User login
Down syndrome in adolescents
Teen years, no doubt, come with expected challenges. For teens with Down syndrome (DS), the challenges are exponentially greater. Although DS is associated with mental retardation, the vast majority of people with DS have only mild to moderate intellectual disability. Still, this can lead to a great deal of internal stress for the adolescent and anxiety and stress for the parents.
Many issues must be considered for the adolescent with DS. Annual surveillance changes as the child ages and the need for intervention do as well. For example, 50% of children with DS are born with congenital heart defect. During infancy, it is important to do echocardiograms to identify and follow specific lesions. Approximately 57% of adolescents with DS will develop mitral valve prolapse and 10% will develop aortic regurgitation.1 Therefore, close evaluation should be done, listening for new onset murmurs, clicks, and unexplained fatigue, and, if these are identified, an echocardiogram should be repeated.

Dysmorphic features such as midfacial hypoplasia, tonsillar hypertrophy, and narrow ear canals also lead to issues that develop in the adolescent years. Chronic otitis, conductive hearing loss because of chronic middle-ear effusion or impacted cerumen, and enlarged tonsils can result in obstructive sleep apnea. As individuals gain weight, these issues are further affected, and a sleep study may be required. Annual hearing screens are recommended.1

Musculoskeletal disorders such as ligamentous laxity and atlantoaxial instability can also present with complications in the adolescent years. Pes planus is a very common finding that can further lead to hip and knee pain. Obesity also further adds to its occurrence (14%-67%).3
Now, the most pressing and, likely, most overlooked issue is the issue of sexuality. We spend a great deal of time educating teens without DS about the risks of unprotected sex and exposures to STIs, but many assume that these issues do not affect teens with DS. Secondary sexual characteristics develop in the same manner and at the same age that they do in children without DS. Therefore, it is a safe assumption that sexual curiosity and arousal do as well. Given that there can be varying levels of mental impairment, the approach to sex education needs to be developmentally appropriate. Normalizing the feelings and having discussions on appropriate and inappropriate expression are important.
As with all teens, acceptance and inclusion are of utmost importance. Physical and learning disabilities set them apart despite shared sexual and emotional development. This can lead to anxiety, depression, and behavior issues. Understanding that these are real issues for the adolescent with DS is important when providing the appropriate resources and support.
Management of the menstrual cycle can add new challenges for both the adolescent and the parent and, thus, should be investigated during health maintenance visits. Amenorrhea can result from introduction of hormonal therapy and should be considered. Sexual abuse also is increased in this age group, so close supervision and awareness of this issue are important.
Assisting parents of children with DS through the teen years is imperative. Making them aware of local support groups and national organizations for children with disabilities will help them navigate these years. The American Academy of Pediatrics has guidelines for health maintenance for DS.2
Dr. Pearce is a pediatrician in Frankfort, Ill. She reported no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com
References
1. J Pediatr Health Care. 2006 May-Jun;20(3):198-205.
2. Pediatrics. 2011. doi: 10.1542/peds.2011-1605.
3. Clin Obes. 2015;5(2):52-9.
Correction, 7/26/17: An earlier version of this article misstated a recommendation about radiologic evaluation of the cervical spine in asymptomatic children
Teen years, no doubt, come with expected challenges. For teens with Down syndrome (DS), the challenges are exponentially greater. Although DS is associated with mental retardation, the vast majority of people with DS have only mild to moderate intellectual disability. Still, this can lead to a great deal of internal stress for the adolescent and anxiety and stress for the parents.
Many issues must be considered for the adolescent with DS. Annual surveillance changes as the child ages and the need for intervention do as well. For example, 50% of children with DS are born with congenital heart defect. During infancy, it is important to do echocardiograms to identify and follow specific lesions. Approximately 57% of adolescents with DS will develop mitral valve prolapse and 10% will develop aortic regurgitation.1 Therefore, close evaluation should be done, listening for new onset murmurs, clicks, and unexplained fatigue, and, if these are identified, an echocardiogram should be repeated.
Dysmorphic features such as midfacial hypoplasia, tonsillar hypertrophy, and narrow ear canals also lead to issues that develop in the adolescent years. Chronic otitis, conductive hearing loss because of chronic middle-ear effusion or impacted cerumen, and enlarged tonsils can result in obstructive sleep apnea. As individuals gain weight, these issues are further affected, and a sleep study may be required. Annual hearing screens are recommended.1
Musculoskeletal disorders such as ligamentous laxity and atlantoaxial instability can also present with complications in the adolescent years. Pes planus is a very common finding that can further lead to hip and knee pain. Obesity also further adds to its occurrence (14%-67%).3
Now, the most pressing and, likely, most overlooked issue is the issue of sexuality. We spend a great deal of time educating teens without DS about the risks of unprotected sex and exposures to STIs, but many assume that these issues do not affect teens with DS. Secondary sexual characteristics develop in the same manner and at the same age that they do in children without DS. Therefore, it is a safe assumption that sexual curiosity and arousal do as well. Given that there can be varying levels of mental impairment, the approach to sex education needs to be developmentally appropriate. Normalizing the feelings and having discussions on appropriate and inappropriate expression are important.
As with all teens, acceptance and inclusion are of utmost importance. Physical and learning disabilities set them apart despite shared sexual and emotional development. This can lead to anxiety, depression, and behavior issues. Understanding that these are real issues for the adolescent with DS is important when providing the appropriate resources and support.
Management of the menstrual cycle can add new challenges for both the adolescent and the parent and, thus, should be investigated during health maintenance visits. Amenorrhea can result from introduction of hormonal therapy and should be considered. Sexual abuse also is increased in this age group, so close supervision and awareness of this issue are important.
Assisting parents of children with DS through the teen years is imperative. Making them aware of local support groups and national organizations for children with disabilities will help them navigate these years. The American Academy of Pediatrics has guidelines for health maintenance for DS.2
Dr. Pearce is a pediatrician in Frankfort, Ill. She reported no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com
References
1. J Pediatr Health Care. 2006 May-Jun;20(3):198-205.
2. Pediatrics. 2011. doi: 10.1542/peds.2011-1605.
3. Clin Obes. 2015;5(2):52-9.
Correction, 7/26/17: An earlier version of this article misstated a recommendation about radiologic evaluation of the cervical spine in asymptomatic children
Teen years, no doubt, come with expected challenges. For teens with Down syndrome (DS), the challenges are exponentially greater. Although DS is associated with mental retardation, the vast majority of people with DS have only mild to moderate intellectual disability. Still, this can lead to a great deal of internal stress for the adolescent and anxiety and stress for the parents.
Many issues must be considered for the adolescent with DS. Annual surveillance changes as the child ages and the need for intervention do as well. For example, 50% of children with DS are born with congenital heart defect. During infancy, it is important to do echocardiograms to identify and follow specific lesions. Approximately 57% of adolescents with DS will develop mitral valve prolapse and 10% will develop aortic regurgitation.1 Therefore, close evaluation should be done, listening for new onset murmurs, clicks, and unexplained fatigue, and, if these are identified, an echocardiogram should be repeated.
Dysmorphic features such as midfacial hypoplasia, tonsillar hypertrophy, and narrow ear canals also lead to issues that develop in the adolescent years. Chronic otitis, conductive hearing loss because of chronic middle-ear effusion or impacted cerumen, and enlarged tonsils can result in obstructive sleep apnea. As individuals gain weight, these issues are further affected, and a sleep study may be required. Annual hearing screens are recommended.1
Musculoskeletal disorders such as ligamentous laxity and atlantoaxial instability can also present with complications in the adolescent years. Pes planus is a very common finding that can further lead to hip and knee pain. Obesity also further adds to its occurrence (14%-67%).3
Now, the most pressing and, likely, most overlooked issue is the issue of sexuality. We spend a great deal of time educating teens without DS about the risks of unprotected sex and exposures to STIs, but many assume that these issues do not affect teens with DS. Secondary sexual characteristics develop in the same manner and at the same age that they do in children without DS. Therefore, it is a safe assumption that sexual curiosity and arousal do as well. Given that there can be varying levels of mental impairment, the approach to sex education needs to be developmentally appropriate. Normalizing the feelings and having discussions on appropriate and inappropriate expression are important.
As with all teens, acceptance and inclusion are of utmost importance. Physical and learning disabilities set them apart despite shared sexual and emotional development. This can lead to anxiety, depression, and behavior issues. Understanding that these are real issues for the adolescent with DS is important when providing the appropriate resources and support.
Management of the menstrual cycle can add new challenges for both the adolescent and the parent and, thus, should be investigated during health maintenance visits. Amenorrhea can result from introduction of hormonal therapy and should be considered. Sexual abuse also is increased in this age group, so close supervision and awareness of this issue are important.
Assisting parents of children with DS through the teen years is imperative. Making them aware of local support groups and national organizations for children with disabilities will help them navigate these years. The American Academy of Pediatrics has guidelines for health maintenance for DS.2
Dr. Pearce is a pediatrician in Frankfort, Ill. She reported no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com
References
1. J Pediatr Health Care. 2006 May-Jun;20(3):198-205.
2. Pediatrics. 2011. doi: 10.1542/peds.2011-1605.
3. Clin Obes. 2015;5(2):52-9.
Correction, 7/26/17: An earlier version of this article misstated a recommendation about radiologic evaluation of the cervical spine in asymptomatic children
Lonely in the middle
Those of us who consider ourselves centrists are feeling pretty lonely right now. It seems everyone else, or at least all of the folks in Washington, have fled to the extreme political poles and left us to search for a patch of middle ground to stand on. It appears that without courageous leadership the silent majority has splintered and gravitated to the tails of what was once a bell-shaped curve.
One issue that might attract support from both sides of the political spectrum emerged from the Nov. 18, 2016, report from the United States Department of Agriculture that listed sweetened drinks as the No. 1 purchase by households participating in SNAP (“Foods Typically Purchased by Supplemental Nutrition Assistance Program (SNAP) Households”). The data reveal that households in this $74 billion program are spending 5% of their food dollars on soft drinks and almost 10% on sweetened beverages – soft drinks, fruit juices, energy drinks, and sweetened teas.

Several states (including Maine), dozens of other municipalities (most notably New York City under Mayor Michael Bloomberg), and a variety of medical groups have asked the USDA to reconsider its guidelines. Arguing that selectively banning certain items would generate too much red tape and be unfair to food stamp recipients, the department has been resistant to change (“In the Shopping Cart of a Food Stamp Household: Lots of Soda,” by Anahad O’Connor, New York Times, Jan. 13, 2017). One has to wonder how much of the department’s hesitancy is a reflection of the millions of dollars the food and beverage industries have invested in lobbying against change.
There are some ultra liberals (or progressives if you prefer) who feel that no one should be deprived of the privilege of buying unhealthy food simply because he or she is poor. At the other end of the spectrum there are conservatives who would prefer to scrap the whole SNAP program because it is a wasteful frill of the welfare state. However, I have to believe that the vast majority of folks on both sides of the political divide believe that feeding the less fortunate is important, but that spending their tax money on junk food and soft drinks is a bad idea.
While we still are learning that the causes of our obesity epidemic are far more complex than we once imagined, I think most people believe that soft drinks and junk food are playing a significant role – even though these same folks may have found it difficult to change their own behavior. According to the New York Times article mentioned above, Kevin Concannon, the USDA undersecretary for food, nutrition, and consumer services, said that instead of restricting food, the USDA has prioritized incentive programs to encourage participants to purchase more nutritious foods. However, a 2014 study of more than 19,000 SNAP recipients by Stanford researchers determined that an incentive program would not affect obesity rates, while banning sugary drinks would “significantly reduce obesity prevalence and type 2 diabetes incidence” (Health Aff. Jun 2014;33[6]:1032-9).
All we need now are a few courageous senators and congressmen to buck the soft drink lobby and bring this issue to the front burner. I have to believe that there are more than enough people, both liberals and conservatives, who would venture together on the middle ground and support removing sweetened drinks from the SNAP program. If I’m correct, it would be a refreshing example of some much needed legislative cooperation. Or, am I just a lonely dreamer longing for some company here in the center?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Those of us who consider ourselves centrists are feeling pretty lonely right now. It seems everyone else, or at least all of the folks in Washington, have fled to the extreme political poles and left us to search for a patch of middle ground to stand on. It appears that without courageous leadership the silent majority has splintered and gravitated to the tails of what was once a bell-shaped curve.
