User login
Service Connection Expanded to Additional Cancers
The US Department of Veterans Affairs (VA) is "lowering the burden of proof" for thousands, making acute and chronic leukemias, multiple myelomas, myelodysplastic syndromes, myelofibrosis, urinary bladder, ureter, and related genitourinary cancers presumptive for service connection.
The Jan. 8 decision included Gulf War veterans, those who served in Somalia or the Southwest Asia theater of operations during the Persian Gulf War on or after Aug. 2, 1990; and post-9/11 veterans, those who served in Afghanistan, Iraq, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, or Uzbekistan and the airspace above these locations during the Gulf War on or after Sept. 11, 2001. It also includes veterans who served at the Karshi-Khanabad (K2) base in Uzbekistan after Sept. 11, 2001.
Veterans no longer must prove their service caused their condition to receive benefits. This landmark decision allows them access to free health care for that condition.
According to the VA, these steps are also part of a comprehensive effort to ensure that K2 veterans—and their survivors—receive the care and benefits they deserve. K2 veterans have higher claim and approval rates than any other cohort of veterans: 13,002 are enrolled in VA health care, and the average K2 veteran is service connected for 14.6 conditions.
The 2022 PACT Act was the largest expansion of veteran benefits in generations. The VA then made millions of veterans eligible for health care and benefits years earlier than called for by the law. It also launched the largest outreach campaign in the history of the VA to encourage veterans to apply.
Nearly 890,000 veterans have signed up for VA health care since the bill was signed into law, a nearly 40% increase over the previous equivalent period, and veterans have submitted > 4.8 million applications for VA benefits (a 42% increase over the previous equivalent period and an all-time record). The VA has delivered > $600 billion in earned benefits directly to veterans, their families, and survivors during that time.
The VA encourages all eligible veterans—including those with previously denied claims—to apply for benefits. To apply for benefits, veterans and survivors may visit VA.gov or call 1-800-MYVA411.
The US Department of Veterans Affairs (VA) is "lowering the burden of proof" for thousands, making acute and chronic leukemias, multiple myelomas, myelodysplastic syndromes, myelofibrosis, urinary bladder, ureter, and related genitourinary cancers presumptive for service connection.
The Jan. 8 decision included Gulf War veterans, those who served in Somalia or the Southwest Asia theater of operations during the Persian Gulf War on or after Aug. 2, 1990; and post-9/11 veterans, those who served in Afghanistan, Iraq, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, or Uzbekistan and the airspace above these locations during the Gulf War on or after Sept. 11, 2001. It also includes veterans who served at the Karshi-Khanabad (K2) base in Uzbekistan after Sept. 11, 2001.
Veterans no longer must prove their service caused their condition to receive benefits. This landmark decision allows them access to free health care for that condition.
According to the VA, these steps are also part of a comprehensive effort to ensure that K2 veterans—and their survivors—receive the care and benefits they deserve. K2 veterans have higher claim and approval rates than any other cohort of veterans: 13,002 are enrolled in VA health care, and the average K2 veteran is service connected for 14.6 conditions.
The 2022 PACT Act was the largest expansion of veteran benefits in generations. The VA then made millions of veterans eligible for health care and benefits years earlier than called for by the law. It also launched the largest outreach campaign in the history of the VA to encourage veterans to apply.
Nearly 890,000 veterans have signed up for VA health care since the bill was signed into law, a nearly 40% increase over the previous equivalent period, and veterans have submitted > 4.8 million applications for VA benefits (a 42% increase over the previous equivalent period and an all-time record). The VA has delivered > $600 billion in earned benefits directly to veterans, their families, and survivors during that time.
The VA encourages all eligible veterans—including those with previously denied claims—to apply for benefits. To apply for benefits, veterans and survivors may visit VA.gov or call 1-800-MYVA411.
The US Department of Veterans Affairs (VA) is "lowering the burden of proof" for thousands, making acute and chronic leukemias, multiple myelomas, myelodysplastic syndromes, myelofibrosis, urinary bladder, ureter, and related genitourinary cancers presumptive for service connection.
The Jan. 8 decision included Gulf War veterans, those who served in Somalia or the Southwest Asia theater of operations during the Persian Gulf War on or after Aug. 2, 1990; and post-9/11 veterans, those who served in Afghanistan, Iraq, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, or Uzbekistan and the airspace above these locations during the Gulf War on or after Sept. 11, 2001. It also includes veterans who served at the Karshi-Khanabad (K2) base in Uzbekistan after Sept. 11, 2001.
Veterans no longer must prove their service caused their condition to receive benefits. This landmark decision allows them access to free health care for that condition.
According to the VA, these steps are also part of a comprehensive effort to ensure that K2 veterans—and their survivors—receive the care and benefits they deserve. K2 veterans have higher claim and approval rates than any other cohort of veterans: 13,002 are enrolled in VA health care, and the average K2 veteran is service connected for 14.6 conditions.
The 2022 PACT Act was the largest expansion of veteran benefits in generations. The VA then made millions of veterans eligible for health care and benefits years earlier than called for by the law. It also launched the largest outreach campaign in the history of the VA to encourage veterans to apply.
Nearly 890,000 veterans have signed up for VA health care since the bill was signed into law, a nearly 40% increase over the previous equivalent period, and veterans have submitted > 4.8 million applications for VA benefits (a 42% increase over the previous equivalent period and an all-time record). The VA has delivered > $600 billion in earned benefits directly to veterans, their families, and survivors during that time.
The VA encourages all eligible veterans—including those with previously denied claims—to apply for benefits. To apply for benefits, veterans and survivors may visit VA.gov or call 1-800-MYVA411.
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
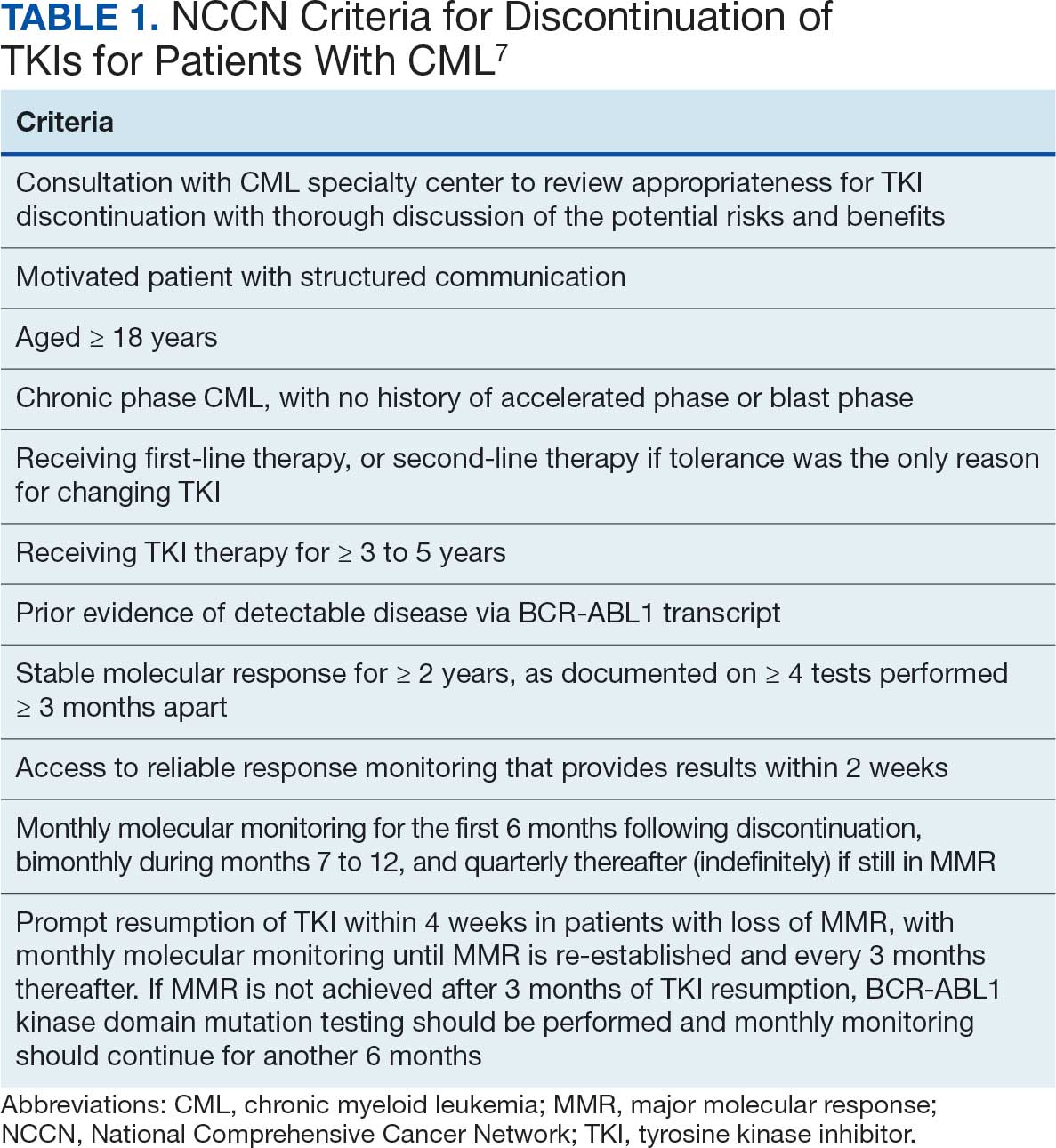
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
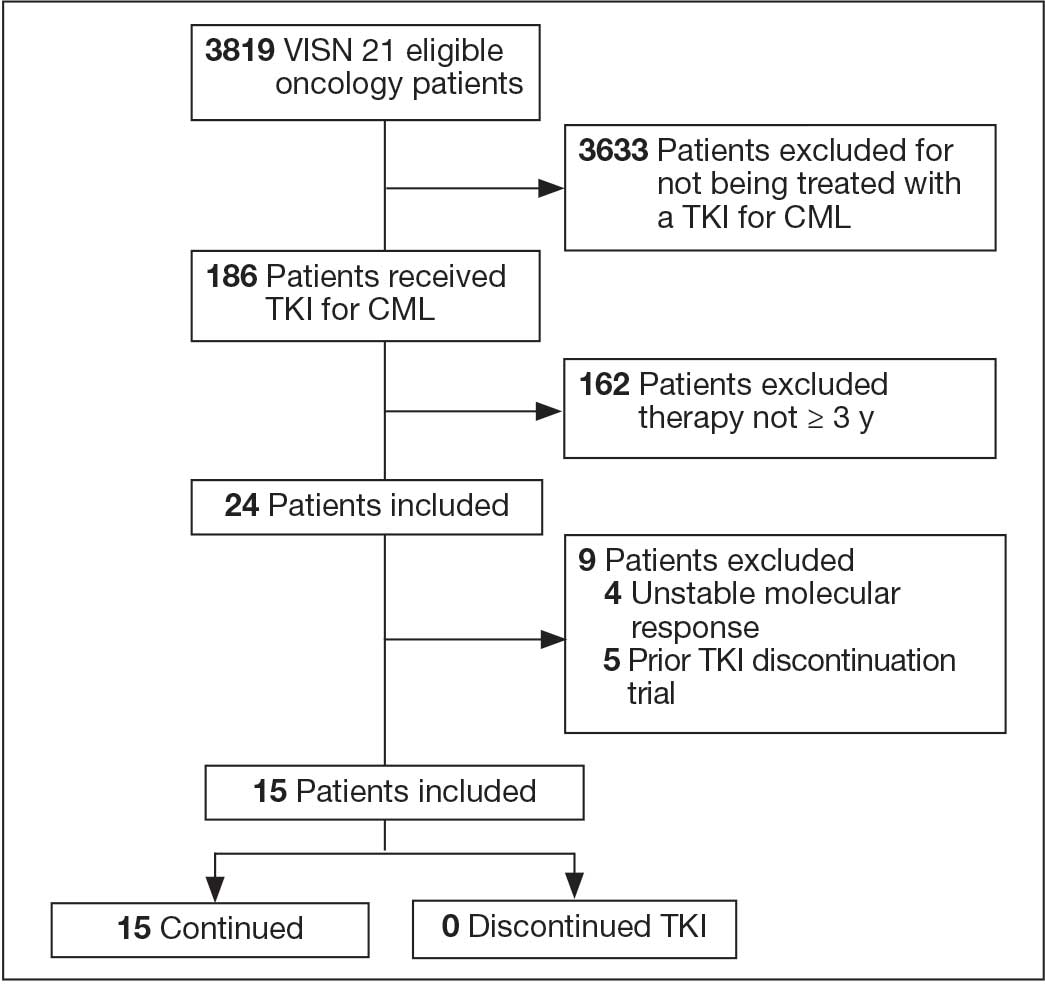
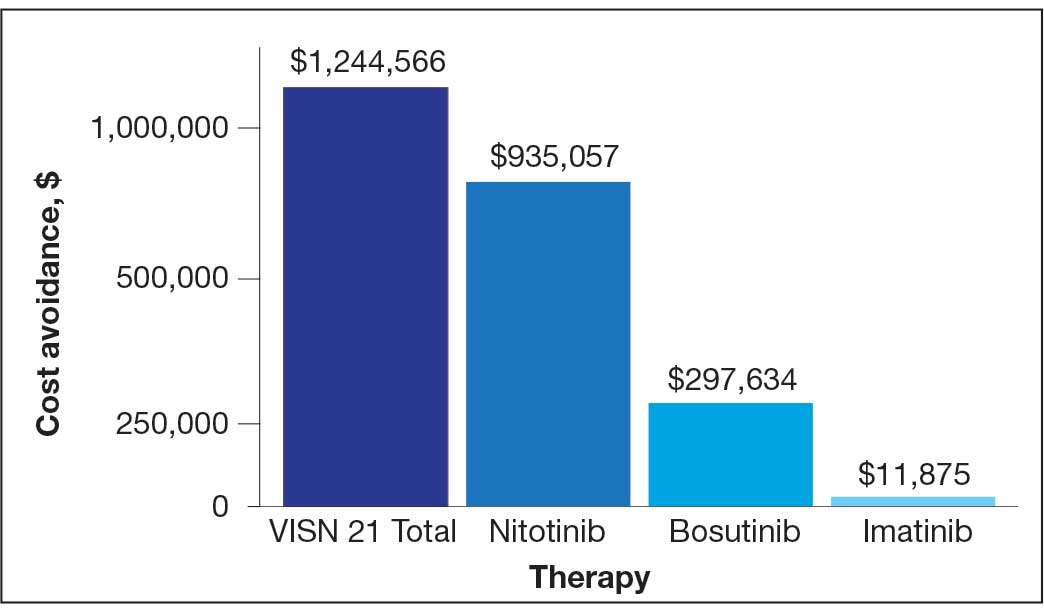
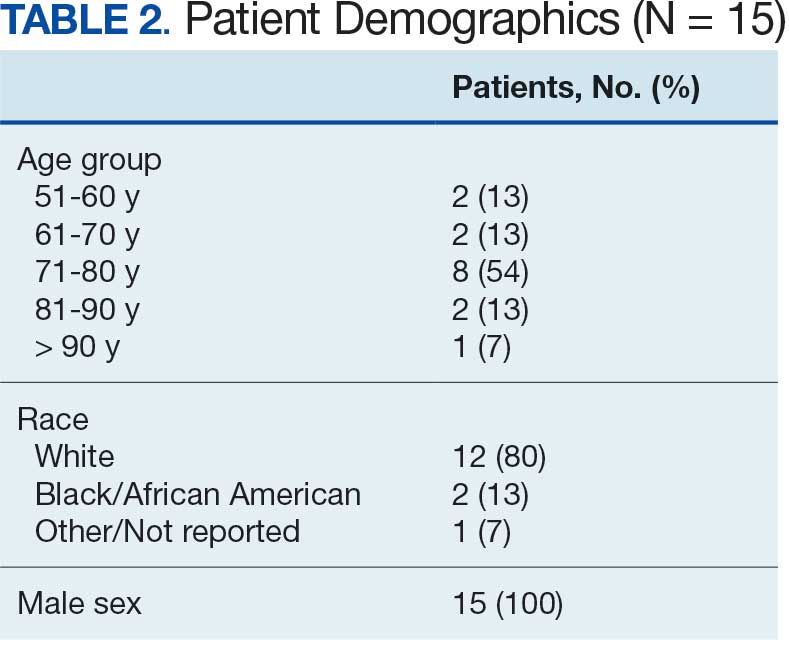
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
New Insights on Treatment of Veterans With CLL From ASH 2025
New Insights on Treatment of Veterans With CLL From ASH 2025

Insights from phase 3 trials presented at the 2025 American Society of Hematology Annual Meeting may expand treatment options for veterans with chronic lymphocytic leukemia (CLL), as discussed by Dr Nicholas Burwick from University of Washington, Seattle.
