User login
Improving education for pediatric cancer caregivers

A new checklist could improve education for parents and other caregivers of children newly diagnosed with cancer, according to a group of nurses.
The checklist is divided into topics that should be taught according to their level of urgency.
The list includes subjects that should be discussed prior to patients’ initial hospital discharge and topics that can be covered later, either within the first month of the patients’ cancer diagnosis or before patients complete therapy.
Cheryl Rodgers, PhD, RN, and her colleagues provided details on this checklist in the Journal of Pediatric Oncology Nursing.
A team of 19 nurses and 2 parent advocates from the Children’s Oncology Group developed the checklist based on existing education checklists, expert recommendations, and team-based activities and discussions.
The checklist is divided into primary, secondary, and tertiary topics.
Primary topics are those that should be discussed with caregivers before they leave the hospital the first time. Examples include home medication dose and frequency, who and when to call for help, preventing infection, and treatment side effects to know before the next appointment.
Secondary topics are those that can be covered during the first month after a child’s cancer diagnosis. Examples include an explanation of what cancer is, an overview of chemotherapy, and more details on the side effects of cancer treatment.
Tertiary topics can be discussed before the child finishes cancer treatment. Examples include details on tests and procedures, risky behaviors to avoid, coping skills, and insurance issues.
Dr Rodgers and her colleagues said this checklist provides nurses with a clear outline of topics that should be discussed with caregivers immediately and topics that can be safely deferred. This could prevent information overload and help caregivers remember the most important information.
A new checklist could improve education for parents and other caregivers of children newly diagnosed with cancer, according to a group of nurses.
The checklist is divided into topics that should be taught according to their level of urgency.
The list includes subjects that should be discussed prior to patients’ initial hospital discharge and topics that can be covered later, either within the first month of the patients’ cancer diagnosis or before patients complete therapy.
Cheryl Rodgers, PhD, RN, and her colleagues provided details on this checklist in the Journal of Pediatric Oncology Nursing.
A team of 19 nurses and 2 parent advocates from the Children’s Oncology Group developed the checklist based on existing education checklists, expert recommendations, and team-based activities and discussions.
The checklist is divided into primary, secondary, and tertiary topics.
Primary topics are those that should be discussed with caregivers before they leave the hospital the first time. Examples include home medication dose and frequency, who and when to call for help, preventing infection, and treatment side effects to know before the next appointment.
Secondary topics are those that can be covered during the first month after a child’s cancer diagnosis. Examples include an explanation of what cancer is, an overview of chemotherapy, and more details on the side effects of cancer treatment.
Tertiary topics can be discussed before the child finishes cancer treatment. Examples include details on tests and procedures, risky behaviors to avoid, coping skills, and insurance issues.
Dr Rodgers and her colleagues said this checklist provides nurses with a clear outline of topics that should be discussed with caregivers immediately and topics that can be safely deferred. This could prevent information overload and help caregivers remember the most important information.
A new checklist could improve education for parents and other caregivers of children newly diagnosed with cancer, according to a group of nurses.
The checklist is divided into topics that should be taught according to their level of urgency.
The list includes subjects that should be discussed prior to patients’ initial hospital discharge and topics that can be covered later, either within the first month of the patients’ cancer diagnosis or before patients complete therapy.
Cheryl Rodgers, PhD, RN, and her colleagues provided details on this checklist in the Journal of Pediatric Oncology Nursing.
A team of 19 nurses and 2 parent advocates from the Children’s Oncology Group developed the checklist based on existing education checklists, expert recommendations, and team-based activities and discussions.
The checklist is divided into primary, secondary, and tertiary topics.
Primary topics are those that should be discussed with caregivers before they leave the hospital the first time. Examples include home medication dose and frequency, who and when to call for help, preventing infection, and treatment side effects to know before the next appointment.
Secondary topics are those that can be covered during the first month after a child’s cancer diagnosis. Examples include an explanation of what cancer is, an overview of chemotherapy, and more details on the side effects of cancer treatment.
Tertiary topics can be discussed before the child finishes cancer treatment. Examples include details on tests and procedures, risky behaviors to avoid, coping skills, and insurance issues.
Dr Rodgers and her colleagues said this checklist provides nurses with a clear outline of topics that should be discussed with caregivers immediately and topics that can be safely deferred. This could prevent information overload and help caregivers remember the most important information.
Psoriasis duration reflects cardiovascular event risk
KAUAI, HAWAII – The recent report that the risk of a major adverse cardiovascular event increases by 1% more than in the general population for each additional year of psoriasis duration is sobering news for physicians who treat pediatric psoriasis.
