User login
HM Group Economics 101
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
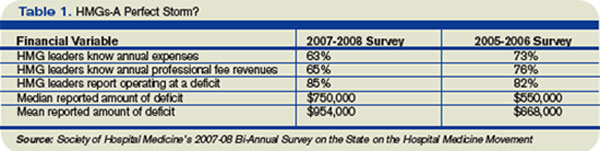
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
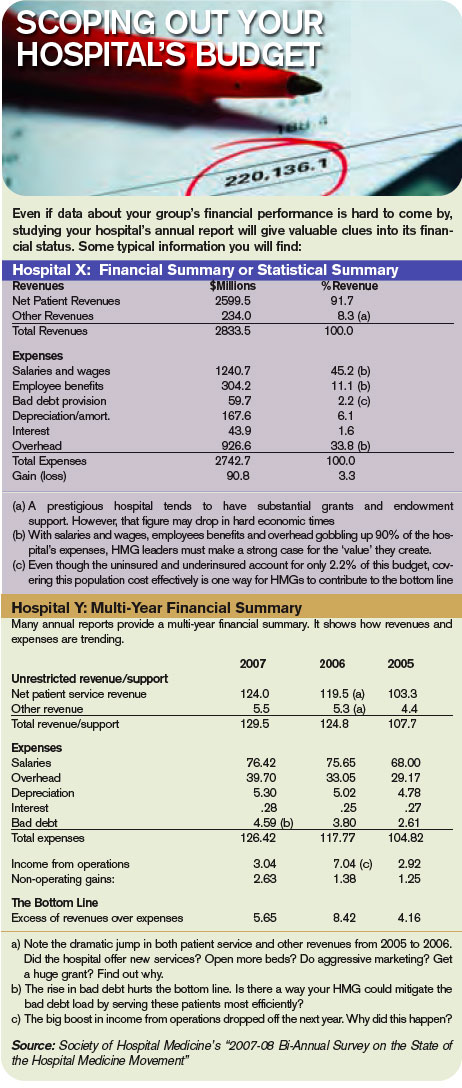
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
Navigate the Winds of Change
When a Catholic group moved to buy Lutheran Medical Center in Wheat Ridge, Colo., just outside of Denver, hospitalist Steven Krebs, MD, had strong objections. Sisters of Charity of Leavenworth Health System already was part-owner of the 400-bed medical center. As the sole owner, it would require the hospital to follow Catholic rules regarding end-of-life care and reproductive health, meaning some medical services would be prohibited.
“It’s really the last hospital before you go into the mountains. There’s no real hospital facility until Vail, almost 100 miles up the road,” Dr. Krebs says. Patients who wanted a tubal ligation, an emergency contraceptive, or other medical services typically not offered in a Catholic hospital would have to travel to receive them—or not receive them at all.
After negotiations failed to produce a satisfactory outcome, Dr. Krebs took the drastic step of becoming part of a lawsuit to stop the sale. In May 2008, Colorado’s governor signed into law a bill that allows the state attorney general to review how the sale of a nonprofit hospital affects patient care. If he believes care will be affected, the attorney general may ask for more information from the sponsors of the transaction or require a public hearing be held before determining whether to approve the transaction.
The sale is pending.
—Steven Krebs, MD, Lutheran Medical Center, Wheat Ridge, Colo.
In an ideal world, patients would get the same excellent care, no matter who owns or runs a hospital. A sale or a change in executive leadership wouldn’t alter the tone of a hospital. As the Colorado case shows, ownership and leadership matter.
Hospitalists who have been through a hospital sale or a change of leadership say it’s possible to influence the process from within, to benefit the hospital, the patients, and the hospitalists themselves, often through simple negotiation and clear communication.
Become a Resource, Partner for Leadership
Established hospitalist programs are in an especially strong bargaining position. “We have a track record we can point to,” says Brian Bossard, MD, director of Inpatient Physician Associates, whose medical center, BryanLGH in Lincoln, Neb., went through a search for a new CEO in early 2008. That track record includes a strong relationship between the hospitalist program and hospital administrators.
When the medical center considered formalizing its hospitalist program in 2002, for example, Dr. Bossard went with administrators to regional and national meetings. “Instead of having competing perspectives on what the costs of the program should be and what the value equation is, we came from a similar perspective,” he explains. “Since that time, that trust has been maintained by coming through on promises, whether it’s being able to manage the volumes or get good results.”
A strong foundation can lead to a well-integrated hospitalist program and positive relationships with the CEO and COO, Dr. Bossard adds. Though he considers the change in CEOs at BryanLGH “a little unsettling,” he says he’s confident his hospitalist program has the support of the hospital community. Perhaps as evidence of that, the hospital hiring committee considered input from hospitalists before making a final selection.
Dr. Bossard plans to present to the new CEO the hospitalist program’s accomplishments, goals, and potential challenges early on, so the CEO can get to know the program. “The [hospitalists] really should try to position themselves, in my view anyway, as sort of an insider with useful information, a leader they can go to to ask what’s really going on in the hospital,” Dr. Bossard says. “Hospitalist programs will grow so rapidly within hospital systems, taking care of 50% to 75%, to sometimes close to 100% of patients. They’re really great sources of information.”
Keep Lines of Communication Open
Strong relationships with hospital leadership creates a stable environment where hospitalists feel valued. It also helps ensure a program can weather almost any storm, says Julia Wright, MD, University of Wisconsin Hospital and Clinics hospitalist director and the director of hospital medicine at UW School of Medicine and Public Health in Madison, Wis. “Once you get to the point where you have value, a mission, a system of operations, and a delivery-of-care plan, then that might translate into some personal ownership in the program that could withstand a change in administration,” she says.
Dr. Wright, who took a five-person hospitalist program and has enlarged it to 13, says she understands the value of communication with hospital executives. She also has a game plan, should executive leadership at her hospital change. “The first thing I would do is sit down and discuss what my mission is,” she says. “Continued dialogue after that is really important.” The dialogue would include meeting with hospital administration regularly, as well as talking about objectives and ways to meet them. “I just know what’s worked to keep our program on track,” she says, “and it’s been very successful.”
Leverage a Change in Administration
At Meriter Hospital in Madison, Wis., Cate Ranheim, MD, director of the hospitalist program, found a change in administration actually benefitted her hospitalists. “Our previous administration was essentially a chief operating officer (COO) who approved—or more often—refused, every request for even the simplest things, from sinks to filing cabinets to call rooms,” she explains. “The former CEO was here for 30-plus years, as was the COO, and was virtually invisible within the institution.”
The COO was a strong advocate for the hospitalist group, but Dr. Ranheim says she still had to go through tough negotiations to get what the group needed. When a new CEO came in and announced an open-door policy, Dr. Ranheim jumped at the opportunity to be heard. “Whenever I need something for the group, I go directly to him, and I have never been refused anything because he knows I am not game-playing or negotiating,” she says. “If I say the group needs something, it really does.”
Dr. Ranheim’s experience actually is fairly common. Executive leadership or ownership changes often create “a window of opportunity to further some agendas,” Dr. Wright points out. “If there’s a group that’s been saying, ‘We really want to start this new initiative and just haven’t been able to get there yet,’ this might be the time to do that.”
Whether the transition is a good time can depend on how comfortable a hospitalist group feels with the new executive. “In my own experience, it’s all about personality,” Dr. Ranheim says. “As hospitalist director, I instantly trusted my new CEO, and that trust has never been violated in either direction.” She adds, “Of course, I still do get everything in writing.”
Pay Attention to National Standards
Whether hospitalists can bring about improvements during a hospital change of ownership or leadership isn’t just based on how much the program improves care or reduces costs at the facility. National standards also should come into play, Dr. Bossard says. “The hospitalist negotiator and the administration need to be comfortable with their command of what the data shows and what their standards are,” he cautions.
At Lutheran Medical Center in Colorado, Dr. Krebs felt strongly the change in ownership would cause patients hardship and go against national standards. Though both sides attempted to collect feedback and reach a compromise, neither came up with a solution that satisfied Dr. Krebs. He felt he had no choice but to seek legal action. (Exempla Healthcare, which manages the medical center, also sued to stop the sale).
“If the parent organization of Jehovah’s Witnesses took over a hospital and declared that no one could have a transfusion, no one would allow that,” Dr. Krebs argues. “If I have a patient that’s a Jehovah’s Witness, and they say, ‘I won’t have a transfusion,’ that’s very important. However, that person doesn’t have the right to impose their belief system on someone else.”
Dr. Krebs says he has the support of his medical community and his hospital, largely because, as a hospitalist, he’s been involved with the community all along. He says any hospitalist who hopes to influence standards of care should get involved, too, by sitting on or chairing a hospital committee, becoming an integral part of the medical community early on, and, above all, providing great care.
“If you leverage the facility you’re in to the Nth degree for income, you’re not going to be viewed as a partner, but as a vendor commodity, and you’ll have very little influence,” Dr. Krebs says. “There’s a benefit to being a hospitalist. You are in a unique position to exert influence on the hospital, because in some ways, both parties need the other to do well.” TH
When a Catholic group moved to buy Lutheran Medical Center in Wheat Ridge, Colo., just outside of Denver, hospitalist Steven Krebs, MD, had strong objections. Sisters of Charity of Leavenworth Health System already was part-owner of the 400-bed medical center. As the sole owner, it would require the hospital to follow Catholic rules regarding end-of-life care and reproductive health, meaning some medical services would be prohibited.
“It’s really the last hospital before you go into the mountains. There’s no real hospital facility until Vail, almost 100 miles up the road,” Dr. Krebs says. Patients who wanted a tubal ligation, an emergency contraceptive, or other medical services typically not offered in a Catholic hospital would have to travel to receive them—or not receive them at all.
After negotiations failed to produce a satisfactory outcome, Dr. Krebs took the drastic step of becoming part of a lawsuit to stop the sale. In May 2008, Colorado’s governor signed into law a bill that allows the state attorney general to review how the sale of a nonprofit hospital affects patient care. If he believes care will be affected, the attorney general may ask for more information from the sponsors of the transaction or require a public hearing be held before determining whether to approve the transaction.
The sale is pending.
—Steven Krebs, MD, Lutheran Medical Center, Wheat Ridge, Colo.
In an ideal world, patients would get the same excellent care, no matter who owns or runs a hospital. A sale or a change in executive leadership wouldn’t alter the tone of a hospital. As the Colorado case shows, ownership and leadership matter.
Hospitalists who have been through a hospital sale or a change of leadership say it’s possible to influence the process from within, to benefit the hospital, the patients, and the hospitalists themselves, often through simple negotiation and clear communication.
Become a Resource, Partner for Leadership
Established hospitalist programs are in an especially strong bargaining position. “We have a track record we can point to,” says Brian Bossard, MD, director of Inpatient Physician Associates, whose medical center, BryanLGH in Lincoln, Neb., went through a search for a new CEO in early 2008. That track record includes a strong relationship between the hospitalist program and hospital administrators.
When the medical center considered formalizing its hospitalist program in 2002, for example, Dr. Bossard went with administrators to regional and national meetings. “Instead of having competing perspectives on what the costs of the program should be and what the value equation is, we came from a similar perspective,” he explains. “Since that time, that trust has been maintained by coming through on promises, whether it’s being able to manage the volumes or get good results.”
A strong foundation can lead to a well-integrated hospitalist program and positive relationships with the CEO and COO, Dr. Bossard adds. Though he considers the change in CEOs at BryanLGH “a little unsettling,” he says he’s confident his hospitalist program has the support of the hospital community. Perhaps as evidence of that, the hospital hiring committee considered input from hospitalists before making a final selection.
Dr. Bossard plans to present to the new CEO the hospitalist program’s accomplishments, goals, and potential challenges early on, so the CEO can get to know the program. “The [hospitalists] really should try to position themselves, in my view anyway, as sort of an insider with useful information, a leader they can go to to ask what’s really going on in the hospital,” Dr. Bossard says. “Hospitalist programs will grow so rapidly within hospital systems, taking care of 50% to 75%, to sometimes close to 100% of patients. They’re really great sources of information.”
Keep Lines of Communication Open
Strong relationships with hospital leadership creates a stable environment where hospitalists feel valued. It also helps ensure a program can weather almost any storm, says Julia Wright, MD, University of Wisconsin Hospital and Clinics hospitalist director and the director of hospital medicine at UW School of Medicine and Public Health in Madison, Wis. “Once you get to the point where you have value, a mission, a system of operations, and a delivery-of-care plan, then that might translate into some personal ownership in the program that could withstand a change in administration,” she says.
Dr. Wright, who took a five-person hospitalist program and has enlarged it to 13, says she understands the value of communication with hospital executives. She also has a game plan, should executive leadership at her hospital change. “The first thing I would do is sit down and discuss what my mission is,” she says. “Continued dialogue after that is really important.” The dialogue would include meeting with hospital administration regularly, as well as talking about objectives and ways to meet them. “I just know what’s worked to keep our program on track,” she says, “and it’s been very successful.”
Leverage a Change in Administration
At Meriter Hospital in Madison, Wis., Cate Ranheim, MD, director of the hospitalist program, found a change in administration actually benefitted her hospitalists. “Our previous administration was essentially a chief operating officer (COO) who approved—or more often—refused, every request for even the simplest things, from sinks to filing cabinets to call rooms,” she explains. “The former CEO was here for 30-plus years, as was the COO, and was virtually invisible within the institution.”
The COO was a strong advocate for the hospitalist group, but Dr. Ranheim says she still had to go through tough negotiations to get what the group needed. When a new CEO came in and announced an open-door policy, Dr. Ranheim jumped at the opportunity to be heard. “Whenever I need something for the group, I go directly to him, and I have never been refused anything because he knows I am not game-playing or negotiating,” she says. “If I say the group needs something, it really does.”
Dr. Ranheim’s experience actually is fairly common. Executive leadership or ownership changes often create “a window of opportunity to further some agendas,” Dr. Wright points out. “If there’s a group that’s been saying, ‘We really want to start this new initiative and just haven’t been able to get there yet,’ this might be the time to do that.”
Whether the transition is a good time can depend on how comfortable a hospitalist group feels with the new executive. “In my own experience, it’s all about personality,” Dr. Ranheim says. “As hospitalist director, I instantly trusted my new CEO, and that trust has never been violated in either direction.” She adds, “Of course, I still do get everything in writing.”
