User login
Mycobacterium tuberculosis: Overcoming one obstacle on the road to elimination
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).

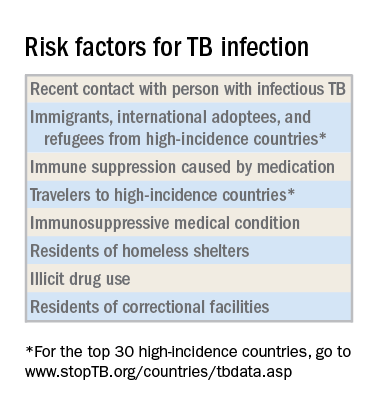
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
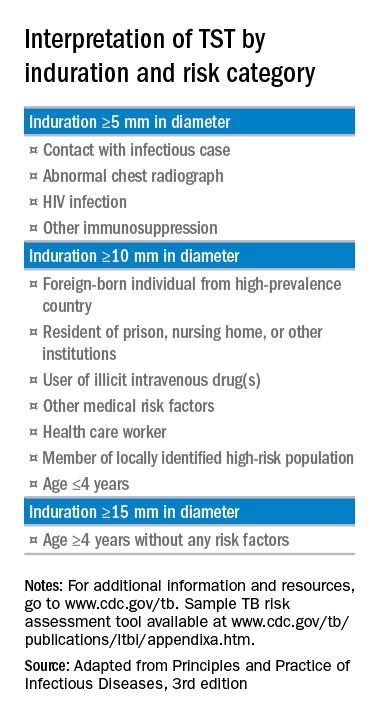
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Cooperation must overcome polarization
Each profession has its own core set of knowledge, skills, and values. For physicians, the core set of knowledge is anatomy, pathophysiology, and pharmacology. Skills include taking a history, the physical exam, and surgical procedures. The core values traditionally have been compassion and altruism. For modern medical practice, I urge adding cooperation as a core value. Medical school and the apprenticeship of residency are designed to teach, role model, foster, develop, and groom these core competencies.
Getting into medical school is highly competitive. Medical training uses methods that are very different than those used to train elite Olympic and professional athletes. Some competitiveness persists in medical school, but in general the faculty emphasizes cooperation rather than competition. The metric is not whether one student or resident is better than another. Gold and silver medals are not awarded. It is about whether each physician-to-be has passed the milestones needed to practice medicine.

But American health care is threatened by the continued polarization of our government and our society. For years both Cleveland Clinic and Dana Farber have held annual fundraising events at Mar-a-Lago. In February 2017, because of that location’s association with President Trump, some people associated with the organizations advocated boycotting those important fund-raisers. These past few months, it seems every action and every purchase has become a political statement. One restaurant mentioned immigrants on its receipt. The action went viral and caused other people to advocate boycotting the restaurant or not tipping the wait staff (“The new political battleground: Your restaurant receipt,” The Washington Post, by Maura Judkis, Feb. 14, 2017).
Secondary boycotts are an ethical quandary. In labor disputes, organized unions can go on strike. In the 1970s, Japanese cars were not welcome in the employee parking lot of a Ford assembly plant. People do vote with their pocketbook. But in labor disputes, there are legal restrictions on secondary boycotts against other companies. People do need to get along with their neighbors and so do businesses. Politics is the art of encouraging cooperation on one project amongst people who disagree about the goals of many other proposed projects. The Preamble to the United States Constitution enumerates the benefits of cooperation.
In any large-scale human endeavor, conflicts arise that may limit cooperation. Accommodating conscientious objection is the safety valve that permits cooperation when dealing with contested government endeavors such as war, abortion, and physician-assisted suicide. It is meant as a last ditch effort to maintain cohesion of both societal and individual moral integrity. But if every proposed action is met with votes divided along party lines, conscientious objection loses its moral high ground.
Judge Neil Gorsuch, the nominee for the U.S. Supreme Court, has a record of supporting religious freedom in Yellowbear v. Lambert (10th Cir. 2014). He would likely support conscientious objection in relation to assisted dying by physicians, contrary to the arguments made recently by bioethicists Julian Savulescu and Udo Schuklenk. In related news, the liberty of physicians to address gun safety was affirmed when a Florida appeals court upheld the overturning of the state’s Privacy of Firearm Owners Act.
Summing up a tumultuous month of medical ethics, I leave you with the words of Voltaire: “Cherish those who seek the truth but beware of those who find it.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
Each profession has its own core set of knowledge, skills, and values. For physicians, the core set of knowledge is anatomy, pathophysiology, and pharmacology. Skills include taking a history, the physical exam, and surgical procedures. The core values traditionally have been compassion and altruism. For modern medical practice, I urge adding cooperation as a core value. Medical school and the apprenticeship of residency are designed to teach, role model, foster, develop, and groom these core competencies.
Getting into medical school is highly competitive. Medical training uses methods that are very different than those used to train elite Olympic and professional athletes. Some competitiveness persists in medical school, but in general the faculty emphasizes cooperation rather than competition. The metric is not whether one student or resident is better than another. Gold and silver medals are not awarded. It is about whether each physician-to-be has passed the milestones needed to practice medicine.
But American health care is threatened by the continued polarization of our government and our society. For years both Cleveland Clinic and Dana Farber have held annual fundraising events at Mar-a-Lago. In February 2017, because of that location’s association with President Trump, some people associated with the organizations advocated boycotting those important fund-raisers. These past few months, it seems every action and every purchase has become a political statement. One restaurant mentioned immigrants on its receipt. The action went viral and caused other people to advocate boycotting the restaurant or not tipping the wait staff (“The new political battleground: Your restaurant receipt,” The Washington Post, by Maura Judkis, Feb. 14, 2017).
Secondary boycotts are an ethical quandary. In labor disputes, organized unions can go on strike. In the 1970s, Japanese cars were not welcome in the employee parking lot of a Ford assembly plant. People do vote with their pocketbook. But in labor disputes, there are legal restrictions on secondary boycotts against other companies. People do need to get along with their neighbors and so do businesses. Politics is the art of encouraging cooperation on one project amongst people who disagree about the goals of many other proposed projects. The Preamble to the United States Constitution enumerates the benefits of cooperation.
In any large-scale human endeavor, conflicts arise that may limit cooperation. Accommodating conscientious objection is the safety valve that permits cooperation when dealing with contested government endeavors such as war, abortion, and physician-assisted suicide. It is meant as a last ditch effort to maintain cohesion of both societal and individual moral integrity. But if every proposed action is met with votes divided along party lines, conscientious objection loses its moral high ground.
Judge Neil Gorsuch, the nominee for the U.S. Supreme Court, has a record of supporting religious freedom in Yellowbear v. Lambert (10th Cir. 2014). He would likely support conscientious objection in relation to assisted dying by physicians, contrary to the arguments made recently by bioethicists Julian Savulescu and Udo Schuklenk. In related news, the liberty of physicians to address gun safety was affirmed when a Florida appeals court upheld the overturning of the state’s Privacy of Firearm Owners Act.
Summing up a tumultuous month of medical ethics, I leave you with the words of Voltaire: “Cherish those who seek the truth but beware of those who find it.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
Each profession has its own core set of knowledge, skills, and values. For physicians, the core set of knowledge is anatomy, pathophysiology, and pharmacology. Skills include taking a history, the physical exam, and surgical procedures. The core values traditionally have been compassion and altruism. For modern medical practice, I urge adding cooperation as a core value. Medical school and the apprenticeship of residency are designed to teach, role model, foster, develop, and groom these core competencies.
Getting into medical school is highly competitive. Medical training uses methods that are very different than those used to train elite Olympic and professional athletes. Some competitiveness persists in medical school, but in general the faculty emphasizes cooperation rather than competition. The metric is not whether one student or resident is better than another. Gold and silver medals are not awarded. It is about whether each physician-to-be has passed the milestones needed to practice medicine.
But American health care is threatened by the continued polarization of our government and our society. For years both Cleveland Clinic and Dana Farber have held annual fundraising events at Mar-a-Lago. In February 2017, because of that location’s association with President Trump, some people associated with the organizations advocated boycotting those important fund-raisers. These past few months, it seems every action and every purchase has become a political statement. One restaurant mentioned immigrants on its receipt. The action went viral and caused other people to advocate boycotting the restaurant or not tipping the wait staff (“The new political battleground: Your restaurant receipt,” The Washington Post, by Maura Judkis, Feb. 14, 2017).
Secondary boycotts are an ethical quandary. In labor disputes, organized unions can go on strike. In the 1970s, Japanese cars were not welcome in the employee parking lot of a Ford assembly plant. People do vote with their pocketbook. But in labor disputes, there are legal restrictions on secondary boycotts against other companies. People do need to get along with their neighbors and so do businesses. Politics is the art of encouraging cooperation on one project amongst people who disagree about the goals of many other proposed projects. The Preamble to the United States Constitution enumerates the benefits of cooperation.
In any large-scale human endeavor, conflicts arise that may limit cooperation. Accommodating conscientious objection is the safety valve that permits cooperation when dealing with contested government endeavors such as war, abortion, and physician-assisted suicide. It is meant as a last ditch effort to maintain cohesion of both societal and individual moral integrity. But if every proposed action is met with votes divided along party lines, conscientious objection loses its moral high ground.
Judge Neil Gorsuch, the nominee for the U.S. Supreme Court, has a record of supporting religious freedom in Yellowbear v. Lambert (10th Cir. 2014). He would likely support conscientious objection in relation to assisted dying by physicians, contrary to the arguments made recently by bioethicists Julian Savulescu and Udo Schuklenk. In related news, the liberty of physicians to address gun safety was affirmed when a Florida appeals court upheld the overturning of the state’s Privacy of Firearm Owners Act.
Summing up a tumultuous month of medical ethics, I leave you with the words of Voltaire: “Cherish those who seek the truth but beware of those who find it.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
Eating disorders in transgender youth
The field of transgender health is growing. What began as a lone German physician in 1918 defying the norms of treating gender identity as a disease now has burgeoned into a field that includes 1,079 PubMed articles,two medical guidelines1,2, and a multitude of books. As we learn more about the complexity of gender and gender identity, we also are discovering potential problems that occur when providing care to our transgender patients. One is eating disorders.
A systematic review by Jones et al. showed only a handful of studies on eating disorders in transgender individuals, most of them restricted to case studies.3 In some situations, the issue of gender identity arises during treatment for an eating disorder, as the individual realizes that body dissatisfaction is due to the gender identity instead of a fear of gaining weight. In other cases, a transgender person in the process of transitioning to the affirmed gender develops an eating disorder.

There are two larger quantitative studies on eating disorders among transgender individuals. One study of 289,024 college students reveals that transgender students, compared to cisgender students, are almost five times as likely to report an eating disorder and two times as likely to use unhealthy compensatory methods (e.g., vomiting) for weight control.4 Another study of almost 2,500 teenagers shows that transgender individuals are almost three times as likely to restrict their eating, almost nine times as likely to take diet pills, and seven times as likely to take laxatives.5
The most commonly suggested reason for the possible elevated risk for eating disorders among transgender individuals is that many of them are trying to achieve the unrealistic standards of the ideal masculine or feminine body type. Another explanation is that eating disorders among transgender individuals are maladaptive coping mechanisms to stress from antitrans stigma and discrimination.4 However, these explanations are not mutually exclusive and could simultaneously drive disordered eating among transgender individuals.