“If I have a 16-year-old who has a 5-year history of psoriasis, what does that mean for when she’s 30 or 40? And should we be intervening more aggressively?” Lawrence F. Eichenfield, MD, asked at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
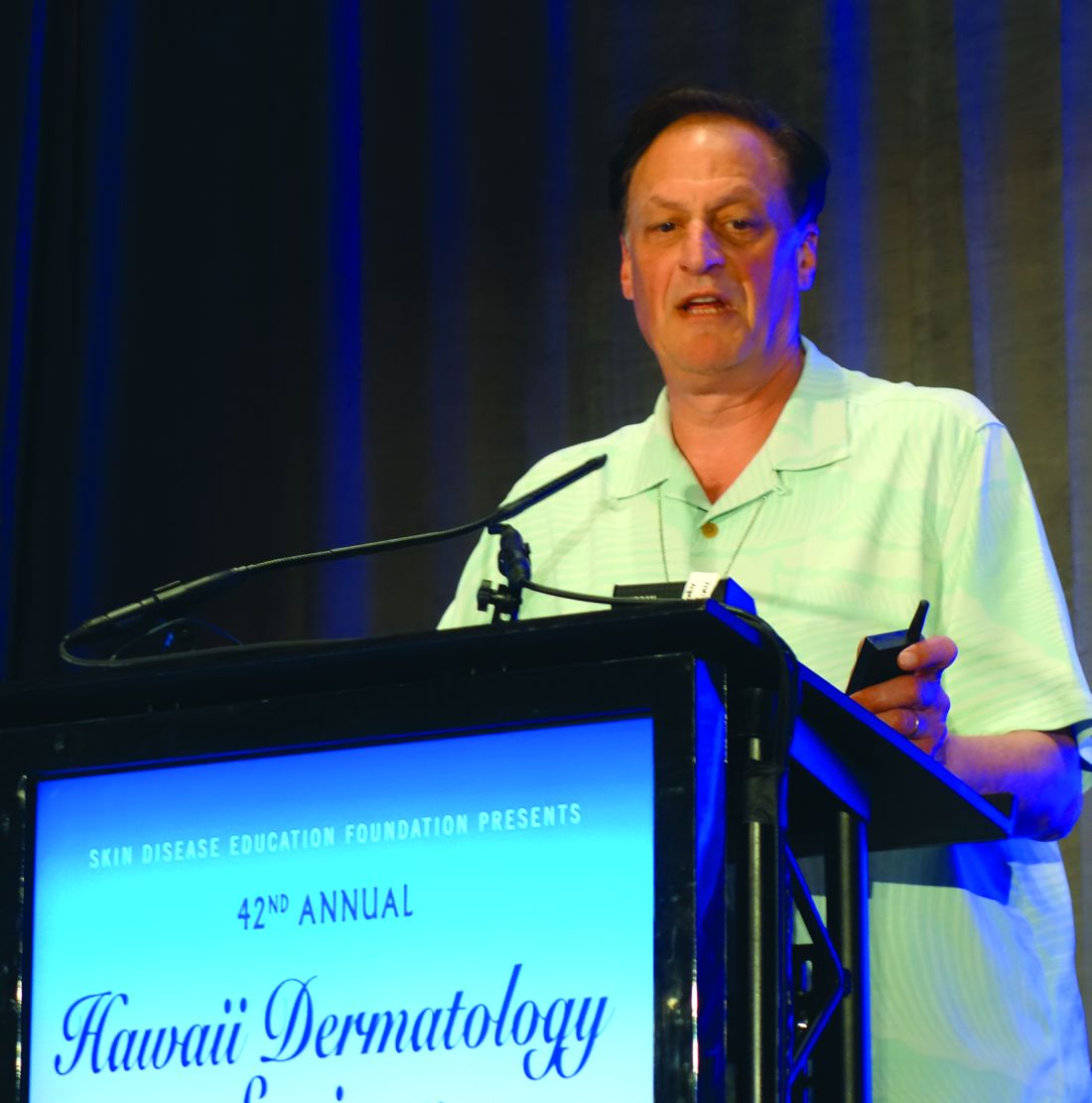
“Even though there’s not a great deal of evidence, there’s some evidence to rationalize early screening in psoriasis,” according to Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego.
Psoriasis develops during childhood in almost one-third of patients.
The pediatric psoriasis screening guidelines describe a simple routine screening program and timeline for early identification of overweight or obesity, type 2 diabetes, hypertension, nonalcoholic fatty liver disease, anxiety, depression, substance abuse, inflammatory bowel disease, and quality of life issues, all of which are encountered with increased frequency in pediatric psoriasis patients. A fasting lipid panel is recommended in children aged 9-11 years with psoriasis and again at age 17-21 years.
“Don’t forget arthritis. For a kid with psoriasis, at every office visit, I ask about morning stiffness or limp. Those are probably the two most sensitive questions in screening for psoriatic arthritis,” according to Dr. Eichenfield.
It has been clear for some time that the skin is not the only organ affected by psoriatic inflammation. The study that quantified the relationship between psoriasis duration and cardiovascular risk – a 1% increase for each year of psoriasis – was a collaboration between investigators at the University of Copenhagen and the University of Pennsylvania, Philadelphia.
The two-part project included aortal imaging of 190 psoriasis patients using fludeoxyglucose F 18 PET/CT scan, which showed a strong relationship between duration of psoriasis and the degree of vascular inflammation. This was bolstered by a population-based study using Danish national registry data on 87,161 psoriasis patients and 4.2 million controls from the general Danish population (J Am Acad Dermatol. 2017 Oct;77[4]:650-56.e3).
Dr. Eichenfield reported serving as a consultant to and/or recipient of research grants from more than a dozen pharmaceutical companies.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – The recent report that the risk of a major adverse cardiovascular event increases by 1% more than in the general population for each additional year of psoriasis duration is sobering news for physicians who treat pediatric psoriasis.
“If I have a 16-year-old who has a 5-year history of psoriasis, what does that mean for when she’s 30 or 40? And should we be intervening more aggressively?” Lawrence F. Eichenfield, MD, asked at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
“Even though there’s not a great deal of evidence, there’s some evidence to rationalize early screening in psoriasis,” according to Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego.
