User login
Residency programs need greater focus on BPD treatment
Borderline personality disorder (BPD) has suffered from underdiagnosis, in part because not enough clinicians know how to handle patients with BPD. “They don’t have the tools to know how to manage these situations effectively,” Lois W. Choi-Kain, MEd, MD, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass., said in an interview.
As a result, the clinician avoids the BPD patient, who feels demeaned and never finds the capacity to get better.
Psychiatry training in residency tends to emphasize biomedical treatments and does not focus enough on learning psychotherapy and other psychosocial treatments, according to Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass.
“This is where I see the need for a greater psychotherapy teaching focus in residency, along with teaching of general principles for working with patients with BPD,” said Dr. Plakun.
In his last phase of his career, BPD pioneer John G. Gunderson, MD, worked with Dr. Choi-Kain to train clinicians on general psychiatric management (GPM), which employs a sensitive, nonattacking approach to diffuse and calm situations with BPD patients.
As interest grows in combining GPM with manual treatments, GPM alone offers a more accessible approach for therapist and patient, said Dr. Choi-Kain, who has been trying to promote its use and do research on its techniques.
“It’s trying to boil it down to make it simple,” she said. As much as evidence-based, manualized approaches have advanced the field, they’re just not that widely available, she said.
Orchestrating treatments such as dialectical behavior therapy and mentalization-based therapy takes a lot of specialization, noted Dr. Choi-Kain. “And because of the amount of work that it involves for both the clinician and the patient, it decreases the capacity that clinicians and systems have to offer treatment to a wider number of patients.”
Learning a manualized treatment for BPD is asking a lot from residents, agreed Dr. Plakun. “Those who want more immersion in treating these patients can pursue further training in residency electives, in postresidency graduate medical education programs or through psychoanalytic training.”
Borderline personality disorder (BPD) has suffered from underdiagnosis, in part because not enough clinicians know how to handle patients with BPD. “They don’t have the tools to know how to manage these situations effectively,” Lois W. Choi-Kain, MEd, MD, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass., said in an interview.
As a result, the clinician avoids the BPD patient, who feels demeaned and never finds the capacity to get better.
Psychiatry training in residency tends to emphasize biomedical treatments and does not focus enough on learning psychotherapy and other psychosocial treatments, according to Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass.
“This is where I see the need for a greater psychotherapy teaching focus in residency, along with teaching of general principles for working with patients with BPD,” said Dr. Plakun.
In his last phase of his career, BPD pioneer John G. Gunderson, MD, worked with Dr. Choi-Kain to train clinicians on general psychiatric management (GPM), which employs a sensitive, nonattacking approach to diffuse and calm situations with BPD patients.
As interest grows in combining GPM with manual treatments, GPM alone offers a more accessible approach for therapist and patient, said Dr. Choi-Kain, who has been trying to promote its use and do research on its techniques.
“It’s trying to boil it down to make it simple,” she said. As much as evidence-based, manualized approaches have advanced the field, they’re just not that widely available, she said.
Orchestrating treatments such as dialectical behavior therapy and mentalization-based therapy takes a lot of specialization, noted Dr. Choi-Kain. “And because of the amount of work that it involves for both the clinician and the patient, it decreases the capacity that clinicians and systems have to offer treatment to a wider number of patients.”
Learning a manualized treatment for BPD is asking a lot from residents, agreed Dr. Plakun. “Those who want more immersion in treating these patients can pursue further training in residency electives, in postresidency graduate medical education programs or through psychoanalytic training.”
Borderline personality disorder (BPD) has suffered from underdiagnosis, in part because not enough clinicians know how to handle patients with BPD. “They don’t have the tools to know how to manage these situations effectively,” Lois W. Choi-Kain, MEd, MD, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass., said in an interview.
As a result, the clinician avoids the BPD patient, who feels demeaned and never finds the capacity to get better.
Psychiatry training in residency tends to emphasize biomedical treatments and does not focus enough on learning psychotherapy and other psychosocial treatments, according to Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass.
“This is where I see the need for a greater psychotherapy teaching focus in residency, along with teaching of general principles for working with patients with BPD,” said Dr. Plakun.
In his last phase of his career, BPD pioneer John G. Gunderson, MD, worked with Dr. Choi-Kain to train clinicians on general psychiatric management (GPM), which employs a sensitive, nonattacking approach to diffuse and calm situations with BPD patients.
As interest grows in combining GPM with manual treatments, GPM alone offers a more accessible approach for therapist and patient, said Dr. Choi-Kain, who has been trying to promote its use and do research on its techniques.
“It’s trying to boil it down to make it simple,” she said. As much as evidence-based, manualized approaches have advanced the field, they’re just not that widely available, she said.
Orchestrating treatments such as dialectical behavior therapy and mentalization-based therapy takes a lot of specialization, noted Dr. Choi-Kain. “And because of the amount of work that it involves for both the clinician and the patient, it decreases the capacity that clinicians and systems have to offer treatment to a wider number of patients.”
Learning a manualized treatment for BPD is asking a lot from residents, agreed Dr. Plakun. “Those who want more immersion in treating these patients can pursue further training in residency electives, in postresidency graduate medical education programs or through psychoanalytic training.”
A new name for BPD?
Michael A. Cummings, MD, has never liked the term “borderline personality disorder” (BPD). In his view, it’s a misnomer and needs to be changed.
“What is it bordering on? It’s not bordering on something, it’s a disorder on its own,” said Dr. Cummings of the department of psychiatry at the University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD grew out of the concept that patients were bordering on something, perhaps becoming bipolar. “In many ways, I don’t think it is even a personality disorder. It appears to be an inherent temperament that evolves into an inability to regulate mood.”
In his view, this puts it in the category of a mood dysregulation disorder.
Changing the label would not necessarily improve treatment, he added. However, transitioning from a pejorative to a more neutral label could make it easier for people to say, “this is just a type of mood disorder. It’s not necessarily easy, but it’s workable,” said Dr. Cummings.
Others in the field contend that the term fits the condition. BPD “describes how it encompasses a lot of complex psychological difficulties, undermining functioning of patients in a specific way,” said Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass. The disorder was identified because of its relationship with other known psychiatric disorders, said Dr. Choi-Kain. “There’s an element of BPD that borders on mood disorders because moods are so unstable with BPD. It also borders on trauma-related disorders. It borders on psychotic disorders because there’s sometimes stress-induced experiences of losing contact with realistic thinking.”
If anything needs to change, it’s the attitude toward the disorder, not the name. “I don’t think the term itself is pejorative. But I think that associations with the term have been very stigmatizing. For a long time, there was an attitude that these patients could not be treated or had negative therapeutic reactions.”
Data suggest that these patients are highly prevalent in clinical settings. “And I interpret that as them seeking the care that they need rather than resisting care or not responding to care,” said Dr. Choi-Kain.
Michael A. Cummings, MD, has never liked the term “borderline personality disorder” (BPD). In his view, it’s a misnomer and needs to be changed.
“What is it bordering on? It’s not bordering on something, it’s a disorder on its own,” said Dr. Cummings of the department of psychiatry at the University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD grew out of the concept that patients were bordering on something, perhaps becoming bipolar. “In many ways, I don’t think it is even a personality disorder. It appears to be an inherent temperament that evolves into an inability to regulate mood.”
In his view, this puts it in the category of a mood dysregulation disorder.
Changing the label would not necessarily improve treatment, he added. However, transitioning from a pejorative to a more neutral label could make it easier for people to say, “this is just a type of mood disorder. It’s not necessarily easy, but it’s workable,” said Dr. Cummings.
Others in the field contend that the term fits the condition. BPD “describes how it encompasses a lot of complex psychological difficulties, undermining functioning of patients in a specific way,” said Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass. The disorder was identified because of its relationship with other known psychiatric disorders, said Dr. Choi-Kain. “There’s an element of BPD that borders on mood disorders because moods are so unstable with BPD. It also borders on trauma-related disorders. It borders on psychotic disorders because there’s sometimes stress-induced experiences of losing contact with realistic thinking.”
If anything needs to change, it’s the attitude toward the disorder, not the name. “I don’t think the term itself is pejorative. But I think that associations with the term have been very stigmatizing. For a long time, there was an attitude that these patients could not be treated or had negative therapeutic reactions.”
Data suggest that these patients are highly prevalent in clinical settings. “And I interpret that as them seeking the care that they need rather than resisting care or not responding to care,” said Dr. Choi-Kain.
Michael A. Cummings, MD, has never liked the term “borderline personality disorder” (BPD). In his view, it’s a misnomer and needs to be changed.
“What is it bordering on? It’s not bordering on something, it’s a disorder on its own,” said Dr. Cummings of the department of psychiatry at the University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD grew out of the concept that patients were bordering on something, perhaps becoming bipolar. “In many ways, I don’t think it is even a personality disorder. It appears to be an inherent temperament that evolves into an inability to regulate mood.”
In his view, this puts it in the category of a mood dysregulation disorder.
Changing the label would not necessarily improve treatment, he added. However, transitioning from a pejorative to a more neutral label could make it easier for people to say, “this is just a type of mood disorder. It’s not necessarily easy, but it’s workable,” said Dr. Cummings.
Others in the field contend that the term fits the condition. BPD “describes how it encompasses a lot of complex psychological difficulties, undermining functioning of patients in a specific way,” said Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute, McLean Hospital, Belmont, Mass. The disorder was identified because of its relationship with other known psychiatric disorders, said Dr. Choi-Kain. “There’s an element of BPD that borders on mood disorders because moods are so unstable with BPD. It also borders on trauma-related disorders. It borders on psychotic disorders because there’s sometimes stress-induced experiences of losing contact with realistic thinking.”
If anything needs to change, it’s the attitude toward the disorder, not the name. “I don’t think the term itself is pejorative. But I think that associations with the term have been very stigmatizing. For a long time, there was an attitude that these patients could not be treated or had negative therapeutic reactions.”
Data suggest that these patients are highly prevalent in clinical settings. “And I interpret that as them seeking the care that they need rather than resisting care or not responding to care,” said Dr. Choi-Kain.
Trust is key in treating borderline personality disorder
Difficulties associated with treating borderline personality disorder (BPD) make for an uneasy alliance between patient and clinician. Deep-seated anxiety and trust issues often lead to patients skipping visits or raging at those who treat them, leaving clinicians frustrated and ready to give up or relying on a pill to make the patient better.
John M. Oldham, MD, MS, recalls one patient he almost lost, a woman who was struggling with aggressive behavior. Initially cooperative and punctual, the patient gradually became distrustful, grilling Dr. Oldham on his training and credentials. “As the questions continued, she slipped from being very cooperative to being enraged and attacking me,” said Dr. Oldham, Distinguished Emeritus Professor in the Menninger department of psychiatry and behavioral sciences at Baylor College in Houston.
Dr. Oldham eventually drew her back in by earning her trust. “There’s no magic to this,” he acknowledged. “You try to be as alert and informed and vigilant for anything you say that produces a negative or concerning reaction in the patient.”
This interactive approach to BPD treatment has been gaining traction in a profession that often looks to medications to alleviate specific symptoms. It’s so effective that it sometimes even surprises the patient, Dr. Oldham noted. “When you approach them like this, they can begin to settle down,” which was the case with the female patient he once treated.
About 1.4% of the U.S. population has BPD, according to the National Institute of Mental Health. Conceptualized by the late John G. Gunderson, MD, BPD initially was seen as floating on the borderline between psychosis and neurosis. Clinicians now understand that this isn’t the case. The patients need, as Dr. Gunderson once pointed out, constant vigilance because of attachment issues and childhood trauma.
A stable therapeutic alliance between patient and physician, sometimes in combination with evidence-based therapies, is a formula for success, some experts say.