Dr Burwick begins with the CLL17 trial examining continuous treatment vs fixed-duration therapy in previously untreated patients. The fixed-duration therapy showed noninferior results. Research pertaining to the veterans population in the phase 2 Benefit VA study may offer further insight on these results.
He next discusses the first study comparing the noncovalent BTKi pirtobrutinib to covalent ibrutinib in both treatment-naive patients and those with relapsed/refractory CLL. Pirtobrutinib demonstrated noninferiority in each subgroup.
Pirtobrutinib was compared to bendamustine plus rituximab in the treatment-naive setting in the next study, showing favorable progression-free survival and a notable trend in overall survival. These two trials could lead to use of a noncovalent BTKi as frontline therapy.
Dr Burwick then turns to 6-year follow-up in the SEQUOIA trial, in which zanubrutinib showed sustained superiority over bendamustine and rituximab. He notes that acalabrutinib is currently the preferred BTKi therapy for veterans with CLL.
Finally, he discusses a study examining combination acalabrutinib and venetoclax, to which obinutuzumab was added either early or late. The rate of infections was significantly higher in the early group, an issue of particular concern in the veterans population.
--
Nicholas R. Burwick, MD, VA Puget Sound Health Care System; Associate Professor, Department of Medicine, Division of Hematology, University of Washington, Seattle; President, AVAHO - Association of VA Hematology/Oncology
Nicholas R. Burwick, MD, has disclosed no relevant financial relationships.
Insights from phase 3 trials presented at the 2025 American Society of Hematology Annual Meeting may expand treatment options for veterans with chronic lymphocytic leukemia (CLL), as discussed by Dr Nicholas Burwick from University of Washington, Seattle.
Dr Burwick begins with the CLL17 trial examining continuous treatment vs fixed-duration therapy in previously untreated patients. The fixed-duration therapy showed noninferior results. Research pertaining to the veterans population in the phase 2 Benefit VA study may offer further insight on these results.
He next discusses the first study comparing the noncovalent BTKi pirtobrutinib to covalent ibrutinib in both treatment-naive patients and those with relapsed/refractory CLL. Pirtobrutinib demonstrated noninferiority in each subgroup.
Pirtobrutinib was compared to bendamustine plus rituximab in the treatment-naive setting in the next study, showing favorable progression-free survival and a notable trend in overall survival. These two trials could lead to use of a noncovalent BTKi as frontline therapy.
Dr Burwick then turns to 6-year follow-up in the SEQUOIA trial, in which zanubrutinib showed sustained superiority over bendamustine and rituximab. He notes that acalabrutinib is currently the preferred BTKi therapy for veterans with CLL.
Finally, he discusses a study examining combination acalabrutinib and venetoclax, to which obinutuzumab was added either early or late. The rate of infections was significantly higher in the early group, an issue of particular concern in the veterans population.
--
Nicholas R. Burwick, MD, VA Puget Sound Health Care System; Associate Professor, Department of Medicine, Division of Hematology, University of Washington, Seattle; President, AVAHO - Association of VA Hematology/Oncology
Nicholas R. Burwick, MD, has disclosed no relevant financial relationships.
Insights from phase 3 trials presented at the 2025 American Society of Hematology Annual Meeting may expand treatment options for veterans with chronic lymphocytic leukemia (CLL), as discussed by Dr Nicholas Burwick from University of Washington, Seattle.
Dr Burwick begins with the CLL17 trial examining continuous treatment vs fixed-duration therapy in previously untreated patients. The fixed-duration therapy showed noninferior results. Research pertaining to the veterans population in the phase 2 Benefit VA study may offer further insight on these results.
He next discusses the first study comparing the noncovalent BTKi pirtobrutinib to covalent ibrutinib in both treatment-naive patients and those with relapsed/refractory CLL. Pirtobrutinib demonstrated noninferiority in each subgroup.
Pirtobrutinib was compared to bendamustine plus rituximab in the treatment-naive setting in the next study, showing favorable progression-free survival and a notable trend in overall survival. These two trials could lead to use of a noncovalent BTKi as frontline therapy.
Dr Burwick then turns to 6-year follow-up in the SEQUOIA trial, in which zanubrutinib showed sustained superiority over bendamustine and rituximab. He notes that acalabrutinib is currently the preferred BTKi therapy for veterans with CLL.
Finally, he discusses a study examining combination acalabrutinib and venetoclax, to which obinutuzumab was added either early or late. The rate of infections was significantly higher in the early group, an issue of particular concern in the veterans population.
--
Nicholas R. Burwick, MD, VA Puget Sound Health Care System; Associate Professor, Department of Medicine, Division of Hematology, University of Washington, Seattle; President, AVAHO - Association of VA Hematology/Oncology
Nicholas R. Burwick, MD, has disclosed no relevant financial relationships.
New Insights on Treatment of Veterans With CLL From ASH 2025
New Insights on Treatment of Veterans With CLL From ASH 2025

FDA Okays CAR T-Cell Therapy for Marginal Zone Lymphoma
The FDA has approved lisocabtagene maraleucel (Breyanzi, Bristol Myers Squibb) for relapsed or refractory marginal zone lymphoma (MZL) in adults after at least two prior lines of systemic therapy.
Lisocabtagene maraleucel (liso–cel) is now the only CD19-directed chimeric antigen receptor (CAR) T–cell therapy approved for MZL. The approval marks liso-cel’s fifth indication, the most of any CD19-directed CAR T–cell therapy, BMS said in a press release.
Prior approvals are also in the relapsed or refractory setting and include large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma.
MZL is a slow-growing subtype of non-Hodgkin lymphoma (NHL), accounting for about 7% of all NHL cases and typically diagnosed in older adults. Prognosis is generally favorable, but in patients who relapse or become refractory, NHL can transform into diffuse large B-cell lymphoma.
Basis for Approval
Liso-cel’s new approval was based on the MZL cohort of the single arm TRANSFORM FL trial, which included 66 patients in the third or later lines; 95.5% responded to the one-time treatment, with 62.1% having a complete response. Responses were durable in 90.1% of patients at 2 years, according to the BMS press release.
In terms of safety, 76% of MZL patients developed cytokine release syndrome, which was grade 3 or worse in 4.5%. Nervous system disorders included headache (21%, grade ≥ 3 in 1.5%), encephalopathy (21%, grade ≥ 3 in 1.5%), tremor (21%), dizziness (16%), and aphasia (10%).
Labeling also warns of hypersensitivity reactions, serious infections, prolonged cytopenias, hypogammaglobulinemia, and secondary malignancies.
Cost of Treatment
One-time treatment costs $567,237.18, according to drugs.com. BMS noted liso-cel is broadly covered by commercial and government insurance programs.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award–winning medical journalist who worked for several major news outlets before joining this news organization. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@mdedge.com
A version of this article first appeared on Medscape.com.
The FDA has approved lisocabtagene maraleucel (Breyanzi, Bristol Myers Squibb) for relapsed or refractory marginal zone lymphoma (MZL) in adults after at least two prior lines of systemic therapy.
Lisocabtagene maraleucel (liso–cel) is now the only CD19-directed chimeric antigen receptor (CAR) T–cell therapy approved for MZL. The approval marks liso-cel’s fifth indication, the most of any CD19-directed CAR T–cell therapy, BMS said in a press release.
Prior approvals are also in the relapsed or refractory setting and include large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma.
MZL is a slow-growing subtype of non-Hodgkin lymphoma (NHL), accounting for about 7% of all NHL cases and typically diagnosed in older adults. Prognosis is generally favorable, but in patients who relapse or become refractory, NHL can transform into diffuse large B-cell lymphoma.
Basis for Approval
Liso-cel’s new approval was based on the MZL cohort of the single arm TRANSFORM FL trial, which included 66 patients in the third or later lines; 95.5% responded to the one-time treatment, with 62.1% having a complete response. Responses were durable in 90.1% of patients at 2 years, according to the BMS press release.
In terms of safety, 76% of MZL patients developed cytokine release syndrome, which was grade 3 or worse in 4.5%. Nervous system disorders included headache (21%, grade ≥ 3 in 1.5%), encephalopathy (21%, grade ≥ 3 in 1.5%), tremor (21%), dizziness (16%), and aphasia (10%).
Labeling also warns of hypersensitivity reactions, serious infections, prolonged cytopenias, hypogammaglobulinemia, and secondary malignancies.
Cost of Treatment
One-time treatment costs $567,237.18, according to drugs.com. BMS noted liso-cel is broadly covered by commercial and government insurance programs.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award–winning medical journalist who worked for several major news outlets before joining this news organization. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@mdedge.com
A version of this article first appeared on Medscape.com.
The FDA has approved lisocabtagene maraleucel (Breyanzi, Bristol Myers Squibb) for relapsed or refractory marginal zone lymphoma (MZL) in adults after at least two prior lines of systemic therapy.
Lisocabtagene maraleucel (liso–cel) is now the only CD19-directed chimeric antigen receptor (CAR) T–cell therapy approved for MZL. The approval marks liso-cel’s fifth indication, the most of any CD19-directed CAR T–cell therapy, BMS said in a press release.
Prior approvals are also in the relapsed or refractory setting and include large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma.
