User login
Link Between PTSD and TBI Is Only the Beginning for MRS Study
April 25, 2014
A fundamental challenge for any study examining the impact of military service on the health of military personnel is establishing a baseline. Whether heart disease or posttraumatic stress disorder (PTSD), the symptoms often appear after (sometimes long after) the service has ended. The longitudinal Marine Resiliency Study (MRS I) and its successor MRS II are seeking to resolve that issue in a novel approach that brings together the Department of Veterans Affairs, U.S. Marine Corps, and Navy Medicine.
In the MRS study, a cohort of about 2,600 Marines (MRS-I) in 4 battalions and about 1,300 Marines (MRS-II) in 2 battalions deployed to Iraq or Afghanistan underwent a scientifically rigorous examination a month prior to deployment. This baseline was established using self-reported questionnaires, clinical interviews, and laboratory examinations. Follow-up examinations were repeated at 3 months (MRS-I and MRS-II) and again at 6 months post-deployment (MRS-I).

The program is ambitious, Dr. Dewleen Baker of the VA San Diego Health Care System told Federal Practitioner. “MRS was designed to provide broad-based (psychosocial, psychophysiological, and biological) prospective, longitudinal data, with a goal toward ultimate integrated analyses of variables, to determine risk and resilience for post-deployment mental health outcomes, i.e,. PTSD and co-occurring disorders,” she explained. “Analyses have just begun, and we are working our way through aspects of the data toward more integrated approaches.”
In one of the first of many reports to come out of MRS, the researchers found that the probability of developing PTSD was highest for participants with severe pre-deployment symptoms, high combat intensity, and deployment-related traumatic brain injury (TBI). Most significant, the researchers found that TBI doubled or nearly doubled the PTSD rates for participants with less severe pre-deployment PTSD symptoms. According to Baker:
By contrast, deployment-related mild TBI increases post-deployment symptom scores by 23%, and moderate-to-severe injuries increase scores by 71%. Our findings suggest that TBI may be a very important risk factor of PTSD, even when accounting for preexisting symptoms and combat intensity.
Our study focused on the impact of pre-deployment symptoms, combat intensity and TBI; however, it is important to consider other factors of psychological risk and resilience. Genes, coping style, and social support are just a few of the many other factors that may influence an individual’s response to stress.
Creating a rigorous cross-agency research study required tact, diligence, and patience from the MRS team. “Each agency has their own unique culture and institutional rules, regulations, and bureaucracy, so ideas, programs, etc, must be vetted across all agencies and reconciled—the various cultures/agencies to be reconciled include DoD, VA and academia.” Baker explained. “In addition in regards to initiation of studies for MRS II, for the past couple years, we also interface with NIMH as well as Headquarters Marine Corps; NIMH has the role of scientific review of MRS-II studies carried out under Headquarters Marine Corps/BUMED funding.”
The MRS-I and II studies may very well provide a template for future studies. The MRS team included a military liaison to work with the active duty Marines and attached Sailors, gather data, schedule meetings, and to report findings. “This study has a lot of experience working within and across these agencies,” Baker noted, “It’s an excellent model for future VA/DOD joint projects.”
April 25, 2014
A fundamental challenge for any study examining the impact of military service on the health of military personnel is establishing a baseline. Whether heart disease or posttraumatic stress disorder (PTSD), the symptoms often appear after (sometimes long after) the service has ended. The longitudinal Marine Resiliency Study (MRS I) and its successor MRS II are seeking to resolve that issue in a novel approach that brings together the Department of Veterans Affairs, U.S. Marine Corps, and Navy Medicine.
In the MRS study, a cohort of about 2,600 Marines (MRS-I) in 4 battalions and about 1,300 Marines (MRS-II) in 2 battalions deployed to Iraq or Afghanistan underwent a scientifically rigorous examination a month prior to deployment. This baseline was established using self-reported questionnaires, clinical interviews, and laboratory examinations. Follow-up examinations were repeated at 3 months (MRS-I and MRS-II) and again at 6 months post-deployment (MRS-I).
The program is ambitious, Dr. Dewleen Baker of the VA San Diego Health Care System told Federal Practitioner. “MRS was designed to provide broad-based (psychosocial, psychophysiological, and biological) prospective, longitudinal data, with a goal toward ultimate integrated analyses of variables, to determine risk and resilience for post-deployment mental health outcomes, i.e,. PTSD and co-occurring disorders,” she explained. “Analyses have just begun, and we are working our way through aspects of the data toward more integrated approaches.”
In one of the first of many reports to come out of MRS, the researchers found that the probability of developing PTSD was highest for participants with severe pre-deployment symptoms, high combat intensity, and deployment-related traumatic brain injury (TBI). Most significant, the researchers found that TBI doubled or nearly doubled the PTSD rates for participants with less severe pre-deployment PTSD symptoms. According to Baker:
By contrast, deployment-related mild TBI increases post-deployment symptom scores by 23%, and moderate-to-severe injuries increase scores by 71%. Our findings suggest that TBI may be a very important risk factor of PTSD, even when accounting for preexisting symptoms and combat intensity.
Our study focused on the impact of pre-deployment symptoms, combat intensity and TBI; however, it is important to consider other factors of psychological risk and resilience. Genes, coping style, and social support are just a few of the many other factors that may influence an individual’s response to stress.
Creating a rigorous cross-agency research study required tact, diligence, and patience from the MRS team. “Each agency has their own unique culture and institutional rules, regulations, and bureaucracy, so ideas, programs, etc, must be vetted across all agencies and reconciled—the various cultures/agencies to be reconciled include DoD, VA and academia.” Baker explained. “In addition in regards to initiation of studies for MRS II, for the past couple years, we also interface with NIMH as well as Headquarters Marine Corps; NIMH has the role of scientific review of MRS-II studies carried out under Headquarters Marine Corps/BUMED funding.”
The MRS-I and II studies may very well provide a template for future studies. The MRS team included a military liaison to work with the active duty Marines and attached Sailors, gather data, schedule meetings, and to report findings. “This study has a lot of experience working within and across these agencies,” Baker noted, “It’s an excellent model for future VA/DOD joint projects.”
April 25, 2014
A fundamental challenge for any study examining the impact of military service on the health of military personnel is establishing a baseline. Whether heart disease or posttraumatic stress disorder (PTSD), the symptoms often appear after (sometimes long after) the service has ended. The longitudinal Marine Resiliency Study (MRS I) and its successor MRS II are seeking to resolve that issue in a novel approach that brings together the Department of Veterans Affairs, U.S. Marine Corps, and Navy Medicine.
In the MRS study, a cohort of about 2,600 Marines (MRS-I) in 4 battalions and about 1,300 Marines (MRS-II) in 2 battalions deployed to Iraq or Afghanistan underwent a scientifically rigorous examination a month prior to deployment. This baseline was established using self-reported questionnaires, clinical interviews, and laboratory examinations. Follow-up examinations were repeated at 3 months (MRS-I and MRS-II) and again at 6 months post-deployment (MRS-I).
The program is ambitious, Dr. Dewleen Baker of the VA San Diego Health Care System told Federal Practitioner. “MRS was designed to provide broad-based (psychosocial, psychophysiological, and biological) prospective, longitudinal data, with a goal toward ultimate integrated analyses of variables, to determine risk and resilience for post-deployment mental health outcomes, i.e,. PTSD and co-occurring disorders,” she explained. “Analyses have just begun, and we are working our way through aspects of the data toward more integrated approaches.”
