User login
Thinking Outside the DRG Box
When choosing quality improvement activities, hospitalists have no shortage of choices. In this column, I offer a strategic guide for hospitalists as they assess where best to spend their energy as the shift to value-based care progresses. This includes the introduction of MACRA, the landmark new payment program for doctors and other clinicians (aka the Medicare Access and CHIP Reauthorization Act of 2015), with its incentives for participation in alternative payment models.
Since 1983, Medicare has reimbursed hospitals using a lump-sum payment known as a diagnosis-related group, or DRG. Since then, hospitals have focused a good deal of their energy on removing needless expenses from the hospitalization to improve their bottom line, recognizing the DRG payment they receive is relatively fixed. To this end, a major strategy has been to use hospitalists to decrease length of stay and “right size” the utilization of in-hospital tests and treatments.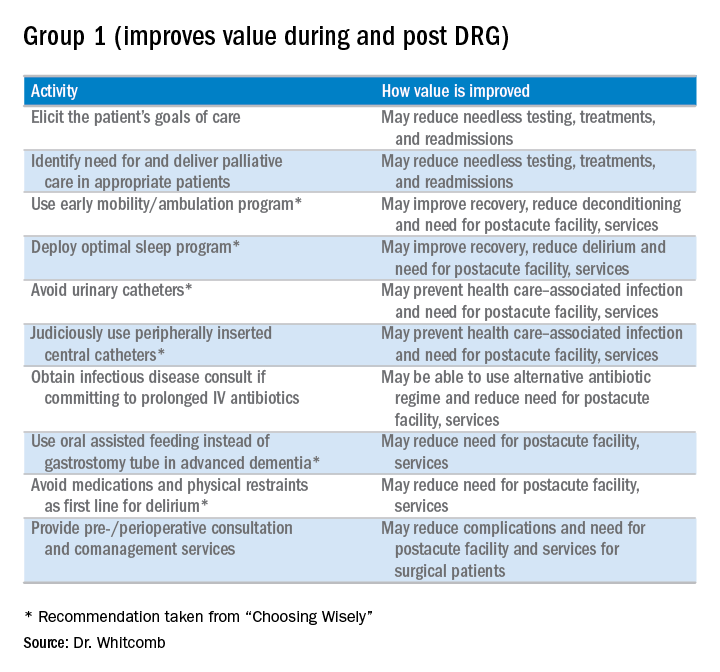
However, things are changing as we enter the era of alternative payment models such as accountable care organizations (ACOs) and bundled payments. The lens Medicare (and, to a great extent, commercial payors) peers through to assess inpatient hospital costs is the DRG payment amount. Beyond that, Medicare has little visibility into the actual costs hospitals incur. Since hospital spending equates to the payment amount for a DRG, it becomes apparent that the incremental opportunity for hospitalists to improve value (quality divided by cost) in alternative payment models stems from payments outside the DRG. Such payments include those related to the post-acute period such as nursing and rehabilitation facilities, readmissions, and part B activity (e.g., consultants and outpatient tests).
What does this mean for hospitalists? MACRA begins in 2019, but initial payments will be based on 2017 performance. The associated advantage of participating in an “advanced alternative payment model” where there is accountability for care beyond the hospitalization is that hospitalists will be rewarded for taking costs out of the post-acute time period.
To be clear, hospitalists should remain agents of in-hospital efficiency and quality. After all, that is how we add value to the hospitals in which we practice. All things being equal, however, hospitalists should focus on practices that will improve value beyond the four walls of the hospital.
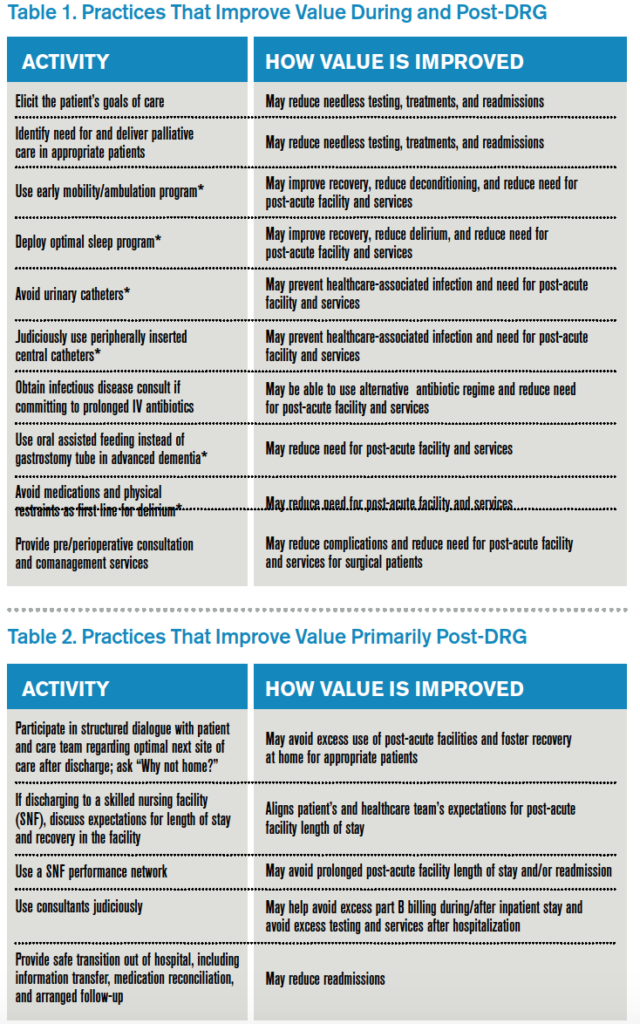
Here is my shortlist of these practices. While there is crossover between the categories, I divide the practices into those that improve value during the DRG period and also post-DRG and those that improve value primarily post-DRG (thanks to Choosing Wisely for contributing to the recommendations with an asterisk1):

Thinking outside the DRG box will require an adjustment to the approach taken by hospitalists because the current demands are often more than enough for a day’s work. Hospitalists will be called upon to innovate and fashion better approaches to care. This will require support by other members of the healthcare team so hospitalists can work smarter, not harder, to meet the requirements of a changing healthcare system. A prerequisite is better payment models that align financial incentives so that providing higher-value care is sustainable and appropriately rewarded.

Reference
Clinician lists. Choosing Wisely website. Accessed October 25, 2016.
When choosing quality improvement activities, hospitalists have no shortage of choices. In this column, I offer a strategic guide for hospitalists as they assess where best to spend their energy as the shift to value-based care progresses. This includes the introduction of MACRA, the landmark new payment program for doctors and other clinicians (aka the Medicare Access and CHIP Reauthorization Act of 2015), with its incentives for participation in alternative payment models.
Since 1983, Medicare has reimbursed hospitals using a lump-sum payment known as a diagnosis-related group, or DRG. Since then, hospitals have focused a good deal of their energy on removing needless expenses from the hospitalization to improve their bottom line, recognizing the DRG payment they receive is relatively fixed. To this end, a major strategy has been to use hospitalists to decrease length of stay and “right size” the utilization of in-hospital tests and treatments.
However, things are changing as we enter the era of alternative payment models such as accountable care organizations (ACOs) and bundled payments. The lens Medicare (and, to a great extent, commercial payors) peers through to assess inpatient hospital costs is the DRG payment amount. Beyond that, Medicare has little visibility into the actual costs hospitals incur. Since hospital spending equates to the payment amount for a DRG, it becomes apparent that the incremental opportunity for hospitalists to improve value (quality divided by cost) in alternative payment models stems from payments outside the DRG. Such payments include those related to the post-acute period such as nursing and rehabilitation facilities, readmissions, and part B activity (e.g., consultants and outpatient tests).
What does this mean for hospitalists? MACRA begins in 2019, but initial payments will be based on 2017 performance. The associated advantage of participating in an “advanced alternative payment model” where there is accountability for care beyond the hospitalization is that hospitalists will be rewarded for taking costs out of the post-acute time period.
To be clear, hospitalists should remain agents of in-hospital efficiency and quality. After all, that is how we add value to the hospitals in which we practice. All things being equal, however, hospitalists should focus on practices that will improve value beyond the four walls of the hospital.
Here is my shortlist of these practices. While there is crossover between the categories, I divide the practices into those that improve value during the DRG period and also post-DRG and those that improve value primarily post-DRG (thanks to Choosing Wisely for contributing to the recommendations with an asterisk1):
Thinking outside the DRG box will require an adjustment to the approach taken by hospitalists because the current demands are often more than enough for a day’s work. Hospitalists will be called upon to innovate and fashion better approaches to care. This will require support by other members of the healthcare team so hospitalists can work smarter, not harder, to meet the requirements of a changing healthcare system. A prerequisite is better payment models that align financial incentives so that providing higher-value care is sustainable and appropriately rewarded.
Reference
Clinician lists. Choosing Wisely website. Accessed October 25, 2016.
When choosing quality improvement activities, hospitalists have no shortage of choices. In this column, I offer a strategic guide for hospitalists as they assess where best to spend their energy as the shift to value-based care progresses. This includes the introduction of MACRA, the landmark new payment program for doctors and other clinicians (aka the Medicare Access and CHIP Reauthorization Act of 2015), with its incentives for participation in alternative payment models.
Since 1983, Medicare has reimbursed hospitals using a lump-sum payment known as a diagnosis-related group, or DRG. Since then, hospitals have focused a good deal of their energy on removing needless expenses from the hospitalization to improve their bottom line, recognizing the DRG payment they receive is relatively fixed. To this end, a major strategy has been to use hospitalists to decrease length of stay and “right size” the utilization of in-hospital tests and treatments.
However, things are changing as we enter the era of alternative payment models such as accountable care organizations (ACOs) and bundled payments. The lens Medicare (and, to a great extent, commercial payors) peers through to assess inpatient hospital costs is the DRG payment amount. Beyond that, Medicare has little visibility into the actual costs hospitals incur. Since hospital spending equates to the payment amount for a DRG, it becomes apparent that the incremental opportunity for hospitalists to improve value (quality divided by cost) in alternative payment models stems from payments outside the DRG. Such payments include those related to the post-acute period such as nursing and rehabilitation facilities, readmissions, and part B activity (e.g., consultants and outpatient tests).
What does this mean for hospitalists? MACRA begins in 2019, but initial payments will be based on 2017 performance. The associated advantage of participating in an “advanced alternative payment model” where there is accountability for care beyond the hospitalization is that hospitalists will be rewarded for taking costs out of the post-acute time period.
To be clear, hospitalists should remain agents of in-hospital efficiency and quality. After all, that is how we add value to the hospitals in which we practice. All things being equal, however, hospitalists should focus on practices that will improve value beyond the four walls of the hospital.
Here is my shortlist of these practices. While there is crossover between the categories, I divide the practices into those that improve value during the DRG period and also post-DRG and those that improve value primarily post-DRG (thanks to Choosing Wisely for contributing to the recommendations with an asterisk1):
Thinking outside the DRG box will require an adjustment to the approach taken by hospitalists because the current demands are often more than enough for a day’s work. Hospitalists will be called upon to innovate and fashion better approaches to care. This will require support by other members of the healthcare team so hospitalists can work smarter, not harder, to meet the requirements of a changing healthcare system. A prerequisite is better payment models that align financial incentives so that providing higher-value care is sustainable and appropriately rewarded.
Reference
Clinician lists. Choosing Wisely website. Accessed October 25, 2016.
Keeping up with New Payment Models

