User login
Breathe2Relax

The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
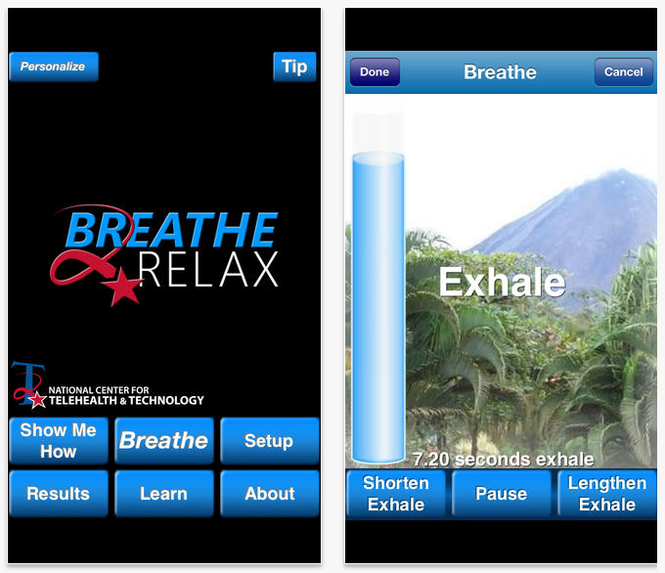
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.

Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.
Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.
Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
Chronic pain and opioid use much higher among soldiers
Rates of chronic pain and opioid use are significantly higher among soldiers, compared with the general population, a survey of 2,597 Army infantry soldiers showed.
The survey, conducted in 2011 after the soldiers had been deployed from combat in Afghanistan or Iraq, found that 44% of the soldiers reported experiencing chronic pain and 15.1% declared that they had used opioids sometime in the past month.
The survey also found that among those reporting opioid use, 44.1%% said they had experienced only mild or no pain in the past month, while among those with chronic pain, only 23.2% had received opioids in the past month, according to a research letter published online June 30 (JAMA 2014 [doi:10.1001/jamainternmed.2014.2726]).
Those with chronic pain were more likely to be aged over 30 years, to be married or have been married, to be injured during combat, to be in higher-intensity combat, or to have experienced posttraumatic stress disorder or major depressive disorder. Use of opioids was associated with "sex, age 25 years or older, being married, rank, injury during combat, chronic pain, and pain severity," wrote Robin L. Toblin, Ph.D., and colleagues.
"These findings suggest a large unmet need for assessment, management, and treatment of chronic pain and related opioid use and misuse in military personnel after combat deployments," said Dr. Toblin of the center for military psychiatry and neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md.
An accompanying editorial contrasted the figures for chronic pain and opioid use in the military with those in the general population – 26% and 4%, respectively (JAMA 2014 June 30 [doi:10.1001/jamainternmed.2014.2114]).
"While chronic pain and opioid use have been a long-standing concern of the military leadership, this study is among the first to quantify the impact of recent wars on the prevalence of pain and narcotic use among soldiers," wrote Dr. Wayne B. Jonas of the Samueli Institute in Alexandria, Va., and the Uniformed Services University of the Health Sciences in Bethesda, Md., and Dr. Eric B. Schoomaker, also of the Samueli Institute.
No conflicts of interest were declared.
Rates of chronic pain and opioid use are significantly higher among soldiers, compared with the general population, a survey of 2,597 Army infantry soldiers showed.
The survey, conducted in 2011 after the soldiers had been deployed from combat in Afghanistan or Iraq, found that 44% of the soldiers reported experiencing chronic pain and 15.1% declared that they had used opioids sometime in the past month.
The survey also found that among those reporting opioid use, 44.1%% said they had experienced only mild or no pain in the past month, while among those with chronic pain, only 23.2% had received opioids in the past month, according to a research letter published online June 30 (JAMA 2014 [doi:10.1001/jamainternmed.2014.2726]).
Those with chronic pain were more likely to be aged over 30 years, to be married or have been married, to be injured during combat, to be in higher-intensity combat, or to have experienced posttraumatic stress disorder or major depressive disorder. Use of opioids was associated with "sex, age 25 years or older, being married, rank, injury during combat, chronic pain, and pain severity," wrote Robin L. Toblin, Ph.D., and colleagues.
"These findings suggest a large unmet need for assessment, management, and treatment of chronic pain and related opioid use and misuse in military personnel after combat deployments," said Dr. Toblin of the center for military psychiatry and neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md.
An accompanying editorial contrasted the figures for chronic pain and opioid use in the military with those in the general population – 26% and 4%, respectively (JAMA 2014 June 30 [doi:10.1001/jamainternmed.2014.2114]).
"While chronic pain and opioid use have been a long-standing concern of the military leadership, this study is among the first to quantify the impact of recent wars on the prevalence of pain and narcotic use among soldiers," wrote Dr. Wayne B. Jonas of the Samueli Institute in Alexandria, Va., and the Uniformed Services University of the Health Sciences in Bethesda, Md., and Dr. Eric B. Schoomaker, also of the Samueli Institute.
No conflicts of interest were declared.
Rates of chronic pain and opioid use are significantly higher among soldiers, compared with the general population, a survey of 2,597 Army infantry soldiers showed.
The survey, conducted in 2011 after the soldiers had been deployed from combat in Afghanistan or Iraq, found that 44% of the soldiers reported experiencing chronic pain and 15.1% declared that they had used opioids sometime in the past month.
The survey also found that among those reporting opioid use, 44.1%% said they had experienced only mild or no pain in the past month, while among those with chronic pain, only 23.2% had received opioids in the past month, according to a research letter published online June 30 (JAMA 2014 [doi:10.1001/jamainternmed.2014.2726]).
Those with chronic pain were more likely to be aged over 30 years, to be married or have been married, to be injured during combat, to be in higher-intensity combat, or to have experienced posttraumatic stress disorder or major depressive disorder. Use of opioids was associated with "sex, age 25 years or older, being married, rank, injury during combat, chronic pain, and pain severity," wrote Robin L. Toblin, Ph.D., and colleagues.
"These findings suggest a large unmet need for assessment, management, and treatment of chronic pain and related opioid use and misuse in military personnel after combat deployments," said Dr. Toblin of the center for military psychiatry and neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md.
An accompanying editorial contrasted the figures for chronic pain and opioid use in the military with those in the general population – 26% and 4%, respectively (JAMA 2014 June 30 [doi:10.1001/jamainternmed.2014.2114]).
"While chronic pain and opioid use have been a long-standing concern of the military leadership, this study is among the first to quantify the impact of recent wars on the prevalence of pain and narcotic use among soldiers," wrote Dr. Wayne B. Jonas of the Samueli Institute in Alexandria, Va., and the Uniformed Services University of the Health Sciences in Bethesda, Md., and Dr. Eric B. Schoomaker, also of the Samueli Institute.
No conflicts of interest were declared.
FROM JAMA
Key clinical point: Prescription practices should be analyzed to make sure that the use of opioids among military personnel "is consistent with standards of care and practice guidelines and nonopioid alternatives are considered whenever possible."
Major finding: A survey has found 44% of soldiers experience chronic pain and 15.1% have used opioids sometime in the past month. Among those reporting opioid use, 44.1% said they had had only mild or no pain in the past month, while among those with chronic pain, only 23.3% had received opioids in the past month.
Data source: A survey of 2,597 soldiers after combat deployment.
Disclosures: No conflicts of interest were declared.
Risk of Vehicle Accidents for Returning Military
Motor vehicle crashes (MVCs) account for almost one-third of deaths among service members every year. One study showed that within 6 months after deployment, military personnel had a 13% increase in at-fault accidents.
Using data from the Millennium Cohort Study and the Military Health System Data Repository, researchers from the Naval Health Research Center in San Diego, California, investigated possible risk factors.The researchers looked at both demographic and military-specific data, including service branch, health status (such as hearing loss and hours of sleep), and whether the individual had been diagnosed with depression, pain, or anxiety.
Of the 13,620 service members included in the study, 6,800 reported combat experiences; 107 had a MVC within 6 months following deployment.
Service members who had an MVC within 6 months postdeployment were more likely to report combat experiences, have more than one deployment, and be deployed for more than 365 cumulative days. Women, service members born after 1980, enlisted rank, African Americans, and those with baseline physical health symptoms and problem drinking were among those at greater risk. After adjusting for all variables, combat experiences nearly doubled the risk, and 3 or more deployments nearly tripled the risk of a MVC in the 6 months after deployment.
The researchers did not find an association between physical health symptoms, such as hearing loss, headache, or confusion, and MVCs, nor did they find a link between mental health symptoms and the severity of scores. That suggests that physical and mental health may not be the primary contributors to the association. In fact, the researchers say, the link between deployment and crashes may be multifactorial. For instance, service members may engage in risky driving behavior to recreate the emotions felt during combat. Although this study did not include questions about the use of seat belts, alcohol while driving, speeding, or other risk-taking behaviors, the researchers point to other studies that say that military personnel may not wear seat belts and may speed because that is what they got used to during deployment. The researchers also say that those who have participated in military combat may be inherent risk takers.
Multiple deployments, the researchers suggest, may instill “greater levels of risky driving behaviors that accumulate over time.” Length of deployment was not as crucial, which may mean that returning home more frequently puts service members in the driver’s seat more often.
The data suggest that a critical “window of time” may exist for preventing MVCs among the recently deployed. The researchers advocate intervention strategies early in the transition home.
Source
Woodall KA, Jacobson IG, Crum-Cianflone NF. Am J Prev Med. 2014;46(4):350–358.
doi: 10.1016/j.amepre.2013.11.015.
Motor vehicle crashes (MVCs) account for almost one-third of deaths among service members every year. One study showed that within 6 months after deployment, military personnel had a 13% increase in at-fault accidents.
Using data from the Millennium Cohort Study and the Military Health System Data Repository, researchers from the Naval Health Research Center in San Diego, California, investigated possible risk factors.The researchers looked at both demographic and military-specific data, including service branch, health status (such as hearing loss and hours of sleep), and whether the individual had been diagnosed with depression, pain, or anxiety.
Of the 13,620 service members included in the study, 6,800 reported combat experiences; 107 had a MVC within 6 months following deployment.
Service members who had an MVC within 6 months postdeployment were more likely to report combat experiences, have more than one deployment, and be deployed for more than 365 cumulative days. Women, service members born after 1980, enlisted rank, African Americans, and those with baseline physical health symptoms and problem drinking were among those at greater risk. After adjusting for all variables, combat experiences nearly doubled the risk, and 3 or more deployments nearly tripled the risk of a MVC in the 6 months after deployment.
The researchers did not find an association between physical health symptoms, such as hearing loss, headache, or confusion, and MVCs, nor did they find a link between mental health symptoms and the severity of scores. That suggests that physical and mental health may not be the primary contributors to the association. In fact, the researchers say, the link between deployment and crashes may be multifactorial. For instance, service members may engage in risky driving behavior to recreate the emotions felt during combat. Although this study did not include questions about the use of seat belts, alcohol while driving, speeding, or other risk-taking behaviors, the researchers point to other studies that say that military personnel may not wear seat belts and may speed because that is what they got used to during deployment. The researchers also say that those who have participated in military combat may be inherent risk takers.
Multiple deployments, the researchers suggest, may instill “greater levels of risky driving behaviors that accumulate over time.” Length of deployment was not as crucial, which may mean that returning home more frequently puts service members in the driver’s seat more often.
The data suggest that a critical “window of time” may exist for preventing MVCs among the recently deployed. The researchers advocate intervention strategies early in the transition home.
Source
Woodall KA, Jacobson IG, Crum-Cianflone NF. Am J Prev Med. 2014;46(4):350–358.
doi: 10.1016/j.amepre.2013.11.015.