MZL is a slow-growing subtype of non-Hodgkin lymphoma (NHL), accounting for about 7% of all NHL cases and typically diagnosed in older adults. Prognosis is generally favorable, but in patients who relapse or become refractory, NHL can transform into diffuse large B-cell lymphoma.
Basis for Approval
Liso-cel’s new approval was based on the MZL cohort of the single arm TRANSFORM FL trial, which included 66 patients in the third or later lines; 95.5% responded to the one-time treatment, with 62.1% having a complete response. Responses were durable in 90.1% of patients at 2 years, according to the BMS press release.
In terms of safety, 76% of MZL patients developed cytokine release syndrome, which was grade 3 or worse in 4.5%. Nervous system disorders included headache (21%, grade ≥ 3 in 1.5%), encephalopathy (21%, grade ≥ 3 in 1.5%), tremor (21%), dizziness (16%), and aphasia (10%).
Labeling also warns of hypersensitivity reactions, serious infections, prolonged cytopenias, hypogammaglobulinemia, and secondary malignancies.
Cost of Treatment
One-time treatment costs $567,237.18, according to drugs.com. BMS noted liso-cel is broadly covered by commercial and government insurance programs.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award–winning medical journalist who worked for several major news outlets before joining this news organization. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@mdedge.com
A version of this article first appeared on Medscape.com.
Agent Orange Exposure and Genetic Factors Independently Raise Risk for Multiple Lymphoma Types
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Last Month in Oncology: FDA Cancer News Roundup
Last month, the United States Food and Drug Administration (FDA) approved two new drugs and two biosimilars as well as halted commercialization for a hemophilia treatment.
Here’s a deeper look of what happened last month.
New Drugs
1. The FDA has approved mirdametinib (Gomekli, SpringWorks Therapeutics, Inc.) for adult and pediatric patients 2 years or older with neurofibromatosis type 1 and symptomatic plexiform neurofibromas that are not amenable to complete resection.
Approval for this agent was based on overall response rate findings from a multicenter, single-arm, phase 2b trial. The trial, which enrolled 58 adults and 56 pediatric patients with this rare disease, reported confirmed overall response rates of 41% among adults and 52% among children.
Adverse reactions occurring in at least 25% of adults included rash, diarrhea, nausea, musculoskeletal pain, vomiting, and fatigue. Mirdametinib can also cause ocular toxicity. Treatment should be withheld, discontinued, or the dosage reduced based on the severity of these adverse reactions, according to the FDA notice.
2. The FDA has approved vimseltinib (Romvimza, Deciphera Pharmaceuticals, LLC) to treat adult patients with symptomatic tenosynovial giant cell tumors who will not benefit from surgical resection.
Vimseltinib was approved based on findings from the MOTION trial, which included 123 patients randomly assigned 2:1 to vimseltinib 30 mg twice weekly or to placebo for 24 weeks. At 25 weeks, the objective response rate was 40% in the vimseltinib arm and 0% in the placebo arm. The median duration of response was not reached in the vimseltinib arm. Patients receiving vimseltinib also demonstrated significant improvements in active range of motion, physical functioning, and pain at this time. After another 6 months of follow-up, 58% of responders had a duration of response of 9 months or longer.
Treatment-emergent adverse events in MOTION were largely of grade 1 or 2. The most common adverse reactions, occurring in at least 20% of patients, included increased aspartate aminotransferase, periorbital edema, fatigue, rash, and cholesterol.
New or Expanded Indications
1. The FDA has approved a supplemental Biologics License Application for brentuximab vedotin (Adcetris, Seagen Inc.), in combination with lenalidomide and rituximab, for adults with relapsed or refractory large B-cell lymphoma, after at least two prior lines of therapy, who are ineligible for stem cell transplant or chimeric antigen receptor T-cell therapy. This includes patients with diffuse large B-cell lymphoma (DLBCL) not otherwise specified, DLBCL arising from indolent lymphoma, or high-grade B-cell lymphoma.
Approval was based on the randomized, double-blind, placebo-controlled ECHELON-3 trial, which randomly assigned patients 1:1 to receive lenalidomide and rituximab plus either brentuximab vedotin or placebo until disease progression or unacceptable toxicity. Researchers reported a median overall survival of 13.8 months in the treatment group vs 8.5 months in the placebo group (hazard ratio, 0.63).
2. The FDA has approved the Biologics License Application for Ospomyv and Xbryk (Samsung Bioepis Co.) — biosimilars referencing denosumab (Prolia and Xgeva, respectively) — to treat osteoporosis and cancer-related bone loss.
Ospomyv and Xbryk have been approved for use in all indications of the approved reference drugs. Specifically, Xbryk is indicated for the prevention of skeletal-related events in patients with bone metastases from solid tumors or multiple myeloma, and Ospomyv is indicated in several populations of patients with osteoporosis at high risk for fracture.
“The FDA approval of Ospomyv and Xbryk marks a key step in improving patient access and alleviating treatment cost for patients with osteoporosis and cancer-related bone loss in the United States,” Byoungin Jung, vice president at Samsung Bioepis, said in the news release.
Drug Commercialization Halt
Pfizer announced last month that it will halt the global development and commercialization of its hemophilia gene therapy fidanacogene elaparvovec (Beqvez). The company cited several reasons for the discontinuation, including low demand from patients and doctors.
Beqvez is a one-time therapy approved in the United States last April to treat adults with moderate to severe hemophilia B, a rare bleeding disorder that affects almost 4 in 100,000 men in the United States.
The significant price tag is one reason hematologists have cited for the low uptake. Another barrier is that “we don’t know the long-term outcomes” associated with the drug, pediatric hematologist Ben Samelson-Jones, MD, PhD, of the Perelman School of Medicine at the University of Pennsylvania and Children’s Hospital of Philadelphia, Philadelphia, told this news organization earlier this year.
Other issues include the prospect of newer treatment advances in the hemophilia space and logistical challenges. “There’s just a lot of logistics to getting an institution ready to provide this type of therapy,” Samelson-Jones added.
A version of this article first appeared on Medscape.com.
Last month, the United States Food and Drug Administration (FDA) approved two new drugs and two biosimilars as well as halted commercialization for a hemophilia treatment.
Here’s a deeper look of what happened last month.
New Drugs
1. The FDA has approved mirdametinib (Gomekli, SpringWorks Therapeutics, Inc.) for adult and pediatric patients 2 years or older with neurofibromatosis type 1 and symptomatic plexiform neurofibromas that are not amenable to complete resection.
Approval for this agent was based on overall response rate findings from a multicenter, single-arm, phase 2b trial. The trial, which enrolled 58 adults and 56 pediatric patients with this rare disease, reported confirmed overall response rates of 41% among adults and 52% among children.
Adverse reactions occurring in at least 25% of adults included rash, diarrhea, nausea, musculoskeletal pain, vomiting, and fatigue. Mirdametinib can also cause ocular toxicity. Treatment should be withheld, discontinued, or the dosage reduced based on the severity of these adverse reactions, according to the FDA notice.
2. The FDA has approved vimseltinib (Romvimza, Deciphera Pharmaceuticals, LLC) to treat adult patients with symptomatic tenosynovial giant cell tumors who will not benefit from surgical resection.
Vimseltinib was approved based on findings from the MOTION trial, which included 123 patients randomly assigned 2:1 to vimseltinib 30 mg twice weekly or to placebo for 24 weeks. At 25 weeks, the objective response rate was 40% in the vimseltinib arm and 0% in the placebo arm. The median duration of response was not reached in the vimseltinib arm. Patients receiving vimseltinib also demonstrated significant improvements in active range of motion, physical functioning, and pain at this time. After another 6 months of follow-up, 58% of responders had a duration of response of 9 months or longer.
Treatment-emergent adverse events in MOTION were largely of grade 1 or 2. The most common adverse reactions, occurring in at least 20% of patients, included increased aspartate aminotransferase, periorbital edema, fatigue, rash, and cholesterol.
New or Expanded Indications
1. The FDA has approved a supplemental Biologics License Application for brentuximab vedotin (Adcetris, Seagen Inc.), in combination with lenalidomide and rituximab, for adults with relapsed or refractory large B-cell lymphoma, after at least two prior lines of therapy, who are ineligible for stem cell transplant or chimeric antigen receptor T-cell therapy. This includes patients with diffuse large B-cell lymphoma (DLBCL) not otherwise specified, DLBCL arising from indolent lymphoma, or high-grade B-cell lymphoma.
Approval was based on the randomized, double-blind, placebo-controlled ECHELON-3 trial, which randomly assigned patients 1:1 to receive lenalidomide and rituximab plus either brentuximab vedotin or placebo until disease progression or unacceptable toxicity. Researchers reported a median overall survival of 13.8 months in the treatment group vs 8.5 months in the placebo group (hazard ratio, 0.63).
2. The FDA has approved the Biologics License Application for Ospomyv and Xbryk (Samsung Bioepis Co.) — biosimilars referencing denosumab (Prolia and Xgeva, respectively) — to treat osteoporosis and cancer-related bone loss.
Ospomyv and Xbryk have been approved for use in all indications of the approved reference drugs. Specifically, Xbryk is indicated for the prevention of skeletal-related events in patients with bone metastases from solid tumors or multiple myeloma, and Ospomyv is indicated in several populations of patients with osteoporosis at high risk for fracture.
“The FDA approval of Ospomyv and Xbryk marks a key step in improving patient access and alleviating treatment cost for patients with osteoporosis and cancer-related bone loss in the United States,” Byoungin Jung, vice president at Samsung Bioepis, said in the news release.
Drug Commercialization Halt
Pfizer announced last month that it will halt the global development and commercialization of its hemophilia gene therapy fidanacogene elaparvovec (Beqvez). The company cited several reasons for the discontinuation, including low demand from patients and doctors.
Beqvez is a one-time therapy approved in the United States last April to treat adults with moderate to severe hemophilia B, a rare bleeding disorder that affects almost 4 in 100,000 men in the United States.
The significant price tag is one reason hematologists have cited for the low uptake. Another barrier is that “we don’t know the long-term outcomes” associated with the drug, pediatric hematologist Ben Samelson-Jones, MD, PhD, of the Perelman School of Medicine at the University of Pennsylvania and Children’s Hospital of Philadelphia, Philadelphia, told this news organization earlier this year.
Other issues include the prospect of newer treatment advances in the hemophilia space and logistical challenges. “There’s just a lot of logistics to getting an institution ready to provide this type of therapy,” Samelson-Jones added.
A version of this article first appeared on Medscape.com.
Last month, the United States Food and Drug Administration (FDA) approved two new drugs and two biosimilars as well as halted commercialization for a hemophilia treatment.
Here’s a deeper look of what happened last month.
New Drugs
1. The FDA has approved mirdametinib (Gomekli, SpringWorks Therapeutics, Inc.) for adult and pediatric patients 2 years or older with neurofibromatosis type 1 and symptomatic plexiform neurofibromas that are not amenable to complete resection.
Approval for this agent was based on overall response rate findings from a multicenter, single-arm, phase 2b trial. The trial, which enrolled 58 adults and 56 pediatric patients with this rare disease, reported confirmed overall response rates of 41% among adults and 52% among children.
Adverse reactions occurring in at least 25% of adults included rash, diarrhea, nausea, musculoskeletal pain, vomiting, and fatigue. Mirdametinib can also cause ocular toxicity. Treatment should be withheld, discontinued, or the dosage reduced based on the severity of these adverse reactions, according to the FDA notice.
2. The FDA has approved vimseltinib (Romvimza, Deciphera Pharmaceuticals, LLC) to treat adult patients with symptomatic tenosynovial giant cell tumors who will not benefit from surgical resection.
Vimseltinib was approved based on findings from the MOTION trial, which included 123 patients randomly assigned 2:1 to vimseltinib 30 mg twice weekly or to placebo for 24 weeks. At 25 weeks, the objective response rate was 40% in the vimseltinib arm and 0% in the placebo arm. The median duration of response was not reached in the vimseltinib arm. Patients receiving vimseltinib also demonstrated significant improvements in active range of motion, physical functioning, and pain at this time. After another 6 months of follow-up, 58% of responders had a duration of response of 9 months or longer.
Treatment-emergent adverse events in MOTION were largely of grade 1 or 2. The most common adverse reactions, occurring in at least 20% of patients, included increased aspartate aminotransferase, periorbital edema, fatigue, rash, and cholesterol.
New or Expanded Indications
1. The FDA has approved a supplemental Biologics License Application for brentuximab vedotin (Adcetris, Seagen Inc.), in combination with lenalidomide and rituximab, for adults with relapsed or refractory large B-cell lymphoma, after at least two prior lines of therapy, who are ineligible for stem cell transplant or chimeric antigen receptor T-cell therapy. This includes patients with diffuse large B-cell lymphoma (DLBCL) not otherwise specified, DLBCL arising from indolent lymphoma, or high-grade B-cell lymphoma.
Approval was based on the randomized, double-blind, placebo-controlled ECHELON-3 trial, which randomly assigned patients 1:1 to receive lenalidomide and rituximab plus either brentuximab vedotin or placebo until disease progression or unacceptable toxicity. Researchers reported a median overall survival of 13.8 months in the treatment group vs 8.5 months in the placebo group (hazard ratio, 0.63).
