User login
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
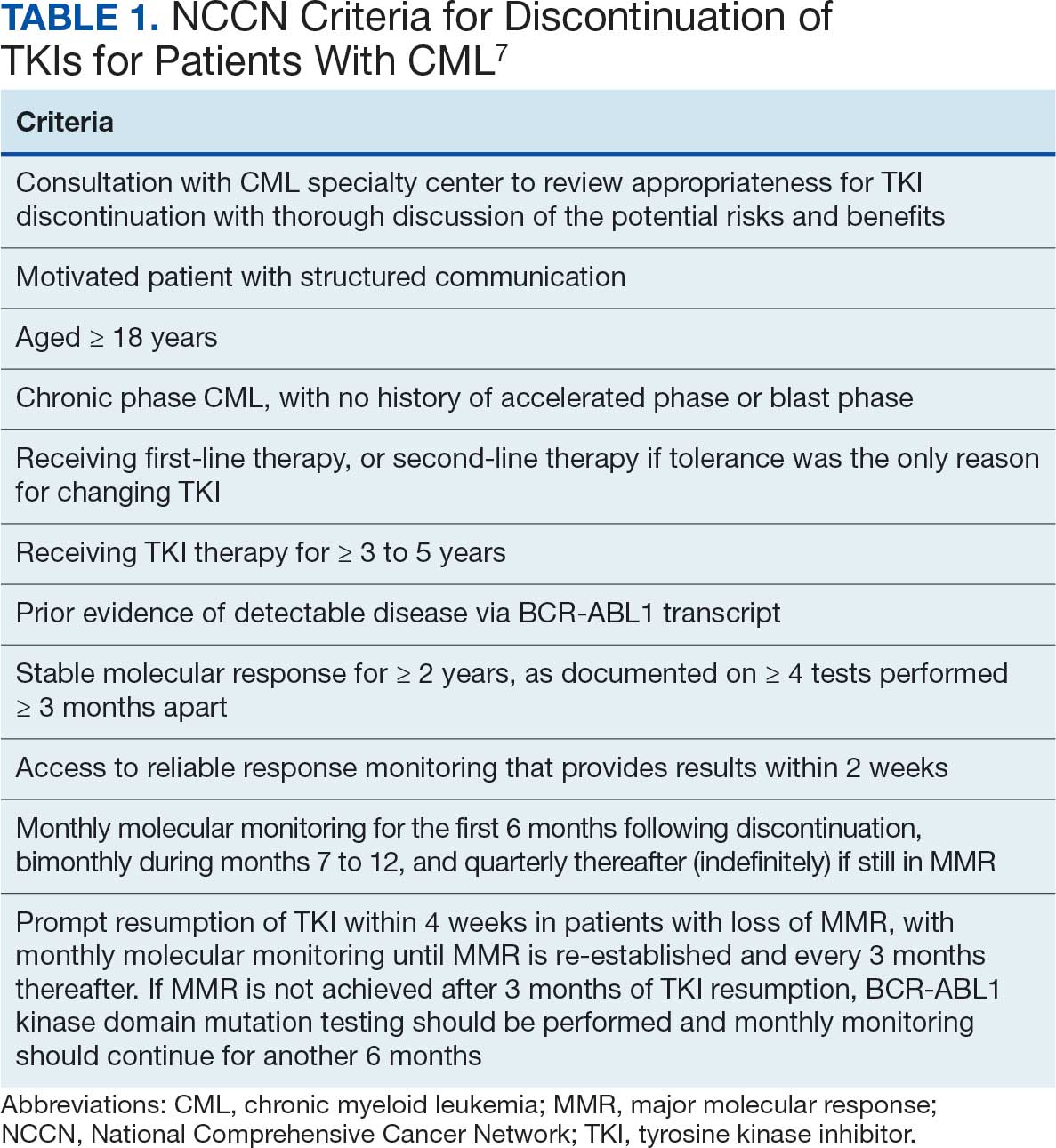
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
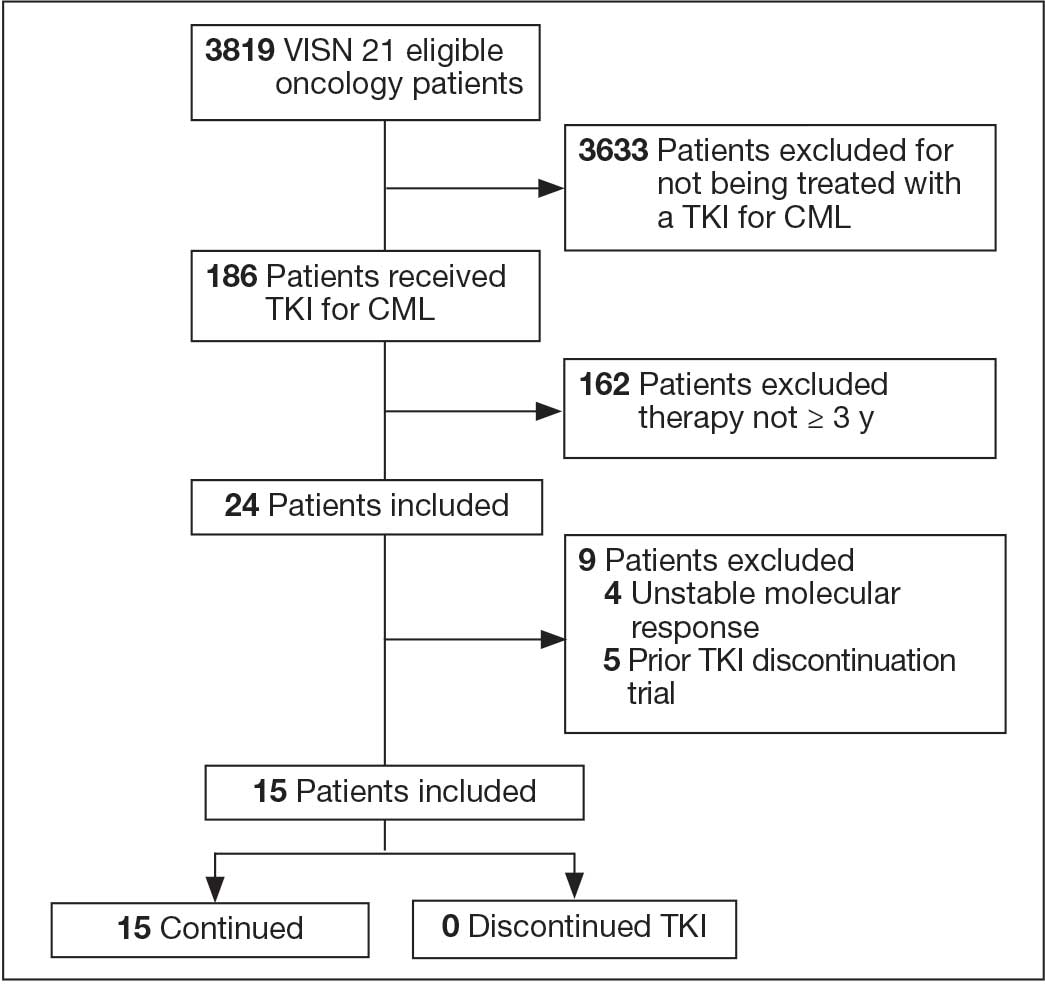
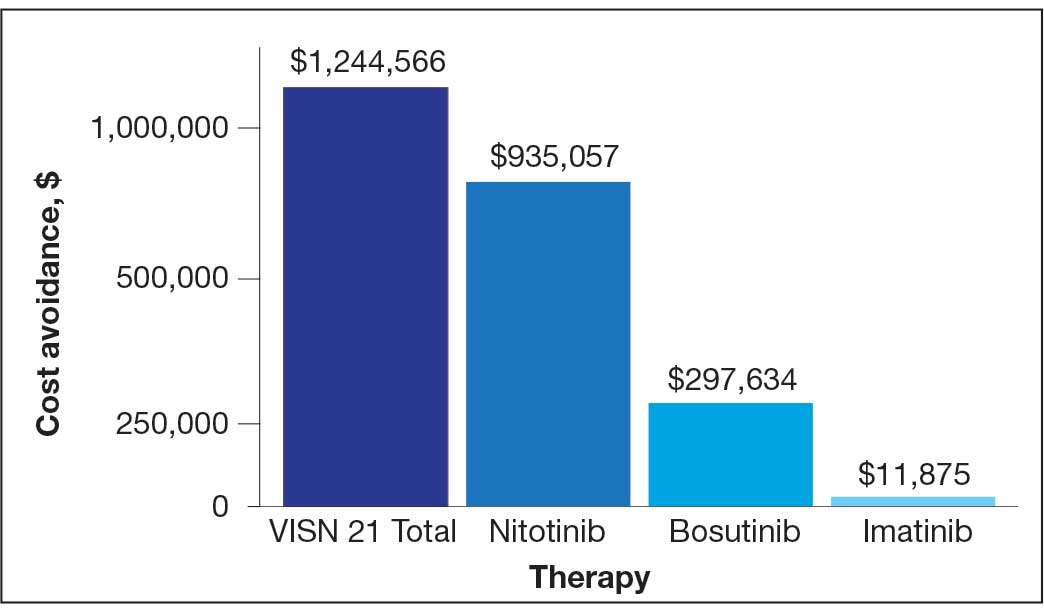
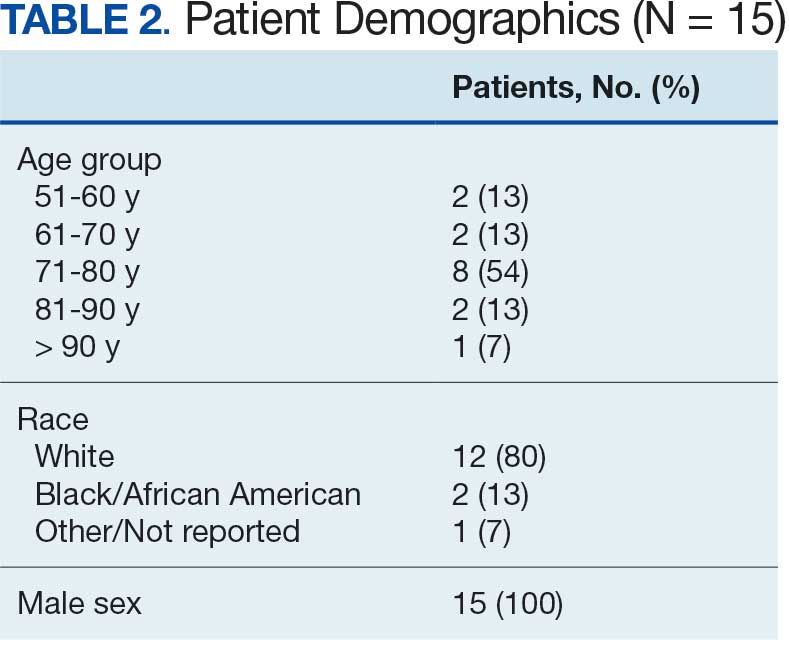
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
New Cancer Drugs: Do Patients Prefer Faster Access or Clinical Benefit?
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
Accelerated Approval of New Frontline TKI Use in CML Raises Questions
In October, the US Food and Drug Administration (FDA) granted accelerated approval to asciminib (Scemblix, Novartis AG) for adult patients with newly diagnosed Philadelphia chromosome–positive CML in chronic phase.
Asciminib is one of the six tyrosine kinase inhibitor (TKI) drugs used for CML, a class that began with the introduction of imatinib (Gleevec) in 2001. By 2016, researchers reported that TKIs had helped make life expectancy in patients with CML approach that of the general population. Physicians and patients now have several options of second-generation TKI drugs that also can be used in newly diagnosed patients, along with the option to begin with the more affordable option of imatinib.
The FDA in 1992 instituted the accelerated approval pathway to try to speed market drugs for serious conditions that fill unmet medical needs.
The agency and companies essentially make bets on promising study results, often using surrogate markers, to allow sales of medicines while waiting for evidence from confirmatory studies. For example, the FDA in August used the accelerated approval process to clear the first T-cell receptor gene therapy for certain advanced forms of sarcoma, a form of cancer with limited treatment options.
The next accelerated approval of a cancer drug was the indication for asciminib as a frontline therapy. The FDA also used accelerated approval for the initial clearance of asciminib in 2021 for use in CML previously treated with two or more TKIs. By 2022, Novartis presented sufficient evidence of the drug’s merit to win full approval for the drug in this use.
The timeline is longer for the expected confirmatory research for asciminib as a frontline therapy, with a 2028 deadline set for this work. The data presented to date on asciminib have not persuaded some oncologists on the need for the speedy approval of frontline use.
“This boils down to a drug that looks as if it’s just as good as other second-generation TKIs,” Mikkael A. Sekeres, MD, MS, chief of the Division of Hematology at the Sylvester Comprehensive Cancer Center, University of Miami Health System, Miami. “I don’t know how they could use the accelerated approval mechanism to get this through.”