A misunderstood condition
Although there is some degree of heritable risk, BPD patients are often the product of an invalidating environment in childhood. “As kids, we’re guided and nurtured by caring adults to provide models of reasonable, trustworthy behavior. If those role models are missing or just so inconsistent and unpredictable, the patient doesn’t end up with a sturdy self-image. Instead, they’re adrift, trying to figure out who will be helpful and be a meaningful, trustworthy companion and adviser,” Dr. Oldham said.
Emotional or affective instability and impulsivity, sometimes impulsive aggression, often characterize their condition. “Brain-imaging studies have revealed that certain nerve pathways that are necessary to regulate emotions are impoverished in patients with BPD,” Dr. Oldham said.
An analogy is a car going too fast, with a runaway engine that’s running too hot – and the brakes don’t work, he added.
“People think these patients are trying to create big drama, that they’re putting on a big show. That’s not accurate,” he continued. These patients don’t have the ability to stop the trigger that leads to their emotional storms. They also don’t have the ability to regulate themselves. “We may say, it’s a beautiful day outside, but I still have to go to work. Someone with BPD may say: It’s a beautiful day; I’m going to the beach,” Dr. Oldham explained.
A person with BPD might sound coherent when arguing with someone else. But their words are driven by the storm they can’t turn off.
This can lead to their own efforts to turn off the intensity. They might become self-injurious or push other people away. It’s one of the ironies of this condition because BPD patients desperately want to trust others but are scared to do so. “They look for any little signal – that someone else will hurt, disappoint, or leave them. Eventually their relationships unravel,” Dr. Oldham saod.
For some, suicide is sometimes a final solution.

Those traits make it difficult for a therapist to connect with a patient. “This is a very difficult group of people to treat and to establish treatment,” said Michael A. Cummings, MD, of the department of psychiatry at University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD patients tend to idealize people who are attempting to help them. When they become frustrated or disappointed in some way, “they then devalue the caregiver or the treatment and not infrequently, fall out of treatment,” Dr. Cummings said. It can be a very taxing experience, particularly for younger, less experienced therapists.
Medication only goes so far
Psychiatrists tend to look at BPD patients as receptor sites for molecules, assessing symptoms they can prescribe for, Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass., said in an interview.
Yet, BPD is not a molecular problem, principally. It’s an interpersonal disorder. When BPD is a co-occurring disorder, as is often the case, the depressive, anxiety, or other disorder can mask the BPD, he added, citing his 2018 paper on tensions in psychiatry between the biomedical and biopsychosocial models (Psychiatr Clin North Am. 2018 Jun;41[2]:237-48).
In one longitudinal study (J Pers Disord. 2005 Oct;19[5]:487-504), the presence of BPD strongly predicted the persistence of depression. BPD comorbid with depression is often a recipe for treatment-resistant depression, which results in higher costs, more utilization of resources, and higher suicide rates. Too often, psychiatrists diagnose the depression but miss the BPD. They keep trying molecular approaches with prescription drugs – even though it’s really the interpersonal issues of BPD that need to be addressed, said Dr. Plakun, who is a member of the Group for the Advancement of Psychiatry’s Psychotherapy Committee, and founder and past leader of the American Psychiatric Association’s Psychotherapy Caucus.
Medication can be helpful as a short-term adjunctive therapy. Long term, it’s not a sustainable approach, said Dr. Oldham. “If a patient is in a particularly stressful period, in the middle of a stormy breakup or having a depressive episode or talking about suicide, a time-limited course of an antidepressant may be helpful,” he said. They could also benefit from an anxiety-related drug or medication to help them sleep.
What you don’t want is for the patient to start relying on medications to help them feel better. The problem is, many are suffering so much that they’ll go to their primary care doctor and say, “I’m suffering from anxiety,” and get an antianxiety drug. Or they’re depressed or in pain and end up with a cocktail of medications. “And that’s just going to make matters worse,” Dr. Oldham said.
Psychotherapy as a first-line approach
APA practice guidelines and others worldwide have all come to the same conclusion about BPD. , who chaired an APA committee that developed an evidence-based practice guideline for patients with BPD.
Psychotherapy keeps the patient from firing you, he asserted. “Because of the lack of trust, they push away. They’re very scared, and this fear also applies to therapist. The goal is to help the patient learn to trust you. To do that, you need to develop a strong therapeutic alliance.”
In crafting the APA’s practice guideline, Dr. Oldham and his colleagues studied a variety of approaches, including mentalization-based therapy (MBT) and dialectical behavior therapy (DBT), which was developed by Marsha Linehan, PhD. Since then, other approaches have demonstrated efficacy in randomized clinical trials, including schema-based therapy (SBT), cognitive-behavioral therapy (CBT), and transference-focused psychotherapy (TFP).

Those treatments might complement the broader goal of establishing a strong alliance with the patient, Dr. Oldham said. Manualized approaches can help prepackage a program that allows clinicians and patients to look at their problems in an objective, nonpejorative way, Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute at McLean Hospital in Belmont, Mass., said in an interview. DBT, for example, focuses on emotion dysregulation. MBT addresses how the patient sees themselves through others and their interactions with others. “It destigmatizes a problem as a clinical entity rather than an interpersonal problem between the patient and the clinician,” Dr. Choi-Kain said.
The choice of approach depends on several factors: the patient’s needs and preferences, and the therapist’s skills and experience, said Dr. Oldham. Some patients don’t do well with DBT because it involves a lot of homework and didactic work. Others do better with TFP because they want to understand what drives their behavior.
Dr. Cummings recalled how one of his patients used TFP to look inward and heal.
He first met the patient when she was in her early 30s. “She had made some progress, but I remember she was still struggling mightily with relationship issues and with identifying her role in relationships,” he said. The patient was becoming increasingly aware that she was going to end up alone and didn’t want that as an outcome.
Adapting to a TFP model, “she worked very hard trying to understand herself as she related to other people, understanding her own emotional volatility, and some of her proneness to behavioral problems,” Dr. Cummings said. The patient also had to learn how to negotiate her relationships to the point where she didn’t end up destroying them and alienating people.
Customizing the treatment
Physicians can choose from one of these manualized forms of treatment to see what’s appropriate and what works for the patient. “You can individualize the treatment, borrowing from these approaches and shaping it based on what your patient needs,” Dr. Oldham recommended.
Recently, the field of psychiatry has seen the benefits of combining manualized, evidence-based approaches with general psychiatric management (GPM), a method conceived by Dr. Gunderson. GPM “reflects a sensitive understanding of mental illness, offering ‘non attacking’ or collaborative work with the patient and a sensitive recognition of appropriate interventions or corrections to help the patient stay in treatment,” said Dr. Oldham.
It aims to conceptualize BPD in a clinically objective way, medicalizing the disorder so it’s something that the patient has, rather than something he or she is, explained Dr. Choi-Kain, who worked with Dr. Gunderson to train clinicians on using this approach. Using a framework that’s compatible with good medical practices, the clinician tries to define the problem together with the patient, “really assessing whether or not the treatment works, setting goals, managing safety, and trying to promote functioning, something we need to pay more attention to with BPD,” she said.
For these patients, the goal is to have positive, corrective experiences in the real world, reinforcing their hopes and what they’re capable of, and an interface with the world that makes them feel like contributors, she said.
Cycle of rupture and repair
Many people with BPD struggle with the desire to find and feel love, but also deal with their rage and hate. Hence, therapists must prepare themselves for the experience of sometimes being hated, said Dr. Plakun. The patient needs to feel they’re in a safe enough space to express those feelings, activating a cycle of “rupture and repair,” he continued.
The key in working with these patients is to avoid any language that will make them feel attacked or criticized, said Dr. Oldham.
A patient may get furious and say “I don’t know what you’re talking about. I didn’t say that.” When in truth, the psychiatrist is flat accurate about what the patient said. Instead of arguing with the patient, a physician can back up and say: “Help me understand what you’re feeling right now. What did I say that made you feel that you couldn’t trust me? Help me understand you. I may have made a mistake,” he advised.
Trust is a key ingredient in an alliance-based intervention for suicidal patients with BPD that Dr. Plakun has frequently written about. A bond he had with a deeply suicidal patient helped her overcome her grief and come to terms with an abusive childhood.
“She had a horrible history of abuse and had BPD and bipolar disorder. Even controlled with medications her life was still awful. She contemplated suicide relentlessly.” Working through her history of sexual abuse, the patient discovered that much of what she and clinicians thought of as a depressive illness was in fact intense grief about the irreparable damage that had taken place during childhood.
Through their work she was able to mourn, and her depression and BPD improved.
Developing a trusting relationship with the patient isn’t a starting point; it’s the goal, he emphasized.
“You don’t prescribe trust to someone. It’s earned.” Through the shared journey of therapy, as the patient suffers from inevitable injuries and ruptures and as the therapist reveals his or her imperfections, opportunities arise to nonjudgmentally examine and repair ruptures. This lead to gains in trust, he said.
It’s not just about genes
Many in the psychiatric and psychological communities tend to develop a very nihilistic view of BPD patients, observed Dr. Cummings. “They’ll say: ‘Oh, well, it’s hopeless. There’s nothing that can be done.’ That isn’t true,” he said.
Epidemiologic studies of these individuals have shown that many of these patients no longer meet the diagnostic criteria for BPD by the time they reach middle age. This means they get better over time, noted Dr. Cummings.
Dr. Plakun’s hope is that the field will evolve in a direction that recognizes the importance of psychosocial treatments like psychotherapy, in addition to biomedical treatments. The drive to medicate still exists, which can contribute to underdiagnosis and undertreatment of BPD, he said. “Although there are manualized, evidence-based treatments, few clinicians learn even one of these for BPD, not to mention those for other disorders.”
In 1996, Francis S. Collins, MD, PhD, the current director of the National Institutes of Health, predicted that the decoding of the human genome would transform treatment of medical and mental disorders [and] “that we would discover the ways in which genes equal disease,” said Dr. Plakun. What the science has since shown, is genes by environmental interaction lead to disease and health.
Nature and nurture both matter. “And I don’t think we’re paying enough attention to the nurture side,” Dr. Plakun said.
The solution is a return to a biopsychosocial model, recognizing that psychotherapy is an essential part of treatment of BPD and other conditions, and an essential clinician skill, he said.
Dr. Oldham is coeditor of the “Textbook of Personality Disorders”, 3rd edition (Washington: American Psychiatric Association Publishing, 2021).Dr. Choi-Kain is coeditor with Dr. Gunderson of “Applications of Good Psychiatric Management for Borderline Personality Disorder: A Practical Guide” (Washington: American Psychiatric Association Publishing, 2019).
Dr. Cummings and Dr. Plakun had no disclosures.
Difficulties associated with treating borderline personality disorder (BPD) make for an uneasy alliance between patient and clinician. Deep-seated anxiety and trust issues often lead to patients skipping visits or raging at those who treat them, leaving clinicians frustrated and ready to give up or relying on a pill to make the patient better.
John M. Oldham, MD, MS, recalls one patient he almost lost, a woman who was struggling with aggressive behavior. Initially cooperative and punctual, the patient gradually became distrustful, grilling Dr. Oldham on his training and credentials. “As the questions continued, she slipped from being very cooperative to being enraged and attacking me,” said Dr. Oldham, Distinguished Emeritus Professor in the Menninger department of psychiatry and behavioral sciences at Baylor College in Houston.
Dr. Oldham eventually drew her back in by earning her trust. “There’s no magic to this,” he acknowledged. “You try to be as alert and informed and vigilant for anything you say that produces a negative or concerning reaction in the patient.”
This interactive approach to BPD treatment has been gaining traction in a profession that often looks to medications to alleviate specific symptoms. It’s so effective that it sometimes even surprises the patient, Dr. Oldham noted. “When you approach them like this, they can begin to settle down,” which was the case with the female patient he once treated.
