User login
Can arterial switch operation impact cognitive deficits?
With dramatic advances of neonatal repair of complex cardiac disease, the population of adults with congenital heart disease (CHD) has increased dramatically, and while studies have shown an increased risk of neurodevelopmental and psychological disorders in these patients, few studies have evaluated their cognitive and psychosocial outcomes. Now, a review of young adults who had an arterial switch operation for transposition of the great arteries in France has found that they have almost twice the rate of cognitive difficulties and more than triple the rate of cognitive impairment as healthy peers.
“Despite satisfactory outcomes in most adults with transposition of the great arteries (TGA), a substantial proportion has cognitive or psychologic difficulties that may reduce their academic success and quality of life,” said lead author David Kalfa, MD, PhD, of Morgan Stanley Children’s Hospital of New York-Presbyterian, Columbia University Medical Center and coauthors in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:1028-35).
The study involved a review of 67 adults aged 18 and older born with TGA between 1984 and 1985 who had an arterial switch operation (ASO) at two hospitals in France: Necker Children’s Hospital in Paris and Marie Lannelongue Hospital in Le Plessis-Robinson. The researchers performed a matched analysis with 43 healthy subjects for age, gender, and education level.
The researchers found that 69% of the TGA patients had an intelligence quotient in the normal range of 85-115. The TGA patients had lower quotients for mean full-scale (94.9 plus or minus 15.3 vs. 103.4 plus or minus 12.3 in healthy subjects; P = 0.003), verbal (96.8 plus or minus 16.2 vs. 102.5 plus or minus 11.5; P =.033) and performance intelligence (93.7 plus or minus 14.6 vs. 103.8 plus or minus 14.3; P less than .001).
The TGA patients also had higher rates of cognitive difficulties, measured as intelligence quotient less than or equal to –1 standard deviation, and cognitive impairment, measured as intelligence quotient less than or equal to –2 standard deviation; 31% vs. 16% (P = .001) for the former and 6% vs. 2% (P = .030) for the latter.
TGA patients with cognitive difficulties had lower educational levels and were also more likely to repeat grades in school, Dr. Kalfa and coauthors noted. “Patients reported an overall satisfactory health-related quality of life,” Dr. Kalfa and coauthors said of the TGA group; “however, those with cognitive or psychologic difficulties reported poorer quality of life.” The researchers identified three predictors of worse outcomes: lower parental socioeconomic and educational status; older age at surgery; and longer hospital stays.
“Our findings suggest that the cognitive morbidities commonly reported in children and adolescents with complex CHD persist into adulthood in individuals with TGA after the ASO,” Dr. Kalfa and coauthors said. Future research should evaluate specific cognitive domains such as attention, memory, and executive functions. “This consideration is important for evaluation of the whole [adult] CHD population because specific cognitive impairments are increasingly documented into adolescence but remain rarely investigated in adulthood,” the researchers said.
Dr. Kalfa and coauthors reported having no financial disclosures.
The findings by Dr. Kalfa and coauthors may point the way to improve cognitive outcomes in children who have the arterial switch operation, said Ryan R. Davies, MD, of A.I duPont Hospital for Children in Wilmington, Del., in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:1036-7.) “Modifiable factors may exist both during the perioperative stage (perfusion strategies, intensive care management) and over the longer term (early neurocognitive assessments and interventions,” Dr. Davies said.
That parental socioeconomic status is associated with cognitive performance suggests early intervention and education “may pay long-term dividends,” Dr. Davies said. Future studies should focus on the impact of specific interventions and identify modifiable developmental factors, he said.

Dr. Kalfa and coauthors have provided an “important start” in that direction, Dr. Davies said. “They have shown that the neurodevelopmental deficits seen early in children with CHD persist into adulthood,” he said. “There are also hints here as to where interventions may be effective in ameliorating those deficits.”
Dr. Davies reported having no financial disclosures.
The findings by Dr. Kalfa and coauthors may point the way to improve cognitive outcomes in children who have the arterial switch operation, said Ryan R. Davies, MD, of A.I duPont Hospital for Children in Wilmington, Del., in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:1036-7.) “Modifiable factors may exist both during the perioperative stage (perfusion strategies, intensive care management) and over the longer term (early neurocognitive assessments and interventions,” Dr. Davies said.
That parental socioeconomic status is associated with cognitive performance suggests early intervention and education “may pay long-term dividends,” Dr. Davies said. Future studies should focus on the impact of specific interventions and identify modifiable developmental factors, he said.
Dr. Kalfa and coauthors have provided an “important start” in that direction, Dr. Davies said. “They have shown that the neurodevelopmental deficits seen early in children with CHD persist into adulthood,” he said. “There are also hints here as to where interventions may be effective in ameliorating those deficits.”
Dr. Davies reported having no financial disclosures.
The findings by Dr. Kalfa and coauthors may point the way to improve cognitive outcomes in children who have the arterial switch operation, said Ryan R. Davies, MD, of A.I duPont Hospital for Children in Wilmington, Del., in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:1036-7.) “Modifiable factors may exist both during the perioperative stage (perfusion strategies, intensive care management) and over the longer term (early neurocognitive assessments and interventions,” Dr. Davies said.
That parental socioeconomic status is associated with cognitive performance suggests early intervention and education “may pay long-term dividends,” Dr. Davies said. Future studies should focus on the impact of specific interventions and identify modifiable developmental factors, he said.
Dr. Kalfa and coauthors have provided an “important start” in that direction, Dr. Davies said. “They have shown that the neurodevelopmental deficits seen early in children with CHD persist into adulthood,” he said. “There are also hints here as to where interventions may be effective in ameliorating those deficits.”
Dr. Davies reported having no financial disclosures.
With dramatic advances of neonatal repair of complex cardiac disease, the population of adults with congenital heart disease (CHD) has increased dramatically, and while studies have shown an increased risk of neurodevelopmental and psychological disorders in these patients, few studies have evaluated their cognitive and psychosocial outcomes. Now, a review of young adults who had an arterial switch operation for transposition of the great arteries in France has found that they have almost twice the rate of cognitive difficulties and more than triple the rate of cognitive impairment as healthy peers.
“Despite satisfactory outcomes in most adults with transposition of the great arteries (TGA), a substantial proportion has cognitive or psychologic difficulties that may reduce their academic success and quality of life,” said lead author David Kalfa, MD, PhD, of Morgan Stanley Children’s Hospital of New York-Presbyterian, Columbia University Medical Center and coauthors in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:1028-35).
The study involved a review of 67 adults aged 18 and older born with TGA between 1984 and 1985 who had an arterial switch operation (ASO) at two hospitals in France: Necker Children’s Hospital in Paris and Marie Lannelongue Hospital in Le Plessis-Robinson. The researchers performed a matched analysis with 43 healthy subjects for age, gender, and education level.
The researchers found that 69% of the TGA patients had an intelligence quotient in the normal range of 85-115. The TGA patients had lower quotients for mean full-scale (94.9 plus or minus 15.3 vs. 103.4 plus or minus 12.3 in healthy subjects; P = 0.003), verbal (96.8 plus or minus 16.2 vs. 102.5 plus or minus 11.5; P =.033) and performance intelligence (93.7 plus or minus 14.6 vs. 103.8 plus or minus 14.3; P less than .001).
The TGA patients also had higher rates of cognitive difficulties, measured as intelligence quotient less than or equal to –1 standard deviation, and cognitive impairment, measured as intelligence quotient less than or equal to –2 standard deviation; 31% vs. 16% (P = .001) for the former and 6% vs. 2% (P = .030) for the latter.
TGA patients with cognitive difficulties had lower educational levels and were also more likely to repeat grades in school, Dr. Kalfa and coauthors noted. “Patients reported an overall satisfactory health-related quality of life,” Dr. Kalfa and coauthors said of the TGA group; “however, those with cognitive or psychologic difficulties reported poorer quality of life.” The researchers identified three predictors of worse outcomes: lower parental socioeconomic and educational status; older age at surgery; and longer hospital stays.
“Our findings suggest that the cognitive morbidities commonly reported in children and adolescents with complex CHD persist into adulthood in individuals with TGA after the ASO,” Dr. Kalfa and coauthors said. Future research should evaluate specific cognitive domains such as attention, memory, and executive functions. “This consideration is important for evaluation of the whole [adult] CHD population because specific cognitive impairments are increasingly documented into adolescence but remain rarely investigated in adulthood,” the researchers said.
Dr. Kalfa and coauthors reported having no financial disclosures.
With dramatic advances of neonatal repair of complex cardiac disease, the population of adults with congenital heart disease (CHD) has increased dramatically, and while studies have shown an increased risk of neurodevelopmental and psychological disorders in these patients, few studies have evaluated their cognitive and psychosocial outcomes. Now, a review of young adults who had an arterial switch operation for transposition of the great arteries in France has found that they have almost twice the rate of cognitive difficulties and more than triple the rate of cognitive impairment as healthy peers.
“Despite satisfactory outcomes in most adults with transposition of the great arteries (TGA), a substantial proportion has cognitive or psychologic difficulties that may reduce their academic success and quality of life,” said lead author David Kalfa, MD, PhD, of Morgan Stanley Children’s Hospital of New York-Presbyterian, Columbia University Medical Center and coauthors in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:1028-35).
The study involved a review of 67 adults aged 18 and older born with TGA between 1984 and 1985 who had an arterial switch operation (ASO) at two hospitals in France: Necker Children’s Hospital in Paris and Marie Lannelongue Hospital in Le Plessis-Robinson. The researchers performed a matched analysis with 43 healthy subjects for age, gender, and education level.
The researchers found that 69% of the TGA patients had an intelligence quotient in the normal range of 85-115. The TGA patients had lower quotients for mean full-scale (94.9 plus or minus 15.3 vs. 103.4 plus or minus 12.3 in healthy subjects; P = 0.003), verbal (96.8 plus or minus 16.2 vs. 102.5 plus or minus 11.5; P =.033) and performance intelligence (93.7 plus or minus 14.6 vs. 103.8 plus or minus 14.3; P less than .001).
The TGA patients also had higher rates of cognitive difficulties, measured as intelligence quotient less than or equal to –1 standard deviation, and cognitive impairment, measured as intelligence quotient less than or equal to –2 standard deviation; 31% vs. 16% (P = .001) for the former and 6% vs. 2% (P = .030) for the latter.
TGA patients with cognitive difficulties had lower educational levels and were also more likely to repeat grades in school, Dr. Kalfa and coauthors noted. “Patients reported an overall satisfactory health-related quality of life,” Dr. Kalfa and coauthors said of the TGA group; “however, those with cognitive or psychologic difficulties reported poorer quality of life.” The researchers identified three predictors of worse outcomes: lower parental socioeconomic and educational status; older age at surgery; and longer hospital stays.
“Our findings suggest that the cognitive morbidities commonly reported in children and adolescents with complex CHD persist into adulthood in individuals with TGA after the ASO,” Dr. Kalfa and coauthors said. Future research should evaluate specific cognitive domains such as attention, memory, and executive functions. “This consideration is important for evaluation of the whole [adult] CHD population because specific cognitive impairments are increasingly documented into adolescence but remain rarely investigated in adulthood,” the researchers said.
