User login
Is There a Relationship Between Facility Peer Review Findings and Quality in the Veterans Health Administration?
Hospital leaders report the most common aim of peer review (PR) is to improve quality and patient safety, thus it is a potentially powerful quality improvement (QI) driver.1 “When conducted systematically and credibly, peer review for quality management can result in both short-term and long-term improvements in patient care by revealing areas for improvement in the provision of care,” Veterans Health Administration (VHA) Directive 1190 states. “This ultimately contributes to organizational improvements.” At the same time, there are anecdotal concerns that PR may be used punitively and driven by case outcomes rather than by accepted best practices supporting QI.
Studies of the PR process suggest these concerns are valid. A key tenet of QI is standardization. PR is problematic in that regard; studies show poor interrater reliability for judgments on care, as well as hindsight bias—the fact that raters are strongly influenced by the outcome of care, not the process of care.2-5 There are concerns that case selection or review process when not standardized may be wielded as punitive too.6 In this study, we sought to identify the relationship between PR findings and subsequent institution quality metrics. If PR does lead to an improvement in quality, or if quality concerns are managed within the PR committee, it should be possible to identify a measurable relationship between the PR process and a facility’s subsequent quality measures.
A handful of studies describe the association between PR and quality of care. Itri and colleagues noted that random, not standardized PR in radiology does not achieve reductions in diagnostic error rate.7 However, adoption of just culture principles in PR resulted in a significant improvement in facility leaders’ self-reports of quality measures at surveyed institutions.8 The same author reported that increases in PR standardization and integration with performance improvement activities could explain up to 18% of objective quality measure variation.9
We sought to determine whether a specific aspect of the PR process, the PR committee judgment of quality of care by clinicians, was related to medical center quality in a cross-sectional study of 136 Veterans Health Administration (VHA) medical centers. The VHA is a good source of study because there are standardized PR processes and training for committee members and reviewers. Our hypothesis was that medical centers with a higher number of Level 2 (“most experienced and competent clinicians might have managed the case differently”) and Level 3 (“most experienced and competent providers would have managed the case differently”) PR findings would also have lower quality metric scores for processes and outcomes of care.
Methods
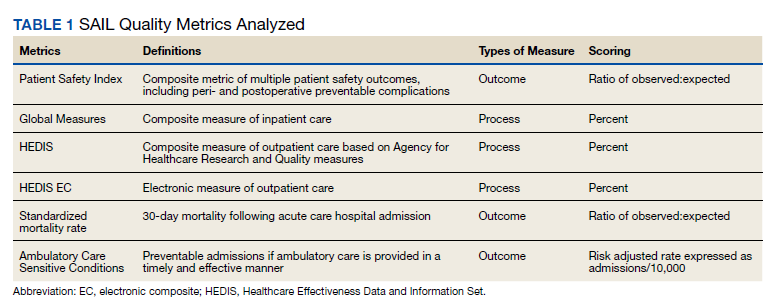
We used PR data from fiscal year 2018 and 2019. VHA PR data are available quarterly and are self-reported by each facility to the VHA Office of Clinical Risk Management. These data are broken down by facility. The following data, when available in both fiscal years 2018 and 2019, were used for this analysis: percent and number of PR that are ranked as level 1, 2, or 3; medical center group (MCG) acuity measure assigned by the VHA (1 is highest, 3 is lowest); and number of PR per 100,000 unique veteran encounters in 2019. Measures of facility quality are drawn from Strategic Analytics for Improvement and Learning (SAIL) data from 2019, which are available quarterly by facility and are rolling for 12 months. SAIL measures processes and outcomes of care. Table 1 indicates which measures are focused on outcomes vs quality processes.
SAS Version 9.2 was used to perform statistical analyses. We used Spearman correlation to estimate the PR and quality relationship.
Results
There were 136 facilities with 2 years of PR data available. The majority of these facilities (89) were highest complexity MCG 1 facilities; 19 were MCG 2, and 28 were MCG 3. Of 13,515 PRs, most of the 9555 PR findings were level 1 (70.7%). The between-facility range of level 2 and 3 findings was large, varying from 3.5% to nearly 70% in 2019 (Table 2). Findings were similar in 2018; facilities level 2 and 3 ratings ranged from 3.6% to 73.5% of all PR findings.
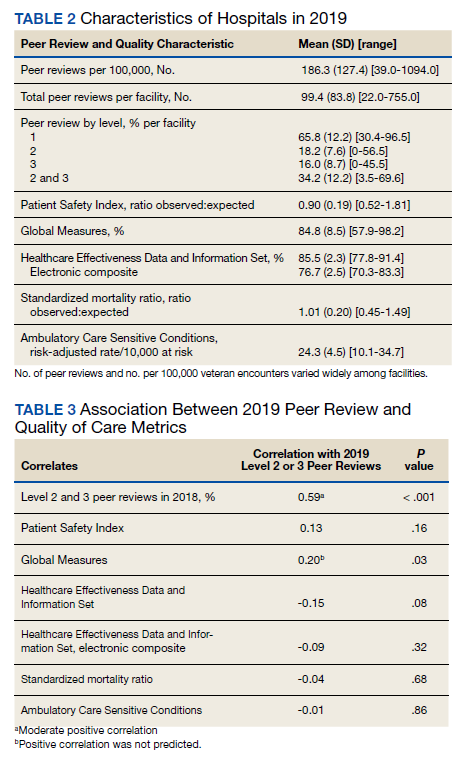
There was no correlation between most quality measures and facility PR findings (Table 3). The only exception was for Global Measures (GM90), an inpatient process of care measure. Unexpectedly, the correlation was positive—facilities with a higher percentage of level 2 and 3 PR findings had better inpatient processes of care SAIL score. The strongest correlation was between 2018 and 2019 PR findings.
Discussion
We hypothesized that a high percentage of level 2 and 3 PR findings would be negatively associated with objective facility measures of care processes in SAIL but we did not see this association. The only quality measure associated with PR findings was GM90, a score of inpatient care processes. However, the association was positive, with better performance associated with more level 2 and 3 PR findings.
The best predictor of the proportion of a facility’s PR findings is the previous year’s PR findings. With an R = 0.59, the previous year findings explain about 35% of the variability in level assignment. Our analysis may describe a new bias in PR, in which committees consistently assign either low or high proportions of level 2 and 3 findings. This correlation could be due to individual PR committee culture or composition, but it does not relate to objective quality measures.
Strengths
For this study we use objective measures of PR processes, the assignment of levels of care.
Limitations
Facilities self-report PR outcomes, so there could be errors in reporting. In addition, this study was cross sectional and not longitudinal and it is possible that change in quality measures over time are correlated with PR findings. Future studies using the VHA PR and SAIL data could evaluate whether changes over time, and perhaps in response to level 2 and 3 findings, would be a more sensitive indicator of the impact of the PR process on quality metrics. Future studies could incorporate the relationship between findings from the All Employee Survey, which is conducted annually, such as psychologic safety, as well as the distance the facility has gone on the high reliability organization journey, with PR findings and SAIL metrics. Finally, PR is focused on the practice of an individual clinician, while SAIL quality metrics reflect facility performance. Interventions possibly stay at the clinician level and do not drive subsequent QI processes.
What does this mean for PR? Since the early 1990s, there have been exhortations from experts to improve PR, by adopting a QI model, or for a deeper integration of PR and QI.1,2,10 Just culture tools, which include QI, are promoted as a means to improve PR.8,11,12 Other studies show PR remains problematic in terms of standardization, incorporation of best practices, redesigning systems of care, or demonstrable improvements to facility safety and care quality.1,4,6,8 Several publications have described interventions to improve PR. Deyo-Svedson discussed a program with standardized training and triggers, much like VHA.13 Itri and colleagues standardized PR in radiology to target areas of known diagnostic error, as well as use the issues assessed in PR to perform QI and education. One example of a successful QI effort involved changing the radiology reporting template to make sure areas that are prone to diagnostic error are addressed.7
Conclusions
Since 35% of PR level variance is correlated with prior year’s results, PR committees should look at increased standardization in reviews and findings. We endorse a strong focus on standardization, application of just culture tools to case reviews, and tighter linkage between process and outcome metrics measured by SAIL and PR case finding. Studies should be performed to pilot interventions to improve the linkage between PR and quality, so that greater and faster gains can be made in quality processes and, leading from this, outcomes. Additionally, future research should investigate why some facilities consistently choose higher or lower PR ratings.
Acknowledgments
We acknowledge Dr. George “Web” Ross for his helpful edits.
1. Edwards MT. In pursuit of quality and safety: an 8-year study of clinical peer review best practices in US hospitals. Int J Qual Health Care. 2018;30(8):602-607. doi:10.1093/intqhc/mzy069
2. Dans PE. Clinical peer Review: burnishing a tarnished icon. Ann Intern Med. 1993;118(7):566-568. doi:10.7326/0003-4819-118-7-199304010-00014
3. Goldman RL. The reliability of peer assessments of quality of care. JAMA. 1992;267(7):958-960. doi:10.1001/jama.1992.03480070074034
4. Swaroop R. Disrupting physician clinical practice peer review. Perm J. 2019;23:18-207. doi:10.7812/TPP/18-207
5. Caplan RA, Posner KL, Cheney FW. Effect of outcome on physician judgments of appropriateness of care. JAMA. 1991;265(15):1957–1960. doi:10.1001/jama.1991.03460150061024
6. Vyas D, Hozain AE. Clinical peer review in the United States: history, legal development and subsequent abuse. World J Gastroenterol. 2014;20(21):6357-6363. doi:10.3748/wjg.v20.i21.6357
7. Itri JN, Donithan A, Patel SH. Random versus nonrandom peer review: a case for more meaningful peer review. J Am Coll Radiol. 2018;15(7):1045-1052. doi:10.1016/j.jacr.2018.03.054
8. Edwards MT. An assessment of the impact of just culture on quality and safety in US hospitals. Am J Med Qual. 2018; 33(5):502-508. doi:10.1177/1062860618768057
9. Edwards MT. The objective impact of clinical peer review on hospital quality and safety. Am J Med Qual. 2011;26(2);110-119. doi:10.1177/1062860610380732
10. Berwick DM. Peer review and quality management: are they compatible?. QRB Qual Rev Bull. 1990;16(7):246-251. doi:10.1016/s0097-5990(16)30377-3
11. Volkar JK, Phrampus P, English D, et al. Institution of just culture physician peer review in an academic medical center. J Patient Saf. 2021;17(7):e689-e693. doi:10.1097/PTS.0000000000000449
12. Burns J, Miller T, Weiss JM, Erdfarb A, Silber D, Goldberg-Stein S. Just culture: practical implementation for radiologist peer review. J Am Coll Radiol. 2019;16(3):384-388. doi:10.1016/j.jacr.2018.10.021
13. Deyo-Svendsen ME, Phillips MR, Albright JK, et al. A systematic approach to clinical peer review in a critical access hospital. Qual Manag Health Care. 2016;25(4):213-218. doi:10.1097/QMH.0000000000000113
Hospital leaders report the most common aim of peer review (PR) is to improve quality and patient safety, thus it is a potentially powerful quality improvement (QI) driver.1 “When conducted systematically and credibly, peer review for quality management can result in both short-term and long-term improvements in patient care by revealing areas for improvement in the provision of care,” Veterans Health Administration (VHA) Directive 1190 states. “This ultimately contributes to organizational improvements.” At the same time, there are anecdotal concerns that PR may be used punitively and driven by case outcomes rather than by accepted best practices supporting QI.
Studies of the PR process suggest these concerns are valid. A key tenet of QI is standardization. PR is problematic in that regard; studies show poor interrater reliability for judgments on care, as well as hindsight bias—the fact that raters are strongly influenced by the outcome of care, not the process of care.2-5 There are concerns that case selection or review process when not standardized may be wielded as punitive too.6 In this study, we sought to identify the relationship between PR findings and subsequent institution quality metrics. If PR does lead to an improvement in quality, or if quality concerns are managed within the PR committee, it should be possible to identify a measurable relationship between the PR process and a facility’s subsequent quality measures.
A handful of studies describe the association between PR and quality of care. Itri and colleagues noted that random, not standardized PR in radiology does not achieve reductions in diagnostic error rate.7 However, adoption of just culture principles in PR resulted in a significant improvement in facility leaders’ self-reports of quality measures at surveyed institutions.8 The same author reported that increases in PR standardization and integration with performance improvement activities could explain up to 18% of objective quality measure variation.9
We sought to determine whether a specific aspect of the PR process, the PR committee judgment of quality of care by clinicians, was related to medical center quality in a cross-sectional study of 136 Veterans Health Administration (VHA) medical centers. The VHA is a good source of study because there are standardized PR processes and training for committee members and reviewers. Our hypothesis was that medical centers with a higher number of Level 2 (“most experienced and competent clinicians might have managed the case differently”) and Level 3 (“most experienced and competent providers would have managed the case differently”) PR findings would also have lower quality metric scores for processes and outcomes of care.
Methods
We used PR data from fiscal year 2018 and 2019. VHA PR data are available quarterly and are self-reported by each facility to the VHA Office of Clinical Risk Management. These data are broken down by facility. The following data, when available in both fiscal years 2018 and 2019, were used for this analysis: percent and number of PR that are ranked as level 1, 2, or 3; medical center group (MCG) acuity measure assigned by the VHA (1 is highest, 3 is lowest); and number of PR per 100,000 unique veteran encounters in 2019. Measures of facility quality are drawn from Strategic Analytics for Improvement and Learning (SAIL) data from 2019, which are available quarterly by facility and are rolling for 12 months. SAIL measures processes and outcomes of care. Table 1 indicates which measures are focused on outcomes vs quality processes.
SAS Version 9.2 was used to perform statistical analyses. We used Spearman correlation to estimate the PR and quality relationship.
Results
There were 136 facilities with 2 years of PR data available. The majority of these facilities (89) were highest complexity MCG 1 facilities; 19 were MCG 2, and 28 were MCG 3. Of 13,515 PRs, most of the 9555 PR findings were level 1 (70.7%). The between-facility range of level 2 and 3 findings was large, varying from 3.5% to nearly 70% in 2019 (Table 2). Findings were similar in 2018; facilities level 2 and 3 ratings ranged from 3.6% to 73.5% of all PR findings.
There was no correlation between most quality measures and facility PR findings (Table 3). The only exception was for Global Measures (GM90), an inpatient process of care measure. Unexpectedly, the correlation was positive—facilities with a higher percentage of level 2 and 3 PR findings had better inpatient processes of care SAIL score. The strongest correlation was between 2018 and 2019 PR findings.
Discussion
We hypothesized that a high percentage of level 2 and 3 PR findings would be negatively associated with objective facility measures of care processes in SAIL but we did not see this association. The only quality measure associated with PR findings was GM90, a score of inpatient care processes. However, the association was positive, with better performance associated with more level 2 and 3 PR findings.
The best predictor of the proportion of a facility’s PR findings is the previous year’s PR findings. With an R = 0.59, the previous year findings explain about 35% of the variability in level assignment. Our analysis may describe a new bias in PR, in which committees consistently assign either low or high proportions of level 2 and 3 findings. This correlation could be due to individual PR committee culture or composition, but it does not relate to objective quality measures.
Strengths
For this study we use objective measures of PR processes, the assignment of levels of care.
Limitations
Facilities self-report PR outcomes, so there could be errors in reporting. In addition, this study was cross sectional and not longitudinal and it is possible that change in quality measures over time are correlated with PR findings. Future studies using the VHA PR and SAIL data could evaluate whether changes over time, and perhaps in response to level 2 and 3 findings, would be a more sensitive indicator of the impact of the PR process on quality metrics. Future studies could incorporate the relationship between findings from the All Employee Survey, which is conducted annually, such as psychologic safety, as well as the distance the facility has gone on the high reliability organization journey, with PR findings and SAIL metrics. Finally, PR is focused on the practice of an individual clinician, while SAIL quality metrics reflect facility performance. Interventions possibly stay at the clinician level and do not drive subsequent QI processes.
What does this mean for PR? Since the early 1990s, there have been exhortations from experts to improve PR, by adopting a QI model, or for a deeper integration of PR and QI.1,2,10 Just culture tools, which include QI, are promoted as a means to improve PR.8,11,12 Other studies show PR remains problematic in terms of standardization, incorporation of best practices, redesigning systems of care, or demonstrable improvements to facility safety and care quality.1,4,6,8 Several publications have described interventions to improve PR. Deyo-Svedson discussed a program with standardized training and triggers, much like VHA.13 Itri and colleagues standardized PR in radiology to target areas of known diagnostic error, as well as use the issues assessed in PR to perform QI and education. One example of a successful QI effort involved changing the radiology reporting template to make sure areas that are prone to diagnostic error are addressed.7
Conclusions
Since 35% of PR level variance is correlated with prior year’s results, PR committees should look at increased standardization in reviews and findings. We endorse a strong focus on standardization, application of just culture tools to case reviews, and tighter linkage between process and outcome metrics measured by SAIL and PR case finding. Studies should be performed to pilot interventions to improve the linkage between PR and quality, so that greater and faster gains can be made in quality processes and, leading from this, outcomes. Additionally, future research should investigate why some facilities consistently choose higher or lower PR ratings.
Acknowledgments
We acknowledge Dr. George “Web” Ross for his helpful edits.
Hospital leaders report the most common aim of peer review (PR) is to improve quality and patient safety, thus it is a potentially powerful quality improvement (QI) driver.1 “When conducted systematically and credibly, peer review for quality management can result in both short-term and long-term improvements in patient care by revealing areas for improvement in the provision of care,” Veterans Health Administration (VHA) Directive 1190 states. “This ultimately contributes to organizational improvements.” At the same time, there are anecdotal concerns that PR may be used punitively and driven by case outcomes rather than by accepted best practices supporting QI.
Studies of the PR process suggest these concerns are valid. A key tenet of QI is standardization. PR is problematic in that regard; studies show poor interrater reliability for judgments on care, as well as hindsight bias—the fact that raters are strongly influenced by the outcome of care, not the process of care.2-5 There are concerns that case selection or review process when not standardized may be wielded as punitive too.6 In this study, we sought to identify the relationship between PR findings and subsequent institution quality metrics. If PR does lead to an improvement in quality, or if quality concerns are managed within the PR committee, it should be possible to identify a measurable relationship between the PR process and a facility’s subsequent quality measures.
A handful of studies describe the association between PR and quality of care. Itri and colleagues noted that random, not standardized PR in radiology does not achieve reductions in diagnostic error rate.7 However, adoption of just culture principles in PR resulted in a significant improvement in facility leaders’ self-reports of quality measures at surveyed institutions.8 The same author reported that increases in PR standardization and integration with performance improvement activities could explain up to 18% of objective quality measure variation.9
We sought to determine whether a specific aspect of the PR process, the PR committee judgment of quality of care by clinicians, was related to medical center quality in a cross-sectional study of 136 Veterans Health Administration (VHA) medical centers. The VHA is a good source of study because there are standardized PR processes and training for committee members and reviewers. Our hypothesis was that medical centers with a higher number of Level 2 (“most experienced and competent clinicians might have managed the case differently”) and Level 3 (“most experienced and competent providers would have managed the case differently”) PR findings would also have lower quality metric scores for processes and outcomes of care.
Methods
We used PR data from fiscal year 2018 and 2019. VHA PR data are available quarterly and are self-reported by each facility to the VHA Office of Clinical Risk Management. These data are broken down by facility. The following data, when available in both fiscal years 2018 and 2019, were used for this analysis: percent and number of PR that are ranked as level 1, 2, or 3; medical center group (MCG) acuity measure assigned by the VHA (1 is highest, 3 is lowest); and number of PR per 100,000 unique veteran encounters in 2019. Measures of facility quality are drawn from Strategic Analytics for Improvement and Learning (SAIL) data from 2019, which are available quarterly by facility and are rolling for 12 months. SAIL measures processes and outcomes of care. Table 1 indicates which measures are focused on outcomes vs quality processes.
SAS Version 9.2 was used to perform statistical analyses. We used Spearman correlation to estimate the PR and quality relationship.
Results
There were 136 facilities with 2 years of PR data available. The majority of these facilities (89) were highest complexity MCG 1 facilities; 19 were MCG 2, and 28 were MCG 3. Of 13,515 PRs, most of the 9555 PR findings were level 1 (70.7%). The between-facility range of level 2 and 3 findings was large, varying from 3.5% to nearly 70% in 2019 (Table 2). Findings were similar in 2018; facilities level 2 and 3 ratings ranged from 3.6% to 73.5% of all PR findings.
There was no correlation between most quality measures and facility PR findings (Table 3). The only exception was for Global Measures (GM90), an inpatient process of care measure. Unexpectedly, the correlation was positive—facilities with a higher percentage of level 2 and 3 PR findings had better inpatient processes of care SAIL score. The strongest correlation was between 2018 and 2019 PR findings.
Discussion
We hypothesized that a high percentage of level 2 and 3 PR findings would be negatively associated with objective facility measures of care processes in SAIL but we did not see this association. The only quality measure associated with PR findings was GM90, a score of inpatient care processes. However, the association was positive, with better performance associated with more level 2 and 3 PR findings.
The best predictor of the proportion of a facility’s PR findings is the previous year’s PR findings. With an R = 0.59, the previous year findings explain about 35% of the variability in level assignment. Our analysis may describe a new bias in PR, in which committees consistently assign either low or high proportions of level 2 and 3 findings. This correlation could be due to individual PR committee culture or composition, but it does not relate to objective quality measures.
Strengths
For this study we use objective measures of PR processes, the assignment of levels of care.
Limitations
Facilities self-report PR outcomes, so there could be errors in reporting. In addition, this study was cross sectional and not longitudinal and it is possible that change in quality measures over time are correlated with PR findings. Future studies using the VHA PR and SAIL data could evaluate whether changes over time, and perhaps in response to level 2 and 3 findings, would be a more sensitive indicator of the impact of the PR process on quality metrics. Future studies could incorporate the relationship between findings from the All Employee Survey, which is conducted annually, such as psychologic safety, as well as the distance the facility has gone on the high reliability organization journey, with PR findings and SAIL metrics. Finally, PR is focused on the practice of an individual clinician, while SAIL quality metrics reflect facility performance. Interventions possibly stay at the clinician level and do not drive subsequent QI processes.
What does this mean for PR? Since the early 1990s, there have been exhortations from experts to improve PR, by adopting a QI model, or for a deeper integration of PR and QI.1,2,10 Just culture tools, which include QI, are promoted as a means to improve PR.8,11,12 Other studies show PR remains problematic in terms of standardization, incorporation of best practices, redesigning systems of care, or demonstrable improvements to facility safety and care quality.1,4,6,8 Several publications have described interventions to improve PR. Deyo-Svedson discussed a program with standardized training and triggers, much like VHA.13 Itri and colleagues standardized PR in radiology to target areas of known diagnostic error, as well as use the issues assessed in PR to perform QI and education. One example of a successful QI effort involved changing the radiology reporting template to make sure areas that are prone to diagnostic error are addressed.7
Conclusions
Since 35% of PR level variance is correlated with prior year’s results, PR committees should look at increased standardization in reviews and findings. We endorse a strong focus on standardization, application of just culture tools to case reviews, and tighter linkage between process and outcome metrics measured by SAIL and PR case finding. Studies should be performed to pilot interventions to improve the linkage between PR and quality, so that greater and faster gains can be made in quality processes and, leading from this, outcomes. Additionally, future research should investigate why some facilities consistently choose higher or lower PR ratings.
Acknowledgments
We acknowledge Dr. George “Web” Ross for his helpful edits.
1. Edwards MT. In pursuit of quality and safety: an 8-year study of clinical peer review best practices in US hospitals. Int J Qual Health Care. 2018;30(8):602-607. doi:10.1093/intqhc/mzy069
2. Dans PE. Clinical peer Review: burnishing a tarnished icon. Ann Intern Med. 1993;118(7):566-568. doi:10.7326/0003-4819-118-7-199304010-00014
3. Goldman RL. The reliability of peer assessments of quality of care. JAMA. 1992;267(7):958-960. doi:10.1001/jama.1992.03480070074034
4. Swaroop R. Disrupting physician clinical practice peer review. Perm J. 2019;23:18-207. doi:10.7812/TPP/18-207
5. Caplan RA, Posner KL, Cheney FW. Effect of outcome on physician judgments of appropriateness of care. JAMA. 1991;265(15):1957–1960. doi:10.1001/jama.1991.03460150061024
6. Vyas D, Hozain AE. Clinical peer review in the United States: history, legal development and subsequent abuse. World J Gastroenterol. 2014;20(21):6357-6363. doi:10.3748/wjg.v20.i21.6357
7. Itri JN, Donithan A, Patel SH. Random versus nonrandom peer review: a case for more meaningful peer review. J Am Coll Radiol. 2018;15(7):1045-1052. doi:10.1016/j.jacr.2018.03.054
8. Edwards MT. An assessment of the impact of just culture on quality and safety in US hospitals. Am J Med Qual. 2018; 33(5):502-508. doi:10.1177/1062860618768057
9. Edwards MT. The objective impact of clinical peer review on hospital quality and safety. Am J Med Qual. 2011;26(2);110-119. doi:10.1177/1062860610380732
10. Berwick DM. Peer review and quality management: are they compatible?. QRB Qual Rev Bull. 1990;16(7):246-251. doi:10.1016/s0097-5990(16)30377-3
11. Volkar JK, Phrampus P, English D, et al. Institution of just culture physician peer review in an academic medical center. J Patient Saf. 2021;17(7):e689-e693. doi:10.1097/PTS.0000000000000449
12. Burns J, Miller T, Weiss JM, Erdfarb A, Silber D, Goldberg-Stein S. Just culture: practical implementation for radiologist peer review. J Am Coll Radiol. 2019;16(3):384-388. doi:10.1016/j.jacr.2018.10.021
13. Deyo-Svendsen ME, Phillips MR, Albright JK, et al. A systematic approach to clinical peer review in a critical access hospital. Qual Manag Health Care. 2016;25(4):213-218. doi:10.1097/QMH.0000000000000113
1. Edwards MT. In pursuit of quality and safety: an 8-year study of clinical peer review best practices in US hospitals. Int J Qual Health Care. 2018;30(8):602-607. doi:10.1093/intqhc/mzy069
2. Dans PE. Clinical peer Review: burnishing a tarnished icon. Ann Intern Med. 1993;118(7):566-568. doi:10.7326/0003-4819-118-7-199304010-00014
3. Goldman RL. The reliability of peer assessments of quality of care. JAMA. 1992;267(7):958-960. doi:10.1001/jama.1992.03480070074034
4. Swaroop R. Disrupting physician clinical practice peer review. Perm J. 2019;23:18-207. doi:10.7812/TPP/18-207
5. Caplan RA, Posner KL, Cheney FW. Effect of outcome on physician judgments of appropriateness of care. JAMA. 1991;265(15):1957–1960. doi:10.1001/jama.1991.03460150061024
6. Vyas D, Hozain AE. Clinical peer review in the United States: history, legal development and subsequent abuse. World J Gastroenterol. 2014;20(21):6357-6363. doi:10.3748/wjg.v20.i21.6357
7. Itri JN, Donithan A, Patel SH. Random versus nonrandom peer review: a case for more meaningful peer review. J Am Coll Radiol. 2018;15(7):1045-1052. doi:10.1016/j.jacr.2018.03.054
8. Edwards MT. An assessment of the impact of just culture on quality and safety in US hospitals. Am J Med Qual. 2018; 33(5):502-508. doi:10.1177/1062860618768057
9. Edwards MT. The objective impact of clinical peer review on hospital quality and safety. Am J Med Qual. 2011;26(2);110-119. doi:10.1177/1062860610380732
10. Berwick DM. Peer review and quality management: are they compatible?. QRB Qual Rev Bull. 1990;16(7):246-251. doi:10.1016/s0097-5990(16)30377-3
11. Volkar JK, Phrampus P, English D, et al. Institution of just culture physician peer review in an academic medical center. J Patient Saf. 2021;17(7):e689-e693. doi:10.1097/PTS.0000000000000449
12. Burns J, Miller T, Weiss JM, Erdfarb A, Silber D, Goldberg-Stein S. Just culture: practical implementation for radiologist peer review. J Am Coll Radiol. 2019;16(3):384-388. doi:10.1016/j.jacr.2018.10.021
13. Deyo-Svendsen ME, Phillips MR, Albright JK, et al. A systematic approach to clinical peer review in a critical access hospital. Qual Manag Health Care. 2016;25(4):213-218. doi:10.1097/QMH.0000000000000113
Green Alerts: Balancing Suicide Risk and Privacy
Contemporary critiques of Memorial and Veterans Day celebrations have emphasized that while ceremonies and celebrations are culturally requisite means of demonstrating a society’s respect and gratitude for those who gave their lives and health in the country’s cause—it is not enough. These holidays have immense symbolic significance to remind the nation of the sacrifice of those who bore arms in its service. An enduring and substantive impact on veterans will require real work done on their behalf. Through its representative institutions, such as the US Departments of Defense (DoD) and Veterans Affairs (VA) and citizens’ voluntary efforts, the public must provide practical assistance to veterans and their families.2
Memorial Day honors our sacred dead who lost their lives defending freedom. In federal practice and the larger community, we are duty-bound to try and restore the things war took from these wounded warriors and in whatever measure is possible to return them to the land of the fully living. Except in memory, we cannot bring back the dead. And while life is the most precious gift, those who survived the battlefield too often lose much that matters to a meaningful human life—friends, family, livelihood, housing, self-worth, peace of heart, soundness of mind, and health of the body.
