User login
Renal Function Caveats
Use of increased numbers of medications and age-related decline in renal function make older patients more susceptible to adverse medication effects. Drug pharmacokinetics change, and it’s important to remember that drug metabolism is affected by a number of processes.
Renal elimination of drugs is based on nephron and renal tubule capacity, which decrease with age.1 Older individuals will not metabolize and excrete drugs as efficiently as younger, healthier individuals.
According to the Centers for Disease Control and Prevention (CDC), there are more than 36 million adults in the United States older than 65, and overall U.S. healthcare costs related to them are projected to increase 25% by 2030.2
Preventing health problems, preserving patient function, and preventing patient injury that can lead to or prolong patient hospitalizations will help contain these costs.
Quartarolo, et al., recently reported that although physicians noted the estimated glomerular filtration rate (GFR) in elderly hospitalized patients, they didn’t modify their prescribing.3 They also noted that drug dose changes in these hospitalized patients are important to prevent dosing errors and adverse reactions.
There are four major age-related pharmacokinetic parameters:
- Usually decreased gastrointestinal absorption changes ;
- Increases or decreases of a drug’s volume of distribution leading to increased blood drug levels and/or plasma-protein-binding changes;
- Usually decreased clearance with increased drug half-life effect (hepatic metabolism changes); and/or
- Decreased clearance (and increased half-life) of renally eliminated drugs.4,5
Renal Effects
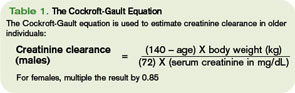
Renal excretion of drugs correlates with creatinine clearance. Because lean body mass decreases as people age, the serum creatinine level is a poor gauge of creatinine clearance in older individuals. Creatinine clearance decreases by 50% between age 25 and 85.6 The Cockroft-Gault equation is used to estimate creatinine clearance in older individuals to assist in renal dosing of drugs (See Table 1, above).
The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative defines chronic kidney disease (CKD) as:
- Kidney damage for three or more months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR, marked by either pathological abnormalities or markers of kidney damage; or
- GFR of 60 mL/min/1.73 m2 or less for three or more months, with or without kidney damage.6
In these patients, adjustment of the drug dose or dosing interval is imperative to attain optimal drug effects and patient outcomes. The same is also true for older adults with decreased renal function, whether diagnosed with CKD or not.
In addition, patients with severe renal insufficiency, including those with CKD, may encounter accumulation of active metabolites, as well as accumulation of the parent drug compound. This can lead to significant toxicity in some cases. Examples of active metabolites include:
- Normeperidine, an active metabolite of meperidine that can lead to central nervous system stimulation including seizures;
- Morphine-6-glucuronide, an active metabolite of morphine and codeine with less analgesic effect. It can lead to a prolonged narcotic effect; or
- N-acetyl-p-benzoquinoneimine, a metabolite of acetaminophen responsible for hepatotoxicity.7
Doses of renally cleared drugs should be adjusted in patients with decreased renal function. Initial dosages can be determined using published guidelines.8 TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Quartarolo JM, Thoelke M, Schafers SJ. Reporting of estimated glomerular filtration rate: effect on physician recognition of chronic kidney disease and prescribing practices for elderly hospitalized patients. J Hosp Med. 2007;2(2):74-78.
- Frye RF, Matzke GR. Drug therapy individualization for patients with renal insufficiency. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:939-952.
- Healthy Aging At-A-Glance 2007. Available at www.cdc.gov/nccdphp/publications/aag/pdf/healthy_aging.pdf. Last accessed Oct. 15, 2007.
- Hanlon JT, Ruby CM, Guay D, et al. Geriatrics. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:79-89.
- Williams CM. Using medications appropriately in older adults. Am Fam Physician. 2002;66(10):1917-1924.
- K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Available at www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_g1.htm. Last accessed Oct. 15, 2007.
- Munar MY, Singh H. Drug dosing adjustments in patients with chronic kidney disease. Am Fam Physician. 2007;75(10):1487-1496.
- Brier ME, Aronoff GR. Drug Prescribing in Renal Failure: Dosing Guidelines for adults. 5th ed. Philadelphia, Pa : American College of Physicians; 2007.
Use of increased numbers of medications and age-related decline in renal function make older patients more susceptible to adverse medication effects. Drug pharmacokinetics change, and it’s important to remember that drug metabolism is affected by a number of processes.
Renal elimination of drugs is based on nephron and renal tubule capacity, which decrease with age.1 Older individuals will not metabolize and excrete drugs as efficiently as younger, healthier individuals.
According to the Centers for Disease Control and Prevention (CDC), there are more than 36 million adults in the United States older than 65, and overall U.S. healthcare costs related to them are projected to increase 25% by 2030.2
Preventing health problems, preserving patient function, and preventing patient injury that can lead to or prolong patient hospitalizations will help contain these costs.
Quartarolo, et al., recently reported that although physicians noted the estimated glomerular filtration rate (GFR) in elderly hospitalized patients, they didn’t modify their prescribing.3 They also noted that drug dose changes in these hospitalized patients are important to prevent dosing errors and adverse reactions.
There are four major age-related pharmacokinetic parameters:
- Usually decreased gastrointestinal absorption changes ;
- Increases or decreases of a drug’s volume of distribution leading to increased blood drug levels and/or plasma-protein-binding changes;
- Usually decreased clearance with increased drug half-life effect (hepatic metabolism changes); and/or
- Decreased clearance (and increased half-life) of renally eliminated drugs.4,5
Renal Effects
Renal excretion of drugs correlates with creatinine clearance. Because lean body mass decreases as people age, the serum creatinine level is a poor gauge of creatinine clearance in older individuals. Creatinine clearance decreases by 50% between age 25 and 85.6 The Cockroft-Gault equation is used to estimate creatinine clearance in older individuals to assist in renal dosing of drugs (See Table 1, above).
The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative defines chronic kidney disease (CKD) as:
- Kidney damage for three or more months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR, marked by either pathological abnormalities or markers of kidney damage; or
- GFR of 60 mL/min/1.73 m2 or less for three or more months, with or without kidney damage.6
In these patients, adjustment of the drug dose or dosing interval is imperative to attain optimal drug effects and patient outcomes. The same is also true for older adults with decreased renal function, whether diagnosed with CKD or not.
In addition, patients with severe renal insufficiency, including those with CKD, may encounter accumulation of active metabolites, as well as accumulation of the parent drug compound. This can lead to significant toxicity in some cases. Examples of active metabolites include:
- Normeperidine, an active metabolite of meperidine that can lead to central nervous system stimulation including seizures;
- Morphine-6-glucuronide, an active metabolite of morphine and codeine with less analgesic effect. It can lead to a prolonged narcotic effect; or
- N-acetyl-p-benzoquinoneimine, a metabolite of acetaminophen responsible for hepatotoxicity.7
Doses of renally cleared drugs should be adjusted in patients with decreased renal function. Initial dosages can be determined using published guidelines.8 TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Quartarolo JM, Thoelke M, Schafers SJ. Reporting of estimated glomerular filtration rate: effect on physician recognition of chronic kidney disease and prescribing practices for elderly hospitalized patients. J Hosp Med. 2007;2(2):74-78.
- Frye RF, Matzke GR. Drug therapy individualization for patients with renal insufficiency. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:939-952.
- Healthy Aging At-A-Glance 2007. Available at www.cdc.gov/nccdphp/publications/aag/pdf/healthy_aging.pdf. Last accessed Oct. 15, 2007.
- Hanlon JT, Ruby CM, Guay D, et al. Geriatrics. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:79-89.
- Williams CM. Using medications appropriately in older adults. Am Fam Physician. 2002;66(10):1917-1924.
- K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Available at www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_g1.htm. Last accessed Oct. 15, 2007.
- Munar MY, Singh H. Drug dosing adjustments in patients with chronic kidney disease. Am Fam Physician. 2007;75(10):1487-1496.
- Brier ME, Aronoff GR. Drug Prescribing in Renal Failure: Dosing Guidelines for adults. 5th ed. Philadelphia, Pa : American College of Physicians; 2007.
Use of increased numbers of medications and age-related decline in renal function make older patients more susceptible to adverse medication effects. Drug pharmacokinetics change, and it’s important to remember that drug metabolism is affected by a number of processes.
Renal elimination of drugs is based on nephron and renal tubule capacity, which decrease with age.1 Older individuals will not metabolize and excrete drugs as efficiently as younger, healthier individuals.
According to the Centers for Disease Control and Prevention (CDC), there are more than 36 million adults in the United States older than 65, and overall U.S. healthcare costs related to them are projected to increase 25% by 2030.2
Preventing health problems, preserving patient function, and preventing patient injury that can lead to or prolong patient hospitalizations will help contain these costs.
Quartarolo, et al., recently reported that although physicians noted the estimated glomerular filtration rate (GFR) in elderly hospitalized patients, they didn’t modify their prescribing.3 They also noted that drug dose changes in these hospitalized patients are important to prevent dosing errors and adverse reactions.
There are four major age-related pharmacokinetic parameters:
- Usually decreased gastrointestinal absorption changes ;
- Increases or decreases of a drug’s volume of distribution leading to increased blood drug levels and/or plasma-protein-binding changes;
- Usually decreased clearance with increased drug half-life effect (hepatic metabolism changes); and/or
- Decreased clearance (and increased half-life) of renally eliminated drugs.4,5
Renal Effects
Renal excretion of drugs correlates with creatinine clearance. Because lean body mass decreases as people age, the serum creatinine level is a poor gauge of creatinine clearance in older individuals. Creatinine clearance decreases by 50% between age 25 and 85.6 The Cockroft-Gault equation is used to estimate creatinine clearance in older individuals to assist in renal dosing of drugs (See Table 1, above).
The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative defines chronic kidney disease (CKD) as:
- Kidney damage for three or more months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR, marked by either pathological abnormalities or markers of kidney damage; or
- GFR of 60 mL/min/1.73 m2 or less for three or more months, with or without kidney damage.6
In these patients, adjustment of the drug dose or dosing interval is imperative to attain optimal drug effects and patient outcomes. The same is also true for older adults with decreased renal function, whether diagnosed with CKD or not.
In addition, patients with severe renal insufficiency, including those with CKD, may encounter accumulation of active metabolites, as well as accumulation of the parent drug compound. This can lead to significant toxicity in some cases. Examples of active metabolites include:
- Normeperidine, an active metabolite of meperidine that can lead to central nervous system stimulation including seizures;
- Morphine-6-glucuronide, an active metabolite of morphine and codeine with less analgesic effect. It can lead to a prolonged narcotic effect; or
- N-acetyl-p-benzoquinoneimine, a metabolite of acetaminophen responsible for hepatotoxicity.7
Doses of renally cleared drugs should be adjusted in patients with decreased renal function. Initial dosages can be determined using published guidelines.8 TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Quartarolo JM, Thoelke M, Schafers SJ. Reporting of estimated glomerular filtration rate: effect on physician recognition of chronic kidney disease and prescribing practices for elderly hospitalized patients. J Hosp Med. 2007;2(2):74-78.
- Frye RF, Matzke GR. Drug therapy individualization for patients with renal insufficiency. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:939-952.
- Healthy Aging At-A-Glance 2007. Available at www.cdc.gov/nccdphp/publications/aag/pdf/healthy_aging.pdf. Last accessed Oct. 15, 2007.
- Hanlon JT, Ruby CM, Guay D, et al. Geriatrics. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002:79-89.
- Williams CM. Using medications appropriately in older adults. Am Fam Physician. 2002;66(10):1917-1924.
- K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Available at www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_g1.htm. Last accessed Oct. 15, 2007.
- Munar MY, Singh H. Drug dosing adjustments in patients with chronic kidney disease. Am Fam Physician. 2007;75(10):1487-1496.
- Brier ME, Aronoff GR. Drug Prescribing in Renal Failure: Dosing Guidelines for adults. 5th ed. Philadelphia, Pa : American College of Physicians; 2007.
Nutrition Mission
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
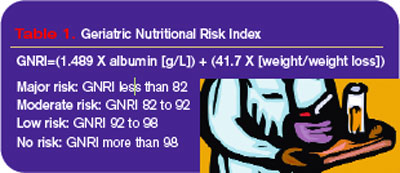
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.
In the Literature
In This Edition
- Treat with antibiotics for seven days or less in adults with community-acquired pneumonia.
- In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux (Arixtra) is safer than with enoxaparin (Lovenox).
- Multislice coronary angiography rules out suspected coronary artery disease.
- Hospitalists in teaching hospitals decrease length of stay in complex patients.
- Epoetin alfa (Procrit/Epogen) use in critically ill patients does not reduce red-cell transfusion but may reduce mortality in trauma.
- Newer antibiotics appear to be more effective for acute exacerbations of chronic bronchitis.
- Low-income patients and patients seen by specialists are less likely to use generic medications.
- Hospitalist-orthopedic comanagement of patients with hip fractures does not negatively affect long-term mortality.
- Probiotics reduce antibiotic and C. difficile-associated diarrhea.
- Healthcare-associated pneumonia closely resembles nosocomial pneumonia.
What Is the Appropriate Duration of Antibiotic Therapy for Adults with CAP?
Background: Community-acquired pneumonia (CAP) is a leading cause of morbidity and mortality, but there is little consensus on the appropriate duration of antibiotic therapy. Current guidelines recommend antibiotic regimens lasting from five to 14 days. Shorter courses of antibiotic therapy may improve patient compliance, reduce risk of medication related adverse effects, and minimize the risk of antimicrobial resistance.
Study design: Meta-analysis.
Synopsis: Authors included 15 randomized controlled trials from 1990 through 2004. They compared the efficacy of short-course (seven days or less) antibiotic monotherapy versus extended regimens (longer than seven days) in patients age 12 or older with mild to moderate CAP. They excluded trials with a significant number of patients with bronchitis, healthcare-associated pneumonias, and chronic obstructive pulmonary disease exacerbations. The primary outcome measure failed to achieve clinical improvement or cure. Secondary outcome measures included mortality, bacteriologic failure, and other adverse events.
The authors found no significant differences in the risk of clinical failure, risk of mortality, risk of bacteriologic failure, or risk of adverse events in the short-course versus extended-course antibiotic regimens. This was consistent among the four antibiotic classes in the study: beta-lactam, fluoroquinolone, ketolide, and macrolide.
Bottom line: This study found no differences between short-course and extended-course antibiotic regimens in the treatment of adults with mild to moderate CAP in regard to clinical success, mortality, bacteriologic success, and adverse events.
Citation: Li JZ, Winston LG, Moore DH, et al. Efficacy of short-course antibiotic regimens for CAP: A meta-analysis. Am J Med. 2007;120(9):783-790.
Is Fondaparinux Superior to Enoxaparin in Non-ST-Elevation Acute Coronary Syndromes?
