User login
Recognizing and treating trigger finger
CASE
A 55-year-old right-hand-dominant woman presented to the clinic with a chief complaint of right ring finger pain and stiffness. There was no history of trauma or prior surgery. She had no tingling or numbness. She had a history of type 2 diabetes that was well controlled. She worked as a clerk for a government office for many years, and her painful, limited finger motion interfered with keyboarding and picking up items. Physical examination revealed tenderness to palpation over the palmar aspect of the metacarpophalangeal joint (MCPJ) of the ring finger with no other joint tenderness or swelling. When she made a fist, her ring finger MCPJ, proximal interphalangeal joint (PIPJ), and distal interphalangeal joint (DIPJ) locked in a flexed position that required manipulation to extend the finger. A firm mass was palpated in the palm with finger flexion that moved into the finger with extension.
Stenosing tenosynovitis, also known as trigger finger (TF), is an inflammatory condition that causes pain in the distal palm and proximal digit with associated limited motion. The most commonly affected digits are the middle and ring fingers of the dominant hand.1 The disorder is particularly noticeable when it inhibits day-to-day functioning.
TF affects 2% to 3% of the general population and up to 20% of patients with diabetes.2,3 Patient age and duration of diabetes are commonly cited as contributing factors, although the effect of well-controlled blood glucose and A1C on the frequency and cure rate of TF has not been established.3,4 TF is most commonly seen in individuals ages 40 to 60 years, with a 6 times’ greater frequency in females than males.5
In the United States, there are an estimated 200,000 cases of TF each year, with initial presentation typically being to a primary care physician.6 For this reason, it is essential for primary care physicians to recognize this common pathology and treat symptoms early to prevent progression and the need for surgical intervention.
An impaired gliding motion of the flexor tendons
In each finger, a tendon sheath, consisting of 5 annular pulleys and 3 cruciate pulleys, forms a tunnel around the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS). The tendon sheath allows for maximum force by eliminating bowstringing of the tendons when the digit is flexed. Deep to the tendons and surrounding the tendons is a synovial membrane that provides nutrition and reduces friction between the tendons and the tendon sheath.7
The FDP is longer and assists in flexion of the MCPJ and the PIPJ. It is the sole flexor of the DIPJ.
In the thumb, the flexor pollicis longus (FPL) is the only flexor within its tendon sheath. The FPL assists in flexion of the MCPJ and flexes the thumb interphalangeal joint (IPJ). The intrinsic muscles (lumbricals and interossei) do not extend into the tendon sheath and do not contribute to TF.
Continue to: TF occurs when
TF occurs when the tendon sheath, most commonly at the first annular pulley (A1), or the flexor tendons thicken due to fibrocartilaginous metaplasia. This results in impaired gliding motion of the flexor tendons.8 The stenosed A1 pulley can lead to pinching of the flexor tendons and cause the formation of a nodule on the FDS tendon at its bifurcation.9 The nodule of the FDS bifurcation moves proximal to the A1 pulley when the finger is flexed. Upon extension, the tendon nodule may get caught on the A1 pulley. This prevents smooth extension and is the source of pain and triggering (FIGURE 1). In a similar manner, thumb triggering is the result of a stenosed A1 pulley creating a nodule on the FPL tendon, which prevents smooth gliding of the FPL.

What you’ll see
TF is characterized by locking, popping, or clicking at the base of the finger or thumb.7,10 A small nodule may be palpated on the palmar aspect of the MCPJ when the finger is flexed. This nodule will then move distally when the finger is extended. Patients will present with the affected digit in a flexed position and will have difficulty extending the digit. In some cases, the patient may have to use the other hand to straighten the affected digit. In more severe cases, the digit may be fixed in a position of flexion or extension. The severity of triggering is commonly graded by the Green’s classification system (see TABLE11).

Is it Dupuytren contracture, trigger finger, or something else?
The differential diagnosis for TF includes Dupuytren contracture, MCPJ sprain, calcific peritendinitis, flexor tenosynovitis, diabetic cheiroarthropathy (DCA), rheumatoid arthritis (RA), osteoarthritis (OA), and crystalline arthropathy (gout).5
Dupuytren contracture is usually nonpainful and manifests with a palpable cord in the palm and a fixed flexion contracture that has progressed over time, with no history of catching.
MCPJ sprain is diagnosed with tenderness of the MCPJ and a history of trauma.
Continue to: Calcific peritendinitis
Calcific peritendinitis is characterized by pain, tenderness, and edema near a joint with calcified deposits seen on radiographs.
Flexor tenosynovitis manifests with fusiform swelling of the digit, tenderness over the flexor tendon sheath, and pain with passive extension of the digit; it is more commonly associated with RA.
DCA, RA, OA, and gout usually affect more than 1 digit. DCA is associated with both type 1 and type 2 diabetes and is characterized by thickened, waxy skin and painless, limited extension of the digits. RA and OA are diagnosed by medical history, lab work, and radiographs. Gout is diagnosed with lab work and aspiration of joint fluid.
A thorough history, physical exam, and review of radiographs must be performed to rule out these other disorders. Once the diagnosis of TF is made, available treatment options should be pursued.
Treatment: A conservative or surgical approach?
Current treatment options include both nonsurgical (conservative) and surgical interventions. Nonsurgical interventions include activity modification, splinting, and corticosteroid injections. While nonsteroidal anti-inflammatory drugs are commonly recommended to resolve the local inflammation secondary to triggering, there is no scientific evidence to support their use at this time.7 Surgical interventions, utilized in more severe cases or after conservative treatment has failed, include percutaneous and open release of the tendon sheath.2,7
Continue to: Conservative treatments
Conservative treatments
Splinting is only an option for digits that retain flexibility (Green’s classification grades I, II, and III). The goal of splinting is to keep the affected digit in extension to avoid repeated friction between the tendon and the tendon sheath.12 This ideally allows any cartilaginous metaplasia or inflammation to resolve, subsequently alleviating symptoms. The recommended length of treatment with splinting ranges from 3 to 12 weeks, with an average of 6 weeks.1
Multiple studies have shown long-term alleviation of symptoms with the use of orthotic devices. A retrospective analysis found that 87% of patients who wore their PIPJ orthotic device both day and night for a minimum of 6 weeks required no further treatment at 1-year follow-up.13 In contrast, MCPJ splinting only at night has been shown to resolve symptoms in just 55% of patients after 6 weeks.14 From a practical standpoint, however, patients are more likely to be compliant with night-only splinting, making it a reasonable option. Splinting does remain efficacious for patients even after 6 months of symptomatology.15
Day and night splinting for approximately 8 weeks using a PIPJ orthotic could be considered as an effective first-line intervention.16 Notably, PIPJ splinting is more functional, as it allows motion of the MCPJ and DIPJ.
An adjunct treatment to splinting is tendon-gliding exercises, including passive IPJ flexion, full finger flexion and extension, and hooking.13 Patients may remove the orthotic device to perform these exercises 3 times a day for 5 repetitions, as well as for activities that are not conducive to splinting.13
Corticosteroid injections. Injections of a corticosteroid and 1% lidocaine in a 1:1 mixture for a total volume of 1 cc can be inserted into the tendon sheath, A1 pulley, or adjacent tissue.17 Steroid injections help to decrease inflammation and pain in the affected area, giving symptom relief lasting a few months in as many as 57% to 87% of patients.18
Continue to: While the location of the injection...
While the location of the injection has been debated, recent literature suggests that symptoms can be effectively alleviated regardless of the specific anatomic injection site, such as intra-sheath or extra-sheath (FIGURE 2).19 This allows flexibility for the clinician, as the injection does not have to be placed within the tendon sheath. Corticosteroids should not be injected into the tendon itself, and the needle tip should be slightly withdrawn if there is resistance while injecting. Patients who are averse to injections have been shown to benefit from needle-free jet lidocaine (J-tip) administration prior to the actual steroid injection.20

A randomized controlled trial comparing dexamethasone to triamcinolone injections found no difference in outcome at the 3-month follow-up (n = 84).17 This may suggest that the choice of corticosteroid is at the clinician’s discretion. In terms of long-term efficacy of steroid injections, it has been shown that 70% of trigger digits had complete resolution of symptoms at a mean follow-up of 8 years after just 1 injection (n = 43).21
Some patients, though, may require additional corticosteroid injections to maintain symptom control. If multiple injections are performed, they should not be given in intervals shorter than 4 months between treatments.5 Furthermore, steroids can be administered safely up to 3 times in the same digit before surgery is recommended.22
A patient’s options should be reconsidered if efficacy is not demonstrated with prior injections. Notably, a lower success rate has been shown in patients with type 2 diabetes (66%) compared to those without diabetes (90%).4,23 This difference in success rates is not well understood, as there is no causal relationship between well-controlled diabetes and TF.4 Complications of corticosteroid injections include local pain, fat atrophy, and hypopigmentation at the site of the injection, as well as short-term elevations in blood glucose levels in patients with diabetes.5,24
Surgical correction (to be discussed) remains superior to steroid injections in terms of cure rate and resolution of symptoms. A randomized controlled trial (n = 165) found that an injection-only group reported 86% and 49% success at 3-month and 12-month follow-up, respectively, compared to 99% success at both 3- and 12-month follow-up for the surgical group. Further, at 12-month follow-up, the median pain scores were significantly higher in the injection group (3; range, 1-9) than in the surgery group (1; range, 1-7).25 If conservative treatment modalities lead to unresolved symptoms or recurrence, referral to a hand specialist for surgery is recommended.
Continue to: Surgical treatments in an office setting
Surgical treatments in an office setting
Procedures for TF can be safely performed under conscious sedation or local anesthesia, with or without a tourniquet.26 Wide-awake procedures with local anesthesia and no tourniquet (WALANT) can be performed in an office-based procedure room rather than the operating room. This increases efficiency for the surgeon, reduces the amount of preparation and recovery time for the patient, and helps to keep costs down.
Percutaneous release involves the insertion of a 16-gauge hypodermic needle into the affected A1 pulley. The needle is used to fray and disrupt the pulley by moving the needle tip over the fibrotic A1 pulley.
However, it is not without possible complications.27 Inadvertent A2 pulley damage is particularly troublesome, as it leads to “bowstringing” or protrusion of the flexor tendon into the palm upon flexion. This can cause pain and failure to fully extend or flex the finger.10 Because the anatomy is not well visualized during the percutaneous approach, incomplete release, neurovascular injury, and iatrogenic injury to the A2 pulley or deep tendon may occur.28 Ultrasound-guided percutaneous release techniques have shown effective clinical outcomes with minimal complications compared to nonguided percutaneous release techniques.29,30
Open release is the gold standard surgical treatment for trigger finger (FIGURE 3). A small incision (1-2 cm) is made directly over or proximal to the A1 pulley in the distal palmar crease at the base of the affected digit. After blunt dissection through the subcutaneous tissue, the A1 pulley is sharply incised. An open approach has the clear benefit of avoiding the digital neurovascular bundles, as well as visualizing the resolution of triggering upon flexion and extension prior to closure. The WALANT procedure has the advantage of allowing the awake patient to actively flex and extend the digit to determine if the A1 release has been successful prior to closure of the incision.

Outcomes and complications of surgery. A recent systematic review and meta-analysis has shown percutaneous techniques to be successful in 94% of cases.27 The success rate of open surgery has been reported at 99% to 100% at varying follow-up intervals up to 1 year.25,30,31 The complication rate for percutaneous release (guided and nonguided) was calculated at 2.2% (n = 2114).27 In another study, the overall complication rate of open releases was calculated at 1% (n = 999).32 When comparing percutaneous release (guided and nonguided) and open release, a meta-analysis found no significant difference in complication rate (RR = 0.84) or failure rate (RR = 0.94).32
Continue to: Several risk factors...
Several risk factors have been associated with postoperative surgical infection, including recent steroid injection (< 80 d), smoking status, increasing age, and pre-operative use of lidocaine with epinephrine.33 Open release has been shown to be an effective and safe treatment modality for patients with and without diabetes alike.34 Overall, definitive surgical correction has been demonstrated to be superior to conservative measures due to a significantly lower rate of recurrence.35
CASE
Given the patient’s presentation with triggering of the digit, tenderness over the A1 pulley, and lack of trauma history, we diagnosed trigger finger in this patient. Potential treatments included splinting, corticosteroid injections, and surgery. After discussion of the risks and benefits of each treatment option, the patient elected to undergo a corticosteroid injection. She was also given a neoprene finger sleeve to wear every night, and in the daytime when possible.
At 12-week follow-up, she noted early improvement in her triggering, which had since recurred. Due to her history of diabetes, the patient was then referred for surgery. She had an open release under local anesthesia. The surgery was uncomplicated, and the abnormality was corrected. At the patient’s 1-year postoperative follow-up visit, there was no evidence of recurrence, and she had regained full active and passive range of motion of her finger.
Acknowledgements
The authors wish to thank Jose Borrero, MD, for contributing his time and creative talents to produce the illustrations in this article.
CORRESPONDENCE
Evan P. Johnson, MD; 506 South Greer Street, Memphis, TN 38111; EvanJohnsonOrtho@gmail.com
1. Lunsford D, Valdes K, Hengy S. Conservative management of trigger finger: a systematic review. J Hand Ther. 2019;32:212-221. doi: 10.1016/j.jht.2017.10.016
2. Makkouk AH, Oetgen ME, Swigart CR, et al. Trigger finger: etiology, evaluation, and treatment. Curr Rev Musculoskelet Med. 2008;1:92-96. doi: 10.1007/s12178-007-9012-1
3. Fitzgibbons PG, Weiss AP. Hand manifestations of diabetes mellitus. J Hand Surg Am. 2008;33:771-775. doi: 10.1016/j.jhsa.2008.01.038
4. Junot HSN, Anderson Hertz AFL, Gustavo Vasconcelos GR, et al. Epidemiology of trigger finger: metabolic syndrome as a new perspective of associated disease. Hand (N Y). 2019:1558944719867135. doi: 10.1177/1558944719867135.
5. Matthews A, Smith K, Read L, et al. Trigger finger: an overview of the treatment options. JAAPA. 2019;32:17-21. doi: 10.1097/01.Jaa.0000550281.42592.97
6. Pencle FJ, Waheed A, Molnar JA. Trigger thumb. StatPearls [Internet]. StatPearls Publishing; 2020. www.ncbi.nlm.nih.gov/books/NBK441854/
7. Giugale JM, Fowler JR. Trigger finger: adult and pediatric treatment strategies. Orthop Clin North Am. 2015;46:561-569. doi: 10.1016/j.ocl.2015.06.014
8. Bianchi S, Gitto S, Draghi F. Ultrasound features of trigger finger: review of the literature. J Ultrasound Med. 2019;38:3141-3154. doi: 10.1002/jum.15025
9. Chuang XL, Ooi CC, Chin ST, et al. What triggers in trigger finger? The flexor tendons at the flexor digitorum superficialis bifurcation. J Plast Reconstr Aesthet Surg. 2017;70:1411-1419. doi: 10.1016/j.bjps.2017.05.037
10. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006;31:135-146. doi: 10.1016/j.jhsa.2005.10.013
11. Chapter 56: Tendinoapthy. In: Wolfe SW, Peterson WC, Kozin SH, Cohen MS. Green’s Operative Hand Surgery. Vol 2. 7th ed. Elsevier; 2017: 1904-1925.