Motor vehicle crashes (MVCs) account for almost one-third of deaths among service members every year. One study showed that within 6 months after deployment, military personnel had a 13% increase in at-fault accidents.
Using data from the Millennium Cohort Study and the Military Health System Data Repository, researchers from the Naval Health Research Center in San Diego, California, investigated possible risk factors.The researchers looked at both demographic and military-specific data, including service branch, health status (such as hearing loss and hours of sleep), and whether the individual had been diagnosed with depression, pain, or anxiety.
Of the 13,620 service members included in the study, 6,800 reported combat experiences; 107 had a MVC within 6 months following deployment.
Service members who had an MVC within 6 months postdeployment were more likely to report combat experiences, have more than one deployment, and be deployed for more than 365 cumulative days. Women, service members born after 1980, enlisted rank, African Americans, and those with baseline physical health symptoms and problem drinking were among those at greater risk. After adjusting for all variables, combat experiences nearly doubled the risk, and 3 or more deployments nearly tripled the risk of a MVC in the 6 months after deployment.
The researchers did not find an association between physical health symptoms, such as hearing loss, headache, or confusion, and MVCs, nor did they find a link between mental health symptoms and the severity of scores. That suggests that physical and mental health may not be the primary contributors to the association. In fact, the researchers say, the link between deployment and crashes may be multifactorial. For instance, service members may engage in risky driving behavior to recreate the emotions felt during combat. Although this study did not include questions about the use of seat belts, alcohol while driving, speeding, or other risk-taking behaviors, the researchers point to other studies that say that military personnel may not wear seat belts and may speed because that is what they got used to during deployment. The researchers also say that those who have participated in military combat may be inherent risk takers.
Multiple deployments, the researchers suggest, may instill “greater levels of risky driving behaviors that accumulate over time.” Length of deployment was not as crucial, which may mean that returning home more frequently puts service members in the driver’s seat more often.
The data suggest that a critical “window of time” may exist for preventing MVCs among the recently deployed. The researchers advocate intervention strategies early in the transition home.
Source
Woodall KA, Jacobson IG, Crum-Cianflone NF. Am J Prev Med. 2014;46(4):350–358.
doi: 10.1016/j.amepre.2013.11.015.
Post-World War II psychiatry: 70 years of momentous change
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
IOM: Military, veterans’ PTSD programs lack consistency, outcomes measures
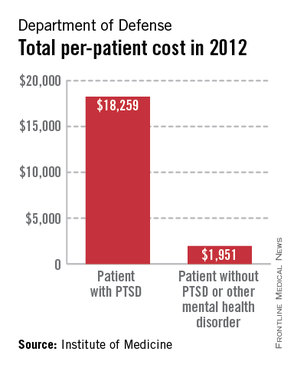
A lack of consistent outcome measures means there is no way to know whether the more than $3 billion spent on treating posttraumatic stress disorder by the Department of Defense and Veterans Affairs in 2012 yielded worthwhile results, according to a report released June 20.
"Given that the DOD and VA are responsible for serving millions of service members, families, and veterans, we found it surprising that no PTSD outcome measures are used consistently to know if these treatments are working," Dr. Sandro Galea, chair of the Institute of Medicine committee tasked by Congress to study PTSD treatment in military and veteran populations, said in a statement.
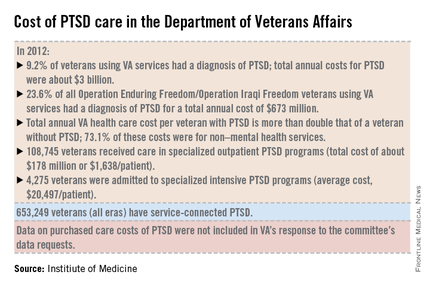
The report notes that currently, "neither the DOD nor the VA knows whether it is providing effective or adequate PTSD care, for which they spent $294 million and more than $3 billion, respectively, in 2012." Similar findings were reported by the IOM in 2012.
"What we found over and over again were really hardworking, well-intentioned people who wanted to do the best they could, but they either didn’t have an administrative structure to support them, or enough staff, or they had an overwhelming number of patients," committee member Dr. Elspeth Cameron Ritchie said during a press briefing.
In addition to better data collection and sharing, the report calls for the development of an adequate workforce to provide mental health care to this growing population.
Although tele-therapies and virtual reality therapies, for which the evidence base is growing, can provide some help, inadequate staffing still leads to a limitation in the number of evidence-based therapies available to patients, said Dr. Ritchie, a retired Army psychiatrist and current professor of psychiatry at Georgetown University in Washington. To wit, the report cited the VA’s failure in 2013 to provide the recommended eight sessions of psychotherapy within 14 weeks to nearly half of all Iraq and Afghanistan war veterans seeking care for a primary diagnosis of PTSD.
The report also calls for the development of evidenced-base treatments, including combination therapies of psychotherapies such as cognitive behavioral therapy, with medications such as SSRIs.
The report recommends that family members be involved in the treatment of PTSD; the recommendation was based on feedback from service members and veterans who said they wanted their loved ones to be actively included.
In addition, the report states that research into PTSD should be focused on current patient needs, and that both departments should actively collaborate with one another and with other government agencies, such as the National Institutes of Health, to fill knowledge gaps.
The number of veterans seeking care for PTSD from the VA has more than doubled from 190,000 (4.3% of all VA users) in 2003 to more than a half million (9.2%) in 2012. Although veterans of all eras are included in the increase, 23.6% (119,500) of those treated for PTSD by the VA in 2012 were veterans of the wars in Iraq and Afghanistan.

In 2013, 528,260 veterans made at least two visits to the VA for PTSD outpatient care; one-quarter were new patients. Although the overall incidence rate for PTSD across all service members is about 1%, the prevalence rose from 0.4% in 2004 to 5% in 2012, with an 8% increase in those who had been deployed previously, according to the report.
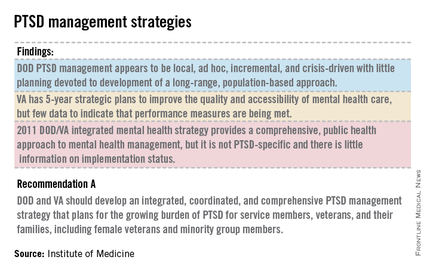
The committee said the DOD approach to PTSD treatment is "local, ad hoc, incremental, and crisis driven, with little planning." While VA programs benefits from better organization and consistency, the lack of data on either department’s delivery methods and outcomes means there is "no way of knowing whether the care they are providing is effective or whether DOD and VA’s expenditures are resulting in high-value health care," according to the report.
The report is based on 4 years of combing through data provided by the DOD and the VA, peer-reviewed literature, government documents, research databases, and testimonies from a variety of DOD and VA experts and providers at military bases and treatment facilities around the country, including six VA medical centers.
On Twitter @whitneymcknight
A lack of consistent outcome measures means there is no way to know whether the more than $3 billion spent on treating posttraumatic stress disorder by the Department of Defense and Veterans Affairs in 2012 yielded worthwhile results, according to a report released June 20.
"Given that the DOD and VA are responsible for serving millions of service members, families, and veterans, we found it surprising that no PTSD outcome measures are used consistently to know if these treatments are working," Dr. Sandro Galea, chair of the Institute of Medicine committee tasked by Congress to study PTSD treatment in military and veteran populations, said in a statement.
The report notes that currently, "neither the DOD nor the VA knows whether it is providing effective or adequate PTSD care, for which they spent $294 million and more than $3 billion, respectively, in 2012." Similar findings were reported by the IOM in 2012.
"What we found over and over again were really hardworking, well-intentioned people who wanted to do the best they could, but they either didn’t have an administrative structure to support them, or enough staff, or they had an overwhelming number of patients," committee member Dr. Elspeth Cameron Ritchie said during a press briefing.
In addition to better data collection and sharing, the report calls for the development of an adequate workforce to provide mental health care to this growing population.
Although tele-therapies and virtual reality therapies, for which the evidence base is growing, can provide some help, inadequate staffing still leads to a limitation in the number of evidence-based therapies available to patients, said Dr. Ritchie, a retired Army psychiatrist and current professor of psychiatry at Georgetown University in Washington. To wit, the report cited the VA’s failure in 2013 to provide the recommended eight sessions of psychotherapy within 14 weeks to nearly half of all Iraq and Afghanistan war veterans seeking care for a primary diagnosis of PTSD.
The report also calls for the development of evidenced-base treatments, including combination therapies of psychotherapies such as cognitive behavioral therapy, with medications such as SSRIs.
The report recommends that family members be involved in the treatment of PTSD; the recommendation was based on feedback from service members and veterans who said they wanted their loved ones to be actively included.
In addition, the report states that research into PTSD should be focused on current patient needs, and that both departments should actively collaborate with one another and with other government agencies, such as the National Institutes of Health, to fill knowledge gaps.
The number of veterans seeking care for PTSD from the VA has more than doubled from 190,000 (4.3% of all VA users) in 2003 to more than a half million (9.2%) in 2012. Although veterans of all eras are included in the increase, 23.6% (119,500) of those treated for PTSD by the VA in 2012 were veterans of the wars in Iraq and Afghanistan.
In 2013, 528,260 veterans made at least two visits to the VA for PTSD outpatient care; one-quarter were new patients. Although the overall incidence rate for PTSD across all service members is about 1%, the prevalence rose from 0.4% in 2004 to 5% in 2012, with an 8% increase in those who had been deployed previously, according to the report.
The committee said the DOD approach to PTSD treatment is "local, ad hoc, incremental, and crisis driven, with little planning." While VA programs benefits from better organization and consistency, the lack of data on either department’s delivery methods and outcomes means there is "no way of knowing whether the care they are providing is effective or whether DOD and VA’s expenditures are resulting in high-value health care," according to the report.
The report is based on 4 years of combing through data provided by the DOD and the VA, peer-reviewed literature, government documents, research databases, and testimonies from a variety of DOD and VA experts and providers at military bases and treatment facilities around the country, including six VA medical centers.
On Twitter @whitneymcknight
A lack of consistent outcome measures means there is no way to know whether the more than $3 billion spent on treating posttraumatic stress disorder by the Department of Defense and Veterans Affairs in 2012 yielded worthwhile results, according to a report released June 20.
"Given that the DOD and VA are responsible for serving millions of service members, families, and veterans, we found it surprising that no PTSD outcome measures are used consistently to know if these treatments are working," Dr. Sandro Galea, chair of the Institute of Medicine committee tasked by Congress to study PTSD treatment in military and veteran populations, said in a statement.
The report notes that currently, "neither the DOD nor the VA knows whether it is providing effective or adequate PTSD care, for which they spent $294 million and more than $3 billion, respectively, in 2012." Similar findings were reported by the IOM in 2012.
"What we found over and over again were really hardworking, well-intentioned people who wanted to do the best they could, but they either didn’t have an administrative structure to support them, or enough staff, or they had an overwhelming number of patients," committee member Dr. Elspeth Cameron Ritchie said during a press briefing.
In addition to better data collection and sharing, the report calls for the development of an adequate workforce to provide mental health care to this growing population.
Although tele-therapies and virtual reality therapies, for which the evidence base is growing, can provide some help, inadequate staffing still leads to a limitation in the number of evidence-based therapies available to patients, said Dr. Ritchie, a retired Army psychiatrist and current professor of psychiatry at Georgetown University in Washington. To wit, the report cited the VA’s failure in 2013 to provide the recommended eight sessions of psychotherapy within 14 weeks to nearly half of all Iraq and Afghanistan war veterans seeking care for a primary diagnosis of PTSD.
