User login
Managing family differences
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.

Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.
Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.
Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
Five-day treatment of ear infections
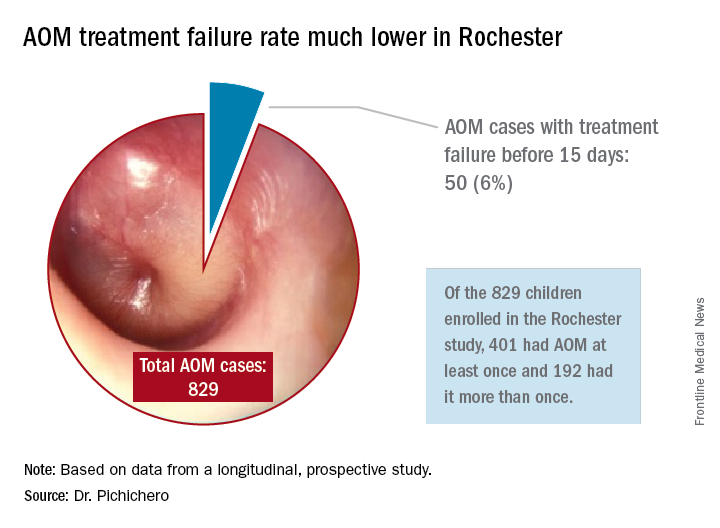
In December 2016, the results of a randomized, controlled trial of 5-day vs. 10-day amoxicillin/clavulanate treatment of acute otitis media (AOM) in children aged 6-23 months was reported by Hoberman et al. in the New England Journal of Medicine (NEJM).1 Predefined criteria for clinical failure were used that considered both symptoms and signs of AOM, assessed on days 12-14 after start of treatment with 5 vs. 10 days of treatment with the antibiotic. The conclusion reached was clear: The clinical failure rate for the 5-day regimen was 34% vs. 16% in the 10-day group, supporting a preference for the 10-day treatment.
I was surprised. The clinical failure rate for the 5-day regimen seemed very high for treatment with amoxicillin/clavulanate. If it is 34% with amoxicillin/clavulanate, then what would it have been with amoxicillin, as recommended by the American Academy of Pediatrics?

So, why did the systematic review conclude that there was a minimal difference between shortened treatments and the standard 10-day when the NEJM study reported such a striking difference?
In Rochester, N.Y., we have been conducting a longitudinal, prospective study of AOM that is NIH-sponsored to better understand the immune response to AOM, especially in otitis-prone children.3,4 In that study we are treating all children aged 6-23 months with amoxicillin/clavulanate using the same dose as used in the study by Hoberman et al. We have two exceptions: If the child has a second AOM within 30 days of a prior episode or they have an eardrum rupture, we treat for 10 days.5 Our clinical failure rate is 6%. Why is the failure rate in Rochester so much lower than that in Pittsburgh and Bardstown, Ky., where the Hoberman et al. study was done?
One possibility is an important difference in our study design, compared with that of the NEJM study. All the children in our prospective study have a tympanocentesis to confirm the clinical diagnosis, and our research has shown that tympanocentesis results in immediate relief of ear pain and reduces the frequency of antibiotic treatment failure about twofold, compared with children diagnosed and treated by the same physicians in the same clinic practice.6 So, if the tympanocentesis is factored out of the equation, the Rochester clinical failure comes out to 14% for 5-day treatment. Why would the children in Rochester not getting a tympanocentesis, being treated with the same antibiotic, same dose, and same definition of clinical failure, during the same time frame, and having the same bacteria with the same antibiotic resistance rates have a clinical failure rate of 14%, compared with the 34% in the NEJM study?
Next question: How does a clinical failure rate of 34% fit according to past studies of shortened course antibiotic treatment of AOM? Besides the systematic review and meta-analysis noted above, in many countries outside the United States the 5-day regimen is standard, so, if health care providers were seeing a 34% failure rate, that would have been noticeable for sure.8 So, if health care providers were seeing a 34% failure rate, would that not have been noticeable? And would not a 16% failure rate, nearly 1 of 5 cases, be noticeable for children treated for 10 days?
Was there something different about the children who were in the Hoberman et al. study and the children treated in countries outside the United States and in our practice in Rochester? My group has collaborated and published on studies of AOM with the Pittsburgh and Kentucky groups, and we have not found significant site to site differences in outcomes, demonstrating that a population difference is unlikely.9-11
Next question: How does a clinical failure rate of 16% fit according to past studies of 10 days’ antibiotic treatment of AOM? It is on target with the meta-analysis and two other recent studies in the NEJM.12,13 However, if the failure rate was 16% with amoxicillin/clavulanate (which is effective against beta-lactamase–producing Haemophilus influenzae and Moraxella catarrhalis, whereas amoxicillin is not), then the predicted failure rate with amoxicillin for 10 days should be double (34%) or triple (51%) had amoxicillin been used as recommended by the AAP in light of the bacterial resistance of otopathogens. That calculation is based on the prevalence of beta-lactamase–producing H. influenzae and M. catarrhalis in the Pittsburgh and Kentucky populations, the same prevalence seen in the Rochester population.” 14
So, I conclude that this wonderful study does not convince me to change my practice from standard use of 5-day amoxicillin/clavulanate treatment of AOM. Besides, outside of a study setting, most parents don’t give the full 10-day treatment. They stop when their child seems normal (a few days after starting treatment) and save the remainder of the medicine in the refrigerator for the next illness to save a trip to the doctor. Plus, in this column, I did not even get into the issue of disturbing the microbiome with longer courses of antibiotic treatment, a topic for a future discussion.
References
1. N Engl J Med. 2016 Dec 22;375(25):2446-56.
2. Cochrane Database Syst Rev. 2010 Sep 8;(9):CD001095.
3. Pediatr Infect Dis J. 2016 Sep;35(9):1027-32.
4. Pediatr Infect Dis J. 2016 Sep;35(9):1033-9.
5. Otolaryngol Head Neck Surg. 2001 Apr;124(4):381-7.
6. Pediatr Infect Dis J. 2013 May;32(5):473-8.
7. Pediatr Infect Dis J. 2006 Mar;25(3):211-8.
8. Pediatr Infect Dis J. 2000 Sep;19(9):929-37.
9. Pediatr Infect Dis J. 1999 Aug;18(8):741-4.
10. Clin Pediatr (Phila). 2008 Nov;47(9):901-6.
11. Drugs. 2012 Oct 22;72(15):1991-7.
12. N Engl J Med. 2011 Jan 13;364(2):105-15.
13. N Engl J Med. 2011 Jan 13;364(2):116-26.
14. Pediatr Infect Dis J. 2016 Aug;35(8):901-6.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no disclosures.
In December 2016, the results of a randomized, controlled trial of 5-day vs. 10-day amoxicillin/clavulanate treatment of acute otitis media (AOM) in children aged 6-23 months was reported by Hoberman et al. in the New England Journal of Medicine (NEJM).1 Predefined criteria for clinical failure were used that considered both symptoms and signs of AOM, assessed on days 12-14 after start of treatment with 5 vs. 10 days of treatment with the antibiotic. The conclusion reached was clear: The clinical failure rate for the 5-day regimen was 34% vs. 16% in the 10-day group, supporting a preference for the 10-day treatment.
I was surprised. The clinical failure rate for the 5-day regimen seemed very high for treatment with amoxicillin/clavulanate. If it is 34% with amoxicillin/clavulanate, then what would it have been with amoxicillin, as recommended by the American Academy of Pediatrics?
So, why did the systematic review conclude that there was a minimal difference between shortened treatments and the standard 10-day when the NEJM study reported such a striking difference?
In Rochester, N.Y., we have been conducting a longitudinal, prospective study of AOM that is NIH-sponsored to better understand the immune response to AOM, especially in otitis-prone children.3,4 In that study we are treating all children aged 6-23 months with amoxicillin/clavulanate using the same dose as used in the study by Hoberman et al. We have two exceptions: If the child has a second AOM within 30 days of a prior episode or they have an eardrum rupture, we treat for 10 days.5 Our clinical failure rate is 6%. Why is the failure rate in Rochester so much lower than that in Pittsburgh and Bardstown, Ky., where the Hoberman et al. study was done?
One possibility is an important difference in our study design, compared with that of the NEJM study. All the children in our prospective study have a tympanocentesis to confirm the clinical diagnosis, and our research has shown that tympanocentesis results in immediate relief of ear pain and reduces the frequency of antibiotic treatment failure about twofold, compared with children diagnosed and treated by the same physicians in the same clinic practice.6 So, if the tympanocentesis is factored out of the equation, the Rochester clinical failure comes out to 14% for 5-day treatment. Why would the children in Rochester not getting a tympanocentesis, being treated with the same antibiotic, same dose, and same definition of clinical failure, during the same time frame, and having the same bacteria with the same antibiotic resistance rates have a clinical failure rate of 14%, compared with the 34% in the NEJM study?
