User login
Safety Concerns with CGRP Monoclonal Antibodies
Editors’ note: For the April edition of Expert Perspectives, we asked 2 leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class. To read a counterargument in which Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of CGRP mAbs, click here.
Lawrence Robbins, MD is an associate professor of neurology at Chicago Medical School and is in private practice in Riverwoods, IL.
Dr. Robbins discloses speaker’s bureau remuneration from AbbVie, Amgen, Biohaven, Impel NeuroPharma, Lundbeck, and Teva.
The calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) were introduced in 2018 as efficacious with few adverse effects. Unfortunately, the phase 3 trials failed to indicate the considerable number of adverse effects that have since been identified. This is a common occurrence with new drugs and mAbs.
There are few adverse events identified in the package insert (PI) for any of the 4 CGRP mAbs, but again that is not restricted to this class. Post-approval, it frequently takes time to piece together the true adverse effect profile. Reasons that phase 3 studies may miss adverse effects include 1) The studies are powered for efficacy but are not powered for adverse effects in terms of both the number of patients and the length of the study; 2) Studies do not use a checklist of likely adverse effects; and 3) Adverse effects become “disaggregated” (for example, 1 person states they have malaise, another tiredness, and another fatigue).
In the ensuing years since the launch of the CGRP mAbs, various lines of evidence pointed to the adverse effects attributed to these mAbs. These include the US Food and Drug Administration (FDA)/FDA Adverse Event Reporting System (FAERS) website, published studies, the collective experience of high prescribers, and filtered comments from patient chat boards. In addition, I have received hundreds of letters from providers and patients regarding serious adverse effects, which are detailed further in this article.
As of March 2022, the FDA/FAERS website has listed approximately 50,000 adverse events in connection with the CGRP mAbs. The number of serious events (hospitalization or life-threatening issues) was about 7000. These large numbers, just 3.75 years after launch, are like those listed for onabotulinumtoxin A after 30 years! Most of the reports involve erenumab. This is because erenumab was approved first and is the most prescribed drug in this class. I do not believe it is more dangerous than the others. Considering that the vast majority of adverse events go unreported, these are staggering numbers. Regarding serious adverse events, only 1% to 10% are actually reported to the FDA. Nobody knows the true percentage of milder adverse events that are actually reported, but in my experience, it is extremely low.
Unfortunately, the FDA/FAERS website lists on only adverse events, not adverse effects, which are just as important to discuss. In my small practice I have observed 4 serious adverse effects in women I believe are attributable to CGRP mAbs. These include a cerebrovascular accident in a 21-year-old patient, a case of reversible cerebral vasoconstrictive syndrome in a 61-year-old patient, severe joint pain in a 66-year-old patient, and a constellation of symptoms that resembled multiple sclerosis in a 30-year-old patient. I have administered onabotulinumtoxinA to thousands of patients for 25 years, with no serious adverse effects.
There have been a number of post-approval articles, studies, and case reports published since the launch of the CGRP mAbs. Many “review” or “meta-analysis” articles tend to repeat the results of the pharma-sponsored studies. They typically characterize the CGRP mAbs as safe, with few adverse events. Long-term safety extension studies almost always conclude that the drug is safe. In my opinion, the results from these studies are not reliable because of their possible ties to phrama.
Other studies tell a different tale. One observational study of erenumab concluded that adverse effects contributed to 33% of the discontinuations. Another study reported that 63.3% of patients taking mAbs described at least 1 adverse effect. A study of patients who had been prescribed erenumab indicated that 48% reported a non-serious adverse event after 3 months.
Neurologists are generally unaware of the dangers posed by CGRP mAbs. In September 2021, I engaged in a debate on this topic during the International 15th World Congress on Controversies in Neurology (CONy). Prior to the debate, the audience members were polled. 94% believed the CGRP mAbs to be safe. After our debate, only 40% felt that these mAbs were safe. I think that the audience, primarily consisting of neurologists, was not informed as to the potential dangers of the CGRP mAbs.
In our practice
For refractory patients, I do prescribe these CGRP mAbs. However, I feel they should only be prescribed after several other, safer options have failed. These include the natural approaches (butterbur, magnesium, riboflavin), several of the standard medications (amitriptyline, beta blockers, topiramate, valproate, angiotensin II receptor blockers), and onabotulinumtoxinA. Additionally, the newer gepants for prevention (rimegepant and atogepant) appear to be safer options than the CGRP mAbs, although we cannot say this definitively at this time.
In 2018, our clinic began a retrospective study that lasted until January 2020. We assessed 119 patients with chronic migraine who had been prescribed one of the CGRP mAbs. This study incorporated the use of a checklist of possible adverse effects. Each of these adverse effects had created a “signal.” We initially asked the patients, “Have you experienced any issues, problems, or side effects due to the CGRP monoclonal antibody?” The patients subsequently were interviewed and asked about each possible adverse effect included on the checklist. The patient and physician determined whether any adverse effect mentioned by the patient was due to the CGRP mAb. After discussing the checklist, 66% of the patients concluded they had experienced 1 additional adverse effect that they attributed to the CGRP mAb and had not originally disclosed in response to the initial question. Most of these patients identified more than 1 additional adverse effect through use of the checklist.
Gathering data
To determine the true adverse event profile post-approval, we rely upon the input of high prescribers, who often can provide this necessary feedback. I have assessed input from headache provider chat boards, private correspondence with many providers, and discussions with colleagues at conferences. The opinions do vary, with some headache providers arguing that there are not that many adverse effects arising from the CGRP mAbs. Many others believe, as I do, that there are a large number of adverse events. In my observations, there is not a consensus among headache providers.
The CGRP patient chat boards are another valuable line of evidence. I have screened 2800 comments from patients regarding adverse events. I filtered these down into 490 “highly believable” comments. Among those, the adverse events described align very well with our other lines of evidence.
If we put all the post-approval lines of evidence together, we come up with the following list of “adverse effect signals” attribututed to the CGRP mAbs. These include constipation (it may be severe; hence the warning in the erenumab PI), injection site reactions, joint pain, anxiety, muscle pain or cramps, hypertension or worsening hypertension (there is a warning in the erenumab PI), nausea (it may be severe; “area postrema syndrome” has occurred), rash, increased headache, fatigue, depression, insomnia, hair loss, tachycardia (and other cardiac arrhythmias), stroke, angina and myocardial infarction, weight gain or loss, irritability, and sexual dysfunction. There are also other adverse events. In his review of the CGRP mAbs, Thomas Moore, a leading expert in adverse events, cited the “sheer number of case reports, and it is likely that AEs of this migraine preventive were underestimated in the clinical trials.”
This discussion has focused on short-term adverse events. We have no idea regarding long-term effects, but I suspect that we will encounter serious ones. Evolution has deemed CGRP to be vital for 450 million years. We ignore evolution at our peril.
CGRP is a powerful vasodilator and protects our cardiovascular and cerebrovascular systems. CGRP resists the onset of hypertension. Wound and burn healing, as well as tissue repair, require CGRP. Bony metabolism and bone healing are partly dependent upon CGRP. CGRP protects from gastrointestinal (GI) ulcers and aids GI motility. CGRP mitigates the effects of sepsis.
CGRP is also involved with flushing, thermoregulation, cold hypersensitivity, protecting the kidneys when under stress, helping regulate insulin release, and mediating the adrenal glucocorticoid response to acute stress (particularly in the mature fetus). Effects on the hypothalamic-pituitary-adrenal axis are worrisome but unknown. CGRP is important as a vasodilator during stress, and the CGRP mAbs have not yet been tested under stress.
The CGRP mAbs have been terrific for many patients, and their efficacy is on par with onabotulinumtoxinA. However, in a short period of time we have witnessed a plethora of serious (and non-serious) adverse effects from short-term use. CGRP plays an important role in many physiologic processes. We have no idea as to the long-term consequences of blocking CGRP and we should proceed with caution.
Editors’ note: For the April edition of Expert Perspectives, we asked 2 leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class. To read a counterargument in which Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of CGRP mAbs, click here.
Lawrence Robbins, MD is an associate professor of neurology at Chicago Medical School and is in private practice in Riverwoods, IL.
Dr. Robbins discloses speaker’s bureau remuneration from AbbVie, Amgen, Biohaven, Impel NeuroPharma, Lundbeck, and Teva.
The calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) were introduced in 2018 as efficacious with few adverse effects. Unfortunately, the phase 3 trials failed to indicate the considerable number of adverse effects that have since been identified. This is a common occurrence with new drugs and mAbs.
There are few adverse events identified in the package insert (PI) for any of the 4 CGRP mAbs, but again that is not restricted to this class. Post-approval, it frequently takes time to piece together the true adverse effect profile. Reasons that phase 3 studies may miss adverse effects include 1) The studies are powered for efficacy but are not powered for adverse effects in terms of both the number of patients and the length of the study; 2) Studies do not use a checklist of likely adverse effects; and 3) Adverse effects become “disaggregated” (for example, 1 person states they have malaise, another tiredness, and another fatigue).
In the ensuing years since the launch of the CGRP mAbs, various lines of evidence pointed to the adverse effects attributed to these mAbs. These include the US Food and Drug Administration (FDA)/FDA Adverse Event Reporting System (FAERS) website, published studies, the collective experience of high prescribers, and filtered comments from patient chat boards. In addition, I have received hundreds of letters from providers and patients regarding serious adverse effects, which are detailed further in this article.
As of March 2022, the FDA/FAERS website has listed approximately 50,000 adverse events in connection with the CGRP mAbs. The number of serious events (hospitalization or life-threatening issues) was about 7000. These large numbers, just 3.75 years after launch, are like those listed for onabotulinumtoxin A after 30 years! Most of the reports involve erenumab. This is because erenumab was approved first and is the most prescribed drug in this class. I do not believe it is more dangerous than the others. Considering that the vast majority of adverse events go unreported, these are staggering numbers. Regarding serious adverse events, only 1% to 10% are actually reported to the FDA. Nobody knows the true percentage of milder adverse events that are actually reported, but in my experience, it is extremely low.
Unfortunately, the FDA/FAERS website lists on only adverse events, not adverse effects, which are just as important to discuss. In my small practice I have observed 4 serious adverse effects in women I believe are attributable to CGRP mAbs. These include a cerebrovascular accident in a 21-year-old patient, a case of reversible cerebral vasoconstrictive syndrome in a 61-year-old patient, severe joint pain in a 66-year-old patient, and a constellation of symptoms that resembled multiple sclerosis in a 30-year-old patient. I have administered onabotulinumtoxinA to thousands of patients for 25 years, with no serious adverse effects.
There have been a number of post-approval articles, studies, and case reports published since the launch of the CGRP mAbs. Many “review” or “meta-analysis” articles tend to repeat the results of the pharma-sponsored studies. They typically characterize the CGRP mAbs as safe, with few adverse events. Long-term safety extension studies almost always conclude that the drug is safe. In my opinion, the results from these studies are not reliable because of their possible ties to phrama.
Other studies tell a different tale. One observational study of erenumab concluded that adverse effects contributed to 33% of the discontinuations. Another study reported that 63.3% of patients taking mAbs described at least 1 adverse effect. A study of patients who had been prescribed erenumab indicated that 48% reported a non-serious adverse event after 3 months.
Neurologists are generally unaware of the dangers posed by CGRP mAbs. In September 2021, I engaged in a debate on this topic during the International 15th World Congress on Controversies in Neurology (CONy). Prior to the debate, the audience members were polled. 94% believed the CGRP mAbs to be safe. After our debate, only 40% felt that these mAbs were safe. I think that the audience, primarily consisting of neurologists, was not informed as to the potential dangers of the CGRP mAbs.
In our practice
For refractory patients, I do prescribe these CGRP mAbs. However, I feel they should only be prescribed after several other, safer options have failed. These include the natural approaches (butterbur, magnesium, riboflavin), several of the standard medications (amitriptyline, beta blockers, topiramate, valproate, angiotensin II receptor blockers), and onabotulinumtoxinA. Additionally, the newer gepants for prevention (rimegepant and atogepant) appear to be safer options than the CGRP mAbs, although we cannot say this definitively at this time.
In 2018, our clinic began a retrospective study that lasted until January 2020. We assessed 119 patients with chronic migraine who had been prescribed one of the CGRP mAbs. This study incorporated the use of a checklist of possible adverse effects. Each of these adverse effects had created a “signal.” We initially asked the patients, “Have you experienced any issues, problems, or side effects due to the CGRP monoclonal antibody?” The patients subsequently were interviewed and asked about each possible adverse effect included on the checklist. The patient and physician determined whether any adverse effect mentioned by the patient was due to the CGRP mAb. After discussing the checklist, 66% of the patients concluded they had experienced 1 additional adverse effect that they attributed to the CGRP mAb and had not originally disclosed in response to the initial question. Most of these patients identified more than 1 additional adverse effect through use of the checklist.
Gathering data
To determine the true adverse event profile post-approval, we rely upon the input of high prescribers, who often can provide this necessary feedback. I have assessed input from headache provider chat boards, private correspondence with many providers, and discussions with colleagues at conferences. The opinions do vary, with some headache providers arguing that there are not that many adverse effects arising from the CGRP mAbs. Many others believe, as I do, that there are a large number of adverse events. In my observations, there is not a consensus among headache providers.
The CGRP patient chat boards are another valuable line of evidence. I have screened 2800 comments from patients regarding adverse events. I filtered these down into 490 “highly believable” comments. Among those, the adverse events described align very well with our other lines of evidence.
If we put all the post-approval lines of evidence together, we come up with the following list of “adverse effect signals” attribututed to the CGRP mAbs. These include constipation (it may be severe; hence the warning in the erenumab PI), injection site reactions, joint pain, anxiety, muscle pain or cramps, hypertension or worsening hypertension (there is a warning in the erenumab PI), nausea (it may be severe; “area postrema syndrome” has occurred), rash, increased headache, fatigue, depression, insomnia, hair loss, tachycardia (and other cardiac arrhythmias), stroke, angina and myocardial infarction, weight gain or loss, irritability, and sexual dysfunction. There are also other adverse events. In his review of the CGRP mAbs, Thomas Moore, a leading expert in adverse events, cited the “sheer number of case reports, and it is likely that AEs of this migraine preventive were underestimated in the clinical trials.”
This discussion has focused on short-term adverse events. We have no idea regarding long-term effects, but I suspect that we will encounter serious ones. Evolution has deemed CGRP to be vital for 450 million years. We ignore evolution at our peril.
CGRP is a powerful vasodilator and protects our cardiovascular and cerebrovascular systems. CGRP resists the onset of hypertension. Wound and burn healing, as well as tissue repair, require CGRP. Bony metabolism and bone healing are partly dependent upon CGRP. CGRP protects from gastrointestinal (GI) ulcers and aids GI motility. CGRP mitigates the effects of sepsis.
CGRP is also involved with flushing, thermoregulation, cold hypersensitivity, protecting the kidneys when under stress, helping regulate insulin release, and mediating the adrenal glucocorticoid response to acute stress (particularly in the mature fetus). Effects on the hypothalamic-pituitary-adrenal axis are worrisome but unknown. CGRP is important as a vasodilator during stress, and the CGRP mAbs have not yet been tested under stress.
The CGRP mAbs have been terrific for many patients, and their efficacy is on par with onabotulinumtoxinA. However, in a short period of time we have witnessed a plethora of serious (and non-serious) adverse effects from short-term use. CGRP plays an important role in many physiologic processes. We have no idea as to the long-term consequences of blocking CGRP and we should proceed with caution.
Editors’ note: For the April edition of Expert Perspectives, we asked 2 leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class. To read a counterargument in which Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of CGRP mAbs, click here.
Lawrence Robbins, MD is an associate professor of neurology at Chicago Medical School and is in private practice in Riverwoods, IL.
Dr. Robbins discloses speaker’s bureau remuneration from AbbVie, Amgen, Biohaven, Impel NeuroPharma, Lundbeck, and Teva.
The calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) were introduced in 2018 as efficacious with few adverse effects. Unfortunately, the phase 3 trials failed to indicate the considerable number of adverse effects that have since been identified. This is a common occurrence with new drugs and mAbs.
There are few adverse events identified in the package insert (PI) for any of the 4 CGRP mAbs, but again that is not restricted to this class. Post-approval, it frequently takes time to piece together the true adverse effect profile. Reasons that phase 3 studies may miss adverse effects include 1) The studies are powered for efficacy but are not powered for adverse effects in terms of both the number of patients and the length of the study; 2) Studies do not use a checklist of likely adverse effects; and 3) Adverse effects become “disaggregated” (for example, 1 person states they have malaise, another tiredness, and another fatigue).
In the ensuing years since the launch of the CGRP mAbs, various lines of evidence pointed to the adverse effects attributed to these mAbs. These include the US Food and Drug Administration (FDA)/FDA Adverse Event Reporting System (FAERS) website, published studies, the collective experience of high prescribers, and filtered comments from patient chat boards. In addition, I have received hundreds of letters from providers and patients regarding serious adverse effects, which are detailed further in this article.
As of March 2022, the FDA/FAERS website has listed approximately 50,000 adverse events in connection with the CGRP mAbs. The number of serious events (hospitalization or life-threatening issues) was about 7000. These large numbers, just 3.75 years after launch, are like those listed for onabotulinumtoxin A after 30 years! Most of the reports involve erenumab. This is because erenumab was approved first and is the most prescribed drug in this class. I do not believe it is more dangerous than the others. Considering that the vast majority of adverse events go unreported, these are staggering numbers. Regarding serious adverse events, only 1% to 10% are actually reported to the FDA. Nobody knows the true percentage of milder adverse events that are actually reported, but in my experience, it is extremely low.
Unfortunately, the FDA/FAERS website lists on only adverse events, not adverse effects, which are just as important to discuss. In my small practice I have observed 4 serious adverse effects in women I believe are attributable to CGRP mAbs. These include a cerebrovascular accident in a 21-year-old patient, a case of reversible cerebral vasoconstrictive syndrome in a 61-year-old patient, severe joint pain in a 66-year-old patient, and a constellation of symptoms that resembled multiple sclerosis in a 30-year-old patient. I have administered onabotulinumtoxinA to thousands of patients for 25 years, with no serious adverse effects.
There have been a number of post-approval articles, studies, and case reports published since the launch of the CGRP mAbs. Many “review” or “meta-analysis” articles tend to repeat the results of the pharma-sponsored studies. They typically characterize the CGRP mAbs as safe, with few adverse events. Long-term safety extension studies almost always conclude that the drug is safe. In my opinion, the results from these studies are not reliable because of their possible ties to phrama.
Other studies tell a different tale. One observational study of erenumab concluded that adverse effects contributed to 33% of the discontinuations. Another study reported that 63.3% of patients taking mAbs described at least 1 adverse effect. A study of patients who had been prescribed erenumab indicated that 48% reported a non-serious adverse event after 3 months.
Neurologists are generally unaware of the dangers posed by CGRP mAbs. In September 2021, I engaged in a debate on this topic during the International 15th World Congress on Controversies in Neurology (CONy). Prior to the debate, the audience members were polled. 94% believed the CGRP mAbs to be safe. After our debate, only 40% felt that these mAbs were safe. I think that the audience, primarily consisting of neurologists, was not informed as to the potential dangers of the CGRP mAbs.
