User login
Attention-Deficit/Hyperactivity Disorder in a VA Polytrauma Clinic
Traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are considered the signature injuries in veterans of the military operations in Iraq and Afghanistan.1 In 2007, the VA implemented the Polytrauma System of Care (PSC) to provide comprehensive screening, evaluation, and treatment of these multifaceted injuries.2,3 The VA defined polytrauma as “two or more injuries to physical regions or organ systems, one of which may be life threatening, resulting in physical, cognitive, psychological, or psychosocial impairments and functional disability.”3 The VA intended the PSC to provide a national system of integrated care to meet the unique needs of these combat service members.
In addition to the comprehensive evaluation and treatment of traumatic injuries, a critical mission of the PSC is to facilitate the reintegration of injured combat veterans into their home communities. Optimal community reintegration requires that the clinician also assess premorbid comorbidities, which may affect postdeployment adjustments. Attention-deficit/hyperactivity disorder (ADHD), with an estimated adult prevalence of 4.4% in the U.S. and 2.5% to 3.4% worldwide, is a common disorder in the general adult population that often is associated with chronic social and vocational adjustment difficulties.4-6 The increasing recognition that this disorder often persists into adulthood is of significance to veterans, largely young and male, who have left military service and are reintegrating into college and community job settings.7 Despite growing interest in adult ADHD, little is known about its prevalence and correlates in the veteran population.
The prevalence of ADHD in the Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) veteran polytrauma population has not been adequately studied. Studies have found that combat veterans with or without confirmed TBI diagnosis commonly have similar overlapping symptoms, such as memory problems, difficulty concentrating, poor attention, and sleep problems associated with other comorbidities such as pain, PTSD, ADHD, and other mental health diagnoses.8-14 Increased awareness of various clinical variables would enhance understanding of the population characteristics and specific needs for education and management.
Related: Preparing the Military Health System for the 21st Century
To begin to address the lack of information about ADHD in the VA polytrauma population, this study aimed to (1) identify the prevalence of ADHD in veterans referred to the Clement J. Zablocki (CJZ) VAMC Polytrauma Clinic (PC) in Milwaukee, Wisconsin; (2) describe demographic characteristics of polytrauma veterans with ADHD; (3) determine the comorbidity relationship between ADHD and TBI, PTSD, depression and anxiety disorders, and substance abuse; and (4) determine whether individuals with ADHD compared with those without ADHD report more physical and emotional symptomatic distress with particular attention given to reports of pain, headaches, and problems with attention and concentration, memory, and sleep.
Methods
The study population consisted of 690 OEF/OIF/OND soldiers and veterans who received a comprehensive TBI evaluation in the CJZVAMC PC from January 1, 2008, to December 31, 2012. Referrals to the PC were made by primary care physicians (PCPs) when OEF/OIF/OND veterans or service members enrolled at a VA facility for health care or transferred their care from another VA facility.
Either a prior diagnosis of TBI established by a qualified provider or positive responses to a 4-question screening tool for TBI prompted a referral to the PC. The 4 questions sought to establish (1) events that may increase risk of TBIs; (2) immediate symptoms following the event; (3) new or worsening symptoms following the event; and (4) current symptoms.1 Referrals to the clinic most commonly came from PCPs at the CJZVAMC and its associated community-based outpatient clinics but occasionally came from mental health service providers.
Study Design
The CJZVAMC Institutional Review Board approved this study. A population database was developed from a review of medical records, clinical interviews of patients, and completion of standard intake forms during the veterans’ initial evaluations in the CJZVAMC PC. The database aimed to abstract patient information relevant for understanding and treating the population seen in the clinic. The database contained information related to demographics, injury parameters, neurobehavioral and PTSD symptoms, past and current mental health disorders, substance abuse history, pain symptoms, and developmental history (eg, ADHD, learning disability).
Related: First Brain Wave Test to Diagnose ADHD
Prior to the PC intake interview, each veteran completed a packet of preclinic questionnaires that included information concerning deployment-related injury exposure and history; the 22-item Neurobehavioral Symptom Inventory (NSI), which assessed physical, cognitive, and emotional symptoms; current pain symptoms; and the Posttraumatic Stress Disorder Checklist-Civilian Version (PCLC).15,16 Intake interviews in the CJZVAMC PC were typically conducted with a minimum of 2 specialties present (physical medicine/rehabilitation and neuropsychology) and occasionally as many as 4 specialties present (also including health psychology and social work). Data collection and abstraction for the database were derived by all specialties present and assisted by the polytrauma program technician.
Diagnoses
The diagnosis of ADHD in a veteran was established through 1 of 2 methods: (1) report of a developmental history of behavioral adjustment difficulties consistent with ADHD that was coupled with formal psychiatric diagnosis and recommended treatment of ADHD in childhood; or (2) current diagnosis of ADHD as identified in the veteran’s active problem list. In most cases of report of developmental diagnosis, the veteran reported having been diagnosed and having received treatment with a stimulant medication for a period of time. In a few cases, the veteran reported having been diagnosed and stimulant medication was recommended, but the veteran’s parents declined the pharmacologic treatment in favor of behavioral treatment strategies.
In cases of current diagnosis, Diagnostic and Statistical Manual of Mental Disorders, Text Revision, 4th Edition (DSM-IV-TR), criteria were applied and supported by formal clinical examinations for ADHD conducted by psychologists, psychiatrists or neuropsychologists, or through VA disability (Compensation and Pension) evaluations where an issue related to ADHD diagnosis was raised.17 There was considerable overlap between these 2 diagnostic criteria (ie, through report of developmental history of diagnosis or formal adult evaluation) with 93% of cases being positive on both diagnostic methods.
Other comorbid psychiatric (eg, depression, anxiety, PTSD, substance abuse) and medical (eg, headache, pain) conditions also were abstracted from the veteran’s medical records at the time of the intake evaluation. Documentation of these conditions was derived from the veteran’s problem list and clinical notes that identified the condition as a diagnostic conclusion or focus of treatment. The comorbid conditions were not otherwise independently documented. Many veterans were taking psychotropic medications for mood, sleep, or chronic pain problems at the time of evaluation in the PC; however, use of medication and their effects were not systematically evaluated.
Statistical Analysis
In addition to documentation of the population prevalence for ADHD, analysis for disproportionate prevalence of comorbid conditions in individuals with ADHD compared with those without ADHD was done through the use of the chi-square test and/or Fisher exact test. For continuous variables, t tests were used to compare individuals with ADHD with individuals without ADHD. To control family-wise type I error to a P value of .05, a false discovery rate (FDR) was applied to studies of demographics, comorbidities, and ratings of symptomatic distress.
Results
The general population characteristics of the 690 veterans and soldiers are summarized in Table 1. The sample was predominantly male (96%), white (88%), and ranged in age from 22 to 55 years with a mean of 28 years. Active-duty service members and reservists from the U.S. Army, Marines, Navy, and Air Force were represented, but most were Army veterans (72%). Most (63%) had a high school education. About two-thirds of the veterans had a single deployment, and the remaining had multiple deployments.

The TBI clinic evaluations found that 58% of the patients had ≥ 1 TBI during their deployments, almost exclusively mild in severity. Seventy-three patients met study criteria for ADHD: 69 with an identified history of diagnosis in childhood and 68 with a current diagnosis, with 93% overlap of these groups. Table 2 provides a breakdown of demographic characteristics, comorbidities, and symptomatic distress in veterans with ADHD compared with those without the diagnosis.

Demographic Characteristics
Veterans with ADHD were found to be slightly younger (2.3 years younger, P = .003) and to have less education (greater frequency of less than high school and high school only, P = .003) compared with those who did not have the diagnosis. No significant group differences in sex, employment/school status, marital status, or number of deployments were identified in veterans with ADHD compared with non-ADHD veterans. Individuals with ADHD did not experience more physical, emotional, or sexual abuse as children than did their non-ADHD counterparts. The prevalence of TBI during deployment was similar in veterans with ADHD compared with that of non-ADHD veterans. There was a trend for veterans with ADHD to have more TBIs prior to military service than in non-ADHD veterans; however, this trend did not reach statistical significance (P = .188).
Comorbidities
After application of the FDR threshold, veterans with ADHD did not show a disproportionate prevalence of mental health diagnoses (eg, PTSD, depression and anxiety disorders, or substance abuse). There was a nonsignificant trend for more veterans with ADHD to report pain during the previous 30 days (P = .035) and more issues with substance abuse (P = .10) than for non-ADHD veterans, but these trends did not meet the FDR threshold of < .05.
Symptomatic Distress
Veterans with ADHD did not report significantly greater levels of distress on either the NSI or the PCLC survey compared with non-ADHD veterans.Not surprisingly, when select symptoms were investigated, veterans with ADHD reported more problems with attention and concentration than for non-ADHD veterans (P = .015). No group differences were identified for sleep issues, headaches, or memory, although there was a trend for the latter (P = .14).
Discussion
In this study, there was a 10.6% prevalence of ADHD in 690 OEF/OIF/OND combat veterans. This rate is considerably higher than estimates of prevalence of ADHD in adults (4.4%) made from a nationwide survey and worldwide prevalence estimates of 2.5% to 3.5%.4-6 Still, the current prevalence finding is consistent with a recent finding of ADHD in previous deploying U.S. soldiers military samples (10.4%).18 The high prevalence of ADHD in the current clinic population argues for increased provider awareness of this condition as a possible factor in postdeployment adjustment assessments.
Changes in prevalence estimates of ADHD may represent increased awareness of the condition over this interval of time, professional drift in the application of diagnostic criteria, or changes in societal attitudes about acceptability in pursuing treatment for the condition. For example, in nationwide surveys in 2003, 2007, and 2011, the CDC identified an increase from 7.8% to 9.5% to 11%, respectively, in diagnoses of ADHD in childhood.19 Also, considering that the current sample was predominantly male and the prevalence of ADHD in males is higher than in females, one might expect a higher ADHD prevalence rate in this study than that in the general population. In this regard, the ADHD prevalence rate in males remains comparable to that estimated by recent CDC survey data.19
When estimating ADHD population prevalence in the future, it is worth noting that a change in the diagnostic criteria for ADHD has occurred in DSM-5. Specifically, the age at which critical symptoms must be present to make the diagnosis of ADHD has been increased from age 7 years to age 12 years, and the number of critical symptoms to meet hyperactivity-impulsivity criteria has been lowered from 6 to 5 in older adolescents and adults.20 These changes in the diagnostic criteria for ADHD will have the net effect of increasing estimates of prevalence of ADHD.
The 73 individuals with an ADHD diagnoses in this study were found to have less education and be slightly younger than were the veterans who did not have an ADHD diagnosis. This finding is not unexpected, as individuals with ADHD are known to struggle in school and often drop out of high school and pursue alternative means of getting an equivalency degree or certification.21 Early departure from high school can be followed by earlier enlistment in the military. Prior studies by Krauss and colleagues found similar findings in an ADHD study of military recruits (ie, they were less likely to have education beyond a high school degree).7
ADHD and TBI
Given problems with attention, impulsivity, and high levels of aggressive behaviors associated with ADHD, individuals with ADHD have been found to be at higher risk for accidental injuries, including TBI, than are individuals without ADHD.21,22 Thus, soldiers with ADHD may be at greater risk for TBI during their time in the military. In the current sample, although veterans with ADHD showed a trend toward having more TBIs prior to joining the military relative to non-ADHD veterans, the veterans with ADHD had a similar rate of TBIs during their time in the military relative to non-ADHD veterans.
Although individuals with ADHD are reported to have a higher prevalence of mental health issues than does the general public, this was not evident in the current sample.21 Veterans with ADHD in this study did not have a disproportionate prevalence of PTSD, depression, anxiety, or substance abuse.
There was a nonsignificant trend for more individuals with an ADHD diagnosis compared with those without the diagnosis to report experiencing pain during the 30 days prior to their evaluation in the PC. Although not statistically significant, this finding would not be unexpected, in that individuals with ADHD are known to show less tolerance for frustration relative to that of the general population.21 In the current study, reports of pain in the ADHD group correlated with reports of being irritable and easily annoyed (r = .27, P = .024), but no correlation was observed with reports of poor frustration tolerance (r = .04, P = .74). Still, of note, > 90% of the OEF/OIF/OND veterans in this study, regardless of their ADHD diagnosis, reported pain symptoms of some type. The high prevalence of pain symptoms in this sample is consistent with a previous study that found pain to be one of the most common problems in polytrauma patients.10
Related: Civilian Stress Compounds Service-Related Stress
Not surprisingly, as shown in Table 2, veterans with ADHD compared with those without the diagnosis reported more problems with attention and concentration. The report of more attentional problems is seemingly not accounted for by group differences in reports of pain in general, headaches, sleep disturbance, or memory problems.
Study Strengths
A large sample of veterans constituted this study, and the data were gathered in consecutive referrals to the CJZVAMC PC over a 5-year period. Also, information on a number of comorbidities were captured simultaneously with the polytrauma and ADHD diagnoses, allowing much greater ability to investigate the interaction of multiple comorbidities as well as lingering reports of symptoms following discharge from active military service.
In these authors’ experience, veterans with ADHD benefit substantially from structured treatment interventions that are focused on developing compensatory skills for their problems with attention and impulsivity. Individuals with ADHD typically have a greater need for assistance with planning and organizing, making decisions, problem solving, and regulating their attention and affect. Individuals with ADHD may benefit from treatment strategies focused on ADHD behaviors in conjunction with traditional treatment strategies frequently used in the PC. These strategies include increased case management, medication trials, education regarding ADHD, vocational assistance, and consideration of both the school and work accommodations.
Studies have shown that treatments with stimulants improve functioning and reduce depression and substance use.21 In this study, < 5% of individuals with ADHD were taking stimulants at the time they were initially assessed in the PC, whereas the majority were taking stimulants after being referred for ADHD evaluation. Thus, identification of veterans with ADHD has clinical relevance in understanding the specific needs that guide development of individualized treatment plans to promote successful community reintegration.
Limitations
One limitation of the study is the lack of available medical records of historical ADHD diagnoses prior to military service. Also, although DSM-IV criteria for ADHD were operational in the psychodiagnostic clinics for these subjects, because the polytrauma study team did not conduct the evaluations in this sample, uniform diagnostic standards may not have been consistently applied when establishing the ADHD diagnosis. There was a 93% agreement between the 2 methods of diagnosis (ie, report of developmental diagnosis or positive adult evaluation), suggesting that diagnostic precision for ADHD in this study was reasonably accurate.
Another significant limitation of this study, apart from establishing medical and psychiatric status at the time of the initial referral to the PC, is the omission of functional outcome assessments regarding success of polytrauma treatment initiatives or ultimate community reintegration of successful psychosocial participation or academic and vocational achievements. Future longitudinal outcome studies are needed to determine whether ADHD has a significant impact on clinical outcomes. Of interest, pain was an overwhelmingly common factor (> 90%) for the military population studied at this site. Some degree of disturbance in attentional capacities is common in patients with chronic pain, which may aggravate ADHD symptoms and vice versa. Further investigations are needed to determine the potential functional impact of pain, including use of pain and psychotropic medications, on ADHD symptoms and the combined effect of these symptoms on overall outcome from rehabilitation and reintegration efforts.
Although these findings suggest that polytrauma veterans with ADHD do not have more psychiatric or physical comorbidities than do veterans without ADHD, it is premature to conclude that community reintegration can be optimally managed in the same way for both groups. Community reintegration of individuals with ADHD will likely be challenging, as these individuals often have struggled with functioning in their communities prior to their military service.
Studies of adult ADHD in the U.S. and in other countries have found that it is often associated with substantial impairment in managing the demands of functioning as an adult in society.4 Although some theorists have speculated that symptoms of ADHD may have been evolutionarily adaptive to survival in select environments (eg, predatory hunting environments), there is no clear evidence to support such adaptive benefits of the symptom in modern combat environments.23,24 Symptoms of ADHD are typically maladaptive to soldiers transitioning to civilian lives.
Conclusions
This investigation described the demographic and clinical characteristics of OEF/OIF/OND veterans referred for evaluation of TBI to the CJZVAMC PC during 5 years of operation from 2008 through 2012. The aim was to increase provider awareness of possible important variables that may influence recovery and community reintegration. This study may help to form the foundation for future lines of research into variables such as ADHD that may influence outcomes of rehabilitation and reintegration interventions.
To better understand the treatment needs of young veterans returning home from the wars in Iraq and Afghanistan, this study sought to identify the prevalence rate of ADHD, a condition known to complicate community adjustment. In this study, there was a 10.6% prevalence of ADHD among the 690 OEF/OIF/OND combat veterans seen over the 5-year period in the CJZVAMC PC, which is substantially higher than prevalence estimates in the U.S. general population but similar to estimates in previous military samples.
Compared with veterans who did not have ADHD, veterans with ADHD were younger, less well educated, and reported more problems with attention and concentration but did not have a greater incidence of military TBI or mental health comorbidities. The high prevalence of ADHD in this group argues for greater awareness of this clinical variable and development of intervention programs tailored to the specific skill deficiencies found in the condition, which can be included as part of the comprehensive treatment interventions.
Veterans with ADHD treated in the PC seem to benefit from structured treatment plans and education to promote self-awareness and veteran-centered self-management for effective symptom reduction and coping strategies. Development of effective integrated treatment options with a focus on educational and vocational resources and assistance could facilitate successful community reintegration. Future studies are needed to further assess outcomes of community reintegration, including academic and occupational outcomes, in this population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358(5):453-463.
2. Screening and Evaluation of Possible Traumatic Brain Injury in Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) Veterans. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-012.
3. Polytrauma System of Care. Washington, DC: Dept of Veterans Affairs; 2013. VHA Handbook 1172.01.
4. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163(4):716-723.
5. Simon V, Czobor P, Bálint S, Mészáros A, Bitter I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. Br J Psychiatry. 2009;194(3):204-211.
6. Fayyad J, De Graaf R, Kessler R, et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry. 2007;190(5):402-409.
7. Krauss MR, Russell RK, Powers TE, Li Y. Accession standards for attention-deficit/hyperactivity disorder: A survival analysis of military recruits, 1995-2000. Mil Med. 2006;171(2):99-102.
8. Vanderploeg RD, Belanger HG, Horner RD, et al. Health outcomes associated with military deployment: Mild traumatic brain injury, blast, trauma, and combat associations in the Florida National Guard. Arch Phys Med Rehabil. 2012;93(11):1887-1895.
9. Theeler BJ, Flynn FG, Erickson JC. Headaches after concussion in US soldiers returning from Iraq or Afghanistan. Headache. 2010;50(8):1262-1272.
10. Sayer NA, Chiros CE, Sigford B, et al. Characteristics and rehabilitation outcomes among patients with blast and other injuries sustained during the Global War on Terror. Arch Phys Med Rehabil. 2008;89(1):163-170.
11. Sayer NA, Rettmann NA, Carlson KF, et al. Veterans with history of mild traumatic brain injury and posttraumatic stress disorder: Challenges from provider perspective. J Rehabil Res Dev. 2009;46(6):703-716.
12. Nampiaparampil DE. Prevalence of chronic pain after traumatic brain injury: A systematic review. JAMA. 2008;300(6):711-719.
13. Halbauer JD, Ashford JW, Zeitzer JM, Adamson MM, Lew HL, Yesavage JA. Neuropsychiatric diagnosis and management of chronic sequelae of war-related mild to moderate traumatic brain injury. J Rehabil Res Dev. 2009;46(6):757-796.
14. Romesser J, Shen S, Reblin M, et al. A preliminary study of the effect of a diagnosis of concussion on PTSD symptoms and other psychiatric variables at the time of treatment seeking among veterans. Mil Med. 2011;176(3):246-252.
15. Cicerone KD, Kalmar K. Persistent postconcussion syndrome: The structure of subjective complaints after mild traumatic brain injury. J Head Trauma Rehabil. 1995;10(3):1-17.
16. Weathers FW, Huska JA, Keane TM. PCL-C for DSM-IV. Boston, MA: National Center for PTSD–Behavioral Science Division; 1991.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision (DSM-IV-TR). 4th ed. Washington, DC: American Psychiatric Association; 2000.
18. Hanson JA, Haub MD, Walker JJ, Johnston DT, Goff BS, Dretsch MN. Attention deficit hyperactivity disorder subtypes and their relation to cognitive functioning, mood states, and combat stress symptomatology in deploying U.S. soldiers. Mil Med. 2012;177(6):655-662.
