User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
LDL cholesterol triglycerides ‘robust’ ASCVD risk marker
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.

The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.

This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.
The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.
This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
High levels of triglyceride molecules in LDL cholesterol are “robustly” linked with an increased risk of atherosclerotic cardiovascular disease, according to a study that used two different methods in two separate cohorts from a large European population study plus a meta-analysis to verify the results.
“There have been some studies in the past, as you can see from our meta-analysis, that found a similar association, but I don’t think most people are convinced that there is really this relationship, and certainly I was not convinced,” lead investigator Børge G. Nordestgaard, MD, DMSc, professor at the University of Copenhagen, said in an interview.
The study enrolled 68,290 patients from the Copenhagen General Population study; 38,081 were assigned to direct automated assay to measure their LDL triglycerides and 30,208 had nuclear magnetic resonance (NMR) spectroscopy. Median follow-up was 3 and 9.2 years for the respective cohorts.
LDL triglycerides carry higher ASCVD risk
In the automated assay group, each 0.1-mmol/L (9 mg/dL)–higher direct LDL triglycerides carried a 22%-38% higher risk for the following outcomes: ASCVD (hazard ratio, 1.26; 95% confidence interval, 1.17-1.35); ischemic heart disease (HR, 1.27; 95% CI, 1.16-1.39); myocardial infarction (HR, 1.28; 95% CI, 1.11-1.48); ischemic stroke (HR, 1.22; 95% CI, 1.08-1.38); and peripheral artery disease (HR, 1.38; 95% CI, 1.21-1.58).
In the group that had NMR spectroscopy to measure LDL triglycerides, risks were similar, ranging from HRs of 1.13 (95% CI, 1.05-1.23) for ischemic stroke to 1.41 (95% CI, 1.31-1.52) for myocardial infarction. The investigators noted that apolipoprotein B levels didn’t entirely explain these results.
The meta-analysis included 18 studies that evaluated varying cardiovascular disease outcomes. It compared random-effects risk ratios for the highest quartile vs. the lowest quartile of LDL triglycerides. They were 1.50 (95% CI, 1.35-1.66) for ASCVD (four studies, 71,526 individuals, 8,576 events); 1.62 (95% CI, 1.37-1.93) for ischemic heart disease (six studies, 107,538 individuals, 9,734 events); 1.30 (95% CI, 1.13-1.49) for ischemic stroke (four studies, 78,026 individuals, 4,273 events); and 1.53 (95% CI, 1.29-1.81) for peripheral artery disease (four studies, 107,511 individuals, 1,848 events). The study was published online in the Journal of the American College of Cardiology.
Results confirm hypothesis the study sought to disprove
The purpose of the study was to actually disprove the hypothesis that the study ended up confirming, Dr. Nordestgaard said. “When we started this study, my idea was that we wanted to show that LDL triglyceride was not related to these diseases, because that didn’t make sense to me,” he said. “I’m so used to the thinking that the cholesterol content of these particles drive atherosclerosis and therefore atherosclerotic cardiovascular disease.”
He noted that LDL can carry both cholesterol and triglycerides, and that larger remnant lipoproteins can carry a substantial amount of triglycerides and a lesser amount of cholesterol. “Those remnants actually transfer into LDL, so they somewhat bring the triglycerides molecules into LDL,” Dr. Nordestgaard said.
The direct automated assay test used in the study to measure LDL triglycerides is not approved for use in the United States by the Food and Drug Administration, according to Denka, the manufacturer of the test.
