User login
Medicare Okays Wound Plasma Gel for Clinical Trial Patients
The Centers for Medicare and Medicaid Services has announced coverage of platelet-rich plasma gel for chronic wounds, but only for patients who are enrolled in clinical trials that meet the agency’s criteria.
"The available evidence does not permit us to conclude that use of autologous PRP improves health outcomes in beneficiaries with chronic diabetic, pressure, and/or venous wounds," the agency wrote in its decision statement Therefore, trials are needed to prove effectiveness.
The decision comes after CMS rejection of coverage since 1992, according to Cytomedix of Gaithersburg, Md., which manufactures a device called AutoloGel that produces PRP from a patient’s own blood. "This determination reverses a nearly 20-year non-coverage determination for PRP and provides for an appropriate research study with practical study designs we are confident will demonstrate that patients treated with our autologous PRP product, the AutoloGel System, experience clinically significant health outcomes," Martin P. Rosendale, CEO of Cytomedix, said in a statement.
Cytomedix submitted another request in October 2011 for CMS review of its PRP therapy, which was approved under the coverage with evidence development (CED) program.
Under the program, services, equipment, and supplies are covered through Medicare and Medicaid while a product is further investigated. CMS noted in its decision that it "is evaluating PRP as a service, and not a specific system for administrating PRP."
In the PRP process, autologous blood is centrifuged to produce a concentrate of platelets and plasma proteins. Individual growth factors are not identified or separated, but additives are used to change the consistency.
Autologous PRP has had many uses over the years, including use as an adhesive in plastic surgery and as filler for acute wounds. It has also been used to treat amateur and professional athletes – such as golfer Tiger Woods, basketball player Kobe Bryant, and baseball star Alex Rodriguez – to help heal tendons and ligaments, and is growing in popularity in the sports world, according to recent consumer news reports.
According to the CMS, to continue being covered for wound healing PRP therapy must show complete wound healing in patients and a reduction of wound size or healing trajectory. It also must help a patient’s ability to return to previous function and normal activities. The studies have to be prospective and enroll Medicare beneficiaries with chronic nonhealing diabetic, pressure, and/or venous wounds who are receiving optimal care, in addition to the therapy.
The agency must receive all pertinent data by August 2014.
Cytomedix said that it has been in talks with CMS about trials. "We look forward to continuing to work with CMS in the coming weeks in further defining the specifics of the protocols for the research studies and clinical questions to be answered through the CED program," said Mr. Rosendale.
The Centers for Medicare and Medicaid Services has announced coverage of platelet-rich plasma gel for chronic wounds, but only for patients who are enrolled in clinical trials that meet the agency’s criteria.
"The available evidence does not permit us to conclude that use of autologous PRP improves health outcomes in beneficiaries with chronic diabetic, pressure, and/or venous wounds," the agency wrote in its decision statement Therefore, trials are needed to prove effectiveness.
The decision comes after CMS rejection of coverage since 1992, according to Cytomedix of Gaithersburg, Md., which manufactures a device called AutoloGel that produces PRP from a patient’s own blood. "This determination reverses a nearly 20-year non-coverage determination for PRP and provides for an appropriate research study with practical study designs we are confident will demonstrate that patients treated with our autologous PRP product, the AutoloGel System, experience clinically significant health outcomes," Martin P. Rosendale, CEO of Cytomedix, said in a statement.
Cytomedix submitted another request in October 2011 for CMS review of its PRP therapy, which was approved under the coverage with evidence development (CED) program.
Under the program, services, equipment, and supplies are covered through Medicare and Medicaid while a product is further investigated. CMS noted in its decision that it "is evaluating PRP as a service, and not a specific system for administrating PRP."
In the PRP process, autologous blood is centrifuged to produce a concentrate of platelets and plasma proteins. Individual growth factors are not identified or separated, but additives are used to change the consistency.
Autologous PRP has had many uses over the years, including use as an adhesive in plastic surgery and as filler for acute wounds. It has also been used to treat amateur and professional athletes – such as golfer Tiger Woods, basketball player Kobe Bryant, and baseball star Alex Rodriguez – to help heal tendons and ligaments, and is growing in popularity in the sports world, according to recent consumer news reports.
According to the CMS, to continue being covered for wound healing PRP therapy must show complete wound healing in patients and a reduction of wound size or healing trajectory. It also must help a patient’s ability to return to previous function and normal activities. The studies have to be prospective and enroll Medicare beneficiaries with chronic nonhealing diabetic, pressure, and/or venous wounds who are receiving optimal care, in addition to the therapy.
The agency must receive all pertinent data by August 2014.
Cytomedix said that it has been in talks with CMS about trials. "We look forward to continuing to work with CMS in the coming weeks in further defining the specifics of the protocols for the research studies and clinical questions to be answered through the CED program," said Mr. Rosendale.
The Centers for Medicare and Medicaid Services has announced coverage of platelet-rich plasma gel for chronic wounds, but only for patients who are enrolled in clinical trials that meet the agency’s criteria.
"The available evidence does not permit us to conclude that use of autologous PRP improves health outcomes in beneficiaries with chronic diabetic, pressure, and/or venous wounds," the agency wrote in its decision statement Therefore, trials are needed to prove effectiveness.
The decision comes after CMS rejection of coverage since 1992, according to Cytomedix of Gaithersburg, Md., which manufactures a device called AutoloGel that produces PRP from a patient’s own blood. "This determination reverses a nearly 20-year non-coverage determination for PRP and provides for an appropriate research study with practical study designs we are confident will demonstrate that patients treated with our autologous PRP product, the AutoloGel System, experience clinically significant health outcomes," Martin P. Rosendale, CEO of Cytomedix, said in a statement.
Cytomedix submitted another request in October 2011 for CMS review of its PRP therapy, which was approved under the coverage with evidence development (CED) program.
Under the program, services, equipment, and supplies are covered through Medicare and Medicaid while a product is further investigated. CMS noted in its decision that it "is evaluating PRP as a service, and not a specific system for administrating PRP."
In the PRP process, autologous blood is centrifuged to produce a concentrate of platelets and plasma proteins. Individual growth factors are not identified or separated, but additives are used to change the consistency.
Autologous PRP has had many uses over the years, including use as an adhesive in plastic surgery and as filler for acute wounds. It has also been used to treat amateur and professional athletes – such as golfer Tiger Woods, basketball player Kobe Bryant, and baseball star Alex Rodriguez – to help heal tendons and ligaments, and is growing in popularity in the sports world, according to recent consumer news reports.
According to the CMS, to continue being covered for wound healing PRP therapy must show complete wound healing in patients and a reduction of wound size or healing trajectory. It also must help a patient’s ability to return to previous function and normal activities. The studies have to be prospective and enroll Medicare beneficiaries with chronic nonhealing diabetic, pressure, and/or venous wounds who are receiving optimal care, in addition to the therapy.
The agency must receive all pertinent data by August 2014.
Cytomedix said that it has been in talks with CMS about trials. "We look forward to continuing to work with CMS in the coming weeks in further defining the specifics of the protocols for the research studies and clinical questions to be answered through the CED program," said Mr. Rosendale.
Vemurafenib After Ipilimumab Linked to Rash
CHICAGO – The sequencing and timing of two new targeted therapies for melanoma may have important implications for the development of serious skin toxicity, according to one center’s experience.
Investigators at Memorial Sloan-Kettering Cancer Center in New York retrospectively identified 16 patients treated there for BRAFV600E-mutant metastatic melanoma who received vemurafenib (Zelboraf) after ipilimumab (Yervoy).
Vemurafenib is an inhibitor of the BRAF kinase. Ipilimumab blocks cytotoxic T-lymphocyte–associated antigen 4 (CTLA 4), which normally acts as a key checkpoint or brake in the immune system.

