User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Thrombolysis not necessary in mild nondisabling stroke: ARAMIS
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
Diabetes drug tied to lower dementia risk
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM NEUROLOGY
‘Only a sociopath could work for a large health system,’ doc says sardonically
A frustrated physician recently voiced some strong words in Medscape’s US Physician Burnout & Depression Report: “Only a sociopath could work for a large health system and not be burned out. Anyone who cares about patients is doomed to burnout.”
Medscape’s report showed that 53% of physicians feel burned out by job requirements; 65% say that burnout has impacted their relationships, and other statistics say that physicians are leaving clinical medicine because of all this pressure.
What is it about being employed by large organizations that can be so negative? In another study, MEMO – Minimizing Error, Maximizing Outcomes – researchers at the University of Wisconsin surveyed more than 400 doctors to learn about how their working environments corresponded with medical errors. More than half of the physicians reported time pressures when conducting physical examinations. Nearly a third felt they needed at least 50% more time than was allotted for this patient care function, and nearly a quarter said they needed at least 50% more time for follow-up appointments.
Some have asked: Can anyone, then, thrive in today’s health care environment and avoid burnout?
Although the frustrated physician noted above may sardonically say that a doctor needs to be sociopathic to enjoy it – lacking in feelings for others – “It’s a very small number of doctors who get in it for the wrong reasons and therefore care about their own benefit and not their patients,” said psychiatrist Wendy Dean, MD, CEO and cofounder of Moral Injury of Healthcare, a nonprofit organization addressing workforce distress in health care. “Those are the outliers.”
The vast majority of physicians do care about their patients – deeply, said Dr. Dean. They struggle under the weight of the health care system and yet must find ways to get through. Today, thriving in an imperfect system requires honing new skills, asking for help when needed, and pushing for systemic and cultural change.
“We’ve been assessing and trying to address burnout for half a century,” said Dr. Dean. “Despite all the good intentions, and people dedicating their entire careers to solving the issue, we’ve barely made a dent.”
With the advent of new technological requirements on the job and more demands from increasingly larger health care organizations, the risk for burnout is higher than ever before. “There’s an increased burden of regulatory-mandated and cumbersome administrative workload per patient,” said Shomron Ben-Horin, MD, cofounder of Evinature. “Often the computer/paperwork before and after a procedure is much longer than the procedure itself.”
Meeting insurance requirements is increasingly cumbersome, too, and preauthorizations and debates with payers over medical approval may put physicians frustratingly in the middle.
“This increases the psychological burden for physicians who may feel responsible for wrongdoing no matter which option they deem better,” Dr. Ben-Horin said. “Add in physician accessibility around the clock via mobile phones, emails, and apps, and you end up on call even if you’re not officially on call.”
Why some physicians suffer more
Some physicians are more likely to suffer burnout than others, said Jessi Gold, MD, assistant professor in the department of psychiatry at Washington University in St. Louis. “The self-valuation concept comes into play here,” she said. “If you make a mistake, do you blame yourself or see it as a growth opportunity? If it’s the former, you’re more likely to burn out.”
Dr. Ben-Horin added that the most patient-centric doctors are the ones who struggle most. “These are the doctors we’d all love to have as a patient,” he said. “But they are burdened by the extra tasks of the job, and they are the most stressed by the environment.”
So too are those physicians who never master compartmentalizing their feelings and emotions. “We learn in training to compartmentalize our emotions,” said Dr. Dean. “You can’t allow yourself to get emotional while performing chest compressions on an 18-year-old kid. So you shut it all away; otherwise, you might lose the patient.”
This turn-off switch becomes automatic, but it also comes at a cost. “When doctors were interviewed about [Buffalo Bills player] Damar Hamlin going into cardiac arrest on the football field, they talked about how a life-and-death situation is so common that they have to put the emotions away, work on the patient, and move onto the next,” said Dr. Dean. “The next patient needs you just as much. We must lock away our feelings and manage the situation.”
Dr. Gold explained that burying feelings, however, is a symptom of burnout. “We have to remove ourselves from the situation to protect ourselves,” she said. “We can’t cry in these situations, but we can’t bury our feelings either.”
Instead, Dr. Gold suggested, a good medium may exist. “You may not be able to address them in the moment, but you should sometime after,” she said.
This is just a starting point on how to remain a dedicated, caring physician without burning out. “The system is pretty broken, and to survive it first means wanting to survive it,” Dr. Gold said. “There’s a lot of focus on resiliency and lack thereof if a physician expresses burnout, but that’s a false notion. Doctors are a resilient bunch but even they get burned out.”
Change for the better must come from several places. One is asking for help, something that can be hard for a group conditioned to keeping a stiff upper lip. “Just because your peers might look healthy (emotionally) doesn’t mean they are,” said Dr. Gold. “We’ve normalized this culture of burying feelings, but that doesn’t mean it’s right.”
Dr. Ben-Horin also advocates diversifying your work. This might include engaging in research and academics, for instance. “This not only makes you a better broad-perspective doctor but allows you to psychologically switch gears on research days,” he said.
The biggest place to make change, however, is within the health care system culture itself. The AMA created a series of recommendations to address burnout at the resident and fellow level, a good starting point to carry through into staff work. The steps include creating a well-being framework, gathering a team to support a well-being program, developing the program in a way to foster fun and connectivity among the staff, fostering individual well-being that addresses emotional and physical well-being, and confronting burnout and creating a sustainable culture of well-being.
On a personal level, it’s essential that physicians keep close tabs on themselves and peers. “Understand the signs and symptoms of burnout by taking stock of where you are emotionally,” said Dr. Gold. “Have a place and time at the end of a hard day to reflect or find a ritual that helps you and stay with it.”
You might also reach out to a therapist or a peer when you’re struggling. Having honest conversations with peers can go a long way. “Find a confidant that allows you to be vulnerable,” Dr. Gold recommended. “Acknowledge that this is hard and that you might need help taking care of yourself. The system needs to change, but we can also learn to survive in the meantime. You don’t have to be a sociopath to make it.”
A version of this article originally appeared on Medscape.com.
A frustrated physician recently voiced some strong words in Medscape’s US Physician Burnout & Depression Report: “Only a sociopath could work for a large health system and not be burned out. Anyone who cares about patients is doomed to burnout.”
Medscape’s report showed that 53% of physicians feel burned out by job requirements; 65% say that burnout has impacted their relationships, and other statistics say that physicians are leaving clinical medicine because of all this pressure.
What is it about being employed by large organizations that can be so negative? In another study, MEMO – Minimizing Error, Maximizing Outcomes – researchers at the University of Wisconsin surveyed more than 400 doctors to learn about how their working environments corresponded with medical errors. More than half of the physicians reported time pressures when conducting physical examinations. Nearly a third felt they needed at least 50% more time than was allotted for this patient care function, and nearly a quarter said they needed at least 50% more time for follow-up appointments.
Some have asked: Can anyone, then, thrive in today’s health care environment and avoid burnout?
Although the frustrated physician noted above may sardonically say that a doctor needs to be sociopathic to enjoy it – lacking in feelings for others – “It’s a very small number of doctors who get in it for the wrong reasons and therefore care about their own benefit and not their patients,” said psychiatrist Wendy Dean, MD, CEO and cofounder of Moral Injury of Healthcare, a nonprofit organization addressing workforce distress in health care. “Those are the outliers.”
The vast majority of physicians do care about their patients – deeply, said Dr. Dean. They struggle under the weight of the health care system and yet must find ways to get through. Today, thriving in an imperfect system requires honing new skills, asking for help when needed, and pushing for systemic and cultural change.
“We’ve been assessing and trying to address burnout for half a century,” said Dr. Dean. “Despite all the good intentions, and people dedicating their entire careers to solving the issue, we’ve barely made a dent.”
With the advent of new technological requirements on the job and more demands from increasingly larger health care organizations, the risk for burnout is higher than ever before. “There’s an increased burden of regulatory-mandated and cumbersome administrative workload per patient,” said Shomron Ben-Horin, MD, cofounder of Evinature. “Often the computer/paperwork before and after a procedure is much longer than the procedure itself.”
Meeting insurance requirements is increasingly cumbersome, too, and preauthorizations and debates with payers over medical approval may put physicians frustratingly in the middle.
“This increases the psychological burden for physicians who may feel responsible for wrongdoing no matter which option they deem better,” Dr. Ben-Horin said. “Add in physician accessibility around the clock via mobile phones, emails, and apps, and you end up on call even if you’re not officially on call.”
Why some physicians suffer more
Some physicians are more likely to suffer burnout than others, said Jessi Gold, MD, assistant professor in the department of psychiatry at Washington University in St. Louis. “The self-valuation concept comes into play here,” she said. “If you make a mistake, do you blame yourself or see it as a growth opportunity? If it’s the former, you’re more likely to burn out.”
Dr. Ben-Horin added that the most patient-centric doctors are the ones who struggle most. “These are the doctors we’d all love to have as a patient,” he said. “But they are burdened by the extra tasks of the job, and they are the most stressed by the environment.”
So too are those physicians who never master compartmentalizing their feelings and emotions. “We learn in training to compartmentalize our emotions,” said Dr. Dean. “You can’t allow yourself to get emotional while performing chest compressions on an 18-year-old kid. So you shut it all away; otherwise, you might lose the patient.”
This turn-off switch becomes automatic, but it also comes at a cost. “When doctors were interviewed about [Buffalo Bills player] Damar Hamlin going into cardiac arrest on the football field, they talked about how a life-and-death situation is so common that they have to put the emotions away, work on the patient, and move onto the next,” said Dr. Dean. “The next patient needs you just as much. We must lock away our feelings and manage the situation.”
Dr. Gold explained that burying feelings, however, is a symptom of burnout. “We have to remove ourselves from the situation to protect ourselves,” she said. “We can’t cry in these situations, but we can’t bury our feelings either.”
Instead, Dr. Gold suggested, a good medium may exist. “You may not be able to address them in the moment, but you should sometime after,” she said.
This is just a starting point on how to remain a dedicated, caring physician without burning out. “The system is pretty broken, and to survive it first means wanting to survive it,” Dr. Gold said. “There’s a lot of focus on resiliency and lack thereof if a physician expresses burnout, but that’s a false notion. Doctors are a resilient bunch but even they get burned out.”
Change for the better must come from several places. One is asking for help, something that can be hard for a group conditioned to keeping a stiff upper lip. “Just because your peers might look healthy (emotionally) doesn’t mean they are,” said Dr. Gold. “We’ve normalized this culture of burying feelings, but that doesn’t mean it’s right.”
Dr. Ben-Horin also advocates diversifying your work. This might include engaging in research and academics, for instance. “This not only makes you a better broad-perspective doctor but allows you to psychologically switch gears on research days,” he said.
The biggest place to make change, however, is within the health care system culture itself. The AMA created a series of recommendations to address burnout at the resident and fellow level, a good starting point to carry through into staff work. The steps include creating a well-being framework, gathering a team to support a well-being program, developing the program in a way to foster fun and connectivity among the staff, fostering individual well-being that addresses emotional and physical well-being, and confronting burnout and creating a sustainable culture of well-being.
On a personal level, it’s essential that physicians keep close tabs on themselves and peers. “Understand the signs and symptoms of burnout by taking stock of where you are emotionally,” said Dr. Gold. “Have a place and time at the end of a hard day to reflect or find a ritual that helps you and stay with it.”
You might also reach out to a therapist or a peer when you’re struggling. Having honest conversations with peers can go a long way. “Find a confidant that allows you to be vulnerable,” Dr. Gold recommended. “Acknowledge that this is hard and that you might need help taking care of yourself. The system needs to change, but we can also learn to survive in the meantime. You don’t have to be a sociopath to make it.”
A version of this article originally appeared on Medscape.com.
A frustrated physician recently voiced some strong words in Medscape’s US Physician Burnout & Depression Report: “Only a sociopath could work for a large health system and not be burned out. Anyone who cares about patients is doomed to burnout.”
Medscape’s report showed that 53% of physicians feel burned out by job requirements; 65% say that burnout has impacted their relationships, and other statistics say that physicians are leaving clinical medicine because of all this pressure.
What is it about being employed by large organizations that can be so negative? In another study, MEMO – Minimizing Error, Maximizing Outcomes – researchers at the University of Wisconsin surveyed more than 400 doctors to learn about how their working environments corresponded with medical errors. More than half of the physicians reported time pressures when conducting physical examinations. Nearly a third felt they needed at least 50% more time than was allotted for this patient care function, and nearly a quarter said they needed at least 50% more time for follow-up appointments.
Some have asked: Can anyone, then, thrive in today’s health care environment and avoid burnout?
Although the frustrated physician noted above may sardonically say that a doctor needs to be sociopathic to enjoy it – lacking in feelings for others – “It’s a very small number of doctors who get in it for the wrong reasons and therefore care about their own benefit and not their patients,” said psychiatrist Wendy Dean, MD, CEO and cofounder of Moral Injury of Healthcare, a nonprofit organization addressing workforce distress in health care. “Those are the outliers.”
The vast majority of physicians do care about their patients – deeply, said Dr. Dean. They struggle under the weight of the health care system and yet must find ways to get through. Today, thriving in an imperfect system requires honing new skills, asking for help when needed, and pushing for systemic and cultural change.
“We’ve been assessing and trying to address burnout for half a century,” said Dr. Dean. “Despite all the good intentions, and people dedicating their entire careers to solving the issue, we’ve barely made a dent.”