19. Visser SN, Danielson ML, Bitsko RH, et al. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003-2011. J Am Acad Child Adolesc Psychiatry. 2014;53(1):34-46.e2.
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Association; 2013.
21. Barkley, RA, Murphy KR, Fischer M. ADHD in Adults: What the Science Says. New York, NY: Guilford Press; 2008.
22. Barkley RA, Cox D. A review of driving risks and impairments associated with attention-deficit/hyperactivity disorder and the effects of stimulant medication on driving performance. J Safety Res. 2007;38(1):113-128.
23. Shelley-Tremblay JF, Rosén LA. Attention deficit hyperactivity disorder: An evolutionary perspective. J Genet Psychol. 1996;157(4):443-453.
24. Jensen PS, Mrazek D, Knapp PK, et al. Evolution and revolution in child psychiatry: ADHD as a disorder of adaptation. J Am Acad Child Adolesc Psychiatry. 1997;36(12):1672-1679.
Traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are considered the signature injuries in veterans of the military operations in Iraq and Afghanistan.1 In 2007, the VA implemented the Polytrauma System of Care (PSC) to provide comprehensive screening, evaluation, and treatment of these multifaceted injuries.2,3 The VA defined polytrauma as “two or more injuries to physical regions or organ systems, one of which may be life threatening, resulting in physical, cognitive, psychological, or psychosocial impairments and functional disability.”3 The VA intended the PSC to provide a national system of integrated care to meet the unique needs of these combat service members.
In addition to the comprehensive evaluation and treatment of traumatic injuries, a critical mission of the PSC is to facilitate the reintegration of injured combat veterans into their home communities. Optimal community reintegration requires that the clinician also assess premorbid comorbidities, which may affect postdeployment adjustments. Attention-deficit/hyperactivity disorder (ADHD), with an estimated adult prevalence of 4.4% in the U.S. and 2.5% to 3.4% worldwide, is a common disorder in the general adult population that often is associated with chronic social and vocational adjustment difficulties.4-6 The increasing recognition that this disorder often persists into adulthood is of significance to veterans, largely young and male, who have left military service and are reintegrating into college and community job settings.7 Despite growing interest in adult ADHD, little is known about its prevalence and correlates in the veteran population.
The prevalence of ADHD in the Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) veteran polytrauma population has not been adequately studied. Studies have found that combat veterans with or without confirmed TBI diagnosis commonly have similar overlapping symptoms, such as memory problems, difficulty concentrating, poor attention, and sleep problems associated with other comorbidities such as pain, PTSD, ADHD, and other mental health diagnoses.8-14 Increased awareness of various clinical variables would enhance understanding of the population characteristics and specific needs for education and management.
Related: Preparing the Military Health System for the 21st Century
To begin to address the lack of information about ADHD in the VA polytrauma population, this study aimed to (1) identify the prevalence of ADHD in veterans referred to the Clement J. Zablocki (CJZ) VAMC Polytrauma Clinic (PC) in Milwaukee, Wisconsin; (2) describe demographic characteristics of polytrauma veterans with ADHD; (3) determine the comorbidity relationship between ADHD and TBI, PTSD, depression and anxiety disorders, and substance abuse; and (4) determine whether individuals with ADHD compared with those without ADHD report more physical and emotional symptomatic distress with particular attention given to reports of pain, headaches, and problems with attention and concentration, memory, and sleep.
Methods
The study population consisted of 690 OEF/OIF/OND soldiers and veterans who received a comprehensive TBI evaluation in the CJZVAMC PC from January 1, 2008, to December 31, 2012. Referrals to the PC were made by primary care physicians (PCPs) when OEF/OIF/OND veterans or service members enrolled at a VA facility for health care or transferred their care from another VA facility.
Either a prior diagnosis of TBI established by a qualified provider or positive responses to a 4-question screening tool for TBI prompted a referral to the PC. The 4 questions sought to establish (1) events that may increase risk of TBIs; (2) immediate symptoms following the event; (3) new or worsening symptoms following the event; and (4) current symptoms.1 Referrals to the clinic most commonly came from PCPs at the CJZVAMC and its associated community-based outpatient clinics but occasionally came from mental health service providers.
Study Design
The CJZVAMC Institutional Review Board approved this study. A population database was developed from a review of medical records, clinical interviews of patients, and completion of standard intake forms during the veterans’ initial evaluations in the CJZVAMC PC. The database aimed to abstract patient information relevant for understanding and treating the population seen in the clinic. The database contained information related to demographics, injury parameters, neurobehavioral and PTSD symptoms, past and current mental health disorders, substance abuse history, pain symptoms, and developmental history (eg, ADHD, learning disability).
Related: First Brain Wave Test to Diagnose ADHD
Prior to the PC intake interview, each veteran completed a packet of preclinic questionnaires that included information concerning deployment-related injury exposure and history; the 22-item Neurobehavioral Symptom Inventory (NSI), which assessed physical, cognitive, and emotional symptoms; current pain symptoms; and the Posttraumatic Stress Disorder Checklist-Civilian Version (PCLC).15,16 Intake interviews in the CJZVAMC PC were typically conducted with a minimum of 2 specialties present (physical medicine/rehabilitation and neuropsychology) and occasionally as many as 4 specialties present (also including health psychology and social work). Data collection and abstraction for the database were derived by all specialties present and assisted by the polytrauma program technician.
Diagnoses
The diagnosis of ADHD in a veteran was established through 1 of 2 methods: (1) report of a developmental history of behavioral adjustment difficulties consistent with ADHD that was coupled with formal psychiatric diagnosis and recommended treatment of ADHD in childhood; or (2) current diagnosis of ADHD as identified in the veteran’s active problem list. In most cases of report of developmental diagnosis, the veteran reported having been diagnosed and having received treatment with a stimulant medication for a period of time. In a few cases, the veteran reported having been diagnosed and stimulant medication was recommended, but the veteran’s parents declined the pharmacologic treatment in favor of behavioral treatment strategies.
In cases of current diagnosis, Diagnostic and Statistical Manual of Mental Disorders, Text Revision, 4th Edition (DSM-IV-TR), criteria were applied and supported by formal clinical examinations for ADHD conducted by psychologists, psychiatrists or neuropsychologists, or through VA disability (Compensation and Pension) evaluations where an issue related to ADHD diagnosis was raised.17 There was considerable overlap between these 2 diagnostic criteria (ie, through report of developmental history of diagnosis or formal adult evaluation) with 93% of cases being positive on both diagnostic methods.
Other comorbid psychiatric (eg, depression, anxiety, PTSD, substance abuse) and medical (eg, headache, pain) conditions also were abstracted from the veteran’s medical records at the time of the intake evaluation. Documentation of these conditions was derived from the veteran’s problem list and clinical notes that identified the condition as a diagnostic conclusion or focus of treatment. The comorbid conditions were not otherwise independently documented. Many veterans were taking psychotropic medications for mood, sleep, or chronic pain problems at the time of evaluation in the PC; however, use of medication and their effects were not systematically evaluated.
Statistical Analysis
In addition to documentation of the population prevalence for ADHD, analysis for disproportionate prevalence of comorbid conditions in individuals with ADHD compared with those without ADHD was done through the use of the chi-square test and/or Fisher exact test. For continuous variables, t tests were used to compare individuals with ADHD with individuals without ADHD. To control family-wise type I error to a P value of .05, a false discovery rate (FDR) was applied to studies of demographics, comorbidities, and ratings of symptomatic distress.
Results
The general population characteristics of the 690 veterans and soldiers are summarized in Table 1. The sample was predominantly male (96%), white (88%), and ranged in age from 22 to 55 years with a mean of 28 years. Active-duty service members and reservists from the U.S. Army, Marines, Navy, and Air Force were represented, but most were Army veterans (72%). Most (63%) had a high school education. About two-thirds of the veterans had a single deployment, and the remaining had multiple deployments.
The TBI clinic evaluations found that 58% of the patients had ≥ 1 TBI during their deployments, almost exclusively mild in severity. Seventy-three patients met study criteria for ADHD: 69 with an identified history of diagnosis in childhood and 68 with a current diagnosis, with 93% overlap of these groups. Table 2 provides a breakdown of demographic characteristics, comorbidities, and symptomatic distress in veterans with ADHD compared with those without the diagnosis.
Demographic Characteristics
Veterans with ADHD were found to be slightly younger (2.3 years younger, P = .003) and to have less education (greater frequency of less than high school and high school only, P = .003) compared with those who did not have the diagnosis. No significant group differences in sex, employment/school status, marital status, or number of deployments were identified in veterans with ADHD compared with non-ADHD veterans. Individuals with ADHD did not experience more physical, emotional, or sexual abuse as children than did their non-ADHD counterparts. The prevalence of TBI during deployment was similar in veterans with ADHD compared with that of non-ADHD veterans. There was a trend for veterans with ADHD to have more TBIs prior to military service than in non-ADHD veterans; however, this trend did not reach statistical significance (P = .188).
Comorbidities
After application of the FDR threshold, veterans with ADHD did not show a disproportionate prevalence of mental health diagnoses (eg, PTSD, depression and anxiety disorders, or substance abuse). There was a nonsignificant trend for more veterans with ADHD to report pain during the previous 30 days (P = .035) and more issues with substance abuse (P = .10) than for non-ADHD veterans, but these trends did not meet the FDR threshold of < .05.
Symptomatic Distress
Veterans with ADHD did not report significantly greater levels of distress on either the NSI or the PCLC survey compared with non-ADHD veterans.Not surprisingly, when select symptoms were investigated, veterans with ADHD reported more problems with attention and concentration than for non-ADHD veterans (P = .015). No group differences were identified for sleep issues, headaches, or memory, although there was a trend for the latter (P = .14).
Discussion
In this study, there was a 10.6% prevalence of ADHD in 690 OEF/OIF/OND combat veterans. This rate is considerably higher than estimates of prevalence of ADHD in adults (4.4%) made from a nationwide survey and worldwide prevalence estimates of 2.5% to 3.5%.4-6 Still, the current prevalence finding is consistent with a recent finding of ADHD in previous deploying U.S. soldiers military samples (10.4%).18 The high prevalence of ADHD in the current clinic population argues for increased provider awareness of this condition as a possible factor in postdeployment adjustment assessments.
Changes in prevalence estimates of ADHD may represent increased awareness of the condition over this interval of time, professional drift in the application of diagnostic criteria, or changes in societal attitudes about acceptability in pursuing treatment for the condition. For example, in nationwide surveys in 2003, 2007, and 2011, the CDC identified an increase from 7.8% to 9.5% to 11%, respectively, in diagnoses of ADHD in childhood.19 Also, considering that the current sample was predominantly male and the prevalence of ADHD in males is higher than in females, one might expect a higher ADHD prevalence rate in this study than that in the general population. In this regard, the ADHD prevalence rate in males remains comparable to that estimated by recent CDC survey data.19
When estimating ADHD population prevalence in the future, it is worth noting that a change in the diagnostic criteria for ADHD has occurred in DSM-5. Specifically, the age at which critical symptoms must be present to make the diagnosis of ADHD has been increased from age 7 years to age 12 years, and the number of critical symptoms to meet hyperactivity-impulsivity criteria has been lowered from 6 to 5 in older adolescents and adults.20 These changes in the diagnostic criteria for ADHD will have the net effect of increasing estimates of prevalence of ADHD.
The 73 individuals with an ADHD diagnoses in this study were found to have less education and be slightly younger than were the veterans who did not have an ADHD diagnosis. This finding is not unexpected, as individuals with ADHD are known to struggle in school and often drop out of high school and pursue alternative means of getting an equivalency degree or certification.21 Early departure from high school can be followed by earlier enlistment in the military. Prior studies by Krauss and colleagues found similar findings in an ADHD study of military recruits (ie, they were less likely to have education beyond a high school degree).7
ADHD and TBI
Given problems with attention, impulsivity, and high levels of aggressive behaviors associated with ADHD, individuals with ADHD have been found to be at higher risk for accidental injuries, including TBI, than are individuals without ADHD.21,22 Thus, soldiers with ADHD may be at greater risk for TBI during their time in the military. In the current sample, although veterans with ADHD showed a trend toward having more TBIs prior to joining the military relative to non-ADHD veterans, the veterans with ADHD had a similar rate of TBIs during their time in the military relative to non-ADHD veterans.
Although individuals with ADHD are reported to have a higher prevalence of mental health issues than does the general public, this was not evident in the current sample.21 Veterans with ADHD in this study did not have a disproportionate prevalence of PTSD, depression, anxiety, or substance abuse.
There was a nonsignificant trend for more individuals with an ADHD diagnosis compared with those without the diagnosis to report experiencing pain during the 30 days prior to their evaluation in the PC. Although not statistically significant, this finding would not be unexpected, in that individuals with ADHD are known to show less tolerance for frustration relative to that of the general population.21 In the current study, reports of pain in the ADHD group correlated with reports of being irritable and easily annoyed (r = .27, P = .024), but no correlation was observed with reports of poor frustration tolerance (r = .04, P = .74). Still, of note, > 90% of the OEF/OIF/OND veterans in this study, regardless of their ADHD diagnosis, reported pain symptoms of some type. The high prevalence of pain symptoms in this sample is consistent with a previous study that found pain to be one of the most common problems in polytrauma patients.10
Related: Civilian Stress Compounds Service-Related Stress
Not surprisingly, as shown in Table 2, veterans with ADHD compared with those without the diagnosis reported more problems with attention and concentration. The report of more attentional problems is seemingly not accounted for by group differences in reports of pain in general, headaches, sleep disturbance, or memory problems.
Study Strengths
A large sample of veterans constituted this study, and the data were gathered in consecutive referrals to the CJZVAMC PC over a 5-year period. Also, information on a number of comorbidities were captured simultaneously with the polytrauma and ADHD diagnoses, allowing much greater ability to investigate the interaction of multiple comorbidities as well as lingering reports of symptoms following discharge from active military service.
In these authors’ experience, veterans with ADHD benefit substantially from structured treatment interventions that are focused on developing compensatory skills for their problems with attention and impulsivity. Individuals with ADHD typically have a greater need for assistance with planning and organizing, making decisions, problem solving, and regulating their attention and affect. Individuals with ADHD may benefit from treatment strategies focused on ADHD behaviors in conjunction with traditional treatment strategies frequently used in the PC. These strategies include increased case management, medication trials, education regarding ADHD, vocational assistance, and consideration of both the school and work accommodations.
Studies have shown that treatments with stimulants improve functioning and reduce depression and substance use.21 In this study, < 5% of individuals with ADHD were taking stimulants at the time they were initially assessed in the PC, whereas the majority were taking stimulants after being referred for ADHD evaluation. Thus, identification of veterans with ADHD has clinical relevance in understanding the specific needs that guide development of individualized treatment plans to promote successful community reintegration.
Limitations
One limitation of the study is the lack of available medical records of historical ADHD diagnoses prior to military service. Also, although DSM-IV criteria for ADHD were operational in the psychodiagnostic clinics for these subjects, because the polytrauma study team did not conduct the evaluations in this sample, uniform diagnostic standards may not have been consistently applied when establishing the ADHD diagnosis. There was a 93% agreement between the 2 methods of diagnosis (ie, report of developmental diagnosis or positive adult evaluation), suggesting that diagnostic precision for ADHD in this study was reasonably accurate.
Another significant limitation of this study, apart from establishing medical and psychiatric status at the time of the initial referral to the PC, is the omission of functional outcome assessments regarding success of polytrauma treatment initiatives or ultimate community reintegration of successful psychosocial participation or academic and vocational achievements. Future longitudinal outcome studies are needed to determine whether ADHD has a significant impact on clinical outcomes. Of interest, pain was an overwhelmingly common factor (> 90%) for the military population studied at this site. Some degree of disturbance in attentional capacities is common in patients with chronic pain, which may aggravate ADHD symptoms and vice versa. Further investigations are needed to determine the potential functional impact of pain, including use of pain and psychotropic medications, on ADHD symptoms and the combined effect of these symptoms on overall outcome from rehabilitation and reintegration efforts.
Although these findings suggest that polytrauma veterans with ADHD do not have more psychiatric or physical comorbidities than do veterans without ADHD, it is premature to conclude that community reintegration can be optimally managed in the same way for both groups. Community reintegration of individuals with ADHD will likely be challenging, as these individuals often have struggled with functioning in their communities prior to their military service.
Studies of adult ADHD in the U.S. and in other countries have found that it is often associated with substantial impairment in managing the demands of functioning as an adult in society.4 Although some theorists have speculated that symptoms of ADHD may have been evolutionarily adaptive to survival in select environments (eg, predatory hunting environments), there is no clear evidence to support such adaptive benefits of the symptom in modern combat environments.23,24 Symptoms of ADHD are typically maladaptive to soldiers transitioning to civilian lives.
Conclusions
This investigation described the demographic and clinical characteristics of OEF/OIF/OND veterans referred for evaluation of TBI to the CJZVAMC PC during 5 years of operation from 2008 through 2012. The aim was to increase provider awareness of possible important variables that may influence recovery and community reintegration. This study may help to form the foundation for future lines of research into variables such as ADHD that may influence outcomes of rehabilitation and reintegration interventions.
To better understand the treatment needs of young veterans returning home from the wars in Iraq and Afghanistan, this study sought to identify the prevalence rate of ADHD, a condition known to complicate community adjustment. In this study, there was a 10.6% prevalence of ADHD among the 690 OEF/OIF/OND combat veterans seen over the 5-year period in the CJZVAMC PC, which is substantially higher than prevalence estimates in the U.S. general population but similar to estimates in previous military samples.
Compared with veterans who did not have ADHD, veterans with ADHD were younger, less well educated, and reported more problems with attention and concentration but did not have a greater incidence of military TBI or mental health comorbidities. The high prevalence of ADHD in this group argues for greater awareness of this clinical variable and development of intervention programs tailored to the specific skill deficiencies found in the condition, which can be included as part of the comprehensive treatment interventions.
Veterans with ADHD treated in the PC seem to benefit from structured treatment plans and education to promote self-awareness and veteran-centered self-management for effective symptom reduction and coping strategies. Development of effective integrated treatment options with a focus on educational and vocational resources and assistance could facilitate successful community reintegration. Future studies are needed to further assess outcomes of community reintegration, including academic and occupational outcomes, in this population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are considered the signature injuries in veterans of the military operations in Iraq and Afghanistan.1 In 2007, the VA implemented the Polytrauma System of Care (PSC) to provide comprehensive screening, evaluation, and treatment of these multifaceted injuries.2,3 The VA defined polytrauma as “two or more injuries to physical regions or organ systems, one of which may be life threatening, resulting in physical, cognitive, psychological, or psychosocial impairments and functional disability.”3 The VA intended the PSC to provide a national system of integrated care to meet the unique needs of these combat service members.
In addition to the comprehensive evaluation and treatment of traumatic injuries, a critical mission of the PSC is to facilitate the reintegration of injured combat veterans into their home communities. Optimal community reintegration requires that the clinician also assess premorbid comorbidities, which may affect postdeployment adjustments. Attention-deficit/hyperactivity disorder (ADHD), with an estimated adult prevalence of 4.4% in the U.S. and 2.5% to 3.4% worldwide, is a common disorder in the general adult population that often is associated with chronic social and vocational adjustment difficulties.4-6 The increasing recognition that this disorder often persists into adulthood is of significance to veterans, largely young and male, who have left military service and are reintegrating into college and community job settings.7 Despite growing interest in adult ADHD, little is known about its prevalence and correlates in the veteran population.
The prevalence of ADHD in the Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) veteran polytrauma population has not been adequately studied. Studies have found that combat veterans with or without confirmed TBI diagnosis commonly have similar overlapping symptoms, such as memory problems, difficulty concentrating, poor attention, and sleep problems associated with other comorbidities such as pain, PTSD, ADHD, and other mental health diagnoses.8-14 Increased awareness of various clinical variables would enhance understanding of the population characteristics and specific needs for education and management.
Related: Preparing the Military Health System for the 21st Century
To begin to address the lack of information about ADHD in the VA polytrauma population, this study aimed to (1) identify the prevalence of ADHD in veterans referred to the Clement J. Zablocki (CJZ) VAMC Polytrauma Clinic (PC) in Milwaukee, Wisconsin; (2) describe demographic characteristics of polytrauma veterans with ADHD; (3) determine the comorbidity relationship between ADHD and TBI, PTSD, depression and anxiety disorders, and substance abuse; and (4) determine whether individuals with ADHD compared with those without ADHD report more physical and emotional symptomatic distress with particular attention given to reports of pain, headaches, and problems with attention and concentration, memory, and sleep.