Pay Attention to National Standards
Whether hospitalists can bring about improvements during a hospital change of ownership or leadership isn’t just based on how much the program improves care or reduces costs at the facility. National standards also should come into play, Dr. Bossard says. “The hospitalist negotiator and the administration need to be comfortable with their command of what the data shows and what their standards are,” he cautions.
At Lutheran Medical Center in Colorado, Dr. Krebs felt strongly the change in ownership would cause patients hardship and go against national standards. Though both sides attempted to collect feedback and reach a compromise, neither came up with a solution that satisfied Dr. Krebs. He felt he had no choice but to seek legal action. (Exempla Healthcare, which manages the medical center, also sued to stop the sale).
“If the parent organization of Jehovah’s Witnesses took over a hospital and declared that no one could have a transfusion, no one would allow that,” Dr. Krebs argues. “If I have a patient that’s a Jehovah’s Witness, and they say, ‘I won’t have a transfusion,’ that’s very important. However, that person doesn’t have the right to impose their belief system on someone else.”
Dr. Krebs says he has the support of his medical community and his hospital, largely because, as a hospitalist, he’s been involved with the community all along. He says any hospitalist who hopes to influence standards of care should get involved, too, by sitting on or chairing a hospital committee, becoming an integral part of the medical community early on, and, above all, providing great care.
“If you leverage the facility you’re in to the Nth degree for income, you’re not going to be viewed as a partner, but as a vendor commodity, and you’ll have very little influence,” Dr. Krebs says. “There’s a benefit to being a hospitalist. You are in a unique position to exert influence on the hospital, because in some ways, both parties need the other to do well.” TH
When a Catholic group moved to buy Lutheran Medical Center in Wheat Ridge, Colo., just outside of Denver, hospitalist Steven Krebs, MD, had strong objections. Sisters of Charity of Leavenworth Health System already was part-owner of the 400-bed medical center. As the sole owner, it would require the hospital to follow Catholic rules regarding end-of-life care and reproductive health, meaning some medical services would be prohibited.
“It’s really the last hospital before you go into the mountains. There’s no real hospital facility until Vail, almost 100 miles up the road,” Dr. Krebs says. Patients who wanted a tubal ligation, an emergency contraceptive, or other medical services typically not offered in a Catholic hospital would have to travel to receive them—or not receive them at all.
After negotiations failed to produce a satisfactory outcome, Dr. Krebs took the drastic step of becoming part of a lawsuit to stop the sale. In May 2008, Colorado’s governor signed into law a bill that allows the state attorney general to review how the sale of a nonprofit hospital affects patient care. If he believes care will be affected, the attorney general may ask for more information from the sponsors of the transaction or require a public hearing be held before determining whether to approve the transaction.
The sale is pending.
—Steven Krebs, MD, Lutheran Medical Center, Wheat Ridge, Colo.
In an ideal world, patients would get the same excellent care, no matter who owns or runs a hospital. A sale or a change in executive leadership wouldn’t alter the tone of a hospital. As the Colorado case shows, ownership and leadership matter.
Hospitalists who have been through a hospital sale or a change of leadership say it’s possible to influence the process from within, to benefit the hospital, the patients, and the hospitalists themselves, often through simple negotiation and clear communication.
Become a Resource, Partner for Leadership
Established hospitalist programs are in an especially strong bargaining position. “We have a track record we can point to,” says Brian Bossard, MD, director of Inpatient Physician Associates, whose medical center, BryanLGH in Lincoln, Neb., went through a search for a new CEO in early 2008. That track record includes a strong relationship between the hospitalist program and hospital administrators.
When the medical center considered formalizing its hospitalist program in 2002, for example, Dr. Bossard went with administrators to regional and national meetings. “Instead of having competing perspectives on what the costs of the program should be and what the value equation is, we came from a similar perspective,” he explains. “Since that time, that trust has been maintained by coming through on promises, whether it’s being able to manage the volumes or get good results.”
A strong foundation can lead to a well-integrated hospitalist program and positive relationships with the CEO and COO, Dr. Bossard adds. Though he considers the change in CEOs at BryanLGH “a little unsettling,” he says he’s confident his hospitalist program has the support of the hospital community. Perhaps as evidence of that, the hospital hiring committee considered input from hospitalists before making a final selection.
Dr. Bossard plans to present to the new CEO the hospitalist program’s accomplishments, goals, and potential challenges early on, so the CEO can get to know the program. “The [hospitalists] really should try to position themselves, in my view anyway, as sort of an insider with useful information, a leader they can go to to ask what’s really going on in the hospital,” Dr. Bossard says. “Hospitalist programs will grow so rapidly within hospital systems, taking care of 50% to 75%, to sometimes close to 100% of patients. They’re really great sources of information.”
Keep Lines of Communication Open
Strong relationships with hospital leadership creates a stable environment where hospitalists feel valued. It also helps ensure a program can weather almost any storm, says Julia Wright, MD, University of Wisconsin Hospital and Clinics hospitalist director and the director of hospital medicine at UW School of Medicine and Public Health in Madison, Wis. “Once you get to the point where you have value, a mission, a system of operations, and a delivery-of-care plan, then that might translate into some personal ownership in the program that could withstand a change in administration,” she says.
Dr. Wright, who took a five-person hospitalist program and has enlarged it to 13, says she understands the value of communication with hospital executives. She also has a game plan, should executive leadership at her hospital change. “The first thing I would do is sit down and discuss what my mission is,” she says. “Continued dialogue after that is really important.” The dialogue would include meeting with hospital administration regularly, as well as talking about objectives and ways to meet them. “I just know what’s worked to keep our program on track,” she says, “and it’s been very successful.”
Leverage a Change in Administration
At Meriter Hospital in Madison, Wis., Cate Ranheim, MD, director of the hospitalist program, found a change in administration actually benefitted her hospitalists. “Our previous administration was essentially a chief operating officer (COO) who approved—or more often—refused, every request for even the simplest things, from sinks to filing cabinets to call rooms,” she explains. “The former CEO was here for 30-plus years, as was the COO, and was virtually invisible within the institution.”
The COO was a strong advocate for the hospitalist group, but Dr. Ranheim says she still had to go through tough negotiations to get what the group needed. When a new CEO came in and announced an open-door policy, Dr. Ranheim jumped at the opportunity to be heard. “Whenever I need something for the group, I go directly to him, and I have never been refused anything because he knows I am not game-playing or negotiating,” she says. “If I say the group needs something, it really does.”
Dr. Ranheim’s experience actually is fairly common. Executive leadership or ownership changes often create “a window of opportunity to further some agendas,” Dr. Wright points out. “If there’s a group that’s been saying, ‘We really want to start this new initiative and just haven’t been able to get there yet,’ this might be the time to do that.”
Whether the transition is a good time can depend on how comfortable a hospitalist group feels with the new executive. “In my own experience, it’s all about personality,” Dr. Ranheim says. “As hospitalist director, I instantly trusted my new CEO, and that trust has never been violated in either direction.” She adds, “Of course, I still do get everything in writing.”
Pay Attention to National Standards
Whether hospitalists can bring about improvements during a hospital change of ownership or leadership isn’t just based on how much the program improves care or reduces costs at the facility. National standards also should come into play, Dr. Bossard says. “The hospitalist negotiator and the administration need to be comfortable with their command of what the data shows and what their standards are,” he cautions.
At Lutheran Medical Center in Colorado, Dr. Krebs felt strongly the change in ownership would cause patients hardship and go against national standards. Though both sides attempted to collect feedback and reach a compromise, neither came up with a solution that satisfied Dr. Krebs. He felt he had no choice but to seek legal action. (Exempla Healthcare, which manages the medical center, also sued to stop the sale).
“If the parent organization of Jehovah’s Witnesses took over a hospital and declared that no one could have a transfusion, no one would allow that,” Dr. Krebs argues. “If I have a patient that’s a Jehovah’s Witness, and they say, ‘I won’t have a transfusion,’ that’s very important. However, that person doesn’t have the right to impose their belief system on someone else.”
Dr. Krebs says he has the support of his medical community and his hospital, largely because, as a hospitalist, he’s been involved with the community all along. He says any hospitalist who hopes to influence standards of care should get involved, too, by sitting on or chairing a hospital committee, becoming an integral part of the medical community early on, and, above all, providing great care.
“If you leverage the facility you’re in to the Nth degree for income, you’re not going to be viewed as a partner, but as a vendor commodity, and you’ll have very little influence,” Dr. Krebs says. “There’s a benefit to being a hospitalist. You are in a unique position to exert influence on the hospital, because in some ways, both parties need the other to do well.” TH
A young pregnant woman with shortness of breath
A 21-year-old woman who is 12 weeks pregnant according to the date of her last menstrual period comes to the emergency department with shortness of breath and chest pain.
One week ago she began experiencing pre-syncope and shortness of breath on minimal exertion and then even at rest on most days. The shortness of breath worsened throughout the week, eventually limiting her daily activities to such a degree that she restricted herself to bed rest.
Her chest pain started today while she was sitting in church, without any apparent provocation. It is right-sided, sharp, and focal, and it does not radiate. At the same time, her shortness of breath was more severe than before, so she immediately came to the emergency department.
This is her third pregnancy; she has had one live birth and one abortion. Her last pregnancy was full-term, with routine prenatal care and no complications. However, so far during this pregnancy, she has had no prenatal care, she has not taken prenatal vitamins, and she has been unable to maintain adequate nutrition because of persistent emesis, which began early in her pregnancy and continues to occur as often as two or three times daily. She has lost 20 pounds over the past 12 weeks.
She says she has no close contacts who are sick, and she has had no fever, diarrhea, dysuria, urinary frequency or urgency, palpitations, swelling of the legs or feet, blurry vision, or increase in neck girth. She says she does not smoke or use alcohol or illicit substances. Her only previous surgery was laser-assisted in situ keratoplasty (LASIK) eye surgery in 1998. She is allergic to seafood only. She has not eaten at any new places recently. She is up to date with her childhood vaccinations. She has no family history of hypercoagulability or venous thrombotic events.
PHYSICAL EXAMINATION
She is breathing rapidly—as fast as 45 breaths per minute. Her temperature is 37.2°C (98.9°F), blood pressure 95/60 mm Hg, oxygen saturation 100% while on 10 L of oxygen using a nonrebreather mask, pulse 102 beats per minute, and weight 55.9 kg (123.2 pounds). She appears alert, oriented, and comfortable, with a thin body habitus. She has no jugular venous distention, neck mass, or thyromegaly. Her lungs are clear to auscultation, with no wheezes or rales. The cardiovascular examination is normal. She has a regular heart rate and rhythm, normal S1 and S2 sounds, and no rubs, clicks, or murmurs. Pulses in the extremities are normal, and she has no peripheral edema. The neurologic examination is normal.
Electrocardiography shows sinus tachycardia with first-degree atrioventricular block.
DIFFERENTIAL DIAGNOSIS
1. At this point, which is the most probable cause of her symptoms?
- Pulmonary embolism
- Peripartum cardiomyopathy
- Acute coronary syndrome
- Aortic dissection
- Expected physiologic changes of pregnancy
Pulmonary embolism would be the most probable diagnosis, given the patient’s pregnancy, shortness of breath, and tachycardia and the pleuritic quality of her chest pain.
Peripartum cardiomyopathy is also a possible cause, as it may present with profound shortness of breath and markedly decreased cardiac function. But it is much less likely in this patient because she is early in her pregnancy, and peripartum cardiomyopathy usually is seen during the last month of gestation or the first months after delivery.
Acute coronary syndrome is unlikely, given her young age and the lack of significant risk factors or a supporting history.
Aortic dissection is unlikely in view of her medical history.
Physiologic changes of pregnancy. Many pregnant women experience a sensation of not being able to catch their breath or expand their lungs fully, as the diaphragm is limited by the gravid abdomen. They also present with dyspnea, fatigue, reduced exercise capacity, peripheral edema, or volume overload.1 However, these changes tend to occur gradually and worsen over time. This patient’s degree of shortness of breath and its sudden onset do not seem like normal physiologic changes of pregnancy.
Other possible causes of dyspnea in a pregnant woman include asthma, pleural empyema, pneumonia, and severe anemia. Asthma should be considered in anyone with a history of wheezing, cough, and dyspnea. Fever and sputum production would support a diagnosis of pneumonia or empyema. In addition, maternal heart disease (eg, endocarditis, pulmonary hypertension) complicates 0.2% to 3% of pregnancies.1
CASE CONTINUED
The emergency department staff decide to evaluate the patient for heart failure and pulmonary embolism.
Bedside echocardiography reveals an ejection fraction of 55% (normal range 50%–75%), normal heart function and size, and no valvular abnormalities.
Chest radiography is normal.
Lower-extremity duplex ultrasonography is negative for deep-vein thrombosis.
The D-dimer level is 380 ng/mL (normal range < 500 ng/mL).
The medical intensive care unit is consulted about the patient’s continued tachypnea and the possible need for intubation. A ventilation-perfusion scan is performed to screen for pulmonary embolism, and it is negative.
An obstetric team performs Doppler ultrasonography at the bedside; a fetal heartbeat can be heard, thus confirming a viable pregnancy.
The patient has normal serum levels of the cardiac enzymes troponin T and creatine kinase-MB fraction, thus all but ruling out myocardial ischemia.
The patient is admitted to the hospital the next day, and a cardiology consult is obtained.
RULING OUT PULMONARY EMBOLISM
2. Has pulmonary embolism been definitively ruled out at this point?
- Yes
- No
The answer is no. The negative ventilation-perfusion scan and normal D-dimer test in this patient are not enough to rule out pulmonary embolism. The diagnosis of pulmonary embolism should be based on the clinician’s estimation of the pretest probability of pulmonary embolism (which is based on presenting signs and symptoms), as well as on a variety of tests, including spiral computed tomography (CT), ventilation-perfusion lung scanning, and serum D-dimer testing. Signs and symptoms that may guide the clinician are chest pain (present in 70% of patients with pulmonary embolism), tachypnea (70%), cough (40%), shortness of breath (25%), and tachycardia (33%).2 A history of pregnancy, malignancy, immobility, or recent surgery may also increase the pretest probability of pulmonary embolism. In many cases, one’s clinical suspicion is highly predictive and is useful in diagnosing pulmonary embolism.