While in medical school, I learned about what was then called GRID (gay-related immune deficiency) and we now know as HIV/AIDS. I thought this condition would become so central to practice in nearly any specialty that I decided to try to keep up with all of the literature on it. It wasn’t yet in textbooks, so I thought it would be very important to keep up with all the new research studies and review articles about it.
I kept in my apartment a growing file of articles photocopied and torn out of journals. But I had badly misjudged the enormity of the task, and within a few years, there were far too many articles for me to read or keep up with in any fashion. Before long, HIV medicine became its own specialty, and while it has always been something I, like any hospitalist, need to know something about, I’ve left it to others to be the real HIV experts.
I was naive to have embarked on the quest. What seemed manageable at first became overwhelming very quickly. The same could be said for trying to keep up with new payment models.
New Professional Fee Reimbursement Models
For decades, most physicians could understand the general concept of how their professional activities generated revenue. But it’s gotten a lot more complicated lately.
The growing prevalence of capitation and other managed-care reimbursement models in the ’80s and ’90s might have been when reimbursement complexity began to increase significantly. But while nearly every doctor in the country heard about managed care, for many, it was something happening elsewhere that never made its way to them.
But for hospitalists, I think the arrival of the Physician Quality Reporting System (PQRS, originally Physician Quality Reporting Initiative, or PQRI) marks the swerve in reimbursement complexity. Some years ago I wrote in these pages about the importance of hospitalists understanding PQRS and described key features of the program.
Like HIV/AIDS medicine literature, the breadth and complexity of reimbursement programs from the Centers for Medicare & Medicaid Services (and other payors) seem to have grown logarithmically since PQRS. The still relatively new bundled payment and MACRA-related models are far more complicated than PQRS. And they change often. Calendar milestones come and go with changes in relevant metrics and performance thresholds, etc. Even the terminology changes frequently. Did you know, for example, that under MIPSi “Advancing Care Information” is essentially a new name for EHR Meaningful Use?
Bundled payments and MACRA are only a small portion of new models implemented over the last few years. There are many others, and dedicated effort is required just to keep track of whether each model influences only physicians (and other providers), only hospitals, or both.
Clinicians’ Responsibility for Keeping Up
My thinking about most hospitalists, or doctors in any specialty, keeping up with all of these models has evolved the same way it did with HIV/AIDS. I think it’s pretty clear that it’s folly to expect most clinicians to know more than the broad outlines of these programs.
Payment models are important. Someone needs to know them in detail, but clinicians should reserve brain cells for clinical knowledge base and focus only on the big picture of payment models. Think how well you’ve done learning and keeping up with CPT coding, observation versus inpatient status determinations, and clinical documentation. You probably still aren’t an expert at these things, so is it wise to set about becoming an expert in new payment models?
Instead, most hospitalists should rely on others to keep up with the precise details of these programs. Most commonly that will mean our employer will appoint or hire one or more people, or engage an outside party, to do this.
Don’t Feel Guilty
It’s common to leave a presentation or doctor’s lounge conversation on payment models feeling like you need to study up on the details of this or that payment model since good performance under that model will be important for your paycheck and to remain a viable “player.” And speakers sometimes intentionally or unintentionally enhance your anxiety about this. Maybe they love to show off what they know, and it’s easy for them to think only about their topic and not keep in mind all of the other stuff you need to know.
It’s terrific if someone in your practice is particularly interested in payment models and chooses to stay on top of them. Just make sure that doesn’t come at the expense of keeping up with changes in clinical practice. Most groups won’t have such a person and should rely on others, including SHM, without feeling the smallest bit of guilt.
SHM is advocating on behalf of hospitalists and working diligently to distill the impact MACRA and its various alternative payment frameworks will have on hospital medicine. With webinars, Q&As, and additional online and print resources, SHM will continue to provide digestible updates for hospitalists and their practices.
The End of Small-Group Physician Practice?
While the intent of these programs is to encourage and reward improvements in clinical practice, keeping up with and managing them is a tax that takes resources away from clinical practice. This is an especially difficult burden for small private practices and may prove to be a significant factor in nearly extinguishing them. There are relatively few small private hospitalist groups,ii but all of them should carefully consider how they will keep up with new reimbursement models.
While in medical school, I learned about what was then called GRID (gay-related immune deficiency) and we now know as HIV/AIDS. I thought this condition would become so central to practice in nearly any specialty that I decided to try to keep up with all of the literature on it. It wasn’t yet in textbooks, so I thought it would be very important to keep up with all the new research studies and review articles about it.
I kept in my apartment a growing file of articles photocopied and torn out of journals. But I had badly misjudged the enormity of the task, and within a few years, there were far too many articles for me to read or keep up with in any fashion. Before long, HIV medicine became its own specialty, and while it has always been something I, like any hospitalist, need to know something about, I’ve left it to others to be the real HIV experts.
I was naive to have embarked on the quest. What seemed manageable at first became overwhelming very quickly. The same could be said for trying to keep up with new payment models.
New Professional Fee Reimbursement Models
For decades, most physicians could understand the general concept of how their professional activities generated revenue. But it’s gotten a lot more complicated lately.
The growing prevalence of capitation and other managed-care reimbursement models in the ’80s and ’90s might have been when reimbursement complexity began to increase significantly. But while nearly every doctor in the country heard about managed care, for many, it was something happening elsewhere that never made its way to them.
But for hospitalists, I think the arrival of the Physician Quality Reporting System (PQRS, originally Physician Quality Reporting Initiative, or PQRI) marks the swerve in reimbursement complexity. Some years ago I wrote in these pages about the importance of hospitalists understanding PQRS and described key features of the program.
Like HIV/AIDS medicine literature, the breadth and complexity of reimbursement programs from the Centers for Medicare & Medicaid Services (and other payors) seem to have grown logarithmically since PQRS. The still relatively new bundled payment and MACRA-related models are far more complicated than PQRS. And they change often. Calendar milestones come and go with changes in relevant metrics and performance thresholds, etc. Even the terminology changes frequently. Did you know, for example, that under MIPSi “Advancing Care Information” is essentially a new name for EHR Meaningful Use?
Bundled payments and MACRA are only a small portion of new models implemented over the last few years. There are many others, and dedicated effort is required just to keep track of whether each model influences only physicians (and other providers), only hospitals, or both.
Clinicians’ Responsibility for Keeping Up
My thinking about most hospitalists, or doctors in any specialty, keeping up with all of these models has evolved the same way it did with HIV/AIDS. I think it’s pretty clear that it’s folly to expect most clinicians to know more than the broad outlines of these programs.
Payment models are important. Someone needs to know them in detail, but clinicians should reserve brain cells for clinical knowledge base and focus only on the big picture of payment models. Think how well you’ve done learning and keeping up with CPT coding, observation versus inpatient status determinations, and clinical documentation. You probably still aren’t an expert at these things, so is it wise to set about becoming an expert in new payment models?
Instead, most hospitalists should rely on others to keep up with the precise details of these programs. Most commonly that will mean our employer will appoint or hire one or more people, or engage an outside party, to do this.
Don’t Feel Guilty
It’s common to leave a presentation or doctor’s lounge conversation on payment models feeling like you need to study up on the details of this or that payment model since good performance under that model will be important for your paycheck and to remain a viable “player.” And speakers sometimes intentionally or unintentionally enhance your anxiety about this. Maybe they love to show off what they know, and it’s easy for them to think only about their topic and not keep in mind all of the other stuff you need to know.
It’s terrific if someone in your practice is particularly interested in payment models and chooses to stay on top of them. Just make sure that doesn’t come at the expense of keeping up with changes in clinical practice. Most groups won’t have such a person and should rely on others, including SHM, without feeling the smallest bit of guilt.
SHM is advocating on behalf of hospitalists and working diligently to distill the impact MACRA and its various alternative payment frameworks will have on hospital medicine. With webinars, Q&As, and additional online and print resources, SHM will continue to provide digestible updates for hospitalists and their practices.
The End of Small-Group Physician Practice?
While the intent of these programs is to encourage and reward improvements in clinical practice, keeping up with and managing them is a tax that takes resources away from clinical practice. This is an especially difficult burden for small private practices and may prove to be a significant factor in nearly extinguishing them. There are relatively few small private hospitalist groups,ii but all of them should carefully consider how they will keep up with new reimbursement models.
While in medical school, I learned about what was then called GRID (gay-related immune deficiency) and we now know as HIV/AIDS. I thought this condition would become so central to practice in nearly any specialty that I decided to try to keep up with all of the literature on it. It wasn’t yet in textbooks, so I thought it would be very important to keep up with all the new research studies and review articles about it.
I kept in my apartment a growing file of articles photocopied and torn out of journals. But I had badly misjudged the enormity of the task, and within a few years, there were far too many articles for me to read or keep up with in any fashion. Before long, HIV medicine became its own specialty, and while it has always been something I, like any hospitalist, need to know something about, I’ve left it to others to be the real HIV experts.
I was naive to have embarked on the quest. What seemed manageable at first became overwhelming very quickly. The same could be said for trying to keep up with new payment models.
New Professional Fee Reimbursement Models
For decades, most physicians could understand the general concept of how their professional activities generated revenue. But it’s gotten a lot more complicated lately.
The growing prevalence of capitation and other managed-care reimbursement models in the ’80s and ’90s might have been when reimbursement complexity began to increase significantly. But while nearly every doctor in the country heard about managed care, for many, it was something happening elsewhere that never made its way to them.
But for hospitalists, I think the arrival of the Physician Quality Reporting System (PQRS, originally Physician Quality Reporting Initiative, or PQRI) marks the swerve in reimbursement complexity. Some years ago I wrote in these pages about the importance of hospitalists understanding PQRS and described key features of the program.
Like HIV/AIDS medicine literature, the breadth and complexity of reimbursement programs from the Centers for Medicare & Medicaid Services (and other payors) seem to have grown logarithmically since PQRS. The still relatively new bundled payment and MACRA-related models are far more complicated than PQRS. And they change often. Calendar milestones come and go with changes in relevant metrics and performance thresholds, etc. Even the terminology changes frequently. Did you know, for example, that under MIPSi “Advancing Care Information” is essentially a new name for EHR Meaningful Use?
Bundled payments and MACRA are only a small portion of new models implemented over the last few years. There are many others, and dedicated effort is required just to keep track of whether each model influences only physicians (and other providers), only hospitals, or both.
Clinicians’ Responsibility for Keeping Up
My thinking about most hospitalists, or doctors in any specialty, keeping up with all of these models has evolved the same way it did with HIV/AIDS. I think it’s pretty clear that it’s folly to expect most clinicians to know more than the broad outlines of these programs.
Payment models are important. Someone needs to know them in detail, but clinicians should reserve brain cells for clinical knowledge base and focus only on the big picture of payment models. Think how well you’ve done learning and keeping up with CPT coding, observation versus inpatient status determinations, and clinical documentation. You probably still aren’t an expert at these things, so is it wise to set about becoming an expert in new payment models?
Instead, most hospitalists should rely on others to keep up with the precise details of these programs. Most commonly that will mean our employer will appoint or hire one or more people, or engage an outside party, to do this.
Don’t Feel Guilty
It’s common to leave a presentation or doctor’s lounge conversation on payment models feeling like you need to study up on the details of this or that payment model since good performance under that model will be important for your paycheck and to remain a viable “player.” And speakers sometimes intentionally or unintentionally enhance your anxiety about this. Maybe they love to show off what they know, and it’s easy for them to think only about their topic and not keep in mind all of the other stuff you need to know.
It’s terrific if someone in your practice is particularly interested in payment models and chooses to stay on top of them. Just make sure that doesn’t come at the expense of keeping up with changes in clinical practice. Most groups won’t have such a person and should rely on others, including SHM, without feeling the smallest bit of guilt.
SHM is advocating on behalf of hospitalists and working diligently to distill the impact MACRA and its various alternative payment frameworks will have on hospital medicine. With webinars, Q&As, and additional online and print resources, SHM will continue to provide digestible updates for hospitalists and their practices.
The End of Small-Group Physician Practice?
While the intent of these programs is to encourage and reward improvements in clinical practice, keeping up with and managing them is a tax that takes resources away from clinical practice. This is an especially difficult burden for small private practices and may prove to be a significant factor in nearly extinguishing them. There are relatively few small private hospitalist groups,ii but all of them should carefully consider how they will keep up with new reimbursement models.
It’s in the nose
There is a lot more going on in the nose besides air going in and out. The nose is where it all begins for pathogenesis for all respiratory infections. The interplay between the commensal microbes, the potential pathogens, innate immunity, and adaptive immunity is much more complex than was previously understood. So what is new?
In our research on acute otitis media, we swab and wash out noses of children aged 6-36 months to isolate the potential pathogens Streptococcus pneumoniae, nontypeable Haemophilus influenza, Moraxella catarrhalis, Staphylococcus aureus, and Group A streptococci. We isolate one or more of these bacteria from most of the children even though they are well. We observe perhaps a half-dozen other species of bacteria on the culture plate. Mostly, we isolate S. pneumoniae, nontypeable H. influenza, or M. catarrhalis and alpha-hemolytic streptococci and corynebacterium species.

We have recently begun to investigate the other microbiota in the nose and found they are indeed plentiful. In a recent screening of a half-dozen children, we found hundreds of different microbes in their noses, so cultures and standard molecular detection methods were just touching the surface. I was asked recently at a medical conference – the American Academy of Pediatrics– Orange County, California, annual CME course – at which I spoke on this topic what I thought would be the most-important area of research in the next decade. I responded, the microbiome. The microbiome is indeed a hot topic. Research over the last decade suggests that 90% of all diseases can be traced in some way to disturbances in the microbiome. What I mean by microbiome is “the totality of microorganisms and their collective genetic material present in or on the human body.” The term is often used interchangeably with “microbiota,” although the former refers to genes of microbes and the latter refers to the microbes themselves. What I mean by “disturbance” is excessive use of antibiotics.
How many microbes are in the nose? We don’t know. But if the gut is any indication, there are thousands of microbes in the nose because the gut has more than 10,000 different microbes. Recognizing that there are hundreds of microbes in the nose and from time to time children get colonized by potential pathogens that can cause otitis media, sinusitis, or pneumonia, how does pathogenesis get started? It starts with a respiratory virus infection. The bacteria need help from the viruses to cause disease. The viruses cause damage to the epithelial cells of the nose, and this gives the bacteria more places to attach when they divide so the amount of bacteria increases exponentially. As the viruses replicate, they more effectively slow down cilia beating, and the nasal mucus thickens. This, too, helps the bacteria and viruses attach to and penetrate epithelial cells in the nose and increase in density on the surface of the cells and inside the cells. The viruses divert and/or suppress the innate immune system, represented by neutrophils that migrate to the nose and discharge their intracellular contents to turn nasal mucus yellow and green. The viruses even down-modulate the adaptive immune system in clever ways that result in fewer potentially protective cytotoxic lymphocytes that kill viruses making their way to the nose, and fewer T cells that discharge cytokines that promote a necessary inflammatory response to clear both bacteria and viruses from the nose and fewer B cells that become plasma cells and release antibodies into the nose.
When the bacteria with potential to cause diseases reach a “pathogenic threshold,” they move, along with mucus, into the middle ear, the sinuses, or down the throat to the lungs, usually with the accompanying respiratory virus. There pathogenesis continues in the otherwise sterile and protected sanctuary of these interconnected respiratory sites. A few days later, we as clinicians observe the symptoms and signs of otitis media, sinusitis, or pneumonia.
What can we do to help the nose? Mostly, we should do no harm, and that has been our failing for decades since the introduction of antibiotics. The allure of antibiotics is great because they have indeed saved many lives and shortened many illnesses when appropriately used. However, too often clinicians have seen patients with yellow and green nasal mucus (or any increased nasal mucus) and diagnosed “a bacterial infection” and prescribed antibiotics. And too often clinicians have seen patients with an annoying cough (or any cough) and diagnosed “a bacterial chest infection” and prescribed antibiotics. The clinicians thought it was the right thing to do because they wanted to help their patient. And they did not want them to come back in a few days with persistence or worsening of symptoms, or worse, seek care from other health care providers elsewhere. So they gave antibiotics.
Well, the paradigm has changed. It is now clearly known that antibiotics can be harmful mainly by damaging the normal, healthy microbiome. The change in healthy homeostasis of the microbiome wrought by antibiotics is greatest in newborns, especially premature newborns, then next worst for infants, and then next worst for young children. These are the age groups where antibiotics are prescribed most frequently! And everyone needs to stop writing those prescriptions for runny noses, yellow and green mucus in the nose, and coughs. All of us need to prescribe antibiotics only when there is an accurate diagnosis of otitis media or sinusitis or bronchopneumonia or lobar pneumonia. And when we do prescribe the antibiotics ,we need to give them for as short a time as possible. But that is a topic for another column.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he has no relevant financial disclosures, and that his research is supported by a grant from the National Institutes of Health National Institute of Deafness and Communication Disorders. Email him at pdnews@frontlinemedcom.com.
There is a lot more going on in the nose besides air going in and out. The nose is where it all begins for pathogenesis for all respiratory infections. The interplay between the commensal microbes, the potential pathogens, innate immunity, and adaptive immunity is much more complex than was previously understood. So what is new?
In our research on acute otitis media, we swab and wash out noses of children aged 6-36 months to isolate the potential pathogens Streptococcus pneumoniae, nontypeable Haemophilus influenza, Moraxella catarrhalis, Staphylococcus aureus, and Group A streptococci. We isolate one or more of these bacteria from most of the children even though they are well. We observe perhaps a half-dozen other species of bacteria on the culture plate. Mostly, we isolate S. pneumoniae, nontypeable H. influenza, or M. catarrhalis and alpha-hemolytic streptococci and corynebacterium species.
We have recently begun to investigate the other microbiota in the nose and found they are indeed plentiful. In a recent screening of a half-dozen children, we found hundreds of different microbes in their noses, so cultures and standard molecular detection methods were just touching the surface. I was asked recently at a medical conference – the American Academy of Pediatrics– Orange County, California, annual CME course – at which I spoke on this topic what I thought would be the most-important area of research in the next decade. I responded, the microbiome. The microbiome is indeed a hot topic. Research over the last decade suggests that 90% of all diseases can be traced in some way to disturbances in the microbiome. What I mean by microbiome is “the totality of microorganisms and their collective genetic material present in or on the human body.” The term is often used interchangeably with “microbiota,” although the former refers to genes of microbes and the latter refers to the microbes themselves. What I mean by “disturbance” is excessive use of antibiotics.
How many microbes are in the nose? We don’t know. But if the gut is any indication, there are thousands of microbes in the nose because the gut has more than 10,000 different microbes. Recognizing that there are hundreds of microbes in the nose and from time to time children get colonized by potential pathogens that can cause otitis media, sinusitis, or pneumonia, how does pathogenesis get started? It starts with a respiratory virus infection. The bacteria need help from the viruses to cause disease. The viruses cause damage to the epithelial cells of the nose, and this gives the bacteria more places to attach when they divide so the amount of bacteria increases exponentially. As the viruses replicate, they more effectively slow down cilia beating, and the nasal mucus thickens. This, too, helps the bacteria and viruses attach to and penetrate epithelial cells in the nose and increase in density on the surface of the cells and inside the cells. The viruses divert and/or suppress the innate immune system, represented by neutrophils that migrate to the nose and discharge their intracellular contents to turn nasal mucus yellow and green. The viruses even down-modulate the adaptive immune system in clever ways that result in fewer potentially protective cytotoxic lymphocytes that kill viruses making their way to the nose, and fewer T cells that discharge cytokines that promote a necessary inflammatory response to clear both bacteria and viruses from the nose and fewer B cells that become plasma cells and release antibodies into the nose.
When the bacteria with potential to cause diseases reach a “pathogenic threshold,” they move, along with mucus, into the middle ear, the sinuses, or down the throat to the lungs, usually with the accompanying respiratory virus. There pathogenesis continues in the otherwise sterile and protected sanctuary of these interconnected respiratory sites. A few days later, we as clinicians observe the symptoms and signs of otitis media, sinusitis, or pneumonia.
What can we do to help the nose? Mostly, we should do no harm, and that has been our failing for decades since the introduction of antibiotics. The allure of antibiotics is great because they have indeed saved many lives and shortened many illnesses when appropriately used. However, too often clinicians have seen patients with yellow and green nasal mucus (or any increased nasal mucus) and diagnosed “a bacterial infection” and prescribed antibiotics. And too often clinicians have seen patients with an annoying cough (or any cough) and diagnosed “a bacterial chest infection” and prescribed antibiotics. The clinicians thought it was the right thing to do because they wanted to help their patient. And they did not want them to come back in a few days with persistence or worsening of symptoms, or worse, seek care from other health care providers elsewhere. So they gave antibiotics.
Well, the paradigm has changed. It is now clearly known that antibiotics can be harmful mainly by damaging the normal, healthy microbiome. The change in healthy homeostasis of the microbiome wrought by antibiotics is greatest in newborns, especially premature newborns, then next worst for infants, and then next worst for young children. These are the age groups where antibiotics are prescribed most frequently! And everyone needs to stop writing those prescriptions for runny noses, yellow and green mucus in the nose, and coughs. All of us need to prescribe antibiotics only when there is an accurate diagnosis of otitis media or sinusitis or bronchopneumonia or lobar pneumonia. And when we do prescribe the antibiotics ,we need to give them for as short a time as possible. But that is a topic for another column.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he has no relevant financial disclosures, and that his research is supported by a grant from the National Institutes of Health National Institute of Deafness and Communication Disorders. Email him at pdnews@frontlinemedcom.com.
There is a lot more going on in the nose besides air going in and out. The nose is where it all begins for pathogenesis for all respiratory infections. The interplay between the commensal microbes, the potential pathogens, innate immunity, and adaptive immunity is much more complex than was previously understood. So what is new?
In our research on acute otitis media, we swab and wash out noses of children aged 6-36 months to isolate the potential pathogens Streptococcus pneumoniae, nontypeable Haemophilus influenza, Moraxella catarrhalis, Staphylococcus aureus, and Group A streptococci. We isolate one or more of these bacteria from most of the children even though they are well. We observe perhaps a half-dozen other species of bacteria on the culture plate. Mostly, we isolate S. pneumoniae, nontypeable H. influenza, or M. catarrhalis and alpha-hemolytic streptococci and corynebacterium species.
We have recently begun to investigate the other microbiota in the nose and found they are indeed plentiful. In a recent screening of a half-dozen children, we found hundreds of different microbes in their noses, so cultures and standard molecular detection methods were just touching the surface. I was asked recently at a medical conference – the American Academy of Pediatrics– Orange County, California, annual CME course – at which I spoke on this topic what I thought would be the most-important area of research in the next decade. I responded, the microbiome. The microbiome is indeed a hot topic. Research over the last decade suggests that 90% of all diseases can be traced in some way to disturbances in the microbiome. What I mean by microbiome is “the totality of microorganisms and their collective genetic material present in or on the human body.” The term is often used interchangeably with “microbiota,” although the former refers to genes of microbes and the latter refers to the microbes themselves. What I mean by “disturbance” is excessive use of antibiotics.
How many microbes are in the nose? We don’t know. But if the gut is any indication, there are thousands of microbes in the nose because the gut has more than 10,000 different microbes. Recognizing that there are hundreds of microbes in the nose and from time to time children get colonized by potential pathogens that can cause otitis media, sinusitis, or pneumonia, how does pathogenesis get started? It starts with a respiratory virus infection. The bacteria need help from the viruses to cause disease. The viruses cause damage to the epithelial cells of the nose, and this gives the bacteria more places to attach when they divide so the amount of bacteria increases exponentially. As the viruses replicate, they more effectively slow down cilia beating, and the nasal mucus thickens. This, too, helps the bacteria and viruses attach to and penetrate epithelial cells in the nose and increase in density on the surface of the cells and inside the cells. The viruses divert and/or suppress the innate immune system, represented by neutrophils that migrate to the nose and discharge their intracellular contents to turn nasal mucus yellow and green. The viruses even down-modulate the adaptive immune system in clever ways that result in fewer potentially protective cytotoxic lymphocytes that kill viruses making their way to the nose, and fewer T cells that discharge cytokines that promote a necessary inflammatory response to clear both bacteria and viruses from the nose and fewer B cells that become plasma cells and release antibodies into the nose.
When the bacteria with potential to cause diseases reach a “pathogenic threshold,” they move, along with mucus, into the middle ear, the sinuses, or down the throat to the lungs, usually with the accompanying respiratory virus. There pathogenesis continues in the otherwise sterile and protected sanctuary of these interconnected respiratory sites. A few days later, we as clinicians observe the symptoms and signs of otitis media, sinusitis, or pneumonia.
What can we do to help the nose? Mostly, we should do no harm, and that has been our failing for decades since the introduction of antibiotics. The allure of antibiotics is great because they have indeed saved many lives and shortened many illnesses when appropriately used. However, too often clinicians have seen patients with yellow and green nasal mucus (or any increased nasal mucus) and diagnosed “a bacterial infection” and prescribed antibiotics. And too often clinicians have seen patients with an annoying cough (or any cough) and diagnosed “a bacterial chest infection” and prescribed antibiotics. The clinicians thought it was the right thing to do because they wanted to help their patient. And they did not want them to come back in a few days with persistence or worsening of symptoms, or worse, seek care from other health care providers elsewhere. So they gave antibiotics.
Well, the paradigm has changed. It is now clearly known that antibiotics can be harmful mainly by damaging the normal, healthy microbiome. The change in healthy homeostasis of the microbiome wrought by antibiotics is greatest in newborns, especially premature newborns, then next worst for infants, and then next worst for young children. These are the age groups where antibiotics are prescribed most frequently! And everyone needs to stop writing those prescriptions for runny noses, yellow and green mucus in the nose, and coughs. All of us need to prescribe antibiotics only when there is an accurate diagnosis of otitis media or sinusitis or bronchopneumonia or lobar pneumonia. And when we do prescribe the antibiotics ,we need to give them for as short a time as possible. But that is a topic for another column.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he has no relevant financial disclosures, and that his research is supported by a grant from the National Institutes of Health National Institute of Deafness and Communication Disorders. Email him at pdnews@frontlinemedcom.com.
VIDEO: The surgical treatment of pelvic congestion
BY CHARLES E. MILLER, MD
Chronic pelvic pain is described as the presence of lower abdominal or pelvic pain for longer than 6 months. It is believed to affect approximately one in six women and 12%-15% of women of reproductive age. The diagnosis and treatment of chronic pelvic pain adds as much as a $2 billion burden to our health system annually.
It was first described clinically in the literature in 1857, while the existence of pelvic varicosities wasn’t documented for nearly another 100 years. Pelvic congestion syndrome (PCS) accounts for 30%-70% of cases presenting with chronic pelvic pain. PCS can be due to pelvic venous insufficiency, characterized by reflux into pelvic veins leading to pelvic varicosities or alternative venous pathways secondary to varicose veins of the leg.
Other etiologies of PCS include nutcracker syndrome (left renal vein compressed between the aorta and the superior mesenteric artery), May-Thurner syndrome (compression of the left common iliac vein by the right common iliac artery) or, less likely, tumor thrombosis of the inferior vena cava, portal vein thrombosis, renal cell carcinoma, left renal thrombosis, or left kidney arterial-venous fistula.