Background: Fondaparinux is a selective factor Xa inhibitor approved by the FDA for the treatment and prevention of venous thromboembolism. The Organization to Assess Strategies for Ischemic Syndromes (OASIS)-5 was a randomized, double-blind trial that demonstrated fondaparinux is similar to enoxaparin in reducing the risk of ischemic events, but substantially reduces major bleeding, long-term mortality, and morbidity.1
Study design: Subgroup analysis of a randomized, controlled trial.
Setting: Hospitals to which patients with non-ST-segment elevation acute coronary syndrome presented.
Synopsis: In a subgroup analysis of 19,979 in the OASIS-5 trial, patients were divided into quartiles based on their estimated creatinine clearance, calculated by using the Modification of Diet in Renal Disease formula.2 Death, myocardial infarction, refractory ischemia, and major bleeding were evaluated separately, and as a composite end point at nine, 30, and 180 days.
At nine days, death, myocardial infarction, or refractory ischemia occurred in 6.7% of patients receiving fondaparinux and 7.4% of those receiving enoxaparin (hazard ratio, 0.90, 95% confidence interval [CI], 0.73 to 1.11); major bleeding occurred in 2.8% and 6.4%, respectively (hazard ratio, 0.42, CI, 0.32 to 0.56). Statistically significant differences in major bleeding persisted at 30 and 180 days.
While there was a trend toward a reduction in the composite end point among all quartiles of glomerular filtration rate (GFR), the differences were statistically significant only among patients with a GFR less than 58 mL/min per 1.73 m2. The authors concluded that the absolute differences in favor of fondaparinux (efficacy and safety) were most apparent in patients with a GFR less than 58 mL/min per 1.73 m2 and were largely the result in a reduction in bleeding events.
The subgroup analysis was not planned before the OASIS-5 data were collected, and the results have not been confirmed elsewhere. For patients managed with an early invasive strategy, catheter thrombosis occurred more often in those who received fondaparinux than enoxaparin alone. Fondaparinux is not FDA approved for this indication.
Bottom line: In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux is associated with a significant reduction in the incidence of major bleeding as compared with enoxaparin.
Citations:
- Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354(14):1464-1476.
- Fox KA, Bassand JP, Mehta SR, et al. Influence of renal function on the efficacy and safety of fondaparinux relative to enoxaparin in non ST-segment elevation acute coronary syndromes. Ann Intern Med. 2007;147(5):304-310.
What’s the Prognosis of Asymptomatic Patients with Suspected Coronary Artery Disease with Normal Multislice Angiogram?
Background: Several studies have demonstrated high sensitivity and negative predictive values for computed tomography (CT) coronary angiography.
Study design: Prospective, sequentially enrolled subjects.
Synopsis: A CT angiogram was given to 182 consecutive patients scheduled for conventional coronary angiography without acute coronary syndrome and insufficient coronary calcification to limit CT angiography. Researchers enrolled 141 because CT angiography was inconclusive or warranted actual conventional angiography.
These normal CT angiogram subjects were followed for a mean time of 14.7 months without loss to follow-up or any mortality. Five subsequently underwent conventional angiography eight to 11 months following CT, and three had clinically significant single-vessel disease. The other two had normal conventional angiograms. There was one myocardial infarction patient who, upon further review of CT, had previously unappreciated right-coronary-artery (RCA) disease. This prospective study demonstrated a 97.2% negative predictive value consistent with previous studies. Mortality, myocardial infarction, and subsequently identified coronary artery disease (CAD) are also consistent with previously published data for conventional angiography.
Bottom line: In this small, prospective study, multislice CT coronary angiography safely rules out suspected CAD.
Citation: Gilard M, Le Gal G, Cornily JC, et al. Midterm prognosis of patients with suspected coronary artery disease and normal multislice computer tomographic findings. Arch Intern Med. 2007;165(15):1687-1689.
Does Epoetin Alfa Reduce Need for Blood Transfusion Therapy in Critically Ill Patients?
Background: Two prior studies demonstrated that the use of epoetin reduced the number of red-cell transfusions in ICU patients without any other clinical benefits. There were possible subgroup differences between trauma and nontrauma patients. This study assessed a reduced dose of epoetin alfa and evaluated clinical outcomes and subgroup differences suggested by the previous studies.
Study design: Prospective, randomized, double-blind, placebo-controlled clinical trial.
Setting: 115 medical centers.
Synopsis: The study group of 1,460 patients underwent stratified randomization into trauma, surgical nontrauma, and medical nontrauma groups. There were no significant differences in transfusion requirements between the epoetin group, the placebo group, or in any subgroup. The mean pre-transfusion hemoglobin was the same in each group.
The epoetin group had a higher-than-baseline hemoglobin level at day 29 (1.6 versus 1.2 g/dL, p<0.001) and a higher absolute hemoglobin (11.2 versus 10.8 g/dL, p<0.001) than the placebo group. Mortality was lower in the epoetin group (8.5% versus 11.4%, p=0.02) and in the trauma subgroup (3.5% versus 6.6%, p=0.04). In two nontrauma groups, point estimates demonstrated similar lower mortality but were not statistically significant.
Thrombotic vascular events were higher in the epoetin group than the placebo group (16.5% versus 11.5%, p=0.008), but post-hoc analyses demonstrated that the effect was only observed in patients who had not received heparin at baseline. There were no other observed differences in length of stay or use of mechanical ventilation.
Bottom line: Epoetin alfa does not reduce red blood cell transfusions in ICU patients but may reduce mortality in trauma patients. Increased thrombotic events may be mitigated with the use of heparin.
Citation: Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med. 2007;357 (10):965-976.
What Patients Benefit Most from Hospitalist Care in an Academic Medical Center?
Background: Hospitalists increasingly serve as teaching attending physicians at many academic medical centers. Studies have shown hospitalists’ care can reduce the length of hospital stay in patients with a limited number of specific diagnoses. It has not been established whether there are other specific patient diagnoses or discharge dispositions that might benefit from hospitalist care in a teaching hospital.
Study design: Retrospective cohort.
Setting: Urban teaching hospital.
Synopsis: The authors examined the patients discharged from a hospitalist and a non-hospitalist teaching attending service at an academic medical center during a two-year period beginning July 1, 2002. The length of hospital stay for patients on the hospitalist teaching attending service was significantly lower than that of the non-hospitalist teaching attending service. This difference was most pronounced in patients with highest overall acuity as measured by diagnosis-related group (DRG) weight and patients who required discharge to nursing facilities.
Bottom line: Medically complex inpatients and inpatients with complex discharge planning needs appear to have a shorter length of hospital stay when under the care of hospitalists serving as teaching attending physicians compared with non-hospitalist teaching attending physicians.
Citation: Southern WN, Berger MA, Bellin EY, et al. Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring. Arch Intern Med. 2007;167(17):1869-1874.
What Influences Use of Generic, Branded Medications?
Background: Expenditures for prescription medications exceeded $250 billion in 2005. Various patient, physician, and payment factors may increase generic drug use in an attempt to reduce costs without affecting quality of care.
Study design: Observational analysis.
Synopsis: This study analyzed initial and subsequent pharmacy claims for 5,399 patients enrolled in a large health plan in the western United States, from 2001-2003. For new prescriptions, 23% were generics. Initiation of generic medications was less likely for patients in poor neighborhoods and for prescriptions written by specialists; pharmacy benefit design and pharmacy type did not have a significant influence.
After initiation of branded medications, 15% switched to generics during the study follow-up. Patients were more likely to switch to generic medications if they were older, if they used mail-order pharmacies, or if they participated in multitier (three or more) co-payment plans.
Bottom line: Low-income patients and patients who see specialists are less likely to initiate generic medications; after initiation on branded medications, patients using mail-order pharmacies or multitier co-payment systems are more likely to switch to generics.
Citation: Shrank WH, Stedman M, Ettner SL, et al. Patient, physician, pharmacy, and pharmacy benefit design factors related to generic medication use. J Gen Intern Med. 2007; 22:1298-1304.
Does Orthopedic Comanagement Increase Mortality in Elderly Hip Fracture Patients?
Background: Prior studies have demonstrated that for patients with hip fracture, a hospitalist-orthopedic comanagement management service reduced time to surgery and length of stay, with no difference in inpatient mortality. This study sought to address whether this applied to long-term mortality as well.
Study design: Retrospective cohort study.
Setting: Tertiary care center.
Synopsis: This study examined 466 patients admitted consecutively to a tertiary care center for surgical repair of a hip fracture, and followed them for one year postoperatively. It compared outcomes for patients admitted to a hospitalist-orthopedic comanagement service (2001-2002) with a standard care group of historical controls admitted to either an orthopedic or general medical teaching service (2000-2001).
One-year survival did not differ between the patients on the hospitalist-orthopedic comanagement service (70.5%) versus those in the standard care group (70.6%). The hospitalist-orthopedic comanagement model was associated with shorter time to surgery and shorter length of stay (8.4 versus 10.6 days). According to multivariate analysis, independent predictors of mortality were: American Society of Anesthesiologists (ASA) class III or IV (hazard ratio 4.2, 95% CI, 2.21, 7.99), admission from a nursing home (hazard ratio 2.24, 95% CI, 1.73, 2.90), and inpatient complications such as renal failure, myocardial infarction, or ICU admission (hazard ratio 1.85, CI 95%, 1.45, 2.35).
The authors note that prior studies demonstrated benefits from hospitalist involvement only after one year of implementation. This study was performed during the first year of the hospitalist-orthopedic comanagement team.
Bottom line: Hospitalist-orthopedic comanagement of patients with hip fracture reduces length of stay and does not negatively affect long-term mortality.
Citation: Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2:219-225.
How Effective Are First-Line, Second-Line Antibiotics for AECB?
Background: Antibiotics are frequently used for treatment of acute exacerbations of chronic bronchitis (AECB). However, in this era of increasing microbial resistance, there are insufficient data comparing the efficacy and safety of first-line antibiotics (ampicillin, amoxicillin, doxycycline, trimethoprim-sulfamethoxazole [Bactrim, Cotrima, Septra]) with second-line antibiotics (amoxicillin-clavulanic acid [Augmentin], macrolides, second- and third-generation cephalosporins, and fluoroquinolones).
Study design: Meta-analysis of randomized controlled trials (RCT).
Synopsis: Authors included 12 RCTs from 1981 to 2000, enrolling 2,261 adult patients comparing the efficacy and toxicity of first-line with second-line antibiotics for AECB in inpatient and outpatient settings. The authors measured treatment success, drug-related adverse events, all-cause mortality and pathogen eradication.
They concluded that administration of first-line antibiotics was associated with lower treatment success than administration of second-line antibiotics (odd ratio [OR] 0.51, 95% CI, 0.34 to 0.75). However, no differences were found with regard to all-cause mortality (OR 0.64, 95% CI, 0.25 to 3.35), adverse effects (OR 0.75, 95% CI, 0.39 to 1.45), or treatment success in microbiologically evaluable patients (OR 0.56, 95% CI, 0.22 to 1.43). Some limitations of this meta-analysis include:
- Inadequate data to stratify patients according to risk factors for poor outcome;
- Trials included inpatients as well as outpatients (likely with varying disease severity); and
- Trials were conducted in different time periods with changing patterns of anti-microbial resistance.
Bottom line: In patients with AECB, second-line antibiotics are more effective than first-line antibiotics with no differences in safety or mortality.
Citation: Dimopoulos G, Siempos II, Korbila IP, et al. Comparison of first-line with second-line antibiotics for acute exacerbations of chronic bronchitis. Chest. 2007;132:447-455.
Do Probiotic Drinks Reduce Antibiotic-Associated Diarrhea?
Background: Patients on antibiotics experience diarrhea as a side effect 5%-25% of the time, of which C. difficile is the cause in 15%-25% of these cases. Probiotics, such as Streptococcus thermophilus, Enterococcus species, Saccharomyces species, and Lactobacillus species are live microorganisms that can safely be used to treat diarrhea associated with antibiotic use.
Study design: Randomized, double-blind, placebo controlled
Setting: Three London hospitals
Synopsis: The study enrolled 135 hospitalized patients over age 50 who were prescribed antibiotics.
The treatment group received a probiotic yogurt drink containing Lactobacillus casei, L. bulgaricus, and S. thermophilus; the placebo group received a sterile milkshake. Subjects consumed the drinks twice daily within 48 hours of starting antibiotic therapy and continued for one week after antibiotic use.
There was a significant reduction of diarrhea in the probiotic group (p=0.007); the number needed to treat (NNT) was five. There was also a significant decrease in diarrhea caused by C. difficile (p=0.001), the secondary outcome, with an NNT of six.
These results may translate into decreased patient morbidity, mortality, healthcare costs, and length of stay. Additional studies are needed to establish the most effective probiotic and dosing for reducing diarrhea.
Bottom line: Twice-daily consumption of probiotic drinks can decrease the risk of antibiotic-induced diarrhea.
Citation: Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomized double blind placebo controlled trial. BMJ. 2007 Jul 14;335(7610):80.
What Organisms Commonly Cause Healthcare-Associated Pneumonia in Nonhospitalized Patients?
Background: Changes in practice patterns have resulted in a large number of patients who regularly interact with healthcare but aren’t admitted to the hospital (e.g., those receiving dialysis or home healthcare). These patients develop nosocomial-type infections rather than infections from traditionally community-acquired organisms.
Study design: Prospective observational for three years.
Setting: A large teaching hospital in Barcelona, Spain.
Synopsis: A total of 727 patients were stratified into community-acquired pneumonia (CAP) or healthcare-associated pneumonia (HCAP) groups based on whether they had:
- Received home intravenous therapy;
- Attended a hospital or hemodialysis clinic or had chemotherapy in the preceding 30 days;
- Were admitted to an acute care facility for at least two days in the preceding 90 days; or
- Resided in a nursing home.
The HCAP group tended to be older, have higher comorbidities (particularly cerebrovascular disease or malignancy), have previously received antibiotics, and have higher pneumonia severity indices.
The putative organisms were similar in both groups with Streptococcus pneumoniae representing the most common pathogen. HCAP patients had higher rates of penicillin, erythromycin, and levofloxacin resistance; aspiration pneumonia; longer lengths of stay; and 30-day mortality. Inappropriate therapy occurred more commonly in the HCAP group (5.6% versus 2.0%). Such therapy was defined as the absence of antibiotics targeting suspect pathogens, the use of antibiotics to which the bacteria were not susceptible, or the failure to start anaerobic coverage for aspiration pneumonia.
Bottom line: Outpatients who come in frequent contact with the healthcare system while presenting with pneumonia are more likely to have drug-resistant organisms similar to those seen in nosocomial pneumonia. Further, they tend to have inappropriate or inadequate antimicrobial therapy, longer hospital stays, and increased risk of death.
Citation: Carratalà J, Mykietiuk A, Fernández-Sabe N, et al. Health care-associated pneumonia requiring hospital admission. Arch Intern Med. 2007;167(13):1393-1399. TH
In This Edition
- Treat with antibiotics for seven days or less in adults with community-acquired pneumonia.
- In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux (Arixtra) is safer than with enoxaparin (Lovenox).
- Multislice coronary angiography rules out suspected coronary artery disease.