Methods
The study population consisted of 690 OEF/OIF/OND soldiers and veterans who received a comprehensive TBI evaluation in the CJZVAMC PC from January 1, 2008, to December 31, 2012. Referrals to the PC were made by primary care physicians (PCPs) when OEF/OIF/OND veterans or service members enrolled at a VA facility for health care or transferred their care from another VA facility.
Either a prior diagnosis of TBI established by a qualified provider or positive responses to a 4-question screening tool for TBI prompted a referral to the PC. The 4 questions sought to establish (1) events that may increase risk of TBIs; (2) immediate symptoms following the event; (3) new or worsening symptoms following the event; and (4) current symptoms.1 Referrals to the clinic most commonly came from PCPs at the CJZVAMC and its associated community-based outpatient clinics but occasionally came from mental health service providers.
Study Design
The CJZVAMC Institutional Review Board approved this study. A population database was developed from a review of medical records, clinical interviews of patients, and completion of standard intake forms during the veterans’ initial evaluations in the CJZVAMC PC. The database aimed to abstract patient information relevant for understanding and treating the population seen in the clinic. The database contained information related to demographics, injury parameters, neurobehavioral and PTSD symptoms, past and current mental health disorders, substance abuse history, pain symptoms, and developmental history (eg, ADHD, learning disability).
Related: First Brain Wave Test to Diagnose ADHD
Prior to the PC intake interview, each veteran completed a packet of preclinic questionnaires that included information concerning deployment-related injury exposure and history; the 22-item Neurobehavioral Symptom Inventory (NSI), which assessed physical, cognitive, and emotional symptoms; current pain symptoms; and the Posttraumatic Stress Disorder Checklist-Civilian Version (PCLC).15,16 Intake interviews in the CJZVAMC PC were typically conducted with a minimum of 2 specialties present (physical medicine/rehabilitation and neuropsychology) and occasionally as many as 4 specialties present (also including health psychology and social work). Data collection and abstraction for the database were derived by all specialties present and assisted by the polytrauma program technician.
Diagnoses
The diagnosis of ADHD in a veteran was established through 1 of 2 methods: (1) report of a developmental history of behavioral adjustment difficulties consistent with ADHD that was coupled with formal psychiatric diagnosis and recommended treatment of ADHD in childhood; or (2) current diagnosis of ADHD as identified in the veteran’s active problem list. In most cases of report of developmental diagnosis, the veteran reported having been diagnosed and having received treatment with a stimulant medication for a period of time. In a few cases, the veteran reported having been diagnosed and stimulant medication was recommended, but the veteran’s parents declined the pharmacologic treatment in favor of behavioral treatment strategies.
In cases of current diagnosis, Diagnostic and Statistical Manual of Mental Disorders, Text Revision, 4th Edition (DSM-IV-TR), criteria were applied and supported by formal clinical examinations for ADHD conducted by psychologists, psychiatrists or neuropsychologists, or through VA disability (Compensation and Pension) evaluations where an issue related to ADHD diagnosis was raised.17 There was considerable overlap between these 2 diagnostic criteria (ie, through report of developmental history of diagnosis or formal adult evaluation) with 93% of cases being positive on both diagnostic methods.
Other comorbid psychiatric (eg, depression, anxiety, PTSD, substance abuse) and medical (eg, headache, pain) conditions also were abstracted from the veteran’s medical records at the time of the intake evaluation. Documentation of these conditions was derived from the veteran’s problem list and clinical notes that identified the condition as a diagnostic conclusion or focus of treatment. The comorbid conditions were not otherwise independently documented. Many veterans were taking psychotropic medications for mood, sleep, or chronic pain problems at the time of evaluation in the PC; however, use of medication and their effects were not systematically evaluated.
Statistical Analysis
In addition to documentation of the population prevalence for ADHD, analysis for disproportionate prevalence of comorbid conditions in individuals with ADHD compared with those without ADHD was done through the use of the chi-square test and/or Fisher exact test. For continuous variables, t tests were used to compare individuals with ADHD with individuals without ADHD. To control family-wise type I error to a P value of .05, a false discovery rate (FDR) was applied to studies of demographics, comorbidities, and ratings of symptomatic distress.
Results
The general population characteristics of the 690 veterans and soldiers are summarized in Table 1. The sample was predominantly male (96%), white (88%), and ranged in age from 22 to 55 years with a mean of 28 years. Active-duty service members and reservists from the U.S. Army, Marines, Navy, and Air Force were represented, but most were Army veterans (72%). Most (63%) had a high school education. About two-thirds of the veterans had a single deployment, and the remaining had multiple deployments.
The TBI clinic evaluations found that 58% of the patients had ≥ 1 TBI during their deployments, almost exclusively mild in severity. Seventy-three patients met study criteria for ADHD: 69 with an identified history of diagnosis in childhood and 68 with a current diagnosis, with 93% overlap of these groups. Table 2 provides a breakdown of demographic characteristics, comorbidities, and symptomatic distress in veterans with ADHD compared with those without the diagnosis.
Demographic Characteristics
Veterans with ADHD were found to be slightly younger (2.3 years younger, P = .003) and to have less education (greater frequency of less than high school and high school only, P = .003) compared with those who did not have the diagnosis. No significant group differences in sex, employment/school status, marital status, or number of deployments were identified in veterans with ADHD compared with non-ADHD veterans. Individuals with ADHD did not experience more physical, emotional, or sexual abuse as children than did their non-ADHD counterparts. The prevalence of TBI during deployment was similar in veterans with ADHD compared with that of non-ADHD veterans. There was a trend for veterans with ADHD to have more TBIs prior to military service than in non-ADHD veterans; however, this trend did not reach statistical significance (P = .188).
Comorbidities
After application of the FDR threshold, veterans with ADHD did not show a disproportionate prevalence of mental health diagnoses (eg, PTSD, depression and anxiety disorders, or substance abuse). There was a nonsignificant trend for more veterans with ADHD to report pain during the previous 30 days (P = .035) and more issues with substance abuse (P = .10) than for non-ADHD veterans, but these trends did not meet the FDR threshold of < .05.
Symptomatic Distress
Veterans with ADHD did not report significantly greater levels of distress on either the NSI or the PCLC survey compared with non-ADHD veterans.Not surprisingly, when select symptoms were investigated, veterans with ADHD reported more problems with attention and concentration than for non-ADHD veterans (P = .015). No group differences were identified for sleep issues, headaches, or memory, although there was a trend for the latter (P = .14).
Discussion
In this study, there was a 10.6% prevalence of ADHD in 690 OEF/OIF/OND combat veterans. This rate is considerably higher than estimates of prevalence of ADHD in adults (4.4%) made from a nationwide survey and worldwide prevalence estimates of 2.5% to 3.5%.4-6 Still, the current prevalence finding is consistent with a recent finding of ADHD in previous deploying U.S. soldiers military samples (10.4%).18 The high prevalence of ADHD in the current clinic population argues for increased provider awareness of this condition as a possible factor in postdeployment adjustment assessments.
Changes in prevalence estimates of ADHD may represent increased awareness of the condition over this interval of time, professional drift in the application of diagnostic criteria, or changes in societal attitudes about acceptability in pursuing treatment for the condition. For example, in nationwide surveys in 2003, 2007, and 2011, the CDC identified an increase from 7.8% to 9.5% to 11%, respectively, in diagnoses of ADHD in childhood.19 Also, considering that the current sample was predominantly male and the prevalence of ADHD in males is higher than in females, one might expect a higher ADHD prevalence rate in this study than that in the general population. In this regard, the ADHD prevalence rate in males remains comparable to that estimated by recent CDC survey data.19
When estimating ADHD population prevalence in the future, it is worth noting that a change in the diagnostic criteria for ADHD has occurred in DSM-5. Specifically, the age at which critical symptoms must be present to make the diagnosis of ADHD has been increased from age 7 years to age 12 years, and the number of critical symptoms to meet hyperactivity-impulsivity criteria has been lowered from 6 to 5 in older adolescents and adults.20 These changes in the diagnostic criteria for ADHD will have the net effect of increasing estimates of prevalence of ADHD.
The 73 individuals with an ADHD diagnoses in this study were found to have less education and be slightly younger than were the veterans who did not have an ADHD diagnosis. This finding is not unexpected, as individuals with ADHD are known to struggle in school and often drop out of high school and pursue alternative means of getting an equivalency degree or certification.21 Early departure from high school can be followed by earlier enlistment in the military. Prior studies by Krauss and colleagues found similar findings in an ADHD study of military recruits (ie, they were less likely to have education beyond a high school degree).7
ADHD and TBI
Given problems with attention, impulsivity, and high levels of aggressive behaviors associated with ADHD, individuals with ADHD have been found to be at higher risk for accidental injuries, including TBI, than are individuals without ADHD.21,22 Thus, soldiers with ADHD may be at greater risk for TBI during their time in the military. In the current sample, although veterans with ADHD showed a trend toward having more TBIs prior to joining the military relative to non-ADHD veterans, the veterans with ADHD had a similar rate of TBIs during their time in the military relative to non-ADHD veterans.
Although individuals with ADHD are reported to have a higher prevalence of mental health issues than does the general public, this was not evident in the current sample.21 Veterans with ADHD in this study did not have a disproportionate prevalence of PTSD, depression, anxiety, or substance abuse.
There was a nonsignificant trend for more individuals with an ADHD diagnosis compared with those without the diagnosis to report experiencing pain during the 30 days prior to their evaluation in the PC. Although not statistically significant, this finding would not be unexpected, in that individuals with ADHD are known to show less tolerance for frustration relative to that of the general population.21 In the current study, reports of pain in the ADHD group correlated with reports of being irritable and easily annoyed (r = .27, P = .024), but no correlation was observed with reports of poor frustration tolerance (r = .04, P = .74). Still, of note, > 90% of the OEF/OIF/OND veterans in this study, regardless of their ADHD diagnosis, reported pain symptoms of some type. The high prevalence of pain symptoms in this sample is consistent with a previous study that found pain to be one of the most common problems in polytrauma patients.10
Related: Civilian Stress Compounds Service-Related Stress
Not surprisingly, as shown in Table 2, veterans with ADHD compared with those without the diagnosis reported more problems with attention and concentration. The report of more attentional problems is seemingly not accounted for by group differences in reports of pain in general, headaches, sleep disturbance, or memory problems.
Study Strengths
A large sample of veterans constituted this study, and the data were gathered in consecutive referrals to the CJZVAMC PC over a 5-year period. Also, information on a number of comorbidities were captured simultaneously with the polytrauma and ADHD diagnoses, allowing much greater ability to investigate the interaction of multiple comorbidities as well as lingering reports of symptoms following discharge from active military service.
In these authors’ experience, veterans with ADHD benefit substantially from structured treatment interventions that are focused on developing compensatory skills for their problems with attention and impulsivity. Individuals with ADHD typically have a greater need for assistance with planning and organizing, making decisions, problem solving, and regulating their attention and affect. Individuals with ADHD may benefit from treatment strategies focused on ADHD behaviors in conjunction with traditional treatment strategies frequently used in the PC. These strategies include increased case management, medication trials, education regarding ADHD, vocational assistance, and consideration of both the school and work accommodations.
Studies have shown that treatments with stimulants improve functioning and reduce depression and substance use.21 In this study, < 5% of individuals with ADHD were taking stimulants at the time they were initially assessed in the PC, whereas the majority were taking stimulants after being referred for ADHD evaluation. Thus, identification of veterans with ADHD has clinical relevance in understanding the specific needs that guide development of individualized treatment plans to promote successful community reintegration.
Limitations
One limitation of the study is the lack of available medical records of historical ADHD diagnoses prior to military service. Also, although DSM-IV criteria for ADHD were operational in the psychodiagnostic clinics for these subjects, because the polytrauma study team did not conduct the evaluations in this sample, uniform diagnostic standards may not have been consistently applied when establishing the ADHD diagnosis. There was a 93% agreement between the 2 methods of diagnosis (ie, report of developmental diagnosis or positive adult evaluation), suggesting that diagnostic precision for ADHD in this study was reasonably accurate.
Another significant limitation of this study, apart from establishing medical and psychiatric status at the time of the initial referral to the PC, is the omission of functional outcome assessments regarding success of polytrauma treatment initiatives or ultimate community reintegration of successful psychosocial participation or academic and vocational achievements. Future longitudinal outcome studies are needed to determine whether ADHD has a significant impact on clinical outcomes. Of interest, pain was an overwhelmingly common factor (> 90%) for the military population studied at this site. Some degree of disturbance in attentional capacities is common in patients with chronic pain, which may aggravate ADHD symptoms and vice versa. Further investigations are needed to determine the potential functional impact of pain, including use of pain and psychotropic medications, on ADHD symptoms and the combined effect of these symptoms on overall outcome from rehabilitation and reintegration efforts.
Although these findings suggest that polytrauma veterans with ADHD do not have more psychiatric or physical comorbidities than do veterans without ADHD, it is premature to conclude that community reintegration can be optimally managed in the same way for both groups. Community reintegration of individuals with ADHD will likely be challenging, as these individuals often have struggled with functioning in their communities prior to their military service.
Studies of adult ADHD in the U.S. and in other countries have found that it is often associated with substantial impairment in managing the demands of functioning as an adult in society.4 Although some theorists have speculated that symptoms of ADHD may have been evolutionarily adaptive to survival in select environments (eg, predatory hunting environments), there is no clear evidence to support such adaptive benefits of the symptom in modern combat environments.23,24 Symptoms of ADHD are typically maladaptive to soldiers transitioning to civilian lives.
Conclusions
This investigation described the demographic and clinical characteristics of OEF/OIF/OND veterans referred for evaluation of TBI to the CJZVAMC PC during 5 years of operation from 2008 through 2012. The aim was to increase provider awareness of possible important variables that may influence recovery and community reintegration. This study may help to form the foundation for future lines of research into variables such as ADHD that may influence outcomes of rehabilitation and reintegration interventions.
To better understand the treatment needs of young veterans returning home from the wars in Iraq and Afghanistan, this study sought to identify the prevalence rate of ADHD, a condition known to complicate community adjustment. In this study, there was a 10.6% prevalence of ADHD among the 690 OEF/OIF/OND combat veterans seen over the 5-year period in the CJZVAMC PC, which is substantially higher than prevalence estimates in the U.S. general population but similar to estimates in previous military samples.
Compared with veterans who did not have ADHD, veterans with ADHD were younger, less well educated, and reported more problems with attention and concentration but did not have a greater incidence of military TBI or mental health comorbidities. The high prevalence of ADHD in this group argues for greater awareness of this clinical variable and development of intervention programs tailored to the specific skill deficiencies found in the condition, which can be included as part of the comprehensive treatment interventions.
Veterans with ADHD treated in the PC seem to benefit from structured treatment plans and education to promote self-awareness and veteran-centered self-management for effective symptom reduction and coping strategies. Development of effective integrated treatment options with a focus on educational and vocational resources and assistance could facilitate successful community reintegration. Future studies are needed to further assess outcomes of community reintegration, including academic and occupational outcomes, in this population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358(5):453-463.
2. Screening and Evaluation of Possible Traumatic Brain Injury in Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) Veterans. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-012.
3. Polytrauma System of Care. Washington, DC: Dept of Veterans Affairs; 2013. VHA Handbook 1172.01.
4. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163(4):716-723.
5. Simon V, Czobor P, Bálint S, Mészáros A, Bitter I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. Br J Psychiatry. 2009;194(3):204-211.
6. Fayyad J, De Graaf R, Kessler R, et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry. 2007;190(5):402-409.
7. Krauss MR, Russell RK, Powers TE, Li Y. Accession standards for attention-deficit/hyperactivity disorder: A survival analysis of military recruits, 1995-2000. Mil Med. 2006;171(2):99-102.
8. Vanderploeg RD, Belanger HG, Horner RD, et al. Health outcomes associated with military deployment: Mild traumatic brain injury, blast, trauma, and combat associations in the Florida National Guard. Arch Phys Med Rehabil. 2012;93(11):1887-1895.
9. Theeler BJ, Flynn FG, Erickson JC. Headaches after concussion in US soldiers returning from Iraq or Afghanistan. Headache. 2010;50(8):1262-1272.
10. Sayer NA, Chiros CE, Sigford B, et al. Characteristics and rehabilitation outcomes among patients with blast and other injuries sustained during the Global War on Terror. Arch Phys Med Rehabil. 2008;89(1):163-170.
11. Sayer NA, Rettmann NA, Carlson KF, et al. Veterans with history of mild traumatic brain injury and posttraumatic stress disorder: Challenges from provider perspective. J Rehabil Res Dev. 2009;46(6):703-716.
12. Nampiaparampil DE. Prevalence of chronic pain after traumatic brain injury: A systematic review. JAMA. 2008;300(6):711-719.
13. Halbauer JD, Ashford JW, Zeitzer JM, Adamson MM, Lew HL, Yesavage JA. Neuropsychiatric diagnosis and management of chronic sequelae of war-related mild to moderate traumatic brain injury. J Rehabil Res Dev. 2009;46(6):757-796.
14. Romesser J, Shen S, Reblin M, et al. A preliminary study of the effect of a diagnosis of concussion on PTSD symptoms and other psychiatric variables at the time of treatment seeking among veterans. Mil Med. 2011;176(3):246-252.
15. Cicerone KD, Kalmar K. Persistent postconcussion syndrome: The structure of subjective complaints after mild traumatic brain injury. J Head Trauma Rehabil. 1995;10(3):1-17.
16. Weathers FW, Huska JA, Keane TM. PCL-C for DSM-IV. Boston, MA: National Center for PTSD–Behavioral Science Division; 1991.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision (DSM-IV-TR). 4th ed. Washington, DC: American Psychiatric Association; 2000.
18. Hanson JA, Haub MD, Walker JJ, Johnston DT, Goff BS, Dretsch MN. Attention deficit hyperactivity disorder subtypes and their relation to cognitive functioning, mood states, and combat stress symptomatology in deploying U.S. soldiers. Mil Med. 2012;177(6):655-662.
19. Visser SN, Danielson ML, Bitsko RH, et al. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003-2011. J Am Acad Child Adolesc Psychiatry. 2014;53(1):34-46.e2.
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Association; 2013.
21. Barkley, RA, Murphy KR, Fischer M. ADHD in Adults: What the Science Says. New York, NY: Guilford Press; 2008.
22. Barkley RA, Cox D. A review of driving risks and impairments associated with attention-deficit/hyperactivity disorder and the effects of stimulant medication on driving performance. J Safety Res. 2007;38(1):113-128.
23. Shelley-Tremblay JF, Rosén LA. Attention deficit hyperactivity disorder: An evolutionary perspective. J Genet Psychol. 1996;157(4):443-453.
24. Jensen PS, Mrazek D, Knapp PK, et al. Evolution and revolution in child psychiatry: ADHD as a disorder of adaptation. J Am Acad Child Adolesc Psychiatry. 1997;36(12):1672-1679.
1. Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358(5):453-463.
2. Screening and Evaluation of Possible Traumatic Brain Injury in Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) Veterans. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-012.
3. Polytrauma System of Care. Washington, DC: Dept of Veterans Affairs; 2013. VHA Handbook 1172.01.
4. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163(4):716-723.
5. Simon V, Czobor P, Bálint S, Mészáros A, Bitter I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. Br J Psychiatry. 2009;194(3):204-211.
6. Fayyad J, De Graaf R, Kessler R, et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry. 2007;190(5):402-409.
7. Krauss MR, Russell RK, Powers TE, Li Y. Accession standards for attention-deficit/hyperactivity disorder: A survival analysis of military recruits, 1995-2000. Mil Med. 2006;171(2):99-102.
8. Vanderploeg RD, Belanger HG, Horner RD, et al. Health outcomes associated with military deployment: Mild traumatic brain injury, blast, trauma, and combat associations in the Florida National Guard. Arch Phys Med Rehabil. 2012;93(11):1887-1895.
9. Theeler BJ, Flynn FG, Erickson JC. Headaches after concussion in US soldiers returning from Iraq or Afghanistan. Headache. 2010;50(8):1262-1272.
