User login
Filling a Gender Gap in Research
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
ICER assesses value of CAR T-cell therapies

The Institute for Clinical and Economic Review (ICER) has made policy recommendations intended to ensure affordability and access to chimeric antigen receptor (CAR) T-cell therapies.
ICER released a Final Evidence Report on tisagenlecleucel (Kymriah, Novartis) and axicabtagene ciloleucel (Yescarta, Kite Pharma/Gilead), 2 CAR T-cell therapies approved in the US to treat B-cell acute lymphoblastic leukemia (B-ALL) and non-Hodgkin lymphoma (NHL), respectively.
The report says the pricing of these therapies aligns with patient benefit, but changes will be needed in future pricing, payment, and delivery mechanisms to ensure patient access without threatening health system affordability.
“Given the currently available evidence, these therapies appear to be effective options for those with B-ALL or NHL, though uncertainty in the evidence raised questions around the long-term value for money,” said Dan Ollendorf, PhD, ICER’s chief scientific officer.
Net health benefit
ICER’s report says tisagenlecleucel provides a net health benefit for children with B-ALL, and both tisagenlecleucel and axicabtagene ciloleucel provide a net health benefit for adults with certain types of NHL. (Novartis is seeking approval for tisagenlecleucel in NHL).
The evidence suggests there is at least a small net health benefit of the CAR T-cell therapies compared to other therapies. The benefit may be substantial, but uncertainties remain.
The data show complete remission (CR), disease-free survival (DFS), and overall survival (OS) rates are superior for NHL patients who receive axicabtagene ciloleucel, compared to patients who receive standard chemoimmunotherapy regimens.
Similarly, B-ALL patients treated with tisagenlecleucel have superior CR, DFS, and OS rates to patients treated with standard therapies. CR and OS rates are also superior in NHL patients treated with tisagenlecleucel, but DFS has not been reported in this population.
The report says there is insufficient evidence to distinguish between the 2 CAR T-cell therapies for the treatment of NHL.
Toxicity and uncertainty
The report highlights the fact that cytokine release syndrome, neurological symptoms, and B-cell aplasia have been observed in patients who receive CAR T-cell therapies. However, these sometimes severe adverse events are generally “manageable.”
In addition to toxicity, the report highlights sources of uncertainty. These include the fact that studies of tisagenlecleucel and axicabtagene ciloleucel are small, single-arm trials with short follow-up; comparisons with historical controls may be misleading; and improvements in the CAR T-cell manufacturing process may change outcomes.
Cost-effectiveness
The report states that the cost-effectiveness of each therapy fell below or within commonly cited thresholds of $50,000 to $150,000 per quality-adjusted life-year (QALY) over a lifetime.
For its analyses, ICER used the wholesale acquisition cost (WAC) plus an assumed hospital mark-up. The analyses were also based on the assumption that survival benefits observed in clinical trials would continue after the trials ended.
For tisagenlecleucel in pediatric B-ALL, the WAC is $475,000. The long-term cost-effectiveness compared to clofarabine is $45,871 per QALY gained.
For axicabtagene ciloleucel in adults with NHL, the WAC is $373,000. The long-term cost-effectiveness compared to salvage chemotherapy is $136,078 per QALY gained. The effectiveness assumptions for chemotherapy were based on an average of salvage chemotherapy regimens from the SCHOLAR-1 trial, and the cost assumptions were based on the cost of the R-DHAP (rituximab, dexamethasone, cytarabine, and cisplatin) regimen.
The report says tisagenlecleucel’s price would remain in alignment with value even if price premiums of 102% to 194% were applied.
Meanwhile, axicabtagene ciloleucel’s price could be increased by up to 11% and remain in alignment with the upper threshold ($150,000 per QALY gained) but would need to be discounted by 28% to align with the lower threshold ($100,000 per QALY gained).
Tisagenlecleucel, as a treatment for B-ALL, is not expected to cross the $915 million threshold for annual budget impact.
However, the short-term costs of axicabtagene ciloleucel for relapsed/refractory NHL could exceed the threshold. Only 38% of the estimated 5900 eligible patients could receive axicabtagene ciloleucel in a year before crossing the threshold.
Because of these findings, ICER issued an “Affordability and Access Alert” for axicabtagene ciloleucel.
This alert is intended to signal when the added costs associated with a new treatment may be difficult for the healthcare system to absorb over the short-term without displacing other needed services or contributing to unsustainable growth in healthcare insurance costs.
“Based on current evidence, both therapies appear to be priced in alignment with their clinical value, but there are potential short-term affordability concerns—for axicabtagene ciloleucel under its current indication and for both treatments should they receive future approvals for broader patient populations,” Dr Ollendorf said.
Panel voting results
ICER’s report was reviewed at a public meeting of the California Technology Assessment Forum on March 2.
Most of the panel said tisagenlecleucel provides intermediate long-term value for money when treating B-ALL. However, the significant uncertainty surrounding the long-term risks and benefits of the therapy precluded a high-value vote.
After deliberating on the value of axicabtagene ciloleucel to treat NHL, the panel’s votes were split between low-value and intermediate-value, driven by similar concerns about long-term uncertainty.
Policy recommendations
Following the voting session, ICER convened a policy roundtable of experts, including physicians, patient advocates, manufacturer representatives, and payer representatives.
Based on the roundtable discussion, ICER developed recommendations for enhanced stakeholder communication, innovative payment models, generation of additional evidence, settings of care, and patient education.
“With many other potentially transformative therapies in the pipeline, stakeholders must collaborate now to develop payment and delivery systems that can ensure timely patient access, manage short-term affordability for expensive one-time treatments, and continue to reward the innovation that brings these new treatments to market,” Dr Ollendorf said.
Some of ICER’s recommendations include:
- When launching novel therapies approved with limited clinical evidence, such as CAR T-cell therapies, manufacturers and payers should consider using a lower launch price that could be increased if substantial clinical benefits are confirmed or using a higher initial price tied to a requirement for refunds or rebates if real-world evidence fails to confirm high expectations.
- Outcomes-based pricing arrangements must be linked to “meaningful clinical outcomes assessed with sufficient follow up.”
- Hospital mark-up for CAR T-cell therapies “should reflect the expected additional cost for care delivered in the hospital, rather than a percentage of the drug cost to avoid perverse incentives in choosing the treatment location.”
- Initially, CAR T-cell therapies should be delivered in “manufacturer-accredited centers to ensure the quality and appropriateness of care.” Later, “centers of excellence accredited by specialty societies” can administer these therapies, as long as providers have “sufficient expertise” to manage serious side effects.
- Centers should ensure that patients understand what to expect from CAR T-cell therapy, including long-term consequences.
- Because additional evidence on CAR T-cell therapies is needed, all patients who receive these therapies should enter into a registry with planned long-term follow-up.
- Studies should determine the optimal timing of CAR T-cell therapy in the sequence of treatments for B-ALL and NHL.
Additional recommendations and more details are available in ICER’s report.
About ICER
ICER is an independent, non-profit research institute that produces reports analyzing evidence on the effectiveness and value of drugs and other medical services.
ICER’s reports include evidence-based calculations of prices for new drugs that reflect the degree of improvement expected in long-term patient outcomes, while also highlighting price levels that might contribute to unaffordable short-term cost growth for the overall healthcare system.
ICER’s reports incorporate input from stakeholders and are the subject of public hearings through 3 core programs: the California Technology Assessment Forum, the Midwest Comparative Effectiveness Public Advisory Council, and the New England Comparative Effectiveness Public Advisory Council.
These independent panels review ICER’s reports at public meetings to deliberate on the evidence and develop recommendations for how patients, clinicians, insurers, and policymakers can improve the quality and value of healthcare.
The Institute for Clinical and Economic Review (ICER) has made policy recommendations intended to ensure affordability and access to chimeric antigen receptor (CAR) T-cell therapies.
ICER released a Final Evidence Report on tisagenlecleucel (Kymriah, Novartis) and axicabtagene ciloleucel (Yescarta, Kite Pharma/Gilead), 2 CAR T-cell therapies approved in the US to treat B-cell acute lymphoblastic leukemia (B-ALL) and non-Hodgkin lymphoma (NHL), respectively.
The report says the pricing of these therapies aligns with patient benefit, but changes will be needed in future pricing, payment, and delivery mechanisms to ensure patient access without threatening health system affordability.
“Given the currently available evidence, these therapies appear to be effective options for those with B-ALL or NHL, though uncertainty in the evidence raised questions around the long-term value for money,” said Dan Ollendorf, PhD, ICER’s chief scientific officer.
Net health benefit
ICER’s report says tisagenlecleucel provides a net health benefit for children with B-ALL, and both tisagenlecleucel and axicabtagene ciloleucel provide a net health benefit for adults with certain types of NHL. (Novartis is seeking approval for tisagenlecleucel in NHL).
The evidence suggests there is at least a small net health benefit of the CAR T-cell therapies compared to other therapies. The benefit may be substantial, but uncertainties remain.
The data show complete remission (CR), disease-free survival (DFS), and overall survival (OS) rates are superior for NHL patients who receive axicabtagene ciloleucel, compared to patients who receive standard chemoimmunotherapy regimens.
Similarly, B-ALL patients treated with tisagenlecleucel have superior CR, DFS, and OS rates to patients treated with standard therapies. CR and OS rates are also superior in NHL patients treated with tisagenlecleucel, but DFS has not been reported in this population.
The report says there is insufficient evidence to distinguish between the 2 CAR T-cell therapies for the treatment of NHL.
Toxicity and uncertainty
The report highlights the fact that cytokine release syndrome, neurological symptoms, and B-cell aplasia have been observed in patients who receive CAR T-cell therapies. However, these sometimes severe adverse events are generally “manageable.”
In addition to toxicity, the report highlights sources of uncertainty. These include the fact that studies of tisagenlecleucel and axicabtagene ciloleucel are small, single-arm trials with short follow-up; comparisons with historical controls may be misleading; and improvements in the CAR T-cell manufacturing process may change outcomes.
Cost-effectiveness
The report states that the cost-effectiveness of each therapy fell below or within commonly cited thresholds of $50,000 to $150,000 per quality-adjusted life-year (QALY) over a lifetime.
For its analyses, ICER used the wholesale acquisition cost (WAC) plus an assumed hospital mark-up. The analyses were also based on the assumption that survival benefits observed in clinical trials would continue after the trials ended.