- Hospitalists in teaching hospitals decrease length of stay in complex patients.
- Epoetin alfa (Procrit/Epogen) use in critically ill patients does not reduce red-cell transfusion but may reduce mortality in trauma.
- Newer antibiotics appear to be more effective for acute exacerbations of chronic bronchitis.
- Low-income patients and patients seen by specialists are less likely to use generic medications.
- Hospitalist-orthopedic comanagement of patients with hip fractures does not negatively affect long-term mortality.
- Probiotics reduce antibiotic and C. difficile-associated diarrhea.
- Healthcare-associated pneumonia closely resembles nosocomial pneumonia.
What Is the Appropriate Duration of Antibiotic Therapy for Adults with CAP?
Background: Community-acquired pneumonia (CAP) is a leading cause of morbidity and mortality, but there is little consensus on the appropriate duration of antibiotic therapy. Current guidelines recommend antibiotic regimens lasting from five to 14 days. Shorter courses of antibiotic therapy may improve patient compliance, reduce risk of medication related adverse effects, and minimize the risk of antimicrobial resistance.
Study design: Meta-analysis.
Synopsis: Authors included 15 randomized controlled trials from 1990 through 2004. They compared the efficacy of short-course (seven days or less) antibiotic monotherapy versus extended regimens (longer than seven days) in patients age 12 or older with mild to moderate CAP. They excluded trials with a significant number of patients with bronchitis, healthcare-associated pneumonias, and chronic obstructive pulmonary disease exacerbations. The primary outcome measure failed to achieve clinical improvement or cure. Secondary outcome measures included mortality, bacteriologic failure, and other adverse events.
The authors found no significant differences in the risk of clinical failure, risk of mortality, risk of bacteriologic failure, or risk of adverse events in the short-course versus extended-course antibiotic regimens. This was consistent among the four antibiotic classes in the study: beta-lactam, fluoroquinolone, ketolide, and macrolide.
Bottom line: This study found no differences between short-course and extended-course antibiotic regimens in the treatment of adults with mild to moderate CAP in regard to clinical success, mortality, bacteriologic success, and adverse events.
Citation: Li JZ, Winston LG, Moore DH, et al. Efficacy of short-course antibiotic regimens for CAP: A meta-analysis. Am J Med. 2007;120(9):783-790.
Is Fondaparinux Superior to Enoxaparin in Non-ST-Elevation Acute Coronary Syndromes?
Background: Fondaparinux is a selective factor Xa inhibitor approved by the FDA for the treatment and prevention of venous thromboembolism. The Organization to Assess Strategies for Ischemic Syndromes (OASIS)-5 was a randomized, double-blind trial that demonstrated fondaparinux is similar to enoxaparin in reducing the risk of ischemic events, but substantially reduces major bleeding, long-term mortality, and morbidity.1
Study design: Subgroup analysis of a randomized, controlled trial.
Setting: Hospitals to which patients with non-ST-segment elevation acute coronary syndrome presented.
Synopsis: In a subgroup analysis of 19,979 in the OASIS-5 trial, patients were divided into quartiles based on their estimated creatinine clearance, calculated by using the Modification of Diet in Renal Disease formula.2 Death, myocardial infarction, refractory ischemia, and major bleeding were evaluated separately, and as a composite end point at nine, 30, and 180 days.
At nine days, death, myocardial infarction, or refractory ischemia occurred in 6.7% of patients receiving fondaparinux and 7.4% of those receiving enoxaparin (hazard ratio, 0.90, 95% confidence interval [CI], 0.73 to 1.11); major bleeding occurred in 2.8% and 6.4%, respectively (hazard ratio, 0.42, CI, 0.32 to 0.56). Statistically significant differences in major bleeding persisted at 30 and 180 days.
While there was a trend toward a reduction in the composite end point among all quartiles of glomerular filtration rate (GFR), the differences were statistically significant only among patients with a GFR less than 58 mL/min per 1.73 m2. The authors concluded that the absolute differences in favor of fondaparinux (efficacy and safety) were most apparent in patients with a GFR less than 58 mL/min per 1.73 m2 and were largely the result in a reduction in bleeding events.
The subgroup analysis was not planned before the OASIS-5 data were collected, and the results have not been confirmed elsewhere. For patients managed with an early invasive strategy, catheter thrombosis occurred more often in those who received fondaparinux than enoxaparin alone. Fondaparinux is not FDA approved for this indication.
Bottom line: In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux is associated with a significant reduction in the incidence of major bleeding as compared with enoxaparin.
Citations:
- Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354(14):1464-1476.
- Fox KA, Bassand JP, Mehta SR, et al. Influence of renal function on the efficacy and safety of fondaparinux relative to enoxaparin in non ST-segment elevation acute coronary syndromes. Ann Intern Med. 2007;147(5):304-310.
What’s the Prognosis of Asymptomatic Patients with Suspected Coronary Artery Disease with Normal Multislice Angiogram?
Background: Several studies have demonstrated high sensitivity and negative predictive values for computed tomography (CT) coronary angiography.
Study design: Prospective, sequentially enrolled subjects.
Synopsis: A CT angiogram was given to 182 consecutive patients scheduled for conventional coronary angiography without acute coronary syndrome and insufficient coronary calcification to limit CT angiography. Researchers enrolled 141 because CT angiography was inconclusive or warranted actual conventional angiography.
These normal CT angiogram subjects were followed for a mean time of 14.7 months without loss to follow-up or any mortality. Five subsequently underwent conventional angiography eight to 11 months following CT, and three had clinically significant single-vessel disease. The other two had normal conventional angiograms. There was one myocardial infarction patient who, upon further review of CT, had previously unappreciated right-coronary-artery (RCA) disease. This prospective study demonstrated a 97.2% negative predictive value consistent with previous studies. Mortality, myocardial infarction, and subsequently identified coronary artery disease (CAD) are also consistent with previously published data for conventional angiography.
Bottom line: In this small, prospective study, multislice CT coronary angiography safely rules out suspected CAD.
Citation: Gilard M, Le Gal G, Cornily JC, et al. Midterm prognosis of patients with suspected coronary artery disease and normal multislice computer tomographic findings. Arch Intern Med. 2007;165(15):1687-1689.
Does Epoetin Alfa Reduce Need for Blood Transfusion Therapy in Critically Ill Patients?
Background: Two prior studies demonstrated that the use of epoetin reduced the number of red-cell transfusions in ICU patients without any other clinical benefits. There were possible subgroup differences between trauma and nontrauma patients. This study assessed a reduced dose of epoetin alfa and evaluated clinical outcomes and subgroup differences suggested by the previous studies.
Study design: Prospective, randomized, double-blind, placebo-controlled clinical trial.
Setting: 115 medical centers.
Synopsis: The study group of 1,460 patients underwent stratified randomization into trauma, surgical nontrauma, and medical nontrauma groups. There were no significant differences in transfusion requirements between the epoetin group, the placebo group, or in any subgroup. The mean pre-transfusion hemoglobin was the same in each group.
The epoetin group had a higher-than-baseline hemoglobin level at day 29 (1.6 versus 1.2 g/dL, p<0.001) and a higher absolute hemoglobin (11.2 versus 10.8 g/dL, p<0.001) than the placebo group. Mortality was lower in the epoetin group (8.5% versus 11.4%, p=0.02) and in the trauma subgroup (3.5% versus 6.6%, p=0.04). In two nontrauma groups, point estimates demonstrated similar lower mortality but were not statistically significant.
Thrombotic vascular events were higher in the epoetin group than the placebo group (16.5% versus 11.5%, p=0.008), but post-hoc analyses demonstrated that the effect was only observed in patients who had not received heparin at baseline. There were no other observed differences in length of stay or use of mechanical ventilation.
Bottom line: Epoetin alfa does not reduce red blood cell transfusions in ICU patients but may reduce mortality in trauma patients. Increased thrombotic events may be mitigated with the use of heparin.
Citation: Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med. 2007;357 (10):965-976.
What Patients Benefit Most from Hospitalist Care in an Academic Medical Center?
Background: Hospitalists increasingly serve as teaching attending physicians at many academic medical centers. Studies have shown hospitalists’ care can reduce the length of hospital stay in patients with a limited number of specific diagnoses. It has not been established whether there are other specific patient diagnoses or discharge dispositions that might benefit from hospitalist care in a teaching hospital.
Study design: Retrospective cohort.
Setting: Urban teaching hospital.
Synopsis: The authors examined the patients discharged from a hospitalist and a non-hospitalist teaching attending service at an academic medical center during a two-year period beginning July 1, 2002. The length of hospital stay for patients on the hospitalist teaching attending service was significantly lower than that of the non-hospitalist teaching attending service. This difference was most pronounced in patients with highest overall acuity as measured by diagnosis-related group (DRG) weight and patients who required discharge to nursing facilities.
Bottom line: Medically complex inpatients and inpatients with complex discharge planning needs appear to have a shorter length of hospital stay when under the care of hospitalists serving as teaching attending physicians compared with non-hospitalist teaching attending physicians.
Citation: Southern WN, Berger MA, Bellin EY, et al. Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring. Arch Intern Med. 2007;167(17):1869-1874.
What Influences Use of Generic, Branded Medications?
Background: Expenditures for prescription medications exceeded $250 billion in 2005. Various patient, physician, and payment factors may increase generic drug use in an attempt to reduce costs without affecting quality of care.
Study design: Observational analysis.
Synopsis: This study analyzed initial and subsequent pharmacy claims for 5,399 patients enrolled in a large health plan in the western United States, from 2001-2003. For new prescriptions, 23% were generics. Initiation of generic medications was less likely for patients in poor neighborhoods and for prescriptions written by specialists; pharmacy benefit design and pharmacy type did not have a significant influence.
After initiation of branded medications, 15% switched to generics during the study follow-up. Patients were more likely to switch to generic medications if they were older, if they used mail-order pharmacies, or if they participated in multitier (three or more) co-payment plans.
Bottom line: Low-income patients and patients who see specialists are less likely to initiate generic medications; after initiation on branded medications, patients using mail-order pharmacies or multitier co-payment systems are more likely to switch to generics.
Citation: Shrank WH, Stedman M, Ettner SL, et al. Patient, physician, pharmacy, and pharmacy benefit design factors related to generic medication use. J Gen Intern Med. 2007; 22:1298-1304.
Does Orthopedic Comanagement Increase Mortality in Elderly Hip Fracture Patients?
Background: Prior studies have demonstrated that for patients with hip fracture, a hospitalist-orthopedic comanagement management service reduced time to surgery and length of stay, with no difference in inpatient mortality. This study sought to address whether this applied to long-term mortality as well.
Study design: Retrospective cohort study.
Setting: Tertiary care center.
Synopsis: This study examined 466 patients admitted consecutively to a tertiary care center for surgical repair of a hip fracture, and followed them for one year postoperatively. It compared outcomes for patients admitted to a hospitalist-orthopedic comanagement service (2001-2002) with a standard care group of historical controls admitted to either an orthopedic or general medical teaching service (2000-2001).
One-year survival did not differ between the patients on the hospitalist-orthopedic comanagement service (70.5%) versus those in the standard care group (70.6%). The hospitalist-orthopedic comanagement model was associated with shorter time to surgery and shorter length of stay (8.4 versus 10.6 days). According to multivariate analysis, independent predictors of mortality were: American Society of Anesthesiologists (ASA) class III or IV (hazard ratio 4.2, 95% CI, 2.21, 7.99), admission from a nursing home (hazard ratio 2.24, 95% CI, 1.73, 2.90), and inpatient complications such as renal failure, myocardial infarction, or ICU admission (hazard ratio 1.85, CI 95%, 1.45, 2.35).
The authors note that prior studies demonstrated benefits from hospitalist involvement only after one year of implementation. This study was performed during the first year of the hospitalist-orthopedic comanagement team.
Bottom line: Hospitalist-orthopedic comanagement of patients with hip fracture reduces length of stay and does not negatively affect long-term mortality.
Citation: Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2:219-225.
How Effective Are First-Line, Second-Line Antibiotics for AECB?
Background: Antibiotics are frequently used for treatment of acute exacerbations of chronic bronchitis (AECB). However, in this era of increasing microbial resistance, there are insufficient data comparing the efficacy and safety of first-line antibiotics (ampicillin, amoxicillin, doxycycline, trimethoprim-sulfamethoxazole [Bactrim, Cotrima, Septra]) with second-line antibiotics (amoxicillin-clavulanic acid [Augmentin], macrolides, second- and third-generation cephalosporins, and fluoroquinolones).
Study design: Meta-analysis of randomized controlled trials (RCT).
Synopsis: Authors included 12 RCTs from 1981 to 2000, enrolling 2,261 adult patients comparing the efficacy and toxicity of first-line with second-line antibiotics for AECB in inpatient and outpatient settings. The authors measured treatment success, drug-related adverse events, all-cause mortality and pathogen eradication.
They concluded that administration of first-line antibiotics was associated with lower treatment success than administration of second-line antibiotics (odd ratio [OR] 0.51, 95% CI, 0.34 to 0.75). However, no differences were found with regard to all-cause mortality (OR 0.64, 95% CI, 0.25 to 3.35), adverse effects (OR 0.75, 95% CI, 0.39 to 1.45), or treatment success in microbiologically evaluable patients (OR 0.56, 95% CI, 0.22 to 1.43). Some limitations of this meta-analysis include:
- Inadequate data to stratify patients according to risk factors for poor outcome;
- Trials included inpatients as well as outpatients (likely with varying disease severity); and
- Trials were conducted in different time periods with changing patterns of anti-microbial resistance.
Bottom line: In patients with AECB, second-line antibiotics are more effective than first-line antibiotics with no differences in safety or mortality.
Citation: Dimopoulos G, Siempos II, Korbila IP, et al. Comparison of first-line with second-line antibiotics for acute exacerbations of chronic bronchitis. Chest. 2007;132:447-455.
Do Probiotic Drinks Reduce Antibiotic-Associated Diarrhea?
Background: Patients on antibiotics experience diarrhea as a side effect 5%-25% of the time, of which C. difficile is the cause in 15%-25% of these cases. Probiotics, such as Streptococcus thermophilus, Enterococcus species, Saccharomyces species, and Lactobacillus species are live microorganisms that can safely be used to treat diarrhea associated with antibiotic use.
Study design: Randomized, double-blind, placebo controlled
Setting: Three London hospitals
Synopsis: The study enrolled 135 hospitalized patients over age 50 who were prescribed antibiotics.
The treatment group received a probiotic yogurt drink containing Lactobacillus casei, L. bulgaricus, and S. thermophilus; the placebo group received a sterile milkshake. Subjects consumed the drinks twice daily within 48 hours of starting antibiotic therapy and continued for one week after antibiotic use.
There was a significant reduction of diarrhea in the probiotic group (p=0.007); the number needed to treat (NNT) was five. There was also a significant decrease in diarrhea caused by C. difficile (p=0.001), the secondary outcome, with an NNT of six.
These results may translate into decreased patient morbidity, mortality, healthcare costs, and length of stay. Additional studies are needed to establish the most effective probiotic and dosing for reducing diarrhea.