About 1.4% of the U.S. population has BPD, according to the National Institute of Mental Health. Conceptualized by the late John G. Gunderson, MD, BPD initially was seen as floating on the borderline between psychosis and neurosis. Clinicians now understand that this isn’t the case. The patients need, as Dr. Gunderson once pointed out, constant vigilance because of attachment issues and childhood trauma.
A stable therapeutic alliance between patient and physician, sometimes in combination with evidence-based therapies, is a formula for success, some experts say.
A misunderstood condition
Although there is some degree of heritable risk, BPD patients are often the product of an invalidating environment in childhood. “As kids, we’re guided and nurtured by caring adults to provide models of reasonable, trustworthy behavior. If those role models are missing or just so inconsistent and unpredictable, the patient doesn’t end up with a sturdy self-image. Instead, they’re adrift, trying to figure out who will be helpful and be a meaningful, trustworthy companion and adviser,” Dr. Oldham said.
Emotional or affective instability and impulsivity, sometimes impulsive aggression, often characterize their condition. “Brain-imaging studies have revealed that certain nerve pathways that are necessary to regulate emotions are impoverished in patients with BPD,” Dr. Oldham said.
An analogy is a car going too fast, with a runaway engine that’s running too hot – and the brakes don’t work, he added.
“People think these patients are trying to create big drama, that they’re putting on a big show. That’s not accurate,” he continued. These patients don’t have the ability to stop the trigger that leads to their emotional storms. They also don’t have the ability to regulate themselves. “We may say, it’s a beautiful day outside, but I still have to go to work. Someone with BPD may say: It’s a beautiful day; I’m going to the beach,” Dr. Oldham explained.
A person with BPD might sound coherent when arguing with someone else. But their words are driven by the storm they can’t turn off.
This can lead to their own efforts to turn off the intensity. They might become self-injurious or push other people away. It’s one of the ironies of this condition because BPD patients desperately want to trust others but are scared to do so. “They look for any little signal – that someone else will hurt, disappoint, or leave them. Eventually their relationships unravel,” Dr. Oldham saod.
For some, suicide is sometimes a final solution.
Those traits make it difficult for a therapist to connect with a patient. “This is a very difficult group of people to treat and to establish treatment,” said Michael A. Cummings, MD, of the department of psychiatry at University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD patients tend to idealize people who are attempting to help them. When they become frustrated or disappointed in some way, “they then devalue the caregiver or the treatment and not infrequently, fall out of treatment,” Dr. Cummings said. It can be a very taxing experience, particularly for younger, less experienced therapists.
Medication only goes so far
Psychiatrists tend to look at BPD patients as receptor sites for molecules, assessing symptoms they can prescribe for, Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass., said in an interview.
Yet, BPD is not a molecular problem, principally. It’s an interpersonal disorder. When BPD is a co-occurring disorder, as is often the case, the depressive, anxiety, or other disorder can mask the BPD, he added, citing his 2018 paper on tensions in psychiatry between the biomedical and biopsychosocial models (Psychiatr Clin North Am. 2018 Jun;41[2]:237-48).
In one longitudinal study (J Pers Disord. 2005 Oct;19[5]:487-504), the presence of BPD strongly predicted the persistence of depression. BPD comorbid with depression is often a recipe for treatment-resistant depression, which results in higher costs, more utilization of resources, and higher suicide rates. Too often, psychiatrists diagnose the depression but miss the BPD. They keep trying molecular approaches with prescription drugs – even though it’s really the interpersonal issues of BPD that need to be addressed, said Dr. Plakun, who is a member of the Group for the Advancement of Psychiatry’s Psychotherapy Committee, and founder and past leader of the American Psychiatric Association’s Psychotherapy Caucus.
Medication can be helpful as a short-term adjunctive therapy. Long term, it’s not a sustainable approach, said Dr. Oldham. “If a patient is in a particularly stressful period, in the middle of a stormy breakup or having a depressive episode or talking about suicide, a time-limited course of an antidepressant may be helpful,” he said. They could also benefit from an anxiety-related drug or medication to help them sleep.
What you don’t want is for the patient to start relying on medications to help them feel better. The problem is, many are suffering so much that they’ll go to their primary care doctor and say, “I’m suffering from anxiety,” and get an antianxiety drug. Or they’re depressed or in pain and end up with a cocktail of medications. “And that’s just going to make matters worse,” Dr. Oldham said.
Psychotherapy as a first-line approach
APA practice guidelines and others worldwide have all come to the same conclusion about BPD. , who chaired an APA committee that developed an evidence-based practice guideline for patients with BPD.
Psychotherapy keeps the patient from firing you, he asserted. “Because of the lack of trust, they push away. They’re very scared, and this fear also applies to therapist. The goal is to help the patient learn to trust you. To do that, you need to develop a strong therapeutic alliance.”
In crafting the APA’s practice guideline, Dr. Oldham and his colleagues studied a variety of approaches, including mentalization-based therapy (MBT) and dialectical behavior therapy (DBT), which was developed by Marsha Linehan, PhD. Since then, other approaches have demonstrated efficacy in randomized clinical trials, including schema-based therapy (SBT), cognitive-behavioral therapy (CBT), and transference-focused psychotherapy (TFP).
Those treatments might complement the broader goal of establishing a strong alliance with the patient, Dr. Oldham said. Manualized approaches can help prepackage a program that allows clinicians and patients to look at their problems in an objective, nonpejorative way, Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute at McLean Hospital in Belmont, Mass., said in an interview. DBT, for example, focuses on emotion dysregulation. MBT addresses how the patient sees themselves through others and their interactions with others. “It destigmatizes a problem as a clinical entity rather than an interpersonal problem between the patient and the clinician,” Dr. Choi-Kain said.
The choice of approach depends on several factors: the patient’s needs and preferences, and the therapist’s skills and experience, said Dr. Oldham. Some patients don’t do well with DBT because it involves a lot of homework and didactic work. Others do better with TFP because they want to understand what drives their behavior.
Dr. Cummings recalled how one of his patients used TFP to look inward and heal.
He first met the patient when she was in her early 30s. “She had made some progress, but I remember she was still struggling mightily with relationship issues and with identifying her role in relationships,” he said. The patient was becoming increasingly aware that she was going to end up alone and didn’t want that as an outcome.
Adapting to a TFP model, “she worked very hard trying to understand herself as she related to other people, understanding her own emotional volatility, and some of her proneness to behavioral problems,” Dr. Cummings said. The patient also had to learn how to negotiate her relationships to the point where she didn’t end up destroying them and alienating people.
Customizing the treatment
Physicians can choose from one of these manualized forms of treatment to see what’s appropriate and what works for the patient. “You can individualize the treatment, borrowing from these approaches and shaping it based on what your patient needs,” Dr. Oldham recommended.
Recently, the field of psychiatry has seen the benefits of combining manualized, evidence-based approaches with general psychiatric management (GPM), a method conceived by Dr. Gunderson. GPM “reflects a sensitive understanding of mental illness, offering ‘non attacking’ or collaborative work with the patient and a sensitive recognition of appropriate interventions or corrections to help the patient stay in treatment,” said Dr. Oldham.
It aims to conceptualize BPD in a clinically objective way, medicalizing the disorder so it’s something that the patient has, rather than something he or she is, explained Dr. Choi-Kain, who worked with Dr. Gunderson to train clinicians on using this approach. Using a framework that’s compatible with good medical practices, the clinician tries to define the problem together with the patient, “really assessing whether or not the treatment works, setting goals, managing safety, and trying to promote functioning, something we need to pay more attention to with BPD,” she said.
For these patients, the goal is to have positive, corrective experiences in the real world, reinforcing their hopes and what they’re capable of, and an interface with the world that makes them feel like contributors, she said.
Cycle of rupture and repair
Many people with BPD struggle with the desire to find and feel love, but also deal with their rage and hate. Hence, therapists must prepare themselves for the experience of sometimes being hated, said Dr. Plakun. The patient needs to feel they’re in a safe enough space to express those feelings, activating a cycle of “rupture and repair,” he continued.
The key in working with these patients is to avoid any language that will make them feel attacked or criticized, said Dr. Oldham.
A patient may get furious and say “I don’t know what you’re talking about. I didn’t say that.” When in truth, the psychiatrist is flat accurate about what the patient said. Instead of arguing with the patient, a physician can back up and say: “Help me understand what you’re feeling right now. What did I say that made you feel that you couldn’t trust me? Help me understand you. I may have made a mistake,” he advised.
Trust is a key ingredient in an alliance-based intervention for suicidal patients with BPD that Dr. Plakun has frequently written about. A bond he had with a deeply suicidal patient helped her overcome her grief and come to terms with an abusive childhood.
“She had a horrible history of abuse and had BPD and bipolar disorder. Even controlled with medications her life was still awful. She contemplated suicide relentlessly.” Working through her history of sexual abuse, the patient discovered that much of what she and clinicians thought of as a depressive illness was in fact intense grief about the irreparable damage that had taken place during childhood.
Through their work she was able to mourn, and her depression and BPD improved.
Developing a trusting relationship with the patient isn’t a starting point; it’s the goal, he emphasized.
“You don’t prescribe trust to someone. It’s earned.” Through the shared journey of therapy, as the patient suffers from inevitable injuries and ruptures and as the therapist reveals his or her imperfections, opportunities arise to nonjudgmentally examine and repair ruptures. This lead to gains in trust, he said.
It’s not just about genes
Many in the psychiatric and psychological communities tend to develop a very nihilistic view of BPD patients, observed Dr. Cummings. “They’ll say: ‘Oh, well, it’s hopeless. There’s nothing that can be done.’ That isn’t true,” he said.
Epidemiologic studies of these individuals have shown that many of these patients no longer meet the diagnostic criteria for BPD by the time they reach middle age. This means they get better over time, noted Dr. Cummings.
Dr. Plakun’s hope is that the field will evolve in a direction that recognizes the importance of psychosocial treatments like psychotherapy, in addition to biomedical treatments. The drive to medicate still exists, which can contribute to underdiagnosis and undertreatment of BPD, he said. “Although there are manualized, evidence-based treatments, few clinicians learn even one of these for BPD, not to mention those for other disorders.”
In 1996, Francis S. Collins, MD, PhD, the current director of the National Institutes of Health, predicted that the decoding of the human genome would transform treatment of medical and mental disorders [and] “that we would discover the ways in which genes equal disease,” said Dr. Plakun. What the science has since shown, is genes by environmental interaction lead to disease and health.
Nature and nurture both matter. “And I don’t think we’re paying enough attention to the nurture side,” Dr. Plakun said.
The solution is a return to a biopsychosocial model, recognizing that psychotherapy is an essential part of treatment of BPD and other conditions, and an essential clinician skill, he said.
Dr. Oldham is coeditor of the “Textbook of Personality Disorders”, 3rd edition (Washington: American Psychiatric Association Publishing, 2021).Dr. Choi-Kain is coeditor with Dr. Gunderson of “Applications of Good Psychiatric Management for Borderline Personality Disorder: A Practical Guide” (Washington: American Psychiatric Association Publishing, 2019).
Dr. Cummings and Dr. Plakun had no disclosures.
Difficulties associated with treating borderline personality disorder (BPD) make for an uneasy alliance between patient and clinician. Deep-seated anxiety and trust issues often lead to patients skipping visits or raging at those who treat them, leaving clinicians frustrated and ready to give up or relying on a pill to make the patient better.
John M. Oldham, MD, MS, recalls one patient he almost lost, a woman who was struggling with aggressive behavior. Initially cooperative and punctual, the patient gradually became distrustful, grilling Dr. Oldham on his training and credentials. “As the questions continued, she slipped from being very cooperative to being enraged and attacking me,” said Dr. Oldham, Distinguished Emeritus Professor in the Menninger department of psychiatry and behavioral sciences at Baylor College in Houston.
Dr. Oldham eventually drew her back in by earning her trust. “There’s no magic to this,” he acknowledged. “You try to be as alert and informed and vigilant for anything you say that produces a negative or concerning reaction in the patient.”
