User login
MDedge Daily News: Why most heart failure may be preventable
Why most heart failure may be preventable. Statins miss the mark in familial high cholesterol. Why mumps outbreaks are on the rise. And how using epileptic drugs in pregnancy affects school test scores.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
Why most heart failure may be preventable. Statins miss the mark in familial high cholesterol. Why mumps outbreaks are on the rise. And how using epileptic drugs in pregnancy affects school test scores.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
Why most heart failure may be preventable. Statins miss the mark in familial high cholesterol. Why mumps outbreaks are on the rise. And how using epileptic drugs in pregnancy affects school test scores.
Listen to the MDedge Daily News podcast for all the details on today’s top news.

Phase 1 results with UCART19 in kids

LISBON—Early results from a phase 1, pediatric trial of UCART19 expand upon results observed in children who received the therapy via a compassionate use program.
Two patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL) received UCART19, a “universal,” donor-derived chimeric antigen receptor (CAR) T-cell therapy, via the program.
Both achieved remission and were still alive at last follow-up, more than 2 years after proceeding to transplant.
In the phase 1 trial, 5 of 6 B-ALL patients have achieved remission and gone on to transplant.
Three of the patients are still alive, and 2 are still negative for minimal residual disease (MRD) at 10 months and 11 months after UCART19 infusion.
However, 2 patients died of progression, and 1 died of transplant-related complications.
Paul Veys, MBBS, of Great Ormond Street Hospital (GOSH) in London, UK, presented these results, from the PALL trial, at the 44th Annual Meeting of the EBMT (abstract OS18-5*).
The trial is sponsored by Servier. In 2015, Servier acquired exclusive rights from Cellectis for UCART19, which is being co-developed by Servier and Pfizer.
Prior experience
Researchers previously reported results with UCART19 in 2 infants with relapsed/refractory B-ALL who had exhausted all other treatment options and received UCART19 via a compassionate use program.
Both patients achieved remission after UCART19 and proceeded to allogeneic hematopoietic stem cell transplant (allo-HSCT).
When these results were published, in January 2017, both patients were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19 infusion.
Dr Veys provided an update, noting that these patients were still alive and in remission at 24 months and 30 months after allo-HSCT.
Phase 1 patients and treatment
Thus far, the phase 1 trial has enrolled and treated 6 patients with relapsed B-ALL. They had a median age of 3.75 (range, 0.8-16.4).
All patients had morphological disease or an MRD level of at least 1 x 10-3 (via flow cytometry and/or qPCR) at baseline.
One patient had received 1 prior therapy, 2 had 3 prior therapies, and 3 had 4 or more prior therapies. Two patients had prior inotuzumab ozogamicin, and 2 had prior allo-HSCT. Both had relapsed within 6 months of allo-HSCT.
Five patients had less than 10% bone marrow blasts prior to lymphodepletion, and 1 had greater than 50% blasts.
Patients underwent lymphodepletion with fludarabine, cyclophosphamide, and alemtuzumab (n=5) or fludarabine and cyclophosphamide (n=1).
The patients received UCART19 at doses of 2 x 107 total cells or 1.1 to 2.3 x 106 cells/kg.
Toxicity
All 6 patients developed cytokine release syndrome (CRS), including grade 1 (n=1), grade 2 (n=4), and grade 3 (n-1) CRS. However, all 6 cases resolved completely.
Three patients had neurotoxic events, 2 grade 1 and 1 grade 2. One patient had grade 3 febrile neutropenia.
Three patients had grade 4 prolonged cytopenia. This was defined as persistent neutropenia and/or thrombocytopenia beyond day 42 after UCART19 infusion, except if the patient had >5% bone marrow blasts.
One patient had grade 1 adenovirus infection, 1 had grade 3 cytomegalovirus infection, 2 had grade 3 BK virus hemorrhagic cystitis, and 1 had grade 4 metapneumovirus infection.
One patient had grade 1 acute cutaneous graft-versus-host disease.
Efficacy
All 6 patients achieved a complete response at day 28 to 42 after UCART19 infusion. Five patients achieved MRD negativity according to flow cytometry, and 3 were MRD-negative according to PCR.
The 5 flow-MRD-negative patients went on to receive an allo-HSCT between 49 days and 62 days after UCART19 infusion. Conditioning consisted of total body irradiation and fludarabine, with or without cyclophosphamide and antithymocyte globulin. All of these patients received a dose of rituximab as well, which was intended to target any remaining UCART19 cells.
Two patients relapsed 3 months after transplant and died at 7 months and 8 months after UCART19 infusion. One of these patients was CD19-, and 1 was CD19+, but both were MRD-positive by PCR prior to receiving their transplant.
A third patient died 2.5 months after allo-HSCT from transplant-related complications, including thrombotic microangiopathy, BK hemorrhagic cystitis, and nephritis.
The remaining 3 patients are still alive at 1.5 months, 10 months, and 11 months after UCART19 infusion. Two are still MRD-negative, and 1 is MRD-positive. The MRD-positive patient has not undergone allo-HSCT.
*Data in the abstract were updated in the presentation.
LISBON—Early results from a phase 1, pediatric trial of UCART19 expand upon results observed in children who received the therapy via a compassionate use program.
Two patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL) received UCART19, a “universal,” donor-derived chimeric antigen receptor (CAR) T-cell therapy, via the program.
Both achieved remission and were still alive at last follow-up, more than 2 years after proceeding to transplant.
In the phase 1 trial, 5 of 6 B-ALL patients have achieved remission and gone on to transplant.
Three of the patients are still alive, and 2 are still negative for minimal residual disease (MRD) at 10 months and 11 months after UCART19 infusion.
However, 2 patients died of progression, and 1 died of transplant-related complications.
Paul Veys, MBBS, of Great Ormond Street Hospital (GOSH) in London, UK, presented these results, from the PALL trial, at the 44th Annual Meeting of the EBMT (abstract OS18-5*).
The trial is sponsored by Servier. In 2015, Servier acquired exclusive rights from Cellectis for UCART19, which is being co-developed by Servier and Pfizer.
Prior experience
Researchers previously reported results with UCART19 in 2 infants with relapsed/refractory B-ALL who had exhausted all other treatment options and received UCART19 via a compassionate use program.
Both patients achieved remission after UCART19 and proceeded to allogeneic hematopoietic stem cell transplant (allo-HSCT).
When these results were published, in January 2017, both patients were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19 infusion.
Dr Veys provided an update, noting that these patients were still alive and in remission at 24 months and 30 months after allo-HSCT.
Phase 1 patients and treatment
Thus far, the phase 1 trial has enrolled and treated 6 patients with relapsed B-ALL. They had a median age of 3.75 (range, 0.8-16.4).
All patients had morphological disease or an MRD level of at least 1 x 10-3 (via flow cytometry and/or qPCR) at baseline.
One patient had received 1 prior therapy, 2 had 3 prior therapies, and 3 had 4 or more prior therapies. Two patients had prior inotuzumab ozogamicin, and 2 had prior allo-HSCT. Both had relapsed within 6 months of allo-HSCT.
Five patients had less than 10% bone marrow blasts prior to lymphodepletion, and 1 had greater than 50% blasts.
Patients underwent lymphodepletion with fludarabine, cyclophosphamide, and alemtuzumab (n=5) or fludarabine and cyclophosphamide (n=1).
The patients received UCART19 at doses of 2 x 107 total cells or 1.1 to 2.3 x 106 cells/kg.
Toxicity
All 6 patients developed cytokine release syndrome (CRS), including grade 1 (n=1), grade 2 (n=4), and grade 3 (n-1) CRS. However, all 6 cases resolved completely.
Three patients had neurotoxic events, 2 grade 1 and 1 grade 2. One patient had grade 3 febrile neutropenia.
Three patients had grade 4 prolonged cytopenia. This was defined as persistent neutropenia and/or thrombocytopenia beyond day 42 after UCART19 infusion, except if the patient had >5% bone marrow blasts.
One patient had grade 1 adenovirus infection, 1 had grade 3 cytomegalovirus infection, 2 had grade 3 BK virus hemorrhagic cystitis, and 1 had grade 4 metapneumovirus infection.
One patient had grade 1 acute cutaneous graft-versus-host disease.
Efficacy
All 6 patients achieved a complete response at day 28 to 42 after UCART19 infusion. Five patients achieved MRD negativity according to flow cytometry, and 3 were MRD-negative according to PCR.
The 5 flow-MRD-negative patients went on to receive an allo-HSCT between 49 days and 62 days after UCART19 infusion. Conditioning consisted of total body irradiation and fludarabine, with or without cyclophosphamide and antithymocyte globulin. All of these patients received a dose of rituximab as well, which was intended to target any remaining UCART19 cells.
Two patients relapsed 3 months after transplant and died at 7 months and 8 months after UCART19 infusion. One of these patients was CD19-, and 1 was CD19+, but both were MRD-positive by PCR prior to receiving their transplant.
A third patient died 2.5 months after allo-HSCT from transplant-related complications, including thrombotic microangiopathy, BK hemorrhagic cystitis, and nephritis.
The remaining 3 patients are still alive at 1.5 months, 10 months, and 11 months after UCART19 infusion. Two are still MRD-negative, and 1 is MRD-positive. The MRD-positive patient has not undergone allo-HSCT.
*Data in the abstract were updated in the presentation.
LISBON—Early results from a phase 1, pediatric trial of UCART19 expand upon results observed in children who received the therapy via a compassionate use program.
Two patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL) received UCART19, a “universal,” donor-derived chimeric antigen receptor (CAR) T-cell therapy, via the program.
Both achieved remission and were still alive at last follow-up, more than 2 years after proceeding to transplant.
In the phase 1 trial, 5 of 6 B-ALL patients have achieved remission and gone on to transplant.
Three of the patients are still alive, and 2 are still negative for minimal residual disease (MRD) at 10 months and 11 months after UCART19 infusion.
However, 2 patients died of progression, and 1 died of transplant-related complications.
Paul Veys, MBBS, of Great Ormond Street Hospital (GOSH) in London, UK, presented these results, from the PALL trial, at the 44th Annual Meeting of the EBMT (abstract OS18-5*).
The trial is sponsored by Servier. In 2015, Servier acquired exclusive rights from Cellectis for UCART19, which is being co-developed by Servier and Pfizer.
Prior experience
Researchers previously reported results with UCART19 in 2 infants with relapsed/refractory B-ALL who had exhausted all other treatment options and received UCART19 via a compassionate use program.
Both patients achieved remission after UCART19 and proceeded to allogeneic hematopoietic stem cell transplant (allo-HSCT).