One such recent initiative of reclamation is the Green Alert. Readers are likely familiar with Amber alerts for abducted children and Silver Alerts for older adults often with cognitive impairment who are lost. The Green Alert is a similar program deploying media and law enforcement to search for missing veterans believed to be vulnerable to harm because of a medical or psychiatric illness related to their service.
In 2017 Wisconsin became the first state to pass Green Alert legislation. The Missing Veterans at Risk Act lists 2 criteria that trigger a Green Alert: There is a reason to believe that the veteran at risk is missing due to a physical or mental health condition or that the veteran at risk is missing due to a physical or mental health condition. Relevant to the readers of Federal Practitioner, in Wisconsin, Green Alerts can be issued on behalf of missing veterans, and active-duty guard and reserve members and thus cover almost all the ranks of US military service.3 When law enforcement receives a report of a missing veteran as defined in the act within 72 hours of their disappearance, a Green Alert is issued. The statute directs the US Department of Justice to permit law enforcement to access the crime notification network to notify the media to broadcast pertinent information about the missing veteran.
As of this writing, Delaware, Kentucky, Connecticut, and Texas have passed similar laws, and legislatures in other states are considering bills, as is Congress.4 The sponsorship of the National Green Alert Act is bipartisan. Its stated purpose is: to develop interagency Green Alert systems that would be used when a veteran “goes missing” and “for other purposes.”5
The program’s potential to reduce the number of veterans who die by suicide every day has understandably attracted the attention of legislators and the public.6 The Cost of War project disclosed the terrible irony that at least 4 times as many post-9/11 service members died by suicide as perished in the combat that Memorial Day traditionally commemorates.7 As with many veteran-related laws, the initial Green Alert in Wisconsin was borne out of tragedy and passed through the heroic advocacy of bereaved and outraged family members.8 The DoD and VA, Congress, veterans service organizations, and the loved ones of servicemembers desperately want to turn this devastating tide of self-destruction through any means possible.
It seems almost a blasphemous betrayal of our public trust to raise ethical questions about Green Alerts. Yet that must happen if we ensure that these laws achieve their intended aims of preventing harm. For many veterans, these laws may indeed be lifesaving. However, a 2019 National Public Radio report suggested that these laws may, in some cases, result in several unintended harms.9 On first reading, it is worthy, even our duty, to extend the public health safety net for children who are victims of abduction and individuals with dementia to vulnerable veterans secondary to the mental and physical wounds of service.
When the service member is located, the alert is canceled. Nevertheless, their data remains in all the protean forms of media now available. In these searches for service members thought to be lost, there is a risk of violating their privacy if too much protected health information is made widely public. These breaches of confidentiality can further exacerbate the already too prevalent stigmatization of mental illness in the military, which has been a formidable obstacle to persuading those in uniform to seek treatment.10 As J.R.R. Tolkien has noted, not every person who “wanders” is lost.1 A veteran may leave his home for some period, even without notifying anyone, without being in grave and imminent danger. The diagnoses we health care professionals assign to patients are wide conceptual nets full of empirical holes: they are poorly predictive and protective mechanisms.11 A broadly written or vague law leaves latitude for bias, discrimination, liability, and fear to drive decisions that to be ethically justifiable require consistency, transparency, equity, and expertise. Much more research is needed to develop situational awareness, scientific accuracy, and clinical reliability to understand when, how, and for whom Green Alerts are genuinely beneficial.
These are not insurmountable questions. The experts and stakeholders appointed to the interagency committee the national Green Alert proposes will work to address these problems. Yet, unless they and we look bravely at the thorny issues these laudable laws present, it will be challenging to achieve their purpose to safeguard the dignity, safety, as well as autonomy and well-being of service members.
1. Tolkien JRR. The Fellowship of the Ring. Ballantine Books; 1974.
2. Constantine J. Here’s how to thank veterans for their service. Accessed April 25, 2022. https://www.military.com/veterans-day/heres-how-to-actually-thank-veterans-for-their-service.html
3. 2017 Wisconsin Act 275. Accessed April 25, 2022. https://docs.legis.wisconsin.gov/2017/related/acts/175
4. Thayer RL. Texas is the third state to approve an alert that helps locate missing vets and service members. Stars and Stripes. August 14, 2019. Accessed April 25, 2022. https://www.stripes.com/texas-is-third-state-to-approve-alert-that-helps-locate-missing-vets-servicemembers-1.594348
5. National Green Alert Act of 2021. HR 2797, 117th Cong (2021). Accessed April 25, 2022. https://www.govinfo.gov/app/details/BILLS-117hr2797ih
6. Suitt TH III. High suicide rates among United States service members and veterans of the post 9/11 wars. June 21, 2021. Accessed April 25, 2022. https://watson.brown.edu/costsofwar/files/cow/imce/papers/2021/Suitt_Suicides_Costs%20of%20War_June%2021%202021.pdf
7. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2021 annual report. September 2021. Accessed April 25, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2021/2021-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-9-8-21.pdf
8. Chamberlin K. Wisconsin becomes the first state with “green alerts” for vulnerable vets. Military Times. March 31, 2018. Accessed April 25, 2022. https://www.militarytimes.com/veterans/2018/03/31/wisconsin-becomes-first-state-with-green-alerts-for-vulnerable-vets/
9. Lawrence Q. Balancing safety and privacy when a veteran goes missing. All Things Considered. National Public Radio. April 9, 2019. Accessed April 25, 2022. https://www.npr.org/2019/04/09/711040850/balancing-safety-and-privacy-when-a-veteran-goes-missing
10. Kim PJ, Thomas JL, Wilk JE, Castro CA, Hoge CW. Stigma, barriers to care, and use of mental health services among active duty and national guard soldiers after combat. Psychiatric Services. 2010;61(6):582-588. doi:10.1176/ps.2010.61.6.582
11. Peterson K, Anderson J, Bourne D. Evidence Brief: Suicide Prevention in Veterans. Department of Veterans Affairs; 2018. Accessed April 25, 2022. https://www.ncbi.nlm.nih.gov/books/NBK535971/
Contemporary critiques of Memorial and Veterans Day celebrations have emphasized that while ceremonies and celebrations are culturally requisite means of demonstrating a society’s respect and gratitude for those who gave their lives and health in the country’s cause—it is not enough. These holidays have immense symbolic significance to remind the nation of the sacrifice of those who bore arms in its service. An enduring and substantive impact on veterans will require real work done on their behalf. Through its representative institutions, such as the US Departments of Defense (DoD) and Veterans Affairs (VA) and citizens’ voluntary efforts, the public must provide practical assistance to veterans and their families.2
Memorial Day honors our sacred dead who lost their lives defending freedom. In federal practice and the larger community, we are duty-bound to try and restore the things war took from these wounded warriors and in whatever measure is possible to return them to the land of the fully living. Except in memory, we cannot bring back the dead. And while life is the most precious gift, those who survived the battlefield too often lose much that matters to a meaningful human life—friends, family, livelihood, housing, self-worth, peace of heart, soundness of mind, and health of the body.
One such recent initiative of reclamation is the Green Alert. Readers are likely familiar with Amber alerts for abducted children and Silver Alerts for older adults often with cognitive impairment who are lost. The Green Alert is a similar program deploying media and law enforcement to search for missing veterans believed to be vulnerable to harm because of a medical or psychiatric illness related to their service.
In 2017 Wisconsin became the first state to pass Green Alert legislation. The Missing Veterans at Risk Act lists 2 criteria that trigger a Green Alert: There is a reason to believe that the veteran at risk is missing due to a physical or mental health condition or that the veteran at risk is missing due to a physical or mental health condition. Relevant to the readers of Federal Practitioner, in Wisconsin, Green Alerts can be issued on behalf of missing veterans, and active-duty guard and reserve members and thus cover almost all the ranks of US military service.3 When law enforcement receives a report of a missing veteran as defined in the act within 72 hours of their disappearance, a Green Alert is issued. The statute directs the US Department of Justice to permit law enforcement to access the crime notification network to notify the media to broadcast pertinent information about the missing veteran.
As of this writing, Delaware, Kentucky, Connecticut, and Texas have passed similar laws, and legislatures in other states are considering bills, as is Congress.4 The sponsorship of the National Green Alert Act is bipartisan. Its stated purpose is: to develop interagency Green Alert systems that would be used when a veteran “goes missing” and “for other purposes.”5
The program’s potential to reduce the number of veterans who die by suicide every day has understandably attracted the attention of legislators and the public.6 The Cost of War project disclosed the terrible irony that at least 4 times as many post-9/11 service members died by suicide as perished in the combat that Memorial Day traditionally commemorates.7 As with many veteran-related laws, the initial Green Alert in Wisconsin was borne out of tragedy and passed through the heroic advocacy of bereaved and outraged family members.8 The DoD and VA, Congress, veterans service organizations, and the loved ones of servicemembers desperately want to turn this devastating tide of self-destruction through any means possible.
It seems almost a blasphemous betrayal of our public trust to raise ethical questions about Green Alerts. Yet that must happen if we ensure that these laws achieve their intended aims of preventing harm. For many veterans, these laws may indeed be lifesaving. However, a 2019 National Public Radio report suggested that these laws may, in some cases, result in several unintended harms.9 On first reading, it is worthy, even our duty, to extend the public health safety net for children who are victims of abduction and individuals with dementia to vulnerable veterans secondary to the mental and physical wounds of service.
When the service member is located, the alert is canceled. Nevertheless, their data remains in all the protean forms of media now available. In these searches for service members thought to be lost, there is a risk of violating their privacy if too much protected health information is made widely public. These breaches of confidentiality can further exacerbate the already too prevalent stigmatization of mental illness in the military, which has been a formidable obstacle to persuading those in uniform to seek treatment.10 As J.R.R. Tolkien has noted, not every person who “wanders” is lost.1 A veteran may leave his home for some period, even without notifying anyone, without being in grave and imminent danger. The diagnoses we health care professionals assign to patients are wide conceptual nets full of empirical holes: they are poorly predictive and protective mechanisms.11 A broadly written or vague law leaves latitude for bias, discrimination, liability, and fear to drive decisions that to be ethically justifiable require consistency, transparency, equity, and expertise. Much more research is needed to develop situational awareness, scientific accuracy, and clinical reliability to understand when, how, and for whom Green Alerts are genuinely beneficial.
These are not insurmountable questions. The experts and stakeholders appointed to the interagency committee the national Green Alert proposes will work to address these problems. Yet, unless they and we look bravely at the thorny issues these laudable laws present, it will be challenging to achieve their purpose to safeguard the dignity, safety, as well as autonomy and well-being of service members.
Contemporary critiques of Memorial and Veterans Day celebrations have emphasized that while ceremonies and celebrations are culturally requisite means of demonstrating a society’s respect and gratitude for those who gave their lives and health in the country’s cause—it is not enough. These holidays have immense symbolic significance to remind the nation of the sacrifice of those who bore arms in its service. An enduring and substantive impact on veterans will require real work done on their behalf. Through its representative institutions, such as the US Departments of Defense (DoD) and Veterans Affairs (VA) and citizens’ voluntary efforts, the public must provide practical assistance to veterans and their families.2
Memorial Day honors our sacred dead who lost their lives defending freedom. In federal practice and the larger community, we are duty-bound to try and restore the things war took from these wounded warriors and in whatever measure is possible to return them to the land of the fully living. Except in memory, we cannot bring back the dead. And while life is the most precious gift, those who survived the battlefield too often lose much that matters to a meaningful human life—friends, family, livelihood, housing, self-worth, peace of heart, soundness of mind, and health of the body.
One such recent initiative of reclamation is the Green Alert. Readers are likely familiar with Amber alerts for abducted children and Silver Alerts for older adults often with cognitive impairment who are lost. The Green Alert is a similar program deploying media and law enforcement to search for missing veterans believed to be vulnerable to harm because of a medical or psychiatric illness related to their service.
In 2017 Wisconsin became the first state to pass Green Alert legislation. The Missing Veterans at Risk Act lists 2 criteria that trigger a Green Alert: There is a reason to believe that the veteran at risk is missing due to a physical or mental health condition or that the veteran at risk is missing due to a physical or mental health condition. Relevant to the readers of Federal Practitioner, in Wisconsin, Green Alerts can be issued on behalf of missing veterans, and active-duty guard and reserve members and thus cover almost all the ranks of US military service.3 When law enforcement receives a report of a missing veteran as defined in the act within 72 hours of their disappearance, a Green Alert is issued. The statute directs the US Department of Justice to permit law enforcement to access the crime notification network to notify the media to broadcast pertinent information about the missing veteran.
As of this writing, Delaware, Kentucky, Connecticut, and Texas have passed similar laws, and legislatures in other states are considering bills, as is Congress.4 The sponsorship of the National Green Alert Act is bipartisan. Its stated purpose is: to develop interagency Green Alert systems that would be used when a veteran “goes missing” and “for other purposes.”5
The program’s potential to reduce the number of veterans who die by suicide every day has understandably attracted the attention of legislators and the public.6 The Cost of War project disclosed the terrible irony that at least 4 times as many post-9/11 service members died by suicide as perished in the combat that Memorial Day traditionally commemorates.7 As with many veteran-related laws, the initial Green Alert in Wisconsin was borne out of tragedy and passed through the heroic advocacy of bereaved and outraged family members.8 The DoD and VA, Congress, veterans service organizations, and the loved ones of servicemembers desperately want to turn this devastating tide of self-destruction through any means possible.
It seems almost a blasphemous betrayal of our public trust to raise ethical questions about Green Alerts. Yet that must happen if we ensure that these laws achieve their intended aims of preventing harm. For many veterans, these laws may indeed be lifesaving. However, a 2019 National Public Radio report suggested that these laws may, in some cases, result in several unintended harms.9 On first reading, it is worthy, even our duty, to extend the public health safety net for children who are victims of abduction and individuals with dementia to vulnerable veterans secondary to the mental and physical wounds of service.
When the service member is located, the alert is canceled. Nevertheless, their data remains in all the protean forms of media now available. In these searches for service members thought to be lost, there is a risk of violating their privacy if too much protected health information is made widely public. These breaches of confidentiality can further exacerbate the already too prevalent stigmatization of mental illness in the military, which has been a formidable obstacle to persuading those in uniform to seek treatment.10 As J.R.R. Tolkien has noted, not every person who “wanders” is lost.1 A veteran may leave his home for some period, even without notifying anyone, without being in grave and imminent danger. The diagnoses we health care professionals assign to patients are wide conceptual nets full of empirical holes: they are poorly predictive and protective mechanisms.11 A broadly written or vague law leaves latitude for bias, discrimination, liability, and fear to drive decisions that to be ethically justifiable require consistency, transparency, equity, and expertise. Much more research is needed to develop situational awareness, scientific accuracy, and clinical reliability to understand when, how, and for whom Green Alerts are genuinely beneficial.
These are not insurmountable questions. The experts and stakeholders appointed to the interagency committee the national Green Alert proposes will work to address these problems. Yet, unless they and we look bravely at the thorny issues these laudable laws present, it will be challenging to achieve their purpose to safeguard the dignity, safety, as well as autonomy and well-being of service members.
1. Tolkien JRR. The Fellowship of the Ring. Ballantine Books; 1974.
2. Constantine J. Here’s how to thank veterans for their service. Accessed April 25, 2022. https://www.military.com/veterans-day/heres-how-to-actually-thank-veterans-for-their-service.html
3. 2017 Wisconsin Act 275. Accessed April 25, 2022. https://docs.legis.wisconsin.gov/2017/related/acts/175
4. Thayer RL. Texas is the third state to approve an alert that helps locate missing vets and service members. Stars and Stripes. August 14, 2019. Accessed April 25, 2022. https://www.stripes.com/texas-is-third-state-to-approve-alert-that-helps-locate-missing-vets-servicemembers-1.594348
5. National Green Alert Act of 2021. HR 2797, 117th Cong (2021). Accessed April 25, 2022. https://www.govinfo.gov/app/details/BILLS-117hr2797ih
6. Suitt TH III. High suicide rates among United States service members and veterans of the post 9/11 wars. June 21, 2021. Accessed April 25, 2022. https://watson.brown.edu/costsofwar/files/cow/imce/papers/2021/Suitt_Suicides_Costs%20of%20War_June%2021%202021.pdf
7. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2021 annual report. September 2021. Accessed April 25, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2021/2021-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-9-8-21.pdf
8. Chamberlin K. Wisconsin becomes the first state with “green alerts” for vulnerable vets. Military Times. March 31, 2018. Accessed April 25, 2022. https://www.militarytimes.com/veterans/2018/03/31/wisconsin-becomes-first-state-with-green-alerts-for-vulnerable-vets/
9. Lawrence Q. Balancing safety and privacy when a veteran goes missing. All Things Considered. National Public Radio. April 9, 2019. Accessed April 25, 2022. https://www.npr.org/2019/04/09/711040850/balancing-safety-and-privacy-when-a-veteran-goes-missing
10. Kim PJ, Thomas JL, Wilk JE, Castro CA, Hoge CW. Stigma, barriers to care, and use of mental health services among active duty and national guard soldiers after combat. Psychiatric Services. 2010;61(6):582-588. doi:10.1176/ps.2010.61.6.582
11. Peterson K, Anderson J, Bourne D. Evidence Brief: Suicide Prevention in Veterans. Department of Veterans Affairs; 2018. Accessed April 25, 2022. https://www.ncbi.nlm.nih.gov/books/NBK535971/
1. Tolkien JRR. The Fellowship of the Ring. Ballantine Books; 1974.
2. Constantine J. Here’s how to thank veterans for their service. Accessed April 25, 2022. https://www.military.com/veterans-day/heres-how-to-actually-thank-veterans-for-their-service.html
3. 2017 Wisconsin Act 275. Accessed April 25, 2022. https://docs.legis.wisconsin.gov/2017/related/acts/175
4. Thayer RL. Texas is the third state to approve an alert that helps locate missing vets and service members. Stars and Stripes. August 14, 2019. Accessed April 25, 2022. https://www.stripes.com/texas-is-third-state-to-approve-alert-that-helps-locate-missing-vets-servicemembers-1.594348
5. National Green Alert Act of 2021. HR 2797, 117th Cong (2021). Accessed April 25, 2022. https://www.govinfo.gov/app/details/BILLS-117hr2797ih
6. Suitt TH III. High suicide rates among United States service members and veterans of the post 9/11 wars. June 21, 2021. Accessed April 25, 2022. https://watson.brown.edu/costsofwar/files/cow/imce/papers/2021/Suitt_Suicides_Costs%20of%20War_June%2021%202021.pdf
7. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2021 annual report. September 2021. Accessed April 25, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2021/2021-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-9-8-21.pdf
8. Chamberlin K. Wisconsin becomes the first state with “green alerts” for vulnerable vets. Military Times. March 31, 2018. Accessed April 25, 2022. https://www.militarytimes.com/veterans/2018/03/31/wisconsin-becomes-first-state-with-green-alerts-for-vulnerable-vets/
9. Lawrence Q. Balancing safety and privacy when a veteran goes missing. All Things Considered. National Public Radio. April 9, 2019. Accessed April 25, 2022. https://www.npr.org/2019/04/09/711040850/balancing-safety-and-privacy-when-a-veteran-goes-missing
10. Kim PJ, Thomas JL, Wilk JE, Castro CA, Hoge CW. Stigma, barriers to care, and use of mental health services among active duty and national guard soldiers after combat. Psychiatric Services. 2010;61(6):582-588. doi:10.1176/ps.2010.61.6.582
11. Peterson K, Anderson J, Bourne D. Evidence Brief: Suicide Prevention in Veterans. Department of Veterans Affairs; 2018. Accessed April 25, 2022. https://www.ncbi.nlm.nih.gov/books/NBK535971/
Study casts doubt on safety, efficacy of L-serine supplementation for AD
When given to patients with AD, L-serine supplements could be driving abnormally increased serine levels in the brain even higher, potentially accelerating neuronal death, according to study author Xu Chen, PhD, of the University of California, San Diego, and colleagues.
This conclusion conflicts with a 2020 study by Juliette Le Douce, PhD, and colleagues, who reported that oral L-serine supplementation may act as a “ready-to-use therapy” for AD, based on their findings that patients with AD had low levels of PHGDH, an enzyme necessary for synthesizing serine, and AD-like mice had low levels of serine.

Writing in Cell Metabolism, Dr. Chen and colleagues framed the present study, and their findings, in this context.
“In contrast to the work of Le Douce et al., here we report that PHGDH mRNA and protein levels are increased in the brains of two mouse models of AD and/or tauopathy, and are also progressively increased in human brains with no, early, and late AD pathology, as well as in people with no, asymptomatic, and symptomatic AD,” they wrote.
They suggested adjusting clinical recommendations for L-serine, the form of the amino acid commonly found in supplements. In the body, L-serine is converted to D-serine, which acts on the NMDA receptor (NMDAR).
‘Long-term use of D-serine contributes to neuronal death’ suggests research
“We feel oral L-serine as a ready-to-use therapy to AD warrants precaution,” Dr. Chen and colleagues wrote. “This is because despite being a cognitive enhancer, some [research] suggests that long-term use of D-serine contributes to neuronal death in AD through excitotoxicity. Furthermore, D-serine, as a co-agonist of NMDAR, would be expected to oppose NMDAR antagonists, which have proven clinical benefits in treating AD.”
According to principal author Sheng Zhong, PhD, of the University of California, San Diego, “Research is needed to test if targeting PHGDH can ameliorate cognitive decline in AD.”
Dr. Zhong also noted that the present findings support the “promise of using a specific RNA in blood as a biomarker for early detection of Alzheimer’s disease.” This approach is currently being validated at UCSD Shiley-Marcos Alzheimer’s Disease Research Center, he added.
Roles of PHGDH and serine in Alzheimer’s disease require further study
Commenting on both studies, Steve W. Barger, PhD, of the University of Arkansas for Medical Sciences, Little Rock, suggested that more work is needed to better understand the roles of PHGDH and serine in AD before clinical applications can be considered.
“In the end, these two studies fail to provide the clarity we need in designing evidence-based therapeutic hypotheses,” Dr. Barger said in an interview. “We still do not have a firm grasp on the role that D-serine plays in AD. Indeed, the evidence regarding even a single enzyme contributing to its levels is ambiguous.”
Dr. Barger, who has published extensively on the topic of neuronal death, with a particular focus on Alzheimer’s disease, noted that “determination of what happens to D-serine levels in AD has been of interest for decades,” but levels of the amino acid have been notoriously challenging to measure because “D-serine can disappear rapidly from the brain and its fluids after death.”
While Dr. Le Douce and colleagues did measure levels of serine in mice, Dr. Barger noted that the study by Dr. Chen and colleagues was conducted with more “quantitatively rigorous methods.” Even though Dr. Chen and colleagues “did not assay the levels of D-serine itself ... the implication of their findings is that PHGDH is poised to elevate this critical neurotransmitter,” leading to their conclusion that serine supplementation is “potentially dangerous.”
At this point, it may be too early to tell, according to Dr. Barger.
He suggested that conclusions drawn from PHGDH levels alone are “always limited,” and conclusions based on serine levels may be equally dubious, considering that the activities and effects of serine “are quite complex,” and may be influenced by other physiologic processes, including the effects of gut bacteria.
Instead, Dr. Barger suggested that changes in PHGDH and serine may be interpreted as signals coming from a more relevant process upstream: glucose metabolism.
“What we can say confidently is that the glucose metabolism that PHGDH connects to D-serine is most definitely a factor in AD,” he said. “Countless studies have documented what now appears to be a universal decline in glucose delivery to the cerebral cortex, even before frank dementia sets in.”
Dr. Barger noted that declining glucose delivery coincides with some of the earliest events in the development of AD, perhaps “linking accumulation of amyloid β-peptide to subsequent neurofibrillary tangles and tissue atrophy.”
Dr. Barger’s own work recently demonstrated that AD is associated with “an irregularity in the insertion of a specific glucose transporter (GLUT1) into the cell surface” of astrocytes.
“It could be more effective to direct therapeutic interventions at these events lying upstream of PHGDH or serine,” he concluded.
The study was partly supported by a Kreuger v. Wyeth research award. The investigators and Dr. Barger reported no conflicts of interest.
When given to patients with AD, L-serine supplements could be driving abnormally increased serine levels in the brain even higher, potentially accelerating neuronal death, according to study author Xu Chen, PhD, of the University of California, San Diego, and colleagues.
This conclusion conflicts with a 2020 study by Juliette Le Douce, PhD, and colleagues, who reported that oral L-serine supplementation may act as a “ready-to-use therapy” for AD, based on their findings that patients with AD had low levels of PHGDH, an enzyme necessary for synthesizing serine, and AD-like mice had low levels of serine.
Writing in Cell Metabolism, Dr. Chen and colleagues framed the present study, and their findings, in this context.
“In contrast to the work of Le Douce et al., here we report that PHGDH mRNA and protein levels are increased in the brains of two mouse models of AD and/or tauopathy, and are also progressively increased in human brains with no, early, and late AD pathology, as well as in people with no, asymptomatic, and symptomatic AD,” they wrote.
They suggested adjusting clinical recommendations for L-serine, the form of the amino acid commonly found in supplements. In the body, L-serine is converted to D-serine, which acts on the NMDA receptor (NMDAR).