To further appreciate the relationship between these two conditions, one must understand their similarities and differences. The Diagnostic Statistical Manual of Mental Disorders V characterizes eating disorders as “a persistent disturbance of eating or eating-related behavior that results in the altered consumption or absorption of food and ... significantly impairs physical health or psychosocial functioning.”6 Anorexia nervosa and bulimia nervosa are driven by fear of gaining weight or by a self-esteem unduly influenced by weight or appearance.6
Gender dysphoria, in comparison, is the distress caused by the incongruence between one’s gender identity and one’s anatomy, along with the desire to have the characteristics of one’s affirmed gender identity. This condition also could severely alter physical and psychosocial functioning,7 partly because of the distress from the incongruence, and partly because of the stress from antitrans stigma and discrimination, as an individual attempts to match the body with the gender identity8 (e.g., wearing clothing to match the gender identity).
The higher risk of developing an eating disorder among transgender individuals makes sense. Dissatisfaction with one’s body characterizes both conditions. The high standards on what is masculine or feminine affects everyone, especially transgender individuals who may feel that they’re “far behind” when they begin to transition to their affirmed gender. In addition, both involve identity. Those who have anorexia nervosa also incorporate this into their own identity.9 This is why treating an eating disorder can be very difficult.
Finally, individuals afflicted by an eating disorder or gender dysphoria engage in certain behaviors to achieve their desired appearance. However, this is where the similarities end. One major distinction between an eating disorder and gender dysphoria is the treatment approach. The goal in treating an eating disorder is to discourage the disordered behavior and encourage healthier eating habits and a more positive body image. Affirming the identity of someone with an eating disorder can be deadly, as it will encourage more disordered eating.10 In contrast, affirming the identity of someone with gender dysphoria through social transition, cross-sex hormones, and/or surgical reassignment is life-saving and therapeutic.11
There is little guidance on how to treat the these disorders simultaneously. What complicates treating both conditions at the same time is that when an eating disorder is accompanied by another mental health disorder (e.g., substance use), one condition over the other is prioritized.12 There is no guidance on whether the eating disorder or gender dysphoria should take priority over the other, or if it is possible to treat both conditions at the same time.
Strandjord et al. suggest a hierarchal approach, in which life-threatening issues (such as suicide or electrolyte disturbances) take priority.13 In addition, if the patient is malnourished, weight restoration should be the initial focus. A patient who is severely malnourished may not have the cognitive capacity nor the physiological ability to manage comorbidities such as anxiety or depression,12 much less have the capacity to process something as complex as gender and gender identity, nor understand the steps necessary for a successful transition to the affirmed gender. However, this does not mean providers should wait to successfully manage an eating disorder before addressing gender dysphoria. Studies have suggested that gender-affirming medical therapies (e.g., cross sex hormones) can be therapeutic for both gender dysphoria and eating disorder symptoms.14 Finally, because of the two ways a transgender patient with an eating disorder can present, I recommend screening for eating disorders in transgender individuals and inquiring about gender identity among those with an eating disorder. Doing so may save a life.
References
1. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
2. Adv Urol. 2012;2012:581712.
3. Int Rev Psychiatry. 2016;28(1):81-94.
4. J Adolesc Health. 2015 Aug;57(2):144-9.
5. J Adolesc Health. 2016. doi: 10.1016/j.jadohealth.2016.08.027.
6. Feeding and Eating Disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
7. Gender Dysphoria. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
8. Psychol Bull. 2003 Sep;129(5):674-97.
9. Int J Law Psychiatry. 2003 Sep-Oct;26(5):533-48.
10. Arch Gen Psychiatry. 2011 Jul;68(7):724-31.
11. Clin Endocrinol (Oxf). 2010 Feb;72(2):214-31.
12. CNS drugs. 2006;20(8):655-63.
13. Int J Eat Disord. 2015 Nov;48(7):942-5.
14. Eat Disord. 2012;20(4):300-11.
The field of transgender health is growing. What began as a lone German physician in 1918 defying the norms of treating gender identity as a disease now has burgeoned into a field that includes 1,079 PubMed articles,two medical guidelines1,2, and a multitude of books. As we learn more about the complexity of gender and gender identity, we also are discovering potential problems that occur when providing care to our transgender patients. One is eating disorders.
A systematic review by Jones et al. showed only a handful of studies on eating disorders in transgender individuals, most of them restricted to case studies.3 In some situations, the issue of gender identity arises during treatment for an eating disorder, as the individual realizes that body dissatisfaction is due to the gender identity instead of a fear of gaining weight. In other cases, a transgender person in the process of transitioning to the affirmed gender develops an eating disorder.
There are two larger quantitative studies on eating disorders among transgender individuals. One study of 289,024 college students reveals that transgender students, compared to cisgender students, are almost five times as likely to report an eating disorder and two times as likely to use unhealthy compensatory methods (e.g., vomiting) for weight control.4 Another study of almost 2,500 teenagers shows that transgender individuals are almost three times as likely to restrict their eating, almost nine times as likely to take diet pills, and seven times as likely to take laxatives.5
The most commonly suggested reason for the possible elevated risk for eating disorders among transgender individuals is that many of them are trying to achieve the unrealistic standards of the ideal masculine or feminine body type. Another explanation is that eating disorders among transgender individuals are maladaptive coping mechanisms to stress from antitrans stigma and discrimination.4 However, these explanations are not mutually exclusive and could simultaneously drive disordered eating among transgender individuals.
To further appreciate the relationship between these two conditions, one must understand their similarities and differences. The Diagnostic Statistical Manual of Mental Disorders V characterizes eating disorders as “a persistent disturbance of eating or eating-related behavior that results in the altered consumption or absorption of food and ... significantly impairs physical health or psychosocial functioning.”6 Anorexia nervosa and bulimia nervosa are driven by fear of gaining weight or by a self-esteem unduly influenced by weight or appearance.6
Gender dysphoria, in comparison, is the distress caused by the incongruence between one’s gender identity and one’s anatomy, along with the desire to have the characteristics of one’s affirmed gender identity. This condition also could severely alter physical and psychosocial functioning,7 partly because of the distress from the incongruence, and partly because of the stress from antitrans stigma and discrimination, as an individual attempts to match the body with the gender identity8 (e.g., wearing clothing to match the gender identity).
The higher risk of developing an eating disorder among transgender individuals makes sense. Dissatisfaction with one’s body characterizes both conditions. The high standards on what is masculine or feminine affects everyone, especially transgender individuals who may feel that they’re “far behind” when they begin to transition to their affirmed gender. In addition, both involve identity. Those who have anorexia nervosa also incorporate this into their own identity.9 This is why treating an eating disorder can be very difficult.
Finally, individuals afflicted by an eating disorder or gender dysphoria engage in certain behaviors to achieve their desired appearance. However, this is where the similarities end. One major distinction between an eating disorder and gender dysphoria is the treatment approach. The goal in treating an eating disorder is to discourage the disordered behavior and encourage healthier eating habits and a more positive body image. Affirming the identity of someone with an eating disorder can be deadly, as it will encourage more disordered eating.10 In contrast, affirming the identity of someone with gender dysphoria through social transition, cross-sex hormones, and/or surgical reassignment is life-saving and therapeutic.11
There is little guidance on how to treat the these disorders simultaneously. What complicates treating both conditions at the same time is that when an eating disorder is accompanied by another mental health disorder (e.g., substance use), one condition over the other is prioritized.12 There is no guidance on whether the eating disorder or gender dysphoria should take priority over the other, or if it is possible to treat both conditions at the same time.
Strandjord et al. suggest a hierarchal approach, in which life-threatening issues (such as suicide or electrolyte disturbances) take priority.13 In addition, if the patient is malnourished, weight restoration should be the initial focus. A patient who is severely malnourished may not have the cognitive capacity nor the physiological ability to manage comorbidities such as anxiety or depression,12 much less have the capacity to process something as complex as gender and gender identity, nor understand the steps necessary for a successful transition to the affirmed gender. However, this does not mean providers should wait to successfully manage an eating disorder before addressing gender dysphoria. Studies have suggested that gender-affirming medical therapies (e.g., cross sex hormones) can be therapeutic for both gender dysphoria and eating disorder symptoms.14 Finally, because of the two ways a transgender patient with an eating disorder can present, I recommend screening for eating disorders in transgender individuals and inquiring about gender identity among those with an eating disorder. Doing so may save a life.
References
1. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
2. Adv Urol. 2012;2012:581712.
3. Int Rev Psychiatry. 2016;28(1):81-94.
4. J Adolesc Health. 2015 Aug;57(2):144-9.
5. J Adolesc Health. 2016. doi: 10.1016/j.jadohealth.2016.08.027.
6. Feeding and Eating Disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
7. Gender Dysphoria. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
8. Psychol Bull. 2003 Sep;129(5):674-97.
9. Int J Law Psychiatry. 2003 Sep-Oct;26(5):533-48.
10. Arch Gen Psychiatry. 2011 Jul;68(7):724-31.
11. Clin Endocrinol (Oxf). 2010 Feb;72(2):214-31.
12. CNS drugs. 2006;20(8):655-63.
13. Int J Eat Disord. 2015 Nov;48(7):942-5.
14. Eat Disord. 2012;20(4):300-11.
The field of transgender health is growing. What began as a lone German physician in 1918 defying the norms of treating gender identity as a disease now has burgeoned into a field that includes 1,079 PubMed articles,two medical guidelines1,2, and a multitude of books. As we learn more about the complexity of gender and gender identity, we also are discovering potential problems that occur when providing care to our transgender patients. One is eating disorders.
A systematic review by Jones et al. showed only a handful of studies on eating disorders in transgender individuals, most of them restricted to case studies.3 In some situations, the issue of gender identity arises during treatment for an eating disorder, as the individual realizes that body dissatisfaction is due to the gender identity instead of a fear of gaining weight. In other cases, a transgender person in the process of transitioning to the affirmed gender develops an eating disorder.
There are two larger quantitative studies on eating disorders among transgender individuals. One study of 289,024 college students reveals that transgender students, compared to cisgender students, are almost five times as likely to report an eating disorder and two times as likely to use unhealthy compensatory methods (e.g., vomiting) for weight control.4 Another study of almost 2,500 teenagers shows that transgender individuals are almost three times as likely to restrict their eating, almost nine times as likely to take diet pills, and seven times as likely to take laxatives.5
The most commonly suggested reason for the possible elevated risk for eating disorders among transgender individuals is that many of them are trying to achieve the unrealistic standards of the ideal masculine or feminine body type. Another explanation is that eating disorders among transgender individuals are maladaptive coping mechanisms to stress from antitrans stigma and discrimination.4 However, these explanations are not mutually exclusive and could simultaneously drive disordered eating among transgender individuals.
To further appreciate the relationship between these two conditions, one must understand their similarities and differences. The Diagnostic Statistical Manual of Mental Disorders V characterizes eating disorders as “a persistent disturbance of eating or eating-related behavior that results in the altered consumption or absorption of food and ... significantly impairs physical health or psychosocial functioning.”6 Anorexia nervosa and bulimia nervosa are driven by fear of gaining weight or by a self-esteem unduly influenced by weight or appearance.6
Gender dysphoria, in comparison, is the distress caused by the incongruence between one’s gender identity and one’s anatomy, along with the desire to have the characteristics of one’s affirmed gender identity. This condition also could severely alter physical and psychosocial functioning,7 partly because of the distress from the incongruence, and partly because of the stress from antitrans stigma and discrimination, as an individual attempts to match the body with the gender identity8 (e.g., wearing clothing to match the gender identity).
The higher risk of developing an eating disorder among transgender individuals makes sense. Dissatisfaction with one’s body characterizes both conditions. The high standards on what is masculine or feminine affects everyone, especially transgender individuals who may feel that they’re “far behind” when they begin to transition to their affirmed gender. In addition, both involve identity. Those who have anorexia nervosa also incorporate this into their own identity.9 This is why treating an eating disorder can be very difficult.