With the advent of new technological requirements on the job and more demands from increasingly larger health care organizations, the risk for burnout is higher than ever before. “There’s an increased burden of regulatory-mandated and cumbersome administrative workload per patient,” said Shomron Ben-Horin, MD, cofounder of Evinature. “Often the computer/paperwork before and after a procedure is much longer than the procedure itself.”
Meeting insurance requirements is increasingly cumbersome, too, and preauthorizations and debates with payers over medical approval may put physicians frustratingly in the middle.
“This increases the psychological burden for physicians who may feel responsible for wrongdoing no matter which option they deem better,” Dr. Ben-Horin said. “Add in physician accessibility around the clock via mobile phones, emails, and apps, and you end up on call even if you’re not officially on call.”
Why some physicians suffer more
Some physicians are more likely to suffer burnout than others, said Jessi Gold, MD, assistant professor in the department of psychiatry at Washington University in St. Louis. “The self-valuation concept comes into play here,” she said. “If you make a mistake, do you blame yourself or see it as a growth opportunity? If it’s the former, you’re more likely to burn out.”
Dr. Ben-Horin added that the most patient-centric doctors are the ones who struggle most. “These are the doctors we’d all love to have as a patient,” he said. “But they are burdened by the extra tasks of the job, and they are the most stressed by the environment.”
So too are those physicians who never master compartmentalizing their feelings and emotions. “We learn in training to compartmentalize our emotions,” said Dr. Dean. “You can’t allow yourself to get emotional while performing chest compressions on an 18-year-old kid. So you shut it all away; otherwise, you might lose the patient.”
This turn-off switch becomes automatic, but it also comes at a cost. “When doctors were interviewed about [Buffalo Bills player] Damar Hamlin going into cardiac arrest on the football field, they talked about how a life-and-death situation is so common that they have to put the emotions away, work on the patient, and move onto the next,” said Dr. Dean. “The next patient needs you just as much. We must lock away our feelings and manage the situation.”
Dr. Gold explained that burying feelings, however, is a symptom of burnout. “We have to remove ourselves from the situation to protect ourselves,” she said. “We can’t cry in these situations, but we can’t bury our feelings either.”
Instead, Dr. Gold suggested, a good medium may exist. “You may not be able to address them in the moment, but you should sometime after,” she said.
This is just a starting point on how to remain a dedicated, caring physician without burning out. “The system is pretty broken, and to survive it first means wanting to survive it,” Dr. Gold said. “There’s a lot of focus on resiliency and lack thereof if a physician expresses burnout, but that’s a false notion. Doctors are a resilient bunch but even they get burned out.”
Change for the better must come from several places. One is asking for help, something that can be hard for a group conditioned to keeping a stiff upper lip. “Just because your peers might look healthy (emotionally) doesn’t mean they are,” said Dr. Gold. “We’ve normalized this culture of burying feelings, but that doesn’t mean it’s right.”
Dr. Ben-Horin also advocates diversifying your work. This might include engaging in research and academics, for instance. “This not only makes you a better broad-perspective doctor but allows you to psychologically switch gears on research days,” he said.
The biggest place to make change, however, is within the health care system culture itself. The AMA created a series of recommendations to address burnout at the resident and fellow level, a good starting point to carry through into staff work. The steps include creating a well-being framework, gathering a team to support a well-being program, developing the program in a way to foster fun and connectivity among the staff, fostering individual well-being that addresses emotional and physical well-being, and confronting burnout and creating a sustainable culture of well-being.
On a personal level, it’s essential that physicians keep close tabs on themselves and peers. “Understand the signs and symptoms of burnout by taking stock of where you are emotionally,” said Dr. Gold. “Have a place and time at the end of a hard day to reflect or find a ritual that helps you and stay with it.”
You might also reach out to a therapist or a peer when you’re struggling. Having honest conversations with peers can go a long way. “Find a confidant that allows you to be vulnerable,” Dr. Gold recommended. “Acknowledge that this is hard and that you might need help taking care of yourself. The system needs to change, but we can also learn to survive in the meantime. You don’t have to be a sociopath to make it.”
A version of this article originally appeared on Medscape.com.
Not always implemented or enforced: Harassment policies at work
Many companies, government agencies, and organizations have implemented policies and procedures to shield employees from sexual and other forms of harassment. The U.S. Department of Health & Human Services and the American Medical Association are just two examples.
Employers can tap a rich lode of guidance and resources to craft these antiharassment policies. The National Institutes of Health’s resource page is a good site for hospitals to check out.
But how effective have official policies proved in deterring harassment in medical workplaces? After all, in a study by the American Association of Medical Colleges, 34% of female faculty said they had experienced sexual harassment irrespective of such policies. And in a recent Medscape survey of more than 3,000 physicians, 27% reported that they had either witnessed or been subjected to sexual harassment or misconduct at work during the past 4 years.
When policies are absent or unenforced
She believes employer rules and policies generally are helpful in establishing who fields harassment complaints and in creating at least some accountability.
On the other hand, policies that don’t recognize anonymous complaints effectively discourage harassment victims from coming forward, Dr. Rohr-Kirchgraber argues. Even those policies that do allow anonymous complaints may have limitations.
For example, the NIH policy on reporting harassment acknowledges that “officials must follow up on all allegations of harassment and cannot guarantee that your identity will not become apparent during the process. Please note that if you remain anonymous, key details about the allegation or concern [may] be omitted. This will limit the NIH’s ability to conduct an inquiry and take corrective action as warranted.”
Risks in pressing a harassment case
A complainant whose name becomes public risks getting a reputation as a problem employee or suffering workplace retaliation, according to Dr. Rohr-Kirchgraber. She recalls a colleague who was on a clinical education track until she lodged a harassment complaint. Abruptly, she was told she was needed on a service with fewer teaching opportunities.
With such risks in mind, respondents to the Medscape survey advised employees in medical workplaces to familiarize themselves with policies and procedures before pressing a case.
“Document everything,” an ophthalmologist urged, including time, place, offender, and witnesses. Present that information to your supervisor, and if nothing is done, hire a lawyer, a gastroenterologist suggested.
But taking the situation to the Equal Employment Opportunity Commission can be complicated, Roberta Gebhard, DO, past AMWA president and founder of its Gender Equity Task Force, told this news organization.
“They talk to the employer and get the employer’s side of the story and eventually render a decision about whether you have a case you can put through and file a lawsuit,” she said. “I don’t know of any other situation in which you need ‘permission’ to file a lawsuit.”
Nevertheless, an attorney can be helpful with cases, and when someone is terminated, a lawyer can possibly have it overturned or converted to a resignation, Dr. Gebhard said.
“And always have a lawyer review your contract before you take the job,” she advised. The lawyer might adjust the contract’s verbiage in ways that can protect one down the road in the event of a potential termination. “It’s money very well spent.”
More education needed
Dr. Rohr-Kirchgraber said that protection against harassment goes beyond the employer’s policies and procedures. Building an overall consciousness of what harassment is should begin with employee onboarding, she said.
“The harasser may not even recognize that what they’re doing or saying is a form of harassment, so we need better education,” Dr. Rohr-Kirchgraber emphasized.
A version of this article originally appeared on Medscape.com.
Many companies, government agencies, and organizations have implemented policies and procedures to shield employees from sexual and other forms of harassment. The U.S. Department of Health & Human Services and the American Medical Association are just two examples.
Employers can tap a rich lode of guidance and resources to craft these antiharassment policies. The National Institutes of Health’s resource page is a good site for hospitals to check out.
But how effective have official policies proved in deterring harassment in medical workplaces? After all, in a study by the American Association of Medical Colleges, 34% of female faculty said they had experienced sexual harassment irrespective of such policies. And in a recent Medscape survey of more than 3,000 physicians, 27% reported that they had either witnessed or been subjected to sexual harassment or misconduct at work during the past 4 years.
When policies are absent or unenforced
She believes employer rules and policies generally are helpful in establishing who fields harassment complaints and in creating at least some accountability.
On the other hand, policies that don’t recognize anonymous complaints effectively discourage harassment victims from coming forward, Dr. Rohr-Kirchgraber argues. Even those policies that do allow anonymous complaints may have limitations.
For example, the NIH policy on reporting harassment acknowledges that “officials must follow up on all allegations of harassment and cannot guarantee that your identity will not become apparent during the process. Please note that if you remain anonymous, key details about the allegation or concern [may] be omitted. This will limit the NIH’s ability to conduct an inquiry and take corrective action as warranted.”
Risks in pressing a harassment case
A complainant whose name becomes public risks getting a reputation as a problem employee or suffering workplace retaliation, according to Dr. Rohr-Kirchgraber. She recalls a colleague who was on a clinical education track until she lodged a harassment complaint. Abruptly, she was told she was needed on a service with fewer teaching opportunities.
With such risks in mind, respondents to the Medscape survey advised employees in medical workplaces to familiarize themselves with policies and procedures before pressing a case.
“Document everything,” an ophthalmologist urged, including time, place, offender, and witnesses. Present that information to your supervisor, and if nothing is done, hire a lawyer, a gastroenterologist suggested.
But taking the situation to the Equal Employment Opportunity Commission can be complicated, Roberta Gebhard, DO, past AMWA president and founder of its Gender Equity Task Force, told this news organization.
“They talk to the employer and get the employer’s side of the story and eventually render a decision about whether you have a case you can put through and file a lawsuit,” she said. “I don’t know of any other situation in which you need ‘permission’ to file a lawsuit.”
Nevertheless, an attorney can be helpful with cases, and when someone is terminated, a lawyer can possibly have it overturned or converted to a resignation, Dr. Gebhard said.
“And always have a lawyer review your contract before you take the job,” she advised. The lawyer might adjust the contract’s verbiage in ways that can protect one down the road in the event of a potential termination. “It’s money very well spent.”
More education needed
Dr. Rohr-Kirchgraber said that protection against harassment goes beyond the employer’s policies and procedures. Building an overall consciousness of what harassment is should begin with employee onboarding, she said.
“The harasser may not even recognize that what they’re doing or saying is a form of harassment, so we need better education,” Dr. Rohr-Kirchgraber emphasized.
A version of this article originally appeared on Medscape.com.
Many companies, government agencies, and organizations have implemented policies and procedures to shield employees from sexual and other forms of harassment. The U.S. Department of Health & Human Services and the American Medical Association are just two examples.
Employers can tap a rich lode of guidance and resources to craft these antiharassment policies. The National Institutes of Health’s resource page is a good site for hospitals to check out.
But how effective have official policies proved in deterring harassment in medical workplaces? After all, in a study by the American Association of Medical Colleges, 34% of female faculty said they had experienced sexual harassment irrespective of such policies. And in a recent Medscape survey of more than 3,000 physicians, 27% reported that they had either witnessed or been subjected to sexual harassment or misconduct at work during the past 4 years.
When policies are absent or unenforced
She believes employer rules and policies generally are helpful in establishing who fields harassment complaints and in creating at least some accountability.
On the other hand, policies that don’t recognize anonymous complaints effectively discourage harassment victims from coming forward, Dr. Rohr-Kirchgraber argues. Even those policies that do allow anonymous complaints may have limitations.
For example, the NIH policy on reporting harassment acknowledges that “officials must follow up on all allegations of harassment and cannot guarantee that your identity will not become apparent during the process. Please note that if you remain anonymous, key details about the allegation or concern [may] be omitted. This will limit the NIH’s ability to conduct an inquiry and take corrective action as warranted.”
Risks in pressing a harassment case
A complainant whose name becomes public risks getting a reputation as a problem employee or suffering workplace retaliation, according to Dr. Rohr-Kirchgraber. She recalls a colleague who was on a clinical education track until she lodged a harassment complaint. Abruptly, she was told she was needed on a service with fewer teaching opportunities.
With such risks in mind, respondents to the Medscape survey advised employees in medical workplaces to familiarize themselves with policies and procedures before pressing a case.
“Document everything,” an ophthalmologist urged, including time, place, offender, and witnesses. Present that information to your supervisor, and if nothing is done, hire a lawyer, a gastroenterologist suggested.
But taking the situation to the Equal Employment Opportunity Commission can be complicated, Roberta Gebhard, DO, past AMWA president and founder of its Gender Equity Task Force, told this news organization.
“They talk to the employer and get the employer’s side of the story and eventually render a decision about whether you have a case you can put through and file a lawsuit,” she said. “I don’t know of any other situation in which you need ‘permission’ to file a lawsuit.”
Nevertheless, an attorney can be helpful with cases, and when someone is terminated, a lawyer can possibly have it overturned or converted to a resignation, Dr. Gebhard said.
“And always have a lawyer review your contract before you take the job,” she advised. The lawyer might adjust the contract’s verbiage in ways that can protect one down the road in the event of a potential termination. “It’s money very well spent.”
More education needed
Dr. Rohr-Kirchgraber said that protection against harassment goes beyond the employer’s policies and procedures. Building an overall consciousness of what harassment is should begin with employee onboarding, she said.
“The harasser may not even recognize that what they’re doing or saying is a form of harassment, so we need better education,” Dr. Rohr-Kirchgraber emphasized.
A version of this article originally appeared on Medscape.com.