Next question: How does a clinical failure rate of 34% fit according to past studies of shortened course antibiotic treatment of AOM? Besides the systematic review and meta-analysis noted above, in many countries outside the United States the 5-day regimen is standard, so, if health care providers were seeing a 34% failure rate, that would have been noticeable for sure.8 So, if health care providers were seeing a 34% failure rate, would that not have been noticeable? And would not a 16% failure rate, nearly 1 of 5 cases, be noticeable for children treated for 10 days?
Was there something different about the children who were in the Hoberman et al. study and the children treated in countries outside the United States and in our practice in Rochester? My group has collaborated and published on studies of AOM with the Pittsburgh and Kentucky groups, and we have not found significant site to site differences in outcomes, demonstrating that a population difference is unlikely.9-11
Next question: How does a clinical failure rate of 16% fit according to past studies of 10 days’ antibiotic treatment of AOM? It is on target with the meta-analysis and two other recent studies in the NEJM.12,13 However, if the failure rate was 16% with amoxicillin/clavulanate (which is effective against beta-lactamase–producing Haemophilus influenzae and Moraxella catarrhalis, whereas amoxicillin is not), then the predicted failure rate with amoxicillin for 10 days should be double (34%) or triple (51%) had amoxicillin been used as recommended by the AAP in light of the bacterial resistance of otopathogens. That calculation is based on the prevalence of beta-lactamase–producing H. influenzae and M. catarrhalis in the Pittsburgh and Kentucky populations, the same prevalence seen in the Rochester population.” 14
So, I conclude that this wonderful study does not convince me to change my practice from standard use of 5-day amoxicillin/clavulanate treatment of AOM. Besides, outside of a study setting, most parents don’t give the full 10-day treatment. They stop when their child seems normal (a few days after starting treatment) and save the remainder of the medicine in the refrigerator for the next illness to save a trip to the doctor. Plus, in this column, I did not even get into the issue of disturbing the microbiome with longer courses of antibiotic treatment, a topic for a future discussion.
References
1. N Engl J Med. 2016 Dec 22;375(25):2446-56.
2. Cochrane Database Syst Rev. 2010 Sep 8;(9):CD001095.
3. Pediatr Infect Dis J. 2016 Sep;35(9):1027-32.
4. Pediatr Infect Dis J. 2016 Sep;35(9):1033-9.
5. Otolaryngol Head Neck Surg. 2001 Apr;124(4):381-7.
6. Pediatr Infect Dis J. 2013 May;32(5):473-8.
7. Pediatr Infect Dis J. 2006 Mar;25(3):211-8.
8. Pediatr Infect Dis J. 2000 Sep;19(9):929-37.
9. Pediatr Infect Dis J. 1999 Aug;18(8):741-4.
10. Clin Pediatr (Phila). 2008 Nov;47(9):901-6.
11. Drugs. 2012 Oct 22;72(15):1991-7.
12. N Engl J Med. 2011 Jan 13;364(2):105-15.
13. N Engl J Med. 2011 Jan 13;364(2):116-26.
14. Pediatr Infect Dis J. 2016 Aug;35(8):901-6.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no disclosures.
In December 2016, the results of a randomized, controlled trial of 5-day vs. 10-day amoxicillin/clavulanate treatment of acute otitis media (AOM) in children aged 6-23 months was reported by Hoberman et al. in the New England Journal of Medicine (NEJM).1 Predefined criteria for clinical failure were used that considered both symptoms and signs of AOM, assessed on days 12-14 after start of treatment with 5 vs. 10 days of treatment with the antibiotic. The conclusion reached was clear: The clinical failure rate for the 5-day regimen was 34% vs. 16% in the 10-day group, supporting a preference for the 10-day treatment.
I was surprised. The clinical failure rate for the 5-day regimen seemed very high for treatment with amoxicillin/clavulanate. If it is 34% with amoxicillin/clavulanate, then what would it have been with amoxicillin, as recommended by the American Academy of Pediatrics?
So, why did the systematic review conclude that there was a minimal difference between shortened treatments and the standard 10-day when the NEJM study reported such a striking difference?
In Rochester, N.Y., we have been conducting a longitudinal, prospective study of AOM that is NIH-sponsored to better understand the immune response to AOM, especially in otitis-prone children.3,4 In that study we are treating all children aged 6-23 months with amoxicillin/clavulanate using the same dose as used in the study by Hoberman et al. We have two exceptions: If the child has a second AOM within 30 days of a prior episode or they have an eardrum rupture, we treat for 10 days.5 Our clinical failure rate is 6%. Why is the failure rate in Rochester so much lower than that in Pittsburgh and Bardstown, Ky., where the Hoberman et al. study was done?
One possibility is an important difference in our study design, compared with that of the NEJM study. All the children in our prospective study have a tympanocentesis to confirm the clinical diagnosis, and our research has shown that tympanocentesis results in immediate relief of ear pain and reduces the frequency of antibiotic treatment failure about twofold, compared with children diagnosed and treated by the same physicians in the same clinic practice.6 So, if the tympanocentesis is factored out of the equation, the Rochester clinical failure comes out to 14% for 5-day treatment. Why would the children in Rochester not getting a tympanocentesis, being treated with the same antibiotic, same dose, and same definition of clinical failure, during the same time frame, and having the same bacteria with the same antibiotic resistance rates have a clinical failure rate of 14%, compared with the 34% in the NEJM study?
Next question: How does a clinical failure rate of 34% fit according to past studies of shortened course antibiotic treatment of AOM? Besides the systematic review and meta-analysis noted above, in many countries outside the United States the 5-day regimen is standard, so, if health care providers were seeing a 34% failure rate, that would have been noticeable for sure.8 So, if health care providers were seeing a 34% failure rate, would that not have been noticeable? And would not a 16% failure rate, nearly 1 of 5 cases, be noticeable for children treated for 10 days?
Was there something different about the children who were in the Hoberman et al. study and the children treated in countries outside the United States and in our practice in Rochester? My group has collaborated and published on studies of AOM with the Pittsburgh and Kentucky groups, and we have not found significant site to site differences in outcomes, demonstrating that a population difference is unlikely.9-11
Next question: How does a clinical failure rate of 16% fit according to past studies of 10 days’ antibiotic treatment of AOM? It is on target with the meta-analysis and two other recent studies in the NEJM.12,13 However, if the failure rate was 16% with amoxicillin/clavulanate (which is effective against beta-lactamase–producing Haemophilus influenzae and Moraxella catarrhalis, whereas amoxicillin is not), then the predicted failure rate with amoxicillin for 10 days should be double (34%) or triple (51%) had amoxicillin been used as recommended by the AAP in light of the bacterial resistance of otopathogens. That calculation is based on the prevalence of beta-lactamase–producing H. influenzae and M. catarrhalis in the Pittsburgh and Kentucky populations, the same prevalence seen in the Rochester population.” 14
So, I conclude that this wonderful study does not convince me to change my practice from standard use of 5-day amoxicillin/clavulanate treatment of AOM. Besides, outside of a study setting, most parents don’t give the full 10-day treatment. They stop when their child seems normal (a few days after starting treatment) and save the remainder of the medicine in the refrigerator for the next illness to save a trip to the doctor. Plus, in this column, I did not even get into the issue of disturbing the microbiome with longer courses of antibiotic treatment, a topic for a future discussion.
References
1. N Engl J Med. 2016 Dec 22;375(25):2446-56.
2. Cochrane Database Syst Rev. 2010 Sep 8;(9):CD001095.
3. Pediatr Infect Dis J. 2016 Sep;35(9):1027-32.
4. Pediatr Infect Dis J. 2016 Sep;35(9):1033-9.
5. Otolaryngol Head Neck Surg. 2001 Apr;124(4):381-7.
6. Pediatr Infect Dis J. 2013 May;32(5):473-8.
7. Pediatr Infect Dis J. 2006 Mar;25(3):211-8.
8. Pediatr Infect Dis J. 2000 Sep;19(9):929-37.
9. Pediatr Infect Dis J. 1999 Aug;18(8):741-4.
10. Clin Pediatr (Phila). 2008 Nov;47(9):901-6.
11. Drugs. 2012 Oct 22;72(15):1991-7.
12. N Engl J Med. 2011 Jan 13;364(2):105-15.
13. N Engl J Med. 2011 Jan 13;364(2):116-26.
14. Pediatr Infect Dis J. 2016 Aug;35(8):901-6.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no disclosures.
Book Review: Psychiatrist rejects ‘physician as cog’ model of care
The title of the book, “Passion for Patients,” by Lee H. Beecher, MD, DLFAPA, FASAM, with writer Dave Racer, MLitt (St. Paul, Minn., Alethos Press, 2017), clearly represents Dr. Beecher’s approach to his professional life: His focal interest has been his patients ever since he went to medical school and started a very long and successful practice.
Dr. Beecher’s years of practice encompass many of the changes that the practice of medicine has seen in the last 50 years.
He attended medical school when an office was the place where a physician and his patients would get together to exchange thoughts, feelings, ideas, and plans so that they would eventually work together directly and unencumbered on the same concepts that they share and that they considered crucial to their relationship.
