User login
No increased intussusception risk from rotavirus vaccine in Africa
Neither the first nor second dose of the monovalent rotavirus vaccine increased the risk of intussusception in the 3 weeks after immunization, a recent study found.
“This finding contrasts with previous studies in high- and upper-middle-income countries, in which an association with intussusception was found,” Jacqueline E. Tate, PhD, of the Centers for Disease Control and Prevention, and her associates reported in the New England Journal of Medicine.
“Given these large health benefits, the absence of increased risk of intussusception after RV1 [monovalent Rotarix vaccine] administration in our study is reassuring,” the authors wrote.
An African Intussusception Surveillance Network at 29 hospitals in Ethiopia, Ghana, Kenya, Malawi, Tanzania, Zambia and Zimbabwe enrolled 1,060 infants younger than age 12 months who experienced intussusception during Feb. 2012-Dec. 2016.
The researchers excluded infants without confirmed record of rotavirus vaccination status or who developed intussusception symptoms when younger than 28 days or older than 245 days. A little more than a third of the remaining 717 infants (36%) were from Ghana, more than half (61%) were male, and their median age was 25 weeks. Only 2% of the children had never received breast milk before developing intussusception symptoms.
The researchers used vaccine cards and clinic records to determine the rotavirus vaccination status for those 717 children with intussusception. The majority of the children (84%) had received both doses of the monovalent rotavirus vaccine. A total of 6% had received only one dose, and 10% received none. Five children received at least one rotavirus vaccine dose after having had intussusception already.
One intussusception case occurred within the first 7 days after the first vaccine dose, and five cases occurred within a week of the second dose. These incidences were no higher than was the background rate of intussusception, so no increased risk of intussusception in the week after either dose was identified, the researchers said.
The relative incidence of intussusception for dose one during days 1-7 was 0.25 (95% confidence interval, less than .001-1.16), and the relative incidence of intussusception for dose two during days 1-7 was 0.76 (95% CI, 0.16-1.87), Dr. Tate and her associates said.
Incidence of intussusception during the period 8-21 days after vaccination included 6 cases after the first dose and 16 cases after the second dose. Intussusception risk in this extended postvaccination period also was no higher than background risk.
“No clustering of cases occurred in any of the risk windows (1-7 days, 8-21 days, or 1-21 days) after receipt of either dose of RV1,” the authors reported.
They offered several possible reasons why no increased intussusception risk with rotavirus vaccination occurred in these countries despite studies in middle- and high-income countries showing an increased risk.
“First, although the exact mechanism is not known, intussusception may be related to intestinal replication of the orally administered, live-vaccine rotavirus strain,” Dr. Tate and her colleagues wrote. “Because oral rotavirus vaccines are less efficacious and shedding of vaccine virus – a potential marker of vaccine replication – is less frequently detected in low-income countries than in high- and middle-income countries, rotavirus vaccination might also be associated with a lower intussusception risk in low-income countries.”
Coadministration of rotavirus vaccination with the first dose of oral polio vaccine, which can reduce the rotavirus vaccine’s immunogenicity, also may play a role. Further, the children in this study were vaccinated against rotavirus at age 6- and 10-weeks-old – earlier than the 8 and 16 weeks in middle- and high-income countries – and intussusception is less common under 2 months old, potentially reducing likelihood of an association. Diet, breastfeeding practices, microbiome, maternal antibody levels, or other factors also may be at play.
The research was funded by the Gavi Alliance through the CDC Foundation. Dr. Cunliffe and Dr. Lopman have received personal fees from GlaxoSmithKline and Takeda Pharmaceutical, respectively. The other authors had no disclosures.
SOURCE: Tate JE et al. N Engl J Med. 2018;378:1521-8.
Neither the first nor second dose of the monovalent rotavirus vaccine increased the risk of intussusception in the 3 weeks after immunization, a recent study found.
“This finding contrasts with previous studies in high- and upper-middle-income countries, in which an association with intussusception was found,” Jacqueline E. Tate, PhD, of the Centers for Disease Control and Prevention, and her associates reported in the New England Journal of Medicine.
“Given these large health benefits, the absence of increased risk of intussusception after RV1 [monovalent Rotarix vaccine] administration in our study is reassuring,” the authors wrote.
An African Intussusception Surveillance Network at 29 hospitals in Ethiopia, Ghana, Kenya, Malawi, Tanzania, Zambia and Zimbabwe enrolled 1,060 infants younger than age 12 months who experienced intussusception during Feb. 2012-Dec. 2016.
The researchers excluded infants without confirmed record of rotavirus vaccination status or who developed intussusception symptoms when younger than 28 days or older than 245 days. A little more than a third of the remaining 717 infants (36%) were from Ghana, more than half (61%) were male, and their median age was 25 weeks. Only 2% of the children had never received breast milk before developing intussusception symptoms.
The researchers used vaccine cards and clinic records to determine the rotavirus vaccination status for those 717 children with intussusception. The majority of the children (84%) had received both doses of the monovalent rotavirus vaccine. A total of 6% had received only one dose, and 10% received none. Five children received at least one rotavirus vaccine dose after having had intussusception already.
One intussusception case occurred within the first 7 days after the first vaccine dose, and five cases occurred within a week of the second dose. These incidences were no higher than was the background rate of intussusception, so no increased risk of intussusception in the week after either dose was identified, the researchers said.
The relative incidence of intussusception for dose one during days 1-7 was 0.25 (95% confidence interval, less than .001-1.16), and the relative incidence of intussusception for dose two during days 1-7 was 0.76 (95% CI, 0.16-1.87), Dr. Tate and her associates said.
Incidence of intussusception during the period 8-21 days after vaccination included 6 cases after the first dose and 16 cases after the second dose. Intussusception risk in this extended postvaccination period also was no higher than background risk.
“No clustering of cases occurred in any of the risk windows (1-7 days, 8-21 days, or 1-21 days) after receipt of either dose of RV1,” the authors reported.
They offered several possible reasons why no increased intussusception risk with rotavirus vaccination occurred in these countries despite studies in middle- and high-income countries showing an increased risk.
“First, although the exact mechanism is not known, intussusception may be related to intestinal replication of the orally administered, live-vaccine rotavirus strain,” Dr. Tate and her colleagues wrote. “Because oral rotavirus vaccines are less efficacious and shedding of vaccine virus – a potential marker of vaccine replication – is less frequently detected in low-income countries than in high- and middle-income countries, rotavirus vaccination might also be associated with a lower intussusception risk in low-income countries.”
Coadministration of rotavirus vaccination with the first dose of oral polio vaccine, which can reduce the rotavirus vaccine’s immunogenicity, also may play a role. Further, the children in this study were vaccinated against rotavirus at age 6- and 10-weeks-old – earlier than the 8 and 16 weeks in middle- and high-income countries – and intussusception is less common under 2 months old, potentially reducing likelihood of an association. Diet, breastfeeding practices, microbiome, maternal antibody levels, or other factors also may be at play.
The research was funded by the Gavi Alliance through the CDC Foundation. Dr. Cunliffe and Dr. Lopman have received personal fees from GlaxoSmithKline and Takeda Pharmaceutical, respectively. The other authors had no disclosures.
SOURCE: Tate JE et al. N Engl J Med. 2018;378:1521-8.
Neither the first nor second dose of the monovalent rotavirus vaccine increased the risk of intussusception in the 3 weeks after immunization, a recent study found.
“This finding contrasts with previous studies in high- and upper-middle-income countries, in which an association with intussusception was found,” Jacqueline E. Tate, PhD, of the Centers for Disease Control and Prevention, and her associates reported in the New England Journal of Medicine.
“Given these large health benefits, the absence of increased risk of intussusception after RV1 [monovalent Rotarix vaccine] administration in our study is reassuring,” the authors wrote.
An African Intussusception Surveillance Network at 29 hospitals in Ethiopia, Ghana, Kenya, Malawi, Tanzania, Zambia and Zimbabwe enrolled 1,060 infants younger than age 12 months who experienced intussusception during Feb. 2012-Dec. 2016.
The researchers excluded infants without confirmed record of rotavirus vaccination status or who developed intussusception symptoms when younger than 28 days or older than 245 days. A little more than a third of the remaining 717 infants (36%) were from Ghana, more than half (61%) were male, and their median age was 25 weeks. Only 2% of the children had never received breast milk before developing intussusception symptoms.
The researchers used vaccine cards and clinic records to determine the rotavirus vaccination status for those 717 children with intussusception. The majority of the children (84%) had received both doses of the monovalent rotavirus vaccine. A total of 6% had received only one dose, and 10% received none. Five children received at least one rotavirus vaccine dose after having had intussusception already.
