User login
Team Approach

Team Approach
Question: We work with a large orthopedic group. We would like to propose a more formal structure to this. We are interested in building business and partnerships. Do you know of any articles or references to support hospitalists doing this, or any sources to show the orthopedic group we can and would improve outcomes and their work life and workload?
Julie Lepzinski, director,
hospitalist medicine group,
Michigan
Dr. Hospitalist responds: I commend you and your hospitalist group for taking the initiative to develop a relationship with your orthopedics colleagues. Many hospitalist groups are exploring such relationships with not only orthopedists but also with other surgical and medical subspecialists.
As you mentioned, the opportunity exists to improve your group’s income and improve orthopedist work life. More importantly, there is a real opportunity to improve the medical care of patients admitted to the hospital primarily with orthopedic problems.
There are published data from an academic medical center on a hospitalist-orthopedics co-management model. Huddleston, et al., studied the effect of such a co-management model on the care of patients after elective hip and knee arthroplasty at the Mayo Clinic.1 They found that “the co-management medical hospitalist-orthopedic team model reduced minor postoperative complication rates with no statistically significant difference in length of stay or cost. The nurses and surgeons strongly preferred the co-management hospitalist model.”
This study would seem to support your notion that orthopedists may prefer the involvement of hospitalists in the care of their patients. Hospitalist involvement reduced minor complications (urinary tract infections, fever, electrolyte abnormalities). However, investigators did not find that hospitalist co-management reduced major postoperative complications (death, myocardial infarction, renal failure requiring hemodialysis) or intermediate ones (heart failure, pulmonary embolus, ileus, pneumonia).
Mayo Clinic hospitalists also studied the impact of a hospitalist-orthopedist co-management model of the care on elderly patients admitted to their hospital with hip fracture.2 Phy, et al., found that, “In elderly patients with hip fracture, a hospitalist model decreased time to surgery, time from surgery to dismissal and length of stay without adversely affecting inpatient deaths or 30-day readmission rates.” This study demonstrated that hospitalist co-management can decrease hospital length of stay in this population of patients.
We should recognize the obvious limitations of these studies. They were done at a single large academic institution with a largely Caucasian population at the turn of the century (2000-2001), early in the hospitalist movement. The hospitalist movement has matured, with approximately 20,000 hospitalists in the country. I hope we will soon see more robust data coming from multicenter trials that include a more diverse population of patients as well as a mix of community and academic institutions.
Start an HMG?
Question: We own a medical clinic in Arizona and are thinking of starting a hospitalist group as a separate business entity. Are you aware of any recommended reading or articles on how to start one, if it’s profitable, and in what shape or form? And most important--regarding the current trends and projections--I wonder if the need has changed, as most hospitals reduce their number of vendors.
Shawn Toloui, president and owner,
1st Care Medical Clinic,
Phoenix, Ariz.
Dr. Hospitalist responds: These are the kind of questions people have been asking since the term “hospitalist” was coined in 1996. Over the past decade, we have seen an explosion in the number of hospitalists in the country. Few folks in the 1990s thought there would be 20,000 hospitalists today.
If I understand you correctly, you are concerned that because many hospitals are reducing their numbers of vendors, this may have an adverse effect on the need for hospitalists. Hospitals will engage in business relationships with hospitalists as long as the hospitalists can bring solutions to problems and fulfill needs. To understand this better, let’s examine the reasons the numbers of hospitalists have grown over the past decade.
Costs: When Medicare started paying hospitals based on diagnosis-related groups (DRGs) in the early ’80s, this forced hospitals to “manage” patients’ length of stay. The DRG system pays a fixed fee regardless of the length of stay but allows for an adjusted higher payment based on a hospital’s case mix index (a measure of how “sick” patients are in a given hospital).
This reimbursement system encourages hospitals to take care of ill patients but also to “manage” their length of stay. It is difficult for doctors to manage any hospitalized patients from outpatient offices, let alone sick patients. Hospitals and payers found that hospitalists are able to manage sick patients and reduce costs, mostly by being available to admit, manage, and discharge patients in a timely manner. This increased throughput of patients also allows hospitals to put another patient in a bed sooner, bringing additional revenue.
Quality: By serendipity, the hospitalist movement coincided with the quality movement. Hospitalists have helped reduce variations in care by working locally to develop and implement clinical-care pathways. Hospitalists have also served as partners for hospitals to achieve compliance with payer quality mandates.
For example, in 2003, Medicare began requiring hospitals to report a handful of diagnosis-based quality measures it called the Core Measures. The number of measures continues to grow. In 2007, Medicare tied hospital reimbursement to performance on the Core Measures. I hear from hospital administrators that they find it easier to educate and work with a small group of hospitalists, rather than a large medical staff, to achieve optimal results on these measures.
Satisfaction: The exodus of primary care physicians (PCPs) from the hospital has fueled much of the growth in hospital medicine. PCPs have found it increasingly difficult to care for hospitalized patients while juggling the demands of a busy outpatient practice. In hospitalists, nurses have found a physician partner who is available physically to work with them in the care of acutely ill patients.
PCPs and nurses have been very satisfied with the hospitalist model of care. Although provider satisfaction is important, satisfaction in healthcare begins and ends with patients. Despite the discontinuity of care of meeting a new provider during hospitalization, patients have been satisfied with hospitalist care. Patients view hospitalists as providers available to provide for their acute needs while also communicating with the patients’ outpatient providers to understand their long-term needs.
I expect the number of hospitalists to grow over the next decade, albeit at a slower pace as most programs begin to fill their available positions. SHM believes the numbers of hospitalists will grow to 40,000.
There are a number of resources that can help you understand how to develop, manage, and grow a hospitalist program. I suggest you visit the “Practice Resources” section of the SHM Web site at www.hospitalmedicine.org. In particular, I recommend the “Best Practices in Managing a Hospital Medicine Program,” held twice a year. The spring program is held in conjunction with the SHM Annual Meeting in San Diego, April 3-5. The fall program is held in conjunction with the University of California, San Francisco’s “Management of the Hospitalized Patient” course in San Francisco. Also, the book Hospitalists: A Guide to Building and Sustaining a Successful Program by SHM Senior Vice President Joe Miller and SHM cofounders John Nelson, MD, and Winthrop F. Whitcomb, MD, is a must read for anybody looking to build a hospitalist program. TH
References
- Huddleston JM, Long KH, Naessens JM, Vanness DJ, Larson D, Trousdale R, Plevak M, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004 July 6;141(1):28-38.
- Phy MP, Vanness DJ, Melton JL, Hallong K, Schleck C, Larson DR, Huddleston PM. et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165:796-801.
Team Approach
Question: We work with a large orthopedic group. We would like to propose a more formal structure to this. We are interested in building business and partnerships. Do you know of any articles or references to support hospitalists doing this, or any sources to show the orthopedic group we can and would improve outcomes and their work life and workload?
Julie Lepzinski, director,
hospitalist medicine group,
Michigan
Dr. Hospitalist responds: I commend you and your hospitalist group for taking the initiative to develop a relationship with your orthopedics colleagues. Many hospitalist groups are exploring such relationships with not only orthopedists but also with other surgical and medical subspecialists.
As you mentioned, the opportunity exists to improve your group’s income and improve orthopedist work life. More importantly, there is a real opportunity to improve the medical care of patients admitted to the hospital primarily with orthopedic problems.
There are published data from an academic medical center on a hospitalist-orthopedics co-management model. Huddleston, et al., studied the effect of such a co-management model on the care of patients after elective hip and knee arthroplasty at the Mayo Clinic.1 They found that “the co-management medical hospitalist-orthopedic team model reduced minor postoperative complication rates with no statistically significant difference in length of stay or cost. The nurses and surgeons strongly preferred the co-management hospitalist model.”
This study would seem to support your notion that orthopedists may prefer the involvement of hospitalists in the care of their patients. Hospitalist involvement reduced minor complications (urinary tract infections, fever, electrolyte abnormalities). However, investigators did not find that hospitalist co-management reduced major postoperative complications (death, myocardial infarction, renal failure requiring hemodialysis) or intermediate ones (heart failure, pulmonary embolus, ileus, pneumonia).
Mayo Clinic hospitalists also studied the impact of a hospitalist-orthopedist co-management model of the care on elderly patients admitted to their hospital with hip fracture.2 Phy, et al., found that, “In elderly patients with hip fracture, a hospitalist model decreased time to surgery, time from surgery to dismissal and length of stay without adversely affecting inpatient deaths or 30-day readmission rates.” This study demonstrated that hospitalist co-management can decrease hospital length of stay in this population of patients.
We should recognize the obvious limitations of these studies. They were done at a single large academic institution with a largely Caucasian population at the turn of the century (2000-2001), early in the hospitalist movement. The hospitalist movement has matured, with approximately 20,000 hospitalists in the country. I hope we will soon see more robust data coming from multicenter trials that include a more diverse population of patients as well as a mix of community and academic institutions.
Start an HMG?
Question: We own a medical clinic in Arizona and are thinking of starting a hospitalist group as a separate business entity. Are you aware of any recommended reading or articles on how to start one, if it’s profitable, and in what shape or form? And most important--regarding the current trends and projections--I wonder if the need has changed, as most hospitals reduce their number of vendors.
Shawn Toloui, president and owner,
1st Care Medical Clinic,
Phoenix, Ariz.
Dr. Hospitalist responds: These are the kind of questions people have been asking since the term “hospitalist” was coined in 1996. Over the past decade, we have seen an explosion in the number of hospitalists in the country. Few folks in the 1990s thought there would be 20,000 hospitalists today.
If I understand you correctly, you are concerned that because many hospitals are reducing their numbers of vendors, this may have an adverse effect on the need for hospitalists. Hospitals will engage in business relationships with hospitalists as long as the hospitalists can bring solutions to problems and fulfill needs. To understand this better, let’s examine the reasons the numbers of hospitalists have grown over the past decade.
Costs: When Medicare started paying hospitals based on diagnosis-related groups (DRGs) in the early ’80s, this forced hospitals to “manage” patients’ length of stay. The DRG system pays a fixed fee regardless of the length of stay but allows for an adjusted higher payment based on a hospital’s case mix index (a measure of how “sick” patients are in a given hospital).
This reimbursement system encourages hospitals to take care of ill patients but also to “manage” their length of stay. It is difficult for doctors to manage any hospitalized patients from outpatient offices, let alone sick patients. Hospitals and payers found that hospitalists are able to manage sick patients and reduce costs, mostly by being available to admit, manage, and discharge patients in a timely manner. This increased throughput of patients also allows hospitals to put another patient in a bed sooner, bringing additional revenue.
Quality: By serendipity, the hospitalist movement coincided with the quality movement. Hospitalists have helped reduce variations in care by working locally to develop and implement clinical-care pathways. Hospitalists have also served as partners for hospitals to achieve compliance with payer quality mandates.
For example, in 2003, Medicare began requiring hospitals to report a handful of diagnosis-based quality measures it called the Core Measures. The number of measures continues to grow. In 2007, Medicare tied hospital reimbursement to performance on the Core Measures. I hear from hospital administrators that they find it easier to educate and work with a small group of hospitalists, rather than a large medical staff, to achieve optimal results on these measures.
Satisfaction: The exodus of primary care physicians (PCPs) from the hospital has fueled much of the growth in hospital medicine. PCPs have found it increasingly difficult to care for hospitalized patients while juggling the demands of a busy outpatient practice. In hospitalists, nurses have found a physician partner who is available physically to work with them in the care of acutely ill patients.
PCPs and nurses have been very satisfied with the hospitalist model of care. Although provider satisfaction is important, satisfaction in healthcare begins and ends with patients. Despite the discontinuity of care of meeting a new provider during hospitalization, patients have been satisfied with hospitalist care. Patients view hospitalists as providers available to provide for their acute needs while also communicating with the patients’ outpatient providers to understand their long-term needs.
I expect the number of hospitalists to grow over the next decade, albeit at a slower pace as most programs begin to fill their available positions. SHM believes the numbers of hospitalists will grow to 40,000.
There are a number of resources that can help you understand how to develop, manage, and grow a hospitalist program. I suggest you visit the “Practice Resources” section of the SHM Web site at www.hospitalmedicine.org. In particular, I recommend the “Best Practices in Managing a Hospital Medicine Program,” held twice a year. The spring program is held in conjunction with the SHM Annual Meeting in San Diego, April 3-5. The fall program is held in conjunction with the University of California, San Francisco’s “Management of the Hospitalized Patient” course in San Francisco. Also, the book Hospitalists: A Guide to Building and Sustaining a Successful Program by SHM Senior Vice President Joe Miller and SHM cofounders John Nelson, MD, and Winthrop F. Whitcomb, MD, is a must read for anybody looking to build a hospitalist program. TH
References
- Huddleston JM, Long KH, Naessens JM, Vanness DJ, Larson D, Trousdale R, Plevak M, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004 July 6;141(1):28-38.
- Phy MP, Vanness DJ, Melton JL, Hallong K, Schleck C, Larson DR, Huddleston PM. et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165:796-801.
Team Approach
Question: We work with a large orthopedic group. We would like to propose a more formal structure to this. We are interested in building business and partnerships. Do you know of any articles or references to support hospitalists doing this, or any sources to show the orthopedic group we can and would improve outcomes and their work life and workload?
Julie Lepzinski, director,
hospitalist medicine group,
Michigan
Dr. Hospitalist responds: I commend you and your hospitalist group for taking the initiative to develop a relationship with your orthopedics colleagues. Many hospitalist groups are exploring such relationships with not only orthopedists but also with other surgical and medical subspecialists.
As you mentioned, the opportunity exists to improve your group’s income and improve orthopedist work life. More importantly, there is a real opportunity to improve the medical care of patients admitted to the hospital primarily with orthopedic problems.
There are published data from an academic medical center on a hospitalist-orthopedics co-management model. Huddleston, et al., studied the effect of such a co-management model on the care of patients after elective hip and knee arthroplasty at the Mayo Clinic.1 They found that “the co-management medical hospitalist-orthopedic team model reduced minor postoperative complication rates with no statistically significant difference in length of stay or cost. The nurses and surgeons strongly preferred the co-management hospitalist model.”
This study would seem to support your notion that orthopedists may prefer the involvement of hospitalists in the care of their patients. Hospitalist involvement reduced minor complications (urinary tract infections, fever, electrolyte abnormalities). However, investigators did not find that hospitalist co-management reduced major postoperative complications (death, myocardial infarction, renal failure requiring hemodialysis) or intermediate ones (heart failure, pulmonary embolus, ileus, pneumonia).
Mayo Clinic hospitalists also studied the impact of a hospitalist-orthopedist co-management model of the care on elderly patients admitted to their hospital with hip fracture.2 Phy, et al., found that, “In elderly patients with hip fracture, a hospitalist model decreased time to surgery, time from surgery to dismissal and length of stay without adversely affecting inpatient deaths or 30-day readmission rates.” This study demonstrated that hospitalist co-management can decrease hospital length of stay in this population of patients.
We should recognize the obvious limitations of these studies. They were done at a single large academic institution with a largely Caucasian population at the turn of the century (2000-2001), early in the hospitalist movement. The hospitalist movement has matured, with approximately 20,000 hospitalists in the country. I hope we will soon see more robust data coming from multicenter trials that include a more diverse population of patients as well as a mix of community and academic institutions.
Start an HMG?
Question: We own a medical clinic in Arizona and are thinking of starting a hospitalist group as a separate business entity. Are you aware of any recommended reading or articles on how to start one, if it’s profitable, and in what shape or form? And most important--regarding the current trends and projections--I wonder if the need has changed, as most hospitals reduce their number of vendors.
Shawn Toloui, president and owner,
1st Care Medical Clinic,
Phoenix, Ariz.
Dr. Hospitalist responds: These are the kind of questions people have been asking since the term “hospitalist” was coined in 1996. Over the past decade, we have seen an explosion in the number of hospitalists in the country. Few folks in the 1990s thought there would be 20,000 hospitalists today.
If I understand you correctly, you are concerned that because many hospitals are reducing their numbers of vendors, this may have an adverse effect on the need for hospitalists. Hospitals will engage in business relationships with hospitalists as long as the hospitalists can bring solutions to problems and fulfill needs. To understand this better, let’s examine the reasons the numbers of hospitalists have grown over the past decade.
Costs: When Medicare started paying hospitals based on diagnosis-related groups (DRGs) in the early ’80s, this forced hospitals to “manage” patients’ length of stay. The DRG system pays a fixed fee regardless of the length of stay but allows for an adjusted higher payment based on a hospital’s case mix index (a measure of how “sick” patients are in a given hospital).
This reimbursement system encourages hospitals to take care of ill patients but also to “manage” their length of stay. It is difficult for doctors to manage any hospitalized patients from outpatient offices, let alone sick patients. Hospitals and payers found that hospitalists are able to manage sick patients and reduce costs, mostly by being available to admit, manage, and discharge patients in a timely manner. This increased throughput of patients also allows hospitals to put another patient in a bed sooner, bringing additional revenue.
Quality: By serendipity, the hospitalist movement coincided with the quality movement. Hospitalists have helped reduce variations in care by working locally to develop and implement clinical-care pathways. Hospitalists have also served as partners for hospitals to achieve compliance with payer quality mandates.
For example, in 2003, Medicare began requiring hospitals to report a handful of diagnosis-based quality measures it called the Core Measures. The number of measures continues to grow. In 2007, Medicare tied hospital reimbursement to performance on the Core Measures. I hear from hospital administrators that they find it easier to educate and work with a small group of hospitalists, rather than a large medical staff, to achieve optimal results on these measures.
Satisfaction: The exodus of primary care physicians (PCPs) from the hospital has fueled much of the growth in hospital medicine. PCPs have found it increasingly difficult to care for hospitalized patients while juggling the demands of a busy outpatient practice. In hospitalists, nurses have found a physician partner who is available physically to work with them in the care of acutely ill patients.
PCPs and nurses have been very satisfied with the hospitalist model of care. Although provider satisfaction is important, satisfaction in healthcare begins and ends with patients. Despite the discontinuity of care of meeting a new provider during hospitalization, patients have been satisfied with hospitalist care. Patients view hospitalists as providers available to provide for their acute needs while also communicating with the patients’ outpatient providers to understand their long-term needs.
I expect the number of hospitalists to grow over the next decade, albeit at a slower pace as most programs begin to fill their available positions. SHM believes the numbers of hospitalists will grow to 40,000.
There are a number of resources that can help you understand how to develop, manage, and grow a hospitalist program. I suggest you visit the “Practice Resources” section of the SHM Web site at www.hospitalmedicine.org. In particular, I recommend the “Best Practices in Managing a Hospital Medicine Program,” held twice a year. The spring program is held in conjunction with the SHM Annual Meeting in San Diego, April 3-5. The fall program is held in conjunction with the University of California, San Francisco’s “Management of the Hospitalized Patient” course in San Francisco. Also, the book Hospitalists: A Guide to Building and Sustaining a Successful Program by SHM Senior Vice President Joe Miller and SHM cofounders John Nelson, MD, and Winthrop F. Whitcomb, MD, is a must read for anybody looking to build a hospitalist program. TH
References
- Huddleston JM, Long KH, Naessens JM, Vanness DJ, Larson D, Trousdale R, Plevak M, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004 July 6;141(1):28-38.
- Phy MP, Vanness DJ, Melton JL, Hallong K, Schleck C, Larson DR, Huddleston PM. et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165:796-801.
Nocturnal Economics

In my previous column, I reviewed different strategies for providing hospitalist practice night coverage based on the size of the group (February 2008, p. 61). I suggested that dedicated nocturnists are a valuable though expensive asset that any practice larger than about six to eight full-time equivalents (FTE) should consider.
This month, I offer additional thoughts about compensation for nocturnists. I’ll demonstrate why adding dedicated night coverage—in which the doctor working at night doesn’t work during the daytime hours the day before or after the night shift—may not increase practice workload significantly.
What follows is adapted from a new book I co-wrote with Joe Miller, senior vice president of SHM, and Win Whitcomb, MD, a hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM.1
Compensation
If all hospitalists provide an equal amount of night coverage in rotation (e.g., each member of a four-person group works 61 nights annually), it’s not necessary to adjust the compensation scheme to reflect night work. A night-shift differential in this situation will not influence a doctor’s annual income relative to that of his partner hospitalists.
