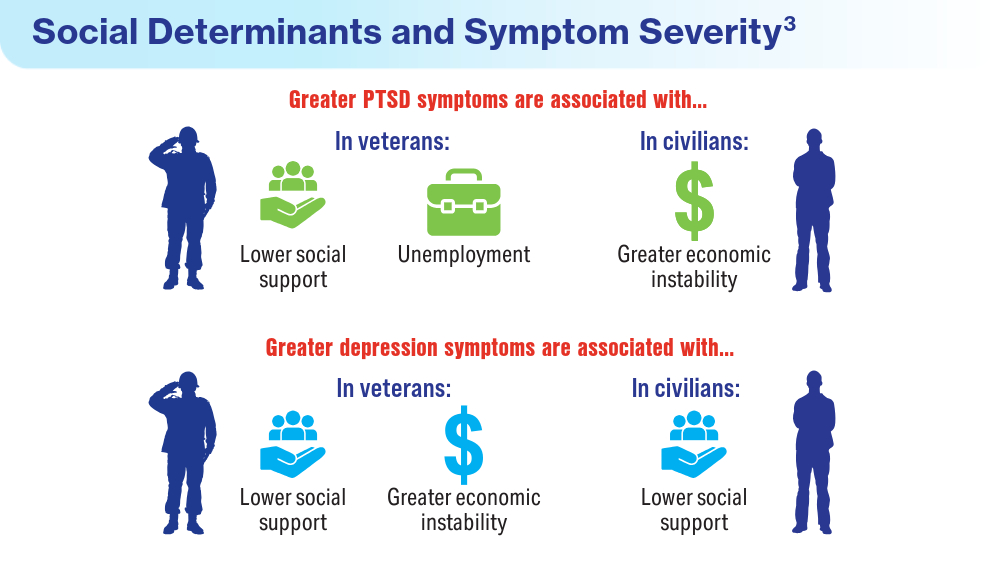
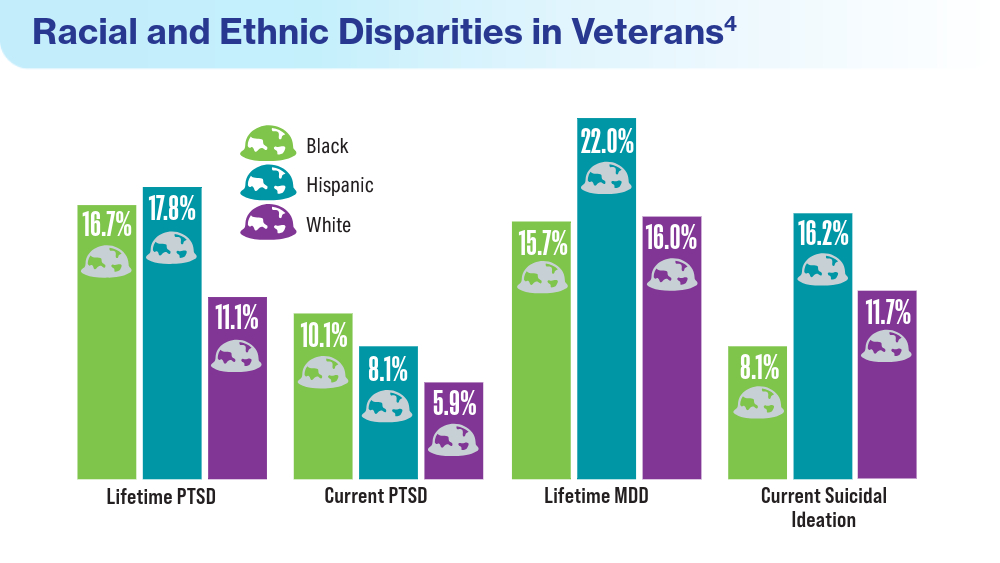
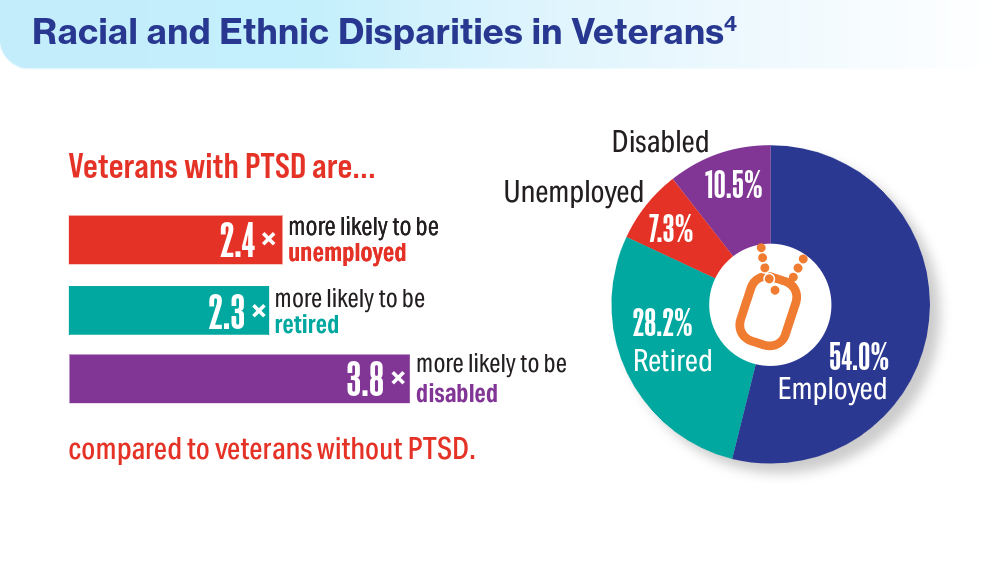
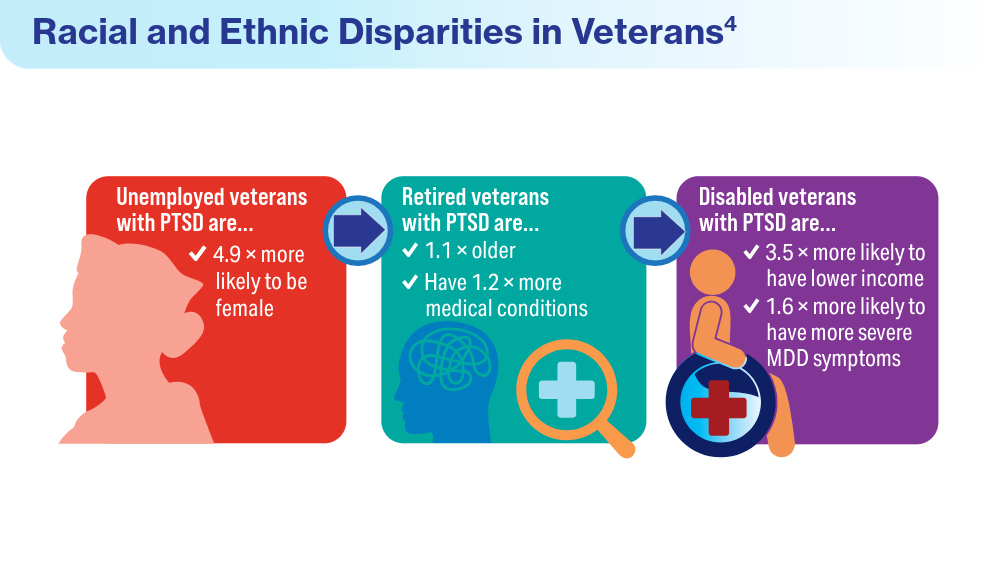
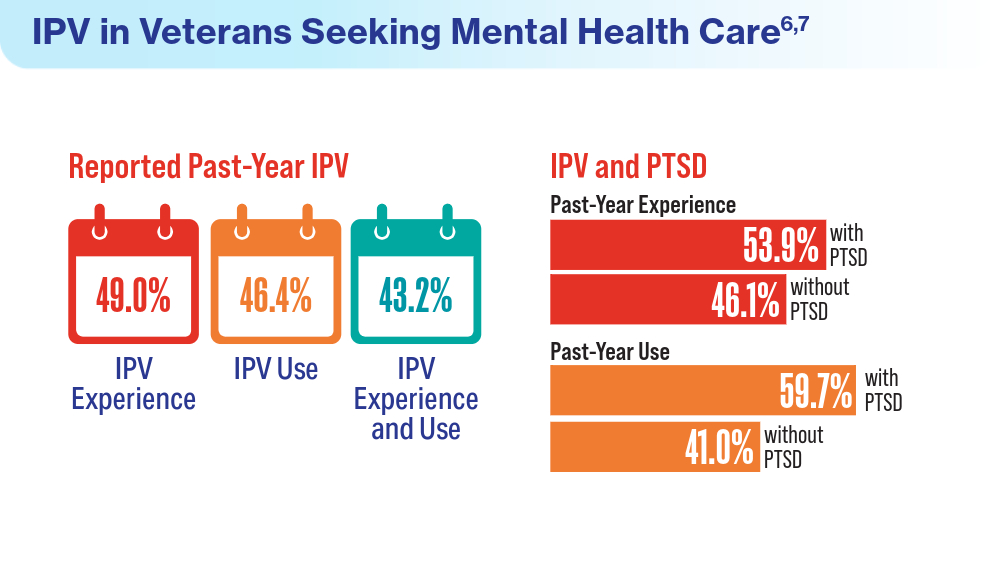
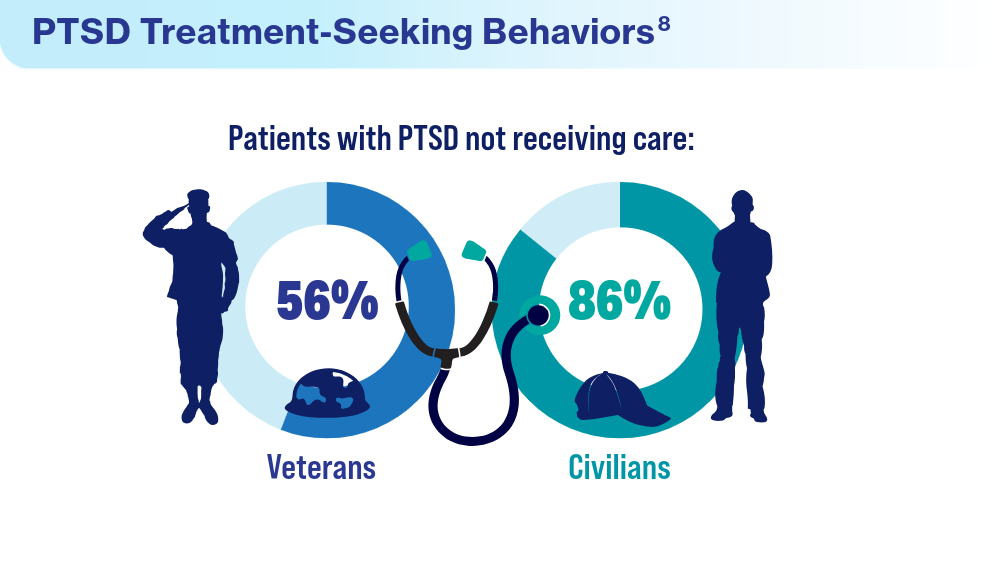
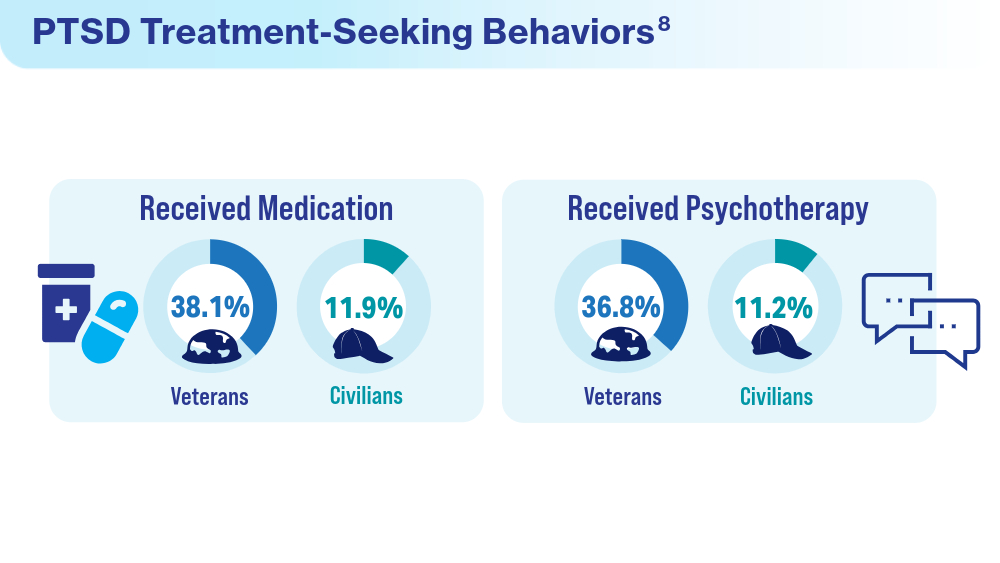
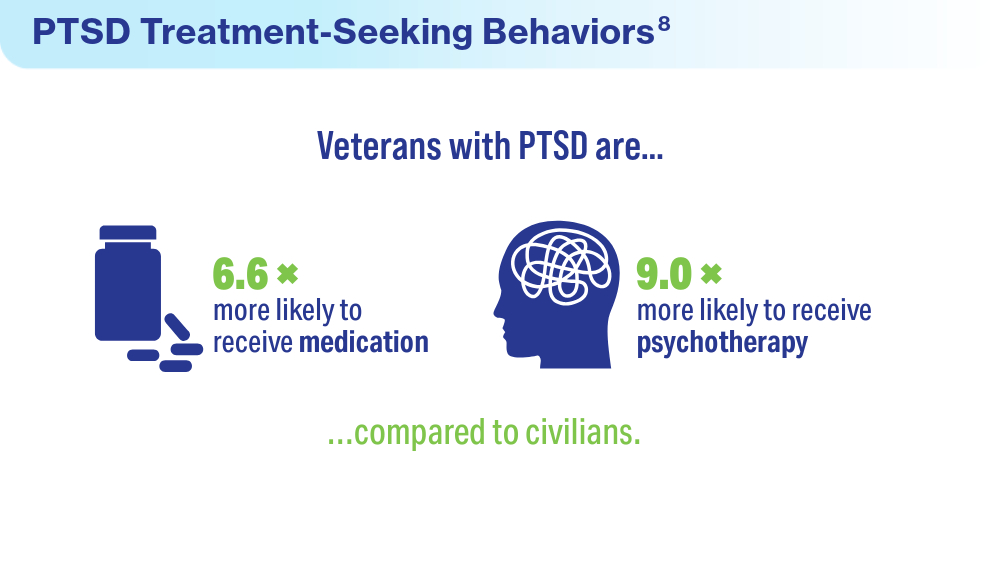
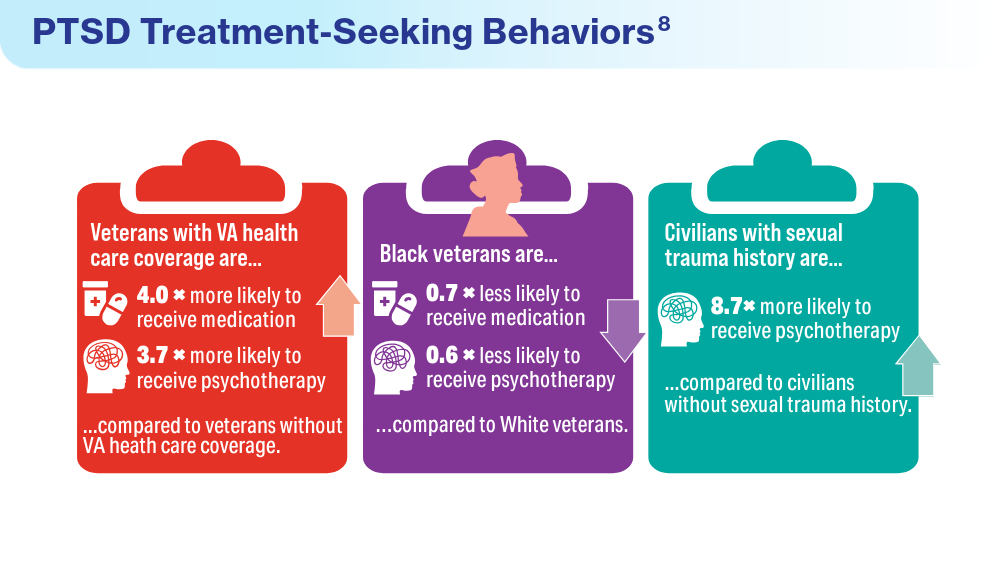
Federal Health Care Data Trends 2024

Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
New Biological Pathway May Explain BPA Exposure, Autism Link
BPA is a potent endocrine disruptor found in polycarbonate plastics and epoxy resins and has been banned by the Food and Drug Administration for use in baby bottles, sippy cups, and infant formula packaging.
“Exposure to BPA has already been shown in some studies to be associated with subsequent autism in offspring,” lead researcher Anne-Louise Ponsonby, PhD, The Florey Institute, Heidelberg, Australia, said in a statement.
“Our work is important because it demonstrates one of the biological mechanisms potentially involved. BPA can disrupt hormone-controlled male fetal brain development in several ways, including silencing a key enzyme, aromatase, that controls neurohormones and is especially important in fetal male brain development. This appears to be part of the autism puzzle,” she said.
Brain aromatase, encoded by CYP19A1, converts neural androgens to neural estrogens and has been implicated in ASD. Postmortem analyses of men with ASD also show markedly reduced aromatase activity.
The findings were published online in Nature Communications.
New Biological Mechanism
For the study, the researchers analyzed data from the Barwon Infant Study in 1067 infants in Australia. At age 7-11 years, 43 children had a confirmed ASD diagnosis, and 249 infants with Child Behavior Checklist (CBCL) data at age 2 years had an autism spectrum problem score above the median.