The accuracy of the tests varies widely, depending on the pretest probability of pulmonary embolism. For instance, in a patient with a high pretest probability but a low-probability ventilation-perfusion scan, the true probability of pulmonary embolism is 40%, but in a patient with a low pretest probability and a low-probability scan, the probability is only 4%.
The Wells criteria can be used to calculate the pretest probability of pulmonary embolism. Given this patient’s tachycardia and clinical presentation, her pretest probability according to the Wells criteria indicates increased risk. However, because her D-dimer test, lower-extremity Doppler test, and ventilation-perfusion scan were normal, pulmonary embolism is less likely.3
However, if one’s clinical suspicion is high enough, further investigation of pulmonary embolism would proceed despite the encouraging test results.
CASE CONTINUED
The cardiology consult team notes that her beta human chorionic gonadotropin (beta-hCG) level is much higher than would be expected at 12 weeks of pregnancy, and so they are concerned about the possibility of a molar pregnancy. In addition, her level of thyroid-stimulating hormone (TSH, or thyrotropin) is markedly low.
HYPERTHYROIDISM IN PREGNANCY
3. Which of the following would not explain this patient’s markedly low TSH level?
- Graves disease
- Molar pregnancy
- TSH-secreting pituitary adenoma
- Gestational transient thyrotoxicosis
- Twin pregnancy
Hyperthyroidism (also called thyrotoxicosis) has many causes, including but not limited to Graves disease, pituitary adenoma, struma ovarii (teratoma), hCG-secreting hydatidiform mole, and thyroid carcinoma (which is rare).4 In most of these disorders, the TSH level is low while the levels of thyroxine (T4), triiodothyronine (T3), or both are high.
Symptoms of hyperthyroidism are the effect of elevated T4 and T3 levels on the target organs themselves. Common symptoms include fever, tachycardia, tremor, stare, sweating, and lid lag. Other symptoms include nervousness, delirium, hypersensitivity to heat, flushing, palpitations, fatigue, weight loss, dyspnea, weakness, increased appetite, swelling of the legs, nausea, vomiting, diarrhea, goiter, tremor, atrial fibrillation, and cardiac failure.4 In its extreme form, called thyroid storm, thyrotoxicosis can be life-threatening. The likelihood of an impending thyroid storm can be assessed by clinical variables such as the patient’s temperature and heart rate and whether he or she has heart failure or gastrointestinal manifestations.5
Graves disease, the most common cause of hyperthyroidism in pregnancy, is due to stimulation of TSH receptors by antibodies against these receptors. Graves disease is possible in this patient, but a subsequent TSH receptor antibody test is negative.
Pituitary adenomas are one of the few causes of hyperthyroidism in which the TSH level is high, not low. Therefore, this is the correct answer.
Gestational transient thyrotoxicosis is a nonautoimmune condition that results in transient hyperthyroidism of variable severity.6 Usually, it occurs in otherwise normal pregnancies without complications, but the initial manifestation is hyper- emesis.6 It can be differentiated from Graves disease by the absence of TSH receptor antibodies and by no history of thyroid disorder.7 Common symptoms of gestational transient thyrotoxicosis include weight loss (or failure to gain weight), tachycardia, and fatigue.
The reason for the transient rise in T4 may be that beta-hCG is structurally similar to TSH (and also to luteinizing hormone and follicle-stimulating hormone), so that it has mild thyroid-stimulating effects.7 Sustained high levels of beta-hCG may in time give rise to the manifestations of thyrotoxicosis.
Molar pregnancy also can cause hyper-thyroidism via elevated levels of beta-hCG. However, twin pregnancy is more common and can produce sustained levels of beta-hCG above 100,000 IU/L. In most cases of twin pregnancy, the TSH level is decreased and the T4 level transiently elevated.6 The elevated beta-hCG and the subsequent thyrotropic manifestations are thought to be directly related, and symptoms resolve when beta-hCG levels go down.6
In most cases of hyperthyroidism in pregnancy, the acute condition can be managed by a short (≤ 2-month) course of a beta-blocker. In rare cases, propylthiouracil treatment may be required. Gestational transient thyrotoxicosis is not associated with detrimental outcomes.
Case continued
Our patient’s TSH level is low and her free T4 and T3 levels are elevated. Her high beta-hCG level may be stimulating the thyroid gland and may account for the low TSH value, as well as for her tachycardia, emesis, shortness of breath, and weight loss.
After an obstetric consult, it is determined that our patient has a viable pregnancy. However, further investigation with transvaginal ultrasonography reveals that she has two viable, single-placenta, intrauterine gestations, separated by a thin chorionic membrane.
Beta-hCG and free T4 levels are significantly higher in twin pregnancies than in single pregnancies, especially in the early stages.6 In our patient, the twin pregnancy led to the elevated beta-hCG, which eventually manifested as thyrotoxicosis, which caused the shortness of breath, hyperemesis, weight loss, tachycardia, and nausea.
Shortness of breath in patients with thyrotoxicosis is well recognized but not well explained. It may be caused by decreased lung compliance, engorged capillaries in the lung, or left ventricular failure, as well as by chest pain due to increased myocardial demand or coronary artery vasospasm.4 The dyspnea is present at rest and during exertion, and the high metabolic rate is thought to lead to an inappropriate response of the ventilatory system.3,8
WHAT TREATMENT?
4. How would you treat this patient at this point?
- No drug therapy, just supportive care
- Propranolol (Inderal)
- Levothyroxine
- Propylthiouracil
Several types of drugs are used to manage hyperthyroidism.
Antithyroid drugs such as propylthiouracil, methimazole (Northyx, Tapazole), and carbimazole block thyroid hormone synthesis by inhibiting thyroid peroxidase. Propylthiouracil also blocks peripheral conversion of T4 to T3. Side effects of these agents include abnormal sense of taste, pruritus, urticaria, agranulocytosis, and hepatotoxicity.4
Usually, hyperthyroidism is treated with propylthiouracil at the smallest effective dose. This has been proven to be safe to the fetus and mother during pregnancy.9 Propylthiouracil and the other drugs in its class cross the placenta, but propylthiouracil crosses at one-quarter the rate of the other two.9
Beta-blockers are effective in the acute phase of thyrotoxicosis against tachycardia, hypertension, and atrial fibrillation. They also decrease conversion of T4 to T3, which is an added benefit. Beta-blockers can be tapered as thyroid hormone levels decrease.
A short course of a short-acting beta-blocker would be an option for our patient and would decrease her symptoms, although she does not have the typical markedly elevated T4 or T3 levels. In the long term, a beta-blocker would present a fetal risk, but short courses can be tolerated without incident.9
Radioactive iodine 131 is used in patients with Graves disease. 131Iodine therapy is safe for most adults, but in pregnancy its use is contraindicated. Fetal thyroid tissue is thought to be present after 10 weeks of gestation and could be damaged by the use of radioactive iodine. Another warning with the use of radioactive iodine is that patients should avoid close contact with other adults for a few days after treatment, and should avoid close contact with children and pregnant women for 2 to 3 weeks after treatment because of the risk of exposure to radiation emanating from the thyroid gland.
Levothyroxine is a treatment for hypothyroidism, not hyperthyroidism.
CASE CONTINUED
Our patient is treated with propranolol and monitored for several days in the hospital, during which her symptoms markedly improve. She is discharged without complications.
TAKE-HOME POINTS
The evaluation of shortness of breath in adult patients can be difficult, given the many possible causes. It is especially challenging in pregnant patients, since normal physiologic changes of pregnancy may produce these symptoms.
In many instances, cardiomyopathy must be suspected if a pregnant patient complains of shortness of breath. However, it is not the only possible cause.
- Dobbenga-Rhodes YA, Prive AM. Assessment and evaluation of the woman with cardiac disease during pregnancy. J Perinat Neonatal Nurs 2006; 20:295–302.
- Carman TL, Deitcher SR. Advances in diagnosing and excluding pulmonary embolism: spiral CT and D-dimer measurement. Cleve Clin J Med 2002; 69:721–729.
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83:416–420.
- Nayak B, Burman K. Thyrotoxicosis and thyroid storm. Endocrinol Metab Clin North Am 2006; 35:663–686.
- Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am 1993; 22:263–277.
- Grün JP, Meuris S, De Nayer P, Glinoer D. The thyrotrophic role of human chorionic gonadotrophin (hCG) in the early stages of twin (versus single) pregnancies. Clin Endocrinol (Oxf) 1997; 46:719–725.
- Glinoer D, De Nayer P, Robyn C, Lejeune B, Kinthaert J, Meuris S. Serum levels of intact human chorionic gonadotropin (HCG) and its free alpha and beta subunits, in relation to maternal thyroid stimulation during normal pregnancy. J Endocrinol Invest 1993; 16:881–888.
- Small D, Gibbons W, Levy RD, de Lucas P, Gregory W, Cosio MG. Exertional dyspnea and ventilation in hyper-thyroidism. Chest 1992; 101:1268–1273.
- Atkins P, Cohen SB, Phillips BJ. Drug therapy for hyper-thyroidism in pregnancy: safety issues for mother and fetus. Drug Saf 2000; 23:229–244.
A 21-year-old woman who is 12 weeks pregnant according to the date of her last menstrual period comes to the emergency department with shortness of breath and chest pain.
One week ago she began experiencing pre-syncope and shortness of breath on minimal exertion and then even at rest on most days. The shortness of breath worsened throughout the week, eventually limiting her daily activities to such a degree that she restricted herself to bed rest.
Her chest pain started today while she was sitting in church, without any apparent provocation. It is right-sided, sharp, and focal, and it does not radiate. At the same time, her shortness of breath was more severe than before, so she immediately came to the emergency department.
This is her third pregnancy; she has had one live birth and one abortion. Her last pregnancy was full-term, with routine prenatal care and no complications. However, so far during this pregnancy, she has had no prenatal care, she has not taken prenatal vitamins, and she has been unable to maintain adequate nutrition because of persistent emesis, which began early in her pregnancy and continues to occur as often as two or three times daily. She has lost 20 pounds over the past 12 weeks.
She says she has no close contacts who are sick, and she has had no fever, diarrhea, dysuria, urinary frequency or urgency, palpitations, swelling of the legs or feet, blurry vision, or increase in neck girth. She says she does not smoke or use alcohol or illicit substances. Her only previous surgery was laser-assisted in situ keratoplasty (LASIK) eye surgery in 1998. She is allergic to seafood only. She has not eaten at any new places recently. She is up to date with her childhood vaccinations. She has no family history of hypercoagulability or venous thrombotic events.
PHYSICAL EXAMINATION
She is breathing rapidly—as fast as 45 breaths per minute. Her temperature is 37.2°C (98.9°F), blood pressure 95/60 mm Hg, oxygen saturation 100% while on 10 L of oxygen using a nonrebreather mask, pulse 102 beats per minute, and weight 55.9 kg (123.2 pounds). She appears alert, oriented, and comfortable, with a thin body habitus. She has no jugular venous distention, neck mass, or thyromegaly. Her lungs are clear to auscultation, with no wheezes or rales. The cardiovascular examination is normal. She has a regular heart rate and rhythm, normal S1 and S2 sounds, and no rubs, clicks, or murmurs. Pulses in the extremities are normal, and she has no peripheral edema. The neurologic examination is normal.
Electrocardiography shows sinus tachycardia with first-degree atrioventricular block.
DIFFERENTIAL DIAGNOSIS
1. At this point, which is the most probable cause of her symptoms?
- Pulmonary embolism
- Peripartum cardiomyopathy
- Acute coronary syndrome
- Aortic dissection
- Expected physiologic changes of pregnancy
Pulmonary embolism would be the most probable diagnosis, given the patient’s pregnancy, shortness of breath, and tachycardia and the pleuritic quality of her chest pain.
Peripartum cardiomyopathy is also a possible cause, as it may present with profound shortness of breath and markedly decreased cardiac function. But it is much less likely in this patient because she is early in her pregnancy, and peripartum cardiomyopathy usually is seen during the last month of gestation or the first months after delivery.
Acute coronary syndrome is unlikely, given her young age and the lack of significant risk factors or a supporting history.
Aortic dissection is unlikely in view of her medical history.
Physiologic changes of pregnancy. Many pregnant women experience a sensation of not being able to catch their breath or expand their lungs fully, as the diaphragm is limited by the gravid abdomen. They also present with dyspnea, fatigue, reduced exercise capacity, peripheral edema, or volume overload.1 However, these changes tend to occur gradually and worsen over time. This patient’s degree of shortness of breath and its sudden onset do not seem like normal physiologic changes of pregnancy.
Other possible causes of dyspnea in a pregnant woman include asthma, pleural empyema, pneumonia, and severe anemia. Asthma should be considered in anyone with a history of wheezing, cough, and dyspnea. Fever and sputum production would support a diagnosis of pneumonia or empyema. In addition, maternal heart disease (eg, endocarditis, pulmonary hypertension) complicates 0.2% to 3% of pregnancies.1
CASE CONTINUED
The emergency department staff decide to evaluate the patient for heart failure and pulmonary embolism.
Bedside echocardiography reveals an ejection fraction of 55% (normal range 50%–75%), normal heart function and size, and no valvular abnormalities.
Chest radiography is normal.
Lower-extremity duplex ultrasonography is negative for deep-vein thrombosis.
The D-dimer level is 380 ng/mL (normal range < 500 ng/mL).
The medical intensive care unit is consulted about the patient’s continued tachypnea and the possible need for intubation. A ventilation-perfusion scan is performed to screen for pulmonary embolism, and it is negative.
An obstetric team performs Doppler ultrasonography at the bedside; a fetal heartbeat can be heard, thus confirming a viable pregnancy.
The patient has normal serum levels of the cardiac enzymes troponin T and creatine kinase-MB fraction, thus all but ruling out myocardial ischemia.
The patient is admitted to the hospital the next day, and a cardiology consult is obtained.