Psoriasis develops during childhood in almost one-third of patients.
The pediatric psoriasis screening guidelines describe a simple routine screening program and timeline for early identification of overweight or obesity, type 2 diabetes, hypertension, nonalcoholic fatty liver disease, anxiety, depression, substance abuse, inflammatory bowel disease, and quality of life issues, all of which are encountered with increased frequency in pediatric psoriasis patients. A fasting lipid panel is recommended in children aged 9-11 years with psoriasis and again at age 17-21 years.
“Don’t forget arthritis. For a kid with psoriasis, at every office visit, I ask about morning stiffness or limp. Those are probably the two most sensitive questions in screening for psoriatic arthritis,” according to Dr. Eichenfield.
It has been clear for some time that the skin is not the only organ affected by psoriatic inflammation. The study that quantified the relationship between psoriasis duration and cardiovascular risk – a 1% increase for each year of psoriasis – was a collaboration between investigators at the University of Copenhagen and the University of Pennsylvania, Philadelphia.
The two-part project included aortal imaging of 190 psoriasis patients using fludeoxyglucose F 18 PET/CT scan, which showed a strong relationship between duration of psoriasis and the degree of vascular inflammation. This was bolstered by a population-based study using Danish national registry data on 87,161 psoriasis patients and 4.2 million controls from the general Danish population (J Am Acad Dermatol. 2017 Oct;77[4]:650-56.e3).
Dr. Eichenfield reported serving as a consultant to and/or recipient of research grants from more than a dozen pharmaceutical companies.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – The recent report that the risk of a major adverse cardiovascular event increases by 1% more than in the general population for each additional year of psoriasis duration is sobering news for physicians who treat pediatric psoriasis.
“If I have a 16-year-old who has a 5-year history of psoriasis, what does that mean for when she’s 30 or 40? And should we be intervening more aggressively?” Lawrence F. Eichenfield, MD, asked at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
“Even though there’s not a great deal of evidence, there’s some evidence to rationalize early screening in psoriasis,” according to Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego.
Psoriasis develops during childhood in almost one-third of patients.
The pediatric psoriasis screening guidelines describe a simple routine screening program and timeline for early identification of overweight or obesity, type 2 diabetes, hypertension, nonalcoholic fatty liver disease, anxiety, depression, substance abuse, inflammatory bowel disease, and quality of life issues, all of which are encountered with increased frequency in pediatric psoriasis patients. A fasting lipid panel is recommended in children aged 9-11 years with psoriasis and again at age 17-21 years.
“Don’t forget arthritis. For a kid with psoriasis, at every office visit, I ask about morning stiffness or limp. Those are probably the two most sensitive questions in screening for psoriatic arthritis,” according to Dr. Eichenfield.
It has been clear for some time that the skin is not the only organ affected by psoriatic inflammation. The study that quantified the relationship between psoriasis duration and cardiovascular risk – a 1% increase for each year of psoriasis – was a collaboration between investigators at the University of Copenhagen and the University of Pennsylvania, Philadelphia.
The two-part project included aortal imaging of 190 psoriasis patients using fludeoxyglucose F 18 PET/CT scan, which showed a strong relationship between duration of psoriasis and the degree of vascular inflammation. This was bolstered by a population-based study using Danish national registry data on 87,161 psoriasis patients and 4.2 million controls from the general Danish population (J Am Acad Dermatol. 2017 Oct;77[4]:650-56.e3).
Dr. Eichenfield reported serving as a consultant to and/or recipient of research grants from more than a dozen pharmaceutical companies.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Self-harm
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.

Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.
Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.
Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Suicide on the minds of many Utah teens
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.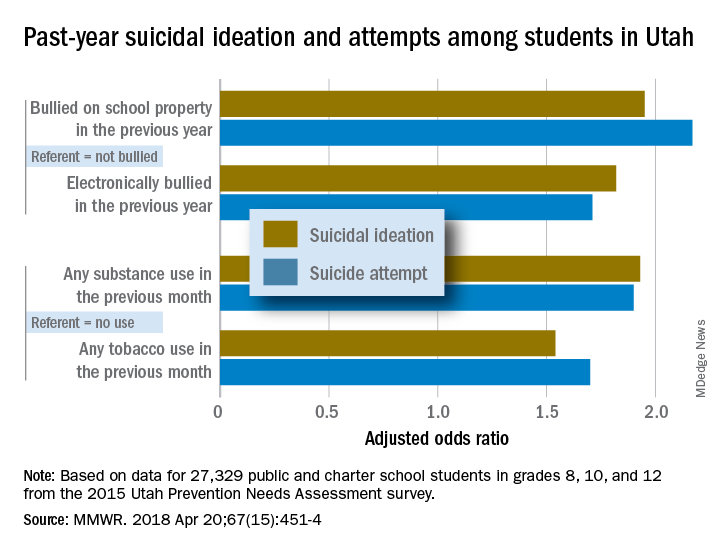
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
FROM MMWR
MenB vaccine receives breakthrough therapy designation for children aged 1-9 years
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
Adolescents, young adults endorse marijuana for IBD
according to study findings.
In a cross-sectional study of 99 patients with IBD aged 13-22 years, 32% of participants reported ever having used marijuana or endorsing use in the past 6 months. Additionally, 42% of patients perceived little to no risk of harm with regular use, reported Edward J. Hoffenberg, MD, of the departments of pediatrics and psychiatry at the University of Colorado, Aurora, and his associates.
