User login
What interventions most effectively protect against contrast media-induced nephropathy?
Case
A 68-year-old diabetic woman hospitalized for non-ST-segment elevation myocardial infarction develops increasing chest pain despite maximal appropriate medical therapy and is referred for urgent coronary angiography. She is normotensive, weighs 60 kg, and is without signs of congestive heart failure on examination. The serum creatinine is 1.6 mg/dL (her baseline). What is her risk for contrast media-induced nephropathy (CIN)? What measures can be undertaken to reduce her risk?
Background
Radiocontrast agents are well-recognized nephrotoxins that can cause a usually reversible, non-oliguric form of renal failure within 24 hours and up to five days following administration. Contrast nephropathy is associated with longer hospital stays and higher mortality. The incidence varies widely according to patient characteristics and the type and quantity of contrast agent used.
The pathogenesis of CIN is not completely understood, but likely represents a combination of contrast-mediated renal vasoconstriction, oxidative damage, and direct cytotoxic effects. Newer low-osmolar or iso-osmolar contrast agents are associated with lower rates of CIN than high-osmolar contrast agents. Multiple pharmacologic strategies for CIN prevention have been investigated, with several important trials published in the past two years. This review summarizes the risk assessment and prophylactic strategies required for optimal protection of patients from CIN.
Assesment of Patient Risk
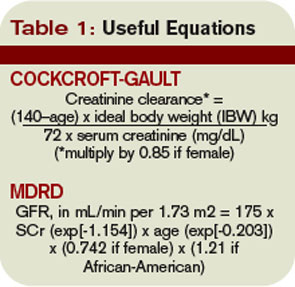
Contrast-induced nephropathy is defined variably in clinical trials, most commonly as a 25% increase in serum creatinine above baseline at 48 hours after contrast administration. The most important risk factor for CIN is pre-existing kidney disease—more specifically, a diminished glomerular filtration rate (GFR) below 60 mL/minute/1.73 m2 body surface area.1 The serum creatinine concentration can be misleading. Advancing age, female gender, low lean body mass, or unstable rising creatinine all can lead to overestimation of the GFR. The Modification of Diet in Renal Disease (MDRD) estimate of GFR and the Cockcroft-Gault estimate of creatinine clearance are calculated in a basic formula. (see Table 1, left)
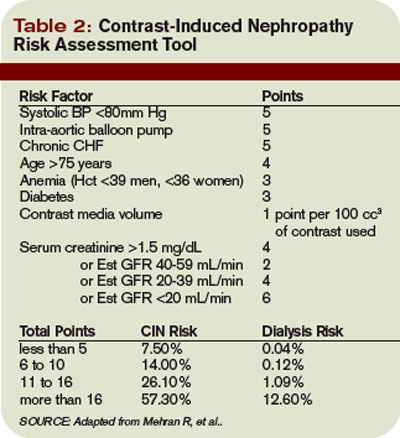
Several other factors have been linked to increased risk for CIN. Table 2 (left) summarizes these risk factors and assigns them various point scores. In general, patients with chronic kidney disease or any of these risk factors should have a serum creatinine drawn before the contrast study to clarify their CIN risk and facilitate decisions regarding prophylaxis. Patients with a score of six or more are at substantial risk for CIN.1
Strategy for Prophylaxis
Low-osmolar and iso-osmolar contrast agents have been associated with lower rates of CIN compared to high-osmolar contrast. However, the referring hospitalist rarely determines the type and volume of contrast used. Fortunately, high-osmolar contrast is used infrequently today. The primary strategy for CIN prophylaxis is to:
1) Determine CIN risk using a validated tool (see Table 2).
2) If “at risk,” consider alternate diagnostic modalities that do not involve the intravenous administration of iodinated contrast. Consider delaying testing with contrast agents until potentially reversible conditions affecting GFR are addressed, such as volume depletion, recent contrast use, or concomitant use of nonsteroidal anti-inflammatory drugs or angiotensin-converting enzyme inhibitors.
