User login
‘Facebuddha’ analyzes psychology of social media through a Buddhist lens
The new book by Ravi Chandra, MD, is a concise introduction to Buddhism, and a forceful exposition on the power and danger of social networking – deftly interwoven with a moving account of the author’s personal life and professional growth as well as his arduous quest for identity.
Social networking has exploded into a major global industry within the last decade, rapidly penetrating and dominating all aspects of our personal and social lives. Instead of promoting social interactions and connections, the lure of instant intimacy often proves illusory. For far too many, the virtual world deepens their sense of isolation and loneliness, fosters jealousy and narcissism, engenders a profound sense of insecurity, and leads to anxiety, depression, and much worse.
By juxtaposing the Buddha with social networking in the book title, Dr. Chandra expresses his hope and faith that Buddhism could serve as an effective tool for harnessing the force unleashed by these powerful new technologies, helping us to put the genie of our invention back into the bottle. Over the millenia, Buddhism has guided societies and individuals to overcome (“transcend”) crises and adversities, and could play a crucial role in negotiating these still largely uncharted territories.
Despite the popularity of terms such as Zen, meditation, transcendence, and mindfulness, Buddhism remains mysterious and exotic to most modern readers, and is laden with misconceptions and prejudices. This is regrettable, since Buddhism is the most clinically relevant of all major philosophical traditions, and its tenets are most compatible with modern neuroscience. The term philosophical is used here because, at its core, Buddhism represents an uncompromisingly rational approach to dealing with the “human condition.” Siddhartha Gautama (Buddha), its founder, admonished against speculating on questions that are “unanswerables,” such as eternity, existence after death, and the origin and ending of the universe. Instead, Siddhartha focused on identifying life’s vicissitudes (Dukkha, “bumpy rides in life,” commonly translated as “suffering”), clarifying forces responsible for these problems, delineating the ultimate goal, and specifying methods for achieving the goal (the “Four Noble Truths”). He then provided systematic paths for solving problems (the “Eightfold Noble Path”). His approaches are akin to what we clinicians strive to do on a daily basis, albeit on a grander scale: diagnosis, pathogenesis, treatment goals, and therapeutic approaches. The framework Siddhartha proposed is austere, rational, practical. It is exactly for this reason that Siddhartha has been called a great physician, a doctor, and a healer.

As a psychiatrist and a practicing Buddhist, Dr. Chandra is well positioned to critically examine these profoundly important issues (Buddhism and social networking), and he did an excellent job in “Facebuddha.” Impressively, Dr. Chandra’s discussions did not take place in a vacuum. They were not just dry intellectual exercises but were embedded in accounts of personal and clinical experiences, demonstrating the relevance of Buddhist thoughts and practices in real life.
Born in South India and raised by a physician mother in half a dozen American cities, Dr. Chandra experienced repeated uprooting and various types of racial/cultural discrimination. His childhood and adolescence were characterized by a long and arduous search for identity. That he has not only survived, but thrived, is a testament to his resilience and resourcefulness. His love of art and poetry played an important role, as did friendships and the support of Asian American communities. But, above all, it was the Buddha’s teachings and examples that have been the most significant sustaining forces in his life. His accounts are a personal testimony to the power of a 2,500-year-old tradition that is still alive and relevant in our postmodern world.
Dr. Chandra’s book is an endearing chronicle of a remarkable personal journey. Readers will appreciate the opportunity to witness glimpses of this journey and may reasonably expect that such explorations will continue, leading to new vistas that are not only fascinating to behold but also relevant to the practice of our profession.
Dr. Lin is professor emeritus of psychiatry, University of California, Los Angeles, and Distinguished Life Fellow, American Psychiatric Association. He was the founding director of the National Institute of Mental Health/Harbor-UCLA Research Center on the Psychobiology of Ethnicity, the Coastal Asian Pacific Mental Health Center, and the Long Beach Asian Pacific Mental Health Center. The honors Dr. Lin has received include the Kun-Po Soo Asian American Award, American Psychiatric Association; William Sargant Lecturer, Royal College of Psychiatrists, Great Britain; and honorary professor, Hunan (China) Medical University. Information about the book can be found at www.facebuddha.co.
The new book by Ravi Chandra, MD, is a concise introduction to Buddhism, and a forceful exposition on the power and danger of social networking – deftly interwoven with a moving account of the author’s personal life and professional growth as well as his arduous quest for identity.
Social networking has exploded into a major global industry within the last decade, rapidly penetrating and dominating all aspects of our personal and social lives. Instead of promoting social interactions and connections, the lure of instant intimacy often proves illusory. For far too many, the virtual world deepens their sense of isolation and loneliness, fosters jealousy and narcissism, engenders a profound sense of insecurity, and leads to anxiety, depression, and much worse.
By juxtaposing the Buddha with social networking in the book title, Dr. Chandra expresses his hope and faith that Buddhism could serve as an effective tool for harnessing the force unleashed by these powerful new technologies, helping us to put the genie of our invention back into the bottle. Over the millenia, Buddhism has guided societies and individuals to overcome (“transcend”) crises and adversities, and could play a crucial role in negotiating these still largely uncharted territories.
Despite the popularity of terms such as Zen, meditation, transcendence, and mindfulness, Buddhism remains mysterious and exotic to most modern readers, and is laden with misconceptions and prejudices. This is regrettable, since Buddhism is the most clinically relevant of all major philosophical traditions, and its tenets are most compatible with modern neuroscience. The term philosophical is used here because, at its core, Buddhism represents an uncompromisingly rational approach to dealing with the “human condition.” Siddhartha Gautama (Buddha), its founder, admonished against speculating on questions that are “unanswerables,” such as eternity, existence after death, and the origin and ending of the universe. Instead, Siddhartha focused on identifying life’s vicissitudes (Dukkha, “bumpy rides in life,” commonly translated as “suffering”), clarifying forces responsible for these problems, delineating the ultimate goal, and specifying methods for achieving the goal (the “Four Noble Truths”). He then provided systematic paths for solving problems (the “Eightfold Noble Path”). His approaches are akin to what we clinicians strive to do on a daily basis, albeit on a grander scale: diagnosis, pathogenesis, treatment goals, and therapeutic approaches. The framework Siddhartha proposed is austere, rational, practical. It is exactly for this reason that Siddhartha has been called a great physician, a doctor, and a healer.
As a psychiatrist and a practicing Buddhist, Dr. Chandra is well positioned to critically examine these profoundly important issues (Buddhism and social networking), and he did an excellent job in “Facebuddha.” Impressively, Dr. Chandra’s discussions did not take place in a vacuum. They were not just dry intellectual exercises but were embedded in accounts of personal and clinical experiences, demonstrating the relevance of Buddhist thoughts and practices in real life.
Born in South India and raised by a physician mother in half a dozen American cities, Dr. Chandra experienced repeated uprooting and various types of racial/cultural discrimination. His childhood and adolescence were characterized by a long and arduous search for identity. That he has not only survived, but thrived, is a testament to his resilience and resourcefulness. His love of art and poetry played an important role, as did friendships and the support of Asian American communities. But, above all, it was the Buddha’s teachings and examples that have been the most significant sustaining forces in his life. His accounts are a personal testimony to the power of a 2,500-year-old tradition that is still alive and relevant in our postmodern world.
Dr. Chandra’s book is an endearing chronicle of a remarkable personal journey. Readers will appreciate the opportunity to witness glimpses of this journey and may reasonably expect that such explorations will continue, leading to new vistas that are not only fascinating to behold but also relevant to the practice of our profession.
Dr. Lin is professor emeritus of psychiatry, University of California, Los Angeles, and Distinguished Life Fellow, American Psychiatric Association. He was the founding director of the National Institute of Mental Health/Harbor-UCLA Research Center on the Psychobiology of Ethnicity, the Coastal Asian Pacific Mental Health Center, and the Long Beach Asian Pacific Mental Health Center. The honors Dr. Lin has received include the Kun-Po Soo Asian American Award, American Psychiatric Association; William Sargant Lecturer, Royal College of Psychiatrists, Great Britain; and honorary professor, Hunan (China) Medical University. Information about the book can be found at www.facebuddha.co.
The new book by Ravi Chandra, MD, is a concise introduction to Buddhism, and a forceful exposition on the power and danger of social networking – deftly interwoven with a moving account of the author’s personal life and professional growth as well as his arduous quest for identity.
Social networking has exploded into a major global industry within the last decade, rapidly penetrating and dominating all aspects of our personal and social lives. Instead of promoting social interactions and connections, the lure of instant intimacy often proves illusory. For far too many, the virtual world deepens their sense of isolation and loneliness, fosters jealousy and narcissism, engenders a profound sense of insecurity, and leads to anxiety, depression, and much worse.
By juxtaposing the Buddha with social networking in the book title, Dr. Chandra expresses his hope and faith that Buddhism could serve as an effective tool for harnessing the force unleashed by these powerful new technologies, helping us to put the genie of our invention back into the bottle. Over the millenia, Buddhism has guided societies and individuals to overcome (“transcend”) crises and adversities, and could play a crucial role in negotiating these still largely uncharted territories.
Despite the popularity of terms such as Zen, meditation, transcendence, and mindfulness, Buddhism remains mysterious and exotic to most modern readers, and is laden with misconceptions and prejudices. This is regrettable, since Buddhism is the most clinically relevant of all major philosophical traditions, and its tenets are most compatible with modern neuroscience. The term philosophical is used here because, at its core, Buddhism represents an uncompromisingly rational approach to dealing with the “human condition.” Siddhartha Gautama (Buddha), its founder, admonished against speculating on questions that are “unanswerables,” such as eternity, existence after death, and the origin and ending of the universe. Instead, Siddhartha focused on identifying life’s vicissitudes (Dukkha, “bumpy rides in life,” commonly translated as “suffering”), clarifying forces responsible for these problems, delineating the ultimate goal, and specifying methods for achieving the goal (the “Four Noble Truths”). He then provided systematic paths for solving problems (the “Eightfold Noble Path”). His approaches are akin to what we clinicians strive to do on a daily basis, albeit on a grander scale: diagnosis, pathogenesis, treatment goals, and therapeutic approaches. The framework Siddhartha proposed is austere, rational, practical. It is exactly for this reason that Siddhartha has been called a great physician, a doctor, and a healer.