Overall, 62 patients had a diagnosis of Crohn’s disease, 27 had ulcerative colitis, and 10 had indeterminate/unknown colitis. Patients in the ever-use group were older (mean, 17 years) than those in the never-use group (mean, 15.9 years). Serum cannabinoids were detected in 50% of patients in the ever-use group. “The detection of serum cannabinoids only in the ever-users is consistent with truthful reporting,” the researchers said.
Additionally, 80% of ever-users and 25% of never users perceived low to no risk of harm with regular use. After adjustment for age, ever-users were 10.7 times more likely to perceive low to no risk of harm (odds ratio, 10.7; P less than .001), the authors reported.
Weekly and daily marijuana use was reported by 52% and 31% of ever-users, respectively; 9% reported daily or almost daily use. Medical reasons for use was endorsed by 57%, and 53% reported physical pain relief as a reason. Nonmedical recreational or psychological reasons for use were reported by 87%. Problems with use were reported by 37% of users, including cravings or strong desire to use (20%), needing to use more to achieve the same effect (17%), and using a larger amount for longer than intended (17%).
“There is a need for further understanding of the potential medical benefits of marijuana use in IBD,” Dr. Hoffenberg and his associates wrote. “Theoretically, a different study design, such as a randomized controlled trial of marijuana use or placebo, could better evaluate the safety and benefit of frequent marijuana use for induction or maintenance of remission.”
Limitations of the study include difficulty determining differences in disease activity between groups because of the large number of patients with inactive or mild disease, as well as the need to group patients with Crohn’s disease and ulcerative colitis together because of the small total number of participants who endorse marijuana use.
The study was funded by the Colorado Department of Public Health and Environment. No conflicts of interest were reported.
SOURCE: Hoffenberg EJ et al. 2018. doi: 10.1016/j.jpeds.2018.03.041.
according to study findings.
In a cross-sectional study of 99 patients with IBD aged 13-22 years, 32% of participants reported ever having used marijuana or endorsing use in the past 6 months. Additionally, 42% of patients perceived little to no risk of harm with regular use, reported Edward J. Hoffenberg, MD, of the departments of pediatrics and psychiatry at the University of Colorado, Aurora, and his associates.
Overall, 62 patients had a diagnosis of Crohn’s disease, 27 had ulcerative colitis, and 10 had indeterminate/unknown colitis. Patients in the ever-use group were older (mean, 17 years) than those in the never-use group (mean, 15.9 years). Serum cannabinoids were detected in 50% of patients in the ever-use group. “The detection of serum cannabinoids only in the ever-users is consistent with truthful reporting,” the researchers said.
Additionally, 80% of ever-users and 25% of never users perceived low to no risk of harm with regular use. After adjustment for age, ever-users were 10.7 times more likely to perceive low to no risk of harm (odds ratio, 10.7; P less than .001), the authors reported.
Weekly and daily marijuana use was reported by 52% and 31% of ever-users, respectively; 9% reported daily or almost daily use. Medical reasons for use was endorsed by 57%, and 53% reported physical pain relief as a reason. Nonmedical recreational or psychological reasons for use were reported by 87%. Problems with use were reported by 37% of users, including cravings or strong desire to use (20%), needing to use more to achieve the same effect (17%), and using a larger amount for longer than intended (17%).
“There is a need for further understanding of the potential medical benefits of marijuana use in IBD,” Dr. Hoffenberg and his associates wrote. “Theoretically, a different study design, such as a randomized controlled trial of marijuana use or placebo, could better evaluate the safety and benefit of frequent marijuana use for induction or maintenance of remission.”
Limitations of the study include difficulty determining differences in disease activity between groups because of the large number of patients with inactive or mild disease, as well as the need to group patients with Crohn’s disease and ulcerative colitis together because of the small total number of participants who endorse marijuana use.
The study was funded by the Colorado Department of Public Health and Environment. No conflicts of interest were reported.
SOURCE: Hoffenberg EJ et al. 2018. doi: 10.1016/j.jpeds.2018.03.041.
according to study findings.
In a cross-sectional study of 99 patients with IBD aged 13-22 years, 32% of participants reported ever having used marijuana or endorsing use in the past 6 months. Additionally, 42% of patients perceived little to no risk of harm with regular use, reported Edward J. Hoffenberg, MD, of the departments of pediatrics and psychiatry at the University of Colorado, Aurora, and his associates.
Overall, 62 patients had a diagnosis of Crohn’s disease, 27 had ulcerative colitis, and 10 had indeterminate/unknown colitis. Patients in the ever-use group were older (mean, 17 years) than those in the never-use group (mean, 15.9 years). Serum cannabinoids were detected in 50% of patients in the ever-use group. “The detection of serum cannabinoids only in the ever-users is consistent with truthful reporting,” the researchers said.
Additionally, 80% of ever-users and 25% of never users perceived low to no risk of harm with regular use. After adjustment for age, ever-users were 10.7 times more likely to perceive low to no risk of harm (odds ratio, 10.7; P less than .001), the authors reported.
Weekly and daily marijuana use was reported by 52% and 31% of ever-users, respectively; 9% reported daily or almost daily use. Medical reasons for use was endorsed by 57%, and 53% reported physical pain relief as a reason. Nonmedical recreational or psychological reasons for use were reported by 87%. Problems with use were reported by 37% of users, including cravings or strong desire to use (20%), needing to use more to achieve the same effect (17%), and using a larger amount for longer than intended (17%).
