User login
‘If this is an emergency, call 911’
This is the mantra that the world hears when they call most, if not all, hospitals and medical clinics for the symptomatic relief of a myriad of health care complaints. Exactly what is the definition of an emergency is uncertain. We all could include severe chest pain, shortness of breath or sudden collapse or loss of consciousness.
To a patient, an emergency might just include the pressing need to speak to their doctor about the occurrence of symptoms and or anxieties that suddenly have occurred. In the past, before the telephone was invented, a friend or family member was sent by horseback or a Ford V8 to find the local doctor. With the advent of the telephone, doctors actually listed their number in a phone directory to facilitate contact with their patient.

Enter the current situation. Many patients still perceive the need to call their doctor for everything from a mild cough or headache or an actual fever to just not feeling well. This perceived patient need to seek expert medical help short of an ambulance ride to the emergency room leads the patient into the frustrating downward spiral associated with this bizarre need to communicate with their doctor.
I presume many patients assume that they may be able to actually talk to their doctor by telephone. They learn, as I have, that presumption is an arcane curiosity. First of all, most of my young colleagues, like most of their generation, do not own a land line and therefore are not listed in any known telephone directory. They work in an environment driven by the pressure to see more and more patients, and at the end of the day they are pretty much ready to “hang it up.” But many in my generation worked hard, and we still answered the telephone, and many of us actually made house calls.
But, should you have your doctor’s telephone number and make the call, you are immediately put in touch with a triage nurse who demands to know the intimate details of your problem in order to assist you in speaking to the doctor. Having divulged your symptoms in their gory details and achieved an appropriate threshold, you will be placed on hold while being connected to the clinic nurse. Once again you will be asked to divulge your intimate symptoms and again will be passed on to the doctor’s physician assistant who is familiar with the innermost knowledge of your doctor. But, again, if you persist you may again be put on hold to talk to your doctor or asked to leave a message with the physician assistant, since the doctor is seeing a patient or does not take calls during office hours. “Perhaps you would like to leave an email, and the doctor will contact you.”
Now, I have to admit that many of my friends find this process acceptable and use a variety of digital devices like “My Chart” to communicate with their doctor. But having grown up in the shadow of the horse and buggy era, and having adapted to the contemporary world, I give my patients my cell phone number. I will give it to you, too.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
This is the mantra that the world hears when they call most, if not all, hospitals and medical clinics for the symptomatic relief of a myriad of health care complaints. Exactly what is the definition of an emergency is uncertain. We all could include severe chest pain, shortness of breath or sudden collapse or loss of consciousness.
To a patient, an emergency might just include the pressing need to speak to their doctor about the occurrence of symptoms and or anxieties that suddenly have occurred. In the past, before the telephone was invented, a friend or family member was sent by horseback or a Ford V8 to find the local doctor. With the advent of the telephone, doctors actually listed their number in a phone directory to facilitate contact with their patient.
Enter the current situation. Many patients still perceive the need to call their doctor for everything from a mild cough or headache or an actual fever to just not feeling well. This perceived patient need to seek expert medical help short of an ambulance ride to the emergency room leads the patient into the frustrating downward spiral associated with this bizarre need to communicate with their doctor.
I presume many patients assume that they may be able to actually talk to their doctor by telephone. They learn, as I have, that presumption is an arcane curiosity. First of all, most of my young colleagues, like most of their generation, do not own a land line and therefore are not listed in any known telephone directory. They work in an environment driven by the pressure to see more and more patients, and at the end of the day they are pretty much ready to “hang it up.” But many in my generation worked hard, and we still answered the telephone, and many of us actually made house calls.
But, should you have your doctor’s telephone number and make the call, you are immediately put in touch with a triage nurse who demands to know the intimate details of your problem in order to assist you in speaking to the doctor. Having divulged your symptoms in their gory details and achieved an appropriate threshold, you will be placed on hold while being connected to the clinic nurse. Once again you will be asked to divulge your intimate symptoms and again will be passed on to the doctor’s physician assistant who is familiar with the innermost knowledge of your doctor. But, again, if you persist you may again be put on hold to talk to your doctor or asked to leave a message with the physician assistant, since the doctor is seeing a patient or does not take calls during office hours. “Perhaps you would like to leave an email, and the doctor will contact you.”
Now, I have to admit that many of my friends find this process acceptable and use a variety of digital devices like “My Chart” to communicate with their doctor. But having grown up in the shadow of the horse and buggy era, and having adapted to the contemporary world, I give my patients my cell phone number. I will give it to you, too.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
This is the mantra that the world hears when they call most, if not all, hospitals and medical clinics for the symptomatic relief of a myriad of health care complaints. Exactly what is the definition of an emergency is uncertain. We all could include severe chest pain, shortness of breath or sudden collapse or loss of consciousness.
To a patient, an emergency might just include the pressing need to speak to their doctor about the occurrence of symptoms and or anxieties that suddenly have occurred. In the past, before the telephone was invented, a friend or family member was sent by horseback or a Ford V8 to find the local doctor. With the advent of the telephone, doctors actually listed their number in a phone directory to facilitate contact with their patient.
Enter the current situation. Many patients still perceive the need to call their doctor for everything from a mild cough or headache or an actual fever to just not feeling well. This perceived patient need to seek expert medical help short of an ambulance ride to the emergency room leads the patient into the frustrating downward spiral associated with this bizarre need to communicate with their doctor.
I presume many patients assume that they may be able to actually talk to their doctor by telephone. They learn, as I have, that presumption is an arcane curiosity. First of all, most of my young colleagues, like most of their generation, do not own a land line and therefore are not listed in any known telephone directory. They work in an environment driven by the pressure to see more and more patients, and at the end of the day they are pretty much ready to “hang it up.” But many in my generation worked hard, and we still answered the telephone, and many of us actually made house calls.
But, should you have your doctor’s telephone number and make the call, you are immediately put in touch with a triage nurse who demands to know the intimate details of your problem in order to assist you in speaking to the doctor. Having divulged your symptoms in their gory details and achieved an appropriate threshold, you will be placed on hold while being connected to the clinic nurse. Once again you will be asked to divulge your intimate symptoms and again will be passed on to the doctor’s physician assistant who is familiar with the innermost knowledge of your doctor. But, again, if you persist you may again be put on hold to talk to your doctor or asked to leave a message with the physician assistant, since the doctor is seeing a patient or does not take calls during office hours. “Perhaps you would like to leave an email, and the doctor will contact you.”
Now, I have to admit that many of my friends find this process acceptable and use a variety of digital devices like “My Chart” to communicate with their doctor. But having grown up in the shadow of the horse and buggy era, and having adapted to the contemporary world, I give my patients my cell phone number. I will give it to you, too.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Hospitalist movers and shakers – March 2018
Jason Blair, DO, recently was named an honorary Fellow by the American College of Osteopathic Internists (ACOI) for excellence in the practice of internal medicine. Dr. Blair currently is a hospitalist at Lake Regional Health System in Osage Beach, Mo.
The degree of Fellow is given to physicians who demonstrate continuing professional accomplishments, scholarship, and professional activities, including teaching, research, and community service. The ACOI represents more than 5,000 osteopathic internists and subspecialists nationwide. Dr. Blair joined Lake Regional in 2017.

Dr. Howell is the division director of the Collaborative Inpatient Medicine Service (CIMS) and a professor of medicine at the Johns Hopkins Bayview Medical Center in Baltimore. He received the award for his work with project EQUIP (Excellence in Quality, Utilization Integration, and Patient-Centered Care) to improve quality and efficiency and to reduce mortality, emergency department boarding, and patient lengths of stay.
David Svec, MD, MBA, has been named the new chief medical officer at Stanford Health Care – ValleyCare in Pleasanton, Calif. Dr. Svec has served as a hospitalist and internal medicine specialist at ValleyCare for the past 6 years. Previously, he was ValleyCare’s medical director of the hospitalist team and a clinical assistant professor of medicine. Dr. Svec helped develop the hospitalist program at ValleyCare and will continue to work in that capacity while advancing into his new role.
As CMO, Dr. Svec will carry on the mission of Stanford Health Care, including increasing innovative programs, monitoring outcome measures, and developing and implementing improvement plans.
Dr. Svec earned Stanford Health Care’s 2016 David A. Rytand Clinical Teaching Award, the 2016 Lawrence Mathers Award: Exceptional Commitment to Teaching/Active Involvement in Medical Student Education, and the 2014 Arthur L. Bloomfield Award for Excellence in Clinical Teaching.
Brent Baboolal, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Baboolal is an internist and a hospitalist serving the Texas Health Presbyterian Hospital in Dallas.
Trained in Grenada, Dr. Baboolal came to the United States in 2009 and began work at Stamford (Conn.) Hospital. He is board certified by the American Board of Internal Medicine and is renowned as a leading internist and hospitalist. He is a former associate professor at the University of Texas School of Nursing.
BUSINESS MOVES
Sound Physicians in Tacoma, Wash., recently announced that it will take over providing hospitalist services for SSM Health DePaul Hospital and SSM Health St. Mary’s Hospital in St. Louis. Sound Physicians already had been running critical care at SSM Health St. Clare Hospital, Fenton, Mo.
SSM Health is a Catholic, faith-based, nonprofit health system serving communities in Illinois, Missouri, Oklahoma, and Wisconsin.
“We have been impressed with their efficiency and professionalism of establishing Sound Physicians’ infrastructure that supports providers and implementing processes to drive improved outcomes,” said Rajiv Patel, MD, vice president of medical affairs for SSM Health DePaul Hospital.
Sound Physicians prides itself on improving quality and lowering costs of acute care for health organizations and facilities. Sound provides emergency medicine, hospital medicine, critical care, transitional care, and advisory services for its partners nationwide.
Pittsburgh-based health leaders Highmark Health and Allegheny Health Network, and Erie, Pa.–based Lecom Health have agreed to establish an affiliation with Warren (Pa.) General Hospital, a full-service, 87-bed facility about an hour from Erie. The agreement will provide Warren General with capital to make improvements to its maternity unit and radiation oncology equipment, among other services.
The partnership includes Warren General agreeing to use Allegheny Health Network (AHN) affiliates for clinical, emergency, and hospitalist services, and Warren General physicians will join the AHN integrated network. AHN, Highmark, and Lecom will assist Warren General with capital investments and community health reinvestment projects.
Hospitalist group Adfinitas Health in Hanover, Md., announced it has acquired a majority interest in Advanced Inpatient Medicine in Lakeville, Pa. Advanced Inpatient Medicine (AIM) provides hospitalist services for four hospitals and several acute care and skilled nursing facilities in Northeastern Pennsylvania.
AIM and its 40 employees join Adfinitas, which has partnership agreements with 14 hospitals and 40 postacute facilities in Maryland, Virginia, and Michigan. AIM and Adfinitas share the theory of integrating advanced practice providers, such as nurse practitioners and physician assistants, into their physician-led care teams.
Jason Blair, DO, recently was named an honorary Fellow by the American College of Osteopathic Internists (ACOI) for excellence in the practice of internal medicine. Dr. Blair currently is a hospitalist at Lake Regional Health System in Osage Beach, Mo.
The degree of Fellow is given to physicians who demonstrate continuing professional accomplishments, scholarship, and professional activities, including teaching, research, and community service. The ACOI represents more than 5,000 osteopathic internists and subspecialists nationwide. Dr. Blair joined Lake Regional in 2017.
Dr. Howell is the division director of the Collaborative Inpatient Medicine Service (CIMS) and a professor of medicine at the Johns Hopkins Bayview Medical Center in Baltimore. He received the award for his work with project EQUIP (Excellence in Quality, Utilization Integration, and Patient-Centered Care) to improve quality and efficiency and to reduce mortality, emergency department boarding, and patient lengths of stay.
David Svec, MD, MBA, has been named the new chief medical officer at Stanford Health Care – ValleyCare in Pleasanton, Calif. Dr. Svec has served as a hospitalist and internal medicine specialist at ValleyCare for the past 6 years. Previously, he was ValleyCare’s medical director of the hospitalist team and a clinical assistant professor of medicine. Dr. Svec helped develop the hospitalist program at ValleyCare and will continue to work in that capacity while advancing into his new role.
As CMO, Dr. Svec will carry on the mission of Stanford Health Care, including increasing innovative programs, monitoring outcome measures, and developing and implementing improvement plans.
Dr. Svec earned Stanford Health Care’s 2016 David A. Rytand Clinical Teaching Award, the 2016 Lawrence Mathers Award: Exceptional Commitment to Teaching/Active Involvement in Medical Student Education, and the 2014 Arthur L. Bloomfield Award for Excellence in Clinical Teaching.
Brent Baboolal, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Baboolal is an internist and a hospitalist serving the Texas Health Presbyterian Hospital in Dallas.
Trained in Grenada, Dr. Baboolal came to the United States in 2009 and began work at Stamford (Conn.) Hospital. He is board certified by the American Board of Internal Medicine and is renowned as a leading internist and hospitalist. He is a former associate professor at the University of Texas School of Nursing.
BUSINESS MOVES
Sound Physicians in Tacoma, Wash., recently announced that it will take over providing hospitalist services for SSM Health DePaul Hospital and SSM Health St. Mary’s Hospital in St. Louis. Sound Physicians already had been running critical care at SSM Health St. Clare Hospital, Fenton, Mo.
SSM Health is a Catholic, faith-based, nonprofit health system serving communities in Illinois, Missouri, Oklahoma, and Wisconsin.
“We have been impressed with their efficiency and professionalism of establishing Sound Physicians’ infrastructure that supports providers and implementing processes to drive improved outcomes,” said Rajiv Patel, MD, vice president of medical affairs for SSM Health DePaul Hospital.
Sound Physicians prides itself on improving quality and lowering costs of acute care for health organizations and facilities. Sound provides emergency medicine, hospital medicine, critical care, transitional care, and advisory services for its partners nationwide.
Pittsburgh-based health leaders Highmark Health and Allegheny Health Network, and Erie, Pa.–based Lecom Health have agreed to establish an affiliation with Warren (Pa.) General Hospital, a full-service, 87-bed facility about an hour from Erie. The agreement will provide Warren General with capital to make improvements to its maternity unit and radiation oncology equipment, among other services.
The partnership includes Warren General agreeing to use Allegheny Health Network (AHN) affiliates for clinical, emergency, and hospitalist services, and Warren General physicians will join the AHN integrated network. AHN, Highmark, and Lecom will assist Warren General with capital investments and community health reinvestment projects.
Hospitalist group Adfinitas Health in Hanover, Md., announced it has acquired a majority interest in Advanced Inpatient Medicine in Lakeville, Pa. Advanced Inpatient Medicine (AIM) provides hospitalist services for four hospitals and several acute care and skilled nursing facilities in Northeastern Pennsylvania.
AIM and its 40 employees join Adfinitas, which has partnership agreements with 14 hospitals and 40 postacute facilities in Maryland, Virginia, and Michigan. AIM and Adfinitas share the theory of integrating advanced practice providers, such as nurse practitioners and physician assistants, into their physician-led care teams.
Jason Blair, DO, recently was named an honorary Fellow by the American College of Osteopathic Internists (ACOI) for excellence in the practice of internal medicine. Dr. Blair currently is a hospitalist at Lake Regional Health System in Osage Beach, Mo.
The degree of Fellow is given to physicians who demonstrate continuing professional accomplishments, scholarship, and professional activities, including teaching, research, and community service. The ACOI represents more than 5,000 osteopathic internists and subspecialists nationwide. Dr. Blair joined Lake Regional in 2017.
Dr. Howell is the division director of the Collaborative Inpatient Medicine Service (CIMS) and a professor of medicine at the Johns Hopkins Bayview Medical Center in Baltimore. He received the award for his work with project EQUIP (Excellence in Quality, Utilization Integration, and Patient-Centered Care) to improve quality and efficiency and to reduce mortality, emergency department boarding, and patient lengths of stay.
David Svec, MD, MBA, has been named the new chief medical officer at Stanford Health Care – ValleyCare in Pleasanton, Calif. Dr. Svec has served as a hospitalist and internal medicine specialist at ValleyCare for the past 6 years. Previously, he was ValleyCare’s medical director of the hospitalist team and a clinical assistant professor of medicine. Dr. Svec helped develop the hospitalist program at ValleyCare and will continue to work in that capacity while advancing into his new role.
As CMO, Dr. Svec will carry on the mission of Stanford Health Care, including increasing innovative programs, monitoring outcome measures, and developing and implementing improvement plans.
Dr. Svec earned Stanford Health Care’s 2016 David A. Rytand Clinical Teaching Award, the 2016 Lawrence Mathers Award: Exceptional Commitment to Teaching/Active Involvement in Medical Student Education, and the 2014 Arthur L. Bloomfield Award for Excellence in Clinical Teaching.