For tisagenlecleucel in pediatric B-ALL, the WAC is $475,000. The long-term cost-effectiveness compared to clofarabine is $45,871 per QALY gained.
For axicabtagene ciloleucel in adults with NHL, the WAC is $373,000. The long-term cost-effectiveness compared to salvage chemotherapy is $136,078 per QALY gained. The effectiveness assumptions for chemotherapy were based on an average of salvage chemotherapy regimens from the SCHOLAR-1 trial, and the cost assumptions were based on the cost of the R-DHAP (rituximab, dexamethasone, cytarabine, and cisplatin) regimen.
The report says tisagenlecleucel’s price would remain in alignment with value even if price premiums of 102% to 194% were applied.
Meanwhile, axicabtagene ciloleucel’s price could be increased by up to 11% and remain in alignment with the upper threshold ($150,000 per QALY gained) but would need to be discounted by 28% to align with the lower threshold ($100,000 per QALY gained).
Tisagenlecleucel, as a treatment for B-ALL, is not expected to cross the $915 million threshold for annual budget impact.
However, the short-term costs of axicabtagene ciloleucel for relapsed/refractory NHL could exceed the threshold. Only 38% of the estimated 5900 eligible patients could receive axicabtagene ciloleucel in a year before crossing the threshold.
Because of these findings, ICER issued an “Affordability and Access Alert” for axicabtagene ciloleucel.
This alert is intended to signal when the added costs associated with a new treatment may be difficult for the healthcare system to absorb over the short-term without displacing other needed services or contributing to unsustainable growth in healthcare insurance costs.
“Based on current evidence, both therapies appear to be priced in alignment with their clinical value, but there are potential short-term affordability concerns—for axicabtagene ciloleucel under its current indication and for both treatments should they receive future approvals for broader patient populations,” Dr Ollendorf said.
Panel voting results
ICER’s report was reviewed at a public meeting of the California Technology Assessment Forum on March 2.
Most of the panel said tisagenlecleucel provides intermediate long-term value for money when treating B-ALL. However, the significant uncertainty surrounding the long-term risks and benefits of the therapy precluded a high-value vote.
After deliberating on the value of axicabtagene ciloleucel to treat NHL, the panel’s votes were split between low-value and intermediate-value, driven by similar concerns about long-term uncertainty.
Policy recommendations
Following the voting session, ICER convened a policy roundtable of experts, including physicians, patient advocates, manufacturer representatives, and payer representatives.
Based on the roundtable discussion, ICER developed recommendations for enhanced stakeholder communication, innovative payment models, generation of additional evidence, settings of care, and patient education.
“With many other potentially transformative therapies in the pipeline, stakeholders must collaborate now to develop payment and delivery systems that can ensure timely patient access, manage short-term affordability for expensive one-time treatments, and continue to reward the innovation that brings these new treatments to market,” Dr Ollendorf said.
Some of ICER’s recommendations include:
- When launching novel therapies approved with limited clinical evidence, such as CAR T-cell therapies, manufacturers and payers should consider using a lower launch price that could be increased if substantial clinical benefits are confirmed or using a higher initial price tied to a requirement for refunds or rebates if real-world evidence fails to confirm high expectations.
- Outcomes-based pricing arrangements must be linked to “meaningful clinical outcomes assessed with sufficient follow up.”
- Hospital mark-up for CAR T-cell therapies “should reflect the expected additional cost for care delivered in the hospital, rather than a percentage of the drug cost to avoid perverse incentives in choosing the treatment location.”
- Initially, CAR T-cell therapies should be delivered in “manufacturer-accredited centers to ensure the quality and appropriateness of care.” Later, “centers of excellence accredited by specialty societies” can administer these therapies, as long as providers have “sufficient expertise” to manage serious side effects.
- Centers should ensure that patients understand what to expect from CAR T-cell therapy, including long-term consequences.
- Because additional evidence on CAR T-cell therapies is needed, all patients who receive these therapies should enter into a registry with planned long-term follow-up.
- Studies should determine the optimal timing of CAR T-cell therapy in the sequence of treatments for B-ALL and NHL.
Additional recommendations and more details are available in ICER’s report.
About ICER
ICER is an independent, non-profit research institute that produces reports analyzing evidence on the effectiveness and value of drugs and other medical services.
ICER’s reports include evidence-based calculations of prices for new drugs that reflect the degree of improvement expected in long-term patient outcomes, while also highlighting price levels that might contribute to unaffordable short-term cost growth for the overall healthcare system.
ICER’s reports incorporate input from stakeholders and are the subject of public hearings through 3 core programs: the California Technology Assessment Forum, the Midwest Comparative Effectiveness Public Advisory Council, and the New England Comparative Effectiveness Public Advisory Council.
These independent panels review ICER’s reports at public meetings to deliberate on the evidence and develop recommendations for how patients, clinicians, insurers, and policymakers can improve the quality and value of healthcare.
The Institute for Clinical and Economic Review (ICER) has made policy recommendations intended to ensure affordability and access to chimeric antigen receptor (CAR) T-cell therapies.
ICER released a Final Evidence Report on tisagenlecleucel (Kymriah, Novartis) and axicabtagene ciloleucel (Yescarta, Kite Pharma/Gilead), 2 CAR T-cell therapies approved in the US to treat B-cell acute lymphoblastic leukemia (B-ALL) and non-Hodgkin lymphoma (NHL), respectively.
The report says the pricing of these therapies aligns with patient benefit, but changes will be needed in future pricing, payment, and delivery mechanisms to ensure patient access without threatening health system affordability.
“Given the currently available evidence, these therapies appear to be effective options for those with B-ALL or NHL, though uncertainty in the evidence raised questions around the long-term value for money,” said Dan Ollendorf, PhD, ICER’s chief scientific officer.
Net health benefit
ICER’s report says tisagenlecleucel provides a net health benefit for children with B-ALL, and both tisagenlecleucel and axicabtagene ciloleucel provide a net health benefit for adults with certain types of NHL. (Novartis is seeking approval for tisagenlecleucel in NHL).
The evidence suggests there is at least a small net health benefit of the CAR T-cell therapies compared to other therapies. The benefit may be substantial, but uncertainties remain.
The data show complete remission (CR), disease-free survival (DFS), and overall survival (OS) rates are superior for NHL patients who receive axicabtagene ciloleucel, compared to patients who receive standard chemoimmunotherapy regimens.
Similarly, B-ALL patients treated with tisagenlecleucel have superior CR, DFS, and OS rates to patients treated with standard therapies. CR and OS rates are also superior in NHL patients treated with tisagenlecleucel, but DFS has not been reported in this population.
The report says there is insufficient evidence to distinguish between the 2 CAR T-cell therapies for the treatment of NHL.
Toxicity and uncertainty
The report highlights the fact that cytokine release syndrome, neurological symptoms, and B-cell aplasia have been observed in patients who receive CAR T-cell therapies. However, these sometimes severe adverse events are generally “manageable.”
In addition to toxicity, the report highlights sources of uncertainty. These include the fact that studies of tisagenlecleucel and axicabtagene ciloleucel are small, single-arm trials with short follow-up; comparisons with historical controls may be misleading; and improvements in the CAR T-cell manufacturing process may change outcomes.
Cost-effectiveness
The report states that the cost-effectiveness of each therapy fell below or within commonly cited thresholds of $50,000 to $150,000 per quality-adjusted life-year (QALY) over a lifetime.
For its analyses, ICER used the wholesale acquisition cost (WAC) plus an assumed hospital mark-up. The analyses were also based on the assumption that survival benefits observed in clinical trials would continue after the trials ended.
For tisagenlecleucel in pediatric B-ALL, the WAC is $475,000. The long-term cost-effectiveness compared to clofarabine is $45,871 per QALY gained.
For axicabtagene ciloleucel in adults with NHL, the WAC is $373,000. The long-term cost-effectiveness compared to salvage chemotherapy is $136,078 per QALY gained. The effectiveness assumptions for chemotherapy were based on an average of salvage chemotherapy regimens from the SCHOLAR-1 trial, and the cost assumptions were based on the cost of the R-DHAP (rituximab, dexamethasone, cytarabine, and cisplatin) regimen.
The report says tisagenlecleucel’s price would remain in alignment with value even if price premiums of 102% to 194% were applied.
Meanwhile, axicabtagene ciloleucel’s price could be increased by up to 11% and remain in alignment with the upper threshold ($150,000 per QALY gained) but would need to be discounted by 28% to align with the lower threshold ($100,000 per QALY gained).
Tisagenlecleucel, as a treatment for B-ALL, is not expected to cross the $915 million threshold for annual budget impact.
However, the short-term costs of axicabtagene ciloleucel for relapsed/refractory NHL could exceed the threshold. Only 38% of the estimated 5900 eligible patients could receive axicabtagene ciloleucel in a year before crossing the threshold.
Because of these findings, ICER issued an “Affordability and Access Alert” for axicabtagene ciloleucel.
This alert is intended to signal when the added costs associated with a new treatment may be difficult for the healthcare system to absorb over the short-term without displacing other needed services or contributing to unsustainable growth in healthcare insurance costs.
“Based on current evidence, both therapies appear to be priced in alignment with their clinical value, but there are potential short-term affordability concerns—for axicabtagene ciloleucel under its current indication and for both treatments should they receive future approvals for broader patient populations,” Dr Ollendorf said.
Panel voting results
ICER’s report was reviewed at a public meeting of the California Technology Assessment Forum on March 2.
Most of the panel said tisagenlecleucel provides intermediate long-term value for money when treating B-ALL. However, the significant uncertainty surrounding the long-term risks and benefits of the therapy precluded a high-value vote.
After deliberating on the value of axicabtagene ciloleucel to treat NHL, the panel’s votes were split between low-value and intermediate-value, driven by similar concerns about long-term uncertainty.
Policy recommendations
Following the voting session, ICER convened a policy roundtable of experts, including physicians, patient advocates, manufacturer representatives, and payer representatives.
Based on the roundtable discussion, ICER developed recommendations for enhanced stakeholder communication, innovative payment models, generation of additional evidence, settings of care, and patient education.
“With many other potentially transformative therapies in the pipeline, stakeholders must collaborate now to develop payment and delivery systems that can ensure timely patient access, manage short-term affordability for expensive one-time treatments, and continue to reward the innovation that brings these new treatments to market,” Dr Ollendorf said.