Sekeres, a former chair of the Oncologic Drugs Advisory Committee, explored concerns and challenges involved with the use of the accelerated approval process in his 2022 book, Drugs and the FDA: Safety, Efficacy, and the Public’s Trust.
“The intent of the accelerated approval mechanism is that you’re bringing a new therapy to treat a serious disease in a way that others haven’t previously, where there aren’t existing options,” Sekeres said.
This is a markedly different situation that exists for CML, where medicines have improved dramatically in the 21st century, unlike many other forms of cancer treated by hematologists.
“As someone who specializes in treating people with leukemia, I’d be happy every clinic day of my life if all of my patients came in with chronic phase, chronic myeloid leukemia,” instead of other cancers lacking these robust treatment options, he said.
With CML, physicians select among TKIs considering side effects and other health conditions patients have, including weighing the impact of financial toxicity in some cases, he said.
“If I have a patient with lower risk chronic phase, chronic myeloid leukemia, I’m treating them with imatinib,” Sekeres said.
Questions About Surrogate Endpoints
Sekeres is not alone in questioning the use of the speedier FDA pathway for a new indication for a TKI in CML.
“Where is the ‘unmet need’ justifying an accelerated approval in this setting?” Timothée Olivier, MD, who is affiliated with both the Hôpitaux universitaires de Genève and the VK Prasad Laboratory funded by Vinay Prasad, MD, MPH, wrote in a November 3 post on X.
Olivier, Prasad, and coauthors in a September correspondence to the American Journal of Hematology raised questions about the study design for a key asciminib study, ASC4FIRST. They noted what they consider a weakness with the endpoints used.
“Molecular milestones like the 48-week MMR [major molecular response] are often used in clinical trials due to their convenience and shorter timeline for assessment,” they wrote. “However, these milestones are not definitive indicators of long-term survival or overall clinical benefit.”
There has been rising concern in recent years about the evidence gap between initial accelerated approvals and the completion of studies that show whether these promising therapies actually help patients live longer or better. Researchers including Bishal Gyawali, MD, PhD, a Medscape Medical News contributor, also have questioned the degree of reliance on surrogate endpoints in accelerated approvals.
In response, the FDA’s Cancer Division and the US Congress have taken steps to try to force drugmakers to more quickly answer the key question in accelerated approvals: Does this medicine produce the expected benefits? For example, the FDA in March appears to have turned down a bid for accelerated approval of a lymphoma drug due to concerns about the timing of completion of confirmatory research.
The use of accelerated approval will continue to be a balancing act, due in part to demand for newer agents, Ravi Bhatia, MD, of the O’Neal Comprehensive Cancer Center at The University of Alabama at Birmingham, told this news organization.
“Accelerated approval of agents for up-front treatment of CML does not appear well justified, given the high degree of efficacy of existing agents,” said Bhatia, vice chair of the National Comprehensive Cancer Network’s Clinical Practice Guidelines in Oncology Panel for Chronic Myeloid Leukemia.
“On the other hand, there is greater urgency for developing agents for patients who have failed existing agents and patients with advanced phase disease, and the use of accelerated approval may be justified in this setting,” Bhatia said.
In an interview with this news organization, Richard A. Larson, MD, a professor in the Department of Hematology/Oncology at The University of Chicago, who is an ASC4FIRST investigator, noted the 96-week follow-up data from the trial will be presented at the annual meeting of the American Society of Hematology in December in San Diego.
Larson said data from this trial will show continued benefit with the frontline use of asciminib. Larson also is an author of a New England Journal of Medicine article in May about the ASC4FIRST trial.
“The data speak for themselves, that asciminib is at least as effective or more so and at least as well tolerated as what’s already on the market,” Larson said. “So their argument, at the end of the day, really boils down to the cost of a new drug and whether we need a new drug.”
From the point of view of patients with cancer, the answer to that is clear, he said.
“If you talk to cancer patients, they’d like to see new drugs become available as quickly as possible. And I think that was the original rationale for the accelerated approval pathway, that a drug that has been shown to be safe and effective in a prospective clinical trial could get accelerated approval based on a surrogate endpoint.”
The remarkable success seen in developing TKI drugs for CML creates difficulties in testing later entrants in this class due to their prolonged survival, Larson said.
“If you look on a population basis, the overall survival of newly diagnosed CML patients with all of these therapeutic options available to them now approximate that of the non-CML population.”
“For most anticancer drugs, the FDA would like to see an overall survival benefit, but patients with newly diagnosed CML are surviving 20 or 30 years, and they’re not dying at an accelerated rate the way they were. So it’d be impractical to require a clinical trial to show a survival benefit, a randomized trial.”
“That’s where the use of a surrogate endpoint, which is the major molecular response at 1 year, has been so valuable, gets the drugs approved, gets them into patients far earlier than if there was a survival end point requirement,” he said.
Larson reported ties with AbbVie, Amgen, Astellas, Celgene, Cellectis, Curis, CVS Caremark, Daiichi Sankyo, ImmunoGen, Jazz, MorphoSys, Rigel, Servier, Forty Seven/Gilead, Novartis, and Rafael Pharmaceuticals. Sekeres disclosed relationships with BMS, Kurome, and Novartis Advisory Boards. Bhatia reported no relevant disclosures.
A version of this article appeared on Medscape.com.
In October, the US Food and Drug Administration (FDA) granted accelerated approval to asciminib (Scemblix, Novartis AG) for adult patients with newly diagnosed Philadelphia chromosome–positive CML in chronic phase.
Asciminib is one of the six tyrosine kinase inhibitor (TKI) drugs used for CML, a class that began with the introduction of imatinib (Gleevec) in 2001. By 2016, researchers reported that TKIs had helped make life expectancy in patients with CML approach that of the general population. Physicians and patients now have several options of second-generation TKI drugs that also can be used in newly diagnosed patients, along with the option to begin with the more affordable option of imatinib.
The FDA in 1992 instituted the accelerated approval pathway to try to speed market drugs for serious conditions that fill unmet medical needs.
The agency and companies essentially make bets on promising study results, often using surrogate markers, to allow sales of medicines while waiting for evidence from confirmatory studies. For example, the FDA in August used the accelerated approval process to clear the first T-cell receptor gene therapy for certain advanced forms of sarcoma, a form of cancer with limited treatment options.
The next accelerated approval of a cancer drug was the indication for asciminib as a frontline therapy. The FDA also used accelerated approval for the initial clearance of asciminib in 2021 for use in CML previously treated with two or more TKIs. By 2022, Novartis presented sufficient evidence of the drug’s merit to win full approval for the drug in this use.
The timeline is longer for the expected confirmatory research for asciminib as a frontline therapy, with a 2028 deadline set for this work. The data presented to date on asciminib have not persuaded some oncologists on the need for the speedy approval of frontline use.
“This boils down to a drug that looks as if it’s just as good as other second-generation TKIs,” Mikkael A. Sekeres, MD, MS, chief of the Division of Hematology at the Sylvester Comprehensive Cancer Center, University of Miami Health System, Miami. “I don’t know how they could use the accelerated approval mechanism to get this through.”
Sekeres, a former chair of the Oncologic Drugs Advisory Committee, explored concerns and challenges involved with the use of the accelerated approval process in his 2022 book, Drugs and the FDA: Safety, Efficacy, and the Public’s Trust.
“The intent of the accelerated approval mechanism is that you’re bringing a new therapy to treat a serious disease in a way that others haven’t previously, where there aren’t existing options,” Sekeres said.
This is a markedly different situation that exists for CML, where medicines have improved dramatically in the 21st century, unlike many other forms of cancer treated by hematologists.
“As someone who specializes in treating people with leukemia, I’d be happy every clinic day of my life if all of my patients came in with chronic phase, chronic myeloid leukemia,” instead of other cancers lacking these robust treatment options, he said.
With CML, physicians select among TKIs considering side effects and other health conditions patients have, including weighing the impact of financial toxicity in some cases, he said.
“If I have a patient with lower risk chronic phase, chronic myeloid leukemia, I’m treating them with imatinib,” Sekeres said.
Questions About Surrogate Endpoints
Sekeres is not alone in questioning the use of the speedier FDA pathway for a new indication for a TKI in CML.
“Where is the ‘unmet need’ justifying an accelerated approval in this setting?” Timothée Olivier, MD, who is affiliated with both the Hôpitaux universitaires de Genève and the VK Prasad Laboratory funded by Vinay Prasad, MD, MPH, wrote in a November 3 post on X.
Olivier, Prasad, and coauthors in a September correspondence to the American Journal of Hematology raised questions about the study design for a key asciminib study, ASC4FIRST. They noted what they consider a weakness with the endpoints used.
“Molecular milestones like the 48-week MMR [major molecular response] are often used in clinical trials due to their convenience and shorter timeline for assessment,” they wrote. “However, these milestones are not definitive indicators of long-term survival or overall clinical benefit.”
There has been rising concern in recent years about the evidence gap between initial accelerated approvals and the completion of studies that show whether these promising therapies actually help patients live longer or better. Researchers including Bishal Gyawali, MD, PhD, a Medscape Medical News contributor, also have questioned the degree of reliance on surrogate endpoints in accelerated approvals.
In response, the FDA’s Cancer Division and the US Congress have taken steps to try to force drugmakers to more quickly answer the key question in accelerated approvals: Does this medicine produce the expected benefits? For example, the FDA in March appears to have turned down a bid for accelerated approval of a lymphoma drug due to concerns about the timing of completion of confirmatory research.
The use of accelerated approval will continue to be a balancing act, due in part to demand for newer agents, Ravi Bhatia, MD, of the O’Neal Comprehensive Cancer Center at The University of Alabama at Birmingham, told this news organization.
“Accelerated approval of agents for up-front treatment of CML does not appear well justified, given the high degree of efficacy of existing agents,” said Bhatia, vice chair of the National Comprehensive Cancer Network’s Clinical Practice Guidelines in Oncology Panel for Chronic Myeloid Leukemia.
“On the other hand, there is greater urgency for developing agents for patients who have failed existing agents and patients with advanced phase disease, and the use of accelerated approval may be justified in this setting,” Bhatia said.
In an interview with this news organization, Richard A. Larson, MD, a professor in the Department of Hematology/Oncology at The University of Chicago, who is an ASC4FIRST investigator, noted the 96-week follow-up data from the trial will be presented at the annual meeting of the American Society of Hematology in December in San Diego.
Larson said data from this trial will show continued benefit with the frontline use of asciminib. Larson also is an author of a New England Journal of Medicine article in May about the ASC4FIRST trial.
“The data speak for themselves, that asciminib is at least as effective or more so and at least as well tolerated as what’s already on the market,” Larson said. “So their argument, at the end of the day, really boils down to the cost of a new drug and whether we need a new drug.”
From the point of view of patients with cancer, the answer to that is clear, he said.
“If you talk to cancer patients, they’d like to see new drugs become available as quickly as possible. And I think that was the original rationale for the accelerated approval pathway, that a drug that has been shown to be safe and effective in a prospective clinical trial could get accelerated approval based on a surrogate endpoint.”
The remarkable success seen in developing TKI drugs for CML creates difficulties in testing later entrants in this class due to their prolonged survival, Larson said.
“If you look on a population basis, the overall survival of newly diagnosed CML patients with all of these therapeutic options available to them now approximate that of the non-CML population.”
“For most anticancer drugs, the FDA would like to see an overall survival benefit, but patients with newly diagnosed CML are surviving 20 or 30 years, and they’re not dying at an accelerated rate the way they were. So it’d be impractical to require a clinical trial to show a survival benefit, a randomized trial.”
“That’s where the use of a surrogate endpoint, which is the major molecular response at 1 year, has been so valuable, gets the drugs approved, gets them into patients far earlier than if there was a survival end point requirement,” he said.
Larson reported ties with AbbVie, Amgen, Astellas, Celgene, Cellectis, Curis, CVS Caremark, Daiichi Sankyo, ImmunoGen, Jazz, MorphoSys, Rigel, Servier, Forty Seven/Gilead, Novartis, and Rafael Pharmaceuticals. Sekeres disclosed relationships with BMS, Kurome, and Novartis Advisory Boards. Bhatia reported no relevant disclosures.
A version of this article appeared on Medscape.com.
In October, the US Food and Drug Administration (FDA) granted accelerated approval to asciminib (Scemblix, Novartis AG) for adult patients with newly diagnosed Philadelphia chromosome–positive CML in chronic phase.
Asciminib is one of the six tyrosine kinase inhibitor (TKI) drugs used for CML, a class that began with the introduction of imatinib (Gleevec) in 2001. By 2016, researchers reported that TKIs had helped make life expectancy in patients with CML approach that of the general population. Physicians and patients now have several options of second-generation TKI drugs that also can be used in newly diagnosed patients, along with the option to begin with the more affordable option of imatinib.
The FDA in 1992 instituted the accelerated approval pathway to try to speed market drugs for serious conditions that fill unmet medical needs.
The agency and companies essentially make bets on promising study results, often using surrogate markers, to allow sales of medicines while waiting for evidence from confirmatory studies. For example, the FDA in August used the accelerated approval process to clear the first T-cell receptor gene therapy for certain advanced forms of sarcoma, a form of cancer with limited treatment options.