The report also calls for the development of evidenced-base treatments, including combination therapies of psychotherapies such as cognitive behavioral therapy, with medications such as SSRIs.
The report recommends that family members be involved in the treatment of PTSD; the recommendation was based on feedback from service members and veterans who said they wanted their loved ones to be actively included.
In addition, the report states that research into PTSD should be focused on current patient needs, and that both departments should actively collaborate with one another and with other government agencies, such as the National Institutes of Health, to fill knowledge gaps.
The number of veterans seeking care for PTSD from the VA has more than doubled from 190,000 (4.3% of all VA users) in 2003 to more than a half million (9.2%) in 2012. Although veterans of all eras are included in the increase, 23.6% (119,500) of those treated for PTSD by the VA in 2012 were veterans of the wars in Iraq and Afghanistan.
In 2013, 528,260 veterans made at least two visits to the VA for PTSD outpatient care; one-quarter were new patients. Although the overall incidence rate for PTSD across all service members is about 1%, the prevalence rose from 0.4% in 2004 to 5% in 2012, with an 8% increase in those who had been deployed previously, according to the report.
The committee said the DOD approach to PTSD treatment is "local, ad hoc, incremental, and crisis driven, with little planning." While VA programs benefits from better organization and consistency, the lack of data on either department’s delivery methods and outcomes means there is "no way of knowing whether the care they are providing is effective or whether DOD and VA’s expenditures are resulting in high-value health care," according to the report.
The report is based on 4 years of combing through data provided by the DOD and the VA, peer-reviewed literature, government documents, research databases, and testimonies from a variety of DOD and VA experts and providers at military bases and treatment facilities around the country, including six VA medical centers.
On Twitter @whitneymcknight
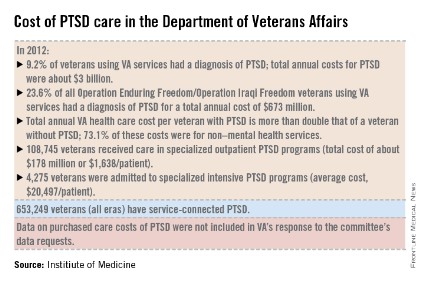
VIDEO: PTSD common in survivors of critical illness
SAN DIEGO – Following an ICU stay, about one-fourth of critical illness survivors are affected by symptoms of posttraumatic stress disorder, a meta-analysis of studies representing 3,437 patients demonstrated.
During a press briefing at an international conference of the American Thoracic Society, Dr. Ann Parker, a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore, discussed the findings and noted that certain patient-related risk factors influenced the association, including younger age, preexisting mental health problems, and post-ICU memories of frightening experiences in the ICU.
On Twitter @dougbrunk
SAN DIEGO – Following an ICU stay, about one-fourth of critical illness survivors are affected by symptoms of posttraumatic stress disorder, a meta-analysis of studies representing 3,437 patients demonstrated.
During a press briefing at an international conference of the American Thoracic Society, Dr. Ann Parker, a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore, discussed the findings and noted that certain patient-related risk factors influenced the association, including younger age, preexisting mental health problems, and post-ICU memories of frightening experiences in the ICU.
On Twitter @dougbrunk
SAN DIEGO – Following an ICU stay, about one-fourth of critical illness survivors are affected by symptoms of posttraumatic stress disorder, a meta-analysis of studies representing 3,437 patients demonstrated.
During a press briefing at an international conference of the American Thoracic Society, Dr. Ann Parker, a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore, discussed the findings and noted that certain patient-related risk factors influenced the association, including younger age, preexisting mental health problems, and post-ICU memories of frightening experiences in the ICU.
On Twitter @dougbrunk
AT ATS 2014
PTSD symptoms a common complication of critical illness
SAN DIEGO – About one-fourth of survivors after critical illness are substantially affected by symptoms of posttraumatic stress syndrome up to 1 year after discharge from the ICU, results from a large meta-analysis demonstrated.
"This incidence is as high as PTSD following other traumatic exposures, such as wartime combat," Dr. Ann Parker said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented. "It is important for clinicians to recognize that patients with preexisting psychological symptoms, receiving benzodiazepines for sedation in the ICU or reporting memories of ‘frightening’ ICU experiences are at increased risk of developing PTSD following critical illness."

In a study led by Dr. Dale M. Needham, medical director of Johns Hopkins University’s critical care physical medicine and rehabilitation program, Dr. Parker and fellow first author Dr. Thiti Sricharoenchai searched PubMed and four other databases to perform a systematic review and meta-analysis of the prevalence of and risk factors for PTSD in survivors of critical illness.
"The number of studies investigating PTSD among critical illness survivors has doubled since the publication of prior reviews [in 2007 and 2008]," said Dr. Parker, who is a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore. "With these additional publications, there is greater similarity between studies regarding the timing of and instruments used for PTSD symptom assessment. As a result, we provide the first meta-analysis yielding a pooled prevalence of clinically important PTSD symptoms."
The researchers evaluated the databases from inception through July 15, 2012, for studies that included adult ICU survivors, used a validated PTSD instrument 1 month or more post-ICU discharge, focused on general ICU populations, and included at least 10 patients with substantial PTSD symptoms. In all, 28 articles on 25 unique cohorts representing a total of 3,437 patients were identified. The most common validated PTSD instrument used in the studies was the Impact of Events Scale (IES), a scoring system that ranges from 0-75, with higher scores indicating greater symptoms.
Dr. Parker reported that among 429 patients who were assessed 1-6 months post-ICU discharge, the pooled mean IES score was 19 and the pooled prevalence of clinically important PTSD symptoms ranged from 23% to 42%. Among 698 patients who were assessed 7-12 months post-ICU discharge, the pooled mean IES score was 17 and the pooled prevalence of clinically important PTSD symptoms ranged from 17% to 34%. In other studies the prevalence of PTSD symptoms ranged from 5% to 62%.
Risk factors for PTSD in critical illness survivors included patient-specific factors, such as younger age and preexisting mental health disorders, as well as ICU-specific factors, including sedation with benzodiazepines and memories of "frightening" experiences in the ICU. In addition, PTSD symptoms were associated with worse quality of life.
"It seems that patients’ memories of their ICU experiences after ICU discharge may play a more important role than the duration of their stay in the ICU or the severity of their illness," Dr. Parker said. "Patients who recalled ‘frightening’ memories were more likely to have substantial PTSD symptoms. These memories may be related to delirium in the ICU, but few studies have attempted to evaluate this theory. There are very few interventions with proven efficacy for reducing PTSD symptoms in critical illness survivors. One intervention that has shown promising results in two European studies is the ICU diary, which has not been rigorously evaluated in North America."
She acknowledged certain limitations of the study, including the fact that differences between studies regarding sample populations and PTSD symptom instruments "make direct comparison difficult. However, the use of meta-analysis to pool the results of the 10 studies using the IES for PTSD symptom assessment strengthens the assertion that PTSD symptoms are highly prevalent among general critical illness survivors."
Neither Dr. Parker nor her associates had relevant financial disclosures.
SAN DIEGO – About one-fourth of survivors after critical illness are substantially affected by symptoms of posttraumatic stress syndrome up to 1 year after discharge from the ICU, results from a large meta-analysis demonstrated.
"This incidence is as high as PTSD following other traumatic exposures, such as wartime combat," Dr. Ann Parker said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented. "It is important for clinicians to recognize that patients with preexisting psychological symptoms, receiving benzodiazepines for sedation in the ICU or reporting memories of ‘frightening’ ICU experiences are at increased risk of developing PTSD following critical illness."
In a study led by Dr. Dale M. Needham, medical director of Johns Hopkins University’s critical care physical medicine and rehabilitation program, Dr. Parker and fellow first author Dr. Thiti Sricharoenchai searched PubMed and four other databases to perform a systematic review and meta-analysis of the prevalence of and risk factors for PTSD in survivors of critical illness.
"The number of studies investigating PTSD among critical illness survivors has doubled since the publication of prior reviews [in 2007 and 2008]," said Dr. Parker, who is a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore. "With these additional publications, there is greater similarity between studies regarding the timing of and instruments used for PTSD symptom assessment. As a result, we provide the first meta-analysis yielding a pooled prevalence of clinically important PTSD symptoms."
The researchers evaluated the databases from inception through July 15, 2012, for studies that included adult ICU survivors, used a validated PTSD instrument 1 month or more post-ICU discharge, focused on general ICU populations, and included at least 10 patients with substantial PTSD symptoms. In all, 28 articles on 25 unique cohorts representing a total of 3,437 patients were identified. The most common validated PTSD instrument used in the studies was the Impact of Events Scale (IES), a scoring system that ranges from 0-75, with higher scores indicating greater symptoms.
Dr. Parker reported that among 429 patients who were assessed 1-6 months post-ICU discharge, the pooled mean IES score was 19 and the pooled prevalence of clinically important PTSD symptoms ranged from 23% to 42%. Among 698 patients who were assessed 7-12 months post-ICU discharge, the pooled mean IES score was 17 and the pooled prevalence of clinically important PTSD symptoms ranged from 17% to 34%. In other studies the prevalence of PTSD symptoms ranged from 5% to 62%.
Risk factors for PTSD in critical illness survivors included patient-specific factors, such as younger age and preexisting mental health disorders, as well as ICU-specific factors, including sedation with benzodiazepines and memories of "frightening" experiences in the ICU. In addition, PTSD symptoms were associated with worse quality of life.
"It seems that patients’ memories of their ICU experiences after ICU discharge may play a more important role than the duration of their stay in the ICU or the severity of their illness," Dr. Parker said. "Patients who recalled ‘frightening’ memories were more likely to have substantial PTSD symptoms. These memories may be related to delirium in the ICU, but few studies have attempted to evaluate this theory. There are very few interventions with proven efficacy for reducing PTSD symptoms in critical illness survivors. One intervention that has shown promising results in two European studies is the ICU diary, which has not been rigorously evaluated in North America."
She acknowledged certain limitations of the study, including the fact that differences between studies regarding sample populations and PTSD symptom instruments "make direct comparison difficult. However, the use of meta-analysis to pool the results of the 10 studies using the IES for PTSD symptom assessment strengthens the assertion that PTSD symptoms are highly prevalent among general critical illness survivors."
Neither Dr. Parker nor her associates had relevant financial disclosures.
SAN DIEGO – About one-fourth of survivors after critical illness are substantially affected by symptoms of posttraumatic stress syndrome up to 1 year after discharge from the ICU, results from a large meta-analysis demonstrated.
"This incidence is as high as PTSD following other traumatic exposures, such as wartime combat," Dr. Ann Parker said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented. "It is important for clinicians to recognize that patients with preexisting psychological symptoms, receiving benzodiazepines for sedation in the ICU or reporting memories of ‘frightening’ ICU experiences are at increased risk of developing PTSD following critical illness."
In a study led by Dr. Dale M. Needham, medical director of Johns Hopkins University’s critical care physical medicine and rehabilitation program, Dr. Parker and fellow first author Dr. Thiti Sricharoenchai searched PubMed and four other databases to perform a systematic review and meta-analysis of the prevalence of and risk factors for PTSD in survivors of critical illness.
"The number of studies investigating PTSD among critical illness survivors has doubled since the publication of prior reviews [in 2007 and 2008]," said Dr. Parker, who is a fellow in pulmonary and critical care medicine at Johns Hopkins University, Baltimore. "With these additional publications, there is greater similarity between studies regarding the timing of and instruments used for PTSD symptom assessment. As a result, we provide the first meta-analysis yielding a pooled prevalence of clinically important PTSD symptoms."