This interactive approach to BPD treatment has been gaining traction in a profession that often looks to medications to alleviate specific symptoms. It’s so effective that it sometimes even surprises the patient, Dr. Oldham noted. “When you approach them like this, they can begin to settle down,” which was the case with the female patient he once treated.
About 1.4% of the U.S. population has BPD, according to the National Institute of Mental Health. Conceptualized by the late John G. Gunderson, MD, BPD initially was seen as floating on the borderline between psychosis and neurosis. Clinicians now understand that this isn’t the case. The patients need, as Dr. Gunderson once pointed out, constant vigilance because of attachment issues and childhood trauma.
A stable therapeutic alliance between patient and physician, sometimes in combination with evidence-based therapies, is a formula for success, some experts say.
A misunderstood condition
Although there is some degree of heritable risk, BPD patients are often the product of an invalidating environment in childhood. “As kids, we’re guided and nurtured by caring adults to provide models of reasonable, trustworthy behavior. If those role models are missing or just so inconsistent and unpredictable, the patient doesn’t end up with a sturdy self-image. Instead, they’re adrift, trying to figure out who will be helpful and be a meaningful, trustworthy companion and adviser,” Dr. Oldham said.
Emotional or affective instability and impulsivity, sometimes impulsive aggression, often characterize their condition. “Brain-imaging studies have revealed that certain nerve pathways that are necessary to regulate emotions are impoverished in patients with BPD,” Dr. Oldham said.
An analogy is a car going too fast, with a runaway engine that’s running too hot – and the brakes don’t work, he added.
“People think these patients are trying to create big drama, that they’re putting on a big show. That’s not accurate,” he continued. These patients don’t have the ability to stop the trigger that leads to their emotional storms. They also don’t have the ability to regulate themselves. “We may say, it’s a beautiful day outside, but I still have to go to work. Someone with BPD may say: It’s a beautiful day; I’m going to the beach,” Dr. Oldham explained.
A person with BPD might sound coherent when arguing with someone else. But their words are driven by the storm they can’t turn off.
This can lead to their own efforts to turn off the intensity. They might become self-injurious or push other people away. It’s one of the ironies of this condition because BPD patients desperately want to trust others but are scared to do so. “They look for any little signal – that someone else will hurt, disappoint, or leave them. Eventually their relationships unravel,” Dr. Oldham saod.
For some, suicide is sometimes a final solution.
Those traits make it difficult for a therapist to connect with a patient. “This is a very difficult group of people to treat and to establish treatment,” said Michael A. Cummings, MD, of the department of psychiatry at University of California, Riverside, and a psychopharmacology consultant with the California Department of State Hospitals’ Psychopharmacology Resource Network.
BPD patients tend to idealize people who are attempting to help them. When they become frustrated or disappointed in some way, “they then devalue the caregiver or the treatment and not infrequently, fall out of treatment,” Dr. Cummings said. It can be a very taxing experience, particularly for younger, less experienced therapists.
Medication only goes so far
Psychiatrists tend to look at BPD patients as receptor sites for molecules, assessing symptoms they can prescribe for, Eric M. Plakun, MD, DLFAPA, FACPsych, medical director/CEO of the Austen Riggs Center in Stockbridge, Mass., said in an interview.
Yet, BPD is not a molecular problem, principally. It’s an interpersonal disorder. When BPD is a co-occurring disorder, as is often the case, the depressive, anxiety, or other disorder can mask the BPD, he added, citing his 2018 paper on tensions in psychiatry between the biomedical and biopsychosocial models (Psychiatr Clin North Am. 2018 Jun;41[2]:237-48).
In one longitudinal study (J Pers Disord. 2005 Oct;19[5]:487-504), the presence of BPD strongly predicted the persistence of depression. BPD comorbid with depression is often a recipe for treatment-resistant depression, which results in higher costs, more utilization of resources, and higher suicide rates. Too often, psychiatrists diagnose the depression but miss the BPD. They keep trying molecular approaches with prescription drugs – even though it’s really the interpersonal issues of BPD that need to be addressed, said Dr. Plakun, who is a member of the Group for the Advancement of Psychiatry’s Psychotherapy Committee, and founder and past leader of the American Psychiatric Association’s Psychotherapy Caucus.
Medication can be helpful as a short-term adjunctive therapy. Long term, it’s not a sustainable approach, said Dr. Oldham. “If a patient is in a particularly stressful period, in the middle of a stormy breakup or having a depressive episode or talking about suicide, a time-limited course of an antidepressant may be helpful,” he said. They could also benefit from an anxiety-related drug or medication to help them sleep.
What you don’t want is for the patient to start relying on medications to help them feel better. The problem is, many are suffering so much that they’ll go to their primary care doctor and say, “I’m suffering from anxiety,” and get an antianxiety drug. Or they’re depressed or in pain and end up with a cocktail of medications. “And that’s just going to make matters worse,” Dr. Oldham said.
Psychotherapy as a first-line approach
APA practice guidelines and others worldwide have all come to the same conclusion about BPD. , who chaired an APA committee that developed an evidence-based practice guideline for patients with BPD.
Psychotherapy keeps the patient from firing you, he asserted. “Because of the lack of trust, they push away. They’re very scared, and this fear also applies to therapist. The goal is to help the patient learn to trust you. To do that, you need to develop a strong therapeutic alliance.”
In crafting the APA’s practice guideline, Dr. Oldham and his colleagues studied a variety of approaches, including mentalization-based therapy (MBT) and dialectical behavior therapy (DBT), which was developed by Marsha Linehan, PhD. Since then, other approaches have demonstrated efficacy in randomized clinical trials, including schema-based therapy (SBT), cognitive-behavioral therapy (CBT), and transference-focused psychotherapy (TFP).
Those treatments might complement the broader goal of establishing a strong alliance with the patient, Dr. Oldham said. Manualized approaches can help prepackage a program that allows clinicians and patients to look at their problems in an objective, nonpejorative way, Lois W. Choi-Kain, MD, MEd, director of the Gunderson Personality Disorders Institute at McLean Hospital in Belmont, Mass., said in an interview. DBT, for example, focuses on emotion dysregulation. MBT addresses how the patient sees themselves through others and their interactions with others. “It destigmatizes a problem as a clinical entity rather than an interpersonal problem between the patient and the clinician,” Dr. Choi-Kain said.
The choice of approach depends on several factors: the patient’s needs and preferences, and the therapist’s skills and experience, said Dr. Oldham. Some patients don’t do well with DBT because it involves a lot of homework and didactic work. Others do better with TFP because they want to understand what drives their behavior.
Dr. Cummings recalled how one of his patients used TFP to look inward and heal.
He first met the patient when she was in her early 30s. “She had made some progress, but I remember she was still struggling mightily with relationship issues and with identifying her role in relationships,” he said. The patient was becoming increasingly aware that she was going to end up alone and didn’t want that as an outcome.
Adapting to a TFP model, “she worked very hard trying to understand herself as she related to other people, understanding her own emotional volatility, and some of her proneness to behavioral problems,” Dr. Cummings said. The patient also had to learn how to negotiate her relationships to the point where she didn’t end up destroying them and alienating people.
Customizing the treatment
Physicians can choose from one of these manualized forms of treatment to see what’s appropriate and what works for the patient. “You can individualize the treatment, borrowing from these approaches and shaping it based on what your patient needs,” Dr. Oldham recommended.
Recently, the field of psychiatry has seen the benefits of combining manualized, evidence-based approaches with general psychiatric management (GPM), a method conceived by Dr. Gunderson. GPM “reflects a sensitive understanding of mental illness, offering ‘non attacking’ or collaborative work with the patient and a sensitive recognition of appropriate interventions or corrections to help the patient stay in treatment,” said Dr. Oldham.
It aims to conceptualize BPD in a clinically objective way, medicalizing the disorder so it’s something that the patient has, rather than something he or she is, explained Dr. Choi-Kain, who worked with Dr. Gunderson to train clinicians on using this approach. Using a framework that’s compatible with good medical practices, the clinician tries to define the problem together with the patient, “really assessing whether or not the treatment works, setting goals, managing safety, and trying to promote functioning, something we need to pay more attention to with BPD,” she said.
For these patients, the goal is to have positive, corrective experiences in the real world, reinforcing their hopes and what they’re capable of, and an interface with the world that makes them feel like contributors, she said.
Cycle of rupture and repair
Many people with BPD struggle with the desire to find and feel love, but also deal with their rage and hate. Hence, therapists must prepare themselves for the experience of sometimes being hated, said Dr. Plakun. The patient needs to feel they’re in a safe enough space to express those feelings, activating a cycle of “rupture and repair,” he continued.
The key in working with these patients is to avoid any language that will make them feel attacked or criticized, said Dr. Oldham.
A patient may get furious and say “I don’t know what you’re talking about. I didn’t say that.” When in truth, the psychiatrist is flat accurate about what the patient said. Instead of arguing with the patient, a physician can back up and say: “Help me understand what you’re feeling right now. What did I say that made you feel that you couldn’t trust me? Help me understand you. I may have made a mistake,” he advised.
Trust is a key ingredient in an alliance-based intervention for suicidal patients with BPD that Dr. Plakun has frequently written about. A bond he had with a deeply suicidal patient helped her overcome her grief and come to terms with an abusive childhood.
“She had a horrible history of abuse and had BPD and bipolar disorder. Even controlled with medications her life was still awful. She contemplated suicide relentlessly.” Working through her history of sexual abuse, the patient discovered that much of what she and clinicians thought of as a depressive illness was in fact intense grief about the irreparable damage that had taken place during childhood.
Through their work she was able to mourn, and her depression and BPD improved.
Developing a trusting relationship with the patient isn’t a starting point; it’s the goal, he emphasized.
“You don’t prescribe trust to someone. It’s earned.” Through the shared journey of therapy, as the patient suffers from inevitable injuries and ruptures and as the therapist reveals his or her imperfections, opportunities arise to nonjudgmentally examine and repair ruptures. This lead to gains in trust, he said.
It’s not just about genes
Many in the psychiatric and psychological communities tend to develop a very nihilistic view of BPD patients, observed Dr. Cummings. “They’ll say: ‘Oh, well, it’s hopeless. There’s nothing that can be done.’ That isn’t true,” he said.
Epidemiologic studies of these individuals have shown that many of these patients no longer meet the diagnostic criteria for BPD by the time they reach middle age. This means they get better over time, noted Dr. Cummings.
Dr. Plakun’s hope is that the field will evolve in a direction that recognizes the importance of psychosocial treatments like psychotherapy, in addition to biomedical treatments. The drive to medicate still exists, which can contribute to underdiagnosis and undertreatment of BPD, he said. “Although there are manualized, evidence-based treatments, few clinicians learn even one of these for BPD, not to mention those for other disorders.”
In 1996, Francis S. Collins, MD, PhD, the current director of the National Institutes of Health, predicted that the decoding of the human genome would transform treatment of medical and mental disorders [and] “that we would discover the ways in which genes equal disease,” said Dr. Plakun. What the science has since shown, is genes by environmental interaction lead to disease and health.
Nature and nurture both matter. “And I don’t think we’re paying enough attention to the nurture side,” Dr. Plakun said.
The solution is a return to a biopsychosocial model, recognizing that psychotherapy is an essential part of treatment of BPD and other conditions, and an essential clinician skill, he said.
Dr. Oldham is coeditor of the “Textbook of Personality Disorders”, 3rd edition (Washington: American Psychiatric Association Publishing, 2021).Dr. Choi-Kain is coeditor with Dr. Gunderson of “Applications of Good Psychiatric Management for Borderline Personality Disorder: A Practical Guide” (Washington: American Psychiatric Association Publishing, 2019).
Dr. Cummings and Dr. Plakun had no disclosures.