Finally, individuals afflicted by an eating disorder or gender dysphoria engage in certain behaviors to achieve their desired appearance. However, this is where the similarities end. One major distinction between an eating disorder and gender dysphoria is the treatment approach. The goal in treating an eating disorder is to discourage the disordered behavior and encourage healthier eating habits and a more positive body image. Affirming the identity of someone with an eating disorder can be deadly, as it will encourage more disordered eating.10 In contrast, affirming the identity of someone with gender dysphoria through social transition, cross-sex hormones, and/or surgical reassignment is life-saving and therapeutic.11
There is little guidance on how to treat the these disorders simultaneously. What complicates treating both conditions at the same time is that when an eating disorder is accompanied by another mental health disorder (e.g., substance use), one condition over the other is prioritized.12 There is no guidance on whether the eating disorder or gender dysphoria should take priority over the other, or if it is possible to treat both conditions at the same time.
Strandjord et al. suggest a hierarchal approach, in which life-threatening issues (such as suicide or electrolyte disturbances) take priority.13 In addition, if the patient is malnourished, weight restoration should be the initial focus. A patient who is severely malnourished may not have the cognitive capacity nor the physiological ability to manage comorbidities such as anxiety or depression,12 much less have the capacity to process something as complex as gender and gender identity, nor understand the steps necessary for a successful transition to the affirmed gender. However, this does not mean providers should wait to successfully manage an eating disorder before addressing gender dysphoria. Studies have suggested that gender-affirming medical therapies (e.g., cross sex hormones) can be therapeutic for both gender dysphoria and eating disorder symptoms.14 Finally, because of the two ways a transgender patient with an eating disorder can present, I recommend screening for eating disorders in transgender individuals and inquiring about gender identity among those with an eating disorder. Doing so may save a life.
References
1. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
2. Adv Urol. 2012;2012:581712.
3. Int Rev Psychiatry. 2016;28(1):81-94.
4. J Adolesc Health. 2015 Aug;57(2):144-9.
5. J Adolesc Health. 2016. doi: 10.1016/j.jadohealth.2016.08.027.
6. Feeding and Eating Disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
7. Gender Dysphoria. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (Washington: American Psychiatric Association, 2013).
8. Psychol Bull. 2003 Sep;129(5):674-97.
9. Int J Law Psychiatry. 2003 Sep-Oct;26(5):533-48.
10. Arch Gen Psychiatry. 2011 Jul;68(7):724-31.
11. Clin Endocrinol (Oxf). 2010 Feb;72(2):214-31.
12. CNS drugs. 2006;20(8):655-63.
13. Int J Eat Disord. 2015 Nov;48(7):942-5.
14. Eat Disord. 2012;20(4):300-11.
Not enough time? Time to rethink
Raising children is a lot like drinking out of a fire hose. Feeding, cleaning, dressing, transporting, teaching, entertaining, protecting, comforting, and managing one child is demanding, but is increased exponentially by multiple children, a spouse, and a job.
In our dataset of more than 74,900 parents of 0- to 3-year-olds completing a routine previsit questionnaire about the “best” and “hardest” parts of parenting their child, the most frequent spontaneous comment for the hardest part was “time-life balance.” The goal of asking these questions is to broaden the agenda for the pediatric visit to address stresses that are highly relevant to the child’s life in the family, and their current well-being and future outcome. The hardest part also rather succinctly captures the stress I hear every day from parents coming to me not only for health supervision, but especially for child behavior problems.

Setting limits on work to free up more time is not possible for everyone. Many people are grateful to have a job at all or need multiple jobs to make ends meet. They may not be in a position to negotiate for fewer tasks, hours, or roles. But others more fortunate may have fallen into a habit of taking on extra duties, taking work home, or simply not examining where they might set limits to preserve time for themselves and their family.
Working parents may need to prepare themselves for the onslaught when they get home. If the returning parent retreats into TV, the computer, or the bedroom, it makes the children feel angry and rejected. The parent who has been managing the household for the preceding hour(s) feels resentful, unappreciated, and often exhausted. I sometimes suggest that the returning parent pause 15 minutes to take a walk before picking children up at day care or go to the gym before coming home to be ready to engage, accept, and be present for whatever happens when they open the door.
Eliciting the “hardest part” can insert a pause for some much-needed problem-solving. Pointing out to parents the value to their child of working on their own time-life balance often gives them needed permission to make changes.
Balancing time for some parents may include setting some privacy for “alone time.” Individual desire to be alone varies, but trouble getting it is universal, especially with young children who don’t even respect a closed bathroom door! Given a young child’s need for contact about every 3-5 minutes, parents need to revise their expectations, wait until after bedtime, get some help, learn to do “token” relaxation, or all of these.
Parents often feel guilty for not attending more to their child, but then feel irritable about getting behind on other chores. It can be useful to cite the fact that mothers at home full time typically spend only 20 minutes of exclusive playtime with their child. I regularly prescribe 15 minutes of “special time” daily to break this irritability cycle for both the parent and child. Getting a babysitter does not mean that the parent has to leave the house and the undone laundry. I often suggest to resource-strapped families that they pay an 8-year-old neighbor to play with their kids for an hour several times per week. While not expecting to leave the child alone with such a “sitter,” one could relax in the tub, read a magazine, or make an uninterrupted phone call to a friend with such help.
The same parents feeling the pinch of too little time often are lacking in social support, a major buffer of stress. Sometimes, the solutions overlap. For example, trading play dates with another family by taking all their kids on a regular basis and vice versa requires no money exchange. Several kids playing together are often easier to care for than one’s own with their usual sibling struggles or boredom. And sharing of this kind can build lasting friendships and social support for the adults. Another often forgotten source of adult rest coupled with social support is religious services that offer “Sunday School.” The service has built-in cues to meditation, the kids make new friends protected by accepting teachers, and the social hour builds social support for the parents.
But we can’t really insert more hours in the day, right? Actually, one of the most valuable suggestions may be for parents to keep a diary of their activities for a few days. The average American in 2015 clocked 147 minutes watching TV, 103 minutes in front of a computer, 151 minutes on smart phones, and 43 minutes with a tablet. These time wasters may not only not feel satisfying or even relaxing, but even prompt anxiety or envy, and certainly take away from sleep, exercise, and intimacy. The American Academy of Pediatrics recently provided a Media Calculator and Family Media Plan intended to help families consider these choices for their child’s media life within all the other required activities of a day (including sleep), but adults could benefit from the same approach to making decisions about how they budget their time.
By mapping out actual time spent, parents can then reevaluate and choose differently. A useful question we might ask frazzled parents is “What fills your tank?” to help them come up with a list of activities that (used to be) regenerative to put on the new schedule. Most people blurt out “go on a cruise” (not practical) when “token” activities can suffice and be immediately possible. Coach them to be creative! Instead of a cruise, take a walk around the block; instead of going to a spa, request a back rub at bedtime; instead of a movie, watch a YouTube clip. When allowing oneself to be fully present to such “tokens,” they can have immense value. The practice of mindfulness (for which many training apps are available) can heighten awareness of each moment and expand the sense of time. Meditation and yoga training both are proven to provide benefits for relaxation and well-being that can be fit into anyone’s day.
While this column is intended to help with pediatric practice, I’ll bet you thought I was talking about you! With the pace of current health care practice and emphasis on “productivity,” many pediatricians are struggling with balancing time for themselves and their families as well. All the ideas just discussed also apply to you, but maybe, just maybe, you have the resources to insist on limits on work you haven’t seized. Cherishing the years when you have children in your life is for you, too, not just your patients. Remember, “The days are long, but the years are short.”
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
Raising children is a lot like drinking out of a fire hose. Feeding, cleaning, dressing, transporting, teaching, entertaining, protecting, comforting, and managing one child is demanding, but is increased exponentially by multiple children, a spouse, and a job.
In our dataset of more than 74,900 parents of 0- to 3-year-olds completing a routine previsit questionnaire about the “best” and “hardest” parts of parenting their child, the most frequent spontaneous comment for the hardest part was “time-life balance.” The goal of asking these questions is to broaden the agenda for the pediatric visit to address stresses that are highly relevant to the child’s life in the family, and their current well-being and future outcome. The hardest part also rather succinctly captures the stress I hear every day from parents coming to me not only for health supervision, but especially for child behavior problems.
Setting limits on work to free up more time is not possible for everyone. Many people are grateful to have a job at all or need multiple jobs to make ends meet. They may not be in a position to negotiate for fewer tasks, hours, or roles. But others more fortunate may have fallen into a habit of taking on extra duties, taking work home, or simply not examining where they might set limits to preserve time for themselves and their family.
Working parents may need to prepare themselves for the onslaught when they get home. If the returning parent retreats into TV, the computer, or the bedroom, it makes the children feel angry and rejected. The parent who has been managing the household for the preceding hour(s) feels resentful, unappreciated, and often exhausted. I sometimes suggest that the returning parent pause 15 minutes to take a walk before picking children up at day care or go to the gym before coming home to be ready to engage, accept, and be present for whatever happens when they open the door.
Eliciting the “hardest part” can insert a pause for some much-needed problem-solving. Pointing out to parents the value to their child of working on their own time-life balance often gives them needed permission to make changes.
Balancing time for some parents may include setting some privacy for “alone time.” Individual desire to be alone varies, but trouble getting it is universal, especially with young children who don’t even respect a closed bathroom door! Given a young child’s need for contact about every 3-5 minutes, parents need to revise their expectations, wait until after bedtime, get some help, learn to do “token” relaxation, or all of these.
Parents often feel guilty for not attending more to their child, but then feel irritable about getting behind on other chores. It can be useful to cite the fact that mothers at home full time typically spend only 20 minutes of exclusive playtime with their child. I regularly prescribe 15 minutes of “special time” daily to break this irritability cycle for both the parent and child. Getting a babysitter does not mean that the parent has to leave the house and the undone laundry. I often suggest to resource-strapped families that they pay an 8-year-old neighbor to play with their kids for an hour several times per week. While not expecting to leave the child alone with such a “sitter,” one could relax in the tub, read a magazine, or make an uninterrupted phone call to a friend with such help.
The same parents feeling the pinch of too little time often are lacking in social support, a major buffer of stress. Sometimes, the solutions overlap. For example, trading play dates with another family by taking all their kids on a regular basis and vice versa requires no money exchange. Several kids playing together are often easier to care for than one’s own with their usual sibling struggles or boredom. And sharing of this kind can build lasting friendships and social support for the adults. Another often forgotten source of adult rest coupled with social support is religious services that offer “Sunday School.” The service has built-in cues to meditation, the kids make new friends protected by accepting teachers, and the social hour builds social support for the parents.
But we can’t really insert more hours in the day, right? Actually, one of the most valuable suggestions may be for parents to keep a diary of their activities for a few days. The average American in 2015 clocked 147 minutes watching TV, 103 minutes in front of a computer, 151 minutes on smart phones, and 43 minutes with a tablet. These time wasters may not only not feel satisfying or even relaxing, but even prompt anxiety or envy, and certainly take away from sleep, exercise, and intimacy. The American Academy of Pediatrics recently provided a Media Calculator and Family Media Plan intended to help families consider these choices for their child’s media life within all the other required activities of a day (including sleep), but adults could benefit from the same approach to making decisions about how they budget their time.
By mapping out actual time spent, parents can then reevaluate and choose differently. A useful question we might ask frazzled parents is “What fills your tank?” to help them come up with a list of activities that (used to be) regenerative to put on the new schedule. Most people blurt out “go on a cruise” (not practical) when “token” activities can suffice and be immediately possible. Coach them to be creative! Instead of a cruise, take a walk around the block; instead of going to a spa, request a back rub at bedtime; instead of a movie, watch a YouTube clip. When allowing oneself to be fully present to such “tokens,” they can have immense value. The practice of mindfulness (for which many training apps are available) can heighten awareness of each moment and expand the sense of time. Meditation and yoga training both are proven to provide benefits for relaxation and well-being that can be fit into anyone’s day.