In one of the first of many reports to come out of MRS, the researchers found that the probability of developing PTSD was highest for participants with severe pre-deployment symptoms, high combat intensity, and deployment-related traumatic brain injury (TBI). Most significant, the researchers found that TBI doubled or nearly doubled the PTSD rates for participants with less severe pre-deployment PTSD symptoms. According to Baker:
By contrast, deployment-related mild TBI increases post-deployment symptom scores by 23%, and moderate-to-severe injuries increase scores by 71%. Our findings suggest that TBI may be a very important risk factor of PTSD, even when accounting for preexisting symptoms and combat intensity.
Our study focused on the impact of pre-deployment symptoms, combat intensity and TBI; however, it is important to consider other factors of psychological risk and resilience. Genes, coping style, and social support are just a few of the many other factors that may influence an individual’s response to stress.
Creating a rigorous cross-agency research study required tact, diligence, and patience from the MRS team. “Each agency has their own unique culture and institutional rules, regulations, and bureaucracy, so ideas, programs, etc, must be vetted across all agencies and reconciled—the various cultures/agencies to be reconciled include DoD, VA and academia.” Baker explained. “In addition in regards to initiation of studies for MRS II, for the past couple years, we also interface with NIMH as well as Headquarters Marine Corps; NIMH has the role of scientific review of MRS-II studies carried out under Headquarters Marine Corps/BUMED funding.”
The MRS-I and II studies may very well provide a template for future studies. The MRS team included a military liaison to work with the active duty Marines and attached Sailors, gather data, schedule meetings, and to report findings. “This study has a lot of experience working within and across these agencies,” Baker noted, “It’s an excellent model for future VA/DOD joint projects.”

AUDIO: Beyond the battlefield: suicide, PTSD, and ‘moral injury’
Military suicide rates for never-deployed service members now surpass rates for those who have been in-country. Is one of the reasons because veterans who’ve served don’t make the time to help welcome new recruits into the fold, leaving them to feel isolated and not a part of the mission?
"The Army itself has been on a very high operations tempo. Troops are deploying all the time. They’re tired," says Col. Elspeth Cameron Ritchie, U.S. Army retired, and a former Army psychiatrist. "When a new solder joins a unit, [he or she] may not be welcomed in the same way as [a soldier] might have been in the past."
But, does the military attract people who are already predisposed to mental health issues, including suicidal ideation? And while most servicemen and -women are sound of mind and body when they start out, if they do encounter mental health issues, many don’t seek the help that is available to them.
In this audio interview, Dr. Ritchie explains why this may be the case, and examines the role stigma does – or doesn’t – play in addressing mental health issues in the military. She also defines what is only now beginning to receive recognition as a factor in posttraumatic stress disorder: moral injury, or the effects of having to kill on order.
Dr. Ritchie also discussed how PTSD entered our lexicon and what utility the diagnosis has for nonservice members.
On Twitter @whitneymcknight
Military suicide rates for never-deployed service members now surpass rates for those who have been in-country. Is one of the reasons because veterans who’ve served don’t make the time to help welcome new recruits into the fold, leaving them to feel isolated and not a part of the mission?
"The Army itself has been on a very high operations tempo. Troops are deploying all the time. They’re tired," says Col. Elspeth Cameron Ritchie, U.S. Army retired, and a former Army psychiatrist. "When a new solder joins a unit, [he or she] may not be welcomed in the same way as [a soldier] might have been in the past."
But, does the military attract people who are already predisposed to mental health issues, including suicidal ideation? And while most servicemen and -women are sound of mind and body when they start out, if they do encounter mental health issues, many don’t seek the help that is available to them.
In this audio interview, Dr. Ritchie explains why this may be the case, and examines the role stigma does – or doesn’t – play in addressing mental health issues in the military. She also defines what is only now beginning to receive recognition as a factor in posttraumatic stress disorder: moral injury, or the effects of having to kill on order.
Dr. Ritchie also discussed how PTSD entered our lexicon and what utility the diagnosis has for nonservice members.
On Twitter @whitneymcknight
Military suicide rates for never-deployed service members now surpass rates for those who have been in-country. Is one of the reasons because veterans who’ve served don’t make the time to help welcome new recruits into the fold, leaving them to feel isolated and not a part of the mission?
"The Army itself has been on a very high operations tempo. Troops are deploying all the time. They’re tired," says Col. Elspeth Cameron Ritchie, U.S. Army retired, and a former Army psychiatrist. "When a new solder joins a unit, [he or she] may not be welcomed in the same way as [a soldier] might have been in the past."
But, does the military attract people who are already predisposed to mental health issues, including suicidal ideation? And while most servicemen and -women are sound of mind and body when they start out, if they do encounter mental health issues, many don’t seek the help that is available to them.
In this audio interview, Dr. Ritchie explains why this may be the case, and examines the role stigma does – or doesn’t – play in addressing mental health issues in the military. She also defines what is only now beginning to receive recognition as a factor in posttraumatic stress disorder: moral injury, or the effects of having to kill on order.
Dr. Ritchie also discussed how PTSD entered our lexicon and what utility the diagnosis has for nonservice members.
On Twitter @whitneymcknight

AUDIO: The 'moral injury' suffered after killing on command
How does killing another person because you’ve been commanded to affect one’s mental health? Does it bring on an existential crisis, and does that contribute to posttraumatic stress disorder?
Col. Elspeth Ritchie, U.S. Army retired and an Army psychiatrist, explains how participating in "vast amounts of death and destruction" affects a person’s ability to cope afterward.
On Twitter @whitneymcknight
How does killing another person because you’ve been commanded to affect one’s mental health? Does it bring on an existential crisis, and does that contribute to posttraumatic stress disorder?
Col. Elspeth Ritchie, U.S. Army retired and an Army psychiatrist, explains how participating in "vast amounts of death and destruction" affects a person’s ability to cope afterward.
On Twitter @whitneymcknight
How does killing another person because you’ve been commanded to affect one’s mental health? Does it bring on an existential crisis, and does that contribute to posttraumatic stress disorder?
Col. Elspeth Ritchie, U.S. Army retired and an Army psychiatrist, explains how participating in "vast amounts of death and destruction" affects a person’s ability to cope afterward.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM CLINICAL PSYCHIATRY NEWS BOARD MEMBER

VIDEO: No longer ‘haunted’: a novel treatment for PTSD
CHICAGO – The driving force behind anxiety is avoidance, according to Barbara Rothbaum, Ph.D., an expert in exposure therapy and a presenter at this year’s annual conference of the Anxiety and Depression Association of America.
"What we think maintains [a person’s] anxiety is avoidance of what they’re scared of," says Dr. Rothbaum in this video. "We help people confront what they’re scared of, in a therapeutic manner."
Particularly in posttraumatic stress disorder, there are two drivers holding anxiety in place, which when addressed by repeatedly immersing a patient in a virtual re-creation of the traumatic event, are relieved so the person can find peace. Many patients say, "It doesn’t haunt me anymore," according to Dr. Rothbaum, professor in the department of psychiatry and behavioral sciences and director of the trauma and anxiety recovery program at Emory University, Atlanta.
In this video, Dr. Rothbaum explores what drives anxiety and how the therapeutic, virtual re-creations of painful memories is helping patients with PTSD accept that although certain things will always be "sad," they need not negate joy and pleasure in life.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
CHICAGO – The driving force behind anxiety is avoidance, according to Barbara Rothbaum, Ph.D., an expert in exposure therapy and a presenter at this year’s annual conference of the Anxiety and Depression Association of America.
