User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
Antipsychotics boosted CVD events in elderly
DALLAS – Elderly patients who started treatment with an antipsychotic drug had a substantially increased risk for a major adverse cardiovascular disease event, especially during the first month on treatment, according to Danish national records from more than 1 million people.
The risk remained elevated even when the analysis focused on elderly people who were aged 70 years or older and were without cardiovascular disease or dementia at the time of their first use of an antipsychotic medication, Dr. Charlotte Andersson and her associates reported in a poster at the American Heart Association scientific sessions.
Treatment was linked with a significantly increased rate of major adverse cardiovascular events (MACE) at some time during follow-up for all eight antipsychotic drugs studied in detail: haloperidol (Haldol), flupentixol (Fluanxol), chlorprothixene, levomepromazine (Nozinan), quetiapine (Seroquel), risperidone (Risperdal), olanzapine, and ziprasidone (Geodon), reported Dr. Andersson, a researcher at Gentofte Hospital in Copenhagen. The MACE association was relatively weak for ziprasidone, but it was robust for the other seven agents.
The study included 1,235,869 Danes aged 70 years or older during 1997-2009 who had not previously been treated with an antipsychotic drug. During the period studied, 100,140 (8%) of these people started treatment with an antipsychotic drug. During follow-up the researchers tallied the incidence of MACE (the combined rate of nonfatal myocardial infarction, nonfatal stroke, and cardiovascular death).
Overall, use of an antipsychotic drug for more than 1 year was linked with a roughly doubled rate of MACE after adjustment for several demographic and clinical factors, including age, gender, diabetes, renal disease, dementia, and schizophrenia. The adjusted relative increase in MACE was even higher during the first 30 days of treatment for most of the eight drugs.
For example, during the first 30 days following the start of treatment, patients treated with any haloperidol dosage had a roughly fivefold increased adjusted MACE rate compared with people not receiving an antipsychotic. The relative risk was highest during the first 30 days in patients on the highest haloperidol dosages, 2 mg/day or more, who had a 10-fold increased MACE rate.
Similar increases in adjusted MACE rates were seen in patients treated with haloperidol for 1-12 months, as well as in those treated for more than a year, although with longer follow-up the adjusted relative risk was about two- to threefold above background. Similar risk patterns also existed in the subgroup of patients who were treated with haloperidol and were free from cardiovascular disease at baseline, as well as in those free from dementia at baseline.
Dr. Andersson and her associates said that they had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
DALLAS – Elderly patients who started treatment with an antipsychotic drug had a substantially increased risk for a major adverse cardiovascular disease event, especially during the first month on treatment, according to Danish national records from more than 1 million people.
The risk remained elevated even when the analysis focused on elderly people who were aged 70 years or older and were without cardiovascular disease or dementia at the time of their first use of an antipsychotic medication, Dr. Charlotte Andersson and her associates reported in a poster at the American Heart Association scientific sessions.
Treatment was linked with a significantly increased rate of major adverse cardiovascular events (MACE) at some time during follow-up for all eight antipsychotic drugs studied in detail: haloperidol (Haldol), flupentixol (Fluanxol), chlorprothixene, levomepromazine (Nozinan), quetiapine (Seroquel), risperidone (Risperdal), olanzapine, and ziprasidone (Geodon), reported Dr. Andersson, a researcher at Gentofte Hospital in Copenhagen. The MACE association was relatively weak for ziprasidone, but it was robust for the other seven agents.
The study included 1,235,869 Danes aged 70 years or older during 1997-2009 who had not previously been treated with an antipsychotic drug. During the period studied, 100,140 (8%) of these people started treatment with an antipsychotic drug. During follow-up the researchers tallied the incidence of MACE (the combined rate of nonfatal myocardial infarction, nonfatal stroke, and cardiovascular death).
Overall, use of an antipsychotic drug for more than 1 year was linked with a roughly doubled rate of MACE after adjustment for several demographic and clinical factors, including age, gender, diabetes, renal disease, dementia, and schizophrenia. The adjusted relative increase in MACE was even higher during the first 30 days of treatment for most of the eight drugs.
For example, during the first 30 days following the start of treatment, patients treated with any haloperidol dosage had a roughly fivefold increased adjusted MACE rate compared with people not receiving an antipsychotic. The relative risk was highest during the first 30 days in patients on the highest haloperidol dosages, 2 mg/day or more, who had a 10-fold increased MACE rate.
Similar increases in adjusted MACE rates were seen in patients treated with haloperidol for 1-12 months, as well as in those treated for more than a year, although with longer follow-up the adjusted relative risk was about two- to threefold above background. Similar risk patterns also existed in the subgroup of patients who were treated with haloperidol and were free from cardiovascular disease at baseline, as well as in those free from dementia at baseline.
Dr. Andersson and her associates said that they had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
DALLAS – Elderly patients who started treatment with an antipsychotic drug had a substantially increased risk for a major adverse cardiovascular disease event, especially during the first month on treatment, according to Danish national records from more than 1 million people.
The risk remained elevated even when the analysis focused on elderly people who were aged 70 years or older and were without cardiovascular disease or dementia at the time of their first use of an antipsychotic medication, Dr. Charlotte Andersson and her associates reported in a poster at the American Heart Association scientific sessions.
Treatment was linked with a significantly increased rate of major adverse cardiovascular events (MACE) at some time during follow-up for all eight antipsychotic drugs studied in detail: haloperidol (Haldol), flupentixol (Fluanxol), chlorprothixene, levomepromazine (Nozinan), quetiapine (Seroquel), risperidone (Risperdal), olanzapine, and ziprasidone (Geodon), reported Dr. Andersson, a researcher at Gentofte Hospital in Copenhagen. The MACE association was relatively weak for ziprasidone, but it was robust for the other seven agents.
The study included 1,235,869 Danes aged 70 years or older during 1997-2009 who had not previously been treated with an antipsychotic drug. During the period studied, 100,140 (8%) of these people started treatment with an antipsychotic drug. During follow-up the researchers tallied the incidence of MACE (the combined rate of nonfatal myocardial infarction, nonfatal stroke, and cardiovascular death).
Overall, use of an antipsychotic drug for more than 1 year was linked with a roughly doubled rate of MACE after adjustment for several demographic and clinical factors, including age, gender, diabetes, renal disease, dementia, and schizophrenia. The adjusted relative increase in MACE was even higher during the first 30 days of treatment for most of the eight drugs.
For example, during the first 30 days following the start of treatment, patients treated with any haloperidol dosage had a roughly fivefold increased adjusted MACE rate compared with people not receiving an antipsychotic. The relative risk was highest during the first 30 days in patients on the highest haloperidol dosages, 2 mg/day or more, who had a 10-fold increased MACE rate.
Similar increases in adjusted MACE rates were seen in patients treated with haloperidol for 1-12 months, as well as in those treated for more than a year, although with longer follow-up the adjusted relative risk was about two- to threefold above background. Similar risk patterns also existed in the subgroup of patients who were treated with haloperidol and were free from cardiovascular disease at baseline, as well as in those free from dementia at baseline.
Dr. Andersson and her associates said that they had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Major finding: Long-term use of an antipsychotic drug by elderly Danes doubled their rate of major cardiovascular adverse events.
Data source: A review of 1,235,869 Danes aged 70 years or older during 1997-2009 who were not receiving an antipsychotic drug at the time they entered the database.
Disclosures: Dr. Andersson and her associates said that they had no disclosures.
Evidence and expertise in writing medical guidelines
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."

The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."
The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."
The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler

‘JNC 8’ relaxes elderly systolic target below 150 mm Hg
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).

The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.

Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).
The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.
Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).
The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.
Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
FROM JAMA

Heart failure exacerbation by saxagliptin called ‘real’
DALLAS – The glycemia-lowering drug saxagliptin led to a "real" excess of hospitalizations for heart failure in a 16,000-patient trial designed to examine the drug’s cardiovascular safety, but given saxagliptin’s overall safety in the study the signal of heart failure exacerbation should not rule out the drug’s use for most patients, even those with preexisting heart failure.
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Benjamin M. Scirica while presenting a poster at the American Heart Association’s scientific sessions. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."