However, if the hospitalist program seeks more flexibility, it may be advisable to pay more for a night of work than a day of work. Under this scheme, hospitalists may trade day and night work among themselves, leading to enhanced satisfaction. For example, Dr. McCartney is willing to work some of Dr. Lennon’s nights because of the income benefit. Dr. Lennon may or may not work some of Dr. McCartney’s days in return.
If the practice has one or more dedicated nocturnists, they will need to realize some benefit to working only nights. This benefit can take many forms:
- The night hospitalist works less often than day doctors (e.g., day doctors work 220 days annually, night doctors work 182);
- The night hospitalist has a lighter patient load (e.g., a night hospitalist in a small practice typically sleeps three to six hours per night shift while the day doctors typically work a busy eight-to-12-hour shift);
- The night doctor earns more than the day doctors; or
- The night doctor has a higher priority in time-off scheduling.
It is common to combine these benefits. For example a night hospitalist might work less often than day doctors, have a lighter patient load, and earn the same annual income. Anecdotal experience shows that having more income or fewer workdays than day doctors is valued more than a reduced patient load.
For most practices, compensating hospitalists based significantly or entirely on their production can be a good idea but might be problematic for a night doctor. It could lead the night doctor to encourage marginal admissions, some of whom would need to be discharged by the daytime hospitalists hours later. In effect, the night hospitalist could say: “I’ll admit anyone I can get my hands on because my income will increase. I’ll leave it for the day doctors to sort out what to do with all these patients tomorrow.”
An Example
A traditional system of night call (such as pager call from home while also working days) is usually cheaper than dedicated night shifts. And while there are many benefits to having dedicated night shifts, increased patient capacity may not be one of them. Consider the following example:
- On any given day, a five-FTE hospitalist practice has three doctors working, one of whom will be on-call that night by pager;
- That will mean 219 worked days per year for each doctor, one-third of which (73) will be on-call. Each hospitalist gets 146 days off per year;
- The practice decides to switch to dedicated night shifts in which the doctors do not work the day before or after a night shift. The practice wants to retain the 146 days off for each hospitalist. This new coverage arrangement is equivalent to adding 365 shifts annually (one for each night); and
- This will require an additional 1.67 FTE hospitalists (1.67 hospitalists at 219 shifts/year=365).
In this example, by switching from on-call coverage to on-site coverage, the practice increased from five FTEs to 6.67 FTEs. If the daytime work was already enough to keep all three doctors busy, adding 1.67 FTEs for dedicated night shifts may not increase practice productivity or revenue significantly. The practice looks much less productive per FTE (6.67 FTEs are now seeing the volume previously handled by five FTEs) and much costlier.
Changing from traditional night call to dedicated night coverage can be expensive because it may require adding staff yet doesn’t usually increase practice capacity significantly. But it offers other benefits such as those listed in Table 1 (see p. TK). Some practices find they must provide dedicated night coverage to recruit hospitalists. Other institutions choose to support it believing it leads to more timely, efficient, higher-quality care. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Miller J, Nelson J, Whitcomb W. Hospitalists: A Guide to Building and Sustaining a Successful Program. Chicago:Health Administration Press;2007:149-150.
In my previous column, I reviewed different strategies for providing hospitalist practice night coverage based on the size of the group (February 2008, p. 61). I suggested that dedicated nocturnists are a valuable though expensive asset that any practice larger than about six to eight full-time equivalents (FTE) should consider.
This month, I offer additional thoughts about compensation for nocturnists. I’ll demonstrate why adding dedicated night coverage—in which the doctor working at night doesn’t work during the daytime hours the day before or after the night shift—may not increase practice workload significantly.
What follows is adapted from a new book I co-wrote with Joe Miller, senior vice president of SHM, and Win Whitcomb, MD, a hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM.1
Compensation
If all hospitalists provide an equal amount of night coverage in rotation (e.g., each member of a four-person group works 61 nights annually), it’s not necessary to adjust the compensation scheme to reflect night work. A night-shift differential in this situation will not influence a doctor’s annual income relative to that of his partner hospitalists.
However, if the hospitalist program seeks more flexibility, it may be advisable to pay more for a night of work than a day of work. Under this scheme, hospitalists may trade day and night work among themselves, leading to enhanced satisfaction. For example, Dr. McCartney is willing to work some of Dr. Lennon’s nights because of the income benefit. Dr. Lennon may or may not work some of Dr. McCartney’s days in return.
If the practice has one or more dedicated nocturnists, they will need to realize some benefit to working only nights. This benefit can take many forms:
- The night hospitalist works less often than day doctors (e.g., day doctors work 220 days annually, night doctors work 182);
- The night hospitalist has a lighter patient load (e.g., a night hospitalist in a small practice typically sleeps three to six hours per night shift while the day doctors typically work a busy eight-to-12-hour shift);
- The night doctor earns more than the day doctors; or
- The night doctor has a higher priority in time-off scheduling.
It is common to combine these benefits. For example a night hospitalist might work less often than day doctors, have a lighter patient load, and earn the same annual income. Anecdotal experience shows that having more income or fewer workdays than day doctors is valued more than a reduced patient load.
For most practices, compensating hospitalists based significantly or entirely on their production can be a good idea but might be problematic for a night doctor. It could lead the night doctor to encourage marginal admissions, some of whom would need to be discharged by the daytime hospitalists hours later. In effect, the night hospitalist could say: “I’ll admit anyone I can get my hands on because my income will increase. I’ll leave it for the day doctors to sort out what to do with all these patients tomorrow.”
An Example
A traditional system of night call (such as pager call from home while also working days) is usually cheaper than dedicated night shifts. And while there are many benefits to having dedicated night shifts, increased patient capacity may not be one of them. Consider the following example:
- On any given day, a five-FTE hospitalist practice has three doctors working, one of whom will be on-call that night by pager;
- That will mean 219 worked days per year for each doctor, one-third of which (73) will be on-call. Each hospitalist gets 146 days off per year;
- The practice decides to switch to dedicated night shifts in which the doctors do not work the day before or after a night shift. The practice wants to retain the 146 days off for each hospitalist. This new coverage arrangement is equivalent to adding 365 shifts annually (one for each night); and
- This will require an additional 1.67 FTE hospitalists (1.67 hospitalists at 219 shifts/year=365).
In this example, by switching from on-call coverage to on-site coverage, the practice increased from five FTEs to 6.67 FTEs. If the daytime work was already enough to keep all three doctors busy, adding 1.67 FTEs for dedicated night shifts may not increase practice productivity or revenue significantly. The practice looks much less productive per FTE (6.67 FTEs are now seeing the volume previously handled by five FTEs) and much costlier.
Changing from traditional night call to dedicated night coverage can be expensive because it may require adding staff yet doesn’t usually increase practice capacity significantly. But it offers other benefits such as those listed in Table 1 (see p. TK). Some practices find they must provide dedicated night coverage to recruit hospitalists. Other institutions choose to support it believing it leads to more timely, efficient, higher-quality care. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Miller J, Nelson J, Whitcomb W. Hospitalists: A Guide to Building and Sustaining a Successful Program. Chicago:Health Administration Press;2007:149-150.
In my previous column, I reviewed different strategies for providing hospitalist practice night coverage based on the size of the group (February 2008, p. 61). I suggested that dedicated nocturnists are a valuable though expensive asset that any practice larger than about six to eight full-time equivalents (FTE) should consider.
This month, I offer additional thoughts about compensation for nocturnists. I’ll demonstrate why adding dedicated night coverage—in which the doctor working at night doesn’t work during the daytime hours the day before or after the night shift—may not increase practice workload significantly.
What follows is adapted from a new book I co-wrote with Joe Miller, senior vice president of SHM, and Win Whitcomb, MD, a hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM.1
Compensation
If all hospitalists provide an equal amount of night coverage in rotation (e.g., each member of a four-person group works 61 nights annually), it’s not necessary to adjust the compensation scheme to reflect night work. A night-shift differential in this situation will not influence a doctor’s annual income relative to that of his partner hospitalists.
However, if the hospitalist program seeks more flexibility, it may be advisable to pay more for a night of work than a day of work. Under this scheme, hospitalists may trade day and night work among themselves, leading to enhanced satisfaction. For example, Dr. McCartney is willing to work some of Dr. Lennon’s nights because of the income benefit. Dr. Lennon may or may not work some of Dr. McCartney’s days in return.
If the practice has one or more dedicated nocturnists, they will need to realize some benefit to working only nights. This benefit can take many forms:
- The night hospitalist works less often than day doctors (e.g., day doctors work 220 days annually, night doctors work 182);
- The night hospitalist has a lighter patient load (e.g., a night hospitalist in a small practice typically sleeps three to six hours per night shift while the day doctors typically work a busy eight-to-12-hour shift);
- The night doctor earns more than the day doctors; or
- The night doctor has a higher priority in time-off scheduling.
It is common to combine these benefits. For example a night hospitalist might work less often than day doctors, have a lighter patient load, and earn the same annual income. Anecdotal experience shows that having more income or fewer workdays than day doctors is valued more than a reduced patient load.
For most practices, compensating hospitalists based significantly or entirely on their production can be a good idea but might be problematic for a night doctor. It could lead the night doctor to encourage marginal admissions, some of whom would need to be discharged by the daytime hospitalists hours later. In effect, the night hospitalist could say: “I’ll admit anyone I can get my hands on because my income will increase. I’ll leave it for the day doctors to sort out what to do with all these patients tomorrow.”
An Example
A traditional system of night call (such as pager call from home while also working days) is usually cheaper than dedicated night shifts. And while there are many benefits to having dedicated night shifts, increased patient capacity may not be one of them. Consider the following example:
- On any given day, a five-FTE hospitalist practice has three doctors working, one of whom will be on-call that night by pager;
- That will mean 219 worked days per year for each doctor, one-third of which (73) will be on-call. Each hospitalist gets 146 days off per year;
- The practice decides to switch to dedicated night shifts in which the doctors do not work the day before or after a night shift. The practice wants to retain the 146 days off for each hospitalist. This new coverage arrangement is equivalent to adding 365 shifts annually (one for each night); and
- This will require an additional 1.67 FTE hospitalists (1.67 hospitalists at 219 shifts/year=365).
In this example, by switching from on-call coverage to on-site coverage, the practice increased from five FTEs to 6.67 FTEs. If the daytime work was already enough to keep all three doctors busy, adding 1.67 FTEs for dedicated night shifts may not increase practice productivity or revenue significantly. The practice looks much less productive per FTE (6.67 FTEs are now seeing the volume previously handled by five FTEs) and much costlier.
Changing from traditional night call to dedicated night coverage can be expensive because it may require adding staff yet doesn’t usually increase practice capacity significantly. But it offers other benefits such as those listed in Table 1 (see p. TK). Some practices find they must provide dedicated night coverage to recruit hospitalists. Other institutions choose to support it believing it leads to more timely, efficient, higher-quality care. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Miller J, Nelson J, Whitcomb W. Hospitalists: A Guide to Building and Sustaining a Successful Program. Chicago:Health Administration Press;2007:149-150.
Lessons of the Deposed

Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
SHM Chooses Greatness

We have reached an important milestone: SHM is 10 years old. As with all such anniversaries, it’s a good a time to reflect upon what we’ve achieved and decide our future objectives.
But to assess SHM’s progress, we must first know more about its past. The society was formed with the following objectives, found in our mission statement and declaration of goals:
Mission Statement
SHM is dedicated to promoting the highest quality care for all hospitalized patients. The society is committed to promoting excellence in the practice of hospital medicine through education, advocacy, and research.
Goals
- Promote high-quality care for all hospitalized patients;
- Promote education and research in hospital medicine;
- Promote teamwork to achieve the best possible care for hospitalized patients;
- Advocate a career path that will attract and retain the highest quality hospitalists;
- Define the competencies, activities, and needs of the hospitalist community; and
- Propose, support, and promote changes to the healthcare system that lead to higher quality, more efficient care for all hospitalized patients.
These are commendable goals, indeed. Achieving them is the responsibility of our Board of Directors, which is tasked with providing governance and guiding the society and its members in accordance with these objectives.
How does the SHM and our board make these real-world choices? Let’s take a closer look at the board and its thinking.
SHM’s bottom line is the care of our patients. It is the fundamental goal that sets us apart from for-profit companies where success is measured purely by financial returns. SHM and other medical societies also differ from for-profits in other fundamental ways. Our boards are composed of unpaid volunteers, and our power structures are diffuse rather than concentrated in a single, powerful CEO.
In addition, our board, like the boards of other medical societies, hires the CEO, provides for the election of board officers, and approves and manages the budget. It also supplies the leadership to guide our programs and evaluate our progress toward the goals it has set. Along with our executive staff, the board also oversees all strategic planning, relationships with other organizations, allocation of resources, membership growth, advocacy, and fundraising.
These functions and responsibilities are all attributes of good social-sector organizations. But our board strives for more than that. We want greatness, as defined by business researcher and author Jim Collins, in his monograph Good to Great and the Social Sectors. Assessing greatness, he says, comes down to one critical question: “How effectively do we deliver on our mission and make a distinctive impact, relative to our resources?”
There are seven key criteria derived from Collins’ research on greatness that you can use to assess the effectiveness of the SHM board.
- Were the activities we engaged in consistent with the mission?
- How much impact did we make, relative to our resources?
- What qualitative and quantitative achievements did the organization reach over the past year?
- Do the board’s actions and decisions endure, even when board members and officers change?
- Is the organization growing in terms of resources (revenues, membership, contributors)?
- Does the board build on its successes?
- Is the board clear about tough choices regarding what it can and cannot do?
It is in SHM’s single-minded allegiance to our mission where our choices have stood out from those of other medical societies. Some other societies spend [time and money] on protecting turf, defending professional fees, or advocating for higher reimbursement. Our prime focus—straight from our mission statement—has always been upon our patients. Our priorities revolve around patients and the hospital care setting. They revolve around how we can improve patient care, preserve resources, advance the education of our members, advance hospital medicine research, and partner with other healthcare professionals.
These are laudatory aims, but we have to remember that we work in an environment of limited—and competing—organizational resources. The board must make hard and sometimes unpopular choices regarding which projects, positions, or initiatives we undertake, and which we must say no to. This is the reality we live with. This is the discipline the board must exercise. We simply cannot do it all. And that means we cannot please everyone all the time.
The board hears its members when they ask, “Why aren’t you doing this?”—“this” being a variety of valuable projects competing for more valuable time and resources.
One of the board’s thornier issues has been deciding whether or not to accept money from Big Pharma, as some other medical organizations do. Other contentious issues include whether to weigh in on appropriate workloads for individual physicians or lobby for more reimbursement, especially from Medicare. Reasonable people can and do have differing opinions on these and other difficult issues. But the board must weigh each issue against our mission and goals and make a final judgment.
The board is responsible not only for what we do but how we do it. We must be thorough in our decision-making to avoid—or at least mitigate—unintended consequences. We must endeavor to always remain ethical in all our positions and dealings. As we focus on these important and difficult issues, the board will hold to one overriding principle: Make SHM a great organization that believes in its core values while constantly adapting to a changing environment.
Collins summed it up this way: “Greatness is not a function of circumstance. Greatness, it turns out, is a matter of conscious choice and discipline.” TH
Dr. Holman is the president of SHM.
We have reached an important milestone: SHM is 10 years old. As with all such anniversaries, it’s a good a time to reflect upon what we’ve achieved and decide our future objectives.
But to assess SHM’s progress, we must first know more about its past. The society was formed with the following objectives, found in our mission statement and declaration of goals:
Mission Statement
SHM is dedicated to promoting the highest quality care for all hospitalized patients. The society is committed to promoting excellence in the practice of hospital medicine through education, advocacy, and research.
Goals
- Promote high-quality care for all hospitalized patients;
- Promote education and research in hospital medicine;
- Promote teamwork to achieve the best possible care for hospitalized patients;
- Advocate a career path that will attract and retain the highest quality hospitalists;
- Define the competencies, activities, and needs of the hospitalist community; and
- Propose, support, and promote changes to the healthcare system that lead to higher quality, more efficient care for all hospitalized patients.
These are commendable goals, indeed. Achieving them is the responsibility of our Board of Directors, which is tasked with providing governance and guiding the society and its members in accordance with these objectives.
How does the SHM and our board make these real-world choices? Let’s take a closer look at the board and its thinking.
SHM’s bottom line is the care of our patients. It is the fundamental goal that sets us apart from for-profit companies where success is measured purely by financial returns. SHM and other medical societies also differ from for-profits in other fundamental ways. Our boards are composed of unpaid volunteers, and our power structures are diffuse rather than concentrated in a single, powerful CEO.
In addition, our board, like the boards of other medical societies, hires the CEO, provides for the election of board officers, and approves and manages the budget. It also supplies the leadership to guide our programs and evaluate our progress toward the goals it has set. Along with our executive staff, the board also oversees all strategic planning, relationships with other organizations, allocation of resources, membership growth, advocacy, and fundraising.
These functions and responsibilities are all attributes of good social-sector organizations. But our board strives for more than that. We want greatness, as defined by business researcher and author Jim Collins, in his monograph Good to Great and the Social Sectors. Assessing greatness, he says, comes down to one critical question: “How effectively do we deliver on our mission and make a distinctive impact, relative to our resources?”
There are seven key criteria derived from Collins’ research on greatness that you can use to assess the effectiveness of the SHM board.
- Were the activities we engaged in consistent with the mission?
- How much impact did we make, relative to our resources?
- What qualitative and quantitative achievements did the organization reach over the past year?
- Do the board’s actions and decisions endure, even when board members and officers change?
- Is the organization growing in terms of resources (revenues, membership, contributors)?
- Does the board build on its successes?
- Is the board clear about tough choices regarding what it can and cannot do?
It is in SHM’s single-minded allegiance to our mission where our choices have stood out from those of other medical societies. Some other societies spend [time and money] on protecting turf, defending professional fees, or advocating for higher reimbursement. Our prime focus—straight from our mission statement—has always been upon our patients. Our priorities revolve around patients and the hospital care setting. They revolve around how we can improve patient care, preserve resources, advance the education of our members, advance hospital medicine research, and partner with other healthcare professionals.
These are laudatory aims, but we have to remember that we work in an environment of limited—and competing—organizational resources. The board must make hard and sometimes unpopular choices regarding which projects, positions, or initiatives we undertake, and which we must say no to. This is the reality we live with. This is the discipline the board must exercise. We simply cannot do it all. And that means we cannot please everyone all the time.
The board hears its members when they ask, “Why aren’t you doing this?”—“this” being a variety of valuable projects competing for more valuable time and resources.
One of the board’s thornier issues has been deciding whether or not to accept money from Big Pharma, as some other medical organizations do. Other contentious issues include whether to weigh in on appropriate workloads for individual physicians or lobby for more reimbursement, especially from Medicare. Reasonable people can and do have differing opinions on these and other difficult issues. But the board must weigh each issue against our mission and goals and make a final judgment.
The board is responsible not only for what we do but how we do it. We must be thorough in our decision-making to avoid—or at least mitigate—unintended consequences. We must endeavor to always remain ethical in all our positions and dealings. As we focus on these important and difficult issues, the board will hold to one overriding principle: Make SHM a great organization that believes in its core values while constantly adapting to a changing environment.
Collins summed it up this way: “Greatness is not a function of circumstance. Greatness, it turns out, is a matter of conscious choice and discipline.” TH
Dr. Holman is the president of SHM.
We have reached an important milestone: SHM is 10 years old. As with all such anniversaries, it’s a good a time to reflect upon what we’ve achieved and decide our future objectives.
But to assess SHM’s progress, we must first know more about its past. The society was formed with the following objectives, found in our mission statement and declaration of goals:
Mission Statement
SHM is dedicated to promoting the highest quality care for all hospitalized patients. The society is committed to promoting excellence in the practice of hospital medicine through education, advocacy, and research.
Goals
- Promote high-quality care for all hospitalized patients;
- Promote education and research in hospital medicine;
- Promote teamwork to achieve the best possible care for hospitalized patients;
- Advocate a career path that will attract and retain the highest quality hospitalists;
- Define the competencies, activities, and needs of the hospitalist community; and
- Propose, support, and promote changes to the healthcare system that lead to higher quality, more efficient care for all hospitalized patients.