Some of ICER’s recommendations include:
- When launching novel therapies approved with limited clinical evidence, such as CAR T-cell therapies, manufacturers and payers should consider using a lower launch price that could be increased if substantial clinical benefits are confirmed or using a higher initial price tied to a requirement for refunds or rebates if real-world evidence fails to confirm high expectations.
- Outcomes-based pricing arrangements must be linked to “meaningful clinical outcomes assessed with sufficient follow up.”
- Hospital mark-up for CAR T-cell therapies “should reflect the expected additional cost for care delivered in the hospital, rather than a percentage of the drug cost to avoid perverse incentives in choosing the treatment location.”
- Initially, CAR T-cell therapies should be delivered in “manufacturer-accredited centers to ensure the quality and appropriateness of care.” Later, “centers of excellence accredited by specialty societies” can administer these therapies, as long as providers have “sufficient expertise” to manage serious side effects.
- Centers should ensure that patients understand what to expect from CAR T-cell therapy, including long-term consequences.
- Because additional evidence on CAR T-cell therapies is needed, all patients who receive these therapies should enter into a registry with planned long-term follow-up.
- Studies should determine the optimal timing of CAR T-cell therapy in the sequence of treatments for B-ALL and NHL.
Additional recommendations and more details are available in ICER’s report.
About ICER
ICER is an independent, non-profit research institute that produces reports analyzing evidence on the effectiveness and value of drugs and other medical services.
ICER’s reports include evidence-based calculations of prices for new drugs that reflect the degree of improvement expected in long-term patient outcomes, while also highlighting price levels that might contribute to unaffordable short-term cost growth for the overall healthcare system.
ICER’s reports incorporate input from stakeholders and are the subject of public hearings through 3 core programs: the California Technology Assessment Forum, the Midwest Comparative Effectiveness Public Advisory Council, and the New England Comparative Effectiveness Public Advisory Council.
These independent panels review ICER’s reports at public meetings to deliberate on the evidence and develop recommendations for how patients, clinicians, insurers, and policymakers can improve the quality and value of healthcare.
Leukemia research pioneer dies at 92
James F. Holland, MD, passed away last week, at the age of 92, due to complications of cardiovascular disease.
Dr Holland has been called a pioneer in the field of leukemia research.
He and his colleagues are credited with using combination chemotherapy to transform pediatric acute lymphoblastic leukemia from an incurable illness to one with a high survival rate.
Dr Holland and his colleagues also developed the 7+3 regimen—3 daily injections of daunorubicin and 7 days of intravenous cytarabine—for patients with acute myeloid leukemia.
Dr Holland was born on May 16, 1925, in Morristown, New Jersey. He graduated from Princeton University in 1944 and earned his medical degree from Columbia University College of Physicians and Surgeons in 1947.
Dr Holland was a captain in the US Army Medical Corps from 1949 to 1951. After that, he worked at Francis Delafield Hospital (which closed in 1975) in New York, New York. He joined the National Cancer Institute (NCI) in 1953. Two years later, he began working at Roswell Park Cancer Institute in Buffalo, New York.
Dr Holland became Roswell Park’s chief of medicine and director of the Cancer Clinical Research Center. But he continued to work with the NCI, conducting research as part of Acute Leukemia Group B, which later became Cancer and Leukemia Group B.
After spending a year on an oncology exchange program in the Soviet Union, Dr Holland started at Mount Sinai in New York, New York, in 1973. While there, he established the Department of Neoplastic Diseases at The Tisch Cancer Institute, Icahn School of Medicine.
Most recently, Dr Holland was a distinguished professor of neoplastic diseases at Mount Sinai. He saw patients but also conducted research on the human mammary tumor virus.
Dr Holland collaborated with Emil Frei III to publish the textbook Cancer Medicine, which is now in its ninth edition. Dr Holland served as president of the American Association for Cancer Research and the American Society of Clinical Oncology. He was a co-founder of the African Organization for Research and Training in Cancer as well.
Dr Holland was married to Jimmie C. Holland, MD, who is credited with founding the field of psycho-oncology. Jimmie passed away in December 2017. The couple is survived by 6 children and 9 grandchildren.
James F. Holland, MD, passed away last week, at the age of 92, due to complications of cardiovascular disease.
Dr Holland has been called a pioneer in the field of leukemia research.
He and his colleagues are credited with using combination chemotherapy to transform pediatric acute lymphoblastic leukemia from an incurable illness to one with a high survival rate.
Dr Holland and his colleagues also developed the 7+3 regimen—3 daily injections of daunorubicin and 7 days of intravenous cytarabine—for patients with acute myeloid leukemia.
Dr Holland was born on May 16, 1925, in Morristown, New Jersey. He graduated from Princeton University in 1944 and earned his medical degree from Columbia University College of Physicians and Surgeons in 1947.
Dr Holland was a captain in the US Army Medical Corps from 1949 to 1951. After that, he worked at Francis Delafield Hospital (which closed in 1975) in New York, New York. He joined the National Cancer Institute (NCI) in 1953. Two years later, he began working at Roswell Park Cancer Institute in Buffalo, New York.
Dr Holland became Roswell Park’s chief of medicine and director of the Cancer Clinical Research Center. But he continued to work with the NCI, conducting research as part of Acute Leukemia Group B, which later became Cancer and Leukemia Group B.
After spending a year on an oncology exchange program in the Soviet Union, Dr Holland started at Mount Sinai in New York, New York, in 1973. While there, he established the Department of Neoplastic Diseases at The Tisch Cancer Institute, Icahn School of Medicine.
Most recently, Dr Holland was a distinguished professor of neoplastic diseases at Mount Sinai. He saw patients but also conducted research on the human mammary tumor virus.
Dr Holland collaborated with Emil Frei III to publish the textbook Cancer Medicine, which is now in its ninth edition. Dr Holland served as president of the American Association for Cancer Research and the American Society of Clinical Oncology. He was a co-founder of the African Organization for Research and Training in Cancer as well.
Dr Holland was married to Jimmie C. Holland, MD, who is credited with founding the field of psycho-oncology. Jimmie passed away in December 2017. The couple is survived by 6 children and 9 grandchildren.
James F. Holland, MD, passed away last week, at the age of 92, due to complications of cardiovascular disease.
Dr Holland has been called a pioneer in the field of leukemia research.
He and his colleagues are credited with using combination chemotherapy to transform pediatric acute lymphoblastic leukemia from an incurable illness to one with a high survival rate.
Dr Holland and his colleagues also developed the 7+3 regimen—3 daily injections of daunorubicin and 7 days of intravenous cytarabine—for patients with acute myeloid leukemia.
Dr Holland was born on May 16, 1925, in Morristown, New Jersey. He graduated from Princeton University in 1944 and earned his medical degree from Columbia University College of Physicians and Surgeons in 1947.
Dr Holland was a captain in the US Army Medical Corps from 1949 to 1951. After that, he worked at Francis Delafield Hospital (which closed in 1975) in New York, New York. He joined the National Cancer Institute (NCI) in 1953. Two years later, he began working at Roswell Park Cancer Institute in Buffalo, New York.
Dr Holland became Roswell Park’s chief of medicine and director of the Cancer Clinical Research Center. But he continued to work with the NCI, conducting research as part of Acute Leukemia Group B, which later became Cancer and Leukemia Group B.
After spending a year on an oncology exchange program in the Soviet Union, Dr Holland started at Mount Sinai in New York, New York, in 1973. While there, he established the Department of Neoplastic Diseases at The Tisch Cancer Institute, Icahn School of Medicine.
Most recently, Dr Holland was a distinguished professor of neoplastic diseases at Mount Sinai. He saw patients but also conducted research on the human mammary tumor virus.
Dr Holland collaborated with Emil Frei III to publish the textbook Cancer Medicine, which is now in its ninth edition. Dr Holland served as president of the American Association for Cancer Research and the American Society of Clinical Oncology. He was a co-founder of the African Organization for Research and Training in Cancer as well.
Dr Holland was married to Jimmie C. Holland, MD, who is credited with founding the field of psycho-oncology. Jimmie passed away in December 2017. The couple is survived by 6 children and 9 grandchildren.
Product approved for hemophilia patients in Japan

Japan’s Ministry of Health, Labour and Welfare (MHLW) has approved the bispecific factor IXa- and factor X-directed antibody emicizumab (Hemlibra), according to Chugai Pharmaceutical Co., Ltd.
Emicizumab is now approved for use in Japan as routine prophylaxis to prevent or reduce the frequency of bleeding episodes in patients with hemophilia A and factor VIII inhibitors.
There are a few conditions for this approval, including requirements for a risk management plan, early phase post-marketing vigilance, and post-marketing drug use surveillance.
A risk management plan is intended to assess measures for appropriate management of the risks associated with a drug, either at regular intervals or in response to the progress of post-marketing surveillance.
According to Japan’s Pharmaceuticals and Medical Devices Agency, a risk management plan must consist of 3 elements:
- Safety specification—Important adverse drug reactions and missing information
- Pharmacovigilance activities—Information collection activities performed in the post-marketing period
- Risk-minimization activities—Safety measures taken to minimize risks, which consists of providing information to healthcare professionals and setting the terms of use for a drug.
For the early phase post-marketing vigilance requirement, Chugai must provide safety information to healthcare professionals and collect information on adverse reactions to emicizumab in the early post-marketing phase.
Post-marketing drug use surveillance for emicizumab will include all patients receiving the product and is scheduled to continue until data is collected from approximately 100 people. The goal is to understand background information on patients receiving emicizumab, as well as to collect safety and efficacy data on the product and take necessary measures for the appropriate use of emicizumab.
The data collected via this surveillance effort will be reviewed to determine whether new surveillance or further safety measures are needed. Results of the surveillance will be reported to the regulatory authorities, and the data will be presented at scientific meetings, according to Chugai.
Phase 3 studies
The MHLW’s approval of emicizumab is based on data from a pair of phase 3 studies—HAVEN 1 and HAVEN 2.
Results from HAVEN 1 were published in NEJM and presented at the 26th ISTH Congress in July 2017. Updated results from HAVEN 2 were presented at the 2017 ASH Annual Meeting in December.
HAVEN 1
This study enrolled 109 patients (age 12 and older) with hemophilia A and factor VIII inhibitors who were previously treated with bypassing agents (BPAs) on-demand or as prophylaxis.
The patients were randomized to receive emicizumab prophylaxis or no prophylaxis. On-demand treatment of breakthrough bleeds with BPAs was allowed.