‘Long-term use of D-serine contributes to neuronal death’ suggests research
“We feel oral L-serine as a ready-to-use therapy to AD warrants precaution,” Dr. Chen and colleagues wrote. “This is because despite being a cognitive enhancer, some [research] suggests that long-term use of D-serine contributes to neuronal death in AD through excitotoxicity. Furthermore, D-serine, as a co-agonist of NMDAR, would be expected to oppose NMDAR antagonists, which have proven clinical benefits in treating AD.”
According to principal author Sheng Zhong, PhD, of the University of California, San Diego, “Research is needed to test if targeting PHGDH can ameliorate cognitive decline in AD.”
Dr. Zhong also noted that the present findings support the “promise of using a specific RNA in blood as a biomarker for early detection of Alzheimer’s disease.” This approach is currently being validated at UCSD Shiley-Marcos Alzheimer’s Disease Research Center, he added.
Roles of PHGDH and serine in Alzheimer’s disease require further study
Commenting on both studies, Steve W. Barger, PhD, of the University of Arkansas for Medical Sciences, Little Rock, suggested that more work is needed to better understand the roles of PHGDH and serine in AD before clinical applications can be considered.
“In the end, these two studies fail to provide the clarity we need in designing evidence-based therapeutic hypotheses,” Dr. Barger said in an interview. “We still do not have a firm grasp on the role that D-serine plays in AD. Indeed, the evidence regarding even a single enzyme contributing to its levels is ambiguous.”
Dr. Barger, who has published extensively on the topic of neuronal death, with a particular focus on Alzheimer’s disease, noted that “determination of what happens to D-serine levels in AD has been of interest for decades,” but levels of the amino acid have been notoriously challenging to measure because “D-serine can disappear rapidly from the brain and its fluids after death.”
While Dr. Le Douce and colleagues did measure levels of serine in mice, Dr. Barger noted that the study by Dr. Chen and colleagues was conducted with more “quantitatively rigorous methods.” Even though Dr. Chen and colleagues “did not assay the levels of D-serine itself ... the implication of their findings is that PHGDH is poised to elevate this critical neurotransmitter,” leading to their conclusion that serine supplementation is “potentially dangerous.”
At this point, it may be too early to tell, according to Dr. Barger.
He suggested that conclusions drawn from PHGDH levels alone are “always limited,” and conclusions based on serine levels may be equally dubious, considering that the activities and effects of serine “are quite complex,” and may be influenced by other physiologic processes, including the effects of gut bacteria.
Instead, Dr. Barger suggested that changes in PHGDH and serine may be interpreted as signals coming from a more relevant process upstream: glucose metabolism.
“What we can say confidently is that the glucose metabolism that PHGDH connects to D-serine is most definitely a factor in AD,” he said. “Countless studies have documented what now appears to be a universal decline in glucose delivery to the cerebral cortex, even before frank dementia sets in.”
Dr. Barger noted that declining glucose delivery coincides with some of the earliest events in the development of AD, perhaps “linking accumulation of amyloid β-peptide to subsequent neurofibrillary tangles and tissue atrophy.”
Dr. Barger’s own work recently demonstrated that AD is associated with “an irregularity in the insertion of a specific glucose transporter (GLUT1) into the cell surface” of astrocytes.
“It could be more effective to direct therapeutic interventions at these events lying upstream of PHGDH or serine,” he concluded.
The study was partly supported by a Kreuger v. Wyeth research award. The investigators and Dr. Barger reported no conflicts of interest.
When given to patients with AD, L-serine supplements could be driving abnormally increased serine levels in the brain even higher, potentially accelerating neuronal death, according to study author Xu Chen, PhD, of the University of California, San Diego, and colleagues.
This conclusion conflicts with a 2020 study by Juliette Le Douce, PhD, and colleagues, who reported that oral L-serine supplementation may act as a “ready-to-use therapy” for AD, based on their findings that patients with AD had low levels of PHGDH, an enzyme necessary for synthesizing serine, and AD-like mice had low levels of serine.
Writing in Cell Metabolism, Dr. Chen and colleagues framed the present study, and their findings, in this context.
“In contrast to the work of Le Douce et al., here we report that PHGDH mRNA and protein levels are increased in the brains of two mouse models of AD and/or tauopathy, and are also progressively increased in human brains with no, early, and late AD pathology, as well as in people with no, asymptomatic, and symptomatic AD,” they wrote.
They suggested adjusting clinical recommendations for L-serine, the form of the amino acid commonly found in supplements. In the body, L-serine is converted to D-serine, which acts on the NMDA receptor (NMDAR).
‘Long-term use of D-serine contributes to neuronal death’ suggests research
“We feel oral L-serine as a ready-to-use therapy to AD warrants precaution,” Dr. Chen and colleagues wrote. “This is because despite being a cognitive enhancer, some [research] suggests that long-term use of D-serine contributes to neuronal death in AD through excitotoxicity. Furthermore, D-serine, as a co-agonist of NMDAR, would be expected to oppose NMDAR antagonists, which have proven clinical benefits in treating AD.”
According to principal author Sheng Zhong, PhD, of the University of California, San Diego, “Research is needed to test if targeting PHGDH can ameliorate cognitive decline in AD.”
Dr. Zhong also noted that the present findings support the “promise of using a specific RNA in blood as a biomarker for early detection of Alzheimer’s disease.” This approach is currently being validated at UCSD Shiley-Marcos Alzheimer’s Disease Research Center, he added.
Roles of PHGDH and serine in Alzheimer’s disease require further study
Commenting on both studies, Steve W. Barger, PhD, of the University of Arkansas for Medical Sciences, Little Rock, suggested that more work is needed to better understand the roles of PHGDH and serine in AD before clinical applications can be considered.
“In the end, these two studies fail to provide the clarity we need in designing evidence-based therapeutic hypotheses,” Dr. Barger said in an interview. “We still do not have a firm grasp on the role that D-serine plays in AD. Indeed, the evidence regarding even a single enzyme contributing to its levels is ambiguous.”
Dr. Barger, who has published extensively on the topic of neuronal death, with a particular focus on Alzheimer’s disease, noted that “determination of what happens to D-serine levels in AD has been of interest for decades,” but levels of the amino acid have been notoriously challenging to measure because “D-serine can disappear rapidly from the brain and its fluids after death.”
While Dr. Le Douce and colleagues did measure levels of serine in mice, Dr. Barger noted that the study by Dr. Chen and colleagues was conducted with more “quantitatively rigorous methods.” Even though Dr. Chen and colleagues “did not assay the levels of D-serine itself ... the implication of their findings is that PHGDH is poised to elevate this critical neurotransmitter,” leading to their conclusion that serine supplementation is “potentially dangerous.”
At this point, it may be too early to tell, according to Dr. Barger.
He suggested that conclusions drawn from PHGDH levels alone are “always limited,” and conclusions based on serine levels may be equally dubious, considering that the activities and effects of serine “are quite complex,” and may be influenced by other physiologic processes, including the effects of gut bacteria.
Instead, Dr. Barger suggested that changes in PHGDH and serine may be interpreted as signals coming from a more relevant process upstream: glucose metabolism.
“What we can say confidently is that the glucose metabolism that PHGDH connects to D-serine is most definitely a factor in AD,” he said. “Countless studies have documented what now appears to be a universal decline in glucose delivery to the cerebral cortex, even before frank dementia sets in.”
Dr. Barger noted that declining glucose delivery coincides with some of the earliest events in the development of AD, perhaps “linking accumulation of amyloid β-peptide to subsequent neurofibrillary tangles and tissue atrophy.”
Dr. Barger’s own work recently demonstrated that AD is associated with “an irregularity in the insertion of a specific glucose transporter (GLUT1) into the cell surface” of astrocytes.
“It could be more effective to direct therapeutic interventions at these events lying upstream of PHGDH or serine,” he concluded.
The study was partly supported by a Kreuger v. Wyeth research award. The investigators and Dr. Barger reported no conflicts of interest.
FROM CELL METABOLISM
Prior authorizations delay TNF inhibitors for children with JIA
Children with juvenile idiopathic arthritis (JIA) who need a tumor necrosis factor (TNF) inhibitor after failing conventional disease-modifying antirheumatic drug (DMARD) treatment often experience insurance delays before beginning the new drug because of prior authorization denials, according to research presented at the 2022 annual meeting of the Childhood Arthritis and Rheumatology Research Alliance (CARRA). The findings were also published as a research letter in JAMA Network Open.
“Prompt escalation to TNF inhibitors is recommended for children with JIA refractory to DMARDs,” author Jordan Roberts, MD, a clinical fellow of the Harvard Medical School Rheumatology Program, Boston, told CARRA attendees. TNF inhibitors are increasingly used as first-line treatment in JIA since growing evidence suggests better outcomes from early treatment with biologics. “Prior authorization requirements that delay TNF inhibitor initiation among children with JIA are common in clinical practice,” Dr. Roberts said, but little evidence exists to understand the extent of this problem and its causes.
The researchers therefore conducted a retrospective cohort study using a search of electronic health records from January 2018 to December 2019 to find all children at a single center with a new diagnosis of nonsystemic JIA. Then the authors pulled the timing of prior authorization requests, approvals, denials, and first TNF inhibitor dose from the medical notes. They also sought out any children who had been recommended a TNF inhibitor but never started one.
The total population included 54 children with an average age of 10 years, about two-thirds of whom had private insurance (63%). The group was predominantly White (63%), although 13% declined to provide race, and 7% were Hispanic. Most subtypes of disease were represented: oligoarticular persistent (28%), oligoarticular extended (2%), polyarticular rheumatoid factor-negative (15%), polyarticular rheumatoid factor-positive (15%), psoriatic arthritis (26%), enthesitis-related arthritis (12%), and undifferentiated arthritis (2%).
The 44 participants with private insurance had an average of two joints with active disease, while the 10 patients with public insurance had an average of four involved joints. Nearly all the patients (91%) had previously taken or were currently taking DMARDs when the prior authorization was submitted, and 61% had received NSAIDs.
All but one of the patients’ insurance plans required a prior authorization. The first prior authorization was denied for about one-third of the public insurance patients (30%) and a quarter of the private insurance patients. About 1 in 5 patients overall (22%) required a written appeal to override the denial, and 4% required peer-to-peer review. Meanwhile, 7% of patients began another medication because of the denial.
It took a median of 3 days for prior authorizations to be approved and a median of 24 days from the time the TNF inhibitor was recommended to the patient receiving the first dose. However, 22% of patients waited at least 2 weeks before the prior authorization was approved, and more than a quarter of the requests took over 30 days before the patient could begin the medication. In the public insurance group in particular, a quarter of children waited at least 19 days for approval and at least 44 days before starting the medication.
In fact, when the researchers looked at the difference in approval time between those who did and did not receive an initial denial, the difference was stark. Median approval time was 16 days when the prior authorization was denied, compared with a median of 5 days when the first prior authorization was approved. Similarly, time to initiation of the drug after recommendation was a median of 35 days for those whose prior authorization was first denied and 17 days for those with an initial approval.
The most common reason for an initial denial was the insurance company requiring a different TNF inhibitor than the one the rheumatologist wanted to prescribe. “These were all children whose rheumatologist has recommended either infliximab or etanercept that were required to use adalimumab instead,” Dr. Roberts said.
The other reasons for initial denial were similarly familiar ones:
- Required submission to another insurer
- Additional documentation required
- Lack of medical necessity
- Prescription was for an indication not approved by the Food and Drug Administration
- Age of patient
- Nonbiologic DMARD required
- NSAID required for step therapy
Only three children who were advised to begin a TNF inhibitor did not do so, including one who was lost to follow-up, one who had injection-related anxiety, and one who had safety concerns about the medication.
“Several children were required to use alternative TNF inhibitors than the one that was recommended due to restricted formularies, which may reduce shared decisionmaking between physicians and families and may not be the optimal clinical choice for an individual child,” Dr. Roberts said in her conclusion. Most children, however, were able to get approval for the TNF inhibitor originally requested, “suggesting that utilization management strategies present barriers to timely care despite appropriate specialty medication requests,” she said. “Therefore, it’s important for us to advocate for access to medications for children with JIA.”
Findings are not surprising
“I have these same experiences at my institution – often insurance will dictate clinical practice, and step therapy is the only option, causing a delay to initiation of TNFi even if we think, as the pediatric rheumatologist, that a child needs this medicine to be initiated on presentation to our clinic,” Nayimisha Balmuri, MD, assistant professor of pediatrics in the division of allergy, immunology, and rheumatology at the Johns Hopkins School of Medicine, Baltimore, told this news organization.
Dr. Balmuri, who was not involved in the study, noted that in her clinic at Johns Hopkins, it is hit or miss if an appeal to insurance companies or to the state (if it is Medicaid coverage) will be successful. “Unfortunately, [we are] mostly unsuccessful, and we have to try another DMARD for 8 to 12 weeks first before trying to get TNFi,” she said.
Dr. Balmuri called for bringing these issues to the attention of state and federal legislators. “It’s so important for us to continue to advocate for our patients at the state and national level! We are the advocates for our patients, and we are uniquely trained to know the best medications to initiate to help patients maximize their chance to reach remission of arthritis. Insurance companies need to hear our voices!”
Dr. Roberts reported grants from CARRA, the Lupus Foundation of America, and the National Institute of Allergy and Infectious Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children with juvenile idiopathic arthritis (JIA) who need a tumor necrosis factor (TNF) inhibitor after failing conventional disease-modifying antirheumatic drug (DMARD) treatment often experience insurance delays before beginning the new drug because of prior authorization denials, according to research presented at the 2022 annual meeting of the Childhood Arthritis and Rheumatology Research Alliance (CARRA). The findings were also published as a research letter in JAMA Network Open.
“Prompt escalation to TNF inhibitors is recommended for children with JIA refractory to DMARDs,” author Jordan Roberts, MD, a clinical fellow of the Harvard Medical School Rheumatology Program, Boston, told CARRA attendees. TNF inhibitors are increasingly used as first-line treatment in JIA since growing evidence suggests better outcomes from early treatment with biologics. “Prior authorization requirements that delay TNF inhibitor initiation among children with JIA are common in clinical practice,” Dr. Roberts said, but little evidence exists to understand the extent of this problem and its causes.
The researchers therefore conducted a retrospective cohort study using a search of electronic health records from January 2018 to December 2019 to find all children at a single center with a new diagnosis of nonsystemic JIA. Then the authors pulled the timing of prior authorization requests, approvals, denials, and first TNF inhibitor dose from the medical notes. They also sought out any children who had been recommended a TNF inhibitor but never started one.
The total population included 54 children with an average age of 10 years, about two-thirds of whom had private insurance (63%). The group was predominantly White (63%), although 13% declined to provide race, and 7% were Hispanic. Most subtypes of disease were represented: oligoarticular persistent (28%), oligoarticular extended (2%), polyarticular rheumatoid factor-negative (15%), polyarticular rheumatoid factor-positive (15%), psoriatic arthritis (26%), enthesitis-related arthritis (12%), and undifferentiated arthritis (2%).
The 44 participants with private insurance had an average of two joints with active disease, while the 10 patients with public insurance had an average of four involved joints. Nearly all the patients (91%) had previously taken or were currently taking DMARDs when the prior authorization was submitted, and 61% had received NSAIDs.
All but one of the patients’ insurance plans required a prior authorization. The first prior authorization was denied for about one-third of the public insurance patients (30%) and a quarter of the private insurance patients. About 1 in 5 patients overall (22%) required a written appeal to override the denial, and 4% required peer-to-peer review. Meanwhile, 7% of patients began another medication because of the denial.
It took a median of 3 days for prior authorizations to be approved and a median of 24 days from the time the TNF inhibitor was recommended to the patient receiving the first dose. However, 22% of patients waited at least 2 weeks before the prior authorization was approved, and more than a quarter of the requests took over 30 days before the patient could begin the medication. In the public insurance group in particular, a quarter of children waited at least 19 days for approval and at least 44 days before starting the medication.
In fact, when the researchers looked at the difference in approval time between those who did and did not receive an initial denial, the difference was stark. Median approval time was 16 days when the prior authorization was denied, compared with a median of 5 days when the first prior authorization was approved. Similarly, time to initiation of the drug after recommendation was a median of 35 days for those whose prior authorization was first denied and 17 days for those with an initial approval.
The most common reason for an initial denial was the insurance company requiring a different TNF inhibitor than the one the rheumatologist wanted to prescribe. “These were all children whose rheumatologist has recommended either infliximab or etanercept that were required to use adalimumab instead,” Dr. Roberts said.
The other reasons for initial denial were similarly familiar ones:
- Required submission to another insurer
- Additional documentation required
- Lack of medical necessity
- Prescription was for an indication not approved by the Food and Drug Administration
- Age of patient
- Nonbiologic DMARD required
- NSAID required for step therapy
Only three children who were advised to begin a TNF inhibitor did not do so, including one who was lost to follow-up, one who had injection-related anxiety, and one who had safety concerns about the medication.
“Several children were required to use alternative TNF inhibitors than the one that was recommended due to restricted formularies, which may reduce shared decisionmaking between physicians and families and may not be the optimal clinical choice for an individual child,” Dr. Roberts said in her conclusion. Most children, however, were able to get approval for the TNF inhibitor originally requested, “suggesting that utilization management strategies present barriers to timely care despite appropriate specialty medication requests,” she said. “Therefore, it’s important for us to advocate for access to medications for children with JIA.”
Findings are not surprising
“I have these same experiences at my institution – often insurance will dictate clinical practice, and step therapy is the only option, causing a delay to initiation of TNFi even if we think, as the pediatric rheumatologist, that a child needs this medicine to be initiated on presentation to our clinic,” Nayimisha Balmuri, MD, assistant professor of pediatrics in the division of allergy, immunology, and rheumatology at the Johns Hopkins School of Medicine, Baltimore, told this news organization.
Dr. Balmuri, who was not involved in the study, noted that in her clinic at Johns Hopkins, it is hit or miss if an appeal to insurance companies or to the state (if it is Medicaid coverage) will be successful. “Unfortunately, [we are] mostly unsuccessful, and we have to try another DMARD for 8 to 12 weeks first before trying to get TNFi,” she said.
Dr. Balmuri called for bringing these issues to the attention of state and federal legislators. “It’s so important for us to continue to advocate for our patients at the state and national level! We are the advocates for our patients, and we are uniquely trained to know the best medications to initiate to help patients maximize their chance to reach remission of arthritis. Insurance companies need to hear our voices!”
Dr. Roberts reported grants from CARRA, the Lupus Foundation of America, and the National Institute of Allergy and Infectious Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children with juvenile idiopathic arthritis (JIA) who need a tumor necrosis factor (TNF) inhibitor after failing conventional disease-modifying antirheumatic drug (DMARD) treatment often experience insurance delays before beginning the new drug because of prior authorization denials, according to research presented at the 2022 annual meeting of the Childhood Arthritis and Rheumatology Research Alliance (CARRA). The findings were also published as a research letter in JAMA Network Open.
“Prompt escalation to TNF inhibitors is recommended for children with JIA refractory to DMARDs,” author Jordan Roberts, MD, a clinical fellow of the Harvard Medical School Rheumatology Program, Boston, told CARRA attendees. TNF inhibitors are increasingly used as first-line treatment in JIA since growing evidence suggests better outcomes from early treatment with biologics. “Prior authorization requirements that delay TNF inhibitor initiation among children with JIA are common in clinical practice,” Dr. Roberts said, but little evidence exists to understand the extent of this problem and its causes.
The researchers therefore conducted a retrospective cohort study using a search of electronic health records from January 2018 to December 2019 to find all children at a single center with a new diagnosis of nonsystemic JIA. Then the authors pulled the timing of prior authorization requests, approvals, denials, and first TNF inhibitor dose from the medical notes. They also sought out any children who had been recommended a TNF inhibitor but never started one.
The total population included 54 children with an average age of 10 years, about two-thirds of whom had private insurance (63%). The group was predominantly White (63%), although 13% declined to provide race, and 7% were Hispanic. Most subtypes of disease were represented: oligoarticular persistent (28%), oligoarticular extended (2%), polyarticular rheumatoid factor-negative (15%), polyarticular rheumatoid factor-positive (15%), psoriatic arthritis (26%), enthesitis-related arthritis (12%), and undifferentiated arthritis (2%).
The 44 participants with private insurance had an average of two joints with active disease, while the 10 patients with public insurance had an average of four involved joints. Nearly all the patients (91%) had previously taken or were currently taking DMARDs when the prior authorization was submitted, and 61% had received NSAIDs.
All but one of the patients’ insurance plans required a prior authorization. The first prior authorization was denied for about one-third of the public insurance patients (30%) and a quarter of the private insurance patients. About 1 in 5 patients overall (22%) required a written appeal to override the denial, and 4% required peer-to-peer review. Meanwhile, 7% of patients began another medication because of the denial.
It took a median of 3 days for prior authorizations to be approved and a median of 24 days from the time the TNF inhibitor was recommended to the patient receiving the first dose. However, 22% of patients waited at least 2 weeks before the prior authorization was approved, and more than a quarter of the requests took over 30 days before the patient could begin the medication. In the public insurance group in particular, a quarter of children waited at least 19 days for approval and at least 44 days before starting the medication.
In fact, when the researchers looked at the difference in approval time between those who did and did not receive an initial denial, the difference was stark. Median approval time was 16 days when the prior authorization was denied, compared with a median of 5 days when the first prior authorization was approved. Similarly, time to initiation of the drug after recommendation was a median of 35 days for those whose prior authorization was first denied and 17 days for those with an initial approval.
The most common reason for an initial denial was the insurance company requiring a different TNF inhibitor than the one the rheumatologist wanted to prescribe. “These were all children whose rheumatologist has recommended either infliximab or etanercept that were required to use adalimumab instead,” Dr. Roberts said.
The other reasons for initial denial were similarly familiar ones:
- Required submission to another insurer
- Additional documentation required
- Lack of medical necessity
- Prescription was for an indication not approved by the Food and Drug Administration
- Age of patient
- Nonbiologic DMARD required
- NSAID required for step therapy
Only three children who were advised to begin a TNF inhibitor did not do so, including one who was lost to follow-up, one who had injection-related anxiety, and one who had safety concerns about the medication.
“Several children were required to use alternative TNF inhibitors than the one that was recommended due to restricted formularies, which may reduce shared decisionmaking between physicians and families and may not be the optimal clinical choice for an individual child,” Dr. Roberts said in her conclusion. Most children, however, were able to get approval for the TNF inhibitor originally requested, “suggesting that utilization management strategies present barriers to timely care despite appropriate specialty medication requests,” she said. “Therefore, it’s important for us to advocate for access to medications for children with JIA.”
Findings are not surprising
“I have these same experiences at my institution – often insurance will dictate clinical practice, and step therapy is the only option, causing a delay to initiation of TNFi even if we think, as the pediatric rheumatologist, that a child needs this medicine to be initiated on presentation to our clinic,” Nayimisha Balmuri, MD, assistant professor of pediatrics in the division of allergy, immunology, and rheumatology at the Johns Hopkins School of Medicine, Baltimore, told this news organization.
Dr. Balmuri, who was not involved in the study, noted that in her clinic at Johns Hopkins, it is hit or miss if an appeal to insurance companies or to the state (if it is Medicaid coverage) will be successful. “Unfortunately, [we are] mostly unsuccessful, and we have to try another DMARD for 8 to 12 weeks first before trying to get TNFi,” she said.
Dr. Balmuri called for bringing these issues to the attention of state and federal legislators. “It’s so important for us to continue to advocate for our patients at the state and national level! We are the advocates for our patients, and we are uniquely trained to know the best medications to initiate to help patients maximize their chance to reach remission of arthritis. Insurance companies need to hear our voices!”
Dr. Roberts reported grants from CARRA, the Lupus Foundation of America, and the National Institute of Allergy and Infectious Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Headache in pregnancy: New ACOG guidelines offer insight
SAN DIEGO – If a medical professional is trying to figure out the best medical treatment for a pregnant woman with headache, it may be helpful to review data from randomized clinical trials (RCTs). Well, make that data from the RCT. There’s just been one, Northwestern Medicine obstetrician-gynecologist Catherine Stika, MD, told colleagues at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Only a single efficacy RCT has examined headache in pregnancy, said Dr. Stika. “Overall, we have very limited data in pregnancy to tell us exactly what to do,” she added.
But ob.gyns. aren’t entirely in the dark, according to medical specialists who spoke at the session. Expert opinion and fetal safety data offer insight into the best treatments, as does a new ACOG clinical practice guideline on headaches during pregnancy and post partum that was coauthored by the speakers.
And there’s some good news: Pregnancy itself is often a good treatment for headaches.
Pregnant women often find relief from one kind of headache – migraine – as their estradiol levels rise, said Laura Mercer, MD, an ob.gyn. at the University of Arizona, Phoenix. “About half of patients will report that migraines are getting better as early as the first trimester, and upwards of 83% will say that their migraines are better by the time they’re in their third trimester,” she said. “What this means for us as obstetricians is that oftentimes we can actually discontinue preventative therapies for patients during pregnancy.”
But simply discontinuing every headache treatment during pregnancy may not be the right approach, Dr. Mercer said. Instead, she said, consider the benefits and risks.
Divalproex sodium (Depakote) and topiramate (Topamax) must be avoided because of fetal risk, she said. “In fact, we will prefer that people stop these medications before they discontinue their contraception if they’re planning on getting pregnant,” she said.
Other medications, such as ACE inhibitors and the herbal remedy feverfew, should not be used at any time during pregnancy, she said.
On the other hand, calcium channel blockers and antihistamines are alright to use in pregnancy, she said. “These two should be considered first-line because there’s no known risks for them.”
Beta-blockers also may be used “with some consideration to the known risks that we’re familiar with when we use them for other indications,” she said.
There are questions about the safety of oral magnesium in pregnancy, although it’s generally considered safe, she added, and “nerve blocks and nerve stimulators seem very promising and have little known risks.”
Dr. Mercer recommended gradually tapering most medications prior to conception. But it’s crucial to stop higher-risk drugs immediately once pregnancy is confirmed, she said.
In regard to acute headache, Dr. Stika urged caution if a patient reports taking a headache medication more than twice a week. “All the medications we use for the treatment of migraine, both in and outside of pregnancy, carry the risk of what’s called medication overuse” that can lead to rebound headaches, she said.
Excedrin Tension Headache may be used for headaches in pregnancy, she said, but not Excedrin Migraine since it includes aspirin. Triptans are not recommended as first-line therapy, she added, and they “should absolutely not be used in any pregnant patient with a history of known cardiac disease or hypertension.”
Dr. Stika added that ACOG advises against the use of drugs that contain butalbital, a barbiturate that’s combined with other agents to treat headache. “Butalbital is the drug that’s most closely associated with getting people into this medication overuse headache,” she said. “It’s even worse than opioids.”
Unlike multiple other countries and the entire European Union, the United States has not banned compounds that contain butalbital, she said.
In some cases, she said, patients may present to triage with vomiting, an inability to keep food down, and persistent headache despite treatment. “This is a really classic presentation.”
The ACOG clinical practice guideline offers a flow chart about what to do, she said. Hydration is key, she said, and various treatment options can help. A referral to neurology may be needed in extreme cases, she said. But “most of the time, you’re able to get rid of her headache.”
Dr. Mercer and Dr. Stika report no disclosures.