Four of the patients (25%) developed a grade 3 maculopapular rash, according to data reported in a poster session at the annual meeting of the American Society of Clinical Oncology.
Biopsy findings suggested these were drug hypersensitivity reactions, and analyses showed that grade 3 rash was much more likely when vemurafenib was given within 1 month of stopping ipilimumab as compared with later (100% vs. 8%, P = .007).
"It’s interesting to speculate that loss of checkpoint inhibition by ipilimumab might predispose patients to drug reactions," lead investigator Dr. James J. Harding commented in an interview, while cautioning that the study was very small and retrospective.
"The take-home message is these agents, both of which improve overall survival, will be used in sequence. It’s not clear if there is a benefit of sequencing one before the other or combining them – that will be studied prospectively," he noted, as in the case of an ongoing phase I-II trial looking at the two drugs together (NCT01400451).
"Until more data are available, it’s possible that there may be a significant maculopapular rash if you give vemurafenib within a month of ipilimumab. In almost all cases, a dose interruption followed by dose reduction is acceptable," he added.
"One thing that people need to remember is that if you give vemurafenib after ipilimumab, you are giving a combination therapy because the ipilimumab half-life is 2 weeks," noted discussant Dr. Mario Sznol, vice-chief of medical oncology with the Yale Medical Group in New Haven, CT.
"I would have hoped that we would have seen really dramatic antitumor effects with this combination, especially in the patients who were treated soon after their last dose of ipilimumab. And in fact that’s not what we saw," he added. "I don’t think this curve [waterfall plot] looks much better than what we would have seen with vemurafenib alone in this population of patients," with no apparent difference for patients receiving vemurafenib within 45 days of ipilimumab and the rest.
"So it’s just a warning that there will be sequence issues and toxicity interactions, and we really need to know the biology when we combine these agents," Dr. Sznol concluded. "We may do better with this combination, but we may not. We may need to use this in combination with other agents."
Of the 16 patients studied, 13 (81%) developed any-grade skin rash on vemurafenib, making this by far the most common adverse event observed. (For comparison, the rate of skin rash with vemurafenib was 37% in the BRIM-3 trial and 52% in the BRIM-2 trial.)
The cases of grade 3 rash developed within 6-8 days of starting vemurafenib and began as a pruritic eruption on the neck or chest that rapidly expanded to involve the back, trunk, and extremities. The incidence seen was triple that in the BRIM-3 trial (25% vs. 8%, P = .02).
Biopsies, performed in two of the four patients, revealed spongiotic and perivascular dermatitis with eosinophils, consistent with drug hypersensitivity reaction.
Although the time elapsed since the prior ipilimumab influenced the development of grade 3 rash, the dose of prior ipilimumab, number of doses, and immune-related adverse events did not.
None of the rashes progressed to anaphylaxis or Stevens-Johnson syndrome. Steroids appeared to be largely ineffective, according to Dr. Harding; one patient developed the rash while already taking steroids, and another was given steroids with little to no improvement.
"We essentially stopped the vemurafenib and then redosed it 11 days later [after the rash resolved]. And, with the exception of one patient, all of the patients tolerated it well and were able to continue," he reported.
The objective overall response rate with vemurafenib was 50%, similar to what was seen in the prior phase II and III trials of the drug.
Dr. Harding disclosed no relevant conflicts of interest. Dr. Sznol disclosed that he is a consultant to Abbott Laboratories, Anaeropharma, BioVex, Bristol-Myers Squibb, Genesis Biopharma, Genzyme, and Prometheus; receives honoraria from Prometheus; and receives research funding from Bristol-Myers Squibb.
CHICAGO – The sequencing and timing of two new targeted therapies for melanoma may have important implications for the development of serious skin toxicity, according to one center’s experience.
Investigators at Memorial Sloan-Kettering Cancer Center in New York retrospectively identified 16 patients treated there for BRAFV600E-mutant metastatic melanoma who received vemurafenib (Zelboraf) after ipilimumab (Yervoy).
Vemurafenib is an inhibitor of the BRAF kinase. Ipilimumab blocks cytotoxic T-lymphocyte–associated antigen 4 (CTLA 4), which normally acts as a key checkpoint or brake in the immune system.
Four of the patients (25%) developed a grade 3 maculopapular rash, according to data reported in a poster session at the annual meeting of the American Society of Clinical Oncology.
Biopsy findings suggested these were drug hypersensitivity reactions, and analyses showed that grade 3 rash was much more likely when vemurafenib was given within 1 month of stopping ipilimumab as compared with later (100% vs. 8%, P = .007).
"It’s interesting to speculate that loss of checkpoint inhibition by ipilimumab might predispose patients to drug reactions," lead investigator Dr. James J. Harding commented in an interview, while cautioning that the study was very small and retrospective.
"The take-home message is these agents, both of which improve overall survival, will be used in sequence. It’s not clear if there is a benefit of sequencing one before the other or combining them – that will be studied prospectively," he noted, as in the case of an ongoing phase I-II trial looking at the two drugs together (NCT01400451).
"Until more data are available, it’s possible that there may be a significant maculopapular rash if you give vemurafenib within a month of ipilimumab. In almost all cases, a dose interruption followed by dose reduction is acceptable," he added.
"One thing that people need to remember is that if you give vemurafenib after ipilimumab, you are giving a combination therapy because the ipilimumab half-life is 2 weeks," noted discussant Dr. Mario Sznol, vice-chief of medical oncology with the Yale Medical Group in New Haven, CT.
"I would have hoped that we would have seen really dramatic antitumor effects with this combination, especially in the patients who were treated soon after their last dose of ipilimumab. And in fact that’s not what we saw," he added. "I don’t think this curve [waterfall plot] looks much better than what we would have seen with vemurafenib alone in this population of patients," with no apparent difference for patients receiving vemurafenib within 45 days of ipilimumab and the rest.
"So it’s just a warning that there will be sequence issues and toxicity interactions, and we really need to know the biology when we combine these agents," Dr. Sznol concluded. "We may do better with this combination, but we may not. We may need to use this in combination with other agents."
Of the 16 patients studied, 13 (81%) developed any-grade skin rash on vemurafenib, making this by far the most common adverse event observed. (For comparison, the rate of skin rash with vemurafenib was 37% in the BRIM-3 trial and 52% in the BRIM-2 trial.)
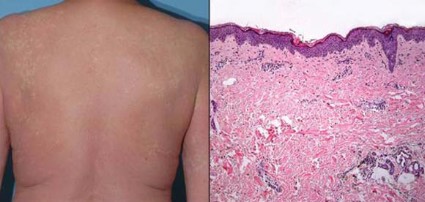
The cases of grade 3 rash developed within 6-8 days of starting vemurafenib and began as a pruritic eruption on the neck or chest that rapidly expanded to involve the back, trunk, and extremities. The incidence seen was triple that in the BRIM-3 trial (25% vs. 8%, P = .02).