When these results were published, in January 2017, both patients were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19 infusion.
Dr Veys provided an update, noting that these patients were still alive and in remission at 24 months and 30 months after allo-HSCT.
Phase 1 patients and treatment
Thus far, the phase 1 trial has enrolled and treated 6 patients with relapsed B-ALL. They had a median age of 3.75 (range, 0.8-16.4).
All patients had morphological disease or an MRD level of at least 1 x 10-3 (via flow cytometry and/or qPCR) at baseline.
One patient had received 1 prior therapy, 2 had 3 prior therapies, and 3 had 4 or more prior therapies. Two patients had prior inotuzumab ozogamicin, and 2 had prior allo-HSCT. Both had relapsed within 6 months of allo-HSCT.
Five patients had less than 10% bone marrow blasts prior to lymphodepletion, and 1 had greater than 50% blasts.
Patients underwent lymphodepletion with fludarabine, cyclophosphamide, and alemtuzumab (n=5) or fludarabine and cyclophosphamide (n=1).
The patients received UCART19 at doses of 2 x 107 total cells or 1.1 to 2.3 x 106 cells/kg.
Toxicity
All 6 patients developed cytokine release syndrome (CRS), including grade 1 (n=1), grade 2 (n=4), and grade 3 (n-1) CRS. However, all 6 cases resolved completely.
Three patients had neurotoxic events, 2 grade 1 and 1 grade 2. One patient had grade 3 febrile neutropenia.
Three patients had grade 4 prolonged cytopenia. This was defined as persistent neutropenia and/or thrombocytopenia beyond day 42 after UCART19 infusion, except if the patient had >5% bone marrow blasts.
One patient had grade 1 adenovirus infection, 1 had grade 3 cytomegalovirus infection, 2 had grade 3 BK virus hemorrhagic cystitis, and 1 had grade 4 metapneumovirus infection.
One patient had grade 1 acute cutaneous graft-versus-host disease.
Efficacy
All 6 patients achieved a complete response at day 28 to 42 after UCART19 infusion. Five patients achieved MRD negativity according to flow cytometry, and 3 were MRD-negative according to PCR.
The 5 flow-MRD-negative patients went on to receive an allo-HSCT between 49 days and 62 days after UCART19 infusion. Conditioning consisted of total body irradiation and fludarabine, with or without cyclophosphamide and antithymocyte globulin. All of these patients received a dose of rituximab as well, which was intended to target any remaining UCART19 cells.
Two patients relapsed 3 months after transplant and died at 7 months and 8 months after UCART19 infusion. One of these patients was CD19-, and 1 was CD19+, but both were MRD-positive by PCR prior to receiving their transplant.
A third patient died 2.5 months after allo-HSCT from transplant-related complications, including thrombotic microangiopathy, BK hemorrhagic cystitis, and nephritis.
The remaining 3 patients are still alive at 1.5 months, 10 months, and 11 months after UCART19 infusion. Two are still MRD-negative, and 1 is MRD-positive. The MRD-positive patient has not undergone allo-HSCT.
*Data in the abstract were updated in the presentation.
CHMP rejects plitidepsin again

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of marketing authorization for plitidepsin (Aplidin).
PharmaMar is seeking approval for plitidepsin to treat adults with multiple myeloma (MM) who have received at least 3 prior treatments, including bortezomib and either lenalidomide or thalidomide.
Plitidepsin is intended to be used in combination with dexamethasone.
This is the second time the CHMP has recommended against authorizing plitidepsin for this indication. The first time was last December.
At that time, PharmaMar asked the CHMP to re-examine its opinion, and the CHMP obliged. The committee confirmed its negative opinion of plitidepsin last week.
The CHMP’s review
Upon its initial review, the CHMP was concerned that data from the main study of plitidepsin in MM—the phase 3 ADMYRE trial—did not demonstrate a sufficient benefit of plitidepsin plus dexamethasone, compared to dexamethasone alone, in MM patients who had received 3 to 6 prior therapies.
The CHMP noted that the data showed a modest increase in progression free-survival (PFS)—around 1 month—with plitidepsin. According to study investigators, the median PFS was 3.8 months in patients who received plitidepsin and 1.9 months in those who received dexamethasone alone. According to an independent review committee, the median PFS was 2.6 months and 1.7 months, respectively.
The CHMP also said improvement in overall survival (OS) was not sufficiently demonstrated in this trial. The median OS was 11.6 months in the plitidepsin arm and 6.4 months in the dexamethasone arm.
Finally, the CHMP noted that severe adverse events were reported more frequently in patients who received plitidepsin. The most common grade 3/4 treatment-related adverse events (in the plitidepsin and dexamethasone arms, respectively) were fatigue (10.8% vs 1.2%), myalgia (5.4% vs 0%), and nausea (3.6% vs 1.2%).
Rates of treatment discontinuation were 9% in the plitidepsin arm, 6.5% in the dexamethasone arm, and 13.5% among patients who crossed over from the dexamethasone arm to the plitidepsin arm. Patients were allowed to cross over if they progressed after at least 8 weeks of treatment.
Based on these data, the CHMP was of the opinion that the benefits of plitidepsin did not outweigh its risks, so the committee recommended refusal of marketing authorization. After re-examination, the CHMP remained of the same opinion.
The European Commission (EC) has the final say on the marketing authorization application for plitidepsin. Though it is not required to do so, the EC typically follows the CHMP’s advice. The EC makes its decision within 67 days of the CHMP’s opinion.
PharmaMar has not announced whether it plans to continue developing plitidepsin for MM patients if the EC refuses to authorize the drug, and the company did not respond to a request for comment.
About plitidepsin
Plitidepsin is an investigational anticancer agent of marine origin, originally obtained from the ascidian Aplidium albicans. The drug specifically binds to eEF1A2 and targets the non-canonical role of this protein, resulting in cancer cell death via apoptosis.
Plitidepsin is currently in clinical development for hematologic malignancies.
In a phase 1b trial (NCT02100657), researchers are evaluating plitidepsin in combination with bortezomib and dexamethasone for patients with relapsed/refractory MM.
In a phase 2 trial (NCT03117361), researchers are investigating plitidepsin in combination with bortezomib and dexamethasone for patients with MM that is refractory to both lenalidomide and bortezomib.
Plitidepsin has received orphan drug designation in the European Union and the US.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of marketing authorization for plitidepsin (Aplidin).
PharmaMar is seeking approval for plitidepsin to treat adults with multiple myeloma (MM) who have received at least 3 prior treatments, including bortezomib and either lenalidomide or thalidomide.
Plitidepsin is intended to be used in combination with dexamethasone.
This is the second time the CHMP has recommended against authorizing plitidepsin for this indication. The first time was last December.
At that time, PharmaMar asked the CHMP to re-examine its opinion, and the CHMP obliged. The committee confirmed its negative opinion of plitidepsin last week.
The CHMP’s review
Upon its initial review, the CHMP was concerned that data from the main study of plitidepsin in MM—the phase 3 ADMYRE trial—did not demonstrate a sufficient benefit of plitidepsin plus dexamethasone, compared to dexamethasone alone, in MM patients who had received 3 to 6 prior therapies.
The CHMP noted that the data showed a modest increase in progression free-survival (PFS)—around 1 month—with plitidepsin. According to study investigators, the median PFS was 3.8 months in patients who received plitidepsin and 1.9 months in those who received dexamethasone alone. According to an independent review committee, the median PFS was 2.6 months and 1.7 months, respectively.
The CHMP also said improvement in overall survival (OS) was not sufficiently demonstrated in this trial. The median OS was 11.6 months in the plitidepsin arm and 6.4 months in the dexamethasone arm.
Finally, the CHMP noted that severe adverse events were reported more frequently in patients who received plitidepsin. The most common grade 3/4 treatment-related adverse events (in the plitidepsin and dexamethasone arms, respectively) were fatigue (10.8% vs 1.2%), myalgia (5.4% vs 0%), and nausea (3.6% vs 1.2%).
Rates of treatment discontinuation were 9% in the plitidepsin arm, 6.5% in the dexamethasone arm, and 13.5% among patients who crossed over from the dexamethasone arm to the plitidepsin arm. Patients were allowed to cross over if they progressed after at least 8 weeks of treatment.
Based on these data, the CHMP was of the opinion that the benefits of plitidepsin did not outweigh its risks, so the committee recommended refusal of marketing authorization. After re-examination, the CHMP remained of the same opinion.
The European Commission (EC) has the final say on the marketing authorization application for plitidepsin. Though it is not required to do so, the EC typically follows the CHMP’s advice. The EC makes its decision within 67 days of the CHMP’s opinion.
PharmaMar has not announced whether it plans to continue developing plitidepsin for MM patients if the EC refuses to authorize the drug, and the company did not respond to a request for comment.
About plitidepsin
Plitidepsin is an investigational anticancer agent of marine origin, originally obtained from the ascidian Aplidium albicans. The drug specifically binds to eEF1A2 and targets the non-canonical role of this protein, resulting in cancer cell death via apoptosis.
Plitidepsin is currently in clinical development for hematologic malignancies.
In a phase 1b trial (NCT02100657), researchers are evaluating plitidepsin in combination with bortezomib and dexamethasone for patients with relapsed/refractory MM.
In a phase 2 trial (NCT03117361), researchers are investigating plitidepsin in combination with bortezomib and dexamethasone for patients with MM that is refractory to both lenalidomide and bortezomib.
Plitidepsin has received orphan drug designation in the European Union and the US.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of marketing authorization for plitidepsin (Aplidin).
PharmaMar is seeking approval for plitidepsin to treat adults with multiple myeloma (MM) who have received at least 3 prior treatments, including bortezomib and either lenalidomide or thalidomide.
Plitidepsin is intended to be used in combination with dexamethasone.
This is the second time the CHMP has recommended against authorizing plitidepsin for this indication. The first time was last December.
At that time, PharmaMar asked the CHMP to re-examine its opinion, and the CHMP obliged. The committee confirmed its negative opinion of plitidepsin last week.
The CHMP’s review
Upon its initial review, the CHMP was concerned that data from the main study of plitidepsin in MM—the phase 3 ADMYRE trial—did not demonstrate a sufficient benefit of plitidepsin plus dexamethasone, compared to dexamethasone alone, in MM patients who had received 3 to 6 prior therapies.
The CHMP noted that the data showed a modest increase in progression free-survival (PFS)—around 1 month—with plitidepsin. According to study investigators, the median PFS was 3.8 months in patients who received plitidepsin and 1.9 months in those who received dexamethasone alone. According to an independent review committee, the median PFS was 2.6 months and 1.7 months, respectively.