SAN DIEGO – If a medical professional is trying to figure out the best medical treatment for a pregnant woman with headache, it may be helpful to review data from randomized clinical trials (RCTs). Well, make that data from the RCT. There’s just been one, Northwestern Medicine obstetrician-gynecologist Catherine Stika, MD, told colleagues at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Only a single efficacy RCT has examined headache in pregnancy, said Dr. Stika. “Overall, we have very limited data in pregnancy to tell us exactly what to do,” she added.
But ob.gyns. aren’t entirely in the dark, according to medical specialists who spoke at the session. Expert opinion and fetal safety data offer insight into the best treatments, as does a new ACOG clinical practice guideline on headaches during pregnancy and post partum that was coauthored by the speakers.
And there’s some good news: Pregnancy itself is often a good treatment for headaches.
Pregnant women often find relief from one kind of headache – migraine – as their estradiol levels rise, said Laura Mercer, MD, an ob.gyn. at the University of Arizona, Phoenix. “About half of patients will report that migraines are getting better as early as the first trimester, and upwards of 83% will say that their migraines are better by the time they’re in their third trimester,” she said. “What this means for us as obstetricians is that oftentimes we can actually discontinue preventative therapies for patients during pregnancy.”
But simply discontinuing every headache treatment during pregnancy may not be the right approach, Dr. Mercer said. Instead, she said, consider the benefits and risks.
Divalproex sodium (Depakote) and topiramate (Topamax) must be avoided because of fetal risk, she said. “In fact, we will prefer that people stop these medications before they discontinue their contraception if they’re planning on getting pregnant,” she said.
Other medications, such as ACE inhibitors and the herbal remedy feverfew, should not be used at any time during pregnancy, she said.
On the other hand, calcium channel blockers and antihistamines are alright to use in pregnancy, she said. “These two should be considered first-line because there’s no known risks for them.”
Beta-blockers also may be used “with some consideration to the known risks that we’re familiar with when we use them for other indications,” she said.
There are questions about the safety of oral magnesium in pregnancy, although it’s generally considered safe, she added, and “nerve blocks and nerve stimulators seem very promising and have little known risks.”
Dr. Mercer recommended gradually tapering most medications prior to conception. But it’s crucial to stop higher-risk drugs immediately once pregnancy is confirmed, she said.
In regard to acute headache, Dr. Stika urged caution if a patient reports taking a headache medication more than twice a week. “All the medications we use for the treatment of migraine, both in and outside of pregnancy, carry the risk of what’s called medication overuse” that can lead to rebound headaches, she said.
Excedrin Tension Headache may be used for headaches in pregnancy, she said, but not Excedrin Migraine since it includes aspirin. Triptans are not recommended as first-line therapy, she added, and they “should absolutely not be used in any pregnant patient with a history of known cardiac disease or hypertension.”
Dr. Stika added that ACOG advises against the use of drugs that contain butalbital, a barbiturate that’s combined with other agents to treat headache. “Butalbital is the drug that’s most closely associated with getting people into this medication overuse headache,” she said. “It’s even worse than opioids.”
Unlike multiple other countries and the entire European Union, the United States has not banned compounds that contain butalbital, she said.
In some cases, she said, patients may present to triage with vomiting, an inability to keep food down, and persistent headache despite treatment. “This is a really classic presentation.”
The ACOG clinical practice guideline offers a flow chart about what to do, she said. Hydration is key, she said, and various treatment options can help. A referral to neurology may be needed in extreme cases, she said. But “most of the time, you’re able to get rid of her headache.”
Dr. Mercer and Dr. Stika report no disclosures.
SAN DIEGO – If a medical professional is trying to figure out the best medical treatment for a pregnant woman with headache, it may be helpful to review data from randomized clinical trials (RCTs). Well, make that data from the RCT. There’s just been one, Northwestern Medicine obstetrician-gynecologist Catherine Stika, MD, told colleagues at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Only a single efficacy RCT has examined headache in pregnancy, said Dr. Stika. “Overall, we have very limited data in pregnancy to tell us exactly what to do,” she added.
But ob.gyns. aren’t entirely in the dark, according to medical specialists who spoke at the session. Expert opinion and fetal safety data offer insight into the best treatments, as does a new ACOG clinical practice guideline on headaches during pregnancy and post partum that was coauthored by the speakers.
And there’s some good news: Pregnancy itself is often a good treatment for headaches.
Pregnant women often find relief from one kind of headache – migraine – as their estradiol levels rise, said Laura Mercer, MD, an ob.gyn. at the University of Arizona, Phoenix. “About half of patients will report that migraines are getting better as early as the first trimester, and upwards of 83% will say that their migraines are better by the time they’re in their third trimester,” she said. “What this means for us as obstetricians is that oftentimes we can actually discontinue preventative therapies for patients during pregnancy.”
But simply discontinuing every headache treatment during pregnancy may not be the right approach, Dr. Mercer said. Instead, she said, consider the benefits and risks.
Divalproex sodium (Depakote) and topiramate (Topamax) must be avoided because of fetal risk, she said. “In fact, we will prefer that people stop these medications before they discontinue their contraception if they’re planning on getting pregnant,” she said.
Other medications, such as ACE inhibitors and the herbal remedy feverfew, should not be used at any time during pregnancy, she said.
On the other hand, calcium channel blockers and antihistamines are alright to use in pregnancy, she said. “These two should be considered first-line because there’s no known risks for them.”
Beta-blockers also may be used “with some consideration to the known risks that we’re familiar with when we use them for other indications,” she said.
There are questions about the safety of oral magnesium in pregnancy, although it’s generally considered safe, she added, and “nerve blocks and nerve stimulators seem very promising and have little known risks.”
Dr. Mercer recommended gradually tapering most medications prior to conception. But it’s crucial to stop higher-risk drugs immediately once pregnancy is confirmed, she said.
In regard to acute headache, Dr. Stika urged caution if a patient reports taking a headache medication more than twice a week. “All the medications we use for the treatment of migraine, both in and outside of pregnancy, carry the risk of what’s called medication overuse” that can lead to rebound headaches, she said.
Excedrin Tension Headache may be used for headaches in pregnancy, she said, but not Excedrin Migraine since it includes aspirin. Triptans are not recommended as first-line therapy, she added, and they “should absolutely not be used in any pregnant patient with a history of known cardiac disease or hypertension.”
Dr. Stika added that ACOG advises against the use of drugs that contain butalbital, a barbiturate that’s combined with other agents to treat headache. “Butalbital is the drug that’s most closely associated with getting people into this medication overuse headache,” she said. “It’s even worse than opioids.”
Unlike multiple other countries and the entire European Union, the United States has not banned compounds that contain butalbital, she said.
In some cases, she said, patients may present to triage with vomiting, an inability to keep food down, and persistent headache despite treatment. “This is a really classic presentation.”
The ACOG clinical practice guideline offers a flow chart about what to do, she said. Hydration is key, she said, and various treatment options can help. A referral to neurology may be needed in extreme cases, she said. But “most of the time, you’re able to get rid of her headache.”
Dr. Mercer and Dr. Stika report no disclosures.
AT ACOG 2022
Bronchoscopic lung reduction boosts survival in severe COPD
Bronchoscopic lung volume reduction significantly increased survival in patients with severe chronic obstructive pulmonary disease, based on data from more than 1,400 individuals.
Previous studies have shown that patients with severe chronic obstructive pulmonary disease (COPD) can benefit from treatment with bronchoscopic lung volume reduction (BLVR) involving lung volume reduction coils or endobronchial valves (EBVs) in terms of improved pulmonary function, lung volume, exercise capacity, and quality of life.
However, data on the impact of the procedure on patient survival are limited, and most previous studies have been small, wrote Jorine E. Hartman, MD, of the University of Groningen, the Netherlands, and colleagues.
In a study published in Respiratory Medicine, the researchers reviewed data from 1,471 patients with severe COPD who had consultations for BLVR at a single center between June 2006 and July 2019. Of these, 483 (33%) underwent a BLVR treatment.
The follow-up period ranged from 633 days to 5,401 days. During this time, 531 patients died (35%); 165 of these (34%) were in the BLVR group.
Overall, the median survival of BLVR patients was significantly longer, compared with those who did not have the procedure, for a difference of approximately 1.7 years (3,133 days vs. 2,503 days, P < .001). No significant differences in survival were noted in BLVR patients treated with coils or EBVs.
The average age of the study population at baseline was 61 years, and 63% were women. Overall, patients treated with BLVR were more likely to be younger and female, with fewer COPD exacerbations but worse pulmonary function, as well as lower body mass index and more evidence of emphysema than the untreated patients, the researchers noted. Patients treated with BLVR also were more likely than untreated patients to have a history of myocardial infarction, percutaneous coronary intervention, or stroke.
However, BLVR was a significant independent predictor of survival after controlling for multiple variables, including age, sex, and disease severity, the researchers noted.
The current study supports existing literature on the value of BLVR for severe COPD but stands out from previous studies by comparing patients who underwent BLVR with those who did not, the researchers noted in their discussion of the findings.
The study findings were limited by several factors, including the fact that the non-treated patients were not eligible for treatment for various reasons that might have impacted survival, the researchers noted. Another limitation was the lack of data on cause of death and other medical events and treatments during the follow-up period, they said.
However, the results were strengthened by the large sample size and long-term follow-up and suggest that “reducing lung volume in patients with COPD and severe hyperinflation and reduced life expectancy may lead to a survival benefit,” they concluded.
The study received no outside funding. Dr. Hartman had no financial conflicts to disclose.
Bronchoscopic lung volume reduction significantly increased survival in patients with severe chronic obstructive pulmonary disease, based on data from more than 1,400 individuals.
Previous studies have shown that patients with severe chronic obstructive pulmonary disease (COPD) can benefit from treatment with bronchoscopic lung volume reduction (BLVR) involving lung volume reduction coils or endobronchial valves (EBVs) in terms of improved pulmonary function, lung volume, exercise capacity, and quality of life.
However, data on the impact of the procedure on patient survival are limited, and most previous studies have been small, wrote Jorine E. Hartman, MD, of the University of Groningen, the Netherlands, and colleagues.
In a study published in Respiratory Medicine, the researchers reviewed data from 1,471 patients with severe COPD who had consultations for BLVR at a single center between June 2006 and July 2019. Of these, 483 (33%) underwent a BLVR treatment.
The follow-up period ranged from 633 days to 5,401 days. During this time, 531 patients died (35%); 165 of these (34%) were in the BLVR group.
Overall, the median survival of BLVR patients was significantly longer, compared with those who did not have the procedure, for a difference of approximately 1.7 years (3,133 days vs. 2,503 days, P < .001). No significant differences in survival were noted in BLVR patients treated with coils or EBVs.
The average age of the study population at baseline was 61 years, and 63% were women. Overall, patients treated with BLVR were more likely to be younger and female, with fewer COPD exacerbations but worse pulmonary function, as well as lower body mass index and more evidence of emphysema than the untreated patients, the researchers noted. Patients treated with BLVR also were more likely than untreated patients to have a history of myocardial infarction, percutaneous coronary intervention, or stroke.
However, BLVR was a significant independent predictor of survival after controlling for multiple variables, including age, sex, and disease severity, the researchers noted.
The current study supports existing literature on the value of BLVR for severe COPD but stands out from previous studies by comparing patients who underwent BLVR with those who did not, the researchers noted in their discussion of the findings.
The study findings were limited by several factors, including the fact that the non-treated patients were not eligible for treatment for various reasons that might have impacted survival, the researchers noted. Another limitation was the lack of data on cause of death and other medical events and treatments during the follow-up period, they said.
However, the results were strengthened by the large sample size and long-term follow-up and suggest that “reducing lung volume in patients with COPD and severe hyperinflation and reduced life expectancy may lead to a survival benefit,” they concluded.
The study received no outside funding. Dr. Hartman had no financial conflicts to disclose.
Bronchoscopic lung volume reduction significantly increased survival in patients with severe chronic obstructive pulmonary disease, based on data from more than 1,400 individuals.
Previous studies have shown that patients with severe chronic obstructive pulmonary disease (COPD) can benefit from treatment with bronchoscopic lung volume reduction (BLVR) involving lung volume reduction coils or endobronchial valves (EBVs) in terms of improved pulmonary function, lung volume, exercise capacity, and quality of life.
However, data on the impact of the procedure on patient survival are limited, and most previous studies have been small, wrote Jorine E. Hartman, MD, of the University of Groningen, the Netherlands, and colleagues.
In a study published in Respiratory Medicine, the researchers reviewed data from 1,471 patients with severe COPD who had consultations for BLVR at a single center between June 2006 and July 2019. Of these, 483 (33%) underwent a BLVR treatment.
The follow-up period ranged from 633 days to 5,401 days. During this time, 531 patients died (35%); 165 of these (34%) were in the BLVR group.
Overall, the median survival of BLVR patients was significantly longer, compared with those who did not have the procedure, for a difference of approximately 1.7 years (3,133 days vs. 2,503 days, P < .001). No significant differences in survival were noted in BLVR patients treated with coils or EBVs.
The average age of the study population at baseline was 61 years, and 63% were women. Overall, patients treated with BLVR were more likely to be younger and female, with fewer COPD exacerbations but worse pulmonary function, as well as lower body mass index and more evidence of emphysema than the untreated patients, the researchers noted. Patients treated with BLVR also were more likely than untreated patients to have a history of myocardial infarction, percutaneous coronary intervention, or stroke.
However, BLVR was a significant independent predictor of survival after controlling for multiple variables, including age, sex, and disease severity, the researchers noted.
The current study supports existing literature on the value of BLVR for severe COPD but stands out from previous studies by comparing patients who underwent BLVR with those who did not, the researchers noted in their discussion of the findings.
The study findings were limited by several factors, including the fact that the non-treated patients were not eligible for treatment for various reasons that might have impacted survival, the researchers noted. Another limitation was the lack of data on cause of death and other medical events and treatments during the follow-up period, they said.
However, the results were strengthened by the large sample size and long-term follow-up and suggest that “reducing lung volume in patients with COPD and severe hyperinflation and reduced life expectancy may lead to a survival benefit,” they concluded.
The study received no outside funding. Dr. Hartman had no financial conflicts to disclose.
FROM RESPIRATORY MEDICINE
Patients asking about APOE gene test results? Here’s what to tell them
Advances in Alzheimer disease (AD) genes and biomarkers now allow older adults to undergo testing and learn about their risk for AD.1 Current routes for doing so include testing in cardiology, screening for enrollment in secondary prevention trials (which use these tests to determine trial eligibility),2 and direct-to-consumer (DTC) services that provide these results as part of large panels.3 Patients may also obtain apolipoprotein (APOE) genotype information as part of an assessment of the risks and benefits of treatment with aducanumab (Aduhelm) or other anti-amyloid therapies that have been developed to stop or slow the progression of AD pathologies.
Expanded access to testing, in combination with limited guidance from DTC companies, suggests more older adults may consult their primary care physicians about this testing. In this narrative review, we use a vignette-driven approach to summarize the current scientific knowledge of the topic and to offer guidance on provider-patient discussions and follow-up.
First, a look at APOE genotyping
In cognitively unimpaired older adults, the APOE gene is a known risk factor for mild cognitive impairment (MCI) or AD.3 A person has 2 alleles of the APOE gene, which has 3 variants: ε2, ε3, and ε4. The combination of alleles conveys varying levels of risk for developing clinical symptoms (TABLE 14), with ε4 increasing risk and ε2 decreasing risk compared to the more common ε3; thus the ε4/ε4 genotype conveys the most risk and the ε2/ε2 the least.

The APOE gene differs from other genes that have been identified in early-onset familial AD. These other genes, which include APP, PSEN1, and PSEN2, are deterministic genes that are fully penetrant. The APOE gene is not deterministic, meaning there is no combination of APOE alleles that are necessary or sufficient to cause late-onset AD dementia.
In clinical trials of amyloid-modifying therapies, the APOE gene has been shown to convey a risk of amyloid-related imaging abnormalities (ARIA).5 That is, in addition to conveying a risk for AD, the gene also conveys a risk for adverse effects of emerging treatments that can result in serious injury or death. This includes the drug aducanumab that was recently approved by the US Food and Drug Administration (FDA).6 In this review, we focus primarily on common clinical scenarios related to APOE. However, in light of the recent controversy over aducanumab and whether the drug should be offered to patients,7-9 we also describe how a patient’s APOE genotype may factor into drug candidacy decisions.
Testing, in clinic and “at home.” To date, practice guidelines have consistently recommended against APOE genetic testing in routine clinical practice. This is primarily due to low clinical prognostic utility and the lack of actionable results. Furthermore, no lifestyle or pharmaceutical interventions based on APOE genotype currently exist (although trials are underway10).
In 2017, the FDA approved marketing of DTC testing for the APOE gene.11 While DTC companies tend to issue standardized test result reports, the content and quality can vary widely. In fact, some provide risk estimates that are too high and too definitive and may not reflect the most recent science.12
Continue to: 7 clinical scenarios and how to approach them
7 clinical scenarios and how to approach them
Six of the following vignettes describe common clinical scenarios in which patients seek medical advice regarding APOE test results. The seventh vignette describes a patient whose APOE genotype may play a role in possible disease-modifying treatments down the road. Each vignette is designed to guide your approach to patient discussions and follow-up. Recommendations and considerations are also summarized in TABLE 213-16.

Vignette 1
Janet W, age 65, comes to the clinic for a new patient visit. She has no concerns about her memory but recently purchased DTC genetic testing to learn about her genetic health risks. Her results showed an APOE ε4/ε4 genotype. She is now concerned about developing AD. Her mother was diagnosed with AD in her 70s.
Several important pieces of information can be conveyed by the primary care physician. First, patients such as Ms. W should be told that the APOE gene is not deterministic; many people, even those with 2 ε4 alleles, never develop dementia. Second, no specific preventive measures or treatments exist based on an individual’s APOE genotype (see Vignette 5 for additional discussion).
In this scenario, patients may ask for numeric quantification of their risk for dementia (see TABLE 14 for estimates). When conveying probabilistic risk, consider using simple percentages or pictographs (eg, out of 100 individuals with an ε4/ε4 genotype, 30 to 55 develop MCI or AD). Additionally, because people tend to exhibit confirmatory bias in thinking about probabilistic risk, providing opposing interpretations of an estimate may help them to consider alternative possibilities.17 For example
There are important caveats to the interpretation of APOE risk estimates. Because APOE risk estimates are probabilistic and averaged across a broader spectrum of people in large population cohorts,4 estimates may not accurately reflect a given individual’s risk. The ranges reflect the uncertainty in the estimates. The uncertainty arises from relatively small samples, the rareness of some genotypes (notably ε4/ε4) even in large samples, and variations in methods and sampling that can lead to differences in estimates beyond statistical variation.
Vignette 2
Eric J, age 85, presents for a new patient visit accompanied by his daughter. He lives independently, volunteers at a senior center several times a week, and exercises regularly, and neither he nor his daughter has any concerns about his memory. As a gift, he recently underwent DTC genetic testing and unexpectedly learned his APOE result, which is ε4/ε4. He wants to know about his chances of developing AD.
Risk conveyed by APOE genotype can be modified by a patient’s age. At age 85, Mr. J is healthy, highly functional, and cognitively unimpaired. Given his age, Mr. J has likely “outlived” much of the risk for dementia attributable to the ε4/ε4 genotype. His risk for dementia remains high, but this risk is likely driven more by age than by his APOE genotype. Data for individuals older than age 80 are limited, and thus risk estimates lack precision. Given Mr. J’s good health and functional status, his physician may want to perform a brief cognitive screening test to serve as a baseline for future evaluations.
Continue to: Vignette 3
Vignette 3
Audrey S is a 60-year-old African American woman who comes to the clinic for her annual visit. Because her father had AD, she recently purchased DTC genetic testing to learn about her APOE genotype and risk for AD. Her results are ε3/ε4. She is wondering what this may mean for her future.
Lack of diversity in research cohorts often limits the generalizability of estimates. For example, both the frequency and impact of APOE ε4 differ across racial groups.18 But most of the data on APOE lifetime risk estimates are from largely White patient samples. While APOE ε4 seems to confer increased risk for AD across sociocultural groups, these effects may be attenuated in African American and Hispanic populations.19,20 If Ms. S is interested in numeric risk estimates, the physician can provide the estimate for ε3/ε4 (20%-25% lifetime risk), with the important caveat that this estimate may not be reflective of her individual risk.
It may be prudent to determine whether Ms. S, at age 60, has subjective memory concerns and if she does, to perform a brief cognitive exam to serve as a baseline for future evaluations. Additionally, while the Genetic Information Nondiscrimination Act (GINA, 2008) prohibits health insurers and employers from discriminating based on genetic testing results, no legal provisions exist regarding long-term care, disability, or life insurance. Documented conversations about APOE test results in the medical record may become part of patients’ applications for these insurance products, and physicians should be cautious before documenting such discussions in the medical record.
Vignette 4
Tina L, age 60, comes to the clinic for a routine wellness visit. She recently developed an interest in genealogy and purchased a DNA testing kit to learn more about her family tree. As part of this testing, she unexpectedly learned that she has an APOE ε4/ε4 genotype. She describes feeling distraught and anxious about what the result means for her future.
Ms. L’s reaction to receiving unexpected genetic results highlights a concern of DTC APOE testing. Her experience is quite different from individuals undergoing medically recommended genetic testing or those who are participating in research studies. They receive comprehensive pre-test counseling by licensed genetic counselors. The counseling includes psychological assessment, education, and discussion of expectations.2
In Ms. L’s case, it may be helpful to explain the limits of APOE lifetime risk estimates (see Vignettes 1-3). But it’s also important to address her concerns. There are behavior scales that can aid the assessment and monitoring of an individual’s well-being. The Impact of Genetic Testing for Alzheimer’s Disease (IGT-AD) scale is a tool that assesses psychological impact. It can help physicians to identify, monitor, and address concerns.21 Other useful tools include the Patient Health Questionnaire-9 (PHQ-9) and the Geriatric Depression Scale (GDS) for depression, and a suicide or self-harm assessment.2,22,23 Finally, a follow-up visit at 2 to 4 weeks may be useful to reassess psychological well-being.
Vignette 4 (cont’d)
Ms. L returns to the clinic 2 weeks later, reporting continued anxiety about her APOE test result and feelings of hopelessness and despair.
Continue to: Some patients struggle...
Some patients struggle with knowing their APOE test result. Test result–related distress is often a combination of depression (as with Ms. L), anger, confusion, and grief.24 Cognitions often include worries about uncertainty, stereotyped threat, and internalized stigma.25,26 These issues can spill over to patient concerns about sharing an APOE test result with others.27
Intolerance of uncertainty is a transdiagnostic risk factor that can influence psychological suffering.28 Brief cognitive behavioral interventions that reinforce routines and encourage healthy and mindful practices may help alleviate patient distress from unexpected genetic test results.29 Interventions that personalize and validate an individual’s experience can help address internalized stigma.30 Referral to a psychologist or psychiatrist could be warranted. Additionally, referral to a genetic counselor may help provide patients with access to added expertise and guidance; useful web-based resources for identifying an appropriate referral include https://medlineplus.gov/genetics/understanding/consult/findingprofessional/ and https://findageneticcounselor.nsgc.org/.
Vignette 5
Bob K, age 65, comes to the clinic for his annual exam. He is a current smoker and says he’s hoping to be more physically active now that he is retired. He says that his mother and grandmother both had AD. He recently purchased DTC genetic testing to learn more about his risk for AD. His learned his APOE genotype is ε3/ε4 and is wondering what he can do to decrease his chances of developing AD.
Mr. K likely would have benefited from pre-test counseling regarding the lack of current therapies to modify one’s genetic risk for AD. A pre-test counseling session often includes education about APOE testing and a brief evaluation to assess psychological readiness to undergo testing. Posttest educational information may help Mr. K avoid predatory advertising of products claiming—without scientific evidence—to modify risk for cognitive decline or to improve cognitive function.
There are several important pieces of information that should be communicated to Mr. K. Emerging evidence from randomized controlled trials suggests that healthy lifestyle modifications may benefit cognition in individuals with APOE ε4 alleles.31 It would be prudent to address proper blood pressure control32 and counsel Mr. K on how he may be able to avoid diabetes through exercise and weight maintenance. Lifestyle recommendations for Mr. K could include: smoking cessation, regular aerobic exercise (eg, 150 min/wk), and a brain-healthy diet (eg, the Mediterranean-DASH Intervention for Neurodegenerative Delay [MIND] diet).13,14 Moreover, dementia prevention also includes appropriately managing depression and chronic illnesses and preventing social isolation and hearing loss.15,16 This information should be thoughtfully conveyed, as these interventions can improve overall (especially cardiovascular) health, as well as mitigating one’s personal risk for AD.
Vignette 6
Juan L, age 45, comes in for his annual physical exam. He has a strong family history of heart disease. His cardiologist recently ordered lipid disorder genetic testing for familial hypercholesterolemia. This panel included APOE testing and showed Mr. L’s genotype is ε2/ε4. He read that the APOE gene can be associated with an increased AD risk and asks for information about his genotype.
Mr. L received genetic testing results that were ordered by a physician for another health purpose. Current recommendations for genetic testing in cardiology advise pre-test genetic counseling.33 But this counseling may not include discussion of the relationship of APOE and risk for MCI or AD. This additional information may be unexpected for Mr. L. Moreover, its significance in the context of his present concerns about cardiovascular disease may influence his reaction.
Continue to: The ε2/ε4 genotype...
The ε2/ε4 genotype is rare. One study showed that in healthy adults, the frequency was 7 in 210 (0.02 [0.01-0.04]).34 Given the rarity of the ε2/ε4 genotype, data about it are sparse. However, since the ε4 allele increases risk but the ε2 allele decreases risk, it is likely that any increase in risk is more modest than with ε3/ε4. In addition, it would help Mr. L to know that AD occurs infrequently before age 60.35 Given his relatively young age, he is unlikely to develop AD any time in the near future. In addition, particularly if he starts early, he might be able to mitigate any increased risk through some of the advice provided to Mr. K in Vignette 5.
Vignette 7
Joe J, age 65, comes to the clinic for a new patient visit. He has no concerns about his memory but has a family history of dementia and recently purchased DTC genetic testing to learn about his genetic health risks. His results showed an APOE ε4/ε4 genotype. He is concerned about developing AD. He heard on the news that there is a drug that can treat AD and wants to know if he is a candidate for this treatment.
Mr. J would benefit from the education provided to Ms. W in Vignette 1. Patients such as Mr. J should be advised that while an APOE ε4/ε4 genotype conveys an increased risk for AD, it is not deterministic of the disease. While there are no specific preventive measures or treatments based on APOE genotype, careful medical care and lifestyle factors can offset some of the risk (see Vignette 5 for discussion).
Recently (and controversially), the FDA approved aducanumab, a drug that targets amyloid.6,36 Of note, brain amyloid is more common in individuals with the APOE ε4/ε4 genotype, such as Mr. J. However, there would be no point in testing Mr. J for brain amyloid because at present the drug is only indicated in symptomatic individuals—and, even in this setting, it is controversial. One reason for the controversy is that aducanumab has potentially severe adverse effects. Patients with the ε4/ε4 genotype should know that this genotype carries increased risk for the most serious adverse event, ARIA—which can include brain edema and microhemorrhages.
What lies ahead?
More research is needed to explore the impact that greater AD gene and biomarker testing will have on the health system and workforce development. In addition, graduate schools and training programs will need to prepare clinicians to address probabilistic risk estimates for common diseases, such as AD. Finally, health systems and medical groups that employ clinicians may want to offer simulated training—similar to the vignettes in this article—as a practice requirement or as continuing medical education. This may also allow health systems or medical groups to put in place frameworks that support clinicians in proactively answering questions for patients and families about APOE and other emerging markers of disease risk.