12. Tarbhai K, Hannah S, von Schroeder HP. Trigger finger treatment: a comparison of 2 splint designs. J Hand Surg Am. 2012;37:243-249, 249.e241. doi: 10.1016/j.jhsa.2011.10.038
13. Valdes K. A retrospective review to determine the long-term efficacy of orthotic devices for trigger finger. J Hand Ther. 2012;25:89-95. doi: 10.1016/j.jht.2011.09.005
14. Drijkoningen T, van Berckel M, Becker SJE, et al. Night splinting for idiopathic trigger digits. Hand (N Y). 2018;13:558-562. doi: 10.1177/1558944717725374
15. Colbourn J, Heath N, Manary S, et al. Effectiveness of splinting for the treatment of trigger finger. J Hand Ther. 2008;21:336-343. doi: 10.1197/j.jht.2008.05.001
16. Teo SH, Ng DCL, Wong YKY. Effectiveness of proximal interphalangeal joint-blocking orthosis vs metacarpophalangeal joint-blocking orthosis in trigger digit management: A randomized clinical trial. J Hand Ther. 2018;32:444-451. doi: 10.1016/j.jht.2018.02.007
17. Ring D, Lozano-Calderon S, Shin R, et al. A prospective randomized controlled trial of injection of dexamethasone versus triamcinolone for idiopathic trigger finger. J Hand Surg Am. 2008;33:516-522; discussion 523-514. doi: 10.1016/j.jhsa.2008.01.001
18. Fleisch SB, Spindler KP, Lee DH. Corticosteroid injections in the treatment of trigger finger: A level I and II systematic review. J Am Acad Orthop Surg. 2007;15:166-171. doi: 10.5435/00124635-200703000-00006
19. Shinomiya R, Sunagawa T, Nakashima Y, et al. Impact of corticosteroid injection site on the treatment success rate of trigger finger: a prospective study comparing ultrasound-guided true intra-sheath and true extra-sheath injections. Ultrasound Med Biol. 2016;42:2203-2208. doi: 10.1016/j.ultrasmedbio.2016.05.015
20. Earp BE, Stanbury SJ, Mora AN, et al. Needle-free jet lidocaine administration for preinjection anesthesia in trigger finger injection: a randomized controlled trial. J Hand Surg Am. 2017;42:618-622. doi: 10.1016/j.jhsa.2017.05.001
21. Castellanos J, Munoz-Mahamud E, Dominguez E, et al. Long-term effectiveness of corticosteroid injections for trigger finger and thumb. J Hand Surg Am. 2015;40:121-126. doi: 10.1016/j.jhsa.2014.09.006
22. Dala-Ali BM, Nakhdjevani A, Lloyd MA, et al. The efficacy of steroid injection in the treatment of trigger finger. Clin Orthop Surg. 2012;4:263-268. doi: 10.4055/cios.2012.4.4.263
23. Griggs SM, Weiss AP, Lane LB, et al. Treatment of trigger finger in patients with diabetes mellitus. J Hand Surg Am. 1995;20:787-789. doi: 10.1016/s0363-5023(05)80432-0
24. Stepan JG, London DA, Boyer MI, et al. Blood glucose levels in diabetic patients following corticosteroid injections into the hand and wrist. J Hand Surg Am. 2014;39:706-712. doi: 10.1016/j.jhsa.2014.01.014
25. Hansen RL, Sondergaard M, Lange J. Open surgery versus ultrasound-guided corticosteroid injection for trigger finger: a randomized controlled trial with 1-year follow-up. J Hand Surg Am. 2017;42:359-366. doi: 10.1016/j.jhsa.2017.02.011
26. Mohd Rashid MZ, Sapuan J, Abdullah S. A randomized controlled trial of trigger finger release under digital anesthesia with (WALANT) and without adrenaline. J Orthop Surg (Hong Kong). 2019;27:2309499019833002. doi: 10.1177/2309499019833002
27. Zhao J-G, Kan S-L, Zhao L, et al. Percutaneous first annular pulley release for trigger digits: a systematic review and meta-analysis of current evidence. J Hand Surg Am. 2014;39:2192-2202. doi: 10.1016/j.jhsa.2014.07.044
28. Guler F, Kose O, Ercan EC, et al. Open versus percutaneous release for the treatment of trigger thumb. Orthopedics. 2013;36:e1290-1294. doi: 10.3928/01477447-20130920-22
29. Wu KC, Chern TC, Jou IM. Ultrasound-assisted percutaneous trigger finger release: it is safe [letter]. Hand (N Y). 2009;4:339. doi: 10.1007/s11552-009-9179-6
30. Nikolaou VS, Malahias M-A, Kaseta M-K, et al. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J Orthop. 2017;8:163-169. doi: 10.5312/wjo.v8.i2.163
31. Lim M-H, Lim K-K, Rasheed MZ, et al. Outcome of open trigger digit release. J Hand Surg Eur Vol. 2007;32:457-459. doi: 10.1016/j.Jhsb.2007.02.016
32. Wang J, Zhao J-G, Liang C-C. Percutaneous release, open surgery, or corticosteroid injection, which is the best treatment method for trigger digits? Clin Orthop Relat Res. 2013;471:1879-1886. doi: 10.1007/s11999-012-2716-6
33. Ng WKY, Olmscheid N, Worhacz K, et al. Steroid injection and open trigger finger release outcomes: a retrospective review of 999 digits. Hand (N Y). 2018;15:399-406. doi: 10.1177/1558944718796559
34. Ho SWL, Chia CY, Rajaratnam V. Characteristics and clinical outcomes of open surgery for trigger digits in diabetes. J Hand Microsurg. 2019;11:80-83. doi: 10.1055/s-0038-1670927
35. Sato ES, dos Santos JB, Belloti JC, et al. Percutaneous release of trigger fingers. Hand Clin. 2014;30:39-45. doi: 10.1016/j.hcl.2013.08.017
CASE
A 55-year-old right-hand-dominant woman presented to the clinic with a chief complaint of right ring finger pain and stiffness. There was no history of trauma or prior surgery. She had no tingling or numbness. She had a history of type 2 diabetes that was well controlled. She worked as a clerk for a government office for many years, and her painful, limited finger motion interfered with keyboarding and picking up items. Physical examination revealed tenderness to palpation over the palmar aspect of the metacarpophalangeal joint (MCPJ) of the ring finger with no other joint tenderness or swelling. When she made a fist, her ring finger MCPJ, proximal interphalangeal joint (PIPJ), and distal interphalangeal joint (DIPJ) locked in a flexed position that required manipulation to extend the finger. A firm mass was palpated in the palm with finger flexion that moved into the finger with extension.
Stenosing tenosynovitis, also known as trigger finger (TF), is an inflammatory condition that causes pain in the distal palm and proximal digit with associated limited motion. The most commonly affected digits are the middle and ring fingers of the dominant hand.1 The disorder is particularly noticeable when it inhibits day-to-day functioning.
TF affects 2% to 3% of the general population and up to 20% of patients with diabetes.2,3 Patient age and duration of diabetes are commonly cited as contributing factors, although the effect of well-controlled blood glucose and A1C on the frequency and cure rate of TF has not been established.3,4 TF is most commonly seen in individuals ages 40 to 60 years, with a 6 times’ greater frequency in females than males.5
In the United States, there are an estimated 200,000 cases of TF each year, with initial presentation typically being to a primary care physician.6 For this reason, it is essential for primary care physicians to recognize this common pathology and treat symptoms early to prevent progression and the need for surgical intervention.
An impaired gliding motion of the flexor tendons
In each finger, a tendon sheath, consisting of 5 annular pulleys and 3 cruciate pulleys, forms a tunnel around the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS). The tendon sheath allows for maximum force by eliminating bowstringing of the tendons when the digit is flexed. Deep to the tendons and surrounding the tendons is a synovial membrane that provides nutrition and reduces friction between the tendons and the tendon sheath.7
The FDP is longer and assists in flexion of the MCPJ and the PIPJ. It is the sole flexor of the DIPJ.
In the thumb, the flexor pollicis longus (FPL) is the only flexor within its tendon sheath. The FPL assists in flexion of the MCPJ and flexes the thumb interphalangeal joint (IPJ). The intrinsic muscles (lumbricals and interossei) do not extend into the tendon sheath and do not contribute to TF.
Continue to: TF occurs when
TF occurs when the tendon sheath, most commonly at the first annular pulley (A1), or the flexor tendons thicken due to fibrocartilaginous metaplasia. This results in impaired gliding motion of the flexor tendons.8 The stenosed A1 pulley can lead to pinching of the flexor tendons and cause the formation of a nodule on the FDS tendon at its bifurcation.9 The nodule of the FDS bifurcation moves proximal to the A1 pulley when the finger is flexed. Upon extension, the tendon nodule may get caught on the A1 pulley. This prevents smooth extension and is the source of pain and triggering (FIGURE 1). In a similar manner, thumb triggering is the result of a stenosed A1 pulley creating a nodule on the FPL tendon, which prevents smooth gliding of the FPL.
What you’ll see
TF is characterized by locking, popping, or clicking at the base of the finger or thumb.7,10 A small nodule may be palpated on the palmar aspect of the MCPJ when the finger is flexed. This nodule will then move distally when the finger is extended. Patients will present with the affected digit in a flexed position and will have difficulty extending the digit. In some cases, the patient may have to use the other hand to straighten the affected digit. In more severe cases, the digit may be fixed in a position of flexion or extension. The severity of triggering is commonly graded by the Green’s classification system (see TABLE11).
Is it Dupuytren contracture, trigger finger, or something else?
The differential diagnosis for TF includes Dupuytren contracture, MCPJ sprain, calcific peritendinitis, flexor tenosynovitis, diabetic cheiroarthropathy (DCA), rheumatoid arthritis (RA), osteoarthritis (OA), and crystalline arthropathy (gout).5
Dupuytren contracture is usually nonpainful and manifests with a palpable cord in the palm and a fixed flexion contracture that has progressed over time, with no history of catching.
MCPJ sprain is diagnosed with tenderness of the MCPJ and a history of trauma.
Continue to: Calcific peritendinitis
Calcific peritendinitis is characterized by pain, tenderness, and edema near a joint with calcified deposits seen on radiographs.
Flexor tenosynovitis manifests with fusiform swelling of the digit, tenderness over the flexor tendon sheath, and pain with passive extension of the digit; it is more commonly associated with RA.
DCA, RA, OA, and gout usually affect more than 1 digit. DCA is associated with both type 1 and type 2 diabetes and is characterized by thickened, waxy skin and painless, limited extension of the digits. RA and OA are diagnosed by medical history, lab work, and radiographs. Gout is diagnosed with lab work and aspiration of joint fluid.
A thorough history, physical exam, and review of radiographs must be performed to rule out these other disorders. Once the diagnosis of TF is made, available treatment options should be pursued.
Treatment: A conservative or surgical approach?
Current treatment options include both nonsurgical (conservative) and surgical interventions. Nonsurgical interventions include activity modification, splinting, and corticosteroid injections. While nonsteroidal anti-inflammatory drugs are commonly recommended to resolve the local inflammation secondary to triggering, there is no scientific evidence to support their use at this time.7 Surgical interventions, utilized in more severe cases or after conservative treatment has failed, include percutaneous and open release of the tendon sheath.2,7
Continue to: Conservative treatments
Conservative treatments
Splinting is only an option for digits that retain flexibility (Green’s classification grades I, II, and III). The goal of splinting is to keep the affected digit in extension to avoid repeated friction between the tendon and the tendon sheath.12 This ideally allows any cartilaginous metaplasia or inflammation to resolve, subsequently alleviating symptoms. The recommended length of treatment with splinting ranges from 3 to 12 weeks, with an average of 6 weeks.1
Multiple studies have shown long-term alleviation of symptoms with the use of orthotic devices. A retrospective analysis found that 87% of patients who wore their PIPJ orthotic device both day and night for a minimum of 6 weeks required no further treatment at 1-year follow-up.13 In contrast, MCPJ splinting only at night has been shown to resolve symptoms in just 55% of patients after 6 weeks.14 From a practical standpoint, however, patients are more likely to be compliant with night-only splinting, making it a reasonable option. Splinting does remain efficacious for patients even after 6 months of symptomatology.15
Day and night splinting for approximately 8 weeks using a PIPJ orthotic could be considered as an effective first-line intervention.16 Notably, PIPJ splinting is more functional, as it allows motion of the MCPJ and DIPJ.
An adjunct treatment to splinting is tendon-gliding exercises, including passive IPJ flexion, full finger flexion and extension, and hooking.13 Patients may remove the orthotic device to perform these exercises 3 times a day for 5 repetitions, as well as for activities that are not conducive to splinting.13
Corticosteroid injections. Injections of a corticosteroid and 1% lidocaine in a 1:1 mixture for a total volume of 1 cc can be inserted into the tendon sheath, A1 pulley, or adjacent tissue.17 Steroid injections help to decrease inflammation and pain in the affected area, giving symptom relief lasting a few months in as many as 57% to 87% of patients.18
Continue to: While the location of the injection...
While the location of the injection has been debated, recent literature suggests that symptoms can be effectively alleviated regardless of the specific anatomic injection site, such as intra-sheath or extra-sheath (FIGURE 2).19 This allows flexibility for the clinician, as the injection does not have to be placed within the tendon sheath. Corticosteroids should not be injected into the tendon itself, and the needle tip should be slightly withdrawn if there is resistance while injecting. Patients who are averse to injections have been shown to benefit from needle-free jet lidocaine (J-tip) administration prior to the actual steroid injection.20
A randomized controlled trial comparing dexamethasone to triamcinolone injections found no difference in outcome at the 3-month follow-up (n = 84).17 This may suggest that the choice of corticosteroid is at the clinician’s discretion. In terms of long-term efficacy of steroid injections, it has been shown that 70% of trigger digits had complete resolution of symptoms at a mean follow-up of 8 years after just 1 injection (n = 43).21
Some patients, though, may require additional corticosteroid injections to maintain symptom control. If multiple injections are performed, they should not be given in intervals shorter than 4 months between treatments.5 Furthermore, steroids can be administered safely up to 3 times in the same digit before surgery is recommended.22
A patient’s options should be reconsidered if efficacy is not demonstrated with prior injections. Notably, a lower success rate has been shown in patients with type 2 diabetes (66%) compared to those without diabetes (90%).4,23 This difference in success rates is not well understood, as there is no causal relationship between well-controlled diabetes and TF.4 Complications of corticosteroid injections include local pain, fat atrophy, and hypopigmentation at the site of the injection, as well as short-term elevations in blood glucose levels in patients with diabetes.5,24
Surgical correction (to be discussed) remains superior to steroid injections in terms of cure rate and resolution of symptoms. A randomized controlled trial (n = 165) found that an injection-only group reported 86% and 49% success at 3-month and 12-month follow-up, respectively, compared to 99% success at both 3- and 12-month follow-up for the surgical group. Further, at 12-month follow-up, the median pain scores were significantly higher in the injection group (3; range, 1-9) than in the surgery group (1; range, 1-7).25 If conservative treatment modalities lead to unresolved symptoms or recurrence, referral to a hand specialist for surgery is recommended.
Continue to: Surgical treatments in an office setting
Surgical treatments in an office setting
Procedures for TF can be safely performed under conscious sedation or local anesthesia, with or without a tourniquet.26 Wide-awake procedures with local anesthesia and no tourniquet (WALANT) can be performed in an office-based procedure room rather than the operating room. This increases efficiency for the surgeon, reduces the amount of preparation and recovery time for the patient, and helps to keep costs down.
Percutaneous release involves the insertion of a 16-gauge hypodermic needle into the affected A1 pulley. The needle is used to fray and disrupt the pulley by moving the needle tip over the fibrotic A1 pulley.
However, it is not without possible complications.27 Inadvertent A2 pulley damage is particularly troublesome, as it leads to “bowstringing” or protrusion of the flexor tendon into the palm upon flexion. This can cause pain and failure to fully extend or flex the finger.10 Because the anatomy is not well visualized during the percutaneous approach, incomplete release, neurovascular injury, and iatrogenic injury to the A2 pulley or deep tendon may occur.28 Ultrasound-guided percutaneous release techniques have shown effective clinical outcomes with minimal complications compared to nonguided percutaneous release techniques.29,30
Open release is the gold standard surgical treatment for trigger finger (FIGURE 3). A small incision (1-2 cm) is made directly over or proximal to the A1 pulley in the distal palmar crease at the base of the affected digit. After blunt dissection through the subcutaneous tissue, the A1 pulley is sharply incised. An open approach has the clear benefit of avoiding the digital neurovascular bundles, as well as visualizing the resolution of triggering upon flexion and extension prior to closure. The WALANT procedure has the advantage of allowing the awake patient to actively flex and extend the digit to determine if the A1 release has been successful prior to closure of the incision.
Outcomes and complications of surgery. A recent systematic review and meta-analysis has shown percutaneous techniques to be successful in 94% of cases.27 The success rate of open surgery has been reported at 99% to 100% at varying follow-up intervals up to 1 year.25,30,31 The complication rate for percutaneous release (guided and nonguided) was calculated at 2.2% (n = 2114).27 In another study, the overall complication rate of open releases was calculated at 1% (n = 999).32 When comparing percutaneous release (guided and nonguided) and open release, a meta-analysis found no significant difference in complication rate (RR = 0.84) or failure rate (RR = 0.94).32
Continue to: Several risk factors...
Several risk factors have been associated with postoperative surgical infection, including recent steroid injection (< 80 d), smoking status, increasing age, and pre-operative use of lidocaine with epinephrine.33 Open release has been shown to be an effective and safe treatment modality for patients with and without diabetes alike.34 Overall, definitive surgical correction has been demonstrated to be superior to conservative measures due to a significantly lower rate of recurrence.35
CASE
Given the patient’s presentation with triggering of the digit, tenderness over the A1 pulley, and lack of trauma history, we diagnosed trigger finger in this patient. Potential treatments included splinting, corticosteroid injections, and surgery. After discussion of the risks and benefits of each treatment option, the patient elected to undergo a corticosteroid injection. She was also given a neoprene finger sleeve to wear every night, and in the daytime when possible.