While this column is intended to help with pediatric practice, I’ll bet you thought I was talking about you! With the pace of current health care practice and emphasis on “productivity,” many pediatricians are struggling with balancing time for themselves and their families as well. All the ideas just discussed also apply to you, but maybe, just maybe, you have the resources to insist on limits on work you haven’t seized. Cherishing the years when you have children in your life is for you, too, not just your patients. Remember, “The days are long, but the years are short.”
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
Raising children is a lot like drinking out of a fire hose. Feeding, cleaning, dressing, transporting, teaching, entertaining, protecting, comforting, and managing one child is demanding, but is increased exponentially by multiple children, a spouse, and a job.
In our dataset of more than 74,900 parents of 0- to 3-year-olds completing a routine previsit questionnaire about the “best” and “hardest” parts of parenting their child, the most frequent spontaneous comment for the hardest part was “time-life balance.” The goal of asking these questions is to broaden the agenda for the pediatric visit to address stresses that are highly relevant to the child’s life in the family, and their current well-being and future outcome. The hardest part also rather succinctly captures the stress I hear every day from parents coming to me not only for health supervision, but especially for child behavior problems.
Setting limits on work to free up more time is not possible for everyone. Many people are grateful to have a job at all or need multiple jobs to make ends meet. They may not be in a position to negotiate for fewer tasks, hours, or roles. But others more fortunate may have fallen into a habit of taking on extra duties, taking work home, or simply not examining where they might set limits to preserve time for themselves and their family.
Working parents may need to prepare themselves for the onslaught when they get home. If the returning parent retreats into TV, the computer, or the bedroom, it makes the children feel angry and rejected. The parent who has been managing the household for the preceding hour(s) feels resentful, unappreciated, and often exhausted. I sometimes suggest that the returning parent pause 15 minutes to take a walk before picking children up at day care or go to the gym before coming home to be ready to engage, accept, and be present for whatever happens when they open the door.
Eliciting the “hardest part” can insert a pause for some much-needed problem-solving. Pointing out to parents the value to their child of working on their own time-life balance often gives them needed permission to make changes.
Balancing time for some parents may include setting some privacy for “alone time.” Individual desire to be alone varies, but trouble getting it is universal, especially with young children who don’t even respect a closed bathroom door! Given a young child’s need for contact about every 3-5 minutes, parents need to revise their expectations, wait until after bedtime, get some help, learn to do “token” relaxation, or all of these.
Parents often feel guilty for not attending more to their child, but then feel irritable about getting behind on other chores. It can be useful to cite the fact that mothers at home full time typically spend only 20 minutes of exclusive playtime with their child. I regularly prescribe 15 minutes of “special time” daily to break this irritability cycle for both the parent and child. Getting a babysitter does not mean that the parent has to leave the house and the undone laundry. I often suggest to resource-strapped families that they pay an 8-year-old neighbor to play with their kids for an hour several times per week. While not expecting to leave the child alone with such a “sitter,” one could relax in the tub, read a magazine, or make an uninterrupted phone call to a friend with such help.
The same parents feeling the pinch of too little time often are lacking in social support, a major buffer of stress. Sometimes, the solutions overlap. For example, trading play dates with another family by taking all their kids on a regular basis and vice versa requires no money exchange. Several kids playing together are often easier to care for than one’s own with their usual sibling struggles or boredom. And sharing of this kind can build lasting friendships and social support for the adults. Another often forgotten source of adult rest coupled with social support is religious services that offer “Sunday School.” The service has built-in cues to meditation, the kids make new friends protected by accepting teachers, and the social hour builds social support for the parents.
But we can’t really insert more hours in the day, right? Actually, one of the most valuable suggestions may be for parents to keep a diary of their activities for a few days. The average American in 2015 clocked 147 minutes watching TV, 103 minutes in front of a computer, 151 minutes on smart phones, and 43 minutes with a tablet. These time wasters may not only not feel satisfying or even relaxing, but even prompt anxiety or envy, and certainly take away from sleep, exercise, and intimacy. The American Academy of Pediatrics recently provided a Media Calculator and Family Media Plan intended to help families consider these choices for their child’s media life within all the other required activities of a day (including sleep), but adults could benefit from the same approach to making decisions about how they budget their time.
By mapping out actual time spent, parents can then reevaluate and choose differently. A useful question we might ask frazzled parents is “What fills your tank?” to help them come up with a list of activities that (used to be) regenerative to put on the new schedule. Most people blurt out “go on a cruise” (not practical) when “token” activities can suffice and be immediately possible. Coach them to be creative! Instead of a cruise, take a walk around the block; instead of going to a spa, request a back rub at bedtime; instead of a movie, watch a YouTube clip. When allowing oneself to be fully present to such “tokens,” they can have immense value. The practice of mindfulness (for which many training apps are available) can heighten awareness of each moment and expand the sense of time. Meditation and yoga training both are proven to provide benefits for relaxation and well-being that can be fit into anyone’s day.
While this column is intended to help with pediatric practice, I’ll bet you thought I was talking about you! With the pace of current health care practice and emphasis on “productivity,” many pediatricians are struggling with balancing time for themselves and their families as well. All the ideas just discussed also apply to you, but maybe, just maybe, you have the resources to insist on limits on work you haven’t seized. Cherishing the years when you have children in your life is for you, too, not just your patients. Remember, “The days are long, but the years are short.”
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
Artificial intelligence, CNN, and diagnosing melanomas
I have a breakthrough article to share with you. It’s about a technology that detects skin cancer. Before I tell you about that, however, I need to teach you a few things. For example, do you know what AI is? How about machine learning? What about CNN? (This column is a nonpolitical arena, so, no, not that CNN).
AI stands for artificial intelligence. We are surrounded by it everywhere – computers, cars, and cell phones all use AI. AI describes a machine with the ability to problem solve, to create, to understand, to learn. These are characteristics we call “intelligence,” hence, artificial intelligence.

You and I intuitively know that a picture of a chair is a chair. This is true of an folding chair, a Barcelona chair, or a Ghost chair. This ability – to intuit – is a hallmark of humans. Computers don’t intuit, they learn. We don’t need to study 3 million chairs to identify chairs. (Nor could we study 3 million pictures of chairs, a feat that would take years.) Computers, in contrast, can review 3 million pictures of chairs. And learn. In minutes.
Not only do computers learn from millions of examples, they also layer learning. For example, one set of programs will look only for lines that appear to be legs of chairs. This information is then passed on to another layer of programming that can look for seats, then another for backs, then another and another until a final layer puts it together. Do these layers remind you of something we all learned in medical school? It is analogous to the mammalian visual cortex! In the brain, one layer of neurons talks with another. In machines, one layer of programs pushes information to another. We call these machine layers “neural networks.” A convoluted neural network or CNN, therefore, describes a complex network that is analogous to brain cortex. The implications are astounding.
Things get interesting when a CNN is given a complex task to learn and a massive observational data set to learn on. With recent advances in chips called GPUs, deeply nested program layers can accomplish difficult tasks like recognizing faces, understanding voices, and avoiding a bicyclist on a foggy day. Self-driving cars, airport security, and voice-activated assistants all rely on this “deep learning.” And they are getting smarter everyday.
So, now when I say a team at Stanford University has used a CNN and deep learning to diagnose melanoma from pictures, you’ll understand what I mean. And you’ll realize computers can do something heretofore unthinkable – make diagnoses as accurately as a doctor. That story should make you both a little giddy and afraid. But wait, there’s more! Read all about it next time.
Dr. Benabio is a partner physician and chief of service for the department of dermatology of the Southern California Permanente Group in San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com . He has no disclosures related to this column.
I have a breakthrough article to share with you. It’s about a technology that detects skin cancer. Before I tell you about that, however, I need to teach you a few things. For example, do you know what AI is? How about machine learning? What about CNN? (This column is a nonpolitical arena, so, no, not that CNN).
AI stands for artificial intelligence. We are surrounded by it everywhere – computers, cars, and cell phones all use AI. AI describes a machine with the ability to problem solve, to create, to understand, to learn. These are characteristics we call “intelligence,” hence, artificial intelligence.
You and I intuitively know that a picture of a chair is a chair. This is true of an folding chair, a Barcelona chair, or a Ghost chair. This ability – to intuit – is a hallmark of humans. Computers don’t intuit, they learn. We don’t need to study 3 million chairs to identify chairs. (Nor could we study 3 million pictures of chairs, a feat that would take years.) Computers, in contrast, can review 3 million pictures of chairs. And learn. In minutes.
Not only do computers learn from millions of examples, they also layer learning. For example, one set of programs will look only for lines that appear to be legs of chairs. This information is then passed on to another layer of programming that can look for seats, then another for backs, then another and another until a final layer puts it together. Do these layers remind you of something we all learned in medical school? It is analogous to the mammalian visual cortex! In the brain, one layer of neurons talks with another. In machines, one layer of programs pushes information to another. We call these machine layers “neural networks.” A convoluted neural network or CNN, therefore, describes a complex network that is analogous to brain cortex. The implications are astounding.
Things get interesting when a CNN is given a complex task to learn and a massive observational data set to learn on. With recent advances in chips called GPUs, deeply nested program layers can accomplish difficult tasks like recognizing faces, understanding voices, and avoiding a bicyclist on a foggy day. Self-driving cars, airport security, and voice-activated assistants all rely on this “deep learning.” And they are getting smarter everyday.
So, now when I say a team at Stanford University has used a CNN and deep learning to diagnose melanoma from pictures, you’ll understand what I mean. And you’ll realize computers can do something heretofore unthinkable – make diagnoses as accurately as a doctor. That story should make you both a little giddy and afraid. But wait, there’s more! Read all about it next time.
Dr. Benabio is a partner physician and chief of service for the department of dermatology of the Southern California Permanente Group in San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com . He has no disclosures related to this column.
I have a breakthrough article to share with you. It’s about a technology that detects skin cancer. Before I tell you about that, however, I need to teach you a few things. For example, do you know what AI is? How about machine learning? What about CNN? (This column is a nonpolitical arena, so, no, not that CNN).
AI stands for artificial intelligence. We are surrounded by it everywhere – computers, cars, and cell phones all use AI. AI describes a machine with the ability to problem solve, to create, to understand, to learn. These are characteristics we call “intelligence,” hence, artificial intelligence.
You and I intuitively know that a picture of a chair is a chair. This is true of an folding chair, a Barcelona chair, or a Ghost chair. This ability – to intuit – is a hallmark of humans. Computers don’t intuit, they learn. We don’t need to study 3 million chairs to identify chairs. (Nor could we study 3 million pictures of chairs, a feat that would take years.) Computers, in contrast, can review 3 million pictures of chairs. And learn. In minutes.
Not only do computers learn from millions of examples, they also layer learning. For example, one set of programs will look only for lines that appear to be legs of chairs. This information is then passed on to another layer of programming that can look for seats, then another for backs, then another and another until a final layer puts it together. Do these layers remind you of something we all learned in medical school? It is analogous to the mammalian visual cortex! In the brain, one layer of neurons talks with another. In machines, one layer of programs pushes information to another. We call these machine layers “neural networks.” A convoluted neural network or CNN, therefore, describes a complex network that is analogous to brain cortex. The implications are astounding.