As a psychiatrist and a practicing Buddhist, Dr. Chandra is well positioned to critically examine these profoundly important issues (Buddhism and social networking), and he did an excellent job in “Facebuddha.” Impressively, Dr. Chandra’s discussions did not take place in a vacuum. They were not just dry intellectual exercises but were embedded in accounts of personal and clinical experiences, demonstrating the relevance of Buddhist thoughts and practices in real life.
Born in South India and raised by a physician mother in half a dozen American cities, Dr. Chandra experienced repeated uprooting and various types of racial/cultural discrimination. His childhood and adolescence were characterized by a long and arduous search for identity. That he has not only survived, but thrived, is a testament to his resilience and resourcefulness. His love of art and poetry played an important role, as did friendships and the support of Asian American communities. But, above all, it was the Buddha’s teachings and examples that have been the most significant sustaining forces in his life. His accounts are a personal testimony to the power of a 2,500-year-old tradition that is still alive and relevant in our postmodern world.
Dr. Chandra’s book is an endearing chronicle of a remarkable personal journey. Readers will appreciate the opportunity to witness glimpses of this journey and may reasonably expect that such explorations will continue, leading to new vistas that are not only fascinating to behold but also relevant to the practice of our profession.
Dr. Lin is professor emeritus of psychiatry, University of California, Los Angeles, and Distinguished Life Fellow, American Psychiatric Association. He was the founding director of the National Institute of Mental Health/Harbor-UCLA Research Center on the Psychobiology of Ethnicity, the Coastal Asian Pacific Mental Health Center, and the Long Beach Asian Pacific Mental Health Center. The honors Dr. Lin has received include the Kun-Po Soo Asian American Award, American Psychiatric Association; William Sargant Lecturer, Royal College of Psychiatrists, Great Britain; and honorary professor, Hunan (China) Medical University. Information about the book can be found at www.facebuddha.co.
The pediatrician detective and high lead levels
I am not going to tell you about the dangers of lead, as it is well known and publicized, but I will tell you my family’s story with lead.
In 2012, 1 year after my younger daughter was born, I took her for her 1-year checkup. As I would do with any of my pediatric patients at this age, I took her for a lead level check. Never during my residency training or my first few years of practice as a pediatrician have I encountered a positive lead level. So when I opened the lab result sheet, I thought I would be shredding it the next moment. Well, that didn’t happen. It turned out that her lead level was 7 mcg/dL! Not too high, but detectable. The only question that kept on coming back over the next month or so was a big WHY? Why my child? Now my older daughter’s lead level was normal at her 1-year visit. We had just moved into a new house before my youngest daughter was born. I thought, it has to do with the house, and since my 1-year-old was putting everything in her mouth at this stage, then she must be getting the lead that way.

So it was not the house or the wall pipes that were contaminated with lead. It was not our food that we cooked, otherwise my nanny’s daughter would have had a high lead level, as she ate the same food we ate almost daily. Our family did not travel recently. So what was it that my family had or ate that my neighbor or nanny’s child did not?
The answer was thyme. It is an herb that we mix with olive oil and spread on dough – I call it Lebanese pizza. That is one thing that my nanny and her child never ate, but we did. It was a long painful month of investigation, elimination, and anxiety. I called the public health department in Phoenix and they stated that lots of imported spices were contaminated with lead. There were two theories as to why this might happen. The first one is that the spice dealers would add lead to increase the weight of the spices to get more money. The second is that the spice fields were close to factories that used lead in their manufacturing, and somehow the lead would contaminate the nearby fields where the spices grew.
The type of thyme we used was bought in Syria and packaged in Lebanon. It was not the pure organic type that we usually got from our grandparents in our southern Lebanese village. This packaged thyme had lot of nuts added to it to give it more flavor.
The public health department official asked that I send her some samples of all the spices that I had. I packed up to ten different spice bags including the thyme. Two weeks later she called me, stating that the lead level allowable in spices must be less than 10, and that our thyme’s lead level was 900!
We got rid of all the spices, and have never eaten that packaged spice again. My kids’ lead levels dropped nicely afterward and back to normal. That is our story with lead. Now it seems like a mini-detective story and even fun, but the anxiety that I experienced until we figured out the cause was not!
Dr. Faddoul is a private practice pediatrician in La Canada Flintridge, Calif.
I am not going to tell you about the dangers of lead, as it is well known and publicized, but I will tell you my family’s story with lead.
In 2012, 1 year after my younger daughter was born, I took her for her 1-year checkup. As I would do with any of my pediatric patients at this age, I took her for a lead level check. Never during my residency training or my first few years of practice as a pediatrician have I encountered a positive lead level. So when I opened the lab result sheet, I thought I would be shredding it the next moment. Well, that didn’t happen. It turned out that her lead level was 7 mcg/dL! Not too high, but detectable. The only question that kept on coming back over the next month or so was a big WHY? Why my child? Now my older daughter’s lead level was normal at her 1-year visit. We had just moved into a new house before my youngest daughter was born. I thought, it has to do with the house, and since my 1-year-old was putting everything in her mouth at this stage, then she must be getting the lead that way.
So it was not the house or the wall pipes that were contaminated with lead. It was not our food that we cooked, otherwise my nanny’s daughter would have had a high lead level, as she ate the same food we ate almost daily. Our family did not travel recently. So what was it that my family had or ate that my neighbor or nanny’s child did not?
The answer was thyme. It is an herb that we mix with olive oil and spread on dough – I call it Lebanese pizza. That is one thing that my nanny and her child never ate, but we did. It was a long painful month of investigation, elimination, and anxiety. I called the public health department in Phoenix and they stated that lots of imported spices were contaminated with lead. There were two theories as to why this might happen. The first one is that the spice dealers would add lead to increase the weight of the spices to get more money. The second is that the spice fields were close to factories that used lead in their manufacturing, and somehow the lead would contaminate the nearby fields where the spices grew.
The type of thyme we used was bought in Syria and packaged in Lebanon. It was not the pure organic type that we usually got from our grandparents in our southern Lebanese village. This packaged thyme had lot of nuts added to it to give it more flavor.
The public health department official asked that I send her some samples of all the spices that I had. I packed up to ten different spice bags including the thyme. Two weeks later she called me, stating that the lead level allowable in spices must be less than 10, and that our thyme’s lead level was 900!
We got rid of all the spices, and have never eaten that packaged spice again. My kids’ lead levels dropped nicely afterward and back to normal. That is our story with lead. Now it seems like a mini-detective story and even fun, but the anxiety that I experienced until we figured out the cause was not!
Dr. Faddoul is a private practice pediatrician in La Canada Flintridge, Calif.
I am not going to tell you about the dangers of lead, as it is well known and publicized, but I will tell you my family’s story with lead.
In 2012, 1 year after my younger daughter was born, I took her for her 1-year checkup. As I would do with any of my pediatric patients at this age, I took her for a lead level check. Never during my residency training or my first few years of practice as a pediatrician have I encountered a positive lead level. So when I opened the lab result sheet, I thought I would be shredding it the next moment. Well, that didn’t happen. It turned out that her lead level was 7 mcg/dL! Not too high, but detectable. The only question that kept on coming back over the next month or so was a big WHY? Why my child? Now my older daughter’s lead level was normal at her 1-year visit. We had just moved into a new house before my youngest daughter was born. I thought, it has to do with the house, and since my 1-year-old was putting everything in her mouth at this stage, then she must be getting the lead that way.
So it was not the house or the wall pipes that were contaminated with lead. It was not our food that we cooked, otherwise my nanny’s daughter would have had a high lead level, as she ate the same food we ate almost daily. Our family did not travel recently. So what was it that my family had or ate that my neighbor or nanny’s child did not?
The answer was thyme. It is an herb that we mix with olive oil and spread on dough – I call it Lebanese pizza. That is one thing that my nanny and her child never ate, but we did. It was a long painful month of investigation, elimination, and anxiety. I called the public health department in Phoenix and they stated that lots of imported spices were contaminated with lead. There were two theories as to why this might happen. The first one is that the spice dealers would add lead to increase the weight of the spices to get more money. The second is that the spice fields were close to factories that used lead in their manufacturing, and somehow the lead would contaminate the nearby fields where the spices grew.
The type of thyme we used was bought in Syria and packaged in Lebanon. It was not the pure organic type that we usually got from our grandparents in our southern Lebanese village. This packaged thyme had lot of nuts added to it to give it more flavor.
The public health department official asked that I send her some samples of all the spices that I had. I packed up to ten different spice bags including the thyme. Two weeks later she called me, stating that the lead level allowable in spices must be less than 10, and that our thyme’s lead level was 900!
We got rid of all the spices, and have never eaten that packaged spice again. My kids’ lead levels dropped nicely afterward and back to normal. That is our story with lead. Now it seems like a mini-detective story and even fun, but the anxiety that I experienced until we figured out the cause was not!
Dr. Faddoul is a private practice pediatrician in La Canada Flintridge, Calif.
Failure to diagnose is a continuing challenge
Question: A middle-aged woman developed cellulitis after sustaining multiple mosquito bites in her lower left leg. The area of infection did not appear to reach the knee, which housed a prosthesis implanted there 3 years earlier. Over the next few days, she had significant knee pain, which was attributed to the surrounding cellulitis. Her pulse rate reached 105 beats per min, and her temperature was 101° F, but she was continued on oral antibiotics as an outpatient. Later that evening, she collapsed at home.
Which of the following is best?
A. Fever and tachycardia alone are enough to make the diagnosis of systemic inflammatory response syndrome (SIRS) and should have raised sepsis as a cause.
B. In septic patients, even a short delay in antibiotic administration can significantly affect morbidity and mortality.
C. Failure to diagnose is the most common basis for a medical malpractice claim.
D. The doctor may have anchored his diagnosis on the mosquito-bite incident, and should have considered a septic joint and/or sepsis in the differential.
