User login
Cervical cancer: A path to eradication
David G. Mutch, MD: The cervical cancer screening guidelines, using Pap testing, have changed significantly since the times of yearly Paps and exams. Coupled with vaccination and new management guidelines (recommending HPV testing, etc), we actually hope that we are on the way to eradicating cervical cancer from our environment.
Screening: Current recommendations
Dr. Mutch: Warner, the American Society of Colposcopy and Cervical Pathology (ASCCP)1 endorses the cervical cancer screening guidelines for several professional organizations, including the American Cancer Society (ACS),2 the US Preventive Services Task Force (USPSTF),3 and the American College of Obstetricians and Gynecologists (ACOG).4 What are the current screening recommendations, as these organizations have disparate views?
Warner Huh, MD: There was a time, around 2012-2013, when for the first time ever, we had significant harmonization of the guidelines between ACOG and the USPSTF and ACS. But in the last 10 years there has been an explosion of data in terms of how to best screen patients.
The move to primary HPV testing. The USPSTF3 initially had recommended looking into primary HPV screening, which is just using HPV testing by itself as the screening modality. But there was a lot of pushback at that time. I think a lot of people thought that we were not prepared to make that leap. Therefore, they endorsed screening with cytology by itself as well as HPV testing by itself, as well as co-testing; but in their recommendations, they made it very clear that they were leaning toward primary HPV screening.
A new patient age to begin screening. In 2020, the ACS put out their new guidelines,2 which are a significant departure from what we are used to—they are recommending that we start screening at 25 years of age. Like you said, Dr. Mutch, it doesn’t seem that long ago when we were screening people at age 18, or within 3 years of sexual intercourse. But the reason for it is that the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already do this.
The other major departure in the ACS guidelines is that they really are asking clinicians and screeners to focus on primary HPV screening. Overall, they have sort of doubled down on why they think primary HPV screening is so important.
ACOG sits sort of in the middle of the other recommendations. ACOG understands the value of primary HPV screening, but I don’t think that they are quite ready to recommend screening at age 25. If you look at their updated guidelines from April 2021,4 they state that we should continue a screening-starting age of 21 years. So there are some disparate views, but I am confident, Dr. Mutch, that in the next 2 to 3 years, there will be greater harmonization of these guidelines and less confusion for our providers. The greatest barrier is understanding the science and the comfort level of clinicians to go with just an HPV test, since for the last 40 years the Pap test has anchored gynecologic care in this country. And it took at least 10 years to get to what I consider to be widespread adoption to co-testing. The other thing that readers should recognize is that the Task Force is actually revisiting their cervical cancer screening guidance now, so expect another major revision.
Reimbursement and access are barriers. Reimbursement is a further real issue. We are now using one less test, but insurance companies may not reimburse when just the HPV test is used. The other issue is access to labs that can do the HPV testing.
Dr. Mutch: We used to see patients yearly and picked up a lot of adjunctive or additional illnesses. Now they are not being seen yearly it could impact negatively their overall health care. We need to understand that cervical cancer screening is simply a test, which should not eliminate other health care.
Dr. Huh: Yes, I think the extended interval between recommended HPV screenings scares people. I have been involved in these screening guidelines (and I can only speak for myself, not for my colleagues), but even I do think we made a leap to a longer interval way too quickly in this country. Screening changes are slow, and sometimes a glacial process. I think it can worry providers when we make rapid changes.
But this is a test that should not anchor the yearly visit. There are plenty of other reasons—and ACOG actually states this4—why patients should come for a wellness exam on a yearly basis. So I think our ObGyns in the United States need to recognize that, but I understand there are underlying concerns that if you extend intervals too long, (a) will patients come back, and (b), as a consequence, is the interval going to miss something in between? Those are real legitimate concerns.
Continue to: Management guidelines...
Management guidelines: The latest
Dr. Mutch: The ASCCP issued new management guidelines in 2019.5 Can you address what you feel are the most important updates?
Dr. Huh: Going back to 2002, we have revised these guidelines every 5 years. For this one, the revision came out a little bit later for various reasons, but the reason we revised it is because we collect new data that we think markedly changes our understanding of the disease process and natural history and the interventions for women that have preinvasive disease of the cervix.
Briefly, I think the biggest changes based on what we were hearing from our providers and users of our apps and algorithms was that our algorithms were becoming way too complicated, and they were. If you look over the last 10 years, the number of branch points on our algorithms basically quadrupled. If we incorporated the new data this time, the algorithms would be unworkable, and you could not use them on your phone because they would be too complicated.
So, we created a system where, in essence, providers have 5 choices for patients:
- treatment
- colposcopy
- follow-up in 1 year
- follow-up in 3 years
- follow-up in 5 years.
Those recommendations are based on what we call “clinically actionable thresholds”—basically, the percent chance of developing immediate CIN3 or worse. That threshold will probably change over time, but what we did is create a system that (a) makes it easier for the provider, (although they have to trust the system—and they can look under the hood and understand how we did this) and (b) allows us to create a foundation where we can add future technologies that use the same rubric or paradigm so that they still wind up getting the same result without having to go to another algorithm.
This new system is probably the most marked change in the history of the ASCCP management guidelines, but we did it to make it ultimately easier for providers going forward for the next 10 to 20 years. There are real opportunities, Dr. Mutch, in terms of how do we integrate this into the electronic medical record (EMR), and how do we pull data so clinicians don’t have to manually enter it.
The other difference is now there is a web-based application. Back in 2012, there were a lot of people that were not using EMRs. Now the majority of the country is, and so they actually are on a browser more than they are on their phone. We actually have an equally robust web platform that allows them to get the information that they need.
Dr. Mutch: I think that is really important—the utility of utilizing a mobile app, if you will, for triaging your patient with a specific test result so that patients are followed up at the proper interval, and that ultimately becomes cost-effective.
Dr. Huh: Yes, the app now is very different than the app that I think people are used to using for the last almost 10 years. You don’t put inputs, pull up the algorithm, and look at the outcome. This is different. You enter the patient’s age. You add their cytology, their HPV results, the clinical scenario that you are in, and then it puts out a recommendation of what to do next. Over time, we want to get away from an algorithm and for our providers to understand what the risk is and how that risk calculation then translates into a clinical recommendation.
Dr. Mutch: I think to utilize an app is almost necessary given the complexity of the triaging process so that it does become, in fact, the most cost-effective way to screen patients.
Dr. Huh: I would agree with that. There is a learning curve for whenever you see new technology. There was a learning curve for even ASCCP leadership as they tried to educate providers. I think people will ultimately see that this is a much better way of managing patients with cervical abnormalities, and I am hoping actually that we will use a similar platform for many other diseases that we manage in women’s health.
Continue to: Chipping away of the yearly exam...
Chipping away of the yearly exam
Dr. Mutch: With this moving away from the yearly exam and Pap test, women may not get yearly examinations. Do you feel that this could affect a stage migration to a higher stage at diagnosis, for instance, of a cervical cancer? Or that it might adversely impact other health issues?
Dr. Huh: I think that’s a good question. I am worried about the interval—I think 5 years is a bit long. I am more worried that patients will miss out on visits because they may think that they need to only come back for their Pap, even though they should be re-educated on that.
COVID-19 has made this a little hard for us to analyze because, clearly, we have had access to care issues. But I am a little concerned that we could see an uptick in invasive cancer rates in this country, including an uptick in the stage and more locally advanced cervical cancer because of the changes in the screening paradigms. But we don’t know that to be the case.
As with all screenings, the bottom line is you have to worry about what the false-negative and false-positive rates of screening are, and that affects everything. I want the readers to know that primary HPV should be used for screenings. It is not perfect, but it is much better than cytology alone. We need to think about how to better adapt screening in the age that we live in.
HPV self-sampling
Dr. Mutch: Could self-sampling for HPV testing, which obviously would be easier for the patient, and certainly useful in terms of screening, address some health care disparities with regard to cervical cancer?
Dr. Huh: The short answer is, yes. Self-sampling is not US Food and Drug Administration-approved in this country. It’s not being widely used without that approval. But there are multiple countries, including the United States, that have done lots of studies on this topic. There are many public health experts and champions for HPV self-sampling. I think we have learned, based on some studies, that the sensitivity is reasonable.6
I live in a part of the country that is woefully underserved; where you are there are pockets in Missouri that are woefully underserved as well. So the issue is, can we reduce these disparities and access to care with something like self-sampling? My personal feeling is I think that we can make a dent in that, and it is never going to fully replace screening, but it at least will allow us to reallocate our resources and attention to those women that are at highest risk for developing cervical cancer or precancer based on the self-sampling result.
I don’t think it will ever replace screening per se, but if we have an abnormal self-sampling test, we might say to that patient, “You really do need to come in to get re-tested or to get re-evaluated.” So it could be a better resource and use of our health care dollars and investments in terms of trying to reduce the incidence of cervical cancer. Of course the verdict is out, but I think there are a lot of people who would love to see this scenario.
If we screen and treat perfectly in this country, we would not even need the HPV vaccine when it comes to cervical cancer. That is how effective screening is. But, up to 50% to 60% of women in this country now still are underscreened or unscreened. We were talking about that number almost 25-30 years ago, Dr. Mutch. So access to screening is a big problem, but the other problem is how do you get patients in to be seen if they have an abnormal screening test? It’s not just about screening. It’s about screening, evaluation, and treatment; all 3 components are really important.
Continue to: Where do we stand with HPV vaccination?...
Where do we stand with HPV vaccination?
Dr. Mutch: Those are great points.
You brought up vaccination. We have a long way to go with regard to that, certainly in the United States, because of the various factions opposed to vaccination and so on. But do you think that vaccination has allowed us to decrease the incidence of cervical cancer?
Dr. Huh: Yes. There is clear evidence from the Nordic countries.7 There is emerging evidence from Australia.8 There is emerging evidence from other industrialized nations that clearly demonstrate vaccination’s positive effect in reducing the incidence of cervical cancer. None of this should be a surprise. Every population-based study that has been published with the HPV vaccine in populations that have a low frequency of vaccination have demonstrated substantial reductions in things like genital warts, abnormal Pap tests, precancer, and now evidence that there is a downward trend in terms of the incidence of cervical cancer.9
I don’t think that there is any debate anymore that vaccination is the way to go. Our challenge is about implementation and getting the vaccine to people. We still have a long way to go with that. There are parts of the world that are so affected by invasive cervical cancers; we need to get the vaccine to those parts of the world.
Dr. Mutch: What are the barriers to vaccination? How can we overcome those barriers?
Dr. Huh: There is a lot of criticism that we are not vaccinating more in the United States. However, the rates of vaccination are going up every single year. The pandemic may have blunted that rise a bit, but if you look at the vaccination curves, they are going up, not down. We need to continue to educate patients, parents, and pediatricians on the importance of vaccination.
Boys still get vaccinated less frequently than girls, so we have some work to do there. I think globally it is the issue of getting the vaccine to people, making sure that vaccine is available. The thing that I think will be the game-changer going forward is whether or not we will have evidence to indicate that 1 dose is as effective as 2 doses or 3 doses. If we can vaccinate boys and girls with just 1 dose, then in the next generation or two, we seriously might eradicate not just cervical cancer but a lot of HPV-related malignancies worldwide.
Educating patients, clinicians is key
Dr. Mutch: So it seems education, education, education, with regard to screening guidelines, with regard to the need for continued examinations, and that HPV testing is only a test, it does not supplant overall care. Finally, education regarding eradication of cervical cancer through vaccination.
Dr. Huh: That summarizes it well. We are still going to screen for cervical cancer. We are still going to vaccinate, and providers are still going to manage abnormal Pap tests. It is confusing because we are changing it up it seems every year or 2, so this conversation you and I are having is particularly important for clinicians to understand the basis of that. There has been an explosion of data that has come out in this area in the last decade.
Dr. Mutch: Thank you, Dr. Huh. I really appreciate your thoughts on this. As you all know, Dr. Huh has been President of the ASCCP and is instrumental in writing and disseminating these guidelines, so we are very grateful that he has consented to agree to come and talk with us today.
Dr. Huh: My pleasure. Thank you for inviting me. This was fun, and I have really enjoyed talking to you and participating. ●
- ASCCP Screening Guidelines. https://www.asccp.org /screening-guidelines. Accessed April 25, 2021.
- Fontham ET, Wolf AM, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guidelines update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
- US Preventive Services Task Force. Screening for cervical cancer. US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320:674-686. doi:10.1001/jama .2018.10897.
- American College of Obstetricians and Gynecologists. Practice Advisory: Updated cervical cancer screening guidelines. April 2022. https://www.acog.org/clinical/clinical-guidance /practice-advisory/articles/2021/04/updated-cervical -cancer-screening-guidelines. Accessed April 25, 2022.
- Perkins RB, Guido RS, Castle PE, et al; 2019 ASCCP RiskBased Management Consensus Guidelines Committee. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24:102-131. doi: 10 34 .1097/LGT.0000000000000525.
- Yeh PT, Kennedy CE, de Vuyst H, et al. Self-sampling for human papillomavirus (HPV) testing: a systematic review and meta-analysis. BMJ Global Health. 2019;4:e001351. doi:10.1136/ bmjgh-2018-001351.
- Kjaer SK, Nygard M, Dillner J, et al. A 12-year follow-up on the long-term effectiveness of the quadrivalent human papillomavirus vaccine in 4 Nordic countries. Clin Infect Dis. 2018;66:339-345. doi: 10.1093/cid/cix797.
- Patel C, Brotherton JM, Pillsbury A, et al. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonvalent vaccine prevent? Euro Surveill. 2018;23:1700737. doi: 10 .2807/1560-7917.
- Falcaro M, Castanon A, Ndlela B, et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. 2021;398:2084-2092. doi.org/10.1016/S0140-6736(21) 02178-4.
David G. Mutch, MD: The cervical cancer screening guidelines, using Pap testing, have changed significantly since the times of yearly Paps and exams. Coupled with vaccination and new management guidelines (recommending HPV testing, etc), we actually hope that we are on the way to eradicating cervical cancer from our environment.
Screening: Current recommendations
Dr. Mutch: Warner, the American Society of Colposcopy and Cervical Pathology (ASCCP)1 endorses the cervical cancer screening guidelines for several professional organizations, including the American Cancer Society (ACS),2 the US Preventive Services Task Force (USPSTF),3 and the American College of Obstetricians and Gynecologists (ACOG).4 What are the current screening recommendations, as these organizations have disparate views?
Warner Huh, MD: There was a time, around 2012-2013, when for the first time ever, we had significant harmonization of the guidelines between ACOG and the USPSTF and ACS. But in the last 10 years there has been an explosion of data in terms of how to best screen patients.
The move to primary HPV testing. The USPSTF3 initially had recommended looking into primary HPV screening, which is just using HPV testing by itself as the screening modality. But there was a lot of pushback at that time. I think a lot of people thought that we were not prepared to make that leap. Therefore, they endorsed screening with cytology by itself as well as HPV testing by itself, as well as co-testing; but in their recommendations, they made it very clear that they were leaning toward primary HPV screening.
A new patient age to begin screening. In 2020, the ACS put out their new guidelines,2 which are a significant departure from what we are used to—they are recommending that we start screening at 25 years of age. Like you said, Dr. Mutch, it doesn’t seem that long ago when we were screening people at age 18, or within 3 years of sexual intercourse. But the reason for it is that the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already do this.
The other major departure in the ACS guidelines is that they really are asking clinicians and screeners to focus on primary HPV screening. Overall, they have sort of doubled down on why they think primary HPV screening is so important.
ACOG sits sort of in the middle of the other recommendations. ACOG understands the value of primary HPV screening, but I don’t think that they are quite ready to recommend screening at age 25. If you look at their updated guidelines from April 2021,4 they state that we should continue a screening-starting age of 21 years. So there are some disparate views, but I am confident, Dr. Mutch, that in the next 2 to 3 years, there will be greater harmonization of these guidelines and less confusion for our providers. The greatest barrier is understanding the science and the comfort level of clinicians to go with just an HPV test, since for the last 40 years the Pap test has anchored gynecologic care in this country. And it took at least 10 years to get to what I consider to be widespread adoption to co-testing. The other thing that readers should recognize is that the Task Force is actually revisiting their cervical cancer screening guidance now, so expect another major revision.
Reimbursement and access are barriers. Reimbursement is a further real issue. We are now using one less test, but insurance companies may not reimburse when just the HPV test is used. The other issue is access to labs that can do the HPV testing.
Dr. Mutch: We used to see patients yearly and picked up a lot of adjunctive or additional illnesses. Now they are not being seen yearly it could impact negatively their overall health care. We need to understand that cervical cancer screening is simply a test, which should not eliminate other health care.
Dr. Huh: Yes, I think the extended interval between recommended HPV screenings scares people. I have been involved in these screening guidelines (and I can only speak for myself, not for my colleagues), but even I do think we made a leap to a longer interval way too quickly in this country. Screening changes are slow, and sometimes a glacial process. I think it can worry providers when we make rapid changes.
But this is a test that should not anchor the yearly visit. There are plenty of other reasons—and ACOG actually states this4—why patients should come for a wellness exam on a yearly basis. So I think our ObGyns in the United States need to recognize that, but I understand there are underlying concerns that if you extend intervals too long, (a) will patients come back, and (b), as a consequence, is the interval going to miss something in between? Those are real legitimate concerns.
Continue to: Management guidelines...
Management guidelines: The latest
Dr. Mutch: The ASCCP issued new management guidelines in 2019.5 Can you address what you feel are the most important updates?
Dr. Huh: Going back to 2002, we have revised these guidelines every 5 years. For this one, the revision came out a little bit later for various reasons, but the reason we revised it is because we collect new data that we think markedly changes our understanding of the disease process and natural history and the interventions for women that have preinvasive disease of the cervix.
Briefly, I think the biggest changes based on what we were hearing from our providers and users of our apps and algorithms was that our algorithms were becoming way too complicated, and they were. If you look over the last 10 years, the number of branch points on our algorithms basically quadrupled. If we incorporated the new data this time, the algorithms would be unworkable, and you could not use them on your phone because they would be too complicated.
So, we created a system where, in essence, providers have 5 choices for patients:
- treatment
- colposcopy
- follow-up in 1 year
- follow-up in 3 years
- follow-up in 5 years.
Those recommendations are based on what we call “clinically actionable thresholds”—basically, the percent chance of developing immediate CIN3 or worse. That threshold will probably change over time, but what we did is create a system that (a) makes it easier for the provider, (although they have to trust the system—and they can look under the hood and understand how we did this) and (b) allows us to create a foundation where we can add future technologies that use the same rubric or paradigm so that they still wind up getting the same result without having to go to another algorithm.
This new system is probably the most marked change in the history of the ASCCP management guidelines, but we did it to make it ultimately easier for providers going forward for the next 10 to 20 years. There are real opportunities, Dr. Mutch, in terms of how do we integrate this into the electronic medical record (EMR), and how do we pull data so clinicians don’t have to manually enter it.
The other difference is now there is a web-based application. Back in 2012, there were a lot of people that were not using EMRs. Now the majority of the country is, and so they actually are on a browser more than they are on their phone. We actually have an equally robust web platform that allows them to get the information that they need.
Dr. Mutch: I think that is really important—the utility of utilizing a mobile app, if you will, for triaging your patient with a specific test result so that patients are followed up at the proper interval, and that ultimately becomes cost-effective.
Dr. Huh: Yes, the app now is very different than the app that I think people are used to using for the last almost 10 years. You don’t put inputs, pull up the algorithm, and look at the outcome. This is different. You enter the patient’s age. You add their cytology, their HPV results, the clinical scenario that you are in, and then it puts out a recommendation of what to do next. Over time, we want to get away from an algorithm and for our providers to understand what the risk is and how that risk calculation then translates into a clinical recommendation.
Dr. Mutch: I think to utilize an app is almost necessary given the complexity of the triaging process so that it does become, in fact, the most cost-effective way to screen patients.
Dr. Huh: I would agree with that. There is a learning curve for whenever you see new technology. There was a learning curve for even ASCCP leadership as they tried to educate providers. I think people will ultimately see that this is a much better way of managing patients with cervical abnormalities, and I am hoping actually that we will use a similar platform for many other diseases that we manage in women’s health.
Continue to: Chipping away of the yearly exam...
Chipping away of the yearly exam
Dr. Mutch: With this moving away from the yearly exam and Pap test, women may not get yearly examinations. Do you feel that this could affect a stage migration to a higher stage at diagnosis, for instance, of a cervical cancer? Or that it might adversely impact other health issues?
Dr. Huh: I think that’s a good question. I am worried about the interval—I think 5 years is a bit long. I am more worried that patients will miss out on visits because they may think that they need to only come back for their Pap, even though they should be re-educated on that.
COVID-19 has made this a little hard for us to analyze because, clearly, we have had access to care issues. But I am a little concerned that we could see an uptick in invasive cancer rates in this country, including an uptick in the stage and more locally advanced cervical cancer because of the changes in the screening paradigms. But we don’t know that to be the case.
As with all screenings, the bottom line is you have to worry about what the false-negative and false-positive rates of screening are, and that affects everything. I want the readers to know that primary HPV should be used for screenings. It is not perfect, but it is much better than cytology alone. We need to think about how to better adapt screening in the age that we live in.
HPV self-sampling
Dr. Mutch: Could self-sampling for HPV testing, which obviously would be easier for the patient, and certainly useful in terms of screening, address some health care disparities with regard to cervical cancer?
Dr. Huh: The short answer is, yes. Self-sampling is not US Food and Drug Administration-approved in this country. It’s not being widely used without that approval. But there are multiple countries, including the United States, that have done lots of studies on this topic. There are many public health experts and champions for HPV self-sampling. I think we have learned, based on some studies, that the sensitivity is reasonable.6
I live in a part of the country that is woefully underserved; where you are there are pockets in Missouri that are woefully underserved as well. So the issue is, can we reduce these disparities and access to care with something like self-sampling? My personal feeling is I think that we can make a dent in that, and it is never going to fully replace screening, but it at least will allow us to reallocate our resources and attention to those women that are at highest risk for developing cervical cancer or precancer based on the self-sampling result.
I don’t think it will ever replace screening per se, but if we have an abnormal self-sampling test, we might say to that patient, “You really do need to come in to get re-tested or to get re-evaluated.” So it could be a better resource and use of our health care dollars and investments in terms of trying to reduce the incidence of cervical cancer. Of course the verdict is out, but I think there are a lot of people who would love to see this scenario.
If we screen and treat perfectly in this country, we would not even need the HPV vaccine when it comes to cervical cancer. That is how effective screening is. But, up to 50% to 60% of women in this country now still are underscreened or unscreened. We were talking about that number almost 25-30 years ago, Dr. Mutch. So access to screening is a big problem, but the other problem is how do you get patients in to be seen if they have an abnormal screening test? It’s not just about screening. It’s about screening, evaluation, and treatment; all 3 components are really important.
Continue to: Where do we stand with HPV vaccination?...
Where do we stand with HPV vaccination?
Dr. Mutch: Those are great points.
You brought up vaccination. We have a long way to go with regard to that, certainly in the United States, because of the various factions opposed to vaccination and so on. But do you think that vaccination has allowed us to decrease the incidence of cervical cancer?
Dr. Huh: Yes. There is clear evidence from the Nordic countries.7 There is emerging evidence from Australia.8 There is emerging evidence from other industrialized nations that clearly demonstrate vaccination’s positive effect in reducing the incidence of cervical cancer. None of this should be a surprise. Every population-based study that has been published with the HPV vaccine in populations that have a low frequency of vaccination have demonstrated substantial reductions in things like genital warts, abnormal Pap tests, precancer, and now evidence that there is a downward trend in terms of the incidence of cervical cancer.9
I don’t think that there is any debate anymore that vaccination is the way to go. Our challenge is about implementation and getting the vaccine to people. We still have a long way to go with that. There are parts of the world that are so affected by invasive cervical cancers; we need to get the vaccine to those parts of the world.