Immunodeficiencies tied to psychiatric disorders in offspring
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.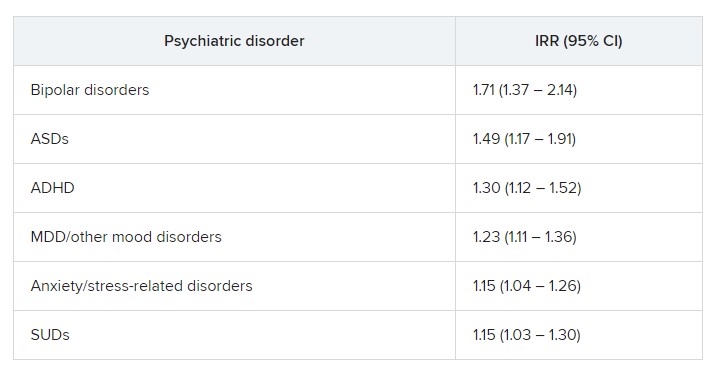
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM JAMA PSYCHIATRY
Slowing, not stopping, Alzheimer’s a better goal for clinical trials?
and may be a more realistic goal for clinical AD drug trials, a new report suggests.
The report is a yearlong undertaking by an expert work group convened by the Alzheimer’s Association and was prompted, in part, by the fallout from the U.S. Food and Drug Administration’s controversial decision to grant aducanumab (Aduhelm) accelerated approval, which came over the objection of an advisory panel that found the drug was ineffective.
The report’s authors call for a “reframing” of how researchers define “clinically meaningful” in randomized controlled trials (RCTs), noting that it’s time to adjust expectations of outcomes from relatively short clinical trials.
“Without lowering the bar, are we expecting too much from a clinical trial by expecting that unless the disease is halted in its tracks and there’s no progression, we failed at treatment?” the report’s lead author and group leader Ronald C. Petersen, MD, PhD, lead author, chair of the work group, and professor of neurology at the Mayo Clinic, Rochester, Minn., told this news organization.
Interpretations of clinical meaningfulness are used in the drug approval process and in decisions about whether an insurer will cover the cost of treatment, the authors note.
While the report doesn’t provide a consensus definition of clinically meaningful benefit, it does offer a starting point for a conversation about how the phrase should be defined in the context of RCTs for disease-modifying therapies (DMTs) in AD, Dr. Petersen said.
“What we tried to do was to put it into some kind of perspective and at least have people reflect on this: If you’re going to design the perfect drug trial in Alzheimer’s disease, what would it be? We wanted to get people to think about it without digging in their heels for or against,” he added.
The report was published online in Alzheimer’s and Dementia: The Journal of the Alzheimer’s Association.
A proactive measure
The expert group began its work in January 2022, less than a year after the FDA approved aducanumab. Since the panel began its work, the FDA has approved a second AD drug, lecanemab (Leqembi), and denied accelerated approval of a third medication, donanemab.
“At the time we started this group, we had one approved treatment, and we just knew that there were others on the way, and we needed to be prepared to have this conversation and be more proactive than reactive,” Christopher Weber, PhD, director of global science initiatives for the Alzheimer’s Association and co-author of the report, said in an interview.
The work group suggests that simply slowing disease progression might be a desired goal for drug trials, especially early on, before cognition and memory are affected.
They also note that a benefit identified during an 18-month clinical trial may ultimately lead to even more meaningful changes over coming years, well beyond the trial’s end.
In addition, the report authors call for the development of better research tools to more accurately assess meaningful change. The Clinical Dementia Rating (CDR) scale is currently the key instrument used as a primary outcome measure in RCTs. However, the report’s authors note that it may not be adequate to measure meaningful change in early-stage disease.
“Developing better tools certainly should be on the radar screen for all of us, because I think we can do better,” Dr. Petersen said. “The CDR, as good as it is and as long as it’s been used in the field, is a pretty blunt instrument, and it’s the result of subjective ratings.”
‘Quality of mind’
Jason Karlawish, MD, professor of medicine, medical ethics, health policy, and neurology at the University of Pennsylvania, Philadelphia, said measuring the actual impact of a drug on a patient’s disease and quality of life has been a hot topic in the AD field for some time, but settling on a definition of “clinically meaningful” that everyone agrees upon will be a challenge.
“I think the idea of ‘clinically meaningful’ is truly a socially constructed idea,” said Dr. Karlawish, co-director of Penn’s Memory Center, who did not work on the report.
“You can come up with objective measures of cognition, but a measure to call something ‘clinically meaningful’ ultimately requires some sort of negotiated social order among clinicians and patients and others who have immediate interest in the health and well-being of the patient.”
Dr. Karlawish added that he’s interested in the conversations the report might prompt and the challenges it could highlight, especially when it comes to how meaningful clinical benefit can be measured, regardless of how it’s defined.
“Hidden in this conversation about clinically meaningful treatments in Alzheimer’s disease is, frankly, not quality of life, but quality of mind,” said Dr. Karlawish. “No measure captures acceptably the very thing that everyone actually cares a lot about and why we view this disease as so dreadful, which is damage to our mind.”
More evidence needed
The development of such tools will take time. What does that mean for drugs already in the pipeline? Members of the work group argue that those trials must move forward at the same time new tools are being created.
“We need to continue to refine, develop better instruments, [and] develop tools that are going to assess the disease in its more subtle features early on, even in the so-called ‘pre-symptomatic’ stage of the disease,” said lead author Dr. Petersen. “We shouldn’t wait for the development of that before intervening if we have a drug that seems to work.”
However, not everyone who agrees with the premise of the report agrees with this position, including Joel S. Perlmutter, MD, professor of neurology, Washington University School of Medicine, St. Louis, who also commented on the report.
As reported by this news organization, Dr. Perlmutter was one of three physicians who resigned from the FDA advisory panel that voted against approving aducanumab after the agency moved forward anyway.
“We have to be careful not to recommend DMTs that we hope will help without strong evidence, especially when potential side effects are not trivial,” Dr. Perlmutter said. “We have to have evidence before making these recommendations so we don’t end up harming people more than helping them.”
The report received no specific funding. Dr. Petersen received consulting fees from Roche, Nestle, Merck, Biogen, Eisai, and Genentech. Full disclosures are included in the original article. Dr. Perlmutter and Dr. Karlawish report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
and may be a more realistic goal for clinical AD drug trials, a new report suggests.
The report is a yearlong undertaking by an expert work group convened by the Alzheimer’s Association and was prompted, in part, by the fallout from the U.S. Food and Drug Administration’s controversial decision to grant aducanumab (Aduhelm) accelerated approval, which came over the objection of an advisory panel that found the drug was ineffective.
The report’s authors call for a “reframing” of how researchers define “clinically meaningful” in randomized controlled trials (RCTs), noting that it’s time to adjust expectations of outcomes from relatively short clinical trials.
“Without lowering the bar, are we expecting too much from a clinical trial by expecting that unless the disease is halted in its tracks and there’s no progression, we failed at treatment?” the report’s lead author and group leader Ronald C. Petersen, MD, PhD, lead author, chair of the work group, and professor of neurology at the Mayo Clinic, Rochester, Minn., told this news organization.
Interpretations of clinical meaningfulness are used in the drug approval process and in decisions about whether an insurer will cover the cost of treatment, the authors note.
While the report doesn’t provide a consensus definition of clinically meaningful benefit, it does offer a starting point for a conversation about how the phrase should be defined in the context of RCTs for disease-modifying therapies (DMTs) in AD, Dr. Petersen said.
“What we tried to do was to put it into some kind of perspective and at least have people reflect on this: If you’re going to design the perfect drug trial in Alzheimer’s disease, what would it be? We wanted to get people to think about it without digging in their heels for or against,” he added.
The report was published online in Alzheimer’s and Dementia: The Journal of the Alzheimer’s Association.
A proactive measure
The expert group began its work in January 2022, less than a year after the FDA approved aducanumab. Since the panel began its work, the FDA has approved a second AD drug, lecanemab (Leqembi), and denied accelerated approval of a third medication, donanemab.
“At the time we started this group, we had one approved treatment, and we just knew that there were others on the way, and we needed to be prepared to have this conversation and be more proactive than reactive,” Christopher Weber, PhD, director of global science initiatives for the Alzheimer’s Association and co-author of the report, said in an interview.
The work group suggests that simply slowing disease progression might be a desired goal for drug trials, especially early on, before cognition and memory are affected.
They also note that a benefit identified during an 18-month clinical trial may ultimately lead to even more meaningful changes over coming years, well beyond the trial’s end.
In addition, the report authors call for the development of better research tools to more accurately assess meaningful change. The Clinical Dementia Rating (CDR) scale is currently the key instrument used as a primary outcome measure in RCTs. However, the report’s authors note that it may not be adequate to measure meaningful change in early-stage disease.
“Developing better tools certainly should be on the radar screen for all of us, because I think we can do better,” Dr. Petersen said. “The CDR, as good as it is and as long as it’s been used in the field, is a pretty blunt instrument, and it’s the result of subjective ratings.”
‘Quality of mind’
Jason Karlawish, MD, professor of medicine, medical ethics, health policy, and neurology at the University of Pennsylvania, Philadelphia, said measuring the actual impact of a drug on a patient’s disease and quality of life has been a hot topic in the AD field for some time, but settling on a definition of “clinically meaningful” that everyone agrees upon will be a challenge.
“I think the idea of ‘clinically meaningful’ is truly a socially constructed idea,” said Dr. Karlawish, co-director of Penn’s Memory Center, who did not work on the report.
“You can come up with objective measures of cognition, but a measure to call something ‘clinically meaningful’ ultimately requires some sort of negotiated social order among clinicians and patients and others who have immediate interest in the health and well-being of the patient.”
Dr. Karlawish added that he’s interested in the conversations the report might prompt and the challenges it could highlight, especially when it comes to how meaningful clinical benefit can be measured, regardless of how it’s defined.
“Hidden in this conversation about clinically meaningful treatments in Alzheimer’s disease is, frankly, not quality of life, but quality of mind,” said Dr. Karlawish. “No measure captures acceptably the very thing that everyone actually cares a lot about and why we view this disease as so dreadful, which is damage to our mind.”
More evidence needed
The development of such tools will take time. What does that mean for drugs already in the pipeline? Members of the work group argue that those trials must move forward at the same time new tools are being created.
“We need to continue to refine, develop better instruments, [and] develop tools that are going to assess the disease in its more subtle features early on, even in the so-called ‘pre-symptomatic’ stage of the disease,” said lead author Dr. Petersen. “We shouldn’t wait for the development of that before intervening if we have a drug that seems to work.”
However, not everyone who agrees with the premise of the report agrees with this position, including Joel S. Perlmutter, MD, professor of neurology, Washington University School of Medicine, St. Louis, who also commented on the report.
As reported by this news organization, Dr. Perlmutter was one of three physicians who resigned from the FDA advisory panel that voted against approving aducanumab after the agency moved forward anyway.
“We have to be careful not to recommend DMTs that we hope will help without strong evidence, especially when potential side effects are not trivial,” Dr. Perlmutter said. “We have to have evidence before making these recommendations so we don’t end up harming people more than helping them.”
The report received no specific funding. Dr. Petersen received consulting fees from Roche, Nestle, Merck, Biogen, Eisai, and Genentech. Full disclosures are included in the original article. Dr. Perlmutter and Dr. Karlawish report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
and may be a more realistic goal for clinical AD drug trials, a new report suggests.
The report is a yearlong undertaking by an expert work group convened by the Alzheimer’s Association and was prompted, in part, by the fallout from the U.S. Food and Drug Administration’s controversial decision to grant aducanumab (Aduhelm) accelerated approval, which came over the objection of an advisory panel that found the drug was ineffective.
The report’s authors call for a “reframing” of how researchers define “clinically meaningful” in randomized controlled trials (RCTs), noting that it’s time to adjust expectations of outcomes from relatively short clinical trials.
“Without lowering the bar, are we expecting too much from a clinical trial by expecting that unless the disease is halted in its tracks and there’s no progression, we failed at treatment?” the report’s lead author and group leader Ronald C. Petersen, MD, PhD, lead author, chair of the work group, and professor of neurology at the Mayo Clinic, Rochester, Minn., told this news organization.
Interpretations of clinical meaningfulness are used in the drug approval process and in decisions about whether an insurer will cover the cost of treatment, the authors note.
While the report doesn’t provide a consensus definition of clinically meaningful benefit, it does offer a starting point for a conversation about how the phrase should be defined in the context of RCTs for disease-modifying therapies (DMTs) in AD, Dr. Petersen said.
“What we tried to do was to put it into some kind of perspective and at least have people reflect on this: If you’re going to design the perfect drug trial in Alzheimer’s disease, what would it be? We wanted to get people to think about it without digging in their heels for or against,” he added.
The report was published online in Alzheimer’s and Dementia: The Journal of the Alzheimer’s Association.
A proactive measure
The expert group began its work in January 2022, less than a year after the FDA approved aducanumab. Since the panel began its work, the FDA has approved a second AD drug, lecanemab (Leqembi), and denied accelerated approval of a third medication, donanemab.
“At the time we started this group, we had one approved treatment, and we just knew that there were others on the way, and we needed to be prepared to have this conversation and be more proactive than reactive,” Christopher Weber, PhD, director of global science initiatives for the Alzheimer’s Association and co-author of the report, said in an interview.
The work group suggests that simply slowing disease progression might be a desired goal for drug trials, especially early on, before cognition and memory are affected.
They also note that a benefit identified during an 18-month clinical trial may ultimately lead to even more meaningful changes over coming years, well beyond the trial’s end.
In addition, the report authors call for the development of better research tools to more accurately assess meaningful change. The Clinical Dementia Rating (CDR) scale is currently the key instrument used as a primary outcome measure in RCTs. However, the report’s authors note that it may not be adequate to measure meaningful change in early-stage disease.