One intussusception case occurred within the first 7 days after the first vaccine dose, and five cases occurred within a week of the second dose. These incidences were no higher than was the background rate of intussusception, so no increased risk of intussusception in the week after either dose was identified, the researchers said.
The relative incidence of intussusception for dose one during days 1-7 was 0.25 (95% confidence interval, less than .001-1.16), and the relative incidence of intussusception for dose two during days 1-7 was 0.76 (95% CI, 0.16-1.87), Dr. Tate and her associates said.
Incidence of intussusception during the period 8-21 days after vaccination included 6 cases after the first dose and 16 cases after the second dose. Intussusception risk in this extended postvaccination period also was no higher than background risk.
“No clustering of cases occurred in any of the risk windows (1-7 days, 8-21 days, or 1-21 days) after receipt of either dose of RV1,” the authors reported.
They offered several possible reasons why no increased intussusception risk with rotavirus vaccination occurred in these countries despite studies in middle- and high-income countries showing an increased risk.
“First, although the exact mechanism is not known, intussusception may be related to intestinal replication of the orally administered, live-vaccine rotavirus strain,” Dr. Tate and her colleagues wrote. “Because oral rotavirus vaccines are less efficacious and shedding of vaccine virus – a potential marker of vaccine replication – is less frequently detected in low-income countries than in high- and middle-income countries, rotavirus vaccination might also be associated with a lower intussusception risk in low-income countries.”
Coadministration of rotavirus vaccination with the first dose of oral polio vaccine, which can reduce the rotavirus vaccine’s immunogenicity, also may play a role. Further, the children in this study were vaccinated against rotavirus at age 6- and 10-weeks-old – earlier than the 8 and 16 weeks in middle- and high-income countries – and intussusception is less common under 2 months old, potentially reducing likelihood of an association. Diet, breastfeeding practices, microbiome, maternal antibody levels, or other factors also may be at play.
The research was funded by the Gavi Alliance through the CDC Foundation. Dr. Cunliffe and Dr. Lopman have received personal fees from GlaxoSmithKline and Takeda Pharmaceutical, respectively. The other authors had no disclosures.
SOURCE: Tate JE et al. N Engl J Med. 2018;378:1521-8.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The relative incidence of intussusception for dose one during days 1-7 was 0.25 (95% confidence interval, less than .001-1.16), and the relative incidence of intussusception for dose two during days 1-7 was 0.76 (95% CI, 0.16-1.87).
Data source: The findings are based on a self-controlled case-series study involving 717 infants with intussusception and confirmed status of rotavirus vaccination, from Ethiopia, Ghana, Kenya, Malawi, Tanzania, Zambia, and Zimbabwe.
Disclosures: The research was funded by the Gavi Alliance through the CDC Foundation. Dr. Cunliffe and Dr. Lopman have received personal fees from GlaxoSmithKline and Takeda Pharmaceutical, respectively. The other authors had no disclosures.
Source: Tate JE et al. N Engl J Med. 2018;378:1521-8.
JADAS appears best for measuring various aspects of JIA activity
Applying clinical Juvenile Arthritis Disease Activity Score criteria to identify clinically inactive disease in patients with juvenile idiopathic arthritis (JIA) resulted in patients with better long-term functional activity and psychosocial health outcomes, compared with patients whose disease state was assessed using Wallace’s preliminary criteria, according to recent research from the multicenter Childhood Arthritis Prospective Study.
“A challenge is in understanding how best to apply these results in the clinical setting,” wrote Stephanie J.W. Shoop-Worrall of the Arthritis Research UK Centre for Epidemiology at the University of Manchester (England) and her coauthors. “As achievement of CID [clinically inactive disease] according to cJADAS10 [clinical Juvenile Arthritis Disease Activity Score assessed in 10 joints] was associated with equivalent or superior outcomes to Wallace’s preliminary criteria and it is more feasible to complete in clinical practice, due to containing only three routinely collected components, one could argue that this is likely to be a superior treatment target for application in clinical practice.”
Investigators applied the cJADAS10 to determine MDA, while CID was assessed using both cJADAS10 and Wallace’s preliminary criteria at 1-year follow-up. Children were categorized based on whether they achieved CID according to cJADAS10 only, whether they did so according to Wallace’s preliminary criteria only, whether they did so according to both cJADAS10 and Wallace’s preliminary criteria, or whether they did not achieve CID according to either; they also were categorized based on whether they achieved MDA but not CID according to cJADAS10. Researchers examined patient function, limited joints, and psychosocial health, as well as annual pain between 1-year and 5-year follow-up. The results were recently published in Arthritis & Rheumatology.
“Wallace’s preliminary criteria includes five components, observed or measured by a physician, which must all be absent or in the normal range, but do not include an assessment by the patient or their proxy,” Ms. Shoop-Worrall and her colleagues wrote. “In contrast, the JADAS and cJADAS include fewer overall components, meaning they may be easier to complete in a routine clinical setting, but do include a patient or proxy subjective assessment of patient wellbeing.”
Of the patients analyzed, 68% had oligoarthritis, while 27% had RF-negative and 5% had RF-positive polyarticular JIA. Over half (56%) of patients did not achieve CID, while 21% had achieved CID through both definitions. A further 23% of patients achieved CID in only one definition – 16% of patients according to cJADAS10 and 7% of patients according to Wallace’s preliminary criteria. Patients who achieved CID had significantly increased odds of having no limited joints according to either cJADAS10 (odds ratio, 3.9; 95% confidence interval, 2.5-6.3) or Wallace’s preliminary criteria (OR, 7.5; 95% CI, 2.9-19.2). Patients had better Child Health Questionnaire psychosocial scores when they achieved CID according to either cJADAS10 (coefficient, 5.3; 95% CI, 0.5-10.1) or both cJADAS10 and Wallace’s preliminary criteria (coefficient, 5.5; 95% CI, 2.2-9.5).
When patients’ function was assessed using the Childhood Health Assessment questionnaire, they had significantly increased odds of having no disability recorded when they achieved CID with either cJADAS10 (OR, 4.5; 95% CI, 2.2-9.5) or both criteria (OR 5.2; 95% CI, 2.7-9.9). Patients assessed with Wallace’s preliminary criteria had “no better Child Health Questionnaire psychosocial scores or Childhood Health Assessment questionnaire scores than those with active disease at 1 year.” Most patients who achieved CID also achieved MDA, but 10% of patients reached MDA without achieving CID.
The researchers noted that reliance on either cJADAS10 or Wallace’s preliminary criteria alone may miss data needed for clinical treatment. Data obtained from cJADAS10 may lead to additional psychological and physiotherapy treatments not seen in Wallace’s preliminary criteria; however, “relying solely on Wallace’s preliminary criteria may guide immunosuppressive therapy very well, but may ignore other symptoms relevant to the patient.”
“As the two scores differ in their components one could argue that they are not capturing the same construct,” Ms. Shoop-Worrall and her associates wrote. “Wallace’s preliminary criteria capture more objective measures of inflammation, whilst the cJADAS10, through inclusion of a patient well-being measure, may also capture other noninflammatory components of the disease, such as chronic pain and fatigue, not captured by Wallace’s preliminary criteria.”
The authors reported having no relevant financial disclosures for this study.
SOURCE: Shoop‐Worrall SJW et al. Arthritis Rheumatol. 2018 April 12. doi: 10.1002/art.40519.
Applying clinical Juvenile Arthritis Disease Activity Score criteria to identify clinically inactive disease in patients with juvenile idiopathic arthritis (JIA) resulted in patients with better long-term functional activity and psychosocial health outcomes, compared with patients whose disease state was assessed using Wallace’s preliminary criteria, according to recent research from the multicenter Childhood Arthritis Prospective Study.
“A challenge is in understanding how best to apply these results in the clinical setting,” wrote Stephanie J.W. Shoop-Worrall of the Arthritis Research UK Centre for Epidemiology at the University of Manchester (England) and her coauthors. “As achievement of CID [clinically inactive disease] according to cJADAS10 [clinical Juvenile Arthritis Disease Activity Score assessed in 10 joints] was associated with equivalent or superior outcomes to Wallace’s preliminary criteria and it is more feasible to complete in clinical practice, due to containing only three routinely collected components, one could argue that this is likely to be a superior treatment target for application in clinical practice.”
Investigators applied the cJADAS10 to determine MDA, while CID was assessed using both cJADAS10 and Wallace’s preliminary criteria at 1-year follow-up. Children were categorized based on whether they achieved CID according to cJADAS10 only, whether they did so according to Wallace’s preliminary criteria only, whether they did so according to both cJADAS10 and Wallace’s preliminary criteria, or whether they did not achieve CID according to either; they also were categorized based on whether they achieved MDA but not CID according to cJADAS10. Researchers examined patient function, limited joints, and psychosocial health, as well as annual pain between 1-year and 5-year follow-up. The results were recently published in Arthritis & Rheumatology.