Patients panic as docs cut off breast cancer drug
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Flurry of cancer drug endorsements from EU panel
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
FDA approves first oral drug for NSCLC with EGFR Exon 20 insertion
The drug is limited to use in patients whose disease has progressed on or after platinum-based chemotherapy and who have had the EGFR Exon 20 insertion mutation detected on an FDA-approved test.
Mobocertinib is the first oral tyrosine kinase inhibitor (TKI) specifically designed to target these mutations, which are less common than the more predominant EGFR mutations in this lung cancer.
“EGFR Exon 20 insertion+ NSCLC is an underserved cancer that we have been unable to target effectively with traditional EGFR TKIs,” said Pasi Jänne, MD, PhD, of the Dana Farber Cancer Institute, Boston, in a press statement from the maker, Takeda.
“The approval of [mobocertinib] marks another important step forward that provides physicians and their patients with a new targeted oral therapy specifically designed for this patient population that has shown clinically meaningful and sustained responses,” Dr. Jänne added.
According to the company, EGFR Exon 20 insertion+ NSCLC makes up approximately 1%-2% of patients with NSCLC and is more common in Asian populations compared with Western populations.
The new approval is based on overall response rate (ORR) and duration of response (DoR) results from a phase 1/2 trial consisting of 114 patients with EGFR Exon 20 insertion+ NSCLC who received prior platinum-based therapy and were treated with the 160-mg dose.
Per an independent review committee, mobocertinib demonstrated a confirmed ORR of 28% and a median DoR of 17.5 months.
Median overall survival was 24 months and median progression-free survival was 7.3 months.
The FDA-approved next-generation sequencing (NGS) companion diagnostic for mobocertinib is Thermo Fisher Scientific’s Oncomine Dx Target Test, which identifies NSCLC patients with EGFR Exon 20 insertions.
“NGS testing is critical for these patients, as it can enable more accurate diagnoses compared to polymerase chain reaction (PCR) testing, which detects less than 50% of EGFR Exon 20 insertions,” according to the company.
Results from the phase 1/2 trial used in the FDA approval were presented at the 2021 American Society of Clinical Oncology Annual Meeting.
The most common adverse reactions (greater than 20%) were diarrhea, rash, nausea, stomatitis, vomiting, decreased appetite, paronychia, fatigue, dry skin, and musculoskeletal pain, according to the company.
The prescribing information includes a boxed warning for QTc prolongation and Torsades de Pointes, and warnings and precautions for interstitial lung disease/pneumonitis, cardiac toxicity, and diarrhea.
“Patients with EGFR Exon 20 insertion+ NSCLC have historically faced a unique set of challenges living with a very rare lung cancer that is not only underdiagnosed but also lacking targeted treatment options that can improve response rates,” said Marcia Horn, executive director, Exon 20 Group at the International Cancer Advocacy Network, in the press statement.
The FDA review was conducted under Project Orbis, an FDA initiative that enables concurrent submission and review of oncology products among international partners.
The new drug was also granted priority review and received breakthrough therapy, fast track, and orphan drug designations from the FDA.
A version of this article first appeared on Medscape.com.
The drug is limited to use in patients whose disease has progressed on or after platinum-based chemotherapy and who have had the EGFR Exon 20 insertion mutation detected on an FDA-approved test.
Mobocertinib is the first oral tyrosine kinase inhibitor (TKI) specifically designed to target these mutations, which are less common than the more predominant EGFR mutations in this lung cancer.
“EGFR Exon 20 insertion+ NSCLC is an underserved cancer that we have been unable to target effectively with traditional EGFR TKIs,” said Pasi Jänne, MD, PhD, of the Dana Farber Cancer Institute, Boston, in a press statement from the maker, Takeda.
“The approval of [mobocertinib] marks another important step forward that provides physicians and their patients with a new targeted oral therapy specifically designed for this patient population that has shown clinically meaningful and sustained responses,” Dr. Jänne added.
According to the company, EGFR Exon 20 insertion+ NSCLC makes up approximately 1%-2% of patients with NSCLC and is more common in Asian populations compared with Western populations.
The new approval is based on overall response rate (ORR) and duration of response (DoR) results from a phase 1/2 trial consisting of 114 patients with EGFR Exon 20 insertion+ NSCLC who received prior platinum-based therapy and were treated with the 160-mg dose.
Per an independent review committee, mobocertinib demonstrated a confirmed ORR of 28% and a median DoR of 17.5 months.
Median overall survival was 24 months and median progression-free survival was 7.3 months.
The FDA-approved next-generation sequencing (NGS) companion diagnostic for mobocertinib is Thermo Fisher Scientific’s Oncomine Dx Target Test, which identifies NSCLC patients with EGFR Exon 20 insertions.
“NGS testing is critical for these patients, as it can enable more accurate diagnoses compared to polymerase chain reaction (PCR) testing, which detects less than 50% of EGFR Exon 20 insertions,” according to the company.
Results from the phase 1/2 trial used in the FDA approval were presented at the 2021 American Society of Clinical Oncology Annual Meeting.
The most common adverse reactions (greater than 20%) were diarrhea, rash, nausea, stomatitis, vomiting, decreased appetite, paronychia, fatigue, dry skin, and musculoskeletal pain, according to the company.
The prescribing information includes a boxed warning for QTc prolongation and Torsades de Pointes, and warnings and precautions for interstitial lung disease/pneumonitis, cardiac toxicity, and diarrhea.
“Patients with EGFR Exon 20 insertion+ NSCLC have historically faced a unique set of challenges living with a very rare lung cancer that is not only underdiagnosed but also lacking targeted treatment options that can improve response rates,” said Marcia Horn, executive director, Exon 20 Group at the International Cancer Advocacy Network, in the press statement.
The FDA review was conducted under Project Orbis, an FDA initiative that enables concurrent submission and review of oncology products among international partners.
The new drug was also granted priority review and received breakthrough therapy, fast track, and orphan drug designations from the FDA.
A version of this article first appeared on Medscape.com.
The drug is limited to use in patients whose disease has progressed on or after platinum-based chemotherapy and who have had the EGFR Exon 20 insertion mutation detected on an FDA-approved test.
Mobocertinib is the first oral tyrosine kinase inhibitor (TKI) specifically designed to target these mutations, which are less common than the more predominant EGFR mutations in this lung cancer.
“EGFR Exon 20 insertion+ NSCLC is an underserved cancer that we have been unable to target effectively with traditional EGFR TKIs,” said Pasi Jänne, MD, PhD, of the Dana Farber Cancer Institute, Boston, in a press statement from the maker, Takeda.
“The approval of [mobocertinib] marks another important step forward that provides physicians and their patients with a new targeted oral therapy specifically designed for this patient population that has shown clinically meaningful and sustained responses,” Dr. Jänne added.
According to the company, EGFR Exon 20 insertion+ NSCLC makes up approximately 1%-2% of patients with NSCLC and is more common in Asian populations compared with Western populations.
The new approval is based on overall response rate (ORR) and duration of response (DoR) results from a phase 1/2 trial consisting of 114 patients with EGFR Exon 20 insertion+ NSCLC who received prior platinum-based therapy and were treated with the 160-mg dose.
Per an independent review committee, mobocertinib demonstrated a confirmed ORR of 28% and a median DoR of 17.5 months.
Median overall survival was 24 months and median progression-free survival was 7.3 months.
The FDA-approved next-generation sequencing (NGS) companion diagnostic for mobocertinib is Thermo Fisher Scientific’s Oncomine Dx Target Test, which identifies NSCLC patients with EGFR Exon 20 insertions.
“NGS testing is critical for these patients, as it can enable more accurate diagnoses compared to polymerase chain reaction (PCR) testing, which detects less than 50% of EGFR Exon 20 insertions,” according to the company.
Results from the phase 1/2 trial used in the FDA approval were presented at the 2021 American Society of Clinical Oncology Annual Meeting.
The most common adverse reactions (greater than 20%) were diarrhea, rash, nausea, stomatitis, vomiting, decreased appetite, paronychia, fatigue, dry skin, and musculoskeletal pain, according to the company.
The prescribing information includes a boxed warning for QTc prolongation and Torsades de Pointes, and warnings and precautions for interstitial lung disease/pneumonitis, cardiac toxicity, and diarrhea.
“Patients with EGFR Exon 20 insertion+ NSCLC have historically faced a unique set of challenges living with a very rare lung cancer that is not only underdiagnosed but also lacking targeted treatment options that can improve response rates,” said Marcia Horn, executive director, Exon 20 Group at the International Cancer Advocacy Network, in the press statement.
The FDA review was conducted under Project Orbis, an FDA initiative that enables concurrent submission and review of oncology products among international partners.
The new drug was also granted priority review and received breakthrough therapy, fast track, and orphan drug designations from the FDA.
A version of this article first appeared on Medscape.com.
Immunotherapy for cancer patients with poor PS needs a rethink
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
EMPEROR-Preserved: Empagliflozin’s HFpEF efficacy catalyzes a heart failure redefinition
Groundbreaking results from the EMPEROR-Preserved trial did more than establish for the first time that a drug, empagliflozin, has clearly proven efficacy for treating patients with heart failure with preserved ejection fraction (HFpEF). The results also helped catalyze a paradigm shift in how heart failure thought leaders think about the role of ejection fraction for making important distinctions among patients with heart failure.

EMPEROR-Preserved may also be the final nail in the coffin for defining patients with heart failure as having HFpEF or heart failure with reduced ejection fraction (HFrEF).
This new consensus essentially throws out left ventricular ejection fraction (EF) as the key metric for matching patients to heart failure treatments. Experts have instead begun suggesting a more unified treatment approach for all heart failure patients regardless of their EF.
‘Forget about ejection fraction’
“We encourage you to forget about ejection fraction,” declared Milton Packer, MD, during discussion at a session of the annual scientific meeting of the Heart Failure Society of America. “We certainly encourage you to forget about an ejection fraction of less than 40%” as having special significance,” added Dr. Packer, a lead investigator for both the EMPEROR-Reduced and EMPEROR-Preserved trials (which researchers combined in a unified analysis with a total of 9,718 patients with heart failure called EMPEROR-Pooled), and a heart failure researcher at Baylor University Medical Center in Dallas.
“The 40% ejection fraction divide is artificial. It was created in 2003 as part of a trial design, but it has no physiological significance,” Dr. Packer explained. A much better way to distinguish systolic and diastolic heart failure is by strain assessment rather than by ejection fraction. “Strain is a measure of myocardial shortening, a measure of what the heart does. Ejection fraction is a measure of volume,” said Dr. Packer. “Sign me up to get rid of ejection fraction,” he added.
“Ejection fraction is not as valuable as we thought for distinguishing the therapeutic benefit” of heart failure drugs, agreed Marvin A. Konstam, MD, professor of medicine at Tufts University and chief physician executive of the CardioVascular Center of Tufts Medical Center, both in Boston, who spoke during a different session at the meeting.

“It would easier if we didn’t spend time parsing this number,” ejection fraction, commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern Medicine in Chicago. “Wouldn’t it be easier if we said that every patient with heart failure needs to receive one agent from each of the four [pillar] drug classes, and put them in a polypill” at reduced dosages, he proposed, envisioning one potential consequence of jettisoning ejection fraction.
The four pillar drug classes, recently identified as essential for patients with HFrEF but until now not endorsed for patients with HFpEF, are the sodium-glucose cotransporter 2 (SGLT2) inhibitors, such as empagliflozin (Jardiance); an angiotensin receptor blocker neprilysin inhibitor compound such as sacubitril/valsartan (Entresto); beta-blockers; and mineralocorticoid receptor antagonists such as spironolactone and eplerenone.
An opportunity for ‘simpler and easier’ treatments
“This is an opportunity to disrupt the way we’ve been doing things and think about something that is simpler and easier,” said Dr. Yancy, who chaired some of the panels serially formed by the American Heart Association and American College of Cardiology to write guidelines for treating heart failure. “An approach that would be easier to implement without worrying about staggering the start of each drug class and an incessant focus on titrating individual elements and taking 6 months to get to a certain place.”