While there appears to be significant literature indicating a long-term success rate of greater than 80% in patients treated by percutaneous endovascular procedures (embolization, stenting), there is far less information on the postsurgical success of blocking the varicose gonadal vein. Nevertheless, our long-term results with gonadal vein clipping is virtually the same as that of our radiological colleagues.
It is a pleasure to welcome Courtney Steller, DO, to this edition of the Master Class in Gynecologic Surgery to discuss the diagnosis and treatment of PCS, with an emphasis on surgical correction.
Dr. Steller is a recent graduate of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. She is currently in private practice and is an associate at the Family Health Centers of San Diego, Calif.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported having no financial disclosures relevant to this column. Email him at obnews@frontlinemedcom.com.
Pelvic congestion syndrome: A treatable cause of pain
BY COURTNEY STELLER, DO
Pelvic congestion syndrome is a poorly understood and underdiagnosed disease. Yet, over the last decade, the syndrome has become less controversial as the etiology has become better understood and as the diagnostic approach has become more specific. Through these advances, treatments have also become increasingly more successful.
This is an important shift, because the chronic pelvic pain experienced by patients with pelvic congestion significantly impacts their quality of life and well-being. As the pain persists, it can become exceedingly difficult to manage. Many patients we have ultimately treated for pelvic congestion syndrome have had years of various work-ups, significant diagnostic investigations, and trials of different treatments without having any cause of their pain identified or achieving any lasting symptom relief.

The pelvic pain in patients with pelvic congestion syndrome (PCS) can be noncyclical or cyclical. It is present most of the time but tends to get worse at the end of the day and after long periods of standing and/or sitting. The pain also may worsen with intercourse, largely afterward. The syndrome tends to occur in premenopausal and multiparous women, but it’s important to appreciate that this is not always the case; we have diagnosed and treated PCS in several young, nulliparous patients as well.
Features and diagnosis
PCS is a disorder of pelvic venous circulation that predominantly affects the ovarian veins. It is sometimes referred to as pelvic vein incompetence or pelvic vascular dysfunction. Just as veins in the legs can enlarge and become varicose, the ovarian veins – and sometimes the internal iliac veins – can become incompetent and unable to effectively return blood back to the heart.
Pregnancy may predispose patients to developing the abnormally dilated and refluxing veins that characterize PCS, as the increase in pelvic vein capacity and uterine compression can lead to significant stasis of blood in the pelvis and subsequent damage to the veins and the venous valves. There also is believed to be an estrogen component to the development of PCS, because estrogen is known to act as a vasodilator. Moreover, a congenital absence and incompetence of venous valves in some cases has been reported.
In a recent study looking at pelvic vein incompetence and symptoms of chronic pelvic pain, these women were reported to have a distinctive symptom profile, with the “most notable” features being the presence of dull pelvic pain that radiates to the upper thighs and is aggravated by prolonged standing and walking – symptoms that are similar to the leg symptoms experienced by patients with severe varicose veins (Eur J Obstet Gynecol Reprod Biol. 2016 Jan;196:21-5).
Other investigators have similarly described the pelvic pain related to PCS as a dull ache or heaviness sensation that is most severe at the end of the day and that is lessened with supine positioning (though not necessarily immediately) and often exacerbated with sexual intercourse, especially post coitus. These descriptions are in line with my experience with PCS. There is usually exquisite tenderness on pelvic exam, especially localized to the adnexa. Patients will often have varicose veins on their upper legs or labia.
Interestingly, it has been repeatedly shown that many women have dilated and incompetent pelvic veins without also having such pathognomonic pain. We therefore cannot treat women based solely on the finding of abnormal veins.
On the other hand we must determine which patients with chronic pelvic pain have PCS. The differential diagnosis for PCS includes endometriosis, adenomyosis chronic pelvic inflammatory disease, adhesive disease, adnexal masses, adnexal torsion, and several nongynecologic diseases including interstitial cystitis and irritable bowel syndrome.
Venography has become the gold standard for diagnosing pelvic congestion. The procedure involves catheterization of the ovarian veins through a femoral or jugular approach. In our experience, the common femoral vein is the more frequently used access point. Using a contrast injection, the interventional radiologist can assess the degree of venous dilation and reflux in the pelvis.

There currently is no consensus on a cutoff for vein diameter or on any validated measures for congestion. According to one report on PCS authored by interventional radiologists, the diagnosis of PCS is confirmed with the venographic findings of ovarian vein diameter greater than 6 mm, retrograde ovarian or pelvic venous flow, presence of several tortuous collateral pelvic venous pathways, and delayed or stagnant clearance on contrast (Semin Intervent Radiol. 2008 Dec;25[4]:361-8).
The criteria vary, however. A recent literature review on pelvic congestion syndrome by Chiara Borghi, MD, and Lucio Dell’Atti, MD, states that incompetent pelvic veins are defined as more than 5-10 mm in diameter (Arch Gynecol Obstet. 2016 Feb;293[2]:291-301).
To more accurately diagnose PCS, our patients undergo tilt-table venography. The patient is placed into a reverse-Trendelenburg upright or semi-upright position to potentially exacerbate any venous reflux or dilation.
Other methods of identifying and diagnosing pelvic congestion have included transabdominal and transvaginal ultrasound, CT, and MRI. While CT and MRI both offer an overview of the pelvic vasculature and are helpful for ruling out other causes of chronic pelvic pain, they have low specificity for pelvic varices, according to the Italian review.
Sonography performed in the supine position, on the other hand, appears to be increasingly viewed as an acceptable screening tool for determining which patients may ultimately benefit from venography. It is also important in evaluation to rule out other pathologies not yet excluded. However, it should not be used for diagnosis of PCS.
Treating PCS
There are two main approaches to treating PCS: venous ligation (a gynecologic surgical approach) and percutaneous transcatheter embolization (performed by interventional radiologists).
The literature and evidence base is still in its infancy, but is growing. In our experience, both approaches lead to good resolution of symptoms over time in the majority of patients, and appear superior to the medical therapies that have been proposed for treating PCS, such as progestins and gonadotropin-releasing hormone agonists. Success rates with medical therapy are more variable and appear to be more short lived.
A review published this year on the effectiveness of embolization of pelvic veins for reducing chronic pelvic pain showed that 75% of women undergoing embolization had symptomatic relief that generally increased over time and was sustained. The authors concluded that embolization appears to be effective for the majority of women, and is safe, although they also noted that the quality of the evidence is low (J Vasc Interv Radiol. 2016 Oct;27[10]:1478-86.e8). Their review was based almost entirely on prospective case series.
Dr. Borghi and Dr. Dell’Atti offered a similar assessment of embolization for PCS, stating in their review article that clinical success has been reported in 70%-85% of patients. They also report nearly equivalent success rates of up to 75% with treatment via surgical ligation of ovarian and/or pelvic vasculature. These findings are from mostly observational data and case series.
Decisions about which approach to take should be individualized. If there are no differences with respect to insurance coverage for the patient, then embolization may be the preferred approach because it is the most minimally invasive technique and can potentially be performed at the time of diagnostic venography, negating the need for a second procedure. A skilled interventional radiologist familiar with the disease and the treatment is necessary. Various embolic agents are utilized, including coils, glues, foams, and other agents that cause sclerosis of the abnormal veins.
In other cases, venous ligation is preferred, especially when an additional gynecologic surgery, such as a cystectomy or myomectomy, is required.
Surgical ligation of ovarian veins was initially performed via laparotomy using a traditional retroperitoneal approach. The surgical goal is to isolate the ovarian vein significantly above the pelvic brim and before the vein becomes substantially dilated. Laparotomy therefore requires a vertical mid-line incision to provide adequate access to the appropriate portion of the ovarian vessels, leading to potentially high morbidity and poor cosmesis.
More recently, gynecologic surgeons skilled in laparoscopy have successfully managed PCS transperitoneally. A few small series of bilateral laparoscopic transperitoneal ligation of ovarian veins have been reported, including one by Tigellio Gargiulo, MD, who clipped both veins in their upper third, near their distal ends at the inferior vena cava (right) and the renal vein (left) (J Am Assoc Gynecol Laparosc. 2003 Nov;10[4]:501-4).
We prefer a robot-assisted laparoscopic approach for most of our patients. Not only does the improved dexterity help while working with sensitive vasculature, but more importantly we are able to use Firefly fluorescence.
The procedure generally is as follows. The uterine adnexa on the affected side is grasped and placed on tension so that the infundibulopelvic (IP) ligament can be visualized as it courses up and above the pelvic brim. The peritoneum immediately over the IP ligament is gently grasped and tented upward, and a small incision is made into the peritoneum, providing access into the retroperitoneum. The ureter should be visualized medial to this dissection.
The peritoneal tissue is then gently dissected off the ovarian vessels. Once the vessels are freed from the peritoneal tissue, the dilated ovarian vein is often clearly visualized. It is important to note that if no venous dilation is seen during laparoscopy, the procedure should not be aborted. Due to the Trendelenburg position that is utilized in gynecologic – and especially laparoscopic – surgery, the venous system sometimes appears falsely “normal” at this time.

Once the ovarian vessels have been isolated, the arteries must be separated from the veins. The adventitial tissue is dissected until the vessels are separated. Great care should be taken to ensure that all movements run parallel to the vessels and not perpendicular, therefore decreasing the risk of bleeding.
This process can be challenging. The surgeon is working with delicate vasculature. Often there are several branches from the vein that have formed due to the abnormal venous system. The best way to approach it is to identify planes and separate those planes in order to isolate individual vessels. If difficulties are still encountered, the surgeon should restart the dissection higher.
Once the dilated ovarian vein is isolated, one to two clips are placed.

