User login
What's Eating You? Pubic Lice (Pthirus pubis)
A shift in referral patterns for HIV/AIDS patients
- Funding for specific training programs on HIV/AIDS care should be targeted to community health centers, where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Purpose With the rapid development (and complex prescribing patterns) of drugs for HIV/AIDS care, it is challenging for physicians to keep current. We conducted a follow-up study to a 1994 cohort study to see how care and referral patterns have changed over the last decade. In this study, we examined how family physicians in Massachusetts were caring for their HIV-infected patients, and explored whether FPs were referring more patients to specialists for care compared with a decade ago.
Methods We designed a cross-sectional survey as an 11-year follow-up to a previous study. It was mailed in 2005 to the active membership of the Massachusetts academy of Family Physicians.
Results Compared with the cohort of 1994, the number of HIV+ patients in individual practices remained about the same, but the number of practices with no AIDS patients was significantly higher. 85.3% of FPs noted that they were more likely to refer HIV/AIDS patients immediately compared with their own practice patterns a decade ago. In this study, 39.0% of current respondents referred HIV+ patients immediately, 57.0% co-managed patients, and 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
Similar changes were seen in regard to care patterns for AIDS patients. among the current cohort, 61.7% reported that they referred patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Conclusions A significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS has occurred over the last decade. The community health center has emerged as a resource for patients with HIV/AIDS. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers.
In June 2008, it will be 27 years since the first reported clusters of Pneumocystis pneumonia cases, which were the earliest published reports of the HIV epidemic.1 There are now more than a million individuals infected with HIV in the United States.2
Since the first antiretroviral drug, azidothymidine (AZT), was approved in 1987, more than a dozen medications have been introduced to treat this illness.2 Care for patients with HIV/AIDS is rapidly evolving—so much so that the International AIDS Society publishes revised treatment guidelines every 2 years.3 The US Department of Health and Human Services also issues frequent guidelines for HIV care.4
Methods
Asking FPs about their HIV/AIDS management practices
This cross-sectional survey was designed as an 11-year follow-up to a previous research study, described in greater detail elsewhere.12
In June 2005, we obtained a membership listing from the Massachusetts Academy of Family Physicians (MAFP). Using the total design methodology described by Dillman,13 a cover letter and survey instrument were mailed to current MAFP members (N=777). Nonresponders were sent a reminder postcard 2 weeks later, and a second survey 2 weeks after that. A final reminder and survey were mailed to the remaining nonrespondents a month later. No incentives were offered for the completion of the survey.
The survey instrument was developed using the original data collection tool from 1994, supplemented by questions assessing any changes in patient management over the previous 11 years. The 31-item survey included questions about the sociodemographic and practice characteristics of the respondents, their patient mix, their education, and their management of patients with HIV/AIDS, as well as a series of Likert-type attitudinal questions assessing their knowledge, access to specialists, and safety concerns regarding HIV.
Outcomes measured: Changes in care and referral patterns
The main outcomes of the survey were changes in the management of patients with HIV/AIDS, particularly regarding referral patterns compared with the previous decade. Univariate and bivariate statistics, frequency and percentile distributions, as well as means and medians, were used to characterize the physician cohort, their practice characteristics, referral patterns, and attitudes. We also examined a variety of relationships (eg, differences by gender, years of practice, and involvement in teaching), including changes from the data we collected in 1994 (using a repeated cross-sectional design approach).
Data were analyzed using SPSS for Windows, version 14 (SPSS, Inc, Chicago, Ill). Depending on the categorical or continuous nature of the data, chi-square and t-tests were used to assess significance at the .05 level. These bivariate analyses were subsequently used to select which independent variables we would include in the stepwise logistic regression analyses.
This study was reviewed by the University of Massachusetts’ Institutional Review Board for the conduct of human subject research and received an exemption from formal review.
Results
Who were the respondents?
In all, 369 completed surveys were returned, along with 44 uncompleted surveys (returned as undeliverable or with an indication that the respondent was no longer practicing), for a response rate of 53.2% (413/777) and a completion rate of 47.4% (369/777).
The respondents included an equal representation of male and female physicians. The majority practiced in non- urban settings (62.6%), and nearly one half (44.8%) had finished their residency since the first survey was sent. Half (54.9%) participated in a solo or single-specialty practice. FPs more often reported teaching medical students regularly (52.9%) than being involved in residency education (30.9%). More than a third (34.2%) reported that ≥15% of their patients participated in “high-risk” behaviors for HIV. (The definition of high-risk was left to the individual respondent.)
Compared with our earlier survey, respondents are now more likely to be female, more likely to be practicing in an urban setting, and slightly more likely to teach medical students. Current respondents also reported that they had fewer patients involved in high-risk behaviors.
The majority (63.8%) indicated that they had at least one HIV+ patient in their practice, with 39.0% also reporting at least one AIDS patient. Compared with the previous cohort studied, HIV+ patient numbers remained about the same; however, the number of practices caring for at least 1 AIDS patient was significantly lower (TABLE 1).
TABLE 1
Demographics of FPs responding (1994 vs 2005)
| SOCIODEMOGRAPHIC AND PRACTICE FACTORS | 1994 SURVEY (N=281)* N(%) | 2005 SURVEY (N=389)* N(%) | P VALUE |
|---|---|---|---|
| Gender | |||
| Male | 205 (74.0%) | 188 (50.9%) | <.0001 |
| Female | 72 (26.0%) | 181 (49.1%) | |
| Year of residency completion | |||
| After 1994 | — | 163 (44.8%) | not tested |
| 1986—1994 | 117 (44.5%) | 107 (29.4%) | |
| Before 1986 | 146 (55.5%) | 94 (25.8%) | |
| Practice location | |||
| Urban | 81 (29.0%) | 135 (37.4%) | |
| Suburban/rural | 198 (71.0%) | 226 (62.6%) | .026 |
| Practice type | |||
| Solo/single specialty | 169 (61.0%) | 200 (54.9%) | |
| Multispecialty/HMO/CHC | 90 (32.5%) | 134 (36.8%) | |
| Hospital-based clinic | 18 (6.5%) | 30 (8.2%) | .289 |
| Teach medical students regularly | |||
| Yes | 127 (45.7%) | 193 (52.9%) | |
| No | 151 (54.3%) | 172 (47.1%) | .071 |
| Teach residents regularly | |||
| Yes | 72 (25.9%) | 112 (30.9%) | |
| No | 206 (74.1%) | 251 (69.1%) | .169 |
| % of patients who engage in high-risk behavior | |||
| ≥15% | 74 (29.4%) | 123 (34.2%) | |
| 6%–14% | 75 (29.8%) | 140 (38.9%) | |
| ≤5% | 103 (40.9%) | 97 (26.9%) | .0012 |
| Number of HIV+ patients in practice | |||
| ≥3 patients | 88 (31.4%) | 89 (24.5%) | |
| 1–2 patients | 103 (36.8%) | 143 (39.3%) | |
| None | 89 (31.8%) | 132 (36.3%) | .136 |
| Number of AIDS patients in practice | |||
| ≥3 patients | 43 (15.5%) | 47 (12.9%) | |
| 1–2 patients | 95 (34.2%) | 95 (26.1%) | |
| None | 140 (50.3%) | 222 (61.0%) | .025 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Some numbers may not total to the individual cohort N because of sporadic missing data. The response rate for the 1994 survey was 60% and for the 2005 survey it was 50%. Percentages are based on the number of responders to each question, not the total number of respondents. | |||
HIV/AIDS care and changing referral patterns
When asked how referral patterns had changed over the past decade, the overwhelming majority (94.4%) reported being far less likely to manage HIV/AIDS patients alone. Just over half (56.2%) of the physicians in the current survey indicated being more likely to co-manage patients, and an impressive 85.3% noted that they were more likely to refer patients immediately compared with their own practice patterns a decade ago.
Changing care patterns for asymptomatic HIV+ patients. A total of 39.0% of current respondents referred patients immediately, 57.0% co-managed patients, while only 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
AIDS patients have similar patterns. Similar changes were seen in regard to care patterns for AIDS patients. Among the current cohort, 61.7% reported that they referred these patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Use of resources. When they were asked which resources they used to help provide care for HIV patients, 39.9% indicated an HIV clinic at the closest teaching hospital (vs 28.4% in 1994); 41.4% noted a specialist at the community hospital where they practiced (vs 52.6% in 1994); and the remainder were fairly equally distributed (in both cohort years) between a local community health center that treats HIV+ patients, a consultant requested by the patient, or an FP colleague (P=.0003).
Which FPs are likely to refer? Given the small number of respondents who manage asymptomatic HIV+ and AIDS patients alone, we focused our analyses between those who refer immediately and those who co-manage care.
Those who reported referring asymptomatic HIV+ patients immediately were less likely to have ≥3 HIV+ or ≥3 AIDS patients in their current practice. They were significantly more likely to be in a group practice and significantly less likely to work at a community health center. They also reported being less likely to teach medical students and residents (TABLE 2).
Similar findings in referral patterns were also seen in the management of symptomatic HIV+/AIDS patients (TABLE 3). In addition, those physicians who immediately refer AIDS patients were also less likely to report that >15% of their patients were involved in high-risk behaviors.
TABLE 2
Care of asymptomatic HIV+ patients—which FPs refer, which co-manage?
| REFER IMMEDIATELY (N=134)* | CO-MANAGE (N=196*) | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 24 (17.9%) | 30 (15.6%) | .001 |
| Single specialty | 58 (43.3%) | 70 (36.5%) | |
| HMO | 3 (2.2%) | 0 (0.0%) | |
| Multispecialty | 22 (16.4%) | 20 (10.4%) | |
| CHC | 14 (10.4%) | 57 (29.7%) | |
| Hospital-based clinic | 13 (9.7%) | 15 (7.8%) | |
| Teach medical students regularly | |||
| Yes | 51 (38.1%) | 118 (61.5%) | <.001 |
| No | 83 (61.9%) | 74 (38.5%) | |
| Teach residents regularly | |||
| Yes | 20 (15.0%) | 78 (40.8%) | <.001 |
| No | 113 (85.0%) | 113 (59.2%) | |
| Number of HIV+ patients in practice | |||
| <3 patients | 121 (91.0%) | 132 (68.0%) | <.001 |
| ≥3 patients | 12 (9.0%) | 62 (32.0%) | |
| Number of AIDS patients in practice | |||
| <3 patients | 128 (96.2%) | 165 (85.1%) | .001 |
| ≥3 patients | 5 (3.8%) | 29 (14.9%) | |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 44 (33.1%) | 44 (23.0%) | .133 |
| 6%—15% | 46 (34.6%) | 78 (40.8%) | |
| >15% | 43 (32.3%) | 69 (36.1%) | |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of the small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Who is caring for HIV/AIDS patients? Those FPs who reported an increase over 11 years in the number of patients with HIV/AIDS in their practices were more likely to practice in a community health center (P<.001), and were more likely to teach medical students (P=.002) and residents (P<.001). Additionally, these FPs reported a higher percentage of patients with high-risk behaviors (P=.008). These FPs were less likely to report that they didn’t have time to care for HIV/AIDS patients (P=.037). They felt more knowledgeable about HIV (P=.005) and AIDS care (P<.001), and were more likely to learn about HIV/AIDS care through formal CME (P=.001).
In contrast, those FPs with <10 HIV/AIDS patients in their practice were more likely to be in rural practices (P=.006), to have been in practice longer (mean, 14.75 vs 12.35 years; P=.042), and to teach medical students (P=.045). There were no differences noted between gender, practice arrangement, or residency education.
TABLE 3
Care of symptomatic HIV+/AIDS patients—which FPs refer, which co-manage?
| Refer IMMEDIATELY (N=134)* | CO-MANAGE (n=196)* | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 37 (17.7%) | 17 (13.7%) | <.001 |
| Single specialty | 91 (43.5%) | 42 (33.9%) | |
| HMO | 3 (1.4%) | 0 (0.0%) | |
| Multispecialty | 34 (16.3%) | 10 (8.1%) | |
| CHC | 25 (12.0%) | 46 (37.1%) | |
| Hospital-based clinic | 19 (9.1%) | 9 (7.2%) | |
| Teach medical students regularly | |||
| Yes | 92 (43.6%) | 82 (67.2%) | |
| No | 119 (56.4%) | 40 (32.8%) | <.001 |
| Teach residents regularly | |||
| Yes | 40 (19.1%) | 60 (49.2%) | |
| No | 169 (80.9%) | 62 (50.8%) | <.001 |
| Number of HIV+ patients in practice | |||
| <3 patients | 180 (86.1%) | 77 (61.6%) | |
| ≥3 patients | 29 (13.9%) | 48 (38.4%) | <.001 |
| Number of AIDS patients in practice | |||
| <3 patients | 203 (97.1%) | 93 (74.4%) | |
| ≥3 patients | 6 (2.9%) | 32 (25.6%) | <.001 |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 67 (32.1%) | 21 (17.2%) | |
| 6%—15% | 83 (39.7%) | 49 (40.2%) | |
| >15% | 59 (28.2%) | 52 (42.6%) | .004 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Multivariate analyses
To identify factors that contributed the most to the immediate referral of asymptomatic HIV+ patients, we employed a stepwise logistic regression analysis based on the results of our bivariate analyses.
FPs were less likely to refer immediately if they were female, practiced in a community health center, had a higher number of HIV patients in their practice, learned about HIV/AIDS care during residency as well as through formal CME programs, taught medical students regularly, and felt more knowledgeable about HIV/AIDS care. They were more likely to refer these patients if they reported having no time to care for HIV/AIDS patients. A similar model was observed for the referral of symptomatic AIDS patients (TABLE 4).
TABLE 4
Multivariate analyses of factors related to referring patients immediately vs co-managing
| INDEPENDENT FACTORS | IMEDIATE REFERRALS FOR ASYMPT OMATIC HIV+ PATIENTS (N=297) OR * (95% CI ) | IMEDIATE REFERRALS FOR SYMPT OMATIC HIV+/AIDS PATIENTS (N=302) OR* (95% CI ) |
|---|---|---|
| Gender | ||
| Male | 1.0 | 1.0 |
| Female | 0.505 (0.283–0.901) | 0.311 (0.168–0.576) |
| Practice location: Community health center | ||
| No | 1.0 | ns† |
| Yes | 0.402 (0.178–0.910) | |
| Number of HIV+ patients in practice | ||
| 4-level ordinal variable: | ||
| 1=None; 2=1-2; 3=3-10; 4≥10 | 0.637 (0.440–0.923) | not in model |
| Number of AIDS patients in practice | ||
| 4-level ordinal variable: | ns† | 0.514 (0.343–0.769) |
| 1=None; 2=1-2; 3=3-10; 4≥10 | ||
| Learned about HIV/AIDS care during residency | ||
| No | 1.0 | ns† |
| Yes | 0.476 (0.243–0.930) | |
| Learned about HIV/AIDS care from formal CME programs | ||
| No | 1.0 | 1.0 |
| Yes | 0.468 (0.257–0.851) | 0.375 (0.204–0.691) |
| Participate in teaching medical students regularly | ||
| No | 1.0 | 1.0 |
| Yes | 0.417 (0.238–0.732) | 0.531 (0.281–1.003) |
| Participate in teaching residents regularly | ||
| No | ns† | 1.0 |
| Yes | 0.537 (0.279–1.035) | |
| Feel knowledgeable about HIV care | ||
| No | 1.0 | 1.0 |
| Yes | 0.345 (0.187–0.638) | 0.357 (0.176–0.728) |
| Have no time in my practice to care for HIV/AIDS patients | ||
| No | 1.0 | 1.0 |
| Yes | 2.076 (1.155–3.729) | 4.306 (2.098–8.838) |
| * An OR of 1.0 reflects the referent category within each of the independent factors. | ||
| † ns = not significant in the stepwise regression model. | ||
| OR, odds ratio; CI, confidence interval; CME, continuing medical education. | ||
Discussion
Referral patterns change with demographics and new treatments
In comparing data with our survey from 1994, we found significant differences in care and referral patterns for HIV/AIDS patients.