In our practice
For refractory patients, I do prescribe these CGRP mAbs. However, I feel they should only be prescribed after several other, safer options have failed. These include the natural approaches (butterbur, magnesium, riboflavin), several of the standard medications (amitriptyline, beta blockers, topiramate, valproate, angiotensin II receptor blockers), and onabotulinumtoxinA. Additionally, the newer gepants for prevention (rimegepant and atogepant) appear to be safer options than the CGRP mAbs, although we cannot say this definitively at this time.
In 2018, our clinic began a retrospective study that lasted until January 2020. We assessed 119 patients with chronic migraine who had been prescribed one of the CGRP mAbs. This study incorporated the use of a checklist of possible adverse effects. Each of these adverse effects had created a “signal.” We initially asked the patients, “Have you experienced any issues, problems, or side effects due to the CGRP monoclonal antibody?” The patients subsequently were interviewed and asked about each possible adverse effect included on the checklist. The patient and physician determined whether any adverse effect mentioned by the patient was due to the CGRP mAb. After discussing the checklist, 66% of the patients concluded they had experienced 1 additional adverse effect that they attributed to the CGRP mAb and had not originally disclosed in response to the initial question. Most of these patients identified more than 1 additional adverse effect through use of the checklist.
Gathering data
To determine the true adverse event profile post-approval, we rely upon the input of high prescribers, who often can provide this necessary feedback. I have assessed input from headache provider chat boards, private correspondence with many providers, and discussions with colleagues at conferences. The opinions do vary, with some headache providers arguing that there are not that many adverse effects arising from the CGRP mAbs. Many others believe, as I do, that there are a large number of adverse events. In my observations, there is not a consensus among headache providers.
The CGRP patient chat boards are another valuable line of evidence. I have screened 2800 comments from patients regarding adverse events. I filtered these down into 490 “highly believable” comments. Among those, the adverse events described align very well with our other lines of evidence.
If we put all the post-approval lines of evidence together, we come up with the following list of “adverse effect signals” attribututed to the CGRP mAbs. These include constipation (it may be severe; hence the warning in the erenumab PI), injection site reactions, joint pain, anxiety, muscle pain or cramps, hypertension or worsening hypertension (there is a warning in the erenumab PI), nausea (it may be severe; “area postrema syndrome” has occurred), rash, increased headache, fatigue, depression, insomnia, hair loss, tachycardia (and other cardiac arrhythmias), stroke, angina and myocardial infarction, weight gain or loss, irritability, and sexual dysfunction. There are also other adverse events. In his review of the CGRP mAbs, Thomas Moore, a leading expert in adverse events, cited the “sheer number of case reports, and it is likely that AEs of this migraine preventive were underestimated in the clinical trials.”
This discussion has focused on short-term adverse events. We have no idea regarding long-term effects, but I suspect that we will encounter serious ones. Evolution has deemed CGRP to be vital for 450 million years. We ignore evolution at our peril.
CGRP is a powerful vasodilator and protects our cardiovascular and cerebrovascular systems. CGRP resists the onset of hypertension. Wound and burn healing, as well as tissue repair, require CGRP. Bony metabolism and bone healing are partly dependent upon CGRP. CGRP protects from gastrointestinal (GI) ulcers and aids GI motility. CGRP mitigates the effects of sepsis.
CGRP is also involved with flushing, thermoregulation, cold hypersensitivity, protecting the kidneys when under stress, helping regulate insulin release, and mediating the adrenal glucocorticoid response to acute stress (particularly in the mature fetus). Effects on the hypothalamic-pituitary-adrenal axis are worrisome but unknown. CGRP is important as a vasodilator during stress, and the CGRP mAbs have not yet been tested under stress.
The CGRP mAbs have been terrific for many patients, and their efficacy is on par with onabotulinumtoxinA. However, in a short period of time we have witnessed a plethora of serious (and non-serious) adverse effects from short-term use. CGRP plays an important role in many physiologic processes. We have no idea as to the long-term consequences of blocking CGRP and we should proceed with caution.
CGRPs: They’ve Been a Long Time Coming
Editors’ note: For the April edition of Expert Perspectives, we asked two leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRPs) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of the CGRP mAbs. To read a counter-argument in which Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class, click here.
Dr. Schim is Co-Director of The Headache Center of Southern California, The Neurology Center. He is Board Member and past President of the Headache Consortium of the Pacific, Board Member and past President, American Heart Association San Diego, a Past President of the California Neurologic Society, and an active member of the American Academy of Neurology, American Stroke Association, and American Headache Society.
The identification of CGRP as a crucial pain signaling molecule in the trigeminal pathway, thereby establishing its link to migraine pain, has transformed care for patients with episodic and chronic migraine. Since 2018, the FDA has approved 4 monoclonal antibodies (mAbs) that either block the CGRP receptor or bind its ligand to prevent attachment to the receptor.
These medications are helping patients with medication overuse headache (MOH) and chronic migraine; one study involving 139 patients showed that half the patients saw their headache days per month cut by half, and migraine days per month cut by 62%. In another small study, 23 patients (47%) with medication overuse headache reported having no MOH issues after 3 months. Most of these patients had a history of medication overuse, but no specific diagnosis of MOH.
In a survey, 277 physicians said that nearly half of their patients had resistant migraine, and 29% had refractory migraine. For these patients, the mAbs have helped restore some normalcy in their lives.
But are these medications safe? Some clinicians posed this question even before the 2018 approval.
It is a valid question. The CGRP neuropeptide is a powerful dilator, establishing vascular homeostasis, organ development in utero, wound healing, and more. It is expressed in the peripheral and central nervous system and found abundantly in neurons and the unmyelinated A-fibers of the peripheral trigeminovascular system and trigeminal ganglion.
So, would blocking CGRP function in one area affect its function in another? So far, I have to say the answer is no. Neither the literature nor my observations say otherwise.
Trials vs the real world
Finding an answer to this question takes more than reading clinical trials data. Participants in these trials do not necessarily represent the real world – no complicated morbidities, no pregnant or lactating women. And trial lengths are generally short.
Thus, it is important to assess the safety of these medications in the real world.
In the trials of the subcutaneous mAbs, local injection site reactions were the most common adverse event. More specifically, erenumab showed increased incidence of constipation, and post-marketing surveillance has revealed some risk of hypertension; pooled analysis from 4 trial phases showed that across treatment groups, 20 people out of 2443 began treatment for hypertension. Some patients enrolled in trials for atogepant, an oral small molecule CGRP receptor agonist, also reported constipation and nausea, suggesting that receptor blockade may result in a higher incidence of GI disturbance. In addition, these medicines on occasion have caused alopecia, fatigue, or achiness.
Eptinezumab is administered intravenously, every 3 months, and thus does not have injection site reactions as a safety concern. In clinical trials, the most common adverse event was nasopharyngitis and hypersensitivity; Datta et al have provided a summary of safety and efficacy.
Raynaud’s and cluster headaches
A retrospective chart review study from the Mayo Clinic looking at individuals with Raynaud’s disease who were treated with CGRP antagonists showed that 5.3% of 169 patients had microvascular complications such as gangrene or autoimmune necrosis. There was no significant difference in demographic characteristics or rheumatologic history among those with Raynaud's who did or did not experience complications. In addition, microvascular complications of migraine therapies have preceded the use of CGRP modulators, as this has been documented in the past with other vasoactive substances such as ergots, triptans, and beta blockers.
In a tolerability and safety study of galcanezumab in patients with chronic cluster headache, with up to 15 months of treatment, the most common treatment emergent adverse events were nasopharyngitis and injection site pain. In this population with 11% to 12% of individuals having baseline hypertension and nearly 63% currently using tobacco, less than 2.5% had any abnormalities on ECG.
Vascular complications including pulmonary embolism, TIA, myocardial infarction, and atrial fibrillation have been reported but with no apparent relation between galcanezumab dosing and onset, with onset following the second to up to the eleventh monthly dose.
Antidrug antibodies can also occur as a complication of exposure to therapeutic antibodies of this class and have been detected in up to 12% of individuals treated. This might lead to therapeutic failure but would not likely be a safety issue.
Anaphylaxis or serious hypersensitivity reactions are uncommon, and in general are the only contraindication to the use of these agents.
Pregnancy registry information is just starting to become available. The number of reports on adverse drug reactions remains limited, and thus it is wise to avoid pregnancy and breastfeeding exposures as best as possible.
FAERS
The FDA adverse event reporting system (FAERS) database does contain reports on adverse events of approved medications. However, even the FDA website warns that the information provided regarding individual cases is unverified and wouldn’t establish causation, considering the confounding variables involved, and this information can be duplicated as well as incomplete. In addition, rates of occurrence cannot be established with reports, as the denominator of exposure is uncertain.
With those caveats established, the most common reports in FAERS concern injection site reactions, more frequent migraine or headache, or drug ineffectiveness. While constipation has been the second most common AE for erenumab, it did not make the top 10 for fremanezumab or galcanezumab, and cardiovascular events have not ranked in the top 10 for any product. Reasons for discontinuing treatment included withdrawal by the patient (147 of 1,890 [8%]) and lack of efficacy (77 of 1,890 [4%]).
As the reader can ascertain, different studies point out different reasons for discontinuing CGRP therapies. Other studies note that the most frequent reasons for discontinuation are lack of efficacy, constipation, and lack of insurance .
Conclusions
These medications have been well received; I believe. Fremanezumab, manufactured by Teva Pharmaceuticals, was approved in September 2018. According to Teva’s 2021 annual report, Ajovy, fremanezumab’s brand name, reached 21% market share in the US and 21% in Europe.
Aimovig, or erenumab, has been prescribed 620,000 times since its approval, according to the Novartis 2021 annual report. Galcanezumab, or Emgality, was approved in 2019, and had 65,300 prescriptions written in the since then. . Adherence to treatment has generally been very high in clinical practice, with the most common reason for a patient to switch being lack of effectiveness, rather than adverse events.
Of note, adverse events of other migraine therapeutics are not insignificant, and considering the pain that people with migraine endure, side effects must be hard to contend with for individuals to stop taking them. Case in point: A year before erenumab was approved, a study was published that looked at medical records for medication persistence in 8,700 chronic migraine patients, who all had been prescribed beta blockers, anti-seizure medications, or antidepressants. By 6 months, only 1 out of 4 patients were still taking the prescribed medicines. By 12 months, that was down to 14%. And about one-third of patients who stopped treatment stayed untreated for at least a year.
The presumed reasons these patients stopped their medications: side effects and-or lack of efficacy.
Migraine is a disabling disorder, for which the mAb class of medications has been highly beneficial for large numbers of patients, with far greater tolerability than prior oral preventives. While no treatments have absolute safety, the overall safety of this class of medications has been very high, leading to much improved clinical outcomes.
Editors’ note: For the April edition of Expert Perspectives, we asked two leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRPs) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of the CGRP mAbs. To read a counter-argument in which Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class, click here.
Dr. Schim is Co-Director of The Headache Center of Southern California, The Neurology Center. He is Board Member and past President of the Headache Consortium of the Pacific, Board Member and past President, American Heart Association San Diego, a Past President of the California Neurologic Society, and an active member of the American Academy of Neurology, American Stroke Association, and American Headache Society.
The identification of CGRP as a crucial pain signaling molecule in the trigeminal pathway, thereby establishing its link to migraine pain, has transformed care for patients with episodic and chronic migraine. Since 2018, the FDA has approved 4 monoclonal antibodies (mAbs) that either block the CGRP receptor or bind its ligand to prevent attachment to the receptor.
These medications are helping patients with medication overuse headache (MOH) and chronic migraine; one study involving 139 patients showed that half the patients saw their headache days per month cut by half, and migraine days per month cut by 62%. In another small study, 23 patients (47%) with medication overuse headache reported having no MOH issues after 3 months. Most of these patients had a history of medication overuse, but no specific diagnosis of MOH.
In a survey, 277 physicians said that nearly half of their patients had resistant migraine, and 29% had refractory migraine. For these patients, the mAbs have helped restore some normalcy in their lives.
But are these medications safe? Some clinicians posed this question even before the 2018 approval.
It is a valid question. The CGRP neuropeptide is a powerful dilator, establishing vascular homeostasis, organ development in utero, wound healing, and more. It is expressed in the peripheral and central nervous system and found abundantly in neurons and the unmyelinated A-fibers of the peripheral trigeminovascular system and trigeminal ganglion.
So, would blocking CGRP function in one area affect its function in another? So far, I have to say the answer is no. Neither the literature nor my observations say otherwise.
Trials vs the real world
Finding an answer to this question takes more than reading clinical trials data. Participants in these trials do not necessarily represent the real world – no complicated morbidities, no pregnant or lactating women. And trial lengths are generally short.
Thus, it is important to assess the safety of these medications in the real world.
In the trials of the subcutaneous mAbs, local injection site reactions were the most common adverse event. More specifically, erenumab showed increased incidence of constipation, and post-marketing surveillance has revealed some risk of hypertension; pooled analysis from 4 trial phases showed that across treatment groups, 20 people out of 2443 began treatment for hypertension. Some patients enrolled in trials for atogepant, an oral small molecule CGRP receptor agonist, also reported constipation and nausea, suggesting that receptor blockade may result in a higher incidence of GI disturbance. In addition, these medicines on occasion have caused alopecia, fatigue, or achiness.
Eptinezumab is administered intravenously, every 3 months, and thus does not have injection site reactions as a safety concern. In clinical trials, the most common adverse event was nasopharyngitis and hypersensitivity; Datta et al have provided a summary of safety and efficacy.
Raynaud’s and cluster headaches
A retrospective chart review study from the Mayo Clinic looking at individuals with Raynaud’s disease who were treated with CGRP antagonists showed that 5.3% of 169 patients had microvascular complications such as gangrene or autoimmune necrosis. There was no significant difference in demographic characteristics or rheumatologic history among those with Raynaud's who did or did not experience complications. In addition, microvascular complications of migraine therapies have preceded the use of CGRP modulators, as this has been documented in the past with other vasoactive substances such as ergots, triptans, and beta blockers.
In a tolerability and safety study of galcanezumab in patients with chronic cluster headache, with up to 15 months of treatment, the most common treatment emergent adverse events were nasopharyngitis and injection site pain. In this population with 11% to 12% of individuals having baseline hypertension and nearly 63% currently using tobacco, less than 2.5% had any abnormalities on ECG.
Vascular complications including pulmonary embolism, TIA, myocardial infarction, and atrial fibrillation have been reported but with no apparent relation between galcanezumab dosing and onset, with onset following the second to up to the eleventh monthly dose.
Antidrug antibodies can also occur as a complication of exposure to therapeutic antibodies of this class and have been detected in up to 12% of individuals treated. This might lead to therapeutic failure but would not likely be a safety issue.
Anaphylaxis or serious hypersensitivity reactions are uncommon, and in general are the only contraindication to the use of these agents.
Pregnancy registry information is just starting to become available. The number of reports on adverse drug reactions remains limited, and thus it is wise to avoid pregnancy and breastfeeding exposures as best as possible.
FAERS
The FDA adverse event reporting system (FAERS) database does contain reports on adverse events of approved medications. However, even the FDA website warns that the information provided regarding individual cases is unverified and wouldn’t establish causation, considering the confounding variables involved, and this information can be duplicated as well as incomplete. In addition, rates of occurrence cannot be established with reports, as the denominator of exposure is uncertain.
With those caveats established, the most common reports in FAERS concern injection site reactions, more frequent migraine or headache, or drug ineffectiveness. While constipation has been the second most common AE for erenumab, it did not make the top 10 for fremanezumab or galcanezumab, and cardiovascular events have not ranked in the top 10 for any product. Reasons for discontinuing treatment included withdrawal by the patient (147 of 1,890 [8%]) and lack of efficacy (77 of 1,890 [4%]).
As the reader can ascertain, different studies point out different reasons for discontinuing CGRP therapies. Other studies note that the most frequent reasons for discontinuation are lack of efficacy, constipation, and lack of insurance .
Conclusions
These medications have been well received; I believe. Fremanezumab, manufactured by Teva Pharmaceuticals, was approved in September 2018. According to Teva’s 2021 annual report, Ajovy, fremanezumab’s brand name, reached 21% market share in the US and 21% in Europe.
Aimovig, or erenumab, has been prescribed 620,000 times since its approval, according to the Novartis 2021 annual report. Galcanezumab, or Emgality, was approved in 2019, and had 65,300 prescriptions written in the since then. . Adherence to treatment has generally been very high in clinical practice, with the most common reason for a patient to switch being lack of effectiveness, rather than adverse events.
Of note, adverse events of other migraine therapeutics are not insignificant, and considering the pain that people with migraine endure, side effects must be hard to contend with for individuals to stop taking them. Case in point: A year before erenumab was approved, a study was published that looked at medical records for medication persistence in 8,700 chronic migraine patients, who all had been prescribed beta blockers, anti-seizure medications, or antidepressants. By 6 months, only 1 out of 4 patients were still taking the prescribed medicines. By 12 months, that was down to 14%. And about one-third of patients who stopped treatment stayed untreated for at least a year.
The presumed reasons these patients stopped their medications: side effects and-or lack of efficacy.
Migraine is a disabling disorder, for which the mAb class of medications has been highly beneficial for large numbers of patients, with far greater tolerability than prior oral preventives. While no treatments have absolute safety, the overall safety of this class of medications has been very high, leading to much improved clinical outcomes.
Editors’ note: For the April edition of Expert Perspectives, we asked two leading neurologists to present differing views on the use of calcitonin gene-related peptide (CGRPs) monoclonal antibodies (mAbs) for the treatment of migraine. Here, Jack D. Schim, MD, of the Neurology Center of Southern California, discusses the observed benefits of the CGRP mAbs. To read a counter-argument in which Lawrence Robbins, MD, of the Robbins Headache Clinic in Riverwoods, IL, discusses potential safety concerns associated with this drug class, click here.
Dr. Schim is Co-Director of The Headache Center of Southern California, The Neurology Center. He is Board Member and past President of the Headache Consortium of the Pacific, Board Member and past President, American Heart Association San Diego, a Past President of the California Neurologic Society, and an active member of the American Academy of Neurology, American Stroke Association, and American Headache Society.
The identification of CGRP as a crucial pain signaling molecule in the trigeminal pathway, thereby establishing its link to migraine pain, has transformed care for patients with episodic and chronic migraine. Since 2018, the FDA has approved 4 monoclonal antibodies (mAbs) that either block the CGRP receptor or bind its ligand to prevent attachment to the receptor.
These medications are helping patients with medication overuse headache (MOH) and chronic migraine; one study involving 139 patients showed that half the patients saw their headache days per month cut by half, and migraine days per month cut by 62%. In another small study, 23 patients (47%) with medication overuse headache reported having no MOH issues after 3 months. Most of these patients had a history of medication overuse, but no specific diagnosis of MOH.
In a survey, 277 physicians said that nearly half of their patients had resistant migraine, and 29% had refractory migraine. For these patients, the mAbs have helped restore some normalcy in their lives.
But are these medications safe? Some clinicians posed this question even before the 2018 approval.
It is a valid question. The CGRP neuropeptide is a powerful dilator, establishing vascular homeostasis, organ development in utero, wound healing, and more. It is expressed in the peripheral and central nervous system and found abundantly in neurons and the unmyelinated A-fibers of the peripheral trigeminovascular system and trigeminal ganglion.
So, would blocking CGRP function in one area affect its function in another? So far, I have to say the answer is no. Neither the literature nor my observations say otherwise.