Bottom line: Twice-daily consumption of probiotic drinks can decrease the risk of antibiotic-induced diarrhea.
Citation: Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomized double blind placebo controlled trial. BMJ. 2007 Jul 14;335(7610):80.
What Organisms Commonly Cause Healthcare-Associated Pneumonia in Nonhospitalized Patients?
Background: Changes in practice patterns have resulted in a large number of patients who regularly interact with healthcare but aren’t admitted to the hospital (e.g., those receiving dialysis or home healthcare). These patients develop nosocomial-type infections rather than infections from traditionally community-acquired organisms.
Study design: Prospective observational for three years.
Setting: A large teaching hospital in Barcelona, Spain.
Synopsis: A total of 727 patients were stratified into community-acquired pneumonia (CAP) or healthcare-associated pneumonia (HCAP) groups based on whether they had:
- Received home intravenous therapy;
- Attended a hospital or hemodialysis clinic or had chemotherapy in the preceding 30 days;
- Were admitted to an acute care facility for at least two days in the preceding 90 days; or
- Resided in a nursing home.
The HCAP group tended to be older, have higher comorbidities (particularly cerebrovascular disease or malignancy), have previously received antibiotics, and have higher pneumonia severity indices.
The putative organisms were similar in both groups with Streptococcus pneumoniae representing the most common pathogen. HCAP patients had higher rates of penicillin, erythromycin, and levofloxacin resistance; aspiration pneumonia; longer lengths of stay; and 30-day mortality. Inappropriate therapy occurred more commonly in the HCAP group (5.6% versus 2.0%). Such therapy was defined as the absence of antibiotics targeting suspect pathogens, the use of antibiotics to which the bacteria were not susceptible, or the failure to start anaerobic coverage for aspiration pneumonia.
Bottom line: Outpatients who come in frequent contact with the healthcare system while presenting with pneumonia are more likely to have drug-resistant organisms similar to those seen in nosocomial pneumonia. Further, they tend to have inappropriate or inadequate antimicrobial therapy, longer hospital stays, and increased risk of death.
Citation: Carratalà J, Mykietiuk A, Fernández-Sabe N, et al. Health care-associated pneumonia requiring hospital admission. Arch Intern Med. 2007;167(13):1393-1399. TH
In This Edition
- Treat with antibiotics for seven days or less in adults with community-acquired pneumonia.
- In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux (Arixtra) is safer than with enoxaparin (Lovenox).
- Multislice coronary angiography rules out suspected coronary artery disease.
- Hospitalists in teaching hospitals decrease length of stay in complex patients.
- Epoetin alfa (Procrit/Epogen) use in critically ill patients does not reduce red-cell transfusion but may reduce mortality in trauma.
- Newer antibiotics appear to be more effective for acute exacerbations of chronic bronchitis.
- Low-income patients and patients seen by specialists are less likely to use generic medications.
- Hospitalist-orthopedic comanagement of patients with hip fractures does not negatively affect long-term mortality.
- Probiotics reduce antibiotic and C. difficile-associated diarrhea.
- Healthcare-associated pneumonia closely resembles nosocomial pneumonia.
What Is the Appropriate Duration of Antibiotic Therapy for Adults with CAP?
Background: Community-acquired pneumonia (CAP) is a leading cause of morbidity and mortality, but there is little consensus on the appropriate duration of antibiotic therapy. Current guidelines recommend antibiotic regimens lasting from five to 14 days. Shorter courses of antibiotic therapy may improve patient compliance, reduce risk of medication related adverse effects, and minimize the risk of antimicrobial resistance.
Study design: Meta-analysis.
Synopsis: Authors included 15 randomized controlled trials from 1990 through 2004. They compared the efficacy of short-course (seven days or less) antibiotic monotherapy versus extended regimens (longer than seven days) in patients age 12 or older with mild to moderate CAP. They excluded trials with a significant number of patients with bronchitis, healthcare-associated pneumonias, and chronic obstructive pulmonary disease exacerbations. The primary outcome measure failed to achieve clinical improvement or cure. Secondary outcome measures included mortality, bacteriologic failure, and other adverse events.
The authors found no significant differences in the risk of clinical failure, risk of mortality, risk of bacteriologic failure, or risk of adverse events in the short-course versus extended-course antibiotic regimens. This was consistent among the four antibiotic classes in the study: beta-lactam, fluoroquinolone, ketolide, and macrolide.
Bottom line: This study found no differences between short-course and extended-course antibiotic regimens in the treatment of adults with mild to moderate CAP in regard to clinical success, mortality, bacteriologic success, and adverse events.
Citation: Li JZ, Winston LG, Moore DH, et al. Efficacy of short-course antibiotic regimens for CAP: A meta-analysis. Am J Med. 2007;120(9):783-790.
Is Fondaparinux Superior to Enoxaparin in Non-ST-Elevation Acute Coronary Syndromes?
Background: Fondaparinux is a selective factor Xa inhibitor approved by the FDA for the treatment and prevention of venous thromboembolism. The Organization to Assess Strategies for Ischemic Syndromes (OASIS)-5 was a randomized, double-blind trial that demonstrated fondaparinux is similar to enoxaparin in reducing the risk of ischemic events, but substantially reduces major bleeding, long-term mortality, and morbidity.1
Study design: Subgroup analysis of a randomized, controlled trial.
Setting: Hospitals to which patients with non-ST-segment elevation acute coronary syndrome presented.
Synopsis: In a subgroup analysis of 19,979 in the OASIS-5 trial, patients were divided into quartiles based on their estimated creatinine clearance, calculated by using the Modification of Diet in Renal Disease formula.2 Death, myocardial infarction, refractory ischemia, and major bleeding were evaluated separately, and as a composite end point at nine, 30, and 180 days.
At nine days, death, myocardial infarction, or refractory ischemia occurred in 6.7% of patients receiving fondaparinux and 7.4% of those receiving enoxaparin (hazard ratio, 0.90, 95% confidence interval [CI], 0.73 to 1.11); major bleeding occurred in 2.8% and 6.4%, respectively (hazard ratio, 0.42, CI, 0.32 to 0.56). Statistically significant differences in major bleeding persisted at 30 and 180 days.
While there was a trend toward a reduction in the composite end point among all quartiles of glomerular filtration rate (GFR), the differences were statistically significant only among patients with a GFR less than 58 mL/min per 1.73 m2. The authors concluded that the absolute differences in favor of fondaparinux (efficacy and safety) were most apparent in patients with a GFR less than 58 mL/min per 1.73 m2 and were largely the result in a reduction in bleeding events.
The subgroup analysis was not planned before the OASIS-5 data were collected, and the results have not been confirmed elsewhere. For patients managed with an early invasive strategy, catheter thrombosis occurred more often in those who received fondaparinux than enoxaparin alone. Fondaparinux is not FDA approved for this indication.
Bottom line: In patients with chronic kidney disease who present with non ST-segment elevation acute coronary syndromes, anticoagulation with fondaparinux is associated with a significant reduction in the incidence of major bleeding as compared with enoxaparin.
Citations:
- Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354(14):1464-1476.
- Fox KA, Bassand JP, Mehta SR, et al. Influence of renal function on the efficacy and safety of fondaparinux relative to enoxaparin in non ST-segment elevation acute coronary syndromes. Ann Intern Med. 2007;147(5):304-310.
What’s the Prognosis of Asymptomatic Patients with Suspected Coronary Artery Disease with Normal Multislice Angiogram?
Background: Several studies have demonstrated high sensitivity and negative predictive values for computed tomography (CT) coronary angiography.
Study design: Prospective, sequentially enrolled subjects.
Synopsis: A CT angiogram was given to 182 consecutive patients scheduled for conventional coronary angiography without acute coronary syndrome and insufficient coronary calcification to limit CT angiography. Researchers enrolled 141 because CT angiography was inconclusive or warranted actual conventional angiography.
These normal CT angiogram subjects were followed for a mean time of 14.7 months without loss to follow-up or any mortality. Five subsequently underwent conventional angiography eight to 11 months following CT, and three had clinically significant single-vessel disease. The other two had normal conventional angiograms. There was one myocardial infarction patient who, upon further review of CT, had previously unappreciated right-coronary-artery (RCA) disease. This prospective study demonstrated a 97.2% negative predictive value consistent with previous studies. Mortality, myocardial infarction, and subsequently identified coronary artery disease (CAD) are also consistent with previously published data for conventional angiography.
Bottom line: In this small, prospective study, multislice CT coronary angiography safely rules out suspected CAD.
Citation: Gilard M, Le Gal G, Cornily JC, et al. Midterm prognosis of patients with suspected coronary artery disease and normal multislice computer tomographic findings. Arch Intern Med. 2007;165(15):1687-1689.
Does Epoetin Alfa Reduce Need for Blood Transfusion Therapy in Critically Ill Patients?
Background: Two prior studies demonstrated that the use of epoetin reduced the number of red-cell transfusions in ICU patients without any other clinical benefits. There were possible subgroup differences between trauma and nontrauma patients. This study assessed a reduced dose of epoetin alfa and evaluated clinical outcomes and subgroup differences suggested by the previous studies.
Study design: Prospective, randomized, double-blind, placebo-controlled clinical trial.
Setting: 115 medical centers.
Synopsis: The study group of 1,460 patients underwent stratified randomization into trauma, surgical nontrauma, and medical nontrauma groups. There were no significant differences in transfusion requirements between the epoetin group, the placebo group, or in any subgroup. The mean pre-transfusion hemoglobin was the same in each group.
The epoetin group had a higher-than-baseline hemoglobin level at day 29 (1.6 versus 1.2 g/dL, p<0.001) and a higher absolute hemoglobin (11.2 versus 10.8 g/dL, p<0.001) than the placebo group. Mortality was lower in the epoetin group (8.5% versus 11.4%, p=0.02) and in the trauma subgroup (3.5% versus 6.6%, p=0.04). In two nontrauma groups, point estimates demonstrated similar lower mortality but were not statistically significant.
Thrombotic vascular events were higher in the epoetin group than the placebo group (16.5% versus 11.5%, p=0.008), but post-hoc analyses demonstrated that the effect was only observed in patients who had not received heparin at baseline. There were no other observed differences in length of stay or use of mechanical ventilation.
Bottom line: Epoetin alfa does not reduce red blood cell transfusions in ICU patients but may reduce mortality in trauma patients. Increased thrombotic events may be mitigated with the use of heparin.
Citation: Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med. 2007;357 (10):965-976.
What Patients Benefit Most from Hospitalist Care in an Academic Medical Center?
Background: Hospitalists increasingly serve as teaching attending physicians at many academic medical centers. Studies have shown hospitalists’ care can reduce the length of hospital stay in patients with a limited number of specific diagnoses. It has not been established whether there are other specific patient diagnoses or discharge dispositions that might benefit from hospitalist care in a teaching hospital.
Study design: Retrospective cohort.
Setting: Urban teaching hospital.
Synopsis: The authors examined the patients discharged from a hospitalist and a non-hospitalist teaching attending service at an academic medical center during a two-year period beginning July 1, 2002. The length of hospital stay for patients on the hospitalist teaching attending service was significantly lower than that of the non-hospitalist teaching attending service. This difference was most pronounced in patients with highest overall acuity as measured by diagnosis-related group (DRG) weight and patients who required discharge to nursing facilities.
Bottom line: Medically complex inpatients and inpatients with complex discharge planning needs appear to have a shorter length of hospital stay when under the care of hospitalists serving as teaching attending physicians compared with non-hospitalist teaching attending physicians.
Citation: Southern WN, Berger MA, Bellin EY, et al. Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring. Arch Intern Med. 2007;167(17):1869-1874.
What Influences Use of Generic, Branded Medications?
Background: Expenditures for prescription medications exceeded $250 billion in 2005. Various patient, physician, and payment factors may increase generic drug use in an attempt to reduce costs without affecting quality of care.
Study design: Observational analysis.
Synopsis: This study analyzed initial and subsequent pharmacy claims for 5,399 patients enrolled in a large health plan in the western United States, from 2001-2003. For new prescriptions, 23% were generics. Initiation of generic medications was less likely for patients in poor neighborhoods and for prescriptions written by specialists; pharmacy benefit design and pharmacy type did not have a significant influence.
After initiation of branded medications, 15% switched to generics during the study follow-up. Patients were more likely to switch to generic medications if they were older, if they used mail-order pharmacies, or if they participated in multitier (three or more) co-payment plans.
Bottom line: Low-income patients and patients who see specialists are less likely to initiate generic medications; after initiation on branded medications, patients using mail-order pharmacies or multitier co-payment systems are more likely to switch to generics.
Citation: Shrank WH, Stedman M, Ettner SL, et al. Patient, physician, pharmacy, and pharmacy benefit design factors related to generic medication use. J Gen Intern Med. 2007; 22:1298-1304.
Does Orthopedic Comanagement Increase Mortality in Elderly Hip Fracture Patients?
Background: Prior studies have demonstrated that for patients with hip fracture, a hospitalist-orthopedic comanagement management service reduced time to surgery and length of stay, with no difference in inpatient mortality. This study sought to address whether this applied to long-term mortality as well.
Study design: Retrospective cohort study.
Setting: Tertiary care center.
Synopsis: This study examined 466 patients admitted consecutively to a tertiary care center for surgical repair of a hip fracture, and followed them for one year postoperatively. It compared outcomes for patients admitted to a hospitalist-orthopedic comanagement service (2001-2002) with a standard care group of historical controls admitted to either an orthopedic or general medical teaching service (2000-2001).
One-year survival did not differ between the patients on the hospitalist-orthopedic comanagement service (70.5%) versus those in the standard care group (70.6%). The hospitalist-orthopedic comanagement model was associated with shorter time to surgery and shorter length of stay (8.4 versus 10.6 days). According to multivariate analysis, independent predictors of mortality were: American Society of Anesthesiologists (ASA) class III or IV (hazard ratio 4.2, 95% CI, 2.21, 7.99), admission from a nursing home (hazard ratio 2.24, 95% CI, 1.73, 2.90), and inpatient complications such as renal failure, myocardial infarction, or ICU admission (hazard ratio 1.85, CI 95%, 1.45, 2.35).
The authors note that prior studies demonstrated benefits from hospitalist involvement only after one year of implementation. This study was performed during the first year of the hospitalist-orthopedic comanagement team.
Bottom line: Hospitalist-orthopedic comanagement of patients with hip fracture reduces length of stay and does not negatively affect long-term mortality.
Citation: Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2:219-225.
How Effective Are First-Line, Second-Line Antibiotics for AECB?
Background: Antibiotics are frequently used for treatment of acute exacerbations of chronic bronchitis (AECB). However, in this era of increasing microbial resistance, there are insufficient data comparing the efficacy and safety of first-line antibiotics (ampicillin, amoxicillin, doxycycline, trimethoprim-sulfamethoxazole [Bactrim, Cotrima, Septra]) with second-line antibiotics (amoxicillin-clavulanic acid [Augmentin], macrolides, second- and third-generation cephalosporins, and fluoroquinolones).
Study design: Meta-analysis of randomized controlled trials (RCT).