The researchers developed a CYP19A1 genetic score for aromatase activity based on five single nucleotide polymorphisms associated with lower estrogen levels. Among 595 children with prenatal BPA and CBCL, those with three or more variants were classified as “low aromatase activity” and the remaining were classified as “high.”
In regression analyses, boys with low aromatase activity and high prenatal BPA exposure (top quartile > 2.18 µg/L) were 3.5 times more likely to have autism symptoms at age 2 years (odds ratio [OR], 3.56; 95% CI, 1.13-11.22).
The odds of a confirmed ASD diagnosis were six times higher at age 9 years only in men with low aromatase activity (OR, 6.24; 95% CI, 1.02-38.26).
The researchers also found that higher BPA levels predicted higher methylation in cord blood across the CYP19A1 brain promoter PI.f region (P = .009).
To replicate the findings, data were used from the Columbia Centre for Children’s Health Study–Mothers and Newborns cohort in the United States. Once again, the BPA level was associated with hypermethylation of the aromatase brain promoter PI.f (P = .0089).
In both cohorts, there was evidence that the effect of increased BPA on brain-derived neurotrophic factor hypermethylation was mediated partly through higher aromatase gene methylation (P = .001).
To validate the findings, the researchers examined human neuroblastoma SH-SY5Y cell lines and found aromatase protein levels were more than halved in the presence of BPA 50 µg/L (P = .01).
Additionally, mouse studies showed that male mice exposed to BPA 50 µg/L mid-gestation and male aromatase knockout mice — but not female mice — had social behavior deficits, such as interacting with a strange mouse, as well as structural and functional brain changes.
“We found that BPA suppresses the aromatase enzyme and is associated with anatomical, neurologic, and behavioral changes in the male mice that may be consistent with autism spectrum disorder,” Wah Chin Boon, PhD, co–lead researcher and research fellow, also with The Florey Institute, said in a statement.
“This is the first time a biological pathway has been identified that might help explain the connection between autism and BPA,” she said.
“In this study, not only were the levels of BPA higher than most people would be exposed to, but in at least one of the experiments the mice were injected with BPA directly, whereas humans would be exposed via food and drink,” observed Oliver Jones, PhD, MSc, professor of chemistry, RMIT University, Melbourne, Australia. “If you ingest the food, it undergoes metabolism before it gets to the bloodstream, which reduces the effective dose.”
Dr. Jones said further studies with larger numbers of participants measuring BPA throughout pregnancy and other chemicals the mother and child were exposed to are needed to be sure of any such link. “Just because there is a possible mechanism in place does not automatically mean that it is activated,” he said.
Dr. Ponsonby pointed out that BPA and other endocrine-disrupting chemicals are “almost impossible for individuals to avoid” and can enter the body through plastic food and drink packaging, home renovation fumes, and sources such as cosmetics.
Fatty Acid Helpful?
Building on earlier observations that 10-hydroxy-2-decenoic acid (10HDA) may have estrogenic modulating activities, the researchers conducted additional studies suggesting that 10HDA may be effective as a competitive ligand that could counteract the effects of BPA on estrogen signaling within cells.
Further, among 3-week-old mice pups prenatally exposed to BPA, daily injections of 10HDA for 3 weeks showed striking and significant improvements in social interaction. Stopping 10HDA resulted in a deficit in social interaction that was again ameliorated by subsequent 10HDA treatment.
“10-hydroxy-2-decenoic acid shows early indications of potential in activating opposing biological pathways to improve autism-like characteristics when administered to animals that have been prenatally exposed to BPA,” Dr. Boon said. “It warrants further studies to see whether this potential treatment could be realized in humans.”
Reached for comment, Dr. Jones said “the human studies are not strong at all,” in large part because BPA levels were tested only once at 36 weeks in the BIS cohort.
“I would argue that if BPA is in the urine, it has been excreted and is no longer in the bloodstream, thus not able to affect the child,” he said. “I’d also argue that a single measurement at 36 weeks cannot give you any idea of the mother’s exposure to BPA over the rest of the pregnancy or what the child was exposed to after birth.”
The study was funded by the Minderoo Foundation, the National Health and Medical Research Council of Australia, the Australian Research Council, and numerous other sponsors. Dr. Boon is a coinventor on “Methods of treating neurodevelopmental diseases and disorders” and is a board member of Meizon Innovation Holdings. Dr. Ponsonby is a scientific adviser to Meizon Innovation Holdings. The remaining authors declared no competing interests.
A version of this article first appeared on Medscape.com.
BPA is a potent endocrine disruptor found in polycarbonate plastics and epoxy resins and has been banned by the Food and Drug Administration for use in baby bottles, sippy cups, and infant formula packaging.
“Exposure to BPA has already been shown in some studies to be associated with subsequent autism in offspring,” lead researcher Anne-Louise Ponsonby, PhD, The Florey Institute, Heidelberg, Australia, said in a statement.
“Our work is important because it demonstrates one of the biological mechanisms potentially involved. BPA can disrupt hormone-controlled male fetal brain development in several ways, including silencing a key enzyme, aromatase, that controls neurohormones and is especially important in fetal male brain development. This appears to be part of the autism puzzle,” she said.
Brain aromatase, encoded by CYP19A1, converts neural androgens to neural estrogens and has been implicated in ASD. Postmortem analyses of men with ASD also show markedly reduced aromatase activity.
The findings were published online in Nature Communications.
New Biological Mechanism
For the study, the researchers analyzed data from the Barwon Infant Study in 1067 infants in Australia. At age 7-11 years, 43 children had a confirmed ASD diagnosis, and 249 infants with Child Behavior Checklist (CBCL) data at age 2 years had an autism spectrum problem score above the median.
The researchers developed a CYP19A1 genetic score for aromatase activity based on five single nucleotide polymorphisms associated with lower estrogen levels. Among 595 children with prenatal BPA and CBCL, those with three or more variants were classified as “low aromatase activity” and the remaining were classified as “high.”