Trials vs the real world
Finding an answer to this question takes more than reading clinical trials data. Participants in these trials do not necessarily represent the real world – no complicated morbidities, no pregnant or lactating women. And trial lengths are generally short.
Thus, it is important to assess the safety of these medications in the real world.
In the trials of the subcutaneous mAbs, local injection site reactions were the most common adverse event. More specifically, erenumab showed increased incidence of constipation, and post-marketing surveillance has revealed some risk of hypertension; pooled analysis from 4 trial phases showed that across treatment groups, 20 people out of 2443 began treatment for hypertension. Some patients enrolled in trials for atogepant, an oral small molecule CGRP receptor agonist, also reported constipation and nausea, suggesting that receptor blockade may result in a higher incidence of GI disturbance. In addition, these medicines on occasion have caused alopecia, fatigue, or achiness.
Eptinezumab is administered intravenously, every 3 months, and thus does not have injection site reactions as a safety concern. In clinical trials, the most common adverse event was nasopharyngitis and hypersensitivity; Datta et al have provided a summary of safety and efficacy.
Raynaud’s and cluster headaches
A retrospective chart review study from the Mayo Clinic looking at individuals with Raynaud’s disease who were treated with CGRP antagonists showed that 5.3% of 169 patients had microvascular complications such as gangrene or autoimmune necrosis. There was no significant difference in demographic characteristics or rheumatologic history among those with Raynaud's who did or did not experience complications. In addition, microvascular complications of migraine therapies have preceded the use of CGRP modulators, as this has been documented in the past with other vasoactive substances such as ergots, triptans, and beta blockers.
In a tolerability and safety study of galcanezumab in patients with chronic cluster headache, with up to 15 months of treatment, the most common treatment emergent adverse events were nasopharyngitis and injection site pain. In this population with 11% to 12% of individuals having baseline hypertension and nearly 63% currently using tobacco, less than 2.5% had any abnormalities on ECG.
Vascular complications including pulmonary embolism, TIA, myocardial infarction, and atrial fibrillation have been reported but with no apparent relation between galcanezumab dosing and onset, with onset following the second to up to the eleventh monthly dose.
Antidrug antibodies can also occur as a complication of exposure to therapeutic antibodies of this class and have been detected in up to 12% of individuals treated. This might lead to therapeutic failure but would not likely be a safety issue.
Anaphylaxis or serious hypersensitivity reactions are uncommon, and in general are the only contraindication to the use of these agents.
Pregnancy registry information is just starting to become available. The number of reports on adverse drug reactions remains limited, and thus it is wise to avoid pregnancy and breastfeeding exposures as best as possible.
FAERS
The FDA adverse event reporting system (FAERS) database does contain reports on adverse events of approved medications. However, even the FDA website warns that the information provided regarding individual cases is unverified and wouldn’t establish causation, considering the confounding variables involved, and this information can be duplicated as well as incomplete. In addition, rates of occurrence cannot be established with reports, as the denominator of exposure is uncertain.
With those caveats established, the most common reports in FAERS concern injection site reactions, more frequent migraine or headache, or drug ineffectiveness. While constipation has been the second most common AE for erenumab, it did not make the top 10 for fremanezumab or galcanezumab, and cardiovascular events have not ranked in the top 10 for any product. Reasons for discontinuing treatment included withdrawal by the patient (147 of 1,890 [8%]) and lack of efficacy (77 of 1,890 [4%]).
As the reader can ascertain, different studies point out different reasons for discontinuing CGRP therapies. Other studies note that the most frequent reasons for discontinuation are lack of efficacy, constipation, and lack of insurance .
Conclusions
These medications have been well received; I believe. Fremanezumab, manufactured by Teva Pharmaceuticals, was approved in September 2018. According to Teva’s 2021 annual report, Ajovy, fremanezumab’s brand name, reached 21% market share in the US and 21% in Europe.
Aimovig, or erenumab, has been prescribed 620,000 times since its approval, according to the Novartis 2021 annual report. Galcanezumab, or Emgality, was approved in 2019, and had 65,300 prescriptions written in the since then. . Adherence to treatment has generally been very high in clinical practice, with the most common reason for a patient to switch being lack of effectiveness, rather than adverse events.
Of note, adverse events of other migraine therapeutics are not insignificant, and considering the pain that people with migraine endure, side effects must be hard to contend with for individuals to stop taking them. Case in point: A year before erenumab was approved, a study was published that looked at medical records for medication persistence in 8,700 chronic migraine patients, who all had been prescribed beta blockers, anti-seizure medications, or antidepressants. By 6 months, only 1 out of 4 patients were still taking the prescribed medicines. By 12 months, that was down to 14%. And about one-third of patients who stopped treatment stayed untreated for at least a year.
The presumed reasons these patients stopped their medications: side effects and-or lack of efficacy.
Migraine is a disabling disorder, for which the mAb class of medications has been highly beneficial for large numbers of patients, with far greater tolerability than prior oral preventives. While no treatments have absolute safety, the overall safety of this class of medications has been very high, leading to much improved clinical outcomes.
Dodging potholes from cancer care to hospice transitions
I’m often in the position of caring for patients after they’ve stopped active cancer treatments, but before they’ve made the decision to enroll in hospice. They remain under my care until they feel emotionally ready, or until their care needs have escalated to the point in which hospice is unavoidable.
Jenny, a mom in her 50s with metastatic pancreatic cancer, stopped coming to the clinic. She lived about 40 minutes away from the clinic and was no longer receiving treatment. The car rides were painful and difficult for her. I held weekly video visits with her for 2 months before she eventually went to hospice and passed away. Before she died, she shared with me her sadness that her oncologist – who had taken care of her for 3 years – had “washed his hands of [me].” She rarely heard from him after their final conversation in the clinic when he informed her that she was no longer a candidate for further therapy. The sense of abandonment Jenny described was visceral and devastating. With her permission, I let her oncology team know how she felt and they reached out to her just 1 week before her death. After she died, her husband told me how meaningful it had been for the whole family to hear from Jenny’s oncologist who told them that she had done everything possible to fight her cancer and that “no stone was left unturned.” Her husband felt this final conversation provided Jenny with the closure she needed to pass away peacefully.

Transitioning from active therapy to symptom management
Switching gears from an all-out pursuit of active therapy to focusing on cancer symptoms is often a scary transition for patients and their families. The transition is often viewed as a movement away from hope and optimism to “giving up the fight.” Whether you agree with the warrior language or not, many patients still describe their journey in these terms and thus, experience enrollment in hospice as a sense of having failed.
The sense of failure can be compounded by feelings of abandonment by oncology providers when they are referred without much guidance or continuity through the hospice enrollment process. Unfortunately, the consequences of suboptimal hospice transitions can be damaging, especially for the mental health and well-being of the patient and their surviving loved ones.
When managed poorly, hospice transitions can easily lead to patient and family harm, which is a claim supported by research. A qualitative study published in 2019 included 92 caregivers of patients with terminal cancer. The authors found three common pathways for end-of-life transitions – a frictionless transition in which the patient and family are well prepared in advance by their oncologist; a more turbulent transition in which patient and family had direct conversations with their oncologist about the incurability of the disease and the lack of efficacy of further treatments, but were given no guidance on prognosis; and a third type of transition marked by abrupt shifts toward end-of-life care occurring in extremis and typically in the hospital.
In the latter two groups, caregivers felt their loved ones died very quickly after stopping treatment, taking them by surprise and leaving them rushing to put end-of-life care plans in place without much support from their oncologists. In the last group, caregivers shared they received their first prognostic information from the hospital or ICU doctor caring for their actively dying loved one, leaving them with a sense of anger and betrayal toward their oncologist for allowing them to be so ill-prepared.
A Japanese survey published in 2018 in The Oncologist of families of cancer patients who had passed away under hospice care over a 2-year period (2012-2014), found that about one-quarter felt abandoned by oncologists. Several factors that were associated with feeling either more or less abandonment. Spouses of patients, patients aged less than 60 years, and patients whose oncologists informed them that there was “nothing more to do” felt more abandoned by oncologists; whereas families for whom the oncologist provided reassurance about the trajectory of care, recommended hospice, and engaged with a palliative care team felt less abandoned by oncologists. Families who felt more abandoned had higher levels of depression and grief when measured with standardized instruments.
‘Don’t just put in the hospice order and walk away’
Fortunately, there are a few low-resource interventions that can improve the quality of care-to-hospice transitions and prevent the sense of abandonment felt by many patients and families.
First, don’t just put in the hospice order and walk away. Designate a staffer in your office to contact hospice directly, ensure all medical records are faxed and received, and update the patient and family on this progress throughout the transition. Taking care of details like these ensures the patient enrolls in hospice in a timely manner and reduces the chance the patient, who is likely to be quite sick at this point, will end up in the hospital despite your best efforts to get hospice involved.
Make sure the patient and family understand that you are still their oncologist and still available to them. If they want to continue care with you, have them name you as the “non–hospice-attending physician” so that you can continue to bill for telemedicine and office visits using the terminal diagnosis (with a billing modifier). This does not mean that you will be expected to manage the patient’s hospice problem list or respond to hospice nurse calls at 2 a.m. – the hospice doctor will still do this. It just ensures that patients do not receive a bill if you continue to see them.
If ongoing office or video visits are too much for the patient and family, consider assigning a member of your team to call the patient and family on a weekly basis to check in and offer support. A small 2018 pilot study aimed at improving communication found that when caregivers of advanced cancer patients transitioning to hospice received weekly supportive phone calls by a member of their oncology team (typically a nurse or nurse practitioner), they felt emotionally supported, had good continuity of care throughout the hospice enrollment, and appreciated the ability to have closure with their oncology team. In other words, a sense of abandonment was prevented and the patient-provider relationship was actually deepened through the transition.
These suggestions are not rocket science – they are simple, obvious ways to try to restore patient-centeredness to a transition that for providers can seem routine, but for patients and families is often the first time they have confronted the reality that death is approaching. That reality is terrifying and overwhelming. Patients and caregivers need our support more during hospice transitions than at any other point during their cancer journey – except perhaps at diagnosis.
As with Jenny, my patient who felt abandoned, all it took was a single call by her oncology team to restore the trust and heal the sense of feeling forsaken by the people who cared for her for years. Sometimes, even just one more phone call can feel like a lot to a chronically overburdened provider – but what a difference a simple call can make.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
I’m often in the position of caring for patients after they’ve stopped active cancer treatments, but before they’ve made the decision to enroll in hospice. They remain under my care until they feel emotionally ready, or until their care needs have escalated to the point in which hospice is unavoidable.
Jenny, a mom in her 50s with metastatic pancreatic cancer, stopped coming to the clinic. She lived about 40 minutes away from the clinic and was no longer receiving treatment. The car rides were painful and difficult for her. I held weekly video visits with her for 2 months before she eventually went to hospice and passed away. Before she died, she shared with me her sadness that her oncologist – who had taken care of her for 3 years – had “washed his hands of [me].” She rarely heard from him after their final conversation in the clinic when he informed her that she was no longer a candidate for further therapy. The sense of abandonment Jenny described was visceral and devastating. With her permission, I let her oncology team know how she felt and they reached out to her just 1 week before her death. After she died, her husband told me how meaningful it had been for the whole family to hear from Jenny’s oncologist who told them that she had done everything possible to fight her cancer and that “no stone was left unturned.” Her husband felt this final conversation provided Jenny with the closure she needed to pass away peacefully.
Transitioning from active therapy to symptom management
Switching gears from an all-out pursuit of active therapy to focusing on cancer symptoms is often a scary transition for patients and their families. The transition is often viewed as a movement away from hope and optimism to “giving up the fight.” Whether you agree with the warrior language or not, many patients still describe their journey in these terms and thus, experience enrollment in hospice as a sense of having failed.
The sense of failure can be compounded by feelings of abandonment by oncology providers when they are referred without much guidance or continuity through the hospice enrollment process. Unfortunately, the consequences of suboptimal hospice transitions can be damaging, especially for the mental health and well-being of the patient and their surviving loved ones.
When managed poorly, hospice transitions can easily lead to patient and family harm, which is a claim supported by research. A qualitative study published in 2019 included 92 caregivers of patients with terminal cancer. The authors found three common pathways for end-of-life transitions – a frictionless transition in which the patient and family are well prepared in advance by their oncologist; a more turbulent transition in which patient and family had direct conversations with their oncologist about the incurability of the disease and the lack of efficacy of further treatments, but were given no guidance on prognosis; and a third type of transition marked by abrupt shifts toward end-of-life care occurring in extremis and typically in the hospital.
In the latter two groups, caregivers felt their loved ones died very quickly after stopping treatment, taking them by surprise and leaving them rushing to put end-of-life care plans in place without much support from their oncologists. In the last group, caregivers shared they received their first prognostic information from the hospital or ICU doctor caring for their actively dying loved one, leaving them with a sense of anger and betrayal toward their oncologist for allowing them to be so ill-prepared.
A Japanese survey published in 2018 in The Oncologist of families of cancer patients who had passed away under hospice care over a 2-year period (2012-2014), found that about one-quarter felt abandoned by oncologists. Several factors that were associated with feeling either more or less abandonment. Spouses of patients, patients aged less than 60 years, and patients whose oncologists informed them that there was “nothing more to do” felt more abandoned by oncologists; whereas families for whom the oncologist provided reassurance about the trajectory of care, recommended hospice, and engaged with a palliative care team felt less abandoned by oncologists. Families who felt more abandoned had higher levels of depression and grief when measured with standardized instruments.
‘Don’t just put in the hospice order and walk away’
Fortunately, there are a few low-resource interventions that can improve the quality of care-to-hospice transitions and prevent the sense of abandonment felt by many patients and families.
First, don’t just put in the hospice order and walk away. Designate a staffer in your office to contact hospice directly, ensure all medical records are faxed and received, and update the patient and family on this progress throughout the transition. Taking care of details like these ensures the patient enrolls in hospice in a timely manner and reduces the chance the patient, who is likely to be quite sick at this point, will end up in the hospital despite your best efforts to get hospice involved.
Make sure the patient and family understand that you are still their oncologist and still available to them. If they want to continue care with you, have them name you as the “non–hospice-attending physician” so that you can continue to bill for telemedicine and office visits using the terminal diagnosis (with a billing modifier). This does not mean that you will be expected to manage the patient’s hospice problem list or respond to hospice nurse calls at 2 a.m. – the hospice doctor will still do this. It just ensures that patients do not receive a bill if you continue to see them.
If ongoing office or video visits are too much for the patient and family, consider assigning a member of your team to call the patient and family on a weekly basis to check in and offer support. A small 2018 pilot study aimed at improving communication found that when caregivers of advanced cancer patients transitioning to hospice received weekly supportive phone calls by a member of their oncology team (typically a nurse or nurse practitioner), they felt emotionally supported, had good continuity of care throughout the hospice enrollment, and appreciated the ability to have closure with their oncology team. In other words, a sense of abandonment was prevented and the patient-provider relationship was actually deepened through the transition.
These suggestions are not rocket science – they are simple, obvious ways to try to restore patient-centeredness to a transition that for providers can seem routine, but for patients and families is often the first time they have confronted the reality that death is approaching. That reality is terrifying and overwhelming. Patients and caregivers need our support more during hospice transitions than at any other point during their cancer journey – except perhaps at diagnosis.
As with Jenny, my patient who felt abandoned, all it took was a single call by her oncology team to restore the trust and heal the sense of feeling forsaken by the people who cared for her for years. Sometimes, even just one more phone call can feel like a lot to a chronically overburdened provider – but what a difference a simple call can make.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
I’m often in the position of caring for patients after they’ve stopped active cancer treatments, but before they’ve made the decision to enroll in hospice. They remain under my care until they feel emotionally ready, or until their care needs have escalated to the point in which hospice is unavoidable.
Jenny, a mom in her 50s with metastatic pancreatic cancer, stopped coming to the clinic. She lived about 40 minutes away from the clinic and was no longer receiving treatment. The car rides were painful and difficult for her. I held weekly video visits with her for 2 months before she eventually went to hospice and passed away. Before she died, she shared with me her sadness that her oncologist – who had taken care of her for 3 years – had “washed his hands of [me].” She rarely heard from him after their final conversation in the clinic when he informed her that she was no longer a candidate for further therapy. The sense of abandonment Jenny described was visceral and devastating. With her permission, I let her oncology team know how she felt and they reached out to her just 1 week before her death. After she died, her husband told me how meaningful it had been for the whole family to hear from Jenny’s oncologist who told them that she had done everything possible to fight her cancer and that “no stone was left unturned.” Her husband felt this final conversation provided Jenny with the closure she needed to pass away peacefully.
Transitioning from active therapy to symptom management
Switching gears from an all-out pursuit of active therapy to focusing on cancer symptoms is often a scary transition for patients and their families. The transition is often viewed as a movement away from hope and optimism to “giving up the fight.” Whether you agree with the warrior language or not, many patients still describe their journey in these terms and thus, experience enrollment in hospice as a sense of having failed.
The sense of failure can be compounded by feelings of abandonment by oncology providers when they are referred without much guidance or continuity through the hospice enrollment process. Unfortunately, the consequences of suboptimal hospice transitions can be damaging, especially for the mental health and well-being of the patient and their surviving loved ones.
When managed poorly, hospice transitions can easily lead to patient and family harm, which is a claim supported by research. A qualitative study published in 2019 included 92 caregivers of patients with terminal cancer. The authors found three common pathways for end-of-life transitions – a frictionless transition in which the patient and family are well prepared in advance by their oncologist; a more turbulent transition in which patient and family had direct conversations with their oncologist about the incurability of the disease and the lack of efficacy of further treatments, but were given no guidance on prognosis; and a third type of transition marked by abrupt shifts toward end-of-life care occurring in extremis and typically in the hospital.
In the latter two groups, caregivers felt their loved ones died very quickly after stopping treatment, taking them by surprise and leaving them rushing to put end-of-life care plans in place without much support from their oncologists. In the last group, caregivers shared they received their first prognostic information from the hospital or ICU doctor caring for their actively dying loved one, leaving them with a sense of anger and betrayal toward their oncologist for allowing them to be so ill-prepared.
A Japanese survey published in 2018 in The Oncologist of families of cancer patients who had passed away under hospice care over a 2-year period (2012-2014), found that about one-quarter felt abandoned by oncologists. Several factors that were associated with feeling either more or less abandonment. Spouses of patients, patients aged less than 60 years, and patients whose oncologists informed them that there was “nothing more to do” felt more abandoned by oncologists; whereas families for whom the oncologist provided reassurance about the trajectory of care, recommended hospice, and engaged with a palliative care team felt less abandoned by oncologists. Families who felt more abandoned had higher levels of depression and grief when measured with standardized instruments.
‘Don’t just put in the hospice order and walk away’
Fortunately, there are a few low-resource interventions that can improve the quality of care-to-hospice transitions and prevent the sense of abandonment felt by many patients and families.
First, don’t just put in the hospice order and walk away. Designate a staffer in your office to contact hospice directly, ensure all medical records are faxed and received, and update the patient and family on this progress throughout the transition. Taking care of details like these ensures the patient enrolls in hospice in a timely manner and reduces the chance the patient, who is likely to be quite sick at this point, will end up in the hospital despite your best efforts to get hospice involved.