FPs are more likely to refer, and right away. FPs are more likely to refer HIV patients immediately, compared with a decade ago; this likely results from many factors. The complexity of this disease and the rapid rate of change in management have been well documented.3
Keeping up-to-date with current practice guidelines and managing complications of treatment protocols can be time-consuming. Also, more physicians in our current survey reported having no AIDS patients in their practices compared with 1994.
The emergence of community health centers. Another interesting finding, based on the results of both our bivariate and multivariate analyses, was to see the community health center emerge as a resource for patients with HIV/AIDS. This may reflect the more urban location of community health centers and the higher prevalence of HIV/AIDS patients in those locales, an increased involvement with teaching, and an increased volume of patients with HIV/AIDS—all resulting in an increased knowledge of HIV/AIDS care. Additionally, community health centers are capable of providing a more comprehensive range of services than a traditional practice, through the support of the Federal Ryan White CARE Act. This likely plays a role in the increasing numbers of such patients being cared for in this setting.
Implications for future training of FPs. Optimal care of HIV patients requires a combination of disease-specific expertise and primary care skills and organization.14 Recent literature demonstrates that generalist physicians are able to develop condition-specific knowledge similar to those with specialty training—if they have a substantial caseload, and if they make an effort to stay current in a particular area.15 Residency training sites, particularly community health centers, will likely emerge as leaders in the training of primary care physicians to care for this disease. The ongoing expertise of faculty in these sites will be a vital aspect of this training.
Limitations of this study Our survey was limited to members of the MAFP, and may not be generalizable to other primary care providers. It also may not be generalizable to other states, given the demographics of Massachusetts and the availability of health care in a more urban environment. The availability of HIV resources and referral centers may vary from state to state.
The survey relied upon self-report and may be prone to either over- or under-reporting of current practice and recall of changes over the past decade.
Also, a higher response rate among male FPs, with females being less likely to refer patients, may have understated the relationship between gender and referral patterns for these patients.
Quality of care? it’s still a question. The quality of care provided by the subset of family physicians that are caring for their HIV/AIDS patients was not studied in this article. As this group continues to train new physicians and provide ongoing care for these patients, it will be important to measure the quality of care being provided.9,16
Will the role of the FP in HIV/AIDS care expand?
Our study demonstrates a significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS over the last decade. This overall shift likely reflects the complexity of caring for these patients.
However, as these patients have longer survival rates, primary care offices will likely be seeing more individuals with HIV disease. While these patients may be followed by specialists, the role of the primary care physician in providing care may well expand. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Acknowledgments
We gratefully acknowledge the survey implementation and data entry efforts of Denise West and the expert review by Jeff Baxter, MD.
Correspondence
Philip O. Fournier, MD, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA 01655; FournieP@ummhc.org
1. Centers for Disease Control and Prevention. Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep 1981;30:250-252.
2. Frame PT. HIV disease in primary care. Prim Care 2004;30:205-237.
3. Hammer SM, Saag MS, Schechter M, et al. Treatment for adult HIV infection 2006. Recommendations of the International AIDS Society—USA Panel. JAMA 2006;296:827-843.
4. US Department of Health and Human Services. Guidelines and Standards. Available at: www.aids.gov/treatment/guidelines/index.html. Accessed January 17, 2008.
5. Sherer RI, Stieglitz K, Narra J, et al. HIV multidisciplinary teams work: Support services improve access to and retention in HIV primary care. AIDS Care 2002;14(Suppl 1):S31-S44.
6. Kitahata MM, Van Rompaey SE, Dillingham PW, et al. Primary care delivery is associated with greater physician experience and improved survival among persons with AIDS. J Gen Intern Med 2003;18:95-103.
7. Sackoff JE, Hanna DB, Pfeiffer MR, Torian L. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New york City. Ann Intern Med 2006;145:397-406.
8. Kirchner J. Who should care for patients with HIV/AIDS? Am Fam Physician 2006;73:290-291.
9. Landon BE, Wilson IB, McInnes K, et al. Physician specialization and the quality of care for human immunodeficiency virus infection. Arch Intern Med 2005;165:1133-1139.
10. Gemson DH, Colombotos J, Elinson J, et al. Acquired immunodeficiency syndrome prevention: Knowledge, attitudes, and practices of primary care physicians. Arch Intern Med 1991;151:1102-1108.
11. Skiest DJ, Keiser P. Human immunodeficiency virus infection in patients older than 50 years: A survey of primary care physicians’ beliefs, practices, and knowledge. Arch Intern Med 1991;151:1102-1108.
12. Fournier PO, Baldor RA, Warfield ME, Frazier B. Patients with HIV/AIDS: Physicians’ knowledge, attitudes, and referral practices. J Fam Pract 1997;44:85-89.
13. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. Hoboken, NJ: John Wiley & Sons; 2000.
14. Hecht FM, Wilson IB, Wu AW, et al. Optimizing care for persons with HIV infection. Ann Intern Med 1999;131:136-143.
15. Wilson IB, Landon BE, Ding L, et al. A national study of the relationship of care site HIV specialization to early adoption of highly active antiretroviral therapy. Med Care 2005;43:12-20.
16. Wilson IB, Landon BE, Hirschhorn LR, et al. Quality of HIV care provided by nurse practitioners, physicians assistants, and physicians. Ann Intern Med 2005;143:729-736.
- Funding for specific training programs on HIV/AIDS care should be targeted to community health centers, where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Purpose With the rapid development (and complex prescribing patterns) of drugs for HIV/AIDS care, it is challenging for physicians to keep current. We conducted a follow-up study to a 1994 cohort study to see how care and referral patterns have changed over the last decade. In this study, we examined how family physicians in Massachusetts were caring for their HIV-infected patients, and explored whether FPs were referring more patients to specialists for care compared with a decade ago.
Methods We designed a cross-sectional survey as an 11-year follow-up to a previous study. It was mailed in 2005 to the active membership of the Massachusetts academy of Family Physicians.
Results Compared with the cohort of 1994, the number of HIV+ patients in individual practices remained about the same, but the number of practices with no AIDS patients was significantly higher. 85.3% of FPs noted that they were more likely to refer HIV/AIDS patients immediately compared with their own practice patterns a decade ago. In this study, 39.0% of current respondents referred HIV+ patients immediately, 57.0% co-managed patients, and 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
Similar changes were seen in regard to care patterns for AIDS patients. among the current cohort, 61.7% reported that they referred patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Conclusions A significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS has occurred over the last decade. The community health center has emerged as a resource for patients with HIV/AIDS. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers.
In June 2008, it will be 27 years since the first reported clusters of Pneumocystis pneumonia cases, which were the earliest published reports of the HIV epidemic.1 There are now more than a million individuals infected with HIV in the United States.2
Since the first antiretroviral drug, azidothymidine (AZT), was approved in 1987, more than a dozen medications have been introduced to treat this illness.2 Care for patients with HIV/AIDS is rapidly evolving—so much so that the International AIDS Society publishes revised treatment guidelines every 2 years.3 The US Department of Health and Human Services also issues frequent guidelines for HIV care.4
Methods
Asking FPs about their HIV/AIDS management practices
This cross-sectional survey was designed as an 11-year follow-up to a previous research study, described in greater detail elsewhere.12
In June 2005, we obtained a membership listing from the Massachusetts Academy of Family Physicians (MAFP). Using the total design methodology described by Dillman,13 a cover letter and survey instrument were mailed to current MAFP members (N=777). Nonresponders were sent a reminder postcard 2 weeks later, and a second survey 2 weeks after that. A final reminder and survey were mailed to the remaining nonrespondents a month later. No incentives were offered for the completion of the survey.
The survey instrument was developed using the original data collection tool from 1994, supplemented by questions assessing any changes in patient management over the previous 11 years. The 31-item survey included questions about the sociodemographic and practice characteristics of the respondents, their patient mix, their education, and their management of patients with HIV/AIDS, as well as a series of Likert-type attitudinal questions assessing their knowledge, access to specialists, and safety concerns regarding HIV.
Outcomes measured: Changes in care and referral patterns
The main outcomes of the survey were changes in the management of patients with HIV/AIDS, particularly regarding referral patterns compared with the previous decade. Univariate and bivariate statistics, frequency and percentile distributions, as well as means and medians, were used to characterize the physician cohort, their practice characteristics, referral patterns, and attitudes. We also examined a variety of relationships (eg, differences by gender, years of practice, and involvement in teaching), including changes from the data we collected in 1994 (using a repeated cross-sectional design approach).
Data were analyzed using SPSS for Windows, version 14 (SPSS, Inc, Chicago, Ill). Depending on the categorical or continuous nature of the data, chi-square and t-tests were used to assess significance at the .05 level. These bivariate analyses were subsequently used to select which independent variables we would include in the stepwise logistic regression analyses.
This study was reviewed by the University of Massachusetts’ Institutional Review Board for the conduct of human subject research and received an exemption from formal review.
Results
Who were the respondents?
In all, 369 completed surveys were returned, along with 44 uncompleted surveys (returned as undeliverable or with an indication that the respondent was no longer practicing), for a response rate of 53.2% (413/777) and a completion rate of 47.4% (369/777).
The respondents included an equal representation of male and female physicians. The majority practiced in non- urban settings (62.6%), and nearly one half (44.8%) had finished their residency since the first survey was sent. Half (54.9%) participated in a solo or single-specialty practice. FPs more often reported teaching medical students regularly (52.9%) than being involved in residency education (30.9%). More than a third (34.2%) reported that ≥15% of their patients participated in “high-risk” behaviors for HIV. (The definition of high-risk was left to the individual respondent.)
Compared with our earlier survey, respondents are now more likely to be female, more likely to be practicing in an urban setting, and slightly more likely to teach medical students. Current respondents also reported that they had fewer patients involved in high-risk behaviors.
The majority (63.8%) indicated that they had at least one HIV+ patient in their practice, with 39.0% also reporting at least one AIDS patient. Compared with the previous cohort studied, HIV+ patient numbers remained about the same; however, the number of practices caring for at least 1 AIDS patient was significantly lower (TABLE 1).
TABLE 1
Demographics of FPs responding (1994 vs 2005)
| SOCIODEMOGRAPHIC AND PRACTICE FACTORS | 1994 SURVEY (N=281)* N(%) | 2005 SURVEY (N=389)* N(%) | P VALUE |
|---|---|---|---|
| Gender | |||
| Male | 205 (74.0%) | 188 (50.9%) | <.0001 |
| Female | 72 (26.0%) | 181 (49.1%) | |
| Year of residency completion | |||
| After 1994 | — | 163 (44.8%) | not tested |
| 1986—1994 | 117 (44.5%) | 107 (29.4%) | |
| Before 1986 | 146 (55.5%) | 94 (25.8%) | |
| Practice location | |||
| Urban | 81 (29.0%) | 135 (37.4%) | |
| Suburban/rural | 198 (71.0%) | 226 (62.6%) | .026 |
| Practice type | |||
| Solo/single specialty | 169 (61.0%) | 200 (54.9%) | |
| Multispecialty/HMO/CHC | 90 (32.5%) | 134 (36.8%) | |
| Hospital-based clinic | 18 (6.5%) | 30 (8.2%) | .289 |
| Teach medical students regularly | |||
| Yes | 127 (45.7%) | 193 (52.9%) | |
| No | 151 (54.3%) | 172 (47.1%) | .071 |
| Teach residents regularly | |||
| Yes | 72 (25.9%) | 112 (30.9%) | |
| No | 206 (74.1%) | 251 (69.1%) | .169 |
| % of patients who engage in high-risk behavior | |||
| ≥15% | 74 (29.4%) | 123 (34.2%) | |
| 6%–14% | 75 (29.8%) | 140 (38.9%) | |
| ≤5% | 103 (40.9%) | 97 (26.9%) | .0012 |
| Number of HIV+ patients in practice | |||
| ≥3 patients | 88 (31.4%) | 89 (24.5%) | |
| 1–2 patients | 103 (36.8%) | 143 (39.3%) | |
| None | 89 (31.8%) | 132 (36.3%) | .136 |
| Number of AIDS patients in practice | |||
| ≥3 patients | 43 (15.5%) | 47 (12.9%) | |
| 1–2 patients | 95 (34.2%) | 95 (26.1%) | |
| None | 140 (50.3%) | 222 (61.0%) | .025 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Some numbers may not total to the individual cohort N because of sporadic missing data. The response rate for the 1994 survey was 60% and for the 2005 survey it was 50%. Percentages are based on the number of responders to each question, not the total number of respondents. | |||
HIV/AIDS care and changing referral patterns
When asked how referral patterns had changed over the past decade, the overwhelming majority (94.4%) reported being far less likely to manage HIV/AIDS patients alone. Just over half (56.2%) of the physicians in the current survey indicated being more likely to co-manage patients, and an impressive 85.3% noted that they were more likely to refer patients immediately compared with their own practice patterns a decade ago.
Changing care patterns for asymptomatic HIV+ patients. A total of 39.0% of current respondents referred patients immediately, 57.0% co-managed patients, while only 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
AIDS patients have similar patterns. Similar changes were seen in regard to care patterns for AIDS patients. Among the current cohort, 61.7% reported that they referred these patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Use of resources. When they were asked which resources they used to help provide care for HIV patients, 39.9% indicated an HIV clinic at the closest teaching hospital (vs 28.4% in 1994); 41.4% noted a specialist at the community hospital where they practiced (vs 52.6% in 1994); and the remainder were fairly equally distributed (in both cohort years) between a local community health center that treats HIV+ patients, a consultant requested by the patient, or an FP colleague (P=.0003).
Which FPs are likely to refer? Given the small number of respondents who manage asymptomatic HIV+ and AIDS patients alone, we focused our analyses between those who refer immediately and those who co-manage care.
Those who reported referring asymptomatic HIV+ patients immediately were less likely to have ≥3 HIV+ or ≥3 AIDS patients in their current practice. They were significantly more likely to be in a group practice and significantly less likely to work at a community health center. They also reported being less likely to teach medical students and residents (TABLE 2).
Similar findings in referral patterns were also seen in the management of symptomatic HIV+/AIDS patients (TABLE 3). In addition, those physicians who immediately refer AIDS patients were also less likely to report that >15% of their patients were involved in high-risk behaviors.
TABLE 2
Care of asymptomatic HIV+ patients—which FPs refer, which co-manage?
| REFER IMMEDIATELY (N=134)* | CO-MANAGE (N=196*) | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 24 (17.9%) | 30 (15.6%) | .001 |
| Single specialty | 58 (43.3%) | 70 (36.5%) | |
| HMO | 3 (2.2%) | 0 (0.0%) | |
| Multispecialty | 22 (16.4%) | 20 (10.4%) | |
| CHC | 14 (10.4%) | 57 (29.7%) | |
| Hospital-based clinic | 13 (9.7%) | 15 (7.8%) | |
| Teach medical students regularly | |||
| Yes | 51 (38.1%) | 118 (61.5%) | <.001 |
| No | 83 (61.9%) | 74 (38.5%) | |
| Teach residents regularly | |||
| Yes | 20 (15.0%) | 78 (40.8%) | <.001 |
| No | 113 (85.0%) | 113 (59.2%) | |
| Number of HIV+ patients in practice | |||
| <3 patients | 121 (91.0%) | 132 (68.0%) | <.001 |
| ≥3 patients | 12 (9.0%) | 62 (32.0%) | |
| Number of AIDS patients in practice | |||
| <3 patients | 128 (96.2%) | 165 (85.1%) | .001 |
| ≥3 patients | 5 (3.8%) | 29 (14.9%) | |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 44 (33.1%) | 44 (23.0%) | .133 |
| 6%—15% | 46 (34.6%) | 78 (40.8%) | |
| >15% | 43 (32.3%) | 69 (36.1%) | |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of the small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Who is caring for HIV/AIDS patients? Those FPs who reported an increase over 11 years in the number of patients with HIV/AIDS in their practices were more likely to practice in a community health center (P<.001), and were more likely to teach medical students (P=.002) and residents (P<.001). Additionally, these FPs reported a higher percentage of patients with high-risk behaviors (P=.008). These FPs were less likely to report that they didn’t have time to care for HIV/AIDS patients (P=.037). They felt more knowledgeable about HIV (P=.005) and AIDS care (P<.001), and were more likely to learn about HIV/AIDS care through formal CME (P=.001).