E. All are correct.
Answer: E. “Failure to diagnose” is a legal term, whereas in medical usage we tend to use terms such “missed diagnosis,” “overlooked condition,” or “diagnostic error.” If such failure is shown to be a breach of the standard of care and is proven to be a proximate cause of the patient’s injury, then a case for medical negligence is made out. Even if the situation is atypical or complex, there still is the duty to refer, if customarily required, to an appropriate specialist, and failure to do so may also constitute negligence.

Diagnostic errors tend to cause the most severe injuries, especially in hospitalized patients. Roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Failure to diagnose occurs in both outpatient and in-hospital settings, recurring examples being myocardial infarction, dissecting aneurysm, pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a records-review study covering a large urban Veterans Affairs facility and an integrated private health care system in a primary care setting, the authors reported that pneumonia, heart failure, acute renal failure, cancer, and urinary tract infections (UTIs) were frequently missed diagnoses.2 They identified 190 diagnostic errors over a 12-month period in 2006-2007, and they attributed them to “process breakdowns” involving the practitioner-patient clinical encounter, referrals, patient factors, follow-up and tracking of diagnostic information, and interpretation of test results. Deficiencies in bedside history taking, physical exam, and test ordering were common; significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Malpractice carriers regularly compile data regarding the nature of their covered losses, and their reports on diagnostic errors, although not subject to the usual scientific peer review, have generally corroborated the published literature.
For example, data from 2009 to 2013 collected by MIEC, a large malpractice mutual insurance company on the West Coast, impute almost half of all general medicine claims to diagnostic errors.3 The cases, frequently involving cancer and heart disease, resulted in high-severity injuries and death. Lapses in clinical judgment, communication, and patient-related behavior issues were the primary contributing factors that affected the diagnosis-related claims. Pitfalls included errors in patient assessment, diagnostic processing, provider follow-up, and referral to specialists.
Recent reports have drawn attention to sepsis, an example of SIRS, as an important missed diagnosis, often with deadly consequences. It has been pointed out that if a sepsis case goes to trial, jurors will immediately learn that mortality rates are increased if antibiotics are delayed, even for a short period. In one study, each hour’s delay increased mortality by 7.6%, mortality being 21.1% if antibiotics were given in the first hour, compared with 58% if delayed by more than 6 hours.4
To avoid suits, physicians should be alert to seemingly minor vital sign changes, such as new tachypnea or tachycardia. Notably, patients can have severe sepsis and septic shock without fever or hypothermia. Uncomplicated sepsis is common and can quickly progress to severe sepsis, with organ failure and septic shock. The Surviving Sepsis Campaign has estimated that more than 750,000 individuals develop severe sepsis in North America each year, with mortality around 50%.
The Sullivan Group,which comprises a team of professionals dedicated to perfecting a system solution that reduces medical error and improves patient safety, recently published a wrongful-death narrative from undiagnosed sepsis.5 The decedent gave birth to her first child after 24 hours of labor, sustaining severe vaginal and rectal tearing. Three days later, she began experiencing chills, nausea, worsening vaginal pain, and fever. Her temperature reached 101.9° F (38.8° C). The following day, 4 days after delivery, she was seen by a nurse practitioner in the emergency department with symptoms of nausea, abdominal and back pain, and fever. She was tachycardic at 115 per minute.
The presence of fever plus tachycardia should have raised the diagnosis of SIRS, especially in view of her abdominal pain and a recent complicated delivery. Instead, the practitioner diagnosed a UTI and discharged her on antibiotics. That same afternoon, she collapsed and was admitted for sepsis. Despite an emergency hysterectomy, her condition worsened, she developed multiple organ failure and septic shock, and died the next day. The source of her sepsis was endometritis, and the jury returned a $20 million verdict for the plaintiff.
Observers of medical errors point to our recurring failure to continue to consider alternatives after forming an initial tentative diagnosis, and warn us about the various cognitive biases familiar to behavioral economists but ignored by many doctors.6 These include anchoring bias, in which one is locked into an aspect of the case; framing bias, in which there is misdirection because of the way the problem was posed; availability bias, in which things are judged by what comes readily to mind, such as a recent experience; and confirmation bias, in which one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary.
In the case outlined earlier, the Sullivan Group noted that the practitioner did not consider sepsis because of cognitive bias, anchoring, and premature closure. The trial documents indicated that the urinalysis did not show bacteria, but the practitioner may have settled – prematurely – on the UTI diagnosis, based on the presence of WBCs in the urine and her obstetrics history. Having anchored on that thought process and prematurely closed her decision making, the practitioner then ignored the elevated white blood cell count with a left shift, and a depressed platelet count of 50,000. Perhaps UTI was a reasonable consideration in the differential, but the working diagnosis of sepsis should have been first and foremost.
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials may have been published in earlier columns in Internal Medicine News, and can be accessed at www.mdedge.com/taxonomy/term/83/path_term/21/latest. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. BMJ Qual Saf. 2013 Aug;22(8):672-80.
2. JAMA Intern Med. 2013 Mar 25;173(6):418-25.
3. MIEC, the Exchange, Issue 8, March 2017.
4. Crit Care Med. 2006 Jun;34(6):1589-96.
5. The Sullivan Group. Case: Avoiding cognitive bias in diagnosing sepsis.
6. Acad Med. 2003 Aug;78(8):775-80.
Question: A middle-aged woman developed cellulitis after sustaining multiple mosquito bites in her lower left leg. The area of infection did not appear to reach the knee, which housed a prosthesis implanted there 3 years earlier. Over the next few days, she had significant knee pain, which was attributed to the surrounding cellulitis. Her pulse rate reached 105 beats per min, and her temperature was 101° F, but she was continued on oral antibiotics as an outpatient. Later that evening, she collapsed at home.
Which of the following is best?
A. Fever and tachycardia alone are enough to make the diagnosis of systemic inflammatory response syndrome (SIRS) and should have raised sepsis as a cause.
B. In septic patients, even a short delay in antibiotic administration can significantly affect morbidity and mortality.
C. Failure to diagnose is the most common basis for a medical malpractice claim.
D. The doctor may have anchored his diagnosis on the mosquito-bite incident, and should have considered a septic joint and/or sepsis in the differential.
E. All are correct.
Answer: E. “Failure to diagnose” is a legal term, whereas in medical usage we tend to use terms such “missed diagnosis,” “overlooked condition,” or “diagnostic error.” If such failure is shown to be a breach of the standard of care and is proven to be a proximate cause of the patient’s injury, then a case for medical negligence is made out. Even if the situation is atypical or complex, there still is the duty to refer, if customarily required, to an appropriate specialist, and failure to do so may also constitute negligence.
Diagnostic errors tend to cause the most severe injuries, especially in hospitalized patients. Roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Failure to diagnose occurs in both outpatient and in-hospital settings, recurring examples being myocardial infarction, dissecting aneurysm, pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a records-review study covering a large urban Veterans Affairs facility and an integrated private health care system in a primary care setting, the authors reported that pneumonia, heart failure, acute renal failure, cancer, and urinary tract infections (UTIs) were frequently missed diagnoses.2 They identified 190 diagnostic errors over a 12-month period in 2006-2007, and they attributed them to “process breakdowns” involving the practitioner-patient clinical encounter, referrals, patient factors, follow-up and tracking of diagnostic information, and interpretation of test results. Deficiencies in bedside history taking, physical exam, and test ordering were common; significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Malpractice carriers regularly compile data regarding the nature of their covered losses, and their reports on diagnostic errors, although not subject to the usual scientific peer review, have generally corroborated the published literature.
For example, data from 2009 to 2013 collected by MIEC, a large malpractice mutual insurance company on the West Coast, impute almost half of all general medicine claims to diagnostic errors.3 The cases, frequently involving cancer and heart disease, resulted in high-severity injuries and death. Lapses in clinical judgment, communication, and patient-related behavior issues were the primary contributing factors that affected the diagnosis-related claims. Pitfalls included errors in patient assessment, diagnostic processing, provider follow-up, and referral to specialists.
Recent reports have drawn attention to sepsis, an example of SIRS, as an important missed diagnosis, often with deadly consequences. It has been pointed out that if a sepsis case goes to trial, jurors will immediately learn that mortality rates are increased if antibiotics are delayed, even for a short period. In one study, each hour’s delay increased mortality by 7.6%, mortality being 21.1% if antibiotics were given in the first hour, compared with 58% if delayed by more than 6 hours.4
To avoid suits, physicians should be alert to seemingly minor vital sign changes, such as new tachypnea or tachycardia. Notably, patients can have severe sepsis and septic shock without fever or hypothermia. Uncomplicated sepsis is common and can quickly progress to severe sepsis, with organ failure and septic shock. The Surviving Sepsis Campaign has estimated that more than 750,000 individuals develop severe sepsis in North America each year, with mortality around 50%.
The Sullivan Group,which comprises a team of professionals dedicated to perfecting a system solution that reduces medical error and improves patient safety, recently published a wrongful-death narrative from undiagnosed sepsis.5 The decedent gave birth to her first child after 24 hours of labor, sustaining severe vaginal and rectal tearing. Three days later, she began experiencing chills, nausea, worsening vaginal pain, and fever. Her temperature reached 101.9° F (38.8° C). The following day, 4 days after delivery, she was seen by a nurse practitioner in the emergency department with symptoms of nausea, abdominal and back pain, and fever. She was tachycardic at 115 per minute.
The presence of fever plus tachycardia should have raised the diagnosis of SIRS, especially in view of her abdominal pain and a recent complicated delivery. Instead, the practitioner diagnosed a UTI and discharged her on antibiotics. That same afternoon, she collapsed and was admitted for sepsis. Despite an emergency hysterectomy, her condition worsened, she developed multiple organ failure and septic shock, and died the next day. The source of her sepsis was endometritis, and the jury returned a $20 million verdict for the plaintiff.
Observers of medical errors point to our recurring failure to continue to consider alternatives after forming an initial tentative diagnosis, and warn us about the various cognitive biases familiar to behavioral economists but ignored by many doctors.6 These include anchoring bias, in which one is locked into an aspect of the case; framing bias, in which there is misdirection because of the way the problem was posed; availability bias, in which things are judged by what comes readily to mind, such as a recent experience; and confirmation bias, in which one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary.