This follow-up analysis of data collected in the SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction) trial occurred because prior reports on the study’s outcomes had shown a small but statistically significant excess incidence of hospitalization for heart failure among the 8,280 patients treated with saxagliptin, compared with the 8,212 patients randomized to placebo.
Researchers ran the SAVOR-TIMI 53 trial in patients with type 2 diabetes and either established cardiovascular disease or multiple risk factors to explicitly test the cardiovascular safety of saxagliptin (Onglyza), a selective dipeptidyl peptidase 4 (DPP-4) inhibitor, following guidance from the Food and Drug Administration in 2009 (N. Engl. J. Med. 2013;369:1317-26). The primary outcome from the study showed no statistically significant difference in the combined rate of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke between the saxagliptin and placebo arms during a median 2.1 years of follow-up. The results also showed saxagliptin met the FDA’s recommended safety criterion for cardiovascular safety in a drug meant to treat type 2 diabetes.
More detailed analyses showed a 0.7% absolute increased risk for hospitalization for heart failure in the saxagliptin-treated patients, compared with the placebo group (a 27% increase in relative risk), and that the largest number of increased hospitalizations occurred among the quartile of patients enrolled in the trial with baseline blood levels of NT–pro-brain natriuretic peptide of at least 333 pg/mL. Further analysis reported for the first time by Dr. Scirica in his poster showed that the greatest excess rate of hospitalization for heart failure occurred during the first 6 months of treatment. After the first 6 months, hospitalization rates for this reason were virtually identical in the two treatment arms of the study, said Dr. Scirica, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School in Boston.
His analysis also compared the impact of saxagliptin on hospitalization for heart failure with the same effect of alogliptin, another DPP-4 inhibitor, in results from the EXAMINE (Examination of Cardiovascular Outcomes With Alogliptin vs. Standard of Care) trial (N. Engl. J. Med. 2013;369:1327-35). In EXAMINE the 2,701 patients who received alogliptin (Nesina) had an absolute 0.6% higher rate of hospitalizations for heart failure (an 18% relative increase) that was not statistically significant. EXAMINE also showed no significantly different rate between alogliptin and placebo treatment for the study’s primary, combined cardiovascular endpoint during a median 1.5 years of treatment in patients with type 2 diabetes and acute coronary syndrome.
"One could look at the alogliptin results and say there was no signal [for increased hospitalization for heart failure], or that there was a signal, although not statistically significant. The only way to know for sure is to see what the next trial shows," said Dr. Deepak L. Bhatt, professor of medicine at Harvard Medical School, a cardiologist at Brigham and Women’s Hospital, and senior investigator for SAVOR-TIMI 53. The TECOS (Sitagliptin Cardiovascular Outcome Study) study using sitagliptin (Januvia), a third DPP-4 inhibitor, is slated to finish at the end of 2014. "Whether this is a drug or class effect still very much has yet to be seen," said Dr. Scirica. The mechanism also remains elusive for the time being.
"The most important message is that future trials [of diabetes drugs] need to prospectively look at heart failure rates, adjudicate heart failure events, and really look for any heart failure effect," Dr. Bhatt said.
SAVOR-TIMI 53 was sponsored by Astra Zeneca and Bristol-Myers Squibb. Dr. Scirica said that he has received honoraria as a consultant or adviser to Gilead, Eisai, Lexicon, Arena, St. Jude’s Medical, Decision Resources, and Boston Clinical research Institute, and that he has received research grants from six other drug companies. Dr. Bhatt said that he has received research grants from six other drug or device companies.
On Twitter @mitchelzoler
DALLAS – The glycemia-lowering drug saxagliptin led to a "real" excess of hospitalizations for heart failure in a 16,000-patient trial designed to examine the drug’s cardiovascular safety, but given saxagliptin’s overall safety in the study the signal of heart failure exacerbation should not rule out the drug’s use for most patients, even those with preexisting heart failure.
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Benjamin M. Scirica while presenting a poster at the American Heart Association’s scientific sessions. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."
This follow-up analysis of data collected in the SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction) trial occurred because prior reports on the study’s outcomes had shown a small but statistically significant excess incidence of hospitalization for heart failure among the 8,280 patients treated with saxagliptin, compared with the 8,212 patients randomized to placebo.
Researchers ran the SAVOR-TIMI 53 trial in patients with type 2 diabetes and either established cardiovascular disease or multiple risk factors to explicitly test the cardiovascular safety of saxagliptin (Onglyza), a selective dipeptidyl peptidase 4 (DPP-4) inhibitor, following guidance from the Food and Drug Administration in 2009 (N. Engl. J. Med. 2013;369:1317-26). The primary outcome from the study showed no statistically significant difference in the combined rate of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke between the saxagliptin and placebo arms during a median 2.1 years of follow-up. The results also showed saxagliptin met the FDA’s recommended safety criterion for cardiovascular safety in a drug meant to treat type 2 diabetes.
More detailed analyses showed a 0.7% absolute increased risk for hospitalization for heart failure in the saxagliptin-treated patients, compared with the placebo group (a 27% increase in relative risk), and that the largest number of increased hospitalizations occurred among the quartile of patients enrolled in the trial with baseline blood levels of NT–pro-brain natriuretic peptide of at least 333 pg/mL. Further analysis reported for the first time by Dr. Scirica in his poster showed that the greatest excess rate of hospitalization for heart failure occurred during the first 6 months of treatment. After the first 6 months, hospitalization rates for this reason were virtually identical in the two treatment arms of the study, said Dr. Scirica, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School in Boston.
His analysis also compared the impact of saxagliptin on hospitalization for heart failure with the same effect of alogliptin, another DPP-4 inhibitor, in results from the EXAMINE (Examination of Cardiovascular Outcomes With Alogliptin vs. Standard of Care) trial (N. Engl. J. Med. 2013;369:1327-35). In EXAMINE the 2,701 patients who received alogliptin (Nesina) had an absolute 0.6% higher rate of hospitalizations for heart failure (an 18% relative increase) that was not statistically significant. EXAMINE also showed no significantly different rate between alogliptin and placebo treatment for the study’s primary, combined cardiovascular endpoint during a median 1.5 years of treatment in patients with type 2 diabetes and acute coronary syndrome.
"One could look at the alogliptin results and say there was no signal [for increased hospitalization for heart failure], or that there was a signal, although not statistically significant. The only way to know for sure is to see what the next trial shows," said Dr. Deepak L. Bhatt, professor of medicine at Harvard Medical School, a cardiologist at Brigham and Women’s Hospital, and senior investigator for SAVOR-TIMI 53. The TECOS (Sitagliptin Cardiovascular Outcome Study) study using sitagliptin (Januvia), a third DPP-4 inhibitor, is slated to finish at the end of 2014. "Whether this is a drug or class effect still very much has yet to be seen," said Dr. Scirica. The mechanism also remains elusive for the time being.
"The most important message is that future trials [of diabetes drugs] need to prospectively look at heart failure rates, adjudicate heart failure events, and really look for any heart failure effect," Dr. Bhatt said.
SAVOR-TIMI 53 was sponsored by Astra Zeneca and Bristol-Myers Squibb. Dr. Scirica said that he has received honoraria as a consultant or adviser to Gilead, Eisai, Lexicon, Arena, St. Jude’s Medical, Decision Resources, and Boston Clinical research Institute, and that he has received research grants from six other drug companies. Dr. Bhatt said that he has received research grants from six other drug or device companies.
On Twitter @mitchelzoler
DALLAS – The glycemia-lowering drug saxagliptin led to a "real" excess of hospitalizations for heart failure in a 16,000-patient trial designed to examine the drug’s cardiovascular safety, but given saxagliptin’s overall safety in the study the signal of heart failure exacerbation should not rule out the drug’s use for most patients, even those with preexisting heart failure.
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Benjamin M. Scirica while presenting a poster at the American Heart Association’s scientific sessions. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."
This follow-up analysis of data collected in the SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction) trial occurred because prior reports on the study’s outcomes had shown a small but statistically significant excess incidence of hospitalization for heart failure among the 8,280 patients treated with saxagliptin, compared with the 8,212 patients randomized to placebo.
Researchers ran the SAVOR-TIMI 53 trial in patients with type 2 diabetes and either established cardiovascular disease or multiple risk factors to explicitly test the cardiovascular safety of saxagliptin (Onglyza), a selective dipeptidyl peptidase 4 (DPP-4) inhibitor, following guidance from the Food and Drug Administration in 2009 (N. Engl. J. Med. 2013;369:1317-26). The primary outcome from the study showed no statistically significant difference in the combined rate of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke between the saxagliptin and placebo arms during a median 2.1 years of follow-up. The results also showed saxagliptin met the FDA’s recommended safety criterion for cardiovascular safety in a drug meant to treat type 2 diabetes.
More detailed analyses showed a 0.7% absolute increased risk for hospitalization for heart failure in the saxagliptin-treated patients, compared with the placebo group (a 27% increase in relative risk), and that the largest number of increased hospitalizations occurred among the quartile of patients enrolled in the trial with baseline blood levels of NT–pro-brain natriuretic peptide of at least 333 pg/mL. Further analysis reported for the first time by Dr. Scirica in his poster showed that the greatest excess rate of hospitalization for heart failure occurred during the first 6 months of treatment. After the first 6 months, hospitalization rates for this reason were virtually identical in the two treatment arms of the study, said Dr. Scirica, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School in Boston.
His analysis also compared the impact of saxagliptin on hospitalization for heart failure with the same effect of alogliptin, another DPP-4 inhibitor, in results from the EXAMINE (Examination of Cardiovascular Outcomes With Alogliptin vs. Standard of Care) trial (N. Engl. J. Med. 2013;369:1327-35). In EXAMINE the 2,701 patients who received alogliptin (Nesina) had an absolute 0.6% higher rate of hospitalizations for heart failure (an 18% relative increase) that was not statistically significant. EXAMINE also showed no significantly different rate between alogliptin and placebo treatment for the study’s primary, combined cardiovascular endpoint during a median 1.5 years of treatment in patients with type 2 diabetes and acute coronary syndrome.
"One could look at the alogliptin results and say there was no signal [for increased hospitalization for heart failure], or that there was a signal, although not statistically significant. The only way to know for sure is to see what the next trial shows," said Dr. Deepak L. Bhatt, professor of medicine at Harvard Medical School, a cardiologist at Brigham and Women’s Hospital, and senior investigator for SAVOR-TIMI 53. The TECOS (Sitagliptin Cardiovascular Outcome Study) study using sitagliptin (Januvia), a third DPP-4 inhibitor, is slated to finish at the end of 2014. "Whether this is a drug or class effect still very much has yet to be seen," said Dr. Scirica. The mechanism also remains elusive for the time being.
"The most important message is that future trials [of diabetes drugs] need to prospectively look at heart failure rates, adjudicate heart failure events, and really look for any heart failure effect," Dr. Bhatt said.
SAVOR-TIMI 53 was sponsored by Astra Zeneca and Bristol-Myers Squibb. Dr. Scirica said that he has received honoraria as a consultant or adviser to Gilead, Eisai, Lexicon, Arena, St. Jude’s Medical, Decision Resources, and Boston Clinical research Institute, and that he has received research grants from six other drug companies. Dr. Bhatt said that he has received research grants from six other drug or device companies.
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Major finding: Treatment with saxagliptin led to a "real" 0.7% increased rate of hospitalization for heart failure, compared with patients on placebo.
Data source: The SAVOR-TIMI 53 study, which randomized 16,492 patients with type 2 diabetes to treatment with saxagliptin or placebo at 788 sites in 26 countries.
Disclosures: SAVOR-TIMI 53 was sponsored by AstraZeneca and Bristol-Myers Squibb. Dr. Scirica said that he has received honoraria as a consultant or adviser to Gilead, Eisai, Lexicon, Arena, St. Jude’s Medical, Decision Resources, and Boston Clinical Research Institute, and that he has received research grants from six other drug companies. Dr. Bhatt said that he has received research grants from six other drug or device companies.

Genetic profiling transforms cancer treatment trials
BRUSSELS – The ballooning list of genetic markers linked with various cancers is spawning a radical shift in the design of oncology treatment trials.
These days, the trend is to incorporate detailed genetic analysis into the trials, so that once the results are in, researchers can try to correlate treatment responses or failures with variations in each tumor’s genetic profile.
Leaders in the field say that, ideally, the tumor of every single patient now entering a cancer treatment trial should undergo a baseline genetic analysis, either using a large panel of targeted genetic markers or full-genome sequencing – although they acknowledge that, for the time being, complete sequencing provides much more information than can be used practically.

This changing paradigm of cancer treatment trial design comes with a major, built-in limitation that seems solvable only by dramatically increasing the scope of patients enrolled in trials: Each mutational cancer "driver" seems specific for just a few percent of patients. That means making statistically meaningful correlations among the responses of patients to various drugs and their tumors’ genetic profiles requires sifting through thousands of patients, far more than usually enroll in treatment trials today.
"The big challenge is to identify the mutations or genetic alterations that help inform the results of clinical trials. There are a lot of potential genetic markers, but very few have been validated. Tumors are being sequenced, and we find lots of mutations; but we don’t yet know what to do with most of this information," said Dr. Francisco J. Esteva, professor of medicine and director of the breast medical oncology program at New York University in an interview during a meeting on markers in cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
"Finding ‘actionable’ mutations is very complicated because of next-generation sequencing," Dr. Esteva added. "We have some very good inhibitor drugs" aimed at certain mutations that can be highly effective in selected patients, "but when we give these drugs to larger populations of patients, the drugs may not work."
Even though a tumor may carry a genetic mutation identified as a cancer driver and thus an effective target for drug treatment in some patients, the mutation may not be the most important driver in other patients.
"Trying to find the mutations or other genetic changes that can be effective targets for treatment sounds simple, but it’s really not so simple," noted Dr. Esteva, an organizer of the meeting, sponsored by the American Society of Clinical Oncology, the European Organization for Research and Treatment of Cancer, and the National Cancer Institute.
"We’ve been in an era where we looked at one genetic marker at a time. Now it’s pretty clear that this approach will not move us forward fast enough," said Dr. Lisa A. Carey, professor and medical director of the breast center at the University of North Carolina in Chapel Hill, and another organizer of the meeting.
"Looking at a full genetic profile of the tumor has great appeal but is also more complicated," Dr. Carey explained. "Today, we have a limited portfolio of genetic markers with known clinical significance and a limited portfolio of drugs. We’ve had some huge success stories [with targeted therapy], but it’s not simple, and it is far from solved."
"Finding a target in a patient’s tumor and having an agent that inhibits the target does not imply clinical benefit," said Dr. Shivaani Kummar, head of early clinical trials development in the division of cancer treatment and diagnosis of the National Cancer Institute.
The enormous volume of genetic information now available from next-generation sequencing, which can supply data on hundreds or even potentially thousands of individual genes for a relatively affordable price, "is affecting trial design, leading to ‘umbrella’ designs that use a variety of genetic markers and panels of several drugs," said Dr. Robert L. Becker Jr., a chief medical officer at the Center for Devices and Radiological Health of the Food and Drug Administration.