10. Sayer NA, Chiros CE, Sigford B, et al. Characteristics and rehabilitation outcomes among patients with blast and other injuries sustained during the Global War on Terror. Arch Phys Med Rehabil. 2008;89(1):163-170.
11. Sayer NA, Rettmann NA, Carlson KF, et al. Veterans with history of mild traumatic brain injury and posttraumatic stress disorder: Challenges from provider perspective. J Rehabil Res Dev. 2009;46(6):703-716.
12. Nampiaparampil DE. Prevalence of chronic pain after traumatic brain injury: A systematic review. JAMA. 2008;300(6):711-719.
13. Halbauer JD, Ashford JW, Zeitzer JM, Adamson MM, Lew HL, Yesavage JA. Neuropsychiatric diagnosis and management of chronic sequelae of war-related mild to moderate traumatic brain injury. J Rehabil Res Dev. 2009;46(6):757-796.
14. Romesser J, Shen S, Reblin M, et al. A preliminary study of the effect of a diagnosis of concussion on PTSD symptoms and other psychiatric variables at the time of treatment seeking among veterans. Mil Med. 2011;176(3):246-252.
15. Cicerone KD, Kalmar K. Persistent postconcussion syndrome: The structure of subjective complaints after mild traumatic brain injury. J Head Trauma Rehabil. 1995;10(3):1-17.
16. Weathers FW, Huska JA, Keane TM. PCL-C for DSM-IV. Boston, MA: National Center for PTSD–Behavioral Science Division; 1991.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision (DSM-IV-TR). 4th ed. Washington, DC: American Psychiatric Association; 2000.
18. Hanson JA, Haub MD, Walker JJ, Johnston DT, Goff BS, Dretsch MN. Attention deficit hyperactivity disorder subtypes and their relation to cognitive functioning, mood states, and combat stress symptomatology in deploying U.S. soldiers. Mil Med. 2012;177(6):655-662.
19. Visser SN, Danielson ML, Bitsko RH, et al. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003-2011. J Am Acad Child Adolesc Psychiatry. 2014;53(1):34-46.e2.
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Association; 2013.
21. Barkley, RA, Murphy KR, Fischer M. ADHD in Adults: What the Science Says. New York, NY: Guilford Press; 2008.
22. Barkley RA, Cox D. A review of driving risks and impairments associated with attention-deficit/hyperactivity disorder and the effects of stimulant medication on driving performance. J Safety Res. 2007;38(1):113-128.
23. Shelley-Tremblay JF, Rosén LA. Attention deficit hyperactivity disorder: An evolutionary perspective. J Genet Psychol. 1996;157(4):443-453.
24. Jensen PS, Mrazek D, Knapp PK, et al. Evolution and revolution in child psychiatry: ADHD as a disorder of adaptation. J Am Acad Child Adolesc Psychiatry. 1997;36(12):1672-1679.
Civilian Stress Compounds Service-Related Stress
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
The stresses of civilian life—job problems, divorce, money—can add to the burden when a service member is already under strain from deployment-related traumatic events, such as being wounded or sexually harassed. Those extramilitary stressors may make it more likely for reserve soldiers to abuse alcohol, say researchers from Columbia University in New York City; University of Michigan in Ann Arbor; Case Western Reserve University in Cleveland, and University of Toledo, both in Ohio.
The researchers surveyed 1,095 members of the Ohio Army National Guard who served mostly in Afghanistan and Iraq from June 2008 to February 2009. They wanted to find out the relative influence of both deployment-related trauma and civilian stress, including the influence of both or either on alcohol abuse.
Almost 60% of soldiers surveyed reported experiencing combat-related traumatic events; 13% of that group was abusing alcohol. Of the 17% who reported being sexually harassed, about 5% were abusing alcohol. Of the nearly 36% of respondents who also experienced civilian stressors, 7.1% were abusing alcohol. In a final model, only civilian stressors were associated with subsequent alcohol use disorder (AUD), independent of deployment-related traumatic events.
Of the respondents, 106 had experienced mental illness personally or in someone close to them, 156 had been through a divorce or breakup, and 105 had been unemployed for ≥ 3 months. While serving, 364 had encountered land mines, water mines, or booby traps; 573 had received hostile incoming fire; and 471 had been attacked by terrorists, insurgents, or civilians.
The civilian stressors found to be most closely associated with AUD were having a family member with a serious drug or alcohol problem (adjusted odds ratio [OR] 1.36; 95% CI, 0.96-1.94), being robbed or having the house broken into (adjusted OR, 1.48; 95% CI, 1.02-2.21), and having problems in getting access to adequate health care (adjusted OR, 1.97; 95% CI, 1.07-3.63). Having experienced sexual harassment was the most closely associated combat trauma.
It was clear to the researchers that the combination of deployment-related trauma and civilian stressors were associated with new onset of AUD. That could mean that adult-onset AUD constitutes a different phenotype from recurrent AUDs, the researchers say. They cite previous research that identified 2 “types” of people who abuse alcohol. One type has a later onset, has “greater malleability to the social environment,” uses alcohol to soothe anxiety, and has less severe alcohol dependence symptoms. The other type turns to alcohol earlier, may be genetically predisposed to alcohol abuse, uses alcohol for its euphoric effect, and has a chronic treatment history.
A consideration when evaluating the findings, the researchers say, is that the soldiers who were interviewed shortly after their deployment may have been misclassified because psychiatric symptoms tend to appear 3 to 4 months after deployment.
Source
Cerdá M, Richards C, Cohen GH, et al. Am J Prev Med. 2014;47(4):461-466.
doi: 10.1016/j.amepre.2014.06.015.
Telemedicine-based collaborative care benefits rural veterans with PTSD
U.S. military veterans living in rural areas who engage in evidence-based psychotherapy and telemedicine-based collaborative care can significantly increase their chances of improving outcomes related to posttraumatic stress disorder, according to a new study.
“Although psychotherapy and pharmacotherapy treatments for PTSD have proven to be efficacious in randomized clinical trials and have been disseminated widely by the [Veterans Health Administration], stigma and geographic barriers often prevent rural veterans from engaging in these evidence-based treatments,” says the study, published in JAMA (2014 Nov. 19 [doi.101001/jamapsychiatry.2014.1575]) and led by John C. Fortney, Ph.D., of the University of Washington’s department of psychiatry and behavioral sciences in Seattle, and his associates.
In a pragmatic, randomized effectiveness trial, Dr. Fortney and his associates recruited outpatients from 11 Department of Veterans Affairs (VA) community-based outpatient clinics (CBOCs) in predominantly rural areas of the United States over the course of 22 months. A total of 265 patients completed baseline interviews and randomization after meeting eligibility criteria, which consisted of meeting diagnostic standards for PTSD; having no medical history of schizophrenia, bipolar disorder, substance dependence, or hearing impairment; having a telephone; not having a life-threatening illness; and lacking capacity to consent.

The 265 subjects were randomized into one of two groups: those receiving usual care (UC), or those receiving the Telemedicine Outreach for PTSD (TOP) treatment developed by the investigators. Patients were mostly unemployed, middle-aged men with severe PTSD symptoms and “other mental health coexisting illnesses,” according to a press release.
Subjects in the UC group received certain health care services, such as psychotropic medications for PTSD prescribed by psychiatrists, evidence-based psychotherapy for PTSD delivered by psychologists or social workers, supportive PTSD-focused therapy delivered by psychologists or social workers (individual and group), and supportive therapy delivered by social workers (individual and group), among others. Subjects in the TOP group, however, received the attention of telephone nurse care managers, including PTSD symptom monitoring and medication regimen adherence monitoring and promotion. In addition, those in the TOP group received access to a telephone pharmacist and telepsychologist.
Subjects were enrolled in a series of 12 cognitive processing therapy sessions for the duration of the study, from Nov. 23, 2009, through Sept. 28, 2011, and attendance was taken at each session. After the sessions concluded, subjects were then followed up on for 12 months.
During that follow-up period after treatments ended, patients who received TOP had significantly larger decreases in Posttraumatic Diagnostic Scale (PDS) scores (from 35.0 to 29.1), compared with those from the UC group (from 33.5 to 32.1) at 6 months (beta = −3.81; P = .002) and 12 months (beta = −2.49; P = .04). At 12 months, TOP subjects also had significantly larger decreases in PDS scores (from 35.0 to 30.1), compared with those who received UC (from 33.5 to 29.1) .
Subjects who attended at least eight cognitive processing therapy sessions were more likely to improve their PDS scores (beta = −3.86 [95% confidence interval, −7.19 to −0.54]; P = .02). However, the authors noted that there were “no significant group differences in the number of PTSD medications prescribed and adherence to medication regimens” was not significant.
“This trial introduces a promising model for managing PTSD in a treatment-resistant population,” Dr. Fortney and his associates wrote. “Findings suggest that telemedicine-based collaborative care can successfully engage this population in evidence-based psychotherapy for PTSD, thereby improving clinical outcomes.”
Among the study limitations cited by the investigators is that the PDS was administered to assess PTSD, rather than the Clinician-Administered PTSD Scale, which is the reference standard.
The authors reported no relevant financial conflicts of interest.
U.S. military veterans living in rural areas who engage in evidence-based psychotherapy and telemedicine-based collaborative care can significantly increase their chances of improving outcomes related to posttraumatic stress disorder, according to a new study.
“Although psychotherapy and pharmacotherapy treatments for PTSD have proven to be efficacious in randomized clinical trials and have been disseminated widely by the [Veterans Health Administration], stigma and geographic barriers often prevent rural veterans from engaging in these evidence-based treatments,” says the study, published in JAMA (2014 Nov. 19 [doi.101001/jamapsychiatry.2014.1575]) and led by John C. Fortney, Ph.D., of the University of Washington’s department of psychiatry and behavioral sciences in Seattle, and his associates.
In a pragmatic, randomized effectiveness trial, Dr. Fortney and his associates recruited outpatients from 11 Department of Veterans Affairs (VA) community-based outpatient clinics (CBOCs) in predominantly rural areas of the United States over the course of 22 months. A total of 265 patients completed baseline interviews and randomization after meeting eligibility criteria, which consisted of meeting diagnostic standards for PTSD; having no medical history of schizophrenia, bipolar disorder, substance dependence, or hearing impairment; having a telephone; not having a life-threatening illness; and lacking capacity to consent.
The 265 subjects were randomized into one of two groups: those receiving usual care (UC), or those receiving the Telemedicine Outreach for PTSD (TOP) treatment developed by the investigators. Patients were mostly unemployed, middle-aged men with severe PTSD symptoms and “other mental health coexisting illnesses,” according to a press release.
Subjects in the UC group received certain health care services, such as psychotropic medications for PTSD prescribed by psychiatrists, evidence-based psychotherapy for PTSD delivered by psychologists or social workers, supportive PTSD-focused therapy delivered by psychologists or social workers (individual and group), and supportive therapy delivered by social workers (individual and group), among others. Subjects in the TOP group, however, received the attention of telephone nurse care managers, including PTSD symptom monitoring and medication regimen adherence monitoring and promotion. In addition, those in the TOP group received access to a telephone pharmacist and telepsychologist.
Subjects were enrolled in a series of 12 cognitive processing therapy sessions for the duration of the study, from Nov. 23, 2009, through Sept. 28, 2011, and attendance was taken at each session. After the sessions concluded, subjects were then followed up on for 12 months.
During that follow-up period after treatments ended, patients who received TOP had significantly larger decreases in Posttraumatic Diagnostic Scale (PDS) scores (from 35.0 to 29.1), compared with those from the UC group (from 33.5 to 32.1) at 6 months (beta = −3.81; P = .002) and 12 months (beta = −2.49; P = .04). At 12 months, TOP subjects also had significantly larger decreases in PDS scores (from 35.0 to 30.1), compared with those who received UC (from 33.5 to 29.1) .
Subjects who attended at least eight cognitive processing therapy sessions were more likely to improve their PDS scores (beta = −3.86 [95% confidence interval, −7.19 to −0.54]; P = .02). However, the authors noted that there were “no significant group differences in the number of PTSD medications prescribed and adherence to medication regimens” was not significant.
“This trial introduces a promising model for managing PTSD in a treatment-resistant population,” Dr. Fortney and his associates wrote. “Findings suggest that telemedicine-based collaborative care can successfully engage this population in evidence-based psychotherapy for PTSD, thereby improving clinical outcomes.”
Among the study limitations cited by the investigators is that the PDS was administered to assess PTSD, rather than the Clinician-Administered PTSD Scale, which is the reference standard.
The authors reported no relevant financial conflicts of interest.
U.S. military veterans living in rural areas who engage in evidence-based psychotherapy and telemedicine-based collaborative care can significantly increase their chances of improving outcomes related to posttraumatic stress disorder, according to a new study.
“Although psychotherapy and pharmacotherapy treatments for PTSD have proven to be efficacious in randomized clinical trials and have been disseminated widely by the [Veterans Health Administration], stigma and geographic barriers often prevent rural veterans from engaging in these evidence-based treatments,” says the study, published in JAMA (2014 Nov. 19 [doi.101001/jamapsychiatry.2014.1575]) and led by John C. Fortney, Ph.D., of the University of Washington’s department of psychiatry and behavioral sciences in Seattle, and his associates.
In a pragmatic, randomized effectiveness trial, Dr. Fortney and his associates recruited outpatients from 11 Department of Veterans Affairs (VA) community-based outpatient clinics (CBOCs) in predominantly rural areas of the United States over the course of 22 months. A total of 265 patients completed baseline interviews and randomization after meeting eligibility criteria, which consisted of meeting diagnostic standards for PTSD; having no medical history of schizophrenia, bipolar disorder, substance dependence, or hearing impairment; having a telephone; not having a life-threatening illness; and lacking capacity to consent.
The 265 subjects were randomized into one of two groups: those receiving usual care (UC), or those receiving the Telemedicine Outreach for PTSD (TOP) treatment developed by the investigators. Patients were mostly unemployed, middle-aged men with severe PTSD symptoms and “other mental health coexisting illnesses,” according to a press release.
Subjects in the UC group received certain health care services, such as psychotropic medications for PTSD prescribed by psychiatrists, evidence-based psychotherapy for PTSD delivered by psychologists or social workers, supportive PTSD-focused therapy delivered by psychologists or social workers (individual and group), and supportive therapy delivered by social workers (individual and group), among others. Subjects in the TOP group, however, received the attention of telephone nurse care managers, including PTSD symptom monitoring and medication regimen adherence monitoring and promotion. In addition, those in the TOP group received access to a telephone pharmacist and telepsychologist.
Subjects were enrolled in a series of 12 cognitive processing therapy sessions for the duration of the study, from Nov. 23, 2009, through Sept. 28, 2011, and attendance was taken at each session. After the sessions concluded, subjects were then followed up on for 12 months.
During that follow-up period after treatments ended, patients who received TOP had significantly larger decreases in Posttraumatic Diagnostic Scale (PDS) scores (from 35.0 to 29.1), compared with those from the UC group (from 33.5 to 32.1) at 6 months (beta = −3.81; P = .002) and 12 months (beta = −2.49; P = .04). At 12 months, TOP subjects also had significantly larger decreases in PDS scores (from 35.0 to 30.1), compared with those who received UC (from 33.5 to 29.1) .
Subjects who attended at least eight cognitive processing therapy sessions were more likely to improve their PDS scores (beta = −3.86 [95% confidence interval, −7.19 to −0.54]; P = .02). However, the authors noted that there were “no significant group differences in the number of PTSD medications prescribed and adherence to medication regimens” was not significant.
“This trial introduces a promising model for managing PTSD in a treatment-resistant population,” Dr. Fortney and his associates wrote. “Findings suggest that telemedicine-based collaborative care can successfully engage this population in evidence-based psychotherapy for PTSD, thereby improving clinical outcomes.”
Among the study limitations cited by the investigators is that the PDS was administered to assess PTSD, rather than the Clinician-Administered PTSD Scale, which is the reference standard.
The authors reported no relevant financial conflicts of interest.
FROM JAMA
Key clinical point: Collaborative care models can “encourage veterans to intiate and adhere to evidence-based psychotherapies for PTSD.”
Major finding: Veterans receiving Telemedicine Outreach for PTSD had significantly larger decreases in Posttraumatic Diagnostic Scale scores (from 35.0 to 29.1), compared with those receiving usual care (from 33.5 to 32.1) at 6 (beta = −3.81; P = .002) and 12 (beta = −2.49; P = .04) months.
Data source: A multisite pragmatic, randomized effectiveness trial developed by the Veterans Health Administration and the National Institute of Mental Health.
Disclosures: The authors reported no financial conflicts of interest.

Recovering From Military Sexual Trauma
Military sexual trauma (MST) refers to experiences of sexual assault or repeated, threatening sexual harassment experienced while on federal active duty or active duty for training. About 1 in 4 women and 1 in 100 men have reported MST to their VA doctors. However, these numbers do not account for those who have not sought health care for their MST experience or who have sought care for MST outside the VA.
Military sexual trauma is:
Military sexual trauma is the term VA uses to refer to sexual assault or sexual harassment that occurred while the veteran was in the military. A victim of MST may have been:
- Involved in sexual activity against his or her will, by physical force or nonphysical pressure. Nonphysical pressure includes threats of negative consequences for refusing to be sexually cooperative, or indirect promises of faster promotions or better treatment in exchange for sex.
- Unable to consent to sexual activities. This includes intoxication by alcohol or other substances.
Other experiences include sexual touching or grabbing, threatening or offensive remarks about a person’s body or sexual activities, as well as threatening and unwelcome sexual advances.
How do I know if I’m at risk?
Military sexual trauma can occur on or off base and while a service member—man or woman—is on or off duty. Those who commit sexual assault or sexual harassment can be men or women, military personnel or civilians, commanding officers or subordinates, strangers, friends, spouses, or intimate partners.
When do I need medical attention?
The VA reports sexual assault is more likely to result in symptoms of PTSD (posttraumatic stress disorder) than are most other types of trauma, including combat. You should seek medical attention from your primary care doctor, a mental health professional, or your VA facility’s MST Coordinator following a MST experience, especially if you experience any of the following symptoms:
- Depression
- Suicidal thoughts
- Feeling angry or irritable most of the time
- Strong emotional reactions
- Feeling emotionally numb
- Trouble falling or staying asleep
- Nightmares
- Trouble focusing
- Difficulty remembering things
- Substance abuse
- Trouble feeling safe or trusting others
- Feeling isolated or disconnected from others
- Headaches
- Gastrointestinal difficulties
- Sexual dysfunction
- Chronic pain
- Chronic fatigue
- Weight or eating problems
Survivors who are not formally diagnosed may still struggle in certain situations with emotional reactions, memories related to their experiences of MST, or other interpersonal issues.
How is MST treated?
Because MST is an experience, not a diagnosis, treatment needs may vary from patient to patient. However, VA provides free, confidential counseling and treatment to male and female veterans for mental and physical health conditions related to experiences of MST. It is important to note that treatment is available even if the MST incident was not reported at the time it happened.
Your doctor may recommend individual therapy, group therapy, or medication, depending on your symptoms. Therapies that may be used to treat MST include:
- Cognitive behavioral therapy. The main goal of this therapy is to help you change your thought patterns, which will help you change the emotions and behavior connected with the MST experience. A counselor might encourage you to reimagine your trauma repeatedly under controlled conditions—an approach called exposure therapy—as a way of learning to cope.
- Stress inoculation (in-ock-you-lay-shun) training. This therapy involves combining stress management strategies with stress-relieving techniques, such as muscle relaxation, breathing retraining, self-dialogue, and thought stopping.
- Group therapy. This therapy enables you to discuss your trauma with others who have had similar experiences.
- Inpatient therapy. Nationwide, there are programs that offer specialized sexual trauma treatment for veterans who need more intense treatment and support, including that for severe depression or substance abuse.
- Medication. If your MST experience resulted in PTSD, your doctor may prescribe medication to help control symptoms of anxiety or to help you sleep. Your doctor will monitor you closely for any possible adverse effects of these medications. It is also possible that an STD (sexually transmitted disease) was passed during the trauma, so your doctor may choose to screen you for an STD. If the test comes back positive, your doctor will prescribe the appropriate drug for treatment.
Services are designed to help veterans at all stages of their recovery, whether that is focusing on strategies for coping with emotions and memories or, for veterans who are ready, talking about their MST experiences in depth.