RULING OUT PULMONARY EMBOLISM
2. Has pulmonary embolism been definitively ruled out at this point?
- Yes
- No
The answer is no. The negative ventilation-perfusion scan and normal D-dimer test in this patient are not enough to rule out pulmonary embolism. The diagnosis of pulmonary embolism should be based on the clinician’s estimation of the pretest probability of pulmonary embolism (which is based on presenting signs and symptoms), as well as on a variety of tests, including spiral computed tomography (CT), ventilation-perfusion lung scanning, and serum D-dimer testing. Signs and symptoms that may guide the clinician are chest pain (present in 70% of patients with pulmonary embolism), tachypnea (70%), cough (40%), shortness of breath (25%), and tachycardia (33%).2 A history of pregnancy, malignancy, immobility, or recent surgery may also increase the pretest probability of pulmonary embolism. In many cases, one’s clinical suspicion is highly predictive and is useful in diagnosing pulmonary embolism.
The accuracy of the tests varies widely, depending on the pretest probability of pulmonary embolism. For instance, in a patient with a high pretest probability but a low-probability ventilation-perfusion scan, the true probability of pulmonary embolism is 40%, but in a patient with a low pretest probability and a low-probability scan, the probability is only 4%.
The Wells criteria can be used to calculate the pretest probability of pulmonary embolism. Given this patient’s tachycardia and clinical presentation, her pretest probability according to the Wells criteria indicates increased risk. However, because her D-dimer test, lower-extremity Doppler test, and ventilation-perfusion scan were normal, pulmonary embolism is less likely.3
However, if one’s clinical suspicion is high enough, further investigation of pulmonary embolism would proceed despite the encouraging test results.
CASE CONTINUED
The cardiology consult team notes that her beta human chorionic gonadotropin (beta-hCG) level is much higher than would be expected at 12 weeks of pregnancy, and so they are concerned about the possibility of a molar pregnancy. In addition, her level of thyroid-stimulating hormone (TSH, or thyrotropin) is markedly low.
HYPERTHYROIDISM IN PREGNANCY
3. Which of the following would not explain this patient’s markedly low TSH level?
- Graves disease
- Molar pregnancy
- TSH-secreting pituitary adenoma
- Gestational transient thyrotoxicosis
- Twin pregnancy
Hyperthyroidism (also called thyrotoxicosis) has many causes, including but not limited to Graves disease, pituitary adenoma, struma ovarii (teratoma), hCG-secreting hydatidiform mole, and thyroid carcinoma (which is rare).4 In most of these disorders, the TSH level is low while the levels of thyroxine (T4), triiodothyronine (T3), or both are high.
Symptoms of hyperthyroidism are the effect of elevated T4 and T3 levels on the target organs themselves. Common symptoms include fever, tachycardia, tremor, stare, sweating, and lid lag. Other symptoms include nervousness, delirium, hypersensitivity to heat, flushing, palpitations, fatigue, weight loss, dyspnea, weakness, increased appetite, swelling of the legs, nausea, vomiting, diarrhea, goiter, tremor, atrial fibrillation, and cardiac failure.4 In its extreme form, called thyroid storm, thyrotoxicosis can be life-threatening. The likelihood of an impending thyroid storm can be assessed by clinical variables such as the patient’s temperature and heart rate and whether he or she has heart failure or gastrointestinal manifestations.5
Graves disease, the most common cause of hyperthyroidism in pregnancy, is due to stimulation of TSH receptors by antibodies against these receptors. Graves disease is possible in this patient, but a subsequent TSH receptor antibody test is negative.
Pituitary adenomas are one of the few causes of hyperthyroidism in which the TSH level is high, not low. Therefore, this is the correct answer.
Gestational transient thyrotoxicosis is a nonautoimmune condition that results in transient hyperthyroidism of variable severity.6 Usually, it occurs in otherwise normal pregnancies without complications, but the initial manifestation is hyper- emesis.6 It can be differentiated from Graves disease by the absence of TSH receptor antibodies and by no history of thyroid disorder.7 Common symptoms of gestational transient thyrotoxicosis include weight loss (or failure to gain weight), tachycardia, and fatigue.
The reason for the transient rise in T4 may be that beta-hCG is structurally similar to TSH (and also to luteinizing hormone and follicle-stimulating hormone), so that it has mild thyroid-stimulating effects.7 Sustained high levels of beta-hCG may in time give rise to the manifestations of thyrotoxicosis.
Molar pregnancy also can cause hyper-thyroidism via elevated levels of beta-hCG. However, twin pregnancy is more common and can produce sustained levels of beta-hCG above 100,000 IU/L. In most cases of twin pregnancy, the TSH level is decreased and the T4 level transiently elevated.6 The elevated beta-hCG and the subsequent thyrotropic manifestations are thought to be directly related, and symptoms resolve when beta-hCG levels go down.6
In most cases of hyperthyroidism in pregnancy, the acute condition can be managed by a short (≤ 2-month) course of a beta-blocker. In rare cases, propylthiouracil treatment may be required. Gestational transient thyrotoxicosis is not associated with detrimental outcomes.
Case continued
Our patient’s TSH level is low and her free T4 and T3 levels are elevated. Her high beta-hCG level may be stimulating the thyroid gland and may account for the low TSH value, as well as for her tachycardia, emesis, shortness of breath, and weight loss.
After an obstetric consult, it is determined that our patient has a viable pregnancy. However, further investigation with transvaginal ultrasonography reveals that she has two viable, single-placenta, intrauterine gestations, separated by a thin chorionic membrane.
Beta-hCG and free T4 levels are significantly higher in twin pregnancies than in single pregnancies, especially in the early stages.6 In our patient, the twin pregnancy led to the elevated beta-hCG, which eventually manifested as thyrotoxicosis, which caused the shortness of breath, hyperemesis, weight loss, tachycardia, and nausea.
Shortness of breath in patients with thyrotoxicosis is well recognized but not well explained. It may be caused by decreased lung compliance, engorged capillaries in the lung, or left ventricular failure, as well as by chest pain due to increased myocardial demand or coronary artery vasospasm.4 The dyspnea is present at rest and during exertion, and the high metabolic rate is thought to lead to an inappropriate response of the ventilatory system.3,8
WHAT TREATMENT?
4. How would you treat this patient at this point?
- No drug therapy, just supportive care
- Propranolol (Inderal)
- Levothyroxine
- Propylthiouracil
Several types of drugs are used to manage hyperthyroidism.
Antithyroid drugs such as propylthiouracil, methimazole (Northyx, Tapazole), and carbimazole block thyroid hormone synthesis by inhibiting thyroid peroxidase. Propylthiouracil also blocks peripheral conversion of T4 to T3. Side effects of these agents include abnormal sense of taste, pruritus, urticaria, agranulocytosis, and hepatotoxicity.4
Usually, hyperthyroidism is treated with propylthiouracil at the smallest effective dose. This has been proven to be safe to the fetus and mother during pregnancy.9 Propylthiouracil and the other drugs in its class cross the placenta, but propylthiouracil crosses at one-quarter the rate of the other two.9
Beta-blockers are effective in the acute phase of thyrotoxicosis against tachycardia, hypertension, and atrial fibrillation. They also decrease conversion of T4 to T3, which is an added benefit. Beta-blockers can be tapered as thyroid hormone levels decrease.
A short course of a short-acting beta-blocker would be an option for our patient and would decrease her symptoms, although she does not have the typical markedly elevated T4 or T3 levels. In the long term, a beta-blocker would present a fetal risk, but short courses can be tolerated without incident.9
Radioactive iodine 131 is used in patients with Graves disease. 131Iodine therapy is safe for most adults, but in pregnancy its use is contraindicated. Fetal thyroid tissue is thought to be present after 10 weeks of gestation and could be damaged by the use of radioactive iodine. Another warning with the use of radioactive iodine is that patients should avoid close contact with other adults for a few days after treatment, and should avoid close contact with children and pregnant women for 2 to 3 weeks after treatment because of the risk of exposure to radiation emanating from the thyroid gland.
Levothyroxine is a treatment for hypothyroidism, not hyperthyroidism.
CASE CONTINUED
Our patient is treated with propranolol and monitored for several days in the hospital, during which her symptoms markedly improve. She is discharged without complications.
TAKE-HOME POINTS
The evaluation of shortness of breath in adult patients can be difficult, given the many possible causes. It is especially challenging in pregnant patients, since normal physiologic changes of pregnancy may produce these symptoms.
In many instances, cardiomyopathy must be suspected if a pregnant patient complains of shortness of breath. However, it is not the only possible cause.
A 21-year-old woman who is 12 weeks pregnant according to the date of her last menstrual period comes to the emergency department with shortness of breath and chest pain.
One week ago she began experiencing pre-syncope and shortness of breath on minimal exertion and then even at rest on most days. The shortness of breath worsened throughout the week, eventually limiting her daily activities to such a degree that she restricted herself to bed rest.
Her chest pain started today while she was sitting in church, without any apparent provocation. It is right-sided, sharp, and focal, and it does not radiate. At the same time, her shortness of breath was more severe than before, so she immediately came to the emergency department.
This is her third pregnancy; she has had one live birth and one abortion. Her last pregnancy was full-term, with routine prenatal care and no complications. However, so far during this pregnancy, she has had no prenatal care, she has not taken prenatal vitamins, and she has been unable to maintain adequate nutrition because of persistent emesis, which began early in her pregnancy and continues to occur as often as two or three times daily. She has lost 20 pounds over the past 12 weeks.
She says she has no close contacts who are sick, and she has had no fever, diarrhea, dysuria, urinary frequency or urgency, palpitations, swelling of the legs or feet, blurry vision, or increase in neck girth. She says she does not smoke or use alcohol or illicit substances. Her only previous surgery was laser-assisted in situ keratoplasty (LASIK) eye surgery in 1998. She is allergic to seafood only. She has not eaten at any new places recently. She is up to date with her childhood vaccinations. She has no family history of hypercoagulability or venous thrombotic events.
PHYSICAL EXAMINATION
She is breathing rapidly—as fast as 45 breaths per minute. Her temperature is 37.2°C (98.9°F), blood pressure 95/60 mm Hg, oxygen saturation 100% while on 10 L of oxygen using a nonrebreather mask, pulse 102 beats per minute, and weight 55.9 kg (123.2 pounds). She appears alert, oriented, and comfortable, with a thin body habitus. She has no jugular venous distention, neck mass, or thyromegaly. Her lungs are clear to auscultation, with no wheezes or rales. The cardiovascular examination is normal. She has a regular heart rate and rhythm, normal S1 and S2 sounds, and no rubs, clicks, or murmurs. Pulses in the extremities are normal, and she has no peripheral edema. The neurologic examination is normal.
Electrocardiography shows sinus tachycardia with first-degree atrioventricular block.
DIFFERENTIAL DIAGNOSIS
1. At this point, which is the most probable cause of her symptoms?
- Pulmonary embolism
- Peripartum cardiomyopathy
- Acute coronary syndrome
- Aortic dissection
- Expected physiologic changes of pregnancy
Pulmonary embolism would be the most probable diagnosis, given the patient’s pregnancy, shortness of breath, and tachycardia and the pleuritic quality of her chest pain.
Peripartum cardiomyopathy is also a possible cause, as it may present with profound shortness of breath and markedly decreased cardiac function. But it is much less likely in this patient because she is early in her pregnancy, and peripartum cardiomyopathy usually is seen during the last month of gestation or the first months after delivery.
Acute coronary syndrome is unlikely, given her young age and the lack of significant risk factors or a supporting history.
Aortic dissection is unlikely in view of her medical history.
Physiologic changes of pregnancy. Many pregnant women experience a sensation of not being able to catch their breath or expand their lungs fully, as the diaphragm is limited by the gravid abdomen. They also present with dyspnea, fatigue, reduced exercise capacity, peripheral edema, or volume overload.1 However, these changes tend to occur gradually and worsen over time. This patient’s degree of shortness of breath and its sudden onset do not seem like normal physiologic changes of pregnancy.
Other possible causes of dyspnea in a pregnant woman include asthma, pleural empyema, pneumonia, and severe anemia. Asthma should be considered in anyone with a history of wheezing, cough, and dyspnea. Fever and sputum production would support a diagnosis of pneumonia or empyema. In addition, maternal heart disease (eg, endocarditis, pulmonary hypertension) complicates 0.2% to 3% of pregnancies.1
CASE CONTINUED
The emergency department staff decide to evaluate the patient for heart failure and pulmonary embolism.
Bedside echocardiography reveals an ejection fraction of 55% (normal range 50%–75%), normal heart function and size, and no valvular abnormalities.
Chest radiography is normal.
Lower-extremity duplex ultrasonography is negative for deep-vein thrombosis.
The D-dimer level is 380 ng/mL (normal range < 500 ng/mL).
The medical intensive care unit is consulted about the patient’s continued tachypnea and the possible need for intubation. A ventilation-perfusion scan is performed to screen for pulmonary embolism, and it is negative.
An obstetric team performs Doppler ultrasonography at the bedside; a fetal heartbeat can be heard, thus confirming a viable pregnancy.
The patient has normal serum levels of the cardiac enzymes troponin T and creatine kinase-MB fraction, thus all but ruling out myocardial ischemia.
The patient is admitted to the hospital the next day, and a cardiology consult is obtained.
RULING OUT PULMONARY EMBOLISM
2. Has pulmonary embolism been definitively ruled out at this point?
- Yes
- No
The answer is no. The negative ventilation-perfusion scan and normal D-dimer test in this patient are not enough to rule out pulmonary embolism. The diagnosis of pulmonary embolism should be based on the clinician’s estimation of the pretest probability of pulmonary embolism (which is based on presenting signs and symptoms), as well as on a variety of tests, including spiral computed tomography (CT), ventilation-perfusion lung scanning, and serum D-dimer testing. Signs and symptoms that may guide the clinician are chest pain (present in 70% of patients with pulmonary embolism), tachypnea (70%), cough (40%), shortness of breath (25%), and tachycardia (33%).2 A history of pregnancy, malignancy, immobility, or recent surgery may also increase the pretest probability of pulmonary embolism. In many cases, one’s clinical suspicion is highly predictive and is useful in diagnosing pulmonary embolism.
The accuracy of the tests varies widely, depending on the pretest probability of pulmonary embolism. For instance, in a patient with a high pretest probability but a low-probability ventilation-perfusion scan, the true probability of pulmonary embolism is 40%, but in a patient with a low pretest probability and a low-probability scan, the probability is only 4%.