The researchers evaluated the databases from inception through July 15, 2012, for studies that included adult ICU survivors, used a validated PTSD instrument 1 month or more post-ICU discharge, focused on general ICU populations, and included at least 10 patients with substantial PTSD symptoms. In all, 28 articles on 25 unique cohorts representing a total of 3,437 patients were identified. The most common validated PTSD instrument used in the studies was the Impact of Events Scale (IES), a scoring system that ranges from 0-75, with higher scores indicating greater symptoms.
Dr. Parker reported that among 429 patients who were assessed 1-6 months post-ICU discharge, the pooled mean IES score was 19 and the pooled prevalence of clinically important PTSD symptoms ranged from 23% to 42%. Among 698 patients who were assessed 7-12 months post-ICU discharge, the pooled mean IES score was 17 and the pooled prevalence of clinically important PTSD symptoms ranged from 17% to 34%. In other studies the prevalence of PTSD symptoms ranged from 5% to 62%.
Risk factors for PTSD in critical illness survivors included patient-specific factors, such as younger age and preexisting mental health disorders, as well as ICU-specific factors, including sedation with benzodiazepines and memories of "frightening" experiences in the ICU. In addition, PTSD symptoms were associated with worse quality of life.
"It seems that patients’ memories of their ICU experiences after ICU discharge may play a more important role than the duration of their stay in the ICU or the severity of their illness," Dr. Parker said. "Patients who recalled ‘frightening’ memories were more likely to have substantial PTSD symptoms. These memories may be related to delirium in the ICU, but few studies have attempted to evaluate this theory. There are very few interventions with proven efficacy for reducing PTSD symptoms in critical illness survivors. One intervention that has shown promising results in two European studies is the ICU diary, which has not been rigorously evaluated in North America."
She acknowledged certain limitations of the study, including the fact that differences between studies regarding sample populations and PTSD symptom instruments "make direct comparison difficult. However, the use of meta-analysis to pool the results of the 10 studies using the IES for PTSD symptom assessment strengthens the assertion that PTSD symptoms are highly prevalent among general critical illness survivors."
Neither Dr. Parker nor her associates had relevant financial disclosures.
AT ATS 2014
Key clinical point: PTSD symptoms affect 25% or more of patients up to a year after a critical illness.
Major finding: Among 429 survivors of critical illness who were assessed 1-6 months post-ICU discharge, the prevalence of clinically important PTSD symptoms ranged from 23% to 42%. Among 698 patients who were assessed 7-12 months post-ICU discharge, prevalence of clinically important PTSD symptoms ranged from 17% to 34%.
Data source: A meta-analysis of 28 articles in the medical literature on 25 unique cohorts representing a total of 3,437 patients.
Disclosures: Neither Dr. Parker nor her associates had relevant financial disclosures.

General screening for suicide not recommended yet
Primary care physicians are not advised to screen general patients for suicide risk at present, because evidence remains insufficient to properly assess the benefits and harms of suicide screening in this setting, according to a clinical guideline updated by the U.S. Preventive Services Task Force and published May 19 online.
Suicide was the 10th leading cause of death in the United States in 2010, and it ranks among the top 5 causes of death in adolescents and young adults. Nevertheless, currently "there is insufficient evidence to conclude that screening adolescents, adults, and older adults in primary care adequately identifies patients at risk for suicide who would not otherwise be identified on the basis of an existing mental health disorder, emotional distress, or previous suicide attempt," said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri–Columbia, and his associates (Ann. Intern. Med. 2014;160:719-26).
They emphasized that screening the general population for depression is a separate issue. Depression screening by primary physicians is recommended for all age groups.

The USPSTF first issued a clinical guideline regarding suicide screening in 2004, when research indicated that 38% of adults – and 50%-70% of adults over age 65 – who committed suicide had visited their primary care provider within 1 month of taking their lives. Later research also showed that nearly 90% of adolescents and children who committed suicide had seen their primary care provider during the preceding year. It was reasoned that primary caregivers might be in a position to intervene and prevent some of these deaths.
At the time of the 2004 Clinical Guideline, the USPSTF concluded that there was insufficient evidence to recommend either for or against clinicians conducting routine screening to detect suicide risk in the general population. After reviewing new data from studies conducted since the last review, the USPSTF again has reached the same conclusion. (The American Academy of Family Physicians published a similar recommendation in January of this year, Dr. LeFevre and his colleagues noted.)
Since the 2004 recommendations, only four studies have assessed the accuracy of screening instruments, and all of them were considered to be only of fair quality. Only one study involved primary care patients of all ages. Two studies involved only adolescents, one involved only the elderly, and one involved depressed patients receiving outpatient mental health services.
Similarly, no studies since the 2004 recommendations have directly assessed whether screening and subsequent referral for treatment improved health outcomes. Few studies have examined treatment efficacy, particularly that of medication; those that have done so were of only fair quality, with small sample sizes, high attrition rates, and extremely low incidences of suicide. The treatments found most effective at reducing the risk of suicide attempts include psychotherapy, specifically cognitive-behavioral therapy and related approaches, Dr. LeFevre wrote. "Although most of these treatments are not customarily administered by primary care providers in the office, patients can be referred to behavioral health providers for them. The primary care provider can play a continued role in the care of these patients by monitoring them during the process, providing follow-up, and coordinating with other care providers," the investigators wrote.
Few studies have assessed the potential harms of screening the general population for suicide, and at this time the possibility cannot be ruled out that a primary caregiver’s inquiring about suicide might actually increase a patient’s distress.
In contrast to the general patient population, certain subsets of patients are at risk for suicide attempts. Primary caregivers "should consider identifying patients with [these] risk factors or those who seem to have high levels of emotional distress and referring them for further evaluation," the USPSTF said.
Risk factors for suicide include:
• Mental health disorders. These include depression, schizophrenia, posttraumatic stress disorder (PTSD), and substance use disorders. "About 87% of patients who die by suicide meet the criteria for one or more mental health disorders." In addition, "depression is probably present in 50%-79% of youths attempting suicide, although it may not always be recognized," the investigators said.
• Older age. Suicide risk begins to rise in both men and women in their 50s and 60s, compared with those in their 30s and 40s, and continues to rise with increasing age. Social isolation, unemployment, grief over a spouse’s death, physical illness or disability, and functional impairment all add to this risk.
• Ethnicity. American Indians and Alaskan natives of all ages have higher-than-average rates of death by suicide. Among adolescents, Hispanic girls are at higher risk than girls of other ethnicities.
• Military service. Veterans who have sustained traumatic brain injury, have separated from the service within the past year, or have PTSD are at particularly high risk of suicide.
"Other important risk factors for suicide attempt include serious adverse childhood events; family history of suicide; prejudice or discrimination associated with being gay, bisexual, or transgender; access to lethal means; and possibly a history of being bullied, sleep disturbances, and such chronic medical conditions as epilepsy and chronic pain. In males, socioeconomic factors such as low income, occupation, and unemployment also are related to suicide risk," Dr. LeFevre and his associates said.
Reprints of the recommendation statement are available here. In addition, resources regarding suicide prevention are available at the Suicide Prevention Resource Center, which is supported by the Substance Abuse and Mental Health Services Administration.
The USPSTF is an independent, voluntary group supported by the U.S. Agency for Healthcare Research and mandated by Congress to make recommendations about the effectiveness of specific preventive care services for patients. Dr. LeFevre and his associates reported no financial conflicts of interest.
Primary care physicians are not advised to screen general patients for suicide risk at present, because evidence remains insufficient to properly assess the benefits and harms of suicide screening in this setting, according to a clinical guideline updated by the U.S. Preventive Services Task Force and published May 19 online.
Suicide was the 10th leading cause of death in the United States in 2010, and it ranks among the top 5 causes of death in adolescents and young adults. Nevertheless, currently "there is insufficient evidence to conclude that screening adolescents, adults, and older adults in primary care adequately identifies patients at risk for suicide who would not otherwise be identified on the basis of an existing mental health disorder, emotional distress, or previous suicide attempt," said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri–Columbia, and his associates (Ann. Intern. Med. 2014;160:719-26).
They emphasized that screening the general population for depression is a separate issue. Depression screening by primary physicians is recommended for all age groups.
The USPSTF first issued a clinical guideline regarding suicide screening in 2004, when research indicated that 38% of adults – and 50%-70% of adults over age 65 – who committed suicide had visited their primary care provider within 1 month of taking their lives. Later research also showed that nearly 90% of adolescents and children who committed suicide had seen their primary care provider during the preceding year. It was reasoned that primary caregivers might be in a position to intervene and prevent some of these deaths.
At the time of the 2004 Clinical Guideline, the USPSTF concluded that there was insufficient evidence to recommend either for or against clinicians conducting routine screening to detect suicide risk in the general population. After reviewing new data from studies conducted since the last review, the USPSTF again has reached the same conclusion. (The American Academy of Family Physicians published a similar recommendation in January of this year, Dr. LeFevre and his colleagues noted.)
Since the 2004 recommendations, only four studies have assessed the accuracy of screening instruments, and all of them were considered to be only of fair quality. Only one study involved primary care patients of all ages. Two studies involved only adolescents, one involved only the elderly, and one involved depressed patients receiving outpatient mental health services.
Similarly, no studies since the 2004 recommendations have directly assessed whether screening and subsequent referral for treatment improved health outcomes. Few studies have examined treatment efficacy, particularly that of medication; those that have done so were of only fair quality, with small sample sizes, high attrition rates, and extremely low incidences of suicide. The treatments found most effective at reducing the risk of suicide attempts include psychotherapy, specifically cognitive-behavioral therapy and related approaches, Dr. LeFevre wrote. "Although most of these treatments are not customarily administered by primary care providers in the office, patients can be referred to behavioral health providers for them. The primary care provider can play a continued role in the care of these patients by monitoring them during the process, providing follow-up, and coordinating with other care providers," the investigators wrote.
Few studies have assessed the potential harms of screening the general population for suicide, and at this time the possibility cannot be ruled out that a primary caregiver’s inquiring about suicide might actually increase a patient’s distress.
In contrast to the general patient population, certain subsets of patients are at risk for suicide attempts. Primary caregivers "should consider identifying patients with [these] risk factors or those who seem to have high levels of emotional distress and referring them for further evaluation," the USPSTF said.
Risk factors for suicide include:
• Mental health disorders. These include depression, schizophrenia, posttraumatic stress disorder (PTSD), and substance use disorders. "About 87% of patients who die by suicide meet the criteria for one or more mental health disorders." In addition, "depression is probably present in 50%-79% of youths attempting suicide, although it may not always be recognized," the investigators said.
• Older age. Suicide risk begins to rise in both men and women in their 50s and 60s, compared with those in their 30s and 40s, and continues to rise with increasing age. Social isolation, unemployment, grief over a spouse’s death, physical illness or disability, and functional impairment all add to this risk.
• Ethnicity. American Indians and Alaskan natives of all ages have higher-than-average rates of death by suicide. Among adolescents, Hispanic girls are at higher risk than girls of other ethnicities.
• Military service. Veterans who have sustained traumatic brain injury, have separated from the service within the past year, or have PTSD are at particularly high risk of suicide.
"Other important risk factors for suicide attempt include serious adverse childhood events; family history of suicide; prejudice or discrimination associated with being gay, bisexual, or transgender; access to lethal means; and possibly a history of being bullied, sleep disturbances, and such chronic medical conditions as epilepsy and chronic pain. In males, socioeconomic factors such as low income, occupation, and unemployment also are related to suicide risk," Dr. LeFevre and his associates said.
Reprints of the recommendation statement are available here. In addition, resources regarding suicide prevention are available at the Suicide Prevention Resource Center, which is supported by the Substance Abuse and Mental Health Services Administration.