Shortly after Dr. Beecher graduated, Medicaid and Medicare came into medical practice, together with progressive limitations, threats, and a great many unwelcome interlopers, whose mission drastically changed the doctor-patient relationship. No matter how one examines the actions of the numerous new participants – be they auditors, insurance companies, employers, or money managers – one of their main missions was to modify, qualify, re-identify, and limit the interaction between the doctor and the patient.

“What is amazing – and contrary to truth – about the current evolution of medical care reform is its manifold references to safeguarding the best interests of the patient,” Dr. Beecher wrote. “On the contrary, the medical care reformers in current vogue see the physician as but one cog in the production of a specified medical care outcome – a cog that must be greased by evidence-based medicine and managed by analytical applications derived from data, cured in the crucible of number crunching, and controlled by payment systems.”
We live in an age when forces other than medical thinking and practice are trying to define what psychiatrists do, how we do it, and whether our effort is worth being paid for. This has created lack of satisfaction in the exercise of psychiatry, early retirements, and lack of growth in many quarters. When one considers that practically all psychiatric endeavors can be traced to the efforts of devoted practitioners interested in improving the profession, one can see that the future might look bleak because people other than psychiatrists define, quantify, and evaluate the practice of our specialty.
“I escaped from managed care into the practice model that had served so well for decades prior to HMOs, [preferred provider organizations], and other externally controlled practice models,” he wrote. “My patients paid me directly.”
Dr. Beecher is a witness and protester, as well as a thinking innovator, coming to defend patients and physicians at a time when they are under attack from precisely the same forces that were supposed to help and support them.
Throughout his book, Dr. Beecher tells us the story of his many points of disagreement with the intruders and his many arguments in favor of patients and doctors, going back to the beginning of the forces that are controlling and destroying their relationship at this time and advocating principled resistance and a careful search for independence. The reader easily accompanies the author to the points when independence blends with excellence – accepting that neither one exists without the other.
Dr. Muñoz, a former president of the American Psychiatric Association, has written eight books and more than 200 articles about various aspects of psychiatry. He is a professor of psychiatry at the University of California, San Diego, and has a private practice. Dr. Muñoz and Dr. Beecher serve on the Editorial Advisory Board of Clinical Psychiatry News.
The title of the book, “Passion for Patients,” by Lee H. Beecher, MD, DLFAPA, FASAM, with writer Dave Racer, MLitt (St. Paul, Minn., Alethos Press, 2017), clearly represents Dr. Beecher’s approach to his professional life: His focal interest has been his patients ever since he went to medical school and started a very long and successful practice.
Dr. Beecher’s years of practice encompass many of the changes that the practice of medicine has seen in the last 50 years.
He attended medical school when an office was the place where a physician and his patients would get together to exchange thoughts, feelings, ideas, and plans so that they would eventually work together directly and unencumbered on the same concepts that they share and that they considered crucial to their relationship.
Shortly after Dr. Beecher graduated, Medicaid and Medicare came into medical practice, together with progressive limitations, threats, and a great many unwelcome interlopers, whose mission drastically changed the doctor-patient relationship. No matter how one examines the actions of the numerous new participants – be they auditors, insurance companies, employers, or money managers – one of their main missions was to modify, qualify, re-identify, and limit the interaction between the doctor and the patient.
“What is amazing – and contrary to truth – about the current evolution of medical care reform is its manifold references to safeguarding the best interests of the patient,” Dr. Beecher wrote. “On the contrary, the medical care reformers in current vogue see the physician as but one cog in the production of a specified medical care outcome – a cog that must be greased by evidence-based medicine and managed by analytical applications derived from data, cured in the crucible of number crunching, and controlled by payment systems.”
We live in an age when forces other than medical thinking and practice are trying to define what psychiatrists do, how we do it, and whether our effort is worth being paid for. This has created lack of satisfaction in the exercise of psychiatry, early retirements, and lack of growth in many quarters. When one considers that practically all psychiatric endeavors can be traced to the efforts of devoted practitioners interested in improving the profession, one can see that the future might look bleak because people other than psychiatrists define, quantify, and evaluate the practice of our specialty.
“I escaped from managed care into the practice model that had served so well for decades prior to HMOs, [preferred provider organizations], and other externally controlled practice models,” he wrote. “My patients paid me directly.”
Dr. Beecher is a witness and protester, as well as a thinking innovator, coming to defend patients and physicians at a time when they are under attack from precisely the same forces that were supposed to help and support them.
Throughout his book, Dr. Beecher tells us the story of his many points of disagreement with the intruders and his many arguments in favor of patients and doctors, going back to the beginning of the forces that are controlling and destroying their relationship at this time and advocating principled resistance and a careful search for independence. The reader easily accompanies the author to the points when independence blends with excellence – accepting that neither one exists without the other.
Dr. Muñoz, a former president of the American Psychiatric Association, has written eight books and more than 200 articles about various aspects of psychiatry. He is a professor of psychiatry at the University of California, San Diego, and has a private practice. Dr. Muñoz and Dr. Beecher serve on the Editorial Advisory Board of Clinical Psychiatry News.
The title of the book, “Passion for Patients,” by Lee H. Beecher, MD, DLFAPA, FASAM, with writer Dave Racer, MLitt (St. Paul, Minn., Alethos Press, 2017), clearly represents Dr. Beecher’s approach to his professional life: His focal interest has been his patients ever since he went to medical school and started a very long and successful practice.
Dr. Beecher’s years of practice encompass many of the changes that the practice of medicine has seen in the last 50 years.
He attended medical school when an office was the place where a physician and his patients would get together to exchange thoughts, feelings, ideas, and plans so that they would eventually work together directly and unencumbered on the same concepts that they share and that they considered crucial to their relationship.
Shortly after Dr. Beecher graduated, Medicaid and Medicare came into medical practice, together with progressive limitations, threats, and a great many unwelcome interlopers, whose mission drastically changed the doctor-patient relationship. No matter how one examines the actions of the numerous new participants – be they auditors, insurance companies, employers, or money managers – one of their main missions was to modify, qualify, re-identify, and limit the interaction between the doctor and the patient.
“What is amazing – and contrary to truth – about the current evolution of medical care reform is its manifold references to safeguarding the best interests of the patient,” Dr. Beecher wrote. “On the contrary, the medical care reformers in current vogue see the physician as but one cog in the production of a specified medical care outcome – a cog that must be greased by evidence-based medicine and managed by analytical applications derived from data, cured in the crucible of number crunching, and controlled by payment systems.”
We live in an age when forces other than medical thinking and practice are trying to define what psychiatrists do, how we do it, and whether our effort is worth being paid for. This has created lack of satisfaction in the exercise of psychiatry, early retirements, and lack of growth in many quarters. When one considers that practically all psychiatric endeavors can be traced to the efforts of devoted practitioners interested in improving the profession, one can see that the future might look bleak because people other than psychiatrists define, quantify, and evaluate the practice of our specialty.
“I escaped from managed care into the practice model that had served so well for decades prior to HMOs, [preferred provider organizations], and other externally controlled practice models,” he wrote. “My patients paid me directly.”
Dr. Beecher is a witness and protester, as well as a thinking innovator, coming to defend patients and physicians at a time when they are under attack from precisely the same forces that were supposed to help and support them.
Throughout his book, Dr. Beecher tells us the story of his many points of disagreement with the intruders and his many arguments in favor of patients and doctors, going back to the beginning of the forces that are controlling and destroying their relationship at this time and advocating principled resistance and a careful search for independence. The reader easily accompanies the author to the points when independence blends with excellence – accepting that neither one exists without the other.
Dr. Muñoz, a former president of the American Psychiatric Association, has written eight books and more than 200 articles about various aspects of psychiatry. He is a professor of psychiatry at the University of California, San Diego, and has a private practice. Dr. Muñoz and Dr. Beecher serve on the Editorial Advisory Board of Clinical Psychiatry News.
Two boys, a dog, and our electronic health records
“Speak clearly, if you speak at all; carve every word before you let it fall.” – Oliver Wendell Holmes Sr.
One of our favorite stories is that of two boys talking to one another with a dog sitting nearby. One boy says to the other, “I taught my dog how to whistle.” Skeptically, the other boy responds, “Really? I don’t hear him whistling.” The first boys then replies, “I said I taught him. I didn’t say he learned!”
We spend a lot of time as physicians going over information with our patients, yet, according to the best data available, they retain only a small portion of what we tell them. Medication adherence rates for chronic disease range from 30% to 70%, showing that many doses of important medications are missed. Patients often don’t even remember the last instructions we give them as they are walking out of the office. This raises questions about both the way we explain information and how we can use the tools at our disposal to enhance the communication so vital to patient outcomes.

Obviously, we need to consider our words carefully and focus on teaching, not just speaking. What sets teaching apart from speaking is consideration of the learner. The better we understand our patients’ perspectives, the better the knowledge transfer will be. A simple way to address this may be better eye contact.