Dr. Mutch: What are the barriers to vaccination? How can we overcome those barriers?
Dr. Huh: There is a lot of criticism that we are not vaccinating more in the United States. However, the rates of vaccination are going up every single year. The pandemic may have blunted that rise a bit, but if you look at the vaccination curves, they are going up, not down. We need to continue to educate patients, parents, and pediatricians on the importance of vaccination.
Boys still get vaccinated less frequently than girls, so we have some work to do there. I think globally it is the issue of getting the vaccine to people, making sure that vaccine is available. The thing that I think will be the game-changer going forward is whether or not we will have evidence to indicate that 1 dose is as effective as 2 doses or 3 doses. If we can vaccinate boys and girls with just 1 dose, then in the next generation or two, we seriously might eradicate not just cervical cancer but a lot of HPV-related malignancies worldwide.
Educating patients, clinicians is key
Dr. Mutch: So it seems education, education, education, with regard to screening guidelines, with regard to the need for continued examinations, and that HPV testing is only a test, it does not supplant overall care. Finally, education regarding eradication of cervical cancer through vaccination.
Dr. Huh: That summarizes it well. We are still going to screen for cervical cancer. We are still going to vaccinate, and providers are still going to manage abnormal Pap tests. It is confusing because we are changing it up it seems every year or 2, so this conversation you and I are having is particularly important for clinicians to understand the basis of that. There has been an explosion of data that has come out in this area in the last decade.
Dr. Mutch: Thank you, Dr. Huh. I really appreciate your thoughts on this. As you all know, Dr. Huh has been President of the ASCCP and is instrumental in writing and disseminating these guidelines, so we are very grateful that he has consented to agree to come and talk with us today.
Dr. Huh: My pleasure. Thank you for inviting me. This was fun, and I have really enjoyed talking to you and participating. ●
David G. Mutch, MD: The cervical cancer screening guidelines, using Pap testing, have changed significantly since the times of yearly Paps and exams. Coupled with vaccination and new management guidelines (recommending HPV testing, etc), we actually hope that we are on the way to eradicating cervical cancer from our environment.
Screening: Current recommendations
Dr. Mutch: Warner, the American Society of Colposcopy and Cervical Pathology (ASCCP)1 endorses the cervical cancer screening guidelines for several professional organizations, including the American Cancer Society (ACS),2 the US Preventive Services Task Force (USPSTF),3 and the American College of Obstetricians and Gynecologists (ACOG).4 What are the current screening recommendations, as these organizations have disparate views?
Warner Huh, MD: There was a time, around 2012-2013, when for the first time ever, we had significant harmonization of the guidelines between ACOG and the USPSTF and ACS. But in the last 10 years there has been an explosion of data in terms of how to best screen patients.
The move to primary HPV testing. The USPSTF3 initially had recommended looking into primary HPV screening, which is just using HPV testing by itself as the screening modality. But there was a lot of pushback at that time. I think a lot of people thought that we were not prepared to make that leap. Therefore, they endorsed screening with cytology by itself as well as HPV testing by itself, as well as co-testing; but in their recommendations, they made it very clear that they were leaning toward primary HPV screening.
A new patient age to begin screening. In 2020, the ACS put out their new guidelines,2 which are a significant departure from what we are used to—they are recommending that we start screening at 25 years of age. Like you said, Dr. Mutch, it doesn’t seem that long ago when we were screening people at age 18, or within 3 years of sexual intercourse. But the reason for it is that the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already do this.
The other major departure in the ACS guidelines is that they really are asking clinicians and screeners to focus on primary HPV screening. Overall, they have sort of doubled down on why they think primary HPV screening is so important.
ACOG sits sort of in the middle of the other recommendations. ACOG understands the value of primary HPV screening, but I don’t think that they are quite ready to recommend screening at age 25. If you look at their updated guidelines from April 2021,4 they state that we should continue a screening-starting age of 21 years. So there are some disparate views, but I am confident, Dr. Mutch, that in the next 2 to 3 years, there will be greater harmonization of these guidelines and less confusion for our providers. The greatest barrier is understanding the science and the comfort level of clinicians to go with just an HPV test, since for the last 40 years the Pap test has anchored gynecologic care in this country. And it took at least 10 years to get to what I consider to be widespread adoption to co-testing. The other thing that readers should recognize is that the Task Force is actually revisiting their cervical cancer screening guidance now, so expect another major revision.
Reimbursement and access are barriers. Reimbursement is a further real issue. We are now using one less test, but insurance companies may not reimburse when just the HPV test is used. The other issue is access to labs that can do the HPV testing.
Dr. Mutch: We used to see patients yearly and picked up a lot of adjunctive or additional illnesses. Now they are not being seen yearly it could impact negatively their overall health care. We need to understand that cervical cancer screening is simply a test, which should not eliminate other health care.
Dr. Huh: Yes, I think the extended interval between recommended HPV screenings scares people. I have been involved in these screening guidelines (and I can only speak for myself, not for my colleagues), but even I do think we made a leap to a longer interval way too quickly in this country. Screening changes are slow, and sometimes a glacial process. I think it can worry providers when we make rapid changes.
But this is a test that should not anchor the yearly visit. There are plenty of other reasons—and ACOG actually states this4—why patients should come for a wellness exam on a yearly basis. So I think our ObGyns in the United States need to recognize that, but I understand there are underlying concerns that if you extend intervals too long, (a) will patients come back, and (b), as a consequence, is the interval going to miss something in between? Those are real legitimate concerns.
Continue to: Management guidelines...
Management guidelines: The latest
Dr. Mutch: The ASCCP issued new management guidelines in 2019.5 Can you address what you feel are the most important updates?
Dr. Huh: Going back to 2002, we have revised these guidelines every 5 years. For this one, the revision came out a little bit later for various reasons, but the reason we revised it is because we collect new data that we think markedly changes our understanding of the disease process and natural history and the interventions for women that have preinvasive disease of the cervix.
Briefly, I think the biggest changes based on what we were hearing from our providers and users of our apps and algorithms was that our algorithms were becoming way too complicated, and they were. If you look over the last 10 years, the number of branch points on our algorithms basically quadrupled. If we incorporated the new data this time, the algorithms would be unworkable, and you could not use them on your phone because they would be too complicated.
So, we created a system where, in essence, providers have 5 choices for patients:
- treatment
- colposcopy
- follow-up in 1 year
- follow-up in 3 years
- follow-up in 5 years.
Those recommendations are based on what we call “clinically actionable thresholds”—basically, the percent chance of developing immediate CIN3 or worse. That threshold will probably change over time, but what we did is create a system that (a) makes it easier for the provider, (although they have to trust the system—and they can look under the hood and understand how we did this) and (b) allows us to create a foundation where we can add future technologies that use the same rubric or paradigm so that they still wind up getting the same result without having to go to another algorithm.
This new system is probably the most marked change in the history of the ASCCP management guidelines, but we did it to make it ultimately easier for providers going forward for the next 10 to 20 years. There are real opportunities, Dr. Mutch, in terms of how do we integrate this into the electronic medical record (EMR), and how do we pull data so clinicians don’t have to manually enter it.
The other difference is now there is a web-based application. Back in 2012, there were a lot of people that were not using EMRs. Now the majority of the country is, and so they actually are on a browser more than they are on their phone. We actually have an equally robust web platform that allows them to get the information that they need.
Dr. Mutch: I think that is really important—the utility of utilizing a mobile app, if you will, for triaging your patient with a specific test result so that patients are followed up at the proper interval, and that ultimately becomes cost-effective.
Dr. Huh: Yes, the app now is very different than the app that I think people are used to using for the last almost 10 years. You don’t put inputs, pull up the algorithm, and look at the outcome. This is different. You enter the patient’s age. You add their cytology, their HPV results, the clinical scenario that you are in, and then it puts out a recommendation of what to do next. Over time, we want to get away from an algorithm and for our providers to understand what the risk is and how that risk calculation then translates into a clinical recommendation.
Dr. Mutch: I think to utilize an app is almost necessary given the complexity of the triaging process so that it does become, in fact, the most cost-effective way to screen patients.
Dr. Huh: I would agree with that. There is a learning curve for whenever you see new technology. There was a learning curve for even ASCCP leadership as they tried to educate providers. I think people will ultimately see that this is a much better way of managing patients with cervical abnormalities, and I am hoping actually that we will use a similar platform for many other diseases that we manage in women’s health.
Continue to: Chipping away of the yearly exam...
Chipping away of the yearly exam
Dr. Mutch: With this moving away from the yearly exam and Pap test, women may not get yearly examinations. Do you feel that this could affect a stage migration to a higher stage at diagnosis, for instance, of a cervical cancer? Or that it might adversely impact other health issues?
Dr. Huh: I think that’s a good question. I am worried about the interval—I think 5 years is a bit long. I am more worried that patients will miss out on visits because they may think that they need to only come back for their Pap, even though they should be re-educated on that.
COVID-19 has made this a little hard for us to analyze because, clearly, we have had access to care issues. But I am a little concerned that we could see an uptick in invasive cancer rates in this country, including an uptick in the stage and more locally advanced cervical cancer because of the changes in the screening paradigms. But we don’t know that to be the case.
As with all screenings, the bottom line is you have to worry about what the false-negative and false-positive rates of screening are, and that affects everything. I want the readers to know that primary HPV should be used for screenings. It is not perfect, but it is much better than cytology alone. We need to think about how to better adapt screening in the age that we live in.
HPV self-sampling
Dr. Mutch: Could self-sampling for HPV testing, which obviously would be easier for the patient, and certainly useful in terms of screening, address some health care disparities with regard to cervical cancer?
Dr. Huh: The short answer is, yes. Self-sampling is not US Food and Drug Administration-approved in this country. It’s not being widely used without that approval. But there are multiple countries, including the United States, that have done lots of studies on this topic. There are many public health experts and champions for HPV self-sampling. I think we have learned, based on some studies, that the sensitivity is reasonable.6
I live in a part of the country that is woefully underserved; where you are there are pockets in Missouri that are woefully underserved as well. So the issue is, can we reduce these disparities and access to care with something like self-sampling? My personal feeling is I think that we can make a dent in that, and it is never going to fully replace screening, but it at least will allow us to reallocate our resources and attention to those women that are at highest risk for developing cervical cancer or precancer based on the self-sampling result.
I don’t think it will ever replace screening per se, but if we have an abnormal self-sampling test, we might say to that patient, “You really do need to come in to get re-tested or to get re-evaluated.” So it could be a better resource and use of our health care dollars and investments in terms of trying to reduce the incidence of cervical cancer. Of course the verdict is out, but I think there are a lot of people who would love to see this scenario.
If we screen and treat perfectly in this country, we would not even need the HPV vaccine when it comes to cervical cancer. That is how effective screening is. But, up to 50% to 60% of women in this country now still are underscreened or unscreened. We were talking about that number almost 25-30 years ago, Dr. Mutch. So access to screening is a big problem, but the other problem is how do you get patients in to be seen if they have an abnormal screening test? It’s not just about screening. It’s about screening, evaluation, and treatment; all 3 components are really important.
Continue to: Where do we stand with HPV vaccination?...
Where do we stand with HPV vaccination?
Dr. Mutch: Those are great points.
You brought up vaccination. We have a long way to go with regard to that, certainly in the United States, because of the various factions opposed to vaccination and so on. But do you think that vaccination has allowed us to decrease the incidence of cervical cancer?
Dr. Huh: Yes. There is clear evidence from the Nordic countries.7 There is emerging evidence from Australia.8 There is emerging evidence from other industrialized nations that clearly demonstrate vaccination’s positive effect in reducing the incidence of cervical cancer. None of this should be a surprise. Every population-based study that has been published with the HPV vaccine in populations that have a low frequency of vaccination have demonstrated substantial reductions in things like genital warts, abnormal Pap tests, precancer, and now evidence that there is a downward trend in terms of the incidence of cervical cancer.9
I don’t think that there is any debate anymore that vaccination is the way to go. Our challenge is about implementation and getting the vaccine to people. We still have a long way to go with that. There are parts of the world that are so affected by invasive cervical cancers; we need to get the vaccine to those parts of the world.
Dr. Mutch: What are the barriers to vaccination? How can we overcome those barriers?
Dr. Huh: There is a lot of criticism that we are not vaccinating more in the United States. However, the rates of vaccination are going up every single year. The pandemic may have blunted that rise a bit, but if you look at the vaccination curves, they are going up, not down. We need to continue to educate patients, parents, and pediatricians on the importance of vaccination.
Boys still get vaccinated less frequently than girls, so we have some work to do there. I think globally it is the issue of getting the vaccine to people, making sure that vaccine is available. The thing that I think will be the game-changer going forward is whether or not we will have evidence to indicate that 1 dose is as effective as 2 doses or 3 doses. If we can vaccinate boys and girls with just 1 dose, then in the next generation or two, we seriously might eradicate not just cervical cancer but a lot of HPV-related malignancies worldwide.
Educating patients, clinicians is key
Dr. Mutch: So it seems education, education, education, with regard to screening guidelines, with regard to the need for continued examinations, and that HPV testing is only a test, it does not supplant overall care. Finally, education regarding eradication of cervical cancer through vaccination.
Dr. Huh: That summarizes it well. We are still going to screen for cervical cancer. We are still going to vaccinate, and providers are still going to manage abnormal Pap tests. It is confusing because we are changing it up it seems every year or 2, so this conversation you and I are having is particularly important for clinicians to understand the basis of that. There has been an explosion of data that has come out in this area in the last decade.
Dr. Mutch: Thank you, Dr. Huh. I really appreciate your thoughts on this. As you all know, Dr. Huh has been President of the ASCCP and is instrumental in writing and disseminating these guidelines, so we are very grateful that he has consented to agree to come and talk with us today.
Dr. Huh: My pleasure. Thank you for inviting me. This was fun, and I have really enjoyed talking to you and participating. ●
- ASCCP Screening Guidelines. https://www.asccp.org /screening-guidelines. Accessed April 25, 2021.
- Fontham ET, Wolf AM, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guidelines update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
- US Preventive Services Task Force. Screening for cervical cancer. US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320:674-686. doi:10.1001/jama .2018.10897.
- American College of Obstetricians and Gynecologists. Practice Advisory: Updated cervical cancer screening guidelines. April 2022. https://www.acog.org/clinical/clinical-guidance /practice-advisory/articles/2021/04/updated-cervical -cancer-screening-guidelines. Accessed April 25, 2022.
- Perkins RB, Guido RS, Castle PE, et al; 2019 ASCCP RiskBased Management Consensus Guidelines Committee. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24:102-131. doi: 10 34 .1097/LGT.0000000000000525.
- Yeh PT, Kennedy CE, de Vuyst H, et al. Self-sampling for human papillomavirus (HPV) testing: a systematic review and meta-analysis. BMJ Global Health. 2019;4:e001351. doi:10.1136/ bmjgh-2018-001351.
- Kjaer SK, Nygard M, Dillner J, et al. A 12-year follow-up on the long-term effectiveness of the quadrivalent human papillomavirus vaccine in 4 Nordic countries. Clin Infect Dis. 2018;66:339-345. doi: 10.1093/cid/cix797.
- Patel C, Brotherton JM, Pillsbury A, et al. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonvalent vaccine prevent? Euro Surveill. 2018;23:1700737. doi: 10 .2807/1560-7917.
- Falcaro M, Castanon A, Ndlela B, et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. 2021;398:2084-2092. doi.org/10.1016/S0140-6736(21) 02178-4.
- ASCCP Screening Guidelines. https://www.asccp.org /screening-guidelines. Accessed April 25, 2021.
- Fontham ET, Wolf AM, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guidelines update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-346. doi:10.3322/caac.21628.
- US Preventive Services Task Force. Screening for cervical cancer. US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320:674-686. doi:10.1001/jama .2018.10897.
- American College of Obstetricians and Gynecologists. Practice Advisory: Updated cervical cancer screening guidelines. April 2022. https://www.acog.org/clinical/clinical-guidance /practice-advisory/articles/2021/04/updated-cervical -cancer-screening-guidelines. Accessed April 25, 2022.
- Perkins RB, Guido RS, Castle PE, et al; 2019 ASCCP RiskBased Management Consensus Guidelines Committee. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24:102-131. doi: 10 34 .1097/LGT.0000000000000525.
- Yeh PT, Kennedy CE, de Vuyst H, et al. Self-sampling for human papillomavirus (HPV) testing: a systematic review and meta-analysis. BMJ Global Health. 2019;4:e001351. doi:10.1136/ bmjgh-2018-001351.
- Kjaer SK, Nygard M, Dillner J, et al. A 12-year follow-up on the long-term effectiveness of the quadrivalent human papillomavirus vaccine in 4 Nordic countries. Clin Infect Dis. 2018;66:339-345. doi: 10.1093/cid/cix797.
- Patel C, Brotherton JM, Pillsbury A, et al. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonvalent vaccine prevent? Euro Surveill. 2018;23:1700737. doi: 10 .2807/1560-7917.
- Falcaro M, Castanon A, Ndlela B, et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. 2021;398:2084-2092. doi.org/10.1016/S0140-6736(21) 02178-4.
Commonly used antibiotics in ObGyn practice
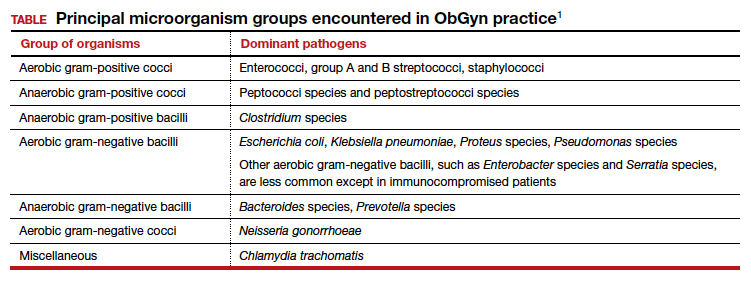
In this article, I provide a simplified, practical review of the principal antibiotics that we use on a daily basis to treat bacterial infections. The antibiotics are listed in alphabetical order, either individually or by group. I focus first on the mechanism of action and spectrum of activity of the drugs used against the usual pelvic pathogens (TABLE).1 I then review their principal adverse effects, relative cost (categorized as low, intermediate, and high), and the key indications for these drugs in obstetrics and gynecology. In a forthcoming 2-part companion article, I will review how to select specific antibiotics and their dosing regimens for the most commonly encountered bacterial infections in our clinical practice.
Aminoglycoside antibiotics
The aminoglycosides include amikacin, gentamicin, plazomicin, and tobramycin.2,3 The 2 agents most commonly used in our specialty are amikacin and gentamicin. The drugs may be administered intramuscularly or intravenously, and they specifically target aerobic gram-negative bacilli. They also provide coverage against staphylococci and gonococci. Ototoxicity and nephrotoxicity are their principal adverse effects.
Aminoglycosides are used primarily as single agents to treat pyelonephritis caused by highly resistant bacteria and in combination with agents such as clindamycin and metronidazole to treat polymicrobial infections, including chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. Of all the aminoglycosides, gentamicin is clearly the least expensive.
Carbapenems
The original carbapenem widely introduced into clinical practice was imipenem-cilastatin. Imipenem, the active antibiotic, inhibits bacterial cell wall synthesis. Cilastatin inhibits renal dehydropeptidase I and, thereby, slows the metabolism of imipenem by the kidney. Other carbapenems include meropenem and ertapenem.
The carbapenems have the widest spectrum of activity against the pelvic pathogens of any antibiotic. They provide excellent coverage of aerobic and anaerobic gram-positive cocci and aerobic and anaerobic gram-negative bacilli. They do not cover methicillin-resistant Staphylococcus aureus (MRSA) and the enterococci very well.
A major adverse effect of the carbapenems is an allergic reaction, including anaphylaxis and Stevens-Johnson syndrome, and there is some minimal cross-sensitivity with the β-lactam antibiotics. Other important, but fortunately rare, adverse effects include neurotoxicity, hepatotoxicity, and Clostridium difficile colitis.4
As a group, the carbapenems are relatively more expensive than most other agents. Their principal application in our specialty is for single-agent treatment of serious polymicrobial infections, such as puerperal endometritis, pelvic cellulitis, and pelvic abscess, especially in patients who have a contraindication to the use of combination antibiotic regimens that include an aminoglycoside.1,2
Cephalosporins
The cephalosporins are β-lactam antibiotics that act by disrupting the synthesis of the bacterial cell wall. They may be administered orally, intramuscularly, and intravenously. The most common adverse effects associated with these agents are an allergic reaction, which can range from a mild rash to anaphylaxis and the Stevens-Johnson syndrome; central nervous system toxicity; and antibiotic-induced diarrhea, including C difficile colitis.1,2,4
This group of antibiotics can be confusing because it includes so many agents, and their spectrum of activity varies. I find it helpful to think about the coverage of these agents as limited spectrum versus intermediate spectrum versus extended spectrum.
The limited-spectrum cephalosporin prototypes are cephalexin (oral administration) and cefazolin (parenteral administration). This group of cephalosporins provides excellent coverage of aerobic and anaerobic gram-positive cocci. They are excellent against staphylococci, except for MRSA. Coverage is moderate for aerobic gram-negative bacilli but only limited for anaerobic gram-negative bacilli. They do not cover the enterococci. In our specialty, their principal application is for treatment of mastitis, urinary tract infections (UTIs), and wound infections and for prophylaxis against group B streptococcus (GBS) infection and post-cesarean infection.2,5 The cost of these drugs is relatively low.
The prototypes of the intermediate-spectrum cephalosporins are cefixime (oral) and ceftriaxone (parenteral). Both drugs have strong activity against aerobic and anaerobic streptococci, Neisseria gonorrhoeae, most aerobic gram-negative bacilli, and Treponema pallidum (principally, ceftriaxone). They are not consistently effective against staphylococci, particularly MRSA, and enterococci. Their key indications in obstetrics and gynecology are treatment of gonorrhea, syphilis (in penicillin-allergic patients), and acute pyelonephritis. Compared with the limited-spectrum cephalosporins, these antibiotics are moderately expensive.1,2
The 3 extended-spectrum cephalosporins used most commonly in our specialty are cefepime, cefotetan, and cefoxitin. These agents are administered intramuscularly and intravenously, and they provide very good coverage against aerobic and anaerobic gram-positive cocci, with the exception of staphylococci and enterococci. They have very good coverage against most gram-negative aerobic bacilli and excellent coverage against anerobic microorganisms. Their primary application in our specialty is for single-agent treatment of polymicrobial infections, such as puerperal endometritis and pelvic cellulitis. When used in combination with doxycycline, they are valuable in treating pelvic inflammatory disease. These drugs are more expensive than the limited-spectrum or intermediate-spectrum agents. They should not be used routinely as prophylaxis for pelvic surgery.1,2,5
Continue to: Fluorinated quinolones...
Fluorinated quinolones
The fluorinated quinolones include several agents, but the 3 most commonly used in our specialty are ciprofloxacin, ofloxacin, and levofloxacin. All 3 drugs can be administered orally; ciprofloxacin and levofloxacin also are available in intravenous formulations. These drugs interfere with bacterial protein synthesis by targeting DNA gyrase, an enzyme that introduces negative supertwists into DNA and separates interlocked DNA molecules.
These drugs provide excellent coverage against gram-negative bacilli, including Haemophilus influenzae; gram-negative cocci, such as N gonorrhoeae, Neisseria meningitidis, and Moraxella catarrhalis; and many staphylococci species. Levofloxacin, but not the other 2 drugs, provides moderate coverage against anaerobes. Ofloxacin and levofloxacin are active against chlamydia. Levofloxacin also covers the mycoplasma organisms that are responsible for atypical pneumonia.