At 12-week follow-up, she noted early improvement in her triggering, which had since recurred. Due to her history of diabetes, the patient was then referred for surgery. She had an open release under local anesthesia. The surgery was uncomplicated, and the abnormality was corrected. At the patient’s 1-year postoperative follow-up visit, there was no evidence of recurrence, and she had regained full active and passive range of motion of her finger.
Acknowledgements
The authors wish to thank Jose Borrero, MD, for contributing his time and creative talents to produce the illustrations in this article.
CORRESPONDENCE
Evan P. Johnson, MD; 506 South Greer Street, Memphis, TN 38111; EvanJohnsonOrtho@gmail.com
CASE
A 55-year-old right-hand-dominant woman presented to the clinic with a chief complaint of right ring finger pain and stiffness. There was no history of trauma or prior surgery. She had no tingling or numbness. She had a history of type 2 diabetes that was well controlled. She worked as a clerk for a government office for many years, and her painful, limited finger motion interfered with keyboarding and picking up items. Physical examination revealed tenderness to palpation over the palmar aspect of the metacarpophalangeal joint (MCPJ) of the ring finger with no other joint tenderness or swelling. When she made a fist, her ring finger MCPJ, proximal interphalangeal joint (PIPJ), and distal interphalangeal joint (DIPJ) locked in a flexed position that required manipulation to extend the finger. A firm mass was palpated in the palm with finger flexion that moved into the finger with extension.
Stenosing tenosynovitis, also known as trigger finger (TF), is an inflammatory condition that causes pain in the distal palm and proximal digit with associated limited motion. The most commonly affected digits are the middle and ring fingers of the dominant hand.1 The disorder is particularly noticeable when it inhibits day-to-day functioning.
TF affects 2% to 3% of the general population and up to 20% of patients with diabetes.2,3 Patient age and duration of diabetes are commonly cited as contributing factors, although the effect of well-controlled blood glucose and A1C on the frequency and cure rate of TF has not been established.3,4 TF is most commonly seen in individuals ages 40 to 60 years, with a 6 times’ greater frequency in females than males.5
In the United States, there are an estimated 200,000 cases of TF each year, with initial presentation typically being to a primary care physician.6 For this reason, it is essential for primary care physicians to recognize this common pathology and treat symptoms early to prevent progression and the need for surgical intervention.
An impaired gliding motion of the flexor tendons
In each finger, a tendon sheath, consisting of 5 annular pulleys and 3 cruciate pulleys, forms a tunnel around the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS). The tendon sheath allows for maximum force by eliminating bowstringing of the tendons when the digit is flexed. Deep to the tendons and surrounding the tendons is a synovial membrane that provides nutrition and reduces friction between the tendons and the tendon sheath.7
The FDP is longer and assists in flexion of the MCPJ and the PIPJ. It is the sole flexor of the DIPJ.
In the thumb, the flexor pollicis longus (FPL) is the only flexor within its tendon sheath. The FPL assists in flexion of the MCPJ and flexes the thumb interphalangeal joint (IPJ). The intrinsic muscles (lumbricals and interossei) do not extend into the tendon sheath and do not contribute to TF.
Continue to: TF occurs when
TF occurs when the tendon sheath, most commonly at the first annular pulley (A1), or the flexor tendons thicken due to fibrocartilaginous metaplasia. This results in impaired gliding motion of the flexor tendons.8 The stenosed A1 pulley can lead to pinching of the flexor tendons and cause the formation of a nodule on the FDS tendon at its bifurcation.9 The nodule of the FDS bifurcation moves proximal to the A1 pulley when the finger is flexed. Upon extension, the tendon nodule may get caught on the A1 pulley. This prevents smooth extension and is the source of pain and triggering (FIGURE 1). In a similar manner, thumb triggering is the result of a stenosed A1 pulley creating a nodule on the FPL tendon, which prevents smooth gliding of the FPL.
What you’ll see
TF is characterized by locking, popping, or clicking at the base of the finger or thumb.7,10 A small nodule may be palpated on the palmar aspect of the MCPJ when the finger is flexed. This nodule will then move distally when the finger is extended. Patients will present with the affected digit in a flexed position and will have difficulty extending the digit. In some cases, the patient may have to use the other hand to straighten the affected digit. In more severe cases, the digit may be fixed in a position of flexion or extension. The severity of triggering is commonly graded by the Green’s classification system (see TABLE11).
Is it Dupuytren contracture, trigger finger, or something else?
The differential diagnosis for TF includes Dupuytren contracture, MCPJ sprain, calcific peritendinitis, flexor tenosynovitis, diabetic cheiroarthropathy (DCA), rheumatoid arthritis (RA), osteoarthritis (OA), and crystalline arthropathy (gout).5
Dupuytren contracture is usually nonpainful and manifests with a palpable cord in the palm and a fixed flexion contracture that has progressed over time, with no history of catching.
MCPJ sprain is diagnosed with tenderness of the MCPJ and a history of trauma.
Continue to: Calcific peritendinitis
Calcific peritendinitis is characterized by pain, tenderness, and edema near a joint with calcified deposits seen on radiographs.
Flexor tenosynovitis manifests with fusiform swelling of the digit, tenderness over the flexor tendon sheath, and pain with passive extension of the digit; it is more commonly associated with RA.
DCA, RA, OA, and gout usually affect more than 1 digit. DCA is associated with both type 1 and type 2 diabetes and is characterized by thickened, waxy skin and painless, limited extension of the digits. RA and OA are diagnosed by medical history, lab work, and radiographs. Gout is diagnosed with lab work and aspiration of joint fluid.
A thorough history, physical exam, and review of radiographs must be performed to rule out these other disorders. Once the diagnosis of TF is made, available treatment options should be pursued.
Treatment: A conservative or surgical approach?
Current treatment options include both nonsurgical (conservative) and surgical interventions. Nonsurgical interventions include activity modification, splinting, and corticosteroid injections. While nonsteroidal anti-inflammatory drugs are commonly recommended to resolve the local inflammation secondary to triggering, there is no scientific evidence to support their use at this time.7 Surgical interventions, utilized in more severe cases or after conservative treatment has failed, include percutaneous and open release of the tendon sheath.2,7
Continue to: Conservative treatments
Conservative treatments
Splinting is only an option for digits that retain flexibility (Green’s classification grades I, II, and III). The goal of splinting is to keep the affected digit in extension to avoid repeated friction between the tendon and the tendon sheath.12 This ideally allows any cartilaginous metaplasia or inflammation to resolve, subsequently alleviating symptoms. The recommended length of treatment with splinting ranges from 3 to 12 weeks, with an average of 6 weeks.1
Multiple studies have shown long-term alleviation of symptoms with the use of orthotic devices. A retrospective analysis found that 87% of patients who wore their PIPJ orthotic device both day and night for a minimum of 6 weeks required no further treatment at 1-year follow-up.13 In contrast, MCPJ splinting only at night has been shown to resolve symptoms in just 55% of patients after 6 weeks.14 From a practical standpoint, however, patients are more likely to be compliant with night-only splinting, making it a reasonable option. Splinting does remain efficacious for patients even after 6 months of symptomatology.15
Day and night splinting for approximately 8 weeks using a PIPJ orthotic could be considered as an effective first-line intervention.16 Notably, PIPJ splinting is more functional, as it allows motion of the MCPJ and DIPJ.
An adjunct treatment to splinting is tendon-gliding exercises, including passive IPJ flexion, full finger flexion and extension, and hooking.13 Patients may remove the orthotic device to perform these exercises 3 times a day for 5 repetitions, as well as for activities that are not conducive to splinting.13
Corticosteroid injections. Injections of a corticosteroid and 1% lidocaine in a 1:1 mixture for a total volume of 1 cc can be inserted into the tendon sheath, A1 pulley, or adjacent tissue.17 Steroid injections help to decrease inflammation and pain in the affected area, giving symptom relief lasting a few months in as many as 57% to 87% of patients.18
Continue to: While the location of the injection...
While the location of the injection has been debated, recent literature suggests that symptoms can be effectively alleviated regardless of the specific anatomic injection site, such as intra-sheath or extra-sheath (FIGURE 2).19 This allows flexibility for the clinician, as the injection does not have to be placed within the tendon sheath. Corticosteroids should not be injected into the tendon itself, and the needle tip should be slightly withdrawn if there is resistance while injecting. Patients who are averse to injections have been shown to benefit from needle-free jet lidocaine (J-tip) administration prior to the actual steroid injection.20
A randomized controlled trial comparing dexamethasone to triamcinolone injections found no difference in outcome at the 3-month follow-up (n = 84).17 This may suggest that the choice of corticosteroid is at the clinician’s discretion. In terms of long-term efficacy of steroid injections, it has been shown that 70% of trigger digits had complete resolution of symptoms at a mean follow-up of 8 years after just 1 injection (n = 43).21
Some patients, though, may require additional corticosteroid injections to maintain symptom control. If multiple injections are performed, they should not be given in intervals shorter than 4 months between treatments.5 Furthermore, steroids can be administered safely up to 3 times in the same digit before surgery is recommended.22
A patient’s options should be reconsidered if efficacy is not demonstrated with prior injections. Notably, a lower success rate has been shown in patients with type 2 diabetes (66%) compared to those without diabetes (90%).4,23 This difference in success rates is not well understood, as there is no causal relationship between well-controlled diabetes and TF.4 Complications of corticosteroid injections include local pain, fat atrophy, and hypopigmentation at the site of the injection, as well as short-term elevations in blood glucose levels in patients with diabetes.5,24
Surgical correction (to be discussed) remains superior to steroid injections in terms of cure rate and resolution of symptoms. A randomized controlled trial (n = 165) found that an injection-only group reported 86% and 49% success at 3-month and 12-month follow-up, respectively, compared to 99% success at both 3- and 12-month follow-up for the surgical group. Further, at 12-month follow-up, the median pain scores were significantly higher in the injection group (3; range, 1-9) than in the surgery group (1; range, 1-7).25 If conservative treatment modalities lead to unresolved symptoms or recurrence, referral to a hand specialist for surgery is recommended.
Continue to: Surgical treatments in an office setting
Surgical treatments in an office setting
Procedures for TF can be safely performed under conscious sedation or local anesthesia, with or without a tourniquet.26 Wide-awake procedures with local anesthesia and no tourniquet (WALANT) can be performed in an office-based procedure room rather than the operating room. This increases efficiency for the surgeon, reduces the amount of preparation and recovery time for the patient, and helps to keep costs down.
Percutaneous release involves the insertion of a 16-gauge hypodermic needle into the affected A1 pulley. The needle is used to fray and disrupt the pulley by moving the needle tip over the fibrotic A1 pulley.
However, it is not without possible complications.27 Inadvertent A2 pulley damage is particularly troublesome, as it leads to “bowstringing” or protrusion of the flexor tendon into the palm upon flexion. This can cause pain and failure to fully extend or flex the finger.10 Because the anatomy is not well visualized during the percutaneous approach, incomplete release, neurovascular injury, and iatrogenic injury to the A2 pulley or deep tendon may occur.28 Ultrasound-guided percutaneous release techniques have shown effective clinical outcomes with minimal complications compared to nonguided percutaneous release techniques.29,30
Open release is the gold standard surgical treatment for trigger finger (FIGURE 3). A small incision (1-2 cm) is made directly over or proximal to the A1 pulley in the distal palmar crease at the base of the affected digit. After blunt dissection through the subcutaneous tissue, the A1 pulley is sharply incised. An open approach has the clear benefit of avoiding the digital neurovascular bundles, as well as visualizing the resolution of triggering upon flexion and extension prior to closure. The WALANT procedure has the advantage of allowing the awake patient to actively flex and extend the digit to determine if the A1 release has been successful prior to closure of the incision.
Outcomes and complications of surgery. A recent systematic review and meta-analysis has shown percutaneous techniques to be successful in 94% of cases.27 The success rate of open surgery has been reported at 99% to 100% at varying follow-up intervals up to 1 year.25,30,31 The complication rate for percutaneous release (guided and nonguided) was calculated at 2.2% (n = 2114).27 In another study, the overall complication rate of open releases was calculated at 1% (n = 999).32 When comparing percutaneous release (guided and nonguided) and open release, a meta-analysis found no significant difference in complication rate (RR = 0.84) or failure rate (RR = 0.94).32
Continue to: Several risk factors...
Several risk factors have been associated with postoperative surgical infection, including recent steroid injection (< 80 d), smoking status, increasing age, and pre-operative use of lidocaine with epinephrine.33 Open release has been shown to be an effective and safe treatment modality for patients with and without diabetes alike.34 Overall, definitive surgical correction has been demonstrated to be superior to conservative measures due to a significantly lower rate of recurrence.35
CASE
Given the patient’s presentation with triggering of the digit, tenderness over the A1 pulley, and lack of trauma history, we diagnosed trigger finger in this patient. Potential treatments included splinting, corticosteroid injections, and surgery. After discussion of the risks and benefits of each treatment option, the patient elected to undergo a corticosteroid injection. She was also given a neoprene finger sleeve to wear every night, and in the daytime when possible.
At 12-week follow-up, she noted early improvement in her triggering, which had since recurred. Due to her history of diabetes, the patient was then referred for surgery. She had an open release under local anesthesia. The surgery was uncomplicated, and the abnormality was corrected. At the patient’s 1-year postoperative follow-up visit, there was no evidence of recurrence, and she had regained full active and passive range of motion of her finger.
Acknowledgements
The authors wish to thank Jose Borrero, MD, for contributing his time and creative talents to produce the illustrations in this article.
CORRESPONDENCE
Evan P. Johnson, MD; 506 South Greer Street, Memphis, TN 38111; EvanJohnsonOrtho@gmail.com
1. Lunsford D, Valdes K, Hengy S. Conservative management of trigger finger: a systematic review. J Hand Ther. 2019;32:212-221. doi: 10.1016/j.jht.2017.10.016
2. Makkouk AH, Oetgen ME, Swigart CR, et al. Trigger finger: etiology, evaluation, and treatment. Curr Rev Musculoskelet Med. 2008;1:92-96. doi: 10.1007/s12178-007-9012-1
3. Fitzgibbons PG, Weiss AP. Hand manifestations of diabetes mellitus. J Hand Surg Am. 2008;33:771-775. doi: 10.1016/j.jhsa.2008.01.038
4. Junot HSN, Anderson Hertz AFL, Gustavo Vasconcelos GR, et al. Epidemiology of trigger finger: metabolic syndrome as a new perspective of associated disease. Hand (N Y). 2019:1558944719867135. doi: 10.1177/1558944719867135.
5. Matthews A, Smith K, Read L, et al. Trigger finger: an overview of the treatment options. JAAPA. 2019;32:17-21. doi: 10.1097/01.Jaa.0000550281.42592.97
6. Pencle FJ, Waheed A, Molnar JA. Trigger thumb. StatPearls [Internet]. StatPearls Publishing; 2020. www.ncbi.nlm.nih.gov/books/NBK441854/
7. Giugale JM, Fowler JR. Trigger finger: adult and pediatric treatment strategies. Orthop Clin North Am. 2015;46:561-569. doi: 10.1016/j.ocl.2015.06.014
8. Bianchi S, Gitto S, Draghi F. Ultrasound features of trigger finger: review of the literature. J Ultrasound Med. 2019;38:3141-3154. doi: 10.1002/jum.15025
9. Chuang XL, Ooi CC, Chin ST, et al. What triggers in trigger finger? The flexor tendons at the flexor digitorum superficialis bifurcation. J Plast Reconstr Aesthet Surg. 2017;70:1411-1419. doi: 10.1016/j.bjps.2017.05.037
10. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006;31:135-146. doi: 10.1016/j.jhsa.2005.10.013
11. Chapter 56: Tendinoapthy. In: Wolfe SW, Peterson WC, Kozin SH, Cohen MS. Green’s Operative Hand Surgery. Vol 2. 7th ed. Elsevier; 2017: 1904-1925.