In the case outlined earlier, the Sullivan Group noted that the practitioner did not consider sepsis because of cognitive bias, anchoring, and premature closure. The trial documents indicated that the urinalysis did not show bacteria, but the practitioner may have settled – prematurely – on the UTI diagnosis, based on the presence of WBCs in the urine and her obstetrics history. Having anchored on that thought process and prematurely closed her decision making, the practitioner then ignored the elevated white blood cell count with a left shift, and a depressed platelet count of 50,000. Perhaps UTI was a reasonable consideration in the differential, but the working diagnosis of sepsis should have been first and foremost.
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials may have been published in earlier columns in Internal Medicine News, and can be accessed at www.mdedge.com/taxonomy/term/83/path_term/21/latest. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. BMJ Qual Saf. 2013 Aug;22(8):672-80.
2. JAMA Intern Med. 2013 Mar 25;173(6):418-25.
3. MIEC, the Exchange, Issue 8, March 2017.
4. Crit Care Med. 2006 Jun;34(6):1589-96.
5. The Sullivan Group. Case: Avoiding cognitive bias in diagnosing sepsis.
6. Acad Med. 2003 Aug;78(8):775-80.
Question: A middle-aged woman developed cellulitis after sustaining multiple mosquito bites in her lower left leg. The area of infection did not appear to reach the knee, which housed a prosthesis implanted there 3 years earlier. Over the next few days, she had significant knee pain, which was attributed to the surrounding cellulitis. Her pulse rate reached 105 beats per min, and her temperature was 101° F, but she was continued on oral antibiotics as an outpatient. Later that evening, she collapsed at home.
Which of the following is best?
A. Fever and tachycardia alone are enough to make the diagnosis of systemic inflammatory response syndrome (SIRS) and should have raised sepsis as a cause.
B. In septic patients, even a short delay in antibiotic administration can significantly affect morbidity and mortality.
C. Failure to diagnose is the most common basis for a medical malpractice claim.
D. The doctor may have anchored his diagnosis on the mosquito-bite incident, and should have considered a septic joint and/or sepsis in the differential.
E. All are correct.
Answer: E. “Failure to diagnose” is a legal term, whereas in medical usage we tend to use terms such “missed diagnosis,” “overlooked condition,” or “diagnostic error.” If such failure is shown to be a breach of the standard of care and is proven to be a proximate cause of the patient’s injury, then a case for medical negligence is made out. Even if the situation is atypical or complex, there still is the duty to refer, if customarily required, to an appropriate specialist, and failure to do so may also constitute negligence.
Diagnostic errors tend to cause the most severe injuries, especially in hospitalized patients. Roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Failure to diagnose occurs in both outpatient and in-hospital settings, recurring examples being myocardial infarction, dissecting aneurysm, pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a records-review study covering a large urban Veterans Affairs facility and an integrated private health care system in a primary care setting, the authors reported that pneumonia, heart failure, acute renal failure, cancer, and urinary tract infections (UTIs) were frequently missed diagnoses.2 They identified 190 diagnostic errors over a 12-month period in 2006-2007, and they attributed them to “process breakdowns” involving the practitioner-patient clinical encounter, referrals, patient factors, follow-up and tracking of diagnostic information, and interpretation of test results. Deficiencies in bedside history taking, physical exam, and test ordering were common; significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Malpractice carriers regularly compile data regarding the nature of their covered losses, and their reports on diagnostic errors, although not subject to the usual scientific peer review, have generally corroborated the published literature.
For example, data from 2009 to 2013 collected by MIEC, a large malpractice mutual insurance company on the West Coast, impute almost half of all general medicine claims to diagnostic errors.3 The cases, frequently involving cancer and heart disease, resulted in high-severity injuries and death. Lapses in clinical judgment, communication, and patient-related behavior issues were the primary contributing factors that affected the diagnosis-related claims. Pitfalls included errors in patient assessment, diagnostic processing, provider follow-up, and referral to specialists.
Recent reports have drawn attention to sepsis, an example of SIRS, as an important missed diagnosis, often with deadly consequences. It has been pointed out that if a sepsis case goes to trial, jurors will immediately learn that mortality rates are increased if antibiotics are delayed, even for a short period. In one study, each hour’s delay increased mortality by 7.6%, mortality being 21.1% if antibiotics were given in the first hour, compared with 58% if delayed by more than 6 hours.4
To avoid suits, physicians should be alert to seemingly minor vital sign changes, such as new tachypnea or tachycardia. Notably, patients can have severe sepsis and septic shock without fever or hypothermia. Uncomplicated sepsis is common and can quickly progress to severe sepsis, with organ failure and septic shock. The Surviving Sepsis Campaign has estimated that more than 750,000 individuals develop severe sepsis in North America each year, with mortality around 50%.
The Sullivan Group,which comprises a team of professionals dedicated to perfecting a system solution that reduces medical error and improves patient safety, recently published a wrongful-death narrative from undiagnosed sepsis.5 The decedent gave birth to her first child after 24 hours of labor, sustaining severe vaginal and rectal tearing. Three days later, she began experiencing chills, nausea, worsening vaginal pain, and fever. Her temperature reached 101.9° F (38.8° C). The following day, 4 days after delivery, she was seen by a nurse practitioner in the emergency department with symptoms of nausea, abdominal and back pain, and fever. She was tachycardic at 115 per minute.
The presence of fever plus tachycardia should have raised the diagnosis of SIRS, especially in view of her abdominal pain and a recent complicated delivery. Instead, the practitioner diagnosed a UTI and discharged her on antibiotics. That same afternoon, she collapsed and was admitted for sepsis. Despite an emergency hysterectomy, her condition worsened, she developed multiple organ failure and septic shock, and died the next day. The source of her sepsis was endometritis, and the jury returned a $20 million verdict for the plaintiff.
Observers of medical errors point to our recurring failure to continue to consider alternatives after forming an initial tentative diagnosis, and warn us about the various cognitive biases familiar to behavioral economists but ignored by many doctors.6 These include anchoring bias, in which one is locked into an aspect of the case; framing bias, in which there is misdirection because of the way the problem was posed; availability bias, in which things are judged by what comes readily to mind, such as a recent experience; and confirmation bias, in which one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary.
In the case outlined earlier, the Sullivan Group noted that the practitioner did not consider sepsis because of cognitive bias, anchoring, and premature closure. The trial documents indicated that the urinalysis did not show bacteria, but the practitioner may have settled – prematurely – on the UTI diagnosis, based on the presence of WBCs in the urine and her obstetrics history. Having anchored on that thought process and prematurely closed her decision making, the practitioner then ignored the elevated white blood cell count with a left shift, and a depressed platelet count of 50,000. Perhaps UTI was a reasonable consideration in the differential, but the working diagnosis of sepsis should have been first and foremost.
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials may have been published in earlier columns in Internal Medicine News, and can be accessed at www.mdedge.com/taxonomy/term/83/path_term/21/latest. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. BMJ Qual Saf. 2013 Aug;22(8):672-80.