Biopsies, performed in two of the four patients, revealed spongiotic and perivascular dermatitis with eosinophils, consistent with drug hypersensitivity reaction.
Although the time elapsed since the prior ipilimumab influenced the development of grade 3 rash, the dose of prior ipilimumab, number of doses, and immune-related adverse events did not.
None of the rashes progressed to anaphylaxis or Stevens-Johnson syndrome. Steroids appeared to be largely ineffective, according to Dr. Harding; one patient developed the rash while already taking steroids, and another was given steroids with little to no improvement.
"We essentially stopped the vemurafenib and then redosed it 11 days later [after the rash resolved]. And, with the exception of one patient, all of the patients tolerated it well and were able to continue," he reported.
The objective overall response rate with vemurafenib was 50%, similar to what was seen in the prior phase II and III trials of the drug.
Dr. Harding disclosed no relevant conflicts of interest. Dr. Sznol disclosed that he is a consultant to Abbott Laboratories, Anaeropharma, BioVex, Bristol-Myers Squibb, Genesis Biopharma, Genzyme, and Prometheus; receives honoraria from Prometheus; and receives research funding from Bristol-Myers Squibb.
CHICAGO – The sequencing and timing of two new targeted therapies for melanoma may have important implications for the development of serious skin toxicity, according to one center’s experience.
Investigators at Memorial Sloan-Kettering Cancer Center in New York retrospectively identified 16 patients treated there for BRAFV600E-mutant metastatic melanoma who received vemurafenib (Zelboraf) after ipilimumab (Yervoy).
Vemurafenib is an inhibitor of the BRAF kinase. Ipilimumab blocks cytotoxic T-lymphocyte–associated antigen 4 (CTLA 4), which normally acts as a key checkpoint or brake in the immune system.
Four of the patients (25%) developed a grade 3 maculopapular rash, according to data reported in a poster session at the annual meeting of the American Society of Clinical Oncology.
Biopsy findings suggested these were drug hypersensitivity reactions, and analyses showed that grade 3 rash was much more likely when vemurafenib was given within 1 month of stopping ipilimumab as compared with later (100% vs. 8%, P = .007).
"It’s interesting to speculate that loss of checkpoint inhibition by ipilimumab might predispose patients to drug reactions," lead investigator Dr. James J. Harding commented in an interview, while cautioning that the study was very small and retrospective.
"The take-home message is these agents, both of which improve overall survival, will be used in sequence. It’s not clear if there is a benefit of sequencing one before the other or combining them – that will be studied prospectively," he noted, as in the case of an ongoing phase I-II trial looking at the two drugs together (NCT01400451).
"Until more data are available, it’s possible that there may be a significant maculopapular rash if you give vemurafenib within a month of ipilimumab. In almost all cases, a dose interruption followed by dose reduction is acceptable," he added.
"One thing that people need to remember is that if you give vemurafenib after ipilimumab, you are giving a combination therapy because the ipilimumab half-life is 2 weeks," noted discussant Dr. Mario Sznol, vice-chief of medical oncology with the Yale Medical Group in New Haven, CT.
"I would have hoped that we would have seen really dramatic antitumor effects with this combination, especially in the patients who were treated soon after their last dose of ipilimumab. And in fact that’s not what we saw," he added. "I don’t think this curve [waterfall plot] looks much better than what we would have seen with vemurafenib alone in this population of patients," with no apparent difference for patients receiving vemurafenib within 45 days of ipilimumab and the rest.
"So it’s just a warning that there will be sequence issues and toxicity interactions, and we really need to know the biology when we combine these agents," Dr. Sznol concluded. "We may do better with this combination, but we may not. We may need to use this in combination with other agents."
Of the 16 patients studied, 13 (81%) developed any-grade skin rash on vemurafenib, making this by far the most common adverse event observed. (For comparison, the rate of skin rash with vemurafenib was 37% in the BRIM-3 trial and 52% in the BRIM-2 trial.)
The cases of grade 3 rash developed within 6-8 days of starting vemurafenib and began as a pruritic eruption on the neck or chest that rapidly expanded to involve the back, trunk, and extremities. The incidence seen was triple that in the BRIM-3 trial (25% vs. 8%, P = .02).
Biopsies, performed in two of the four patients, revealed spongiotic and perivascular dermatitis with eosinophils, consistent with drug hypersensitivity reaction.
Although the time elapsed since the prior ipilimumab influenced the development of grade 3 rash, the dose of prior ipilimumab, number of doses, and immune-related adverse events did not.
None of the rashes progressed to anaphylaxis or Stevens-Johnson syndrome. Steroids appeared to be largely ineffective, according to Dr. Harding; one patient developed the rash while already taking steroids, and another was given steroids with little to no improvement.
"We essentially stopped the vemurafenib and then redosed it 11 days later [after the rash resolved]. And, with the exception of one patient, all of the patients tolerated it well and were able to continue," he reported.
The objective overall response rate with vemurafenib was 50%, similar to what was seen in the prior phase II and III trials of the drug.
Dr. Harding disclosed no relevant conflicts of interest. Dr. Sznol disclosed that he is a consultant to Abbott Laboratories, Anaeropharma, BioVex, Bristol-Myers Squibb, Genesis Biopharma, Genzyme, and Prometheus; receives honoraria from Prometheus; and receives research funding from Bristol-Myers Squibb.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Four patients (25%) developed grade 3 maculopapular skin rash that histologically had features of a drug hypersensitivity rash.
Data Source: A single-center retrospective case series of 16 patients with BRAFV600E-mutant metastatic melanoma treated with vemurafenib after ipilimumab
Disclosures: Dr. Harding disclosed no relevant conflicts of interest. Dr. Sznol disclosed that he is a consultant to Abbott Laboratories, Anaeropharma Science, BioVex, Bristol-Myers Squibb, Genesis Biopharma, Genzyme, and Prometheus; receives honoraria from Prometheus; and receives research funding from Bristol-Myers Squibb.
Kaposi's Sarcoma Makes Unwelcome Return
Kaposi's sarcoma is making a comeback in aging HIV patients, even among those with well-controlled disease. Dr. Kieron S. Leslie, an associate clinical professor of dermatology at the University of California, San Francisco, discusses the cancer's return and its implications for patients with HIV.
Kaposi's sarcoma is making a comeback in aging HIV patients, even among those with well-controlled disease. Dr. Kieron S. Leslie, an associate clinical professor of dermatology at the University of California, San Francisco, discusses the cancer's return and its implications for patients with HIV.
Kaposi's sarcoma is making a comeback in aging HIV patients, even among those with well-controlled disease. Dr. Kieron S. Leslie, an associate clinical professor of dermatology at the University of California, San Francisco, discusses the cancer's return and its implications for patients with HIV.