12. Tarbhai K, Hannah S, von Schroeder HP. Trigger finger treatment: a comparison of 2 splint designs. J Hand Surg Am. 2012;37:243-249, 249.e241. doi: 10.1016/j.jhsa.2011.10.038
13. Valdes K. A retrospective review to determine the long-term efficacy of orthotic devices for trigger finger. J Hand Ther. 2012;25:89-95. doi: 10.1016/j.jht.2011.09.005
14. Drijkoningen T, van Berckel M, Becker SJE, et al. Night splinting for idiopathic trigger digits. Hand (N Y). 2018;13:558-562. doi: 10.1177/1558944717725374
15. Colbourn J, Heath N, Manary S, et al. Effectiveness of splinting for the treatment of trigger finger. J Hand Ther. 2008;21:336-343. doi: 10.1197/j.jht.2008.05.001
16. Teo SH, Ng DCL, Wong YKY. Effectiveness of proximal interphalangeal joint-blocking orthosis vs metacarpophalangeal joint-blocking orthosis in trigger digit management: A randomized clinical trial. J Hand Ther. 2018;32:444-451. doi: 10.1016/j.jht.2018.02.007
17. Ring D, Lozano-Calderon S, Shin R, et al. A prospective randomized controlled trial of injection of dexamethasone versus triamcinolone for idiopathic trigger finger. J Hand Surg Am. 2008;33:516-522; discussion 523-514. doi: 10.1016/j.jhsa.2008.01.001
18. Fleisch SB, Spindler KP, Lee DH. Corticosteroid injections in the treatment of trigger finger: A level I and II systematic review. J Am Acad Orthop Surg. 2007;15:166-171. doi: 10.5435/00124635-200703000-00006
19. Shinomiya R, Sunagawa T, Nakashima Y, et al. Impact of corticosteroid injection site on the treatment success rate of trigger finger: a prospective study comparing ultrasound-guided true intra-sheath and true extra-sheath injections. Ultrasound Med Biol. 2016;42:2203-2208. doi: 10.1016/j.ultrasmedbio.2016.05.015
20. Earp BE, Stanbury SJ, Mora AN, et al. Needle-free jet lidocaine administration for preinjection anesthesia in trigger finger injection: a randomized controlled trial. J Hand Surg Am. 2017;42:618-622. doi: 10.1016/j.jhsa.2017.05.001
21. Castellanos J, Munoz-Mahamud E, Dominguez E, et al. Long-term effectiveness of corticosteroid injections for trigger finger and thumb. J Hand Surg Am. 2015;40:121-126. doi: 10.1016/j.jhsa.2014.09.006
22. Dala-Ali BM, Nakhdjevani A, Lloyd MA, et al. The efficacy of steroid injection in the treatment of trigger finger. Clin Orthop Surg. 2012;4:263-268. doi: 10.4055/cios.2012.4.4.263
23. Griggs SM, Weiss AP, Lane LB, et al. Treatment of trigger finger in patients with diabetes mellitus. J Hand Surg Am. 1995;20:787-789. doi: 10.1016/s0363-5023(05)80432-0
24. Stepan JG, London DA, Boyer MI, et al. Blood glucose levels in diabetic patients following corticosteroid injections into the hand and wrist. J Hand Surg Am. 2014;39:706-712. doi: 10.1016/j.jhsa.2014.01.014
25. Hansen RL, Sondergaard M, Lange J. Open surgery versus ultrasound-guided corticosteroid injection for trigger finger: a randomized controlled trial with 1-year follow-up. J Hand Surg Am. 2017;42:359-366. doi: 10.1016/j.jhsa.2017.02.011
26. Mohd Rashid MZ, Sapuan J, Abdullah S. A randomized controlled trial of trigger finger release under digital anesthesia with (WALANT) and without adrenaline. J Orthop Surg (Hong Kong). 2019;27:2309499019833002. doi: 10.1177/2309499019833002
27. Zhao J-G, Kan S-L, Zhao L, et al. Percutaneous first annular pulley release for trigger digits: a systematic review and meta-analysis of current evidence. J Hand Surg Am. 2014;39:2192-2202. doi: 10.1016/j.jhsa.2014.07.044
28. Guler F, Kose O, Ercan EC, et al. Open versus percutaneous release for the treatment of trigger thumb. Orthopedics. 2013;36:e1290-1294. doi: 10.3928/01477447-20130920-22
29. Wu KC, Chern TC, Jou IM. Ultrasound-assisted percutaneous trigger finger release: it is safe [letter]. Hand (N Y). 2009;4:339. doi: 10.1007/s11552-009-9179-6
30. Nikolaou VS, Malahias M-A, Kaseta M-K, et al. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J Orthop. 2017;8:163-169. doi: 10.5312/wjo.v8.i2.163
31. Lim M-H, Lim K-K, Rasheed MZ, et al. Outcome of open trigger digit release. J Hand Surg Eur Vol. 2007;32:457-459. doi: 10.1016/j.Jhsb.2007.02.016
32. Wang J, Zhao J-G, Liang C-C. Percutaneous release, open surgery, or corticosteroid injection, which is the best treatment method for trigger digits? Clin Orthop Relat Res. 2013;471:1879-1886. doi: 10.1007/s11999-012-2716-6
33. Ng WKY, Olmscheid N, Worhacz K, et al. Steroid injection and open trigger finger release outcomes: a retrospective review of 999 digits. Hand (N Y). 2018;15:399-406. doi: 10.1177/1558944718796559
34. Ho SWL, Chia CY, Rajaratnam V. Characteristics and clinical outcomes of open surgery for trigger digits in diabetes. J Hand Microsurg. 2019;11:80-83. doi: 10.1055/s-0038-1670927
35. Sato ES, dos Santos JB, Belloti JC, et al. Percutaneous release of trigger fingers. Hand Clin. 2014;30:39-45. doi: 10.1016/j.hcl.2013.08.017
1. Lunsford D, Valdes K, Hengy S. Conservative management of trigger finger: a systematic review. J Hand Ther. 2019;32:212-221. doi: 10.1016/j.jht.2017.10.016
2. Makkouk AH, Oetgen ME, Swigart CR, et al. Trigger finger: etiology, evaluation, and treatment. Curr Rev Musculoskelet Med. 2008;1:92-96. doi: 10.1007/s12178-007-9012-1
3. Fitzgibbons PG, Weiss AP. Hand manifestations of diabetes mellitus. J Hand Surg Am. 2008;33:771-775. doi: 10.1016/j.jhsa.2008.01.038
4. Junot HSN, Anderson Hertz AFL, Gustavo Vasconcelos GR, et al. Epidemiology of trigger finger: metabolic syndrome as a new perspective of associated disease. Hand (N Y). 2019:1558944719867135. doi: 10.1177/1558944719867135.
5. Matthews A, Smith K, Read L, et al. Trigger finger: an overview of the treatment options. JAAPA. 2019;32:17-21. doi: 10.1097/01.Jaa.0000550281.42592.97
6. Pencle FJ, Waheed A, Molnar JA. Trigger thumb. StatPearls [Internet]. StatPearls Publishing; 2020. www.ncbi.nlm.nih.gov/books/NBK441854/
7. Giugale JM, Fowler JR. Trigger finger: adult and pediatric treatment strategies. Orthop Clin North Am. 2015;46:561-569. doi: 10.1016/j.ocl.2015.06.014
8. Bianchi S, Gitto S, Draghi F. Ultrasound features of trigger finger: review of the literature. J Ultrasound Med. 2019;38:3141-3154. doi: 10.1002/jum.15025
9. Chuang XL, Ooi CC, Chin ST, et al. What triggers in trigger finger? The flexor tendons at the flexor digitorum superficialis bifurcation. J Plast Reconstr Aesthet Surg. 2017;70:1411-1419. doi: 10.1016/j.bjps.2017.05.037
10. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006;31:135-146. doi: 10.1016/j.jhsa.2005.10.013
11. Chapter 56: Tendinoapthy. In: Wolfe SW, Peterson WC, Kozin SH, Cohen MS. Green’s Operative Hand Surgery. Vol 2. 7th ed. Elsevier; 2017: 1904-1925.
12. Tarbhai K, Hannah S, von Schroeder HP. Trigger finger treatment: a comparison of 2 splint designs. J Hand Surg Am. 2012;37:243-249, 249.e241. doi: 10.1016/j.jhsa.2011.10.038
13. Valdes K. A retrospective review to determine the long-term efficacy of orthotic devices for trigger finger. J Hand Ther. 2012;25:89-95. doi: 10.1016/j.jht.2011.09.005
14. Drijkoningen T, van Berckel M, Becker SJE, et al. Night splinting for idiopathic trigger digits. Hand (N Y). 2018;13:558-562. doi: 10.1177/1558944717725374
15. Colbourn J, Heath N, Manary S, et al. Effectiveness of splinting for the treatment of trigger finger. J Hand Ther. 2008;21:336-343. doi: 10.1197/j.jht.2008.05.001
16. Teo SH, Ng DCL, Wong YKY. Effectiveness of proximal interphalangeal joint-blocking orthosis vs metacarpophalangeal joint-blocking orthosis in trigger digit management: A randomized clinical trial. J Hand Ther. 2018;32:444-451. doi: 10.1016/j.jht.2018.02.007
17. Ring D, Lozano-Calderon S, Shin R, et al. A prospective randomized controlled trial of injection of dexamethasone versus triamcinolone for idiopathic trigger finger. J Hand Surg Am. 2008;33:516-522; discussion 523-514. doi: 10.1016/j.jhsa.2008.01.001
18. Fleisch SB, Spindler KP, Lee DH. Corticosteroid injections in the treatment of trigger finger: A level I and II systematic review. J Am Acad Orthop Surg. 2007;15:166-171. doi: 10.5435/00124635-200703000-00006
19. Shinomiya R, Sunagawa T, Nakashima Y, et al. Impact of corticosteroid injection site on the treatment success rate of trigger finger: a prospective study comparing ultrasound-guided true intra-sheath and true extra-sheath injections. Ultrasound Med Biol. 2016;42:2203-2208. doi: 10.1016/j.ultrasmedbio.2016.05.015
20. Earp BE, Stanbury SJ, Mora AN, et al. Needle-free jet lidocaine administration for preinjection anesthesia in trigger finger injection: a randomized controlled trial. J Hand Surg Am. 2017;42:618-622. doi: 10.1016/j.jhsa.2017.05.001
21. Castellanos J, Munoz-Mahamud E, Dominguez E, et al. Long-term effectiveness of corticosteroid injections for trigger finger and thumb. J Hand Surg Am. 2015;40:121-126. doi: 10.1016/j.jhsa.2014.09.006
22. Dala-Ali BM, Nakhdjevani A, Lloyd MA, et al. The efficacy of steroid injection in the treatment of trigger finger. Clin Orthop Surg. 2012;4:263-268. doi: 10.4055/cios.2012.4.4.263
23. Griggs SM, Weiss AP, Lane LB, et al. Treatment of trigger finger in patients with diabetes mellitus. J Hand Surg Am. 1995;20:787-789. doi: 10.1016/s0363-5023(05)80432-0
24. Stepan JG, London DA, Boyer MI, et al. Blood glucose levels in diabetic patients following corticosteroid injections into the hand and wrist. J Hand Surg Am. 2014;39:706-712. doi: 10.1016/j.jhsa.2014.01.014
25. Hansen RL, Sondergaard M, Lange J. Open surgery versus ultrasound-guided corticosteroid injection for trigger finger: a randomized controlled trial with 1-year follow-up. J Hand Surg Am. 2017;42:359-366. doi: 10.1016/j.jhsa.2017.02.011
26. Mohd Rashid MZ, Sapuan J, Abdullah S. A randomized controlled trial of trigger finger release under digital anesthesia with (WALANT) and without adrenaline. J Orthop Surg (Hong Kong). 2019;27:2309499019833002. doi: 10.1177/2309499019833002
27. Zhao J-G, Kan S-L, Zhao L, et al. Percutaneous first annular pulley release for trigger digits: a systematic review and meta-analysis of current evidence. J Hand Surg Am. 2014;39:2192-2202. doi: 10.1016/j.jhsa.2014.07.044
28. Guler F, Kose O, Ercan EC, et al. Open versus percutaneous release for the treatment of trigger thumb. Orthopedics. 2013;36:e1290-1294. doi: 10.3928/01477447-20130920-22
29. Wu KC, Chern TC, Jou IM. Ultrasound-assisted percutaneous trigger finger release: it is safe [letter]. Hand (N Y). 2009;4:339. doi: 10.1007/s11552-009-9179-6
30. Nikolaou VS, Malahias M-A, Kaseta M-K, et al. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J Orthop. 2017;8:163-169. doi: 10.5312/wjo.v8.i2.163
31. Lim M-H, Lim K-K, Rasheed MZ, et al. Outcome of open trigger digit release. J Hand Surg Eur Vol. 2007;32:457-459. doi: 10.1016/j.Jhsb.2007.02.016
32. Wang J, Zhao J-G, Liang C-C. Percutaneous release, open surgery, or corticosteroid injection, which is the best treatment method for trigger digits? Clin Orthop Relat Res. 2013;471:1879-1886. doi: 10.1007/s11999-012-2716-6
33. Ng WKY, Olmscheid N, Worhacz K, et al. Steroid injection and open trigger finger release outcomes: a retrospective review of 999 digits. Hand (N Y). 2018;15:399-406. doi: 10.1177/1558944718796559
34. Ho SWL, Chia CY, Rajaratnam V. Characteristics and clinical outcomes of open surgery for trigger digits in diabetes. J Hand Microsurg. 2019;11:80-83. doi: 10.1055/s-0038-1670927
35. Sato ES, dos Santos JB, Belloti JC, et al. Percutaneous release of trigger fingers. Hand Clin. 2014;30:39-45. doi: 10.1016/j.hcl.2013.08.017
PRACTICE RECOMMENDATIONS
› Recommend splinting as a first-line conservative treatment for trigger finger if there is not a fixed contracture. B
› Prescribe corticosteroids, which may completely resolve trigger finger in the majority of patients without diabetes. A
› Refer patients for surgical release if they do not respond to conservative management. The surgical success rate is as high as 99%. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series

Do carotid artery calcifications seen on radiographs predict stenosis in asymptomatic adults?
EVIDENCE SUMMARY
Mixed results, quality issues do not support screening asymptomatic patients
A meta-analysis (12 observational studies; n = 1002) compared the diagnostic accuracy of
In a retrospective cohort study (n = 778) from the United States, researchers identified carotid artery calcifications on routine dental radiographs in patients ≥ 55 years old and prospectively performed duplex ultrasound (DUS) to assess for significant carotid stenosis (≥ 50%).2 Twenty-seven patients (3.5%) had carotid artery calcifications on radiographs, and 20 of those patients underwent DUS of bilateral carotid arteries (40 sides). Of 26 sides with calcifications on radiograph, 13 (50%) had stenosis confirmed with DUS. Of the 14 sides without calcification on radiograph, 3 (21%) had stenosis on DUS. The positive predictive value for calcification on PR predicting significant carotid stenosis was between 40% and 80%.
In a cross-sectional study from Sweden, investigators sought surgical candidates for asymptomatic carotid endarterectomy and performed PRs of 1182 patients.3 Calcifications were found in 176 people; 117 of them were eligible for asymptomatic carotid endarterectomy (ages 18-74; no cancer or other serious comorbidity; and no prior stroke or transient ischemic attack) and underwent ultrasound to assess for significant carotid stenosis (≥ 50%). Of the 117 participants who underwent ultrasound, 8 (6.8%; 95% CI, 2.2%-11.5%), all men, were found to have significant carotid stenosis. Compared to a sex- and age-matched reference group (n = 119) with no calcifications on PR, the prevalence of carotid stenosis was significantly higher in men (12.5%; 95% CI, 4.2%-20.8%) and in patients who were current smokers (19%; 95% CI, 0.7%-37.4%), were taking cholesterol medications (13.1%; 95% CI 4.4%-21.8%), and had a cardiovascular event history (15.9%; 95% CI, 7%-27.2%).
Recommendations from others
The US Preventive Services Task Force (USPSTF) and the American Academy of Family Physicians do not mention carotid screening with radiographs but recommend against
Editor’s takeaway
If you see calcification of the carotid artery on an x-ray of an asymptomatic patient, ignore it. The positive and negative predictive values for carotid stenosis are poor, and you should not pursue further testing.