We have all heard the expression “the eyes are a window to the soul.” Yet, we now have computers that acts as a virtual shades, covering that window and drawing our gaze away from our patients. These shades can blind us to important clues, impeding communication and leading to misunderstanding, missed opportunity, and even patient harm. This is why some practices have chosen to use scribes to handle documentation, freeing up physicians’ eyes and addressing another obstacle to communication: time.
One of the most cited complaints from physicians is lack of time. There is an ever-growing demand on us to see more patients, manage more data, and “check off more boxes” to meet bureaucratic requirements. It should come as no surprise that these impede good patient care. We are thankful that attempts to modernize payment models are recognizing this problem. For example, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) helps to blaze the trail by focusing on care quality, practice improvement, and patient satisfaction for incentive payments. While these are early steps, they certainly point to a future more concerned with value than with volume.
As we move toward that future, we need to acknowledge that information technology can be both the problem and the answer. The current state of health IT is far from perfect. The tools we use have been designed, seemingly, around financial performance or developed to meet government requirements. It appears that neither physicians nor patients were consulted to ensure their usability or utility. Step No. 1 was getting EHRs out there. Steps 2-10 will be making them useful to clinicians, patients, and health care systems. Part of that utility will come in their ability to enhance communication.
Take patient portals, for example. The “meaningful use program” set as a requirement the ability for patients to “view, download, or transmit” their health information through electronic means. EHR vendors complied with this request but seem to have missed the intent of the measure. Patients accessing the information often are confronted with a morass of technical jargon and unfamiliar medical terms, which may even be offensive. For example, we recently spoke to a parent of a teenager with moderate intellectual disabilities. A hold-out ICD-9 code on the teen’s chart translated to her portal as “318.0 – Imbecile.” Her mother was appropriately upset, and she decided to leave the practice.
As we begin to understand technology’s advantages – and learn its pitfalls – we believe EHR vendors must enhance their offerings while engaging both providers and patients in the process of improvement. We also believe physicians need to leverage the entire care team to realize the software’s full potential. This approach may present new challenges in communication, but it also presents new opportunities. We hope that this collaborative approach will allow physicians to have more time to spend connecting with patients, leading to enhanced understanding and satisfaction.
Our knowledge of human health and disease is growing more sophisticated and so is the challenge of imparting that knowledge to patients. It is critical to find ways to do so that are relevant and understandable and give patients the tools they need to reinforce and remember what we say. This is one of the promises that we are just beginning to see fulfilled by modern EHR technology. Unlike the boy who was trying to teach his dog to whistle, our words have deep impact, and our roles as educators have never been more important.
This article was updated 3/24/17.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
“Speak clearly, if you speak at all; carve every word before you let it fall.” – Oliver Wendell Holmes Sr.
One of our favorite stories is that of two boys talking to one another with a dog sitting nearby. One boy says to the other, “I taught my dog how to whistle.” Skeptically, the other boy responds, “Really? I don’t hear him whistling.” The first boys then replies, “I said I taught him. I didn’t say he learned!”
We spend a lot of time as physicians going over information with our patients, yet, according to the best data available, they retain only a small portion of what we tell them. Medication adherence rates for chronic disease range from 30% to 70%, showing that many doses of important medications are missed. Patients often don’t even remember the last instructions we give them as they are walking out of the office. This raises questions about both the way we explain information and how we can use the tools at our disposal to enhance the communication so vital to patient outcomes.
Obviously, we need to consider our words carefully and focus on teaching, not just speaking. What sets teaching apart from speaking is consideration of the learner. The better we understand our patients’ perspectives, the better the knowledge transfer will be. A simple way to address this may be better eye contact.
We have all heard the expression “the eyes are a window to the soul.” Yet, we now have computers that acts as a virtual shades, covering that window and drawing our gaze away from our patients. These shades can blind us to important clues, impeding communication and leading to misunderstanding, missed opportunity, and even patient harm. This is why some practices have chosen to use scribes to handle documentation, freeing up physicians’ eyes and addressing another obstacle to communication: time.
One of the most cited complaints from physicians is lack of time. There is an ever-growing demand on us to see more patients, manage more data, and “check off more boxes” to meet bureaucratic requirements. It should come as no surprise that these impede good patient care. We are thankful that attempts to modernize payment models are recognizing this problem. For example, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) helps to blaze the trail by focusing on care quality, practice improvement, and patient satisfaction for incentive payments. While these are early steps, they certainly point to a future more concerned with value than with volume.
As we move toward that future, we need to acknowledge that information technology can be both the problem and the answer. The current state of health IT is far from perfect. The tools we use have been designed, seemingly, around financial performance or developed to meet government requirements. It appears that neither physicians nor patients were consulted to ensure their usability or utility. Step No. 1 was getting EHRs out there. Steps 2-10 will be making them useful to clinicians, patients, and health care systems. Part of that utility will come in their ability to enhance communication.
Take patient portals, for example. The “meaningful use program” set as a requirement the ability for patients to “view, download, or transmit” their health information through electronic means. EHR vendors complied with this request but seem to have missed the intent of the measure. Patients accessing the information often are confronted with a morass of technical jargon and unfamiliar medical terms, which may even be offensive. For example, we recently spoke to a parent of a teenager with moderate intellectual disabilities. A hold-out ICD-9 code on the teen’s chart translated to her portal as “318.0 – Imbecile.” Her mother was appropriately upset, and she decided to leave the practice.
As we begin to understand technology’s advantages – and learn its pitfalls – we believe EHR vendors must enhance their offerings while engaging both providers and patients in the process of improvement. We also believe physicians need to leverage the entire care team to realize the software’s full potential. This approach may present new challenges in communication, but it also presents new opportunities. We hope that this collaborative approach will allow physicians to have more time to spend connecting with patients, leading to enhanced understanding and satisfaction.
Our knowledge of human health and disease is growing more sophisticated and so is the challenge of imparting that knowledge to patients. It is critical to find ways to do so that are relevant and understandable and give patients the tools they need to reinforce and remember what we say. This is one of the promises that we are just beginning to see fulfilled by modern EHR technology. Unlike the boy who was trying to teach his dog to whistle, our words have deep impact, and our roles as educators have never been more important.
This article was updated 3/24/17.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
“Speak clearly, if you speak at all; carve every word before you let it fall.” – Oliver Wendell Holmes Sr.
One of our favorite stories is that of two boys talking to one another with a dog sitting nearby. One boy says to the other, “I taught my dog how to whistle.” Skeptically, the other boy responds, “Really? I don’t hear him whistling.” The first boys then replies, “I said I taught him. I didn’t say he learned!”
We spend a lot of time as physicians going over information with our patients, yet, according to the best data available, they retain only a small portion of what we tell them. Medication adherence rates for chronic disease range from 30% to 70%, showing that many doses of important medications are missed. Patients often don’t even remember the last instructions we give them as they are walking out of the office. This raises questions about both the way we explain information and how we can use the tools at our disposal to enhance the communication so vital to patient outcomes.
Obviously, we need to consider our words carefully and focus on teaching, not just speaking. What sets teaching apart from speaking is consideration of the learner. The better we understand our patients’ perspectives, the better the knowledge transfer will be. A simple way to address this may be better eye contact.
We have all heard the expression “the eyes are a window to the soul.” Yet, we now have computers that acts as a virtual shades, covering that window and drawing our gaze away from our patients. These shades can blind us to important clues, impeding communication and leading to misunderstanding, missed opportunity, and even patient harm. This is why some practices have chosen to use scribes to handle documentation, freeing up physicians’ eyes and addressing another obstacle to communication: time.
One of the most cited complaints from physicians is lack of time. There is an ever-growing demand on us to see more patients, manage more data, and “check off more boxes” to meet bureaucratic requirements. It should come as no surprise that these impede good patient care. We are thankful that attempts to modernize payment models are recognizing this problem. For example, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) helps to blaze the trail by focusing on care quality, practice improvement, and patient satisfaction for incentive payments. While these are early steps, they certainly point to a future more concerned with value than with volume.
As we move toward that future, we need to acknowledge that information technology can be both the problem and the answer. The current state of health IT is far from perfect. The tools we use have been designed, seemingly, around financial performance or developed to meet government requirements. It appears that neither physicians nor patients were consulted to ensure their usability or utility. Step No. 1 was getting EHRs out there. Steps 2-10 will be making them useful to clinicians, patients, and health care systems. Part of that utility will come in their ability to enhance communication.
Take patient portals, for example. The “meaningful use program” set as a requirement the ability for patients to “view, download, or transmit” their health information through electronic means. EHR vendors complied with this request but seem to have missed the intent of the measure. Patients accessing the information often are confronted with a morass of technical jargon and unfamiliar medical terms, which may even be offensive. For example, we recently spoke to a parent of a teenager with moderate intellectual disabilities. A hold-out ICD-9 code on the teen’s chart translated to her portal as “318.0 – Imbecile.” Her mother was appropriately upset, and she decided to leave the practice.