The use of the Copenhagen General Population Study cohorts is a strength of the study because it has 100% follow-up with all patients, Dr. Nordestgaard said. The meta-analysis is another strength. “So we can show real clearly, not only in our two prospective studies, but also added to the former ones in the literature: All say exactly the same thing: High LDL triglycerides carry a high risk for ASCVD and its components.”
A limitation Dr. Nordestgaard acknowledged: The study doesn’t explain the causal relationship between high LDL triglycerides and ASCVD. But the study provides “very sound evidence that there’s a relationship,” he added. The study population was also a White, Danish population that lacked ethnic and racial diversity.
Next step is finding a treatment
The Danish study essentially confirms what the Atherosclerosis Risk in Community Study (ARIC) found with regard to LDL triglycerides, said Christie M. Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston, and an ARIC investigator.
This study is the “first step” to coming up with a test to identify risk, he said. “These data are pretty convincing, when you throw in the data in this study plus all the meta-analyses data, that LDL triglycerides, when they’re elevated, identify individuals at increased risk for an atherosclerotic cardiovascular event.”
The next step, he said, is coming up with a treatment for people with elevated HDL triglyceride. “That’s where we don’t have as much data because this test hasn’t been used. I’m pretty sure that statins are going to work fine for these people, because they lower LDL cholesterol and they also lower triglycerides, and some of the data have shown already that they reduce the LDL remnant,” Dr. Ballantyne said.
The Danish study provides enough of a basis for pursuing future studies to better understand the effect of statins on LDL triglyceride levels, Dr. Ballantyne added.
The study received funding from the Novo Nordisk Foundation and the Danish Heart Foundation, along with institutional support. Dr. Nordestgaard has no relevant disclosures. Dr. Ballantyne disclosed receiving research support from Denka.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Spikes out: A COVID mystery
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.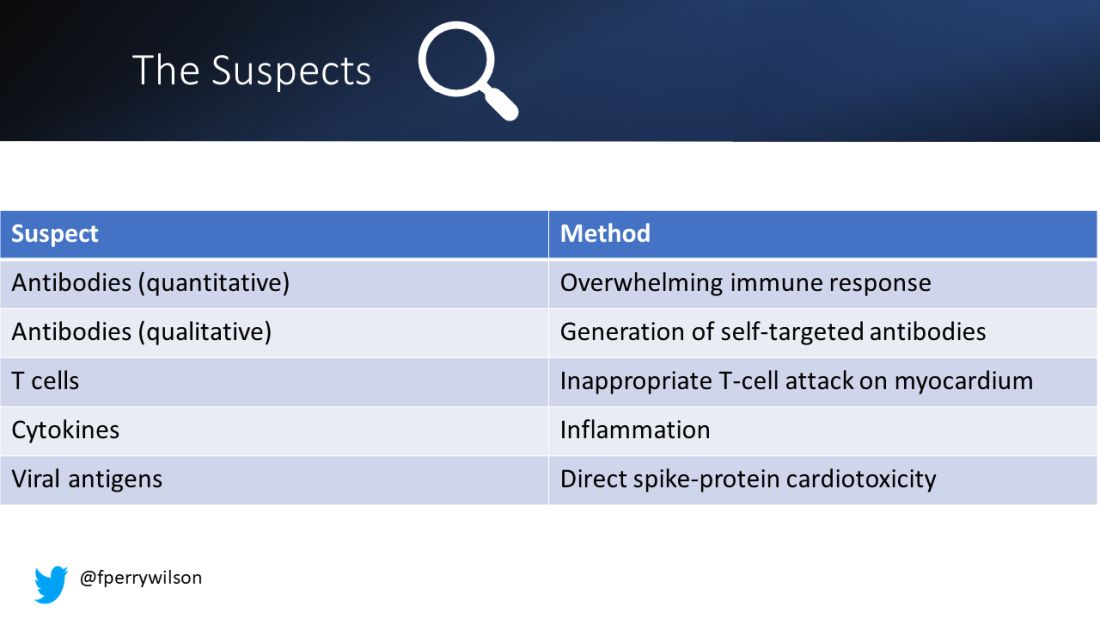
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.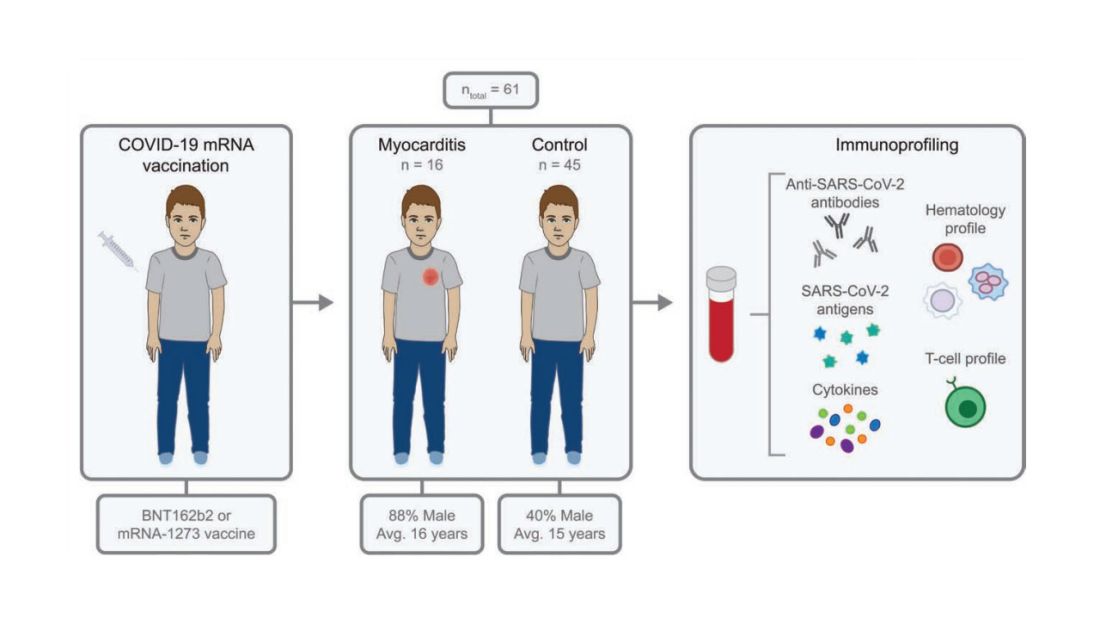
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.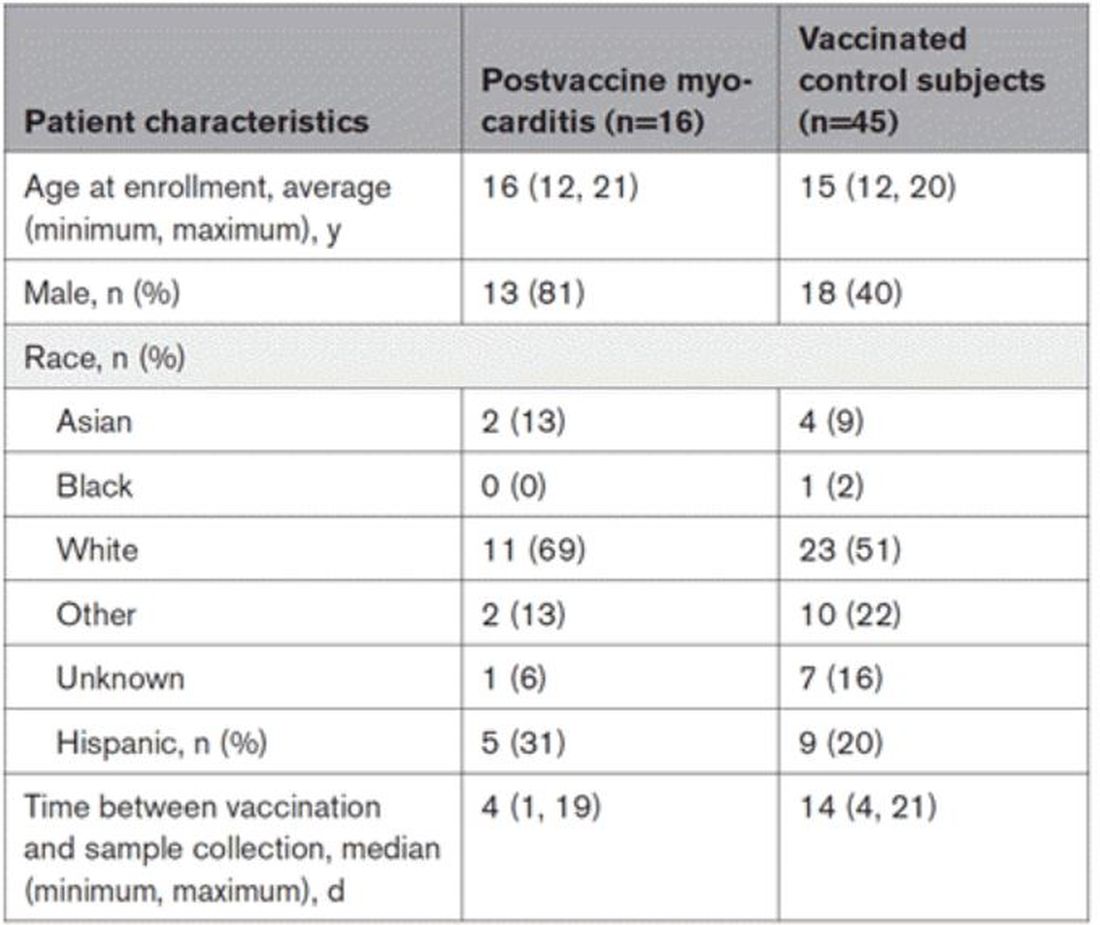
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.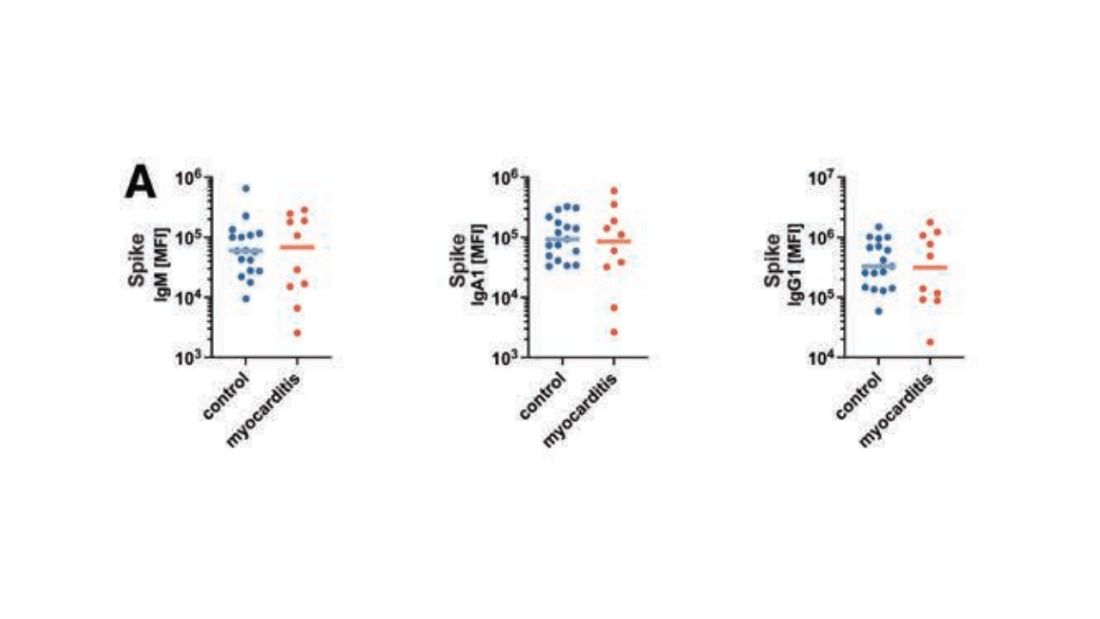
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.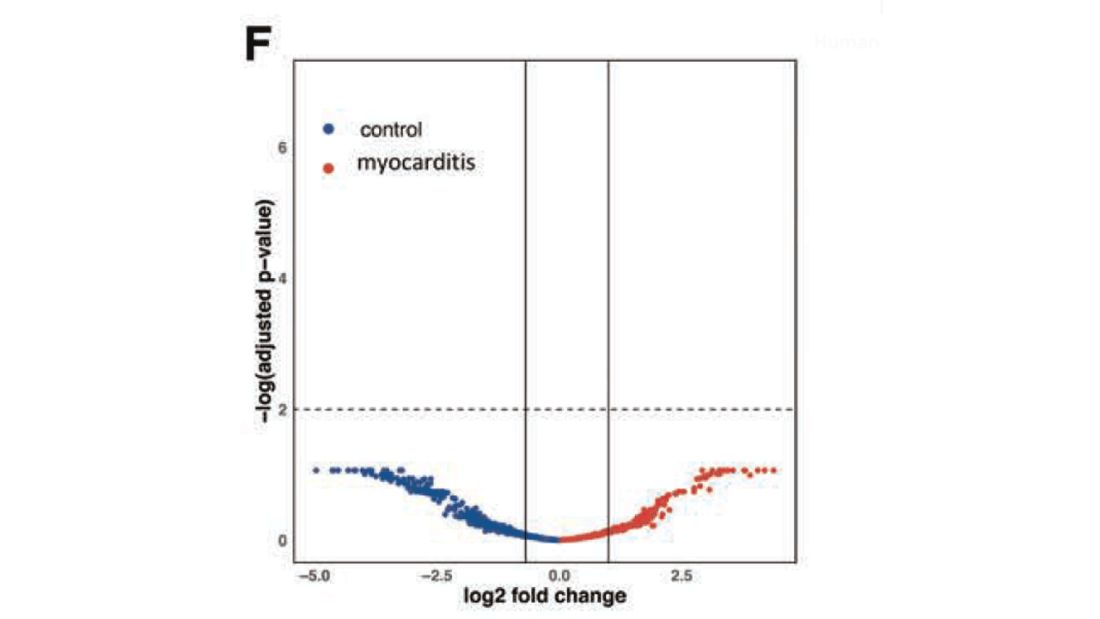
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.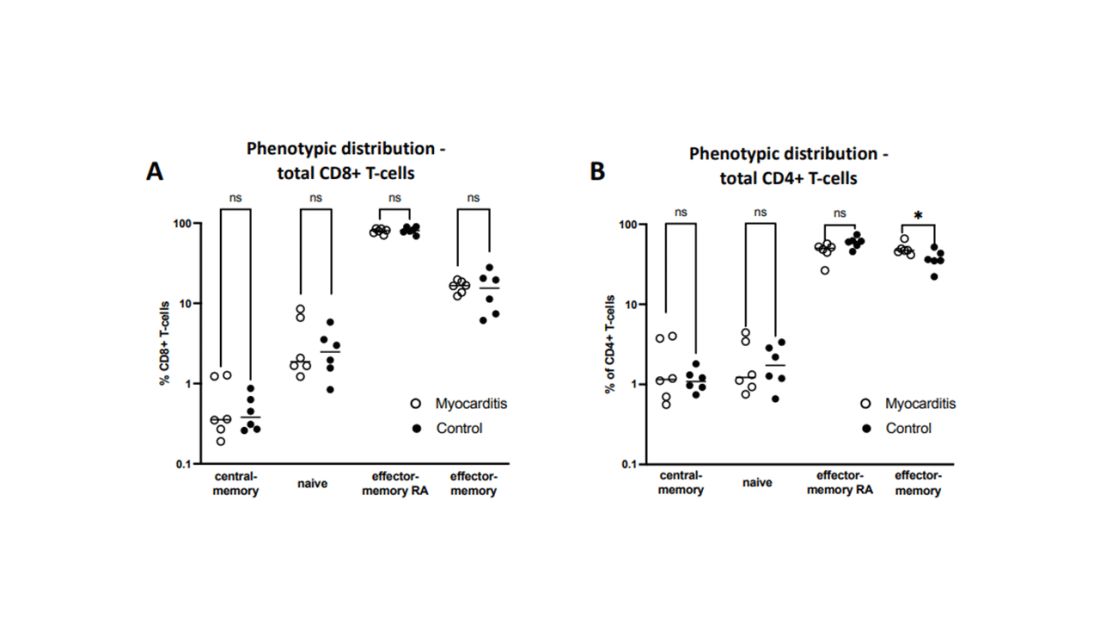
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.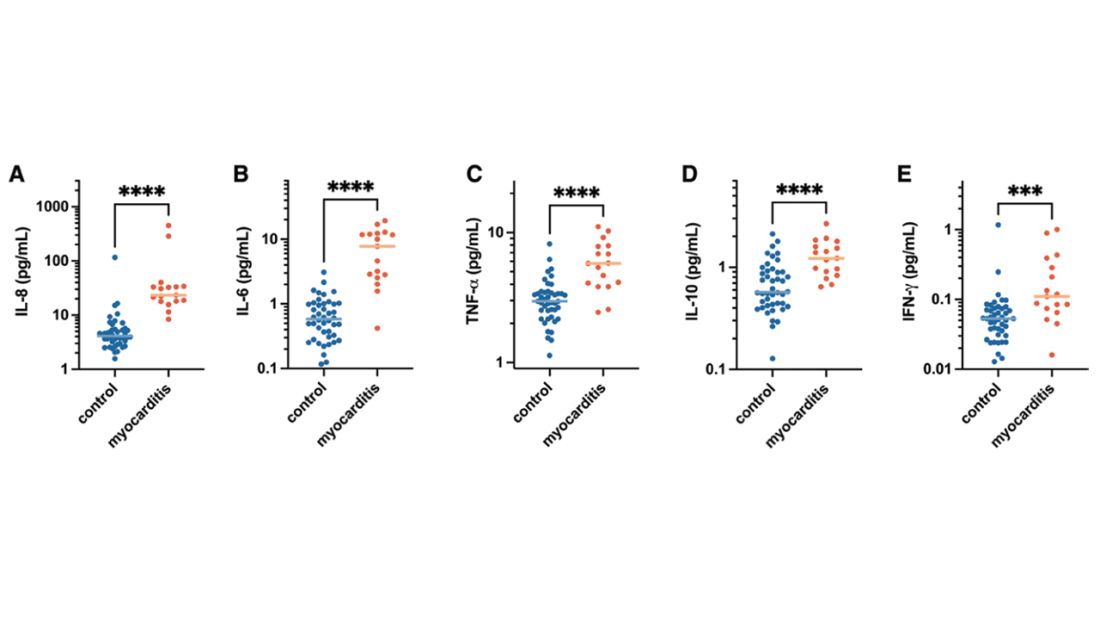
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.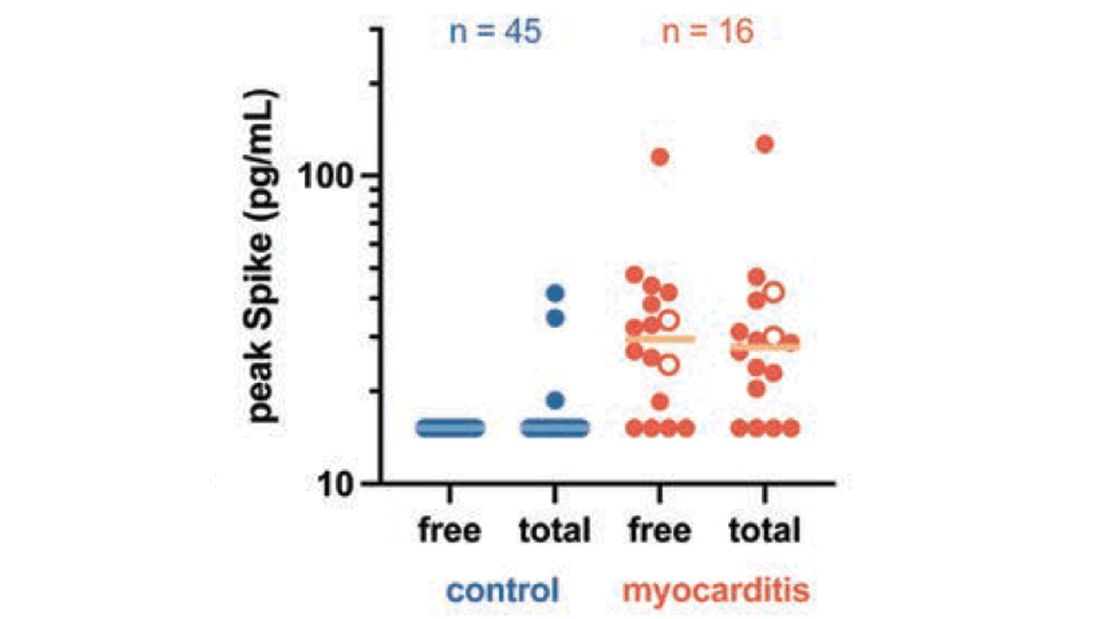
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
New Omicron subvariant is ‘crazy infectious,’ COVID expert warns
“It’s crazy infectious,” said Paula Cannon, PhD, a virologist at the University of Southern California, Los Angeles. “All the things that have protected you for the past couple of years, I don’t think are going to protect you against this new crop of variants.”
XBB.1.5 is spreading quickly in the United States. It accounted for 27.6% of cases in the country in the week ending on Jan. 7, up from about 1% of cases at one point in December, according to the Centers for Disease Control and Prevention. It’s especially prevalent in the Northeast, now accounting for more than 70% of the cases in that region.
It’s spreading across the globe, too. Maria Van Kerkhove, PhD, technical lead of the World Health Organization, has called XBB.1.5 is “the most transmissible subvariant that has been detected yet.”