The next accelerated approval of a cancer drug was the indication for asciminib as a frontline therapy. The FDA also used accelerated approval for the initial clearance of asciminib in 2021 for use in CML previously treated with two or more TKIs. By 2022, Novartis presented sufficient evidence of the drug’s merit to win full approval for the drug in this use.
The timeline is longer for the expected confirmatory research for asciminib as a frontline therapy, with a 2028 deadline set for this work. The data presented to date on asciminib have not persuaded some oncologists on the need for the speedy approval of frontline use.
“This boils down to a drug that looks as if it’s just as good as other second-generation TKIs,” Mikkael A. Sekeres, MD, MS, chief of the Division of Hematology at the Sylvester Comprehensive Cancer Center, University of Miami Health System, Miami. “I don’t know how they could use the accelerated approval mechanism to get this through.”
Sekeres, a former chair of the Oncologic Drugs Advisory Committee, explored concerns and challenges involved with the use of the accelerated approval process in his 2022 book, Drugs and the FDA: Safety, Efficacy, and the Public’s Trust.
“The intent of the accelerated approval mechanism is that you’re bringing a new therapy to treat a serious disease in a way that others haven’t previously, where there aren’t existing options,” Sekeres said.
This is a markedly different situation that exists for CML, where medicines have improved dramatically in the 21st century, unlike many other forms of cancer treated by hematologists.
“As someone who specializes in treating people with leukemia, I’d be happy every clinic day of my life if all of my patients came in with chronic phase, chronic myeloid leukemia,” instead of other cancers lacking these robust treatment options, he said.
With CML, physicians select among TKIs considering side effects and other health conditions patients have, including weighing the impact of financial toxicity in some cases, he said.
“If I have a patient with lower risk chronic phase, chronic myeloid leukemia, I’m treating them with imatinib,” Sekeres said.
Questions About Surrogate Endpoints
Sekeres is not alone in questioning the use of the speedier FDA pathway for a new indication for a TKI in CML.
“Where is the ‘unmet need’ justifying an accelerated approval in this setting?” Timothée Olivier, MD, who is affiliated with both the Hôpitaux universitaires de Genève and the VK Prasad Laboratory funded by Vinay Prasad, MD, MPH, wrote in a November 3 post on X.
Olivier, Prasad, and coauthors in a September correspondence to the American Journal of Hematology raised questions about the study design for a key asciminib study, ASC4FIRST. They noted what they consider a weakness with the endpoints used.
“Molecular milestones like the 48-week MMR [major molecular response] are often used in clinical trials due to their convenience and shorter timeline for assessment,” they wrote. “However, these milestones are not definitive indicators of long-term survival or overall clinical benefit.”
There has been rising concern in recent years about the evidence gap between initial accelerated approvals and the completion of studies that show whether these promising therapies actually help patients live longer or better. Researchers including Bishal Gyawali, MD, PhD, a Medscape Medical News contributor, also have questioned the degree of reliance on surrogate endpoints in accelerated approvals.
In response, the FDA’s Cancer Division and the US Congress have taken steps to try to force drugmakers to more quickly answer the key question in accelerated approvals: Does this medicine produce the expected benefits? For example, the FDA in March appears to have turned down a bid for accelerated approval of a lymphoma drug due to concerns about the timing of completion of confirmatory research.
The use of accelerated approval will continue to be a balancing act, due in part to demand for newer agents, Ravi Bhatia, MD, of the O’Neal Comprehensive Cancer Center at The University of Alabama at Birmingham, told this news organization.
“Accelerated approval of agents for up-front treatment of CML does not appear well justified, given the high degree of efficacy of existing agents,” said Bhatia, vice chair of the National Comprehensive Cancer Network’s Clinical Practice Guidelines in Oncology Panel for Chronic Myeloid Leukemia.
“On the other hand, there is greater urgency for developing agents for patients who have failed existing agents and patients with advanced phase disease, and the use of accelerated approval may be justified in this setting,” Bhatia said.
In an interview with this news organization, Richard A. Larson, MD, a professor in the Department of Hematology/Oncology at The University of Chicago, who is an ASC4FIRST investigator, noted the 96-week follow-up data from the trial will be presented at the annual meeting of the American Society of Hematology in December in San Diego.
Larson said data from this trial will show continued benefit with the frontline use of asciminib. Larson also is an author of a New England Journal of Medicine article in May about the ASC4FIRST trial.
“The data speak for themselves, that asciminib is at least as effective or more so and at least as well tolerated as what’s already on the market,” Larson said. “So their argument, at the end of the day, really boils down to the cost of a new drug and whether we need a new drug.”
From the point of view of patients with cancer, the answer to that is clear, he said.
“If you talk to cancer patients, they’d like to see new drugs become available as quickly as possible. And I think that was the original rationale for the accelerated approval pathway, that a drug that has been shown to be safe and effective in a prospective clinical trial could get accelerated approval based on a surrogate endpoint.”
The remarkable success seen in developing TKI drugs for CML creates difficulties in testing later entrants in this class due to their prolonged survival, Larson said.
“If you look on a population basis, the overall survival of newly diagnosed CML patients with all of these therapeutic options available to them now approximate that of the non-CML population.”
“For most anticancer drugs, the FDA would like to see an overall survival benefit, but patients with newly diagnosed CML are surviving 20 or 30 years, and they’re not dying at an accelerated rate the way they were. So it’d be impractical to require a clinical trial to show a survival benefit, a randomized trial.”
“That’s where the use of a surrogate endpoint, which is the major molecular response at 1 year, has been so valuable, gets the drugs approved, gets them into patients far earlier than if there was a survival end point requirement,” he said.
Larson reported ties with AbbVie, Amgen, Astellas, Celgene, Cellectis, Curis, CVS Caremark, Daiichi Sankyo, ImmunoGen, Jazz, MorphoSys, Rigel, Servier, Forty Seven/Gilead, Novartis, and Rafael Pharmaceuticals. Sekeres disclosed relationships with BMS, Kurome, and Novartis Advisory Boards. Bhatia reported no relevant disclosures.
A version of this article appeared on Medscape.com.
Inside the Patient-Oncologist Bond: Why It’s Often So Strong
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
From Mexico City to the Heights of Leukemia Medicine
His work has helped transform CML into an often-survivable disease instead of one that took the lives of most patients within 5 years.
“It’s been remarkable to see the evolution in CML and to be part of that transition as a fellow, as faculty, and as leader of some of the trials,” said Cortes, who directs the Georgia Cancer Center at Augusta University. “I’m the luckiest person in the world.”
In an interview, Cortes talked about his youth in Mexico, his research path, and his close connections to cancer medicine in Latin America.
Q: You grew up in Mexico City. What was your family like?
A: “My father grew up very poor in a small town in Michoacán in the southwest part of Mexico. In Mexico City, he had a tiny grocery store in an old-fashioned market, and we were lower middle class.
One of the things I learned was to work hard. There’s nobody I know who worked as hard as my father. He opened his store every day of the year, [Mexican] Independence Day or New Year’s or Christmas. He worked hard so we could have a better life than he did.
We learned English from a very young age. My elementary school was called Westminster School because he wanted a school where we would learn English.
As for my mother, she stayed with us [at home] and made sure we did our homework and were taken care of. I learned about being honest and dedicating to what you were doing.”
Q: You trained at the Salvador Zubirán National Institute of Health Sciences and Nutrition in Mexico City. Then what happened?
A: “Through encouragement by my dermatologist older brother and a mentor at the institution where I was training as a hematologist, I decided to come to the United States.
My initial focus was going to be on coagulation and thrombosis. I came to Houston (Texas) for a fellowship at the University of Texas Health Science Center.
Then I started doing my rotation for the malignant part of the fellowship at MD Anderson Cancer Center [Houston]. One of my first rotations was with Susan M. O’Brien, [MD,] who became my greatest mentor throughout my career. I really enjoyed my rotation. I thought she was great clinically, and she was doing research and teaching. That’s what I wanted for my career.”
Q: What drew you to leukemia specifically?
A: “Dr O’Brien worked in leukemia during my initial rotation, and I really loved it. It was hard work, but it was very inspiring to see the clinical research and the things you could for patients. She had a lot of joy doing that.
I told my program director I’d change and transfer to MD Anderson, and I ended up staying at MD Anderson for 23 years.”
Q: What was leukemia research like in those days?
A: “We didn’t have the understanding of the biology and the new drugs that we have now. When I started in Mexico, we didn’t even have hydroxyurea. What we were doing was much more basic. But still, the field sounded like a great field to be involved with because they were doing so many trials and had an outstanding database.
Because of the influence of Dr [Moshe] Talpaz, [MD,] I started getting very involved with CML. In my initial years as a young faculty, I started working with him on interferon. Then imatinib appeared. I saw even from the phase 1 study how impressive the outcomes were in patients who had no response to anything and were in bad shape.”
Q: What CML medications have you worked on?
A: “I’ve been involved with all of them. Imatinib early on, then I led trials with dasatinib and nilotinib. Then, I led the registration trials of bosutinib and ponatinib. More recently, I was part of the development of asciminib.”
Q: What were some of the biggest challenges in CML research?
A: “We had an opportunity to do a lot of analysis about TKIs [tyrosine kinase inhibitors] when these were new drugs. It was a very steep curve of learning, how to monitor and manage side effects.
Then patients were starting to have resistance to two to three TKIs. Ponatinib came along, and it was an incredibly effective drug. But after it was approved, we started to recognize the occurrence of heart attacks and strokes.
That was unexpected and not something that was known for any TKI. It was a big challenge. The drug was taken off the market for some time, and trials were put on hold by the FDA [US Food and Drug Administration].
We scrambled to understand the mechanism of action. For a year or two, it was a stressful time. But eventually we moved past it, and we learned a lot.”
Q: What sort of work have you done in Latin America?
A: “I’ve always been very close to Latin America. I have many good friends and colleagues there, and I’ve always been interested in working with them.
We’ve done research and studies and created an organization called Latin American Leukemia Net to develop more trials in Latin America. The most rewarding thing has been the educational programs for patients that we’ve done, helping them understand the disease, the treatments, and the goals of treatment.
We’ve conducted a number of programs, and they have been effective, well-attended, and well received. I still work with my colleagues to develop local guidelines and do collaborative research.”
Q: What convinced you to leave MD Anderson for Georgia?
A: “I never thought I’d leave MD Anderson. I had my well-oiled machine of clinical trials, my clinic, and my fellowship program. But the one thing that I wanted to see if I could try next was to develop an institution.
That was the goal here, to take the Georgia Cancer Center to NCI [National Cancer Institute] designation. So, I thought, ‘That’s a nice challenge.’ It may be a good opportunity to try a different aspect of what it means to be an oncologist.
There are days that you think, ‘What am I doing here?’ when you have to deal with budgets and personnel and all these things. But it’s part of the process. It’s still good to know that we have a goal, and that we’re going to make it.
Also, I still see my patients, and I enjoy that I still do some research and mentoring.”
Q: What’s the current state of CML treatment?
A: “Many patients have a pretty much normal life expectancy while [on therapy]. Still, one of the goals of many patients is to stop therapy. But that’s a reality only for a small percentage of patients. How can we make that happen for more patients?”
Q: By stopping therapy, do you mean curing the cancer?
A: “Yes, pretty much. You have a good response, you stop the therapy, and it doesn’t come back.
There are also patients who really don’t do well. We hear about CML being with a disease with such a good outcome, but we have patients for whom nothing works. Is it a matter of [needing] another TKI, or do we need to look at something else?”
Q: What do you see on the horizon?
A: “We are developing new approaches like combination therapies. We’re scratching the surface on that. We need to understand which combinations work, and where and when.
And we can make more efficient uses of the drugs we have now in terms of which ones to use when, the doses, the safety profiles. I think we can do better.”
Cortes disclosed consulting for Amphivena, Astellas, Bio-Path, BioLineRx, Bristol Myers Squibb, Daiichi Sankyo, Jazz, Novartis, Pfizer, and Takeda and research funding from Astellas Pharma, Bristol Myers Squibb, Daiichi Sankyo, Immunogen, Jazz, Merus, Novartis, Pfizer, Sun Pharma, Takeda, Tolero and Trovagene.
A version of this article appeared on Medscape.com.
His work has helped transform CML into an often-survivable disease instead of one that took the lives of most patients within 5 years.
“It’s been remarkable to see the evolution in CML and to be part of that transition as a fellow, as faculty, and as leader of some of the trials,” said Cortes, who directs the Georgia Cancer Center at Augusta University. “I’m the luckiest person in the world.”
In an interview, Cortes talked about his youth in Mexico, his research path, and his close connections to cancer medicine in Latin America.
Q: You grew up in Mexico City. What was your family like?
A: “My father grew up very poor in a small town in Michoacán in the southwest part of Mexico. In Mexico City, he had a tiny grocery store in an old-fashioned market, and we were lower middle class.
One of the things I learned was to work hard. There’s nobody I know who worked as hard as my father. He opened his store every day of the year, [Mexican] Independence Day or New Year’s or Christmas. He worked hard so we could have a better life than he did.