In contrast, those FPs with <10 HIV/AIDS patients in their practice were more likely to be in rural practices (P=.006), to have been in practice longer (mean, 14.75 vs 12.35 years; P=.042), and to teach medical students (P=.045). There were no differences noted between gender, practice arrangement, or residency education.
TABLE 3
Care of symptomatic HIV+/AIDS patients—which FPs refer, which co-manage?
| Refer IMMEDIATELY (N=134)* | CO-MANAGE (n=196)* | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 37 (17.7%) | 17 (13.7%) | <.001 |
| Single specialty | 91 (43.5%) | 42 (33.9%) | |
| HMO | 3 (1.4%) | 0 (0.0%) | |
| Multispecialty | 34 (16.3%) | 10 (8.1%) | |
| CHC | 25 (12.0%) | 46 (37.1%) | |
| Hospital-based clinic | 19 (9.1%) | 9 (7.2%) | |
| Teach medical students regularly | |||
| Yes | 92 (43.6%) | 82 (67.2%) | |
| No | 119 (56.4%) | 40 (32.8%) | <.001 |
| Teach residents regularly | |||
| Yes | 40 (19.1%) | 60 (49.2%) | |
| No | 169 (80.9%) | 62 (50.8%) | <.001 |
| Number of HIV+ patients in practice | |||
| <3 patients | 180 (86.1%) | 77 (61.6%) | |
| ≥3 patients | 29 (13.9%) | 48 (38.4%) | <.001 |
| Number of AIDS patients in practice | |||
| <3 patients | 203 (97.1%) | 93 (74.4%) | |
| ≥3 patients | 6 (2.9%) | 32 (25.6%) | <.001 |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 67 (32.1%) | 21 (17.2%) | |
| 6%—15% | 83 (39.7%) | 49 (40.2%) | |
| >15% | 59 (28.2%) | 52 (42.6%) | .004 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Multivariate analyses
To identify factors that contributed the most to the immediate referral of asymptomatic HIV+ patients, we employed a stepwise logistic regression analysis based on the results of our bivariate analyses.
FPs were less likely to refer immediately if they were female, practiced in a community health center, had a higher number of HIV patients in their practice, learned about HIV/AIDS care during residency as well as through formal CME programs, taught medical students regularly, and felt more knowledgeable about HIV/AIDS care. They were more likely to refer these patients if they reported having no time to care for HIV/AIDS patients. A similar model was observed for the referral of symptomatic AIDS patients (TABLE 4).
TABLE 4
Multivariate analyses of factors related to referring patients immediately vs co-managing
| INDEPENDENT FACTORS | IMEDIATE REFERRALS FOR ASYMPT OMATIC HIV+ PATIENTS (N=297) OR * (95% CI ) | IMEDIATE REFERRALS FOR SYMPT OMATIC HIV+/AIDS PATIENTS (N=302) OR* (95% CI ) |
|---|---|---|
| Gender | ||
| Male | 1.0 | 1.0 |
| Female | 0.505 (0.283–0.901) | 0.311 (0.168–0.576) |
| Practice location: Community health center | ||
| No | 1.0 | ns† |
| Yes | 0.402 (0.178–0.910) | |
| Number of HIV+ patients in practice | ||
| 4-level ordinal variable: | ||
| 1=None; 2=1-2; 3=3-10; 4≥10 | 0.637 (0.440–0.923) | not in model |
| Number of AIDS patients in practice | ||
| 4-level ordinal variable: | ns† | 0.514 (0.343–0.769) |
| 1=None; 2=1-2; 3=3-10; 4≥10 | ||
| Learned about HIV/AIDS care during residency | ||
| No | 1.0 | ns† |
| Yes | 0.476 (0.243–0.930) | |
| Learned about HIV/AIDS care from formal CME programs | ||
| No | 1.0 | 1.0 |
| Yes | 0.468 (0.257–0.851) | 0.375 (0.204–0.691) |
| Participate in teaching medical students regularly | ||
| No | 1.0 | 1.0 |
| Yes | 0.417 (0.238–0.732) | 0.531 (0.281–1.003) |
| Participate in teaching residents regularly | ||
| No | ns† | 1.0 |
| Yes | 0.537 (0.279–1.035) | |
| Feel knowledgeable about HIV care | ||
| No | 1.0 | 1.0 |
| Yes | 0.345 (0.187–0.638) | 0.357 (0.176–0.728) |
| Have no time in my practice to care for HIV/AIDS patients | ||
| No | 1.0 | 1.0 |
| Yes | 2.076 (1.155–3.729) | 4.306 (2.098–8.838) |
| * An OR of 1.0 reflects the referent category within each of the independent factors. | ||
| † ns = not significant in the stepwise regression model. | ||
| OR, odds ratio; CI, confidence interval; CME, continuing medical education. | ||
Discussion
Referral patterns change with demographics and new treatments
In comparing data with our survey from 1994, we found significant differences in care and referral patterns for HIV/AIDS patients.
FPs are more likely to refer, and right away. FPs are more likely to refer HIV patients immediately, compared with a decade ago; this likely results from many factors. The complexity of this disease and the rapid rate of change in management have been well documented.3
Keeping up-to-date with current practice guidelines and managing complications of treatment protocols can be time-consuming. Also, more physicians in our current survey reported having no AIDS patients in their practices compared with 1994.
The emergence of community health centers. Another interesting finding, based on the results of both our bivariate and multivariate analyses, was to see the community health center emerge as a resource for patients with HIV/AIDS. This may reflect the more urban location of community health centers and the higher prevalence of HIV/AIDS patients in those locales, an increased involvement with teaching, and an increased volume of patients with HIV/AIDS—all resulting in an increased knowledge of HIV/AIDS care. Additionally, community health centers are capable of providing a more comprehensive range of services than a traditional practice, through the support of the Federal Ryan White CARE Act. This likely plays a role in the increasing numbers of such patients being cared for in this setting.
Implications for future training of FPs. Optimal care of HIV patients requires a combination of disease-specific expertise and primary care skills and organization.14 Recent literature demonstrates that generalist physicians are able to develop condition-specific knowledge similar to those with specialty training—if they have a substantial caseload, and if they make an effort to stay current in a particular area.15 Residency training sites, particularly community health centers, will likely emerge as leaders in the training of primary care physicians to care for this disease. The ongoing expertise of faculty in these sites will be a vital aspect of this training.
Limitations of this study Our survey was limited to members of the MAFP, and may not be generalizable to other primary care providers. It also may not be generalizable to other states, given the demographics of Massachusetts and the availability of health care in a more urban environment. The availability of HIV resources and referral centers may vary from state to state.
The survey relied upon self-report and may be prone to either over- or under-reporting of current practice and recall of changes over the past decade.
Also, a higher response rate among male FPs, with females being less likely to refer patients, may have understated the relationship between gender and referral patterns for these patients.
Quality of care? it’s still a question. The quality of care provided by the subset of family physicians that are caring for their HIV/AIDS patients was not studied in this article. As this group continues to train new physicians and provide ongoing care for these patients, it will be important to measure the quality of care being provided.9,16
Will the role of the FP in HIV/AIDS care expand?
Our study demonstrates a significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS over the last decade. This overall shift likely reflects the complexity of caring for these patients.
However, as these patients have longer survival rates, primary care offices will likely be seeing more individuals with HIV disease. While these patients may be followed by specialists, the role of the primary care physician in providing care may well expand. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Acknowledgments
We gratefully acknowledge the survey implementation and data entry efforts of Denise West and the expert review by Jeff Baxter, MD.
Correspondence
Philip O. Fournier, MD, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA 01655; FournieP@ummhc.org
- Funding for specific training programs on HIV/AIDS care should be targeted to community health centers, where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Purpose With the rapid development (and complex prescribing patterns) of drugs for HIV/AIDS care, it is challenging for physicians to keep current. We conducted a follow-up study to a 1994 cohort study to see how care and referral patterns have changed over the last decade. In this study, we examined how family physicians in Massachusetts were caring for their HIV-infected patients, and explored whether FPs were referring more patients to specialists for care compared with a decade ago.
Methods We designed a cross-sectional survey as an 11-year follow-up to a previous study. It was mailed in 2005 to the active membership of the Massachusetts academy of Family Physicians.
Results Compared with the cohort of 1994, the number of HIV+ patients in individual practices remained about the same, but the number of practices with no AIDS patients was significantly higher. 85.3% of FPs noted that they were more likely to refer HIV/AIDS patients immediately compared with their own practice patterns a decade ago. In this study, 39.0% of current respondents referred HIV+ patients immediately, 57.0% co-managed patients, and 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
Similar changes were seen in regard to care patterns for AIDS patients. among the current cohort, 61.7% reported that they referred patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Conclusions A significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS has occurred over the last decade. The community health center has emerged as a resource for patients with HIV/AIDS. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers.
In June 2008, it will be 27 years since the first reported clusters of Pneumocystis pneumonia cases, which were the earliest published reports of the HIV epidemic.1 There are now more than a million individuals infected with HIV in the United States.2
Since the first antiretroviral drug, azidothymidine (AZT), was approved in 1987, more than a dozen medications have been introduced to treat this illness.2 Care for patients with HIV/AIDS is rapidly evolving—so much so that the International AIDS Society publishes revised treatment guidelines every 2 years.3 The US Department of Health and Human Services also issues frequent guidelines for HIV care.4
Methods
Asking FPs about their HIV/AIDS management practices
This cross-sectional survey was designed as an 11-year follow-up to a previous research study, described in greater detail elsewhere.12
In June 2005, we obtained a membership listing from the Massachusetts Academy of Family Physicians (MAFP). Using the total design methodology described by Dillman,13 a cover letter and survey instrument were mailed to current MAFP members (N=777). Nonresponders were sent a reminder postcard 2 weeks later, and a second survey 2 weeks after that. A final reminder and survey were mailed to the remaining nonrespondents a month later. No incentives were offered for the completion of the survey.
The survey instrument was developed using the original data collection tool from 1994, supplemented by questions assessing any changes in patient management over the previous 11 years. The 31-item survey included questions about the sociodemographic and practice characteristics of the respondents, their patient mix, their education, and their management of patients with HIV/AIDS, as well as a series of Likert-type attitudinal questions assessing their knowledge, access to specialists, and safety concerns regarding HIV.
Outcomes measured: Changes in care and referral patterns
The main outcomes of the survey were changes in the management of patients with HIV/AIDS, particularly regarding referral patterns compared with the previous decade. Univariate and bivariate statistics, frequency and percentile distributions, as well as means and medians, were used to characterize the physician cohort, their practice characteristics, referral patterns, and attitudes. We also examined a variety of relationships (eg, differences by gender, years of practice, and involvement in teaching), including changes from the data we collected in 1994 (using a repeated cross-sectional design approach).
Data were analyzed using SPSS for Windows, version 14 (SPSS, Inc, Chicago, Ill). Depending on the categorical or continuous nature of the data, chi-square and t-tests were used to assess significance at the .05 level. These bivariate analyses were subsequently used to select which independent variables we would include in the stepwise logistic regression analyses.
This study was reviewed by the University of Massachusetts’ Institutional Review Board for the conduct of human subject research and received an exemption from formal review.
Results
Who were the respondents?
In all, 369 completed surveys were returned, along with 44 uncompleted surveys (returned as undeliverable or with an indication that the respondent was no longer practicing), for a response rate of 53.2% (413/777) and a completion rate of 47.4% (369/777).
The respondents included an equal representation of male and female physicians. The majority practiced in non- urban settings (62.6%), and nearly one half (44.8%) had finished their residency since the first survey was sent. Half (54.9%) participated in a solo or single-specialty practice. FPs more often reported teaching medical students regularly (52.9%) than being involved in residency education (30.9%). More than a third (34.2%) reported that ≥15% of their patients participated in “high-risk” behaviors for HIV. (The definition of high-risk was left to the individual respondent.)
Compared with our earlier survey, respondents are now more likely to be female, more likely to be practicing in an urban setting, and slightly more likely to teach medical students. Current respondents also reported that they had fewer patients involved in high-risk behaviors.
The majority (63.8%) indicated that they had at least one HIV+ patient in their practice, with 39.0% also reporting at least one AIDS patient. Compared with the previous cohort studied, HIV+ patient numbers remained about the same; however, the number of practices caring for at least 1 AIDS patient was significantly lower (TABLE 1).
TABLE 1
Demographics of FPs responding (1994 vs 2005)
| SOCIODEMOGRAPHIC AND PRACTICE FACTORS | 1994 SURVEY (N=281)* N(%) | 2005 SURVEY (N=389)* N(%) | P VALUE |
|---|---|---|---|
| Gender | |||
| Male | 205 (74.0%) | 188 (50.9%) | <.0001 |
| Female | 72 (26.0%) | 181 (49.1%) | |
| Year of residency completion | |||
| After 1994 | — | 163 (44.8%) | not tested |
| 1986—1994 | 117 (44.5%) | 107 (29.4%) | |
| Before 1986 | 146 (55.5%) | 94 (25.8%) | |
| Practice location | |||
| Urban | 81 (29.0%) | 135 (37.4%) | |
| Suburban/rural | 198 (71.0%) | 226 (62.6%) | .026 |
| Practice type | |||
| Solo/single specialty | 169 (61.0%) | 200 (54.9%) | |
| Multispecialty/HMO/CHC | 90 (32.5%) | 134 (36.8%) | |
| Hospital-based clinic | 18 (6.5%) | 30 (8.2%) | .289 |
| Teach medical students regularly | |||
| Yes | 127 (45.7%) | 193 (52.9%) | |
| No | 151 (54.3%) | 172 (47.1%) | .071 |
| Teach residents regularly | |||
| Yes | 72 (25.9%) | 112 (30.9%) | |
| No | 206 (74.1%) | 251 (69.1%) | .169 |
| % of patients who engage in high-risk behavior | |||
| ≥15% | 74 (29.4%) | 123 (34.2%) | |
| 6%–14% | 75 (29.8%) | 140 (38.9%) | |
| ≤5% | 103 (40.9%) | 97 (26.9%) | .0012 |
| Number of HIV+ patients in practice | |||
| ≥3 patients | 88 (31.4%) | 89 (24.5%) | |
| 1–2 patients | 103 (36.8%) | 143 (39.3%) | |
| None | 89 (31.8%) | 132 (36.3%) | .136 |
| Number of AIDS patients in practice | |||
| ≥3 patients | 43 (15.5%) | 47 (12.9%) | |
| 1–2 patients | 95 (34.2%) | 95 (26.1%) | |
| None | 140 (50.3%) | 222 (61.0%) | .025 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Some numbers may not total to the individual cohort N because of sporadic missing data. The response rate for the 1994 survey was 60% and for the 2005 survey it was 50%. Percentages are based on the number of responders to each question, not the total number of respondents. | |||
HIV/AIDS care and changing referral patterns
When asked how referral patterns had changed over the past decade, the overwhelming majority (94.4%) reported being far less likely to manage HIV/AIDS patients alone. Just over half (56.2%) of the physicians in the current survey indicated being more likely to co-manage patients, and an impressive 85.3% noted that they were more likely to refer patients immediately compared with their own practice patterns a decade ago.