Ashish Jha, MD, the White House COVID-19 response coordinator, tweeted a few days ago that the spread of XBB.1.5 is “stunning” but cautioned that it’s unclear if the symptoms of infection will be more severe than for previous variants.
“Whether we’ll have an XBB.1.5 wave (and if yes, how big) will depend on many factors including immunity of the population, people’s actions, etc.,” he tweeted.
He urged people to get up to date on their boosters, wear a snug-fitting mask, and avoid crowded indoor spaces. He noted that people who haven’t been infected recently or haven’t gotten the bivalent booster likely have little protection against infection.
The symptoms for XBB.1.5 appear to be the same as for other versions of COVID-19. However, it’s less common for people infected with XBB.1.5 to report losing their sense of taste and smell, USA Today reported.
A version of this article first appeared on WebMD.com.
“It’s crazy infectious,” said Paula Cannon, PhD, a virologist at the University of Southern California, Los Angeles. “All the things that have protected you for the past couple of years, I don’t think are going to protect you against this new crop of variants.”
XBB.1.5 is spreading quickly in the United States. It accounted for 27.6% of cases in the country in the week ending on Jan. 7, up from about 1% of cases at one point in December, according to the Centers for Disease Control and Prevention. It’s especially prevalent in the Northeast, now accounting for more than 70% of the cases in that region.
It’s spreading across the globe, too. Maria Van Kerkhove, PhD, technical lead of the World Health Organization, has called XBB.1.5 is “the most transmissible subvariant that has been detected yet.”
Ashish Jha, MD, the White House COVID-19 response coordinator, tweeted a few days ago that the spread of XBB.1.5 is “stunning” but cautioned that it’s unclear if the symptoms of infection will be more severe than for previous variants.
“Whether we’ll have an XBB.1.5 wave (and if yes, how big) will depend on many factors including immunity of the population, people’s actions, etc.,” he tweeted.
He urged people to get up to date on their boosters, wear a snug-fitting mask, and avoid crowded indoor spaces. He noted that people who haven’t been infected recently or haven’t gotten the bivalent booster likely have little protection against infection.
The symptoms for XBB.1.5 appear to be the same as for other versions of COVID-19. However, it’s less common for people infected with XBB.1.5 to report losing their sense of taste and smell, USA Today reported.
A version of this article first appeared on WebMD.com.
“It’s crazy infectious,” said Paula Cannon, PhD, a virologist at the University of Southern California, Los Angeles. “All the things that have protected you for the past couple of years, I don’t think are going to protect you against this new crop of variants.”
XBB.1.5 is spreading quickly in the United States. It accounted for 27.6% of cases in the country in the week ending on Jan. 7, up from about 1% of cases at one point in December, according to the Centers for Disease Control and Prevention. It’s especially prevalent in the Northeast, now accounting for more than 70% of the cases in that region.
It’s spreading across the globe, too. Maria Van Kerkhove, PhD, technical lead of the World Health Organization, has called XBB.1.5 is “the most transmissible subvariant that has been detected yet.”
Ashish Jha, MD, the White House COVID-19 response coordinator, tweeted a few days ago that the spread of XBB.1.5 is “stunning” but cautioned that it’s unclear if the symptoms of infection will be more severe than for previous variants.
“Whether we’ll have an XBB.1.5 wave (and if yes, how big) will depend on many factors including immunity of the population, people’s actions, etc.,” he tweeted.
He urged people to get up to date on their boosters, wear a snug-fitting mask, and avoid crowded indoor spaces. He noted that people who haven’t been infected recently or haven’t gotten the bivalent booster likely have little protection against infection.
The symptoms for XBB.1.5 appear to be the same as for other versions of COVID-19. However, it’s less common for people infected with XBB.1.5 to report losing their sense of taste and smell, USA Today reported.
A version of this article first appeared on WebMD.com.
Autopsies show COVID virus invades entire body
A study on the subject was published in the journal Nature. The researchers completed autopsies from April 2020 to March 2021 of 44 unvaccinated people who had severe COVID-19. The median age was 62.5 years old, and 30% were female. Extensive brain sampling was done for 11 cases.
Because of its nature as a respiratory illness, SARS-CoV-2 was most widespread in the respiratory system such as in the lungs. But it was also found in 79 other body locations, including the heart, kidneys, liver, muscles, nerves, reproductive tract, and eyes.
The researchers said their work shows the SARS-CoV-2 “is capable of infecting and replicating within the human brain.” They also said their results indicate the virus spreads via the blood early during infection, which “seeds the virus throughout the body following infection of the respiratory tract.”
The authors noted that, while the virus was found outside the respiratory tract, they did not find signs of inflammation beyond the respiratory system.
The results will help narrow down treatments for long COVID, and particularly support the idea of using the antiviral drug Paxlovid to treat long COVID, according to a blog post from the National Institute of Allergy and Infectious Diseases. A clinical trial is already underway examining the treatment, and results are expected in January 2024.
A version of this article first appeared on WebMD.com.
A study on the subject was published in the journal Nature. The researchers completed autopsies from April 2020 to March 2021 of 44 unvaccinated people who had severe COVID-19. The median age was 62.5 years old, and 30% were female. Extensive brain sampling was done for 11 cases.
Because of its nature as a respiratory illness, SARS-CoV-2 was most widespread in the respiratory system such as in the lungs. But it was also found in 79 other body locations, including the heart, kidneys, liver, muscles, nerves, reproductive tract, and eyes.
The researchers said their work shows the SARS-CoV-2 “is capable of infecting and replicating within the human brain.” They also said their results indicate the virus spreads via the blood early during infection, which “seeds the virus throughout the body following infection of the respiratory tract.”
The authors noted that, while the virus was found outside the respiratory tract, they did not find signs of inflammation beyond the respiratory system.
The results will help narrow down treatments for long COVID, and particularly support the idea of using the antiviral drug Paxlovid to treat long COVID, according to a blog post from the National Institute of Allergy and Infectious Diseases. A clinical trial is already underway examining the treatment, and results are expected in January 2024.
A version of this article first appeared on WebMD.com.
A study on the subject was published in the journal Nature. The researchers completed autopsies from April 2020 to March 2021 of 44 unvaccinated people who had severe COVID-19. The median age was 62.5 years old, and 30% were female. Extensive brain sampling was done for 11 cases.
Because of its nature as a respiratory illness, SARS-CoV-2 was most widespread in the respiratory system such as in the lungs. But it was also found in 79 other body locations, including the heart, kidneys, liver, muscles, nerves, reproductive tract, and eyes.
The researchers said their work shows the SARS-CoV-2 “is capable of infecting and replicating within the human brain.” They also said their results indicate the virus spreads via the blood early during infection, which “seeds the virus throughout the body following infection of the respiratory tract.”
The authors noted that, while the virus was found outside the respiratory tract, they did not find signs of inflammation beyond the respiratory system.
The results will help narrow down treatments for long COVID, and particularly support the idea of using the antiviral drug Paxlovid to treat long COVID, according to a blog post from the National Institute of Allergy and Infectious Diseases. A clinical trial is already underway examining the treatment, and results are expected in January 2024.
A version of this article first appeared on WebMD.com.
FROM NATURE
Modified Atkins diet beneficial in drug-resistant epilepsy
, new research shows.
In a randomized prospective study, the number of seizures per month dropped by more than half in one-quarter of patients following the high-fat, low-carb diet; and 5% of the group were free from all seizure activity after 6 months.
Both adults and adolescents reported benefits from the diet, which is a less strict version of a traditional ketogenic diet that many patients find difficult to follow. The modified Atkins diet includes foods such as leafy green vegetables and eggs, chicken, fish, bacon, and other animal proteins.
“The use of an exchange list and recipe booklet with local recipes and spices helped in the initiation of modified Atkins diet with the flexibility of meal choices and ease of administration,” said coinvestigator Manjari Tripathi, MD, DM, department of neurology, All India Institute of Medical Science, New Delhi.
“As items were everyday household ingredients in proportion to the requirement of the modified Atkins diet, this diet is possible in low-income countries also,” Dr. Tripathi added.
The findings were published online in the journal Neurology.
Low carbs, high benefit
The modified Atkins diet includes around 65% fat, 25% protein, and 10% carbohydrates. Unlike a traditional ketogenic diet, the modified Atkins diet includes no restrictions on protein, calories, or fluids.
Researchers have long known that ketogenic and Atkins diets are associated with reduced seizure activity in adolescents with epilepsy. But previous studies were small, and many were retrospective analyses.
The current investigators enrolled 160 patients (80 adults, 80 adolescents) aged 10-55 years whose epilepsy was not controlled despite using at least three antiseizure medications at maximum tolerated doses.
The intervention group received training in the modified Atkins diet and were given a food exchange list, sample menu, and recipe booklet. Carbohydrate intake was restricted to 20 grams per day.
Participants took supplemental multivitamins and minerals, kept a food diary, logged seizure activity, and measured urine ketone levels three times a day. They also received weekly check-up phone calls to ensure diet adherence.
The control group received a normal diet with no carbohydrate restrictions. All participants continued their prescribed antiseizure therapy throughout the trial.
Primary outcome met
The primary study outcome was a reduction in seizures of more than 50%. At 6 months, 26.2% of the intervention group had reached that goal, compared with just 2.5% of the control group (P < .001).
When the median number of seizures in the modified Atkins diet group was analyzed, the frequency dropped in the intervention group from 37.5 per month at baseline to 27.5 per month after 3 months of the modified Atkins diet and to 21.5 per month after 6 months.
Adding the modified Atkins diet had a larger effect on seizure activity in adults than in adolescents. At the end of 6 months, 36% of adolescents on the modified Atkins diet had more than a 50% reduction in seizures, while 57.1% of adults on the diet reached that level.
Quality-of-life scores were also higher in the intervention group.
By the end of the trial, 5% of patients on the modified Atkins diet had no seizure activity at all versus none of the control group. In fact, the median number of seizures increased in the control group during the study.
The mean morning and evening levels of urine ketosis in the intervention group were 58.3 ± 8.0 mg/dL and 62.2 ± 22.6 mg/dL, respectively, suggesting satisfactory diet adherence. There was no significant difference between groups in weight loss.
Dr. Tripathi noted that 33% of participants did not complete the study because of poor tolerance of the diet, lack of benefit, or the inability to follow up – in part due to COVID-19. However, she said tolerance of the modified Atkins diet was better than what has been reported with the ketogenic diet.
“Though the exact mechanism by which such a diet protects against seizures is unknown, there is evidence that it causes effects on intermediary metabolism that influences the dynamics of the major inhibitory and excitatory neurotransmitter systems in the brain,” Dr. Tripathi said.
Benefits outweigh cost
Commenting on the research findings, Mackenzie Cervenka, MD, professor of neurology and director of the Adult Epilepsy Diet Center at Johns Hopkins University, Baltimore, noted that the study is the first randomized controlled trial of this size to demonstrate a benefit from adding the modified Atkins diet to standard antiseizure therapy in treatment-resistant epilepsy.
“Importantly, the study also showed improvement in quality of life and behavior over standard-of-care therapies without significant adverse effects,” said Dr. Cervenka, who was not part of the research.
The investigators noted that the flexibility of the modified Atkins diet allows more variation in menu options and a greater intake of protein, making it easier to follow than a traditional ketogenic diet.
One area of debate, however, is whether these diets are manageable for individuals with low income. Poultry, meat, and fish, all of which are staples of a modified Atkins diet, can be more expensive than other high-carb options such as pasta and rice.
“While some of the foods such as protein sources that patients purchase when they are on a ketogenic diet therapy can be more expensive, if you take into account the cost of antiseizure medications and other antiseizure treatments, hospital visits, and missed work related to seizures, et cetera, the overall financial benefits of seizure reduction with incorporating a ketogenic diet therapy may outweigh these costs,” Dr. Cervenka said.
“There are also low-cost foods that can be used since there is a great deal of flexibility with a modified Atkins diet,” she added.
The study was funded by the Centre of Excellence for Epilepsy, which is funded by the Department of Biotechnology, Government of India. Dr. Tripathi and Dr. Cervenka report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
In a randomized prospective study, the number of seizures per month dropped by more than half in one-quarter of patients following the high-fat, low-carb diet; and 5% of the group were free from all seizure activity after 6 months.
Both adults and adolescents reported benefits from the diet, which is a less strict version of a traditional ketogenic diet that many patients find difficult to follow. The modified Atkins diet includes foods such as leafy green vegetables and eggs, chicken, fish, bacon, and other animal proteins.