The USPSTF is an independent, voluntary group supported by the U.S. Agency for Healthcare Research and mandated by Congress to make recommendations about the effectiveness of specific preventive care services for patients. Dr. LeFevre and his associates reported no financial conflicts of interest.
Primary care physicians are not advised to screen general patients for suicide risk at present, because evidence remains insufficient to properly assess the benefits and harms of suicide screening in this setting, according to a clinical guideline updated by the U.S. Preventive Services Task Force and published May 19 online.
Suicide was the 10th leading cause of death in the United States in 2010, and it ranks among the top 5 causes of death in adolescents and young adults. Nevertheless, currently "there is insufficient evidence to conclude that screening adolescents, adults, and older adults in primary care adequately identifies patients at risk for suicide who would not otherwise be identified on the basis of an existing mental health disorder, emotional distress, or previous suicide attempt," said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri–Columbia, and his associates (Ann. Intern. Med. 2014;160:719-26).
They emphasized that screening the general population for depression is a separate issue. Depression screening by primary physicians is recommended for all age groups.
The USPSTF first issued a clinical guideline regarding suicide screening in 2004, when research indicated that 38% of adults – and 50%-70% of adults over age 65 – who committed suicide had visited their primary care provider within 1 month of taking their lives. Later research also showed that nearly 90% of adolescents and children who committed suicide had seen their primary care provider during the preceding year. It was reasoned that primary caregivers might be in a position to intervene and prevent some of these deaths.
At the time of the 2004 Clinical Guideline, the USPSTF concluded that there was insufficient evidence to recommend either for or against clinicians conducting routine screening to detect suicide risk in the general population. After reviewing new data from studies conducted since the last review, the USPSTF again has reached the same conclusion. (The American Academy of Family Physicians published a similar recommendation in January of this year, Dr. LeFevre and his colleagues noted.)
Since the 2004 recommendations, only four studies have assessed the accuracy of screening instruments, and all of them were considered to be only of fair quality. Only one study involved primary care patients of all ages. Two studies involved only adolescents, one involved only the elderly, and one involved depressed patients receiving outpatient mental health services.
Similarly, no studies since the 2004 recommendations have directly assessed whether screening and subsequent referral for treatment improved health outcomes. Few studies have examined treatment efficacy, particularly that of medication; those that have done so were of only fair quality, with small sample sizes, high attrition rates, and extremely low incidences of suicide. The treatments found most effective at reducing the risk of suicide attempts include psychotherapy, specifically cognitive-behavioral therapy and related approaches, Dr. LeFevre wrote. "Although most of these treatments are not customarily administered by primary care providers in the office, patients can be referred to behavioral health providers for them. The primary care provider can play a continued role in the care of these patients by monitoring them during the process, providing follow-up, and coordinating with other care providers," the investigators wrote.
Few studies have assessed the potential harms of screening the general population for suicide, and at this time the possibility cannot be ruled out that a primary caregiver’s inquiring about suicide might actually increase a patient’s distress.
In contrast to the general patient population, certain subsets of patients are at risk for suicide attempts. Primary caregivers "should consider identifying patients with [these] risk factors or those who seem to have high levels of emotional distress and referring them for further evaluation," the USPSTF said.
Risk factors for suicide include:
• Mental health disorders. These include depression, schizophrenia, posttraumatic stress disorder (PTSD), and substance use disorders. "About 87% of patients who die by suicide meet the criteria for one or more mental health disorders." In addition, "depression is probably present in 50%-79% of youths attempting suicide, although it may not always be recognized," the investigators said.
• Older age. Suicide risk begins to rise in both men and women in their 50s and 60s, compared with those in their 30s and 40s, and continues to rise with increasing age. Social isolation, unemployment, grief over a spouse’s death, physical illness or disability, and functional impairment all add to this risk.
• Ethnicity. American Indians and Alaskan natives of all ages have higher-than-average rates of death by suicide. Among adolescents, Hispanic girls are at higher risk than girls of other ethnicities.
• Military service. Veterans who have sustained traumatic brain injury, have separated from the service within the past year, or have PTSD are at particularly high risk of suicide.
"Other important risk factors for suicide attempt include serious adverse childhood events; family history of suicide; prejudice or discrimination associated with being gay, bisexual, or transgender; access to lethal means; and possibly a history of being bullied, sleep disturbances, and such chronic medical conditions as epilepsy and chronic pain. In males, socioeconomic factors such as low income, occupation, and unemployment also are related to suicide risk," Dr. LeFevre and his associates said.
Reprints of the recommendation statement are available here. In addition, resources regarding suicide prevention are available at the Suicide Prevention Resource Center, which is supported by the Substance Abuse and Mental Health Services Administration.
The USPSTF is an independent, voluntary group supported by the U.S. Agency for Healthcare Research and mandated by Congress to make recommendations about the effectiveness of specific preventive care services for patients. Dr. LeFevre and his associates reported no financial conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: The most effective way to reduce suicide attempts is to refer patients who are at risk to behavioral health providers.
Major finding: There is insufficient evidence to conclude that screening adolescents, adults, and older adults in primary care adequately identifies patients at risk for suicide who would not otherwise be identified on the basis of an existing mental health disorder, emotional distress, or previous suicide attempt.
Data source: A comprehensive review of the literature since 2004 regarding screening tools for suicide risk and treatment outcomes for patients identified by such screening.
Disclosures: The USPSTF is an independent, voluntary group supported by the U.S. Agency for Healthcare Research and mandated by Congress to make recommendations about the effectiveness of specific preventive care services for patients. Dr. LeFevre and his associates reported no financial conflicts of interest.

Treating PTSD and its effects here at home
Providing sensitive mental health treatment to patients who have served in the military requires better understanding of this unique culture. Toward that end, this news organization recently sat down with Col. (Ret.) Elspeth Cameron Ritchie, former chief of psychiatry for the U.S. Army and the current chief clinical officer in the department of behavioral health for the District of Columbia. The following is an edited transcript of a discussion with Dr. Ritchie*.
Question: Why are there more suicides among service members who’ve never deployed than in those who have been in-country?

Dr. Ritchie: For many years, there was a relatively stable suicide rate at about 10 per 100,000 troops per year. Starting in 2004, the rate more than doubled, so that by 2010, 2011, and 2013, we had very high suicide rates for the military. The suicide pattern also shifted over time. In the beginning, there was a lot of concern that the rates were related to deployment; although in individual cases, the deployment may have caused some stresses, by and large the suicides did not seem to be directly related to individual deployment, and now more than half the suicides occur in those who’ve never deployed.
Why is that? Well, it’s complex, but one of the reasons I look at is that the army itself has been on a high operations tempo, so troops are deploying all the time; they’re tired, so one of the things that’s going on is that when a new soldier joins a unit, they might not be welcomed in the same way as they would have been in the past, because everyone’s so busy. So, that’s one piece of it.
But, let me go big picture. For a long time, the stressors that led to suicide have been all about failed relationships and also getting into trouble at work or having financial troubles. And that pattern has stayed the same over time, but the number of troops who have suicided has risen over time.
Question: So it’s the social structure of the military driving this, at least in part?
Dr. Ritchie: That’s one of the drivers. The people are just so busy, by that I mean the units, who have so busy going back and forth. So, for example, if you look at the 101st Division at Fort Campbell, they have been in and out of the theater of war almost every other year for a long time, they’re slowing down now a little, and they had a very high suicide rate for a number of years. And that’s not dissimilar to the other bases like Fort Stewart and Fort Hood; they are all deploying troops very rapidly in and out of the theater of war.
Question: Does the military need to sensitize its troops to welcoming in recruits?
Dr. Ritchie: The military has been very concerned about the suicide rate, and they have done a lot about it, with perhaps the beginning of some success in that the suicide rate among active duty troops is starting to level off, but the rate is rising in the Reserves and National Guard. But, for example, there was a Department of the Army task force to look at this, and it started out as suicide prevention, but then they added risk reduction, and they then added health promotion as part of it. Then there was the Department of Defense task force with many, many recommendations. And basically, the easy recommendations are all done. Recommendations that are harder to do, like ending the conflicts of wars, well, the wars are finally winding down, but that’s not something you can just "stop," and as the military, it’s your job to go to war.

Question: Is the military screening recruits well enough? Maybe they are coming in with too many problems to begin with.
Dr. Ritchie: There already is quite a bit of screening. There are some misconceptions about that. As a matter of fact, there is a bill going to Congress about that now, that calls for adding mental health screening. There already is a history and physical done as a young recruit tries to enter the military, and they’re asked about mental health problems. But one of the realities is that if you’re motivated to come into the service, you’re probably not going to talk about your mental health problems, because you’re worried that will disqualify you from service. Already, only about a third of people who apply to the military are able to make the mental health and physical standards. So, there is a screening.
We have tried pen-and-paper screenings for 100 years, literally, since World War I, and what we’ve found is that generally, they don’t work. Again, these are based on self-report. If somebody fills out a piece of paper that asks about suicidal ideation, if the person wants to get into the military, they’re not going to answer that. And the military doesn’t have access to previous records unless the person chooses to offer them.
Let me add to that, the best screen is basic training. So, remember when a recruit comes in, they have 8 to 13 weeks, depending on the service, of very intense interaction with other recruits, and with the drill sergeants, and about 8% of troops actually wash out of basic training. What we’ve tried over and over to do is to develop a paper-and-pencil screen, but it either isn’t sensitive or isn’t specific enough.
Question: What about "checkpoint" screenings that you do periodically after some time in the service?
Dr. Ritchie: As people come back from deployment, they are screened, and 3 to 6 months later, they have a postdeployment reassessment because we realized that people weren’t going to tell the truth as they were coming back home because they just wanted to go home. So, we asked them again. And, there is a yearly assessment done, but again, a lot of what this relies on is the soldier’s willingness to share what’s really going on. There are questions for depression, and suicidal ideation, and posttraumatic stress disorder as part of the whole assessment process.
Question: But will they answer truthfully at all times, regardless of how they feel about deployment, because they are afraid of being stigmatized?
Dr. Ritchie: Remember that this is an all-volunteer army, and we’ve been at war since 9/11/2001, so troops who have been in the service know they’re going to be deployed and want to be deployed. And with the difficult economy, they want to stay in the service and they want to be promoted. So, they are concerned if they answer "yes" to a mental health question, they will be made to see a psychiatrist, which might have an impact on their career, or they won’t be allowed to deploy. So, there is a lot of motivation to minimize symptoms.
Now, that’s true of people who want to make the military a career. I have also seen that people who have decided to leave the military, or the military has decided that the person shouldn’t stay, then there is often a lot of incentive to answer yes to all the mental and physical health symptoms. For example, on your retirement physical, you’re told, "Make sure you put down every condition you’ve got because you want to have access to the VA" and maybe you’ll get disability or get compensated. So you’ll often see underreporting if a soldier wants to stay on active duty, and perhaps there’s some embellishment of symptoms as they’re going out the door.
Question: What about therapies that are said to address other physical symptoms, like acupuncture, but which are actually addressing the mental health aspect as well?
Dr. Ritchie: There are two main types of evidence-based therapies for PTSD. There’s the cognitive-behavioral therapy, which has cognitive processing therapy as part of it, and there is exposure-based therapy, as evidence-based psychotherapies. And then there are medications – the selective serotonin reuptake inhibitors for PTSD – as well. However, many, many service members don’t want to take medication, and/or they don’t want to go and talk to someone about their trauma. In most cases, these are young men, and young men often don’t want to talk about anything, much less their feelings or a traumatic experience where perhaps one of their friends was killed or wounded. So, I have gotten very interested in the various forms of integrative medicine – such as acupuncture, yoga, mindfulness – which many of our troops really enjoy doing. They probably don’t treat the PTSD by themselves, but they provide a bridge to treatment.