The Wells criteria can be used to calculate the pretest probability of pulmonary embolism. Given this patient’s tachycardia and clinical presentation, her pretest probability according to the Wells criteria indicates increased risk. However, because her D-dimer test, lower-extremity Doppler test, and ventilation-perfusion scan were normal, pulmonary embolism is less likely.3
However, if one’s clinical suspicion is high enough, further investigation of pulmonary embolism would proceed despite the encouraging test results.
CASE CONTINUED
The cardiology consult team notes that her beta human chorionic gonadotropin (beta-hCG) level is much higher than would be expected at 12 weeks of pregnancy, and so they are concerned about the possibility of a molar pregnancy. In addition, her level of thyroid-stimulating hormone (TSH, or thyrotropin) is markedly low.
HYPERTHYROIDISM IN PREGNANCY
3. Which of the following would not explain this patient’s markedly low TSH level?
- Graves disease
- Molar pregnancy
- TSH-secreting pituitary adenoma
- Gestational transient thyrotoxicosis
- Twin pregnancy
Hyperthyroidism (also called thyrotoxicosis) has many causes, including but not limited to Graves disease, pituitary adenoma, struma ovarii (teratoma), hCG-secreting hydatidiform mole, and thyroid carcinoma (which is rare).4 In most of these disorders, the TSH level is low while the levels of thyroxine (T4), triiodothyronine (T3), or both are high.
Symptoms of hyperthyroidism are the effect of elevated T4 and T3 levels on the target organs themselves. Common symptoms include fever, tachycardia, tremor, stare, sweating, and lid lag. Other symptoms include nervousness, delirium, hypersensitivity to heat, flushing, palpitations, fatigue, weight loss, dyspnea, weakness, increased appetite, swelling of the legs, nausea, vomiting, diarrhea, goiter, tremor, atrial fibrillation, and cardiac failure.4 In its extreme form, called thyroid storm, thyrotoxicosis can be life-threatening. The likelihood of an impending thyroid storm can be assessed by clinical variables such as the patient’s temperature and heart rate and whether he or she has heart failure or gastrointestinal manifestations.5
Graves disease, the most common cause of hyperthyroidism in pregnancy, is due to stimulation of TSH receptors by antibodies against these receptors. Graves disease is possible in this patient, but a subsequent TSH receptor antibody test is negative.
Pituitary adenomas are one of the few causes of hyperthyroidism in which the TSH level is high, not low. Therefore, this is the correct answer.
Gestational transient thyrotoxicosis is a nonautoimmune condition that results in transient hyperthyroidism of variable severity.6 Usually, it occurs in otherwise normal pregnancies without complications, but the initial manifestation is hyper- emesis.6 It can be differentiated from Graves disease by the absence of TSH receptor antibodies and by no history of thyroid disorder.7 Common symptoms of gestational transient thyrotoxicosis include weight loss (or failure to gain weight), tachycardia, and fatigue.
The reason for the transient rise in T4 may be that beta-hCG is structurally similar to TSH (and also to luteinizing hormone and follicle-stimulating hormone), so that it has mild thyroid-stimulating effects.7 Sustained high levels of beta-hCG may in time give rise to the manifestations of thyrotoxicosis.
Molar pregnancy also can cause hyper-thyroidism via elevated levels of beta-hCG. However, twin pregnancy is more common and can produce sustained levels of beta-hCG above 100,000 IU/L. In most cases of twin pregnancy, the TSH level is decreased and the T4 level transiently elevated.6 The elevated beta-hCG and the subsequent thyrotropic manifestations are thought to be directly related, and symptoms resolve when beta-hCG levels go down.6
In most cases of hyperthyroidism in pregnancy, the acute condition can be managed by a short (≤ 2-month) course of a beta-blocker. In rare cases, propylthiouracil treatment may be required. Gestational transient thyrotoxicosis is not associated with detrimental outcomes.
Case continued
Our patient’s TSH level is low and her free T4 and T3 levels are elevated. Her high beta-hCG level may be stimulating the thyroid gland and may account for the low TSH value, as well as for her tachycardia, emesis, shortness of breath, and weight loss.
After an obstetric consult, it is determined that our patient has a viable pregnancy. However, further investigation with transvaginal ultrasonography reveals that she has two viable, single-placenta, intrauterine gestations, separated by a thin chorionic membrane.
Beta-hCG and free T4 levels are significantly higher in twin pregnancies than in single pregnancies, especially in the early stages.6 In our patient, the twin pregnancy led to the elevated beta-hCG, which eventually manifested as thyrotoxicosis, which caused the shortness of breath, hyperemesis, weight loss, tachycardia, and nausea.
Shortness of breath in patients with thyrotoxicosis is well recognized but not well explained. It may be caused by decreased lung compliance, engorged capillaries in the lung, or left ventricular failure, as well as by chest pain due to increased myocardial demand or coronary artery vasospasm.4 The dyspnea is present at rest and during exertion, and the high metabolic rate is thought to lead to an inappropriate response of the ventilatory system.3,8
WHAT TREATMENT?
4. How would you treat this patient at this point?
- No drug therapy, just supportive care
- Propranolol (Inderal)
- Levothyroxine
- Propylthiouracil
Several types of drugs are used to manage hyperthyroidism.
Antithyroid drugs such as propylthiouracil, methimazole (Northyx, Tapazole), and carbimazole block thyroid hormone synthesis by inhibiting thyroid peroxidase. Propylthiouracil also blocks peripheral conversion of T4 to T3. Side effects of these agents include abnormal sense of taste, pruritus, urticaria, agranulocytosis, and hepatotoxicity.4
Usually, hyperthyroidism is treated with propylthiouracil at the smallest effective dose. This has been proven to be safe to the fetus and mother during pregnancy.9 Propylthiouracil and the other drugs in its class cross the placenta, but propylthiouracil crosses at one-quarter the rate of the other two.9
Beta-blockers are effective in the acute phase of thyrotoxicosis against tachycardia, hypertension, and atrial fibrillation. They also decrease conversion of T4 to T3, which is an added benefit. Beta-blockers can be tapered as thyroid hormone levels decrease.
A short course of a short-acting beta-blocker would be an option for our patient and would decrease her symptoms, although she does not have the typical markedly elevated T4 or T3 levels. In the long term, a beta-blocker would present a fetal risk, but short courses can be tolerated without incident.9
Radioactive iodine 131 is used in patients with Graves disease. 131Iodine therapy is safe for most adults, but in pregnancy its use is contraindicated. Fetal thyroid tissue is thought to be present after 10 weeks of gestation and could be damaged by the use of radioactive iodine. Another warning with the use of radioactive iodine is that patients should avoid close contact with other adults for a few days after treatment, and should avoid close contact with children and pregnant women for 2 to 3 weeks after treatment because of the risk of exposure to radiation emanating from the thyroid gland.
Levothyroxine is a treatment for hypothyroidism, not hyperthyroidism.
CASE CONTINUED
Our patient is treated with propranolol and monitored for several days in the hospital, during which her symptoms markedly improve. She is discharged without complications.
TAKE-HOME POINTS
The evaluation of shortness of breath in adult patients can be difficult, given the many possible causes. It is especially challenging in pregnant patients, since normal physiologic changes of pregnancy may produce these symptoms.
In many instances, cardiomyopathy must be suspected if a pregnant patient complains of shortness of breath. However, it is not the only possible cause.
- Dobbenga-Rhodes YA, Prive AM. Assessment and evaluation of the woman with cardiac disease during pregnancy. J Perinat Neonatal Nurs 2006; 20:295–302.
- Carman TL, Deitcher SR. Advances in diagnosing and excluding pulmonary embolism: spiral CT and D-dimer measurement. Cleve Clin J Med 2002; 69:721–729.
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83:416–420.
- Nayak B, Burman K. Thyrotoxicosis and thyroid storm. Endocrinol Metab Clin North Am 2006; 35:663–686.
- Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am 1993; 22:263–277.
- Grün JP, Meuris S, De Nayer P, Glinoer D. The thyrotrophic role of human chorionic gonadotrophin (hCG) in the early stages of twin (versus single) pregnancies. Clin Endocrinol (Oxf) 1997; 46:719–725.
- Glinoer D, De Nayer P, Robyn C, Lejeune B, Kinthaert J, Meuris S. Serum levels of intact human chorionic gonadotropin (HCG) and its free alpha and beta subunits, in relation to maternal thyroid stimulation during normal pregnancy. J Endocrinol Invest 1993; 16:881–888.
- Small D, Gibbons W, Levy RD, de Lucas P, Gregory W, Cosio MG. Exertional dyspnea and ventilation in hyper-thyroidism. Chest 1992; 101:1268–1273.
- Atkins P, Cohen SB, Phillips BJ. Drug therapy for hyper-thyroidism in pregnancy: safety issues for mother and fetus. Drug Saf 2000; 23:229–244.
- Dobbenga-Rhodes YA, Prive AM. Assessment and evaluation of the woman with cardiac disease during pregnancy. J Perinat Neonatal Nurs 2006; 20:295–302.
- Carman TL, Deitcher SR. Advances in diagnosing and excluding pulmonary embolism: spiral CT and D-dimer measurement. Cleve Clin J Med 2002; 69:721–729.
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83:416–420.
- Nayak B, Burman K. Thyrotoxicosis and thyroid storm. Endocrinol Metab Clin North Am 2006; 35:663–686.
- Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am 1993; 22:263–277.
- Grün JP, Meuris S, De Nayer P, Glinoer D. The thyrotrophic role of human chorionic gonadotrophin (hCG) in the early stages of twin (versus single) pregnancies. Clin Endocrinol (Oxf) 1997; 46:719–725.
- Glinoer D, De Nayer P, Robyn C, Lejeune B, Kinthaert J, Meuris S. Serum levels of intact human chorionic gonadotropin (HCG) and its free alpha and beta subunits, in relation to maternal thyroid stimulation during normal pregnancy. J Endocrinol Invest 1993; 16:881–888.
- Small D, Gibbons W, Levy RD, de Lucas P, Gregory W, Cosio MG. Exertional dyspnea and ventilation in hyper-thyroidism. Chest 1992; 101:1268–1273.
- Atkins P, Cohen SB, Phillips BJ. Drug therapy for hyper-thyroidism in pregnancy: safety issues for mother and fetus. Drug Saf 2000; 23:229–244.
The hospital guy redux

You responded to the parts of Dr. Lansdale’s commentary that struck a personal chord. Almost all responders shared his frustration. Many wrote that the American payer system fails to appropriately reward internists and primary care providers and called for restructuring the Medicare and third-party payer systems. Some of you took umbrage at his contention that hospitals are not safe, and that health care delivery systems do not always place quality care above economic imperatives as new programs and “centers of excellence” are implemented. And some of you reacted to the issues of physician satisfaction and difficulties in providing quality care in hospitals regulated by multiple agencies that generate unfunded mandates, while the hospitals already require high numbers of patients in order to survive financially.
I recently did a stint as rheumatology consultant at my hospital, and Dr. Lansdale’s commentary was fresh in my mind. I noticed with satisfaction that the physicians and nurses were using foam antiseptic on their hands. I noted the new checks on verbal orders and a successful emphasis on preventing deep vein thrombosis and bedsores. But I also noted more patient hand-offs between house staff and faculty, and difficulty in finding doctors who actually knew the patient (or doctors that patients recognized as being responsible for their care).
The electronic medical record is legible and available from all over the hospital, and I could tell who signed the notes. But many notes were actually cut-and-pasted from earlier notes, and thus I couldn’t always be sure who actually had said what and when. Technology is not an immediate panacea for the problem of limited physician time!
The house staff “lab” in the hospital with its microscope was closed due to regulatory concerns; thus, there was no easy way to look at a freshly spun urine sample for evidence of glomerulonephritis. This turned out to be a detriment to effective patient care: urine samples sent to the regular laboratory (with the usual transportation delay) rarely if ever reveal cellular casts. But we found creative, if inefficient, ways to deal with this and other problems.
At the end of the day, I realized that I still enjoy my time in the hospital. Patients’ problems can be presented to house staff and students at the bedside and their diagnoses and therapies discussed in real time. Junior physicians can observe how senior physicians talk to patients and families, including the many ways we have learned to say “I don’t know,” and learn to appreciate the value of a well-directed physical examination. There is still a synergy and intellectual satisfaction in being one of a group of senior consultants discussing the care of a shared patient who has complex medical problems.
With rational and caring involvement, individual physicians can alter the trajectory of patient management and remain the primary patient advocates within a health care system that can’t always easily deliver the quality that everyone desires. Caring, patient-focused physicians must remain in charge of health care delivery, lest we pay attention only to the financial and regulatory problems.
Tom, I am older and even more cynical than I was when we roamed the hospital together every third night and never went home on our post-call day until the last laboratory result had been checked and the last transfusion had been given. We inefficiently examined every patient’s urine ourselves (even from those being admitted for cardiac catheterization), and we had to convince patients of the (apparent) need for the urgent 3 AM blood draw to evaluate their 100.5° fever before we prepped the area and drew the blood. We drew blood for sedimentation rates and checked rapid plasma reagins at every admission and checked for urinary light chains in everyone with an elevated creatinine level and anemia, “just to be sure.” We blindly placed Swan-Ganz catheters to monitor many hypotensive patients in the intensive care units, and we aspirated pleural effusions on the basis of our percussive examination. We talked to patients and accepted enormous individual responsibility for their care, but we were also frequently numbed by the overwhelming intensity of the training and the practice.
I am all too aware of the many forces that are eroding physician-patient relationships and that can corrupt patient care in the name of efficiency, financial necessity, marketing advantage, or regulatory compliance. Many of these forces I hope to help change. But I remain a hospital guy because I can still make a difference. I still feel honored that patients entrust their care to me as we attempt to navigate our evolving and, yes, sometimes treacherous medical system. Evading the crocodiles and fighting insurance companies are now in my job description.
In this issue we run two letters in response to Dr. Lansdale’s commentary. In December we will publish more letters, though due to space limitations some will be abridged. We plan to run full text of many of the letters online at www.ccjm.org in December.