"What we think maintains [a person’s] anxiety is avoidance of what they’re scared of," says Dr. Rothbaum in this video. "We help people confront what they’re scared of, in a therapeutic manner."
Particularly in posttraumatic stress disorder, there are two drivers holding anxiety in place, which when addressed by repeatedly immersing a patient in a virtual re-creation of the traumatic event, are relieved so the person can find peace. Many patients say, "It doesn’t haunt me anymore," according to Dr. Rothbaum, professor in the department of psychiatry and behavioral sciences and director of the trauma and anxiety recovery program at Emory University, Atlanta.
In this video, Dr. Rothbaum explores what drives anxiety and how the therapeutic, virtual re-creations of painful memories is helping patients with PTSD accept that although certain things will always be "sad," they need not negate joy and pleasure in life.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
CHICAGO – The driving force behind anxiety is avoidance, according to Barbara Rothbaum, Ph.D., an expert in exposure therapy and a presenter at this year’s annual conference of the Anxiety and Depression Association of America.
"What we think maintains [a person’s] anxiety is avoidance of what they’re scared of," says Dr. Rothbaum in this video. "We help people confront what they’re scared of, in a therapeutic manner."
Particularly in posttraumatic stress disorder, there are two drivers holding anxiety in place, which when addressed by repeatedly immersing a patient in a virtual re-creation of the traumatic event, are relieved so the person can find peace. Many patients say, "It doesn’t haunt me anymore," according to Dr. Rothbaum, professor in the department of psychiatry and behavioral sciences and director of the trauma and anxiety recovery program at Emory University, Atlanta.
In this video, Dr. Rothbaum explores what drives anxiety and how the therapeutic, virtual re-creations of painful memories is helping patients with PTSD accept that although certain things will always be "sad," they need not negate joy and pleasure in life.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE AADA ANNUAL CONFERENCE
Warriors at Ease
The art of yoga has been practiced for thousands of years and most recently has been incorporated into medical practice as a holistic approach to healing. Veterans return from war with a unique set of physical and mental limitations, and for them a unique healing strategy must be established.
One piece of the healing puzzle is alternative therapy, and to accommodate wounded warriors, Warriors at Ease was established. With resources available at http://warriorsatease.com, Warriors at Ease “brings the healing power of yoga and meditation to military communities around the world, especially those affected by combat stress, PTSD [posttraumatic stress disorder], and trauma.”
This website offers information on earning certification to teach yoga and meditation in military communities, including why, how, and where. Webinars and residential trainings are offered on such topics as Fundamentals, Teaching Trauma-Sensitive Meditation, and Advanced Skills for Addressing Combat-Related Issues. A certified instructor can also be found through the zip code search function.
The art of yoga has been practiced for thousands of years and most recently has been incorporated into medical practice as a holistic approach to healing. Veterans return from war with a unique set of physical and mental limitations, and for them a unique healing strategy must be established.
One piece of the healing puzzle is alternative therapy, and to accommodate wounded warriors, Warriors at Ease was established. With resources available at http://warriorsatease.com, Warriors at Ease “brings the healing power of yoga and meditation to military communities around the world, especially those affected by combat stress, PTSD [posttraumatic stress disorder], and trauma.”
This website offers information on earning certification to teach yoga and meditation in military communities, including why, how, and where. Webinars and residential trainings are offered on such topics as Fundamentals, Teaching Trauma-Sensitive Meditation, and Advanced Skills for Addressing Combat-Related Issues. A certified instructor can also be found through the zip code search function.
The art of yoga has been practiced for thousands of years and most recently has been incorporated into medical practice as a holistic approach to healing. Veterans return from war with a unique set of physical and mental limitations, and for them a unique healing strategy must be established.
One piece of the healing puzzle is alternative therapy, and to accommodate wounded warriors, Warriors at Ease was established. With resources available at http://warriorsatease.com, Warriors at Ease “brings the healing power of yoga and meditation to military communities around the world, especially those affected by combat stress, PTSD [posttraumatic stress disorder], and trauma.”
This website offers information on earning certification to teach yoga and meditation in military communities, including why, how, and where. Webinars and residential trainings are offered on such topics as Fundamentals, Teaching Trauma-Sensitive Meditation, and Advanced Skills for Addressing Combat-Related Issues. A certified instructor can also be found through the zip code search function.
Peptic Ulcer Bleeding; PTSD and Metabolic Syndrome
ACE Fit; I Want to Work on My...; Heart360
Hearing voices, time traveling, and being hit with a high-heeled shoe
CASE Grief and confusion
Mr. P, age 47, is arrested for entering the apartment of a woman he does not know and tossing her belongings out the window. When he is assessed to determine if he can participate in his legal defense, examiners find an attentive, courteous man who is baffled by his own behavior.
Mr. P says that he had been “stressed out” after the recent death of his grandmother, with whom he was close. He says he entered the apartment because voices told him to do so. He has no recent history of substance abuse or psychiatric hospitalizations, but he had a similar episode of “confusion” years before, when another close family member died.
Mr. P is found not fit to stand trial and the charges are dropped. He accepts haloperidol, 10 mg/d, and benztropine, 2 mg/d, and is transferred to a hospital for psychiatric treatment.
On interview, Mr. P is well groomed, soft-spoken, and shy, without formal thought disorder. Physical exam and routine lab tests are within normal limits. He says that 18 months before his arrest, he and his frail grandmother moved to a large city in hopes that he would find a wife. Both depended on the grandmother’s Social Security benefits while he cared for her.
In the 2 months after she died, he reports that he felt sad and alone and slept poorly, but made efforts to find a job and keep his apartment. When his efforts failed and he lost the apartment, he stayed with various friends for a few days at a time, then spent several days in the subway before ending up on the streets.
His arrest on the current charge occurred 4 days after he began walking the streets.
a) continue haloperidol to treat psychotic symptoms
b) discontinue haloperidol and observe him
c) add an antidepressant to haloperidol
HISTORY Imagining nonsense
Mr. P cannot explain why he started “trashing” the woman’s apartment, but says he entered it because he thought it was his apartment. With embarrassment and regret, he admits he has been depressed and confused, “imagining things”—“foolish things,” he admits—such as being in a different “time zone.”
Contradicting his earlier statements, Mr. P now admits that he had “a few beers” and denies that he experienced auditory hallucinations, saying he only talks to himself. He now says that within 2 days after his arrest, he was “all over it.” Mr. P denies current symptoms, including hallucinations, but, when pressed, waffles, then admits to a strange belief: that some people, including him, can move from one “time zone” to another.
Mr. P says he was treated for psychiatric problems 4 years earlier when his parents were killed in a car crash. By his recollection, his reaction to their death was similar to his reaction to his grandmother’s death: He became upset and wandered the streets for a few days, “moving between time zones” and talking to himself but not experiencing hallucinations. After he was taken to a hospital and “given an injection,” he calmed down and was released. Within a few days he recovered and returned to supporting himself and caring for his grandmother. Mr. P says the idea of travelling between “time zones” is embarrassing and nonsensical but adds that he was affected in this way because he “bickered” with his mother.
Mr. P’s grandmother raised him until he was age 15, although he frequently visited his parents, who lived nearby and worked during the day. Mr. P initially denies substance abuse, then admits to smoking marijuana every day for about a year before admission. He also admits to cocaine abuse in his 20s. He denies a history of suicide attempts.