"Is the current model for development of diagnostic markers and drugs sustainable?’" Dr. Becker asked. "Next-generation sequencing is different, because it can query an almost unlimited number of analytes in a single assay."
At the meeting, a series of researchers from the United States and Europe described and discussed several recently designed drug treatment trials prospectively structured to collect wide-ranging genetic data from the tumors of enrolled patients.
One example is the MATCH (Molecular Analysis for Therapy Choice) trial, expected to start in 2014 with a goal of enrolling about 1,000 patients with solid tumors that have progressed following initial treatment with at least one drug. The investigators will use targeted mutations or amplifications as well as whole exome sequencing to try to better assign patients to their next regimen, said Dr. Kummar.
"It’s a new paradigm of trial design for cancer," said Dr. Esteva. "Going forward, all major drug trials should be designed" to include genetic analyses.
But the MATCH trial, as well as several others outlined at the meeting, will require casting large nets to find adequate numbers of appropriate patients to enroll.
"It’s a small subset of patients with each type of mutation, so getting the sample size required to get information about treatments will require a community effort," said Dr. Esteva. "It’s very important to have a lot of patients to get meaningful results." Progressing from studies with relatively small numbers of patients at academic centers to the larger populations of patients treated by community oncologists "will be one of the biggest challenges," he said.
Incorporating routine genetic analyses into trials and into routine practice also raises other issues, Dr. Carey noted. "Does the tumor evolve during treatment, so that what was found with testing at baseline is no longer the disease being treated?"
Once genetic profiling of tumors becomes routine, another challenge will be efficiently and reliably alerting physicians and patients when a genetic marker that had no known clinical consequence when it was first found in a patient’s tumor is subsequently discovered to be effectively treated with a targeted drug, she said.
And no consensus has emerged on whether it’s best to do genetic assessments of tumors using specimens collected by direct biopsy or by collecting tumor cells or tumor DNA circulating in a patient’s blood, Dr. Carey cautioned.
For now, the key step is making genetic analysis a routine part of every cancer-treatment trial. "We need tumor analyses for every patient," she said. "We should get correlates for 100% of cancers."
Dr. Becker, Dr. Carey, Dr. Esteva, and Dr. Kummar all said that they had no disclosures.
On Twitter @mitchelzoler
BRUSSELS – The ballooning list of genetic markers linked with various cancers is spawning a radical shift in the design of oncology treatment trials.
These days, the trend is to incorporate detailed genetic analysis into the trials, so that once the results are in, researchers can try to correlate treatment responses or failures with variations in each tumor’s genetic profile.
Leaders in the field say that, ideally, the tumor of every single patient now entering a cancer treatment trial should undergo a baseline genetic analysis, either using a large panel of targeted genetic markers or full-genome sequencing – although they acknowledge that, for the time being, complete sequencing provides much more information than can be used practically.
This changing paradigm of cancer treatment trial design comes with a major, built-in limitation that seems solvable only by dramatically increasing the scope of patients enrolled in trials: Each mutational cancer "driver" seems specific for just a few percent of patients. That means making statistically meaningful correlations among the responses of patients to various drugs and their tumors’ genetic profiles requires sifting through thousands of patients, far more than usually enroll in treatment trials today.
"The big challenge is to identify the mutations or genetic alterations that help inform the results of clinical trials. There are a lot of potential genetic markers, but very few have been validated. Tumors are being sequenced, and we find lots of mutations; but we don’t yet know what to do with most of this information," said Dr. Francisco J. Esteva, professor of medicine and director of the breast medical oncology program at New York University in an interview during a meeting on markers in cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
"Finding ‘actionable’ mutations is very complicated because of next-generation sequencing," Dr. Esteva added. "We have some very good inhibitor drugs" aimed at certain mutations that can be highly effective in selected patients, "but when we give these drugs to larger populations of patients, the drugs may not work."
Even though a tumor may carry a genetic mutation identified as a cancer driver and thus an effective target for drug treatment in some patients, the mutation may not be the most important driver in other patients.
"Trying to find the mutations or other genetic changes that can be effective targets for treatment sounds simple, but it’s really not so simple," noted Dr. Esteva, an organizer of the meeting, sponsored by the American Society of Clinical Oncology, the European Organization for Research and Treatment of Cancer, and the National Cancer Institute.
"We’ve been in an era where we looked at one genetic marker at a time. Now it’s pretty clear that this approach will not move us forward fast enough," said Dr. Lisa A. Carey, professor and medical director of the breast center at the University of North Carolina in Chapel Hill, and another organizer of the meeting.
"Looking at a full genetic profile of the tumor has great appeal but is also more complicated," Dr. Carey explained. "Today, we have a limited portfolio of genetic markers with known clinical significance and a limited portfolio of drugs. We’ve had some huge success stories [with targeted therapy], but it’s not simple, and it is far from solved."
"Finding a target in a patient’s tumor and having an agent that inhibits the target does not imply clinical benefit," said Dr. Shivaani Kummar, head of early clinical trials development in the division of cancer treatment and diagnosis of the National Cancer Institute.
The enormous volume of genetic information now available from next-generation sequencing, which can supply data on hundreds or even potentially thousands of individual genes for a relatively affordable price, "is affecting trial design, leading to ‘umbrella’ designs that use a variety of genetic markers and panels of several drugs," said Dr. Robert L. Becker Jr., a chief medical officer at the Center for Devices and Radiological Health of the Food and Drug Administration.
"Is the current model for development of diagnostic markers and drugs sustainable?’" Dr. Becker asked. "Next-generation sequencing is different, because it can query an almost unlimited number of analytes in a single assay."
At the meeting, a series of researchers from the United States and Europe described and discussed several recently designed drug treatment trials prospectively structured to collect wide-ranging genetic data from the tumors of enrolled patients.
One example is the MATCH (Molecular Analysis for Therapy Choice) trial, expected to start in 2014 with a goal of enrolling about 1,000 patients with solid tumors that have progressed following initial treatment with at least one drug. The investigators will use targeted mutations or amplifications as well as whole exome sequencing to try to better assign patients to their next regimen, said Dr. Kummar.
"It’s a new paradigm of trial design for cancer," said Dr. Esteva. "Going forward, all major drug trials should be designed" to include genetic analyses.
But the MATCH trial, as well as several others outlined at the meeting, will require casting large nets to find adequate numbers of appropriate patients to enroll.
"It’s a small subset of patients with each type of mutation, so getting the sample size required to get information about treatments will require a community effort," said Dr. Esteva. "It’s very important to have a lot of patients to get meaningful results." Progressing from studies with relatively small numbers of patients at academic centers to the larger populations of patients treated by community oncologists "will be one of the biggest challenges," he said.
Incorporating routine genetic analyses into trials and into routine practice also raises other issues, Dr. Carey noted. "Does the tumor evolve during treatment, so that what was found with testing at baseline is no longer the disease being treated?"
Once genetic profiling of tumors becomes routine, another challenge will be efficiently and reliably alerting physicians and patients when a genetic marker that had no known clinical consequence when it was first found in a patient’s tumor is subsequently discovered to be effectively treated with a targeted drug, she said.
And no consensus has emerged on whether it’s best to do genetic assessments of tumors using specimens collected by direct biopsy or by collecting tumor cells or tumor DNA circulating in a patient’s blood, Dr. Carey cautioned.
For now, the key step is making genetic analysis a routine part of every cancer-treatment trial. "We need tumor analyses for every patient," she said. "We should get correlates for 100% of cancers."
Dr. Becker, Dr. Carey, Dr. Esteva, and Dr. Kummar all said that they had no disclosures.
On Twitter @mitchelzoler
BRUSSELS – The ballooning list of genetic markers linked with various cancers is spawning a radical shift in the design of oncology treatment trials.
These days, the trend is to incorporate detailed genetic analysis into the trials, so that once the results are in, researchers can try to correlate treatment responses or failures with variations in each tumor’s genetic profile.
Leaders in the field say that, ideally, the tumor of every single patient now entering a cancer treatment trial should undergo a baseline genetic analysis, either using a large panel of targeted genetic markers or full-genome sequencing – although they acknowledge that, for the time being, complete sequencing provides much more information than can be used practically.
This changing paradigm of cancer treatment trial design comes with a major, built-in limitation that seems solvable only by dramatically increasing the scope of patients enrolled in trials: Each mutational cancer "driver" seems specific for just a few percent of patients. That means making statistically meaningful correlations among the responses of patients to various drugs and their tumors’ genetic profiles requires sifting through thousands of patients, far more than usually enroll in treatment trials today.
"The big challenge is to identify the mutations or genetic alterations that help inform the results of clinical trials. There are a lot of potential genetic markers, but very few have been validated. Tumors are being sequenced, and we find lots of mutations; but we don’t yet know what to do with most of this information," said Dr. Francisco J. Esteva, professor of medicine and director of the breast medical oncology program at New York University in an interview during a meeting on markers in cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
"Finding ‘actionable’ mutations is very complicated because of next-generation sequencing," Dr. Esteva added. "We have some very good inhibitor drugs" aimed at certain mutations that can be highly effective in selected patients, "but when we give these drugs to larger populations of patients, the drugs may not work."
Even though a tumor may carry a genetic mutation identified as a cancer driver and thus an effective target for drug treatment in some patients, the mutation may not be the most important driver in other patients.
"Trying to find the mutations or other genetic changes that can be effective targets for treatment sounds simple, but it’s really not so simple," noted Dr. Esteva, an organizer of the meeting, sponsored by the American Society of Clinical Oncology, the European Organization for Research and Treatment of Cancer, and the National Cancer Institute.
"We’ve been in an era where we looked at one genetic marker at a time. Now it’s pretty clear that this approach will not move us forward fast enough," said Dr. Lisa A. Carey, professor and medical director of the breast center at the University of North Carolina in Chapel Hill, and another organizer of the meeting.
"Looking at a full genetic profile of the tumor has great appeal but is also more complicated," Dr. Carey explained. "Today, we have a limited portfolio of genetic markers with known clinical significance and a limited portfolio of drugs. We’ve had some huge success stories [with targeted therapy], but it’s not simple, and it is far from solved."
"Finding a target in a patient’s tumor and having an agent that inhibits the target does not imply clinical benefit," said Dr. Shivaani Kummar, head of early clinical trials development in the division of cancer treatment and diagnosis of the National Cancer Institute.
The enormous volume of genetic information now available from next-generation sequencing, which can supply data on hundreds or even potentially thousands of individual genes for a relatively affordable price, "is affecting trial design, leading to ‘umbrella’ designs that use a variety of genetic markers and panels of several drugs," said Dr. Robert L. Becker Jr., a chief medical officer at the Center for Devices and Radiological Health of the Food and Drug Administration.
"Is the current model for development of diagnostic markers and drugs sustainable?’" Dr. Becker asked. "Next-generation sequencing is different, because it can query an almost unlimited number of analytes in a single assay."
At the meeting, a series of researchers from the United States and Europe described and discussed several recently designed drug treatment trials prospectively structured to collect wide-ranging genetic data from the tumors of enrolled patients.
One example is the MATCH (Molecular Analysis for Therapy Choice) trial, expected to start in 2014 with a goal of enrolling about 1,000 patients with solid tumors that have progressed following initial treatment with at least one drug. The investigators will use targeted mutations or amplifications as well as whole exome sequencing to try to better assign patients to their next regimen, said Dr. Kummar.
"It’s a new paradigm of trial design for cancer," said Dr. Esteva. "Going forward, all major drug trials should be designed" to include genetic analyses.
But the MATCH trial, as well as several others outlined at the meeting, will require casting large nets to find adequate numbers of appropriate patients to enroll.
"It’s a small subset of patients with each type of mutation, so getting the sample size required to get information about treatments will require a community effort," said Dr. Esteva. "It’s very important to have a lot of patients to get meaningful results." Progressing from studies with relatively small numbers of patients at academic centers to the larger populations of patients treated by community oncologists "will be one of the biggest challenges," he said.
Incorporating routine genetic analyses into trials and into routine practice also raises other issues, Dr. Carey noted. "Does the tumor evolve during treatment, so that what was found with testing at baseline is no longer the disease being treated?"
Once genetic profiling of tumors becomes routine, another challenge will be efficiently and reliably alerting physicians and patients when a genetic marker that had no known clinical consequence when it was first found in a patient’s tumor is subsequently discovered to be effectively treated with a targeted drug, she said.
And no consensus has emerged on whether it’s best to do genetic assessments of tumors using specimens collected by direct biopsy or by collecting tumor cells or tumor DNA circulating in a patient’s blood, Dr. Carey cautioned.
For now, the key step is making genetic analysis a routine part of every cancer-treatment trial. "We need tumor analyses for every patient," she said. "We should get correlates for 100% of cancers."
Dr. Becker, Dr. Carey, Dr. Esteva, and Dr. Kummar all said that they had no disclosures.
On Twitter @mitchelzoler
EXPERT ANALYSIS AT THE MARKERS IN CANCER MEETING

Substrate ablation shows no advantage for A fib
DALLAS – A substrate-based ablation strategy failed to show an efficacy advantage over conventional circumferential pulmonary vein isolation for eliminating persistent or paroxysmal atrial fibrillation in a multicenter randomized trial with 232 patients.
High-frequency source ablation (HFSA), a strategy that targets rotors in the atrial substrate responsible for maintaining fibrillation episodes, did not reach statistical significance for noninferiority compared with circumferential pulmonary vein isolation (CPVI) after 6 months in patients with paroxysmal atrial fibrillation (AF), the study’s primary endpoint, Dr. Felipe Atienza said at the American Heart Association scientific sessions.

In enrolled patients with persistent atrial fibrillation, adding HFSA to CPVI "offered no incremental value with a trend for an increase in complications," after 6 months in a study designed to test superiority, said Dr. Atienza, an electrophysiologist at Gregorio Marañón University Hospital in Madrid.
But a ray of promise came from 1-year follow-up of the paroxysmal atrial fibrillation patients, half of the patients enrolled in the study. (The other patients had persistent atrial fibrillation.) At that time, HFSA treatment achieved statistically significant noninferiority compared with CPVI for freedom from atrial fibrillation and freedom from atrial tachyarrhythmia, with a significantly lower rate of serious adverse events.
Although the results mean that pulmonary vein isolation remains the standard of care for treating atrial fibrillation patients who fail to respond to drug treatment, substrate-based ablation showed enough potential in the study to remain a viable candidate for further testing, experts said.
"In this trial, HFSA did not improve outcomes in patients with paroxysmal or persistent AF, but the fact that HFSA treatment was equivalent to CPVI in patients with paroxysmal AF keeps the AF substrate and trigger argument alive," commented Dr. Mark S. Link, professor and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center Boston, and designated discussant for the report.
"The way to go is to run further investigations like this to try to find and eliminate the substrates of atrial fibrillation instead of ablating everywhere," said Dr. Atienza.
The RADAR-AF (Radiofrequency Ablation of Drivers of Atrial Fibrillation) trial enrolled 115 patients with paroxysmal AF and 117 patients with persistent AF at 11 hospitals in Spain. The researchers randomized the patients with paroxysmal AF to treatment with either HFSA or CPVI; they randomized patients with persistent AF to treatment with both HFSA and CPVI or to CPVI alone. They used software developed by St. Jude Medical to identify the sites for HFSA.
The study’s primary endpoint was freedom from AF while off of antiarrhythmic drugs at 6 months. In the paroxysmal patients, this endpoint was reached by 73% of patients treated with HFSA and 83% treated with CPVI, which failed to meet the prespecified criteria for noninferiority. However, after 1 year the rate of freedom from AF was 69% in patients in both groups, and the rate of freedom from atrial tachyarrhythmia in both groups was 59%, rates that met the criteria for noninferiority. In addition, after 1 year the cumulative rate of serious adverse events was 9% in the HFSA group and 24% in the CPVI group, a statistically significant difference.
Among the patients with persistent atrial fibrillation, the rate of freedom from AF after 6 months was 61% in patients treated with both techniques and 60% in those treated with CPVI alone, which failed to show superiority. Efficacy rates were also similar in both arms after 1 year, and the rate of serious adverse events was 24% in patients treated with both HFSA and CPVI, compared with 10% among those treated by CPVI only.
The RADAR-AF trial was sponsored by St. Jude Medical, which developed the rotor-mapping software used for substrate ablation in the study. Dr. Atienza and Dr. Link said they had no relevant financial disclosures.
On Twitter @mitchelzoler
The hypothesis underlying the RADAR-AF trial is that while atrial fibrillation is initiated by focal triggers, it is maintained in the atrial substrate, specifically by rotors in the substrate. The concept is that if you can ablate the substrate correctly, it will prevent episodes of sustained atrial fibrillation and move us beyond the ceiling we currently have with pulmonary vein isolation, which has about a 70% success rate.