You responded to the parts of Dr. Lansdale’s commentary that struck a personal chord. Almost all responders shared his frustration. Many wrote that the American payer system fails to appropriately reward internists and primary care providers and called for restructuring the Medicare and third-party payer systems. Some of you took umbrage at his contention that hospitals are not safe, and that health care delivery systems do not always place quality care above economic imperatives as new programs and “centers of excellence” are implemented. And some of you reacted to the issues of physician satisfaction and difficulties in providing quality care in hospitals regulated by multiple agencies that generate unfunded mandates, while the hospitals already require high numbers of patients in order to survive financially.
I recently did a stint as rheumatology consultant at my hospital, and Dr. Lansdale’s commentary was fresh in my mind. I noticed with satisfaction that the physicians and nurses were using foam antiseptic on their hands. I noted the new checks on verbal orders and a successful emphasis on preventing deep vein thrombosis and bedsores. But I also noted more patient hand-offs between house staff and faculty, and difficulty in finding doctors who actually knew the patient (or doctors that patients recognized as being responsible for their care).
The electronic medical record is legible and available from all over the hospital, and I could tell who signed the notes. But many notes were actually cut-and-pasted from earlier notes, and thus I couldn’t always be sure who actually had said what and when. Technology is not an immediate panacea for the problem of limited physician time!
The house staff “lab” in the hospital with its microscope was closed due to regulatory concerns; thus, there was no easy way to look at a freshly spun urine sample for evidence of glomerulonephritis. This turned out to be a detriment to effective patient care: urine samples sent to the regular laboratory (with the usual transportation delay) rarely if ever reveal cellular casts. But we found creative, if inefficient, ways to deal with this and other problems.
At the end of the day, I realized that I still enjoy my time in the hospital. Patients’ problems can be presented to house staff and students at the bedside and their diagnoses and therapies discussed in real time. Junior physicians can observe how senior physicians talk to patients and families, including the many ways we have learned to say “I don’t know,” and learn to appreciate the value of a well-directed physical examination. There is still a synergy and intellectual satisfaction in being one of a group of senior consultants discussing the care of a shared patient who has complex medical problems.
With rational and caring involvement, individual physicians can alter the trajectory of patient management and remain the primary patient advocates within a health care system that can’t always easily deliver the quality that everyone desires. Caring, patient-focused physicians must remain in charge of health care delivery, lest we pay attention only to the financial and regulatory problems.
Tom, I am older and even more cynical than I was when we roamed the hospital together every third night and never went home on our post-call day until the last laboratory result had been checked and the last transfusion had been given. We inefficiently examined every patient’s urine ourselves (even from those being admitted for cardiac catheterization), and we had to convince patients of the (apparent) need for the urgent 3 AM blood draw to evaluate their 100.5° fever before we prepped the area and drew the blood. We drew blood for sedimentation rates and checked rapid plasma reagins at every admission and checked for urinary light chains in everyone with an elevated creatinine level and anemia, “just to be sure.” We blindly placed Swan-Ganz catheters to monitor many hypotensive patients in the intensive care units, and we aspirated pleural effusions on the basis of our percussive examination. We talked to patients and accepted enormous individual responsibility for their care, but we were also frequently numbed by the overwhelming intensity of the training and the practice.
I am all too aware of the many forces that are eroding physician-patient relationships and that can corrupt patient care in the name of efficiency, financial necessity, marketing advantage, or regulatory compliance. Many of these forces I hope to help change. But I remain a hospital guy because I can still make a difference. I still feel honored that patients entrust their care to me as we attempt to navigate our evolving and, yes, sometimes treacherous medical system. Evading the crocodiles and fighting insurance companies are now in my job description.
In this issue we run two letters in response to Dr. Lansdale’s commentary. In December we will publish more letters, though due to space limitations some will be abridged. We plan to run full text of many of the letters online at www.ccjm.org in December.
You responded to the parts of Dr. Lansdale’s commentary that struck a personal chord. Almost all responders shared his frustration. Many wrote that the American payer system fails to appropriately reward internists and primary care providers and called for restructuring the Medicare and third-party payer systems. Some of you took umbrage at his contention that hospitals are not safe, and that health care delivery systems do not always place quality care above economic imperatives as new programs and “centers of excellence” are implemented. And some of you reacted to the issues of physician satisfaction and difficulties in providing quality care in hospitals regulated by multiple agencies that generate unfunded mandates, while the hospitals already require high numbers of patients in order to survive financially.
I recently did a stint as rheumatology consultant at my hospital, and Dr. Lansdale’s commentary was fresh in my mind. I noticed with satisfaction that the physicians and nurses were using foam antiseptic on their hands. I noted the new checks on verbal orders and a successful emphasis on preventing deep vein thrombosis and bedsores. But I also noted more patient hand-offs between house staff and faculty, and difficulty in finding doctors who actually knew the patient (or doctors that patients recognized as being responsible for their care).
The electronic medical record is legible and available from all over the hospital, and I could tell who signed the notes. But many notes were actually cut-and-pasted from earlier notes, and thus I couldn’t always be sure who actually had said what and when. Technology is not an immediate panacea for the problem of limited physician time!
The house staff “lab” in the hospital with its microscope was closed due to regulatory concerns; thus, there was no easy way to look at a freshly spun urine sample for evidence of glomerulonephritis. This turned out to be a detriment to effective patient care: urine samples sent to the regular laboratory (with the usual transportation delay) rarely if ever reveal cellular casts. But we found creative, if inefficient, ways to deal with this and other problems.
At the end of the day, I realized that I still enjoy my time in the hospital. Patients’ problems can be presented to house staff and students at the bedside and their diagnoses and therapies discussed in real time. Junior physicians can observe how senior physicians talk to patients and families, including the many ways we have learned to say “I don’t know,” and learn to appreciate the value of a well-directed physical examination. There is still a synergy and intellectual satisfaction in being one of a group of senior consultants discussing the care of a shared patient who has complex medical problems.
With rational and caring involvement, individual physicians can alter the trajectory of patient management and remain the primary patient advocates within a health care system that can’t always easily deliver the quality that everyone desires. Caring, patient-focused physicians must remain in charge of health care delivery, lest we pay attention only to the financial and regulatory problems.
Tom, I am older and even more cynical than I was when we roamed the hospital together every third night and never went home on our post-call day until the last laboratory result had been checked and the last transfusion had been given. We inefficiently examined every patient’s urine ourselves (even from those being admitted for cardiac catheterization), and we had to convince patients of the (apparent) need for the urgent 3 AM blood draw to evaluate their 100.5° fever before we prepped the area and drew the blood. We drew blood for sedimentation rates and checked rapid plasma reagins at every admission and checked for urinary light chains in everyone with an elevated creatinine level and anemia, “just to be sure.” We blindly placed Swan-Ganz catheters to monitor many hypotensive patients in the intensive care units, and we aspirated pleural effusions on the basis of our percussive examination. We talked to patients and accepted enormous individual responsibility for their care, but we were also frequently numbed by the overwhelming intensity of the training and the practice.
I am all too aware of the many forces that are eroding physician-patient relationships and that can corrupt patient care in the name of efficiency, financial necessity, marketing advantage, or regulatory compliance. Many of these forces I hope to help change. But I remain a hospital guy because I can still make a difference. I still feel honored that patients entrust their care to me as we attempt to navigate our evolving and, yes, sometimes treacherous medical system. Evading the crocodiles and fighting insurance companies are now in my job description.
In this issue we run two letters in response to Dr. Lansdale’s commentary. In December we will publish more letters, though due to space limitations some will be abridged. We plan to run full text of many of the letters online at www.ccjm.org in December.
Resuming Continuous Antiretroviral Therapy After Episodic Treatment
Atypical Presentation of Infiltrating Mucinous Carcinoma of the Breast
Benzoyl Peroxide Cleansers for the Treatment of Acne Vulgaris: Status Report on Available Data
A Diagnostic Pearl in Allergic Contact Dermatitis to Fragrances: The Atomizer Sign (See Erratum. 2009;83:49)
Did PSA finding get lost in the shuffle?...Woman sent home from ER dies of aneurysm...more
Did PSA finding get lost in the shuffle?
A SCREENING PROSTATE-SPECIFIC ANTIGEN (PSA) TEST ordered for a 76-year-old man by his primary care physician was within normal limits at 3.1. Two years later, the patient saw a urologist, who diagnosed renal cysts and bladder trabeculation based on a CT scan. Five months after that, the primary care physician ordered a second screening PSA, which was elevated at 12.
About a week later, the primary care physician noted that the patient was scheduled to see the urologist the next day, but didn’t indicate that the urologist had been informed of the elevated PSA or that the patient had been told of its significance. A letter from the primary care physician to the urologist after the patient’s visit stated that the patient was being treated for microscopic hematuria but didn’t mention elevated PSA. A letter several weeks later from the urologist to the primary care physician discussed the patient’s elevated PSA. The primary care physician didn’t contact the urologist to follow up on the finding, however.
After a year of testing, the urologist concluded that the hematuria was probably related to the kidney, or perhaps the prostate, and started the patient on dutasteride, which helped the bleeding. Two months after the start of treatment, the urologist ordered a PSA test, which was extremely elevated. A subsequent biopsy revealed adenocarcinoma, and a bone scan showed metastatic bony disease, which hadn’t shown up on a bone scan done 6 months before. The patient died 2 years later. The cause of death was listed as cardiopulmonary arrest, cardiogenic shock, and myocardial infarction.
PLAINTIFF’S CLAIM The plaintiff’s claim focused on the handling of the PSA test, though the specifics of the claim were not detailed in the case summary.
DOCTOR’S DEFENSE The primary care physician claimed that his nurse told the patient after the second PSA test that the PSA was 12 and encouraged the patient to see the urologist to discuss the elevated level. The physician also claimed that he had faxed the elevated PSA test result to the urologist and that the patient was reminded of the elevated PSA during his visit to the urologist. No information about the urologist’s defense was available.
VERDICT $325,000 Massachusetts settlement.
COMMENT Coordination of care and documentation of communication are keys to good patient care—and avoiding lawsuits.
Woman sent home from ER dies of aneurysm
SEVERE HEADACHES prompted a 38-year-old woman to visit her family physician, who referred her to a neurologist; an appointment was scheduled for more than a month later. A month after seeing the family physician, the patient went to the emergency room complaining of a severe headache.
A CT scan ordered by the ER physician showed a large mass in the patient’s brain. The ER physician gave the patient the scan report, told her to see her family doctor, and sent her home without consulting a neurosurgeon. Later that day, the aneurysm ruptured; the patient’s family took her to the hospital, where she died the next morning.
PLAINTIFF’S CLAIM The family physician should have ordered a CT scan, which would have revealed the aneurysm. The ER physician should have ordered an immediate neurologic consult, which would have led to surgical repair of the leaking aneurysm. Either measure would have saved the patient’s life.
DOCTOR’S DEFENSE The family physician claimed that the patient’s complaints weren’t urgent and he made a proper referral. The ER physician claimed that the patient wouldn’t have lived even if he’d arranged an immediate consult.
VERDICT $1.5 million Michigan verdict against the ER physician.
COMMENT This case illustrates the value of clearly documenting referrals and suggesting follow-up if a change in symptoms occurs.
Jaundiced newborn dies after slip-ups
AN INFANT BORN AT 36 WEEKS and the baby’s 20-year-old mother were discharged from the hospital fewer than 48 hours after delivery, with an appointment with a visiting nurse for the following day and a pediatrician 3 days later. Hospital medical records reported infrequent breast feeding, significant decrease in weight, and a bruise on the back of the infant’s head.
The visiting nurse who examined the baby noted moderate facial jaundice, mild jaundice in the groin, and slight jaundice in the sclera of the eyes, as well as the bruise on the back of the head. The nurse didn’t notify the pediatrician of the jaundice. The mother said that when she voiced concern about the jaundice, the nurse told her to feed the infant more often and expose her to sunlight.
The day after the nurse’s visit, the parents noticed that the baby was more jaundiced and had started to arch her back, grunt, and whine. The mother called the pediatrician’s office that day and reported the symptoms; the nurse told her that the pediatrician felt that he didn’t need to see the baby before her appointment the following day. As the symptoms worsened, the mother called the pediatrician’s office 3 more times before 6 PM, speaking with 2 nurses, neither of whom took a medical history.
The mother called again after the office had closed. A nurse arranged for the infant to be seen at the hospital, where the baby was admitted with a critically low temperature, decreased muscle tone, arching of the back, and an elevated bilirubin level of 35.4 mg/dL. Despite phototherapy and intubation, the infant’s condition deteriorated, and she was airlifted to another medical facility for more advanced care. The baby was given cardiopulmonary resuscitation on arrival, but died 4 hours later of acute bilirubin encephalopathy.
PLAINTIFF’S CLAIM In light of her symptoms, the baby shouldn’t have been discharged from the hospital. The visiting nurse should have reported the baby’s symptoms to the pediatrician or recommended that the parents take the baby to the doctor right away. The nurses in the pediatrician’s office were negligent in not taking a full medical history. The pediatrician should have seen the baby immediately. He failed to recognize the symptoms of possible hyperbilirubinemia, a medical emergency.
DOCTOR’S DEFENSE No information about the doctor’s or nurses’ defense is available.
VERDICT $460,000 Massachusetts settlement.
COMMENT This case illustrates, once again, the importance of care coordination and sharing information on a timely basis.
Did PSA finding get lost in the shuffle?
A SCREENING PROSTATE-SPECIFIC ANTIGEN (PSA) TEST ordered for a 76-year-old man by his primary care physician was within normal limits at 3.1. Two years later, the patient saw a urologist, who diagnosed renal cysts and bladder trabeculation based on a CT scan. Five months after that, the primary care physician ordered a second screening PSA, which was elevated at 12.
About a week later, the primary care physician noted that the patient was scheduled to see the urologist the next day, but didn’t indicate that the urologist had been informed of the elevated PSA or that the patient had been told of its significance. A letter from the primary care physician to the urologist after the patient’s visit stated that the patient was being treated for microscopic hematuria but didn’t mention elevated PSA. A letter several weeks later from the urologist to the primary care physician discussed the patient’s elevated PSA. The primary care physician didn’t contact the urologist to follow up on the finding, however.