“Wallace’s preliminary criteria includes five components, observed or measured by a physician, which must all be absent or in the normal range, but do not include an assessment by the patient or their proxy,” Ms. Shoop-Worrall and her colleagues wrote. “In contrast, the JADAS and cJADAS include fewer overall components, meaning they may be easier to complete in a routine clinical setting, but do include a patient or proxy subjective assessment of patient wellbeing.”
Of the patients analyzed, 68% had oligoarthritis, while 27% had RF-negative and 5% had RF-positive polyarticular JIA. Over half (56%) of patients did not achieve CID, while 21% had achieved CID through both definitions. A further 23% of patients achieved CID in only one definition – 16% of patients according to cJADAS10 and 7% of patients according to Wallace’s preliminary criteria. Patients who achieved CID had significantly increased odds of having no limited joints according to either cJADAS10 (odds ratio, 3.9; 95% confidence interval, 2.5-6.3) or Wallace’s preliminary criteria (OR, 7.5; 95% CI, 2.9-19.2). Patients had better Child Health Questionnaire psychosocial scores when they achieved CID according to either cJADAS10 (coefficient, 5.3; 95% CI, 0.5-10.1) or both cJADAS10 and Wallace’s preliminary criteria (coefficient, 5.5; 95% CI, 2.2-9.5).
When patients’ function was assessed using the Childhood Health Assessment questionnaire, they had significantly increased odds of having no disability recorded when they achieved CID with either cJADAS10 (OR, 4.5; 95% CI, 2.2-9.5) or both criteria (OR 5.2; 95% CI, 2.7-9.9). Patients assessed with Wallace’s preliminary criteria had “no better Child Health Questionnaire psychosocial scores or Childhood Health Assessment questionnaire scores than those with active disease at 1 year.” Most patients who achieved CID also achieved MDA, but 10% of patients reached MDA without achieving CID.
The researchers noted that reliance on either cJADAS10 or Wallace’s preliminary criteria alone may miss data needed for clinical treatment. Data obtained from cJADAS10 may lead to additional psychological and physiotherapy treatments not seen in Wallace’s preliminary criteria; however, “relying solely on Wallace’s preliminary criteria may guide immunosuppressive therapy very well, but may ignore other symptoms relevant to the patient.”
“As the two scores differ in their components one could argue that they are not capturing the same construct,” Ms. Shoop-Worrall and her associates wrote. “Wallace’s preliminary criteria capture more objective measures of inflammation, whilst the cJADAS10, through inclusion of a patient well-being measure, may also capture other noninflammatory components of the disease, such as chronic pain and fatigue, not captured by Wallace’s preliminary criteria.”
The authors reported having no relevant financial disclosures for this study.
SOURCE: Shoop‐Worrall SJW et al. Arthritis Rheumatol. 2018 April 12. doi: 10.1002/art.40519.
Applying clinical Juvenile Arthritis Disease Activity Score criteria to identify clinically inactive disease in patients with juvenile idiopathic arthritis (JIA) resulted in patients with better long-term functional activity and psychosocial health outcomes, compared with patients whose disease state was assessed using Wallace’s preliminary criteria, according to recent research from the multicenter Childhood Arthritis Prospective Study.
“A challenge is in understanding how best to apply these results in the clinical setting,” wrote Stephanie J.W. Shoop-Worrall of the Arthritis Research UK Centre for Epidemiology at the University of Manchester (England) and her coauthors. “As achievement of CID [clinically inactive disease] according to cJADAS10 [clinical Juvenile Arthritis Disease Activity Score assessed in 10 joints] was associated with equivalent or superior outcomes to Wallace’s preliminary criteria and it is more feasible to complete in clinical practice, due to containing only three routinely collected components, one could argue that this is likely to be a superior treatment target for application in clinical practice.”
Investigators applied the cJADAS10 to determine MDA, while CID was assessed using both cJADAS10 and Wallace’s preliminary criteria at 1-year follow-up. Children were categorized based on whether they achieved CID according to cJADAS10 only, whether they did so according to Wallace’s preliminary criteria only, whether they did so according to both cJADAS10 and Wallace’s preliminary criteria, or whether they did not achieve CID according to either; they also were categorized based on whether they achieved MDA but not CID according to cJADAS10. Researchers examined patient function, limited joints, and psychosocial health, as well as annual pain between 1-year and 5-year follow-up. The results were recently published in Arthritis & Rheumatology.
“Wallace’s preliminary criteria includes five components, observed or measured by a physician, which must all be absent or in the normal range, but do not include an assessment by the patient or their proxy,” Ms. Shoop-Worrall and her colleagues wrote. “In contrast, the JADAS and cJADAS include fewer overall components, meaning they may be easier to complete in a routine clinical setting, but do include a patient or proxy subjective assessment of patient wellbeing.”
Of the patients analyzed, 68% had oligoarthritis, while 27% had RF-negative and 5% had RF-positive polyarticular JIA. Over half (56%) of patients did not achieve CID, while 21% had achieved CID through both definitions. A further 23% of patients achieved CID in only one definition – 16% of patients according to cJADAS10 and 7% of patients according to Wallace’s preliminary criteria. Patients who achieved CID had significantly increased odds of having no limited joints according to either cJADAS10 (odds ratio, 3.9; 95% confidence interval, 2.5-6.3) or Wallace’s preliminary criteria (OR, 7.5; 95% CI, 2.9-19.2). Patients had better Child Health Questionnaire psychosocial scores when they achieved CID according to either cJADAS10 (coefficient, 5.3; 95% CI, 0.5-10.1) or both cJADAS10 and Wallace’s preliminary criteria (coefficient, 5.5; 95% CI, 2.2-9.5).
When patients’ function was assessed using the Childhood Health Assessment questionnaire, they had significantly increased odds of having no disability recorded when they achieved CID with either cJADAS10 (OR, 4.5; 95% CI, 2.2-9.5) or both criteria (OR 5.2; 95% CI, 2.7-9.9). Patients assessed with Wallace’s preliminary criteria had “no better Child Health Questionnaire psychosocial scores or Childhood Health Assessment questionnaire scores than those with active disease at 1 year.” Most patients who achieved CID also achieved MDA, but 10% of patients reached MDA without achieving CID.
The researchers noted that reliance on either cJADAS10 or Wallace’s preliminary criteria alone may miss data needed for clinical treatment. Data obtained from cJADAS10 may lead to additional psychological and physiotherapy treatments not seen in Wallace’s preliminary criteria; however, “relying solely on Wallace’s preliminary criteria may guide immunosuppressive therapy very well, but may ignore other symptoms relevant to the patient.”
“As the two scores differ in their components one could argue that they are not capturing the same construct,” Ms. Shoop-Worrall and her associates wrote. “Wallace’s preliminary criteria capture more objective measures of inflammation, whilst the cJADAS10, through inclusion of a patient well-being measure, may also capture other noninflammatory components of the disease, such as chronic pain and fatigue, not captured by Wallace’s preliminary criteria.”
The authors reported having no relevant financial disclosures for this study.
SOURCE: Shoop‐Worrall SJW et al. Arthritis Rheumatol. 2018 April 12. doi: 10.1002/art.40519.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Defining CID state using clinical JADAS criteria as a treatment target improved functional ability and psychosocial health, compared with that of patients defined using Wallace’s preliminary criteria.
Major finding: At 1-year follow-up, 16% of children achieved CID with cJADAS10 only and 7% with Wallace’s preliminary criteria only, while 21% of patients achieved CID when both definitions were used.
Story details: A prospective inception cohort of 832 children from eight pediatric and adolescent rheumatology centers in the United Kingdom recruited to the Childhood Arthritis Prospective Study during 2001-2011.
Disclosures: The authors reported having no financial disclosures.
Source: Shoop‐Worrall SJW et al. Arthritis Rheumatol. 2018 April 12. doi: 10.1002/art.40519.

New regimen looks good in stage IV favorable histology Wilms
Tailoring chemoradiation therapy while minimizing anthracycline exposure produced strong survival results in stage IV favorable histology Wilms tumor (FHWT), according to new results from the Children’s Oncology Group AREN0533 study.
In the new regimen, patients whose isolated lung nodules completely respond to 6 weeks of vincristine/dactinomycin/doxorubicin (DD4A) therapy continue DD4A and forgo lung radiation therapy (RT), explained David B. Dix, MBChB, of British Columbia Children’s Hospital, Vancouver, B.C., and his associates. Incomplete responders and patients with loss of heterozygosity at chromosomes 1p/16q receive lung RT plus boosted chemotherapy consisting of DD4 plus four cycles of cyclophosphamide/etoposide (Regimen M).