As we begin to understand technology’s advantages – and learn its pitfalls – we believe EHR vendors must enhance their offerings while engaging both providers and patients in the process of improvement. We also believe physicians need to leverage the entire care team to realize the software’s full potential. This approach may present new challenges in communication, but it also presents new opportunities. We hope that this collaborative approach will allow physicians to have more time to spend connecting with patients, leading to enhanced understanding and satisfaction.
Our knowledge of human health and disease is growing more sophisticated and so is the challenge of imparting that knowledge to patients. It is critical to find ways to do so that are relevant and understandable and give patients the tools they need to reinforce and remember what we say. This is one of the promises that we are just beginning to see fulfilled by modern EHR technology. Unlike the boy who was trying to teach his dog to whistle, our words have deep impact, and our roles as educators have never been more important.
This article was updated 3/24/17.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
Depression and deep brain stimulation: ‘Furor therapeuticus redux’
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
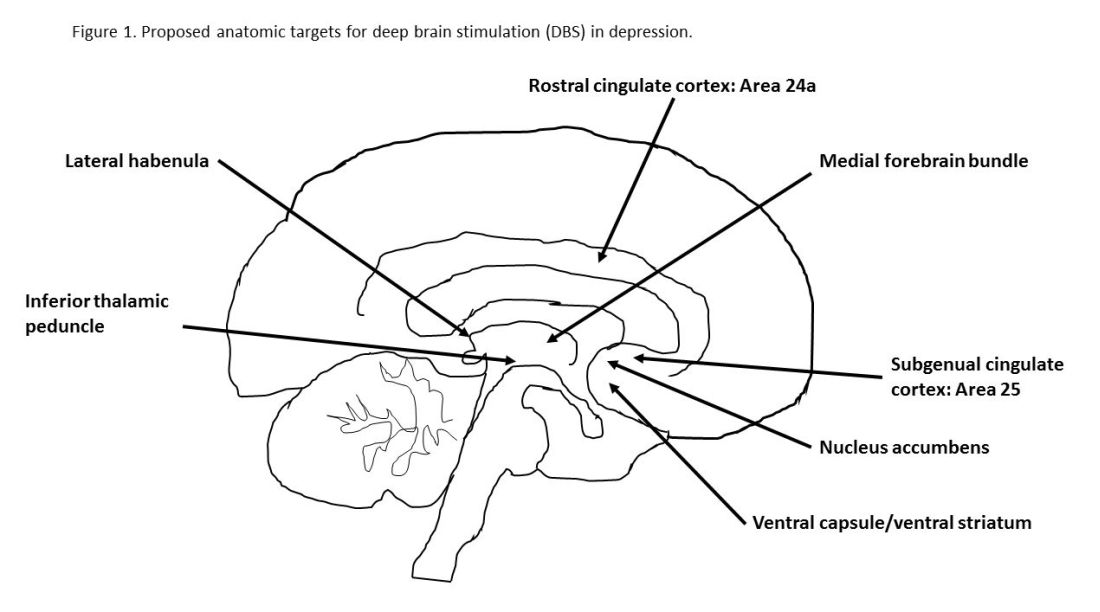
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Japan could benefit from hospital medicine expansion, leadership
The need for hospitalists continues to increase in Japan. There are approximately 9,000 hospitals in Japan, and approximately 80% of these hospitals are small- to medium-sized hospitals (<300 beds) where the need for hospital medicine is greatest. Historically, internal medicine subspecialists from nearly all subspecialties served as the primary attending physicians of hospitalized patients because inpatient internal medicine physicians, or hospitalists, did not exist.
Most subspecialists caring for hospitalized patients learned to practice internal medicine “on the fly” because they were not required to complete training in internal medicine before pursuing a subspecialty. After medical school, all graduates are required to complete a 2-year internship known as the National Obligatory Initial Postgraduate Clinical Training Program (NOIPCTP). The level of training during the NOIPCTP is similar to the third and fourth years of medical school in the United States.

The aging population and increasing complexity of hospitalized patients are the two main drivers of hospital medicine in Japan. Recently, the number of patients who have had adverse events because of inpatient medical errors has risen, and the transparency of these adverse events is making the need for hospitalists more apparent. In addition to improving the day-to-day medical management of hospitalized patients, hospitalists are needed to serve as champions of quality improvement, patient safety, and hospital throughput.
Leaders of the Japanese health care system recognize the need to improve the quality of inpatient care. The first step is to establish internal medicine as a specialty with dedicated internal medicine residency training programs. The Japanese Board of Medical Specialties approved establishing standardized, 3-year internal medicine residency training programs starting this spring, but that decision has been met with resistance for various reasons, namely concern for creating a disparity due to the shortage of internists in rural areas. Therefore, launch of this initiative has been postponed until April 2018.
In the meantime, the concept of hospital-based internists has been gradually gaining the support of subspecialists in Japan. Hospitalists are anticipated to work as the primary medical team leaders, directing and coordinating care among subspecialists in the future.
Despite its gradual spread, there are several challenges to growth. First, there are many terms for hospitalists, such as “hospital general practitioners” and “general internal medicine physicians.” A unified term for hospitalists would foster acceptance among Japanese physicians.
Additionally, some physicians, namely subspecialists, still question whether hospitalists are needed in Japan (even though potential loss of clinical revenue is not a significant concern among subspecialists).
Another challenge is lack of standardized training programs that define the skillset of hospitalists. Standardization of internal medicine training will also improve efficiency of communication between hospitalists and subspecialists.
An important milestone in the Japanese hospital medicine movement was the establishment of a society of hospitalists, known as the Japanese Hospitalist Network (JHN). The JHN has a quarterly publication (Hospitalist) targeted at junior faculty and residents that reviews topics in hospital medicine.
The JHN is affiliated with a larger society, the Japanese Society of Hospital General Medicine (JSHGM), which holds meetings twice a year. A unique offering at the next JSHGM meeting in March is a point-of-care ultrasound training workshop. Although this is the first such workshop for hospitalists in Japan, there are many training courses designed for the country’s hospitalists.
The emergence of such courses in Japan has paralleled the increasing need for hospitalists in Japan. We hope these courses for hospitalists will pave the road for the continued growth of hospital medicine in Japan.
Toru Yamada, MD
Dr. Yamada is an internist in the department of general medicine/family and community medicine at Nagoya (Japan) University and practices at Tokyo Bay Urayasu Ichikawa Medical Center in Chiba.
Taro Minami, MD
Dr. Minami is assistant professor of medicine in the division of pulmonary, critical care, and sleep medicine at Brown University in Providence, R.I., and director of ultrasound and simulation training at Memorial Hospital of Rhode Island.
Nilam J. Soni, MD, MS, FHM
Dr. Soni is associate professor of medicine in the division of hospital medicine at the University of Texas, San Antonio, and a hospitalist with the South Texas Veterans Health Care System in San Antonio.
The need for hospitalists continues to increase in Japan. There are approximately 9,000 hospitals in Japan, and approximately 80% of these hospitals are small- to medium-sized hospitals (<300 beds) where the need for hospital medicine is greatest. Historically, internal medicine subspecialists from nearly all subspecialties served as the primary attending physicians of hospitalized patients because inpatient internal medicine physicians, or hospitalists, did not exist.
Most subspecialists caring for hospitalized patients learned to practice internal medicine “on the fly” because they were not required to complete training in internal medicine before pursuing a subspecialty. After medical school, all graduates are required to complete a 2-year internship known as the National Obligatory Initial Postgraduate Clinical Training Program (NOIPCTP). The level of training during the NOIPCTP is similar to the third and fourth years of medical school in the United States.
The aging population and increasing complexity of hospitalized patients are the two main drivers of hospital medicine in Japan. Recently, the number of patients who have had adverse events because of inpatient medical errors has risen, and the transparency of these adverse events is making the need for hospitalists more apparent. In addition to improving the day-to-day medical management of hospitalized patients, hospitalists are needed to serve as champions of quality improvement, patient safety, and hospital throughput.
Leaders of the Japanese health care system recognize the need to improve the quality of inpatient care. The first step is to establish internal medicine as a specialty with dedicated internal medicine residency training programs. The Japanese Board of Medical Specialties approved establishing standardized, 3-year internal medicine residency training programs starting this spring, but that decision has been met with resistance for various reasons, namely concern for creating a disparity due to the shortage of internists in rural areas. Therefore, launch of this initiative has been postponed until April 2018.
In the meantime, the concept of hospital-based internists has been gradually gaining the support of subspecialists in Japan. Hospitalists are anticipated to work as the primary medical team leaders, directing and coordinating care among subspecialists in the future.
Despite its gradual spread, there are several challenges to growth. First, there are many terms for hospitalists, such as “hospital general practitioners” and “general internal medicine physicians.” A unified term for hospitalists would foster acceptance among Japanese physicians.
Additionally, some physicians, namely subspecialists, still question whether hospitalists are needed in Japan (even though potential loss of clinical revenue is not a significant concern among subspecialists).
Another challenge is lack of standardized training programs that define the skillset of hospitalists. Standardization of internal medicine training will also improve efficiency of communication between hospitalists and subspecialists.