Brent Baboolal, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Baboolal is an internist and a hospitalist serving the Texas Health Presbyterian Hospital in Dallas.
Trained in Grenada, Dr. Baboolal came to the United States in 2009 and began work at Stamford (Conn.) Hospital. He is board certified by the American Board of Internal Medicine and is renowned as a leading internist and hospitalist. He is a former associate professor at the University of Texas School of Nursing.
BUSINESS MOVES
Sound Physicians in Tacoma, Wash., recently announced that it will take over providing hospitalist services for SSM Health DePaul Hospital and SSM Health St. Mary’s Hospital in St. Louis. Sound Physicians already had been running critical care at SSM Health St. Clare Hospital, Fenton, Mo.
SSM Health is a Catholic, faith-based, nonprofit health system serving communities in Illinois, Missouri, Oklahoma, and Wisconsin.
“We have been impressed with their efficiency and professionalism of establishing Sound Physicians’ infrastructure that supports providers and implementing processes to drive improved outcomes,” said Rajiv Patel, MD, vice president of medical affairs for SSM Health DePaul Hospital.
Sound Physicians prides itself on improving quality and lowering costs of acute care for health organizations and facilities. Sound provides emergency medicine, hospital medicine, critical care, transitional care, and advisory services for its partners nationwide.
Pittsburgh-based health leaders Highmark Health and Allegheny Health Network, and Erie, Pa.–based Lecom Health have agreed to establish an affiliation with Warren (Pa.) General Hospital, a full-service, 87-bed facility about an hour from Erie. The agreement will provide Warren General with capital to make improvements to its maternity unit and radiation oncology equipment, among other services.
The partnership includes Warren General agreeing to use Allegheny Health Network (AHN) affiliates for clinical, emergency, and hospitalist services, and Warren General physicians will join the AHN integrated network. AHN, Highmark, and Lecom will assist Warren General with capital investments and community health reinvestment projects.
Hospitalist group Adfinitas Health in Hanover, Md., announced it has acquired a majority interest in Advanced Inpatient Medicine in Lakeville, Pa. Advanced Inpatient Medicine (AIM) provides hospitalist services for four hospitals and several acute care and skilled nursing facilities in Northeastern Pennsylvania.
AIM and its 40 employees join Adfinitas, which has partnership agreements with 14 hospitals and 40 postacute facilities in Maryland, Virginia, and Michigan. AIM and Adfinitas share the theory of integrating advanced practice providers, such as nurse practitioners and physician assistants, into their physician-led care teams.
Learn About New ABS Continuous Certification Program
The American Board of Surgery has announced the details of its new Continuous Certification Program, shaped by surgeon feedback and designed to provide greater value, flexibility and convenience in maintaining ABS board certification. Instead of taking one recertification exam every 10 years, surgeons will use the new program to demonstrate their surgical knowledge on a continual basis. General surgeons will follow the new assessment this year; members of other ABS specialties will do so over the next few years.
The American Board of Surgery has announced the details of its new Continuous Certification Program, shaped by surgeon feedback and designed to provide greater value, flexibility and convenience in maintaining ABS board certification. Instead of taking one recertification exam every 10 years, surgeons will use the new program to demonstrate their surgical knowledge on a continual basis. General surgeons will follow the new assessment this year; members of other ABS specialties will do so over the next few years.
The American Board of Surgery has announced the details of its new Continuous Certification Program, shaped by surgeon feedback and designed to provide greater value, flexibility and convenience in maintaining ABS board certification. Instead of taking one recertification exam every 10 years, surgeons will use the new program to demonstrate their surgical knowledge on a continual basis. General surgeons will follow the new assessment this year; members of other ABS specialties will do so over the next few years.
Deadline is March 30 to Apply for Council, Committee Spots
SVS members who want to serve on an SVS Council or Committee must complete the brief application by Friday, March 30, 2018. Please note: Members must create a new account; SVS log-in credentials will not work.
SVS members who want to serve on an SVS Council or Committee must complete the brief application by Friday, March 30, 2018. Please note: Members must create a new account; SVS log-in credentials will not work.
SVS members who want to serve on an SVS Council or Committee must complete the brief application by Friday, March 30, 2018. Please note: Members must create a new account; SVS log-in credentials will not work.
Children with autism, younger siblings are undervaccinated
according to findings published March 26 in JAMA Pediatrics.
In a matched cohort study of 3,729 children with autism spectrum disorder (ASD) and 592,907 children without ASD, children with ASD were significantly less likely than children without ASD to be fully vaccinated for vaccines recommended at 4-6 years of age (adjusted rate ratio = 0.87; 95% confidence interval 0.85-0.88; P less than .05), wrote Ousseny Zerbo, PhD, of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and his coauthors.
ASD was defined based on ICD-9-CM codes 299.0, 299.8, and 299.9 in EHRs at least twice from birth until either the patient’s 6th birthday or follow-up, whichever came first. Assessment included the Centers for Disease Control and Prevention’s ACIP (Advisory Committee Immunization Practices)–recommended vaccinations for ages 4-6 years and 11-12 years. Children who received all doses within the ACIP-recommended age limits were considered fully vaccinated, the investigators said.
Only 81.6% of children with ASD had received all recommended doses between ages 4 and 6 years, compared with 94.1% of children without ASD. For the MMR vaccine, 84.0% of children with ASD aged 4-6 years were vaccinated, compared with 95.9% of children without ASD. For vaccines recommended at 11-12 years of age, the proportion of children with and without ASD receiving all vaccines were 77.5% and 76.9%, respectively, and adjusted RR was not significant, Dr. Zerbo and colleagues reported.
In all age groups, the proportion of fully vaccinated children was lower among the younger siblings of children with ASD, compared with the younger siblings of children without ASD. The largest differences in vaccination rates were seen in children aged 1-11 months and 1-2 years, with 73.2% of ASD siblings and 85% of non-ASD siblings aged 1-11 months being fully vaccinated (aRR, 0.86; 95% confidence interval, 0.82-0.89), and 60.2% of ASD siblings and 70.7% of non-ASD siblings aged 1-2 years being fully vaccinated (aRR, 0.84; 95% CI, 0.79-0.89), the authors noted.
Although most parents vaccinate their children in accordance with the ACIP-recommended schedule, the results of this study suggest that for siblings of children with ASD, “the ASD diagnosis of the older sibling may have contributed to the undervaccination of the younger children,” Dr. Zerbo and his colleagues wrote.
“Children with ASD and their younger siblings were undervaccinated, compared with the general population, suggesting that they are at increased risk of vaccine-preventable diseases,” they wrote. “New strategies, including establishing or promoting a better dialogue among parents, health care professionals, and public health authorities, may be needed to increase vaccine uptake in populations with low uptake.”
The study was funded in part by a CDC grant. Dr. Zerbo had no relevant financial disclosures. Some authors disclosed relationships with MedImmune, GlaxoSmithKline, and other pharmaceutical companies.
SOURCE: Zerbo, O et al. JAMA Pediatr. 2018, Mar 26. doi: 10.1001/jamapediatrics.2018.0082.
according to findings published March 26 in JAMA Pediatrics.
In a matched cohort study of 3,729 children with autism spectrum disorder (ASD) and 592,907 children without ASD, children with ASD were significantly less likely than children without ASD to be fully vaccinated for vaccines recommended at 4-6 years of age (adjusted rate ratio = 0.87; 95% confidence interval 0.85-0.88; P less than .05), wrote Ousseny Zerbo, PhD, of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and his coauthors.
ASD was defined based on ICD-9-CM codes 299.0, 299.8, and 299.9 in EHRs at least twice from birth until either the patient’s 6th birthday or follow-up, whichever came first. Assessment included the Centers for Disease Control and Prevention’s ACIP (Advisory Committee Immunization Practices)–recommended vaccinations for ages 4-6 years and 11-12 years. Children who received all doses within the ACIP-recommended age limits were considered fully vaccinated, the investigators said.
Only 81.6% of children with ASD had received all recommended doses between ages 4 and 6 years, compared with 94.1% of children without ASD. For the MMR vaccine, 84.0% of children with ASD aged 4-6 years were vaccinated, compared with 95.9% of children without ASD. For vaccines recommended at 11-12 years of age, the proportion of children with and without ASD receiving all vaccines were 77.5% and 76.9%, respectively, and adjusted RR was not significant, Dr. Zerbo and colleagues reported.
In all age groups, the proportion of fully vaccinated children was lower among the younger siblings of children with ASD, compared with the younger siblings of children without ASD. The largest differences in vaccination rates were seen in children aged 1-11 months and 1-2 years, with 73.2% of ASD siblings and 85% of non-ASD siblings aged 1-11 months being fully vaccinated (aRR, 0.86; 95% confidence interval, 0.82-0.89), and 60.2% of ASD siblings and 70.7% of non-ASD siblings aged 1-2 years being fully vaccinated (aRR, 0.84; 95% CI, 0.79-0.89), the authors noted.
Although most parents vaccinate their children in accordance with the ACIP-recommended schedule, the results of this study suggest that for siblings of children with ASD, “the ASD diagnosis of the older sibling may have contributed to the undervaccination of the younger children,” Dr. Zerbo and his colleagues wrote.
“Children with ASD and their younger siblings were undervaccinated, compared with the general population, suggesting that they are at increased risk of vaccine-preventable diseases,” they wrote. “New strategies, including establishing or promoting a better dialogue among parents, health care professionals, and public health authorities, may be needed to increase vaccine uptake in populations with low uptake.”
The study was funded in part by a CDC grant. Dr. Zerbo had no relevant financial disclosures. Some authors disclosed relationships with MedImmune, GlaxoSmithKline, and other pharmaceutical companies.
SOURCE: Zerbo, O et al. JAMA Pediatr. 2018, Mar 26. doi: 10.1001/jamapediatrics.2018.0082.
according to findings published March 26 in JAMA Pediatrics.
In a matched cohort study of 3,729 children with autism spectrum disorder (ASD) and 592,907 children without ASD, children with ASD were significantly less likely than children without ASD to be fully vaccinated for vaccines recommended at 4-6 years of age (adjusted rate ratio = 0.87; 95% confidence interval 0.85-0.88; P less than .05), wrote Ousseny Zerbo, PhD, of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and his coauthors.
ASD was defined based on ICD-9-CM codes 299.0, 299.8, and 299.9 in EHRs at least twice from birth until either the patient’s 6th birthday or follow-up, whichever came first. Assessment included the Centers for Disease Control and Prevention’s ACIP (Advisory Committee Immunization Practices)–recommended vaccinations for ages 4-6 years and 11-12 years. Children who received all doses within the ACIP-recommended age limits were considered fully vaccinated, the investigators said.
Only 81.6% of children with ASD had received all recommended doses between ages 4 and 6 years, compared with 94.1% of children without ASD. For the MMR vaccine, 84.0% of children with ASD aged 4-6 years were vaccinated, compared with 95.9% of children without ASD. For vaccines recommended at 11-12 years of age, the proportion of children with and without ASD receiving all vaccines were 77.5% and 76.9%, respectively, and adjusted RR was not significant, Dr. Zerbo and colleagues reported.
In all age groups, the proportion of fully vaccinated children was lower among the younger siblings of children with ASD, compared with the younger siblings of children without ASD. The largest differences in vaccination rates were seen in children aged 1-11 months and 1-2 years, with 73.2% of ASD siblings and 85% of non-ASD siblings aged 1-11 months being fully vaccinated (aRR, 0.86; 95% confidence interval, 0.82-0.89), and 60.2% of ASD siblings and 70.7% of non-ASD siblings aged 1-2 years being fully vaccinated (aRR, 0.84; 95% CI, 0.79-0.89), the authors noted.
Although most parents vaccinate their children in accordance with the ACIP-recommended schedule, the results of this study suggest that for siblings of children with ASD, “the ASD diagnosis of the older sibling may have contributed to the undervaccination of the younger children,” Dr. Zerbo and his colleagues wrote.
“Children with ASD and their younger siblings were undervaccinated, compared with the general population, suggesting that they are at increased risk of vaccine-preventable diseases,” they wrote. “New strategies, including establishing or promoting a better dialogue among parents, health care professionals, and public health authorities, may be needed to increase vaccine uptake in populations with low uptake.”
The study was funded in part by a CDC grant. Dr. Zerbo had no relevant financial disclosures. Some authors disclosed relationships with MedImmune, GlaxoSmithKline, and other pharmaceutical companies.
SOURCE: Zerbo, O et al. JAMA Pediatr. 2018, Mar 26. doi: 10.1001/jamapediatrics.2018.0082.
FROM JAMA PEDIATRICS
Key clinical point: After receiving a diagnosis of ASD, children and their younger siblings were undervaccinated.
Major finding: Only 81.6% of children with ASD had received all recommended doses between ages 4 and 6 years, compared with 94.1% of children without ASD.
Study details: A matched cohort study of 3,729 children with ASD and 592,907 children without.
Disclosures: The study was funded in part by a CDC grant. Dr. Zerbo had no relevant financial disclosures. Some authors disclosed relationships with MedImmune, GlaxoSmithKline, and other pharmaceutical companies.
Source: Zerbo O et al. JAMA Pediatr. 2018 Mar 26. doi: 10.1001/jamapediatrics.2018.0082.
Office-based screen predicts dementia in Parkinson’s disease
A simple, office-based screening tool was at least as effective as biomarker-based assessments in predicting which patients with Parkinson’s disease are likely to develop dementia in an international study.
The eight-item scale “is a short and easily-administered office tool that despite its simplicity can nonetheless accurately screen for dementia risk in Parkinson’s disease,” investigators noted in reporting the results of an international multicenter study in 607 patients with Parkinson’s disease but free of dementia at baseline. The results of the study, testing the predictive validity of the Montreal Parkinson’s Risk of Dementia Scale, were published online in JAMA Neurology.
Compared with patients in the low-risk group, those in the high-risk group had a 20-fold higher risk of dementia, and those in the intermediate risk group had a 10-fold higher risk (P less than 0.001).
A positive screen result – a cut-off of four or above – showed a sensitivity of 77.1% and a specificity of 87.2%. The positive predictive value was 43.9% and the negative predictive value was 96.7%, and the overall area under the receiver operating characteristic curve was 0.877.
Benjamin K. Dawson, from the department of neurology and neurosurgery at McGill University, Montreal, and coauthors said a previous study using a combination of lumbar puncture, dopamine transporter scanning with [123I]FP-CIT single photon emission CT (DaTscan), and clinical markers had an area under the curve of 0.80, while clinical-genetic risk score that included an analysis of GBA mutations had reported an AUC of 0.88.
The Montreal Parkinson’s Risk of Dementia Scale includes eight items: age below 70 years, male sex, falls and/or freezing, bilateral disease onset, history suggestive of rapid eye movement sleep behavior disorder, orthostatic hypotension, mild cognitive impairment, and visual hallucinations.
The authors noted that the risk scores were lower when the cohort was limited to patients without mild cognitive impairment. Because sex was also such a strong risk factor for dementia, the authors divided the results according to sex and found that the scale did perform somewhat better in men.
The authors commented that the main advantage of the Montreal Parkinson Risk of Dementia Scale was its practicality in an office-based clinical setting.
“Featuring demographic data as well as motor and nonmotor signs, the items of the scale are already often screened for in a routine office visit of a patient with [Parkinson’s disease], with no need for biological samples, neuroimaging, or genetic testing,” they wrote. “Therefore, compiling results is rapid for the clinician during a single outpatient office visit, and the results are available without delay or requirement for statistical software.”
The study was supported by the Fonds de la Recherche Sante Quebec and the Canadian Institute of Health Research. One author declared travel and speaking fees and consultancies with the pharmaceutical, and he and two other authors declared a range of grants from other funding bodies including Fonds de la Recherche Sante Quebec. No other conflicts of interest were declared.
SOURCE: Dawson B et al. JAMA Neurol. 2018 Mar 26. doi:10.1001/jamaneurol.2018.0254.
A simple, office-based screening tool was at least as effective as biomarker-based assessments in predicting which patients with Parkinson’s disease are likely to develop dementia in an international study.
The eight-item scale “is a short and easily-administered office tool that despite its simplicity can nonetheless accurately screen for dementia risk in Parkinson’s disease,” investigators noted in reporting the results of an international multicenter study in 607 patients with Parkinson’s disease but free of dementia at baseline. The results of the study, testing the predictive validity of the Montreal Parkinson’s Risk of Dementia Scale, were published online in JAMA Neurology.
Compared with patients in the low-risk group, those in the high-risk group had a 20-fold higher risk of dementia, and those in the intermediate risk group had a 10-fold higher risk (P less than 0.001).