Among 133 assessable complete responders who received the DD4A regimen and were followed for a median of 4.7 years, 4-year event-free survival (EFS) was 79.5% (95% confidence interval, 71%-88%) and 4-year overall survival (OS) was 96% (95% CI, 92%-100%), Dr. Dix and his associates wrote. The report was published in the Journal of Clinical Oncology.
Among 159 incomplete responders receiving Regimen M, 4-year EFS was 88.5% (95% CI, 82%-95%) and 4-year OS was 95% (95% CI, 91%-100%). Regimen M produced superior EFS and OS (P less than .001 for both comparisons) than the protocol used in the National Wilms Tumor Study (NWTS) 5 study, in which all patients with lung metastases received DD4A plus RT, regardless of lung nodule response. “These results provide a benchmark for future studies,” Dr. Dix and his associates concluded.
Most patients with FHWT have pulmonary metastases and historically have fared worse than peers with localized disease. Until now, patients have had two main treatment options. The Society of Pediatric Oncology (SIOP) protocol focuses on pre-nephrectomy DD4A and forgoes lung RT if chemotherapy or surgical resection achieves lung nodule CR. Patients in the most recently reported SIOP trial (93-01) received a high cumulative anthracycline dose of 350 mg/m2 and had 5-year EFS of 77% and 5-year OS of 87%. The second option – the NWTS protocol – more than halves the cumulative doxorubicin dose (150 mg/m2), but all patients undergo lung RT.
In contrast, the AREN0533 protocol involved cumulative doxorubicin doses of 150 mg/m2 for DD4A and 195 mg/m2 for Regimen M. Among complete responders, the expected event rate was 15% and the actual rate was 20% (P = .05). Among incomplete responders, observed and expected event rates were 25% and. 12%, respectively (P less than .001). The higher-than-expected event rates might stem from lower chemotherapy doses, but the SIOP study also did not include central image review and may have defined CR less stringently, Dr. Dix and his coinvestigators said.
They concluded that AREN0533 showed “excellent” survival results for patients with CR and that certain late risks of Regimen M – including an increased risk of leukemia from exposure to cyclophosphamide and etoposide – should be balanced against its superior 4-year EFS.
Funders included the National Cancer Institute, National Institutes of Health, and St. Baldrick’s Foundation. Senior author Jeffrey S. Dome, MD, PhD, disclosed intellectual property with Rockland Immunochemicals. Three coinvestigators disclosed ties to healthcare and pharmaceutical companies.
SOURCE: Dix DB et al. J Clin Oncol. 2018 Apr 11. doi: 10.1200/JCO. 2017.77.1931.
Tailoring chemoradiation therapy while minimizing anthracycline exposure produced strong survival results in stage IV favorable histology Wilms tumor (FHWT), according to new results from the Children’s Oncology Group AREN0533 study.
In the new regimen, patients whose isolated lung nodules completely respond to 6 weeks of vincristine/dactinomycin/doxorubicin (DD4A) therapy continue DD4A and forgo lung radiation therapy (RT), explained David B. Dix, MBChB, of British Columbia Children’s Hospital, Vancouver, B.C., and his associates. Incomplete responders and patients with loss of heterozygosity at chromosomes 1p/16q receive lung RT plus boosted chemotherapy consisting of DD4 plus four cycles of cyclophosphamide/etoposide (Regimen M).
Among 133 assessable complete responders who received the DD4A regimen and were followed for a median of 4.7 years, 4-year event-free survival (EFS) was 79.5% (95% confidence interval, 71%-88%) and 4-year overall survival (OS) was 96% (95% CI, 92%-100%), Dr. Dix and his associates wrote. The report was published in the Journal of Clinical Oncology.
Among 159 incomplete responders receiving Regimen M, 4-year EFS was 88.5% (95% CI, 82%-95%) and 4-year OS was 95% (95% CI, 91%-100%). Regimen M produced superior EFS and OS (P less than .001 for both comparisons) than the protocol used in the National Wilms Tumor Study (NWTS) 5 study, in which all patients with lung metastases received DD4A plus RT, regardless of lung nodule response. “These results provide a benchmark for future studies,” Dr. Dix and his associates concluded.
Most patients with FHWT have pulmonary metastases and historically have fared worse than peers with localized disease. Until now, patients have had two main treatment options. The Society of Pediatric Oncology (SIOP) protocol focuses on pre-nephrectomy DD4A and forgoes lung RT if chemotherapy or surgical resection achieves lung nodule CR. Patients in the most recently reported SIOP trial (93-01) received a high cumulative anthracycline dose of 350 mg/m2 and had 5-year EFS of 77% and 5-year OS of 87%. The second option – the NWTS protocol – more than halves the cumulative doxorubicin dose (150 mg/m2), but all patients undergo lung RT.
In contrast, the AREN0533 protocol involved cumulative doxorubicin doses of 150 mg/m2 for DD4A and 195 mg/m2 for Regimen M. Among complete responders, the expected event rate was 15% and the actual rate was 20% (P = .05). Among incomplete responders, observed and expected event rates were 25% and. 12%, respectively (P less than .001). The higher-than-expected event rates might stem from lower chemotherapy doses, but the SIOP study also did not include central image review and may have defined CR less stringently, Dr. Dix and his coinvestigators said.
They concluded that AREN0533 showed “excellent” survival results for patients with CR and that certain late risks of Regimen M – including an increased risk of leukemia from exposure to cyclophosphamide and etoposide – should be balanced against its superior 4-year EFS.
Funders included the National Cancer Institute, National Institutes of Health, and St. Baldrick’s Foundation. Senior author Jeffrey S. Dome, MD, PhD, disclosed intellectual property with Rockland Immunochemicals. Three coinvestigators disclosed ties to healthcare and pharmaceutical companies.
SOURCE: Dix DB et al. J Clin Oncol. 2018 Apr 11. doi: 10.1200/JCO. 2017.77.1931.
Tailoring chemoradiation therapy while minimizing anthracycline exposure produced strong survival results in stage IV favorable histology Wilms tumor (FHWT), according to new results from the Children’s Oncology Group AREN0533 study.
In the new regimen, patients whose isolated lung nodules completely respond to 6 weeks of vincristine/dactinomycin/doxorubicin (DD4A) therapy continue DD4A and forgo lung radiation therapy (RT), explained David B. Dix, MBChB, of British Columbia Children’s Hospital, Vancouver, B.C., and his associates. Incomplete responders and patients with loss of heterozygosity at chromosomes 1p/16q receive lung RT plus boosted chemotherapy consisting of DD4 plus four cycles of cyclophosphamide/etoposide (Regimen M).
Among 133 assessable complete responders who received the DD4A regimen and were followed for a median of 4.7 years, 4-year event-free survival (EFS) was 79.5% (95% confidence interval, 71%-88%) and 4-year overall survival (OS) was 96% (95% CI, 92%-100%), Dr. Dix and his associates wrote. The report was published in the Journal of Clinical Oncology.
Among 159 incomplete responders receiving Regimen M, 4-year EFS was 88.5% (95% CI, 82%-95%) and 4-year OS was 95% (95% CI, 91%-100%). Regimen M produced superior EFS and OS (P less than .001 for both comparisons) than the protocol used in the National Wilms Tumor Study (NWTS) 5 study, in which all patients with lung metastases received DD4A plus RT, regardless of lung nodule response. “These results provide a benchmark for future studies,” Dr. Dix and his associates concluded.
Most patients with FHWT have pulmonary metastases and historically have fared worse than peers with localized disease. Until now, patients have had two main treatment options. The Society of Pediatric Oncology (SIOP) protocol focuses on pre-nephrectomy DD4A and forgoes lung RT if chemotherapy or surgical resection achieves lung nodule CR. Patients in the most recently reported SIOP trial (93-01) received a high cumulative anthracycline dose of 350 mg/m2 and had 5-year EFS of 77% and 5-year OS of 87%. The second option – the NWTS protocol – more than halves the cumulative doxorubicin dose (150 mg/m2), but all patients undergo lung RT.
In contrast, the AREN0533 protocol involved cumulative doxorubicin doses of 150 mg/m2 for DD4A and 195 mg/m2 for Regimen M. Among complete responders, the expected event rate was 15% and the actual rate was 20% (P = .05). Among incomplete responders, observed and expected event rates were 25% and. 12%, respectively (P less than .001). The higher-than-expected event rates might stem from lower chemotherapy doses, but the SIOP study also did not include central image review and may have defined CR less stringently, Dr. Dix and his coinvestigators said.
They concluded that AREN0533 showed “excellent” survival results for patients with CR and that certain late risks of Regimen M – including an increased risk of leukemia from exposure to cyclophosphamide and etoposide – should be balanced against its superior 4-year EFS.