In regression analyses, boys with low aromatase activity and high prenatal BPA exposure (top quartile > 2.18 µg/L) were 3.5 times more likely to have autism symptoms at age 2 years (odds ratio [OR], 3.56; 95% CI, 1.13-11.22).
The odds of a confirmed ASD diagnosis were six times higher at age 9 years only in men with low aromatase activity (OR, 6.24; 95% CI, 1.02-38.26).
The researchers also found that higher BPA levels predicted higher methylation in cord blood across the CYP19A1 brain promoter PI.f region (P = .009).
To replicate the findings, data were used from the Columbia Centre for Children’s Health Study–Mothers and Newborns cohort in the United States. Once again, the BPA level was associated with hypermethylation of the aromatase brain promoter PI.f (P = .0089).
In both cohorts, there was evidence that the effect of increased BPA on brain-derived neurotrophic factor hypermethylation was mediated partly through higher aromatase gene methylation (P = .001).
To validate the findings, the researchers examined human neuroblastoma SH-SY5Y cell lines and found aromatase protein levels were more than halved in the presence of BPA 50 µg/L (P = .01).
Additionally, mouse studies showed that male mice exposed to BPA 50 µg/L mid-gestation and male aromatase knockout mice — but not female mice — had social behavior deficits, such as interacting with a strange mouse, as well as structural and functional brain changes.
“We found that BPA suppresses the aromatase enzyme and is associated with anatomical, neurologic, and behavioral changes in the male mice that may be consistent with autism spectrum disorder,” Wah Chin Boon, PhD, co–lead researcher and research fellow, also with The Florey Institute, said in a statement.
“This is the first time a biological pathway has been identified that might help explain the connection between autism and BPA,” she said.
“In this study, not only were the levels of BPA higher than most people would be exposed to, but in at least one of the experiments the mice were injected with BPA directly, whereas humans would be exposed via food and drink,” observed Oliver Jones, PhD, MSc, professor of chemistry, RMIT University, Melbourne, Australia. “If you ingest the food, it undergoes metabolism before it gets to the bloodstream, which reduces the effective dose.”
Dr. Jones said further studies with larger numbers of participants measuring BPA throughout pregnancy and other chemicals the mother and child were exposed to are needed to be sure of any such link. “Just because there is a possible mechanism in place does not automatically mean that it is activated,” he said.
Dr. Ponsonby pointed out that BPA and other endocrine-disrupting chemicals are “almost impossible for individuals to avoid” and can enter the body through plastic food and drink packaging, home renovation fumes, and sources such as cosmetics.
Fatty Acid Helpful?
Building on earlier observations that 10-hydroxy-2-decenoic acid (10HDA) may have estrogenic modulating activities, the researchers conducted additional studies suggesting that 10HDA may be effective as a competitive ligand that could counteract the effects of BPA on estrogen signaling within cells.
Further, among 3-week-old mice pups prenatally exposed to BPA, daily injections of 10HDA for 3 weeks showed striking and significant improvements in social interaction. Stopping 10HDA resulted in a deficit in social interaction that was again ameliorated by subsequent 10HDA treatment.
“10-hydroxy-2-decenoic acid shows early indications of potential in activating opposing biological pathways to improve autism-like characteristics when administered to animals that have been prenatally exposed to BPA,” Dr. Boon said. “It warrants further studies to see whether this potential treatment could be realized in humans.”
Reached for comment, Dr. Jones said “the human studies are not strong at all,” in large part because BPA levels were tested only once at 36 weeks in the BIS cohort.
“I would argue that if BPA is in the urine, it has been excreted and is no longer in the bloodstream, thus not able to affect the child,” he said. “I’d also argue that a single measurement at 36 weeks cannot give you any idea of the mother’s exposure to BPA over the rest of the pregnancy or what the child was exposed to after birth.”
The study was funded by the Minderoo Foundation, the National Health and Medical Research Council of Australia, the Australian Research Council, and numerous other sponsors. Dr. Boon is a coinventor on “Methods of treating neurodevelopmental diseases and disorders” and is a board member of Meizon Innovation Holdings. Dr. Ponsonby is a scientific adviser to Meizon Innovation Holdings. The remaining authors declared no competing interests.
A version of this article first appeared on Medscape.com.
BPA is a potent endocrine disruptor found in polycarbonate plastics and epoxy resins and has been banned by the Food and Drug Administration for use in baby bottles, sippy cups, and infant formula packaging.
“Exposure to BPA has already been shown in some studies to be associated with subsequent autism in offspring,” lead researcher Anne-Louise Ponsonby, PhD, The Florey Institute, Heidelberg, Australia, said in a statement.
“Our work is important because it demonstrates one of the biological mechanisms potentially involved. BPA can disrupt hormone-controlled male fetal brain development in several ways, including silencing a key enzyme, aromatase, that controls neurohormones and is especially important in fetal male brain development. This appears to be part of the autism puzzle,” she said.
Brain aromatase, encoded by CYP19A1, converts neural androgens to neural estrogens and has been implicated in ASD. Postmortem analyses of men with ASD also show markedly reduced aromatase activity.
The findings were published online in Nature Communications.
New Biological Mechanism
For the study, the researchers analyzed data from the Barwon Infant Study in 1067 infants in Australia. At age 7-11 years, 43 children had a confirmed ASD diagnosis, and 249 infants with Child Behavior Checklist (CBCL) data at age 2 years had an autism spectrum problem score above the median.
The researchers developed a CYP19A1 genetic score for aromatase activity based on five single nucleotide polymorphisms associated with lower estrogen levels. Among 595 children with prenatal BPA and CBCL, those with three or more variants were classified as “low aromatase activity” and the remaining were classified as “high.”
In regression analyses, boys with low aromatase activity and high prenatal BPA exposure (top quartile > 2.18 µg/L) were 3.5 times more likely to have autism symptoms at age 2 years (odds ratio [OR], 3.56; 95% CI, 1.13-11.22).
The odds of a confirmed ASD diagnosis were six times higher at age 9 years only in men with low aromatase activity (OR, 6.24; 95% CI, 1.02-38.26).