2. The FDA has approved the Biologics License Application for Ospomyv and Xbryk (Samsung Bioepis Co.) — biosimilars referencing denosumab (Prolia and Xgeva, respectively) — to treat osteoporosis and cancer-related bone loss.
Ospomyv and Xbryk have been approved for use in all indications of the approved reference drugs. Specifically, Xbryk is indicated for the prevention of skeletal-related events in patients with bone metastases from solid tumors or multiple myeloma, and Ospomyv is indicated in several populations of patients with osteoporosis at high risk for fracture.
“The FDA approval of Ospomyv and Xbryk marks a key step in improving patient access and alleviating treatment cost for patients with osteoporosis and cancer-related bone loss in the United States,” Byoungin Jung, vice president at Samsung Bioepis, said in the news release.
Drug Commercialization Halt
Pfizer announced last month that it will halt the global development and commercialization of its hemophilia gene therapy fidanacogene elaparvovec (Beqvez). The company cited several reasons for the discontinuation, including low demand from patients and doctors.
Beqvez is a one-time therapy approved in the United States last April to treat adults with moderate to severe hemophilia B, a rare bleeding disorder that affects almost 4 in 100,000 men in the United States.
The significant price tag is one reason hematologists have cited for the low uptake. Another barrier is that “we don’t know the long-term outcomes” associated with the drug, pediatric hematologist Ben Samelson-Jones, MD, PhD, of the Perelman School of Medicine at the University of Pennsylvania and Children’s Hospital of Philadelphia, Philadelphia, told this news organization earlier this year.
Other issues include the prospect of newer treatment advances in the hemophilia space and logistical challenges. “There’s just a lot of logistics to getting an institution ready to provide this type of therapy,” Samelson-Jones added.
A version of this article first appeared on Medscape.com.
Cellular Therapies for Solid Tumors: The Next Big Thing?
The cutting edge of treating solid tumors with cell therapies got notably sharper in 2024.
First came the US Food and Drug Administration (FDA) approval in February 2024 of the tumor-infiltrating lymphocyte (TIL) therapy lifileucel in unresectable or metastatic melanoma that had progressed on prior immunotherapy, the first cellular therapy for any solid tumor. Then came the August FDA approval of afamitresgene autoleucel in unresectable or metastatic synovial sarcoma with failed chemotherapy, the first engineered T-cell therapy for cancers in soft tissue.
“This was a pipe dream just a decade ago,” Alison Betof Warner, MD, PhD, lead author of a lifileucel study (NCT05640193), said in an interview with Medscape Medical News. “At the start of 2024, we had no approvals of these kinds of products in solid cancers. Now we have two.”
As the director of Solid Tumor Cell Therapy and leader of Stanford Medicine’s Melanoma and Cutaneous Oncology Clinical Research Group, Betof Warner has been at the forefront of developing commercial cell therapy using tumor-infiltrating lymphocytes (TILs).
“The approval of lifileucel increases confidence that we can get these therapies across the regulatory finish line and to patients,” Betof Warner said during the interview. She was not involved in the development of afamitresgene autoleucel.
‘Reverse Engineering’
In addition to her contributions to the work that led to lifileucel’s approval, Betof Warner was the lead author on the first consensus guidelines on management and best practices for tumor-infiltrating lymphocyte cell therapy.
Betof Warner began studying TILs after doing research with her mentors in immuno-oncology, Jedd D. Wolchok and Michael A. Postow. Their investigations — including one that Betof Warner coauthored — into how monoclonal antibodies and checkpoint inhibitors, such as ipilimumab or nivolumab, might extend the lives of people with advanced unresectable or metastatic melanoma inspired her to push further to find ways to minimize treatment while maximizing outcomes for patients. Betof Warner’s interest overall, she said in the interview, is in capitalizing on what can be learned about how the immune system controls cancer.
“What we know is that the immune system has the ability to kill cancer,” Betof Warner said. “Therefore we need to be thinking about how we can increase immune surveillance. How can we enhance that before a patient develops advanced cancer?
Betof Warner said that although TILs are now standard treatment in melanoma, there is about a 30% response rate compared with about a 50% response rate in immunotherapy, and the latter is easier for the patient to withstand.
“Antibodies on the frontline are better than going through a surgery and then waiting weeks to get your therapy,” Betof Warner said in the interview. “You can come into my clinic and get an antibody therapy in 30 minutes and go straight to work. TILs require patients to be in the hospital for weeks at a time and out of work for months at a time.”
In an effort to combine therapies to maximize best outcomes, a phase 3 trial (NCT05727904) is currently recruiting. The TILVANCE-301 trial will compare immunotherapy plus adoptive cell therapy vs immunotherapy alone in untreated unresectable or metastatic melanoma. Betof Warner is not a part of this study.
Cell Therapies Include CAR T Cells and TCRT
In general, adoptive T-cell therapies such as TILs involve the isolation of autologous immune cells that are removed from the body and either expanded or modified to optimize their efficacy in fighting antigens, before their transfer to the patient as a living drug by infusion.
In addition to TILs, adoptive cell therapies for antitumor therapeutics include chimeric antigen receptor (CAR) T cells and engineered T-cell receptor therapy (TCRT).
In CAR T-cell therapy and TCRT, naive T cells are harvested from the patient’s blood then engineered to target a tumor. In TIL therapy, tumor-specific T cells are taken from the patient’s tumor. Once extracted, the respective cells are expanded billions of times and then delivered back to the patient’s body, said Betof Warner.
“The main promise of this approach is to generate responses in what we know as ‘cold’ tumors, or tumors that do not have a lot of endogenous T-cell infiltration or where the T cells are not working well, to bring in tumor targeting T cells and then trigger an immune response,” Betof Warner told an audience at the American Society of Clinical Oncology (ASCO) 2024 annual meeting.
TIL patients also receive interleukin (IL)-2 infusions to further stimulate the cells. In patients being treated with TCRT, they either receive low or no IL-2, Betof Warner said in her ASCO presentation, “Adopting Cutting-Edge Cell Therapies in Melanoma,” part of the session Beyond the Tip of the Iceberg: Next-Generation Cell-Based Therapies.
Decades in the Making
The National Cancer Institute began investigating TILs in the late 1980s, with the current National Cancer Institute (NCI) surgery chief, Steven Rosenberg, MD, PhD, leading the first-ever trials that showed TILs could shrink tumors in people with advanced melanoma.
Since then, NCI staff and others have also investigated TILs beyond melanoma and additional cell therapies based on CAR T cells and TCRT for antitumor therapeutics.
“TCRs are different from CAR Ts because they go after intracellular antigens instead of extracellular antigens,” said Betof Warner. “That has appeal because many of the tumor antigens we’re looking for will be intracellular.”
Because CAR T cells only target extracellular antigens, their utility is somewhat limited. Although several CAR T-cell therapies exist for blood cancers, there currently are no approved CAR T-cell therapies for solid tumors. However, several trials of CAR T cells in gastrointestinal cancers and melanoma are ongoing, said Betof Warner, who is not a part of these studies.
“We are starting to see early-phase efficacy in pediatric gliomas,” Betof Warner said, mentioning a study conducted by colleagues at Stanford who demonstrated potential for anti-GD2 CAR T-cell therapy in deadly pediatric diffuse midline gliomas, tumors on the spine and brain.
In their study, nine out of 11 participants (median age, 15 years) showed benefit from the cell therapy, with one participant’s tumors resolving completely. The results paved the way for the FDA to grant a Regenerative Medicine Advanced Therapy designation for use of anti-GD2 CAR T cells in H3K27M-positive diffuse midline gliomas.
The investigators are now recruiting for a phase 1 trial (NCT04196413). Results of the initial study were published in Nature last month.
Another lesser-known cell therapy expected to advance at some point in the future for solid tumors is use of the body’s natural killer (NK) cells. “They’ve been known about for a long time, but they are more difficult to regulate, which is one reason why it has taken longer to make NK cell therapies,” said Betof Warner, who is not involved in the study of NK cells. “One of their advantages is that, potentially, there could be an ‘off the shelf’ NK product. They don’t necessarily have to be made with autologous cells.”
Risk-Benefit Profiles Depend on Mechanism of Action
If the corresponding TCR sequence of a tumor antigen is known, said Betof Warner, it is possible to use leukapheresis to generate naive circulating lymphocytes. Once infused, the manufactured TCRTs will activate in the body the same as native cells because the signaling is the same.
An advantage to TCRT compared with CAR T-cell therapy is that it targets intracellular proteins, which are significantly present in the tumor, Betof Warner said in her presentation at ASCO 2024. She clarified that tumors will usually be screened for the presence of this antigen before a patient is selected for treatment with that particular therapy, because not all antigens are highly expressed in every tumor.
“Furthermore, the tumor antigen has to be presented by a major histocompatibility complex, meaning there are human leukocyte antigen restrictions, which impacts patient selection,” she said.
A risk with both TCRT and CAR T-cell therapy, according to Betof Warner, is that because there are often shared antigens between tumor and normal tissues, on-target/off-tumor toxicity is a risk.
“TILs are different because they are nonengineered, at least not for antigen recognition. They are polyclonal and go after multiple targets,” Betof Warner said. “TCRs and CARs are engineered to go after one target. So, TILs have much lower rates of on-tumor/off-target effects, vs when you engineer a very high affinity receptor like a TCR or CAR.”
A good example of how this amplification of TCR affinity can lead to poor outcomes is in metastatic melanoma, said Betof Warner.
In investigations (NCI-07-C-0174 and NCI-07-C-0175) of TCRT in metastatic melanoma, for example, the researchers were targeting MART-1 or gp100, which are expressed in melanocytes.
“The problem was that these antigens are also expressed in the eyes and ears, so it caused eye inflammation and hearing loss in a number of patients because it wasn’t specific enough for the tumor,” said Betof Warner. “So, if that target is highly expressed on normal tissue, then you have a high risk.”
Promise of PRAME
Betof Warner said the most promising TCRT at present is the investigational autologous cell therapy IMA203 (NCT03688124), which targets the preferentially expressed antigen (PRAME). Although PRAME is found in many tumors, this testis antigen does not tend to express in normal, healthy adult tissues. Betof Warner is not affiliated with this study.
“It’s maybe the most exciting TCRT cell in melanoma,” Betof Warner told her audience at the ASCO 2024 meeting. Because the expression rate of PRAME in cutaneous and uveal melanoma is at or above 95% and 90%, respectively, she said “it is a really good target in melanoma.”
Phase 1a results reported in late 2023 from a first-in-human trial of IMA203 involving 13 persons with highly advanced melanoma and a median of 5.5 previous treatments showed a 50% objective response rate in the 12 evaluable results. The duration of response ranged between 2.2 and 14.7 months (median follow-up, 14 months).
The safety profile of the treatment was favorable, with no grade 3 adverse events occurring in more than 10% of the cohort, and no grade 5 adverse events at all.
Phase 1b results published in October by maker Immatics showed that in 28 heavily pretreated metastatic melanoma patients, IMA203 had a confirmed objective response rate of 54% with a median duration of response of 12.1 months, while maintaining a favorable tolerability profile.
Accelerated Approvals, Boxed Warnings
The FDA granted accelerated approvals for both lifileucel, the TIL therapy, and afamitresgene autoleucel, the TCRT.
Both were approved with boxed warnings. Lifileucel’s warning is for treatment-related mortality, prolonged severe cytopenia, severe infection, and cardiopulmonary and renal impairment. Afamitresgene autoleucel’s boxed warning is for serious or fatal cytokine release syndrome, which may be severe or life-threatening.
With these approvals, the bar is now raised on TILs and TCRTs, said Betof Warner.
The lifileucel trial studied 73 patients whose melanoma had continued to metastasize despite treatment with a programmed cell death protein (PD-1)/ programmed death-ligand (PD-L1)–targeted immune checkpoint inhibitor and a BRAF inhibitor (if appropriate based on tumor mutation status), and whose lifileucel dose was at least 7.5 billion cells (the approved dose). The cohort also received a median of six IL-2 (aldesleukin) doses.
The objective response rate was 31.5% (95% CI, 21.1-43.4), and median duration of response was not reached (lower bound of 95% CI, 4.1).
In the afamitresgene autoleucel study, 44 of 52 patients with synovial sarcoma received leukapheresis and a single infusion of afamitresgene autoleucel.
The overall response rate was 43.2% (95% CI, 28.4-59.0). The median time to response was 4.9 weeks (95% CI, 4.4-8), and the median duration of response was 6 months (lower bound of 95% CI, 4.6). Among patients who were responsive to the treatment, 45.6% and 39.0% had a duration of response of 6 months or longer and 12 months or longer, respectively.
New Hope for Patients
Betof Warner and her colleagues are now recruiting for an open-label, phase 1/2 investigation of the safety and efficacy of the TIL therapy OBX-115 in adult advanced solid tumors in melanoma or non–small cell lung cancer. The first-in-human results of a previous trial were presented at the ASCO 2024 meeting, and OBX-115 received FDA fast track designation in July.