Things get interesting when a CNN is given a complex task to learn and a massive observational data set to learn on. With recent advances in chips called GPUs, deeply nested program layers can accomplish difficult tasks like recognizing faces, understanding voices, and avoiding a bicyclist on a foggy day. Self-driving cars, airport security, and voice-activated assistants all rely on this “deep learning.” And they are getting smarter everyday.
So, now when I say a team at Stanford University has used a CNN and deep learning to diagnose melanoma from pictures, you’ll understand what I mean. And you’ll realize computers can do something heretofore unthinkable – make diagnoses as accurately as a doctor. That story should make you both a little giddy and afraid. But wait, there’s more! Read all about it next time.
Dr. Benabio is a partner physician and chief of service for the department of dermatology of the Southern California Permanente Group in San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com . He has no disclosures related to this column.
Why can’t my patient have that miracle drug?
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.

Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.
Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.
Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
Open vs. endovascular for chronic mesenteric ischemia
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.

As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2

Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.
As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2
Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.
As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2
Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
FOUND IN TRANSLATION Minimal nomenclature and maximum sensitivity complicate MRD measures
In hematologic malignancies, there is a deep and direct connection between each individual patient, that patient’s symptoms, the visible cells that cause the disease, and the direct measurements and assessments of those cells. The totality of these factors helps to determine the diagnosis and treatment plan. As a butterfly needle often is sufficient for obtaining a diagnostic tumor biopsy, it is not surprising that these same diagnostic techniques are now standardly being used to monitor disease response.
The techniques differ in their limits of detection, however. With sequencing depths able to reliably detect variant allele frequencies of less than 10%, even when patients’ overt leukemia may no longer be detectable, clinicians may be left to ponder what to do with persistent “preleukemic” or “rising clones.”1-3

These patients, now more appropriately stratified for risk of recurrence, are in desperate need of better care algorithms. Standard MRD assessment by flow cytometric analysis is able to detect less than 1 x 10-4 cells. While it can be applied to most patients, its sensitivity will likely be surpassed by new and emerging genomic assays. Real time quantitative polymerase chain reaction (RT-qPCR) and next generation sequencing (NGS) require a leukemia-specific abnormality but have the potential for far greater sensitivity with deeper sequencing techniques.
Long-term follow up data in acute promyelocytic leukemia (APL) provides the illustrative example where morphologic remission is not durable in the setting of a persistent PML-RARa transcript and therapeutic goals for PCR negativity irrespective of morphology are standard. Pathologic fusion proteins are ideal for marker-driven therapy, but are found in only about 50% of patients, mainly those with APL and Philadelphia chromosome-positive leukemias.
With driver mutations identified in the majority of patients, we can be hopeful that NGS negativity may be a useful clinical endpoint. In work presented at ASH 2016 by Bartlomiej M Getta, MBBS, of Memorial Sloan Kettering Cancer Center, New York, and his colleagues, patients with concordant MRD positivity by flow cytometry and NGS had inferior outcomes, even after allogeneic transplant, compared to patients with MRD positivity on one assay but not both.5 Nonetheless, caution should be taken in early adoption of NGS as a independent marker of MRD status for two main reasons: 1) False positives and lack of standardization make current interpretation difficult. 2) The presence of “preleukemic” clones remains enigmatic – and no matter the nomenclature used, can a DNMT3A or IDH-mutant clone really be deemed “clonal hematopoiesis of indeterminate potential” when a patient has already had clonal transformation?
Conversely, not all patients reported in the work by Klco2 and Getta ultimately relapse. Thus, while it would be preferred to clear all mutant clones, as a therapeutic goal this likely would subject many patients to unnecessary toxicity. One half of the patients reported by Getta were disease free at a year with concordant flow and NGS positive MRD while patients with NGS positivity alone had outcomes equivalent to those of MRD-negative patients, highlighting that certain persistent clones in NGS-only, MRD-positive patients might be amenable to immunotherapy, either with checkpoint inhibitors or allogeneic transplant. Insight into which clones remain quiescent and which are more sinister will require more investigation, but there does seem to be an additive role to NGS-positivity, whereby all MRD is not created equal and the precision and clinical utility of MRD status will likely take on nuanced nomenclature.
References
1. Jan, M. et al. Clonal evolution of preleukemic hematopoietic stem cells precedes human acute myeloid leukemia. Science Translational Medicine 4, 149ra118, doi: 10.1126/scitranslmed.3004315 (2012).
2. Klco, J. M. et al. Association Between Mutation Clearance After Induction Therapy and Outcomes in Acute Myeloid Leukemia. JAMA 2015;314:811-22. doi: 10.1001/jama.2015.9643.
3. Wong, T. N. et al. Rapid expansion of preexisting nonleukemic hematopoietic clones frequently follows induction therapy for de novo AML. Blood 2016;127:893-7. doi: 10.1182/blood-2015-10-677021 (2016).
4. Lane, A. A. et al. Results from Ongoing Phase II Trial of SL-401 As Consolidation Therapy in Patients with Acute Myeloid Leukemia (AML) in Remission with High Relapse Risk Including Minimal Residual Disease (MRD), Abstract 215, ASH 2016.
5. Getta, B. M. et al. Multicolor Flow Cytometry and Multi-Gene Next Generation Sequencing Are Complimentary and Highly Predictive for Relapse in Acute Myeloid Leukemia Following Allogeneic Hematopoietic Stem Cell Transplant, Abstract 834, ASH 2016.
Dr. Viny is with the Memorial Sloan-Kettering Cancer Center, New York, where he is a clinical instructor, on the staff of the leukemia service, and a clinical researcher in The Ross Levine Lab. Contact Dr. Viny at vinya@mskcc.org.
In hematologic malignancies, there is a deep and direct connection between each individual patient, that patient’s symptoms, the visible cells that cause the disease, and the direct measurements and assessments of those cells. The totality of these factors helps to determine the diagnosis and treatment plan. As a butterfly needle often is sufficient for obtaining a diagnostic tumor biopsy, it is not surprising that these same diagnostic techniques are now standardly being used to monitor disease response.
The techniques differ in their limits of detection, however. With sequencing depths able to reliably detect variant allele frequencies of less than 10%, even when patients’ overt leukemia may no longer be detectable, clinicians may be left to ponder what to do with persistent “preleukemic” or “rising clones.”1-3
These patients, now more appropriately stratified for risk of recurrence, are in desperate need of better care algorithms. Standard MRD assessment by flow cytometric analysis is able to detect less than 1 x 10-4 cells. While it can be applied to most patients, its sensitivity will likely be surpassed by new and emerging genomic assays. Real time quantitative polymerase chain reaction (RT-qPCR) and next generation sequencing (NGS) require a leukemia-specific abnormality but have the potential for far greater sensitivity with deeper sequencing techniques.
Long-term follow up data in acute promyelocytic leukemia (APL) provides the illustrative example where morphologic remission is not durable in the setting of a persistent PML-RARa transcript and therapeutic goals for PCR negativity irrespective of morphology are standard. Pathologic fusion proteins are ideal for marker-driven therapy, but are found in only about 50% of patients, mainly those with APL and Philadelphia chromosome-positive leukemias.
With driver mutations identified in the majority of patients, we can be hopeful that NGS negativity may be a useful clinical endpoint. In work presented at ASH 2016 by Bartlomiej M Getta, MBBS, of Memorial Sloan Kettering Cancer Center, New York, and his colleagues, patients with concordant MRD positivity by flow cytometry and NGS had inferior outcomes, even after allogeneic transplant, compared to patients with MRD positivity on one assay but not both.5 Nonetheless, caution should be taken in early adoption of NGS as a independent marker of MRD status for two main reasons: 1) False positives and lack of standardization make current interpretation difficult. 2) The presence of “preleukemic” clones remains enigmatic – and no matter the nomenclature used, can a DNMT3A or IDH-mutant clone really be deemed “clonal hematopoiesis of indeterminate potential” when a patient has already had clonal transformation?
Conversely, not all patients reported in the work by Klco2 and Getta ultimately relapse. Thus, while it would be preferred to clear all mutant clones, as a therapeutic goal this likely would subject many patients to unnecessary toxicity. One half of the patients reported by Getta were disease free at a year with concordant flow and NGS positive MRD while patients with NGS positivity alone had outcomes equivalent to those of MRD-negative patients, highlighting that certain persistent clones in NGS-only, MRD-positive patients might be amenable to immunotherapy, either with checkpoint inhibitors or allogeneic transplant. Insight into which clones remain quiescent and which are more sinister will require more investigation, but there does seem to be an additive role to NGS-positivity, whereby all MRD is not created equal and the precision and clinical utility of MRD status will likely take on nuanced nomenclature.
References
1. Jan, M. et al. Clonal evolution of preleukemic hematopoietic stem cells precedes human acute myeloid leukemia. Science Translational Medicine 4, 149ra118, doi: 10.1126/scitranslmed.3004315 (2012).
2. Klco, J. M. et al. Association Between Mutation Clearance After Induction Therapy and Outcomes in Acute Myeloid Leukemia. JAMA 2015;314:811-22. doi: 10.1001/jama.2015.9643.
3. Wong, T. N. et al. Rapid expansion of preexisting nonleukemic hematopoietic clones frequently follows induction therapy for de novo AML. Blood 2016;127:893-7. doi: 10.1182/blood-2015-10-677021 (2016).
4. Lane, A. A. et al. Results from Ongoing Phase II Trial of SL-401 As Consolidation Therapy in Patients with Acute Myeloid Leukemia (AML) in Remission with High Relapse Risk Including Minimal Residual Disease (MRD), Abstract 215, ASH 2016.
5. Getta, B. M. et al. Multicolor Flow Cytometry and Multi-Gene Next Generation Sequencing Are Complimentary and Highly Predictive for Relapse in Acute Myeloid Leukemia Following Allogeneic Hematopoietic Stem Cell Transplant, Abstract 834, ASH 2016.
Dr. Viny is with the Memorial Sloan-Kettering Cancer Center, New York, where he is a clinical instructor, on the staff of the leukemia service, and a clinical researcher in The Ross Levine Lab. Contact Dr. Viny at vinya@mskcc.org.
In hematologic malignancies, there is a deep and direct connection between each individual patient, that patient’s symptoms, the visible cells that cause the disease, and the direct measurements and assessments of those cells. The totality of these factors helps to determine the diagnosis and treatment plan. As a butterfly needle often is sufficient for obtaining a diagnostic tumor biopsy, it is not surprising that these same diagnostic techniques are now standardly being used to monitor disease response.
The techniques differ in their limits of detection, however. With sequencing depths able to reliably detect variant allele frequencies of less than 10%, even when patients’ overt leukemia may no longer be detectable, clinicians may be left to ponder what to do with persistent “preleukemic” or “rising clones.”1-3
These patients, now more appropriately stratified for risk of recurrence, are in desperate need of better care algorithms. Standard MRD assessment by flow cytometric analysis is able to detect less than 1 x 10-4 cells. While it can be applied to most patients, its sensitivity will likely be surpassed by new and emerging genomic assays. Real time quantitative polymerase chain reaction (RT-qPCR) and next generation sequencing (NGS) require a leukemia-specific abnormality but have the potential for far greater sensitivity with deeper sequencing techniques.
Long-term follow up data in acute promyelocytic leukemia (APL) provides the illustrative example where morphologic remission is not durable in the setting of a persistent PML-RARa transcript and therapeutic goals for PCR negativity irrespective of morphology are standard. Pathologic fusion proteins are ideal for marker-driven therapy, but are found in only about 50% of patients, mainly those with APL and Philadelphia chromosome-positive leukemias.