An important milestone in the Japanese hospital medicine movement was the establishment of a society of hospitalists, known as the Japanese Hospitalist Network (JHN). The JHN has a quarterly publication (Hospitalist) targeted at junior faculty and residents that reviews topics in hospital medicine.
The JHN is affiliated with a larger society, the Japanese Society of Hospital General Medicine (JSHGM), which holds meetings twice a year. A unique offering at the next JSHGM meeting in March is a point-of-care ultrasound training workshop. Although this is the first such workshop for hospitalists in Japan, there are many training courses designed for the country’s hospitalists.
The emergence of such courses in Japan has paralleled the increasing need for hospitalists in Japan. We hope these courses for hospitalists will pave the road for the continued growth of hospital medicine in Japan.
Toru Yamada, MD
Dr. Yamada is an internist in the department of general medicine/family and community medicine at Nagoya (Japan) University and practices at Tokyo Bay Urayasu Ichikawa Medical Center in Chiba.
Taro Minami, MD
Dr. Minami is assistant professor of medicine in the division of pulmonary, critical care, and sleep medicine at Brown University in Providence, R.I., and director of ultrasound and simulation training at Memorial Hospital of Rhode Island.
Nilam J. Soni, MD, MS, FHM
Dr. Soni is associate professor of medicine in the division of hospital medicine at the University of Texas, San Antonio, and a hospitalist with the South Texas Veterans Health Care System in San Antonio.
The need for hospitalists continues to increase in Japan. There are approximately 9,000 hospitals in Japan, and approximately 80% of these hospitals are small- to medium-sized hospitals (<300 beds) where the need for hospital medicine is greatest. Historically, internal medicine subspecialists from nearly all subspecialties served as the primary attending physicians of hospitalized patients because inpatient internal medicine physicians, or hospitalists, did not exist.
Most subspecialists caring for hospitalized patients learned to practice internal medicine “on the fly” because they were not required to complete training in internal medicine before pursuing a subspecialty. After medical school, all graduates are required to complete a 2-year internship known as the National Obligatory Initial Postgraduate Clinical Training Program (NOIPCTP). The level of training during the NOIPCTP is similar to the third and fourth years of medical school in the United States.
The aging population and increasing complexity of hospitalized patients are the two main drivers of hospital medicine in Japan. Recently, the number of patients who have had adverse events because of inpatient medical errors has risen, and the transparency of these adverse events is making the need for hospitalists more apparent. In addition to improving the day-to-day medical management of hospitalized patients, hospitalists are needed to serve as champions of quality improvement, patient safety, and hospital throughput.
Leaders of the Japanese health care system recognize the need to improve the quality of inpatient care. The first step is to establish internal medicine as a specialty with dedicated internal medicine residency training programs. The Japanese Board of Medical Specialties approved establishing standardized, 3-year internal medicine residency training programs starting this spring, but that decision has been met with resistance for various reasons, namely concern for creating a disparity due to the shortage of internists in rural areas. Therefore, launch of this initiative has been postponed until April 2018.
In the meantime, the concept of hospital-based internists has been gradually gaining the support of subspecialists in Japan. Hospitalists are anticipated to work as the primary medical team leaders, directing and coordinating care among subspecialists in the future.
Despite its gradual spread, there are several challenges to growth. First, there are many terms for hospitalists, such as “hospital general practitioners” and “general internal medicine physicians.” A unified term for hospitalists would foster acceptance among Japanese physicians.
Additionally, some physicians, namely subspecialists, still question whether hospitalists are needed in Japan (even though potential loss of clinical revenue is not a significant concern among subspecialists).
Another challenge is lack of standardized training programs that define the skillset of hospitalists. Standardization of internal medicine training will also improve efficiency of communication between hospitalists and subspecialists.
An important milestone in the Japanese hospital medicine movement was the establishment of a society of hospitalists, known as the Japanese Hospitalist Network (JHN). The JHN has a quarterly publication (Hospitalist) targeted at junior faculty and residents that reviews topics in hospital medicine.
The JHN is affiliated with a larger society, the Japanese Society of Hospital General Medicine (JSHGM), which holds meetings twice a year. A unique offering at the next JSHGM meeting in March is a point-of-care ultrasound training workshop. Although this is the first such workshop for hospitalists in Japan, there are many training courses designed for the country’s hospitalists.
The emergence of such courses in Japan has paralleled the increasing need for hospitalists in Japan. We hope these courses for hospitalists will pave the road for the continued growth of hospital medicine in Japan.
Toru Yamada, MD
Dr. Yamada is an internist in the department of general medicine/family and community medicine at Nagoya (Japan) University and practices at Tokyo Bay Urayasu Ichikawa Medical Center in Chiba.
Taro Minami, MD
Dr. Minami is assistant professor of medicine in the division of pulmonary, critical care, and sleep medicine at Brown University in Providence, R.I., and director of ultrasound and simulation training at Memorial Hospital of Rhode Island.
Nilam J. Soni, MD, MS, FHM
Dr. Soni is associate professor of medicine in the division of hospital medicine at the University of Texas, San Antonio, and a hospitalist with the South Texas Veterans Health Care System in San Antonio.
Moving toward safer morcellation techniques
For minimally invasive surgeons throughout the world, particularly in the United States, as well as the patients we treat, April 17, 2014, is our day of infamy. It was on this day that the Food and Drug Administration recommended against the use of the electronic power morcellator. The basis of the agency’s decision was the concern about inadvertent spread of sarcomatous tissue. Many hospitals, medical centers, and hospital systems subsequently banned the use of power morcellation. With such bans, a subsequent study by Wright et al. noted a decrease in the percentage of both laparoscopic and vaginal hysterectomy (JAMA. 2016 Aug 23-30;316[8]:877-8). This is concerning when you consider that the complication rate for abdominal hysterectomy is around 17%, compared with about 4% for the minimally invasive procedure.

For this edition of the Master Class in Gynecologic Surgery, I have asked Tony Shibley, MD, to describe the PneumoLiner, the first FDA-approved bag for the purpose of contained laparoscopic morcellation. Dr. Shibley, who is in private practice in the Minneapolis area, first came to national attention because of his expertise in single-port surgery. He has been performing power morcellation in a contained system for 5 years and is the thought leader behind the design and creation of the PneumoLiner.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported receiving research funds from Espiner Medical Inc., and being a consultant to Olympus, which manufacturers the PneumoLiner.
For minimally invasive surgeons throughout the world, particularly in the United States, as well as the patients we treat, April 17, 2014, is our day of infamy. It was on this day that the Food and Drug Administration recommended against the use of the electronic power morcellator. The basis of the agency’s decision was the concern about inadvertent spread of sarcomatous tissue. Many hospitals, medical centers, and hospital systems subsequently banned the use of power morcellation. With such bans, a subsequent study by Wright et al. noted a decrease in the percentage of both laparoscopic and vaginal hysterectomy (JAMA. 2016 Aug 23-30;316[8]:877-8). This is concerning when you consider that the complication rate for abdominal hysterectomy is around 17%, compared with about 4% for the minimally invasive procedure.
For this edition of the Master Class in Gynecologic Surgery, I have asked Tony Shibley, MD, to describe the PneumoLiner, the first FDA-approved bag for the purpose of contained laparoscopic morcellation. Dr. Shibley, who is in private practice in the Minneapolis area, first came to national attention because of his expertise in single-port surgery. He has been performing power morcellation in a contained system for 5 years and is the thought leader behind the design and creation of the PneumoLiner.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported receiving research funds from Espiner Medical Inc., and being a consultant to Olympus, which manufacturers the PneumoLiner.
For minimally invasive surgeons throughout the world, particularly in the United States, as well as the patients we treat, April 17, 2014, is our day of infamy. It was on this day that the Food and Drug Administration recommended against the use of the electronic power morcellator. The basis of the agency’s decision was the concern about inadvertent spread of sarcomatous tissue. Many hospitals, medical centers, and hospital systems subsequently banned the use of power morcellation. With such bans, a subsequent study by Wright et al. noted a decrease in the percentage of both laparoscopic and vaginal hysterectomy (JAMA. 2016 Aug 23-30;316[8]:877-8). This is concerning when you consider that the complication rate for abdominal hysterectomy is around 17%, compared with about 4% for the minimally invasive procedure.
For this edition of the Master Class in Gynecologic Surgery, I have asked Tony Shibley, MD, to describe the PneumoLiner, the first FDA-approved bag for the purpose of contained laparoscopic morcellation. Dr. Shibley, who is in private practice in the Minneapolis area, first came to national attention because of his expertise in single-port surgery. He has been performing power morcellation in a contained system for 5 years and is the thought leader behind the design and creation of the PneumoLiner.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported receiving research funds from Espiner Medical Inc., and being a consultant to Olympus, which manufacturers the PneumoLiner.