Funders included the National Cancer Institute, National Institutes of Health, and St. Baldrick’s Foundation. Senior author Jeffrey S. Dome, MD, PhD, disclosed intellectual property with Rockland Immunochemicals. Three coinvestigators disclosed ties to healthcare and pharmaceutical companies.
SOURCE: Dix DB et al. J Clin Oncol. 2018 Apr 11. doi: 10.1200/JCO. 2017.77.1931.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Tailored chemoradiation therapy that reduces anthracycline exposure produced good outcomes in stage IV favorable histology Wilms tumor.
Major finding: Four-year event-free survival rates were 79.5% among complete responders and 89% among incomplete responders.
Study details: Study of 292 patients from AREN0533 (Treatment of Newly Diagnosed Higher-Risk Favorable Histology Wilms Tumors).
Disclosures: Funders included the National Cancer Institute, National Institutes of Health, and St. Baldrick’s Foundation. Senior author Jeffrey S. Dome, MD, PhD, disclosed intellectual property with Rockland Immunochemicals. Three coinvestigators disclosed ties to health care and pharmaceutical companies.
Source: Dix DB et al. J Clin Oncol. 2018 Apr 16. doi: 10.1200/JCO.2017.77.1931.
FDA approves burosumab to treat X-linked hypophosphatemia
The Food and Drug Administration has approved burosumab to treat X-linked hypophosphatemia, a rare, heritable form of rickets, in adults and children at least 1 year of age. Burosumab received expedited review by the FDA as a breakthrough therapy, and it also has been designated an orphan drug.
X-linked hypophosphatemia (XLH) “differs from other forms of rickets in that vitamin D therapy is not effective. This is the first FDA-approved medication for the treatment of XLH and a real breakthrough for those living with this serious disease,” said Julie Beitz, MD, in an FDA press release announcing the approval of the fully human monoclonal antibody. Dr. Beitz is director of the Office of Drug Evaluation III in the FDA’s Center for Drug Evaluation and Research.
Four clinical trials formed the basis for the FDA’s approval of burosumab. A pivotal randomized, placebo-controlled, double-blind study of adults with XLH that randomized 134 patients 1:1 to subcutaneous burosumab or placebo found that normal phosphorus levels were achieved in 94% of adults receiving burosumab, compared with 8% of those who received placebo.
For children, biweekly burosumab resulted in normal phosphorus levels for 94%-100% of participants. Significant skeletal radiographic improvement also was seen for adults and children taking burosumab.
In both adults and children, burosumab had a good safety profile, with no significant changes in serum or urine levels of calcium or in serum levels of intact parathyroid hormone.
X-linked hypophosphatemia is variable in severity; many patients with XLH will have bone pain, bowed legs, and a waddling gait; enthesopathy with associated joint pain; and dental problems and pain. Many also have short stature and, unlike rickets caused by dietary deficiency and some malabsorption problems, XLH is not improved by conventional vitamin D therapy.
The rare disorder, affecting about 3,000 children and 12,000 adults in the United States, is caused by a mutation in the PHEX gene, with resultant overactivity of fibroblast growth factor 23 (FGF23). Burosumab binds FGF23, increasing renal tubular reabsorption of phosphorus and 1,25-dihydroxycholecalciferol, also called calcitriol.
Previously, XLH had been treated by frequent oral supplementation with phosphate and calcitriol. Burosumab will be marketed by Ultragenyx Pharmaceutical as Crysvita. It is given as a once-monthly or biweekly subcutaneous injection.
The Food and Drug Administration has approved burosumab to treat X-linked hypophosphatemia, a rare, heritable form of rickets, in adults and children at least 1 year of age. Burosumab received expedited review by the FDA as a breakthrough therapy, and it also has been designated an orphan drug.
X-linked hypophosphatemia (XLH) “differs from other forms of rickets in that vitamin D therapy is not effective. This is the first FDA-approved medication for the treatment of XLH and a real breakthrough for those living with this serious disease,” said Julie Beitz, MD, in an FDA press release announcing the approval of the fully human monoclonal antibody. Dr. Beitz is director of the Office of Drug Evaluation III in the FDA’s Center for Drug Evaluation and Research.
Four clinical trials formed the basis for the FDA’s approval of burosumab. A pivotal randomized, placebo-controlled, double-blind study of adults with XLH that randomized 134 patients 1:1 to subcutaneous burosumab or placebo found that normal phosphorus levels were achieved in 94% of adults receiving burosumab, compared with 8% of those who received placebo.
For children, biweekly burosumab resulted in normal phosphorus levels for 94%-100% of participants. Significant skeletal radiographic improvement also was seen for adults and children taking burosumab.
In both adults and children, burosumab had a good safety profile, with no significant changes in serum or urine levels of calcium or in serum levels of intact parathyroid hormone.
X-linked hypophosphatemia is variable in severity; many patients with XLH will have bone pain, bowed legs, and a waddling gait; enthesopathy with associated joint pain; and dental problems and pain. Many also have short stature and, unlike rickets caused by dietary deficiency and some malabsorption problems, XLH is not improved by conventional vitamin D therapy.
The rare disorder, affecting about 3,000 children and 12,000 adults in the United States, is caused by a mutation in the PHEX gene, with resultant overactivity of fibroblast growth factor 23 (FGF23). Burosumab binds FGF23, increasing renal tubular reabsorption of phosphorus and 1,25-dihydroxycholecalciferol, also called calcitriol.
Previously, XLH had been treated by frequent oral supplementation with phosphate and calcitriol. Burosumab will be marketed by Ultragenyx Pharmaceutical as Crysvita. It is given as a once-monthly or biweekly subcutaneous injection.
The Food and Drug Administration has approved burosumab to treat X-linked hypophosphatemia, a rare, heritable form of rickets, in adults and children at least 1 year of age. Burosumab received expedited review by the FDA as a breakthrough therapy, and it also has been designated an orphan drug.
X-linked hypophosphatemia (XLH) “differs from other forms of rickets in that vitamin D therapy is not effective. This is the first FDA-approved medication for the treatment of XLH and a real breakthrough for those living with this serious disease,” said Julie Beitz, MD, in an FDA press release announcing the approval of the fully human monoclonal antibody. Dr. Beitz is director of the Office of Drug Evaluation III in the FDA’s Center for Drug Evaluation and Research.
Four clinical trials formed the basis for the FDA’s approval of burosumab. A pivotal randomized, placebo-controlled, double-blind study of adults with XLH that randomized 134 patients 1:1 to subcutaneous burosumab or placebo found that normal phosphorus levels were achieved in 94% of adults receiving burosumab, compared with 8% of those who received placebo.
For children, biweekly burosumab resulted in normal phosphorus levels for 94%-100% of participants. Significant skeletal radiographic improvement also was seen for adults and children taking burosumab.
In both adults and children, burosumab had a good safety profile, with no significant changes in serum or urine levels of calcium or in serum levels of intact parathyroid hormone.
X-linked hypophosphatemia is variable in severity; many patients with XLH will have bone pain, bowed legs, and a waddling gait; enthesopathy with associated joint pain; and dental problems and pain. Many also have short stature and, unlike rickets caused by dietary deficiency and some malabsorption problems, XLH is not improved by conventional vitamin D therapy.
The rare disorder, affecting about 3,000 children and 12,000 adults in the United States, is caused by a mutation in the PHEX gene, with resultant overactivity of fibroblast growth factor 23 (FGF23). Burosumab binds FGF23, increasing renal tubular reabsorption of phosphorus and 1,25-dihydroxycholecalciferol, also called calcitriol.
Previously, XLH had been treated by frequent oral supplementation with phosphate and calcitriol. Burosumab will be marketed by Ultragenyx Pharmaceutical as Crysvita. It is given as a once-monthly or biweekly subcutaneous injection.
Top AAN picks from Clinical Neurology News’ medical editor
Standout presentations at this year’s American Academy of Neurology annual meeting range from targeting tau in Alzheimer’s disease, to new treatments for spinal muscular atrophy, to the controversial topic of allowing your child to play contact sports, but all are sure to have an impact, according to Clinical Neurology News Medical Editor Richard J. Caselli, MD.
“There are a lot of good talks and papers being presented, and it is impossible without having seen and heard them all to accurately predict what will be the real standouts, but from a purely personal perspective, and with all due apologies to any others not mentioned below, these are some of the ones I think could have large and, in some cases, almost immediate impact or potential impact,” said Dr. Caselli, professor of neurology at the Mayo Clinic Arizona in Scottsdale and also associate director and clinical core director of the Arizona Alzheimer’s Disease Center.