The CHMP also said improvement in overall survival (OS) was not sufficiently demonstrated in this trial. The median OS was 11.6 months in the plitidepsin arm and 6.4 months in the dexamethasone arm.
Finally, the CHMP noted that severe adverse events were reported more frequently in patients who received plitidepsin. The most common grade 3/4 treatment-related adverse events (in the plitidepsin and dexamethasone arms, respectively) were fatigue (10.8% vs 1.2%), myalgia (5.4% vs 0%), and nausea (3.6% vs 1.2%).
Rates of treatment discontinuation were 9% in the plitidepsin arm, 6.5% in the dexamethasone arm, and 13.5% among patients who crossed over from the dexamethasone arm to the plitidepsin arm. Patients were allowed to cross over if they progressed after at least 8 weeks of treatment.
Based on these data, the CHMP was of the opinion that the benefits of plitidepsin did not outweigh its risks, so the committee recommended refusal of marketing authorization. After re-examination, the CHMP remained of the same opinion.
The European Commission (EC) has the final say on the marketing authorization application for plitidepsin. Though it is not required to do so, the EC typically follows the CHMP’s advice. The EC makes its decision within 67 days of the CHMP’s opinion.
PharmaMar has not announced whether it plans to continue developing plitidepsin for MM patients if the EC refuses to authorize the drug, and the company did not respond to a request for comment.
About plitidepsin
Plitidepsin is an investigational anticancer agent of marine origin, originally obtained from the ascidian Aplidium albicans. The drug specifically binds to eEF1A2 and targets the non-canonical role of this protein, resulting in cancer cell death via apoptosis.
Plitidepsin is currently in clinical development for hematologic malignancies.
In a phase 1b trial (NCT02100657), researchers are evaluating plitidepsin in combination with bortezomib and dexamethasone for patients with relapsed/refractory MM.
In a phase 2 trial (NCT03117361), researchers are investigating plitidepsin in combination with bortezomib and dexamethasone for patients with MM that is refractory to both lenalidomide and bortezomib.
Plitidepsin has received orphan drug designation in the European Union and the US.
CHMP recommends approval for generic prasugrel

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended granting marketing authorization to a generic version of prasugrel called Prasugrel Mylan.
Mylan S.A.S. is seeking approval for this product to be co-administered with acetylsalicylic acid for the prevention of atherothrombotic events in adults with acute coronary syndrome (ie, unstable angina, non-ST segment elevation myocardial infarction, or ST segment elevation myocardial infarction) undergoing primary or delayed percutaneous coronary intervention.
The CHMP’s opinion on Prasugrel Mylan will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
If approved, Prasugrel Mylan will be available as 5 mg and 10 mg film-coated tablets.
Prasugrel is an inhibitor of platelet activation and aggregation that acts through the irreversible binding of its active metabolite to the P2Y12 class of ADP receptors on platelets.
Since platelets participate in the initiation and/or evolution of thrombotic complications of atherosclerotic disease, inhibition of platelet function can reduce the risk of cardiovascular events such as death, myocardial infarction, or stroke.
Prasugrel Mylan is a generic of Efient, which has been authorized in the European Union since 2009.
According to the CHMP, studies have demonstrated that Prasugrel Mylan is of “satisfactory quality” and bioequivalent to Efient.
In the TRITON–TIMI 38 study, treatment with prasugrel (Efient) was associated with significantly reduced rates of ischemic events, including stent thrombosis, when compared to treatment with clopidogrel in patients with moderate- to high-risk acute coronary syndromes with scheduled percutaneous coronary intervention.
However, prasugrel was also associated with an increased risk of major bleeding, including fatal bleeding. Still, there was no significant difference in mortality between the treatment groups.
These results were published in NEJM in 2007.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended granting marketing authorization to a generic version of prasugrel called Prasugrel Mylan.
Mylan S.A.S. is seeking approval for this product to be co-administered with acetylsalicylic acid for the prevention of atherothrombotic events in adults with acute coronary syndrome (ie, unstable angina, non-ST segment elevation myocardial infarction, or ST segment elevation myocardial infarction) undergoing primary or delayed percutaneous coronary intervention.
The CHMP’s opinion on Prasugrel Mylan will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
If approved, Prasugrel Mylan will be available as 5 mg and 10 mg film-coated tablets.
Prasugrel is an inhibitor of platelet activation and aggregation that acts through the irreversible binding of its active metabolite to the P2Y12 class of ADP receptors on platelets.
Since platelets participate in the initiation and/or evolution of thrombotic complications of atherosclerotic disease, inhibition of platelet function can reduce the risk of cardiovascular events such as death, myocardial infarction, or stroke.
Prasugrel Mylan is a generic of Efient, which has been authorized in the European Union since 2009.
According to the CHMP, studies have demonstrated that Prasugrel Mylan is of “satisfactory quality” and bioequivalent to Efient.
In the TRITON–TIMI 38 study, treatment with prasugrel (Efient) was associated with significantly reduced rates of ischemic events, including stent thrombosis, when compared to treatment with clopidogrel in patients with moderate- to high-risk acute coronary syndromes with scheduled percutaneous coronary intervention.
However, prasugrel was also associated with an increased risk of major bleeding, including fatal bleeding. Still, there was no significant difference in mortality between the treatment groups.
These results were published in NEJM in 2007.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended granting marketing authorization to a generic version of prasugrel called Prasugrel Mylan.
Mylan S.A.S. is seeking approval for this product to be co-administered with acetylsalicylic acid for the prevention of atherothrombotic events in adults with acute coronary syndrome (ie, unstable angina, non-ST segment elevation myocardial infarction, or ST segment elevation myocardial infarction) undergoing primary or delayed percutaneous coronary intervention.
The CHMP’s opinion on Prasugrel Mylan will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
If approved, Prasugrel Mylan will be available as 5 mg and 10 mg film-coated tablets.
Prasugrel is an inhibitor of platelet activation and aggregation that acts through the irreversible binding of its active metabolite to the P2Y12 class of ADP receptors on platelets.
Since platelets participate in the initiation and/or evolution of thrombotic complications of atherosclerotic disease, inhibition of platelet function can reduce the risk of cardiovascular events such as death, myocardial infarction, or stroke.
Prasugrel Mylan is a generic of Efient, which has been authorized in the European Union since 2009.
According to the CHMP, studies have demonstrated that Prasugrel Mylan is of “satisfactory quality” and bioequivalent to Efient.
In the TRITON–TIMI 38 study, treatment with prasugrel (Efient) was associated with significantly reduced rates of ischemic events, including stent thrombosis, when compared to treatment with clopidogrel in patients with moderate- to high-risk acute coronary syndromes with scheduled percutaneous coronary intervention.
However, prasugrel was also associated with an increased risk of major bleeding, including fatal bleeding. Still, there was no significant difference in mortality between the treatment groups.
These results were published in NEJM in 2007.
Survival worse with alcohol-related HCC, compared with other types
Hepatocellular carcinoma (HCC) related to alcohol use tends to be diagnosed at a later stage than HCC from other causes, which contributes to reduced overall survival among patients with alcoholic HCC, investigators in a prospective French study said.
Among 894 patients diagnosed with HCC, the adjusted median overall survival was 5.7 months for those with alcoholic HCC, compared with 9.7 months for those with nonalcoholic HCC (P = .0002), reported Charlotte E. Costentin, MD, of the Hopital Henri Mondor in Creteil, France, and colleagues.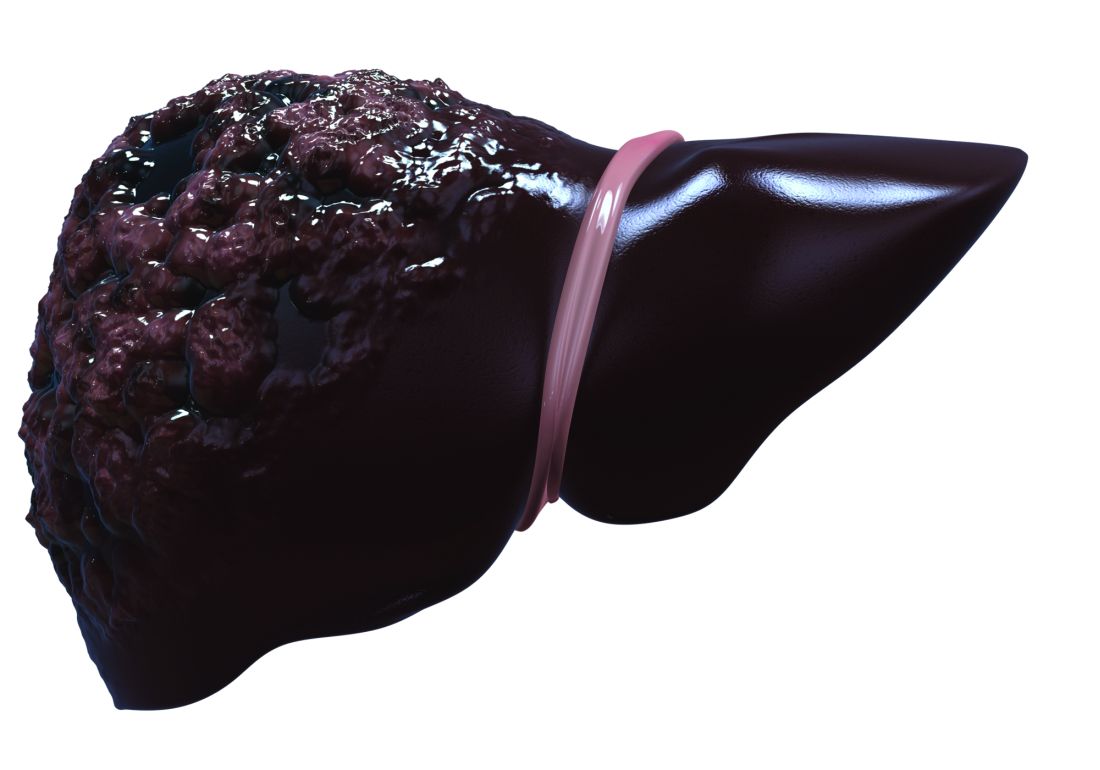
“Various assumptions can be made to explain why patients with alcohol-related HCC have reduced survival in comparison with patients with non–alcohol-related HCC: a diagnosis at a later stage due to lower rates of HCC screening, worse liver function and/or ongoing alcohol consumption preventing curative options, and discrimination against alcoholic patients leading to less aggressive treatment options,” they wrote in a study published online in Cancer.