Skin Cancer Drug Steps Into New Alzheimer's Study
The first human trial of bexarotene, the skin cancer drug shown to clear beta-amyloid brain plaques in mice with Alzheimer’s-like pathology, will commence sometime in September.
The phase Ib trial will randomize 12 healthy subjects to placebo or bexarotene (Targretin), Gary E. Landreth, Ph.D., said in an interview.

Researchers will obtain hourly samples of cerebrospinal fluid and blood for 36 hours after administration of the drug, looking for signs that bexarotene increases natural clearance of the beta-amyloid protein, said Dr. Landreth of Case Western Reserve University, Cleveland.
"If our hypothesis is correct, the drug should accelerate the synthesis and steady-state levels of apolipoprotein E," a protein that helps break down soluble beta-amyloid, he said. Hungry microglia are bexarotene’s second punch; in mice, the drug activated these cells to scavenge beta-amyloid plaques.
If these two events also occur in humans, Dr. Landreth said, "we will have a reason to go forward" into phase II trials.
Media stories about Dr. Landreth’s research sparked a firestorm of dialogue on Alzheimer’s Internet forums and message boards this spring. Families discussed traveling to Canada for bexarotene, and begging their family doctors for a prescription.
Two opinion pieces in the Aug. 9 issue of the New England Journal of Medicine tackled the thorny problem physicians may face when desperate families come looking for answers.
"Writing an off-label prescription is completely permissible and would fulfill family members’ desire to try anything to help their loved ones," wrote Dr. Steven D. Pearson of Massachusetts General Hospital’s Institute for Technology Assessment, Boston, and his colleagues. But in the case of bexarotene, they asked, "is it the right thing to do?"
In the second editorial, Frank M. LaFerla, Ph.D., of the University of California, Irvine, warned against overenthusiasm: "Only a well-designed and carefully executed clinical trial will reveal whether this class of drug lives up to its promise. Until such trials are performed, it would be a mistake to offer this treatment to Alzheimer’s patients."
Dr. Landreth agrees. Although relatively benign, bexarotene can cause hypothyroidism and dyslipidemia in cancer patients. Although volunteers in the upcoming trial will almost certainly experience neither of these, "there is no guarantee at all that it would be safe in an Alzheimer’s population," he said. "I have absolutely no idea what could happen when this drug interacts with a diseased brain. If you remove the plaque, then what happens? Do you end up with holes in the brain? This is the question that keeps me up at night."
Dr. Landreth and his colleague, Paige Cramer, hold a U.S. provisional patent application for bexarotene as a potential therapy for Alzheimer’s disease and have founded ReXceptor Inc., which has licensing options from the university to use bexarotene to treat Alzheimer’s disease.
The first human trial of bexarotene, the skin cancer drug shown to clear beta-amyloid brain plaques in mice with Alzheimer’s-like pathology, will commence sometime in September.
The phase Ib trial will randomize 12 healthy subjects to placebo or bexarotene (Targretin), Gary E. Landreth, Ph.D., said in an interview.
Researchers will obtain hourly samples of cerebrospinal fluid and blood for 36 hours after administration of the drug, looking for signs that bexarotene increases natural clearance of the beta-amyloid protein, said Dr. Landreth of Case Western Reserve University, Cleveland.
"If our hypothesis is correct, the drug should accelerate the synthesis and steady-state levels of apolipoprotein E," a protein that helps break down soluble beta-amyloid, he said. Hungry microglia are bexarotene’s second punch; in mice, the drug activated these cells to scavenge beta-amyloid plaques.
If these two events also occur in humans, Dr. Landreth said, "we will have a reason to go forward" into phase II trials.
Media stories about Dr. Landreth’s research sparked a firestorm of dialogue on Alzheimer’s Internet forums and message boards this spring. Families discussed traveling to Canada for bexarotene, and begging their family doctors for a prescription.
Two opinion pieces in the Aug. 9 issue of the New England Journal of Medicine tackled the thorny problem physicians may face when desperate families come looking for answers.
"Writing an off-label prescription is completely permissible and would fulfill family members’ desire to try anything to help their loved ones," wrote Dr. Steven D. Pearson of Massachusetts General Hospital’s Institute for Technology Assessment, Boston, and his colleagues. But in the case of bexarotene, they asked, "is it the right thing to do?"
In the second editorial, Frank M. LaFerla, Ph.D., of the University of California, Irvine, warned against overenthusiasm: "Only a well-designed and carefully executed clinical trial will reveal whether this class of drug lives up to its promise. Until such trials are performed, it would be a mistake to offer this treatment to Alzheimer’s patients."
Dr. Landreth agrees. Although relatively benign, bexarotene can cause hypothyroidism and dyslipidemia in cancer patients. Although volunteers in the upcoming trial will almost certainly experience neither of these, "there is no guarantee at all that it would be safe in an Alzheimer’s population," he said. "I have absolutely no idea what could happen when this drug interacts with a diseased brain. If you remove the plaque, then what happens? Do you end up with holes in the brain? This is the question that keeps me up at night."
Dr. Landreth and his colleague, Paige Cramer, hold a U.S. provisional patent application for bexarotene as a potential therapy for Alzheimer’s disease and have founded ReXceptor Inc., which has licensing options from the university to use bexarotene to treat Alzheimer’s disease.
The first human trial of bexarotene, the skin cancer drug shown to clear beta-amyloid brain plaques in mice with Alzheimer’s-like pathology, will commence sometime in September.
The phase Ib trial will randomize 12 healthy subjects to placebo or bexarotene (Targretin), Gary E. Landreth, Ph.D., said in an interview.
Researchers will obtain hourly samples of cerebrospinal fluid and blood for 36 hours after administration of the drug, looking for signs that bexarotene increases natural clearance of the beta-amyloid protein, said Dr. Landreth of Case Western Reserve University, Cleveland.
"If our hypothesis is correct, the drug should accelerate the synthesis and steady-state levels of apolipoprotein E," a protein that helps break down soluble beta-amyloid, he said. Hungry microglia are bexarotene’s second punch; in mice, the drug activated these cells to scavenge beta-amyloid plaques.
If these two events also occur in humans, Dr. Landreth said, "we will have a reason to go forward" into phase II trials.
Media stories about Dr. Landreth’s research sparked a firestorm of dialogue on Alzheimer’s Internet forums and message boards this spring. Families discussed traveling to Canada for bexarotene, and begging their family doctors for a prescription.
Two opinion pieces in the Aug. 9 issue of the New England Journal of Medicine tackled the thorny problem physicians may face when desperate families come looking for answers.
"Writing an off-label prescription is completely permissible and would fulfill family members’ desire to try anything to help their loved ones," wrote Dr. Steven D. Pearson of Massachusetts General Hospital’s Institute for Technology Assessment, Boston, and his colleagues. But in the case of bexarotene, they asked, "is it the right thing to do?"
In the second editorial, Frank M. LaFerla, Ph.D., of the University of California, Irvine, warned against overenthusiasm: "Only a well-designed and carefully executed clinical trial will reveal whether this class of drug lives up to its promise. Until such trials are performed, it would be a mistake to offer this treatment to Alzheimer’s patients."
Dr. Landreth agrees. Although relatively benign, bexarotene can cause hypothyroidism and dyslipidemia in cancer patients. Although volunteers in the upcoming trial will almost certainly experience neither of these, "there is no guarantee at all that it would be safe in an Alzheimer’s population," he said. "I have absolutely no idea what could happen when this drug interacts with a diseased brain. If you remove the plaque, then what happens? Do you end up with holes in the brain? This is the question that keeps me up at night."
Dr. Landreth and his colleague, Paige Cramer, hold a U.S. provisional patent application for bexarotene as a potential therapy for Alzheimer’s disease and have founded ReXceptor Inc., which has licensing options from the university to use bexarotene to treat Alzheimer’s disease.