CORRESPONDENCE
Shana Stites, University of Pennsylvania, 3615 Chestnut Street, Philadelphia, PA 19104; Stites@UPenn.edu
1. Jack CR, Bennett DA, Blennow K, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement J Alzheimers Assoc. 2018;14:535-562. doi: 10.1016/j.jalz.2018.02.018 PMCID:PMC5958625
2. Langlois CM, Bradbury A, Wood EM, et al. Alzheimer’s Prevention Initiative Generation Program: development of an APOE genetic counseling and disclosure process in the context of clinical trials. Alzheimers Dement Transl Res Clin Interv. 2019;5:705-716. doi: 10.1016/j.trci.2019.09.013
3. Frank L, Wesson Ashford J, Bayley PJ, et al. Genetic risk of Alzheimer’s disease: three wishes now that the genie is out of the bottle. J Alzheimers Dis. 2018;66:421-423. doi: 10.3233/JAD-180629
4. Qian J, Wolters FJ, Beiser A, et al. APOE-related risk of mild cognitive impairment and dementia for prevention trials: an analysis of four cohorts. PLOS Med. 2017;14:e1002254. doi: 10.1371/journal.pmed.1002254
5. Sperling RA, Jack CR, Black SE, et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer’s Association Research Roundtable Workgroup. Alzheimers Dement. 2011;7:367-385. doi: 10.1016/j.jalz.2011.05.2351
6. FDA. November 6, 2020: Meeting of the Peripheral and Central Nervous System Drugs Advisory Committee Meeting Announcement. Published November 12, 2020. Accessed January 14, 2021. www.fda.gov/advisory-committees/advisory-committee-calendar/november-6-2020-meeting-peripheral-and-central-nervous-system-drugs-advisory-committee-meeting
7. Cummings J. Why aducanumab is important. Nat Med. 2021;27:1498-1498. doi: 10.1038/s41591-021-01478-4
8. Alexander GC, Karlawish J. The problem of aducanumab for the treatment of Alzheimer disease. Ann Intern Med. 2021;174:1303-1304. doi: 10.7326/M21-2603
9. Mullard A. More Alzheimer’s drugs head for FDA review: what scientists are watching. Nature. 2021;599:544-545. doi: 10.1038/d41586-021-03410-9
10. Rosenberg A, Mangialasche F, Ngandu T, et al. Multidomain interventions to prevent cognitive impairment, Alzheimer’s disease, and dementia: from finger to world-wide fingers. J Prev Alzheimers Dis. 2019:1-8. doi: 10.14283/jpad.2019.41
11. FDA. Commissioner of the FDA allows marketing of first direct-to-consumer tests that provide genetic risk information for certain conditions. Published March 24, 2020. Accessed November 7, 2020. www.fda.gov/news-events/press-announcements/fda-allows-marketing-first-direct-consumer-tests-provide-genetic-risk-information-certain-conditions
12. Blell M, Hunter MA. Direct-to-consumer genetic testing’s red herring: “genetic ancestry” and personalized medicine. Front Med. 2019;6:48. doi: 10.3389/fmed.2019.00048
13. Ekstrand B, Scheers N, Rasmussen MK, et al. Brain foods - the role of diet in brain performance and health. Nutr Rev. 2021;79:693-708. doi: 10.1093/nutrit/nuaa091
14. Cherian L, Wang Y, Fakuda K, et al. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diet slows cognitive decline after stroke. J Prev Alzheimers Dis. 2019;6:267-273. doi: 10.14283/jpad.2019.28
15. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet. 2020;396:413-446. doi: 10.1016/S0140-6736(20)30367-6
16. Livingston PG, Sommerlad A, Orgeta V, et al. The Lancet International Commission on Dementia Prevention and Care. 2017. Accessed March 30, 2022. https://discovery.ucl.ac.uk/id/eprint/1567635/1/Livingston_Dementia_prevention_intervention_care.pdf
17. Peters U. What is the function of confirmation bias? Erkenntnis. April 2020. doi: 10.1007/s10670-020-00252-1
18. Barnes LL, Bennett DA. Cognitive resilience in APOE*ε4 carriers—is race important? Nat Rev Neurol. 2015;11:190-191. doi: 10.1038/nrneurol.2015.38
19. Farrer LA. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease: a meta-analysis. JAMA. 1997;278:1349. doi: 10.1001/jama.1997.03550160069041
20. Evans DA, Bennett DA, Wilson RS, et al. Incidence of Alzheimer disease in a biracial urban community: relation to apolipoprotein E allele status. Arch Neurol. 2003;60:185. doi: 10.1001/archneur.60.2.185
21. Chung WW, Chen CA, Cupples LA, et al. A new scale measuring psychologic impact of genetic susceptibility testing for Alzheimer disease. Alzheimer Dis Assoc Disord. 2009;23:50-56. doi: 10.1097/WAD.0b013e318188429e
22. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi: 10.1046/j.1525-1497.2001.016009606.x
23. Yesavage JA, Sheikh JI. 9/Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5:165-173. doi: 10.1300/J018v05n01_09
24. Green RC, Roberts JS, Cupples LA, et al. Disclosure of APOE genotype for risk of Alzheimer’s disease. N Engl J Med. 2009;361:245-254. doi: 10.1056/NEJMoa0809578
25. Lineweaver TT, Bondi MW, Galasko D, et al. Effect of knowledge of APOE genotype on subjective and objective memory performance in healthy older adults. Am J Psychiatry. 2014;171:201-208. doi: 10.1176/appi.ajp.2013.12121590
26. Karlawish J. Understanding the impact of learning an amyloid PET scan result: preliminary findings from the SOKRATES study. Alzheimers Dement J Alzheimers Assoc. 2016;12:P325. doi: 10.1016/j.jalz.2016.06.594
27. Stites SD. Cognitively healthy individuals want to know their risk for Alzheimer’s disease: what should we do? J Alzheimers Dis. 2018;62:499-502. doi: 10.3233/JAD-171089
28. Milne S, Lomax C, Freeston MH. A review of the relationship between intolerance of uncertainty and threat appraisal in anxiety. Cogn Behav Ther. 2019;12:e38. doi: 10.1017/S1754470X19000230
29. Hebert EA, Dugas MJ. Behavioral experiments for intolerance of uncertainty: challenging the unknown in the treatment of generalized anxiety disorder. Cogn Behav Pract. 2019;26:421-436. doi: 10.1016/j.cbpra.2018.07.007
30. Stites SD, Karlawish, J. Stigma of Alzheimer’s disease dementia: considerations for practice. Pract Neurol. Published June 2018. Accessed January 31, 2019. http://practicalneurology.com/2018/06/stigma-of-alzheimers-disease-dementia/
31. Solomon A, Turunen H, Ngandu T, et al. Effect of the apolipoprotein E genotype on cognitive change during a multidomain lifestyle intervention: a subgroup analysis of a randomized clinical trial. JAMA Neurol. 2018;75:462. doi: 10.1001/jamaneurol.2017.4365
32. Peters R, Warwick J, Anstey KJ, et al. Blood pressure and dementia: what the SPRINT-MIND trial adds and what we still need to know. Neurology. 2019;92:1017-1018. doi: 10.1212/WNL.0000000000007543
33. Musunuru K, Hershberger RE, Day SM, et al. Genetic testing for inherited cardiovascular diseases: a Scientific Statement from the American Heart Association. Circ Genom Precis Med. 2020;13: e000067. doi: 10.1161/HCG.0000000000000067
34. Margaglione M, Seripa D, Gravina C, et al. Prevalence of apolipoprotein E alleles in healthy subjects and survivors of ischemic stroke. Stroke. 1998;29:399-403. doi: 10.1161/01.STR.29.2.399
35. National Institute on Aging. Alzheimer’s disease genetics fact sheet. Reviewed December 24, 2019. Accessed April 10, 2022. www.nia.nih.gov/health/alzheimers-disease-genetics-fact-sheet
36. Belluck P, Kaplan S, Robbins R. How Aduhelm, an unproven Alzheimer’s drug, got approved. The New York Times. Published July 19, 2021. Updated Oct. 20, 2021. Accessed December 1, 2021. www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html
Advances in Alzheimer disease (AD) genes and biomarkers now allow older adults to undergo testing and learn about their risk for AD.1 Current routes for doing so include testing in cardiology, screening for enrollment in secondary prevention trials (which use these tests to determine trial eligibility),2 and direct-to-consumer (DTC) services that provide these results as part of large panels.3 Patients may also obtain apolipoprotein (APOE) genotype information as part of an assessment of the risks and benefits of treatment with aducanumab (Aduhelm) or other anti-amyloid therapies that have been developed to stop or slow the progression of AD pathologies.
Expanded access to testing, in combination with limited guidance from DTC companies, suggests more older adults may consult their primary care physicians about this testing. In this narrative review, we use a vignette-driven approach to summarize the current scientific knowledge of the topic and to offer guidance on provider-patient discussions and follow-up.
First, a look at APOE genotyping
In cognitively unimpaired older adults, the APOE gene is a known risk factor for mild cognitive impairment (MCI) or AD.3 A person has 2 alleles of the APOE gene, which has 3 variants: ε2, ε3, and ε4. The combination of alleles conveys varying levels of risk for developing clinical symptoms (TABLE 14), with ε4 increasing risk and ε2 decreasing risk compared to the more common ε3; thus the ε4/ε4 genotype conveys the most risk and the ε2/ε2 the least.
The APOE gene differs from other genes that have been identified in early-onset familial AD. These other genes, which include APP, PSEN1, and PSEN2, are deterministic genes that are fully penetrant. The APOE gene is not deterministic, meaning there is no combination of APOE alleles that are necessary or sufficient to cause late-onset AD dementia.
In clinical trials of amyloid-modifying therapies, the APOE gene has been shown to convey a risk of amyloid-related imaging abnormalities (ARIA).5 That is, in addition to conveying a risk for AD, the gene also conveys a risk for adverse effects of emerging treatments that can result in serious injury or death. This includes the drug aducanumab that was recently approved by the US Food and Drug Administration (FDA).6 In this review, we focus primarily on common clinical scenarios related to APOE. However, in light of the recent controversy over aducanumab and whether the drug should be offered to patients,7-9 we also describe how a patient’s APOE genotype may factor into drug candidacy decisions.
Testing, in clinic and “at home.” To date, practice guidelines have consistently recommended against APOE genetic testing in routine clinical practice. This is primarily due to low clinical prognostic utility and the lack of actionable results. Furthermore, no lifestyle or pharmaceutical interventions based on APOE genotype currently exist (although trials are underway10).
In 2017, the FDA approved marketing of DTC testing for the APOE gene.11 While DTC companies tend to issue standardized test result reports, the content and quality can vary widely. In fact, some provide risk estimates that are too high and too definitive and may not reflect the most recent science.12
Continue to: 7 clinical scenarios and how to approach them
7 clinical scenarios and how to approach them
Six of the following vignettes describe common clinical scenarios in which patients seek medical advice regarding APOE test results. The seventh vignette describes a patient whose APOE genotype may play a role in possible disease-modifying treatments down the road. Each vignette is designed to guide your approach to patient discussions and follow-up. Recommendations and considerations are also summarized in TABLE 213-16.
Vignette 1
Janet W, age 65, comes to the clinic for a new patient visit. She has no concerns about her memory but recently purchased DTC genetic testing to learn about her genetic health risks. Her results showed an APOE ε4/ε4 genotype. She is now concerned about developing AD. Her mother was diagnosed with AD in her 70s.
Several important pieces of information can be conveyed by the primary care physician. First, patients such as Ms. W should be told that the APOE gene is not deterministic; many people, even those with 2 ε4 alleles, never develop dementia. Second, no specific preventive measures or treatments exist based on an individual’s APOE genotype (see Vignette 5 for additional discussion).
In this scenario, patients may ask for numeric quantification of their risk for dementia (see TABLE 14 for estimates). When conveying probabilistic risk, consider using simple percentages or pictographs (eg, out of 100 individuals with an ε4/ε4 genotype, 30 to 55 develop MCI or AD). Additionally, because people tend to exhibit confirmatory bias in thinking about probabilistic risk, providing opposing interpretations of an estimate may help them to consider alternative possibilities.17 For example
There are important caveats to the interpretation of APOE risk estimates. Because APOE risk estimates are probabilistic and averaged across a broader spectrum of people in large population cohorts,4 estimates may not accurately reflect a given individual’s risk. The ranges reflect the uncertainty in the estimates. The uncertainty arises from relatively small samples, the rareness of some genotypes (notably ε4/ε4) even in large samples, and variations in methods and sampling that can lead to differences in estimates beyond statistical variation.
Vignette 2
Eric J, age 85, presents for a new patient visit accompanied by his daughter. He lives independently, volunteers at a senior center several times a week, and exercises regularly, and neither he nor his daughter has any concerns about his memory. As a gift, he recently underwent DTC genetic testing and unexpectedly learned his APOE result, which is ε4/ε4. He wants to know about his chances of developing AD.
Risk conveyed by APOE genotype can be modified by a patient’s age. At age 85, Mr. J is healthy, highly functional, and cognitively unimpaired. Given his age, Mr. J has likely “outlived” much of the risk for dementia attributable to the ε4/ε4 genotype. His risk for dementia remains high, but this risk is likely driven more by age than by his APOE genotype. Data for individuals older than age 80 are limited, and thus risk estimates lack precision. Given Mr. J’s good health and functional status, his physician may want to perform a brief cognitive screening test to serve as a baseline for future evaluations.
Continue to: Vignette 3
Vignette 3
Audrey S is a 60-year-old African American woman who comes to the clinic for her annual visit. Because her father had AD, she recently purchased DTC genetic testing to learn about her APOE genotype and risk for AD. Her results are ε3/ε4. She is wondering what this may mean for her future.
Lack of diversity in research cohorts often limits the generalizability of estimates. For example, both the frequency and impact of APOE ε4 differ across racial groups.18 But most of the data on APOE lifetime risk estimates are from largely White patient samples. While APOE ε4 seems to confer increased risk for AD across sociocultural groups, these effects may be attenuated in African American and Hispanic populations.19,20 If Ms. S is interested in numeric risk estimates, the physician can provide the estimate for ε3/ε4 (20%-25% lifetime risk), with the important caveat that this estimate may not be reflective of her individual risk.
It may be prudent to determine whether Ms. S, at age 60, has subjective memory concerns and if she does, to perform a brief cognitive exam to serve as a baseline for future evaluations. Additionally, while the Genetic Information Nondiscrimination Act (GINA, 2008) prohibits health insurers and employers from discriminating based on genetic testing results, no legal provisions exist regarding long-term care, disability, or life insurance. Documented conversations about APOE test results in the medical record may become part of patients’ applications for these insurance products, and physicians should be cautious before documenting such discussions in the medical record.
Vignette 4
Tina L, age 60, comes to the clinic for a routine wellness visit. She recently developed an interest in genealogy and purchased a DNA testing kit to learn more about her family tree. As part of this testing, she unexpectedly learned that she has an APOE ε4/ε4 genotype. She describes feeling distraught and anxious about what the result means for her future.
Ms. L’s reaction to receiving unexpected genetic results highlights a concern of DTC APOE testing. Her experience is quite different from individuals undergoing medically recommended genetic testing or those who are participating in research studies. They receive comprehensive pre-test counseling by licensed genetic counselors. The counseling includes psychological assessment, education, and discussion of expectations.2
In Ms. L’s case, it may be helpful to explain the limits of APOE lifetime risk estimates (see Vignettes 1-3). But it’s also important to address her concerns. There are behavior scales that can aid the assessment and monitoring of an individual’s well-being. The Impact of Genetic Testing for Alzheimer’s Disease (IGT-AD) scale is a tool that assesses psychological impact. It can help physicians to identify, monitor, and address concerns.21 Other useful tools include the Patient Health Questionnaire-9 (PHQ-9) and the Geriatric Depression Scale (GDS) for depression, and a suicide or self-harm assessment.2,22,23 Finally, a follow-up visit at 2 to 4 weeks may be useful to reassess psychological well-being.
Vignette 4 (cont’d)
Ms. L returns to the clinic 2 weeks later, reporting continued anxiety about her APOE test result and feelings of hopelessness and despair.
Continue to: Some patients struggle...
Some patients struggle with knowing their APOE test result. Test result–related distress is often a combination of depression (as with Ms. L), anger, confusion, and grief.24 Cognitions often include worries about uncertainty, stereotyped threat, and internalized stigma.25,26 These issues can spill over to patient concerns about sharing an APOE test result with others.27
Intolerance of uncertainty is a transdiagnostic risk factor that can influence psychological suffering.28 Brief cognitive behavioral interventions that reinforce routines and encourage healthy and mindful practices may help alleviate patient distress from unexpected genetic test results.29 Interventions that personalize and validate an individual’s experience can help address internalized stigma.30 Referral to a psychologist or psychiatrist could be warranted. Additionally, referral to a genetic counselor may help provide patients with access to added expertise and guidance; useful web-based resources for identifying an appropriate referral include https://medlineplus.gov/genetics/understanding/consult/findingprofessional/ and https://findageneticcounselor.nsgc.org/.
Vignette 5
Bob K, age 65, comes to the clinic for his annual exam. He is a current smoker and says he’s hoping to be more physically active now that he is retired. He says that his mother and grandmother both had AD. He recently purchased DTC genetic testing to learn more about his risk for AD. His learned his APOE genotype is ε3/ε4 and is wondering what he can do to decrease his chances of developing AD.
Mr. K likely would have benefited from pre-test counseling regarding the lack of current therapies to modify one’s genetic risk for AD. A pre-test counseling session often includes education about APOE testing and a brief evaluation to assess psychological readiness to undergo testing. Posttest educational information may help Mr. K avoid predatory advertising of products claiming—without scientific evidence—to modify risk for cognitive decline or to improve cognitive function.
There are several important pieces of information that should be communicated to Mr. K. Emerging evidence from randomized controlled trials suggests that healthy lifestyle modifications may benefit cognition in individuals with APOE ε4 alleles.31 It would be prudent to address proper blood pressure control32 and counsel Mr. K on how he may be able to avoid diabetes through exercise and weight maintenance. Lifestyle recommendations for Mr. K could include: smoking cessation, regular aerobic exercise (eg, 150 min/wk), and a brain-healthy diet (eg, the Mediterranean-DASH Intervention for Neurodegenerative Delay [MIND] diet).13,14 Moreover, dementia prevention also includes appropriately managing depression and chronic illnesses and preventing social isolation and hearing loss.15,16 This information should be thoughtfully conveyed, as these interventions can improve overall (especially cardiovascular) health, as well as mitigating one’s personal risk for AD.
Vignette 6
Juan L, age 45, comes in for his annual physical exam. He has a strong family history of heart disease. His cardiologist recently ordered lipid disorder genetic testing for familial hypercholesterolemia. This panel included APOE testing and showed Mr. L’s genotype is ε2/ε4. He read that the APOE gene can be associated with an increased AD risk and asks for information about his genotype.
Mr. L received genetic testing results that were ordered by a physician for another health purpose. Current recommendations for genetic testing in cardiology advise pre-test genetic counseling.33 But this counseling may not include discussion of the relationship of APOE and risk for MCI or AD. This additional information may be unexpected for Mr. L. Moreover, its significance in the context of his present concerns about cardiovascular disease may influence his reaction.
Continue to: The ε2/ε4 genotype...
The ε2/ε4 genotype is rare. One study showed that in healthy adults, the frequency was 7 in 210 (0.02 [0.01-0.04]).34 Given the rarity of the ε2/ε4 genotype, data about it are sparse. However, since the ε4 allele increases risk but the ε2 allele decreases risk, it is likely that any increase in risk is more modest than with ε3/ε4. In addition, it would help Mr. L to know that AD occurs infrequently before age 60.35 Given his relatively young age, he is unlikely to develop AD any time in the near future. In addition, particularly if he starts early, he might be able to mitigate any increased risk through some of the advice provided to Mr. K in Vignette 5.
Vignette 7
Joe J, age 65, comes to the clinic for a new patient visit. He has no concerns about his memory but has a family history of dementia and recently purchased DTC genetic testing to learn about his genetic health risks. His results showed an APOE ε4/ε4 genotype. He is concerned about developing AD. He heard on the news that there is a drug that can treat AD and wants to know if he is a candidate for this treatment.
Mr. J would benefit from the education provided to Ms. W in Vignette 1. Patients such as Mr. J should be advised that while an APOE ε4/ε4 genotype conveys an increased risk for AD, it is not deterministic of the disease. While there are no specific preventive measures or treatments based on APOE genotype, careful medical care and lifestyle factors can offset some of the risk (see Vignette 5 for discussion).
Recently (and controversially), the FDA approved aducanumab, a drug that targets amyloid.6,36 Of note, brain amyloid is more common in individuals with the APOE ε4/ε4 genotype, such as Mr. J. However, there would be no point in testing Mr. J for brain amyloid because at present the drug is only indicated in symptomatic individuals—and, even in this setting, it is controversial. One reason for the controversy is that aducanumab has potentially severe adverse effects. Patients with the ε4/ε4 genotype should know that this genotype carries increased risk for the most serious adverse event, ARIA—which can include brain edema and microhemorrhages.
What lies ahead?
More research is needed to explore the impact that greater AD gene and biomarker testing will have on the health system and workforce development. In addition, graduate schools and training programs will need to prepare clinicians to address probabilistic risk estimates for common diseases, such as AD. Finally, health systems and medical groups that employ clinicians may want to offer simulated training—similar to the vignettes in this article—as a practice requirement or as continuing medical education. This may also allow health systems or medical groups to put in place frameworks that support clinicians in proactively answering questions for patients and families about APOE and other emerging markers of disease risk.
CORRESPONDENCE
Shana Stites, University of Pennsylvania, 3615 Chestnut Street, Philadelphia, PA 19104; Stites@UPenn.edu
Advances in Alzheimer disease (AD) genes and biomarkers now allow older adults to undergo testing and learn about their risk for AD.1 Current routes for doing so include testing in cardiology, screening for enrollment in secondary prevention trials (which use these tests to determine trial eligibility),2 and direct-to-consumer (DTC) services that provide these results as part of large panels.3 Patients may also obtain apolipoprotein (APOE) genotype information as part of an assessment of the risks and benefits of treatment with aducanumab (Aduhelm) or other anti-amyloid therapies that have been developed to stop or slow the progression of AD pathologies.
Expanded access to testing, in combination with limited guidance from DTC companies, suggests more older adults may consult their primary care physicians about this testing. In this narrative review, we use a vignette-driven approach to summarize the current scientific knowledge of the topic and to offer guidance on provider-patient discussions and follow-up.
First, a look at APOE genotyping
In cognitively unimpaired older adults, the APOE gene is a known risk factor for mild cognitive impairment (MCI) or AD.3 A person has 2 alleles of the APOE gene, which has 3 variants: ε2, ε3, and ε4. The combination of alleles conveys varying levels of risk for developing clinical symptoms (TABLE 14), with ε4 increasing risk and ε2 decreasing risk compared to the more common ε3; thus the ε4/ε4 genotype conveys the most risk and the ε2/ε2 the least.
The APOE gene differs from other genes that have been identified in early-onset familial AD. These other genes, which include APP, PSEN1, and PSEN2, are deterministic genes that are fully penetrant. The APOE gene is not deterministic, meaning there is no combination of APOE alleles that are necessary or sufficient to cause late-onset AD dementia.
In clinical trials of amyloid-modifying therapies, the APOE gene has been shown to convey a risk of amyloid-related imaging abnormalities (ARIA).5 That is, in addition to conveying a risk for AD, the gene also conveys a risk for adverse effects of emerging treatments that can result in serious injury or death. This includes the drug aducanumab that was recently approved by the US Food and Drug Administration (FDA).6 In this review, we focus primarily on common clinical scenarios related to APOE. However, in light of the recent controversy over aducanumab and whether the drug should be offered to patients,7-9 we also describe how a patient’s APOE genotype may factor into drug candidacy decisions.
Testing, in clinic and “at home.” To date, practice guidelines have consistently recommended against APOE genetic testing in routine clinical practice. This is primarily due to low clinical prognostic utility and the lack of actionable results. Furthermore, no lifestyle or pharmaceutical interventions based on APOE genotype currently exist (although trials are underway10).
In 2017, the FDA approved marketing of DTC testing for the APOE gene.11 While DTC companies tend to issue standardized test result reports, the content and quality can vary widely. In fact, some provide risk estimates that are too high and too definitive and may not reflect the most recent science.12
Continue to: 7 clinical scenarios and how to approach them
7 clinical scenarios and how to approach them
Six of the following vignettes describe common clinical scenarios in which patients seek medical advice regarding APOE test results. The seventh vignette describes a patient whose APOE genotype may play a role in possible disease-modifying treatments down the road. Each vignette is designed to guide your approach to patient discussions and follow-up. Recommendations and considerations are also summarized in TABLE 213-16.
Vignette 1
Janet W, age 65, comes to the clinic for a new patient visit. She has no concerns about her memory but recently purchased DTC genetic testing to learn about her genetic health risks. Her results showed an APOE ε4/ε4 genotype. She is now concerned about developing AD. Her mother was diagnosed with AD in her 70s.
Several important pieces of information can be conveyed by the primary care physician. First, patients such as Ms. W should be told that the APOE gene is not deterministic; many people, even those with 2 ε4 alleles, never develop dementia. Second, no specific preventive measures or treatments exist based on an individual’s APOE genotype (see Vignette 5 for additional discussion).
In this scenario, patients may ask for numeric quantification of their risk for dementia (see TABLE 14 for estimates). When conveying probabilistic risk, consider using simple percentages or pictographs (eg, out of 100 individuals with an ε4/ε4 genotype, 30 to 55 develop MCI or AD). Additionally, because people tend to exhibit confirmatory bias in thinking about probabilistic risk, providing opposing interpretations of an estimate may help them to consider alternative possibilities.17 For example
There are important caveats to the interpretation of APOE risk estimates. Because APOE risk estimates are probabilistic and averaged across a broader spectrum of people in large population cohorts,4 estimates may not accurately reflect a given individual’s risk. The ranges reflect the uncertainty in the estimates. The uncertainty arises from relatively small samples, the rareness of some genotypes (notably ε4/ε4) even in large samples, and variations in methods and sampling that can lead to differences in estimates beyond statistical variation.
Vignette 2
Eric J, age 85, presents for a new patient visit accompanied by his daughter. He lives independently, volunteers at a senior center several times a week, and exercises regularly, and neither he nor his daughter has any concerns about his memory. As a gift, he recently underwent DTC genetic testing and unexpectedly learned his APOE result, which is ε4/ε4. He wants to know about his chances of developing AD.
Risk conveyed by APOE genotype can be modified by a patient’s age. At age 85, Mr. J is healthy, highly functional, and cognitively unimpaired. Given his age, Mr. J has likely “outlived” much of the risk for dementia attributable to the ε4/ε4 genotype. His risk for dementia remains high, but this risk is likely driven more by age than by his APOE genotype. Data for individuals older than age 80 are limited, and thus risk estimates lack precision. Given Mr. J’s good health and functional status, his physician may want to perform a brief cognitive screening test to serve as a baseline for future evaluations.