3) Provide pharmacologic and intravenous fluid prophylaxis as described below.
Pharmacologic Prophylaxis
Multiple agents have been investigated in the prevention of CIN: mannitol, furosemide, theophylline, fenoldopam, dopamine, N-acetylcysteine, and others. The most effective noteworthy of these is N-acetylcysteine (NAC). The first major trial of NAC for CIN prevention was published in 2000.2 Since then, more than two dozen studies, mostly randomized controlled trials (RCTs), and nearly a dozen meta-analyses have been published, with inconsistent results.
Of particular note, systematic reviews and meta-analyses have reached differing conclusions on the overall efficacy of NAC in the prevention of CIN. One recent study including NAC trials published before June 2006 concluded there has been “significant publication bias throughout the life cycle of this clinical question … further amplified by meta-analyses.”3 It has been estimated a single trial enrolling 1,800 patients (about 10 times larger than most completed trials) would be needed to definitively answer this question.4 The latest meta-analysis includes at least one large RCT of NAC not included in prior meta-analyses and concludes that NAC is effective in the prevention of CIN.5 The pooled relative risk for CIN was 0.62 (95% C.I. 0.44-0.88). These investigators concluded there was no significant publication bias.
Taken together, the primary literature and secondary meta-analyses suggest that NAC is probably effective in the prevention of CIN, although there may be some publication bias. Practically speaking, NAC is essentially without side effects, and the likelihood that it affords some degree of protection suggests it should be used routinely, unless or until larger studies demonstrate otherwise. A NAC dose of 1,200 mg twice daily beginning the day prior and continuing through the day of contrast administration was part of the successful protocol published by Brigouri, et al., in 2007.
Intravenous Crystalloids Trials
A landmark trial published in 1994 showed half-normal saline in 5% dextrose given 12 hours before and 12 hours after administering a radiocontrast agent was superior to half-normal saline plus mannitol or half-normal saline plus furosemide in preventing CIN.6 This regimen remained the standard of care until 2002, when a large RCT compared half- normal saline in 5% dextrose to isotonic normal saline in 1,620 patients undergoing coronary angioplasty.7 About 20% of the patients had underlying renal dysfunction and about 15% were diabetic. The rate of CIN decreased from 2% (14/698) to 0.7% (5/685), a modest-but-statistically-significant difference. After this study, practice generally shifted to using normal saline at 1 mL/kg/hr 12 hours before and 12 hours after contrast procedures. One notable review article published in 2006 concluded that isotonic saline was the best-proven strategy for the prevention of CIN.8
How does intravenous sodium chloride reduce the rate of CIN? The mechanism is unclear, but it may work simply by treating subclinical states of volume depletion. But as free radical oxidation has been implicated in the pathophysiology of CIN, investigators hypothesized that alkalinizing the urine (reducing free radical formation) with isotonic sodium bicarbonate might better protect patients from CIN than saline. In 2004, the first trial demonstrating the efficacy of bicarbonate was stopped early after the rate of CIN had decreased from 13.6% (8/59) in the saline arm to 1.7% (1/60) in the bicarbonate arm.9 The editorial accompanying this small trial cautioned “prospective confirmation should be required before accepting new therapies into routine clinical practice.”
In 2007, four prospective trials comparing various hydration regimens were published; each concluding that bicarbonate is superior to saline. The largest of these studies was the REMEDIAL trial.10 Patients were referred for coronary angiography and had a baseline serum creatinine of 2.0 mg/dl or higher or an estimated GFR below 40 mL/minute/1.73 m2 (or both). In double-blind fashion, patients were randomized to one of three preventative strategies: normal saline plus NAC (n=111), sodium bicarbonate plus NAC (n=108), or normal saline plus NAC plus ascorbic acid (n=107). The primary endpoint was defined as a 25% or higher increase in serum creatinine at 48 hours. This occurred in 9.9% (11/111) of the normal saline plus NAC group, 1.9% (2/108) of the sodium bicarbonate plus NAC group, and 10.3% (11/107) of the normal saline plus NAC plus ascorbic acid group (p=0.019 for sodium bicarbonate plus NAC versus normal saline plus NAC).