These are commendable goals, indeed. Achieving them is the responsibility of our Board of Directors, which is tasked with providing governance and guiding the society and its members in accordance with these objectives.
How does the SHM and our board make these real-world choices? Let’s take a closer look at the board and its thinking.
SHM’s bottom line is the care of our patients. It is the fundamental goal that sets us apart from for-profit companies where success is measured purely by financial returns. SHM and other medical societies also differ from for-profits in other fundamental ways. Our boards are composed of unpaid volunteers, and our power structures are diffuse rather than concentrated in a single, powerful CEO.
In addition, our board, like the boards of other medical societies, hires the CEO, provides for the election of board officers, and approves and manages the budget. It also supplies the leadership to guide our programs and evaluate our progress toward the goals it has set. Along with our executive staff, the board also oversees all strategic planning, relationships with other organizations, allocation of resources, membership growth, advocacy, and fundraising.
These functions and responsibilities are all attributes of good social-sector organizations. But our board strives for more than that. We want greatness, as defined by business researcher and author Jim Collins, in his monograph Good to Great and the Social Sectors. Assessing greatness, he says, comes down to one critical question: “How effectively do we deliver on our mission and make a distinctive impact, relative to our resources?”
There are seven key criteria derived from Collins’ research on greatness that you can use to assess the effectiveness of the SHM board.
- Were the activities we engaged in consistent with the mission?
- How much impact did we make, relative to our resources?
- What qualitative and quantitative achievements did the organization reach over the past year?
- Do the board’s actions and decisions endure, even when board members and officers change?
- Is the organization growing in terms of resources (revenues, membership, contributors)?
- Does the board build on its successes?
- Is the board clear about tough choices regarding what it can and cannot do?
It is in SHM’s single-minded allegiance to our mission where our choices have stood out from those of other medical societies. Some other societies spend [time and money] on protecting turf, defending professional fees, or advocating for higher reimbursement. Our prime focus—straight from our mission statement—has always been upon our patients. Our priorities revolve around patients and the hospital care setting. They revolve around how we can improve patient care, preserve resources, advance the education of our members, advance hospital medicine research, and partner with other healthcare professionals.
These are laudatory aims, but we have to remember that we work in an environment of limited—and competing—organizational resources. The board must make hard and sometimes unpopular choices regarding which projects, positions, or initiatives we undertake, and which we must say no to. This is the reality we live with. This is the discipline the board must exercise. We simply cannot do it all. And that means we cannot please everyone all the time.
The board hears its members when they ask, “Why aren’t you doing this?”—“this” being a variety of valuable projects competing for more valuable time and resources.
One of the board’s thornier issues has been deciding whether or not to accept money from Big Pharma, as some other medical organizations do. Other contentious issues include whether to weigh in on appropriate workloads for individual physicians or lobby for more reimbursement, especially from Medicare. Reasonable people can and do have differing opinions on these and other difficult issues. But the board must weigh each issue against our mission and goals and make a final judgment.
The board is responsible not only for what we do but how we do it. We must be thorough in our decision-making to avoid—or at least mitigate—unintended consequences. We must endeavor to always remain ethical in all our positions and dealings. As we focus on these important and difficult issues, the board will hold to one overriding principle: Make SHM a great organization that believes in its core values while constantly adapting to a changing environment.
Collins summed it up this way: “Greatness is not a function of circumstance. Greatness, it turns out, is a matter of conscious choice and discipline.” TH
Dr. Holman is the president of SHM.
One for the Ages
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.

The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.

The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.
The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.
The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.
The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.
The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
What is the target blood glucose for noncritical care patients?
Case
A 65-year-old obese (100 kg) man with type 2 diabetes, hypertension, and a pack-a-day smoking habit is admitted with moderately severe bilobar pneumonia. His condition is manifest by fever, cough, chills, leukocytosis, and a modest oxygen requirement. You order oxygen, intravenous (IV) fluids, diet, and appropriate antibiotics while continuing the history and chart review. The patient uses metformin and glyburide, and his home glucose readings are generally in the 160 to 180 mg/dL range. An HbA1c level performed three months ago was 9.8, leading to an increased dose of glyburide. As you finish the history, the nurse reports a glucose reading of 198 mg/dL. What is the target blood glucose for noncritical care adult inpatients?
Overview
Diabetes mellitus is an epidemic in the United States. At least 9.3% of adults older than 20 (more than 20 million people) have diabetes. Approximately 30% are unaware they have diabetes.1 Concurrent with the increasing prevalence of diabetes in the U.S. from 1980 through 2003, the number of hospital discharges with diabetes as any listed diagnosis more than doubled between 1980 and 2003. These trends are expected to accelerate.2 Studies suggest 26% of inpatients have diabetes and 12% have pre-diabetes, previously undiagnosed diabetes, or stress hyperglycemia.3
Review of the Data
A full review of the evidence is beyond the scope of this article. What follows is a sampling of the most representative or influential critical care studies.
Physiology
Fluid and electrolyte balance, left ventricular (LV) function, leukocyte action, wound healing, endothelial function, and immunoglobulin function are all impaired with hyperglycemia.
A prothrombotic state and enhanced platelet aggregation have been demonstrated with even mild elevations of blood glucose.
The mechanisms are multifactorial and complex and involve metabolic derangements leading to oxidative stress, release of free fatty acids, and counter-regulatory hormones.4-6
Observational Studies
A strong and consistent association with hyperglycemia and adverse outcomes is seen in a wide variety of critical care and peri-operative settings. Trauma survival, stroke survival and function, and the incidence of post-operative infections are all adversely affected by hyperglycemia.7-10 Acute myocardial infarction (MI) mortality, acute MI infarct size, and LV dysfunction are also consistently adversely affected in these studies.11-13
This association is typically present in hyperglycemic patients whether they have a diagnosis of diabetes or not, and the association is often even stronger in those lacking a pre-existing diagnosis. Dysfunction typically is detectable at only modest elevations of blood glucose and becomes more marked in a dose response relationship.
Uncontrolled Interventional Studies
The Portland Diabetic Project is a prospective, non-randomized, observational study of 5,510 consecutive diabetic cardiac surgery patients.14-15 The three-day blood glucose average (3-BG) has been progressively reduced for the population through the use of continuous insulin infusion (CII).
The last reported glycemic target is less than 130 mg/dL, and the current glycemic target is less than 110 mg/dL. Both CII for three days and a favorable 3-BG were independently associated with improved mortality, deep sternal-wound infection rates, and length of stay. Mortality and deep sternal-wound infection rates for diabetic patients with well-controlled glucose levels are equal to patients without diabetes.
Another study compared 800 mixed medical-surgical ICU patients with tight glycemic control (mean BG 130.7 mg/dL) to historical controls with a mean glucose of 152.3 mg/dL. The insulin infusion group had associated significant reductions in mortality and median length of ICU stay.16
Randomized Controlled Trials and Meta-Analyses
In the first Diabetes and Insulin-Glucose study (DIGAMI 1), patients with acute MI received IV insulin therapy for 24 hours, followed by multiple daily injections for three months or longer. The insulin group had lower glucose values and a 29% reduction in mortality at one year and 28% reduction at 3.4 years compared with the control group.17-18
In the most influential study to date, van den Berghe, et al., randomized 1,548 surgical intensive-care unit (ICU) patients to either intensive (IT) or conventional (CT) insulin therapy.19 The glycemic target in the IT arm was 80 to 110 mg/dL (mean glucose attained was 103 mg/dL), while the CT arm had a mean glucose level of 153 mg/dL. The IT group enjoyed substantial reductions in both ICU and total in-hospital mortality, as well as reductions in blood stream infections, acute renal failure, transfusions and the duration of mechanical ventilation (p<0.01 for all).
While a similar study in a medical ICU did not achieve statistical significance in the overall intention-to-treat analysis for mortality, it did demonstrate reductions in mortality in patients with at least three days of ICU treatment and significant reductions in morbidity.20
A meta-analysis of these two studies demonstrated a relative risk reduction in mortality (23.6 to 20.4%) and morbidity in all patients treated with intensive insulin therapy.21
A separate meta-analysis of 35 clinical trials evaluating the effect of intensive insulin infusion therapy on mortality in critically ill inpatients revealed a 15% reduction in short-term mortality.22
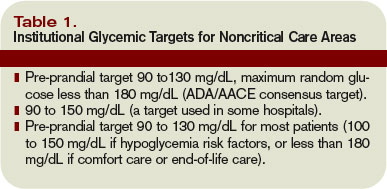
Noncritical Care Settings
There are no randomized controlled trials establishing the optimal glycemic target for noncritical care inpatients. There are a number of observational and pilot studies that reinforce the studies performed in critical care settings.
In a retrospective review of almost 1,900 general medical-surgical admissions, Umpierrez, et al., reported an 18-fold increase in mortality in hyperglycemic patients without prior history of diabetes and a 2.5-fold increase in mortality in patients with known diabetes compared to controls. These associations persisted with adjustment for severity of illness.23
A variety of observational and pilot studies associate hyperglycemia with poor outcomes in community acquired pneumonia, renal transplant, and the durability of remission in acute lymphocytic leukemia.24-25
Guidelines and Recommendations
Spurred by the emerging controlled trial evidence, the American Association of Clinical Endocrinologists (AACE) convened a consensus conference involving nine organizations, including SHM. Recommendations for the management of inpatient hyperglycemia included stringent glycemic targets for critical care and noncritical care areas.26 The American Diabetes Association (ADA) produced an excellent technical review on inpatient diabetes that provided the basis for ADA Clinical Practice Guideline glycemic targets.27 The glycemic targets recommended are shown in Table 1 (above).
Caveats
Before accepting these recommended glycemic targets, review the shortcomings of the literature supporting them and consider institutional and individual patient factors that might modify the glycemic target.
Insulin has beneficial vascular and anti-inflammatory effects in its own right, making it difficult in some studies to distinguish the benefit of glucose lowering from the benefit of the insulin used to attain improved control.
The majority of studies supporting inpatient glycemic targets are observational or non-randomized. Some use admission blood glucose concentrations as the sole measure of glucose control.
While most of these studies used valid methods to control for severity of illness and co-morbidities, these methods are not perfect. In some cases, hyperglycemia may have been a marker of a more stressed and sick patient rather than an independent source of adverse outcome.
The dramatic results from the first van den Berghe study have proved difficult to replicate, in part because other investigators have had difficulty achieving stringent glycemic targets safely. Two international multicenter studies recently stopped enrollment due to excess rates of hypoglycemia, but the studies have not yet been published in final form.28-29
Finally, it bears repeating that the proposed glucose targets for noncritically ill patients are based on essentially no clinical trial data in that population. In part, the glycemic targets reflect the evidence derived from landmark outpatient randomized trials.30-31 In the outpatient setting, insulin requirements and nutritional intake are far more reliable than the inpatient setting, where the iatrogenic induction of excessive hypoglycemia is a valid concern.
Safe Glycemic Control
Rapidly fluctuating nutritional status, changing insulin requirements, varied levels of expertise, and hand-offs between geographic locations and providers are all common in the inpatient setting.
Aggressively pursuing glycemic targets without having systems and safeguards in place could lead to net harm.
The AACE recently identified these barriers and recommended a multidisciplinary team approach, reliable metrics, and a standardized method for insulin protocols, orders, and hypoglycemia prevention and treatment techniques.32
Both the AACE and SHM have produced toolkits to assist institutions to safely achieve improved glycemic control and care.33-34 The SHM Glycemic Control Task Force recently summarized key concepts to emphasize in formulating protocols and order sets in the noncritical care setting (see Table 2, left).
Stringent glycemic targets recommended by the ADA and the AACE may be appropriately moderated in centers that do not yet have the systems in place to achieve those goals safely.
Your glycemic target need not be identical to the ADA and AACE glycemic targets but should be similar to them. Examples of glycemic targets for noncritically ill inpatients are shown in Table 3 (see p. 48).
The glycemic target should be actionable, in that some institutionally endorsed action should result when a patient’s glycemic target is consistently not met.
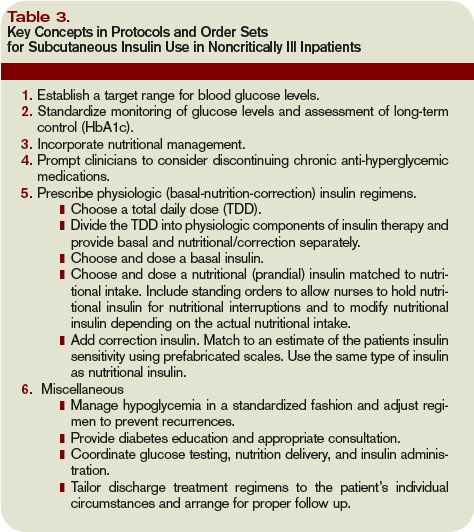
Back to the Case
Your patient has an active infection, a glucose of 198 mg/dL and an elevated HbA1c. You hold the oral agents and start a basal bolus insulin regimen.
You generate an estimate for a safe insulin total daily dose of 60 units (100 kg x 0.6 units per kg for an obese, type 2 diabetes patient), and administer half as basal insulin, with the remaining 30 units distributed as rapid acting insulin in three divided doses. Your orders include routine glucose monitoring, and you plan to adjust the insulin daily as needed to adhere to the institutional glycemic target for noncritically ill patients of 90 to 150 mg/dL. TH
Dr. Maynard is the division chief for hospital medicine at the University of California, San Diego. He is the leader of SHM’s Glycemic Control Task Force and a leader of the VTE Prevention Collaborative.
References
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health And Nutrition Examination Survey 1999-2002. Diabetes Care. 2006;29(6):1263-1268.
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, 2005. Available at www.cdc.gov/diabetes/pubs/factsheet05.htm. Last accessed September 18, 2007.
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982.
- Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, Hirsch IB, the Diabetes In Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals (Technical Review). Diabetes Care. 2004;27:553–591.
- Zarich SW. Mechanism by which hyperglycemia plays a role in the setting of acute cardiovascular illness. Rev Cardiovasc Med. 2006;7 (Suppl 2):S35-43.
- Hansen T, Thiel S, Wouters P, Christiansen J, VandenBerghe B. Intensive insulin therapy exerts anti-inflammatory effects in critically ill patients and counteracts the adverse effect of low mannose-gind lectin levels. J Clin Endocrinol Metab. 2003;88:1082-1088.
- Yendamuri S, Fulda GJ, Tinkoff GH. Admission hyperglycemia as a prognostic indicator in trauma. J Trauma. 2003;55:33-38.
- Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein H. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–
- 2432.
- Bruno A, Williams LS, Kent TA. How important is hyperglycemia during acute brain infarction? Neurologist 2004;10(4):195-200.
- Pomposelli JJ, Baxter JK, Babineau TJ, et al. Early postoperative glucose control predicts nosocomial infection rate in diabetic patients. J Parenter Enteral Nutr.1998;22(2):77-81.
- Ainla T, Baburin A, Teesalu R, Rahu M. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med. 2005;22(10):1321-1325.
- Timmer JR, van der Horst IC, Ottervanger JP, et al. Prognostic value of admission glucose in non-diabetic patients with myocardial infarction. Am Heart J. 2004;148:399-404.
- Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355:773–778.
- Furnary AP, Wu Y. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland Diabetic Project. Endocr Pract. 2006:12 (Suppl 3): 22-26.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007–1021.
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471–1478.
- Malmberg K. Prospective randomised study of intensive insulin treatment on long-term survival after acute myocardial infarction inpatients with diabetes mellitus. BMJ. 1997;314:1512–1515.
- Malmberg K, Norhammar A, Wedel H, Ryden L. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626–2632.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449-461.
- Van den Berghe G, Wilmer A, Milants I, et al. Intensive insulin therapy in mixed medical/surgical intensive care units: benefit versus harm. Diabetes. 2006;55(11):3151-3159.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004;164(18):2005-2011.
- McAlister FA, Majumdar SR, Blitz S, Rowe BH, Romney J, Marrie TJ. The relation between hyperglycemia and outcomes in 2,471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care. 2005;28(4):810-815.
- Thomas M, Mathew T, Russ G, Rao M, Moran J. Early peri-operative glycaemic control and allograft rejection in patients with diabetes mellitus: a pilot study. Transplantation. 2001;72(7):1321-1324.
- Weiser MA, Cabanillas ME, Konopleva M, et al. Relation between the duration of remission and hyperglycemia during induction chemotherapy for acute lymphocytic leukemia with a hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone/methotrexate-cytarabine regimen. Cancer. 2004;100(6):1179-1185.
- Garber AJ, Moghissi ES, Bransome ED Jr, et al., American College of Endocrinology Task Force on Inpatient Diabetes Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract. 2004;10:77–82.
- Standards of medical care in diabetes-2006. Diabetes Care. 2006;29 (Suppl. 1):S4-S42.
- Vanhorebeek I, Langouche L, Van den Berghe G. Tight blood glucose control with insulin in the ICU: facts and controversies. Chest. 2007;132(1):268-278.
- Devos P, Preiser JC. Current controversies around tight glucose control in critically ill patients. Curr Opin Clin Nutr Metab Care. 2007;10(2):206-209.
- The Diabetes Control and Complications Trial Research Group (DCCT). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977-986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853.
- American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control: a call to action. Diabetes Care. 2006;29(8):1955-1962.
- American Association of Clinical Endocrinologists Inpatient Glycemic Control Resource Center 2007. Available at http://resources.aace.com/index.asp. Last accessed December 18, 2007.
- Society of Hospital Medicine Glycemic Control Resource Room. Available at www.hospitalmedicine.org/ResourceRoomRedesign/GlycemicControl.cfm. Last accessed Nov. 25, 2007.
Case
A 65-year-old obese (100 kg) man with type 2 diabetes, hypertension, and a pack-a-day smoking habit is admitted with moderately severe bilobar pneumonia. His condition is manifest by fever, cough, chills, leukocytosis, and a modest oxygen requirement. You order oxygen, intravenous (IV) fluids, diet, and appropriate antibiotics while continuing the history and chart review. The patient uses metformin and glyburide, and his home glucose readings are generally in the 160 to 180 mg/dL range. An HbA1c level performed three months ago was 9.8, leading to an increased dose of glyburide. As you finish the history, the nurse reports a glucose reading of 198 mg/dL. What is the target blood glucose for noncritical care adult inpatients?
Overview
Diabetes mellitus is an epidemic in the United States. At least 9.3% of adults older than 20 (more than 20 million people) have diabetes. Approximately 30% are unaware they have diabetes.1 Concurrent with the increasing prevalence of diabetes in the U.S. from 1980 through 2003, the number of hospital discharges with diabetes as any listed diagnosis more than doubled between 1980 and 2003. These trends are expected to accelerate.2 Studies suggest 26% of inpatients have diabetes and 12% have pre-diabetes, previously undiagnosed diabetes, or stress hyperglycemia.3
Review of the Data
A full review of the evidence is beyond the scope of this article. What follows is a sampling of the most representative or influential critical care studies.
Physiology
Fluid and electrolyte balance, left ventricular (LV) function, leukocyte action, wound healing, endothelial function, and immunoglobulin function are all impaired with hyperglycemia.
A prothrombotic state and enhanced platelet aggregation have been demonstrated with even mild elevations of blood glucose.
The mechanisms are multifactorial and complex and involve metabolic derangements leading to oxidative stress, release of free fatty acids, and counter-regulatory hormones.4-6
Observational Studies
A strong and consistent association with hyperglycemia and adverse outcomes is seen in a wide variety of critical care and peri-operative settings. Trauma survival, stroke survival and function, and the incidence of post-operative infections are all adversely affected by hyperglycemia.7-10 Acute myocardial infarction (MI) mortality, acute MI infarct size, and LV dysfunction are also consistently adversely affected in these studies.11-13
This association is typically present in hyperglycemic patients whether they have a diagnosis of diabetes or not, and the association is often even stronger in those lacking a pre-existing diagnosis. Dysfunction typically is detectable at only modest elevations of blood glucose and becomes more marked in a dose response relationship.
Uncontrolled Interventional Studies
The Portland Diabetic Project is a prospective, non-randomized, observational study of 5,510 consecutive diabetic cardiac surgery patients.14-15 The three-day blood glucose average (3-BG) has been progressively reduced for the population through the use of continuous insulin infusion (CII).