“There is a need for further understanding of the potential medical benefits of marijuana use in IBD,” Dr. Hoffenberg and his associates wrote. “Theoretically, a different study design, such as a randomized controlled trial of marijuana use or placebo, could better evaluate the safety and benefit of frequent marijuana use for induction or maintenance of remission.”
Limitations of the study include difficulty determining differences in disease activity between groups because of the large number of patients with inactive or mild disease, as well as the need to group patients with Crohn’s disease and ulcerative colitis together because of the small total number of participants who endorse marijuana use.
The study was funded by the Colorado Department of Public Health and Environment. No conflicts of interest were reported.
SOURCE: Hoffenberg EJ et al. 2018. doi: 10.1016/j.jpeds.2018.03.041.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: Many adolescents and young adults with IBD use marijuana and perceive little to no harm from regular use.
Major finding: Of the participants in the study, 32% reported ever having used marijuana or endorsing use in the past 6 months, and 42% perceived little to no risk of harm with regular use.
Study details: A cross-sectional study of 99 IBD patients aged 13-22 years at Children’s Hospital Colorado.
Disclosures: The study was funded by the Colorado Department of Public Health and Environment. No conflicts of interest were reported.
Source: Hoffenberg EJ et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2018.03.041.
E-cigarette use in teens increases risk of cannabis use
, reported Hongying Dai, PhD, of Children’s Mercy Kansas City (Mo.), and her associates.
In an analysis of data from the Population Assessment of Tobacco and Health (PATH) survey, 11,996 participants aged 12-17 years completed both the wave 1 and wave 2 surveys. Researchers found one in four adolescents (26.6%) who used e-cigarettes at wave 1 reported marijuana use at wave 2, compared with 7.7% of adolescents who never used e-cigarettes at wave 1 (P less than .05). E-cigarette users at wave 1 were more likely to report marijuana use in the past 12 months at wave 2 (adjusted odds ratio = 1.9). In addition, 2.8% of participants who had never used marijuana at wave 1 reported heavy use of marijuana at wave 2.
“Our study revealed that e-cigarette use was associated with an increased risk of subsequent marijuana use among youth, with a stronger temporal association among younger adolescents,” the researchers concluded. “With these findings, we suggest that the widespread use of e-cigarettes among youth may have implications for the uptake of other drugs of abuse beyond nicotine and tobacco products.”
SOURCE: Dai H et al. Pediatrics. 2018;141(5):e20173787.
, reported Hongying Dai, PhD, of Children’s Mercy Kansas City (Mo.), and her associates.
In an analysis of data from the Population Assessment of Tobacco and Health (PATH) survey, 11,996 participants aged 12-17 years completed both the wave 1 and wave 2 surveys. Researchers found one in four adolescents (26.6%) who used e-cigarettes at wave 1 reported marijuana use at wave 2, compared with 7.7% of adolescents who never used e-cigarettes at wave 1 (P less than .05). E-cigarette users at wave 1 were more likely to report marijuana use in the past 12 months at wave 2 (adjusted odds ratio = 1.9). In addition, 2.8% of participants who had never used marijuana at wave 1 reported heavy use of marijuana at wave 2.
“Our study revealed that e-cigarette use was associated with an increased risk of subsequent marijuana use among youth, with a stronger temporal association among younger adolescents,” the researchers concluded. “With these findings, we suggest that the widespread use of e-cigarettes among youth may have implications for the uptake of other drugs of abuse beyond nicotine and tobacco products.”
SOURCE: Dai H et al. Pediatrics. 2018;141(5):e20173787.
, reported Hongying Dai, PhD, of Children’s Mercy Kansas City (Mo.), and her associates.
In an analysis of data from the Population Assessment of Tobacco and Health (PATH) survey, 11,996 participants aged 12-17 years completed both the wave 1 and wave 2 surveys. Researchers found one in four adolescents (26.6%) who used e-cigarettes at wave 1 reported marijuana use at wave 2, compared with 7.7% of adolescents who never used e-cigarettes at wave 1 (P less than .05). E-cigarette users at wave 1 were more likely to report marijuana use in the past 12 months at wave 2 (adjusted odds ratio = 1.9). In addition, 2.8% of participants who had never used marijuana at wave 1 reported heavy use of marijuana at wave 2.
“Our study revealed that e-cigarette use was associated with an increased risk of subsequent marijuana use among youth, with a stronger temporal association among younger adolescents,” the researchers concluded. “With these findings, we suggest that the widespread use of e-cigarettes among youth may have implications for the uptake of other drugs of abuse beyond nicotine and tobacco products.”
SOURCE: Dai H et al. Pediatrics. 2018;141(5):e20173787.
FROM PEDIATRICS
New JIA guidelines emphasize treating to target
– a strategy made possible with new therapies that have transformed treatment in recent years, including earlier treatment with methotrexate, expanding use of intra-articular glucocorticoids, and especially disease-modifying antibodies.
The guidelines, published online April 11 in the Annals of the Rheumatic Diseases, are a departure from some others in that there is very little research supporting the approach they advocate. But there is precedent in adult disease. Research in adults with rheumatoid arthritis has shown that achievement of low levels of disease activity through frequent adjustments of therapy improves patient outcomes, no matter the treatment used.