The sodium bicarbonate regimen was the same as that reported by Merten in 2004—namely, 154 mEq/L of sodium bicarbonate in 5% dextrose solution, given at 3 mL/kg/hr for one hour before contrast administration and 1 mL/kg/hr for six hours afterward. The saline regimen (154 mEq/L) was the same as that reported by Mueller in 2002—1 mL/kg/hr for 12 hours before contrast administration and 12 hours afterward. All patients received NAC at a dose of 1,200 mg twice daily the day before and the day of contrast administration. It is not possible to conclude from this trial whether sodium bicarbonate without NAC would have been as effective as the regimen studied. Ascorbic acid was included in this trial as another antioxidant to compare with NAC. The three other RCTs published in 2007 are summarized in Table 3 (see p. 21).11,12,13
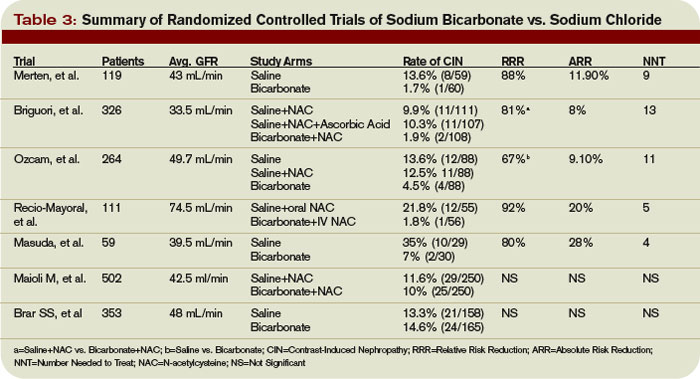
Recently, two large RCTs of saline versus bicarbonate concluded there was no difference between the two.14,15 These trials were the largest to date, each of them single center and unblinded, and using slightly different methods than the REMEDIAL trial. CIN also was defined more broadly as a 0.5mg/dL or 25% change in creatinine within five days after contrast. Follow-up was only 88% in one trial. Nevertheless, these two new trials reach quite different conclusions than those before. Table 3 (see p. 21) summarizes seven RCTs of saline versus bicarbonate in the prevention of CIN. Differences in design and methods, definitions of CIN, completeness of follow-up, and severity of renal dysfunction among patients studied, make direct comparisons among these trials difficult. But as five of the seven RCTs of saline versus bicarbonate have concluded that bicarbonate is superior, and none have concluded saline is superior, this author recommends that at the present time intravenous sodium bicarbonate be used according to the Merten protocol when providing IVF for the prevention of CIN.
Back to the Case
The patient in the vignette has an estimated GFR of about 32 mL/min by the MDRD equation. With this level of renal dysfunction, the presence of diabetes mellitus, mellitus and assuming at least a 100 cc contrast bolus with the angiography, her risk for CIN is about 14% (eight points on the Mehran scale illustrated in Table 21). Alternatives to coronary angiography are limited in this example, and pharmacologic and IVF measures to prevent CIN are indicated. Borrowing from the regimen used in the REMEDIAL trial, she should ideally receive NAC 1200 mg orally BID for two days, starting one day prior to the procedure (in this case, would begin as soon as the risk for CIN is appreciated and continue for four doses). More importantly, she should receive sodium bicarbonate 154mEq/L at a rate of 3 mL/kg/hr one hour prior to contrast and 1 mL/kg/hr during and for six hours following the contrast procedure.