One issue that might attract support from both sides of the political spectrum emerged from the Nov. 18, 2016, report from the United States Department of Agriculture that listed sweetened drinks as the No. 1 purchase by households participating in SNAP (“Foods Typically Purchased by Supplemental Nutrition Assistance Program (SNAP) Households”). The data reveal that households in this $74 billion program are spending 5% of their food dollars on soft drinks and almost 10% on sweetened beverages – soft drinks, fruit juices, energy drinks, and sweetened teas.
Several states (including Maine), dozens of other municipalities (most notably New York City under Mayor Michael Bloomberg), and a variety of medical groups have asked the USDA to reconsider its guidelines. Arguing that selectively banning certain items would generate too much red tape and be unfair to food stamp recipients, the department has been resistant to change (“In the Shopping Cart of a Food Stamp Household: Lots of Soda,” by Anahad O’Connor, New York Times, Jan. 13, 2017). One has to wonder how much of the department’s hesitancy is a reflection of the millions of dollars the food and beverage industries have invested in lobbying against change.
There are some ultra liberals (or progressives if you prefer) who feel that no one should be deprived of the privilege of buying unhealthy food simply because he or she is poor. At the other end of the spectrum there are conservatives who would prefer to scrap the whole SNAP program because it is a wasteful frill of the welfare state. However, I have to believe that the vast majority of folks on both sides of the political divide believe that feeding the less fortunate is important, but that spending their tax money on junk food and soft drinks is a bad idea.
While we still are learning that the causes of our obesity epidemic are far more complex than we once imagined, I think most people believe that soft drinks and junk food are playing a significant role – even though these same folks may have found it difficult to change their own behavior. According to the New York Times article mentioned above, Kevin Concannon, the USDA undersecretary for food, nutrition, and consumer services, said that instead of restricting food, the USDA has prioritized incentive programs to encourage participants to purchase more nutritious foods. However, a 2014 study of more than 19,000 SNAP recipients by Stanford researchers determined that an incentive program would not affect obesity rates, while banning sugary drinks would “significantly reduce obesity prevalence and type 2 diabetes incidence” (Health Aff. Jun 2014;33[6]:1032-9).
All we need now are a few courageous senators and congressmen to buck the soft drink lobby and bring this issue to the front burner. I have to believe that there are more than enough people, both liberals and conservatives, who would venture together on the middle ground and support removing sweetened drinks from the SNAP program. If I’m correct, it would be a refreshing example of some much needed legislative cooperation. Or, am I just a lonely dreamer longing for some company here in the center?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Those of us who consider ourselves centrists are feeling pretty lonely right now. It seems everyone else, or at least all of the folks in Washington, have fled to the extreme political poles and left us to search for a patch of middle ground to stand on. It appears that without courageous leadership the silent majority has splintered and gravitated to the tails of what was once a bell-shaped curve.
One issue that might attract support from both sides of the political spectrum emerged from the Nov. 18, 2016, report from the United States Department of Agriculture that listed sweetened drinks as the No. 1 purchase by households participating in SNAP (“Foods Typically Purchased by Supplemental Nutrition Assistance Program (SNAP) Households”). The data reveal that households in this $74 billion program are spending 5% of their food dollars on soft drinks and almost 10% on sweetened beverages – soft drinks, fruit juices, energy drinks, and sweetened teas.
Several states (including Maine), dozens of other municipalities (most notably New York City under Mayor Michael Bloomberg), and a variety of medical groups have asked the USDA to reconsider its guidelines. Arguing that selectively banning certain items would generate too much red tape and be unfair to food stamp recipients, the department has been resistant to change (“In the Shopping Cart of a Food Stamp Household: Lots of Soda,” by Anahad O’Connor, New York Times, Jan. 13, 2017). One has to wonder how much of the department’s hesitancy is a reflection of the millions of dollars the food and beverage industries have invested in lobbying against change.
There are some ultra liberals (or progressives if you prefer) who feel that no one should be deprived of the privilege of buying unhealthy food simply because he or she is poor. At the other end of the spectrum there are conservatives who would prefer to scrap the whole SNAP program because it is a wasteful frill of the welfare state. However, I have to believe that the vast majority of folks on both sides of the political divide believe that feeding the less fortunate is important, but that spending their tax money on junk food and soft drinks is a bad idea.
While we still are learning that the causes of our obesity epidemic are far more complex than we once imagined, I think most people believe that soft drinks and junk food are playing a significant role – even though these same folks may have found it difficult to change their own behavior. According to the New York Times article mentioned above, Kevin Concannon, the USDA undersecretary for food, nutrition, and consumer services, said that instead of restricting food, the USDA has prioritized incentive programs to encourage participants to purchase more nutritious foods. However, a 2014 study of more than 19,000 SNAP recipients by Stanford researchers determined that an incentive program would not affect obesity rates, while banning sugary drinks would “significantly reduce obesity prevalence and type 2 diabetes incidence” (Health Aff. Jun 2014;33[6]:1032-9).
All we need now are a few courageous senators and congressmen to buck the soft drink lobby and bring this issue to the front burner. I have to believe that there are more than enough people, both liberals and conservatives, who would venture together on the middle ground and support removing sweetened drinks from the SNAP program. If I’m correct, it would be a refreshing example of some much needed legislative cooperation. Or, am I just a lonely dreamer longing for some company here in the center?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
The power of interaction – Supporting language and play development
Engaging caregivers in the management and treatment of early childhood developmental challenges is a critical component of effective intervention.1 Family-centered care helps to promote positive outcomes with early intervention (across developmental domains), and there’s increasing evidence that parent-training programs can be effective in promoting skill generalization and targeting core impairments in toddlers with autism.2
Furthermore, a 2014 randomized controlled trial revealed that individual Early Social Interaction (ESI) with home coaching using the SCERTS (Social Communication, Emotional Regulation, and Transactional Support) curriculum was associated with improvement of a range of child outcomes, compared with group ESI. The authors commented on the importance of individualized parent coaching in natural environments as a way to improve social components of communication and receptive language for toddlers with autism.3
For many parents and at-home caregivers, however, engaging in home-based and parent-delivered interventions can be overwhelming and anxiety-provoking, as well as complicated by other barriers (competing responsibilities, cultural beliefs, and so on). Additionally, these interventions can themselves be a source of stress for some families.

Case
Jake is a 3-year-old boy with a history of global developmental delays, who presents with particular struggles: relating his expressive communication, ability to engage peers in an age-appropriate manner, and capacity to self-regulate when frustrated. He and his family participated in an comprehensive autism diagnostic assessment. In reviewing the history and presentation, considerable challenges in the two core symptom domains that characterize an autism spectrum disorder were noted. A diagnosis of autism was provided, and treatment recommendations were discussed. “What can I do at home to help Jake learn?” his mother asked, noting that, with one-on-one attention, he does seem to demonstrate increased responsiveness, less use of echolalic language, and improved eye contact.
Discussion
To complement the autism services that Jake would likely qualify for through an Early Education program, in-home interaction and play to ensure skill development was discussed at length with his mother, who readily acknowledged her own care-giving struggles that, in part, are informed by her own mental health troubles.
We openly explored Jake’s mother’s perceived challenges in engaging with her son at home and developed initial recommendations for interaction that didn’t risk overwhelming her. We impressed upon Jake’s mother that, regardless of a child’s developmental profile, toddlers use play to learn and she can be Jake’s “favorite toy.” After all, “play is really the work of childhood,” as Fred Rogers said.
With all children, back-and-forth interactions serve as the foundation for future development. Using scaffolding techniques, parent support is a primary driver of “how children develop cognitive, language, social-emotional, and higher-level thinking skills.”4 In particular, the quality of parental interaction can influence language development, and, when considering children with autism, there are several recommendations for what parents can do to help build social, play, and communication skills.5 The Hanen Program is a great resource for providers and parents to learn more about parent engagement in early learning, the power of building communication through everyday experiences and attention to responsiveness, and the use of a child’s strengths to help make family interactions more meaningful and enjoyable. Additionally, the 2012 book “An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn” by Sally Rogers, PhD, et al. is an easy-to-read text for parents and caregivers for learning effective and practical strategies for engaging their child with autism.
With Jake and his mother, our team offered the following in-home recommendations:
- Try to keep interaction fun. Be enthusiastic when encouraging Jake’s attempts to communicate.
- Teach Jake song-gesture games. Encourage him to produce routine, predictable gestures to keep the song going (in imitation of mom). Using songs with vowel emphasis is encouraged (for example: Farmer in the Dell with “E I E I OOOOO”).
- Encourage Jake to produce responsive gestures in play and daily routines not involving songs, such as open arms to receive a ball, reaching to mom when about to be tickled, or having his arms up to have his shirt taken off.
- Capitalize on Jake’s natural desires and personal preferences. Activate a wind-up toy, let it deactivate, and then hand it to Jake.
- Initiate a familiar social game with Jake until he expresses pleasure. Then stop the game and wait for him to initiate continuance.
- Adapt the environment so that Jake will need to frequently request objects of assistance to make choices (place favorite toys in clear containers which may be difficult to open so that he must request help).
Clinical pearl
The United States Department of Education recognizes the importance of family engagement in a child’s early years. Their 2015 policy statement notes that “families are their children’s first and most important teachers, advocates, and nurturers. As such, strong family engagement is central – not supplemental – to the success of early childhood systems and programs that promote children’s healthy development, learning, and wellness.”
By recognizing this principle, primary care providers are in a position to talk with parents about how much youth learn through play and regular interaction. This especially holds true for children with autism. Developing in-home strategies to facilitate active engagement, even strategies that may not be a formal component of a home-based intervention program, are instrumental in fostering positive family- and child-based outcomes and wellness.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic. Email him at pdnews@frontlinemedcom.com.
References
1. Annu Rev Clin Psychol. 2010;6:447-68.
2. J Autism Dev Disord. 2010 Sep;40(9):1045-56.
3. Pediatrics. 2014 Dec;134(6):1084-93.
4. JAMA Pediatr. 2016 Feb;170(2):112-3.
5. Child Dev. 2012 Sep-Oct;83(5):1762-74.
Engaging caregivers in the management and treatment of early childhood developmental challenges is a critical component of effective intervention.1 Family-centered care helps to promote positive outcomes with early intervention (across developmental domains), and there’s increasing evidence that parent-training programs can be effective in promoting skill generalization and targeting core impairments in toddlers with autism.2
Furthermore, a 2014 randomized controlled trial revealed that individual Early Social Interaction (ESI) with home coaching using the SCERTS (Social Communication, Emotional Regulation, and Transactional Support) curriculum was associated with improvement of a range of child outcomes, compared with group ESI. The authors commented on the importance of individualized parent coaching in natural environments as a way to improve social components of communication and receptive language for toddlers with autism.3
For many parents and at-home caregivers, however, engaging in home-based and parent-delivered interventions can be overwhelming and anxiety-provoking, as well as complicated by other barriers (competing responsibilities, cultural beliefs, and so on). Additionally, these interventions can themselves be a source of stress for some families.
Case
Jake is a 3-year-old boy with a history of global developmental delays, who presents with particular struggles: relating his expressive communication, ability to engage peers in an age-appropriate manner, and capacity to self-regulate when frustrated. He and his family participated in an comprehensive autism diagnostic assessment. In reviewing the history and presentation, considerable challenges in the two core symptom domains that characterize an autism spectrum disorder were noted. A diagnosis of autism was provided, and treatment recommendations were discussed. “What can I do at home to help Jake learn?” his mother asked, noting that, with one-on-one attention, he does seem to demonstrate increased responsiveness, less use of echolalic language, and improved eye contact.
Discussion
To complement the autism services that Jake would likely qualify for through an Early Education program, in-home interaction and play to ensure skill development was discussed at length with his mother, who readily acknowledged her own care-giving struggles that, in part, are informed by her own mental health troubles.