The author’s observations
Mr. P reported only 2 episodes of “confusion” (or psychosis) and strange behavior in his life, both precipitated by the loss of a loved one, and at least 1 while under the influence of alcohol and Cannabis. He gave an inconsistent and ambiguous history of auditory hallucinations associated with episodes of confusion. He believes that time travel is possible, an idea that he acknowledged is nonsense. This alone was not enough to warrant long-term antipsychotic treatment. The most likely diagnosis seemed to be brief psychotic episode induced by Cannabis and the stressors of homelessness and his grandmother’s death.
EVALUATION Changing stories
No longer taking haloperidol, Mr. P continues to deny hallucinations and depressed mood, but keeps to himself. Nine days after admission he becomes tearful after he informs his aunt of his grandmother’s death in a telephone call, then approaches a nurse and complains of sadness and auditory hallucinations.
Mr. P confesses that he denied hallucinations on admission because he feared he would remain in the hospital for years if he revealed the truth that he had been experiencing auditory hallucinations almost continuously from age 10. He reports that the voices distracted him when he worked; seem to be male; often spoke gibberish; and alternate between deprecating and positive and supportive. Mr. P is reluctant to disclose more about what the voices actually say, although he acknowledges that they are not commenting or conversing with him, and that he has never believed the voices were his own thoughts but did believe that they came from inside his brain.
With haloperidol, the voices stopped. They resumed, however, when haloperidol was discontinued.
When we ask what happened to him at age 10, Mr. P shrugs.
a) childhood onset schizophrenia
b) substance abuse
c) posttraumatic stress disorder (PTSD)
d) none
The author’s observations
In community samples of children and adolescents, auditory hallucinations are not rare and usually do not cause distress or dysfunction. In a study of 3,870 children age 7 and 8,1 9% endorsed auditory hallucinations. Most heard 1 voice, once a week or less, at low volume. In 85% of children who experienced hallucinations, they caused minimal or no suffering; 97% reported minimal or no interference with daily functioning. Among children who experienced auditory hallucinations at age 7 or 8, 24% continued to hallucinate 5 years later.2 Persistent hallucinations were associated with more problematic behaviors at baseline and follow up.
In a group of 12-year-old twins, 4.2% reported auditory hallucinations.3 In that study, hallucinations were not related to Cannabis use; rather, they were heritable and related to risk factors such as cognitive impairment; behavioral, emotional, and educational problems at age 5; and a history of physical abuse and self-harm at age 12. The authors noted that these are risk factors and correlates of schizophrenia, but are not specific to schizophrenia.
Hallucinations and delusions have been found in 4% to 8% of children and adolescents referred for psychiatric treatment,4 far more than the prevalence of childhood-onset schizophrenia (0.01% of children).5 Psychotic symptoms in children have been associated with bipolar disorder, but also with anxiety disorders, obsessive-compulsive disorder, PTSD, pervasive developmental disorder, conduct disorder, and substance abuse.4
Childhood-onset schizophrenia is rare and would require that Mr. P have a diagnosis of schizophrenia as an adult. It is possible that Mr. P’s childhood symptoms were related to substance abuse but he was not asked for this history because it seemed unlikely in a 10-year-old boy. A PTSD diagnosis requires a traumatic event, which Mr. P did not reveal. It is possible that at age 10 he did not have a psychiatric disorder.
a) PTSD
b) dissociative disorder
c) borderline personality disorder
d) chronic schizophrenia
e) no psychiatric diagnosis
Among adults in the general population, 10% to 15% report auditory hallucinations.6 Hallucinations could be caused by substance abuse or psychiatric conditions other than schizophrenia; however, in adults—as in children—auditory hallucinations can occur in the absence of these conditions (Table 1) and rarely cause distress or dysfunction.6 In Sommer and colleagues’6 study of 103 healthy persons, none who heard voices had disorganization or negative symptoms. Those who heard voices had significantly more schizotypal symptoms and more childhood trauma, including emotional, physical, and sexual abuse, than those who did not hear voices.6
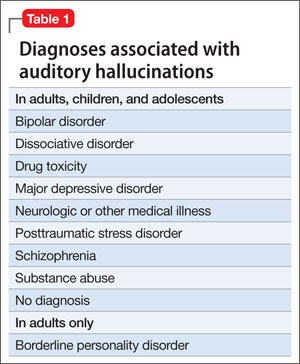
Conditions associated with hallucinations
PTSD is associated with auditory hallucinations and other psychotic symptoms.7 Most studies are of combat veterans with PTSD, in whom auditory hallucinations and delusions were associated with major depressive disorder, not a thought disorder or inappropriate affect.8 In a community sample,9 psychotic symptoms—particularly auditory hallucinations—were associated with PTSD. Subjects with PTSD and psychotic symptoms were more likely to have other psychiatric disorders, including major depressive disorder and substance use disorder, than patients with PTSD but no psychotic symptoms; however, the relationship between PTSD and psychosis remained after controlling for other psychiatric disorders.
Hallucinations can occur in persons with dissociative disorders in the absence of distinct personality states.10 Hallucinations have been seen transiently and chronically in persons with borderline personality disorder and can be associated with comorbid conditions such as substance abuse disorders, mood disorders, and PTSD.11
Mr. P lacked the reduced capacity for interpersonal relationships required for a schizotypal personality disorder diagnosis. A diagnosis of PTSD or dissociative disorder requires a history of trauma, which Mr. P did not report.
“Time travelling” with incomprehensible behavior could be interpreted as dissociation, but dissociative fugue or dissociative disorder not otherwise specified (NOS) cannot be diagnosed if symptoms might be the direct effect of a substance, such as Cannabis. Mr. P admitted to substance abuse. We can rule out borderline personality disorder because he did not display or admit to tempestuous interpersonal relationships.
A schizophrenia diagnosis requires the presence of auditory hallucinations that commented on his behavior or conversed among themselves, a second psychotic symptom for ≥1 month, or negative symptoms, which Mr. P lacked (unless belief in time travel is considered delusional).
Last, a physician might have considered malingering or a factitious disorder when Mr. P was found not able to participate in his own defense, but this seemed less likely after he revealed that he experienced auditory hallucinations since age 10.
HISTORY Bad beatings
With a few days of beginning risperidone, 4 mg/d, Mr. P reports that his hallucinations have stopped and he feels less sad. He reveals that, at age 10, when the hallucinations began, his mother hit him over the head with a high-heeled shoe, causing a scalp laceration that required a visit to the emergency room for suturing. His mother beat Mr. P for as long as he could remember. She beat him “bad” at least twice weekly, and he was taken to the hospital 7 or 8 times for injury, but she also beat him “constantly” with a belt buckle, sometimes striking his head. She instructed him to tell nobody.
The author’s observations
Auditory hallucinations in adults have been associated with childhood abuse, particularly childhood sexual abuse,12 in clinical and non-clinical samples.13 Some argue13 that child abuse itself causes hallucinations and other psychotic symptoms.
OUTCOME Depressed and sleepless
Mr. P admits that he had been smoking marijuana 2 to 3 times daily for a year. He also reports insomnia, sleeping approximately 4 hours a night and spending hours awake in bed thinking of his grandmother, with depressed mood and tearfulness. He denies suicidal ideas and hallucinations. He is treated for depressive disorder NOS first with amitriptyline, 50 mg at bedtime, for sleep, then paroxetine, 20 mg/d, for depressive symptoms, in addition to risperidone, 4 mg/d. Although Mr. P does not describe re-experiencing his childhood trauma, avoidance of stimuli associated with the trauma, or symptoms of increased arousal (except for insomnia), the treatment team did not ask, so it remains uncertain if he has PTSD (Table 2).