The last reported glycemic target is less than 130 mg/dL, and the current glycemic target is less than 110 mg/dL. Both CII for three days and a favorable 3-BG were independently associated with improved mortality, deep sternal-wound infection rates, and length of stay. Mortality and deep sternal-wound infection rates for diabetic patients with well-controlled glucose levels are equal to patients without diabetes.
Another study compared 800 mixed medical-surgical ICU patients with tight glycemic control (mean BG 130.7 mg/dL) to historical controls with a mean glucose of 152.3 mg/dL. The insulin infusion group had associated significant reductions in mortality and median length of ICU stay.16
Randomized Controlled Trials and Meta-Analyses
In the first Diabetes and Insulin-Glucose study (DIGAMI 1), patients with acute MI received IV insulin therapy for 24 hours, followed by multiple daily injections for three months or longer. The insulin group had lower glucose values and a 29% reduction in mortality at one year and 28% reduction at 3.4 years compared with the control group.17-18
In the most influential study to date, van den Berghe, et al., randomized 1,548 surgical intensive-care unit (ICU) patients to either intensive (IT) or conventional (CT) insulin therapy.19 The glycemic target in the IT arm was 80 to 110 mg/dL (mean glucose attained was 103 mg/dL), while the CT arm had a mean glucose level of 153 mg/dL. The IT group enjoyed substantial reductions in both ICU and total in-hospital mortality, as well as reductions in blood stream infections, acute renal failure, transfusions and the duration of mechanical ventilation (p<0.01 for all).
While a similar study in a medical ICU did not achieve statistical significance in the overall intention-to-treat analysis for mortality, it did demonstrate reductions in mortality in patients with at least three days of ICU treatment and significant reductions in morbidity.20
A meta-analysis of these two studies demonstrated a relative risk reduction in mortality (23.6 to 20.4%) and morbidity in all patients treated with intensive insulin therapy.21
A separate meta-analysis of 35 clinical trials evaluating the effect of intensive insulin infusion therapy on mortality in critically ill inpatients revealed a 15% reduction in short-term mortality.22
Noncritical Care Settings
There are no randomized controlled trials establishing the optimal glycemic target for noncritical care inpatients. There are a number of observational and pilot studies that reinforce the studies performed in critical care settings.
In a retrospective review of almost 1,900 general medical-surgical admissions, Umpierrez, et al., reported an 18-fold increase in mortality in hyperglycemic patients without prior history of diabetes and a 2.5-fold increase in mortality in patients with known diabetes compared to controls. These associations persisted with adjustment for severity of illness.23
A variety of observational and pilot studies associate hyperglycemia with poor outcomes in community acquired pneumonia, renal transplant, and the durability of remission in acute lymphocytic leukemia.24-25
Guidelines and Recommendations
Spurred by the emerging controlled trial evidence, the American Association of Clinical Endocrinologists (AACE) convened a consensus conference involving nine organizations, including SHM. Recommendations for the management of inpatient hyperglycemia included stringent glycemic targets for critical care and noncritical care areas.26 The American Diabetes Association (ADA) produced an excellent technical review on inpatient diabetes that provided the basis for ADA Clinical Practice Guideline glycemic targets.27 The glycemic targets recommended are shown in Table 1 (above).
Caveats
Before accepting these recommended glycemic targets, review the shortcomings of the literature supporting them and consider institutional and individual patient factors that might modify the glycemic target.
Insulin has beneficial vascular and anti-inflammatory effects in its own right, making it difficult in some studies to distinguish the benefit of glucose lowering from the benefit of the insulin used to attain improved control.
The majority of studies supporting inpatient glycemic targets are observational or non-randomized. Some use admission blood glucose concentrations as the sole measure of glucose control.
While most of these studies used valid methods to control for severity of illness and co-morbidities, these methods are not perfect. In some cases, hyperglycemia may have been a marker of a more stressed and sick patient rather than an independent source of adverse outcome.
The dramatic results from the first van den Berghe study have proved difficult to replicate, in part because other investigators have had difficulty achieving stringent glycemic targets safely. Two international multicenter studies recently stopped enrollment due to excess rates of hypoglycemia, but the studies have not yet been published in final form.28-29
Finally, it bears repeating that the proposed glucose targets for noncritically ill patients are based on essentially no clinical trial data in that population. In part, the glycemic targets reflect the evidence derived from landmark outpatient randomized trials.30-31 In the outpatient setting, insulin requirements and nutritional intake are far more reliable than the inpatient setting, where the iatrogenic induction of excessive hypoglycemia is a valid concern.
Safe Glycemic Control
Rapidly fluctuating nutritional status, changing insulin requirements, varied levels of expertise, and hand-offs between geographic locations and providers are all common in the inpatient setting.
Aggressively pursuing glycemic targets without having systems and safeguards in place could lead to net harm.
The AACE recently identified these barriers and recommended a multidisciplinary team approach, reliable metrics, and a standardized method for insulin protocols, orders, and hypoglycemia prevention and treatment techniques.32
Both the AACE and SHM have produced toolkits to assist institutions to safely achieve improved glycemic control and care.33-34 The SHM Glycemic Control Task Force recently summarized key concepts to emphasize in formulating protocols and order sets in the noncritical care setting (see Table 2, left).
Stringent glycemic targets recommended by the ADA and the AACE may be appropriately moderated in centers that do not yet have the systems in place to achieve those goals safely.
Your glycemic target need not be identical to the ADA and AACE glycemic targets but should be similar to them. Examples of glycemic targets for noncritically ill inpatients are shown in Table 3 (see p. 48).
The glycemic target should be actionable, in that some institutionally endorsed action should result when a patient’s glycemic target is consistently not met.
Back to the Case
Your patient has an active infection, a glucose of 198 mg/dL and an elevated HbA1c. You hold the oral agents and start a basal bolus insulin regimen.
You generate an estimate for a safe insulin total daily dose of 60 units (100 kg x 0.6 units per kg for an obese, type 2 diabetes patient), and administer half as basal insulin, with the remaining 30 units distributed as rapid acting insulin in three divided doses. Your orders include routine glucose monitoring, and you plan to adjust the insulin daily as needed to adhere to the institutional glycemic target for noncritically ill patients of 90 to 150 mg/dL. TH
Dr. Maynard is the division chief for hospital medicine at the University of California, San Diego. He is the leader of SHM’s Glycemic Control Task Force and a leader of the VTE Prevention Collaborative.
References
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health And Nutrition Examination Survey 1999-2002. Diabetes Care. 2006;29(6):1263-1268.
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, 2005. Available at www.cdc.gov/diabetes/pubs/factsheet05.htm. Last accessed September 18, 2007.
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982.
- Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, Hirsch IB, the Diabetes In Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals (Technical Review). Diabetes Care. 2004;27:553–591.
- Zarich SW. Mechanism by which hyperglycemia plays a role in the setting of acute cardiovascular illness. Rev Cardiovasc Med. 2006;7 (Suppl 2):S35-43.
- Hansen T, Thiel S, Wouters P, Christiansen J, VandenBerghe B. Intensive insulin therapy exerts anti-inflammatory effects in critically ill patients and counteracts the adverse effect of low mannose-gind lectin levels. J Clin Endocrinol Metab. 2003;88:1082-1088.
- Yendamuri S, Fulda GJ, Tinkoff GH. Admission hyperglycemia as a prognostic indicator in trauma. J Trauma. 2003;55:33-38.
- Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein H. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–
- 2432.
- Bruno A, Williams LS, Kent TA. How important is hyperglycemia during acute brain infarction? Neurologist 2004;10(4):195-200.
- Pomposelli JJ, Baxter JK, Babineau TJ, et al. Early postoperative glucose control predicts nosocomial infection rate in diabetic patients. J Parenter Enteral Nutr.1998;22(2):77-81.
- Ainla T, Baburin A, Teesalu R, Rahu M. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med. 2005;22(10):1321-1325.
- Timmer JR, van der Horst IC, Ottervanger JP, et al. Prognostic value of admission glucose in non-diabetic patients with myocardial infarction. Am Heart J. 2004;148:399-404.
- Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355:773–778.
- Furnary AP, Wu Y. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland Diabetic Project. Endocr Pract. 2006:12 (Suppl 3): 22-26.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007–1021.
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471–1478.
- Malmberg K. Prospective randomised study of intensive insulin treatment on long-term survival after acute myocardial infarction inpatients with diabetes mellitus. BMJ. 1997;314:1512–1515.
- Malmberg K, Norhammar A, Wedel H, Ryden L. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626–2632.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449-461.
- Van den Berghe G, Wilmer A, Milants I, et al. Intensive insulin therapy in mixed medical/surgical intensive care units: benefit versus harm. Diabetes. 2006;55(11):3151-3159.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004;164(18):2005-2011.
- McAlister FA, Majumdar SR, Blitz S, Rowe BH, Romney J, Marrie TJ. The relation between hyperglycemia and outcomes in 2,471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care. 2005;28(4):810-815.
- Thomas M, Mathew T, Russ G, Rao M, Moran J. Early peri-operative glycaemic control and allograft rejection in patients with diabetes mellitus: a pilot study. Transplantation. 2001;72(7):1321-1324.
- Weiser MA, Cabanillas ME, Konopleva M, et al. Relation between the duration of remission and hyperglycemia during induction chemotherapy for acute lymphocytic leukemia with a hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone/methotrexate-cytarabine regimen. Cancer. 2004;100(6):1179-1185.
- Garber AJ, Moghissi ES, Bransome ED Jr, et al., American College of Endocrinology Task Force on Inpatient Diabetes Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract. 2004;10:77–82.
- Standards of medical care in diabetes-2006. Diabetes Care. 2006;29 (Suppl. 1):S4-S42.
- Vanhorebeek I, Langouche L, Van den Berghe G. Tight blood glucose control with insulin in the ICU: facts and controversies. Chest. 2007;132(1):268-278.
- Devos P, Preiser JC. Current controversies around tight glucose control in critically ill patients. Curr Opin Clin Nutr Metab Care. 2007;10(2):206-209.
- The Diabetes Control and Complications Trial Research Group (DCCT). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977-986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853.
- American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control: a call to action. Diabetes Care. 2006;29(8):1955-1962.
- American Association of Clinical Endocrinologists Inpatient Glycemic Control Resource Center 2007. Available at http://resources.aace.com/index.asp. Last accessed December 18, 2007.
- Society of Hospital Medicine Glycemic Control Resource Room. Available at www.hospitalmedicine.org/ResourceRoomRedesign/GlycemicControl.cfm. Last accessed Nov. 25, 2007.
Case
A 65-year-old obese (100 kg) man with type 2 diabetes, hypertension, and a pack-a-day smoking habit is admitted with moderately severe bilobar pneumonia. His condition is manifest by fever, cough, chills, leukocytosis, and a modest oxygen requirement. You order oxygen, intravenous (IV) fluids, diet, and appropriate antibiotics while continuing the history and chart review. The patient uses metformin and glyburide, and his home glucose readings are generally in the 160 to 180 mg/dL range. An HbA1c level performed three months ago was 9.8, leading to an increased dose of glyburide. As you finish the history, the nurse reports a glucose reading of 198 mg/dL. What is the target blood glucose for noncritical care adult inpatients?
Overview
Diabetes mellitus is an epidemic in the United States. At least 9.3% of adults older than 20 (more than 20 million people) have diabetes. Approximately 30% are unaware they have diabetes.1 Concurrent with the increasing prevalence of diabetes in the U.S. from 1980 through 2003, the number of hospital discharges with diabetes as any listed diagnosis more than doubled between 1980 and 2003. These trends are expected to accelerate.2 Studies suggest 26% of inpatients have diabetes and 12% have pre-diabetes, previously undiagnosed diabetes, or stress hyperglycemia.3
Review of the Data
A full review of the evidence is beyond the scope of this article. What follows is a sampling of the most representative or influential critical care studies.
Physiology
Fluid and electrolyte balance, left ventricular (LV) function, leukocyte action, wound healing, endothelial function, and immunoglobulin function are all impaired with hyperglycemia.
A prothrombotic state and enhanced platelet aggregation have been demonstrated with even mild elevations of blood glucose.
The mechanisms are multifactorial and complex and involve metabolic derangements leading to oxidative stress, release of free fatty acids, and counter-regulatory hormones.4-6
Observational Studies
A strong and consistent association with hyperglycemia and adverse outcomes is seen in a wide variety of critical care and peri-operative settings. Trauma survival, stroke survival and function, and the incidence of post-operative infections are all adversely affected by hyperglycemia.7-10 Acute myocardial infarction (MI) mortality, acute MI infarct size, and LV dysfunction are also consistently adversely affected in these studies.11-13
This association is typically present in hyperglycemic patients whether they have a diagnosis of diabetes or not, and the association is often even stronger in those lacking a pre-existing diagnosis. Dysfunction typically is detectable at only modest elevations of blood glucose and becomes more marked in a dose response relationship.
Uncontrolled Interventional Studies
The Portland Diabetic Project is a prospective, non-randomized, observational study of 5,510 consecutive diabetic cardiac surgery patients.14-15 The three-day blood glucose average (3-BG) has been progressively reduced for the population through the use of continuous insulin infusion (CII).
The last reported glycemic target is less than 130 mg/dL, and the current glycemic target is less than 110 mg/dL. Both CII for three days and a favorable 3-BG were independently associated with improved mortality, deep sternal-wound infection rates, and length of stay. Mortality and deep sternal-wound infection rates for diabetic patients with well-controlled glucose levels are equal to patients without diabetes.
Another study compared 800 mixed medical-surgical ICU patients with tight glycemic control (mean BG 130.7 mg/dL) to historical controls with a mean glucose of 152.3 mg/dL. The insulin infusion group had associated significant reductions in mortality and median length of ICU stay.16
Randomized Controlled Trials and Meta-Analyses
In the first Diabetes and Insulin-Glucose study (DIGAMI 1), patients with acute MI received IV insulin therapy for 24 hours, followed by multiple daily injections for three months or longer. The insulin group had lower glucose values and a 29% reduction in mortality at one year and 28% reduction at 3.4 years compared with the control group.17-18
In the most influential study to date, van den Berghe, et al., randomized 1,548 surgical intensive-care unit (ICU) patients to either intensive (IT) or conventional (CT) insulin therapy.19 The glycemic target in the IT arm was 80 to 110 mg/dL (mean glucose attained was 103 mg/dL), while the CT arm had a mean glucose level of 153 mg/dL. The IT group enjoyed substantial reductions in both ICU and total in-hospital mortality, as well as reductions in blood stream infections, acute renal failure, transfusions and the duration of mechanical ventilation (p<0.01 for all).
While a similar study in a medical ICU did not achieve statistical significance in the overall intention-to-treat analysis for mortality, it did demonstrate reductions in mortality in patients with at least three days of ICU treatment and significant reductions in morbidity.20
A meta-analysis of these two studies demonstrated a relative risk reduction in mortality (23.6 to 20.4%) and morbidity in all patients treated with intensive insulin therapy.21
A separate meta-analysis of 35 clinical trials evaluating the effect of intensive insulin infusion therapy on mortality in critically ill inpatients revealed a 15% reduction in short-term mortality.22
Noncritical Care Settings
There are no randomized controlled trials establishing the optimal glycemic target for noncritical care inpatients. There are a number of observational and pilot studies that reinforce the studies performed in critical care settings.
In a retrospective review of almost 1,900 general medical-surgical admissions, Umpierrez, et al., reported an 18-fold increase in mortality in hyperglycemic patients without prior history of diabetes and a 2.5-fold increase in mortality in patients with known diabetes compared to controls. These associations persisted with adjustment for severity of illness.23
A variety of observational and pilot studies associate hyperglycemia with poor outcomes in community acquired pneumonia, renal transplant, and the durability of remission in acute lymphocytic leukemia.24-25
Guidelines and Recommendations
Spurred by the emerging controlled trial evidence, the American Association of Clinical Endocrinologists (AACE) convened a consensus conference involving nine organizations, including SHM. Recommendations for the management of inpatient hyperglycemia included stringent glycemic targets for critical care and noncritical care areas.26 The American Diabetes Association (ADA) produced an excellent technical review on inpatient diabetes that provided the basis for ADA Clinical Practice Guideline glycemic targets.27 The glycemic targets recommended are shown in Table 1 (above).
Caveats
Before accepting these recommended glycemic targets, review the shortcomings of the literature supporting them and consider institutional and individual patient factors that might modify the glycemic target.
Insulin has beneficial vascular and anti-inflammatory effects in its own right, making it difficult in some studies to distinguish the benefit of glucose lowering from the benefit of the insulin used to attain improved control.
The majority of studies supporting inpatient glycemic targets are observational or non-randomized. Some use admission blood glucose concentrations as the sole measure of glucose control.
While most of these studies used valid methods to control for severity of illness and co-morbidities, these methods are not perfect. In some cases, hyperglycemia may have been a marker of a more stressed and sick patient rather than an independent source of adverse outcome.
The dramatic results from the first van den Berghe study have proved difficult to replicate, in part because other investigators have had difficulty achieving stringent glycemic targets safely. Two international multicenter studies recently stopped enrollment due to excess rates of hypoglycemia, but the studies have not yet been published in final form.28-29
Finally, it bears repeating that the proposed glucose targets for noncritically ill patients are based on essentially no clinical trial data in that population. In part, the glycemic targets reflect the evidence derived from landmark outpatient randomized trials.30-31 In the outpatient setting, insulin requirements and nutritional intake are far more reliable than the inpatient setting, where the iatrogenic induction of excessive hypoglycemia is a valid concern.
Safe Glycemic Control
Rapidly fluctuating nutritional status, changing insulin requirements, varied levels of expertise, and hand-offs between geographic locations and providers are all common in the inpatient setting.
Aggressively pursuing glycemic targets without having systems and safeguards in place could lead to net harm.
The AACE recently identified these barriers and recommended a multidisciplinary team approach, reliable metrics, and a standardized method for insulin protocols, orders, and hypoglycemia prevention and treatment techniques.32
Both the AACE and SHM have produced toolkits to assist institutions to safely achieve improved glycemic control and care.33-34 The SHM Glycemic Control Task Force recently summarized key concepts to emphasize in formulating protocols and order sets in the noncritical care setting (see Table 2, left).
Stringent glycemic targets recommended by the ADA and the AACE may be appropriately moderated in centers that do not yet have the systems in place to achieve those goals safely.
Your glycemic target need not be identical to the ADA and AACE glycemic targets but should be similar to them. Examples of glycemic targets for noncritically ill inpatients are shown in Table 3 (see p. 48).
The glycemic target should be actionable, in that some institutionally endorsed action should result when a patient’s glycemic target is consistently not met.
Back to the Case
Your patient has an active infection, a glucose of 198 mg/dL and an elevated HbA1c. You hold the oral agents and start a basal bolus insulin regimen.
You generate an estimate for a safe insulin total daily dose of 60 units (100 kg x 0.6 units per kg for an obese, type 2 diabetes patient), and administer half as basal insulin, with the remaining 30 units distributed as rapid acting insulin in three divided doses. Your orders include routine glucose monitoring, and you plan to adjust the insulin daily as needed to adhere to the institutional glycemic target for noncritically ill patients of 90 to 150 mg/dL. TH
Dr. Maynard is the division chief for hospital medicine at the University of California, San Diego. He is the leader of SHM’s Glycemic Control Task Force and a leader of the VTE Prevention Collaborative.
References
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health And Nutrition Examination Survey 1999-2002. Diabetes Care. 2006;29(6):1263-1268.
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, 2005. Available at www.cdc.gov/diabetes/pubs/factsheet05.htm. Last accessed September 18, 2007.
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982.
- Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, Hirsch IB, the Diabetes In Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals (Technical Review). Diabetes Care. 2004;27:553–591.
- Zarich SW. Mechanism by which hyperglycemia plays a role in the setting of acute cardiovascular illness. Rev Cardiovasc Med. 2006;7 (Suppl 2):S35-43.
- Hansen T, Thiel S, Wouters P, Christiansen J, VandenBerghe B. Intensive insulin therapy exerts anti-inflammatory effects in critically ill patients and counteracts the adverse effect of low mannose-gind lectin levels. J Clin Endocrinol Metab. 2003;88:1082-1088.