KIT Inhibition Promising for Select Few
ORLANDO – Patients who express a KIT genetic abnormality represent a small minority of those with melanoma, but there is a lot of interest in the development of specific inhibitors, said Dr. Richard D. Carvajal at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery.
Studies from Dr. Carvajal and other researchers indicate that inhibitors could significantly prolong median progression-free survival for patients who have amplification, overexpression, or a mutation of this genetic driver of melanoma.

In his phase II study of Novartis’ imatinib (Gleevec) for patients with melanoma and KIT alterations, 4 of 25 evaluable patients responded, for an overall durable response rate of 16%. Median progression-free survival was "pretty modest at 3 to 3.5 months," Dr. Carvajal said. Two patients had a complete response to therapy, and another two achieved a partial response (JAMA 2011;305:2327-34).
"So the question is: Can we better select patients likely to respond?" Dr. Carvajal asked at the meeting. "Certainly this is not vemurafenib [Zelboraf], where we get a response in 50% of patients. It could be due to variability in KIT mutations," said Dr. Carvajal, a medical oncologist specializing in melanoma and sarcomas at Memorial Sloan-Kettering Cancer Center in New York.
Only 3% of patients with melanoma harbor a KIT mutation. "You have to have a mutation in KIT; otherwise, the patient is not going to respond to imatinib," he said. The study was preceded by three negative clinical trials in unselected patients (before the mutation was identified).
In another phase II study enrolling only patients with KIT alterations, investigators reported that 10 of 43 patients responded to treatment with imatinib, for a 23% overall response rate (J. Clin. Oncol. 2011;29:2904-9).
Studies are underway with potential KIT inhibitors other than imatinib, including Pfizer’s sunitinib (Sutent), Novartis’ nilotinib (Tasigna), and Bristol-Myers Squibb’s dasatinib (Sprycel).
Sunitinib
Sunitinib is "reasonably promising" for melanoma patients with KIT mutations, said Dr. David Minor, of the California Pacific Center for Melanoma Research and Treatment at the University of California, San Francisco.
He and his colleagues conducted gene sequencing of tumors from 90 patients with advanced melanoma. The findings revealed that 11% featured a KIT mutation (Clin. Cancer Res. 2012:18:1457-63).
Ten of 12 patients treated with sunitinib were evaluable – 4 with KIT mutations and 6 with KIT amplification or overexpression. Although the mutation was a significant predictor of shortened survival time, treatment with sunitinib was associated with complete remission in 1 patient for 15 months and 2 partial responses for 1 and 7 months, he noted. A KIT mutation might be more clinically relevant because there were no complete responses and only one partial response in patients with KIT amplification or overexpression. Dr. Minor is director of inpatient oncology at the California Pacific Medical Center.
Nilotinib
Because only a small percentage of melanoma patients harbor a KIT mutation, conducting large efficacy studies remains a challenge, Dr. Carvajal said. "Indeed, a randomized, phase III trial of nilotinib versus DTIC [dacarbazine] in KIT-mutant melanoma was designed to be the definitive study demonstrating improved outcomes with nilotinib versus DTIC," he said. However, after patient accrual began for the TEAM (Tasigna Efficacy in Advanced Melanoma) trial in 2010, researchers reported difficulty enrolling a sufficient number of patients with metastatic or inoperable melanoma and a KIT mutation. Therefore, they redesigned the study into a single-arm phase II trial of nilotinib alone.
Researchers at the University of Pittsburgh also termed nilotinib a promising agent for melanoma patients with relevant KIT mutations in a review article (Expert Opin. Investig. Drugs 2012;21:861-9).
Dasatinib
Dr. Harriet Kluger and her colleagues at Yale University in New Haven, Conn., reported mixed efficacy for dasatinib in a phase II study (Cancer 2011;117:2202-8).
"At this point I would say that other than in the setting of patients with c-KIT mutations in their tumors, which is still being studied, dasatinib is not a promising agent for this disease," Dr. Kluger said in an interview. She is on the medical oncology faculty at Yale.
She and her colleagues studied 36 evaluable patients with stage 3 or 4 unresectable melanoma. Dasatinib was associated with two partial responses (24 weeks and 64 weeks) and three minor responses. Another patient who initially responded discontinued because of noncompliance. The median progression-free survival was 8 weeks, and the 6-month progression-free survival was 13%. Some activity of dasatinib was observed in a small subset of patients without KIT mutations, suggesting that more research is needed to identify predictive biomarkers for response to this inhibitor.
The KIT gene is located on chromosome 4 and codes for a family of proteins, the receptor tyrosine kinases. KIT function is essential for normal melanocyte genesis and migration. KIT protein signaling also is important for the development of reproductive germ cells, early hematopoietic stem cells, immune mast cells, and interstitial cells of Cajal located in the gastrointestinal tract.
Available data suggest that patients with mutations affecting exons 11 or 13 of KIT may be more likely to achieve clinical benefit with KIT inhibition, Dr. Carvajal said. He added that greater expression of the mutant KIT allele, compared with the wild type, may be a marker of tumors more "addicted" to KIT activation and that may be more susceptible to inhibition.
"This work is still fairly new," he said.
Dr. Carvajal is a consultant to Novartis. Dr. Minor and Dr. Kluger said that they had no relevant disclosures.
ORLANDO – Patients who express a KIT genetic abnormality represent a small minority of those with melanoma, but there is a lot of interest in the development of specific inhibitors, said Dr. Richard D. Carvajal at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery.
Studies from Dr. Carvajal and other researchers indicate that inhibitors could significantly prolong median progression-free survival for patients who have amplification, overexpression, or a mutation of this genetic driver of melanoma.
In his phase II study of Novartis’ imatinib (Gleevec) for patients with melanoma and KIT alterations, 4 of 25 evaluable patients responded, for an overall durable response rate of 16%. Median progression-free survival was "pretty modest at 3 to 3.5 months," Dr. Carvajal said. Two patients had a complete response to therapy, and another two achieved a partial response (JAMA 2011;305:2327-34).
"So the question is: Can we better select patients likely to respond?" Dr. Carvajal asked at the meeting. "Certainly this is not vemurafenib [Zelboraf], where we get a response in 50% of patients. It could be due to variability in KIT mutations," said Dr. Carvajal, a medical oncologist specializing in melanoma and sarcomas at Memorial Sloan-Kettering Cancer Center in New York.
Only 3% of patients with melanoma harbor a KIT mutation. "You have to have a mutation in KIT; otherwise, the patient is not going to respond to imatinib," he said. The study was preceded by three negative clinical trials in unselected patients (before the mutation was identified).
In another phase II study enrolling only patients with KIT alterations, investigators reported that 10 of 43 patients responded to treatment with imatinib, for a 23% overall response rate (J. Clin. Oncol. 2011;29:2904-9).
Studies are underway with potential KIT inhibitors other than imatinib, including Pfizer’s sunitinib (Sutent), Novartis’ nilotinib (Tasigna), and Bristol-Myers Squibb’s dasatinib (Sprycel).
Sunitinib
Sunitinib is "reasonably promising" for melanoma patients with KIT mutations, said Dr. David Minor, of the California Pacific Center for Melanoma Research and Treatment at the University of California, San Francisco.
He and his colleagues conducted gene sequencing of tumors from 90 patients with advanced melanoma. The findings revealed that 11% featured a KIT mutation (Clin. Cancer Res. 2012:18:1457-63).
Ten of 12 patients treated with sunitinib were evaluable – 4 with KIT mutations and 6 with KIT amplification or overexpression. Although the mutation was a significant predictor of shortened survival time, treatment with sunitinib was associated with complete remission in 1 patient for 15 months and 2 partial responses for 1 and 7 months, he noted. A KIT mutation might be more clinically relevant because there were no complete responses and only one partial response in patients with KIT amplification or overexpression. Dr. Minor is director of inpatient oncology at the California Pacific Medical Center.
Nilotinib
Because only a small percentage of melanoma patients harbor a KIT mutation, conducting large efficacy studies remains a challenge, Dr. Carvajal said. "Indeed, a randomized, phase III trial of nilotinib versus DTIC [dacarbazine] in KIT-mutant melanoma was designed to be the definitive study demonstrating improved outcomes with nilotinib versus DTIC," he said. However, after patient accrual began for the TEAM (Tasigna Efficacy in Advanced Melanoma) trial in 2010, researchers reported difficulty enrolling a sufficient number of patients with metastatic or inoperable melanoma and a KIT mutation. Therefore, they redesigned the study into a single-arm phase II trial of nilotinib alone.
Researchers at the University of Pittsburgh also termed nilotinib a promising agent for melanoma patients with relevant KIT mutations in a review article (Expert Opin. Investig. Drugs 2012;21:861-9).
Dasatinib
Dr. Harriet Kluger and her colleagues at Yale University in New Haven, Conn., reported mixed efficacy for dasatinib in a phase II study (Cancer 2011;117:2202-8).
"At this point I would say that other than in the setting of patients with c-KIT mutations in their tumors, which is still being studied, dasatinib is not a promising agent for this disease," Dr. Kluger said in an interview. She is on the medical oncology faculty at Yale.
She and her colleagues studied 36 evaluable patients with stage 3 or 4 unresectable melanoma. Dasatinib was associated with two partial responses (24 weeks and 64 weeks) and three minor responses. Another patient who initially responded discontinued because of noncompliance. The median progression-free survival was 8 weeks, and the 6-month progression-free survival was 13%. Some activity of dasatinib was observed in a small subset of patients without KIT mutations, suggesting that more research is needed to identify predictive biomarkers for response to this inhibitor.
The KIT gene is located on chromosome 4 and codes for a family of proteins, the receptor tyrosine kinases. KIT function is essential for normal melanocyte genesis and migration. KIT protein signaling also is important for the development of reproductive germ cells, early hematopoietic stem cells, immune mast cells, and interstitial cells of Cajal located in the gastrointestinal tract.
Available data suggest that patients with mutations affecting exons 11 or 13 of KIT may be more likely to achieve clinical benefit with KIT inhibition, Dr. Carvajal said. He added that greater expression of the mutant KIT allele, compared with the wild type, may be a marker of tumors more "addicted" to KIT activation and that may be more susceptible to inhibition.
"This work is still fairly new," he said.
Dr. Carvajal is a consultant to Novartis. Dr. Minor and Dr. Kluger said that they had no relevant disclosures.
ORLANDO – Patients who express a KIT genetic abnormality represent a small minority of those with melanoma, but there is a lot of interest in the development of specific inhibitors, said Dr. Richard D. Carvajal at the annual meeting of the Florida Society of Dermatology and Dermatologic Surgery.
Studies from Dr. Carvajal and other researchers indicate that inhibitors could significantly prolong median progression-free survival for patients who have amplification, overexpression, or a mutation of this genetic driver of melanoma.
In his phase II study of Novartis’ imatinib (Gleevec) for patients with melanoma and KIT alterations, 4 of 25 evaluable patients responded, for an overall durable response rate of 16%. Median progression-free survival was "pretty modest at 3 to 3.5 months," Dr. Carvajal said. Two patients had a complete response to therapy, and another two achieved a partial response (JAMA 2011;305:2327-34).
"So the question is: Can we better select patients likely to respond?" Dr. Carvajal asked at the meeting. "Certainly this is not vemurafenib [Zelboraf], where we get a response in 50% of patients. It could be due to variability in KIT mutations," said Dr. Carvajal, a medical oncologist specializing in melanoma and sarcomas at Memorial Sloan-Kettering Cancer Center in New York.
Only 3% of patients with melanoma harbor a KIT mutation. "You have to have a mutation in KIT; otherwise, the patient is not going to respond to imatinib," he said. The study was preceded by three negative clinical trials in unselected patients (before the mutation was identified).
In another phase II study enrolling only patients with KIT alterations, investigators reported that 10 of 43 patients responded to treatment with imatinib, for a 23% overall response rate (J. Clin. Oncol. 2011;29:2904-9).
Studies are underway with potential KIT inhibitors other than imatinib, including Pfizer’s sunitinib (Sutent), Novartis’ nilotinib (Tasigna), and Bristol-Myers Squibb’s dasatinib (Sprycel).
Sunitinib
Sunitinib is "reasonably promising" for melanoma patients with KIT mutations, said Dr. David Minor, of the California Pacific Center for Melanoma Research and Treatment at the University of California, San Francisco.
He and his colleagues conducted gene sequencing of tumors from 90 patients with advanced melanoma. The findings revealed that 11% featured a KIT mutation (Clin. Cancer Res. 2012:18:1457-63).
Ten of 12 patients treated with sunitinib were evaluable – 4 with KIT mutations and 6 with KIT amplification or overexpression. Although the mutation was a significant predictor of shortened survival time, treatment with sunitinib was associated with complete remission in 1 patient for 15 months and 2 partial responses for 1 and 7 months, he noted. A KIT mutation might be more clinically relevant because there were no complete responses and only one partial response in patients with KIT amplification or overexpression. Dr. Minor is director of inpatient oncology at the California Pacific Medical Center.
Nilotinib
Because only a small percentage of melanoma patients harbor a KIT mutation, conducting large efficacy studies remains a challenge, Dr. Carvajal said. "Indeed, a randomized, phase III trial of nilotinib versus DTIC [dacarbazine] in KIT-mutant melanoma was designed to be the definitive study demonstrating improved outcomes with nilotinib versus DTIC," he said. However, after patient accrual began for the TEAM (Tasigna Efficacy in Advanced Melanoma) trial in 2010, researchers reported difficulty enrolling a sufficient number of patients with metastatic or inoperable melanoma and a KIT mutation. Therefore, they redesigned the study into a single-arm phase II trial of nilotinib alone.
Researchers at the University of Pittsburgh also termed nilotinib a promising agent for melanoma patients with relevant KIT mutations in a review article (Expert Opin. Investig. Drugs 2012;21:861-9).
Dasatinib
Dr. Harriet Kluger and her colleagues at Yale University in New Haven, Conn., reported mixed efficacy for dasatinib in a phase II study (Cancer 2011;117:2202-8).
"At this point I would say that other than in the setting of patients with c-KIT mutations in their tumors, which is still being studied, dasatinib is not a promising agent for this disease," Dr. Kluger said in an interview. She is on the medical oncology faculty at Yale.
She and her colleagues studied 36 evaluable patients with stage 3 or 4 unresectable melanoma. Dasatinib was associated with two partial responses (24 weeks and 64 weeks) and three minor responses. Another patient who initially responded discontinued because of noncompliance. The median progression-free survival was 8 weeks, and the 6-month progression-free survival was 13%. Some activity of dasatinib was observed in a small subset of patients without KIT mutations, suggesting that more research is needed to identify predictive biomarkers for response to this inhibitor.
The KIT gene is located on chromosome 4 and codes for a family of proteins, the receptor tyrosine kinases. KIT function is essential for normal melanocyte genesis and migration. KIT protein signaling also is important for the development of reproductive germ cells, early hematopoietic stem cells, immune mast cells, and interstitial cells of Cajal located in the gastrointestinal tract.
Available data suggest that patients with mutations affecting exons 11 or 13 of KIT may be more likely to achieve clinical benefit with KIT inhibition, Dr. Carvajal said. He added that greater expression of the mutant KIT allele, compared with the wild type, may be a marker of tumors more "addicted" to KIT activation and that may be more susceptible to inhibition.
"This work is still fairly new," he said.
Dr. Carvajal is a consultant to Novartis. Dr. Minor and Dr. Kluger said that they had no relevant disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE FLORIDA SOCIETY OF DERMATOLOGY AND DERMATOLOGIC SURGERY