When Mr. P is discharged to a clinic, he smiles easily and is positive and supportive with other patients. He spruces up his appearance by wearing jewelry and works in the hospital kitchen.
Bottom Line
Chronic auditory hallucinations are associated with psychiatric illnesses other than chronic schizophrenia, particularly those resulting from trauma such as posttraumatic stress disorder. They can also occur in the absence of diagnosable psychiatric illness and rarely cause distress or functional impairment. Auditory hallucinations in adults have been associated with childhood abuse.
Related Resources
- Moskowitz A, Schafer I, Dorahy MJ. Psychosis, trauma and dissociation: emerging perspectives on severe psychopathology. West Sussex, UK: John Wiley and Sons, Ltd.; 2008.
- The International Hearing Voices Network. www.intervoiceonline.org.
Drug Brand Names
Amitriptyline • Elavil Paroxetine • Paxil
Benztropine • Cogentin Risperidone • Risperdal
Haloperidol • Haldol
Disclosure
Dr. Crowner reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Barthel-Velthuis AA, Jenner JA, van de Willige G, et al Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
2. Bartels-Velthuis AA, van de Willige G, Jenner JA, et al. Course of auditory vocal hallucinations in childhood: 5-year follow-up study. Br J Psychiatry. 2011;199(4):296-302.
3. Polanczyk G, Moffitt TE, Arsensault L, et al. Etiological and clinical features of childhood psychotic symptoms: results from a birth cohort. Arch Gen Psychiatry. 2010;67(4):328-338.
4. Biederman J, Pety C, Faracone SV, et al. Phenomenology of childhood psychosis: Findings from a large sample of psychiatrically referred youth. J Nerv Ment Dis 2004;192(9):607-614.
5. American Academy of Child and Adolescent Psychiatry. Practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry. 2001;40(suppl 7):4SS-23S.
6. Sommer IEC, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; Who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
7. Butler RW, Mueser KT, Sprock J, et al. Positive symptoms of psychosis in posttraumatic stress disorder. Biol Psychiatry. 1996;39:839-844.
8. David D, Kutcher GS, Jackson EI, et al Psychotic symptoms in combat-related posttraumatic stress disorder. J Clin Psychiatry. 1999;60(1):29-32.
9. Sareen J, Cox BJ, Goodwin RD, et al. Co-occurrence of posttraumatic stress disorder with positive psychotic symptoms in a nationally representative sample. J Trauma Stress. 2005;18(4):313-322.
10. Sar V, Akyuv G, Dogan O. Prevalence of dissociative disorders among women in the general population. Psychiatry Res. 2007;149:169-176.
11. Barnow S, Arens EA, Sieswerda S, et al. Borderline personality disorder and psychosis: a review. Curr Psychiatry Rep. 2010;12(3):186-195.
12. Bebbington P, Jonas S, Kuipers E, et al. Childhood sexual abuse and psychosis: data from a cross-sectional national psychiatric survey in England. Br J Psychiatry. 2011;199(1):29-37.
13. Read J, van Os J, Morrison AP, et al. Childhood trauma, psychosis and schizophrenia: a literature review with theoretical and clinical implications. Acta Psychiatr Scand. 2005;112(5):330-350.
CASE Grief and confusion
Mr. P, age 47, is arrested for entering the apartment of a woman he does not know and tossing her belongings out the window. When he is assessed to determine if he can participate in his legal defense, examiners find an attentive, courteous man who is baffled by his own behavior.
Mr. P says that he had been “stressed out” after the recent death of his grandmother, with whom he was close. He says he entered the apartment because voices told him to do so. He has no recent history of substance abuse or psychiatric hospitalizations, but he had a similar episode of “confusion” years before, when another close family member died.
Mr. P is found not fit to stand trial and the charges are dropped. He accepts haloperidol, 10 mg/d, and benztropine, 2 mg/d, and is transferred to a hospital for psychiatric treatment.
On interview, Mr. P is well groomed, soft-spoken, and shy, without formal thought disorder. Physical exam and routine lab tests are within normal limits. He says that 18 months before his arrest, he and his frail grandmother moved to a large city in hopes that he would find a wife. Both depended on the grandmother’s Social Security benefits while he cared for her.
In the 2 months after she died, he reports that he felt sad and alone and slept poorly, but made efforts to find a job and keep his apartment. When his efforts failed and he lost the apartment, he stayed with various friends for a few days at a time, then spent several days in the subway before ending up on the streets.
His arrest on the current charge occurred 4 days after he began walking the streets.
a) continue haloperidol to treat psychotic symptoms
b) discontinue haloperidol and observe him
c) add an antidepressant to haloperidol
HISTORY Imagining nonsense
Mr. P cannot explain why he started “trashing” the woman’s apartment, but says he entered it because he thought it was his apartment. With embarrassment and regret, he admits he has been depressed and confused, “imagining things”—“foolish things,” he admits—such as being in a different “time zone.”
Contradicting his earlier statements, Mr. P now admits that he had “a few beers” and denies that he experienced auditory hallucinations, saying he only talks to himself. He now says that within 2 days after his arrest, he was “all over it.” Mr. P denies current symptoms, including hallucinations, but, when pressed, waffles, then admits to a strange belief: that some people, including him, can move from one “time zone” to another.
Mr. P says he was treated for psychiatric problems 4 years earlier when his parents were killed in a car crash. By his recollection, his reaction to their death was similar to his reaction to his grandmother’s death: He became upset and wandered the streets for a few days, “moving between time zones” and talking to himself but not experiencing hallucinations. After he was taken to a hospital and “given an injection,” he calmed down and was released. Within a few days he recovered and returned to supporting himself and caring for his grandmother. Mr. P says the idea of travelling between “time zones” is embarrassing and nonsensical but adds that he was affected in this way because he “bickered” with his mother.
Mr. P’s grandmother raised him until he was age 15, although he frequently visited his parents, who lived nearby and worked during the day. Mr. P initially denies substance abuse, then admits to smoking marijuana every day for about a year before admission. He also admits to cocaine abuse in his 20s. He denies a history of suicide attempts.
The author’s observations
Mr. P reported only 2 episodes of “confusion” (or psychosis) and strange behavior in his life, both precipitated by the loss of a loved one, and at least 1 while under the influence of alcohol and Cannabis. He gave an inconsistent and ambiguous history of auditory hallucinations associated with episodes of confusion. He believes that time travel is possible, an idea that he acknowledged is nonsense. This alone was not enough to warrant long-term antipsychotic treatment. The most likely diagnosis seemed to be brief psychotic episode induced by Cannabis and the stressors of homelessness and his grandmother’s death.
EVALUATION Changing stories
No longer taking haloperidol, Mr. P continues to deny hallucinations and depressed mood, but keeps to himself. Nine days after admission he becomes tearful after he informs his aunt of his grandmother’s death in a telephone call, then approaches a nurse and complains of sadness and auditory hallucinations.
Mr. P confesses that he denied hallucinations on admission because he feared he would remain in the hospital for years if he revealed the truth that he had been experiencing auditory hallucinations almost continuously from age 10. He reports that the voices distracted him when he worked; seem to be male; often spoke gibberish; and alternate between deprecating and positive and supportive. Mr. P is reluctant to disclose more about what the voices actually say, although he acknowledges that they are not commenting or conversing with him, and that he has never believed the voices were his own thoughts but did believe that they came from inside his brain.