- Yendamuri S, Fulda GJ, Tinkoff GH. Admission hyperglycemia as a prognostic indicator in trauma. J Trauma. 2003;55:33-38.
- Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein H. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–
- 2432.
- Bruno A, Williams LS, Kent TA. How important is hyperglycemia during acute brain infarction? Neurologist 2004;10(4):195-200.
- Pomposelli JJ, Baxter JK, Babineau TJ, et al. Early postoperative glucose control predicts nosocomial infection rate in diabetic patients. J Parenter Enteral Nutr.1998;22(2):77-81.
- Ainla T, Baburin A, Teesalu R, Rahu M. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med. 2005;22(10):1321-1325.
- Timmer JR, van der Horst IC, Ottervanger JP, et al. Prognostic value of admission glucose in non-diabetic patients with myocardial infarction. Am Heart J. 2004;148:399-404.
- Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355:773–778.
- Furnary AP, Wu Y. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland Diabetic Project. Endocr Pract. 2006:12 (Suppl 3): 22-26.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007–1021.
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471–1478.
- Malmberg K. Prospective randomised study of intensive insulin treatment on long-term survival after acute myocardial infarction inpatients with diabetes mellitus. BMJ. 1997;314:1512–1515.
- Malmberg K, Norhammar A, Wedel H, Ryden L. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626–2632.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449-461.
- Van den Berghe G, Wilmer A, Milants I, et al. Intensive insulin therapy in mixed medical/surgical intensive care units: benefit versus harm. Diabetes. 2006;55(11):3151-3159.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004;164(18):2005-2011.
- McAlister FA, Majumdar SR, Blitz S, Rowe BH, Romney J, Marrie TJ. The relation between hyperglycemia and outcomes in 2,471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care. 2005;28(4):810-815.
- Thomas M, Mathew T, Russ G, Rao M, Moran J. Early peri-operative glycaemic control and allograft rejection in patients with diabetes mellitus: a pilot study. Transplantation. 2001;72(7):1321-1324.
- Weiser MA, Cabanillas ME, Konopleva M, et al. Relation between the duration of remission and hyperglycemia during induction chemotherapy for acute lymphocytic leukemia with a hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone/methotrexate-cytarabine regimen. Cancer. 2004;100(6):1179-1185.
- Garber AJ, Moghissi ES, Bransome ED Jr, et al., American College of Endocrinology Task Force on Inpatient Diabetes Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract. 2004;10:77–82.
- Standards of medical care in diabetes-2006. Diabetes Care. 2006;29 (Suppl. 1):S4-S42.
- Vanhorebeek I, Langouche L, Van den Berghe G. Tight blood glucose control with insulin in the ICU: facts and controversies. Chest. 2007;132(1):268-278.
- Devos P, Preiser JC. Current controversies around tight glucose control in critically ill patients. Curr Opin Clin Nutr Metab Care. 2007;10(2):206-209.
- The Diabetes Control and Complications Trial Research Group (DCCT). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977-986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853.
- American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control: a call to action. Diabetes Care. 2006;29(8):1955-1962.
- American Association of Clinical Endocrinologists Inpatient Glycemic Control Resource Center 2007. Available at http://resources.aace.com/index.asp. Last accessed December 18, 2007.
- Society of Hospital Medicine Glycemic Control Resource Room. Available at www.hospitalmedicine.org/ResourceRoomRedesign/GlycemicControl.cfm. Last accessed Nov. 25, 2007.
Make a Move
As elderly patients suffering functional decline and immobility face prolonged hospital stays, placement in nursing homes, and increased risk of mortality, hospitalists must focus on one mission: Keep them moving.#1
With today’s emphasis on cost containment and quality assurance, keeping patients moving is one small step toward improving the quality of a patient’s hospitalization.
At the core of elders’ quality of life is independent mobility. When mobility is lost, a patient’s ability to socialize with peers and family, perform activities of daily living (ADLs), and participate in decisions regarding their well-being is severely compromised.
Most hospital admissions begin with the assignment of a patient to a bed. Although acute illness, medications, and a new environment all take their toll on patient functionality, simply putting a patient in recline has a significant impact.
If a young healthy person is ordered to rest for more than 72 hours, muscle mass and strength decrease, gait speed slows, and coordination becomes impaired.#2 If that patient is put to bed for more than 72 hours, organs other than the musculoskeletal system become compromised. Cardiovascular deconditioning with resting tachycardia and orthostatic hypotension, glucose intolerance, venous thromboembolism, hypercalcemia and osteoporosis, constipation and fecal impaction, pressure ulcers, and even depression can occur.3# Imagine then how elderly patients would fare.
Unfortunately, the independence of elderly patients is continually undermined by the same environment that offers treatment and care—the inpatient ward. And staff and patient family members are at fault.#4
Establish a Baseline
Teaching patients to move autonomously requires extra nursing time. Most on the nursing staff find it easier to provide a bedpan rather than assist a patient to the bathroom. When assisted ambulation is offered, patients may resist.
Families may hinder the resumption of mobility by performing tasks for patients instead of encouraging them to do them themselves. Further, changes in mobility are difficult to quantify and communicate due to limited mobility terminology in nursing practice and limited physician time. When a pre-admission functional status is not clearly documented, hospital staff often assumes that the patient’s compromised state is little changed from its baseline.
With so many barriers to patient mobility, obtaining an accurate assessment of a patient’s functional status two weeks prior to admission is key in establishing a plan for helping elderly patients regain mobility.
Ideally, one should speak to the patient as well as someone closely involved with the patient’s care who can verify or clarify the patient’s description of his or her prior activities. Significant information to obtain includes which ADLs the patient can independently perform, how far the patient can ambulate and with what assistive devices, and whether glasses, hearing aids, specially fitted shoes and orthotics, and knee braces are normally required for ambulation.#5
Though no screening tool has been validated as an absolute predictor of inpatient functional decline, lower functional status before admission, cognitive impairment, depression, advanced age, and prolonged length of hospital stay have been associated with loss of independence. Their presence may warrant a more aggressive regimen for regaining mobility.
Set the Stage
Before calling in a transfer to inpatient rehab, there are several steps one can take to maximize the return of function. By optimizing a patient’s functional capabilities during the admission, you enable them to integrate necessary skills into a daily routine—something they’re unlikely to learn at a rehabilitation center. Take these steps:6
- Control pain. Adequate analgesia is imperative for regaining mobility. Opiates and opiate agonists may be necessary for optimal control. Constipation should be expected and treated, and patients should be closely monitored for orthostasis, confusion, and urinary retention;
- Get the patient to a chair with assistive devices nearby. This includes canes, braces, walkers, orthopedic shoes, glasses, and hearing aids;
- Minimize IVs, catheters, and drains. Those that cannot be removed can be taped to minimize their interference with ambulation. Regular clothes, particularly jogging suits, promote ambulation and comfort;
- Coordinate with nursing department so the patient has periods of activity and rest. A walk down the corridor should be followed by a commensurate period of minimal activity, not a two-hour nap;
- Encourage sleep hygiene. Daytime activities can be maximized only when preceded by a restful night’s sleep. Limiting caffeinated beverages, restricting television time, and encouraging relaxing evening activities like reading may be necessary to ensure adequate sleep. Well-rested patients are better equipped to challenge themselves physically during the day and are less at risk for the side effects associated with sleeping medications;
- Give early referral to physical and occupational therapies. Even if the patient can barely tolerate sitting in a chair, a passive range of motion exercises for all joints should be undertaken daily. Additionally, active resistance exercises may be feasible for even debilitated patients if they receive daily assistance and continual encouragement. With persistence, skeletal muscles and the cardiovascular and pulmonary systems will show more endurance.#
Follow Progress
Accurately following a patient’s progress in regaining mobility requires the use of an assessment tool. The Elderly Mobility Scale (EMS) is useful for assessing improvements in mobility of elderly patients receiving physical therapy.
Balance, range of motion, and ambulation are scored initially, and the scores are updated during daily physical therapy. A review of this assessment tool was published in the Journal of Ageing this year, with the authors concluding that the EMS is a valid, reliable scale that can be readily applied during daily clinical work.7# Further, a review in Clinical Rehabilitation found the EMS to be a reliable test of motor function in elderly patients with a range of functional levels.#8 This assessment falls short in its lack of predictive validity in terms of falls or discharge destination.
Elderly patients suffer more hospital-associated falls than those younger than 65. According to a 2000 article from the British Medical Journal, patients older than 65 were seven times as likely to experience a preventable fall while in the hospital compared with younger age groups.#9
Patient factors that contribute to falls include age-related changes in postural control, impaired gait, decreased visual acuity, medications, the presence of acute and chronic diseases that affect sensory input, the central nervous system, and coordination. Osteoporosis is also an important factor—pathologic fractures often precede a fall. Environmental factors include poor lighting, obtrusive furniture, slippery floors, loose floor coverings, and bathrooms without handrails or grab bars.
The items most commonly included in fall risk-assessment tools include:10
- Comorbid patient characteristics or conditions associated with falling, such as cognitive impairment;
- History of a fall;
- Mobility impairment;
- Incontinence;
- Medications affecting balance/cognition and polypharmacy;
- Sensory deficits; and
- Advanced age.
The presence of more than three of these items identifies a patient at high risk for falling. But calculating a fall assessment includes not only identifying relevant risk factors, but also performing a focused physical exam. In ambulatory patients, the timed “get up and go” test is a useful predictor of falls. The patient is observed as she rises from a chair, walks 10 feet, then returns to the chair. If the patient requires more than 16 seconds to complete the task, he or she is at greater risk for a fall.
Early Intervention
While management depends on the underlying etiology of the fall, some generally acceptable practices are effective:
- Maintain a safe physical environment. Making sure spills are cleaned up quickly and walkways are kept free of obstruction is as important as maintaining adequate lighting in all areas where older adults will walk;
- Avoid use of restraints. Though restraints are often employed to prevent falls, they have not proved effective in medical trials. It has been demonstrated that their use increases the injury associated with falls, and several restraint-reduction projects have demonstrated that restraints can be removed without a significant increase in falls or injuries;
- Deal with medication side effects. The side effects of CNS altering drugs, and drugs affecting postural blood pressure, balance, and gait should be expected and addressed. Polypharmacy should be minimized;
- Watch patients closely. High risk patients should be positioned by the nursing station so that their visibility to the staff is maximized; and
- Promote mobility. There has been considerable research demonstrating the positive effect of exercise on reducing fall risk among community-residing older adults. While no study to date has addressed the impact of exercise in the hospital-based community, improved balance, mobility, and flexibility have been documented in nursing home residents receiving aggressive physical therapy. TH
Dr. Landis is a frequent contributor to The Hospitalist.
References
- Hoogerduijn JG, Schuurmans MJ, Duijnstee MS, et al. A systematic review of predictors and screening instruments to identify older hospitalized patients at risk for functional decline. J Clin Nurs. 2007 Jan;16(1):46-57.
- Callen BL, Mahoney JE, Wells TJ, et al. Admission and discharge mobility of frail hospitalized older adults. MedSurg Nursing 2004:13(3):156-163.
- Resnick NM, Marcantonio ER. How should clinical care of the aged differ? Lancet 2002; 350:1157-1167.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient. ACS surgery: principles and practice. Medscape 2005.
- Miller KE, Zylstra RG, Standridge JB. The geriatric patient: a systematic approach to maintaining health. Am Fam Physician. 2000;61(4):1080-1098.
- Rydwik E, Frändin K, Akner G. Effects of physical training on physical performance in institutionalized elderly patients with multiple diagnoses. Age Ageing. 2004 Jan;33(1):13-23.
- Kuys SS , Brauer SG. Validation and reliability of the Modified Elderly Mobility Scale. Australas J Ageing 2006; 25(3):140-144.
- Spilg EG, Martin BJ, Mitchell SL, et al. A comparison of mobility assessments in a geriatric day hospital. Clin Rehabil. 2001 Jun;15(3):296-300.
- Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population based review of medical records. BMJ 2000;320(7237):741-744
- Gray-Miceli DL, Capezuti E. A nursing guide to the prevention and management of falls in geriatric patients in long-term care settings. Medscape; May 19, 2005.
As elderly patients suffering functional decline and immobility face prolonged hospital stays, placement in nursing homes, and increased risk of mortality, hospitalists must focus on one mission: Keep them moving.#1
With today’s emphasis on cost containment and quality assurance, keeping patients moving is one small step toward improving the quality of a patient’s hospitalization.
At the core of elders’ quality of life is independent mobility. When mobility is lost, a patient’s ability to socialize with peers and family, perform activities of daily living (ADLs), and participate in decisions regarding their well-being is severely compromised.
Most hospital admissions begin with the assignment of a patient to a bed. Although acute illness, medications, and a new environment all take their toll on patient functionality, simply putting a patient in recline has a significant impact.
If a young healthy person is ordered to rest for more than 72 hours, muscle mass and strength decrease, gait speed slows, and coordination becomes impaired.#2 If that patient is put to bed for more than 72 hours, organs other than the musculoskeletal system become compromised. Cardiovascular deconditioning with resting tachycardia and orthostatic hypotension, glucose intolerance, venous thromboembolism, hypercalcemia and osteoporosis, constipation and fecal impaction, pressure ulcers, and even depression can occur.3# Imagine then how elderly patients would fare.
Unfortunately, the independence of elderly patients is continually undermined by the same environment that offers treatment and care—the inpatient ward. And staff and patient family members are at fault.#4
Establish a Baseline
Teaching patients to move autonomously requires extra nursing time. Most on the nursing staff find it easier to provide a bedpan rather than assist a patient to the bathroom. When assisted ambulation is offered, patients may resist.
Families may hinder the resumption of mobility by performing tasks for patients instead of encouraging them to do them themselves. Further, changes in mobility are difficult to quantify and communicate due to limited mobility terminology in nursing practice and limited physician time. When a pre-admission functional status is not clearly documented, hospital staff often assumes that the patient’s compromised state is little changed from its baseline.
With so many barriers to patient mobility, obtaining an accurate assessment of a patient’s functional status two weeks prior to admission is key in establishing a plan for helping elderly patients regain mobility.
Ideally, one should speak to the patient as well as someone closely involved with the patient’s care who can verify or clarify the patient’s description of his or her prior activities. Significant information to obtain includes which ADLs the patient can independently perform, how far the patient can ambulate and with what assistive devices, and whether glasses, hearing aids, specially fitted shoes and orthotics, and knee braces are normally required for ambulation.#5
Though no screening tool has been validated as an absolute predictor of inpatient functional decline, lower functional status before admission, cognitive impairment, depression, advanced age, and prolonged length of hospital stay have been associated with loss of independence. Their presence may warrant a more aggressive regimen for regaining mobility.
Set the Stage
Before calling in a transfer to inpatient rehab, there are several steps one can take to maximize the return of function. By optimizing a patient’s functional capabilities during the admission, you enable them to integrate necessary skills into a daily routine—something they’re unlikely to learn at a rehabilitation center. Take these steps:6
- Control pain. Adequate analgesia is imperative for regaining mobility. Opiates and opiate agonists may be necessary for optimal control. Constipation should be expected and treated, and patients should be closely monitored for orthostasis, confusion, and urinary retention;
- Get the patient to a chair with assistive devices nearby. This includes canes, braces, walkers, orthopedic shoes, glasses, and hearing aids;
- Minimize IVs, catheters, and drains. Those that cannot be removed can be taped to minimize their interference with ambulation. Regular clothes, particularly jogging suits, promote ambulation and comfort;
- Coordinate with nursing department so the patient has periods of activity and rest. A walk down the corridor should be followed by a commensurate period of minimal activity, not a two-hour nap;
- Encourage sleep hygiene. Daytime activities can be maximized only when preceded by a restful night’s sleep. Limiting caffeinated beverages, restricting television time, and encouraging relaxing evening activities like reading may be necessary to ensure adequate sleep. Well-rested patients are better equipped to challenge themselves physically during the day and are less at risk for the side effects associated with sleeping medications;
- Give early referral to physical and occupational therapies. Even if the patient can barely tolerate sitting in a chair, a passive range of motion exercises for all joints should be undertaken daily. Additionally, active resistance exercises may be feasible for even debilitated patients if they receive daily assistance and continual encouragement. With persistence, skeletal muscles and the cardiovascular and pulmonary systems will show more endurance.#
Follow Progress
Accurately following a patient’s progress in regaining mobility requires the use of an assessment tool. The Elderly Mobility Scale (EMS) is useful for assessing improvements in mobility of elderly patients receiving physical therapy.
Balance, range of motion, and ambulation are scored initially, and the scores are updated during daily physical therapy. A review of this assessment tool was published in the Journal of Ageing this year, with the authors concluding that the EMS is a valid, reliable scale that can be readily applied during daily clinical work.7# Further, a review in Clinical Rehabilitation found the EMS to be a reliable test of motor function in elderly patients with a range of functional levels.#8 This assessment falls short in its lack of predictive validity in terms of falls or discharge destination.
Elderly patients suffer more hospital-associated falls than those younger than 65. According to a 2000 article from the British Medical Journal, patients older than 65 were seven times as likely to experience a preventable fall while in the hospital compared with younger age groups.#9
Patient factors that contribute to falls include age-related changes in postural control, impaired gait, decreased visual acuity, medications, the presence of acute and chronic diseases that affect sensory input, the central nervous system, and coordination. Osteoporosis is also an important factor—pathologic fractures often precede a fall. Environmental factors include poor lighting, obtrusive furniture, slippery floors, loose floor coverings, and bathrooms without handrails or grab bars.
The items most commonly included in fall risk-assessment tools include:10
- Comorbid patient characteristics or conditions associated with falling, such as cognitive impairment;
- History of a fall;
- Mobility impairment;
- Incontinence;
- Medications affecting balance/cognition and polypharmacy;
- Sensory deficits; and
- Advanced age.
The presence of more than three of these items identifies a patient at high risk for falling. But calculating a fall assessment includes not only identifying relevant risk factors, but also performing a focused physical exam. In ambulatory patients, the timed “get up and go” test is a useful predictor of falls. The patient is observed as she rises from a chair, walks 10 feet, then returns to the chair. If the patient requires more than 16 seconds to complete the task, he or she is at greater risk for a fall.
Early Intervention
While management depends on the underlying etiology of the fall, some generally acceptable practices are effective:
- Maintain a safe physical environment. Making sure spills are cleaned up quickly and walkways are kept free of obstruction is as important as maintaining adequate lighting in all areas where older adults will walk;
- Avoid use of restraints. Though restraints are often employed to prevent falls, they have not proved effective in medical trials. It has been demonstrated that their use increases the injury associated with falls, and several restraint-reduction projects have demonstrated that restraints can be removed without a significant increase in falls or injuries;
- Deal with medication side effects. The side effects of CNS altering drugs, and drugs affecting postural blood pressure, balance, and gait should be expected and addressed. Polypharmacy should be minimized;
- Watch patients closely. High risk patients should be positioned by the nursing station so that their visibility to the staff is maximized; and
- Promote mobility. There has been considerable research demonstrating the positive effect of exercise on reducing fall risk among community-residing older adults. While no study to date has addressed the impact of exercise in the hospital-based community, improved balance, mobility, and flexibility have been documented in nursing home residents receiving aggressive physical therapy. TH
Dr. Landis is a frequent contributor to The Hospitalist.
References
- Hoogerduijn JG, Schuurmans MJ, Duijnstee MS, et al. A systematic review of predictors and screening instruments to identify older hospitalized patients at risk for functional decline. J Clin Nurs. 2007 Jan;16(1):46-57.
- Callen BL, Mahoney JE, Wells TJ, et al. Admission and discharge mobility of frail hospitalized older adults. MedSurg Nursing 2004:13(3):156-163.
- Resnick NM, Marcantonio ER. How should clinical care of the aged differ? Lancet 2002; 350:1157-1167.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient. ACS surgery: principles and practice. Medscape 2005.
- Miller KE, Zylstra RG, Standridge JB. The geriatric patient: a systematic approach to maintaining health. Am Fam Physician. 2000;61(4):1080-1098.
- Rydwik E, Frändin K, Akner G. Effects of physical training on physical performance in institutionalized elderly patients with multiple diagnoses. Age Ageing. 2004 Jan;33(1):13-23.