2. JAMA Intern Med. 2013 Mar 25;173(6):418-25.
3. MIEC, the Exchange, Issue 8, March 2017.
4. Crit Care Med. 2006 Jun;34(6):1589-96.
5. The Sullivan Group. Case: Avoiding cognitive bias in diagnosing sepsis.
6. Acad Med. 2003 Aug;78(8):775-80.
Morbidly adherent placenta: A multidisciplinary approach
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
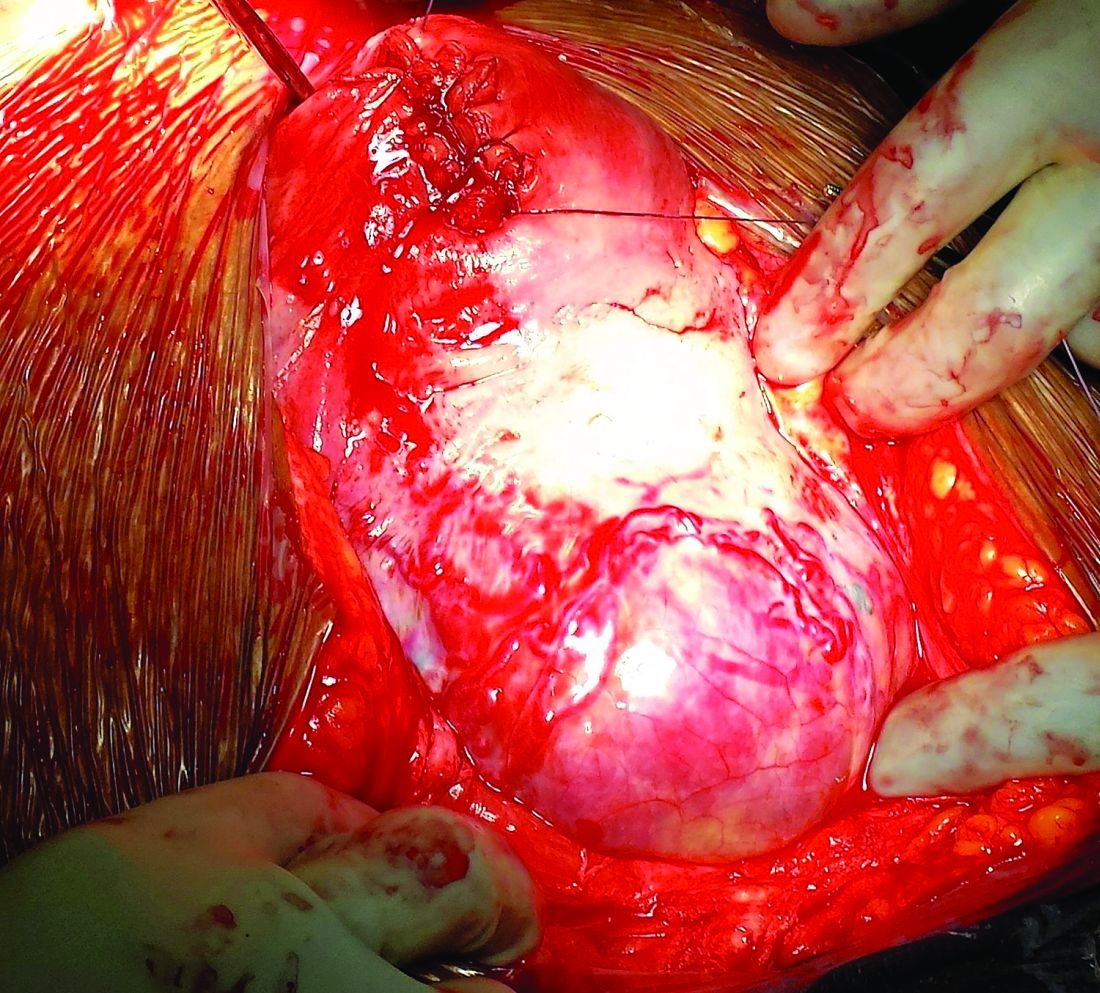
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
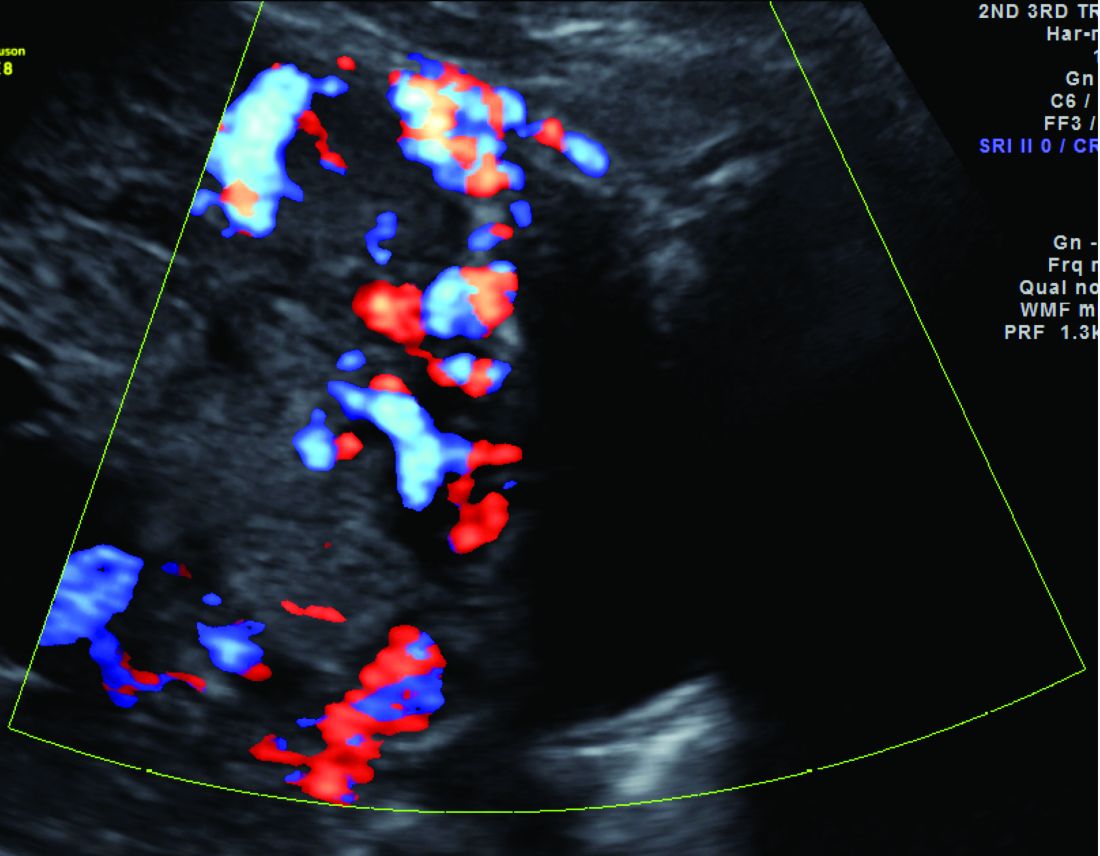
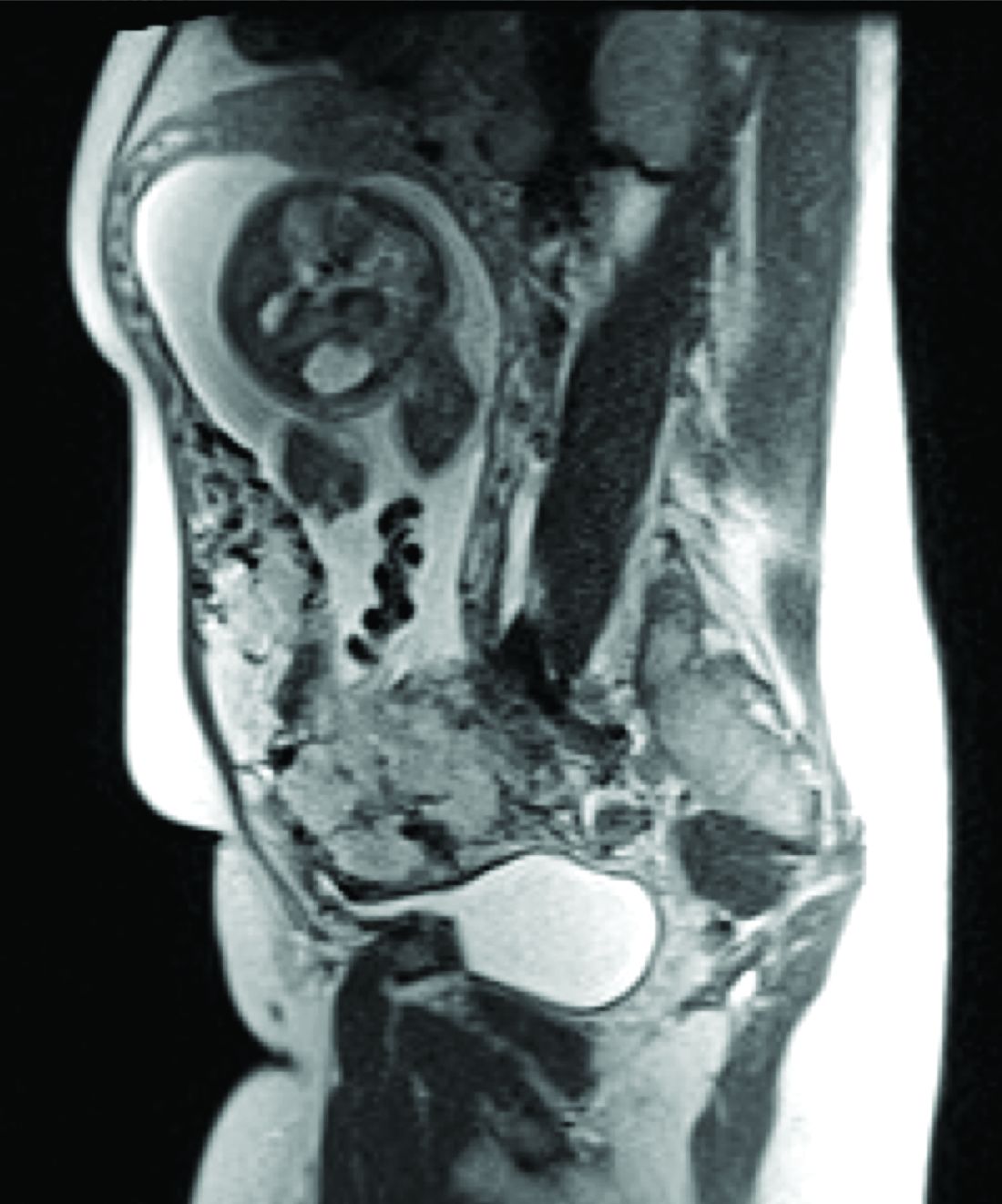
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.

In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.
In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.
In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
Multidisciplinary teams offer key to complex deliveries
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.

The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Strategies to evaluate postmenopausal bleeding
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.

Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Coordinating data collection in a QI project
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
I am currently working with my mentor, Dr. Ian Jenkins, an attending in the Division of Hospital Medicine at the University of California, San Diego, to start piloting data collection on our project to cut catheter-associated urinary tract infections (CAUTI). We have contacted a number of potential units to recruit for CAUTI prevention efforts, but we are hoping to do a preliminary trial of data collection to better estimate the amount of time it takes to gather data for an individual unit.
I am quickly learning that conducting a successful quality improvement project requires one to be forward-looking in an attempt to identify challenges before they arise. With respect to coordinating data collection, it may have been helpful for us to initially meet with hospital staff to identify the best staff for coordinating data collection efforts (i.e. physician, nurse, trainee) within each individual unit. This could potentially have helped us to also better communicate and recruit individuals to partner with us for our project.
I am continuing to enjoy the challenges of performing a quality improvement project. One skill that I have developed is learning how to be forward-thinking in my approach to research in an attempt to handle challenges prospectively, as opposed to retrospectively. This has helped me improve everything from how I think about data collection to how I think about displaying results. I am truly grateful to my mentor Dr. Jenkins for his help in this regard.
Victor Ekuta is a third-year medical student at UC San Diego.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
I am currently working with my mentor, Dr. Ian Jenkins, an attending in the Division of Hospital Medicine at the University of California, San Diego, to start piloting data collection on our project to cut catheter-associated urinary tract infections (CAUTI). We have contacted a number of potential units to recruit for CAUTI prevention efforts, but we are hoping to do a preliminary trial of data collection to better estimate the amount of time it takes to gather data for an individual unit.
I am quickly learning that conducting a successful quality improvement project requires one to be forward-looking in an attempt to identify challenges before they arise. With respect to coordinating data collection, it may have been helpful for us to initially meet with hospital staff to identify the best staff for coordinating data collection efforts (i.e. physician, nurse, trainee) within each individual unit. This could potentially have helped us to also better communicate and recruit individuals to partner with us for our project.
I am continuing to enjoy the challenges of performing a quality improvement project. One skill that I have developed is learning how to be forward-thinking in my approach to research in an attempt to handle challenges prospectively, as opposed to retrospectively. This has helped me improve everything from how I think about data collection to how I think about displaying results. I am truly grateful to my mentor Dr. Jenkins for his help in this regard.