There was a significant reduction in treated bleeds of 87% with emicizumab prophylaxis compared to no prophylaxis (95% CI: 72.3; 94.3, P<0.0001). And there was an 80% reduction in all bleeds with emicizumab (95% CI: 62.5; 89.8, P<0.0001).
Adverse events (AEs) occurring in at least 5% of patients treated with emicizumab were local injection site reactions, headache, fatigue, upper respiratory tract infection, and arthralgia.
Two patients experienced thromboembolic events (TEs). Three had thrombotic microangiopathy (TMA) while receiving emicizumab prophylaxis and more than 100 u/kg/day of activated prothrombin complex concentrate, on average, for 24 hours or more before the event. Two of these patients had also received recombinant factor VIIa.
Neither TE required anticoagulation therapy, and 1 patient restarted emicizumab. The cases of TMA observed were transient, and 1 patient restarted emicizumab.
HAVEN 2
In this single-arm trial, researchers evaluated emicizumab prophylaxis in 60 patients, ages 1 to 17, who had hemophilia A with factor VIII inhibitors.
The efficacy analysis included 57 patients who were younger than 12. The 3 older patients were only included in the safety analysis.
Of the 57 patients, 64.9% had 0 bleeds, 94.7% had 0 treated bleeds, and 98.2% had 0 treated spontaneous bleeds and 0 treated joint bleeds. None of the patients had treated target joint bleeds.
Forty patients had a total of 201 AEs. The most common of these were viral upper respiratory tract infections (16.7%) and injection site reactions (16.7%).
There were no TEs or TMA events, and none of the patients tested positive for anti-drug antibodies. None of the 7 serious AEs in this trial were considered treatment-related.
Japan’s Ministry of Health, Labour and Welfare (MHLW) has approved the bispecific factor IXa- and factor X-directed antibody emicizumab (Hemlibra), according to Chugai Pharmaceutical Co., Ltd.
Emicizumab is now approved for use in Japan as routine prophylaxis to prevent or reduce the frequency of bleeding episodes in patients with hemophilia A and factor VIII inhibitors.
There are a few conditions for this approval, including requirements for a risk management plan, early phase post-marketing vigilance, and post-marketing drug use surveillance.
A risk management plan is intended to assess measures for appropriate management of the risks associated with a drug, either at regular intervals or in response to the progress of post-marketing surveillance.
According to Japan’s Pharmaceuticals and Medical Devices Agency, a risk management plan must consist of 3 elements:
- Safety specification—Important adverse drug reactions and missing information
- Pharmacovigilance activities—Information collection activities performed in the post-marketing period
- Risk-minimization activities—Safety measures taken to minimize risks, which consists of providing information to healthcare professionals and setting the terms of use for a drug.
For the early phase post-marketing vigilance requirement, Chugai must provide safety information to healthcare professionals and collect information on adverse reactions to emicizumab in the early post-marketing phase.
Post-marketing drug use surveillance for emicizumab will include all patients receiving the product and is scheduled to continue until data is collected from approximately 100 people. The goal is to understand background information on patients receiving emicizumab, as well as to collect safety and efficacy data on the product and take necessary measures for the appropriate use of emicizumab.
The data collected via this surveillance effort will be reviewed to determine whether new surveillance or further safety measures are needed. Results of the surveillance will be reported to the regulatory authorities, and the data will be presented at scientific meetings, according to Chugai.
Phase 3 studies
The MHLW’s approval of emicizumab is based on data from a pair of phase 3 studies—HAVEN 1 and HAVEN 2.
Results from HAVEN 1 were published in NEJM and presented at the 26th ISTH Congress in July 2017. Updated results from HAVEN 2 were presented at the 2017 ASH Annual Meeting in December.
HAVEN 1
This study enrolled 109 patients (age 12 and older) with hemophilia A and factor VIII inhibitors who were previously treated with bypassing agents (BPAs) on-demand or as prophylaxis.
The patients were randomized to receive emicizumab prophylaxis or no prophylaxis. On-demand treatment of breakthrough bleeds with BPAs was allowed.
There was a significant reduction in treated bleeds of 87% with emicizumab prophylaxis compared to no prophylaxis (95% CI: 72.3; 94.3, P<0.0001). And there was an 80% reduction in all bleeds with emicizumab (95% CI: 62.5; 89.8, P<0.0001).
Adverse events (AEs) occurring in at least 5% of patients treated with emicizumab were local injection site reactions, headache, fatigue, upper respiratory tract infection, and arthralgia.
Two patients experienced thromboembolic events (TEs). Three had thrombotic microangiopathy (TMA) while receiving emicizumab prophylaxis and more than 100 u/kg/day of activated prothrombin complex concentrate, on average, for 24 hours or more before the event. Two of these patients had also received recombinant factor VIIa.
Neither TE required anticoagulation therapy, and 1 patient restarted emicizumab. The cases of TMA observed were transient, and 1 patient restarted emicizumab.
HAVEN 2
In this single-arm trial, researchers evaluated emicizumab prophylaxis in 60 patients, ages 1 to 17, who had hemophilia A with factor VIII inhibitors.
The efficacy analysis included 57 patients who were younger than 12. The 3 older patients were only included in the safety analysis.
Of the 57 patients, 64.9% had 0 bleeds, 94.7% had 0 treated bleeds, and 98.2% had 0 treated spontaneous bleeds and 0 treated joint bleeds. None of the patients had treated target joint bleeds.
Forty patients had a total of 201 AEs. The most common of these were viral upper respiratory tract infections (16.7%) and injection site reactions (16.7%).
There were no TEs or TMA events, and none of the patients tested positive for anti-drug antibodies. None of the 7 serious AEs in this trial were considered treatment-related.
Japan’s Ministry of Health, Labour and Welfare (MHLW) has approved the bispecific factor IXa- and factor X-directed antibody emicizumab (Hemlibra), according to Chugai Pharmaceutical Co., Ltd.
Emicizumab is now approved for use in Japan as routine prophylaxis to prevent or reduce the frequency of bleeding episodes in patients with hemophilia A and factor VIII inhibitors.
There are a few conditions for this approval, including requirements for a risk management plan, early phase post-marketing vigilance, and post-marketing drug use surveillance.
A risk management plan is intended to assess measures for appropriate management of the risks associated with a drug, either at regular intervals or in response to the progress of post-marketing surveillance.
According to Japan’s Pharmaceuticals and Medical Devices Agency, a risk management plan must consist of 3 elements:
- Safety specification—Important adverse drug reactions and missing information
- Pharmacovigilance activities—Information collection activities performed in the post-marketing period
- Risk-minimization activities—Safety measures taken to minimize risks, which consists of providing information to healthcare professionals and setting the terms of use for a drug.
For the early phase post-marketing vigilance requirement, Chugai must provide safety information to healthcare professionals and collect information on adverse reactions to emicizumab in the early post-marketing phase.
Post-marketing drug use surveillance for emicizumab will include all patients receiving the product and is scheduled to continue until data is collected from approximately 100 people. The goal is to understand background information on patients receiving emicizumab, as well as to collect safety and efficacy data on the product and take necessary measures for the appropriate use of emicizumab.
The data collected via this surveillance effort will be reviewed to determine whether new surveillance or further safety measures are needed. Results of the surveillance will be reported to the regulatory authorities, and the data will be presented at scientific meetings, according to Chugai.
Phase 3 studies
The MHLW’s approval of emicizumab is based on data from a pair of phase 3 studies—HAVEN 1 and HAVEN 2.
Results from HAVEN 1 were published in NEJM and presented at the 26th ISTH Congress in July 2017. Updated results from HAVEN 2 were presented at the 2017 ASH Annual Meeting in December.
HAVEN 1
This study enrolled 109 patients (age 12 and older) with hemophilia A and factor VIII inhibitors who were previously treated with bypassing agents (BPAs) on-demand or as prophylaxis.
The patients were randomized to receive emicizumab prophylaxis or no prophylaxis. On-demand treatment of breakthrough bleeds with BPAs was allowed.
There was a significant reduction in treated bleeds of 87% with emicizumab prophylaxis compared to no prophylaxis (95% CI: 72.3; 94.3, P<0.0001). And there was an 80% reduction in all bleeds with emicizumab (95% CI: 62.5; 89.8, P<0.0001).
Adverse events (AEs) occurring in at least 5% of patients treated with emicizumab were local injection site reactions, headache, fatigue, upper respiratory tract infection, and arthralgia.
Two patients experienced thromboembolic events (TEs). Three had thrombotic microangiopathy (TMA) while receiving emicizumab prophylaxis and more than 100 u/kg/day of activated prothrombin complex concentrate, on average, for 24 hours or more before the event. Two of these patients had also received recombinant factor VIIa.
Neither TE required anticoagulation therapy, and 1 patient restarted emicizumab. The cases of TMA observed were transient, and 1 patient restarted emicizumab.
HAVEN 2
In this single-arm trial, researchers evaluated emicizumab prophylaxis in 60 patients, ages 1 to 17, who had hemophilia A with factor VIII inhibitors.
The efficacy analysis included 57 patients who were younger than 12. The 3 older patients were only included in the safety analysis.
Of the 57 patients, 64.9% had 0 bleeds, 94.7% had 0 treated bleeds, and 98.2% had 0 treated spontaneous bleeds and 0 treated joint bleeds. None of the patients had treated target joint bleeds.
Forty patients had a total of 201 AEs. The most common of these were viral upper respiratory tract infections (16.7%) and injection site reactions (16.7%).
There were no TEs or TMA events, and none of the patients tested positive for anti-drug antibodies. None of the 7 serious AEs in this trial were considered treatment-related.
FDA clears software for immunohematology labs

The US Food and Drug Administration (FDA) has granted 510(k) clearance for ORTHO CONNECT V2.0, a software system developed by Ortho Clinical Diagnostics.
ORTHO CONNECT V2.0 is middleware designed to keep large quantities of data accessible and consistent across multiple instruments and laboratory systems.
ORTHO CONNECT V2.0 works with other products Ortho Clinical Diagnostics has developed for immunohematology labs.
The software is now available for purchase in the US.
According to Ortho Clinical Diagnostics, ORTHO CONNECT V2.0 is comprehensive, integrated, and customizable middleware (software that acts as a bridge between an operating system or database and application).
ORTHO CONNECT V2.0 centralizes laboratory operations and workflow across hospitals and networks, allowing blood banks and their data to be managed through one central terminal. The software can link all Ortho Clinical Diagnostics instruments to lab information systems through a single interface.