After a year of testing, the urologist concluded that the hematuria was probably related to the kidney, or perhaps the prostate, and started the patient on dutasteride, which helped the bleeding. Two months after the start of treatment, the urologist ordered a PSA test, which was extremely elevated. A subsequent biopsy revealed adenocarcinoma, and a bone scan showed metastatic bony disease, which hadn’t shown up on a bone scan done 6 months before. The patient died 2 years later. The cause of death was listed as cardiopulmonary arrest, cardiogenic shock, and myocardial infarction.
PLAINTIFF’S CLAIM The plaintiff’s claim focused on the handling of the PSA test, though the specifics of the claim were not detailed in the case summary.
DOCTOR’S DEFENSE The primary care physician claimed that his nurse told the patient after the second PSA test that the PSA was 12 and encouraged the patient to see the urologist to discuss the elevated level. The physician also claimed that he had faxed the elevated PSA test result to the urologist and that the patient was reminded of the elevated PSA during his visit to the urologist. No information about the urologist’s defense was available.
VERDICT $325,000 Massachusetts settlement.
COMMENT Coordination of care and documentation of communication are keys to good patient care—and avoiding lawsuits.
Woman sent home from ER dies of aneurysm
SEVERE HEADACHES prompted a 38-year-old woman to visit her family physician, who referred her to a neurologist; an appointment was scheduled for more than a month later. A month after seeing the family physician, the patient went to the emergency room complaining of a severe headache.
A CT scan ordered by the ER physician showed a large mass in the patient’s brain. The ER physician gave the patient the scan report, told her to see her family doctor, and sent her home without consulting a neurosurgeon. Later that day, the aneurysm ruptured; the patient’s family took her to the hospital, where she died the next morning.
PLAINTIFF’S CLAIM The family physician should have ordered a CT scan, which would have revealed the aneurysm. The ER physician should have ordered an immediate neurologic consult, which would have led to surgical repair of the leaking aneurysm. Either measure would have saved the patient’s life.
DOCTOR’S DEFENSE The family physician claimed that the patient’s complaints weren’t urgent and he made a proper referral. The ER physician claimed that the patient wouldn’t have lived even if he’d arranged an immediate consult.
VERDICT $1.5 million Michigan verdict against the ER physician.
COMMENT This case illustrates the value of clearly documenting referrals and suggesting follow-up if a change in symptoms occurs.
Jaundiced newborn dies after slip-ups
AN INFANT BORN AT 36 WEEKS and the baby’s 20-year-old mother were discharged from the hospital fewer than 48 hours after delivery, with an appointment with a visiting nurse for the following day and a pediatrician 3 days later. Hospital medical records reported infrequent breast feeding, significant decrease in weight, and a bruise on the back of the infant’s head.
The visiting nurse who examined the baby noted moderate facial jaundice, mild jaundice in the groin, and slight jaundice in the sclera of the eyes, as well as the bruise on the back of the head. The nurse didn’t notify the pediatrician of the jaundice. The mother said that when she voiced concern about the jaundice, the nurse told her to feed the infant more often and expose her to sunlight.
The day after the nurse’s visit, the parents noticed that the baby was more jaundiced and had started to arch her back, grunt, and whine. The mother called the pediatrician’s office that day and reported the symptoms; the nurse told her that the pediatrician felt that he didn’t need to see the baby before her appointment the following day. As the symptoms worsened, the mother called the pediatrician’s office 3 more times before 6 PM, speaking with 2 nurses, neither of whom took a medical history.
The mother called again after the office had closed. A nurse arranged for the infant to be seen at the hospital, where the baby was admitted with a critically low temperature, decreased muscle tone, arching of the back, and an elevated bilirubin level of 35.4 mg/dL. Despite phototherapy and intubation, the infant’s condition deteriorated, and she was airlifted to another medical facility for more advanced care. The baby was given cardiopulmonary resuscitation on arrival, but died 4 hours later of acute bilirubin encephalopathy.
PLAINTIFF’S CLAIM In light of her symptoms, the baby shouldn’t have been discharged from the hospital. The visiting nurse should have reported the baby’s symptoms to the pediatrician or recommended that the parents take the baby to the doctor right away. The nurses in the pediatrician’s office were negligent in not taking a full medical history. The pediatrician should have seen the baby immediately. He failed to recognize the symptoms of possible hyperbilirubinemia, a medical emergency.
DOCTOR’S DEFENSE No information about the doctor’s or nurses’ defense is available.
VERDICT $460,000 Massachusetts settlement.
COMMENT This case illustrates, once again, the importance of care coordination and sharing information on a timely basis.
Did PSA finding get lost in the shuffle?
A SCREENING PROSTATE-SPECIFIC ANTIGEN (PSA) TEST ordered for a 76-year-old man by his primary care physician was within normal limits at 3.1. Two years later, the patient saw a urologist, who diagnosed renal cysts and bladder trabeculation based on a CT scan. Five months after that, the primary care physician ordered a second screening PSA, which was elevated at 12.
About a week later, the primary care physician noted that the patient was scheduled to see the urologist the next day, but didn’t indicate that the urologist had been informed of the elevated PSA or that the patient had been told of its significance. A letter from the primary care physician to the urologist after the patient’s visit stated that the patient was being treated for microscopic hematuria but didn’t mention elevated PSA. A letter several weeks later from the urologist to the primary care physician discussed the patient’s elevated PSA. The primary care physician didn’t contact the urologist to follow up on the finding, however.
After a year of testing, the urologist concluded that the hematuria was probably related to the kidney, or perhaps the prostate, and started the patient on dutasteride, which helped the bleeding. Two months after the start of treatment, the urologist ordered a PSA test, which was extremely elevated. A subsequent biopsy revealed adenocarcinoma, and a bone scan showed metastatic bony disease, which hadn’t shown up on a bone scan done 6 months before. The patient died 2 years later. The cause of death was listed as cardiopulmonary arrest, cardiogenic shock, and myocardial infarction.
PLAINTIFF’S CLAIM The plaintiff’s claim focused on the handling of the PSA test, though the specifics of the claim were not detailed in the case summary.
DOCTOR’S DEFENSE The primary care physician claimed that his nurse told the patient after the second PSA test that the PSA was 12 and encouraged the patient to see the urologist to discuss the elevated level. The physician also claimed that he had faxed the elevated PSA test result to the urologist and that the patient was reminded of the elevated PSA during his visit to the urologist. No information about the urologist’s defense was available.
VERDICT $325,000 Massachusetts settlement.
COMMENT Coordination of care and documentation of communication are keys to good patient care—and avoiding lawsuits.
Woman sent home from ER dies of aneurysm
SEVERE HEADACHES prompted a 38-year-old woman to visit her family physician, who referred her to a neurologist; an appointment was scheduled for more than a month later. A month after seeing the family physician, the patient went to the emergency room complaining of a severe headache.
A CT scan ordered by the ER physician showed a large mass in the patient’s brain. The ER physician gave the patient the scan report, told her to see her family doctor, and sent her home without consulting a neurosurgeon. Later that day, the aneurysm ruptured; the patient’s family took her to the hospital, where she died the next morning.
PLAINTIFF’S CLAIM The family physician should have ordered a CT scan, which would have revealed the aneurysm. The ER physician should have ordered an immediate neurologic consult, which would have led to surgical repair of the leaking aneurysm. Either measure would have saved the patient’s life.
DOCTOR’S DEFENSE The family physician claimed that the patient’s complaints weren’t urgent and he made a proper referral. The ER physician claimed that the patient wouldn’t have lived even if he’d arranged an immediate consult.
VERDICT $1.5 million Michigan verdict against the ER physician.
COMMENT This case illustrates the value of clearly documenting referrals and suggesting follow-up if a change in symptoms occurs.
Jaundiced newborn dies after slip-ups
AN INFANT BORN AT 36 WEEKS and the baby’s 20-year-old mother were discharged from the hospital fewer than 48 hours after delivery, with an appointment with a visiting nurse for the following day and a pediatrician 3 days later. Hospital medical records reported infrequent breast feeding, significant decrease in weight, and a bruise on the back of the infant’s head.
The visiting nurse who examined the baby noted moderate facial jaundice, mild jaundice in the groin, and slight jaundice in the sclera of the eyes, as well as the bruise on the back of the head. The nurse didn’t notify the pediatrician of the jaundice. The mother said that when she voiced concern about the jaundice, the nurse told her to feed the infant more often and expose her to sunlight.
The day after the nurse’s visit, the parents noticed that the baby was more jaundiced and had started to arch her back, grunt, and whine. The mother called the pediatrician’s office that day and reported the symptoms; the nurse told her that the pediatrician felt that he didn’t need to see the baby before her appointment the following day. As the symptoms worsened, the mother called the pediatrician’s office 3 more times before 6 PM, speaking with 2 nurses, neither of whom took a medical history.
The mother called again after the office had closed. A nurse arranged for the infant to be seen at the hospital, where the baby was admitted with a critically low temperature, decreased muscle tone, arching of the back, and an elevated bilirubin level of 35.4 mg/dL. Despite phototherapy and intubation, the infant’s condition deteriorated, and she was airlifted to another medical facility for more advanced care. The baby was given cardiopulmonary resuscitation on arrival, but died 4 hours later of acute bilirubin encephalopathy.
PLAINTIFF’S CLAIM In light of her symptoms, the baby shouldn’t have been discharged from the hospital. The visiting nurse should have reported the baby’s symptoms to the pediatrician or recommended that the parents take the baby to the doctor right away. The nurses in the pediatrician’s office were negligent in not taking a full medical history. The pediatrician should have seen the baby immediately. He failed to recognize the symptoms of possible hyperbilirubinemia, a medical emergency.
DOCTOR’S DEFENSE No information about the doctor’s or nurses’ defense is available.
VERDICT $460,000 Massachusetts settlement.
COMMENT This case illustrates, once again, the importance of care coordination and sharing information on a timely basis.
USPSTF scales back approach to lipid screening for women
When patients reached a certain age (36 for men, 46 for women), it used to mean that it was time, in the eyes of the United States Preventive Services Task Force (USPSTF), to screen for lipid disorders. But that’s changed for female patients.
The USPSTF’s latest recommendations (TABLE 1) on screening for lipid disorders in adults1 call for screening women only when coronary heart disease (CHD) risk factors are present, regardless of their age. (See TABLE 2 for a list of CHD risk factors.) That’s a major shift from the 2001 recommendation, which stated that all women over age 45 should be screened and women ages 20 to 45 should be screened if they were at elevated risk.
The recommendations for men remain the same: All men older than 35 should be screened, as should men who are between the ages of 20 and 35 who have other CHD risks.
TABLE 1
USPSTF lipid disorder screening recommendations at a glance
| Screening men • The United States Preventive Services Task Force (USPSTF) strongly recommends screening men ages 35 and older for lipid disorders. Grade A recommendation |
| • The USPSTF recommends screening men ages 20 to 35 for lipid disorders if they are at increased risk for coronary heart disease (CHD). Grade B recommendation |
| Screening women at increased risk • The USPSTF strongly recommends screening women ages 45 and older for lipid disorders if they are at increased risk for CHD. Grade A recommendation |
| • The USPSTF recommends screening women ages 20 to 45 for lipid disorders if they are at increased risk for CHD. Grade B recommendation |
| Screening young men and all women not at increased risk • The USPSTF makes no recommendation for or against routine screening for lipid disorders in men between the ages of 20 and 35, or in women ages 20 and older who are not at increased risk for CHD. Grade C recommendation |
TABLE 2
Risk factors for CHD
| • Diabetes |
| • Personal history of coronary heart disease (CHD) or noncoronary atherosclerosis (eg, abdominal aortic aneurysm, peripheral artery disease, and carotid artery stenosis) |
| • A family history of cardiovascular disease before age 50 in male relatives or age 60 in female relatives |
| • Tobacco use |
| • Hypertension |
| • Obesity (body mass index ≥30) |
A different approach from NIH and AHA
The revised updated recommendation for women over age 45 was based on 2 systematic evidence reviews2,3 that concluded, while treatment clearly benefits women with other risk factors, benefit has not been proven for women who are otherwise CHD risk free.
The recommendation for women conflicts with those of the National Institutes of Health and the American Heart Association; both recommend screening all adults starting at age 20—regardless of risk.
Screening those without risk isn’t ruled out
It is important to note that the task force is not recommending against screening in women (or men between the ages of 20 and 35) who do not have other CHD risks. The task force makes a C recommendation with wording that states, “The USPSTF makes no recommendation for or against routine provision of [the service]. The USPSTF found at least fair evidence that [the service] can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation” (TABLE 3).
The task force chose not to use the new wording for a C recommendation, adopted in 2007, which reads, “The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small.”
It is also important to realize that a large proportion of women have another CHD risk and will not fall into the C category recommendation.
TABLE 3
USPSTF recommendation categories
| A—Strongly recommended: The United States Preventive Services Task Force (USPSTF) strongly recommends that clinicians provide the service to eligible patients. The USPSTF found good evidence that the service improves important health outcomes and concludes that benefits substantially outweigh harms. |
| B—Recommended: The USPSTF recommends that clinicians provide the service to eligible patients. The USPSTF found at least fair evidence that the service improves important health outcomes and concludes that benefits outweigh harms. |
| C—No recommendation: The USPSTF makes no recommendation for or against routine provision of the service. The USPSTF found at least fair evidence that the service can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation. |
| D—Not recommended: The USPSTF recommends against routinely providing the service to asymptomatic patients. The USPSTF found at least fair evidence that the service is ineffective or that harms outweigh benefits. |
| I—Insufficient evidence to make a recommendation: The USPSTF concludes that the evidence is insufficient to recommend for or against routinely providing the service. Evidence that the service is effective is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
No need to look at triglycerides initially
The task force recommends screening with a fasting or nonfasting serum sample for total cholesterol and high-density lipoprotein cholesterol. The task force does not recommend including a triglyceride level because there is mixed and inclusive evidence that triglyceride levels are independently associated with CHD risk and scant evidence that treating isolated elevated triglyceride levels reduces the occurrence of CHD events. This approach also conflicts with other organizations that recommend screening with fasting lipid profiles that include a triglyceride level.
The task force states that an abnormal initial screen should be confirmed by a repeat test and, if confirmed, a fasting lipid panel should be obtained. Wide adoption of the task force recommendations would result in considerable savings in cost and patient inconvenience by avoiding complete fasting lipid panels as the initial screen.