Make sure the patient and family understand that you are still their oncologist and still available to them. If they want to continue care with you, have them name you as the “non–hospice-attending physician” so that you can continue to bill for telemedicine and office visits using the terminal diagnosis (with a billing modifier). This does not mean that you will be expected to manage the patient’s hospice problem list or respond to hospice nurse calls at 2 a.m. – the hospice doctor will still do this. It just ensures that patients do not receive a bill if you continue to see them.
If ongoing office or video visits are too much for the patient and family, consider assigning a member of your team to call the patient and family on a weekly basis to check in and offer support. A small 2018 pilot study aimed at improving communication found that when caregivers of advanced cancer patients transitioning to hospice received weekly supportive phone calls by a member of their oncology team (typically a nurse or nurse practitioner), they felt emotionally supported, had good continuity of care throughout the hospice enrollment, and appreciated the ability to have closure with their oncology team. In other words, a sense of abandonment was prevented and the patient-provider relationship was actually deepened through the transition.
These suggestions are not rocket science – they are simple, obvious ways to try to restore patient-centeredness to a transition that for providers can seem routine, but for patients and families is often the first time they have confronted the reality that death is approaching. That reality is terrifying and overwhelming. Patients and caregivers need our support more during hospice transitions than at any other point during their cancer journey – except perhaps at diagnosis.
As with Jenny, my patient who felt abandoned, all it took was a single call by her oncology team to restore the trust and heal the sense of feeling forsaken by the people who cared for her for years. Sometimes, even just one more phone call can feel like a lot to a chronically overburdened provider – but what a difference a simple call can make.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
‘Critical window’ to intervene for weight issues in early childhood
Signs of cardiometabolic damage in children who are overweight appear as early as 6-8 years of age, but were not evident in preschoolers, providing a window of opportunity for intervention, show the latest results from a long-running Danish study of childhood weight.
The proportion of children who were overweight (nearly 14% in 2015) was similar between the two groups – those of preschool age (2-5 years) and school age (6-8 years) – but only the latter showed significant signs of cardiometabolic abnormalities.
The results, published in Obesity Research & Clinical Practice, are the latest in a series of many findings from the HOLBAEK study (formerly known as The Danish Childhood Obesity Biobank) that have emerged since it began in 2007. They were presented, along with a meta-analysis of much of their work, at the European Congress on Obesity (ECO) 2022.
“When comparing children with and without overweight, there were only barely significant differences among the preschool children,” said investigator Christine Frithioff-Bøjsøe, MD, but in contrast, “the school children with overweight exhibited significantly higher systolic blood pressure, glucose, insulin, and higher HDL cholesterol,” among other markers, she noted.
“Detection needs to start as early as age 2-5 years because if you wait just a few years longer these children will show early signs of disease starting to take hold. This could provide a critical window to detect and manage overweight,” said Frithioff-Bøjsøe, PhD, of the Children’s Obesity Clinic, Copenhagen University, Hospital Holbaek, Denmark.
Asked to comment, Aaron S. Kelly, PhD, professor of pediatrics, codirector, University of Minnesota Center for Pediatric Obesity Medicine in Minneapolis, said: “Recent results from HOLBAEK highlight the critical importance of identifying obesity early in life, before its complications spring up.
“Ideally, we should be in the business of managing and reducing excess adiposity as soon as it surfaces with the goal of preventing the onset of cardiometabolic risk factors, not watchful waiting and hoping for the best.”
Routine dental visits checked overweight
In the newest study, the researchers trained dental assistants to measure weight and height and carried out body mass index assessments during routine appointments.
A total of 335 preschool and 657 school-age children were recruited for the study. Of these, 40% attended additional hospital-based examinations including blood pressure measurement and a blood sample. Children were reexamined approximately 1 year later.
Systolic blood pressure, for example, was significantly higher in 6- to 8-year-olds with overweight compared to those of normal weight (P = .001). There was no significant difference between systolic blood pressure of 2.5- to 5-year-olds without and with overweight.
Likewise, with insulin resistance, there was no significant difference between preschoolers with and without overweight. However, in schoolchildren, homoeostasis model of assessment–insulin resistance (HOMA-IR) was significantly higher in those with overweight, at 2.2, compared to those without, at 0.9 (P < .001).
Also, during follow-up (around a year later), the prevalence of overweight did not change in preschool children but increased from 13.7% to 17.0% in schoolchildren.
The researchers noted that, in Europe, it is the primary health care sector that has continuous contact with the pediatric population, with the potential for early evaluation of children at risk. Their decision to use dental health care assistants to assess weight in this particular study is novel, but feasible, they observed.
Danish model for treating overweight and obesity is ‘game-changing’
As part of the HOLBAEK initiative, clinical data and biological samples have been collected from children and adolescents receiving treatment at The Children’s Obesity Clinic, Holbaek Hospital, using a population-based cohort as a reference group. Data have been collected on about 8,000 children and adolescents so far.
Jens-Christian Holm, PhD, along with colleague and research assistant Maria Frauland, both from Copenhagen University, Hospital Holbaek, presented a review of the HOLBAEK studies (2007-2021) at ECO 2022. They said the results highlight the importance of taking an integrated approach to managing children and adolescents with obesity.
The review, which included 82 papers, found a wide variety of obesity-related complications already present at a young age in some of the cross-sectional studies, including dyslipidemia in 28% of children with obesity, hepatic steatosis in 31%, obstructive sleep apnea in 45%, and prehypertension or hypertension in 52%.
The family-based interventional weight management programs adopted by HOLBAEK showed a 75% reduction in the “degree of obesity,” which comprised a measure of dyslipidemia, hypertension, hepatic steatosis, sleep apnea, and parental obesity.
“The HOLBAEK method is a holistic approach where we integrate everything,” Dr. Holm told this news organization.
Ms. Frauland said: “The HOLBAEK study has provided important insights into childhood overweight. It has highlighted that obesity is a serious multisystem disease that can be managed and treated effectively, reducing the degree of overweight and improving overweight-related complications.”
Dr. Kelly, the U.S. pediatrician, applauded the HOLBAEK philosophy, which emphasizes that obesity is not the fault of the child or parent, but rather the manifestation of dysregulated energy metabolism. “The recognition that obesity is a biologically driven, chronic, refractory, and relapsing disease is interwoven into the approach, which shifts the responsibility to the care provider for ensuring positive outcomes of treatment.
“Highlighting this fact to the parents and child can be game-changing since it removes the blame and shame associated with obesity and unburdens the family by framing the problem in a different light,” Dr. Kelly stressed.
Dr. Frithioff-Bøjsøe has reported no relevant financial relationships. Dr. Holm has an obesity management company called Holm. Dr. Kelly serves as an unpaid consultant for Novo Nordisk, Vivus, Eli Lilly, and Boehringer Ingelheim and receives donated drug/placebo from Vivus for a clinical trial funded by the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Signs of cardiometabolic damage in children who are overweight appear as early as 6-8 years of age, but were not evident in preschoolers, providing a window of opportunity for intervention, show the latest results from a long-running Danish study of childhood weight.
The proportion of children who were overweight (nearly 14% in 2015) was similar between the two groups – those of preschool age (2-5 years) and school age (6-8 years) – but only the latter showed significant signs of cardiometabolic abnormalities.
The results, published in Obesity Research & Clinical Practice, are the latest in a series of many findings from the HOLBAEK study (formerly known as The Danish Childhood Obesity Biobank) that have emerged since it began in 2007. They were presented, along with a meta-analysis of much of their work, at the European Congress on Obesity (ECO) 2022.
“When comparing children with and without overweight, there were only barely significant differences among the preschool children,” said investigator Christine Frithioff-Bøjsøe, MD, but in contrast, “the school children with overweight exhibited significantly higher systolic blood pressure, glucose, insulin, and higher HDL cholesterol,” among other markers, she noted.
“Detection needs to start as early as age 2-5 years because if you wait just a few years longer these children will show early signs of disease starting to take hold. This could provide a critical window to detect and manage overweight,” said Frithioff-Bøjsøe, PhD, of the Children’s Obesity Clinic, Copenhagen University, Hospital Holbaek, Denmark.
Asked to comment, Aaron S. Kelly, PhD, professor of pediatrics, codirector, University of Minnesota Center for Pediatric Obesity Medicine in Minneapolis, said: “Recent results from HOLBAEK highlight the critical importance of identifying obesity early in life, before its complications spring up.
“Ideally, we should be in the business of managing and reducing excess adiposity as soon as it surfaces with the goal of preventing the onset of cardiometabolic risk factors, not watchful waiting and hoping for the best.”
Routine dental visits checked overweight
In the newest study, the researchers trained dental assistants to measure weight and height and carried out body mass index assessments during routine appointments.
A total of 335 preschool and 657 school-age children were recruited for the study. Of these, 40% attended additional hospital-based examinations including blood pressure measurement and a blood sample. Children were reexamined approximately 1 year later.
Systolic blood pressure, for example, was significantly higher in 6- to 8-year-olds with overweight compared to those of normal weight (P = .001). There was no significant difference between systolic blood pressure of 2.5- to 5-year-olds without and with overweight.
Likewise, with insulin resistance, there was no significant difference between preschoolers with and without overweight. However, in schoolchildren, homoeostasis model of assessment–insulin resistance (HOMA-IR) was significantly higher in those with overweight, at 2.2, compared to those without, at 0.9 (P < .001).
Also, during follow-up (around a year later), the prevalence of overweight did not change in preschool children but increased from 13.7% to 17.0% in schoolchildren.
The researchers noted that, in Europe, it is the primary health care sector that has continuous contact with the pediatric population, with the potential for early evaluation of children at risk. Their decision to use dental health care assistants to assess weight in this particular study is novel, but feasible, they observed.
Danish model for treating overweight and obesity is ‘game-changing’
As part of the HOLBAEK initiative, clinical data and biological samples have been collected from children and adolescents receiving treatment at The Children’s Obesity Clinic, Holbaek Hospital, using a population-based cohort as a reference group. Data have been collected on about 8,000 children and adolescents so far.
Jens-Christian Holm, PhD, along with colleague and research assistant Maria Frauland, both from Copenhagen University, Hospital Holbaek, presented a review of the HOLBAEK studies (2007-2021) at ECO 2022. They said the results highlight the importance of taking an integrated approach to managing children and adolescents with obesity.
The review, which included 82 papers, found a wide variety of obesity-related complications already present at a young age in some of the cross-sectional studies, including dyslipidemia in 28% of children with obesity, hepatic steatosis in 31%, obstructive sleep apnea in 45%, and prehypertension or hypertension in 52%.
The family-based interventional weight management programs adopted by HOLBAEK showed a 75% reduction in the “degree of obesity,” which comprised a measure of dyslipidemia, hypertension, hepatic steatosis, sleep apnea, and parental obesity.
“The HOLBAEK method is a holistic approach where we integrate everything,” Dr. Holm told this news organization.
Ms. Frauland said: “The HOLBAEK study has provided important insights into childhood overweight. It has highlighted that obesity is a serious multisystem disease that can be managed and treated effectively, reducing the degree of overweight and improving overweight-related complications.”
Dr. Kelly, the U.S. pediatrician, applauded the HOLBAEK philosophy, which emphasizes that obesity is not the fault of the child or parent, but rather the manifestation of dysregulated energy metabolism. “The recognition that obesity is a biologically driven, chronic, refractory, and relapsing disease is interwoven into the approach, which shifts the responsibility to the care provider for ensuring positive outcomes of treatment.
“Highlighting this fact to the parents and child can be game-changing since it removes the blame and shame associated with obesity and unburdens the family by framing the problem in a different light,” Dr. Kelly stressed.
Dr. Frithioff-Bøjsøe has reported no relevant financial relationships. Dr. Holm has an obesity management company called Holm. Dr. Kelly serves as an unpaid consultant for Novo Nordisk, Vivus, Eli Lilly, and Boehringer Ingelheim and receives donated drug/placebo from Vivus for a clinical trial funded by the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Signs of cardiometabolic damage in children who are overweight appear as early as 6-8 years of age, but were not evident in preschoolers, providing a window of opportunity for intervention, show the latest results from a long-running Danish study of childhood weight.
The proportion of children who were overweight (nearly 14% in 2015) was similar between the two groups – those of preschool age (2-5 years) and school age (6-8 years) – but only the latter showed significant signs of cardiometabolic abnormalities.
The results, published in Obesity Research & Clinical Practice, are the latest in a series of many findings from the HOLBAEK study (formerly known as The Danish Childhood Obesity Biobank) that have emerged since it began in 2007. They were presented, along with a meta-analysis of much of their work, at the European Congress on Obesity (ECO) 2022.
“When comparing children with and without overweight, there were only barely significant differences among the preschool children,” said investigator Christine Frithioff-Bøjsøe, MD, but in contrast, “the school children with overweight exhibited significantly higher systolic blood pressure, glucose, insulin, and higher HDL cholesterol,” among other markers, she noted.
“Detection needs to start as early as age 2-5 years because if you wait just a few years longer these children will show early signs of disease starting to take hold. This could provide a critical window to detect and manage overweight,” said Frithioff-Bøjsøe, PhD, of the Children’s Obesity Clinic, Copenhagen University, Hospital Holbaek, Denmark.
Asked to comment, Aaron S. Kelly, PhD, professor of pediatrics, codirector, University of Minnesota Center for Pediatric Obesity Medicine in Minneapolis, said: “Recent results from HOLBAEK highlight the critical importance of identifying obesity early in life, before its complications spring up.
“Ideally, we should be in the business of managing and reducing excess adiposity as soon as it surfaces with the goal of preventing the onset of cardiometabolic risk factors, not watchful waiting and hoping for the best.”
Routine dental visits checked overweight
In the newest study, the researchers trained dental assistants to measure weight and height and carried out body mass index assessments during routine appointments.
A total of 335 preschool and 657 school-age children were recruited for the study. Of these, 40% attended additional hospital-based examinations including blood pressure measurement and a blood sample. Children were reexamined approximately 1 year later.
Systolic blood pressure, for example, was significantly higher in 6- to 8-year-olds with overweight compared to those of normal weight (P = .001). There was no significant difference between systolic blood pressure of 2.5- to 5-year-olds without and with overweight.
Likewise, with insulin resistance, there was no significant difference between preschoolers with and without overweight. However, in schoolchildren, homoeostasis model of assessment–insulin resistance (HOMA-IR) was significantly higher in those with overweight, at 2.2, compared to those without, at 0.9 (P < .001).
Also, during follow-up (around a year later), the prevalence of overweight did not change in preschool children but increased from 13.7% to 17.0% in schoolchildren.
The researchers noted that, in Europe, it is the primary health care sector that has continuous contact with the pediatric population, with the potential for early evaluation of children at risk. Their decision to use dental health care assistants to assess weight in this particular study is novel, but feasible, they observed.
Danish model for treating overweight and obesity is ‘game-changing’
As part of the HOLBAEK initiative, clinical data and biological samples have been collected from children and adolescents receiving treatment at The Children’s Obesity Clinic, Holbaek Hospital, using a population-based cohort as a reference group. Data have been collected on about 8,000 children and adolescents so far.
Jens-Christian Holm, PhD, along with colleague and research assistant Maria Frauland, both from Copenhagen University, Hospital Holbaek, presented a review of the HOLBAEK studies (2007-2021) at ECO 2022. They said the results highlight the importance of taking an integrated approach to managing children and adolescents with obesity.
The review, which included 82 papers, found a wide variety of obesity-related complications already present at a young age in some of the cross-sectional studies, including dyslipidemia in 28% of children with obesity, hepatic steatosis in 31%, obstructive sleep apnea in 45%, and prehypertension or hypertension in 52%.
The family-based interventional weight management programs adopted by HOLBAEK showed a 75% reduction in the “degree of obesity,” which comprised a measure of dyslipidemia, hypertension, hepatic steatosis, sleep apnea, and parental obesity.
“The HOLBAEK method is a holistic approach where we integrate everything,” Dr. Holm told this news organization.
Ms. Frauland said: “The HOLBAEK study has provided important insights into childhood overweight. It has highlighted that obesity is a serious multisystem disease that can be managed and treated effectively, reducing the degree of overweight and improving overweight-related complications.”
Dr. Kelly, the U.S. pediatrician, applauded the HOLBAEK philosophy, which emphasizes that obesity is not the fault of the child or parent, but rather the manifestation of dysregulated energy metabolism. “The recognition that obesity is a biologically driven, chronic, refractory, and relapsing disease is interwoven into the approach, which shifts the responsibility to the care provider for ensuring positive outcomes of treatment.
“Highlighting this fact to the parents and child can be game-changing since it removes the blame and shame associated with obesity and unburdens the family by framing the problem in a different light,” Dr. Kelly stressed.
Dr. Frithioff-Bøjsøe has reported no relevant financial relationships. Dr. Holm has an obesity management company called Holm. Dr. Kelly serves as an unpaid consultant for Novo Nordisk, Vivus, Eli Lilly, and Boehringer Ingelheim and receives donated drug/placebo from Vivus for a clinical trial funded by the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM OBESITY RESEARCH & CLINICAL PRACTICE
Telehealth continues to loom large, say experts
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
AT INTERNAL MEDICINE 2022
Pick your sunscreen carefully: 75% don’t pass muster
Just in time for Memorial Day outings, a new report on sunscreens is out.
The news isn’t all sunny. , a nonprofit research and advocacy group that just issued its 16th annual Guide to Sunscreens.
In response, dermatologists, including the president of the American Academy of Dermatology, say that although some concerns have been raised about the safety of some sunscreen ingredients, sunscreens themselves remain an important tool in the fight against skin cancer. According to the Skin Cancer Foundation, 1 in 5 Americans will get skin cancer by age 70. Melanoma, the most deadly, has a 5-year survival rate of 99% if caught early.
2022 report
Overall, the Environmental Working Group found that about 1 in 4 sunscreens, or about 500 products, met their standards for providing adequate sun protection and avoiding ingredients linked to known health harms. Products meant for babies and children did slightly better, with about 1 in 3 meeting the standards. The group evaluated mineral sunscreens, also called physical sunscreens, and non-mineral sunscreens, also called chemical sunscreens. Mineral sunscreens contain zinc oxide or titanium dioxide and sit on the skin to deflect the sun’s rays. Chemical sunscreens, with ingredients such as oxybenzone or avobenzone, are partially absorbed into the skin.
Among the group’s concerns:
- The use of oxybenzone in the non-mineral sunscreens. About 30% of the non-mineral sunscreens have it, says Carla Burns, senior director for cosmetic science for the Environmental Working Group. Oxybenzone is a potential hormone disrupter and a skin sensitizer that may harm children and adults, she says. Some progress has been made, as the group found oxybenzone in 66% of the non-mineral sunscreens it reviewed in 2019. (The FDA is seeking more information on oxybenzone and many other sunscreen ingredients.)
- Contamination of sunscreens with benzene, which has been linked to leukemia and other blood disorders, according to the National Cancer Institute. But industry experts stress that that chemical is found in trace amounts in personal care products and does not pose a safety concern. “Benzene is a chemical that is ubiquitous in the environment and not an intentionally added ingredient in personal care products. People worldwide are exposed daily to benzene from indoor and outdoor sources, including air, drinking water, and food and beverages,” the Personal Care Products Council, an industry group, said in a statement.
- Protection from ultraviolet A (UVA) rays is often inadequate, according to research published last year by the Environmental Working Group.