Usually the artery is clearly distinct from the vein as it is smaller, more elastic, and can be seen pulsing. However, occasionally it is difficult to distinguish. In these cases, assistance with the da Vinci surgical system is useful: Indocyanine green (ICG) dye can be injected intravenously and visualized with a near-infrared light on the da Vinci platform. The dye is then seen glowing green as it first courses through the artery and then the vein.
For patients who have been found on venography to have bilateral disease, we perform the ligation procedure bilaterally. Once ligation is complete, the more competent collateral veins in the pelvis will assume more of the venous circulation.
In our experience, patients have ultimately noted substantial pain relief after these procedures, both with the endoscopic embolization and the surgical ligation. Patients are counseled that it can take several months to notice a relief in the pain.
In rare cases, pelvic congestion is related to extrinsic compression. For instance, the left renal vein can become compressed between the aorta and the superior mesenteric artery (the nutcracker syndrome), or the left common iliac vein can be compressed between the overlying right internal iliac artery and the underlying vertebral body (May-Thurner syndrome). Both of these conditions can lead to secondary PCS.
Such complex conditions are usually treated by vascular surgeons. May-Thurner syndrome is treated via stenting, while nutcracker syndrome can be treated with stenting or transposition of the renal vein to the distal vena cava.
Dr. Steller is an associate at the Family Health Centers of San Diego. She reported having no relevant financial disclosures.
BY CHARLES E. MILLER, MD
Chronic pelvic pain is described as the presence of lower abdominal or pelvic pain for longer than 6 months. It is believed to affect approximately one in six women and 12%-15% of women of reproductive age. The diagnosis and treatment of chronic pelvic pain adds as much as a $2 billion burden to our health system annually.
It was first described clinically in the literature in 1857, while the existence of pelvic varicosities wasn’t documented for nearly another 100 years. Pelvic congestion syndrome (PCS) accounts for 30%-70% of cases presenting with chronic pelvic pain. PCS can be due to pelvic venous insufficiency, characterized by reflux into pelvic veins leading to pelvic varicosities or alternative venous pathways secondary to varicose veins of the leg.
Other etiologies of PCS include nutcracker syndrome (left renal vein compressed between the aorta and the superior mesenteric artery), May-Thurner syndrome (compression of the left common iliac vein by the right common iliac artery) or, less likely, tumor thrombosis of the inferior vena cava, portal vein thrombosis, renal cell carcinoma, left renal thrombosis, or left kidney arterial-venous fistula.
While there appears to be significant literature indicating a long-term success rate of greater than 80% in patients treated by percutaneous endovascular procedures (embolization, stenting), there is far less information on the postsurgical success of blocking the varicose gonadal vein. Nevertheless, our long-term results with gonadal vein clipping is virtually the same as that of our radiological colleagues.
It is a pleasure to welcome Courtney Steller, DO, to this edition of the Master Class in Gynecologic Surgery to discuss the diagnosis and treatment of PCS, with an emphasis on surgical correction.
Dr. Steller is a recent graduate of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. She is currently in private practice and is an associate at the Family Health Centers of San Diego, Calif.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported having no financial disclosures relevant to this column. Email him at obnews@frontlinemedcom.com.
Pelvic congestion syndrome: A treatable cause of pain
BY COURTNEY STELLER, DO
Pelvic congestion syndrome is a poorly understood and underdiagnosed disease. Yet, over the last decade, the syndrome has become less controversial as the etiology has become better understood and as the diagnostic approach has become more specific. Through these advances, treatments have also become increasingly more successful.
This is an important shift, because the chronic pelvic pain experienced by patients with pelvic congestion significantly impacts their quality of life and well-being. As the pain persists, it can become exceedingly difficult to manage. Many patients we have ultimately treated for pelvic congestion syndrome have had years of various work-ups, significant diagnostic investigations, and trials of different treatments without having any cause of their pain identified or achieving any lasting symptom relief.
The pelvic pain in patients with pelvic congestion syndrome (PCS) can be noncyclical or cyclical. It is present most of the time but tends to get worse at the end of the day and after long periods of standing and/or sitting. The pain also may worsen with intercourse, largely afterward. The syndrome tends to occur in premenopausal and multiparous women, but it’s important to appreciate that this is not always the case; we have diagnosed and treated PCS in several young, nulliparous patients as well.
Features and diagnosis
PCS is a disorder of pelvic venous circulation that predominantly affects the ovarian veins. It is sometimes referred to as pelvic vein incompetence or pelvic vascular dysfunction. Just as veins in the legs can enlarge and become varicose, the ovarian veins – and sometimes the internal iliac veins – can become incompetent and unable to effectively return blood back to the heart.
Pregnancy may predispose patients to developing the abnormally dilated and refluxing veins that characterize PCS, as the increase in pelvic vein capacity and uterine compression can lead to significant stasis of blood in the pelvis and subsequent damage to the veins and the venous valves. There also is believed to be an estrogen component to the development of PCS, because estrogen is known to act as a vasodilator. Moreover, a congenital absence and incompetence of venous valves in some cases has been reported.
In a recent study looking at pelvic vein incompetence and symptoms of chronic pelvic pain, these women were reported to have a distinctive symptom profile, with the “most notable” features being the presence of dull pelvic pain that radiates to the upper thighs and is aggravated by prolonged standing and walking – symptoms that are similar to the leg symptoms experienced by patients with severe varicose veins (Eur J Obstet Gynecol Reprod Biol. 2016 Jan;196:21-5).
Other investigators have similarly described the pelvic pain related to PCS as a dull ache or heaviness sensation that is most severe at the end of the day and that is lessened with supine positioning (though not necessarily immediately) and often exacerbated with sexual intercourse, especially post coitus. These descriptions are in line with my experience with PCS. There is usually exquisite tenderness on pelvic exam, especially localized to the adnexa. Patients will often have varicose veins on their upper legs or labia.
Interestingly, it has been repeatedly shown that many women have dilated and incompetent pelvic veins without also having such pathognomonic pain. We therefore cannot treat women based solely on the finding of abnormal veins.
On the other hand we must determine which patients with chronic pelvic pain have PCS. The differential diagnosis for PCS includes endometriosis, adenomyosis chronic pelvic inflammatory disease, adhesive disease, adnexal masses, adnexal torsion, and several nongynecologic diseases including interstitial cystitis and irritable bowel syndrome.
Venography has become the gold standard for diagnosing pelvic congestion. The procedure involves catheterization of the ovarian veins through a femoral or jugular approach. In our experience, the common femoral vein is the more frequently used access point. Using a contrast injection, the interventional radiologist can assess the degree of venous dilation and reflux in the pelvis.
There currently is no consensus on a cutoff for vein diameter or on any validated measures for congestion. According to one report on PCS authored by interventional radiologists, the diagnosis of PCS is confirmed with the venographic findings of ovarian vein diameter greater than 6 mm, retrograde ovarian or pelvic venous flow, presence of several tortuous collateral pelvic venous pathways, and delayed or stagnant clearance on contrast (Semin Intervent Radiol. 2008 Dec;25[4]:361-8).
The criteria vary, however. A recent literature review on pelvic congestion syndrome by Chiara Borghi, MD, and Lucio Dell’Atti, MD, states that incompetent pelvic veins are defined as more than 5-10 mm in diameter (Arch Gynecol Obstet. 2016 Feb;293[2]:291-301).
To more accurately diagnose PCS, our patients undergo tilt-table venography. The patient is placed into a reverse-Trendelenburg upright or semi-upright position to potentially exacerbate any venous reflux or dilation.
Other methods of identifying and diagnosing pelvic congestion have included transabdominal and transvaginal ultrasound, CT, and MRI. While CT and MRI both offer an overview of the pelvic vasculature and are helpful for ruling out other causes of chronic pelvic pain, they have low specificity for pelvic varices, according to the Italian review.
Sonography performed in the supine position, on the other hand, appears to be increasingly viewed as an acceptable screening tool for determining which patients may ultimately benefit from venography. It is also important in evaluation to rule out other pathologies not yet excluded. However, it should not be used for diagnosis of PCS.
Treating PCS
There are two main approaches to treating PCS: venous ligation (a gynecologic surgical approach) and percutaneous transcatheter embolization (performed by interventional radiologists).
The literature and evidence base is still in its infancy, but is growing. In our experience, both approaches lead to good resolution of symptoms over time in the majority of patients, and appear superior to the medical therapies that have been proposed for treating PCS, such as progestins and gonadotropin-releasing hormone agonists. Success rates with medical therapy are more variable and appear to be more short lived.
A review published this year on the effectiveness of embolization of pelvic veins for reducing chronic pelvic pain showed that 75% of women undergoing embolization had symptomatic relief that generally increased over time and was sustained. The authors concluded that embolization appears to be effective for the majority of women, and is safe, although they also noted that the quality of the evidence is low (J Vasc Interv Radiol. 2016 Oct;27[10]:1478-86.e8). Their review was based almost entirely on prospective case series.
Dr. Borghi and Dr. Dell’Atti offered a similar assessment of embolization for PCS, stating in their review article that clinical success has been reported in 70%-85% of patients. They also report nearly equivalent success rates of up to 75% with treatment via surgical ligation of ovarian and/or pelvic vasculature. These findings are from mostly observational data and case series.
Decisions about which approach to take should be individualized. If there are no differences with respect to insurance coverage for the patient, then embolization may be the preferred approach because it is the most minimally invasive technique and can potentially be performed at the time of diagnostic venography, negating the need for a second procedure. A skilled interventional radiologist familiar with the disease and the treatment is necessary. Various embolic agents are utilized, including coils, glues, foams, and other agents that cause sclerosis of the abnormal veins.
In other cases, venous ligation is preferred, especially when an additional gynecologic surgery, such as a cystectomy or myomectomy, is required.
Surgical ligation of ovarian veins was initially performed via laparotomy using a traditional retroperitoneal approach. The surgical goal is to isolate the ovarian vein significantly above the pelvic brim and before the vein becomes substantially dilated. Laparotomy therefore requires a vertical mid-line incision to provide adequate access to the appropriate portion of the ovarian vessels, leading to potentially high morbidity and poor cosmesis.
More recently, gynecologic surgeons skilled in laparoscopy have successfully managed PCS transperitoneally. A few small series of bilateral laparoscopic transperitoneal ligation of ovarian veins have been reported, including one by Tigellio Gargiulo, MD, who clipped both veins in their upper third, near their distal ends at the inferior vena cava (right) and the renal vein (left) (J Am Assoc Gynecol Laparosc. 2003 Nov;10[4]:501-4).
We prefer a robot-assisted laparoscopic approach for most of our patients. Not only does the improved dexterity help while working with sensitive vasculature, but more importantly we are able to use Firefly fluorescence.
The procedure generally is as follows. The uterine adnexa on the affected side is grasped and placed on tension so that the infundibulopelvic (IP) ligament can be visualized as it courses up and above the pelvic brim. The peritoneum immediately over the IP ligament is gently grasped and tented upward, and a small incision is made into the peritoneum, providing access into the retroperitoneum. The ureter should be visualized medial to this dissection.
The peritoneal tissue is then gently dissected off the ovarian vessels. Once the vessels are freed from the peritoneal tissue, the dilated ovarian vein is often clearly visualized. It is important to note that if no venous dilation is seen during laparoscopy, the procedure should not be aborted. Due to the Trendelenburg position that is utilized in gynecologic – and especially laparoscopic – surgery, the venous system sometimes appears falsely “normal” at this time.
Once the ovarian vessels have been isolated, the arteries must be separated from the veins. The adventitial tissue is dissected until the vessels are separated. Great care should be taken to ensure that all movements run parallel to the vessels and not perpendicular, therefore decreasing the risk of bleeding.
This process can be challenging. The surgeon is working with delicate vasculature. Often there are several branches from the vein that have formed due to the abnormal venous system. The best way to approach it is to identify planes and separate those planes in order to isolate individual vessels. If difficulties are still encountered, the surgeon should restart the dissection higher.
Once the dilated ovarian vein is isolated, one to two clips are placed.
Usually the artery is clearly distinct from the vein as it is smaller, more elastic, and can be seen pulsing. However, occasionally it is difficult to distinguish. In these cases, assistance with the da Vinci surgical system is useful: Indocyanine green (ICG) dye can be injected intravenously and visualized with a near-infrared light on the da Vinci platform. The dye is then seen glowing green as it first courses through the artery and then the vein.
For patients who have been found on venography to have bilateral disease, we perform the ligation procedure bilaterally. Once ligation is complete, the more competent collateral veins in the pelvis will assume more of the venous circulation.
In our experience, patients have ultimately noted substantial pain relief after these procedures, both with the endoscopic embolization and the surgical ligation. Patients are counseled that it can take several months to notice a relief in the pain.
In rare cases, pelvic congestion is related to extrinsic compression. For instance, the left renal vein can become compressed between the aorta and the superior mesenteric artery (the nutcracker syndrome), or the left common iliac vein can be compressed between the overlying right internal iliac artery and the underlying vertebral body (May-Thurner syndrome). Both of these conditions can lead to secondary PCS.
Such complex conditions are usually treated by vascular surgeons. May-Thurner syndrome is treated via stenting, while nutcracker syndrome can be treated with stenting or transposition of the renal vein to the distal vena cava.
Dr. Steller is an associate at the Family Health Centers of San Diego. She reported having no relevant financial disclosures.
BY CHARLES E. MILLER, MD
Chronic pelvic pain is described as the presence of lower abdominal or pelvic pain for longer than 6 months. It is believed to affect approximately one in six women and 12%-15% of women of reproductive age. The diagnosis and treatment of chronic pelvic pain adds as much as a $2 billion burden to our health system annually.
It was first described clinically in the literature in 1857, while the existence of pelvic varicosities wasn’t documented for nearly another 100 years. Pelvic congestion syndrome (PCS) accounts for 30%-70% of cases presenting with chronic pelvic pain. PCS can be due to pelvic venous insufficiency, characterized by reflux into pelvic veins leading to pelvic varicosities or alternative venous pathways secondary to varicose veins of the leg.
Other etiologies of PCS include nutcracker syndrome (left renal vein compressed between the aorta and the superior mesenteric artery), May-Thurner syndrome (compression of the left common iliac vein by the right common iliac artery) or, less likely, tumor thrombosis of the inferior vena cava, portal vein thrombosis, renal cell carcinoma, left renal thrombosis, or left kidney arterial-venous fistula.
While there appears to be significant literature indicating a long-term success rate of greater than 80% in patients treated by percutaneous endovascular procedures (embolization, stenting), there is far less information on the postsurgical success of blocking the varicose gonadal vein. Nevertheless, our long-term results with gonadal vein clipping is virtually the same as that of our radiological colleagues.
It is a pleasure to welcome Courtney Steller, DO, to this edition of the Master Class in Gynecologic Surgery to discuss the diagnosis and treatment of PCS, with an emphasis on surgical correction.
Dr. Steller is a recent graduate of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill. She is currently in private practice and is an associate at the Family Health Centers of San Diego, Calif.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, and past president of the AAGL and the International Society for Gynecologic Endoscopy. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. He reported having no financial disclosures relevant to this column. Email him at obnews@frontlinemedcom.com.
Pelvic congestion syndrome: A treatable cause of pain
BY COURTNEY STELLER, DO
Pelvic congestion syndrome is a poorly understood and underdiagnosed disease. Yet, over the last decade, the syndrome has become less controversial as the etiology has become better understood and as the diagnostic approach has become more specific. Through these advances, treatments have also become increasingly more successful.
This is an important shift, because the chronic pelvic pain experienced by patients with pelvic congestion significantly impacts their quality of life and well-being. As the pain persists, it can become exceedingly difficult to manage. Many patients we have ultimately treated for pelvic congestion syndrome have had years of various work-ups, significant diagnostic investigations, and trials of different treatments without having any cause of their pain identified or achieving any lasting symptom relief.
The pelvic pain in patients with pelvic congestion syndrome (PCS) can be noncyclical or cyclical. It is present most of the time but tends to get worse at the end of the day and after long periods of standing and/or sitting. The pain also may worsen with intercourse, largely afterward. The syndrome tends to occur in premenopausal and multiparous women, but it’s important to appreciate that this is not always the case; we have diagnosed and treated PCS in several young, nulliparous patients as well.
Features and diagnosis
PCS is a disorder of pelvic venous circulation that predominantly affects the ovarian veins. It is sometimes referred to as pelvic vein incompetence or pelvic vascular dysfunction. Just as veins in the legs can enlarge and become varicose, the ovarian veins – and sometimes the internal iliac veins – can become incompetent and unable to effectively return blood back to the heart.
Pregnancy may predispose patients to developing the abnormally dilated and refluxing veins that characterize PCS, as the increase in pelvic vein capacity and uterine compression can lead to significant stasis of blood in the pelvis and subsequent damage to the veins and the venous valves. There also is believed to be an estrogen component to the development of PCS, because estrogen is known to act as a vasodilator. Moreover, a congenital absence and incompetence of venous valves in some cases has been reported.
In a recent study looking at pelvic vein incompetence and symptoms of chronic pelvic pain, these women were reported to have a distinctive symptom profile, with the “most notable” features being the presence of dull pelvic pain that radiates to the upper thighs and is aggravated by prolonged standing and walking – symptoms that are similar to the leg symptoms experienced by patients with severe varicose veins (Eur J Obstet Gynecol Reprod Biol. 2016 Jan;196:21-5).
Other investigators have similarly described the pelvic pain related to PCS as a dull ache or heaviness sensation that is most severe at the end of the day and that is lessened with supine positioning (though not necessarily immediately) and often exacerbated with sexual intercourse, especially post coitus. These descriptions are in line with my experience with PCS. There is usually exquisite tenderness on pelvic exam, especially localized to the adnexa. Patients will often have varicose veins on their upper legs or labia.
Interestingly, it has been repeatedly shown that many women have dilated and incompetent pelvic veins without also having such pathognomonic pain. We therefore cannot treat women based solely on the finding of abnormal veins.
On the other hand we must determine which patients with chronic pelvic pain have PCS. The differential diagnosis for PCS includes endometriosis, adenomyosis chronic pelvic inflammatory disease, adhesive disease, adnexal masses, adnexal torsion, and several nongynecologic diseases including interstitial cystitis and irritable bowel syndrome.
Venography has become the gold standard for diagnosing pelvic congestion. The procedure involves catheterization of the ovarian veins through a femoral or jugular approach. In our experience, the common femoral vein is the more frequently used access point. Using a contrast injection, the interventional radiologist can assess the degree of venous dilation and reflux in the pelvis.
There currently is no consensus on a cutoff for vein diameter or on any validated measures for congestion. According to one report on PCS authored by interventional radiologists, the diagnosis of PCS is confirmed with the venographic findings of ovarian vein diameter greater than 6 mm, retrograde ovarian or pelvic venous flow, presence of several tortuous collateral pelvic venous pathways, and delayed or stagnant clearance on contrast (Semin Intervent Radiol. 2008 Dec;25[4]:361-8).
The criteria vary, however. A recent literature review on pelvic congestion syndrome by Chiara Borghi, MD, and Lucio Dell’Atti, MD, states that incompetent pelvic veins are defined as more than 5-10 mm in diameter (Arch Gynecol Obstet. 2016 Feb;293[2]:291-301).
To more accurately diagnose PCS, our patients undergo tilt-table venography. The patient is placed into a reverse-Trendelenburg upright or semi-upright position to potentially exacerbate any venous reflux or dilation.
Other methods of identifying and diagnosing pelvic congestion have included transabdominal and transvaginal ultrasound, CT, and MRI. While CT and MRI both offer an overview of the pelvic vasculature and are helpful for ruling out other causes of chronic pelvic pain, they have low specificity for pelvic varices, according to the Italian review.
Sonography performed in the supine position, on the other hand, appears to be increasingly viewed as an acceptable screening tool for determining which patients may ultimately benefit from venography. It is also important in evaluation to rule out other pathologies not yet excluded. However, it should not be used for diagnosis of PCS.
Treating PCS
There are two main approaches to treating PCS: venous ligation (a gynecologic surgical approach) and percutaneous transcatheter embolization (performed by interventional radiologists).
The literature and evidence base is still in its infancy, but is growing. In our experience, both approaches lead to good resolution of symptoms over time in the majority of patients, and appear superior to the medical therapies that have been proposed for treating PCS, such as progestins and gonadotropin-releasing hormone agonists. Success rates with medical therapy are more variable and appear to be more short lived.
A review published this year on the effectiveness of embolization of pelvic veins for reducing chronic pelvic pain showed that 75% of women undergoing embolization had symptomatic relief that generally increased over time and was sustained. The authors concluded that embolization appears to be effective for the majority of women, and is safe, although they also noted that the quality of the evidence is low (J Vasc Interv Radiol. 2016 Oct;27[10]:1478-86.e8). Their review was based almost entirely on prospective case series.
Dr. Borghi and Dr. Dell’Atti offered a similar assessment of embolization for PCS, stating in their review article that clinical success has been reported in 70%-85% of patients. They also report nearly equivalent success rates of up to 75% with treatment via surgical ligation of ovarian and/or pelvic vasculature. These findings are from mostly observational data and case series.
Decisions about which approach to take should be individualized. If there are no differences with respect to insurance coverage for the patient, then embolization may be the preferred approach because it is the most minimally invasive technique and can potentially be performed at the time of diagnostic venography, negating the need for a second procedure. A skilled interventional radiologist familiar with the disease and the treatment is necessary. Various embolic agents are utilized, including coils, glues, foams, and other agents that cause sclerosis of the abnormal veins.
In other cases, venous ligation is preferred, especially when an additional gynecologic surgery, such as a cystectomy or myomectomy, is required.
Surgical ligation of ovarian veins was initially performed via laparotomy using a traditional retroperitoneal approach. The surgical goal is to isolate the ovarian vein significantly above the pelvic brim and before the vein becomes substantially dilated. Laparotomy therefore requires a vertical mid-line incision to provide adequate access to the appropriate portion of the ovarian vessels, leading to potentially high morbidity and poor cosmesis.
More recently, gynecologic surgeons skilled in laparoscopy have successfully managed PCS transperitoneally. A few small series of bilateral laparoscopic transperitoneal ligation of ovarian veins have been reported, including one by Tigellio Gargiulo, MD, who clipped both veins in their upper third, near their distal ends at the inferior vena cava (right) and the renal vein (left) (J Am Assoc Gynecol Laparosc. 2003 Nov;10[4]:501-4).
We prefer a robot-assisted laparoscopic approach for most of our patients. Not only does the improved dexterity help while working with sensitive vasculature, but more importantly we are able to use Firefly fluorescence.
The procedure generally is as follows. The uterine adnexa on the affected side is grasped and placed on tension so that the infundibulopelvic (IP) ligament can be visualized as it courses up and above the pelvic brim. The peritoneum immediately over the IP ligament is gently grasped and tented upward, and a small incision is made into the peritoneum, providing access into the retroperitoneum. The ureter should be visualized medial to this dissection.
The peritoneal tissue is then gently dissected off the ovarian vessels. Once the vessels are freed from the peritoneal tissue, the dilated ovarian vein is often clearly visualized. It is important to note that if no venous dilation is seen during laparoscopy, the procedure should not be aborted. Due to the Trendelenburg position that is utilized in gynecologic – and especially laparoscopic – surgery, the venous system sometimes appears falsely “normal” at this time.
Once the ovarian vessels have been isolated, the arteries must be separated from the veins. The adventitial tissue is dissected until the vessels are separated. Great care should be taken to ensure that all movements run parallel to the vessels and not perpendicular, therefore decreasing the risk of bleeding.
This process can be challenging. The surgeon is working with delicate vasculature. Often there are several branches from the vein that have formed due to the abnormal venous system. The best way to approach it is to identify planes and separate those planes in order to isolate individual vessels. If difficulties are still encountered, the surgeon should restart the dissection higher.
Once the dilated ovarian vein is isolated, one to two clips are placed.
Usually the artery is clearly distinct from the vein as it is smaller, more elastic, and can be seen pulsing. However, occasionally it is difficult to distinguish. In these cases, assistance with the da Vinci surgical system is useful: Indocyanine green (ICG) dye can be injected intravenously and visualized with a near-infrared light on the da Vinci platform. The dye is then seen glowing green as it first courses through the artery and then the vein.
For patients who have been found on venography to have bilateral disease, we perform the ligation procedure bilaterally. Once ligation is complete, the more competent collateral veins in the pelvis will assume more of the venous circulation.
In our experience, patients have ultimately noted substantial pain relief after these procedures, both with the endoscopic embolization and the surgical ligation. Patients are counseled that it can take several months to notice a relief in the pain.
In rare cases, pelvic congestion is related to extrinsic compression. For instance, the left renal vein can become compressed between the aorta and the superior mesenteric artery (the nutcracker syndrome), or the left common iliac vein can be compressed between the overlying right internal iliac artery and the underlying vertebral body (May-Thurner syndrome). Both of these conditions can lead to secondary PCS.
Such complex conditions are usually treated by vascular surgeons. May-Thurner syndrome is treated via stenting, while nutcracker syndrome can be treated with stenting or transposition of the renal vein to the distal vena cava.
Dr. Steller is an associate at the Family Health Centers of San Diego. She reported having no relevant financial disclosures.