|
Mitchel L. Zoler/IMNG Medical Media
|
The results from RADAR-AF do not kill the notion that the substrate is important, especially because in patients with paroxysmal atrial fibrillation just ablating the substrate did as well after 1 year as standard pulmonary vein isolation.
The findings also indicate that the technique tested for identifying rotors in the substrate is inadequate, and we need a better way to do this. Several ongoing clinical trials are looking at this. We just do not have adequate tools right now to know where to ablate the substrate.
The most important thing is that the RADAR-AF results produced a signal that the substrate is important.
Dr. Mark S. Link is professor of medicine and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center in Boston. He made these comments as the designated discussant for the report and during a press conference. He said he had no relevant financial disclosures.
RADAR-AF, Radiofrequency Ablation of Drivers of Atrial Fibrillation trial,
The hypothesis underlying the RADAR-AF trial is that while atrial fibrillation is initiated by focal triggers, it is maintained in the atrial substrate, specifically by rotors in the substrate. The concept is that if you can ablate the substrate correctly, it will prevent episodes of sustained atrial fibrillation and move us beyond the ceiling we currently have with pulmonary vein isolation, which has about a 70% success rate.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The results from RADAR-AF do not kill the notion that the substrate is important, especially because in patients with paroxysmal atrial fibrillation just ablating the substrate did as well after 1 year as standard pulmonary vein isolation.
The findings also indicate that the technique tested for identifying rotors in the substrate is inadequate, and we need a better way to do this. Several ongoing clinical trials are looking at this. We just do not have adequate tools right now to know where to ablate the substrate.
The most important thing is that the RADAR-AF results produced a signal that the substrate is important.
Dr. Mark S. Link is professor of medicine and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center in Boston. He made these comments as the designated discussant for the report and during a press conference. He said he had no relevant financial disclosures.
The hypothesis underlying the RADAR-AF trial is that while atrial fibrillation is initiated by focal triggers, it is maintained in the atrial substrate, specifically by rotors in the substrate. The concept is that if you can ablate the substrate correctly, it will prevent episodes of sustained atrial fibrillation and move us beyond the ceiling we currently have with pulmonary vein isolation, which has about a 70% success rate.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The results from RADAR-AF do not kill the notion that the substrate is important, especially because in patients with paroxysmal atrial fibrillation just ablating the substrate did as well after 1 year as standard pulmonary vein isolation.
The findings also indicate that the technique tested for identifying rotors in the substrate is inadequate, and we need a better way to do this. Several ongoing clinical trials are looking at this. We just do not have adequate tools right now to know where to ablate the substrate.
The most important thing is that the RADAR-AF results produced a signal that the substrate is important.
Dr. Mark S. Link is professor of medicine and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center in Boston. He made these comments as the designated discussant for the report and during a press conference. He said he had no relevant financial disclosures.
DALLAS – A substrate-based ablation strategy failed to show an efficacy advantage over conventional circumferential pulmonary vein isolation for eliminating persistent or paroxysmal atrial fibrillation in a multicenter randomized trial with 232 patients.
High-frequency source ablation (HFSA), a strategy that targets rotors in the atrial substrate responsible for maintaining fibrillation episodes, did not reach statistical significance for noninferiority compared with circumferential pulmonary vein isolation (CPVI) after 6 months in patients with paroxysmal atrial fibrillation (AF), the study’s primary endpoint, Dr. Felipe Atienza said at the American Heart Association scientific sessions.
In enrolled patients with persistent atrial fibrillation, adding HFSA to CPVI "offered no incremental value with a trend for an increase in complications," after 6 months in a study designed to test superiority, said Dr. Atienza, an electrophysiologist at Gregorio Marañón University Hospital in Madrid.
But a ray of promise came from 1-year follow-up of the paroxysmal atrial fibrillation patients, half of the patients enrolled in the study. (The other patients had persistent atrial fibrillation.) At that time, HFSA treatment achieved statistically significant noninferiority compared with CPVI for freedom from atrial fibrillation and freedom from atrial tachyarrhythmia, with a significantly lower rate of serious adverse events.
Although the results mean that pulmonary vein isolation remains the standard of care for treating atrial fibrillation patients who fail to respond to drug treatment, substrate-based ablation showed enough potential in the study to remain a viable candidate for further testing, experts said.
"In this trial, HFSA did not improve outcomes in patients with paroxysmal or persistent AF, but the fact that HFSA treatment was equivalent to CPVI in patients with paroxysmal AF keeps the AF substrate and trigger argument alive," commented Dr. Mark S. Link, professor and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center Boston, and designated discussant for the report.
"The way to go is to run further investigations like this to try to find and eliminate the substrates of atrial fibrillation instead of ablating everywhere," said Dr. Atienza.
The RADAR-AF (Radiofrequency Ablation of Drivers of Atrial Fibrillation) trial enrolled 115 patients with paroxysmal AF and 117 patients with persistent AF at 11 hospitals in Spain. The researchers randomized the patients with paroxysmal AF to treatment with either HFSA or CPVI; they randomized patients with persistent AF to treatment with both HFSA and CPVI or to CPVI alone. They used software developed by St. Jude Medical to identify the sites for HFSA.
The study’s primary endpoint was freedom from AF while off of antiarrhythmic drugs at 6 months. In the paroxysmal patients, this endpoint was reached by 73% of patients treated with HFSA and 83% treated with CPVI, which failed to meet the prespecified criteria for noninferiority. However, after 1 year the rate of freedom from AF was 69% in patients in both groups, and the rate of freedom from atrial tachyarrhythmia in both groups was 59%, rates that met the criteria for noninferiority. In addition, after 1 year the cumulative rate of serious adverse events was 9% in the HFSA group and 24% in the CPVI group, a statistically significant difference.
Among the patients with persistent atrial fibrillation, the rate of freedom from AF after 6 months was 61% in patients treated with both techniques and 60% in those treated with CPVI alone, which failed to show superiority. Efficacy rates were also similar in both arms after 1 year, and the rate of serious adverse events was 24% in patients treated with both HFSA and CPVI, compared with 10% among those treated by CPVI only.
The RADAR-AF trial was sponsored by St. Jude Medical, which developed the rotor-mapping software used for substrate ablation in the study. Dr. Atienza and Dr. Link said they had no relevant financial disclosures.
On Twitter @mitchelzoler
DALLAS – A substrate-based ablation strategy failed to show an efficacy advantage over conventional circumferential pulmonary vein isolation for eliminating persistent or paroxysmal atrial fibrillation in a multicenter randomized trial with 232 patients.
High-frequency source ablation (HFSA), a strategy that targets rotors in the atrial substrate responsible for maintaining fibrillation episodes, did not reach statistical significance for noninferiority compared with circumferential pulmonary vein isolation (CPVI) after 6 months in patients with paroxysmal atrial fibrillation (AF), the study’s primary endpoint, Dr. Felipe Atienza said at the American Heart Association scientific sessions.
In enrolled patients with persistent atrial fibrillation, adding HFSA to CPVI "offered no incremental value with a trend for an increase in complications," after 6 months in a study designed to test superiority, said Dr. Atienza, an electrophysiologist at Gregorio Marañón University Hospital in Madrid.
But a ray of promise came from 1-year follow-up of the paroxysmal atrial fibrillation patients, half of the patients enrolled in the study. (The other patients had persistent atrial fibrillation.) At that time, HFSA treatment achieved statistically significant noninferiority compared with CPVI for freedom from atrial fibrillation and freedom from atrial tachyarrhythmia, with a significantly lower rate of serious adverse events.
Although the results mean that pulmonary vein isolation remains the standard of care for treating atrial fibrillation patients who fail to respond to drug treatment, substrate-based ablation showed enough potential in the study to remain a viable candidate for further testing, experts said.
"In this trial, HFSA did not improve outcomes in patients with paroxysmal or persistent AF, but the fact that HFSA treatment was equivalent to CPVI in patients with paroxysmal AF keeps the AF substrate and trigger argument alive," commented Dr. Mark S. Link, professor and codirector of the New England Cardiac Arrhythmia Center at Tufts Medical Center Boston, and designated discussant for the report.
"The way to go is to run further investigations like this to try to find and eliminate the substrates of atrial fibrillation instead of ablating everywhere," said Dr. Atienza.
The RADAR-AF (Radiofrequency Ablation of Drivers of Atrial Fibrillation) trial enrolled 115 patients with paroxysmal AF and 117 patients with persistent AF at 11 hospitals in Spain. The researchers randomized the patients with paroxysmal AF to treatment with either HFSA or CPVI; they randomized patients with persistent AF to treatment with both HFSA and CPVI or to CPVI alone. They used software developed by St. Jude Medical to identify the sites for HFSA.
The study’s primary endpoint was freedom from AF while off of antiarrhythmic drugs at 6 months. In the paroxysmal patients, this endpoint was reached by 73% of patients treated with HFSA and 83% treated with CPVI, which failed to meet the prespecified criteria for noninferiority. However, after 1 year the rate of freedom from AF was 69% in patients in both groups, and the rate of freedom from atrial tachyarrhythmia in both groups was 59%, rates that met the criteria for noninferiority. In addition, after 1 year the cumulative rate of serious adverse events was 9% in the HFSA group and 24% in the CPVI group, a statistically significant difference.
Among the patients with persistent atrial fibrillation, the rate of freedom from AF after 6 months was 61% in patients treated with both techniques and 60% in those treated with CPVI alone, which failed to show superiority. Efficacy rates were also similar in both arms after 1 year, and the rate of serious adverse events was 24% in patients treated with both HFSA and CPVI, compared with 10% among those treated by CPVI only.
The RADAR-AF trial was sponsored by St. Jude Medical, which developed the rotor-mapping software used for substrate ablation in the study. Dr. Atienza and Dr. Link said they had no relevant financial disclosures.
On Twitter @mitchelzoler
RADAR-AF, Radiofrequency Ablation of Drivers of Atrial Fibrillation trial,
RADAR-AF, Radiofrequency Ablation of Drivers of Atrial Fibrillation trial,
AT THE AHA SCIENTIFIC SESSIONS
Major finding: Substrate ablation failed to show efficacy compared with conventional pulmonary vein isolation for patients with atrial fibrillation.
Data source: The RADAR-AF trial, which enrolled 232 patients with paroxysmal or persistent atrial fibrillation at 11 Spanish Hospitals.
Disclosures: The study was sponsored by St. Jude Medical, which developed the rotor-mapping software used for substrate ablation in the study. Dr. Atienza and Dr. Link said they had no relevant financial disclosures.

Guideline authors, AHA-ACC leaders confident in risk calculator
DALLAS – In the face of high-profile criticism of the new U.S. cholesterol-management guidelines released by the American College of Cardiology and American Heart Association on Nov. 12, the physicians who crafted the guidelines, as well as the leadership of the two organizations, stood firmly behind the work, reiterating that it is a big step forward in the battle against atherosclerotic cardiovascular disease.
During a last-minute press conference called on Monday morning, Nov. 18, to address concerns that first bubbled up over the prior weekend, a series of representatives from the guideline-writing panel stressed that the new cardiovascular-risk-calculation formula introduced in the guidelines reflected the best and most comprehensive evidence available today. They also stressed that the guidelines do not advocate simply using the formula and a rigid risk-threshold to decide whether or not a patient should receive a statin, but instead tell physicians and their patients to use the risk calculator as the starting point for a discussion of the risks and benefits that statin treatment might pose for each person.

"I think these are these are the most carefully vetted guidelines ever published," said Dr. Mariell Jessup, AHA president. "We’re confident that they are based on the best evidence."
"We intend to move forward with implementation of these guidelines," said Dr. Sidney Smith, professor of medicine at the University of North Carolina in Chapel Hill and chair of the ACC/AHA subcommittee on prevention guidelines.
The controversy began with an analysis run by two Harvard researchers starting on the day the guidelines and risk calculator came out that applied the new risk calculator to three databases at their immediate disposal, the Women’s Health Study, the Physicians’ Health Study, and the Women’s Health Initiative Observational Study. They found that the risk calculator overestimated the 10-year rate of atherosclerotic cardiovascular disease (ASCVD) event by 75%-150%, doubling the actual, observed risk in these three cohorts. The authors of the analysis, Dr. Paul M. Ridker and Nancy R. Cook, Sc.D., of Harvard Medical School and Brigham and Women’s Hospital, both in Boston, published their results in a brief article published online in the Lancet on Nov. 19.