Dr. Kalfa and coauthors reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: A substantial proportion of young adults who had transposition of the great arteries have cognitive or psychological difficulties.
Major finding: Cognitive difficulties were significantly more frequent in the study population than the general population, 31% vs. 16%.
Data source: Age-, gender-, and education level–matched population of 67 young adults with transposition of the great arteries and 43 healthy subjects.
Disclosures: Dr. Kalfa and coauthors reported having no financial disclosures.
Nature versus nurture: 50 years of a popular debate
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7

In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7
In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7
In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
One in four ‘control’ mothers in NAS study tests positive for drug use
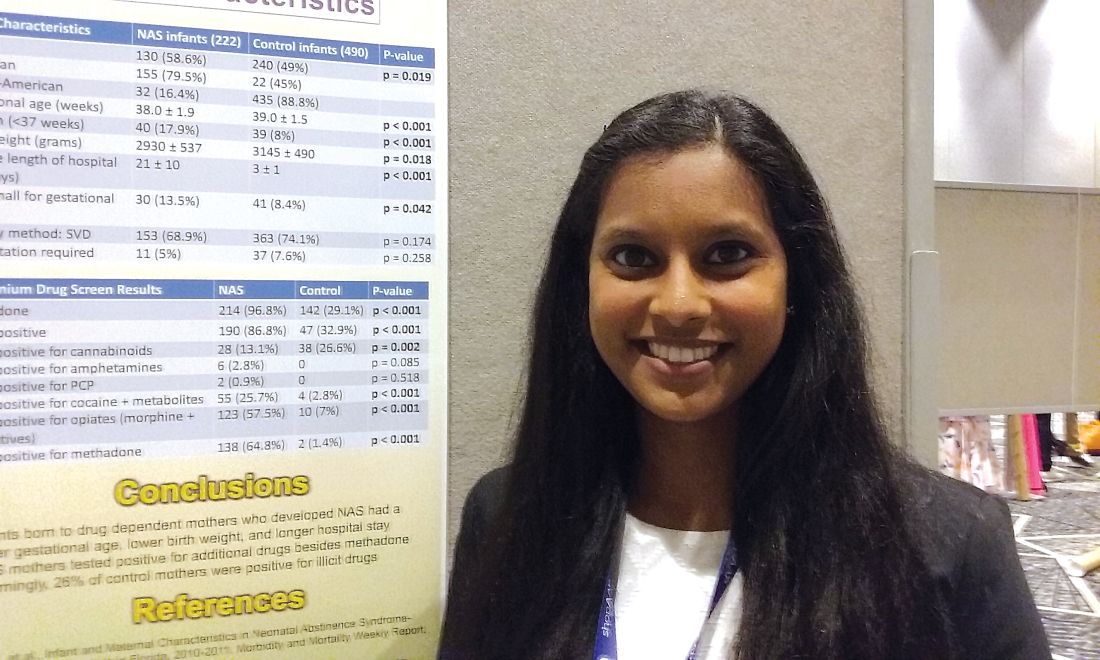
CHICAGO – A study that compares babies who develop neonatal abstinence syndrome (NAS) with a control group of healthy newborns found largely what researchers expected to see – lower gestational ages, lower birth weights, and substance use in 100% of the mothers in the affected group. It’s when they looked at the control group of healthy newborns and their mothers that they got a surprise.
“Something that was very alarming in our study is [that] one in four of the control mothers was also positive for illicit drugs. That is something we definitely didn’t expect,” said Pallavi Karunakaran MD, a pediatric resident at Children’s Hospital of Michigan in Detroit.
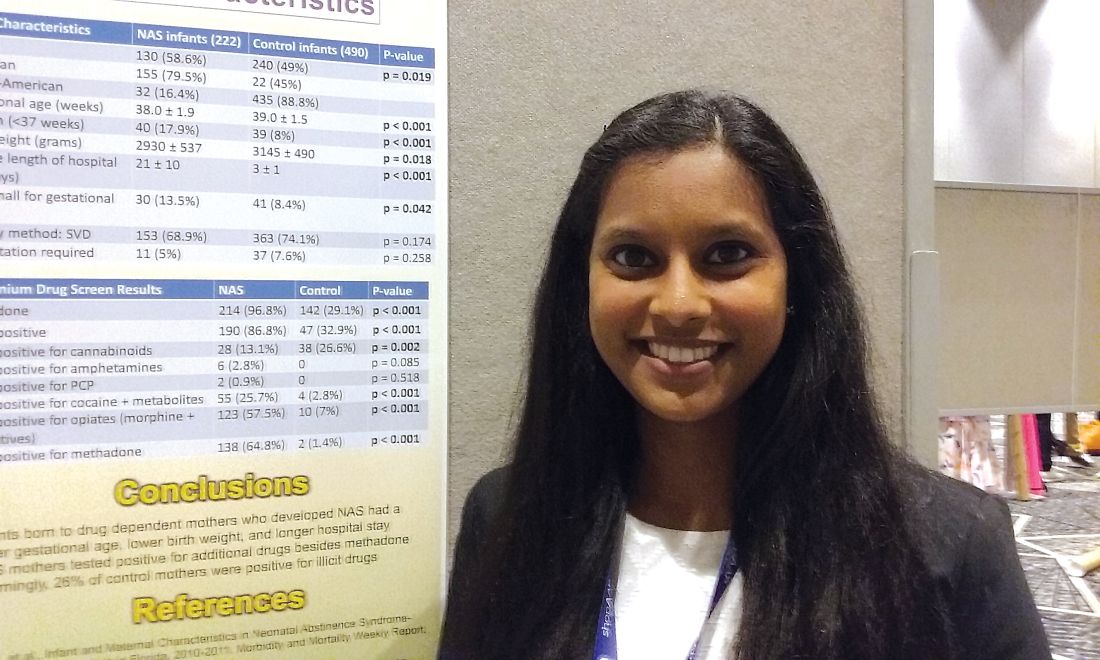
The investigators also looked at maternal characteristics in both groups, with data available on 198 mothers whose babies developed the syndrome and 490 controls. “Interestingly enough, we expected that the mothers of the NAS babies would have some kind of drug use, [but] a lot of the NAS cohort mothers tested positive for additional drugs, other than methadone, which is usually how babies end up developing neonatal abstinence syndrome,” Dr. Karunakaran said at the annual meeting of the American Academy of Pediatrics. Drug use in mothers of affected babies included opioids among 81% (including methadone for 70%); heroin, 42%; cocaine, 29%; marijuana, 26%; benzodiazepines, 18%; buprenorphine, 6%; and barbiturates, 2%.
Among the control group mothers, drug use included marijuana among 20.4%; opioids, 1.8%; cocaine, 1.2%; benzodiazepines, 0.6%; heroin, 0.2%; and barbiturates, 0.2%.
Mean gestational age for affected infants was 38 weeks versus 39 weeks in controls, a significant difference (P less than .001). Mean birth weight for affected infants was 2,930 grams versus 3,145 grams in controls (P = .018). The average length of hospital stay was 21 days for infants who developed NAS, compared with 3 days among control infants (P less than .001). Mean Apgar scores were not significantly different between groups.
“The next step in terms of taking care of our population – is we’re trying to see how we can catch those one in four control mothers who are having well babies because we want to make sure we’re also taking care of them while they’re pregnant,” Dr. Karunakaran said. “If they’re involved in drug use, we want to get them the right resources and the right doctors they may need.”
Dr. Karunakaran had no relevant financial disclosures.
CHICAGO – A study that compares babies who develop neonatal abstinence syndrome (NAS) with a control group of healthy newborns found largely what researchers expected to see – lower gestational ages, lower birth weights, and substance use in 100% of the mothers in the affected group. It’s when they looked at the control group of healthy newborns and their mothers that they got a surprise.
“Something that was very alarming in our study is [that] one in four of the control mothers was also positive for illicit drugs. That is something we definitely didn’t expect,” said Pallavi Karunakaran MD, a pediatric resident at Children’s Hospital of Michigan in Detroit.
The investigators also looked at maternal characteristics in both groups, with data available on 198 mothers whose babies developed the syndrome and 490 controls. “Interestingly enough, we expected that the mothers of the NAS babies would have some kind of drug use, [but] a lot of the NAS cohort mothers tested positive for additional drugs, other than methadone, which is usually how babies end up developing neonatal abstinence syndrome,” Dr. Karunakaran said at the annual meeting of the American Academy of Pediatrics. Drug use in mothers of affected babies included opioids among 81% (including methadone for 70%); heroin, 42%; cocaine, 29%; marijuana, 26%; benzodiazepines, 18%; buprenorphine, 6%; and barbiturates, 2%.
Among the control group mothers, drug use included marijuana among 20.4%; opioids, 1.8%; cocaine, 1.2%; benzodiazepines, 0.6%; heroin, 0.2%; and barbiturates, 0.2%.
Mean gestational age for affected infants was 38 weeks versus 39 weeks in controls, a significant difference (P less than .001). Mean birth weight for affected infants was 2,930 grams versus 3,145 grams in controls (P = .018). The average length of hospital stay was 21 days for infants who developed NAS, compared with 3 days among control infants (P less than .001). Mean Apgar scores were not significantly different between groups.
“The next step in terms of taking care of our population – is we’re trying to see how we can catch those one in four control mothers who are having well babies because we want to make sure we’re also taking care of them while they’re pregnant,” Dr. Karunakaran said. “If they’re involved in drug use, we want to get them the right resources and the right doctors they may need.”
Dr. Karunakaran had no relevant financial disclosures.
CHICAGO – A study that compares babies who develop neonatal abstinence syndrome (NAS) with a control group of healthy newborns found largely what researchers expected to see – lower gestational ages, lower birth weights, and substance use in 100% of the mothers in the affected group. It’s when they looked at the control group of healthy newborns and their mothers that they got a surprise.
“Something that was very alarming in our study is [that] one in four of the control mothers was also positive for illicit drugs. That is something we definitely didn’t expect,” said Pallavi Karunakaran MD, a pediatric resident at Children’s Hospital of Michigan in Detroit.
The investigators also looked at maternal characteristics in both groups, with data available on 198 mothers whose babies developed the syndrome and 490 controls. “Interestingly enough, we expected that the mothers of the NAS babies would have some kind of drug use, [but] a lot of the NAS cohort mothers tested positive for additional drugs, other than methadone, which is usually how babies end up developing neonatal abstinence syndrome,” Dr. Karunakaran said at the annual meeting of the American Academy of Pediatrics. Drug use in mothers of affected babies included opioids among 81% (including methadone for 70%); heroin, 42%; cocaine, 29%; marijuana, 26%; benzodiazepines, 18%; buprenorphine, 6%; and barbiturates, 2%.
Among the control group mothers, drug use included marijuana among 20.4%; opioids, 1.8%; cocaine, 1.2%; benzodiazepines, 0.6%; heroin, 0.2%; and barbiturates, 0.2%.