1. Schroder AGD, de Araujo CM, Guariza-Filho O, et al. Diagnostic accuracy of panoramic radiography in the detection of calcified carotid artery atheroma: a meta-analysis. Clin Oral Investig. 2019;23:2021-2040. https://doi.org/10.1007/s00784-019-02880-6
2. Almog DM, Horev T, Illig KA, et al. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:768-773. doi: 10.1067/moe.2002.128965
3. Johansson EP, Ahlqvist J, Garoff M, et al. Ultrasound screening for asymptomatic carotid stenosis in subjects with calcifications in the area of the carotid arteries on panoramic radiographs: a cross-sectional study. BMC Cardiovasc Disord. 2011;11:44. doi: 10.1186/1471-2261-11-44
4. USPSTF. Carotid artery stenosis: screening. Updated February 2, 2021. Accessed September 1, 2021. www.uspreventiveservicestaskforce.org/uspstf/recommendation/carotid-artery-stenosis-screening
5. American Academy of Family Physicians. Don’t screen for carotid artery stenosis (CAS) in asymptomatic adult patients. Choosing Wisely website. Published February 21, 2013. Accessed August 29, 2020. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-carotid-artery-stenosis/
EVIDENCE SUMMARY
Mixed results, quality issues do not support screening asymptomatic patients
A meta-analysis (12 observational studies; n = 1002) compared the diagnostic accuracy of
In a retrospective cohort study (n = 778) from the United States, researchers identified carotid artery calcifications on routine dental radiographs in patients ≥ 55 years old and prospectively performed duplex ultrasound (DUS) to assess for significant carotid stenosis (≥ 50%).2 Twenty-seven patients (3.5%) had carotid artery calcifications on radiographs, and 20 of those patients underwent DUS of bilateral carotid arteries (40 sides). Of 26 sides with calcifications on radiograph, 13 (50%) had stenosis confirmed with DUS. Of the 14 sides without calcification on radiograph, 3 (21%) had stenosis on DUS. The positive predictive value for calcification on PR predicting significant carotid stenosis was between 40% and 80%.
In a cross-sectional study from Sweden, investigators sought surgical candidates for asymptomatic carotid endarterectomy and performed PRs of 1182 patients.3 Calcifications were found in 176 people; 117 of them were eligible for asymptomatic carotid endarterectomy (ages 18-74; no cancer or other serious comorbidity; and no prior stroke or transient ischemic attack) and underwent ultrasound to assess for significant carotid stenosis (≥ 50%). Of the 117 participants who underwent ultrasound, 8 (6.8%; 95% CI, 2.2%-11.5%), all men, were found to have significant carotid stenosis. Compared to a sex- and age-matched reference group (n = 119) with no calcifications on PR, the prevalence of carotid stenosis was significantly higher in men (12.5%; 95% CI, 4.2%-20.8%) and in patients who were current smokers (19%; 95% CI, 0.7%-37.4%), were taking cholesterol medications (13.1%; 95% CI 4.4%-21.8%), and had a cardiovascular event history (15.9%; 95% CI, 7%-27.2%).
Recommendations from others
The US Preventive Services Task Force (USPSTF) and the American Academy of Family Physicians do not mention carotid screening with radiographs but recommend against
Editor’s takeaway
If you see calcification of the carotid artery on an x-ray of an asymptomatic patient, ignore it. The positive and negative predictive values for carotid stenosis are poor, and you should not pursue further testing.
EVIDENCE SUMMARY
Mixed results, quality issues do not support screening asymptomatic patients
A meta-analysis (12 observational studies; n = 1002) compared the diagnostic accuracy of
In a retrospective cohort study (n = 778) from the United States, researchers identified carotid artery calcifications on routine dental radiographs in patients ≥ 55 years old and prospectively performed duplex ultrasound (DUS) to assess for significant carotid stenosis (≥ 50%).2 Twenty-seven patients (3.5%) had carotid artery calcifications on radiographs, and 20 of those patients underwent DUS of bilateral carotid arteries (40 sides). Of 26 sides with calcifications on radiograph, 13 (50%) had stenosis confirmed with DUS. Of the 14 sides without calcification on radiograph, 3 (21%) had stenosis on DUS. The positive predictive value for calcification on PR predicting significant carotid stenosis was between 40% and 80%.
In a cross-sectional study from Sweden, investigators sought surgical candidates for asymptomatic carotid endarterectomy and performed PRs of 1182 patients.3 Calcifications were found in 176 people; 117 of them were eligible for asymptomatic carotid endarterectomy (ages 18-74; no cancer or other serious comorbidity; and no prior stroke or transient ischemic attack) and underwent ultrasound to assess for significant carotid stenosis (≥ 50%). Of the 117 participants who underwent ultrasound, 8 (6.8%; 95% CI, 2.2%-11.5%), all men, were found to have significant carotid stenosis. Compared to a sex- and age-matched reference group (n = 119) with no calcifications on PR, the prevalence of carotid stenosis was significantly higher in men (12.5%; 95% CI, 4.2%-20.8%) and in patients who were current smokers (19%; 95% CI, 0.7%-37.4%), were taking cholesterol medications (13.1%; 95% CI 4.4%-21.8%), and had a cardiovascular event history (15.9%; 95% CI, 7%-27.2%).
Recommendations from others
The US Preventive Services Task Force (USPSTF) and the American Academy of Family Physicians do not mention carotid screening with radiographs but recommend against
Editor’s takeaway
If you see calcification of the carotid artery on an x-ray of an asymptomatic patient, ignore it. The positive and negative predictive values for carotid stenosis are poor, and you should not pursue further testing.
1. Schroder AGD, de Araujo CM, Guariza-Filho O, et al. Diagnostic accuracy of panoramic radiography in the detection of calcified carotid artery atheroma: a meta-analysis. Clin Oral Investig. 2019;23:2021-2040. https://doi.org/10.1007/s00784-019-02880-6
2. Almog DM, Horev T, Illig KA, et al. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:768-773. doi: 10.1067/moe.2002.128965
3. Johansson EP, Ahlqvist J, Garoff M, et al. Ultrasound screening for asymptomatic carotid stenosis in subjects with calcifications in the area of the carotid arteries on panoramic radiographs: a cross-sectional study. BMC Cardiovasc Disord. 2011;11:44. doi: 10.1186/1471-2261-11-44
4. USPSTF. Carotid artery stenosis: screening. Updated February 2, 2021. Accessed September 1, 2021. www.uspreventiveservicestaskforce.org/uspstf/recommendation/carotid-artery-stenosis-screening
5. American Academy of Family Physicians. Don’t screen for carotid artery stenosis (CAS) in asymptomatic adult patients. Choosing Wisely website. Published February 21, 2013. Accessed August 29, 2020. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-carotid-artery-stenosis/
1. Schroder AGD, de Araujo CM, Guariza-Filho O, et al. Diagnostic accuracy of panoramic radiography in the detection of calcified carotid artery atheroma: a meta-analysis. Clin Oral Investig. 2019;23:2021-2040. https://doi.org/10.1007/s00784-019-02880-6
2. Almog DM, Horev T, Illig KA, et al. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:768-773. doi: 10.1067/moe.2002.128965
3. Johansson EP, Ahlqvist J, Garoff M, et al. Ultrasound screening for asymptomatic carotid stenosis in subjects with calcifications in the area of the carotid arteries on panoramic radiographs: a cross-sectional study. BMC Cardiovasc Disord. 2011;11:44. doi: 10.1186/1471-2261-11-44
4. USPSTF. Carotid artery stenosis: screening. Updated February 2, 2021. Accessed September 1, 2021. www.uspreventiveservicestaskforce.org/uspstf/recommendation/carotid-artery-stenosis-screening
5. American Academy of Family Physicians. Don’t screen for carotid artery stenosis (CAS) in asymptomatic adult patients. Choosing Wisely website. Published February 21, 2013. Accessed August 29, 2020. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-carotid-artery-stenosis/
EVIDENCE-BASED ANSWER:
Not very well. In asymptomatic patients, carotid artery calcification seen on radiograph has a positive predictive value of 70% and a negative predictive value of 75% for carotid artery stenosis (strength of recommendation [SOR]: B, systematic review of observational studies with heterogeneous results and a retrospective cohort study). Carotid calcifications on radiographs may be more predictive of carotid stenosis in people with atherosclerotic risk factors (SOR: C, cross-sectional study). Harms outweigh benefits in screening for carotid artery stenosis in asymptomatic adults (SOR: B, multiple cohort studies); therefore, incidental radiographic carotid artery calcifications in asymptomatic patients should not prompt further testing.

FDA approves topical ruxolitinib for atopic dermatitis, first JAK inhibitor for this indication in the U.S.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.

The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.
The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.
The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
Supreme Court sets date for case that challenges Roe v. Wade
The Supreme Court will hear arguments in a major Mississippi abortion case on Dec. 1, which could challenge the landmark Roe v. Wade decision that guarantees a woman’s right to an abortion.
On Sept. 20, the court issued its calendar for arguments that will be heard in late November and early December, The Associated Press reported.
The Mississippi case, Dobbs v. Jackson Women’s Health Organization, is seeking to overturn Roe v. Wade by asking the Supreme Court to uphold a ban on most abortions after the 15th week of pregnancy. The state also said the court should overrule the 1992 decision in Planned Parenthood v. Casey that prevents states from banning abortion before viability, which is around 24 weeks of pregnancy.
Earlier in September, the Supreme Court allowed a Texas law to take effect that bans abortions after cardiac activity can be detected, which is around 6 weeks of pregnancy and often before many women know they’re pregnant. The court, which was split 5-4, didn’t rule on the constitutional nature of the law, instead declining to block its enforcement.
Hundreds of legal briefs have been filed on both sides of the case, the AP reported. On Sept. 20, more than 500 women athletes, including members of the Women’s National Basketball Players Association, the National Women’s Soccer League Players Association, and Olympic medalists, filed a brief that said an abortion ban would be devastating for female athletes.
The Mississippi law was enacted in 2018 but was blocked after a challenge at the federal court level. The state’s only abortion clinic, Jackson Women’s Health Organization, remains open and offers abortions up to 16 weeks of pregnancy, the AP reported. About 100 abortions a year are completed after 15 weeks, the organization said.
More than 90% of abortions in the United States occur in the first 13 weeks of pregnancy, the AP said.
The Supreme Court justices will return to the courtroom in October to hear arguments now that all of them have been vaccinated, the AP reported. The justices had been hearing cases by phone during the pandemic.
The public won’t be able to attend sessions, but the court will allow live audio of the session.
A version of this article first appeared on WebMD.com.
The Supreme Court will hear arguments in a major Mississippi abortion case on Dec. 1, which could challenge the landmark Roe v. Wade decision that guarantees a woman’s right to an abortion.
On Sept. 20, the court issued its calendar for arguments that will be heard in late November and early December, The Associated Press reported.
The Mississippi case, Dobbs v. Jackson Women’s Health Organization, is seeking to overturn Roe v. Wade by asking the Supreme Court to uphold a ban on most abortions after the 15th week of pregnancy. The state also said the court should overrule the 1992 decision in Planned Parenthood v. Casey that prevents states from banning abortion before viability, which is around 24 weeks of pregnancy.
Earlier in September, the Supreme Court allowed a Texas law to take effect that bans abortions after cardiac activity can be detected, which is around 6 weeks of pregnancy and often before many women know they’re pregnant. The court, which was split 5-4, didn’t rule on the constitutional nature of the law, instead declining to block its enforcement.
Hundreds of legal briefs have been filed on both sides of the case, the AP reported. On Sept. 20, more than 500 women athletes, including members of the Women’s National Basketball Players Association, the National Women’s Soccer League Players Association, and Olympic medalists, filed a brief that said an abortion ban would be devastating for female athletes.
The Mississippi law was enacted in 2018 but was blocked after a challenge at the federal court level. The state’s only abortion clinic, Jackson Women’s Health Organization, remains open and offers abortions up to 16 weeks of pregnancy, the AP reported. About 100 abortions a year are completed after 15 weeks, the organization said.
More than 90% of abortions in the United States occur in the first 13 weeks of pregnancy, the AP said.
The Supreme Court justices will return to the courtroom in October to hear arguments now that all of them have been vaccinated, the AP reported. The justices had been hearing cases by phone during the pandemic.
The public won’t be able to attend sessions, but the court will allow live audio of the session.
A version of this article first appeared on WebMD.com.
The Supreme Court will hear arguments in a major Mississippi abortion case on Dec. 1, which could challenge the landmark Roe v. Wade decision that guarantees a woman’s right to an abortion.
On Sept. 20, the court issued its calendar for arguments that will be heard in late November and early December, The Associated Press reported.
The Mississippi case, Dobbs v. Jackson Women’s Health Organization, is seeking to overturn Roe v. Wade by asking the Supreme Court to uphold a ban on most abortions after the 15th week of pregnancy. The state also said the court should overrule the 1992 decision in Planned Parenthood v. Casey that prevents states from banning abortion before viability, which is around 24 weeks of pregnancy.
Earlier in September, the Supreme Court allowed a Texas law to take effect that bans abortions after cardiac activity can be detected, which is around 6 weeks of pregnancy and often before many women know they’re pregnant. The court, which was split 5-4, didn’t rule on the constitutional nature of the law, instead declining to block its enforcement.
Hundreds of legal briefs have been filed on both sides of the case, the AP reported. On Sept. 20, more than 500 women athletes, including members of the Women’s National Basketball Players Association, the National Women’s Soccer League Players Association, and Olympic medalists, filed a brief that said an abortion ban would be devastating for female athletes.
The Mississippi law was enacted in 2018 but was blocked after a challenge at the federal court level. The state’s only abortion clinic, Jackson Women’s Health Organization, remains open and offers abortions up to 16 weeks of pregnancy, the AP reported. About 100 abortions a year are completed after 15 weeks, the organization said.
More than 90% of abortions in the United States occur in the first 13 weeks of pregnancy, the AP said.
The Supreme Court justices will return to the courtroom in October to hear arguments now that all of them have been vaccinated, the AP reported. The justices had been hearing cases by phone during the pandemic.
The public won’t be able to attend sessions, but the court will allow live audio of the session.
A version of this article first appeared on WebMD.com.
Most community-based oncologists skip biomarker testing
A recent survey shows that fewer than half of community oncologists use biomarker testing to guide patient discussions about treatment, which compares with 73% of academic clinicians.
The findings, reported at the 2020 World Conference on Lung Cancer, which was rescheduled for January 2021, highlight the potential for unequal application of the latest advances in cancer genomics and targeted therapies throughout the health care system, which could worsen existing disparities in underserved populations, according to Leigh Boehmer, PharmD, medical director for the Association of Community Cancer Centers, Rockville, Md.
The survey – a mixed-methods approach for assessing practice patterns, attitudes, barriers, and resource needs related to biomarker testing among clinicians – was developed by the ACCC in partnership with the LUNGevity Foundation and administered to clinicians caring for patients with non–small cell lung cancer who are uninsured or covered by Medicaid.
Of 99 respondents, more than 85% were physicians and 68% worked in a community setting. Only 40% indicated they were very familiar or extremely familiar with 2018 Molecular Testing Guidelines for Lung Cancer from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology.
Clinicians were most confident about selecting appropriate tests to use, interpreting test results, and prognosticating based on test results, with 77%, 74%, and 74%, respectively, saying they are very confident or extremely confident in those areas. They were less confident about determining when to order testing and in coordinating care across the multidisciplinary team, with 59% and 64%, respectively, saying they were very confident or extremely confident in those areas, Dr. Boehmer reported at the conference.
The shortcomings with respect to communication across teams were echoed in two focus groups convened to further validate the survey results, he noted.
As for the reasons why clinicians ordered biomarker testing, 88% and 82% of community and academic clinicians, respectively, said they did so to help make targeted treatment decisions.
“Only 48% of community clinicians indicated that they use biomarker testing to guide patient discussions, compared to 73% of academic clinicians,” he said. “That finding was considered statistically significant.”
With respect to decision-making about biomarker testing, 41% said they prefer to share the responsibility with patients, whereas 52% said they prefer to make the final decision.
“Shedding further light on this situation, focus group participants expressed that patients lacked comprehension and interest about what testing entails and what testing means for their treatment options,” Dr. Boehmer noted.
In order to make more informed decisions about biomarker testing, respondents said they need more information on financial resources for patient assistance (26%) and education around both published guidelines and practical implications of the clinical data (21%).
When asked about patients’ information needs, 23% said their patients need psychosocial support, 22% said they need financial assistance, and 9% said their patients have no additional resource needs.
However, only 27% said they provide patients with resources related to psychosocial support services, and only 44% share financial assistance information, he said.
Further, the fact that 9% said their patients need no additional resources represents “a disconnect” from the findings of the survey and focus groups, he added.
“We believe that this study identifies key areas of ongoing clinician need related to biomarker testing, including things like increased guideline familiarity, practical applications of guideline-concordant testing, and … how to optimally coordinate multidisciplinary care delivery,” Dr. Boehmer said. “Professional organizations … in partnership with patient advocacy organizations or groups should focus on developing those patient education materials … and tools for improving patient-clinician discussions about biomarker testing.”
The ACCC will be working with the LUNGevity Foundation and the Center for Business Models in Healthcare to develop an intervention to ensure that such discussions are “easily integrated into the care process for every patient,” he noted.