Continue to: Vignette 3
Vignette 3
Audrey S is a 60-year-old African American woman who comes to the clinic for her annual visit. Because her father had AD, she recently purchased DTC genetic testing to learn about her APOE genotype and risk for AD. Her results are ε3/ε4. She is wondering what this may mean for her future.
Lack of diversity in research cohorts often limits the generalizability of estimates. For example, both the frequency and impact of APOE ε4 differ across racial groups.18 But most of the data on APOE lifetime risk estimates are from largely White patient samples. While APOE ε4 seems to confer increased risk for AD across sociocultural groups, these effects may be attenuated in African American and Hispanic populations.19,20 If Ms. S is interested in numeric risk estimates, the physician can provide the estimate for ε3/ε4 (20%-25% lifetime risk), with the important caveat that this estimate may not be reflective of her individual risk.
It may be prudent to determine whether Ms. S, at age 60, has subjective memory concerns and if she does, to perform a brief cognitive exam to serve as a baseline for future evaluations. Additionally, while the Genetic Information Nondiscrimination Act (GINA, 2008) prohibits health insurers and employers from discriminating based on genetic testing results, no legal provisions exist regarding long-term care, disability, or life insurance. Documented conversations about APOE test results in the medical record may become part of patients’ applications for these insurance products, and physicians should be cautious before documenting such discussions in the medical record.
Vignette 4
Tina L, age 60, comes to the clinic for a routine wellness visit. She recently developed an interest in genealogy and purchased a DNA testing kit to learn more about her family tree. As part of this testing, she unexpectedly learned that she has an APOE ε4/ε4 genotype. She describes feeling distraught and anxious about what the result means for her future.
Ms. L’s reaction to receiving unexpected genetic results highlights a concern of DTC APOE testing. Her experience is quite different from individuals undergoing medically recommended genetic testing or those who are participating in research studies. They receive comprehensive pre-test counseling by licensed genetic counselors. The counseling includes psychological assessment, education, and discussion of expectations.2
In Ms. L’s case, it may be helpful to explain the limits of APOE lifetime risk estimates (see Vignettes 1-3). But it’s also important to address her concerns. There are behavior scales that can aid the assessment and monitoring of an individual’s well-being. The Impact of Genetic Testing for Alzheimer’s Disease (IGT-AD) scale is a tool that assesses psychological impact. It can help physicians to identify, monitor, and address concerns.21 Other useful tools include the Patient Health Questionnaire-9 (PHQ-9) and the Geriatric Depression Scale (GDS) for depression, and a suicide or self-harm assessment.2,22,23 Finally, a follow-up visit at 2 to 4 weeks may be useful to reassess psychological well-being.
Vignette 4 (cont’d)
Ms. L returns to the clinic 2 weeks later, reporting continued anxiety about her APOE test result and feelings of hopelessness and despair.
Continue to: Some patients struggle...
Some patients struggle with knowing their APOE test result. Test result–related distress is often a combination of depression (as with Ms. L), anger, confusion, and grief.24 Cognitions often include worries about uncertainty, stereotyped threat, and internalized stigma.25,26 These issues can spill over to patient concerns about sharing an APOE test result with others.27
Intolerance of uncertainty is a transdiagnostic risk factor that can influence psychological suffering.28 Brief cognitive behavioral interventions that reinforce routines and encourage healthy and mindful practices may help alleviate patient distress from unexpected genetic test results.29 Interventions that personalize and validate an individual’s experience can help address internalized stigma.30 Referral to a psychologist or psychiatrist could be warranted. Additionally, referral to a genetic counselor may help provide patients with access to added expertise and guidance; useful web-based resources for identifying an appropriate referral include https://medlineplus.gov/genetics/understanding/consult/findingprofessional/ and https://findageneticcounselor.nsgc.org/.
Vignette 5
Bob K, age 65, comes to the clinic for his annual exam. He is a current smoker and says he’s hoping to be more physically active now that he is retired. He says that his mother and grandmother both had AD. He recently purchased DTC genetic testing to learn more about his risk for AD. His learned his APOE genotype is ε3/ε4 and is wondering what he can do to decrease his chances of developing AD.
Mr. K likely would have benefited from pre-test counseling regarding the lack of current therapies to modify one’s genetic risk for AD. A pre-test counseling session often includes education about APOE testing and a brief evaluation to assess psychological readiness to undergo testing. Posttest educational information may help Mr. K avoid predatory advertising of products claiming—without scientific evidence—to modify risk for cognitive decline or to improve cognitive function.
There are several important pieces of information that should be communicated to Mr. K. Emerging evidence from randomized controlled trials suggests that healthy lifestyle modifications may benefit cognition in individuals with APOE ε4 alleles.31 It would be prudent to address proper blood pressure control32 and counsel Mr. K on how he may be able to avoid diabetes through exercise and weight maintenance. Lifestyle recommendations for Mr. K could include: smoking cessation, regular aerobic exercise (eg, 150 min/wk), and a brain-healthy diet (eg, the Mediterranean-DASH Intervention for Neurodegenerative Delay [MIND] diet).13,14 Moreover, dementia prevention also includes appropriately managing depression and chronic illnesses and preventing social isolation and hearing loss.15,16 This information should be thoughtfully conveyed, as these interventions can improve overall (especially cardiovascular) health, as well as mitigating one’s personal risk for AD.
Vignette 6
Juan L, age 45, comes in for his annual physical exam. He has a strong family history of heart disease. His cardiologist recently ordered lipid disorder genetic testing for familial hypercholesterolemia. This panel included APOE testing and showed Mr. L’s genotype is ε2/ε4. He read that the APOE gene can be associated with an increased AD risk and asks for information about his genotype.
Mr. L received genetic testing results that were ordered by a physician for another health purpose. Current recommendations for genetic testing in cardiology advise pre-test genetic counseling.33 But this counseling may not include discussion of the relationship of APOE and risk for MCI or AD. This additional information may be unexpected for Mr. L. Moreover, its significance in the context of his present concerns about cardiovascular disease may influence his reaction.
Continue to: The ε2/ε4 genotype...
The ε2/ε4 genotype is rare. One study showed that in healthy adults, the frequency was 7 in 210 (0.02 [0.01-0.04]).34 Given the rarity of the ε2/ε4 genotype, data about it are sparse. However, since the ε4 allele increases risk but the ε2 allele decreases risk, it is likely that any increase in risk is more modest than with ε3/ε4. In addition, it would help Mr. L to know that AD occurs infrequently before age 60.35 Given his relatively young age, he is unlikely to develop AD any time in the near future. In addition, particularly if he starts early, he might be able to mitigate any increased risk through some of the advice provided to Mr. K in Vignette 5.
Vignette 7
Joe J, age 65, comes to the clinic for a new patient visit. He has no concerns about his memory but has a family history of dementia and recently purchased DTC genetic testing to learn about his genetic health risks. His results showed an APOE ε4/ε4 genotype. He is concerned about developing AD. He heard on the news that there is a drug that can treat AD and wants to know if he is a candidate for this treatment.
Mr. J would benefit from the education provided to Ms. W in Vignette 1. Patients such as Mr. J should be advised that while an APOE ε4/ε4 genotype conveys an increased risk for AD, it is not deterministic of the disease. While there are no specific preventive measures or treatments based on APOE genotype, careful medical care and lifestyle factors can offset some of the risk (see Vignette 5 for discussion).
Recently (and controversially), the FDA approved aducanumab, a drug that targets amyloid.6,36 Of note, brain amyloid is more common in individuals with the APOE ε4/ε4 genotype, such as Mr. J. However, there would be no point in testing Mr. J for brain amyloid because at present the drug is only indicated in symptomatic individuals—and, even in this setting, it is controversial. One reason for the controversy is that aducanumab has potentially severe adverse effects. Patients with the ε4/ε4 genotype should know that this genotype carries increased risk for the most serious adverse event, ARIA—which can include brain edema and microhemorrhages.
What lies ahead?
More research is needed to explore the impact that greater AD gene and biomarker testing will have on the health system and workforce development. In addition, graduate schools and training programs will need to prepare clinicians to address probabilistic risk estimates for common diseases, such as AD. Finally, health systems and medical groups that employ clinicians may want to offer simulated training—similar to the vignettes in this article—as a practice requirement or as continuing medical education. This may also allow health systems or medical groups to put in place frameworks that support clinicians in proactively answering questions for patients and families about APOE and other emerging markers of disease risk.
CORRESPONDENCE
Shana Stites, University of Pennsylvania, 3615 Chestnut Street, Philadelphia, PA 19104; Stites@UPenn.edu
1. Jack CR, Bennett DA, Blennow K, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement J Alzheimers Assoc. 2018;14:535-562. doi: 10.1016/j.jalz.2018.02.018 PMCID:PMC5958625
2. Langlois CM, Bradbury A, Wood EM, et al. Alzheimer’s Prevention Initiative Generation Program: development of an APOE genetic counseling and disclosure process in the context of clinical trials. Alzheimers Dement Transl Res Clin Interv. 2019;5:705-716. doi: 10.1016/j.trci.2019.09.013
3. Frank L, Wesson Ashford J, Bayley PJ, et al. Genetic risk of Alzheimer’s disease: three wishes now that the genie is out of the bottle. J Alzheimers Dis. 2018;66:421-423. doi: 10.3233/JAD-180629
4. Qian J, Wolters FJ, Beiser A, et al. APOE-related risk of mild cognitive impairment and dementia for prevention trials: an analysis of four cohorts. PLOS Med. 2017;14:e1002254. doi: 10.1371/journal.pmed.1002254
5. Sperling RA, Jack CR, Black SE, et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer’s Association Research Roundtable Workgroup. Alzheimers Dement. 2011;7:367-385. doi: 10.1016/j.jalz.2011.05.2351
6. FDA. November 6, 2020: Meeting of the Peripheral and Central Nervous System Drugs Advisory Committee Meeting Announcement. Published November 12, 2020. Accessed January 14, 2021. www.fda.gov/advisory-committees/advisory-committee-calendar/november-6-2020-meeting-peripheral-and-central-nervous-system-drugs-advisory-committee-meeting
7. Cummings J. Why aducanumab is important. Nat Med. 2021;27:1498-1498. doi: 10.1038/s41591-021-01478-4
8. Alexander GC, Karlawish J. The problem of aducanumab for the treatment of Alzheimer disease. Ann Intern Med. 2021;174:1303-1304. doi: 10.7326/M21-2603
9. Mullard A. More Alzheimer’s drugs head for FDA review: what scientists are watching. Nature. 2021;599:544-545. doi: 10.1038/d41586-021-03410-9
10. Rosenberg A, Mangialasche F, Ngandu T, et al. Multidomain interventions to prevent cognitive impairment, Alzheimer’s disease, and dementia: from finger to world-wide fingers. J Prev Alzheimers Dis. 2019:1-8. doi: 10.14283/jpad.2019.41
11. FDA. Commissioner of the FDA allows marketing of first direct-to-consumer tests that provide genetic risk information for certain conditions. Published March 24, 2020. Accessed November 7, 2020. www.fda.gov/news-events/press-announcements/fda-allows-marketing-first-direct-consumer-tests-provide-genetic-risk-information-certain-conditions
12. Blell M, Hunter MA. Direct-to-consumer genetic testing’s red herring: “genetic ancestry” and personalized medicine. Front Med. 2019;6:48. doi: 10.3389/fmed.2019.00048
13. Ekstrand B, Scheers N, Rasmussen MK, et al. Brain foods - the role of diet in brain performance and health. Nutr Rev. 2021;79:693-708. doi: 10.1093/nutrit/nuaa091
14. Cherian L, Wang Y, Fakuda K, et al. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diet slows cognitive decline after stroke. J Prev Alzheimers Dis. 2019;6:267-273. doi: 10.14283/jpad.2019.28
15. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet. 2020;396:413-446. doi: 10.1016/S0140-6736(20)30367-6
16. Livingston PG, Sommerlad A, Orgeta V, et al. The Lancet International Commission on Dementia Prevention and Care. 2017. Accessed March 30, 2022. https://discovery.ucl.ac.uk/id/eprint/1567635/1/Livingston_Dementia_prevention_intervention_care.pdf
17. Peters U. What is the function of confirmation bias? Erkenntnis. April 2020. doi: 10.1007/s10670-020-00252-1
18. Barnes LL, Bennett DA. Cognitive resilience in APOE*ε4 carriers—is race important? Nat Rev Neurol. 2015;11:190-191. doi: 10.1038/nrneurol.2015.38
19. Farrer LA. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease: a meta-analysis. JAMA. 1997;278:1349. doi: 10.1001/jama.1997.03550160069041
20. Evans DA, Bennett DA, Wilson RS, et al. Incidence of Alzheimer disease in a biracial urban community: relation to apolipoprotein E allele status. Arch Neurol. 2003;60:185. doi: 10.1001/archneur.60.2.185
21. Chung WW, Chen CA, Cupples LA, et al. A new scale measuring psychologic impact of genetic susceptibility testing for Alzheimer disease. Alzheimer Dis Assoc Disord. 2009;23:50-56. doi: 10.1097/WAD.0b013e318188429e
22. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi: 10.1046/j.1525-1497.2001.016009606.x
23. Yesavage JA, Sheikh JI. 9/Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5:165-173. doi: 10.1300/J018v05n01_09
24. Green RC, Roberts JS, Cupples LA, et al. Disclosure of APOE genotype for risk of Alzheimer’s disease. N Engl J Med. 2009;361:245-254. doi: 10.1056/NEJMoa0809578
25. Lineweaver TT, Bondi MW, Galasko D, et al. Effect of knowledge of APOE genotype on subjective and objective memory performance in healthy older adults. Am J Psychiatry. 2014;171:201-208. doi: 10.1176/appi.ajp.2013.12121590
26. Karlawish J. Understanding the impact of learning an amyloid PET scan result: preliminary findings from the SOKRATES study. Alzheimers Dement J Alzheimers Assoc. 2016;12:P325. doi: 10.1016/j.jalz.2016.06.594
27. Stites SD. Cognitively healthy individuals want to know their risk for Alzheimer’s disease: what should we do? J Alzheimers Dis. 2018;62:499-502. doi: 10.3233/JAD-171089
28. Milne S, Lomax C, Freeston MH. A review of the relationship between intolerance of uncertainty and threat appraisal in anxiety. Cogn Behav Ther. 2019;12:e38. doi: 10.1017/S1754470X19000230
29. Hebert EA, Dugas MJ. Behavioral experiments for intolerance of uncertainty: challenging the unknown in the treatment of generalized anxiety disorder. Cogn Behav Pract. 2019;26:421-436. doi: 10.1016/j.cbpra.2018.07.007
30. Stites SD, Karlawish, J. Stigma of Alzheimer’s disease dementia: considerations for practice. Pract Neurol. Published June 2018. Accessed January 31, 2019. http://practicalneurology.com/2018/06/stigma-of-alzheimers-disease-dementia/
31. Solomon A, Turunen H, Ngandu T, et al. Effect of the apolipoprotein E genotype on cognitive change during a multidomain lifestyle intervention: a subgroup analysis of a randomized clinical trial. JAMA Neurol. 2018;75:462. doi: 10.1001/jamaneurol.2017.4365
32. Peters R, Warwick J, Anstey KJ, et al. Blood pressure and dementia: what the SPRINT-MIND trial adds and what we still need to know. Neurology. 2019;92:1017-1018. doi: 10.1212/WNL.0000000000007543
33. Musunuru K, Hershberger RE, Day SM, et al. Genetic testing for inherited cardiovascular diseases: a Scientific Statement from the American Heart Association. Circ Genom Precis Med. 2020;13: e000067. doi: 10.1161/HCG.0000000000000067
34. Margaglione M, Seripa D, Gravina C, et al. Prevalence of apolipoprotein E alleles in healthy subjects and survivors of ischemic stroke. Stroke. 1998;29:399-403. doi: 10.1161/01.STR.29.2.399
35. National Institute on Aging. Alzheimer’s disease genetics fact sheet. Reviewed December 24, 2019. Accessed April 10, 2022. www.nia.nih.gov/health/alzheimers-disease-genetics-fact-sheet
36. Belluck P, Kaplan S, Robbins R. How Aduhelm, an unproven Alzheimer’s drug, got approved. The New York Times. Published July 19, 2021. Updated Oct. 20, 2021. Accessed December 1, 2021. www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html
1. Jack CR, Bennett DA, Blennow K, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement J Alzheimers Assoc. 2018;14:535-562. doi: 10.1016/j.jalz.2018.02.018 PMCID:PMC5958625
2. Langlois CM, Bradbury A, Wood EM, et al. Alzheimer’s Prevention Initiative Generation Program: development of an APOE genetic counseling and disclosure process in the context of clinical trials. Alzheimers Dement Transl Res Clin Interv. 2019;5:705-716. doi: 10.1016/j.trci.2019.09.013
3. Frank L, Wesson Ashford J, Bayley PJ, et al. Genetic risk of Alzheimer’s disease: three wishes now that the genie is out of the bottle. J Alzheimers Dis. 2018;66:421-423. doi: 10.3233/JAD-180629
4. Qian J, Wolters FJ, Beiser A, et al. APOE-related risk of mild cognitive impairment and dementia for prevention trials: an analysis of four cohorts. PLOS Med. 2017;14:e1002254. doi: 10.1371/journal.pmed.1002254
5. Sperling RA, Jack CR, Black SE, et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer’s Association Research Roundtable Workgroup. Alzheimers Dement. 2011;7:367-385. doi: 10.1016/j.jalz.2011.05.2351
6. FDA. November 6, 2020: Meeting of the Peripheral and Central Nervous System Drugs Advisory Committee Meeting Announcement. Published November 12, 2020. Accessed January 14, 2021. www.fda.gov/advisory-committees/advisory-committee-calendar/november-6-2020-meeting-peripheral-and-central-nervous-system-drugs-advisory-committee-meeting
7. Cummings J. Why aducanumab is important. Nat Med. 2021;27:1498-1498. doi: 10.1038/s41591-021-01478-4
8. Alexander GC, Karlawish J. The problem of aducanumab for the treatment of Alzheimer disease. Ann Intern Med. 2021;174:1303-1304. doi: 10.7326/M21-2603
9. Mullard A. More Alzheimer’s drugs head for FDA review: what scientists are watching. Nature. 2021;599:544-545. doi: 10.1038/d41586-021-03410-9
10. Rosenberg A, Mangialasche F, Ngandu T, et al. Multidomain interventions to prevent cognitive impairment, Alzheimer’s disease, and dementia: from finger to world-wide fingers. J Prev Alzheimers Dis. 2019:1-8. doi: 10.14283/jpad.2019.41
11. FDA. Commissioner of the FDA allows marketing of first direct-to-consumer tests that provide genetic risk information for certain conditions. Published March 24, 2020. Accessed November 7, 2020. www.fda.gov/news-events/press-announcements/fda-allows-marketing-first-direct-consumer-tests-provide-genetic-risk-information-certain-conditions
12. Blell M, Hunter MA. Direct-to-consumer genetic testing’s red herring: “genetic ancestry” and personalized medicine. Front Med. 2019;6:48. doi: 10.3389/fmed.2019.00048
13. Ekstrand B, Scheers N, Rasmussen MK, et al. Brain foods - the role of diet in brain performance and health. Nutr Rev. 2021;79:693-708. doi: 10.1093/nutrit/nuaa091
14. Cherian L, Wang Y, Fakuda K, et al. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diet slows cognitive decline after stroke. J Prev Alzheimers Dis. 2019;6:267-273. doi: 10.14283/jpad.2019.28
15. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet. 2020;396:413-446. doi: 10.1016/S0140-6736(20)30367-6
16. Livingston PG, Sommerlad A, Orgeta V, et al. The Lancet International Commission on Dementia Prevention and Care. 2017. Accessed March 30, 2022. https://discovery.ucl.ac.uk/id/eprint/1567635/1/Livingston_Dementia_prevention_intervention_care.pdf
17. Peters U. What is the function of confirmation bias? Erkenntnis. April 2020. doi: 10.1007/s10670-020-00252-1
18. Barnes LL, Bennett DA. Cognitive resilience in APOE*ε4 carriers—is race important? Nat Rev Neurol. 2015;11:190-191. doi: 10.1038/nrneurol.2015.38
19. Farrer LA. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease: a meta-analysis. JAMA. 1997;278:1349. doi: 10.1001/jama.1997.03550160069041
20. Evans DA, Bennett DA, Wilson RS, et al. Incidence of Alzheimer disease in a biracial urban community: relation to apolipoprotein E allele status. Arch Neurol. 2003;60:185. doi: 10.1001/archneur.60.2.185
21. Chung WW, Chen CA, Cupples LA, et al. A new scale measuring psychologic impact of genetic susceptibility testing for Alzheimer disease. Alzheimer Dis Assoc Disord. 2009;23:50-56. doi: 10.1097/WAD.0b013e318188429e
22. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi: 10.1046/j.1525-1497.2001.016009606.x
23. Yesavage JA, Sheikh JI. 9/Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5:165-173. doi: 10.1300/J018v05n01_09
24. Green RC, Roberts JS, Cupples LA, et al. Disclosure of APOE genotype for risk of Alzheimer’s disease. N Engl J Med. 2009;361:245-254. doi: 10.1056/NEJMoa0809578
25. Lineweaver TT, Bondi MW, Galasko D, et al. Effect of knowledge of APOE genotype on subjective and objective memory performance in healthy older adults. Am J Psychiatry. 2014;171:201-208. doi: 10.1176/appi.ajp.2013.12121590
26. Karlawish J. Understanding the impact of learning an amyloid PET scan result: preliminary findings from the SOKRATES study. Alzheimers Dement J Alzheimers Assoc. 2016;12:P325. doi: 10.1016/j.jalz.2016.06.594
27. Stites SD. Cognitively healthy individuals want to know their risk for Alzheimer’s disease: what should we do? J Alzheimers Dis. 2018;62:499-502. doi: 10.3233/JAD-171089
28. Milne S, Lomax C, Freeston MH. A review of the relationship between intolerance of uncertainty and threat appraisal in anxiety. Cogn Behav Ther. 2019;12:e38. doi: 10.1017/S1754470X19000230
29. Hebert EA, Dugas MJ. Behavioral experiments for intolerance of uncertainty: challenging the unknown in the treatment of generalized anxiety disorder. Cogn Behav Pract. 2019;26:421-436. doi: 10.1016/j.cbpra.2018.07.007
30. Stites SD, Karlawish, J. Stigma of Alzheimer’s disease dementia: considerations for practice. Pract Neurol. Published June 2018. Accessed January 31, 2019. http://practicalneurology.com/2018/06/stigma-of-alzheimers-disease-dementia/
31. Solomon A, Turunen H, Ngandu T, et al. Effect of the apolipoprotein E genotype on cognitive change during a multidomain lifestyle intervention: a subgroup analysis of a randomized clinical trial. JAMA Neurol. 2018;75:462. doi: 10.1001/jamaneurol.2017.4365
32. Peters R, Warwick J, Anstey KJ, et al. Blood pressure and dementia: what the SPRINT-MIND trial adds and what we still need to know. Neurology. 2019;92:1017-1018. doi: 10.1212/WNL.0000000000007543
33. Musunuru K, Hershberger RE, Day SM, et al. Genetic testing for inherited cardiovascular diseases: a Scientific Statement from the American Heart Association. Circ Genom Precis Med. 2020;13: e000067. doi: 10.1161/HCG.0000000000000067
34. Margaglione M, Seripa D, Gravina C, et al. Prevalence of apolipoprotein E alleles in healthy subjects and survivors of ischemic stroke. Stroke. 1998;29:399-403. doi: 10.1161/01.STR.29.2.399
35. National Institute on Aging. Alzheimer’s disease genetics fact sheet. Reviewed December 24, 2019. Accessed April 10, 2022. www.nia.nih.gov/health/alzheimers-disease-genetics-fact-sheet
36. Belluck P, Kaplan S, Robbins R. How Aduhelm, an unproven Alzheimer’s drug, got approved. The New York Times. Published July 19, 2021. Updated Oct. 20, 2021. Accessed December 1, 2021. www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html

Ex–hospital porter a neglected giant of cancer research
We have a half-forgotten Indian immigrant to thank – a hospital night porter turned biochemist –for revolutionizing treatment of leukemia, the once deadly childhood scourge that is still the most common pediatric cancer.
Dr. Yellapragada SubbaRow has been called the “father of chemotherapy” for developing methotrexate, a powerful, inexpensive therapy for leukemia and other diseases, and he is celebrated for additional scientific achievements. Yet Dr. SubbaRow’s life was marked more by struggle than glory.
Born poor in southeastern India, he nearly succumbed to a tropical disease that killed two older brothers, and he didn’t focus on schoolwork until his father died. Later, prejudice dogged his years as an immigrant to the United States, and a blood clot took his life at the age of 53.
Scientifically, however, Dr. SubbaRow (pronounced sue-buh-rao) triumphed, despite mammoth challenges and a lack of recognition that persists to this day. National Cancer Research Month is a fitting time to look back on his extraordinary life and work and pay tribute to his accomplishments.
‘Yella,’ folic acid, and a paradigm shift
No one appreciates Dr. SubbaRow more than a cadre of Indian-born physicians who have kept his legacy alive in journal articles, presentations, and a Pulitzer Prize-winning book. Among them is author and oncologist Siddhartha Mukherjee, MD, who chronicled Dr. SubbaRow’s achievements in his New York Times No. 1 bestseller, “The Emperor of All Maladies: A Biography of Cancer.”
As Dr. Mukherjee wrote, Dr. SubbaRow was a “pioneer in many ways, a physician turned cellular physiologist, a chemist who had accidentally wandered into biology.” (Per Indian tradition, SubbaRow is the doctor’s first name, and Yellapragada is his surname, but medical literature uses SubbaRow as his cognomen, with some variations in spelling. Dr. Mukherjee wrote that his friends called him “Yella.”)
Dr. SubbaRow came to the United States in 1923, after enduring a difficult childhood and young adulthood. He’d survived bouts of religious fervor, childhood rebellion (including a bid to run away from home and become a banana trader), and a failed arranged marriage. His wife bore him a child who died in infancy. He left it all behind.
In Boston, medical officials rejected his degree. Broke, he worked for a time as a night porter at Brigham and Women’s Hospital in Boston, changing sheets and cleaning urinals. To a poor but proud high-caste Indian Brahmin, the culture shock of carrying out these tasks must have been especially jarring.
Dr. SubbaRow went on to earn a diploma from Harvard Medical School, also in Boston, and became a junior faculty member. As a foreigner, Dr. Mukherjee wrote, Dr. SubbaRow was a “reclusive, nocturnal, heavily accented vegetarian,” so different from his colleagues that advancement seemed impossible. Despite his pioneering biochemistry work, Harvard later declined to offer Dr. SubbaRow a tenured faculty position.
By the early 1940s, he took a job at an upstate New York pharmaceutical company called Lederle Labs (later purchased by Pfizer). At Lederle, Dr. SubbaRow strove to synthesize the vitamin known as folic acid. He ended up creating a kind of antivitamin, a lookalike that acted like folic acid but only succeeded in gumming up the works in receptors. But what good would it do to stop the body from absorbing folic acid? Plenty, it turned out.
Discoveries pile up, but credit and fame prove elusive
Dr. SubbaRow was no stranger to producing landmark biological work. He’d previously codiscovered phosphocreatine and ATP, which are crucial to muscular contractions. However, “in 1935, he had to disown the extent of his role in the discovery of the color test related to phosphorus, instead giving the credit to his co-author, who was being considered for promotion to a full professorship at Harvard,” wrote author Gerald Posner in his 2020 book, “Pharma: Greed, Lies and the Poisoning of America.”