Mean gestational age for affected infants was 38 weeks versus 39 weeks in controls, a significant difference (P less than .001). Mean birth weight for affected infants was 2,930 grams versus 3,145 grams in controls (P = .018). The average length of hospital stay was 21 days for infants who developed NAS, compared with 3 days among control infants (P less than .001). Mean Apgar scores were not significantly different between groups.
“The next step in terms of taking care of our population – is we’re trying to see how we can catch those one in four control mothers who are having well babies because we want to make sure we’re also taking care of them while they’re pregnant,” Dr. Karunakaran said. “If they’re involved in drug use, we want to get them the right resources and the right doctors they may need.”
Dr. Karunakaran had no relevant financial disclosures.
AT AAP 2017
Key clinical point: Investigators studied mothers whose babies developed NAS and were surprised when almost 25% of women in the control group also tested positive for illicit drug use.
Major finding: Among the control mothers, drug use included marijuana 20.4%, opioids 1.8%, cocaine 1.2%, benzodiazepines 0.6%, heroin 0.2%, and barbiturates 0.2%.
Data source: Chart review of 222 infants who developed neonatal abstinence syndrome, compared with 490 controls.
Disclosures: Dr. Karunakaran had no relevant financial disclosures.
SCD drug receives rare pediatric disease designation

The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to Altemia™ soft gelatin capsules for the treatment of children with sickle cell disease (SCD).
Altemia (formerly SC411) is being developed by Sancilio Pharmaceuticals Company, Inc. (SPCI) to treat SCD patients between the ages of 5 and 17 years.
Altemia consists of a mixture of fatty acids, primarily in the form of Ethyl Cervonate™ (a proprietary blend of docosahexaenoic acid and other omega-3 fatty acids), and surface active agents formulated using Advanced Lipid Technologies®.
According to SPCI, Advanced Lipid Technologies are proprietary formulation and manufacturing techniques used to create lipophilic drug products capable of increased bioavailability, avoidance of the first pass effect, and elimination of the food effects commonly associated with oral administration.
Altemia is designed to replenish the lipids destroyed by sickle hemoglobin. The product is intended to be taken once daily to reduce vaso-occlusive crises, anemia, organ damage, and other complications of SCD.
Altemia also has orphan drug designation from the FDA.
SPCI is currently conducting a phase 2 trial of Altemia. In this randomized, double-blind, placebo-controlled trial, researchers are evaluating the efficacy and safety of Altemia in pediatric patients with SCD.
The company plans to report top-line results from the study, known as the SCOT trial, early in the fourth quarter of this year.
About rare pediatric disease designation
Rare pediatric disease designation is granted to drugs that show promise to treat diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 or younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, if a drug with rare pediatric disease designation is approved, the drug’s developer may qualify for a voucher that can be redeemed to obtain priority review for any subsequent marketing application. ![]()
The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to Altemia™ soft gelatin capsules for the treatment of children with sickle cell disease (SCD).
Altemia (formerly SC411) is being developed by Sancilio Pharmaceuticals Company, Inc. (SPCI) to treat SCD patients between the ages of 5 and 17 years.
Altemia consists of a mixture of fatty acids, primarily in the form of Ethyl Cervonate™ (a proprietary blend of docosahexaenoic acid and other omega-3 fatty acids), and surface active agents formulated using Advanced Lipid Technologies®.
According to SPCI, Advanced Lipid Technologies are proprietary formulation and manufacturing techniques used to create lipophilic drug products capable of increased bioavailability, avoidance of the first pass effect, and elimination of the food effects commonly associated with oral administration.
Altemia is designed to replenish the lipids destroyed by sickle hemoglobin. The product is intended to be taken once daily to reduce vaso-occlusive crises, anemia, organ damage, and other complications of SCD.
Altemia also has orphan drug designation from the FDA.
SPCI is currently conducting a phase 2 trial of Altemia. In this randomized, double-blind, placebo-controlled trial, researchers are evaluating the efficacy and safety of Altemia in pediatric patients with SCD.
The company plans to report top-line results from the study, known as the SCOT trial, early in the fourth quarter of this year.
About rare pediatric disease designation
Rare pediatric disease designation is granted to drugs that show promise to treat diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 or younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, if a drug with rare pediatric disease designation is approved, the drug’s developer may qualify for a voucher that can be redeemed to obtain priority review for any subsequent marketing application. ![]()
The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to Altemia™ soft gelatin capsules for the treatment of children with sickle cell disease (SCD).
Altemia (formerly SC411) is being developed by Sancilio Pharmaceuticals Company, Inc. (SPCI) to treat SCD patients between the ages of 5 and 17 years.
Altemia consists of a mixture of fatty acids, primarily in the form of Ethyl Cervonate™ (a proprietary blend of docosahexaenoic acid and other omega-3 fatty acids), and surface active agents formulated using Advanced Lipid Technologies®.
According to SPCI, Advanced Lipid Technologies are proprietary formulation and manufacturing techniques used to create lipophilic drug products capable of increased bioavailability, avoidance of the first pass effect, and elimination of the food effects commonly associated with oral administration.
Altemia is designed to replenish the lipids destroyed by sickle hemoglobin. The product is intended to be taken once daily to reduce vaso-occlusive crises, anemia, organ damage, and other complications of SCD.
Altemia also has orphan drug designation from the FDA.
SPCI is currently conducting a phase 2 trial of Altemia. In this randomized, double-blind, placebo-controlled trial, researchers are evaluating the efficacy and safety of Altemia in pediatric patients with SCD.
The company plans to report top-line results from the study, known as the SCOT trial, early in the fourth quarter of this year.
About rare pediatric disease designation
Rare pediatric disease designation is granted to drugs that show promise to treat diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 or younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, if a drug with rare pediatric disease designation is approved, the drug’s developer may qualify for a voucher that can be redeemed to obtain priority review for any subsequent marketing application. ![]()
Make teen suicide screenings a part of everyday practice
CHICAGO – at the annual meeting of the American Academy of Pediatrics.
An estimated 2 million teenagers, aged 15-19 years, have attempted suicide within the past year, based on data from the Centers for Disease Control and Prevention. According to the CDC’s 1991-2015 High School Youth Risk Behavior Survey data, nearly a third of students (30%) have felt so sad or helpless nearly daily for at least 2 weeks that they stopped doing their normal activities, and 18% had seriously considered suicide within the past year. One in seven (15%) had made a plan for attempting suicide, 9% had attempted suicide at least once, and 3% attempted suicide that required medical treatment. About twice as many females as males had considered, planned, and/or attempted suicide.

“The offspring of suicide attempters have a sixfold higher risk of suicide than their peers whose parents have not attempted suicide,” Dr. Cody said. Other major risk factors include a history of being bullied, a history of abuse, and a history of substance abuse, particularly alcohol and opioids.
Once you identify a patient at risk for suicide, Dr. Cody advised that you should follow a suicide assessment management protocol, such as the one developed by Angela Stanley, PsyD, of the Medical College of Wisconsin and the Children’s Hospital of Wisconsin, both in Milwaukee. Doctors should identify the teen’s intensity of suicidal ideation, ask how far they are in their plans, ascertain their access to means, create a safety plan, refer the patient for mental health care, and follow up frequently.
Dr. Cody emphasized that “suicide contracts” and “safety plans” are different things. Suicide pacts are agreements not to hurt oneself, whereas safety plans include concrete, collaborative, proactive steps a person will take if experiencing suicidal thoughts.
“There is no evidence that contracts prevent suicide, but a lot of research shows that safety or crisis plans are much more effective at preventing a person from committing suicide,” Dr. Cody stated.
The first step of screening is asking a patient directly whether they have ever wished they were dead or had thoughts about killing themselves.
“Some pediatricians are afraid to ask the questions because they’re afraid they’re going to put the idea of suicide in the child’s head, but there is no evidence that screening puts kids at risk,” Dr. Cody said. The other reason you may feel uneasy asking about self-harm is not knowing what to do if a teen says that she is feeling suicidal. That’s where an assessment protocol helps.
If a patient has considered suicide more than a month prior, it shouldn’t be ignored, although the situation may require less urgency but further follow-up. For those with more recent suicidal ideation but without a plan or intent, Dr. Cody recommends following up within 2 weeks because the adolescent’s situation may change.
For those with suicidal ideation and a plan, you should ask three questions:
- What ways of killing yourself have you thought about?
- How likely is it you will follow through on your plan?
- When you think about killing yourself, what stops you?
These questions can help you determine risk acuity: The more specific, realistic, available, and lethal a plan is, the more acute the risk. You then should ask questions to try to determine how likely the teen is to follow through, such as asking about his future plans, his connectedness with others, and his religious beliefs.
Asking about a plan helps determine how much access the patient has to a lethal, realistic means. Firearms are responsible for 52% of teen suicides, followed by hanging/suffocation (25%) and poisoning (16%).
“This is why it’s a really important part of social history to screen for guns in the house,” Dr. Cody told attendees. “I know it’s been really controversial, but it’s something that’s really important, especially if you have an adolescent in the house that’s having suicidal ideation.”
Teens with suicidal ideation and a plan but no intent require a safety plan along with follow-up within 1 week. Those with a plan and intent, or those with no intent but an unwillingness agree to a safety plan, should be immediately hospitalized, Dr. Cody said.
These suicide screenings should occur at annual well-child visits, Dr. Cody said, but they also should be done at acute visits; basically, any time you see your preteen and adolescent patients. Ideally, these should take place during alone time, without any parents present.
You also should share resources with your patients, including the National Suicide Prevention Lifeline at 1-800-273-8255 and the Crisis TextLine at 741741.
Dr. Cody reported having no disclosures, and no external funding was used for the presentation.
CHICAGO – at the annual meeting of the American Academy of Pediatrics.
An estimated 2 million teenagers, aged 15-19 years, have attempted suicide within the past year, based on data from the Centers for Disease Control and Prevention. According to the CDC’s 1991-2015 High School Youth Risk Behavior Survey data, nearly a third of students (30%) have felt so sad or helpless nearly daily for at least 2 weeks that they stopped doing their normal activities, and 18% had seriously considered suicide within the past year. One in seven (15%) had made a plan for attempting suicide, 9% had attempted suicide at least once, and 3% attempted suicide that required medical treatment. About twice as many females as males had considered, planned, and/or attempted suicide.
“The offspring of suicide attempters have a sixfold higher risk of suicide than their peers whose parents have not attempted suicide,” Dr. Cody said. Other major risk factors include a history of being bullied, a history of abuse, and a history of substance abuse, particularly alcohol and opioids.
Once you identify a patient at risk for suicide, Dr. Cody advised that you should follow a suicide assessment management protocol, such as the one developed by Angela Stanley, PsyD, of the Medical College of Wisconsin and the Children’s Hospital of Wisconsin, both in Milwaukee. Doctors should identify the teen’s intensity of suicidal ideation, ask how far they are in their plans, ascertain their access to means, create a safety plan, refer the patient for mental health care, and follow up frequently.
Dr. Cody emphasized that “suicide contracts” and “safety plans” are different things. Suicide pacts are agreements not to hurt oneself, whereas safety plans include concrete, collaborative, proactive steps a person will take if experiencing suicidal thoughts.
“There is no evidence that contracts prevent suicide, but a lot of research shows that safety or crisis plans are much more effective at preventing a person from committing suicide,” Dr. Cody stated.
The first step of screening is asking a patient directly whether they have ever wished they were dead or had thoughts about killing themselves.
“Some pediatricians are afraid to ask the questions because they’re afraid they’re going to put the idea of suicide in the child’s head, but there is no evidence that screening puts kids at risk,” Dr. Cody said. The other reason you may feel uneasy asking about self-harm is not knowing what to do if a teen says that she is feeling suicidal. That’s where an assessment protocol helps.
If a patient has considered suicide more than a month prior, it shouldn’t be ignored, although the situation may require less urgency but further follow-up. For those with more recent suicidal ideation but without a plan or intent, Dr. Cody recommends following up within 2 weeks because the adolescent’s situation may change.
For those with suicidal ideation and a plan, you should ask three questions:
- What ways of killing yourself have you thought about?
- How likely is it you will follow through on your plan?
- When you think about killing yourself, what stops you?
These questions can help you determine risk acuity: The more specific, realistic, available, and lethal a plan is, the more acute the risk. You then should ask questions to try to determine how likely the teen is to follow through, such as asking about his future plans, his connectedness with others, and his religious beliefs.
Asking about a plan helps determine how much access the patient has to a lethal, realistic means. Firearms are responsible for 52% of teen suicides, followed by hanging/suffocation (25%) and poisoning (16%).
“This is why it’s a really important part of social history to screen for guns in the house,” Dr. Cody told attendees. “I know it’s been really controversial, but it’s something that’s really important, especially if you have an adolescent in the house that’s having suicidal ideation.”
Teens with suicidal ideation and a plan but no intent require a safety plan along with follow-up within 1 week. Those with a plan and intent, or those with no intent but an unwillingness agree to a safety plan, should be immediately hospitalized, Dr. Cody said.
These suicide screenings should occur at annual well-child visits, Dr. Cody said, but they also should be done at acute visits; basically, any time you see your preteen and adolescent patients. Ideally, these should take place during alone time, without any parents present.
You also should share resources with your patients, including the National Suicide Prevention Lifeline at 1-800-273-8255 and the Crisis TextLine at 741741.
Dr. Cody reported having no disclosures, and no external funding was used for the presentation.
CHICAGO – at the annual meeting of the American Academy of Pediatrics.
An estimated 2 million teenagers, aged 15-19 years, have attempted suicide within the past year, based on data from the Centers for Disease Control and Prevention. According to the CDC’s 1991-2015 High School Youth Risk Behavior Survey data, nearly a third of students (30%) have felt so sad or helpless nearly daily for at least 2 weeks that they stopped doing their normal activities, and 18% had seriously considered suicide within the past year. One in seven (15%) had made a plan for attempting suicide, 9% had attempted suicide at least once, and 3% attempted suicide that required medical treatment. About twice as many females as males had considered, planned, and/or attempted suicide.
“The offspring of suicide attempters have a sixfold higher risk of suicide than their peers whose parents have not attempted suicide,” Dr. Cody said. Other major risk factors include a history of being bullied, a history of abuse, and a history of substance abuse, particularly alcohol and opioids.
Once you identify a patient at risk for suicide, Dr. Cody advised that you should follow a suicide assessment management protocol, such as the one developed by Angela Stanley, PsyD, of the Medical College of Wisconsin and the Children’s Hospital of Wisconsin, both in Milwaukee. Doctors should identify the teen’s intensity of suicidal ideation, ask how far they are in their plans, ascertain their access to means, create a safety plan, refer the patient for mental health care, and follow up frequently.
Dr. Cody emphasized that “suicide contracts” and “safety plans” are different things. Suicide pacts are agreements not to hurt oneself, whereas safety plans include concrete, collaborative, proactive steps a person will take if experiencing suicidal thoughts.
“There is no evidence that contracts prevent suicide, but a lot of research shows that safety or crisis plans are much more effective at preventing a person from committing suicide,” Dr. Cody stated.
The first step of screening is asking a patient directly whether they have ever wished they were dead or had thoughts about killing themselves.
“Some pediatricians are afraid to ask the questions because they’re afraid they’re going to put the idea of suicide in the child’s head, but there is no evidence that screening puts kids at risk,” Dr. Cody said. The other reason you may feel uneasy asking about self-harm is not knowing what to do if a teen says that she is feeling suicidal. That’s where an assessment protocol helps.
If a patient has considered suicide more than a month prior, it shouldn’t be ignored, although the situation may require less urgency but further follow-up. For those with more recent suicidal ideation but without a plan or intent, Dr. Cody recommends following up within 2 weeks because the adolescent’s situation may change.
For those with suicidal ideation and a plan, you should ask three questions:
- What ways of killing yourself have you thought about?
- How likely is it you will follow through on your plan?
- When you think about killing yourself, what stops you?
These questions can help you determine risk acuity: The more specific, realistic, available, and lethal a plan is, the more acute the risk. You then should ask questions to try to determine how likely the teen is to follow through, such as asking about his future plans, his connectedness with others, and his religious beliefs.
Asking about a plan helps determine how much access the patient has to a lethal, realistic means. Firearms are responsible for 52% of teen suicides, followed by hanging/suffocation (25%) and poisoning (16%).
“This is why it’s a really important part of social history to screen for guns in the house,” Dr. Cody told attendees. “I know it’s been really controversial, but it’s something that’s really important, especially if you have an adolescent in the house that’s having suicidal ideation.”
Teens with suicidal ideation and a plan but no intent require a safety plan along with follow-up within 1 week. Those with a plan and intent, or those with no intent but an unwillingness agree to a safety plan, should be immediately hospitalized, Dr. Cody said.
These suicide screenings should occur at annual well-child visits, Dr. Cody said, but they also should be done at acute visits; basically, any time you see your preteen and adolescent patients. Ideally, these should take place during alone time, without any parents present.
You also should share resources with your patients, including the National Suicide Prevention Lifeline at 1-800-273-8255 and the Crisis TextLine at 741741.
Dr. Cody reported having no disclosures, and no external funding was used for the presentation.
EXPERT ANALYSIS FROM AAP 2017

When is it really recurrent strep throat?
CHICAGO – When a child is sitting in your exam room with recurrent strep pharyngitis, the first question to ask yourself is “Is it real?”
According to pediatric infectious disease specialist John Bradley, MD, the answer to that question comes with careful attention to the history and clinical presentation, but titers and viral polymerase chain reaction tests can also help clarify the diagnosis.
Although that involves some detective work and perhaps some legwork by the provider or the office staff, it’s worth the effort, especially in an era of increased concerns about antimicrobial stewardship, said Dr. Bradley during an antimicrobial update session at the annual meeting of the American Academy of Pediatrics.
“Are the episodes really documented by you in your office?” asked Dr. Bradley. If so, the job is easier. If not, it’s important to differentiate whether documentation of the strep infection was done by culture, whether it was done by an extremely sensitive rapid test, or whether any testing has been done at all, said Dr. Bradley, chief of the division of infectious diseases at the University of California, San Diego.
Somehow, said Dr. Bradley, it’s still true that all group A streptococci are susceptible to penicillin, but penicillin does not always work. There’s about a 10% failure rate for reasons that are not completely understood. Perhaps some individuals have other oropharyngeal flora that produce beta-lactamases, thereby negating penicillin’s efficacy against the strep, he added.
One very good clue as to whether the child has recurrent strep is the appearance of the throat, said Dr. Bradley. A viral illness also can produce a very red posterior oropharynx, so – unless there’s frank pus – it’s unlikely to be strep pharyngitis.
Some patients will, in fact, have recurrent strep, but some patients who might even have positive rapid strep tests may actually be carriers.
So, “what the heck is the carrier state?” asked Dr. Bradley. Although a rapid strep test will occasionally be positive, he explained, the culture is only weakly positive, with growth that’s usually less than 1+. The child who’s a carrier is not symptomatic, will not have an elevated antistreptolysin O titer, and is not contagious. Also, the child will not respond to penicillin treatment.
How can clinicians differentiate recurrent strep from a child with frequent viral illnesses who’s a carrier?
“For the standard case of ‘recurrent strep,’ please get cultures and document the density of group A strep to rule out the carrier state,” said Dr. Bradley. Having parents text pictures of the throat during an episode – for which his facility has a secure portal – can save families an office visit. A negative antistreptolysin O titer can help rule out a recurrent infection, he added.
When a child is having recurrent bouts of pharyngitis, but the clinical picture isn’t clearly consistent with strep, physicians can consider submitting multiplex viral polymerase chain reaction tests. “This can give the family an alternative diagnosis” and reassure parents that it’s safe to hold off on antibiotics, noted Dr. Bradley.
Culturing between episodes of pharyngitis, when the patient is asymptomatic, can also help determine whether a child is a carrier. Sometimes, it makes sense to culture the whole family, and there have also been reports of family pets being Group A strep reservoirs, said Dr. Bradley.
For recurrent infection, choose a broad spectrum agent that will knock back both Group A strep and the oral flora that may be producing beta-lactamases or adhesion molecules that negate penicillin’s efficacy. One logical choice is clindamycin for 10 days, although some strains are resistant. Another good choice is amoxicillin/clavulanate for 10 days or 10 days of a cephalosporin. Penicillin can still be used if it’s augmented by oral rifampin during the last 4 days of the 10-day course.
Long-term prophylaxis can also be considered for stubborn recurrences, he noted.
Dr. Bradley reported no relevant conflicts of interest.
CHICAGO – When a child is sitting in your exam room with recurrent strep pharyngitis, the first question to ask yourself is “Is it real?”
According to pediatric infectious disease specialist John Bradley, MD, the answer to that question comes with careful attention to the history and clinical presentation, but titers and viral polymerase chain reaction tests can also help clarify the diagnosis.
Although that involves some detective work and perhaps some legwork by the provider or the office staff, it’s worth the effort, especially in an era of increased concerns about antimicrobial stewardship, said Dr. Bradley during an antimicrobial update session at the annual meeting of the American Academy of Pediatrics.
“Are the episodes really documented by you in your office?” asked Dr. Bradley. If so, the job is easier. If not, it’s important to differentiate whether documentation of the strep infection was done by culture, whether it was done by an extremely sensitive rapid test, or whether any testing has been done at all, said Dr. Bradley, chief of the division of infectious diseases at the University of California, San Diego.
Somehow, said Dr. Bradley, it’s still true that all group A streptococci are susceptible to penicillin, but penicillin does not always work. There’s about a 10% failure rate for reasons that are not completely understood. Perhaps some individuals have other oropharyngeal flora that produce beta-lactamases, thereby negating penicillin’s efficacy against the strep, he added.
One very good clue as to whether the child has recurrent strep is the appearance of the throat, said Dr. Bradley. A viral illness also can produce a very red posterior oropharynx, so – unless there’s frank pus – it’s unlikely to be strep pharyngitis.
Some patients will, in fact, have recurrent strep, but some patients who might even have positive rapid strep tests may actually be carriers.
So, “what the heck is the carrier state?” asked Dr. Bradley. Although a rapid strep test will occasionally be positive, he explained, the culture is only weakly positive, with growth that’s usually less than 1+. The child who’s a carrier is not symptomatic, will not have an elevated antistreptolysin O titer, and is not contagious. Also, the child will not respond to penicillin treatment.
How can clinicians differentiate recurrent strep from a child with frequent viral illnesses who’s a carrier?
“For the standard case of ‘recurrent strep,’ please get cultures and document the density of group A strep to rule out the carrier state,” said Dr. Bradley. Having parents text pictures of the throat during an episode – for which his facility has a secure portal – can save families an office visit. A negative antistreptolysin O titer can help rule out a recurrent infection, he added.
When a child is having recurrent bouts of pharyngitis, but the clinical picture isn’t clearly consistent with strep, physicians can consider submitting multiplex viral polymerase chain reaction tests. “This can give the family an alternative diagnosis” and reassure parents that it’s safe to hold off on antibiotics, noted Dr. Bradley.
Culturing between episodes of pharyngitis, when the patient is asymptomatic, can also help determine whether a child is a carrier. Sometimes, it makes sense to culture the whole family, and there have also been reports of family pets being Group A strep reservoirs, said Dr. Bradley.
For recurrent infection, choose a broad spectrum agent that will knock back both Group A strep and the oral flora that may be producing beta-lactamases or adhesion molecules that negate penicillin’s efficacy. One logical choice is clindamycin for 10 days, although some strains are resistant. Another good choice is amoxicillin/clavulanate for 10 days or 10 days of a cephalosporin. Penicillin can still be used if it’s augmented by oral rifampin during the last 4 days of the 10-day course.
Long-term prophylaxis can also be considered for stubborn recurrences, he noted.
Dr. Bradley reported no relevant conflicts of interest.
CHICAGO – When a child is sitting in your exam room with recurrent strep pharyngitis, the first question to ask yourself is “Is it real?”
According to pediatric infectious disease specialist John Bradley, MD, the answer to that question comes with careful attention to the history and clinical presentation, but titers and viral polymerase chain reaction tests can also help clarify the diagnosis.
Although that involves some detective work and perhaps some legwork by the provider or the office staff, it’s worth the effort, especially in an era of increased concerns about antimicrobial stewardship, said Dr. Bradley during an antimicrobial update session at the annual meeting of the American Academy of Pediatrics.
“Are the episodes really documented by you in your office?” asked Dr. Bradley. If so, the job is easier. If not, it’s important to differentiate whether documentation of the strep infection was done by culture, whether it was done by an extremely sensitive rapid test, or whether any testing has been done at all, said Dr. Bradley, chief of the division of infectious diseases at the University of California, San Diego.
Somehow, said Dr. Bradley, it’s still true that all group A streptococci are susceptible to penicillin, but penicillin does not always work. There’s about a 10% failure rate for reasons that are not completely understood. Perhaps some individuals have other oropharyngeal flora that produce beta-lactamases, thereby negating penicillin’s efficacy against the strep, he added.
One very good clue as to whether the child has recurrent strep is the appearance of the throat, said Dr. Bradley. A viral illness also can produce a very red posterior oropharynx, so – unless there’s frank pus – it’s unlikely to be strep pharyngitis.
Some patients will, in fact, have recurrent strep, but some patients who might even have positive rapid strep tests may actually be carriers.
So, “what the heck is the carrier state?” asked Dr. Bradley. Although a rapid strep test will occasionally be positive, he explained, the culture is only weakly positive, with growth that’s usually less than 1+. The child who’s a carrier is not symptomatic, will not have an elevated antistreptolysin O titer, and is not contagious. Also, the child will not respond to penicillin treatment.
How can clinicians differentiate recurrent strep from a child with frequent viral illnesses who’s a carrier?
“For the standard case of ‘recurrent strep,’ please get cultures and document the density of group A strep to rule out the carrier state,” said Dr. Bradley. Having parents text pictures of the throat during an episode – for which his facility has a secure portal – can save families an office visit. A negative antistreptolysin O titer can help rule out a recurrent infection, he added.
When a child is having recurrent bouts of pharyngitis, but the clinical picture isn’t clearly consistent with strep, physicians can consider submitting multiplex viral polymerase chain reaction tests. “This can give the family an alternative diagnosis” and reassure parents that it’s safe to hold off on antibiotics, noted Dr. Bradley.
Culturing between episodes of pharyngitis, when the patient is asymptomatic, can also help determine whether a child is a carrier. Sometimes, it makes sense to culture the whole family, and there have also been reports of family pets being Group A strep reservoirs, said Dr. Bradley.
For recurrent infection, choose a broad spectrum agent that will knock back both Group A strep and the oral flora that may be producing beta-lactamases or adhesion molecules that negate penicillin’s efficacy. One logical choice is clindamycin for 10 days, although some strains are resistant. Another good choice is amoxicillin/clavulanate for 10 days or 10 days of a cephalosporin. Penicillin can still be used if it’s augmented by oral rifampin during the last 4 days of the 10-day course.
Long-term prophylaxis can also be considered for stubborn recurrences, he noted.
Dr. Bradley reported no relevant conflicts of interest.
EXPERT ANALYSIS FROM AAP 2017
Survival in lupus patients has plateaued
The major improvement in survival that patients with systemic lupus erythematosus (SLE) have experienced from 1950 to the mid-1990s has plateaued ever since, reported Maria Tektonidou, MD, and her colleagues. The study was published in Annals of the Rheumatic Diseases.
Dr. Tektonidou of National and Kapodistrian University of Athens and her coauthors at the U.S. National Institute of Arthritis and Musculoskeletal and Skin Diseases performed a meta-analysis on studies examining survival in adult and pediatric SLE patients from the 1950s to the mid-1990s. Ultimately, they analyzed 125 adult studies, including 82 from high-income countries and 43 from low- to middle-income countries (LMIC), and 51 pediatric studies, of which 33 were from high-income countries and 18 from LMIC.
In adult studies, researchers found that both high-income and LMIC experienced gradual increases in survival from the 1950s to mid-1990s. After this period of time, the survival estimates stabilized. “In 2008–2016, the 5-year, 10-year, and 15-year survival estimates in high-income countries were 0.95 (95% credible interval, 0.94 to 0.96), 0.89 (0.88 to 0.90) and 0.82 (0.81 to 0.83), respectively” (Ann Rheum Dis. 2017 Aug 9. doi: 10.1136/annrheumdis-2017-211663).
Although there were no data for LMIC prior to 1970, researchers identified survival trends similar to those in high-income countries in more recent years. Over the same time period between 2008 and 2016, “the 5-year, 10-year, and 15-year survival estimates in LMIC were 0.92 (0.91 to 0.93), 0.85 (0.84 to 0.87) and 0.79 (0.78 to 0.81), respectively,” according to the report.
Unlike the steady improvement seen over a 40-year period with adult studies, pediatric SLE patients in high-income countries experienced dramatic increases in survival rates from the 1960s to the 1970s, followed by slower increases in survival rates. The researchers reported that between 2008 and 2016,“the 5-year and 10-year survival estimates from high-income countries were 0.99 (0.98 to 1.00) and 0.97 (0.96 to 0.98), respectively.”
LMIC had significantly worse survival in pediatric SLE patients than did their wealthy counterparts. “Survival persistently lagged [behind] that of high-income countries” between 1980 and 2000. Dr. Tektonidou and her associates found that “5-year and 10-year survival estimates from LMIC were 0.85 (0.83 to 0.88) and 0.79 (0.76 to 0.82), respectively.” Due to the small number of studies reporting 15-year survival rates, this time point was not included in the pediatric analysis.
The researchers also analyzed the cause of death for adult and pediatric SLE patients in both high-income countries and LMIC. High-income countries showed lower rates of SLE-associated deaths over time in adults, although infection-related deaths increased in adults in both high-income countries and LMIC. There were not enough studies and data to assess cause of death in pediatric studies in high-income countries, but pediatric patients in LMIC had an upward trend in SLE-associated deaths.
The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. The researchers reported having no relevant financial disclosures.
The major improvement in survival that patients with systemic lupus erythematosus (SLE) have experienced from 1950 to the mid-1990s has plateaued ever since, reported Maria Tektonidou, MD, and her colleagues. The study was published in Annals of the Rheumatic Diseases.
Dr. Tektonidou of National and Kapodistrian University of Athens and her coauthors at the U.S. National Institute of Arthritis and Musculoskeletal and Skin Diseases performed a meta-analysis on studies examining survival in adult and pediatric SLE patients from the 1950s to the mid-1990s. Ultimately, they analyzed 125 adult studies, including 82 from high-income countries and 43 from low- to middle-income countries (LMIC), and 51 pediatric studies, of which 33 were from high-income countries and 18 from LMIC.
In adult studies, researchers found that both high-income and LMIC experienced gradual increases in survival from the 1950s to mid-1990s. After this period of time, the survival estimates stabilized. “In 2008–2016, the 5-year, 10-year, and 15-year survival estimates in high-income countries were 0.95 (95% credible interval, 0.94 to 0.96), 0.89 (0.88 to 0.90) and 0.82 (0.81 to 0.83), respectively” (Ann Rheum Dis. 2017 Aug 9. doi: 10.1136/annrheumdis-2017-211663).
Although there were no data for LMIC prior to 1970, researchers identified survival trends similar to those in high-income countries in more recent years. Over the same time period between 2008 and 2016, “the 5-year, 10-year, and 15-year survival estimates in LMIC were 0.92 (0.91 to 0.93), 0.85 (0.84 to 0.87) and 0.79 (0.78 to 0.81), respectively,” according to the report.
Unlike the steady improvement seen over a 40-year period with adult studies, pediatric SLE patients in high-income countries experienced dramatic increases in survival rates from the 1960s to the 1970s, followed by slower increases in survival rates. The researchers reported that between 2008 and 2016,“the 5-year and 10-year survival estimates from high-income countries were 0.99 (0.98 to 1.00) and 0.97 (0.96 to 0.98), respectively.”
LMIC had significantly worse survival in pediatric SLE patients than did their wealthy counterparts. “Survival persistently lagged [behind] that of high-income countries” between 1980 and 2000. Dr. Tektonidou and her associates found that “5-year and 10-year survival estimates from LMIC were 0.85 (0.83 to 0.88) and 0.79 (0.76 to 0.82), respectively.” Due to the small number of studies reporting 15-year survival rates, this time point was not included in the pediatric analysis.
The researchers also analyzed the cause of death for adult and pediatric SLE patients in both high-income countries and LMIC. High-income countries showed lower rates of SLE-associated deaths over time in adults, although infection-related deaths increased in adults in both high-income countries and LMIC. There were not enough studies and data to assess cause of death in pediatric studies in high-income countries, but pediatric patients in LMIC had an upward trend in SLE-associated deaths.
The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. The researchers reported having no relevant financial disclosures.
The major improvement in survival that patients with systemic lupus erythematosus (SLE) have experienced from 1950 to the mid-1990s has plateaued ever since, reported Maria Tektonidou, MD, and her colleagues. The study was published in Annals of the Rheumatic Diseases.
Dr. Tektonidou of National and Kapodistrian University of Athens and her coauthors at the U.S. National Institute of Arthritis and Musculoskeletal and Skin Diseases performed a meta-analysis on studies examining survival in adult and pediatric SLE patients from the 1950s to the mid-1990s. Ultimately, they analyzed 125 adult studies, including 82 from high-income countries and 43 from low- to middle-income countries (LMIC), and 51 pediatric studies, of which 33 were from high-income countries and 18 from LMIC.
In adult studies, researchers found that both high-income and LMIC experienced gradual increases in survival from the 1950s to mid-1990s. After this period of time, the survival estimates stabilized. “In 2008–2016, the 5-year, 10-year, and 15-year survival estimates in high-income countries were 0.95 (95% credible interval, 0.94 to 0.96), 0.89 (0.88 to 0.90) and 0.82 (0.81 to 0.83), respectively” (Ann Rheum Dis. 2017 Aug 9. doi: 10.1136/annrheumdis-2017-211663).
Although there were no data for LMIC prior to 1970, researchers identified survival trends similar to those in high-income countries in more recent years. Over the same time period between 2008 and 2016, “the 5-year, 10-year, and 15-year survival estimates in LMIC were 0.92 (0.91 to 0.93), 0.85 (0.84 to 0.87) and 0.79 (0.78 to 0.81), respectively,” according to the report.
Unlike the steady improvement seen over a 40-year period with adult studies, pediatric SLE patients in high-income countries experienced dramatic increases in survival rates from the 1960s to the 1970s, followed by slower increases in survival rates. The researchers reported that between 2008 and 2016,“the 5-year and 10-year survival estimates from high-income countries were 0.99 (0.98 to 1.00) and 0.97 (0.96 to 0.98), respectively.”
LMIC had significantly worse survival in pediatric SLE patients than did their wealthy counterparts. “Survival persistently lagged [behind] that of high-income countries” between 1980 and 2000. Dr. Tektonidou and her associates found that “5-year and 10-year survival estimates from LMIC were 0.85 (0.83 to 0.88) and 0.79 (0.76 to 0.82), respectively.” Due to the small number of studies reporting 15-year survival rates, this time point was not included in the pediatric analysis.
The researchers also analyzed the cause of death for adult and pediatric SLE patients in both high-income countries and LMIC. High-income countries showed lower rates of SLE-associated deaths over time in adults, although infection-related deaths increased in adults in both high-income countries and LMIC. There were not enough studies and data to assess cause of death in pediatric studies in high-income countries, but pediatric patients in LMIC had an upward trend in SLE-associated deaths.
The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. The researchers reported having no relevant financial disclosures.
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point:
Major finding: Five-year survival for SLE in adults and children in high-income countries is greater than 0.95.
Data source: Systematic literature review and Bayesian meta-analysis of 171 published cohort studies of survival in SLE patients from 1950 to the present.
Disclosures: The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. The researchers reported having no relevant financial disclosures.
Endocrine Society updates treatment guidelines for transgender persons
Previous clinical recommendations on caring for transgender individuals have advised that hormone treatment begin no earlier than age 16 years, but
“Sixteen is the typical age cutoff in many areas of the world for some decision-making capacity from a legal perspective, but when you think about hormones and puberty, 16 is pretty late,” Joshua D. Safer, MD, one of the task force members who authored the guideline, said in an interview. “If we’re going to use biology for guidance, then hormone interventions for transgender kids should begin occurring earlier, when puberty really happens, like around age 12, 13, or 14. However, we’re in a situation where we lack a test. We can’t diagnose anybody as transgender with excellent confidence, outside of talking to those kids. When we start talking about hormone therapies, we talk about some things that will be irreversible. That’s a fraught place to go, but we recognize that people are going to treat kids under 16 in many instances.”
Over several years, Dr. Safer and nine other task force members, chaired by Wylie Hembree, MD, of the College of Physicians and Surgeons at Columbia University, New York, worked to establish a framework for the appropriate treatment of transgender individuals. The efforts of the task force were framed around a durable biological underpinning to gender identity. “That’s state of the art right now,” said Dr. Safer, who is the medical director of the Center for Transgender Medicine and Surgery at Boston University Medical Center. “People think there’s debate about whether there’s a substantial biological component. I think that the data are pretty strong, so I don’t think there’s a lot of debate about that in the scientific world. The debate is more about what that biology might be. That’s all over the map.”
That notion of a biological basis for gender identity contributed to a second major change from the Endocrine Society’s 2009 guideline, which recommended that the diagnosis of gender identity disorder be made by a mental health professional. The current guideline states that for the care of peripubertal youths and older adolescents, “we recommend that an expert multidisciplinary team comprised of medical professionals and mental health professionals manage this treatment. The treating physician must confirm the criteria for treatment used by the referring mental health practitioner and collaborate with them in decisions about gender-affirming surgery in older adolescents.” Meanwhile, for adult gender-dysphoric/gender-incongruent persons, “the treating clinicians (collectively) should have expertise in transgender-specific diagnostic criteria, mental health, primary care, hormone treatment, and surgery, as needed by the patient.” Dr. Safer described this new approach as “a major change in terms of trying to gain access to care by liberalizing the variety of those in the medical community who can be associated with the diagnosis, at least on the adult side.”
A number of associations cosponsored the guideline, including the American Association of Clinical Endocrinologists, American Society of Andrology, European Society for Paediatric Endocrinology, European Society of Endocrinology, Pediatric Endocrine Society, and World Professional Association for Transgender Health. Other key recommendations from the guideline include:
- All individuals seeking gender-affirming medical treatment should receive information and counsel on options for fertility preservation prior to initiating puberty suppression in adolescents and prior to treating with hormonal therapy of the affirmed gender in both adolescents and adults.
- Removal of gonads may be considered when high doses of sex steroids are required to suppress the body’s secretion of hormones and/or to reduce steroid levels in advanced age.
- During sex-steroid treatment, clinicians should monitor, in both transgender males (female to male) and transgender females (male to female), prolactin, metabolic disorders, and bone loss, as well as cancer risks in individuals who have not undergone surgical treatment.
Concurrent with the release of the new guideline, the Endocrine Society issued a position statement that calls on federal and private insurers to cover medical interventions for transgender individuals as prescribed by a physician. “I live in Massachusetts, where our insurance commissioner deemed insurance coverage obligatory for transgender individuals as of 2015,” said Dr. Safer, who is also director of the endocrinology fellowship training program at Boston University. “I’ve spoken to the medical directors of our large insurers, like Blue Cross/Blue Shield. What’s notable is that there has been no push back [on coverage for transgender individuals] from the insurance companies. These services are not expensive: the primary care, the mental health care, and the hormones. Many of the patients are not opting for surgeries. The theme of their concern was to get their [health insurance] policies right as quickly as possible so that they could stop wasting time talking about it, and they could focus their energy on other, more expensive health care concerns.”
In the guideline, Dr. Safer and the other task force members called for more rigorous evaluations of the effectiveness and safety of endocrine and surgical protocols in the future. “Specifically, endocrine treatment protocols for GD/gender incongruence should include the careful assessment of the following: (1) the effects of prolonged delay of puberty in adolescents on bone health, gonadal function, and the brain (including effects on cognitive, emotional, social, and sexual development); (2) the effects of treatment in adults on sex hormone levels; (3) the requirement for and the effects of progestins and other agents used to suppress endogenous sex steroids during treatment; and (4) the risks and benefits of gender-affirming hormone treatment in older transgender people.”
Dr. Safer reported having no financial disclosures.
Previous clinical recommendations on caring for transgender individuals have advised that hormone treatment begin no earlier than age 16 years, but
“Sixteen is the typical age cutoff in many areas of the world for some decision-making capacity from a legal perspective, but when you think about hormones and puberty, 16 is pretty late,” Joshua D. Safer, MD, one of the task force members who authored the guideline, said in an interview. “If we’re going to use biology for guidance, then hormone interventions for transgender kids should begin occurring earlier, when puberty really happens, like around age 12, 13, or 14. However, we’re in a situation where we lack a test. We can’t diagnose anybody as transgender with excellent confidence, outside of talking to those kids. When we start talking about hormone therapies, we talk about some things that will be irreversible. That’s a fraught place to go, but we recognize that people are going to treat kids under 16 in many instances.”
Over several years, Dr. Safer and nine other task force members, chaired by Wylie Hembree, MD, of the College of Physicians and Surgeons at Columbia University, New York, worked to establish a framework for the appropriate treatment of transgender individuals. The efforts of the task force were framed around a durable biological underpinning to gender identity. “That’s state of the art right now,” said Dr. Safer, who is the medical director of the Center for Transgender Medicine and Surgery at Boston University Medical Center. “People think there’s debate about whether there’s a substantial biological component. I think that the data are pretty strong, so I don’t think there’s a lot of debate about that in the scientific world. The debate is more about what that biology might be. That’s all over the map.”
That notion of a biological basis for gender identity contributed to a second major change from the Endocrine Society’s 2009 guideline, which recommended that the diagnosis of gender identity disorder be made by a mental health professional. The current guideline states that for the care of peripubertal youths and older adolescents, “we recommend that an expert multidisciplinary team comprised of medical professionals and mental health professionals manage this treatment. The treating physician must confirm the criteria for treatment used by the referring mental health practitioner and collaborate with them in decisions about gender-affirming surgery in older adolescents.” Meanwhile, for adult gender-dysphoric/gender-incongruent persons, “the treating clinicians (collectively) should have expertise in transgender-specific diagnostic criteria, mental health, primary care, hormone treatment, and surgery, as needed by the patient.” Dr. Safer described this new approach as “a major change in terms of trying to gain access to care by liberalizing the variety of those in the medical community who can be associated with the diagnosis, at least on the adult side.”
A number of associations cosponsored the guideline, including the American Association of Clinical Endocrinologists, American Society of Andrology, European Society for Paediatric Endocrinology, European Society of Endocrinology, Pediatric Endocrine Society, and World Professional Association for Transgender Health. Other key recommendations from the guideline include:
- All individuals seeking gender-affirming medical treatment should receive information and counsel on options for fertility preservation prior to initiating puberty suppression in adolescents and prior to treating with hormonal therapy of the affirmed gender in both adolescents and adults.
- Removal of gonads may be considered when high doses of sex steroids are required to suppress the body’s secretion of hormones and/or to reduce steroid levels in advanced age.
- During sex-steroid treatment, clinicians should monitor, in both transgender males (female to male) and transgender females (male to female), prolactin, metabolic disorders, and bone loss, as well as cancer risks in individuals who have not undergone surgical treatment.