We learned English from a very young age. My elementary school was called Westminster School because he wanted a school where we would learn English.
As for my mother, she stayed with us [at home] and made sure we did our homework and were taken care of. I learned about being honest and dedicating to what you were doing.”
Q: You trained at the Salvador Zubirán National Institute of Health Sciences and Nutrition in Mexico City. Then what happened?
A: “Through encouragement by my dermatologist older brother and a mentor at the institution where I was training as a hematologist, I decided to come to the United States.
My initial focus was going to be on coagulation and thrombosis. I came to Houston (Texas) for a fellowship at the University of Texas Health Science Center.
Then I started doing my rotation for the malignant part of the fellowship at MD Anderson Cancer Center [Houston]. One of my first rotations was with Susan M. O’Brien, [MD,] who became my greatest mentor throughout my career. I really enjoyed my rotation. I thought she was great clinically, and she was doing research and teaching. That’s what I wanted for my career.”
Q: What drew you to leukemia specifically?
A: “Dr O’Brien worked in leukemia during my initial rotation, and I really loved it. It was hard work, but it was very inspiring to see the clinical research and the things you could for patients. She had a lot of joy doing that.
I told my program director I’d change and transfer to MD Anderson, and I ended up staying at MD Anderson for 23 years.”
Q: What was leukemia research like in those days?
A: “We didn’t have the understanding of the biology and the new drugs that we have now. When I started in Mexico, we didn’t even have hydroxyurea. What we were doing was much more basic. But still, the field sounded like a great field to be involved with because they were doing so many trials and had an outstanding database.
Because of the influence of Dr [Moshe] Talpaz, [MD,] I started getting very involved with CML. In my initial years as a young faculty, I started working with him on interferon. Then imatinib appeared. I saw even from the phase 1 study how impressive the outcomes were in patients who had no response to anything and were in bad shape.”
Q: What CML medications have you worked on?
A: “I’ve been involved with all of them. Imatinib early on, then I led trials with dasatinib and nilotinib. Then, I led the registration trials of bosutinib and ponatinib. More recently, I was part of the development of asciminib.”
Q: What were some of the biggest challenges in CML research?
A: “We had an opportunity to do a lot of analysis about TKIs [tyrosine kinase inhibitors] when these were new drugs. It was a very steep curve of learning, how to monitor and manage side effects.
Then patients were starting to have resistance to two to three TKIs. Ponatinib came along, and it was an incredibly effective drug. But after it was approved, we started to recognize the occurrence of heart attacks and strokes.
That was unexpected and not something that was known for any TKI. It was a big challenge. The drug was taken off the market for some time, and trials were put on hold by the FDA [US Food and Drug Administration].
We scrambled to understand the mechanism of action. For a year or two, it was a stressful time. But eventually we moved past it, and we learned a lot.”
Q: What sort of work have you done in Latin America?
A: “I’ve always been very close to Latin America. I have many good friends and colleagues there, and I’ve always been interested in working with them.
We’ve done research and studies and created an organization called Latin American Leukemia Net to develop more trials in Latin America. The most rewarding thing has been the educational programs for patients that we’ve done, helping them understand the disease, the treatments, and the goals of treatment.
We’ve conducted a number of programs, and they have been effective, well-attended, and well received. I still work with my colleagues to develop local guidelines and do collaborative research.”
Q: What convinced you to leave MD Anderson for Georgia?
A: “I never thought I’d leave MD Anderson. I had my well-oiled machine of clinical trials, my clinic, and my fellowship program. But the one thing that I wanted to see if I could try next was to develop an institution.
That was the goal here, to take the Georgia Cancer Center to NCI [National Cancer Institute] designation. So, I thought, ‘That’s a nice challenge.’ It may be a good opportunity to try a different aspect of what it means to be an oncologist.
There are days that you think, ‘What am I doing here?’ when you have to deal with budgets and personnel and all these things. But it’s part of the process. It’s still good to know that we have a goal, and that we’re going to make it.
Also, I still see my patients, and I enjoy that I still do some research and mentoring.”
Q: What’s the current state of CML treatment?
A: “Many patients have a pretty much normal life expectancy while [on therapy]. Still, one of the goals of many patients is to stop therapy. But that’s a reality only for a small percentage of patients. How can we make that happen for more patients?”
Q: By stopping therapy, do you mean curing the cancer?
A: “Yes, pretty much. You have a good response, you stop the therapy, and it doesn’t come back.
There are also patients who really don’t do well. We hear about CML being with a disease with such a good outcome, but we have patients for whom nothing works. Is it a matter of [needing] another TKI, or do we need to look at something else?”
Q: What do you see on the horizon?
A: “We are developing new approaches like combination therapies. We’re scratching the surface on that. We need to understand which combinations work, and where and when.
And we can make more efficient uses of the drugs we have now in terms of which ones to use when, the doses, the safety profiles. I think we can do better.”
Cortes disclosed consulting for Amphivena, Astellas, Bio-Path, BioLineRx, Bristol Myers Squibb, Daiichi Sankyo, Jazz, Novartis, Pfizer, and Takeda and research funding from Astellas Pharma, Bristol Myers Squibb, Daiichi Sankyo, Immunogen, Jazz, Merus, Novartis, Pfizer, Sun Pharma, Takeda, Tolero and Trovagene.
A version of this article appeared on Medscape.com.
His work has helped transform CML into an often-survivable disease instead of one that took the lives of most patients within 5 years.
“It’s been remarkable to see the evolution in CML and to be part of that transition as a fellow, as faculty, and as leader of some of the trials,” said Cortes, who directs the Georgia Cancer Center at Augusta University. “I’m the luckiest person in the world.”
In an interview, Cortes talked about his youth in Mexico, his research path, and his close connections to cancer medicine in Latin America.
Q: You grew up in Mexico City. What was your family like?
A: “My father grew up very poor in a small town in Michoacán in the southwest part of Mexico. In Mexico City, he had a tiny grocery store in an old-fashioned market, and we were lower middle class.
One of the things I learned was to work hard. There’s nobody I know who worked as hard as my father. He opened his store every day of the year, [Mexican] Independence Day or New Year’s or Christmas. He worked hard so we could have a better life than he did.
We learned English from a very young age. My elementary school was called Westminster School because he wanted a school where we would learn English.
As for my mother, she stayed with us [at home] and made sure we did our homework and were taken care of. I learned about being honest and dedicating to what you were doing.”
Q: You trained at the Salvador Zubirán National Institute of Health Sciences and Nutrition in Mexico City. Then what happened?
A: “Through encouragement by my dermatologist older brother and a mentor at the institution where I was training as a hematologist, I decided to come to the United States.
My initial focus was going to be on coagulation and thrombosis. I came to Houston (Texas) for a fellowship at the University of Texas Health Science Center.
Then I started doing my rotation for the malignant part of the fellowship at MD Anderson Cancer Center [Houston]. One of my first rotations was with Susan M. O’Brien, [MD,] who became my greatest mentor throughout my career. I really enjoyed my rotation. I thought she was great clinically, and she was doing research and teaching. That’s what I wanted for my career.”
Q: What drew you to leukemia specifically?
A: “Dr O’Brien worked in leukemia during my initial rotation, and I really loved it. It was hard work, but it was very inspiring to see the clinical research and the things you could for patients. She had a lot of joy doing that.
I told my program director I’d change and transfer to MD Anderson, and I ended up staying at MD Anderson for 23 years.”
Q: What was leukemia research like in those days?
A: “We didn’t have the understanding of the biology and the new drugs that we have now. When I started in Mexico, we didn’t even have hydroxyurea. What we were doing was much more basic. But still, the field sounded like a great field to be involved with because they were doing so many trials and had an outstanding database.
Because of the influence of Dr [Moshe] Talpaz, [MD,] I started getting very involved with CML. In my initial years as a young faculty, I started working with him on interferon. Then imatinib appeared. I saw even from the phase 1 study how impressive the outcomes were in patients who had no response to anything and were in bad shape.”
Q: What CML medications have you worked on?
A: “I’ve been involved with all of them. Imatinib early on, then I led trials with dasatinib and nilotinib. Then, I led the registration trials of bosutinib and ponatinib. More recently, I was part of the development of asciminib.”
Q: What were some of the biggest challenges in CML research?
A: “We had an opportunity to do a lot of analysis about TKIs [tyrosine kinase inhibitors] when these were new drugs. It was a very steep curve of learning, how to monitor and manage side effects.
Then patients were starting to have resistance to two to three TKIs. Ponatinib came along, and it was an incredibly effective drug. But after it was approved, we started to recognize the occurrence of heart attacks and strokes.
That was unexpected and not something that was known for any TKI. It was a big challenge. The drug was taken off the market for some time, and trials were put on hold by the FDA [US Food and Drug Administration].
We scrambled to understand the mechanism of action. For a year or two, it was a stressful time. But eventually we moved past it, and we learned a lot.”
Q: What sort of work have you done in Latin America?
A: “I’ve always been very close to Latin America. I have many good friends and colleagues there, and I’ve always been interested in working with them.
We’ve done research and studies and created an organization called Latin American Leukemia Net to develop more trials in Latin America. The most rewarding thing has been the educational programs for patients that we’ve done, helping them understand the disease, the treatments, and the goals of treatment.
We’ve conducted a number of programs, and they have been effective, well-attended, and well received. I still work with my colleagues to develop local guidelines and do collaborative research.”
Q: What convinced you to leave MD Anderson for Georgia?
A: “I never thought I’d leave MD Anderson. I had my well-oiled machine of clinical trials, my clinic, and my fellowship program. But the one thing that I wanted to see if I could try next was to develop an institution.
That was the goal here, to take the Georgia Cancer Center to NCI [National Cancer Institute] designation. So, I thought, ‘That’s a nice challenge.’ It may be a good opportunity to try a different aspect of what it means to be an oncologist.
There are days that you think, ‘What am I doing here?’ when you have to deal with budgets and personnel and all these things. But it’s part of the process. It’s still good to know that we have a goal, and that we’re going to make it.
Also, I still see my patients, and I enjoy that I still do some research and mentoring.”
Q: What’s the current state of CML treatment?
A: “Many patients have a pretty much normal life expectancy while [on therapy]. Still, one of the goals of many patients is to stop therapy. But that’s a reality only for a small percentage of patients. How can we make that happen for more patients?”
Q: By stopping therapy, do you mean curing the cancer?
A: “Yes, pretty much. You have a good response, you stop the therapy, and it doesn’t come back.
There are also patients who really don’t do well. We hear about CML being with a disease with such a good outcome, but we have patients for whom nothing works. Is it a matter of [needing] another TKI, or do we need to look at something else?”
Q: What do you see on the horizon?
A: “We are developing new approaches like combination therapies. We’re scratching the surface on that. We need to understand which combinations work, and where and when.
And we can make more efficient uses of the drugs we have now in terms of which ones to use when, the doses, the safety profiles. I think we can do better.”
Cortes disclosed consulting for Amphivena, Astellas, Bio-Path, BioLineRx, Bristol Myers Squibb, Daiichi Sankyo, Jazz, Novartis, Pfizer, and Takeda and research funding from Astellas Pharma, Bristol Myers Squibb, Daiichi Sankyo, Immunogen, Jazz, Merus, Novartis, Pfizer, Sun Pharma, Takeda, Tolero and Trovagene.
A version of this article appeared on Medscape.com.
For Radiation ‘Downwinders,’ Cancer Compensation Is On Hold
As of 2022, more than 40,000 patients with cancer successfully applied for $2.6 billion in compensation. Recipients included “downwinders” who were eligible for $50,000 each if they lived in certain areas of Nevada, Utah, and Arizona during specified nuclear testing periods and developed a covered form of cancer.
In June 2024, however, the Radiation Exposure Compensation Program expired amid infighting among Republicans in Congress over whether to expand it. For now, no one can make a claim, even though many downwinders are still alive and continue to be diagnosed with covered cancers decades after they were exposed in the 1940s, 1950s, and 1960s.
There’s a glimmer of good news. The federal government continues to support free medical screenings for eligible people, including certain downwinders and uranium workers. Meanwhile, there are still important roles for clinicians across the country to play as politicians figure out what — if anything — to do next regarding those exposed to radiation.
“We are still here. We can still screen people,” Zachary Davis, program director for the Radiation Exposure Screening and Education Program, The University of New Mexico, in Albuquerque, New Mexico, said in an interview.
Still-Unfolding Legacy of Radiation Exposure
No one knew just how far radiation would spread when the first nuclear bomb was tested in New Mexico in July 1945. Would it cover the state? The entire Southwest? The whole nation?
It also wasn’t clear how radiation would affect people’s health. “There was an awareness that some cancers were caused by radiation, but there wasn’t a cohesive understanding of what the problem was,” Joseph Shonka, PhD, a health physicist who studies radiation exposure and has worked for decades in nuclear engineering, said in an interview.
Now, nearly eight decades later, scientists are still figuring out the full extent of radioactive fallout from nuclear testing. Just last year, a study suggested that radiation from 94 nuclear weapon tests in the Southwest from 1945 to 1962 reached 46 states along with Canada and Mexico.