What can I do to cope?
When trauma survivors take direct action to cope with their stress reactions, they put themselves in a position of power. This is called active coping, which involves accepting the impact the trauma had on your life and taking direct action to make improvements.
It is important to remember that recovery is a process and takes time. Healing from trauma, including MST, does not happen all at once, and healing does not mean that you must forget the experience. Instead, it means you have less pain and fewer bad feelings when you think about the experience, and any associated symptoms will over time bother you less.
Discussing your trauma with other survivors in a controlled setting can help you learn that you are not alone or weak. In addition, surrounding yourself with people you can talk to about your MST experience may help you feel more understood. You may even choose to distract yourself with positive recreational or work activities.
When you experience unwanted or distressing memories, remind yourself that they are just memories, and talk about them with someone you trust. If you feel that the trauma is happening again, which is known as a flashback, keep your eyes open and remind yourself where you presently are and that the trauma happened in the past.
Although VA and DoD are working to put an end to MST, it is an ongoing problem that affects a large percentage of women and men who proudly serve in the armed forces. For information on how to access free VA services and to determine your eligibility in MST benefits, visit http://www.mentalhealth.va.gov/msthome.asp.
Military sexual trauma (MST) refers to experiences of sexual assault or repeated, threatening sexual harassment experienced while on federal active duty or active duty for training. About 1 in 4 women and 1 in 100 men have reported MST to their VA doctors. However, these numbers do not account for those who have not sought health care for their MST experience or who have sought care for MST outside the VA.
Military sexual trauma is:
Military sexual trauma is the term VA uses to refer to sexual assault or sexual harassment that occurred while the veteran was in the military. A victim of MST may have been:
- Involved in sexual activity against his or her will, by physical force or nonphysical pressure. Nonphysical pressure includes threats of negative consequences for refusing to be sexually cooperative, or indirect promises of faster promotions or better treatment in exchange for sex.
- Unable to consent to sexual activities. This includes intoxication by alcohol or other substances.
Other experiences include sexual touching or grabbing, threatening or offensive remarks about a person’s body or sexual activities, as well as threatening and unwelcome sexual advances.
How do I know if I’m at risk?
Military sexual trauma can occur on or off base and while a service member—man or woman—is on or off duty. Those who commit sexual assault or sexual harassment can be men or women, military personnel or civilians, commanding officers or subordinates, strangers, friends, spouses, or intimate partners.
When do I need medical attention?
The VA reports sexual assault is more likely to result in symptoms of PTSD (posttraumatic stress disorder) than are most other types of trauma, including combat. You should seek medical attention from your primary care doctor, a mental health professional, or your VA facility’s MST Coordinator following a MST experience, especially if you experience any of the following symptoms:
- Depression
- Suicidal thoughts
- Feeling angry or irritable most of the time
- Strong emotional reactions
- Feeling emotionally numb
- Trouble falling or staying asleep
- Nightmares
- Trouble focusing
- Difficulty remembering things
- Substance abuse
- Trouble feeling safe or trusting others
- Feeling isolated or disconnected from others
- Headaches
- Gastrointestinal difficulties
- Sexual dysfunction
- Chronic pain
- Chronic fatigue
- Weight or eating problems
Survivors who are not formally diagnosed may still struggle in certain situations with emotional reactions, memories related to their experiences of MST, or other interpersonal issues.
How is MST treated?
Because MST is an experience, not a diagnosis, treatment needs may vary from patient to patient. However, VA provides free, confidential counseling and treatment to male and female veterans for mental and physical health conditions related to experiences of MST. It is important to note that treatment is available even if the MST incident was not reported at the time it happened.
Your doctor may recommend individual therapy, group therapy, or medication, depending on your symptoms. Therapies that may be used to treat MST include:
- Cognitive behavioral therapy. The main goal of this therapy is to help you change your thought patterns, which will help you change the emotions and behavior connected with the MST experience. A counselor might encourage you to reimagine your trauma repeatedly under controlled conditions—an approach called exposure therapy—as a way of learning to cope.
- Stress inoculation (in-ock-you-lay-shun) training. This therapy involves combining stress management strategies with stress-relieving techniques, such as muscle relaxation, breathing retraining, self-dialogue, and thought stopping.
- Group therapy. This therapy enables you to discuss your trauma with others who have had similar experiences.
- Inpatient therapy. Nationwide, there are programs that offer specialized sexual trauma treatment for veterans who need more intense treatment and support, including that for severe depression or substance abuse.
- Medication. If your MST experience resulted in PTSD, your doctor may prescribe medication to help control symptoms of anxiety or to help you sleep. Your doctor will monitor you closely for any possible adverse effects of these medications. It is also possible that an STD (sexually transmitted disease) was passed during the trauma, so your doctor may choose to screen you for an STD. If the test comes back positive, your doctor will prescribe the appropriate drug for treatment.
Services are designed to help veterans at all stages of their recovery, whether that is focusing on strategies for coping with emotions and memories or, for veterans who are ready, talking about their MST experiences in depth.
What can I do to cope?
When trauma survivors take direct action to cope with their stress reactions, they put themselves in a position of power. This is called active coping, which involves accepting the impact the trauma had on your life and taking direct action to make improvements.
It is important to remember that recovery is a process and takes time. Healing from trauma, including MST, does not happen all at once, and healing does not mean that you must forget the experience. Instead, it means you have less pain and fewer bad feelings when you think about the experience, and any associated symptoms will over time bother you less.
Discussing your trauma with other survivors in a controlled setting can help you learn that you are not alone or weak. In addition, surrounding yourself with people you can talk to about your MST experience may help you feel more understood. You may even choose to distract yourself with positive recreational or work activities.
When you experience unwanted or distressing memories, remind yourself that they are just memories, and talk about them with someone you trust. If you feel that the trauma is happening again, which is known as a flashback, keep your eyes open and remind yourself where you presently are and that the trauma happened in the past.
Although VA and DoD are working to put an end to MST, it is an ongoing problem that affects a large percentage of women and men who proudly serve in the armed forces. For information on how to access free VA services and to determine your eligibility in MST benefits, visit http://www.mentalhealth.va.gov/msthome.asp.
Military sexual trauma (MST) refers to experiences of sexual assault or repeated, threatening sexual harassment experienced while on federal active duty or active duty for training. About 1 in 4 women and 1 in 100 men have reported MST to their VA doctors. However, these numbers do not account for those who have not sought health care for their MST experience or who have sought care for MST outside the VA.
Military sexual trauma is:
Military sexual trauma is the term VA uses to refer to sexual assault or sexual harassment that occurred while the veteran was in the military. A victim of MST may have been:
- Involved in sexual activity against his or her will, by physical force or nonphysical pressure. Nonphysical pressure includes threats of negative consequences for refusing to be sexually cooperative, or indirect promises of faster promotions or better treatment in exchange for sex.
- Unable to consent to sexual activities. This includes intoxication by alcohol or other substances.
Other experiences include sexual touching or grabbing, threatening or offensive remarks about a person’s body or sexual activities, as well as threatening and unwelcome sexual advances.
How do I know if I’m at risk?
Military sexual trauma can occur on or off base and while a service member—man or woman—is on or off duty. Those who commit sexual assault or sexual harassment can be men or women, military personnel or civilians, commanding officers or subordinates, strangers, friends, spouses, or intimate partners.
When do I need medical attention?
The VA reports sexual assault is more likely to result in symptoms of PTSD (posttraumatic stress disorder) than are most other types of trauma, including combat. You should seek medical attention from your primary care doctor, a mental health professional, or your VA facility’s MST Coordinator following a MST experience, especially if you experience any of the following symptoms:
- Depression
- Suicidal thoughts
- Feeling angry or irritable most of the time
- Strong emotional reactions
- Feeling emotionally numb
- Trouble falling or staying asleep
- Nightmares
- Trouble focusing
- Difficulty remembering things
- Substance abuse
- Trouble feeling safe or trusting others
- Feeling isolated or disconnected from others
- Headaches
- Gastrointestinal difficulties
- Sexual dysfunction
- Chronic pain
- Chronic fatigue
- Weight or eating problems
Survivors who are not formally diagnosed may still struggle in certain situations with emotional reactions, memories related to their experiences of MST, or other interpersonal issues.
How is MST treated?
Because MST is an experience, not a diagnosis, treatment needs may vary from patient to patient. However, VA provides free, confidential counseling and treatment to male and female veterans for mental and physical health conditions related to experiences of MST. It is important to note that treatment is available even if the MST incident was not reported at the time it happened.
Your doctor may recommend individual therapy, group therapy, or medication, depending on your symptoms. Therapies that may be used to treat MST include:
- Cognitive behavioral therapy. The main goal of this therapy is to help you change your thought patterns, which will help you change the emotions and behavior connected with the MST experience. A counselor might encourage you to reimagine your trauma repeatedly under controlled conditions—an approach called exposure therapy—as a way of learning to cope.
- Stress inoculation (in-ock-you-lay-shun) training. This therapy involves combining stress management strategies with stress-relieving techniques, such as muscle relaxation, breathing retraining, self-dialogue, and thought stopping.
- Group therapy. This therapy enables you to discuss your trauma with others who have had similar experiences.
- Inpatient therapy. Nationwide, there are programs that offer specialized sexual trauma treatment for veterans who need more intense treatment and support, including that for severe depression or substance abuse.
- Medication. If your MST experience resulted in PTSD, your doctor may prescribe medication to help control symptoms of anxiety or to help you sleep. Your doctor will monitor you closely for any possible adverse effects of these medications. It is also possible that an STD (sexually transmitted disease) was passed during the trauma, so your doctor may choose to screen you for an STD. If the test comes back positive, your doctor will prescribe the appropriate drug for treatment.
Services are designed to help veterans at all stages of their recovery, whether that is focusing on strategies for coping with emotions and memories or, for veterans who are ready, talking about their MST experiences in depth.
What can I do to cope?
When trauma survivors take direct action to cope with their stress reactions, they put themselves in a position of power. This is called active coping, which involves accepting the impact the trauma had on your life and taking direct action to make improvements.
It is important to remember that recovery is a process and takes time. Healing from trauma, including MST, does not happen all at once, and healing does not mean that you must forget the experience. Instead, it means you have less pain and fewer bad feelings when you think about the experience, and any associated symptoms will over time bother you less.
Discussing your trauma with other survivors in a controlled setting can help you learn that you are not alone or weak. In addition, surrounding yourself with people you can talk to about your MST experience may help you feel more understood. You may even choose to distract yourself with positive recreational or work activities.
When you experience unwanted or distressing memories, remind yourself that they are just memories, and talk about them with someone you trust. If you feel that the trauma is happening again, which is known as a flashback, keep your eyes open and remind yourself where you presently are and that the trauma happened in the past.
Although VA and DoD are working to put an end to MST, it is an ongoing problem that affects a large percentage of women and men who proudly serve in the armed forces. For information on how to access free VA services and to determine your eligibility in MST benefits, visit http://www.mentalhealth.va.gov/msthome.asp.

How Effective Is Group Cognitive Behavioral Therapy to Treat PTSD?
Anxiety is a necessary and natural reaction to trauma, but, sometimes, anxiety symptoms become excessive and problematic, as experienced with posttraumatic stress disorder (PTSD). Some patients who struggle with PTSD endure a relentless apprehension so intense that it keeps them from participating in everyday activities, such as attending work and partaking in social activities. Associated anxiety symptoms severely impair everyday function and include increased heart rate, sweating, intrusive images, poor attention, fear, or insomnia. Posttraumatic stress disorder symptoms often lead to occupational dysfunction, relationship difficulty, and numerous other functional impairments.
Approximately 300,000 veterans meet the criteria for PTSD related to ongoing or recent wars.1 The veteran does not bear the personal and functional burden alone; however, the financial load is felt throughout society. One recent study suggests that for veterans diagnosed with PTSD, the first 2 years after deployment cost society an estimated $7,000 per individial.2 Current research suggests that this potentially debilitating disorder occurs in about 14% of Operation Iraqi Freedom/Operation Enduring Freedom combat troops, whereas the similar U.S. demographic population experiences PTSD at a rate of about 7%.1,3 The ongoing military trauma exposures are compelling the mental health community to establish efficient and effective treatment options.4,5
Several treatment strategies exist to reduce PTSD symptoms, but health care professionals must seek a balance between therapeutic benefit and cost. The treatment of PTSD is diverse and variable; however, in the most recent Clinical Practice Guideline (CPG) for PTSD, the VA and DoD specifically endorse some psychotherapeutic interventions while dissuading the use of others.6 Of note, the VA and DoD CPG strongly encourages Stress Inoculation Training (SIT) and similar cognitive therapies aimed at guiding patients through the process of consciously understanding the relationship between thoughts and feelings and then modifying thoughts to appropriately manage stressors.6 Meanwhile, group psychotherapy has been determined to be “somewhat helpful.”6 Even though cognitive- and group-based therapies have long been established as efficacious for numerous psychological disorders (depression, obsessive compulsive disorder, eating disorders, etc), neither the American Group Psychotherapy Association nor the VA and DoD CPG directly endorse the use of group cognitive behavioral therapy (GCBT) for the treatment of PTSD.6,7 However, both VA and DoD mental health providers commonly practice CBT and various group psychotherapies for the treatment of PTSD.
Despite the widespread use of CBT, there is a gap in the clinical understanding of the evidence supporting GCBT for PTSD. The goal of this synthesis was to understand the efficacy of treating PTSD symptoms with group psychotherapy. To begin this investigation, the following PICO (population, intervention, comparison, outcome) question was asked: In adults diagnosed with PTSD, how effective is group cognitive behavioral therapy in reducing PTSD-related symptoms?
Methods
Research articles addressing the use of GCBT in PTSD were obtained via database searches that took place during October 2012 (Table). Searched databases included the Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews Randomized Controlled Trials, Psychological Information (PsycINFO), and Public Medicine (PubMed).
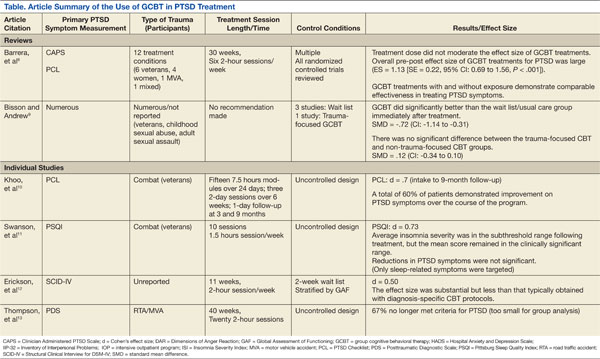
The PubMed database was searched using the following MeSH (medical subject heading) terms: “psychotherapy, group” and “stress disorders, post-traumatic” and “cognitive therapy.” Limitations were set to include only patients aged ≥ 18 years, results in English, those involving human subjects, and articles published within the past 5 years. A manual search of references was also conducted, and relevant articles were retained.
Articles that addressed primary substance abuse, other DSM Axis I disorders, intimate partner violence, or family issues were excluded from the evidence sample due to concerns of an alternate treatment focus. Articles with a focus on telehealth or alternative medicine were considered confounding to the scope of this review were also excluded. It was also noted that the term CBT is used collectively for an umbrella of treatments; however, treatments that focused on elements other than the components of CBT being delivered in a group were not included. To prevent duplication of the results, research from an inclusive review was not considered individually.
SUMMARY OF EVIDENCE
Six works fulfilled the PICO criteria and were of sufficient quality to be synthesized. Of the 6 articles retained for synthesis, 2 were high-level reviews. Both reviews supported the use of GCBT for PTSD treatment. Barrera and colleagues reported an overall large effect size regardless of the presence of exposure in-group among the 12 treatment conditions and 651 study participants.8 These researchers also reported that in-group exposure did not further traumatize other group members.
Similarly, although a notably older and smaller review, Bisson and Andrew reported a significant standard mean deviation between 4 GCBT treatment and wait list controls. These reviewers did not find a significant difference between trauma- and nontrauma-focused treatment groups. The reviews also noted that individual psychotherapy and/or pharmacotherapy was most often continued throughout the reviewed studies.8,9
The 4 other studies contribute substantively to this synthesis but arguably represent lower evidence quality. A large longitudinal study of 496 Australian veterans reported a large effect size that was sustained 9 months after treatment began.10 These researchers used an intensive outpatient program that included medication and other treatment modalities as the basis for GCBT delivery. They reported that the majority of the patients revealed improvement in PTSD symptoms.
Another study sampled a similar group of 10 combat veterans but focused particular attention on sleep-related PTSD symptoms of insomnia, nightmares, and sleep quality.11 Although these researchers were unable to report a significant difference in overall PTSD symptoms for the 8 subjects who completed the protocol, they did find a large effect size on insomnia severity and a medium effect size on sleep quality. Regular treatment, including medication, continued throughout this study.
Other researchers reported a medium effect size on PTSD symptoms while using GCBT in a heterogeneous group with various anxiety disorders, including obsessive compulsive disorder, generalized anxiety disorder, social phobia, panic disorders, and PTSD.12 Although reporting similar results as all other included studies, this study has some significant limitations, including a 26% dropout rate among the 152 participants. The final study included for synthesis reported a remarkable 67% elimination of the PTSD diagnosis among 6 motor vehicle accident survivors in the small, uncontrolled study.13 Concomitant treatments, including medications, were not reported in detail for these 4 studies except as mentioned.
As a whole, the 6 studies revealed some appreciable commonalities. Time since diagnosis did not seem to influence the results. Attrition was consistently found to be similar to other PTSD treatments. The reported session topics were loosely based on common CBT tenets (ie, education, challenging cognitions, and relaxation techniques) and were typically similar among treatment groups, including the use of homework.
DISCUSSION
As the diagnosis of PTSD increases to unfamiliar levels, GCBT has the potential to be helpful to clinicians and patients seeking alternatives to their current treatments.1,4,14 The reported results imply that GCBT can be useful in PTSD symptom reduction. This could be particularly useful to VA and military providers or rural providers operating with limited resources.
Treatment protocols are not well established and should be approached with care prior to the establishment of CBT treatment groups for those diagnosed with PTSD. Session overviews and descriptions, such as those mentioned in Thompson and colleagues, could provide a reference point for future use.13
Also worth considering, CBT can be an ambiguous term requiring deliberate definition within treatment protocols. As noted in the VA and DoD CPG, exposure- and trauma-focused treatment designs can be efficacious, but these elements do not seem to be required within the GCBT treatment setting.
The current research also suggests GCBT efficacy regardless of the index trauma. This does not suggest that heterogeneous groups were frequently studied nor can conclusions be drawn regarding heterogeneous treatment groups. Elements such as group size and session length are inconsistently reported and require specific consideration as well. There is a distinct lack of research directly comparing individual CBT with GCBT directly, which prohibits meaningful conclusions regarding PTSD symptom reduction. This research gap may well have influenced the recommendations within the VA and DoD CPG. Although some higher quality studies exist, many of the published reports on GCBT have noteworthy design flaw, such as inadequate controls and statistical analysis.
LIMITATIONS
There are some limitations to this literature synthesis. Although the search was limited to the past 5 years, the inclusion of reviews accounts for older evidence. As alluded to earlier, the lack of a standardized GCBT treatment protocol challenges results comparisons as well. The consequent treatment variations make direct interstudy comparison and synthesis difficult. Similarly, outcome measures varied between studies. Also, group psychotherapy is well established and accepted. Therefore, much of the supporting research was accomplished outside the parameters of this literature search. This empirical view of group psychotherapy among mental health providers may also contribute to the lack of available research.
It is also worth noting that studies finding neutral or negative results are often unpublished. This publication bias could account for the lack of available evidence. The research reports do not consistently report therapist qualifications; however, board certificates in group psychotherapy and CBT are undeniably variables available for debate. The inclusion of uncontrolled trials limits these findings as well. Although the above limitations are not exhaustive, they do provide necessary caveats to future generalizations.
FUTURE IMPLICATIONS
Perhaps the most important information to gain from future research is that of treatment outcomes. Studies that include a detailed outcome evaluation could reveal patient satisfaction, efficacy, and financial considerations. In the presence of adequate supportive data, GCBT could contribute outcome data regarding trauma survivor symptom normalization, peer support formation, access to care, treatment efficiency, and health care resources utilization. As noted in Barrera and colleagues, future analysis will require a greater volume of trials with an overall increase in methodological rigor.8
Current research has demonstrated a solid base from which to spawn specific treatment protocols. The available research is investigational in terms of treatment procedures. Replication of these studies could dictate treatment protocol and contribute substantively to future VA and DoD CPG updates. Future researchers should consider the use of a standard PTSD symptom assessment tool to make interstudy comparisons more meaningful. The length of treatment and exposure elements should be targeted specifically in future research as these components currently vary the most.