Changing care patterns for asymptomatic HIV+ patients. A total of 39.0% of current respondents referred patients immediately, 57.0% co-managed patients, while only 4.1% managed these patients alone (the data for the 1994 cohort was 7.0%, 45.8%, and 47.2%, respectively; P<.0001).
AIDS patients have similar patterns. Similar changes were seen in regard to care patterns for AIDS patients. Among the current cohort, 61.7% reported that they referred these patients immediately, compared with only 18.3% in 1994; 36.8% noted that they co-managed these patients (vs 74.3% in 1994); and only 1.5% reported that they managed these patients alone (vs 7.4% in 1994; P<.0001).
Use of resources. When they were asked which resources they used to help provide care for HIV patients, 39.9% indicated an HIV clinic at the closest teaching hospital (vs 28.4% in 1994); 41.4% noted a specialist at the community hospital where they practiced (vs 52.6% in 1994); and the remainder were fairly equally distributed (in both cohort years) between a local community health center that treats HIV+ patients, a consultant requested by the patient, or an FP colleague (P=.0003).
Which FPs are likely to refer? Given the small number of respondents who manage asymptomatic HIV+ and AIDS patients alone, we focused our analyses between those who refer immediately and those who co-manage care.
Those who reported referring asymptomatic HIV+ patients immediately were less likely to have ≥3 HIV+ or ≥3 AIDS patients in their current practice. They were significantly more likely to be in a group practice and significantly less likely to work at a community health center. They also reported being less likely to teach medical students and residents (TABLE 2).
Similar findings in referral patterns were also seen in the management of symptomatic HIV+/AIDS patients (TABLE 3). In addition, those physicians who immediately refer AIDS patients were also less likely to report that >15% of their patients were involved in high-risk behaviors.
TABLE 2
Care of asymptomatic HIV+ patients—which FPs refer, which co-manage?
| REFER IMMEDIATELY (N=134)* | CO-MANAGE (N=196*) | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 24 (17.9%) | 30 (15.6%) | .001 |
| Single specialty | 58 (43.3%) | 70 (36.5%) | |
| HMO | 3 (2.2%) | 0 (0.0%) | |
| Multispecialty | 22 (16.4%) | 20 (10.4%) | |
| CHC | 14 (10.4%) | 57 (29.7%) | |
| Hospital-based clinic | 13 (9.7%) | 15 (7.8%) | |
| Teach medical students regularly | |||
| Yes | 51 (38.1%) | 118 (61.5%) | <.001 |
| No | 83 (61.9%) | 74 (38.5%) | |
| Teach residents regularly | |||
| Yes | 20 (15.0%) | 78 (40.8%) | <.001 |
| No | 113 (85.0%) | 113 (59.2%) | |
| Number of HIV+ patients in practice | |||
| <3 patients | 121 (91.0%) | 132 (68.0%) | <.001 |
| ≥3 patients | 12 (9.0%) | 62 (32.0%) | |
| Number of AIDS patients in practice | |||
| <3 patients | 128 (96.2%) | 165 (85.1%) | .001 |
| ≥3 patients | 5 (3.8%) | 29 (14.9%) | |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 44 (33.1%) | 44 (23.0%) | .133 |
| 6%—15% | 46 (34.6%) | 78 (40.8%) | |
| >15% | 43 (32.3%) | 69 (36.1%) | |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of the small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Who is caring for HIV/AIDS patients? Those FPs who reported an increase over 11 years in the number of patients with HIV/AIDS in their practices were more likely to practice in a community health center (P<.001), and were more likely to teach medical students (P=.002) and residents (P<.001). Additionally, these FPs reported a higher percentage of patients with high-risk behaviors (P=.008). These FPs were less likely to report that they didn’t have time to care for HIV/AIDS patients (P=.037). They felt more knowledgeable about HIV (P=.005) and AIDS care (P<.001), and were more likely to learn about HIV/AIDS care through formal CME (P=.001).
In contrast, those FPs with <10 HIV/AIDS patients in their practice were more likely to be in rural practices (P=.006), to have been in practice longer (mean, 14.75 vs 12.35 years; P=.042), and to teach medical students (P=.045). There were no differences noted between gender, practice arrangement, or residency education.
TABLE 3
Care of symptomatic HIV+/AIDS patients—which FPs refer, which co-manage?
| Refer IMMEDIATELY (N=134)* | CO-MANAGE (n=196)* | P VALUE | |
|---|---|---|---|
| Practice type | |||
| Solo practice | 37 (17.7%) | 17 (13.7%) | <.001 |
| Single specialty | 91 (43.5%) | 42 (33.9%) | |
| HMO | 3 (1.4%) | 0 (0.0%) | |
| Multispecialty | 34 (16.3%) | 10 (8.1%) | |
| CHC | 25 (12.0%) | 46 (37.1%) | |
| Hospital-based clinic | 19 (9.1%) | 9 (7.2%) | |
| Teach medical students regularly | |||
| Yes | 92 (43.6%) | 82 (67.2%) | |
| No | 119 (56.4%) | 40 (32.8%) | <.001 |
| Teach residents regularly | |||
| Yes | 40 (19.1%) | 60 (49.2%) | |
| No | 169 (80.9%) | 62 (50.8%) | <.001 |
| Number of HIV+ patients in practice | |||
| <3 patients | 180 (86.1%) | 77 (61.6%) | |
| ≥3 patients | 29 (13.9%) | 48 (38.4%) | <.001 |
| Number of AIDS patients in practice | |||
| <3 patients | 203 (97.1%) | 93 (74.4%) | |
| ≥3 patients | 6 (2.9%) | 32 (25.6%) | <.001 |
| % of patients who engage in high-risk behavior | |||
| 0%—5% | 67 (32.1%) | 21 (17.2%) | |
| 6%—15% | 83 (39.7%) | 49 (40.2%) | |
| >15% | 59 (28.2%) | 52 (42.6%) | .004 |
| HMO, health maintenance organization; CHC, community health center. | |||
| * Total N=369. We removed those physicians who noted “manage alone” because of small sample size. Each item’s total may not be the total number of respondents due to unanswered questions. Percentages are based on the total number of responders to each question, not the total number of respondents. | |||
Multivariate analyses
To identify factors that contributed the most to the immediate referral of asymptomatic HIV+ patients, we employed a stepwise logistic regression analysis based on the results of our bivariate analyses.
FPs were less likely to refer immediately if they were female, practiced in a community health center, had a higher number of HIV patients in their practice, learned about HIV/AIDS care during residency as well as through formal CME programs, taught medical students regularly, and felt more knowledgeable about HIV/AIDS care. They were more likely to refer these patients if they reported having no time to care for HIV/AIDS patients. A similar model was observed for the referral of symptomatic AIDS patients (TABLE 4).
TABLE 4
Multivariate analyses of factors related to referring patients immediately vs co-managing
| INDEPENDENT FACTORS | IMEDIATE REFERRALS FOR ASYMPT OMATIC HIV+ PATIENTS (N=297) OR * (95% CI ) | IMEDIATE REFERRALS FOR SYMPT OMATIC HIV+/AIDS PATIENTS (N=302) OR* (95% CI ) |
|---|---|---|
| Gender | ||
| Male | 1.0 | 1.0 |
| Female | 0.505 (0.283–0.901) | 0.311 (0.168–0.576) |
| Practice location: Community health center | ||
| No | 1.0 | ns† |
| Yes | 0.402 (0.178–0.910) | |
| Number of HIV+ patients in practice | ||
| 4-level ordinal variable: | ||
| 1=None; 2=1-2; 3=3-10; 4≥10 | 0.637 (0.440–0.923) | not in model |
| Number of AIDS patients in practice | ||
| 4-level ordinal variable: | ns† | 0.514 (0.343–0.769) |
| 1=None; 2=1-2; 3=3-10; 4≥10 | ||
| Learned about HIV/AIDS care during residency | ||
| No | 1.0 | ns† |
| Yes | 0.476 (0.243–0.930) | |
| Learned about HIV/AIDS care from formal CME programs | ||
| No | 1.0 | 1.0 |
| Yes | 0.468 (0.257–0.851) | 0.375 (0.204–0.691) |
| Participate in teaching medical students regularly | ||
| No | 1.0 | 1.0 |
| Yes | 0.417 (0.238–0.732) | 0.531 (0.281–1.003) |
| Participate in teaching residents regularly | ||
| No | ns† | 1.0 |
| Yes | 0.537 (0.279–1.035) | |
| Feel knowledgeable about HIV care | ||
| No | 1.0 | 1.0 |
| Yes | 0.345 (0.187–0.638) | 0.357 (0.176–0.728) |
| Have no time in my practice to care for HIV/AIDS patients | ||
| No | 1.0 | 1.0 |
| Yes | 2.076 (1.155–3.729) | 4.306 (2.098–8.838) |
| * An OR of 1.0 reflects the referent category within each of the independent factors. | ||
| † ns = not significant in the stepwise regression model. | ||
| OR, odds ratio; CI, confidence interval; CME, continuing medical education. | ||
Discussion
Referral patterns change with demographics and new treatments
In comparing data with our survey from 1994, we found significant differences in care and referral patterns for HIV/AIDS patients.
FPs are more likely to refer, and right away. FPs are more likely to refer HIV patients immediately, compared with a decade ago; this likely results from many factors. The complexity of this disease and the rapid rate of change in management have been well documented.3
Keeping up-to-date with current practice guidelines and managing complications of treatment protocols can be time-consuming. Also, more physicians in our current survey reported having no AIDS patients in their practices compared with 1994.
The emergence of community health centers. Another interesting finding, based on the results of both our bivariate and multivariate analyses, was to see the community health center emerge as a resource for patients with HIV/AIDS. This may reflect the more urban location of community health centers and the higher prevalence of HIV/AIDS patients in those locales, an increased involvement with teaching, and an increased volume of patients with HIV/AIDS—all resulting in an increased knowledge of HIV/AIDS care. Additionally, community health centers are capable of providing a more comprehensive range of services than a traditional practice, through the support of the Federal Ryan White CARE Act. This likely plays a role in the increasing numbers of such patients being cared for in this setting.
Implications for future training of FPs. Optimal care of HIV patients requires a combination of disease-specific expertise and primary care skills and organization.14 Recent literature demonstrates that generalist physicians are able to develop condition-specific knowledge similar to those with specialty training—if they have a substantial caseload, and if they make an effort to stay current in a particular area.15 Residency training sites, particularly community health centers, will likely emerge as leaders in the training of primary care physicians to care for this disease. The ongoing expertise of faculty in these sites will be a vital aspect of this training.
Limitations of this study Our survey was limited to members of the MAFP, and may not be generalizable to other primary care providers. It also may not be generalizable to other states, given the demographics of Massachusetts and the availability of health care in a more urban environment. The availability of HIV resources and referral centers may vary from state to state.
The survey relied upon self-report and may be prone to either over- or under-reporting of current practice and recall of changes over the past decade.
Also, a higher response rate among male FPs, with females being less likely to refer patients, may have understated the relationship between gender and referral patterns for these patients.
Quality of care? it’s still a question. The quality of care provided by the subset of family physicians that are caring for their HIV/AIDS patients was not studied in this article. As this group continues to train new physicians and provide ongoing care for these patients, it will be important to measure the quality of care being provided.9,16
Will the role of the FP in HIV/AIDS care expand?
Our study demonstrates a significant shift amongst FPs with regard to their referral patterns for patients with HIV/AIDS over the last decade. This overall shift likely reflects the complexity of caring for these patients.
However, as these patients have longer survival rates, primary care offices will likely be seeing more individuals with HIV disease. While these patients may be followed by specialists, the role of the primary care physician in providing care may well expand. Funding for specific training programs on HIV/AIDS care should be targeted to community health centers where there is sufficient volume of HIV patients and an already demonstrated expertise amongst clinical faculty.
Acknowledgments
We gratefully acknowledge the survey implementation and data entry efforts of Denise West and the expert review by Jeff Baxter, MD.
Correspondence
Philip O. Fournier, MD, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA 01655; FournieP@ummhc.org
1. Centers for Disease Control and Prevention. Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep 1981;30:250-252.
2. Frame PT. HIV disease in primary care. Prim Care 2004;30:205-237.
3. Hammer SM, Saag MS, Schechter M, et al. Treatment for adult HIV infection 2006. Recommendations of the International AIDS Society—USA Panel. JAMA 2006;296:827-843.
4. US Department of Health and Human Services. Guidelines and Standards. Available at: www.aids.gov/treatment/guidelines/index.html. Accessed January 17, 2008.
5. Sherer RI, Stieglitz K, Narra J, et al. HIV multidisciplinary teams work: Support services improve access to and retention in HIV primary care. AIDS Care 2002;14(Suppl 1):S31-S44.
6. Kitahata MM, Van Rompaey SE, Dillingham PW, et al. Primary care delivery is associated with greater physician experience and improved survival among persons with AIDS. J Gen Intern Med 2003;18:95-103.
7. Sackoff JE, Hanna DB, Pfeiffer MR, Torian L. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New york City. Ann Intern Med 2006;145:397-406.
8. Kirchner J. Who should care for patients with HIV/AIDS? Am Fam Physician 2006;73:290-291.
9. Landon BE, Wilson IB, McInnes K, et al. Physician specialization and the quality of care for human immunodeficiency virus infection. Arch Intern Med 2005;165:1133-1139.
10. Gemson DH, Colombotos J, Elinson J, et al. Acquired immunodeficiency syndrome prevention: Knowledge, attitudes, and practices of primary care physicians. Arch Intern Med 1991;151:1102-1108.
11. Skiest DJ, Keiser P. Human immunodeficiency virus infection in patients older than 50 years: A survey of primary care physicians’ beliefs, practices, and knowledge. Arch Intern Med 1991;151:1102-1108.
12. Fournier PO, Baldor RA, Warfield ME, Frazier B. Patients with HIV/AIDS: Physicians’ knowledge, attitudes, and referral practices. J Fam Pract 1997;44:85-89.
13. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. Hoboken, NJ: John Wiley & Sons; 2000.
14. Hecht FM, Wilson IB, Wu AW, et al. Optimizing care for persons with HIV infection. Ann Intern Med 1999;131:136-143.
15. Wilson IB, Landon BE, Ding L, et al. A national study of the relationship of care site HIV specialization to early adoption of highly active antiretroviral therapy. Med Care 2005;43:12-20.
16. Wilson IB, Landon BE, Hirschhorn LR, et al. Quality of HIV care provided by nurse practitioners, physicians assistants, and physicians. Ann Intern Med 2005;143:729-736.
1. Centers for Disease Control and Prevention. Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep 1981;30:250-252.
2. Frame PT. HIV disease in primary care. Prim Care 2004;30:205-237.
3. Hammer SM, Saag MS, Schechter M, et al. Treatment for adult HIV infection 2006. Recommendations of the International AIDS Society—USA Panel. JAMA 2006;296:827-843.
4. US Department of Health and Human Services. Guidelines and Standards. Available at: www.aids.gov/treatment/guidelines/index.html. Accessed January 17, 2008.
5. Sherer RI, Stieglitz K, Narra J, et al. HIV multidisciplinary teams work: Support services improve access to and retention in HIV primary care. AIDS Care 2002;14(Suppl 1):S31-S44.
6. Kitahata MM, Van Rompaey SE, Dillingham PW, et al. Primary care delivery is associated with greater physician experience and improved survival among persons with AIDS. J Gen Intern Med 2003;18:95-103.
7. Sackoff JE, Hanna DB, Pfeiffer MR, Torian L. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New york City. Ann Intern Med 2006;145:397-406.