“The use of an exchange list and recipe booklet with local recipes and spices helped in the initiation of modified Atkins diet with the flexibility of meal choices and ease of administration,” said coinvestigator Manjari Tripathi, MD, DM, department of neurology, All India Institute of Medical Science, New Delhi.
“As items were everyday household ingredients in proportion to the requirement of the modified Atkins diet, this diet is possible in low-income countries also,” Dr. Tripathi added.
The findings were published online in the journal Neurology.
Low carbs, high benefit
The modified Atkins diet includes around 65% fat, 25% protein, and 10% carbohydrates. Unlike a traditional ketogenic diet, the modified Atkins diet includes no restrictions on protein, calories, or fluids.
Researchers have long known that ketogenic and Atkins diets are associated with reduced seizure activity in adolescents with epilepsy. But previous studies were small, and many were retrospective analyses.
The current investigators enrolled 160 patients (80 adults, 80 adolescents) aged 10-55 years whose epilepsy was not controlled despite using at least three antiseizure medications at maximum tolerated doses.
The intervention group received training in the modified Atkins diet and were given a food exchange list, sample menu, and recipe booklet. Carbohydrate intake was restricted to 20 grams per day.
Participants took supplemental multivitamins and minerals, kept a food diary, logged seizure activity, and measured urine ketone levels three times a day. They also received weekly check-up phone calls to ensure diet adherence.
The control group received a normal diet with no carbohydrate restrictions. All participants continued their prescribed antiseizure therapy throughout the trial.
Primary outcome met
The primary study outcome was a reduction in seizures of more than 50%. At 6 months, 26.2% of the intervention group had reached that goal, compared with just 2.5% of the control group (P < .001).
When the median number of seizures in the modified Atkins diet group was analyzed, the frequency dropped in the intervention group from 37.5 per month at baseline to 27.5 per month after 3 months of the modified Atkins diet and to 21.5 per month after 6 months.
Adding the modified Atkins diet had a larger effect on seizure activity in adults than in adolescents. At the end of 6 months, 36% of adolescents on the modified Atkins diet had more than a 50% reduction in seizures, while 57.1% of adults on the diet reached that level.
Quality-of-life scores were also higher in the intervention group.
By the end of the trial, 5% of patients on the modified Atkins diet had no seizure activity at all versus none of the control group. In fact, the median number of seizures increased in the control group during the study.
The mean morning and evening levels of urine ketosis in the intervention group were 58.3 ± 8.0 mg/dL and 62.2 ± 22.6 mg/dL, respectively, suggesting satisfactory diet adherence. There was no significant difference between groups in weight loss.
Dr. Tripathi noted that 33% of participants did not complete the study because of poor tolerance of the diet, lack of benefit, or the inability to follow up – in part due to COVID-19. However, she said tolerance of the modified Atkins diet was better than what has been reported with the ketogenic diet.
“Though the exact mechanism by which such a diet protects against seizures is unknown, there is evidence that it causes effects on intermediary metabolism that influences the dynamics of the major inhibitory and excitatory neurotransmitter systems in the brain,” Dr. Tripathi said.
Benefits outweigh cost
Commenting on the research findings, Mackenzie Cervenka, MD, professor of neurology and director of the Adult Epilepsy Diet Center at Johns Hopkins University, Baltimore, noted that the study is the first randomized controlled trial of this size to demonstrate a benefit from adding the modified Atkins diet to standard antiseizure therapy in treatment-resistant epilepsy.
“Importantly, the study also showed improvement in quality of life and behavior over standard-of-care therapies without significant adverse effects,” said Dr. Cervenka, who was not part of the research.
The investigators noted that the flexibility of the modified Atkins diet allows more variation in menu options and a greater intake of protein, making it easier to follow than a traditional ketogenic diet.
One area of debate, however, is whether these diets are manageable for individuals with low income. Poultry, meat, and fish, all of which are staples of a modified Atkins diet, can be more expensive than other high-carb options such as pasta and rice.
“While some of the foods such as protein sources that patients purchase when they are on a ketogenic diet therapy can be more expensive, if you take into account the cost of antiseizure medications and other antiseizure treatments, hospital visits, and missed work related to seizures, et cetera, the overall financial benefits of seizure reduction with incorporating a ketogenic diet therapy may outweigh these costs,” Dr. Cervenka said.
“There are also low-cost foods that can be used since there is a great deal of flexibility with a modified Atkins diet,” she added.
The study was funded by the Centre of Excellence for Epilepsy, which is funded by the Department of Biotechnology, Government of India. Dr. Tripathi and Dr. Cervenka report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
In a randomized prospective study, the number of seizures per month dropped by more than half in one-quarter of patients following the high-fat, low-carb diet; and 5% of the group were free from all seizure activity after 6 months.
Both adults and adolescents reported benefits from the diet, which is a less strict version of a traditional ketogenic diet that many patients find difficult to follow. The modified Atkins diet includes foods such as leafy green vegetables and eggs, chicken, fish, bacon, and other animal proteins.
“The use of an exchange list and recipe booklet with local recipes and spices helped in the initiation of modified Atkins diet with the flexibility of meal choices and ease of administration,” said coinvestigator Manjari Tripathi, MD, DM, department of neurology, All India Institute of Medical Science, New Delhi.
“As items were everyday household ingredients in proportion to the requirement of the modified Atkins diet, this diet is possible in low-income countries also,” Dr. Tripathi added.
The findings were published online in the journal Neurology.
Low carbs, high benefit
The modified Atkins diet includes around 65% fat, 25% protein, and 10% carbohydrates. Unlike a traditional ketogenic diet, the modified Atkins diet includes no restrictions on protein, calories, or fluids.
Researchers have long known that ketogenic and Atkins diets are associated with reduced seizure activity in adolescents with epilepsy. But previous studies were small, and many were retrospective analyses.
The current investigators enrolled 160 patients (80 adults, 80 adolescents) aged 10-55 years whose epilepsy was not controlled despite using at least three antiseizure medications at maximum tolerated doses.
The intervention group received training in the modified Atkins diet and were given a food exchange list, sample menu, and recipe booklet. Carbohydrate intake was restricted to 20 grams per day.
Participants took supplemental multivitamins and minerals, kept a food diary, logged seizure activity, and measured urine ketone levels three times a day. They also received weekly check-up phone calls to ensure diet adherence.
The control group received a normal diet with no carbohydrate restrictions. All participants continued their prescribed antiseizure therapy throughout the trial.
Primary outcome met
The primary study outcome was a reduction in seizures of more than 50%. At 6 months, 26.2% of the intervention group had reached that goal, compared with just 2.5% of the control group (P < .001).
When the median number of seizures in the modified Atkins diet group was analyzed, the frequency dropped in the intervention group from 37.5 per month at baseline to 27.5 per month after 3 months of the modified Atkins diet and to 21.5 per month after 6 months.
Adding the modified Atkins diet had a larger effect on seizure activity in adults than in adolescents. At the end of 6 months, 36% of adolescents on the modified Atkins diet had more than a 50% reduction in seizures, while 57.1% of adults on the diet reached that level.
Quality-of-life scores were also higher in the intervention group.
By the end of the trial, 5% of patients on the modified Atkins diet had no seizure activity at all versus none of the control group. In fact, the median number of seizures increased in the control group during the study.
The mean morning and evening levels of urine ketosis in the intervention group were 58.3 ± 8.0 mg/dL and 62.2 ± 22.6 mg/dL, respectively, suggesting satisfactory diet adherence. There was no significant difference between groups in weight loss.
Dr. Tripathi noted that 33% of participants did not complete the study because of poor tolerance of the diet, lack of benefit, or the inability to follow up – in part due to COVID-19. However, she said tolerance of the modified Atkins diet was better than what has been reported with the ketogenic diet.
“Though the exact mechanism by which such a diet protects against seizures is unknown, there is evidence that it causes effects on intermediary metabolism that influences the dynamics of the major inhibitory and excitatory neurotransmitter systems in the brain,” Dr. Tripathi said.
Benefits outweigh cost
Commenting on the research findings, Mackenzie Cervenka, MD, professor of neurology and director of the Adult Epilepsy Diet Center at Johns Hopkins University, Baltimore, noted that the study is the first randomized controlled trial of this size to demonstrate a benefit from adding the modified Atkins diet to standard antiseizure therapy in treatment-resistant epilepsy.
“Importantly, the study also showed improvement in quality of life and behavior over standard-of-care therapies without significant adverse effects,” said Dr. Cervenka, who was not part of the research.
The investigators noted that the flexibility of the modified Atkins diet allows more variation in menu options and a greater intake of protein, making it easier to follow than a traditional ketogenic diet.
One area of debate, however, is whether these diets are manageable for individuals with low income. Poultry, meat, and fish, all of which are staples of a modified Atkins diet, can be more expensive than other high-carb options such as pasta and rice.
“While some of the foods such as protein sources that patients purchase when they are on a ketogenic diet therapy can be more expensive, if you take into account the cost of antiseizure medications and other antiseizure treatments, hospital visits, and missed work related to seizures, et cetera, the overall financial benefits of seizure reduction with incorporating a ketogenic diet therapy may outweigh these costs,” Dr. Cervenka said.
“There are also low-cost foods that can be used since there is a great deal of flexibility with a modified Atkins diet,” she added.
The study was funded by the Centre of Excellence for Epilepsy, which is funded by the Department of Biotechnology, Government of India. Dr. Tripathi and Dr. Cervenka report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
‘Low-value’ prostate cancer screening prevalent in primary care
Yet a new study shows that testing for prostate-specific antigen (PSA) and also digital rectal examinations (DRE) are both carried out frequently in older men, even when there is no indication for such testing.
“As a man ages, the risk for a false-positive result increases,” said lead author Chris Gillette, PhD, associate professor of physician assistant studies at Wake Forest University, Winston-Salem, N.C., in a statement
The study authors looked at primary care visits for men who were age 70 or older, and found that, per 100 visits, there were 6.7 PSA tests and 1.6 DRE performed.
Dr. Gillette and colleagues emphasized the importance of their findings. Whereas prior studies have relied on commercially insured men or patient-reported rates of PSA testing, they used a nationally representative clinical dataset that is much more inclusive, as it includes men who are also uninsured or insured through traditional Medicare.
The study was published online in the Journal of the American Board of Family Medicine.
Screening for prostate cancer has been much debated, and the guidelines have changed in recent years. In the period 2012-2018, the U.S. Preventive Services Task Force recommended against PSA-based screening in all men, but then the guidelines changed, and the USPSTF subsequently endorsed individualized screening in those aged 55-69 years after a shared decision-making discussion. That same 2018 update also recommends against PSA screening in men over the age of 70.
In addition, the American Urological Association has recommended against PSA-based prostate cancer screening for men over the age of 70 since 2013.
Previous studies have shown that clinicians are not adhering to the guidelines. An analysis conducted in March 2022 found that about one in four accredited U.S. cancer centers fails to follow national guidelines for PSA testing to screen for prostate cancer. Contrary to national guidelines, which advocate shared decision-making, 22% of centers recommend all men universally initiate PSA screening at either age 50 or 55 and another 4% of centers recommend this before age 50, earlier than the guidelines advise.
In the current study, Dr. Gillette and colleagues conducted a secondary analysis of the National Ambulatory Medical Care Survey datasets from 2013 to 2016 and 2018. The dataset is a nationally representative sample of visits to nonfederal, office-based physician clinics. This analysis was restricted to male patients aged 70 years and older who visited a primary care clinic.
The team found that health care professionals who order a lot of tests are more likely to order low-value screening such as PSA and DRE.
The data also showed that when there were a higher number of services ordered/provided, the patients were significantly more likely to receive a low-value PSA (odds ratio, 1.49) and a low-value DRE (OR, 1.37). In contrast, patients who had more previous visits to the clinician were less likely to receive a low-value DRE (OR, 0.92).
Overall, there a decline in low-value PSA screening after 2014, but this trend was not seen for DRE during primary care visits.
Speculating as to why these low-value tests are being carried out, Dr. Gillette suggested that health care professionals might be responding to patient requests when ordering these screening tests, or they may be using what’s known as a “shotgun” approach to medical testing where all possible tests are ordered during a medical visit.
“However, as health care systems move toward a more value-based care system – where the benefit of services provided outweighs any risks – clinicians need to engage patients in these discussions on the complexity of this testing,” he commented. “Ultimately, when and if to screen is a decision best left between a provider and the patient.”
There was no outside funding and the authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Yet a new study shows that testing for prostate-specific antigen (PSA) and also digital rectal examinations (DRE) are both carried out frequently in older men, even when there is no indication for such testing.