And, perhaps they do treat the symptoms themselves. Certainly, service members have reported vast improvements from acupuncture, from stellate ganglion block, from yoga. They say: "It cools my brain so I can concentrate on other things."
Question: Please explain to us how stellate ganglion block, which is an anesthesia, is used to treat PTSD.
Dr. Ritchie: It is an anesthetic technique used for pain, where lidocaine is injected into the stellate ganglion by an anesthesiologist. It has been seen to dramatically reduce PTSD symptoms in some. There is not yet a robust body of literature, but there are certainly a lot of very promising case studies and anecdotal reports on it.
Question: So, how does a soldier who would like to try these integrative therapies to help minimize their discomfort and anguish without overtly asking and risking being stigmatized, go about receiving them?
Dr. Ritchie: Good question. To be honest, it’s highly variable as to what their access is to those treatments. At a place like the NICoE (National Intrepid Center of Excellence) in Bethesda at the new Walter Reed Military Medical Center, there is a very intense program that includes art therapy, acupuncture, and virtual reality exposure therapy. There are also other facilities, such as one in San Diego, but if a service member doesn’t have access to these facilities it might be difficult to get this kind of treatment.
Question: How does the Veterans Health Administration deal with this?
Dr. Ritchie: I need to separate what I have just been talking about, which is to deal with the military health care system, from the VA. There is a lot of confusion over this. They are not the same health care system; they’re very different. When someone is on active duty, by and large they will be seen in the military health care system. If someone is a veteran, they may or may not be able to be seen in the VA depending on their priority level, their income, whether they had a disability, whether they had a service-related condition, et cetera.
The larger question is, how does the VA deal with PTSD? Well, I think the VA does a really good job providing evidence-based therapies, and in other cases, it’s quite overwhelmed by the number of veterans coming to it for treatment. It’s hard, because many people will say that the VA is 141 different hospitals, and it has centers and clinics, so it’s highly variable.
Question: So, if I am a service member seeking treatment without stigma, would I go to a community-based clinician?
Dr. Ritchie: The military actually has been quite active in trying to provide confidential treatment. Military OneSource has a website and phone number to call to refer troops to resources. Although a military member can go on his or her own to a community doctor for treatment, they’re not really supposed to, although certainly people do it.
On every base, there are chaplains and a mental health clinic, and there are other programs such as resiliency training, like the Comprehensive Soldier Fitness Program, and other programs that try to provide treatment while minimizing stigma, and to reach out to the service member who might not be willing to reach out to the military. So, the military is trying, but it’s not easy. It’s not as simple as hiring 20 more psychologists, because a lot of people are worried about their career and so won’t come into a clinic.
I didn’t talk about this before, but the army also uses therapy dogs, or animal-assisted therapy, because a lot of times the soldier won’t come talk to you as a shrink, but they will come talk to you about their dog. So, there are a lot of bridges that can be made.
Question: Well, then is there really a stigma? Or if it’s there, is it really as impactful as a soldier might fear?
Dr. Ritchie: I wish I could say that there is no reality behind the stigma, but there is a reality there. If someone is known to seek mental health treatment, some people will think less of them. This is true elsewhere in law enforcement and in the civilian world. So the approach taken in many cases in the military is to combine mental health with primary care, because if someone goes into the primary care clinic, that’s a lot less stigmatizing than sitting in the mental health clinic. But simply saying that stigma should end doesn’t work.
This is a downsizing military, and there is lots of talk about troop cuts, especially in the Army, so you don’t want to be the one who has something less than perfect on your record.
Question: Let’s back up to something you said before about the purpose of a soldier being to win wars. If the military is scaling back, are troops worried they won’t have that job to do any more, and maybe are wondering about their purpose, so that there is an existential component to the anguish these service members face? In other words, is the term "posttraumatic stress disorder" wholly appropriate to explain what is happening before some of these people try, and in some cases, succeed, to take their lives?
Dr. Ritchie: There is a term I will throw in here that I think will help the discussion. Moral injury. It’s related, but not the same as PTSD, which is a diagnosis in the DSM-IV and DSM-5, while "moral injury" is not. Moral injury refers to the feelings of guilt and shame that might be related to killing others or having your friends killed: being tainted by being at war.
So when I look at PTSD, it isn’t as a risk factor for suicide itself. As we talked about, more than half of the suicides now happen in those who have not deployed. PTSD does factor in, in the sense that it can contribute to the breakup of relationships, the feeling that you don’t fit in, and those are risk factors for suicide. So, I am not saying PTSD is unrelated, but if you look at the number of completed suicides, only 10% had a PTSD diagnosis. More could have had PTSD, and it just wasn’t in their records. But, back to the question about existential angst, I think it’s around having seen vast amounts of death and destruction.
Question: Is that your point of view, or does the military recognize this?
Dr. Ritchie: There is increasing recognition, but there are no systematic studies that have been done on it yet. And, the issue about asking people if they’ve killed is difficult, because in many of these cases there is a gray area. If someone is shooting at you, there is no question that you can defend yourself, but people worry whether they have committed a war crime, so it’s difficult to study this scientifically without getting into questions about ethics and legal quandaries.
Question: So language is very important. PTSD used to be called "shell shock." When did it broaden out to become PTSD and become used to address anything that traumatizes a person, not just soldiers?
Dr. Ritchie: Here’s a brief answer. We have called PTSD many things: shell shock, battle fatigue, combat neurosis, and combat stress injury. There have been many names. The term PTSD began in 1980, after the Vietnam War. And a lot of the concepts were based on soldiers and service members from that war. It also encompasses other trauma, the largest amount of literature being on sexual assault victims and disaster victims.
The diagnosis was upgraded in the DSM-5, meaning that there were more symptoms added to the classic symptoms, which were hypervigilance – being jumpy and nervous, the flashbacks and memories, and the numbness, and being detached. Now, the symptoms include sleep difficulties, depression, irritability, cognitive difficulties, and somatic reactions. So, it’s a wider diagnosis now, and it will be interesting to see how that affects the prevalence of the disorder.
Question: People have been traumatized since the beginning of humanity, and have needed to cope with it. That’s where the existentialism comes in. Does PTSD offer an opportunity to find meaning in life that wasn’t seen before?
Dr. Ritchie: Certainly, people talk about posttraumatic growth. People used to join the army because it "made a man out of you." I think there are certainly good things that come out of military service on all kinds of levels. Seeing trauma and being around trauma don’t mean you are scarred for life. You can grow as a result of the experience.
Question: Barbara Rothbaum, Ph.D., a leading expert in exposure therapy, says that the trauma will always be sad, but that it doesn’t mean you can’t feel joy again. People forget that you can come out the other side – that PTSD isn’t permanently debilitating.
Dr. Ritchie: PTSD has a range of severity. Dr. Robert Ursano at the Center for the Study of Traumatic Stress in Bethesda, likened it to being the common cold of psychiatry. A lot of people are exposed, have symptoms; most become better quickly, but in some it becomes chronic bronchitis or pneumonia. So, it’s important to recognize there is both a range in the severity of the trauma and people’s reaction to it.
It’s also important to remember that people who are going to combat now are well trained, well armed, and in combat gear, and they are expecting traumatic things. That’s different than if you’ve been the victim of sexual assault, and you’re surprised and feel vulnerable and helpless. So, I think the vast majority of those who experience the psychological effects of war go on to grow from the experience.
–Interview by Whitney McKnight
*CORRECTION, 4/30/2014: An earlier version of this article misidentified Col. (Ret.) Elspeth Cameron Ritchie.
Providing sensitive mental health treatment to patients who have served in the military requires better understanding of this unique culture. Toward that end, this news organization recently sat down with Col. (Ret.) Elspeth Cameron Ritchie, former chief of psychiatry for the U.S. Army and the current chief clinical officer in the department of behavioral health for the District of Columbia. The following is an edited transcript of a discussion with Dr. Ritchie*.
Question: Why are there more suicides among service members who’ve never deployed than in those who have been in-country?
Dr. Ritchie: For many years, there was a relatively stable suicide rate at about 10 per 100,000 troops per year. Starting in 2004, the rate more than doubled, so that by 2010, 2011, and 2013, we had very high suicide rates for the military. The suicide pattern also shifted over time. In the beginning, there was a lot of concern that the rates were related to deployment; although in individual cases, the deployment may have caused some stresses, by and large the suicides did not seem to be directly related to individual deployment, and now more than half the suicides occur in those who’ve never deployed.
Why is that? Well, it’s complex, but one of the reasons I look at is that the army itself has been on a high operations tempo, so troops are deploying all the time; they’re tired, so one of the things that’s going on is that when a new soldier joins a unit, they might not be welcomed in the same way as they would have been in the past, because everyone’s so busy. So, that’s one piece of it.
But, let me go big picture. For a long time, the stressors that led to suicide have been all about failed relationships and also getting into trouble at work or having financial troubles. And that pattern has stayed the same over time, but the number of troops who have suicided has risen over time.
Question: So it’s the social structure of the military driving this, at least in part?
Dr. Ritchie: That’s one of the drivers. The people are just so busy, by that I mean the units, who have so busy going back and forth. So, for example, if you look at the 101st Division at Fort Campbell, they have been in and out of the theater of war almost every other year for a long time, they’re slowing down now a little, and they had a very high suicide rate for a number of years. And that’s not dissimilar to the other bases like Fort Stewart and Fort Hood; they are all deploying troops very rapidly in and out of the theater of war.
Question: Does the military need to sensitize its troops to welcoming in recruits?
Dr. Ritchie: The military has been very concerned about the suicide rate, and they have done a lot about it, with perhaps the beginning of some success in that the suicide rate among active duty troops is starting to level off, but the rate is rising in the Reserves and National Guard. But, for example, there was a Department of the Army task force to look at this, and it started out as suicide prevention, but then they added risk reduction, and they then added health promotion as part of it. Then there was the Department of Defense task force with many, many recommendations. And basically, the easy recommendations are all done. Recommendations that are harder to do, like ending the conflicts of wars, well, the wars are finally winding down, but that’s not something you can just "stop," and as the military, it’s your job to go to war.
Question: Is the military screening recruits well enough? Maybe they are coming in with too many problems to begin with.
Dr. Ritchie: There already is quite a bit of screening. There are some misconceptions about that. As a matter of fact, there is a bill going to Congress about that now, that calls for adding mental health screening. There already is a history and physical done as a young recruit tries to enter the military, and they’re asked about mental health problems. But one of the realities is that if you’re motivated to come into the service, you’re probably not going to talk about your mental health problems, because you’re worried that will disqualify you from service. Already, only about a third of people who apply to the military are able to make the mental health and physical standards. So, there is a screening.
We have tried pen-and-paper screenings for 100 years, literally, since World War I, and what we’ve found is that generally, they don’t work. Again, these are based on self-report. If somebody fills out a piece of paper that asks about suicidal ideation, if the person wants to get into the military, they’re not going to answer that. And the military doesn’t have access to previous records unless the person chooses to offer them.
Let me add to that, the best screen is basic training. So, remember when a recruit comes in, they have 8 to 13 weeks, depending on the service, of very intense interaction with other recruits, and with the drill sergeants, and about 8% of troops actually wash out of basic training. What we’ve tried over and over to do is to develop a paper-and-pencil screen, but it either isn’t sensitive or isn’t specific enough.
Question: What about "checkpoint" screenings that you do periodically after some time in the service?