Such efforts are important for ensuring that clinicians are informed about the value of biomarker testing and about guidelines for testing so that patients receive the best possible care, said invited discussant Joshua Sabari, MD, of New York University Langone Health’s Perlmutter Cancer Center.
“I know that, in clinic, when meeting a new patient with non–small cell lung cancer, it’s critical to understand the driver alteration, not only for prognosis, but also for goals-of-care discussion, as well as potential treatment option,” Dr. Sabari said.
Dr. Boehmer reported consulting for Pfizer. Dr. Sabari reported consulting and advisory board membership for multiple pharmaceutical companies.
A recent survey shows that fewer than half of community oncologists use biomarker testing to guide patient discussions about treatment, which compares with 73% of academic clinicians.
The findings, reported at the 2020 World Conference on Lung Cancer, which was rescheduled for January 2021, highlight the potential for unequal application of the latest advances in cancer genomics and targeted therapies throughout the health care system, which could worsen existing disparities in underserved populations, according to Leigh Boehmer, PharmD, medical director for the Association of Community Cancer Centers, Rockville, Md.
The survey – a mixed-methods approach for assessing practice patterns, attitudes, barriers, and resource needs related to biomarker testing among clinicians – was developed by the ACCC in partnership with the LUNGevity Foundation and administered to clinicians caring for patients with non–small cell lung cancer who are uninsured or covered by Medicaid.
Of 99 respondents, more than 85% were physicians and 68% worked in a community setting. Only 40% indicated they were very familiar or extremely familiar with 2018 Molecular Testing Guidelines for Lung Cancer from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology.
Clinicians were most confident about selecting appropriate tests to use, interpreting test results, and prognosticating based on test results, with 77%, 74%, and 74%, respectively, saying they are very confident or extremely confident in those areas. They were less confident about determining when to order testing and in coordinating care across the multidisciplinary team, with 59% and 64%, respectively, saying they were very confident or extremely confident in those areas, Dr. Boehmer reported at the conference.
The shortcomings with respect to communication across teams were echoed in two focus groups convened to further validate the survey results, he noted.
As for the reasons why clinicians ordered biomarker testing, 88% and 82% of community and academic clinicians, respectively, said they did so to help make targeted treatment decisions.
“Only 48% of community clinicians indicated that they use biomarker testing to guide patient discussions, compared to 73% of academic clinicians,” he said. “That finding was considered statistically significant.”
With respect to decision-making about biomarker testing, 41% said they prefer to share the responsibility with patients, whereas 52% said they prefer to make the final decision.
“Shedding further light on this situation, focus group participants expressed that patients lacked comprehension and interest about what testing entails and what testing means for their treatment options,” Dr. Boehmer noted.
In order to make more informed decisions about biomarker testing, respondents said they need more information on financial resources for patient assistance (26%) and education around both published guidelines and practical implications of the clinical data (21%).
When asked about patients’ information needs, 23% said their patients need psychosocial support, 22% said they need financial assistance, and 9% said their patients have no additional resource needs.
However, only 27% said they provide patients with resources related to psychosocial support services, and only 44% share financial assistance information, he said.
Further, the fact that 9% said their patients need no additional resources represents “a disconnect” from the findings of the survey and focus groups, he added.
“We believe that this study identifies key areas of ongoing clinician need related to biomarker testing, including things like increased guideline familiarity, practical applications of guideline-concordant testing, and … how to optimally coordinate multidisciplinary care delivery,” Dr. Boehmer said. “Professional organizations … in partnership with patient advocacy organizations or groups should focus on developing those patient education materials … and tools for improving patient-clinician discussions about biomarker testing.”
The ACCC will be working with the LUNGevity Foundation and the Center for Business Models in Healthcare to develop an intervention to ensure that such discussions are “easily integrated into the care process for every patient,” he noted.
Such efforts are important for ensuring that clinicians are informed about the value of biomarker testing and about guidelines for testing so that patients receive the best possible care, said invited discussant Joshua Sabari, MD, of New York University Langone Health’s Perlmutter Cancer Center.
“I know that, in clinic, when meeting a new patient with non–small cell lung cancer, it’s critical to understand the driver alteration, not only for prognosis, but also for goals-of-care discussion, as well as potential treatment option,” Dr. Sabari said.
Dr. Boehmer reported consulting for Pfizer. Dr. Sabari reported consulting and advisory board membership for multiple pharmaceutical companies.
A recent survey shows that fewer than half of community oncologists use biomarker testing to guide patient discussions about treatment, which compares with 73% of academic clinicians.
The findings, reported at the 2020 World Conference on Lung Cancer, which was rescheduled for January 2021, highlight the potential for unequal application of the latest advances in cancer genomics and targeted therapies throughout the health care system, which could worsen existing disparities in underserved populations, according to Leigh Boehmer, PharmD, medical director for the Association of Community Cancer Centers, Rockville, Md.
The survey – a mixed-methods approach for assessing practice patterns, attitudes, barriers, and resource needs related to biomarker testing among clinicians – was developed by the ACCC in partnership with the LUNGevity Foundation and administered to clinicians caring for patients with non–small cell lung cancer who are uninsured or covered by Medicaid.
Of 99 respondents, more than 85% were physicians and 68% worked in a community setting. Only 40% indicated they were very familiar or extremely familiar with 2018 Molecular Testing Guidelines for Lung Cancer from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology.
Clinicians were most confident about selecting appropriate tests to use, interpreting test results, and prognosticating based on test results, with 77%, 74%, and 74%, respectively, saying they are very confident or extremely confident in those areas. They were less confident about determining when to order testing and in coordinating care across the multidisciplinary team, with 59% and 64%, respectively, saying they were very confident or extremely confident in those areas, Dr. Boehmer reported at the conference.
The shortcomings with respect to communication across teams were echoed in two focus groups convened to further validate the survey results, he noted.
As for the reasons why clinicians ordered biomarker testing, 88% and 82% of community and academic clinicians, respectively, said they did so to help make targeted treatment decisions.
“Only 48% of community clinicians indicated that they use biomarker testing to guide patient discussions, compared to 73% of academic clinicians,” he said. “That finding was considered statistically significant.”
With respect to decision-making about biomarker testing, 41% said they prefer to share the responsibility with patients, whereas 52% said they prefer to make the final decision.
“Shedding further light on this situation, focus group participants expressed that patients lacked comprehension and interest about what testing entails and what testing means for their treatment options,” Dr. Boehmer noted.
In order to make more informed decisions about biomarker testing, respondents said they need more information on financial resources for patient assistance (26%) and education around both published guidelines and practical implications of the clinical data (21%).
When asked about patients’ information needs, 23% said their patients need psychosocial support, 22% said they need financial assistance, and 9% said their patients have no additional resource needs.
However, only 27% said they provide patients with resources related to psychosocial support services, and only 44% share financial assistance information, he said.
Further, the fact that 9% said their patients need no additional resources represents “a disconnect” from the findings of the survey and focus groups, he added.
“We believe that this study identifies key areas of ongoing clinician need related to biomarker testing, including things like increased guideline familiarity, practical applications of guideline-concordant testing, and … how to optimally coordinate multidisciplinary care delivery,” Dr. Boehmer said. “Professional organizations … in partnership with patient advocacy organizations or groups should focus on developing those patient education materials … and tools for improving patient-clinician discussions about biomarker testing.”
The ACCC will be working with the LUNGevity Foundation and the Center for Business Models in Healthcare to develop an intervention to ensure that such discussions are “easily integrated into the care process for every patient,” he noted.
Such efforts are important for ensuring that clinicians are informed about the value of biomarker testing and about guidelines for testing so that patients receive the best possible care, said invited discussant Joshua Sabari, MD, of New York University Langone Health’s Perlmutter Cancer Center.
“I know that, in clinic, when meeting a new patient with non–small cell lung cancer, it’s critical to understand the driver alteration, not only for prognosis, but also for goals-of-care discussion, as well as potential treatment option,” Dr. Sabari said.
Dr. Boehmer reported consulting for Pfizer. Dr. Sabari reported consulting and advisory board membership for multiple pharmaceutical companies.
REPORTING FROM WCLC 2020
Nurses ‘at the breaking point,’ consider quitting due to COVID issues: Survey
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
Decline in child COVID may signal end of latest surge
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.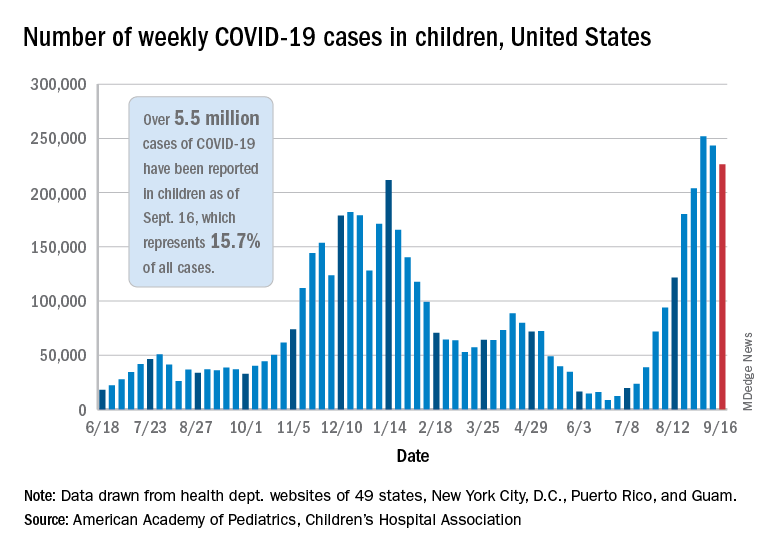
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
Cancer risk after radioiodine for hyperthyroidism ‘small’: Meta-analysis
Amid ongoing debate over potential adverse effects of radioactive iodine (RAI) in the treatment of hyperthyroidism, a new meta-analysis shows no significant increase in the risk of cancer or cancer mortality in the vast majority of cases, with an increased dose-response risk with higher doses shown in some studies.
“These findings suggest that radiation-induced cancer risks following RAI therapy for hyperthyroidism are small and, in observational studies, may only be detectable at higher levels of administered dose,” report the authors of the analysis, published Sept. 27 in JAMA Network Open.
In a commentary published along with the study, Bernadette Biondi, MD, noted that, despite some limitations, “the current analysis from recent literature studies is reassuring on the potential negative effects of RAI”.
“These data can help reduce anxiety in both patients and clinicians as to the risk of cancer after RAI.”
Martin A. Walter, MD, agreed. “When including nearly a half-million patients into the analysis, there is no significant increase of risk for secondary cancers after radioiodine therapy for hyperthyroidism,” Dr. Walter, who was a coauthor on the American Thyroid Association’s guidelines for the diagnosis and management of hyperthyroidism (Thyroid. 2016 Oct;26:1343-421), told this news organization.
“For me, this paper is rather reassuring of the safety of the therapy,” he added.
Though used in the treatment of hyperthyroidism for more than 7 decades, the frequent use of RAI continues to generate concern of potential carcinogenic effects, with some previous studies linking the treatment with subsequent malignant neoplasms, while others have shown no risk.
However, the potential role of a dose-response effect on the cancer risk has not been well explored, the authors note.
For their meta-analysis, Sung Ryul Shim, PhD, of the department of preventive medicine, Korea University, Seoul, South Korea, and colleagues identified 12 studies including 479,452 participants that involved evaluation of cancer incidence and mortality with exposure versus nonexposure to RAI therapy for hyperthyroidism.
Overall, the results showed no significant difference in the pooled cancer incidence ratio between those who were and were not exposed to RAI therapy (incidence ratio, 1.02), and there also were no significant differences in mortality (IR, 0.98).
There were no increases in the risk of any specific cancers with the exception of thyroid cancer, which had a higher incidence among those with RAI treatment (1.86), and more than twice the risk of mortality (2.22).
Two studies did report a linear dose-response association between RAI for hyperthyroidism and breast cancer mortality (1.35 per 370 MBq; P = .03) and solid cancer mortality (1.14 per 370 MBq; P = .01).
Among them was a 2019 study, using data on nearly 19,000 patients from the multicenter Cooperative Thyrotoxicosis Therapy Follow-up Study, showing a dose-response effect on solid-cancer mortality that the study authors described as “modest.”
“For every 1,000 patients with hyperthyroidism receiving typical doses to the stomach (150-250 mGy), an estimated lifetime excess of 19-32 solid cancer deaths could occur,” the study concluded.
Caveats surrounding the issue include that hyperthyroidism itself has been associated with an increased risk of cancer, suggesting a potential role of an excess of thyroid hormone excess on cancer risk.
“The underlying conditions of the thyroid gland could be another possible reason for the increased risk of malignant thyroid tumor after RAI for hyperthyroidism,” the investigators of the current study write.
“Thyroid-stimulating hormone and thyroid-stimulating antibodies, present in Graves disease, may play a role in carcinogenesis and tumoral growth, and hyperthyroidism is associated with a high incidence of thyroid carcinoma,” they add.
Tumors developing from hyperthyroid tissue show aggressive behavior, they add, and note that an increased overall risk of cancer and greater cancer mortality has been also reported with the alternative of antithyroid drug therapy when compared with RAI.
Nevertheless, considering the dose-response risk observed in the two studies, the authors and Dr. Bondi agree that more rigorous studies are needed to investigate the issue.
“The limited quality of the evidence in the literature on the adverse effects of RAI underlines the need for future randomized clinical trials in this area,” writes Dr. Bondi, of the department of clinical medicine and surgery, University of Naples (Italy) Federico II, in her editorial.
In further commenting, Dr. Walter, of the department of nuclear medicine, University Hospital, University of Geneva, agreed that the benefits of treatment need to be weighed against the risks.
“There is always caution used when deciding for a medical therapy, including radioiodine therapy,” he added. “It has to be emphasized though, that poorly controlled hyperthyroidism is a serious condition that, for instance, can lead to arrhythmia, and that in elderly patients is associated with increased mortality,” Dr, Walter cautioned.
“Statistically significant does not always mean clinically relevant, and the benefits clearly outweigh the risks.”
The authors, Dr. Bondi, and Dr. Walter had no disclosures to report.
Amid ongoing debate over potential adverse effects of radioactive iodine (RAI) in the treatment of hyperthyroidism, a new meta-analysis shows no significant increase in the risk of cancer or cancer mortality in the vast majority of cases, with an increased dose-response risk with higher doses shown in some studies.
“These findings suggest that radiation-induced cancer risks following RAI therapy for hyperthyroidism are small and, in observational studies, may only be detectable at higher levels of administered dose,” report the authors of the analysis, published Sept. 27 in JAMA Network Open.
In a commentary published along with the study, Bernadette Biondi, MD, noted that, despite some limitations, “the current analysis from recent literature studies is reassuring on the potential negative effects of RAI”.
“These data can help reduce anxiety in both patients and clinicians as to the risk of cancer after RAI.”
Martin A. Walter, MD, agreed. “When including nearly a half-million patients into the analysis, there is no significant increase of risk for secondary cancers after radioiodine therapy for hyperthyroidism,” Dr. Walter, who was a coauthor on the American Thyroid Association’s guidelines for the diagnosis and management of hyperthyroidism (Thyroid. 2016 Oct;26:1343-421), told this news organization.
“For me, this paper is rather reassuring of the safety of the therapy,” he added.
Though used in the treatment of hyperthyroidism for more than 7 decades, the frequent use of RAI continues to generate concern of potential carcinogenic effects, with some previous studies linking the treatment with subsequent malignant neoplasms, while others have shown no risk.
However, the potential role of a dose-response effect on the cancer risk has not been well explored, the authors note.
For their meta-analysis, Sung Ryul Shim, PhD, of the department of preventive medicine, Korea University, Seoul, South Korea, and colleagues identified 12 studies including 479,452 participants that involved evaluation of cancer incidence and mortality with exposure versus nonexposure to RAI therapy for hyperthyroidism.
Overall, the results showed no significant difference in the pooled cancer incidence ratio between those who were and were not exposed to RAI therapy (incidence ratio, 1.02), and there also were no significant differences in mortality (IR, 0.98).
There were no increases in the risk of any specific cancers with the exception of thyroid cancer, which had a higher incidence among those with RAI treatment (1.86), and more than twice the risk of mortality (2.22).
Two studies did report a linear dose-response association between RAI for hyperthyroidism and breast cancer mortality (1.35 per 370 MBq; P = .03) and solid cancer mortality (1.14 per 370 MBq; P = .01).
Among them was a 2019 study, using data on nearly 19,000 patients from the multicenter Cooperative Thyrotoxicosis Therapy Follow-up Study, showing a dose-response effect on solid-cancer mortality that the study authors described as “modest.”
“For every 1,000 patients with hyperthyroidism receiving typical doses to the stomach (150-250 mGy), an estimated lifetime excess of 19-32 solid cancer deaths could occur,” the study concluded.