Bottom Line
Contrast nephropathy risk varies inversely with GFR and can be estimated according to a validated tool. Patients at risk for CIN should be identified early and offered NAC and sodium bicarbonate, if there are no alternatives to administering intravenous contrast. Intravenous saline also is effective, but may not be as effective as bicarbonate. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado Denver and the associate chief, Medical Service, at the Denver VA Medical Center.
References
1. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393-1399.
2. Tepel M, van der Giet M, Schwarzfeld C, et al. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med. 2000;343:180-184.
3. Vaitkus PT and Brar C. N-Acetylcysteine in the prevention of contrast-induced nephropathy: publication bias perpetuated by meta-analyses. Am Heart J. 2007;153:275-280.
4. Bagshaw SM, McAlister FA, Manns BJ, Ghali WA. Acetylcysteine in the prevention of contrast-induced nephropathy: a case study of the pitfalls in the evolution of evidence. Arch Intern Med. 2006;166:161-166.
5. Kelly AM, Dwamena B, Cronin P, Bernstein SJ and Carlos RC. Meta-analysis: effectiveness of drugs for preventing contrast-induced nephropathy. Ann Intern Med. 2008;148:284-294.
6. Solomon R, Werner C, Mann D, et al. Effects of saline, mannitol, and furosemide on acute decreases in renal function induced by radiocontrast agents. N Engl J Med. 1994;331:14-16.
7. Mueller C, Buerkle G, Buettner HJ, et al. Prevention of contrast-media associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Arch Intern Med. 2002;162:329-336.
8. Barrett BJ and Parfrey PS. Preventing nephropathy induced by contrast medium. N Engl J Med. 2006;354:379-386.
9. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with bicarbonate: a randomized controlled trial. JAMA. 2004;291:2328-2334.
10. Brigouri C, Airoldi F, D.Andrea, et al. Renal insufficiency following contrast media administration trial (remedial): a randomized comparison of 3 preventive strategies. Circulation. 2007;115:1211-1217.
11. Masuda M, Yamada T, Mine T, et al. Comparison of usefulness of sodium bicarbonate versus sodium chloride to prevent contrast-induced nephropathy in patients undergoing an emergent coronary procedure. Am J Cardiol. 2007;100:781-786.
12. Recio-Mayoral A, Chaparro M, Prado B, et al. The reno-protective effect of hydration with sodium bicarbonate plus n-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the reno study. J Am Coll Cardiol. 2007;49:1283-1288.
13. Ozcan EE, Guneri S, Akdeniz B, et al. Sodium bicarbonate, n-acetylcysteine, and saline for the prevention of radiocontrast-induced nephropathy. a comparison of 3 regimens for protecting contrast-induced nephropathy (sic) in patients undergoing coronary procedures. a single center prospective controlled trial. Am Heart J. 2007;154:539-544.
14. Maioli M, Toso A, Leoncini M, et al. Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. J Am Coll Cardiol. 2008;52:599-604.
15. Brar SS, Shen AYJ, Jorgensen MB, et al. Sodium bicarbonate vs. sodium chloride for the prevention of contrast medium-induced nephropathy in patients undergoing coronary angiography: a randomized trial. JAMA. 2008;300:1038-1046.
Case
A 68-year-old diabetic woman hospitalized for non-ST-segment elevation myocardial infarction develops increasing chest pain despite maximal appropriate medical therapy and is referred for urgent coronary angiography. She is normotensive, weighs 60 kg, and is without signs of congestive heart failure on examination. The serum creatinine is 1.6 mg/dL (her baseline). What is her risk for contrast media-induced nephropathy (CIN)? What measures can be undertaken to reduce her risk?
Background
Radiocontrast agents are well-recognized nephrotoxins that can cause a usually reversible, non-oliguric form of renal failure within 24 hours and up to five days following administration. Contrast nephropathy is associated with longer hospital stays and higher mortality. The incidence varies widely according to patient characteristics and the type and quantity of contrast agent used.