8. Kirchner J. Who should care for patients with HIV/AIDS? Am Fam Physician 2006;73:290-291.
9. Landon BE, Wilson IB, McInnes K, et al. Physician specialization and the quality of care for human immunodeficiency virus infection. Arch Intern Med 2005;165:1133-1139.
10. Gemson DH, Colombotos J, Elinson J, et al. Acquired immunodeficiency syndrome prevention: Knowledge, attitudes, and practices of primary care physicians. Arch Intern Med 1991;151:1102-1108.
11. Skiest DJ, Keiser P. Human immunodeficiency virus infection in patients older than 50 years: A survey of primary care physicians’ beliefs, practices, and knowledge. Arch Intern Med 1991;151:1102-1108.
12. Fournier PO, Baldor RA, Warfield ME, Frazier B. Patients with HIV/AIDS: Physicians’ knowledge, attitudes, and referral practices. J Fam Pract 1997;44:85-89.
13. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. Hoboken, NJ: John Wiley & Sons; 2000.
14. Hecht FM, Wilson IB, Wu AW, et al. Optimizing care for persons with HIV infection. Ann Intern Med 1999;131:136-143.
15. Wilson IB, Landon BE, Ding L, et al. A national study of the relationship of care site HIV specialization to early adoption of highly active antiretroviral therapy. Med Care 2005;43:12-20.
16. Wilson IB, Landon BE, Hirschhorn LR, et al. Quality of HIV care provided by nurse practitioners, physicians assistants, and physicians. Ann Intern Med 2005;143:729-736.
REIMBURSEMENT ADVISER
In the July 2007 issue of OBG Management, I wrote an article about the Medicare Physician Quality Reporting Initiative (PQRI) program, which could have earned you as much as a 1.5% bonus at the end of that year (read this article). For 2008, there are many more quality measures for which you can qualify.
For example, there are now measures for screening, such as colon cancer screening and mammography. And more:
- New measure 113 allows you to note that you documented the result of a fecal occult blood test
- If you document, at the time of a problem visit, the result of a recent mammogram, you can report measure 112
- Measures 114 and 115 relate to inquiring about a patient’s tobacco use and then advising her to quit—activities customarily performed by ObGyns.
For details on how to participate in this program (and to see how easy it is to report measures), visit the Centers for Medicare & Medicaid Services (CMS) at www.cms.hhs.gov/PQRI/35_2008PQRI-Information.asp. Download “2008 PRQI Quality Measure Specifications.”
For coding tips on managing obstetric anal sphincter injury, see this issue’s cover article
Reimbursement for repair of your surgical injury?
When the injury occurs during the surgery and is repaired at that time, Medicare does not allow the surgeon who caused the injury to bill separately for repairing it. If another physician is called in to make the repair, however, he (she) is reimbursed for the work. According to Medicare’s General Correct Coding Policies for National Correct Coding Initiative Policy Manual for Medicare Services, “When a complication described by codes defining complications arises during an operative session…a separate service for treating the complication is not to be reported.”
A return to the operating room for a complication would be reimbursed, however; report this by adding a modifier -78 to the surgical code for the complication repair (for example, 49002 [re-opening of a recent laparotomy for hemorrhage exploration]).
Most private payers allow separate billing for repair of iatrogenic injury.
In the July 2007 issue of OBG Management, I wrote an article about the Medicare Physician Quality Reporting Initiative (PQRI) program, which could have earned you as much as a 1.5% bonus at the end of that year (read this article). For 2008, there are many more quality measures for which you can qualify.
For example, there are now measures for screening, such as colon cancer screening and mammography. And more:
- New measure 113 allows you to note that you documented the result of a fecal occult blood test
- If you document, at the time of a problem visit, the result of a recent mammogram, you can report measure 112
- Measures 114 and 115 relate to inquiring about a patient’s tobacco use and then advising her to quit—activities customarily performed by ObGyns.
For details on how to participate in this program (and to see how easy it is to report measures), visit the Centers for Medicare & Medicaid Services (CMS) at www.cms.hhs.gov/PQRI/35_2008PQRI-Information.asp. Download “2008 PRQI Quality Measure Specifications.”
For coding tips on managing obstetric anal sphincter injury, see this issue’s cover article
Reimbursement for repair of your surgical injury?
When the injury occurs during the surgery and is repaired at that time, Medicare does not allow the surgeon who caused the injury to bill separately for repairing it. If another physician is called in to make the repair, however, he (she) is reimbursed for the work. According to Medicare’s General Correct Coding Policies for National Correct Coding Initiative Policy Manual for Medicare Services, “When a complication described by codes defining complications arises during an operative session…a separate service for treating the complication is not to be reported.”
A return to the operating room for a complication would be reimbursed, however; report this by adding a modifier -78 to the surgical code for the complication repair (for example, 49002 [re-opening of a recent laparotomy for hemorrhage exploration]).
Most private payers allow separate billing for repair of iatrogenic injury.
In the July 2007 issue of OBG Management, I wrote an article about the Medicare Physician Quality Reporting Initiative (PQRI) program, which could have earned you as much as a 1.5% bonus at the end of that year (read this article). For 2008, there are many more quality measures for which you can qualify.
For example, there are now measures for screening, such as colon cancer screening and mammography. And more:
- New measure 113 allows you to note that you documented the result of a fecal occult blood test
- If you document, at the time of a problem visit, the result of a recent mammogram, you can report measure 112
- Measures 114 and 115 relate to inquiring about a patient’s tobacco use and then advising her to quit—activities customarily performed by ObGyns.
For details on how to participate in this program (and to see how easy it is to report measures), visit the Centers for Medicare & Medicaid Services (CMS) at www.cms.hhs.gov/PQRI/35_2008PQRI-Information.asp. Download “2008 PRQI Quality Measure Specifications.”
For coding tips on managing obstetric anal sphincter injury, see this issue’s cover article
Reimbursement for repair of your surgical injury?
When the injury occurs during the surgery and is repaired at that time, Medicare does not allow the surgeon who caused the injury to bill separately for repairing it. If another physician is called in to make the repair, however, he (she) is reimbursed for the work. According to Medicare’s General Correct Coding Policies for National Correct Coding Initiative Policy Manual for Medicare Services, “When a complication described by codes defining complications arises during an operative session…a separate service for treating the complication is not to be reported.”
A return to the operating room for a complication would be reimbursed, however; report this by adding a modifier -78 to the surgical code for the complication repair (for example, 49002 [re-opening of a recent laparotomy for hemorrhage exploration]).
Most private payers allow separate billing for repair of iatrogenic injury.
Was the patient still suicidal?
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Tips to make documentation easier, faster, and more satisfying
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at douglas.mossman@dowdenhealth.com.
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at douglas.mossman@dowdenhealth.com.
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at douglas.mossman@dowdenhealth.com.
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
C. immitis Meningitis Can Be Elusive Diagnosis
SAN FRANCISCO – Hydrocephalus is an easy clue to potential Coccidioides immitis meningitis, but a subacute course of the disease can make it much more difficult to pin down the diagnosis, Dr. Parvin Azimi said at the annual meeting of the American Academy of Pediatrics.
She described two cases of chronic meningitis that illustrate different manifestations of C. immitis. The first patient, a 16-year-old African American boy, had a history of exposure to soil in endemic areas, the likely source of his fungal infection, said Dr. Azimi, director of infectious diseases at Children's Hospital and Research Center, Oakland, Calif. The patient presented with a 5-week history of headache, vomiting, and decreased energy, with no response to treatment with oral amoxicillin. He had a fever higher than 100° F with a stiff neck, flat affect, and lethargy.
A spinal tap showed that the cerebral spinal fluid (CSF) had a high protein level (148 mg/dL) and a low glucose level (15 mg/dL). The RBC count was 3/mcL and the WBC count was 380/mcL with 25% polymorphonuclear leukocytes (PMNs), 66% lymphocytes, and 9% monocytes. Gram stain and culture were negative for bacteria.
“Obviously, the spinal fluid findings look very much like TB,” so clinicians did a work-up for tuberculosis, she said. A purified protein derivative (PPD) skin test for tuberculosis produced no induration, although “that doesn't mean the patient doesn't have TB,” she acknowledged. Chest x-ray, cranial CT scan, and EEG were all normal.
The teenager had been traveling to Corpus Christi, Tex., where he collected insects and played with his pet tarantula and puppy during his visit. He sought help for his symptoms at a Texas hospital and was sent home to California with a diagnosis of viral meningitis.
The headaches and vomiting continued. A repeat spinal tap 3 weeks after the first one showed that the CSF protein level had increased (176 mg/dL) and the glucose level decreased (9 mg/dL). The RBC was 1/mcL and the WBC was 737/mcL with 33% PMNs, 51% lymphocytes, 15% monocytes, and 1% macrocytes.
Infectious disease consultants were called in at this point. They ordered fungal, parasitic, and acid-fast bacilli studies and started the patient on empiric therapy for presumed TB meningitis pending results of cultures. The CSF was negative for cryptococcal antigen and amebic trophozoites, ruling these out of the differential diagnosis, Dr. Azimi said. An HIV test was negative.
Finally, the CSF and sera were found to be reactive to C. immitis antibodies.
In the second case described by Dr. Azimi, a 19-month-old Filipino-Latino boy from Antioch, Calif., presented with a 6-month history of decreased activity, clinging behavior, and poor growth. In the past 6 days, he'd had lethargy, frequent falls, and difficulty walking. On physical exam, he was mildly feverish and irritable, and refused to stand or walk.
A head CT scan showed hydrocephalus “that was significant enough that it prompted surgeons to place a shunt quickly” to provide decompression, she said. Hydrocephalus is a well-known complication of Coccidioides meningitis.
The patient's CSF showed highly elevated protein (319 mg/dL) and low glucose (25 mg/dL). The RBC was 340/mcL and the WBC was 117/mcL with 65% lymphocytes and 4% PMNs, among other findings. CSF Gram stain and cultures were negative, as were a chest x-ray and PPD skin test for TB.
As in the first patient with subacute disease, this patient's CSF and sera were reactive for C. immitis antibodies.
Fewer than 1% of cases of Coccidioides infection become disseminated, but half of disseminated cases have CNS involvement, Dr. Azimi said. Oral fluconazole is the treatment of choice, continued for life. Stopping therapy risks a recurrence in 35% of cases.
{kind=link}
Fewer than 1% of cases become disseminated, but half of those cases have CNS involvement. DR. AZIMI
SAN FRANCISCO – Hydrocephalus is an easy clue to potential Coccidioides immitis meningitis, but a subacute course of the disease can make it much more difficult to pin down the diagnosis, Dr. Parvin Azimi said at the annual meeting of the American Academy of Pediatrics.
She described two cases of chronic meningitis that illustrate different manifestations of C. immitis. The first patient, a 16-year-old African American boy, had a history of exposure to soil in endemic areas, the likely source of his fungal infection, said Dr. Azimi, director of infectious diseases at Children's Hospital and Research Center, Oakland, Calif. The patient presented with a 5-week history of headache, vomiting, and decreased energy, with no response to treatment with oral amoxicillin. He had a fever higher than 100° F with a stiff neck, flat affect, and lethargy.
A spinal tap showed that the cerebral spinal fluid (CSF) had a high protein level (148 mg/dL) and a low glucose level (15 mg/dL). The RBC count was 3/mcL and the WBC count was 380/mcL with 25% polymorphonuclear leukocytes (PMNs), 66% lymphocytes, and 9% monocytes. Gram stain and culture were negative for bacteria.
“Obviously, the spinal fluid findings look very much like TB,” so clinicians did a work-up for tuberculosis, she said. A purified protein derivative (PPD) skin test for tuberculosis produced no induration, although “that doesn't mean the patient doesn't have TB,” she acknowledged. Chest x-ray, cranial CT scan, and EEG were all normal.
The teenager had been traveling to Corpus Christi, Tex., where he collected insects and played with his pet tarantula and puppy during his visit. He sought help for his symptoms at a Texas hospital and was sent home to California with a diagnosis of viral meningitis.
The headaches and vomiting continued. A repeat spinal tap 3 weeks after the first one showed that the CSF protein level had increased (176 mg/dL) and the glucose level decreased (9 mg/dL). The RBC was 1/mcL and the WBC was 737/mcL with 33% PMNs, 51% lymphocytes, 15% monocytes, and 1% macrocytes.
Infectious disease consultants were called in at this point. They ordered fungal, parasitic, and acid-fast bacilli studies and started the patient on empiric therapy for presumed TB meningitis pending results of cultures. The CSF was negative for cryptococcal antigen and amebic trophozoites, ruling these out of the differential diagnosis, Dr. Azimi said. An HIV test was negative.
Finally, the CSF and sera were found to be reactive to C. immitis antibodies.
In the second case described by Dr. Azimi, a 19-month-old Filipino-Latino boy from Antioch, Calif., presented with a 6-month history of decreased activity, clinging behavior, and poor growth. In the past 6 days, he'd had lethargy, frequent falls, and difficulty walking. On physical exam, he was mildly feverish and irritable, and refused to stand or walk.
A head CT scan showed hydrocephalus “that was significant enough that it prompted surgeons to place a shunt quickly” to provide decompression, she said. Hydrocephalus is a well-known complication of Coccidioides meningitis.
The patient's CSF showed highly elevated protein (319 mg/dL) and low glucose (25 mg/dL). The RBC was 340/mcL and the WBC was 117/mcL with 65% lymphocytes and 4% PMNs, among other findings. CSF Gram stain and cultures were negative, as were a chest x-ray and PPD skin test for TB.
As in the first patient with subacute disease, this patient's CSF and sera were reactive for C. immitis antibodies.
Fewer than 1% of cases of Coccidioides infection become disseminated, but half of disseminated cases have CNS involvement, Dr. Azimi said. Oral fluconazole is the treatment of choice, continued for life. Stopping therapy risks a recurrence in 35% of cases.
Fewer than 1% of cases become disseminated, but half of those cases have CNS involvement. DR. AZIMI
SAN FRANCISCO – Hydrocephalus is an easy clue to potential Coccidioides immitis meningitis, but a subacute course of the disease can make it much more difficult to pin down the diagnosis, Dr. Parvin Azimi said at the annual meeting of the American Academy of Pediatrics.
She described two cases of chronic meningitis that illustrate different manifestations of C. immitis. The first patient, a 16-year-old African American boy, had a history of exposure to soil in endemic areas, the likely source of his fungal infection, said Dr. Azimi, director of infectious diseases at Children's Hospital and Research Center, Oakland, Calif. The patient presented with a 5-week history of headache, vomiting, and decreased energy, with no response to treatment with oral amoxicillin. He had a fever higher than 100° F with a stiff neck, flat affect, and lethargy.
A spinal tap showed that the cerebral spinal fluid (CSF) had a high protein level (148 mg/dL) and a low glucose level (15 mg/dL). The RBC count was 3/mcL and the WBC count was 380/mcL with 25% polymorphonuclear leukocytes (PMNs), 66% lymphocytes, and 9% monocytes. Gram stain and culture were negative for bacteria.
“Obviously, the spinal fluid findings look very much like TB,” so clinicians did a work-up for tuberculosis, she said. A purified protein derivative (PPD) skin test for tuberculosis produced no induration, although “that doesn't mean the patient doesn't have TB,” she acknowledged. Chest x-ray, cranial CT scan, and EEG were all normal.
The teenager had been traveling to Corpus Christi, Tex., where he collected insects and played with his pet tarantula and puppy during his visit. He sought help for his symptoms at a Texas hospital and was sent home to California with a diagnosis of viral meningitis.
The headaches and vomiting continued. A repeat spinal tap 3 weeks after the first one showed that the CSF protein level had increased (176 mg/dL) and the glucose level decreased (9 mg/dL). The RBC was 1/mcL and the WBC was 737/mcL with 33% PMNs, 51% lymphocytes, 15% monocytes, and 1% macrocytes.