Targeting tau in Alzheimer’s

The measuring of plasma tau to detect preclinical Alzheimer’s, as is described in the abstract from Pase and colleagues, is an “intriguing” approach, Dr. Caselli said. In that study, higher plasma tau levels were observed across correlates of preclinical Alzheimer’s: poorer cognitive function and smaller hippocampal volumes on MRI. Plasma tau level was also a strong predictor of future dementia. It will be presented Friday, April 27, 1:00-3:00 in S48, “Novel Biomarkers in Aging and Dementia.”
Focus continues on SMA
More advancements continue to be made in the treatment of various forms of spinal muscular trophy. In Monday morning’s Presidential Plenary Session, Richard Finkel’s presentation in receipt of the Sidney Carter Award in Child Neurology, should chart the development, current state, and future of antisense oligonucleotide therapy for SMA.
In the Emerging Science poster program on Wednesday, April 25, attendees will get an update on trial results for a different approach to the treatment of SMA using AVXS-101 gene replacement therapy for SMA type 1. John W. Day, MD, PhD, will provide longer-term outcomes after last year’s presentation of results in 15 patients.
Big news in stroke
Gregory Albers, MD, will describe in the Clinical Trials Plenary Session how new evidence from stroke thrombectomy trials such as DEFUSE 3 have led to new recommendations for extending the time window for thrombectomy. The results of DEFUSE 3 were first reported in January at the International Stroke Conference.
Other plenary presentations
In Wednesday’s Frontiers in Neuroscience Session, Dr. Caselli recommended Alan Evans’ discussion of the development and current and upcoming work to use and update the giant, freely accessible “BigBrain” High Resolution 3D Digital Human Brain Atlas.
In the always “fun and interesting” Controversies in Neurology on the morning of Thursday, April 26, the debate on “Should We Use Biomarkers Alone For Diagnosis of Alzheimer’s?” takes on greater interest now that the National Institute on Aging and the Alzheimer’s Association have defined Alzheimer’s disease as a diagnosis based on biomarkers. The separate debate of “Would You Let Your Child Play Contact Sports?” should also bring lots of interesting questions to the forefront of attendees’ minds.
Dr. Steven R. Messé’s talk, “Finally, Some Closure on PFO Closure,” at the Neurology Year in Review on Friday morning, April 27, is “of immediate relevance” as recent clinical trials have begun to determine patient groups for whom PFO closure appears worthwhile, Dr. Caselli said.
He has no relevant disclosures.
Standout presentations at this year’s American Academy of Neurology annual meeting range from targeting tau in Alzheimer’s disease, to new treatments for spinal muscular atrophy, to the controversial topic of allowing your child to play contact sports, but all are sure to have an impact, according to Clinical Neurology News Medical Editor Richard J. Caselli, MD.
“There are a lot of good talks and papers being presented, and it is impossible without having seen and heard them all to accurately predict what will be the real standouts, but from a purely personal perspective, and with all due apologies to any others not mentioned below, these are some of the ones I think could have large and, in some cases, almost immediate impact or potential impact,” said Dr. Caselli, professor of neurology at the Mayo Clinic Arizona in Scottsdale and also associate director and clinical core director of the Arizona Alzheimer’s Disease Center.
Targeting tau in Alzheimer’s
The measuring of plasma tau to detect preclinical Alzheimer’s, as is described in the abstract from Pase and colleagues, is an “intriguing” approach, Dr. Caselli said. In that study, higher plasma tau levels were observed across correlates of preclinical Alzheimer’s: poorer cognitive function and smaller hippocampal volumes on MRI. Plasma tau level was also a strong predictor of future dementia. It will be presented Friday, April 27, 1:00-3:00 in S48, “Novel Biomarkers in Aging and Dementia.”
Focus continues on SMA
More advancements continue to be made in the treatment of various forms of spinal muscular trophy. In Monday morning’s Presidential Plenary Session, Richard Finkel’s presentation in receipt of the Sidney Carter Award in Child Neurology, should chart the development, current state, and future of antisense oligonucleotide therapy for SMA.
In the Emerging Science poster program on Wednesday, April 25, attendees will get an update on trial results for a different approach to the treatment of SMA using AVXS-101 gene replacement therapy for SMA type 1. John W. Day, MD, PhD, will provide longer-term outcomes after last year’s presentation of results in 15 patients.
Big news in stroke
Gregory Albers, MD, will describe in the Clinical Trials Plenary Session how new evidence from stroke thrombectomy trials such as DEFUSE 3 have led to new recommendations for extending the time window for thrombectomy. The results of DEFUSE 3 were first reported in January at the International Stroke Conference.
Other plenary presentations
In Wednesday’s Frontiers in Neuroscience Session, Dr. Caselli recommended Alan Evans’ discussion of the development and current and upcoming work to use and update the giant, freely accessible “BigBrain” High Resolution 3D Digital Human Brain Atlas.
In the always “fun and interesting” Controversies in Neurology on the morning of Thursday, April 26, the debate on “Should We Use Biomarkers Alone For Diagnosis of Alzheimer’s?” takes on greater interest now that the National Institute on Aging and the Alzheimer’s Association have defined Alzheimer’s disease as a diagnosis based on biomarkers. The separate debate of “Would You Let Your Child Play Contact Sports?” should also bring lots of interesting questions to the forefront of attendees’ minds.
Dr. Steven R. Messé’s talk, “Finally, Some Closure on PFO Closure,” at the Neurology Year in Review on Friday morning, April 27, is “of immediate relevance” as recent clinical trials have begun to determine patient groups for whom PFO closure appears worthwhile, Dr. Caselli said.
He has no relevant disclosures.
Standout presentations at this year’s American Academy of Neurology annual meeting range from targeting tau in Alzheimer’s disease, to new treatments for spinal muscular atrophy, to the controversial topic of allowing your child to play contact sports, but all are sure to have an impact, according to Clinical Neurology News Medical Editor Richard J. Caselli, MD.
“There are a lot of good talks and papers being presented, and it is impossible without having seen and heard them all to accurately predict what will be the real standouts, but from a purely personal perspective, and with all due apologies to any others not mentioned below, these are some of the ones I think could have large and, in some cases, almost immediate impact or potential impact,” said Dr. Caselli, professor of neurology at the Mayo Clinic Arizona in Scottsdale and also associate director and clinical core director of the Arizona Alzheimer’s Disease Center.
Targeting tau in Alzheimer’s
The measuring of plasma tau to detect preclinical Alzheimer’s, as is described in the abstract from Pase and colleagues, is an “intriguing” approach, Dr. Caselli said. In that study, higher plasma tau levels were observed across correlates of preclinical Alzheimer’s: poorer cognitive function and smaller hippocampal volumes on MRI. Plasma tau level was also a strong predictor of future dementia. It will be presented Friday, April 27, 1:00-3:00 in S48, “Novel Biomarkers in Aging and Dementia.”
Focus continues on SMA
More advancements continue to be made in the treatment of various forms of spinal muscular trophy. In Monday morning’s Presidential Plenary Session, Richard Finkel’s presentation in receipt of the Sidney Carter Award in Child Neurology, should chart the development, current state, and future of antisense oligonucleotide therapy for SMA.
In the Emerging Science poster program on Wednesday, April 25, attendees will get an update on trial results for a different approach to the treatment of SMA using AVXS-101 gene replacement therapy for SMA type 1. John W. Day, MD, PhD, will provide longer-term outcomes after last year’s presentation of results in 15 patients.
Big news in stroke
Gregory Albers, MD, will describe in the Clinical Trials Plenary Session how new evidence from stroke thrombectomy trials such as DEFUSE 3 have led to new recommendations for extending the time window for thrombectomy. The results of DEFUSE 3 were first reported in January at the International Stroke Conference.
Other plenary presentations
In Wednesday’s Frontiers in Neuroscience Session, Dr. Caselli recommended Alan Evans’ discussion of the development and current and upcoming work to use and update the giant, freely accessible “BigBrain” High Resolution 3D Digital Human Brain Atlas.
In the always “fun and interesting” Controversies in Neurology on the morning of Thursday, April 26, the debate on “Should We Use Biomarkers Alone For Diagnosis of Alzheimer’s?” takes on greater interest now that the National Institute on Aging and the Alzheimer’s Association have defined Alzheimer’s disease as a diagnosis based on biomarkers. The separate debate of “Would You Let Your Child Play Contact Sports?” should also bring lots of interesting questions to the forefront of attendees’ minds.
Dr. Steven R. Messé’s talk, “Finally, Some Closure on PFO Closure,” at the Neurology Year in Review on Friday morning, April 27, is “of immediate relevance” as recent clinical trials have begun to determine patient groups for whom PFO closure appears worthwhile, Dr. Caselli said.
He has no relevant disclosures.