Postoperative pain in women with preexisting chronic pain
Chronic pain disorders have reached epidemic levels in the United States, with the Institute of Medicine reporting more than 100 million Americans affected and health care costs more than $500 billion annually.1 Although many pain disorders are confined to the abdomen or pelvis (chronic pelvic pain, vulvodynia, irritable bowel syndrome, and bladder pain syndrome), others present with global symptoms (fibromyalgia and chronic fatigue syndrome). Women are more likely to be diagnosed with a chronic pain condition and more likely to seek treatment for chronic pain, including undergoing a surgical intervention. In fact, chronic pelvic pain alone affects upward of 20% of women in the United States, and, of the 400,000 hysterectomies performed each year (54.2%, abdominal; 16.7%, vaginal; and 16.8%, laparoscopic/robotic assisted), approximately 15% are for chronic pain.2
Neurobiology of pain
Perioperative pain control, specifically in women with preexisting pain disorders, can provide an additional challenge. Unlike acute pain, chronic pain (lasting more than 6 months) is associated with an amplified pain response of the central nervous system. This abnormal pain processing, known as centralization of pain, may result in a decrease of the inhibitory pain pathways and/or an increase of the amplification pathways, often augmenting the pain response of the original peripheral insult, specifically surgery. Because of these physiologic changes, a multimodal approach to perioperative pain should be offered, especially in women with preexisting pain. The approach ideally ought to target the different mechanisms of actions in both the peripheral and central nervous systems to provide an overall reduction in pain perception.

Preoperative visit
Perhaps the most underutilized opportunity to optimize postoperative pain is a proactive, preoperative approach. Preoperative education, including goal setting of postoperative pain expectations, has been associated with a significant reduction in postoperative opioid use, less preoperative anxiety, and a decreased length of surgical stay.3 While it is unknown exactly when this should be provided to the patient in the treatment course, it should occur prior to the day of surgery to allow for appropriate intervention.
The use of a shared decision-making model between the clinician and the chronic pain patient in the development of a pain management plan has been highly successful in improving pain outcomes in the outpatient setting.4 A similar method can be applied to the preoperative course as well. A detailed history (including the use of an opioid risk assessment tool) allows the clinician to identify patients at risk for opioid misuse and abuse. This is also an opportunity to review a plan for an opioid taper with the patient and the prescriber, if the postoperative plan includes opioid reduction/cessation. The preoperative visit may be an opportunity to adjust centrally acting medications (antidepressants, anticonvulsants) before surgery or to reduce the dose or frequency of high-risk medications, such as benzodiazepines.

Perioperative strategy
One of the most impactful ways for us, as surgeons, to reduce tissue injury and decrease pain from surgery is by offering a minimally invasive approach. The benefits of minimally invasive surgery are well established, resulting in improved perioperative pain control, decreased blood loss, lower infection rates, decreased length of hospital stay, and a faster recovery, compared with laparotomy. Because patients with chronic pain disorders are at increased risk of greater acute postoperative pain and have an elevated risk for the development of chronic postsurgical pain, a minimally invasive surgical approach should be prioritized, when available.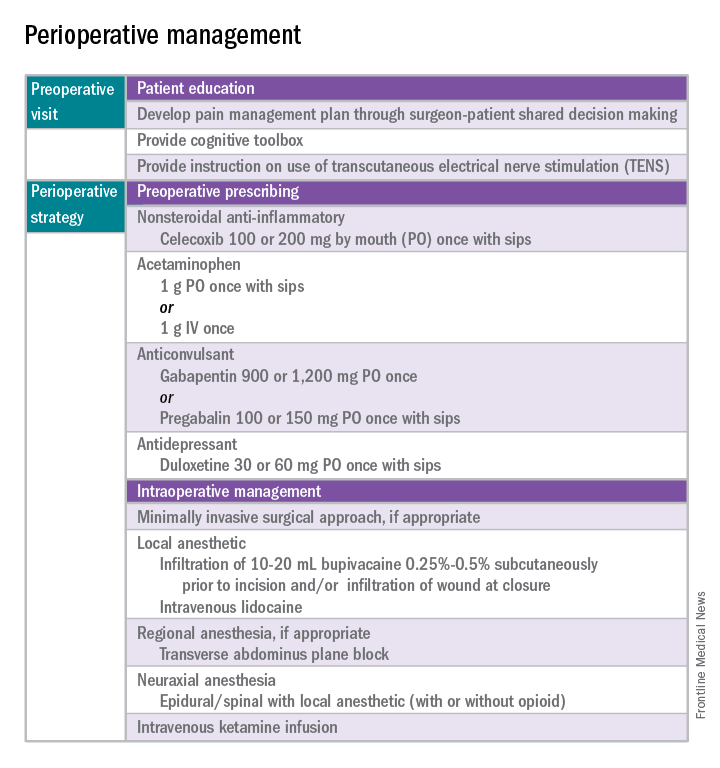
Perioperative multimodal drug therapy is associated with significant decreases in opioid consumption and reductions in acute postoperative pain.6 Recently, a multidisciplinary expert panel from the American Pain Society devised an evidence-based clinical practice guideline for postoperative pain.7 While there is no consensus as to the best regimen specific to gynecologic surgery, the general principles are similar across disciplines.
The postoperative period
Opioid-tolerant patients may experience greater pain during the first 24 hours postoperatively and require an increase in opioids, compared with opioid-naive patients.8 In the event that a postoperative patient does not respond as expected to the usual course, that patient should be evaluated for barriers to routine postoperative care, such as a surgical complication, opioid tolerance, or psychological distress. Surgeons should be aggressive with pain management immediately after surgery, even in the opioid-tolerant patient, and make short-term adjustments as needed based on the pain response. These patients will require pain medications beyond their baseline dose. Additionally, if an opioid taper is not planned in a chronic opioid user, work with the patient and the long-term opioid prescriber in restarting baseline opioid therapy outside of the acute surgical window. 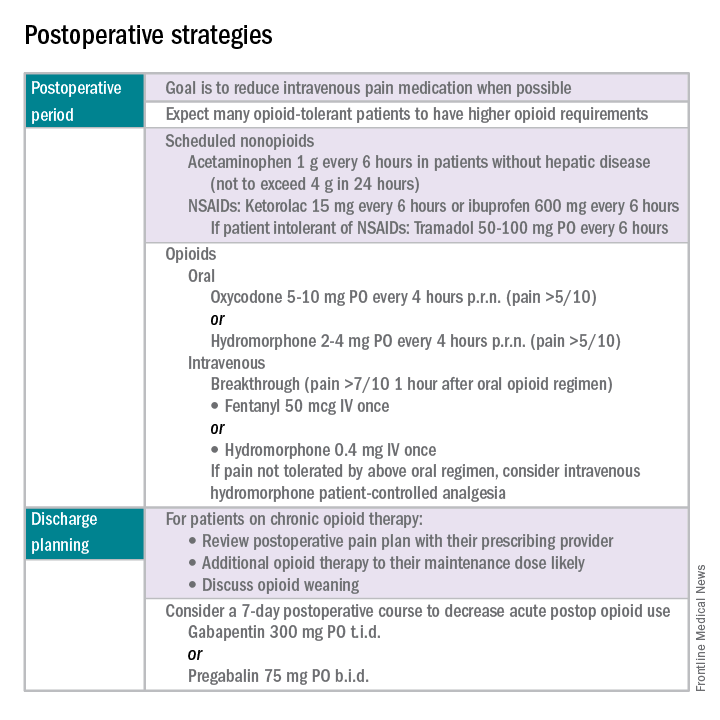
References
1. Institute of Medicine. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press, 2011.
2. Obstet Gynecol. 2013 Aug;122(2 Pt 1):233-41.
3. N Engl J Med. 1964 Apr 16;270:825-7.
4. J Pain Symptom Manage. 1999 Jul;18(1):38-48.
5. Pain. 2010 Dec;151(3):694-702.
6. Anesthesiology. 2005 Dec;103(6):1296-304.
7. J Pain. 2016 Feb;17(2):131-57.
8. Pharmacotherapy. 2008 Dec;28(12):1453-60.
Dr. Carey is the director of minimally invasive gynecologic surgery at the University of North Carolina at Chapel Hill, and specializes in the medical and surgical management of pelvic pain disorders. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC–Chapel Hill. They reported having no relevant financial disclosures.
Chronic pain disorders have reached epidemic levels in the United States, with the Institute of Medicine reporting more than 100 million Americans affected and health care costs more than $500 billion annually.1 Although many pain disorders are confined to the abdomen or pelvis (chronic pelvic pain, vulvodynia, irritable bowel syndrome, and bladder pain syndrome), others present with global symptoms (fibromyalgia and chronic fatigue syndrome). Women are more likely to be diagnosed with a chronic pain condition and more likely to seek treatment for chronic pain, including undergoing a surgical intervention. In fact, chronic pelvic pain alone affects upward of 20% of women in the United States, and, of the 400,000 hysterectomies performed each year (54.2%, abdominal; 16.7%, vaginal; and 16.8%, laparoscopic/robotic assisted), approximately 15% are for chronic pain.2
Neurobiology of pain
Perioperative pain control, specifically in women with preexisting pain disorders, can provide an additional challenge. Unlike acute pain, chronic pain (lasting more than 6 months) is associated with an amplified pain response of the central nervous system. This abnormal pain processing, known as centralization of pain, may result in a decrease of the inhibitory pain pathways and/or an increase of the amplification pathways, often augmenting the pain response of the original peripheral insult, specifically surgery. Because of these physiologic changes, a multimodal approach to perioperative pain should be offered, especially in women with preexisting pain. The approach ideally ought to target the different mechanisms of actions in both the peripheral and central nervous systems to provide an overall reduction in pain perception.