Acting as an intermediary between instruments and lab information systems, ORTHO CONNECT V2.0 allows labs to exchange data, perform data management, and complete regulatory process tasks that are not easily performed alone. All test results on connected analyzers can be viewed and verified no matter the location.
ORTHO CONNECT V2.0 enables the ORTHO VISION® and ORTHO VISION® Max immunohematology analyzers, which test blood for transfusion compatibility, to integrate with a hospital’s laboratory information systems through a single validated connection to exchange data and simplify processes.
“Ortho [Clinical Diagnostics] is focused on diminishing the complexities of immunohematology testing while improving safety, speed, and efficiency throughout the blood bank,” said Robert Yates, the company’s chief operating officer.
“ORTHO CONNECT does just that, bringing improved functionality to laboratory information systems that are often relatively rigid and outdated. It’s the perfect complement to our ORTHO VISION platform of analyzers.”
The US Food and Drug Administration (FDA) has granted 510(k) clearance for ORTHO CONNECT V2.0, a software system developed by Ortho Clinical Diagnostics.
ORTHO CONNECT V2.0 is middleware designed to keep large quantities of data accessible and consistent across multiple instruments and laboratory systems.
ORTHO CONNECT V2.0 works with other products Ortho Clinical Diagnostics has developed for immunohematology labs.
The software is now available for purchase in the US.
According to Ortho Clinical Diagnostics, ORTHO CONNECT V2.0 is comprehensive, integrated, and customizable middleware (software that acts as a bridge between an operating system or database and application).
ORTHO CONNECT V2.0 centralizes laboratory operations and workflow across hospitals and networks, allowing blood banks and their data to be managed through one central terminal. The software can link all Ortho Clinical Diagnostics instruments to lab information systems through a single interface.
Acting as an intermediary between instruments and lab information systems, ORTHO CONNECT V2.0 allows labs to exchange data, perform data management, and complete regulatory process tasks that are not easily performed alone. All test results on connected analyzers can be viewed and verified no matter the location.
ORTHO CONNECT V2.0 enables the ORTHO VISION® and ORTHO VISION® Max immunohematology analyzers, which test blood for transfusion compatibility, to integrate with a hospital’s laboratory information systems through a single validated connection to exchange data and simplify processes.
“Ortho [Clinical Diagnostics] is focused on diminishing the complexities of immunohematology testing while improving safety, speed, and efficiency throughout the blood bank,” said Robert Yates, the company’s chief operating officer.
“ORTHO CONNECT does just that, bringing improved functionality to laboratory information systems that are often relatively rigid and outdated. It’s the perfect complement to our ORTHO VISION platform of analyzers.”
The US Food and Drug Administration (FDA) has granted 510(k) clearance for ORTHO CONNECT V2.0, a software system developed by Ortho Clinical Diagnostics.
ORTHO CONNECT V2.0 is middleware designed to keep large quantities of data accessible and consistent across multiple instruments and laboratory systems.
ORTHO CONNECT V2.0 works with other products Ortho Clinical Diagnostics has developed for immunohematology labs.
The software is now available for purchase in the US.
According to Ortho Clinical Diagnostics, ORTHO CONNECT V2.0 is comprehensive, integrated, and customizable middleware (software that acts as a bridge between an operating system or database and application).
ORTHO CONNECT V2.0 centralizes laboratory operations and workflow across hospitals and networks, allowing blood banks and their data to be managed through one central terminal. The software can link all Ortho Clinical Diagnostics instruments to lab information systems through a single interface.
Acting as an intermediary between instruments and lab information systems, ORTHO CONNECT V2.0 allows labs to exchange data, perform data management, and complete regulatory process tasks that are not easily performed alone. All test results on connected analyzers can be viewed and verified no matter the location.
ORTHO CONNECT V2.0 enables the ORTHO VISION® and ORTHO VISION® Max immunohematology analyzers, which test blood for transfusion compatibility, to integrate with a hospital’s laboratory information systems through a single validated connection to exchange data and simplify processes.
“Ortho [Clinical Diagnostics] is focused on diminishing the complexities of immunohematology testing while improving safety, speed, and efficiency throughout the blood bank,” said Robert Yates, the company’s chief operating officer.
“ORTHO CONNECT does just that, bringing improved functionality to laboratory information systems that are often relatively rigid and outdated. It’s the perfect complement to our ORTHO VISION platform of analyzers.”
Congressional budget includes AGA wins
AGA spends a lot of time on Capitol Hill advocating to help gastroenterologists in practice better care for their patients and receive fair reimbursement. Therefore, we were pleased that the budget deal passed by Congress and signed by the president in February included several policy victories that AGA has been working diligently on for many years.
IPAB repeal

AGA, and all of organized medicine, have long opposed the Independent Payment Advisory Board (IPAB) that was created as part of the Affordable Care Act. IPAB is an unelected, unaccountable board whose sole purpose is to cut Medicare spending from providers should Medicare reach a certain threshold of spending. Since hospitals are exempt from their purview, physicians would be particularly vulnerable to cuts. However, repealing IPAB has had bipartisan support over the years, and we applaud Congress for listening to us and the medical community and taking action.
Misvalued codes
AGA and the physician community were also successful in removing a provision that would have extended the misvalued codes initiative for the next two years to reallocate savings from potentially overvalued codes. AGA, the Alliance of Specialty Medicine and the AMA opposed the original provision expanding the misvalued codes initiative and have argued that virtually all codes under the fee schedule, including gastroenterology, have been reevaluated and have already faced significant cuts. In the final agreement, Congress eliminated recapturing savings from the misvalued codes initiative and instead lowered overall updates for physician reimbursement under Medicare by .25 percent for 1 year. Although AGA would prefer this reduction not be included, it is much better than the misvalued codes provision, which disproportionately impacts specialties, like gastroenterology.
Geographic Practice Cost Index
The budget agreement extends the work for the Geographic Practice Cost Index (GPCI) floor for two additional years, which avoids a decrease in Medicare reimbursement for physicians that practice in rural areas. The work GPCI is a variable that Medicare uses to adjust the work component of physician payment based on where they live. A work GPCI floor of 1.0 protects physicians in low-cost, often rural areas, from being paid less for the work they do.
Meaningful use standards
The package addresses electronic health record (EHR) standards and eases requirements for physicians. The language removes the mandate that meaningful use standards become more stringent over time, which is a major financial burden for physician practices. The language also gives physicians more time to submit and receive a hardship exemption from the current EHR standards that would apply to meaningful use and the Quality Payment Program’s advancing care information performance category.
Biosimilars coverage under Medicare Part D
The agreement also levels the playing field between biologics and biosimilars by adding biosimilars to the Medicare Coverage Gap Discount Program. Additionally, by providing the 50 percent discount equally, beneficiary out-of-pocket costs will be reduced and the Medicare program will save money as a result of covering the less expensive medication.
AGA and the medical community have fought long and hard for these provisions and are happy to see them finally being implemented. We thank all of our members who have worked along with us to ensure that the voice of gastroenterology continues to be heard on Capitol Hill.
AGA spends a lot of time on Capitol Hill advocating to help gastroenterologists in practice better care for their patients and receive fair reimbursement. Therefore, we were pleased that the budget deal passed by Congress and signed by the president in February included several policy victories that AGA has been working diligently on for many years.
IPAB repeal
AGA, and all of organized medicine, have long opposed the Independent Payment Advisory Board (IPAB) that was created as part of the Affordable Care Act. IPAB is an unelected, unaccountable board whose sole purpose is to cut Medicare spending from providers should Medicare reach a certain threshold of spending. Since hospitals are exempt from their purview, physicians would be particularly vulnerable to cuts. However, repealing IPAB has had bipartisan support over the years, and we applaud Congress for listening to us and the medical community and taking action.
Misvalued codes
AGA and the physician community were also successful in removing a provision that would have extended the misvalued codes initiative for the next two years to reallocate savings from potentially overvalued codes. AGA, the Alliance of Specialty Medicine and the AMA opposed the original provision expanding the misvalued codes initiative and have argued that virtually all codes under the fee schedule, including gastroenterology, have been reevaluated and have already faced significant cuts. In the final agreement, Congress eliminated recapturing savings from the misvalued codes initiative and instead lowered overall updates for physician reimbursement under Medicare by .25 percent for 1 year. Although AGA would prefer this reduction not be included, it is much better than the misvalued codes provision, which disproportionately impacts specialties, like gastroenterology.
Geographic Practice Cost Index
The budget agreement extends the work for the Geographic Practice Cost Index (GPCI) floor for two additional years, which avoids a decrease in Medicare reimbursement for physicians that practice in rural areas. The work GPCI is a variable that Medicare uses to adjust the work component of physician payment based on where they live. A work GPCI floor of 1.0 protects physicians in low-cost, often rural areas, from being paid less for the work they do.
Meaningful use standards
The package addresses electronic health record (EHR) standards and eases requirements for physicians. The language removes the mandate that meaningful use standards become more stringent over time, which is a major financial burden for physician practices. The language also gives physicians more time to submit and receive a hardship exemption from the current EHR standards that would apply to meaningful use and the Quality Payment Program’s advancing care information performance category.
Biosimilars coverage under Medicare Part D
The agreement also levels the playing field between biologics and biosimilars by adding biosimilars to the Medicare Coverage Gap Discount Program. Additionally, by providing the 50 percent discount equally, beneficiary out-of-pocket costs will be reduced and the Medicare program will save money as a result of covering the less expensive medication.
AGA and the medical community have fought long and hard for these provisions and are happy to see them finally being implemented. We thank all of our members who have worked along with us to ensure that the voice of gastroenterology continues to be heard on Capitol Hill.
AGA spends a lot of time on Capitol Hill advocating to help gastroenterologists in practice better care for their patients and receive fair reimbursement. Therefore, we were pleased that the budget deal passed by Congress and signed by the president in February included several policy victories that AGA has been working diligently on for many years.
IPAB repeal
AGA, and all of organized medicine, have long opposed the Independent Payment Advisory Board (IPAB) that was created as part of the Affordable Care Act. IPAB is an unelected, unaccountable board whose sole purpose is to cut Medicare spending from providers should Medicare reach a certain threshold of spending. Since hospitals are exempt from their purview, physicians would be particularly vulnerable to cuts. However, repealing IPAB has had bipartisan support over the years, and we applaud Congress for listening to us and the medical community and taking action.