With driver mutations identified in the majority of patients, we can be hopeful that NGS negativity may be a useful clinical endpoint. In work presented at ASH 2016 by Bartlomiej M Getta, MBBS, of Memorial Sloan Kettering Cancer Center, New York, and his colleagues, patients with concordant MRD positivity by flow cytometry and NGS had inferior outcomes, even after allogeneic transplant, compared to patients with MRD positivity on one assay but not both.5 Nonetheless, caution should be taken in early adoption of NGS as a independent marker of MRD status for two main reasons: 1) False positives and lack of standardization make current interpretation difficult. 2) The presence of “preleukemic” clones remains enigmatic – and no matter the nomenclature used, can a DNMT3A or IDH-mutant clone really be deemed “clonal hematopoiesis of indeterminate potential” when a patient has already had clonal transformation?
Conversely, not all patients reported in the work by Klco2 and Getta ultimately relapse. Thus, while it would be preferred to clear all mutant clones, as a therapeutic goal this likely would subject many patients to unnecessary toxicity. One half of the patients reported by Getta were disease free at a year with concordant flow and NGS positive MRD while patients with NGS positivity alone had outcomes equivalent to those of MRD-negative patients, highlighting that certain persistent clones in NGS-only, MRD-positive patients might be amenable to immunotherapy, either with checkpoint inhibitors or allogeneic transplant. Insight into which clones remain quiescent and which are more sinister will require more investigation, but there does seem to be an additive role to NGS-positivity, whereby all MRD is not created equal and the precision and clinical utility of MRD status will likely take on nuanced nomenclature.
References
1. Jan, M. et al. Clonal evolution of preleukemic hematopoietic stem cells precedes human acute myeloid leukemia. Science Translational Medicine 4, 149ra118, doi: 10.1126/scitranslmed.3004315 (2012).
2. Klco, J. M. et al. Association Between Mutation Clearance After Induction Therapy and Outcomes in Acute Myeloid Leukemia. JAMA 2015;314:811-22. doi: 10.1001/jama.2015.9643.
3. Wong, T. N. et al. Rapid expansion of preexisting nonleukemic hematopoietic clones frequently follows induction therapy for de novo AML. Blood 2016;127:893-7. doi: 10.1182/blood-2015-10-677021 (2016).
4. Lane, A. A. et al. Results from Ongoing Phase II Trial of SL-401 As Consolidation Therapy in Patients with Acute Myeloid Leukemia (AML) in Remission with High Relapse Risk Including Minimal Residual Disease (MRD), Abstract 215, ASH 2016.
5. Getta, B. M. et al. Multicolor Flow Cytometry and Multi-Gene Next Generation Sequencing Are Complimentary and Highly Predictive for Relapse in Acute Myeloid Leukemia Following Allogeneic Hematopoietic Stem Cell Transplant, Abstract 834, ASH 2016.
Dr. Viny is with the Memorial Sloan-Kettering Cancer Center, New York, where he is a clinical instructor, on the staff of the leukemia service, and a clinical researcher in The Ross Levine Lab. Contact Dr. Viny at vinya@mskcc.org.
Professional time
As I write this article, the snow is piling up outside. While Cleveland’s west side citizens are raking up the last of fallen leaves, its east siders will dig out of 2 feet of snow. The lake effect is affecting us. The snow plow trucks vainly clear a path only for it to disappear in minutes. There seems to be no end to the torrents of white flakes that are each unique and tiny, but in aggregate uniform and overwhelming.
A blizzard of patients awaits my return from the annual meeting of the American Society of Hematology in San Diego. Like snowflakes, they are each unique, but in aggregate can be overwhelming. Plowing through a clinic, we go from patient to patient knowing that we will eventually see them all, then return to our offices or home to finish the labor of charting.

For some physicians, this is a daily reality. Whether patients in the clinic, or cases in the queue, some hematologists revisit the storm every day. Most, however, are engaged in an academic practice where at least some respite from direct patient care is offered. Whether teaching medical students, analyzing data, participating in administrative meetings, or writing manuscripts, most of us do something more beyond the clinic. We do this during our “protected time.”
But what are we protected from? Patients and their concerns? Really, this is what we want to be protected from?
“Protected” is the wrong word. The time we spend pursuing academics is really “professional” time. Some centers call it administrative time, but this also falls short. Time allotted to nonclinical activities keeps us fresh, sharpens our intellect, and ultimately helps our patients. Professional time helps prevent burnout by making us more present when we are in clinic. Professional time allows for scientific inquiry to advance treatments, and encourages continuing education to remain at the cutting edge of technology. Professional time, though, competes with patient time and that tension can drive disengagement.
Patients, and their problems, do not operate according to half-day clinic schedules. When there exists any professional time, patient time is always interfering. The interference becomes more acute as academic success increases and the allotted professional time seems inadequate. Hematologists then start to blame patients for interfering with their careers. A pernicious disdain for patient care may develop because it interrupts the academic motivations that drive many physicians once they get a taste of success. Manifestations of this attitude include dread of inpatient service, negotiations to reduce clinic time for research, and refusal to see or sometimes even talk to patients when not assigned to clinic. The more successful the academic hematologist becomes, the less he or she wants to be troubled with patients without whom professional success could not have been achieved.
The professional and patient time balance is as important to recognize as work and life balance, as one tension directly impacts the other. When nature sends a snowstorm, a warm home allows survival, but if one never ventures from home, the beauty and grandeur of nature is lost. True satisfaction comes from a balance of the two and no one person knows how best to accomplish it. I believe we can learn to manage our professional and patient time better by exchanging ideas and best practices. Please email me at kalaycm@ccf.org with your ideas and we will post as many as we can on the Hematology News website for all to learn from.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
As I write this article, the snow is piling up outside. While Cleveland’s west side citizens are raking up the last of fallen leaves, its east siders will dig out of 2 feet of snow. The lake effect is affecting us. The snow plow trucks vainly clear a path only for it to disappear in minutes. There seems to be no end to the torrents of white flakes that are each unique and tiny, but in aggregate uniform and overwhelming.
A blizzard of patients awaits my return from the annual meeting of the American Society of Hematology in San Diego. Like snowflakes, they are each unique, but in aggregate can be overwhelming. Plowing through a clinic, we go from patient to patient knowing that we will eventually see them all, then return to our offices or home to finish the labor of charting.
For some physicians, this is a daily reality. Whether patients in the clinic, or cases in the queue, some hematologists revisit the storm every day. Most, however, are engaged in an academic practice where at least some respite from direct patient care is offered. Whether teaching medical students, analyzing data, participating in administrative meetings, or writing manuscripts, most of us do something more beyond the clinic. We do this during our “protected time.”
But what are we protected from? Patients and their concerns? Really, this is what we want to be protected from?
“Protected” is the wrong word. The time we spend pursuing academics is really “professional” time. Some centers call it administrative time, but this also falls short. Time allotted to nonclinical activities keeps us fresh, sharpens our intellect, and ultimately helps our patients. Professional time helps prevent burnout by making us more present when we are in clinic. Professional time allows for scientific inquiry to advance treatments, and encourages continuing education to remain at the cutting edge of technology. Professional time, though, competes with patient time and that tension can drive disengagement.
Patients, and their problems, do not operate according to half-day clinic schedules. When there exists any professional time, patient time is always interfering. The interference becomes more acute as academic success increases and the allotted professional time seems inadequate. Hematologists then start to blame patients for interfering with their careers. A pernicious disdain for patient care may develop because it interrupts the academic motivations that drive many physicians once they get a taste of success. Manifestations of this attitude include dread of inpatient service, negotiations to reduce clinic time for research, and refusal to see or sometimes even talk to patients when not assigned to clinic. The more successful the academic hematologist becomes, the less he or she wants to be troubled with patients without whom professional success could not have been achieved.
The professional and patient time balance is as important to recognize as work and life balance, as one tension directly impacts the other. When nature sends a snowstorm, a warm home allows survival, but if one never ventures from home, the beauty and grandeur of nature is lost. True satisfaction comes from a balance of the two and no one person knows how best to accomplish it. I believe we can learn to manage our professional and patient time better by exchanging ideas and best practices. Please email me at kalaycm@ccf.org with your ideas and we will post as many as we can on the Hematology News website for all to learn from.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
As I write this article, the snow is piling up outside. While Cleveland’s west side citizens are raking up the last of fallen leaves, its east siders will dig out of 2 feet of snow. The lake effect is affecting us. The snow plow trucks vainly clear a path only for it to disappear in minutes. There seems to be no end to the torrents of white flakes that are each unique and tiny, but in aggregate uniform and overwhelming.
A blizzard of patients awaits my return from the annual meeting of the American Society of Hematology in San Diego. Like snowflakes, they are each unique, but in aggregate can be overwhelming. Plowing through a clinic, we go from patient to patient knowing that we will eventually see them all, then return to our offices or home to finish the labor of charting.
For some physicians, this is a daily reality. Whether patients in the clinic, or cases in the queue, some hematologists revisit the storm every day. Most, however, are engaged in an academic practice where at least some respite from direct patient care is offered. Whether teaching medical students, analyzing data, participating in administrative meetings, or writing manuscripts, most of us do something more beyond the clinic. We do this during our “protected time.”
But what are we protected from? Patients and their concerns? Really, this is what we want to be protected from?
“Protected” is the wrong word. The time we spend pursuing academics is really “professional” time. Some centers call it administrative time, but this also falls short. Time allotted to nonclinical activities keeps us fresh, sharpens our intellect, and ultimately helps our patients. Professional time helps prevent burnout by making us more present when we are in clinic. Professional time allows for scientific inquiry to advance treatments, and encourages continuing education to remain at the cutting edge of technology. Professional time, though, competes with patient time and that tension can drive disengagement.
Patients, and their problems, do not operate according to half-day clinic schedules. When there exists any professional time, patient time is always interfering. The interference becomes more acute as academic success increases and the allotted professional time seems inadequate. Hematologists then start to blame patients for interfering with their careers. A pernicious disdain for patient care may develop because it interrupts the academic motivations that drive many physicians once they get a taste of success. Manifestations of this attitude include dread of inpatient service, negotiations to reduce clinic time for research, and refusal to see or sometimes even talk to patients when not assigned to clinic. The more successful the academic hematologist becomes, the less he or she wants to be troubled with patients without whom professional success could not have been achieved.
The professional and patient time balance is as important to recognize as work and life balance, as one tension directly impacts the other. When nature sends a snowstorm, a warm home allows survival, but if one never ventures from home, the beauty and grandeur of nature is lost. True satisfaction comes from a balance of the two and no one person knows how best to accomplish it. I believe we can learn to manage our professional and patient time better by exchanging ideas and best practices. Please email me at kalaycm@ccf.org with your ideas and we will post as many as we can on the Hematology News website for all to learn from.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.

SVS (Specialty of Vascular Surgery): Why, How, and When
The November 2016 issue of Annals of Vascular Surgery was devoted entirely to the history of the American Board of Vascular Surgery (ABVS) and the unsuccessful attempt to establish an independent specialty of Vascular Surgery. The manuscript is methodically detailed by founders of the ABVS, James Stanley, MD, and Frank Veith, MD, and supplemented by commentaries from past board members as well as thought leaders in vascular surgery. In an attempt to maintain neutrality, readers are also provided with many of the documents that were either supportive or contrary to the development of the ABVS. Most senior vascular surgeons will recall the intense discussion and sometimes acrimonious arguments that accompanied the progress of the Board and its failed attempt to be recognized by the American Board of Medical Specialties (ABMS).
Younger vascular surgeons may not realize that the ABVS was ever established. Some may not even realize that, until relatively recently, vascular surgeons were not able to claim board certification even if they had completed a fellowship. Accordingly, as an historical document detailing an important aspect of the evolution of our specialty, this edition of Annals of Vascular surgery is a must read.