As a group, the fluorinated quinolones are moderately expensive. The most likely adverse effects with these agents are gastrointestinal (GI) upset, headache, agitation, and sleep disturbance. Allergic reactions are rare. These drugs are of primary value in our specialty in treating gonorrhea, chlamydia, complicated UTIs, and respiratory tract infections.1,2,6
The penicillins
Penicillin
Penicillin, a β-lactam antibiotic, was one of the first antibiotics developed and employed in clinical practice. It may be administered orally, intramuscularly, and intravenously. Penicillin exerts its effect by interfering with bacterial cell wall synthesis. Its principal spectrum of activity is against aerobic streptococci, such as group A and B streptococcus; most anaerobic gram-positive cocci that are present in the vaginal flora; some anaerobic gram-negative bacilli; and T pallidum. Penicillin is not effective against the majority of staphylococci species, enterococci, or aerobic gram-negative bacilli, such as Escherichia coli.
Penicillin’s major adverse effect is an allergic reaction, experienced by less than 10% of recipients.7 Most reactions are mild and are characterized by a morbilliform skin rash. However, some reactions are severe and take the form of an urticarial skin eruption, laryngospasm, bronchospasm, and overt anaphylaxis. The cost of both oral and parenteral penicillin formulations is very low. In obstetrics and gynecology, penicillin is used primarily for the treatment of group A and B streptococci infections, clostridial infections, and syphilis.1,2
Ampicillin and amoxicillin
The β-lactam antibiotics ampicillin and amoxicillin also act by interfering with bacterial cell wall synthesis. Amoxicillin is administered orally; ampicillin may be administered orally, intramuscularly, and intravenously. Their spectrum of activity includes group A and B streptococci, enterococci, most anaerobic gram-positive cocci, some anaerobic gram-negative bacilli, many aerobic gram-negative bacilli, and clostridial organisms.
Like penicillin, ampicillin and amoxicillin may cause allergic reactions that range from mild rashes to anaphylaxis. Unlike the more narrow-spectrum penicillin, they may cause antibiotic-associated diarrhea, including C difficile colitis,4 and they may eliminate part of the normal vaginal flora and stimulate an overgrowth of yeast organisms in the vagina. The cost of ampicillin and amoxicillin is very low. These 2 agents are used primarily for treatment of group A and B streptococci infections and some UTIs, particularly those caused by enterococci.1,2
Dicloxacillin sodium
This penicillin derivative disrupts bacterial cell wall synthesis and targets primarily aerobic gram-positive cocci, particularly staphylococci species. The antibiotic is not active against MRSA. The principal adverse effects of dicloxacillin sodium are an allergic reaction and GI upset. The drug is very inexpensive.
The key application for dicloxacillin sodium in our specialty is for treatment of puerperal mastitis.1
Continue to: Extended-spectrum penicillins...
Extended-spectrum penicillins
Three interesting combination extended-spectrum penicillins are used widely in our specialty. They are ampicillin/sulbactam, amoxicillin/clavulanate, and piperacillin/tazobactam. Ampicillin/sulbactam may be administered intramuscularly and intravenously. Piperacillin/tazobactam is administered intravenously; amoxicillin/clavulanate is administered orally.
Clavulanate, sulbactam, and tazobactam are β-lactamase inhibitors. When added to the parent antibiotic (amoxicillin, ampicillin, and piperacillin, respectively), they significantly enhance the parent drug’s spectrum of activity. These agents interfere with bacterial cell wall synthesis. They provide excellent coverage of aerobic gram-positive cocci, including enterococci; anaerobic gram-positive cocci; anaerobic gram-negative bacilli; and aerobic gram-negative bacilli. Their principal adverse effects include allergic reactions and antibiotic-associated diarrhea. They are moderately expensive.
The principal application of ampicillin/sulbactam and piperacillin/tazobactam in our specialty is as single agents for treatment of puerperal endometritis, postoperative pelvic cellulitis, and pyelonephritis. The usual role for amoxicillin/clavulanate is for oral treatment of complicated UTIs, including pyelonephritis in early pregnancy, and for outpatient therapy of mild to moderately severe endometritis following delivery or pregnancy termination.
Macrolides, monobactams, and additional antibiotics
Azithromycin
Azithromycin is a macrolide antibiotic that is in the same class as erythromycin and clindamycin. In our specialty, it has largely replaced erythromycin because of its more convenient dosage schedule and its better tolerability. It inhibits bacterial protein synthesis, and it is available in both an oral and intravenous formulation.
Azithromycin has an excellent spectrum of activity against the 3 major microorganisms that cause otitis media, sinusitis, and bronchitis: Streptococcus pneumoniae, H influenzae, and M catarrhalis. It also provides excellent coverage of Chlamydia trachomatis, Mycoplasma pneumoniae, and genital mycoplasmas; in high doses it provides modest coverage against gonorrhea.8 Unlike erythromycin, it has minimal GI toxicity and is usually very well tolerated by most patients. One unusual, but very important, adverse effect of the drug is prolongation of the Q-T interval.9
Azithromycin is now available in generic form and is relatively inexpensive. As a single agent, its principal applications in our specialty are for treatment of respiratory tract infections such as otitis media, sinusitis, and acute bronchitis and for treatment of chlamydia urethritis and endocervicitis.8,10 In combination with ampicillin, azithromycin is used as prophylaxis in patients with preterm premature rupture of membranes (PPROM), and, in combination with cefazolin, it is used for prophylaxis in patients undergoing cesarean delivery.1,2,5
Aztreonam
Aztreonam is a monobactam antibiotic. Like the cephalosporins and penicillins, aztreonam inhibits bacterial cell wall synthesis. It may be administered intramuscularly and intravenously, and its principal spectrum of activity is against aerobic gram-negative bacilli, which is similar to the aminoglycosides’ spectrum.
Aztreonam’s most likely adverse effects include phlebitis at the injection site, allergy, GI upset, and diarrhea. The drug is moderately expensive. In our specialty, aztreonam could be used as a single agent, in lieu of an aminoglycoside, for treatment of pyelonephritis caused by an unusually resistant organism. It also could be used in combination with clindamycin or metronidazole plus ampicillin for treatment of polymicrobial infections, such as chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Continue to: Clindamycin...
Clindamycin
A macrolide antibiotic, clindamycin exerts its antibacterial effect by interfering with bacterial protein synthesis. It can be administered orally and intravenously. Its key spectrum of activity in our specialty includes GBS, staphylococci, and anaerobes. However, clindamycin is not active against enterococci or aerobic gram-negative bacilli. GI upset and antibiotic-induced diarrhea are its principal adverse effects, and clindamycin is one of the most important causes of C difficile colitis. Although it is available in a generic formulation, this drug is still relatively expensive.
Clindamycin’s principal application in our specialty is for treating staphylococcal infections, such as wound infections and mastitis. It is particularly effective against MRSA infections. When used in combination with an aminoglycoside such as gentamicin, clindamycin provides excellent treatment for chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. In fact, for many years, the combination of clindamycin plus gentamicin has been considered the gold standard for the treatment of polymicrobial, mixed aerobic-anaerobic pelvic infections.1,2
Doxycycline
Doxycycline, a tetracycline, exerts its antibacterial effect by inhibiting bacterial protein synthesis. The drug targets a broad range of pelvic pathogens, including C trachomatis and N gonorrhoeae, and it may be administered both orally and intravenously. Doxycycline’s principal adverse effects include headache, GI upset, and photosensitivity. By disrupting the normal bowel and vaginal flora, the drug also can cause diarrhea and vulvovaginal moniliasis. In addition, it can cause permanent discoloration of the teeth, and, for this reason, doxycycline should not be used in pregnant or lactating women or in young children.
Although doxycycline has been available in generic formulation for many years, it remains relatively expensive. As a single agent, its principal application in our specialty is for treatment of chlamydia infection. It may be used as prophylaxis for surgical procedures, such as hysterectomy and pregnancy terminations. In combination with an extended-spectrum cephalosporin, it also may be used to treat pelvic inflammatory disease.2,8,10
Metronidazole
Metronidazole, a nitroimidazole derivative, exerts its antibacterial effect by disrupting bacterial protein synthesis. The drug may be administered topically, orally, and intravenously. Its primary spectrum of activity is against anerobic microorganisms. It is also active against Giardia and Trichomonas vaginalis.
Metronidazole’s most common adverse effects are GI upset, a metallic taste in the mouth, and a disulfiram-like effect when taken with alcohol. The cost of oral and intravenous metronidazole is relatively low; ironically, the cost of topical metronidazole is relatively high. In our specialty, the principal applications of oral metronidazole are as a single agent for treatment of bacterial vaginosis and trichomoniasis. When combined with ampicillin plus an aminoglycoside, intravenous metronidazole provides excellent coverage against the diverse anaerobic microorganisms that cause chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Trimethoprim-sulfamethoxazole (TMP-SMX)
This antibiotic combination (an antifolate and a sulfonamide) inhibits sequential steps in the synthesis of folic acid, an essential nutrient in bacterial metabolism. It is available in both an intravenous and oral formulation. TMP-SMX has a broad spectrum of activity against the aerobic gram-negative bacilli that cause UTIs in women. In addition, it provides excellent coverage against staphylococci, including MRSA; Pneumocystis jirovecii; and Toxoplasma gondii.
The medication’s principal toxicity is an allergic reaction. Some reactions are quite severe, such as the Stevens-Johnson syndrome. TMP-SMX is relatively inexpensive, particularly the oral formulation. The most common indications for TMP-SMX in our specialty are for treatment of UTIs, mastitis, and wound infections.1,2,11 In HIV-infected patients, the drug provides excellent prophylaxis against recurrent Pneumocystis and Toxoplasma infections. TMP-SMX should not be used in the first trimester of pregnancy because it has been linked to several birth defects, including neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia.12
Nitrofurantoin
Usually administered orally as nitrofurantoin monohydrate macrocrystals, nitrofurantoin exerts its antibacterial effect primarily by inhibiting protein synthesis. Its principal spectrum of activity is against the aerobic gram-negative bacilli, with the exception of Proteus species. Nitrofurantoin’s most common adverse effects are GI upset, headache, vertigo, drowsiness, and allergic reactions. The drug is relatively inexpensive.
Nitrofurantoin is an excellent agent for the treatment of lower UTIs.11 It is not well concentrated in the renal parenchyma or blood, however, so it should not be used to treat pyelonephritis. As a general rule, nitrofurantoin should not be used in the first trimester of pregnancy because it has been associated with eye, heart, and facial cleft defects in the fetus.12
Vancomycin
Vancomycin exerts its antibacterial effect by inhibiting cell wall synthesis. It may be administered both orally and intravenously, and it specifically targets aerobic gram-positive cocci, particularly methicillin-sensitive and methicillin-resistant staphylococci. Vancomycin’s most important adverse effects include GI upset, nephrotoxicity, ototoxicity, and severe allergic reactions, such as anaphylaxis, Stevens-Johnson syndrome, and exfoliative dermatitis (the “red man” syndrome). The drug is moderately expensive.13
In its oral formulation, vancomycin’s principal application in our discipline is for treating C difficile colitis. In its intravenous formulation, it is used primarily as a single agent for GBS prophylaxis in penicillin-allergic patients, and it is used in combination with other antibiotics, such as clindamycin plus gentamicin, for treating patients with deep-seated incisional (wound) infections.1,2,13,14 ●
- Duff P. Maternal and perinatal infection in pregnancy: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe’s Obstetrics: Normal and Problem Pregnancies, 8th ed. Elsevier; 2020: chapter 58.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.
- Wagenlehner FME, Cloutier DJ, Komirenko AS, et al; EPIC Study Group. Once-daily plazomicin for complicated urinary tract infections. N Engl J Med. 2019;380:729-740.
- Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372:1539-1548.
- Duff P. Prevention of infection after cesarean delivery. Clin Obstet Gynecol. 2019;62:758-770.
- Hooper DC, Wolfson JS. Fluoroquinolone antimicrobial agents. N Engl J Med. 1991;324:384-394.
- Castells M, Khan DA, Phillips EJ. Penicillin allergy. N Engl J Med. 2019 381:2338-2351.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.
- Ray WA, Murray KT, Hall K, et al. Azithromycin and the risk of cardiovascular death. N Engl J Med. 2012;366:1881-1890.
- Workowski KA, Bolan GA. Sexually transmitted disease treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64(RR3):1-137.
- Duff P. UTIs in pregnancy: managing urethritis, asymptomatic bacteriuria, cystitis, and pyelonephritis. OBG Manag. 2022;34(1):42-46.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects prevalence study. Arch Pediatr Adolesc Med. 2009;163:978985.
- Alvarez-Arango S, Ogunwole SM, Sequist TD, et al. Vancomycin infusion reaction—moving beyond “red man syndrome.” N Engl J Med. 2021;384:1283-1286.
- Finley TA, Duff P. Antibiotics for treatment of staphylococcal infections in the obstetric patient. Clin Obstet Gynecol. 2019;62:790-803.

Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The author reports no financial relationships relevant to this article.
In this article, I provide a simplified, practical review of the principal antibiotics that we use on a daily basis to treat bacterial infections. The antibiotics are listed in alphabetical order, either individually or by group. I focus first on the mechanism of action and spectrum of activity of the drugs used against the usual pelvic pathogens (TABLE).1 I then review their principal adverse effects, relative cost (categorized as low, intermediate, and high), and the key indications for these drugs in obstetrics and gynecology. In a forthcoming 2-part companion article, I will review how to select specific antibiotics and their dosing regimens for the most commonly encountered bacterial infections in our clinical practice.
Aminoglycoside antibiotics
The aminoglycosides include amikacin, gentamicin, plazomicin, and tobramycin.2,3 The 2 agents most commonly used in our specialty are amikacin and gentamicin. The drugs may be administered intramuscularly or intravenously, and they specifically target aerobic gram-negative bacilli. They also provide coverage against staphylococci and gonococci. Ototoxicity and nephrotoxicity are their principal adverse effects.
Aminoglycosides are used primarily as single agents to treat pyelonephritis caused by highly resistant bacteria and in combination with agents such as clindamycin and metronidazole to treat polymicrobial infections, including chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. Of all the aminoglycosides, gentamicin is clearly the least expensive.
Carbapenems
The original carbapenem widely introduced into clinical practice was imipenem-cilastatin. Imipenem, the active antibiotic, inhibits bacterial cell wall synthesis. Cilastatin inhibits renal dehydropeptidase I and, thereby, slows the metabolism of imipenem by the kidney. Other carbapenems include meropenem and ertapenem.
The carbapenems have the widest spectrum of activity against the pelvic pathogens of any antibiotic. They provide excellent coverage of aerobic and anaerobic gram-positive cocci and aerobic and anaerobic gram-negative bacilli. They do not cover methicillin-resistant Staphylococcus aureus (MRSA) and the enterococci very well.
A major adverse effect of the carbapenems is an allergic reaction, including anaphylaxis and Stevens-Johnson syndrome, and there is some minimal cross-sensitivity with the β-lactam antibiotics. Other important, but fortunately rare, adverse effects include neurotoxicity, hepatotoxicity, and Clostridium difficile colitis.4
As a group, the carbapenems are relatively more expensive than most other agents. Their principal application in our specialty is for single-agent treatment of serious polymicrobial infections, such as puerperal endometritis, pelvic cellulitis, and pelvic abscess, especially in patients who have a contraindication to the use of combination antibiotic regimens that include an aminoglycoside.1,2
Cephalosporins
The cephalosporins are β-lactam antibiotics that act by disrupting the synthesis of the bacterial cell wall. They may be administered orally, intramuscularly, and intravenously. The most common adverse effects associated with these agents are an allergic reaction, which can range from a mild rash to anaphylaxis and the Stevens-Johnson syndrome; central nervous system toxicity; and antibiotic-induced diarrhea, including C difficile colitis.1,2,4
This group of antibiotics can be confusing because it includes so many agents, and their spectrum of activity varies. I find it helpful to think about the coverage of these agents as limited spectrum versus intermediate spectrum versus extended spectrum.
The limited-spectrum cephalosporin prototypes are cephalexin (oral administration) and cefazolin (parenteral administration). This group of cephalosporins provides excellent coverage of aerobic and anaerobic gram-positive cocci. They are excellent against staphylococci, except for MRSA. Coverage is moderate for aerobic gram-negative bacilli but only limited for anaerobic gram-negative bacilli. They do not cover the enterococci. In our specialty, their principal application is for treatment of mastitis, urinary tract infections (UTIs), and wound infections and for prophylaxis against group B streptococcus (GBS) infection and post-cesarean infection.2,5 The cost of these drugs is relatively low.
The prototypes of the intermediate-spectrum cephalosporins are cefixime (oral) and ceftriaxone (parenteral). Both drugs have strong activity against aerobic and anaerobic streptococci, Neisseria gonorrhoeae, most aerobic gram-negative bacilli, and Treponema pallidum (principally, ceftriaxone). They are not consistently effective against staphylococci, particularly MRSA, and enterococci. Their key indications in obstetrics and gynecology are treatment of gonorrhea, syphilis (in penicillin-allergic patients), and acute pyelonephritis. Compared with the limited-spectrum cephalosporins, these antibiotics are moderately expensive.1,2
The 3 extended-spectrum cephalosporins used most commonly in our specialty are cefepime, cefotetan, and cefoxitin. These agents are administered intramuscularly and intravenously, and they provide very good coverage against aerobic and anaerobic gram-positive cocci, with the exception of staphylococci and enterococci. They have very good coverage against most gram-negative aerobic bacilli and excellent coverage against anerobic microorganisms. Their primary application in our specialty is for single-agent treatment of polymicrobial infections, such as puerperal endometritis and pelvic cellulitis. When used in combination with doxycycline, they are valuable in treating pelvic inflammatory disease. These drugs are more expensive than the limited-spectrum or intermediate-spectrum agents. They should not be used routinely as prophylaxis for pelvic surgery.1,2,5
Continue to: Fluorinated quinolones...
Fluorinated quinolones
The fluorinated quinolones include several agents, but the 3 most commonly used in our specialty are ciprofloxacin, ofloxacin, and levofloxacin. All 3 drugs can be administered orally; ciprofloxacin and levofloxacin also are available in intravenous formulations. These drugs interfere with bacterial protein synthesis by targeting DNA gyrase, an enzyme that introduces negative supertwists into DNA and separates interlocked DNA molecules.
These drugs provide excellent coverage against gram-negative bacilli, including Haemophilus influenzae; gram-negative cocci, such as N gonorrhoeae, Neisseria meningitidis, and Moraxella catarrhalis; and many staphylococci species. Levofloxacin, but not the other 2 drugs, provides moderate coverage against anaerobes. Ofloxacin and levofloxacin are active against chlamydia. Levofloxacin also covers the mycoplasma organisms that are responsible for atypical pneumonia.
As a group, the fluorinated quinolones are moderately expensive. The most likely adverse effects with these agents are gastrointestinal (GI) upset, headache, agitation, and sleep disturbance. Allergic reactions are rare. These drugs are of primary value in our specialty in treating gonorrhea, chlamydia, complicated UTIs, and respiratory tract infections.1,2,6
The penicillins
Penicillin
Penicillin, a β-lactam antibiotic, was one of the first antibiotics developed and employed in clinical practice. It may be administered orally, intramuscularly, and intravenously. Penicillin exerts its effect by interfering with bacterial cell wall synthesis. Its principal spectrum of activity is against aerobic streptococci, such as group A and B streptococcus; most anaerobic gram-positive cocci that are present in the vaginal flora; some anaerobic gram-negative bacilli; and T pallidum. Penicillin is not effective against the majority of staphylococci species, enterococci, or aerobic gram-negative bacilli, such as Escherichia coli.
Penicillin’s major adverse effect is an allergic reaction, experienced by less than 10% of recipients.7 Most reactions are mild and are characterized by a morbilliform skin rash. However, some reactions are severe and take the form of an urticarial skin eruption, laryngospasm, bronchospasm, and overt anaphylaxis. The cost of both oral and parenteral penicillin formulations is very low. In obstetrics and gynecology, penicillin is used primarily for the treatment of group A and B streptococci infections, clostridial infections, and syphilis.1,2
Ampicillin and amoxicillin
The β-lactam antibiotics ampicillin and amoxicillin also act by interfering with bacterial cell wall synthesis. Amoxicillin is administered orally; ampicillin may be administered orally, intramuscularly, and intravenously. Their spectrum of activity includes group A and B streptococci, enterococci, most anaerobic gram-positive cocci, some anaerobic gram-negative bacilli, many aerobic gram-negative bacilli, and clostridial organisms.
Like penicillin, ampicillin and amoxicillin may cause allergic reactions that range from mild rashes to anaphylaxis. Unlike the more narrow-spectrum penicillin, they may cause antibiotic-associated diarrhea, including C difficile colitis,4 and they may eliminate part of the normal vaginal flora and stimulate an overgrowth of yeast organisms in the vagina. The cost of ampicillin and amoxicillin is very low. These 2 agents are used primarily for treatment of group A and B streptococci infections and some UTIs, particularly those caused by enterococci.1,2
Dicloxacillin sodium
This penicillin derivative disrupts bacterial cell wall synthesis and targets primarily aerobic gram-positive cocci, particularly staphylococci species. The antibiotic is not active against MRSA. The principal adverse effects of dicloxacillin sodium are an allergic reaction and GI upset. The drug is very inexpensive.
The key application for dicloxacillin sodium in our specialty is for treatment of puerperal mastitis.1
Continue to: Extended-spectrum penicillins...
Extended-spectrum penicillins
Three interesting combination extended-spectrum penicillins are used widely in our specialty. They are ampicillin/sulbactam, amoxicillin/clavulanate, and piperacillin/tazobactam. Ampicillin/sulbactam may be administered intramuscularly and intravenously. Piperacillin/tazobactam is administered intravenously; amoxicillin/clavulanate is administered orally.
Clavulanate, sulbactam, and tazobactam are β-lactamase inhibitors. When added to the parent antibiotic (amoxicillin, ampicillin, and piperacillin, respectively), they significantly enhance the parent drug’s spectrum of activity. These agents interfere with bacterial cell wall synthesis. They provide excellent coverage of aerobic gram-positive cocci, including enterococci; anaerobic gram-positive cocci; anaerobic gram-negative bacilli; and aerobic gram-negative bacilli. Their principal adverse effects include allergic reactions and antibiotic-associated diarrhea. They are moderately expensive.
The principal application of ampicillin/sulbactam and piperacillin/tazobactam in our specialty is as single agents for treatment of puerperal endometritis, postoperative pelvic cellulitis, and pyelonephritis. The usual role for amoxicillin/clavulanate is for oral treatment of complicated UTIs, including pyelonephritis in early pregnancy, and for outpatient therapy of mild to moderately severe endometritis following delivery or pregnancy termination.
Macrolides, monobactams, and additional antibiotics
Azithromycin
Azithromycin is a macrolide antibiotic that is in the same class as erythromycin and clindamycin. In our specialty, it has largely replaced erythromycin because of its more convenient dosage schedule and its better tolerability. It inhibits bacterial protein synthesis, and it is available in both an oral and intravenous formulation.
Azithromycin has an excellent spectrum of activity against the 3 major microorganisms that cause otitis media, sinusitis, and bronchitis: Streptococcus pneumoniae, H influenzae, and M catarrhalis. It also provides excellent coverage of Chlamydia trachomatis, Mycoplasma pneumoniae, and genital mycoplasmas; in high doses it provides modest coverage against gonorrhea.8 Unlike erythromycin, it has minimal GI toxicity and is usually very well tolerated by most patients. One unusual, but very important, adverse effect of the drug is prolongation of the Q-T interval.9
Azithromycin is now available in generic form and is relatively inexpensive. As a single agent, its principal applications in our specialty are for treatment of respiratory tract infections such as otitis media, sinusitis, and acute bronchitis and for treatment of chlamydia urethritis and endocervicitis.8,10 In combination with ampicillin, azithromycin is used as prophylaxis in patients with preterm premature rupture of membranes (PPROM), and, in combination with cefazolin, it is used for prophylaxis in patients undergoing cesarean delivery.1,2,5
Aztreonam
Aztreonam is a monobactam antibiotic. Like the cephalosporins and penicillins, aztreonam inhibits bacterial cell wall synthesis. It may be administered intramuscularly and intravenously, and its principal spectrum of activity is against aerobic gram-negative bacilli, which is similar to the aminoglycosides’ spectrum.