‘Committed’ takes a nonpatronizing approach to involuntary care
Psychiatrists are trained to view involuntary treatment as an unpleasant means to a desirable end, a necessary evil. And we make the assumption that patients who are helped by the care they receive involuntarily will ultimately be grateful for that care.
Dinah Miller, MD, and Annette Hanson, MD, were inspired to write “Committed: The Battle Over Involuntary Psychiatric Care,” when they discovered that this assumption is false, that there are no clear data about the long-term effects of involuntary care, and that many patients whose mental illnesses improved as the result of involuntary care were terribly traumatized by their experiences of being forced into treatment. In writing “Committed,” Dr. Miller and Dr. Hanson set out to understand those experiences, and the contexts, both psychiatric and legal, in which they occurred.

There are two main cases that help tell the “Committed” “story,” Eleanor and Lily. Both were hospitalized involuntarily for psychotic episodes; both improved psychiatrically because of hospitalization; and both currently are functioning well. But years later, Eleanor is still resentful and traumatized, and Lily is grateful.
One of the many strengths of “Committed” is in the open-minded, nonpatronizing way it approaches differences in perspective. Numerous patients were interviewed for the book, and their complaints are taken seriously, not simply dismissed as manifestations of psychosis or “borderline traits.” At the same time, Dr. Miller and Dr. Hanson are well aware of distortions and errors in memory, as well as misperceptions about care, and they share their questioning of patients’ stories.
Another strength of “Committed” is that it does not shy away from controversy. It takes an honest look at the gamut of positions with regard to involuntary treatment, from Dr. E. Fuller Torrey’s Treatment Advocacy Center, which takes the view that it is a disservice not to force patients who are unaware that they are ill into treatment, to the Church of Scientology’s Citizens Commission on Human Rights, which doesn’t believe in the existence of mental illness, and therefore views involuntary treatment as unacceptable under any circumstance. The authors genuinely try to understand each group’s rationale, but they are also courageous enough to state their own position: that involuntary care should be avoided if at all possible but is sometimes necessary as a last resort. They also make the invaluable point that simply placing someone in a locked ward, or assigning him to involuntary outpatient care, will accomplish nothing if there are no adequate services to support his long-term care plan, and that those services require funding.
The book’s one drawback for me is the authors’ choice to break up Eleanor’s and Lily’s cases into segments. I found it a little difficult to pick up where the case had been left off several chapters earlier. But the reason for this choice is clearly that it allows the reader to consider an individual topic in the context of that topic’s application to the main cases.
“Committed” is easy to read and well-written, even waxing poetic at times. In describing Lily, Dr. Miller writes, “Her right cheek was punctuated by the best of dimples.” It is written in such a way that it is easily understandable by a lay person but still has a plethora of information that will be new and useful to mental health professionals. In fact, I am flabbergasted by the amount of research that went into writing it.
Committed bravely addresses the complex question of what it means to take away someone’s rights, not because she committed a crime, but because her mind is not working “normally.” It is an excellent book that should be required reading for anyone interested in the concept of autonomy, which is to say, everyone.
Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York City.
Psychiatrists are trained to view involuntary treatment as an unpleasant means to a desirable end, a necessary evil. And we make the assumption that patients who are helped by the care they receive involuntarily will ultimately be grateful for that care.
Dinah Miller, MD, and Annette Hanson, MD, were inspired to write “Committed: The Battle Over Involuntary Psychiatric Care,” when they discovered that this assumption is false, that there are no clear data about the long-term effects of involuntary care, and that many patients whose mental illnesses improved as the result of involuntary care were terribly traumatized by their experiences of being forced into treatment. In writing “Committed,” Dr. Miller and Dr. Hanson set out to understand those experiences, and the contexts, both psychiatric and legal, in which they occurred.
There are two main cases that help tell the “Committed” “story,” Eleanor and Lily. Both were hospitalized involuntarily for psychotic episodes; both improved psychiatrically because of hospitalization; and both currently are functioning well. But years later, Eleanor is still resentful and traumatized, and Lily is grateful.
One of the many strengths of “Committed” is in the open-minded, nonpatronizing way it approaches differences in perspective. Numerous patients were interviewed for the book, and their complaints are taken seriously, not simply dismissed as manifestations of psychosis or “borderline traits.” At the same time, Dr. Miller and Dr. Hanson are well aware of distortions and errors in memory, as well as misperceptions about care, and they share their questioning of patients’ stories.
Another strength of “Committed” is that it does not shy away from controversy. It takes an honest look at the gamut of positions with regard to involuntary treatment, from Dr. E. Fuller Torrey’s Treatment Advocacy Center, which takes the view that it is a disservice not to force patients who are unaware that they are ill into treatment, to the Church of Scientology’s Citizens Commission on Human Rights, which doesn’t believe in the existence of mental illness, and therefore views involuntary treatment as unacceptable under any circumstance. The authors genuinely try to understand each group’s rationale, but they are also courageous enough to state their own position: that involuntary care should be avoided if at all possible but is sometimes necessary as a last resort. They also make the invaluable point that simply placing someone in a locked ward, or assigning him to involuntary outpatient care, will accomplish nothing if there are no adequate services to support his long-term care plan, and that those services require funding.
The book’s one drawback for me is the authors’ choice to break up Eleanor’s and Lily’s cases into segments. I found it a little difficult to pick up where the case had been left off several chapters earlier. But the reason for this choice is clearly that it allows the reader to consider an individual topic in the context of that topic’s application to the main cases.
“Committed” is easy to read and well-written, even waxing poetic at times. In describing Lily, Dr. Miller writes, “Her right cheek was punctuated by the best of dimples.” It is written in such a way that it is easily understandable by a lay person but still has a plethora of information that will be new and useful to mental health professionals. In fact, I am flabbergasted by the amount of research that went into writing it.
Committed bravely addresses the complex question of what it means to take away someone’s rights, not because she committed a crime, but because her mind is not working “normally.” It is an excellent book that should be required reading for anyone interested in the concept of autonomy, which is to say, everyone.
Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York City.
Psychiatrists are trained to view involuntary treatment as an unpleasant means to a desirable end, a necessary evil. And we make the assumption that patients who are helped by the care they receive involuntarily will ultimately be grateful for that care.
Dinah Miller, MD, and Annette Hanson, MD, were inspired to write “Committed: The Battle Over Involuntary Psychiatric Care,” when they discovered that this assumption is false, that there are no clear data about the long-term effects of involuntary care, and that many patients whose mental illnesses improved as the result of involuntary care were terribly traumatized by their experiences of being forced into treatment. In writing “Committed,” Dr. Miller and Dr. Hanson set out to understand those experiences, and the contexts, both psychiatric and legal, in which they occurred.
There are two main cases that help tell the “Committed” “story,” Eleanor and Lily. Both were hospitalized involuntarily for psychotic episodes; both improved psychiatrically because of hospitalization; and both currently are functioning well. But years later, Eleanor is still resentful and traumatized, and Lily is grateful.
One of the many strengths of “Committed” is in the open-minded, nonpatronizing way it approaches differences in perspective. Numerous patients were interviewed for the book, and their complaints are taken seriously, not simply dismissed as manifestations of psychosis or “borderline traits.” At the same time, Dr. Miller and Dr. Hanson are well aware of distortions and errors in memory, as well as misperceptions about care, and they share their questioning of patients’ stories.
Another strength of “Committed” is that it does not shy away from controversy. It takes an honest look at the gamut of positions with regard to involuntary treatment, from Dr. E. Fuller Torrey’s Treatment Advocacy Center, which takes the view that it is a disservice not to force patients who are unaware that they are ill into treatment, to the Church of Scientology’s Citizens Commission on Human Rights, which doesn’t believe in the existence of mental illness, and therefore views involuntary treatment as unacceptable under any circumstance. The authors genuinely try to understand each group’s rationale, but they are also courageous enough to state their own position: that involuntary care should be avoided if at all possible but is sometimes necessary as a last resort. They also make the invaluable point that simply placing someone in a locked ward, or assigning him to involuntary outpatient care, will accomplish nothing if there are no adequate services to support his long-term care plan, and that those services require funding.
The book’s one drawback for me is the authors’ choice to break up Eleanor’s and Lily’s cases into segments. I found it a little difficult to pick up where the case had been left off several chapters earlier. But the reason for this choice is clearly that it allows the reader to consider an individual topic in the context of that topic’s application to the main cases.
“Committed” is easy to read and well-written, even waxing poetic at times. In describing Lily, Dr. Miller writes, “Her right cheek was punctuated by the best of dimples.” It is written in such a way that it is easily understandable by a lay person but still has a plethora of information that will be new and useful to mental health professionals. In fact, I am flabbergasted by the amount of research that went into writing it.
Committed bravely addresses the complex question of what it means to take away someone’s rights, not because she committed a crime, but because her mind is not working “normally.” It is an excellent book that should be required reading for anyone interested in the concept of autonomy, which is to say, everyone.
Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York City.
A Quick Lesson on Bundled Payments
The Centers for Medicare & Medicaid Services (CMS) has too many new payment models for a practicing doctor to keep up with them all. But there are three that I think are most important for hospitalists to know something about: hospital value-based purchasing, MACRA-related models, and bundled payments. Here, I’ll focus on the latter, which unlike the first two, influences payment to both hospitals and physicians (as well as other providers).
Bundles for Different Diagnoses
Bundled payment programs are the most visible of CMS’s episode payment models (EPMs). There are currently voluntary bundle models (called Bundled Payments for Care Improvement, or BPCI) across many different diagnoses. And in some locales, there is a mandatory bundle program for hip and knee replacements that began in March 2016 (called Comprehensive Care for Joint Replacement, or CCJR or just CJR).
These programs are set to expand significantly in the next few years. The Surgical Hip and Femur Fracture Treatment (SHFFT) becomes active in 2017 in some locales. It will essentially add hip and femur fractures requiring surgery to the existing CJR program. New bundles for acute myocardial infarction, either managed medically or with percutaneous coronary intervention (PCI), and coronary bypass surgery will become mandatory in some parts of the country beginning July 2017.
How the Programs Work
CMS totals all Medicare dollars paid per patient historically for the relevant bundle. This includes payments to the hospital (e.g., the DRG payment) and all fees paid to physicians, therapists, visiting nurses, skilled nursing facilities, etc., from the time of hospital admission through 90 days after discharge. It then sets a target spend (or price) for that diagnosis that is about 3% below the historical average. Because it is based on the past track record of a hospital and its market (or region), the price will vary from place to place.
If, going forward, the Medicare spend for each patient is below the target, CMS pays that amount to the hospital. But if the spend is above the target, the hospital pays some or all of that amount to CMS. Presumably, hospitals will have negotiated with others, such as physicians, how such an “upside” or penalty payment will be divided between them.
It’s worth noting that all parties continue to bill, and are paid by Medicare, via the same fee-for-service arrangements currently in place. It is only at the time of a “true up” that an upside is paid or penalty assessed. And hospitals are eligible for upside payments only if they perform above a threshold on a few quality and patient satisfaction metrics.
The details of these programs are incredibly complicated, and I’m intentionally providing a very simple description of them here. I think that nearly all practicing clinicians should not try to learn and keep up with all of the precise details. They change often! Instead, it’s best to focus on the big picture only and rely on others at the hospital to keep track of the details.
Ways to Lower the Spend
These programs are intended to provide a significant financial incentive to find lower-cost ways to care for patients while still ensuring good care. Any successful effort to lower the cost should start by analyzing just what Medicare spends on each element of care over the more than 90 days each patient is in the bundle. For example, for hip and knee replacement patients, nearly half of the spend goes toward post-hospital services such as a skilled nursing facility and home nursing visits. So the best opportunity to reduce the spend may be to reduce utilization of these services where appropriate.
For patients in the bundles for coronary artery bypass grafting and acute myocardial infarction treated with PCI, only about 10% of the total spend goes to post-hospital services. For these, it might be more effective to focus cost reductions on other things.
Each organization will need to make its own decisions regarding where to focus cost-reduction efforts across the bundle. For many of us, that will mean moving away from a focus on traditional hospitalist-related cost-containment efforts like length of stay or pharmacy costs and instead looking at the bigger picture, including use of post-hospital services.
Some Things to Watch
I expect there will be a number of side effects of these payment models that hospitalists will care about. Doctors in different specialties, for example, might change their minds about whether they want to serve as attending physicians for “bundle patients.” One scenario is that if orthopedists have an opportunity to realize a significant financial upside, they may prefer to serve as attendings for hip fracture patients rather than leaving to hospitalists financially important decisions such as whether patients are discharged to a skilled nursing facility or home. We’ll just have to see how that plays out and be prepared to advocate for our position if different from other specialties.
Successful performance in bundles requires effective coordination of care across settings, and I’m hopeful this will benefit patients. Hospitals and skilled nursing facilities, for example, will need to work together more effectively to curb unnecessary days in the facilities and to reduce readmissions. Many hospitals have already begun developing a preferred network of skilled nursing facilities for referrals that is based on demonstrating good care and low returns to the hospital. Your hospital has probably already started doing this work even if you haven’t heard about it yet.
For me, one of the most concerning outcomes of bundles is the negotiations between providers regarding how an upside or penalty is to be shared among them. I suspect this won’t be contentious initially, but as the dollars at stake grow, it could lead to increasingly stressful negotiations and relationships.
And, lastly, like any payment model, bundles are “gameable,” especially bundles for medical diagnoses such as congestive heart failure or pneumonia, which can be gamed by lowering the threshold for admitting less-sick patients to inpatient status. The spend for these patients, who are less likely to require expensive post-hospital services or be readmitted, will lower the average spend in the bundle, increasing the chance of an upside payment for the providers. TH