Synopsis: Authors included 12 RCTs from 1981 to 2000, enrolling 2,261 adult patients comparing the efficacy and toxicity of first-line with second-line antibiotics for AECB in inpatient and outpatient settings. The authors measured treatment success, drug-related adverse events, all-cause mortality and pathogen eradication.
They concluded that administration of first-line antibiotics was associated with lower treatment success than administration of second-line antibiotics (odd ratio [OR] 0.51, 95% CI, 0.34 to 0.75). However, no differences were found with regard to all-cause mortality (OR 0.64, 95% CI, 0.25 to 3.35), adverse effects (OR 0.75, 95% CI, 0.39 to 1.45), or treatment success in microbiologically evaluable patients (OR 0.56, 95% CI, 0.22 to 1.43). Some limitations of this meta-analysis include:
- Inadequate data to stratify patients according to risk factors for poor outcome;
- Trials included inpatients as well as outpatients (likely with varying disease severity); and
- Trials were conducted in different time periods with changing patterns of anti-microbial resistance.
Bottom line: In patients with AECB, second-line antibiotics are more effective than first-line antibiotics with no differences in safety or mortality.
Citation: Dimopoulos G, Siempos II, Korbila IP, et al. Comparison of first-line with second-line antibiotics for acute exacerbations of chronic bronchitis. Chest. 2007;132:447-455.
Do Probiotic Drinks Reduce Antibiotic-Associated Diarrhea?
Background: Patients on antibiotics experience diarrhea as a side effect 5%-25% of the time, of which C. difficile is the cause in 15%-25% of these cases. Probiotics, such as Streptococcus thermophilus, Enterococcus species, Saccharomyces species, and Lactobacillus species are live microorganisms that can safely be used to treat diarrhea associated with antibiotic use.
Study design: Randomized, double-blind, placebo controlled
Setting: Three London hospitals
Synopsis: The study enrolled 135 hospitalized patients over age 50 who were prescribed antibiotics.
The treatment group received a probiotic yogurt drink containing Lactobacillus casei, L. bulgaricus, and S. thermophilus; the placebo group received a sterile milkshake. Subjects consumed the drinks twice daily within 48 hours of starting antibiotic therapy and continued for one week after antibiotic use.
There was a significant reduction of diarrhea in the probiotic group (p=0.007); the number needed to treat (NNT) was five. There was also a significant decrease in diarrhea caused by C. difficile (p=0.001), the secondary outcome, with an NNT of six.
These results may translate into decreased patient morbidity, mortality, healthcare costs, and length of stay. Additional studies are needed to establish the most effective probiotic and dosing for reducing diarrhea.
Bottom line: Twice-daily consumption of probiotic drinks can decrease the risk of antibiotic-induced diarrhea.
Citation: Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomized double blind placebo controlled trial. BMJ. 2007 Jul 14;335(7610):80.
What Organisms Commonly Cause Healthcare-Associated Pneumonia in Nonhospitalized Patients?
Background: Changes in practice patterns have resulted in a large number of patients who regularly interact with healthcare but aren’t admitted to the hospital (e.g., those receiving dialysis or home healthcare). These patients develop nosocomial-type infections rather than infections from traditionally community-acquired organisms.
Study design: Prospective observational for three years.
Setting: A large teaching hospital in Barcelona, Spain.
Synopsis: A total of 727 patients were stratified into community-acquired pneumonia (CAP) or healthcare-associated pneumonia (HCAP) groups based on whether they had:
- Received home intravenous therapy;
- Attended a hospital or hemodialysis clinic or had chemotherapy in the preceding 30 days;
- Were admitted to an acute care facility for at least two days in the preceding 90 days; or
- Resided in a nursing home.
The HCAP group tended to be older, have higher comorbidities (particularly cerebrovascular disease or malignancy), have previously received antibiotics, and have higher pneumonia severity indices.
The putative organisms were similar in both groups with Streptococcus pneumoniae representing the most common pathogen. HCAP patients had higher rates of penicillin, erythromycin, and levofloxacin resistance; aspiration pneumonia; longer lengths of stay; and 30-day mortality. Inappropriate therapy occurred more commonly in the HCAP group (5.6% versus 2.0%). Such therapy was defined as the absence of antibiotics targeting suspect pathogens, the use of antibiotics to which the bacteria were not susceptible, or the failure to start anaerobic coverage for aspiration pneumonia.
Bottom line: Outpatients who come in frequent contact with the healthcare system while presenting with pneumonia are more likely to have drug-resistant organisms similar to those seen in nosocomial pneumonia. Further, they tend to have inappropriate or inadequate antimicrobial therapy, longer hospital stays, and increased risk of death.
Citation: Carratalà J, Mykietiuk A, Fernández-Sabe N, et al. Health care-associated pneumonia requiring hospital admission. Arch Intern Med. 2007;167(13):1393-1399. TH
SHM Behind the Scenes
You may have noticed a new look to SHM’s Web site. To the naked eye, many of these changes might appear subtle. Behind the nuanced changes to the graphical interface, the content now resides in a completely different structure that allows users to more easily find information and resources.
Why the change? As SHM’s interactive services manager, I have spent a lot of time trying to find pages of content on the SHM Web site that need to be added, updated, or removed. This is not a task for the faint of heart, considering there are more than 10,000 active pages on the SHM Web site.
About a year ago, after a particularly head-splitting day of trying to find an obscure piece of information, I concluded: “There has got to be a better way to organize the information on this site!” After discussions with key stakeholders, we concluded it was time to completely reorganize our Web site. As a reward for bringing this to everyone’s attention, I was chosen to head the endeavor.
After a couple of minutes of pondering the sheer magnitude of the effort I thought for a moment about taking an extended leave of absence. It would have been easy to sit in my cubicle and pound out a new architecture I thought would work well for the organization’s needs. But the reality was that just about everybody would need a say in the process.
As one of the most prominent faces of the organization, the Web site projects the core of SHM. Its online presence is a major tool for finding and engaging members, promoting SHM’s major initiatives and letting the world know exactly what the hospital medicine movement is about. Because of this, it was imperative that all the individuals involved in making the Society what it is were involved in the process of creating an information architecture for the Web site that would best serve the needs of all our users.
Right from the beginning of the process, it was clear that in order to create an information structure that worked for the organization as a whole, everyone would need to understand the importance of each other’s stake in the content on the Web site. Once there was an across-the-board understanding of the key pieces and groups of information on the site, it would be easier to implement structural changes that made sense to the organization as a whole.
Buy-in needed to occur at a high level early on. From the beginning of this project, I saw an opportunity to use many of the teaching and group-participation skills I learned as a Peace Corp volunteer in Ukraine. Not surprisingly, much of what I used to engage individuals, generate discussions and create ideas actually worked better in a roomful of SHM staff than it did in a classroom packed with hormone driven teenagers who were more interested in knowing if I personally knew Britney Spears than speaking English.
The initial brainstorming and idea-gathering sessions we held laid a solid foundation for restructuring the site’s navigation and information architecture, making it easier to navigate and more engaging for the end-user.
In the end, brute force, hard work, and group collaboration got the job done. Without the contribution and dedication of countless members of the SHM staff and community, this project would not have become a reality.
SHM now boasts a site that is cleaner, easier to navigate, and better showcases SHM’s role as the heart of the hospital medicine movement. A Web site, like many other things in life, is always a work in progress. But we feel confident that what you see today is a significant improvement over its predecessor.
Stop by www.hospitalmedicine.org to check out the result of this organization-wide effort. Comments and suggestions are always welcome as we continue to strive to improve the user experience. E-mail me at bhansen@hospitalmedicine.org.
You may have noticed a new look to SHM’s Web site. To the naked eye, many of these changes might appear subtle. Behind the nuanced changes to the graphical interface, the content now resides in a completely different structure that allows users to more easily find information and resources.
Why the change? As SHM’s interactive services manager, I have spent a lot of time trying to find pages of content on the SHM Web site that need to be added, updated, or removed. This is not a task for the faint of heart, considering there are more than 10,000 active pages on the SHM Web site.
About a year ago, after a particularly head-splitting day of trying to find an obscure piece of information, I concluded: “There has got to be a better way to organize the information on this site!” After discussions with key stakeholders, we concluded it was time to completely reorganize our Web site. As a reward for bringing this to everyone’s attention, I was chosen to head the endeavor.
After a couple of minutes of pondering the sheer magnitude of the effort I thought for a moment about taking an extended leave of absence. It would have been easy to sit in my cubicle and pound out a new architecture I thought would work well for the organization’s needs. But the reality was that just about everybody would need a say in the process.
As one of the most prominent faces of the organization, the Web site projects the core of SHM. Its online presence is a major tool for finding and engaging members, promoting SHM’s major initiatives and letting the world know exactly what the hospital medicine movement is about. Because of this, it was imperative that all the individuals involved in making the Society what it is were involved in the process of creating an information architecture for the Web site that would best serve the needs of all our users.
Right from the beginning of the process, it was clear that in order to create an information structure that worked for the organization as a whole, everyone would need to understand the importance of each other’s stake in the content on the Web site. Once there was an across-the-board understanding of the key pieces and groups of information on the site, it would be easier to implement structural changes that made sense to the organization as a whole.
Buy-in needed to occur at a high level early on. From the beginning of this project, I saw an opportunity to use many of the teaching and group-participation skills I learned as a Peace Corp volunteer in Ukraine. Not surprisingly, much of what I used to engage individuals, generate discussions and create ideas actually worked better in a roomful of SHM staff than it did in a classroom packed with hormone driven teenagers who were more interested in knowing if I personally knew Britney Spears than speaking English.
The initial brainstorming and idea-gathering sessions we held laid a solid foundation for restructuring the site’s navigation and information architecture, making it easier to navigate and more engaging for the end-user.
In the end, brute force, hard work, and group collaboration got the job done. Without the contribution and dedication of countless members of the SHM staff and community, this project would not have become a reality.
SHM now boasts a site that is cleaner, easier to navigate, and better showcases SHM’s role as the heart of the hospital medicine movement. A Web site, like many other things in life, is always a work in progress. But we feel confident that what you see today is a significant improvement over its predecessor.
Stop by www.hospitalmedicine.org to check out the result of this organization-wide effort. Comments and suggestions are always welcome as we continue to strive to improve the user experience. E-mail me at bhansen@hospitalmedicine.org.
You may have noticed a new look to SHM’s Web site. To the naked eye, many of these changes might appear subtle. Behind the nuanced changes to the graphical interface, the content now resides in a completely different structure that allows users to more easily find information and resources.
Why the change? As SHM’s interactive services manager, I have spent a lot of time trying to find pages of content on the SHM Web site that need to be added, updated, or removed. This is not a task for the faint of heart, considering there are more than 10,000 active pages on the SHM Web site.
About a year ago, after a particularly head-splitting day of trying to find an obscure piece of information, I concluded: “There has got to be a better way to organize the information on this site!” After discussions with key stakeholders, we concluded it was time to completely reorganize our Web site. As a reward for bringing this to everyone’s attention, I was chosen to head the endeavor.
After a couple of minutes of pondering the sheer magnitude of the effort I thought for a moment about taking an extended leave of absence. It would have been easy to sit in my cubicle and pound out a new architecture I thought would work well for the organization’s needs. But the reality was that just about everybody would need a say in the process.
As one of the most prominent faces of the organization, the Web site projects the core of SHM. Its online presence is a major tool for finding and engaging members, promoting SHM’s major initiatives and letting the world know exactly what the hospital medicine movement is about. Because of this, it was imperative that all the individuals involved in making the Society what it is were involved in the process of creating an information architecture for the Web site that would best serve the needs of all our users.
Right from the beginning of the process, it was clear that in order to create an information structure that worked for the organization as a whole, everyone would need to understand the importance of each other’s stake in the content on the Web site. Once there was an across-the-board understanding of the key pieces and groups of information on the site, it would be easier to implement structural changes that made sense to the organization as a whole.
Buy-in needed to occur at a high level early on. From the beginning of this project, I saw an opportunity to use many of the teaching and group-participation skills I learned as a Peace Corp volunteer in Ukraine. Not surprisingly, much of what I used to engage individuals, generate discussions and create ideas actually worked better in a roomful of SHM staff than it did in a classroom packed with hormone driven teenagers who were more interested in knowing if I personally knew Britney Spears than speaking English.
The initial brainstorming and idea-gathering sessions we held laid a solid foundation for restructuring the site’s navigation and information architecture, making it easier to navigate and more engaging for the end-user.
In the end, brute force, hard work, and group collaboration got the job done. Without the contribution and dedication of countless members of the SHM staff and community, this project would not have become a reality.
SHM now boasts a site that is cleaner, easier to navigate, and better showcases SHM’s role as the heart of the hospital medicine movement. A Web site, like many other things in life, is always a work in progress. But we feel confident that what you see today is a significant improvement over its predecessor.
Stop by www.hospitalmedicine.org to check out the result of this organization-wide effort. Comments and suggestions are always welcome as we continue to strive to improve the user experience. E-mail me at bhansen@hospitalmedicine.org.
All Eyes on San Diego
SHM’s Annual Meeting highlights hospital medicine as a distinct field within internal medicine. Being able to, year after year, incorporate core clinical topics, evidence-based practice, quality-related content, and career development into three days is only possible because of the foundation laid from previous meetings over the past 10 years.
Expectations about the role of hospitalists have taken shape through recommendations from education summits and national experts on healthcare policy, and via publications like the Journal of Hospital Medicine and The Core Competencies in Hospital Medicine. The Annual Meeting Committee’s goal was to define a program that facilitates hospitalists in achieving that role.