Activists believe the tests triggered untold number of cancer cases in residents who were exposed in downwind areas:
“My brother died of stomach cancer; my mom died of bone cancer. One of my sisters is surviving brain tumors, and the other one is surviving thyroid cancer,” one New Mexico man recently told ABC-TV’s “Nightline.”
In Idaho, a downwinder advocate told Idaho Capital Sun that everyone who attended a reception for her newly married parents in 1952 — just weeks after a nuclear test — developed cancer or “weird medical complications.” That included her parents, who both had cancer. Her two older brothers, born in 1953 and 1955, also developed cancer, and she’s tracked many other cases in the small town of Emmett.
In Utah, another downwinder advocate told Utah News Dispatch that cancer was common in Salt Lake City neighborhood, where she grew up, which was exposed to fallout. She developed thyroid cancer, her younger sister developed stomach cancer, and an older sister died of lupus, which is connected to radiation exposure. But Salt Lake City isn’t in one of the regions of Utah covered by the federal compensation program, so the advocate can’t get a $50,000 payment.
Downwinders who lived in New Mexico, Idaho, and the Salt Lake City area of Utah are not covered by the federal compensation program. That means none of these people or their descendants are eligible for payments — yet.
Decades After Nuclear Testing, the Government Responds
In 1990, Congress passed the Radiation Exposure Compensation Act, which allowed compensation to people with cancer at several levels. It was later expanded. Downwinders — including those who’ve moved elsewhere over the years — were eligible for $50,000. Onsite participants in nuclear testing could get $75,000. Uranium miners, millers, and ore transporters in 11 states west of the Mississippi River could get $100,000.
Among downwinders, eligible cancers included blood cancers (leukemias with the exception of chronic lymphocytic leukemia, multiple myeloma, and non-Hodgkin’s lymphomas) and a long list of solid organ cancers such as thyroid, breast, stomach, brain, lung, colon, and liver cancers.
“When it comes to blood-related cancers, we do see leukemias, lymphomas, and multiple myeloma, but these cancers were more likely to occur sooner after fallout exposure,” said Laura Shaw, MD, principal investigator who oversees the radiation exposure screening program at the University of Nevada, Las Vegas. “At this point, we see more pancreatic, thyroid, lung, stomach, bladder, and breast cancer.”
The compensation program had major limitations, critics said. “It left out a lot of communities that were exposed,” said Lilly Adams, senior outreach coordinator with the Union of Concerned Scientists (UCS), which supports expanding the program. A national nonprofit organization, UCS was founded more than 50 years ago by scientists and students at the Massachusetts Institute of Technology.
“You have this pretty small amount of one-time compensation, and that’s it,” Adams said in an interview. “You can’t get reimbursed for medical costs or lost wages.” Still, “as flawed as the program is, it’s really valuable for the people who are eligible,” she noted.
Now Congress Is Divided on Next Steps
Some lawmakers have recognized the need to do more for those who developed cancer that’s potentially linked to radiation exposure. As the June 2024 expiration of the Radiation Exposure Compensation Act loomed, Democrats and Republicans in Congress worked together to extend and expand the program.
They introduced a bill for higher compensation — $100,000 per person — and the widening of covered downwinder areas to all of Arizona, Nevada, and Utah (which had only been partially covered), along with all of Colorado, Idaho, New Mexico, Montana, and Guam. Under the legislation, the program also would expand to cover some uranium workers who were on the job after 1971 and residents exposed to nuclear waste in Kentucky, Missouri, and Tennessee.
In March, the new legislation easily passed the US Senate by a vote of 69-30, with support from both political parties — but the Republican-led House hasn’t taken it up. As a result, the Radiation Exposure Compensation Act expired in June, and no one can submit new applications for compensation.
A spokesman for House Speaker Mike Johnson told Missouri Independent “unfortunately, the current Senate bill is estimated to cost $50-$60 billion in new mandatory spending with no offsets and was supported by only 20 of 49 Republicans in the Senate.”
Adams rejected these arguments. “The government spends literally trillions of dollars on our nuclear weapons. Whether or not you support that spending, the human cost of building those weapons should be factored in,” she said. She added that she hopes the House will act by the end of the year to pass the bill, but that’s uncertain.
As Compensation Is On Hold, Medical Screening Continues
A major benefit is still available for downwinders and uranium workers: Free medical screening and referrals for medical treatment. The Radiation Exposure Screening and Education Program’s funding has not been affected by the congressional impasse, so screenings are continuing for eligible people exposed to radiation.
Radiation exposure clinics offer screening in Arizona, Colorado, Nevada, New Mexico, and Utah, and health providers can get funding to offer screening in other affected states.
In Nevada, “we hold screening clinics throughout the state: Caliente, Ely, and Winnemucca. Also, in Reno and Las Vegas, which are not in designated downwind areas, but many downwinders have migrated there,” said Shaw in an interview. Among downwinders, “our youngest patients are in their 60s and range up to a few in their 90s,” she said.
Patients fill out questionnaires that ask about their medical problems, family history, and medications. “Ely patients in particular seem to have extensive family histories of cancer, and this may be due to their location directly downwind of the Nevada Test Site,” Shaw said. (Ely is a remote town in central eastern Nevada near the Utah border.)
The screenings cover both cancer and noncancer conditions. Shaw said clinicians often diagnose problems other than the covered cancers — new cases of atrial fibrillation, diabetes, and hypertension. “We see a ton of prostate and skin cancer” but don’t make patients eligible for the compensation program because they’re not covered, she said.
Even as compensation is on hold, doctors can get the word out that screenings are still available, Shaw said. “We continue to get contacted by individuals who in these communities who have never heard of this program, even though we’ve been holding clinics since 2005,” Shaw said. “Despite outreach activities and advertising through newspapers and radio, we find the most successful method of reaching these patients is through word of mouth — either from other patients or their doctors. That is why we feel it is so important to reach other physicians as well.”
Affected Patients Don’t Just Live in the West
On the outreach front, clinicians in states outside of the western US region can be helpful, too. Shaw urged oncologists nationwide to ask older patients where they lived in the 1950s and 1960s. “Did they live in Nevada, Arizona, Utah, and other Western states that are downwind? They may qualify for needed services and future compensation.”
With regard to compensation, she noted that applicants need to prove that they lived in affected areas many decades ago. And, of course, they must prove that they’ve had cancer. Locating residency records “has often been an enormous challenge.” Old utility bills, pay stubs, and high school annuals can be helpful, “but these records tend to disappear. People and their families throw stuff away.”
Even proving a cancer diagnosis can be a challenge because records can be missing. In Nevada, the law says clinicians only need to keep medical records for 5 years, Shaw said. “Imaging and pathology reports are destroyed. Patients that have been diagnosed with cancer can’t prove it.”
Shaw said she hopes oncologists will offer these messages to patients: “Be an advocate for your own health and keep copies of your own records. Discuss your diagnosis with your family and contact a cancer registry if you are diagnosed with cancer.”
A version of this article appeared on Medscape.com.
As of 2022, more than 40,000 patients with cancer successfully applied for $2.6 billion in compensation. Recipients included “downwinders” who were eligible for $50,000 each if they lived in certain areas of Nevada, Utah, and Arizona during specified nuclear testing periods and developed a covered form of cancer.
In June 2024, however, the Radiation Exposure Compensation Program expired amid infighting among Republicans in Congress over whether to expand it. For now, no one can make a claim, even though many downwinders are still alive and continue to be diagnosed with covered cancers decades after they were exposed in the 1940s, 1950s, and 1960s.
There’s a glimmer of good news. The federal government continues to support free medical screenings for eligible people, including certain downwinders and uranium workers. Meanwhile, there are still important roles for clinicians across the country to play as politicians figure out what — if anything — to do next regarding those exposed to radiation.
“We are still here. We can still screen people,” Zachary Davis, program director for the Radiation Exposure Screening and Education Program, The University of New Mexico, in Albuquerque, New Mexico, said in an interview.
Still-Unfolding Legacy of Radiation Exposure
No one knew just how far radiation would spread when the first nuclear bomb was tested in New Mexico in July 1945. Would it cover the state? The entire Southwest? The whole nation?
It also wasn’t clear how radiation would affect people’s health. “There was an awareness that some cancers were caused by radiation, but there wasn’t a cohesive understanding of what the problem was,” Joseph Shonka, PhD, a health physicist who studies radiation exposure and has worked for decades in nuclear engineering, said in an interview.
Now, nearly eight decades later, scientists are still figuring out the full extent of radioactive fallout from nuclear testing. Just last year, a study suggested that radiation from 94 nuclear weapon tests in the Southwest from 1945 to 1962 reached 46 states along with Canada and Mexico.
Activists believe the tests triggered untold number of cancer cases in residents who were exposed in downwind areas:
“My brother died of stomach cancer; my mom died of bone cancer. One of my sisters is surviving brain tumors, and the other one is surviving thyroid cancer,” one New Mexico man recently told ABC-TV’s “Nightline.”
In Idaho, a downwinder advocate told Idaho Capital Sun that everyone who attended a reception for her newly married parents in 1952 — just weeks after a nuclear test — developed cancer or “weird medical complications.” That included her parents, who both had cancer. Her two older brothers, born in 1953 and 1955, also developed cancer, and she’s tracked many other cases in the small town of Emmett.
In Utah, another downwinder advocate told Utah News Dispatch that cancer was common in Salt Lake City neighborhood, where she grew up, which was exposed to fallout. She developed thyroid cancer, her younger sister developed stomach cancer, and an older sister died of lupus, which is connected to radiation exposure. But Salt Lake City isn’t in one of the regions of Utah covered by the federal compensation program, so the advocate can’t get a $50,000 payment.
Downwinders who lived in New Mexico, Idaho, and the Salt Lake City area of Utah are not covered by the federal compensation program. That means none of these people or their descendants are eligible for payments — yet.
Decades After Nuclear Testing, the Government Responds
In 1990, Congress passed the Radiation Exposure Compensation Act, which allowed compensation to people with cancer at several levels. It was later expanded. Downwinders — including those who’ve moved elsewhere over the years — were eligible for $50,000. Onsite participants in nuclear testing could get $75,000. Uranium miners, millers, and ore transporters in 11 states west of the Mississippi River could get $100,000.
Among downwinders, eligible cancers included blood cancers (leukemias with the exception of chronic lymphocytic leukemia, multiple myeloma, and non-Hodgkin’s lymphomas) and a long list of solid organ cancers such as thyroid, breast, stomach, brain, lung, colon, and liver cancers.
“When it comes to blood-related cancers, we do see leukemias, lymphomas, and multiple myeloma, but these cancers were more likely to occur sooner after fallout exposure,” said Laura Shaw, MD, principal investigator who oversees the radiation exposure screening program at the University of Nevada, Las Vegas. “At this point, we see more pancreatic, thyroid, lung, stomach, bladder, and breast cancer.”
The compensation program had major limitations, critics said. “It left out a lot of communities that were exposed,” said Lilly Adams, senior outreach coordinator with the Union of Concerned Scientists (UCS), which supports expanding the program. A national nonprofit organization, UCS was founded more than 50 years ago by scientists and students at the Massachusetts Institute of Technology.
“You have this pretty small amount of one-time compensation, and that’s it,” Adams said in an interview. “You can’t get reimbursed for medical costs or lost wages.” Still, “as flawed as the program is, it’s really valuable for the people who are eligible,” she noted.
Now Congress Is Divided on Next Steps
Some lawmakers have recognized the need to do more for those who developed cancer that’s potentially linked to radiation exposure. As the June 2024 expiration of the Radiation Exposure Compensation Act loomed, Democrats and Republicans in Congress worked together to extend and expand the program.
They introduced a bill for higher compensation — $100,000 per person — and the widening of covered downwinder areas to all of Arizona, Nevada, and Utah (which had only been partially covered), along with all of Colorado, Idaho, New Mexico, Montana, and Guam. Under the legislation, the program also would expand to cover some uranium workers who were on the job after 1971 and residents exposed to nuclear waste in Kentucky, Missouri, and Tennessee.
In March, the new legislation easily passed the US Senate by a vote of 69-30, with support from both political parties — but the Republican-led House hasn’t taken it up. As a result, the Radiation Exposure Compensation Act expired in June, and no one can submit new applications for compensation.
A spokesman for House Speaker Mike Johnson told Missouri Independent “unfortunately, the current Senate bill is estimated to cost $50-$60 billion in new mandatory spending with no offsets and was supported by only 20 of 49 Republicans in the Senate.”
Adams rejected these arguments. “The government spends literally trillions of dollars on our nuclear weapons. Whether or not you support that spending, the human cost of building those weapons should be factored in,” she said. She added that she hopes the House will act by the end of the year to pass the bill, but that’s uncertain.
As Compensation Is On Hold, Medical Screening Continues
A major benefit is still available for downwinders and uranium workers: Free medical screening and referrals for medical treatment. The Radiation Exposure Screening and Education Program’s funding has not been affected by the congressional impasse, so screenings are continuing for eligible people exposed to radiation.