Results from EMPEROR-Preserved and the combined EMPEROR-Pooled analysis triggered these paradigm-shifting sentiments by showing clear evidence that treatment with empagliflozin exerts consistent benefit – and is consistently safe – for patients with heart failure across a spectrum of EFs, from less than 25% to 64%, though its performance in patients with HFpEF and EFs of 65% or greater in the EMPEROR-Preserved trial remains unclear.
The consequence is that clinicians should feel comfortable prescribing empagliflozin to most patients with heart failure without regard to EF, even patients with EF values in the mid-60% range.
The EMPEROR-Preserved results showed a clear signal of attenuated benefit among patients with an EF of 65% or greater “on a population basis,” stressed Dr. Packer. “But on an individual basis, ejection fraction is not that reproducible, so measuring ejection fraction will not help you determine whom to treat or not treat. “

“There is significant variability” measuring EF using the most common modality, echocardiography, noted Javed Butler, MD, an EMPEROR coinvestigator who also spoke at the meeting session. A person with a measured EF of 65% could actually have a value that may be as low as 58% or as high as about 72%, noted Dr. Butler, who is professor and chair of medicine at the University of Mississippi, Jackson. The upshot is that any patient diagnosed with heart failure should receive an SGLT2 inhibitor “irrespective of their ejection fraction,” Dr. Butler advised.
“Ejection fraction is very crude, and probably not sufficient to identify a phenotype,” for treatment, said Dr. Yancy. “The real takeaway may be that we need to revisit what we call HFrEF, and then let that be the new standard for treatment.”
“Is [an EF of] 60% the new 40%?” asked Dr. Packer, implying that the answer was yes.
Results from several trials suggest redefining HFrEF
The idea that patients without traditionally defined HFrEF – an EF of 40% or less – could also benefit from other classes of heart failure drugs has been gestating for a while, and then rose to a new level with the August 2021 report of results from EMPEROR-Preserved. Two years ago, in September 2019, Dr. Butler, Dr. Packer, and a third colleague advanced the notion of redefining HFrEF by raising the ejection fraction ceiling in a published commentary.
They cited the experience with the angiotensin receptor blocker candesartan in a post hoc analysis of data collected in the CHARM-Preserved trial, which showed a strong signal of benefit in the subgroup of patients with EFs of 41%-49%, but not in those with an EF of 50% or higher. This finding prompted Dr. Konstam to express doubts about relying on EF to define heart failure subgroups in trials and guide management in a commentary published more than 3 years ago.
Another crack in the traditional EF framework came from analysis of results from the TOPCAT trial that tested spironolactone as a treatment for patients with HFpEF, according to the 2019 opinion published by Dr. Butler and Dr. Packer. Once again a post hoc analysis, this time using data from TOPCAT, suggested a benefit from the mineralocorticoid receptor antagonist spironolactone in patients with heart failure and an EF of 45%-49% (45% was the minimum EF for enrollment into the study).
Recently, data from a third trial that tested sacubitril/valsartan in patients with HFpEF, PARAGON-HF, showed benefit among patients with EFs below the study median of 57%. This finding led the Food and Drug Administration in February 2021 to amend its initial approval for sacubitril/valsartan by removing a specific EF ceiling from the drug’s indication and instead saying that patient’s receiving the drug should have a “below normal” EF.
Writing in a recent commentary, Dr. Yancy called the FDA’s action on sacubitril/valsartan “reasonable,” and that the subgroup assessment of data from the PARAGON-HF trial creates a “new, reasonably evidence-based therapy for HFpEF.” He also predicted that guideline-writing panels will “likely align with a permissive statement of indication” for sacubitril/valsartan in patients with HFpEF, especially those with EFs of less than 57%.
The idea of using an SGLT2 inhibitor like empagliflozin on all heart failure patients, and also adding agents like sacubitril/valsartan and spironolactone in patients with HFpEF and EFs in the mid-50% range or lower may take some time to catch on, but it already has one influential advocate.
“If a patient has HFpEF with an EF of less than 55%, use quadruple-class therapy,” summed up Dr. Butler during the HFSA session, while also suggesting prescribing an SGLT2 inhibitor to essentially all patients with heart failure regardless of their EF.
The EMPEROR-Preserved and EMPEROR-Reduced trials and the EMPEROR-Pooled analysis were sponsored by Boehringer Ingelheim and Lilly, the companies that jointly market empagliflozin (Jardiance). Dr. Packer has had financial relationships with BI and Lilly and numerous other companies. Dr. Konstam has served on data monitoring committees for trials funded by Boehringer Ingelheim and by Amgen, Luitpold, and Pfizer, and has been a consultant to Arena, LivaNova, Merck, SC Pharma, and Takeda. Dr. Yancy had no disclosures. Dr. Butler has had financial relationships with Boehringer Ingelheim and numerous other companies.
Groundbreaking results from the EMPEROR-Preserved trial did more than establish for the first time that a drug, empagliflozin, has clearly proven efficacy for treating patients with heart failure with preserved ejection fraction (HFpEF). The results also helped catalyze a paradigm shift in how heart failure thought leaders think about the role of ejection fraction for making important distinctions among patients with heart failure.
EMPEROR-Preserved may also be the final nail in the coffin for defining patients with heart failure as having HFpEF or heart failure with reduced ejection fraction (HFrEF).
This new consensus essentially throws out left ventricular ejection fraction (EF) as the key metric for matching patients to heart failure treatments. Experts have instead begun suggesting a more unified treatment approach for all heart failure patients regardless of their EF.
‘Forget about ejection fraction’
“We encourage you to forget about ejection fraction,” declared Milton Packer, MD, during discussion at a session of the annual scientific meeting of the Heart Failure Society of America. “We certainly encourage you to forget about an ejection fraction of less than 40%” as having special significance,” added Dr. Packer, a lead investigator for both the EMPEROR-Reduced and EMPEROR-Preserved trials (which researchers combined in a unified analysis with a total of 9,718 patients with heart failure called EMPEROR-Pooled), and a heart failure researcher at Baylor University Medical Center in Dallas.
“The 40% ejection fraction divide is artificial. It was created in 2003 as part of a trial design, but it has no physiological significance,” Dr. Packer explained. A much better way to distinguish systolic and diastolic heart failure is by strain assessment rather than by ejection fraction. “Strain is a measure of myocardial shortening, a measure of what the heart does. Ejection fraction is a measure of volume,” said Dr. Packer. “Sign me up to get rid of ejection fraction,” he added.
“Ejection fraction is not as valuable as we thought for distinguishing the therapeutic benefit” of heart failure drugs, agreed Marvin A. Konstam, MD, professor of medicine at Tufts University and chief physician executive of the CardioVascular Center of Tufts Medical Center, both in Boston, who spoke during a different session at the meeting.
“It would easier if we didn’t spend time parsing this number,” ejection fraction, commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern Medicine in Chicago. “Wouldn’t it be easier if we said that every patient with heart failure needs to receive one agent from each of the four [pillar] drug classes, and put them in a polypill” at reduced dosages, he proposed, envisioning one potential consequence of jettisoning ejection fraction.
The four pillar drug classes, recently identified as essential for patients with HFrEF but until now not endorsed for patients with HFpEF, are the sodium-glucose cotransporter 2 (SGLT2) inhibitors, such as empagliflozin (Jardiance); an angiotensin receptor blocker neprilysin inhibitor compound such as sacubitril/valsartan (Entresto); beta-blockers; and mineralocorticoid receptor antagonists such as spironolactone and eplerenone.
An opportunity for ‘simpler and easier’ treatments
“This is an opportunity to disrupt the way we’ve been doing things and think about something that is simpler and easier,” said Dr. Yancy, who chaired some of the panels serially formed by the American Heart Association and American College of Cardiology to write guidelines for treating heart failure. “An approach that would be easier to implement without worrying about staggering the start of each drug class and an incessant focus on titrating individual elements and taking 6 months to get to a certain place.”
Results from EMPEROR-Preserved and the combined EMPEROR-Pooled analysis triggered these paradigm-shifting sentiments by showing clear evidence that treatment with empagliflozin exerts consistent benefit – and is consistently safe – for patients with heart failure across a spectrum of EFs, from less than 25% to 64%, though its performance in patients with HFpEF and EFs of 65% or greater in the EMPEROR-Preserved trial remains unclear.
The consequence is that clinicians should feel comfortable prescribing empagliflozin to most patients with heart failure without regard to EF, even patients with EF values in the mid-60% range.
The EMPEROR-Preserved results showed a clear signal of attenuated benefit among patients with an EF of 65% or greater “on a population basis,” stressed Dr. Packer. “But on an individual basis, ejection fraction is not that reproducible, so measuring ejection fraction will not help you determine whom to treat or not treat. “
“There is significant variability” measuring EF using the most common modality, echocardiography, noted Javed Butler, MD, an EMPEROR coinvestigator who also spoke at the meeting session. A person with a measured EF of 65% could actually have a value that may be as low as 58% or as high as about 72%, noted Dr. Butler, who is professor and chair of medicine at the University of Mississippi, Jackson. The upshot is that any patient diagnosed with heart failure should receive an SGLT2 inhibitor “irrespective of their ejection fraction,” Dr. Butler advised.
“Ejection fraction is very crude, and probably not sufficient to identify a phenotype,” for treatment, said Dr. Yancy. “The real takeaway may be that we need to revisit what we call HFrEF, and then let that be the new standard for treatment.”
“Is [an EF of] 60% the new 40%?” asked Dr. Packer, implying that the answer was yes.
Results from several trials suggest redefining HFrEF
The idea that patients without traditionally defined HFrEF – an EF of 40% or less – could also benefit from other classes of heart failure drugs has been gestating for a while, and then rose to a new level with the August 2021 report of results from EMPEROR-Preserved. Two years ago, in September 2019, Dr. Butler, Dr. Packer, and a third colleague advanced the notion of redefining HFrEF by raising the ejection fraction ceiling in a published commentary.
They cited the experience with the angiotensin receptor blocker candesartan in a post hoc analysis of data collected in the CHARM-Preserved trial, which showed a strong signal of benefit in the subgroup of patients with EFs of 41%-49%, but not in those with an EF of 50% or higher. This finding prompted Dr. Konstam to express doubts about relying on EF to define heart failure subgroups in trials and guide management in a commentary published more than 3 years ago.
Another crack in the traditional EF framework came from analysis of results from the TOPCAT trial that tested spironolactone as a treatment for patients with HFpEF, according to the 2019 opinion published by Dr. Butler and Dr. Packer. Once again a post hoc analysis, this time using data from TOPCAT, suggested a benefit from the mineralocorticoid receptor antagonist spironolactone in patients with heart failure and an EF of 45%-49% (45% was the minimum EF for enrollment into the study).
Recently, data from a third trial that tested sacubitril/valsartan in patients with HFpEF, PARAGON-HF, showed benefit among patients with EFs below the study median of 57%. This finding led the Food and Drug Administration in February 2021 to amend its initial approval for sacubitril/valsartan by removing a specific EF ceiling from the drug’s indication and instead saying that patient’s receiving the drug should have a “below normal” EF.
Writing in a recent commentary, Dr. Yancy called the FDA’s action on sacubitril/valsartan “reasonable,” and that the subgroup assessment of data from the PARAGON-HF trial creates a “new, reasonably evidence-based therapy for HFpEF.” He also predicted that guideline-writing panels will “likely align with a permissive statement of indication” for sacubitril/valsartan in patients with HFpEF, especially those with EFs of less than 57%.
The idea of using an SGLT2 inhibitor like empagliflozin on all heart failure patients, and also adding agents like sacubitril/valsartan and spironolactone in patients with HFpEF and EFs in the mid-50% range or lower may take some time to catch on, but it already has one influential advocate.