Products on the ‘best’ list
The Environmental Working Group found that 282 recreational sunscreens met its criteria. Among them:
- Coral Safe Sunscreen Lotion, SPF 30
- Neutrogena Sheer Zinc Mineral Sunscreen Lotion, SPF 30
- Mad Hippie Facial Sunscreen Lotion, SPF 30+
The group chose 86 non-mineral sunscreens as better options, including:
- Alba Botanica Hawaiian Sunscreen Lotion, Aloe Vera, SPF 30
- Banana Boat Sport Ultra Sunscreen Stick, SPF 50+
- Black Girl Sunscreen Melanin Boosting Moisturizing Sunscreen Lotion, SPF 30
And 70 sunscreens made the kids’ best list, including:
- True Baby Everyday Play Sunscreen Lotion, SPF 30+
- Sun Biologic Kids’ Sunscreen Stick, SPF 30+
- Kiss My Face Organic Kids’ Defense Sunscreen Lotion, SPF 30
Industry response, FDA actions
In a statement, Alexandra Kowcz, chief scientist at the Personal Care Products Council, pointed out that “as part of a daily safe-sun regimen, sunscreen products help prevent sunburn and reduce skin cancer risk. It is unfortunate that as Americans spend more time outdoors, the Environmental Working Group’s (EWG) 2022 Guide to Sunscreens resorts to fear-mongering with misleading information that could keep consumers from using sunscreens altogether.”
The FDA has asked for more information about certain ingredients to further evaluate products, she says, and industry is working with the agency. The FDA says it is attempting to improve the quality, safety and effectiveness of over-the-counter sunscreen products. In September, 2021, the FDA issued a proposal for regulating OTC sunscreen products, as required under the CARES (Coronavirus Aid, Relief and Economic Security) Act. The effective date for the final order can’t be earlier than September 2022, the CARES Act says.
Dermatologists weigh in
“Every time something like this gets published, my patients come in hysterical,” says Michele Green, MD, a New York City dermatologist who reviewed the report for WebMD. She acknowledges that more research is needed on some sunscreen ingredients. “We really do not know the long-term consequence of oxybenzone,” she says.
Her advice: If her patients have melasma (a skin condition with brown patches on the face), she advises them to use both a chemical and a mineral sunscreen. “I don’t tell my patients in general not to use the chemical [sunscreens].”
For children, she says, the mineral sunscreens may be preferred. On her own children, who are teens, she uses the mineral sunscreens, due to possible concern about hormone disruption.
In a statement, Mark D. Kaufmann, MD, president of the American Academy of Dermatology, says that “sunscreen is an important part of a comprehensive sun protection strategy.”
Besides a broad-spectrum, water-resistant sunscreen with an SPF of 30 or higher for exposed skin, the academy recommends seeking shade and wearing sun-protective clothing to reduce skin cancer risk.
A version of this article first appeared on WebMD.com.
Just in time for Memorial Day outings, a new report on sunscreens is out.
The news isn’t all sunny. , a nonprofit research and advocacy group that just issued its 16th annual Guide to Sunscreens.
In response, dermatologists, including the president of the American Academy of Dermatology, say that although some concerns have been raised about the safety of some sunscreen ingredients, sunscreens themselves remain an important tool in the fight against skin cancer. According to the Skin Cancer Foundation, 1 in 5 Americans will get skin cancer by age 70. Melanoma, the most deadly, has a 5-year survival rate of 99% if caught early.
2022 report
Overall, the Environmental Working Group found that about 1 in 4 sunscreens, or about 500 products, met their standards for providing adequate sun protection and avoiding ingredients linked to known health harms. Products meant for babies and children did slightly better, with about 1 in 3 meeting the standards. The group evaluated mineral sunscreens, also called physical sunscreens, and non-mineral sunscreens, also called chemical sunscreens. Mineral sunscreens contain zinc oxide or titanium dioxide and sit on the skin to deflect the sun’s rays. Chemical sunscreens, with ingredients such as oxybenzone or avobenzone, are partially absorbed into the skin.
Among the group’s concerns:
- The use of oxybenzone in the non-mineral sunscreens. About 30% of the non-mineral sunscreens have it, says Carla Burns, senior director for cosmetic science for the Environmental Working Group. Oxybenzone is a potential hormone disrupter and a skin sensitizer that may harm children and adults, she says. Some progress has been made, as the group found oxybenzone in 66% of the non-mineral sunscreens it reviewed in 2019. (The FDA is seeking more information on oxybenzone and many other sunscreen ingredients.)
- Contamination of sunscreens with benzene, which has been linked to leukemia and other blood disorders, according to the National Cancer Institute. But industry experts stress that that chemical is found in trace amounts in personal care products and does not pose a safety concern. “Benzene is a chemical that is ubiquitous in the environment and not an intentionally added ingredient in personal care products. People worldwide are exposed daily to benzene from indoor and outdoor sources, including air, drinking water, and food and beverages,” the Personal Care Products Council, an industry group, said in a statement.
- Protection from ultraviolet A (UVA) rays is often inadequate, according to research published last year by the Environmental Working Group.
Products on the ‘best’ list
The Environmental Working Group found that 282 recreational sunscreens met its criteria. Among them:
- Coral Safe Sunscreen Lotion, SPF 30
- Neutrogena Sheer Zinc Mineral Sunscreen Lotion, SPF 30
- Mad Hippie Facial Sunscreen Lotion, SPF 30+
The group chose 86 non-mineral sunscreens as better options, including:
- Alba Botanica Hawaiian Sunscreen Lotion, Aloe Vera, SPF 30
- Banana Boat Sport Ultra Sunscreen Stick, SPF 50+
- Black Girl Sunscreen Melanin Boosting Moisturizing Sunscreen Lotion, SPF 30
And 70 sunscreens made the kids’ best list, including:
- True Baby Everyday Play Sunscreen Lotion, SPF 30+
- Sun Biologic Kids’ Sunscreen Stick, SPF 30+
- Kiss My Face Organic Kids’ Defense Sunscreen Lotion, SPF 30
Industry response, FDA actions
In a statement, Alexandra Kowcz, chief scientist at the Personal Care Products Council, pointed out that “as part of a daily safe-sun regimen, sunscreen products help prevent sunburn and reduce skin cancer risk. It is unfortunate that as Americans spend more time outdoors, the Environmental Working Group’s (EWG) 2022 Guide to Sunscreens resorts to fear-mongering with misleading information that could keep consumers from using sunscreens altogether.”
The FDA has asked for more information about certain ingredients to further evaluate products, she says, and industry is working with the agency. The FDA says it is attempting to improve the quality, safety and effectiveness of over-the-counter sunscreen products. In September, 2021, the FDA issued a proposal for regulating OTC sunscreen products, as required under the CARES (Coronavirus Aid, Relief and Economic Security) Act. The effective date for the final order can’t be earlier than September 2022, the CARES Act says.
Dermatologists weigh in
“Every time something like this gets published, my patients come in hysterical,” says Michele Green, MD, a New York City dermatologist who reviewed the report for WebMD. She acknowledges that more research is needed on some sunscreen ingredients. “We really do not know the long-term consequence of oxybenzone,” she says.
Her advice: If her patients have melasma (a skin condition with brown patches on the face), she advises them to use both a chemical and a mineral sunscreen. “I don’t tell my patients in general not to use the chemical [sunscreens].”
For children, she says, the mineral sunscreens may be preferred. On her own children, who are teens, she uses the mineral sunscreens, due to possible concern about hormone disruption.
In a statement, Mark D. Kaufmann, MD, president of the American Academy of Dermatology, says that “sunscreen is an important part of a comprehensive sun protection strategy.”
Besides a broad-spectrum, water-resistant sunscreen with an SPF of 30 or higher for exposed skin, the academy recommends seeking shade and wearing sun-protective clothing to reduce skin cancer risk.
A version of this article first appeared on WebMD.com.
Just in time for Memorial Day outings, a new report on sunscreens is out.
The news isn’t all sunny. , a nonprofit research and advocacy group that just issued its 16th annual Guide to Sunscreens.
In response, dermatologists, including the president of the American Academy of Dermatology, say that although some concerns have been raised about the safety of some sunscreen ingredients, sunscreens themselves remain an important tool in the fight against skin cancer. According to the Skin Cancer Foundation, 1 in 5 Americans will get skin cancer by age 70. Melanoma, the most deadly, has a 5-year survival rate of 99% if caught early.
2022 report
Overall, the Environmental Working Group found that about 1 in 4 sunscreens, or about 500 products, met their standards for providing adequate sun protection and avoiding ingredients linked to known health harms. Products meant for babies and children did slightly better, with about 1 in 3 meeting the standards. The group evaluated mineral sunscreens, also called physical sunscreens, and non-mineral sunscreens, also called chemical sunscreens. Mineral sunscreens contain zinc oxide or titanium dioxide and sit on the skin to deflect the sun’s rays. Chemical sunscreens, with ingredients such as oxybenzone or avobenzone, are partially absorbed into the skin.
Among the group’s concerns:
- The use of oxybenzone in the non-mineral sunscreens. About 30% of the non-mineral sunscreens have it, says Carla Burns, senior director for cosmetic science for the Environmental Working Group. Oxybenzone is a potential hormone disrupter and a skin sensitizer that may harm children and adults, she says. Some progress has been made, as the group found oxybenzone in 66% of the non-mineral sunscreens it reviewed in 2019. (The FDA is seeking more information on oxybenzone and many other sunscreen ingredients.)
- Contamination of sunscreens with benzene, which has been linked to leukemia and other blood disorders, according to the National Cancer Institute. But industry experts stress that that chemical is found in trace amounts in personal care products and does not pose a safety concern. “Benzene is a chemical that is ubiquitous in the environment and not an intentionally added ingredient in personal care products. People worldwide are exposed daily to benzene from indoor and outdoor sources, including air, drinking water, and food and beverages,” the Personal Care Products Council, an industry group, said in a statement.
- Protection from ultraviolet A (UVA) rays is often inadequate, according to research published last year by the Environmental Working Group.
Products on the ‘best’ list
The Environmental Working Group found that 282 recreational sunscreens met its criteria. Among them:
- Coral Safe Sunscreen Lotion, SPF 30
- Neutrogena Sheer Zinc Mineral Sunscreen Lotion, SPF 30
- Mad Hippie Facial Sunscreen Lotion, SPF 30+
The group chose 86 non-mineral sunscreens as better options, including:
- Alba Botanica Hawaiian Sunscreen Lotion, Aloe Vera, SPF 30
- Banana Boat Sport Ultra Sunscreen Stick, SPF 50+
- Black Girl Sunscreen Melanin Boosting Moisturizing Sunscreen Lotion, SPF 30
And 70 sunscreens made the kids’ best list, including:
- True Baby Everyday Play Sunscreen Lotion, SPF 30+
- Sun Biologic Kids’ Sunscreen Stick, SPF 30+
- Kiss My Face Organic Kids’ Defense Sunscreen Lotion, SPF 30
Industry response, FDA actions
In a statement, Alexandra Kowcz, chief scientist at the Personal Care Products Council, pointed out that “as part of a daily safe-sun regimen, sunscreen products help prevent sunburn and reduce skin cancer risk. It is unfortunate that as Americans spend more time outdoors, the Environmental Working Group’s (EWG) 2022 Guide to Sunscreens resorts to fear-mongering with misleading information that could keep consumers from using sunscreens altogether.”
The FDA has asked for more information about certain ingredients to further evaluate products, she says, and industry is working with the agency. The FDA says it is attempting to improve the quality, safety and effectiveness of over-the-counter sunscreen products. In September, 2021, the FDA issued a proposal for regulating OTC sunscreen products, as required under the CARES (Coronavirus Aid, Relief and Economic Security) Act. The effective date for the final order can’t be earlier than September 2022, the CARES Act says.
Dermatologists weigh in
“Every time something like this gets published, my patients come in hysterical,” says Michele Green, MD, a New York City dermatologist who reviewed the report for WebMD. She acknowledges that more research is needed on some sunscreen ingredients. “We really do not know the long-term consequence of oxybenzone,” she says.
Her advice: If her patients have melasma (a skin condition with brown patches on the face), she advises them to use both a chemical and a mineral sunscreen. “I don’t tell my patients in general not to use the chemical [sunscreens].”
For children, she says, the mineral sunscreens may be preferred. On her own children, who are teens, she uses the mineral sunscreens, due to possible concern about hormone disruption.
In a statement, Mark D. Kaufmann, MD, president of the American Academy of Dermatology, says that “sunscreen is an important part of a comprehensive sun protection strategy.”
Besides a broad-spectrum, water-resistant sunscreen with an SPF of 30 or higher for exposed skin, the academy recommends seeking shade and wearing sun-protective clothing to reduce skin cancer risk.
A version of this article first appeared on WebMD.com.
Calorie counting and exercise ‘of limited value’ for obesity weight loss
Counting calories, joining a gym, and taking part in exercise programs are popular methods used by people in the United Kingdom who want to shed some pounds, but they seem to be fairly ineffective strategies, according to an investigation.
A survey of adults with obesity from six countries in western Europe found that most who set out to reduce a meaningful amount of weight failed in their attempt.
The preliminary results, presented in two posters at the European Congress on Obesity, underlined the need for better support and solutions for weight management, the authors suggested.
Marc Evans, MB, BCh, a consultant physician in diabetes and endocrinology, from University Hospital, Cardiff, Wales, who led the analysis, said that, “while obesity’s impact on health is well known, our finding that a sizable proportion of adults with obesity appear at elevated risk of hospitalization or surgery due to multiple underlying illnesses, undoubtedly adds a sense of urgency to tackling Europe’s growing obesity epidemic.”
The study, which also involved analytics consultancy firm Lane Clark & Peacock, conducted a cross-sectional survey of 1,850 adults. Of those 500 were from the UK, and the remainder from France, Germany, Italy, Spain, and Sweden.
All participants had a body mass index of 30 kg/m2, or higher. More specifically, 56.3%; were classified as obesity class I, 26.8% obesity class II, and 16.9% obesity class III.
Obesity-related conditions
In total, 25.7% of participants reported no obesity-related health conditions, 28.4% had one condition, 19.6% had two, and 26.3% had three or more. The most common comorbidities were hypertension, dyslipidemia, and type 2 diabetes.
Overall, 78.6% of respondents reported having tried to lose weight in the previous year. Asked in a questionnaire about how they had tried to achieve this, the responses indicated that the most common strategies were:
- Calorie-controlled/restricted diet (71.9%)
- Exercise program course (21.9%)
- Pharmaceutical treatment/medication (12.3%)
- Joined a gym (12%)
- Digital health app (9.7%)
Among other participants, 8.1% said they had used alternative treatments, 7.6% a weight loss service, and 2.1% cognitive-behavioral therapy.
Analysis of the survey results showed that 78% of the individuals who attempted to lose weight did not achieve a clinically meaningful loss of 5% or more of their body weight, while some actually weighed more afterward.
Exercise and restricted diet
Notably, while exercise and calorie-controlled or restricted diets were among the most popular weight-loss methods in U.K. participants, they were amongst the least successful strategies. For instance, while 26.5% of adults who controlled their diet said they had lost weight, 17.1% reported their weight had increased. For those who took part in an exercise program, 33.3% said they lost weight, but 15.5% said they gained weight.
Signing up for gym membership also scored poorly, with 27% shedding weight, compared with 32.4% who put weight on.
“Our survey results indicate that, while the majority of adults with obesity are actively trying to reduce their weight, using a variety of strategies, most are unsuccessful,” said Dr. Evans.
Further studies were needed to assess whether people who lose weight succeed in maintaining their weight loss, the authors said.
The conference posters have yet to be published in a journal but were peer reviewed by the ECO selection committee.
The studies were sponsored by Novo Nordisk, a researcher into and manufacturer of diabetes and obesity medications, and employer of several of the coauthors.
A version of this article first appeared on Medscape UK/Univadis.
Counting calories, joining a gym, and taking part in exercise programs are popular methods used by people in the United Kingdom who want to shed some pounds, but they seem to be fairly ineffective strategies, according to an investigation.
A survey of adults with obesity from six countries in western Europe found that most who set out to reduce a meaningful amount of weight failed in their attempt.
The preliminary results, presented in two posters at the European Congress on Obesity, underlined the need for better support and solutions for weight management, the authors suggested.
Marc Evans, MB, BCh, a consultant physician in diabetes and endocrinology, from University Hospital, Cardiff, Wales, who led the analysis, said that, “while obesity’s impact on health is well known, our finding that a sizable proportion of adults with obesity appear at elevated risk of hospitalization or surgery due to multiple underlying illnesses, undoubtedly adds a sense of urgency to tackling Europe’s growing obesity epidemic.”
The study, which also involved analytics consultancy firm Lane Clark & Peacock, conducted a cross-sectional survey of 1,850 adults. Of those 500 were from the UK, and the remainder from France, Germany, Italy, Spain, and Sweden.
All participants had a body mass index of 30 kg/m2, or higher. More specifically, 56.3%; were classified as obesity class I, 26.8% obesity class II, and 16.9% obesity class III.
Obesity-related conditions
In total, 25.7% of participants reported no obesity-related health conditions, 28.4% had one condition, 19.6% had two, and 26.3% had three or more. The most common comorbidities were hypertension, dyslipidemia, and type 2 diabetes.
Overall, 78.6% of respondents reported having tried to lose weight in the previous year. Asked in a questionnaire about how they had tried to achieve this, the responses indicated that the most common strategies were:
- Calorie-controlled/restricted diet (71.9%)
- Exercise program course (21.9%)
- Pharmaceutical treatment/medication (12.3%)
- Joined a gym (12%)
- Digital health app (9.7%)
Among other participants, 8.1% said they had used alternative treatments, 7.6% a weight loss service, and 2.1% cognitive-behavioral therapy.
Analysis of the survey results showed that 78% of the individuals who attempted to lose weight did not achieve a clinically meaningful loss of 5% or more of their body weight, while some actually weighed more afterward.
Exercise and restricted diet
Notably, while exercise and calorie-controlled or restricted diets were among the most popular weight-loss methods in U.K. participants, they were amongst the least successful strategies. For instance, while 26.5% of adults who controlled their diet said they had lost weight, 17.1% reported their weight had increased. For those who took part in an exercise program, 33.3% said they lost weight, but 15.5% said they gained weight.
Signing up for gym membership also scored poorly, with 27% shedding weight, compared with 32.4% who put weight on.
“Our survey results indicate that, while the majority of adults with obesity are actively trying to reduce their weight, using a variety of strategies, most are unsuccessful,” said Dr. Evans.
Further studies were needed to assess whether people who lose weight succeed in maintaining their weight loss, the authors said.
The conference posters have yet to be published in a journal but were peer reviewed by the ECO selection committee.
The studies were sponsored by Novo Nordisk, a researcher into and manufacturer of diabetes and obesity medications, and employer of several of the coauthors.
A version of this article first appeared on Medscape UK/Univadis.
Counting calories, joining a gym, and taking part in exercise programs are popular methods used by people in the United Kingdom who want to shed some pounds, but they seem to be fairly ineffective strategies, according to an investigation.
A survey of adults with obesity from six countries in western Europe found that most who set out to reduce a meaningful amount of weight failed in their attempt.
The preliminary results, presented in two posters at the European Congress on Obesity, underlined the need for better support and solutions for weight management, the authors suggested.