The 2008 meeting April 3-5 in San Diego will feature:
- National leaders in hospital medicine and healthcare;
- Six precourses addressing timely and relevant topics; and
- Seven tracks addressing clinical, operational, quality, academic, and pediatric issues.
Issues that have broad appeal and present challenges for hospitalists will be addressed in three widely anticipated keynotes:
Quality: Don Berwick, MD, MPP, FRCP, president and CEO, Institute for Healthcare Improvement (IHI) and architect of both the 100,000 Lives and 5 Million Lives campaigns;
The future of healthcare: Ian Morrison, PhD, president emeritus and health advisory panel chair, Institute for the Future, and an internationally known author on long-term forecasting with particular emphasis on healthcare;
Thriving in the face of comanagement, non-teaching services, transparency, and the reality of perpetual change: Robert Wachter, MD, professor and chief of the division of hospital medicine, associate chairman of the department of medicine, University of California, San Francisco.
The future of hospital medicine: opportunities and challenges: A special plenary session presented by a panel of hospital medicine leaders who will share perspectives from:
- The large hospitalist company;
- The large hospital company as an employer;
- The hospital CEO; and
- The individual hospital employed/associated hospital medicine group.
The following program elements are only a few of the many highlights of “Hospital Medicine 2008”:
The Evidence-Based Rapid-Fire Track: This track was developed in response from last year’s attendees. It is designed to provide participants—new or old attendees, academic or community caregivers—with “rapid bursts” of content and to address specific questions framed by the committee, based on the highest level of medical evidence available.
Research, Innovations, and Clinical Vignettes (RIV) Competition: Building on a new feature from “Hospital Medicine 2007,” a nationally renowned professor will again tour the poster session and comment on the entries, meet with academic hospitalists, attend forums, and generally be a “visiting professor” for the duration of the meeting. Additionally, SHM’s RIV Committee, along with staff, are working on arrangements for junior faculty to interact with senior researchers during times that run concurrent with non-plenary sessions. Senior hospitalists with expertise in quality-improvement research will also provide individual feedback to authors at the poster sessions. Mini poster presentation sessions will provide a way for residents to highlight their work, and there will be new, separate receptions for the posters (April 3) and exhibits (April 4).
More networking: Networking provides a critical outlet to interact with senior hospitalists, find out what others are doing to advance their careers, and seek mentorship. In addition to the networking opportunities incorporated in the RIV Competition, other networking opportunities include the exhibits, President’s Luncheon and additional receptions, and two new special-interest forums on com-anagement and consultative medicine and international hospital medicine.
The Annual Meeting Committee sought improvements in developing and implementing this year’s program. Committee brainstorming sessions for this year’s meeting focused on:
- Balancing what works with innovation;
- Making the meeting more valuable to clinical educators and researchers, and more applicable to community hospitalists; and
- Showing national leaders the extraordinary talent behind and work of SHM.
A key innovation was a successful “call for speakers.” Submissions were sought for three breakout sessions to create additional opportunity for members to play an active role in “Hospital Medicine 2008.” Based on submissions, sessions were added on the following topics:
- “Prevention, Management, and Treatment of Acute Delirium”;
- “Designing Compensation and Bonus Plans to Drive Desired Behavior”; and
- “Acute Coronary Syndrome Trials and Tribulations.”
Changes for “Hospital Medicine 2008” reflect the volunteerism of many professionals and would not have been possible without the mentorship and expertise of seasoned veteran leaders in hospital medicine, as well as the feedback and participation of hospitalists providing daily inpatient care. As part of a continuous quality-improvement initiative, rules of engagement were developed so speakers would have useful information up front.
The success of the SHM Annual Meeting depends upon the participation and leadership of SHM members, staff, committees, and task forces, as well as the SHM Board. My thanks goes out to them all for their efforts in once again creating a top-flight program.
For more information on “Hospital Medicine 2008,” and to register, visit www.hospitalmedicine.org/hospitalmedicine2008.
SHM’s Annual Meeting highlights hospital medicine as a distinct field within internal medicine. Being able to, year after year, incorporate core clinical topics, evidence-based practice, quality-related content, and career development into three days is only possible because of the foundation laid from previous meetings over the past 10 years.
Expectations about the role of hospitalists have taken shape through recommendations from education summits and national experts on healthcare policy, and via publications like the Journal of Hospital Medicine and The Core Competencies in Hospital Medicine. The Annual Meeting Committee’s goal was to define a program that facilitates hospitalists in achieving that role.
The 2008 meeting April 3-5 in San Diego will feature:
- National leaders in hospital medicine and healthcare;
- Six precourses addressing timely and relevant topics; and
- Seven tracks addressing clinical, operational, quality, academic, and pediatric issues.
Issues that have broad appeal and present challenges for hospitalists will be addressed in three widely anticipated keynotes:
Quality: Don Berwick, MD, MPP, FRCP, president and CEO, Institute for Healthcare Improvement (IHI) and architect of both the 100,000 Lives and 5 Million Lives campaigns;
The future of healthcare: Ian Morrison, PhD, president emeritus and health advisory panel chair, Institute for the Future, and an internationally known author on long-term forecasting with particular emphasis on healthcare;
Thriving in the face of comanagement, non-teaching services, transparency, and the reality of perpetual change: Robert Wachter, MD, professor and chief of the division of hospital medicine, associate chairman of the department of medicine, University of California, San Francisco.
The future of hospital medicine: opportunities and challenges: A special plenary session presented by a panel of hospital medicine leaders who will share perspectives from:
- The large hospitalist company;
- The large hospital company as an employer;
- The hospital CEO; and
- The individual hospital employed/associated hospital medicine group.
The following program elements are only a few of the many highlights of “Hospital Medicine 2008”:
The Evidence-Based Rapid-Fire Track: This track was developed in response from last year’s attendees. It is designed to provide participants—new or old attendees, academic or community caregivers—with “rapid bursts” of content and to address specific questions framed by the committee, based on the highest level of medical evidence available.
Research, Innovations, and Clinical Vignettes (RIV) Competition: Building on a new feature from “Hospital Medicine 2007,” a nationally renowned professor will again tour the poster session and comment on the entries, meet with academic hospitalists, attend forums, and generally be a “visiting professor” for the duration of the meeting. Additionally, SHM’s RIV Committee, along with staff, are working on arrangements for junior faculty to interact with senior researchers during times that run concurrent with non-plenary sessions. Senior hospitalists with expertise in quality-improvement research will also provide individual feedback to authors at the poster sessions. Mini poster presentation sessions will provide a way for residents to highlight their work, and there will be new, separate receptions for the posters (April 3) and exhibits (April 4).
More networking: Networking provides a critical outlet to interact with senior hospitalists, find out what others are doing to advance their careers, and seek mentorship. In addition to the networking opportunities incorporated in the RIV Competition, other networking opportunities include the exhibits, President’s Luncheon and additional receptions, and two new special-interest forums on com-anagement and consultative medicine and international hospital medicine.
The Annual Meeting Committee sought improvements in developing and implementing this year’s program. Committee brainstorming sessions for this year’s meeting focused on:
- Balancing what works with innovation;
- Making the meeting more valuable to clinical educators and researchers, and more applicable to community hospitalists; and
- Showing national leaders the extraordinary talent behind and work of SHM.
A key innovation was a successful “call for speakers.” Submissions were sought for three breakout sessions to create additional opportunity for members to play an active role in “Hospital Medicine 2008.” Based on submissions, sessions were added on the following topics:
- “Prevention, Management, and Treatment of Acute Delirium”;
- “Designing Compensation and Bonus Plans to Drive Desired Behavior”; and
- “Acute Coronary Syndrome Trials and Tribulations.”
Changes for “Hospital Medicine 2008” reflect the volunteerism of many professionals and would not have been possible without the mentorship and expertise of seasoned veteran leaders in hospital medicine, as well as the feedback and participation of hospitalists providing daily inpatient care. As part of a continuous quality-improvement initiative, rules of engagement were developed so speakers would have useful information up front.
The success of the SHM Annual Meeting depends upon the participation and leadership of SHM members, staff, committees, and task forces, as well as the SHM Board. My thanks goes out to them all for their efforts in once again creating a top-flight program.
For more information on “Hospital Medicine 2008,” and to register, visit www.hospitalmedicine.org/hospitalmedicine2008.
SHM’s Annual Meeting highlights hospital medicine as a distinct field within internal medicine. Being able to, year after year, incorporate core clinical topics, evidence-based practice, quality-related content, and career development into three days is only possible because of the foundation laid from previous meetings over the past 10 years.
Expectations about the role of hospitalists have taken shape through recommendations from education summits and national experts on healthcare policy, and via publications like the Journal of Hospital Medicine and The Core Competencies in Hospital Medicine. The Annual Meeting Committee’s goal was to define a program that facilitates hospitalists in achieving that role.
The 2008 meeting April 3-5 in San Diego will feature:
- National leaders in hospital medicine and healthcare;
- Six precourses addressing timely and relevant topics; and
- Seven tracks addressing clinical, operational, quality, academic, and pediatric issues.
Issues that have broad appeal and present challenges for hospitalists will be addressed in three widely anticipated keynotes:
Quality: Don Berwick, MD, MPP, FRCP, president and CEO, Institute for Healthcare Improvement (IHI) and architect of both the 100,000 Lives and 5 Million Lives campaigns;
The future of healthcare: Ian Morrison, PhD, president emeritus and health advisory panel chair, Institute for the Future, and an internationally known author on long-term forecasting with particular emphasis on healthcare;
Thriving in the face of comanagement, non-teaching services, transparency, and the reality of perpetual change: Robert Wachter, MD, professor and chief of the division of hospital medicine, associate chairman of the department of medicine, University of California, San Francisco.
The future of hospital medicine: opportunities and challenges: A special plenary session presented by a panel of hospital medicine leaders who will share perspectives from:
- The large hospitalist company;
- The large hospital company as an employer;
- The hospital CEO; and
- The individual hospital employed/associated hospital medicine group.
The following program elements are only a few of the many highlights of “Hospital Medicine 2008”:
The Evidence-Based Rapid-Fire Track: This track was developed in response from last year’s attendees. It is designed to provide participants—new or old attendees, academic or community caregivers—with “rapid bursts” of content and to address specific questions framed by the committee, based on the highest level of medical evidence available.
Research, Innovations, and Clinical Vignettes (RIV) Competition: Building on a new feature from “Hospital Medicine 2007,” a nationally renowned professor will again tour the poster session and comment on the entries, meet with academic hospitalists, attend forums, and generally be a “visiting professor” for the duration of the meeting. Additionally, SHM’s RIV Committee, along with staff, are working on arrangements for junior faculty to interact with senior researchers during times that run concurrent with non-plenary sessions. Senior hospitalists with expertise in quality-improvement research will also provide individual feedback to authors at the poster sessions. Mini poster presentation sessions will provide a way for residents to highlight their work, and there will be new, separate receptions for the posters (April 3) and exhibits (April 4).
More networking: Networking provides a critical outlet to interact with senior hospitalists, find out what others are doing to advance their careers, and seek mentorship. In addition to the networking opportunities incorporated in the RIV Competition, other networking opportunities include the exhibits, President’s Luncheon and additional receptions, and two new special-interest forums on com-anagement and consultative medicine and international hospital medicine.
The Annual Meeting Committee sought improvements in developing and implementing this year’s program. Committee brainstorming sessions for this year’s meeting focused on:
- Balancing what works with innovation;
- Making the meeting more valuable to clinical educators and researchers, and more applicable to community hospitalists; and
- Showing national leaders the extraordinary talent behind and work of SHM.
A key innovation was a successful “call for speakers.” Submissions were sought for three breakout sessions to create additional opportunity for members to play an active role in “Hospital Medicine 2008.” Based on submissions, sessions were added on the following topics:
- “Prevention, Management, and Treatment of Acute Delirium”;
- “Designing Compensation and Bonus Plans to Drive Desired Behavior”; and
- “Acute Coronary Syndrome Trials and Tribulations.”
Changes for “Hospital Medicine 2008” reflect the volunteerism of many professionals and would not have been possible without the mentorship and expertise of seasoned veteran leaders in hospital medicine, as well as the feedback and participation of hospitalists providing daily inpatient care. As part of a continuous quality-improvement initiative, rules of engagement were developed so speakers would have useful information up front.
The success of the SHM Annual Meeting depends upon the participation and leadership of SHM members, staff, committees, and task forces, as well as the SHM Board. My thanks goes out to them all for their efforts in once again creating a top-flight program.
For more information on “Hospital Medicine 2008,” and to register, visit www.hospitalmedicine.org/hospitalmedicine2008.
Hospitalists Find Writing Makes Them Better Doctors
When people hear that Ruben J. Nazario, MD, a pediatric hospitalist at Kentucky Children’s Hospital in Lexington, writes in his spare time, they assume he writes for children. “But my writing is very non-pediatric,” he says. “I’m two people in one.”
A native of Puerto Rico, Dr. Nazario primarily writes poetry in English and stories in Spanish. His short stories and novels deal with what he calls “the fun stuff”: passion, violence, death.
For example, a speck of tomato sauce falling on the floor when his wife served him a plate of spaghetti became the inspiration for a story in which the same thing happens. But in his story, the characters argue and the husband licks up the sauce from the floor. “That part didn’t really happen,” he laughs.
One might imagine writing as merely a hobby or diversion for practicing hospitalists. But those who indulge in the craft say it hones their medical skills.
Ron Grant, MD, pediatric hospitalist at the University of Arizona Medical Center in Tucson says writing affects his mood, which subsequently affects his practice. “It allows you to speak out [about] frustrations that arise, interesting situations that arise, and I find that very valuable,” he says.
The therapeutic experience is common to hospitalist writers.
Sandi Verbin, MD, a pediatric hospitalist at Holy Redeemer Hospital in Meadowbrook, Pa., says writing brings out her sense of humor, which helps with everything in medical practice. “Fortunately, with pediatrics, most of our patients get better,” she says.
But of course that’s not always the case. When a 7-year-old patient, who was in his care on and off for three years during his training, died of leukemia, Randy Ferrance, MD, a hospitalist at Riverside Tappahannock Hospital in Va., filtered the experience into a story.