Nevertheless, the time for aggressive treatment in children has come, according to Karen Onel, MD, chief of the division of pediatric rheumatology at the Hospital for Special Surgery, New York. She pointed out that joint and organ damage resulting from JIA can be permanent. “These guidelines are meant to be fluid, but we need to be committed to getting patients into remission as quickly as possible. Anything less than that is not OK,” said Dr. Onel, who did not participate in drafting the guidelines.
The guidelines make almost no mention of specific treatments, with the exception of an admonition to avoid long-term systemic glucocorticoid therapy. “It’s addressing a philosophy of care that is different than what most of us do in our daily practice,” Dr. Lovell said. The lack of medication specifics also ensures that the guidelines will be useful in a wide range of settings, since specific drugs may be unavailable in some countries, or unaffordable due to insurance considerations.
The guidelines and the community at large are battling a historical perception of JIA as a childhood disease that patients outgrow. That has led to conservative approaches to therapy in an attempt to spare children from toxicity. But with new treatment options, that approach is outdated. “We have an issue in pediatrics where many people feel, including families, that you should wait until the child is old enough to make these decisions on their own. But the reality is that if [JIA] is not fixed in childhood, it won’t be fixed in adulthood,” Dr. Onel said.
About half of JIA cases are handled by rheumatologists who primarily work with adults, and they tend to favor toxicity-sparing regimens. These practitioners must be convinced to be more aggressive in their treatment, but parents are critical as well. The guidelines emphasize communicating with parents the rationale behind a chosen treatment target, along with information on the disease and the benefits and risks of the medications to be prescribed. Parents may struggle to understand the need for aggressive treatment, especially those with young children.
Parents may even be socially stigmatized by peers who think dietary change and exercise should be sufficient. “It’s really unfair. Nobody says to a parent of a child with cancer that they are treating their children with poison. The same holds true for other childhood chronic diseases. For whatever reason, the risk of permanent disability from childhood arthritis is understated,” Dr. Onel said.
A call for research
The primary target called for in the guidelines is clinically inactive disease (CID), defined as an absence of signs and symptoms of inflammatory disease activity, including extra-articular manifestations. An alternative target is minimal or low disease activity (LDA), which may be a more appropriate goal in patients with long-standing disease. Whatever the target, patients should be tracked at each clinical visit using a validated composite instrument, though the committee did not recommend one specifically.
Frequency of assessments may range from weekly to monthly or every 3 months, depending on the disease state. Within 3 months, the guidelines call for a minimum 50% improvement in disease activity, and by 6 months, clinicians should aim to achieve the target of clinical remission or LDA.
“It’s really important that clinicians systematically collect information on disease activity at every encounter. The next step is making sure we have some way of measuring outcomes. That might require a registry. It’s not easy to just start doing this. You need to have a plan in place,” said Esi Morgan, MD, of the department of rheumatology at Cincinnati Children’s Hospital Medical Center, and also a member of the guideline committee.
It remains to be seen how effective treatment to target will be, but Dr. Lovell hopes the guidelines will encourage research to provide definitive answers. “I think the recommendation is to just get on with it. Start doing trials utilizing a treat-to-target approach, and do them in a formal enough fashion that you can compare it to routine care in kids with JIA so you can assess the impact,” Dr. Lovell said.
Confidence is high. “There are many examples [of treating to target], so we can be confident this will work. What’s slightly different is applying this across the many subtypes of JIA. There are many categories, so it makes it a little more complex in terms of telling people what to do. But it’s definitely worth doing. We just need to solve the problem of how to address those issues,” Dr. Morgan said.
One key question is whether CID or LDA is the best target for functional outcomes. The UK Childhood Arthritis Prospective Study examined this question among 832 JIA patients and found that only achievement of CID on the clinical Juvenile Arthritis Disease Activity Score (cJADAS) was associated with an improvement in functional ability and psychosocial health at 1 year. Both endpoints were associated with greater absence of limited joints.
Another challenge is to determine what instrument to use to track disease activity and treatment response. Instruments include Wallace’s preliminary criteria, the American College of Rheumatology preliminary criteria, the Childhood Health Assessment Questionnaire (CHAQ), and the JADAS. All can be time consuming, which is a problem in a busy clinic. “That’s the work we need to do now: Figuring out what the best, easiest, most predictive instrument is going to be,” Dr. Onel said.
Dr. Lovell and Dr. Onel have no financial disclosures. Dr. Morgan is chair of the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN), which has received grants from Novartis and Medac Pharma.
SOURCE: Ravelli A et al. Ann Rheum Dis. 2018 Apr 11. doi: 10.1136/annrheumdis-2018-213030.
– a strategy made possible with new therapies that have transformed treatment in recent years, including earlier treatment with methotrexate, expanding use of intra-articular glucocorticoids, and especially disease-modifying antibodies.
The guidelines, published online April 11 in the Annals of the Rheumatic Diseases, are a departure from some others in that there is very little research supporting the approach they advocate. But there is precedent in adult disease. Research in adults with rheumatoid arthritis has shown that achievement of low levels of disease activity through frequent adjustments of therapy improves patient outcomes, no matter the treatment used.
Nevertheless, the time for aggressive treatment in children has come, according to Karen Onel, MD, chief of the division of pediatric rheumatology at the Hospital for Special Surgery, New York. She pointed out that joint and organ damage resulting from JIA can be permanent. “These guidelines are meant to be fluid, but we need to be committed to getting patients into remission as quickly as possible. Anything less than that is not OK,” said Dr. Onel, who did not participate in drafting the guidelines.