Cogent arguments both for and against an independent specialty were made by the leaders of our specialty at the time that the ABVS was being developed. Unfortunately, this did not lead to a uniform policy but rather long-standing, rancorous, and bitter divisions that in all probability prevented the ABVS from being recognized by the ABMS. Despite this failure, the debate around this issue elevated the stature of vascular surgery when the American Board of Surgery conceded that vascular surgeons could now claim “Board certification in vascular surgery” without having to be trained in general surgery. However, all important modifications to the current design of vascular residency and fellowship programs still need to be decided by the American Board of Surgery and its associated Residency Review Committee for Surgery (RRC-S). Further, many hospital administrators subordinate vascular surgery by insisting that vascular surgeons' interests be controlled by general or cardiothoracic surgeons.
Most notably, this issue of Annals reignites fundamental questions that are at the heart of our existence as vascular surgeons. For example, has vascular surgery matured sufficiently to be considered a distinct specialty equivalent to other surgical specialties such as orthopedics, colorectal, urology, and otolaryngology surgery? If so, why did this not occur earlier? Does it warrant becoming independent from the American Board of Surgery such that only vascular surgeons will be in control of training programs, graduate education, and the practice of vascular surgery at universities, hospitals, and community practices? More significantly, why should these institutions, health agencies and the lay public care that there is a separate independent specialty – vascular surgery? The answer to these questions becomes apparent by an analysis of four historic elements that have changed since the ABVS was being formulated.
First, and perhaps most importantly, the argument for an ABVS occurred when vascular surgery had just entered the endovascular revolution. How difficult it must have been for those early vascular surgeons to realize that within a few years perhaps upward of 70%-80% of all procedures would not be performed in a standard operating room but rather an angiography suite, cath lab, or hybrid room? Could they envisage an era where abdominal aneurysms were treated not only without a laparotomy scar but even without a groin incision? That carotid endarterectomy may be replaced by a stent or that varicose veins would be abolished by an outpatient laser procedure? Without such foresight, general surgeons and even those early vascular surgeons had to believe that vascular surgery, as then practiced, required general surgery training.
A second historical reality that impacted the progress of the ABVS was the fragmentation of the governance of vascular surgeons on both a local and national level. Locally, university surgeons, assuming that vascular surgery was an intrinsic part of general surgery, may have been concerned that their leadership roles would be diminished if they were relegated to division heads rather than department chairs. Nationally, there existed three bodies representing vascular surgeons, each with its own leadership and motivations. These were the Society for Vascular Surgery (SVS), the North American chapter of the International Society for Cardiovascular Surgery (NA-ISCVS) which later changed its name to the American Association for Vascular Surgery (AAVS) and the Society for Clinical Vascular Surgery (SCVS).
The SVS at the time was predominantly an academic association with its primary goal being the annual meeting. The SCVS was a casual community of predominantly private practice surgeons. The AAVS was the most representative but it did not have the infrastructure to be a dominant force. Further, there also existed the Association of Program Directors in Vascular Surgery (APDVS). This division was compounded by the formation of the ABVS. Despite three polls of vascular surgeons, the majority of which supported an independent specialty, the divided leadership of these various organizations refused to abide by the voice of their respective memberships. The destructive internecine arguments that developed are detailed in the Annals manuscript, and this disunion of the vascular community and its leadership clearly hampered a collective identity.
Thirdly, the members of the ABVS argued that an independent specialty was necessary in order to train vascular surgeons in the evolving field of endovascular procedures. However, many established leaders balked at this proposal and resisted incorporating such training into their programs. Their refusal to assist in the education of endo-competent vascular surgeons and the development of an independent specialty allowed cardiologists and interventional radiologists to infiltrate the field. Now, the argument for an independent specialty of vascular surgery is not so much with general surgeons but rather with Cardiologists and interventional radiologists.
Fourth, the ABS at the time still considered itself an authoritative Board protective of an all-encompassing General surgery. Its leaders feared that separation of vascular surgery would lead to a stampede with other subspecialties such as pediatric and hand surgery clamoring for independence.
It is not surprising that there was little chance that the ABVS would succeed. However, much can be learned from this historical review that predicts a new initiative in today’s healthcare environment will likely be successful and benefit not only vascular surgeons but also their patients.
In this modern era the practice of vascular surgery involves multiple disciplines and various forms of therapy. As I have frequently claimed, vascular surgeons “operate, medicate, and dilate”. When so much of what vascular surgeons do is beyond the realm of open surgery, wouldn’t most agree that vascular surgery should not be controlled by a governing body, the ABS, whose primary motivation remains operative therapy?
On the other hand, the current ABS recognizes all its subspecialties are similarly morphing away from general surgery and so the ABS is evolving into a Federation of quasi-independent boards. Accordingly, it is likely to be less resistant to a fully independent vascular specialty board existing under its umbrella organization.
Concomitantly, heads of divisions of vascular surgery in universities as well as community practice hospitals can no longer rely on the largesse of chairpersons of general or cardiothoracic surgery since most will not have clinical vascular experience. Accordingly, these vascular surgeons must have complete autonomy with titles and positions elevated to chairs of a department rather than a division.
Vascular surgeons should also acknowledge that they can no longer claim total control of vascular patients. Vascular internists, cardiologists, interventional radiologists and even interventional nephrologists are all involved. An attempt to block further inroads will alienate these other specialties who in turn will attempt to deny us independent specialty designation. We need to work in conjunction, while remaining the only specialty that can offer all forms of therapy. By providing quality care vascular surgeons will gain the respect of government, insurance agencies and our patients and thus support for our independent status.
Although our small specialty of probably no more than 3000 active vascular surgeons is still represented by many differing societies, the SVS has now become the de facto union of vascular surgeons. It has the ability to bring together all factions and it has the finances, the manpower and the organizational structure to represent all vascular surgeons on the national and international level. As such it is already recognized by governmental and commercial agencies as the authoritative voice of vascular surgeons. The SVS, which has built a strong relationship with the APDVS, is also in a strong position to support and facilitate the undergraduate and postgraduate training of vascular surgeons and strengthen all aspects of an independent specialty of vascular surgery. Although there may still be disagreements about whether vascular surgery should be an independent specialty, the SVS should be the organization that serves as “convener” and ultimately implements the decision of the majority of vascular surgeons. It may be appropriate that the SVS Executive Committee authorizes one more survey of its membership to determine whether we continue to seek independent specialty designation and to approve it as a binding membership referendum.
The plusses and minuses should be carefully defined and much thought given to how the questions in the opinion poll are defined. Whatever the results, they should stand, and be implemented.
Finally, as a practicing vascular surgeon and not necessarily in my role as medical editor of the Vascular Specialist I would like to thank Dr. Timothy M. Sullivan and the Annals of Vascular Surgery for publication of this review and Drs. Stanley and Veith for providing us with the gift of historical perspective. Now our goal should not be to repeat history, but rather to learn from our past experiences. I am sure most will commend Drs. Stanley and Veith and all the other vascular surgeons who dedicated so much of their time in the pursuit of an independent vascular specialty.
However, we should not demonize those that held a contrary view, for most were a product of their times. As recent Nobel Laureate Bob Dylan has written, “The times they are a’changing,” and they are changing in our favor. ■
The November 2016 issue of Annals of Vascular Surgery was devoted entirely to the history of the American Board of Vascular Surgery (ABVS) and the unsuccessful attempt to establish an independent specialty of Vascular Surgery. The manuscript is methodically detailed by founders of the ABVS, James Stanley, MD, and Frank Veith, MD, and supplemented by commentaries from past board members as well as thought leaders in vascular surgery. In an attempt to maintain neutrality, readers are also provided with many of the documents that were either supportive or contrary to the development of the ABVS. Most senior vascular surgeons will recall the intense discussion and sometimes acrimonious arguments that accompanied the progress of the Board and its failed attempt to be recognized by the American Board of Medical Specialties (ABMS).
Younger vascular surgeons may not realize that the ABVS was ever established. Some may not even realize that, until relatively recently, vascular surgeons were not able to claim board certification even if they had completed a fellowship. Accordingly, as an historical document detailing an important aspect of the evolution of our specialty, this edition of Annals of Vascular surgery is a must read.
Cogent arguments both for and against an independent specialty were made by the leaders of our specialty at the time that the ABVS was being developed. Unfortunately, this did not lead to a uniform policy but rather long-standing, rancorous, and bitter divisions that in all probability prevented the ABVS from being recognized by the ABMS. Despite this failure, the debate around this issue elevated the stature of vascular surgery when the American Board of Surgery conceded that vascular surgeons could now claim “Board certification in vascular surgery” without having to be trained in general surgery. However, all important modifications to the current design of vascular residency and fellowship programs still need to be decided by the American Board of Surgery and its associated Residency Review Committee for Surgery (RRC-S). Further, many hospital administrators subordinate vascular surgery by insisting that vascular surgeons' interests be controlled by general or cardiothoracic surgeons.
Most notably, this issue of Annals reignites fundamental questions that are at the heart of our existence as vascular surgeons. For example, has vascular surgery matured sufficiently to be considered a distinct specialty equivalent to other surgical specialties such as orthopedics, colorectal, urology, and otolaryngology surgery? If so, why did this not occur earlier? Does it warrant becoming independent from the American Board of Surgery such that only vascular surgeons will be in control of training programs, graduate education, and the practice of vascular surgery at universities, hospitals, and community practices? More significantly, why should these institutions, health agencies and the lay public care that there is a separate independent specialty – vascular surgery? The answer to these questions becomes apparent by an analysis of four historic elements that have changed since the ABVS was being formulated.
First, and perhaps most importantly, the argument for an ABVS occurred when vascular surgery had just entered the endovascular revolution. How difficult it must have been for those early vascular surgeons to realize that within a few years perhaps upward of 70%-80% of all procedures would not be performed in a standard operating room but rather an angiography suite, cath lab, or hybrid room? Could they envisage an era where abdominal aneurysms were treated not only without a laparotomy scar but even without a groin incision? That carotid endarterectomy may be replaced by a stent or that varicose veins would be abolished by an outpatient laser procedure? Without such foresight, general surgeons and even those early vascular surgeons had to believe that vascular surgery, as then practiced, required general surgery training.
A second historical reality that impacted the progress of the ABVS was the fragmentation of the governance of vascular surgeons on both a local and national level. Locally, university surgeons, assuming that vascular surgery was an intrinsic part of general surgery, may have been concerned that their leadership roles would be diminished if they were relegated to division heads rather than department chairs. Nationally, there existed three bodies representing vascular surgeons, each with its own leadership and motivations. These were the Society for Vascular Surgery (SVS), the North American chapter of the International Society for Cardiovascular Surgery (NA-ISCVS) which later changed its name to the American Association for Vascular Surgery (AAVS) and the Society for Clinical Vascular Surgery (SCVS).
The SVS at the time was predominantly an academic association with its primary goal being the annual meeting. The SCVS was a casual community of predominantly private practice surgeons. The AAVS was the most representative but it did not have the infrastructure to be a dominant force. Further, there also existed the Association of Program Directors in Vascular Surgery (APDVS). This division was compounded by the formation of the ABVS. Despite three polls of vascular surgeons, the majority of which supported an independent specialty, the divided leadership of these various organizations refused to abide by the voice of their respective memberships. The destructive internecine arguments that developed are detailed in the Annals manuscript, and this disunion of the vascular community and its leadership clearly hampered a collective identity.
Thirdly, the members of the ABVS argued that an independent specialty was necessary in order to train vascular surgeons in the evolving field of endovascular procedures. However, many established leaders balked at this proposal and resisted incorporating such training into their programs. Their refusal to assist in the education of endo-competent vascular surgeons and the development of an independent specialty allowed cardiologists and interventional radiologists to infiltrate the field. Now, the argument for an independent specialty of vascular surgery is not so much with general surgeons but rather with Cardiologists and interventional radiologists.