“Developing better tools certainly should be on the radar screen for all of us, because I think we can do better,” Dr. Petersen said. “The CDR, as good as it is and as long as it’s been used in the field, is a pretty blunt instrument, and it’s the result of subjective ratings.”
‘Quality of mind’
Jason Karlawish, MD, professor of medicine, medical ethics, health policy, and neurology at the University of Pennsylvania, Philadelphia, said measuring the actual impact of a drug on a patient’s disease and quality of life has been a hot topic in the AD field for some time, but settling on a definition of “clinically meaningful” that everyone agrees upon will be a challenge.
“I think the idea of ‘clinically meaningful’ is truly a socially constructed idea,” said Dr. Karlawish, co-director of Penn’s Memory Center, who did not work on the report.
“You can come up with objective measures of cognition, but a measure to call something ‘clinically meaningful’ ultimately requires some sort of negotiated social order among clinicians and patients and others who have immediate interest in the health and well-being of the patient.”
Dr. Karlawish added that he’s interested in the conversations the report might prompt and the challenges it could highlight, especially when it comes to how meaningful clinical benefit can be measured, regardless of how it’s defined.
“Hidden in this conversation about clinically meaningful treatments in Alzheimer’s disease is, frankly, not quality of life, but quality of mind,” said Dr. Karlawish. “No measure captures acceptably the very thing that everyone actually cares a lot about and why we view this disease as so dreadful, which is damage to our mind.”
More evidence needed
The development of such tools will take time. What does that mean for drugs already in the pipeline? Members of the work group argue that those trials must move forward at the same time new tools are being created.
“We need to continue to refine, develop better instruments, [and] develop tools that are going to assess the disease in its more subtle features early on, even in the so-called ‘pre-symptomatic’ stage of the disease,” said lead author Dr. Petersen. “We shouldn’t wait for the development of that before intervening if we have a drug that seems to work.”
However, not everyone who agrees with the premise of the report agrees with this position, including Joel S. Perlmutter, MD, professor of neurology, Washington University School of Medicine, St. Louis, who also commented on the report.
As reported by this news organization, Dr. Perlmutter was one of three physicians who resigned from the FDA advisory panel that voted against approving aducanumab after the agency moved forward anyway.
“We have to be careful not to recommend DMTs that we hope will help without strong evidence, especially when potential side effects are not trivial,” Dr. Perlmutter said. “We have to have evidence before making these recommendations so we don’t end up harming people more than helping them.”
The report received no specific funding. Dr. Petersen received consulting fees from Roche, Nestle, Merck, Biogen, Eisai, and Genentech. Full disclosures are included in the original article. Dr. Perlmutter and Dr. Karlawish report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ALZHEIMER’S AND DEMENTIA
Novel celery seed–derived drug may improve stroke outcomes
a new report suggests.
Patients treated with butylphthalide had fewer severe neurologic symptoms and better function 90 days after the stroke, compared with those receiving placebo.
Butylphthalide is approved and available for use in China, where the study was conducted. However, the medication hasn’t been approved for use by the U.S. Food and Drug Administration.
“Patients who received butylphthalide had less severe neurological symptoms and a better living status at 90 days post stroke, compared to those who received the placebo,” said coauthor Baixue Jia, MD, an attending physician in interventional neuroradiology at the Beijing Tiantan Hospital of Capital Medical University and a faculty member at the China National Clinical Research Center for Neurological Diseases in Beijing. “If the results are confirmed in other trials, this may lead to more options to treat strokes caused by clots.”
The study was presented at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Studying stroke outcomes
The researchers described butylphthalide as a cerebroprotective drug that was originally extracted from seeds of Apium graveolens. In China, previous studies have shown that the drug has cerebroprotective effects in animal models of ischemia-reperfusion, they noted.
In this randomized, double-blind, placebo-controlled trial, Dr. Jia and colleagues evaluated whether treatment with butylphthalide could improve 90-day outcomes for adults with acute ischemic stroke who received intravenous recombinant tissue plasminogen activator (tPA), endovascular treatment, or both.
The participants were treated at one of 59 medical centers in China between July 2018 and February 2022. Those who had minimal stroke symptoms on their initial exam, defined as a score of 0-3 on the National Institutes of Health Stroke Scale, or had severe stroke symptoms, defined as having a score of 26 or higher on the NIHSS, were excluded from the study.
Along with an initial revascularization intervention chosen by their physician, participants were randomly selected to receive either butylphthalide or a placebo daily for 90 days. The drug was administered through daily intravenous injections for the first 14 days, after which patients received oral capsules for 76 days.
The research team defined the outcomes as “favorable” if a patient fell into one of the following categories 90 days after the stroke: an initially mild to moderate stroke (NIHSS, 4-7) and no symptoms after treatment, defined as a score of 0 on the Modified Rankin Scale (mRS), which measures disability and dependence; an initially moderate to serious stroke (NIHSS, 8-14) and no residual symptoms or mild symptoms that don’t impair the ability to perform routine activities of daily living without assistance (mRS, 0-1); or an initially serious to severe stroke (NIHSS, 15-25) and no remaining symptoms or a slight disability that impairs some activities but allows one to conduct daily living without assistance (mRS, 0-2).
Secondary outcomes included symptomatic intracranial hemorrhage, recurrent stroke, and mortality.
Among the 1,216 participants, 607 were assigned to the treatment group, and 609 were assigned to the placebo group. The average age was 66 years, and 68% were men.
Overall, participants in the butylphthalide group were 70% more likely to have a favorable 90-day outcome, compared with the placebo group. Favorable outcomes occurred in 344 patients (56.7%) in the butylphthalide group, compared with 268 patients (44%) in the placebo group (odds ratio, 1.70; 95% confidence interval, 1.35-2.14; P < .001).
In addition, butylphthalide improved function equally well for the patients who initially received tPA, those who received endovascular treatment, and those who received both tPA and endovascular treatment.
Secondary events, such as recurrent stroke and intracranial hemorrhage, weren’t significantly different between the butylphthalide and placebo groups.
Ongoing questions
Dr. Jia and colleagues noted the need to understand how butylphthalide works in the brain. Animal studies have suggested several possible mechanisms, but it remains unclear.
“The next step should be investigating the exact mechanisms of butylphthalide in humans,” Dr. Jia said.
Additional research should assess the medication in other populations, the authors noted, particularly because the study involved participants who received initial treatment with tPA, endovascular treatment, or both. The results may not be generalizable to stroke patients who receive other treatments or to populations outside of China.
“While these are interesting results, this is only one relatively small study on a fairly select population in China. Butylphthalide, a medication initially compounded from celery seed, is not ready for use in standard stroke treatment,” said Daniel Lackland, DrPH, professor of neurology and director of the division of translational neurosciences and population studies at the Medical University of South Carolina, Charleston.
Dr. Lackland, who wasn’t involved with the study, is a member of the American Stroke Association’s Stroke Council. Although butylphthalide was originally extracted from seeds, he noted, it’s not what patients would find commercially available.
“The medication used in this study is not the same as celery seed or celery seed extract supplements,” he said. “Stroke survivors should always consult with their neurologist or healthcare professional regarding diet after a stroke.”
The study was funded by the National Key Technology Research and Development Program of the Ministry of Science and Technology of the People’s Republic of China and Shijiazhuang Pharmaceutical Group dl-3-butylphthalide Pharmaceutical. Several authors are employed with Beijing Tiantan Hospital and the Beijing Institute of Brain Disorders. Dr. Lackland reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new report suggests.
Patients treated with butylphthalide had fewer severe neurologic symptoms and better function 90 days after the stroke, compared with those receiving placebo.
Butylphthalide is approved and available for use in China, where the study was conducted. However, the medication hasn’t been approved for use by the U.S. Food and Drug Administration.
“Patients who received butylphthalide had less severe neurological symptoms and a better living status at 90 days post stroke, compared to those who received the placebo,” said coauthor Baixue Jia, MD, an attending physician in interventional neuroradiology at the Beijing Tiantan Hospital of Capital Medical University and a faculty member at the China National Clinical Research Center for Neurological Diseases in Beijing. “If the results are confirmed in other trials, this may lead to more options to treat strokes caused by clots.”
The study was presented at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Studying stroke outcomes
The researchers described butylphthalide as a cerebroprotective drug that was originally extracted from seeds of Apium graveolens. In China, previous studies have shown that the drug has cerebroprotective effects in animal models of ischemia-reperfusion, they noted.
In this randomized, double-blind, placebo-controlled trial, Dr. Jia and colleagues evaluated whether treatment with butylphthalide could improve 90-day outcomes for adults with acute ischemic stroke who received intravenous recombinant tissue plasminogen activator (tPA), endovascular treatment, or both.
The participants were treated at one of 59 medical centers in China between July 2018 and February 2022. Those who had minimal stroke symptoms on their initial exam, defined as a score of 0-3 on the National Institutes of Health Stroke Scale, or had severe stroke symptoms, defined as having a score of 26 or higher on the NIHSS, were excluded from the study.
Along with an initial revascularization intervention chosen by their physician, participants were randomly selected to receive either butylphthalide or a placebo daily for 90 days. The drug was administered through daily intravenous injections for the first 14 days, after which patients received oral capsules for 76 days.
The research team defined the outcomes as “favorable” if a patient fell into one of the following categories 90 days after the stroke: an initially mild to moderate stroke (NIHSS, 4-7) and no symptoms after treatment, defined as a score of 0 on the Modified Rankin Scale (mRS), which measures disability and dependence; an initially moderate to serious stroke (NIHSS, 8-14) and no residual symptoms or mild symptoms that don’t impair the ability to perform routine activities of daily living without assistance (mRS, 0-1); or an initially serious to severe stroke (NIHSS, 15-25) and no remaining symptoms or a slight disability that impairs some activities but allows one to conduct daily living without assistance (mRS, 0-2).
Secondary outcomes included symptomatic intracranial hemorrhage, recurrent stroke, and mortality.
Among the 1,216 participants, 607 were assigned to the treatment group, and 609 were assigned to the placebo group. The average age was 66 years, and 68% were men.
Overall, participants in the butylphthalide group were 70% more likely to have a favorable 90-day outcome, compared with the placebo group. Favorable outcomes occurred in 344 patients (56.7%) in the butylphthalide group, compared with 268 patients (44%) in the placebo group (odds ratio, 1.70; 95% confidence interval, 1.35-2.14; P < .001).
In addition, butylphthalide improved function equally well for the patients who initially received tPA, those who received endovascular treatment, and those who received both tPA and endovascular treatment.
Secondary events, such as recurrent stroke and intracranial hemorrhage, weren’t significantly different between the butylphthalide and placebo groups.
Ongoing questions
Dr. Jia and colleagues noted the need to understand how butylphthalide works in the brain. Animal studies have suggested several possible mechanisms, but it remains unclear.
“The next step should be investigating the exact mechanisms of butylphthalide in humans,” Dr. Jia said.
Additional research should assess the medication in other populations, the authors noted, particularly because the study involved participants who received initial treatment with tPA, endovascular treatment, or both. The results may not be generalizable to stroke patients who receive other treatments or to populations outside of China.
“While these are interesting results, this is only one relatively small study on a fairly select population in China. Butylphthalide, a medication initially compounded from celery seed, is not ready for use in standard stroke treatment,” said Daniel Lackland, DrPH, professor of neurology and director of the division of translational neurosciences and population studies at the Medical University of South Carolina, Charleston.
Dr. Lackland, who wasn’t involved with the study, is a member of the American Stroke Association’s Stroke Council. Although butylphthalide was originally extracted from seeds, he noted, it’s not what patients would find commercially available.
“The medication used in this study is not the same as celery seed or celery seed extract supplements,” he said. “Stroke survivors should always consult with their neurologist or healthcare professional regarding diet after a stroke.”
The study was funded by the National Key Technology Research and Development Program of the Ministry of Science and Technology of the People’s Republic of China and Shijiazhuang Pharmaceutical Group dl-3-butylphthalide Pharmaceutical. Several authors are employed with Beijing Tiantan Hospital and the Beijing Institute of Brain Disorders. Dr. Lackland reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new report suggests.
Patients treated with butylphthalide had fewer severe neurologic symptoms and better function 90 days after the stroke, compared with those receiving placebo.
Butylphthalide is approved and available for use in China, where the study was conducted. However, the medication hasn’t been approved for use by the U.S. Food and Drug Administration.
“Patients who received butylphthalide had less severe neurological symptoms and a better living status at 90 days post stroke, compared to those who received the placebo,” said coauthor Baixue Jia, MD, an attending physician in interventional neuroradiology at the Beijing Tiantan Hospital of Capital Medical University and a faculty member at the China National Clinical Research Center for Neurological Diseases in Beijing. “If the results are confirmed in other trials, this may lead to more options to treat strokes caused by clots.”
The study was presented at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Studying stroke outcomes
The researchers described butylphthalide as a cerebroprotective drug that was originally extracted from seeds of Apium graveolens. In China, previous studies have shown that the drug has cerebroprotective effects in animal models of ischemia-reperfusion, they noted.
In this randomized, double-blind, placebo-controlled trial, Dr. Jia and colleagues evaluated whether treatment with butylphthalide could improve 90-day outcomes for adults with acute ischemic stroke who received intravenous recombinant tissue plasminogen activator (tPA), endovascular treatment, or both.
The participants were treated at one of 59 medical centers in China between July 2018 and February 2022. Those who had minimal stroke symptoms on their initial exam, defined as a score of 0-3 on the National Institutes of Health Stroke Scale, or had severe stroke symptoms, defined as having a score of 26 or higher on the NIHSS, were excluded from the study.