“The piece was mostly biographical, but I put it in a fictional context,” says Dr. Ferrance. “I wrote it to say some of the things that I never did say, and work through things I never had worked through, with the patient and family. Writing helps me to clear my head and put things in a better perspective. It’s worth the time I carve out. It doesn’t affect the medical end of things, but it helps my ability to continue doing what I do.”
Many hospitalist writers say their art makes them more empathetic.
Joseph Geskey, DO, the division chief of pediatric hospital medicine at Penn State M.S. Hershey Medical Center in Pa., has published poetry in the Journal of the American Medical Association, an anthology in a book, essays, and fiction. “Writing allows you to clarify your thoughts, so it allows for some epiphanies, not only [regarding] writing but about life in general,” he says.
Preliminary studies suggest writing may have medical benefits such as reducing stress catecholamines and inflammatory markers. Though hard data are still to come, Dr. Geskey believes writing has made him a better physician. He says he is more patient, a better listener, and lets patients digress in their stories, revealing information he might not otherwise have learned. “If I’m able to use my rudimentary senses in my writing to evoke a scene or an image, how do I use those same senses to color in my interaction with patients, to help them feel better?” he asks.
The Trend Grows
There are a number of doctors who teach creative writing around the country, and writing workshops for physicians are popping up in and outside medical education curricula.
In Durham, N.C., Dr. Geskey participated in a Duke University poetry and medicine conference that he describes as “probably the most creative three or four days of my life.”
For three years, Bryan R. Fine, MD, MPH, pediatric hospitalist at Children’s National Medical Center in Washington, D.C., ran a creative writing elective for fourth-year medical students at George Washington University. Dr. Fine often writes during down time at work, especially on the night shift. He writes stories, nonfiction essays, and songs, which he performs publicly on occasion, including a few weeks each year at Club Med and other Caribbean locales.
Dr. Verbin has taken seminars in writing for children. “I’ve made some baby steps in that direction, but progress has been slow and mostly relegated to someday,’” she says.
In 1998, Dr. Grant left the University of Arizona, where he was practicing as a hospitalist for Cleo Hardin, MD, section chief of pediatric hospital medicine and herself a writer. (She is revising a memoir she wrote a couple years ago and beginning a novel about mothers and daughters). He traveled to Israel and Poland and wrote about that experience, then realized he wanted more. He returned to his school to pursue a master’s in creative writing. A year ago, at Dr. Hardin’s urging, he returned to medicine, now describing himself as a part-time hospitalist and full-time writer.
“I was overwhelmed by a lot of strange sensations when I went back to the hospital—all of which really informed my writing,” says Dr. Grant.
He is working on a memoir about leaving medicine after becoming uncomfortable with the ethical and personal dilemmas he faced as a pediatrician and as a father. “It’s hard to watch children die, but unbearable when you have children of your own,” he says.
Dr. Grant works nights, teaches medical students an elective in creative writing, and occasionally teaches at a community college. His most exciting teaching outlet is as an instructor in the Czech Republic at the prestigious Prague Summer Program, a study-abroad program offered through Western Michigan University. Those who take his the two-week memoir-writing workshop bring complete manuscripts for review and critique.
“The whole philosophy behind teaching writing and taking humanities classes is that there are unexplored areas of the brain that get withered as you go through medical school and residency,” Dr. Grant says. “Re-exploring that creative side allows us to become better physicians. Becoming more in touch with your own humanity allows you to be a more human practitioner, Even though I only practice part time, I’m certainly different as a practitioner than I was before [I started writing].”
As a full-time writer, Dr. Grant is the exception. But Dr. Nazario recalls a quote from physician Anton Chekhov that may sum things up for other hospitalist writers: “Medicine is my lawful wife, and literature is my mistress. When I get fed up with one, I spend the night with the other.” TH
Andrea Sattinger is a medical writer based in North Carolina.
When people hear that Ruben J. Nazario, MD, a pediatric hospitalist at Kentucky Children’s Hospital in Lexington, writes in his spare time, they assume he writes for children. “But my writing is very non-pediatric,” he says. “I’m two people in one.”
A native of Puerto Rico, Dr. Nazario primarily writes poetry in English and stories in Spanish. His short stories and novels deal with what he calls “the fun stuff”: passion, violence, death.
For example, a speck of tomato sauce falling on the floor when his wife served him a plate of spaghetti became the inspiration for a story in which the same thing happens. But in his story, the characters argue and the husband licks up the sauce from the floor. “That part didn’t really happen,” he laughs.
One might imagine writing as merely a hobby or diversion for practicing hospitalists. But those who indulge in the craft say it hones their medical skills.
Ron Grant, MD, pediatric hospitalist at the University of Arizona Medical Center in Tucson says writing affects his mood, which subsequently affects his practice. “It allows you to speak out [about] frustrations that arise, interesting situations that arise, and I find that very valuable,” he says.
The therapeutic experience is common to hospitalist writers.
Sandi Verbin, MD, a pediatric hospitalist at Holy Redeemer Hospital in Meadowbrook, Pa., says writing brings out her sense of humor, which helps with everything in medical practice. “Fortunately, with pediatrics, most of our patients get better,” she says.
But of course that’s not always the case. When a 7-year-old patient, who was in his care on and off for three years during his training, died of leukemia, Randy Ferrance, MD, a hospitalist at Riverside Tappahannock Hospital in Va., filtered the experience into a story.
“The piece was mostly biographical, but I put it in a fictional context,” says Dr. Ferrance. “I wrote it to say some of the things that I never did say, and work through things I never had worked through, with the patient and family. Writing helps me to clear my head and put things in a better perspective. It’s worth the time I carve out. It doesn’t affect the medical end of things, but it helps my ability to continue doing what I do.”
Many hospitalist writers say their art makes them more empathetic.
Joseph Geskey, DO, the division chief of pediatric hospital medicine at Penn State M.S. Hershey Medical Center in Pa., has published poetry in the Journal of the American Medical Association, an anthology in a book, essays, and fiction. “Writing allows you to clarify your thoughts, so it allows for some epiphanies, not only [regarding] writing but about life in general,” he says.
Preliminary studies suggest writing may have medical benefits such as reducing stress catecholamines and inflammatory markers. Though hard data are still to come, Dr. Geskey believes writing has made him a better physician. He says he is more patient, a better listener, and lets patients digress in their stories, revealing information he might not otherwise have learned. “If I’m able to use my rudimentary senses in my writing to evoke a scene or an image, how do I use those same senses to color in my interaction with patients, to help them feel better?” he asks.
The Trend Grows
There are a number of doctors who teach creative writing around the country, and writing workshops for physicians are popping up in and outside medical education curricula.
In Durham, N.C., Dr. Geskey participated in a Duke University poetry and medicine conference that he describes as “probably the most creative three or four days of my life.”
For three years, Bryan R. Fine, MD, MPH, pediatric hospitalist at Children’s National Medical Center in Washington, D.C., ran a creative writing elective for fourth-year medical students at George Washington University. Dr. Fine often writes during down time at work, especially on the night shift. He writes stories, nonfiction essays, and songs, which he performs publicly on occasion, including a few weeks each year at Club Med and other Caribbean locales.
Dr. Verbin has taken seminars in writing for children. “I’ve made some baby steps in that direction, but progress has been slow and mostly relegated to someday,’” she says.
In 1998, Dr. Grant left the University of Arizona, where he was practicing as a hospitalist for Cleo Hardin, MD, section chief of pediatric hospital medicine and herself a writer. (She is revising a memoir she wrote a couple years ago and beginning a novel about mothers and daughters). He traveled to Israel and Poland and wrote about that experience, then realized he wanted more. He returned to his school to pursue a master’s in creative writing. A year ago, at Dr. Hardin’s urging, he returned to medicine, now describing himself as a part-time hospitalist and full-time writer.
“I was overwhelmed by a lot of strange sensations when I went back to the hospital—all of which really informed my writing,” says Dr. Grant.
He is working on a memoir about leaving medicine after becoming uncomfortable with the ethical and personal dilemmas he faced as a pediatrician and as a father. “It’s hard to watch children die, but unbearable when you have children of your own,” he says.
Dr. Grant works nights, teaches medical students an elective in creative writing, and occasionally teaches at a community college. His most exciting teaching outlet is as an instructor in the Czech Republic at the prestigious Prague Summer Program, a study-abroad program offered through Western Michigan University. Those who take his the two-week memoir-writing workshop bring complete manuscripts for review and critique.
“The whole philosophy behind teaching writing and taking humanities classes is that there are unexplored areas of the brain that get withered as you go through medical school and residency,” Dr. Grant says. “Re-exploring that creative side allows us to become better physicians. Becoming more in touch with your own humanity allows you to be a more human practitioner, Even though I only practice part time, I’m certainly different as a practitioner than I was before [I started writing].”
As a full-time writer, Dr. Grant is the exception. But Dr. Nazario recalls a quote from physician Anton Chekhov that may sum things up for other hospitalist writers: “Medicine is my lawful wife, and literature is my mistress. When I get fed up with one, I spend the night with the other.” TH
Andrea Sattinger is a medical writer based in North Carolina.
When people hear that Ruben J. Nazario, MD, a pediatric hospitalist at Kentucky Children’s Hospital in Lexington, writes in his spare time, they assume he writes for children. “But my writing is very non-pediatric,” he says. “I’m two people in one.”
A native of Puerto Rico, Dr. Nazario primarily writes poetry in English and stories in Spanish. His short stories and novels deal with what he calls “the fun stuff”: passion, violence, death.
For example, a speck of tomato sauce falling on the floor when his wife served him a plate of spaghetti became the inspiration for a story in which the same thing happens. But in his story, the characters argue and the husband licks up the sauce from the floor. “That part didn’t really happen,” he laughs.
One might imagine writing as merely a hobby or diversion for practicing hospitalists. But those who indulge in the craft say it hones their medical skills.
Ron Grant, MD, pediatric hospitalist at the University of Arizona Medical Center in Tucson says writing affects his mood, which subsequently affects his practice. “It allows you to speak out [about] frustrations that arise, interesting situations that arise, and I find that very valuable,” he says.
The therapeutic experience is common to hospitalist writers.
Sandi Verbin, MD, a pediatric hospitalist at Holy Redeemer Hospital in Meadowbrook, Pa., says writing brings out her sense of humor, which helps with everything in medical practice. “Fortunately, with pediatrics, most of our patients get better,” she says.
But of course that’s not always the case. When a 7-year-old patient, who was in his care on and off for three years during his training, died of leukemia, Randy Ferrance, MD, a hospitalist at Riverside Tappahannock Hospital in Va., filtered the experience into a story.
“The piece was mostly biographical, but I put it in a fictional context,” says Dr. Ferrance. “I wrote it to say some of the things that I never did say, and work through things I never had worked through, with the patient and family. Writing helps me to clear my head and put things in a better perspective. It’s worth the time I carve out. It doesn’t affect the medical end of things, but it helps my ability to continue doing what I do.”
Many hospitalist writers say their art makes them more empathetic.
Joseph Geskey, DO, the division chief of pediatric hospital medicine at Penn State M.S. Hershey Medical Center in Pa., has published poetry in the Journal of the American Medical Association, an anthology in a book, essays, and fiction. “Writing allows you to clarify your thoughts, so it allows for some epiphanies, not only [regarding] writing but about life in general,” he says.
Preliminary studies suggest writing may have medical benefits such as reducing stress catecholamines and inflammatory markers. Though hard data are still to come, Dr. Geskey believes writing has made him a better physician. He says he is more patient, a better listener, and lets patients digress in their stories, revealing information he might not otherwise have learned. “If I’m able to use my rudimentary senses in my writing to evoke a scene or an image, how do I use those same senses to color in my interaction with patients, to help them feel better?” he asks.
The Trend Grows
There are a number of doctors who teach creative writing around the country, and writing workshops for physicians are popping up in and outside medical education curricula.
In Durham, N.C., Dr. Geskey participated in a Duke University poetry and medicine conference that he describes as “probably the most creative three or four days of my life.”
For three years, Bryan R. Fine, MD, MPH, pediatric hospitalist at Children’s National Medical Center in Washington, D.C., ran a creative writing elective for fourth-year medical students at George Washington University. Dr. Fine often writes during down time at work, especially on the night shift. He writes stories, nonfiction essays, and songs, which he performs publicly on occasion, including a few weeks each year at Club Med and other Caribbean locales.
Dr. Verbin has taken seminars in writing for children. “I’ve made some baby steps in that direction, but progress has been slow and mostly relegated to someday,’” she says.
In 1998, Dr. Grant left the University of Arizona, where he was practicing as a hospitalist for Cleo Hardin, MD, section chief of pediatric hospital medicine and herself a writer. (She is revising a memoir she wrote a couple years ago and beginning a novel about mothers and daughters). He traveled to Israel and Poland and wrote about that experience, then realized he wanted more. He returned to his school to pursue a master’s in creative writing. A year ago, at Dr. Hardin’s urging, he returned to medicine, now describing himself as a part-time hospitalist and full-time writer.
“I was overwhelmed by a lot of strange sensations when I went back to the hospital—all of which really informed my writing,” says Dr. Grant.
He is working on a memoir about leaving medicine after becoming uncomfortable with the ethical and personal dilemmas he faced as a pediatrician and as a father. “It’s hard to watch children die, but unbearable when you have children of your own,” he says.
Dr. Grant works nights, teaches medical students an elective in creative writing, and occasionally teaches at a community college. His most exciting teaching outlet is as an instructor in the Czech Republic at the prestigious Prague Summer Program, a study-abroad program offered through Western Michigan University. Those who take his the two-week memoir-writing workshop bring complete manuscripts for review and critique.
“The whole philosophy behind teaching writing and taking humanities classes is that there are unexplored areas of the brain that get withered as you go through medical school and residency,” Dr. Grant says. “Re-exploring that creative side allows us to become better physicians. Becoming more in touch with your own humanity allows you to be a more human practitioner, Even though I only practice part time, I’m certainly different as a practitioner than I was before [I started writing].”
As a full-time writer, Dr. Grant is the exception. But Dr. Nazario recalls a quote from physician Anton Chekhov that may sum things up for other hospitalist writers: “Medicine is my lawful wife, and literature is my mistress. When I get fed up with one, I spend the night with the other.” TH
Andrea Sattinger is a medical writer based in North Carolina.
Team Hospitalist at Work for you
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist

R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston

Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.

Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas

Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.

William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia

David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.

Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia

Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.

Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.

Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.

Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison

David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist
R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston
Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.
Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas
Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia
David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.
Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia
Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.
Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.
Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.
Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison
David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist
R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston
Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.
Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas
Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia
David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.
Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia
Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.
Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.
Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.
Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison
David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
The STAR*D study: Treating depression in the real world
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
KEY POINTS
- Remission (ie, complete relief from a depressive episode) rather than response (merely substantial improvement) should be the goal of treatment, as it is associated with a better prognosis and better function.
- Should the first treatment fail, either switching treat mentor augmenting the current treatment is reasonable.
- For most patients, remission will require repeated trials of sufficiently sustained, vigorously dosed antidepressant medication. Physicians should give maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- After two well-delivered medication trials, the likelihood of remission substantially decreases. Such patients likely require more complicated regimens. Given the thin existing database, these patients are best referred to a psychiatrist for more complex treatments.
- With persistent and vigorous treatment, most patients will enter remission: about 33% after one step, 50% after two steps, 60% after three steps, and 70% after four steps (assuming patients stay in treatment).
Masquerade: Nonspinal musculoskeletal disorders that mimic spinal conditions
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1

Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together

Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1
Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together
Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1
Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together
Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
KEY POINTS
- Neck pain is commonly caused by shoulder problems such as rotator cuff disease, glenohumeral arthritis, and humeral head osteonecrosis.
- Brachial neuritis involves acute, severe neck or shoulder pain, followed by weakness as pain resolves.
- Low back pain can be caused by hip or spine arthritis, femoral head osteonecrosis, an occult or impending femoral neck fracture, hip dysplasia, piriformis syndrome, and bursitis.
- Bony and soft tissue masses can be detected with imaging studies.
- Peripheral nerve compression can mimic cervical or lumbar spine radiculopathy. Electromyography and eliciting symptoms by tapping over the compressed nerve aid in making a diagnosis.
- Patients with human immunodeficiency virus infection, alcoholism, or corticosteroid use are at increased risk of developing osteonecrosis of the humeral or femoral head.
Fluid restriction is superior in acute lung injury and ARDS
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
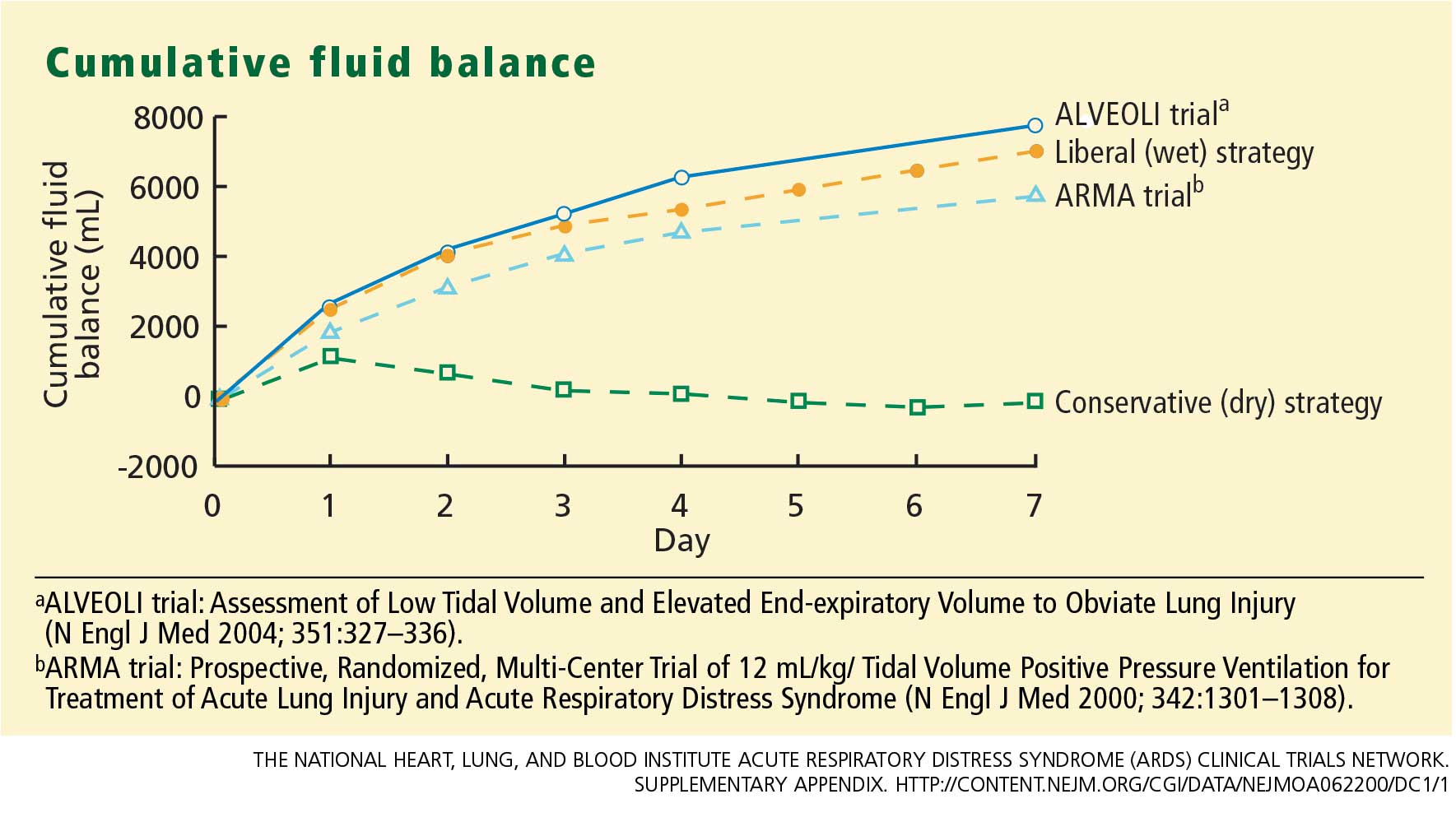
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
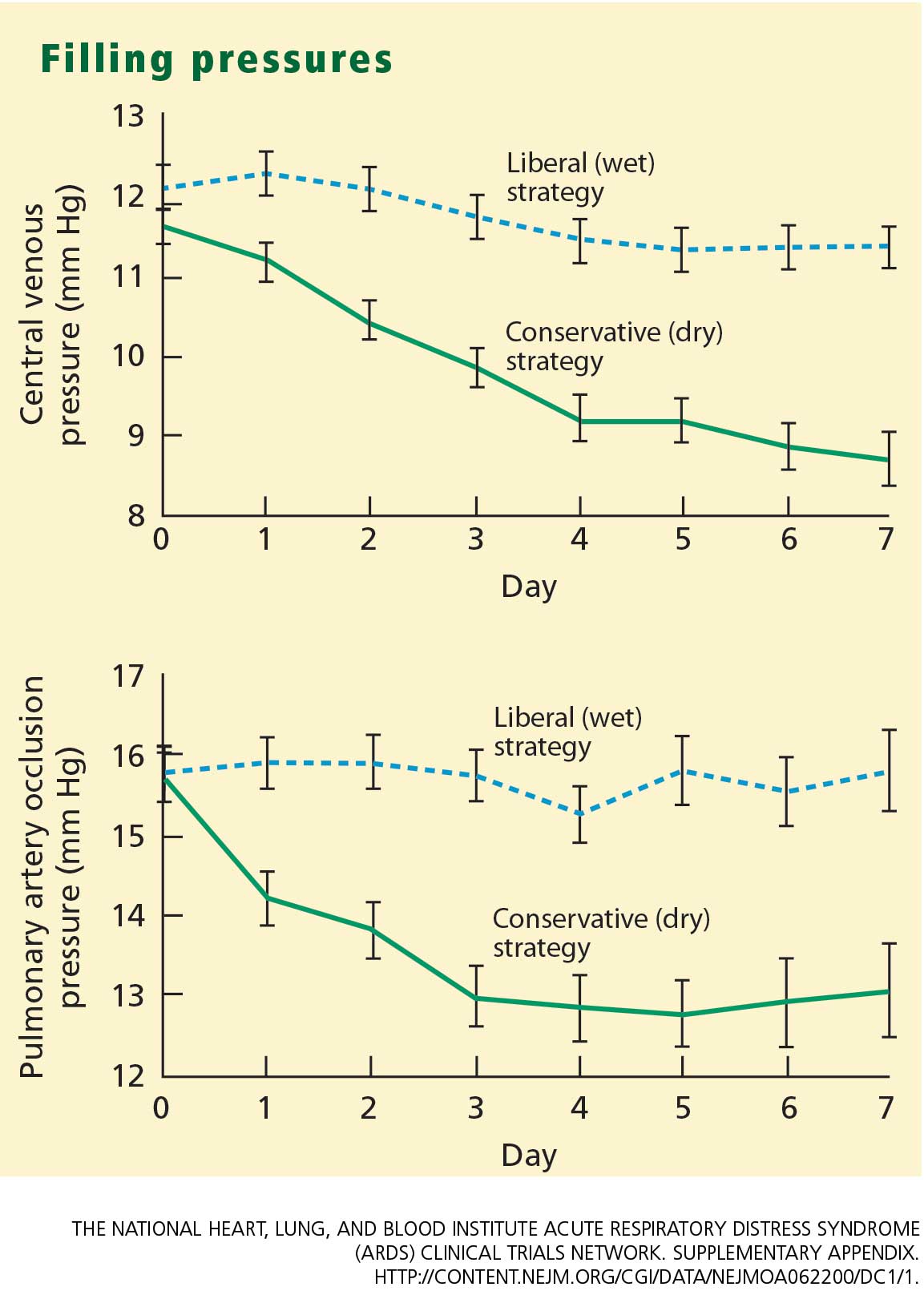
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
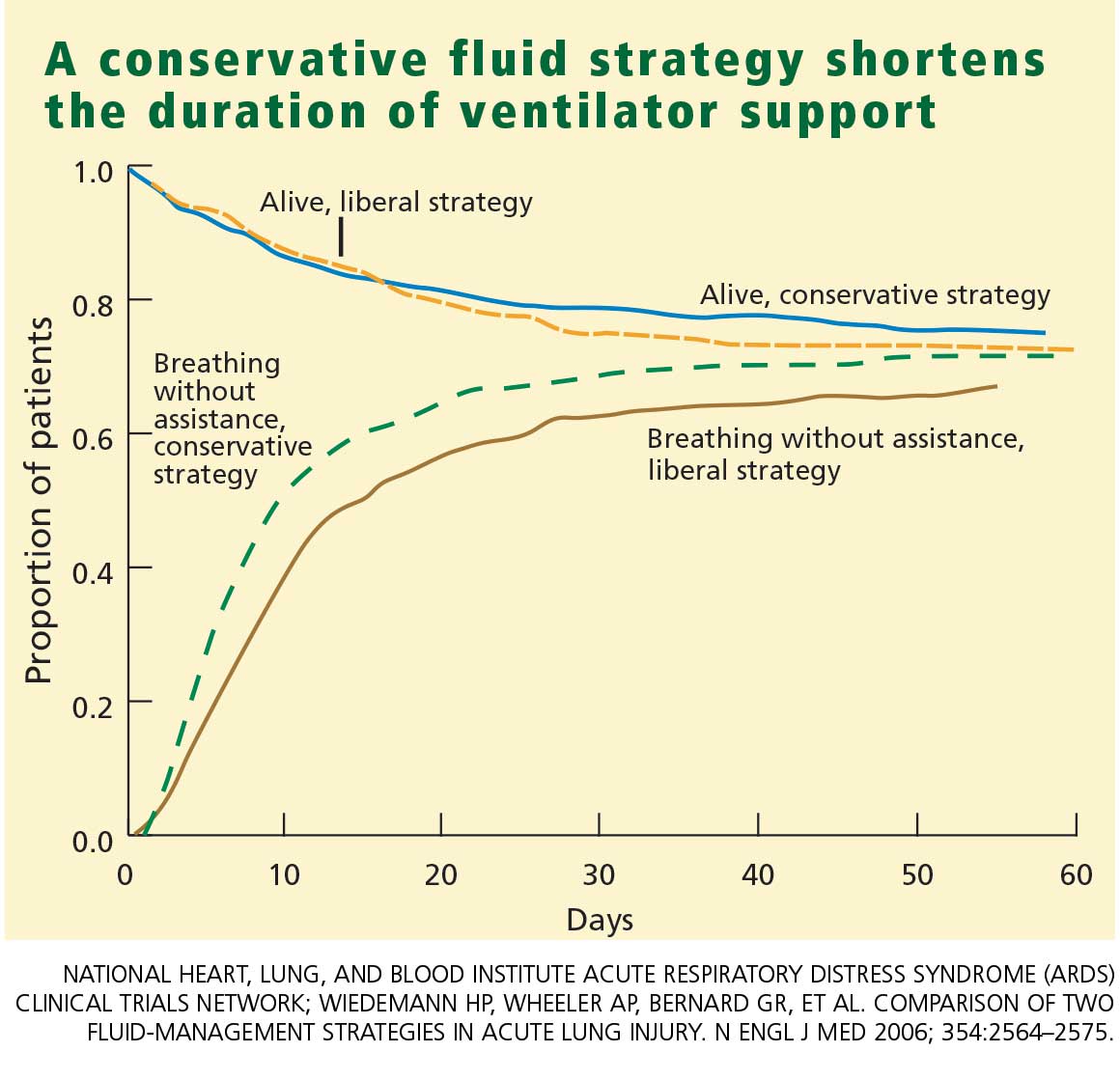
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
KEY POINTS
- In the conservative-strategy group, the target filling pressures were a pulmonary artery occlusion pressure less than 8 mm Hg for those with a pulmonary artery catheter and a central venous pressure less than 4 mm Hg for those with only a central venous catheter. Pressures were brought into these ranges by diuresis.
- The conservative-strategy group did not experience more frequent need for dialysis or more shock.
- Although the number of adverse events—particularly ,metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group, the overall incidence was low.