Based on their calculations, "it is possible that as many as 40% to 50% of the 33 million Americans targeted by the new guidelines for statin therapy do not actually have risk thresholds exceeding the 7.5% level suggested for treatment," the two researchers wrote. "Miscalibration to this extent should be reconciled and addressed ... before these new prediction models are widely implemented."
Their analysis was made available to the New York Times over the weekend, which led to a prominent story in the newspaper’s Nov. 18 edition that called this overestimate by the risk calculator a "major embarrassment," and quoted some prominent cardiologists who also called for a delay in implementation of the new guidelines and risk calculator.
The researchers who devised the calculator responded by acknowledging the flaws in the device, something they had already done in their manuscript, but stressed that it represented a major improvement over the risk calculator from the prior guidelines, the third edition of the Adult Treatment Panel (ATP III) used for the past 12 years, particularly because of its inclusion of strokes as a ASCVD endpoint and its reliance on databases that had substantial numbers of African Americans, two major features missing from ATP III.
A risk calculator "will never be perfect, but this is a huge step ahead from where we were 12 years ago," said Dr. Donald Lloyd-Jones, professor of preventive medicine at Northwestern University in Chicago and cochair of the panel that developed the risk calculator. "We made it better for women [by including stroke as an outcome], for African Americans, and for white men, too. We feel very confident that we are in a great place now, but as more data become available, we’re very happy to see if we can improve it further. You can certainly criticize the calculator, but I don’t know of anything that’s better," he said in an interview.
Other experts who led development of the new guidelines also stressed that they do not call for blindly prescribing a statin to every person whose risk calculates at or above 7.5%.
"No one said that patients automatically get a statin. We said that there needs to be a risk discussion between the patient and physician, because sometimes the numbers make sense and sometimes they don’t," said Dr. Neil Stone, Robert Bonow Professor in the division of medicine-cardiology at Northwestern University and chair of the ACC/AHA panel that wrote the new guidelines. "For the first time, we built into the guidelines the unique judgment of physicians, and patients’ personal preferences." Risk calculation "is the start of a discussion" between a physician and patient, not the endpoint. He also noted that the guidelines included a built-in "buffer" because "we had evidence that statins are effective even for patients with a 5% risk" for an ASCVD event over the subsequent 10 years.
The guidelines say that it is "reasonable to offer" statin treatment to a middle-age person with a 7.5% or greater 10-year risk for a ASCVD event and no other risks that warrant statin treatment and that before starting statin treatment, it is "reasonable" for a physician and patient to have a discussion that covers the patient’s individual risk level, the potential risks and benefits of statin treatment, and patient preference.
Aside from their critique of the risk calculator, Dr. Ridker and Dr. Cook applauded the overall guidelines in their commentary, calling them "a major step in the right direction."
On Twitter @mitchelzoler
DALLAS – In the face of high-profile criticism of the new U.S. cholesterol-management guidelines released by the American College of Cardiology and American Heart Association on Nov. 12, the physicians who crafted the guidelines, as well as the leadership of the two organizations, stood firmly behind the work, reiterating that it is a big step forward in the battle against atherosclerotic cardiovascular disease.
During a last-minute press conference called on Monday morning, Nov. 18, to address concerns that first bubbled up over the prior weekend, a series of representatives from the guideline-writing panel stressed that the new cardiovascular-risk-calculation formula introduced in the guidelines reflected the best and most comprehensive evidence available today. They also stressed that the guidelines do not advocate simply using the formula and a rigid risk-threshold to decide whether or not a patient should receive a statin, but instead tell physicians and their patients to use the risk calculator as the starting point for a discussion of the risks and benefits that statin treatment might pose for each person.
"I think these are these are the most carefully vetted guidelines ever published," said Dr. Mariell Jessup, AHA president. "We’re confident that they are based on the best evidence."
"We intend to move forward with implementation of these guidelines," said Dr. Sidney Smith, professor of medicine at the University of North Carolina in Chapel Hill and chair of the ACC/AHA subcommittee on prevention guidelines.
The controversy began with an analysis run by two Harvard researchers starting on the day the guidelines and risk calculator came out that applied the new risk calculator to three databases at their immediate disposal, the Women’s Health Study, the Physicians’ Health Study, and the Women’s Health Initiative Observational Study. They found that the risk calculator overestimated the 10-year rate of atherosclerotic cardiovascular disease (ASCVD) event by 75%-150%, doubling the actual, observed risk in these three cohorts. The authors of the analysis, Dr. Paul M. Ridker and Nancy R. Cook, Sc.D., of Harvard Medical School and Brigham and Women’s Hospital, both in Boston, published their results in a brief article published online in the Lancet on Nov. 19.
Based on their calculations, "it is possible that as many as 40% to 50% of the 33 million Americans targeted by the new guidelines for statin therapy do not actually have risk thresholds exceeding the 7.5% level suggested for treatment," the two researchers wrote. "Miscalibration to this extent should be reconciled and addressed ... before these new prediction models are widely implemented."
Their analysis was made available to the New York Times over the weekend, which led to a prominent story in the newspaper’s Nov. 18 edition that called this overestimate by the risk calculator a "major embarrassment," and quoted some prominent cardiologists who also called for a delay in implementation of the new guidelines and risk calculator.
The researchers who devised the calculator responded by acknowledging the flaws in the device, something they had already done in their manuscript, but stressed that it represented a major improvement over the risk calculator from the prior guidelines, the third edition of the Adult Treatment Panel (ATP III) used for the past 12 years, particularly because of its inclusion of strokes as a ASCVD endpoint and its reliance on databases that had substantial numbers of African Americans, two major features missing from ATP III.
A risk calculator "will never be perfect, but this is a huge step ahead from where we were 12 years ago," said Dr. Donald Lloyd-Jones, professor of preventive medicine at Northwestern University in Chicago and cochair of the panel that developed the risk calculator. "We made it better for women [by including stroke as an outcome], for African Americans, and for white men, too. We feel very confident that we are in a great place now, but as more data become available, we’re very happy to see if we can improve it further. You can certainly criticize the calculator, but I don’t know of anything that’s better," he said in an interview.
Other experts who led development of the new guidelines also stressed that they do not call for blindly prescribing a statin to every person whose risk calculates at or above 7.5%.
"No one said that patients automatically get a statin. We said that there needs to be a risk discussion between the patient and physician, because sometimes the numbers make sense and sometimes they don’t," said Dr. Neil Stone, Robert Bonow Professor in the division of medicine-cardiology at Northwestern University and chair of the ACC/AHA panel that wrote the new guidelines. "For the first time, we built into the guidelines the unique judgment of physicians, and patients’ personal preferences." Risk calculation "is the start of a discussion" between a physician and patient, not the endpoint. He also noted that the guidelines included a built-in "buffer" because "we had evidence that statins are effective even for patients with a 5% risk" for an ASCVD event over the subsequent 10 years.
The guidelines say that it is "reasonable to offer" statin treatment to a middle-age person with a 7.5% or greater 10-year risk for a ASCVD event and no other risks that warrant statin treatment and that before starting statin treatment, it is "reasonable" for a physician and patient to have a discussion that covers the patient’s individual risk level, the potential risks and benefits of statin treatment, and patient preference.
Aside from their critique of the risk calculator, Dr. Ridker and Dr. Cook applauded the overall guidelines in their commentary, calling them "a major step in the right direction."
On Twitter @mitchelzoler
DALLAS – In the face of high-profile criticism of the new U.S. cholesterol-management guidelines released by the American College of Cardiology and American Heart Association on Nov. 12, the physicians who crafted the guidelines, as well as the leadership of the two organizations, stood firmly behind the work, reiterating that it is a big step forward in the battle against atherosclerotic cardiovascular disease.
During a last-minute press conference called on Monday morning, Nov. 18, to address concerns that first bubbled up over the prior weekend, a series of representatives from the guideline-writing panel stressed that the new cardiovascular-risk-calculation formula introduced in the guidelines reflected the best and most comprehensive evidence available today. They also stressed that the guidelines do not advocate simply using the formula and a rigid risk-threshold to decide whether or not a patient should receive a statin, but instead tell physicians and their patients to use the risk calculator as the starting point for a discussion of the risks and benefits that statin treatment might pose for each person.
"I think these are these are the most carefully vetted guidelines ever published," said Dr. Mariell Jessup, AHA president. "We’re confident that they are based on the best evidence."
"We intend to move forward with implementation of these guidelines," said Dr. Sidney Smith, professor of medicine at the University of North Carolina in Chapel Hill and chair of the ACC/AHA subcommittee on prevention guidelines.
The controversy began with an analysis run by two Harvard researchers starting on the day the guidelines and risk calculator came out that applied the new risk calculator to three databases at their immediate disposal, the Women’s Health Study, the Physicians’ Health Study, and the Women’s Health Initiative Observational Study. They found that the risk calculator overestimated the 10-year rate of atherosclerotic cardiovascular disease (ASCVD) event by 75%-150%, doubling the actual, observed risk in these three cohorts. The authors of the analysis, Dr. Paul M. Ridker and Nancy R. Cook, Sc.D., of Harvard Medical School and Brigham and Women’s Hospital, both in Boston, published their results in a brief article published online in the Lancet on Nov. 19.
Based on their calculations, "it is possible that as many as 40% to 50% of the 33 million Americans targeted by the new guidelines for statin therapy do not actually have risk thresholds exceeding the 7.5% level suggested for treatment," the two researchers wrote. "Miscalibration to this extent should be reconciled and addressed ... before these new prediction models are widely implemented."
Their analysis was made available to the New York Times over the weekend, which led to a prominent story in the newspaper’s Nov. 18 edition that called this overestimate by the risk calculator a "major embarrassment," and quoted some prominent cardiologists who also called for a delay in implementation of the new guidelines and risk calculator.
The researchers who devised the calculator responded by acknowledging the flaws in the device, something they had already done in their manuscript, but stressed that it represented a major improvement over the risk calculator from the prior guidelines, the third edition of the Adult Treatment Panel (ATP III) used for the past 12 years, particularly because of its inclusion of strokes as a ASCVD endpoint and its reliance on databases that had substantial numbers of African Americans, two major features missing from ATP III.
A risk calculator "will never be perfect, but this is a huge step ahead from where we were 12 years ago," said Dr. Donald Lloyd-Jones, professor of preventive medicine at Northwestern University in Chicago and cochair of the panel that developed the risk calculator. "We made it better for women [by including stroke as an outcome], for African Americans, and for white men, too. We feel very confident that we are in a great place now, but as more data become available, we’re very happy to see if we can improve it further. You can certainly criticize the calculator, but I don’t know of anything that’s better," he said in an interview.
Other experts who led development of the new guidelines also stressed that they do not call for blindly prescribing a statin to every person whose risk calculates at or above 7.5%.
"No one said that patients automatically get a statin. We said that there needs to be a risk discussion between the patient and physician, because sometimes the numbers make sense and sometimes they don’t," said Dr. Neil Stone, Robert Bonow Professor in the division of medicine-cardiology at Northwestern University and chair of the ACC/AHA panel that wrote the new guidelines. "For the first time, we built into the guidelines the unique judgment of physicians, and patients’ personal preferences." Risk calculation "is the start of a discussion" between a physician and patient, not the endpoint. He also noted that the guidelines included a built-in "buffer" because "we had evidence that statins are effective even for patients with a 5% risk" for an ASCVD event over the subsequent 10 years.
The guidelines say that it is "reasonable to offer" statin treatment to a middle-age person with a 7.5% or greater 10-year risk for a ASCVD event and no other risks that warrant statin treatment and that before starting statin treatment, it is "reasonable" for a physician and patient to have a discussion that covers the patient’s individual risk level, the potential risks and benefits of statin treatment, and patient preference.
Aside from their critique of the risk calculator, Dr. Ridker and Dr. Cook applauded the overall guidelines in their commentary, calling them "a major step in the right direction."
On Twitter @mitchelzoler
EXPERT OPINION AT THE AHA SCIENTIFIC SESSIONS

BP therapy didn’t boost survival in ischemic stroke
DALLAS – Immediate blood pressure reduction in hypertensive acute ischemic stroke patients did not reduce death and disability after 14 days, but the strategy was safe and did not worsen patient’s 14-day outcomes, a randomized controlled study has shown.
The findings suggest that, among patients with relatively mild acute ischemic strokes and a systolic blood pressure of 140-219 mm Hg, "the decision to lower blood pressure with antihypertensive treatment should be based on individual clinical judgment," Dr. Jiang He said at the American Heart Association scientific sessions.
Elevated blood pressure immediately following an ischemic stroke poses a risk of hemorrhagic conversion or cerebral edema, but an elevated blood pressure also might be protective by forcing more blood into the penumbra around the stroke site. Blood pressure reduction measures are not appropriate for patients treated by reperfusion, but they are considered necessary for patients with "markedly elevated" blood pressure, generally defined as a systolic pressure of 220 mm Hg or higher, he said.
U.S. guidelines on stroke management published earlier this year noted that the data to guide recommendations for treating less severe arterial hypertension, in the range studied in this trial, are "inconclusive or conflicting," and that "the benefit of treating arterial hypertension in the setting of acute ischemic stroke is not well established" (Stroke 2013;44:870-947). Some U.S. clinicians, however, take steps to reduce moderately elevated blood pressure in acute ischemic stroke patients, especially when systolic pressures are at or close to 200 mm Hg.
Based on the new findings, Dr. Sila proposed in her formal comments a strategy for managing patients with mild ischemic strokes who do not undergo reperfusion treatment and have a systolic pressure of 140-219 mm Hg more than 15 hours after their stroke onset and no major-vessel stenosis or occlusion. She suggested that a "reasonable" goal was to lower blood pressure by 10%-15% over the first 24 hours of treatment, with a goal blood pressure of less than 140/90 mm Hg within the next 7 days.
The China Antihypertensive Trial in Acute Ischemic Stroke (CATIS) randomized 4,071 patients aged 22 years or older with a confirmed ischemic stroke who did not undergo reperfusion treatment at 26 hospitals in China. Their average age was 62 years, they were seen an average of 15 hours after their stroke onset, and they had a median National Institutes of Health Stroke Scale score of 4.
The 2,038 patients randomized to blood pressure reduction received an intravenous angiotensin-converting enzyme inhibitor, enalapril, as their first-line treatment, followed by a calcium channel blocker as second-line treatment and a diuretic as a third-line agent. The objective was to reduce systolic pressure by 10%-25% within the first 24 hours, with a goal blood pressure of less than 140/90 mm Hg after 7 days.
The treatments were effective, resulting in an average 13% reduction in blood pressure in treated patients after 24 hours (an average drop of 22 mm Hg), and an average systolic pressure of 137 mm Hg after 7 days. The control patients had an average 7% reduction in their systolic pressure, an average reduction of 13 mm Hg after 24 hours, and an average systolic pressure of 147 mm Hg after 7 days. All of the differences were significant.
The study’s primary endpoint was the rate of death or major disability (a modified Rankin score of 3 or higher) at 14 days or at the time of hospital discharge. This endpoint occurred in 34% of patients in both the intervention and control arms, reported Dr. He, professor of epidemiology at Tulane University in New Orleans. After 14 days or at discharge, the average modified Rankin score was 2 for patients in both treatment arms.
The report by Dr. He and his associates was published online in JAMA (2013 Nov. 17 [doi:10.1001/jama.2013.282543]) concurrently with his presentation.
Dr. He and Dr. Sila said that they had no disclosures.
On Twitter @mitchelzoler
Elevated blood pressure occurs in most patients with acute ischemic stroke, and it may be harmful but might also be protective. The results of this study, the largest reported trial of blood pressure management in acute ischemic stroke patients, add something to our clinical judgment for the subset of patients who match those enrolled in the study: patients beyond the hyper-acute phase with a mild stroke (average NIH Stroke Scale score of 4), no major-vessel occlusions, moderately elevated blood pressure, and no reperfusion treatment.