We openly explored Jake’s mother’s perceived challenges in engaging with her son at home and developed initial recommendations for interaction that didn’t risk overwhelming her. We impressed upon Jake’s mother that, regardless of a child’s developmental profile, toddlers use play to learn and she can be Jake’s “favorite toy.” After all, “play is really the work of childhood,” as Fred Rogers said.
With all children, back-and-forth interactions serve as the foundation for future development. Using scaffolding techniques, parent support is a primary driver of “how children develop cognitive, language, social-emotional, and higher-level thinking skills.”4 In particular, the quality of parental interaction can influence language development, and, when considering children with autism, there are several recommendations for what parents can do to help build social, play, and communication skills.5 The Hanen Program is a great resource for providers and parents to learn more about parent engagement in early learning, the power of building communication through everyday experiences and attention to responsiveness, and the use of a child’s strengths to help make family interactions more meaningful and enjoyable. Additionally, the 2012 book “An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn” by Sally Rogers, PhD, et al. is an easy-to-read text for parents and caregivers for learning effective and practical strategies for engaging their child with autism.
With Jake and his mother, our team offered the following in-home recommendations:
- Try to keep interaction fun. Be enthusiastic when encouraging Jake’s attempts to communicate.
- Teach Jake song-gesture games. Encourage him to produce routine, predictable gestures to keep the song going (in imitation of mom). Using songs with vowel emphasis is encouraged (for example: Farmer in the Dell with “E I E I OOOOO”).
- Encourage Jake to produce responsive gestures in play and daily routines not involving songs, such as open arms to receive a ball, reaching to mom when about to be tickled, or having his arms up to have his shirt taken off.
- Capitalize on Jake’s natural desires and personal preferences. Activate a wind-up toy, let it deactivate, and then hand it to Jake.
- Initiate a familiar social game with Jake until he expresses pleasure. Then stop the game and wait for him to initiate continuance.
- Adapt the environment so that Jake will need to frequently request objects of assistance to make choices (place favorite toys in clear containers which may be difficult to open so that he must request help).
Clinical pearl
The United States Department of Education recognizes the importance of family engagement in a child’s early years. Their 2015 policy statement notes that “families are their children’s first and most important teachers, advocates, and nurturers. As such, strong family engagement is central – not supplemental – to the success of early childhood systems and programs that promote children’s healthy development, learning, and wellness.”
By recognizing this principle, primary care providers are in a position to talk with parents about how much youth learn through play and regular interaction. This especially holds true for children with autism. Developing in-home strategies to facilitate active engagement, even strategies that may not be a formal component of a home-based intervention program, are instrumental in fostering positive family- and child-based outcomes and wellness.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic. Email him at pdnews@frontlinemedcom.com.
References
1. Annu Rev Clin Psychol. 2010;6:447-68.
2. J Autism Dev Disord. 2010 Sep;40(9):1045-56.
3. Pediatrics. 2014 Dec;134(6):1084-93.
4. JAMA Pediatr. 2016 Feb;170(2):112-3.
5. Child Dev. 2012 Sep-Oct;83(5):1762-74.
Engaging caregivers in the management and treatment of early childhood developmental challenges is a critical component of effective intervention.1 Family-centered care helps to promote positive outcomes with early intervention (across developmental domains), and there’s increasing evidence that parent-training programs can be effective in promoting skill generalization and targeting core impairments in toddlers with autism.2
Furthermore, a 2014 randomized controlled trial revealed that individual Early Social Interaction (ESI) with home coaching using the SCERTS (Social Communication, Emotional Regulation, and Transactional Support) curriculum was associated with improvement of a range of child outcomes, compared with group ESI. The authors commented on the importance of individualized parent coaching in natural environments as a way to improve social components of communication and receptive language for toddlers with autism.3
For many parents and at-home caregivers, however, engaging in home-based and parent-delivered interventions can be overwhelming and anxiety-provoking, as well as complicated by other barriers (competing responsibilities, cultural beliefs, and so on). Additionally, these interventions can themselves be a source of stress for some families.
Case
Jake is a 3-year-old boy with a history of global developmental delays, who presents with particular struggles: relating his expressive communication, ability to engage peers in an age-appropriate manner, and capacity to self-regulate when frustrated. He and his family participated in an comprehensive autism diagnostic assessment. In reviewing the history and presentation, considerable challenges in the two core symptom domains that characterize an autism spectrum disorder were noted. A diagnosis of autism was provided, and treatment recommendations were discussed. “What can I do at home to help Jake learn?” his mother asked, noting that, with one-on-one attention, he does seem to demonstrate increased responsiveness, less use of echolalic language, and improved eye contact.
Discussion
To complement the autism services that Jake would likely qualify for through an Early Education program, in-home interaction and play to ensure skill development was discussed at length with his mother, who readily acknowledged her own care-giving struggles that, in part, are informed by her own mental health troubles.
We openly explored Jake’s mother’s perceived challenges in engaging with her son at home and developed initial recommendations for interaction that didn’t risk overwhelming her. We impressed upon Jake’s mother that, regardless of a child’s developmental profile, toddlers use play to learn and she can be Jake’s “favorite toy.” After all, “play is really the work of childhood,” as Fred Rogers said.
With all children, back-and-forth interactions serve as the foundation for future development. Using scaffolding techniques, parent support is a primary driver of “how children develop cognitive, language, social-emotional, and higher-level thinking skills.”4 In particular, the quality of parental interaction can influence language development, and, when considering children with autism, there are several recommendations for what parents can do to help build social, play, and communication skills.5 The Hanen Program is a great resource for providers and parents to learn more about parent engagement in early learning, the power of building communication through everyday experiences and attention to responsiveness, and the use of a child’s strengths to help make family interactions more meaningful and enjoyable. Additionally, the 2012 book “An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn” by Sally Rogers, PhD, et al. is an easy-to-read text for parents and caregivers for learning effective and practical strategies for engaging their child with autism.
With Jake and his mother, our team offered the following in-home recommendations:
- Try to keep interaction fun. Be enthusiastic when encouraging Jake’s attempts to communicate.
- Teach Jake song-gesture games. Encourage him to produce routine, predictable gestures to keep the song going (in imitation of mom). Using songs with vowel emphasis is encouraged (for example: Farmer in the Dell with “E I E I OOOOO”).
- Encourage Jake to produce responsive gestures in play and daily routines not involving songs, such as open arms to receive a ball, reaching to mom when about to be tickled, or having his arms up to have his shirt taken off.
- Capitalize on Jake’s natural desires and personal preferences. Activate a wind-up toy, let it deactivate, and then hand it to Jake.
- Initiate a familiar social game with Jake until he expresses pleasure. Then stop the game and wait for him to initiate continuance.
- Adapt the environment so that Jake will need to frequently request objects of assistance to make choices (place favorite toys in clear containers which may be difficult to open so that he must request help).
Clinical pearl
The United States Department of Education recognizes the importance of family engagement in a child’s early years. Their 2015 policy statement notes that “families are their children’s first and most important teachers, advocates, and nurturers. As such, strong family engagement is central – not supplemental – to the success of early childhood systems and programs that promote children’s healthy development, learning, and wellness.”
By recognizing this principle, primary care providers are in a position to talk with parents about how much youth learn through play and regular interaction. This especially holds true for children with autism. Developing in-home strategies to facilitate active engagement, even strategies that may not be a formal component of a home-based intervention program, are instrumental in fostering positive family- and child-based outcomes and wellness.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic. Email him at pdnews@frontlinemedcom.com.
References
1. Annu Rev Clin Psychol. 2010;6:447-68.
2. J Autism Dev Disord. 2010 Sep;40(9):1045-56.
3. Pediatrics. 2014 Dec;134(6):1084-93.
4. JAMA Pediatr. 2016 Feb;170(2):112-3.
5. Child Dev. 2012 Sep-Oct;83(5):1762-74.
How you can help avoid catastrophic cuts to dermatology
It seems like only yesterday we were celebrating the elimination of the Medicare sustainable growth rate and the continuation of “global periods.” Now we are facing the elimination of the global payment periods again, and if we don’t bill the proper CPT code (99024) for our follow-up visits, during an upcoming survey period, it will indeed be a challenge for the specialty.
You may not know it, but there is payment for follow-up visits – global periods – built into codes dermatologists frequently use. As you can see, a large part of our specialty is vulnerable, from destruction of actinics and warts, to malignant and benign excisions, to destructions, to reconstructive surgery. This is real money, about a billion (yes, with a “b”) paid to dermatologists every year in Medicare alone.

These embedded visits vary from one (actinic destruction) to five (full thickness graft of the nose) and make up a major part of your reimbursement. As part of MACRA (Medicare Access and CHIP Reauthorization Act), the CMS was directed to investigate the validity of these embedded visits.1
The CMS has decided to complete this data gathering by how often the CPT code 99024 is billed.
I am not worried that we don’t provide these visits. I know we do, but I am terribly worried that we won’t correctly report these visits and won’t get credit for them.
The problem is that 99024 pays nothing, it is simply a notation to indicate that the patient was seen in follow up. Since it pays nothing, and since billing anything has an inherent expense, and since 30% of dermatologists are still on paper claims, most dermatologists have never used this code and may not start. In addition, groups of under 10 physicians are not required to report, but can, and you must! Seventy percent of our members are in groups of under 10. That means there will be no data collected on most of these codes, which are almost all performed by dermatologists, the great majority of the time.
Let me say it clearly here: If you do not start filing 99024 every time you see a patient in follow-up (and perhaps for telephone follow-ups), the amount you are paid to perform the original procedure will be cut by 30%-75%. Since the CMS will erroneously think you are not seeing these follow-up patients, they will pull these embedded payments out of the codes. You will have to start billing patients (think additional copays and deductibles) for every suture removal and wound check visit.
Data on 99024 will be collected in only nine states (Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island). It will start July 1 and no one knows how long it will continue.
So, start preparing. You will not be penalized for adding this nonpaying code to every follow-up when you do not bill an evaluation and management code. I note that one electronic medical record vendor (Modernizing Medicine) has already started populating its bills with 99024. Good for them! You must report follow-up visits no matter the size of your practice. Report early and report often. Your future depends on it.