The investigators looked at data on clinical features and treatment allocation of patients in the CHANGH cohort (cohorte de Carcinomes Hepatocelulaires de l’Association des hepato-Gastroenterologues des Hopitaux Generaux), a prospective, observational cohort study.
Of 1,207 patients with complete data, 582 had isolated alcohol-related HCC, and 312 had non–alcohol-related HCC, which was caused by either nonalcoholic fatty liver, hepatitis C infections, hepatitis B infections, hemochromatosis, or other etiologies.
As noted before, the median overall survival adjusted for lead-time bias (the length of time between the detection of a disease and its usual diagnosis) was significantly shorter for patients with alcohol-related HCC.
In univariate analysis, alcohol-related HCC, compared with non–alcohol-related HCC, was an independent risk factor for worse overall survival (hazard ratio, 1.39; P = .0002).
Among patients in the alcohol-related HCC group, median overall survival adjusted for lead-time was 5.8 months for patients who had been abstinent for a median of 1 year, compared with 5.0 months for the nonabstinent patients, a difference that was not statistically significant.
In multivariate analysis, factors significantly associated with worse overall survival included advanced HCC at diagnosis (diffuse or metastatic HCC and/or macrovascular invasion), alkaline phosphatase score, alpha-fetoprotein levels, creatinine, performance status, Child-Pugh score, age plus alcohol-related disease, and male sex plus alcohol-related disease. However, alcohol-related versus non–alcohol-related HCC was no longer statistically significant in multivariate analysis.
They noted that for 199 patients who were diagnosed with HCC as part of a cirrhosis follow-up program, the median overall survival adjusted for lead-time was 11.7 months, compared with 5.4 months for patients whose HCC was detected incidentally (P less than .0001).
The investigators noted that other studies have shown that screening rates for HCC are lower in alcohol abusers and that the most common reason for a lack of screening was failure of clinician to order surveillance in patients with known cirrhosis. In addition, alcoholic patients are less likely to be compliant with screening.
“Importantly, Bucci et al (Aliment Pharmacol Ther. 2016 Feb;43[3]:385-99) observed similar survival between alcoholic patients and patients with hepatitis C virus among patients undergoing HCC surveillance according to guidelines. The poorer prognosis of alcohol-related HCC is, therefore, very likely to be related to an advanced stage at diagnosis due to screening failure instead of greater cancer aggressiveness,” they wrote.
“To improve prognosis of liver cancer in the alcoholic population, efforts should be made to implement effective screening programs for both cirrhosis and liver cancer and to improve access to alcoholism treatment services,” Dr. Costentin said in press release. “A smaller tumor burden and a better liver function at diagnosis should translate into higher rates of patients with alcohol-related liver cancer amenable to curative treatment such as tumor resection or ablation and liver transplantation.”
Dr. Costentin did not report conflicts of interest. Several of her coauthors reported personal fees from various companies outside the submitted work.
SOURCE: Costentin CE at al. Cancer. doi: 10.1002/cncr.31215.
Hepatocellular carcinoma (HCC) related to alcohol use tends to be diagnosed at a later stage than HCC from other causes, which contributes to reduced overall survival among patients with alcoholic HCC, investigators in a prospective French study said.
Among 894 patients diagnosed with HCC, the adjusted median overall survival was 5.7 months for those with alcoholic HCC, compared with 9.7 months for those with nonalcoholic HCC (P = .0002), reported Charlotte E. Costentin, MD, of the Hopital Henri Mondor in Creteil, France, and colleagues.
“Various assumptions can be made to explain why patients with alcohol-related HCC have reduced survival in comparison with patients with non–alcohol-related HCC: a diagnosis at a later stage due to lower rates of HCC screening, worse liver function and/or ongoing alcohol consumption preventing curative options, and discrimination against alcoholic patients leading to less aggressive treatment options,” they wrote in a study published online in Cancer.
The investigators looked at data on clinical features and treatment allocation of patients in the CHANGH cohort (cohorte de Carcinomes Hepatocelulaires de l’Association des hepato-Gastroenterologues des Hopitaux Generaux), a prospective, observational cohort study.
Of 1,207 patients with complete data, 582 had isolated alcohol-related HCC, and 312 had non–alcohol-related HCC, which was caused by either nonalcoholic fatty liver, hepatitis C infections, hepatitis B infections, hemochromatosis, or other etiologies.
As noted before, the median overall survival adjusted for lead-time bias (the length of time between the detection of a disease and its usual diagnosis) was significantly shorter for patients with alcohol-related HCC.
In univariate analysis, alcohol-related HCC, compared with non–alcohol-related HCC, was an independent risk factor for worse overall survival (hazard ratio, 1.39; P = .0002).
Among patients in the alcohol-related HCC group, median overall survival adjusted for lead-time was 5.8 months for patients who had been abstinent for a median of 1 year, compared with 5.0 months for the nonabstinent patients, a difference that was not statistically significant.
In multivariate analysis, factors significantly associated with worse overall survival included advanced HCC at diagnosis (diffuse or metastatic HCC and/or macrovascular invasion), alkaline phosphatase score, alpha-fetoprotein levels, creatinine, performance status, Child-Pugh score, age plus alcohol-related disease, and male sex plus alcohol-related disease. However, alcohol-related versus non–alcohol-related HCC was no longer statistically significant in multivariate analysis.
They noted that for 199 patients who were diagnosed with HCC as part of a cirrhosis follow-up program, the median overall survival adjusted for lead-time was 11.7 months, compared with 5.4 months for patients whose HCC was detected incidentally (P less than .0001).
The investigators noted that other studies have shown that screening rates for HCC are lower in alcohol abusers and that the most common reason for a lack of screening was failure of clinician to order surveillance in patients with known cirrhosis. In addition, alcoholic patients are less likely to be compliant with screening.
“Importantly, Bucci et al (Aliment Pharmacol Ther. 2016 Feb;43[3]:385-99) observed similar survival between alcoholic patients and patients with hepatitis C virus among patients undergoing HCC surveillance according to guidelines. The poorer prognosis of alcohol-related HCC is, therefore, very likely to be related to an advanced stage at diagnosis due to screening failure instead of greater cancer aggressiveness,” they wrote.
“To improve prognosis of liver cancer in the alcoholic population, efforts should be made to implement effective screening programs for both cirrhosis and liver cancer and to improve access to alcoholism treatment services,” Dr. Costentin said in press release. “A smaller tumor burden and a better liver function at diagnosis should translate into higher rates of patients with alcohol-related liver cancer amenable to curative treatment such as tumor resection or ablation and liver transplantation.”
Dr. Costentin did not report conflicts of interest. Several of her coauthors reported personal fees from various companies outside the submitted work.
SOURCE: Costentin CE at al. Cancer. doi: 10.1002/cncr.31215.
Hepatocellular carcinoma (HCC) related to alcohol use tends to be diagnosed at a later stage than HCC from other causes, which contributes to reduced overall survival among patients with alcoholic HCC, investigators in a prospective French study said.
Among 894 patients diagnosed with HCC, the adjusted median overall survival was 5.7 months for those with alcoholic HCC, compared with 9.7 months for those with nonalcoholic HCC (P = .0002), reported Charlotte E. Costentin, MD, of the Hopital Henri Mondor in Creteil, France, and colleagues.
“Various assumptions can be made to explain why patients with alcohol-related HCC have reduced survival in comparison with patients with non–alcohol-related HCC: a diagnosis at a later stage due to lower rates of HCC screening, worse liver function and/or ongoing alcohol consumption preventing curative options, and discrimination against alcoholic patients leading to less aggressive treatment options,” they wrote in a study published online in Cancer.
The investigators looked at data on clinical features and treatment allocation of patients in the CHANGH cohort (cohorte de Carcinomes Hepatocelulaires de l’Association des hepato-Gastroenterologues des Hopitaux Generaux), a prospective, observational cohort study.
Of 1,207 patients with complete data, 582 had isolated alcohol-related HCC, and 312 had non–alcohol-related HCC, which was caused by either nonalcoholic fatty liver, hepatitis C infections, hepatitis B infections, hemochromatosis, or other etiologies.
As noted before, the median overall survival adjusted for lead-time bias (the length of time between the detection of a disease and its usual diagnosis) was significantly shorter for patients with alcohol-related HCC.
In univariate analysis, alcohol-related HCC, compared with non–alcohol-related HCC, was an independent risk factor for worse overall survival (hazard ratio, 1.39; P = .0002).
Among patients in the alcohol-related HCC group, median overall survival adjusted for lead-time was 5.8 months for patients who had been abstinent for a median of 1 year, compared with 5.0 months for the nonabstinent patients, a difference that was not statistically significant.
In multivariate analysis, factors significantly associated with worse overall survival included advanced HCC at diagnosis (diffuse or metastatic HCC and/or macrovascular invasion), alkaline phosphatase score, alpha-fetoprotein levels, creatinine, performance status, Child-Pugh score, age plus alcohol-related disease, and male sex plus alcohol-related disease. However, alcohol-related versus non–alcohol-related HCC was no longer statistically significant in multivariate analysis.
They noted that for 199 patients who were diagnosed with HCC as part of a cirrhosis follow-up program, the median overall survival adjusted for lead-time was 11.7 months, compared with 5.4 months for patients whose HCC was detected incidentally (P less than .0001).
The investigators noted that other studies have shown that screening rates for HCC are lower in alcohol abusers and that the most common reason for a lack of screening was failure of clinician to order surveillance in patients with known cirrhosis. In addition, alcoholic patients are less likely to be compliant with screening.
“Importantly, Bucci et al (Aliment Pharmacol Ther. 2016 Feb;43[3]:385-99) observed similar survival between alcoholic patients and patients with hepatitis C virus among patients undergoing HCC surveillance according to guidelines. The poorer prognosis of alcohol-related HCC is, therefore, very likely to be related to an advanced stage at diagnosis due to screening failure instead of greater cancer aggressiveness,” they wrote.
“To improve prognosis of liver cancer in the alcoholic population, efforts should be made to implement effective screening programs for both cirrhosis and liver cancer and to improve access to alcoholism treatment services,” Dr. Costentin said in press release. “A smaller tumor burden and a better liver function at diagnosis should translate into higher rates of patients with alcohol-related liver cancer amenable to curative treatment such as tumor resection or ablation and liver transplantation.”
Dr. Costentin did not report conflicts of interest. Several of her coauthors reported personal fees from various companies outside the submitted work.
SOURCE: Costentin CE at al. Cancer. doi: 10.1002/cncr.31215.
FROM CANCER
Key clinical point: Patients with HCC from alcohol or other causes had better survival if they were under surveillance for cirrhosis.