With haloperidol, the voices stopped. They resumed, however, when haloperidol was discontinued.
When we ask what happened to him at age 10, Mr. P shrugs.
a) childhood onset schizophrenia
b) substance abuse
c) posttraumatic stress disorder (PTSD)
d) none
The author’s observations
In community samples of children and adolescents, auditory hallucinations are not rare and usually do not cause distress or dysfunction. In a study of 3,870 children age 7 and 8,1 9% endorsed auditory hallucinations. Most heard 1 voice, once a week or less, at low volume. In 85% of children who experienced hallucinations, they caused minimal or no suffering; 97% reported minimal or no interference with daily functioning. Among children who experienced auditory hallucinations at age 7 or 8, 24% continued to hallucinate 5 years later.2 Persistent hallucinations were associated with more problematic behaviors at baseline and follow up.
In a group of 12-year-old twins, 4.2% reported auditory hallucinations.3 In that study, hallucinations were not related to Cannabis use; rather, they were heritable and related to risk factors such as cognitive impairment; behavioral, emotional, and educational problems at age 5; and a history of physical abuse and self-harm at age 12. The authors noted that these are risk factors and correlates of schizophrenia, but are not specific to schizophrenia.
Hallucinations and delusions have been found in 4% to 8% of children and adolescents referred for psychiatric treatment,4 far more than the prevalence of childhood-onset schizophrenia (0.01% of children).5 Psychotic symptoms in children have been associated with bipolar disorder, but also with anxiety disorders, obsessive-compulsive disorder, PTSD, pervasive developmental disorder, conduct disorder, and substance abuse.4
Childhood-onset schizophrenia is rare and would require that Mr. P have a diagnosis of schizophrenia as an adult. It is possible that Mr. P’s childhood symptoms were related to substance abuse but he was not asked for this history because it seemed unlikely in a 10-year-old boy. A PTSD diagnosis requires a traumatic event, which Mr. P did not reveal. It is possible that at age 10 he did not have a psychiatric disorder.
a) PTSD
b) dissociative disorder
c) borderline personality disorder
d) chronic schizophrenia
e) no psychiatric diagnosis
Among adults in the general population, 10% to 15% report auditory hallucinations.6 Hallucinations could be caused by substance abuse or psychiatric conditions other than schizophrenia; however, in adults—as in children—auditory hallucinations can occur in the absence of these conditions (Table 1) and rarely cause distress or dysfunction.6 In Sommer and colleagues’6 study of 103 healthy persons, none who heard voices had disorganization or negative symptoms. Those who heard voices had significantly more schizotypal symptoms and more childhood trauma, including emotional, physical, and sexual abuse, than those who did not hear voices.6
Conditions associated with hallucinations
PTSD is associated with auditory hallucinations and other psychotic symptoms.7 Most studies are of combat veterans with PTSD, in whom auditory hallucinations and delusions were associated with major depressive disorder, not a thought disorder or inappropriate affect.8 In a community sample,9 psychotic symptoms—particularly auditory hallucinations—were associated with PTSD. Subjects with PTSD and psychotic symptoms were more likely to have other psychiatric disorders, including major depressive disorder and substance use disorder, than patients with PTSD but no psychotic symptoms; however, the relationship between PTSD and psychosis remained after controlling for other psychiatric disorders.
Hallucinations can occur in persons with dissociative disorders in the absence of distinct personality states.10 Hallucinations have been seen transiently and chronically in persons with borderline personality disorder and can be associated with comorbid conditions such as substance abuse disorders, mood disorders, and PTSD.11
Mr. P lacked the reduced capacity for interpersonal relationships required for a schizotypal personality disorder diagnosis. A diagnosis of PTSD or dissociative disorder requires a history of trauma, which Mr. P did not report.
“Time travelling” with incomprehensible behavior could be interpreted as dissociation, but dissociative fugue or dissociative disorder not otherwise specified (NOS) cannot be diagnosed if symptoms might be the direct effect of a substance, such as Cannabis. Mr. P admitted to substance abuse. We can rule out borderline personality disorder because he did not display or admit to tempestuous interpersonal relationships.
A schizophrenia diagnosis requires the presence of auditory hallucinations that commented on his behavior or conversed among themselves, a second psychotic symptom for ≥1 month, or negative symptoms, which Mr. P lacked (unless belief in time travel is considered delusional).
Last, a physician might have considered malingering or a factitious disorder when Mr. P was found not able to participate in his own defense, but this seemed less likely after he revealed that he experienced auditory hallucinations since age 10.
HISTORY Bad beatings
With a few days of beginning risperidone, 4 mg/d, Mr. P reports that his hallucinations have stopped and he feels less sad. He reveals that, at age 10, when the hallucinations began, his mother hit him over the head with a high-heeled shoe, causing a scalp laceration that required a visit to the emergency room for suturing. His mother beat Mr. P for as long as he could remember. She beat him “bad” at least twice weekly, and he was taken to the hospital 7 or 8 times for injury, but she also beat him “constantly” with a belt buckle, sometimes striking his head. She instructed him to tell nobody.
The author’s observations
Auditory hallucinations in adults have been associated with childhood abuse, particularly childhood sexual abuse,12 in clinical and non-clinical samples.13 Some argue13 that child abuse itself causes hallucinations and other psychotic symptoms.
OUTCOME Depressed and sleepless
Mr. P admits that he had been smoking marijuana 2 to 3 times daily for a year. He also reports insomnia, sleeping approximately 4 hours a night and spending hours awake in bed thinking of his grandmother, with depressed mood and tearfulness. He denies suicidal ideas and hallucinations. He is treated for depressive disorder NOS first with amitriptyline, 50 mg at bedtime, for sleep, then paroxetine, 20 mg/d, for depressive symptoms, in addition to risperidone, 4 mg/d. Although Mr. P does not describe re-experiencing his childhood trauma, avoidance of stimuli associated with the trauma, or symptoms of increased arousal (except for insomnia), the treatment team did not ask, so it remains uncertain if he has PTSD (Table 2).
When Mr. P is discharged to a clinic, he smiles easily and is positive and supportive with other patients. He spruces up his appearance by wearing jewelry and works in the hospital kitchen.
Bottom Line
Chronic auditory hallucinations are associated with psychiatric illnesses other than chronic schizophrenia, particularly those resulting from trauma such as posttraumatic stress disorder. They can also occur in the absence of diagnosable psychiatric illness and rarely cause distress or functional impairment. Auditory hallucinations in adults have been associated with childhood abuse.
Related Resources
- Moskowitz A, Schafer I, Dorahy MJ. Psychosis, trauma and dissociation: emerging perspectives on severe psychopathology. West Sussex, UK: John Wiley and Sons, Ltd.; 2008.
- The International Hearing Voices Network. www.intervoiceonline.org.
Drug Brand Names
Amitriptyline • Elavil Paroxetine • Paxil
Benztropine • Cogentin Risperidone • Risperdal
Haloperidol • Haldol
Disclosure
Dr. Crowner reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE Grief and confusion
Mr. P, age 47, is arrested for entering the apartment of a woman he does not know and tossing her belongings out the window. When he is assessed to determine if he can participate in his legal defense, examiners find an attentive, courteous man who is baffled by his own behavior.
Mr. P says that he had been “stressed out” after the recent death of his grandmother, with whom he was close. He says he entered the apartment because voices told him to do so. He has no recent history of substance abuse or psychiatric hospitalizations, but he had a similar episode of “confusion” years before, when another close family member died.