A positive screen result – a cut-off of four or above – showed a sensitivity of 77.1% and a specificity of 87.2%. The positive predictive value was 43.9% and the negative predictive value was 96.7%, and the overall area under the receiver operating characteristic curve was 0.877.
Benjamin K. Dawson, from the department of neurology and neurosurgery at McGill University, Montreal, and coauthors said a previous study using a combination of lumbar puncture, dopamine transporter scanning with [123I]FP-CIT single photon emission CT (DaTscan), and clinical markers had an area under the curve of 0.80, while clinical-genetic risk score that included an analysis of GBA mutations had reported an AUC of 0.88.
The Montreal Parkinson’s Risk of Dementia Scale includes eight items: age below 70 years, male sex, falls and/or freezing, bilateral disease onset, history suggestive of rapid eye movement sleep behavior disorder, orthostatic hypotension, mild cognitive impairment, and visual hallucinations.
The authors noted that the risk scores were lower when the cohort was limited to patients without mild cognitive impairment. Because sex was also such a strong risk factor for dementia, the authors divided the results according to sex and found that the scale did perform somewhat better in men.
The authors commented that the main advantage of the Montreal Parkinson Risk of Dementia Scale was its practicality in an office-based clinical setting.
“Featuring demographic data as well as motor and nonmotor signs, the items of the scale are already often screened for in a routine office visit of a patient with [Parkinson’s disease], with no need for biological samples, neuroimaging, or genetic testing,” they wrote. “Therefore, compiling results is rapid for the clinician during a single outpatient office visit, and the results are available without delay or requirement for statistical software.”
The study was supported by the Fonds de la Recherche Sante Quebec and the Canadian Institute of Health Research. One author declared travel and speaking fees and consultancies with the pharmaceutical, and he and two other authors declared a range of grants from other funding bodies including Fonds de la Recherche Sante Quebec. No other conflicts of interest were declared.
SOURCE: Dawson B et al. JAMA Neurol. 2018 Mar 26. doi:10.1001/jamaneurol.2018.0254.
A simple, office-based screening tool was at least as effective as biomarker-based assessments in predicting which patients with Parkinson’s disease are likely to develop dementia in an international study.
The eight-item scale “is a short and easily-administered office tool that despite its simplicity can nonetheless accurately screen for dementia risk in Parkinson’s disease,” investigators noted in reporting the results of an international multicenter study in 607 patients with Parkinson’s disease but free of dementia at baseline. The results of the study, testing the predictive validity of the Montreal Parkinson’s Risk of Dementia Scale, were published online in JAMA Neurology.
Compared with patients in the low-risk group, those in the high-risk group had a 20-fold higher risk of dementia, and those in the intermediate risk group had a 10-fold higher risk (P less than 0.001).
A positive screen result – a cut-off of four or above – showed a sensitivity of 77.1% and a specificity of 87.2%. The positive predictive value was 43.9% and the negative predictive value was 96.7%, and the overall area under the receiver operating characteristic curve was 0.877.
Benjamin K. Dawson, from the department of neurology and neurosurgery at McGill University, Montreal, and coauthors said a previous study using a combination of lumbar puncture, dopamine transporter scanning with [123I]FP-CIT single photon emission CT (DaTscan), and clinical markers had an area under the curve of 0.80, while clinical-genetic risk score that included an analysis of GBA mutations had reported an AUC of 0.88.
The Montreal Parkinson’s Risk of Dementia Scale includes eight items: age below 70 years, male sex, falls and/or freezing, bilateral disease onset, history suggestive of rapid eye movement sleep behavior disorder, orthostatic hypotension, mild cognitive impairment, and visual hallucinations.
The authors noted that the risk scores were lower when the cohort was limited to patients without mild cognitive impairment. Because sex was also such a strong risk factor for dementia, the authors divided the results according to sex and found that the scale did perform somewhat better in men.
The authors commented that the main advantage of the Montreal Parkinson Risk of Dementia Scale was its practicality in an office-based clinical setting.
“Featuring demographic data as well as motor and nonmotor signs, the items of the scale are already often screened for in a routine office visit of a patient with [Parkinson’s disease], with no need for biological samples, neuroimaging, or genetic testing,” they wrote. “Therefore, compiling results is rapid for the clinician during a single outpatient office visit, and the results are available without delay or requirement for statistical software.”
The study was supported by the Fonds de la Recherche Sante Quebec and the Canadian Institute of Health Research. One author declared travel and speaking fees and consultancies with the pharmaceutical, and he and two other authors declared a range of grants from other funding bodies including Fonds de la Recherche Sante Quebec. No other conflicts of interest were declared.
SOURCE: Dawson B et al. JAMA Neurol. 2018 Mar 26. doi:10.1001/jamaneurol.2018.0254.
FROM JAMA NEUROLOGY
Key clinical point: An eight-item screen predicts dementia in Parkinson’s disease.
Major finding: The screening tool has an area under the curve of 0.88.
Study details: An international multicenter study in 607 patients with Parkinson’s disease.
Disclosures: The study was supported by the Fonds de la Recherche Sante Quebec and the Canadian Institute of Health Research. One author declared travel and speaking fees and consultancies with the pharmaceutical, and he and two other authors declared a range of grants from other funding bodies including Fonds de la Recherche Sante Quebec. No other conflicts of interest were declared.
Source: Dawson BK et al. JAMA Neurol. 2018 Mar 26. doi:10.1001/jamaneurol.2018.0254.
Study using U.K. data quantifies infection risk associated with psoriasis
Psoriasis was linked to increased risk of serious infection, with more severe disease associated with increased infection risk, in a study that used electronic medical records of patients in the United Kingdom.
The most common serious infections were lower respiratory tract, skin and soft tissue, and upper respiratory tract infections; and the most common opportunistic infection was tuberculosis, reported Junko Takeshita, MD, PhD, of the departments of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, and her coauthors.
They identified 199,700 psoriasis patients and 954,315 healthy patients from THIN (the Health Improvement Network), a medical records database in the United Kingdom. Of the psoriasis patients, 187,258 had mild disease and 12,442 had moderate to severe disease; almost 70% of patients with moderate to severe disease were treated with methotrexate.
Adjusted hazard ratios for serious infection were 1.21 (95% confidence interval, 1.18-1.23) for psoriasis patients overall, 1.18 (95% confidence interval, 1.16-1.21) for those with mild psoriasis, and 1.63 (95% CI, 1.52-1.75) for those with moderate to severe psoriasis, Dr. Takeshita and her coauthors wrote in the Journal of Investigative Dermatology.
Among all psoriasis patients, the attributable risk of serious infection was 16.2 per 10,000 person-years, compared with 14.4 per 10,000 person-years among those with mild psoriasis, and 49.5 per 10,000 person-years, among those with moderate to severe disease.
The investigators also analyzed data from a nested cohort – the iHOPE (Incident Health Outcomes and Psoriasis Events) study – of 8,569 psoriasis patients, with mild (less than 3% of body surface area involvement) or moderate to severe disease (3% or greater BSA), and 83,540 matched patients without psoriasis.
The adjusted HR for serious infection was 1.21 (95% CI, 1.09-1.35) for all psoriasis patients, 1.16 (95% CI, 0.99-1.35) for those with mild disease, and 1.27 (95% CI, 1.10-1.47) for those with moderate to severe disease. When patients who had received immunosuppressive treatment were excluded from the analysis, hazard ratios were similar among the different psoriasis groups, at 1.18 for all psoriasis patients (95% CI, 1.05-1.32), 1.15 among those with mild disease (95% CI, 0.99-1.34), and 1.21 for those with moderate to severe disease (95% CI, 1.03-1.42).
“Importantly, the risk of serious infection was observed to be similar in both the full THIN and iHOPE cohorts with the exception of the moderate to severe psoriasis subgroup among whom the risk of serious infection was attenuated but still significantly elevated in the iHOPE versus full THIN cohort,” they observed.
In the THIN cohort, the most common opportunistic infection “by far” was tuberculosis, with incidence rates of 1.05, 0.94, and 3.00 per 10,000 person-years among all psoriasis patients, patients with mild disease, and patients with moderate to severe disease, respectively, compared with 1.15 for those without psoriasis.
Patients with moderate to severe disease had an increased risk of opportunistic infection (HR, 1.57; 95% CI, 1.06-2.34), but rates were similar among those with mild disease and those without psoriasis, Dr. Takeshita and her colleagues reported. But the opportunistic infection risk was “substantially attenuated” when patients who had received immunosuppressive treatment were excluded (HR, 1.17; 95% CI, 0.44-3.12).
Patients with moderate to severe disease also had the greatest risk of herpes zoster (HR, 1.17; 95% CI, 1.06-1.30). While the increased risk of herpes zoster was smaller in patients with mild psoriasis, it was still significant (HR, 1.07; 95% CI, 1.05-1.10). Again, when exclusion of patients who had received immunosuppressive therapies, the risk for herpes zoster associated with moderate to severe psoriasis no longer was elevated (HR, 0.97; 95% CI, 0.76-1.23).
“Our findings suggest that psoriasis is associated with an increased risk of serious infection, and more severe psoriasis, whether defined by treatment pattern or by BSA involvement, is a predictor of greater serious infection risk,” the authors wrote. Clinicians should ensure that patients, especially those with severe disease and those who receive immunosuppressive treatment, are vaccinated against influenza and pneumonia, and “should also consider herpes zoster vaccination with the new nonlive vaccine.”
“Future studies will be important to further characterize the risk of various infections among patients with psoriasis, compare the risk of infection associated with psoriasis to that of other chronic diseases, and delineate the pathophysiologic mechanisms that contribute to the increased risk of infections associated with psoriasis and its therapies,” they concluded.
The study was funded by an unrestricted Pfizer grant. Dr. Takeshita has received a research grant (to the Trustees of the University of Pennsylvania) from Pfizer for unrelated work payment for continuing medical education work related to psoriasis supported indirectly by Eli Lilly and Novartis. Other authors’ disclosures included servings as a consultant for Bristol-Myers Squibb, Novartis, Pfizer, Coherus, and other pharmaceutical companies.
dermnews@mdedge.com
SOURCE: Takeshita J et al. J Invest Dermatol. 2018 Mar 2. doi: 10.1016/j.jid.2018.01.039.
Psoriasis was linked to increased risk of serious infection, with more severe disease associated with increased infection risk, in a study that used electronic medical records of patients in the United Kingdom.
The most common serious infections were lower respiratory tract, skin and soft tissue, and upper respiratory tract infections; and the most common opportunistic infection was tuberculosis, reported Junko Takeshita, MD, PhD, of the departments of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, and her coauthors.
They identified 199,700 psoriasis patients and 954,315 healthy patients from THIN (the Health Improvement Network), a medical records database in the United Kingdom. Of the psoriasis patients, 187,258 had mild disease and 12,442 had moderate to severe disease; almost 70% of patients with moderate to severe disease were treated with methotrexate.
Adjusted hazard ratios for serious infection were 1.21 (95% confidence interval, 1.18-1.23) for psoriasis patients overall, 1.18 (95% confidence interval, 1.16-1.21) for those with mild psoriasis, and 1.63 (95% CI, 1.52-1.75) for those with moderate to severe psoriasis, Dr. Takeshita and her coauthors wrote in the Journal of Investigative Dermatology.
Among all psoriasis patients, the attributable risk of serious infection was 16.2 per 10,000 person-years, compared with 14.4 per 10,000 person-years among those with mild psoriasis, and 49.5 per 10,000 person-years, among those with moderate to severe disease.
The investigators also analyzed data from a nested cohort – the iHOPE (Incident Health Outcomes and Psoriasis Events) study – of 8,569 psoriasis patients, with mild (less than 3% of body surface area involvement) or moderate to severe disease (3% or greater BSA), and 83,540 matched patients without psoriasis.
The adjusted HR for serious infection was 1.21 (95% CI, 1.09-1.35) for all psoriasis patients, 1.16 (95% CI, 0.99-1.35) for those with mild disease, and 1.27 (95% CI, 1.10-1.47) for those with moderate to severe disease. When patients who had received immunosuppressive treatment were excluded from the analysis, hazard ratios were similar among the different psoriasis groups, at 1.18 for all psoriasis patients (95% CI, 1.05-1.32), 1.15 among those with mild disease (95% CI, 0.99-1.34), and 1.21 for those with moderate to severe disease (95% CI, 1.03-1.42).
“Importantly, the risk of serious infection was observed to be similar in both the full THIN and iHOPE cohorts with the exception of the moderate to severe psoriasis subgroup among whom the risk of serious infection was attenuated but still significantly elevated in the iHOPE versus full THIN cohort,” they observed.
In the THIN cohort, the most common opportunistic infection “by far” was tuberculosis, with incidence rates of 1.05, 0.94, and 3.00 per 10,000 person-years among all psoriasis patients, patients with mild disease, and patients with moderate to severe disease, respectively, compared with 1.15 for those without psoriasis.
Patients with moderate to severe disease had an increased risk of opportunistic infection (HR, 1.57; 95% CI, 1.06-2.34), but rates were similar among those with mild disease and those without psoriasis, Dr. Takeshita and her colleagues reported. But the opportunistic infection risk was “substantially attenuated” when patients who had received immunosuppressive treatment were excluded (HR, 1.17; 95% CI, 0.44-3.12).
Patients with moderate to severe disease also had the greatest risk of herpes zoster (HR, 1.17; 95% CI, 1.06-1.30). While the increased risk of herpes zoster was smaller in patients with mild psoriasis, it was still significant (HR, 1.07; 95% CI, 1.05-1.10). Again, when exclusion of patients who had received immunosuppressive therapies, the risk for herpes zoster associated with moderate to severe psoriasis no longer was elevated (HR, 0.97; 95% CI, 0.76-1.23).
“Our findings suggest that psoriasis is associated with an increased risk of serious infection, and more severe psoriasis, whether defined by treatment pattern or by BSA involvement, is a predictor of greater serious infection risk,” the authors wrote. Clinicians should ensure that patients, especially those with severe disease and those who receive immunosuppressive treatment, are vaccinated against influenza and pneumonia, and “should also consider herpes zoster vaccination with the new nonlive vaccine.”
“Future studies will be important to further characterize the risk of various infections among patients with psoriasis, compare the risk of infection associated with psoriasis to that of other chronic diseases, and delineate the pathophysiologic mechanisms that contribute to the increased risk of infections associated with psoriasis and its therapies,” they concluded.
The study was funded by an unrestricted Pfizer grant. Dr. Takeshita has received a research grant (to the Trustees of the University of Pennsylvania) from Pfizer for unrelated work payment for continuing medical education work related to psoriasis supported indirectly by Eli Lilly and Novartis. Other authors’ disclosures included servings as a consultant for Bristol-Myers Squibb, Novartis, Pfizer, Coherus, and other pharmaceutical companies.
dermnews@mdedge.com
SOURCE: Takeshita J et al. J Invest Dermatol. 2018 Mar 2. doi: 10.1016/j.jid.2018.01.039.
Psoriasis was linked to increased risk of serious infection, with more severe disease associated with increased infection risk, in a study that used electronic medical records of patients in the United Kingdom.
The most common serious infections were lower respiratory tract, skin and soft tissue, and upper respiratory tract infections; and the most common opportunistic infection was tuberculosis, reported Junko Takeshita, MD, PhD, of the departments of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, and her coauthors.
They identified 199,700 psoriasis patients and 954,315 healthy patients from THIN (the Health Improvement Network), a medical records database in the United Kingdom. Of the psoriasis patients, 187,258 had mild disease and 12,442 had moderate to severe disease; almost 70% of patients with moderate to severe disease were treated with methotrexate.
Adjusted hazard ratios for serious infection were 1.21 (95% confidence interval, 1.18-1.23) for psoriasis patients overall, 1.18 (95% confidence interval, 1.16-1.21) for those with mild psoriasis, and 1.63 (95% CI, 1.52-1.75) for those with moderate to severe psoriasis, Dr. Takeshita and her coauthors wrote in the Journal of Investigative Dermatology.
Among all psoriasis patients, the attributable risk of serious infection was 16.2 per 10,000 person-years, compared with 14.4 per 10,000 person-years among those with mild psoriasis, and 49.5 per 10,000 person-years, among those with moderate to severe disease.
The investigators also analyzed data from a nested cohort – the iHOPE (Incident Health Outcomes and Psoriasis Events) study – of 8,569 psoriasis patients, with mild (less than 3% of body surface area involvement) or moderate to severe disease (3% or greater BSA), and 83,540 matched patients without psoriasis.
The adjusted HR for serious infection was 1.21 (95% CI, 1.09-1.35) for all psoriasis patients, 1.16 (95% CI, 0.99-1.35) for those with mild disease, and 1.27 (95% CI, 1.10-1.47) for those with moderate to severe disease. When patients who had received immunosuppressive treatment were excluded from the analysis, hazard ratios were similar among the different psoriasis groups, at 1.18 for all psoriasis patients (95% CI, 1.05-1.32), 1.15 among those with mild disease (95% CI, 0.99-1.34), and 1.21 for those with moderate to severe disease (95% CI, 1.03-1.42).