|
Mitchel L. Zoler/IMNG Medical Media
|
In this trial, an average blood pressure reduction of 12.7% after 24 hours did not improve the primary endpoint but it did not worsen recovery. That is reassuring. It shows that we can push the envelope a little in our use of blood pressure reduction. In current U.S. practice, some clinicians will try to reduce blood pressure in patients with moderately elevated pressure. Many U.S. stroke units are comfortable with blood pressure monitoring and with the target of less than 180 mm Hg used for patients treated with tissue plasminogen activator. These protocols are often also applied to ischemic stroke patients not treated with fibrinolysis because it is part of their usual practice.
My take on the findings is that, for the types of patients enrolled in this study, this strategy of more active blood pressure management to get pressure down to a goal level could be a safe option.
Dr. Cathy Sila is professor of neurology and director of the stroke and cerebrovascular center at Case Medical Center in Cleveland. She made these comments as the designated discussant for the report and in an interview.
Elevated blood pressure occurs in most patients with acute ischemic stroke, and it may be harmful but might also be protective. The results of this study, the largest reported trial of blood pressure management in acute ischemic stroke patients, add something to our clinical judgment for the subset of patients who match those enrolled in the study: patients beyond the hyper-acute phase with a mild stroke (average NIH Stroke Scale score of 4), no major-vessel occlusions, moderately elevated blood pressure, and no reperfusion treatment.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
In this trial, an average blood pressure reduction of 12.7% after 24 hours did not improve the primary endpoint but it did not worsen recovery. That is reassuring. It shows that we can push the envelope a little in our use of blood pressure reduction. In current U.S. practice, some clinicians will try to reduce blood pressure in patients with moderately elevated pressure. Many U.S. stroke units are comfortable with blood pressure monitoring and with the target of less than 180 mm Hg used for patients treated with tissue plasminogen activator. These protocols are often also applied to ischemic stroke patients not treated with fibrinolysis because it is part of their usual practice.
My take on the findings is that, for the types of patients enrolled in this study, this strategy of more active blood pressure management to get pressure down to a goal level could be a safe option.
Dr. Cathy Sila is professor of neurology and director of the stroke and cerebrovascular center at Case Medical Center in Cleveland. She made these comments as the designated discussant for the report and in an interview.
Elevated blood pressure occurs in most patients with acute ischemic stroke, and it may be harmful but might also be protective. The results of this study, the largest reported trial of blood pressure management in acute ischemic stroke patients, add something to our clinical judgment for the subset of patients who match those enrolled in the study: patients beyond the hyper-acute phase with a mild stroke (average NIH Stroke Scale score of 4), no major-vessel occlusions, moderately elevated blood pressure, and no reperfusion treatment.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
In this trial, an average blood pressure reduction of 12.7% after 24 hours did not improve the primary endpoint but it did not worsen recovery. That is reassuring. It shows that we can push the envelope a little in our use of blood pressure reduction. In current U.S. practice, some clinicians will try to reduce blood pressure in patients with moderately elevated pressure. Many U.S. stroke units are comfortable with blood pressure monitoring and with the target of less than 180 mm Hg used for patients treated with tissue plasminogen activator. These protocols are often also applied to ischemic stroke patients not treated with fibrinolysis because it is part of their usual practice.
My take on the findings is that, for the types of patients enrolled in this study, this strategy of more active blood pressure management to get pressure down to a goal level could be a safe option.
Dr. Cathy Sila is professor of neurology and director of the stroke and cerebrovascular center at Case Medical Center in Cleveland. She made these comments as the designated discussant for the report and in an interview.
DALLAS – Immediate blood pressure reduction in hypertensive acute ischemic stroke patients did not reduce death and disability after 14 days, but the strategy was safe and did not worsen patient’s 14-day outcomes, a randomized controlled study has shown.
The findings suggest that, among patients with relatively mild acute ischemic strokes and a systolic blood pressure of 140-219 mm Hg, "the decision to lower blood pressure with antihypertensive treatment should be based on individual clinical judgment," Dr. Jiang He said at the American Heart Association scientific sessions.
Elevated blood pressure immediately following an ischemic stroke poses a risk of hemorrhagic conversion or cerebral edema, but an elevated blood pressure also might be protective by forcing more blood into the penumbra around the stroke site. Blood pressure reduction measures are not appropriate for patients treated by reperfusion, but they are considered necessary for patients with "markedly elevated" blood pressure, generally defined as a systolic pressure of 220 mm Hg or higher, he said.
U.S. guidelines on stroke management published earlier this year noted that the data to guide recommendations for treating less severe arterial hypertension, in the range studied in this trial, are "inconclusive or conflicting," and that "the benefit of treating arterial hypertension in the setting of acute ischemic stroke is not well established" (Stroke 2013;44:870-947). Some U.S. clinicians, however, take steps to reduce moderately elevated blood pressure in acute ischemic stroke patients, especially when systolic pressures are at or close to 200 mm Hg.
Based on the new findings, Dr. Sila proposed in her formal comments a strategy for managing patients with mild ischemic strokes who do not undergo reperfusion treatment and have a systolic pressure of 140-219 mm Hg more than 15 hours after their stroke onset and no major-vessel stenosis or occlusion. She suggested that a "reasonable" goal was to lower blood pressure by 10%-15% over the first 24 hours of treatment, with a goal blood pressure of less than 140/90 mm Hg within the next 7 days.
The China Antihypertensive Trial in Acute Ischemic Stroke (CATIS) randomized 4,071 patients aged 22 years or older with a confirmed ischemic stroke who did not undergo reperfusion treatment at 26 hospitals in China. Their average age was 62 years, they were seen an average of 15 hours after their stroke onset, and they had a median National Institutes of Health Stroke Scale score of 4.
The 2,038 patients randomized to blood pressure reduction received an intravenous angiotensin-converting enzyme inhibitor, enalapril, as their first-line treatment, followed by a calcium channel blocker as second-line treatment and a diuretic as a third-line agent. The objective was to reduce systolic pressure by 10%-25% within the first 24 hours, with a goal blood pressure of less than 140/90 mm Hg after 7 days.
The treatments were effective, resulting in an average 13% reduction in blood pressure in treated patients after 24 hours (an average drop of 22 mm Hg), and an average systolic pressure of 137 mm Hg after 7 days. The control patients had an average 7% reduction in their systolic pressure, an average reduction of 13 mm Hg after 24 hours, and an average systolic pressure of 147 mm Hg after 7 days. All of the differences were significant.
The study’s primary endpoint was the rate of death or major disability (a modified Rankin score of 3 or higher) at 14 days or at the time of hospital discharge. This endpoint occurred in 34% of patients in both the intervention and control arms, reported Dr. He, professor of epidemiology at Tulane University in New Orleans. After 14 days or at discharge, the average modified Rankin score was 2 for patients in both treatment arms.
The report by Dr. He and his associates was published online in JAMA (2013 Nov. 17 [doi:10.1001/jama.2013.282543]) concurrently with his presentation.
Dr. He and Dr. Sila said that they had no disclosures.
On Twitter @mitchelzoler
DALLAS – Immediate blood pressure reduction in hypertensive acute ischemic stroke patients did not reduce death and disability after 14 days, but the strategy was safe and did not worsen patient’s 14-day outcomes, a randomized controlled study has shown.
The findings suggest that, among patients with relatively mild acute ischemic strokes and a systolic blood pressure of 140-219 mm Hg, "the decision to lower blood pressure with antihypertensive treatment should be based on individual clinical judgment," Dr. Jiang He said at the American Heart Association scientific sessions.
Elevated blood pressure immediately following an ischemic stroke poses a risk of hemorrhagic conversion or cerebral edema, but an elevated blood pressure also might be protective by forcing more blood into the penumbra around the stroke site. Blood pressure reduction measures are not appropriate for patients treated by reperfusion, but they are considered necessary for patients with "markedly elevated" blood pressure, generally defined as a systolic pressure of 220 mm Hg or higher, he said.
U.S. guidelines on stroke management published earlier this year noted that the data to guide recommendations for treating less severe arterial hypertension, in the range studied in this trial, are "inconclusive or conflicting," and that "the benefit of treating arterial hypertension in the setting of acute ischemic stroke is not well established" (Stroke 2013;44:870-947). Some U.S. clinicians, however, take steps to reduce moderately elevated blood pressure in acute ischemic stroke patients, especially when systolic pressures are at or close to 200 mm Hg.
Based on the new findings, Dr. Sila proposed in her formal comments a strategy for managing patients with mild ischemic strokes who do not undergo reperfusion treatment and have a systolic pressure of 140-219 mm Hg more than 15 hours after their stroke onset and no major-vessel stenosis or occlusion. She suggested that a "reasonable" goal was to lower blood pressure by 10%-15% over the first 24 hours of treatment, with a goal blood pressure of less than 140/90 mm Hg within the next 7 days.
The China Antihypertensive Trial in Acute Ischemic Stroke (CATIS) randomized 4,071 patients aged 22 years or older with a confirmed ischemic stroke who did not undergo reperfusion treatment at 26 hospitals in China. Their average age was 62 years, they were seen an average of 15 hours after their stroke onset, and they had a median National Institutes of Health Stroke Scale score of 4.
The 2,038 patients randomized to blood pressure reduction received an intravenous angiotensin-converting enzyme inhibitor, enalapril, as their first-line treatment, followed by a calcium channel blocker as second-line treatment and a diuretic as a third-line agent. The objective was to reduce systolic pressure by 10%-25% within the first 24 hours, with a goal blood pressure of less than 140/90 mm Hg after 7 days.
The treatments were effective, resulting in an average 13% reduction in blood pressure in treated patients after 24 hours (an average drop of 22 mm Hg), and an average systolic pressure of 137 mm Hg after 7 days. The control patients had an average 7% reduction in their systolic pressure, an average reduction of 13 mm Hg after 24 hours, and an average systolic pressure of 147 mm Hg after 7 days. All of the differences were significant.
The study’s primary endpoint was the rate of death or major disability (a modified Rankin score of 3 or higher) at 14 days or at the time of hospital discharge. This endpoint occurred in 34% of patients in both the intervention and control arms, reported Dr. He, professor of epidemiology at Tulane University in New Orleans. After 14 days or at discharge, the average modified Rankin score was 2 for patients in both treatment arms.
The report by Dr. He and his associates was published online in JAMA (2013 Nov. 17 [doi:10.1001/jama.2013.282543]) concurrently with his presentation.
Dr. He and Dr. Sila said that they had no disclosures.
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Major finding: Blood pressure lowering resulted in a similar rate of death and major disability as placebo after 14 days.
Data source: The CATIS trial randomized 4,071 patients with mild acute ischemic strokes to a blood pressure-lowering strategy or placebo at 26 Chinese hospitals.
Disclosures: Dr. He and Dr. Sila said that they had no disclosures.