Victor Ekuta is a third-year medical student at UC San Diego.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
I am currently working with my mentor, Dr. Ian Jenkins, an attending in the Division of Hospital Medicine at the University of California, San Diego, to start piloting data collection on our project to cut catheter-associated urinary tract infections (CAUTI). We have contacted a number of potential units to recruit for CAUTI prevention efforts, but we are hoping to do a preliminary trial of data collection to better estimate the amount of time it takes to gather data for an individual unit.
I am quickly learning that conducting a successful quality improvement project requires one to be forward-looking in an attempt to identify challenges before they arise. With respect to coordinating data collection, it may have been helpful for us to initially meet with hospital staff to identify the best staff for coordinating data collection efforts (i.e. physician, nurse, trainee) within each individual unit. This could potentially have helped us to also better communicate and recruit individuals to partner with us for our project.
I am continuing to enjoy the challenges of performing a quality improvement project. One skill that I have developed is learning how to be forward-thinking in my approach to research in an attempt to handle challenges prospectively, as opposed to retrospectively. This has helped me improve everything from how I think about data collection to how I think about displaying results. I am truly grateful to my mentor Dr. Jenkins for his help in this regard.
Victor Ekuta is a third-year medical student at UC San Diego.
Review of plant phenolics, part 3: Nonflavonoid compounds
Polyphenols are widely distributed in the plant kingdom, and are found in copious supply in multiple vegetables, fruits, herbs, grains, tea, coffee beans, honey, and red wine, for example. They are an especially important source of antioxidants and are increasingly the focus of research due to their potent and diverse biologic activities. In the conclusion to my three-part review of polyphenols, this column identifies representative compounds from the classes of nonflavonoid polyphenols and provides a brief update on research.

Phenolic acids: ferulic acid
Derived from curcumin, ferulic acid is noted for exhibiting multiple biologic activities, including antiapoptotic, anticarcinogenic, antidiabetic, hepatoprotective, and cardioprotective, among others. Its beneficial effects are thought to be mediated through its antioxidant and anti-inflammatory characteristics.1 In a small 2008 study, a stable formulation of 15% l-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid was applied topically to normal-appearing human skin for 4 days and was found to impart significant photoprotection against solar-simulated UV radiation and was especially effective at diminishing thymine dimer mutations, which are linked to skin cancer. The authors also noted that the mechanism of action of this antioxidant formulation differs from that of sunscreens and, therefore, may serve as a supplement to such products.2 (It is worth noting that ferulic acid has been approved as a sunscreen agent in Japan.3)
In 2015, Ambothi et al. used Swiss albino mice to assess the photochemopreventive effects of ferulic acid against chronic (30-week) UVB, finding the intraperitoneal and topical administration of the phenolic acid effective in significantly lowering the incidence of UVB-induced tumor volume and weight in the mice skin.4 The next year, Hahn et al. reported that pretreatment with ferulic acid protects human dermal fibroblasts from UVA-induced photodamage.5 Also in 2016, Chaiprasongsuk et al. found that several dietary phenolics, including ferulic acid, deliver protection against UVA-induced melanogenesis through indirect regulation of the Nrf2-ARE pathway.6 
Lignans: flaxseed
Flaxseed lignans, which exhibit a wide range of biologic activities, are best known for their antioxidant properties.7 In a 2017 study using atopic dermatitis–induced NC/Nga mice, Yang et al. found that fermented flaxseed oil administered orally was successful in relieving symptoms such as erythema, edema, pruritus, and epithelial damage.8 Two years earlier, Draganescu et al. developed a topical flaxseed extract formulation that displayed wound healing capabilities on Wistar rats.7 Emulsions produced from the oils and seeds of transgenic flax have also been found to protect against oxidative stress in hamster fibroblasts, with investigators suggesting that the emulsions have potential to protect the skin against such damage.8
Stilbenes: resveratrol
The antioxidant potency of resveratrol has been cited for conferring a wide range of salutary effects, including antitumorigenic as well as antiaging activity. In 2008, a resveratrol-based skin care formulation intended to combat photoaging was reported to exhibit 17-fold greater antioxidant activity than idebenone.9 In a different study that year, resveratrol, the primary active polyphenolic constituent in red wine, was assessed in terms of topical/transdermal delivery viability, given previously established benefits shown via systemic administration. Several hydrogel systems used as resveratrol vehicles were shown to be safe and effective methods for cutaneously delivering the therapeutic effects of this antioxidant.10 Since then, resveratrol has been demonstrated to penetrate the skin via topical administration, reinforcing the antioxidant system of the stratum corneum and delivering increases of antioxidants to human epidermal tissue.11
In 2014, Farris et al. showed that a proprietary topical antioxidant blend of resveratrol, baicalin, and vitamin E applied topically at night yielded statistically significant amelioration of fine lines and wrinkles, as well as skin firmness, elasticity, laxity, hyperpigmentation, radiance, and roughness over a 12-week period.12 Resveratrol has also been shown in mice to suppress the inflammatory response and improve survival from severe burns with bacterial infections.13 
Hydrolyzable tannins: ellagic acid
Ellagic acid, a dimer of gallic acid, has been reported to impart anti-inflammatory, antitumor, immunomodulatory, and antifungal activities.14-16 Ortiz-Ruiz et al. have noted that while ellagic acid is used as a whitening agent, it can act as a substrate to rather than an inhibitor of tyrosinase, as it is oxidized by the enzyme to an unstable o-quinone. However, as a potent antioxidant, ellagic acid can block melanogenesis by reducing o-quinones and semiquinones.17
In a double-blind, placebo-controlled, 4-week trial to assess the effects of orally administered ellagic acid–rich pomegranate extract on the pigmentation of 13 women after UV exposure, with healthy volunteers randomly assigned to high-dose, low-dose, and control groups, luminance values decreased by 1.73% in the high-dose group and 1.35% in the low-dose group, as compared with the control group, and stains and freckles were reported to be diminished.18 A 2016 study in human dermal fibroblasts by Baek et al. suggested that ellagic acid displays antiphotoaging activity, as the polyphenol protected against UVB-induced oxidative stress potentially through an Nrf2-dependent pathway.15
Condensed tannins (Proanthocyanidins): pycnogenol
Pycnogenol has been used in an antioxidant mixture also including vitamins C and E, as well as evening primrose that when orally administered for 10 weeks to female SKH-1 hairless mice exposed three times weekly to UVB irradiation demonstrated the capacity to significantly inhibit wrinkle formation by markedly suppressing UVB-induced MMP activity while promoting collagen production.19 In a 2012 study of 112 women with mild to moderate photoaging, orally administered pycnogenol was shown to yield significant reductions in clinical grading of skin photoaging scores.20 Four years later, a review by Grether-Beck et al. suggested that oral administration of pycnogenol imparts photoprotection, diminishes hyperpigmentation, and improves skin barrier function and the stability of the extracellular matrix.21
Lignins: various woody plants
Recognized as efficient natural scavengers of reactive oxygen species, lignins are complex phenolic polymers that are abundant in nature, particularly in various tree species and agricultural products. In 2004, Dizhbite et al. isolated lignin samples from deciduous and coniferous trees to assess their capacity as natural antioxidants. Samples were assessed against the 1,1-diphenyl-2-picrylhydrazyl (DPPH) radical in homogeneous conditions, with the commercially available kraft lignin noted for displaying antibacterial activity associated with its radical-scavenging properties.22 Four years later, Ugartondo et al. studied several lignins and reported a strong antioxidant capacity at various concentrations that were innocuous to normal human cells and stable when exposed to UVA. The investigators concluded that lignins may be viable for inclusion in cosmetic and topical medical formulations.23
Conclusion
A brief survey of the polyphenolic landscape obviously cannot do the subject justice. From the dermatologic perspective, this diverse family of compounds factor into the skin care formulations becoming more prevalent in the established armamentarium, as well as the direct-to-consumer market. Given the increasing attention paid here and elsewhere to the impact of diet on the skin, the status of this dynamic class of polyphenolic compounds, which includes several antioxidants and is found in numerous plants, appears to be well deserved and warrants much more research.
Dr. Baumann is a private practice dermatologist, researcher, author and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Food Chem Toxicol. 2017 May;103:41-55.
2. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
3. J Pharm Biomed Anal. 2008 Mar 13;46(4):645-52.
4. Food Chem Toxicol. 2015 Aug;82:72-8.
5. Ann Dermatol. 2016 Dec;28(6):740-8.
6. Redox Biol. 2016 Aug;8:79-90.
7. Int J Biol Macromol. 2015 Jan;72:614-23.
8. Evid Based Complement Alternat Med. 2017;2017:5469125.
9. J Cosmet Dermatol. 2008 Mar;7(1):2-7.
10. Biol Pharm Bull. 2008 May;31(5):955-62.
11. Arch Dermatol Res. 2017 Aug;309(6):423-31.
12. J Drugs Dermatol. 2014 Dec;13(12):1467-72.
13. Inflammation. 2015;38(3):1273-80.
14. Dermatol Ther. 2012 May-Jun;25(3):252-9.
15. Korean J Physiol Pharmacol. 2016 May;20(3):269-77.
16. Phytother Res. 2015 Jul;29(7):1019-25.
17. J Dermatol Sci. 2016 May;82(2):115-22.
18. J Nutr Sci Vitaminol (Tokyo). 2006 Oct;52(5):383-8.
19. Photodermatol Photoimmunol Photomed. 2007 Oct;23(5):155-62.
20. Clin Interv Aging. 2012;7:275-86.
21. Skin Pharmacol Physiol. 2016;29(1):13-7.
22. Bioresour Technol. 2004 Dec;95(3):309-17.
23. Bioresour Technol. 2008 Sep;99(14):6683-7.
Polyphenols are widely distributed in the plant kingdom, and are found in copious supply in multiple vegetables, fruits, herbs, grains, tea, coffee beans, honey, and red wine, for example. They are an especially important source of antioxidants and are increasingly the focus of research due to their potent and diverse biologic activities. In the conclusion to my three-part review of polyphenols, this column identifies representative compounds from the classes of nonflavonoid polyphenols and provides a brief update on research.