“Importantly, the risk of serious infection was observed to be similar in both the full THIN and iHOPE cohorts with the exception of the moderate to severe psoriasis subgroup among whom the risk of serious infection was attenuated but still significantly elevated in the iHOPE versus full THIN cohort,” they observed.
In the THIN cohort, the most common opportunistic infection “by far” was tuberculosis, with incidence rates of 1.05, 0.94, and 3.00 per 10,000 person-years among all psoriasis patients, patients with mild disease, and patients with moderate to severe disease, respectively, compared with 1.15 for those without psoriasis.
Patients with moderate to severe disease had an increased risk of opportunistic infection (HR, 1.57; 95% CI, 1.06-2.34), but rates were similar among those with mild disease and those without psoriasis, Dr. Takeshita and her colleagues reported. But the opportunistic infection risk was “substantially attenuated” when patients who had received immunosuppressive treatment were excluded (HR, 1.17; 95% CI, 0.44-3.12).
Patients with moderate to severe disease also had the greatest risk of herpes zoster (HR, 1.17; 95% CI, 1.06-1.30). While the increased risk of herpes zoster was smaller in patients with mild psoriasis, it was still significant (HR, 1.07; 95% CI, 1.05-1.10). Again, when exclusion of patients who had received immunosuppressive therapies, the risk for herpes zoster associated with moderate to severe psoriasis no longer was elevated (HR, 0.97; 95% CI, 0.76-1.23).
“Our findings suggest that psoriasis is associated with an increased risk of serious infection, and more severe psoriasis, whether defined by treatment pattern or by BSA involvement, is a predictor of greater serious infection risk,” the authors wrote. Clinicians should ensure that patients, especially those with severe disease and those who receive immunosuppressive treatment, are vaccinated against influenza and pneumonia, and “should also consider herpes zoster vaccination with the new nonlive vaccine.”
“Future studies will be important to further characterize the risk of various infections among patients with psoriasis, compare the risk of infection associated with psoriasis to that of other chronic diseases, and delineate the pathophysiologic mechanisms that contribute to the increased risk of infections associated with psoriasis and its therapies,” they concluded.
The study was funded by an unrestricted Pfizer grant. Dr. Takeshita has received a research grant (to the Trustees of the University of Pennsylvania) from Pfizer for unrelated work payment for continuing medical education work related to psoriasis supported indirectly by Eli Lilly and Novartis. Other authors’ disclosures included servings as a consultant for Bristol-Myers Squibb, Novartis, Pfizer, Coherus, and other pharmaceutical companies.
dermnews@mdedge.com
SOURCE: Takeshita J et al. J Invest Dermatol. 2018 Mar 2. doi: 10.1016/j.jid.2018.01.039.
Key clinical point: Psoriasis is linked to risk of serious infection, with increased risk in more severe disease.
Major finding: Hazard ratios for serious infection were 1.21 (95% CI, 1.18-1.23) for psoriasis overall, 1.18 (95% CI, 1.16-1.21) for mild psoriasis, and 1.63 (95% CI, 1.52-1.75) for moderate to severe psoriasis.
Study details: The evaluation included data on 199,700 patients with psoriasis and 954,315 patients without psoriasis in a U.K. electronic medical records database.
Disclosures: The study was funded by an unrestricted Pfizer grant. Dr. Takeshita has received a research grant (to the Trustees of the University of Pennsylvania) from Pfizer for unrelated work payment for continuing medical education work related to psoriasis supported indirectly by Eli Lilly and Novartis. Other authors’ disclosures included servings as a consultant for Bristol-Myers Squibb, Novartis, Pfizer, Coherus, and other pharmaceutical companies.
Source: Takeshita J et al. J Invest Dermatol. 2018 Mar 2. doi: 10.1016/j.jid.2018.01.039.
mainbar
Psoriasis was linked to increased risk of serious infection, with more severe disease associated with increased infection risk, in a study that used electronic medical records of patients in the United Kingdom.
The most common serious infections were lower respiratory tract, skin and soft tissue, and upper respiratory tract infections; and the most common opportunistic infection was tuberculosis, reported Junko Takeshita, MD, PhD, of the departments of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, and her coauthors.
Adjusted hazard ratios for serious infection were 1.21 (95% confidence interval, 1.18-1.23) for psoriasis patients overall, 1.18 (95% confidence interval, 1.16-1.21) for those with mild psoriasis, and 1.63 (95% CI, 1.52-1.75) for those with moderate to severe psoriasis, Dr. Takeshita and her coauthors wrote in the Journal of Investigative Dermatology.
Among all psoriasis patients, the attributable risk of serious infection was 16.2 per 10,000 person-years, compared with 14.4 per 10,000 person-years among those with mild psoriasis, and 49.5 per 10,000 person-years, among those with moderate to severe disease.
The investigators also analyzed data from a nested cohort – the iHOPE (Incident Health Outcomes and Psoriasis Events) study – of 8,569 psoriasis patients, with mild (less than 3% of body surface area involvement) or moderate to severe disease (3% or greater BSA), and 83,540 matched patients without psoriasis. The adjusted HR for serious infection was 1.21 (95% CI, 1.09-1.35) for all psoriasis patients, 1.16 (95% CI, 0.99-1.35) for those with mild disease, and 1.27 (95% CI, 1.10-1.47) for those with moderate to severe disease. When patients who had received immunosuppressive treatment were excluded from the analysis, hazard ratios were similar among the different psoriasis groups, at 1.18 for all psoriasis patients (95% CI, 1.05-1.32), 1.15 among those with mild disease (95% CI, 0.99-1.34), and 1.21 for those with moderate to severe disease (95% CI, 1.03-1.42).
“Importantly, the risk of serious infection was observed to be similar in both the full THIN and iHOPE cohorts with the exception of the moderate to severe psoriasis subgroup among whom the risk of serious infection was attenuated but still significantly elevated in the iHOPE versus full THIN cohort,” they observed.
In the THIN cohort, the most common opportunistic infection “by far” was tuberculosis, with incidence rates of 1.05, 0.94, and 3.00 per 10,000 person-years among all psoriasis patients, patients with mild disease, and patients with moderate to severe disease, respectively, compared with 1.15 for those without psoriasis.
Patients with moderate to severe disease had an increased risk of opportunistic infection (HR, 1.57; 95% CI, 1.06-2.34), but rates were similar among those with mild disease and those without psoriasis, Dr. Takeshita and her colleagues reported. But the opportunistic infection risk was “substantially attenuated” when patients who had received immunosuppressive treatment were excluded (HR, 1.17; 95% CI, 0.44-3.12).
Patients with moderate to severe disease also had the greatest risk of herpes zoster (HR, 1.17; 95% CI, 1.06-1.30). While the increased risk of herpes zoster was smaller in patients with mild psoriasis, it was still significant (HR, 1.07; 95% CI, 1.05-1.10). Again, when exclusion of patients who had received immunosuppressive therapies, the risk for herpes zoster associated with moderate to severe psoriasis no longer was elevated (HR, 0.97; 95% CI, 0.76-1.23).
“Our findings suggest that psoriasis is associated with an increased risk of serious infection, and more severe psoriasis, whether defined by treatment pattern or by BSA involvement, is a predictor of greater serious infection risk,” the authors wrote. Clinicians should ensure that patients, especially those with severe disease and those who receive immunosuppressive treatment, are vaccinated against influenza and pneumonia, and “should also consider herpes zoster vaccination with the new nonlive vaccine.”
“Future studies will be important to further characterize the risk of various infections among patients with psoriasis, compare the risk of infection associated with psoriasis to that of other chronic diseases, and delineate the pathophysiologic mechanisms that contribute to the increased risk of infections associated with psoriasis and its therapies,” they concluded.
The study was funded by an unrestricted Pfizer grant. Dr. Takeshita has received a research grant (to the Trustees of the University of Pennsylvania) from Pfizer for unrelated work payment for continuing medical education work related to psoriasis supported indirectly by Eli Lilly and Novartis. Other authors’ disclosures included servings as a consultant for Bristol-Myers Squibb, Novartis, Pfizer, Coherus, and other pharmaceutical companies.
SOURCE: Takeshita J et al. J Invest Dermatol. 2018 Mar 2. doi: 10.1016/j.jid.2018.01.039.
Drug pricing proposals raise red flags with specialists
White House proposals to help lower drug prices are being met with concerns by a group of specialists.
In a March 14 letter to Department of Health & Human Services Secretary Alex Azar, a group of nine specialty medical organizations highlighted four recent proposals that could have an unintended consequence of limiting access.
The specialty groups that signed onto the letter are the American Academy of Dermatology Association, American Academy of Neurology, American Academy of Ophthalmology, American Academy of Physical Medicine and Rehabilitation, American College of Gastroenterology, American College of Rheumatology, American Gastroenterological Association, American Urological Association, and the Infectious Diseases Society of America.
The groups focused on issues pertaining to four proposals highlighted in the White House’s proposed fiscal year 2019 budget and the February 2018 report from the Council of Economic Advisors titled, “Reforming Biopharmaceutical Pricing at Home and Abroad.”
The first proposal relates to changing the requirement that Medicare Part D prescription drug plans cover at least two drugs per category to covering only one as a way to provide more flexibility and potential negotiation power, while at the same time expanding the ability to use utilization management tools.
“We worry this could create access issues for patients on high cost biologic medications,” the groups said in the letter. “We believe Part D benefits should not limit patients’ access to the medical therapy judged by the treating physician to be the most efficacious choice.”
“We worry that moving Part B drugs into Part D may lead to access issues and force patients into higher cost sites of care,” the groups said.
Third, the White House is proposing to cut Part B drug reimbursement to physicians from the current average sales price plus 6% down to ASP+3% for new drugs.
The groups said that with the budget sequestration currently in place, “the existing Part B payment structure does not adequately cover the costs of obtaining and providing these complex therapies in an outpatient setting. If additional payment cuts or negative changes are implemented or activated through demonstration projects, many patients would be forced into more expensive, less convenient settings to receive their therapies – if an alternative setting is available at all in their areas.”
Finally, the groups mention a proposal that would introduce physician reimbursement that is not tied to drug pricing. But this option is not expanded upon in the Council of Economic Advisors report.
“We request more clarity on any potential policies that would affect physician reimbursement,” the groups said. “Physicians have no control over the cost of drugs or ancillary services, nor over the severity of illness and comorbidities that drive the need for such services.”
The groups did support a few of the recommendations from the two documents, including requiring Medicare Part D plans to apply a substantial portion of the rebate at point of sale, establishing a Part D out-of-pocket maximum in the catastrophic phase to better protect beneficiaries against high drug costs, decreasing the consolidation by pharmacy benefit managers and others in the supply chain, and providing the Centers for Medicare & Medicaid Services with guidance on how drug-related value-based contracts and price reporting would affect other price regulations.
“We appreciate HHS’ continued focus on transparency and patient-centered care,” the groups said. “Knowing that HHS is committed to transforming the health care delivery system and the Medicare program by putting a strong focus on patient-centered care, so providers can direct their time and resources to patients and improving outcomes, is reassuring to our providers.”
White House proposals to help lower drug prices are being met with concerns by a group of specialists.
In a March 14 letter to Department of Health & Human Services Secretary Alex Azar, a group of nine specialty medical organizations highlighted four recent proposals that could have an unintended consequence of limiting access.
The specialty groups that signed onto the letter are the American Academy of Dermatology Association, American Academy of Neurology, American Academy of Ophthalmology, American Academy of Physical Medicine and Rehabilitation, American College of Gastroenterology, American College of Rheumatology, American Gastroenterological Association, American Urological Association, and the Infectious Diseases Society of America.
The groups focused on issues pertaining to four proposals highlighted in the White House’s proposed fiscal year 2019 budget and the February 2018 report from the Council of Economic Advisors titled, “Reforming Biopharmaceutical Pricing at Home and Abroad.”
The first proposal relates to changing the requirement that Medicare Part D prescription drug plans cover at least two drugs per category to covering only one as a way to provide more flexibility and potential negotiation power, while at the same time expanding the ability to use utilization management tools.
“We worry this could create access issues for patients on high cost biologic medications,” the groups said in the letter. “We believe Part D benefits should not limit patients’ access to the medical therapy judged by the treating physician to be the most efficacious choice.”
“We worry that moving Part B drugs into Part D may lead to access issues and force patients into higher cost sites of care,” the groups said.
Third, the White House is proposing to cut Part B drug reimbursement to physicians from the current average sales price plus 6% down to ASP+3% for new drugs.
The groups said that with the budget sequestration currently in place, “the existing Part B payment structure does not adequately cover the costs of obtaining and providing these complex therapies in an outpatient setting. If additional payment cuts or negative changes are implemented or activated through demonstration projects, many patients would be forced into more expensive, less convenient settings to receive their therapies – if an alternative setting is available at all in their areas.”
Finally, the groups mention a proposal that would introduce physician reimbursement that is not tied to drug pricing. But this option is not expanded upon in the Council of Economic Advisors report.
“We request more clarity on any potential policies that would affect physician reimbursement,” the groups said. “Physicians have no control over the cost of drugs or ancillary services, nor over the severity of illness and comorbidities that drive the need for such services.”
The groups did support a few of the recommendations from the two documents, including requiring Medicare Part D plans to apply a substantial portion of the rebate at point of sale, establishing a Part D out-of-pocket maximum in the catastrophic phase to better protect beneficiaries against high drug costs, decreasing the consolidation by pharmacy benefit managers and others in the supply chain, and providing the Centers for Medicare & Medicaid Services with guidance on how drug-related value-based contracts and price reporting would affect other price regulations.
“We appreciate HHS’ continued focus on transparency and patient-centered care,” the groups said. “Knowing that HHS is committed to transforming the health care delivery system and the Medicare program by putting a strong focus on patient-centered care, so providers can direct their time and resources to patients and improving outcomes, is reassuring to our providers.”
White House proposals to help lower drug prices are being met with concerns by a group of specialists.
In a March 14 letter to Department of Health & Human Services Secretary Alex Azar, a group of nine specialty medical organizations highlighted four recent proposals that could have an unintended consequence of limiting access.
The specialty groups that signed onto the letter are the American Academy of Dermatology Association, American Academy of Neurology, American Academy of Ophthalmology, American Academy of Physical Medicine and Rehabilitation, American College of Gastroenterology, American College of Rheumatology, American Gastroenterological Association, American Urological Association, and the Infectious Diseases Society of America.
The groups focused on issues pertaining to four proposals highlighted in the White House’s proposed fiscal year 2019 budget and the February 2018 report from the Council of Economic Advisors titled, “Reforming Biopharmaceutical Pricing at Home and Abroad.”
The first proposal relates to changing the requirement that Medicare Part D prescription drug plans cover at least two drugs per category to covering only one as a way to provide more flexibility and potential negotiation power, while at the same time expanding the ability to use utilization management tools.
“We worry this could create access issues for patients on high cost biologic medications,” the groups said in the letter. “We believe Part D benefits should not limit patients’ access to the medical therapy judged by the treating physician to be the most efficacious choice.”
“We worry that moving Part B drugs into Part D may lead to access issues and force patients into higher cost sites of care,” the groups said.
Third, the White House is proposing to cut Part B drug reimbursement to physicians from the current average sales price plus 6% down to ASP+3% for new drugs.
The groups said that with the budget sequestration currently in place, “the existing Part B payment structure does not adequately cover the costs of obtaining and providing these complex therapies in an outpatient setting. If additional payment cuts or negative changes are implemented or activated through demonstration projects, many patients would be forced into more expensive, less convenient settings to receive their therapies – if an alternative setting is available at all in their areas.”
Finally, the groups mention a proposal that would introduce physician reimbursement that is not tied to drug pricing. But this option is not expanded upon in the Council of Economic Advisors report.
“We request more clarity on any potential policies that would affect physician reimbursement,” the groups said. “Physicians have no control over the cost of drugs or ancillary services, nor over the severity of illness and comorbidities that drive the need for such services.”
The groups did support a few of the recommendations from the two documents, including requiring Medicare Part D plans to apply a substantial portion of the rebate at point of sale, establishing a Part D out-of-pocket maximum in the catastrophic phase to better protect beneficiaries against high drug costs, decreasing the consolidation by pharmacy benefit managers and others in the supply chain, and providing the Centers for Medicare & Medicaid Services with guidance on how drug-related value-based contracts and price reporting would affect other price regulations.