Major finding: Adjusted median overall survival was 5.7 months with alcohol-related HCC versus 9.7 months for nonalcoholic HCC (P = .0002).
Study details: Analysis of data from a prospective observational cohort of 1,207 patients with HCC in France.
Disclosures: The study was supported by the Association Nationale des Hepato-Gastroenterologues des Hopitaux Généraux group and Roche Pharmaceuticals. Dr. Constentin did not report conflicts of interest. Several of her coauthors reported personal fees from various companies outside the submitted work.
Source: Costentin CE at al. Cancer. doi: 10.1002/cncr.31215.
Abstract: Don't demonise prescription opioids
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Roehr, B., BMJ 359:j4727, October 19, 2017
The author, a biomedical journalist from Washington, DC, explains how a zero-tolerance policy to opioid prescribing will impede the delivery of care for patients with severe pain. He notes that he has used hydrocodone daily for nearly ten years for nerve damage due to knee replacement and spinal surgeries, and suggests that reports of the opioid epidemic “crisis” represent overblown rhetoric from persons with an interest in promoting a “war on drugs” agenda. In fact, research shows that while 38% of the US population used a prescription opioid in 2015, few of whom were being treated for cancer, only 0.8% were classified as drug abusers. The author considers himself dependent on hydrocodone in the same way that he is dependent on his blood pressure medication, and states that hydrocodone allows him to remain relatively pain-free and productive but without adverse effects. The dramatic rise in opioid-related deaths is fueled in part by fentanyl and other illicit street drugs. In fact, he contends that CDC mortality data are methodologically flawed because deaths due to street drugs including heroin are combined with deaths due to prescription opioids, while in fact prescription drug deaths have been decreasing over the past few years. Efforts to control the opioid supply with prescribing limits, prosecution of “pill mills,” and tamper-resistant formulations were all in place before the recent increases in opioid-related deaths. The author disputes the concept of opioids as gateway drugs, stating that the gateway theory has long been disproven, yet he acknowledges that patients who lose access to prescription opioids may turn to more accessible, black-market options such as street drugs containing fentanyl. He concludes that denial of opioids to everyone because some are abusers will mean that many patients with legitimate need will suffer unnecessarily. 4 references (bobroehr@aol.com – no reprints)
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Roehr, B., BMJ 359:j4727, October 19, 2017
The author, a biomedical journalist from Washington, DC, explains how a zero-tolerance policy to opioid prescribing will impede the delivery of care for patients with severe pain. He notes that he has used hydrocodone daily for nearly ten years for nerve damage due to knee replacement and spinal surgeries, and suggests that reports of the opioid epidemic “crisis” represent overblown rhetoric from persons with an interest in promoting a “war on drugs” agenda. In fact, research shows that while 38% of the US population used a prescription opioid in 2015, few of whom were being treated for cancer, only 0.8% were classified as drug abusers. The author considers himself dependent on hydrocodone in the same way that he is dependent on his blood pressure medication, and states that hydrocodone allows him to remain relatively pain-free and productive but without adverse effects. The dramatic rise in opioid-related deaths is fueled in part by fentanyl and other illicit street drugs. In fact, he contends that CDC mortality data are methodologically flawed because deaths due to street drugs including heroin are combined with deaths due to prescription opioids, while in fact prescription drug deaths have been decreasing over the past few years. Efforts to control the opioid supply with prescribing limits, prosecution of “pill mills,” and tamper-resistant formulations were all in place before the recent increases in opioid-related deaths. The author disputes the concept of opioids as gateway drugs, stating that the gateway theory has long been disproven, yet he acknowledges that patients who lose access to prescription opioids may turn to more accessible, black-market options such as street drugs containing fentanyl. He concludes that denial of opioids to everyone because some are abusers will mean that many patients with legitimate need will suffer unnecessarily. 4 references (bobroehr@aol.com – no reprints)
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Roehr, B., BMJ 359:j4727, October 19, 2017
The author, a biomedical journalist from Washington, DC, explains how a zero-tolerance policy to opioid prescribing will impede the delivery of care for patients with severe pain. He notes that he has used hydrocodone daily for nearly ten years for nerve damage due to knee replacement and spinal surgeries, and suggests that reports of the opioid epidemic “crisis” represent overblown rhetoric from persons with an interest in promoting a “war on drugs” agenda. In fact, research shows that while 38% of the US population used a prescription opioid in 2015, few of whom were being treated for cancer, only 0.8% were classified as drug abusers. The author considers himself dependent on hydrocodone in the same way that he is dependent on his blood pressure medication, and states that hydrocodone allows him to remain relatively pain-free and productive but without adverse effects. The dramatic rise in opioid-related deaths is fueled in part by fentanyl and other illicit street drugs. In fact, he contends that CDC mortality data are methodologically flawed because deaths due to street drugs including heroin are combined with deaths due to prescription opioids, while in fact prescription drug deaths have been decreasing over the past few years. Efforts to control the opioid supply with prescribing limits, prosecution of “pill mills,” and tamper-resistant formulations were all in place before the recent increases in opioid-related deaths. The author disputes the concept of opioids as gateway drugs, stating that the gateway theory has long been disproven, yet he acknowledges that patients who lose access to prescription opioids may turn to more accessible, black-market options such as street drugs containing fentanyl. He concludes that denial of opioids to everyone because some are abusers will mean that many patients with legitimate need will suffer unnecessarily. 4 references (bobroehr@aol.com – no reprints)
Learn more about the Primary Care Medical Abstracts and podcasts, for which you can earn up to 9 CME credits per month.
Copyright © The Center for Medical Education

Newborn with multiple plaques

Giant congenital nevus was diagnosed in this patient. Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis. Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), or giant (>40 cm).
Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi, which are rare, are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair. CMN can cover any part of the body and occur independent of skin color and other ethnic factors.
CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations are part of the differential diagnosis for CMN and have individual location and color characteristics that set them apart clinically.
Patients with CMN are at increased risk for neurocutaneous melanosis (NCM; a melanocyte proliferation in the central nervous system) and melanoma. Magnetic resonance imaging (MRI) is helpful to exclude NCM. Treatment options for patients with large and giant CMN include early curettage, local excision, dermabrasion, and laser therapy. (There is, however, considerable debate about the value of surgery.) The newborn in the case underwent an MRI and the results were normal. At 4 months of age, he hadn’t developed any neurologic symptoms. The child’s nevi continue to grow and he sees his family physician for routine well-child visits and a dermatologist annually to monitor the nevi.
Adapted from: Karnes J, Griffin C. Large plaques on a baby boy. J Fam Pract. 2016;65:407-409.
Giant congenital nevus was diagnosed in this patient. Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis. Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), or giant (>40 cm).
Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi, which are rare, are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair. CMN can cover any part of the body and occur independent of skin color and other ethnic factors.
CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations are part of the differential diagnosis for CMN and have individual location and color characteristics that set them apart clinically.
Patients with CMN are at increased risk for neurocutaneous melanosis (NCM; a melanocyte proliferation in the central nervous system) and melanoma. Magnetic resonance imaging (MRI) is helpful to exclude NCM. Treatment options for patients with large and giant CMN include early curettage, local excision, dermabrasion, and laser therapy. (There is, however, considerable debate about the value of surgery.) The newborn in the case underwent an MRI and the results were normal. At 4 months of age, he hadn’t developed any neurologic symptoms. The child’s nevi continue to grow and he sees his family physician for routine well-child visits and a dermatologist annually to monitor the nevi.
Adapted from: Karnes J, Griffin C. Large plaques on a baby boy. J Fam Pract. 2016;65:407-409.
Giant congenital nevus was diagnosed in this patient. Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis. Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), or giant (>40 cm).
Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi, which are rare, are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair. CMN can cover any part of the body and occur independent of skin color and other ethnic factors.
CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations are part of the differential diagnosis for CMN and have individual location and color characteristics that set them apart clinically.
Patients with CMN are at increased risk for neurocutaneous melanosis (NCM; a melanocyte proliferation in the central nervous system) and melanoma. Magnetic resonance imaging (MRI) is helpful to exclude NCM. Treatment options for patients with large and giant CMN include early curettage, local excision, dermabrasion, and laser therapy. (There is, however, considerable debate about the value of surgery.) The newborn in the case underwent an MRI and the results were normal. At 4 months of age, he hadn’t developed any neurologic symptoms. The child’s nevi continue to grow and he sees his family physician for routine well-child visits and a dermatologist annually to monitor the nevi.
Adapted from: Karnes J, Griffin C. Large plaques on a baby boy. J Fam Pract. 2016;65:407-409.

Nivolumab helps some with advanced NSCLC reach 5-year mark
Some patients with previously treated advanced non-small cell lung cancer (NSCLC), a malignancy with a historically dim prognosis, survived at least 5 years after receiving the immune checkpoint inhibitor nivolumab (Opdivo) in an early phase 1 trial.
For 129 patients with NSCLC treated with nivolumab in the CA209-003 trial, the estimated 5 year overall survival (OS) was 16%. Twelve patients who did not receive any subsequent therapy following completion of nivolumab were alive with no evidence of disease at the 5-year follow-up mark, reported Scott Gettinger, MD, of the Yale Cancer Center in New Haven, Connecticut, and colleagues.
“Considering the historically low 5-year survival rate for patients with metastatic lung cancer, the estimated 5-year OS rate of 16% from the time of nivolumab treatment initiation observed in this cohort of heavily pretreated patients with advanced NSCLC constitutes a milestone in the advancement of lung cancer treatment,” they wrote in the Journal of Clinical Oncology. In the NSCLC cohort of the phase 1 dose-escalation and expansion study, 129 patients with heavily pretreated advanced NSCLC received nivolumab in doses of 1, 3, or 10 mg/kg intravenously once every 2 weeks in 8-week cycles for up to 96 weeks. The investigators previously reportedthat after a median follow-up of 39 weeks, the median overall survival across all three dose groups was 9.9 months. For 37 patients treated at the 3 mg/kg dose chosen for further development, the median 1-, 2-, and 3-year OS rates were 56%, 42%, and 27%, respectively.
In the current study, they followed the patients out to a minimum of 58.25 months. The median OS was 9.9 months, and the estimated 5-year OS rate, as noted before, was 16%. The 5-year OS rates for patients with squamous histology cancers was 16%, and the rate for patients with nonsquamous histology was 15%.
In all, 16 patients survived at least 5 years, with the longest follow-up out to 88.6 months. Two of the patients died before the database lock in November 2016, one from disease progression, and one from chronic obstructive pulmonary disease.