Radiation exposure clinics offer screening in Arizona, Colorado, Nevada, New Mexico, and Utah, and health providers can get funding to offer screening in other affected states.
In Nevada, “we hold screening clinics throughout the state: Caliente, Ely, and Winnemucca. Also, in Reno and Las Vegas, which are not in designated downwind areas, but many downwinders have migrated there,” said Shaw in an interview. Among downwinders, “our youngest patients are in their 60s and range up to a few in their 90s,” she said.
Patients fill out questionnaires that ask about their medical problems, family history, and medications. “Ely patients in particular seem to have extensive family histories of cancer, and this may be due to their location directly downwind of the Nevada Test Site,” Shaw said. (Ely is a remote town in central eastern Nevada near the Utah border.)
The screenings cover both cancer and noncancer conditions. Shaw said clinicians often diagnose problems other than the covered cancers — new cases of atrial fibrillation, diabetes, and hypertension. “We see a ton of prostate and skin cancer” but don’t make patients eligible for the compensation program because they’re not covered, she said.
Even as compensation is on hold, doctors can get the word out that screenings are still available, Shaw said. “We continue to get contacted by individuals who in these communities who have never heard of this program, even though we’ve been holding clinics since 2005,” Shaw said. “Despite outreach activities and advertising through newspapers and radio, we find the most successful method of reaching these patients is through word of mouth — either from other patients or their doctors. That is why we feel it is so important to reach other physicians as well.”
Affected Patients Don’t Just Live in the West
On the outreach front, clinicians in states outside of the western US region can be helpful, too. Shaw urged oncologists nationwide to ask older patients where they lived in the 1950s and 1960s. “Did they live in Nevada, Arizona, Utah, and other Western states that are downwind? They may qualify for needed services and future compensation.”
With regard to compensation, she noted that applicants need to prove that they lived in affected areas many decades ago. And, of course, they must prove that they’ve had cancer. Locating residency records “has often been an enormous challenge.” Old utility bills, pay stubs, and high school annuals can be helpful, “but these records tend to disappear. People and their families throw stuff away.”
Even proving a cancer diagnosis can be a challenge because records can be missing. In Nevada, the law says clinicians only need to keep medical records for 5 years, Shaw said. “Imaging and pathology reports are destroyed. Patients that have been diagnosed with cancer can’t prove it.”
Shaw said she hopes oncologists will offer these messages to patients: “Be an advocate for your own health and keep copies of your own records. Discuss your diagnosis with your family and contact a cancer registry if you are diagnosed with cancer.”
A version of this article appeared on Medscape.com.
As of 2022, more than 40,000 patients with cancer successfully applied for $2.6 billion in compensation. Recipients included “downwinders” who were eligible for $50,000 each if they lived in certain areas of Nevada, Utah, and Arizona during specified nuclear testing periods and developed a covered form of cancer.
In June 2024, however, the Radiation Exposure Compensation Program expired amid infighting among Republicans in Congress over whether to expand it. For now, no one can make a claim, even though many downwinders are still alive and continue to be diagnosed with covered cancers decades after they were exposed in the 1940s, 1950s, and 1960s.
There’s a glimmer of good news. The federal government continues to support free medical screenings for eligible people, including certain downwinders and uranium workers. Meanwhile, there are still important roles for clinicians across the country to play as politicians figure out what — if anything — to do next regarding those exposed to radiation.
“We are still here. We can still screen people,” Zachary Davis, program director for the Radiation Exposure Screening and Education Program, The University of New Mexico, in Albuquerque, New Mexico, said in an interview.
Still-Unfolding Legacy of Radiation Exposure
No one knew just how far radiation would spread when the first nuclear bomb was tested in New Mexico in July 1945. Would it cover the state? The entire Southwest? The whole nation?
It also wasn’t clear how radiation would affect people’s health. “There was an awareness that some cancers were caused by radiation, but there wasn’t a cohesive understanding of what the problem was,” Joseph Shonka, PhD, a health physicist who studies radiation exposure and has worked for decades in nuclear engineering, said in an interview.
Now, nearly eight decades later, scientists are still figuring out the full extent of radioactive fallout from nuclear testing. Just last year, a study suggested that radiation from 94 nuclear weapon tests in the Southwest from 1945 to 1962 reached 46 states along with Canada and Mexico.
Activists believe the tests triggered untold number of cancer cases in residents who were exposed in downwind areas:
“My brother died of stomach cancer; my mom died of bone cancer. One of my sisters is surviving brain tumors, and the other one is surviving thyroid cancer,” one New Mexico man recently told ABC-TV’s “Nightline.”
In Idaho, a downwinder advocate told Idaho Capital Sun that everyone who attended a reception for her newly married parents in 1952 — just weeks after a nuclear test — developed cancer or “weird medical complications.” That included her parents, who both had cancer. Her two older brothers, born in 1953 and 1955, also developed cancer, and she’s tracked many other cases in the small town of Emmett.
In Utah, another downwinder advocate told Utah News Dispatch that cancer was common in Salt Lake City neighborhood, where she grew up, which was exposed to fallout. She developed thyroid cancer, her younger sister developed stomach cancer, and an older sister died of lupus, which is connected to radiation exposure. But Salt Lake City isn’t in one of the regions of Utah covered by the federal compensation program, so the advocate can’t get a $50,000 payment.
Downwinders who lived in New Mexico, Idaho, and the Salt Lake City area of Utah are not covered by the federal compensation program. That means none of these people or their descendants are eligible for payments — yet.
Decades After Nuclear Testing, the Government Responds
In 1990, Congress passed the Radiation Exposure Compensation Act, which allowed compensation to people with cancer at several levels. It was later expanded. Downwinders — including those who’ve moved elsewhere over the years — were eligible for $50,000. Onsite participants in nuclear testing could get $75,000. Uranium miners, millers, and ore transporters in 11 states west of the Mississippi River could get $100,000.
Among downwinders, eligible cancers included blood cancers (leukemias with the exception of chronic lymphocytic leukemia, multiple myeloma, and non-Hodgkin’s lymphomas) and a long list of solid organ cancers such as thyroid, breast, stomach, brain, lung, colon, and liver cancers.
“When it comes to blood-related cancers, we do see leukemias, lymphomas, and multiple myeloma, but these cancers were more likely to occur sooner after fallout exposure,” said Laura Shaw, MD, principal investigator who oversees the radiation exposure screening program at the University of Nevada, Las Vegas. “At this point, we see more pancreatic, thyroid, lung, stomach, bladder, and breast cancer.”
The compensation program had major limitations, critics said. “It left out a lot of communities that were exposed,” said Lilly Adams, senior outreach coordinator with the Union of Concerned Scientists (UCS), which supports expanding the program. A national nonprofit organization, UCS was founded more than 50 years ago by scientists and students at the Massachusetts Institute of Technology.
“You have this pretty small amount of one-time compensation, and that’s it,” Adams said in an interview. “You can’t get reimbursed for medical costs or lost wages.” Still, “as flawed as the program is, it’s really valuable for the people who are eligible,” she noted.
Now Congress Is Divided on Next Steps
Some lawmakers have recognized the need to do more for those who developed cancer that’s potentially linked to radiation exposure. As the June 2024 expiration of the Radiation Exposure Compensation Act loomed, Democrats and Republicans in Congress worked together to extend and expand the program.
They introduced a bill for higher compensation — $100,000 per person — and the widening of covered downwinder areas to all of Arizona, Nevada, and Utah (which had only been partially covered), along with all of Colorado, Idaho, New Mexico, Montana, and Guam. Under the legislation, the program also would expand to cover some uranium workers who were on the job after 1971 and residents exposed to nuclear waste in Kentucky, Missouri, and Tennessee.
In March, the new legislation easily passed the US Senate by a vote of 69-30, with support from both political parties — but the Republican-led House hasn’t taken it up. As a result, the Radiation Exposure Compensation Act expired in June, and no one can submit new applications for compensation.
A spokesman for House Speaker Mike Johnson told Missouri Independent “unfortunately, the current Senate bill is estimated to cost $50-$60 billion in new mandatory spending with no offsets and was supported by only 20 of 49 Republicans in the Senate.”
Adams rejected these arguments. “The government spends literally trillions of dollars on our nuclear weapons. Whether or not you support that spending, the human cost of building those weapons should be factored in,” she said. She added that she hopes the House will act by the end of the year to pass the bill, but that’s uncertain.
As Compensation Is On Hold, Medical Screening Continues
A major benefit is still available for downwinders and uranium workers: Free medical screening and referrals for medical treatment. The Radiation Exposure Screening and Education Program’s funding has not been affected by the congressional impasse, so screenings are continuing for eligible people exposed to radiation.
Radiation exposure clinics offer screening in Arizona, Colorado, Nevada, New Mexico, and Utah, and health providers can get funding to offer screening in other affected states.
In Nevada, “we hold screening clinics throughout the state: Caliente, Ely, and Winnemucca. Also, in Reno and Las Vegas, which are not in designated downwind areas, but many downwinders have migrated there,” said Shaw in an interview. Among downwinders, “our youngest patients are in their 60s and range up to a few in their 90s,” she said.
Patients fill out questionnaires that ask about their medical problems, family history, and medications. “Ely patients in particular seem to have extensive family histories of cancer, and this may be due to their location directly downwind of the Nevada Test Site,” Shaw said. (Ely is a remote town in central eastern Nevada near the Utah border.)
The screenings cover both cancer and noncancer conditions. Shaw said clinicians often diagnose problems other than the covered cancers — new cases of atrial fibrillation, diabetes, and hypertension. “We see a ton of prostate and skin cancer” but don’t make patients eligible for the compensation program because they’re not covered, she said.
Even as compensation is on hold, doctors can get the word out that screenings are still available, Shaw said. “We continue to get contacted by individuals who in these communities who have never heard of this program, even though we’ve been holding clinics since 2005,” Shaw said. “Despite outreach activities and advertising through newspapers and radio, we find the most successful method of reaching these patients is through word of mouth — either from other patients or their doctors. That is why we feel it is so important to reach other physicians as well.”
Affected Patients Don’t Just Live in the West
On the outreach front, clinicians in states outside of the western US region can be helpful, too. Shaw urged oncologists nationwide to ask older patients where they lived in the 1950s and 1960s. “Did they live in Nevada, Arizona, Utah, and other Western states that are downwind? They may qualify for needed services and future compensation.”
With regard to compensation, she noted that applicants need to prove that they lived in affected areas many decades ago. And, of course, they must prove that they’ve had cancer. Locating residency records “has often been an enormous challenge.” Old utility bills, pay stubs, and high school annuals can be helpful, “but these records tend to disappear. People and their families throw stuff away.”
Even proving a cancer diagnosis can be a challenge because records can be missing. In Nevada, the law says clinicians only need to keep medical records for 5 years, Shaw said. “Imaging and pathology reports are destroyed. Patients that have been diagnosed with cancer can’t prove it.”
Shaw said she hopes oncologists will offer these messages to patients: “Be an advocate for your own health and keep copies of your own records. Discuss your diagnosis with your family and contact a cancer registry if you are diagnosed with cancer.”
A version of this article appeared on Medscape.com.
Popular Weight Loss Drugs Now for Patients With Cancer?
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.
Does Medicare Advantage Offer Higher-Value Chemotherapy?
TOPLINE:
METHODOLOGY:
- Private Medicare Advantage plans enroll more than half of the Medicare population, but it is unknown if or how the cost restrictions they impose affect chemotherapy, which accounts for a large portion of cancer care costs.
- Researchers conducted a cohort study using national Medicare data from January 2015 to December 2019 to look at Medicare Advantage enrollment and treatment patterns for patients with cancer receiving chemotherapy.
- The study included 96,501 Medicare Advantage enrollees and 206,274 traditional Medicare beneficiaries who initiated chemotherapy between January 2016 and December 2019 (mean age, ~73 years; ~56% women; Hispanic individuals, 15% and 8%; Black individuals, 15% and 8%; and White individuals, 75% and 86%, respectively).
- Resource use and care quality were measured during a 6-month period following chemotherapy initiation, and survival days were measured 18 months after beginning chemotherapy.
- Resource use measures included hospital inpatient services, outpatient care, prescription drugs, hospice services, and chemotherapy services. Quality measures included chemotherapy-related emergency visits and hospital admissions, as well as avoidable emergency visits and preventable hospitalizations.
TAKEAWAY:
- Medicare Advantage plans had lower resource use than traditional Medicare per enrollee with cancer undergoing chemotherapy ($8718 lower; 95% CI, $8343-$9094).
- The lower resource use was largely caused by fewer chemotherapy visits and less expensive chemotherapy per visit in Medicare Advantage plans ($5032 lower; 95% CI, $4772-$5293).
- Medicare Advantage enrollees had 2.5 percentage points fewer chemotherapy-related emergency department visits and 0.7 percentage points fewer chemotherapy-related hospitalizations than traditional Medicare beneficiaries.
- There was no clinically meaningful difference in survival between Medicare Advantage and traditional Medicare beneficiaries during the 18 months following chemotherapy initiation.