Mr. P is found not fit to stand trial and the charges are dropped. He accepts haloperidol, 10 mg/d, and benztropine, 2 mg/d, and is transferred to a hospital for psychiatric treatment.
On interview, Mr. P is well groomed, soft-spoken, and shy, without formal thought disorder. Physical exam and routine lab tests are within normal limits. He says that 18 months before his arrest, he and his frail grandmother moved to a large city in hopes that he would find a wife. Both depended on the grandmother’s Social Security benefits while he cared for her.
In the 2 months after she died, he reports that he felt sad and alone and slept poorly, but made efforts to find a job and keep his apartment. When his efforts failed and he lost the apartment, he stayed with various friends for a few days at a time, then spent several days in the subway before ending up on the streets.
His arrest on the current charge occurred 4 days after he began walking the streets.
a) continue haloperidol to treat psychotic symptoms
b) discontinue haloperidol and observe him
c) add an antidepressant to haloperidol
HISTORY Imagining nonsense
Mr. P cannot explain why he started “trashing” the woman’s apartment, but says he entered it because he thought it was his apartment. With embarrassment and regret, he admits he has been depressed and confused, “imagining things”—“foolish things,” he admits—such as being in a different “time zone.”
Contradicting his earlier statements, Mr. P now admits that he had “a few beers” and denies that he experienced auditory hallucinations, saying he only talks to himself. He now says that within 2 days after his arrest, he was “all over it.” Mr. P denies current symptoms, including hallucinations, but, when pressed, waffles, then admits to a strange belief: that some people, including him, can move from one “time zone” to another.
Mr. P says he was treated for psychiatric problems 4 years earlier when his parents were killed in a car crash. By his recollection, his reaction to their death was similar to his reaction to his grandmother’s death: He became upset and wandered the streets for a few days, “moving between time zones” and talking to himself but not experiencing hallucinations. After he was taken to a hospital and “given an injection,” he calmed down and was released. Within a few days he recovered and returned to supporting himself and caring for his grandmother. Mr. P says the idea of travelling between “time zones” is embarrassing and nonsensical but adds that he was affected in this way because he “bickered” with his mother.
Mr. P’s grandmother raised him until he was age 15, although he frequently visited his parents, who lived nearby and worked during the day. Mr. P initially denies substance abuse, then admits to smoking marijuana every day for about a year before admission. He also admits to cocaine abuse in his 20s. He denies a history of suicide attempts.
The author’s observations
Mr. P reported only 2 episodes of “confusion” (or psychosis) and strange behavior in his life, both precipitated by the loss of a loved one, and at least 1 while under the influence of alcohol and Cannabis. He gave an inconsistent and ambiguous history of auditory hallucinations associated with episodes of confusion. He believes that time travel is possible, an idea that he acknowledged is nonsense. This alone was not enough to warrant long-term antipsychotic treatment. The most likely diagnosis seemed to be brief psychotic episode induced by Cannabis and the stressors of homelessness and his grandmother’s death.
EVALUATION Changing stories
No longer taking haloperidol, Mr. P continues to deny hallucinations and depressed mood, but keeps to himself. Nine days after admission he becomes tearful after he informs his aunt of his grandmother’s death in a telephone call, then approaches a nurse and complains of sadness and auditory hallucinations.
Mr. P confesses that he denied hallucinations on admission because he feared he would remain in the hospital for years if he revealed the truth that he had been experiencing auditory hallucinations almost continuously from age 10. He reports that the voices distracted him when he worked; seem to be male; often spoke gibberish; and alternate between deprecating and positive and supportive. Mr. P is reluctant to disclose more about what the voices actually say, although he acknowledges that they are not commenting or conversing with him, and that he has never believed the voices were his own thoughts but did believe that they came from inside his brain.
With haloperidol, the voices stopped. They resumed, however, when haloperidol was discontinued.
When we ask what happened to him at age 10, Mr. P shrugs.
a) childhood onset schizophrenia
b) substance abuse
c) posttraumatic stress disorder (PTSD)
d) none
The author’s observations
In community samples of children and adolescents, auditory hallucinations are not rare and usually do not cause distress or dysfunction. In a study of 3,870 children age 7 and 8,1 9% endorsed auditory hallucinations. Most heard 1 voice, once a week or less, at low volume. In 85% of children who experienced hallucinations, they caused minimal or no suffering; 97% reported minimal or no interference with daily functioning. Among children who experienced auditory hallucinations at age 7 or 8, 24% continued to hallucinate 5 years later.2 Persistent hallucinations were associated with more problematic behaviors at baseline and follow up.
In a group of 12-year-old twins, 4.2% reported auditory hallucinations.3 In that study, hallucinations were not related to Cannabis use; rather, they were heritable and related to risk factors such as cognitive impairment; behavioral, emotional, and educational problems at age 5; and a history of physical abuse and self-harm at age 12. The authors noted that these are risk factors and correlates of schizophrenia, but are not specific to schizophrenia.
Hallucinations and delusions have been found in 4% to 8% of children and adolescents referred for psychiatric treatment,4 far more than the prevalence of childhood-onset schizophrenia (0.01% of children).5 Psychotic symptoms in children have been associated with bipolar disorder, but also with anxiety disorders, obsessive-compulsive disorder, PTSD, pervasive developmental disorder, conduct disorder, and substance abuse.4
Childhood-onset schizophrenia is rare and would require that Mr. P have a diagnosis of schizophrenia as an adult. It is possible that Mr. P’s childhood symptoms were related to substance abuse but he was not asked for this history because it seemed unlikely in a 10-year-old boy. A PTSD diagnosis requires a traumatic event, which Mr. P did not reveal. It is possible that at age 10 he did not have a psychiatric disorder.
a) PTSD
b) dissociative disorder
c) borderline personality disorder
d) chronic schizophrenia
e) no psychiatric diagnosis
Among adults in the general population, 10% to 15% report auditory hallucinations.6 Hallucinations could be caused by substance abuse or psychiatric conditions other than schizophrenia; however, in adults—as in children—auditory hallucinations can occur in the absence of these conditions (Table 1) and rarely cause distress or dysfunction.6 In Sommer and colleagues’6 study of 103 healthy persons, none who heard voices had disorganization or negative symptoms. Those who heard voices had significantly more schizotypal symptoms and more childhood trauma, including emotional, physical, and sexual abuse, than those who did not hear voices.6
Conditions associated with hallucinations
PTSD is associated with auditory hallucinations and other psychotic symptoms.7 Most studies are of combat veterans with PTSD, in whom auditory hallucinations and delusions were associated with major depressive disorder, not a thought disorder or inappropriate affect.8 In a community sample,9 psychotic symptoms—particularly auditory hallucinations—were associated with PTSD. Subjects with PTSD and psychotic symptoms were more likely to have other psychiatric disorders, including major depressive disorder and substance use disorder, than patients with PTSD but no psychotic symptoms; however, the relationship between PTSD and psychosis remained after controlling for other psychiatric disorders.
Hallucinations can occur in persons with dissociative disorders in the absence of distinct personality states.10 Hallucinations have been seen transiently and chronically in persons with borderline personality disorder and can be associated with comorbid conditions such as substance abuse disorders, mood disorders, and PTSD.11
Mr. P lacked the reduced capacity for interpersonal relationships required for a schizotypal personality disorder diagnosis. A diagnosis of PTSD or dissociative disorder requires a history of trauma, which Mr. P did not report.