The pathogenesis of CIN is not completely understood, but likely represents a combination of contrast-mediated renal vasoconstriction, oxidative damage, and direct cytotoxic effects. Newer low-osmolar or iso-osmolar contrast agents are associated with lower rates of CIN than high-osmolar contrast agents. Multiple pharmacologic strategies for CIN prevention have been investigated, with several important trials published in the past two years. This review summarizes the risk assessment and prophylactic strategies required for optimal protection of patients from CIN.
Assesment of Patient Risk
Contrast-induced nephropathy is defined variably in clinical trials, most commonly as a 25% increase in serum creatinine above baseline at 48 hours after contrast administration. The most important risk factor for CIN is pre-existing kidney disease—more specifically, a diminished glomerular filtration rate (GFR) below 60 mL/minute/1.73 m2 body surface area.1 The serum creatinine concentration can be misleading. Advancing age, female gender, low lean body mass, or unstable rising creatinine all can lead to overestimation of the GFR. The Modification of Diet in Renal Disease (MDRD) estimate of GFR and the Cockcroft-Gault estimate of creatinine clearance are calculated in a basic formula. (see Table 1, left)
Several other factors have been linked to increased risk for CIN. Table 2 (left) summarizes these risk factors and assigns them various point scores. In general, patients with chronic kidney disease or any of these risk factors should have a serum creatinine drawn before the contrast study to clarify their CIN risk and facilitate decisions regarding prophylaxis. Patients with a score of six or more are at substantial risk for CIN.1
Strategy for Prophylaxis
Low-osmolar and iso-osmolar contrast agents have been associated with lower rates of CIN compared to high-osmolar contrast. However, the referring hospitalist rarely determines the type and volume of contrast used. Fortunately, high-osmolar contrast is used infrequently today. The primary strategy for CIN prophylaxis is to:
1) Determine CIN risk using a validated tool (see Table 2).
2) If “at risk,” consider alternate diagnostic modalities that do not involve the intravenous administration of iodinated contrast. Consider delaying testing with contrast agents until potentially reversible conditions affecting GFR are addressed, such as volume depletion, recent contrast use, or concomitant use of nonsteroidal anti-inflammatory drugs or angiotensin-converting enzyme inhibitors.
3) Provide pharmacologic and intravenous fluid prophylaxis as described below.
Pharmacologic Prophylaxis
Multiple agents have been investigated in the prevention of CIN: mannitol, furosemide, theophylline, fenoldopam, dopamine, N-acetylcysteine, and others. The most effective noteworthy of these is N-acetylcysteine (NAC). The first major trial of NAC for CIN prevention was published in 2000.2 Since then, more than two dozen studies, mostly randomized controlled trials (RCTs), and nearly a dozen meta-analyses have been published, with inconsistent results.
Of particular note, systematic reviews and meta-analyses have reached differing conclusions on the overall efficacy of NAC in the prevention of CIN. One recent study including NAC trials published before June 2006 concluded there has been “significant publication bias throughout the life cycle of this clinical question … further amplified by meta-analyses.”3 It has been estimated a single trial enrolling 1,800 patients (about 10 times larger than most completed trials) would be needed to definitively answer this question.4 The latest meta-analysis includes at least one large RCT of NAC not included in prior meta-analyses and concludes that NAC is effective in the prevention of CIN.5 The pooled relative risk for CIN was 0.62 (95% C.I. 0.44-0.88). These investigators concluded there was no significant publication bias.
Taken together, the primary literature and secondary meta-analyses suggest that NAC is probably effective in the prevention of CIN, although there may be some publication bias. Practically speaking, NAC is essentially without side effects, and the likelihood that it affords some degree of protection suggests it should be used routinely, unless or until larger studies demonstrate otherwise. A NAC dose of 1,200 mg twice daily beginning the day prior and continuing through the day of contrast administration was part of the successful protocol published by Brigouri, et al., in 2007.