- Kuys SS , Brauer SG. Validation and reliability of the Modified Elderly Mobility Scale. Australas J Ageing 2006; 25(3):140-144.
- Spilg EG, Martin BJ, Mitchell SL, et al. A comparison of mobility assessments in a geriatric day hospital. Clin Rehabil. 2001 Jun;15(3):296-300.
- Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population based review of medical records. BMJ 2000;320(7237):741-744
- Gray-Miceli DL, Capezuti E. A nursing guide to the prevention and management of falls in geriatric patients in long-term care settings. Medscape; May 19, 2005.
As elderly patients suffering functional decline and immobility face prolonged hospital stays, placement in nursing homes, and increased risk of mortality, hospitalists must focus on one mission: Keep them moving.#1
With today’s emphasis on cost containment and quality assurance, keeping patients moving is one small step toward improving the quality of a patient’s hospitalization.
At the core of elders’ quality of life is independent mobility. When mobility is lost, a patient’s ability to socialize with peers and family, perform activities of daily living (ADLs), and participate in decisions regarding their well-being is severely compromised.
Most hospital admissions begin with the assignment of a patient to a bed. Although acute illness, medications, and a new environment all take their toll on patient functionality, simply putting a patient in recline has a significant impact.
If a young healthy person is ordered to rest for more than 72 hours, muscle mass and strength decrease, gait speed slows, and coordination becomes impaired.#2 If that patient is put to bed for more than 72 hours, organs other than the musculoskeletal system become compromised. Cardiovascular deconditioning with resting tachycardia and orthostatic hypotension, glucose intolerance, venous thromboembolism, hypercalcemia and osteoporosis, constipation and fecal impaction, pressure ulcers, and even depression can occur.3# Imagine then how elderly patients would fare.
Unfortunately, the independence of elderly patients is continually undermined by the same environment that offers treatment and care—the inpatient ward. And staff and patient family members are at fault.#4
Establish a Baseline
Teaching patients to move autonomously requires extra nursing time. Most on the nursing staff find it easier to provide a bedpan rather than assist a patient to the bathroom. When assisted ambulation is offered, patients may resist.
Families may hinder the resumption of mobility by performing tasks for patients instead of encouraging them to do them themselves. Further, changes in mobility are difficult to quantify and communicate due to limited mobility terminology in nursing practice and limited physician time. When a pre-admission functional status is not clearly documented, hospital staff often assumes that the patient’s compromised state is little changed from its baseline.
With so many barriers to patient mobility, obtaining an accurate assessment of a patient’s functional status two weeks prior to admission is key in establishing a plan for helping elderly patients regain mobility.
Ideally, one should speak to the patient as well as someone closely involved with the patient’s care who can verify or clarify the patient’s description of his or her prior activities. Significant information to obtain includes which ADLs the patient can independently perform, how far the patient can ambulate and with what assistive devices, and whether glasses, hearing aids, specially fitted shoes and orthotics, and knee braces are normally required for ambulation.#5
Though no screening tool has been validated as an absolute predictor of inpatient functional decline, lower functional status before admission, cognitive impairment, depression, advanced age, and prolonged length of hospital stay have been associated with loss of independence. Their presence may warrant a more aggressive regimen for regaining mobility.
Set the Stage
Before calling in a transfer to inpatient rehab, there are several steps one can take to maximize the return of function. By optimizing a patient’s functional capabilities during the admission, you enable them to integrate necessary skills into a daily routine—something they’re unlikely to learn at a rehabilitation center. Take these steps:6
- Control pain. Adequate analgesia is imperative for regaining mobility. Opiates and opiate agonists may be necessary for optimal control. Constipation should be expected and treated, and patients should be closely monitored for orthostasis, confusion, and urinary retention;
- Get the patient to a chair with assistive devices nearby. This includes canes, braces, walkers, orthopedic shoes, glasses, and hearing aids;
- Minimize IVs, catheters, and drains. Those that cannot be removed can be taped to minimize their interference with ambulation. Regular clothes, particularly jogging suits, promote ambulation and comfort;
- Coordinate with nursing department so the patient has periods of activity and rest. A walk down the corridor should be followed by a commensurate period of minimal activity, not a two-hour nap;
- Encourage sleep hygiene. Daytime activities can be maximized only when preceded by a restful night’s sleep. Limiting caffeinated beverages, restricting television time, and encouraging relaxing evening activities like reading may be necessary to ensure adequate sleep. Well-rested patients are better equipped to challenge themselves physically during the day and are less at risk for the side effects associated with sleeping medications;
- Give early referral to physical and occupational therapies. Even if the patient can barely tolerate sitting in a chair, a passive range of motion exercises for all joints should be undertaken daily. Additionally, active resistance exercises may be feasible for even debilitated patients if they receive daily assistance and continual encouragement. With persistence, skeletal muscles and the cardiovascular and pulmonary systems will show more endurance.#
Follow Progress
Accurately following a patient’s progress in regaining mobility requires the use of an assessment tool. The Elderly Mobility Scale (EMS) is useful for assessing improvements in mobility of elderly patients receiving physical therapy.
Balance, range of motion, and ambulation are scored initially, and the scores are updated during daily physical therapy. A review of this assessment tool was published in the Journal of Ageing this year, with the authors concluding that the EMS is a valid, reliable scale that can be readily applied during daily clinical work.7# Further, a review in Clinical Rehabilitation found the EMS to be a reliable test of motor function in elderly patients with a range of functional levels.#8 This assessment falls short in its lack of predictive validity in terms of falls or discharge destination.
Elderly patients suffer more hospital-associated falls than those younger than 65. According to a 2000 article from the British Medical Journal, patients older than 65 were seven times as likely to experience a preventable fall while in the hospital compared with younger age groups.#9
Patient factors that contribute to falls include age-related changes in postural control, impaired gait, decreased visual acuity, medications, the presence of acute and chronic diseases that affect sensory input, the central nervous system, and coordination. Osteoporosis is also an important factor—pathologic fractures often precede a fall. Environmental factors include poor lighting, obtrusive furniture, slippery floors, loose floor coverings, and bathrooms without handrails or grab bars.
The items most commonly included in fall risk-assessment tools include:10
- Comorbid patient characteristics or conditions associated with falling, such as cognitive impairment;
- History of a fall;
- Mobility impairment;
- Incontinence;
- Medications affecting balance/cognition and polypharmacy;
- Sensory deficits; and
- Advanced age.
The presence of more than three of these items identifies a patient at high risk for falling. But calculating a fall assessment includes not only identifying relevant risk factors, but also performing a focused physical exam. In ambulatory patients, the timed “get up and go” test is a useful predictor of falls. The patient is observed as she rises from a chair, walks 10 feet, then returns to the chair. If the patient requires more than 16 seconds to complete the task, he or she is at greater risk for a fall.
Early Intervention
While management depends on the underlying etiology of the fall, some generally acceptable practices are effective:
- Maintain a safe physical environment. Making sure spills are cleaned up quickly and walkways are kept free of obstruction is as important as maintaining adequate lighting in all areas where older adults will walk;
- Avoid use of restraints. Though restraints are often employed to prevent falls, they have not proved effective in medical trials. It has been demonstrated that their use increases the injury associated with falls, and several restraint-reduction projects have demonstrated that restraints can be removed without a significant increase in falls or injuries;
- Deal with medication side effects. The side effects of CNS altering drugs, and drugs affecting postural blood pressure, balance, and gait should be expected and addressed. Polypharmacy should be minimized;
- Watch patients closely. High risk patients should be positioned by the nursing station so that their visibility to the staff is maximized; and
- Promote mobility. There has been considerable research demonstrating the positive effect of exercise on reducing fall risk among community-residing older adults. While no study to date has addressed the impact of exercise in the hospital-based community, improved balance, mobility, and flexibility have been documented in nursing home residents receiving aggressive physical therapy. TH
Dr. Landis is a frequent contributor to The Hospitalist.
References
- Hoogerduijn JG, Schuurmans MJ, Duijnstee MS, et al. A systematic review of predictors and screening instruments to identify older hospitalized patients at risk for functional decline. J Clin Nurs. 2007 Jan;16(1):46-57.
- Callen BL, Mahoney JE, Wells TJ, et al. Admission and discharge mobility of frail hospitalized older adults. MedSurg Nursing 2004:13(3):156-163.
- Resnick NM, Marcantonio ER. How should clinical care of the aged differ? Lancet 2002; 350:1157-1167.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient. ACS surgery: principles and practice. Medscape 2005.
- Miller KE, Zylstra RG, Standridge JB. The geriatric patient: a systematic approach to maintaining health. Am Fam Physician. 2000;61(4):1080-1098.
- Rydwik E, Frändin K, Akner G. Effects of physical training on physical performance in institutionalized elderly patients with multiple diagnoses. Age Ageing. 2004 Jan;33(1):13-23.
- Kuys SS , Brauer SG. Validation and reliability of the Modified Elderly Mobility Scale. Australas J Ageing 2006; 25(3):140-144.
- Spilg EG, Martin BJ, Mitchell SL, et al. A comparison of mobility assessments in a geriatric day hospital. Clin Rehabil. 2001 Jun;15(3):296-300.
- Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population based review of medical records. BMJ 2000;320(7237):741-744
- Gray-Miceli DL, Capezuti E. A nursing guide to the prevention and management of falls in geriatric patients in long-term care settings. Medscape; May 19, 2005.
Subtle Skills
Hospitalists with a hunger for taking on administrative roles often pursue an advanced degree. But whether it’s to assume a leadership role or just do a better job, it’s the not-altogether-obvious skills that can help hospitalists improve their careers and job satisfaction.
By refining communication styles, being receptive to mentoring, or learning how to influence decision-makers, hospitalists can convey competence to their peers and superiors. Intangible strengths such as these will help the hospitalist who wishes to carve a niche as a quality-improvement researcher, director of a medical education clerkship, patient safety officer, or medical director.
Who Needs What
The administrative skills hospitalists need depend on their career goals. Those who reflect on their career goals, identify their core values, and consider what is feasible at different stages in their lives can more quickly build the abilities they’ll need. This self-awareness is perhaps the first skill to develop.
The setting and practice model hospitalists work in also influences which skills they may need.
“Although the skills needed in different settings may be fundamentally the same, the politics differ between a community hospital and a teaching hospital,” says Sayeed Khan, MD, director of the hospitalist program of Lakeside Medical Group. “Communication skills may be even more crucial in a community hospital, where it’s less understood what a hospitalist is.” Such ability to educate people in Hospitalist 101 is yet another skill a savvy administrator or administrator-to-be should hone.
Hospitalists also need to understand quality control and other measures—and what the numbers mean.
For example, says Dr. Khan, it’s valuable to know:
- What it means to have good bed days at the end of the month and an average length of stay of 3.3 days;
- How that compares with other groups in other hospitals; and
- The implications of those measures in terms of outcomes, dollar costs, and savings to the hospital as well as the group—and how that translates for the patient.
“Those are the types of figures that many hospitalists don’t really understand,” says Dr. Khan.
But hospitalists can learn by observing and studying. “I’m a good example of that in that I do not have a formal business background,” Dr. Khan says. “Along with the literature, networking with other people, particularly at the SHM annual meeting, can help hospitalists gain a better understanding of what these numbers mean and what the benchmarks are.”
He believes administrative skills can be divided into two categories: those related to metrics (the math behind what hospitalists do) and those related to patient care.
In regard to patient care, effective committee participation is an administrative ability that can influence the standard of care. For example, Dr. Khan is participating in committee work in the area of maintaining patients’ glycemic control.
“Historically, that issue was not well addressed,” he says. It is now recognized that patients who have tight glycemic control do much better while hospitalized, irrespective of whether they have diabetes. “But it’s difficult to get other clinicians to change their practice styles,” says Dr. Khan. “You can implement change in your own practice, and others can learn by example. But if you are on a committee that designs new protocols and those get implemented, then you’ve directly changed how medicine is practiced at that hospital.”
Being able to win buy-in for your ideas makes that possible. “Purely speaking, committee participation is not an administrative role,” says Dr. Khan. “But it is an administrative skill in that it is outside the scope of what’s normally required for a hospitalist.”
Get Help
Honing one’s receptivity to mentorship is another vital ability for the upwardly mobile hospitalist. Mentors can direct inexperienced physicians to resources that may help them develop proficiency. A mentor who has grappled with the same issues can help open doors to opportunities hospitalists may not know about.
As she reflects on her early career, when she had no mentors and no administrative experience, Sylvia C.W. McKean, MD, realizes she could have used guidance and advocacy. Effective mentorship helps hospitalists reach their goals faster with fewer impediments, she says.
“Mentorship is critical,” says Dr. McKean, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service of Brigham and Women’s Hospital in Boston. “But knowing how to receive the information you’re getting and how to apply it to your own specific professional goals can really help you develop the skills that will help you move your career forward. Informal mentorship is one area where there has been less opportunity for women in the past, resulting in more promotions for men.”
Other skills women may especially need are learning the written and unwritten rules of promotion, being more assertive in finding out what they are, and developing diplomacy—including learning to say no with finesse.
“The reality is that if you are in an environment that has predominantly male leadership, it is important for [a woman] to have male advocates to support whatever it is that you are trying to do,” says Dr. McKean. “In some instances they may have to speak for you.”
Efficiency and setting priorities are also important skills.
“I learned very early on that efficiency was critical to managing several roles—administrative, patient care, and raising three boys,” says Dr. McKean. “There were some things, however, that in retrospect I did not need to do. For example, I did my own home-improvement tasks instead of hiring someone else to do them. For women in particular, you don’t have to be a super everything. At different phases in your life your priorities will vary. Get help so that you’re not spending time doing tasks that don’t further your goals.”
Communication
Facility with communication, of course, is paramount in every aspect of medicine. Being poised, articulate, concise, and persuasive to get your message across, says Dr. McKean, goes a long way toward advancing one’s career.
“It took me a long time to realize this,” says Dr. McKean. “For example, whenever I generated reports I tried to have as much information in there as possible because I thought it would look like I was very knowledgeable. A one-page document that summarizes the key points is often more effective in getting people’s attention.”
Another subset of communication is skill at public speaking, which may lead to being invited to give lectures.
Dr. Khan believes shy, less-articulate clinicians can begin to improve their public speaking by serving on committees. “Unless the committee is a committee of two, that is the appropriate forum to begin voicing your opinions and expertise on a particular matter,” he says. “There’s a certain comfort level built into that because you’re not necessarily speaking on a topic you are unfamiliar with.”
Another intangible administrative skill, he says, is the ability to deal with people from different walks of life. Some highly placed hospital administrators don’t have clinical backgrounds and will require explanations of clinical situations that mesh with their business understanding.
Time Management
Organization is a critical administrative skill no matter what career path a hospitalist follows.
“As hospitalists we are typically juggling more than one thing at one time,” Dr. Khan says. “As a hospitalist who is involved in administrative tasks, if you’re not organized, that is a path to failure.”
Strive to hire the right people for clerical and administrative staff positions. They will fill in the weak spots to keep you on track and present a good image as your front person. But having a good clerical or administrative assistant doesn’t let you off the hook; you, too, must demonstrate solid time management. Make sure you take good notes at committees, quickly access data or documentation, and research and report back well.
The Interpersonal
Robert L. Benak, MD, a hospitalist and medical director of Champlain Valley Physicians Hospital (CVPH) Medical Center, a 341-bed acute care hospital and 54-bed skilled nursing facility in Plattsburgh, N.Y., thinks the most important intangible skills involve managing relationships.
Again, self-reflection helps. “Understand what your personality is like on a calm day and what it is like on a stressful day,” he says.
He says it’s critical to be able to negotiate with others. “Understanding what lies underneath, what common and different interests the two negotiating partners have helps you focus on getting the best compromise of conflicting interests to resolve a disagreement in an amicable and effective way,” he says.
Dr. Benak, who joined SHM around the time his group started in October 2006, thanks the SHM Leadership Academy for strengthening his interpersonal skills. He has tried to bring home what he learned to his group of five hospitalists.
Recently, he had to determine whether to designate a patient with abdominal pain as a surgical or medical patient. Dr. Benak invoked his “ability to sit down with the orthopedic surgeon and general surgeon, recognizing that they’ve got legitimate interests and concerns, as do I, and figuring out what works well for us, and more importantly, what works best for the patient.”
That ability to compromise is indispensable to growth as a hospitalist, he says.
“I was a chemistry major in college and loved working with concrete, though sometimes complicated, problems where you’re either right or you’re wrong,” he says. “I’ve come to see that giving up being right, and giving up any sense of entitlement I may feel in having the principal position, are skills. Even if you think the other person is being unreasonable, you have to accept that as a fact and figure out how to cope with that in a way that is a credit to yourself and your program.” TH
Andrea Sattinger is a medical writer based in North Carolina.
Hospitalists with a hunger for taking on administrative roles often pursue an advanced degree. But whether it’s to assume a leadership role or just do a better job, it’s the not-altogether-obvious skills that can help hospitalists improve their careers and job satisfaction.
By refining communication styles, being receptive to mentoring, or learning how to influence decision-makers, hospitalists can convey competence to their peers and superiors. Intangible strengths such as these will help the hospitalist who wishes to carve a niche as a quality-improvement researcher, director of a medical education clerkship, patient safety officer, or medical director.
Who Needs What
The administrative skills hospitalists need depend on their career goals. Those who reflect on their career goals, identify their core values, and consider what is feasible at different stages in their lives can more quickly build the abilities they’ll need. This self-awareness is perhaps the first skill to develop.
The setting and practice model hospitalists work in also influences which skills they may need.
“Although the skills needed in different settings may be fundamentally the same, the politics differ between a community hospital and a teaching hospital,” says Sayeed Khan, MD, director of the hospitalist program of Lakeside Medical Group. “Communication skills may be even more crucial in a community hospital, where it’s less understood what a hospitalist is.” Such ability to educate people in Hospitalist 101 is yet another skill a savvy administrator or administrator-to-be should hone.
Hospitalists also need to understand quality control and other measures—and what the numbers mean.
For example, says Dr. Khan, it’s valuable to know:
- What it means to have good bed days at the end of the month and an average length of stay of 3.3 days;
- How that compares with other groups in other hospitals; and
- The implications of those measures in terms of outcomes, dollar costs, and savings to the hospital as well as the group—and how that translates for the patient.
“Those are the types of figures that many hospitalists don’t really understand,” says Dr. Khan.
But hospitalists can learn by observing and studying. “I’m a good example of that in that I do not have a formal business background,” Dr. Khan says. “Along with the literature, networking with other people, particularly at the SHM annual meeting, can help hospitalists gain a better understanding of what these numbers mean and what the benchmarks are.”
He believes administrative skills can be divided into two categories: those related to metrics (the math behind what hospitalists do) and those related to patient care.
In regard to patient care, effective committee participation is an administrative ability that can influence the standard of care. For example, Dr. Khan is participating in committee work in the area of maintaining patients’ glycemic control.
“Historically, that issue was not well addressed,” he says. It is now recognized that patients who have tight glycemic control do much better while hospitalized, irrespective of whether they have diabetes. “But it’s difficult to get other clinicians to change their practice styles,” says Dr. Khan. “You can implement change in your own practice, and others can learn by example. But if you are on a committee that designs new protocols and those get implemented, then you’ve directly changed how medicine is practiced at that hospital.”
Being able to win buy-in for your ideas makes that possible. “Purely speaking, committee participation is not an administrative role,” says Dr. Khan. “But it is an administrative skill in that it is outside the scope of what’s normally required for a hospitalist.”
Get Help
Honing one’s receptivity to mentorship is another vital ability for the upwardly mobile hospitalist. Mentors can direct inexperienced physicians to resources that may help them develop proficiency. A mentor who has grappled with the same issues can help open doors to opportunities hospitalists may not know about.
As she reflects on her early career, when she had no mentors and no administrative experience, Sylvia C.W. McKean, MD, realizes she could have used guidance and advocacy. Effective mentorship helps hospitalists reach their goals faster with fewer impediments, she says.
“Mentorship is critical,” says Dr. McKean, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service of Brigham and Women’s Hospital in Boston. “But knowing how to receive the information you’re getting and how to apply it to your own specific professional goals can really help you develop the skills that will help you move your career forward. Informal mentorship is one area where there has been less opportunity for women in the past, resulting in more promotions for men.”