The Centers for Medicare & Medicaid Services (CMS) has too many new payment models for a practicing doctor to keep up with them all. But there are three that I think are most important for hospitalists to know something about: hospital value-based purchasing, MACRA-related models, and bundled payments. Here, I’ll focus on the latter, which unlike the first two, influences payment to both hospitals and physicians (as well as other providers).
Bundles for Different Diagnoses
Bundled payment programs are the most visible of CMS’s episode payment models (EPMs). There are currently voluntary bundle models (called Bundled Payments for Care Improvement, or BPCI) across many different diagnoses. And in some locales, there is a mandatory bundle program for hip and knee replacements that began in March 2016 (called Comprehensive Care for Joint Replacement, or CCJR or just CJR).
These programs are set to expand significantly in the next few years. The Surgical Hip and Femur Fracture Treatment (SHFFT) becomes active in 2017 in some locales. It will essentially add hip and femur fractures requiring surgery to the existing CJR program. New bundles for acute myocardial infarction, either managed medically or with percutaneous coronary intervention (PCI), and coronary bypass surgery will become mandatory in some parts of the country beginning July 2017.
How the Programs Work
CMS totals all Medicare dollars paid per patient historically for the relevant bundle. This includes payments to the hospital (e.g., the DRG payment) and all fees paid to physicians, therapists, visiting nurses, skilled nursing facilities, etc., from the time of hospital admission through 90 days after discharge. It then sets a target spend (or price) for that diagnosis that is about 3% below the historical average. Because it is based on the past track record of a hospital and its market (or region), the price will vary from place to place.
If, going forward, the Medicare spend for each patient is below the target, CMS pays that amount to the hospital. But if the spend is above the target, the hospital pays some or all of that amount to CMS. Presumably, hospitals will have negotiated with others, such as physicians, how such an “upside” or penalty payment will be divided between them.
It’s worth noting that all parties continue to bill, and are paid by Medicare, via the same fee-for-service arrangements currently in place. It is only at the time of a “true up” that an upside is paid or penalty assessed. And hospitals are eligible for upside payments only if they perform above a threshold on a few quality and patient satisfaction metrics.
The details of these programs are incredibly complicated, and I’m intentionally providing a very simple description of them here. I think that nearly all practicing clinicians should not try to learn and keep up with all of the precise details. They change often! Instead, it’s best to focus on the big picture only and rely on others at the hospital to keep track of the details.
Ways to Lower the Spend
These programs are intended to provide a significant financial incentive to find lower-cost ways to care for patients while still ensuring good care. Any successful effort to lower the cost should start by analyzing just what Medicare spends on each element of care over the more than 90 days each patient is in the bundle. For example, for hip and knee replacement patients, nearly half of the spend goes toward post-hospital services such as a skilled nursing facility and home nursing visits. So the best opportunity to reduce the spend may be to reduce utilization of these services where appropriate.
For patients in the bundles for coronary artery bypass grafting and acute myocardial infarction treated with PCI, only about 10% of the total spend goes to post-hospital services. For these, it might be more effective to focus cost reductions on other things.
Each organization will need to make its own decisions regarding where to focus cost-reduction efforts across the bundle. For many of us, that will mean moving away from a focus on traditional hospitalist-related cost-containment efforts like length of stay or pharmacy costs and instead looking at the bigger picture, including use of post-hospital services.
Some Things to Watch
I expect there will be a number of side effects of these payment models that hospitalists will care about. Doctors in different specialties, for example, might change their minds about whether they want to serve as attending physicians for “bundle patients.” One scenario is that if orthopedists have an opportunity to realize a significant financial upside, they may prefer to serve as attendings for hip fracture patients rather than leaving to hospitalists financially important decisions such as whether patients are discharged to a skilled nursing facility or home. We’ll just have to see how that plays out and be prepared to advocate for our position if different from other specialties.
Successful performance in bundles requires effective coordination of care across settings, and I’m hopeful this will benefit patients. Hospitals and skilled nursing facilities, for example, will need to work together more effectively to curb unnecessary days in the facilities and to reduce readmissions. Many hospitals have already begun developing a preferred network of skilled nursing facilities for referrals that is based on demonstrating good care and low returns to the hospital. Your hospital has probably already started doing this work even if you haven’t heard about it yet.
For me, one of the most concerning outcomes of bundles is the negotiations between providers regarding how an upside or penalty is to be shared among them. I suspect this won’t be contentious initially, but as the dollars at stake grow, it could lead to increasingly stressful negotiations and relationships.
And, lastly, like any payment model, bundles are “gameable,” especially bundles for medical diagnoses such as congestive heart failure or pneumonia, which can be gamed by lowering the threshold for admitting less-sick patients to inpatient status. The spend for these patients, who are less likely to require expensive post-hospital services or be readmitted, will lower the average spend in the bundle, increasing the chance of an upside payment for the providers. TH
The Centers for Medicare & Medicaid Services (CMS) has too many new payment models for a practicing doctor to keep up with them all. But there are three that I think are most important for hospitalists to know something about: hospital value-based purchasing, MACRA-related models, and bundled payments. Here, I’ll focus on the latter, which unlike the first two, influences payment to both hospitals and physicians (as well as other providers).
Bundles for Different Diagnoses
Bundled payment programs are the most visible of CMS’s episode payment models (EPMs). There are currently voluntary bundle models (called Bundled Payments for Care Improvement, or BPCI) across many different diagnoses. And in some locales, there is a mandatory bundle program for hip and knee replacements that began in March 2016 (called Comprehensive Care for Joint Replacement, or CCJR or just CJR).
These programs are set to expand significantly in the next few years. The Surgical Hip and Femur Fracture Treatment (SHFFT) becomes active in 2017 in some locales. It will essentially add hip and femur fractures requiring surgery to the existing CJR program. New bundles for acute myocardial infarction, either managed medically or with percutaneous coronary intervention (PCI), and coronary bypass surgery will become mandatory in some parts of the country beginning July 2017.
How the Programs Work
CMS totals all Medicare dollars paid per patient historically for the relevant bundle. This includes payments to the hospital (e.g., the DRG payment) and all fees paid to physicians, therapists, visiting nurses, skilled nursing facilities, etc., from the time of hospital admission through 90 days after discharge. It then sets a target spend (or price) for that diagnosis that is about 3% below the historical average. Because it is based on the past track record of a hospital and its market (or region), the price will vary from place to place.
If, going forward, the Medicare spend for each patient is below the target, CMS pays that amount to the hospital. But if the spend is above the target, the hospital pays some or all of that amount to CMS. Presumably, hospitals will have negotiated with others, such as physicians, how such an “upside” or penalty payment will be divided between them.
It’s worth noting that all parties continue to bill, and are paid by Medicare, via the same fee-for-service arrangements currently in place. It is only at the time of a “true up” that an upside is paid or penalty assessed. And hospitals are eligible for upside payments only if they perform above a threshold on a few quality and patient satisfaction metrics.
The details of these programs are incredibly complicated, and I’m intentionally providing a very simple description of them here. I think that nearly all practicing clinicians should not try to learn and keep up with all of the precise details. They change often! Instead, it’s best to focus on the big picture only and rely on others at the hospital to keep track of the details.
Ways to Lower the Spend
These programs are intended to provide a significant financial incentive to find lower-cost ways to care for patients while still ensuring good care. Any successful effort to lower the cost should start by analyzing just what Medicare spends on each element of care over the more than 90 days each patient is in the bundle. For example, for hip and knee replacement patients, nearly half of the spend goes toward post-hospital services such as a skilled nursing facility and home nursing visits. So the best opportunity to reduce the spend may be to reduce utilization of these services where appropriate.
For patients in the bundles for coronary artery bypass grafting and acute myocardial infarction treated with PCI, only about 10% of the total spend goes to post-hospital services. For these, it might be more effective to focus cost reductions on other things.
Each organization will need to make its own decisions regarding where to focus cost-reduction efforts across the bundle. For many of us, that will mean moving away from a focus on traditional hospitalist-related cost-containment efforts like length of stay or pharmacy costs and instead looking at the bigger picture, including use of post-hospital services.
Some Things to Watch
I expect there will be a number of side effects of these payment models that hospitalists will care about. Doctors in different specialties, for example, might change their minds about whether they want to serve as attending physicians for “bundle patients.” One scenario is that if orthopedists have an opportunity to realize a significant financial upside, they may prefer to serve as attendings for hip fracture patients rather than leaving to hospitalists financially important decisions such as whether patients are discharged to a skilled nursing facility or home. We’ll just have to see how that plays out and be prepared to advocate for our position if different from other specialties.
Successful performance in bundles requires effective coordination of care across settings, and I’m hopeful this will benefit patients. Hospitals and skilled nursing facilities, for example, will need to work together more effectively to curb unnecessary days in the facilities and to reduce readmissions. Many hospitals have already begun developing a preferred network of skilled nursing facilities for referrals that is based on demonstrating good care and low returns to the hospital. Your hospital has probably already started doing this work even if you haven’t heard about it yet.
For me, one of the most concerning outcomes of bundles is the negotiations between providers regarding how an upside or penalty is to be shared among them. I suspect this won’t be contentious initially, but as the dollars at stake grow, it could lead to increasingly stressful negotiations and relationships.
And, lastly, like any payment model, bundles are “gameable,” especially bundles for medical diagnoses such as congestive heart failure or pneumonia, which can be gamed by lowering the threshold for admitting less-sick patients to inpatient status. The spend for these patients, who are less likely to require expensive post-hospital services or be readmitted, will lower the average spend in the bundle, increasing the chance of an upside payment for the providers. TH
‘Doc in a box’ vs.’tele-teaming’: Contending models of telepsychiatric care
As articulated by Steve Daviss, MD, DFAPA, in the inaugural column of Techiatry, the adoption and diffusion of telepsychiatry (live two-way interactive videoconferencing) have not been as rapid and universal as expected from those of us immersed in the field.
Despite having yet to achieve its full promise, telepsychiatry has reached maturity, and is being widely deployed and used across multiple systems, settings, and applications, albeit at times in an uneven, unsystematic manner. Emerging over the past decade of development are two distinct models/approaches to telepsychiatry, which I refer to as “doc in a box” and “tele-teaming.” Those models coexist, compete, and conflict within and across organizations. The dynamic between those two models highlights a larger emergent dialogue within psychiatry around psychiatrists’ core clinical roles and functions in our evolving health care systems.