Intravenous Crystalloids Trials
A landmark trial published in 1994 showed half-normal saline in 5% dextrose given 12 hours before and 12 hours after administering a radiocontrast agent was superior to half-normal saline plus mannitol or half-normal saline plus furosemide in preventing CIN.6 This regimen remained the standard of care until 2002, when a large RCT compared half- normal saline in 5% dextrose to isotonic normal saline in 1,620 patients undergoing coronary angioplasty.7 About 20% of the patients had underlying renal dysfunction and about 15% were diabetic. The rate of CIN decreased from 2% (14/698) to 0.7% (5/685), a modest-but-statistically-significant difference. After this study, practice generally shifted to using normal saline at 1 mL/kg/hr 12 hours before and 12 hours after contrast procedures. One notable review article published in 2006 concluded that isotonic saline was the best-proven strategy for the prevention of CIN.8
How does intravenous sodium chloride reduce the rate of CIN? The mechanism is unclear, but it may work simply by treating subclinical states of volume depletion. But as free radical oxidation has been implicated in the pathophysiology of CIN, investigators hypothesized that alkalinizing the urine (reducing free radical formation) with isotonic sodium bicarbonate might better protect patients from CIN than saline. In 2004, the first trial demonstrating the efficacy of bicarbonate was stopped early after the rate of CIN had decreased from 13.6% (8/59) in the saline arm to 1.7% (1/60) in the bicarbonate arm.9 The editorial accompanying this small trial cautioned “prospective confirmation should be required before accepting new therapies into routine clinical practice.”
In 2007, four prospective trials comparing various hydration regimens were published; each concluding that bicarbonate is superior to saline. The largest of these studies was the REMEDIAL trial.10 Patients were referred for coronary angiography and had a baseline serum creatinine of 2.0 mg/dl or higher or an estimated GFR below 40 mL/minute/1.73 m2 (or both). In double-blind fashion, patients were randomized to one of three preventative strategies: normal saline plus NAC (n=111), sodium bicarbonate plus NAC (n=108), or normal saline plus NAC plus ascorbic acid (n=107). The primary endpoint was defined as a 25% or higher increase in serum creatinine at 48 hours. This occurred in 9.9% (11/111) of the normal saline plus NAC group, 1.9% (2/108) of the sodium bicarbonate plus NAC group, and 10.3% (11/107) of the normal saline plus NAC plus ascorbic acid group (p=0.019 for sodium bicarbonate plus NAC versus normal saline plus NAC).
The sodium bicarbonate regimen was the same as that reported by Merten in 2004—namely, 154 mEq/L of sodium bicarbonate in 5% dextrose solution, given at 3 mL/kg/hr for one hour before contrast administration and 1 mL/kg/hr for six hours afterward. The saline regimen (154 mEq/L) was the same as that reported by Mueller in 2002—1 mL/kg/hr for 12 hours before contrast administration and 12 hours afterward. All patients received NAC at a dose of 1,200 mg twice daily the day before and the day of contrast administration. It is not possible to conclude from this trial whether sodium bicarbonate without NAC would have been as effective as the regimen studied. Ascorbic acid was included in this trial as another antioxidant to compare with NAC. The three other RCTs published in 2007 are summarized in Table 3 (see p. 21).11,12,13
Recently, two large RCTs of saline versus bicarbonate concluded there was no difference between the two.14,15 These trials were the largest to date, each of them single center and unblinded, and using slightly different methods than the REMEDIAL trial. CIN also was defined more broadly as a 0.5mg/dL or 25% change in creatinine within five days after contrast. Follow-up was only 88% in one trial. Nevertheless, these two new trials reach quite different conclusions than those before. Table 3 (see p. 21) summarizes seven RCTs of saline versus bicarbonate in the prevention of CIN. Differences in design and methods, definitions of CIN, completeness of follow-up, and severity of renal dysfunction among patients studied, make direct comparisons among these trials difficult. But as five of the seven RCTs of saline versus bicarbonate have concluded that bicarbonate is superior, and none have concluded saline is superior, this author recommends that at the present time intravenous sodium bicarbonate be used according to the Merten protocol when providing IVF for the prevention of CIN.