“I think the results are really promising,” said Betof Warner. “This is an engineered TIL that does not require administering IL-2 to the patient. There were four out of the nine patients who responded to the treatment and there were no dose-limiting toxicities, no cytokine and no intracranial — all of which is excellent.”
For Betof Warner, the possibility that by using their own immune system, patients with advanced and refractory cancers could soon have a one-time treatment with a cell therapy rather than innumerable bouts of chemotherapy pushes her onward.
“The idea that we can treat cancer one time and have it not recur for years — that’s pushing the start of saying there’s a cure of cancer. That a person could move on from cancer like they move on from an infection. That is the potential of this work. We’re not there yet, but that’s where we need to think and dream big,” she said.
Betof Warner disclosed consulting/advisory roles with BluePath Solutions, Bristol-Myers Squibb/Medarex, Immatics, Instil Bio, Iovance Biotherapeutics, Lyell Immunopharma, Merck, Novartis, and Pfizer and research funding and travel expenses from Iovance Biotherapeutics.
A version of this article appeared on Medscape.com.
The cutting edge of treating solid tumors with cell therapies got notably sharper in 2024.
First came the US Food and Drug Administration (FDA) approval in February 2024 of the tumor-infiltrating lymphocyte (TIL) therapy lifileucel in unresectable or metastatic melanoma that had progressed on prior immunotherapy, the first cellular therapy for any solid tumor. Then came the August FDA approval of afamitresgene autoleucel in unresectable or metastatic synovial sarcoma with failed chemotherapy, the first engineered T-cell therapy for cancers in soft tissue.
“This was a pipe dream just a decade ago,” Alison Betof Warner, MD, PhD, lead author of a lifileucel study (NCT05640193), said in an interview with Medscape Medical News. “At the start of 2024, we had no approvals of these kinds of products in solid cancers. Now we have two.”
As the director of Solid Tumor Cell Therapy and leader of Stanford Medicine’s Melanoma and Cutaneous Oncology Clinical Research Group, Betof Warner has been at the forefront of developing commercial cell therapy using tumor-infiltrating lymphocytes (TILs).
“The approval of lifileucel increases confidence that we can get these therapies across the regulatory finish line and to patients,” Betof Warner said during the interview. She was not involved in the development of afamitresgene autoleucel.
‘Reverse Engineering’
In addition to her contributions to the work that led to lifileucel’s approval, Betof Warner was the lead author on the first consensus guidelines on management and best practices for tumor-infiltrating lymphocyte cell therapy.
Betof Warner began studying TILs after doing research with her mentors in immuno-oncology, Jedd D. Wolchok and Michael A. Postow. Their investigations — including one that Betof Warner coauthored — into how monoclonal antibodies and checkpoint inhibitors, such as ipilimumab or nivolumab, might extend the lives of people with advanced unresectable or metastatic melanoma inspired her to push further to find ways to minimize treatment while maximizing outcomes for patients. Betof Warner’s interest overall, she said in the interview, is in capitalizing on what can be learned about how the immune system controls cancer.
“What we know is that the immune system has the ability to kill cancer,” Betof Warner said. “Therefore we need to be thinking about how we can increase immune surveillance. How can we enhance that before a patient develops advanced cancer?
Betof Warner said that although TILs are now standard treatment in melanoma, there is about a 30% response rate compared with about a 50% response rate in immunotherapy, and the latter is easier for the patient to withstand.
“Antibodies on the frontline are better than going through a surgery and then waiting weeks to get your therapy,” Betof Warner said in the interview. “You can come into my clinic and get an antibody therapy in 30 minutes and go straight to work. TILs require patients to be in the hospital for weeks at a time and out of work for months at a time.”
In an effort to combine therapies to maximize best outcomes, a phase 3 trial (NCT05727904) is currently recruiting. The TILVANCE-301 trial will compare immunotherapy plus adoptive cell therapy vs immunotherapy alone in untreated unresectable or metastatic melanoma. Betof Warner is not a part of this study.
Cell Therapies Include CAR T Cells and TCRT
In general, adoptive T-cell therapies such as TILs involve the isolation of autologous immune cells that are removed from the body and either expanded or modified to optimize their efficacy in fighting antigens, before their transfer to the patient as a living drug by infusion.
In addition to TILs, adoptive cell therapies for antitumor therapeutics include chimeric antigen receptor (CAR) T cells and engineered T-cell receptor therapy (TCRT).
In CAR T-cell therapy and TCRT, naive T cells are harvested from the patient’s blood then engineered to target a tumor. In TIL therapy, tumor-specific T cells are taken from the patient’s tumor. Once extracted, the respective cells are expanded billions of times and then delivered back to the patient’s body, said Betof Warner.
“The main promise of this approach is to generate responses in what we know as ‘cold’ tumors, or tumors that do not have a lot of endogenous T-cell infiltration or where the T cells are not working well, to bring in tumor targeting T cells and then trigger an immune response,” Betof Warner told an audience at the American Society of Clinical Oncology (ASCO) 2024 annual meeting.
TIL patients also receive interleukin (IL)-2 infusions to further stimulate the cells. In patients being treated with TCRT, they either receive low or no IL-2, Betof Warner said in her ASCO presentation, “Adopting Cutting-Edge Cell Therapies in Melanoma,” part of the session Beyond the Tip of the Iceberg: Next-Generation Cell-Based Therapies.
Decades in the Making
The National Cancer Institute began investigating TILs in the late 1980s, with the current National Cancer Institute (NCI) surgery chief, Steven Rosenberg, MD, PhD, leading the first-ever trials that showed TILs could shrink tumors in people with advanced melanoma.
Since then, NCI staff and others have also investigated TILs beyond melanoma and additional cell therapies based on CAR T cells and TCRT for antitumor therapeutics.
“TCRs are different from CAR Ts because they go after intracellular antigens instead of extracellular antigens,” said Betof Warner. “That has appeal because many of the tumor antigens we’re looking for will be intracellular.”
Because CAR T cells only target extracellular antigens, their utility is somewhat limited. Although several CAR T-cell therapies exist for blood cancers, there currently are no approved CAR T-cell therapies for solid tumors. However, several trials of CAR T cells in gastrointestinal cancers and melanoma are ongoing, said Betof Warner, who is not a part of these studies.
“We are starting to see early-phase efficacy in pediatric gliomas,” Betof Warner said, mentioning a study conducted by colleagues at Stanford who demonstrated potential for anti-GD2 CAR T-cell therapy in deadly pediatric diffuse midline gliomas, tumors on the spine and brain.
In their study, nine out of 11 participants (median age, 15 years) showed benefit from the cell therapy, with one participant’s tumors resolving completely. The results paved the way for the FDA to grant a Regenerative Medicine Advanced Therapy designation for use of anti-GD2 CAR T cells in H3K27M-positive diffuse midline gliomas.
The investigators are now recruiting for a phase 1 trial (NCT04196413). Results of the initial study were published in Nature last month.
Another lesser-known cell therapy expected to advance at some point in the future for solid tumors is use of the body’s natural killer (NK) cells. “They’ve been known about for a long time, but they are more difficult to regulate, which is one reason why it has taken longer to make NK cell therapies,” said Betof Warner, who is not involved in the study of NK cells. “One of their advantages is that, potentially, there could be an ‘off the shelf’ NK product. They don’t necessarily have to be made with autologous cells.”
Risk-Benefit Profiles Depend on Mechanism of Action
If the corresponding TCR sequence of a tumor antigen is known, said Betof Warner, it is possible to use leukapheresis to generate naive circulating lymphocytes. Once infused, the manufactured TCRTs will activate in the body the same as native cells because the signaling is the same.
An advantage to TCRT compared with CAR T-cell therapy is that it targets intracellular proteins, which are significantly present in the tumor, Betof Warner said in her presentation at ASCO 2024. She clarified that tumors will usually be screened for the presence of this antigen before a patient is selected for treatment with that particular therapy, because not all antigens are highly expressed in every tumor.
“Furthermore, the tumor antigen has to be presented by a major histocompatibility complex, meaning there are human leukocyte antigen restrictions, which impacts patient selection,” she said.
A risk with both TCRT and CAR T-cell therapy, according to Betof Warner, is that because there are often shared antigens between tumor and normal tissues, on-target/off-tumor toxicity is a risk.
“TILs are different because they are nonengineered, at least not for antigen recognition. They are polyclonal and go after multiple targets,” Betof Warner said. “TCRs and CARs are engineered to go after one target. So, TILs have much lower rates of on-tumor/off-target effects, vs when you engineer a very high affinity receptor like a TCR or CAR.”
A good example of how this amplification of TCR affinity can lead to poor outcomes is in metastatic melanoma, said Betof Warner.
In investigations (NCI-07-C-0174 and NCI-07-C-0175) of TCRT in metastatic melanoma, for example, the researchers were targeting MART-1 or gp100, which are expressed in melanocytes.
“The problem was that these antigens are also expressed in the eyes and ears, so it caused eye inflammation and hearing loss in a number of patients because it wasn’t specific enough for the tumor,” said Betof Warner. “So, if that target is highly expressed on normal tissue, then you have a high risk.”
Promise of PRAME
Betof Warner said the most promising TCRT at present is the investigational autologous cell therapy IMA203 (NCT03688124), which targets the preferentially expressed antigen (PRAME). Although PRAME is found in many tumors, this testis antigen does not tend to express in normal, healthy adult tissues. Betof Warner is not affiliated with this study.
“It’s maybe the most exciting TCRT cell in melanoma,” Betof Warner told her audience at the ASCO 2024 meeting. Because the expression rate of PRAME in cutaneous and uveal melanoma is at or above 95% and 90%, respectively, she said “it is a really good target in melanoma.”
Phase 1a results reported in late 2023 from a first-in-human trial of IMA203 involving 13 persons with highly advanced melanoma and a median of 5.5 previous treatments showed a 50% objective response rate in the 12 evaluable results. The duration of response ranged between 2.2 and 14.7 months (median follow-up, 14 months).
The safety profile of the treatment was favorable, with no grade 3 adverse events occurring in more than 10% of the cohort, and no grade 5 adverse events at all.
Phase 1b results published in October by maker Immatics showed that in 28 heavily pretreated metastatic melanoma patients, IMA203 had a confirmed objective response rate of 54% with a median duration of response of 12.1 months, while maintaining a favorable tolerability profile.
Accelerated Approvals, Boxed Warnings
The FDA granted accelerated approvals for both lifileucel, the TIL therapy, and afamitresgene autoleucel, the TCRT.
Both were approved with boxed warnings. Lifileucel’s warning is for treatment-related mortality, prolonged severe cytopenia, severe infection, and cardiopulmonary and renal impairment. Afamitresgene autoleucel’s boxed warning is for serious or fatal cytokine release syndrome, which may be severe or life-threatening.
With these approvals, the bar is now raised on TILs and TCRTs, said Betof Warner.
The lifileucel trial studied 73 patients whose melanoma had continued to metastasize despite treatment with a programmed cell death protein (PD-1)/ programmed death-ligand (PD-L1)–targeted immune checkpoint inhibitor and a BRAF inhibitor (if appropriate based on tumor mutation status), and whose lifileucel dose was at least 7.5 billion cells (the approved dose). The cohort also received a median of six IL-2 (aldesleukin) doses.
The objective response rate was 31.5% (95% CI, 21.1-43.4), and median duration of response was not reached (lower bound of 95% CI, 4.1).
In the afamitresgene autoleucel study, 44 of 52 patients with synovial sarcoma received leukapheresis and a single infusion of afamitresgene autoleucel.
The overall response rate was 43.2% (95% CI, 28.4-59.0). The median time to response was 4.9 weeks (95% CI, 4.4-8), and the median duration of response was 6 months (lower bound of 95% CI, 4.6). Among patients who were responsive to the treatment, 45.6% and 39.0% had a duration of response of 6 months or longer and 12 months or longer, respectively.
New Hope for Patients
Betof Warner and her colleagues are now recruiting for an open-label, phase 1/2 investigation of the safety and efficacy of the TIL therapy OBX-115 in adult advanced solid tumors in melanoma or non–small cell lung cancer. The first-in-human results of a previous trial were presented at the ASCO 2024 meeting, and OBX-115 received FDA fast track designation in July.
“I think the results are really promising,” said Betof Warner. “This is an engineered TIL that does not require administering IL-2 to the patient. There were four out of the nine patients who responded to the treatment and there were no dose-limiting toxicities, no cytokine and no intracranial — all of which is excellent.”
For Betof Warner, the possibility that by using their own immune system, patients with advanced and refractory cancers could soon have a one-time treatment with a cell therapy rather than innumerable bouts of chemotherapy pushes her onward.
“The idea that we can treat cancer one time and have it not recur for years — that’s pushing the start of saying there’s a cure of cancer. That a person could move on from cancer like they move on from an infection. That is the potential of this work. We’re not there yet, but that’s where we need to think and dream big,” she said.