“As a man ages, the risk for a false-positive result increases,” said lead author Chris Gillette, PhD, associate professor of physician assistant studies at Wake Forest University, Winston-Salem, N.C., in a statement
The study authors looked at primary care visits for men who were age 70 or older, and found that, per 100 visits, there were 6.7 PSA tests and 1.6 DRE performed.
Dr. Gillette and colleagues emphasized the importance of their findings. Whereas prior studies have relied on commercially insured men or patient-reported rates of PSA testing, they used a nationally representative clinical dataset that is much more inclusive, as it includes men who are also uninsured or insured through traditional Medicare.
The study was published online in the Journal of the American Board of Family Medicine.
Screening for prostate cancer has been much debated, and the guidelines have changed in recent years. In the period 2012-2018, the U.S. Preventive Services Task Force recommended against PSA-based screening in all men, but then the guidelines changed, and the USPSTF subsequently endorsed individualized screening in those aged 55-69 years after a shared decision-making discussion. That same 2018 update also recommends against PSA screening in men over the age of 70.
In addition, the American Urological Association has recommended against PSA-based prostate cancer screening for men over the age of 70 since 2013.
Previous studies have shown that clinicians are not adhering to the guidelines. An analysis conducted in March 2022 found that about one in four accredited U.S. cancer centers fails to follow national guidelines for PSA testing to screen for prostate cancer. Contrary to national guidelines, which advocate shared decision-making, 22% of centers recommend all men universally initiate PSA screening at either age 50 or 55 and another 4% of centers recommend this before age 50, earlier than the guidelines advise.
In the current study, Dr. Gillette and colleagues conducted a secondary analysis of the National Ambulatory Medical Care Survey datasets from 2013 to 2016 and 2018. The dataset is a nationally representative sample of visits to nonfederal, office-based physician clinics. This analysis was restricted to male patients aged 70 years and older who visited a primary care clinic.
The team found that health care professionals who order a lot of tests are more likely to order low-value screening such as PSA and DRE.
The data also showed that when there were a higher number of services ordered/provided, the patients were significantly more likely to receive a low-value PSA (odds ratio, 1.49) and a low-value DRE (OR, 1.37). In contrast, patients who had more previous visits to the clinician were less likely to receive a low-value DRE (OR, 0.92).
Overall, there a decline in low-value PSA screening after 2014, but this trend was not seen for DRE during primary care visits.
Speculating as to why these low-value tests are being carried out, Dr. Gillette suggested that health care professionals might be responding to patient requests when ordering these screening tests, or they may be using what’s known as a “shotgun” approach to medical testing where all possible tests are ordered during a medical visit.
“However, as health care systems move toward a more value-based care system – where the benefit of services provided outweighs any risks – clinicians need to engage patients in these discussions on the complexity of this testing,” he commented. “Ultimately, when and if to screen is a decision best left between a provider and the patient.”
There was no outside funding and the authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Yet a new study shows that testing for prostate-specific antigen (PSA) and also digital rectal examinations (DRE) are both carried out frequently in older men, even when there is no indication for such testing.
“As a man ages, the risk for a false-positive result increases,” said lead author Chris Gillette, PhD, associate professor of physician assistant studies at Wake Forest University, Winston-Salem, N.C., in a statement
The study authors looked at primary care visits for men who were age 70 or older, and found that, per 100 visits, there were 6.7 PSA tests and 1.6 DRE performed.
Dr. Gillette and colleagues emphasized the importance of their findings. Whereas prior studies have relied on commercially insured men or patient-reported rates of PSA testing, they used a nationally representative clinical dataset that is much more inclusive, as it includes men who are also uninsured or insured through traditional Medicare.
The study was published online in the Journal of the American Board of Family Medicine.
Screening for prostate cancer has been much debated, and the guidelines have changed in recent years. In the period 2012-2018, the U.S. Preventive Services Task Force recommended against PSA-based screening in all men, but then the guidelines changed, and the USPSTF subsequently endorsed individualized screening in those aged 55-69 years after a shared decision-making discussion. That same 2018 update also recommends against PSA screening in men over the age of 70.
In addition, the American Urological Association has recommended against PSA-based prostate cancer screening for men over the age of 70 since 2013.
Previous studies have shown that clinicians are not adhering to the guidelines. An analysis conducted in March 2022 found that about one in four accredited U.S. cancer centers fails to follow national guidelines for PSA testing to screen for prostate cancer. Contrary to national guidelines, which advocate shared decision-making, 22% of centers recommend all men universally initiate PSA screening at either age 50 or 55 and another 4% of centers recommend this before age 50, earlier than the guidelines advise.
In the current study, Dr. Gillette and colleagues conducted a secondary analysis of the National Ambulatory Medical Care Survey datasets from 2013 to 2016 and 2018. The dataset is a nationally representative sample of visits to nonfederal, office-based physician clinics. This analysis was restricted to male patients aged 70 years and older who visited a primary care clinic.
The team found that health care professionals who order a lot of tests are more likely to order low-value screening such as PSA and DRE.
The data also showed that when there were a higher number of services ordered/provided, the patients were significantly more likely to receive a low-value PSA (odds ratio, 1.49) and a low-value DRE (OR, 1.37). In contrast, patients who had more previous visits to the clinician were less likely to receive a low-value DRE (OR, 0.92).
Overall, there a decline in low-value PSA screening after 2014, but this trend was not seen for DRE during primary care visits.
Speculating as to why these low-value tests are being carried out, Dr. Gillette suggested that health care professionals might be responding to patient requests when ordering these screening tests, or they may be using what’s known as a “shotgun” approach to medical testing where all possible tests are ordered during a medical visit.
“However, as health care systems move toward a more value-based care system – where the benefit of services provided outweighs any risks – clinicians need to engage patients in these discussions on the complexity of this testing,” he commented. “Ultimately, when and if to screen is a decision best left between a provider and the patient.”
There was no outside funding and the authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN BOARD OF FAMILY MEDICINE
Screen all patients for cannabis use before surgery: Guideline
All patients who undergo procedures that require regional or general anesthesia should be asked if, how often, and in what forms they use the drug, according to recommendations from the American Society of Regional Anesthesia and Pain Medicine.
One reason: Patients who regularly use cannabis may experience worse pain and nausea after surgery and may require more opioid analgesia, the group said.
The society’s recommendations – published in Regional Anesthesia and Pain Medicine – are the first guidelines in the United States to cover cannabis use as it relates to surgery, the group said.
Possible interactions
Use of cannabis has increased in recent years, and researchers have been concerned that the drug may interact with anesthesia and complicate pain management. Few studies have evaluated interactions between cannabis and anesthetic agents, however, according to the authors of the new guidelines.
“With the rising prevalence of both medical and recreational cannabis use in the general population, anesthesiologists, surgeons, and perioperative physicians must have an understanding of the effects of cannabis on physiology in order to provide safe perioperative care,” the guideline said.
“Before surgery, anesthesiologists should ask patients if they use cannabis – whether medicinally or recreationally – and be prepared to possibly change the anesthesia plan or delay the procedure in certain situations,” Samer Narouze, MD, PhD, ASRA president and senior author of the guidelines, said in a news release about the recommendations.
Although some patients may use cannabis to relieve pain, research shows that “regular users may have more pain and nausea after surgery, not less, and may need more medications, including opioids, to manage the discomfort,” said Dr. Narouze, chairman of the Center for Pain Medicine at Western Reserve Hospital in Cuyahoga Falls, Ohio.
Risks for vomiting, heart attack
The new recommendations were created by a committee of 13 experts, including anesthesiologists, chronic pain physicians, and a patient advocate. Shalini Shah, MD, vice chair of anesthesiology at the University of California, Irvine, was lead author of the document.
Four of 21 recommendations were classified as grade A, meaning that following them would be expected to provide substantial benefits. Those recommendations are to screen all patients before surgery; postpone elective surgery for patients who have altered mental status or impaired decision-making capacity at the time of surgery; counsel frequent, heavy users about the potential for cannabis use to impair postoperative pain control; and counsel pregnant patients about the risks of cannabis use to unborn children.
The authors cited studies to support their recommendations, including one showing that long-term cannabis use was associated with a 20% increase in the incidence of postoperative nausea and vomiting, a leading complaint of surgery patients. Other research has shown that cannabis use is linked to more pain and use of opioids after surgery.
Other recommendations include delaying elective surgery for at least 2 hours after a patient has smoked cannabis, owing to an increased risk for heart attack, and considering adjustment of ventilation settings during surgery for regular smokers of cannabis. Research has shown that smoking cannabis may be a rare trigger for myocardial infarction and is associated with airway inflammation and self-reported respiratory symptoms.
Nevertheless, doctors should not conduct universal toxicology screening, given a lack of evidence supporting this practice, the guideline stated.
The authors did not have enough information to make recommendations about reducing cannabis use before surgery or adjusting opioid prescriptions after surgery for patients who use cannabis, they said.
Kenneth Finn, MD, president of the American Board of Pain Medicine, welcomed the publication of the new guidelines. Dr. Finn, who practices at Springs Rehabilitation in Colorado Springs, has edited a textbook about cannabis in medicine and founded the International Academy on the Science and Impact of Cannabis.
“The vast majority of medical providers really have no idea about cannabis and what its impacts are on the human body,” Dr. Finn said.
For one, it can interact with numerous other drugs, including warfarin.
Guideline coauthor Eugene R. Viscusi, MD, professor of anesthesiology at the Sidney Kimmel Medical College, Philadelphia, emphasized that, while cannabis may be perceived as “natural,” it should not be considered differently from manufactured drugs.
Cannabis and cannabinoids represent “a class of very potent and pharmacologically active compounds,” Dr. Viscusi said in an interview. While researchers continue to assess possible medically beneficial effects of cannabis compounds, clinicians also need to be aware of the risks.
“The literature continues to emerge, and while we are always hopeful for good news, as physicians, we need to be very well versed on potential risks, especially in a high-risk situation like surgery,” he said.
Dr. Shah has consulted for companies that develop medical devices and drugs. Dr. Finn is the editor of the textbook, “Cannabis in Medicine: An Evidence-Based Approach” (Springer: New York, 2020), for which he receives royalties.
A version of this article first appeared on Medscape.com.
All patients who undergo procedures that require regional or general anesthesia should be asked if, how often, and in what forms they use the drug, according to recommendations from the American Society of Regional Anesthesia and Pain Medicine.
One reason: Patients who regularly use cannabis may experience worse pain and nausea after surgery and may require more opioid analgesia, the group said.
The society’s recommendations – published in Regional Anesthesia and Pain Medicine – are the first guidelines in the United States to cover cannabis use as it relates to surgery, the group said.
Possible interactions
Use of cannabis has increased in recent years, and researchers have been concerned that the drug may interact with anesthesia and complicate pain management. Few studies have evaluated interactions between cannabis and anesthetic agents, however, according to the authors of the new guidelines.
“With the rising prevalence of both medical and recreational cannabis use in the general population, anesthesiologists, surgeons, and perioperative physicians must have an understanding of the effects of cannabis on physiology in order to provide safe perioperative care,” the guideline said.
“Before surgery, anesthesiologists should ask patients if they use cannabis – whether medicinally or recreationally – and be prepared to possibly change the anesthesia plan or delay the procedure in certain situations,” Samer Narouze, MD, PhD, ASRA president and senior author of the guidelines, said in a news release about the recommendations.
Although some patients may use cannabis to relieve pain, research shows that “regular users may have more pain and nausea after surgery, not less, and may need more medications, including opioids, to manage the discomfort,” said Dr. Narouze, chairman of the Center for Pain Medicine at Western Reserve Hospital in Cuyahoga Falls, Ohio.
Risks for vomiting, heart attack
The new recommendations were created by a committee of 13 experts, including anesthesiologists, chronic pain physicians, and a patient advocate. Shalini Shah, MD, vice chair of anesthesiology at the University of California, Irvine, was lead author of the document.
Four of 21 recommendations were classified as grade A, meaning that following them would be expected to provide substantial benefits. Those recommendations are to screen all patients before surgery; postpone elective surgery for patients who have altered mental status or impaired decision-making capacity at the time of surgery; counsel frequent, heavy users about the potential for cannabis use to impair postoperative pain control; and counsel pregnant patients about the risks of cannabis use to unborn children.
The authors cited studies to support their recommendations, including one showing that long-term cannabis use was associated with a 20% increase in the incidence of postoperative nausea and vomiting, a leading complaint of surgery patients. Other research has shown that cannabis use is linked to more pain and use of opioids after surgery.
Other recommendations include delaying elective surgery for at least 2 hours after a patient has smoked cannabis, owing to an increased risk for heart attack, and considering adjustment of ventilation settings during surgery for regular smokers of cannabis. Research has shown that smoking cannabis may be a rare trigger for myocardial infarction and is associated with airway inflammation and self-reported respiratory symptoms.