Dr. Ritchie: As people come back from deployment, they are screened, and 3 to 6 months later, they have a postdeployment reassessment because we realized that people weren’t going to tell the truth as they were coming back home because they just wanted to go home. So, we asked them again. And, there is a yearly assessment done, but again, a lot of what this relies on is the soldier’s willingness to share what’s really going on. There are questions for depression, and suicidal ideation, and posttraumatic stress disorder as part of the whole assessment process.
Question: But will they answer truthfully at all times, regardless of how they feel about deployment, because they are afraid of being stigmatized?
Dr. Ritchie: Remember that this is an all-volunteer army, and we’ve been at war since 9/11/2001, so troops who have been in the service know they’re going to be deployed and want to be deployed. And with the difficult economy, they want to stay in the service and they want to be promoted. So, they are concerned if they answer "yes" to a mental health question, they will be made to see a psychiatrist, which might have an impact on their career, or they won’t be allowed to deploy. So, there is a lot of motivation to minimize symptoms.
Now, that’s true of people who want to make the military a career. I have also seen that people who have decided to leave the military, or the military has decided that the person shouldn’t stay, then there is often a lot of incentive to answer yes to all the mental and physical health symptoms. For example, on your retirement physical, you’re told, "Make sure you put down every condition you’ve got because you want to have access to the VA" and maybe you’ll get disability or get compensated. So you’ll often see underreporting if a soldier wants to stay on active duty, and perhaps there’s some embellishment of symptoms as they’re going out the door.
Question: What about therapies that are said to address other physical symptoms, like acupuncture, but which are actually addressing the mental health aspect as well?
Dr. Ritchie: There are two main types of evidence-based therapies for PTSD. There’s the cognitive-behavioral therapy, which has cognitive processing therapy as part of it, and there is exposure-based therapy, as evidence-based psychotherapies. And then there are medications – the selective serotonin reuptake inhibitors for PTSD – as well. However, many, many service members don’t want to take medication, and/or they don’t want to go and talk to someone about their trauma. In most cases, these are young men, and young men often don’t want to talk about anything, much less their feelings or a traumatic experience where perhaps one of their friends was killed or wounded. So, I have gotten very interested in the various forms of integrative medicine – such as acupuncture, yoga, mindfulness – which many of our troops really enjoy doing. They probably don’t treat the PTSD by themselves, but they provide a bridge to treatment.
And, perhaps they do treat the symptoms themselves. Certainly, service members have reported vast improvements from acupuncture, from stellate ganglion block, from yoga. They say: "It cools my brain so I can concentrate on other things."
Question: Please explain to us how stellate ganglion block, which is an anesthesia, is used to treat PTSD.
Dr. Ritchie: It is an anesthetic technique used for pain, where lidocaine is injected into the stellate ganglion by an anesthesiologist. It has been seen to dramatically reduce PTSD symptoms in some. There is not yet a robust body of literature, but there are certainly a lot of very promising case studies and anecdotal reports on it.
Question: So, how does a soldier who would like to try these integrative therapies to help minimize their discomfort and anguish without overtly asking and risking being stigmatized, go about receiving them?
Dr. Ritchie: Good question. To be honest, it’s highly variable as to what their access is to those treatments. At a place like the NICoE (National Intrepid Center of Excellence) in Bethesda at the new Walter Reed Military Medical Center, there is a very intense program that includes art therapy, acupuncture, and virtual reality exposure therapy. There are also other facilities, such as one in San Diego, but if a service member doesn’t have access to these facilities it might be difficult to get this kind of treatment.
Question: How does the Veterans Health Administration deal with this?
Dr. Ritchie: I need to separate what I have just been talking about, which is to deal with the military health care system, from the VA. There is a lot of confusion over this. They are not the same health care system; they’re very different. When someone is on active duty, by and large they will be seen in the military health care system. If someone is a veteran, they may or may not be able to be seen in the VA depending on their priority level, their income, whether they had a disability, whether they had a service-related condition, et cetera.
The larger question is, how does the VA deal with PTSD? Well, I think the VA does a really good job providing evidence-based therapies, and in other cases, it’s quite overwhelmed by the number of veterans coming to it for treatment. It’s hard, because many people will say that the VA is 141 different hospitals, and it has centers and clinics, so it’s highly variable.
Question: So, if I am a service member seeking treatment without stigma, would I go to a community-based clinician?
Dr. Ritchie: The military actually has been quite active in trying to provide confidential treatment. Military OneSource has a website and phone number to call to refer troops to resources. Although a military member can go on his or her own to a community doctor for treatment, they’re not really supposed to, although certainly people do it.
On every base, there are chaplains and a mental health clinic, and there are other programs such as resiliency training, like the Comprehensive Soldier Fitness Program, and other programs that try to provide treatment while minimizing stigma, and to reach out to the service member who might not be willing to reach out to the military. So, the military is trying, but it’s not easy. It’s not as simple as hiring 20 more psychologists, because a lot of people are worried about their career and so won’t come into a clinic.
I didn’t talk about this before, but the army also uses therapy dogs, or animal-assisted therapy, because a lot of times the soldier won’t come talk to you as a shrink, but they will come talk to you about their dog. So, there are a lot of bridges that can be made.
Question: Well, then is there really a stigma? Or if it’s there, is it really as impactful as a soldier might fear?
Dr. Ritchie: I wish I could say that there is no reality behind the stigma, but there is a reality there. If someone is known to seek mental health treatment, some people will think less of them. This is true elsewhere in law enforcement and in the civilian world. So the approach taken in many cases in the military is to combine mental health with primary care, because if someone goes into the primary care clinic, that’s a lot less stigmatizing than sitting in the mental health clinic. But simply saying that stigma should end doesn’t work.
This is a downsizing military, and there is lots of talk about troop cuts, especially in the Army, so you don’t want to be the one who has something less than perfect on your record.
Question: Let’s back up to something you said before about the purpose of a soldier being to win wars. If the military is scaling back, are troops worried they won’t have that job to do any more, and maybe are wondering about their purpose, so that there is an existential component to the anguish these service members face? In other words, is the term "posttraumatic stress disorder" wholly appropriate to explain what is happening before some of these people try, and in some cases, succeed, to take their lives?
Dr. Ritchie: There is a term I will throw in here that I think will help the discussion. Moral injury. It’s related, but not the same as PTSD, which is a diagnosis in the DSM-IV and DSM-5, while "moral injury" is not. Moral injury refers to the feelings of guilt and shame that might be related to killing others or having your friends killed: being tainted by being at war.
So when I look at PTSD, it isn’t as a risk factor for suicide itself. As we talked about, more than half of the suicides now happen in those who have not deployed. PTSD does factor in, in the sense that it can contribute to the breakup of relationships, the feeling that you don’t fit in, and those are risk factors for suicide. So, I am not saying PTSD is unrelated, but if you look at the number of completed suicides, only 10% had a PTSD diagnosis. More could have had PTSD, and it just wasn’t in their records. But, back to the question about existential angst, I think it’s around having seen vast amounts of death and destruction.
Question: Is that your point of view, or does the military recognize this?
Dr. Ritchie: There is increasing recognition, but there are no systematic studies that have been done on it yet. And, the issue about asking people if they’ve killed is difficult, because in many of these cases there is a gray area. If someone is shooting at you, there is no question that you can defend yourself, but people worry whether they have committed a war crime, so it’s difficult to study this scientifically without getting into questions about ethics and legal quandaries.
Question: So language is very important. PTSD used to be called "shell shock." When did it broaden out to become PTSD and become used to address anything that traumatizes a person, not just soldiers?
Dr. Ritchie: Here’s a brief answer. We have called PTSD many things: shell shock, battle fatigue, combat neurosis, and combat stress injury. There have been many names. The term PTSD began in 1980, after the Vietnam War. And a lot of the concepts were based on soldiers and service members from that war. It also encompasses other trauma, the largest amount of literature being on sexual assault victims and disaster victims.
The diagnosis was upgraded in the DSM-5, meaning that there were more symptoms added to the classic symptoms, which were hypervigilance – being jumpy and nervous, the flashbacks and memories, and the numbness, and being detached. Now, the symptoms include sleep difficulties, depression, irritability, cognitive difficulties, and somatic reactions. So, it’s a wider diagnosis now, and it will be interesting to see how that affects the prevalence of the disorder.
Question: People have been traumatized since the beginning of humanity, and have needed to cope with it. That’s where the existentialism comes in. Does PTSD offer an opportunity to find meaning in life that wasn’t seen before?
Dr. Ritchie: Certainly, people talk about posttraumatic growth. People used to join the army because it "made a man out of you." I think there are certainly good things that come out of military service on all kinds of levels. Seeing trauma and being around trauma don’t mean you are scarred for life. You can grow as a result of the experience.
Question: Barbara Rothbaum, Ph.D., a leading expert in exposure therapy, says that the trauma will always be sad, but that it doesn’t mean you can’t feel joy again. People forget that you can come out the other side – that PTSD isn’t permanently debilitating.
Dr. Ritchie: PTSD has a range of severity. Dr. Robert Ursano at the Center for the Study of Traumatic Stress in Bethesda, likened it to being the common cold of psychiatry. A lot of people are exposed, have symptoms; most become better quickly, but in some it becomes chronic bronchitis or pneumonia. So, it’s important to recognize there is both a range in the severity of the trauma and people’s reaction to it.
It’s also important to remember that people who are going to combat now are well trained, well armed, and in combat gear, and they are expecting traumatic things. That’s different than if you’ve been the victim of sexual assault, and you’re surprised and feel vulnerable and helpless. So, I think the vast majority of those who experience the psychological effects of war go on to grow from the experience.
–Interview by Whitney McKnight
*CORRECTION, 4/30/2014: An earlier version of this article misidentified Col. (Ret.) Elspeth Cameron Ritchie.
Providing sensitive mental health treatment to patients who have served in the military requires better understanding of this unique culture. Toward that end, this news organization recently sat down with Col. (Ret.) Elspeth Cameron Ritchie, former chief of psychiatry for the U.S. Army and the current chief clinical officer in the department of behavioral health for the District of Columbia. The following is an edited transcript of a discussion with Dr. Ritchie*.
Question: Why are there more suicides among service members who’ve never deployed than in those who have been in-country?
Dr. Ritchie: For many years, there was a relatively stable suicide rate at about 10 per 100,000 troops per year. Starting in 2004, the rate more than doubled, so that by 2010, 2011, and 2013, we had very high suicide rates for the military. The suicide pattern also shifted over time. In the beginning, there was a lot of concern that the rates were related to deployment; although in individual cases, the deployment may have caused some stresses, by and large the suicides did not seem to be directly related to individual deployment, and now more than half the suicides occur in those who’ve never deployed.
Why is that? Well, it’s complex, but one of the reasons I look at is that the army itself has been on a high operations tempo, so troops are deploying all the time; they’re tired, so one of the things that’s going on is that when a new soldier joins a unit, they might not be welcomed in the same way as they would have been in the past, because everyone’s so busy. So, that’s one piece of it.
But, let me go big picture. For a long time, the stressors that led to suicide have been all about failed relationships and also getting into trouble at work or having financial troubles. And that pattern has stayed the same over time, but the number of troops who have suicided has risen over time.
Question: So it’s the social structure of the military driving this, at least in part?
Dr. Ritchie: That’s one of the drivers. The people are just so busy, by that I mean the units, who have so busy going back and forth. So, for example, if you look at the 101st Division at Fort Campbell, they have been in and out of the theater of war almost every other year for a long time, they’re slowing down now a little, and they had a very high suicide rate for a number of years. And that’s not dissimilar to the other bases like Fort Stewart and Fort Hood; they are all deploying troops very rapidly in and out of the theater of war.
Question: Does the military need to sensitize its troops to welcoming in recruits?