The researchers also found that higher BPA levels predicted higher methylation in cord blood across the CYP19A1 brain promoter PI.f region (P = .009).
To replicate the findings, data were used from the Columbia Centre for Children’s Health Study–Mothers and Newborns cohort in the United States. Once again, the BPA level was associated with hypermethylation of the aromatase brain promoter PI.f (P = .0089).
In both cohorts, there was evidence that the effect of increased BPA on brain-derived neurotrophic factor hypermethylation was mediated partly through higher aromatase gene methylation (P = .001).
To validate the findings, the researchers examined human neuroblastoma SH-SY5Y cell lines and found aromatase protein levels were more than halved in the presence of BPA 50 µg/L (P = .01).
Additionally, mouse studies showed that male mice exposed to BPA 50 µg/L mid-gestation and male aromatase knockout mice — but not female mice — had social behavior deficits, such as interacting with a strange mouse, as well as structural and functional brain changes.
“We found that BPA suppresses the aromatase enzyme and is associated with anatomical, neurologic, and behavioral changes in the male mice that may be consistent with autism spectrum disorder,” Wah Chin Boon, PhD, co–lead researcher and research fellow, also with The Florey Institute, said in a statement.
“This is the first time a biological pathway has been identified that might help explain the connection between autism and BPA,” she said.
“In this study, not only were the levels of BPA higher than most people would be exposed to, but in at least one of the experiments the mice were injected with BPA directly, whereas humans would be exposed via food and drink,” observed Oliver Jones, PhD, MSc, professor of chemistry, RMIT University, Melbourne, Australia. “If you ingest the food, it undergoes metabolism before it gets to the bloodstream, which reduces the effective dose.”
Dr. Jones said further studies with larger numbers of participants measuring BPA throughout pregnancy and other chemicals the mother and child were exposed to are needed to be sure of any such link. “Just because there is a possible mechanism in place does not automatically mean that it is activated,” he said.
Dr. Ponsonby pointed out that BPA and other endocrine-disrupting chemicals are “almost impossible for individuals to avoid” and can enter the body through plastic food and drink packaging, home renovation fumes, and sources such as cosmetics.
Fatty Acid Helpful?
Building on earlier observations that 10-hydroxy-2-decenoic acid (10HDA) may have estrogenic modulating activities, the researchers conducted additional studies suggesting that 10HDA may be effective as a competitive ligand that could counteract the effects of BPA on estrogen signaling within cells.
Further, among 3-week-old mice pups prenatally exposed to BPA, daily injections of 10HDA for 3 weeks showed striking and significant improvements in social interaction. Stopping 10HDA resulted in a deficit in social interaction that was again ameliorated by subsequent 10HDA treatment.
“10-hydroxy-2-decenoic acid shows early indications of potential in activating opposing biological pathways to improve autism-like characteristics when administered to animals that have been prenatally exposed to BPA,” Dr. Boon said. “It warrants further studies to see whether this potential treatment could be realized in humans.”
Reached for comment, Dr. Jones said “the human studies are not strong at all,” in large part because BPA levels were tested only once at 36 weeks in the BIS cohort.
“I would argue that if BPA is in the urine, it has been excreted and is no longer in the bloodstream, thus not able to affect the child,” he said. “I’d also argue that a single measurement at 36 weeks cannot give you any idea of the mother’s exposure to BPA over the rest of the pregnancy or what the child was exposed to after birth.”
The study was funded by the Minderoo Foundation, the National Health and Medical Research Council of Australia, the Australian Research Council, and numerous other sponsors. Dr. Boon is a coinventor on “Methods of treating neurodevelopmental diseases and disorders” and is a board member of Meizon Innovation Holdings. Dr. Ponsonby is a scientific adviser to Meizon Innovation Holdings. The remaining authors declared no competing interests.
A version of this article first appeared on Medscape.com.
FROM NATURE COMMUNICATIONS
Sexual Arousal Cream Promising in Some Subsets of Women
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
FROM OBSTETRICS & GYNECOLOGY
Navigating Election Anxiety: How Worry Affects the Brain
Once again, America is deeply divided before a national election, with people on each side convinced of the horrors that will be visited upon us if the other side wins.
’Tis the season — and regrettably, not to be jolly but to be worried.
As a neuroscientist, I am especially aware of the deleterious mental and physical impact of chronic worry on our citizenry. That’s because worry is not “all in your head.” We modern humans live in a world of worry which appears to be progressively growing.
Flight or Fight
Worry stems from the brain’s rather remarkable ability to foresee and reflexively respond to threat. Our “fight or flight” brain machinery probably arose in our vertebrate ancestors more than 300 million years ago. The fact that we have machinery akin to that possessed by lizards or tigers or shrews is testimony to its crucial contribution to our species’ survival.
As the phrase “fight or flight” suggests, a brain that senses trouble immediately biases certain body and brain functions. As it shifts into a higher-alert mode, it increases the energy supplies in our blood and supports other changes that facilitate faster and stronger reactions, while it shuts down less essential processes which do not contribute to hiding, fighting, or running like hell.
This hyperreactive response is initiated in the amygdala in the anterior brain, which identifies “what’s happening” as immediately or potentially threatening. The now-activated amygdala generates a response in the hypothalamus that provokes an immediate increase of adrenaline and cortisol in the body, and cortisol and noradrenaline in the brain. Both sharply speed up our physical and neurologic reactivity. In the brain, that is achieved by increasing the level of excitability of neurons across the forebrain. Depending on the perceived level of threat, an excitable brain will be just a little or a lot more “on alert,” just a little or a lot faster to respond, and just a little or a lot better at remembering the specific “warning” events that trigger this lizard-brain response.
Alas, this machinery was designed to be engaged every so often when a potentially dangerous surprise arises in life. When the worry and stress are persistent, the brain experiences a kind of neurologic “burn-out” of its fight versus flight machinery.
Dangers of Nonstop Anxiety and Stress
A consistently stressed-out brain turns down its production and release of noradrenaline, and the brain becomes less attentive, less engaged. This sets the brain on the path to an anxiety (and then a depressive) disorder, and, in the longer term, to cognitive losses in memory and executive control systems, and to emotional distortions that can lead to substance abuse or other addictions.