Betof Warner disclosed consulting/advisory roles with BluePath Solutions, Bristol-Myers Squibb/Medarex, Immatics, Instil Bio, Iovance Biotherapeutics, Lyell Immunopharma, Merck, Novartis, and Pfizer and research funding and travel expenses from Iovance Biotherapeutics.
A version of this article appeared on Medscape.com.
The cutting edge of treating solid tumors with cell therapies got notably sharper in 2024.
First came the US Food and Drug Administration (FDA) approval in February 2024 of the tumor-infiltrating lymphocyte (TIL) therapy lifileucel in unresectable or metastatic melanoma that had progressed on prior immunotherapy, the first cellular therapy for any solid tumor. Then came the August FDA approval of afamitresgene autoleucel in unresectable or metastatic synovial sarcoma with failed chemotherapy, the first engineered T-cell therapy for cancers in soft tissue.
“This was a pipe dream just a decade ago,” Alison Betof Warner, MD, PhD, lead author of a lifileucel study (NCT05640193), said in an interview with Medscape Medical News. “At the start of 2024, we had no approvals of these kinds of products in solid cancers. Now we have two.”
As the director of Solid Tumor Cell Therapy and leader of Stanford Medicine’s Melanoma and Cutaneous Oncology Clinical Research Group, Betof Warner has been at the forefront of developing commercial cell therapy using tumor-infiltrating lymphocytes (TILs).
“The approval of lifileucel increases confidence that we can get these therapies across the regulatory finish line and to patients,” Betof Warner said during the interview. She was not involved in the development of afamitresgene autoleucel.
‘Reverse Engineering’
In addition to her contributions to the work that led to lifileucel’s approval, Betof Warner was the lead author on the first consensus guidelines on management and best practices for tumor-infiltrating lymphocyte cell therapy.
Betof Warner began studying TILs after doing research with her mentors in immuno-oncology, Jedd D. Wolchok and Michael A. Postow. Their investigations — including one that Betof Warner coauthored — into how monoclonal antibodies and checkpoint inhibitors, such as ipilimumab or nivolumab, might extend the lives of people with advanced unresectable or metastatic melanoma inspired her to push further to find ways to minimize treatment while maximizing outcomes for patients. Betof Warner’s interest overall, she said in the interview, is in capitalizing on what can be learned about how the immune system controls cancer.
“What we know is that the immune system has the ability to kill cancer,” Betof Warner said. “Therefore we need to be thinking about how we can increase immune surveillance. How can we enhance that before a patient develops advanced cancer?
Betof Warner said that although TILs are now standard treatment in melanoma, there is about a 30% response rate compared with about a 50% response rate in immunotherapy, and the latter is easier for the patient to withstand.
“Antibodies on the frontline are better than going through a surgery and then waiting weeks to get your therapy,” Betof Warner said in the interview. “You can come into my clinic and get an antibody therapy in 30 minutes and go straight to work. TILs require patients to be in the hospital for weeks at a time and out of work for months at a time.”
In an effort to combine therapies to maximize best outcomes, a phase 3 trial (NCT05727904) is currently recruiting. The TILVANCE-301 trial will compare immunotherapy plus adoptive cell therapy vs immunotherapy alone in untreated unresectable or metastatic melanoma. Betof Warner is not a part of this study.
Cell Therapies Include CAR T Cells and TCRT
In general, adoptive T-cell therapies such as TILs involve the isolation of autologous immune cells that are removed from the body and either expanded or modified to optimize their efficacy in fighting antigens, before their transfer to the patient as a living drug by infusion.
In addition to TILs, adoptive cell therapies for antitumor therapeutics include chimeric antigen receptor (CAR) T cells and engineered T-cell receptor therapy (TCRT).
In CAR T-cell therapy and TCRT, naive T cells are harvested from the patient’s blood then engineered to target a tumor. In TIL therapy, tumor-specific T cells are taken from the patient’s tumor. Once extracted, the respective cells are expanded billions of times and then delivered back to the patient’s body, said Betof Warner.
“The main promise of this approach is to generate responses in what we know as ‘cold’ tumors, or tumors that do not have a lot of endogenous T-cell infiltration or where the T cells are not working well, to bring in tumor targeting T cells and then trigger an immune response,” Betof Warner told an audience at the American Society of Clinical Oncology (ASCO) 2024 annual meeting.
TIL patients also receive interleukin (IL)-2 infusions to further stimulate the cells. In patients being treated with TCRT, they either receive low or no IL-2, Betof Warner said in her ASCO presentation, “Adopting Cutting-Edge Cell Therapies in Melanoma,” part of the session Beyond the Tip of the Iceberg: Next-Generation Cell-Based Therapies.
Decades in the Making
The National Cancer Institute began investigating TILs in the late 1980s, with the current National Cancer Institute (NCI) surgery chief, Steven Rosenberg, MD, PhD, leading the first-ever trials that showed TILs could shrink tumors in people with advanced melanoma.
Since then, NCI staff and others have also investigated TILs beyond melanoma and additional cell therapies based on CAR T cells and TCRT for antitumor therapeutics.
“TCRs are different from CAR Ts because they go after intracellular antigens instead of extracellular antigens,” said Betof Warner. “That has appeal because many of the tumor antigens we’re looking for will be intracellular.”
Because CAR T cells only target extracellular antigens, their utility is somewhat limited. Although several CAR T-cell therapies exist for blood cancers, there currently are no approved CAR T-cell therapies for solid tumors. However, several trials of CAR T cells in gastrointestinal cancers and melanoma are ongoing, said Betof Warner, who is not a part of these studies.
“We are starting to see early-phase efficacy in pediatric gliomas,” Betof Warner said, mentioning a study conducted by colleagues at Stanford who demonstrated potential for anti-GD2 CAR T-cell therapy in deadly pediatric diffuse midline gliomas, tumors on the spine and brain.
In their study, nine out of 11 participants (median age, 15 years) showed benefit from the cell therapy, with one participant’s tumors resolving completely. The results paved the way for the FDA to grant a Regenerative Medicine Advanced Therapy designation for use of anti-GD2 CAR T cells in H3K27M-positive diffuse midline gliomas.
The investigators are now recruiting for a phase 1 trial (NCT04196413). Results of the initial study were published in Nature last month.
Another lesser-known cell therapy expected to advance at some point in the future for solid tumors is use of the body’s natural killer (NK) cells. “They’ve been known about for a long time, but they are more difficult to regulate, which is one reason why it has taken longer to make NK cell therapies,” said Betof Warner, who is not involved in the study of NK cells. “One of their advantages is that, potentially, there could be an ‘off the shelf’ NK product. They don’t necessarily have to be made with autologous cells.”
Risk-Benefit Profiles Depend on Mechanism of Action
If the corresponding TCR sequence of a tumor antigen is known, said Betof Warner, it is possible to use leukapheresis to generate naive circulating lymphocytes. Once infused, the manufactured TCRTs will activate in the body the same as native cells because the signaling is the same.
An advantage to TCRT compared with CAR T-cell therapy is that it targets intracellular proteins, which are significantly present in the tumor, Betof Warner said in her presentation at ASCO 2024. She clarified that tumors will usually be screened for the presence of this antigen before a patient is selected for treatment with that particular therapy, because not all antigens are highly expressed in every tumor.
“Furthermore, the tumor antigen has to be presented by a major histocompatibility complex, meaning there are human leukocyte antigen restrictions, which impacts patient selection,” she said.
A risk with both TCRT and CAR T-cell therapy, according to Betof Warner, is that because there are often shared antigens between tumor and normal tissues, on-target/off-tumor toxicity is a risk.
“TILs are different because they are nonengineered, at least not for antigen recognition. They are polyclonal and go after multiple targets,” Betof Warner said. “TCRs and CARs are engineered to go after one target. So, TILs have much lower rates of on-tumor/off-target effects, vs when you engineer a very high affinity receptor like a TCR or CAR.”
A good example of how this amplification of TCR affinity can lead to poor outcomes is in metastatic melanoma, said Betof Warner.
In investigations (NCI-07-C-0174 and NCI-07-C-0175) of TCRT in metastatic melanoma, for example, the researchers were targeting MART-1 or gp100, which are expressed in melanocytes.
“The problem was that these antigens are also expressed in the eyes and ears, so it caused eye inflammation and hearing loss in a number of patients because it wasn’t specific enough for the tumor,” said Betof Warner. “So, if that target is highly expressed on normal tissue, then you have a high risk.”
Promise of PRAME
Betof Warner said the most promising TCRT at present is the investigational autologous cell therapy IMA203 (NCT03688124), which targets the preferentially expressed antigen (PRAME). Although PRAME is found in many tumors, this testis antigen does not tend to express in normal, healthy adult tissues. Betof Warner is not affiliated with this study.
“It’s maybe the most exciting TCRT cell in melanoma,” Betof Warner told her audience at the ASCO 2024 meeting. Because the expression rate of PRAME in cutaneous and uveal melanoma is at or above 95% and 90%, respectively, she said “it is a really good target in melanoma.”
Phase 1a results reported in late 2023 from a first-in-human trial of IMA203 involving 13 persons with highly advanced melanoma and a median of 5.5 previous treatments showed a 50% objective response rate in the 12 evaluable results. The duration of response ranged between 2.2 and 14.7 months (median follow-up, 14 months).
The safety profile of the treatment was favorable, with no grade 3 adverse events occurring in more than 10% of the cohort, and no grade 5 adverse events at all.
Phase 1b results published in October by maker Immatics showed that in 28 heavily pretreated metastatic melanoma patients, IMA203 had a confirmed objective response rate of 54% with a median duration of response of 12.1 months, while maintaining a favorable tolerability profile.
Accelerated Approvals, Boxed Warnings
The FDA granted accelerated approvals for both lifileucel, the TIL therapy, and afamitresgene autoleucel, the TCRT.
Both were approved with boxed warnings. Lifileucel’s warning is for treatment-related mortality, prolonged severe cytopenia, severe infection, and cardiopulmonary and renal impairment. Afamitresgene autoleucel’s boxed warning is for serious or fatal cytokine release syndrome, which may be severe or life-threatening.
With these approvals, the bar is now raised on TILs and TCRTs, said Betof Warner.
The lifileucel trial studied 73 patients whose melanoma had continued to metastasize despite treatment with a programmed cell death protein (PD-1)/ programmed death-ligand (PD-L1)–targeted immune checkpoint inhibitor and a BRAF inhibitor (if appropriate based on tumor mutation status), and whose lifileucel dose was at least 7.5 billion cells (the approved dose). The cohort also received a median of six IL-2 (aldesleukin) doses.
The objective response rate was 31.5% (95% CI, 21.1-43.4), and median duration of response was not reached (lower bound of 95% CI, 4.1).
In the afamitresgene autoleucel study, 44 of 52 patients with synovial sarcoma received leukapheresis and a single infusion of afamitresgene autoleucel.
The overall response rate was 43.2% (95% CI, 28.4-59.0). The median time to response was 4.9 weeks (95% CI, 4.4-8), and the median duration of response was 6 months (lower bound of 95% CI, 4.6). Among patients who were responsive to the treatment, 45.6% and 39.0% had a duration of response of 6 months or longer and 12 months or longer, respectively.
New Hope for Patients
Betof Warner and her colleagues are now recruiting for an open-label, phase 1/2 investigation of the safety and efficacy of the TIL therapy OBX-115 in adult advanced solid tumors in melanoma or non–small cell lung cancer. The first-in-human results of a previous trial were presented at the ASCO 2024 meeting, and OBX-115 received FDA fast track designation in July.
“I think the results are really promising,” said Betof Warner. “This is an engineered TIL that does not require administering IL-2 to the patient. There were four out of the nine patients who responded to the treatment and there were no dose-limiting toxicities, no cytokine and no intracranial — all of which is excellent.”
For Betof Warner, the possibility that by using their own immune system, patients with advanced and refractory cancers could soon have a one-time treatment with a cell therapy rather than innumerable bouts of chemotherapy pushes her onward.
“The idea that we can treat cancer one time and have it not recur for years — that’s pushing the start of saying there’s a cure of cancer. That a person could move on from cancer like they move on from an infection. That is the potential of this work. We’re not there yet, but that’s where we need to think and dream big,” she said.
Betof Warner disclosed consulting/advisory roles with BluePath Solutions, Bristol-Myers Squibb/Medarex, Immatics, Instil Bio, Iovance Biotherapeutics, Lyell Immunopharma, Merck, Novartis, and Pfizer and research funding and travel expenses from Iovance Biotherapeutics.
A version of this article appeared on Medscape.com.
New Cancer Drugs: Do Patients Prefer Faster Access or Clinical Benefit?
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
Inside the Patient-Oncologist Bond: Why It’s Often So Strong
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Outpatient CAR T: Safe, Effective, Accessible
In one recent study, an industry-funded phase 2 trial, researchers found similar outcomes from outpatient and inpatient CAR T-cell therapy for relapsed/refractory large B-cell lymphoma with lisocabtagene maraleucel (Breyanzi).