“Time travelling” with incomprehensible behavior could be interpreted as dissociation, but dissociative fugue or dissociative disorder not otherwise specified (NOS) cannot be diagnosed if symptoms might be the direct effect of a substance, such as Cannabis. Mr. P admitted to substance abuse. We can rule out borderline personality disorder because he did not display or admit to tempestuous interpersonal relationships.
A schizophrenia diagnosis requires the presence of auditory hallucinations that commented on his behavior or conversed among themselves, a second psychotic symptom for ≥1 month, or negative symptoms, which Mr. P lacked (unless belief in time travel is considered delusional).
Last, a physician might have considered malingering or a factitious disorder when Mr. P was found not able to participate in his own defense, but this seemed less likely after he revealed that he experienced auditory hallucinations since age 10.
HISTORY Bad beatings
With a few days of beginning risperidone, 4 mg/d, Mr. P reports that his hallucinations have stopped and he feels less sad. He reveals that, at age 10, when the hallucinations began, his mother hit him over the head with a high-heeled shoe, causing a scalp laceration that required a visit to the emergency room for suturing. His mother beat Mr. P for as long as he could remember. She beat him “bad” at least twice weekly, and he was taken to the hospital 7 or 8 times for injury, but she also beat him “constantly” with a belt buckle, sometimes striking his head. She instructed him to tell nobody.
The author’s observations
Auditory hallucinations in adults have been associated with childhood abuse, particularly childhood sexual abuse,12 in clinical and non-clinical samples.13 Some argue13 that child abuse itself causes hallucinations and other psychotic symptoms.
OUTCOME Depressed and sleepless
Mr. P admits that he had been smoking marijuana 2 to 3 times daily for a year. He also reports insomnia, sleeping approximately 4 hours a night and spending hours awake in bed thinking of his grandmother, with depressed mood and tearfulness. He denies suicidal ideas and hallucinations. He is treated for depressive disorder NOS first with amitriptyline, 50 mg at bedtime, for sleep, then paroxetine, 20 mg/d, for depressive symptoms, in addition to risperidone, 4 mg/d. Although Mr. P does not describe re-experiencing his childhood trauma, avoidance of stimuli associated with the trauma, or symptoms of increased arousal (except for insomnia), the treatment team did not ask, so it remains uncertain if he has PTSD (Table 2).
When Mr. P is discharged to a clinic, he smiles easily and is positive and supportive with other patients. He spruces up his appearance by wearing jewelry and works in the hospital kitchen.
Bottom Line
Chronic auditory hallucinations are associated with psychiatric illnesses other than chronic schizophrenia, particularly those resulting from trauma such as posttraumatic stress disorder. They can also occur in the absence of diagnosable psychiatric illness and rarely cause distress or functional impairment. Auditory hallucinations in adults have been associated with childhood abuse.
Related Resources
- Moskowitz A, Schafer I, Dorahy MJ. Psychosis, trauma and dissociation: emerging perspectives on severe psychopathology. West Sussex, UK: John Wiley and Sons, Ltd.; 2008.
- The International Hearing Voices Network. www.intervoiceonline.org.
Drug Brand Names
Amitriptyline • Elavil Paroxetine • Paxil
Benztropine • Cogentin Risperidone • Risperdal
Haloperidol • Haldol
Disclosure
Dr. Crowner reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Barthel-Velthuis AA, Jenner JA, van de Willige G, et al Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
2. Bartels-Velthuis AA, van de Willige G, Jenner JA, et al. Course of auditory vocal hallucinations in childhood: 5-year follow-up study. Br J Psychiatry. 2011;199(4):296-302.
3. Polanczyk G, Moffitt TE, Arsensault L, et al. Etiological and clinical features of childhood psychotic symptoms: results from a birth cohort. Arch Gen Psychiatry. 2010;67(4):328-338.
4. Biederman J, Pety C, Faracone SV, et al. Phenomenology of childhood psychosis: Findings from a large sample of psychiatrically referred youth. J Nerv Ment Dis 2004;192(9):607-614.
5. American Academy of Child and Adolescent Psychiatry. Practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry. 2001;40(suppl 7):4SS-23S.
6. Sommer IEC, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; Who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
7. Butler RW, Mueser KT, Sprock J, et al. Positive symptoms of psychosis in posttraumatic stress disorder. Biol Psychiatry. 1996;39:839-844.
8. David D, Kutcher GS, Jackson EI, et al Psychotic symptoms in combat-related posttraumatic stress disorder. J Clin Psychiatry. 1999;60(1):29-32.
9. Sareen J, Cox BJ, Goodwin RD, et al. Co-occurrence of posttraumatic stress disorder with positive psychotic symptoms in a nationally representative sample. J Trauma Stress. 2005;18(4):313-322.
10. Sar V, Akyuv G, Dogan O. Prevalence of dissociative disorders among women in the general population. Psychiatry Res. 2007;149:169-176.
11. Barnow S, Arens EA, Sieswerda S, et al. Borderline personality disorder and psychosis: a review. Curr Psychiatry Rep. 2010;12(3):186-195.
12. Bebbington P, Jonas S, Kuipers E, et al. Childhood sexual abuse and psychosis: data from a cross-sectional national psychiatric survey in England. Br J Psychiatry. 2011;199(1):29-37.
13. Read J, van Os J, Morrison AP, et al. Childhood trauma, psychosis and schizophrenia: a literature review with theoretical and clinical implications. Acta Psychiatr Scand. 2005;112(5):330-350.
1. Barthel-Velthuis AA, Jenner JA, van de Willige G, et al Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
2. Bartels-Velthuis AA, van de Willige G, Jenner JA, et al. Course of auditory vocal hallucinations in childhood: 5-year follow-up study. Br J Psychiatry. 2011;199(4):296-302.
3. Polanczyk G, Moffitt TE, Arsensault L, et al. Etiological and clinical features of childhood psychotic symptoms: results from a birth cohort. Arch Gen Psychiatry. 2010;67(4):328-338.
4. Biederman J, Pety C, Faracone SV, et al. Phenomenology of childhood psychosis: Findings from a large sample of psychiatrically referred youth. J Nerv Ment Dis 2004;192(9):607-614.
5. American Academy of Child and Adolescent Psychiatry. Practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry. 2001;40(suppl 7):4SS-23S.
6. Sommer IEC, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; Who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
7. Butler RW, Mueser KT, Sprock J, et al. Positive symptoms of psychosis in posttraumatic stress disorder. Biol Psychiatry. 1996;39:839-844.
8. David D, Kutcher GS, Jackson EI, et al Psychotic symptoms in combat-related posttraumatic stress disorder. J Clin Psychiatry. 1999;60(1):29-32.
9. Sareen J, Cox BJ, Goodwin RD, et al. Co-occurrence of posttraumatic stress disorder with positive psychotic symptoms in a nationally representative sample. J Trauma Stress. 2005;18(4):313-322.
10. Sar V, Akyuv G, Dogan O. Prevalence of dissociative disorders among women in the general population. Psychiatry Res. 2007;149:169-176.
11. Barnow S, Arens EA, Sieswerda S, et al. Borderline personality disorder and psychosis: a review. Curr Psychiatry Rep. 2010;12(3):186-195.
12. Bebbington P, Jonas S, Kuipers E, et al. Childhood sexual abuse and psychosis: data from a cross-sectional national psychiatric survey in England. Br J Psychiatry. 2011;199(1):29-37.
13. Read J, van Os J, Morrison AP, et al. Childhood trauma, psychosis and schizophrenia: a literature review with theoretical and clinical implications. Acta Psychiatr Scand. 2005;112(5):330-350.