Along with an initial revascularization intervention chosen by their physician, participants were randomly selected to receive either butylphthalide or a placebo daily for 90 days. The drug was administered through daily intravenous injections for the first 14 days, after which patients received oral capsules for 76 days.
The research team defined the outcomes as “favorable” if a patient fell into one of the following categories 90 days after the stroke: an initially mild to moderate stroke (NIHSS, 4-7) and no symptoms after treatment, defined as a score of 0 on the Modified Rankin Scale (mRS), which measures disability and dependence; an initially moderate to serious stroke (NIHSS, 8-14) and no residual symptoms or mild symptoms that don’t impair the ability to perform routine activities of daily living without assistance (mRS, 0-1); or an initially serious to severe stroke (NIHSS, 15-25) and no remaining symptoms or a slight disability that impairs some activities but allows one to conduct daily living without assistance (mRS, 0-2).
Secondary outcomes included symptomatic intracranial hemorrhage, recurrent stroke, and mortality.
Among the 1,216 participants, 607 were assigned to the treatment group, and 609 were assigned to the placebo group. The average age was 66 years, and 68% were men.
Overall, participants in the butylphthalide group were 70% more likely to have a favorable 90-day outcome, compared with the placebo group. Favorable outcomes occurred in 344 patients (56.7%) in the butylphthalide group, compared with 268 patients (44%) in the placebo group (odds ratio, 1.70; 95% confidence interval, 1.35-2.14; P < .001).
In addition, butylphthalide improved function equally well for the patients who initially received tPA, those who received endovascular treatment, and those who received both tPA and endovascular treatment.
Secondary events, such as recurrent stroke and intracranial hemorrhage, weren’t significantly different between the butylphthalide and placebo groups.
Ongoing questions
Dr. Jia and colleagues noted the need to understand how butylphthalide works in the brain. Animal studies have suggested several possible mechanisms, but it remains unclear.
“The next step should be investigating the exact mechanisms of butylphthalide in humans,” Dr. Jia said.
Additional research should assess the medication in other populations, the authors noted, particularly because the study involved participants who received initial treatment with tPA, endovascular treatment, or both. The results may not be generalizable to stroke patients who receive other treatments or to populations outside of China.
“While these are interesting results, this is only one relatively small study on a fairly select population in China. Butylphthalide, a medication initially compounded from celery seed, is not ready for use in standard stroke treatment,” said Daniel Lackland, DrPH, professor of neurology and director of the division of translational neurosciences and population studies at the Medical University of South Carolina, Charleston.
Dr. Lackland, who wasn’t involved with the study, is a member of the American Stroke Association’s Stroke Council. Although butylphthalide was originally extracted from seeds, he noted, it’s not what patients would find commercially available.
“The medication used in this study is not the same as celery seed or celery seed extract supplements,” he said. “Stroke survivors should always consult with their neurologist or healthcare professional regarding diet after a stroke.”
The study was funded by the National Key Technology Research and Development Program of the Ministry of Science and Technology of the People’s Republic of China and Shijiazhuang Pharmaceutical Group dl-3-butylphthalide Pharmaceutical. Several authors are employed with Beijing Tiantan Hospital and the Beijing Institute of Brain Disorders. Dr. Lackland reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
What’s new in brain health?
This transcript has been edited for clarity.
Dear colleagues, I am Christoph Diener from the medical faculty of the University of Duisburg-Essen in Germany.
Treatment of tension-type headache
I would like to start with headache. You are all aware that we have several new studies regarding the prevention of migraine, but very few studies involving nondrug treatments for tension-type headache.
A working group in Göttingen, Germany, conducted a study in people with frequent episodic and chronic tension-type headache. The first of the four randomized groups received traditional Chinese acupuncture for 3 months. The second group received physical therapy and exercise for 1 hour per week for 12 weeks. The third group received a combination of acupuncture and exercise. The last was a control group that received only standard care.
The outcome parameters of tension-type headache were evaluated after 6 months and again after 12 months. Previously, these same researchers published that the intensity but not the frequency of tension-type headache was reduced by active therapy.
In Cephalalgia, they published the outcome for the endpoints of depression, anxiety, and quality of life. Acupuncture, exercise, and the combination of the two improved depression, anxiety, and quality of life. This shows that nonmedical treatment is effective in people with frequent episodic and chronic tension-type headache.
Headache after COVID-19
The next study was published in Headache and discusses headache after COVID-19. In this review of published studies, more than 50% of people with COVID-19 develop headache. It is more frequent in young patients and people with preexisting primary headaches, such as migraine and tension-type headache. Prognosis is usually good, but some patients develop new, daily persistent headache, which is a major problem because treatment is unclear. We desperately need studies investigating how to treat this new, daily persistent headache after COVID-19.
SSRIs during COVID-19 infection
The next study also focuses on COVID-19. We have conflicting results from several studies suggesting that selective serotonin reuptake inhibitors might be effective in people with mild COVID-19 infection. This hypothesis was tested in a study in Brazil and was published in JAMA, The study included 1,288 outpatients with mild COVID-19 who either received 50 mg of fluvoxamine twice daily for 10 days or placebo. There was no benefit of the treatment for any outcome.
Preventing dementia with antihypertensive treatment
The next study was published in the European Heart Journal and addresses the question of whether effective antihypertensive treatment in elderly persons can prevent dementia. This is a meta-analysis of five placebo-controlled trials with more than 28,000 patients. The meta-analysis clearly shows that treating hypertension in elderly patients does prevent dementia. The benefit is higher if the blood pressure is lowered by a larger amount which also stays true for elderly patients. There is no negative impact of lowering blood pressure in this population.
Antiplatelet therapy
The next study was published in Stroke and reexamines whether resumption of antiplatelet therapy should be early or late in people who had an intracerebral hemorrhage while on antiplatelet therapy. In the Taiwanese Health Registry, this was studied in 1,584 patients. The researchers divided participants into groups based on whether antiplatelet therapy was resumed within 30 days or after 30 days. In 1 year, the rate of recurrent intracerebral hemorrhage was 3.2%. There was no difference whether antiplatelet therapy was resumed early or late.
Regular exercise in Parkinson’s disease
The final study is a review of nonmedical therapy. This meta-analysis of 19 randomized trials looked at the benefit of regular exercise in patients with Parkinson’s disease and depression. The analysis clearly showed that rigorous and moderate exercise improved depression in patients with Parkinson’s disease. This is very important because exercise improves not only the symptoms of Parkinson’s disease but also comorbid depression while presenting no serious adverse events or side effects.
Dr. Diener is a professor in the department of neurology at Stroke Center–Headache Center, University Duisburg-Essen, Germany. He disclosed ties with Abbott, Addex Pharma, Alder, Allergan, Almirall, Amgen, Autonomic Technology, AstraZeneca, Bayer Vital, Berlin Chemie, Bristol-Myers Squibb, Boehringer Ingelheim, Chordate, CoAxia, Corimmun, Covidien, Coherex, CoLucid, Daiichi Sankyo, D-Pharm, Electrocore, Fresenius, GlaxoSmithKline, Grunenthal, Janssen-Cilag, Labrys Biologics Lilly, La Roche, Lundbeck, 3M Medica, MSD, Medtronic, Menarini, MindFrame, Minster, Neuroscore, Neurobiological Technologies, Novartis, Novo Nordisk, Johnson & Johnson, Knoll, Paion, Parke-Davis, Pierre Fabre, Pfizer Inc, Schaper and Brummer, Sanofi-Aventis, Schering-Plough, Servier, Solvay, St. Jude, Talecris, Thrombogenics, WebMD Global, Weber and Weber, Wyeth, and Yamanouchi. Dr. Diener has served as editor of Aktuelle Neurologie, Arzneimitteltherapie, Kopfschmerz News, Stroke News, and the Treatment Guidelines of the German Neurological Society; as co-editor of Cephalalgia; and on the editorial board of The Lancet Neurology, Stroke, European Neurology, and Cerebrovascular Disorders. The department of neurology in Essen is supported by the German Research Council, the German Ministry of Education and Research, European Union, National Institutes of Health, Bertelsmann Foundation, and Heinz Nixdorf Foundation. Dr. Diener has no ownership interest and does not own stocks in any pharmaceutical company. A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Dear colleagues, I am Christoph Diener from the medical faculty of the University of Duisburg-Essen in Germany.
Treatment of tension-type headache
I would like to start with headache. You are all aware that we have several new studies regarding the prevention of migraine, but very few studies involving nondrug treatments for tension-type headache.
A working group in Göttingen, Germany, conducted a study in people with frequent episodic and chronic tension-type headache. The first of the four randomized groups received traditional Chinese acupuncture for 3 months. The second group received physical therapy and exercise for 1 hour per week for 12 weeks. The third group received a combination of acupuncture and exercise. The last was a control group that received only standard care.
The outcome parameters of tension-type headache were evaluated after 6 months and again after 12 months. Previously, these same researchers published that the intensity but not the frequency of tension-type headache was reduced by active therapy.
In Cephalalgia, they published the outcome for the endpoints of depression, anxiety, and quality of life. Acupuncture, exercise, and the combination of the two improved depression, anxiety, and quality of life. This shows that nonmedical treatment is effective in people with frequent episodic and chronic tension-type headache.
Headache after COVID-19
The next study was published in Headache and discusses headache after COVID-19. In this review of published studies, more than 50% of people with COVID-19 develop headache. It is more frequent in young patients and people with preexisting primary headaches, such as migraine and tension-type headache. Prognosis is usually good, but some patients develop new, daily persistent headache, which is a major problem because treatment is unclear. We desperately need studies investigating how to treat this new, daily persistent headache after COVID-19.
SSRIs during COVID-19 infection
The next study also focuses on COVID-19. We have conflicting results from several studies suggesting that selective serotonin reuptake inhibitors might be effective in people with mild COVID-19 infection. This hypothesis was tested in a study in Brazil and was published in JAMA, The study included 1,288 outpatients with mild COVID-19 who either received 50 mg of fluvoxamine twice daily for 10 days or placebo. There was no benefit of the treatment for any outcome.
Preventing dementia with antihypertensive treatment
The next study was published in the European Heart Journal and addresses the question of whether effective antihypertensive treatment in elderly persons can prevent dementia. This is a meta-analysis of five placebo-controlled trials with more than 28,000 patients. The meta-analysis clearly shows that treating hypertension in elderly patients does prevent dementia. The benefit is higher if the blood pressure is lowered by a larger amount which also stays true for elderly patients. There is no negative impact of lowering blood pressure in this population.
Antiplatelet therapy
The next study was published in Stroke and reexamines whether resumption of antiplatelet therapy should be early or late in people who had an intracerebral hemorrhage while on antiplatelet therapy. In the Taiwanese Health Registry, this was studied in 1,584 patients. The researchers divided participants into groups based on whether antiplatelet therapy was resumed within 30 days or after 30 days. In 1 year, the rate of recurrent intracerebral hemorrhage was 3.2%. There was no difference whether antiplatelet therapy was resumed early or late.
Regular exercise in Parkinson’s disease
The final study is a review of nonmedical therapy. This meta-analysis of 19 randomized trials looked at the benefit of regular exercise in patients with Parkinson’s disease and depression. The analysis clearly showed that rigorous and moderate exercise improved depression in patients with Parkinson’s disease. This is very important because exercise improves not only the symptoms of Parkinson’s disease but also comorbid depression while presenting no serious adverse events or side effects.
Dr. Diener is a professor in the department of neurology at Stroke Center–Headache Center, University Duisburg-Essen, Germany. He disclosed ties with Abbott, Addex Pharma, Alder, Allergan, Almirall, Amgen, Autonomic Technology, AstraZeneca, Bayer Vital, Berlin Chemie, Bristol-Myers Squibb, Boehringer Ingelheim, Chordate, CoAxia, Corimmun, Covidien, Coherex, CoLucid, Daiichi Sankyo, D-Pharm, Electrocore, Fresenius, GlaxoSmithKline, Grunenthal, Janssen-Cilag, Labrys Biologics Lilly, La Roche, Lundbeck, 3M Medica, MSD, Medtronic, Menarini, MindFrame, Minster, Neuroscore, Neurobiological Technologies, Novartis, Novo Nordisk, Johnson & Johnson, Knoll, Paion, Parke-Davis, Pierre Fabre, Pfizer Inc, Schaper and Brummer, Sanofi-Aventis, Schering-Plough, Servier, Solvay, St. Jude, Talecris, Thrombogenics, WebMD Global, Weber and Weber, Wyeth, and Yamanouchi. Dr. Diener has served as editor of Aktuelle Neurologie, Arzneimitteltherapie, Kopfschmerz News, Stroke News, and the Treatment Guidelines of the German Neurological Society; as co-editor of Cephalalgia; and on the editorial board of The Lancet Neurology, Stroke, European Neurology, and Cerebrovascular Disorders. The department of neurology in Essen is supported by the German Research Council, the German Ministry of Education and Research, European Union, National Institutes of Health, Bertelsmann Foundation, and Heinz Nixdorf Foundation. Dr. Diener has no ownership interest and does not own stocks in any pharmaceutical company. A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Dear colleagues, I am Christoph Diener from the medical faculty of the University of Duisburg-Essen in Germany.
Treatment of tension-type headache
I would like to start with headache. You are all aware that we have several new studies regarding the prevention of migraine, but very few studies involving nondrug treatments for tension-type headache.