Concurrent with the release of the new guideline, the Endocrine Society issued a position statement that calls on federal and private insurers to cover medical interventions for transgender individuals as prescribed by a physician. “I live in Massachusetts, where our insurance commissioner deemed insurance coverage obligatory for transgender individuals as of 2015,” said Dr. Safer, who is also director of the endocrinology fellowship training program at Boston University. “I’ve spoken to the medical directors of our large insurers, like Blue Cross/Blue Shield. What’s notable is that there has been no push back [on coverage for transgender individuals] from the insurance companies. These services are not expensive: the primary care, the mental health care, and the hormones. Many of the patients are not opting for surgeries. The theme of their concern was to get their [health insurance] policies right as quickly as possible so that they could stop wasting time talking about it, and they could focus their energy on other, more expensive health care concerns.”
In the guideline, Dr. Safer and the other task force members called for more rigorous evaluations of the effectiveness and safety of endocrine and surgical protocols in the future. “Specifically, endocrine treatment protocols for GD/gender incongruence should include the careful assessment of the following: (1) the effects of prolonged delay of puberty in adolescents on bone health, gonadal function, and the brain (including effects on cognitive, emotional, social, and sexual development); (2) the effects of treatment in adults on sex hormone levels; (3) the requirement for and the effects of progestins and other agents used to suppress endogenous sex steroids during treatment; and (4) the risks and benefits of gender-affirming hormone treatment in older transgender people.”
Dr. Safer reported having no financial disclosures.
Previous clinical recommendations on caring for transgender individuals have advised that hormone treatment begin no earlier than age 16 years, but
“Sixteen is the typical age cutoff in many areas of the world for some decision-making capacity from a legal perspective, but when you think about hormones and puberty, 16 is pretty late,” Joshua D. Safer, MD, one of the task force members who authored the guideline, said in an interview. “If we’re going to use biology for guidance, then hormone interventions for transgender kids should begin occurring earlier, when puberty really happens, like around age 12, 13, or 14. However, we’re in a situation where we lack a test. We can’t diagnose anybody as transgender with excellent confidence, outside of talking to those kids. When we start talking about hormone therapies, we talk about some things that will be irreversible. That’s a fraught place to go, but we recognize that people are going to treat kids under 16 in many instances.”
Over several years, Dr. Safer and nine other task force members, chaired by Wylie Hembree, MD, of the College of Physicians and Surgeons at Columbia University, New York, worked to establish a framework for the appropriate treatment of transgender individuals. The efforts of the task force were framed around a durable biological underpinning to gender identity. “That’s state of the art right now,” said Dr. Safer, who is the medical director of the Center for Transgender Medicine and Surgery at Boston University Medical Center. “People think there’s debate about whether there’s a substantial biological component. I think that the data are pretty strong, so I don’t think there’s a lot of debate about that in the scientific world. The debate is more about what that biology might be. That’s all over the map.”
That notion of a biological basis for gender identity contributed to a second major change from the Endocrine Society’s 2009 guideline, which recommended that the diagnosis of gender identity disorder be made by a mental health professional. The current guideline states that for the care of peripubertal youths and older adolescents, “we recommend that an expert multidisciplinary team comprised of medical professionals and mental health professionals manage this treatment. The treating physician must confirm the criteria for treatment used by the referring mental health practitioner and collaborate with them in decisions about gender-affirming surgery in older adolescents.” Meanwhile, for adult gender-dysphoric/gender-incongruent persons, “the treating clinicians (collectively) should have expertise in transgender-specific diagnostic criteria, mental health, primary care, hormone treatment, and surgery, as needed by the patient.” Dr. Safer described this new approach as “a major change in terms of trying to gain access to care by liberalizing the variety of those in the medical community who can be associated with the diagnosis, at least on the adult side.”
A number of associations cosponsored the guideline, including the American Association of Clinical Endocrinologists, American Society of Andrology, European Society for Paediatric Endocrinology, European Society of Endocrinology, Pediatric Endocrine Society, and World Professional Association for Transgender Health. Other key recommendations from the guideline include:
- All individuals seeking gender-affirming medical treatment should receive information and counsel on options for fertility preservation prior to initiating puberty suppression in adolescents and prior to treating with hormonal therapy of the affirmed gender in both adolescents and adults.
- Removal of gonads may be considered when high doses of sex steroids are required to suppress the body’s secretion of hormones and/or to reduce steroid levels in advanced age.
- During sex-steroid treatment, clinicians should monitor, in both transgender males (female to male) and transgender females (male to female), prolactin, metabolic disorders, and bone loss, as well as cancer risks in individuals who have not undergone surgical treatment.
Concurrent with the release of the new guideline, the Endocrine Society issued a position statement that calls on federal and private insurers to cover medical interventions for transgender individuals as prescribed by a physician. “I live in Massachusetts, where our insurance commissioner deemed insurance coverage obligatory for transgender individuals as of 2015,” said Dr. Safer, who is also director of the endocrinology fellowship training program at Boston University. “I’ve spoken to the medical directors of our large insurers, like Blue Cross/Blue Shield. What’s notable is that there has been no push back [on coverage for transgender individuals] from the insurance companies. These services are not expensive: the primary care, the mental health care, and the hormones. Many of the patients are not opting for surgeries. The theme of their concern was to get their [health insurance] policies right as quickly as possible so that they could stop wasting time talking about it, and they could focus their energy on other, more expensive health care concerns.”
In the guideline, Dr. Safer and the other task force members called for more rigorous evaluations of the effectiveness and safety of endocrine and surgical protocols in the future. “Specifically, endocrine treatment protocols for GD/gender incongruence should include the careful assessment of the following: (1) the effects of prolonged delay of puberty in adolescents on bone health, gonadal function, and the brain (including effects on cognitive, emotional, social, and sexual development); (2) the effects of treatment in adults on sex hormone levels; (3) the requirement for and the effects of progestins and other agents used to suppress endogenous sex steroids during treatment; and (4) the risks and benefits of gender-affirming hormone treatment in older transgender people.”
Dr. Safer reported having no financial disclosures.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
PHM17 session summary: Career Development (K Award) grants
Session
Career Development (K Award) grants: What are they, why should I apply, and how do I get funded?
Presenters
Christopher Bonafide, MD, MSCE; Patrick Brady, MD, MS; Kavita Parikh, MD, MSHS; Raj Srivastava, MD, MPH, SFHM; Derek Williams, MD, MPH
Session Summary
Pediatric hospital medicine, in its relative infancy, is attracting a cohort of academicians dedicated to advancing the care of hospitalized children. While other pediatric subspecialties have long reserved a significant proportion of fellowship training for research, pediatric hospitalist research has instead developed from the work of scholarly pioneers in the industry.

More colloquially known as K Awards, NIH Career Development Awards exist to financially support early-career clinical, translational, and basic science investigators through a closely mentored career development and research plan. The result? A mutually beneficial initiative lasting 3-5 years aligning the interests of the early-career investigator, hosting institution, and NIH. The realm of grant funding is confusing and can be intimidating, particularly for early-career investigators in a rapidly growing field of practice. Presenters at this session addressed the stigma of applying for K awards head on.
Who should apply for an NIH Career Development Award?
Competitive applicants for a Career Development Award are ideally interested in embarking on a career dedicated to research of some type, although exactly what that entails can and certainly may change over time.
What does the NIH Career Development Award provide?
The award funds a significant portion of your salary to provide protected time dedicated to your research and career development. Removing this financial barrier allows the investigator to become fully immersed in maturation as an independent investigator. The presenters were quick to caution that applicants (along with department and division chairs) should be aware that the award does not cover your entire salary; early-career investigators truly need dedication from their department and/or division to be successful.
Why apply for an NIH Career Development Award?
Clinical, translational, and basic science research takes time to complete, and the skills needed to be a successful investigator are not intuitive. Rather, they require close mentorship and practice. A career development award organizes and prioritizes an early-career investigator’s approach to obtaining research independence. Applying for an NIH Career Development Award helps identify the applicant’s experiential and knowledge gaps and, more importantly, develops a plan for how these deficits will be addressed over the course of the research project. This formative process ideally allows the early-career investigator to be more competitive in seeking larger grant funding.
Interested in pursuing a career development award? Dr. Bonafide and Dr. Srivastava offered the valuable advice that an applicant’s proposed research is only part of the equation for funding success. Equally important is your ability to identify your weaknesses as they pertain to research (and how you will address these weaknesses) as well as to find your mentorship team. You and your fellow awardees should surround yourselves with mentors who will address specific needs, which, in some circumstances, may require creativity and collaboration to augment the experience gained from others.
Key takeaway for PHM
As we recognize the growing complexities of caring for the hospitalized child, opportunities for clinical, translational, and basic science are expanding rapidly. Embracing the benefits of formalizing your research training early can lead to a successful and satisfying academic career in the long term.
Dr. Morrison is a Pediatric Hospital Medicine Fellow at Johns Hopkins All Children’s Hospital, St. Petersburg, Fla.
Session
Career Development (K Award) grants: What are they, why should I apply, and how do I get funded?
Presenters
Christopher Bonafide, MD, MSCE; Patrick Brady, MD, MS; Kavita Parikh, MD, MSHS; Raj Srivastava, MD, MPH, SFHM; Derek Williams, MD, MPH
Session Summary
Pediatric hospital medicine, in its relative infancy, is attracting a cohort of academicians dedicated to advancing the care of hospitalized children. While other pediatric subspecialties have long reserved a significant proportion of fellowship training for research, pediatric hospitalist research has instead developed from the work of scholarly pioneers in the industry.
More colloquially known as K Awards, NIH Career Development Awards exist to financially support early-career clinical, translational, and basic science investigators through a closely mentored career development and research plan. The result? A mutually beneficial initiative lasting 3-5 years aligning the interests of the early-career investigator, hosting institution, and NIH. The realm of grant funding is confusing and can be intimidating, particularly for early-career investigators in a rapidly growing field of practice. Presenters at this session addressed the stigma of applying for K awards head on.
Who should apply for an NIH Career Development Award?
Competitive applicants for a Career Development Award are ideally interested in embarking on a career dedicated to research of some type, although exactly what that entails can and certainly may change over time.
What does the NIH Career Development Award provide?
The award funds a significant portion of your salary to provide protected time dedicated to your research and career development. Removing this financial barrier allows the investigator to become fully immersed in maturation as an independent investigator. The presenters were quick to caution that applicants (along with department and division chairs) should be aware that the award does not cover your entire salary; early-career investigators truly need dedication from their department and/or division to be successful.
Why apply for an NIH Career Development Award?
Clinical, translational, and basic science research takes time to complete, and the skills needed to be a successful investigator are not intuitive. Rather, they require close mentorship and practice. A career development award organizes and prioritizes an early-career investigator’s approach to obtaining research independence. Applying for an NIH Career Development Award helps identify the applicant’s experiential and knowledge gaps and, more importantly, develops a plan for how these deficits will be addressed over the course of the research project. This formative process ideally allows the early-career investigator to be more competitive in seeking larger grant funding.
Interested in pursuing a career development award? Dr. Bonafide and Dr. Srivastava offered the valuable advice that an applicant’s proposed research is only part of the equation for funding success. Equally important is your ability to identify your weaknesses as they pertain to research (and how you will address these weaknesses) as well as to find your mentorship team. You and your fellow awardees should surround yourselves with mentors who will address specific needs, which, in some circumstances, may require creativity and collaboration to augment the experience gained from others.