Among 10 long-term survivors who had quantifiable expression of the programmed death-1 ligand 1 (PD-L1), seven had at least 1% PD-L1 expression at baseline.
Of the 16 5-year survivors, 12 (75%) had a partial response to nivolumab according to RECIST (Response Evaluation Criteria in Solid Tumors), version 1. Two others had stable disease, and two had disease progression at the best response.
In all, nine of the 5-year survivors had completed the maximum 96 weeks of nivolumab, four had discontinued due to adverse events, and three had stopped because of disease progression.
“The findings from CA209-003 indicate some patients can derive long-term benefit from nivolumab treatment that is limited to 2 years; however, the question of optimal treatment duration remains to be formally addressed in a prospective controlled trial,” Dr. Gettinger and associates wrote.
The study was supported by Bristol-Myers Squibb and Ono Pharmaceuticals. Dr. Gettinger and multiple co-authors reported consulting/advisory roles and research funding with BMS and other relationships with multiple companies. Several co-authors are BMS employees.
SOURCE: : Getting S et al. J Clin Oncol. 2018 Mar 23 doi: 10.1200/JCO.2017.77.0412 .
Some patients with previously treated advanced non-small cell lung cancer (NSCLC), a malignancy with a historically dim prognosis, survived at least 5 years after receiving the immune checkpoint inhibitor nivolumab (Opdivo) in an early phase 1 trial.
For 129 patients with NSCLC treated with nivolumab in the CA209-003 trial, the estimated 5 year overall survival (OS) was 16%. Twelve patients who did not receive any subsequent therapy following completion of nivolumab were alive with no evidence of disease at the 5-year follow-up mark, reported Scott Gettinger, MD, of the Yale Cancer Center in New Haven, Connecticut, and colleagues.
“Considering the historically low 5-year survival rate for patients with metastatic lung cancer, the estimated 5-year OS rate of 16% from the time of nivolumab treatment initiation observed in this cohort of heavily pretreated patients with advanced NSCLC constitutes a milestone in the advancement of lung cancer treatment,” they wrote in the Journal of Clinical Oncology. In the NSCLC cohort of the phase 1 dose-escalation and expansion study, 129 patients with heavily pretreated advanced NSCLC received nivolumab in doses of 1, 3, or 10 mg/kg intravenously once every 2 weeks in 8-week cycles for up to 96 weeks. The investigators previously reportedthat after a median follow-up of 39 weeks, the median overall survival across all three dose groups was 9.9 months. For 37 patients treated at the 3 mg/kg dose chosen for further development, the median 1-, 2-, and 3-year OS rates were 56%, 42%, and 27%, respectively.
In the current study, they followed the patients out to a minimum of 58.25 months. The median OS was 9.9 months, and the estimated 5-year OS rate, as noted before, was 16%. The 5-year OS rates for patients with squamous histology cancers was 16%, and the rate for patients with nonsquamous histology was 15%.
In all, 16 patients survived at least 5 years, with the longest follow-up out to 88.6 months. Two of the patients died before the database lock in November 2016, one from disease progression, and one from chronic obstructive pulmonary disease.
Among 10 long-term survivors who had quantifiable expression of the programmed death-1 ligand 1 (PD-L1), seven had at least 1% PD-L1 expression at baseline.
Of the 16 5-year survivors, 12 (75%) had a partial response to nivolumab according to RECIST (Response Evaluation Criteria in Solid Tumors), version 1. Two others had stable disease, and two had disease progression at the best response.
In all, nine of the 5-year survivors had completed the maximum 96 weeks of nivolumab, four had discontinued due to adverse events, and three had stopped because of disease progression.
“The findings from CA209-003 indicate some patients can derive long-term benefit from nivolumab treatment that is limited to 2 years; however, the question of optimal treatment duration remains to be formally addressed in a prospective controlled trial,” Dr. Gettinger and associates wrote.
The study was supported by Bristol-Myers Squibb and Ono Pharmaceuticals. Dr. Gettinger and multiple co-authors reported consulting/advisory roles and research funding with BMS and other relationships with multiple companies. Several co-authors are BMS employees.
SOURCE: : Getting S et al. J Clin Oncol. 2018 Mar 23 doi: 10.1200/JCO.2017.77.0412 .
Some patients with previously treated advanced non-small cell lung cancer (NSCLC), a malignancy with a historically dim prognosis, survived at least 5 years after receiving the immune checkpoint inhibitor nivolumab (Opdivo) in an early phase 1 trial.
For 129 patients with NSCLC treated with nivolumab in the CA209-003 trial, the estimated 5 year overall survival (OS) was 16%. Twelve patients who did not receive any subsequent therapy following completion of nivolumab were alive with no evidence of disease at the 5-year follow-up mark, reported Scott Gettinger, MD, of the Yale Cancer Center in New Haven, Connecticut, and colleagues.
“Considering the historically low 5-year survival rate for patients with metastatic lung cancer, the estimated 5-year OS rate of 16% from the time of nivolumab treatment initiation observed in this cohort of heavily pretreated patients with advanced NSCLC constitutes a milestone in the advancement of lung cancer treatment,” they wrote in the Journal of Clinical Oncology. In the NSCLC cohort of the phase 1 dose-escalation and expansion study, 129 patients with heavily pretreated advanced NSCLC received nivolumab in doses of 1, 3, or 10 mg/kg intravenously once every 2 weeks in 8-week cycles for up to 96 weeks. The investigators previously reportedthat after a median follow-up of 39 weeks, the median overall survival across all three dose groups was 9.9 months. For 37 patients treated at the 3 mg/kg dose chosen for further development, the median 1-, 2-, and 3-year OS rates were 56%, 42%, and 27%, respectively.
In the current study, they followed the patients out to a minimum of 58.25 months. The median OS was 9.9 months, and the estimated 5-year OS rate, as noted before, was 16%. The 5-year OS rates for patients with squamous histology cancers was 16%, and the rate for patients with nonsquamous histology was 15%.
In all, 16 patients survived at least 5 years, with the longest follow-up out to 88.6 months. Two of the patients died before the database lock in November 2016, one from disease progression, and one from chronic obstructive pulmonary disease.
Among 10 long-term survivors who had quantifiable expression of the programmed death-1 ligand 1 (PD-L1), seven had at least 1% PD-L1 expression at baseline.
Of the 16 5-year survivors, 12 (75%) had a partial response to nivolumab according to RECIST (Response Evaluation Criteria in Solid Tumors), version 1. Two others had stable disease, and two had disease progression at the best response.
In all, nine of the 5-year survivors had completed the maximum 96 weeks of nivolumab, four had discontinued due to adverse events, and three had stopped because of disease progression.
“The findings from CA209-003 indicate some patients can derive long-term benefit from nivolumab treatment that is limited to 2 years; however, the question of optimal treatment duration remains to be formally addressed in a prospective controlled trial,” Dr. Gettinger and associates wrote.
The study was supported by Bristol-Myers Squibb and Ono Pharmaceuticals. Dr. Gettinger and multiple co-authors reported consulting/advisory roles and research funding with BMS and other relationships with multiple companies. Several co-authors are BMS employees.
SOURCE: : Getting S et al. J Clin Oncol. 2018 Mar 23 doi: 10.1200/JCO.2017.77.0412 .
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The programmed death-1 inhibitor nivolumab (Opdivo) is associated with long-term survival in a subset of patients with heavily pre-treated advanced non-small cell lung cancer (NSCLC).Major finding: The estimated 5-year overall survival rate was 16%.Study details: Follow-up study of 129 patients with NSCLC treated with nivolumab in a phase 1 study.
Disclosures: The study was supported by Bristol-Myers Squibb and Ono Pharmaceuticals. Dr. Gettinger and multiple co-authors reported consulting/advisory roles and research finding with BMS and other relationships with multiple companies. Several co-authors are BMS employees.
Source: Gettinger S et al. J Clin Oncol. 2018 Mar 23 doi: 10.1200/JCO.2017.77.0412.
Hot Threads in ACS Communities
Your colleagues have a lot to say to each other. Here are the top discussion threads in ACS Communities this week:
1. ABS Continuous Certification Program (General Surgery)
2. ACS Leadership Response to ABS Continuous Certification Program (General Surgery)
3. Update on ACS Violence Prevention Strategy (General Surgery)
4. FNA parathyroid? (Endocrine Surgery)
5. Risk reduction mastectomy with mastectomy for unilateral breast cancer (Breast Surgery)
6. First mammogram after treatment (Breast Surgery)
7. Transferring for “pt preference” (Rural Surgery)
8. Where will the Gen X surgeon work? (Young Fellows)
9. Hiatal hernias and the sleeve (Bariatric Surgery)
10. Level 3 trauma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org, click “Communities” on the blue bar, select “All Communities,” and then click the “Join” button next to the communities you’d like to join. If you have any questions, please send them to acscommunities@facs.org.
Your colleagues have a lot to say to each other. Here are the top discussion threads in ACS Communities this week:
1. ABS Continuous Certification Program (General Surgery)
2. ACS Leadership Response to ABS Continuous Certification Program (General Surgery)
3. Update on ACS Violence Prevention Strategy (General Surgery)
4. FNA parathyroid? (Endocrine Surgery)
5. Risk reduction mastectomy with mastectomy for unilateral breast cancer (Breast Surgery)
6. First mammogram after treatment (Breast Surgery)
7. Transferring for “pt preference” (Rural Surgery)
8. Where will the Gen X surgeon work? (Young Fellows)
9. Hiatal hernias and the sleeve (Bariatric Surgery)
10. Level 3 trauma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org, click “Communities” on the blue bar, select “All Communities,” and then click the “Join” button next to the communities you’d like to join. If you have any questions, please send them to acscommunities@facs.org.
Your colleagues have a lot to say to each other. Here are the top discussion threads in ACS Communities this week:
1. ABS Continuous Certification Program (General Surgery)
2. ACS Leadership Response to ABS Continuous Certification Program (General Surgery)
3. Update on ACS Violence Prevention Strategy (General Surgery)
4. FNA parathyroid? (Endocrine Surgery)
5. Risk reduction mastectomy with mastectomy for unilateral breast cancer (Breast Surgery)
6. First mammogram after treatment (Breast Surgery)
7. Transferring for “pt preference” (Rural Surgery)
8. Where will the Gen X surgeon work? (Young Fellows)
9. Hiatal hernias and the sleeve (Bariatric Surgery)
10. Level 3 trauma (Trauma Surgery)
To join communities, log in to ACS Communities at http://acscommunities.facs.org, click “Communities” on the blue bar, select “All Communities,” and then click the “Join” button next to the communities you’d like to join. If you have any questions, please send them to acscommunities@facs.org.