Dr. Ritchie: The military has been very concerned about the suicide rate, and they have done a lot about it, with perhaps the beginning of some success in that the suicide rate among active duty troops is starting to level off, but the rate is rising in the Reserves and National Guard. But, for example, there was a Department of the Army task force to look at this, and it started out as suicide prevention, but then they added risk reduction, and they then added health promotion as part of it. Then there was the Department of Defense task force with many, many recommendations. And basically, the easy recommendations are all done. Recommendations that are harder to do, like ending the conflicts of wars, well, the wars are finally winding down, but that’s not something you can just "stop," and as the military, it’s your job to go to war.
Question: Is the military screening recruits well enough? Maybe they are coming in with too many problems to begin with.
Dr. Ritchie: There already is quite a bit of screening. There are some misconceptions about that. As a matter of fact, there is a bill going to Congress about that now, that calls for adding mental health screening. There already is a history and physical done as a young recruit tries to enter the military, and they’re asked about mental health problems. But one of the realities is that if you’re motivated to come into the service, you’re probably not going to talk about your mental health problems, because you’re worried that will disqualify you from service. Already, only about a third of people who apply to the military are able to make the mental health and physical standards. So, there is a screening.
We have tried pen-and-paper screenings for 100 years, literally, since World War I, and what we’ve found is that generally, they don’t work. Again, these are based on self-report. If somebody fills out a piece of paper that asks about suicidal ideation, if the person wants to get into the military, they’re not going to answer that. And the military doesn’t have access to previous records unless the person chooses to offer them.
Let me add to that, the best screen is basic training. So, remember when a recruit comes in, they have 8 to 13 weeks, depending on the service, of very intense interaction with other recruits, and with the drill sergeants, and about 8% of troops actually wash out of basic training. What we’ve tried over and over to do is to develop a paper-and-pencil screen, but it either isn’t sensitive or isn’t specific enough.
Question: What about "checkpoint" screenings that you do periodically after some time in the service?
Dr. Ritchie: As people come back from deployment, they are screened, and 3 to 6 months later, they have a postdeployment reassessment because we realized that people weren’t going to tell the truth as they were coming back home because they just wanted to go home. So, we asked them again. And, there is a yearly assessment done, but again, a lot of what this relies on is the soldier’s willingness to share what’s really going on. There are questions for depression, and suicidal ideation, and posttraumatic stress disorder as part of the whole assessment process.
Question: But will they answer truthfully at all times, regardless of how they feel about deployment, because they are afraid of being stigmatized?
Dr. Ritchie: Remember that this is an all-volunteer army, and we’ve been at war since 9/11/2001, so troops who have been in the service know they’re going to be deployed and want to be deployed. And with the difficult economy, they want to stay in the service and they want to be promoted. So, they are concerned if they answer "yes" to a mental health question, they will be made to see a psychiatrist, which might have an impact on their career, or they won’t be allowed to deploy. So, there is a lot of motivation to minimize symptoms.
Now, that’s true of people who want to make the military a career. I have also seen that people who have decided to leave the military, or the military has decided that the person shouldn’t stay, then there is often a lot of incentive to answer yes to all the mental and physical health symptoms. For example, on your retirement physical, you’re told, "Make sure you put down every condition you’ve got because you want to have access to the VA" and maybe you’ll get disability or get compensated. So you’ll often see underreporting if a soldier wants to stay on active duty, and perhaps there’s some embellishment of symptoms as they’re going out the door.
Question: What about therapies that are said to address other physical symptoms, like acupuncture, but which are actually addressing the mental health aspect as well?
Dr. Ritchie: There are two main types of evidence-based therapies for PTSD. There’s the cognitive-behavioral therapy, which has cognitive processing therapy as part of it, and there is exposure-based therapy, as evidence-based psychotherapies. And then there are medications – the selective serotonin reuptake inhibitors for PTSD – as well. However, many, many service members don’t want to take medication, and/or they don’t want to go and talk to someone about their trauma. In most cases, these are young men, and young men often don’t want to talk about anything, much less their feelings or a traumatic experience where perhaps one of their friends was killed or wounded. So, I have gotten very interested in the various forms of integrative medicine – such as acupuncture, yoga, mindfulness – which many of our troops really enjoy doing. They probably don’t treat the PTSD by themselves, but they provide a bridge to treatment.
And, perhaps they do treat the symptoms themselves. Certainly, service members have reported vast improvements from acupuncture, from stellate ganglion block, from yoga. They say: "It cools my brain so I can concentrate on other things."
Question: Please explain to us how stellate ganglion block, which is an anesthesia, is used to treat PTSD.
Dr. Ritchie: It is an anesthetic technique used for pain, where lidocaine is injected into the stellate ganglion by an anesthesiologist. It has been seen to dramatically reduce PTSD symptoms in some. There is not yet a robust body of literature, but there are certainly a lot of very promising case studies and anecdotal reports on it.
Question: So, how does a soldier who would like to try these integrative therapies to help minimize their discomfort and anguish without overtly asking and risking being stigmatized, go about receiving them?
Dr. Ritchie: Good question. To be honest, it’s highly variable as to what their access is to those treatments. At a place like the NICoE (National Intrepid Center of Excellence) in Bethesda at the new Walter Reed Military Medical Center, there is a very intense program that includes art therapy, acupuncture, and virtual reality exposure therapy. There are also other facilities, such as one in San Diego, but if a service member doesn’t have access to these facilities it might be difficult to get this kind of treatment.
Question: How does the Veterans Health Administration deal with this?
Dr. Ritchie: I need to separate what I have just been talking about, which is to deal with the military health care system, from the VA. There is a lot of confusion over this. They are not the same health care system; they’re very different. When someone is on active duty, by and large they will be seen in the military health care system. If someone is a veteran, they may or may not be able to be seen in the VA depending on their priority level, their income, whether they had a disability, whether they had a service-related condition, et cetera.
The larger question is, how does the VA deal with PTSD? Well, I think the VA does a really good job providing evidence-based therapies, and in other cases, it’s quite overwhelmed by the number of veterans coming to it for treatment. It’s hard, because many people will say that the VA is 141 different hospitals, and it has centers and clinics, so it’s highly variable.
Question: So, if I am a service member seeking treatment without stigma, would I go to a community-based clinician?
Dr. Ritchie: The military actually has been quite active in trying to provide confidential treatment. Military OneSource has a website and phone number to call to refer troops to resources. Although a military member can go on his or her own to a community doctor for treatment, they’re not really supposed to, although certainly people do it.
On every base, there are chaplains and a mental health clinic, and there are other programs such as resiliency training, like the Comprehensive Soldier Fitness Program, and other programs that try to provide treatment while minimizing stigma, and to reach out to the service member who might not be willing to reach out to the military. So, the military is trying, but it’s not easy. It’s not as simple as hiring 20 more psychologists, because a lot of people are worried about their career and so won’t come into a clinic.
I didn’t talk about this before, but the army also uses therapy dogs, or animal-assisted therapy, because a lot of times the soldier won’t come talk to you as a shrink, but they will come talk to you about their dog. So, there are a lot of bridges that can be made.
Question: Well, then is there really a stigma? Or if it’s there, is it really as impactful as a soldier might fear?
Dr. Ritchie: I wish I could say that there is no reality behind the stigma, but there is a reality there. If someone is known to seek mental health treatment, some people will think less of them. This is true elsewhere in law enforcement and in the civilian world. So the approach taken in many cases in the military is to combine mental health with primary care, because if someone goes into the primary care clinic, that’s a lot less stigmatizing than sitting in the mental health clinic. But simply saying that stigma should end doesn’t work.
This is a downsizing military, and there is lots of talk about troop cuts, especially in the Army, so you don’t want to be the one who has something less than perfect on your record.
Question: Let’s back up to something you said before about the purpose of a soldier being to win wars. If the military is scaling back, are troops worried they won’t have that job to do any more, and maybe are wondering about their purpose, so that there is an existential component to the anguish these service members face? In other words, is the term "posttraumatic stress disorder" wholly appropriate to explain what is happening before some of these people try, and in some cases, succeed, to take their lives?
Dr. Ritchie: There is a term I will throw in here that I think will help the discussion. Moral injury. It’s related, but not the same as PTSD, which is a diagnosis in the DSM-IV and DSM-5, while "moral injury" is not. Moral injury refers to the feelings of guilt and shame that might be related to killing others or having your friends killed: being tainted by being at war.
So when I look at PTSD, it isn’t as a risk factor for suicide itself. As we talked about, more than half of the suicides now happen in those who have not deployed. PTSD does factor in, in the sense that it can contribute to the breakup of relationships, the feeling that you don’t fit in, and those are risk factors for suicide. So, I am not saying PTSD is unrelated, but if you look at the number of completed suicides, only 10% had a PTSD diagnosis. More could have had PTSD, and it just wasn’t in their records. But, back to the question about existential angst, I think it’s around having seen vast amounts of death and destruction.
Question: Is that your point of view, or does the military recognize this?
Dr. Ritchie: There is increasing recognition, but there are no systematic studies that have been done on it yet. And, the issue about asking people if they’ve killed is difficult, because in many of these cases there is a gray area. If someone is shooting at you, there is no question that you can defend yourself, but people worry whether they have committed a war crime, so it’s difficult to study this scientifically without getting into questions about ethics and legal quandaries.
Question: So language is very important. PTSD used to be called "shell shock." When did it broaden out to become PTSD and become used to address anything that traumatizes a person, not just soldiers?
Dr. Ritchie: Here’s a brief answer. We have called PTSD many things: shell shock, battle fatigue, combat neurosis, and combat stress injury. There have been many names. The term PTSD began in 1980, after the Vietnam War. And a lot of the concepts were based on soldiers and service members from that war. It also encompasses other trauma, the largest amount of literature being on sexual assault victims and disaster victims.
The diagnosis was upgraded in the DSM-5, meaning that there were more symptoms added to the classic symptoms, which were hypervigilance – being jumpy and nervous, the flashbacks and memories, and the numbness, and being detached. Now, the symptoms include sleep difficulties, depression, irritability, cognitive difficulties, and somatic reactions. So, it’s a wider diagnosis now, and it will be interesting to see how that affects the prevalence of the disorder.
Question: People have been traumatized since the beginning of humanity, and have needed to cope with it. That’s where the existentialism comes in. Does PTSD offer an opportunity to find meaning in life that wasn’t seen before?
Dr. Ritchie: Certainly, people talk about posttraumatic growth. People used to join the army because it "made a man out of you." I think there are certainly good things that come out of military service on all kinds of levels. Seeing trauma and being around trauma don’t mean you are scarred for life. You can grow as a result of the experience.
Question: Barbara Rothbaum, Ph.D., a leading expert in exposure therapy, says that the trauma will always be sad, but that it doesn’t mean you can’t feel joy again. People forget that you can come out the other side – that PTSD isn’t permanently debilitating.
Dr. Ritchie: PTSD has a range of severity. Dr. Robert Ursano at the Center for the Study of Traumatic Stress in Bethesda, likened it to being the common cold of psychiatry. A lot of people are exposed, have symptoms; most become better quickly, but in some it becomes chronic bronchitis or pneumonia. So, it’s important to recognize there is both a range in the severity of the trauma and people’s reaction to it.
It’s also important to remember that people who are going to combat now are well trained, well armed, and in combat gear, and they are expecting traumatic things. That’s different than if you’ve been the victim of sexual assault, and you’re surprised and feel vulnerable and helpless. So, I think the vast majority of those who experience the psychological effects of war go on to grow from the experience.
–Interview by Whitney McKnight
*CORRECTION, 4/30/2014: An earlier version of this article misidentified Col. (Ret.) Elspeth Cameron Ritchie.

100 years of solicitude: Do global traumatic events have a transgenerational effect?
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.