Infectious disease consultants were called in at this point. They ordered fungal, parasitic, and acid-fast bacilli studies and started the patient on empiric therapy for presumed TB meningitis pending results of cultures. The CSF was negative for cryptococcal antigen and amebic trophozoites, ruling these out of the differential diagnosis, Dr. Azimi said. An HIV test was negative.
Finally, the CSF and sera were found to be reactive to C. immitis antibodies.
In the second case described by Dr. Azimi, a 19-month-old Filipino-Latino boy from Antioch, Calif., presented with a 6-month history of decreased activity, clinging behavior, and poor growth. In the past 6 days, he'd had lethargy, frequent falls, and difficulty walking. On physical exam, he was mildly feverish and irritable, and refused to stand or walk.
A head CT scan showed hydrocephalus “that was significant enough that it prompted surgeons to place a shunt quickly” to provide decompression, she said. Hydrocephalus is a well-known complication of Coccidioides meningitis.
The patient's CSF showed highly elevated protein (319 mg/dL) and low glucose (25 mg/dL). The RBC was 340/mcL and the WBC was 117/mcL with 65% lymphocytes and 4% PMNs, among other findings. CSF Gram stain and cultures were negative, as were a chest x-ray and PPD skin test for TB.
As in the first patient with subacute disease, this patient's CSF and sera were reactive for C. immitis antibodies.
Fewer than 1% of cases of Coccidioides infection become disseminated, but half of disseminated cases have CNS involvement, Dr. Azimi said. Oral fluconazole is the treatment of choice, continued for life. Stopping therapy risks a recurrence in 35% of cases.
Fewer than 1% of cases become disseminated, but half of those cases have CNS involvement. DR. AZIMI
Docs Around the Clock

Docs Around the Clock
Our hospitalist group presently takes out-of-house call at night, but our hospital is pressuring us to move into the hospital 24/7. What should we do?
Afraid of the Dark,
Provo, Utah
Dr. Hospitalist responds: It can be a real challenge to find sufficient providers to staff the hospital nightly. But I encourage you to take this step. I believe there is a quality advantage to having hospitalists in house 24/7 versus having physicians on call at night from outside the hospital.
Hospitalized patients are no less likely to become acutely ill at night as during the day. From a quality perspective, it has never made sense to me why hospitals do not routinely have a physician in house 24/7. Many hospitals say they cannot afford to pay a physician to work in house at night because there are few opportunities to generate revenue. But in today’s environment, can you afford not to have a hospitalist in at night?
Hospitals without hospitalists in at night often encounter issues with patient throughput each morning. Nurses are waiting for physician orders, and physicians are scrambling to write admission notes on patients admitted overnight. This delays morning discharges and admissions, leading to other problems including overcrowding in the emergency department.
Hospitalized patients are now sicker than ever. Delays in evaluations can mean adverse outcomes. Just because the doctor is not in the hospital does not relieve them of any responsibility if a patient suffers an adverse outcome as a result of delay in care. Patients and payers are not only scrutinizing the care patients receive in the hospital but also paying based on performance. Can you and your hospital afford to not provide the timeliest care possible?
Right Night Solution?
Do you think it is better to have dedicated nocturnist(s) or have hospitalist staff members take turns working nights?
Sleepless in San Diego
Dr. Hospitalist responds: There are advantages and disadvantages of having a dedicated nocturnist versus having a rotation model with regular hospitalist staff members taking turns working nights in the hospital. If your hospital has different groups of nurses for days and nights, there may be an advantage to having nocturnists.
This model allows the doctors and nurses to work closely and develop a cohesive team. This would be more difficult if the doctor at night changes frequently. Using nocturnists to staff nights can also make daytime staffing easier or more difficult.
Consider this analogy. At the end of this baseball season, the New York Yankees faced the decision of whether or not to re-sign arguably the best player on the planet, Alex Rodriguez. With A-Rod’s high price tag ($30 million-plus annually), would the Yankees be better served taking this money and signing several players (because we assume no single player could match his talent)? What would happen if they signed A-Rod and he got hurt? Wouldn’t that leave a hole in the lineup the size of the Milky Way?
How different are nocturnists in today’s hospitalist workplace? Most hospitalist programs covet them. They can do things others can’t—work a large number of nights on the schedule. This means fewer or no nights for colleagues, which makes them happier. Nocturnists command a high salary, and if one leaves for your program for any reason, they leave a gaping hole in the schedule.
My advice is to hire a nocturnist but don’t rely solely on nocturnists to cover nights. Covering your night schedule with a mix of nocturnists and staff hospitalists will allow everyone to appreciate the nocturnist but won’t put you in the uncomfortable position of relying solely on nocturnists to keep your program running effectively.

Performance Anxiety
I just started working as a hospitalist. I was told that the federal government surveys patients about the care I provide in the hospital. Is this true?
Newbie in Fort Lauderdale
Dr. Hospitalist responds: I believe you are referring to the Consumer Assessment of Healthcare Providers and Systems (CAHPS) hospital survey. It is a standardized instrument designed to measure patients’ perspective of care in acute care hospitals.
Hospital participation is optional. Many hospitals survey patients about their perceptions of care after they leave the hospital. Press Ganey Associates works with hospitals nationwide to conduct the surveys. The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission encourage hospitals to incorporate the CAHPS questions into any other surveys being performed. The survey has 27 questions that cover seven topic areas:
- Communication with doctors;
- Communication with nurses;
- Hospital staff responsiveness;
- Pain management;
- Communication about medicines;
- Hospital environment; and
- Discharge information.
Three questions ask about communication with doctors:
- How often did the doctors treat you with courtesy and respect?
- How often did doctors listen carefully to you?
- How often did doctors explain things so you could understand?
The survey will produce data that not only will “allow comparison between hospitals, it will create an incentive for hospitals to improve quality of care and to increase accountability by increasing transparency.” Data collection for the initial period from October 2006 to June 2007 will be publicly reported in March 2008 on the Hospital Compare Web site: www.hospitalcompare.hhs.gov. For additional information, go to www.hcaphsonline.org. TH
Docs Around the Clock
Our hospitalist group presently takes out-of-house call at night, but our hospital is pressuring us to move into the hospital 24/7. What should we do?
Afraid of the Dark,
Provo, Utah
Dr. Hospitalist responds: It can be a real challenge to find sufficient providers to staff the hospital nightly. But I encourage you to take this step. I believe there is a quality advantage to having hospitalists in house 24/7 versus having physicians on call at night from outside the hospital.
Hospitalized patients are no less likely to become acutely ill at night as during the day. From a quality perspective, it has never made sense to me why hospitals do not routinely have a physician in house 24/7. Many hospitals say they cannot afford to pay a physician to work in house at night because there are few opportunities to generate revenue. But in today’s environment, can you afford not to have a hospitalist in at night?
Hospitals without hospitalists in at night often encounter issues with patient throughput each morning. Nurses are waiting for physician orders, and physicians are scrambling to write admission notes on patients admitted overnight. This delays morning discharges and admissions, leading to other problems including overcrowding in the emergency department.
Hospitalized patients are now sicker than ever. Delays in evaluations can mean adverse outcomes. Just because the doctor is not in the hospital does not relieve them of any responsibility if a patient suffers an adverse outcome as a result of delay in care. Patients and payers are not only scrutinizing the care patients receive in the hospital but also paying based on performance. Can you and your hospital afford to not provide the timeliest care possible?
Right Night Solution?
Do you think it is better to have dedicated nocturnist(s) or have hospitalist staff members take turns working nights?
Sleepless in San Diego
Dr. Hospitalist responds: There are advantages and disadvantages of having a dedicated nocturnist versus having a rotation model with regular hospitalist staff members taking turns working nights in the hospital. If your hospital has different groups of nurses for days and nights, there may be an advantage to having nocturnists.
This model allows the doctors and nurses to work closely and develop a cohesive team. This would be more difficult if the doctor at night changes frequently. Using nocturnists to staff nights can also make daytime staffing easier or more difficult.
Consider this analogy. At the end of this baseball season, the New York Yankees faced the decision of whether or not to re-sign arguably the best player on the planet, Alex Rodriguez. With A-Rod’s high price tag ($30 million-plus annually), would the Yankees be better served taking this money and signing several players (because we assume no single player could match his talent)? What would happen if they signed A-Rod and he got hurt? Wouldn’t that leave a hole in the lineup the size of the Milky Way?
How different are nocturnists in today’s hospitalist workplace? Most hospitalist programs covet them. They can do things others can’t—work a large number of nights on the schedule. This means fewer or no nights for colleagues, which makes them happier. Nocturnists command a high salary, and if one leaves for your program for any reason, they leave a gaping hole in the schedule.
My advice is to hire a nocturnist but don’t rely solely on nocturnists to cover nights. Covering your night schedule with a mix of nocturnists and staff hospitalists will allow everyone to appreciate the nocturnist but won’t put you in the uncomfortable position of relying solely on nocturnists to keep your program running effectively.
Performance Anxiety
I just started working as a hospitalist. I was told that the federal government surveys patients about the care I provide in the hospital. Is this true?
Newbie in Fort Lauderdale
Dr. Hospitalist responds: I believe you are referring to the Consumer Assessment of Healthcare Providers and Systems (CAHPS) hospital survey. It is a standardized instrument designed to measure patients’ perspective of care in acute care hospitals.
Hospital participation is optional. Many hospitals survey patients about their perceptions of care after they leave the hospital. Press Ganey Associates works with hospitals nationwide to conduct the surveys. The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission encourage hospitals to incorporate the CAHPS questions into any other surveys being performed. The survey has 27 questions that cover seven topic areas:
- Communication with doctors;
- Communication with nurses;
- Hospital staff responsiveness;
- Pain management;
- Communication about medicines;
- Hospital environment; and
- Discharge information.
Three questions ask about communication with doctors:
- How often did the doctors treat you with courtesy and respect?
- How often did doctors listen carefully to you?
- How often did doctors explain things so you could understand?
The survey will produce data that not only will “allow comparison between hospitals, it will create an incentive for hospitals to improve quality of care and to increase accountability by increasing transparency.” Data collection for the initial period from October 2006 to June 2007 will be publicly reported in March 2008 on the Hospital Compare Web site: www.hospitalcompare.hhs.gov. For additional information, go to www.hcaphsonline.org. TH
Docs Around the Clock
Our hospitalist group presently takes out-of-house call at night, but our hospital is pressuring us to move into the hospital 24/7. What should we do?
Afraid of the Dark,
Provo, Utah
Dr. Hospitalist responds: It can be a real challenge to find sufficient providers to staff the hospital nightly. But I encourage you to take this step. I believe there is a quality advantage to having hospitalists in house 24/7 versus having physicians on call at night from outside the hospital.
Hospitalized patients are no less likely to become acutely ill at night as during the day. From a quality perspective, it has never made sense to me why hospitals do not routinely have a physician in house 24/7. Many hospitals say they cannot afford to pay a physician to work in house at night because there are few opportunities to generate revenue. But in today’s environment, can you afford not to have a hospitalist in at night?
Hospitals without hospitalists in at night often encounter issues with patient throughput each morning. Nurses are waiting for physician orders, and physicians are scrambling to write admission notes on patients admitted overnight. This delays morning discharges and admissions, leading to other problems including overcrowding in the emergency department.
Hospitalized patients are now sicker than ever. Delays in evaluations can mean adverse outcomes. Just because the doctor is not in the hospital does not relieve them of any responsibility if a patient suffers an adverse outcome as a result of delay in care. Patients and payers are not only scrutinizing the care patients receive in the hospital but also paying based on performance. Can you and your hospital afford to not provide the timeliest care possible?
Right Night Solution?
Do you think it is better to have dedicated nocturnist(s) or have hospitalist staff members take turns working nights?
Sleepless in San Diego
Dr. Hospitalist responds: There are advantages and disadvantages of having a dedicated nocturnist versus having a rotation model with regular hospitalist staff members taking turns working nights in the hospital. If your hospital has different groups of nurses for days and nights, there may be an advantage to having nocturnists.
This model allows the doctors and nurses to work closely and develop a cohesive team. This would be more difficult if the doctor at night changes frequently. Using nocturnists to staff nights can also make daytime staffing easier or more difficult.
Consider this analogy. At the end of this baseball season, the New York Yankees faced the decision of whether or not to re-sign arguably the best player on the planet, Alex Rodriguez. With A-Rod’s high price tag ($30 million-plus annually), would the Yankees be better served taking this money and signing several players (because we assume no single player could match his talent)? What would happen if they signed A-Rod and he got hurt? Wouldn’t that leave a hole in the lineup the size of the Milky Way?
How different are nocturnists in today’s hospitalist workplace? Most hospitalist programs covet them. They can do things others can’t—work a large number of nights on the schedule. This means fewer or no nights for colleagues, which makes them happier. Nocturnists command a high salary, and if one leaves for your program for any reason, they leave a gaping hole in the schedule.
My advice is to hire a nocturnist but don’t rely solely on nocturnists to cover nights. Covering your night schedule with a mix of nocturnists and staff hospitalists will allow everyone to appreciate the nocturnist but won’t put you in the uncomfortable position of relying solely on nocturnists to keep your program running effectively.
Performance Anxiety
I just started working as a hospitalist. I was told that the federal government surveys patients about the care I provide in the hospital. Is this true?
Newbie in Fort Lauderdale
Dr. Hospitalist responds: I believe you are referring to the Consumer Assessment of Healthcare Providers and Systems (CAHPS) hospital survey. It is a standardized instrument designed to measure patients’ perspective of care in acute care hospitals.
Hospital participation is optional. Many hospitals survey patients about their perceptions of care after they leave the hospital. Press Ganey Associates works with hospitals nationwide to conduct the surveys. The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission encourage hospitals to incorporate the CAHPS questions into any other surveys being performed. The survey has 27 questions that cover seven topic areas:
- Communication with doctors;
- Communication with nurses;
- Hospital staff responsiveness;
- Pain management;
- Communication about medicines;
- Hospital environment; and
- Discharge information.
Three questions ask about communication with doctors:
- How often did the doctors treat you with courtesy and respect?
- How often did doctors listen carefully to you?
- How often did doctors explain things so you could understand?
The survey will produce data that not only will “allow comparison between hospitals, it will create an incentive for hospitals to improve quality of care and to increase accountability by increasing transparency.” Data collection for the initial period from October 2006 to June 2007 will be publicly reported in March 2008 on the Hospital Compare Web site: www.hospitalcompare.hhs.gov. For additional information, go to www.hcaphsonline.org. TH
Avoid Bottlenecks

I enjoy hearing about the value hospitalists provide our healthcare system. These stories come from peer-reviewed research, magazine articles, local newspapers, and even the occasional blog. When I talk to hospitalists from around the country, they are often eager to tell of their success and how they made it happen.
Not as often, I also hear about problems that may be a result of the hospitalist model. I think any successful practice, and our field as a whole, must remain open to the weaknesses in the hospitalist model and work continuously to address them. Issues like disruptions in care and poor communication between hospitalists and outpatient providers get a reasonable amount of attention and seem to be on most groups’ radar screens. But there are some potential problems I don’t hear discussed often, and I’m not aware of any significant research that has been published or presented to analyze them. I’ll review two such potential problems here.
ED Throughput
Are hospitalists sometimes the cause of a bottleneck in the emergency department (ED)? Hospitalist practice is nearly always credited with improving throughput at a hospital, including in the ED. But many hospitalist practices could impede throughput by delaying patients from leaving the ED when there are multiple simultaneous admissions. Consider the following scenarios:
The pre-hospitalist era: It is 7:30 p.m. and the ED has four patients ready for hand-off to an admitting doctor. There are several primary care groups at the hospital, and each has a doctor on call. Of the four patients needing admission, two go to Dr. Emerson from group A, one goes to Dr. Lake from group B, and one to Dr. Palmer from group C. Because the on-call doctor for these groups is home, he/she provides admitting orders by phone and may or may not see the patient that night. Of course, waiting until the next day to see the patient can be risky. In many cases the ED would have admitting orders on all four patients quickly, say within 30 minutes, and can send the patients up to the floor as soon as the bed is ready.