“We appreciate HHS’ continued focus on transparency and patient-centered care,” the groups said. “Knowing that HHS is committed to transforming the health care delivery system and the Medicare program by putting a strong focus on patient-centered care, so providers can direct their time and resources to patients and improving outcomes, is reassuring to our providers.”
Violaceous Plaques and Papulonodules on the Umbilicus
The Diagnosis: Cutaneous Deposits Of Myeloma
Cutaneous deposits of myeloma are a rare skin manifestation of multiple myeloma that typically occur in less than 5% of patients.1,2 The lesions represent monoclonal proliferations of plasma cells and arise from direct extension of a neoplastic mass or less commonly from hematogenous or lymphatic spread. This secondary cutaneous involvement by plasma cell myeloma has been referred to in the literature as metastatic or extramedullary cutaneous plasmacytoma.1,2 This condition must be distinguished from cutaneous plasma cell infiltrates without underlying bone marrow involvement, classified by the World Health Organization as primary cutaneous marginal zone B-cell lymphoma and previously referred to as primary cutaneous plasmacytoma.3
Clinically, cutaneous deposits of myeloma manifest as erythematous to violaceous papules, plaques, or nodules with a smooth surface and firm consistency.1,2 The lesions typically occur on the trunk and less commonly on the head, neck, arms, and legs. In a review of 83 cases of metastatic cutaneous plasmacytoma and primary cutaneous plasmacytoma in multiple myeloma, Kato et al4 found that 52% (43/83) of cases occurred in IgG myelomas and 23% (19/83) in IgA myelomas.
In our patient, a 4-mm punch biopsy of an umbilical plaque demonstrated a dense infiltrate of atypical plasmacytoid cells through the full thickness of the dermis with nuclear pleomorphism, prominent nucleoli, and frequent mitoses (Figure 1). Immunohistochemical staining was positive for IgA λ light chain (Figure 2A) and CD138 (Figure 2B) and was negative for CD20, which was consistent with the patient's known plasma cell myeloma. Positron emission tomography revealed progression of underlying disease compared to prior studies with hypermetabolic mediastinal, retroperitoneal, and pelvic side wall lymphadenopathy, as well as extensive hypermetabolic soft tissue masses with involvement of the periumbilical region.
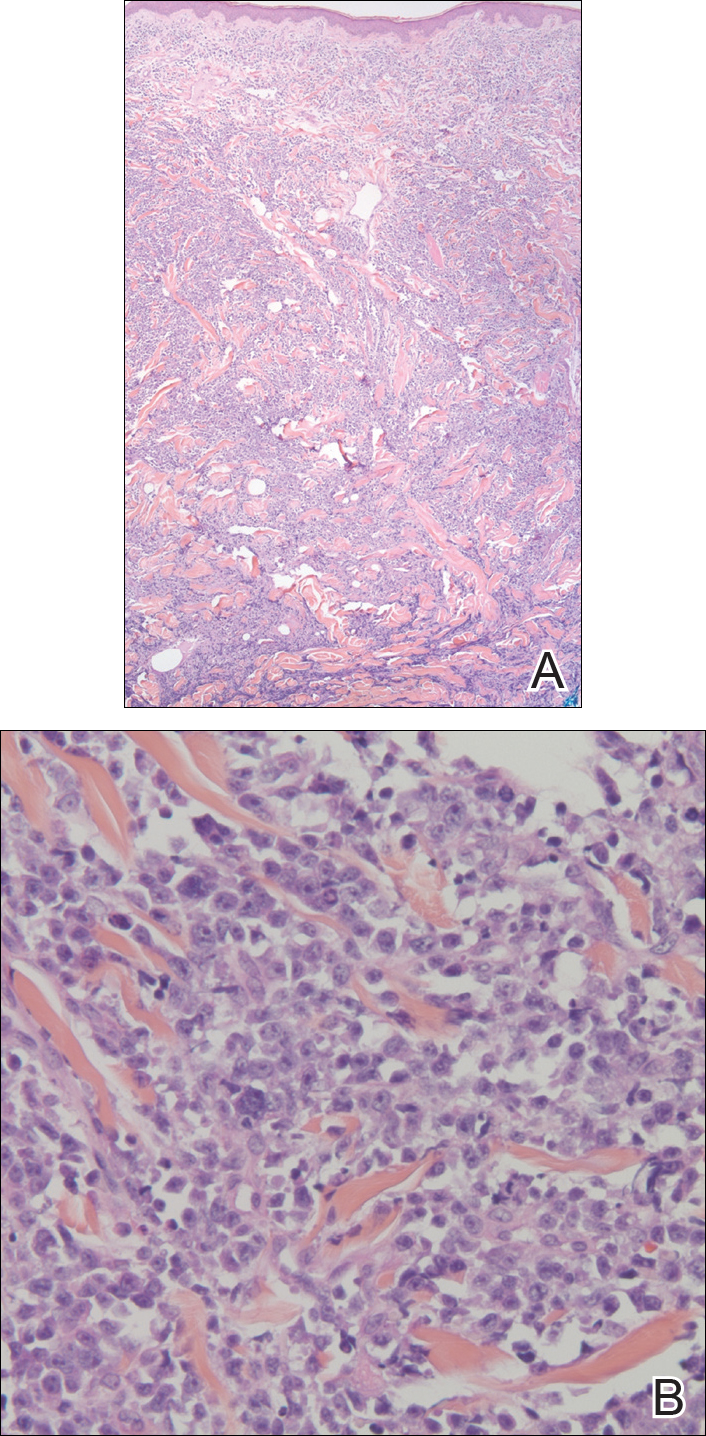
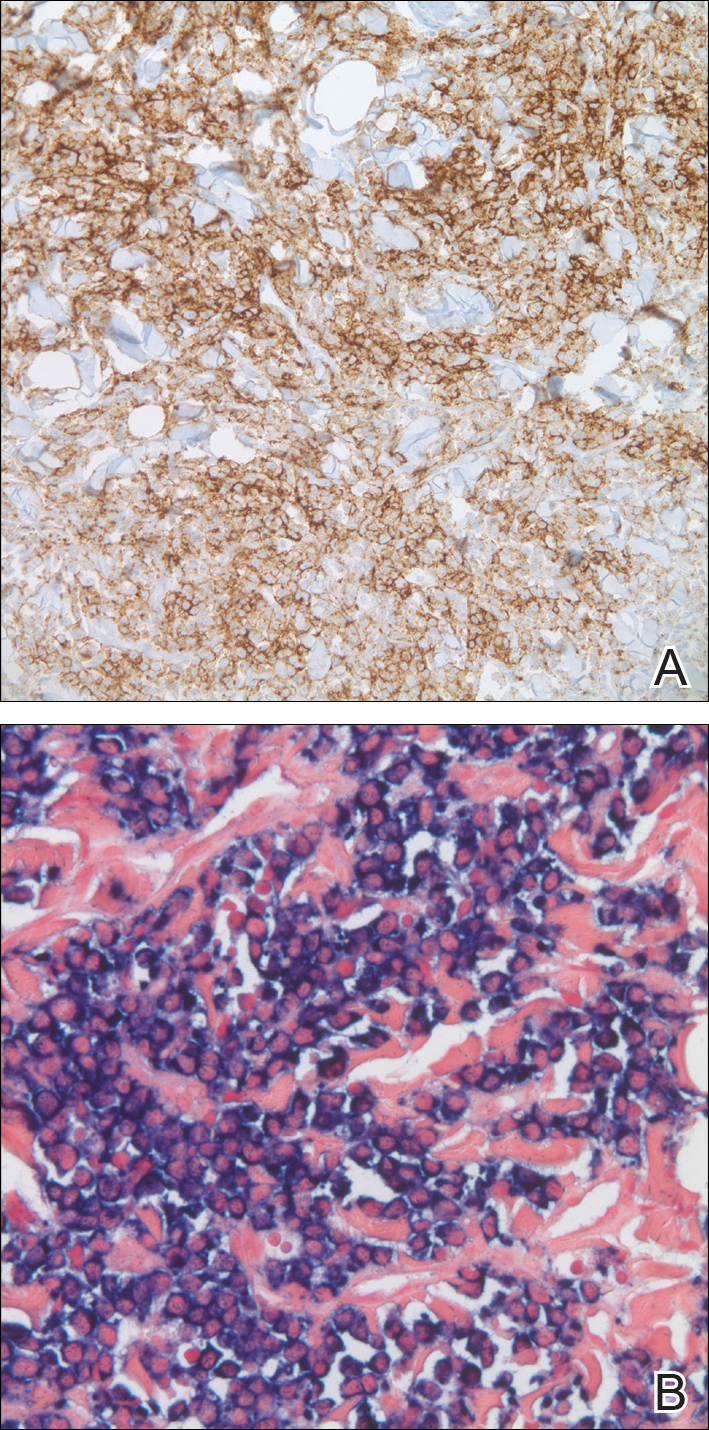
The differential diagnosis for violaceous periumbilical plaques includes cutaneous marginal zone B-cell lymphoma (primary or secondary) or T-cell lymphoma (primary or secondary), cutaneous metastases from solid organ or hematologic malignancies (eg, Sister Mary Joseph nodule), AIDS-associated Kaposi sarcoma (plum-colored plaques that may be extensive), and cutaneous endometriosis (umbilical nodules that may develop in women after surgical excision of endometrial tissue).
The mainstay of therapy for secondary cutaneous involvement of plasma cell myeloma includes treatment with chemotherapy and local radiotherapy.1,2,5 After the diagnosis of cutaneous deposits of myeloma was made in our patient, he was treated with bortezomib, cyclophosphamide with dexamethasone, and local radiotherapy to symptomatic bony lesions; however, he was unresponsive to therapy and the disease progressed with numerous extramedullary lesions of the mediastinum, gastrointestinal tract, and retroperitoneum 2 months later. The patient developed hydronephrosis from external renal compression necessitating nephrostomy tube and malignant pleural effusions requiring intubation. He experienced rapid clinical decline and died 3 months after the initial presentation due to multiorgan failure.
Cutaneous deposits of myeloma are a sign of underlying disease progression in plasma cell myeloma and often herald a fulminant course (eg, death within 12 months of presentation), as seen in our patient.5 Clinicians should be aware of this rare manifestation of plasma cell myeloma and pursue aggressive therapy given the poor prognostic nature of these cutaneous findings.
- Jorizzo JL, Gammon WR, Briggaman RA. Cutaneous plasmacytomas: a review and presentation of an unusual case. J Am Acad Dermatol. 1979;1:59-66.
- Bayer-Garner IB, Smoller BR. The spectrum of cutaneous disease in multiple myeloma. J Am Acad Dermatol. 2003;48:497-507.
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768-3785.
- Kato N, Kimura K, Yasukawa K, et al. Metastatic cutaneous plasmacytoma: a case report associated with IgA lambda multiple myeloma and a review of the literature of metastatic cutaneous plasmacytomas associated with multiple myeloma and primary cutaneous plasmacytomas. J Dermatol. 1999;26:587-594.
- Sanal SM, Yaylaci M, Mangold KA, et al. Extensive extramedullary disease in myeloma. an uncommon variant with features of poor prognosis and dedifferentiation. Cancer. 1996;77:1298-1302.
The Diagnosis: Cutaneous Deposits Of Myeloma
Cutaneous deposits of myeloma are a rare skin manifestation of multiple myeloma that typically occur in less than 5% of patients.1,2 The lesions represent monoclonal proliferations of plasma cells and arise from direct extension of a neoplastic mass or less commonly from hematogenous or lymphatic spread. This secondary cutaneous involvement by plasma cell myeloma has been referred to in the literature as metastatic or extramedullary cutaneous plasmacytoma.1,2 This condition must be distinguished from cutaneous plasma cell infiltrates without underlying bone marrow involvement, classified by the World Health Organization as primary cutaneous marginal zone B-cell lymphoma and previously referred to as primary cutaneous plasmacytoma.3
Clinically, cutaneous deposits of myeloma manifest as erythematous to violaceous papules, plaques, or nodules with a smooth surface and firm consistency.1,2 The lesions typically occur on the trunk and less commonly on the head, neck, arms, and legs. In a review of 83 cases of metastatic cutaneous plasmacytoma and primary cutaneous plasmacytoma in multiple myeloma, Kato et al4 found that 52% (43/83) of cases occurred in IgG myelomas and 23% (19/83) in IgA myelomas.
In our patient, a 4-mm punch biopsy of an umbilical plaque demonstrated a dense infiltrate of atypical plasmacytoid cells through the full thickness of the dermis with nuclear pleomorphism, prominent nucleoli, and frequent mitoses (Figure 1). Immunohistochemical staining was positive for IgA λ light chain (Figure 2A) and CD138 (Figure 2B) and was negative for CD20, which was consistent with the patient's known plasma cell myeloma. Positron emission tomography revealed progression of underlying disease compared to prior studies with hypermetabolic mediastinal, retroperitoneal, and pelvic side wall lymphadenopathy, as well as extensive hypermetabolic soft tissue masses with involvement of the periumbilical region.
The differential diagnosis for violaceous periumbilical plaques includes cutaneous marginal zone B-cell lymphoma (primary or secondary) or T-cell lymphoma (primary or secondary), cutaneous metastases from solid organ or hematologic malignancies (eg, Sister Mary Joseph nodule), AIDS-associated Kaposi sarcoma (plum-colored plaques that may be extensive), and cutaneous endometriosis (umbilical nodules that may develop in women after surgical excision of endometrial tissue).
The mainstay of therapy for secondary cutaneous involvement of plasma cell myeloma includes treatment with chemotherapy and local radiotherapy.1,2,5 After the diagnosis of cutaneous deposits of myeloma was made in our patient, he was treated with bortezomib, cyclophosphamide with dexamethasone, and local radiotherapy to symptomatic bony lesions; however, he was unresponsive to therapy and the disease progressed with numerous extramedullary lesions of the mediastinum, gastrointestinal tract, and retroperitoneum 2 months later. The patient developed hydronephrosis from external renal compression necessitating nephrostomy tube and malignant pleural effusions requiring intubation. He experienced rapid clinical decline and died 3 months after the initial presentation due to multiorgan failure.
Cutaneous deposits of myeloma are a sign of underlying disease progression in plasma cell myeloma and often herald a fulminant course (eg, death within 12 months of presentation), as seen in our patient.5 Clinicians should be aware of this rare manifestation of plasma cell myeloma and pursue aggressive therapy given the poor prognostic nature of these cutaneous findings.
The Diagnosis: Cutaneous Deposits Of Myeloma
Cutaneous deposits of myeloma are a rare skin manifestation of multiple myeloma that typically occur in less than 5% of patients.1,2 The lesions represent monoclonal proliferations of plasma cells and arise from direct extension of a neoplastic mass or less commonly from hematogenous or lymphatic spread. This secondary cutaneous involvement by plasma cell myeloma has been referred to in the literature as metastatic or extramedullary cutaneous plasmacytoma.1,2 This condition must be distinguished from cutaneous plasma cell infiltrates without underlying bone marrow involvement, classified by the World Health Organization as primary cutaneous marginal zone B-cell lymphoma and previously referred to as primary cutaneous plasmacytoma.3
Clinically, cutaneous deposits of myeloma manifest as erythematous to violaceous papules, plaques, or nodules with a smooth surface and firm consistency.1,2 The lesions typically occur on the trunk and less commonly on the head, neck, arms, and legs. In a review of 83 cases of metastatic cutaneous plasmacytoma and primary cutaneous plasmacytoma in multiple myeloma, Kato et al4 found that 52% (43/83) of cases occurred in IgG myelomas and 23% (19/83) in IgA myelomas.
In our patient, a 4-mm punch biopsy of an umbilical plaque demonstrated a dense infiltrate of atypical plasmacytoid cells through the full thickness of the dermis with nuclear pleomorphism, prominent nucleoli, and frequent mitoses (Figure 1). Immunohistochemical staining was positive for IgA λ light chain (Figure 2A) and CD138 (Figure 2B) and was negative for CD20, which was consistent with the patient's known plasma cell myeloma. Positron emission tomography revealed progression of underlying disease compared to prior studies with hypermetabolic mediastinal, retroperitoneal, and pelvic side wall lymphadenopathy, as well as extensive hypermetabolic soft tissue masses with involvement of the periumbilical region.
The differential diagnosis for violaceous periumbilical plaques includes cutaneous marginal zone B-cell lymphoma (primary or secondary) or T-cell lymphoma (primary or secondary), cutaneous metastases from solid organ or hematologic malignancies (eg, Sister Mary Joseph nodule), AIDS-associated Kaposi sarcoma (plum-colored plaques that may be extensive), and cutaneous endometriosis (umbilical nodules that may develop in women after surgical excision of endometrial tissue).