The guidelines make almost no mention of specific treatments, with the exception of an admonition to avoid long-term systemic glucocorticoid therapy. “It’s addressing a philosophy of care that is different than what most of us do in our daily practice,” Dr. Lovell said. The lack of medication specifics also ensures that the guidelines will be useful in a wide range of settings, since specific drugs may be unavailable in some countries, or unaffordable due to insurance considerations.
The guidelines and the community at large are battling a historical perception of JIA as a childhood disease that patients outgrow. That has led to conservative approaches to therapy in an attempt to spare children from toxicity. But with new treatment options, that approach is outdated. “We have an issue in pediatrics where many people feel, including families, that you should wait until the child is old enough to make these decisions on their own. But the reality is that if [JIA] is not fixed in childhood, it won’t be fixed in adulthood,” Dr. Onel said.
About half of JIA cases are handled by rheumatologists who primarily work with adults, and they tend to favor toxicity-sparing regimens. These practitioners must be convinced to be more aggressive in their treatment, but parents are critical as well. The guidelines emphasize communicating with parents the rationale behind a chosen treatment target, along with information on the disease and the benefits and risks of the medications to be prescribed. Parents may struggle to understand the need for aggressive treatment, especially those with young children.
Parents may even be socially stigmatized by peers who think dietary change and exercise should be sufficient. “It’s really unfair. Nobody says to a parent of a child with cancer that they are treating their children with poison. The same holds true for other childhood chronic diseases. For whatever reason, the risk of permanent disability from childhood arthritis is understated,” Dr. Onel said.
A call for research
The primary target called for in the guidelines is clinically inactive disease (CID), defined as an absence of signs and symptoms of inflammatory disease activity, including extra-articular manifestations. An alternative target is minimal or low disease activity (LDA), which may be a more appropriate goal in patients with long-standing disease. Whatever the target, patients should be tracked at each clinical visit using a validated composite instrument, though the committee did not recommend one specifically.
Frequency of assessments may range from weekly to monthly or every 3 months, depending on the disease state. Within 3 months, the guidelines call for a minimum 50% improvement in disease activity, and by 6 months, clinicians should aim to achieve the target of clinical remission or LDA.
“It’s really important that clinicians systematically collect information on disease activity at every encounter. The next step is making sure we have some way of measuring outcomes. That might require a registry. It’s not easy to just start doing this. You need to have a plan in place,” said Esi Morgan, MD, of the department of rheumatology at Cincinnati Children’s Hospital Medical Center, and also a member of the guideline committee.
It remains to be seen how effective treatment to target will be, but Dr. Lovell hopes the guidelines will encourage research to provide definitive answers. “I think the recommendation is to just get on with it. Start doing trials utilizing a treat-to-target approach, and do them in a formal enough fashion that you can compare it to routine care in kids with JIA so you can assess the impact,” Dr. Lovell said.
Confidence is high. “There are many examples [of treating to target], so we can be confident this will work. What’s slightly different is applying this across the many subtypes of JIA. There are many categories, so it makes it a little more complex in terms of telling people what to do. But it’s definitely worth doing. We just need to solve the problem of how to address those issues,” Dr. Morgan said.
One key question is whether CID or LDA is the best target for functional outcomes. The UK Childhood Arthritis Prospective Study examined this question among 832 JIA patients and found that only achievement of CID on the clinical Juvenile Arthritis Disease Activity Score (cJADAS) was associated with an improvement in functional ability and psychosocial health at 1 year. Both endpoints were associated with greater absence of limited joints.
Another challenge is to determine what instrument to use to track disease activity and treatment response. Instruments include Wallace’s preliminary criteria, the American College of Rheumatology preliminary criteria, the Childhood Health Assessment Questionnaire (CHAQ), and the JADAS. All can be time consuming, which is a problem in a busy clinic. “That’s the work we need to do now: Figuring out what the best, easiest, most predictive instrument is going to be,” Dr. Onel said.
Dr. Lovell and Dr. Onel have no financial disclosures. Dr. Morgan is chair of the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN), which has received grants from Novartis and Medac Pharma.
SOURCE: Ravelli A et al. Ann Rheum Dis. 2018 Apr 11. doi: 10.1136/annrheumdis-2018-213030.
– a strategy made possible with new therapies that have transformed treatment in recent years, including earlier treatment with methotrexate, expanding use of intra-articular glucocorticoids, and especially disease-modifying antibodies.
The guidelines, published online April 11 in the Annals of the Rheumatic Diseases, are a departure from some others in that there is very little research supporting the approach they advocate. But there is precedent in adult disease. Research in adults with rheumatoid arthritis has shown that achievement of low levels of disease activity through frequent adjustments of therapy improves patient outcomes, no matter the treatment used.
Nevertheless, the time for aggressive treatment in children has come, according to Karen Onel, MD, chief of the division of pediatric rheumatology at the Hospital for Special Surgery, New York. She pointed out that joint and organ damage resulting from JIA can be permanent. “These guidelines are meant to be fluid, but we need to be committed to getting patients into remission as quickly as possible. Anything less than that is not OK,” said Dr. Onel, who did not participate in drafting the guidelines.
The guidelines make almost no mention of specific treatments, with the exception of an admonition to avoid long-term systemic glucocorticoid therapy. “It’s addressing a philosophy of care that is different than what most of us do in our daily practice,” Dr. Lovell said. The lack of medication specifics also ensures that the guidelines will be useful in a wide range of settings, since specific drugs may be unavailable in some countries, or unaffordable due to insurance considerations.