Houston-area oncologist Kirtan Nautiyal, MD, who paid tribute to Dr. SubbaRow in a 2018 article, contended that “with his Indian instinct for self-effacement, he had irreparably sabotaged his own career.”
Dr. SubbaRow and his team also developed “the first effective treatment of filariasis, which causes elephantiasis of the lower limbs and genitals in millions of people, mainly in tropical countries,” Dr. Nautiyal wrote. “Later in the decade, his antibiotic program generated polymyxin, the first effective treatment against the class of bacteria called Gram negatives, and aureomycin, the first “broad-spectrum’ antibiotic.” (Aureomycin is also the first tetracycline antibiotic.)
Dr. SubbaRow’s discovery of a folic acid antagonist would again go largely unheralded. But first came the realization that folic acid made childhood leukemia worse, not better, and the prospect that this process could potentially be reversed.
Rise of methotrexate and fall of leukemia
In Boston, Sidney Farber, MD, a Boston pathologist, was desperate to help Robert Sandler, a 2-year-old leukemia patient. Dr. Farber contacted his ex-colleague Dr. SubbaRow to request a supply of aminopterin, an early version of methotrexate that Dr. SubbaRow and his team had developed. Dr. Farber injected Robert with the substance and within 3 days, the toddler’s white blood count started falling – fast. He stopped bleeding, resumed eating, and once again seemed almost identical to his twin brother, as Dr. Mukherjee wrote in his book.
Leukemia had never gone into remission before. Unfortunately, the treatment only worked temporarily. Robert, like other children treated with the drug, relapsed and died within months. But Dr. Farber “saw a door open” – a chemical, a kind of chemotherapy, that could turn back cancer. In the case of folic acid antagonists, they do so by stopping cancer cells from replicating.
Methotrexate, a related agent synthesized by Dr. SubbaRow, would become a mainstay of leukemia treatment and begin to produce long-term remission from acute lymphoblastic leukemia in 1970, when combination chemotherapy was developed.
Other cancers fell to methotrexate treatment. “Previous assumptions that cancer was nearly always fatal were revised, and the field of medical oncology (treatment of cancer with chemotherapy), which had not previously existed, was formally established in 1971,” according to the National Cancer Institute’s history of methotrexate. This account does not mention Dr. SubbaRow.
Death takes the doctor, but his legacy remains
In biographies, as well as his own words, Dr. SubbaRow comes across as a prickly, hard-driving workaholic who had little interest in intimate human connections. “It is not good to ask in every letter when I will be back,” he wrote to his wife back in India, before cutting off ties completely in the early 1930s. “I will come as early as possible. ... I do not want to write anything more.”
It seems, as his biographer S.P.K. Gupta noted, that “he was quite determined that the time allotted to him on Earth should be completely devoted to finding cures for ailments that plagued mankind.”
Still, Dr. SubbaRow’s research team was devoted to him, and he had plenty of reasons to be bitter, such as the prejudice and isolation he encountered in the United States and earlier, in British-run India. According to Mr. Posner’s book, even as a young medical student, Dr. SubbaRow heeded the call of Indian independence activist Mohandas Gandhi. He “refused the British surgical gown given him at school and instead donned a traditional and simple cotton Khadi. That act of defiance cost SubbaRow the college degree that was necessary for him to get into the State Medical College.”
During the last year of his life, Dr. SubbaRow faced yet another humiliation: In his landmark 1948 study about aminopterin as a treatment for leukemia, his colleague Dr. Farber failed to credit him, an “astonishing omission” as Yaddanapudi Ravindranath, MBBS, a pediatric hematologist/oncologist at Wayne State University, Detroit, put it. “From everything I know, Dr. Farber spent the rest of his career apologizing and trying to make amends for it,” Dr. Ravindranath said in an interview.
A career cut short, and a lasting legacy
In 1948, at the age of 53, Dr. SubbaRow suddenly died. “Many think Dr. SubbaRow would have won [the] Nobel Prize had he lived a few years longer,” said Dr. Ravindranath.
Like Dr. SubbaRow, Dr. Ravindranath was born in Andhra Pradesh state, near the city of Chennai formerly known as Madras. “Being a compatriot, in a way I continue his legacy, and I am obviously proud of him,” said Dr. Ravindranath, who has conducted his own landmark research regarding methotrexate and leukemia.
Nearly 75 years after Dr. SubbaRow’s death, Indian-born physicians like Dr. Ravindranath continue to honor him in print, trying to ensure that he’s not forgotten. Methotrexate remains a crucial treatment for leukemia, along with a long list of other ailments, including psoriasis.
Recognition for “Yella” may have come late and infrequently, but a Lederle Laboratories research library named after him offered Dr. SubbaRow a kind of immortality. A plaque there memorialized him in stone as a scientist, teacher, philosopher, and humanitarian, featuring the quote: “Science simply prolongs life. Religion deepens it.”
By all accounts, Dr. SubbaRow was a man of science and faith who had faith in science.
We have a half-forgotten Indian immigrant to thank – a hospital night porter turned biochemist –for revolutionizing treatment of leukemia, the once deadly childhood scourge that is still the most common pediatric cancer.
Dr. Yellapragada SubbaRow has been called the “father of chemotherapy” for developing methotrexate, a powerful, inexpensive therapy for leukemia and other diseases, and he is celebrated for additional scientific achievements. Yet Dr. SubbaRow’s life was marked more by struggle than glory.
Born poor in southeastern India, he nearly succumbed to a tropical disease that killed two older brothers, and he didn’t focus on schoolwork until his father died. Later, prejudice dogged his years as an immigrant to the United States, and a blood clot took his life at the age of 53.
Scientifically, however, Dr. SubbaRow (pronounced sue-buh-rao) triumphed, despite mammoth challenges and a lack of recognition that persists to this day. National Cancer Research Month is a fitting time to look back on his extraordinary life and work and pay tribute to his accomplishments.
‘Yella,’ folic acid, and a paradigm shift
No one appreciates Dr. SubbaRow more than a cadre of Indian-born physicians who have kept his legacy alive in journal articles, presentations, and a Pulitzer Prize-winning book. Among them is author and oncologist Siddhartha Mukherjee, MD, who chronicled Dr. SubbaRow’s achievements in his New York Times No. 1 bestseller, “The Emperor of All Maladies: A Biography of Cancer.”
As Dr. Mukherjee wrote, Dr. SubbaRow was a “pioneer in many ways, a physician turned cellular physiologist, a chemist who had accidentally wandered into biology.” (Per Indian tradition, SubbaRow is the doctor’s first name, and Yellapragada is his surname, but medical literature uses SubbaRow as his cognomen, with some variations in spelling. Dr. Mukherjee wrote that his friends called him “Yella.”)
Dr. SubbaRow came to the United States in 1923, after enduring a difficult childhood and young adulthood. He’d survived bouts of religious fervor, childhood rebellion (including a bid to run away from home and become a banana trader), and a failed arranged marriage. His wife bore him a child who died in infancy. He left it all behind.
In Boston, medical officials rejected his degree. Broke, he worked for a time as a night porter at Brigham and Women’s Hospital in Boston, changing sheets and cleaning urinals. To a poor but proud high-caste Indian Brahmin, the culture shock of carrying out these tasks must have been especially jarring.
Dr. SubbaRow went on to earn a diploma from Harvard Medical School, also in Boston, and became a junior faculty member. As a foreigner, Dr. Mukherjee wrote, Dr. SubbaRow was a “reclusive, nocturnal, heavily accented vegetarian,” so different from his colleagues that advancement seemed impossible. Despite his pioneering biochemistry work, Harvard later declined to offer Dr. SubbaRow a tenured faculty position.
By the early 1940s, he took a job at an upstate New York pharmaceutical company called Lederle Labs (later purchased by Pfizer). At Lederle, Dr. SubbaRow strove to synthesize the vitamin known as folic acid. He ended up creating a kind of antivitamin, a lookalike that acted like folic acid but only succeeded in gumming up the works in receptors. But what good would it do to stop the body from absorbing folic acid? Plenty, it turned out.
Discoveries pile up, but credit and fame prove elusive
Dr. SubbaRow was no stranger to producing landmark biological work. He’d previously codiscovered phosphocreatine and ATP, which are crucial to muscular contractions. However, “in 1935, he had to disown the extent of his role in the discovery of the color test related to phosphorus, instead giving the credit to his co-author, who was being considered for promotion to a full professorship at Harvard,” wrote author Gerald Posner in his 2020 book, “Pharma: Greed, Lies and the Poisoning of America.”
Houston-area oncologist Kirtan Nautiyal, MD, who paid tribute to Dr. SubbaRow in a 2018 article, contended that “with his Indian instinct for self-effacement, he had irreparably sabotaged his own career.”
Dr. SubbaRow and his team also developed “the first effective treatment of filariasis, which causes elephantiasis of the lower limbs and genitals in millions of people, mainly in tropical countries,” Dr. Nautiyal wrote. “Later in the decade, his antibiotic program generated polymyxin, the first effective treatment against the class of bacteria called Gram negatives, and aureomycin, the first “broad-spectrum’ antibiotic.” (Aureomycin is also the first tetracycline antibiotic.)
Dr. SubbaRow’s discovery of a folic acid antagonist would again go largely unheralded. But first came the realization that folic acid made childhood leukemia worse, not better, and the prospect that this process could potentially be reversed.
Rise of methotrexate and fall of leukemia
In Boston, Sidney Farber, MD, a Boston pathologist, was desperate to help Robert Sandler, a 2-year-old leukemia patient. Dr. Farber contacted his ex-colleague Dr. SubbaRow to request a supply of aminopterin, an early version of methotrexate that Dr. SubbaRow and his team had developed. Dr. Farber injected Robert with the substance and within 3 days, the toddler’s white blood count started falling – fast. He stopped bleeding, resumed eating, and once again seemed almost identical to his twin brother, as Dr. Mukherjee wrote in his book.
Leukemia had never gone into remission before. Unfortunately, the treatment only worked temporarily. Robert, like other children treated with the drug, relapsed and died within months. But Dr. Farber “saw a door open” – a chemical, a kind of chemotherapy, that could turn back cancer. In the case of folic acid antagonists, they do so by stopping cancer cells from replicating.
Methotrexate, a related agent synthesized by Dr. SubbaRow, would become a mainstay of leukemia treatment and begin to produce long-term remission from acute lymphoblastic leukemia in 1970, when combination chemotherapy was developed.
Other cancers fell to methotrexate treatment. “Previous assumptions that cancer was nearly always fatal were revised, and the field of medical oncology (treatment of cancer with chemotherapy), which had not previously existed, was formally established in 1971,” according to the National Cancer Institute’s history of methotrexate. This account does not mention Dr. SubbaRow.
Death takes the doctor, but his legacy remains
In biographies, as well as his own words, Dr. SubbaRow comes across as a prickly, hard-driving workaholic who had little interest in intimate human connections. “It is not good to ask in every letter when I will be back,” he wrote to his wife back in India, before cutting off ties completely in the early 1930s. “I will come as early as possible. ... I do not want to write anything more.”
It seems, as his biographer S.P.K. Gupta noted, that “he was quite determined that the time allotted to him on Earth should be completely devoted to finding cures for ailments that plagued mankind.”
Still, Dr. SubbaRow’s research team was devoted to him, and he had plenty of reasons to be bitter, such as the prejudice and isolation he encountered in the United States and earlier, in British-run India. According to Mr. Posner’s book, even as a young medical student, Dr. SubbaRow heeded the call of Indian independence activist Mohandas Gandhi. He “refused the British surgical gown given him at school and instead donned a traditional and simple cotton Khadi. That act of defiance cost SubbaRow the college degree that was necessary for him to get into the State Medical College.”
During the last year of his life, Dr. SubbaRow faced yet another humiliation: In his landmark 1948 study about aminopterin as a treatment for leukemia, his colleague Dr. Farber failed to credit him, an “astonishing omission” as Yaddanapudi Ravindranath, MBBS, a pediatric hematologist/oncologist at Wayne State University, Detroit, put it. “From everything I know, Dr. Farber spent the rest of his career apologizing and trying to make amends for it,” Dr. Ravindranath said in an interview.
A career cut short, and a lasting legacy
In 1948, at the age of 53, Dr. SubbaRow suddenly died. “Many think Dr. SubbaRow would have won [the] Nobel Prize had he lived a few years longer,” said Dr. Ravindranath.
Like Dr. SubbaRow, Dr. Ravindranath was born in Andhra Pradesh state, near the city of Chennai formerly known as Madras. “Being a compatriot, in a way I continue his legacy, and I am obviously proud of him,” said Dr. Ravindranath, who has conducted his own landmark research regarding methotrexate and leukemia.
Nearly 75 years after Dr. SubbaRow’s death, Indian-born physicians like Dr. Ravindranath continue to honor him in print, trying to ensure that he’s not forgotten. Methotrexate remains a crucial treatment for leukemia, along with a long list of other ailments, including psoriasis.
Recognition for “Yella” may have come late and infrequently, but a Lederle Laboratories research library named after him offered Dr. SubbaRow a kind of immortality. A plaque there memorialized him in stone as a scientist, teacher, philosopher, and humanitarian, featuring the quote: “Science simply prolongs life. Religion deepens it.”
By all accounts, Dr. SubbaRow was a man of science and faith who had faith in science.
We have a half-forgotten Indian immigrant to thank – a hospital night porter turned biochemist –for revolutionizing treatment of leukemia, the once deadly childhood scourge that is still the most common pediatric cancer.
Dr. Yellapragada SubbaRow has been called the “father of chemotherapy” for developing methotrexate, a powerful, inexpensive therapy for leukemia and other diseases, and he is celebrated for additional scientific achievements. Yet Dr. SubbaRow’s life was marked more by struggle than glory.
Born poor in southeastern India, he nearly succumbed to a tropical disease that killed two older brothers, and he didn’t focus on schoolwork until his father died. Later, prejudice dogged his years as an immigrant to the United States, and a blood clot took his life at the age of 53.
Scientifically, however, Dr. SubbaRow (pronounced sue-buh-rao) triumphed, despite mammoth challenges and a lack of recognition that persists to this day. National Cancer Research Month is a fitting time to look back on his extraordinary life and work and pay tribute to his accomplishments.
‘Yella,’ folic acid, and a paradigm shift
No one appreciates Dr. SubbaRow more than a cadre of Indian-born physicians who have kept his legacy alive in journal articles, presentations, and a Pulitzer Prize-winning book. Among them is author and oncologist Siddhartha Mukherjee, MD, who chronicled Dr. SubbaRow’s achievements in his New York Times No. 1 bestseller, “The Emperor of All Maladies: A Biography of Cancer.”
As Dr. Mukherjee wrote, Dr. SubbaRow was a “pioneer in many ways, a physician turned cellular physiologist, a chemist who had accidentally wandered into biology.” (Per Indian tradition, SubbaRow is the doctor’s first name, and Yellapragada is his surname, but medical literature uses SubbaRow as his cognomen, with some variations in spelling. Dr. Mukherjee wrote that his friends called him “Yella.”)
Dr. SubbaRow came to the United States in 1923, after enduring a difficult childhood and young adulthood. He’d survived bouts of religious fervor, childhood rebellion (including a bid to run away from home and become a banana trader), and a failed arranged marriage. His wife bore him a child who died in infancy. He left it all behind.
In Boston, medical officials rejected his degree. Broke, he worked for a time as a night porter at Brigham and Women’s Hospital in Boston, changing sheets and cleaning urinals. To a poor but proud high-caste Indian Brahmin, the culture shock of carrying out these tasks must have been especially jarring.
Dr. SubbaRow went on to earn a diploma from Harvard Medical School, also in Boston, and became a junior faculty member. As a foreigner, Dr. Mukherjee wrote, Dr. SubbaRow was a “reclusive, nocturnal, heavily accented vegetarian,” so different from his colleagues that advancement seemed impossible. Despite his pioneering biochemistry work, Harvard later declined to offer Dr. SubbaRow a tenured faculty position.
By the early 1940s, he took a job at an upstate New York pharmaceutical company called Lederle Labs (later purchased by Pfizer). At Lederle, Dr. SubbaRow strove to synthesize the vitamin known as folic acid. He ended up creating a kind of antivitamin, a lookalike that acted like folic acid but only succeeded in gumming up the works in receptors. But what good would it do to stop the body from absorbing folic acid? Plenty, it turned out.
Discoveries pile up, but credit and fame prove elusive
Dr. SubbaRow was no stranger to producing landmark biological work. He’d previously codiscovered phosphocreatine and ATP, which are crucial to muscular contractions. However, “in 1935, he had to disown the extent of his role in the discovery of the color test related to phosphorus, instead giving the credit to his co-author, who was being considered for promotion to a full professorship at Harvard,” wrote author Gerald Posner in his 2020 book, “Pharma: Greed, Lies and the Poisoning of America.”
Houston-area oncologist Kirtan Nautiyal, MD, who paid tribute to Dr. SubbaRow in a 2018 article, contended that “with his Indian instinct for self-effacement, he had irreparably sabotaged his own career.”
Dr. SubbaRow and his team also developed “the first effective treatment of filariasis, which causes elephantiasis of the lower limbs and genitals in millions of people, mainly in tropical countries,” Dr. Nautiyal wrote. “Later in the decade, his antibiotic program generated polymyxin, the first effective treatment against the class of bacteria called Gram negatives, and aureomycin, the first “broad-spectrum’ antibiotic.” (Aureomycin is also the first tetracycline antibiotic.)
Dr. SubbaRow’s discovery of a folic acid antagonist would again go largely unheralded. But first came the realization that folic acid made childhood leukemia worse, not better, and the prospect that this process could potentially be reversed.
Rise of methotrexate and fall of leukemia
In Boston, Sidney Farber, MD, a Boston pathologist, was desperate to help Robert Sandler, a 2-year-old leukemia patient. Dr. Farber contacted his ex-colleague Dr. SubbaRow to request a supply of aminopterin, an early version of methotrexate that Dr. SubbaRow and his team had developed. Dr. Farber injected Robert with the substance and within 3 days, the toddler’s white blood count started falling – fast. He stopped bleeding, resumed eating, and once again seemed almost identical to his twin brother, as Dr. Mukherjee wrote in his book.
Leukemia had never gone into remission before. Unfortunately, the treatment only worked temporarily. Robert, like other children treated with the drug, relapsed and died within months. But Dr. Farber “saw a door open” – a chemical, a kind of chemotherapy, that could turn back cancer. In the case of folic acid antagonists, they do so by stopping cancer cells from replicating.
Methotrexate, a related agent synthesized by Dr. SubbaRow, would become a mainstay of leukemia treatment and begin to produce long-term remission from acute lymphoblastic leukemia in 1970, when combination chemotherapy was developed.
Other cancers fell to methotrexate treatment. “Previous assumptions that cancer was nearly always fatal were revised, and the field of medical oncology (treatment of cancer with chemotherapy), which had not previously existed, was formally established in 1971,” according to the National Cancer Institute’s history of methotrexate. This account does not mention Dr. SubbaRow.
Death takes the doctor, but his legacy remains
In biographies, as well as his own words, Dr. SubbaRow comes across as a prickly, hard-driving workaholic who had little interest in intimate human connections. “It is not good to ask in every letter when I will be back,” he wrote to his wife back in India, before cutting off ties completely in the early 1930s. “I will come as early as possible. ... I do not want to write anything more.”
It seems, as his biographer S.P.K. Gupta noted, that “he was quite determined that the time allotted to him on Earth should be completely devoted to finding cures for ailments that plagued mankind.”
Still, Dr. SubbaRow’s research team was devoted to him, and he had plenty of reasons to be bitter, such as the prejudice and isolation he encountered in the United States and earlier, in British-run India. According to Mr. Posner’s book, even as a young medical student, Dr. SubbaRow heeded the call of Indian independence activist Mohandas Gandhi. He “refused the British surgical gown given him at school and instead donned a traditional and simple cotton Khadi. That act of defiance cost SubbaRow the college degree that was necessary for him to get into the State Medical College.”
During the last year of his life, Dr. SubbaRow faced yet another humiliation: In his landmark 1948 study about aminopterin as a treatment for leukemia, his colleague Dr. Farber failed to credit him, an “astonishing omission” as Yaddanapudi Ravindranath, MBBS, a pediatric hematologist/oncologist at Wayne State University, Detroit, put it. “From everything I know, Dr. Farber spent the rest of his career apologizing and trying to make amends for it,” Dr. Ravindranath said in an interview.
A career cut short, and a lasting legacy
In 1948, at the age of 53, Dr. SubbaRow suddenly died. “Many think Dr. SubbaRow would have won [the] Nobel Prize had he lived a few years longer,” said Dr. Ravindranath.
Like Dr. SubbaRow, Dr. Ravindranath was born in Andhra Pradesh state, near the city of Chennai formerly known as Madras. “Being a compatriot, in a way I continue his legacy, and I am obviously proud of him,” said Dr. Ravindranath, who has conducted his own landmark research regarding methotrexate and leukemia.
Nearly 75 years after Dr. SubbaRow’s death, Indian-born physicians like Dr. Ravindranath continue to honor him in print, trying to ensure that he’s not forgotten. Methotrexate remains a crucial treatment for leukemia, along with a long list of other ailments, including psoriasis.
Recognition for “Yella” may have come late and infrequently, but a Lederle Laboratories research library named after him offered Dr. SubbaRow a kind of immortality. A plaque there memorialized him in stone as a scientist, teacher, philosopher, and humanitarian, featuring the quote: “Science simply prolongs life. Religion deepens it.”
By all accounts, Dr. SubbaRow was a man of science and faith who had faith in science.
PPIs should be used ‘judiciously’ in patients with cirrhosis
In a retrospective study to evaluate the impact of proton pump inhibitors (PPIs) on all-cause mortality in patients with cirrhosis, researchers found reduced mortality only in those hospitalized for gastrointestinal bleeding. They reported increased liver-related mortality associated with PPIs in all other patients with cirrhosis.
Patients on PPIs had an 18% reduction in all-cause mortality versus other patients if they had gastrointestinal bleeding. But in those without bleeding, PPIs were associated with a 23% increase in liver-related mortality.
Further analysis suggested that the mortality increase could be related to a 21% increased risk for severe infection with PPI exposure in patients with cirrhosis, as well as a 64% increased risk for decompensation.
“My takeaway from this study is that there should be a nuanced understanding of PPIs and cirrhosis,” corresponding author Nadim Mahmud, MD, MS, University of Pennsylvania, Philadelphia, said in an interview, adding that, if they are to be used in this setting, there should be “a very compelling indication.”
Based on the new analysis, Dr. Mahmud explained, in a patient with cirrhosis hospitalized with a potentially ulcer-related upper gastrointestinal bleed, “we shouldn’t be afraid” to use PPIs “out of fear of potential infection or decompensation because our data demonstrate pretty strongly that that sort of patient may have a mortality benefit.”
In contrast, patients with cirrhosis and “vague abdominal discomfort” are often started on a PPI “just to see if that helps,” Dr. Mahmud said, and they may stay on the medication “in perpetuity, just because they’re so ubiquitously prescribed.”
“In that patient, we should recognize that there is a potential risk of increased infection and decompensation,” he said. There “should be an active effort to deprescribe the PPI or at the very least reduce it to the minimum dose needed for efficacy, if it’s treating a symptom.”
The research was published online in Gastroenterology.
Looking at the big picture of PPIs in people with cirrhosis
The authors noted that the half-life of PPIs is “prolonged in patients with cirrhosis” and that alterations in the gastrointestinal microbiota as a result of gastric acid suppression “may allow for bacterial overgrowth and translocation,” thus increasing the risk for infections.
However, studies of the impact of PPIs on adverse outcomes in patients with cirrhosis have often been hampered by numerous limitations, such as small sample sizes, a “limited ability to control for complex confounding,” or a “narrow focus” on hospitalized patients.
To overcome these problems, the team retrospectively examined data from the Veterans Outcomes and Costs Associated with Liver Diseases cohort, including all adults with incident cirrhosis between January 2008 and June 2021.
They excluded patients with Fibrosis-4 scores less than 1.45 at baseline, as well as those with prior liver transplantation, decompensated cirrhosis at baseline, a diagnosis of hepatocellular carcinoma within 6 months of the index date, and less than 6 months of follow-up.
In all, 76,251 patients with incident cirrhosis met the inclusion criteria, 21% of whom were on a PPI at baseline. The most commonly used PPIs were omeprazole (76.7%), followed by pantoprazole (22.2%) and lansoprazole (0.1%).
Those taking the drugs were more likely than other patients to be White, have metabolic and cardiovascular comorbidities, have a higher median body mass index, and were more likely to have cirrhosis because of alcohol-related liver disease or metabolic-associated fatty liver disease.
Over 49 months of follow-up, all-cause mortality was recorded for 37.5% of patients, of whom 59% experienced non–liver-related death and 41% liver-related mortality.
Multivariate analysis revealed that PPI exposure was not associated with all-cause mortality overall but was significantly associated with reduced all-cause mortality in patients with hospitalization for gastrointestinal bleeding, at a hazard ratio of 0.88.
However, PPI exposure in patients without gastrointestinal bleeding was associated with an increased risk for liver-related mortality (HR, 1.23), but a reduced risk for non–liver-related mortality (HR, 0.88).
Dr. Mahmud and colleagues found that PPI exposure was significantly associated with severe infection (HR, 1.21) and cirrhosis decompensation (HR, 1.64).
The authors suggested that these increased risks “may mediate the observed increased in liver-related mortality.”
Large study suggests limited protective PPI indication
Nancy S. Reau, MD, chair of hepatology at Rush Medical College, Chicago, said that “multiple studies” point to a link between PPI exposure and infection in cirrhosis.
“Although this is a retrospective study, it is very large so we should give credit to the associations,” she said in an interview. She was not involved with the current study.
“The most important message is that we need to be judicious with our therapy,” Dr. Reau added, qualifying that “everything is a risk-benefit ratio.”
“PPI use in cirrhosis has a role but should not overstep its boundary,” she explained. “More simply, if the PPI is indicated, you should not avoid it in a patient with cirrhosis. On the other hand, if you have a patient with advanced liver disease who is chronically taking a PPI, you should question its indication.
Paul Martin, MD, chief of the division of hepatology, University of Miami Health Systems, said in an interview that, when it comes to PPI use in patients with cirrhosis, “judicious is the right word. They should be clearly used if there’s a bona fide indication ... and probably for a finite period of time.”
In a common scenario, “a patient is put on a PPI after they’ve undergone endoscopy with obliteration of varices, and the thought is that PPIs help the ulcers induced by the banding to heal,” said Dr. Martin, who was not associated with the research. “This paper didn’t specifically tease out whether that’s beneficial or not, but it certainly suggests, in patients with a history of gastrointestinal bleeding, that PPIs are still beneficial.”
Dr. Mahmud is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One coauthor is supported by a National Institutes of Health K23 grant; another is supported by a VA Merit Grant and by a National Cancer Institute R01; a third has received unrelated support from Gilead, Glycotest, and Bayer and also is supported by VA Merit Grants. Dr. Reau and Dr. Martin disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a retrospective study to evaluate the impact of proton pump inhibitors (PPIs) on all-cause mortality in patients with cirrhosis, researchers found reduced mortality only in those hospitalized for gastrointestinal bleeding. They reported increased liver-related mortality associated with PPIs in all other patients with cirrhosis.