Another recent study reported that outpatient treatment of B cell non-Hodgkin lymphoma with tisagenlecleucel (Kymriah) had similar efficacy to inpatient treatment. Meanwhile, a 2023 review of CAR T-cell therapy in various settings found similar outcomes in outpatient and inpatient treatment.
“The future of CAR T-cell therapy lies in balancing safety with accessibility,” said Rayne Rouce, MD, a pediatric oncologist at Texas Children’s Cancer Center in Houston, Texas, in an interview. “Expanding CAR T-cell therapy beyond large medical centers is a critical next step.”
Great Outcomes, Low Access
Since 2017, the FDA has approved six CAR T-cell therapies, which target cancer by harnessing the power of a patient’s own T cells. As an Oregon Health & Sciences University/Knight Cancer Center website explains, T cells are removed from the patient’s body, “genetically modified to make the chimeric antigen receptor, or CAR, [which] protein binds to specific proteins on the surface of cancer cells.”
Modified cells are grown and then infused back into the body, where they “multiply and may be able to destroy all the cancer cells.”
As Rouce puts it, “CAR T-cells have revolutionized the treatment of relapsed or refractory blood cancers.” One or more of the therapies have been approved to treat types of lymphoblastic leukemia, B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and multiple myeloma.
A 2023 review of clinical trial data reported complete response rates of 40%-54% in aggressive B-cell lymphoma, 67% in mantle cell lymphoma, and 69%-74% in indolent B cell lymphoma.
“Commercialization of CAR T-cell therapy brought hope that access would expand beyond the major academic medical centers with the highly specialized infrastructure and advanced laboratories required to manufacture and ultimately treat patients,” Rouce said. “However, it quickly became clear that patients who are underinsured or uninsured — or who live outside the network of the well-resourced institutions that house these therapies — are still unable to access these potentially life-saving therapies.”
A 2024 report estimated the cost of CAR T-cell therapy as $700,000-$1 million and said only a small percentage of those who could benefit from the treatment actually get it. For example, an estimated 10,000 patients with diffuse large B-cell lymphoma alone could benefit from CAR T therapy annually, but a survey of 200 US healthcare centers in 2021 found that 1900 procedures were performed overall for all indications.
Distance to Treatment Is a Major Obstacle
Even if patients have insurance plans willing to cover CAR T-cell therapy, they may not be able get care. While more than 150 US centers are certified to administer the therapy, “distance to major medical centers with CAR T capabilities is a major obstacle,” Yuliya Linhares, MD, chief of lymphoma at Miami Cancer Institute in Miami, Florida, said in an interview.
“I have had patients who chose to not proceed with CAR T therapy due to inability to travel the distance to the medical center for pre-CAR T appointments and assessments and a lack of caretakers who are available to stay nearby,” Linhares said.
Indeed, the challenges facing patients in rural and underserved urban areas can be overwhelming, Hoda Badr, PhD, professor of medicine at Baylor College of Medicine in Houston, Texas, said in an interview.
“They must take time off work, arrange accommodations near treatment sites, and manage travel costs, all of which strain limited financial resources. The inability to afford these additional expenses can lead to delays in receiving care or patients forgoing the treatment altogether,” Badr said. She added that “the psychological and social burden of being away from family and community support systems during treatment can intensify the stress of an already difficult situation.”
A statistic tells the story of the urban/community divide. CAR T-cell therapy administration at academic centers after leukapheresis — the separation and collection of white blood cells — is reported to be at around 90%, while it’s only 47% in community-based practices that have to refer patients elsewhere, Linhares noted.
Researchers Explore CAR T-Cell Therapy in the Community
Linhares is lead author of the phase 2 trial that explored administration of lisocabtagene maraleucel in 82 patients with relapsed/refractory large B-cell lymphoma. The findings were published Sept. 30 in Blood Advances.
The OUTREACH trial, funded by Juno/Bristol-Myers Squibb, treated patients in the third line and beyond at community medical centers (outpatient-monitored, 70%; inpatient-monitored, 30%). The trial didn’t require facilities to be certified by the Foundation for the Accreditation of Cellular Therapy (FACT); all had to be non-tertiary cancer centers that weren’t associated with a university. In order to administer therapy on the outpatient basis, the centers had to have phase 1 or hematopoietic stem cell transplant capabilities.
As Linhares explained, 72% of participating centers hadn’t provided CAR T-cell therapy before, and 44% did not have FACT accreditation. “About 32% of patients received CAR T at CAR T naive sites, while 70% of patients received CAR T as outpatients. Investigators had to decide whether patients qualified for the outpatient observation or had to be admitted for the inpatient observation,” she noted.
Community Outcomes Were Comparable to Major Trial
As for the results, grade 3 or higher adverse events occurred at a similar frequency among outpatients and inpatients at 74% and 76%, Linhares said. There were no grade 5 adverse events, and 25% of patients treated as outpatients were never hospitalized.
Response rates were similar to those in the major TRANSCEND trial with the objective response rates rate of 80% and complete response rates of 54%.
“Overall,” Linhares said, “our study demonstrated that with the availability of standard operating procedures, specially trained staff and a multidisciplinary team trained in CAR T toxicity management, inpatient and outpatient CAR T administration is feasible at specialized community medical centers.”
In 2023, another study examined patients with B-cell non-Hodgkin lymphoma who were treated on an outpatient basis with tisagenlecleucel. Researchers reported that outpatient therapy was “feasible and associated with similar efficacy outcomes as inpatient treatment.”
And a 2023 systematic literature review identified 11 studies that reported outpatient vs inpatient outcomes in CAR T-cell therapy and found “comparable response rates (80-82% in outpatient and 72-80% in inpatient).” Costs were cheaper in the outpatient setting.
Research findings like these are good news, Baylor College of Medicine’s Badr said. “Outpatient administration could help to scale the availability of this therapy to a broader range of healthcare settings, including those serving underserved populations. Findings indicate promising safety profiles, which is encouraging for expanding access.”
Not Every Patient Can Tolerate Outpatient Care
Linhares noted that the patients who received outpatient care in the lisocabtagene maraleucel study were in better shape than those in the inpatient group. Those selected for inpatient care had “higher disease risk characteristics, including high grade B cell lymphoma histology, higher disease burden, and having received bridging therapy. This points to the fact that the investigators properly selected patients who were at a higher risk of complications for inpatient observation. Additionally, some patients stayed as inpatient due to social factors, which increases length of stay independently of disease characteristics.”
Specifically, reasons for inpatient monitoring were disease characteristics (48%) including tumor burden and risk of adverse events; psychosocial factors (32%) including lack of caregiver support or transportation; COVID-19 precautions (8%); pre-infusion adverse events (8%) of fever and vasovagal reaction; and principal investigator decision (4%) due to limited hospital experience with CAR T-cell therapy.
Texas Children’s Cancer Center’s Rouce said “certain patients, particularly those with higher risk for complications or those who require intensive monitoring, may not be suited for outpatient CAR T-cell therapy. This may be due to other comorbidities or baseline factors known to predispose to CAR T-related toxicities. However, evidence-based risk mitigation algorithms may still allow closely monitored outpatient treatment, with recognition that hospital admission for incipient side effects may be necessary.”
What’s Next for Access to Therapy?
Rouce noted that her institution, like many others, is offering CAR T-cell therapy on an outpatient basis. “Additionally, continued scientific innovation, such as immediately available, off-the-shelf cell therapies and inducible safety switches, will ultimately improve access,” she said.
Linhares noted a recent advance and highlighted research that’s now in progress. “CAR Ts now have an indication as a second-line therapy in relapsed/refractory large B-cell lymphoma, and there are ongoing clinical trials that will potentially move CAR Ts into the first line,” she said. “Some trials are exploring allogeneic, readily available off-the-shelf CAR T for the treatment of minimal residual disease positive large B-cell lymphoma after completion of first-line therapy.”
These potential advances “are increasing the need for CAR T-capable medical centers,” Linhares noted. “More and more medical centers with expert hematology teams are becoming CAR T-certified, with more patients having access to CAR T.”
Still, she said, “I don’t think access is nearly as good as it should be. Many patients in rural areas are still unable to get this life-saving treatment. “However, “it is very possible that other novel targeted therapies, such as bispecific antibodies, will be used in place of CAR T in areas with poor CAR T access. Bispecific antibody efficacy in various B cell lymphoma histologies are being currently explored.”
Rouce discloses relationships with Novartis and Pfizer. Linhares reports ties with Kyowa Kirin, AbbVie, ADC, BeiGene, Genentech, Gilead, GlaxoSmithKline, Seagen, and TG. Badr has no disclosures.
A version of this article appeared on Medscape.com.
In one recent study, an industry-funded phase 2 trial, researchers found similar outcomes from outpatient and inpatient CAR T-cell therapy for relapsed/refractory large B-cell lymphoma with lisocabtagene maraleucel (Breyanzi).
Another recent study reported that outpatient treatment of B cell non-Hodgkin lymphoma with tisagenlecleucel (Kymriah) had similar efficacy to inpatient treatment. Meanwhile, a 2023 review of CAR T-cell therapy in various settings found similar outcomes in outpatient and inpatient treatment.
“The future of CAR T-cell therapy lies in balancing safety with accessibility,” said Rayne Rouce, MD, a pediatric oncologist at Texas Children’s Cancer Center in Houston, Texas, in an interview. “Expanding CAR T-cell therapy beyond large medical centers is a critical next step.”
Great Outcomes, Low Access
Since 2017, the FDA has approved six CAR T-cell therapies, which target cancer by harnessing the power of a patient’s own T cells. As an Oregon Health & Sciences University/Knight Cancer Center website explains, T cells are removed from the patient’s body, “genetically modified to make the chimeric antigen receptor, or CAR, [which] protein binds to specific proteins on the surface of cancer cells.”
Modified cells are grown and then infused back into the body, where they “multiply and may be able to destroy all the cancer cells.”
As Rouce puts it, “CAR T-cells have revolutionized the treatment of relapsed or refractory blood cancers.” One or more of the therapies have been approved to treat types of lymphoblastic leukemia, B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and multiple myeloma.
A 2023 review of clinical trial data reported complete response rates of 40%-54% in aggressive B-cell lymphoma, 67% in mantle cell lymphoma, and 69%-74% in indolent B cell lymphoma.
“Commercialization of CAR T-cell therapy brought hope that access would expand beyond the major academic medical centers with the highly specialized infrastructure and advanced laboratories required to manufacture and ultimately treat patients,” Rouce said. “However, it quickly became clear that patients who are underinsured or uninsured — or who live outside the network of the well-resourced institutions that house these therapies — are still unable to access these potentially life-saving therapies.”
A 2024 report estimated the cost of CAR T-cell therapy as $700,000-$1 million and said only a small percentage of those who could benefit from the treatment actually get it. For example, an estimated 10,000 patients with diffuse large B-cell lymphoma alone could benefit from CAR T therapy annually, but a survey of 200 US healthcare centers in 2021 found that 1900 procedures were performed overall for all indications.
Distance to Treatment Is a Major Obstacle
Even if patients have insurance plans willing to cover CAR T-cell therapy, they may not be able get care. While more than 150 US centers are certified to administer the therapy, “distance to major medical centers with CAR T capabilities is a major obstacle,” Yuliya Linhares, MD, chief of lymphoma at Miami Cancer Institute in Miami, Florida, said in an interview.
“I have had patients who chose to not proceed with CAR T therapy due to inability to travel the distance to the medical center for pre-CAR T appointments and assessments and a lack of caretakers who are available to stay nearby,” Linhares said.
Indeed, the challenges facing patients in rural and underserved urban areas can be overwhelming, Hoda Badr, PhD, professor of medicine at Baylor College of Medicine in Houston, Texas, said in an interview.
“They must take time off work, arrange accommodations near treatment sites, and manage travel costs, all of which strain limited financial resources. The inability to afford these additional expenses can lead to delays in receiving care or patients forgoing the treatment altogether,” Badr said. She added that “the psychological and social burden of being away from family and community support systems during treatment can intensify the stress of an already difficult situation.”
A statistic tells the story of the urban/community divide. CAR T-cell therapy administration at academic centers after leukapheresis — the separation and collection of white blood cells — is reported to be at around 90%, while it’s only 47% in community-based practices that have to refer patients elsewhere, Linhares noted.
Researchers Explore CAR T-Cell Therapy in the Community
Linhares is lead author of the phase 2 trial that explored administration of lisocabtagene maraleucel in 82 patients with relapsed/refractory large B-cell lymphoma. The findings were published Sept. 30 in Blood Advances.
The OUTREACH trial, funded by Juno/Bristol-Myers Squibb, treated patients in the third line and beyond at community medical centers (outpatient-monitored, 70%; inpatient-monitored, 30%). The trial didn’t require facilities to be certified by the Foundation for the Accreditation of Cellular Therapy (FACT); all had to be non-tertiary cancer centers that weren’t associated with a university. In order to administer therapy on the outpatient basis, the centers had to have phase 1 or hematopoietic stem cell transplant capabilities.