The mainstay of therapy for secondary cutaneous involvement of plasma cell myeloma includes treatment with chemotherapy and local radiotherapy.1,2,5 After the diagnosis of cutaneous deposits of myeloma was made in our patient, he was treated with bortezomib, cyclophosphamide with dexamethasone, and local radiotherapy to symptomatic bony lesions; however, he was unresponsive to therapy and the disease progressed with numerous extramedullary lesions of the mediastinum, gastrointestinal tract, and retroperitoneum 2 months later. The patient developed hydronephrosis from external renal compression necessitating nephrostomy tube and malignant pleural effusions requiring intubation. He experienced rapid clinical decline and died 3 months after the initial presentation due to multiorgan failure.
Cutaneous deposits of myeloma are a sign of underlying disease progression in plasma cell myeloma and often herald a fulminant course (eg, death within 12 months of presentation), as seen in our patient.5 Clinicians should be aware of this rare manifestation of plasma cell myeloma and pursue aggressive therapy given the poor prognostic nature of these cutaneous findings.
- Jorizzo JL, Gammon WR, Briggaman RA. Cutaneous plasmacytomas: a review and presentation of an unusual case. J Am Acad Dermatol. 1979;1:59-66.
- Bayer-Garner IB, Smoller BR. The spectrum of cutaneous disease in multiple myeloma. J Am Acad Dermatol. 2003;48:497-507.
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768-3785.
- Kato N, Kimura K, Yasukawa K, et al. Metastatic cutaneous plasmacytoma: a case report associated with IgA lambda multiple myeloma and a review of the literature of metastatic cutaneous plasmacytomas associated with multiple myeloma and primary cutaneous plasmacytomas. J Dermatol. 1999;26:587-594.
- Sanal SM, Yaylaci M, Mangold KA, et al. Extensive extramedullary disease in myeloma. an uncommon variant with features of poor prognosis and dedifferentiation. Cancer. 1996;77:1298-1302.
- Jorizzo JL, Gammon WR, Briggaman RA. Cutaneous plasmacytomas: a review and presentation of an unusual case. J Am Acad Dermatol. 1979;1:59-66.
- Bayer-Garner IB, Smoller BR. The spectrum of cutaneous disease in multiple myeloma. J Am Acad Dermatol. 2003;48:497-507.
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768-3785.
- Kato N, Kimura K, Yasukawa K, et al. Metastatic cutaneous plasmacytoma: a case report associated with IgA lambda multiple myeloma and a review of the literature of metastatic cutaneous plasmacytomas associated with multiple myeloma and primary cutaneous plasmacytomas. J Dermatol. 1999;26:587-594.
- Sanal SM, Yaylaci M, Mangold KA, et al. Extensive extramedullary disease in myeloma. an uncommon variant with features of poor prognosis and dedifferentiation. Cancer. 1996;77:1298-1302.

A 75-year-old man presented for evaluation of lesions on the umbilicus and lower abdomen that had developed over the past 4 weeks and were asymptomatic. His medical history was notable for plasma cell myeloma (stage III, IgA λ light chain restricted), deep vein thrombosis, and a 30-year history of smoking (20 packs per year). On physical examination, violaceous plaques and papulonodules were noted on the umbilicus. The lesions had a firm consistency and smooth surface without epidermal change. Violaceous papulonodules and subcutaneous plaques were noted on the lower abdomen. The lesions were nontender to palpation. Bilateral edema of the legs also was noted. The remainder of the skin was normal and there was no cervical, axillary, or inguinal lymphadenopathy.

Focusing on Inattention: The Diagnostic Accuracy of Brief Measures of Inattention for Detecting Delirium
Delirium is an acute neurocognitive disorder1 that affects up to 25% of older emergency department (ED) and hospitalized patients.2-4 The relationship between delirium and adverse outcomes is well documented.5-7 Delirium is a strong predictor of increased length of mechanical ventilation, longer intensive care unit and hospital stays, increased risk of falls, long-term cognitive impairment, and mortality.8-13 Delirium is frequently missed by healthcare professionals2,14-16 and goes undetected in up to 3 out of 4 patients by bedside nurses and medical practitioners in many hospital settings.14,17-22 A significant barrier to recognizing delirium is the absence of brief delirium assessments.
In an effort to improve delirium recognition in the acute care setting, there has been a concerted effort to develop and validate brief delirium assessments. To address this unmet need, 4 ‘A’s Test (4AT), the Brief Confusion Assessment Method (bCAM), and the 3-minute diagnostic assessment for CAM-defined delirium (3D-CAM) are 1- to 3-minute delirium assessments that were validated in acutely ill older patients.23 However, 1 to 3 minutes may still be too long in busy clinical environments, and briefer (<30 seconds) delirium assessments may be needed.
One potential more-rapid method to screen for delirium is to specifically test for the presence of inattention, which is a cardinal feature of delirium.24,25 Inattention can be ascertained by having the patient recite the months backwards, recite the days of the week backwards, or spell a word backwards.26 Recent studies have evaluated the diagnostic accuracy of reciting the months of the year backwards for delirium. O’Regan et al.27 evaluated the diagnostic accuracy of the month of the year backwards from December to July (MOTYB-6) and observed that this task was 84% sensitive and 90% specific for delirium in older patients. However, they performed the reference standard delirium assessments in patients who had a positive MOTYB-6, which can overestimate sensitivity and underestimate specificity (verification bias).28 Fick et al.29 examined the diagnostic accuracy of 20 individual elements of the 3D-CAM and observed that reciting the months of the year backwards from December to January (MOTYB-12) was 83% sensitive and 69% specific for delirium. However, this was an exploratory study that was designed to identify an element of the 3D-CAM that had the best diagnostic accuracy.
To address these limitations, we sought to evaluate the diagnostic performance of the MOTYB-6 and MOTYB-12 for delirium as diagnosed by a reference standard. We also explored other brief tests of inattention such as spelling a word (“LUNCH”) backwards, reciting the days of the week backwards, 10-letter vigilance “A” task, and 5 picture recognition task.
METHODS
Study Design and Setting
This was a preplanned secondary analysis of a prospective observational study that validated 3 delirium assessments.30,31 This study was conducted at a tertiary care, academic ED. The local institutional review board (IRB) reviewed and approved this study. Informed consent from the patient or an authorized surrogate was obtained whenever possible. Because this was an observational study and posed minimal risk to the patient, the IRB granted a waiver of consent for patients who were both unable to provide consent and were without an authorized surrogate available in the ED or by phone.
Selection of Participants
We enrolled a convenience sample of patients between June 2010 and February 2012 Monday through Friday from 8
Research assistants approached patients who met inclusion criteria and determined if any exclusion criteria were present. If none of the exclusion criteria were present, then the research assistant reviewed the informed consent document with the patient or authorized surrogate if the patient was not capable of providing consent. If a patient was not capable of providing consent and no authorized surrogate was available, then the patient was enrolled (under the waiver of consent) as long as the patient assented to be a part of the study. Once the patient was enrolled, the research assistant contacted the physician rater and reference standard psychiatrists to approach the patient.
Measures of Inattention
An emergency physician (JHH) who had no formal training in the mental status assessment of elders administered a cognitive battery to the patient, including tests of inattention. The following inattention tasks were administered:
- Spell the word “LUNCH” backwards.30 Patients were initially allowed to spell the word “LUNCH” forwards. Patients who were unable to perform the task were assigned 5 errors.
- Recite the months of the year backwards from December to July.23,26,27,30,32 Patients who were unable to perform the task were assigned 6 errors.
- Recite the days of the week backwards.23,26,33 Patients who were unable to perform the task were assigned 7 errors.
- Ten-letter vigilance “A” task.34 The patient was given a series of 10 letters (“S-A-V-E-A-H-A-A-R-T”) every 3 seconds and was asked to squeeze the rater’s hand every time the patient heard the letter “A.” Patients who were unable to perform the task were assigned 10 errors.
- Five picture recognition task.34 Patients were shown 5 objects on picture cards. Afterwards, patients were shown 10 pictures with the previously shown objects intermingled. The patient had to identify which objects were seen previously in the first 5 pictures. Patients who were unable to perform the task were assigned 10 errors.
- Recite the months of the year backwards from December to January.29 Patients who were unable to perform the task were assigned 12 errors.
Reference Standard for Delirium
A comprehensive consultation-liaison psychiatrist assessment was the reference standard for delirium; the diagnosis of delirium was based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria.35 Three psychiatrists who each had an average of 11 years of clinical experience and regularly diagnosed delirium as part of their daily clinical practice were available to perform these assessments. To arrive at the diagnosis of delirium, they interviewed those who best understood the patient’s mental status (eg, the patient’s family members or caregivers, physician, and nurses). They also reviewed the patient’s medical record and radiology and laboratory test results. They performed bedside cognitive testing that included, but was not limited to, the Mini-Mental State Examination, Clock Drawing Test, Luria hand sequencing task, and tests for verbal fluency. A focused neurological examination was also performed (ie, screening for paraphasic errors, tremors, tone, asterixis, frontal release signs, etc.), and they also evaluated the patient for affective lability, hallucinations, and level of alertness. If the presence of delirium was still questionable, then confrontational naming, proverb interpretation or similarities, and assessments for apraxias were performed at the discretion of the psychiatrist. The psychiatrists were blinded to the physician’s assessments, and the assessments were conducted within 3 hours of each other.
Additional Variables Collected
Using medical record review, comorbidity burden, severity of illness, and premorbid cognition were ascertained. The Charlson Comorbidity Index, a weighted index that takes into account the number and seriousness of 19 preexisting comorbid conditions, was used to quantify comorbidity burden; higher scores indicate higher comorbid burden.36,37 The Acute Physiology Score of the Acute Physiology and Chronic Health Evaluation II was used to quantify severity of illness.38 This score is based upon the initial values of 12 routine physiologic measurements such as vital sign and laboratory abnormalities; higher scores represent higher severities of illness.38 The medical record was reviewed to ascertain the presence of premorbid cognitive impairment; any documentation of dementia in the patient’s clinical problem list or physician history and physical examination from the outpatient or inpatient settings was considered positive. The medical record review was performed by a research assistant and was double-checked for accuracy by one of the investigators (JHH).
Data Analyses
Measures of central tendency and dispersion for continuous variables were reported as medians and interquartile ranges. Categorical variables were reported as proportions. Receiver operating characteristic curves were constructed for each inattention task. Area under the receiver operating characteristic curves (AUC) was reported to provide a global measure of diagnostic accuracy. Sensitivities, specificities, positive likelihood ratios (PLRs), and negative likelihood ratios (NLRs) with their 95% CIs were calculated using the psychiatrist’s assessment as the reference standard.39 Cut-points with PLRs greater than 10 (strongly increased the likelihood of delirium) or NLRs less than 0.1 (strongly decreased the likelihood of delirium) were preferentially reported whenever possible.
All statistical analyses were performed with open source R statistical software version 3.0.1 (http://www.r-project.org/), SAS 9.4 (SAS Institute, Cary, NC), and Microsoft Excel 2010 (Microsoft Inc., Redmond, WA).
RESULTS
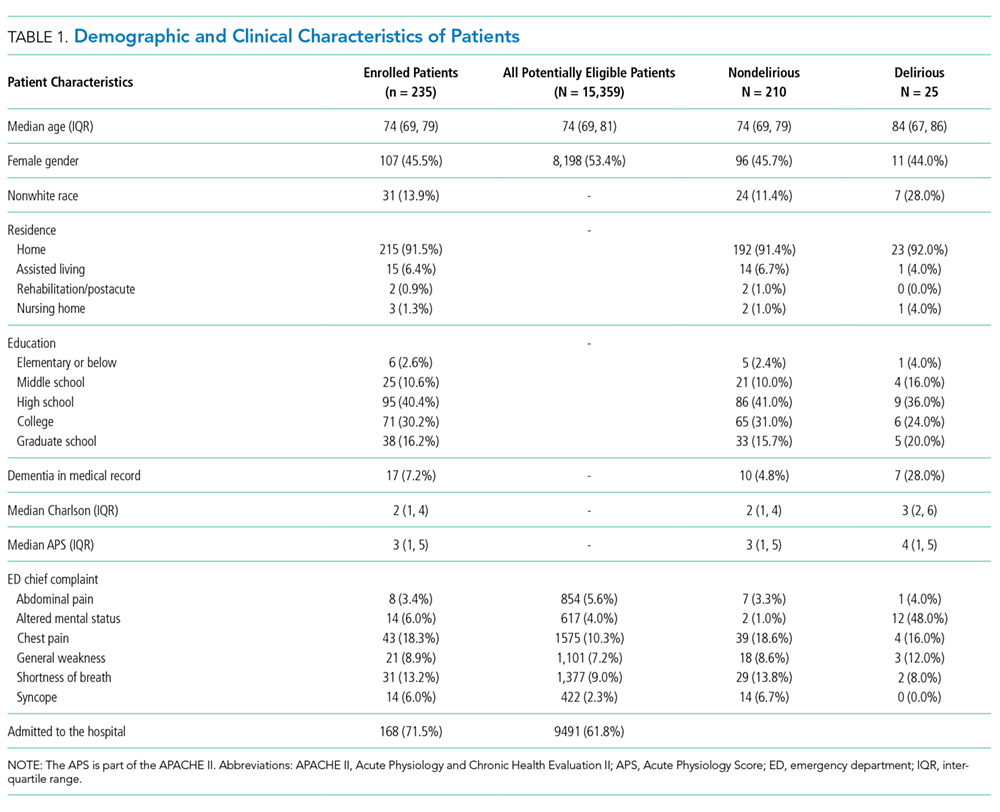
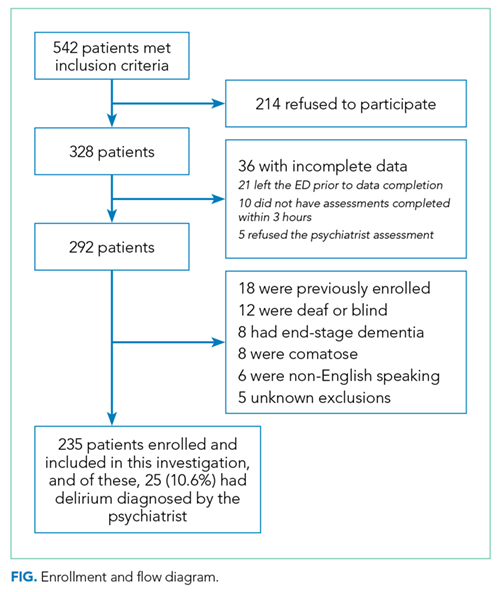
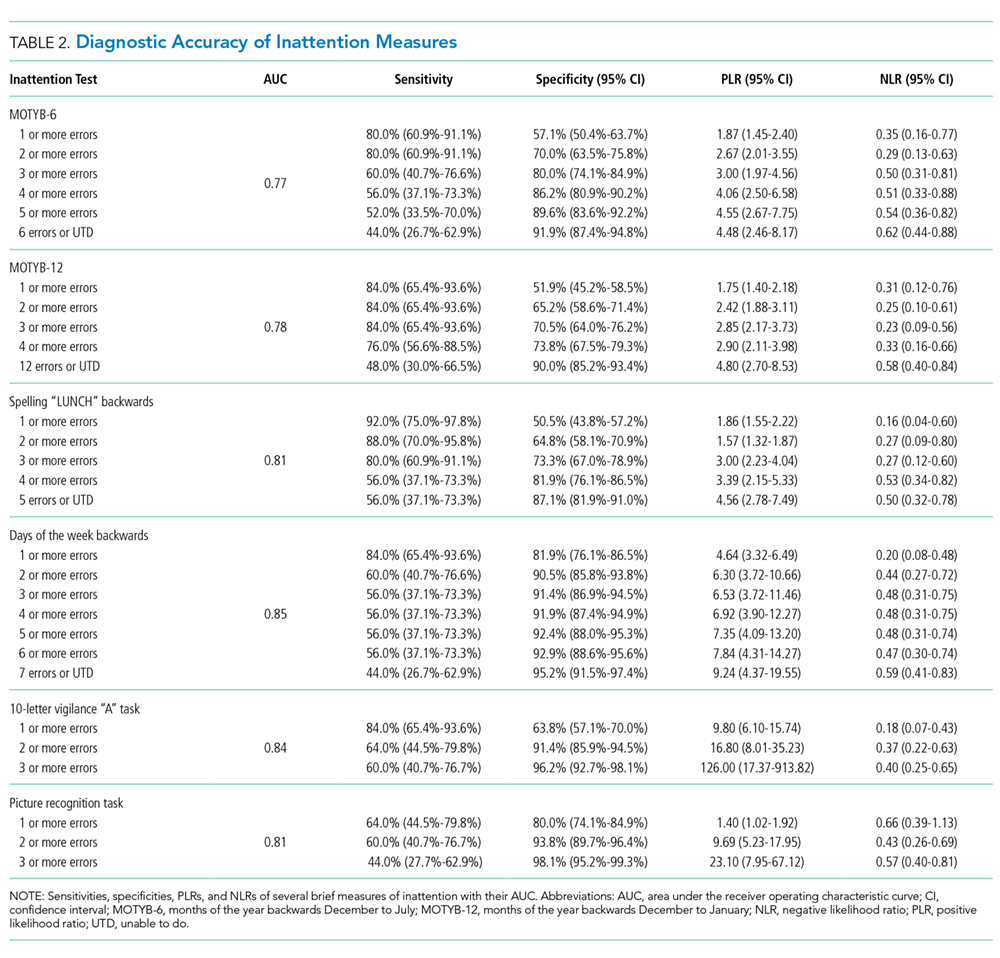
DISCUSSION
Delirium is frequently missed by healthcare providers because it is not routinely screened for in the acute care setting. To help address this deficiency of care, we evaluated several brief measures of inattention that take less than 30 seconds to complete. We observed that any errors made on the MOTYB-6 and MOTYB-12 tasks had very good sensitivities (80% and 84%) but were limited by their modest specificities (approximately 50%) for delirium. As a result, these assessments have limited clinical utility as standalone delirium screens. We also explored other commonly used brief measures of inattention and at a variety of error cutoffs. Reciting the days of the week backwards appeared to best balance sensitivity and specificity. None of the inattention measures could convincingly rule out delirium (NLR < 0.10), but the vigilance “A” and picture recognition tasks may have clinical utility in ruling in delirium (PLR > 10). Overall, all the inattention tasks, including MOTYB-6 and MOTYB-12, had very good diagnostic performances based upon their AUC. However, achieving a high sensitivity often had to be sacrificed for specificity or, alternatively, achieving a high specificity had to be sacrificed for sensitivity.