Phenolic acids: ferulic acid
Derived from curcumin, ferulic acid is noted for exhibiting multiple biologic activities, including antiapoptotic, anticarcinogenic, antidiabetic, hepatoprotective, and cardioprotective, among others. Its beneficial effects are thought to be mediated through its antioxidant and anti-inflammatory characteristics.1 In a small 2008 study, a stable formulation of 15% l-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid was applied topically to normal-appearing human skin for 4 days and was found to impart significant photoprotection against solar-simulated UV radiation and was especially effective at diminishing thymine dimer mutations, which are linked to skin cancer. The authors also noted that the mechanism of action of this antioxidant formulation differs from that of sunscreens and, therefore, may serve as a supplement to such products.2 (It is worth noting that ferulic acid has been approved as a sunscreen agent in Japan.3)
In 2015, Ambothi et al. used Swiss albino mice to assess the photochemopreventive effects of ferulic acid against chronic (30-week) UVB, finding the intraperitoneal and topical administration of the phenolic acid effective in significantly lowering the incidence of UVB-induced tumor volume and weight in the mice skin.4 The next year, Hahn et al. reported that pretreatment with ferulic acid protects human dermal fibroblasts from UVA-induced photodamage.5 Also in 2016, Chaiprasongsuk et al. found that several dietary phenolics, including ferulic acid, deliver protection against UVA-induced melanogenesis through indirect regulation of the Nrf2-ARE pathway.6
Lignans: flaxseed
Flaxseed lignans, which exhibit a wide range of biologic activities, are best known for their antioxidant properties.7 In a 2017 study using atopic dermatitis–induced NC/Nga mice, Yang et al. found that fermented flaxseed oil administered orally was successful in relieving symptoms such as erythema, edema, pruritus, and epithelial damage.8 Two years earlier, Draganescu et al. developed a topical flaxseed extract formulation that displayed wound healing capabilities on Wistar rats.7 Emulsions produced from the oils and seeds of transgenic flax have also been found to protect against oxidative stress in hamster fibroblasts, with investigators suggesting that the emulsions have potential to protect the skin against such damage.8
Stilbenes: resveratrol
The antioxidant potency of resveratrol has been cited for conferring a wide range of salutary effects, including antitumorigenic as well as antiaging activity. In 2008, a resveratrol-based skin care formulation intended to combat photoaging was reported to exhibit 17-fold greater antioxidant activity than idebenone.9 In a different study that year, resveratrol, the primary active polyphenolic constituent in red wine, was assessed in terms of topical/transdermal delivery viability, given previously established benefits shown via systemic administration. Several hydrogel systems used as resveratrol vehicles were shown to be safe and effective methods for cutaneously delivering the therapeutic effects of this antioxidant.10 Since then, resveratrol has been demonstrated to penetrate the skin via topical administration, reinforcing the antioxidant system of the stratum corneum and delivering increases of antioxidants to human epidermal tissue.11
In 2014, Farris et al. showed that a proprietary topical antioxidant blend of resveratrol, baicalin, and vitamin E applied topically at night yielded statistically significant amelioration of fine lines and wrinkles, as well as skin firmness, elasticity, laxity, hyperpigmentation, radiance, and roughness over a 12-week period.12 Resveratrol has also been shown in mice to suppress the inflammatory response and improve survival from severe burns with bacterial infections.13
Hydrolyzable tannins: ellagic acid
Ellagic acid, a dimer of gallic acid, has been reported to impart anti-inflammatory, antitumor, immunomodulatory, and antifungal activities.14-16 Ortiz-Ruiz et al. have noted that while ellagic acid is used as a whitening agent, it can act as a substrate to rather than an inhibitor of tyrosinase, as it is oxidized by the enzyme to an unstable o-quinone. However, as a potent antioxidant, ellagic acid can block melanogenesis by reducing o-quinones and semiquinones.17
In a double-blind, placebo-controlled, 4-week trial to assess the effects of orally administered ellagic acid–rich pomegranate extract on the pigmentation of 13 women after UV exposure, with healthy volunteers randomly assigned to high-dose, low-dose, and control groups, luminance values decreased by 1.73% in the high-dose group and 1.35% in the low-dose group, as compared with the control group, and stains and freckles were reported to be diminished.18 A 2016 study in human dermal fibroblasts by Baek et al. suggested that ellagic acid displays antiphotoaging activity, as the polyphenol protected against UVB-induced oxidative stress potentially through an Nrf2-dependent pathway.15
Condensed tannins (Proanthocyanidins): pycnogenol
Pycnogenol has been used in an antioxidant mixture also including vitamins C and E, as well as evening primrose that when orally administered for 10 weeks to female SKH-1 hairless mice exposed three times weekly to UVB irradiation demonstrated the capacity to significantly inhibit wrinkle formation by markedly suppressing UVB-induced MMP activity while promoting collagen production.19 In a 2012 study of 112 women with mild to moderate photoaging, orally administered pycnogenol was shown to yield significant reductions in clinical grading of skin photoaging scores.20 Four years later, a review by Grether-Beck et al. suggested that oral administration of pycnogenol imparts photoprotection, diminishes hyperpigmentation, and improves skin barrier function and the stability of the extracellular matrix.21
Lignins: various woody plants
Recognized as efficient natural scavengers of reactive oxygen species, lignins are complex phenolic polymers that are abundant in nature, particularly in various tree species and agricultural products. In 2004, Dizhbite et al. isolated lignin samples from deciduous and coniferous trees to assess their capacity as natural antioxidants. Samples were assessed against the 1,1-diphenyl-2-picrylhydrazyl (DPPH) radical in homogeneous conditions, with the commercially available kraft lignin noted for displaying antibacterial activity associated with its radical-scavenging properties.22 Four years later, Ugartondo et al. studied several lignins and reported a strong antioxidant capacity at various concentrations that were innocuous to normal human cells and stable when exposed to UVA. The investigators concluded that lignins may be viable for inclusion in cosmetic and topical medical formulations.23
Conclusion
A brief survey of the polyphenolic landscape obviously cannot do the subject justice. From the dermatologic perspective, this diverse family of compounds factor into the skin care formulations becoming more prevalent in the established armamentarium, as well as the direct-to-consumer market. Given the increasing attention paid here and elsewhere to the impact of diet on the skin, the status of this dynamic class of polyphenolic compounds, which includes several antioxidants and is found in numerous plants, appears to be well deserved and warrants much more research.
Dr. Baumann is a private practice dermatologist, researcher, author and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Food Chem Toxicol. 2017 May;103:41-55.
2. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
3. J Pharm Biomed Anal. 2008 Mar 13;46(4):645-52.
4. Food Chem Toxicol. 2015 Aug;82:72-8.
5. Ann Dermatol. 2016 Dec;28(6):740-8.
6. Redox Biol. 2016 Aug;8:79-90.
7. Int J Biol Macromol. 2015 Jan;72:614-23.
8. Evid Based Complement Alternat Med. 2017;2017:5469125.
9. J Cosmet Dermatol. 2008 Mar;7(1):2-7.
10. Biol Pharm Bull. 2008 May;31(5):955-62.
11. Arch Dermatol Res. 2017 Aug;309(6):423-31.
12. J Drugs Dermatol. 2014 Dec;13(12):1467-72.
13. Inflammation. 2015;38(3):1273-80.
14. Dermatol Ther. 2012 May-Jun;25(3):252-9.
15. Korean J Physiol Pharmacol. 2016 May;20(3):269-77.
16. Phytother Res. 2015 Jul;29(7):1019-25.
17. J Dermatol Sci. 2016 May;82(2):115-22.
18. J Nutr Sci Vitaminol (Tokyo). 2006 Oct;52(5):383-8.
19. Photodermatol Photoimmunol Photomed. 2007 Oct;23(5):155-62.
20. Clin Interv Aging. 2012;7:275-86.
21. Skin Pharmacol Physiol. 2016;29(1):13-7.
22. Bioresour Technol. 2004 Dec;95(3):309-17.
23. Bioresour Technol. 2008 Sep;99(14):6683-7.
Polyphenols are widely distributed in the plant kingdom, and are found in copious supply in multiple vegetables, fruits, herbs, grains, tea, coffee beans, honey, and red wine, for example. They are an especially important source of antioxidants and are increasingly the focus of research due to their potent and diverse biologic activities. In the conclusion to my three-part review of polyphenols, this column identifies representative compounds from the classes of nonflavonoid polyphenols and provides a brief update on research.