Common procedures on which the CMS is collecting postoperative visit data
10040 Acne surgery
10060 Drainage of skin abscess
10061 Drainage of skin abscess
10120 Remove foreign body
10140 Drainage of hematoma/fluid
10160 Puncture drainage of lesion
10180 Complex drainage wound
11200 Removal of skin tags <w/15
11400 Exc tr-ext b9+marg 0.5 cm<
11401 Exc tr-ext b9+marg 0.6-1 cm
11402 Exc tr-ext b9+marg 1.1-2 cm
11403 Exc tr-ext b9+marg 2.1-3cm/<
11404 Exc tr-ext b9+marg 3.1-4 cm
11406 Exc tr-ext b9+marg >4.0 cm
11420 Exc h-f-nk-sp b9+marg 0.5/<
11421 Exc h-f-nk-sp b9+marg 0.6-1
11422 Exc h-f-nk-sp b9+marg 1.1-2
11423 Exc h-f-nk-sp b9+marg 2.1-3
11440 Exc face-mm b9+marg 0.5 cm/<
11441 Exc face-mm b9+marg 0.6-1 cm
11442 Exc face-mm b9+marg 1.1-2 cm
11443 Exc face-mm b9+marg 2.1-3 cm
11601 Exc tr-ext mal+marg 0.6-1 cm
11602 Exc tr-ext mal+marg 1.1-2 cm
11603 Exc tr-ext mal+marg 2.1-3 cm
11604 Exc tr-ext mal+marg 3.1-4 cm
11606 Exc tr-ext mal+marg >4 cm
11621 Exc s/n/h/f/g mal+mrg 0.6-1
11622 Exc s/n/h/f/g mal+mrg 1.1-2
11623 Exc s/n/h/f/g mal+mrg 2.1-3
11640 Exc f/e/e/n/l mal+mrg 0.5cm<
11641 Exc f/e/e/n/l mal+mrg 0.6-1
11642 Exc f/e/e/n/l mal+mrg 1.1-2
11643 Exc f/e/e/n/l mal+mrg 2.1-3
11644 Exc f/e/e/n/l mal+mrg 3.1-4
11646 Exc f/e/e/n/l mal+mrg >4 cm
11750 Removal of nail bed
11765 Excision of nail fold toe
12031 Intmd rpr s/a/t/ext 2.5 cm/<
12032 Intmd rpr s/a/t/ext 2.6-7.5
12034 Intmd rpr s/tr/ext 7.6-12.5
12041 Intmd rpr n-hf/genit 2.5cm/<
12042 Intmd rpr n-hf/genit2.6-7.5
12051 Intmd rpr face/mm 2.5 cm/<
12052 Intmd rpr face/mm 2.6-5.0 cm
13101 Cmplx rpr trunk 2.6-7.5 cm
13121 Cmplx rpr s/a/l 2.6-7.5 cm
13131 Cmplx rpr f/c/c/m/n/ax/g/h/f
13132 Cmplx rpr f/c/c/m/n/ax/g/h/f
13151 Cmplx rpr e/n/e/l 1.1-2.5 cm
13152 Cmplx rpr e/n/e/l 2.6-7.5 cm
13160 Late closure of wound
14020 Tis trnfr s/a/l 10 sq cm/<
14021 Tis trnfr s/a/l 10.1-30 sqcm
14040 Tis trnfr f/c/c/m/n/a/g/h/f
14041 Tis trnfr f/c/c/m/n/a/g/h/f
14060 Tis trnfr e/n/e/l 10 sq cm/<
14061 Tis trnfr e/n/e/l10.1-30sqcm
14301 Tis trnfr any 30.1-60 sq cm
15100 Skin splt grft trnk/arm/leg
15120 Skn splt a-grft fac/nck/hf/g
15240 Skin full grft face/genit/hf
15260 Skin full graft een & lips
15732 Muscle-skin graft head/neck
15734 Muscle-skin graft trunk
15823 Revision of upper eyelid
17000 Destruct premalg lesion
17004 Destroy premal lesions 15/>
17110 Destruct b9 lesion 1-14
17111 Destruct lesion 15 or more
17260 Destruction of skin lesions
17261 Destruction of skin lesions
17262 Destruction of skin lesions
17263 Destruction of skin lesions
17270 Destruction of skin lesions
17271 Destruction of skin lesions
17272 Destruction of skin lesions
17273 Destruction of skin lesions
17280 Destruction of skin lesions
17281 Destruction of skin lesions
17282 Destruction of skin lesions
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
References
1. Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
It seems like only yesterday we were celebrating the elimination of the Medicare sustainable growth rate and the continuation of “global periods.” Now we are facing the elimination of the global payment periods again, and if we don’t bill the proper CPT code (99024) for our follow-up visits, during an upcoming survey period, it will indeed be a challenge for the specialty.
You may not know it, but there is payment for follow-up visits – global periods – built into codes dermatologists frequently use. As you can see, a large part of our specialty is vulnerable, from destruction of actinics and warts, to malignant and benign excisions, to destructions, to reconstructive surgery. This is real money, about a billion (yes, with a “b”) paid to dermatologists every year in Medicare alone.
These embedded visits vary from one (actinic destruction) to five (full thickness graft of the nose) and make up a major part of your reimbursement. As part of MACRA (Medicare Access and CHIP Reauthorization Act), the CMS was directed to investigate the validity of these embedded visits.1
The CMS has decided to complete this data gathering by how often the CPT code 99024 is billed.
I am not worried that we don’t provide these visits. I know we do, but I am terribly worried that we won’t correctly report these visits and won’t get credit for them.
The problem is that 99024 pays nothing, it is simply a notation to indicate that the patient was seen in follow up. Since it pays nothing, and since billing anything has an inherent expense, and since 30% of dermatologists are still on paper claims, most dermatologists have never used this code and may not start. In addition, groups of under 10 physicians are not required to report, but can, and you must! Seventy percent of our members are in groups of under 10. That means there will be no data collected on most of these codes, which are almost all performed by dermatologists, the great majority of the time.
Let me say it clearly here: If you do not start filing 99024 every time you see a patient in follow-up (and perhaps for telephone follow-ups), the amount you are paid to perform the original procedure will be cut by 30%-75%. Since the CMS will erroneously think you are not seeing these follow-up patients, they will pull these embedded payments out of the codes. You will have to start billing patients (think additional copays and deductibles) for every suture removal and wound check visit.
Data on 99024 will be collected in only nine states (Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island). It will start July 1 and no one knows how long it will continue.
So, start preparing. You will not be penalized for adding this nonpaying code to every follow-up when you do not bill an evaluation and management code. I note that one electronic medical record vendor (Modernizing Medicine) has already started populating its bills with 99024. Good for them! You must report follow-up visits no matter the size of your practice. Report early and report often. Your future depends on it.
Common procedures on which the CMS is collecting postoperative visit data
10040 Acne surgery
10060 Drainage of skin abscess
10061 Drainage of skin abscess
10120 Remove foreign body
10140 Drainage of hematoma/fluid
10160 Puncture drainage of lesion
10180 Complex drainage wound
11200 Removal of skin tags <w/15
11400 Exc tr-ext b9+marg 0.5 cm<
11401 Exc tr-ext b9+marg 0.6-1 cm
11402 Exc tr-ext b9+marg 1.1-2 cm
11403 Exc tr-ext b9+marg 2.1-3cm/<
11404 Exc tr-ext b9+marg 3.1-4 cm
11406 Exc tr-ext b9+marg >4.0 cm
11420 Exc h-f-nk-sp b9+marg 0.5/<
11421 Exc h-f-nk-sp b9+marg 0.6-1
11422 Exc h-f-nk-sp b9+marg 1.1-2
11423 Exc h-f-nk-sp b9+marg 2.1-3
11440 Exc face-mm b9+marg 0.5 cm/<
11441 Exc face-mm b9+marg 0.6-1 cm
11442 Exc face-mm b9+marg 1.1-2 cm
11443 Exc face-mm b9+marg 2.1-3 cm
11601 Exc tr-ext mal+marg 0.6-1 cm
11602 Exc tr-ext mal+marg 1.1-2 cm
11603 Exc tr-ext mal+marg 2.1-3 cm
11604 Exc tr-ext mal+marg 3.1-4 cm
11606 Exc tr-ext mal+marg >4 cm
11621 Exc s/n/h/f/g mal+mrg 0.6-1
11622 Exc s/n/h/f/g mal+mrg 1.1-2
11623 Exc s/n/h/f/g mal+mrg 2.1-3
11640 Exc f/e/e/n/l mal+mrg 0.5cm<
11641 Exc f/e/e/n/l mal+mrg 0.6-1
11642 Exc f/e/e/n/l mal+mrg 1.1-2
11643 Exc f/e/e/n/l mal+mrg 2.1-3
11644 Exc f/e/e/n/l mal+mrg 3.1-4
11646 Exc f/e/e/n/l mal+mrg >4 cm
11750 Removal of nail bed
11765 Excision of nail fold toe
12031 Intmd rpr s/a/t/ext 2.5 cm/<
12032 Intmd rpr s/a/t/ext 2.6-7.5
12034 Intmd rpr s/tr/ext 7.6-12.5
12041 Intmd rpr n-hf/genit 2.5cm/<
12042 Intmd rpr n-hf/genit2.6-7.5
12051 Intmd rpr face/mm 2.5 cm/<
12052 Intmd rpr face/mm 2.6-5.0 cm
13101 Cmplx rpr trunk 2.6-7.5 cm
13121 Cmplx rpr s/a/l 2.6-7.5 cm
13131 Cmplx rpr f/c/c/m/n/ax/g/h/f
13132 Cmplx rpr f/c/c/m/n/ax/g/h/f
13151 Cmplx rpr e/n/e/l 1.1-2.5 cm
13152 Cmplx rpr e/n/e/l 2.6-7.5 cm
13160 Late closure of wound
14020 Tis trnfr s/a/l 10 sq cm/<
14021 Tis trnfr s/a/l 10.1-30 sqcm
14040 Tis trnfr f/c/c/m/n/a/g/h/f
14041 Tis trnfr f/c/c/m/n/a/g/h/f
14060 Tis trnfr e/n/e/l 10 sq cm/<
14061 Tis trnfr e/n/e/l10.1-30sqcm
14301 Tis trnfr any 30.1-60 sq cm
15100 Skin splt grft trnk/arm/leg
15120 Skn splt a-grft fac/nck/hf/g
15240 Skin full grft face/genit/hf
15260 Skin full graft een & lips
15732 Muscle-skin graft head/neck
15734 Muscle-skin graft trunk
15823 Revision of upper eyelid
17000 Destruct premalg lesion
17004 Destroy premal lesions 15/>
17110 Destruct b9 lesion 1-14
17111 Destruct lesion 15 or more
17260 Destruction of skin lesions
17261 Destruction of skin lesions
17262 Destruction of skin lesions
17263 Destruction of skin lesions
17270 Destruction of skin lesions
17271 Destruction of skin lesions
17272 Destruction of skin lesions
17273 Destruction of skin lesions
17280 Destruction of skin lesions
17281 Destruction of skin lesions
17282 Destruction of skin lesions
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
References
1. Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
It seems like only yesterday we were celebrating the elimination of the Medicare sustainable growth rate and the continuation of “global periods.” Now we are facing the elimination of the global payment periods again, and if we don’t bill the proper CPT code (99024) for our follow-up visits, during an upcoming survey period, it will indeed be a challenge for the specialty.
You may not know it, but there is payment for follow-up visits – global periods – built into codes dermatologists frequently use. As you can see, a large part of our specialty is vulnerable, from destruction of actinics and warts, to malignant and benign excisions, to destructions, to reconstructive surgery. This is real money, about a billion (yes, with a “b”) paid to dermatologists every year in Medicare alone.
These embedded visits vary from one (actinic destruction) to five (full thickness graft of the nose) and make up a major part of your reimbursement. As part of MACRA (Medicare Access and CHIP Reauthorization Act), the CMS was directed to investigate the validity of these embedded visits.1
The CMS has decided to complete this data gathering by how often the CPT code 99024 is billed.
I am not worried that we don’t provide these visits. I know we do, but I am terribly worried that we won’t correctly report these visits and won’t get credit for them.
The problem is that 99024 pays nothing, it is simply a notation to indicate that the patient was seen in follow up. Since it pays nothing, and since billing anything has an inherent expense, and since 30% of dermatologists are still on paper claims, most dermatologists have never used this code and may not start. In addition, groups of under 10 physicians are not required to report, but can, and you must! Seventy percent of our members are in groups of under 10. That means there will be no data collected on most of these codes, which are almost all performed by dermatologists, the great majority of the time.
Let me say it clearly here: If you do not start filing 99024 every time you see a patient in follow-up (and perhaps for telephone follow-ups), the amount you are paid to perform the original procedure will be cut by 30%-75%. Since the CMS will erroneously think you are not seeing these follow-up patients, they will pull these embedded payments out of the codes. You will have to start billing patients (think additional copays and deductibles) for every suture removal and wound check visit.
Data on 99024 will be collected in only nine states (Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island). It will start July 1 and no one knows how long it will continue.
So, start preparing. You will not be penalized for adding this nonpaying code to every follow-up when you do not bill an evaluation and management code. I note that one electronic medical record vendor (Modernizing Medicine) has already started populating its bills with 99024. Good for them! You must report follow-up visits no matter the size of your practice. Report early and report often. Your future depends on it.