Aztreonam’s most likely adverse effects include phlebitis at the injection site, allergy, GI upset, and diarrhea. The drug is moderately expensive. In our specialty, aztreonam could be used as a single agent, in lieu of an aminoglycoside, for treatment of pyelonephritis caused by an unusually resistant organism. It also could be used in combination with clindamycin or metronidazole plus ampicillin for treatment of polymicrobial infections, such as chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Continue to: Clindamycin...
Clindamycin
A macrolide antibiotic, clindamycin exerts its antibacterial effect by interfering with bacterial protein synthesis. It can be administered orally and intravenously. Its key spectrum of activity in our specialty includes GBS, staphylococci, and anaerobes. However, clindamycin is not active against enterococci or aerobic gram-negative bacilli. GI upset and antibiotic-induced diarrhea are its principal adverse effects, and clindamycin is one of the most important causes of C difficile colitis. Although it is available in a generic formulation, this drug is still relatively expensive.
Clindamycin’s principal application in our specialty is for treating staphylococcal infections, such as wound infections and mastitis. It is particularly effective against MRSA infections. When used in combination with an aminoglycoside such as gentamicin, clindamycin provides excellent treatment for chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. In fact, for many years, the combination of clindamycin plus gentamicin has been considered the gold standard for the treatment of polymicrobial, mixed aerobic-anaerobic pelvic infections.1,2
Doxycycline
Doxycycline, a tetracycline, exerts its antibacterial effect by inhibiting bacterial protein synthesis. The drug targets a broad range of pelvic pathogens, including C trachomatis and N gonorrhoeae, and it may be administered both orally and intravenously. Doxycycline’s principal adverse effects include headache, GI upset, and photosensitivity. By disrupting the normal bowel and vaginal flora, the drug also can cause diarrhea and vulvovaginal moniliasis. In addition, it can cause permanent discoloration of the teeth, and, for this reason, doxycycline should not be used in pregnant or lactating women or in young children.
Although doxycycline has been available in generic formulation for many years, it remains relatively expensive. As a single agent, its principal application in our specialty is for treatment of chlamydia infection. It may be used as prophylaxis for surgical procedures, such as hysterectomy and pregnancy terminations. In combination with an extended-spectrum cephalosporin, it also may be used to treat pelvic inflammatory disease.2,8,10
Metronidazole
Metronidazole, a nitroimidazole derivative, exerts its antibacterial effect by disrupting bacterial protein synthesis. The drug may be administered topically, orally, and intravenously. Its primary spectrum of activity is against anerobic microorganisms. It is also active against Giardia and Trichomonas vaginalis.
Metronidazole’s most common adverse effects are GI upset, a metallic taste in the mouth, and a disulfiram-like effect when taken with alcohol. The cost of oral and intravenous metronidazole is relatively low; ironically, the cost of topical metronidazole is relatively high. In our specialty, the principal applications of oral metronidazole are as a single agent for treatment of bacterial vaginosis and trichomoniasis. When combined with ampicillin plus an aminoglycoside, intravenous metronidazole provides excellent coverage against the diverse anaerobic microorganisms that cause chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Trimethoprim-sulfamethoxazole (TMP-SMX)
This antibiotic combination (an antifolate and a sulfonamide) inhibits sequential steps in the synthesis of folic acid, an essential nutrient in bacterial metabolism. It is available in both an intravenous and oral formulation. TMP-SMX has a broad spectrum of activity against the aerobic gram-negative bacilli that cause UTIs in women. In addition, it provides excellent coverage against staphylococci, including MRSA; Pneumocystis jirovecii; and Toxoplasma gondii.
The medication’s principal toxicity is an allergic reaction. Some reactions are quite severe, such as the Stevens-Johnson syndrome. TMP-SMX is relatively inexpensive, particularly the oral formulation. The most common indications for TMP-SMX in our specialty are for treatment of UTIs, mastitis, and wound infections.1,2,11 In HIV-infected patients, the drug provides excellent prophylaxis against recurrent Pneumocystis and Toxoplasma infections. TMP-SMX should not be used in the first trimester of pregnancy because it has been linked to several birth defects, including neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia.12
Nitrofurantoin
Usually administered orally as nitrofurantoin monohydrate macrocrystals, nitrofurantoin exerts its antibacterial effect primarily by inhibiting protein synthesis. Its principal spectrum of activity is against the aerobic gram-negative bacilli, with the exception of Proteus species. Nitrofurantoin’s most common adverse effects are GI upset, headache, vertigo, drowsiness, and allergic reactions. The drug is relatively inexpensive.
Nitrofurantoin is an excellent agent for the treatment of lower UTIs.11 It is not well concentrated in the renal parenchyma or blood, however, so it should not be used to treat pyelonephritis. As a general rule, nitrofurantoin should not be used in the first trimester of pregnancy because it has been associated with eye, heart, and facial cleft defects in the fetus.12
Vancomycin
Vancomycin exerts its antibacterial effect by inhibiting cell wall synthesis. It may be administered both orally and intravenously, and it specifically targets aerobic gram-positive cocci, particularly methicillin-sensitive and methicillin-resistant staphylococci. Vancomycin’s most important adverse effects include GI upset, nephrotoxicity, ototoxicity, and severe allergic reactions, such as anaphylaxis, Stevens-Johnson syndrome, and exfoliative dermatitis (the “red man” syndrome). The drug is moderately expensive.13
In its oral formulation, vancomycin’s principal application in our discipline is for treating C difficile colitis. In its intravenous formulation, it is used primarily as a single agent for GBS prophylaxis in penicillin-allergic patients, and it is used in combination with other antibiotics, such as clindamycin plus gentamicin, for treating patients with deep-seated incisional (wound) infections.1,2,13,14 ●
In this article, I provide a simplified, practical review of the principal antibiotics that we use on a daily basis to treat bacterial infections. The antibiotics are listed in alphabetical order, either individually or by group. I focus first on the mechanism of action and spectrum of activity of the drugs used against the usual pelvic pathogens (TABLE).1 I then review their principal adverse effects, relative cost (categorized as low, intermediate, and high), and the key indications for these drugs in obstetrics and gynecology. In a forthcoming 2-part companion article, I will review how to select specific antibiotics and their dosing regimens for the most commonly encountered bacterial infections in our clinical practice.
Aminoglycoside antibiotics
The aminoglycosides include amikacin, gentamicin, plazomicin, and tobramycin.2,3 The 2 agents most commonly used in our specialty are amikacin and gentamicin. The drugs may be administered intramuscularly or intravenously, and they specifically target aerobic gram-negative bacilli. They also provide coverage against staphylococci and gonococci. Ototoxicity and nephrotoxicity are their principal adverse effects.
Aminoglycosides are used primarily as single agents to treat pyelonephritis caused by highly resistant bacteria and in combination with agents such as clindamycin and metronidazole to treat polymicrobial infections, including chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. Of all the aminoglycosides, gentamicin is clearly the least expensive.
Carbapenems
The original carbapenem widely introduced into clinical practice was imipenem-cilastatin. Imipenem, the active antibiotic, inhibits bacterial cell wall synthesis. Cilastatin inhibits renal dehydropeptidase I and, thereby, slows the metabolism of imipenem by the kidney. Other carbapenems include meropenem and ertapenem.
The carbapenems have the widest spectrum of activity against the pelvic pathogens of any antibiotic. They provide excellent coverage of aerobic and anaerobic gram-positive cocci and aerobic and anaerobic gram-negative bacilli. They do not cover methicillin-resistant Staphylococcus aureus (MRSA) and the enterococci very well.
A major adverse effect of the carbapenems is an allergic reaction, including anaphylaxis and Stevens-Johnson syndrome, and there is some minimal cross-sensitivity with the β-lactam antibiotics. Other important, but fortunately rare, adverse effects include neurotoxicity, hepatotoxicity, and Clostridium difficile colitis.4
As a group, the carbapenems are relatively more expensive than most other agents. Their principal application in our specialty is for single-agent treatment of serious polymicrobial infections, such as puerperal endometritis, pelvic cellulitis, and pelvic abscess, especially in patients who have a contraindication to the use of combination antibiotic regimens that include an aminoglycoside.1,2
Cephalosporins
The cephalosporins are β-lactam antibiotics that act by disrupting the synthesis of the bacterial cell wall. They may be administered orally, intramuscularly, and intravenously. The most common adverse effects associated with these agents are an allergic reaction, which can range from a mild rash to anaphylaxis and the Stevens-Johnson syndrome; central nervous system toxicity; and antibiotic-induced diarrhea, including C difficile colitis.1,2,4
This group of antibiotics can be confusing because it includes so many agents, and their spectrum of activity varies. I find it helpful to think about the coverage of these agents as limited spectrum versus intermediate spectrum versus extended spectrum.
The limited-spectrum cephalosporin prototypes are cephalexin (oral administration) and cefazolin (parenteral administration). This group of cephalosporins provides excellent coverage of aerobic and anaerobic gram-positive cocci. They are excellent against staphylococci, except for MRSA. Coverage is moderate for aerobic gram-negative bacilli but only limited for anaerobic gram-negative bacilli. They do not cover the enterococci. In our specialty, their principal application is for treatment of mastitis, urinary tract infections (UTIs), and wound infections and for prophylaxis against group B streptococcus (GBS) infection and post-cesarean infection.2,5 The cost of these drugs is relatively low.
The prototypes of the intermediate-spectrum cephalosporins are cefixime (oral) and ceftriaxone (parenteral). Both drugs have strong activity against aerobic and anaerobic streptococci, Neisseria gonorrhoeae, most aerobic gram-negative bacilli, and Treponema pallidum (principally, ceftriaxone). They are not consistently effective against staphylococci, particularly MRSA, and enterococci. Their key indications in obstetrics and gynecology are treatment of gonorrhea, syphilis (in penicillin-allergic patients), and acute pyelonephritis. Compared with the limited-spectrum cephalosporins, these antibiotics are moderately expensive.1,2
The 3 extended-spectrum cephalosporins used most commonly in our specialty are cefepime, cefotetan, and cefoxitin. These agents are administered intramuscularly and intravenously, and they provide very good coverage against aerobic and anaerobic gram-positive cocci, with the exception of staphylococci and enterococci. They have very good coverage against most gram-negative aerobic bacilli and excellent coverage against anerobic microorganisms. Their primary application in our specialty is for single-agent treatment of polymicrobial infections, such as puerperal endometritis and pelvic cellulitis. When used in combination with doxycycline, they are valuable in treating pelvic inflammatory disease. These drugs are more expensive than the limited-spectrum or intermediate-spectrum agents. They should not be used routinely as prophylaxis for pelvic surgery.1,2,5
Continue to: Fluorinated quinolones...
Fluorinated quinolones
The fluorinated quinolones include several agents, but the 3 most commonly used in our specialty are ciprofloxacin, ofloxacin, and levofloxacin. All 3 drugs can be administered orally; ciprofloxacin and levofloxacin also are available in intravenous formulations. These drugs interfere with bacterial protein synthesis by targeting DNA gyrase, an enzyme that introduces negative supertwists into DNA and separates interlocked DNA molecules.
These drugs provide excellent coverage against gram-negative bacilli, including Haemophilus influenzae; gram-negative cocci, such as N gonorrhoeae, Neisseria meningitidis, and Moraxella catarrhalis; and many staphylococci species. Levofloxacin, but not the other 2 drugs, provides moderate coverage against anaerobes. Ofloxacin and levofloxacin are active against chlamydia. Levofloxacin also covers the mycoplasma organisms that are responsible for atypical pneumonia.
As a group, the fluorinated quinolones are moderately expensive. The most likely adverse effects with these agents are gastrointestinal (GI) upset, headache, agitation, and sleep disturbance. Allergic reactions are rare. These drugs are of primary value in our specialty in treating gonorrhea, chlamydia, complicated UTIs, and respiratory tract infections.1,2,6
The penicillins
Penicillin
Penicillin, a β-lactam antibiotic, was one of the first antibiotics developed and employed in clinical practice. It may be administered orally, intramuscularly, and intravenously. Penicillin exerts its effect by interfering with bacterial cell wall synthesis. Its principal spectrum of activity is against aerobic streptococci, such as group A and B streptococcus; most anaerobic gram-positive cocci that are present in the vaginal flora; some anaerobic gram-negative bacilli; and T pallidum. Penicillin is not effective against the majority of staphylococci species, enterococci, or aerobic gram-negative bacilli, such as Escherichia coli.
Penicillin’s major adverse effect is an allergic reaction, experienced by less than 10% of recipients.7 Most reactions are mild and are characterized by a morbilliform skin rash. However, some reactions are severe and take the form of an urticarial skin eruption, laryngospasm, bronchospasm, and overt anaphylaxis. The cost of both oral and parenteral penicillin formulations is very low. In obstetrics and gynecology, penicillin is used primarily for the treatment of group A and B streptococci infections, clostridial infections, and syphilis.1,2
Ampicillin and amoxicillin
The β-lactam antibiotics ampicillin and amoxicillin also act by interfering with bacterial cell wall synthesis. Amoxicillin is administered orally; ampicillin may be administered orally, intramuscularly, and intravenously. Their spectrum of activity includes group A and B streptococci, enterococci, most anaerobic gram-positive cocci, some anaerobic gram-negative bacilli, many aerobic gram-negative bacilli, and clostridial organisms.
Like penicillin, ampicillin and amoxicillin may cause allergic reactions that range from mild rashes to anaphylaxis. Unlike the more narrow-spectrum penicillin, they may cause antibiotic-associated diarrhea, including C difficile colitis,4 and they may eliminate part of the normal vaginal flora and stimulate an overgrowth of yeast organisms in the vagina. The cost of ampicillin and amoxicillin is very low. These 2 agents are used primarily for treatment of group A and B streptococci infections and some UTIs, particularly those caused by enterococci.1,2
Dicloxacillin sodium
This penicillin derivative disrupts bacterial cell wall synthesis and targets primarily aerobic gram-positive cocci, particularly staphylococci species. The antibiotic is not active against MRSA. The principal adverse effects of dicloxacillin sodium are an allergic reaction and GI upset. The drug is very inexpensive.
The key application for dicloxacillin sodium in our specialty is for treatment of puerperal mastitis.1
Continue to: Extended-spectrum penicillins...
Extended-spectrum penicillins
Three interesting combination extended-spectrum penicillins are used widely in our specialty. They are ampicillin/sulbactam, amoxicillin/clavulanate, and piperacillin/tazobactam. Ampicillin/sulbactam may be administered intramuscularly and intravenously. Piperacillin/tazobactam is administered intravenously; amoxicillin/clavulanate is administered orally.
Clavulanate, sulbactam, and tazobactam are β-lactamase inhibitors. When added to the parent antibiotic (amoxicillin, ampicillin, and piperacillin, respectively), they significantly enhance the parent drug’s spectrum of activity. These agents interfere with bacterial cell wall synthesis. They provide excellent coverage of aerobic gram-positive cocci, including enterococci; anaerobic gram-positive cocci; anaerobic gram-negative bacilli; and aerobic gram-negative bacilli. Their principal adverse effects include allergic reactions and antibiotic-associated diarrhea. They are moderately expensive.
The principal application of ampicillin/sulbactam and piperacillin/tazobactam in our specialty is as single agents for treatment of puerperal endometritis, postoperative pelvic cellulitis, and pyelonephritis. The usual role for amoxicillin/clavulanate is for oral treatment of complicated UTIs, including pyelonephritis in early pregnancy, and for outpatient therapy of mild to moderately severe endometritis following delivery or pregnancy termination.
Macrolides, monobactams, and additional antibiotics
Azithromycin
Azithromycin is a macrolide antibiotic that is in the same class as erythromycin and clindamycin. In our specialty, it has largely replaced erythromycin because of its more convenient dosage schedule and its better tolerability. It inhibits bacterial protein synthesis, and it is available in both an oral and intravenous formulation.
Azithromycin has an excellent spectrum of activity against the 3 major microorganisms that cause otitis media, sinusitis, and bronchitis: Streptococcus pneumoniae, H influenzae, and M catarrhalis. It also provides excellent coverage of Chlamydia trachomatis, Mycoplasma pneumoniae, and genital mycoplasmas; in high doses it provides modest coverage against gonorrhea.8 Unlike erythromycin, it has minimal GI toxicity and is usually very well tolerated by most patients. One unusual, but very important, adverse effect of the drug is prolongation of the Q-T interval.9
Azithromycin is now available in generic form and is relatively inexpensive. As a single agent, its principal applications in our specialty are for treatment of respiratory tract infections such as otitis media, sinusitis, and acute bronchitis and for treatment of chlamydia urethritis and endocervicitis.8,10 In combination with ampicillin, azithromycin is used as prophylaxis in patients with preterm premature rupture of membranes (PPROM), and, in combination with cefazolin, it is used for prophylaxis in patients undergoing cesarean delivery.1,2,5
Aztreonam
Aztreonam is a monobactam antibiotic. Like the cephalosporins and penicillins, aztreonam inhibits bacterial cell wall synthesis. It may be administered intramuscularly and intravenously, and its principal spectrum of activity is against aerobic gram-negative bacilli, which is similar to the aminoglycosides’ spectrum.
Aztreonam’s most likely adverse effects include phlebitis at the injection site, allergy, GI upset, and diarrhea. The drug is moderately expensive. In our specialty, aztreonam could be used as a single agent, in lieu of an aminoglycoside, for treatment of pyelonephritis caused by an unusually resistant organism. It also could be used in combination with clindamycin or metronidazole plus ampicillin for treatment of polymicrobial infections, such as chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Continue to: Clindamycin...
Clindamycin
A macrolide antibiotic, clindamycin exerts its antibacterial effect by interfering with bacterial protein synthesis. It can be administered orally and intravenously. Its key spectrum of activity in our specialty includes GBS, staphylococci, and anaerobes. However, clindamycin is not active against enterococci or aerobic gram-negative bacilli. GI upset and antibiotic-induced diarrhea are its principal adverse effects, and clindamycin is one of the most important causes of C difficile colitis. Although it is available in a generic formulation, this drug is still relatively expensive.
Clindamycin’s principal application in our specialty is for treating staphylococcal infections, such as wound infections and mastitis. It is particularly effective against MRSA infections. When used in combination with an aminoglycoside such as gentamicin, clindamycin provides excellent treatment for chorioamnionitis, puerperal endometritis, and pelvic inflammatory disease. In fact, for many years, the combination of clindamycin plus gentamicin has been considered the gold standard for the treatment of polymicrobial, mixed aerobic-anaerobic pelvic infections.1,2
Doxycycline
Doxycycline, a tetracycline, exerts its antibacterial effect by inhibiting bacterial protein synthesis. The drug targets a broad range of pelvic pathogens, including C trachomatis and N gonorrhoeae, and it may be administered both orally and intravenously. Doxycycline’s principal adverse effects include headache, GI upset, and photosensitivity. By disrupting the normal bowel and vaginal flora, the drug also can cause diarrhea and vulvovaginal moniliasis. In addition, it can cause permanent discoloration of the teeth, and, for this reason, doxycycline should not be used in pregnant or lactating women or in young children.
Although doxycycline has been available in generic formulation for many years, it remains relatively expensive. As a single agent, its principal application in our specialty is for treatment of chlamydia infection. It may be used as prophylaxis for surgical procedures, such as hysterectomy and pregnancy terminations. In combination with an extended-spectrum cephalosporin, it also may be used to treat pelvic inflammatory disease.2,8,10
Metronidazole
Metronidazole, a nitroimidazole derivative, exerts its antibacterial effect by disrupting bacterial protein synthesis. The drug may be administered topically, orally, and intravenously. Its primary spectrum of activity is against anerobic microorganisms. It is also active against Giardia and Trichomonas vaginalis.
Metronidazole’s most common adverse effects are GI upset, a metallic taste in the mouth, and a disulfiram-like effect when taken with alcohol. The cost of oral and intravenous metronidazole is relatively low; ironically, the cost of topical metronidazole is relatively high. In our specialty, the principal applications of oral metronidazole are as a single agent for treatment of bacterial vaginosis and trichomoniasis. When combined with ampicillin plus an aminoglycoside, intravenous metronidazole provides excellent coverage against the diverse anaerobic microorganisms that cause chorioamnionitis, puerperal endometritis, and pelvic cellulitis.1,2
Trimethoprim-sulfamethoxazole (TMP-SMX)
This antibiotic combination (an antifolate and a sulfonamide) inhibits sequential steps in the synthesis of folic acid, an essential nutrient in bacterial metabolism. It is available in both an intravenous and oral formulation. TMP-SMX has a broad spectrum of activity against the aerobic gram-negative bacilli that cause UTIs in women. In addition, it provides excellent coverage against staphylococci, including MRSA; Pneumocystis jirovecii; and Toxoplasma gondii.
The medication’s principal toxicity is an allergic reaction. Some reactions are quite severe, such as the Stevens-Johnson syndrome. TMP-SMX is relatively inexpensive, particularly the oral formulation. The most common indications for TMP-SMX in our specialty are for treatment of UTIs, mastitis, and wound infections.1,2,11 In HIV-infected patients, the drug provides excellent prophylaxis against recurrent Pneumocystis and Toxoplasma infections. TMP-SMX should not be used in the first trimester of pregnancy because it has been linked to several birth defects, including neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia.12
Nitrofurantoin
Usually administered orally as nitrofurantoin monohydrate macrocrystals, nitrofurantoin exerts its antibacterial effect primarily by inhibiting protein synthesis. Its principal spectrum of activity is against the aerobic gram-negative bacilli, with the exception of Proteus species. Nitrofurantoin’s most common adverse effects are GI upset, headache, vertigo, drowsiness, and allergic reactions. The drug is relatively inexpensive.
Nitrofurantoin is an excellent agent for the treatment of lower UTIs.11 It is not well concentrated in the renal parenchyma or blood, however, so it should not be used to treat pyelonephritis. As a general rule, nitrofurantoin should not be used in the first trimester of pregnancy because it has been associated with eye, heart, and facial cleft defects in the fetus.12
Vancomycin
Vancomycin exerts its antibacterial effect by inhibiting cell wall synthesis. It may be administered both orally and intravenously, and it specifically targets aerobic gram-positive cocci, particularly methicillin-sensitive and methicillin-resistant staphylococci. Vancomycin’s most important adverse effects include GI upset, nephrotoxicity, ototoxicity, and severe allergic reactions, such as anaphylaxis, Stevens-Johnson syndrome, and exfoliative dermatitis (the “red man” syndrome). The drug is moderately expensive.13
In its oral formulation, vancomycin’s principal application in our discipline is for treating C difficile colitis. In its intravenous formulation, it is used primarily as a single agent for GBS prophylaxis in penicillin-allergic patients, and it is used in combination with other antibiotics, such as clindamycin plus gentamicin, for treating patients with deep-seated incisional (wound) infections.1,2,13,14 ●
- Duff P. Maternal and perinatal infection in pregnancy: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe’s Obstetrics: Normal and Problem Pregnancies, 8th ed. Elsevier; 2020: chapter 58.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.
- Wagenlehner FME, Cloutier DJ, Komirenko AS, et al; EPIC Study Group. Once-daily plazomicin for complicated urinary tract infections. N Engl J Med. 2019;380:729-740.
- Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372:1539-1548.
- Duff P. Prevention of infection after cesarean delivery. Clin Obstet Gynecol. 2019;62:758-770.
- Hooper DC, Wolfson JS. Fluoroquinolone antimicrobial agents. N Engl J Med. 1991;324:384-394.
- Castells M, Khan DA, Phillips EJ. Penicillin allergy. N Engl J Med. 2019 381:2338-2351.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.
- Ray WA, Murray KT, Hall K, et al. Azithromycin and the risk of cardiovascular death. N Engl J Med. 2012;366:1881-1890.
- Workowski KA, Bolan GA. Sexually transmitted disease treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64(RR3):1-137.
- Duff P. UTIs in pregnancy: managing urethritis, asymptomatic bacteriuria, cystitis, and pyelonephritis. OBG Manag. 2022;34(1):42-46.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects prevalence study. Arch Pediatr Adolesc Med. 2009;163:978985.
- Alvarez-Arango S, Ogunwole SM, Sequist TD, et al. Vancomycin infusion reaction—moving beyond “red man syndrome.” N Engl J Med. 2021;384:1283-1286.
- Finley TA, Duff P. Antibiotics for treatment of staphylococcal infections in the obstetric patient. Clin Obstet Gynecol. 2019;62:790-803.
- Duff P. Maternal and perinatal infection in pregnancy: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe’s Obstetrics: Normal and Problem Pregnancies, 8th ed. Elsevier; 2020: chapter 58.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.
- Wagenlehner FME, Cloutier DJ, Komirenko AS, et al; EPIC Study Group. Once-daily plazomicin for complicated urinary tract infections. N Engl J Med. 2019;380:729-740.
- Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372:1539-1548.
- Duff P. Prevention of infection after cesarean delivery. Clin Obstet Gynecol. 2019;62:758-770.
- Hooper DC, Wolfson JS. Fluoroquinolone antimicrobial agents. N Engl J Med. 1991;324:384-394.
- Castells M, Khan DA, Phillips EJ. Penicillin allergy. N Engl J Med. 2019 381:2338-2351.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.
- Ray WA, Murray KT, Hall K, et al. Azithromycin and the risk of cardiovascular death. N Engl J Med. 2012;366:1881-1890.
- Workowski KA, Bolan GA. Sexually transmitted disease treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64(RR3):1-137.
- Duff P. UTIs in pregnancy: managing urethritis, asymptomatic bacteriuria, cystitis, and pyelonephritis. OBG Manag. 2022;34(1):42-46.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects prevalence study. Arch Pediatr Adolesc Med. 2009;163:978985.
- Alvarez-Arango S, Ogunwole SM, Sequist TD, et al. Vancomycin infusion reaction—moving beyond “red man syndrome.” N Engl J Med. 2021;384:1283-1286.
- Finley TA, Duff P. Antibiotics for treatment of staphylococcal infections in the obstetric patient. Clin Obstet Gynecol. 2019;62:790-803.
Can US “pattern recognition” of classic adnexal lesions reduce surgery, and even referrals for other imaging, in average-risk women?
Gupta A, Jha P, Baran TM, et al. Ovarian cancer detection in average-risk women: classic- versus nonclassic-appearing adnexal lesions at US. Radiology. 2022;212338. doi: 10.1148/radiol.212338.
Expert commentary
Gupta and colleagues conducted a multicenter, retrospective review of 970 adnexal lesions among 878 women—75% were premenopausal and 25% were postmenopausal.
Imaging details
The lesions were characterized by pattern recognition as “classic” (simple cysts, endometriomas, hemorrhagic cysts, or dermoids) or “nonclassic.” Out of 673 classic lesions, there were 4 malignancies (0.6%), of which 1 was an endometrioma and 3 were classified as simple cysts. However, out of 297 nonclassic lesions (multilocular, unilocular with solid areas or wall irregularity, or mostly solid), 32% (33/103) were malignant when vascularity was present, while 8% (16/184) were malignant when no intralesional vascularity was appreciated.
The authors pointed out that, especially because their study was retrospective, there was no standardization of scan technique or equipment employed. However, this point adds credibility to the “real world” nature of such imaging.
Other data corroborate findings
Other studies have looked at pattern recognition in efforts to optimize a conservative approach to benign masses and referral to oncology for suspected malignant masses, as described above. This was the main cornerstone of the International Consensus Conference,2 which also identified next steps for indeterminate masses, including evidence-based risk assessment algorithms and referral (to an expert imager or gynecologic oncologist). A multicenter trial in Europe3 found that ultrasound experience substantially impacts on diagnostic performance when adnexal masses are classified using pattern recognition. This occurred in a stepwise fashion with increasing accuracy directly related to the level of expertise. Shetty and colleagues4 found that pattern recognition performed better than the risk of malignancy index (sensitivities of 95% and 79%, respectively). ●
While the concept of pattern recognition for some “classic” benign ovarian masses has been around for some time, this is the first time a large United States–based study (albeit retrospective) has corroborated that when ultrasonography reveals a classic, or “almost certainly benign” finding, patients can be reassured that the lesion is benign, thereby avoiding extensive further workup. When a lesion is “nonclassic” in appearance and without any blood flow, further imaging with follow-up magnetic resonance imaging or repeat ultrasound could be considered. In women with a nonclassic lesion with blood flow, particularly in older women, referral to a gynecologic oncologic surgeon will help ensure expeditious treatment of possible ovarian cancer.
- Boll D, Geomini PM, Brölmann HA. The pre-operative assessment of the adnexal mass: the accuracy of clinical estimates versus clinical prediction rules. BJOG. 2003;110:519-523.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36:849-863. doi: 10.1002/jum.14197.
- Van Holsbeke C, Daemen A, Yazbek J, et al. Ultrasound experience substantially impacts on diagnostic performance and confidence when adnexal masses are classified using pattern recognition. Gynecol Obstet Invest. 2010;69:160-168. doi: 10.1159/000265012.
- Shetty J, Reddy G, Pandey D. Role of sonographic grayscale pattern recognition in the diagnosis of adnexal masses. J Clin Diagn Res. 2017;11:QC12-QC15. doi: 10.7860 /JCDR/2017/28533.10614.
Gupta A, Jha P, Baran TM, et al. Ovarian cancer detection in average-risk women: classic- versus nonclassic-appearing adnexal lesions at US. Radiology. 2022;212338. doi: 10.1148/radiol.212338.
Expert commentary
Gupta and colleagues conducted a multicenter, retrospective review of 970 adnexal lesions among 878 women—75% were premenopausal and 25% were postmenopausal.
Imaging details
The lesions were characterized by pattern recognition as “classic” (simple cysts, endometriomas, hemorrhagic cysts, or dermoids) or “nonclassic.” Out of 673 classic lesions, there were 4 malignancies (0.6%), of which 1 was an endometrioma and 3 were classified as simple cysts. However, out of 297 nonclassic lesions (multilocular, unilocular with solid areas or wall irregularity, or mostly solid), 32% (33/103) were malignant when vascularity was present, while 8% (16/184) were malignant when no intralesional vascularity was appreciated.
The authors pointed out that, especially because their study was retrospective, there was no standardization of scan technique or equipment employed. However, this point adds credibility to the “real world” nature of such imaging.
Other data corroborate findings
Other studies have looked at pattern recognition in efforts to optimize a conservative approach to benign masses and referral to oncology for suspected malignant masses, as described above. This was the main cornerstone of the International Consensus Conference,2 which also identified next steps for indeterminate masses, including evidence-based risk assessment algorithms and referral (to an expert imager or gynecologic oncologist). A multicenter trial in Europe3 found that ultrasound experience substantially impacts on diagnostic performance when adnexal masses are classified using pattern recognition. This occurred in a stepwise fashion with increasing accuracy directly related to the level of expertise. Shetty and colleagues4 found that pattern recognition performed better than the risk of malignancy index (sensitivities of 95% and 79%, respectively). ●
While the concept of pattern recognition for some “classic” benign ovarian masses has been around for some time, this is the first time a large United States–based study (albeit retrospective) has corroborated that when ultrasonography reveals a classic, or “almost certainly benign” finding, patients can be reassured that the lesion is benign, thereby avoiding extensive further workup. When a lesion is “nonclassic” in appearance and without any blood flow, further imaging with follow-up magnetic resonance imaging or repeat ultrasound could be considered. In women with a nonclassic lesion with blood flow, particularly in older women, referral to a gynecologic oncologic surgeon will help ensure expeditious treatment of possible ovarian cancer.
Gupta A, Jha P, Baran TM, et al. Ovarian cancer detection in average-risk women: classic- versus nonclassic-appearing adnexal lesions at US. Radiology. 2022;212338. doi: 10.1148/radiol.212338.
Expert commentary
Gupta and colleagues conducted a multicenter, retrospective review of 970 adnexal lesions among 878 women—75% were premenopausal and 25% were postmenopausal.
Imaging details
The lesions were characterized by pattern recognition as “classic” (simple cysts, endometriomas, hemorrhagic cysts, or dermoids) or “nonclassic.” Out of 673 classic lesions, there were 4 malignancies (0.6%), of which 1 was an endometrioma and 3 were classified as simple cysts. However, out of 297 nonclassic lesions (multilocular, unilocular with solid areas or wall irregularity, or mostly solid), 32% (33/103) were malignant when vascularity was present, while 8% (16/184) were malignant when no intralesional vascularity was appreciated.
The authors pointed out that, especially because their study was retrospective, there was no standardization of scan technique or equipment employed. However, this point adds credibility to the “real world” nature of such imaging.
Other data corroborate findings
Other studies have looked at pattern recognition in efforts to optimize a conservative approach to benign masses and referral to oncology for suspected malignant masses, as described above. This was the main cornerstone of the International Consensus Conference,2 which also identified next steps for indeterminate masses, including evidence-based risk assessment algorithms and referral (to an expert imager or gynecologic oncologist). A multicenter trial in Europe3 found that ultrasound experience substantially impacts on diagnostic performance when adnexal masses are classified using pattern recognition. This occurred in a stepwise fashion with increasing accuracy directly related to the level of expertise. Shetty and colleagues4 found that pattern recognition performed better than the risk of malignancy index (sensitivities of 95% and 79%, respectively). ●
While the concept of pattern recognition for some “classic” benign ovarian masses has been around for some time, this is the first time a large United States–based study (albeit retrospective) has corroborated that when ultrasonography reveals a classic, or “almost certainly benign” finding, patients can be reassured that the lesion is benign, thereby avoiding extensive further workup. When a lesion is “nonclassic” in appearance and without any blood flow, further imaging with follow-up magnetic resonance imaging or repeat ultrasound could be considered. In women with a nonclassic lesion with blood flow, particularly in older women, referral to a gynecologic oncologic surgeon will help ensure expeditious treatment of possible ovarian cancer.
- Boll D, Geomini PM, Brölmann HA. The pre-operative assessment of the adnexal mass: the accuracy of clinical estimates versus clinical prediction rules. BJOG. 2003;110:519-523.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36:849-863. doi: 10.1002/jum.14197.
- Van Holsbeke C, Daemen A, Yazbek J, et al. Ultrasound experience substantially impacts on diagnostic performance and confidence when adnexal masses are classified using pattern recognition. Gynecol Obstet Invest. 2010;69:160-168. doi: 10.1159/000265012.
- Shetty J, Reddy G, Pandey D. Role of sonographic grayscale pattern recognition in the diagnosis of adnexal masses. J Clin Diagn Res. 2017;11:QC12-QC15. doi: 10.7860 /JCDR/2017/28533.10614.
- Boll D, Geomini PM, Brölmann HA. The pre-operative assessment of the adnexal mass: the accuracy of clinical estimates versus clinical prediction rules. BJOG. 2003;110:519-523.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36:849-863. doi: 10.1002/jum.14197.
- Van Holsbeke C, Daemen A, Yazbek J, et al. Ultrasound experience substantially impacts on diagnostic performance and confidence when adnexal masses are classified using pattern recognition. Gynecol Obstet Invest. 2010;69:160-168. doi: 10.1159/000265012.
- Shetty J, Reddy G, Pandey D. Role of sonographic grayscale pattern recognition in the diagnosis of adnexal masses. J Clin Diagn Res. 2017;11:QC12-QC15. doi: 10.7860 /JCDR/2017/28533.10614.

Optimize detection and treatment of iron deficiency in pregnancy
During pregnancy, anemia and iron deficiency are prevalent because the fetus depletes maternal iron stores. Iron deficiency and iron deficiency anemia are not synonymous. Effective screening for iron deficiency in the first trimester of pregnancy requires the measurement of a sensitive and specific biomarker of iron deficiency, such as ferritin. Limiting the measurement of ferritin to the subset of patients with anemia will result in missing many cases of iron deficiency. By the time iron deficiency causes anemia, a severe deficiency is present. Detecting iron deficiency in pregnancy and promptly treating the deficiency will reduce the number of women with anemia in the third trimester and at birth.
Diagnosis of anemia
Anemia in pregnancy is diagnosed by a hemoglobin level and hematocrit concentration below 11 g/dL and 33%, respectively, in the first and third trimesters and below 10.5 g/dL and 32%, respectively, in the second trimester.1 The prevalence of anemia in the first, second, and third trimesters is approximately 3%, 2%, and 11%, respectively.2 At a hemoglobin concentration <11 g/dL, severe maternal morbidity rises significantly.3 The laboratory evaluation of pregnant women with anemia may require assessment of iron stores, measurement of folate and cobalamin (vitamin B12), and hemoglobin electrophoresis, if indicated.
Diagnosis of iron deficiency
Iron deficiency anemia is diagnosed by a ferritin level below 30 ng/mL.4,5 Normal iron stores and iron insufficiency are indicated by ferritin levels 45 to 150 ng/mL and 30 to 44 ng/mL, respectively.4,5 Ferritin is an acute phase reactant, and patients with inflammation or chronic illnesses may have iron deficiency and a normal ferritin level. For these patients, a transferrin saturation (TSAT) <16% would support a diagnosis of iron deficiency.6 TSAT is calculated from measurement of serum iron and total iron binding capacity. TSAT saturation may be elevated by iron supplements, which increase serum iron. If measurement of TSAT is necessary, interference with the measurement accuracy can be minimized by not taking an iron supplement on the day of testing.
Iron deficiency is present in approximately 50% of pregnant women.7,8 The greatest prevalence of iron deficiency in pregnancy is observed in non-Hispanic Black females, followed by Hispanic females. Non-Hispanic White females had the lowest prevalence of iron deficiency.2
Fetal needs for iron often cause the depletion of maternal iron stores. Many pregnant women who have a normal ferritin level in the first trimester will develop iron deficiency in the third trimester, even with the usual recommended daily oral iron supplementation. We recommend measuring ferritin and hemoglobin at the first prenatal visit and again between 24 and 28 weeks’ gestation.
Impact of maternal anemia on maternal and newborn health
Iron plays a critical role in maternal health and fetal development independent of its role in red blood cell formation. Many proteins critical to maternal health and fetal development contain iron, including hemoglobin, myoglobin, cytochromes, ribonucleotide reductase, peroxidases, lipoxygenases, and cyclooxygenases. In the fetus, iron plays an important role in myelination of nerves, dendrite arborization, and synthesis of monoamine neurotransmitters.9
Many studies report that maternal anemia is associated with severe maternal morbidity and adverse newborn outcomes. The current literature must be interpreted with caution because socioeconomic factors influence iron stores. Iron deficiency and anemia is more common among economically and socially disadvantaged populations.10-12 It is possible that repleting iron stores, alone, without addressing social determinants of health, including food and housing insecurity, may be insufficient to improve maternal and newborn health.
Maternal anemia is a risk factor for severe maternal morbidity and adverse newborn outcomes.3,13-18 In a study of 515,270 live births in British Columbia between 2004 and 2016, maternal anemia was diagnosed in 12.8% of mothers.15 Maternal morbidity at birth was increased among patients with mild anemia (hemoglobin concentration of 9 to 10.9 g/dL), including higher rates of intrapartum transfusion (adjusted odds ratio [OR], 2.45; 95% confidence interval [CI], 1.74-3.45), cesarean birth (aOR, 1.17; 95% CI, 1.14-1.19), and chorioamnionitis (aOR, 1.35; 95% CI, 1.27-1.44). Newborn morbidity was also increased among newborns of mothers with mild anemia (hemoglobin concentrations of 9 to 10.9 g/dL), including birth before 37 weeks’ gestation (aOR, 1.09; 95% CI, 1.05-1.12), birth before 32 weeks’ gestation (aOR, 1.30; 95% CI, 1.21-1.39), admission to the intensive care unit (aOR, 1.21; 95% CI, 1.17-1.25), and respiratory distress syndrome (aOR, 1.35; 95% CI, 1.24-1.46).15 Adverse maternal and newborn outcomes were more prevalent among mothers with moderate (hemoglobin concentrations of 7 to 8.9 g/dL) or severe anemia (hemoglobin concentrations of <7 g/dL), compared with mild anemia. For example, compared with mothers with no anemia, mothers with moderate anemia had an increased risk of birth <37 weeks (aOR, 2.26) and birth <32 weeks (aOR, 3.95).15
In a study of 166,566 US pregnant patients, 6.1% were diagnosed with anemia.18 Patients with anemia were more likely to have antepartum thrombosis, preeclampsia, eclampsia, a cesarean birth, postpartum hemorrhage, a blood transfusion, and postpartum thrombosis.18 In this study, the newborns of mothers with anemia were more likely to have a diagnosis of antenatal or intrapartum fetal distress, a 5-minute Apgar score <7, and an admission to the neonatal intensive care unit.
Continue to: Maternal anemia and neurodevelopmental disorders in children...
Maternal anemia and neurodevelopmental disorders in children
Some experts, but not all, believe that iron deficiency during pregnancy may adversely impact fetal neurodevelopment and result in childhood behavior issues. All experts agree that more research is needed to understand if maternal anemia causes mental health issues in newborns. In one meta-analysis, among 20 studies of the association of maternal iron deficiency and newborn neurodevelopment, approximately half the studies reported that low maternal ferritin levels were associated with lower childhood performance on standardized tests of cognitive, motor, verbal, and memory function.19 Another systematic review concluded that the evidence linking maternal iron deficiency and child neurodevelopment is equivocal.20
In a study of 532,232 nonadoptive children born in Sweden from 1987 to 2010, maternal anemia was associated with an increased risk of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and intellectual disability (ID).21 In Sweden maternal hemoglobin concentration is measured at 10, 25, and 37 weeks of gestation, permitting comparisons of anemia diagnosed early and late in pregnancy with neurodevelopmental outcomes. The association between anemia and neurodevelopmental disorders was greatest if anemia was diagnosed within the first 30 weeks of pregnancy. Compared with mothers without anemia, maternal anemia diagnosed within the first 30 weeks of pregnancy was associated with higher childhood rates of ASD (4.9% vs 3.5%), ADHD (9.3% vs 7.1%), and ID (3.1% vs 1.3%).21 The differences persisted in analyses that controlled for socioeconomic, maternal, and pregnancy-related factors. In a matched sibling comparison, the diagnosis of maternal anemia within the first 30 weeks of gestation was associated with an increased risk of ASD (OR, 2.25; 95% CI, 1.24-4.11) and ID (OR, 2.59; 95% CI, 1.08-6.22) but not ADHD.21 Other studies have also reported a relationship between maternal anemia and intellectual disability.22,23
Measurement of hemoglobin will identify anemia, but hemoglobin measurement is not sufficiently sensitive to identify most cases of iron deficiency. Measuring ferritin can help to identify cases of iron deficiency before the onset of anemia, permitting early treatment of the nutrient deficiency. In pregnancy, iron deficiency is the prelude to developing anemia. Waiting until anemia occurs to diagnose and treat iron deficiency is suboptimal and may miss a critical window of fetal development that is dependent on maternal iron stores. During pregnancy, ferritin levels decrease as much as 80% between the first and third trimesters, as the fetus utilizes maternal iron stores for its growth.24 We recommend the measurement of ferritin and hemoglobin at the first prenatal visit and again at 24 to 28 weeks’ gestation to optimize early detection and treatment of iron deficiency and reduce the frequency of anemia prior to birth. ●
- American College of Obstetricians and Gynecologists. Anemia in pregnancy. ACOG Practice Bulletin No 233. Obstet Gynecol. 2021;138:e55-64.
- Mei Z, Cogswell ME, Looker AC, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1996-2006. Am J Clin Nutr. 2011;93:1312-1320.
- Ray JG, Davidson AJF, Berger H, et al. Haemoglobin levels in early pregnancy and severe maternal morbidity: population-based cohort study. BJOG. 2020;127:1154-1164.
- Mast AE, Blinder MA, Gronowski AM, et al. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin Chem. 1998;44:45-51.
- Parvord S, Daru J, Prasannan N, et al. UK Guidelines on the management of iron deficiency in pregnancy. Br J Haematol. 2020;188:819-830.
- Camaschell C. Iron-deficiency anemia. N Engl J Med. 2015;372:1832-1843.
- Auerbach M, Abernathy J, Juul S, et al. Prevalence of iron deficiency in first trimester, nonanemic pregnant women. J Matern Fetal Neonatal Med. 2021;34:1002-1005.
- Teichman J, Nisenbaum R, Lausman A, et al. Suboptimal iron deficiency screening in pregnancy and the impact of socioeconomic status in high-resource setting. Blood Adv. 2021;5:4666-4673.
- Georgieff MK. Long-term brain and behavioral consequences of early iron deficiency. Nutr Rev. 2011;69(suppl 1):S43-S48.
- Bodnar LM, Scanlon KS, Freedman DS, et al. High prevalence of postpartum anemia among low-income women in the United States. Am J Obstet Gynecol. 2001;185:438-443.
- Dondi A, PIccinno V, Morigi F, et al. Food insecurity and major diet-related morbidities in migrating children: a systematic review. Nutrients. 2020;12:379.
- Bodnar LM, Cogswell ME, Scanlon KS. Low income postpartum women are at risk of iron deficiency. J Nutr. 2002;132:2298-2302.
- Drukker L, Hants Y, Farkash R, et al. Iron deficiency anemia at admission for labor and delivery is associated with an increased risk for cesarean section and adverse maternal and neonatal outcomes. Transfusion. 2015;55:2799-2806.
- Rahman MM, Abe SK, Rahman S, et al. Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis. Am J Clin Nutr. 2016;103:495-504.
- Smith C, Teng F, Branch E, et al. Maternal and perinatal morbidity and mortality associated with anemia in pregnancy. Obstet Gynecol. 2019;134:1234-1244.
- Parks S, Hoffman MK, Goudar SS, et al. Maternal anaemia and maternal, fetal and neonatal outcomes in a prospective cohort study in India and Pakistan. BJOG. 2019;126:737-743.
- Guignard J, Deneux-Tharaux C, Seco A, et al. Gestational anemia and severe acute maternal morbidity: a population based study. Anesthesia. 2021;76:61-71.
- Harrison RK, Lauhon SR, Colvin ZA, et al. Maternal anemia and severe maternal mortality in a US cohort. Am J Obstet Gynecol MFM. 2021;3:100395.
- Quesada-Pinedo HG, Cassel F, Duijts L, et al. Maternal iron status in pregnancy and child health outcomes after birth: a systematic review and meta-analysis. Nutrients. 2021;13:2221.
- McCann S, Perapoch Amado M, Moore SE. The role of iron in brain development: a systematic review. Nutrients. 2020;12:2001.
- Wiegersma AM, Dalman C, Lee BK, et al. Association of prenatal maternal anemia with neurodevelopmental disorders. JAMA Psychiatry. 2019;76:1294-1304.
- Leonard H, de Klerk N, Bourke J, et al. Maternal health in pregnancy and intellectual disability in the offspring: a population-based study. Ann Epidemiol. 2006;16:448-454.