IN PRACTICE:
“Our new finding is that MA [Medicare Advantage] plans had lower resource use than TM [traditional Medicare] among enrollees with cancer undergoing chemotherapy — a serious condition managed by specialists and requiring expensive treatments. This suggests that MA’s cost advantages over TM are not limited to conditions for which low-cost primary care management can avoid costly services,” the authors wrote.
SOURCE:
The study was led by Yamini Kalidindi, PhD, McDermott+ Consulting, Washington, DC. It was published online on September 20, 2024, in JAMA Network Open (doi: 10.1001/jamanetworkopen.2024.34707), with a commentary.
LIMITATIONS:
The study’s findings may be affected by unobserved patient characteristics despite the use of inverse-probability weighting. The exclusion of Medicare Advantage enrollees in contracts with incomplete encounter data limits the generalizability of the results. The study does not apply to beneficiaries without Part D drug coverage. Quality measures were limited to those available from claims and encounter data, lacking information on patients’ cancer stage. The 18-month measure of survival might not adequately capture survival differences associated with early-stage cancers. The study did not measure whether patient care followed recommended guidelines.
DISCLOSURES:
Various authors reported grants from the National Institute on Aging, the National Institutes of Health, The Commonwealth Fund, Arnold Ventures, the National Cancer Institute, the Department of Defense, and the National Institute of Health Care Management. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Private Medicare Advantage plans enroll more than half of the Medicare population, but it is unknown if or how the cost restrictions they impose affect chemotherapy, which accounts for a large portion of cancer care costs.
- Researchers conducted a cohort study using national Medicare data from January 2015 to December 2019 to look at Medicare Advantage enrollment and treatment patterns for patients with cancer receiving chemotherapy.
- The study included 96,501 Medicare Advantage enrollees and 206,274 traditional Medicare beneficiaries who initiated chemotherapy between January 2016 and December 2019 (mean age, ~73 years; ~56% women; Hispanic individuals, 15% and 8%; Black individuals, 15% and 8%; and White individuals, 75% and 86%, respectively).
- Resource use and care quality were measured during a 6-month period following chemotherapy initiation, and survival days were measured 18 months after beginning chemotherapy.
- Resource use measures included hospital inpatient services, outpatient care, prescription drugs, hospice services, and chemotherapy services. Quality measures included chemotherapy-related emergency visits and hospital admissions, as well as avoidable emergency visits and preventable hospitalizations.
TAKEAWAY:
- Medicare Advantage plans had lower resource use than traditional Medicare per enrollee with cancer undergoing chemotherapy ($8718 lower; 95% CI, $8343-$9094).
- The lower resource use was largely caused by fewer chemotherapy visits and less expensive chemotherapy per visit in Medicare Advantage plans ($5032 lower; 95% CI, $4772-$5293).
- Medicare Advantage enrollees had 2.5 percentage points fewer chemotherapy-related emergency department visits and 0.7 percentage points fewer chemotherapy-related hospitalizations than traditional Medicare beneficiaries.
- There was no clinically meaningful difference in survival between Medicare Advantage and traditional Medicare beneficiaries during the 18 months following chemotherapy initiation.
IN PRACTICE:
“Our new finding is that MA [Medicare Advantage] plans had lower resource use than TM [traditional Medicare] among enrollees with cancer undergoing chemotherapy — a serious condition managed by specialists and requiring expensive treatments. This suggests that MA’s cost advantages over TM are not limited to conditions for which low-cost primary care management can avoid costly services,” the authors wrote.
SOURCE:
The study was led by Yamini Kalidindi, PhD, McDermott+ Consulting, Washington, DC. It was published online on September 20, 2024, in JAMA Network Open (doi: 10.1001/jamanetworkopen.2024.34707), with a commentary.
LIMITATIONS:
The study’s findings may be affected by unobserved patient characteristics despite the use of inverse-probability weighting. The exclusion of Medicare Advantage enrollees in contracts with incomplete encounter data limits the generalizability of the results. The study does not apply to beneficiaries without Part D drug coverage. Quality measures were limited to those available from claims and encounter data, lacking information on patients’ cancer stage. The 18-month measure of survival might not adequately capture survival differences associated with early-stage cancers. The study did not measure whether patient care followed recommended guidelines.
DISCLOSURES:
Various authors reported grants from the National Institute on Aging, the National Institutes of Health, The Commonwealth Fund, Arnold Ventures, the National Cancer Institute, the Department of Defense, and the National Institute of Health Care Management. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Private Medicare Advantage plans enroll more than half of the Medicare population, but it is unknown if or how the cost restrictions they impose affect chemotherapy, which accounts for a large portion of cancer care costs.
- Researchers conducted a cohort study using national Medicare data from January 2015 to December 2019 to look at Medicare Advantage enrollment and treatment patterns for patients with cancer receiving chemotherapy.
- The study included 96,501 Medicare Advantage enrollees and 206,274 traditional Medicare beneficiaries who initiated chemotherapy between January 2016 and December 2019 (mean age, ~73 years; ~56% women; Hispanic individuals, 15% and 8%; Black individuals, 15% and 8%; and White individuals, 75% and 86%, respectively).
- Resource use and care quality were measured during a 6-month period following chemotherapy initiation, and survival days were measured 18 months after beginning chemotherapy.
- Resource use measures included hospital inpatient services, outpatient care, prescription drugs, hospice services, and chemotherapy services. Quality measures included chemotherapy-related emergency visits and hospital admissions, as well as avoidable emergency visits and preventable hospitalizations.
TAKEAWAY:
- Medicare Advantage plans had lower resource use than traditional Medicare per enrollee with cancer undergoing chemotherapy ($8718 lower; 95% CI, $8343-$9094).
- The lower resource use was largely caused by fewer chemotherapy visits and less expensive chemotherapy per visit in Medicare Advantage plans ($5032 lower; 95% CI, $4772-$5293).
- Medicare Advantage enrollees had 2.5 percentage points fewer chemotherapy-related emergency department visits and 0.7 percentage points fewer chemotherapy-related hospitalizations than traditional Medicare beneficiaries.
- There was no clinically meaningful difference in survival between Medicare Advantage and traditional Medicare beneficiaries during the 18 months following chemotherapy initiation.
IN PRACTICE:
“Our new finding is that MA [Medicare Advantage] plans had lower resource use than TM [traditional Medicare] among enrollees with cancer undergoing chemotherapy — a serious condition managed by specialists and requiring expensive treatments. This suggests that MA’s cost advantages over TM are not limited to conditions for which low-cost primary care management can avoid costly services,” the authors wrote.
SOURCE:
The study was led by Yamini Kalidindi, PhD, McDermott+ Consulting, Washington, DC. It was published online on September 20, 2024, in JAMA Network Open (doi: 10.1001/jamanetworkopen.2024.34707), with a commentary.
LIMITATIONS:
The study’s findings may be affected by unobserved patient characteristics despite the use of inverse-probability weighting. The exclusion of Medicare Advantage enrollees in contracts with incomplete encounter data limits the generalizability of the results. The study does not apply to beneficiaries without Part D drug coverage. Quality measures were limited to those available from claims and encounter data, lacking information on patients’ cancer stage. The 18-month measure of survival might not adequately capture survival differences associated with early-stage cancers. The study did not measure whether patient care followed recommended guidelines.
DISCLOSURES:
Various authors reported grants from the National Institute on Aging, the National Institutes of Health, The Commonwealth Fund, Arnold Ventures, the National Cancer Institute, the Department of Defense, and the National Institute of Health Care Management. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
AACR Cancer Progress Report: Big Strides and Big Gaps
The AACR’s 216-page report — an annual endeavor now in its 14th year — focused on the “tremendous” strides made in cancer care, prevention, and early detection and highlighted areas where more research and attention are warranted.
One key area is funding. For the first time since 2016, federal funding for the National Institutes of Health (NIH) and National Cancer Institute (NCI) decreased in the past year. The cuts followed nearly a decade of funding increases that saw the NIH budget expand by nearly $15 billion, and that allowed for a “rapid pace and broad scope” of advances in cancer, AACR’s chief executive officer Margaret Foti, MD, PhD, said during a press briefing.
These recent cuts “threaten to curtail the medical progress seen in recent years and stymie future advancements,” said Dr. Foti, who called on Congress to commit to funding cancer research at significant and consistent levels to “maintain the momentum of progress against cancer.”
Inside the Report: Big Progress
Overall, advances in prevention, early detection, and treatment have helped catch more cancers earlier and save lives.
According to the AACR report, the age-adjusted overall cancer death rate in the United States fell by 33% between 1991 and 2021, meaning about 4.1 million cancer deaths were averted. The overall cancer death rate for children and adolescents has declined by 24% in the past 2 decades. The 5-year relative survival rate for children diagnosed with cancer in the US has improved from 58% for those diagnosed in the mid-1970s to 85% for those diagnosed between 2013 and 2019.
The past fiscal year has seen many new approvals for cancer drugs, diagnostics, and screening tests. From July 1, 2023, to June 30, 2024, the Food and Drug Administration (FDA) approved 15 new anticancer therapeutics, as well as 15 new indications for previously approved agents, one new imaging agent, several artificial intelligence (AI) tools to improve early cancer detection and diagnosis, and two minimally invasive tests for assessing inherited cancer risk or early cancer detection, according to the report.
“Cancer diagnostics are becoming more sophisticated,” AACR president Patricia M. LoRusso, DO, PhD, said during the briefing. “New technologies, such as spatial transcriptomics, are helping us study tumors at a cellular level, and helping to unveil things that we did not initially even begin to understand or think of. AI-based approaches are beginning to transform cancer detection, diagnosis, clinical decision-making, and treatment response monitoring.”
The report also highlights the significant progress in many childhood and adolescent/young adult cancers, Dr. LoRusso noted. These include FDA approvals for two new molecularly targeted therapeutics: tovorafenib for children with certain types of brain tumor and repotrectinib for children with a wide array of cancer types that have a specific genetic alteration known as NTRK gene fusion. It also includes an expanded approval for eflornithine to reduce the risk for relapse in children with high-risk neuroblastoma.
“Decades — decades — of basic research discoveries, have led to these clinical breakthroughs,” she stressed. “These gains against cancer are because of the rapid progress in our ability to decode the cancer genome, which has opened new and innovative avenues for drug development.”
The Gaps
Even with progress in cancer prevention, early detection, and treatment, cancer remains a significant issue.
“In 2024, it is estimated that more than 2 million new cases of cancer will be diagnosed in the United States. More than 611,000 people will die from the disease,” according to the report.
The 2024 report shows that incidence rates for some cancers are increasing in the United States, including vaccine-preventable cancers such as human papillomavirus (HPV)–associated oral cancers and, in young adults, cervical cancers. A recent analysis also found that overall cervical cancer incidence among women aged 30-34 years increased by 2.5% a year between 2012 and 2019.
Furthermore, despite clear evidence demonstrating that the HPV vaccine reduces cervical cancer incidence, uptake has remained poor, with only 38.6% of US children and adolescents aged 9-17 years receiving at least one dose of the vaccine in 2022.
Early-onset cancers are also increasing. Rates of breast, colorectal, and other cancers are on the rise in adults younger than 50 years, the report noted.
The report also pointed to data that 40% of all cancer cases in the United States can be attributed to preventable factors, such as smoking, excess body weight, and alcohol. However, our understanding of these risk factors has improved. Excessive levels of alcohol consumption have, for instance, been shown to increase the risk for six different types of cancer: certain types of head and neck cancer, esophageal squamous cell carcinoma, and breast, colorectal, liver, and stomach cancers.
Financial toxicity remains prevalent as well.
The report explains that financial hardship following a cancer diagnosis is widespread, and the effects can last for years. In fact, more than 40% of patients can spend their entire life savings within the first 2 years of cancer treatment. Among adult survivors of childhood cancers, 20.7% had trouble paying their medical bills, 29.9% said they had been sent to debt collection for unpaid bills, 14.1% had forgone medical care, and 26.8% could not afford nutritious meals.
For young cancer survivors, the lifetime costs associated with a diagnosis of cancer are substantial, reaching an average of $259,324 per person.
On a global level, it is estimated that from 2020 to 2050, the cumulative economic burden of cancer will be $25.2 trillion.
The Path Forward
Despite these challenges, Dr. LoRusso said, “it is unquestionable that we are in a time of unparalleled opportunities in cancer research.
“I am excited about what the future holds for cancer research, and especially for patient care,” she said.
However, funding commitments are needed to avoid impeding this momentum and losing a “talented and creative young workforce” that has brought new ideas and new technologies to the table.
Continued robust funding will help “to markedly improve cancer care, increase cancer survivorship, spur economic growth, and maintain the United States’ position as the global leader in science and medical research,” she added.
The AACR report specifically calls on Congress to:
- Appropriate at least $51.3 billion in fiscal year 2025 for the base budget of the NIH and at least $7.934 billion for the NCI.
- Provide $3.6 billion in dedicated funding for Cancer Moonshot activities through fiscal year 2026 in addition to other funding, consistent with the President’s fiscal year 2025 budget.