Nevertheless, doctors should not conduct universal toxicology screening, given a lack of evidence supporting this practice, the guideline stated.
The authors did not have enough information to make recommendations about reducing cannabis use before surgery or adjusting opioid prescriptions after surgery for patients who use cannabis, they said.
Kenneth Finn, MD, president of the American Board of Pain Medicine, welcomed the publication of the new guidelines. Dr. Finn, who practices at Springs Rehabilitation in Colorado Springs, has edited a textbook about cannabis in medicine and founded the International Academy on the Science and Impact of Cannabis.
“The vast majority of medical providers really have no idea about cannabis and what its impacts are on the human body,” Dr. Finn said.
For one, it can interact with numerous other drugs, including warfarin.
Guideline coauthor Eugene R. Viscusi, MD, professor of anesthesiology at the Sidney Kimmel Medical College, Philadelphia, emphasized that, while cannabis may be perceived as “natural,” it should not be considered differently from manufactured drugs.
Cannabis and cannabinoids represent “a class of very potent and pharmacologically active compounds,” Dr. Viscusi said in an interview. While researchers continue to assess possible medically beneficial effects of cannabis compounds, clinicians also need to be aware of the risks.
“The literature continues to emerge, and while we are always hopeful for good news, as physicians, we need to be very well versed on potential risks, especially in a high-risk situation like surgery,” he said.
Dr. Shah has consulted for companies that develop medical devices and drugs. Dr. Finn is the editor of the textbook, “Cannabis in Medicine: An Evidence-Based Approach” (Springer: New York, 2020), for which he receives royalties.
A version of this article first appeared on Medscape.com.
All patients who undergo procedures that require regional or general anesthesia should be asked if, how often, and in what forms they use the drug, according to recommendations from the American Society of Regional Anesthesia and Pain Medicine.
One reason: Patients who regularly use cannabis may experience worse pain and nausea after surgery and may require more opioid analgesia, the group said.
The society’s recommendations – published in Regional Anesthesia and Pain Medicine – are the first guidelines in the United States to cover cannabis use as it relates to surgery, the group said.
Possible interactions
Use of cannabis has increased in recent years, and researchers have been concerned that the drug may interact with anesthesia and complicate pain management. Few studies have evaluated interactions between cannabis and anesthetic agents, however, according to the authors of the new guidelines.
“With the rising prevalence of both medical and recreational cannabis use in the general population, anesthesiologists, surgeons, and perioperative physicians must have an understanding of the effects of cannabis on physiology in order to provide safe perioperative care,” the guideline said.
“Before surgery, anesthesiologists should ask patients if they use cannabis – whether medicinally or recreationally – and be prepared to possibly change the anesthesia plan or delay the procedure in certain situations,” Samer Narouze, MD, PhD, ASRA president and senior author of the guidelines, said in a news release about the recommendations.
Although some patients may use cannabis to relieve pain, research shows that “regular users may have more pain and nausea after surgery, not less, and may need more medications, including opioids, to manage the discomfort,” said Dr. Narouze, chairman of the Center for Pain Medicine at Western Reserve Hospital in Cuyahoga Falls, Ohio.
Risks for vomiting, heart attack
The new recommendations were created by a committee of 13 experts, including anesthesiologists, chronic pain physicians, and a patient advocate. Shalini Shah, MD, vice chair of anesthesiology at the University of California, Irvine, was lead author of the document.
Four of 21 recommendations were classified as grade A, meaning that following them would be expected to provide substantial benefits. Those recommendations are to screen all patients before surgery; postpone elective surgery for patients who have altered mental status or impaired decision-making capacity at the time of surgery; counsel frequent, heavy users about the potential for cannabis use to impair postoperative pain control; and counsel pregnant patients about the risks of cannabis use to unborn children.
The authors cited studies to support their recommendations, including one showing that long-term cannabis use was associated with a 20% increase in the incidence of postoperative nausea and vomiting, a leading complaint of surgery patients. Other research has shown that cannabis use is linked to more pain and use of opioids after surgery.
Other recommendations include delaying elective surgery for at least 2 hours after a patient has smoked cannabis, owing to an increased risk for heart attack, and considering adjustment of ventilation settings during surgery for regular smokers of cannabis. Research has shown that smoking cannabis may be a rare trigger for myocardial infarction and is associated with airway inflammation and self-reported respiratory symptoms.
Nevertheless, doctors should not conduct universal toxicology screening, given a lack of evidence supporting this practice, the guideline stated.
The authors did not have enough information to make recommendations about reducing cannabis use before surgery or adjusting opioid prescriptions after surgery for patients who use cannabis, they said.
Kenneth Finn, MD, president of the American Board of Pain Medicine, welcomed the publication of the new guidelines. Dr. Finn, who practices at Springs Rehabilitation in Colorado Springs, has edited a textbook about cannabis in medicine and founded the International Academy on the Science and Impact of Cannabis.
“The vast majority of medical providers really have no idea about cannabis and what its impacts are on the human body,” Dr. Finn said.
For one, it can interact with numerous other drugs, including warfarin.
Guideline coauthor Eugene R. Viscusi, MD, professor of anesthesiology at the Sidney Kimmel Medical College, Philadelphia, emphasized that, while cannabis may be perceived as “natural,” it should not be considered differently from manufactured drugs.
Cannabis and cannabinoids represent “a class of very potent and pharmacologically active compounds,” Dr. Viscusi said in an interview. While researchers continue to assess possible medically beneficial effects of cannabis compounds, clinicians also need to be aware of the risks.
“The literature continues to emerge, and while we are always hopeful for good news, as physicians, we need to be very well versed on potential risks, especially in a high-risk situation like surgery,” he said.
Dr. Shah has consulted for companies that develop medical devices and drugs. Dr. Finn is the editor of the textbook, “Cannabis in Medicine: An Evidence-Based Approach” (Springer: New York, 2020), for which he receives royalties.
A version of this article first appeared on Medscape.com.
FROM REGIONAL ANETHESIA AND MEDICINE
Is thrombolysis safe for stroke patients on DOACs?
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
From JAMA Neurology
Advanced Primary Care program boosts COVID-19 results
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
FROM JAMA NETWORK OPEN
Cancer clinics begin to accommodate patients demanding new cancer detection tests
Doug Flora, MD, knows the value of early cancer detection because it helped him survive kidney cancer 5 years ago. But as a medical oncologist and hematologist, and the executive medical director of oncology services at St. Elizabeth Healthcare in Edgewood, Ky., he also knows that a new era of early cancer detection testing poses big challenges for his network of six hospitals and 169 specialty and primary care offices throughout Kentucky, Ohio, and Indiana.
Multicancer early detection (MCED) tests are finally a reality and could be a potential game changer because they can screen for the possibility of up to 50 different cancers in asymptomatic individuals with one blood draw. They represent one of the fastest growing segments in medical diagnostics with a projected value of $2.77 billion by 2030, according to the market research firm Grand View Research.
These tests are different from traditional liquid biopsies, which are designed to identify actionable gene mutations to help inform treatment decisions of patients already diagnosed with cancer. Instead, MCED tests work to detect fragments of circulating free DNA that have been shed by tumors and released into the bloodstream. Detecting these cancer signals could indicate that an individual has cancer well before they ever develop symptoms.
For some cancer types, particularly those commonly diagnosed at advanced stages or those without general population screening tests, MCED testing could have a significant impact.
In its new report, Grand View Research highlights nine “prominent players” active in the MCED market; of these, two have been granted breakthrough device designation by the Food and Drug Administration: OverC MCDBT by Burning Rock on Jan. 3, 2023, and Galleri by Grail in 2019. Galleri was launched in June 2021 and can be obtained with a prescription at a cost of $949.
Yet, while patients are asking for these tests and primary care physicians are prescribing them, oncologists are grappling with how to manage the first patients whose tests tell them they may have cancer.
Ordering the tests may seem straightforward, but in reality, it is not. In fact, they are so new that most health systems have no internal guidelines for physicians. Guidelines would address when the tests should be prescribed, and whether a patient should undergo more testing or be referred to an oncologist.
Clinical trials underway
There are currently at least 17 clinical trials underway to investigate the performance and clinical utility of MCED tests. Six of these involve Grail, including NHS-Galleri, the largest study to date of 140,000 participants in the United Kingdom where participants will be followed for 3 years with annual visits at 12 and 24 months. And, the National Cancer Institute is spearheading a clinical trial of its own, according to a search of ClinicalTrials.gov.
In September 2022, Grail presented findings from its pivotal PATHFINDER study at the annual meeting of the European Society of Medical Oncology. Researchers reported that cancer signals were detected in 1.4% (92) of 6,621 participants enrolled in the study. Of the 92, 35 people were diagnosed with 36 cancers: 19 were solid tumors (2 oropharyngeal, 5 breast, l liver, 1 intrahepatic bile duct, 2 colon/rectum, 2 prostate, 1 lung, 1 pancreas, 1 small intestine, 1 uterus, 1 ovary and 1 bone) and 17 hematologic cancers (1 plasma cell myeloma/disorders, 2 lymphoid leukemia, 2 Waldenström’s macroglobulinemia, and 12 lymphoma).
Almost half of newly diagnosed cases were cancers in stage 1 or 2. Of stage 1 cancers, three were solid tumors and four were hematologic cancers. Of stage 2 cancers, three were solid tumors and four were hematologic cancers. All other cancers were in stage 3 and 4 or were listed as recurrent or no stage. Deb Schrag, MD, MPH, chair of the department of medicine at Memorial Sloan Kettering Cancer Center in New York, who presented the results from PATHFINDER at ESMO, reported that, of all diagnosed cancers, only breast, colon/rectum, prostate, and lung have established screening protocols.
The findings were so striking that the meeting scientific co-chair, Fabrice André, MD, PhD, told ESMO the oncology field must prepare for an onslaught of new patients.
“Within the next 5 years, we will need more doctors, surgeons and nurses with more diagnostic and treatment infrastructures to care for the rising number of people who will be identified by multicancer early detection tests,” said Dr. André, who is director of research at Gustave Roussy Cancer Center, Villejuif, France, and future president of ESMO (2025-2026). “We need to involve all stakeholders in deciding new pathways of care. We need to agree who will be tested and when and where tests will be carried out, and to anticipate the changes that will happen as a result of these tests.”
But first, he urged, the need for comparative trials “across all types of cancer to find out if having an early detection test affects morbidity and mortality. We also need to know how the tests benefit patients, and how to discuss the results with them,” Dr. André said.
Demand may burden health systems
Dr. Flora suggested that companies like Grail are rushing their product to market without conducting long-term sizable clinical trials.
“These diagnostic companies are a billion dollar publicly traded or venture capital-funded companies that are losing millions of dollars a quarter as they’re scaling up these tests. So, there is some pressure on the sales forces ... to start moving product long before the science has met our lowest areas for entry,” Dr. Flora said. “They are aggressively marketing to a primary care audience that knows nothing about MCEDs. It’s a sales-driven development solving a problem we all believe is real, but we don’t know if it actually solves the problem.”
There are many unanswered questions, he said. Among these include whether the tests do indeed extend survival. “What they’re suggesting – that is if the blood test detects it – that we’re going to save your life. That’s not yet been proven. This is where the providers are pushing back against these industry types to say: ‘This is the wild west right now.’ It’s very irresponsible to go out there and try to sell hundreds of millions of dollars of product to doctors who have never studied genetics,” Dr. Flora said.
Grail’s chief medical officer Jeff Venstrom, MD, however, said physicians don’t need a background in genetic testing to order or interpret Galleri because it’s not a genetic test. Genetic tests look for genetic variants associated with cancer risk, which Galleri does not. MCED tests rely on genomic profiling to identify alterations in tumors.
“Maybe there’s still confusion in the market, which is common for new technologies when they’re initially launched. This is not a 23andMe test. We do not report germline mutations that have implications for cancer risk. We’re using this blood sample to test for the presence or absence of a cancer signal. The test result is very clear and simple: One area of the report says ‘yes’ or ‘no.’ It is a binary result that says if a signal is detected or not. The second provides additional information around where that signal could be coming from,” he said.
Galleri could fill a huge unmet need in cancer prevention, Dr. Venstrom said. Not only could it detect cancer at an earlier stage, but it could serve as a screening tool for cancers like pancreatic cancer in which screening is not available.
The test is not intended to replace standard of care screening, he said. The ordering provider should have a conversation with the patient about overall cancer risk. “Are you smoking? What’s your risk of obesity-associated cancers? Do you have a family history of cancer? I think this should all be in the context of a good conversation around preventative care,” he said.