New psychoactive drug nomenclature system devised
BARCELONA – Neuropsychopharmacologists want to change the way you describe psychoactive drugs.
A team of representatives from four international neuropsychopharmacology groups is finishing a first draft of its proposed new system for drug classification and nomenclature that – in its current form – describes each of approximately 120 psychoactive drugs by five different parameters, or axes, including neurobiologic activity, efficacy, and approved indications worldwide. The goal is a new, Web-based framework for classifying and identifying drugs that is more consistent, informative, and transparent than the existing nomenclature.
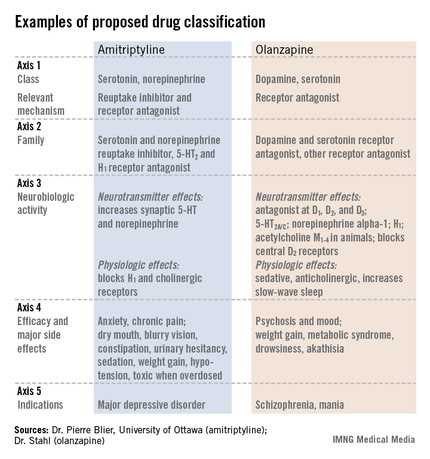
"We expect drug nomenclature to reflect current scientific knowledge, give useful pharmacologic information to clinicians, and give patients a rationale for using a drug," but the existing nomenclature does not accomplish those goals, said Dr. Joseph Zohar, director of psychiatry at Sheba Medical Center in Tel Hashomer, Israel, and a member of the nomenclature group. "Existing nomenclature dates from the 1960s; no wonder it does not reflect current understanding. Drugs called antidepressants are often prescribed to patients with anxiety disorders. Patients ask, why give me an antidepressant if I have anxiety? Antipsychotics are prescribed to patients with depression, and they ask why they are getting an antipsychotic? The nomenclature is confusing," Dr. Zohar said at a session at the annual congress of the European College of Neuropsychopharmacology devoted to presenting the new nomenclature system to congress participants.
"We want to rationalize classification and have it better reflect science. We want to focus on mechanisms; knowing the entire profile of medications will help make more informed choices," he said.
"It’s getting people to think more about what drugs do. If people understood drugs better, they would use them better," said Dr. David J. Nutt, professor of neuropsychopharmacology at Imperial College London and another member of the nomenclature group. "The shorthands we currently use [for classifying psychoactive drugs] may be useful, but we need to determine what’s not useful" and get rid of it.
Leadership from the European College of Neuropsychopharmacology (ECNP) arranged for a panel with two representatives each from the American College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, the Asian College of Neuropsychopharmacology, and the ECNP. A draft version of the nomenclature document should appear for comment on the ECNP website by early next year, and the current plan is to publish a finalized version before the end of next year. But the panel members stressed that since the document will primarily be Web-based, it will be open to frequent revision.
"This is the first step in a long process. We’re trying to wake up a 50-year-old nomenclature into a living document that will be used over the next decades and may someday merge with DSM [Diagnostic and Statistical Manual of Mental Disorders]," said Dr. Stephen M. Stahl, a panel member and psychiatrist affiliated with the University of California, San Diego.
The format the panel has in place currently describes every psychoactive drug in terms of five axes: class and relevant mechanisms; family; neurobiologic activity, neurotransmitter effects, and physiologic effects; efficacy and major side effects; and approved and licenses indications in the major countries and regions that perform drug licensing. Some of the collaborators on the panel published an explanation of the five axes template online in September (Euro. Neuropsychopharmacol. 2013 [doi:10.1016/j.euroneuro.2013.08.004]).