Caveats surrounding the issue include that hyperthyroidism itself has been associated with an increased risk of cancer, suggesting a potential role of an excess of thyroid hormone excess on cancer risk.
“The underlying conditions of the thyroid gland could be another possible reason for the increased risk of malignant thyroid tumor after RAI for hyperthyroidism,” the investigators of the current study write.
“Thyroid-stimulating hormone and thyroid-stimulating antibodies, present in Graves disease, may play a role in carcinogenesis and tumoral growth, and hyperthyroidism is associated with a high incidence of thyroid carcinoma,” they add.
Tumors developing from hyperthyroid tissue show aggressive behavior, they add, and note that an increased overall risk of cancer and greater cancer mortality has been also reported with the alternative of antithyroid drug therapy when compared with RAI.
Nevertheless, considering the dose-response risk observed in the two studies, the authors and Dr. Bondi agree that more rigorous studies are needed to investigate the issue.
“The limited quality of the evidence in the literature on the adverse effects of RAI underlines the need for future randomized clinical trials in this area,” writes Dr. Bondi, of the department of clinical medicine and surgery, University of Naples (Italy) Federico II, in her editorial.
In further commenting, Dr. Walter, of the department of nuclear medicine, University Hospital, University of Geneva, agreed that the benefits of treatment need to be weighed against the risks.
“There is always caution used when deciding for a medical therapy, including radioiodine therapy,” he added. “It has to be emphasized though, that poorly controlled hyperthyroidism is a serious condition that, for instance, can lead to arrhythmia, and that in elderly patients is associated with increased mortality,” Dr, Walter cautioned.
“Statistically significant does not always mean clinically relevant, and the benefits clearly outweigh the risks.”
The authors, Dr. Bondi, and Dr. Walter had no disclosures to report.
Amid ongoing debate over potential adverse effects of radioactive iodine (RAI) in the treatment of hyperthyroidism, a new meta-analysis shows no significant increase in the risk of cancer or cancer mortality in the vast majority of cases, with an increased dose-response risk with higher doses shown in some studies.
“These findings suggest that radiation-induced cancer risks following RAI therapy for hyperthyroidism are small and, in observational studies, may only be detectable at higher levels of administered dose,” report the authors of the analysis, published Sept. 27 in JAMA Network Open.
In a commentary published along with the study, Bernadette Biondi, MD, noted that, despite some limitations, “the current analysis from recent literature studies is reassuring on the potential negative effects of RAI”.
“These data can help reduce anxiety in both patients and clinicians as to the risk of cancer after RAI.”
Martin A. Walter, MD, agreed. “When including nearly a half-million patients into the analysis, there is no significant increase of risk for secondary cancers after radioiodine therapy for hyperthyroidism,” Dr. Walter, who was a coauthor on the American Thyroid Association’s guidelines for the diagnosis and management of hyperthyroidism (Thyroid. 2016 Oct;26:1343-421), told this news organization.
“For me, this paper is rather reassuring of the safety of the therapy,” he added.
Though used in the treatment of hyperthyroidism for more than 7 decades, the frequent use of RAI continues to generate concern of potential carcinogenic effects, with some previous studies linking the treatment with subsequent malignant neoplasms, while others have shown no risk.
However, the potential role of a dose-response effect on the cancer risk has not been well explored, the authors note.
For their meta-analysis, Sung Ryul Shim, PhD, of the department of preventive medicine, Korea University, Seoul, South Korea, and colleagues identified 12 studies including 479,452 participants that involved evaluation of cancer incidence and mortality with exposure versus nonexposure to RAI therapy for hyperthyroidism.
Overall, the results showed no significant difference in the pooled cancer incidence ratio between those who were and were not exposed to RAI therapy (incidence ratio, 1.02), and there also were no significant differences in mortality (IR, 0.98).
There were no increases in the risk of any specific cancers with the exception of thyroid cancer, which had a higher incidence among those with RAI treatment (1.86), and more than twice the risk of mortality (2.22).
Two studies did report a linear dose-response association between RAI for hyperthyroidism and breast cancer mortality (1.35 per 370 MBq; P = .03) and solid cancer mortality (1.14 per 370 MBq; P = .01).
Among them was a 2019 study, using data on nearly 19,000 patients from the multicenter Cooperative Thyrotoxicosis Therapy Follow-up Study, showing a dose-response effect on solid-cancer mortality that the study authors described as “modest.”
“For every 1,000 patients with hyperthyroidism receiving typical doses to the stomach (150-250 mGy), an estimated lifetime excess of 19-32 solid cancer deaths could occur,” the study concluded.
Caveats surrounding the issue include that hyperthyroidism itself has been associated with an increased risk of cancer, suggesting a potential role of an excess of thyroid hormone excess on cancer risk.
“The underlying conditions of the thyroid gland could be another possible reason for the increased risk of malignant thyroid tumor after RAI for hyperthyroidism,” the investigators of the current study write.
“Thyroid-stimulating hormone and thyroid-stimulating antibodies, present in Graves disease, may play a role in carcinogenesis and tumoral growth, and hyperthyroidism is associated with a high incidence of thyroid carcinoma,” they add.
Tumors developing from hyperthyroid tissue show aggressive behavior, they add, and note that an increased overall risk of cancer and greater cancer mortality has been also reported with the alternative of antithyroid drug therapy when compared with RAI.
Nevertheless, considering the dose-response risk observed in the two studies, the authors and Dr. Bondi agree that more rigorous studies are needed to investigate the issue.
“The limited quality of the evidence in the literature on the adverse effects of RAI underlines the need for future randomized clinical trials in this area,” writes Dr. Bondi, of the department of clinical medicine and surgery, University of Naples (Italy) Federico II, in her editorial.
In further commenting, Dr. Walter, of the department of nuclear medicine, University Hospital, University of Geneva, agreed that the benefits of treatment need to be weighed against the risks.
“There is always caution used when deciding for a medical therapy, including radioiodine therapy,” he added. “It has to be emphasized though, that poorly controlled hyperthyroidism is a serious condition that, for instance, can lead to arrhythmia, and that in elderly patients is associated with increased mortality,” Dr, Walter cautioned.
“Statistically significant does not always mean clinically relevant, and the benefits clearly outweigh the risks.”
The authors, Dr. Bondi, and Dr. Walter had no disclosures to report.
FROM JAMA OPEN NETWORK
How to engage soldiers, veterans in psychiatric treatment
Deployments in places such as Afghanistan and Iraq, and traumatic events such as the Sept. 11, 2001, attacks affect everyone, but military personnel and veterans face unique circumstances that can present challenges to treatment. Much progress has been made in recent years in treating people with posttraumatic stress disorder and helping them recover after traumatic events.

To explore some of those changes and challenges, this news organization interviewed Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH, who retired from the Army in 2010 after assignments and missions that took her to Korea, Somalia, Iraq, and Cuba, about her approaches to treating soldiers and veterans.
Dr. Ritchie is chief of psychiatry at Medstar Washington Hospital Center, and a professor of psychiatry at the Uniformed Services University of the Health Sciences in Bethesda, Md., and at Georgetown University and George Washington University, both in Washington.
She is the author of 250 publications, including the book, “Forensic and Ethical Issues in Military Behavioral Health” (Fort Sam Houston, Tex.: Borden Institute, 2015). In addition, Dr. Ritchie is coeditor of “Post-Traumatic Stress Disorder and Related Diseases in Combat Veterans” (New York: Springer, 2015) and “Psychiatrists in Combat, Clinicians Experience in the War Zone” (New York: Springer, 2017).
Question: What are some of the interventions available in the aftermath of traumatic events?
Answer: What we thought the standard of care should be after a traumatic event was to have what’s called a critical incident stress debriefing (CISD). It was basically getting the members of the group who had been traumatized by a school shooting or plane crash, or the Oklahoma City bombing, getting them all together literally a few hours after the event, and having them tell what happened. And the idea is to get it all out. But what we discovered is that this could actually make people worse, because you’d be hearing not only about your own trauma, but other people’s traumas, and that it was too soon for the event.

So prior to 9/11, we had organized a conference, which was held in October 2001, just a month after 9/11. At that conference, we worked on mass violence and early intervention, which is the name of the book that came out from the (National Institute of Mental Health) as a result. It focused on basic principles of safety and security and communication, and knowing where your family was, rather than reliving the trauma. Now, we did think that sometimes you could have a CISD that would be helpful, but only when it was people who knew each other well, like an ED group who would work with each other or soldiers who served together.
Q: What was your involvement in the aftermath of the Sept. 11 attacks?
A: At the time of 9/11, I was assigned at the Pentagon, but I wasn’t there. When the plane hit, I was actually across the river at the Navy’s Bureau of Medicine and Surgery. And then for the next 3 weeks, all I did was work at the Pentagon. We used some of these principles of early intervention but not focusing on telling us what happened right afterward. We focused on how the service members and their families were coping in the here and now, and how they could support each other.
We knew that soldiers would not come out of their offices to go to a therapist. They are too strong for that. So, we did what was called “therapy by walking around.” We went to the service members’ offices.
There was also a Family Assistance Center. That was for the families of the people who died. And that was very helpful because you had all the services there in one place – medical care, mental health care, therapy dogs, massage, the people who collected the DNA to identify remains. You had it in one place, the Sheraton in Crystal City, Va.. That has become a model now, especially for mass transportation fatalities. There are a lot more in the literature about Family Assistance Centers now, mainly formed by the National Transportation Safety Board.
Right after 9/11, we went to war in Afghanistan, and later in Iraq, and we had a lot of soldiers who developed both PTSD and traumatic brain injury (TBI). One of the good things that the military can do is they can really innovate with both medical treatment and mental health treatment because they don’t have to ask for an insurance company to pay for it. So for some years, starting in about 2004, Congress allocated a large sum of money every year to the Department of Defense to focus on treatment for PTSD and TBI.
And as a result of that, a couple of things happened. One was that the treatments that we had, we were able to study much better, exposure therapy and cognitive-behavioral therapy. We were able to do large trials, and then we continued with the use of medications when necessary. There are only two (Food and Drug Administration)–approved medicines for the treatment of PTSD: sertraline and paroxetine, but many others are used.
We also learned what didn’t work and what soldiers would not take. Most of these medications have sexual side effects. If you’re a young, healthy soldier, you really don’t want to be taking something that causes you erectile dysfunction, or in women a loss of libido. So many people wouldn’t take these therapies. As for exposure therapy, if you got into it and completed the program, usually your PTSD symptoms went down. But many people couldn’t complete it. In the exposure therapy, you’re talking about whatever trauma you’ve been through – maybe your best friend died next to you, and you don’t want to talk about that all the time.
When I talk to patients about this, I say the first bucket is medication, the second bucket is therapy, and the third bucket is everything else. And everything else includes meditation, yoga, exercise, and it also involves working with animals. There are programs where you’re paired with a service dog, who helps calm you down, and you feel protected.
One of my favorites is called Warrior Canine Connection, where a soldier with PTSD trains a puppy to become a service animal. And in the training of the dog, you have to learn to control your emotions, you have to modulate your voice, you have to appear calm. Often soldiers have a background that they’re familiar with animals, especially dogs. So that’s been very successful.
A couple of other (treatments) to mention one is called stellate ganglion block, where a little lidocaine is injected into the back of the cervical spine. It was used initially for pain control, and they found that it was actually very helpful for PTSD. Another thing we’ve learned is that pain and PTSD often go hand in hand, because if you’re in pain, you’ll be feeling awful, you won’t sleep well, you’ll have more nightmares. But if you can control both of them together, then that’s going to help.
Q: One issue that veterans may face is moral injury. Can you talk about that?
A: Moral injury is a term that was first used after Vietnam. Moral injury is not a psychiatric diagnosis. It is feelings of shame and guilt that can be very corrosive and can lead to suicide. It overlaps with PTSD. You feel either you’ve let yourself down, or the government has let you down. And this can be very corrosive. Another thing that could happen is, say, you switched your tour of duty with a buddy, and he got killed and you didn’t. A very common scenario is you’re manning a checkpoint, and a car comes at you and doesn’t stop like it’s supposed to. You do what you’ve been trained to do, which is open fire, and check on the car afterward. And there’s four little kids and their parents in the car all dead. And that is something that even though that was your sort of duty, that it still eats at you because you have kids the same age as the ones who were dead in the car.
You can still have these feelings of shame and guilt, and it will often bleed into your relationships with your family. And that can lead to distance and divorce, which is a further risk factor for suicide.
Q: Are there are any specific treatments that have been designed for moral injury, different from PTSD or other conditions?
A: The Armed Services has set up a number of intensive programs at different places, and each is a little bit different. They usually integrate moral injury in with some of the other treatments. There was one at Fort Bliss, Tex., that had reiki; they had art therapy. And they had the chaplains working on moral injury. So there’s no medical treatment for it, but there certainly is talking about it, and for some people to go to a chaplain can be very helpful.
There’s a Military Health System Centers of Excellence, which is a place by the new Walter Reed on the campus, they have a marvelous wall full of masks. And the masks have been painted by soldiers with usually a combination of PTSD, TBI, and although it’s not an official psychiatric diagnosis, moral injury. They’re able to draw and paint. Another thing that’s been used quite a bit as writing therapy, and journaling, and just writing down how you feel about something, because you can do that without retraumatizing anybody else, except perhaps if you are working with a therapist.
Q: For therapists who are treating soldiers, veterans, are there specific challenges that they should be aware of? Are these patients maybe different from the patients that they might otherwise see? Are there specific pieces of advice as to how to engage them?
A: There are a few things that are different. One is that many people in the military are not used to talking about their feelings. And that’s especially if you’ve got a young man who only grunts and says: “Hooah!” That is going to be hard to break through. And that’s why some of these other ways of reaching somebody is very effective. Also, the military likes to have physical activity; they’re usually not comfortable sitting in a chair. If you’re a civilian psychiatrist, I don’t expect you to go bungee jumping with your patients. But what I’d recommend is that you recommend to your patients that they stay active.
Another thing about veterans is that they like to be self-sufficient. They really don’t like to ask for help, although they might ask for help for their buddy. After the Pentagon and 9/11, when I was working with senior officers, they never needed any help. No, but their buddy over here might, so I could help them in the guise of providing care for their buddy in a group setting. We could work with everybody and enhance cohesion, morale, bonding, “we’re all in this together” type of feeling.
I think one thing that’s really improved is that there is less stigma around PTSD. People are more willing to present for help, and some people have called PTSD the Purple Heart of mental disorders. People don’t feel like it’s as bad as having depression or anxiety. Even though PTSD often has depression and anxiety components to it – they run hand in hand – still, it’s sort of more honorable if you’ve been at war and have gotten PTSD.
Q: How have you been faring yourself, in the face of the 9/11 anniversary and recent events in Afghanistan?
A: (The Sept. 11 weekend) was very sad for me – and a lot of my colleagues [with] the combination of the 20th anniversary of 9/11, and the recent development. Fortunately, I have friends and people I can talk to. I walked with a colleague of mine who was in the Army. I’m following my own rule of the three buckets, so we took a walk around the hospital center for about 45 minutes, and we have five fish ponds here. And we went and looked at the fish, and talked to the fish. At the National Rehab Hospital, they were playing the guitar. So there’s are a variety of things that people can do.
Deployments in places such as Afghanistan and Iraq, and traumatic events such as the Sept. 11, 2001, attacks affect everyone, but military personnel and veterans face unique circumstances that can present challenges to treatment. Much progress has been made in recent years in treating people with posttraumatic stress disorder and helping them recover after traumatic events.
To explore some of those changes and challenges, this news organization interviewed Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH, who retired from the Army in 2010 after assignments and missions that took her to Korea, Somalia, Iraq, and Cuba, about her approaches to treating soldiers and veterans.
Dr. Ritchie is chief of psychiatry at Medstar Washington Hospital Center, and a professor of psychiatry at the Uniformed Services University of the Health Sciences in Bethesda, Md., and at Georgetown University and George Washington University, both in Washington.
She is the author of 250 publications, including the book, “Forensic and Ethical Issues in Military Behavioral Health” (Fort Sam Houston, Tex.: Borden Institute, 2015). In addition, Dr. Ritchie is coeditor of “Post-Traumatic Stress Disorder and Related Diseases in Combat Veterans” (New York: Springer, 2015) and “Psychiatrists in Combat, Clinicians Experience in the War Zone” (New York: Springer, 2017).
Question: What are some of the interventions available in the aftermath of traumatic events?