- Drassinower D, Lavery JA, Friedman AM, et al. The effect of maternal hematocrit on offspring IQ at 4 and 7 years of age: a secondary analysis. BJOG. 2016;123:2087-2093.
- Horton KD, Adetona O, Aguilar-Villalobos M, et al. Changes in the concentration of biochemical indicators of diet and nutritional status of pregnant women across pregnancy trimesters in Trujillo, Peru 2004-2005. Nutrition J. 2013;12:80.

Dr. Nawal is Chair, Department of Obstetrics and Gynecology and Founding Director, African Women’s Health Center, Brigham and Women’s Hospital, and Kate Macy Ladd Professorship, Harvard Medical School, Boston, Massachusetts.

Dr. Barbieri is Chair Emeritus, Department of Obstetrics and Gynecology, and Chief of Obstetrics, Brigham and Women’s Hospital, and Kate Macy Ladd Distinguished Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
Dr. Nawal is Chair, Department of Obstetrics and Gynecology and Founding Director, African Women’s Health Center, Brigham and Women’s Hospital, and Kate Macy Ladd Professorship, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri is Chair Emeritus, Department of Obstetrics and Gynecology, and Chief of Obstetrics, Brigham and Women’s Hospital, and Kate Macy Ladd Distinguished Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
Dr. Nawal is Chair, Department of Obstetrics and Gynecology and Founding Director, African Women’s Health Center, Brigham and Women’s Hospital, and Kate Macy Ladd Professorship, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri is Chair Emeritus, Department of Obstetrics and Gynecology, and Chief of Obstetrics, Brigham and Women’s Hospital, and Kate Macy Ladd Distinguished Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
During pregnancy, anemia and iron deficiency are prevalent because the fetus depletes maternal iron stores. Iron deficiency and iron deficiency anemia are not synonymous. Effective screening for iron deficiency in the first trimester of pregnancy requires the measurement of a sensitive and specific biomarker of iron deficiency, such as ferritin. Limiting the measurement of ferritin to the subset of patients with anemia will result in missing many cases of iron deficiency. By the time iron deficiency causes anemia, a severe deficiency is present. Detecting iron deficiency in pregnancy and promptly treating the deficiency will reduce the number of women with anemia in the third trimester and at birth.
Diagnosis of anemia
Anemia in pregnancy is diagnosed by a hemoglobin level and hematocrit concentration below 11 g/dL and 33%, respectively, in the first and third trimesters and below 10.5 g/dL and 32%, respectively, in the second trimester.1 The prevalence of anemia in the first, second, and third trimesters is approximately 3%, 2%, and 11%, respectively.2 At a hemoglobin concentration <11 g/dL, severe maternal morbidity rises significantly.3 The laboratory evaluation of pregnant women with anemia may require assessment of iron stores, measurement of folate and cobalamin (vitamin B12), and hemoglobin electrophoresis, if indicated.
Diagnosis of iron deficiency
Iron deficiency anemia is diagnosed by a ferritin level below 30 ng/mL.4,5 Normal iron stores and iron insufficiency are indicated by ferritin levels 45 to 150 ng/mL and 30 to 44 ng/mL, respectively.4,5 Ferritin is an acute phase reactant, and patients with inflammation or chronic illnesses may have iron deficiency and a normal ferritin level. For these patients, a transferrin saturation (TSAT) <16% would support a diagnosis of iron deficiency.6 TSAT is calculated from measurement of serum iron and total iron binding capacity. TSAT saturation may be elevated by iron supplements, which increase serum iron. If measurement of TSAT is necessary, interference with the measurement accuracy can be minimized by not taking an iron supplement on the day of testing.
Iron deficiency is present in approximately 50% of pregnant women.7,8 The greatest prevalence of iron deficiency in pregnancy is observed in non-Hispanic Black females, followed by Hispanic females. Non-Hispanic White females had the lowest prevalence of iron deficiency.2
Fetal needs for iron often cause the depletion of maternal iron stores. Many pregnant women who have a normal ferritin level in the first trimester will develop iron deficiency in the third trimester, even with the usual recommended daily oral iron supplementation. We recommend measuring ferritin and hemoglobin at the first prenatal visit and again between 24 and 28 weeks’ gestation.
Impact of maternal anemia on maternal and newborn health
Iron plays a critical role in maternal health and fetal development independent of its role in red blood cell formation. Many proteins critical to maternal health and fetal development contain iron, including hemoglobin, myoglobin, cytochromes, ribonucleotide reductase, peroxidases, lipoxygenases, and cyclooxygenases. In the fetus, iron plays an important role in myelination of nerves, dendrite arborization, and synthesis of monoamine neurotransmitters.9
Many studies report that maternal anemia is associated with severe maternal morbidity and adverse newborn outcomes. The current literature must be interpreted with caution because socioeconomic factors influence iron stores. Iron deficiency and anemia is more common among economically and socially disadvantaged populations.10-12 It is possible that repleting iron stores, alone, without addressing social determinants of health, including food and housing insecurity, may be insufficient to improve maternal and newborn health.
Maternal anemia is a risk factor for severe maternal morbidity and adverse newborn outcomes.3,13-18 In a study of 515,270 live births in British Columbia between 2004 and 2016, maternal anemia was diagnosed in 12.8% of mothers.15 Maternal morbidity at birth was increased among patients with mild anemia (hemoglobin concentration of 9 to 10.9 g/dL), including higher rates of intrapartum transfusion (adjusted odds ratio [OR], 2.45; 95% confidence interval [CI], 1.74-3.45), cesarean birth (aOR, 1.17; 95% CI, 1.14-1.19), and chorioamnionitis (aOR, 1.35; 95% CI, 1.27-1.44). Newborn morbidity was also increased among newborns of mothers with mild anemia (hemoglobin concentrations of 9 to 10.9 g/dL), including birth before 37 weeks’ gestation (aOR, 1.09; 95% CI, 1.05-1.12), birth before 32 weeks’ gestation (aOR, 1.30; 95% CI, 1.21-1.39), admission to the intensive care unit (aOR, 1.21; 95% CI, 1.17-1.25), and respiratory distress syndrome (aOR, 1.35; 95% CI, 1.24-1.46).15 Adverse maternal and newborn outcomes were more prevalent among mothers with moderate (hemoglobin concentrations of 7 to 8.9 g/dL) or severe anemia (hemoglobin concentrations of <7 g/dL), compared with mild anemia. For example, compared with mothers with no anemia, mothers with moderate anemia had an increased risk of birth <37 weeks (aOR, 2.26) and birth <32 weeks (aOR, 3.95).15
In a study of 166,566 US pregnant patients, 6.1% were diagnosed with anemia.18 Patients with anemia were more likely to have antepartum thrombosis, preeclampsia, eclampsia, a cesarean birth, postpartum hemorrhage, a blood transfusion, and postpartum thrombosis.18 In this study, the newborns of mothers with anemia were more likely to have a diagnosis of antenatal or intrapartum fetal distress, a 5-minute Apgar score <7, and an admission to the neonatal intensive care unit.
Continue to: Maternal anemia and neurodevelopmental disorders in children...
Maternal anemia and neurodevelopmental disorders in children
Some experts, but not all, believe that iron deficiency during pregnancy may adversely impact fetal neurodevelopment and result in childhood behavior issues. All experts agree that more research is needed to understand if maternal anemia causes mental health issues in newborns. In one meta-analysis, among 20 studies of the association of maternal iron deficiency and newborn neurodevelopment, approximately half the studies reported that low maternal ferritin levels were associated with lower childhood performance on standardized tests of cognitive, motor, verbal, and memory function.19 Another systematic review concluded that the evidence linking maternal iron deficiency and child neurodevelopment is equivocal.20
In a study of 532,232 nonadoptive children born in Sweden from 1987 to 2010, maternal anemia was associated with an increased risk of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and intellectual disability (ID).21 In Sweden maternal hemoglobin concentration is measured at 10, 25, and 37 weeks of gestation, permitting comparisons of anemia diagnosed early and late in pregnancy with neurodevelopmental outcomes. The association between anemia and neurodevelopmental disorders was greatest if anemia was diagnosed within the first 30 weeks of pregnancy. Compared with mothers without anemia, maternal anemia diagnosed within the first 30 weeks of pregnancy was associated with higher childhood rates of ASD (4.9% vs 3.5%), ADHD (9.3% vs 7.1%), and ID (3.1% vs 1.3%).21 The differences persisted in analyses that controlled for socioeconomic, maternal, and pregnancy-related factors. In a matched sibling comparison, the diagnosis of maternal anemia within the first 30 weeks of gestation was associated with an increased risk of ASD (OR, 2.25; 95% CI, 1.24-4.11) and ID (OR, 2.59; 95% CI, 1.08-6.22) but not ADHD.21 Other studies have also reported a relationship between maternal anemia and intellectual disability.22,23
Measurement of hemoglobin will identify anemia, but hemoglobin measurement is not sufficiently sensitive to identify most cases of iron deficiency. Measuring ferritin can help to identify cases of iron deficiency before the onset of anemia, permitting early treatment of the nutrient deficiency. In pregnancy, iron deficiency is the prelude to developing anemia. Waiting until anemia occurs to diagnose and treat iron deficiency is suboptimal and may miss a critical window of fetal development that is dependent on maternal iron stores. During pregnancy, ferritin levels decrease as much as 80% between the first and third trimesters, as the fetus utilizes maternal iron stores for its growth.24 We recommend the measurement of ferritin and hemoglobin at the first prenatal visit and again at 24 to 28 weeks’ gestation to optimize early detection and treatment of iron deficiency and reduce the frequency of anemia prior to birth. ●
During pregnancy, anemia and iron deficiency are prevalent because the fetus depletes maternal iron stores. Iron deficiency and iron deficiency anemia are not synonymous. Effective screening for iron deficiency in the first trimester of pregnancy requires the measurement of a sensitive and specific biomarker of iron deficiency, such as ferritin. Limiting the measurement of ferritin to the subset of patients with anemia will result in missing many cases of iron deficiency. By the time iron deficiency causes anemia, a severe deficiency is present. Detecting iron deficiency in pregnancy and promptly treating the deficiency will reduce the number of women with anemia in the third trimester and at birth.
Diagnosis of anemia
Anemia in pregnancy is diagnosed by a hemoglobin level and hematocrit concentration below 11 g/dL and 33%, respectively, in the first and third trimesters and below 10.5 g/dL and 32%, respectively, in the second trimester.1 The prevalence of anemia in the first, second, and third trimesters is approximately 3%, 2%, and 11%, respectively.2 At a hemoglobin concentration <11 g/dL, severe maternal morbidity rises significantly.3 The laboratory evaluation of pregnant women with anemia may require assessment of iron stores, measurement of folate and cobalamin (vitamin B12), and hemoglobin electrophoresis, if indicated.
Diagnosis of iron deficiency
Iron deficiency anemia is diagnosed by a ferritin level below 30 ng/mL.4,5 Normal iron stores and iron insufficiency are indicated by ferritin levels 45 to 150 ng/mL and 30 to 44 ng/mL, respectively.4,5 Ferritin is an acute phase reactant, and patients with inflammation or chronic illnesses may have iron deficiency and a normal ferritin level. For these patients, a transferrin saturation (TSAT) <16% would support a diagnosis of iron deficiency.6 TSAT is calculated from measurement of serum iron and total iron binding capacity. TSAT saturation may be elevated by iron supplements, which increase serum iron. If measurement of TSAT is necessary, interference with the measurement accuracy can be minimized by not taking an iron supplement on the day of testing.
Iron deficiency is present in approximately 50% of pregnant women.7,8 The greatest prevalence of iron deficiency in pregnancy is observed in non-Hispanic Black females, followed by Hispanic females. Non-Hispanic White females had the lowest prevalence of iron deficiency.2
Fetal needs for iron often cause the depletion of maternal iron stores. Many pregnant women who have a normal ferritin level in the first trimester will develop iron deficiency in the third trimester, even with the usual recommended daily oral iron supplementation. We recommend measuring ferritin and hemoglobin at the first prenatal visit and again between 24 and 28 weeks’ gestation.
Impact of maternal anemia on maternal and newborn health
Iron plays a critical role in maternal health and fetal development independent of its role in red blood cell formation. Many proteins critical to maternal health and fetal development contain iron, including hemoglobin, myoglobin, cytochromes, ribonucleotide reductase, peroxidases, lipoxygenases, and cyclooxygenases. In the fetus, iron plays an important role in myelination of nerves, dendrite arborization, and synthesis of monoamine neurotransmitters.9
Many studies report that maternal anemia is associated with severe maternal morbidity and adverse newborn outcomes. The current literature must be interpreted with caution because socioeconomic factors influence iron stores. Iron deficiency and anemia is more common among economically and socially disadvantaged populations.10-12 It is possible that repleting iron stores, alone, without addressing social determinants of health, including food and housing insecurity, may be insufficient to improve maternal and newborn health.
Maternal anemia is a risk factor for severe maternal morbidity and adverse newborn outcomes.3,13-18 In a study of 515,270 live births in British Columbia between 2004 and 2016, maternal anemia was diagnosed in 12.8% of mothers.15 Maternal morbidity at birth was increased among patients with mild anemia (hemoglobin concentration of 9 to 10.9 g/dL), including higher rates of intrapartum transfusion (adjusted odds ratio [OR], 2.45; 95% confidence interval [CI], 1.74-3.45), cesarean birth (aOR, 1.17; 95% CI, 1.14-1.19), and chorioamnionitis (aOR, 1.35; 95% CI, 1.27-1.44). Newborn morbidity was also increased among newborns of mothers with mild anemia (hemoglobin concentrations of 9 to 10.9 g/dL), including birth before 37 weeks’ gestation (aOR, 1.09; 95% CI, 1.05-1.12), birth before 32 weeks’ gestation (aOR, 1.30; 95% CI, 1.21-1.39), admission to the intensive care unit (aOR, 1.21; 95% CI, 1.17-1.25), and respiratory distress syndrome (aOR, 1.35; 95% CI, 1.24-1.46).15 Adverse maternal and newborn outcomes were more prevalent among mothers with moderate (hemoglobin concentrations of 7 to 8.9 g/dL) or severe anemia (hemoglobin concentrations of <7 g/dL), compared with mild anemia. For example, compared with mothers with no anemia, mothers with moderate anemia had an increased risk of birth <37 weeks (aOR, 2.26) and birth <32 weeks (aOR, 3.95).15
In a study of 166,566 US pregnant patients, 6.1% were diagnosed with anemia.18 Patients with anemia were more likely to have antepartum thrombosis, preeclampsia, eclampsia, a cesarean birth, postpartum hemorrhage, a blood transfusion, and postpartum thrombosis.18 In this study, the newborns of mothers with anemia were more likely to have a diagnosis of antenatal or intrapartum fetal distress, a 5-minute Apgar score <7, and an admission to the neonatal intensive care unit.
Continue to: Maternal anemia and neurodevelopmental disorders in children...
Maternal anemia and neurodevelopmental disorders in children
Some experts, but not all, believe that iron deficiency during pregnancy may adversely impact fetal neurodevelopment and result in childhood behavior issues. All experts agree that more research is needed to understand if maternal anemia causes mental health issues in newborns. In one meta-analysis, among 20 studies of the association of maternal iron deficiency and newborn neurodevelopment, approximately half the studies reported that low maternal ferritin levels were associated with lower childhood performance on standardized tests of cognitive, motor, verbal, and memory function.19 Another systematic review concluded that the evidence linking maternal iron deficiency and child neurodevelopment is equivocal.20
In a study of 532,232 nonadoptive children born in Sweden from 1987 to 2010, maternal anemia was associated with an increased risk of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and intellectual disability (ID).21 In Sweden maternal hemoglobin concentration is measured at 10, 25, and 37 weeks of gestation, permitting comparisons of anemia diagnosed early and late in pregnancy with neurodevelopmental outcomes. The association between anemia and neurodevelopmental disorders was greatest if anemia was diagnosed within the first 30 weeks of pregnancy. Compared with mothers without anemia, maternal anemia diagnosed within the first 30 weeks of pregnancy was associated with higher childhood rates of ASD (4.9% vs 3.5%), ADHD (9.3% vs 7.1%), and ID (3.1% vs 1.3%).21 The differences persisted in analyses that controlled for socioeconomic, maternal, and pregnancy-related factors. In a matched sibling comparison, the diagnosis of maternal anemia within the first 30 weeks of gestation was associated with an increased risk of ASD (OR, 2.25; 95% CI, 1.24-4.11) and ID (OR, 2.59; 95% CI, 1.08-6.22) but not ADHD.21 Other studies have also reported a relationship between maternal anemia and intellectual disability.22,23
Measurement of hemoglobin will identify anemia, but hemoglobin measurement is not sufficiently sensitive to identify most cases of iron deficiency. Measuring ferritin can help to identify cases of iron deficiency before the onset of anemia, permitting early treatment of the nutrient deficiency. In pregnancy, iron deficiency is the prelude to developing anemia. Waiting until anemia occurs to diagnose and treat iron deficiency is suboptimal and may miss a critical window of fetal development that is dependent on maternal iron stores. During pregnancy, ferritin levels decrease as much as 80% between the first and third trimesters, as the fetus utilizes maternal iron stores for its growth.24 We recommend the measurement of ferritin and hemoglobin at the first prenatal visit and again at 24 to 28 weeks’ gestation to optimize early detection and treatment of iron deficiency and reduce the frequency of anemia prior to birth. ●
- American College of Obstetricians and Gynecologists. Anemia in pregnancy. ACOG Practice Bulletin No 233. Obstet Gynecol. 2021;138:e55-64.
- Mei Z, Cogswell ME, Looker AC, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1996-2006. Am J Clin Nutr. 2011;93:1312-1320.
- Ray JG, Davidson AJF, Berger H, et al. Haemoglobin levels in early pregnancy and severe maternal morbidity: population-based cohort study. BJOG. 2020;127:1154-1164.
- Mast AE, Blinder MA, Gronowski AM, et al. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin Chem. 1998;44:45-51.
- Parvord S, Daru J, Prasannan N, et al. UK Guidelines on the management of iron deficiency in pregnancy. Br J Haematol. 2020;188:819-830.
- Camaschell C. Iron-deficiency anemia. N Engl J Med. 2015;372:1832-1843.
- Auerbach M, Abernathy J, Juul S, et al. Prevalence of iron deficiency in first trimester, nonanemic pregnant women. J Matern Fetal Neonatal Med. 2021;34:1002-1005.
- Teichman J, Nisenbaum R, Lausman A, et al. Suboptimal iron deficiency screening in pregnancy and the impact of socioeconomic status in high-resource setting. Blood Adv. 2021;5:4666-4673.
- Georgieff MK. Long-term brain and behavioral consequences of early iron deficiency. Nutr Rev. 2011;69(suppl 1):S43-S48.
- Bodnar LM, Scanlon KS, Freedman DS, et al. High prevalence of postpartum anemia among low-income women in the United States. Am J Obstet Gynecol. 2001;185:438-443.
- Dondi A, PIccinno V, Morigi F, et al. Food insecurity and major diet-related morbidities in migrating children: a systematic review. Nutrients. 2020;12:379.
- Bodnar LM, Cogswell ME, Scanlon KS. Low income postpartum women are at risk of iron deficiency. J Nutr. 2002;132:2298-2302.
- Drukker L, Hants Y, Farkash R, et al. Iron deficiency anemia at admission for labor and delivery is associated with an increased risk for cesarean section and adverse maternal and neonatal outcomes. Transfusion. 2015;55:2799-2806.
- Rahman MM, Abe SK, Rahman S, et al. Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis. Am J Clin Nutr. 2016;103:495-504.
- Smith C, Teng F, Branch E, et al. Maternal and perinatal morbidity and mortality associated with anemia in pregnancy. Obstet Gynecol. 2019;134:1234-1244.
- Parks S, Hoffman MK, Goudar SS, et al. Maternal anaemia and maternal, fetal and neonatal outcomes in a prospective cohort study in India and Pakistan. BJOG. 2019;126:737-743.
- Guignard J, Deneux-Tharaux C, Seco A, et al. Gestational anemia and severe acute maternal morbidity: a population based study. Anesthesia. 2021;76:61-71.
- Harrison RK, Lauhon SR, Colvin ZA, et al. Maternal anemia and severe maternal mortality in a US cohort. Am J Obstet Gynecol MFM. 2021;3:100395.
- Quesada-Pinedo HG, Cassel F, Duijts L, et al. Maternal iron status in pregnancy and child health outcomes after birth: a systematic review and meta-analysis. Nutrients. 2021;13:2221.
- McCann S, Perapoch Amado M, Moore SE. The role of iron in brain development: a systematic review. Nutrients. 2020;12:2001.
- Wiegersma AM, Dalman C, Lee BK, et al. Association of prenatal maternal anemia with neurodevelopmental disorders. JAMA Psychiatry. 2019;76:1294-1304.
- Leonard H, de Klerk N, Bourke J, et al. Maternal health in pregnancy and intellectual disability in the offspring: a population-based study. Ann Epidemiol. 2006;16:448-454.
- Drassinower D, Lavery JA, Friedman AM, et al. The effect of maternal hematocrit on offspring IQ at 4 and 7 years of age: a secondary analysis. BJOG. 2016;123:2087-2093.
- Horton KD, Adetona O, Aguilar-Villalobos M, et al. Changes in the concentration of biochemical indicators of diet and nutritional status of pregnant women across pregnancy trimesters in Trujillo, Peru 2004-2005. Nutrition J. 2013;12:80.
- American College of Obstetricians and Gynecologists. Anemia in pregnancy. ACOG Practice Bulletin No 233. Obstet Gynecol. 2021;138:e55-64.
- Mei Z, Cogswell ME, Looker AC, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1996-2006. Am J Clin Nutr. 2011;93:1312-1320.
- Ray JG, Davidson AJF, Berger H, et al. Haemoglobin levels in early pregnancy and severe maternal morbidity: population-based cohort study. BJOG. 2020;127:1154-1164.
- Mast AE, Blinder MA, Gronowski AM, et al. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin Chem. 1998;44:45-51.
- Parvord S, Daru J, Prasannan N, et al. UK Guidelines on the management of iron deficiency in pregnancy. Br J Haematol. 2020;188:819-830.
- Camaschell C. Iron-deficiency anemia. N Engl J Med. 2015;372:1832-1843.
- Auerbach M, Abernathy J, Juul S, et al. Prevalence of iron deficiency in first trimester, nonanemic pregnant women. J Matern Fetal Neonatal Med. 2021;34:1002-1005.
- Teichman J, Nisenbaum R, Lausman A, et al. Suboptimal iron deficiency screening in pregnancy and the impact of socioeconomic status in high-resource setting. Blood Adv. 2021;5:4666-4673.
- Georgieff MK. Long-term brain and behavioral consequences of early iron deficiency. Nutr Rev. 2011;69(suppl 1):S43-S48.
- Bodnar LM, Scanlon KS, Freedman DS, et al. High prevalence of postpartum anemia among low-income women in the United States. Am J Obstet Gynecol. 2001;185:438-443.
- Dondi A, PIccinno V, Morigi F, et al. Food insecurity and major diet-related morbidities in migrating children: a systematic review. Nutrients. 2020;12:379.
- Bodnar LM, Cogswell ME, Scanlon KS. Low income postpartum women are at risk of iron deficiency. J Nutr. 2002;132:2298-2302.
- Drukker L, Hants Y, Farkash R, et al. Iron deficiency anemia at admission for labor and delivery is associated with an increased risk for cesarean section and adverse maternal and neonatal outcomes. Transfusion. 2015;55:2799-2806.
- Rahman MM, Abe SK, Rahman S, et al. Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis. Am J Clin Nutr. 2016;103:495-504.