The guidelines and the community at large are battling a historical perception of JIA as a childhood disease that patients outgrow. That has led to conservative approaches to therapy in an attempt to spare children from toxicity. But with new treatment options, that approach is outdated. “We have an issue in pediatrics where many people feel, including families, that you should wait until the child is old enough to make these decisions on their own. But the reality is that if [JIA] is not fixed in childhood, it won’t be fixed in adulthood,” Dr. Onel said.
About half of JIA cases are handled by rheumatologists who primarily work with adults, and they tend to favor toxicity-sparing regimens. These practitioners must be convinced to be more aggressive in their treatment, but parents are critical as well. The guidelines emphasize communicating with parents the rationale behind a chosen treatment target, along with information on the disease and the benefits and risks of the medications to be prescribed. Parents may struggle to understand the need for aggressive treatment, especially those with young children.
Parents may even be socially stigmatized by peers who think dietary change and exercise should be sufficient. “It’s really unfair. Nobody says to a parent of a child with cancer that they are treating their children with poison. The same holds true for other childhood chronic diseases. For whatever reason, the risk of permanent disability from childhood arthritis is understated,” Dr. Onel said.
A call for research
The primary target called for in the guidelines is clinically inactive disease (CID), defined as an absence of signs and symptoms of inflammatory disease activity, including extra-articular manifestations. An alternative target is minimal or low disease activity (LDA), which may be a more appropriate goal in patients with long-standing disease. Whatever the target, patients should be tracked at each clinical visit using a validated composite instrument, though the committee did not recommend one specifically.
Frequency of assessments may range from weekly to monthly or every 3 months, depending on the disease state. Within 3 months, the guidelines call for a minimum 50% improvement in disease activity, and by 6 months, clinicians should aim to achieve the target of clinical remission or LDA.
“It’s really important that clinicians systematically collect information on disease activity at every encounter. The next step is making sure we have some way of measuring outcomes. That might require a registry. It’s not easy to just start doing this. You need to have a plan in place,” said Esi Morgan, MD, of the department of rheumatology at Cincinnati Children’s Hospital Medical Center, and also a member of the guideline committee.
It remains to be seen how effective treatment to target will be, but Dr. Lovell hopes the guidelines will encourage research to provide definitive answers. “I think the recommendation is to just get on with it. Start doing trials utilizing a treat-to-target approach, and do them in a formal enough fashion that you can compare it to routine care in kids with JIA so you can assess the impact,” Dr. Lovell said.
Confidence is high. “There are many examples [of treating to target], so we can be confident this will work. What’s slightly different is applying this across the many subtypes of JIA. There are many categories, so it makes it a little more complex in terms of telling people what to do. But it’s definitely worth doing. We just need to solve the problem of how to address those issues,” Dr. Morgan said.
One key question is whether CID or LDA is the best target for functional outcomes. The UK Childhood Arthritis Prospective Study examined this question among 832 JIA patients and found that only achievement of CID on the clinical Juvenile Arthritis Disease Activity Score (cJADAS) was associated with an improvement in functional ability and psychosocial health at 1 year. Both endpoints were associated with greater absence of limited joints.
Another challenge is to determine what instrument to use to track disease activity and treatment response. Instruments include Wallace’s preliminary criteria, the American College of Rheumatology preliminary criteria, the Childhood Health Assessment Questionnaire (CHAQ), and the JADAS. All can be time consuming, which is a problem in a busy clinic. “That’s the work we need to do now: Figuring out what the best, easiest, most predictive instrument is going to be,” Dr. Onel said.
Dr. Lovell and Dr. Onel have no financial disclosures. Dr. Morgan is chair of the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN), which has received grants from Novartis and Medac Pharma.
SOURCE: Ravelli A et al. Ann Rheum Dis. 2018 Apr 11. doi: 10.1136/annrheumdis-2018-213030.
FROM ANNALS OF THE RHEUMATIC DISEASES

New rankings focus on child health care
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.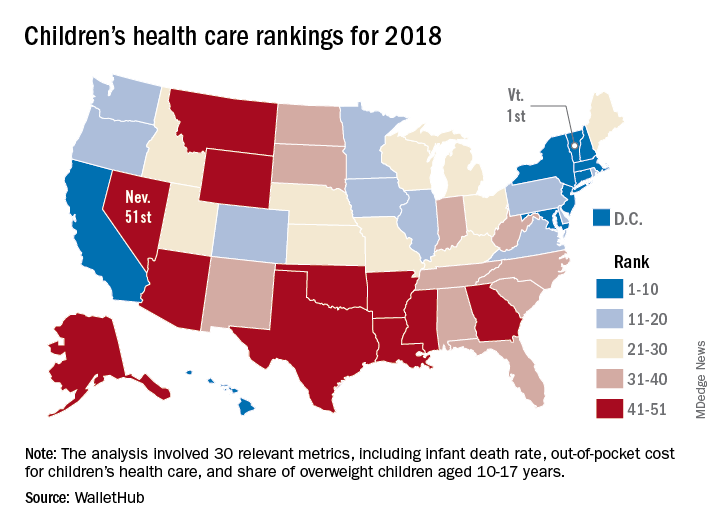
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
FDA panel recommends CBD for pediatric seizure disorders
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING