User login
The cost of leadership
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.

Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.
Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.
Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
A spike in syphilis puts prenatal care in focus
Fifteen years ago, reported cases of syphilis in the United States were so infrequent that public health officials thought it might join the ranks of malaria, polio, and smallpox as an eradicated disease. That turned out to be wishful thinking.
According to data from the Centers for Disease Control and Prevention, between 2012 and 2015, the overall rates of syphilis in the United States increased by 48%, while the rates of primary and secondary infection among women spiked by 56%. That was a compelling enough rise, but fresh data from the agency indicate that the overall rates of syphilis increased by 17.6% between 2015 and 2016, and by 74% between 2012 and 2016. 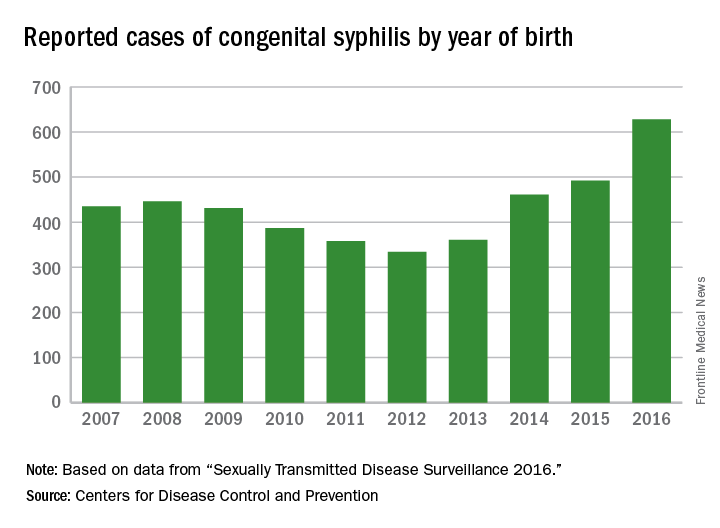
These trends prompted the CDC to launch a “call to action” educational campaign in an effort to curb the rising syphilis rates. The United States Preventive Services Task Force also is taking action. It recently posted a research plan on screening pregnant women for syphilis that will form the basis of a forthcoming evidence review and, potentially, new recommendations.

observed in all regions of the United States during the same time period, said Dr. Kidd, who coauthored a 2015 Morbidity and Mortality Weekly Report on the topic (MMWR. 2015 Nov 13;64[44]:1241-5). That analysis found that during 2012-2014, the number of reported CS cases in the United States increased from 334 to 458, which represents a rate increase from 8.4 to 11.6 cases per 100,000 live births. This contrasted with earlier data, which found that the overall rate of reported CS had decreased from 10.5 to 8.4 cases per 100,000 live births during 2008-2012.
In 2016, there were 628 reported cases of CS, including 41 syphilitic stillbirths, according to the CDC.
“Congenital syphilis rates tend to track female syphilis rates; so as female rates go up, we know we’re going to see a rise in congenital syphilis rates,” Dr. Kidd said. “One way to prevent syphilis is to prevent female syphilis altogether. Another way is to prevent the transmission from mother to infant when you have a pregnant woman with syphilis.”
Lack of prenatal care
CDC guidelines recommend that all pregnant women undergo routine serologic screening for syphilis during their first prenatal visit. Additional testing at 28 weeks’ gestation and again at delivery is warranted for women who are at increased risk or live in communities with increased prevalence of syphilis infection. That approach may seem sensible, but such prevention measures are ineffective when mothers don’t receive any prenatal care or receive it late, which happens in about half of all CS cases, Dr. Kidd said.
Inconsistent, inadequate, or a total absence of prenatal care is “probably the biggest risk factor for vertical transmission, especially among high-risk populations, where there is an increased background prevalence of syphilis in childbearing women,” said Robert Maupin, MD, professor of clinical obstetrics and gynecology in the section of maternal-fetal medicine at Louisiana State University Health Sciences Center, New Orleans.

To complicate matters, women who receive no or inconsistent prenatal care face an increased risk for preterm birth, Dr. Maupin noted. So while a clinician might follow CDC recommendations that pregnant women with confirmed or suspected syphilis complete a course of long-acting penicillin G for at least 30 days or longer before the child is born, “the timing of being able to implement effective prevention and treatment prior to that 30-day window can sometimes be compromised by the fact that she ends up delivering prematurely,” he said. “If someone’s not adequately linked to consistent prenatal care, she may not complete that full course of prevention. Additionally, patterns of care are often fragmented, meaning that patients may go to one clinic or one provider, may not return, and may end up switching to a different clinic. That translates into a potential lag in implementing treatment or making a diagnosis in the first place, and that may be disruptive in the context of our attempted prevention measures.”
Precise reasons why some pregnant women in the United States receive no or inadequate prenatal care remain unclear.
“Anecdotally, in the West, I hear that women with drug abuse histories or drug abuse issues [are vulnerable], or they may be homeless or have mental health issues,” Dr. Kidd said. “In other areas of the country, people feel that it’s more of an insurance or access to care issue, but we don’t have data on that here at the CDC.”
Repeat screening
In 2015, a large analysis of women who were commercially-insured or Medicaid-insured found that more than 95% who received prenatal care were screened for syphilis at least once during pregnancy (Obstet Gynecol. 2015;125[5]:1211-6). However, CDC data of CS cases shows that about 15% of their mothers are infected during pregnancy, which would occur after that first screening test.
“That’s where the repeat screening early in the third trimester and at delivery becomes the real issue,” Dr. Kidd said. “For high-risk women, including those who live in the high morbidity areas, they should be screened again later in pregnancy. Many ob.gyns. may not be aware of that recommendation, or may not be aware they’re in an area that does have a high syphilis morbidity, and that the pregnant women who are seeing them may be at increased risk of syphilis.”
Dr. Maupin, who is associate dean of diversity and community engagement at LSU Health Sciences Center, advised clinicians to view CS with the same sense of urgency that existed in previous years with perinatal HIV transmission.
“In the last decade and a half we’ve seen a substantial decline in perinatal HIV transmission because of intensive efforts on the public health side in terms of both screening and use of treatment,” he said. “If we look at this with a similar level of contemporary urgency, it will bear similar fruit over time. Additionally, from a maternal-fetal medicine standpoint, the more effectively we treat and/or control diseases and comorbidities prior to pregnancy, the less likely those things will have an adverse impact on the health and well-being of the newborn.”
Steps you can take to curb CS
In its “call to action” on syphilis, the Centers for Disease Control and Prevention cited several practical ways that clinicians can combat the spread of congenital syphilis (CS).
1. Complete a sexual history for your patients. The CDC recommends following this with STD counseling for those at risk and contraception counseling for women at risk of unintended pregnancy.
2. Test all pregnant women for syphilis. This should be done at the first prenatal visit, with repeat screening for pregnant women at high risk and in areas of high prevalence at the beginning of the third trimester and again at delivery.
3. Treat women infected with syphilis immediately. If a woman has syphilis or suspected syphilis, she should be treated with long-acting penicillin G, especially if she is pregnant. CDC also calls for testing and treating the infected woman’s sex partner(s) to avoid reinfection.
4. Confirm syphilis testing at delivery. Before discharging the mother or infant from the hospital, check that the mother has been tested for syphilis at least once during pregnancy or at delivery. All women who deliver a stillborn infant should be tested for syphilis.
5. Report CS cases to the local or state health department within 24 hours.
Fifteen years ago, reported cases of syphilis in the United States were so infrequent that public health officials thought it might join the ranks of malaria, polio, and smallpox as an eradicated disease. That turned out to be wishful thinking.
According to data from the Centers for Disease Control and Prevention, between 2012 and 2015, the overall rates of syphilis in the United States increased by 48%, while the rates of primary and secondary infection among women spiked by 56%. That was a compelling enough rise, but fresh data from the agency indicate that the overall rates of syphilis increased by 17.6% between 2015 and 2016, and by 74% between 2012 and 2016.
These trends prompted the CDC to launch a “call to action” educational campaign in an effort to curb the rising syphilis rates. The United States Preventive Services Task Force also is taking action. It recently posted a research plan on screening pregnant women for syphilis that will form the basis of a forthcoming evidence review and, potentially, new recommendations.
observed in all regions of the United States during the same time period, said Dr. Kidd, who coauthored a 2015 Morbidity and Mortality Weekly Report on the topic (MMWR. 2015 Nov 13;64[44]:1241-5). That analysis found that during 2012-2014, the number of reported CS cases in the United States increased from 334 to 458, which represents a rate increase from 8.4 to 11.6 cases per 100,000 live births. This contrasted with earlier data, which found that the overall rate of reported CS had decreased from 10.5 to 8.4 cases per 100,000 live births during 2008-2012.
In 2016, there were 628 reported cases of CS, including 41 syphilitic stillbirths, according to the CDC.
“Congenital syphilis rates tend to track female syphilis rates; so as female rates go up, we know we’re going to see a rise in congenital syphilis rates,” Dr. Kidd said. “One way to prevent syphilis is to prevent female syphilis altogether. Another way is to prevent the transmission from mother to infant when you have a pregnant woman with syphilis.”
Lack of prenatal care
CDC guidelines recommend that all pregnant women undergo routine serologic screening for syphilis during their first prenatal visit. Additional testing at 28 weeks’ gestation and again at delivery is warranted for women who are at increased risk or live in communities with increased prevalence of syphilis infection. That approach may seem sensible, but such prevention measures are ineffective when mothers don’t receive any prenatal care or receive it late, which happens in about half of all CS cases, Dr. Kidd said.
Inconsistent, inadequate, or a total absence of prenatal care is “probably the biggest risk factor for vertical transmission, especially among high-risk populations, where there is an increased background prevalence of syphilis in childbearing women,” said Robert Maupin, MD, professor of clinical obstetrics and gynecology in the section of maternal-fetal medicine at Louisiana State University Health Sciences Center, New Orleans.
To complicate matters, women who receive no or inconsistent prenatal care face an increased risk for preterm birth, Dr. Maupin noted. So while a clinician might follow CDC recommendations that pregnant women with confirmed or suspected syphilis complete a course of long-acting penicillin G for at least 30 days or longer before the child is born, “the timing of being able to implement effective prevention and treatment prior to that 30-day window can sometimes be compromised by the fact that she ends up delivering prematurely,” he said. “If someone’s not adequately linked to consistent prenatal care, she may not complete that full course of prevention. Additionally, patterns of care are often fragmented, meaning that patients may go to one clinic or one provider, may not return, and may end up switching to a different clinic. That translates into a potential lag in implementing treatment or making a diagnosis in the first place, and that may be disruptive in the context of our attempted prevention measures.”
Precise reasons why some pregnant women in the United States receive no or inadequate prenatal care remain unclear.
“Anecdotally, in the West, I hear that women with drug abuse histories or drug abuse issues [are vulnerable], or they may be homeless or have mental health issues,” Dr. Kidd said. “In other areas of the country, people feel that it’s more of an insurance or access to care issue, but we don’t have data on that here at the CDC.”
Repeat screening
In 2015, a large analysis of women who were commercially-insured or Medicaid-insured found that more than 95% who received prenatal care were screened for syphilis at least once during pregnancy (Obstet Gynecol. 2015;125[5]:1211-6). However, CDC data of CS cases shows that about 15% of their mothers are infected during pregnancy, which would occur after that first screening test.
“That’s where the repeat screening early in the third trimester and at delivery becomes the real issue,” Dr. Kidd said. “For high-risk women, including those who live in the high morbidity areas, they should be screened again later in pregnancy. Many ob.gyns. may not be aware of that recommendation, or may not be aware they’re in an area that does have a high syphilis morbidity, and that the pregnant women who are seeing them may be at increased risk of syphilis.”
Dr. Maupin, who is associate dean of diversity and community engagement at LSU Health Sciences Center, advised clinicians to view CS with the same sense of urgency that existed in previous years with perinatal HIV transmission.
“In the last decade and a half we’ve seen a substantial decline in perinatal HIV transmission because of intensive efforts on the public health side in terms of both screening and use of treatment,” he said. “If we look at this with a similar level of contemporary urgency, it will bear similar fruit over time. Additionally, from a maternal-fetal medicine standpoint, the more effectively we treat and/or control diseases and comorbidities prior to pregnancy, the less likely those things will have an adverse impact on the health and well-being of the newborn.”
Steps you can take to curb CS
In its “call to action” on syphilis, the Centers for Disease Control and Prevention cited several practical ways that clinicians can combat the spread of congenital syphilis (CS).
1. Complete a sexual history for your patients. The CDC recommends following this with STD counseling for those at risk and contraception counseling for women at risk of unintended pregnancy.
2. Test all pregnant women for syphilis. This should be done at the first prenatal visit, with repeat screening for pregnant women at high risk and in areas of high prevalence at the beginning of the third trimester and again at delivery.
3. Treat women infected with syphilis immediately. If a woman has syphilis or suspected syphilis, she should be treated with long-acting penicillin G, especially if she is pregnant. CDC also calls for testing and treating the infected woman’s sex partner(s) to avoid reinfection.
4. Confirm syphilis testing at delivery. Before discharging the mother or infant from the hospital, check that the mother has been tested for syphilis at least once during pregnancy or at delivery. All women who deliver a stillborn infant should be tested for syphilis.
5. Report CS cases to the local or state health department within 24 hours.
Fifteen years ago, reported cases of syphilis in the United States were so infrequent that public health officials thought it might join the ranks of malaria, polio, and smallpox as an eradicated disease. That turned out to be wishful thinking.
According to data from the Centers for Disease Control and Prevention, between 2012 and 2015, the overall rates of syphilis in the United States increased by 48%, while the rates of primary and secondary infection among women spiked by 56%. That was a compelling enough rise, but fresh data from the agency indicate that the overall rates of syphilis increased by 17.6% between 2015 and 2016, and by 74% between 2012 and 2016.
These trends prompted the CDC to launch a “call to action” educational campaign in an effort to curb the rising syphilis rates. The United States Preventive Services Task Force also is taking action. It recently posted a research plan on screening pregnant women for syphilis that will form the basis of a forthcoming evidence review and, potentially, new recommendations.
observed in all regions of the United States during the same time period, said Dr. Kidd, who coauthored a 2015 Morbidity and Mortality Weekly Report on the topic (MMWR. 2015 Nov 13;64[44]:1241-5). That analysis found that during 2012-2014, the number of reported CS cases in the United States increased from 334 to 458, which represents a rate increase from 8.4 to 11.6 cases per 100,000 live births. This contrasted with earlier data, which found that the overall rate of reported CS had decreased from 10.5 to 8.4 cases per 100,000 live births during 2008-2012.
In 2016, there were 628 reported cases of CS, including 41 syphilitic stillbirths, according to the CDC.
“Congenital syphilis rates tend to track female syphilis rates; so as female rates go up, we know we’re going to see a rise in congenital syphilis rates,” Dr. Kidd said. “One way to prevent syphilis is to prevent female syphilis altogether. Another way is to prevent the transmission from mother to infant when you have a pregnant woman with syphilis.”
Lack of prenatal care
CDC guidelines recommend that all pregnant women undergo routine serologic screening for syphilis during their first prenatal visit. Additional testing at 28 weeks’ gestation and again at delivery is warranted for women who are at increased risk or live in communities with increased prevalence of syphilis infection. That approach may seem sensible, but such prevention measures are ineffective when mothers don’t receive any prenatal care or receive it late, which happens in about half of all CS cases, Dr. Kidd said.
Inconsistent, inadequate, or a total absence of prenatal care is “probably the biggest risk factor for vertical transmission, especially among high-risk populations, where there is an increased background prevalence of syphilis in childbearing women,” said Robert Maupin, MD, professor of clinical obstetrics and gynecology in the section of maternal-fetal medicine at Louisiana State University Health Sciences Center, New Orleans.
To complicate matters, women who receive no or inconsistent prenatal care face an increased risk for preterm birth, Dr. Maupin noted. So while a clinician might follow CDC recommendations that pregnant women with confirmed or suspected syphilis complete a course of long-acting penicillin G for at least 30 days or longer before the child is born, “the timing of being able to implement effective prevention and treatment prior to that 30-day window can sometimes be compromised by the fact that she ends up delivering prematurely,” he said. “If someone’s not adequately linked to consistent prenatal care, she may not complete that full course of prevention. Additionally, patterns of care are often fragmented, meaning that patients may go to one clinic or one provider, may not return, and may end up switching to a different clinic. That translates into a potential lag in implementing treatment or making a diagnosis in the first place, and that may be disruptive in the context of our attempted prevention measures.”
Precise reasons why some pregnant women in the United States receive no or inadequate prenatal care remain unclear.
“Anecdotally, in the West, I hear that women with drug abuse histories or drug abuse issues [are vulnerable], or they may be homeless or have mental health issues,” Dr. Kidd said. “In other areas of the country, people feel that it’s more of an insurance or access to care issue, but we don’t have data on that here at the CDC.”
Repeat screening
In 2015, a large analysis of women who were commercially-insured or Medicaid-insured found that more than 95% who received prenatal care were screened for syphilis at least once during pregnancy (Obstet Gynecol. 2015;125[5]:1211-6). However, CDC data of CS cases shows that about 15% of their mothers are infected during pregnancy, which would occur after that first screening test.
“That’s where the repeat screening early in the third trimester and at delivery becomes the real issue,” Dr. Kidd said. “For high-risk women, including those who live in the high morbidity areas, they should be screened again later in pregnancy. Many ob.gyns. may not be aware of that recommendation, or may not be aware they’re in an area that does have a high syphilis morbidity, and that the pregnant women who are seeing them may be at increased risk of syphilis.”
Dr. Maupin, who is associate dean of diversity and community engagement at LSU Health Sciences Center, advised clinicians to view CS with the same sense of urgency that existed in previous years with perinatal HIV transmission.
“In the last decade and a half we’ve seen a substantial decline in perinatal HIV transmission because of intensive efforts on the public health side in terms of both screening and use of treatment,” he said. “If we look at this with a similar level of contemporary urgency, it will bear similar fruit over time. Additionally, from a maternal-fetal medicine standpoint, the more effectively we treat and/or control diseases and comorbidities prior to pregnancy, the less likely those things will have an adverse impact on the health and well-being of the newborn.”
Steps you can take to curb CS
In its “call to action” on syphilis, the Centers for Disease Control and Prevention cited several practical ways that clinicians can combat the spread of congenital syphilis (CS).
1. Complete a sexual history for your patients. The CDC recommends following this with STD counseling for those at risk and contraception counseling for women at risk of unintended pregnancy.
2. Test all pregnant women for syphilis. This should be done at the first prenatal visit, with repeat screening for pregnant women at high risk and in areas of high prevalence at the beginning of the third trimester and again at delivery.
3. Treat women infected with syphilis immediately. If a woman has syphilis or suspected syphilis, she should be treated with long-acting penicillin G, especially if she is pregnant. CDC also calls for testing and treating the infected woman’s sex partner(s) to avoid reinfection.
4. Confirm syphilis testing at delivery. Before discharging the mother or infant from the hospital, check that the mother has been tested for syphilis at least once during pregnancy or at delivery. All women who deliver a stillborn infant should be tested for syphilis.
5. Report CS cases to the local or state health department within 24 hours.
Study shows childhood IBD increased cancer risk in adulthood
Children who had developed inflammatory bowel disease had an 18-fold greater risk of gastrointestinal cancers in later life, a new study suggests.
The cohort study found that the risk of all cancers was elevated in individuals with childhood-onset inflammatory bowel disease, but particularly in those with primary sclerosing cholangitis and ulcerative colitis.
Researchers followed 9,405 patients with childhood-onset inflammatory bowel disease to a mean age of 27 years using a Swedish national patient register (BMJ. 2017 Sep 21. doi: 10.1136/bmj.j3951).
Analysis revealed that individuals with childhood-onset inflammatory bowel disease had double the risk of any cancer, compared with the general population (hazard ratio, 2.2; 95% confidence interval, 2.0-2.5), and a 2.7-fold greater risk of developing cancer before the age of 18 years.
Primary sclerosing cholangitis was associated with a sixfold greater risk of cancer, ulcerative colitis was associated with a 2.6-fold greater risk, and patients who had had colitis for 10 years or more had a nearly fourfold greater risk of cancer (HR, 3.9).
The study also found that childhood-onset inflammatory bowel disease was associated with an 18-fold greater risk of gastrointestinal cancer, compared with the general population, matched for age, sex, birth year, and county.
The risk was particularly high in patients with ulcerative colitis, who showed a 33-fold higher risk of colorectal cancer, while patients with Crohn’s disease had a nearly 6-fold higher risk.
“Colorectal cancer is a major cause of cancer mortality in the population, and even a moderately increased incidence is likely to have a large effect on patients with inflammatory bowel disease,” wrote Ola Olén, MD, of Karolinska Institutet, Stockholm, and coauthors.
When the researchers looked in more detail at the type of cancers, they saw the greatest increases in risk were for colorectal cancer (HR, 19.5) and small intestinal cancer (HR, 12.8), while the risk of liver cancer was 134 times higher (95% CI, 59.6-382).
The researchers also saw a 2.7-fold increased risk of lymphoid neoplasms associated with childhood inflammatory bowel disease, particularly in individuals with ulcerative colitis or Crohn’s disease. The most common lymphoid neoplasms were non-Hodgkin lymphomas, followed by Hodgkin lymphomas.
Commenting on possible explanations for the associations seen in the study, the authors said that patients with inflammatory bowel disease may have their gastrointestinal cancers diagnosed earlier than the general population because of regular endoscopies.
They also said that thiopurines and TNF inhibitors – both used to treat inflammatory bowel disease – could not be ruled out as a possible cause of the increase in cancer risk, but their study was not powered to pick up such an effect.
“Instead, we suggest that extent and duration of chronic inflammation might be the main driving mechanisms underlying the increased risk of cancer,” they wrote.
The authors noted that their study did not include data on the smoking status of individuals, which could be significant, because smoking is known to reduce the risk of ulcerative colitis and increase the risk of Crohn’s disease and cancer. However, they pointed out that the majority of patients would not have been smoking at the time of their initial inflammatory bowel disease diagnosis, and would have been unlikely to take up the habit after their diagnosis.
With the observation that the risk of cancer in inflammatory bowel disease was higher in patients who were younger when diagnosed with the disease, the authors suggested that age of onset be considered when designing surveillance strategies for cancer in this group.
The Stockholm County Council and the Karolinska Institutet, the Swedish Cancer Society, the Swedish Research Council, and the Swedish Foundation for Strategic Research supported the study. One author received grants from the Swedish Medical Society, Magtarmfonden, the Jane and Dan Olsson Foundation, the Mjölkdroppen Foundation, the Bengt Ihre Research Fellowship in gastroenterology, and the Karolinska Institutet Foundations. No conflicts of interest were declared.
Children who had developed inflammatory bowel disease had an 18-fold greater risk of gastrointestinal cancers in later life, a new study suggests.
The cohort study found that the risk of all cancers was elevated in individuals with childhood-onset inflammatory bowel disease, but particularly in those with primary sclerosing cholangitis and ulcerative colitis.
Researchers followed 9,405 patients with childhood-onset inflammatory bowel disease to a mean age of 27 years using a Swedish national patient register (BMJ. 2017 Sep 21. doi: 10.1136/bmj.j3951).
Analysis revealed that individuals with childhood-onset inflammatory bowel disease had double the risk of any cancer, compared with the general population (hazard ratio, 2.2; 95% confidence interval, 2.0-2.5), and a 2.7-fold greater risk of developing cancer before the age of 18 years.
Primary sclerosing cholangitis was associated with a sixfold greater risk of cancer, ulcerative colitis was associated with a 2.6-fold greater risk, and patients who had had colitis for 10 years or more had a nearly fourfold greater risk of cancer (HR, 3.9).
The study also found that childhood-onset inflammatory bowel disease was associated with an 18-fold greater risk of gastrointestinal cancer, compared with the general population, matched for age, sex, birth year, and county.
The risk was particularly high in patients with ulcerative colitis, who showed a 33-fold higher risk of colorectal cancer, while patients with Crohn’s disease had a nearly 6-fold higher risk.
“Colorectal cancer is a major cause of cancer mortality in the population, and even a moderately increased incidence is likely to have a large effect on patients with inflammatory bowel disease,” wrote Ola Olén, MD, of Karolinska Institutet, Stockholm, and coauthors.
When the researchers looked in more detail at the type of cancers, they saw the greatest increases in risk were for colorectal cancer (HR, 19.5) and small intestinal cancer (HR, 12.8), while the risk of liver cancer was 134 times higher (95% CI, 59.6-382).
The researchers also saw a 2.7-fold increased risk of lymphoid neoplasms associated with childhood inflammatory bowel disease, particularly in individuals with ulcerative colitis or Crohn’s disease. The most common lymphoid neoplasms were non-Hodgkin lymphomas, followed by Hodgkin lymphomas.
Commenting on possible explanations for the associations seen in the study, the authors said that patients with inflammatory bowel disease may have their gastrointestinal cancers diagnosed earlier than the general population because of regular endoscopies.
They also said that thiopurines and TNF inhibitors – both used to treat inflammatory bowel disease – could not be ruled out as a possible cause of the increase in cancer risk, but their study was not powered to pick up such an effect.
“Instead, we suggest that extent and duration of chronic inflammation might be the main driving mechanisms underlying the increased risk of cancer,” they wrote.
The authors noted that their study did not include data on the smoking status of individuals, which could be significant, because smoking is known to reduce the risk of ulcerative colitis and increase the risk of Crohn’s disease and cancer. However, they pointed out that the majority of patients would not have been smoking at the time of their initial inflammatory bowel disease diagnosis, and would have been unlikely to take up the habit after their diagnosis.
With the observation that the risk of cancer in inflammatory bowel disease was higher in patients who were younger when diagnosed with the disease, the authors suggested that age of onset be considered when designing surveillance strategies for cancer in this group.
The Stockholm County Council and the Karolinska Institutet, the Swedish Cancer Society, the Swedish Research Council, and the Swedish Foundation for Strategic Research supported the study. One author received grants from the Swedish Medical Society, Magtarmfonden, the Jane and Dan Olsson Foundation, the Mjölkdroppen Foundation, the Bengt Ihre Research Fellowship in gastroenterology, and the Karolinska Institutet Foundations. No conflicts of interest were declared.
Children who had developed inflammatory bowel disease had an 18-fold greater risk of gastrointestinal cancers in later life, a new study suggests.
The cohort study found that the risk of all cancers was elevated in individuals with childhood-onset inflammatory bowel disease, but particularly in those with primary sclerosing cholangitis and ulcerative colitis.
Researchers followed 9,405 patients with childhood-onset inflammatory bowel disease to a mean age of 27 years using a Swedish national patient register (BMJ. 2017 Sep 21. doi: 10.1136/bmj.j3951).
Analysis revealed that individuals with childhood-onset inflammatory bowel disease had double the risk of any cancer, compared with the general population (hazard ratio, 2.2; 95% confidence interval, 2.0-2.5), and a 2.7-fold greater risk of developing cancer before the age of 18 years.
Primary sclerosing cholangitis was associated with a sixfold greater risk of cancer, ulcerative colitis was associated with a 2.6-fold greater risk, and patients who had had colitis for 10 years or more had a nearly fourfold greater risk of cancer (HR, 3.9).
The study also found that childhood-onset inflammatory bowel disease was associated with an 18-fold greater risk of gastrointestinal cancer, compared with the general population, matched for age, sex, birth year, and county.
The risk was particularly high in patients with ulcerative colitis, who showed a 33-fold higher risk of colorectal cancer, while patients with Crohn’s disease had a nearly 6-fold higher risk.
“Colorectal cancer is a major cause of cancer mortality in the population, and even a moderately increased incidence is likely to have a large effect on patients with inflammatory bowel disease,” wrote Ola Olén, MD, of Karolinska Institutet, Stockholm, and coauthors.
When the researchers looked in more detail at the type of cancers, they saw the greatest increases in risk were for colorectal cancer (HR, 19.5) and small intestinal cancer (HR, 12.8), while the risk of liver cancer was 134 times higher (95% CI, 59.6-382).
The researchers also saw a 2.7-fold increased risk of lymphoid neoplasms associated with childhood inflammatory bowel disease, particularly in individuals with ulcerative colitis or Crohn’s disease. The most common lymphoid neoplasms were non-Hodgkin lymphomas, followed by Hodgkin lymphomas.
Commenting on possible explanations for the associations seen in the study, the authors said that patients with inflammatory bowel disease may have their gastrointestinal cancers diagnosed earlier than the general population because of regular endoscopies.
They also said that thiopurines and TNF inhibitors – both used to treat inflammatory bowel disease – could not be ruled out as a possible cause of the increase in cancer risk, but their study was not powered to pick up such an effect.
“Instead, we suggest that extent and duration of chronic inflammation might be the main driving mechanisms underlying the increased risk of cancer,” they wrote.
The authors noted that their study did not include data on the smoking status of individuals, which could be significant, because smoking is known to reduce the risk of ulcerative colitis and increase the risk of Crohn’s disease and cancer. However, they pointed out that the majority of patients would not have been smoking at the time of their initial inflammatory bowel disease diagnosis, and would have been unlikely to take up the habit after their diagnosis.
With the observation that the risk of cancer in inflammatory bowel disease was higher in patients who were younger when diagnosed with the disease, the authors suggested that age of onset be considered when designing surveillance strategies for cancer in this group.
The Stockholm County Council and the Karolinska Institutet, the Swedish Cancer Society, the Swedish Research Council, and the Swedish Foundation for Strategic Research supported the study. One author received grants from the Swedish Medical Society, Magtarmfonden, the Jane and Dan Olsson Foundation, the Mjölkdroppen Foundation, the Bengt Ihre Research Fellowship in gastroenterology, and the Karolinska Institutet Foundations. No conflicts of interest were declared.
FROM BMJ
Key clinical point: Childhood inflammatory bowel disease was associated with significant increases in the risk of cancer – particularly gastrointestinal cancer – in later life.
Major finding: Individuals diagnosed with inflammatory bowel disease in childhood have an 18-fold greater risk of gastrointestinal cancer, and a twofold higher risk of any cancer, compared with the general population.
Data source: A cohort study of 9,405 patients with childhood-onset inflammatory bowel disease.
Disclosures: The Stockholm County Council and the Karolinska Institutet, the Swedish Cancer Society, the Swedish Research Council, and the Swedish Foundation for Strategic Research supported the study. One author received grants from the Swedish Medical Society, Magtarmfonden, the Jane and Dan Olsson Foundation, the Mjölkdroppen Foundation, the Bengt Ihre Research Fellowship in gastroenterology, and the Karolinska Institutet Foundations. No conflicts of interest were declared.
Inclusive sexual health counseling and care
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.

Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.

Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
New AAP policy recommends flu vaccination regardless of egg allergy
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.

Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.
Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.
Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
AT AAP 2017
Salmonella infections: The source may be as close as your patient’s backyard
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates

Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates
Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates
Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Rapid genomic testing can diagnose critically ill infants
Rapid, targeted genomic sequencing shows promise in quickly diagnosing critically ill infants for whom standard clinical work-ups were unsuccessful, according to Cleo C. van Diemen, PhD, of the University of Groningen (the Netherlands), and associates.
Over the course of 1 year, 23 critically ill infants younger than 12 months who had no clear diagnosis after standard clinical work-ups underwent rapid, targeted genomics, with 7 receiving a genetic diagnosis. The median turnaround time was 12 days, falling from roughly 3 weeks at the beginning of the study to a maximum of 8 days by the end of the study.
Compound heterozygous mutations in the EPG5, RMND1, and EIF2B5 genes allowed for diagnoses of Vici syndrome, combined oxidative phosphorylation deficiency-11, and vanishing white matter, respectively. Homozygous mutations in the KLHL41, GFER, and GLB1 genes allowed for diagnoses of nemaline myopathy, progressive mitochondrial myopathy, and GM1-gangliosidosis, respectively. In addition, a 1p36.33p36.32 microdeletion was discovered in an infant with cardiomyopathy.
“The clinical relevance of rapid genome diagnostics lies in the fact that these results can be used in the clinical decisions made in caring for critically ill children in ICUs, in better genetic counseling of the parents, and in guiding their future reproductive choices,” the investigators noted.
Find the full study in Pediatrics (2017 Sep 22. doi: 10.1542/ peds.2016-2854).
Rapid, targeted genomic sequencing shows promise in quickly diagnosing critically ill infants for whom standard clinical work-ups were unsuccessful, according to Cleo C. van Diemen, PhD, of the University of Groningen (the Netherlands), and associates.
Over the course of 1 year, 23 critically ill infants younger than 12 months who had no clear diagnosis after standard clinical work-ups underwent rapid, targeted genomics, with 7 receiving a genetic diagnosis. The median turnaround time was 12 days, falling from roughly 3 weeks at the beginning of the study to a maximum of 8 days by the end of the study.
Compound heterozygous mutations in the EPG5, RMND1, and EIF2B5 genes allowed for diagnoses of Vici syndrome, combined oxidative phosphorylation deficiency-11, and vanishing white matter, respectively. Homozygous mutations in the KLHL41, GFER, and GLB1 genes allowed for diagnoses of nemaline myopathy, progressive mitochondrial myopathy, and GM1-gangliosidosis, respectively. In addition, a 1p36.33p36.32 microdeletion was discovered in an infant with cardiomyopathy.
“The clinical relevance of rapid genome diagnostics lies in the fact that these results can be used in the clinical decisions made in caring for critically ill children in ICUs, in better genetic counseling of the parents, and in guiding their future reproductive choices,” the investigators noted.
Find the full study in Pediatrics (2017 Sep 22. doi: 10.1542/ peds.2016-2854).
Rapid, targeted genomic sequencing shows promise in quickly diagnosing critically ill infants for whom standard clinical work-ups were unsuccessful, according to Cleo C. van Diemen, PhD, of the University of Groningen (the Netherlands), and associates.
Over the course of 1 year, 23 critically ill infants younger than 12 months who had no clear diagnosis after standard clinical work-ups underwent rapid, targeted genomics, with 7 receiving a genetic diagnosis. The median turnaround time was 12 days, falling from roughly 3 weeks at the beginning of the study to a maximum of 8 days by the end of the study.
Compound heterozygous mutations in the EPG5, RMND1, and EIF2B5 genes allowed for diagnoses of Vici syndrome, combined oxidative phosphorylation deficiency-11, and vanishing white matter, respectively. Homozygous mutations in the KLHL41, GFER, and GLB1 genes allowed for diagnoses of nemaline myopathy, progressive mitochondrial myopathy, and GM1-gangliosidosis, respectively. In addition, a 1p36.33p36.32 microdeletion was discovered in an infant with cardiomyopathy.
“The clinical relevance of rapid genome diagnostics lies in the fact that these results can be used in the clinical decisions made in caring for critically ill children in ICUs, in better genetic counseling of the parents, and in guiding their future reproductive choices,” the investigators noted.
Find the full study in Pediatrics (2017 Sep 22. doi: 10.1542/ peds.2016-2854).
FROM PEDIATRICS
RAS derangement linked to CVD risk in adolescents born preterm
SAN FRANCISCO – The renin-angiotensin system (RAS) is out of balance in adolescents born prematurely, according to investigators from Wake Forest School of Medicine in Winston-Salem, N.C.
Among other findings, the amount of circulating angiotensin 1-7, a vasodilator that counteracts the vasoconstrictive and other effects of angiotensin II, was lower relative to angiotensin II in 175 subjects born preterm and assessed at age 14 years, compared with 51 controls born at term.
The findings suggest a possible explanation for why people born prematurely have an increased risk for hypertension and cardiovascular disease, which has been a mystery. If the findings pan out with additional research, they also suggest potential therapeutic targets to attenuate the risk, namely upregulating angiotensin 1-7 and blocking angiotensin II, either at birth or later.

“If you could give medications to shift the balance in the RAS back to what it should be, then maybe you could prevent some of the changes that we see at age 14. With the current treatments, that’s difficult; ACE inhibitors and angiotensin II receptor blockers are (generally) not used in the neonatal period because they can precipitate acute kidney injury.” For older patients, “there’s no indication to use these medications in a subtle situation like we have here,” Dr. South said in an interview at a hypertension science meeting jointly sponsored by the American Heart Association and the American Society of Hypertension.
The direct manipulation of angiotensin 1-7 remains, for now, largely in the realm of clinical research.
The preterm subjects had lower plasma angiotensin II and lower angiotensin 1-7 concentrations, compared with their term peers, but an overall increase in the angiotensin II/angiotensin 1-7 ratio (4.2 vs. 2.4). Preterm subjects also had increased urinary excretion of angiotensin 1-7. The findings were statistically significant, and adjusted for potential confounders.
The differences were exaggerated in obese subjects, about a third in both groups. Obesity is known to be associated with increased angiotensin II activity.
The drop in angiotensin 1-7 was greater in preterm girls than in boys, which was curious because female sex is normally associated with decreased angiotensin II activity, and estrogen normally upregulates angiotensin 1-7; perhaps in prematurity, there’s a breakdown in the normal response to estrogen, Dr. South said.
Whatever the case, it’s possible the risk of hypertension and cardiovascular disease from preterm birth might be especially high in obese patients and women, he said.
The preterm group had a mean gestational age of 28 weeks, and a mean birth weight of 1.1 kg. The term group was born at a mean of 40 weeks, with a mean birth weight of 3.5 kg. At age 14 years, preterm subjects were shorter and weighed less than their peers.
Mean systolic and diastolic blood pressures were higher in the preterm group, and 21 preterm subjects (12%) had blood pressures at or above 120/80 mm Hg, vs. one subject (2%) in the term group.
Maternal hypertension and smoking during pregnancy, and C-section delivery, were far more common in the preterm group, as was Medicaid use at age 14 years. There were slightly more girls than boys in both groups, and just over 40% of the subjects in each were black.
The Wake Forest team continues to follow their preterm subjects, who are now in their mid-twenties. “If we can correlate what we found at age 14 with” early development of disease, “it will give us more of an indication that this is actually true causation, not just an association,” Dr. South said.
The investigators had no industry disclosures. The work was funded in part by the National Institutes of Health.
aotto@frontlinemedcom.com
SAN FRANCISCO – The renin-angiotensin system (RAS) is out of balance in adolescents born prematurely, according to investigators from Wake Forest School of Medicine in Winston-Salem, N.C.
Among other findings, the amount of circulating angiotensin 1-7, a vasodilator that counteracts the vasoconstrictive and other effects of angiotensin II, was lower relative to angiotensin II in 175 subjects born preterm and assessed at age 14 years, compared with 51 controls born at term.
The findings suggest a possible explanation for why people born prematurely have an increased risk for hypertension and cardiovascular disease, which has been a mystery. If the findings pan out with additional research, they also suggest potential therapeutic targets to attenuate the risk, namely upregulating angiotensin 1-7 and blocking angiotensin II, either at birth or later.
“If you could give medications to shift the balance in the RAS back to what it should be, then maybe you could prevent some of the changes that we see at age 14. With the current treatments, that’s difficult; ACE inhibitors and angiotensin II receptor blockers are (generally) not used in the neonatal period because they can precipitate acute kidney injury.” For older patients, “there’s no indication to use these medications in a subtle situation like we have here,” Dr. South said in an interview at a hypertension science meeting jointly sponsored by the American Heart Association and the American Society of Hypertension.
The direct manipulation of angiotensin 1-7 remains, for now, largely in the realm of clinical research.
The preterm subjects had lower plasma angiotensin II and lower angiotensin 1-7 concentrations, compared with their term peers, but an overall increase in the angiotensin II/angiotensin 1-7 ratio (4.2 vs. 2.4). Preterm subjects also had increased urinary excretion of angiotensin 1-7. The findings were statistically significant, and adjusted for potential confounders.
The differences were exaggerated in obese subjects, about a third in both groups. Obesity is known to be associated with increased angiotensin II activity.
The drop in angiotensin 1-7 was greater in preterm girls than in boys, which was curious because female sex is normally associated with decreased angiotensin II activity, and estrogen normally upregulates angiotensin 1-7; perhaps in prematurity, there’s a breakdown in the normal response to estrogen, Dr. South said.
Whatever the case, it’s possible the risk of hypertension and cardiovascular disease from preterm birth might be especially high in obese patients and women, he said.
The preterm group had a mean gestational age of 28 weeks, and a mean birth weight of 1.1 kg. The term group was born at a mean of 40 weeks, with a mean birth weight of 3.5 kg. At age 14 years, preterm subjects were shorter and weighed less than their peers.
Mean systolic and diastolic blood pressures were higher in the preterm group, and 21 preterm subjects (12%) had blood pressures at or above 120/80 mm Hg, vs. one subject (2%) in the term group.
Maternal hypertension and smoking during pregnancy, and C-section delivery, were far more common in the preterm group, as was Medicaid use at age 14 years. There were slightly more girls than boys in both groups, and just over 40% of the subjects in each were black.
The Wake Forest team continues to follow their preterm subjects, who are now in their mid-twenties. “If we can correlate what we found at age 14 with” early development of disease, “it will give us more of an indication that this is actually true causation, not just an association,” Dr. South said.
The investigators had no industry disclosures. The work was funded in part by the National Institutes of Health.
aotto@frontlinemedcom.com
SAN FRANCISCO – The renin-angiotensin system (RAS) is out of balance in adolescents born prematurely, according to investigators from Wake Forest School of Medicine in Winston-Salem, N.C.
Among other findings, the amount of circulating angiotensin 1-7, a vasodilator that counteracts the vasoconstrictive and other effects of angiotensin II, was lower relative to angiotensin II in 175 subjects born preterm and assessed at age 14 years, compared with 51 controls born at term.
The findings suggest a possible explanation for why people born prematurely have an increased risk for hypertension and cardiovascular disease, which has been a mystery. If the findings pan out with additional research, they also suggest potential therapeutic targets to attenuate the risk, namely upregulating angiotensin 1-7 and blocking angiotensin II, either at birth or later.
“If you could give medications to shift the balance in the RAS back to what it should be, then maybe you could prevent some of the changes that we see at age 14. With the current treatments, that’s difficult; ACE inhibitors and angiotensin II receptor blockers are (generally) not used in the neonatal period because they can precipitate acute kidney injury.” For older patients, “there’s no indication to use these medications in a subtle situation like we have here,” Dr. South said in an interview at a hypertension science meeting jointly sponsored by the American Heart Association and the American Society of Hypertension.