- Smith C, Teng F, Branch E, et al. Maternal and perinatal morbidity and mortality associated with anemia in pregnancy. Obstet Gynecol. 2019;134:1234-1244.
- Parks S, Hoffman MK, Goudar SS, et al. Maternal anaemia and maternal, fetal and neonatal outcomes in a prospective cohort study in India and Pakistan. BJOG. 2019;126:737-743.
- Guignard J, Deneux-Tharaux C, Seco A, et al. Gestational anemia and severe acute maternal morbidity: a population based study. Anesthesia. 2021;76:61-71.
- Harrison RK, Lauhon SR, Colvin ZA, et al. Maternal anemia and severe maternal mortality in a US cohort. Am J Obstet Gynecol MFM. 2021;3:100395.
- Quesada-Pinedo HG, Cassel F, Duijts L, et al. Maternal iron status in pregnancy and child health outcomes after birth: a systematic review and meta-analysis. Nutrients. 2021;13:2221.
- McCann S, Perapoch Amado M, Moore SE. The role of iron in brain development: a systematic review. Nutrients. 2020;12:2001.
- Wiegersma AM, Dalman C, Lee BK, et al. Association of prenatal maternal anemia with neurodevelopmental disorders. JAMA Psychiatry. 2019;76:1294-1304.
- Leonard H, de Klerk N, Bourke J, et al. Maternal health in pregnancy and intellectual disability in the offspring: a population-based study. Ann Epidemiol. 2006;16:448-454.
- Drassinower D, Lavery JA, Friedman AM, et al. The effect of maternal hematocrit on offspring IQ at 4 and 7 years of age: a secondary analysis. BJOG. 2016;123:2087-2093.
- Horton KD, Adetona O, Aguilar-Villalobos M, et al. Changes in the concentration of biochemical indicators of diet and nutritional status of pregnant women across pregnancy trimesters in Trujillo, Peru 2004-2005. Nutrition J. 2013;12:80.

TNF blockers beat newer biologics in Crohn’s disease: Meta-analysis
Tumor necrosis factor (TNF)–alpha inhibitors achieve better endoscopic healing than the newer biologic drugs vedolizumab (Entyvio) and ustekinumab (Stelara) in moderate to severe Crohn’s disease, a new meta-analysis suggests.
The advantage for the TNF blockers infliximab (Remicade) and adalimumab (Humira) came in treating larger ileal ulcers and colonic disease.
This finding could help physicians choose among the four biologic drugs approved in recent years in the United States, Canada, and Western Europe to treat this disease. None of these drugs has emerged as clearly superior to all the others.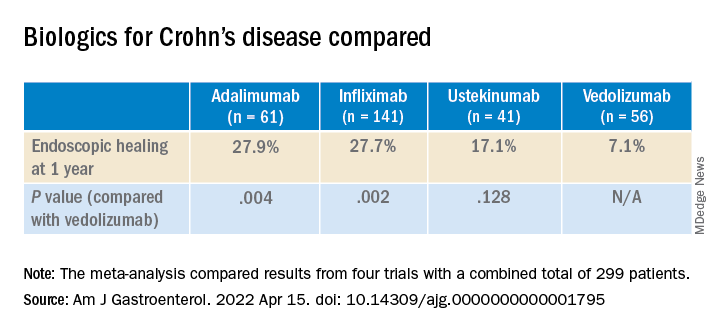
“For patients with high-risk or difficult-to-treat disease, such as those with larger ileal ulcers, the use of anti-TNF may be preferable as a first-line option,” said lead author Neeraj Narula, MD, MPH, of the department of medicine at McMaster University in Toronto, in an email to this news organization.
The study was published online in the American Journal of Gastroenterology.
Few head-to-head trials
In contrast to the TNF blockers infliximab and adalimumab, ustekinumab blocks interleukin-12 and interleukin-23, and vedolizumab blocks integrin–alpha4-beta7.
Only one trial, SEAVUE, has compared any of these drugs head to head for the treatment of Crohn’s disease. This trial found no difference between ustekinumab and adalimumab in rates of clinical remission or endoscopic healing. However, the patients in the trial had a relatively low baseline Simple Endoscopic Score for Crohn’s disease (SES-CD).
In the VARSITY trial, vedolizumab showed better results than adalimumab in clinical remission and endoscopic improvement, but that trial involved patients with ulcerative colitis.
“None of these medications are clearly head and shoulders above the rest; they all work in similar ways,” said Simon Hong, MD, of the Inflammatory Bowel Disease Center at New York University Langone Health, who was not involved in the study. “It’s not clear, at least from a rigorous scientific standpoint, which is better.”
Four biologic drugs compared
In their meta-analysis, Dr. Narula and colleagues compared results from four previous trials, which combined had a total of 299 patients. The investigators assessed the difference in results for specific ileocolonic segments. They focused on endoscopic healing because it is believed to be a more reliable indicator of long-term health than symptoms, which are more susceptible to the placebo effect.
Although the rates of endoscopic healing were low overall, they were significantly better for the TNF blockers than with the newer drugs. The difference between ustekinumab and vedolizumab was not statistically significant.
Among patients with a baseline ileal SES-CD of 3 or greater, the researchers found no significant differences between biologics for 1-year ileal endoscopic healing.
But in patients with ileal ulcers larger than 0.5 cm, the ulcers disappeared after a year in 40.8% of patients who took infliximab vs. 30% of those who took adalimumab, 17.7% of those who took ustekinumab, and 8.7% of those who took vedolizumab. Compared to vedolizumab, the difference was statistically significant for infliximab (P = .045) but not for adalimumab (P = .077) or ustekinumab (P = .259).
Among those patients who had at least one colonic segment with an SES-CD of 3 or greater, the patients taking adalimumab did the best, with 62.5% achieving endoscopic healing of the colon. The rate with infliximab was 52.4%. For vedolizumab, the rate was 31.3%, and for ustekinumab, it was 29.0%. Only the differences between the TNF blockers and the newer biologics were statistically significant for this comparison.
In general, the ileum does not heal as well as the colon, Dr. Narula and colleagues note.
“This confirms, or at least supports, our experience,” Dr. Hong told this news organization. The explanation for the greater efficacy of the TNF blockers could be their more systemic mechanism of action, he said.
The study authors acknowledge that their meta-analysis cannot take the place of true head-to-head trials.
“Safety, convenience, and cost of therapy all are relevant factors that impact decision-making, and the availability of biosimilar TNF-alpha antagonist therapies in routine practice adds additional consideration for cost-effectiveness in population health decisions,” Dr. Narula said.
The study was self-funded. Dr. Narula has received honoraria from Janssen, AbbVie, Takeda, Pfizer, Merck, Sandoz, Novartis, and Ferring. Dr. Hong reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Tumor necrosis factor (TNF)–alpha inhibitors achieve better endoscopic healing than the newer biologic drugs vedolizumab (Entyvio) and ustekinumab (Stelara) in moderate to severe Crohn’s disease, a new meta-analysis suggests.
The advantage for the TNF blockers infliximab (Remicade) and adalimumab (Humira) came in treating larger ileal ulcers and colonic disease.
This finding could help physicians choose among the four biologic drugs approved in recent years in the United States, Canada, and Western Europe to treat this disease. None of these drugs has emerged as clearly superior to all the others.
“For patients with high-risk or difficult-to-treat disease, such as those with larger ileal ulcers, the use of anti-TNF may be preferable as a first-line option,” said lead author Neeraj Narula, MD, MPH, of the department of medicine at McMaster University in Toronto, in an email to this news organization.
The study was published online in the American Journal of Gastroenterology.
Few head-to-head trials
In contrast to the TNF blockers infliximab and adalimumab, ustekinumab blocks interleukin-12 and interleukin-23, and vedolizumab blocks integrin–alpha4-beta7.
Only one trial, SEAVUE, has compared any of these drugs head to head for the treatment of Crohn’s disease. This trial found no difference between ustekinumab and adalimumab in rates of clinical remission or endoscopic healing. However, the patients in the trial had a relatively low baseline Simple Endoscopic Score for Crohn’s disease (SES-CD).
In the VARSITY trial, vedolizumab showed better results than adalimumab in clinical remission and endoscopic improvement, but that trial involved patients with ulcerative colitis.
“None of these medications are clearly head and shoulders above the rest; they all work in similar ways,” said Simon Hong, MD, of the Inflammatory Bowel Disease Center at New York University Langone Health, who was not involved in the study. “It’s not clear, at least from a rigorous scientific standpoint, which is better.”
Four biologic drugs compared
In their meta-analysis, Dr. Narula and colleagues compared results from four previous trials, which combined had a total of 299 patients. The investigators assessed the difference in results for specific ileocolonic segments. They focused on endoscopic healing because it is believed to be a more reliable indicator of long-term health than symptoms, which are more susceptible to the placebo effect.
Although the rates of endoscopic healing were low overall, they were significantly better for the TNF blockers than with the newer drugs. The difference between ustekinumab and vedolizumab was not statistically significant.
Among patients with a baseline ileal SES-CD of 3 or greater, the researchers found no significant differences between biologics for 1-year ileal endoscopic healing.
But in patients with ileal ulcers larger than 0.5 cm, the ulcers disappeared after a year in 40.8% of patients who took infliximab vs. 30% of those who took adalimumab, 17.7% of those who took ustekinumab, and 8.7% of those who took vedolizumab. Compared to vedolizumab, the difference was statistically significant for infliximab (P = .045) but not for adalimumab (P = .077) or ustekinumab (P = .259).
Among those patients who had at least one colonic segment with an SES-CD of 3 or greater, the patients taking adalimumab did the best, with 62.5% achieving endoscopic healing of the colon. The rate with infliximab was 52.4%. For vedolizumab, the rate was 31.3%, and for ustekinumab, it was 29.0%. Only the differences between the TNF blockers and the newer biologics were statistically significant for this comparison.
In general, the ileum does not heal as well as the colon, Dr. Narula and colleagues note.
“This confirms, or at least supports, our experience,” Dr. Hong told this news organization. The explanation for the greater efficacy of the TNF blockers could be their more systemic mechanism of action, he said.
The study authors acknowledge that their meta-analysis cannot take the place of true head-to-head trials.
“Safety, convenience, and cost of therapy all are relevant factors that impact decision-making, and the availability of biosimilar TNF-alpha antagonist therapies in routine practice adds additional consideration for cost-effectiveness in population health decisions,” Dr. Narula said.
The study was self-funded. Dr. Narula has received honoraria from Janssen, AbbVie, Takeda, Pfizer, Merck, Sandoz, Novartis, and Ferring. Dr. Hong reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Tumor necrosis factor (TNF)–alpha inhibitors achieve better endoscopic healing than the newer biologic drugs vedolizumab (Entyvio) and ustekinumab (Stelara) in moderate to severe Crohn’s disease, a new meta-analysis suggests.
The advantage for the TNF blockers infliximab (Remicade) and adalimumab (Humira) came in treating larger ileal ulcers and colonic disease.
This finding could help physicians choose among the four biologic drugs approved in recent years in the United States, Canada, and Western Europe to treat this disease. None of these drugs has emerged as clearly superior to all the others.
“For patients with high-risk or difficult-to-treat disease, such as those with larger ileal ulcers, the use of anti-TNF may be preferable as a first-line option,” said lead author Neeraj Narula, MD, MPH, of the department of medicine at McMaster University in Toronto, in an email to this news organization.
The study was published online in the American Journal of Gastroenterology.
Few head-to-head trials
In contrast to the TNF blockers infliximab and adalimumab, ustekinumab blocks interleukin-12 and interleukin-23, and vedolizumab blocks integrin–alpha4-beta7.
Only one trial, SEAVUE, has compared any of these drugs head to head for the treatment of Crohn’s disease. This trial found no difference between ustekinumab and adalimumab in rates of clinical remission or endoscopic healing. However, the patients in the trial had a relatively low baseline Simple Endoscopic Score for Crohn’s disease (SES-CD).
In the VARSITY trial, vedolizumab showed better results than adalimumab in clinical remission and endoscopic improvement, but that trial involved patients with ulcerative colitis.
“None of these medications are clearly head and shoulders above the rest; they all work in similar ways,” said Simon Hong, MD, of the Inflammatory Bowel Disease Center at New York University Langone Health, who was not involved in the study. “It’s not clear, at least from a rigorous scientific standpoint, which is better.”
Four biologic drugs compared
In their meta-analysis, Dr. Narula and colleagues compared results from four previous trials, which combined had a total of 299 patients. The investigators assessed the difference in results for specific ileocolonic segments. They focused on endoscopic healing because it is believed to be a more reliable indicator of long-term health than symptoms, which are more susceptible to the placebo effect.
Although the rates of endoscopic healing were low overall, they were significantly better for the TNF blockers than with the newer drugs. The difference between ustekinumab and vedolizumab was not statistically significant.
Among patients with a baseline ileal SES-CD of 3 or greater, the researchers found no significant differences between biologics for 1-year ileal endoscopic healing.
But in patients with ileal ulcers larger than 0.5 cm, the ulcers disappeared after a year in 40.8% of patients who took infliximab vs. 30% of those who took adalimumab, 17.7% of those who took ustekinumab, and 8.7% of those who took vedolizumab. Compared to vedolizumab, the difference was statistically significant for infliximab (P = .045) but not for adalimumab (P = .077) or ustekinumab (P = .259).
Among those patients who had at least one colonic segment with an SES-CD of 3 or greater, the patients taking adalimumab did the best, with 62.5% achieving endoscopic healing of the colon. The rate with infliximab was 52.4%. For vedolizumab, the rate was 31.3%, and for ustekinumab, it was 29.0%. Only the differences between the TNF blockers and the newer biologics were statistically significant for this comparison.
In general, the ileum does not heal as well as the colon, Dr. Narula and colleagues note.
“This confirms, or at least supports, our experience,” Dr. Hong told this news organization. The explanation for the greater efficacy of the TNF blockers could be their more systemic mechanism of action, he said.
The study authors acknowledge that their meta-analysis cannot take the place of true head-to-head trials.
“Safety, convenience, and cost of therapy all are relevant factors that impact decision-making, and the availability of biosimilar TNF-alpha antagonist therapies in routine practice adds additional consideration for cost-effectiveness in population health decisions,” Dr. Narula said.
The study was self-funded. Dr. Narula has received honoraria from Janssen, AbbVie, Takeda, Pfizer, Merck, Sandoz, Novartis, and Ferring. Dr. Hong reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
DOJ complaint flags HCV drug denials for people with addiction
A complaint filed with the U.S. Department of Justice (DOJ) alleges that Alabama’s Medicaid program is illegally denying curative drug treatment for hepatitis C virus (HCV) infection to people with substance use disorder.
The complaint was filed May 9 by the Center for Health Law and Policy Innovation (CHLPI) of Harvard Law School, in partnership with AIDS Alabama.
It alleges that Alabama Medicaid has a policy of denying HCV treatment to people who have used illegal drugs or alcohol in the past 6 months.
CHLPI and AIDS Alabama argue that these restrictions violate the Americans With Disabilities Act, which protects people who are disabled because of substance use disorder.
“Forced sobriety policies don’t just unfairly prevent people with substance use disorder from accessing life-saving treatment; they also severely hamper public health efforts to stop the spread of the disease,” Kevin Costello, CHLPI’s litigation director, said in a statement.
“These policies are rooted in stigma, not science, and they violate antidiscrimination provisions of the Americans With Disabilities Act,” Mr. Costello said.
Filing an administrative complaint against Alabama is “an important milestone in fighting sobriety restrictions,” he added.
Morally wrong
Kathie Hiers, CEO of AIDS Alabama, noted that Alabama’s health outcomes are among the worst in the nation.
“Policies that prevent adequate medical care from being provided must end. HCV now has a cure, and withholding that cure from Alabamians based on a moral judgment is wrong and certainly doesn’t follow the science,” Ms. Hiers added.
Direct-acting antiviral (DAA) therapy can cure up to 99% of people living with HCV.
The complaint against Alabama Medicaid builds on CHLPI’s successful policy advocacy and litigation campaigns to expand access to DAA therapy in state Medicaid programs across the country.
Since 2017, 19 states have removed treatment restrictions that were based on drug or alcohol use. In other states, however, “severe, illegal sobriety restrictions remain,” according to CHLPI.
Alabama, Mississippi, Arkansas, South Carolina, and South Dakota still require Medicaid enrollees with HCV to prove they have not used drugs or alcohol for 6 months before they can receive treatment. Iowa, North Dakota, and West Virginia have a 3-month abstinence requirement.
The American Association for the Study of Liver Diseases and the Infectious Diseases Society of America recommend DAA therapy for all patients with chronic HCV infection, regardless of drug or alcohol use.
CHLPI intends to expand this “enforcement campaign” to all states where sobriety restrictions persist.
A version of this article first appeared on Medscape.com.
A complaint filed with the U.S. Department of Justice (DOJ) alleges that Alabama’s Medicaid program is illegally denying curative drug treatment for hepatitis C virus (HCV) infection to people with substance use disorder.
The complaint was filed May 9 by the Center for Health Law and Policy Innovation (CHLPI) of Harvard Law School, in partnership with AIDS Alabama.
It alleges that Alabama Medicaid has a policy of denying HCV treatment to people who have used illegal drugs or alcohol in the past 6 months.
CHLPI and AIDS Alabama argue that these restrictions violate the Americans With Disabilities Act, which protects people who are disabled because of substance use disorder.
“Forced sobriety policies don’t just unfairly prevent people with substance use disorder from accessing life-saving treatment; they also severely hamper public health efforts to stop the spread of the disease,” Kevin Costello, CHLPI’s litigation director, said in a statement.
“These policies are rooted in stigma, not science, and they violate antidiscrimination provisions of the Americans With Disabilities Act,” Mr. Costello said.
Filing an administrative complaint against Alabama is “an important milestone in fighting sobriety restrictions,” he added.
Morally wrong
Kathie Hiers, CEO of AIDS Alabama, noted that Alabama’s health outcomes are among the worst in the nation.
“Policies that prevent adequate medical care from being provided must end. HCV now has a cure, and withholding that cure from Alabamians based on a moral judgment is wrong and certainly doesn’t follow the science,” Ms. Hiers added.
Direct-acting antiviral (DAA) therapy can cure up to 99% of people living with HCV.
The complaint against Alabama Medicaid builds on CHLPI’s successful policy advocacy and litigation campaigns to expand access to DAA therapy in state Medicaid programs across the country.
Since 2017, 19 states have removed treatment restrictions that were based on drug or alcohol use. In other states, however, “severe, illegal sobriety restrictions remain,” according to CHLPI.
Alabama, Mississippi, Arkansas, South Carolina, and South Dakota still require Medicaid enrollees with HCV to prove they have not used drugs or alcohol for 6 months before they can receive treatment. Iowa, North Dakota, and West Virginia have a 3-month abstinence requirement.
The American Association for the Study of Liver Diseases and the Infectious Diseases Society of America recommend DAA therapy for all patients with chronic HCV infection, regardless of drug or alcohol use.
CHLPI intends to expand this “enforcement campaign” to all states where sobriety restrictions persist.
A version of this article first appeared on Medscape.com.
A complaint filed with the U.S. Department of Justice (DOJ) alleges that Alabama’s Medicaid program is illegally denying curative drug treatment for hepatitis C virus (HCV) infection to people with substance use disorder.
The complaint was filed May 9 by the Center for Health Law and Policy Innovation (CHLPI) of Harvard Law School, in partnership with AIDS Alabama.
It alleges that Alabama Medicaid has a policy of denying HCV treatment to people who have used illegal drugs or alcohol in the past 6 months.
CHLPI and AIDS Alabama argue that these restrictions violate the Americans With Disabilities Act, which protects people who are disabled because of substance use disorder.
“Forced sobriety policies don’t just unfairly prevent people with substance use disorder from accessing life-saving treatment; they also severely hamper public health efforts to stop the spread of the disease,” Kevin Costello, CHLPI’s litigation director, said in a statement.
“These policies are rooted in stigma, not science, and they violate antidiscrimination provisions of the Americans With Disabilities Act,” Mr. Costello said.
Filing an administrative complaint against Alabama is “an important milestone in fighting sobriety restrictions,” he added.
Morally wrong
Kathie Hiers, CEO of AIDS Alabama, noted that Alabama’s health outcomes are among the worst in the nation.
“Policies that prevent adequate medical care from being provided must end. HCV now has a cure, and withholding that cure from Alabamians based on a moral judgment is wrong and certainly doesn’t follow the science,” Ms. Hiers added.
Direct-acting antiviral (DAA) therapy can cure up to 99% of people living with HCV.
The complaint against Alabama Medicaid builds on CHLPI’s successful policy advocacy and litigation campaigns to expand access to DAA therapy in state Medicaid programs across the country.
Since 2017, 19 states have removed treatment restrictions that were based on drug or alcohol use. In other states, however, “severe, illegal sobriety restrictions remain,” according to CHLPI.
Alabama, Mississippi, Arkansas, South Carolina, and South Dakota still require Medicaid enrollees with HCV to prove they have not used drugs or alcohol for 6 months before they can receive treatment. Iowa, North Dakota, and West Virginia have a 3-month abstinence requirement.
The American Association for the Study of Liver Diseases and the Infectious Diseases Society of America recommend DAA therapy for all patients with chronic HCV infection, regardless of drug or alcohol use.
CHLPI intends to expand this “enforcement campaign” to all states where sobriety restrictions persist.
A version of this article first appeared on Medscape.com.
Small bowel entrapment during vaginal reconstructive surgery

1931 state law makes abortion a felony if Roe falls, warns Michigan Attorney General
When Stephanie Mejia Arciñiega drove her friend to a Planned Parenthood clinic in Ann Arbor, Mich., they were surrounded by anti-abortion protesters as soon as they tried to park.
“They come up to your car super fast,” Ms. Mejia Arciñiega said. “You don’t want to run their feet over, so we had to stop and be like, ‘OK, no thank you.’ But then they started throwing a bunch of papers and resources at us. We tried to go inside, but we couldn’t.”
The clinic, which offers abortion care as well as birth control, cancer screenings, and STD treatment, has long been the target of anti-abortion protesters. Protesters’ efforts to limit abortions in the state may soon get a huge boost, if the Supreme Court strikes down Roe v. Wade.
In Michigan, this would have an immediate impact. Overnight, nearly all abortions would become a felony carrying a penalty of up to 4 years, even in cases of rape and incest. That’s because an old state law, last updated in 1931, was never repealed, even after Roe made it unenforceable in 1973.
Michigan Attorney General Dana Nessel, a Democrat, said she won’t enforce the law if it springs back into effect. But Michigan has 83 local county prosecutors, and Ms. Nessel said they could enforce the 1931 law. “I don’t think that I have the authority to tell the duly elected county prosecutors what they can and what they cannot charge,” Ms. Nessel told journalists.
Ms. Mejia Arciñiega, 18, who drove her friend to the Ann Arbor clinic, said she never imagined a world where abortion is illegal. “You wouldn’t think that in 2022, we’d be worrying about women’s rights, reproduction rights,” she said. “You wouldn’t want someone young that isn’t ready [to] have to have a baby because the law says ‘No.’ It’s not fair.”
The way the old state law is written, Ms. Nessel said, it’s possible that prosecutors could go after anyone who provides an abortion, as well as those who take medications to end their own pregnancies.
That could “create a scenario where if a woman has self-aborted and she seeks medical care after that, will the doctor then have to report that to law enforcement?”
Speaking to reporters, Ms. Nessel also discussed the abortion she had years ago – one that would be illegal in the state if Roe falls. She was pregnant with triplets and doctors told her the embryos weren’t growing in utero, she said.
“And I was told very, very specifically that there was no way that all three would make it to term. But if I aborted one, that it was possible that the other two might live,” Ms. Nessel said. “I took my doctor’s advice … And you know what? It turned out that he was right. And now I have two beautiful sons.”