The doc in a box model, as captured in early telepsychiatry services in the 1990s and early 2000s, focused on the virtual insertion of a solo psychiatrist into a distant setting. The services involved core psychiatric activities, such as diagnosis and assessment, with a heavy emphasis on pharmacologic management.
Not surprisingly, those services paralleled what was occurring for the rest of psychiatry at the time and were driven by the closer alignment of psychiatry with a biologic framework – and most importantly, reimbursement models that favored pharmacologic interventions and management. The subsequent rise of viable commercial telepsychiatry companies has continued offering this model driven by demands of the marketplace. While there is a legitimate place and need for such services, the phrase “doc in a box” narrows the scope of psychiatric practice, and reinforces current systems of health care structure and funding.
I proffer the phrase “tele-teaming” to denote telepsychiatric care that virtually embeds a psychiatrist as a member of a care team at a distant location. The use of telepsychiatry in integrated care is the clearest example of this. In integrated care, a psychiatrist works as part of a larger behavioral and medical team that may include case managers, social workers, psychologists, nurses, and family physicians to render care to patients in primary care clinics. The psychiatrist performs consultative, direct care, and supervisory roles in the context of the integrated care team, focusing on more holistic and population-based approaches to treatment.
Telepsychiatry, as well as other technologies (for example, electronic medical records, email, and patient registries), enables and enhances integrated care. Telepsychiatry allows smaller primary care practices, which on their own could not support a full-time psychiatrist, to create a full virtual team across multiple sites.
Tele-teaming as a concept is not limited to integrated care. Other notable examples include the use of telepsychiatry in substance rehabilitation facilities, long-term nursing homes, and psychiatric emergency services as a component of ERs. Tele-teaming and doc in a box models are not about the settings or populations to which they provide care, but the structure and philosophy of the psychiatric service.
As an illustration, imagine a rural community mental health center whose long-term psychiatric care provider retires. The center could set up a contract with a psychiatrist to provide medication management services for its patients through telepsychiatry. The psychiatrist, armed with a pen or eprescribing credentials, could provide several days a week of medication management. Treatment planning, therapy, and care coordination could be segmented off to other providers from the center (psychologists, social workers, and case managers). The psychiatrist’s time could be maximized by having the psychiatrist manage prescriptions, with communication between the patients’ various providers through a shared electronic medical record, as in the doc in a box model.
Alternatively, the center could set up a service where the psychiatrist became a virtual team member working to provide complete assessments, treatment planning, supervision, and psychiatric consultation, as well as pharmacologic management. Although in this scenario, the psychiatrist still could devote time to managing prescriptions, she/he also could spend time in team meetings, supervision, and seeing patients, often with her colleagues. In addition, the psychiatrist could work to coordinate care beyond the EMR, for example, through tele-teaming. Either of these scenarios can and do occur with in-person care as well, and the choice of which model to use would not be decided by the technology but by the underlying health care system in which it is being used.
Telepsychiatry begins to become transformative when it’s leveraged to shift, change, or innovate the model of care delivery. Historically, telepsychiatry has been thought of as a solution to patient access issues and as a way to address workforce shortages. The real promise of telepsychiatry in the form of tele-teaming is how it can begin to fundamentally change how care is delivered. The triple aim calls for decreased costs, improved health care for individuals, and a focus on population health.
We know that most Americans with major mental health issues will be seen in primary care, and that providing behavioral health care in primary care settings leads to lower overall health care costs, and improved behavioral and general health outcomes. Telepsychiatry will be essential in the further dissemination and expansion of integrated care, not only in rural and underserved areas, but across large health care systems. Tele-teaming will be essential in other arenas as well, as psychiatry faces the future challenges of an aging and decreasing (per capita) workforce. Team approaches help maximize psychiatrists’ role in the health care system, and help magnify the number of patients their skills and training can support.
Team approaches also help to broaden the scope of psychiatric practice and reclaim psychiatry’s place within the house of medicine. Telepsychiatry, if structured correctly, helps increase flexibility for psychiatrists. It expands the settings available to practice and provides more opportunities to engage in team-based care. Both the doc in a box and tele-teaming models have arisen from forces in the health care marketplace. The differing application of those two models across and within health care systems illustrates overall tensions within psychiatry about the current and future roles of psychiatrists.
Telepsychiatry is a powerful tool that can be leveraged to shape models of psychiatric care delivery or reinforce our existing structures. Which models are embraced will affect how psychiatry continues to evolve and address the challenges before the specialty.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry, and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center and associate professor of psychiatry at the University of Colorado at Denver, Aurora.
As articulated by Steve Daviss, MD, DFAPA, in the inaugural column of Techiatry, the adoption and diffusion of telepsychiatry (live two-way interactive videoconferencing) have not been as rapid and universal as expected from those of us immersed in the field.
Despite having yet to achieve its full promise, telepsychiatry has reached maturity, and is being widely deployed and used across multiple systems, settings, and applications, albeit at times in an uneven, unsystematic manner. Emerging over the past decade of development are two distinct models/approaches to telepsychiatry, which I refer to as “doc in a box” and “tele-teaming.” Those models coexist, compete, and conflict within and across organizations. The dynamic between those two models highlights a larger emergent dialogue within psychiatry around psychiatrists’ core clinical roles and functions in our evolving health care systems.
The doc in a box model, as captured in early telepsychiatry services in the 1990s and early 2000s, focused on the virtual insertion of a solo psychiatrist into a distant setting. The services involved core psychiatric activities, such as diagnosis and assessment, with a heavy emphasis on pharmacologic management.
Not surprisingly, those services paralleled what was occurring for the rest of psychiatry at the time and were driven by the closer alignment of psychiatry with a biologic framework – and most importantly, reimbursement models that favored pharmacologic interventions and management. The subsequent rise of viable commercial telepsychiatry companies has continued offering this model driven by demands of the marketplace. While there is a legitimate place and need for such services, the phrase “doc in a box” narrows the scope of psychiatric practice, and reinforces current systems of health care structure and funding.
I proffer the phrase “tele-teaming” to denote telepsychiatric care that virtually embeds a psychiatrist as a member of a care team at a distant location. The use of telepsychiatry in integrated care is the clearest example of this. In integrated care, a psychiatrist works as part of a larger behavioral and medical team that may include case managers, social workers, psychologists, nurses, and family physicians to render care to patients in primary care clinics. The psychiatrist performs consultative, direct care, and supervisory roles in the context of the integrated care team, focusing on more holistic and population-based approaches to treatment.
Telepsychiatry, as well as other technologies (for example, electronic medical records, email, and patient registries), enables and enhances integrated care. Telepsychiatry allows smaller primary care practices, which on their own could not support a full-time psychiatrist, to create a full virtual team across multiple sites.
Tele-teaming as a concept is not limited to integrated care. Other notable examples include the use of telepsychiatry in substance rehabilitation facilities, long-term nursing homes, and psychiatric emergency services as a component of ERs. Tele-teaming and doc in a box models are not about the settings or populations to which they provide care, but the structure and philosophy of the psychiatric service.
As an illustration, imagine a rural community mental health center whose long-term psychiatric care provider retires. The center could set up a contract with a psychiatrist to provide medication management services for its patients through telepsychiatry. The psychiatrist, armed with a pen or eprescribing credentials, could provide several days a week of medication management. Treatment planning, therapy, and care coordination could be segmented off to other providers from the center (psychologists, social workers, and case managers). The psychiatrist’s time could be maximized by having the psychiatrist manage prescriptions, with communication between the patients’ various providers through a shared electronic medical record, as in the doc in a box model.
Alternatively, the center could set up a service where the psychiatrist became a virtual team member working to provide complete assessments, treatment planning, supervision, and psychiatric consultation, as well as pharmacologic management. Although in this scenario, the psychiatrist still could devote time to managing prescriptions, she/he also could spend time in team meetings, supervision, and seeing patients, often with her colleagues. In addition, the psychiatrist could work to coordinate care beyond the EMR, for example, through tele-teaming. Either of these scenarios can and do occur with in-person care as well, and the choice of which model to use would not be decided by the technology but by the underlying health care system in which it is being used.
Telepsychiatry begins to become transformative when it’s leveraged to shift, change, or innovate the model of care delivery. Historically, telepsychiatry has been thought of as a solution to patient access issues and as a way to address workforce shortages. The real promise of telepsychiatry in the form of tele-teaming is how it can begin to fundamentally change how care is delivered. The triple aim calls for decreased costs, improved health care for individuals, and a focus on population health.
We know that most Americans with major mental health issues will be seen in primary care, and that providing behavioral health care in primary care settings leads to lower overall health care costs, and improved behavioral and general health outcomes. Telepsychiatry will be essential in the further dissemination and expansion of integrated care, not only in rural and underserved areas, but across large health care systems. Tele-teaming will be essential in other arenas as well, as psychiatry faces the future challenges of an aging and decreasing (per capita) workforce. Team approaches help maximize psychiatrists’ role in the health care system, and help magnify the number of patients their skills and training can support.
Team approaches also help to broaden the scope of psychiatric practice and reclaim psychiatry’s place within the house of medicine. Telepsychiatry, if structured correctly, helps increase flexibility for psychiatrists. It expands the settings available to practice and provides more opportunities to engage in team-based care. Both the doc in a box and tele-teaming models have arisen from forces in the health care marketplace. The differing application of those two models across and within health care systems illustrates overall tensions within psychiatry about the current and future roles of psychiatrists.
Telepsychiatry is a powerful tool that can be leveraged to shape models of psychiatric care delivery or reinforce our existing structures. Which models are embraced will affect how psychiatry continues to evolve and address the challenges before the specialty.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry, and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center and associate professor of psychiatry at the University of Colorado at Denver, Aurora.
As articulated by Steve Daviss, MD, DFAPA, in the inaugural column of Techiatry, the adoption and diffusion of telepsychiatry (live two-way interactive videoconferencing) have not been as rapid and universal as expected from those of us immersed in the field.
Despite having yet to achieve its full promise, telepsychiatry has reached maturity, and is being widely deployed and used across multiple systems, settings, and applications, albeit at times in an uneven, unsystematic manner. Emerging over the past decade of development are two distinct models/approaches to telepsychiatry, which I refer to as “doc in a box” and “tele-teaming.” Those models coexist, compete, and conflict within and across organizations. The dynamic between those two models highlights a larger emergent dialogue within psychiatry around psychiatrists’ core clinical roles and functions in our evolving health care systems.
The doc in a box model, as captured in early telepsychiatry services in the 1990s and early 2000s, focused on the virtual insertion of a solo psychiatrist into a distant setting. The services involved core psychiatric activities, such as diagnosis and assessment, with a heavy emphasis on pharmacologic management.
Not surprisingly, those services paralleled what was occurring for the rest of psychiatry at the time and were driven by the closer alignment of psychiatry with a biologic framework – and most importantly, reimbursement models that favored pharmacologic interventions and management. The subsequent rise of viable commercial telepsychiatry companies has continued offering this model driven by demands of the marketplace. While there is a legitimate place and need for such services, the phrase “doc in a box” narrows the scope of psychiatric practice, and reinforces current systems of health care structure and funding.
I proffer the phrase “tele-teaming” to denote telepsychiatric care that virtually embeds a psychiatrist as a member of a care team at a distant location. The use of telepsychiatry in integrated care is the clearest example of this. In integrated care, a psychiatrist works as part of a larger behavioral and medical team that may include case managers, social workers, psychologists, nurses, and family physicians to render care to patients in primary care clinics. The psychiatrist performs consultative, direct care, and supervisory roles in the context of the integrated care team, focusing on more holistic and population-based approaches to treatment.
Telepsychiatry, as well as other technologies (for example, electronic medical records, email, and patient registries), enables and enhances integrated care. Telepsychiatry allows smaller primary care practices, which on their own could not support a full-time psychiatrist, to create a full virtual team across multiple sites.
Tele-teaming as a concept is not limited to integrated care. Other notable examples include the use of telepsychiatry in substance rehabilitation facilities, long-term nursing homes, and psychiatric emergency services as a component of ERs. Tele-teaming and doc in a box models are not about the settings or populations to which they provide care, but the structure and philosophy of the psychiatric service.
As an illustration, imagine a rural community mental health center whose long-term psychiatric care provider retires. The center could set up a contract with a psychiatrist to provide medication management services for its patients through telepsychiatry. The psychiatrist, armed with a pen or eprescribing credentials, could provide several days a week of medication management. Treatment planning, therapy, and care coordination could be segmented off to other providers from the center (psychologists, social workers, and case managers). The psychiatrist’s time could be maximized by having the psychiatrist manage prescriptions, with communication between the patients’ various providers through a shared electronic medical record, as in the doc in a box model.
Alternatively, the center could set up a service where the psychiatrist became a virtual team member working to provide complete assessments, treatment planning, supervision, and psychiatric consultation, as well as pharmacologic management. Although in this scenario, the psychiatrist still could devote time to managing prescriptions, she/he also could spend time in team meetings, supervision, and seeing patients, often with her colleagues. In addition, the psychiatrist could work to coordinate care beyond the EMR, for example, through tele-teaming. Either of these scenarios can and do occur with in-person care as well, and the choice of which model to use would not be decided by the technology but by the underlying health care system in which it is being used.
Telepsychiatry begins to become transformative when it’s leveraged to shift, change, or innovate the model of care delivery. Historically, telepsychiatry has been thought of as a solution to patient access issues and as a way to address workforce shortages. The real promise of telepsychiatry in the form of tele-teaming is how it can begin to fundamentally change how care is delivered. The triple aim calls for decreased costs, improved health care for individuals, and a focus on population health.
We know that most Americans with major mental health issues will be seen in primary care, and that providing behavioral health care in primary care settings leads to lower overall health care costs, and improved behavioral and general health outcomes. Telepsychiatry will be essential in the further dissemination and expansion of integrated care, not only in rural and underserved areas, but across large health care systems. Tele-teaming will be essential in other arenas as well, as psychiatry faces the future challenges of an aging and decreasing (per capita) workforce. Team approaches help maximize psychiatrists’ role in the health care system, and help magnify the number of patients their skills and training can support.
Team approaches also help to broaden the scope of psychiatric practice and reclaim psychiatry’s place within the house of medicine. Telepsychiatry, if structured correctly, helps increase flexibility for psychiatrists. It expands the settings available to practice and provides more opportunities to engage in team-based care. Both the doc in a box and tele-teaming models have arisen from forces in the health care marketplace. The differing application of those two models across and within health care systems illustrates overall tensions within psychiatry about the current and future roles of psychiatrists.
Telepsychiatry is a powerful tool that can be leveraged to shape models of psychiatric care delivery or reinforce our existing structures. Which models are embraced will affect how psychiatry continues to evolve and address the challenges before the specialty.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry, and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center and associate professor of psychiatry at the University of Colorado at Denver, Aurora.
Editorial: Transitioning to College with Epilepsy
Nikesh Ardeshna, MD
Dr. Ardeshna is the Medical Director of Adult Epilepsy Services at Royal Oak Hospital, Beaumont Health , in Royal Oak, Michigan.
Starting college is both an exciting and stressful experience for new students. For people with epilepsy, going to college raises some specific and unique concerns compared to those without the condition . The purpose of this article is to look at some of the challenges for people with epilepsy and some potential solutions. The overall theme is that it is better to be prepared ahead of time.
The main goal of the person with epilepsy at college is to ensure that a breakthrough seizure does not occur, as this could lead to serious consequences (injuries, sprains, strains, and a change in lifestyle). However, it is equally important to ensure that an individual with epilepsy has a quality life.
For most students, attending college is one of life’s milestones. College is a new environment, with some new pressures that include academic success, making new friends (fitting in), participation in extracurricular activities (both academic and not), and taking personal responsibility of what may considered basic yet essential daily activities, such as meal preparation, laundry, etc.
Some of these issues may be of lesser concern, depending on the distance from college to home; however the struggle to maintain independence is common regardless how far away the college campus is from home.
If college is far from home, it may be better for the individual with epilepsy to establish care with a local neurologist, or preferably, a local epileptologist. This is helpful in case of emergency. Ideally, prescriptions should be transferred to a nearby pharmacy before refills are due. It is also beneficial to coordinate follow up visits if needed with the original neurologist/epileptologist at term breaks and vacations. If there is an increase in seizure frequency or side effects patients should contact their physician as soon as possible and not simply wait for the next trip home. It is advisable for people with epilepsy to keep a wallet card or similar such item with them that lists medications names and doses as well as emergency contact numbers. If the patient is traveling by air or bus, mediations should be packed in hand luggage, not checked baggage, to avoid the possible of delayed arrival at the destination.
As class times may differ in a college environment, individuals with epilepsy should ensure they remain complaint with their medication and not miss doses. This may mean remembering to carry the medication with them, and keeping an extra supply at the dormitory/residence in case of emergency.
For individuals with epilepsy, stressors, such as decreased sleep/sleep deprivation, missed meals, over exertion, dehydration can lead to breakthrough seizures (even in those who are compliant with their antiepileptic drugs [AEDs]). Sleep deprivation and missed meals can be somewhat common in a college atmosphere, especially around examination time. People with epilepsy should ensure they get adequate sleep, do not miss meals, and are adequately hydrated (more so when participating in sports).
Use of alcohol and or illicit substances should be avoided as these can reduce seizure threshold, reduce the effectiveness of AEDs, and lead to breakthrough seizures.
For people with epilepsy, there may be an underlying anxiety of if and when a breakthrough seizure may occur. However, it is important to note that for the college student, this fear should not prevent him or her from achieving their full potential.
Nikesh Ardeshna, MD
Dr. Ardeshna is the Medical Director of Adult Epilepsy Services at Royal Oak Hospital, Beaumont Health , in Royal Oak, Michigan.
Starting college is both an exciting and stressful experience for new students. For people with epilepsy, going to college raises some specific and unique concerns compared to those without the condition . The purpose of this article is to look at some of the challenges for people with epilepsy and some potential solutions. The overall theme is that it is better to be prepared ahead of time.
The main goal of the person with epilepsy at college is to ensure that a breakthrough seizure does not occur, as this could lead to serious consequences (injuries, sprains, strains, and a change in lifestyle). However, it is equally important to ensure that an individual with epilepsy has a quality life.
For most students, attending college is one of life’s milestones. College is a new environment, with some new pressures that include academic success, making new friends (fitting in), participation in extracurricular activities (both academic and not), and taking personal responsibility of what may considered basic yet essential daily activities, such as meal preparation, laundry, etc.
Some of these issues may be of lesser concern, depending on the distance from college to home; however the struggle to maintain independence is common regardless how far away the college campus is from home.
If college is far from home, it may be better for the individual with epilepsy to establish care with a local neurologist, or preferably, a local epileptologist. This is helpful in case of emergency. Ideally, prescriptions should be transferred to a nearby pharmacy before refills are due. It is also beneficial to coordinate follow up visits if needed with the original neurologist/epileptologist at term breaks and vacations. If there is an increase in seizure frequency or side effects patients should contact their physician as soon as possible and not simply wait for the next trip home. It is advisable for people with epilepsy to keep a wallet card or similar such item with them that lists medications names and doses as well as emergency contact numbers. If the patient is traveling by air or bus, mediations should be packed in hand luggage, not checked baggage, to avoid the possible of delayed arrival at the destination.
As class times may differ in a college environment, individuals with epilepsy should ensure they remain complaint with their medication and not miss doses. This may mean remembering to carry the medication with them, and keeping an extra supply at the dormitory/residence in case of emergency.
For individuals with epilepsy, stressors, such as decreased sleep/sleep deprivation, missed meals, over exertion, dehydration can lead to breakthrough seizures (even in those who are compliant with their antiepileptic drugs [AEDs]). Sleep deprivation and missed meals can be somewhat common in a college atmosphere, especially around examination time. People with epilepsy should ensure they get adequate sleep, do not miss meals, and are adequately hydrated (more so when participating in sports).
Use of alcohol and or illicit substances should be avoided as these can reduce seizure threshold, reduce the effectiveness of AEDs, and lead to breakthrough seizures.
For people with epilepsy, there may be an underlying anxiety of if and when a breakthrough seizure may occur. However, it is important to note that for the college student, this fear should not prevent him or her from achieving their full potential.
Nikesh Ardeshna, MD
Dr. Ardeshna is the Medical Director of Adult Epilepsy Services at Royal Oak Hospital, Beaumont Health , in Royal Oak, Michigan.
Starting college is both an exciting and stressful experience for new students. For people with epilepsy, going to college raises some specific and unique concerns compared to those without the condition . The purpose of this article is to look at some of the challenges for people with epilepsy and some potential solutions. The overall theme is that it is better to be prepared ahead of time.
The main goal of the person with epilepsy at college is to ensure that a breakthrough seizure does not occur, as this could lead to serious consequences (injuries, sprains, strains, and a change in lifestyle). However, it is equally important to ensure that an individual with epilepsy has a quality life.
For most students, attending college is one of life’s milestones. College is a new environment, with some new pressures that include academic success, making new friends (fitting in), participation in extracurricular activities (both academic and not), and taking personal responsibility of what may considered basic yet essential daily activities, such as meal preparation, laundry, etc.
Some of these issues may be of lesser concern, depending on the distance from college to home; however the struggle to maintain independence is common regardless how far away the college campus is from home.
If college is far from home, it may be better for the individual with epilepsy to establish care with a local neurologist, or preferably, a local epileptologist. This is helpful in case of emergency. Ideally, prescriptions should be transferred to a nearby pharmacy before refills are due. It is also beneficial to coordinate follow up visits if needed with the original neurologist/epileptologist at term breaks and vacations. If there is an increase in seizure frequency or side effects patients should contact their physician as soon as possible and not simply wait for the next trip home. It is advisable for people with epilepsy to keep a wallet card or similar such item with them that lists medications names and doses as well as emergency contact numbers. If the patient is traveling by air or bus, mediations should be packed in hand luggage, not checked baggage, to avoid the possible of delayed arrival at the destination.
As class times may differ in a college environment, individuals with epilepsy should ensure they remain complaint with their medication and not miss doses. This may mean remembering to carry the medication with them, and keeping an extra supply at the dormitory/residence in case of emergency.
For individuals with epilepsy, stressors, such as decreased sleep/sleep deprivation, missed meals, over exertion, dehydration can lead to breakthrough seizures (even in those who are compliant with their antiepileptic drugs [AEDs]). Sleep deprivation and missed meals can be somewhat common in a college atmosphere, especially around examination time. People with epilepsy should ensure they get adequate sleep, do not miss meals, and are adequately hydrated (more so when participating in sports).
Use of alcohol and or illicit substances should be avoided as these can reduce seizure threshold, reduce the effectiveness of AEDs, and lead to breakthrough seizures.
For people with epilepsy, there may be an underlying anxiety of if and when a breakthrough seizure may occur. However, it is important to note that for the college student, this fear should not prevent him or her from achieving their full potential.
Surveys Are Not the Most Effective Way to Improve Patient Satisfaction