As Linhares explained, 72% of participating centers hadn’t provided CAR T-cell therapy before, and 44% did not have FACT accreditation. “About 32% of patients received CAR T at CAR T naive sites, while 70% of patients received CAR T as outpatients. Investigators had to decide whether patients qualified for the outpatient observation or had to be admitted for the inpatient observation,” she noted.
Community Outcomes Were Comparable to Major Trial
As for the results, grade 3 or higher adverse events occurred at a similar frequency among outpatients and inpatients at 74% and 76%, Linhares said. There were no grade 5 adverse events, and 25% of patients treated as outpatients were never hospitalized.
Response rates were similar to those in the major TRANSCEND trial with the objective response rates rate of 80% and complete response rates of 54%.
“Overall,” Linhares said, “our study demonstrated that with the availability of standard operating procedures, specially trained staff and a multidisciplinary team trained in CAR T toxicity management, inpatient and outpatient CAR T administration is feasible at specialized community medical centers.”
In 2023, another study examined patients with B-cell non-Hodgkin lymphoma who were treated on an outpatient basis with tisagenlecleucel. Researchers reported that outpatient therapy was “feasible and associated with similar efficacy outcomes as inpatient treatment.”
And a 2023 systematic literature review identified 11 studies that reported outpatient vs inpatient outcomes in CAR T-cell therapy and found “comparable response rates (80-82% in outpatient and 72-80% in inpatient).” Costs were cheaper in the outpatient setting.
Research findings like these are good news, Baylor College of Medicine’s Badr said. “Outpatient administration could help to scale the availability of this therapy to a broader range of healthcare settings, including those serving underserved populations. Findings indicate promising safety profiles, which is encouraging for expanding access.”
Not Every Patient Can Tolerate Outpatient Care
Linhares noted that the patients who received outpatient care in the lisocabtagene maraleucel study were in better shape than those in the inpatient group. Those selected for inpatient care had “higher disease risk characteristics, including high grade B cell lymphoma histology, higher disease burden, and having received bridging therapy. This points to the fact that the investigators properly selected patients who were at a higher risk of complications for inpatient observation. Additionally, some patients stayed as inpatient due to social factors, which increases length of stay independently of disease characteristics.”
Specifically, reasons for inpatient monitoring were disease characteristics (48%) including tumor burden and risk of adverse events; psychosocial factors (32%) including lack of caregiver support or transportation; COVID-19 precautions (8%); pre-infusion adverse events (8%) of fever and vasovagal reaction; and principal investigator decision (4%) due to limited hospital experience with CAR T-cell therapy.
Texas Children’s Cancer Center’s Rouce said “certain patients, particularly those with higher risk for complications or those who require intensive monitoring, may not be suited for outpatient CAR T-cell therapy. This may be due to other comorbidities or baseline factors known to predispose to CAR T-related toxicities. However, evidence-based risk mitigation algorithms may still allow closely monitored outpatient treatment, with recognition that hospital admission for incipient side effects may be necessary.”
What’s Next for Access to Therapy?
Rouce noted that her institution, like many others, is offering CAR T-cell therapy on an outpatient basis. “Additionally, continued scientific innovation, such as immediately available, off-the-shelf cell therapies and inducible safety switches, will ultimately improve access,” she said.
Linhares noted a recent advance and highlighted research that’s now in progress. “CAR Ts now have an indication as a second-line therapy in relapsed/refractory large B-cell lymphoma, and there are ongoing clinical trials that will potentially move CAR Ts into the first line,” she said. “Some trials are exploring allogeneic, readily available off-the-shelf CAR T for the treatment of minimal residual disease positive large B-cell lymphoma after completion of first-line therapy.”
These potential advances “are increasing the need for CAR T-capable medical centers,” Linhares noted. “More and more medical centers with expert hematology teams are becoming CAR T-certified, with more patients having access to CAR T.”
Still, she said, “I don’t think access is nearly as good as it should be. Many patients in rural areas are still unable to get this life-saving treatment. “However, “it is very possible that other novel targeted therapies, such as bispecific antibodies, will be used in place of CAR T in areas with poor CAR T access. Bispecific antibody efficacy in various B cell lymphoma histologies are being currently explored.”
Rouce discloses relationships with Novartis and Pfizer. Linhares reports ties with Kyowa Kirin, AbbVie, ADC, BeiGene, Genentech, Gilead, GlaxoSmithKline, Seagen, and TG. Badr has no disclosures.
A version of this article appeared on Medscape.com.
In one recent study, an industry-funded phase 2 trial, researchers found similar outcomes from outpatient and inpatient CAR T-cell therapy for relapsed/refractory large B-cell lymphoma with lisocabtagene maraleucel (Breyanzi).
Another recent study reported that outpatient treatment of B cell non-Hodgkin lymphoma with tisagenlecleucel (Kymriah) had similar efficacy to inpatient treatment. Meanwhile, a 2023 review of CAR T-cell therapy in various settings found similar outcomes in outpatient and inpatient treatment.
“The future of CAR T-cell therapy lies in balancing safety with accessibility,” said Rayne Rouce, MD, a pediatric oncologist at Texas Children’s Cancer Center in Houston, Texas, in an interview. “Expanding CAR T-cell therapy beyond large medical centers is a critical next step.”
Great Outcomes, Low Access
Since 2017, the FDA has approved six CAR T-cell therapies, which target cancer by harnessing the power of a patient’s own T cells. As an Oregon Health & Sciences University/Knight Cancer Center website explains, T cells are removed from the patient’s body, “genetically modified to make the chimeric antigen receptor, or CAR, [which] protein binds to specific proteins on the surface of cancer cells.”
Modified cells are grown and then infused back into the body, where they “multiply and may be able to destroy all the cancer cells.”
As Rouce puts it, “CAR T-cells have revolutionized the treatment of relapsed or refractory blood cancers.” One or more of the therapies have been approved to treat types of lymphoblastic leukemia, B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and multiple myeloma.
A 2023 review of clinical trial data reported complete response rates of 40%-54% in aggressive B-cell lymphoma, 67% in mantle cell lymphoma, and 69%-74% in indolent B cell lymphoma.
“Commercialization of CAR T-cell therapy brought hope that access would expand beyond the major academic medical centers with the highly specialized infrastructure and advanced laboratories required to manufacture and ultimately treat patients,” Rouce said. “However, it quickly became clear that patients who are underinsured or uninsured — or who live outside the network of the well-resourced institutions that house these therapies — are still unable to access these potentially life-saving therapies.”
A 2024 report estimated the cost of CAR T-cell therapy as $700,000-$1 million and said only a small percentage of those who could benefit from the treatment actually get it. For example, an estimated 10,000 patients with diffuse large B-cell lymphoma alone could benefit from CAR T therapy annually, but a survey of 200 US healthcare centers in 2021 found that 1900 procedures were performed overall for all indications.
Distance to Treatment Is a Major Obstacle
Even if patients have insurance plans willing to cover CAR T-cell therapy, they may not be able get care. While more than 150 US centers are certified to administer the therapy, “distance to major medical centers with CAR T capabilities is a major obstacle,” Yuliya Linhares, MD, chief of lymphoma at Miami Cancer Institute in Miami, Florida, said in an interview.
“I have had patients who chose to not proceed with CAR T therapy due to inability to travel the distance to the medical center for pre-CAR T appointments and assessments and a lack of caretakers who are available to stay nearby,” Linhares said.
Indeed, the challenges facing patients in rural and underserved urban areas can be overwhelming, Hoda Badr, PhD, professor of medicine at Baylor College of Medicine in Houston, Texas, said in an interview.
“They must take time off work, arrange accommodations near treatment sites, and manage travel costs, all of which strain limited financial resources. The inability to afford these additional expenses can lead to delays in receiving care or patients forgoing the treatment altogether,” Badr said. She added that “the psychological and social burden of being away from family and community support systems during treatment can intensify the stress of an already difficult situation.”
A statistic tells the story of the urban/community divide. CAR T-cell therapy administration at academic centers after leukapheresis — the separation and collection of white blood cells — is reported to be at around 90%, while it’s only 47% in community-based practices that have to refer patients elsewhere, Linhares noted.
Researchers Explore CAR T-Cell Therapy in the Community
Linhares is lead author of the phase 2 trial that explored administration of lisocabtagene maraleucel in 82 patients with relapsed/refractory large B-cell lymphoma. The findings were published Sept. 30 in Blood Advances.
The OUTREACH trial, funded by Juno/Bristol-Myers Squibb, treated patients in the third line and beyond at community medical centers (outpatient-monitored, 70%; inpatient-monitored, 30%). The trial didn’t require facilities to be certified by the Foundation for the Accreditation of Cellular Therapy (FACT); all had to be non-tertiary cancer centers that weren’t associated with a university. In order to administer therapy on the outpatient basis, the centers had to have phase 1 or hematopoietic stem cell transplant capabilities.
As Linhares explained, 72% of participating centers hadn’t provided CAR T-cell therapy before, and 44% did not have FACT accreditation. “About 32% of patients received CAR T at CAR T naive sites, while 70% of patients received CAR T as outpatients. Investigators had to decide whether patients qualified for the outpatient observation or had to be admitted for the inpatient observation,” she noted.
Community Outcomes Were Comparable to Major Trial
As for the results, grade 3 or higher adverse events occurred at a similar frequency among outpatients and inpatients at 74% and 76%, Linhares said. There were no grade 5 adverse events, and 25% of patients treated as outpatients were never hospitalized.
Response rates were similar to those in the major TRANSCEND trial with the objective response rates rate of 80% and complete response rates of 54%.
“Overall,” Linhares said, “our study demonstrated that with the availability of standard operating procedures, specially trained staff and a multidisciplinary team trained in CAR T toxicity management, inpatient and outpatient CAR T administration is feasible at specialized community medical centers.”
In 2023, another study examined patients with B-cell non-Hodgkin lymphoma who were treated on an outpatient basis with tisagenlecleucel. Researchers reported that outpatient therapy was “feasible and associated with similar efficacy outcomes as inpatient treatment.”
And a 2023 systematic literature review identified 11 studies that reported outpatient vs inpatient outcomes in CAR T-cell therapy and found “comparable response rates (80-82% in outpatient and 72-80% in inpatient).” Costs were cheaper in the outpatient setting.
Research findings like these are good news, Baylor College of Medicine’s Badr said. “Outpatient administration could help to scale the availability of this therapy to a broader range of healthcare settings, including those serving underserved populations. Findings indicate promising safety profiles, which is encouraging for expanding access.”
Not Every Patient Can Tolerate Outpatient Care
Linhares noted that the patients who received outpatient care in the lisocabtagene maraleucel study were in better shape than those in the inpatient group. Those selected for inpatient care had “higher disease risk characteristics, including high grade B cell lymphoma histology, higher disease burden, and having received bridging therapy. This points to the fact that the investigators properly selected patients who were at a higher risk of complications for inpatient observation. Additionally, some patients stayed as inpatient due to social factors, which increases length of stay independently of disease characteristics.”
Specifically, reasons for inpatient monitoring were disease characteristics (48%) including tumor burden and risk of adverse events; psychosocial factors (32%) including lack of caregiver support or transportation; COVID-19 precautions (8%); pre-infusion adverse events (8%) of fever and vasovagal reaction; and principal investigator decision (4%) due to limited hospital experience with CAR T-cell therapy.
Texas Children’s Cancer Center’s Rouce said “certain patients, particularly those with higher risk for complications or those who require intensive monitoring, may not be suited for outpatient CAR T-cell therapy. This may be due to other comorbidities or baseline factors known to predispose to CAR T-related toxicities. However, evidence-based risk mitigation algorithms may still allow closely monitored outpatient treatment, with recognition that hospital admission for incipient side effects may be necessary.”
What’s Next for Access to Therapy?
Rouce noted that her institution, like many others, is offering CAR T-cell therapy on an outpatient basis. “Additionally, continued scientific innovation, such as immediately available, off-the-shelf cell therapies and inducible safety switches, will ultimately improve access,” she said.
Linhares noted a recent advance and highlighted research that’s now in progress. “CAR Ts now have an indication as a second-line therapy in relapsed/refractory large B-cell lymphoma, and there are ongoing clinical trials that will potentially move CAR Ts into the first line,” she said. “Some trials are exploring allogeneic, readily available off-the-shelf CAR T for the treatment of minimal residual disease positive large B-cell lymphoma after completion of first-line therapy.”
These potential advances “are increasing the need for CAR T-capable medical centers,” Linhares noted. “More and more medical centers with expert hematology teams are becoming CAR T-certified, with more patients having access to CAR T.”
Still, she said, “I don’t think access is nearly as good as it should be. Many patients in rural areas are still unable to get this life-saving treatment. “However, “it is very possible that other novel targeted therapies, such as bispecific antibodies, will be used in place of CAR T in areas with poor CAR T access. Bispecific antibody efficacy in various B cell lymphoma histologies are being currently explored.”
Rouce discloses relationships with Novartis and Pfizer. Linhares reports ties with Kyowa Kirin, AbbVie, ADC, BeiGene, Genentech, Gilead, GlaxoSmithKline, Seagen, and TG. Badr has no disclosures.
A version of this article appeared on Medscape.com.