Anxiety, depression prevalent in children with comorbid autism and ADHD
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.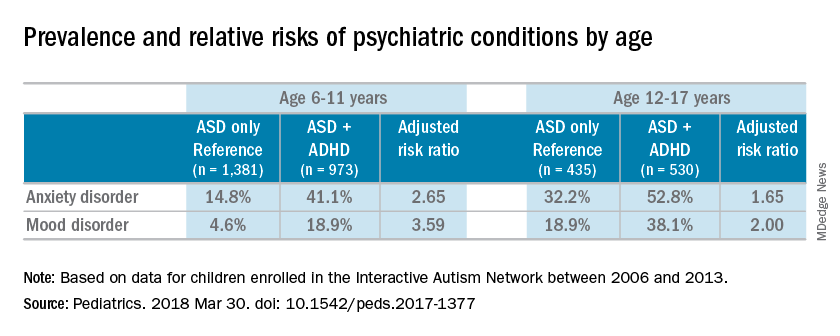
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
FROM PEDIATRICS
Key clinical point: “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
Major finding: Sixteen percent of the children with autistic spectrum disorder had a mood disorder, and 31% had an anxiety disorder.
Study details: A cross-sectional analysis of information on 3,319 patients, obtained between 2006 and 2013 in the Interactive Autism Network (IAN), an online autism research registry that uses parent report information.
Disclosures: None of the study authors reported relevant financial disclosures. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
Source: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
Pot peaks in breast milk 1 hour after smoking
The levels of delta-9-tetrahydrocannabinol in breast milk peak around 1 hour after smoking, according to a pilot pharmacokinetic study.
Eight mothers who were either occasional or chronic cannabis smokers, and who exclusively breastfed their infants, were directed to smoke a preweighed, standardized amount of “Prezidential Kush” from a preselected Denver dispensary after initially discontinuing for 24 hours. Researchers collected breast milk samples from just before smoking, and at 20 minutes, 1 hour, 2 hours, and 4 hours after smoking, according to a paper published in the May issue of Obstetrics & Gynecology.
This translated to an estimated relative infant dose of 2.5% of the maternal dose, or 8 mcg per kilogram per day.
“It remains unclear what exposure to cannabis products during this critical neurobehavioral development period will mean for the infant,” wrote Teresa Baker, MD, of Texas Tech University Health Sciences Center, and her coauthors. “These questions will require an enormous effort to determine.”
Concentrations of delta-9-tetrahydrocannabinol metabolites 11-OH-delta-9-tetrahydrocannabinol and 11-Nor-9-carboxy-delta-9-tetrahydrocannabinol were too low to be detected.
The authors noted that these metabolites are known to be more water soluble and polar than delta-9-tetrahydrocannabinol itself, which may make it more difficult for them to enter the breast milk compartment.
Two of the participants had a low but measurable concentration of delta-9-tetrahydrocannabinol at zero time (the samples collected just before smoking), suggesting some residual accumulation of it from prior heavy use or use close to the start of breast milk collection.
“Although the transfer of delta-9-tetrahydrocannabinol into the plasma compartment is almost instantaneous, the transfer of delta-9-tetrahydrocannabinol into breast milk in our study appears to be slightly slower than the transfer into the plasma compartment,” the authors wrote.
The women in the study were all 2-5 months postpartum. The authors noted that in these women who were exclusively breastfeeding, the breast milk compartment, along with drug entry and exit, “remains fairly consistent.”
The researchers also noted that the lack of corresponding plasma samples was a major limitation of the study, but because of the nature of the study, anonymity was important.
No conflicts of interest were declared.
SOURCE: Baker T et al. Obstet Gynecol. 2018;131:783-8.
The levels of delta-9-tetrahydrocannabinol in breast milk peak around 1 hour after smoking, according to a pilot pharmacokinetic study.
Eight mothers who were either occasional or chronic cannabis smokers, and who exclusively breastfed their infants, were directed to smoke a preweighed, standardized amount of “Prezidential Kush” from a preselected Denver dispensary after initially discontinuing for 24 hours. Researchers collected breast milk samples from just before smoking, and at 20 minutes, 1 hour, 2 hours, and 4 hours after smoking, according to a paper published in the May issue of Obstetrics & Gynecology.
This translated to an estimated relative infant dose of 2.5% of the maternal dose, or 8 mcg per kilogram per day.
“It remains unclear what exposure to cannabis products during this critical neurobehavioral development period will mean for the infant,” wrote Teresa Baker, MD, of Texas Tech University Health Sciences Center, and her coauthors. “These questions will require an enormous effort to determine.”
Concentrations of delta-9-tetrahydrocannabinol metabolites 11-OH-delta-9-tetrahydrocannabinol and 11-Nor-9-carboxy-delta-9-tetrahydrocannabinol were too low to be detected.
The authors noted that these metabolites are known to be more water soluble and polar than delta-9-tetrahydrocannabinol itself, which may make it more difficult for them to enter the breast milk compartment.
Two of the participants had a low but measurable concentration of delta-9-tetrahydrocannabinol at zero time (the samples collected just before smoking), suggesting some residual accumulation of it from prior heavy use or use close to the start of breast milk collection.
“Although the transfer of delta-9-tetrahydrocannabinol into the plasma compartment is almost instantaneous, the transfer of delta-9-tetrahydrocannabinol into breast milk in our study appears to be slightly slower than the transfer into the plasma compartment,” the authors wrote.
The women in the study were all 2-5 months postpartum. The authors noted that in these women who were exclusively breastfeeding, the breast milk compartment, along with drug entry and exit, “remains fairly consistent.”
The researchers also noted that the lack of corresponding plasma samples was a major limitation of the study, but because of the nature of the study, anonymity was important.
No conflicts of interest were declared.
SOURCE: Baker T et al. Obstet Gynecol. 2018;131:783-8.
The levels of delta-9-tetrahydrocannabinol in breast milk peak around 1 hour after smoking, according to a pilot pharmacokinetic study.
Eight mothers who were either occasional or chronic cannabis smokers, and who exclusively breastfed their infants, were directed to smoke a preweighed, standardized amount of “Prezidential Kush” from a preselected Denver dispensary after initially discontinuing for 24 hours. Researchers collected breast milk samples from just before smoking, and at 20 minutes, 1 hour, 2 hours, and 4 hours after smoking, according to a paper published in the May issue of Obstetrics & Gynecology.
This translated to an estimated relative infant dose of 2.5% of the maternal dose, or 8 mcg per kilogram per day.
“It remains unclear what exposure to cannabis products during this critical neurobehavioral development period will mean for the infant,” wrote Teresa Baker, MD, of Texas Tech University Health Sciences Center, and her coauthors. “These questions will require an enormous effort to determine.”
Concentrations of delta-9-tetrahydrocannabinol metabolites 11-OH-delta-9-tetrahydrocannabinol and 11-Nor-9-carboxy-delta-9-tetrahydrocannabinol were too low to be detected.
The authors noted that these metabolites are known to be more water soluble and polar than delta-9-tetrahydrocannabinol itself, which may make it more difficult for them to enter the breast milk compartment.
Two of the participants had a low but measurable concentration of delta-9-tetrahydrocannabinol at zero time (the samples collected just before smoking), suggesting some residual accumulation of it from prior heavy use or use close to the start of breast milk collection.
“Although the transfer of delta-9-tetrahydrocannabinol into the plasma compartment is almost instantaneous, the transfer of delta-9-tetrahydrocannabinol into breast milk in our study appears to be slightly slower than the transfer into the plasma compartment,” the authors wrote.
The women in the study were all 2-5 months postpartum. The authors noted that in these women who were exclusively breastfeeding, the breast milk compartment, along with drug entry and exit, “remains fairly consistent.”
The researchers also noted that the lack of corresponding plasma samples was a major limitation of the study, but because of the nature of the study, anonymity was important.
No conflicts of interest were declared.
SOURCE: Baker T et al. Obstet Gynecol. 2018;131:783-8.
FROM OBSTETRICS & GYNECOLOGY
Key clinical point: Cannabinoid levels peak in breast milk 1 hour after smoking.
Major finding: Breastfeeding infants ingest around 2.5% of the maternal dose in breast milk.
Study details: A pilot pharmacokinetic study in eight women.
Disclosures: No conflicts of interest were declared.
Source: Baker T et al. Obstet Gynecol. 2018;131:783-8.
MDedge Daily News: Is rosacea a red flag for deeper dangers?
MedPAC wants to curb low-value care. Statins cut sepsis patients’ risk of death. And why reading aloud to kids can cut hyperactivity.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
MedPAC wants to curb low-value care. Statins cut sepsis patients’ risk of death. And why reading aloud to kids can cut hyperactivity.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
MedPAC wants to curb low-value care. Statins cut sepsis patients’ risk of death. And why reading aloud to kids can cut hyperactivity.