- Appropriate at least $472.4 million in fiscal year 2025 for the CDC’s Division of Cancer Prevention to support comprehensive cancer control, central cancer registries, and screening and awareness programs for specific cancers.
- Allocate $55 million in funding for the Oncology Center of Excellence at FDA in fiscal year 2025 to provide regulators with the staff and tools necessary to conduct expedited review of cancer-related medical products.
By working together with Congress and other stakeholders, “we will be able to accelerate the pace of progress and make major strides toward the lifesaving goal of preventing and curing all cancers at the earliest possible time,” Dr. Foti said. “I believe if we do that ... one day we will win this war on cancer.”
A version of this article first appeared on Medscape.com.
The AACR’s 216-page report — an annual endeavor now in its 14th year — focused on the “tremendous” strides made in cancer care, prevention, and early detection and highlighted areas where more research and attention are warranted.
One key area is funding. For the first time since 2016, federal funding for the National Institutes of Health (NIH) and National Cancer Institute (NCI) decreased in the past year. The cuts followed nearly a decade of funding increases that saw the NIH budget expand by nearly $15 billion, and that allowed for a “rapid pace and broad scope” of advances in cancer, AACR’s chief executive officer Margaret Foti, MD, PhD, said during a press briefing.
These recent cuts “threaten to curtail the medical progress seen in recent years and stymie future advancements,” said Dr. Foti, who called on Congress to commit to funding cancer research at significant and consistent levels to “maintain the momentum of progress against cancer.”
Inside the Report: Big Progress
Overall, advances in prevention, early detection, and treatment have helped catch more cancers earlier and save lives.
According to the AACR report, the age-adjusted overall cancer death rate in the United States fell by 33% between 1991 and 2021, meaning about 4.1 million cancer deaths were averted. The overall cancer death rate for children and adolescents has declined by 24% in the past 2 decades. The 5-year relative survival rate for children diagnosed with cancer in the US has improved from 58% for those diagnosed in the mid-1970s to 85% for those diagnosed between 2013 and 2019.
The past fiscal year has seen many new approvals for cancer drugs, diagnostics, and screening tests. From July 1, 2023, to June 30, 2024, the Food and Drug Administration (FDA) approved 15 new anticancer therapeutics, as well as 15 new indications for previously approved agents, one new imaging agent, several artificial intelligence (AI) tools to improve early cancer detection and diagnosis, and two minimally invasive tests for assessing inherited cancer risk or early cancer detection, according to the report.
“Cancer diagnostics are becoming more sophisticated,” AACR president Patricia M. LoRusso, DO, PhD, said during the briefing. “New technologies, such as spatial transcriptomics, are helping us study tumors at a cellular level, and helping to unveil things that we did not initially even begin to understand or think of. AI-based approaches are beginning to transform cancer detection, diagnosis, clinical decision-making, and treatment response monitoring.”
The report also highlights the significant progress in many childhood and adolescent/young adult cancers, Dr. LoRusso noted. These include FDA approvals for two new molecularly targeted therapeutics: tovorafenib for children with certain types of brain tumor and repotrectinib for children with a wide array of cancer types that have a specific genetic alteration known as NTRK gene fusion. It also includes an expanded approval for eflornithine to reduce the risk for relapse in children with high-risk neuroblastoma.
“Decades — decades — of basic research discoveries, have led to these clinical breakthroughs,” she stressed. “These gains against cancer are because of the rapid progress in our ability to decode the cancer genome, which has opened new and innovative avenues for drug development.”
The Gaps
Even with progress in cancer prevention, early detection, and treatment, cancer remains a significant issue.
“In 2024, it is estimated that more than 2 million new cases of cancer will be diagnosed in the United States. More than 611,000 people will die from the disease,” according to the report.
The 2024 report shows that incidence rates for some cancers are increasing in the United States, including vaccine-preventable cancers such as human papillomavirus (HPV)–associated oral cancers and, in young adults, cervical cancers. A recent analysis also found that overall cervical cancer incidence among women aged 30-34 years increased by 2.5% a year between 2012 and 2019.
Furthermore, despite clear evidence demonstrating that the HPV vaccine reduces cervical cancer incidence, uptake has remained poor, with only 38.6% of US children and adolescents aged 9-17 years receiving at least one dose of the vaccine in 2022.
Early-onset cancers are also increasing. Rates of breast, colorectal, and other cancers are on the rise in adults younger than 50 years, the report noted.
The report also pointed to data that 40% of all cancer cases in the United States can be attributed to preventable factors, such as smoking, excess body weight, and alcohol. However, our understanding of these risk factors has improved. Excessive levels of alcohol consumption have, for instance, been shown to increase the risk for six different types of cancer: certain types of head and neck cancer, esophageal squamous cell carcinoma, and breast, colorectal, liver, and stomach cancers.
Financial toxicity remains prevalent as well.
The report explains that financial hardship following a cancer diagnosis is widespread, and the effects can last for years. In fact, more than 40% of patients can spend their entire life savings within the first 2 years of cancer treatment. Among adult survivors of childhood cancers, 20.7% had trouble paying their medical bills, 29.9% said they had been sent to debt collection for unpaid bills, 14.1% had forgone medical care, and 26.8% could not afford nutritious meals.
For young cancer survivors, the lifetime costs associated with a diagnosis of cancer are substantial, reaching an average of $259,324 per person.
On a global level, it is estimated that from 2020 to 2050, the cumulative economic burden of cancer will be $25.2 trillion.
The Path Forward
Despite these challenges, Dr. LoRusso said, “it is unquestionable that we are in a time of unparalleled opportunities in cancer research.
“I am excited about what the future holds for cancer research, and especially for patient care,” she said.
However, funding commitments are needed to avoid impeding this momentum and losing a “talented and creative young workforce” that has brought new ideas and new technologies to the table.
Continued robust funding will help “to markedly improve cancer care, increase cancer survivorship, spur economic growth, and maintain the United States’ position as the global leader in science and medical research,” she added.
The AACR report specifically calls on Congress to:
- Appropriate at least $51.3 billion in fiscal year 2025 for the base budget of the NIH and at least $7.934 billion for the NCI.
- Provide $3.6 billion in dedicated funding for Cancer Moonshot activities through fiscal year 2026 in addition to other funding, consistent with the President’s fiscal year 2025 budget.
- Appropriate at least $472.4 million in fiscal year 2025 for the CDC’s Division of Cancer Prevention to support comprehensive cancer control, central cancer registries, and screening and awareness programs for specific cancers.
- Allocate $55 million in funding for the Oncology Center of Excellence at FDA in fiscal year 2025 to provide regulators with the staff and tools necessary to conduct expedited review of cancer-related medical products.
By working together with Congress and other stakeholders, “we will be able to accelerate the pace of progress and make major strides toward the lifesaving goal of preventing and curing all cancers at the earliest possible time,” Dr. Foti said. “I believe if we do that ... one day we will win this war on cancer.”
A version of this article first appeared on Medscape.com.
The AACR’s 216-page report — an annual endeavor now in its 14th year — focused on the “tremendous” strides made in cancer care, prevention, and early detection and highlighted areas where more research and attention are warranted.
One key area is funding. For the first time since 2016, federal funding for the National Institutes of Health (NIH) and National Cancer Institute (NCI) decreased in the past year. The cuts followed nearly a decade of funding increases that saw the NIH budget expand by nearly $15 billion, and that allowed for a “rapid pace and broad scope” of advances in cancer, AACR’s chief executive officer Margaret Foti, MD, PhD, said during a press briefing.
These recent cuts “threaten to curtail the medical progress seen in recent years and stymie future advancements,” said Dr. Foti, who called on Congress to commit to funding cancer research at significant and consistent levels to “maintain the momentum of progress against cancer.”
Inside the Report: Big Progress
Overall, advances in prevention, early detection, and treatment have helped catch more cancers earlier and save lives.
According to the AACR report, the age-adjusted overall cancer death rate in the United States fell by 33% between 1991 and 2021, meaning about 4.1 million cancer deaths were averted. The overall cancer death rate for children and adolescents has declined by 24% in the past 2 decades. The 5-year relative survival rate for children diagnosed with cancer in the US has improved from 58% for those diagnosed in the mid-1970s to 85% for those diagnosed between 2013 and 2019.
The past fiscal year has seen many new approvals for cancer drugs, diagnostics, and screening tests. From July 1, 2023, to June 30, 2024, the Food and Drug Administration (FDA) approved 15 new anticancer therapeutics, as well as 15 new indications for previously approved agents, one new imaging agent, several artificial intelligence (AI) tools to improve early cancer detection and diagnosis, and two minimally invasive tests for assessing inherited cancer risk or early cancer detection, according to the report.
“Cancer diagnostics are becoming more sophisticated,” AACR president Patricia M. LoRusso, DO, PhD, said during the briefing. “New technologies, such as spatial transcriptomics, are helping us study tumors at a cellular level, and helping to unveil things that we did not initially even begin to understand or think of. AI-based approaches are beginning to transform cancer detection, diagnosis, clinical decision-making, and treatment response monitoring.”
The report also highlights the significant progress in many childhood and adolescent/young adult cancers, Dr. LoRusso noted. These include FDA approvals for two new molecularly targeted therapeutics: tovorafenib for children with certain types of brain tumor and repotrectinib for children with a wide array of cancer types that have a specific genetic alteration known as NTRK gene fusion. It also includes an expanded approval for eflornithine to reduce the risk for relapse in children with high-risk neuroblastoma.
“Decades — decades — of basic research discoveries, have led to these clinical breakthroughs,” she stressed. “These gains against cancer are because of the rapid progress in our ability to decode the cancer genome, which has opened new and innovative avenues for drug development.”
The Gaps
Even with progress in cancer prevention, early detection, and treatment, cancer remains a significant issue.
“In 2024, it is estimated that more than 2 million new cases of cancer will be diagnosed in the United States. More than 611,000 people will die from the disease,” according to the report.
The 2024 report shows that incidence rates for some cancers are increasing in the United States, including vaccine-preventable cancers such as human papillomavirus (HPV)–associated oral cancers and, in young adults, cervical cancers. A recent analysis also found that overall cervical cancer incidence among women aged 30-34 years increased by 2.5% a year between 2012 and 2019.
Furthermore, despite clear evidence demonstrating that the HPV vaccine reduces cervical cancer incidence, uptake has remained poor, with only 38.6% of US children and adolescents aged 9-17 years receiving at least one dose of the vaccine in 2022.
Early-onset cancers are also increasing. Rates of breast, colorectal, and other cancers are on the rise in adults younger than 50 years, the report noted.
The report also pointed to data that 40% of all cancer cases in the United States can be attributed to preventable factors, such as smoking, excess body weight, and alcohol. However, our understanding of these risk factors has improved. Excessive levels of alcohol consumption have, for instance, been shown to increase the risk for six different types of cancer: certain types of head and neck cancer, esophageal squamous cell carcinoma, and breast, colorectal, liver, and stomach cancers.
Financial toxicity remains prevalent as well.
The report explains that financial hardship following a cancer diagnosis is widespread, and the effects can last for years. In fact, more than 40% of patients can spend their entire life savings within the first 2 years of cancer treatment. Among adult survivors of childhood cancers, 20.7% had trouble paying their medical bills, 29.9% said they had been sent to debt collection for unpaid bills, 14.1% had forgone medical care, and 26.8% could not afford nutritious meals.
For young cancer survivors, the lifetime costs associated with a diagnosis of cancer are substantial, reaching an average of $259,324 per person.
On a global level, it is estimated that from 2020 to 2050, the cumulative economic burden of cancer will be $25.2 trillion.
The Path Forward
Despite these challenges, Dr. LoRusso said, “it is unquestionable that we are in a time of unparalleled opportunities in cancer research.
“I am excited about what the future holds for cancer research, and especially for patient care,” she said.
However, funding commitments are needed to avoid impeding this momentum and losing a “talented and creative young workforce” that has brought new ideas and new technologies to the table.
Continued robust funding will help “to markedly improve cancer care, increase cancer survivorship, spur economic growth, and maintain the United States’ position as the global leader in science and medical research,” she added.
The AACR report specifically calls on Congress to:
- Appropriate at least $51.3 billion in fiscal year 2025 for the base budget of the NIH and at least $7.934 billion for the NCI.
- Provide $3.6 billion in dedicated funding for Cancer Moonshot activities through fiscal year 2026 in addition to other funding, consistent with the President’s fiscal year 2025 budget.
- Appropriate at least $472.4 million in fiscal year 2025 for the CDC’s Division of Cancer Prevention to support comprehensive cancer control, central cancer registries, and screening and awareness programs for specific cancers.
- Allocate $55 million in funding for the Oncology Center of Excellence at FDA in fiscal year 2025 to provide regulators with the staff and tools necessary to conduct expedited review of cancer-related medical products.
By working together with Congress and other stakeholders, “we will be able to accelerate the pace of progress and make major strides toward the lifesaving goal of preventing and curing all cancers at the earliest possible time,” Dr. Foti said. “I believe if we do that ... one day we will win this war on cancer.”
A version of this article first appeared on Medscape.com.
Cancer Risk: Are Pesticides the New Smoking?
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.