The military represents an obvious avenue for future research due to increased PTSD diagnosis in recent years. Although the etiology of the increase in PTSD is unclear and most likely multifactorial (decreased resilience, increased awareness, increased pursuit of secondary gains, etc), the need for treatment options is apparent.1 Group cohesion has been shown to be a core component of successful group psychotherapy, so military members who are accustomed to unit cohesion might represent a uniquely suitable population for this modality.15 Interestingly and for reasons not currently understood, veterans do not see effects of therapy as large as their civilian counterparts.8 This underscores the need for further evaluation of military-specific outcomes.
CONCLUSIONS
Although the available evidence is not robust, results do support the careful use of GCBT as an effective treatment for PTSD symptom reduction.8 Group psychotherapy has been generally regarded as an efficacious and cost-effective method to achieve similar outcomes to individual therapy. Increasing PTSD prevalence compels mental health care providers to explore all available treatment options. The potential for GCBT as an option is exciting, especially for mental health providers and those with limited resources. Rising health care standards and the current national fiscal situation is dictating a reevaluation of treatment options; so perhaps all health care providers will soon consider the use of GCBT.
As with any group assignment, the clinician should carefully consider the individual’s suitability and desire for group participation.16 With GCBT, providers could facilitate the relief of relentless apprehension and functional impairment for several patients simultaneously. Although there are many details left to explore regarding the use of GCBT for PTSD, the therapy’s foundation for use as a PTSD treatment is apparent.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Litz B, Schlenger W. Posttraumatic stress disorder in service members and new veterans of the Iraq and Afghanistan wars: A bibliography and critique. PTSD Res Q. 2009;20(1):1-3.
2. Tanielian T. Assessing combat exposure and post-traumatic stress disorder in troops and estimating the costs to society: Implications from the RAND Invisible Wounds of War Study. http://www.rand.org/pubs/testimonies/CT321.html. Published 2009. Accessed September 29, 2014.
3. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
4. Cukor J, Spitalnick J, Difede J, Rizzo A, Rothbaum BO. Emerging treatments for PTSD. Clinical Psychol Rev. 2009;29(8):715-726.
5. Hoge CW. Interventions for war-related posttraumatic stress disorder: Meeting veterans where they are. JAMA. 2011;306(5):549-551.
6. Veterans Health Administration, Department of Defense. VA/DoD Clinical Practice Guideline: Management of Post-Traumatic Stress, Version 2.0. Washington, DC: Veterans Health Administration and Department of Defense; 2010.
7. Burlingame GM, Fuhriman A, Mosier J. The differential effectiveness of group psychotherapy: A meta-analytic perspective. Group Dyn. 2003;7(1):3-12.
8. Barrera TL, Mott JM, Hofstein RF, Teng EJ. A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clin Psychol Rev. 2013;33(1):24-32.
9. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2007;(3):CD003388.
10. Khoo A, Dent MT, Oei TS. (2011). Group cognitive behaviour therapy for military service-related post-traumatic stress disorder: Effectiveness, sustainability and repeatability. Aust N Z J Psychiatry. 2011;45(8):663-672.
11. Swanson LM, Favorite TK, Horin E, Arnedt JT. A combined group treatment for nightmares and insomnia in combat veterans: A pilot study. J Trauma Stress. 2009;22(6):639-642.
12. Erickson DH, Janeck A, Tallman K. A cognitive-behavioral group for patients with various anxiety disorders. Psychiatr Serv. 2007;58(9):1205-1211.
13. Thompson AR, Wilde E, Boon K. The development of group CBT for the treatment of road-traffic-accident-related post-traumatic stress disorder: A pilot study. Cognitive Behav Therapist. 2010;2(1):32-42.
14. Slade T, Johnston A, Oakley-Browne MA, Andrews G, Whiteford H. 2007 National Survey of Mental Health and Wellbeing: Methods and key findings. Aust N Z J Psychiatry. 2009;43(7):594-605.
15. Crowe TP, Grenyer BF. Is therapist alliance or whole group cohesion more influential in group psychotherapy outcomes? Clin Psychol Psychother. 2008;15(4):239-246.
16. Leszcz M, Kobos JC. Evidence-based group psychotherapy: Using AGPA’s practice guidelines to enhance clinical effectiveness. J Clin Psychol. 2008;64(11):1238-1260.
Anxiety is a necessary and natural reaction to trauma, but, sometimes, anxiety symptoms become excessive and problematic, as experienced with posttraumatic stress disorder (PTSD). Some patients who struggle with PTSD endure a relentless apprehension so intense that it keeps them from participating in everyday activities, such as attending work and partaking in social activities. Associated anxiety symptoms severely impair everyday function and include increased heart rate, sweating, intrusive images, poor attention, fear, or insomnia. Posttraumatic stress disorder symptoms often lead to occupational dysfunction, relationship difficulty, and numerous other functional impairments.
Approximately 300,000 veterans meet the criteria for PTSD related to ongoing or recent wars.1 The veteran does not bear the personal and functional burden alone; however, the financial load is felt throughout society. One recent study suggests that for veterans diagnosed with PTSD, the first 2 years after deployment cost society an estimated $7,000 per individial.2 Current research suggests that this potentially debilitating disorder occurs in about 14% of Operation Iraqi Freedom/Operation Enduring Freedom combat troops, whereas the similar U.S. demographic population experiences PTSD at a rate of about 7%.1,3 The ongoing military trauma exposures are compelling the mental health community to establish efficient and effective treatment options.4,5
Several treatment strategies exist to reduce PTSD symptoms, but health care professionals must seek a balance between therapeutic benefit and cost. The treatment of PTSD is diverse and variable; however, in the most recent Clinical Practice Guideline (CPG) for PTSD, the VA and DoD specifically endorse some psychotherapeutic interventions while dissuading the use of others.6 Of note, the VA and DoD CPG strongly encourages Stress Inoculation Training (SIT) and similar cognitive therapies aimed at guiding patients through the process of consciously understanding the relationship between thoughts and feelings and then modifying thoughts to appropriately manage stressors.6 Meanwhile, group psychotherapy has been determined to be “somewhat helpful.”6 Even though cognitive- and group-based therapies have long been established as efficacious for numerous psychological disorders (depression, obsessive compulsive disorder, eating disorders, etc), neither the American Group Psychotherapy Association nor the VA and DoD CPG directly endorse the use of group cognitive behavioral therapy (GCBT) for the treatment of PTSD.6,7 However, both VA and DoD mental health providers commonly practice CBT and various group psychotherapies for the treatment of PTSD.
Despite the widespread use of CBT, there is a gap in the clinical understanding of the evidence supporting GCBT for PTSD. The goal of this synthesis was to understand the efficacy of treating PTSD symptoms with group psychotherapy. To begin this investigation, the following PICO (population, intervention, comparison, outcome) question was asked: In adults diagnosed with PTSD, how effective is group cognitive behavioral therapy in reducing PTSD-related symptoms?
Methods
Research articles addressing the use of GCBT in PTSD were obtained via database searches that took place during October 2012 (Table). Searched databases included the Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews Randomized Controlled Trials, Psychological Information (PsycINFO), and Public Medicine (PubMed).
The PubMed database was searched using the following MeSH (medical subject heading) terms: “psychotherapy, group” and “stress disorders, post-traumatic” and “cognitive therapy.” Limitations were set to include only patients aged ≥ 18 years, results in English, those involving human subjects, and articles published within the past 5 years. A manual search of references was also conducted, and relevant articles were retained.
Articles that addressed primary substance abuse, other DSM Axis I disorders, intimate partner violence, or family issues were excluded from the evidence sample due to concerns of an alternate treatment focus. Articles with a focus on telehealth or alternative medicine were considered confounding to the scope of this review were also excluded. It was also noted that the term CBT is used collectively for an umbrella of treatments; however, treatments that focused on elements other than the components of CBT being delivered in a group were not included. To prevent duplication of the results, research from an inclusive review was not considered individually.
SUMMARY OF EVIDENCE
Six works fulfilled the PICO criteria and were of sufficient quality to be synthesized. Of the 6 articles retained for synthesis, 2 were high-level reviews. Both reviews supported the use of GCBT for PTSD treatment. Barrera and colleagues reported an overall large effect size regardless of the presence of exposure in-group among the 12 treatment conditions and 651 study participants.8 These researchers also reported that in-group exposure did not further traumatize other group members.
Similarly, although a notably older and smaller review, Bisson and Andrew reported a significant standard mean deviation between 4 GCBT treatment and wait list controls. These reviewers did not find a significant difference between trauma- and nontrauma-focused treatment groups. The reviews also noted that individual psychotherapy and/or pharmacotherapy was most often continued throughout the reviewed studies.8,9
The 4 other studies contribute substantively to this synthesis but arguably represent lower evidence quality. A large longitudinal study of 496 Australian veterans reported a large effect size that was sustained 9 months after treatment began.10 These researchers used an intensive outpatient program that included medication and other treatment modalities as the basis for GCBT delivery. They reported that the majority of the patients revealed improvement in PTSD symptoms.
Another study sampled a similar group of 10 combat veterans but focused particular attention on sleep-related PTSD symptoms of insomnia, nightmares, and sleep quality.11 Although these researchers were unable to report a significant difference in overall PTSD symptoms for the 8 subjects who completed the protocol, they did find a large effect size on insomnia severity and a medium effect size on sleep quality. Regular treatment, including medication, continued throughout this study.
Other researchers reported a medium effect size on PTSD symptoms while using GCBT in a heterogeneous group with various anxiety disorders, including obsessive compulsive disorder, generalized anxiety disorder, social phobia, panic disorders, and PTSD.12 Although reporting similar results as all other included studies, this study has some significant limitations, including a 26% dropout rate among the 152 participants. The final study included for synthesis reported a remarkable 67% elimination of the PTSD diagnosis among 6 motor vehicle accident survivors in the small, uncontrolled study.13 Concomitant treatments, including medications, were not reported in detail for these 4 studies except as mentioned.
As a whole, the 6 studies revealed some appreciable commonalities. Time since diagnosis did not seem to influence the results. Attrition was consistently found to be similar to other PTSD treatments. The reported session topics were loosely based on common CBT tenets (ie, education, challenging cognitions, and relaxation techniques) and were typically similar among treatment groups, including the use of homework.
DISCUSSION
As the diagnosis of PTSD increases to unfamiliar levels, GCBT has the potential to be helpful to clinicians and patients seeking alternatives to their current treatments.1,4,14 The reported results imply that GCBT can be useful in PTSD symptom reduction. This could be particularly useful to VA and military providers or rural providers operating with limited resources.
Treatment protocols are not well established and should be approached with care prior to the establishment of CBT treatment groups for those diagnosed with PTSD. Session overviews and descriptions, such as those mentioned in Thompson and colleagues, could provide a reference point for future use.13
Also worth considering, CBT can be an ambiguous term requiring deliberate definition within treatment protocols. As noted in the VA and DoD CPG, exposure- and trauma-focused treatment designs can be efficacious, but these elements do not seem to be required within the GCBT treatment setting.
The current research also suggests GCBT efficacy regardless of the index trauma. This does not suggest that heterogeneous groups were frequently studied nor can conclusions be drawn regarding heterogeneous treatment groups. Elements such as group size and session length are inconsistently reported and require specific consideration as well. There is a distinct lack of research directly comparing individual CBT with GCBT directly, which prohibits meaningful conclusions regarding PTSD symptom reduction. This research gap may well have influenced the recommendations within the VA and DoD CPG. Although some higher quality studies exist, many of the published reports on GCBT have noteworthy design flaw, such as inadequate controls and statistical analysis.
LIMITATIONS
There are some limitations to this literature synthesis. Although the search was limited to the past 5 years, the inclusion of reviews accounts for older evidence. As alluded to earlier, the lack of a standardized GCBT treatment protocol challenges results comparisons as well. The consequent treatment variations make direct interstudy comparison and synthesis difficult. Similarly, outcome measures varied between studies. Also, group psychotherapy is well established and accepted. Therefore, much of the supporting research was accomplished outside the parameters of this literature search. This empirical view of group psychotherapy among mental health providers may also contribute to the lack of available research.
It is also worth noting that studies finding neutral or negative results are often unpublished. This publication bias could account for the lack of available evidence. The research reports do not consistently report therapist qualifications; however, board certificates in group psychotherapy and CBT are undeniably variables available for debate. The inclusion of uncontrolled trials limits these findings as well. Although the above limitations are not exhaustive, they do provide necessary caveats to future generalizations.
FUTURE IMPLICATIONS
Perhaps the most important information to gain from future research is that of treatment outcomes. Studies that include a detailed outcome evaluation could reveal patient satisfaction, efficacy, and financial considerations. In the presence of adequate supportive data, GCBT could contribute outcome data regarding trauma survivor symptom normalization, peer support formation, access to care, treatment efficiency, and health care resources utilization. As noted in Barrera and colleagues, future analysis will require a greater volume of trials with an overall increase in methodological rigor.8
Current research has demonstrated a solid base from which to spawn specific treatment protocols. The available research is investigational in terms of treatment procedures. Replication of these studies could dictate treatment protocol and contribute substantively to future VA and DoD CPG updates. Future researchers should consider the use of a standard PTSD symptom assessment tool to make interstudy comparisons more meaningful. The length of treatment and exposure elements should be targeted specifically in future research as these components currently vary the most.
The military represents an obvious avenue for future research due to increased PTSD diagnosis in recent years. Although the etiology of the increase in PTSD is unclear and most likely multifactorial (decreased resilience, increased awareness, increased pursuit of secondary gains, etc), the need for treatment options is apparent.1 Group cohesion has been shown to be a core component of successful group psychotherapy, so military members who are accustomed to unit cohesion might represent a uniquely suitable population for this modality.15 Interestingly and for reasons not currently understood, veterans do not see effects of therapy as large as their civilian counterparts.8 This underscores the need for further evaluation of military-specific outcomes.
CONCLUSIONS
Although the available evidence is not robust, results do support the careful use of GCBT as an effective treatment for PTSD symptom reduction.8 Group psychotherapy has been generally regarded as an efficacious and cost-effective method to achieve similar outcomes to individual therapy. Increasing PTSD prevalence compels mental health care providers to explore all available treatment options. The potential for GCBT as an option is exciting, especially for mental health providers and those with limited resources. Rising health care standards and the current national fiscal situation is dictating a reevaluation of treatment options; so perhaps all health care providers will soon consider the use of GCBT.
As with any group assignment, the clinician should carefully consider the individual’s suitability and desire for group participation.16 With GCBT, providers could facilitate the relief of relentless apprehension and functional impairment for several patients simultaneously. Although there are many details left to explore regarding the use of GCBT for PTSD, the therapy’s foundation for use as a PTSD treatment is apparent.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Anxiety is a necessary and natural reaction to trauma, but, sometimes, anxiety symptoms become excessive and problematic, as experienced with posttraumatic stress disorder (PTSD). Some patients who struggle with PTSD endure a relentless apprehension so intense that it keeps them from participating in everyday activities, such as attending work and partaking in social activities. Associated anxiety symptoms severely impair everyday function and include increased heart rate, sweating, intrusive images, poor attention, fear, or insomnia. Posttraumatic stress disorder symptoms often lead to occupational dysfunction, relationship difficulty, and numerous other functional impairments.
Approximately 300,000 veterans meet the criteria for PTSD related to ongoing or recent wars.1 The veteran does not bear the personal and functional burden alone; however, the financial load is felt throughout society. One recent study suggests that for veterans diagnosed with PTSD, the first 2 years after deployment cost society an estimated $7,000 per individial.2 Current research suggests that this potentially debilitating disorder occurs in about 14% of Operation Iraqi Freedom/Operation Enduring Freedom combat troops, whereas the similar U.S. demographic population experiences PTSD at a rate of about 7%.1,3 The ongoing military trauma exposures are compelling the mental health community to establish efficient and effective treatment options.4,5
Several treatment strategies exist to reduce PTSD symptoms, but health care professionals must seek a balance between therapeutic benefit and cost. The treatment of PTSD is diverse and variable; however, in the most recent Clinical Practice Guideline (CPG) for PTSD, the VA and DoD specifically endorse some psychotherapeutic interventions while dissuading the use of others.6 Of note, the VA and DoD CPG strongly encourages Stress Inoculation Training (SIT) and similar cognitive therapies aimed at guiding patients through the process of consciously understanding the relationship between thoughts and feelings and then modifying thoughts to appropriately manage stressors.6 Meanwhile, group psychotherapy has been determined to be “somewhat helpful.”6 Even though cognitive- and group-based therapies have long been established as efficacious for numerous psychological disorders (depression, obsessive compulsive disorder, eating disorders, etc), neither the American Group Psychotherapy Association nor the VA and DoD CPG directly endorse the use of group cognitive behavioral therapy (GCBT) for the treatment of PTSD.6,7 However, both VA and DoD mental health providers commonly practice CBT and various group psychotherapies for the treatment of PTSD.
Despite the widespread use of CBT, there is a gap in the clinical understanding of the evidence supporting GCBT for PTSD. The goal of this synthesis was to understand the efficacy of treating PTSD symptoms with group psychotherapy. To begin this investigation, the following PICO (population, intervention, comparison, outcome) question was asked: In adults diagnosed with PTSD, how effective is group cognitive behavioral therapy in reducing PTSD-related symptoms?
Methods
Research articles addressing the use of GCBT in PTSD were obtained via database searches that took place during October 2012 (Table). Searched databases included the Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews Randomized Controlled Trials, Psychological Information (PsycINFO), and Public Medicine (PubMed).
The PubMed database was searched using the following MeSH (medical subject heading) terms: “psychotherapy, group” and “stress disorders, post-traumatic” and “cognitive therapy.” Limitations were set to include only patients aged ≥ 18 years, results in English, those involving human subjects, and articles published within the past 5 years. A manual search of references was also conducted, and relevant articles were retained.
Articles that addressed primary substance abuse, other DSM Axis I disorders, intimate partner violence, or family issues were excluded from the evidence sample due to concerns of an alternate treatment focus. Articles with a focus on telehealth or alternative medicine were considered confounding to the scope of this review were also excluded. It was also noted that the term CBT is used collectively for an umbrella of treatments; however, treatments that focused on elements other than the components of CBT being delivered in a group were not included. To prevent duplication of the results, research from an inclusive review was not considered individually.
SUMMARY OF EVIDENCE
Six works fulfilled the PICO criteria and were of sufficient quality to be synthesized. Of the 6 articles retained for synthesis, 2 were high-level reviews. Both reviews supported the use of GCBT for PTSD treatment. Barrera and colleagues reported an overall large effect size regardless of the presence of exposure in-group among the 12 treatment conditions and 651 study participants.8 These researchers also reported that in-group exposure did not further traumatize other group members.
Similarly, although a notably older and smaller review, Bisson and Andrew reported a significant standard mean deviation between 4 GCBT treatment and wait list controls. These reviewers did not find a significant difference between trauma- and nontrauma-focused treatment groups. The reviews also noted that individual psychotherapy and/or pharmacotherapy was most often continued throughout the reviewed studies.8,9
The 4 other studies contribute substantively to this synthesis but arguably represent lower evidence quality. A large longitudinal study of 496 Australian veterans reported a large effect size that was sustained 9 months after treatment began.10 These researchers used an intensive outpatient program that included medication and other treatment modalities as the basis for GCBT delivery. They reported that the majority of the patients revealed improvement in PTSD symptoms.
Another study sampled a similar group of 10 combat veterans but focused particular attention on sleep-related PTSD symptoms of insomnia, nightmares, and sleep quality.11 Although these researchers were unable to report a significant difference in overall PTSD symptoms for the 8 subjects who completed the protocol, they did find a large effect size on insomnia severity and a medium effect size on sleep quality. Regular treatment, including medication, continued throughout this study.