Phenolic acids: ferulic acid
Derived from curcumin, ferulic acid is noted for exhibiting multiple biologic activities, including antiapoptotic, anticarcinogenic, antidiabetic, hepatoprotective, and cardioprotective, among others. Its beneficial effects are thought to be mediated through its antioxidant and anti-inflammatory characteristics.1 In a small 2008 study, a stable formulation of 15% l-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid was applied topically to normal-appearing human skin for 4 days and was found to impart significant photoprotection against solar-simulated UV radiation and was especially effective at diminishing thymine dimer mutations, which are linked to skin cancer. The authors also noted that the mechanism of action of this antioxidant formulation differs from that of sunscreens and, therefore, may serve as a supplement to such products.2 (It is worth noting that ferulic acid has been approved as a sunscreen agent in Japan.3)
In 2015, Ambothi et al. used Swiss albino mice to assess the photochemopreventive effects of ferulic acid against chronic (30-week) UVB, finding the intraperitoneal and topical administration of the phenolic acid effective in significantly lowering the incidence of UVB-induced tumor volume and weight in the mice skin.4 The next year, Hahn et al. reported that pretreatment with ferulic acid protects human dermal fibroblasts from UVA-induced photodamage.5 Also in 2016, Chaiprasongsuk et al. found that several dietary phenolics, including ferulic acid, deliver protection against UVA-induced melanogenesis through indirect regulation of the Nrf2-ARE pathway.6
Lignans: flaxseed
Flaxseed lignans, which exhibit a wide range of biologic activities, are best known for their antioxidant properties.7 In a 2017 study using atopic dermatitis–induced NC/Nga mice, Yang et al. found that fermented flaxseed oil administered orally was successful in relieving symptoms such as erythema, edema, pruritus, and epithelial damage.8 Two years earlier, Draganescu et al. developed a topical flaxseed extract formulation that displayed wound healing capabilities on Wistar rats.7 Emulsions produced from the oils and seeds of transgenic flax have also been found to protect against oxidative stress in hamster fibroblasts, with investigators suggesting that the emulsions have potential to protect the skin against such damage.8
Stilbenes: resveratrol
The antioxidant potency of resveratrol has been cited for conferring a wide range of salutary effects, including antitumorigenic as well as antiaging activity. In 2008, a resveratrol-based skin care formulation intended to combat photoaging was reported to exhibit 17-fold greater antioxidant activity than idebenone.9 In a different study that year, resveratrol, the primary active polyphenolic constituent in red wine, was assessed in terms of topical/transdermal delivery viability, given previously established benefits shown via systemic administration. Several hydrogel systems used as resveratrol vehicles were shown to be safe and effective methods for cutaneously delivering the therapeutic effects of this antioxidant.10 Since then, resveratrol has been demonstrated to penetrate the skin via topical administration, reinforcing the antioxidant system of the stratum corneum and delivering increases of antioxidants to human epidermal tissue.11
In 2014, Farris et al. showed that a proprietary topical antioxidant blend of resveratrol, baicalin, and vitamin E applied topically at night yielded statistically significant amelioration of fine lines and wrinkles, as well as skin firmness, elasticity, laxity, hyperpigmentation, radiance, and roughness over a 12-week period.12 Resveratrol has also been shown in mice to suppress the inflammatory response and improve survival from severe burns with bacterial infections.13
Hydrolyzable tannins: ellagic acid
Ellagic acid, a dimer of gallic acid, has been reported to impart anti-inflammatory, antitumor, immunomodulatory, and antifungal activities.14-16 Ortiz-Ruiz et al. have noted that while ellagic acid is used as a whitening agent, it can act as a substrate to rather than an inhibitor of tyrosinase, as it is oxidized by the enzyme to an unstable o-quinone. However, as a potent antioxidant, ellagic acid can block melanogenesis by reducing o-quinones and semiquinones.17
In a double-blind, placebo-controlled, 4-week trial to assess the effects of orally administered ellagic acid–rich pomegranate extract on the pigmentation of 13 women after UV exposure, with healthy volunteers randomly assigned to high-dose, low-dose, and control groups, luminance values decreased by 1.73% in the high-dose group and 1.35% in the low-dose group, as compared with the control group, and stains and freckles were reported to be diminished.18 A 2016 study in human dermal fibroblasts by Baek et al. suggested that ellagic acid displays antiphotoaging activity, as the polyphenol protected against UVB-induced oxidative stress potentially through an Nrf2-dependent pathway.15
Condensed tannins (Proanthocyanidins): pycnogenol
Pycnogenol has been used in an antioxidant mixture also including vitamins C and E, as well as evening primrose that when orally administered for 10 weeks to female SKH-1 hairless mice exposed three times weekly to UVB irradiation demonstrated the capacity to significantly inhibit wrinkle formation by markedly suppressing UVB-induced MMP activity while promoting collagen production.19 In a 2012 study of 112 women with mild to moderate photoaging, orally administered pycnogenol was shown to yield significant reductions in clinical grading of skin photoaging scores.20 Four years later, a review by Grether-Beck et al. suggested that oral administration of pycnogenol imparts photoprotection, diminishes hyperpigmentation, and improves skin barrier function and the stability of the extracellular matrix.21
Lignins: various woody plants
Recognized as efficient natural scavengers of reactive oxygen species, lignins are complex phenolic polymers that are abundant in nature, particularly in various tree species and agricultural products. In 2004, Dizhbite et al. isolated lignin samples from deciduous and coniferous trees to assess their capacity as natural antioxidants. Samples were assessed against the 1,1-diphenyl-2-picrylhydrazyl (DPPH) radical in homogeneous conditions, with the commercially available kraft lignin noted for displaying antibacterial activity associated with its radical-scavenging properties.22 Four years later, Ugartondo et al. studied several lignins and reported a strong antioxidant capacity at various concentrations that were innocuous to normal human cells and stable when exposed to UVA. The investigators concluded that lignins may be viable for inclusion in cosmetic and topical medical formulations.23
Conclusion
A brief survey of the polyphenolic landscape obviously cannot do the subject justice. From the dermatologic perspective, this diverse family of compounds factor into the skin care formulations becoming more prevalent in the established armamentarium, as well as the direct-to-consumer market. Given the increasing attention paid here and elsewhere to the impact of diet on the skin, the status of this dynamic class of polyphenolic compounds, which includes several antioxidants and is found in numerous plants, appears to be well deserved and warrants much more research.
Dr. Baumann is a private practice dermatologist, researcher, author and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Food Chem Toxicol. 2017 May;103:41-55.
2. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
3. J Pharm Biomed Anal. 2008 Mar 13;46(4):645-52.
4. Food Chem Toxicol. 2015 Aug;82:72-8.
5. Ann Dermatol. 2016 Dec;28(6):740-8.
6. Redox Biol. 2016 Aug;8:79-90.
7. Int J Biol Macromol. 2015 Jan;72:614-23.
8. Evid Based Complement Alternat Med. 2017;2017:5469125.
9. J Cosmet Dermatol. 2008 Mar;7(1):2-7.
10. Biol Pharm Bull. 2008 May;31(5):955-62.
11. Arch Dermatol Res. 2017 Aug;309(6):423-31.
12. J Drugs Dermatol. 2014 Dec;13(12):1467-72.
13. Inflammation. 2015;38(3):1273-80.
14. Dermatol Ther. 2012 May-Jun;25(3):252-9.
15. Korean J Physiol Pharmacol. 2016 May;20(3):269-77.
16. Phytother Res. 2015 Jul;29(7):1019-25.
17. J Dermatol Sci. 2016 May;82(2):115-22.
18. J Nutr Sci Vitaminol (Tokyo). 2006 Oct;52(5):383-8.
19. Photodermatol Photoimmunol Photomed. 2007 Oct;23(5):155-62.
20. Clin Interv Aging. 2012;7:275-86.
21. Skin Pharmacol Physiol. 2016;29(1):13-7.
22. Bioresour Technol. 2004 Dec;95(3):309-17.
23. Bioresour Technol. 2008 Sep;99(14):6683-7.

Identifying the right database
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Vanderbilt University Medical Center will be converting to the most common electronic medical record (EMR) systems used today: Epic. Until that time, Vanderbilt used a homegrown system to keep track of patient data. The “system” was actual comprised of a few separate programs that integrated data, depending on the functions being accessed and who was accessing them.

For many research projects across the hospital, including my own, we are going to be limiting ourselves to data from the time period when our homegrown EMR was functioning. This is thinking a few steps ahead, but it would be interesting to see if our model, once validated, performed similarly in a new EMR environment. Unfortunately, this is thinking a few too many steps ahead for me, as I will have graduated (hopefully) by the time the new EMR is up and running reliably enough for EMR-based research like this project.
The first step in our study was identifying the right database to use, and now the next step will be extracting the data we need. Moving forward, I am continuing to work with my mentors, Dr. Eduard Vasilevskis and Dr. Jesse Ehrenfeld closely. We resubmitted our IRB application now that we have identified how we can pull the data we need, and we identified a few specialized patient populations for whom a separate scoring tool might be useful (e.g., stroke patients). I am looking forward to learning the particulars how our dataset will be built. The potential for finding the answers to many patient-care questions probably lies in the EMR data we already have, but you need to know how to get them to study them.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Vanderbilt University Medical Center will be converting to the most common electronic medical record (EMR) systems used today: Epic. Until that time, Vanderbilt used a homegrown system to keep track of patient data. The “system” was actual comprised of a few separate programs that integrated data, depending on the functions being accessed and who was accessing them.
For many research projects across the hospital, including my own, we are going to be limiting ourselves to data from the time period when our homegrown EMR was functioning. This is thinking a few steps ahead, but it would be interesting to see if our model, once validated, performed similarly in a new EMR environment. Unfortunately, this is thinking a few too many steps ahead for me, as I will have graduated (hopefully) by the time the new EMR is up and running reliably enough for EMR-based research like this project.
The first step in our study was identifying the right database to use, and now the next step will be extracting the data we need. Moving forward, I am continuing to work with my mentors, Dr. Eduard Vasilevskis and Dr. Jesse Ehrenfeld closely. We resubmitted our IRB application now that we have identified how we can pull the data we need, and we identified a few specialized patient populations for whom a separate scoring tool might be useful (e.g., stroke patients). I am looking forward to learning the particulars how our dataset will be built. The potential for finding the answers to many patient-care questions probably lies in the EMR data we already have, but you need to know how to get them to study them.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Vanderbilt University Medical Center will be converting to the most common electronic medical record (EMR) systems used today: Epic. Until that time, Vanderbilt used a homegrown system to keep track of patient data. The “system” was actual comprised of a few separate programs that integrated data, depending on the functions being accessed and who was accessing them.
For many research projects across the hospital, including my own, we are going to be limiting ourselves to data from the time period when our homegrown EMR was functioning. This is thinking a few steps ahead, but it would be interesting to see if our model, once validated, performed similarly in a new EMR environment. Unfortunately, this is thinking a few too many steps ahead for me, as I will have graduated (hopefully) by the time the new EMR is up and running reliably enough for EMR-based research like this project.
The first step in our study was identifying the right database to use, and now the next step will be extracting the data we need. Moving forward, I am continuing to work with my mentors, Dr. Eduard Vasilevskis and Dr. Jesse Ehrenfeld closely. We resubmitted our IRB application now that we have identified how we can pull the data we need, and we identified a few specialized patient populations for whom a separate scoring tool might be useful (e.g., stroke patients). I am looking forward to learning the particulars how our dataset will be built. The potential for finding the answers to many patient-care questions probably lies in the EMR data we already have, but you need to know how to get them to study them.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Children and trauma: How Sesame Street can help
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.

When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.

In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.

No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.
When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.
In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.
No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.
When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.
In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.
No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.