Misvalued codes
AGA and the physician community were also successful in removing a provision that would have extended the misvalued codes initiative for the next two years to reallocate savings from potentially overvalued codes. AGA, the Alliance of Specialty Medicine and the AMA opposed the original provision expanding the misvalued codes initiative and have argued that virtually all codes under the fee schedule, including gastroenterology, have been reevaluated and have already faced significant cuts. In the final agreement, Congress eliminated recapturing savings from the misvalued codes initiative and instead lowered overall updates for physician reimbursement under Medicare by .25 percent for 1 year. Although AGA would prefer this reduction not be included, it is much better than the misvalued codes provision, which disproportionately impacts specialties, like gastroenterology.
Geographic Practice Cost Index
The budget agreement extends the work for the Geographic Practice Cost Index (GPCI) floor for two additional years, which avoids a decrease in Medicare reimbursement for physicians that practice in rural areas. The work GPCI is a variable that Medicare uses to adjust the work component of physician payment based on where they live. A work GPCI floor of 1.0 protects physicians in low-cost, often rural areas, from being paid less for the work they do.
Meaningful use standards
The package addresses electronic health record (EHR) standards and eases requirements for physicians. The language removes the mandate that meaningful use standards become more stringent over time, which is a major financial burden for physician practices. The language also gives physicians more time to submit and receive a hardship exemption from the current EHR standards that would apply to meaningful use and the Quality Payment Program’s advancing care information performance category.
Biosimilars coverage under Medicare Part D
The agreement also levels the playing field between biologics and biosimilars by adding biosimilars to the Medicare Coverage Gap Discount Program. Additionally, by providing the 50 percent discount equally, beneficiary out-of-pocket costs will be reduced and the Medicare program will save money as a result of covering the less expensive medication.
AGA and the medical community have fought long and hard for these provisions and are happy to see them finally being implemented. We thank all of our members who have worked along with us to ensure that the voice of gastroenterology continues to be heard on Capitol Hill.

In utero exposure to valproate and other AEDs linked to low test scores
In utero exposure to some antiepileptic drugs was linked to decreased educational achievement at the age of 7 years, in results of a matched-case control study.
Compared with controls, children exposed in the womb to sodium valproate alone, or to multiple antiepileptics (AEDs), had lower scores on U.K standardized tests routinely administered to 7-year-olds, according to results published in the Journal of Neurology, Neurosurgery & Psychiatry.
The results provide evidence showing that in utero exposure to some AEDs may lead to developmental issues in children, according to lead author Arron S. Lacey, Wales Epilepsy Research Network, Swansea University Medical School, Swansea, England, and coauthors.
“Women with epilepsy should be informed of this risk, and alternative treatment regimens should be discussed before their pregnancy with a physician that specializes in epilepsy,” Dr. Lacey concluded in a discussion of their study results.
In the United Kingdom, already-stringent guidance on valproate in pregnancy was strengthened on March 23 when the European Medicines Agency announced new measures designed to avoid valproate exposure in pregnancy because of risk of malformations and developmental issues. The measures include a ban on valproate-containing medicines for the treatment of epilepsy during pregnancy unless no other effective treatment is available.
The risks of AEDs, and valproate in particular, in pregnancy have been documented in multiple studies suggesting that exposure may lead to cognitive impairment, neurodevelopmental disorders, and impaired IQ. However, the available data are largely from psychometric studies, Dr. Lacey and colleagues noted in their report. “It is important to know whether the psychometric differences demonstrated in research conditions translate to children in the community,” they wrote.
To address this, Dr. Lacey and coinvestigators conducted a study of standardized academic test results in children in Wales born to mothers with epilepsy who had been prescribed AEDs during pregnancy. They reviewed health records and identified 440 AED-exposed children who had available results for Key Stage 1 tests for mathematics, language, and science at the age of 7 years.
Among children whose mothers had been prescribed valproate during pregnancy, the proportion achieving U.K. minimum standards for all subjects was 12.7% lower than a matched control group, investigators said.
Children of mothers who had been prescribed multiple AEDs had an even lower proportion achieving the minimum standard for all subjects, at 20.7% less than the control group, they added.
By contrast, children whose mothers were prescribed carbamazepine did not have any significant differences in educational achievement, compared with controls.
Some previous studies found as association between exposure to carbamazepine and cognitive impairment, while others found no such association. “Our study supports the latter, with no evidence of decreased educational attainment at school age,” the investigators said in their article.
Some study authors reported competing interests related to Eisai, Sanofi, UCB, and others.
SOURCE: Lacey AS et al. J Neurol Neurosurg Psychiatry. 2018 Mar 25. doi: 10.1136/jnnp-201-317515.
Performing a matched-case control study that links health records and national educational data is an innovative approach to assessing educational achievement in children born to mothers with epilepsy, according to Richard F.M. Chin, MD.
Lacey and colleagues demonstrated that in utero exposure to sodium valproate alone or antiepileptic drugs in combination was associated with significant decreases in educational achievement in national educational tests given to 7-year-old children, Dr Chin wrote in an editorial.
That finding may not seem new, given that multiple previous studies have linked in utero antiepileptic exposure to lower IQ, more frequent behavioral issues, and higher risk of psychiatric disorders. However, previous studies depended on detailed, resource-intensive, one-on-one assessments, or parent responses to questionnaires with potentially biased responses, Dr. Chin said. In contrast, Lacey and colleagues incorporating validated epilepsy diagnoses and made use of already available educational attainment data from the epilepsy cases and matched controls.
Because of that, their results may be more likely than previous studies to be representative of the general population, according to Dr. Chin.
“Such a relatively cost-effective and efficient approach has vast potential to be applicable for a number of other conditions and is at the heart of the emerging health informatics revolution,” he wrote.
Richard F.M. Chin is with the Muir Maxwell Epilepsy Centre, University of Edinburgh, Scotland. These comments are derived from his editorial published in the Journal of Neurology, Neurosurgery & Psychiatry (2018 Mar 25. doi: 10.1136/jnnp-2017-317924 ). Dr. Chin declared no competing interests related to the editorial.
Performing a matched-case control study that links health records and national educational data is an innovative approach to assessing educational achievement in children born to mothers with epilepsy, according to Richard F.M. Chin, MD.
Lacey and colleagues demonstrated that in utero exposure to sodium valproate alone or antiepileptic drugs in combination was associated with significant decreases in educational achievement in national educational tests given to 7-year-old children, Dr Chin wrote in an editorial.
That finding may not seem new, given that multiple previous studies have linked in utero antiepileptic exposure to lower IQ, more frequent behavioral issues, and higher risk of psychiatric disorders. However, previous studies depended on detailed, resource-intensive, one-on-one assessments, or parent responses to questionnaires with potentially biased responses, Dr. Chin said. In contrast, Lacey and colleagues incorporating validated epilepsy diagnoses and made use of already available educational attainment data from the epilepsy cases and matched controls.
Because of that, their results may be more likely than previous studies to be representative of the general population, according to Dr. Chin.
“Such a relatively cost-effective and efficient approach has vast potential to be applicable for a number of other conditions and is at the heart of the emerging health informatics revolution,” he wrote.
Richard F.M. Chin is with the Muir Maxwell Epilepsy Centre, University of Edinburgh, Scotland. These comments are derived from his editorial published in the Journal of Neurology, Neurosurgery & Psychiatry (2018 Mar 25. doi: 10.1136/jnnp-2017-317924 ). Dr. Chin declared no competing interests related to the editorial.
Performing a matched-case control study that links health records and national educational data is an innovative approach to assessing educational achievement in children born to mothers with epilepsy, according to Richard F.M. Chin, MD.
Lacey and colleagues demonstrated that in utero exposure to sodium valproate alone or antiepileptic drugs in combination was associated with significant decreases in educational achievement in national educational tests given to 7-year-old children, Dr Chin wrote in an editorial.
That finding may not seem new, given that multiple previous studies have linked in utero antiepileptic exposure to lower IQ, more frequent behavioral issues, and higher risk of psychiatric disorders. However, previous studies depended on detailed, resource-intensive, one-on-one assessments, or parent responses to questionnaires with potentially biased responses, Dr. Chin said. In contrast, Lacey and colleagues incorporating validated epilepsy diagnoses and made use of already available educational attainment data from the epilepsy cases and matched controls.
Because of that, their results may be more likely than previous studies to be representative of the general population, according to Dr. Chin.
“Such a relatively cost-effective and efficient approach has vast potential to be applicable for a number of other conditions and is at the heart of the emerging health informatics revolution,” he wrote.
Richard F.M. Chin is with the Muir Maxwell Epilepsy Centre, University of Edinburgh, Scotland. These comments are derived from his editorial published in the Journal of Neurology, Neurosurgery & Psychiatry (2018 Mar 25. doi: 10.1136/jnnp-2017-317924 ). Dr. Chin declared no competing interests related to the editorial.
In utero exposure to some antiepileptic drugs was linked to decreased educational achievement at the age of 7 years, in results of a matched-case control study.
Compared with controls, children exposed in the womb to sodium valproate alone, or to multiple antiepileptics (AEDs), had lower scores on U.K standardized tests routinely administered to 7-year-olds, according to results published in the Journal of Neurology, Neurosurgery & Psychiatry.
The results provide evidence showing that in utero exposure to some AEDs may lead to developmental issues in children, according to lead author Arron S. Lacey, Wales Epilepsy Research Network, Swansea University Medical School, Swansea, England, and coauthors.
“Women with epilepsy should be informed of this risk, and alternative treatment regimens should be discussed before their pregnancy with a physician that specializes in epilepsy,” Dr. Lacey concluded in a discussion of their study results.
In the United Kingdom, already-stringent guidance on valproate in pregnancy was strengthened on March 23 when the European Medicines Agency announced new measures designed to avoid valproate exposure in pregnancy because of risk of malformations and developmental issues. The measures include a ban on valproate-containing medicines for the treatment of epilepsy during pregnancy unless no other effective treatment is available.
The risks of AEDs, and valproate in particular, in pregnancy have been documented in multiple studies suggesting that exposure may lead to cognitive impairment, neurodevelopmental disorders, and impaired IQ. However, the available data are largely from psychometric studies, Dr. Lacey and colleagues noted in their report. “It is important to know whether the psychometric differences demonstrated in research conditions translate to children in the community,” they wrote.
To address this, Dr. Lacey and coinvestigators conducted a study of standardized academic test results in children in Wales born to mothers with epilepsy who had been prescribed AEDs during pregnancy. They reviewed health records and identified 440 AED-exposed children who had available results for Key Stage 1 tests for mathematics, language, and science at the age of 7 years.