Other researchers reported a medium effect size on PTSD symptoms while using GCBT in a heterogeneous group with various anxiety disorders, including obsessive compulsive disorder, generalized anxiety disorder, social phobia, panic disorders, and PTSD.12 Although reporting similar results as all other included studies, this study has some significant limitations, including a 26% dropout rate among the 152 participants. The final study included for synthesis reported a remarkable 67% elimination of the PTSD diagnosis among 6 motor vehicle accident survivors in the small, uncontrolled study.13 Concomitant treatments, including medications, were not reported in detail for these 4 studies except as mentioned.
As a whole, the 6 studies revealed some appreciable commonalities. Time since diagnosis did not seem to influence the results. Attrition was consistently found to be similar to other PTSD treatments. The reported session topics were loosely based on common CBT tenets (ie, education, challenging cognitions, and relaxation techniques) and were typically similar among treatment groups, including the use of homework.
DISCUSSION
As the diagnosis of PTSD increases to unfamiliar levels, GCBT has the potential to be helpful to clinicians and patients seeking alternatives to their current treatments.1,4,14 The reported results imply that GCBT can be useful in PTSD symptom reduction. This could be particularly useful to VA and military providers or rural providers operating with limited resources.
Treatment protocols are not well established and should be approached with care prior to the establishment of CBT treatment groups for those diagnosed with PTSD. Session overviews and descriptions, such as those mentioned in Thompson and colleagues, could provide a reference point for future use.13
Also worth considering, CBT can be an ambiguous term requiring deliberate definition within treatment protocols. As noted in the VA and DoD CPG, exposure- and trauma-focused treatment designs can be efficacious, but these elements do not seem to be required within the GCBT treatment setting.
The current research also suggests GCBT efficacy regardless of the index trauma. This does not suggest that heterogeneous groups were frequently studied nor can conclusions be drawn regarding heterogeneous treatment groups. Elements such as group size and session length are inconsistently reported and require specific consideration as well. There is a distinct lack of research directly comparing individual CBT with GCBT directly, which prohibits meaningful conclusions regarding PTSD symptom reduction. This research gap may well have influenced the recommendations within the VA and DoD CPG. Although some higher quality studies exist, many of the published reports on GCBT have noteworthy design flaw, such as inadequate controls and statistical analysis.
LIMITATIONS
There are some limitations to this literature synthesis. Although the search was limited to the past 5 years, the inclusion of reviews accounts for older evidence. As alluded to earlier, the lack of a standardized GCBT treatment protocol challenges results comparisons as well. The consequent treatment variations make direct interstudy comparison and synthesis difficult. Similarly, outcome measures varied between studies. Also, group psychotherapy is well established and accepted. Therefore, much of the supporting research was accomplished outside the parameters of this literature search. This empirical view of group psychotherapy among mental health providers may also contribute to the lack of available research.
It is also worth noting that studies finding neutral or negative results are often unpublished. This publication bias could account for the lack of available evidence. The research reports do not consistently report therapist qualifications; however, board certificates in group psychotherapy and CBT are undeniably variables available for debate. The inclusion of uncontrolled trials limits these findings as well. Although the above limitations are not exhaustive, they do provide necessary caveats to future generalizations.
FUTURE IMPLICATIONS
Perhaps the most important information to gain from future research is that of treatment outcomes. Studies that include a detailed outcome evaluation could reveal patient satisfaction, efficacy, and financial considerations. In the presence of adequate supportive data, GCBT could contribute outcome data regarding trauma survivor symptom normalization, peer support formation, access to care, treatment efficiency, and health care resources utilization. As noted in Barrera and colleagues, future analysis will require a greater volume of trials with an overall increase in methodological rigor.8
Current research has demonstrated a solid base from which to spawn specific treatment protocols. The available research is investigational in terms of treatment procedures. Replication of these studies could dictate treatment protocol and contribute substantively to future VA and DoD CPG updates. Future researchers should consider the use of a standard PTSD symptom assessment tool to make interstudy comparisons more meaningful. The length of treatment and exposure elements should be targeted specifically in future research as these components currently vary the most.
The military represents an obvious avenue for future research due to increased PTSD diagnosis in recent years. Although the etiology of the increase in PTSD is unclear and most likely multifactorial (decreased resilience, increased awareness, increased pursuit of secondary gains, etc), the need for treatment options is apparent.1 Group cohesion has been shown to be a core component of successful group psychotherapy, so military members who are accustomed to unit cohesion might represent a uniquely suitable population for this modality.15 Interestingly and for reasons not currently understood, veterans do not see effects of therapy as large as their civilian counterparts.8 This underscores the need for further evaluation of military-specific outcomes.
CONCLUSIONS
Although the available evidence is not robust, results do support the careful use of GCBT as an effective treatment for PTSD symptom reduction.8 Group psychotherapy has been generally regarded as an efficacious and cost-effective method to achieve similar outcomes to individual therapy. Increasing PTSD prevalence compels mental health care providers to explore all available treatment options. The potential for GCBT as an option is exciting, especially for mental health providers and those with limited resources. Rising health care standards and the current national fiscal situation is dictating a reevaluation of treatment options; so perhaps all health care providers will soon consider the use of GCBT.
As with any group assignment, the clinician should carefully consider the individual’s suitability and desire for group participation.16 With GCBT, providers could facilitate the relief of relentless apprehension and functional impairment for several patients simultaneously. Although there are many details left to explore regarding the use of GCBT for PTSD, the therapy’s foundation for use as a PTSD treatment is apparent.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Litz B, Schlenger W. Posttraumatic stress disorder in service members and new veterans of the Iraq and Afghanistan wars: A bibliography and critique. PTSD Res Q. 2009;20(1):1-3.
2. Tanielian T. Assessing combat exposure and post-traumatic stress disorder in troops and estimating the costs to society: Implications from the RAND Invisible Wounds of War Study. http://www.rand.org/pubs/testimonies/CT321.html. Published 2009. Accessed September 29, 2014.
3. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
4. Cukor J, Spitalnick J, Difede J, Rizzo A, Rothbaum BO. Emerging treatments for PTSD. Clinical Psychol Rev. 2009;29(8):715-726.
5. Hoge CW. Interventions for war-related posttraumatic stress disorder: Meeting veterans where they are. JAMA. 2011;306(5):549-551.
6. Veterans Health Administration, Department of Defense. VA/DoD Clinical Practice Guideline: Management of Post-Traumatic Stress, Version 2.0. Washington, DC: Veterans Health Administration and Department of Defense; 2010.
7. Burlingame GM, Fuhriman A, Mosier J. The differential effectiveness of group psychotherapy: A meta-analytic perspective. Group Dyn. 2003;7(1):3-12.
8. Barrera TL, Mott JM, Hofstein RF, Teng EJ. A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clin Psychol Rev. 2013;33(1):24-32.
9. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2007;(3):CD003388.
10. Khoo A, Dent MT, Oei TS. (2011). Group cognitive behaviour therapy for military service-related post-traumatic stress disorder: Effectiveness, sustainability and repeatability. Aust N Z J Psychiatry. 2011;45(8):663-672.
11. Swanson LM, Favorite TK, Horin E, Arnedt JT. A combined group treatment for nightmares and insomnia in combat veterans: A pilot study. J Trauma Stress. 2009;22(6):639-642.
12. Erickson DH, Janeck A, Tallman K. A cognitive-behavioral group for patients with various anxiety disorders. Psychiatr Serv. 2007;58(9):1205-1211.
13. Thompson AR, Wilde E, Boon K. The development of group CBT for the treatment of road-traffic-accident-related post-traumatic stress disorder: A pilot study. Cognitive Behav Therapist. 2010;2(1):32-42.
14. Slade T, Johnston A, Oakley-Browne MA, Andrews G, Whiteford H. 2007 National Survey of Mental Health and Wellbeing: Methods and key findings. Aust N Z J Psychiatry. 2009;43(7):594-605.
15. Crowe TP, Grenyer BF. Is therapist alliance or whole group cohesion more influential in group psychotherapy outcomes? Clin Psychol Psychother. 2008;15(4):239-246.
16. Leszcz M, Kobos JC. Evidence-based group psychotherapy: Using AGPA’s practice guidelines to enhance clinical effectiveness. J Clin Psychol. 2008;64(11):1238-1260.
1. Litz B, Schlenger W. Posttraumatic stress disorder in service members and new veterans of the Iraq and Afghanistan wars: A bibliography and critique. PTSD Res Q. 2009;20(1):1-3.
2. Tanielian T. Assessing combat exposure and post-traumatic stress disorder in troops and estimating the costs to society: Implications from the RAND Invisible Wounds of War Study. http://www.rand.org/pubs/testimonies/CT321.html. Published 2009. Accessed September 29, 2014.
3. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
4. Cukor J, Spitalnick J, Difede J, Rizzo A, Rothbaum BO. Emerging treatments for PTSD. Clinical Psychol Rev. 2009;29(8):715-726.
5. Hoge CW. Interventions for war-related posttraumatic stress disorder: Meeting veterans where they are. JAMA. 2011;306(5):549-551.
6. Veterans Health Administration, Department of Defense. VA/DoD Clinical Practice Guideline: Management of Post-Traumatic Stress, Version 2.0. Washington, DC: Veterans Health Administration and Department of Defense; 2010.
7. Burlingame GM, Fuhriman A, Mosier J. The differential effectiveness of group psychotherapy: A meta-analytic perspective. Group Dyn. 2003;7(1):3-12.
8. Barrera TL, Mott JM, Hofstein RF, Teng EJ. A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clin Psychol Rev. 2013;33(1):24-32.
9. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2007;(3):CD003388.
10. Khoo A, Dent MT, Oei TS. (2011). Group cognitive behaviour therapy for military service-related post-traumatic stress disorder: Effectiveness, sustainability and repeatability. Aust N Z J Psychiatry. 2011;45(8):663-672.
11. Swanson LM, Favorite TK, Horin E, Arnedt JT. A combined group treatment for nightmares and insomnia in combat veterans: A pilot study. J Trauma Stress. 2009;22(6):639-642.
12. Erickson DH, Janeck A, Tallman K. A cognitive-behavioral group for patients with various anxiety disorders. Psychiatr Serv. 2007;58(9):1205-1211.
13. Thompson AR, Wilde E, Boon K. The development of group CBT for the treatment of road-traffic-accident-related post-traumatic stress disorder: A pilot study. Cognitive Behav Therapist. 2010;2(1):32-42.
14. Slade T, Johnston A, Oakley-Browne MA, Andrews G, Whiteford H. 2007 National Survey of Mental Health and Wellbeing: Methods and key findings. Aust N Z J Psychiatry. 2009;43(7):594-605.
15. Crowe TP, Grenyer BF. Is therapist alliance or whole group cohesion more influential in group psychotherapy outcomes? Clin Psychol Psychother. 2008;15(4):239-246.
16. Leszcz M, Kobos JC. Evidence-based group psychotherapy: Using AGPA’s practice guidelines to enhance clinical effectiveness. J Clin Psychol. 2008;64(11):1238-1260.
Memory problems more common in psychogenic nonepileptic seizures plus PTSD
Individuals suffering from psychogenic nonepileptic seizures with posttraumatic stress disorder have significant verbal and visual memory impairments, and a greater likelihood of a history of substance abuse than individuals without PTSD, even if those individuals have a history of trauma, investigators have found in a case-control study.
“Up to 90% of patients with PNESs [psychogenic nonepileptic seizures] have been reported to have histories of significant traumatic experiences, with particularly high instances of childhood sexual and physical abuse, compared with control groups and the general population,” wrote Lorna Myers, Ph.D., of the Northeast Regional Epilepsy Group, New York, and her associates.
Those with psychogenic nonepileptic seizures and PTSD had the highest rates of psychiatric medication use, substance abuse, history of rape, and history of physical abuse, compared with individuals who had psychogenic nonepileptic seizures without a diagnosis of PTSD but with a history of trauma, and individuals with psychogenic nonepileptic seizures and no history of trauma, according to the study (Epilepsy & Behavior 2014;37:82-6).
Investigators for the study – which enrolled 17 people with psychogenic nonepileptic seizures and PTSD, 29 people with psychogenic nonepileptic seizures and a history of trauma but no PTSD, and 17 individuals with psychogenic nonepileptic seizures but no PTSD or trauma history – also found that those with psychogenic nonepileptic seizures and PTSD scored lowest in delayed narrative memory, and showed the highest scores for self-perceived verbal memory, visuospatial memory, and overall Memory Complaints Inventory.
Dr. Myers and her associates cited several limitations. For example, they did not collect data on the patients’ ethnic or racial backgrounds, which suggests that information on “PNES pathology and neuropsychological functions” might have been missed.
The authors declared no conflicts of interest.
Individuals suffering from psychogenic nonepileptic seizures with posttraumatic stress disorder have significant verbal and visual memory impairments, and a greater likelihood of a history of substance abuse than individuals without PTSD, even if those individuals have a history of trauma, investigators have found in a case-control study.
“Up to 90% of patients with PNESs [psychogenic nonepileptic seizures] have been reported to have histories of significant traumatic experiences, with particularly high instances of childhood sexual and physical abuse, compared with control groups and the general population,” wrote Lorna Myers, Ph.D., of the Northeast Regional Epilepsy Group, New York, and her associates.
Those with psychogenic nonepileptic seizures and PTSD had the highest rates of psychiatric medication use, substance abuse, history of rape, and history of physical abuse, compared with individuals who had psychogenic nonepileptic seizures without a diagnosis of PTSD but with a history of trauma, and individuals with psychogenic nonepileptic seizures and no history of trauma, according to the study (Epilepsy & Behavior 2014;37:82-6).
Investigators for the study – which enrolled 17 people with psychogenic nonepileptic seizures and PTSD, 29 people with psychogenic nonepileptic seizures and a history of trauma but no PTSD, and 17 individuals with psychogenic nonepileptic seizures but no PTSD or trauma history – also found that those with psychogenic nonepileptic seizures and PTSD scored lowest in delayed narrative memory, and showed the highest scores for self-perceived verbal memory, visuospatial memory, and overall Memory Complaints Inventory.
Dr. Myers and her associates cited several limitations. For example, they did not collect data on the patients’ ethnic or racial backgrounds, which suggests that information on “PNES pathology and neuropsychological functions” might have been missed.
The authors declared no conflicts of interest.
Individuals suffering from psychogenic nonepileptic seizures with posttraumatic stress disorder have significant verbal and visual memory impairments, and a greater likelihood of a history of substance abuse than individuals without PTSD, even if those individuals have a history of trauma, investigators have found in a case-control study.
“Up to 90% of patients with PNESs [psychogenic nonepileptic seizures] have been reported to have histories of significant traumatic experiences, with particularly high instances of childhood sexual and physical abuse, compared with control groups and the general population,” wrote Lorna Myers, Ph.D., of the Northeast Regional Epilepsy Group, New York, and her associates.
Those with psychogenic nonepileptic seizures and PTSD had the highest rates of psychiatric medication use, substance abuse, history of rape, and history of physical abuse, compared with individuals who had psychogenic nonepileptic seizures without a diagnosis of PTSD but with a history of trauma, and individuals with psychogenic nonepileptic seizures and no history of trauma, according to the study (Epilepsy & Behavior 2014;37:82-6).
Investigators for the study – which enrolled 17 people with psychogenic nonepileptic seizures and PTSD, 29 people with psychogenic nonepileptic seizures and a history of trauma but no PTSD, and 17 individuals with psychogenic nonepileptic seizures but no PTSD or trauma history – also found that those with psychogenic nonepileptic seizures and PTSD scored lowest in delayed narrative memory, and showed the highest scores for self-perceived verbal memory, visuospatial memory, and overall Memory Complaints Inventory.
Dr. Myers and her associates cited several limitations. For example, they did not collect data on the patients’ ethnic or racial backgrounds, which suggests that information on “PNES pathology and neuropsychological functions” might have been missed.
The authors declared no conflicts of interest.
FROM EPILEPSY & BEHAVIOR
Key clinical point: Individuals with psychogenic nonepileptic seizures and PTSD have worse memory problems and higher rates of substance abuse.
Major finding: Substance abuse, memory problems, and history of trauma were more likely in psychogenic nonepileptic seizures plus PTSD than without PTSD.
Data source: Case-control study among 17 people with psychogenic nonepileptic seizures and PTSD, 29 people with psychogenic nonepileptic seizures and a history of trauma but no PTSD, and 17 individuals with psychogenic nonepileptic seizures but no PTSD or trauma history.
Disclosures: The authors declared no conflicts of interest.
Inspiring Americans
With the understanding that healing after war is a long-term process, Welcome Back Veterans (http://www.welcomebackveterans.org), founded by Major League Baseball Charities, the nonprofit McCormick Foundation, and the charitable Entertainment Industry Foundation, was created to “inspire Americans to reach out and help our returning veterans and their families.”
Welcome Back Veterans offers resources on PTSD, including an overview and related statistics, a detailed symptoms list, treatment information, support group names and phone numbers, and a reading list of books on PTSD, all vetted by the organization.
Highlighted veteran stories are posted in the Latest News, which are also accessible via e-mail sign-ups and RSS feeds. A robust list of family resources is available, as well as many inspiring active-duty military personnel and veteran videos.
In addition to the online resources provided for free on the website, Welcome Back Veterans is funding programs at various institutions throughout the U.S. The McCormick Foundation donation page may be accessed directly through
the homepage of Welcome Back Veterans.
With the understanding that healing after war is a long-term process, Welcome Back Veterans (http://www.welcomebackveterans.org), founded by Major League Baseball Charities, the nonprofit McCormick Foundation, and the charitable Entertainment Industry Foundation, was created to “inspire Americans to reach out and help our returning veterans and their families.”
Welcome Back Veterans offers resources on PTSD, including an overview and related statistics, a detailed symptoms list, treatment information, support group names and phone numbers, and a reading list of books on PTSD, all vetted by the organization.
Highlighted veteran stories are posted in the Latest News, which are also accessible via e-mail sign-ups and RSS feeds. A robust list of family resources is available, as well as many inspiring active-duty military personnel and veteran videos.
In addition to the online resources provided for free on the website, Welcome Back Veterans is funding programs at various institutions throughout the U.S. The McCormick Foundation donation page may be accessed directly through
the homepage of Welcome Back Veterans.
With the understanding that healing after war is a long-term process, Welcome Back Veterans (http://www.welcomebackveterans.org), founded by Major League Baseball Charities, the nonprofit McCormick Foundation, and the charitable Entertainment Industry Foundation, was created to “inspire Americans to reach out and help our returning veterans and their families.”
Welcome Back Veterans offers resources on PTSD, including an overview and related statistics, a detailed symptoms list, treatment information, support group names and phone numbers, and a reading list of books on PTSD, all vetted by the organization.
Highlighted veteran stories are posted in the Latest News, which are also accessible via e-mail sign-ups and RSS feeds. A robust list of family resources is available, as well as many inspiring active-duty military personnel and veteran videos.
In addition to the online resources provided for free on the website, Welcome Back Veterans is funding programs at various institutions throughout the U.S. The McCormick Foundation donation page may be accessed directly through
the homepage of Welcome Back Veterans.
Early data indicate D-cycloserine augments effects of virtual reality treatment for PTSD
WASHINGTON – The use of D-cycloserine has promise as a way to augment the beneficial effects of virtual reality therapy of posttraumatic stress disorder, results of two recently published studies show. The results were discussed during a symposium at the annual convention of the American Psychological Association.
In one study of Iraq and Afghanistan veterans, the use of D-cycloserine (DCS) did not provide an advantage overall, compared with alprazolam or placebo. However, DCS was associated with favorable effects on cortisol and startle reactivity, compared with the other two groups, said one of the authors, Tanja Jovanovic, Ph.D. In another trial, a small proof-of concept study, the PTSD remission rate 6 months after treatment was almost 70% among those treated with a combination of virtual reality (VR) therapy and DCS, compared with 17% among those treated with VR therapy and placebo.
DCS, an NMDA (N-methyl-D-aspartate)-receptor partial agonist approved as an antibacterial by the Food and Drug Administration, has been found to enhance exposure therapy for conditions that include social anxiety and acrophobia in previous studies. NMDA also has been found to facilitate extinction learning in animal studies, said Dr. Jovanovic director of the neurophysiology laboratory at the Grady Trauma Project at Emory University, Atlanta.