Common procedures on which the CMS is collecting postoperative visit data
10040 Acne surgery
10060 Drainage of skin abscess
10061 Drainage of skin abscess
10120 Remove foreign body
10140 Drainage of hematoma/fluid
10160 Puncture drainage of lesion
10180 Complex drainage wound
11200 Removal of skin tags <w/15
11400 Exc tr-ext b9+marg 0.5 cm<
11401 Exc tr-ext b9+marg 0.6-1 cm
11402 Exc tr-ext b9+marg 1.1-2 cm
11403 Exc tr-ext b9+marg 2.1-3cm/<
11404 Exc tr-ext b9+marg 3.1-4 cm
11406 Exc tr-ext b9+marg >4.0 cm
11420 Exc h-f-nk-sp b9+marg 0.5/<
11421 Exc h-f-nk-sp b9+marg 0.6-1
11422 Exc h-f-nk-sp b9+marg 1.1-2
11423 Exc h-f-nk-sp b9+marg 2.1-3
11440 Exc face-mm b9+marg 0.5 cm/<
11441 Exc face-mm b9+marg 0.6-1 cm
11442 Exc face-mm b9+marg 1.1-2 cm
11443 Exc face-mm b9+marg 2.1-3 cm
11601 Exc tr-ext mal+marg 0.6-1 cm
11602 Exc tr-ext mal+marg 1.1-2 cm
11603 Exc tr-ext mal+marg 2.1-3 cm
11604 Exc tr-ext mal+marg 3.1-4 cm
11606 Exc tr-ext mal+marg >4 cm
11621 Exc s/n/h/f/g mal+mrg 0.6-1
11622 Exc s/n/h/f/g mal+mrg 1.1-2
11623 Exc s/n/h/f/g mal+mrg 2.1-3
11640 Exc f/e/e/n/l mal+mrg 0.5cm<
11641 Exc f/e/e/n/l mal+mrg 0.6-1
11642 Exc f/e/e/n/l mal+mrg 1.1-2
11643 Exc f/e/e/n/l mal+mrg 2.1-3
11644 Exc f/e/e/n/l mal+mrg 3.1-4
11646 Exc f/e/e/n/l mal+mrg >4 cm
11750 Removal of nail bed
11765 Excision of nail fold toe
12031 Intmd rpr s/a/t/ext 2.5 cm/<
12032 Intmd rpr s/a/t/ext 2.6-7.5
12034 Intmd rpr s/tr/ext 7.6-12.5
12041 Intmd rpr n-hf/genit 2.5cm/<
12042 Intmd rpr n-hf/genit2.6-7.5
12051 Intmd rpr face/mm 2.5 cm/<
12052 Intmd rpr face/mm 2.6-5.0 cm
13101 Cmplx rpr trunk 2.6-7.5 cm
13121 Cmplx rpr s/a/l 2.6-7.5 cm
13131 Cmplx rpr f/c/c/m/n/ax/g/h/f
13132 Cmplx rpr f/c/c/m/n/ax/g/h/f
13151 Cmplx rpr e/n/e/l 1.1-2.5 cm
13152 Cmplx rpr e/n/e/l 2.6-7.5 cm
13160 Late closure of wound
14020 Tis trnfr s/a/l 10 sq cm/<
14021 Tis trnfr s/a/l 10.1-30 sqcm
14040 Tis trnfr f/c/c/m/n/a/g/h/f
14041 Tis trnfr f/c/c/m/n/a/g/h/f
14060 Tis trnfr e/n/e/l 10 sq cm/<
14061 Tis trnfr e/n/e/l10.1-30sqcm
14301 Tis trnfr any 30.1-60 sq cm
15100 Skin splt grft trnk/arm/leg
15120 Skn splt a-grft fac/nck/hf/g
15240 Skin full grft face/genit/hf
15260 Skin full graft een & lips
15732 Muscle-skin graft head/neck
15734 Muscle-skin graft trunk
15823 Revision of upper eyelid
17000 Destruct premalg lesion
17004 Destroy premal lesions 15/>
17110 Destruct b9 lesion 1-14
17111 Destruct lesion 15 or more
17260 Destruction of skin lesions
17261 Destruction of skin lesions
17262 Destruction of skin lesions
17263 Destruction of skin lesions
17270 Destruction of skin lesions
17271 Destruction of skin lesions
17272 Destruction of skin lesions
17273 Destruction of skin lesions
17280 Destruction of skin lesions
17281 Destruction of skin lesions
17282 Destruction of skin lesions
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at dermnews@frontlinemedcom.com.
References
1. Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
Update on malpractice trends
Question: Recent developments in malpractice include the following:
A. Severity and frequency rates continue to rise.
B. Apology laws appear to be very effective in reducing claims.
C. Litigation surrounds whether an assistant may obtain a patient’s informed consent on behalf of the doctor.
D. A and B.
E. A, B, and C.
Answer: C. Over the past decade, malpractice claims have in fact diminished, accompanied by a leveling or reduction in premiums.1 Rates have plummeted to roughly half of previous levels, averaging six claims per 100 doctors in 2016.
According to The Doctors Company, internists paid an average premium of $15,853, compared with an average of $19,900 in 2006, general surgeons $52,905 instead of $68,186, and obstetricians $72,999, a drop from $93,230. Even claims-plagued Florida’s Dade County has seen a dramatic drop in internist premiums by some $27,000, down to $47,707.2

The latest attack on MICRA, in 2015, concerned a wrongful death suit brought by a woman whose mother died from hemorrhagic complications related to Coumadin use following heart surgery.4 Her constitutional challenges included violation of equal protection, due process, and the right to a jury trial. But these were essentially all grounded on an entitlement to recover additional noneconomic damages sufficient to cover attorney fees. The trial court had reduced her $1 million noneconomic damages to $250,000 as required by MICRA. A California appeals court rejected her claim as being “contrary to many well-established legal principles.”
Disclosure of medical errors is a relative newcomer as an ethical and effective way of thwarting potential malpractice claims. Many states have enacted so-called “apology laws,” an outgrowth of the communication and resolution programs popularized by the Lexington (Ky.) VA Medical Center, University of Michigan Health System, Harvard’s affiliated institutions, and Colorado’s COPIC Insurance.
Apology laws disallow statements of sympathy from being admitted into evidence. In some cases, these laws may assist the physician. For example, the Ohio Supreme Court has ruled that a surgeon’s comments and alleged admission of guilt (“I take full responsibility for this” regarding accidentally sectioning the common bile duct) were properly shielded from discovery by the state’s apology statute, even though the incident took place before the law went into effect.5
However, apology laws do vary from state to state, and some do not shield admissions regarding causation of error or fault.
A recent study suggests that apology laws don’t work. A Vanderbilt University study published online used a unique dataset covering all malpractice claims for 90% of physicians practicing in a single specialty across the country.6 The findings revealed that, for physicians who do not regularly perform surgery, apology laws actually increased the probability of facing a lawsuit. For surgeons, apology laws do not have a substantial effect on the probability of facing a claim or the average payment made to resolve a claim.
The study’s authors concluded that “apology laws are not substitutes for specific physician disclosure programs, and that the experiences of these types of programs are not generalizable to the physician population at large. In other words, simply being allowed to apologize is not enough to reduce malpractice risk.”
In the informed consent arena, the latest development in the law revolves around whether a physician assistant, in lieu of the surgeon himself, can obtain informed consent from a patient.
In Shinal v. Toms,7 Megan Shinal underwent surgery to remove a craniopharyngioma, but it regrew and required re-exploration by Dr. Steven Toms. Dr. Toms testified that Ms. Shinal had agreed that he would determine during the surgery whether he should remove the entire tumor or perform a partial resection. The operation was complicated by a carotid artery perforation, which left the patient with impaired vision and ambulation.
The complaint asserted that Dr. Toms’s physician assistant, not Dr. Toms himself, had provided the actual discussion during the informed consent process, and thus the patient’s consent was invalid.
The jury was allowed to consider the information provided by the doctor’s support staff, and the Superior Court of Pennsylvania affirmed the validity of the patient’s consent, holding that consent is based on the scope of information relayed rather than the identity of the individual communicating the information. This carefully watched case is now on final appeal before the Supreme Court of Pennsylvania.
At a personal level, physicians dread the stress surrounding medical malpractice litigation. The process frontally attacks their competence and consumes much time and energy, notwithstanding there being little or no exposure of personal assets because of insurance protection. Virtually all doctors practice defensive medicine, which has been defined as “deviation from sound medical practice that is induced primarily by a threat of liability.”
At a societal level, defensive medicine is reported to add substantially to the nation’s medical bill. The figure tossed around is $12 billion to $50 billion a year, based mostly on estimates by the American Medical Association and an older study extrapolating potential Medicare savings from litigation over heart disease.8
A more recent report continues to emphasize the high cost of defensive medicine.9 Jackson Healthcare invited 138,686 physicians to participate in a confidential online survey to quantify the costs and impact of defensive medicine. More than 3,000 physicians spanning all states and medical specialties completed the survey; however, this represented only a 2.21% response rate.
The authors concluded that defensive medicine is a significant force driving the high cost of health care in the United States, and that physicians estimate the cost of defensive medicine to be in the $650 billion to $850 billion range, or between 26% and 34% of annual health care costs.
Skeptics question the way the profession defines defensive medicine, pointing out that malpractice concerns may not be the primary reason, as most interventions add some marginal value to patient care. There may also be conflicting motivations of physicians, such as financial or other personal rewards.
Above all, there is no acceptable method for measuring the extent and use of defensive medicine, and survey reports are apt to be misleading because of bias and the lack of controls and baseline data.
Looking ahead, what can we expect for malpractice law under the Trump administration? Tom Price, MD, a former Republican congressman from Georgia, is an orthopedic surgeon and the new secretary of the Department of Health & Human Services. He has previously spoken passionately about tort reforms such as defensive medicine, damage caps, health tribunals, and practice guidelines. Many states have already incorporated some of these measures into their own tort reforms – with salutary results. It remains to be seen whether HHS will deem any omnibus federal legislation necessary at this point.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from my earlier columns in Internal Medicine News. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. JAMA. 2014 Nov 26;312(20):2146-55.
2. “Malpractice 2017: Do We Need Reform?” Internal Medicine News, March 1, 2017, page 1.
3. Fein v. Permanente, 38 Cal.3d 137 (1985).
4. Chan v. Curran, 237 CA 4th 601 (2015).
5. Estate of Johnson v. Randall Smith, Inc., 135 Ohio St.3d 440 (2013).
6. Available at https://papers.ssrn.com/sol3/papers2.cfm?abstract_id=2883693.
7. Shinal v. Toms, 122 A. 3d 1066 (Pa. Super. Ct. 2015).
8. Q J Econ. (1996) 111 (2): 353-390.
9. Available at www.jacksonhealthcare.com/media/8968/defensivemedicine_ebook_final.pdf.
Question: Recent developments in malpractice include the following:
A. Severity and frequency rates continue to rise.
B. Apology laws appear to be very effective in reducing claims.
C. Litigation surrounds whether an assistant may obtain a patient’s informed consent on behalf of the doctor.
D. A and B.
E. A, B, and C.
Answer: C. Over the past decade, malpractice claims have in fact diminished, accompanied by a leveling or reduction in premiums.1 Rates have plummeted to roughly half of previous levels, averaging six claims per 100 doctors in 2016.
According to The Doctors Company, internists paid an average premium of $15,853, compared with an average of $19,900 in 2006, general surgeons $52,905 instead of $68,186, and obstetricians $72,999, a drop from $93,230. Even claims-plagued Florida’s Dade County has seen a dramatic drop in internist premiums by some $27,000, down to $47,707.2
The latest attack on MICRA, in 2015, concerned a wrongful death suit brought by a woman whose mother died from hemorrhagic complications related to Coumadin use following heart surgery.4 Her constitutional challenges included violation of equal protection, due process, and the right to a jury trial. But these were essentially all grounded on an entitlement to recover additional noneconomic damages sufficient to cover attorney fees. The trial court had reduced her $1 million noneconomic damages to $250,000 as required by MICRA. A California appeals court rejected her claim as being “contrary to many well-established legal principles.”
Disclosure of medical errors is a relative newcomer as an ethical and effective way of thwarting potential malpractice claims. Many states have enacted so-called “apology laws,” an outgrowth of the communication and resolution programs popularized by the Lexington (Ky.) VA Medical Center, University of Michigan Health System, Harvard’s affiliated institutions, and Colorado’s COPIC Insurance.
Apology laws disallow statements of sympathy from being admitted into evidence. In some cases, these laws may assist the physician. For example, the Ohio Supreme Court has ruled that a surgeon’s comments and alleged admission of guilt (“I take full responsibility for this” regarding accidentally sectioning the common bile duct) were properly shielded from discovery by the state’s apology statute, even though the incident took place before the law went into effect.5
However, apology laws do vary from state to state, and some do not shield admissions regarding causation of error or fault.
A recent study suggests that apology laws don’t work. A Vanderbilt University study published online used a unique dataset covering all malpractice claims for 90% of physicians practicing in a single specialty across the country.6 The findings revealed that, for physicians who do not regularly perform surgery, apology laws actually increased the probability of facing a lawsuit. For surgeons, apology laws do not have a substantial effect on the probability of facing a claim or the average payment made to resolve a claim.