Key takeaway for PHM
As we recognize the growing complexities of caring for the hospitalized child, opportunities for clinical, translational, and basic science are expanding rapidly. Embracing the benefits of formalizing your research training early can lead to a successful and satisfying academic career in the long term.
Dr. Morrison is a Pediatric Hospital Medicine Fellow at Johns Hopkins All Children’s Hospital, St. Petersburg, Fla.
Session
Career Development (K Award) grants: What are they, why should I apply, and how do I get funded?
Presenters
Christopher Bonafide, MD, MSCE; Patrick Brady, MD, MS; Kavita Parikh, MD, MSHS; Raj Srivastava, MD, MPH, SFHM; Derek Williams, MD, MPH
Session Summary
Pediatric hospital medicine, in its relative infancy, is attracting a cohort of academicians dedicated to advancing the care of hospitalized children. While other pediatric subspecialties have long reserved a significant proportion of fellowship training for research, pediatric hospitalist research has instead developed from the work of scholarly pioneers in the industry.
More colloquially known as K Awards, NIH Career Development Awards exist to financially support early-career clinical, translational, and basic science investigators through a closely mentored career development and research plan. The result? A mutually beneficial initiative lasting 3-5 years aligning the interests of the early-career investigator, hosting institution, and NIH. The realm of grant funding is confusing and can be intimidating, particularly for early-career investigators in a rapidly growing field of practice. Presenters at this session addressed the stigma of applying for K awards head on.
Who should apply for an NIH Career Development Award?
Competitive applicants for a Career Development Award are ideally interested in embarking on a career dedicated to research of some type, although exactly what that entails can and certainly may change over time.
What does the NIH Career Development Award provide?
The award funds a significant portion of your salary to provide protected time dedicated to your research and career development. Removing this financial barrier allows the investigator to become fully immersed in maturation as an independent investigator. The presenters were quick to caution that applicants (along with department and division chairs) should be aware that the award does not cover your entire salary; early-career investigators truly need dedication from their department and/or division to be successful.
Why apply for an NIH Career Development Award?
Clinical, translational, and basic science research takes time to complete, and the skills needed to be a successful investigator are not intuitive. Rather, they require close mentorship and practice. A career development award organizes and prioritizes an early-career investigator’s approach to obtaining research independence. Applying for an NIH Career Development Award helps identify the applicant’s experiential and knowledge gaps and, more importantly, develops a plan for how these deficits will be addressed over the course of the research project. This formative process ideally allows the early-career investigator to be more competitive in seeking larger grant funding.
Interested in pursuing a career development award? Dr. Bonafide and Dr. Srivastava offered the valuable advice that an applicant’s proposed research is only part of the equation for funding success. Equally important is your ability to identify your weaknesses as they pertain to research (and how you will address these weaknesses) as well as to find your mentorship team. You and your fellow awardees should surround yourselves with mentors who will address specific needs, which, in some circumstances, may require creativity and collaboration to augment the experience gained from others.
Key takeaway for PHM
As we recognize the growing complexities of caring for the hospitalized child, opportunities for clinical, translational, and basic science are expanding rapidly. Embracing the benefits of formalizing your research training early can lead to a successful and satisfying academic career in the long term.
Dr. Morrison is a Pediatric Hospital Medicine Fellow at Johns Hopkins All Children’s Hospital, St. Petersburg, Fla.
Teens smoking more pot than cigarettes
CHICAGO – The challenge of addressing marijuana use by children and teens is increasing with its wider availability; 29 states have now legalized cannabis for medical use, and 8 of them plus the District of Columbia have legalized recreational marijuana use.
“Past-month marijuana use is now higher than past-month use of cigarettes” based on teens’ responses to surveys from the National Institute on Drug Abuse (NIDA), Karen M. Wilson, MD, said at the annual meeting of the American Academy of Pediatrics.

Dr. Wilson emphasized the importance of discussing drug use and attitudes about drug use with young teens, as well as educating them about risks.
Recent research suggests the brain does not fully mature until the mid-20s, and marijuana has been shown to impair working memory, cognitive flexibility, learning, attention, and verbal functions. Marijuana may alter the developing brain in ways that cannot be repaired in those who halt use at an older age, said Dr. Wilson, division chief of general pediatrics and vice-chair for clinical and translational research at the Icahn School of Medicine at Mount Sinai, New York. Marijuana use becomes an addictive behavior in 9% of users, and this addictive behavior is more likely to persist in those who begin to use marijuana at a young age.
“Whether it’s alcohol or marijuana or tobacco, even if they’re only using it on the weekends,” the behavior can progress to addictive behavior, she said. Discussions should determine how much cannabis is used, how often, and why it is used.
“Kids may be self-medicating if they have depression, anxiety, or chronic pain,” Dr. Wilson said. “That could be something you could provide a more appropriate pharmacological intervention for.”
Motivational interviewing – a collaborative, person-centered form of guiding to elicit and strengthen motivation for change – can be the impetus for discussion about whether young patients can try quitting for a short time to show they can do it.
One challenge of discouraging and reducing teens’ marijuana use is the increasing diversity of products and consumption methods. From candy and baked goods to electronic “vaping” products and dissolvable strips similar to breath mints, it’s difficult to keep up. Dr. Wilson showed an image of a new product that looks exactly like a medical inhaler.
Couse of marijuana with tobacco also presents challenges since researchers have little data on how dual use may affect the ability to quit using either drug. “Joints,” rolled in paper, contain only marijuana, but a “blunt” is marijuana rolled in a tobacco leaf, and “spliffs” contain both marijuana and tobacco. Both blunts and spliffs, therefore, include nicotine which is addictive.
Other inhaled substances that can potentially damage the lungs include “lung juice,” a herbal product marketed to “clean out” the lungs. “We should encourage teens to get clean lungs by not inhaling things that aren’t good for you.”
Dr. Wilson reported having no disclosures, and no external funding was used for the presentation.
CHICAGO – The challenge of addressing marijuana use by children and teens is increasing with its wider availability; 29 states have now legalized cannabis for medical use, and 8 of them plus the District of Columbia have legalized recreational marijuana use.
“Past-month marijuana use is now higher than past-month use of cigarettes” based on teens’ responses to surveys from the National Institute on Drug Abuse (NIDA), Karen M. Wilson, MD, said at the annual meeting of the American Academy of Pediatrics.
Dr. Wilson emphasized the importance of discussing drug use and attitudes about drug use with young teens, as well as educating them about risks.
Recent research suggests the brain does not fully mature until the mid-20s, and marijuana has been shown to impair working memory, cognitive flexibility, learning, attention, and verbal functions. Marijuana may alter the developing brain in ways that cannot be repaired in those who halt use at an older age, said Dr. Wilson, division chief of general pediatrics and vice-chair for clinical and translational research at the Icahn School of Medicine at Mount Sinai, New York. Marijuana use becomes an addictive behavior in 9% of users, and this addictive behavior is more likely to persist in those who begin to use marijuana at a young age.
“Whether it’s alcohol or marijuana or tobacco, even if they’re only using it on the weekends,” the behavior can progress to addictive behavior, she said. Discussions should determine how much cannabis is used, how often, and why it is used.
“Kids may be self-medicating if they have depression, anxiety, or chronic pain,” Dr. Wilson said. “That could be something you could provide a more appropriate pharmacological intervention for.”
Motivational interviewing – a collaborative, person-centered form of guiding to elicit and strengthen motivation for change – can be the impetus for discussion about whether young patients can try quitting for a short time to show they can do it.
One challenge of discouraging and reducing teens’ marijuana use is the increasing diversity of products and consumption methods. From candy and baked goods to electronic “vaping” products and dissolvable strips similar to breath mints, it’s difficult to keep up. Dr. Wilson showed an image of a new product that looks exactly like a medical inhaler.
Couse of marijuana with tobacco also presents challenges since researchers have little data on how dual use may affect the ability to quit using either drug. “Joints,” rolled in paper, contain only marijuana, but a “blunt” is marijuana rolled in a tobacco leaf, and “spliffs” contain both marijuana and tobacco. Both blunts and spliffs, therefore, include nicotine which is addictive.
Other inhaled substances that can potentially damage the lungs include “lung juice,” a herbal product marketed to “clean out” the lungs. “We should encourage teens to get clean lungs by not inhaling things that aren’t good for you.”
Dr. Wilson reported having no disclosures, and no external funding was used for the presentation.
CHICAGO – The challenge of addressing marijuana use by children and teens is increasing with its wider availability; 29 states have now legalized cannabis for medical use, and 8 of them plus the District of Columbia have legalized recreational marijuana use.
“Past-month marijuana use is now higher than past-month use of cigarettes” based on teens’ responses to surveys from the National Institute on Drug Abuse (NIDA), Karen M. Wilson, MD, said at the annual meeting of the American Academy of Pediatrics.
Dr. Wilson emphasized the importance of discussing drug use and attitudes about drug use with young teens, as well as educating them about risks.
Recent research suggests the brain does not fully mature until the mid-20s, and marijuana has been shown to impair working memory, cognitive flexibility, learning, attention, and verbal functions. Marijuana may alter the developing brain in ways that cannot be repaired in those who halt use at an older age, said Dr. Wilson, division chief of general pediatrics and vice-chair for clinical and translational research at the Icahn School of Medicine at Mount Sinai, New York. Marijuana use becomes an addictive behavior in 9% of users, and this addictive behavior is more likely to persist in those who begin to use marijuana at a young age.
“Whether it’s alcohol or marijuana or tobacco, even if they’re only using it on the weekends,” the behavior can progress to addictive behavior, she said. Discussions should determine how much cannabis is used, how often, and why it is used.
“Kids may be self-medicating if they have depression, anxiety, or chronic pain,” Dr. Wilson said. “That could be something you could provide a more appropriate pharmacological intervention for.”
Motivational interviewing – a collaborative, person-centered form of guiding to elicit and strengthen motivation for change – can be the impetus for discussion about whether young patients can try quitting for a short time to show they can do it.
One challenge of discouraging and reducing teens’ marijuana use is the increasing diversity of products and consumption methods. From candy and baked goods to electronic “vaping” products and dissolvable strips similar to breath mints, it’s difficult to keep up. Dr. Wilson showed an image of a new product that looks exactly like a medical inhaler.
Couse of marijuana with tobacco also presents challenges since researchers have little data on how dual use may affect the ability to quit using either drug. “Joints,” rolled in paper, contain only marijuana, but a “blunt” is marijuana rolled in a tobacco leaf, and “spliffs” contain both marijuana and tobacco. Both blunts and spliffs, therefore, include nicotine which is addictive.
Other inhaled substances that can potentially damage the lungs include “lung juice,” a herbal product marketed to “clean out” the lungs. “We should encourage teens to get clean lungs by not inhaling things that aren’t good for you.”
Dr. Wilson reported having no disclosures, and no external funding was used for the presentation.
EXPERT ANALYSIS FROM AAP 2017