Back to the Case
The patient in the vignette has an estimated GFR of about 32 mL/min by the MDRD equation. With this level of renal dysfunction, the presence of diabetes mellitus, mellitus and assuming at least a 100 cc contrast bolus with the angiography, her risk for CIN is about 14% (eight points on the Mehran scale illustrated in Table 21). Alternatives to coronary angiography are limited in this example, and pharmacologic and IVF measures to prevent CIN are indicated. Borrowing from the regimen used in the REMEDIAL trial, she should ideally receive NAC 1200 mg orally BID for two days, starting one day prior to the procedure (in this case, would begin as soon as the risk for CIN is appreciated and continue for four doses). More importantly, she should receive sodium bicarbonate 154mEq/L at a rate of 3 mL/kg/hr one hour prior to contrast and 1 mL/kg/hr during and for six hours following the contrast procedure.
Bottom Line
Contrast nephropathy risk varies inversely with GFR and can be estimated according to a validated tool. Patients at risk for CIN should be identified early and offered NAC and sodium bicarbonate, if there are no alternatives to administering intravenous contrast. Intravenous saline also is effective, but may not be as effective as bicarbonate. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado Denver and the associate chief, Medical Service, at the Denver VA Medical Center.
References
1. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393-1399.
2. Tepel M, van der Giet M, Schwarzfeld C, et al. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med. 2000;343:180-184.
3. Vaitkus PT and Brar C. N-Acetylcysteine in the prevention of contrast-induced nephropathy: publication bias perpetuated by meta-analyses. Am Heart J. 2007;153:275-280.
4. Bagshaw SM, McAlister FA, Manns BJ, Ghali WA. Acetylcysteine in the prevention of contrast-induced nephropathy: a case study of the pitfalls in the evolution of evidence. Arch Intern Med. 2006;166:161-166.
5. Kelly AM, Dwamena B, Cronin P, Bernstein SJ and Carlos RC. Meta-analysis: effectiveness of drugs for preventing contrast-induced nephropathy. Ann Intern Med. 2008;148:284-294.
6. Solomon R, Werner C, Mann D, et al. Effects of saline, mannitol, and furosemide on acute decreases in renal function induced by radiocontrast agents. N Engl J Med. 1994;331:14-16.
7. Mueller C, Buerkle G, Buettner HJ, et al. Prevention of contrast-media associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Arch Intern Med. 2002;162:329-336.
8. Barrett BJ and Parfrey PS. Preventing nephropathy induced by contrast medium. N Engl J Med. 2006;354:379-386.
9. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with bicarbonate: a randomized controlled trial. JAMA. 2004;291:2328-2334.
10. Brigouri C, Airoldi F, D.Andrea, et al. Renal insufficiency following contrast media administration trial (remedial): a randomized comparison of 3 preventive strategies. Circulation. 2007;115:1211-1217.
11. Masuda M, Yamada T, Mine T, et al. Comparison of usefulness of sodium bicarbonate versus sodium chloride to prevent contrast-induced nephropathy in patients undergoing an emergent coronary procedure. Am J Cardiol. 2007;100:781-786.
12. Recio-Mayoral A, Chaparro M, Prado B, et al. The reno-protective effect of hydration with sodium bicarbonate plus n-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the reno study. J Am Coll Cardiol. 2007;49:1283-1288.
13. Ozcan EE, Guneri S, Akdeniz B, et al. Sodium bicarbonate, n-acetylcysteine, and saline for the prevention of radiocontrast-induced nephropathy. a comparison of 3 regimens for protecting contrast-induced nephropathy (sic) in patients undergoing coronary procedures. a single center prospective controlled trial. Am Heart J. 2007;154:539-544.
14. Maioli M, Toso A, Leoncini M, et al. Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. J Am Coll Cardiol. 2008;52:599-604.