Patients on PPIs had an 18% reduction in all-cause mortality versus other patients if they had gastrointestinal bleeding. But in those without bleeding, PPIs were associated with a 23% increase in liver-related mortality.
Further analysis suggested that the mortality increase could be related to a 21% increased risk for severe infection with PPI exposure in patients with cirrhosis, as well as a 64% increased risk for decompensation.
“My takeaway from this study is that there should be a nuanced understanding of PPIs and cirrhosis,” corresponding author Nadim Mahmud, MD, MS, University of Pennsylvania, Philadelphia, said in an interview, adding that, if they are to be used in this setting, there should be “a very compelling indication.”
Based on the new analysis, Dr. Mahmud explained, in a patient with cirrhosis hospitalized with a potentially ulcer-related upper gastrointestinal bleed, “we shouldn’t be afraid” to use PPIs “out of fear of potential infection or decompensation because our data demonstrate pretty strongly that that sort of patient may have a mortality benefit.”
In contrast, patients with cirrhosis and “vague abdominal discomfort” are often started on a PPI “just to see if that helps,” Dr. Mahmud said, and they may stay on the medication “in perpetuity, just because they’re so ubiquitously prescribed.”
“In that patient, we should recognize that there is a potential risk of increased infection and decompensation,” he said. There “should be an active effort to deprescribe the PPI or at the very least reduce it to the minimum dose needed for efficacy, if it’s treating a symptom.”
The research was published online in Gastroenterology.
Looking at the big picture of PPIs in people with cirrhosis
The authors noted that the half-life of PPIs is “prolonged in patients with cirrhosis” and that alterations in the gastrointestinal microbiota as a result of gastric acid suppression “may allow for bacterial overgrowth and translocation,” thus increasing the risk for infections.
However, studies of the impact of PPIs on adverse outcomes in patients with cirrhosis have often been hampered by numerous limitations, such as small sample sizes, a “limited ability to control for complex confounding,” or a “narrow focus” on hospitalized patients.
To overcome these problems, the team retrospectively examined data from the Veterans Outcomes and Costs Associated with Liver Diseases cohort, including all adults with incident cirrhosis between January 2008 and June 2021.
They excluded patients with Fibrosis-4 scores less than 1.45 at baseline, as well as those with prior liver transplantation, decompensated cirrhosis at baseline, a diagnosis of hepatocellular carcinoma within 6 months of the index date, and less than 6 months of follow-up.
In all, 76,251 patients with incident cirrhosis met the inclusion criteria, 21% of whom were on a PPI at baseline. The most commonly used PPIs were omeprazole (76.7%), followed by pantoprazole (22.2%) and lansoprazole (0.1%).
Those taking the drugs were more likely than other patients to be White, have metabolic and cardiovascular comorbidities, have a higher median body mass index, and were more likely to have cirrhosis because of alcohol-related liver disease or metabolic-associated fatty liver disease.
Over 49 months of follow-up, all-cause mortality was recorded for 37.5% of patients, of whom 59% experienced non–liver-related death and 41% liver-related mortality.
Multivariate analysis revealed that PPI exposure was not associated with all-cause mortality overall but was significantly associated with reduced all-cause mortality in patients with hospitalization for gastrointestinal bleeding, at a hazard ratio of 0.88.
However, PPI exposure in patients without gastrointestinal bleeding was associated with an increased risk for liver-related mortality (HR, 1.23), but a reduced risk for non–liver-related mortality (HR, 0.88).
Dr. Mahmud and colleagues found that PPI exposure was significantly associated with severe infection (HR, 1.21) and cirrhosis decompensation (HR, 1.64).
The authors suggested that these increased risks “may mediate the observed increased in liver-related mortality.”
Large study suggests limited protective PPI indication
Nancy S. Reau, MD, chair of hepatology at Rush Medical College, Chicago, said that “multiple studies” point to a link between PPI exposure and infection in cirrhosis.
“Although this is a retrospective study, it is very large so we should give credit to the associations,” she said in an interview. She was not involved with the current study.
“The most important message is that we need to be judicious with our therapy,” Dr. Reau added, qualifying that “everything is a risk-benefit ratio.”
“PPI use in cirrhosis has a role but should not overstep its boundary,” she explained. “More simply, if the PPI is indicated, you should not avoid it in a patient with cirrhosis. On the other hand, if you have a patient with advanced liver disease who is chronically taking a PPI, you should question its indication.
Paul Martin, MD, chief of the division of hepatology, University of Miami Health Systems, said in an interview that, when it comes to PPI use in patients with cirrhosis, “judicious is the right word. They should be clearly used if there’s a bona fide indication ... and probably for a finite period of time.”
In a common scenario, “a patient is put on a PPI after they’ve undergone endoscopy with obliteration of varices, and the thought is that PPIs help the ulcers induced by the banding to heal,” said Dr. Martin, who was not associated with the research. “This paper didn’t specifically tease out whether that’s beneficial or not, but it certainly suggests, in patients with a history of gastrointestinal bleeding, that PPIs are still beneficial.”
Dr. Mahmud is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One coauthor is supported by a National Institutes of Health K23 grant; another is supported by a VA Merit Grant and by a National Cancer Institute R01; a third has received unrelated support from Gilead, Glycotest, and Bayer and also is supported by VA Merit Grants. Dr. Reau and Dr. Martin disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a retrospective study to evaluate the impact of proton pump inhibitors (PPIs) on all-cause mortality in patients with cirrhosis, researchers found reduced mortality only in those hospitalized for gastrointestinal bleeding. They reported increased liver-related mortality associated with PPIs in all other patients with cirrhosis.
Patients on PPIs had an 18% reduction in all-cause mortality versus other patients if they had gastrointestinal bleeding. But in those without bleeding, PPIs were associated with a 23% increase in liver-related mortality.
Further analysis suggested that the mortality increase could be related to a 21% increased risk for severe infection with PPI exposure in patients with cirrhosis, as well as a 64% increased risk for decompensation.
“My takeaway from this study is that there should be a nuanced understanding of PPIs and cirrhosis,” corresponding author Nadim Mahmud, MD, MS, University of Pennsylvania, Philadelphia, said in an interview, adding that, if they are to be used in this setting, there should be “a very compelling indication.”
Based on the new analysis, Dr. Mahmud explained, in a patient with cirrhosis hospitalized with a potentially ulcer-related upper gastrointestinal bleed, “we shouldn’t be afraid” to use PPIs “out of fear of potential infection or decompensation because our data demonstrate pretty strongly that that sort of patient may have a mortality benefit.”
In contrast, patients with cirrhosis and “vague abdominal discomfort” are often started on a PPI “just to see if that helps,” Dr. Mahmud said, and they may stay on the medication “in perpetuity, just because they’re so ubiquitously prescribed.”
“In that patient, we should recognize that there is a potential risk of increased infection and decompensation,” he said. There “should be an active effort to deprescribe the PPI or at the very least reduce it to the minimum dose needed for efficacy, if it’s treating a symptom.”
The research was published online in Gastroenterology.
Looking at the big picture of PPIs in people with cirrhosis
The authors noted that the half-life of PPIs is “prolonged in patients with cirrhosis” and that alterations in the gastrointestinal microbiota as a result of gastric acid suppression “may allow for bacterial overgrowth and translocation,” thus increasing the risk for infections.
However, studies of the impact of PPIs on adverse outcomes in patients with cirrhosis have often been hampered by numerous limitations, such as small sample sizes, a “limited ability to control for complex confounding,” or a “narrow focus” on hospitalized patients.
To overcome these problems, the team retrospectively examined data from the Veterans Outcomes and Costs Associated with Liver Diseases cohort, including all adults with incident cirrhosis between January 2008 and June 2021.
They excluded patients with Fibrosis-4 scores less than 1.45 at baseline, as well as those with prior liver transplantation, decompensated cirrhosis at baseline, a diagnosis of hepatocellular carcinoma within 6 months of the index date, and less than 6 months of follow-up.
In all, 76,251 patients with incident cirrhosis met the inclusion criteria, 21% of whom were on a PPI at baseline. The most commonly used PPIs were omeprazole (76.7%), followed by pantoprazole (22.2%) and lansoprazole (0.1%).
Those taking the drugs were more likely than other patients to be White, have metabolic and cardiovascular comorbidities, have a higher median body mass index, and were more likely to have cirrhosis because of alcohol-related liver disease or metabolic-associated fatty liver disease.
Over 49 months of follow-up, all-cause mortality was recorded for 37.5% of patients, of whom 59% experienced non–liver-related death and 41% liver-related mortality.
Multivariate analysis revealed that PPI exposure was not associated with all-cause mortality overall but was significantly associated with reduced all-cause mortality in patients with hospitalization for gastrointestinal bleeding, at a hazard ratio of 0.88.
However, PPI exposure in patients without gastrointestinal bleeding was associated with an increased risk for liver-related mortality (HR, 1.23), but a reduced risk for non–liver-related mortality (HR, 0.88).
Dr. Mahmud and colleagues found that PPI exposure was significantly associated with severe infection (HR, 1.21) and cirrhosis decompensation (HR, 1.64).
The authors suggested that these increased risks “may mediate the observed increased in liver-related mortality.”
Large study suggests limited protective PPI indication
Nancy S. Reau, MD, chair of hepatology at Rush Medical College, Chicago, said that “multiple studies” point to a link between PPI exposure and infection in cirrhosis.
“Although this is a retrospective study, it is very large so we should give credit to the associations,” she said in an interview. She was not involved with the current study.
“The most important message is that we need to be judicious with our therapy,” Dr. Reau added, qualifying that “everything is a risk-benefit ratio.”
“PPI use in cirrhosis has a role but should not overstep its boundary,” she explained. “More simply, if the PPI is indicated, you should not avoid it in a patient with cirrhosis. On the other hand, if you have a patient with advanced liver disease who is chronically taking a PPI, you should question its indication.
Paul Martin, MD, chief of the division of hepatology, University of Miami Health Systems, said in an interview that, when it comes to PPI use in patients with cirrhosis, “judicious is the right word. They should be clearly used if there’s a bona fide indication ... and probably for a finite period of time.”
In a common scenario, “a patient is put on a PPI after they’ve undergone endoscopy with obliteration of varices, and the thought is that PPIs help the ulcers induced by the banding to heal,” said Dr. Martin, who was not associated with the research. “This paper didn’t specifically tease out whether that’s beneficial or not, but it certainly suggests, in patients with a history of gastrointestinal bleeding, that PPIs are still beneficial.”
Dr. Mahmud is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. One coauthor is supported by a National Institutes of Health K23 grant; another is supported by a VA Merit Grant and by a National Cancer Institute R01; a third has received unrelated support from Gilead, Glycotest, and Bayer and also is supported by VA Merit Grants. Dr. Reau and Dr. Martin disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM GASTROENTEROLOGY
Decentralizing PrEP offers a road map for retention
Good solutions have great road maps.
For HIV preexposure prophylaxis (PrEP), the road map might just be that of contraceptive care. Once an onerous process, over time contraceptive care exploded into a range of options across a broad landscape in terms of approach and accessibility.
How then do organizations help vulnerable patients navigate their PrEP journeys using the contraceptive road map as a guide?
That’s what researchers at the University of Washington were intent on demonstrating, according to Julie Dombrowski, MD, MPH, an infectious disease specialist at the University of Washington, Seattle, and deputy director of the HIV/STD Program, Public Health for the city of Seattle and King County, Wash.
“The same sorts of things that happened with oral contraceptive pills – which initially required you to see a gynecologist and get a Pap smear – over time, became much more available,” said Dr. Dombrowski, coauthor of a new study published online in the Journal of Acquired Immune Deficiency Syndrome.
“The basic idea is that PrEP is not medically complicated; it can be easily protocolized,” she told this news organization.
Decentralizing HIV PrEP
In addition to her responsibilities at University of Washington, Dr. Dombrowski provides clinical services at the Public Health Sexual Health Clinic (PHSKC) at Seattle’s Harborview Medical Center – a dual-county center that provides confidential STI and HIV evaluation, screening, testing, and treatment on a walk-in basis for a sliding fee.
Sexual health clinics are ideal environments for reaching large numbers of patients, but strategies for integrating PrEP successfully into what are commonly one-time appointments have not been well-described or broadly adopted.
“Sexual health clinics in general are STD specialty clinics with walk-in access to care; often, patients come into a clinic, get seen, diagnosed, and treated, and they don’t necessarily come back,” said Dr. Dombrowski.
She said that, because most operations have been set up around same-day treatment, to offer PrEP and successfully change outcomes, there needs to be a shift in the current model toward one that promotes an ongoing relationship with the patients.
So, she and her colleagues decided to see what would happen if they implemented a decentralized PrEP model in their clinic over a 6-year period. They established a protocol that moves from an initial consultation with a clinician to review risk behaviors, ascertain HIV status, and acquire a PrEP prescription, to ongoing interactions with an STI and PrEP-trained disease intervention specialist (DIS).
As the clinic’s PrEP program coordinators, these specialists enroll patients in PrEP drug assistance programs, verify prescription fills, provide follow-up visits and adherence and adverse events assessments, and collect specimens.
“[Disease intervention specialists] are frontline public health workers who ensure that people diagnosed with HIV or an STI – or who’ve been exposed – get necessary testing and treatment,” explained Dr. Dombrowski. “They’re very similar to patient navigators.”
At the same time, clinicians remain the key providers for annual appointments, new symptoms, STI diagnoses, adverse drug reactions, and missed doses. Licensed medical providers review all labs.
Shifting responsibilities, better PrEP initiation, retention rates
After establishing the PrEP services protocol, the University of Washington team then assessed retention rates among PrEP patients who attended an initial visit (1,387) from October 2014 to December 2019. Follow-up continued through February 2020. (For study purposes, PrEP discontinuation was defined as either stopping PrEP after initiation or as lost to follow-up, i.e., either not attending a follow-up visit or not responding to more than three DIS calls or text messages).
Just over half of the participants were aged 20-29 years, and a third were aged 30-39. More than 9 out of 10 (93%) were men who sleep with men (MSM), 55% White, 26% Hispanic/Latinx, and 10% Black.
Over the course of the study, 6,887 PrEP visits were recorded. Quarterly visits increased concurrently with the program expansion, from 31 visits in 2014 to 623 in the fourth quarter (Q4) of 2019. Likewise, while 57% of visits overall were with a clinician, DIS visits increased from 3% in Q4 of 2014 to 45% in Q4 of 2019, an increase of 1,400% in 5 years.
Significant numbers of patients also initiated PrEP in the clinic, especially when prescribing practices were expanded to be part of routine, walk-in visits.
Retention rates also improved, with 43% (510/1,190) of patients still on PrEP at the end of the analysis period. Forty-one percent (490) discontinued PrEP, 21% within 3 months of initiation, and 72% within a year; another 16% moved, transferred care, or tested positive, and were considered “censored.” However, as of July 31, 2021, 54% (265) of the 490 patients who had discontinued PrEP returned to the clinic for a restart visit, 93% of whom refilled their restart prescription.
“This is really basic preventative care and is actually quite easy to do,” noted Sarah Schmalzle, MD, assistant professor of medicine and medical director of the Thrive Program at the Institute of Human Virology at the University of Maryland, Baltimore. Dr. Schmalzle was not involved in the study.
Dr. Schmalzle practices in inner-city Baltimore, so she and her colleagues have been thorough in terms of setting up PrEP (and postexposure prophylaxis, PEP) programs to ensure that patients access PrEP wherever they want to. But she also said that PrEP is only a part of the sexual wellness and prevention toolbox, and ideally, part of a whole prevention program.
“Focusing on how to get the prescription out is great but the rest is having ongoing and accurate sexual health conversations, healthy conversations about sex and prevention, to have [an] algorithm in place that says, ‘Here’s your PrEP, this is the next time that you need an appointment, the next time you need labs, I’m going to check your adherence, etc.’ ”
Both Dr. Dombrowski and Dr. Schmalzle emphasized that decentralization is not a one-size model; flexibility is key, especially when it comes to who is providing PrEP
“People overcomplicate PrEP and clinicians do this too,” said Dr. Dombrowski. “If we are going to successfully increase PrEP and improve the patient experience, we need to decrease the requirement for clinician involvement.”
Dr. Dombrowski has disclosed no relevant financial relationships. Dr. Schmalzle receives grant funding from Gilead Sciences.
A version of this article first appeared on Medscape.com.
Good solutions have great road maps.
For HIV preexposure prophylaxis (PrEP), the road map might just be that of contraceptive care. Once an onerous process, over time contraceptive care exploded into a range of options across a broad landscape in terms of approach and accessibility.
How then do organizations help vulnerable patients navigate their PrEP journeys using the contraceptive road map as a guide?
That’s what researchers at the University of Washington were intent on demonstrating, according to Julie Dombrowski, MD, MPH, an infectious disease specialist at the University of Washington, Seattle, and deputy director of the HIV/STD Program, Public Health for the city of Seattle and King County, Wash.
“The same sorts of things that happened with oral contraceptive pills – which initially required you to see a gynecologist and get a Pap smear – over time, became much more available,” said Dr. Dombrowski, coauthor of a new study published online in the Journal of Acquired Immune Deficiency Syndrome.
“The basic idea is that PrEP is not medically complicated; it can be easily protocolized,” she told this news organization.
Decentralizing HIV PrEP
In addition to her responsibilities at University of Washington, Dr. Dombrowski provides clinical services at the Public Health Sexual Health Clinic (PHSKC) at Seattle’s Harborview Medical Center – a dual-county center that provides confidential STI and HIV evaluation, screening, testing, and treatment on a walk-in basis for a sliding fee.
Sexual health clinics are ideal environments for reaching large numbers of patients, but strategies for integrating PrEP successfully into what are commonly one-time appointments have not been well-described or broadly adopted.
“Sexual health clinics in general are STD specialty clinics with walk-in access to care; often, patients come into a clinic, get seen, diagnosed, and treated, and they don’t necessarily come back,” said Dr. Dombrowski.
She said that, because most operations have been set up around same-day treatment, to offer PrEP and successfully change outcomes, there needs to be a shift in the current model toward one that promotes an ongoing relationship with the patients.
So, she and her colleagues decided to see what would happen if they implemented a decentralized PrEP model in their clinic over a 6-year period. They established a protocol that moves from an initial consultation with a clinician to review risk behaviors, ascertain HIV status, and acquire a PrEP prescription, to ongoing interactions with an STI and PrEP-trained disease intervention specialist (DIS).
As the clinic’s PrEP program coordinators, these specialists enroll patients in PrEP drug assistance programs, verify prescription fills, provide follow-up visits and adherence and adverse events assessments, and collect specimens.
“[Disease intervention specialists] are frontline public health workers who ensure that people diagnosed with HIV or an STI – or who’ve been exposed – get necessary testing and treatment,” explained Dr. Dombrowski. “They’re very similar to patient navigators.”
At the same time, clinicians remain the key providers for annual appointments, new symptoms, STI diagnoses, adverse drug reactions, and missed doses. Licensed medical providers review all labs.
Shifting responsibilities, better PrEP initiation, retention rates
After establishing the PrEP services protocol, the University of Washington team then assessed retention rates among PrEP patients who attended an initial visit (1,387) from October 2014 to December 2019. Follow-up continued through February 2020. (For study purposes, PrEP discontinuation was defined as either stopping PrEP after initiation or as lost to follow-up, i.e., either not attending a follow-up visit or not responding to more than three DIS calls or text messages).
Just over half of the participants were aged 20-29 years, and a third were aged 30-39. More than 9 out of 10 (93%) were men who sleep with men (MSM), 55% White, 26% Hispanic/Latinx, and 10% Black.
Over the course of the study, 6,887 PrEP visits were recorded. Quarterly visits increased concurrently with the program expansion, from 31 visits in 2014 to 623 in the fourth quarter (Q4) of 2019. Likewise, while 57% of visits overall were with a clinician, DIS visits increased from 3% in Q4 of 2014 to 45% in Q4 of 2019, an increase of 1,400% in 5 years.
Significant numbers of patients also initiated PrEP in the clinic, especially when prescribing practices were expanded to be part of routine, walk-in visits.
Retention rates also improved, with 43% (510/1,190) of patients still on PrEP at the end of the analysis period. Forty-one percent (490) discontinued PrEP, 21% within 3 months of initiation, and 72% within a year; another 16% moved, transferred care, or tested positive, and were considered “censored.” However, as of July 31, 2021, 54% (265) of the 490 patients who had discontinued PrEP returned to the clinic for a restart visit, 93% of whom refilled their restart prescription.
“This is really basic preventative care and is actually quite easy to do,” noted Sarah Schmalzle, MD, assistant professor of medicine and medical director of the Thrive Program at the Institute of Human Virology at the University of Maryland, Baltimore. Dr. Schmalzle was not involved in the study.
Dr. Schmalzle practices in inner-city Baltimore, so she and her colleagues have been thorough in terms of setting up PrEP (and postexposure prophylaxis, PEP) programs to ensure that patients access PrEP wherever they want to. But she also said that PrEP is only a part of the sexual wellness and prevention toolbox, and ideally, part of a whole prevention program.
“Focusing on how to get the prescription out is great but the rest is having ongoing and accurate sexual health conversations, healthy conversations about sex and prevention, to have [an] algorithm in place that says, ‘Here’s your PrEP, this is the next time that you need an appointment, the next time you need labs, I’m going to check your adherence, etc.’ ”
Both Dr. Dombrowski and Dr. Schmalzle emphasized that decentralization is not a one-size model; flexibility is key, especially when it comes to who is providing PrEP
“People overcomplicate PrEP and clinicians do this too,” said Dr. Dombrowski. “If we are going to successfully increase PrEP and improve the patient experience, we need to decrease the requirement for clinician involvement.”
Dr. Dombrowski has disclosed no relevant financial relationships. Dr. Schmalzle receives grant funding from Gilead Sciences.
A version of this article first appeared on Medscape.com.
Good solutions have great road maps.
For HIV preexposure prophylaxis (PrEP), the road map might just be that of contraceptive care. Once an onerous process, over time contraceptive care exploded into a range of options across a broad landscape in terms of approach and accessibility.
How then do organizations help vulnerable patients navigate their PrEP journeys using the contraceptive road map as a guide?
That’s what researchers at the University of Washington were intent on demonstrating, according to Julie Dombrowski, MD, MPH, an infectious disease specialist at the University of Washington, Seattle, and deputy director of the HIV/STD Program, Public Health for the city of Seattle and King County, Wash.
“The same sorts of things that happened with oral contraceptive pills – which initially required you to see a gynecologist and get a Pap smear – over time, became much more available,” said Dr. Dombrowski, coauthor of a new study published online in the Journal of Acquired Immune Deficiency Syndrome.
“The basic idea is that PrEP is not medically complicated; it can be easily protocolized,” she told this news organization.
Decentralizing HIV PrEP
In addition to her responsibilities at University of Washington, Dr. Dombrowski provides clinical services at the Public Health Sexual Health Clinic (PHSKC) at Seattle’s Harborview Medical Center – a dual-county center that provides confidential STI and HIV evaluation, screening, testing, and treatment on a walk-in basis for a sliding fee.
Sexual health clinics are ideal environments for reaching large numbers of patients, but strategies for integrating PrEP successfully into what are commonly one-time appointments have not been well-described or broadly adopted.
“Sexual health clinics in general are STD specialty clinics with walk-in access to care; often, patients come into a clinic, get seen, diagnosed, and treated, and they don’t necessarily come back,” said Dr. Dombrowski.
She said that, because most operations have been set up around same-day treatment, to offer PrEP and successfully change outcomes, there needs to be a shift in the current model toward one that promotes an ongoing relationship with the patients.
So, she and her colleagues decided to see what would happen if they implemented a decentralized PrEP model in their clinic over a 6-year period. They established a protocol that moves from an initial consultation with a clinician to review risk behaviors, ascertain HIV status, and acquire a PrEP prescription, to ongoing interactions with an STI and PrEP-trained disease intervention specialist (DIS).
As the clinic’s PrEP program coordinators, these specialists enroll patients in PrEP drug assistance programs, verify prescription fills, provide follow-up visits and adherence and adverse events assessments, and collect specimens.
“[Disease intervention specialists] are frontline public health workers who ensure that people diagnosed with HIV or an STI – or who’ve been exposed – get necessary testing and treatment,” explained Dr. Dombrowski. “They’re very similar to patient navigators.”
At the same time, clinicians remain the key providers for annual appointments, new symptoms, STI diagnoses, adverse drug reactions, and missed doses. Licensed medical providers review all labs.
Shifting responsibilities, better PrEP initiation, retention rates
After establishing the PrEP services protocol, the University of Washington team then assessed retention rates among PrEP patients who attended an initial visit (1,387) from October 2014 to December 2019. Follow-up continued through February 2020. (For study purposes, PrEP discontinuation was defined as either stopping PrEP after initiation or as lost to follow-up, i.e., either not attending a follow-up visit or not responding to more than three DIS calls or text messages).
Just over half of the participants were aged 20-29 years, and a third were aged 30-39. More than 9 out of 10 (93%) were men who sleep with men (MSM), 55% White, 26% Hispanic/Latinx, and 10% Black.
Over the course of the study, 6,887 PrEP visits were recorded. Quarterly visits increased concurrently with the program expansion, from 31 visits in 2014 to 623 in the fourth quarter (Q4) of 2019. Likewise, while 57% of visits overall were with a clinician, DIS visits increased from 3% in Q4 of 2014 to 45% in Q4 of 2019, an increase of 1,400% in 5 years.
Significant numbers of patients also initiated PrEP in the clinic, especially when prescribing practices were expanded to be part of routine, walk-in visits.
Retention rates also improved, with 43% (510/1,190) of patients still on PrEP at the end of the analysis period. Forty-one percent (490) discontinued PrEP, 21% within 3 months of initiation, and 72% within a year; another 16% moved, transferred care, or tested positive, and were considered “censored.” However, as of July 31, 2021, 54% (265) of the 490 patients who had discontinued PrEP returned to the clinic for a restart visit, 93% of whom refilled their restart prescription.
“This is really basic preventative care and is actually quite easy to do,” noted Sarah Schmalzle, MD, assistant professor of medicine and medical director of the Thrive Program at the Institute of Human Virology at the University of Maryland, Baltimore. Dr. Schmalzle was not involved in the study.
Dr. Schmalzle practices in inner-city Baltimore, so she and her colleagues have been thorough in terms of setting up PrEP (and postexposure prophylaxis, PEP) programs to ensure that patients access PrEP wherever they want to. But she also said that PrEP is only a part of the sexual wellness and prevention toolbox, and ideally, part of a whole prevention program.
“Focusing on how to get the prescription out is great but the rest is having ongoing and accurate sexual health conversations, healthy conversations about sex and prevention, to have [an] algorithm in place that says, ‘Here’s your PrEP, this is the next time that you need an appointment, the next time you need labs, I’m going to check your adherence, etc.’ ”
Both Dr. Dombrowski and Dr. Schmalzle emphasized that decentralization is not a one-size model; flexibility is key, especially when it comes to who is providing PrEP
“People overcomplicate PrEP and clinicians do this too,” said Dr. Dombrowski. “If we are going to successfully increase PrEP and improve the patient experience, we need to decrease the requirement for clinician involvement.”
Dr. Dombrowski has disclosed no relevant financial relationships. Dr. Schmalzle receives grant funding from Gilead Sciences.
A version of this article first appeared on Medscape.com.