Among children whose mothers had been prescribed valproate during pregnancy, the proportion achieving U.K. minimum standards for all subjects was 12.7% lower than a matched control group, investigators said.
Children of mothers who had been prescribed multiple AEDs had an even lower proportion achieving the minimum standard for all subjects, at 20.7% less than the control group, they added.
By contrast, children whose mothers were prescribed carbamazepine did not have any significant differences in educational achievement, compared with controls.
Some previous studies found as association between exposure to carbamazepine and cognitive impairment, while others found no such association. “Our study supports the latter, with no evidence of decreased educational attainment at school age,” the investigators said in their article.
Some study authors reported competing interests related to Eisai, Sanofi, UCB, and others.
SOURCE: Lacey AS et al. J Neurol Neurosurg Psychiatry. 2018 Mar 25. doi: 10.1136/jnnp-201-317515.
In utero exposure to some antiepileptic drugs was linked to decreased educational achievement at the age of 7 years, in results of a matched-case control study.
Compared with controls, children exposed in the womb to sodium valproate alone, or to multiple antiepileptics (AEDs), had lower scores on U.K standardized tests routinely administered to 7-year-olds, according to results published in the Journal of Neurology, Neurosurgery & Psychiatry.
The results provide evidence showing that in utero exposure to some AEDs may lead to developmental issues in children, according to lead author Arron S. Lacey, Wales Epilepsy Research Network, Swansea University Medical School, Swansea, England, and coauthors.
“Women with epilepsy should be informed of this risk, and alternative treatment regimens should be discussed before their pregnancy with a physician that specializes in epilepsy,” Dr. Lacey concluded in a discussion of their study results.
In the United Kingdom, already-stringent guidance on valproate in pregnancy was strengthened on March 23 when the European Medicines Agency announced new measures designed to avoid valproate exposure in pregnancy because of risk of malformations and developmental issues. The measures include a ban on valproate-containing medicines for the treatment of epilepsy during pregnancy unless no other effective treatment is available.
The risks of AEDs, and valproate in particular, in pregnancy have been documented in multiple studies suggesting that exposure may lead to cognitive impairment, neurodevelopmental disorders, and impaired IQ. However, the available data are largely from psychometric studies, Dr. Lacey and colleagues noted in their report. “It is important to know whether the psychometric differences demonstrated in research conditions translate to children in the community,” they wrote.
To address this, Dr. Lacey and coinvestigators conducted a study of standardized academic test results in children in Wales born to mothers with epilepsy who had been prescribed AEDs during pregnancy. They reviewed health records and identified 440 AED-exposed children who had available results for Key Stage 1 tests for mathematics, language, and science at the age of 7 years.
Among children whose mothers had been prescribed valproate during pregnancy, the proportion achieving U.K. minimum standards for all subjects was 12.7% lower than a matched control group, investigators said.
Children of mothers who had been prescribed multiple AEDs had an even lower proportion achieving the minimum standard for all subjects, at 20.7% less than the control group, they added.
By contrast, children whose mothers were prescribed carbamazepine did not have any significant differences in educational achievement, compared with controls.
Some previous studies found as association between exposure to carbamazepine and cognitive impairment, while others found no such association. “Our study supports the latter, with no evidence of decreased educational attainment at school age,” the investigators said in their article.
Some study authors reported competing interests related to Eisai, Sanofi, UCB, and others.
SOURCE: Lacey AS et al. J Neurol Neurosurg Psychiatry. 2018 Mar 25. doi: 10.1136/jnnp-201-317515.
FROM THE JOURNAL OF NEUROLOGY, NEUROSURGERY & PSYCHIATRY
Key clinical point: In utero exposure to sodium valproate or to multiple antiepileptic drugs was associated with decreased educational achievement at the age of 7 years.
Major finding: Compared with a control group, the proportion of 7-year-old students achieving U.K. minimum standards for all subjects was 12.7% lower in children born to mothers with epilepsy prescribed valproate during pregnancy.
Study details: An analysis of standardized national test scores for 440 U.K. children who had been born to mothers with epilepsy, compared with test scores for a matched control group.
Disclosures: Some study authors reported competing interests related to Eisai, Sanofi, UCB, and others.
Source: Lacey AS et al. J Neurol Neurosurg Psychiatry. 2018 Mar 25. doi: 10.1136/jnnp-201-317515.
Obesity in adults continues to rise
according to data from the National Health and Nutrition Examination Survey.
The age-standardized prevalence of obesity – defined as a body mass index of 30 or more – among adults aged 20 years and over increased from 33.7% for the 2-year period of 2007-2008 to 39.6% in 2015-2016, while the prevalence of severe obesity – defined as a body mass index of 40 kg/m2 or more – went from 5.7% to 7.7% over that same period, Craig M. Hales, MD, and his associates at the Centers for Disease Control and Prevention in Hyattsville, Md., and Atlanta said in a research letter published in JAMA.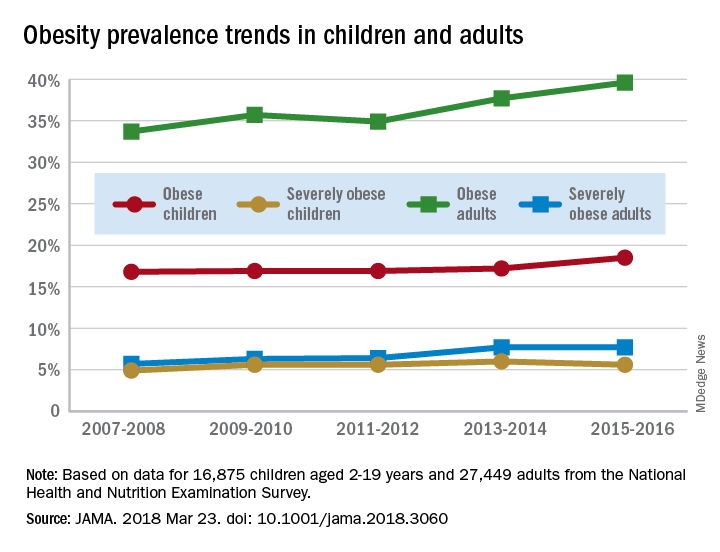
The prevalence of obesity in children aged 2-19 years – defined as BMI at or above the sex-specific 95th percentile – increased, but not significantly, from 16.8% in 2007-2008 to 18.5% in 2015-2016, with most of that increase coming in the last 2 years. Severe obesity – BMI at or above 120% of the sex-specific 95th percentile – rose from 4.9% to 5.6% over those 10 years, but the last 2-year period saw the rate drop from 6% in 2013-2014, the investigators reported.
For the most recent reporting period, boys were more likely than girls to be obese (19.1% vs. 17.8%) and severely obese (6.3% vs. 4.9%), and both obesity and severe obesity were more common with increasing age. Obesity prevalence went from 13.9% in those aged 2-5 years to 20.6% in 12- to 19-year-olds, and severe obesity was 1.8% in the youngest group and 7.7% in the oldest, with the middle-age group (6-11 years) in the middle in both categories, they said
Among the adults, obesity was more common in women than men (41.1% vs. 37.9%) for 2015-2016, as was severe obesity (9.7% vs. 5.6%). Obesity and severe obesity were both highest in those aged 40-59 years, but obesity prevalence was lowest in the younger group (20-39 years) and severe obesity was least common in the older group (60 years and older), Dr. Hales and his associates said.
The analysis involved 16,875 children and 27,449 adults over the 10-year period. The investigators did not report any conflicts of interest.
SOURCE: Hales CM et al. JAMA 2018 Mar 23. doi: 10.1001/jama.2018.3060.
according to data from the National Health and Nutrition Examination Survey.
The age-standardized prevalence of obesity – defined as a body mass index of 30 or more – among adults aged 20 years and over increased from 33.7% for the 2-year period of 2007-2008 to 39.6% in 2015-2016, while the prevalence of severe obesity – defined as a body mass index of 40 kg/m2 or more – went from 5.7% to 7.7% over that same period, Craig M. Hales, MD, and his associates at the Centers for Disease Control and Prevention in Hyattsville, Md., and Atlanta said in a research letter published in JAMA.
The prevalence of obesity in children aged 2-19 years – defined as BMI at or above the sex-specific 95th percentile – increased, but not significantly, from 16.8% in 2007-2008 to 18.5% in 2015-2016, with most of that increase coming in the last 2 years. Severe obesity – BMI at or above 120% of the sex-specific 95th percentile – rose from 4.9% to 5.6% over those 10 years, but the last 2-year period saw the rate drop from 6% in 2013-2014, the investigators reported.
For the most recent reporting period, boys were more likely than girls to be obese (19.1% vs. 17.8%) and severely obese (6.3% vs. 4.9%), and both obesity and severe obesity were more common with increasing age. Obesity prevalence went from 13.9% in those aged 2-5 years to 20.6% in 12- to 19-year-olds, and severe obesity was 1.8% in the youngest group and 7.7% in the oldest, with the middle-age group (6-11 years) in the middle in both categories, they said
Among the adults, obesity was more common in women than men (41.1% vs. 37.9%) for 2015-2016, as was severe obesity (9.7% vs. 5.6%). Obesity and severe obesity were both highest in those aged 40-59 years, but obesity prevalence was lowest in the younger group (20-39 years) and severe obesity was least common in the older group (60 years and older), Dr. Hales and his associates said.
The analysis involved 16,875 children and 27,449 adults over the 10-year period. The investigators did not report any conflicts of interest.
SOURCE: Hales CM et al. JAMA 2018 Mar 23. doi: 10.1001/jama.2018.3060.
according to data from the National Health and Nutrition Examination Survey.
The age-standardized prevalence of obesity – defined as a body mass index of 30 or more – among adults aged 20 years and over increased from 33.7% for the 2-year period of 2007-2008 to 39.6% in 2015-2016, while the prevalence of severe obesity – defined as a body mass index of 40 kg/m2 or more – went from 5.7% to 7.7% over that same period, Craig M. Hales, MD, and his associates at the Centers for Disease Control and Prevention in Hyattsville, Md., and Atlanta said in a research letter published in JAMA.
The prevalence of obesity in children aged 2-19 years – defined as BMI at or above the sex-specific 95th percentile – increased, but not significantly, from 16.8% in 2007-2008 to 18.5% in 2015-2016, with most of that increase coming in the last 2 years. Severe obesity – BMI at or above 120% of the sex-specific 95th percentile – rose from 4.9% to 5.6% over those 10 years, but the last 2-year period saw the rate drop from 6% in 2013-2014, the investigators reported.