The hospitalist era: Things can happen differently when hospitalists are at this hospital. All daytime hospitalists are typically signed out to a single night hospitalist (nocturnist) at 7:30 p.m. when the ED has four patients to admit. This solo nocturnist might show up almost immediately after being notified about the admissions by the ED doctor and promptly start seeing the first of the four admissions. But it might take him/her three or four hours or more to finish admitting all four patients. By that time there are probably additional admissions waiting. The ED might end up keeping each patient much longer than in the first scenario.
The difference in these two scenarios is the availability of several doctors to admit patients simultaneously in the pre-hospitalist era. These doctors may be replaced by a single hospitalist who admits patients one at a time.
A clear benefit of the hospitalist system described in this example is that patients are seen in person by the hospitalist at the time of admission, rather than admitted over the phone by the primary care physician (PCP) and perhaps not seen in person by the PCP until the next day. Yet this may come at a cost of creating a bottleneck that didn’t exist in the pre-hospitalist era.
Think about whether this is a common problem in your practice. Several strategies might help minimize this bottleneck. The most common approach in a practice of more than about 10 hospitalists is to ensure that there is more than one hospitalist available to admit patients until 10 or 11 p.m. when admission volume typically subsides. This has led some groups to develop an evening “swing shift” from late afternoon until about 10 or 11 p.m.
Large groups may decide to dedicate one hospitalist entirely to the ED from sometime in the morning (e.g., 11 a.m.) until near midnight. This person is available to respond quickly to ED admissions and consult with ED doctors regarding management and disposition of borderline cases. While ED staff are usually thrilled to have a hospitalist for the day, that hospitalist often will need to get help from other hospitalists when several patients must be admitted at the same time. And hospitalist-patient continuity suffers because the patient will nearly always need to be handed off to a different hospitalist for follow-up visits.
Marginal Admissions
Do hospitalists increase the number of marginal or potentially avoidable admissions?
The pre-hospitalist era: The ED physician sees a patient of Dr. Bernstein’s at 1 a.m. and is having trouble deciding whether admission is the best approach. The ED doctor gets Dr. Bernstein or his on-call partner, Dr. Copeland, on the phone and learns this patient is well known to the practice and can be seen in the outpatient office early the next morning. Admission is unnecessary.
The hospitalist era: The ED physician sees the same patient at 1 a.m. Because there is a reasonable chance admission is the best approach, he decides to call the hospitalist first rather than the patient’s PCP. Neither the ED doctor nor the hospitalist knows the patient well, and they are unaware outpatient follow-up with the PCP next morning is an option. After all, most PCPs are already “booked up” and probably unable to work someone in on such short notice. And, it’s tough to be sure the PCP would have all the relevant records regarding the data gathered and decisions made during the ED visit. So the hospitalist and ED doctor agree the best approach is to admit this patient to observation status, when in the pre-hospitalist era the patient might have been safely discharged from the ED for outpatient follow-up.
I fear this is a reasonably common scenario for many hospitalist practices. And yet these marginal admissions are often discharged the next day, lowering the overall length of stay (LOS) for hospitalist patients. By admitting marginal patients, some of whom might have been safely discharged from the ED in the pre-hospitalist era, a hospitalist practice can improve its overall LOS. The hospitalists might be patting themselves on the back for such good performance on LOS by admitting patients who could be discharged.
These two problems are difficult to quantify. If you’re confident these aren’t an issue for your practice, you deserve lots of credit. But I think most practices should think carefully about both issues and work to minimize how often they occur. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
I enjoy hearing about the value hospitalists provide our healthcare system. These stories come from peer-reviewed research, magazine articles, local newspapers, and even the occasional blog. When I talk to hospitalists from around the country, they are often eager to tell of their success and how they made it happen.
Not as often, I also hear about problems that may be a result of the hospitalist model. I think any successful practice, and our field as a whole, must remain open to the weaknesses in the hospitalist model and work continuously to address them. Issues like disruptions in care and poor communication between hospitalists and outpatient providers get a reasonable amount of attention and seem to be on most groups’ radar screens. But there are some potential problems I don’t hear discussed often, and I’m not aware of any significant research that has been published or presented to analyze them. I’ll review two such potential problems here.
ED Throughput
Are hospitalists sometimes the cause of a bottleneck in the emergency department (ED)? Hospitalist practice is nearly always credited with improving throughput at a hospital, including in the ED. But many hospitalist practices could impede throughput by delaying patients from leaving the ED when there are multiple simultaneous admissions. Consider the following scenarios:
The pre-hospitalist era: It is 7:30 p.m. and the ED has four patients ready for hand-off to an admitting doctor. There are several primary care groups at the hospital, and each has a doctor on call. Of the four patients needing admission, two go to Dr. Emerson from group A, one goes to Dr. Lake from group B, and one to Dr. Palmer from group C. Because the on-call doctor for these groups is home, he/she provides admitting orders by phone and may or may not see the patient that night. Of course, waiting until the next day to see the patient can be risky. In many cases the ED would have admitting orders on all four patients quickly, say within 30 minutes, and can send the patients up to the floor as soon as the bed is ready.
The hospitalist era: Things can happen differently when hospitalists are at this hospital. All daytime hospitalists are typically signed out to a single night hospitalist (nocturnist) at 7:30 p.m. when the ED has four patients to admit. This solo nocturnist might show up almost immediately after being notified about the admissions by the ED doctor and promptly start seeing the first of the four admissions. But it might take him/her three or four hours or more to finish admitting all four patients. By that time there are probably additional admissions waiting. The ED might end up keeping each patient much longer than in the first scenario.
The difference in these two scenarios is the availability of several doctors to admit patients simultaneously in the pre-hospitalist era. These doctors may be replaced by a single hospitalist who admits patients one at a time.
A clear benefit of the hospitalist system described in this example is that patients are seen in person by the hospitalist at the time of admission, rather than admitted over the phone by the primary care physician (PCP) and perhaps not seen in person by the PCP until the next day. Yet this may come at a cost of creating a bottleneck that didn’t exist in the pre-hospitalist era.
Think about whether this is a common problem in your practice. Several strategies might help minimize this bottleneck. The most common approach in a practice of more than about 10 hospitalists is to ensure that there is more than one hospitalist available to admit patients until 10 or 11 p.m. when admission volume typically subsides. This has led some groups to develop an evening “swing shift” from late afternoon until about 10 or 11 p.m.
Large groups may decide to dedicate one hospitalist entirely to the ED from sometime in the morning (e.g., 11 a.m.) until near midnight. This person is available to respond quickly to ED admissions and consult with ED doctors regarding management and disposition of borderline cases. While ED staff are usually thrilled to have a hospitalist for the day, that hospitalist often will need to get help from other hospitalists when several patients must be admitted at the same time. And hospitalist-patient continuity suffers because the patient will nearly always need to be handed off to a different hospitalist for follow-up visits.
Marginal Admissions
Do hospitalists increase the number of marginal or potentially avoidable admissions?
The pre-hospitalist era: The ED physician sees a patient of Dr. Bernstein’s at 1 a.m. and is having trouble deciding whether admission is the best approach. The ED doctor gets Dr. Bernstein or his on-call partner, Dr. Copeland, on the phone and learns this patient is well known to the practice and can be seen in the outpatient office early the next morning. Admission is unnecessary.
The hospitalist era: The ED physician sees the same patient at 1 a.m. Because there is a reasonable chance admission is the best approach, he decides to call the hospitalist first rather than the patient’s PCP. Neither the ED doctor nor the hospitalist knows the patient well, and they are unaware outpatient follow-up with the PCP next morning is an option. After all, most PCPs are already “booked up” and probably unable to work someone in on such short notice. And, it’s tough to be sure the PCP would have all the relevant records regarding the data gathered and decisions made during the ED visit. So the hospitalist and ED doctor agree the best approach is to admit this patient to observation status, when in the pre-hospitalist era the patient might have been safely discharged from the ED for outpatient follow-up.
I fear this is a reasonably common scenario for many hospitalist practices. And yet these marginal admissions are often discharged the next day, lowering the overall length of stay (LOS) for hospitalist patients. By admitting marginal patients, some of whom might have been safely discharged from the ED in the pre-hospitalist era, a hospitalist practice can improve its overall LOS. The hospitalists might be patting themselves on the back for such good performance on LOS by admitting patients who could be discharged.
These two problems are difficult to quantify. If you’re confident these aren’t an issue for your practice, you deserve lots of credit. But I think most practices should think carefully about both issues and work to minimize how often they occur. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
I enjoy hearing about the value hospitalists provide our healthcare system. These stories come from peer-reviewed research, magazine articles, local newspapers, and even the occasional blog. When I talk to hospitalists from around the country, they are often eager to tell of their success and how they made it happen.
Not as often, I also hear about problems that may be a result of the hospitalist model. I think any successful practice, and our field as a whole, must remain open to the weaknesses in the hospitalist model and work continuously to address them. Issues like disruptions in care and poor communication between hospitalists and outpatient providers get a reasonable amount of attention and seem to be on most groups’ radar screens. But there are some potential problems I don’t hear discussed often, and I’m not aware of any significant research that has been published or presented to analyze them. I’ll review two such potential problems here.
ED Throughput
Are hospitalists sometimes the cause of a bottleneck in the emergency department (ED)? Hospitalist practice is nearly always credited with improving throughput at a hospital, including in the ED. But many hospitalist practices could impede throughput by delaying patients from leaving the ED when there are multiple simultaneous admissions. Consider the following scenarios:
The pre-hospitalist era: It is 7:30 p.m. and the ED has four patients ready for hand-off to an admitting doctor. There are several primary care groups at the hospital, and each has a doctor on call. Of the four patients needing admission, two go to Dr. Emerson from group A, one goes to Dr. Lake from group B, and one to Dr. Palmer from group C. Because the on-call doctor for these groups is home, he/she provides admitting orders by phone and may or may not see the patient that night. Of course, waiting until the next day to see the patient can be risky. In many cases the ED would have admitting orders on all four patients quickly, say within 30 minutes, and can send the patients up to the floor as soon as the bed is ready.
The hospitalist era: Things can happen differently when hospitalists are at this hospital. All daytime hospitalists are typically signed out to a single night hospitalist (nocturnist) at 7:30 p.m. when the ED has four patients to admit. This solo nocturnist might show up almost immediately after being notified about the admissions by the ED doctor and promptly start seeing the first of the four admissions. But it might take him/her three or four hours or more to finish admitting all four patients. By that time there are probably additional admissions waiting. The ED might end up keeping each patient much longer than in the first scenario.
The difference in these two scenarios is the availability of several doctors to admit patients simultaneously in the pre-hospitalist era. These doctors may be replaced by a single hospitalist who admits patients one at a time.
A clear benefit of the hospitalist system described in this example is that patients are seen in person by the hospitalist at the time of admission, rather than admitted over the phone by the primary care physician (PCP) and perhaps not seen in person by the PCP until the next day. Yet this may come at a cost of creating a bottleneck that didn’t exist in the pre-hospitalist era.
Think about whether this is a common problem in your practice. Several strategies might help minimize this bottleneck. The most common approach in a practice of more than about 10 hospitalists is to ensure that there is more than one hospitalist available to admit patients until 10 or 11 p.m. when admission volume typically subsides. This has led some groups to develop an evening “swing shift” from late afternoon until about 10 or 11 p.m.
Large groups may decide to dedicate one hospitalist entirely to the ED from sometime in the morning (e.g., 11 a.m.) until near midnight. This person is available to respond quickly to ED admissions and consult with ED doctors regarding management and disposition of borderline cases. While ED staff are usually thrilled to have a hospitalist for the day, that hospitalist often will need to get help from other hospitalists when several patients must be admitted at the same time. And hospitalist-patient continuity suffers because the patient will nearly always need to be handed off to a different hospitalist for follow-up visits.
Marginal Admissions
Do hospitalists increase the number of marginal or potentially avoidable admissions?
The pre-hospitalist era: The ED physician sees a patient of Dr. Bernstein’s at 1 a.m. and is having trouble deciding whether admission is the best approach. The ED doctor gets Dr. Bernstein or his on-call partner, Dr. Copeland, on the phone and learns this patient is well known to the practice and can be seen in the outpatient office early the next morning. Admission is unnecessary.
The hospitalist era: The ED physician sees the same patient at 1 a.m. Because there is a reasonable chance admission is the best approach, he decides to call the hospitalist first rather than the patient’s PCP. Neither the ED doctor nor the hospitalist knows the patient well, and they are unaware outpatient follow-up with the PCP next morning is an option. After all, most PCPs are already “booked up” and probably unable to work someone in on such short notice. And, it’s tough to be sure the PCP would have all the relevant records regarding the data gathered and decisions made during the ED visit. So the hospitalist and ED doctor agree the best approach is to admit this patient to observation status, when in the pre-hospitalist era the patient might have been safely discharged from the ED for outpatient follow-up.
I fear this is a reasonably common scenario for many hospitalist practices. And yet these marginal admissions are often discharged the next day, lowering the overall length of stay (LOS) for hospitalist patients. By admitting marginal patients, some of whom might have been safely discharged from the ED in the pre-hospitalist era, a hospitalist practice can improve its overall LOS. The hospitalists might be patting themselves on the back for such good performance on LOS by admitting patients who could be discharged.
These two problems are difficult to quantify. If you’re confident these aren’t an issue for your practice, you deserve lots of credit. But I think most practices should think carefully about both issues and work to minimize how often they occur. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Fight the Losing Battle

With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
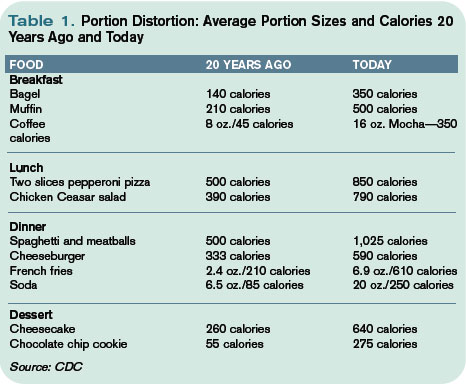
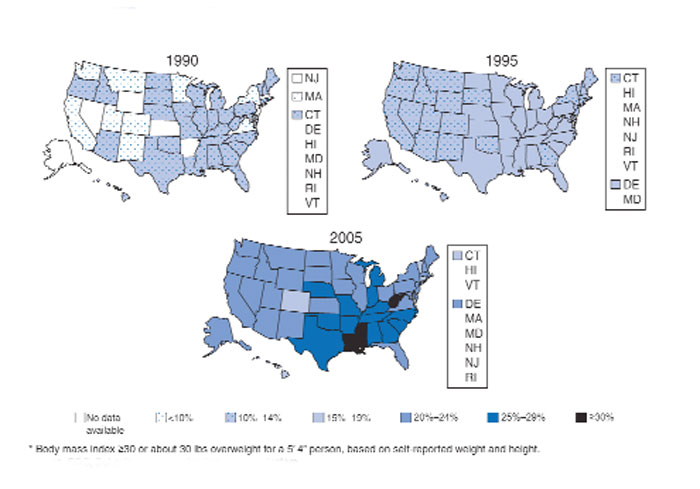
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
In The Driver’s Seat

It’s a refrain I have heard too many times in too many places: “Don’t do it.”