Planning and prep in Boston
In Boston, Aparna Parikh, MD, an oncologist who specializes in gastrointestinal cancers, agreed that MCED testing has forced her team at the Mass General Cancer Center global cancer care program to think outside of the box.
“We’re a major academic center and it’s not easy [because] this is all uncharted territory,” she said. “We all recognize there are more tests coming, and they are here to stay. As a health system, we have to be ready to manage not only the tests, but patient anxieties, and all the complexities that come with it. We just don’t know yet how to best navigate.”
Although Dr. Parikh’s center has set up a working group tasked with organizing an outpatient clinic for patients with positive MCED tests, the current system is haphazard.
“Right now, it gets bounced around between people,” she explained. “Sometimes, patients are getting referred to the oncology team rather than the primary care team to try to sort out where the cancer signal is coming from, that is, if it’s not immediately obvious. No one really knows who should be the right person to own it,” Dr. Parikh said. While the test is supposed to give tissue-specific results, “it’s not perfect” and sometimes imaging and other work-ups are needed to locate the source of the signa.
“A group of four or five oncologists get looped in and then we’re trying to sort it out on a case-by-case basis, but understanding that with more and more tests coming, that kind of ad hoc approach isn’t going to be sufficient. We need a happy medium between the primary care and the disease specific oncologist, someone who can kind of help think through the diagnostic workup until they have a cancer diagnosis to get them to the right place,” Dr. Parikh said.
Dr. Venstrom said Grail is committed to providing support to clinicians in these situations. “We’re doing everything we can with our medical education forums. We have this pretty intense and extensive postpositive suite of resources,” he explained. “Some of our doctors on staff call the ordering provider within 24 hours just to clarify if there are any questions or confusion from the report. For example, if it suggests the signal is coming from the lung, we provide additional support around additional workups.”
Out-of-pocket test may widen disparities in care
With the exception of a few health insurance companies that have committed to covering some of the cost for the test, Galleri is an out-of-pocket expense.
Dr. Venstrom acknowledged that broad insurance coverage for the Galleri test remains a hurdle, although “we’ve secured coverage for a handful of companies of self-insured employers and forward-thinking insurers.” This includes partnerships with Point32Health, and Alignment Health, among others, he said.
There is also growing support among more than 400 cancer organizations for the Multi-Cancer Early Detection Screening Coverage Act to accelerate coverage for Medicare beneficiaries. “We are constantly trying to understand the evidence that’s needed for payors to make sure that we get the broadest access possible for this test,” he said.
The first positive test result
Back at St. Elizabeth Healthcare where they’ve only seen one positive MCED test result thus far, Dr. Flora is more concerned about patients giving informed consent before they even get the test. “When the reps started hammering our primary care doctors, we sent communiques throughout the system saying that we would very much like to regulate this to make sure that before our patients receive accidental harm, that they at least have a conversation with somebody who understands the test,” he explained.
All 15 patients who requested the test at the hospital were first required to discuss the implications with a genetic counselor who is part of the system. “We are really pro–cancer screening,” he said, but added his hospital is “not pumped” about the Galleri test. “We’re being very cautious about overstatements made by sales guys to our primary care doctors, so we’re letting our own precision medicine people handle it.”
There’s a similar system in place at Community Health Network, a nonprofit health system with nine hospitals and 1,300 employee providers throughout Central Indiana. Patrick McGill, MD, a primary care physician and chief analytics officer for the network says they have streamlined patients with positive tests through their high-risk oncology clinic. “They don’t go straight to a medical oncologist which I know some systems are struggling with,” he said. “They get additional testing, whether it’s imaging they might need or other lab testing. We’ve had a few lung positives, and a few leukemia positives which might go straight to medical oncology. I think we had one breast that was positive so she got additional breast imaging.”
Through its foundation, CHN will offer 2,000 tests free of charge. “We decided to take cost off the table with this funding,” Dr. McGill said. “A lot of health systems I talk to are always concerned that insurance doesn’t cover it and it’s cost prohibitive. Is it creating additional disparities because only people who can afford it can get the test?”
Dr. Schrag serves as an uncompensated advisor for Grail. Previously, while with the Dana-Farber Cancer Institute, she received research funding from Grail.
Doug Flora, MD, knows the value of early cancer detection because it helped him survive kidney cancer 5 years ago. But as a medical oncologist and hematologist, and the executive medical director of oncology services at St. Elizabeth Healthcare in Edgewood, Ky., he also knows that a new era of early cancer detection testing poses big challenges for his network of six hospitals and 169 specialty and primary care offices throughout Kentucky, Ohio, and Indiana.
Multicancer early detection (MCED) tests are finally a reality and could be a potential game changer because they can screen for the possibility of up to 50 different cancers in asymptomatic individuals with one blood draw. They represent one of the fastest growing segments in medical diagnostics with a projected value of $2.77 billion by 2030, according to the market research firm Grand View Research.
These tests are different from traditional liquid biopsies, which are designed to identify actionable gene mutations to help inform treatment decisions of patients already diagnosed with cancer. Instead, MCED tests work to detect fragments of circulating free DNA that have been shed by tumors and released into the bloodstream. Detecting these cancer signals could indicate that an individual has cancer well before they ever develop symptoms.
For some cancer types, particularly those commonly diagnosed at advanced stages or those without general population screening tests, MCED testing could have a significant impact.
In its new report, Grand View Research highlights nine “prominent players” active in the MCED market; of these, two have been granted breakthrough device designation by the Food and Drug Administration: OverC MCDBT by Burning Rock on Jan. 3, 2023, and Galleri by Grail in 2019. Galleri was launched in June 2021 and can be obtained with a prescription at a cost of $949.
Yet, while patients are asking for these tests and primary care physicians are prescribing them, oncologists are grappling with how to manage the first patients whose tests tell them they may have cancer.
Ordering the tests may seem straightforward, but in reality, it is not. In fact, they are so new that most health systems have no internal guidelines for physicians. Guidelines would address when the tests should be prescribed, and whether a patient should undergo more testing or be referred to an oncologist.
Clinical trials underway
There are currently at least 17 clinical trials underway to investigate the performance and clinical utility of MCED tests. Six of these involve Grail, including NHS-Galleri, the largest study to date of 140,000 participants in the United Kingdom where participants will be followed for 3 years with annual visits at 12 and 24 months. And, the National Cancer Institute is spearheading a clinical trial of its own, according to a search of ClinicalTrials.gov.
In September 2022, Grail presented findings from its pivotal PATHFINDER study at the annual meeting of the European Society of Medical Oncology. Researchers reported that cancer signals were detected in 1.4% (92) of 6,621 participants enrolled in the study. Of the 92, 35 people were diagnosed with 36 cancers: 19 were solid tumors (2 oropharyngeal, 5 breast, l liver, 1 intrahepatic bile duct, 2 colon/rectum, 2 prostate, 1 lung, 1 pancreas, 1 small intestine, 1 uterus, 1 ovary and 1 bone) and 17 hematologic cancers (1 plasma cell myeloma/disorders, 2 lymphoid leukemia, 2 Waldenström’s macroglobulinemia, and 12 lymphoma).
Almost half of newly diagnosed cases were cancers in stage 1 or 2. Of stage 1 cancers, three were solid tumors and four were hematologic cancers. Of stage 2 cancers, three were solid tumors and four were hematologic cancers. All other cancers were in stage 3 and 4 or were listed as recurrent or no stage. Deb Schrag, MD, MPH, chair of the department of medicine at Memorial Sloan Kettering Cancer Center in New York, who presented the results from PATHFINDER at ESMO, reported that, of all diagnosed cancers, only breast, colon/rectum, prostate, and lung have established screening protocols.
The findings were so striking that the meeting scientific co-chair, Fabrice André, MD, PhD, told ESMO the oncology field must prepare for an onslaught of new patients.
“Within the next 5 years, we will need more doctors, surgeons and nurses with more diagnostic and treatment infrastructures to care for the rising number of people who will be identified by multicancer early detection tests,” said Dr. André, who is director of research at Gustave Roussy Cancer Center, Villejuif, France, and future president of ESMO (2025-2026). “We need to involve all stakeholders in deciding new pathways of care. We need to agree who will be tested and when and where tests will be carried out, and to anticipate the changes that will happen as a result of these tests.”
But first, he urged, the need for comparative trials “across all types of cancer to find out if having an early detection test affects morbidity and mortality. We also need to know how the tests benefit patients, and how to discuss the results with them,” Dr. André said.
Demand may burden health systems
Dr. Flora suggested that companies like Grail are rushing their product to market without conducting long-term sizable clinical trials.
“These diagnostic companies are a billion dollar publicly traded or venture capital-funded companies that are losing millions of dollars a quarter as they’re scaling up these tests. So, there is some pressure on the sales forces ... to start moving product long before the science has met our lowest areas for entry,” Dr. Flora said. “They are aggressively marketing to a primary care audience that knows nothing about MCEDs. It’s a sales-driven development solving a problem we all believe is real, but we don’t know if it actually solves the problem.”
There are many unanswered questions, he said. Among these include whether the tests do indeed extend survival. “What they’re suggesting – that is if the blood test detects it – that we’re going to save your life. That’s not yet been proven. This is where the providers are pushing back against these industry types to say: ‘This is the wild west right now.’ It’s very irresponsible to go out there and try to sell hundreds of millions of dollars of product to doctors who have never studied genetics,” Dr. Flora said.
Grail’s chief medical officer Jeff Venstrom, MD, however, said physicians don’t need a background in genetic testing to order or interpret Galleri because it’s not a genetic test. Genetic tests look for genetic variants associated with cancer risk, which Galleri does not. MCED tests rely on genomic profiling to identify alterations in tumors.
“Maybe there’s still confusion in the market, which is common for new technologies when they’re initially launched. This is not a 23andMe test. We do not report germline mutations that have implications for cancer risk. We’re using this blood sample to test for the presence or absence of a cancer signal. The test result is very clear and simple: One area of the report says ‘yes’ or ‘no.’ It is a binary result that says if a signal is detected or not. The second provides additional information around where that signal could be coming from,” he said.
Galleri could fill a huge unmet need in cancer prevention, Dr. Venstrom said. Not only could it detect cancer at an earlier stage, but it could serve as a screening tool for cancers like pancreatic cancer in which screening is not available.
The test is not intended to replace standard of care screening, he said. The ordering provider should have a conversation with the patient about overall cancer risk. “Are you smoking? What’s your risk of obesity-associated cancers? Do you have a family history of cancer? I think this should all be in the context of a good conversation around preventative care,” he said.
Planning and prep in Boston
In Boston, Aparna Parikh, MD, an oncologist who specializes in gastrointestinal cancers, agreed that MCED testing has forced her team at the Mass General Cancer Center global cancer care program to think outside of the box.
“We’re a major academic center and it’s not easy [because] this is all uncharted territory,” she said. “We all recognize there are more tests coming, and they are here to stay. As a health system, we have to be ready to manage not only the tests, but patient anxieties, and all the complexities that come with it. We just don’t know yet how to best navigate.”
Although Dr. Parikh’s center has set up a working group tasked with organizing an outpatient clinic for patients with positive MCED tests, the current system is haphazard.
“Right now, it gets bounced around between people,” she explained. “Sometimes, patients are getting referred to the oncology team rather than the primary care team to try to sort out where the cancer signal is coming from, that is, if it’s not immediately obvious. No one really knows who should be the right person to own it,” Dr. Parikh said. While the test is supposed to give tissue-specific results, “it’s not perfect” and sometimes imaging and other work-ups are needed to locate the source of the signa.
“A group of four or five oncologists get looped in and then we’re trying to sort it out on a case-by-case basis, but understanding that with more and more tests coming, that kind of ad hoc approach isn’t going to be sufficient. We need a happy medium between the primary care and the disease specific oncologist, someone who can kind of help think through the diagnostic workup until they have a cancer diagnosis to get them to the right place,” Dr. Parikh said.
Dr. Venstrom said Grail is committed to providing support to clinicians in these situations. “We’re doing everything we can with our medical education forums. We have this pretty intense and extensive postpositive suite of resources,” he explained. “Some of our doctors on staff call the ordering provider within 24 hours just to clarify if there are any questions or confusion from the report. For example, if it suggests the signal is coming from the lung, we provide additional support around additional workups.”
Out-of-pocket test may widen disparities in care
With the exception of a few health insurance companies that have committed to covering some of the cost for the test, Galleri is an out-of-pocket expense.