In the study, 156 veterans of the Iraq and Afghanistan wars were randomized to treatment with DCS (50 mg), alprazolam (0.25 mg), or placebo plus five sessions of virtual reality exposure therapy (after an introductory VR session). Assessments of patients – which included evaluation of PTSD symptoms, psychophysiologic responses, and cortisol reactivity – were performed before treatment and 3, 6, and 12 months after treatment. Monitoring included placing electrodes under the eye to measure the contraction of the eye blink muscle and skin conductance testing during exposure to the VR scenes (two convoy explosion scenes and a city scene), said Dr. Jovanovic, one of the authors of the study, which was published in June (Am. J. Psychiatry 2014;171:640-8).
After five series of VR treatment, PTSD symptoms significantly decreased in all three groups after treatment, based on changes on the Clinician-Administered PTSD Scale (CAPS) score, but the greatest degree of reduction in symptoms at 12 months was observed in the DCS group, she said. Those treated with DCS "showed the biggest decline and actually maintained those gains at 6 months, which we did not see with the other groups."
In addition, those treated with DCS had a reduction in cortisol and startle reactivity that was greater than the changes observed in the two other groups. The magnitude of startle reactivity at baseline was related to the change in the CAPS score 6 months later, "so those gains they are maintaining at 6 months are predicted by their initial response to the virtual reality session pretreatment ... the more reactive, the better they got," Dr. Jovanovic reported.
The same also was true for skin conductance findings: The more reactive they were at baseline in this measure, the more improved the patients were at follow-up, but this association was only evident in the DCS-treated patients, Dr. Jovanovic said.
Measurements of cortisol levels before exposure to the VR scenes, immediately afterward, and 15 minutes afterward determined that cortisol reactivity was attenuated with treatment. Cortisol reactivity significantly dropped in all three groups, from before treatment to the 6-month follow-up but was the lowest in the DCS-treated patients. In the alprazolam-treated group, the higher the cortisol reactivity was before treatment, the worse the outcomes were with treatment, the reverse of what was seen with other psychophysiological measures, she added.
During the same symposium on the use of VR in the treatment of PTSD, JoAnn Difede, Ph.D., professor of psychiatry, Cornell University, New York, described the use of DCS "as a cognitive enhancer" for treatment of people with PTSD related to the World Trade Center attacks in 2001. "We see this as very promising," she said.
In one double-blind, proof-of-concept study, 25 people with PTSD were randomized to DCS (100 mg) or placebo administered 90 minutes before weekly sessions of VR therapy, timed so that plasma concentrations would peak during the session. In the placebo group, 3 dropped out, but none of the 13 patients in the DCS group dropped out (Neuropsychopharmacology 2014; 39:1052-8).
Six months after treatment, 9 of the 13 patients (69%) in the DCS group were in remission, compared with 2 of the 12 (17%) on placebo plus VR exposure. Remission was defined as a CAPS total score of 20 or less, and minimal or no impairment in social, occupational, and other important areas of function, as judged by an independent blinded assessor.
Dr. Difede, also director of the program for anxiety and traumatic stress studies at New York-Presbyterian Hospital, said the two groups began to diverge at the third session, and those who received DCS continued to improve 6 months later. A post-hoc analysis identified a "drastic improvement" in anger and sleep among those treated with DCS, a finding that she and her associates plan to look at more closely. The study presented by Dr. Jovanovic was funded by the National Institute of Mental Health. Dr. Difede received partial funding support from DeWitt-Wallace Fund of the New York Community Trust. The trust was not involved in the design, data collection, or in any other aspects of the study.
WASHINGTON – The use of D-cycloserine has promise as a way to augment the beneficial effects of virtual reality therapy of posttraumatic stress disorder, results of two recently published studies show. The results were discussed during a symposium at the annual convention of the American Psychological Association.
In one study of Iraq and Afghanistan veterans, the use of D-cycloserine (DCS) did not provide an advantage overall, compared with alprazolam or placebo. However, DCS was associated with favorable effects on cortisol and startle reactivity, compared with the other two groups, said one of the authors, Tanja Jovanovic, Ph.D. In another trial, a small proof-of concept study, the PTSD remission rate 6 months after treatment was almost 70% among those treated with a combination of virtual reality (VR) therapy and DCS, compared with 17% among those treated with VR therapy and placebo.
DCS, an NMDA (N-methyl-D-aspartate)-receptor partial agonist approved as an antibacterial by the Food and Drug Administration, has been found to enhance exposure therapy for conditions that include social anxiety and acrophobia in previous studies. NMDA also has been found to facilitate extinction learning in animal studies, said Dr. Jovanovic director of the neurophysiology laboratory at the Grady Trauma Project at Emory University, Atlanta.
In the study, 156 veterans of the Iraq and Afghanistan wars were randomized to treatment with DCS (50 mg), alprazolam (0.25 mg), or placebo plus five sessions of virtual reality exposure therapy (after an introductory VR session). Assessments of patients – which included evaluation of PTSD symptoms, psychophysiologic responses, and cortisol reactivity – were performed before treatment and 3, 6, and 12 months after treatment. Monitoring included placing electrodes under the eye to measure the contraction of the eye blink muscle and skin conductance testing during exposure to the VR scenes (two convoy explosion scenes and a city scene), said Dr. Jovanovic, one of the authors of the study, which was published in June (Am. J. Psychiatry 2014;171:640-8).
After five series of VR treatment, PTSD symptoms significantly decreased in all three groups after treatment, based on changes on the Clinician-Administered PTSD Scale (CAPS) score, but the greatest degree of reduction in symptoms at 12 months was observed in the DCS group, she said. Those treated with DCS "showed the biggest decline and actually maintained those gains at 6 months, which we did not see with the other groups."
In addition, those treated with DCS had a reduction in cortisol and startle reactivity that was greater than the changes observed in the two other groups. The magnitude of startle reactivity at baseline was related to the change in the CAPS score 6 months later, "so those gains they are maintaining at 6 months are predicted by their initial response to the virtual reality session pretreatment ... the more reactive, the better they got," Dr. Jovanovic reported.
The same also was true for skin conductance findings: The more reactive they were at baseline in this measure, the more improved the patients were at follow-up, but this association was only evident in the DCS-treated patients, Dr. Jovanovic said.
Measurements of cortisol levels before exposure to the VR scenes, immediately afterward, and 15 minutes afterward determined that cortisol reactivity was attenuated with treatment. Cortisol reactivity significantly dropped in all three groups, from before treatment to the 6-month follow-up but was the lowest in the DCS-treated patients. In the alprazolam-treated group, the higher the cortisol reactivity was before treatment, the worse the outcomes were with treatment, the reverse of what was seen with other psychophysiological measures, she added.
During the same symposium on the use of VR in the treatment of PTSD, JoAnn Difede, Ph.D., professor of psychiatry, Cornell University, New York, described the use of DCS "as a cognitive enhancer" for treatment of people with PTSD related to the World Trade Center attacks in 2001. "We see this as very promising," she said.
In one double-blind, proof-of-concept study, 25 people with PTSD were randomized to DCS (100 mg) or placebo administered 90 minutes before weekly sessions of VR therapy, timed so that plasma concentrations would peak during the session. In the placebo group, 3 dropped out, but none of the 13 patients in the DCS group dropped out (Neuropsychopharmacology 2014; 39:1052-8).
Six months after treatment, 9 of the 13 patients (69%) in the DCS group were in remission, compared with 2 of the 12 (17%) on placebo plus VR exposure. Remission was defined as a CAPS total score of 20 or less, and minimal or no impairment in social, occupational, and other important areas of function, as judged by an independent blinded assessor.
Dr. Difede, also director of the program for anxiety and traumatic stress studies at New York-Presbyterian Hospital, said the two groups began to diverge at the third session, and those who received DCS continued to improve 6 months later. A post-hoc analysis identified a "drastic improvement" in anger and sleep among those treated with DCS, a finding that she and her associates plan to look at more closely. The study presented by Dr. Jovanovic was funded by the National Institute of Mental Health. Dr. Difede received partial funding support from DeWitt-Wallace Fund of the New York Community Trust. The trust was not involved in the design, data collection, or in any other aspects of the study.
WASHINGTON – The use of D-cycloserine has promise as a way to augment the beneficial effects of virtual reality therapy of posttraumatic stress disorder, results of two recently published studies show. The results were discussed during a symposium at the annual convention of the American Psychological Association.
In one study of Iraq and Afghanistan veterans, the use of D-cycloserine (DCS) did not provide an advantage overall, compared with alprazolam or placebo. However, DCS was associated with favorable effects on cortisol and startle reactivity, compared with the other two groups, said one of the authors, Tanja Jovanovic, Ph.D. In another trial, a small proof-of concept study, the PTSD remission rate 6 months after treatment was almost 70% among those treated with a combination of virtual reality (VR) therapy and DCS, compared with 17% among those treated with VR therapy and placebo.
DCS, an NMDA (N-methyl-D-aspartate)-receptor partial agonist approved as an antibacterial by the Food and Drug Administration, has been found to enhance exposure therapy for conditions that include social anxiety and acrophobia in previous studies. NMDA also has been found to facilitate extinction learning in animal studies, said Dr. Jovanovic director of the neurophysiology laboratory at the Grady Trauma Project at Emory University, Atlanta.
In the study, 156 veterans of the Iraq and Afghanistan wars were randomized to treatment with DCS (50 mg), alprazolam (0.25 mg), or placebo plus five sessions of virtual reality exposure therapy (after an introductory VR session). Assessments of patients – which included evaluation of PTSD symptoms, psychophysiologic responses, and cortisol reactivity – were performed before treatment and 3, 6, and 12 months after treatment. Monitoring included placing electrodes under the eye to measure the contraction of the eye blink muscle and skin conductance testing during exposure to the VR scenes (two convoy explosion scenes and a city scene), said Dr. Jovanovic, one of the authors of the study, which was published in June (Am. J. Psychiatry 2014;171:640-8).
After five series of VR treatment, PTSD symptoms significantly decreased in all three groups after treatment, based on changes on the Clinician-Administered PTSD Scale (CAPS) score, but the greatest degree of reduction in symptoms at 12 months was observed in the DCS group, she said. Those treated with DCS "showed the biggest decline and actually maintained those gains at 6 months, which we did not see with the other groups."
In addition, those treated with DCS had a reduction in cortisol and startle reactivity that was greater than the changes observed in the two other groups. The magnitude of startle reactivity at baseline was related to the change in the CAPS score 6 months later, "so those gains they are maintaining at 6 months are predicted by their initial response to the virtual reality session pretreatment ... the more reactive, the better they got," Dr. Jovanovic reported.
The same also was true for skin conductance findings: The more reactive they were at baseline in this measure, the more improved the patients were at follow-up, but this association was only evident in the DCS-treated patients, Dr. Jovanovic said.
Measurements of cortisol levels before exposure to the VR scenes, immediately afterward, and 15 minutes afterward determined that cortisol reactivity was attenuated with treatment. Cortisol reactivity significantly dropped in all three groups, from before treatment to the 6-month follow-up but was the lowest in the DCS-treated patients. In the alprazolam-treated group, the higher the cortisol reactivity was before treatment, the worse the outcomes were with treatment, the reverse of what was seen with other psychophysiological measures, she added.
During the same symposium on the use of VR in the treatment of PTSD, JoAnn Difede, Ph.D., professor of psychiatry, Cornell University, New York, described the use of DCS "as a cognitive enhancer" for treatment of people with PTSD related to the World Trade Center attacks in 2001. "We see this as very promising," she said.
In one double-blind, proof-of-concept study, 25 people with PTSD were randomized to DCS (100 mg) or placebo administered 90 minutes before weekly sessions of VR therapy, timed so that plasma concentrations would peak during the session. In the placebo group, 3 dropped out, but none of the 13 patients in the DCS group dropped out (Neuropsychopharmacology 2014; 39:1052-8).
Six months after treatment, 9 of the 13 patients (69%) in the DCS group were in remission, compared with 2 of the 12 (17%) on placebo plus VR exposure. Remission was defined as a CAPS total score of 20 or less, and minimal or no impairment in social, occupational, and other important areas of function, as judged by an independent blinded assessor.
Dr. Difede, also director of the program for anxiety and traumatic stress studies at New York-Presbyterian Hospital, said the two groups began to diverge at the third session, and those who received DCS continued to improve 6 months later. A post-hoc analysis identified a "drastic improvement" in anger and sleep among those treated with DCS, a finding that she and her associates plan to look at more closely. The study presented by Dr. Jovanovic was funded by the National Institute of Mental Health. Dr. Difede received partial funding support from DeWitt-Wallace Fund of the New York Community Trust. The trust was not involved in the design, data collection, or in any other aspects of the study.
EXPERT ANALYSIS AT THE 2014 APA CONVENTION
PTSD ‘updates’ in DSM-5 concerning
As a seasoned psychiatrist, I try to take most events in stride. My main reaction to unsettling events is to flatten down and take my own pulse.
However, when I saw the article in the Lancet Psychiatry (2014 Aug. 14 [doi:10.1016/S2215-0366(14)70235-4]) by my longtime colleague, Col. (Ret.) Charles W. Hoge, M.D., and his coauthors, my pulse went way up, and "Oh, my God" was my very unscientific reaction.

As readers may recall, the new definition of posttraumatic stress disorder raises the number of symptoms from 17 to 20, and 8 of those original symptoms were substantially reworded. In addition, PTSD was moved in the new manual from an anxiety disorder to disorders related to trauma and stressors.
In their study, Dr. Hoge and his coauthors administered surveys to soldiers looking at DSM-IV-TR and DSM-5 criteria. In brief, about a third of soldiers who met DSM-IV-TR criteria for PTSD did not meet DSM-5 criteria. Almost a third were in the opposite camp, meeting DSM-5 but not the older criteria, wrote Dr. Hoge of the Center for Psychiatry and Neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md. The main issue is about criterion C and the splitting up of avoidance symptoms from depressive symptoms.
Why was my reaction so strong? I had thought that the new criteria would widen those eligible for the diagnosis. Instead, it eliminates almost a third of them, mainly because they did not meet the avoidant criteria. (Please read the article for the full complex details.)
In the disability system in the military and Veterans Affairs system, the diagnosis of PTSD carries major weight. So what will happen if the criteria exclude them?

The good news is that both Veterans Affairs and the Department of Defense have made it clear that service members and veterans who already have the diagnosis according to the DSM-IV will not have it changed as a result of DSM-5, so the new definition mostly pertains to those newly seeking care or benefits now. It remains unclear what diagnosis should be used for those veterans who clearly would have met the previous definition (which has been used for more than 25 years), but not the new one. The DSM-5 recommends the use of adjustment disorder in this case, but some experts are concerned that the use of this diagnosis for this purpose will have negative effects. A major issue is that service members can be separated without benefits for an adjustment disorder. Questions also remain about whether adjustment disorder should have even been paired with PTSD in the same chapter in the new DSM-5.
In the accompanying commentary, Dr. Alexander C. McFarlane, of the Centre for Traumatic Studies at the University of Adelaide, Australia, warns about the negative consequences of the change in definition (Lancet Psychiatry 2014 Aug. 14 [doi:10.1016/S2215-0366(14)70321-9]. He also urges caution when the new diagnosis is used in forensic or disability evaluations.
I recommend that readers review this important article and commentary, and that the military and the VA also take a cautious approach.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.
As a seasoned psychiatrist, I try to take most events in stride. My main reaction to unsettling events is to flatten down and take my own pulse.
However, when I saw the article in the Lancet Psychiatry (2014 Aug. 14 [doi:10.1016/S2215-0366(14)70235-4]) by my longtime colleague, Col. (Ret.) Charles W. Hoge, M.D., and his coauthors, my pulse went way up, and "Oh, my God" was my very unscientific reaction.
As readers may recall, the new definition of posttraumatic stress disorder raises the number of symptoms from 17 to 20, and 8 of those original symptoms were substantially reworded. In addition, PTSD was moved in the new manual from an anxiety disorder to disorders related to trauma and stressors.
In their study, Dr. Hoge and his coauthors administered surveys to soldiers looking at DSM-IV-TR and DSM-5 criteria. In brief, about a third of soldiers who met DSM-IV-TR criteria for PTSD did not meet DSM-5 criteria. Almost a third were in the opposite camp, meeting DSM-5 but not the older criteria, wrote Dr. Hoge of the Center for Psychiatry and Neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md. The main issue is about criterion C and the splitting up of avoidance symptoms from depressive symptoms.
Why was my reaction so strong? I had thought that the new criteria would widen those eligible for the diagnosis. Instead, it eliminates almost a third of them, mainly because they did not meet the avoidant criteria. (Please read the article for the full complex details.)
In the disability system in the military and Veterans Affairs system, the diagnosis of PTSD carries major weight. So what will happen if the criteria exclude them?
The good news is that both Veterans Affairs and the Department of Defense have made it clear that service members and veterans who already have the diagnosis according to the DSM-IV will not have it changed as a result of DSM-5, so the new definition mostly pertains to those newly seeking care or benefits now. It remains unclear what diagnosis should be used for those veterans who clearly would have met the previous definition (which has been used for more than 25 years), but not the new one. The DSM-5 recommends the use of adjustment disorder in this case, but some experts are concerned that the use of this diagnosis for this purpose will have negative effects. A major issue is that service members can be separated without benefits for an adjustment disorder. Questions also remain about whether adjustment disorder should have even been paired with PTSD in the same chapter in the new DSM-5.
In the accompanying commentary, Dr. Alexander C. McFarlane, of the Centre for Traumatic Studies at the University of Adelaide, Australia, warns about the negative consequences of the change in definition (Lancet Psychiatry 2014 Aug. 14 [doi:10.1016/S2215-0366(14)70321-9]. He also urges caution when the new diagnosis is used in forensic or disability evaluations.
I recommend that readers review this important article and commentary, and that the military and the VA also take a cautious approach.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.
As a seasoned psychiatrist, I try to take most events in stride. My main reaction to unsettling events is to flatten down and take my own pulse.
However, when I saw the article in the Lancet Psychiatry (2014 Aug. 14 [doi:10.1016/S2215-0366(14)70235-4]) by my longtime colleague, Col. (Ret.) Charles W. Hoge, M.D., and his coauthors, my pulse went way up, and "Oh, my God" was my very unscientific reaction.
As readers may recall, the new definition of posttraumatic stress disorder raises the number of symptoms from 17 to 20, and 8 of those original symptoms were substantially reworded. In addition, PTSD was moved in the new manual from an anxiety disorder to disorders related to trauma and stressors.
In their study, Dr. Hoge and his coauthors administered surveys to soldiers looking at DSM-IV-TR and DSM-5 criteria. In brief, about a third of soldiers who met DSM-IV-TR criteria for PTSD did not meet DSM-5 criteria. Almost a third were in the opposite camp, meeting DSM-5 but not the older criteria, wrote Dr. Hoge of the Center for Psychiatry and Neuroscience at the Walter Reed Army Institute of Research in Silver Spring, Md. The main issue is about criterion C and the splitting up of avoidance symptoms from depressive symptoms.
Why was my reaction so strong? I had thought that the new criteria would widen those eligible for the diagnosis. Instead, it eliminates almost a third of them, mainly because they did not meet the avoidant criteria. (Please read the article for the full complex details.)
In the disability system in the military and Veterans Affairs system, the diagnosis of PTSD carries major weight. So what will happen if the criteria exclude them?
The good news is that both Veterans Affairs and the Department of Defense have made it clear that service members and veterans who already have the diagnosis according to the DSM-IV will not have it changed as a result of DSM-5, so the new definition mostly pertains to those newly seeking care or benefits now. It remains unclear what diagnosis should be used for those veterans who clearly would have met the previous definition (which has been used for more than 25 years), but not the new one. The DSM-5 recommends the use of adjustment disorder in this case, but some experts are concerned that the use of this diagnosis for this purpose will have negative effects. A major issue is that service members can be separated without benefits for an adjustment disorder. Questions also remain about whether adjustment disorder should have even been paired with PTSD in the same chapter in the new DSM-5.
In the accompanying commentary, Dr. Alexander C. McFarlane, of the Centre for Traumatic Studies at the University of Adelaide, Australia, warns about the negative consequences of the change in definition (Lancet Psychiatry 2014 Aug. 14 [doi:10.1016/S2215-0366(14)70321-9]. He also urges caution when the new diagnosis is used in forensic or disability evaluations.
I recommend that readers review this important article and commentary, and that the military and the VA also take a cautious approach.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.

VIDEO: Dementia risk spikes in older veterans with sleep disorders, PTSD
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
AT AAIC 2014