Preoperative visit
Perhaps the most underutilized opportunity to optimize postoperative pain is a proactive, preoperative approach. Preoperative education, including goal setting of postoperative pain expectations, has been associated with a significant reduction in postoperative opioid use, less preoperative anxiety, and a decreased length of surgical stay.3 While it is unknown exactly when this should be provided to the patient in the treatment course, it should occur prior to the day of surgery to allow for appropriate intervention.
The use of a shared decision-making model between the clinician and the chronic pain patient in the development of a pain management plan has been highly successful in improving pain outcomes in the outpatient setting.4 A similar method can be applied to the preoperative course as well. A detailed history (including the use of an opioid risk assessment tool) allows the clinician to identify patients at risk for opioid misuse and abuse. This is also an opportunity to review a plan for an opioid taper with the patient and the prescriber, if the postoperative plan includes opioid reduction/cessation. The preoperative visit may be an opportunity to adjust centrally acting medications (antidepressants, anticonvulsants) before surgery or to reduce the dose or frequency of high-risk medications, such as benzodiazepines.
Perioperative strategy
One of the most impactful ways for us, as surgeons, to reduce tissue injury and decrease pain from surgery is by offering a minimally invasive approach. The benefits of minimally invasive surgery are well established, resulting in improved perioperative pain control, decreased blood loss, lower infection rates, decreased length of hospital stay, and a faster recovery, compared with laparotomy. Because patients with chronic pain disorders are at increased risk of greater acute postoperative pain and have an elevated risk for the development of chronic postsurgical pain, a minimally invasive surgical approach should be prioritized, when available.
Perioperative multimodal drug therapy is associated with significant decreases in opioid consumption and reductions in acute postoperative pain.6 Recently, a multidisciplinary expert panel from the American Pain Society devised an evidence-based clinical practice guideline for postoperative pain.7 While there is no consensus as to the best regimen specific to gynecologic surgery, the general principles are similar across disciplines.
The postoperative period
Opioid-tolerant patients may experience greater pain during the first 24 hours postoperatively and require an increase in opioids, compared with opioid-naive patients.8 In the event that a postoperative patient does not respond as expected to the usual course, that patient should be evaluated for barriers to routine postoperative care, such as a surgical complication, opioid tolerance, or psychological distress. Surgeons should be aggressive with pain management immediately after surgery, even in the opioid-tolerant patient, and make short-term adjustments as needed based on the pain response. These patients will require pain medications beyond their baseline dose. Additionally, if an opioid taper is not planned in a chronic opioid user, work with the patient and the long-term opioid prescriber in restarting baseline opioid therapy outside of the acute surgical window.
References
1. Institute of Medicine. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press, 2011.
2. Obstet Gynecol. 2013 Aug;122(2 Pt 1):233-41.
3. N Engl J Med. 1964 Apr 16;270:825-7.
4. J Pain Symptom Manage. 1999 Jul;18(1):38-48.
5. Pain. 2010 Dec;151(3):694-702.
6. Anesthesiology. 2005 Dec;103(6):1296-304.
7. J Pain. 2016 Feb;17(2):131-57.
8. Pharmacotherapy. 2008 Dec;28(12):1453-60.
Dr. Carey is the director of minimally invasive gynecologic surgery at the University of North Carolina at Chapel Hill, and specializes in the medical and surgical management of pelvic pain disorders. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC–Chapel Hill. They reported having no relevant financial disclosures.
Chronic pain disorders have reached epidemic levels in the United States, with the Institute of Medicine reporting more than 100 million Americans affected and health care costs more than $500 billion annually.1 Although many pain disorders are confined to the abdomen or pelvis (chronic pelvic pain, vulvodynia, irritable bowel syndrome, and bladder pain syndrome), others present with global symptoms (fibromyalgia and chronic fatigue syndrome). Women are more likely to be diagnosed with a chronic pain condition and more likely to seek treatment for chronic pain, including undergoing a surgical intervention. In fact, chronic pelvic pain alone affects upward of 20% of women in the United States, and, of the 400,000 hysterectomies performed each year (54.2%, abdominal; 16.7%, vaginal; and 16.8%, laparoscopic/robotic assisted), approximately 15% are for chronic pain.2
Neurobiology of pain
Perioperative pain control, specifically in women with preexisting pain disorders, can provide an additional challenge. Unlike acute pain, chronic pain (lasting more than 6 months) is associated with an amplified pain response of the central nervous system. This abnormal pain processing, known as centralization of pain, may result in a decrease of the inhibitory pain pathways and/or an increase of the amplification pathways, often augmenting the pain response of the original peripheral insult, specifically surgery. Because of these physiologic changes, a multimodal approach to perioperative pain should be offered, especially in women with preexisting pain. The approach ideally ought to target the different mechanisms of actions in both the peripheral and central nervous systems to provide an overall reduction in pain perception.
Preoperative visit
Perhaps the most underutilized opportunity to optimize postoperative pain is a proactive, preoperative approach. Preoperative education, including goal setting of postoperative pain expectations, has been associated with a significant reduction in postoperative opioid use, less preoperative anxiety, and a decreased length of surgical stay.3 While it is unknown exactly when this should be provided to the patient in the treatment course, it should occur prior to the day of surgery to allow for appropriate intervention.
The use of a shared decision-making model between the clinician and the chronic pain patient in the development of a pain management plan has been highly successful in improving pain outcomes in the outpatient setting.4 A similar method can be applied to the preoperative course as well. A detailed history (including the use of an opioid risk assessment tool) allows the clinician to identify patients at risk for opioid misuse and abuse. This is also an opportunity to review a plan for an opioid taper with the patient and the prescriber, if the postoperative plan includes opioid reduction/cessation. The preoperative visit may be an opportunity to adjust centrally acting medications (antidepressants, anticonvulsants) before surgery or to reduce the dose or frequency of high-risk medications, such as benzodiazepines.
Perioperative strategy
One of the most impactful ways for us, as surgeons, to reduce tissue injury and decrease pain from surgery is by offering a minimally invasive approach. The benefits of minimally invasive surgery are well established, resulting in improved perioperative pain control, decreased blood loss, lower infection rates, decreased length of hospital stay, and a faster recovery, compared with laparotomy. Because patients with chronic pain disorders are at increased risk of greater acute postoperative pain and have an elevated risk for the development of chronic postsurgical pain, a minimally invasive surgical approach should be prioritized, when available.
Perioperative multimodal drug therapy is associated with significant decreases in opioid consumption and reductions in acute postoperative pain.6 Recently, a multidisciplinary expert panel from the American Pain Society devised an evidence-based clinical practice guideline for postoperative pain.7 While there is no consensus as to the best regimen specific to gynecologic surgery, the general principles are similar across disciplines.
The postoperative period
Opioid-tolerant patients may experience greater pain during the first 24 hours postoperatively and require an increase in opioids, compared with opioid-naive patients.8 In the event that a postoperative patient does not respond as expected to the usual course, that patient should be evaluated for barriers to routine postoperative care, such as a surgical complication, opioid tolerance, or psychological distress. Surgeons should be aggressive with pain management immediately after surgery, even in the opioid-tolerant patient, and make short-term adjustments as needed based on the pain response. These patients will require pain medications beyond their baseline dose. Additionally, if an opioid taper is not planned in a chronic opioid user, work with the patient and the long-term opioid prescriber in restarting baseline opioid therapy outside of the acute surgical window.
References
1. Institute of Medicine. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press, 2011.
2. Obstet Gynecol. 2013 Aug;122(2 Pt 1):233-41.
3. N Engl J Med. 1964 Apr 16;270:825-7.
4. J Pain Symptom Manage. 1999 Jul;18(1):38-48.
5. Pain. 2010 Dec;151(3):694-702.
6. Anesthesiology. 2005 Dec;103(6):1296-304.
7. J Pain. 2016 Feb;17(2):131-57.
8. Pharmacotherapy. 2008 Dec;28(12):1453-60.
Dr. Carey is the director of minimally invasive gynecologic surgery at the University of North Carolina at Chapel Hill, and specializes in the medical and surgical management of pelvic pain disorders. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC–Chapel Hill. They reported having no relevant financial disclosures.
When the iPad is on the other foot
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.

“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)

When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at dermnews@frontlinemedcom.com.
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.
“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)
When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at dermnews@frontlinemedcom.com.
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.
“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)
When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at dermnews@frontlinemedcom.com.
Adverse childhood experiences
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.

Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.
Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.
Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.