Reducing SNF Readmissions: At What Cost?
The landscape of postacute care in skilled nursing facilities (SNFs) in the United States is evolving. As the population ages, a growing number of elderly persons are being discharged to SNFs at an enormous cost and with clear evidence of disappointing outcomes. The reaction to these trends includes payment reforms that “bundle” hospital and postacute care, act as incentives to discourage SNFs, or penalize SNFs for undesired patient outcomes. Hospitalists are expected to increasingly feel the effect of these reforms.1
Thus, hospitals are demonstrating renewed interest in reducing readmissions from SNFs. In this issue of Journal of Hospital Medicine, Rosen and colleagues present the results of the Enhanced Care Program (ECP), a multicomponent intervention consisting of 9 nurse practitioners (NPs), a pharmacist, a pharmacy technician, a nurse educator, a program administrator, and a medical director.2 These providers are deployed to 8 SNFs around a large teaching hospital, providing direct clinical care as well as 24/7 call availability for enrolled patients, robust medication reconciliation, and monthly education for SNF nursing staff. A unique aspect of this model was that individual attending physicians in the associated SNFs could decide whether to enroll their patients in the model; patients not enrolled represented a contemporaneous control cohort. The authors found a nearly 30% reduction in the odds of 30-day readmission (OR 0.71 [0.60–0.85] after adjustment), which was robust to multiple sensitivity analyses, including a propensity-matched cohort comparison. The authors should be commended for working to mitigate these potential confounders, thereby strengthening their conclusions. Such a large reduction in readmissions reflects their high underlying prevalence (23% in the nonintervention cohort).
This report closely follows the evaluation of a similar program at the Cleveland Clinic called Connected Care Model (CCM), in which 4 physicians and 5 NPs or physician assistants provided care, including 24/7 call availability, in 7 associated SNFs.3 In a retrospective pre-post analysis comparing the 30-day readmission rates of these SNFs with those of others in the network, similar reductions in readmissions were observed. ECP and CCM represent important extensions of a much larger body of evidence, from the Evercare model4 to the Initiative to Reduce Avoidable Hospitalizations demonstration project, which suggests that adding NPs to nursing homes reduces hospitalizations.5
However, several factors have to be considered before disseminating ECP or CCM. First, other promising “proof of concept” quality improvement studies were not efficacious when rigorously tested in nursing homes.6 Second, these programs are representative of large academic medical centers, which may establish different relationships with different SNFs compared with smaller or less well-resourced hospitals. As the Initiative to Reduce Hospitalizations demonstrated, even a fundamentally similar intervention can have extremely different results depending on the nursing homes involved,5 and the science behind establishing effective hospital–SNF partnerships is still in its infancy.7 Third, both studies have significant methodological limitations, including most importantly that they are conducted within SNFs selected to be part of their hospitals’ network.
These significant early efforts also present an opportunity to reconsider the underlying assumption of these models: that adding more supervisory clinicians to SNFs is the right approach to reduce hospitalizations. Although adding resources is an attractive “plug and play” solution for many problems in healthcare delivery, placing only 1 NP in each of the 15,583 certified nursing facilities in the United States would employ fully 10% of the entire NP workforce. Amid rising concerns about costs related to our aging population, these interventions face substantial headwinds toward becoming the standard of care without demonstrating cost effectiveness. Furthermore, many SNF directors might suggest that hospitals and hospitalists working with them to address fundamental (but much more intransigent) problems in SNFs, such as high staff turnover, low concentration of highly skilled staff (RNs and MDs), regulatory burden, and hospitals using SNFs like stepdown units, could represent a generalizable and sustainable solution.
We realize that this argument is tricky for hospitalists because its underlying logic (care has become too complex, patients are too sick, and dedicated personnel are needed) also played a major role in establishing our existence. One possibility is that like hospitalists, NPs and a growing cadre of “SNFists” will become major drivers of quality improvement, education, and leadership locally at these facilities, thereby leading to sustainable change.8 Similarly, current conditions may drive recognition that a specific set of skills is required to function effectively in the SNF environment,9 just as we believe hospitalists need unique skills to excel in today’s hospital environment.
Studies such as that of Rosen et al. are valuable for JHM because they prompt us to recognize that we as hospitalists have much to share and learn from nursing homes and the dedicated practitioners who work there. In fact, we argue that few places in the healthcare system are more in need of innovation than hospital–nursing home relationships, and hospitalists do not just have a vested clinical interest; in many ways, we see a mirror of our own development as a “specialty.” We encourage hospitals and hospitalists to take up this challenge on behalf of some of the most vulnerable patients in our system during critical times in their care trajectory. As the Commission for Long-Term Care (www.ltccommission.org) wrote in its final report to Congress: “The need is great. The time to act is now.”
Disclosures
Dr. Burke is supported by a VA Health Services Research and Development (HSR&D) Career Development Award. All opinions are those of the authors and do not necessarily represent those of the Department of Veterans Affairs. Dr. Greysen has nothing to disclose.
1. Burke RE, Cumbler E, Coleman EA, Levy C. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017;12(1):46-51. 10.3810/hp.2012.02.958. PubMed
2. Rosen BT, Halbert RJ, Hart K, Diniz MA, Isonaka S, Black JT. The enhanced care program: Impact of a care transitions program on 30-day hospital readmissions for patients discharged from an acute care facility to skilled nursing facilities. J Hosp Med. 2018;13(4):229-235.
3. Rothberg MB. Impact of a connected care model on 30-day readmission rates from skilled nursing facilities. J Hosp Med. 2017;12(4):238-244. 10.12788/jhm.2710. PubMed
4. Kane RL, Keckhafer G, Flood S, Bershadsky B, Siadaty MS. The effect of Evercare on hospital use. J Am Geriatr Soc. 2003;51(10):1427-1434. 10.1046/j.1532-5415.2003.51461.x. PubMed
5. Ingber MJ, Feng Z, Khatutsky G, et al. Initiative to reduce avoidable hospitalizations among nursing facility residents shows promising results. Health Aff Proj Hope. 2017;36(3):441-450. 10.1377/hlthaff.2016.1310. PubMed
6. Kane RL, Huckfeldt P, Tappen R, et al. Effects of an intervention to reduce hospitalizations from nursing homes: A randomized implementation trial of the INTERACT Program. JAMA Intern Med. 2017;177(9):1257-1264. 10.1001/jamainternmed.2017.2657. PubMed
7. Lage DE, Rusinak D, Carr D, Grabowski DC, Ackerly DC. Creating a network of high-quality skilled nursing facilities: preliminary data on the postacute care quality improvement experiences of an accountable care organization. J Am Geriatr Soc. 2015;63(4):804-808. 10.1111/jgs.13351. PubMed
8. Ryskina KL, Polsky D, Werner RM. Physicians and advanced practitioners specializing in nursing home care. JAMA. 2017;318(20):2040-2042. 10.1001/jama.2017.13378. PubMed
9. Gillespie SM, Levy CR, Katz PR. What exactly is an “SNF-ist?” JAMA Intern Med. 2018;178(1):153-154. 10.1001/jamainternmed.2017.7212. PubMed
The landscape of postacute care in skilled nursing facilities (SNFs) in the United States is evolving. As the population ages, a growing number of elderly persons are being discharged to SNFs at an enormous cost and with clear evidence of disappointing outcomes. The reaction to these trends includes payment reforms that “bundle” hospital and postacute care, act as incentives to discourage SNFs, or penalize SNFs for undesired patient outcomes. Hospitalists are expected to increasingly feel the effect of these reforms.1
Thus, hospitals are demonstrating renewed interest in reducing readmissions from SNFs. In this issue of Journal of Hospital Medicine, Rosen and colleagues present the results of the Enhanced Care Program (ECP), a multicomponent intervention consisting of 9 nurse practitioners (NPs), a pharmacist, a pharmacy technician, a nurse educator, a program administrator, and a medical director.2 These providers are deployed to 8 SNFs around a large teaching hospital, providing direct clinical care as well as 24/7 call availability for enrolled patients, robust medication reconciliation, and monthly education for SNF nursing staff. A unique aspect of this model was that individual attending physicians in the associated SNFs could decide whether to enroll their patients in the model; patients not enrolled represented a contemporaneous control cohort. The authors found a nearly 30% reduction in the odds of 30-day readmission (OR 0.71 [0.60–0.85] after adjustment), which was robust to multiple sensitivity analyses, including a propensity-matched cohort comparison. The authors should be commended for working to mitigate these potential confounders, thereby strengthening their conclusions. Such a large reduction in readmissions reflects their high underlying prevalence (23% in the nonintervention cohort).
This report closely follows the evaluation of a similar program at the Cleveland Clinic called Connected Care Model (CCM), in which 4 physicians and 5 NPs or physician assistants provided care, including 24/7 call availability, in 7 associated SNFs.3 In a retrospective pre-post analysis comparing the 30-day readmission rates of these SNFs with those of others in the network, similar reductions in readmissions were observed. ECP and CCM represent important extensions of a much larger body of evidence, from the Evercare model4 to the Initiative to Reduce Avoidable Hospitalizations demonstration project, which suggests that adding NPs to nursing homes reduces hospitalizations.5
However, several factors have to be considered before disseminating ECP or CCM. First, other promising “proof of concept” quality improvement studies were not efficacious when rigorously tested in nursing homes.6 Second, these programs are representative of large academic medical centers, which may establish different relationships with different SNFs compared with smaller or less well-resourced hospitals. As the Initiative to Reduce Hospitalizations demonstrated, even a fundamentally similar intervention can have extremely different results depending on the nursing homes involved,5 and the science behind establishing effective hospital–SNF partnerships is still in its infancy.7 Third, both studies have significant methodological limitations, including most importantly that they are conducted within SNFs selected to be part of their hospitals’ network.
These significant early efforts also present an opportunity to reconsider the underlying assumption of these models: that adding more supervisory clinicians to SNFs is the right approach to reduce hospitalizations. Although adding resources is an attractive “plug and play” solution for many problems in healthcare delivery, placing only 1 NP in each of the 15,583 certified nursing facilities in the United States would employ fully 10% of the entire NP workforce. Amid rising concerns about costs related to our aging population, these interventions face substantial headwinds toward becoming the standard of care without demonstrating cost effectiveness. Furthermore, many SNF directors might suggest that hospitals and hospitalists working with them to address fundamental (but much more intransigent) problems in SNFs, such as high staff turnover, low concentration of highly skilled staff (RNs and MDs), regulatory burden, and hospitals using SNFs like stepdown units, could represent a generalizable and sustainable solution.