The study’s authors concluded that “apology laws are not substitutes for specific physician disclosure programs, and that the experiences of these types of programs are not generalizable to the physician population at large. In other words, simply being allowed to apologize is not enough to reduce malpractice risk.”
In the informed consent arena, the latest development in the law revolves around whether a physician assistant, in lieu of the surgeon himself, can obtain informed consent from a patient.
In Shinal v. Toms,7 Megan Shinal underwent surgery to remove a craniopharyngioma, but it regrew and required re-exploration by Dr. Steven Toms. Dr. Toms testified that Ms. Shinal had agreed that he would determine during the surgery whether he should remove the entire tumor or perform a partial resection. The operation was complicated by a carotid artery perforation, which left the patient with impaired vision and ambulation.
The complaint asserted that Dr. Toms’s physician assistant, not Dr. Toms himself, had provided the actual discussion during the informed consent process, and thus the patient’s consent was invalid.
The jury was allowed to consider the information provided by the doctor’s support staff, and the Superior Court of Pennsylvania affirmed the validity of the patient’s consent, holding that consent is based on the scope of information relayed rather than the identity of the individual communicating the information. This carefully watched case is now on final appeal before the Supreme Court of Pennsylvania.
At a personal level, physicians dread the stress surrounding medical malpractice litigation. The process frontally attacks their competence and consumes much time and energy, notwithstanding there being little or no exposure of personal assets because of insurance protection. Virtually all doctors practice defensive medicine, which has been defined as “deviation from sound medical practice that is induced primarily by a threat of liability.”
At a societal level, defensive medicine is reported to add substantially to the nation’s medical bill. The figure tossed around is $12 billion to $50 billion a year, based mostly on estimates by the American Medical Association and an older study extrapolating potential Medicare savings from litigation over heart disease.8
A more recent report continues to emphasize the high cost of defensive medicine.9 Jackson Healthcare invited 138,686 physicians to participate in a confidential online survey to quantify the costs and impact of defensive medicine. More than 3,000 physicians spanning all states and medical specialties completed the survey; however, this represented only a 2.21% response rate.
The authors concluded that defensive medicine is a significant force driving the high cost of health care in the United States, and that physicians estimate the cost of defensive medicine to be in the $650 billion to $850 billion range, or between 26% and 34% of annual health care costs.
Skeptics question the way the profession defines defensive medicine, pointing out that malpractice concerns may not be the primary reason, as most interventions add some marginal value to patient care. There may also be conflicting motivations of physicians, such as financial or other personal rewards.
Above all, there is no acceptable method for measuring the extent and use of defensive medicine, and survey reports are apt to be misleading because of bias and the lack of controls and baseline data.
Looking ahead, what can we expect for malpractice law under the Trump administration? Tom Price, MD, a former Republican congressman from Georgia, is an orthopedic surgeon and the new secretary of the Department of Health & Human Services. He has previously spoken passionately about tort reforms such as defensive medicine, damage caps, health tribunals, and practice guidelines. Many states have already incorporated some of these measures into their own tort reforms – with salutary results. It remains to be seen whether HHS will deem any omnibus federal legislation necessary at this point.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from my earlier columns in Internal Medicine News. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. JAMA. 2014 Nov 26;312(20):2146-55.
2. “Malpractice 2017: Do We Need Reform?” Internal Medicine News, March 1, 2017, page 1.
3. Fein v. Permanente, 38 Cal.3d 137 (1985).
4. Chan v. Curran, 237 CA 4th 601 (2015).
5. Estate of Johnson v. Randall Smith, Inc., 135 Ohio St.3d 440 (2013).
6. Available at https://papers.ssrn.com/sol3/papers2.cfm?abstract_id=2883693.
7. Shinal v. Toms, 122 A. 3d 1066 (Pa. Super. Ct. 2015).
8. Q J Econ. (1996) 111 (2): 353-390.
9. Available at www.jacksonhealthcare.com/media/8968/defensivemedicine_ebook_final.pdf.
Question: Recent developments in malpractice include the following:
A. Severity and frequency rates continue to rise.
B. Apology laws appear to be very effective in reducing claims.
C. Litigation surrounds whether an assistant may obtain a patient’s informed consent on behalf of the doctor.
D. A and B.
E. A, B, and C.
Answer: C. Over the past decade, malpractice claims have in fact diminished, accompanied by a leveling or reduction in premiums.1 Rates have plummeted to roughly half of previous levels, averaging six claims per 100 doctors in 2016.
According to The Doctors Company, internists paid an average premium of $15,853, compared with an average of $19,900 in 2006, general surgeons $52,905 instead of $68,186, and obstetricians $72,999, a drop from $93,230. Even claims-plagued Florida’s Dade County has seen a dramatic drop in internist premiums by some $27,000, down to $47,707.2
The latest attack on MICRA, in 2015, concerned a wrongful death suit brought by a woman whose mother died from hemorrhagic complications related to Coumadin use following heart surgery.4 Her constitutional challenges included violation of equal protection, due process, and the right to a jury trial. But these were essentially all grounded on an entitlement to recover additional noneconomic damages sufficient to cover attorney fees. The trial court had reduced her $1 million noneconomic damages to $250,000 as required by MICRA. A California appeals court rejected her claim as being “contrary to many well-established legal principles.”
Disclosure of medical errors is a relative newcomer as an ethical and effective way of thwarting potential malpractice claims. Many states have enacted so-called “apology laws,” an outgrowth of the communication and resolution programs popularized by the Lexington (Ky.) VA Medical Center, University of Michigan Health System, Harvard’s affiliated institutions, and Colorado’s COPIC Insurance.
Apology laws disallow statements of sympathy from being admitted into evidence. In some cases, these laws may assist the physician. For example, the Ohio Supreme Court has ruled that a surgeon’s comments and alleged admission of guilt (“I take full responsibility for this” regarding accidentally sectioning the common bile duct) were properly shielded from discovery by the state’s apology statute, even though the incident took place before the law went into effect.5
However, apology laws do vary from state to state, and some do not shield admissions regarding causation of error or fault.
A recent study suggests that apology laws don’t work. A Vanderbilt University study published online used a unique dataset covering all malpractice claims for 90% of physicians practicing in a single specialty across the country.6 The findings revealed that, for physicians who do not regularly perform surgery, apology laws actually increased the probability of facing a lawsuit. For surgeons, apology laws do not have a substantial effect on the probability of facing a claim or the average payment made to resolve a claim.
The study’s authors concluded that “apology laws are not substitutes for specific physician disclosure programs, and that the experiences of these types of programs are not generalizable to the physician population at large. In other words, simply being allowed to apologize is not enough to reduce malpractice risk.”
In the informed consent arena, the latest development in the law revolves around whether a physician assistant, in lieu of the surgeon himself, can obtain informed consent from a patient.
In Shinal v. Toms,7 Megan Shinal underwent surgery to remove a craniopharyngioma, but it regrew and required re-exploration by Dr. Steven Toms. Dr. Toms testified that Ms. Shinal had agreed that he would determine during the surgery whether he should remove the entire tumor or perform a partial resection. The operation was complicated by a carotid artery perforation, which left the patient with impaired vision and ambulation.
The complaint asserted that Dr. Toms’s physician assistant, not Dr. Toms himself, had provided the actual discussion during the informed consent process, and thus the patient’s consent was invalid.
The jury was allowed to consider the information provided by the doctor’s support staff, and the Superior Court of Pennsylvania affirmed the validity of the patient’s consent, holding that consent is based on the scope of information relayed rather than the identity of the individual communicating the information. This carefully watched case is now on final appeal before the Supreme Court of Pennsylvania.
At a personal level, physicians dread the stress surrounding medical malpractice litigation. The process frontally attacks their competence and consumes much time and energy, notwithstanding there being little or no exposure of personal assets because of insurance protection. Virtually all doctors practice defensive medicine, which has been defined as “deviation from sound medical practice that is induced primarily by a threat of liability.”
At a societal level, defensive medicine is reported to add substantially to the nation’s medical bill. The figure tossed around is $12 billion to $50 billion a year, based mostly on estimates by the American Medical Association and an older study extrapolating potential Medicare savings from litigation over heart disease.8
A more recent report continues to emphasize the high cost of defensive medicine.9 Jackson Healthcare invited 138,686 physicians to participate in a confidential online survey to quantify the costs and impact of defensive medicine. More than 3,000 physicians spanning all states and medical specialties completed the survey; however, this represented only a 2.21% response rate.
The authors concluded that defensive medicine is a significant force driving the high cost of health care in the United States, and that physicians estimate the cost of defensive medicine to be in the $650 billion to $850 billion range, or between 26% and 34% of annual health care costs.
Skeptics question the way the profession defines defensive medicine, pointing out that malpractice concerns may not be the primary reason, as most interventions add some marginal value to patient care. There may also be conflicting motivations of physicians, such as financial or other personal rewards.
Above all, there is no acceptable method for measuring the extent and use of defensive medicine, and survey reports are apt to be misleading because of bias and the lack of controls and baseline data.
Looking ahead, what can we expect for malpractice law under the Trump administration? Tom Price, MD, a former Republican congressman from Georgia, is an orthopedic surgeon and the new secretary of the Department of Health & Human Services. He has previously spoken passionately about tort reforms such as defensive medicine, damage caps, health tribunals, and practice guidelines. Many states have already incorporated some of these measures into their own tort reforms – with salutary results. It remains to be seen whether HHS will deem any omnibus federal legislation necessary at this point.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from my earlier columns in Internal Medicine News. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. JAMA. 2014 Nov 26;312(20):2146-55.
2. “Malpractice 2017: Do We Need Reform?” Internal Medicine News, March 1, 2017, page 1.
3. Fein v. Permanente, 38 Cal.3d 137 (1985).
4. Chan v. Curran, 237 CA 4th 601 (2015).
5. Estate of Johnson v. Randall Smith, Inc., 135 Ohio St.3d 440 (2013).
6. Available at https://papers.ssrn.com/sol3/papers2.cfm?abstract_id=2883693.
7. Shinal v. Toms, 122 A. 3d 1066 (Pa. Super. Ct. 2015).
8. Q J Econ. (1996) 111 (2): 353-390.
9. Available at www.jacksonhealthcare.com/media/8968/defensivemedicine_ebook_final.pdf.
The power of words in aesthetic procedures and healing patients
The words we choose to use prior to procedures can positively or negatively impact a patient’s experience during a procedure and their decision to have the procedure performed. A practical example would include using the word discomfort instead of pain to describe pain that may be associated with a procedure. The root word of discomfort is comfort, which the mind focuses on and creates less of an anxious state than pain.
Obviously, the need to provide proper and realistic expectations, as well as risks and benefits, is of utmost importance when obtaining informed consent. The words used can put a patient’s mind at ease or cause further anxiety about ideas of needles, scalpels, pain, risk of infection, and bleeding that are part of our everyday procedures.

Judith Thomas, DDS, a dentist in Virginia who is trained in clinical hypnosis, once described the power of the word but. People will often put more emphasis in their minds on what is said after the word but than on what is said before. For example, in a romantic relationship context, saying “I love you, but you drive me crazy” has a different impact than “You drive me crazy, but I love you.” The focus tends to stay on the “I love you” portion more when it is said last, after the “but.”
The same phenomenon can happen when we discuss procedures with our patients. When a medical assistant performs phlebotomy or when we as doctors are about to perform an injection, instead of saying this is going to hurt, another way to phrase it would be “In a moment you may feel something, but it doesn’t have to bother you” or “You may experience some discomfort, but it will resolve quickly.” Something I’ve said for years to patients before surgery is “You may feel a little stinging as the anesthetic goes in, after that you may feel me touching you, but nothing uncomfortable.” I guess I had been intuitively using this technique for years, without knowing the impact of the word “but.” Perhaps now that I am more mindful of it, I will be even more mindful of how I phrase these terms. We, in addition to our nurses and medical assistants, can use these techniques to enhance patient comfort and the patient’s experience.