Listen to the MDedge Daily News podcast for all the details on today’s top news.

Make the Diagnosis - May 2018
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.

Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.

Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to dermnews@mdedge.com. This case and photo were submitted by Dr. Bilu Martin.
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.
Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to dermnews@mdedge.com. This case and photo were submitted by Dr. Bilu Martin.
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.
Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to dermnews@mdedge.com. This case and photo were submitted by Dr. Bilu Martin.
Eating disorders put teens at risk for depression, bullying
Disordered eating behavior may put adolescents at greater risk for both depression and peer bullying, data from a longitudinal study of 612 teens show.
“Questions remain as to whether clinically significant disordered eating behavior is an antecedent or consequent of bullying by peers among adolescent girls and boys,” wrote Kirsty S. Lee, PhD, and Tracy Vaillancourt, PhD, of the University of Ottawa.
In a study published online April 11 in JAMA Psychiatry, the researchers reviewed data on adolescents aged 13-17 years who were enrolled in the McMaster Teen Study, a longitudinal study of Canadian teens examining bullying, academic achievement, and mental health. The average age of the study participants was 13 years; 54% were girls, and 71% were white.
At each annual follow-up during the 5-year study period, bullying was significantly concurrently associated with both disordered eating behavior (such as vomiting after eating) and depressive symptoms (P less than .01). In addition, disordered eating was significantly longitudinally associated with depression at every time point (P less than .02) and with peer bullying at two points (P less than .04) during the 5-year study (grades 8-9 and grades 10-11). However, no longitudinal association appeared between peer bullying and depression.
The participants completed a questionnaire each year between grades 7 and 11. The researchers assessed eating disordered behavior using the Short Screen for Eating Disorders; bullying was assessed by providing the teens with a standard definition of bullying to accompany questions about their experiences. Depression was assessed via the Behavior Assessment System for Children, second edition. A cascade model was used to show the relationships among the factors over time.
“At every time point, adolescent girls reported greater bullying by peers, depressive symptoms, and disordered eating behavior than adolescent boys, except in grade 7 when there were no sex differences in disordered eating behavior,” the researchers noted.
The results were consistent with data from previous cross-sectional studies with regard to the stronger associations in girls vs. boys, the researchers said. However, contrary to previous research, they found no mediating effect of depression on the association between peer bullying and disordered eating behavior, and no longitudinal associations between peer bullying and depression.
The findings were limited by several factors, including the inability to analyze different types of eating disorders and the use of self-reports to assess bullying, the researchers said. However, the results support the value of targeting disordered eating behavior to help reduce the risk of other mental health problems, they noted.
, which can reduce symptoms of disordered eating and other psychopathologic symptoms,” they wrote.
The researchers had no financial conflicts to disclose. The study was supported in part by the Ontario Mental Health Foundation, the Canadian Institute of Health Research, and the Social Sciences and Humanities Research Council of Canada.
SOURCE: Lee KS and Vaillancourt T. JAMA Psychiatry 2018 Apr 11. doi: 10.1001/jamapsychiatry.2018.0284.
Disordered eating behavior may put adolescents at greater risk for both depression and peer bullying, data from a longitudinal study of 612 teens show.
“Questions remain as to whether clinically significant disordered eating behavior is an antecedent or consequent of bullying by peers among adolescent girls and boys,” wrote Kirsty S. Lee, PhD, and Tracy Vaillancourt, PhD, of the University of Ottawa.
In a study published online April 11 in JAMA Psychiatry, the researchers reviewed data on adolescents aged 13-17 years who were enrolled in the McMaster Teen Study, a longitudinal study of Canadian teens examining bullying, academic achievement, and mental health. The average age of the study participants was 13 years; 54% were girls, and 71% were white.
At each annual follow-up during the 5-year study period, bullying was significantly concurrently associated with both disordered eating behavior (such as vomiting after eating) and depressive symptoms (P less than .01). In addition, disordered eating was significantly longitudinally associated with depression at every time point (P less than .02) and with peer bullying at two points (P less than .04) during the 5-year study (grades 8-9 and grades 10-11). However, no longitudinal association appeared between peer bullying and depression.
The participants completed a questionnaire each year between grades 7 and 11. The researchers assessed eating disordered behavior using the Short Screen for Eating Disorders; bullying was assessed by providing the teens with a standard definition of bullying to accompany questions about their experiences. Depression was assessed via the Behavior Assessment System for Children, second edition. A cascade model was used to show the relationships among the factors over time.
“At every time point, adolescent girls reported greater bullying by peers, depressive symptoms, and disordered eating behavior than adolescent boys, except in grade 7 when there were no sex differences in disordered eating behavior,” the researchers noted.
The results were consistent with data from previous cross-sectional studies with regard to the stronger associations in girls vs. boys, the researchers said. However, contrary to previous research, they found no mediating effect of depression on the association between peer bullying and disordered eating behavior, and no longitudinal associations between peer bullying and depression.
The findings were limited by several factors, including the inability to analyze different types of eating disorders and the use of self-reports to assess bullying, the researchers said. However, the results support the value of targeting disordered eating behavior to help reduce the risk of other mental health problems, they noted.
, which can reduce symptoms of disordered eating and other psychopathologic symptoms,” they wrote.
The researchers had no financial conflicts to disclose. The study was supported in part by the Ontario Mental Health Foundation, the Canadian Institute of Health Research, and the Social Sciences and Humanities Research Council of Canada.
SOURCE: Lee KS and Vaillancourt T. JAMA Psychiatry 2018 Apr 11. doi: 10.1001/jamapsychiatry.2018.0284.
Disordered eating behavior may put adolescents at greater risk for both depression and peer bullying, data from a longitudinal study of 612 teens show.
“Questions remain as to whether clinically significant disordered eating behavior is an antecedent or consequent of bullying by peers among adolescent girls and boys,” wrote Kirsty S. Lee, PhD, and Tracy Vaillancourt, PhD, of the University of Ottawa.
In a study published online April 11 in JAMA Psychiatry, the researchers reviewed data on adolescents aged 13-17 years who were enrolled in the McMaster Teen Study, a longitudinal study of Canadian teens examining bullying, academic achievement, and mental health. The average age of the study participants was 13 years; 54% were girls, and 71% were white.
At each annual follow-up during the 5-year study period, bullying was significantly concurrently associated with both disordered eating behavior (such as vomiting after eating) and depressive symptoms (P less than .01). In addition, disordered eating was significantly longitudinally associated with depression at every time point (P less than .02) and with peer bullying at two points (P less than .04) during the 5-year study (grades 8-9 and grades 10-11). However, no longitudinal association appeared between peer bullying and depression.
The participants completed a questionnaire each year between grades 7 and 11. The researchers assessed eating disordered behavior using the Short Screen for Eating Disorders; bullying was assessed by providing the teens with a standard definition of bullying to accompany questions about their experiences. Depression was assessed via the Behavior Assessment System for Children, second edition. A cascade model was used to show the relationships among the factors over time.
“At every time point, adolescent girls reported greater bullying by peers, depressive symptoms, and disordered eating behavior than adolescent boys, except in grade 7 when there were no sex differences in disordered eating behavior,” the researchers noted.
The results were consistent with data from previous cross-sectional studies with regard to the stronger associations in girls vs. boys, the researchers said. However, contrary to previous research, they found no mediating effect of depression on the association between peer bullying and disordered eating behavior, and no longitudinal associations between peer bullying and depression.
The findings were limited by several factors, including the inability to analyze different types of eating disorders and the use of self-reports to assess bullying, the researchers said. However, the results support the value of targeting disordered eating behavior to help reduce the risk of other mental health problems, they noted.
, which can reduce symptoms of disordered eating and other psychopathologic symptoms,” they wrote.
The researchers had no financial conflicts to disclose. The study was supported in part by the Ontario Mental Health Foundation, the Canadian Institute of Health Research, and the Social Sciences and Humanities Research Council of Canada.
SOURCE: Lee KS and Vaillancourt T. JAMA Psychiatry 2018 Apr 11. doi: 10.1001/jamapsychiatry.2018.0284.
FROM JAMA PSYCHIATRY
Key clinical point: Teens who demonstrate disordered eating behavior may be at increased risk for depression and peer bullying.
Major finding: Disordered eating was longitudinally linked to depression and peer bullying (P less than .02).
Study details: A 5-year longitudinal study of 612 adolescents.
Disclosures: The researchers had no financial conflicts to disclose. The study was supported in part by the Ontario Mental Health Foundation, the Canadian Institute of Health Research, and the Social Sciences and Humanities Research Council of Canada.
Source: Lee KS and Vaillancourt T. JAMA Psychiatry 2018 Apr 11. doi: 10.1001/jamapsychiatry.2018.0284.