Photoprotection for Preventing Skin Cancer and Premature Skin Aging
Dr. Hale discusses how regular sunscreen use can diminish the chances of developing future skin cancers and can slow the process of premature skin aging. For more information, read Dr. Hale's article in the May 2012 issue, "Sunscreens and Photoaging: An Update."

Dr. Hale discusses how regular sunscreen use can diminish the chances of developing future skin cancers and can slow the process of premature skin aging. For more information, read Dr. Hale's article in the May 2012 issue, "Sunscreens and Photoaging: An Update."
Dr. Hale discusses how regular sunscreen use can diminish the chances of developing future skin cancers and can slow the process of premature skin aging. For more information, read Dr. Hale's article in the May 2012 issue, "Sunscreens and Photoaging: An Update."

Melanoma Sinks Hook Into Coral Reef Trout
Riddle me this: How is a fish like a canary?
As you know, miners used canaries underground, where they functioned as warning systems – when toxic gases leaked into the shaft, the birds would die, signaling a need for the minors to leave the shaft.
Today, it seems prudent to heed the plight of the Great Barrier Reef coral trout, Plectropomus leopardus.

According to Dr. Michael Sweet, a marine research associate at Newcastle (Australia) University, 15% of coral trout caught in two reef locations in Australia were found to have skin cancer. This is the first report of melanoma occurring in a wild fish population, he noted.
Coral trout are a valuable food and sport fish that live at a depth of up to 30 m in unpolluted, clear water – well within the 60-m reach of Australia’s strong UVB radiation, wrote Dr. Sweet.
Several decades ago, there was no problem. But today, a hovering ozone hole seems to have compromised the fish’s health, he noted.
After he heard of coral trout with dark skin lesions, Dr. Sweet went reef fishing. He and his colleagues pulled in 136; 20 of the fish showed visible skin lesions that were raised and darkly pigmented. He took samples from each fish and tested them for microbial, fungal, and parasitic infections (PLoS ONE 2012 Aug. 1 [doi: 10.1371/journal.pone.0041989])
The fish had no infections or disease. But, histologically, they showed disorganized pleomorphic cells, melanocytes, epithelioid-like cells, melanophores, and macromelanophore cells, consistent with lesions induced in a fish cancer model.
The fishes’ behavior seemed unaffected, and all the lesions appeared to be stage I or II. But that isn’t necessarily reassuring, Dr. Sweet reported. Fish exhibiting stage III, IV, or V cancers may show behavioral differences in the wild and may, therefore, have not been caught.
So – other than a general concern for the health of the Great Barrier Reef – why should we care about wild fish developing melanoma?
Jen Makin, a research and evaluation manager for Australia’s SunSmart program, cited unsettling figures about the Australian UV situation and skin cancer (Health Promot. J. Austr. 2011;22:S39-41).
"It is estimated that nearly 450,000 Australians get skin cancer every year," she wrote – 95% of the cancers are directly related to UV radiation.
The ozone layer is slowly recovering its health, but an ever-hotter Earth may undo that skin-protecting change. "Before recovery, it is expected that higher levels of UV radiation will continue in most Australian regions, with an associated higher risk of skin cancer. Indeed, recent data show increases in surface UV radiation throughout Australia since the 1970s. Second, mean temperatures in Australia have increased over the past 30 years and are projected to rise further by 2030," she wrote.
In hot weather, adults spend more time outdoors, are less likely to cover up, and are more likely to get burned. And – as the coral trout have proved – there seem to be few places to hide.
–Michele Sullivan (on Twitter @Alz_Gal)
Riddle me this: How is a fish like a canary?
As you know, miners used canaries underground, where they functioned as warning systems – when toxic gases leaked into the shaft, the birds would die, signaling a need for the minors to leave the shaft.
Today, it seems prudent to heed the plight of the Great Barrier Reef coral trout, Plectropomus leopardus.
According to Dr. Michael Sweet, a marine research associate at Newcastle (Australia) University, 15% of coral trout caught in two reef locations in Australia were found to have skin cancer. This is the first report of melanoma occurring in a wild fish population, he noted.
Coral trout are a valuable food and sport fish that live at a depth of up to 30 m in unpolluted, clear water – well within the 60-m reach of Australia’s strong UVB radiation, wrote Dr. Sweet.
Several decades ago, there was no problem. But today, a hovering ozone hole seems to have compromised the fish’s health, he noted.
After he heard of coral trout with dark skin lesions, Dr. Sweet went reef fishing. He and his colleagues pulled in 136; 20 of the fish showed visible skin lesions that were raised and darkly pigmented. He took samples from each fish and tested them for microbial, fungal, and parasitic infections (PLoS ONE 2012 Aug. 1 [doi: 10.1371/journal.pone.0041989])
The fish had no infections or disease. But, histologically, they showed disorganized pleomorphic cells, melanocytes, epithelioid-like cells, melanophores, and macromelanophore cells, consistent with lesions induced in a fish cancer model.
The fishes’ behavior seemed unaffected, and all the lesions appeared to be stage I or II. But that isn’t necessarily reassuring, Dr. Sweet reported. Fish exhibiting stage III, IV, or V cancers may show behavioral differences in the wild and may, therefore, have not been caught.
So – other than a general concern for the health of the Great Barrier Reef – why should we care about wild fish developing melanoma?
Jen Makin, a research and evaluation manager for Australia’s SunSmart program, cited unsettling figures about the Australian UV situation and skin cancer (Health Promot. J. Austr. 2011;22:S39-41).
"It is estimated that nearly 450,000 Australians get skin cancer every year," she wrote – 95% of the cancers are directly related to UV radiation.
The ozone layer is slowly recovering its health, but an ever-hotter Earth may undo that skin-protecting change. "Before recovery, it is expected that higher levels of UV radiation will continue in most Australian regions, with an associated higher risk of skin cancer. Indeed, recent data show increases in surface UV radiation throughout Australia since the 1970s. Second, mean temperatures in Australia have increased over the past 30 years and are projected to rise further by 2030," she wrote.