According to the American Society of Clinical Hypnosis, physicians and dentists used the power of words through hypnosis as anesthesia before the first chemical general anesthetic agent, ether, was used for surgery in the 1840s, followed by chloroform. Prior to this time, British and Scottish physicians John Elliotson, James Esdaile, and James Braid performed over 3,000 procedures and surgeries with clinical hypnosis alone. Some may argue that the ancient Egyptians also used hypnosis for their well-described surgeries, as no other anesthetic has been documented. Moreover, there is evidence of “sleep temples” that the ancient Egyptians used for healing.1
This article is not to suggest that our words should replace anesthesia. Many advances in anesthesia and pain control have been made since the time of chloroform. However, being mindful of our words can aid and assist in our surgical and aesthetic procedures where less anesthesia is used: Patients feel more comfortable, they heal faster, and overall, they have a more positive outcome and pleasant physician-patient experience.2
For patients, the skill of the doctor and the outcome of the procedure are of the utmost importance, but, especially in aesthetic dermatology, where some of our procedures are repeated or performed periodically, the positive impact of the entire experience will entrust them with your care long term.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
1. Mutter, C.B. (1998). History of Hypnosis. (pp. 10-12) “Hypnotic Induction and Suggestion.” Chicago: American Society of Clinical Hypnosis.
2. Burns. 2010 Aug;36(5):639-46.
The words we choose to use prior to procedures can positively or negatively impact a patient’s experience during a procedure and their decision to have the procedure performed. A practical example would include using the word discomfort instead of pain to describe pain that may be associated with a procedure. The root word of discomfort is comfort, which the mind focuses on and creates less of an anxious state than pain.
Obviously, the need to provide proper and realistic expectations, as well as risks and benefits, is of utmost importance when obtaining informed consent. The words used can put a patient’s mind at ease or cause further anxiety about ideas of needles, scalpels, pain, risk of infection, and bleeding that are part of our everyday procedures.
Judith Thomas, DDS, a dentist in Virginia who is trained in clinical hypnosis, once described the power of the word but. People will often put more emphasis in their minds on what is said after the word but than on what is said before. For example, in a romantic relationship context, saying “I love you, but you drive me crazy” has a different impact than “You drive me crazy, but I love you.” The focus tends to stay on the “I love you” portion more when it is said last, after the “but.”
The same phenomenon can happen when we discuss procedures with our patients. When a medical assistant performs phlebotomy or when we as doctors are about to perform an injection, instead of saying this is going to hurt, another way to phrase it would be “In a moment you may feel something, but it doesn’t have to bother you” or “You may experience some discomfort, but it will resolve quickly.” Something I’ve said for years to patients before surgery is “You may feel a little stinging as the anesthetic goes in, after that you may feel me touching you, but nothing uncomfortable.” I guess I had been intuitively using this technique for years, without knowing the impact of the word “but.” Perhaps now that I am more mindful of it, I will be even more mindful of how I phrase these terms. We, in addition to our nurses and medical assistants, can use these techniques to enhance patient comfort and the patient’s experience.
According to the American Society of Clinical Hypnosis, physicians and dentists used the power of words through hypnosis as anesthesia before the first chemical general anesthetic agent, ether, was used for surgery in the 1840s, followed by chloroform. Prior to this time, British and Scottish physicians John Elliotson, James Esdaile, and James Braid performed over 3,000 procedures and surgeries with clinical hypnosis alone. Some may argue that the ancient Egyptians also used hypnosis for their well-described surgeries, as no other anesthetic has been documented. Moreover, there is evidence of “sleep temples” that the ancient Egyptians used for healing.1
This article is not to suggest that our words should replace anesthesia. Many advances in anesthesia and pain control have been made since the time of chloroform. However, being mindful of our words can aid and assist in our surgical and aesthetic procedures where less anesthesia is used: Patients feel more comfortable, they heal faster, and overall, they have a more positive outcome and pleasant physician-patient experience.2
For patients, the skill of the doctor and the outcome of the procedure are of the utmost importance, but, especially in aesthetic dermatology, where some of our procedures are repeated or performed periodically, the positive impact of the entire experience will entrust them with your care long term.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
1. Mutter, C.B. (1998). History of Hypnosis. (pp. 10-12) “Hypnotic Induction and Suggestion.” Chicago: American Society of Clinical Hypnosis.
2. Burns. 2010 Aug;36(5):639-46.
The words we choose to use prior to procedures can positively or negatively impact a patient’s experience during a procedure and their decision to have the procedure performed. A practical example would include using the word discomfort instead of pain to describe pain that may be associated with a procedure. The root word of discomfort is comfort, which the mind focuses on and creates less of an anxious state than pain.
Obviously, the need to provide proper and realistic expectations, as well as risks and benefits, is of utmost importance when obtaining informed consent. The words used can put a patient’s mind at ease or cause further anxiety about ideas of needles, scalpels, pain, risk of infection, and bleeding that are part of our everyday procedures.
Judith Thomas, DDS, a dentist in Virginia who is trained in clinical hypnosis, once described the power of the word but. People will often put more emphasis in their minds on what is said after the word but than on what is said before. For example, in a romantic relationship context, saying “I love you, but you drive me crazy” has a different impact than “You drive me crazy, but I love you.” The focus tends to stay on the “I love you” portion more when it is said last, after the “but.”
The same phenomenon can happen when we discuss procedures with our patients. When a medical assistant performs phlebotomy or when we as doctors are about to perform an injection, instead of saying this is going to hurt, another way to phrase it would be “In a moment you may feel something, but it doesn’t have to bother you” or “You may experience some discomfort, but it will resolve quickly.” Something I’ve said for years to patients before surgery is “You may feel a little stinging as the anesthetic goes in, after that you may feel me touching you, but nothing uncomfortable.” I guess I had been intuitively using this technique for years, without knowing the impact of the word “but.” Perhaps now that I am more mindful of it, I will be even more mindful of how I phrase these terms. We, in addition to our nurses and medical assistants, can use these techniques to enhance patient comfort and the patient’s experience.
According to the American Society of Clinical Hypnosis, physicians and dentists used the power of words through hypnosis as anesthesia before the first chemical general anesthetic agent, ether, was used for surgery in the 1840s, followed by chloroform. Prior to this time, British and Scottish physicians John Elliotson, James Esdaile, and James Braid performed over 3,000 procedures and surgeries with clinical hypnosis alone. Some may argue that the ancient Egyptians also used hypnosis for their well-described surgeries, as no other anesthetic has been documented. Moreover, there is evidence of “sleep temples” that the ancient Egyptians used for healing.1
This article is not to suggest that our words should replace anesthesia. Many advances in anesthesia and pain control have been made since the time of chloroform. However, being mindful of our words can aid and assist in our surgical and aesthetic procedures where less anesthesia is used: Patients feel more comfortable, they heal faster, and overall, they have a more positive outcome and pleasant physician-patient experience.2
For patients, the skill of the doctor and the outcome of the procedure are of the utmost importance, but, especially in aesthetic dermatology, where some of our procedures are repeated or performed periodically, the positive impact of the entire experience will entrust them with your care long term.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
1. Mutter, C.B. (1998). History of Hypnosis. (pp. 10-12) “Hypnotic Induction and Suggestion.” Chicago: American Society of Clinical Hypnosis.
2. Burns. 2010 Aug;36(5):639-46.
Hold your breath
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).

And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11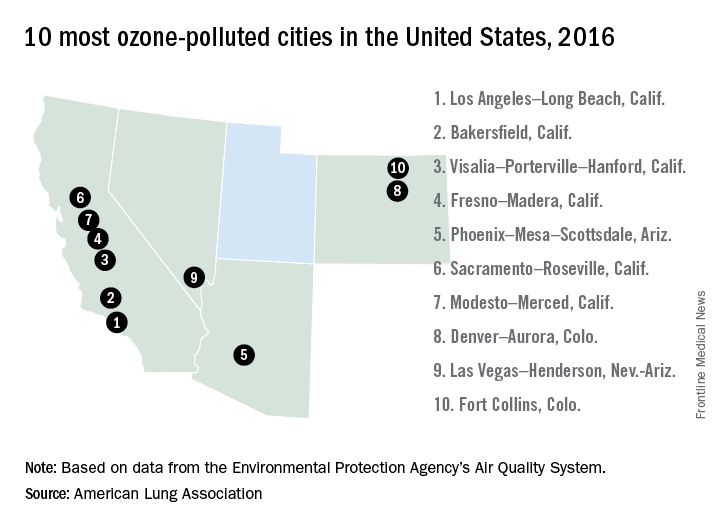
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).
And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).
And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
Music in the OR
I am sure that even though Theodor Billroth and Johannes Brahms were close friends, Billroth never listened to music in his operating room. I’m pretty sure because the Victrola was invented around 1906 and the first commercial radio broadcast was in 1920. So unless Billroth hired a Viennese string quartet to play in his amphitheater, it is likely the operating room was a pretty quiet place.
Radios were the size of a small refrigerator into the 1940s when Bell Laboratories’ invention of the transistor technology permitted small units to play tinny music through speakers about 2 inches across. So, I would guess that Alfred Blalock didn’t listen to Elvis Presley or Buddy Holly during his pioneering days at Hopkins.
By the late 1960s high-quality, recorded music was available on 8-track tapes invented by the Lear Jet Corporation. Music at that point was literally available everywhere and the OR became a theater once more for some surgeons. Cassette tapes followed, and Johnny Paycheck echoed in the heart room where I trained in Dallas – usually at high volume. When Apple changed the world with the iPod in 2001 and then the Internet streaming services emerged, it became possible to take out a gall bladder accompanied by Vladimir Horowitz or Madonna. And it happens routinely.
As I write this, I am listening to a jazz streaming station. Music is one of the most important elements of my life. Yet, my operating room has had music on only one occasion since I became an attending surgeon. I love music too much for it to be in my OR. It not only relaxes me, which may not be entirely a good thing in surgery, but it engages my intellect, taking up needed CPU time which might be useful in avoiding catastrophe for the patient before me.
Not long ago this subject was the focus of a discussion thread on the ACS Communities. Many reported that they never listen to music in the OR, others said it was essential to their performance, and still others took a middle ground. Everyone said the music shouldn’t be loud; however, I can recall visiting a number of operating rooms in which loud was the standard volume setting. Most respondents spoke in terms of what they needed and like. Several felt that as captain of the SS Operating Room they had the final say of whether, what, and when music would be played.
I noted in the conversation justification, defensiveness, authoritarianism mixed with personal insight that is so characteristic of many surgeons. Of course, there isn’t a “right” answer here any more than there is in a number of OR traditions. The evidence is all over the place except when it comes to volume. There, it is clear that loud music causes or exacerbates communications errors due to inability of the OR team to hear one another or distraction of the team from their primary task.
Music affects everyone in the OR. It represents one of many operating room components that hold the potential of both betterment of care or endangerment of the patient. To say that music in the OR is wrong is like saying propellers on aircraft are somehow wrong. Among the most serious injuries at general aviation airports is individuals walking into a spinning propeller; however, without the propeller the plane can’t fly and deliver its benefits enjoyed at large. The problem isn’t that propellers are evil. It is that they are invisible to the victim who ignores their dangers.
My point is that music is an example of the need for us to be aware of the primary and secondary effects of even the small things we do in the OR because innocuous as they seem, they have potential dangers. The Council on Surgical and Perioperative Care of which the ACS is a member, has more data and resources on their homepage (cspsteam.org) for those interested in the subject on distractions in the OR.
So, what I’ve learned through listening to the music of my colleagues opinions is that when it comes to music, we need to be aware of the spinning propeller of noise pollution in the OR. Many invisible dangers inhabit the OR. Take a moment and listen for them.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
I am sure that even though Theodor Billroth and Johannes Brahms were close friends, Billroth never listened to music in his operating room. I’m pretty sure because the Victrola was invented around 1906 and the first commercial radio broadcast was in 1920. So unless Billroth hired a Viennese string quartet to play in his amphitheater, it is likely the operating room was a pretty quiet place.
Radios were the size of a small refrigerator into the 1940s when Bell Laboratories’ invention of the transistor technology permitted small units to play tinny music through speakers about 2 inches across. So, I would guess that Alfred Blalock didn’t listen to Elvis Presley or Buddy Holly during his pioneering days at Hopkins.