Inattention has been shown to be the cardinal feature for delirium,40 and its assessment using cognitive testing has been recommended to help identify the presence of delirium according to an expert consensus panel.26 The diagnostic performance of the MOTYB-12 observed in our study is similar to a study by Fick et al., who reported that MOTYB-12 had very good sensitivity (83%) but had modest specificity (69%) with a cutoff of 1 or more errors. Hendry et al. observed that the MOTYB-12 was 91% sensitive and 50% specific using a cutoff of 4 or more errors. With regard to the MOTYB-6, our reported specificity was different from what was observed by O’Regan et al.27 Using 1 or more errors as a cutoff, they observed a much higher specificity for delirium than we did (90% vs 57%). Discordant observations regarding the diagnostic accuracy for other inattention tasks also exist. We observed that making any error on the days of the week backwards task was 84% sensitive and 82% specific for delirium, whereas Fick et al. observed a sensitivity and specificity of 50% and 94%, respectively. For the vigilance “A” task, we observed that making 2 or more errors over a series of 10 letters was 64.0% sensitive and 91.4% specific for delirium, whereas Pompei et al.41 observed that making 2 or more errors over a series of 60 letters was 51% sensitive and 77% specific for delirium.
The abovementioned discordant findings may be driven by spectrum bias, wherein the sensitivities and specificities for each inattention task may differ in different subgroups. As a result, differences in the age distribution, proportion of college graduates, history of dementia, and susceptibility to delirium can influence overall sensitivity and specificity. Objective measures of delirium, including the inattention screens studied, are particularly prone to spectrum bias.31,34 However, the strength of this approach is that the assessment of inattention becomes less reliant upon clinical judgment and allows it to be used by raters from a wide range of clinical backgrounds. On the other hand, a subjective interpretation of these inattention tasks may allow the rater to capture the subtleties of inattention (ie, decreased speed of performance in a highly intelligent and well-educated patient without dementia). The disadvantage of this approach, however, is that it is more dependent on clinical judgment and may have decreased diagnostic accuracy in those with less clinical experience or with limited training.14,42,43 These factors must be carefully considered when determining which delirium assessment to use.
Additional research is required to determine the clinical utility of these brief inattention assessments. These findings need to be further validated in larger studies, and the optimal cutoff of each task for different subgroup of patients (eg, demented vs nondemented) needs to be further clarified. It is not completely clear whether these inattention tests can serve as standalone assessments. Depending on the cutoff used, some of these assessments may have unacceptable false negative or false positive rates that may lead to increased adverse patient outcomes or increased resource utilization, respectively. Additional components or assessments may be needed to improve the diagnostic accuracy of these assessments. In addition to understanding these inattention assessments’ diagnostic accuracies, their ability to predict adverse outcomes also needs to be investigated. While a previous study observed that making any error on the MOTYB-12 task was associated with increased physical restraint use and prolonged hospital length of stay,44 these assessments’ ability to prognosticate long-term outcomes such as mortality or long-term cognition or function need to be studied. Lastly, studies should also evaluate how easily implementable these assessments are and whether improved delirium recognition leads to improved patient outcomes.
This study has several notable limitations. Though planned a priori, this was a secondary analysis of a larger investigation designed to validate 3 delirium assessments. Our sample size was also relatively small, causing our 95% CIs to overlap in most cases and limiting the statistical power to truly determine whether one measure is better than the other. We also asked the patient to recite the months backwards from December to July as well as recite the months backwards from December to January. It is possible that the patient may have performed better at going from December to January because of learning effect. Our reference standard for delirium was based upon DSM-IV-TR criteria. The new DSM-V criteria may be more restrictive and may slightly change the sensitivities and specificities of the inattention tasks. We enrolled a convenience sample and enrolled patients who were more likely to be male, have cardiovascular chief complaints, and be admitted to the hospital; as a result, selection bias may have been introduced. Lastly, this study was conducted in a single center and enrolled patients who were 65 years and older. Our findings may not be generalizable to other settings and in those who are less than 65 years of age.
CONCLUSIONS
The MOTYB-6 and MOTYB-12 tasks had very good sensitivities but modest specificities (approximately 50%) using any error made as a cutoff; increasing cutoff to 2 errors and 3 errors, respectively, improved their specificities (approximately 70%) with minimal impact to their sensitivities. Reciting the days of the week backwards, spelling the word “LUNCH” backwards, and the 10-letter vigilance “A” task appeared to perform the best in ruling out delirium but only moderately decreased the likelihood of delirium. The 10-letter Vigilance “A” and picture recognition task
Disclosure
This study was funded by the Emergency Medicine Foundation Career Development Award, National Institutes of Health K23AG032355, and National Center for Research Resources, Grant UL1 RR024975-01. The authors report no financial conflicts of interest.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association; 2013.
33. Hamrick I, Hafiz R, Cummings DM. Use of days of the week in a modified mini-mental state exam (M-MMSE) for detecting geriatric cognitive impairment. J Am Board Fam Med. 2013;26(4):429-435.
Delirium is an acute neurocognitive disorder1 that affects up to 25% of older emergency department (ED) and hospitalized patients.2-4 The relationship between delirium and adverse outcomes is well documented.5-7 Delirium is a strong predictor of increased length of mechanical ventilation, longer intensive care unit and hospital stays, increased risk of falls, long-term cognitive impairment, and mortality.8-13 Delirium is frequently missed by healthcare professionals2,14-16 and goes undetected in up to 3 out of 4 patients by bedside nurses and medical practitioners in many hospital settings.14,17-22 A significant barrier to recognizing delirium is the absence of brief delirium assessments.
In an effort to improve delirium recognition in the acute care setting, there has been a concerted effort to develop and validate brief delirium assessments. To address this unmet need, 4 ‘A’s Test (4AT), the Brief Confusion Assessment Method (bCAM), and the 3-minute diagnostic assessment for CAM-defined delirium (3D-CAM) are 1- to 3-minute delirium assessments that were validated in acutely ill older patients.23 However, 1 to 3 minutes may still be too long in busy clinical environments, and briefer (<30 seconds) delirium assessments may be needed.
One potential more-rapid method to screen for delirium is to specifically test for the presence of inattention, which is a cardinal feature of delirium.24,25 Inattention can be ascertained by having the patient recite the months backwards, recite the days of the week backwards, or spell a word backwards.26 Recent studies have evaluated the diagnostic accuracy of reciting the months of the year backwards for delirium. O’Regan et al.27 evaluated the diagnostic accuracy of the month of the year backwards from December to July (MOTYB-6) and observed that this task was 84% sensitive and 90% specific for delirium in older patients. However, they performed the reference standard delirium assessments in patients who had a positive MOTYB-6, which can overestimate sensitivity and underestimate specificity (verification bias).28 Fick et al.29 examined the diagnostic accuracy of 20 individual elements of the 3D-CAM and observed that reciting the months of the year backwards from December to January (MOTYB-12) was 83% sensitive and 69% specific for delirium. However, this was an exploratory study that was designed to identify an element of the 3D-CAM that had the best diagnostic accuracy.
To address these limitations, we sought to evaluate the diagnostic performance of the MOTYB-6 and MOTYB-12 for delirium as diagnosed by a reference standard. We also explored other brief tests of inattention such as spelling a word (“LUNCH”) backwards, reciting the days of the week backwards, 10-letter vigilance “A” task, and 5 picture recognition task.
METHODS
Study Design and Setting
This was a preplanned secondary analysis of a prospective observational study that validated 3 delirium assessments.30,31 This study was conducted at a tertiary care, academic ED. The local institutional review board (IRB) reviewed and approved this study. Informed consent from the patient or an authorized surrogate was obtained whenever possible. Because this was an observational study and posed minimal risk to the patient, the IRB granted a waiver of consent for patients who were both unable to provide consent and were without an authorized surrogate available in the ED or by phone.
Selection of Participants
We enrolled a convenience sample of patients between June 2010 and February 2012 Monday through Friday from 8
Research assistants approached patients who met inclusion criteria and determined if any exclusion criteria were present. If none of the exclusion criteria were present, then the research assistant reviewed the informed consent document with the patient or authorized surrogate if the patient was not capable of providing consent. If a patient was not capable of providing consent and no authorized surrogate was available, then the patient was enrolled (under the waiver of consent) as long as the patient assented to be a part of the study. Once the patient was enrolled, the research assistant contacted the physician rater and reference standard psychiatrists to approach the patient.
Measures of Inattention
An emergency physician (JHH) who had no formal training in the mental status assessment of elders administered a cognitive battery to the patient, including tests of inattention. The following inattention tasks were administered:
- Spell the word “LUNCH” backwards.30 Patients were initially allowed to spell the word “LUNCH” forwards. Patients who were unable to perform the task were assigned 5 errors.
- Recite the months of the year backwards from December to July.23,26,27,30,32 Patients who were unable to perform the task were assigned 6 errors.
- Recite the days of the week backwards.23,26,33 Patients who were unable to perform the task were assigned 7 errors.
- Ten-letter vigilance “A” task.34 The patient was given a series of 10 letters (“S-A-V-E-A-H-A-A-R-T”) every 3 seconds and was asked to squeeze the rater’s hand every time the patient heard the letter “A.” Patients who were unable to perform the task were assigned 10 errors.
- Five picture recognition task.34 Patients were shown 5 objects on picture cards. Afterwards, patients were shown 10 pictures with the previously shown objects intermingled. The patient had to identify which objects were seen previously in the first 5 pictures. Patients who were unable to perform the task were assigned 10 errors.
- Recite the months of the year backwards from December to January.29 Patients who were unable to perform the task were assigned 12 errors.
Reference Standard for Delirium
A comprehensive consultation-liaison psychiatrist assessment was the reference standard for delirium; the diagnosis of delirium was based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria.35 Three psychiatrists who each had an average of 11 years of clinical experience and regularly diagnosed delirium as part of their daily clinical practice were available to perform these assessments. To arrive at the diagnosis of delirium, they interviewed those who best understood the patient’s mental status (eg, the patient’s family members or caregivers, physician, and nurses). They also reviewed the patient’s medical record and radiology and laboratory test results. They performed bedside cognitive testing that included, but was not limited to, the Mini-Mental State Examination, Clock Drawing Test, Luria hand sequencing task, and tests for verbal fluency. A focused neurological examination was also performed (ie, screening for paraphasic errors, tremors, tone, asterixis, frontal release signs, etc.), and they also evaluated the patient for affective lability, hallucinations, and level of alertness. If the presence of delirium was still questionable, then confrontational naming, proverb interpretation or similarities, and assessments for apraxias were performed at the discretion of the psychiatrist. The psychiatrists were blinded to the physician’s assessments, and the assessments were conducted within 3 hours of each other.
Additional Variables Collected
Using medical record review, comorbidity burden, severity of illness, and premorbid cognition were ascertained. The Charlson Comorbidity Index, a weighted index that takes into account the number and seriousness of 19 preexisting comorbid conditions, was used to quantify comorbidity burden; higher scores indicate higher comorbid burden.36,37 The Acute Physiology Score of the Acute Physiology and Chronic Health Evaluation II was used to quantify severity of illness.38 This score is based upon the initial values of 12 routine physiologic measurements such as vital sign and laboratory abnormalities; higher scores represent higher severities of illness.38 The medical record was reviewed to ascertain the presence of premorbid cognitive impairment; any documentation of dementia in the patient’s clinical problem list or physician history and physical examination from the outpatient or inpatient settings was considered positive. The medical record review was performed by a research assistant and was double-checked for accuracy by one of the investigators (JHH).
Data Analyses
Measures of central tendency and dispersion for continuous variables were reported as medians and interquartile ranges. Categorical variables were reported as proportions. Receiver operating characteristic curves were constructed for each inattention task. Area under the receiver operating characteristic curves (AUC) was reported to provide a global measure of diagnostic accuracy. Sensitivities, specificities, positive likelihood ratios (PLRs), and negative likelihood ratios (NLRs) with their 95% CIs were calculated using the psychiatrist’s assessment as the reference standard.39 Cut-points with PLRs greater than 10 (strongly increased the likelihood of delirium) or NLRs less than 0.1 (strongly decreased the likelihood of delirium) were preferentially reported whenever possible.
All statistical analyses were performed with open source R statistical software version 3.0.1 (http://www.r-project.org/), SAS 9.4 (SAS Institute, Cary, NC), and Microsoft Excel 2010 (Microsoft Inc., Redmond, WA).
RESULTS
DISCUSSION
Delirium is frequently missed by healthcare providers because it is not routinely screened for in the acute care setting. To help address this deficiency of care, we evaluated several brief measures of inattention that take less than 30 seconds to complete. We observed that any errors made on the MOTYB-6 and MOTYB-12 tasks had very good sensitivities (80% and 84%) but were limited by their modest specificities (approximately 50%) for delirium. As a result, these assessments have limited clinical utility as standalone delirium screens. We also explored other commonly used brief measures of inattention and at a variety of error cutoffs. Reciting the days of the week backwards appeared to best balance sensitivity and specificity. None of the inattention measures could convincingly rule out delirium (NLR < 0.10), but the vigilance “A” and picture recognition tasks may have clinical utility in ruling in delirium (PLR > 10). Overall, all the inattention tasks, including MOTYB-6 and MOTYB-12, had very good diagnostic performances based upon their AUC. However, achieving a high sensitivity often had to be sacrificed for specificity or, alternatively, achieving a high specificity had to be sacrificed for sensitivity.
Inattention has been shown to be the cardinal feature for delirium,40 and its assessment using cognitive testing has been recommended to help identify the presence of delirium according to an expert consensus panel.26 The diagnostic performance of the MOTYB-12 observed in our study is similar to a study by Fick et al., who reported that MOTYB-12 had very good sensitivity (83%) but had modest specificity (69%) with a cutoff of 1 or more errors. Hendry et al. observed that the MOTYB-12 was 91% sensitive and 50% specific using a cutoff of 4 or more errors. With regard to the MOTYB-6, our reported specificity was different from what was observed by O’Regan et al.27 Using 1 or more errors as a cutoff, they observed a much higher specificity for delirium than we did (90% vs 57%). Discordant observations regarding the diagnostic accuracy for other inattention tasks also exist. We observed that making any error on the days of the week backwards task was 84% sensitive and 82% specific for delirium, whereas Fick et al. observed a sensitivity and specificity of 50% and 94%, respectively. For the vigilance “A” task, we observed that making 2 or more errors over a series of 10 letters was 64.0% sensitive and 91.4% specific for delirium, whereas Pompei et al.41 observed that making 2 or more errors over a series of 60 letters was 51% sensitive and 77% specific for delirium.