A working group in Göttingen, Germany, conducted a study in people with frequent episodic and chronic tension-type headache. The first of the four randomized groups received traditional Chinese acupuncture for 3 months. The second group received physical therapy and exercise for 1 hour per week for 12 weeks. The third group received a combination of acupuncture and exercise. The last was a control group that received only standard care.
The outcome parameters of tension-type headache were evaluated after 6 months and again after 12 months. Previously, these same researchers published that the intensity but not the frequency of tension-type headache was reduced by active therapy.
In Cephalalgia, they published the outcome for the endpoints of depression, anxiety, and quality of life. Acupuncture, exercise, and the combination of the two improved depression, anxiety, and quality of life. This shows that nonmedical treatment is effective in people with frequent episodic and chronic tension-type headache.
Headache after COVID-19
The next study was published in Headache and discusses headache after COVID-19. In this review of published studies, more than 50% of people with COVID-19 develop headache. It is more frequent in young patients and people with preexisting primary headaches, such as migraine and tension-type headache. Prognosis is usually good, but some patients develop new, daily persistent headache, which is a major problem because treatment is unclear. We desperately need studies investigating how to treat this new, daily persistent headache after COVID-19.
SSRIs during COVID-19 infection
The next study also focuses on COVID-19. We have conflicting results from several studies suggesting that selective serotonin reuptake inhibitors might be effective in people with mild COVID-19 infection. This hypothesis was tested in a study in Brazil and was published in JAMA, The study included 1,288 outpatients with mild COVID-19 who either received 50 mg of fluvoxamine twice daily for 10 days or placebo. There was no benefit of the treatment for any outcome.
Preventing dementia with antihypertensive treatment
The next study was published in the European Heart Journal and addresses the question of whether effective antihypertensive treatment in elderly persons can prevent dementia. This is a meta-analysis of five placebo-controlled trials with more than 28,000 patients. The meta-analysis clearly shows that treating hypertension in elderly patients does prevent dementia. The benefit is higher if the blood pressure is lowered by a larger amount which also stays true for elderly patients. There is no negative impact of lowering blood pressure in this population.
Antiplatelet therapy
The next study was published in Stroke and reexamines whether resumption of antiplatelet therapy should be early or late in people who had an intracerebral hemorrhage while on antiplatelet therapy. In the Taiwanese Health Registry, this was studied in 1,584 patients. The researchers divided participants into groups based on whether antiplatelet therapy was resumed within 30 days or after 30 days. In 1 year, the rate of recurrent intracerebral hemorrhage was 3.2%. There was no difference whether antiplatelet therapy was resumed early or late.
Regular exercise in Parkinson’s disease
The final study is a review of nonmedical therapy. This meta-analysis of 19 randomized trials looked at the benefit of regular exercise in patients with Parkinson’s disease and depression. The analysis clearly showed that rigorous and moderate exercise improved depression in patients with Parkinson’s disease. This is very important because exercise improves not only the symptoms of Parkinson’s disease but also comorbid depression while presenting no serious adverse events or side effects.
Dr. Diener is a professor in the department of neurology at Stroke Center–Headache Center, University Duisburg-Essen, Germany. He disclosed ties with Abbott, Addex Pharma, Alder, Allergan, Almirall, Amgen, Autonomic Technology, AstraZeneca, Bayer Vital, Berlin Chemie, Bristol-Myers Squibb, Boehringer Ingelheim, Chordate, CoAxia, Corimmun, Covidien, Coherex, CoLucid, Daiichi Sankyo, D-Pharm, Electrocore, Fresenius, GlaxoSmithKline, Grunenthal, Janssen-Cilag, Labrys Biologics Lilly, La Roche, Lundbeck, 3M Medica, MSD, Medtronic, Menarini, MindFrame, Minster, Neuroscore, Neurobiological Technologies, Novartis, Novo Nordisk, Johnson & Johnson, Knoll, Paion, Parke-Davis, Pierre Fabre, Pfizer Inc, Schaper and Brummer, Sanofi-Aventis, Schering-Plough, Servier, Solvay, St. Jude, Talecris, Thrombogenics, WebMD Global, Weber and Weber, Wyeth, and Yamanouchi. Dr. Diener has served as editor of Aktuelle Neurologie, Arzneimitteltherapie, Kopfschmerz News, Stroke News, and the Treatment Guidelines of the German Neurological Society; as co-editor of Cephalalgia; and on the editorial board of The Lancet Neurology, Stroke, European Neurology, and Cerebrovascular Disorders. The department of neurology in Essen is supported by the German Research Council, the German Ministry of Education and Research, European Union, National Institutes of Health, Bertelsmann Foundation, and Heinz Nixdorf Foundation. Dr. Diener has no ownership interest and does not own stocks in any pharmaceutical company. A version of this article originally appeared on Medscape.com.
Drug combo promising in vascular cognitive impairment: LACI-2 trial results
and is seen as a new therapeutic approach for patients with cerebral small-vessel disease. The drugs – isosorbide mononitrate and cilostazol – stabilize endothelial function, which is a new therapeutic target for patients with small-vessel disease stroke.
The phase 2 LACI-2 study, evaluating these drugs individually and in combination in patients with lacunar stroke, showed promising trends toward reductions in recurrent stroke, cognitive impairment, and dependency, some of which became significant when the drugs were given together. There was also some suggestion of positive impacts on mood and quality of life.
“Isosorbide mononitrate was associated with a reduction in recurrent stroke, a tendency toward a reduction in dependency and a reduction in cognitive impairment, and cilostazol also seemed to reduce dependency,” study investigator Joanna M. Wardlaw, MD, professor of applied neuroimaging at Edinburgh University, reported.
“When used together, they seemed to have more benefits than either drug on its own. So this is good preliminary evidence that the drugs are working together in a positive way,” she said. But she cautioned that these potential benefits will need to be confirmed in a larger phase 3 trial.
The LACI-2 study was presented at the International Stroke Conference by Dr. Wardlaw and coinvestigator Philip Bath, DSc, professor of medicine at the University of Nottingham (England).
They both highlighted the effect seen on cognitive impairment at the conference presented by the American Stroke Association, a division of the American Heart Association.
“We saw a significant reduction in the number of patients with cognitive impairment with the two drugs together in this phase 2 study,” Dr. Wardlaw said. “This is very encouraging since no study has previously found any medications that positively affect cognitive impairment in small-vessel disease strokes. We cautiously hope that these medications may have wider implications for other types of small-vessel disease as well.”
Dr. Bath added: “The results on cognitive impairment are particularly important. Many patients rate cognitive impairment as one of the most dreaded outcomes of a stroke even if they also have quite significant physical disability. People simply don’t want to lose their memory and thinking ability.”
“The results of LACI-2 also raise interesting questions about whether these drugs would be beneficial for other types of small-vessel disease which do not present as stroke, but maybe may manifest as headaches or memory impairment,” he noted.
‘Very intriguing results’
Outside experts were enthusiastic about these preliminary results. In an ISC highlights presentation, program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “It is refreshing to finally see some positive signals in studies in small-vessel stroke. This is an area where we haven’t had answers for a long time.”
He described the reduction in cognitive impairment seen in the study as “very intriguing and very important.”
“I think we have underestimated the burden that cognitive impairment has in stroke, and the burden in general in society of vascular cognitive impairment. This is a very promising approach that definitely deserves to be investigated more thoroughly in a larger trial.”
Commenting on the study findings, Mitchell Elkind, MD, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said this study “provides evidence that points us in at least two important directions.”
“First, it suggests that endothelial dysfunction, or problems with the lining of the blood vessels, may be an important contributor to small-vessel disease and the cognitive decline that often accompanies it. This is a new mechanism of action and different from blood clotting, blood pressure, and other conventional targets of treatment,” Dr. Elkind said.
“Second, and more generally, it suggests that stroke trials, particularly in the subtype of small-vessel disease, can and should explore not only the incidence of recurrent acute events but also the steady decline that occurs after stroke. Poststroke cognitive decline is a relatively new area of stroke research.”
Dr. Wardlaw noted that lacunar stroke is a common type of ischemic stroke, but it has been rather neglected in terms of research. It is assumed to be caused by atherosclerosis of the small vessel but there is now mounting evidence suggesting that it is a result of problems in the endothelium of the small vessels.
“We looked for potential available drugs that targeted endothelial dysfunction. Both the drugs we tested are already widely used – isosorbide mononitrate for the treatment of coronary artery disease and angina, and cilostazol, mainly in Asia, for stroke prevention,” she said.
LACI-2 was primarily a feasibility study looking at whether it was possible to recruit enough patients who had had a lacunar stroke and would take the drugs, individually or in combination, for up to a year. Outcomes were investigated on an exploratory basis. The study enrolled 363 patients who had experienced lacunar stroke from 26 stroke centers throughout the United Kingdom. They were randomly assigned to one of four treatment groups for 1 year:
- 40-60 mg/day of oral isosorbide mononitrate alone.
- 200 mg/day of oral cilostazol alone.
- Both medications.
- Neither medication.
Patients completed phone surveys at 6 and 12 months to assess health status, including recurrent stroke, myocardial infarction, cognitive tests, symptoms, quality of life surveys, and they also had brain imaging at 12 months.
Results showed 98% of patients were still taking their study medication at 1 year, and the drugs appeared to be safe on top of usual care with few deaths or hemorrhages in the study.
The composite outcome including recurrent stroke, MI, cognitive impairment, dependency (modified Rankin score > 2) and death was reduced by 20% in the isosorbide mononitrate–alone group (adjusted hazard ratio, 0.80; 95% confidence interval, 0.59-1.09).
The composite endpoint was reduced by 23% in the cilostazol group (aHR, 0.77; 95% CI, 0.57-1.05) and by 42% in the combination group (aHR, 0.58, 95% CI, 0.36-0.92) compared with those taking neither drug.
Isosorbide mononitrate alone showed trends toward a reduction in recurrent stroke, cognitive impairment, and dependency, whereas cilostazol alone reduced dependency with a trend toward a reduction in cognitive impairment. When used together, the drugs showed large reductions in cognitive impairment (aHR, 0.44; 95% CI, 0.19-0.99) and dependency (aHR ,0.14; 95% CI, 0.03-0.59).
During the highlights session, Dr. Jovin commented: “It is obvious that the investigators have put a lot of thought into the design of this trial. Presumably because of the composite score they were able to increase the power. We are used to trials which require thousands of patients, but here we are able to see significant results, although exploratory, with just a few hundred patients.”
Dr. Bath stressed that this was only a phase 2 study. “We now need to see if we can confirm these results in a larger phase 3 study.” That study, LACI-3, is planned to start later this year. He also suggested that it would be interesting to investigate whether these drugs would work in other types of ischemic stroke such as those caused by large-artery disease or cardioembolic strokes, as well as other forms of small-vessel disease such as patients with vascular cognitive impairment.
“There are many areas to investigate in future. It might be that in a few years’ time these drugs may be standard of care across many different forms of small-vessel disease,” he said.
Dr. Wardlaw noted that lacunar strokes are generally quite mild strokes, which could be one of the reasons why they have not been the target of much research to date. But Dr. Bath added: “While they may be labeled as a mild stroke on the NIHSS scale, patients can still be quite badly affected. About half of patients with a lacunar stroke develop cognitive impairment and eventually dementia – that is certainly not mild.”
The study was funded primarily by the British Heart Foundation, with support from the UK Alzheimer’s Society, the UK Dementia Research Institute, the Stroke Association, the Fondation Leducq, NHS Research Scotland, and the UK National Institutes of Health Research Clinical Research Networks. Dr. Bath is an adviser to CoMind, DiaMedica, Phagenesis, and Roche. Dr. Wardlaw reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
and is seen as a new therapeutic approach for patients with cerebral small-vessel disease. The drugs – isosorbide mononitrate and cilostazol – stabilize endothelial function, which is a new therapeutic target for patients with small-vessel disease stroke.
The phase 2 LACI-2 study, evaluating these drugs individually and in combination in patients with lacunar stroke, showed promising trends toward reductions in recurrent stroke, cognitive impairment, and dependency, some of which became significant when the drugs were given together. There was also some suggestion of positive impacts on mood and quality of life.
“Isosorbide mononitrate was associated with a reduction in recurrent stroke, a tendency toward a reduction in dependency and a reduction in cognitive impairment, and cilostazol also seemed to reduce dependency,” study investigator Joanna M. Wardlaw, MD, professor of applied neuroimaging at Edinburgh University, reported.
“When used together, they seemed to have more benefits than either drug on its own. So this is good preliminary evidence that the drugs are working together in a positive way,” she said. But she cautioned that these potential benefits will need to be confirmed in a larger phase 3 trial.
The LACI-2 study was presented at the International Stroke Conference by Dr. Wardlaw and coinvestigator Philip Bath, DSc, professor of medicine at the University of Nottingham (England).
They both highlighted the effect seen on cognitive impairment at the conference presented by the American Stroke Association, a division of the American Heart Association.
“We saw a significant reduction in the number of patients with cognitive impairment with the two drugs together in this phase 2 study,” Dr. Wardlaw said. “This is very encouraging since no study has previously found any medications that positively affect cognitive impairment in small-vessel disease strokes. We cautiously hope that these medications may have wider implications for other types of small-vessel disease as well.”
Dr. Bath added: “The results on cognitive impairment are particularly important. Many patients rate cognitive impairment as one of the most dreaded outcomes of a stroke even if they also have quite significant physical disability. People simply don’t want to lose their memory and thinking ability.”
“The results of LACI-2 also raise interesting questions about whether these drugs would be beneficial for other types of small-vessel disease which do not present as stroke, but maybe may manifest as headaches or memory impairment,” he noted.