The direct manipulation of angiotensin 1-7 remains, for now, largely in the realm of clinical research.
The preterm subjects had lower plasma angiotensin II and lower angiotensin 1-7 concentrations, compared with their term peers, but an overall increase in the angiotensin II/angiotensin 1-7 ratio (4.2 vs. 2.4). Preterm subjects also had increased urinary excretion of angiotensin 1-7. The findings were statistically significant, and adjusted for potential confounders.
The differences were exaggerated in obese subjects, about a third in both groups. Obesity is known to be associated with increased angiotensin II activity.
The drop in angiotensin 1-7 was greater in preterm girls than in boys, which was curious because female sex is normally associated with decreased angiotensin II activity, and estrogen normally upregulates angiotensin 1-7; perhaps in prematurity, there’s a breakdown in the normal response to estrogen, Dr. South said.
Whatever the case, it’s possible the risk of hypertension and cardiovascular disease from preterm birth might be especially high in obese patients and women, he said.
The preterm group had a mean gestational age of 28 weeks, and a mean birth weight of 1.1 kg. The term group was born at a mean of 40 weeks, with a mean birth weight of 3.5 kg. At age 14 years, preterm subjects were shorter and weighed less than their peers.
Mean systolic and diastolic blood pressures were higher in the preterm group, and 21 preterm subjects (12%) had blood pressures at or above 120/80 mm Hg, vs. one subject (2%) in the term group.
Maternal hypertension and smoking during pregnancy, and C-section delivery, were far more common in the preterm group, as was Medicaid use at age 14 years. There were slightly more girls than boys in both groups, and just over 40% of the subjects in each were black.
The Wake Forest team continues to follow their preterm subjects, who are now in their mid-twenties. “If we can correlate what we found at age 14 with” early development of disease, “it will give us more of an indication that this is actually true causation, not just an association,” Dr. South said.
The investigators had no industry disclosures. The work was funded in part by the National Institutes of Health.
aotto@frontlinemedcom.com
AT THE AHA/ASH JOINT SCIENTIFIC HYPERTENSION MEETING
Key clinical point:
Major finding: The preterm subjects had lower plasma angiotensin II and lower angiotensin 1-7 concentrations, compared with their term peers, but an overall increase in the angiotensin II/angiotensin 1-7 ratio (4.2 vs. 2.4).
Data source: Comparison of 175 subjects born preterm to 51 controls born at term, assessed at age 14 years.
Disclosures: The investigators had no industry disclosures. The work was funded in part by the National Institutes of Health.
Alternative therapies
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.

Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.

Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.
Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.
Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
With inpatient flu shots, providers’ attitude problem may outweigh parents’
reported Suchitra Rao, MD, of the University of Colorado, Aurora, and her colleagues.
Surveys assessing attitudes toward inpatient influenza vaccination were given to parents/caregivers of general pediatric inpatients and to inpatient physicians, residents, nurses, physician assistants, and nurse practitioners at Children’s Hospital Colorado in Aurora between October 2014 and March 2015. Response rates were 95% of the 1,053 parents/caregivers and 58% of the 339 providers.
The parents agreed that the flu is a serious disease (92%), that flu vaccines work (58%), that flu vaccines are safe (76%), and that the vaccines are needed annually (76%), the Dr. Rao and her colleagues found.
The providers thought the most common barriers to vaccination were parental refusal because of child illness (80%) and family misconceptions about the vaccine (74%). Also, 54% of providers forgot to ask about flu vaccination status and 46% forgot to order flu vaccines.
When asked what interventions might increase flu vaccination rates in the inpatient setting, 73% of providers agreed that personal reminders might help increase vaccination rates, but only 48% thought that provider education might help do so.
Read more in the journal Influenza and Other Respiratory Viruses (2017 Sep 5. doi: 10.1111/irv.12482.)
reported Suchitra Rao, MD, of the University of Colorado, Aurora, and her colleagues.
Surveys assessing attitudes toward inpatient influenza vaccination were given to parents/caregivers of general pediatric inpatients and to inpatient physicians, residents, nurses, physician assistants, and nurse practitioners at Children’s Hospital Colorado in Aurora between October 2014 and March 2015. Response rates were 95% of the 1,053 parents/caregivers and 58% of the 339 providers.
The parents agreed that the flu is a serious disease (92%), that flu vaccines work (58%), that flu vaccines are safe (76%), and that the vaccines are needed annually (76%), the Dr. Rao and her colleagues found.
The providers thought the most common barriers to vaccination were parental refusal because of child illness (80%) and family misconceptions about the vaccine (74%). Also, 54% of providers forgot to ask about flu vaccination status and 46% forgot to order flu vaccines.
When asked what interventions might increase flu vaccination rates in the inpatient setting, 73% of providers agreed that personal reminders might help increase vaccination rates, but only 48% thought that provider education might help do so.
Read more in the journal Influenza and Other Respiratory Viruses (2017 Sep 5. doi: 10.1111/irv.12482.)
reported Suchitra Rao, MD, of the University of Colorado, Aurora, and her colleagues.
Surveys assessing attitudes toward inpatient influenza vaccination were given to parents/caregivers of general pediatric inpatients and to inpatient physicians, residents, nurses, physician assistants, and nurse practitioners at Children’s Hospital Colorado in Aurora between October 2014 and March 2015. Response rates were 95% of the 1,053 parents/caregivers and 58% of the 339 providers.
The parents agreed that the flu is a serious disease (92%), that flu vaccines work (58%), that flu vaccines are safe (76%), and that the vaccines are needed annually (76%), the Dr. Rao and her colleagues found.
The providers thought the most common barriers to vaccination were parental refusal because of child illness (80%) and family misconceptions about the vaccine (74%). Also, 54% of providers forgot to ask about flu vaccination status and 46% forgot to order flu vaccines.
When asked what interventions might increase flu vaccination rates in the inpatient setting, 73% of providers agreed that personal reminders might help increase vaccination rates, but only 48% thought that provider education might help do so.
Read more in the journal Influenza and Other Respiratory Viruses (2017 Sep 5. doi: 10.1111/irv.12482.)