The optimal frequency of screening is not established and the task force states that every 5 years is reasonable, although more frequent testing might be considered for those with high normal values, and less frequent intervals for those with optimal cholesterol levels and healthy lifestyles.
Treatment: Look beyond lifestyle
The screening recommendations are accompanied by a discussion of clinical considerations and a description of an approach to treatment for those with lipid disorders. The main point the task force makes is that all CHD risks should be addressed, and that lifestyle changes alone rarely reduce elevated cholesterol to an optimal level. (For more on the treatment of hyperlipidemia, see the National Heart, Lung, and Blood Institute’s Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [Adult Treatment Panel III] at http://www.nhlbi.nih.gov/guidelines/cholesterol/index.htm.)
Time to rethink conventional opinion
The updated task force recommendations are a reminder that many widely used guidelines, including those on the prevention of CHD, are based on a lack of high-level evidence. Thus, it is not surprising that a rigorously evidence-based analysis, as preformed by the USPSTF, will frequently result in recommendations that are at variance with common practice and conventional opinion.
1. U.S. Preventive Services Task Force (USPSTF). Screening for lipid disorders in adults: recommendation statement. June 2008. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipidrs.htm. Accessed September 26, 2008.
2. Grady D, Chaput L, Kristof M. Systematic Review of Lipid Lowering Treatment to Reduce Risk of Coronary Heart Disease in Women. Rockville, Md: Agency for Healthcare Research and Quality; 2003.
3. Helfand M, Carson S. Screening for lipid disorders in adults: selective update of 2001 U.S. Preventive Services Task Force Review. June 2008. AHRQ publication number 08-05114-EF-1. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipides.pdf. Accessed September 26, 2008.
When patients reached a certain age (36 for men, 46 for women), it used to mean that it was time, in the eyes of the United States Preventive Services Task Force (USPSTF), to screen for lipid disorders. But that’s changed for female patients.
The USPSTF’s latest recommendations (TABLE 1) on screening for lipid disorders in adults1 call for screening women only when coronary heart disease (CHD) risk factors are present, regardless of their age. (See TABLE 2 for a list of CHD risk factors.) That’s a major shift from the 2001 recommendation, which stated that all women over age 45 should be screened and women ages 20 to 45 should be screened if they were at elevated risk.
The recommendations for men remain the same: All men older than 35 should be screened, as should men who are between the ages of 20 and 35 who have other CHD risks.
TABLE 1
USPSTF lipid disorder screening recommendations at a glance
| Screening men • The United States Preventive Services Task Force (USPSTF) strongly recommends screening men ages 35 and older for lipid disorders. Grade A recommendation |
| • The USPSTF recommends screening men ages 20 to 35 for lipid disorders if they are at increased risk for coronary heart disease (CHD). Grade B recommendation |
| Screening women at increased risk • The USPSTF strongly recommends screening women ages 45 and older for lipid disorders if they are at increased risk for CHD. Grade A recommendation |
| • The USPSTF recommends screening women ages 20 to 45 for lipid disorders if they are at increased risk for CHD. Grade B recommendation |
| Screening young men and all women not at increased risk • The USPSTF makes no recommendation for or against routine screening for lipid disorders in men between the ages of 20 and 35, or in women ages 20 and older who are not at increased risk for CHD. Grade C recommendation |
TABLE 2
Risk factors for CHD
| • Diabetes |
| • Personal history of coronary heart disease (CHD) or noncoronary atherosclerosis (eg, abdominal aortic aneurysm, peripheral artery disease, and carotid artery stenosis) |
| • A family history of cardiovascular disease before age 50 in male relatives or age 60 in female relatives |
| • Tobacco use |
| • Hypertension |
| • Obesity (body mass index ≥30) |
A different approach from NIH and AHA
The revised updated recommendation for women over age 45 was based on 2 systematic evidence reviews2,3 that concluded, while treatment clearly benefits women with other risk factors, benefit has not been proven for women who are otherwise CHD risk free.
The recommendation for women conflicts with those of the National Institutes of Health and the American Heart Association; both recommend screening all adults starting at age 20—regardless of risk.
Screening those without risk isn’t ruled out
It is important to note that the task force is not recommending against screening in women (or men between the ages of 20 and 35) who do not have other CHD risks. The task force makes a C recommendation with wording that states, “The USPSTF makes no recommendation for or against routine provision of [the service]. The USPSTF found at least fair evidence that [the service] can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation” (TABLE 3).
The task force chose not to use the new wording for a C recommendation, adopted in 2007, which reads, “The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small.”
It is also important to realize that a large proportion of women have another CHD risk and will not fall into the C category recommendation.
TABLE 3
USPSTF recommendation categories
| A—Strongly recommended: The United States Preventive Services Task Force (USPSTF) strongly recommends that clinicians provide the service to eligible patients. The USPSTF found good evidence that the service improves important health outcomes and concludes that benefits substantially outweigh harms. |
| B—Recommended: The USPSTF recommends that clinicians provide the service to eligible patients. The USPSTF found at least fair evidence that the service improves important health outcomes and concludes that benefits outweigh harms. |
| C—No recommendation: The USPSTF makes no recommendation for or against routine provision of the service. The USPSTF found at least fair evidence that the service can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation. |
| D—Not recommended: The USPSTF recommends against routinely providing the service to asymptomatic patients. The USPSTF found at least fair evidence that the service is ineffective or that harms outweigh benefits. |
| I—Insufficient evidence to make a recommendation: The USPSTF concludes that the evidence is insufficient to recommend for or against routinely providing the service. Evidence that the service is effective is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
No need to look at triglycerides initially
The task force recommends screening with a fasting or nonfasting serum sample for total cholesterol and high-density lipoprotein cholesterol. The task force does not recommend including a triglyceride level because there is mixed and inclusive evidence that triglyceride levels are independently associated with CHD risk and scant evidence that treating isolated elevated triglyceride levels reduces the occurrence of CHD events. This approach also conflicts with other organizations that recommend screening with fasting lipid profiles that include a triglyceride level.
The task force states that an abnormal initial screen should be confirmed by a repeat test and, if confirmed, a fasting lipid panel should be obtained. Wide adoption of the task force recommendations would result in considerable savings in cost and patient inconvenience by avoiding complete fasting lipid panels as the initial screen.
The optimal frequency of screening is not established and the task force states that every 5 years is reasonable, although more frequent testing might be considered for those with high normal values, and less frequent intervals for those with optimal cholesterol levels and healthy lifestyles.
Treatment: Look beyond lifestyle
The screening recommendations are accompanied by a discussion of clinical considerations and a description of an approach to treatment for those with lipid disorders. The main point the task force makes is that all CHD risks should be addressed, and that lifestyle changes alone rarely reduce elevated cholesterol to an optimal level. (For more on the treatment of hyperlipidemia, see the National Heart, Lung, and Blood Institute’s Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [Adult Treatment Panel III] at http://www.nhlbi.nih.gov/guidelines/cholesterol/index.htm.)
Time to rethink conventional opinion
The updated task force recommendations are a reminder that many widely used guidelines, including those on the prevention of CHD, are based on a lack of high-level evidence. Thus, it is not surprising that a rigorously evidence-based analysis, as preformed by the USPSTF, will frequently result in recommendations that are at variance with common practice and conventional opinion.
When patients reached a certain age (36 for men, 46 for women), it used to mean that it was time, in the eyes of the United States Preventive Services Task Force (USPSTF), to screen for lipid disorders. But that’s changed for female patients.
The USPSTF’s latest recommendations (TABLE 1) on screening for lipid disorders in adults1 call for screening women only when coronary heart disease (CHD) risk factors are present, regardless of their age. (See TABLE 2 for a list of CHD risk factors.) That’s a major shift from the 2001 recommendation, which stated that all women over age 45 should be screened and women ages 20 to 45 should be screened if they were at elevated risk.
The recommendations for men remain the same: All men older than 35 should be screened, as should men who are between the ages of 20 and 35 who have other CHD risks.
TABLE 1
USPSTF lipid disorder screening recommendations at a glance
| Screening men • The United States Preventive Services Task Force (USPSTF) strongly recommends screening men ages 35 and older for lipid disorders. Grade A recommendation |
| • The USPSTF recommends screening men ages 20 to 35 for lipid disorders if they are at increased risk for coronary heart disease (CHD). Grade B recommendation |
| Screening women at increased risk • The USPSTF strongly recommends screening women ages 45 and older for lipid disorders if they are at increased risk for CHD. Grade A recommendation |
| • The USPSTF recommends screening women ages 20 to 45 for lipid disorders if they are at increased risk for CHD. Grade B recommendation |
| Screening young men and all women not at increased risk • The USPSTF makes no recommendation for or against routine screening for lipid disorders in men between the ages of 20 and 35, or in women ages 20 and older who are not at increased risk for CHD. Grade C recommendation |
TABLE 2
Risk factors for CHD
| • Diabetes |
| • Personal history of coronary heart disease (CHD) or noncoronary atherosclerosis (eg, abdominal aortic aneurysm, peripheral artery disease, and carotid artery stenosis) |
| • A family history of cardiovascular disease before age 50 in male relatives or age 60 in female relatives |
| • Tobacco use |
| • Hypertension |
| • Obesity (body mass index ≥30) |
A different approach from NIH and AHA
The revised updated recommendation for women over age 45 was based on 2 systematic evidence reviews2,3 that concluded, while treatment clearly benefits women with other risk factors, benefit has not been proven for women who are otherwise CHD risk free.
The recommendation for women conflicts with those of the National Institutes of Health and the American Heart Association; both recommend screening all adults starting at age 20—regardless of risk.
Screening those without risk isn’t ruled out
It is important to note that the task force is not recommending against screening in women (or men between the ages of 20 and 35) who do not have other CHD risks. The task force makes a C recommendation with wording that states, “The USPSTF makes no recommendation for or against routine provision of [the service]. The USPSTF found at least fair evidence that [the service] can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation” (TABLE 3).
The task force chose not to use the new wording for a C recommendation, adopted in 2007, which reads, “The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small.”
It is also important to realize that a large proportion of women have another CHD risk and will not fall into the C category recommendation.
TABLE 3
USPSTF recommendation categories
| A—Strongly recommended: The United States Preventive Services Task Force (USPSTF) strongly recommends that clinicians provide the service to eligible patients. The USPSTF found good evidence that the service improves important health outcomes and concludes that benefits substantially outweigh harms. |
| B—Recommended: The USPSTF recommends that clinicians provide the service to eligible patients. The USPSTF found at least fair evidence that the service improves important health outcomes and concludes that benefits outweigh harms. |
| C—No recommendation: The USPSTF makes no recommendation for or against routine provision of the service. The USPSTF found at least fair evidence that the service can improve health outcomes but concludes that the balance of benefits and harms is too close to justify a general recommendation. |
| D—Not recommended: The USPSTF recommends against routinely providing the service to asymptomatic patients. The USPSTF found at least fair evidence that the service is ineffective or that harms outweigh benefits. |
| I—Insufficient evidence to make a recommendation: The USPSTF concludes that the evidence is insufficient to recommend for or against routinely providing the service. Evidence that the service is effective is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
No need to look at triglycerides initially
The task force recommends screening with a fasting or nonfasting serum sample for total cholesterol and high-density lipoprotein cholesterol. The task force does not recommend including a triglyceride level because there is mixed and inclusive evidence that triglyceride levels are independently associated with CHD risk and scant evidence that treating isolated elevated triglyceride levels reduces the occurrence of CHD events. This approach also conflicts with other organizations that recommend screening with fasting lipid profiles that include a triglyceride level.
The task force states that an abnormal initial screen should be confirmed by a repeat test and, if confirmed, a fasting lipid panel should be obtained. Wide adoption of the task force recommendations would result in considerable savings in cost and patient inconvenience by avoiding complete fasting lipid panels as the initial screen.
The optimal frequency of screening is not established and the task force states that every 5 years is reasonable, although more frequent testing might be considered for those with high normal values, and less frequent intervals for those with optimal cholesterol levels and healthy lifestyles.
Treatment: Look beyond lifestyle
The screening recommendations are accompanied by a discussion of clinical considerations and a description of an approach to treatment for those with lipid disorders. The main point the task force makes is that all CHD risks should be addressed, and that lifestyle changes alone rarely reduce elevated cholesterol to an optimal level. (For more on the treatment of hyperlipidemia, see the National Heart, Lung, and Blood Institute’s Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [Adult Treatment Panel III] at http://www.nhlbi.nih.gov/guidelines/cholesterol/index.htm.)
Time to rethink conventional opinion
The updated task force recommendations are a reminder that many widely used guidelines, including those on the prevention of CHD, are based on a lack of high-level evidence. Thus, it is not surprising that a rigorously evidence-based analysis, as preformed by the USPSTF, will frequently result in recommendations that are at variance with common practice and conventional opinion.
1. U.S. Preventive Services Task Force (USPSTF). Screening for lipid disorders in adults: recommendation statement. June 2008. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipidrs.htm. Accessed September 26, 2008.
2. Grady D, Chaput L, Kristof M. Systematic Review of Lipid Lowering Treatment to Reduce Risk of Coronary Heart Disease in Women. Rockville, Md: Agency for Healthcare Research and Quality; 2003.
3. Helfand M, Carson S. Screening for lipid disorders in adults: selective update of 2001 U.S. Preventive Services Task Force Review. June 2008. AHRQ publication number 08-05114-EF-1. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipides.pdf. Accessed September 26, 2008.
1. U.S. Preventive Services Task Force (USPSTF). Screening for lipid disorders in adults: recommendation statement. June 2008. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipidrs.htm. Accessed September 26, 2008.
2. Grady D, Chaput L, Kristof M. Systematic Review of Lipid Lowering Treatment to Reduce Risk of Coronary Heart Disease in Women. Rockville, Md: Agency for Healthcare Research and Quality; 2003.
3. Helfand M, Carson S. Screening for lipid disorders in adults: selective update of 2001 U.S. Preventive Services Task Force Review. June 2008. AHRQ publication number 08-05114-EF-1. Available at: http://www.ahrq.gov/clinic/uspstf08/lipid/lipides.pdf. Accessed September 26, 2008.