Marc Evans, MB, BCh, a consultant physician in diabetes and endocrinology, from University Hospital, Cardiff, Wales, who led the analysis, said that, “while obesity’s impact on health is well known, our finding that a sizable proportion of adults with obesity appear at elevated risk of hospitalization or surgery due to multiple underlying illnesses, undoubtedly adds a sense of urgency to tackling Europe’s growing obesity epidemic.”
The study, which also involved analytics consultancy firm Lane Clark & Peacock, conducted a cross-sectional survey of 1,850 adults. Of those 500 were from the UK, and the remainder from France, Germany, Italy, Spain, and Sweden.
All participants had a body mass index of 30 kg/m2, or higher. More specifically, 56.3%; were classified as obesity class I, 26.8% obesity class II, and 16.9% obesity class III.
Obesity-related conditions
In total, 25.7% of participants reported no obesity-related health conditions, 28.4% had one condition, 19.6% had two, and 26.3% had three or more. The most common comorbidities were hypertension, dyslipidemia, and type 2 diabetes.
Overall, 78.6% of respondents reported having tried to lose weight in the previous year. Asked in a questionnaire about how they had tried to achieve this, the responses indicated that the most common strategies were:
- Calorie-controlled/restricted diet (71.9%)
- Exercise program course (21.9%)
- Pharmaceutical treatment/medication (12.3%)
- Joined a gym (12%)
- Digital health app (9.7%)
Among other participants, 8.1% said they had used alternative treatments, 7.6% a weight loss service, and 2.1% cognitive-behavioral therapy.
Analysis of the survey results showed that 78% of the individuals who attempted to lose weight did not achieve a clinically meaningful loss of 5% or more of their body weight, while some actually weighed more afterward.
Exercise and restricted diet
Notably, while exercise and calorie-controlled or restricted diets were among the most popular weight-loss methods in U.K. participants, they were amongst the least successful strategies. For instance, while 26.5% of adults who controlled their diet said they had lost weight, 17.1% reported their weight had increased. For those who took part in an exercise program, 33.3% said they lost weight, but 15.5% said they gained weight.
Signing up for gym membership also scored poorly, with 27% shedding weight, compared with 32.4% who put weight on.
“Our survey results indicate that, while the majority of adults with obesity are actively trying to reduce their weight, using a variety of strategies, most are unsuccessful,” said Dr. Evans.
Further studies were needed to assess whether people who lose weight succeed in maintaining their weight loss, the authors said.
The conference posters have yet to be published in a journal but were peer reviewed by the ECO selection committee.
The studies were sponsored by Novo Nordisk, a researcher into and manufacturer of diabetes and obesity medications, and employer of several of the coauthors.
A version of this article first appeared on Medscape UK/Univadis.
FROM ECO 2022
Three-parent IVF now legal in two countries
: the United Kingdom and Australia.
Australia’s senate passed a bill on March 30 amending pre-existing laws to allow the procedure in certain circumstances.
The goal of this procedure is to prevent genetic disorders caused by defective mitochondria, the power plants inside our cells that provide energy for normal growth and development. When mitochondria don’t produce any energy at all, the resulting genetic disorders are quickly fatal. When mitochondria make only a little energy, children can have severe illnesses and disabilities.
“The outcomes from this problem are really severe, and it’s highly likely that the baby will be very sick or die,” says Arthur Caplan, PhD, head of the division of medical ethics at the New York University Grossman School of Medicine.
Mitochondria have a little bit of DNA, and children inherit them from their mother. To avoid children inheriting this damaged genetic material, mitochondrial donation, also known as three-parent in vitro fertilization (IVF), takes the nucleus, which contains most of the DNA that makes us who we are, from an egg of the mother and puts it into a donated egg from a woman with healthy mitochondria.
The egg is then fertilized with sperm through IVF, and the resulting embryo has genetic material from two women and one man.
One ethical conundrum about mitochondrial donation is that any child conceived this way would inherit modified DNA and pass that along to their own children.
“I think it’s likely that we are going to go down this road to repair disease,” Dr. Caplan says. “I don’t think all genetic engineering of embryos is wrong, but we have to draw the line between enhancement versus treating disease.”
For couples who want a child that shares at least some of their own DNA, there are other ways to have a child without damaged mitochondria. One option would be genetic screening of their embryos to find healthy embryos without this defect, which would work for some women who have relatively few mitochondrial mutations. Another alternative is using a donor egg from a woman with healthy mitochondria.
Mitochondrial donation may appeal to couples who want their children to have a genetic connection to both parents, Dr. Caplan says. But prospective parents also need to be aware that this procedure is relatively new and, unlike egg donation, doesn’t have a long track record of success.
“It looks promising, but we don’t have the full safety picture yet, and we’re not going to start to get it for another decade or so,” Dr. Caplan cautions. “I do think it’s worth offering as one option, but you also have to get people to think about how important it is to have a biological child together and make sure that they understand that even if we try this technique, we don’t know the long-term outcomes for children yet.”
A version of this article first appeared on WebMD.com.
: the United Kingdom and Australia.
Australia’s senate passed a bill on March 30 amending pre-existing laws to allow the procedure in certain circumstances.
The goal of this procedure is to prevent genetic disorders caused by defective mitochondria, the power plants inside our cells that provide energy for normal growth and development. When mitochondria don’t produce any energy at all, the resulting genetic disorders are quickly fatal. When mitochondria make only a little energy, children can have severe illnesses and disabilities.
“The outcomes from this problem are really severe, and it’s highly likely that the baby will be very sick or die,” says Arthur Caplan, PhD, head of the division of medical ethics at the New York University Grossman School of Medicine.
Mitochondria have a little bit of DNA, and children inherit them from their mother. To avoid children inheriting this damaged genetic material, mitochondrial donation, also known as three-parent in vitro fertilization (IVF), takes the nucleus, which contains most of the DNA that makes us who we are, from an egg of the mother and puts it into a donated egg from a woman with healthy mitochondria.
The egg is then fertilized with sperm through IVF, and the resulting embryo has genetic material from two women and one man.
One ethical conundrum about mitochondrial donation is that any child conceived this way would inherit modified DNA and pass that along to their own children.
“I think it’s likely that we are going to go down this road to repair disease,” Dr. Caplan says. “I don’t think all genetic engineering of embryos is wrong, but we have to draw the line between enhancement versus treating disease.”
For couples who want a child that shares at least some of their own DNA, there are other ways to have a child without damaged mitochondria. One option would be genetic screening of their embryos to find healthy embryos without this defect, which would work for some women who have relatively few mitochondrial mutations. Another alternative is using a donor egg from a woman with healthy mitochondria.
Mitochondrial donation may appeal to couples who want their children to have a genetic connection to both parents, Dr. Caplan says. But prospective parents also need to be aware that this procedure is relatively new and, unlike egg donation, doesn’t have a long track record of success.
“It looks promising, but we don’t have the full safety picture yet, and we’re not going to start to get it for another decade or so,” Dr. Caplan cautions. “I do think it’s worth offering as one option, but you also have to get people to think about how important it is to have a biological child together and make sure that they understand that even if we try this technique, we don’t know the long-term outcomes for children yet.”
A version of this article first appeared on WebMD.com.
: the United Kingdom and Australia.
Australia’s senate passed a bill on March 30 amending pre-existing laws to allow the procedure in certain circumstances.
The goal of this procedure is to prevent genetic disorders caused by defective mitochondria, the power plants inside our cells that provide energy for normal growth and development. When mitochondria don’t produce any energy at all, the resulting genetic disorders are quickly fatal. When mitochondria make only a little energy, children can have severe illnesses and disabilities.
“The outcomes from this problem are really severe, and it’s highly likely that the baby will be very sick or die,” says Arthur Caplan, PhD, head of the division of medical ethics at the New York University Grossman School of Medicine.
Mitochondria have a little bit of DNA, and children inherit them from their mother. To avoid children inheriting this damaged genetic material, mitochondrial donation, also known as three-parent in vitro fertilization (IVF), takes the nucleus, which contains most of the DNA that makes us who we are, from an egg of the mother and puts it into a donated egg from a woman with healthy mitochondria.
The egg is then fertilized with sperm through IVF, and the resulting embryo has genetic material from two women and one man.
One ethical conundrum about mitochondrial donation is that any child conceived this way would inherit modified DNA and pass that along to their own children.
“I think it’s likely that we are going to go down this road to repair disease,” Dr. Caplan says. “I don’t think all genetic engineering of embryos is wrong, but we have to draw the line between enhancement versus treating disease.”
For couples who want a child that shares at least some of their own DNA, there are other ways to have a child without damaged mitochondria. One option would be genetic screening of their embryos to find healthy embryos without this defect, which would work for some women who have relatively few mitochondrial mutations. Another alternative is using a donor egg from a woman with healthy mitochondria.
Mitochondrial donation may appeal to couples who want their children to have a genetic connection to both parents, Dr. Caplan says. But prospective parents also need to be aware that this procedure is relatively new and, unlike egg donation, doesn’t have a long track record of success.
“It looks promising, but we don’t have the full safety picture yet, and we’re not going to start to get it for another decade or so,” Dr. Caplan cautions. “I do think it’s worth offering as one option, but you also have to get people to think about how important it is to have a biological child together and make sure that they understand that even if we try this technique, we don’t know the long-term outcomes for children yet.”
A version of this article first appeared on WebMD.com.
Natriuretic Peptide Screening for Primary Prevention or Early Detection of Heart Failure: A Pharmacist-Driven Team-Based Approach
Heart failure (HF) is one of the leading causes of hospitalizations and the most expensive Medicare diagnosis. Its prevalence continues to rise with a projected increase of 46% from 2012 to 2030 resulting in > 8 million people aged ≥ 18 years with HF in the United States. Despite improvements in therapy, mortality remains unacceptably high with a 50% mortality rate within 5 years. Early detection strategies are needed to identify patients at risk of developing HF to delay the disease course and improve survival.1,2
Emerging data indicates that natriuretic peptide biomarker-based screening using B-type natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-proBNP) and early intervention for patients at risk of HF could prevent development of left ventricular dysfunction or new-onset HF.3-5 The 2013 St. Vincent’s Screening to Prevent Heart Failure (STOP-HF) trial is the largest study to date to evaluate BNP as a screening tool for patients at risk for HF.4 Patients at risk of HF who did not have established left ventricular systolic dysfunction or symptomatic HF were assigned randomly to usual primary care or BNP screening. Patients with BNP levels ≥ 50 pg/mL underwent echocardiogram and were referred to a cardiovascular specialty service for management. The cardiovascular specialty clinic included a team of registered nurses, nurse practitioners, pharmacists, dieticians, palliative care specialists, and cardiologists. Individuals in the intervention group showed increased renin-angiotensin system (RAS) inhibitor use at follow-up (control, 49.6%; intervention, 59.6%; P = .01). All patients received coaching by a nurse who emphasized individual risk, importance of medication adherence, and healthy lifestyle behaviors. After a mean follow-up of 4.2 years, 59 of 677 participants (8.7%) in the control group and 37 of 697 (5.3%) in the intervention group (odds ratio [OR], 0.55; 95% CI, 0.37 to 0.82; P = .003) met the primary end point of left ventricular dysfunction with or without HF. BNP-based screening in conjunction with collaborative care reduced rates of left ventricular dysfunction and HF.
In the 2013 PONTIAC trial, patients with type 2 diabetes mellitus (T2DM) without cardiac disease but with NT-proBNP levels > 125 pg/mL were randomized to usual diabetes care or intensified care at a cardiac outpatient clinic for initiation and increase of RAS inhibitors and β blockers.5 After 2 years, patients randomized to the intensified care group showed a 65% risk reduction of the primary endpoint of hospitalization or death from cardiac disease (P = .04).
Based on this evidence, the 2017 focused update of the American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Failure Society of America (HFSA) guideline for managing HF added a IIa recommendation for natriuretic peptide biomarker screening in those at risk of developing HF.6 The guideline recommends biomarker screening in conjunction with team-based care, including a cardiovascular specialist, and guideline-directed management and therapy to prevent development of left ventricular dysfunction or new-onset HF.
Although ordering a natriuretic peptide biomarker laboratory test is straightforward, the variability of team-based care across institutions and health systems makes it difficult to standardize screening and interventions for patients at risk for HF. We developed and piloted a process using clinical pharmacists in primary care for natriuretic peptide biomarker screening and risk factor reduction within the established patient aligned care team (PACT) framework at a US Department of Veterans Affairs (VA) medical center. In this paper, we describe our implementation process including descriptive preliminary outcomes.
Methods
The PACT team-based approach in primary care clinics is similar to the patient-centered medical home framework. A PACT includes the veteran patient and an interdisciplinary team of health professionals composed of their primary care practitioner (PCP), registered nurse care manager, clinical pharmacist, and other clinical and administrative staff. The PACT clinical pharmacist has prescriptive authority within a scope of practice to provide postdiagnostic chronic disease state management including management of T2DM, hypertension, HF, chronic obstructive pulmonary disease, anticoagulation, tobacco cessation, and atherosclerotic cardiovascular disease (ASCVD) risk reduction. Clinical pharmacists can prescribe and adjust medications and order laboratory tests.
Our institution, Clement J. Zablocki VA Medical Center (CJZVAMC) in Milwaukee, Wisconsin, has a specialty HF clinic that primarily manages ACC/AHA Stage C HF patients. The HF clinic uses a team-based approach to collaborate and coordinate care for the veteran. The HF team is comprised of cardiology specialists, registered nurses, clinical pharmacists, dietitians, and administrative staff. Two PACT clinical pharmacists also staff the HF clinic at CJZVAMC and work collaboratively to initiate, adjust, and optimize veterans’ HF medication regimens.
Two primary care PACT panels were selected for this project. Before implementation, a pharmacy resident and 3 PACT clinical pharmacists (2 of whom also staff the HF clinic) met with a HF cardiology specialist and 2 PACT PCPs to finalize the team-based process and workflow. PCPs were presented with the evidence-based background, purpose, and project design, which included patient identification, NT-proBNP laboratory test ordering, medication adjustment schedules, and protocol for ordering echocardiograms (Figure). Templated notes were created to allow for consistent documentation in patients’ electronic health record. A telephone script also was written for the initial telephone call to patients to explain in patient-friendly terms the implications of an elevated NT-proBNP level, the echocardiogram procedure, and recommendations for risk reduction.
Patient Selection
Patients aged ≥ 18 years with hypertension, taking antihypertensive medication for ≥ 1 month, or diagnosed with T2DM for ≥ 6 months were included. Using the parameters provided in the STOP-HF trial, patients with evidence or history of left ventricular dysfunction, defined as a left ventricular ejection fraction (EF) < 50% or an E/e’ ratio > 15 in the setting of normal EF, or symptomatic HF were excluded. Patients with a diagnosis causing life expectancy < 1 year were excluded, which was determined based on review of the patient’s chart or discussion with the PCP.
A clinical pharmacist screened patients with an upcoming PCP appointment between September 2019 and January 2020 for eligibility. For patients who met criteria, the clinical pharmacist ordered a NT-proBNP laboratory test to their already scheduled tests and entered a templated note into the patient’s chart to alert the PCP of the test. NT-proBNP was used rather than BNP because it was the natriuretic peptide laboratory test available at CJZVAMC during this time. Patients with NT-proBNP < 125 pg/mL received usual care from their PCPs. Patients with NT-proBNP ≥ 125 pg/mL received a follow-up phone call from a clinical pharmacist to discuss the laboratory test result with recommendations for initiation or increase of RAS inhibitors and an echocardiogram. If the patient agreed to an echocardiogram, the PCP was notified to order the test. For patients aged > 80 years with elevated NT-proBNP, risk vs benefit and patient-specific goals of care were discussed with the PCP. For patients whose echocardiograms revealed left ventricular dysfunction, initiation or adjustment of β blockers was considered. During RAS inhibitor increase, the clinical pharmacists provided a review of the patient’s risk factors and optimized management of hypertension, T2DM, ASCVD risk reduction, oral nonsteroidal anti-inflammatory drug (NSAID) reduction, and tobacco cessation.
Outcome Measures
Outcome measures included the percentage of patients who met inclusion/exclusion criteria and had an elevated NT-proBNP level, percent change in RAS inhibitor prescriptions and optimized dosing after intervention, frequency of left ventricular dysfunction visualized with echocardiograms, and quantification of pharmacist interventions in disease state management. Descriptive statistics were used to analyze demographic data, RAS inhibitors prescriptions before and after intervention, echocardiogram results, pharmacist recommendations, and acceptance rates of disease state management.
Results
Between September 2019 and January 2020, 570 patients from 2 PACT teams were screened. Of the 570 patients, 246 met inclusion criteria with upcoming appointments. Of these, 24 were excluded, 10 for EF < 50%, 13 for E/e’ > 15 in setting of normal EF, and 1 for hypertension diagnosis without an antihypertensive regimen or elevated blood pressure. The remaining 222 patients had an NT-proBNP level ordered and drawn and 73 (32.9%) patients had an NT-proBNP ≥ 125 pg/mL. Baseline characteristics are described in Table 1.
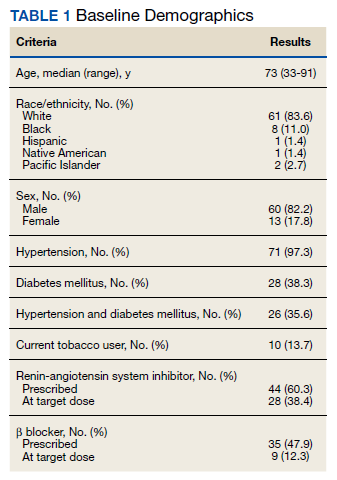
Data was collected through March 2020 (due to COVID-19) found that among the 73 patients with elevated NT-proBNP: 14 had an echocardiogram within the past year without evidence of left ventricular dysfunction; 39 had echocardiograms ordered; and 19 had echocardiograms completed by March 2020. Among the 19 echocardiograms, 16 (84%) showed no evidence of left ventricular dysfunction, 2 (11%) revealed mildly reduced EF (40% to 50%), and 1 (5%) revealed a reduced EF (< 40%). These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
Patients prescribed RAS inhibitors increased from 44 to 50. The number of patients who were able to have their RAS inhibitor dosage adjusted increased from 28 to 31. For the 3 patients with mildly reduced or reduced EF, management with β blockers was based on RAS inhibitor adjustment toleration. One patient with mildly reduced EF was switched from metoprolol tartrate to metoprolol succinate.
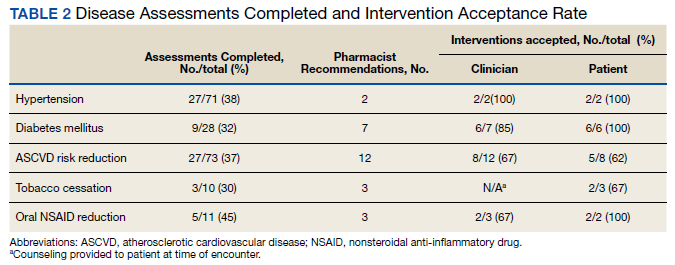
Clinical pharmacists completed disease state assessments to optimize management of hypertension, T2DM, ASCVD risk reduction, oral NSAID reduction, and tobacco cessation (Table 2). Interventions clinical pharmacists recommended for hypertension, in addition to RAS inhibitor management, included initiation and adjustment of amlodipine. For T2DM, interventions included initiation of metformin and initiation or adjustment of empagliflozin. For ASCVD risk reduction, interventions included starting a statin or adjusting statin therapies to appropriate intensities based on clinical ASCVD 10-year risk. Tobacco cessation interventions included pharmacotherapies, counseling, and education with written materials. Pharmacists counseled patients to minimize or eliminate NSAID use and, when appropriate, discontinued active oral NSAID prescriptions.