For the most recent reporting period, boys were more likely than girls to be obese (19.1% vs. 17.8%) and severely obese (6.3% vs. 4.9%), and both obesity and severe obesity were more common with increasing age. Obesity prevalence went from 13.9% in those aged 2-5 years to 20.6% in 12- to 19-year-olds, and severe obesity was 1.8% in the youngest group and 7.7% in the oldest, with the middle-age group (6-11 years) in the middle in both categories, they said
Among the adults, obesity was more common in women than men (41.1% vs. 37.9%) for 2015-2016, as was severe obesity (9.7% vs. 5.6%). Obesity and severe obesity were both highest in those aged 40-59 years, but obesity prevalence was lowest in the younger group (20-39 years) and severe obesity was least common in the older group (60 years and older), Dr. Hales and his associates said.
The analysis involved 16,875 children and 27,449 adults over the 10-year period. The investigators did not report any conflicts of interest.
SOURCE: Hales CM et al. JAMA 2018 Mar 23. doi: 10.1001/jama.2018.3060.
FROM JAMA
Switching to tenofovir alafenamide may benefit HBV patients
PHILADELPHIA – Tenofovir alafenamide, the newest kid on the block for treatment of chronic hepatitis B, not only has less bone and renal effects than tenofovir disoproxil, but now also appears to improve those parameters in patients switched over from the older tenofovir formulation, according to Paul Kwo, MD.
“Renal function, as well as hip and spine bone mineral density measurements, all improve after you flip,” said Dr. Kwo, director of hepatology at Stanford (Calif.) University.

Dr. Kwo described some of the latest data on the newer tenofovir formulation in a hepatitis B update he gave at the conference, jointly provided by Rutgers and Global Academy for Medical Education.
Tenofovir alafenamide, a nucleoside analogue reverse transcriptase inhibitor, was approved in November 2016 for treatment of adults with chronic hepatitis B virus (HBV) infection and compensated liver disease.
It has similar efficacy to tenofovir disoproxil, with fewer bone and renal effects, according to results of two large international phase 3 trials.
Some of the latest data, presented in October 2017 at The Liver Meeting in Washington, show that switching patients from tenofovir disoproxil to tenofovir alafenamide improved creatinine clearance and increased rates of alanine aminotransferase normalization, with sustained rates of virologic control, over 48 weeks of treatment.
Similar results were seen for bone mineral density. “It goes up over time, and you approach bone mineral density levels that are similar to [levels in] those who are on tenofovir alafenamide long term,” Dr. Kwo said, commenting on results of the study.
Compared with tenofovir disoproxil, tenofovir alafenamide is a slightly different prodrug of tenofovir, according to Dr. Kwo.
The approved dose of tenofovir alafenamide is 25 mg, compared with 300 mg for tenofovir disoproxil. “It’s more stable in the serum, so you don’t need higher levels, and you have fewer off-target effects,” Dr. Kwo said.
The two agents are “Coke and Pepsi” in terms of efficacy, he added, noting that comparative studies showed similar efficacy on endpoints of percentage HBV DNA less than 29 IU/mL and log10 HBV DNA change.
Very low rates of resistance are seen with first-line therapies for chronic hepatitis B, including entecavir and tenofovir disoproxil. “We wouldn’t expect (tenofovir alafenamide) to be any different, but nonetheless the surveillance has to happen,” Dr. Kwo said.
Tenofovir alafenamide is not yet listed in the official recommendations of the American Association for the Study of Liver Diseases, but it is in current guidelines from the European Association for the Study of the Liver.
The published EASL guidelines provide guidance on how tenofovir alafenamide fits into the treatment armamentarium for HBV.
Going by the EASL recommendations, age greater than 60 years, bone disease, and renal alterations are all good reasons to use tenofovir alafenamide as first-line therapy for hepatitis B, according to Dr. Kwo.
Dr. Kwo reported disclosures related to AbbVie, Allergan, Bristol-Myers Squibb, Conatus Pharmaceuticals, Dova Pharmaceuticals, DURECT, Gilead Sciences, Merck, and Shionogi.
Global Academy and this news organization are owned by the same company.
PHILADELPHIA – Tenofovir alafenamide, the newest kid on the block for treatment of chronic hepatitis B, not only has less bone and renal effects than tenofovir disoproxil, but now also appears to improve those parameters in patients switched over from the older tenofovir formulation, according to Paul Kwo, MD.
“Renal function, as well as hip and spine bone mineral density measurements, all improve after you flip,” said Dr. Kwo, director of hepatology at Stanford (Calif.) University.
Dr. Kwo described some of the latest data on the newer tenofovir formulation in a hepatitis B update he gave at the conference, jointly provided by Rutgers and Global Academy for Medical Education.
Tenofovir alafenamide, a nucleoside analogue reverse transcriptase inhibitor, was approved in November 2016 for treatment of adults with chronic hepatitis B virus (HBV) infection and compensated liver disease.
It has similar efficacy to tenofovir disoproxil, with fewer bone and renal effects, according to results of two large international phase 3 trials.
Some of the latest data, presented in October 2017 at The Liver Meeting in Washington, show that switching patients from tenofovir disoproxil to tenofovir alafenamide improved creatinine clearance and increased rates of alanine aminotransferase normalization, with sustained rates of virologic control, over 48 weeks of treatment.
Similar results were seen for bone mineral density. “It goes up over time, and you approach bone mineral density levels that are similar to [levels in] those who are on tenofovir alafenamide long term,” Dr. Kwo said, commenting on results of the study.
Compared with tenofovir disoproxil, tenofovir alafenamide is a slightly different prodrug of tenofovir, according to Dr. Kwo.
The approved dose of tenofovir alafenamide is 25 mg, compared with 300 mg for tenofovir disoproxil. “It’s more stable in the serum, so you don’t need higher levels, and you have fewer off-target effects,” Dr. Kwo said.
The two agents are “Coke and Pepsi” in terms of efficacy, he added, noting that comparative studies showed similar efficacy on endpoints of percentage HBV DNA less than 29 IU/mL and log10 HBV DNA change.
Very low rates of resistance are seen with first-line therapies for chronic hepatitis B, including entecavir and tenofovir disoproxil. “We wouldn’t expect (tenofovir alafenamide) to be any different, but nonetheless the surveillance has to happen,” Dr. Kwo said.
Tenofovir alafenamide is not yet listed in the official recommendations of the American Association for the Study of Liver Diseases, but it is in current guidelines from the European Association for the Study of the Liver.
The published EASL guidelines provide guidance on how tenofovir alafenamide fits into the treatment armamentarium for HBV.
Going by the EASL recommendations, age greater than 60 years, bone disease, and renal alterations are all good reasons to use tenofovir alafenamide as first-line therapy for hepatitis B, according to Dr. Kwo.
Dr. Kwo reported disclosures related to AbbVie, Allergan, Bristol-Myers Squibb, Conatus Pharmaceuticals, Dova Pharmaceuticals, DURECT, Gilead Sciences, Merck, and Shionogi.
Global Academy and this news organization are owned by the same company.
PHILADELPHIA – Tenofovir alafenamide, the newest kid on the block for treatment of chronic hepatitis B, not only has less bone and renal effects than tenofovir disoproxil, but now also appears to improve those parameters in patients switched over from the older tenofovir formulation, according to Paul Kwo, MD.
“Renal function, as well as hip and spine bone mineral density measurements, all improve after you flip,” said Dr. Kwo, director of hepatology at Stanford (Calif.) University.
Dr. Kwo described some of the latest data on the newer tenofovir formulation in a hepatitis B update he gave at the conference, jointly provided by Rutgers and Global Academy for Medical Education.
Tenofovir alafenamide, a nucleoside analogue reverse transcriptase inhibitor, was approved in November 2016 for treatment of adults with chronic hepatitis B virus (HBV) infection and compensated liver disease.
It has similar efficacy to tenofovir disoproxil, with fewer bone and renal effects, according to results of two large international phase 3 trials.
Some of the latest data, presented in October 2017 at The Liver Meeting in Washington, show that switching patients from tenofovir disoproxil to tenofovir alafenamide improved creatinine clearance and increased rates of alanine aminotransferase normalization, with sustained rates of virologic control, over 48 weeks of treatment.
Similar results were seen for bone mineral density. “It goes up over time, and you approach bone mineral density levels that are similar to [levels in] those who are on tenofovir alafenamide long term,” Dr. Kwo said, commenting on results of the study.
Compared with tenofovir disoproxil, tenofovir alafenamide is a slightly different prodrug of tenofovir, according to Dr. Kwo.
The approved dose of tenofovir alafenamide is 25 mg, compared with 300 mg for tenofovir disoproxil. “It’s more stable in the serum, so you don’t need higher levels, and you have fewer off-target effects,” Dr. Kwo said.
The two agents are “Coke and Pepsi” in terms of efficacy, he added, noting that comparative studies showed similar efficacy on endpoints of percentage HBV DNA less than 29 IU/mL and log10 HBV DNA change.
Very low rates of resistance are seen with first-line therapies for chronic hepatitis B, including entecavir and tenofovir disoproxil. “We wouldn’t expect (tenofovir alafenamide) to be any different, but nonetheless the surveillance has to happen,” Dr. Kwo said.
Tenofovir alafenamide is not yet listed in the official recommendations of the American Association for the Study of Liver Diseases, but it is in current guidelines from the European Association for the Study of the Liver.
The published EASL guidelines provide guidance on how tenofovir alafenamide fits into the treatment armamentarium for HBV.
Going by the EASL recommendations, age greater than 60 years, bone disease, and renal alterations are all good reasons to use tenofovir alafenamide as first-line therapy for hepatitis B, according to Dr. Kwo.
Dr. Kwo reported disclosures related to AbbVie, Allergan, Bristol-Myers Squibb, Conatus Pharmaceuticals, Dova Pharmaceuticals, DURECT, Gilead Sciences, Merck, and Shionogi.
Global Academy and this news organization are owned by the same company.
EXPERT ANALYSIS FROM DIGESTIVE DISEASES: NEW ADVANCES
Major message: Most heart failure is preventable
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
EXPERT ANALYSIS FROM THE ANNUAL CARDIOVASCULAR CONFERENCE AT SNOWMASS