“If a patient has HFpEF with an EF of less than 55%, use quadruple-class therapy,” summed up Dr. Butler during the HFSA session, while also suggesting prescribing an SGLT2 inhibitor to essentially all patients with heart failure regardless of their EF.
The EMPEROR-Preserved and EMPEROR-Reduced trials and the EMPEROR-Pooled analysis were sponsored by Boehringer Ingelheim and Lilly, the companies that jointly market empagliflozin (Jardiance). Dr. Packer has had financial relationships with BI and Lilly and numerous other companies. Dr. Konstam has served on data monitoring committees for trials funded by Boehringer Ingelheim and by Amgen, Luitpold, and Pfizer, and has been a consultant to Arena, LivaNova, Merck, SC Pharma, and Takeda. Dr. Yancy had no disclosures. Dr. Butler has had financial relationships with Boehringer Ingelheim and numerous other companies.
Groundbreaking results from the EMPEROR-Preserved trial did more than establish for the first time that a drug, empagliflozin, has clearly proven efficacy for treating patients with heart failure with preserved ejection fraction (HFpEF). The results also helped catalyze a paradigm shift in how heart failure thought leaders think about the role of ejection fraction for making important distinctions among patients with heart failure.
EMPEROR-Preserved may also be the final nail in the coffin for defining patients with heart failure as having HFpEF or heart failure with reduced ejection fraction (HFrEF).
This new consensus essentially throws out left ventricular ejection fraction (EF) as the key metric for matching patients to heart failure treatments. Experts have instead begun suggesting a more unified treatment approach for all heart failure patients regardless of their EF.
‘Forget about ejection fraction’
“We encourage you to forget about ejection fraction,” declared Milton Packer, MD, during discussion at a session of the annual scientific meeting of the Heart Failure Society of America. “We certainly encourage you to forget about an ejection fraction of less than 40%” as having special significance,” added Dr. Packer, a lead investigator for both the EMPEROR-Reduced and EMPEROR-Preserved trials (which researchers combined in a unified analysis with a total of 9,718 patients with heart failure called EMPEROR-Pooled), and a heart failure researcher at Baylor University Medical Center in Dallas.
“The 40% ejection fraction divide is artificial. It was created in 2003 as part of a trial design, but it has no physiological significance,” Dr. Packer explained. A much better way to distinguish systolic and diastolic heart failure is by strain assessment rather than by ejection fraction. “Strain is a measure of myocardial shortening, a measure of what the heart does. Ejection fraction is a measure of volume,” said Dr. Packer. “Sign me up to get rid of ejection fraction,” he added.
“Ejection fraction is not as valuable as we thought for distinguishing the therapeutic benefit” of heart failure drugs, agreed Marvin A. Konstam, MD, professor of medicine at Tufts University and chief physician executive of the CardioVascular Center of Tufts Medical Center, both in Boston, who spoke during a different session at the meeting.
“It would easier if we didn’t spend time parsing this number,” ejection fraction, commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern Medicine in Chicago. “Wouldn’t it be easier if we said that every patient with heart failure needs to receive one agent from each of the four [pillar] drug classes, and put them in a polypill” at reduced dosages, he proposed, envisioning one potential consequence of jettisoning ejection fraction.
The four pillar drug classes, recently identified as essential for patients with HFrEF but until now not endorsed for patients with HFpEF, are the sodium-glucose cotransporter 2 (SGLT2) inhibitors, such as empagliflozin (Jardiance); an angiotensin receptor blocker neprilysin inhibitor compound such as sacubitril/valsartan (Entresto); beta-blockers; and mineralocorticoid receptor antagonists such as spironolactone and eplerenone.
An opportunity for ‘simpler and easier’ treatments
“This is an opportunity to disrupt the way we’ve been doing things and think about something that is simpler and easier,” said Dr. Yancy, who chaired some of the panels serially formed by the American Heart Association and American College of Cardiology to write guidelines for treating heart failure. “An approach that would be easier to implement without worrying about staggering the start of each drug class and an incessant focus on titrating individual elements and taking 6 months to get to a certain place.”
Results from EMPEROR-Preserved and the combined EMPEROR-Pooled analysis triggered these paradigm-shifting sentiments by showing clear evidence that treatment with empagliflozin exerts consistent benefit – and is consistently safe – for patients with heart failure across a spectrum of EFs, from less than 25% to 64%, though its performance in patients with HFpEF and EFs of 65% or greater in the EMPEROR-Preserved trial remains unclear.
The consequence is that clinicians should feel comfortable prescribing empagliflozin to most patients with heart failure without regard to EF, even patients with EF values in the mid-60% range.
The EMPEROR-Preserved results showed a clear signal of attenuated benefit among patients with an EF of 65% or greater “on a population basis,” stressed Dr. Packer. “But on an individual basis, ejection fraction is not that reproducible, so measuring ejection fraction will not help you determine whom to treat or not treat. “
“There is significant variability” measuring EF using the most common modality, echocardiography, noted Javed Butler, MD, an EMPEROR coinvestigator who also spoke at the meeting session. A person with a measured EF of 65% could actually have a value that may be as low as 58% or as high as about 72%, noted Dr. Butler, who is professor and chair of medicine at the University of Mississippi, Jackson. The upshot is that any patient diagnosed with heart failure should receive an SGLT2 inhibitor “irrespective of their ejection fraction,” Dr. Butler advised.
“Ejection fraction is very crude, and probably not sufficient to identify a phenotype,” for treatment, said Dr. Yancy. “The real takeaway may be that we need to revisit what we call HFrEF, and then let that be the new standard for treatment.”
“Is [an EF of] 60% the new 40%?” asked Dr. Packer, implying that the answer was yes.
Results from several trials suggest redefining HFrEF
The idea that patients without traditionally defined HFrEF – an EF of 40% or less – could also benefit from other classes of heart failure drugs has been gestating for a while, and then rose to a new level with the August 2021 report of results from EMPEROR-Preserved. Two years ago, in September 2019, Dr. Butler, Dr. Packer, and a third colleague advanced the notion of redefining HFrEF by raising the ejection fraction ceiling in a published commentary.
They cited the experience with the angiotensin receptor blocker candesartan in a post hoc analysis of data collected in the CHARM-Preserved trial, which showed a strong signal of benefit in the subgroup of patients with EFs of 41%-49%, but not in those with an EF of 50% or higher. This finding prompted Dr. Konstam to express doubts about relying on EF to define heart failure subgroups in trials and guide management in a commentary published more than 3 years ago.
Another crack in the traditional EF framework came from analysis of results from the TOPCAT trial that tested spironolactone as a treatment for patients with HFpEF, according to the 2019 opinion published by Dr. Butler and Dr. Packer. Once again a post hoc analysis, this time using data from TOPCAT, suggested a benefit from the mineralocorticoid receptor antagonist spironolactone in patients with heart failure and an EF of 45%-49% (45% was the minimum EF for enrollment into the study).
Recently, data from a third trial that tested sacubitril/valsartan in patients with HFpEF, PARAGON-HF, showed benefit among patients with EFs below the study median of 57%. This finding led the Food and Drug Administration in February 2021 to amend its initial approval for sacubitril/valsartan by removing a specific EF ceiling from the drug’s indication and instead saying that patient’s receiving the drug should have a “below normal” EF.
Writing in a recent commentary, Dr. Yancy called the FDA’s action on sacubitril/valsartan “reasonable,” and that the subgroup assessment of data from the PARAGON-HF trial creates a “new, reasonably evidence-based therapy for HFpEF.” He also predicted that guideline-writing panels will “likely align with a permissive statement of indication” for sacubitril/valsartan in patients with HFpEF, especially those with EFs of less than 57%.
The idea of using an SGLT2 inhibitor like empagliflozin on all heart failure patients, and also adding agents like sacubitril/valsartan and spironolactone in patients with HFpEF and EFs in the mid-50% range or lower may take some time to catch on, but it already has one influential advocate.
“If a patient has HFpEF with an EF of less than 55%, use quadruple-class therapy,” summed up Dr. Butler during the HFSA session, while also suggesting prescribing an SGLT2 inhibitor to essentially all patients with heart failure regardless of their EF.
The EMPEROR-Preserved and EMPEROR-Reduced trials and the EMPEROR-Pooled analysis were sponsored by Boehringer Ingelheim and Lilly, the companies that jointly market empagliflozin (Jardiance). Dr. Packer has had financial relationships with BI and Lilly and numerous other companies. Dr. Konstam has served on data monitoring committees for trials funded by Boehringer Ingelheim and by Amgen, Luitpold, and Pfizer, and has been a consultant to Arena, LivaNova, Merck, SC Pharma, and Takeda. Dr. Yancy had no disclosures. Dr. Butler has had financial relationships with Boehringer Ingelheim and numerous other companies.
FROM HFSA 2021
Survey: Nursing shortages affect safety during labor and delivery
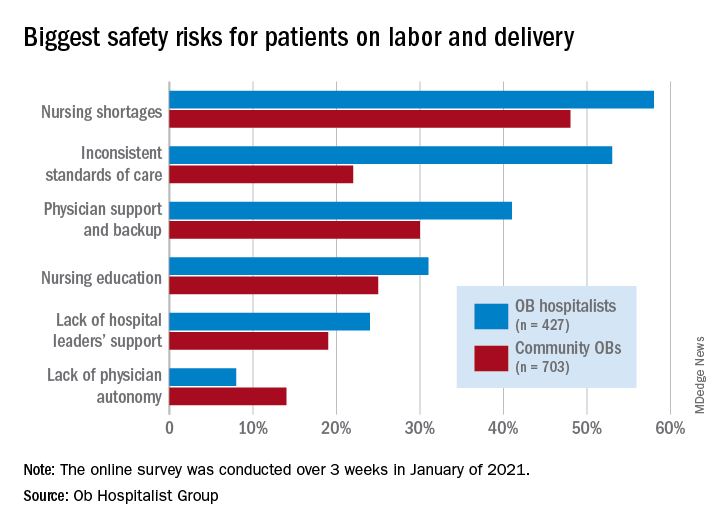
Just over 58% of the 1,130 respondents put nursing shortages ahead of physician support and backup (39.0%), inconsistent standards of care (38.5%), and nursing education (31.1%) as the most important challenge to patient safety, the Ob Hospitalist Group (OBHG) said in a new report.
“The survey reveals some startling gaps in physician and patient support all along the care continuum in obstetrics and OB hospitalist programs filling them,” said Lenny Castiglione, the CEO of OBHG, a national network of over 1,000 obstetric hospitalists. “As pressure builds on ob. units to improve care and reduce costs, and as clinical resources are stretched in the continuing battle against COVID-19 and its variants, health systems need to take serious measures to fill these gaps through staff recruitment, retention, and training.”
The national shortage of nurses is expected to get worse over the coming years as Baby Boomers’ need for health care increases and the large population (over 1 million) of older registered nurses retires by 2030, the OBHG said based on projections from the American Association of Colleges of Nursing.
Ob. hospitalists were somewhat more likely to see the nursing shortage as a major problem, compared with community-based Obs (58% vs. 48%), but the biggest difference in perception of safety risk between the two groups (53% for hospitalists vs. 22% for community physicians) involved inconsistent standards of care. “This is likely due to the ob. hospitalists’ 24/7 presence on the unit, and their visibility into the care provided across the unit,” the report noted.
Priorities for the future
Participants also were asked to rank each of seven focus areas on a scale of 0 (lowest priority) to 3 (highest) by its importance in the next 5 years. Maternal mortality was identified as the highest priority by 59.2% of physicians, followed by gaps in access to care between patient populations (38.0%), rural health care (26.5%), and ob.gyn. shortage (26.4%), the OBHG said.
A number of respondents noted the increase in high-risk patients, many of whom are obese and/or older and have comorbidities. “We know that the risk of C-sections increases relative to maternal weight. We need to focus on maternal morbidity and mortality,” one physician wrote in the open-ended response section.