We realize that this argument is tricky for hospitalists because its underlying logic (care has become too complex, patients are too sick, and dedicated personnel are needed) also played a major role in establishing our existence. One possibility is that like hospitalists, NPs and a growing cadre of “SNFists” will become major drivers of quality improvement, education, and leadership locally at these facilities, thereby leading to sustainable change.8 Similarly, current conditions may drive recognition that a specific set of skills is required to function effectively in the SNF environment,9 just as we believe hospitalists need unique skills to excel in today’s hospital environment.
Studies such as that of Rosen et al. are valuable for JHM because they prompt us to recognize that we as hospitalists have much to share and learn from nursing homes and the dedicated practitioners who work there. In fact, we argue that few places in the healthcare system are more in need of innovation than hospital–nursing home relationships, and hospitalists do not just have a vested clinical interest; in many ways, we see a mirror of our own development as a “specialty.” We encourage hospitals and hospitalists to take up this challenge on behalf of some of the most vulnerable patients in our system during critical times in their care trajectory. As the Commission for Long-Term Care (www.ltccommission.org) wrote in its final report to Congress: “The need is great. The time to act is now.”
Disclosures
Dr. Burke is supported by a VA Health Services Research and Development (HSR&D) Career Development Award. All opinions are those of the authors and do not necessarily represent those of the Department of Veterans Affairs. Dr. Greysen has nothing to disclose.
The landscape of postacute care in skilled nursing facilities (SNFs) in the United States is evolving. As the population ages, a growing number of elderly persons are being discharged to SNFs at an enormous cost and with clear evidence of disappointing outcomes. The reaction to these trends includes payment reforms that “bundle” hospital and postacute care, act as incentives to discourage SNFs, or penalize SNFs for undesired patient outcomes. Hospitalists are expected to increasingly feel the effect of these reforms.1
Thus, hospitals are demonstrating renewed interest in reducing readmissions from SNFs. In this issue of Journal of Hospital Medicine, Rosen and colleagues present the results of the Enhanced Care Program (ECP), a multicomponent intervention consisting of 9 nurse practitioners (NPs), a pharmacist, a pharmacy technician, a nurse educator, a program administrator, and a medical director.2 These providers are deployed to 8 SNFs around a large teaching hospital, providing direct clinical care as well as 24/7 call availability for enrolled patients, robust medication reconciliation, and monthly education for SNF nursing staff. A unique aspect of this model was that individual attending physicians in the associated SNFs could decide whether to enroll their patients in the model; patients not enrolled represented a contemporaneous control cohort. The authors found a nearly 30% reduction in the odds of 30-day readmission (OR 0.71 [0.60–0.85] after adjustment), which was robust to multiple sensitivity analyses, including a propensity-matched cohort comparison. The authors should be commended for working to mitigate these potential confounders, thereby strengthening their conclusions. Such a large reduction in readmissions reflects their high underlying prevalence (23% in the nonintervention cohort).
This report closely follows the evaluation of a similar program at the Cleveland Clinic called Connected Care Model (CCM), in which 4 physicians and 5 NPs or physician assistants provided care, including 24/7 call availability, in 7 associated SNFs.3 In a retrospective pre-post analysis comparing the 30-day readmission rates of these SNFs with those of others in the network, similar reductions in readmissions were observed. ECP and CCM represent important extensions of a much larger body of evidence, from the Evercare model4 to the Initiative to Reduce Avoidable Hospitalizations demonstration project, which suggests that adding NPs to nursing homes reduces hospitalizations.5
However, several factors have to be considered before disseminating ECP or CCM. First, other promising “proof of concept” quality improvement studies were not efficacious when rigorously tested in nursing homes.6 Second, these programs are representative of large academic medical centers, which may establish different relationships with different SNFs compared with smaller or less well-resourced hospitals. As the Initiative to Reduce Hospitalizations demonstrated, even a fundamentally similar intervention can have extremely different results depending on the nursing homes involved,5 and the science behind establishing effective hospital–SNF partnerships is still in its infancy.7 Third, both studies have significant methodological limitations, including most importantly that they are conducted within SNFs selected to be part of their hospitals’ network.
These significant early efforts also present an opportunity to reconsider the underlying assumption of these models: that adding more supervisory clinicians to SNFs is the right approach to reduce hospitalizations. Although adding resources is an attractive “plug and play” solution for many problems in healthcare delivery, placing only 1 NP in each of the 15,583 certified nursing facilities in the United States would employ fully 10% of the entire NP workforce. Amid rising concerns about costs related to our aging population, these interventions face substantial headwinds toward becoming the standard of care without demonstrating cost effectiveness. Furthermore, many SNF directors might suggest that hospitals and hospitalists working with them to address fundamental (but much more intransigent) problems in SNFs, such as high staff turnover, low concentration of highly skilled staff (RNs and MDs), regulatory burden, and hospitals using SNFs like stepdown units, could represent a generalizable and sustainable solution.
We realize that this argument is tricky for hospitalists because its underlying logic (care has become too complex, patients are too sick, and dedicated personnel are needed) also played a major role in establishing our existence. One possibility is that like hospitalists, NPs and a growing cadre of “SNFists” will become major drivers of quality improvement, education, and leadership locally at these facilities, thereby leading to sustainable change.8 Similarly, current conditions may drive recognition that a specific set of skills is required to function effectively in the SNF environment,9 just as we believe hospitalists need unique skills to excel in today’s hospital environment.
Studies such as that of Rosen et al. are valuable for JHM because they prompt us to recognize that we as hospitalists have much to share and learn from nursing homes and the dedicated practitioners who work there. In fact, we argue that few places in the healthcare system are more in need of innovation than hospital–nursing home relationships, and hospitalists do not just have a vested clinical interest; in many ways, we see a mirror of our own development as a “specialty.” We encourage hospitals and hospitalists to take up this challenge on behalf of some of the most vulnerable patients in our system during critical times in their care trajectory. As the Commission for Long-Term Care (www.ltccommission.org) wrote in its final report to Congress: “The need is great. The time to act is now.”
Disclosures
Dr. Burke is supported by a VA Health Services Research and Development (HSR&D) Career Development Award. All opinions are those of the authors and do not necessarily represent those of the Department of Veterans Affairs. Dr. Greysen has nothing to disclose.
1. Burke RE, Cumbler E, Coleman EA, Levy C. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017;12(1):46-51. 10.3810/hp.2012.02.958. PubMed
2. Rosen BT, Halbert RJ, Hart K, Diniz MA, Isonaka S, Black JT. The enhanced care program: Impact of a care transitions program on 30-day hospital readmissions for patients discharged from an acute care facility to skilled nursing facilities. J Hosp Med. 2018;13(4):229-235.
3. Rothberg MB. Impact of a connected care model on 30-day readmission rates from skilled nursing facilities. J Hosp Med. 2017;12(4):238-244. 10.12788/jhm.2710. PubMed
4. Kane RL, Keckhafer G, Flood S, Bershadsky B, Siadaty MS. The effect of Evercare on hospital use. J Am Geriatr Soc. 2003;51(10):1427-1434. 10.1046/j.1532-5415.2003.51461.x. PubMed
5. Ingber MJ, Feng Z, Khatutsky G, et al. Initiative to reduce avoidable hospitalizations among nursing facility residents shows promising results. Health Aff Proj Hope. 2017;36(3):441-450. 10.1377/hlthaff.2016.1310. PubMed
6. Kane RL, Huckfeldt P, Tappen R, et al. Effects of an intervention to reduce hospitalizations from nursing homes: A randomized implementation trial of the INTERACT Program. JAMA Intern Med. 2017;177(9):1257-1264. 10.1001/jamainternmed.2017.2657. PubMed
7. Lage DE, Rusinak D, Carr D, Grabowski DC, Ackerly DC. Creating a network of high-quality skilled nursing facilities: preliminary data on the postacute care quality improvement experiences of an accountable care organization. J Am Geriatr Soc. 2015;63(4):804-808. 10.1111/jgs.13351. PubMed
8. Ryskina KL, Polsky D, Werner RM. Physicians and advanced practitioners specializing in nursing home care. JAMA. 2017;318(20):2040-2042. 10.1001/jama.2017.13378. PubMed
9. Gillespie SM, Levy CR, Katz PR. What exactly is an “SNF-ist?” JAMA Intern Med. 2018;178(1):153-154. 10.1001/jamainternmed.2017.7212. PubMed
1. Burke RE, Cumbler E, Coleman EA, Levy C. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017;12(1):46-51. 10.3810/hp.2012.02.958. PubMed
2. Rosen BT, Halbert RJ, Hart K, Diniz MA, Isonaka S, Black JT. The enhanced care program: Impact of a care transitions program on 30-day hospital readmissions for patients discharged from an acute care facility to skilled nursing facilities. J Hosp Med. 2018;13(4):229-235.
3. Rothberg MB. Impact of a connected care model on 30-day readmission rates from skilled nursing facilities. J Hosp Med. 2017;12(4):238-244. 10.12788/jhm.2710. PubMed
4. Kane RL, Keckhafer G, Flood S, Bershadsky B, Siadaty MS. The effect of Evercare on hospital use. J Am Geriatr Soc. 2003;51(10):1427-1434. 10.1046/j.1532-5415.2003.51461.x. PubMed
5. Ingber MJ, Feng Z, Khatutsky G, et al. Initiative to reduce avoidable hospitalizations among nursing facility residents shows promising results. Health Aff Proj Hope. 2017;36(3):441-450. 10.1377/hlthaff.2016.1310. PubMed
6. Kane RL, Huckfeldt P, Tappen R, et al. Effects of an intervention to reduce hospitalizations from nursing homes: A randomized implementation trial of the INTERACT Program. JAMA Intern Med. 2017;177(9):1257-1264. 10.1001/jamainternmed.2017.2657. PubMed
7. Lage DE, Rusinak D, Carr D, Grabowski DC, Ackerly DC. Creating a network of high-quality skilled nursing facilities: preliminary data on the postacute care quality improvement experiences of an accountable care organization. J Am Geriatr Soc. 2015;63(4):804-808. 10.1111/jgs.13351. PubMed
8. Ryskina KL, Polsky D, Werner RM. Physicians and advanced practitioners specializing in nursing home care. JAMA. 2017;318(20):2040-2042. 10.1001/jama.2017.13378. PubMed
9. Gillespie SM, Levy CR, Katz PR. What exactly is an “SNF-ist?” JAMA Intern Med. 2018;178(1):153-154. 10.1001/jamainternmed.2017.7212. PubMed
© 2018 Society of Hospital Medicine