Dr. Venstrom acknowledged that broad insurance coverage for the Galleri test remains a hurdle, although “we’ve secured coverage for a handful of companies of self-insured employers and forward-thinking insurers.” This includes partnerships with Point32Health, and Alignment Health, among others, he said.
There is also growing support among more than 400 cancer organizations for the Multi-Cancer Early Detection Screening Coverage Act to accelerate coverage for Medicare beneficiaries. “We are constantly trying to understand the evidence that’s needed for payors to make sure that we get the broadest access possible for this test,” he said.
The first positive test result
Back at St. Elizabeth Healthcare where they’ve only seen one positive MCED test result thus far, Dr. Flora is more concerned about patients giving informed consent before they even get the test. “When the reps started hammering our primary care doctors, we sent communiques throughout the system saying that we would very much like to regulate this to make sure that before our patients receive accidental harm, that they at least have a conversation with somebody who understands the test,” he explained.
All 15 patients who requested the test at the hospital were first required to discuss the implications with a genetic counselor who is part of the system. “We are really pro–cancer screening,” he said, but added his hospital is “not pumped” about the Galleri test. “We’re being very cautious about overstatements made by sales guys to our primary care doctors, so we’re letting our own precision medicine people handle it.”
There’s a similar system in place at Community Health Network, a nonprofit health system with nine hospitals and 1,300 employee providers throughout Central Indiana. Patrick McGill, MD, a primary care physician and chief analytics officer for the network says they have streamlined patients with positive tests through their high-risk oncology clinic. “They don’t go straight to a medical oncologist which I know some systems are struggling with,” he said. “They get additional testing, whether it’s imaging they might need or other lab testing. We’ve had a few lung positives, and a few leukemia positives which might go straight to medical oncology. I think we had one breast that was positive so she got additional breast imaging.”
Through its foundation, CHN will offer 2,000 tests free of charge. “We decided to take cost off the table with this funding,” Dr. McGill said. “A lot of health systems I talk to are always concerned that insurance doesn’t cover it and it’s cost prohibitive. Is it creating additional disparities because only people who can afford it can get the test?”
Dr. Schrag serves as an uncompensated advisor for Grail. Previously, while with the Dana-Farber Cancer Institute, she received research funding from Grail.
Doug Flora, MD, knows the value of early cancer detection because it helped him survive kidney cancer 5 years ago. But as a medical oncologist and hematologist, and the executive medical director of oncology services at St. Elizabeth Healthcare in Edgewood, Ky., he also knows that a new era of early cancer detection testing poses big challenges for his network of six hospitals and 169 specialty and primary care offices throughout Kentucky, Ohio, and Indiana.
Multicancer early detection (MCED) tests are finally a reality and could be a potential game changer because they can screen for the possibility of up to 50 different cancers in asymptomatic individuals with one blood draw. They represent one of the fastest growing segments in medical diagnostics with a projected value of $2.77 billion by 2030, according to the market research firm Grand View Research.
These tests are different from traditional liquid biopsies, which are designed to identify actionable gene mutations to help inform treatment decisions of patients already diagnosed with cancer. Instead, MCED tests work to detect fragments of circulating free DNA that have been shed by tumors and released into the bloodstream. Detecting these cancer signals could indicate that an individual has cancer well before they ever develop symptoms.
For some cancer types, particularly those commonly diagnosed at advanced stages or those without general population screening tests, MCED testing could have a significant impact.
In its new report, Grand View Research highlights nine “prominent players” active in the MCED market; of these, two have been granted breakthrough device designation by the Food and Drug Administration: OverC MCDBT by Burning Rock on Jan. 3, 2023, and Galleri by Grail in 2019. Galleri was launched in June 2021 and can be obtained with a prescription at a cost of $949.
Yet, while patients are asking for these tests and primary care physicians are prescribing them, oncologists are grappling with how to manage the first patients whose tests tell them they may have cancer.
Ordering the tests may seem straightforward, but in reality, it is not. In fact, they are so new that most health systems have no internal guidelines for physicians. Guidelines would address when the tests should be prescribed, and whether a patient should undergo more testing or be referred to an oncologist.
Clinical trials underway
There are currently at least 17 clinical trials underway to investigate the performance and clinical utility of MCED tests. Six of these involve Grail, including NHS-Galleri, the largest study to date of 140,000 participants in the United Kingdom where participants will be followed for 3 years with annual visits at 12 and 24 months. And, the National Cancer Institute is spearheading a clinical trial of its own, according to a search of ClinicalTrials.gov.
In September 2022, Grail presented findings from its pivotal PATHFINDER study at the annual meeting of the European Society of Medical Oncology. Researchers reported that cancer signals were detected in 1.4% (92) of 6,621 participants enrolled in the study. Of the 92, 35 people were diagnosed with 36 cancers: 19 were solid tumors (2 oropharyngeal, 5 breast, l liver, 1 intrahepatic bile duct, 2 colon/rectum, 2 prostate, 1 lung, 1 pancreas, 1 small intestine, 1 uterus, 1 ovary and 1 bone) and 17 hematologic cancers (1 plasma cell myeloma/disorders, 2 lymphoid leukemia, 2 Waldenström’s macroglobulinemia, and 12 lymphoma).
Almost half of newly diagnosed cases were cancers in stage 1 or 2. Of stage 1 cancers, three were solid tumors and four were hematologic cancers. Of stage 2 cancers, three were solid tumors and four were hematologic cancers. All other cancers were in stage 3 and 4 or were listed as recurrent or no stage. Deb Schrag, MD, MPH, chair of the department of medicine at Memorial Sloan Kettering Cancer Center in New York, who presented the results from PATHFINDER at ESMO, reported that, of all diagnosed cancers, only breast, colon/rectum, prostate, and lung have established screening protocols.
The findings were so striking that the meeting scientific co-chair, Fabrice André, MD, PhD, told ESMO the oncology field must prepare for an onslaught of new patients.
“Within the next 5 years, we will need more doctors, surgeons and nurses with more diagnostic and treatment infrastructures to care for the rising number of people who will be identified by multicancer early detection tests,” said Dr. André, who is director of research at Gustave Roussy Cancer Center, Villejuif, France, and future president of ESMO (2025-2026). “We need to involve all stakeholders in deciding new pathways of care. We need to agree who will be tested and when and where tests will be carried out, and to anticipate the changes that will happen as a result of these tests.”
But first, he urged, the need for comparative trials “across all types of cancer to find out if having an early detection test affects morbidity and mortality. We also need to know how the tests benefit patients, and how to discuss the results with them,” Dr. André said.
Demand may burden health systems
Dr. Flora suggested that companies like Grail are rushing their product to market without conducting long-term sizable clinical trials.
“These diagnostic companies are a billion dollar publicly traded or venture capital-funded companies that are losing millions of dollars a quarter as they’re scaling up these tests. So, there is some pressure on the sales forces ... to start moving product long before the science has met our lowest areas for entry,” Dr. Flora said. “They are aggressively marketing to a primary care audience that knows nothing about MCEDs. It’s a sales-driven development solving a problem we all believe is real, but we don’t know if it actually solves the problem.”
There are many unanswered questions, he said. Among these include whether the tests do indeed extend survival. “What they’re suggesting – that is if the blood test detects it – that we’re going to save your life. That’s not yet been proven. This is where the providers are pushing back against these industry types to say: ‘This is the wild west right now.’ It’s very irresponsible to go out there and try to sell hundreds of millions of dollars of product to doctors who have never studied genetics,” Dr. Flora said.
Grail’s chief medical officer Jeff Venstrom, MD, however, said physicians don’t need a background in genetic testing to order or interpret Galleri because it’s not a genetic test. Genetic tests look for genetic variants associated with cancer risk, which Galleri does not. MCED tests rely on genomic profiling to identify alterations in tumors.
“Maybe there’s still confusion in the market, which is common for new technologies when they’re initially launched. This is not a 23andMe test. We do not report germline mutations that have implications for cancer risk. We’re using this blood sample to test for the presence or absence of a cancer signal. The test result is very clear and simple: One area of the report says ‘yes’ or ‘no.’ It is a binary result that says if a signal is detected or not. The second provides additional information around where that signal could be coming from,” he said.
Galleri could fill a huge unmet need in cancer prevention, Dr. Venstrom said. Not only could it detect cancer at an earlier stage, but it could serve as a screening tool for cancers like pancreatic cancer in which screening is not available.
The test is not intended to replace standard of care screening, he said. The ordering provider should have a conversation with the patient about overall cancer risk. “Are you smoking? What’s your risk of obesity-associated cancers? Do you have a family history of cancer? I think this should all be in the context of a good conversation around preventative care,” he said.
Planning and prep in Boston
In Boston, Aparna Parikh, MD, an oncologist who specializes in gastrointestinal cancers, agreed that MCED testing has forced her team at the Mass General Cancer Center global cancer care program to think outside of the box.
“We’re a major academic center and it’s not easy [because] this is all uncharted territory,” she said. “We all recognize there are more tests coming, and they are here to stay. As a health system, we have to be ready to manage not only the tests, but patient anxieties, and all the complexities that come with it. We just don’t know yet how to best navigate.”
Although Dr. Parikh’s center has set up a working group tasked with organizing an outpatient clinic for patients with positive MCED tests, the current system is haphazard.
“Right now, it gets bounced around between people,” she explained. “Sometimes, patients are getting referred to the oncology team rather than the primary care team to try to sort out where the cancer signal is coming from, that is, if it’s not immediately obvious. No one really knows who should be the right person to own it,” Dr. Parikh said. While the test is supposed to give tissue-specific results, “it’s not perfect” and sometimes imaging and other work-ups are needed to locate the source of the signa.
“A group of four or five oncologists get looped in and then we’re trying to sort it out on a case-by-case basis, but understanding that with more and more tests coming, that kind of ad hoc approach isn’t going to be sufficient. We need a happy medium between the primary care and the disease specific oncologist, someone who can kind of help think through the diagnostic workup until they have a cancer diagnosis to get them to the right place,” Dr. Parikh said.
Dr. Venstrom said Grail is committed to providing support to clinicians in these situations. “We’re doing everything we can with our medical education forums. We have this pretty intense and extensive postpositive suite of resources,” he explained. “Some of our doctors on staff call the ordering provider within 24 hours just to clarify if there are any questions or confusion from the report. For example, if it suggests the signal is coming from the lung, we provide additional support around additional workups.”
Out-of-pocket test may widen disparities in care
With the exception of a few health insurance companies that have committed to covering some of the cost for the test, Galleri is an out-of-pocket expense.
Dr. Venstrom acknowledged that broad insurance coverage for the Galleri test remains a hurdle, although “we’ve secured coverage for a handful of companies of self-insured employers and forward-thinking insurers.” This includes partnerships with Point32Health, and Alignment Health, among others, he said.
There is also growing support among more than 400 cancer organizations for the Multi-Cancer Early Detection Screening Coverage Act to accelerate coverage for Medicare beneficiaries. “We are constantly trying to understand the evidence that’s needed for payors to make sure that we get the broadest access possible for this test,” he said.
The first positive test result
Back at St. Elizabeth Healthcare where they’ve only seen one positive MCED test result thus far, Dr. Flora is more concerned about patients giving informed consent before they even get the test. “When the reps started hammering our primary care doctors, we sent communiques throughout the system saying that we would very much like to regulate this to make sure that before our patients receive accidental harm, that they at least have a conversation with somebody who understands the test,” he explained.
All 15 patients who requested the test at the hospital were first required to discuss the implications with a genetic counselor who is part of the system. “We are really pro–cancer screening,” he said, but added his hospital is “not pumped” about the Galleri test. “We’re being very cautious about overstatements made by sales guys to our primary care doctors, so we’re letting our own precision medicine people handle it.”
There’s a similar system in place at Community Health Network, a nonprofit health system with nine hospitals and 1,300 employee providers throughout Central Indiana. Patrick McGill, MD, a primary care physician and chief analytics officer for the network says they have streamlined patients with positive tests through their high-risk oncology clinic. “They don’t go straight to a medical oncologist which I know some systems are struggling with,” he said. “They get additional testing, whether it’s imaging they might need or other lab testing. We’ve had a few lung positives, and a few leukemia positives which might go straight to medical oncology. I think we had one breast that was positive so she got additional breast imaging.”
Through its foundation, CHN will offer 2,000 tests free of charge. “We decided to take cost off the table with this funding,” Dr. McGill said. “A lot of health systems I talk to are always concerned that insurance doesn’t cover it and it’s cost prohibitive. Is it creating additional disparities because only people who can afford it can get the test?”
Dr. Schrag serves as an uncompensated advisor for Grail. Previously, while with the Dana-Farber Cancer Institute, she received research funding from Grail.