Answer: What we thought the standard of care should be after a traumatic event was to have what’s called a critical incident stress debriefing (CISD). It was basically getting the members of the group who had been traumatized by a school shooting or plane crash, or the Oklahoma City bombing, getting them all together literally a few hours after the event, and having them tell what happened. And the idea is to get it all out. But what we discovered is that this could actually make people worse, because you’d be hearing not only about your own trauma, but other people’s traumas, and that it was too soon for the event.
So prior to 9/11, we had organized a conference, which was held in October 2001, just a month after 9/11. At that conference, we worked on mass violence and early intervention, which is the name of the book that came out from the (National Institute of Mental Health) as a result. It focused on basic principles of safety and security and communication, and knowing where your family was, rather than reliving the trauma. Now, we did think that sometimes you could have a CISD that would be helpful, but only when it was people who knew each other well, like an ED group who would work with each other or soldiers who served together.
Q: What was your involvement in the aftermath of the Sept. 11 attacks?
A: At the time of 9/11, I was assigned at the Pentagon, but I wasn’t there. When the plane hit, I was actually across the river at the Navy’s Bureau of Medicine and Surgery. And then for the next 3 weeks, all I did was work at the Pentagon. We used some of these principles of early intervention but not focusing on telling us what happened right afterward. We focused on how the service members and their families were coping in the here and now, and how they could support each other.
We knew that soldiers would not come out of their offices to go to a therapist. They are too strong for that. So, we did what was called “therapy by walking around.” We went to the service members’ offices.
There was also a Family Assistance Center. That was for the families of the people who died. And that was very helpful because you had all the services there in one place – medical care, mental health care, therapy dogs, massage, the people who collected the DNA to identify remains. You had it in one place, the Sheraton in Crystal City, Va.. That has become a model now, especially for mass transportation fatalities. There are a lot more in the literature about Family Assistance Centers now, mainly formed by the National Transportation Safety Board.
Right after 9/11, we went to war in Afghanistan, and later in Iraq, and we had a lot of soldiers who developed both PTSD and traumatic brain injury (TBI). One of the good things that the military can do is they can really innovate with both medical treatment and mental health treatment because they don’t have to ask for an insurance company to pay for it. So for some years, starting in about 2004, Congress allocated a large sum of money every year to the Department of Defense to focus on treatment for PTSD and TBI.
And as a result of that, a couple of things happened. One was that the treatments that we had, we were able to study much better, exposure therapy and cognitive-behavioral therapy. We were able to do large trials, and then we continued with the use of medications when necessary. There are only two (Food and Drug Administration)–approved medicines for the treatment of PTSD: sertraline and paroxetine, but many others are used.
We also learned what didn’t work and what soldiers would not take. Most of these medications have sexual side effects. If you’re a young, healthy soldier, you really don’t want to be taking something that causes you erectile dysfunction, or in women a loss of libido. So many people wouldn’t take these therapies. As for exposure therapy, if you got into it and completed the program, usually your PTSD symptoms went down. But many people couldn’t complete it. In the exposure therapy, you’re talking about whatever trauma you’ve been through – maybe your best friend died next to you, and you don’t want to talk about that all the time.
When I talk to patients about this, I say the first bucket is medication, the second bucket is therapy, and the third bucket is everything else. And everything else includes meditation, yoga, exercise, and it also involves working with animals. There are programs where you’re paired with a service dog, who helps calm you down, and you feel protected.
One of my favorites is called Warrior Canine Connection, where a soldier with PTSD trains a puppy to become a service animal. And in the training of the dog, you have to learn to control your emotions, you have to modulate your voice, you have to appear calm. Often soldiers have a background that they’re familiar with animals, especially dogs. So that’s been very successful.
A couple of other (treatments) to mention one is called stellate ganglion block, where a little lidocaine is injected into the back of the cervical spine. It was used initially for pain control, and they found that it was actually very helpful for PTSD. Another thing we’ve learned is that pain and PTSD often go hand in hand, because if you’re in pain, you’ll be feeling awful, you won’t sleep well, you’ll have more nightmares. But if you can control both of them together, then that’s going to help.
Q: One issue that veterans may face is moral injury. Can you talk about that?
A: Moral injury is a term that was first used after Vietnam. Moral injury is not a psychiatric diagnosis. It is feelings of shame and guilt that can be very corrosive and can lead to suicide. It overlaps with PTSD. You feel either you’ve let yourself down, or the government has let you down. And this can be very corrosive. Another thing that could happen is, say, you switched your tour of duty with a buddy, and he got killed and you didn’t. A very common scenario is you’re manning a checkpoint, and a car comes at you and doesn’t stop like it’s supposed to. You do what you’ve been trained to do, which is open fire, and check on the car afterward. And there’s four little kids and their parents in the car all dead. And that is something that even though that was your sort of duty, that it still eats at you because you have kids the same age as the ones who were dead in the car.
You can still have these feelings of shame and guilt, and it will often bleed into your relationships with your family. And that can lead to distance and divorce, which is a further risk factor for suicide.
Q: Are there are any specific treatments that have been designed for moral injury, different from PTSD or other conditions?
A: The Armed Services has set up a number of intensive programs at different places, and each is a little bit different. They usually integrate moral injury in with some of the other treatments. There was one at Fort Bliss, Tex., that had reiki; they had art therapy. And they had the chaplains working on moral injury. So there’s no medical treatment for it, but there certainly is talking about it, and for some people to go to a chaplain can be very helpful.
There’s a Military Health System Centers of Excellence, which is a place by the new Walter Reed on the campus, they have a marvelous wall full of masks. And the masks have been painted by soldiers with usually a combination of PTSD, TBI, and although it’s not an official psychiatric diagnosis, moral injury. They’re able to draw and paint. Another thing that’s been used quite a bit as writing therapy, and journaling, and just writing down how you feel about something, because you can do that without retraumatizing anybody else, except perhaps if you are working with a therapist.
Q: For therapists who are treating soldiers, veterans, are there specific challenges that they should be aware of? Are these patients maybe different from the patients that they might otherwise see? Are there specific pieces of advice as to how to engage them?
A: There are a few things that are different. One is that many people in the military are not used to talking about their feelings. And that’s especially if you’ve got a young man who only grunts and says: “Hooah!” That is going to be hard to break through. And that’s why some of these other ways of reaching somebody is very effective. Also, the military likes to have physical activity; they’re usually not comfortable sitting in a chair. If you’re a civilian psychiatrist, I don’t expect you to go bungee jumping with your patients. But what I’d recommend is that you recommend to your patients that they stay active.
Another thing about veterans is that they like to be self-sufficient. They really don’t like to ask for help, although they might ask for help for their buddy. After the Pentagon and 9/11, when I was working with senior officers, they never needed any help. No, but their buddy over here might, so I could help them in the guise of providing care for their buddy in a group setting. We could work with everybody and enhance cohesion, morale, bonding, “we’re all in this together” type of feeling.
I think one thing that’s really improved is that there is less stigma around PTSD. People are more willing to present for help, and some people have called PTSD the Purple Heart of mental disorders. People don’t feel like it’s as bad as having depression or anxiety. Even though PTSD often has depression and anxiety components to it – they run hand in hand – still, it’s sort of more honorable if you’ve been at war and have gotten PTSD.
Q: How have you been faring yourself, in the face of the 9/11 anniversary and recent events in Afghanistan?
A: (The Sept. 11 weekend) was very sad for me – and a lot of my colleagues [with] the combination of the 20th anniversary of 9/11, and the recent development. Fortunately, I have friends and people I can talk to. I walked with a colleague of mine who was in the Army. I’m following my own rule of the three buckets, so we took a walk around the hospital center for about 45 minutes, and we have five fish ponds here. And we went and looked at the fish, and talked to the fish. At the National Rehab Hospital, they were playing the guitar. So there’s are a variety of things that people can do.
Deployments in places such as Afghanistan and Iraq, and traumatic events such as the Sept. 11, 2001, attacks affect everyone, but military personnel and veterans face unique circumstances that can present challenges to treatment. Much progress has been made in recent years in treating people with posttraumatic stress disorder and helping them recover after traumatic events.
To explore some of those changes and challenges, this news organization interviewed Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH, who retired from the Army in 2010 after assignments and missions that took her to Korea, Somalia, Iraq, and Cuba, about her approaches to treating soldiers and veterans.
Dr. Ritchie is chief of psychiatry at Medstar Washington Hospital Center, and a professor of psychiatry at the Uniformed Services University of the Health Sciences in Bethesda, Md., and at Georgetown University and George Washington University, both in Washington.
She is the author of 250 publications, including the book, “Forensic and Ethical Issues in Military Behavioral Health” (Fort Sam Houston, Tex.: Borden Institute, 2015). In addition, Dr. Ritchie is coeditor of “Post-Traumatic Stress Disorder and Related Diseases in Combat Veterans” (New York: Springer, 2015) and “Psychiatrists in Combat, Clinicians Experience in the War Zone” (New York: Springer, 2017).
Question: What are some of the interventions available in the aftermath of traumatic events?
Answer: What we thought the standard of care should be after a traumatic event was to have what’s called a critical incident stress debriefing (CISD). It was basically getting the members of the group who had been traumatized by a school shooting or plane crash, or the Oklahoma City bombing, getting them all together literally a few hours after the event, and having them tell what happened. And the idea is to get it all out. But what we discovered is that this could actually make people worse, because you’d be hearing not only about your own trauma, but other people’s traumas, and that it was too soon for the event.
So prior to 9/11, we had organized a conference, which was held in October 2001, just a month after 9/11. At that conference, we worked on mass violence and early intervention, which is the name of the book that came out from the (National Institute of Mental Health) as a result. It focused on basic principles of safety and security and communication, and knowing where your family was, rather than reliving the trauma. Now, we did think that sometimes you could have a CISD that would be helpful, but only when it was people who knew each other well, like an ED group who would work with each other or soldiers who served together.
Q: What was your involvement in the aftermath of the Sept. 11 attacks?
A: At the time of 9/11, I was assigned at the Pentagon, but I wasn’t there. When the plane hit, I was actually across the river at the Navy’s Bureau of Medicine and Surgery. And then for the next 3 weeks, all I did was work at the Pentagon. We used some of these principles of early intervention but not focusing on telling us what happened right afterward. We focused on how the service members and their families were coping in the here and now, and how they could support each other.
We knew that soldiers would not come out of their offices to go to a therapist. They are too strong for that. So, we did what was called “therapy by walking around.” We went to the service members’ offices.
There was also a Family Assistance Center. That was for the families of the people who died. And that was very helpful because you had all the services there in one place – medical care, mental health care, therapy dogs, massage, the people who collected the DNA to identify remains. You had it in one place, the Sheraton in Crystal City, Va.. That has become a model now, especially for mass transportation fatalities. There are a lot more in the literature about Family Assistance Centers now, mainly formed by the National Transportation Safety Board.
Right after 9/11, we went to war in Afghanistan, and later in Iraq, and we had a lot of soldiers who developed both PTSD and traumatic brain injury (TBI). One of the good things that the military can do is they can really innovate with both medical treatment and mental health treatment because they don’t have to ask for an insurance company to pay for it. So for some years, starting in about 2004, Congress allocated a large sum of money every year to the Department of Defense to focus on treatment for PTSD and TBI.
And as a result of that, a couple of things happened. One was that the treatments that we had, we were able to study much better, exposure therapy and cognitive-behavioral therapy. We were able to do large trials, and then we continued with the use of medications when necessary. There are only two (Food and Drug Administration)–approved medicines for the treatment of PTSD: sertraline and paroxetine, but many others are used.
We also learned what didn’t work and what soldiers would not take. Most of these medications have sexual side effects. If you’re a young, healthy soldier, you really don’t want to be taking something that causes you erectile dysfunction, or in women a loss of libido. So many people wouldn’t take these therapies. As for exposure therapy, if you got into it and completed the program, usually your PTSD symptoms went down. But many people couldn’t complete it. In the exposure therapy, you’re talking about whatever trauma you’ve been through – maybe your best friend died next to you, and you don’t want to talk about that all the time.
When I talk to patients about this, I say the first bucket is medication, the second bucket is therapy, and the third bucket is everything else. And everything else includes meditation, yoga, exercise, and it also involves working with animals. There are programs where you’re paired with a service dog, who helps calm you down, and you feel protected.
One of my favorites is called Warrior Canine Connection, where a soldier with PTSD trains a puppy to become a service animal. And in the training of the dog, you have to learn to control your emotions, you have to modulate your voice, you have to appear calm. Often soldiers have a background that they’re familiar with animals, especially dogs. So that’s been very successful.
A couple of other (treatments) to mention one is called stellate ganglion block, where a little lidocaine is injected into the back of the cervical spine. It was used initially for pain control, and they found that it was actually very helpful for PTSD. Another thing we’ve learned is that pain and PTSD often go hand in hand, because if you’re in pain, you’ll be feeling awful, you won’t sleep well, you’ll have more nightmares. But if you can control both of them together, then that’s going to help.
Q: One issue that veterans may face is moral injury. Can you talk about that?
A: Moral injury is a term that was first used after Vietnam. Moral injury is not a psychiatric diagnosis. It is feelings of shame and guilt that can be very corrosive and can lead to suicide. It overlaps with PTSD. You feel either you’ve let yourself down, or the government has let you down. And this can be very corrosive. Another thing that could happen is, say, you switched your tour of duty with a buddy, and he got killed and you didn’t. A very common scenario is you’re manning a checkpoint, and a car comes at you and doesn’t stop like it’s supposed to. You do what you’ve been trained to do, which is open fire, and check on the car afterward. And there’s four little kids and their parents in the car all dead. And that is something that even though that was your sort of duty, that it still eats at you because you have kids the same age as the ones who were dead in the car.
You can still have these feelings of shame and guilt, and it will often bleed into your relationships with your family. And that can lead to distance and divorce, which is a further risk factor for suicide.
Q: Are there are any specific treatments that have been designed for moral injury, different from PTSD or other conditions?
A: The Armed Services has set up a number of intensive programs at different places, and each is a little bit different. They usually integrate moral injury in with some of the other treatments. There was one at Fort Bliss, Tex., that had reiki; they had art therapy. And they had the chaplains working on moral injury. So there’s no medical treatment for it, but there certainly is talking about it, and for some people to go to a chaplain can be very helpful.
There’s a Military Health System Centers of Excellence, which is a place by the new Walter Reed on the campus, they have a marvelous wall full of masks. And the masks have been painted by soldiers with usually a combination of PTSD, TBI, and although it’s not an official psychiatric diagnosis, moral injury. They’re able to draw and paint. Another thing that’s been used quite a bit as writing therapy, and journaling, and just writing down how you feel about something, because you can do that without retraumatizing anybody else, except perhaps if you are working with a therapist.
Q: For therapists who are treating soldiers, veterans, are there specific challenges that they should be aware of? Are these patients maybe different from the patients that they might otherwise see? Are there specific pieces of advice as to how to engage them?
A: There are a few things that are different. One is that many people in the military are not used to talking about their feelings. And that’s especially if you’ve got a young man who only grunts and says: “Hooah!” That is going to be hard to break through. And that’s why some of these other ways of reaching somebody is very effective. Also, the military likes to have physical activity; they’re usually not comfortable sitting in a chair. If you’re a civilian psychiatrist, I don’t expect you to go bungee jumping with your patients. But what I’d recommend is that you recommend to your patients that they stay active.
Another thing about veterans is that they like to be self-sufficient. They really don’t like to ask for help, although they might ask for help for their buddy. After the Pentagon and 9/11, when I was working with senior officers, they never needed any help. No, but their buddy over here might, so I could help them in the guise of providing care for their buddy in a group setting. We could work with everybody and enhance cohesion, morale, bonding, “we’re all in this together” type of feeling.
I think one thing that’s really improved is that there is less stigma around PTSD. People are more willing to present for help, and some people have called PTSD the Purple Heart of mental disorders. People don’t feel like it’s as bad as having depression or anxiety. Even though PTSD often has depression and anxiety components to it – they run hand in hand – still, it’s sort of more honorable if you’ve been at war and have gotten PTSD.
Q: How have you been faring yourself, in the face of the 9/11 anniversary and recent events in Afghanistan?
A: (The Sept. 11 weekend) was very sad for me – and a lot of my colleagues [with] the combination of the 20th anniversary of 9/11, and the recent development. Fortunately, I have friends and people I can talk to. I walked with a colleague of mine who was in the Army. I’m following my own rule of the three buckets, so we took a walk around the hospital center for about 45 minutes, and we have five fish ponds here. And we went and looked at the fish, and talked to the fish. At the National Rehab Hospital, they were playing the guitar. So there’s are a variety of things that people can do.
Twelve-month overall survival benefit with ribociclib for metastatic breast cancer
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
FROM ESMO 2021