When compared with the community obs., the hospitalists were much more likely to assign top priority over the next 5 years to maternal mortality (73% vs. 50%) and to gaps in access between patient populations (51% vs. 30%), according to the OBHG survey, which was conducted in January of 2021.
How will practice change in 5 years?
As for changes coming to obstetrical care over the next 5 years, respondents gave their strongest prediction to increased use of telemedicine, with 81.2% saying it would increase and just 14.4% predicting no change. The focus on subspecialization is expected to increase by 79.4% of participants (16.5% said no change), and 75.7% said that use of mid-level providers would rise (20.6% said no change), the survey data show.
The move toward mid-level providers was noted in many of the open-ended responses. “There is nothing mid-level about the midwifery care my colleagues provide our patients. They are experts in their field,” one physician wrote, but another said, “just because I foresee a shift toward increasing utilization of mid-levels and primary care practitioners for women’s health does not mean I endorse this trend.”
Just over 58% of the 1,130 respondents put nursing shortages ahead of physician support and backup (39.0%), inconsistent standards of care (38.5%), and nursing education (31.1%) as the most important challenge to patient safety, the Ob Hospitalist Group (OBHG) said in a new report.
“The survey reveals some startling gaps in physician and patient support all along the care continuum in obstetrics and OB hospitalist programs filling them,” said Lenny Castiglione, the CEO of OBHG, a national network of over 1,000 obstetric hospitalists. “As pressure builds on ob. units to improve care and reduce costs, and as clinical resources are stretched in the continuing battle against COVID-19 and its variants, health systems need to take serious measures to fill these gaps through staff recruitment, retention, and training.”
The national shortage of nurses is expected to get worse over the coming years as Baby Boomers’ need for health care increases and the large population (over 1 million) of older registered nurses retires by 2030, the OBHG said based on projections from the American Association of Colleges of Nursing.
Ob. hospitalists were somewhat more likely to see the nursing shortage as a major problem, compared with community-based Obs (58% vs. 48%), but the biggest difference in perception of safety risk between the two groups (53% for hospitalists vs. 22% for community physicians) involved inconsistent standards of care. “This is likely due to the ob. hospitalists’ 24/7 presence on the unit, and their visibility into the care provided across the unit,” the report noted.
Priorities for the future
Participants also were asked to rank each of seven focus areas on a scale of 0 (lowest priority) to 3 (highest) by its importance in the next 5 years. Maternal mortality was identified as the highest priority by 59.2% of physicians, followed by gaps in access to care between patient populations (38.0%), rural health care (26.5%), and ob.gyn. shortage (26.4%), the OBHG said.
A number of respondents noted the increase in high-risk patients, many of whom are obese and/or older and have comorbidities. “We know that the risk of C-sections increases relative to maternal weight. We need to focus on maternal morbidity and mortality,” one physician wrote in the open-ended response section.
When compared with the community obs., the hospitalists were much more likely to assign top priority over the next 5 years to maternal mortality (73% vs. 50%) and to gaps in access between patient populations (51% vs. 30%), according to the OBHG survey, which was conducted in January of 2021.
How will practice change in 5 years?
As for changes coming to obstetrical care over the next 5 years, respondents gave their strongest prediction to increased use of telemedicine, with 81.2% saying it would increase and just 14.4% predicting no change. The focus on subspecialization is expected to increase by 79.4% of participants (16.5% said no change), and 75.7% said that use of mid-level providers would rise (20.6% said no change), the survey data show.
The move toward mid-level providers was noted in many of the open-ended responses. “There is nothing mid-level about the midwifery care my colleagues provide our patients. They are experts in their field,” one physician wrote, but another said, “just because I foresee a shift toward increasing utilization of mid-levels and primary care practitioners for women’s health does not mean I endorse this trend.”
Just over 58% of the 1,130 respondents put nursing shortages ahead of physician support and backup (39.0%), inconsistent standards of care (38.5%), and nursing education (31.1%) as the most important challenge to patient safety, the Ob Hospitalist Group (OBHG) said in a new report.
“The survey reveals some startling gaps in physician and patient support all along the care continuum in obstetrics and OB hospitalist programs filling them,” said Lenny Castiglione, the CEO of OBHG, a national network of over 1,000 obstetric hospitalists. “As pressure builds on ob. units to improve care and reduce costs, and as clinical resources are stretched in the continuing battle against COVID-19 and its variants, health systems need to take serious measures to fill these gaps through staff recruitment, retention, and training.”
The national shortage of nurses is expected to get worse over the coming years as Baby Boomers’ need for health care increases and the large population (over 1 million) of older registered nurses retires by 2030, the OBHG said based on projections from the American Association of Colleges of Nursing.
Ob. hospitalists were somewhat more likely to see the nursing shortage as a major problem, compared with community-based Obs (58% vs. 48%), but the biggest difference in perception of safety risk between the two groups (53% for hospitalists vs. 22% for community physicians) involved inconsistent standards of care. “This is likely due to the ob. hospitalists’ 24/7 presence on the unit, and their visibility into the care provided across the unit,” the report noted.
Priorities for the future
Participants also were asked to rank each of seven focus areas on a scale of 0 (lowest priority) to 3 (highest) by its importance in the next 5 years. Maternal mortality was identified as the highest priority by 59.2% of physicians, followed by gaps in access to care between patient populations (38.0%), rural health care (26.5%), and ob.gyn. shortage (26.4%), the OBHG said.
A number of respondents noted the increase in high-risk patients, many of whom are obese and/or older and have comorbidities. “We know that the risk of C-sections increases relative to maternal weight. We need to focus on maternal morbidity and mortality,” one physician wrote in the open-ended response section.
When compared with the community obs., the hospitalists were much more likely to assign top priority over the next 5 years to maternal mortality (73% vs. 50%) and to gaps in access between patient populations (51% vs. 30%), according to the OBHG survey, which was conducted in January of 2021.
How will practice change in 5 years?
As for changes coming to obstetrical care over the next 5 years, respondents gave their strongest prediction to increased use of telemedicine, with 81.2% saying it would increase and just 14.4% predicting no change. The focus on subspecialization is expected to increase by 79.4% of participants (16.5% said no change), and 75.7% said that use of mid-level providers would rise (20.6% said no change), the survey data show.
The move toward mid-level providers was noted in many of the open-ended responses. “There is nothing mid-level about the midwifery care my colleagues provide our patients. They are experts in their field,” one physician wrote, but another said, “just because I foresee a shift toward increasing utilization of mid-levels and primary care practitioners for women’s health does not mean I endorse this trend.”
Navigating parenthood as pediatricians
PHM 2021 session
The Baby at Work or the Baby at Home: Navigating Parenthood as Pediatricians

Presenters
Jessica Gold, MD; Dana Foradori, MD, MEd; Nivedita Srinivas, MD; Honora Burnett, MD; Julie Pantaleoni, MD; and Barrett Fromme, MD, MHPE
Session summary
A group of physician-mothers from multiple academic children’s hospitals came together in a storytelling format to discuss topics relating to being a parent and pediatric hospitalist. Through short and poignant stories, the presenters shared their experiences and reviewed recent literature and policy changes relating to the topic. This mini-plenary focused on three themes:
1. Easing the transition back to work after the birth of a child.
2. Coping with the tension between being a parent and pediatrician.
3. The role that divisions, departments, and institutions can play in supporting parents and promoting workplace engagement.
The session concluded with a robust question-and-answer portion where participants built upon the themes above and shared their own experiences as pediatric hospitalist parents.
Key takeaways
- “Use your voice.” Physicians who are parents must continue having conversations about the challenging aspects of being a parent and hospitalist and advocate for the changes they would like to see.
- There will always be tension as a physician parent, but we can learn to embrace it while also learning how to ask for help, set boundaries, and share when we are struggling.
- There are numerous challenges for hospitalists who are parents because of poor parental leave policies in the United States, but this is slowly changing. For example, starting in July 2021, the ACGME mandated 6 weeks of parental leave during training without having to extend training.
- “You are not alone.” The presenters emphasized that their reason for hosting this session was to shed light on this topic and let all pediatric hospitalist parents know that they are not alone in this experience.
Dr. Scott is a second-year pediatric hospital medicine fellow at New York–Presbyterian Columbia/Cornell. Her academic interests are in curriculum development and evaluation in medical education with a focus on telemedicine.
PHM 2021 session
The Baby at Work or the Baby at Home: Navigating Parenthood as Pediatricians
Presenters
Jessica Gold, MD; Dana Foradori, MD, MEd; Nivedita Srinivas, MD; Honora Burnett, MD; Julie Pantaleoni, MD; and Barrett Fromme, MD, MHPE
Session summary
A group of physician-mothers from multiple academic children’s hospitals came together in a storytelling format to discuss topics relating to being a parent and pediatric hospitalist. Through short and poignant stories, the presenters shared their experiences and reviewed recent literature and policy changes relating to the topic. This mini-plenary focused on three themes:
1. Easing the transition back to work after the birth of a child.
2. Coping with the tension between being a parent and pediatrician.
3. The role that divisions, departments, and institutions can play in supporting parents and promoting workplace engagement.
The session concluded with a robust question-and-answer portion where participants built upon the themes above and shared their own experiences as pediatric hospitalist parents.
Key takeaways
- “Use your voice.” Physicians who are parents must continue having conversations about the challenging aspects of being a parent and hospitalist and advocate for the changes they would like to see.
- There will always be tension as a physician parent, but we can learn to embrace it while also learning how to ask for help, set boundaries, and share when we are struggling.
- There are numerous challenges for hospitalists who are parents because of poor parental leave policies in the United States, but this is slowly changing. For example, starting in July 2021, the ACGME mandated 6 weeks of parental leave during training without having to extend training.
- “You are not alone.” The presenters emphasized that their reason for hosting this session was to shed light on this topic and let all pediatric hospitalist parents know that they are not alone in this experience.
Dr. Scott is a second-year pediatric hospital medicine fellow at New York–Presbyterian Columbia/Cornell. Her academic interests are in curriculum development and evaluation in medical education with a focus on telemedicine.
PHM 2021 session
The Baby at Work or the Baby at Home: Navigating Parenthood as Pediatricians
Presenters
Jessica Gold, MD; Dana Foradori, MD, MEd; Nivedita Srinivas, MD; Honora Burnett, MD; Julie Pantaleoni, MD; and Barrett Fromme, MD, MHPE
Session summary
A group of physician-mothers from multiple academic children’s hospitals came together in a storytelling format to discuss topics relating to being a parent and pediatric hospitalist. Through short and poignant stories, the presenters shared their experiences and reviewed recent literature and policy changes relating to the topic. This mini-plenary focused on three themes:
1. Easing the transition back to work after the birth of a child.
2. Coping with the tension between being a parent and pediatrician.
3. The role that divisions, departments, and institutions can play in supporting parents and promoting workplace engagement.
The session concluded with a robust question-and-answer portion where participants built upon the themes above and shared their own experiences as pediatric hospitalist parents.
Key takeaways
- “Use your voice.” Physicians who are parents must continue having conversations about the challenging aspects of being a parent and hospitalist and advocate for the changes they would like to see.
- There will always be tension as a physician parent, but we can learn to embrace it while also learning how to ask for help, set boundaries, and share when we are struggling.
- There are numerous challenges for hospitalists who are parents because of poor parental leave policies in the United States, but this is slowly changing. For example, starting in July 2021, the ACGME mandated 6 weeks of parental leave during training without having to extend training.
- “You are not alone.” The presenters emphasized that their reason for hosting this session was to shed light on this topic and let all pediatric hospitalist parents know that they are not alone in this experience.
Dr. Scott is a second-year pediatric hospital medicine fellow at New York–Presbyterian Columbia/Cornell. Her academic interests are in curriculum development and evaluation in medical education with a focus on telemedicine.