The abovementioned discordant findings may be driven by spectrum bias, wherein the sensitivities and specificities for each inattention task may differ in different subgroups. As a result, differences in the age distribution, proportion of college graduates, history of dementia, and susceptibility to delirium can influence overall sensitivity and specificity. Objective measures of delirium, including the inattention screens studied, are particularly prone to spectrum bias.31,34 However, the strength of this approach is that the assessment of inattention becomes less reliant upon clinical judgment and allows it to be used by raters from a wide range of clinical backgrounds. On the other hand, a subjective interpretation of these inattention tasks may allow the rater to capture the subtleties of inattention (ie, decreased speed of performance in a highly intelligent and well-educated patient without dementia). The disadvantage of this approach, however, is that it is more dependent on clinical judgment and may have decreased diagnostic accuracy in those with less clinical experience or with limited training.14,42,43 These factors must be carefully considered when determining which delirium assessment to use.
Additional research is required to determine the clinical utility of these brief inattention assessments. These findings need to be further validated in larger studies, and the optimal cutoff of each task for different subgroup of patients (eg, demented vs nondemented) needs to be further clarified. It is not completely clear whether these inattention tests can serve as standalone assessments. Depending on the cutoff used, some of these assessments may have unacceptable false negative or false positive rates that may lead to increased adverse patient outcomes or increased resource utilization, respectively. Additional components or assessments may be needed to improve the diagnostic accuracy of these assessments. In addition to understanding these inattention assessments’ diagnostic accuracies, their ability to predict adverse outcomes also needs to be investigated. While a previous study observed that making any error on the MOTYB-12 task was associated with increased physical restraint use and prolonged hospital length of stay,44 these assessments’ ability to prognosticate long-term outcomes such as mortality or long-term cognition or function need to be studied. Lastly, studies should also evaluate how easily implementable these assessments are and whether improved delirium recognition leads to improved patient outcomes.
This study has several notable limitations. Though planned a priori, this was a secondary analysis of a larger investigation designed to validate 3 delirium assessments. Our sample size was also relatively small, causing our 95% CIs to overlap in most cases and limiting the statistical power to truly determine whether one measure is better than the other. We also asked the patient to recite the months backwards from December to July as well as recite the months backwards from December to January. It is possible that the patient may have performed better at going from December to January because of learning effect. Our reference standard for delirium was based upon DSM-IV-TR criteria. The new DSM-V criteria may be more restrictive and may slightly change the sensitivities and specificities of the inattention tasks. We enrolled a convenience sample and enrolled patients who were more likely to be male, have cardiovascular chief complaints, and be admitted to the hospital; as a result, selection bias may have been introduced. Lastly, this study was conducted in a single center and enrolled patients who were 65 years and older. Our findings may not be generalizable to other settings and in those who are less than 65 years of age.
CONCLUSIONS
The MOTYB-6 and MOTYB-12 tasks had very good sensitivities but modest specificities (approximately 50%) using any error made as a cutoff; increasing cutoff to 2 errors and 3 errors, respectively, improved their specificities (approximately 70%) with minimal impact to their sensitivities. Reciting the days of the week backwards, spelling the word “LUNCH” backwards, and the 10-letter vigilance “A” task appeared to perform the best in ruling out delirium but only moderately decreased the likelihood of delirium. The 10-letter Vigilance “A” and picture recognition task
Disclosure
This study was funded by the Emergency Medicine Foundation Career Development Award, National Institutes of Health K23AG032355, and National Center for Research Resources, Grant UL1 RR024975-01. The authors report no financial conflicts of interest.
Delirium is an acute neurocognitive disorder1 that affects up to 25% of older emergency department (ED) and hospitalized patients.2-4 The relationship between delirium and adverse outcomes is well documented.5-7 Delirium is a strong predictor of increased length of mechanical ventilation, longer intensive care unit and hospital stays, increased risk of falls, long-term cognitive impairment, and mortality.8-13 Delirium is frequently missed by healthcare professionals2,14-16 and goes undetected in up to 3 out of 4 patients by bedside nurses and medical practitioners in many hospital settings.14,17-22 A significant barrier to recognizing delirium is the absence of brief delirium assessments.
In an effort to improve delirium recognition in the acute care setting, there has been a concerted effort to develop and validate brief delirium assessments. To address this unmet need, 4 ‘A’s Test (4AT), the Brief Confusion Assessment Method (bCAM), and the 3-minute diagnostic assessment for CAM-defined delirium (3D-CAM) are 1- to 3-minute delirium assessments that were validated in acutely ill older patients.23 However, 1 to 3 minutes may still be too long in busy clinical environments, and briefer (<30 seconds) delirium assessments may be needed.
One potential more-rapid method to screen for delirium is to specifically test for the presence of inattention, which is a cardinal feature of delirium.24,25 Inattention can be ascertained by having the patient recite the months backwards, recite the days of the week backwards, or spell a word backwards.26 Recent studies have evaluated the diagnostic accuracy of reciting the months of the year backwards for delirium. O’Regan et al.27 evaluated the diagnostic accuracy of the month of the year backwards from December to July (MOTYB-6) and observed that this task was 84% sensitive and 90% specific for delirium in older patients. However, they performed the reference standard delirium assessments in patients who had a positive MOTYB-6, which can overestimate sensitivity and underestimate specificity (verification bias).28 Fick et al.29 examined the diagnostic accuracy of 20 individual elements of the 3D-CAM and observed that reciting the months of the year backwards from December to January (MOTYB-12) was 83% sensitive and 69% specific for delirium. However, this was an exploratory study that was designed to identify an element of the 3D-CAM that had the best diagnostic accuracy.
To address these limitations, we sought to evaluate the diagnostic performance of the MOTYB-6 and MOTYB-12 for delirium as diagnosed by a reference standard. We also explored other brief tests of inattention such as spelling a word (“LUNCH”) backwards, reciting the days of the week backwards, 10-letter vigilance “A” task, and 5 picture recognition task.
METHODS
Study Design and Setting
This was a preplanned secondary analysis of a prospective observational study that validated 3 delirium assessments.30,31 This study was conducted at a tertiary care, academic ED. The local institutional review board (IRB) reviewed and approved this study. Informed consent from the patient or an authorized surrogate was obtained whenever possible. Because this was an observational study and posed minimal risk to the patient, the IRB granted a waiver of consent for patients who were both unable to provide consent and were without an authorized surrogate available in the ED or by phone.
Selection of Participants
We enrolled a convenience sample of patients between June 2010 and February 2012 Monday through Friday from 8
Research assistants approached patients who met inclusion criteria and determined if any exclusion criteria were present. If none of the exclusion criteria were present, then the research assistant reviewed the informed consent document with the patient or authorized surrogate if the patient was not capable of providing consent. If a patient was not capable of providing consent and no authorized surrogate was available, then the patient was enrolled (under the waiver of consent) as long as the patient assented to be a part of the study. Once the patient was enrolled, the research assistant contacted the physician rater and reference standard psychiatrists to approach the patient.
Measures of Inattention
An emergency physician (JHH) who had no formal training in the mental status assessment of elders administered a cognitive battery to the patient, including tests of inattention. The following inattention tasks were administered:
- Spell the word “LUNCH” backwards.30 Patients were initially allowed to spell the word “LUNCH” forwards. Patients who were unable to perform the task were assigned 5 errors.
- Recite the months of the year backwards from December to July.23,26,27,30,32 Patients who were unable to perform the task were assigned 6 errors.
- Recite the days of the week backwards.23,26,33 Patients who were unable to perform the task were assigned 7 errors.
- Ten-letter vigilance “A” task.34 The patient was given a series of 10 letters (“S-A-V-E-A-H-A-A-R-T”) every 3 seconds and was asked to squeeze the rater’s hand every time the patient heard the letter “A.” Patients who were unable to perform the task were assigned 10 errors.
- Five picture recognition task.34 Patients were shown 5 objects on picture cards. Afterwards, patients were shown 10 pictures with the previously shown objects intermingled. The patient had to identify which objects were seen previously in the first 5 pictures. Patients who were unable to perform the task were assigned 10 errors.
- Recite the months of the year backwards from December to January.29 Patients who were unable to perform the task were assigned 12 errors.
Reference Standard for Delirium
A comprehensive consultation-liaison psychiatrist assessment was the reference standard for delirium; the diagnosis of delirium was based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria.35 Three psychiatrists who each had an average of 11 years of clinical experience and regularly diagnosed delirium as part of their daily clinical practice were available to perform these assessments. To arrive at the diagnosis of delirium, they interviewed those who best understood the patient’s mental status (eg, the patient’s family members or caregivers, physician, and nurses). They also reviewed the patient’s medical record and radiology and laboratory test results. They performed bedside cognitive testing that included, but was not limited to, the Mini-Mental State Examination, Clock Drawing Test, Luria hand sequencing task, and tests for verbal fluency. A focused neurological examination was also performed (ie, screening for paraphasic errors, tremors, tone, asterixis, frontal release signs, etc.), and they also evaluated the patient for affective lability, hallucinations, and level of alertness. If the presence of delirium was still questionable, then confrontational naming, proverb interpretation or similarities, and assessments for apraxias were performed at the discretion of the psychiatrist. The psychiatrists were blinded to the physician’s assessments, and the assessments were conducted within 3 hours of each other.
Additional Variables Collected
Using medical record review, comorbidity burden, severity of illness, and premorbid cognition were ascertained. The Charlson Comorbidity Index, a weighted index that takes into account the number and seriousness of 19 preexisting comorbid conditions, was used to quantify comorbidity burden; higher scores indicate higher comorbid burden.36,37 The Acute Physiology Score of the Acute Physiology and Chronic Health Evaluation II was used to quantify severity of illness.38 This score is based upon the initial values of 12 routine physiologic measurements such as vital sign and laboratory abnormalities; higher scores represent higher severities of illness.38 The medical record was reviewed to ascertain the presence of premorbid cognitive impairment; any documentation of dementia in the patient’s clinical problem list or physician history and physical examination from the outpatient or inpatient settings was considered positive. The medical record review was performed by a research assistant and was double-checked for accuracy by one of the investigators (JHH).
Data Analyses
Measures of central tendency and dispersion for continuous variables were reported as medians and interquartile ranges. Categorical variables were reported as proportions. Receiver operating characteristic curves were constructed for each inattention task. Area under the receiver operating characteristic curves (AUC) was reported to provide a global measure of diagnostic accuracy. Sensitivities, specificities, positive likelihood ratios (PLRs), and negative likelihood ratios (NLRs) with their 95% CIs were calculated using the psychiatrist’s assessment as the reference standard.39 Cut-points with PLRs greater than 10 (strongly increased the likelihood of delirium) or NLRs less than 0.1 (strongly decreased the likelihood of delirium) were preferentially reported whenever possible.
All statistical analyses were performed with open source R statistical software version 3.0.1 (http://www.r-project.org/), SAS 9.4 (SAS Institute, Cary, NC), and Microsoft Excel 2010 (Microsoft Inc., Redmond, WA).
RESULTS
DISCUSSION
Delirium is frequently missed by healthcare providers because it is not routinely screened for in the acute care setting. To help address this deficiency of care, we evaluated several brief measures of inattention that take less than 30 seconds to complete. We observed that any errors made on the MOTYB-6 and MOTYB-12 tasks had very good sensitivities (80% and 84%) but were limited by their modest specificities (approximately 50%) for delirium. As a result, these assessments have limited clinical utility as standalone delirium screens. We also explored other commonly used brief measures of inattention and at a variety of error cutoffs. Reciting the days of the week backwards appeared to best balance sensitivity and specificity. None of the inattention measures could convincingly rule out delirium (NLR < 0.10), but the vigilance “A” and picture recognition tasks may have clinical utility in ruling in delirium (PLR > 10). Overall, all the inattention tasks, including MOTYB-6 and MOTYB-12, had very good diagnostic performances based upon their AUC. However, achieving a high sensitivity often had to be sacrificed for specificity or, alternatively, achieving a high specificity had to be sacrificed for sensitivity.
Inattention has been shown to be the cardinal feature for delirium,40 and its assessment using cognitive testing has been recommended to help identify the presence of delirium according to an expert consensus panel.26 The diagnostic performance of the MOTYB-12 observed in our study is similar to a study by Fick et al., who reported that MOTYB-12 had very good sensitivity (83%) but had modest specificity (69%) with a cutoff of 1 or more errors. Hendry et al. observed that the MOTYB-12 was 91% sensitive and 50% specific using a cutoff of 4 or more errors. With regard to the MOTYB-6, our reported specificity was different from what was observed by O’Regan et al.27 Using 1 or more errors as a cutoff, they observed a much higher specificity for delirium than we did (90% vs 57%). Discordant observations regarding the diagnostic accuracy for other inattention tasks also exist. We observed that making any error on the days of the week backwards task was 84% sensitive and 82% specific for delirium, whereas Fick et al. observed a sensitivity and specificity of 50% and 94%, respectively. For the vigilance “A” task, we observed that making 2 or more errors over a series of 10 letters was 64.0% sensitive and 91.4% specific for delirium, whereas Pompei et al.41 observed that making 2 or more errors over a series of 60 letters was 51% sensitive and 77% specific for delirium.
The abovementioned discordant findings may be driven by spectrum bias, wherein the sensitivities and specificities for each inattention task may differ in different subgroups. As a result, differences in the age distribution, proportion of college graduates, history of dementia, and susceptibility to delirium can influence overall sensitivity and specificity. Objective measures of delirium, including the inattention screens studied, are particularly prone to spectrum bias.31,34 However, the strength of this approach is that the assessment of inattention becomes less reliant upon clinical judgment and allows it to be used by raters from a wide range of clinical backgrounds. On the other hand, a subjective interpretation of these inattention tasks may allow the rater to capture the subtleties of inattention (ie, decreased speed of performance in a highly intelligent and well-educated patient without dementia). The disadvantage of this approach, however, is that it is more dependent on clinical judgment and may have decreased diagnostic accuracy in those with less clinical experience or with limited training.14,42,43 These factors must be carefully considered when determining which delirium assessment to use.
Additional research is required to determine the clinical utility of these brief inattention assessments. These findings need to be further validated in larger studies, and the optimal cutoff of each task for different subgroup of patients (eg, demented vs nondemented) needs to be further clarified. It is not completely clear whether these inattention tests can serve as standalone assessments. Depending on the cutoff used, some of these assessments may have unacceptable false negative or false positive rates that may lead to increased adverse patient outcomes or increased resource utilization, respectively. Additional components or assessments may be needed to improve the diagnostic accuracy of these assessments. In addition to understanding these inattention assessments’ diagnostic accuracies, their ability to predict adverse outcomes also needs to be investigated. While a previous study observed that making any error on the MOTYB-12 task was associated with increased physical restraint use and prolonged hospital length of stay,44 these assessments’ ability to prognosticate long-term outcomes such as mortality or long-term cognition or function need to be studied. Lastly, studies should also evaluate how easily implementable these assessments are and whether improved delirium recognition leads to improved patient outcomes.
This study has several notable limitations. Though planned a priori, this was a secondary analysis of a larger investigation designed to validate 3 delirium assessments. Our sample size was also relatively small, causing our 95% CIs to overlap in most cases and limiting the statistical power to truly determine whether one measure is better than the other. We also asked the patient to recite the months backwards from December to July as well as recite the months backwards from December to January. It is possible that the patient may have performed better at going from December to January because of learning effect. Our reference standard for delirium was based upon DSM-IV-TR criteria. The new DSM-V criteria may be more restrictive and may slightly change the sensitivities and specificities of the inattention tasks. We enrolled a convenience sample and enrolled patients who were more likely to be male, have cardiovascular chief complaints, and be admitted to the hospital; as a result, selection bias may have been introduced. Lastly, this study was conducted in a single center and enrolled patients who were 65 years and older. Our findings may not be generalizable to other settings and in those who are less than 65 years of age.
CONCLUSIONS
The MOTYB-6 and MOTYB-12 tasks had very good sensitivities but modest specificities (approximately 50%) using any error made as a cutoff; increasing cutoff to 2 errors and 3 errors, respectively, improved their specificities (approximately 70%) with minimal impact to their sensitivities. Reciting the days of the week backwards, spelling the word “LUNCH” backwards, and the 10-letter vigilance “A” task appeared to perform the best in ruling out delirium but only moderately decreased the likelihood of delirium. The 10-letter Vigilance “A” and picture recognition task
Disclosure
This study was funded by the Emergency Medicine Foundation Career Development Award, National Institutes of Health K23AG032355, and National Center for Research Resources, Grant UL1 RR024975-01. The authors report no financial conflicts of interest.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association; 2013.
33. Hamrick I, Hafiz R, Cummings DM. Use of days of the week in a modified mini-mental state exam (M-MMSE) for detecting geriatric cognitive impairment. J Am Board Fam Med. 2013;26(4):429-435.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association; 2013.
33. Hamrick I, Hafiz R, Cummings DM. Use of days of the week in a modified mini-mental state exam (M-MMSE) for detecting geriatric cognitive impairment. J Am Board Fam Med. 2013;26(4):429-435.
© 2018 Society of Hospital Medicine