By the late 1960s high-quality, recorded music was available on 8-track tapes invented by the Lear Jet Corporation. Music at that point was literally available everywhere and the OR became a theater once more for some surgeons. Cassette tapes followed, and Johnny Paycheck echoed in the heart room where I trained in Dallas – usually at high volume. When Apple changed the world with the iPod in 2001 and then the Internet streaming services emerged, it became possible to take out a gall bladder accompanied by Vladimir Horowitz or Madonna. And it happens routinely.
As I write this, I am listening to a jazz streaming station. Music is one of the most important elements of my life. Yet, my operating room has had music on only one occasion since I became an attending surgeon. I love music too much for it to be in my OR. It not only relaxes me, which may not be entirely a good thing in surgery, but it engages my intellect, taking up needed CPU time which might be useful in avoiding catastrophe for the patient before me.
Not long ago this subject was the focus of a discussion thread on the ACS Communities. Many reported that they never listen to music in the OR, others said it was essential to their performance, and still others took a middle ground. Everyone said the music shouldn’t be loud; however, I can recall visiting a number of operating rooms in which loud was the standard volume setting. Most respondents spoke in terms of what they needed and like. Several felt that as captain of the SS Operating Room they had the final say of whether, what, and when music would be played.
I noted in the conversation justification, defensiveness, authoritarianism mixed with personal insight that is so characteristic of many surgeons. Of course, there isn’t a “right” answer here any more than there is in a number of OR traditions. The evidence is all over the place except when it comes to volume. There, it is clear that loud music causes or exacerbates communications errors due to inability of the OR team to hear one another or distraction of the team from their primary task.
Music affects everyone in the OR. It represents one of many operating room components that hold the potential of both betterment of care or endangerment of the patient. To say that music in the OR is wrong is like saying propellers on aircraft are somehow wrong. Among the most serious injuries at general aviation airports is individuals walking into a spinning propeller; however, without the propeller the plane can’t fly and deliver its benefits enjoyed at large. The problem isn’t that propellers are evil. It is that they are invisible to the victim who ignores their dangers.
My point is that music is an example of the need for us to be aware of the primary and secondary effects of even the small things we do in the OR because innocuous as they seem, they have potential dangers. The Council on Surgical and Perioperative Care of which the ACS is a member, has more data and resources on their homepage (cspsteam.org) for those interested in the subject on distractions in the OR.
So, what I’ve learned through listening to the music of my colleagues opinions is that when it comes to music, we need to be aware of the spinning propeller of noise pollution in the OR. Many invisible dangers inhabit the OR. Take a moment and listen for them.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
I am sure that even though Theodor Billroth and Johannes Brahms were close friends, Billroth never listened to music in his operating room. I’m pretty sure because the Victrola was invented around 1906 and the first commercial radio broadcast was in 1920. So unless Billroth hired a Viennese string quartet to play in his amphitheater, it is likely the operating room was a pretty quiet place.
Radios were the size of a small refrigerator into the 1940s when Bell Laboratories’ invention of the transistor technology permitted small units to play tinny music through speakers about 2 inches across. So, I would guess that Alfred Blalock didn’t listen to Elvis Presley or Buddy Holly during his pioneering days at Hopkins.
By the late 1960s high-quality, recorded music was available on 8-track tapes invented by the Lear Jet Corporation. Music at that point was literally available everywhere and the OR became a theater once more for some surgeons. Cassette tapes followed, and Johnny Paycheck echoed in the heart room where I trained in Dallas – usually at high volume. When Apple changed the world with the iPod in 2001 and then the Internet streaming services emerged, it became possible to take out a gall bladder accompanied by Vladimir Horowitz or Madonna. And it happens routinely.
As I write this, I am listening to a jazz streaming station. Music is one of the most important elements of my life. Yet, my operating room has had music on only one occasion since I became an attending surgeon. I love music too much for it to be in my OR. It not only relaxes me, which may not be entirely a good thing in surgery, but it engages my intellect, taking up needed CPU time which might be useful in avoiding catastrophe for the patient before me.
Not long ago this subject was the focus of a discussion thread on the ACS Communities. Many reported that they never listen to music in the OR, others said it was essential to their performance, and still others took a middle ground. Everyone said the music shouldn’t be loud; however, I can recall visiting a number of operating rooms in which loud was the standard volume setting. Most respondents spoke in terms of what they needed and like. Several felt that as captain of the SS Operating Room they had the final say of whether, what, and when music would be played.
I noted in the conversation justification, defensiveness, authoritarianism mixed with personal insight that is so characteristic of many surgeons. Of course, there isn’t a “right” answer here any more than there is in a number of OR traditions. The evidence is all over the place except when it comes to volume. There, it is clear that loud music causes or exacerbates communications errors due to inability of the OR team to hear one another or distraction of the team from their primary task.
Music affects everyone in the OR. It represents one of many operating room components that hold the potential of both betterment of care or endangerment of the patient. To say that music in the OR is wrong is like saying propellers on aircraft are somehow wrong. Among the most serious injuries at general aviation airports is individuals walking into a spinning propeller; however, without the propeller the plane can’t fly and deliver its benefits enjoyed at large. The problem isn’t that propellers are evil. It is that they are invisible to the victim who ignores their dangers.
My point is that music is an example of the need for us to be aware of the primary and secondary effects of even the small things we do in the OR because innocuous as they seem, they have potential dangers. The Council on Surgical and Perioperative Care of which the ACS is a member, has more data and resources on their homepage (cspsteam.org) for those interested in the subject on distractions in the OR.
So, what I’ve learned through listening to the music of my colleagues opinions is that when it comes to music, we need to be aware of the spinning propeller of noise pollution in the OR. Many invisible dangers inhabit the OR. Take a moment and listen for them.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.

Contract negotiations
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.

Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.
Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.
Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.

Surveillance
A few weeks ago I received an email from a pediatrician thanking me for supporting her decision to quit work so that she could be home when her teenage son came home from school. She felt that by being home during her son’s adolescence, not only had she provided him a secure base but she also had helped protect him from a drug-dominated culture that permeated the community where they lived. While I hadn’t touched on it in my column, “Perfect Attendance” (Pediatric News, March 2017), this pediatrician’s experience highlights another benefit of a parental presence during those potentially stormy adolescent years.
In a recent article in the New York Times (“Teenagers Do Dumb Things, but There Are Ways to Limit Recklessness,” by Lisa Damour, March 8, 2017), Dr. Laurence Steinberg, a psychology professor at Temple University, is quoted as saying that “the context in which kids grow up must matter a great deal, and that recklessness isn’t the inevitable byproduct of the period’s biology.”
As writer Lisa Damour cogently states in her article, “For teenagers to find trouble, temptation must meet opportunity.”
Here in Brunswick, high school students finish their school day at 2:10 pm. If the student doesn’t play on a sports team and even if his or her home is at the end of the longest bus route, he or she is going to be home before 3 p.m. ... probably unsupervised. And stuff happens.
Although I may have been unsupervised, I was – or at least I believed that I was – always under constant surveillance. In the 1950s and 1960s, the population of Pleasantville, N.Y. was 5,000 and my mother had me convinced that she knew 4,000 of them. She recounted enough little things she had heard to make me believe that I was being watched by 8,000 eyes. She and the other mothers in town were masters of information sharing long before anyone had heard of networking.
These were not helicopter mothers hovering over every shady corner of our lives. They were simply concerned parents and fellow citizens going about their daily business who were not afraid to say something if they saw something. My mother’s apparent omniscience was a powerful deterrent to my adolescent recklessness. Only after I could afford to buy a car did I feel I could escape her surveillance network. And even then I wasn’t always sure.
The Internet has opened opportunities for mischief that are several orders of magnitude greater than the ones my friends and I sought to exploit in the 1950s and 1960s. However, parents today do have tools with which they can create a surveillance network to protect adolescents from their biologically predetermined urges. They simply need to have to courage to use them and not be afraid to say something if they see something.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
A few weeks ago I received an email from a pediatrician thanking me for supporting her decision to quit work so that she could be home when her teenage son came home from school. She felt that by being home during her son’s adolescence, not only had she provided him a secure base but she also had helped protect him from a drug-dominated culture that permeated the community where they lived. While I hadn’t touched on it in my column, “Perfect Attendance” (Pediatric News, March 2017), this pediatrician’s experience highlights another benefit of a parental presence during those potentially stormy adolescent years.
In a recent article in the New York Times (“Teenagers Do Dumb Things, but There Are Ways to Limit Recklessness,” by Lisa Damour, March 8, 2017), Dr. Laurence Steinberg, a psychology professor at Temple University, is quoted as saying that “the context in which kids grow up must matter a great deal, and that recklessness isn’t the inevitable byproduct of the period’s biology.”
As writer Lisa Damour cogently states in her article, “For teenagers to find trouble, temptation must meet opportunity.”
Here in Brunswick, high school students finish their school day at 2:10 pm. If the student doesn’t play on a sports team and even if his or her home is at the end of the longest bus route, he or she is going to be home before 3 p.m. ... probably unsupervised. And stuff happens.
Although I may have been unsupervised, I was – or at least I believed that I was – always under constant surveillance. In the 1950s and 1960s, the population of Pleasantville, N.Y. was 5,000 and my mother had me convinced that she knew 4,000 of them. She recounted enough little things she had heard to make me believe that I was being watched by 8,000 eyes. She and the other mothers in town were masters of information sharing long before anyone had heard of networking.
These were not helicopter mothers hovering over every shady corner of our lives. They were simply concerned parents and fellow citizens going about their daily business who were not afraid to say something if they saw something. My mother’s apparent omniscience was a powerful deterrent to my adolescent recklessness. Only after I could afford to buy a car did I feel I could escape her surveillance network. And even then I wasn’t always sure.
The Internet has opened opportunities for mischief that are several orders of magnitude greater than the ones my friends and I sought to exploit in the 1950s and 1960s. However, parents today do have tools with which they can create a surveillance network to protect adolescents from their biologically predetermined urges. They simply need to have to courage to use them and not be afraid to say something if they see something.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
A few weeks ago I received an email from a pediatrician thanking me for supporting her decision to quit work so that she could be home when her teenage son came home from school. She felt that by being home during her son’s adolescence, not only had she provided him a secure base but she also had helped protect him from a drug-dominated culture that permeated the community where they lived. While I hadn’t touched on it in my column, “Perfect Attendance” (Pediatric News, March 2017), this pediatrician’s experience highlights another benefit of a parental presence during those potentially stormy adolescent years.
In a recent article in the New York Times (“Teenagers Do Dumb Things, but There Are Ways to Limit Recklessness,” by Lisa Damour, March 8, 2017), Dr. Laurence Steinberg, a psychology professor at Temple University, is quoted as saying that “the context in which kids grow up must matter a great deal, and that recklessness isn’t the inevitable byproduct of the period’s biology.”
As writer Lisa Damour cogently states in her article, “For teenagers to find trouble, temptation must meet opportunity.”
Here in Brunswick, high school students finish their school day at 2:10 pm. If the student doesn’t play on a sports team and even if his or her home is at the end of the longest bus route, he or she is going to be home before 3 p.m. ... probably unsupervised. And stuff happens.
Although I may have been unsupervised, I was – or at least I believed that I was – always under constant surveillance. In the 1950s and 1960s, the population of Pleasantville, N.Y. was 5,000 and my mother had me convinced that she knew 4,000 of them. She recounted enough little things she had heard to make me believe that I was being watched by 8,000 eyes. She and the other mothers in town were masters of information sharing long before anyone had heard of networking.
These were not helicopter mothers hovering over every shady corner of our lives. They were simply concerned parents and fellow citizens going about their daily business who were not afraid to say something if they saw something. My mother’s apparent omniscience was a powerful deterrent to my adolescent recklessness. Only after I could afford to buy a car did I feel I could escape her surveillance network. And even then I wasn’t always sure.
The Internet has opened opportunities for mischief that are several orders of magnitude greater than the ones my friends and I sought to exploit in the 1950s and 1960s. However, parents today do have tools with which they can create a surveillance network to protect adolescents from their biologically predetermined urges. They simply need to have to courage to use them and not be afraid to say something if they see something.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.