In hot weather, adults spend more time outdoors, are less likely to cover up, and are more likely to get burned. And – as the coral trout have proved – there seem to be few places to hide.
–Michele Sullivan (on Twitter @Alz_Gal)
Riddle me this: How is a fish like a canary?
As you know, miners used canaries underground, where they functioned as warning systems – when toxic gases leaked into the shaft, the birds would die, signaling a need for the minors to leave the shaft.
Today, it seems prudent to heed the plight of the Great Barrier Reef coral trout, Plectropomus leopardus.
According to Dr. Michael Sweet, a marine research associate at Newcastle (Australia) University, 15% of coral trout caught in two reef locations in Australia were found to have skin cancer. This is the first report of melanoma occurring in a wild fish population, he noted.
Coral trout are a valuable food and sport fish that live at a depth of up to 30 m in unpolluted, clear water – well within the 60-m reach of Australia’s strong UVB radiation, wrote Dr. Sweet.
Several decades ago, there was no problem. But today, a hovering ozone hole seems to have compromised the fish’s health, he noted.
After he heard of coral trout with dark skin lesions, Dr. Sweet went reef fishing. He and his colleagues pulled in 136; 20 of the fish showed visible skin lesions that were raised and darkly pigmented. He took samples from each fish and tested them for microbial, fungal, and parasitic infections (PLoS ONE 2012 Aug. 1 [doi: 10.1371/journal.pone.0041989])
The fish had no infections or disease. But, histologically, they showed disorganized pleomorphic cells, melanocytes, epithelioid-like cells, melanophores, and macromelanophore cells, consistent with lesions induced in a fish cancer model.
The fishes’ behavior seemed unaffected, and all the lesions appeared to be stage I or II. But that isn’t necessarily reassuring, Dr. Sweet reported. Fish exhibiting stage III, IV, or V cancers may show behavioral differences in the wild and may, therefore, have not been caught.
So – other than a general concern for the health of the Great Barrier Reef – why should we care about wild fish developing melanoma?
Jen Makin, a research and evaluation manager for Australia’s SunSmart program, cited unsettling figures about the Australian UV situation and skin cancer (Health Promot. J. Austr. 2011;22:S39-41).
"It is estimated that nearly 450,000 Australians get skin cancer every year," she wrote – 95% of the cancers are directly related to UV radiation.
The ozone layer is slowly recovering its health, but an ever-hotter Earth may undo that skin-protecting change. "Before recovery, it is expected that higher levels of UV radiation will continue in most Australian regions, with an associated higher risk of skin cancer. Indeed, recent data show increases in surface UV radiation throughout Australia since the 1970s. Second, mean temperatures in Australia have increased over the past 30 years and are projected to rise further by 2030," she wrote.
In hot weather, adults spend more time outdoors, are less likely to cover up, and are more likely to get burned. And – as the coral trout have proved – there seem to be few places to hide.
–Michele Sullivan (on Twitter @Alz_Gal)

Pregnancy-Related Cancers: Rise Is Largely Unrelated to Delayed Childbearing
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.

After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
postponing childbearing, pregnancy-associated cancer,
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
postponing childbearing, pregnancy-associated cancer,
postponing childbearing, pregnancy-associated cancer,
AT THE ANNUAL MEETING OF THE SOCIETY FOR PEDIATRIC AND PERINATAL EPIDEMIOLOGIC RESEARCH

A Musical Marketing Plan: The Skinny Podcast
In this month's program, Dr. Jeffrey Curtis discusses his study, which found new evidence supporting the safety of the shingles vaccine for patients on biologics.
Then, Dr. Jonathan Silverberg talks about the best climates for children with eczema.

Dr. Bruce Brod of the American Academy of Dermatology reports on which states have the toughest laws on indoor tanning, and he highlights the latest legislation on the matter.
Meanwhile, Dr. Lily Talakoub talks about a common summer skin condition, Pityrosporum folliculitis, and Dr. Alan Rockoff presents his musical marketing plan.
Don't miss another episode of The Skinny Podcast; subscribe for free on iTunes!
In this month's program, Dr. Jeffrey Curtis discusses his study, which found new evidence supporting the safety of the shingles vaccine for patients on biologics.
Then, Dr. Jonathan Silverberg talks about the best climates for children with eczema.
Dr. Bruce Brod of the American Academy of Dermatology reports on which states have the toughest laws on indoor tanning, and he highlights the latest legislation on the matter.
Meanwhile, Dr. Lily Talakoub talks about a common summer skin condition, Pityrosporum folliculitis, and Dr. Alan Rockoff presents his musical marketing plan.
Don't miss another episode of The Skinny Podcast; subscribe for free on iTunes!
In this month's program, Dr. Jeffrey Curtis discusses his study, which found new evidence supporting the safety of the shingles vaccine for patients on biologics.
Then, Dr. Jonathan Silverberg talks about the best climates for children with eczema.
Dr. Bruce Brod of the American Academy of Dermatology reports on which states have the toughest laws on indoor tanning, and he highlights the latest legislation on the matter.
Meanwhile, Dr. Lily Talakoub talks about a common summer skin condition, Pityrosporum folliculitis, and Dr. Alan Rockoff presents his musical marketing plan.
Don't miss another episode of The Skinny Podcast; subscribe for free on iTunes!
Let Lip Defect Size Drive Treatment
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.

"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."

He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."

For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.
"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."
He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."
For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.
"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."
He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."
For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
AT A MEETING ON SUPERFICIAL ANATOMY AND CUTANEOUS SURGERY