Fourth, the ABS at the time still considered itself an authoritative Board protective of an all-encompassing General surgery. Its leaders feared that separation of vascular surgery would lead to a stampede with other subspecialties such as pediatric and hand surgery clamoring for independence.
It is not surprising that there was little chance that the ABVS would succeed. However, much can be learned from this historical review that predicts a new initiative in today’s healthcare environment will likely be successful and benefit not only vascular surgeons but also their patients.
In this modern era the practice of vascular surgery involves multiple disciplines and various forms of therapy. As I have frequently claimed, vascular surgeons “operate, medicate, and dilate”. When so much of what vascular surgeons do is beyond the realm of open surgery, wouldn’t most agree that vascular surgery should not be controlled by a governing body, the ABS, whose primary motivation remains operative therapy?
On the other hand, the current ABS recognizes all its subspecialties are similarly morphing away from general surgery and so the ABS is evolving into a Federation of quasi-independent boards. Accordingly, it is likely to be less resistant to a fully independent vascular specialty board existing under its umbrella organization.
Concomitantly, heads of divisions of vascular surgery in universities as well as community practice hospitals can no longer rely on the largesse of chairpersons of general or cardiothoracic surgery since most will not have clinical vascular experience. Accordingly, these vascular surgeons must have complete autonomy with titles and positions elevated to chairs of a department rather than a division.
Vascular surgeons should also acknowledge that they can no longer claim total control of vascular patients. Vascular internists, cardiologists, interventional radiologists and even interventional nephrologists are all involved. An attempt to block further inroads will alienate these other specialties who in turn will attempt to deny us independent specialty designation. We need to work in conjunction, while remaining the only specialty that can offer all forms of therapy. By providing quality care vascular surgeons will gain the respect of government, insurance agencies and our patients and thus support for our independent status.
Although our small specialty of probably no more than 3000 active vascular surgeons is still represented by many differing societies, the SVS has now become the de facto union of vascular surgeons. It has the ability to bring together all factions and it has the finances, the manpower and the organizational structure to represent all vascular surgeons on the national and international level. As such it is already recognized by governmental and commercial agencies as the authoritative voice of vascular surgeons. The SVS, which has built a strong relationship with the APDVS, is also in a strong position to support and facilitate the undergraduate and postgraduate training of vascular surgeons and strengthen all aspects of an independent specialty of vascular surgery. Although there may still be disagreements about whether vascular surgery should be an independent specialty, the SVS should be the organization that serves as “convener” and ultimately implements the decision of the majority of vascular surgeons. It may be appropriate that the SVS Executive Committee authorizes one more survey of its membership to determine whether we continue to seek independent specialty designation and to approve it as a binding membership referendum.
The plusses and minuses should be carefully defined and much thought given to how the questions in the opinion poll are defined. Whatever the results, they should stand, and be implemented.
Finally, as a practicing vascular surgeon and not necessarily in my role as medical editor of the Vascular Specialist I would like to thank Dr. Timothy M. Sullivan and the Annals of Vascular Surgery for publication of this review and Drs. Stanley and Veith for providing us with the gift of historical perspective. Now our goal should not be to repeat history, but rather to learn from our past experiences. I am sure most will commend Drs. Stanley and Veith and all the other vascular surgeons who dedicated so much of their time in the pursuit of an independent vascular specialty.
However, we should not demonize those that held a contrary view, for most were a product of their times. As recent Nobel Laureate Bob Dylan has written, “The times they are a’changing,” and they are changing in our favor. ■
The November 2016 issue of Annals of Vascular Surgery was devoted entirely to the history of the American Board of Vascular Surgery (ABVS) and the unsuccessful attempt to establish an independent specialty of Vascular Surgery. The manuscript is methodically detailed by founders of the ABVS, James Stanley, MD, and Frank Veith, MD, and supplemented by commentaries from past board members as well as thought leaders in vascular surgery. In an attempt to maintain neutrality, readers are also provided with many of the documents that were either supportive or contrary to the development of the ABVS. Most senior vascular surgeons will recall the intense discussion and sometimes acrimonious arguments that accompanied the progress of the Board and its failed attempt to be recognized by the American Board of Medical Specialties (ABMS).
Younger vascular surgeons may not realize that the ABVS was ever established. Some may not even realize that, until relatively recently, vascular surgeons were not able to claim board certification even if they had completed a fellowship. Accordingly, as an historical document detailing an important aspect of the evolution of our specialty, this edition of Annals of Vascular surgery is a must read.
Cogent arguments both for and against an independent specialty were made by the leaders of our specialty at the time that the ABVS was being developed. Unfortunately, this did not lead to a uniform policy but rather long-standing, rancorous, and bitter divisions that in all probability prevented the ABVS from being recognized by the ABMS. Despite this failure, the debate around this issue elevated the stature of vascular surgery when the American Board of Surgery conceded that vascular surgeons could now claim “Board certification in vascular surgery” without having to be trained in general surgery. However, all important modifications to the current design of vascular residency and fellowship programs still need to be decided by the American Board of Surgery and its associated Residency Review Committee for Surgery (RRC-S). Further, many hospital administrators subordinate vascular surgery by insisting that vascular surgeons' interests be controlled by general or cardiothoracic surgeons.
Most notably, this issue of Annals reignites fundamental questions that are at the heart of our existence as vascular surgeons. For example, has vascular surgery matured sufficiently to be considered a distinct specialty equivalent to other surgical specialties such as orthopedics, colorectal, urology, and otolaryngology surgery? If so, why did this not occur earlier? Does it warrant becoming independent from the American Board of Surgery such that only vascular surgeons will be in control of training programs, graduate education, and the practice of vascular surgery at universities, hospitals, and community practices? More significantly, why should these institutions, health agencies and the lay public care that there is a separate independent specialty – vascular surgery? The answer to these questions becomes apparent by an analysis of four historic elements that have changed since the ABVS was being formulated.
First, and perhaps most importantly, the argument for an ABVS occurred when vascular surgery had just entered the endovascular revolution. How difficult it must have been for those early vascular surgeons to realize that within a few years perhaps upward of 70%-80% of all procedures would not be performed in a standard operating room but rather an angiography suite, cath lab, or hybrid room? Could they envisage an era where abdominal aneurysms were treated not only without a laparotomy scar but even without a groin incision? That carotid endarterectomy may be replaced by a stent or that varicose veins would be abolished by an outpatient laser procedure? Without such foresight, general surgeons and even those early vascular surgeons had to believe that vascular surgery, as then practiced, required general surgery training.
A second historical reality that impacted the progress of the ABVS was the fragmentation of the governance of vascular surgeons on both a local and national level. Locally, university surgeons, assuming that vascular surgery was an intrinsic part of general surgery, may have been concerned that their leadership roles would be diminished if they were relegated to division heads rather than department chairs. Nationally, there existed three bodies representing vascular surgeons, each with its own leadership and motivations. These were the Society for Vascular Surgery (SVS), the North American chapter of the International Society for Cardiovascular Surgery (NA-ISCVS) which later changed its name to the American Association for Vascular Surgery (AAVS) and the Society for Clinical Vascular Surgery (SCVS).
The SVS at the time was predominantly an academic association with its primary goal being the annual meeting. The SCVS was a casual community of predominantly private practice surgeons. The AAVS was the most representative but it did not have the infrastructure to be a dominant force. Further, there also existed the Association of Program Directors in Vascular Surgery (APDVS). This division was compounded by the formation of the ABVS. Despite three polls of vascular surgeons, the majority of which supported an independent specialty, the divided leadership of these various organizations refused to abide by the voice of their respective memberships. The destructive internecine arguments that developed are detailed in the Annals manuscript, and this disunion of the vascular community and its leadership clearly hampered a collective identity.
Thirdly, the members of the ABVS argued that an independent specialty was necessary in order to train vascular surgeons in the evolving field of endovascular procedures. However, many established leaders balked at this proposal and resisted incorporating such training into their programs. Their refusal to assist in the education of endo-competent vascular surgeons and the development of an independent specialty allowed cardiologists and interventional radiologists to infiltrate the field. Now, the argument for an independent specialty of vascular surgery is not so much with general surgeons but rather with Cardiologists and interventional radiologists.
Fourth, the ABS at the time still considered itself an authoritative Board protective of an all-encompassing General surgery. Its leaders feared that separation of vascular surgery would lead to a stampede with other subspecialties such as pediatric and hand surgery clamoring for independence.
It is not surprising that there was little chance that the ABVS would succeed. However, much can be learned from this historical review that predicts a new initiative in today’s healthcare environment will likely be successful and benefit not only vascular surgeons but also their patients.
In this modern era the practice of vascular surgery involves multiple disciplines and various forms of therapy. As I have frequently claimed, vascular surgeons “operate, medicate, and dilate”. When so much of what vascular surgeons do is beyond the realm of open surgery, wouldn’t most agree that vascular surgery should not be controlled by a governing body, the ABS, whose primary motivation remains operative therapy?
On the other hand, the current ABS recognizes all its subspecialties are similarly morphing away from general surgery and so the ABS is evolving into a Federation of quasi-independent boards. Accordingly, it is likely to be less resistant to a fully independent vascular specialty board existing under its umbrella organization.
Concomitantly, heads of divisions of vascular surgery in universities as well as community practice hospitals can no longer rely on the largesse of chairpersons of general or cardiothoracic surgery since most will not have clinical vascular experience. Accordingly, these vascular surgeons must have complete autonomy with titles and positions elevated to chairs of a department rather than a division.
Vascular surgeons should also acknowledge that they can no longer claim total control of vascular patients. Vascular internists, cardiologists, interventional radiologists and even interventional nephrologists are all involved. An attempt to block further inroads will alienate these other specialties who in turn will attempt to deny us independent specialty designation. We need to work in conjunction, while remaining the only specialty that can offer all forms of therapy. By providing quality care vascular surgeons will gain the respect of government, insurance agencies and our patients and thus support for our independent status.
Although our small specialty of probably no more than 3000 active vascular surgeons is still represented by many differing societies, the SVS has now become the de facto union of vascular surgeons. It has the ability to bring together all factions and it has the finances, the manpower and the organizational structure to represent all vascular surgeons on the national and international level. As such it is already recognized by governmental and commercial agencies as the authoritative voice of vascular surgeons. The SVS, which has built a strong relationship with the APDVS, is also in a strong position to support and facilitate the undergraduate and postgraduate training of vascular surgeons and strengthen all aspects of an independent specialty of vascular surgery. Although there may still be disagreements about whether vascular surgery should be an independent specialty, the SVS should be the organization that serves as “convener” and ultimately implements the decision of the majority of vascular surgeons. It may be appropriate that the SVS Executive Committee authorizes one more survey of its membership to determine whether we continue to seek independent specialty designation and to approve it as a binding membership referendum.
The plusses and minuses should be carefully defined and much thought given to how the questions in the opinion poll are defined. Whatever the results, they should stand, and be implemented.
Finally, as a practicing vascular surgeon and not necessarily in my role as medical editor of the Vascular Specialist I would like to thank Dr. Timothy M. Sullivan and the Annals of Vascular Surgery for publication of this review and Drs. Stanley and Veith for providing us with the gift of historical perspective. Now our goal should not be to repeat history, but rather to learn from our past experiences. I am sure most will commend Drs. Stanley and Veith and all the other vascular surgeons who dedicated so much of their time in the pursuit of an independent vascular specialty.
However, we should not demonize those that held a contrary view, for most were a product of their times. As recent Nobel Laureate Bob Dylan has written, “The times they are a’changing,” and they are changing in our favor. ■