You have probably heard it, too—that plaintive cry from some practicing physicians trying to discourage young people from entering a career in medicine. I understand why so many doctors seem so pessimistic about medicine’s future. They’re grappling with a healthcare industry that struggles with overwhelming complexity. They face unrelenting cost pressures, misaligned incentives and policies, massive shortfalls in quality and service, fragmented systems, and disunity among peers.
I understand the pessimism, but I cannot agree with it. At the midpoint of my term as SHM president, I reflect upon the strengths that distinguish our specialty and our society from the general malaise of the broader healthcare industry. These strengths compel me to redouble my resolve to deliver on the promise of hospital medicine.
What is that promise? Hospitalists are poised to lead the way toward a better healthcare system in two critical ways. They are situated to help advance quality control and they are uniquely situated to promote medicine as a team effort, a shared vision with the hospital.
Now, quality control and teamwork are not in the standard curriculum. Medical school training focuses on disease. But in the real world of the hospital, quality control and the teamwork it takes to ensure it are vital issues. This is where hospitalists must prove themselves. This is where our special skills align with the priorities of hospital CEOs nationwide. We must advance the quality agenda and engage other physicians in a shared vision with the hospital.
These factors set us apart from other specialties and allow us to lead from the core of our strength. We lead:
- Through quality rather than narrow professional self-interests;
- While valuing the team over the individual; and
- With openness and inclusiveness to all medical personnel involved patient care, from pharmacists to nurses, to nonphysician providers, to management.
This is our great promise—but only if we exercise it. As the brilliant author and scientist Johann Wolfgang von Goethe cautioned 200 years ago: “Knowing is not enough. We must apply.”
Honesty requires physicians to admit there is sometimes a gap between what we know and what we apply. Many quality metrics measure our performance. For example, we know we must get aspirin to a heart attack victim quickly. But the clinical strides that dictate the care patients ought to get must be moved into the operational area, where optimal care is sometimes lacking.
We next need to work out the systems to ensure that care, turning best practices into routine practice. Hospitalists are in the vanguard on that front, just as other specialties have been on the cutting edge of academic medicine. Our specialty will always need to weigh in on the development and vetting of quality and safety metrics related to hospital care.
We are also poised to advance the implementation and application of systems that drive improvement in those metrics.
Ours is a young specialty—the average hospitalist is 37, the leadership 41. While we have accomplished much in our 10 years of existence, there is much more to do. Hospitalists must meet the extraordinarily high expectations of hospitals and the other physicians who work in them. We must help manage emergency patients, surgical patients, and the in-hospital patient census of primary care physicians.
But there is a shortage of physicians in our specialty because demand is so great. It’s hard to sustain our growth as a specialty and work on quality control at the same time.
We are in the financial crosshairs, as well. Administrators want to see value—that is, money saved. But the fact that we see and manage patients does not generate savings per se because insurance companies do not allow reimbursement as such for our services. “Prove your value,” they say. “Show us the money.” That translates into driving down length of stay, cutting nursing expenses, and reducing pharmacy costs though better quality control and more coordinated care.
But administrators also know that to accomplish these goals and bring other physicians on board, their best ally is the hospitalist.
Our patients demand more of us, too. In “Zen and the Art of Physician Autonomy Maintenance” in Annals of Internal Medicine in 2003, author Jim Reinertsen clearly stated the public’s perspective. “You claim that your profession is based on science … now show us that you can use all the science you know, for our benefit,” he writes. He asks us to “join together—as a profession—with our colleagues, in venues large and small to decide on and apply the best science.”
It is the least we can do as physicians. But in practice, working together to apply the best science is difficult.
All of which brings me to my final point: SHM’s commitment to our members. In October, SHM sponsored two summits, the first on healthcare quality, the second on leadership development. Two themes emerged. First, it takes an unwavering commitment to teamwork to accomplish anything of substance. Second, the educational needs of our workforce are tremendous. SHM’s focus on acquiring skills and applying knowledge are the society’s greatest accomplishment and greatest ongoing opportunity. To that end, we are working on four fronts.
First, we are developing alliances with other like-minded organizations such as the Case Management Association of America, the American Nursing Association, the American Hospital Association, and the Institute for Healthcare Improvement. Through these alliances we hope to foster the teams that will improve the monitoring of parameters of hospital care, and the care itself.
Second, we are committed to creating the tools to equip hospitalists to make the changes that will lead to improvements in the front lines of hospital medicine. We have taken several such steps. SHM has developed a discharge checklist for physicians to use before sending patients home or to other facilities. The checklist, somewhat like those used by pilots, ensures nothing is forgotten or overlooked upon discharge. We believe it will become an invaluable tool.
SHM has also added Resource Rooms to our Web site (www.hospitalmedicine.org). Here, our members can look up and download information on disease states like heart failure or venous thromboembolism.
Third, SHM is funding a group of quality-control mentors available to visit hospitals. These mentors will evaluate and advise on quality-control programs at SHM’s expense.
Finally, SHM wants to train its next generation of leaders. Quality control is a never-ending quest; it can always be better. That is what we at SHM strive for. That is what we owe our patients.
All these tools have one goal: Make quality easy. With so many other pressures of physicians and hospital staff, making it easy is also the key to making it work.
“Knowing is not enough,” Goethe said. “We must apply.” I say: “Willing is not enough. We must do.” TH
Dr. Holman is president of SHM.
It’s a refrain I have heard too many times in too many places: “Don’t do it.”
You have probably heard it, too—that plaintive cry from some practicing physicians trying to discourage young people from entering a career in medicine. I understand why so many doctors seem so pessimistic about medicine’s future. They’re grappling with a healthcare industry that struggles with overwhelming complexity. They face unrelenting cost pressures, misaligned incentives and policies, massive shortfalls in quality and service, fragmented systems, and disunity among peers.
I understand the pessimism, but I cannot agree with it. At the midpoint of my term as SHM president, I reflect upon the strengths that distinguish our specialty and our society from the general malaise of the broader healthcare industry. These strengths compel me to redouble my resolve to deliver on the promise of hospital medicine.
What is that promise? Hospitalists are poised to lead the way toward a better healthcare system in two critical ways. They are situated to help advance quality control and they are uniquely situated to promote medicine as a team effort, a shared vision with the hospital.
Now, quality control and teamwork are not in the standard curriculum. Medical school training focuses on disease. But in the real world of the hospital, quality control and the teamwork it takes to ensure it are vital issues. This is where hospitalists must prove themselves. This is where our special skills align with the priorities of hospital CEOs nationwide. We must advance the quality agenda and engage other physicians in a shared vision with the hospital.
These factors set us apart from other specialties and allow us to lead from the core of our strength. We lead:
- Through quality rather than narrow professional self-interests;
- While valuing the team over the individual; and
- With openness and inclusiveness to all medical personnel involved patient care, from pharmacists to nurses, to nonphysician providers, to management.
This is our great promise—but only if we exercise it. As the brilliant author and scientist Johann Wolfgang von Goethe cautioned 200 years ago: “Knowing is not enough. We must apply.”
Honesty requires physicians to admit there is sometimes a gap between what we know and what we apply. Many quality metrics measure our performance. For example, we know we must get aspirin to a heart attack victim quickly. But the clinical strides that dictate the care patients ought to get must be moved into the operational area, where optimal care is sometimes lacking.
We next need to work out the systems to ensure that care, turning best practices into routine practice. Hospitalists are in the vanguard on that front, just as other specialties have been on the cutting edge of academic medicine. Our specialty will always need to weigh in on the development and vetting of quality and safety metrics related to hospital care.
We are also poised to advance the implementation and application of systems that drive improvement in those metrics.
Ours is a young specialty—the average hospitalist is 37, the leadership 41. While we have accomplished much in our 10 years of existence, there is much more to do. Hospitalists must meet the extraordinarily high expectations of hospitals and the other physicians who work in them. We must help manage emergency patients, surgical patients, and the in-hospital patient census of primary care physicians.
But there is a shortage of physicians in our specialty because demand is so great. It’s hard to sustain our growth as a specialty and work on quality control at the same time.
We are in the financial crosshairs, as well. Administrators want to see value—that is, money saved. But the fact that we see and manage patients does not generate savings per se because insurance companies do not allow reimbursement as such for our services. “Prove your value,” they say. “Show us the money.” That translates into driving down length of stay, cutting nursing expenses, and reducing pharmacy costs though better quality control and more coordinated care.
But administrators also know that to accomplish these goals and bring other physicians on board, their best ally is the hospitalist.
Our patients demand more of us, too. In “Zen and the Art of Physician Autonomy Maintenance” in Annals of Internal Medicine in 2003, author Jim Reinertsen clearly stated the public’s perspective. “You claim that your profession is based on science … now show us that you can use all the science you know, for our benefit,” he writes. He asks us to “join together—as a profession—with our colleagues, in venues large and small to decide on and apply the best science.”
It is the least we can do as physicians. But in practice, working together to apply the best science is difficult.
All of which brings me to my final point: SHM’s commitment to our members. In October, SHM sponsored two summits, the first on healthcare quality, the second on leadership development. Two themes emerged. First, it takes an unwavering commitment to teamwork to accomplish anything of substance. Second, the educational needs of our workforce are tremendous. SHM’s focus on acquiring skills and applying knowledge are the society’s greatest accomplishment and greatest ongoing opportunity. To that end, we are working on four fronts.
First, we are developing alliances with other like-minded organizations such as the Case Management Association of America, the American Nursing Association, the American Hospital Association, and the Institute for Healthcare Improvement. Through these alliances we hope to foster the teams that will improve the monitoring of parameters of hospital care, and the care itself.
Second, we are committed to creating the tools to equip hospitalists to make the changes that will lead to improvements in the front lines of hospital medicine. We have taken several such steps. SHM has developed a discharge checklist for physicians to use before sending patients home or to other facilities. The checklist, somewhat like those used by pilots, ensures nothing is forgotten or overlooked upon discharge. We believe it will become an invaluable tool.
SHM has also added Resource Rooms to our Web site (www.hospitalmedicine.org). Here, our members can look up and download information on disease states like heart failure or venous thromboembolism.
Third, SHM is funding a group of quality-control mentors available to visit hospitals. These mentors will evaluate and advise on quality-control programs at SHM’s expense.
Finally, SHM wants to train its next generation of leaders. Quality control is a never-ending quest; it can always be better. That is what we at SHM strive for. That is what we owe our patients.
All these tools have one goal: Make quality easy. With so many other pressures of physicians and hospital staff, making it easy is also the key to making it work.
“Knowing is not enough,” Goethe said. “We must apply.” I say: “Willing is not enough. We must do.” TH
Dr. Holman is president of SHM.
It’s a refrain I have heard too many times in too many places: “Don’t do it.”
You have probably heard it, too—that plaintive cry from some practicing physicians trying to discourage young people from entering a career in medicine. I understand why so many doctors seem so pessimistic about medicine’s future. They’re grappling with a healthcare industry that struggles with overwhelming complexity. They face unrelenting cost pressures, misaligned incentives and policies, massive shortfalls in quality and service, fragmented systems, and disunity among peers.
I understand the pessimism, but I cannot agree with it. At the midpoint of my term as SHM president, I reflect upon the strengths that distinguish our specialty and our society from the general malaise of the broader healthcare industry. These strengths compel me to redouble my resolve to deliver on the promise of hospital medicine.
What is that promise? Hospitalists are poised to lead the way toward a better healthcare system in two critical ways. They are situated to help advance quality control and they are uniquely situated to promote medicine as a team effort, a shared vision with the hospital.
Now, quality control and teamwork are not in the standard curriculum. Medical school training focuses on disease. But in the real world of the hospital, quality control and the teamwork it takes to ensure it are vital issues. This is where hospitalists must prove themselves. This is where our special skills align with the priorities of hospital CEOs nationwide. We must advance the quality agenda and engage other physicians in a shared vision with the hospital.
These factors set us apart from other specialties and allow us to lead from the core of our strength. We lead:
- Through quality rather than narrow professional self-interests;
- While valuing the team over the individual; and
- With openness and inclusiveness to all medical personnel involved patient care, from pharmacists to nurses, to nonphysician providers, to management.
This is our great promise—but only if we exercise it. As the brilliant author and scientist Johann Wolfgang von Goethe cautioned 200 years ago: “Knowing is not enough. We must apply.”
Honesty requires physicians to admit there is sometimes a gap between what we know and what we apply. Many quality metrics measure our performance. For example, we know we must get aspirin to a heart attack victim quickly. But the clinical strides that dictate the care patients ought to get must be moved into the operational area, where optimal care is sometimes lacking.
We next need to work out the systems to ensure that care, turning best practices into routine practice. Hospitalists are in the vanguard on that front, just as other specialties have been on the cutting edge of academic medicine. Our specialty will always need to weigh in on the development and vetting of quality and safety metrics related to hospital care.
We are also poised to advance the implementation and application of systems that drive improvement in those metrics.
Ours is a young specialty—the average hospitalist is 37, the leadership 41. While we have accomplished much in our 10 years of existence, there is much more to do. Hospitalists must meet the extraordinarily high expectations of hospitals and the other physicians who work in them. We must help manage emergency patients, surgical patients, and the in-hospital patient census of primary care physicians.
But there is a shortage of physicians in our specialty because demand is so great. It’s hard to sustain our growth as a specialty and work on quality control at the same time.
We are in the financial crosshairs, as well. Administrators want to see value—that is, money saved. But the fact that we see and manage patients does not generate savings per se because insurance companies do not allow reimbursement as such for our services. “Prove your value,” they say. “Show us the money.” That translates into driving down length of stay, cutting nursing expenses, and reducing pharmacy costs though better quality control and more coordinated care.
But administrators also know that to accomplish these goals and bring other physicians on board, their best ally is the hospitalist.
Our patients demand more of us, too. In “Zen and the Art of Physician Autonomy Maintenance” in Annals of Internal Medicine in 2003, author Jim Reinertsen clearly stated the public’s perspective. “You claim that your profession is based on science … now show us that you can use all the science you know, for our benefit,” he writes. He asks us to “join together—as a profession—with our colleagues, in venues large and small to decide on and apply the best science.”
It is the least we can do as physicians. But in practice, working together to apply the best science is difficult.
All of which brings me to my final point: SHM’s commitment to our members. In October, SHM sponsored two summits, the first on healthcare quality, the second on leadership development. Two themes emerged. First, it takes an unwavering commitment to teamwork to accomplish anything of substance. Second, the educational needs of our workforce are tremendous. SHM’s focus on acquiring skills and applying knowledge are the society’s greatest accomplishment and greatest ongoing opportunity. To that end, we are working on four fronts.
First, we are developing alliances with other like-minded organizations such as the Case Management Association of America, the American Nursing Association, the American Hospital Association, and the Institute for Healthcare Improvement. Through these alliances we hope to foster the teams that will improve the monitoring of parameters of hospital care, and the care itself.
Second, we are committed to creating the tools to equip hospitalists to make the changes that will lead to improvements in the front lines of hospital medicine. We have taken several such steps. SHM has developed a discharge checklist for physicians to use before sending patients home or to other facilities. The checklist, somewhat like those used by pilots, ensures nothing is forgotten or overlooked upon discharge. We believe it will become an invaluable tool.
SHM has also added Resource Rooms to our Web site (www.hospitalmedicine.org). Here, our members can look up and download information on disease states like heart failure or venous thromboembolism.
Third, SHM is funding a group of quality-control mentors available to visit hospitals. These mentors will evaluate and advise on quality-control programs at SHM’s expense.
Finally, SHM wants to train its next generation of leaders. Quality control is a never-ending quest; it can always be better. That is what we at SHM strive for. That is what we owe our patients.
All these tools have one goal: Make quality easy. With so many other pressures of physicians and hospital staff, making it easy is also the key to making it work.
“Knowing is not enough,” Goethe said. “We must apply.” I say: “Willing is not enough. We must do.” TH
Dr. Holman is president of SHM.