Other skills women may especially need are learning the written and unwritten rules of promotion, being more assertive in finding out what they are, and developing diplomacy—including learning to say no with finesse.
“The reality is that if you are in an environment that has predominantly male leadership, it is important for [a woman] to have male advocates to support whatever it is that you are trying to do,” says Dr. McKean. “In some instances they may have to speak for you.”
Efficiency and setting priorities are also important skills.
“I learned very early on that efficiency was critical to managing several roles—administrative, patient care, and raising three boys,” says Dr. McKean. “There were some things, however, that in retrospect I did not need to do. For example, I did my own home-improvement tasks instead of hiring someone else to do them. For women in particular, you don’t have to be a super everything. At different phases in your life your priorities will vary. Get help so that you’re not spending time doing tasks that don’t further your goals.”
Communication
Facility with communication, of course, is paramount in every aspect of medicine. Being poised, articulate, concise, and persuasive to get your message across, says Dr. McKean, goes a long way toward advancing one’s career.
“It took me a long time to realize this,” says Dr. McKean. “For example, whenever I generated reports I tried to have as much information in there as possible because I thought it would look like I was very knowledgeable. A one-page document that summarizes the key points is often more effective in getting people’s attention.”
Another subset of communication is skill at public speaking, which may lead to being invited to give lectures.
Dr. Khan believes shy, less-articulate clinicians can begin to improve their public speaking by serving on committees. “Unless the committee is a committee of two, that is the appropriate forum to begin voicing your opinions and expertise on a particular matter,” he says. “There’s a certain comfort level built into that because you’re not necessarily speaking on a topic you are unfamiliar with.”
Another intangible administrative skill, he says, is the ability to deal with people from different walks of life. Some highly placed hospital administrators don’t have clinical backgrounds and will require explanations of clinical situations that mesh with their business understanding.
Time Management
Organization is a critical administrative skill no matter what career path a hospitalist follows.
“As hospitalists we are typically juggling more than one thing at one time,” Dr. Khan says. “As a hospitalist who is involved in administrative tasks, if you’re not organized, that is a path to failure.”
Strive to hire the right people for clerical and administrative staff positions. They will fill in the weak spots to keep you on track and present a good image as your front person. But having a good clerical or administrative assistant doesn’t let you off the hook; you, too, must demonstrate solid time management. Make sure you take good notes at committees, quickly access data or documentation, and research and report back well.
The Interpersonal
Robert L. Benak, MD, a hospitalist and medical director of Champlain Valley Physicians Hospital (CVPH) Medical Center, a 341-bed acute care hospital and 54-bed skilled nursing facility in Plattsburgh, N.Y., thinks the most important intangible skills involve managing relationships.
Again, self-reflection helps. “Understand what your personality is like on a calm day and what it is like on a stressful day,” he says.
He says it’s critical to be able to negotiate with others. “Understanding what lies underneath, what common and different interests the two negotiating partners have helps you focus on getting the best compromise of conflicting interests to resolve a disagreement in an amicable and effective way,” he says.
Dr. Benak, who joined SHM around the time his group started in October 2006, thanks the SHM Leadership Academy for strengthening his interpersonal skills. He has tried to bring home what he learned to his group of five hospitalists.
Recently, he had to determine whether to designate a patient with abdominal pain as a surgical or medical patient. Dr. Benak invoked his “ability to sit down with the orthopedic surgeon and general surgeon, recognizing that they’ve got legitimate interests and concerns, as do I, and figuring out what works well for us, and more importantly, what works best for the patient.”
That ability to compromise is indispensable to growth as a hospitalist, he says.
“I was a chemistry major in college and loved working with concrete, though sometimes complicated, problems where you’re either right or you’re wrong,” he says. “I’ve come to see that giving up being right, and giving up any sense of entitlement I may feel in having the principal position, are skills. Even if you think the other person is being unreasonable, you have to accept that as a fact and figure out how to cope with that in a way that is a credit to yourself and your program.” TH
Andrea Sattinger is a medical writer based in North Carolina.
Hospitalists with a hunger for taking on administrative roles often pursue an advanced degree. But whether it’s to assume a leadership role or just do a better job, it’s the not-altogether-obvious skills that can help hospitalists improve their careers and job satisfaction.
By refining communication styles, being receptive to mentoring, or learning how to influence decision-makers, hospitalists can convey competence to their peers and superiors. Intangible strengths such as these will help the hospitalist who wishes to carve a niche as a quality-improvement researcher, director of a medical education clerkship, patient safety officer, or medical director.
Who Needs What
The administrative skills hospitalists need depend on their career goals. Those who reflect on their career goals, identify their core values, and consider what is feasible at different stages in their lives can more quickly build the abilities they’ll need. This self-awareness is perhaps the first skill to develop.
The setting and practice model hospitalists work in also influences which skills they may need.
“Although the skills needed in different settings may be fundamentally the same, the politics differ between a community hospital and a teaching hospital,” says Sayeed Khan, MD, director of the hospitalist program of Lakeside Medical Group. “Communication skills may be even more crucial in a community hospital, where it’s less understood what a hospitalist is.” Such ability to educate people in Hospitalist 101 is yet another skill a savvy administrator or administrator-to-be should hone.
Hospitalists also need to understand quality control and other measures—and what the numbers mean.
For example, says Dr. Khan, it’s valuable to know:
- What it means to have good bed days at the end of the month and an average length of stay of 3.3 days;
- How that compares with other groups in other hospitals; and
- The implications of those measures in terms of outcomes, dollar costs, and savings to the hospital as well as the group—and how that translates for the patient.
“Those are the types of figures that many hospitalists don’t really understand,” says Dr. Khan.
But hospitalists can learn by observing and studying. “I’m a good example of that in that I do not have a formal business background,” Dr. Khan says. “Along with the literature, networking with other people, particularly at the SHM annual meeting, can help hospitalists gain a better understanding of what these numbers mean and what the benchmarks are.”
He believes administrative skills can be divided into two categories: those related to metrics (the math behind what hospitalists do) and those related to patient care.
In regard to patient care, effective committee participation is an administrative ability that can influence the standard of care. For example, Dr. Khan is participating in committee work in the area of maintaining patients’ glycemic control.
“Historically, that issue was not well addressed,” he says. It is now recognized that patients who have tight glycemic control do much better while hospitalized, irrespective of whether they have diabetes. “But it’s difficult to get other clinicians to change their practice styles,” says Dr. Khan. “You can implement change in your own practice, and others can learn by example. But if you are on a committee that designs new protocols and those get implemented, then you’ve directly changed how medicine is practiced at that hospital.”
Being able to win buy-in for your ideas makes that possible. “Purely speaking, committee participation is not an administrative role,” says Dr. Khan. “But it is an administrative skill in that it is outside the scope of what’s normally required for a hospitalist.”
Get Help
Honing one’s receptivity to mentorship is another vital ability for the upwardly mobile hospitalist. Mentors can direct inexperienced physicians to resources that may help them develop proficiency. A mentor who has grappled with the same issues can help open doors to opportunities hospitalists may not know about.
As she reflects on her early career, when she had no mentors and no administrative experience, Sylvia C.W. McKean, MD, realizes she could have used guidance and advocacy. Effective mentorship helps hospitalists reach their goals faster with fewer impediments, she says.
“Mentorship is critical,” says Dr. McKean, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service of Brigham and Women’s Hospital in Boston. “But knowing how to receive the information you’re getting and how to apply it to your own specific professional goals can really help you develop the skills that will help you move your career forward. Informal mentorship is one area where there has been less opportunity for women in the past, resulting in more promotions for men.”
Other skills women may especially need are learning the written and unwritten rules of promotion, being more assertive in finding out what they are, and developing diplomacy—including learning to say no with finesse.
“The reality is that if you are in an environment that has predominantly male leadership, it is important for [a woman] to have male advocates to support whatever it is that you are trying to do,” says Dr. McKean. “In some instances they may have to speak for you.”
Efficiency and setting priorities are also important skills.
“I learned very early on that efficiency was critical to managing several roles—administrative, patient care, and raising three boys,” says Dr. McKean. “There were some things, however, that in retrospect I did not need to do. For example, I did my own home-improvement tasks instead of hiring someone else to do them. For women in particular, you don’t have to be a super everything. At different phases in your life your priorities will vary. Get help so that you’re not spending time doing tasks that don’t further your goals.”
Communication
Facility with communication, of course, is paramount in every aspect of medicine. Being poised, articulate, concise, and persuasive to get your message across, says Dr. McKean, goes a long way toward advancing one’s career.
“It took me a long time to realize this,” says Dr. McKean. “For example, whenever I generated reports I tried to have as much information in there as possible because I thought it would look like I was very knowledgeable. A one-page document that summarizes the key points is often more effective in getting people’s attention.”
Another subset of communication is skill at public speaking, which may lead to being invited to give lectures.
Dr. Khan believes shy, less-articulate clinicians can begin to improve their public speaking by serving on committees. “Unless the committee is a committee of two, that is the appropriate forum to begin voicing your opinions and expertise on a particular matter,” he says. “There’s a certain comfort level built into that because you’re not necessarily speaking on a topic you are unfamiliar with.”
Another intangible administrative skill, he says, is the ability to deal with people from different walks of life. Some highly placed hospital administrators don’t have clinical backgrounds and will require explanations of clinical situations that mesh with their business understanding.
Time Management
Organization is a critical administrative skill no matter what career path a hospitalist follows.
“As hospitalists we are typically juggling more than one thing at one time,” Dr. Khan says. “As a hospitalist who is involved in administrative tasks, if you’re not organized, that is a path to failure.”
Strive to hire the right people for clerical and administrative staff positions. They will fill in the weak spots to keep you on track and present a good image as your front person. But having a good clerical or administrative assistant doesn’t let you off the hook; you, too, must demonstrate solid time management. Make sure you take good notes at committees, quickly access data or documentation, and research and report back well.
The Interpersonal
Robert L. Benak, MD, a hospitalist and medical director of Champlain Valley Physicians Hospital (CVPH) Medical Center, a 341-bed acute care hospital and 54-bed skilled nursing facility in Plattsburgh, N.Y., thinks the most important intangible skills involve managing relationships.
Again, self-reflection helps. “Understand what your personality is like on a calm day and what it is like on a stressful day,” he says.
He says it’s critical to be able to negotiate with others. “Understanding what lies underneath, what common and different interests the two negotiating partners have helps you focus on getting the best compromise of conflicting interests to resolve a disagreement in an amicable and effective way,” he says.
Dr. Benak, who joined SHM around the time his group started in October 2006, thanks the SHM Leadership Academy for strengthening his interpersonal skills. He has tried to bring home what he learned to his group of five hospitalists.
Recently, he had to determine whether to designate a patient with abdominal pain as a surgical or medical patient. Dr. Benak invoked his “ability to sit down with the orthopedic surgeon and general surgeon, recognizing that they’ve got legitimate interests and concerns, as do I, and figuring out what works well for us, and more importantly, what works best for the patient.”
That ability to compromise is indispensable to growth as a hospitalist, he says.
“I was a chemistry major in college and loved working with concrete, though sometimes complicated, problems where you’re either right or you’re wrong,” he says. “I’ve come to see that giving up being right, and giving up any sense of entitlement I may feel in having the principal position, are skills. Even if you think the other person is being unreasonable, you have to accept that as a fact and figure out how to cope with that in a way that is a credit to yourself and your program.” TH
Andrea Sattinger is a medical writer based in North Carolina.
Hospitalists on Top
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.

Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.
Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.
Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Safety Sentries
At Mercy Hospital in Iowa City, Iowa, the implementation of safety and quality systems is “stirring up the pot,” says Mercy hospitalist and medical director Martin Izakovic, MD.
He has been recruited to supervise Mercy’s latest safety initiatives, including electronic medical records, pay-for-performance measures, development of treatment protocols, standardization of care, and deep-vein thrombosis prophylaxis.
Hospitalists at Mercy face the challenges their peers around the country face in their quest to improve quality and safeguard patients. The leader in these areas needs to be a role model and respected peer for the physicians he or she must lead day after day, says Dr. Izakovic.
How do hospitalists, who are so well-positioned to become leaders in patient safety, develop in that direction?
“The biggest challenge I see is the spectrum of polarization between clinicians and administrators,” he says. “One of the most important qualities that a patient safety officer needs is the ability to overbridge the doctors on one hand and the administrators on the other.”
What They Need
A patient safety officer (PSO) requires a critical mix of clinical and administrative skills, says Peter B. Angood, MD, vice president and chief patient safety officer for The Joint Commission, in Oakbrook, Ill.
On the clinical side, the hospitalist who wishes to be a PSO needs more than awareness of safety and quality improvement processes. He or she must be knowledgeable about and conversant in safety science in industries beyond healthcare. That expertise needs to encompass leadership, behaviors and cultures, human factors, and process redesign or systems engineering. Important, too, is training in how to corral the pieces of an organization and ensure they operate well together.
An understanding of organizational behavior is of great value. The potential PSO should understand how the key players interact: the board of directors with chief executives, chief executives with senior management, senior management with all staff (including the allied professionals), and medical staff with the organization as a whole.
“Because safety is a systemwide process, the patient safety [person] is pivotal in forming a hub from which much of the quality, safety, and process improvement occurs,” says Dr. Angood.

Jason Adelman, MD, MS, former hospitalist and current PSO at Montefiore Medical Center in New York City, says developing patient safety leaders should embrace technology. “Pay attention to the latest and greatest ideas, products, and services,” he urges. “Come up with strategic plans to implement in healthcare, get the information quickly into the hands of physicians, have physicians report, and include forcing functions [whereby computers will not process to completion when key data are missing].”
Above all, the patient safety officer must train to be a change agent. “Influencing patient safety means you have to be there in the capital-allocation process,” says David Shulkin, MD, chief executive officer at Beth Israel Medical Center in New York City. “You have to be there when they’re designing facilities. You have to understand your human resource policies and the skill sets and aptitudes of the people that the hospital is hiring. To be a good patient safety officer, the training needs to involve broad exposure with a slant toward operations.”
Build a Bridge
As a young physician who wanted to develop as a leader in the field of quality and safety, Dr. Shulkin had to forge his own path. In 1992, after he became chief medical officer (CMO) at the Hospital of the University of Pennsylvania in Philadelphia, he fielded several inquiries a month from young physicians who wanted to pursue a similar career. In response to that need, he designed a quality improvement/patient safety fellowship at his school.
David Bernard, MD, now chief medical officer at Beth Israel, had been practicing medicine for 30 years when at age 50 he took a year’s leave of absence from Boston University and enrolled as Dr. Shulkin’s first fellow in 1994. Dr. Bernard, a nephrologist, was a vice dean in the school of medicine at Boston University Medical Center, a hospital vice president for clinical affairs, and a senior clinician in his specialty group.
Drs. Shulkin and Bernard left the University of Pennsylvania in 1999 to take the concepts of quality transparency to a higher level and formed DoctorQuality Inc. in Conshohocken, Pa. To continue their work, DoctorQuality funded the fellowship. In 2005 when Dr. Shulkin went to Beth Israel in New York, the fellowship was restarted as the Don Hoskins Quality Improvement/Patient Safety program and funded for five years with private philanthropy.
Modeled after graduate medical education, the fellowship is predominantly hands-on. Fellows work on real projects alongside professionals in management, quality, and safety.

Under the Hood
Giving trainees the inside view into the intricacies of how to change physician behavior and cultural issues in hospitals is the backbone of Beth Israel’s program. Fellows see what clinicians rarely see: the real-world complexity of hospitals, why there is so much inertia, and the reasons changing systems can be so difficult. Fellows learn how almost every hospital issue involves financial, personnel, facility, policy and political considerations. By allowing entrée into the executive offices, the fellow gets to hear the many different perspectives when people react to an issue.
“After a quality-improvement meeting, for instance, where people are positioning and requesting different things rather than taking action,” says Dr. Shulkin, “the fellow gets to hear the behind-the-scenes analysis—how executives sometimes label people and develop strategies to overcome some of these barriers.”
Understanding how administrators, directors of social work, or nurses, for instance, view situations and understand their culture helps the leader be more effective.
“To get both leadership and clinician buy-in, and to get leadership to motivate clinicians to participate in system changes, you also need to be politically savvy,” says Dr. Adelman. “Plenty of people resist change. The PSO needs to come off as sincere, passionate, and smart, and has to be able to answer people’s tough questions.”
It can take an ambassador’s touch to make headway in the traditional physician culture.
“The patient safety officers, the chief medical officers, often have to function as diplomats,” says Dr. Angood. “This physician engagement piece is one of the most complicated issues out there, and it arises because physicians historically are trained to be autonomous, to be independent, and to expect that institutions are there to serve them.”
—Latha Sivaprasad, MD, Don Hoskins Quality Improvement/Patient Safety fellow, Beth Israel Medical Center, New York City
One Hospitalist’s View
When Latha Sivaprasad, MD, current Don Hoskins fellow at Beth Israel, started her fellowship six months ago, she was astonished how little she knew about patient safety and quality. Although she felt she knew the day-to-day deficiencies in the hospital and on the front line—and despite having practiced in three other hospitals—she wasn’t prepared to learn what she hadn’t known she didn’t know.
“In my five years as a hospitalist, I knew very little about patient safety and quality—to my shock now,” she says. “Since I’ve been a fellow here, I realize how much I had been underutilized and how much more I could have contributed to making my respective hospitals run more safely.”
Understanding people’s motivations and meeting their needs to make a hospital safer is an intricate process.
“I think it is important for hospitalists to understand how complicated and time-consuming system changes are,” she says. “You do not have that perspective as a clinician. You think that change can occur from a memo or from good intentions to do the right thing.”
She has learned to think about the bigger world outside the clinical portion of running a hospital.
“To be a change agent you really need to appreciate the hospital from the penthouse view, which is what this fellowship provides,” she says. “You need to have access to every meeting, every record, every clinician, and every senior executive to put the pieces of the puzzle together to understand how things change.”
The hospital is working to apply the Toyota method of employee involvement to the issue of how an obstetric patient progresses from triage in the emergency department (ED) to labor and delivery, and how much time passes before the triage the patient is discharged or admitted. Their focus first targeted convening the right group to discuss the issue and identify the details of the problem, then put a plan in place to track ED triage. They looked for ways to make that process more efficient, met again to determine how to implement a new version of that process, then tracked the difference. “All of this was a multihour ordeal,” she says.
It’s exhilarating, frustrating, and intriguing—and sometimes discouraging. “It’s very tedious making change, and I didn’t appreciate that before the fellowship,” she says.
Dr. Sivaprasad advises hospitalists that to be effective in patient safety efforts means being a problem solver, highly empathetic, sensitive to others, and above all, extremely patient. But results often emerge slowly.
“You must have several things brewing at once because if certain programs’ changes are taking time, you need to complete the loop on something else,” she advises.
The Ideal Candidate
Of the 20 fellows Dr. Shulkin has mentored, about half were older and more experienced than he was. Reflecting on the successful fellows and those who benefited less makes him think the distinction of experience and age is less important than the individual’s personality.
“What is important is the personality and motivation and self-directedness of the fellow,” says Dr. Shulkin. “This is a very autonomous fellowship. One of the pluses and minuses of working with senior executives is that they are very busy; they don’t have time the way traditional academic program directors or residency directors do to think, ‘Where are my fellows and what are they doing?’”
Those who will get the most out of this type of experience know how to be delicately assertive yet drive their own agendas.
To Drs. Shulkin and Bernard, a good patient safety leader is naturally curious about what makes healthcare organizations tick. The ideal candidate has an appreciation for hospital financing and the science behind physician behavior change, and the capacity to be a good listener. The trainee also needs to put aside his or her ego while transitioning from a physician in charge to stepping back into the student role to learn the new language and environment.
—David Shulkin, MD, chief executive officer, Beth Israel Medical Center, New York City
Where to Begin

The institution sponsoring the development of the patient safety officer is just as important as who that candidate is.
“The administration has to have a visionary leadership that recognizes that healthcare quality and safety is the way you do business,” says Dr. Bernard. “You have to be in an institution that is not just paying lip service to moving quality and safety. It has to be part of the fabric of the institution.”
The institution also has to be able to offer a variety of experiences, making this kind of training difficult in a nonacademic setting.