Discussion
We included patients diagnosed with T2DM and hypertension for several reasons. Most patients (62%) studied in the STOP-HF trial were diagnosed with hypertension. Also, T2DM represented the patient population enrolled in the PONTIAC trial. Guidance from the European Society of Cardiology recommends use of natriuretic peptides in high-risk populations, such as patients with DM and hypertension, to help target initiation of preventive measures.7 Lastly, T2DM and hypertension patients were easily identified using population management software available at the VA.
The percentage of patients in this project with risk factors for HF and an elevated NT-proBNP were similar to the elevated levels described in the STOP-HF trial. In our project, 32.9% of patients had elevated NT-proBNP levels, similar to the 41.6% of patients in STOP-HF. Among the completed echocardiograms, 16% revealed mildly reduced or reduced EF. These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
In addition to early identification of reduced EF, this project allowed a targeted approach to identifying patients for risk factor reduction. Between the 2 PACT teams, 246 patients with T2DM and/or hypertension were seen from September 2019 to January 2020. By using natriuretic peptide screening, the clinical pharmacists were able to prioritize and focus risk factor management on patients at higher risk. Pharmacists were then able to intervene for all risk factors assessed: hypertension, T2DM, ASCVD risk reduction, NSAID use reduction, and tobacco cessation.
During the implementation period, VA criteria of use of the angiotensin receptor-neprilysin inhibitor, sacubitril/valsartan, was restricted to VA cardiology. For patients with reduced EF, it was up to the PCP’s discretion to consult cardiology for further follow-up. In November 2020, the VA removed the restriction to cardiology and PCPs were able to order sacubitril/valsartan. Although not included in the Figure at the time of project implementation, the clinical pharmacist could now transition a patient with reduced EF from a RAS inhibitor to sacubitril/valsartan and adjust to target dosages.
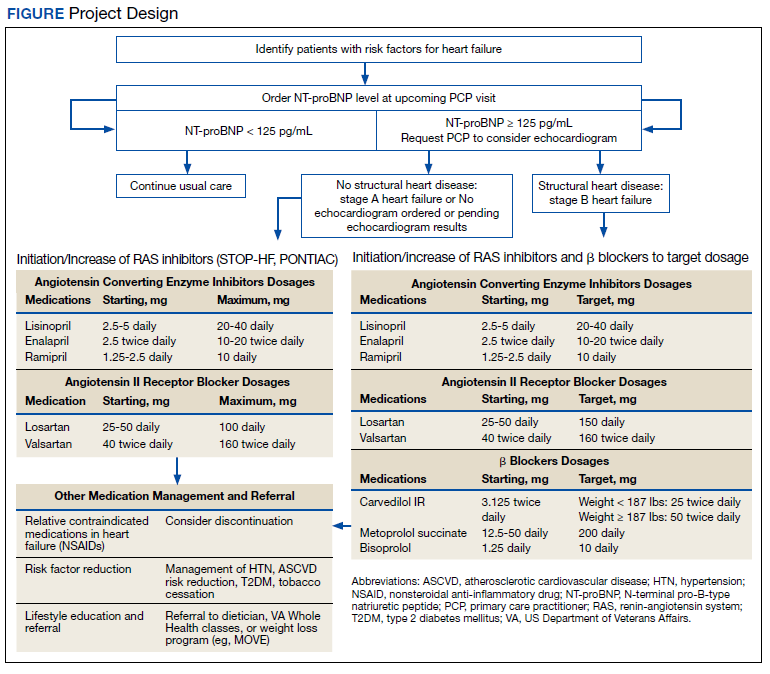
Clinical pharmacists involved in this project had established working relationships with each of the PACT members before project initiation. The PACT employed the clinical pharmacists regularly for chronic disease state management. This facilitated adoption of the natriuretic peptide screening process and PCP buy-in and support. The PCPs agreed to discuss adding a NT-proBNP laboratory test with the patient, when possible, during their in-person appointment and informed the patient that a pharmacist would call if the result was elevated. This warm hand-off facilitated the patient’s reception to the clinical pharmacists’ recommendations after an elevated NT-proBNP result. We also reported PCPs’ high acceptance rate of pharmacist recommendations and interventions for disease state management. These high acceptance rates reflect the established working relationships between clinical pharmacists and the PACT.
Development of templated notes, medication adjustment schedules, and telephone script allowed for consistent implementation into the PACT panels. This process could be duplicated and adopted into other PACTs who want to use a clinical pharmacist to facilitate natriuretic peptide screening and risk factor reduction. The findings from this project can be extrapolated to other team-based care such as the patient-centered medical home model because these programs exhibit many similarities. Both health care models centralize patient care and use interdisciplinary care teams to promote continuity, care coordination, and access to achieve optimized patient outcomes.
Cost was an important factor to consider when implementing this project. With an increase in prescriptions and elective, outpatient echocardiograms, higher outpatient cost is expected. A cost-effectiveness analysis in the STOP-HF trial found an overall cost benefit by reducing the number of patients diagnosed with left ventricular dysfunction or HF and emergency hospitalizations for cardiac events in those who received collaborative care after natriuretic peptide testing.8 These cost savings offset increased outpatient costs.
Limitations
Participants were identified initially through a computer-generated list of patients with hypertension or T2DM without a HF diagnosis documented in their problem list. This problem list is manually updated by PCPs. Although we reviewed records for exclusion criteria, eligible patients might have been excluded. The use and interpretation of an NT-proBNP level is not specific to cardiac disease. Elevations can be seen with increased age, kidney dysfunction, and pulmonary disease. Additionally, an NT-proBNP level might be falsely low in patients who are overweight or obese. Because of the relatively short period of time, we could not analyze associations with HF diagnosis or progression, hospitalizations due to HF, or mortality. Regarding external validity, because of the pre-established interdisciplinary clinic settings and VA pharmacists’ scope of practice with prescriptive authority, implementing this project might have been better received by PCPs and allowed for higher acceptance rates of pharmacist interventions at the VA compared with a community setting.
Conclusions
The ACC/AHA/HFSA guidelines recommended use of natriuretic peptide biomarker screening in conjunction with team-based care for those at risk of developing HF. We describe our process for implementing team-based care using clinical pharmacists in primary care. Our process provides a targeted approach to identifying patients for risk factor reduction through comprehensive medication management and could be replicated by other primary care clinics using a patient-centered medical home model.
Acknowledgments
We would like to acknowledge Dr. Sara Hariman, Dr. Payal Sanghani, and Dr. Cecilia Scholcoff for their support and collaboration with the project.
1. Braunwald E. Heart failure. J Am Coll Cardiol HF. 2013;1(1):1-20. doi: 10.1016/j.jchf.2012.10.002
2. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619. doi:10.1161/HHF.0b013e318291329a
3. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74(11):1893-1900.
4. Ledwidge M, Gallagher J, Conlon C, et al. Natriuretic peptide-based screening and collaborative care for heart failure: the STOP-HF randomized trial. JAMA. 2013;310(1):66-74. doi:10.1001/jama.2013.7588
5. Huelsmann M, Neuhold S, Resl M, et al. PONTIAC (NT-proBNP selected prevention of cardiac events in a population of diabetic patients without a history of cardiac disease): a prospective randomized controlled trial. J Am Coll Cardiol. 2013;62(15):1365-1372. doi:10.1016/j.jacc.2013.05.069
6. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776-803. doi:10.1016/j.jacc.2017.04.025
7. Mueller C, McDonald K, de Boer RA, et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eu J Heart Fail. 2019;21:715-731. doi:10.1002/ejhf.1494
8. Ledwidge MT, O’Connell E, Gallagher J, et al; Heart Failure Association of the European Society of Cardiology. Cost-effectiveness of natriuretic peptide-based screening and collaborative care: a report from the STOP-HF (St. Vincent’s Screening to Prevent Heart Failure) study. Eur J Heart Fail. 2015;17(7):672-679.
Heart failure (HF) is one of the leading causes of hospitalizations and the most expensive Medicare diagnosis. Its prevalence continues to rise with a projected increase of 46% from 2012 to 2030 resulting in > 8 million people aged ≥ 18 years with HF in the United States. Despite improvements in therapy, mortality remains unacceptably high with a 50% mortality rate within 5 years. Early detection strategies are needed to identify patients at risk of developing HF to delay the disease course and improve survival.1,2
Emerging data indicates that natriuretic peptide biomarker-based screening using B-type natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-proBNP) and early intervention for patients at risk of HF could prevent development of left ventricular dysfunction or new-onset HF.3-5 The 2013 St. Vincent’s Screening to Prevent Heart Failure (STOP-HF) trial is the largest study to date to evaluate BNP as a screening tool for patients at risk for HF.4 Patients at risk of HF who did not have established left ventricular systolic dysfunction or symptomatic HF were assigned randomly to usual primary care or BNP screening. Patients with BNP levels ≥ 50 pg/mL underwent echocardiogram and were referred to a cardiovascular specialty service for management. The cardiovascular specialty clinic included a team of registered nurses, nurse practitioners, pharmacists, dieticians, palliative care specialists, and cardiologists. Individuals in the intervention group showed increased renin-angiotensin system (RAS) inhibitor use at follow-up (control, 49.6%; intervention, 59.6%; P = .01). All patients received coaching by a nurse who emphasized individual risk, importance of medication adherence, and healthy lifestyle behaviors. After a mean follow-up of 4.2 years, 59 of 677 participants (8.7%) in the control group and 37 of 697 (5.3%) in the intervention group (odds ratio [OR], 0.55; 95% CI, 0.37 to 0.82; P = .003) met the primary end point of left ventricular dysfunction with or without HF. BNP-based screening in conjunction with collaborative care reduced rates of left ventricular dysfunction and HF.
In the 2013 PONTIAC trial, patients with type 2 diabetes mellitus (T2DM) without cardiac disease but with NT-proBNP levels > 125 pg/mL were randomized to usual diabetes care or intensified care at a cardiac outpatient clinic for initiation and increase of RAS inhibitors and β blockers.5 After 2 years, patients randomized to the intensified care group showed a 65% risk reduction of the primary endpoint of hospitalization or death from cardiac disease (P = .04).
Based on this evidence, the 2017 focused update of the American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Failure Society of America (HFSA) guideline for managing HF added a IIa recommendation for natriuretic peptide biomarker screening in those at risk of developing HF.6 The guideline recommends biomarker screening in conjunction with team-based care, including a cardiovascular specialist, and guideline-directed management and therapy to prevent development of left ventricular dysfunction or new-onset HF.
Although ordering a natriuretic peptide biomarker laboratory test is straightforward, the variability of team-based care across institutions and health systems makes it difficult to standardize screening and interventions for patients at risk for HF. We developed and piloted a process using clinical pharmacists in primary care for natriuretic peptide biomarker screening and risk factor reduction within the established patient aligned care team (PACT) framework at a US Department of Veterans Affairs (VA) medical center. In this paper, we describe our implementation process including descriptive preliminary outcomes.
Methods
The PACT team-based approach in primary care clinics is similar to the patient-centered medical home framework. A PACT includes the veteran patient and an interdisciplinary team of health professionals composed of their primary care practitioner (PCP), registered nurse care manager, clinical pharmacist, and other clinical and administrative staff. The PACT clinical pharmacist has prescriptive authority within a scope of practice to provide postdiagnostic chronic disease state management including management of T2DM, hypertension, HF, chronic obstructive pulmonary disease, anticoagulation, tobacco cessation, and atherosclerotic cardiovascular disease (ASCVD) risk reduction. Clinical pharmacists can prescribe and adjust medications and order laboratory tests.
Our institution, Clement J. Zablocki VA Medical Center (CJZVAMC) in Milwaukee, Wisconsin, has a specialty HF clinic that primarily manages ACC/AHA Stage C HF patients. The HF clinic uses a team-based approach to collaborate and coordinate care for the veteran. The HF team is comprised of cardiology specialists, registered nurses, clinical pharmacists, dietitians, and administrative staff. Two PACT clinical pharmacists also staff the HF clinic at CJZVAMC and work collaboratively to initiate, adjust, and optimize veterans’ HF medication regimens.
Two primary care PACT panels were selected for this project. Before implementation, a pharmacy resident and 3 PACT clinical pharmacists (2 of whom also staff the HF clinic) met with a HF cardiology specialist and 2 PACT PCPs to finalize the team-based process and workflow. PCPs were presented with the evidence-based background, purpose, and project design, which included patient identification, NT-proBNP laboratory test ordering, medication adjustment schedules, and protocol for ordering echocardiograms (Figure). Templated notes were created to allow for consistent documentation in patients’ electronic health record. A telephone script also was written for the initial telephone call to patients to explain in patient-friendly terms the implications of an elevated NT-proBNP level, the echocardiogram procedure, and recommendations for risk reduction.
Patient Selection
Patients aged ≥ 18 years with hypertension, taking antihypertensive medication for ≥ 1 month, or diagnosed with T2DM for ≥ 6 months were included. Using the parameters provided in the STOP-HF trial, patients with evidence or history of left ventricular dysfunction, defined as a left ventricular ejection fraction (EF) < 50% or an E/e’ ratio > 15 in the setting of normal EF, or symptomatic HF were excluded. Patients with a diagnosis causing life expectancy < 1 year were excluded, which was determined based on review of the patient’s chart or discussion with the PCP.
A clinical pharmacist screened patients with an upcoming PCP appointment between September 2019 and January 2020 for eligibility. For patients who met criteria, the clinical pharmacist ordered a NT-proBNP laboratory test to their already scheduled tests and entered a templated note into the patient’s chart to alert the PCP of the test. NT-proBNP was used rather than BNP because it was the natriuretic peptide laboratory test available at CJZVAMC during this time. Patients with NT-proBNP < 125 pg/mL received usual care from their PCPs. Patients with NT-proBNP ≥ 125 pg/mL received a follow-up phone call from a clinical pharmacist to discuss the laboratory test result with recommendations for initiation or increase of RAS inhibitors and an echocardiogram. If the patient agreed to an echocardiogram, the PCP was notified to order the test. For patients aged > 80 years with elevated NT-proBNP, risk vs benefit and patient-specific goals of care were discussed with the PCP. For patients whose echocardiograms revealed left ventricular dysfunction, initiation or adjustment of β blockers was considered. During RAS inhibitor increase, the clinical pharmacists provided a review of the patient’s risk factors and optimized management of hypertension, T2DM, ASCVD risk reduction, oral nonsteroidal anti-inflammatory drug (NSAID) reduction, and tobacco cessation.
Outcome Measures
Outcome measures included the percentage of patients who met inclusion/exclusion criteria and had an elevated NT-proBNP level, percent change in RAS inhibitor prescriptions and optimized dosing after intervention, frequency of left ventricular dysfunction visualized with echocardiograms, and quantification of pharmacist interventions in disease state management. Descriptive statistics were used to analyze demographic data, RAS inhibitors prescriptions before and after intervention, echocardiogram results, pharmacist recommendations, and acceptance rates of disease state management.
Results
Between September 2019 and January 2020, 570 patients from 2 PACT teams were screened. Of the 570 patients, 246 met inclusion criteria with upcoming appointments. Of these, 24 were excluded, 10 for EF < 50%, 13 for E/e’ > 15 in setting of normal EF, and 1 for hypertension diagnosis without an antihypertensive regimen or elevated blood pressure. The remaining 222 patients had an NT-proBNP level ordered and drawn and 73 (32.9%) patients had an NT-proBNP ≥ 125 pg/mL. Baseline characteristics are described in Table 1.
Data was collected through March 2020 (due to COVID-19) found that among the 73 patients with elevated NT-proBNP: 14 had an echocardiogram within the past year without evidence of left ventricular dysfunction; 39 had echocardiograms ordered; and 19 had echocardiograms completed by March 2020. Among the 19 echocardiograms, 16 (84%) showed no evidence of left ventricular dysfunction, 2 (11%) revealed mildly reduced EF (40% to 50%), and 1 (5%) revealed a reduced EF (< 40%). These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
Patients prescribed RAS inhibitors increased from 44 to 50. The number of patients who were able to have their RAS inhibitor dosage adjusted increased from 28 to 31. For the 3 patients with mildly reduced or reduced EF, management with β blockers was based on RAS inhibitor adjustment toleration. One patient with mildly reduced EF was switched from metoprolol tartrate to metoprolol succinate.
Clinical pharmacists completed disease state assessments to optimize management of hypertension, T2DM, ASCVD risk reduction, oral NSAID reduction, and tobacco cessation (Table 2). Interventions clinical pharmacists recommended for hypertension, in addition to RAS inhibitor management, included initiation and adjustment of amlodipine. For T2DM, interventions included initiation of metformin and initiation or adjustment of empagliflozin. For ASCVD risk reduction, interventions included starting a statin or adjusting statin therapies to appropriate intensities based on clinical ASCVD 10-year risk. Tobacco cessation interventions included pharmacotherapies, counseling, and education with written materials. Pharmacists counseled patients to minimize or eliminate NSAID use and, when appropriate, discontinued active oral NSAID prescriptions.
Discussion
We included patients diagnosed with T2DM and hypertension for several reasons. Most patients (62%) studied in the STOP-HF trial were diagnosed with hypertension. Also, T2DM represented the patient population enrolled in the PONTIAC trial. Guidance from the European Society of Cardiology recommends use of natriuretic peptides in high-risk populations, such as patients with DM and hypertension, to help target initiation of preventive measures.7 Lastly, T2DM and hypertension patients were easily identified using population management software available at the VA.
The percentage of patients in this project with risk factors for HF and an elevated NT-proBNP were similar to the elevated levels described in the STOP-HF trial. In our project, 32.9% of patients had elevated NT-proBNP levels, similar to the 41.6% of patients in STOP-HF. Among the completed echocardiograms, 16% revealed mildly reduced or reduced EF. These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
In addition to early identification of reduced EF, this project allowed a targeted approach to identifying patients for risk factor reduction. Between the 2 PACT teams, 246 patients with T2DM and/or hypertension were seen from September 2019 to January 2020. By using natriuretic peptide screening, the clinical pharmacists were able to prioritize and focus risk factor management on patients at higher risk. Pharmacists were then able to intervene for all risk factors assessed: hypertension, T2DM, ASCVD risk reduction, NSAID use reduction, and tobacco cessation.
During the implementation period, VA criteria of use of the angiotensin receptor-neprilysin inhibitor, sacubitril/valsartan, was restricted to VA cardiology. For patients with reduced EF, it was up to the PCP’s discretion to consult cardiology for further follow-up. In November 2020, the VA removed the restriction to cardiology and PCPs were able to order sacubitril/valsartan. Although not included in the Figure at the time of project implementation, the clinical pharmacist could now transition a patient with reduced EF from a RAS inhibitor to sacubitril/valsartan and adjust to target dosages.
Clinical pharmacists involved in this project had established working relationships with each of the PACT members before project initiation. The PACT employed the clinical pharmacists regularly for chronic disease state management. This facilitated adoption of the natriuretic peptide screening process and PCP buy-in and support. The PCPs agreed to discuss adding a NT-proBNP laboratory test with the patient, when possible, during their in-person appointment and informed the patient that a pharmacist would call if the result was elevated. This warm hand-off facilitated the patient’s reception to the clinical pharmacists’ recommendations after an elevated NT-proBNP result. We also reported PCPs’ high acceptance rate of pharmacist recommendations and interventions for disease state management. These high acceptance rates reflect the established working relationships between clinical pharmacists and the PACT.