Our political distress is but one source of persistent worry and stress. Worry is a modern plague. The head counts of individuals seeking psychiatric or psychological health are at an all-time high in the United States. Near-universal low-level stressors, such as 2 years of COVID, insecurities about the changing demands of our professional and private lives, and a deeply divided body politic are unequivocally affecting American brain health.
The brain also collaborates in our body’s response to stress. Its regulation of hormonal responses and its autonomic nervous system’s mediated responses contribute to elevated blood sugar levels, to craving high-sugar foods, to elevated blood pressure, and to weaker immune responses. This all contributes to higher risks for cardiovascular and other dietary- and immune system–related disease. And ultimately, to shorter lifespans.
Strategies to Address Neurologic Changes Arising From Chronic Stress
There are many things you can try to bring your worry back to a manageable (and even productive) level.
- Engage in a “reset” strategy several times a day to bring your amygdala and locus coeruleus back under control. It takes a minute (or five) of calm, positive meditation to take your brain to a happy, optimistic place. Or use a mindfulness exercise to quiet down that overactive amygdala.
- Talk to people. Keeping your worries to yourself can compound them. Hashing through your concerns with a family member, friend, professional coach, or therapist can help put them in perspective and may allow you to come up with strategies to identify and neurologically respond to your sources of stress.
- Exercise, both physically and mentally. Do what works for you, whether it’s a run, a long walk, pumping iron, playing racquetball — anything that promotes physical release. Exercise your brain too. Engage in a project or activity that is mentally demanding. Personally, I like to garden and do online brain exercises. There’s nothing quite like yanking out weeds or hitting a new personal best at a cognitive exercise for me to notch a sense of accomplishment to counterbalance the unresolved issues driving my worry.
- Accept the uncertainty. Life is full of uncertainty. To paraphrase from Yale theologian Reinhold Niebuhr’s “Serenity Prayer”: Have the serenity to accept what you cannot help, the courage to change what you can, and the wisdom to recognize one from the other.
And, please, be assured that you’ll make it through this election season.
Dr. Merzenich, professor emeritus, Department of Neuroscience, University of California San Francisco, disclosed ties with Posit Science. He is often credited with discovering lifelong plasticity, with being the first to harness plasticity for human benefit (in his co-invention of the cochlear implant), and for pioneering the field of plasticity-based computerized brain exercise. He is a Kavli Laureate in Neuroscience, and he has been honored by each of the US National Academies of Sciences, Engineering, and Medicine. He may be most widely known for a series of specials on the brain on public television. His current focus is BrainHQ, a brain exercise app.
A version of this article appeared on Medscape.com.
Once again, America is deeply divided before a national election, with people on each side convinced of the horrors that will be visited upon us if the other side wins.
’Tis the season — and regrettably, not to be jolly but to be worried.
As a neuroscientist, I am especially aware of the deleterious mental and physical impact of chronic worry on our citizenry. That’s because worry is not “all in your head.” We modern humans live in a world of worry which appears to be progressively growing.
Flight or Fight
Worry stems from the brain’s rather remarkable ability to foresee and reflexively respond to threat. Our “fight or flight” brain machinery probably arose in our vertebrate ancestors more than 300 million years ago. The fact that we have machinery akin to that possessed by lizards or tigers or shrews is testimony to its crucial contribution to our species’ survival.
As the phrase “fight or flight” suggests, a brain that senses trouble immediately biases certain body and brain functions. As it shifts into a higher-alert mode, it increases the energy supplies in our blood and supports other changes that facilitate faster and stronger reactions, while it shuts down less essential processes which do not contribute to hiding, fighting, or running like hell.
This hyperreactive response is initiated in the amygdala in the anterior brain, which identifies “what’s happening” as immediately or potentially threatening. The now-activated amygdala generates a response in the hypothalamus that provokes an immediate increase of adrenaline and cortisol in the body, and cortisol and noradrenaline in the brain. Both sharply speed up our physical and neurologic reactivity. In the brain, that is achieved by increasing the level of excitability of neurons across the forebrain. Depending on the perceived level of threat, an excitable brain will be just a little or a lot more “on alert,” just a little or a lot faster to respond, and just a little or a lot better at remembering the specific “warning” events that trigger this lizard-brain response.
Alas, this machinery was designed to be engaged every so often when a potentially dangerous surprise arises in life. When the worry and stress are persistent, the brain experiences a kind of neurologic “burn-out” of its fight versus flight machinery.
Dangers of Nonstop Anxiety and Stress
A consistently stressed-out brain turns down its production and release of noradrenaline, and the brain becomes less attentive, less engaged. This sets the brain on the path to an anxiety (and then a depressive) disorder, and, in the longer term, to cognitive losses in memory and executive control systems, and to emotional distortions that can lead to substance abuse or other addictions.
Our political distress is but one source of persistent worry and stress. Worry is a modern plague. The head counts of individuals seeking psychiatric or psychological health are at an all-time high in the United States. Near-universal low-level stressors, such as 2 years of COVID, insecurities about the changing demands of our professional and private lives, and a deeply divided body politic are unequivocally affecting American brain health.
The brain also collaborates in our body’s response to stress. Its regulation of hormonal responses and its autonomic nervous system’s mediated responses contribute to elevated blood sugar levels, to craving high-sugar foods, to elevated blood pressure, and to weaker immune responses. This all contributes to higher risks for cardiovascular and other dietary- and immune system–related disease. And ultimately, to shorter lifespans.
Strategies to Address Neurologic Changes Arising From Chronic Stress
There are many things you can try to bring your worry back to a manageable (and even productive) level.
- Engage in a “reset” strategy several times a day to bring your amygdala and locus coeruleus back under control. It takes a minute (or five) of calm, positive meditation to take your brain to a happy, optimistic place. Or use a mindfulness exercise to quiet down that overactive amygdala.
- Talk to people. Keeping your worries to yourself can compound them. Hashing through your concerns with a family member, friend, professional coach, or therapist can help put them in perspective and may allow you to come up with strategies to identify and neurologically respond to your sources of stress.