What started with a car dealership survey has become a near avalanche of surveys from my credit card, bank, airlines, hotels, and other businesses. Each starts by assuring me that it will take only a minute or two to complete the survey, but if I completed every survey sent my way, it would add up to a significant amount of time. So I’ve stopped responding to nearly all of them, not so much as a form of protest but as part of my overall time-management efforts.
I imagine many of our patients see surveys from hospitals and other healthcare providers similarly: just another one to add to the pile. Patients in their 80s and 90s—a significant portion of hospitalist patients—probably interact a lot less with companies that send satisfaction surveys and so might be more attentive to ones from healthcare organizations. But I suspect that a reasonable portion of older patients rely on a family member to complete them, and this person, often a son or daughter, probably does get a lot of similar surveys. Surely, survey fatigue is influencing the results at least a little.
Healthcare Surveys: HCAHPS
For all the surveying going on, I find it pretty difficult to use HCAHPS results to guide patient-satisfaction improvement efforts. Sure, I can see how individual doctors or different physician groups score compared to one another and try to model my behaviors after the high performers. That is a really valuable thing to do, but it doesn’t get to the granular level I’d like.
One would hope the three physician-specific HCAHPS questions would support drilling down to more actionable information. But every hospitalist group I’ve seen always has the same pattern, scoring from lowest to highest as follows:
- How often did doctors explain things in a way you could understand?
- How often did doctors listen carefully to you?
- How often did doctors treat you with courtesy and respect?
So I don’t think the difference in scores on these questions is very useful in guiding improvement efforts.
Looking beyond HCAHPS
For a few years, our hospitalist group added a very short survey to the brochure describing the practice. I still think that was good idea to ensure accurate attribution and more granular information, but it didn’t yield much value in practice because of a low response rate. Ultimately, we stopped using it because of our hospital risk manager’s concern any such survey could be construed as “coaching” patients in their HCAHPS responses, something the Centers for Medicare & Medicaid Services forbids.
Mark Rudolph, MD, vice president of physician development and patient experience at Sound Physicians, told me about their experience with their employed RNs using tablet computers to survey every patient the day following hospital admission (i.e., while patients were still in the hospital). It seems to me this could be a really valuable tool to provide very granular feedback at the outset of a patient stay when there is still time to address areas in which the patient is less satisfied. They found that for about 30% of patients, the survey uncovered something that could be fixed, such as providing another blanket, determining what time a test was likely to be done, etc. I bet for most patients the fact that a nurse cared enough to ask how things are going and try to remedy problems improved their HCAPHS scores.
Yet after some experience with this approach, Sound Physicians found that, for a number of reasons, this wasn’t as valuable as hoped. They now survey a smaller sample of patients and sometimes adjust the questions based on the known or suspected strengths and weaknesses of individual providers. For one doctor, for example, the survey might ask whether the doctor spent enough time with the patient; for another, it might ask if the doctor spoke clearly, etc.
Dr. Rudolph thinks having someone such as the lead hospitalist observe the doctor while on rounds might ultimately prove more valuable than administering a survey. It will be interesting to see how his group and others around the country evolve their approach to better understand each provider’s strengths and weaknesses and most effective ways to improve patient satisfaction.
How to Improve Patient Satisfaction?
In my April 2012 column, I wrote about several things for hospitalists to consider including in their patient-satisfaction improvement plan. And, of course, there are a lot of additional sources of ideas available just by searching the Internet.
I find it difficult to consistently implement a bundle of multiple different habits, such as always sitting or always rounding with the patient’s bedside nurse, etc. I acknowledge these are proven valuable strategies to improve scores, but I still find it hard to do them consistently.
For some of us, it might be better to pick one thing to focus on. And while I don’t have research data to prove it, I think the single most valuable thing to improve patient satisfaction with hospitalists is to phone patients after discharge. It isn’t as difficult as most assume, and it often leads patients (or the family member you reach) to thank you profusely for the call. I think hospitalists can really benefit from more expressions of gratitude from patients and families, and these calls often provide it.
I’ve learned a few lessons about making post-discharge calls that are detailed in my August 2012 column. TH
What started with a car dealership survey has become a near avalanche of surveys from my credit card, bank, airlines, hotels, and other businesses. Each starts by assuring me that it will take only a minute or two to complete the survey, but if I completed every survey sent my way, it would add up to a significant amount of time. So I’ve stopped responding to nearly all of them, not so much as a form of protest but as part of my overall time-management efforts.
I imagine many of our patients see surveys from hospitals and other healthcare providers similarly: just another one to add to the pile. Patients in their 80s and 90s—a significant portion of hospitalist patients—probably interact a lot less with companies that send satisfaction surveys and so might be more attentive to ones from healthcare organizations. But I suspect that a reasonable portion of older patients rely on a family member to complete them, and this person, often a son or daughter, probably does get a lot of similar surveys. Surely, survey fatigue is influencing the results at least a little.
Healthcare Surveys: HCAHPS
For all the surveying going on, I find it pretty difficult to use HCAHPS results to guide patient-satisfaction improvement efforts. Sure, I can see how individual doctors or different physician groups score compared to one another and try to model my behaviors after the high performers. That is a really valuable thing to do, but it doesn’t get to the granular level I’d like.
One would hope the three physician-specific HCAHPS questions would support drilling down to more actionable information. But every hospitalist group I’ve seen always has the same pattern, scoring from lowest to highest as follows:
- How often did doctors explain things in a way you could understand?
- How often did doctors listen carefully to you?
- How often did doctors treat you with courtesy and respect?
So I don’t think the difference in scores on these questions is very useful in guiding improvement efforts.
Looking beyond HCAHPS
For a few years, our hospitalist group added a very short survey to the brochure describing the practice. I still think that was good idea to ensure accurate attribution and more granular information, but it didn’t yield much value in practice because of a low response rate. Ultimately, we stopped using it because of our hospital risk manager’s concern any such survey could be construed as “coaching” patients in their HCAHPS responses, something the Centers for Medicare & Medicaid Services forbids.
Mark Rudolph, MD, vice president of physician development and patient experience at Sound Physicians, told me about their experience with their employed RNs using tablet computers to survey every patient the day following hospital admission (i.e., while patients were still in the hospital). It seems to me this could be a really valuable tool to provide very granular feedback at the outset of a patient stay when there is still time to address areas in which the patient is less satisfied. They found that for about 30% of patients, the survey uncovered something that could be fixed, such as providing another blanket, determining what time a test was likely to be done, etc. I bet for most patients the fact that a nurse cared enough to ask how things are going and try to remedy problems improved their HCAPHS scores.
Yet after some experience with this approach, Sound Physicians found that, for a number of reasons, this wasn’t as valuable as hoped. They now survey a smaller sample of patients and sometimes adjust the questions based on the known or suspected strengths and weaknesses of individual providers. For one doctor, for example, the survey might ask whether the doctor spent enough time with the patient; for another, it might ask if the doctor spoke clearly, etc.
Dr. Rudolph thinks having someone such as the lead hospitalist observe the doctor while on rounds might ultimately prove more valuable than administering a survey. It will be interesting to see how his group and others around the country evolve their approach to better understand each provider’s strengths and weaknesses and most effective ways to improve patient satisfaction.
How to Improve Patient Satisfaction?
In my April 2012 column, I wrote about several things for hospitalists to consider including in their patient-satisfaction improvement plan. And, of course, there are a lot of additional sources of ideas available just by searching the Internet.
I find it difficult to consistently implement a bundle of multiple different habits, such as always sitting or always rounding with the patient’s bedside nurse, etc. I acknowledge these are proven valuable strategies to improve scores, but I still find it hard to do them consistently.
For some of us, it might be better to pick one thing to focus on. And while I don’t have research data to prove it, I think the single most valuable thing to improve patient satisfaction with hospitalists is to phone patients after discharge. It isn’t as difficult as most assume, and it often leads patients (or the family member you reach) to thank you profusely for the call. I think hospitalists can really benefit from more expressions of gratitude from patients and families, and these calls often provide it.
I’ve learned a few lessons about making post-discharge calls that are detailed in my August 2012 column. TH
What started with a car dealership survey has become a near avalanche of surveys from my credit card, bank, airlines, hotels, and other businesses. Each starts by assuring me that it will take only a minute or two to complete the survey, but if I completed every survey sent my way, it would add up to a significant amount of time. So I’ve stopped responding to nearly all of them, not so much as a form of protest but as part of my overall time-management efforts.
I imagine many of our patients see surveys from hospitals and other healthcare providers similarly: just another one to add to the pile. Patients in their 80s and 90s—a significant portion of hospitalist patients—probably interact a lot less with companies that send satisfaction surveys and so might be more attentive to ones from healthcare organizations. But I suspect that a reasonable portion of older patients rely on a family member to complete them, and this person, often a son or daughter, probably does get a lot of similar surveys. Surely, survey fatigue is influencing the results at least a little.
Healthcare Surveys: HCAHPS
For all the surveying going on, I find it pretty difficult to use HCAHPS results to guide patient-satisfaction improvement efforts. Sure, I can see how individual doctors or different physician groups score compared to one another and try to model my behaviors after the high performers. That is a really valuable thing to do, but it doesn’t get to the granular level I’d like.
One would hope the three physician-specific HCAHPS questions would support drilling down to more actionable information. But every hospitalist group I’ve seen always has the same pattern, scoring from lowest to highest as follows:
- How often did doctors explain things in a way you could understand?
- How often did doctors listen carefully to you?
- How often did doctors treat you with courtesy and respect?
So I don’t think the difference in scores on these questions is very useful in guiding improvement efforts.
Looking beyond HCAHPS
For a few years, our hospitalist group added a very short survey to the brochure describing the practice. I still think that was good idea to ensure accurate attribution and more granular information, but it didn’t yield much value in practice because of a low response rate. Ultimately, we stopped using it because of our hospital risk manager’s concern any such survey could be construed as “coaching” patients in their HCAHPS responses, something the Centers for Medicare & Medicaid Services forbids.
Mark Rudolph, MD, vice president of physician development and patient experience at Sound Physicians, told me about their experience with their employed RNs using tablet computers to survey every patient the day following hospital admission (i.e., while patients were still in the hospital). It seems to me this could be a really valuable tool to provide very granular feedback at the outset of a patient stay when there is still time to address areas in which the patient is less satisfied. They found that for about 30% of patients, the survey uncovered something that could be fixed, such as providing another blanket, determining what time a test was likely to be done, etc. I bet for most patients the fact that a nurse cared enough to ask how things are going and try to remedy problems improved their HCAPHS scores.
Yet after some experience with this approach, Sound Physicians found that, for a number of reasons, this wasn’t as valuable as hoped. They now survey a smaller sample of patients and sometimes adjust the questions based on the known or suspected strengths and weaknesses of individual providers. For one doctor, for example, the survey might ask whether the doctor spent enough time with the patient; for another, it might ask if the doctor spoke clearly, etc.
Dr. Rudolph thinks having someone such as the lead hospitalist observe the doctor while on rounds might ultimately prove more valuable than administering a survey. It will be interesting to see how his group and others around the country evolve their approach to better understand each provider’s strengths and weaknesses and most effective ways to improve patient satisfaction.
How to Improve Patient Satisfaction?
In my April 2012 column, I wrote about several things for hospitalists to consider including in their patient-satisfaction improvement plan. And, of course, there are a lot of additional sources of ideas available just by searching the Internet.
I find it difficult to consistently implement a bundle of multiple different habits, such as always sitting or always rounding with the patient’s bedside nurse, etc. I acknowledge these are proven valuable strategies to improve scores, but I still find it hard to do them consistently.
For some of us, it might be better to pick one thing to focus on. And while I don’t have research data to prove it, I think the single most valuable thing to improve patient satisfaction with hospitalists is to phone patients after discharge. It isn’t as difficult as most assume, and it often leads patients (or the family member you reach) to thank you profusely for the call. I think hospitalists can really benefit from more expressions of gratitude from patients and families, and these calls often provide it.
I’ve learned a few lessons about making post-discharge calls that are detailed in my August 2012 column. TH

The Problem of ‘Is’ and ‘Ought’ for Surgeons
Many years ago during medical school, I took time out to pursue graduate studies in philosophy. At that time, I took a number of courses that explored various approaches to the philosophical questions of morality and ethics. My ultimate goal, even back then, was to focus on ethical issues in the practice of medicine.
I often found the philosophical discussions from the “giants” in philosophy were not always easy to apply to everyday problems. After completing my graduate studies in philosophy and nearing the end of medical school, I found that I was drawn to surgery. Not surprisingly, many surgical faculty that I interviewed with for my residency saw little application of my philosophy studies to the practice of surgery. Although I felt confident that ethics was central to the practice of surgery, I let pass the general suggestions from many senior surgeons that surgery and philosophical analysis have little in common.

In recent years, however, I have increasingly seen an area of overlap that I believe will be central to the future of surgery. The options for the treatment of critically ill surgical patients across all areas of surgery have increased dramatically. Just in the area of cardiovascular disease, patients with failing hearts have the option of mechanical assist devices. Patients with multiple comorbidities and vascular problems can have numerous endovascular procedures done that years ago would have been unthinkable. Consider a patient with a ventricular assist device on a ventilator who is being dialyzed. Such a patient may be supported for weeks or months beyond what was possible just a few decades ago.
Whereas our surgical forefathers were constantly asking the question, “What can be done for this patient?” those caring for critically ill patients today must repeatedly ask, “What should we do for this patient?” Years ago, the statement, “there is nothing more that we can offer” was much more commonly heard than it is today. The critical question for today – “What should be done?” – is often more challenging and nuanced than “what can be done?” Whenever we ask “what should be done?” we must take into account the values of the patient and weigh the possible outcomes and the inherent risks of the possible interventions with the patient’s goals.
The current necessity to answer “what should be done?” has several striking parallels with the classical philosophical problem of “is” and “ought.” Over the centuries, many philosophers have considered whether we can derive an “ought” from an “is.” In other words, just because one can show that something is the case in the world, it does not automatically follow that it ought to be that way. David Hume, the Scottish philosopher (1711-1776), famously argued that there is a tremendous difference between statements about what is and statements about what ought to be. In particular, Hume argued that we cannot logically derive an “ought” from an “is.”
Despite the centuries that have passed since Hume’s days, I believe that his analysis has much to teach modern surgery. Just because we can undertake many interventions for our patients, it does not follow that we should undertake all of those interventions. A central aspect of what many of us refer to commonly as “surgical judgment” is deciding among the many possible interventions for a patient, what specific ones ought we offer. Although this entire discussion may seem theoretical (and possibly even arcane) to some surgeons, I firmly believe that one of the greatest challenges to the future of surgery is whether surgeons are willing to address the question of what should be done for every patient.
Excellent surgeons have traditionally been seen as having both technical mastery and sound judgment. In the current era in which surgeons are increasingly pushed to do more cases and maximize RVUs, multiple forces are encouraging surgeons to increasingly become pure technicians. Technicians can answer the question “what can be done?” However, “what should be done for this specific patient?” is a question that only a physician can answer. In the decades to come, we must ensure that surgeons continue to engage in the harder questions of “what should be done?” so that we do not forget that “is” and “ought” are different. The mastery of surgery involves not only the technical expertise that can be applied on behalf of a patient, but also the appreciation and understanding of the patient’s values so that surgeons can make recommendations about what should be done for their patients.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Many years ago during medical school, I took time out to pursue graduate studies in philosophy. At that time, I took a number of courses that explored various approaches to the philosophical questions of morality and ethics. My ultimate goal, even back then, was to focus on ethical issues in the practice of medicine.
I often found the philosophical discussions from the “giants” in philosophy were not always easy to apply to everyday problems. After completing my graduate studies in philosophy and nearing the end of medical school, I found that I was drawn to surgery. Not surprisingly, many surgical faculty that I interviewed with for my residency saw little application of my philosophy studies to the practice of surgery. Although I felt confident that ethics was central to the practice of surgery, I let pass the general suggestions from many senior surgeons that surgery and philosophical analysis have little in common.
In recent years, however, I have increasingly seen an area of overlap that I believe will be central to the future of surgery. The options for the treatment of critically ill surgical patients across all areas of surgery have increased dramatically. Just in the area of cardiovascular disease, patients with failing hearts have the option of mechanical assist devices. Patients with multiple comorbidities and vascular problems can have numerous endovascular procedures done that years ago would have been unthinkable. Consider a patient with a ventricular assist device on a ventilator who is being dialyzed. Such a patient may be supported for weeks or months beyond what was possible just a few decades ago.
Whereas our surgical forefathers were constantly asking the question, “What can be done for this patient?” those caring for critically ill patients today must repeatedly ask, “What should we do for this patient?” Years ago, the statement, “there is nothing more that we can offer” was much more commonly heard than it is today. The critical question for today – “What should be done?” – is often more challenging and nuanced than “what can be done?” Whenever we ask “what should be done?” we must take into account the values of the patient and weigh the possible outcomes and the inherent risks of the possible interventions with the patient’s goals.
The current necessity to answer “what should be done?” has several striking parallels with the classical philosophical problem of “is” and “ought.” Over the centuries, many philosophers have considered whether we can derive an “ought” from an “is.” In other words, just because one can show that something is the case in the world, it does not automatically follow that it ought to be that way. David Hume, the Scottish philosopher (1711-1776), famously argued that there is a tremendous difference between statements about what is and statements about what ought to be. In particular, Hume argued that we cannot logically derive an “ought” from an “is.”
Despite the centuries that have passed since Hume’s days, I believe that his analysis has much to teach modern surgery. Just because we can undertake many interventions for our patients, it does not follow that we should undertake all of those interventions. A central aspect of what many of us refer to commonly as “surgical judgment” is deciding among the many possible interventions for a patient, what specific ones ought we offer. Although this entire discussion may seem theoretical (and possibly even arcane) to some surgeons, I firmly believe that one of the greatest challenges to the future of surgery is whether surgeons are willing to address the question of what should be done for every patient.
Excellent surgeons have traditionally been seen as having both technical mastery and sound judgment. In the current era in which surgeons are increasingly pushed to do more cases and maximize RVUs, multiple forces are encouraging surgeons to increasingly become pure technicians. Technicians can answer the question “what can be done?” However, “what should be done for this specific patient?” is a question that only a physician can answer. In the decades to come, we must ensure that surgeons continue to engage in the harder questions of “what should be done?” so that we do not forget that “is” and “ought” are different. The mastery of surgery involves not only the technical expertise that can be applied on behalf of a patient, but also the appreciation and understanding of the patient’s values so that surgeons can make recommendations about what should be done for their patients.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Many years ago during medical school, I took time out to pursue graduate studies in philosophy. At that time, I took a number of courses that explored various approaches to the philosophical questions of morality and ethics. My ultimate goal, even back then, was to focus on ethical issues in the practice of medicine.
I often found the philosophical discussions from the “giants” in philosophy were not always easy to apply to everyday problems. After completing my graduate studies in philosophy and nearing the end of medical school, I found that I was drawn to surgery. Not surprisingly, many surgical faculty that I interviewed with for my residency saw little application of my philosophy studies to the practice of surgery. Although I felt confident that ethics was central to the practice of surgery, I let pass the general suggestions from many senior surgeons that surgery and philosophical analysis have little in common.
In recent years, however, I have increasingly seen an area of overlap that I believe will be central to the future of surgery. The options for the treatment of critically ill surgical patients across all areas of surgery have increased dramatically. Just in the area of cardiovascular disease, patients with failing hearts have the option of mechanical assist devices. Patients with multiple comorbidities and vascular problems can have numerous endovascular procedures done that years ago would have been unthinkable. Consider a patient with a ventricular assist device on a ventilator who is being dialyzed. Such a patient may be supported for weeks or months beyond what was possible just a few decades ago.
Whereas our surgical forefathers were constantly asking the question, “What can be done for this patient?” those caring for critically ill patients today must repeatedly ask, “What should we do for this patient?” Years ago, the statement, “there is nothing more that we can offer” was much more commonly heard than it is today. The critical question for today – “What should be done?” – is often more challenging and nuanced than “what can be done?” Whenever we ask “what should be done?” we must take into account the values of the patient and weigh the possible outcomes and the inherent risks of the possible interventions with the patient’s goals.
The current necessity to answer “what should be done?” has several striking parallels with the classical philosophical problem of “is” and “ought.” Over the centuries, many philosophers have considered whether we can derive an “ought” from an “is.” In other words, just because one can show that something is the case in the world, it does not automatically follow that it ought to be that way. David Hume, the Scottish philosopher (1711-1776), famously argued that there is a tremendous difference between statements about what is and statements about what ought to be. In particular, Hume argued that we cannot logically derive an “ought” from an “is.”
Despite the centuries that have passed since Hume’s days, I believe that his analysis has much to teach modern surgery. Just because we can undertake many interventions for our patients, it does not follow that we should undertake all of those interventions. A central aspect of what many of us refer to commonly as “surgical judgment” is deciding among the many possible interventions for a patient, what specific ones ought we offer. Although this entire discussion may seem theoretical (and possibly even arcane) to some surgeons, I firmly believe that one of the greatest challenges to the future of surgery is whether surgeons are willing to address the question of what should be done for every patient.
Excellent surgeons have traditionally been seen as having both technical mastery and sound judgment. In the current era in which surgeons are increasingly pushed to do more cases and maximize RVUs, multiple forces are encouraging surgeons to increasingly become pure technicians. Technicians can answer the question “what can be done?” However, “what should be done for this specific patient?” is a question that only a physician can answer. In the decades to come, we must ensure that surgeons continue to engage in the harder questions of “what should be done?” so that we do not forget that “is” and “ought” are different. The mastery of surgery involves not only the technical expertise that can be applied on behalf of a patient, but also the appreciation and understanding of the patient’s values so that surgeons can make recommendations about what should be done for their patients.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