Development of templated notes, medication adjustment schedules, and telephone script allowed for consistent implementation into the PACT panels. This process could be duplicated and adopted into other PACTs who want to use a clinical pharmacist to facilitate natriuretic peptide screening and risk factor reduction. The findings from this project can be extrapolated to other team-based care such as the patient-centered medical home model because these programs exhibit many similarities. Both health care models centralize patient care and use interdisciplinary care teams to promote continuity, care coordination, and access to achieve optimized patient outcomes.
Cost was an important factor to consider when implementing this project. With an increase in prescriptions and elective, outpatient echocardiograms, higher outpatient cost is expected. A cost-effectiveness analysis in the STOP-HF trial found an overall cost benefit by reducing the number of patients diagnosed with left ventricular dysfunction or HF and emergency hospitalizations for cardiac events in those who received collaborative care after natriuretic peptide testing.8 These cost savings offset increased outpatient costs.
Limitations
Participants were identified initially through a computer-generated list of patients with hypertension or T2DM without a HF diagnosis documented in their problem list. This problem list is manually updated by PCPs. Although we reviewed records for exclusion criteria, eligible patients might have been excluded. The use and interpretation of an NT-proBNP level is not specific to cardiac disease. Elevations can be seen with increased age, kidney dysfunction, and pulmonary disease. Additionally, an NT-proBNP level might be falsely low in patients who are overweight or obese. Because of the relatively short period of time, we could not analyze associations with HF diagnosis or progression, hospitalizations due to HF, or mortality. Regarding external validity, because of the pre-established interdisciplinary clinic settings and VA pharmacists’ scope of practice with prescriptive authority, implementing this project might have been better received by PCPs and allowed for higher acceptance rates of pharmacist interventions at the VA compared with a community setting.
Conclusions
The ACC/AHA/HFSA guidelines recommended use of natriuretic peptide biomarker screening in conjunction with team-based care for those at risk of developing HF. We describe our process for implementing team-based care using clinical pharmacists in primary care. Our process provides a targeted approach to identifying patients for risk factor reduction through comprehensive medication management and could be replicated by other primary care clinics using a patient-centered medical home model.
Acknowledgments
We would like to acknowledge Dr. Sara Hariman, Dr. Payal Sanghani, and Dr. Cecilia Scholcoff for their support and collaboration with the project.
Heart failure (HF) is one of the leading causes of hospitalizations and the most expensive Medicare diagnosis. Its prevalence continues to rise with a projected increase of 46% from 2012 to 2030 resulting in > 8 million people aged ≥ 18 years with HF in the United States. Despite improvements in therapy, mortality remains unacceptably high with a 50% mortality rate within 5 years. Early detection strategies are needed to identify patients at risk of developing HF to delay the disease course and improve survival.1,2
Emerging data indicates that natriuretic peptide biomarker-based screening using B-type natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-proBNP) and early intervention for patients at risk of HF could prevent development of left ventricular dysfunction or new-onset HF.3-5 The 2013 St. Vincent’s Screening to Prevent Heart Failure (STOP-HF) trial is the largest study to date to evaluate BNP as a screening tool for patients at risk for HF.4 Patients at risk of HF who did not have established left ventricular systolic dysfunction or symptomatic HF were assigned randomly to usual primary care or BNP screening. Patients with BNP levels ≥ 50 pg/mL underwent echocardiogram and were referred to a cardiovascular specialty service for management. The cardiovascular specialty clinic included a team of registered nurses, nurse practitioners, pharmacists, dieticians, palliative care specialists, and cardiologists. Individuals in the intervention group showed increased renin-angiotensin system (RAS) inhibitor use at follow-up (control, 49.6%; intervention, 59.6%; P = .01). All patients received coaching by a nurse who emphasized individual risk, importance of medication adherence, and healthy lifestyle behaviors. After a mean follow-up of 4.2 years, 59 of 677 participants (8.7%) in the control group and 37 of 697 (5.3%) in the intervention group (odds ratio [OR], 0.55; 95% CI, 0.37 to 0.82; P = .003) met the primary end point of left ventricular dysfunction with or without HF. BNP-based screening in conjunction with collaborative care reduced rates of left ventricular dysfunction and HF.
In the 2013 PONTIAC trial, patients with type 2 diabetes mellitus (T2DM) without cardiac disease but with NT-proBNP levels > 125 pg/mL were randomized to usual diabetes care or intensified care at a cardiac outpatient clinic for initiation and increase of RAS inhibitors and β blockers.5 After 2 years, patients randomized to the intensified care group showed a 65% risk reduction of the primary endpoint of hospitalization or death from cardiac disease (P = .04).
Based on this evidence, the 2017 focused update of the American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Failure Society of America (HFSA) guideline for managing HF added a IIa recommendation for natriuretic peptide biomarker screening in those at risk of developing HF.6 The guideline recommends biomarker screening in conjunction with team-based care, including a cardiovascular specialist, and guideline-directed management and therapy to prevent development of left ventricular dysfunction or new-onset HF.
Although ordering a natriuretic peptide biomarker laboratory test is straightforward, the variability of team-based care across institutions and health systems makes it difficult to standardize screening and interventions for patients at risk for HF. We developed and piloted a process using clinical pharmacists in primary care for natriuretic peptide biomarker screening and risk factor reduction within the established patient aligned care team (PACT) framework at a US Department of Veterans Affairs (VA) medical center. In this paper, we describe our implementation process including descriptive preliminary outcomes.
Methods
The PACT team-based approach in primary care clinics is similar to the patient-centered medical home framework. A PACT includes the veteran patient and an interdisciplinary team of health professionals composed of their primary care practitioner (PCP), registered nurse care manager, clinical pharmacist, and other clinical and administrative staff. The PACT clinical pharmacist has prescriptive authority within a scope of practice to provide postdiagnostic chronic disease state management including management of T2DM, hypertension, HF, chronic obstructive pulmonary disease, anticoagulation, tobacco cessation, and atherosclerotic cardiovascular disease (ASCVD) risk reduction. Clinical pharmacists can prescribe and adjust medications and order laboratory tests.
Our institution, Clement J. Zablocki VA Medical Center (CJZVAMC) in Milwaukee, Wisconsin, has a specialty HF clinic that primarily manages ACC/AHA Stage C HF patients. The HF clinic uses a team-based approach to collaborate and coordinate care for the veteran. The HF team is comprised of cardiology specialists, registered nurses, clinical pharmacists, dietitians, and administrative staff. Two PACT clinical pharmacists also staff the HF clinic at CJZVAMC and work collaboratively to initiate, adjust, and optimize veterans’ HF medication regimens.
Two primary care PACT panels were selected for this project. Before implementation, a pharmacy resident and 3 PACT clinical pharmacists (2 of whom also staff the HF clinic) met with a HF cardiology specialist and 2 PACT PCPs to finalize the team-based process and workflow. PCPs were presented with the evidence-based background, purpose, and project design, which included patient identification, NT-proBNP laboratory test ordering, medication adjustment schedules, and protocol for ordering echocardiograms (Figure). Templated notes were created to allow for consistent documentation in patients’ electronic health record. A telephone script also was written for the initial telephone call to patients to explain in patient-friendly terms the implications of an elevated NT-proBNP level, the echocardiogram procedure, and recommendations for risk reduction.
Patient Selection
Patients aged ≥ 18 years with hypertension, taking antihypertensive medication for ≥ 1 month, or diagnosed with T2DM for ≥ 6 months were included. Using the parameters provided in the STOP-HF trial, patients with evidence or history of left ventricular dysfunction, defined as a left ventricular ejection fraction (EF) < 50% or an E/e’ ratio > 15 in the setting of normal EF, or symptomatic HF were excluded. Patients with a diagnosis causing life expectancy < 1 year were excluded, which was determined based on review of the patient’s chart or discussion with the PCP.
A clinical pharmacist screened patients with an upcoming PCP appointment between September 2019 and January 2020 for eligibility. For patients who met criteria, the clinical pharmacist ordered a NT-proBNP laboratory test to their already scheduled tests and entered a templated note into the patient’s chart to alert the PCP of the test. NT-proBNP was used rather than BNP because it was the natriuretic peptide laboratory test available at CJZVAMC during this time. Patients with NT-proBNP < 125 pg/mL received usual care from their PCPs. Patients with NT-proBNP ≥ 125 pg/mL received a follow-up phone call from a clinical pharmacist to discuss the laboratory test result with recommendations for initiation or increase of RAS inhibitors and an echocardiogram. If the patient agreed to an echocardiogram, the PCP was notified to order the test. For patients aged > 80 years with elevated NT-proBNP, risk vs benefit and patient-specific goals of care were discussed with the PCP. For patients whose echocardiograms revealed left ventricular dysfunction, initiation or adjustment of β blockers was considered. During RAS inhibitor increase, the clinical pharmacists provided a review of the patient’s risk factors and optimized management of hypertension, T2DM, ASCVD risk reduction, oral nonsteroidal anti-inflammatory drug (NSAID) reduction, and tobacco cessation.
Outcome Measures
Outcome measures included the percentage of patients who met inclusion/exclusion criteria and had an elevated NT-proBNP level, percent change in RAS inhibitor prescriptions and optimized dosing after intervention, frequency of left ventricular dysfunction visualized with echocardiograms, and quantification of pharmacist interventions in disease state management. Descriptive statistics were used to analyze demographic data, RAS inhibitors prescriptions before and after intervention, echocardiogram results, pharmacist recommendations, and acceptance rates of disease state management.
Results
Between September 2019 and January 2020, 570 patients from 2 PACT teams were screened. Of the 570 patients, 246 met inclusion criteria with upcoming appointments. Of these, 24 were excluded, 10 for EF < 50%, 13 for E/e’ > 15 in setting of normal EF, and 1 for hypertension diagnosis without an antihypertensive regimen or elevated blood pressure. The remaining 222 patients had an NT-proBNP level ordered and drawn and 73 (32.9%) patients had an NT-proBNP ≥ 125 pg/mL. Baseline characteristics are described in Table 1.
Data was collected through March 2020 (due to COVID-19) found that among the 73 patients with elevated NT-proBNP: 14 had an echocardiogram within the past year without evidence of left ventricular dysfunction; 39 had echocardiograms ordered; and 19 had echocardiograms completed by March 2020. Among the 19 echocardiograms, 16 (84%) showed no evidence of left ventricular dysfunction, 2 (11%) revealed mildly reduced EF (40% to 50%), and 1 (5%) revealed a reduced EF (< 40%). These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
Patients prescribed RAS inhibitors increased from 44 to 50. The number of patients who were able to have their RAS inhibitor dosage adjusted increased from 28 to 31. For the 3 patients with mildly reduced or reduced EF, management with β blockers was based on RAS inhibitor adjustment toleration. One patient with mildly reduced EF was switched from metoprolol tartrate to metoprolol succinate.
Clinical pharmacists completed disease state assessments to optimize management of hypertension, T2DM, ASCVD risk reduction, oral NSAID reduction, and tobacco cessation (Table 2). Interventions clinical pharmacists recommended for hypertension, in addition to RAS inhibitor management, included initiation and adjustment of amlodipine. For T2DM, interventions included initiation of metformin and initiation or adjustment of empagliflozin. For ASCVD risk reduction, interventions included starting a statin or adjusting statin therapies to appropriate intensities based on clinical ASCVD 10-year risk. Tobacco cessation interventions included pharmacotherapies, counseling, and education with written materials. Pharmacists counseled patients to minimize or eliminate NSAID use and, when appropriate, discontinued active oral NSAID prescriptions.
Discussion
We included patients diagnosed with T2DM and hypertension for several reasons. Most patients (62%) studied in the STOP-HF trial were diagnosed with hypertension. Also, T2DM represented the patient population enrolled in the PONTIAC trial. Guidance from the European Society of Cardiology recommends use of natriuretic peptides in high-risk populations, such as patients with DM and hypertension, to help target initiation of preventive measures.7 Lastly, T2DM and hypertension patients were easily identified using population management software available at the VA.
The percentage of patients in this project with risk factors for HF and an elevated NT-proBNP were similar to the elevated levels described in the STOP-HF trial. In our project, 32.9% of patients had elevated NT-proBNP levels, similar to the 41.6% of patients in STOP-HF. Among the completed echocardiograms, 16% revealed mildly reduced or reduced EF. These patients were identified early in the disease course before symptom onset and received intervention with RAS inhibitors and disease state management.
In addition to early identification of reduced EF, this project allowed a targeted approach to identifying patients for risk factor reduction. Between the 2 PACT teams, 246 patients with T2DM and/or hypertension were seen from September 2019 to January 2020. By using natriuretic peptide screening, the clinical pharmacists were able to prioritize and focus risk factor management on patients at higher risk. Pharmacists were then able to intervene for all risk factors assessed: hypertension, T2DM, ASCVD risk reduction, NSAID use reduction, and tobacco cessation.
During the implementation period, VA criteria of use of the angiotensin receptor-neprilysin inhibitor, sacubitril/valsartan, was restricted to VA cardiology. For patients with reduced EF, it was up to the PCP’s discretion to consult cardiology for further follow-up. In November 2020, the VA removed the restriction to cardiology and PCPs were able to order sacubitril/valsartan. Although not included in the Figure at the time of project implementation, the clinical pharmacist could now transition a patient with reduced EF from a RAS inhibitor to sacubitril/valsartan and adjust to target dosages.
Clinical pharmacists involved in this project had established working relationships with each of the PACT members before project initiation. The PACT employed the clinical pharmacists regularly for chronic disease state management. This facilitated adoption of the natriuretic peptide screening process and PCP buy-in and support. The PCPs agreed to discuss adding a NT-proBNP laboratory test with the patient, when possible, during their in-person appointment and informed the patient that a pharmacist would call if the result was elevated. This warm hand-off facilitated the patient’s reception to the clinical pharmacists’ recommendations after an elevated NT-proBNP result. We also reported PCPs’ high acceptance rate of pharmacist recommendations and interventions for disease state management. These high acceptance rates reflect the established working relationships between clinical pharmacists and the PACT.
Development of templated notes, medication adjustment schedules, and telephone script allowed for consistent implementation into the PACT panels. This process could be duplicated and adopted into other PACTs who want to use a clinical pharmacist to facilitate natriuretic peptide screening and risk factor reduction. The findings from this project can be extrapolated to other team-based care such as the patient-centered medical home model because these programs exhibit many similarities. Both health care models centralize patient care and use interdisciplinary care teams to promote continuity, care coordination, and access to achieve optimized patient outcomes.
Cost was an important factor to consider when implementing this project. With an increase in prescriptions and elective, outpatient echocardiograms, higher outpatient cost is expected. A cost-effectiveness analysis in the STOP-HF trial found an overall cost benefit by reducing the number of patients diagnosed with left ventricular dysfunction or HF and emergency hospitalizations for cardiac events in those who received collaborative care after natriuretic peptide testing.8 These cost savings offset increased outpatient costs.
Limitations
Participants were identified initially through a computer-generated list of patients with hypertension or T2DM without a HF diagnosis documented in their problem list. This problem list is manually updated by PCPs. Although we reviewed records for exclusion criteria, eligible patients might have been excluded. The use and interpretation of an NT-proBNP level is not specific to cardiac disease. Elevations can be seen with increased age, kidney dysfunction, and pulmonary disease. Additionally, an NT-proBNP level might be falsely low in patients who are overweight or obese. Because of the relatively short period of time, we could not analyze associations with HF diagnosis or progression, hospitalizations due to HF, or mortality. Regarding external validity, because of the pre-established interdisciplinary clinic settings and VA pharmacists’ scope of practice with prescriptive authority, implementing this project might have been better received by PCPs and allowed for higher acceptance rates of pharmacist interventions at the VA compared with a community setting.
Conclusions
The ACC/AHA/HFSA guidelines recommended use of natriuretic peptide biomarker screening in conjunction with team-based care for those at risk of developing HF. We describe our process for implementing team-based care using clinical pharmacists in primary care. Our process provides a targeted approach to identifying patients for risk factor reduction through comprehensive medication management and could be replicated by other primary care clinics using a patient-centered medical home model.
Acknowledgments
We would like to acknowledge Dr. Sara Hariman, Dr. Payal Sanghani, and Dr. Cecilia Scholcoff for their support and collaboration with the project.
1. Braunwald E. Heart failure. J Am Coll Cardiol HF. 2013;1(1):1-20. doi: 10.1016/j.jchf.2012.10.002
2. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619. doi:10.1161/HHF.0b013e318291329a
3. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74(11):1893-1900.
4. Ledwidge M, Gallagher J, Conlon C, et al. Natriuretic peptide-based screening and collaborative care for heart failure: the STOP-HF randomized trial. JAMA. 2013;310(1):66-74. doi:10.1001/jama.2013.7588
5. Huelsmann M, Neuhold S, Resl M, et al. PONTIAC (NT-proBNP selected prevention of cardiac events in a population of diabetic patients without a history of cardiac disease): a prospective randomized controlled trial. J Am Coll Cardiol. 2013;62(15):1365-1372. doi:10.1016/j.jacc.2013.05.069
6. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776-803. doi:10.1016/j.jacc.2017.04.025
7. Mueller C, McDonald K, de Boer RA, et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eu J Heart Fail. 2019;21:715-731. doi:10.1002/ejhf.1494
8. Ledwidge MT, O’Connell E, Gallagher J, et al; Heart Failure Association of the European Society of Cardiology. Cost-effectiveness of natriuretic peptide-based screening and collaborative care: a report from the STOP-HF (St. Vincent’s Screening to Prevent Heart Failure) study. Eur J Heart Fail. 2015;17(7):672-679.
1. Braunwald E. Heart failure. J Am Coll Cardiol HF. 2013;1(1):1-20. doi: 10.1016/j.jchf.2012.10.002
2. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619. doi:10.1161/HHF.0b013e318291329a
3. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74(11):1893-1900.
4. Ledwidge M, Gallagher J, Conlon C, et al. Natriuretic peptide-based screening and collaborative care for heart failure: the STOP-HF randomized trial. JAMA. 2013;310(1):66-74. doi:10.1001/jama.2013.7588
5. Huelsmann M, Neuhold S, Resl M, et al. PONTIAC (NT-proBNP selected prevention of cardiac events in a population of diabetic patients without a history of cardiac disease): a prospective randomized controlled trial. J Am Coll Cardiol. 2013;62(15):1365-1372. doi:10.1016/j.jacc.2013.05.069
6. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776-803. doi:10.1016/j.jacc.2017.04.025
7. Mueller C, McDonald K, de Boer RA, et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eu J Heart Fail. 2019;21:715-731. doi:10.1002/ejhf.1494
8. Ledwidge MT, O’Connell E, Gallagher J, et al; Heart Failure Association of the European Society of Cardiology. Cost-effectiveness of natriuretic peptide-based screening and collaborative care: a report from the STOP-HF (St. Vincent’s Screening to Prevent Heart Failure) study. Eur J Heart Fail. 2015;17(7):672-679.
New toolkit offers help for climate change anxiety
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.

“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.

As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”

Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.
“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.
As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”
Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.
“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.
As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”
Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.