All this information for each drug "should tell you everything you need to know to make a rational decision about what to do with the drug," Dr. Nutt said.
"We need to be very humble about these medications and what they do. You have multiple things going on simultaneously," said Dr. Stahl, also founder of the Neuroscience Education Institute in San Diego. "The second-generation antipsychotics are the most complicated drugs in medicine; one patient’s side effect is another’s therapeutic effect.
"We propose that it is no longer appropriate to name all drugs that treat psychosis as ‘antipsychotics.’ We propose a multiaxial classification system based on pharmacologic mechanisms of action. A mechanism-based nomenclature may clarify the differing mechanisms of individual agents, especially actions in psychosis versus mood disorders. This approach has the potential to better inform those who work with drugs that treat depression, and prevent confusion with other drugs that treat both psychosis and multiple additional disorders such as depression and mania. This approach is also a strategy for naming drugs yet to be discovered that target novel mechanisms of action."
"What we don’t want is industry or a regulator to define a new glycine-reuptake blocker as an antipsychotic," Dr. Nutt said.
Several panel members stressed that the five-axis format will allow a diverse list of useful information.
"We don’t want to be constrained by the approved indications," Dr. Nutt said. "This is an opportunity to document off-label indications and to link to the evidence for off-label uses," said Dr. Guy Goodwin, chairman of psychiatry at the University of Oxford (England) and another collaborator on the panel.
The audience of about 150 congress attendees at the session seemed persuaded by the speakers. At the session’s end, in an electronic vote, 67% said they fully agreed, and another 26% said they partly agreed, that the existing nomenclature needs revision. Asked whether the proposed nomenclature was a step in the right direction, 48% said they fully agreed, and another 39% said they partly agreed. Another question asked what feature should drive a drug’s top-line definition. Sixty percent of the audience said pharmacologic action, and an additional 29% voted in favor of clinical indication.
Dr. Zohar said he has been an adviser or consultant to or received research support from eight drug companies. Dr. Nutt said he has been an adviser or consultant to eight drug companies. Dr. Stahl said he has been an adviser or consultant to more than 30 drug companies. Dr. Goodwin said he had been an adviser or consultant to 12 drug companies.
On Twitter @mitchelzoler
BARCELONA – Neuropsychopharmacologists want to change the way you describe psychoactive drugs.
A team of representatives from four international neuropsychopharmacology groups is finishing a first draft of its proposed new system for drug classification and nomenclature that – in its current form – describes each of approximately 120 psychoactive drugs by five different parameters, or axes, including neurobiologic activity, efficacy, and approved indications worldwide. The goal is a new, Web-based framework for classifying and identifying drugs that is more consistent, informative, and transparent than the existing nomenclature.
"We expect drug nomenclature to reflect current scientific knowledge, give useful pharmacologic information to clinicians, and give patients a rationale for using a drug," but the existing nomenclature does not accomplish those goals, said Dr. Joseph Zohar, director of psychiatry at Sheba Medical Center in Tel Hashomer, Israel, and a member of the nomenclature group. "Existing nomenclature dates from the 1960s; no wonder it does not reflect current understanding. Drugs called antidepressants are often prescribed to patients with anxiety disorders. Patients ask, why give me an antidepressant if I have anxiety? Antipsychotics are prescribed to patients with depression, and they ask why they are getting an antipsychotic? The nomenclature is confusing," Dr. Zohar said at a session at the annual congress of the European College of Neuropsychopharmacology devoted to presenting the new nomenclature system to congress participants.
"We want to rationalize classification and have it better reflect science. We want to focus on mechanisms; knowing the entire profile of medications will help make more informed choices," he said.
"It’s getting people to think more about what drugs do. If people understood drugs better, they would use them better," said Dr. David J. Nutt, professor of neuropsychopharmacology at Imperial College London and another member of the nomenclature group. "The shorthands we currently use [for classifying psychoactive drugs] may be useful, but we need to determine what’s not useful" and get rid of it.
Leadership from the European College of Neuropsychopharmacology (ECNP) arranged for a panel with two representatives each from the American College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, the Asian College of Neuropsychopharmacology, and the ECNP. A draft version of the nomenclature document should appear for comment on the ECNP website by early next year, and the current plan is to publish a finalized version before the end of next year. But the panel members stressed that since the document will primarily be Web-based, it will be open to frequent revision.
"This is the first step in a long process. We’re trying to wake up a 50-year-old nomenclature into a living document that will be used over the next decades and may someday merge with DSM [Diagnostic and Statistical Manual of Mental Disorders]," said Dr. Stephen M. Stahl, a panel member and psychiatrist affiliated with the University of California, San Diego.
The format the panel has in place currently describes every psychoactive drug in terms of five axes: class and relevant mechanisms; family; neurobiologic activity, neurotransmitter effects, and physiologic effects; efficacy and major side effects; and approved and licenses indications in the major countries and regions that perform drug licensing. Some of the collaborators on the panel published an explanation of the five axes template online in September (Euro. Neuropsychopharmacol. 2013 [doi:10.1016/j.euroneuro.2013.08.004]).
All this information for each drug "should tell you everything you need to know to make a rational decision about what to do with the drug," Dr. Nutt said.
"We need to be very humble about these medications and what they do. You have multiple things going on simultaneously," said Dr. Stahl, also founder of the Neuroscience Education Institute in San Diego. "The second-generation antipsychotics are the most complicated drugs in medicine; one patient’s side effect is another’s therapeutic effect.
"We propose that it is no longer appropriate to name all drugs that treat psychosis as ‘antipsychotics.’ We propose a multiaxial classification system based on pharmacologic mechanisms of action. A mechanism-based nomenclature may clarify the differing mechanisms of individual agents, especially actions in psychosis versus mood disorders. This approach has the potential to better inform those who work with drugs that treat depression, and prevent confusion with other drugs that treat both psychosis and multiple additional disorders such as depression and mania. This approach is also a strategy for naming drugs yet to be discovered that target novel mechanisms of action."
"What we don’t want is industry or a regulator to define a new glycine-reuptake blocker as an antipsychotic," Dr. Nutt said.
Several panel members stressed that the five-axis format will allow a diverse list of useful information.
"We don’t want to be constrained by the approved indications," Dr. Nutt said. "This is an opportunity to document off-label indications and to link to the evidence for off-label uses," said Dr. Guy Goodwin, chairman of psychiatry at the University of Oxford (England) and another collaborator on the panel.
The audience of about 150 congress attendees at the session seemed persuaded by the speakers. At the session’s end, in an electronic vote, 67% said they fully agreed, and another 26% said they partly agreed, that the existing nomenclature needs revision. Asked whether the proposed nomenclature was a step in the right direction, 48% said they fully agreed, and another 39% said they partly agreed. Another question asked what feature should drive a drug’s top-line definition. Sixty percent of the audience said pharmacologic action, and an additional 29% voted in favor of clinical indication.
Dr. Zohar said he has been an adviser or consultant to or received research support from eight drug companies. Dr. Nutt said he has been an adviser or consultant to eight drug companies. Dr. Stahl said he has been an adviser or consultant to more than 30 drug companies. Dr. Goodwin said he had been an adviser or consultant to 12 drug companies.
On Twitter @mitchelzoler
BARCELONA – Neuropsychopharmacologists want to change the way you describe psychoactive drugs.
A team of representatives from four international neuropsychopharmacology groups is finishing a first draft of its proposed new system for drug classification and nomenclature that – in its current form – describes each of approximately 120 psychoactive drugs by five different parameters, or axes, including neurobiologic activity, efficacy, and approved indications worldwide. The goal is a new, Web-based framework for classifying and identifying drugs that is more consistent, informative, and transparent than the existing nomenclature.
"We expect drug nomenclature to reflect current scientific knowledge, give useful pharmacologic information to clinicians, and give patients a rationale for using a drug," but the existing nomenclature does not accomplish those goals, said Dr. Joseph Zohar, director of psychiatry at Sheba Medical Center in Tel Hashomer, Israel, and a member of the nomenclature group. "Existing nomenclature dates from the 1960s; no wonder it does not reflect current understanding. Drugs called antidepressants are often prescribed to patients with anxiety disorders. Patients ask, why give me an antidepressant if I have anxiety? Antipsychotics are prescribed to patients with depression, and they ask why they are getting an antipsychotic? The nomenclature is confusing," Dr. Zohar said at a session at the annual congress of the European College of Neuropsychopharmacology devoted to presenting the new nomenclature system to congress participants.
"We want to rationalize classification and have it better reflect science. We want to focus on mechanisms; knowing the entire profile of medications will help make more informed choices," he said.
"It’s getting people to think more about what drugs do. If people understood drugs better, they would use them better," said Dr. David J. Nutt, professor of neuropsychopharmacology at Imperial College London and another member of the nomenclature group. "The shorthands we currently use [for classifying psychoactive drugs] may be useful, but we need to determine what’s not useful" and get rid of it.
Leadership from the European College of Neuropsychopharmacology (ECNP) arranged for a panel with two representatives each from the American College of Neuropsychopharmacology, the International College of Neuropsychopharmacology, the Asian College of Neuropsychopharmacology, and the ECNP. A draft version of the nomenclature document should appear for comment on the ECNP website by early next year, and the current plan is to publish a finalized version before the end of next year. But the panel members stressed that since the document will primarily be Web-based, it will be open to frequent revision.
"This is the first step in a long process. We’re trying to wake up a 50-year-old nomenclature into a living document that will be used over the next decades and may someday merge with DSM [Diagnostic and Statistical Manual of Mental Disorders]," said Dr. Stephen M. Stahl, a panel member and psychiatrist affiliated with the University of California, San Diego.
The format the panel has in place currently describes every psychoactive drug in terms of five axes: class and relevant mechanisms; family; neurobiologic activity, neurotransmitter effects, and physiologic effects; efficacy and major side effects; and approved and licenses indications in the major countries and regions that perform drug licensing. Some of the collaborators on the panel published an explanation of the five axes template online in September (Euro. Neuropsychopharmacol. 2013 [doi:10.1016/j.euroneuro.2013.08.004]).
All this information for each drug "should tell you everything you need to know to make a rational decision about what to do with the drug," Dr. Nutt said.
"We need to be very humble about these medications and what they do. You have multiple things going on simultaneously," said Dr. Stahl, also founder of the Neuroscience Education Institute in San Diego. "The second-generation antipsychotics are the most complicated drugs in medicine; one patient’s side effect is another’s therapeutic effect.
"We propose that it is no longer appropriate to name all drugs that treat psychosis as ‘antipsychotics.’ We propose a multiaxial classification system based on pharmacologic mechanisms of action. A mechanism-based nomenclature may clarify the differing mechanisms of individual agents, especially actions in psychosis versus mood disorders. This approach has the potential to better inform those who work with drugs that treat depression, and prevent confusion with other drugs that treat both psychosis and multiple additional disorders such as depression and mania. This approach is also a strategy for naming drugs yet to be discovered that target novel mechanisms of action."
"What we don’t want is industry or a regulator to define a new glycine-reuptake blocker as an antipsychotic," Dr. Nutt said.
Several panel members stressed that the five-axis format will allow a diverse list of useful information.
"We don’t want to be constrained by the approved indications," Dr. Nutt said. "This is an opportunity to document off-label indications and to link to the evidence for off-label uses," said Dr. Guy Goodwin, chairman of psychiatry at the University of Oxford (England) and another collaborator on the panel.
The audience of about 150 congress attendees at the session seemed persuaded by the speakers. At the session’s end, in an electronic vote, 67% said they fully agreed, and another 26% said they partly agreed, that the existing nomenclature needs revision. Asked whether the proposed nomenclature was a step in the right direction, 48% said they fully agreed, and another 39% said they partly agreed. Another question asked what feature should drive a drug’s top-line definition. Sixty percent of the audience said pharmacologic action, and an additional 29% voted in favor of clinical indication.
Dr. Zohar said he has been an adviser or consultant to or received research support from eight drug companies. Dr. Nutt said he has been an adviser or consultant to eight drug companies. Dr. Stahl said he has been an adviser or consultant to more than 30 drug companies. Dr. Goodwin said he had been an adviser or consultant to 12 drug companies.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE ECNP CONGRESS
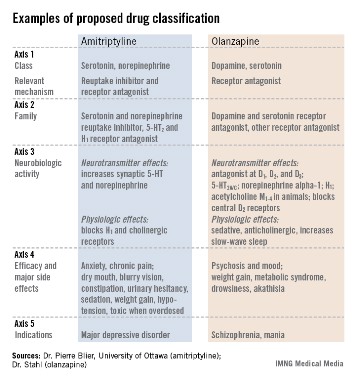
Second-generation antipsychotics cause modest extrapyramidal symptoms
BARCELONA – The greatest risk that patients with schizophrenia will develop extrapyramidal symptoms while on treatment with a second-generation antipsychotic drug comes during the first few weeks of treatment, and then substantially resolves during the rest of the first year on treatment, according to findings from a multicenter European trial with 498 patients.
In addition, the risk level varies from drug to drug, and some extrapyramidal symptoms are rare, with no treatment-related episodes of dystonia and dyskinesia, including tardive dyskinesia, during the year on treatment, Dr. Janusz K. Rybakowski said at the annual congress of the European College of Neuropsychopharmacology.
"Generally, it can be stated that extrapyramidal symptoms are not much of a problem for patients taking second-generation antipsychotic drugs except for the problem of akathisia with ziprasidone treatment, which should be taken into account" when considering which drug to prescribe, said Dr. Rybakowski, professor and head of adult psychiatry at Poznañ (Poland) University.
In the study, 24% of newly diagnosed schizophrenia patients who received ziprasidone as their initial treatment developed akathisia by 1 month after starting treatment. However, among patients who remained in the study and on ziprasidone treatment for 1 year, the prevalence of akathisia fell to less than 9%, he reported. The analysis also documented the rates at which patients developed parkinsonian symptoms.
Second-generation antipsychotics "have to be looked at for their risk-benefit profile," commented Dr. W. Wolfgang Fleischhacker, professor and director of psychiatry at the Medical University of Innsbruck, Austria, and a EUFEST (European First Episode of Schizophrenia Trial) coinvestigator. "Some of these drugs have problems, but they are also effective. Some may have problems causing metabolic syndrome but not extrapyramidal symptoms, and vise versa. And we lack good predictors" for which patients will develop significant adverse effects on treatment. "Even if olanzapine is the biggest offender with regard to metabolic disturbances, probably only 40% of patients are affected. So we can’t judge these drugs generally; we need to closely monitor patients" to see which ones actually develop a significant adverse effect on treatment, Dr. Fleischhacker said.
Dr. Rybakowski and his associates used data collected in EUFEST, which enrolled 498 patients at 50 centers in Europe and in Israel (Lancet 2008;371:1085-97). The investigators randomized patients to treatment with olanzapine, quetiapine, amisulpride, ziprasidone, or to the first-generation antipsychotic haloperidol.
After 1 month, the incidence of parkinsonian symptoms ranged from 4% among those on olanzapine to 13% of those on ziprasidone (and 26% for those on haloperidol). But by 12 months, the rate had dropped to zero among patients on olanzapine and also dropped among all other patients. At 1 year, the highest rate, 9%, was among patients on haloperidol. After 1 month, the incidence of akathisia ranged from 3% among those on olanzapine to 24% for those on ziprasidone (and 21% for patients on haloperidol); after 12 months, the rate fell to zero in patients on olanzapine or amisulpride and was highest, at 7%, among patients on quetiapine.
Although no patients on any second-generation drug developed new symptoms of dystonia or dyskinesia, a few on haloperidol developed dyskinesia.
The percent of patients receiving an anticholinergic drug at 1 month to treat their extrapyramidal symptoms ranged from 13% of those on ziprasidone, 10% on amisulpride, 3% on olanzapine, 2% on quetiapine, and 24% on haloperidol. After 12 months, the rate of anticholinergic drug use fell to a high of 11% on haloperidol and 6% for amisulpride. Patients on all the other second-generation antipsychotics had lower rates of anticholinergic drug use.
EUFEST was sponsored by AstraZeneca, Sanofi-Aventis, and Pfizer. Dr. Rybakowski said he has been a consultant to Adamed, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen-Cilag, Lundbeck, Sanofi-Aventis, and Servier. Dr. Fleischhacker has received honoraria as a speaker or consultant to Bristol-Myers Squibb, Janssen, Lundbeck, MedAvante, Merck, Otsuka, Pfizer, and Roche.
On Twitter @mitchelzoler
BARCELONA – The greatest risk that patients with schizophrenia will develop extrapyramidal symptoms while on treatment with a second-generation antipsychotic drug comes during the first few weeks of treatment, and then substantially resolves during the rest of the first year on treatment, according to findings from a multicenter European trial with 498 patients.
In addition, the risk level varies from drug to drug, and some extrapyramidal symptoms are rare, with no treatment-related episodes of dystonia and dyskinesia, including tardive dyskinesia, during the year on treatment, Dr. Janusz K. Rybakowski said at the annual congress of the European College of Neuropsychopharmacology.
"Generally, it can be stated that extrapyramidal symptoms are not much of a problem for patients taking second-generation antipsychotic drugs except for the problem of akathisia with ziprasidone treatment, which should be taken into account" when considering which drug to prescribe, said Dr. Rybakowski, professor and head of adult psychiatry at Poznañ (Poland) University.
In the study, 24% of newly diagnosed schizophrenia patients who received ziprasidone as their initial treatment developed akathisia by 1 month after starting treatment. However, among patients who remained in the study and on ziprasidone treatment for 1 year, the prevalence of akathisia fell to less than 9%, he reported. The analysis also documented the rates at which patients developed parkinsonian symptoms.
Second-generation antipsychotics "have to be looked at for their risk-benefit profile," commented Dr. W. Wolfgang Fleischhacker, professor and director of psychiatry at the Medical University of Innsbruck, Austria, and a EUFEST (European First Episode of Schizophrenia Trial) coinvestigator. "Some of these drugs have problems, but they are also effective. Some may have problems causing metabolic syndrome but not extrapyramidal symptoms, and vise versa. And we lack good predictors" for which patients will develop significant adverse effects on treatment. "Even if olanzapine is the biggest offender with regard to metabolic disturbances, probably only 40% of patients are affected. So we can’t judge these drugs generally; we need to closely monitor patients" to see which ones actually develop a significant adverse effect on treatment, Dr. Fleischhacker said.
Dr. Rybakowski and his associates used data collected in EUFEST, which enrolled 498 patients at 50 centers in Europe and in Israel (Lancet 2008;371:1085-97). The investigators randomized patients to treatment with olanzapine, quetiapine, amisulpride, ziprasidone, or to the first-generation antipsychotic haloperidol.
After 1 month, the incidence of parkinsonian symptoms ranged from 4% among those on olanzapine to 13% of those on ziprasidone (and 26% for those on haloperidol). But by 12 months, the rate had dropped to zero among patients on olanzapine and also dropped among all other patients. At 1 year, the highest rate, 9%, was among patients on haloperidol. After 1 month, the incidence of akathisia ranged from 3% among those on olanzapine to 24% for those on ziprasidone (and 21% for patients on haloperidol); after 12 months, the rate fell to zero in patients on olanzapine or amisulpride and was highest, at 7%, among patients on quetiapine.
Although no patients on any second-generation drug developed new symptoms of dystonia or dyskinesia, a few on haloperidol developed dyskinesia.
The percent of patients receiving an anticholinergic drug at 1 month to treat their extrapyramidal symptoms ranged from 13% of those on ziprasidone, 10% on amisulpride, 3% on olanzapine, 2% on quetiapine, and 24% on haloperidol. After 12 months, the rate of anticholinergic drug use fell to a high of 11% on haloperidol and 6% for amisulpride. Patients on all the other second-generation antipsychotics had lower rates of anticholinergic drug use.
EUFEST was sponsored by AstraZeneca, Sanofi-Aventis, and Pfizer. Dr. Rybakowski said he has been a consultant to Adamed, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen-Cilag, Lundbeck, Sanofi-Aventis, and Servier. Dr. Fleischhacker has received honoraria as a speaker or consultant to Bristol-Myers Squibb, Janssen, Lundbeck, MedAvante, Merck, Otsuka, Pfizer, and Roche.
On Twitter @mitchelzoler
BARCELONA – The greatest risk that patients with schizophrenia will develop extrapyramidal symptoms while on treatment with a second-generation antipsychotic drug comes during the first few weeks of treatment, and then substantially resolves during the rest of the first year on treatment, according to findings from a multicenter European trial with 498 patients.
In addition, the risk level varies from drug to drug, and some extrapyramidal symptoms are rare, with no treatment-related episodes of dystonia and dyskinesia, including tardive dyskinesia, during the year on treatment, Dr. Janusz K. Rybakowski said at the annual congress of the European College of Neuropsychopharmacology.
"Generally, it can be stated that extrapyramidal symptoms are not much of a problem for patients taking second-generation antipsychotic drugs except for the problem of akathisia with ziprasidone treatment, which should be taken into account" when considering which drug to prescribe, said Dr. Rybakowski, professor and head of adult psychiatry at Poznañ (Poland) University.
In the study, 24% of newly diagnosed schizophrenia patients who received ziprasidone as their initial treatment developed akathisia by 1 month after starting treatment. However, among patients who remained in the study and on ziprasidone treatment for 1 year, the prevalence of akathisia fell to less than 9%, he reported. The analysis also documented the rates at which patients developed parkinsonian symptoms.
Second-generation antipsychotics "have to be looked at for their risk-benefit profile," commented Dr. W. Wolfgang Fleischhacker, professor and director of psychiatry at the Medical University of Innsbruck, Austria, and a EUFEST (European First Episode of Schizophrenia Trial) coinvestigator. "Some of these drugs have problems, but they are also effective. Some may have problems causing metabolic syndrome but not extrapyramidal symptoms, and vise versa. And we lack good predictors" for which patients will develop significant adverse effects on treatment. "Even if olanzapine is the biggest offender with regard to metabolic disturbances, probably only 40% of patients are affected. So we can’t judge these drugs generally; we need to closely monitor patients" to see which ones actually develop a significant adverse effect on treatment, Dr. Fleischhacker said.
Dr. Rybakowski and his associates used data collected in EUFEST, which enrolled 498 patients at 50 centers in Europe and in Israel (Lancet 2008;371:1085-97). The investigators randomized patients to treatment with olanzapine, quetiapine, amisulpride, ziprasidone, or to the first-generation antipsychotic haloperidol.
After 1 month, the incidence of parkinsonian symptoms ranged from 4% among those on olanzapine to 13% of those on ziprasidone (and 26% for those on haloperidol). But by 12 months, the rate had dropped to zero among patients on olanzapine and also dropped among all other patients. At 1 year, the highest rate, 9%, was among patients on haloperidol. After 1 month, the incidence of akathisia ranged from 3% among those on olanzapine to 24% for those on ziprasidone (and 21% for patients on haloperidol); after 12 months, the rate fell to zero in patients on olanzapine or amisulpride and was highest, at 7%, among patients on quetiapine.
Although no patients on any second-generation drug developed new symptoms of dystonia or dyskinesia, a few on haloperidol developed dyskinesia.
The percent of patients receiving an anticholinergic drug at 1 month to treat their extrapyramidal symptoms ranged from 13% of those on ziprasidone, 10% on amisulpride, 3% on olanzapine, 2% on quetiapine, and 24% on haloperidol. After 12 months, the rate of anticholinergic drug use fell to a high of 11% on haloperidol and 6% for amisulpride. Patients on all the other second-generation antipsychotics had lower rates of anticholinergic drug use.
EUFEST was sponsored by AstraZeneca, Sanofi-Aventis, and Pfizer. Dr. Rybakowski said he has been a consultant to Adamed, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen-Cilag, Lundbeck, Sanofi-Aventis, and Servier. Dr. Fleischhacker has received honoraria as a speaker or consultant to Bristol-Myers Squibb, Janssen, Lundbeck, MedAvante, Merck, Otsuka, Pfizer, and Roche.
On Twitter @mitchelzoler
AT THE ECNP CONGRESS
Major finding: Ziprasidone caused the highest incidence of extrapyramidal symptoms: a 24% akathisia rate and 13% parkinsonian-symptom rate after 1 month.
Data source: EUFEST, a multicenter, randomized study with 498 patients with first-episode schizophrenia.
Disclosures: EUFEST was sponsored by AstraZeneca, Sanofi-Aventis, and Pfizer. Dr. Rybakowski said that he has been a consultant to Adamed, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen-Cilag, Lundbeck, Sanofi-Aventis, and Servier. Dr. Fleischhacker has received honoraria as a speaker or consultant to Bristol-Myers Squibb, Janssen, Lundbeck, MedAvante, Merck, Otsuka, Pfizer, and Roche.