‘Very intriguing results’
Outside experts were enthusiastic about these preliminary results. In an ISC highlights presentation, program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “It is refreshing to finally see some positive signals in studies in small-vessel stroke. This is an area where we haven’t had answers for a long time.”
He described the reduction in cognitive impairment seen in the study as “very intriguing and very important.”
“I think we have underestimated the burden that cognitive impairment has in stroke, and the burden in general in society of vascular cognitive impairment. This is a very promising approach that definitely deserves to be investigated more thoroughly in a larger trial.”
Commenting on the study findings, Mitchell Elkind, MD, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said this study “provides evidence that points us in at least two important directions.”
“First, it suggests that endothelial dysfunction, or problems with the lining of the blood vessels, may be an important contributor to small-vessel disease and the cognitive decline that often accompanies it. This is a new mechanism of action and different from blood clotting, blood pressure, and other conventional targets of treatment,” Dr. Elkind said.
“Second, and more generally, it suggests that stroke trials, particularly in the subtype of small-vessel disease, can and should explore not only the incidence of recurrent acute events but also the steady decline that occurs after stroke. Poststroke cognitive decline is a relatively new area of stroke research.”
Dr. Wardlaw noted that lacunar stroke is a common type of ischemic stroke, but it has been rather neglected in terms of research. It is assumed to be caused by atherosclerosis of the small vessel but there is now mounting evidence suggesting that it is a result of problems in the endothelium of the small vessels.
“We looked for potential available drugs that targeted endothelial dysfunction. Both the drugs we tested are already widely used – isosorbide mononitrate for the treatment of coronary artery disease and angina, and cilostazol, mainly in Asia, for stroke prevention,” she said.
LACI-2 was primarily a feasibility study looking at whether it was possible to recruit enough patients who had had a lacunar stroke and would take the drugs, individually or in combination, for up to a year. Outcomes were investigated on an exploratory basis. The study enrolled 363 patients who had experienced lacunar stroke from 26 stroke centers throughout the United Kingdom. They were randomly assigned to one of four treatment groups for 1 year:
- 40-60 mg/day of oral isosorbide mononitrate alone.
- 200 mg/day of oral cilostazol alone.
- Both medications.
- Neither medication.
Patients completed phone surveys at 6 and 12 months to assess health status, including recurrent stroke, myocardial infarction, cognitive tests, symptoms, quality of life surveys, and they also had brain imaging at 12 months.
Results showed 98% of patients were still taking their study medication at 1 year, and the drugs appeared to be safe on top of usual care with few deaths or hemorrhages in the study.
The composite outcome including recurrent stroke, MI, cognitive impairment, dependency (modified Rankin score > 2) and death was reduced by 20% in the isosorbide mononitrate–alone group (adjusted hazard ratio, 0.80; 95% confidence interval, 0.59-1.09).
The composite endpoint was reduced by 23% in the cilostazol group (aHR, 0.77; 95% CI, 0.57-1.05) and by 42% in the combination group (aHR, 0.58, 95% CI, 0.36-0.92) compared with those taking neither drug.
Isosorbide mononitrate alone showed trends toward a reduction in recurrent stroke, cognitive impairment, and dependency, whereas cilostazol alone reduced dependency with a trend toward a reduction in cognitive impairment. When used together, the drugs showed large reductions in cognitive impairment (aHR, 0.44; 95% CI, 0.19-0.99) and dependency (aHR ,0.14; 95% CI, 0.03-0.59).
During the highlights session, Dr. Jovin commented: “It is obvious that the investigators have put a lot of thought into the design of this trial. Presumably because of the composite score they were able to increase the power. We are used to trials which require thousands of patients, but here we are able to see significant results, although exploratory, with just a few hundred patients.”
Dr. Bath stressed that this was only a phase 2 study. “We now need to see if we can confirm these results in a larger phase 3 study.” That study, LACI-3, is planned to start later this year. He also suggested that it would be interesting to investigate whether these drugs would work in other types of ischemic stroke such as those caused by large-artery disease or cardioembolic strokes, as well as other forms of small-vessel disease such as patients with vascular cognitive impairment.
“There are many areas to investigate in future. It might be that in a few years’ time these drugs may be standard of care across many different forms of small-vessel disease,” he said.
Dr. Wardlaw noted that lacunar strokes are generally quite mild strokes, which could be one of the reasons why they have not been the target of much research to date. But Dr. Bath added: “While they may be labeled as a mild stroke on the NIHSS scale, patients can still be quite badly affected. About half of patients with a lacunar stroke develop cognitive impairment and eventually dementia – that is certainly not mild.”
The study was funded primarily by the British Heart Foundation, with support from the UK Alzheimer’s Society, the UK Dementia Research Institute, the Stroke Association, the Fondation Leducq, NHS Research Scotland, and the UK National Institutes of Health Research Clinical Research Networks. Dr. Bath is an adviser to CoMind, DiaMedica, Phagenesis, and Roche. Dr. Wardlaw reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
and is seen as a new therapeutic approach for patients with cerebral small-vessel disease. The drugs – isosorbide mononitrate and cilostazol – stabilize endothelial function, which is a new therapeutic target for patients with small-vessel disease stroke.
The phase 2 LACI-2 study, evaluating these drugs individually and in combination in patients with lacunar stroke, showed promising trends toward reductions in recurrent stroke, cognitive impairment, and dependency, some of which became significant when the drugs were given together. There was also some suggestion of positive impacts on mood and quality of life.
“Isosorbide mononitrate was associated with a reduction in recurrent stroke, a tendency toward a reduction in dependency and a reduction in cognitive impairment, and cilostazol also seemed to reduce dependency,” study investigator Joanna M. Wardlaw, MD, professor of applied neuroimaging at Edinburgh University, reported.
“When used together, they seemed to have more benefits than either drug on its own. So this is good preliminary evidence that the drugs are working together in a positive way,” she said. But she cautioned that these potential benefits will need to be confirmed in a larger phase 3 trial.
The LACI-2 study was presented at the International Stroke Conference by Dr. Wardlaw and coinvestigator Philip Bath, DSc, professor of medicine at the University of Nottingham (England).
They both highlighted the effect seen on cognitive impairment at the conference presented by the American Stroke Association, a division of the American Heart Association.
“We saw a significant reduction in the number of patients with cognitive impairment with the two drugs together in this phase 2 study,” Dr. Wardlaw said. “This is very encouraging since no study has previously found any medications that positively affect cognitive impairment in small-vessel disease strokes. We cautiously hope that these medications may have wider implications for other types of small-vessel disease as well.”
Dr. Bath added: “The results on cognitive impairment are particularly important. Many patients rate cognitive impairment as one of the most dreaded outcomes of a stroke even if they also have quite significant physical disability. People simply don’t want to lose their memory and thinking ability.”
“The results of LACI-2 also raise interesting questions about whether these drugs would be beneficial for other types of small-vessel disease which do not present as stroke, but maybe may manifest as headaches or memory impairment,” he noted.
‘Very intriguing results’
Outside experts were enthusiastic about these preliminary results. In an ISC highlights presentation, program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “It is refreshing to finally see some positive signals in studies in small-vessel stroke. This is an area where we haven’t had answers for a long time.”
He described the reduction in cognitive impairment seen in the study as “very intriguing and very important.”
“I think we have underestimated the burden that cognitive impairment has in stroke, and the burden in general in society of vascular cognitive impairment. This is a very promising approach that definitely deserves to be investigated more thoroughly in a larger trial.”
Commenting on the study findings, Mitchell Elkind, MD, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said this study “provides evidence that points us in at least two important directions.”
“First, it suggests that endothelial dysfunction, or problems with the lining of the blood vessels, may be an important contributor to small-vessel disease and the cognitive decline that often accompanies it. This is a new mechanism of action and different from blood clotting, blood pressure, and other conventional targets of treatment,” Dr. Elkind said.
“Second, and more generally, it suggests that stroke trials, particularly in the subtype of small-vessel disease, can and should explore not only the incidence of recurrent acute events but also the steady decline that occurs after stroke. Poststroke cognitive decline is a relatively new area of stroke research.”
Dr. Wardlaw noted that lacunar stroke is a common type of ischemic stroke, but it has been rather neglected in terms of research. It is assumed to be caused by atherosclerosis of the small vessel but there is now mounting evidence suggesting that it is a result of problems in the endothelium of the small vessels.
“We looked for potential available drugs that targeted endothelial dysfunction. Both the drugs we tested are already widely used – isosorbide mononitrate for the treatment of coronary artery disease and angina, and cilostazol, mainly in Asia, for stroke prevention,” she said.
LACI-2 was primarily a feasibility study looking at whether it was possible to recruit enough patients who had had a lacunar stroke and would take the drugs, individually or in combination, for up to a year. Outcomes were investigated on an exploratory basis. The study enrolled 363 patients who had experienced lacunar stroke from 26 stroke centers throughout the United Kingdom. They were randomly assigned to one of four treatment groups for 1 year:
- 40-60 mg/day of oral isosorbide mononitrate alone.
- 200 mg/day of oral cilostazol alone.
- Both medications.
- Neither medication.
Patients completed phone surveys at 6 and 12 months to assess health status, including recurrent stroke, myocardial infarction, cognitive tests, symptoms, quality of life surveys, and they also had brain imaging at 12 months.
Results showed 98% of patients were still taking their study medication at 1 year, and the drugs appeared to be safe on top of usual care with few deaths or hemorrhages in the study.
The composite outcome including recurrent stroke, MI, cognitive impairment, dependency (modified Rankin score > 2) and death was reduced by 20% in the isosorbide mononitrate–alone group (adjusted hazard ratio, 0.80; 95% confidence interval, 0.59-1.09).
The composite endpoint was reduced by 23% in the cilostazol group (aHR, 0.77; 95% CI, 0.57-1.05) and by 42% in the combination group (aHR, 0.58, 95% CI, 0.36-0.92) compared with those taking neither drug.
Isosorbide mononitrate alone showed trends toward a reduction in recurrent stroke, cognitive impairment, and dependency, whereas cilostazol alone reduced dependency with a trend toward a reduction in cognitive impairment. When used together, the drugs showed large reductions in cognitive impairment (aHR, 0.44; 95% CI, 0.19-0.99) and dependency (aHR ,0.14; 95% CI, 0.03-0.59).
During the highlights session, Dr. Jovin commented: “It is obvious that the investigators have put a lot of thought into the design of this trial. Presumably because of the composite score they were able to increase the power. We are used to trials which require thousands of patients, but here we are able to see significant results, although exploratory, with just a few hundred patients.”
Dr. Bath stressed that this was only a phase 2 study. “We now need to see if we can confirm these results in a larger phase 3 study.” That study, LACI-3, is planned to start later this year. He also suggested that it would be interesting to investigate whether these drugs would work in other types of ischemic stroke such as those caused by large-artery disease or cardioembolic strokes, as well as other forms of small-vessel disease such as patients with vascular cognitive impairment.
“There are many areas to investigate in future. It might be that in a few years’ time these drugs may be standard of care across many different forms of small-vessel disease,” he said.
Dr. Wardlaw noted that lacunar strokes are generally quite mild strokes, which could be one of the reasons why they have not been the target of much research to date. But Dr. Bath added: “While they may be labeled as a mild stroke on the NIHSS scale, patients can still be quite badly affected. About half of patients with a lacunar stroke develop cognitive impairment and eventually dementia – that is certainly not mild.”
The study was funded primarily by the British Heart Foundation, with support from the UK Alzheimer’s Society, the UK Dementia Research Institute, the Stroke Association, the Fondation Leducq, NHS Research Scotland, and the UK National Institutes of Health Research Clinical Research Networks. Dr. Bath is an adviser to CoMind, DiaMedica, Phagenesis, and Roche. Dr. Wardlaw reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
Tenecteplase noninferior to alteplase for ischemic stroke: TRACE-2
, a new study has found. “This was a pivotal trial in establishing the safety and efficacy of tenecteplase as an alternative to alteplase in the thrombolytic treatment of acute ischemic stroke within 4.5 hours in Asian patients,” said study author Shuya Li, MD, associate chief physician, department of neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing.
The findings in this all-Chinese population should have an impact on the use of tenecteplase going forward, said Dr. Li. “The results provide further evidence to support a worldwide switch to tenecteplase as the preferred thrombolytic for acute ischemic stroke.”
The findings were presented at the 2023 International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Single bolus
Use of alteplase (tissue plasminogen activator [tPA]) has for years been the main approach to thrombolytic reperfusion therapy for patients with acute stroke, but tenecteplase has recently emerged as a potential successor.
Tenecteplase is a tPA produced by recombinant DNA technology. It has a relatively long half-life and can be delivered in a single bolus instead of requiring an hour-long infusion, as is the case with alteplase.
The phase 3 noninferiority Tenecteplase Reperfusion Therapy in Acute ischemic Cerebrovascular Events (TRACE-2) trial – the first of its kind in an Asian population – included 1,430 adult ischemic stroke patients at 53 Chinese centers. Patients had to have a National Institutes of Health Stroke Scale (NIHSS) score of 5-25 and either not be eligible for or have refused endovascular therapy.
The mean age of study participants was about 66 years, and the percentage of women was about 31%. The mean baseline NIHSS score was 7 in both groups, and the symptom-onset-to-needle time was similar at 180 minutes for the tenecteplase group and 178.5 minutes for the alteplase group.
Researchers randomly assigned patients to receive tenecteplase or alteplase within 4.5 hours of symptom onset.