- Exercise, both physically and mentally. Do what works for you, whether it’s a run, a long walk, pumping iron, playing racquetball — anything that promotes physical release. Exercise your brain too. Engage in a project or activity that is mentally demanding. Personally, I like to garden and do online brain exercises. There’s nothing quite like yanking out weeds or hitting a new personal best at a cognitive exercise for me to notch a sense of accomplishment to counterbalance the unresolved issues driving my worry.
- Accept the uncertainty. Life is full of uncertainty. To paraphrase from Yale theologian Reinhold Niebuhr’s “Serenity Prayer”: Have the serenity to accept what you cannot help, the courage to change what you can, and the wisdom to recognize one from the other.
And, please, be assured that you’ll make it through this election season.
Dr. Merzenich, professor emeritus, Department of Neuroscience, University of California San Francisco, disclosed ties with Posit Science. He is often credited with discovering lifelong plasticity, with being the first to harness plasticity for human benefit (in his co-invention of the cochlear implant), and for pioneering the field of plasticity-based computerized brain exercise. He is a Kavli Laureate in Neuroscience, and he has been honored by each of the US National Academies of Sciences, Engineering, and Medicine. He may be most widely known for a series of specials on the brain on public television. His current focus is BrainHQ, a brain exercise app.
A version of this article appeared on Medscape.com.
Once again, America is deeply divided before a national election, with people on each side convinced of the horrors that will be visited upon us if the other side wins.
’Tis the season — and regrettably, not to be jolly but to be worried.
As a neuroscientist, I am especially aware of the deleterious mental and physical impact of chronic worry on our citizenry. That’s because worry is not “all in your head.” We modern humans live in a world of worry which appears to be progressively growing.
Flight or Fight
Worry stems from the brain’s rather remarkable ability to foresee and reflexively respond to threat. Our “fight or flight” brain machinery probably arose in our vertebrate ancestors more than 300 million years ago. The fact that we have machinery akin to that possessed by lizards or tigers or shrews is testimony to its crucial contribution to our species’ survival.
As the phrase “fight or flight” suggests, a brain that senses trouble immediately biases certain body and brain functions. As it shifts into a higher-alert mode, it increases the energy supplies in our blood and supports other changes that facilitate faster and stronger reactions, while it shuts down less essential processes which do not contribute to hiding, fighting, or running like hell.
This hyperreactive response is initiated in the amygdala in the anterior brain, which identifies “what’s happening” as immediately or potentially threatening. The now-activated amygdala generates a response in the hypothalamus that provokes an immediate increase of adrenaline and cortisol in the body, and cortisol and noradrenaline in the brain. Both sharply speed up our physical and neurologic reactivity. In the brain, that is achieved by increasing the level of excitability of neurons across the forebrain. Depending on the perceived level of threat, an excitable brain will be just a little or a lot more “on alert,” just a little or a lot faster to respond, and just a little or a lot better at remembering the specific “warning” events that trigger this lizard-brain response.
Alas, this machinery was designed to be engaged every so often when a potentially dangerous surprise arises in life. When the worry and stress are persistent, the brain experiences a kind of neurologic “burn-out” of its fight versus flight machinery.
Dangers of Nonstop Anxiety and Stress
A consistently stressed-out brain turns down its production and release of noradrenaline, and the brain becomes less attentive, less engaged. This sets the brain on the path to an anxiety (and then a depressive) disorder, and, in the longer term, to cognitive losses in memory and executive control systems, and to emotional distortions that can lead to substance abuse or other addictions.
Our political distress is but one source of persistent worry and stress. Worry is a modern plague. The head counts of individuals seeking psychiatric or psychological health are at an all-time high in the United States. Near-universal low-level stressors, such as 2 years of COVID, insecurities about the changing demands of our professional and private lives, and a deeply divided body politic are unequivocally affecting American brain health.
The brain also collaborates in our body’s response to stress. Its regulation of hormonal responses and its autonomic nervous system’s mediated responses contribute to elevated blood sugar levels, to craving high-sugar foods, to elevated blood pressure, and to weaker immune responses. This all contributes to higher risks for cardiovascular and other dietary- and immune system–related disease. And ultimately, to shorter lifespans.
Strategies to Address Neurologic Changes Arising From Chronic Stress
There are many things you can try to bring your worry back to a manageable (and even productive) level.
- Engage in a “reset” strategy several times a day to bring your amygdala and locus coeruleus back under control. It takes a minute (or five) of calm, positive meditation to take your brain to a happy, optimistic place. Or use a mindfulness exercise to quiet down that overactive amygdala.
- Talk to people. Keeping your worries to yourself can compound them. Hashing through your concerns with a family member, friend, professional coach, or therapist can help put them in perspective and may allow you to come up with strategies to identify and neurologically respond to your sources of stress.
- Exercise, both physically and mentally. Do what works for you, whether it’s a run, a long walk, pumping iron, playing racquetball — anything that promotes physical release. Exercise your brain too. Engage in a project or activity that is mentally demanding. Personally, I like to garden and do online brain exercises. There’s nothing quite like yanking out weeds or hitting a new personal best at a cognitive exercise for me to notch a sense of accomplishment to counterbalance the unresolved issues driving my worry.
- Accept the uncertainty. Life is full of uncertainty. To paraphrase from Yale theologian Reinhold Niebuhr’s “Serenity Prayer”: Have the serenity to accept what you cannot help, the courage to change what you can, and the wisdom to recognize one from the other.
And, please, be assured that you’ll make it through this election season.
Dr. Merzenich, professor emeritus, Department of Neuroscience, University of California San Francisco, disclosed ties with Posit Science. He is often credited with discovering lifelong plasticity, with being the first to harness plasticity for human benefit (in his co-invention of the cochlear implant), and for pioneering the field of plasticity-based computerized brain exercise. He is a Kavli Laureate in Neuroscience, and he has been honored by each of the US National Academies of Sciences, Engineering, and Medicine. He may be most widely known for a series of specials on the brain on public television. His current focus is BrainHQ, a brain exercise app.
A version of this article appeared on Medscape.com.