For those interested in pursuing this area of leadership, the natural first step is to meet with the CMO or CEO to explore whether the individual’s and hospital’s interests can be aligned.
“But you can’t force it,” warns Dr. Shulkin. “If that is not a natural fit, if the CMO or CEO doesn’t see their role as, or have an interest in, training faculty people; or if they don’t have the expertise to do it, it’s not going to be a good experience. In those cases, the hospitalist should look elsewhere. An increasing number of centers can offer this kind of experience for a year,” he says. “Then the hospitalist might return to their institution to take on a leadership role there.”
Creating a costly infrastructure to train a patient safety officer is not required. What is necessary is chemistry in the mentor-trainee relationship.
“This is the first time in my postgraduate career that I actually have consistently committed mentors who care about how I am molded as a physician and what my ultimate contribution to the medical field will be,” says Dr. Sivaprasad. TH
Andrea Sattinger is a medical writer based in North Carolina.
At Mercy Hospital in Iowa City, Iowa, the implementation of safety and quality systems is “stirring up the pot,” says Mercy hospitalist and medical director Martin Izakovic, MD.
He has been recruited to supervise Mercy’s latest safety initiatives, including electronic medical records, pay-for-performance measures, development of treatment protocols, standardization of care, and deep-vein thrombosis prophylaxis.
Hospitalists at Mercy face the challenges their peers around the country face in their quest to improve quality and safeguard patients. The leader in these areas needs to be a role model and respected peer for the physicians he or she must lead day after day, says Dr. Izakovic.
How do hospitalists, who are so well-positioned to become leaders in patient safety, develop in that direction?
“The biggest challenge I see is the spectrum of polarization between clinicians and administrators,” he says. “One of the most important qualities that a patient safety officer needs is the ability to overbridge the doctors on one hand and the administrators on the other.”
What They Need
A patient safety officer (PSO) requires a critical mix of clinical and administrative skills, says Peter B. Angood, MD, vice president and chief patient safety officer for The Joint Commission, in Oakbrook, Ill.
On the clinical side, the hospitalist who wishes to be a PSO needs more than awareness of safety and quality improvement processes. He or she must be knowledgeable about and conversant in safety science in industries beyond healthcare. That expertise needs to encompass leadership, behaviors and cultures, human factors, and process redesign or systems engineering. Important, too, is training in how to corral the pieces of an organization and ensure they operate well together.
An understanding of organizational behavior is of great value. The potential PSO should understand how the key players interact: the board of directors with chief executives, chief executives with senior management, senior management with all staff (including the allied professionals), and medical staff with the organization as a whole.
“Because safety is a systemwide process, the patient safety [person] is pivotal in forming a hub from which much of the quality, safety, and process improvement occurs,” says Dr. Angood.
Jason Adelman, MD, MS, former hospitalist and current PSO at Montefiore Medical Center in New York City, says developing patient safety leaders should embrace technology. “Pay attention to the latest and greatest ideas, products, and services,” he urges. “Come up with strategic plans to implement in healthcare, get the information quickly into the hands of physicians, have physicians report, and include forcing functions [whereby computers will not process to completion when key data are missing].”
Above all, the patient safety officer must train to be a change agent. “Influencing patient safety means you have to be there in the capital-allocation process,” says David Shulkin, MD, chief executive officer at Beth Israel Medical Center in New York City. “You have to be there when they’re designing facilities. You have to understand your human resource policies and the skill sets and aptitudes of the people that the hospital is hiring. To be a good patient safety officer, the training needs to involve broad exposure with a slant toward operations.”
Build a Bridge
As a young physician who wanted to develop as a leader in the field of quality and safety, Dr. Shulkin had to forge his own path. In 1992, after he became chief medical officer (CMO) at the Hospital of the University of Pennsylvania in Philadelphia, he fielded several inquiries a month from young physicians who wanted to pursue a similar career. In response to that need, he designed a quality improvement/patient safety fellowship at his school.
David Bernard, MD, now chief medical officer at Beth Israel, had been practicing medicine for 30 years when at age 50 he took a year’s leave of absence from Boston University and enrolled as Dr. Shulkin’s first fellow in 1994. Dr. Bernard, a nephrologist, was a vice dean in the school of medicine at Boston University Medical Center, a hospital vice president for clinical affairs, and a senior clinician in his specialty group.
Drs. Shulkin and Bernard left the University of Pennsylvania in 1999 to take the concepts of quality transparency to a higher level and formed DoctorQuality Inc. in Conshohocken, Pa. To continue their work, DoctorQuality funded the fellowship. In 2005 when Dr. Shulkin went to Beth Israel in New York, the fellowship was restarted as the Don Hoskins Quality Improvement/Patient Safety program and funded for five years with private philanthropy.
Modeled after graduate medical education, the fellowship is predominantly hands-on. Fellows work on real projects alongside professionals in management, quality, and safety.
Under the Hood
Giving trainees the inside view into the intricacies of how to change physician behavior and cultural issues in hospitals is the backbone of Beth Israel’s program. Fellows see what clinicians rarely see: the real-world complexity of hospitals, why there is so much inertia, and the reasons changing systems can be so difficult. Fellows learn how almost every hospital issue involves financial, personnel, facility, policy and political considerations. By allowing entrée into the executive offices, the fellow gets to hear the many different perspectives when people react to an issue.
“After a quality-improvement meeting, for instance, where people are positioning and requesting different things rather than taking action,” says Dr. Shulkin, “the fellow gets to hear the behind-the-scenes analysis—how executives sometimes label people and develop strategies to overcome some of these barriers.”
Understanding how administrators, directors of social work, or nurses, for instance, view situations and understand their culture helps the leader be more effective.
“To get both leadership and clinician buy-in, and to get leadership to motivate clinicians to participate in system changes, you also need to be politically savvy,” says Dr. Adelman. “Plenty of people resist change. The PSO needs to come off as sincere, passionate, and smart, and has to be able to answer people’s tough questions.”
It can take an ambassador’s touch to make headway in the traditional physician culture.
“The patient safety officers, the chief medical officers, often have to function as diplomats,” says Dr. Angood. “This physician engagement piece is one of the most complicated issues out there, and it arises because physicians historically are trained to be autonomous, to be independent, and to expect that institutions are there to serve them.”
—Latha Sivaprasad, MD, Don Hoskins Quality Improvement/Patient Safety fellow, Beth Israel Medical Center, New York City
One Hospitalist’s View
When Latha Sivaprasad, MD, current Don Hoskins fellow at Beth Israel, started her fellowship six months ago, she was astonished how little she knew about patient safety and quality. Although she felt she knew the day-to-day deficiencies in the hospital and on the front line—and despite having practiced in three other hospitals—she wasn’t prepared to learn what she hadn’t known she didn’t know.
“In my five years as a hospitalist, I knew very little about patient safety and quality—to my shock now,” she says. “Since I’ve been a fellow here, I realize how much I had been underutilized and how much more I could have contributed to making my respective hospitals run more safely.”
Understanding people’s motivations and meeting their needs to make a hospital safer is an intricate process.
“I think it is important for hospitalists to understand how complicated and time-consuming system changes are,” she says. “You do not have that perspective as a clinician. You think that change can occur from a memo or from good intentions to do the right thing.”
She has learned to think about the bigger world outside the clinical portion of running a hospital.
“To be a change agent you really need to appreciate the hospital from the penthouse view, which is what this fellowship provides,” she says. “You need to have access to every meeting, every record, every clinician, and every senior executive to put the pieces of the puzzle together to understand how things change.”
The hospital is working to apply the Toyota method of employee involvement to the issue of how an obstetric patient progresses from triage in the emergency department (ED) to labor and delivery, and how much time passes before the triage the patient is discharged or admitted. Their focus first targeted convening the right group to discuss the issue and identify the details of the problem, then put a plan in place to track ED triage. They looked for ways to make that process more efficient, met again to determine how to implement a new version of that process, then tracked the difference. “All of this was a multihour ordeal,” she says.
It’s exhilarating, frustrating, and intriguing—and sometimes discouraging. “It’s very tedious making change, and I didn’t appreciate that before the fellowship,” she says.
Dr. Sivaprasad advises hospitalists that to be effective in patient safety efforts means being a problem solver, highly empathetic, sensitive to others, and above all, extremely patient. But results often emerge slowly.
“You must have several things brewing at once because if certain programs’ changes are taking time, you need to complete the loop on something else,” she advises.
The Ideal Candidate
Of the 20 fellows Dr. Shulkin has mentored, about half were older and more experienced than he was. Reflecting on the successful fellows and those who benefited less makes him think the distinction of experience and age is less important than the individual’s personality.
“What is important is the personality and motivation and self-directedness of the fellow,” says Dr. Shulkin. “This is a very autonomous fellowship. One of the pluses and minuses of working with senior executives is that they are very busy; they don’t have time the way traditional academic program directors or residency directors do to think, ‘Where are my fellows and what are they doing?’”
Those who will get the most out of this type of experience know how to be delicately assertive yet drive their own agendas.
To Drs. Shulkin and Bernard, a good patient safety leader is naturally curious about what makes healthcare organizations tick. The ideal candidate has an appreciation for hospital financing and the science behind physician behavior change, and the capacity to be a good listener. The trainee also needs to put aside his or her ego while transitioning from a physician in charge to stepping back into the student role to learn the new language and environment.
—David Shulkin, MD, chief executive officer, Beth Israel Medical Center, New York City
Where to Begin
The institution sponsoring the development of the patient safety officer is just as important as who that candidate is.
“The administration has to have a visionary leadership that recognizes that healthcare quality and safety is the way you do business,” says Dr. Bernard. “You have to be in an institution that is not just paying lip service to moving quality and safety. It has to be part of the fabric of the institution.”
The institution also has to be able to offer a variety of experiences, making this kind of training difficult in a nonacademic setting.
For those interested in pursuing this area of leadership, the natural first step is to meet with the CMO or CEO to explore whether the individual’s and hospital’s interests can be aligned.
“But you can’t force it,” warns Dr. Shulkin. “If that is not a natural fit, if the CMO or CEO doesn’t see their role as, or have an interest in, training faculty people; or if they don’t have the expertise to do it, it’s not going to be a good experience. In those cases, the hospitalist should look elsewhere. An increasing number of centers can offer this kind of experience for a year,” he says. “Then the hospitalist might return to their institution to take on a leadership role there.”
Creating a costly infrastructure to train a patient safety officer is not required. What is necessary is chemistry in the mentor-trainee relationship.
“This is the first time in my postgraduate career that I actually have consistently committed mentors who care about how I am molded as a physician and what my ultimate contribution to the medical field will be,” says Dr. Sivaprasad. TH
Andrea Sattinger is a medical writer based in North Carolina.
At Mercy Hospital in Iowa City, Iowa, the implementation of safety and quality systems is “stirring up the pot,” says Mercy hospitalist and medical director Martin Izakovic, MD.
He has been recruited to supervise Mercy’s latest safety initiatives, including electronic medical records, pay-for-performance measures, development of treatment protocols, standardization of care, and deep-vein thrombosis prophylaxis.
Hospitalists at Mercy face the challenges their peers around the country face in their quest to improve quality and safeguard patients. The leader in these areas needs to be a role model and respected peer for the physicians he or she must lead day after day, says Dr. Izakovic.
How do hospitalists, who are so well-positioned to become leaders in patient safety, develop in that direction?
“The biggest challenge I see is the spectrum of polarization between clinicians and administrators,” he says. “One of the most important qualities that a patient safety officer needs is the ability to overbridge the doctors on one hand and the administrators on the other.”
What They Need
A patient safety officer (PSO) requires a critical mix of clinical and administrative skills, says Peter B. Angood, MD, vice president and chief patient safety officer for The Joint Commission, in Oakbrook, Ill.
On the clinical side, the hospitalist who wishes to be a PSO needs more than awareness of safety and quality improvement processes. He or she must be knowledgeable about and conversant in safety science in industries beyond healthcare. That expertise needs to encompass leadership, behaviors and cultures, human factors, and process redesign or systems engineering. Important, too, is training in how to corral the pieces of an organization and ensure they operate well together.
An understanding of organizational behavior is of great value. The potential PSO should understand how the key players interact: the board of directors with chief executives, chief executives with senior management, senior management with all staff (including the allied professionals), and medical staff with the organization as a whole.
“Because safety is a systemwide process, the patient safety [person] is pivotal in forming a hub from which much of the quality, safety, and process improvement occurs,” says Dr. Angood.
Jason Adelman, MD, MS, former hospitalist and current PSO at Montefiore Medical Center in New York City, says developing patient safety leaders should embrace technology. “Pay attention to the latest and greatest ideas, products, and services,” he urges. “Come up with strategic plans to implement in healthcare, get the information quickly into the hands of physicians, have physicians report, and include forcing functions [whereby computers will not process to completion when key data are missing].”
Above all, the patient safety officer must train to be a change agent. “Influencing patient safety means you have to be there in the capital-allocation process,” says David Shulkin, MD, chief executive officer at Beth Israel Medical Center in New York City. “You have to be there when they’re designing facilities. You have to understand your human resource policies and the skill sets and aptitudes of the people that the hospital is hiring. To be a good patient safety officer, the training needs to involve broad exposure with a slant toward operations.”
Build a Bridge
As a young physician who wanted to develop as a leader in the field of quality and safety, Dr. Shulkin had to forge his own path. In 1992, after he became chief medical officer (CMO) at the Hospital of the University of Pennsylvania in Philadelphia, he fielded several inquiries a month from young physicians who wanted to pursue a similar career. In response to that need, he designed a quality improvement/patient safety fellowship at his school.
David Bernard, MD, now chief medical officer at Beth Israel, had been practicing medicine for 30 years when at age 50 he took a year’s leave of absence from Boston University and enrolled as Dr. Shulkin’s first fellow in 1994. Dr. Bernard, a nephrologist, was a vice dean in the school of medicine at Boston University Medical Center, a hospital vice president for clinical affairs, and a senior clinician in his specialty group.
Drs. Shulkin and Bernard left the University of Pennsylvania in 1999 to take the concepts of quality transparency to a higher level and formed DoctorQuality Inc. in Conshohocken, Pa. To continue their work, DoctorQuality funded the fellowship. In 2005 when Dr. Shulkin went to Beth Israel in New York, the fellowship was restarted as the Don Hoskins Quality Improvement/Patient Safety program and funded for five years with private philanthropy.
Modeled after graduate medical education, the fellowship is predominantly hands-on. Fellows work on real projects alongside professionals in management, quality, and safety.
Under the Hood
Giving trainees the inside view into the intricacies of how to change physician behavior and cultural issues in hospitals is the backbone of Beth Israel’s program. Fellows see what clinicians rarely see: the real-world complexity of hospitals, why there is so much inertia, and the reasons changing systems can be so difficult. Fellows learn how almost every hospital issue involves financial, personnel, facility, policy and political considerations. By allowing entrée into the executive offices, the fellow gets to hear the many different perspectives when people react to an issue.
“After a quality-improvement meeting, for instance, where people are positioning and requesting different things rather than taking action,” says Dr. Shulkin, “the fellow gets to hear the behind-the-scenes analysis—how executives sometimes label people and develop strategies to overcome some of these barriers.”
Understanding how administrators, directors of social work, or nurses, for instance, view situations and understand their culture helps the leader be more effective.
“To get both leadership and clinician buy-in, and to get leadership to motivate clinicians to participate in system changes, you also need to be politically savvy,” says Dr. Adelman. “Plenty of people resist change. The PSO needs to come off as sincere, passionate, and smart, and has to be able to answer people’s tough questions.”
It can take an ambassador’s touch to make headway in the traditional physician culture.
“The patient safety officers, the chief medical officers, often have to function as diplomats,” says Dr. Angood. “This physician engagement piece is one of the most complicated issues out there, and it arises because physicians historically are trained to be autonomous, to be independent, and to expect that institutions are there to serve them.”
—Latha Sivaprasad, MD, Don Hoskins Quality Improvement/Patient Safety fellow, Beth Israel Medical Center, New York City
One Hospitalist’s View
When Latha Sivaprasad, MD, current Don Hoskins fellow at Beth Israel, started her fellowship six months ago, she was astonished how little she knew about patient safety and quality. Although she felt she knew the day-to-day deficiencies in the hospital and on the front line—and despite having practiced in three other hospitals—she wasn’t prepared to learn what she hadn’t known she didn’t know.
“In my five years as a hospitalist, I knew very little about patient safety and quality—to my shock now,” she says. “Since I’ve been a fellow here, I realize how much I had been underutilized and how much more I could have contributed to making my respective hospitals run more safely.”
Understanding people’s motivations and meeting their needs to make a hospital safer is an intricate process.
“I think it is important for hospitalists to understand how complicated and time-consuming system changes are,” she says. “You do not have that perspective as a clinician. You think that change can occur from a memo or from good intentions to do the right thing.”
She has learned to think about the bigger world outside the clinical portion of running a hospital.
“To be a change agent you really need to appreciate the hospital from the penthouse view, which is what this fellowship provides,” she says. “You need to have access to every meeting, every record, every clinician, and every senior executive to put the pieces of the puzzle together to understand how things change.”
The hospital is working to apply the Toyota method of employee involvement to the issue of how an obstetric patient progresses from triage in the emergency department (ED) to labor and delivery, and how much time passes before the triage the patient is discharged or admitted. Their focus first targeted convening the right group to discuss the issue and identify the details of the problem, then put a plan in place to track ED triage. They looked for ways to make that process more efficient, met again to determine how to implement a new version of that process, then tracked the difference. “All of this was a multihour ordeal,” she says.
It’s exhilarating, frustrating, and intriguing—and sometimes discouraging. “It’s very tedious making change, and I didn’t appreciate that before the fellowship,” she says.
Dr. Sivaprasad advises hospitalists that to be effective in patient safety efforts means being a problem solver, highly empathetic, sensitive to others, and above all, extremely patient. But results often emerge slowly.
“You must have several things brewing at once because if certain programs’ changes are taking time, you need to complete the loop on something else,” she advises.
The Ideal Candidate
Of the 20 fellows Dr. Shulkin has mentored, about half were older and more experienced than he was. Reflecting on the successful fellows and those who benefited less makes him think the distinction of experience and age is less important than the individual’s personality.
“What is important is the personality and motivation and self-directedness of the fellow,” says Dr. Shulkin. “This is a very autonomous fellowship. One of the pluses and minuses of working with senior executives is that they are very busy; they don’t have time the way traditional academic program directors or residency directors do to think, ‘Where are my fellows and what are they doing?’”
Those who will get the most out of this type of experience know how to be delicately assertive yet drive their own agendas.
To Drs. Shulkin and Bernard, a good patient safety leader is naturally curious about what makes healthcare organizations tick. The ideal candidate has an appreciation for hospital financing and the science behind physician behavior change, and the capacity to be a good listener. The trainee also needs to put aside his or her ego while transitioning from a physician in charge to stepping back into the student role to learn the new language and environment.
—David Shulkin, MD, chief executive officer, Beth Israel Medical Center, New York City
Where to Begin
The institution sponsoring the development of the patient safety officer is just as important as who that candidate is.
“The administration has to have a visionary leadership that recognizes that healthcare quality and safety is the way you do business,” says Dr. Bernard. “You have to be in an institution that is not just paying lip service to moving quality and safety. It has to be part of the fabric of the institution.”
The institution also has to be able to offer a variety of experiences, making this kind of training difficult in a nonacademic setting.
For those interested in pursuing this area of leadership, the natural first step is to meet with the CMO or CEO to explore whether the individual’s and hospital’s interests can be aligned.
“But you can’t force it,” warns Dr. Shulkin. “If that is not a natural fit, if the CMO or CEO doesn’t see their role as, or have an interest in, training faculty people; or if they don’t have the expertise to do it, it’s not going to be a good experience. In those cases, the hospitalist should look elsewhere. An increasing number of centers can offer this kind of experience for a year,” he says. “Then the hospitalist might return to their institution to take on a leadership role there.”
Creating a costly infrastructure to train a patient safety officer is not required. What is necessary is chemistry in the mentor-trainee relationship.
“This is the first time in my postgraduate career that I actually have consistently committed mentors who care about how I am molded as a physician and what my ultimate contribution to the medical field will be,” says Dr. Sivaprasad. TH
Andrea Sattinger is a medical writer based in North Carolina.