Those in the tenecteplase group received 0.25 mg/kg of the drug in a single IV bolus (maximum dose, 25 mg). Control group members who were treated with alteplase were given the drug as a 10% bolus, with the remainder given as a 1-hour infusion (0.9 mg/kg with a maximum dose of 90 mg).
Showed noninferiority
The primary efficacy outcome was a modified Rankins scale (mRS) score of 0-1 at 90 days, which is considered excellent function. About 62% of tenecteplase patients and 58% of alteplase patients attained this outcome (risk ratio, 1.09; 95% confidence interval, 1.00-1.18).
The P value was .001 for noninferiority and .06 for superiority, but Dr. Li explained that these values may change when considering the site effect.
There were no statistically significant differences between the two drugs on secondary outcomes of favorable function. For example, 73% of tenecteplase patients and 72% of alteplase patients had an mRS score of 0-2 at 3 months, and 50% in the tenecteplase and 49% in the alteplase group improved by 4 or more points on the NIHSS, or had a score of 1 or less, at 24 hours.
The groups also had comparable scores on the European quality-of-life visual analogue scale and on the Barthel index, which measures functional independence related to personal care and mobility.
Tenecteplase also turned out to be as safe at alteplase. About 2% in both groups had symptomatic intracranial hemorrhage within 36 hours, and both groups had that same percentage for such hemorrhages within 90 days. As well, the groups had a similar rate of any intracranial hemorrhage within 90 days (6% and 7%).
The mortality rate was 7% in the tenecteplase group, compared with 5% in the alteplase group.
Adverse events (AEs) occurred in 86% and 87%, and serious AEs in 16% and 15%, of the tenecteplase and alteplase groups, respectively, again with no statistically significant differences.
The research team aims to test the effectiveness of tenecteplase in other stroke patients, including those with minor strokes, those receiving thrombolysis in a later window, and those receiving endovascular therapy, said Dr. Li.
Strong evidence
Commenting on the study findings, Larry B. Goldstein, MD, professor and chair of neurology, University of Kentucky, Lexington, said it is important to determine the efficacy of tenecteplase among Asians, as they represent “an entirely different population” with unique concerns, such as bleeding complications from anticoagulants.
He noted an advantage of tenecteplase is ease of administration. “You don’t have to go through the loading dose and then the 1-hour infusion,” which poses an “additional hassle” when transferring patients between institutions, he said.
However, he noted that a possible “downside” to having both drugs available in the emergency department is “using the wrong drug at the wrong dose” because of their similar sounding names.
Also commenting on the study, Tudor G. Jovin, MD, professor and chair, department of neurology, Rowan University, Camden, N.J., said he welcomes another trial that confirms that these two drugs are biologically similar.
“I’m very glad this trial was done because it adds another very strong piece of evidence of equivalency.”
But the two drugs are not the same in some important respects, said Dr. Jovin, whose center switched to using tenecteplase almost 3 years ago. That switch has resulted in cutting 17 minutes from the door-to-needle time “which is quite significant,” he said.
“There’s no question that once we used tenecteplase in lieu of tPA, it’s been just so much easier to administer and affects the interhospital transfer protocols, because you’re not transferring the patient with a critical care IV. It’s a win-win situation for everyone.”
The study received funding from the National Science and Technology Major Project, the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences, the National Natural Science Foundation of China, and the China Shijiazhuang Pharmaceutical Company Recomgen Pharmaceutical (Guangzhou). Dr. Li, Dr. Goldstein, and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study has found. “This was a pivotal trial in establishing the safety and efficacy of tenecteplase as an alternative to alteplase in the thrombolytic treatment of acute ischemic stroke within 4.5 hours in Asian patients,” said study author Shuya Li, MD, associate chief physician, department of neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing.
The findings in this all-Chinese population should have an impact on the use of tenecteplase going forward, said Dr. Li. “The results provide further evidence to support a worldwide switch to tenecteplase as the preferred thrombolytic for acute ischemic stroke.”
The findings were presented at the 2023 International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Single bolus
Use of alteplase (tissue plasminogen activator [tPA]) has for years been the main approach to thrombolytic reperfusion therapy for patients with acute stroke, but tenecteplase has recently emerged as a potential successor.
Tenecteplase is a tPA produced by recombinant DNA technology. It has a relatively long half-life and can be delivered in a single bolus instead of requiring an hour-long infusion, as is the case with alteplase.
The phase 3 noninferiority Tenecteplase Reperfusion Therapy in Acute ischemic Cerebrovascular Events (TRACE-2) trial – the first of its kind in an Asian population – included 1,430 adult ischemic stroke patients at 53 Chinese centers. Patients had to have a National Institutes of Health Stroke Scale (NIHSS) score of 5-25 and either not be eligible for or have refused endovascular therapy.
The mean age of study participants was about 66 years, and the percentage of women was about 31%. The mean baseline NIHSS score was 7 in both groups, and the symptom-onset-to-needle time was similar at 180 minutes for the tenecteplase group and 178.5 minutes for the alteplase group.
Researchers randomly assigned patients to receive tenecteplase or alteplase within 4.5 hours of symptom onset.
Those in the tenecteplase group received 0.25 mg/kg of the drug in a single IV bolus (maximum dose, 25 mg). Control group members who were treated with alteplase were given the drug as a 10% bolus, with the remainder given as a 1-hour infusion (0.9 mg/kg with a maximum dose of 90 mg).
Showed noninferiority
The primary efficacy outcome was a modified Rankins scale (mRS) score of 0-1 at 90 days, which is considered excellent function. About 62% of tenecteplase patients and 58% of alteplase patients attained this outcome (risk ratio, 1.09; 95% confidence interval, 1.00-1.18).
The P value was .001 for noninferiority and .06 for superiority, but Dr. Li explained that these values may change when considering the site effect.
There were no statistically significant differences between the two drugs on secondary outcomes of favorable function. For example, 73% of tenecteplase patients and 72% of alteplase patients had an mRS score of 0-2 at 3 months, and 50% in the tenecteplase and 49% in the alteplase group improved by 4 or more points on the NIHSS, or had a score of 1 or less, at 24 hours.
The groups also had comparable scores on the European quality-of-life visual analogue scale and on the Barthel index, which measures functional independence related to personal care and mobility.
Tenecteplase also turned out to be as safe at alteplase. About 2% in both groups had symptomatic intracranial hemorrhage within 36 hours, and both groups had that same percentage for such hemorrhages within 90 days. As well, the groups had a similar rate of any intracranial hemorrhage within 90 days (6% and 7%).
The mortality rate was 7% in the tenecteplase group, compared with 5% in the alteplase group.
Adverse events (AEs) occurred in 86% and 87%, and serious AEs in 16% and 15%, of the tenecteplase and alteplase groups, respectively, again with no statistically significant differences.
The research team aims to test the effectiveness of tenecteplase in other stroke patients, including those with minor strokes, those receiving thrombolysis in a later window, and those receiving endovascular therapy, said Dr. Li.
Strong evidence
Commenting on the study findings, Larry B. Goldstein, MD, professor and chair of neurology, University of Kentucky, Lexington, said it is important to determine the efficacy of tenecteplase among Asians, as they represent “an entirely different population” with unique concerns, such as bleeding complications from anticoagulants.
He noted an advantage of tenecteplase is ease of administration. “You don’t have to go through the loading dose and then the 1-hour infusion,” which poses an “additional hassle” when transferring patients between institutions, he said.
However, he noted that a possible “downside” to having both drugs available in the emergency department is “using the wrong drug at the wrong dose” because of their similar sounding names.
Also commenting on the study, Tudor G. Jovin, MD, professor and chair, department of neurology, Rowan University, Camden, N.J., said he welcomes another trial that confirms that these two drugs are biologically similar.
“I’m very glad this trial was done because it adds another very strong piece of evidence of equivalency.”
But the two drugs are not the same in some important respects, said Dr. Jovin, whose center switched to using tenecteplase almost 3 years ago. That switch has resulted in cutting 17 minutes from the door-to-needle time “which is quite significant,” he said.
“There’s no question that once we used tenecteplase in lieu of tPA, it’s been just so much easier to administer and affects the interhospital transfer protocols, because you’re not transferring the patient with a critical care IV. It’s a win-win situation for everyone.”
The study received funding from the National Science and Technology Major Project, the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences, the National Natural Science Foundation of China, and the China Shijiazhuang Pharmaceutical Company Recomgen Pharmaceutical (Guangzhou). Dr. Li, Dr. Goldstein, and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study has found. “This was a pivotal trial in establishing the safety and efficacy of tenecteplase as an alternative to alteplase in the thrombolytic treatment of acute ischemic stroke within 4.5 hours in Asian patients,” said study author Shuya Li, MD, associate chief physician, department of neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing.
The findings in this all-Chinese population should have an impact on the use of tenecteplase going forward, said Dr. Li. “The results provide further evidence to support a worldwide switch to tenecteplase as the preferred thrombolytic for acute ischemic stroke.”
The findings were presented at the 2023 International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
Single bolus
Use of alteplase (tissue plasminogen activator [tPA]) has for years been the main approach to thrombolytic reperfusion therapy for patients with acute stroke, but tenecteplase has recently emerged as a potential successor.
Tenecteplase is a tPA produced by recombinant DNA technology. It has a relatively long half-life and can be delivered in a single bolus instead of requiring an hour-long infusion, as is the case with alteplase.
The phase 3 noninferiority Tenecteplase Reperfusion Therapy in Acute ischemic Cerebrovascular Events (TRACE-2) trial – the first of its kind in an Asian population – included 1,430 adult ischemic stroke patients at 53 Chinese centers. Patients had to have a National Institutes of Health Stroke Scale (NIHSS) score of 5-25 and either not be eligible for or have refused endovascular therapy.
The mean age of study participants was about 66 years, and the percentage of women was about 31%. The mean baseline NIHSS score was 7 in both groups, and the symptom-onset-to-needle time was similar at 180 minutes for the tenecteplase group and 178.5 minutes for the alteplase group.
Researchers randomly assigned patients to receive tenecteplase or alteplase within 4.5 hours of symptom onset.
Those in the tenecteplase group received 0.25 mg/kg of the drug in a single IV bolus (maximum dose, 25 mg). Control group members who were treated with alteplase were given the drug as a 10% bolus, with the remainder given as a 1-hour infusion (0.9 mg/kg with a maximum dose of 90 mg).
Showed noninferiority
The primary efficacy outcome was a modified Rankins scale (mRS) score of 0-1 at 90 days, which is considered excellent function. About 62% of tenecteplase patients and 58% of alteplase patients attained this outcome (risk ratio, 1.09; 95% confidence interval, 1.00-1.18).
The P value was .001 for noninferiority and .06 for superiority, but Dr. Li explained that these values may change when considering the site effect.
There were no statistically significant differences between the two drugs on secondary outcomes of favorable function. For example, 73% of tenecteplase patients and 72% of alteplase patients had an mRS score of 0-2 at 3 months, and 50% in the tenecteplase and 49% in the alteplase group improved by 4 or more points on the NIHSS, or had a score of 1 or less, at 24 hours.
The groups also had comparable scores on the European quality-of-life visual analogue scale and on the Barthel index, which measures functional independence related to personal care and mobility.
Tenecteplase also turned out to be as safe at alteplase. About 2% in both groups had symptomatic intracranial hemorrhage within 36 hours, and both groups had that same percentage for such hemorrhages within 90 days. As well, the groups had a similar rate of any intracranial hemorrhage within 90 days (6% and 7%).
The mortality rate was 7% in the tenecteplase group, compared with 5% in the alteplase group.
Adverse events (AEs) occurred in 86% and 87%, and serious AEs in 16% and 15%, of the tenecteplase and alteplase groups, respectively, again with no statistically significant differences.
The research team aims to test the effectiveness of tenecteplase in other stroke patients, including those with minor strokes, those receiving thrombolysis in a later window, and those receiving endovascular therapy, said Dr. Li.
Strong evidence
Commenting on the study findings, Larry B. Goldstein, MD, professor and chair of neurology, University of Kentucky, Lexington, said it is important to determine the efficacy of tenecteplase among Asians, as they represent “an entirely different population” with unique concerns, such as bleeding complications from anticoagulants.
He noted an advantage of tenecteplase is ease of administration. “You don’t have to go through the loading dose and then the 1-hour infusion,” which poses an “additional hassle” when transferring patients between institutions, he said.
However, he noted that a possible “downside” to having both drugs available in the emergency department is “using the wrong drug at the wrong dose” because of their similar sounding names.
Also commenting on the study, Tudor G. Jovin, MD, professor and chair, department of neurology, Rowan University, Camden, N.J., said he welcomes another trial that confirms that these two drugs are biologically similar.
“I’m very glad this trial was done because it adds another very strong piece of evidence of equivalency.”
But the two drugs are not the same in some important respects, said Dr. Jovin, whose center switched to using tenecteplase almost 3 years ago. That switch has resulted in cutting 17 minutes from the door-to-needle time “which is quite significant,” he said.
“There’s no question that once we used tenecteplase in lieu of tPA, it’s been just so much easier to administer and affects the interhospital transfer protocols, because you’re not transferring the patient with a critical care IV. It’s a win-win situation for everyone.”
The study received funding from the National Science and Technology Major Project, the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences, the National Natural Science Foundation of China, and the China Shijiazhuang Pharmaceutical Company Recomgen Pharmaceutical (Guangzhou). Dr. Li, Dr. Goldstein, and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ISC 2023