The 1931 law allows just one exemption: Abortions “to preserve the life” of the woman. Yet doctors say they have no idea how to interpret that. Consider a woman who has severe heart disease with a 20%-30% chance of dying during pregnancy.
“Is that enough of a chance?” asked Dr. Lisa Harris, a University of Michigan professor and ob.gyn., speaking on Michigan Radio’s Stateside. “I hate to even put it that way, but is that enough of a chance of dying that that person would qualify under Michigan’s ban for a lifesaving abortion? Or would their risk of dying need to be 50% or 100%?”
Or what if a pregnant person has cancer and needs to end the pregnancy to begin chemotherapy? “There’s not an imminent risk of dying, but there might be a risk of dying years later if they didn’t have chemotherapy,” Dr. Harris said. “So these are the kind of situations doctors are wondering about.”
It’s also unclear whether a woman whose pregnancy would become life-threatening only in its later stages would be required to delay termination until then.
“We see people with things like kidney disease or other problems, where they’re actually OK during early pregnancy. But if the pregnancy were to continue and they were to give birth, then they would have a very high chance of dying,” Dr. Harris explained.
The state legislature is controlled by Republicans, but Michigan Gov. Gretchen Whitmer, a Democrat, filed a preemptive lawsuit seeking to block the 1931 law from taking effect. Planned Parenthood filed a similar suit as well. And a campaign to collect enough signatures is underway to put abortion on the ballot in November. But that would be months after the U.S. Supreme Court makes its final ruling on Roe, which is expected in late June or early July.
In the meantime, the confusion and uncertainty caused by the 1931 law could be enough for some health care professionals to stop offering abortions, Ms. Nessel said.
“I think that this will have the kind of chilling effect that doctors just simply will not perform this procedure really under any set of circumstances, because they don’t want to get dragged into court,” she said. “They don’t want to face the possibility of being prosecuted and the possibility of going to jail or prison. So I think that, honestly, you’ll have doctors that really have to violate their Hippocratic oath and just say, ‘I’m sorry, I can’t help you.’ ”
This story is part of a partnership that includes Michigan Radio, NPR and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. Kate Wells is a reporter with Michigan Radio.
When Stephanie Mejia Arciñiega drove her friend to a Planned Parenthood clinic in Ann Arbor, Mich., they were surrounded by anti-abortion protesters as soon as they tried to park.
“They come up to your car super fast,” Ms. Mejia Arciñiega said. “You don’t want to run their feet over, so we had to stop and be like, ‘OK, no thank you.’ But then they started throwing a bunch of papers and resources at us. We tried to go inside, but we couldn’t.”
The clinic, which offers abortion care as well as birth control, cancer screenings, and STD treatment, has long been the target of anti-abortion protesters. Protesters’ efforts to limit abortions in the state may soon get a huge boost, if the Supreme Court strikes down Roe v. Wade.
In Michigan, this would have an immediate impact. Overnight, nearly all abortions would become a felony carrying a penalty of up to 4 years, even in cases of rape and incest. That’s because an old state law, last updated in 1931, was never repealed, even after Roe made it unenforceable in 1973.
Michigan Attorney General Dana Nessel, a Democrat, said she won’t enforce the law if it springs back into effect. But Michigan has 83 local county prosecutors, and Ms. Nessel said they could enforce the 1931 law. “I don’t think that I have the authority to tell the duly elected county prosecutors what they can and what they cannot charge,” Ms. Nessel told journalists.
Ms. Mejia Arciñiega, 18, who drove her friend to the Ann Arbor clinic, said she never imagined a world where abortion is illegal. “You wouldn’t think that in 2022, we’d be worrying about women’s rights, reproduction rights,” she said. “You wouldn’t want someone young that isn’t ready [to] have to have a baby because the law says ‘No.’ It’s not fair.”
The way the old state law is written, Ms. Nessel said, it’s possible that prosecutors could go after anyone who provides an abortion, as well as those who take medications to end their own pregnancies.
That could “create a scenario where if a woman has self-aborted and she seeks medical care after that, will the doctor then have to report that to law enforcement?”
Speaking to reporters, Ms. Nessel also discussed the abortion she had years ago – one that would be illegal in the state if Roe falls. She was pregnant with triplets and doctors told her the embryos weren’t growing in utero, she said.
“And I was told very, very specifically that there was no way that all three would make it to term. But if I aborted one, that it was possible that the other two might live,” Ms. Nessel said. “I took my doctor’s advice … And you know what? It turned out that he was right. And now I have two beautiful sons.”
The 1931 law allows just one exemption: Abortions “to preserve the life” of the woman. Yet doctors say they have no idea how to interpret that. Consider a woman who has severe heart disease with a 20%-30% chance of dying during pregnancy.
“Is that enough of a chance?” asked Dr. Lisa Harris, a University of Michigan professor and ob.gyn., speaking on Michigan Radio’s Stateside. “I hate to even put it that way, but is that enough of a chance of dying that that person would qualify under Michigan’s ban for a lifesaving abortion? Or would their risk of dying need to be 50% or 100%?”
Or what if a pregnant person has cancer and needs to end the pregnancy to begin chemotherapy? “There’s not an imminent risk of dying, but there might be a risk of dying years later if they didn’t have chemotherapy,” Dr. Harris said. “So these are the kind of situations doctors are wondering about.”
It’s also unclear whether a woman whose pregnancy would become life-threatening only in its later stages would be required to delay termination until then.
“We see people with things like kidney disease or other problems, where they’re actually OK during early pregnancy. But if the pregnancy were to continue and they were to give birth, then they would have a very high chance of dying,” Dr. Harris explained.
The state legislature is controlled by Republicans, but Michigan Gov. Gretchen Whitmer, a Democrat, filed a preemptive lawsuit seeking to block the 1931 law from taking effect. Planned Parenthood filed a similar suit as well. And a campaign to collect enough signatures is underway to put abortion on the ballot in November. But that would be months after the U.S. Supreme Court makes its final ruling on Roe, which is expected in late June or early July.
In the meantime, the confusion and uncertainty caused by the 1931 law could be enough for some health care professionals to stop offering abortions, Ms. Nessel said.
“I think that this will have the kind of chilling effect that doctors just simply will not perform this procedure really under any set of circumstances, because they don’t want to get dragged into court,” she said. “They don’t want to face the possibility of being prosecuted and the possibility of going to jail or prison. So I think that, honestly, you’ll have doctors that really have to violate their Hippocratic oath and just say, ‘I’m sorry, I can’t help you.’ ”
This story is part of a partnership that includes Michigan Radio, NPR and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. Kate Wells is a reporter with Michigan Radio.
When Stephanie Mejia Arciñiega drove her friend to a Planned Parenthood clinic in Ann Arbor, Mich., they were surrounded by anti-abortion protesters as soon as they tried to park.
“They come up to your car super fast,” Ms. Mejia Arciñiega said. “You don’t want to run their feet over, so we had to stop and be like, ‘OK, no thank you.’ But then they started throwing a bunch of papers and resources at us. We tried to go inside, but we couldn’t.”
The clinic, which offers abortion care as well as birth control, cancer screenings, and STD treatment, has long been the target of anti-abortion protesters. Protesters’ efforts to limit abortions in the state may soon get a huge boost, if the Supreme Court strikes down Roe v. Wade.
In Michigan, this would have an immediate impact. Overnight, nearly all abortions would become a felony carrying a penalty of up to 4 years, even in cases of rape and incest. That’s because an old state law, last updated in 1931, was never repealed, even after Roe made it unenforceable in 1973.
Michigan Attorney General Dana Nessel, a Democrat, said she won’t enforce the law if it springs back into effect. But Michigan has 83 local county prosecutors, and Ms. Nessel said they could enforce the 1931 law. “I don’t think that I have the authority to tell the duly elected county prosecutors what they can and what they cannot charge,” Ms. Nessel told journalists.
Ms. Mejia Arciñiega, 18, who drove her friend to the Ann Arbor clinic, said she never imagined a world where abortion is illegal. “You wouldn’t think that in 2022, we’d be worrying about women’s rights, reproduction rights,” she said. “You wouldn’t want someone young that isn’t ready [to] have to have a baby because the law says ‘No.’ It’s not fair.”
The way the old state law is written, Ms. Nessel said, it’s possible that prosecutors could go after anyone who provides an abortion, as well as those who take medications to end their own pregnancies.
That could “create a scenario where if a woman has self-aborted and she seeks medical care after that, will the doctor then have to report that to law enforcement?”
Speaking to reporters, Ms. Nessel also discussed the abortion she had years ago – one that would be illegal in the state if Roe falls. She was pregnant with triplets and doctors told her the embryos weren’t growing in utero, she said.
“And I was told very, very specifically that there was no way that all three would make it to term. But if I aborted one, that it was possible that the other two might live,” Ms. Nessel said. “I took my doctor’s advice … And you know what? It turned out that he was right. And now I have two beautiful sons.”
The 1931 law allows just one exemption: Abortions “to preserve the life” of the woman. Yet doctors say they have no idea how to interpret that. Consider a woman who has severe heart disease with a 20%-30% chance of dying during pregnancy.
“Is that enough of a chance?” asked Dr. Lisa Harris, a University of Michigan professor and ob.gyn., speaking on Michigan Radio’s Stateside. “I hate to even put it that way, but is that enough of a chance of dying that that person would qualify under Michigan’s ban for a lifesaving abortion? Or would their risk of dying need to be 50% or 100%?”
Or what if a pregnant person has cancer and needs to end the pregnancy to begin chemotherapy? “There’s not an imminent risk of dying, but there might be a risk of dying years later if they didn’t have chemotherapy,” Dr. Harris said. “So these are the kind of situations doctors are wondering about.”
It’s also unclear whether a woman whose pregnancy would become life-threatening only in its later stages would be required to delay termination until then.
“We see people with things like kidney disease or other problems, where they’re actually OK during early pregnancy. But if the pregnancy were to continue and they were to give birth, then they would have a very high chance of dying,” Dr. Harris explained.
The state legislature is controlled by Republicans, but Michigan Gov. Gretchen Whitmer, a Democrat, filed a preemptive lawsuit seeking to block the 1931 law from taking effect. Planned Parenthood filed a similar suit as well. And a campaign to collect enough signatures is underway to put abortion on the ballot in November. But that would be months after the U.S. Supreme Court makes its final ruling on Roe, which is expected in late June or early July.
In the meantime, the confusion and uncertainty caused by the 1931 law could be enough for some health care professionals to stop offering abortions, Ms. Nessel said.
“I think that this will have the kind of chilling effect that doctors just simply will not perform this procedure really under any set of circumstances, because they don’t want to get dragged into court,” she said. “They don’t want to face the possibility of being prosecuted and the possibility of going to jail or prison. So I think that, honestly, you’ll have doctors that really have to violate their Hippocratic oath and just say, ‘I’m sorry, I can’t help you.’ ”
This story is part of a partnership that includes Michigan Radio, NPR and KHN. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. Kate Wells is a reporter with Michigan Radio.
COVID-19 patients remain sedentary after hospital discharge
After hospitalization, COVID-19 patients 9 hours per day of sedentary time at 3-6 months after discharge, according to data from 37 individuals.
COVID-19 patients experience a wide range of clinical manifestations, and roughly half of those who were hospitalized for COVID-19 report persisting symptoms both physical and mental up to a year after discharge, Bram van Bakel, MD, of Radboud University Medical Center, Nijmegen, the Netherlands, said in a presentation at the presentation at the annual congress of the European Association of Preventive Cardiology.
However, data on physical activity patterns and the impact on recovery after postinfection hospital discharge are limited, he said. Dr. van Bakel and colleagues aimed to assess physical activity, sedentary behavior, and sleep duration in COVID-19 patients at 3-6 months after hospital discharge to explore the association with patient characteristics, disease severity and cardiac dysfunction.
“We hypothesized that COVID-19 survivors will demonstrate low volumes of physical activity and a high sedentary time, especially those with a more severe disease course,” such as longer hospital duration and admission to intensive care, cardiac dysfunction, and persistent symptoms at 3-6 months post discharge, he said.
Dr. van Bakel and colleagues enrolled 37 adult patients in a cross-sectional cohort study. They objectively assessed physical activity, sedentary behavior, and sleep duration for 24 hrs/day during 8 subsequent days in COVID-19 survivors at 3-6 months post hospitalization. The average age of the patients was 60 years, 78% were male, and the average assessment time was 125 days after hospital discharge.
The researchers compared activity patterns based on patient and disease characteristics, cardiac biomarker release during hospitalization, abnormal transthoracic echocardiogram regarding left and right ventricular function and volumes at 3-6 months of follow-up, and the persistence of symptoms after discharge.
Overall, patients spent a median of 4.2 hours per day in light-intensity physical activity, and 1 hour per day in moderate to vigorous physical activity. The overall median time spent sitting was 9.8 hours per day; this was accumulated in approximately 6 prolonged sitting periods of 30 minutes or more and 41.1 short sitting periods of less than 30 minutes.
The median sleep duration was 9.8 hours per day; sleep duration was significantly higher in women, compared with men (9.2 vs. 8.5 hours/day; P = .03), and in patients with persistent symptoms, compared with those without persistent symptoms (9.1 hrs/day vs. 8.3 hrs/day; P = .02). No other differences in activity or sitting patterns appeared among subgroups. Sedentary time of 10 hours or more per day overall puts individuals at increased risk for detrimental health effects, Dr. van Bakel said.
The study findings were limited by the small sample and cross-sectional design, he noted.
However, the results suggest that COVID-19 patients spent most of their time sedentary within the first 3-6 months after hospital discharge. The similar activity patterns across subgroups support a uniform approach to rehabilitation for these patients to target persisting symptoms and prevent long-term health consequences, said Dr. van Bakel. Further studies are warranted in a larger cohort with a prospective design and longitudinal follow-up.
The current study “highlights the need for ongoing rehabilitation in severe COVID-19 survivors after hospitalization to restore premorbid function and endurance,” Alba Miranda Azola, MD, of Johns Hopkins University, Baltimore, said in an interview.
“The findings regarding inactivity are not surprising,” said Dr. Azola. “Immobility during hospitalization results in muscle atrophy and marked decreased endurance. The need for prolonged use of sedation and paralytics during intensive care stays of severe COVID-19 patients is associated with critical illness myopathy. Also, many patients continue to experience hypoxia and dyspnea on exertion for several months after leaving the hospital. The functional impairments and limited activity tolerance often preclude patients from engaging on outpatient rehabilitation programs.
“I do think it surprising that the level of inactivity observed was independent of disease severity and patient factors, but it definitely speaks to the importance of establishing post hospitalization follow-up care that focuses on restoring function and mobility,” Dr. Azola noted.
The study findings may have long-term clinical implications, as COVID-19 survivors who experience functional decline that limits activity and who continue to lead a sedentary lifestyle may be at increased risk for health issues such as heart disease and type 2 diabetes, Dr. Azola said.
Rigorous research is needed to study the functional and health impact of rehabilitation interventions during and after hospitalization, she emphasized. “Additionally, studies are needed on innovative rehabilitation interventions that improve accessibility to services to patients.”
The study received no outside funding. The researchers and Dr. Azola had no financial conflicts to disclose. Dr. Azola had no financial conflicts to disclose.
After hospitalization, COVID-19 patients 9 hours per day of sedentary time at 3-6 months after discharge, according to data from 37 individuals.
COVID-19 patients experience a wide range of clinical manifestations, and roughly half of those who were hospitalized for COVID-19 report persisting symptoms both physical and mental up to a year after discharge, Bram van Bakel, MD, of Radboud University Medical Center, Nijmegen, the Netherlands, said in a presentation at the presentation at the annual congress of the European Association of Preventive Cardiology.
However, data on physical activity patterns and the impact on recovery after postinfection hospital discharge are limited, he said. Dr. van Bakel and colleagues aimed to assess physical activity, sedentary behavior, and sleep duration in COVID-19 patients at 3-6 months after hospital discharge to explore the association with patient characteristics, disease severity and cardiac dysfunction.
“We hypothesized that COVID-19 survivors will demonstrate low volumes of physical activity and a high sedentary time, especially those with a more severe disease course,” such as longer hospital duration and admission to intensive care, cardiac dysfunction, and persistent symptoms at 3-6 months post discharge, he said.
Dr. van Bakel and colleagues enrolled 37 adult patients in a cross-sectional cohort study. They objectively assessed physical activity, sedentary behavior, and sleep duration for 24 hrs/day during 8 subsequent days in COVID-19 survivors at 3-6 months post hospitalization. The average age of the patients was 60 years, 78% were male, and the average assessment time was 125 days after hospital discharge.
The researchers compared activity patterns based on patient and disease characteristics, cardiac biomarker release during hospitalization, abnormal transthoracic echocardiogram regarding left and right ventricular function and volumes at 3-6 months of follow-up, and the persistence of symptoms after discharge.
Overall, patients spent a median of 4.2 hours per day in light-intensity physical activity, and 1 hour per day in moderate to vigorous physical activity. The overall median time spent sitting was 9.8 hours per day; this was accumulated in approximately 6 prolonged sitting periods of 30 minutes or more and 41.1 short sitting periods of less than 30 minutes.
The median sleep duration was 9.8 hours per day; sleep duration was significantly higher in women, compared with men (9.2 vs. 8.5 hours/day; P = .03), and in patients with persistent symptoms, compared with those without persistent symptoms (9.1 hrs/day vs. 8.3 hrs/day; P = .02). No other differences in activity or sitting patterns appeared among subgroups. Sedentary time of 10 hours or more per day overall puts individuals at increased risk for detrimental health effects, Dr. van Bakel said.
The study findings were limited by the small sample and cross-sectional design, he noted.
However, the results suggest that COVID-19 patients spent most of their time sedentary within the first 3-6 months after hospital discharge. The similar activity patterns across subgroups support a uniform approach to rehabilitation for these patients to target persisting symptoms and prevent long-term health consequences, said Dr. van Bakel. Further studies are warranted in a larger cohort with a prospective design and longitudinal follow-up.
The current study “highlights the need for ongoing rehabilitation in severe COVID-19 survivors after hospitalization to restore premorbid function and endurance,” Alba Miranda Azola, MD, of Johns Hopkins University, Baltimore, said in an interview.
“The findings regarding inactivity are not surprising,” said Dr. Azola. “Immobility during hospitalization results in muscle atrophy and marked decreased endurance. The need for prolonged use of sedation and paralytics during intensive care stays of severe COVID-19 patients is associated with critical illness myopathy. Also, many patients continue to experience hypoxia and dyspnea on exertion for several months after leaving the hospital. The functional impairments and limited activity tolerance often preclude patients from engaging on outpatient rehabilitation programs.
“I do think it surprising that the level of inactivity observed was independent of disease severity and patient factors, but it definitely speaks to the importance of establishing post hospitalization follow-up care that focuses on restoring function and mobility,” Dr. Azola noted.
The study findings may have long-term clinical implications, as COVID-19 survivors who experience functional decline that limits activity and who continue to lead a sedentary lifestyle may be at increased risk for health issues such as heart disease and type 2 diabetes, Dr. Azola said.
Rigorous research is needed to study the functional and health impact of rehabilitation interventions during and after hospitalization, she emphasized. “Additionally, studies are needed on innovative rehabilitation interventions that improve accessibility to services to patients.”
The study received no outside funding. The researchers and Dr. Azola had no financial conflicts to disclose. Dr. Azola had no financial conflicts to disclose.
After hospitalization, COVID-19 patients 9 hours per day of sedentary time at 3-6 months after discharge, according to data from 37 individuals.
COVID-19 patients experience a wide range of clinical manifestations, and roughly half of those who were hospitalized for COVID-19 report persisting symptoms both physical and mental up to a year after discharge, Bram van Bakel, MD, of Radboud University Medical Center, Nijmegen, the Netherlands, said in a presentation at the presentation at the annual congress of the European Association of Preventive Cardiology.
However, data on physical activity patterns and the impact on recovery after postinfection hospital discharge are limited, he said. Dr. van Bakel and colleagues aimed to assess physical activity, sedentary behavior, and sleep duration in COVID-19 patients at 3-6 months after hospital discharge to explore the association with patient characteristics, disease severity and cardiac dysfunction.
“We hypothesized that COVID-19 survivors will demonstrate low volumes of physical activity and a high sedentary time, especially those with a more severe disease course,” such as longer hospital duration and admission to intensive care, cardiac dysfunction, and persistent symptoms at 3-6 months post discharge, he said.
Dr. van Bakel and colleagues enrolled 37 adult patients in a cross-sectional cohort study. They objectively assessed physical activity, sedentary behavior, and sleep duration for 24 hrs/day during 8 subsequent days in COVID-19 survivors at 3-6 months post hospitalization. The average age of the patients was 60 years, 78% were male, and the average assessment time was 125 days after hospital discharge.
The researchers compared activity patterns based on patient and disease characteristics, cardiac biomarker release during hospitalization, abnormal transthoracic echocardiogram regarding left and right ventricular function and volumes at 3-6 months of follow-up, and the persistence of symptoms after discharge.
Overall, patients spent a median of 4.2 hours per day in light-intensity physical activity, and 1 hour per day in moderate to vigorous physical activity. The overall median time spent sitting was 9.8 hours per day; this was accumulated in approximately 6 prolonged sitting periods of 30 minutes or more and 41.1 short sitting periods of less than 30 minutes.
The median sleep duration was 9.8 hours per day; sleep duration was significantly higher in women, compared with men (9.2 vs. 8.5 hours/day; P = .03), and in patients with persistent symptoms, compared with those without persistent symptoms (9.1 hrs/day vs. 8.3 hrs/day; P = .02). No other differences in activity or sitting patterns appeared among subgroups. Sedentary time of 10 hours or more per day overall puts individuals at increased risk for detrimental health effects, Dr. van Bakel said.
The study findings were limited by the small sample and cross-sectional design, he noted.
However, the results suggest that COVID-19 patients spent most of their time sedentary within the first 3-6 months after hospital discharge. The similar activity patterns across subgroups support a uniform approach to rehabilitation for these patients to target persisting symptoms and prevent long-term health consequences, said Dr. van Bakel. Further studies are warranted in a larger cohort with a prospective design and longitudinal follow-up.
The current study “highlights the need for ongoing rehabilitation in severe COVID-19 survivors after hospitalization to restore premorbid function and endurance,” Alba Miranda Azola, MD, of Johns Hopkins University, Baltimore, said in an interview.
“The findings regarding inactivity are not surprising,” said Dr. Azola. “Immobility during hospitalization results in muscle atrophy and marked decreased endurance. The need for prolonged use of sedation and paralytics during intensive care stays of severe COVID-19 patients is associated with critical illness myopathy. Also, many patients continue to experience hypoxia and dyspnea on exertion for several months after leaving the hospital. The functional impairments and limited activity tolerance often preclude patients from engaging on outpatient rehabilitation programs.
“I do think it surprising that the level of inactivity observed was independent of disease severity and patient factors, but it definitely speaks to the importance of establishing post hospitalization follow-up care that focuses on restoring function and mobility,” Dr. Azola noted.
The study findings may have long-term clinical implications, as COVID-19 survivors who experience functional decline that limits activity and who continue to lead a sedentary lifestyle may be at increased risk for health issues such as heart disease and type 2 diabetes, Dr. Azola said.
Rigorous research is needed to study the functional and health impact of rehabilitation interventions during and after hospitalization, she emphasized. “Additionally, studies are needed on innovative rehabilitation interventions that improve accessibility to services to patients.”
The study received no outside funding. The researchers and Dr. Azola had no financial conflicts to disclose. Dr. Azola had no financial conflicts to disclose.
FROM ESC PREVENTIVE CARDIOLOGY 2022
Grit your teeth for a lesser-known complication of diabetes
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM BMJ ENDOCRINE DISORDERS