15. Brar SS, Shen AYJ, Jorgensen MB, et al. Sodium bicarbonate vs. sodium chloride for the prevention of contrast medium-induced nephropathy in patients undergoing coronary angiography: a randomized trial. JAMA. 2008;300:1038-1046.
Case
A 68-year-old diabetic woman hospitalized for non-ST-segment elevation myocardial infarction develops increasing chest pain despite maximal appropriate medical therapy and is referred for urgent coronary angiography. She is normotensive, weighs 60 kg, and is without signs of congestive heart failure on examination. The serum creatinine is 1.6 mg/dL (her baseline). What is her risk for contrast media-induced nephropathy (CIN)? What measures can be undertaken to reduce her risk?
Background
Radiocontrast agents are well-recognized nephrotoxins that can cause a usually reversible, non-oliguric form of renal failure within 24 hours and up to five days following administration. Contrast nephropathy is associated with longer hospital stays and higher mortality. The incidence varies widely according to patient characteristics and the type and quantity of contrast agent used.
The pathogenesis of CIN is not completely understood, but likely represents a combination of contrast-mediated renal vasoconstriction, oxidative damage, and direct cytotoxic effects. Newer low-osmolar or iso-osmolar contrast agents are associated with lower rates of CIN than high-osmolar contrast agents. Multiple pharmacologic strategies for CIN prevention have been investigated, with several important trials published in the past two years. This review summarizes the risk assessment and prophylactic strategies required for optimal protection of patients from CIN.
Assesment of Patient Risk
Contrast-induced nephropathy is defined variably in clinical trials, most commonly as a 25% increase in serum creatinine above baseline at 48 hours after contrast administration. The most important risk factor for CIN is pre-existing kidney disease—more specifically, a diminished glomerular filtration rate (GFR) below 60 mL/minute/1.73 m2 body surface area.1 The serum creatinine concentration can be misleading. Advancing age, female gender, low lean body mass, or unstable rising creatinine all can lead to overestimation of the GFR. The Modification of Diet in Renal Disease (MDRD) estimate of GFR and the Cockcroft-Gault estimate of creatinine clearance are calculated in a basic formula. (see Table 1, left)
Several other factors have been linked to increased risk for CIN. Table 2 (left) summarizes these risk factors and assigns them various point scores. In general, patients with chronic kidney disease or any of these risk factors should have a serum creatinine drawn before the contrast study to clarify their CIN risk and facilitate decisions regarding prophylaxis. Patients with a score of six or more are at substantial risk for CIN.1
Strategy for Prophylaxis
Low-osmolar and iso-osmolar contrast agents have been associated with lower rates of CIN compared to high-osmolar contrast. However, the referring hospitalist rarely determines the type and volume of contrast used. Fortunately, high-osmolar contrast is used infrequently today. The primary strategy for CIN prophylaxis is to:
1) Determine CIN risk using a validated tool (see Table 2).
2) If “at risk,” consider alternate diagnostic modalities that do not involve the intravenous administration of iodinated contrast. Consider delaying testing with contrast agents until potentially reversible conditions affecting GFR are addressed, such as volume depletion, recent contrast use, or concomitant use of nonsteroidal anti-inflammatory drugs or angiotensin-converting enzyme inhibitors.
3) Provide pharmacologic and intravenous fluid prophylaxis as described below.
Pharmacologic Prophylaxis
Multiple agents have been investigated in the prevention of CIN: mannitol, furosemide, theophylline, fenoldopam, dopamine, N-acetylcysteine, and others. The most effective noteworthy of these is N-acetylcysteine (NAC). The first major trial of NAC for CIN prevention was published in 2000.2 Since then, more than two dozen studies, mostly randomized controlled trials (RCTs), and nearly a dozen meta-analyses have been published, with inconsistent results.
Of particular note, systematic reviews and meta-analyses have reached differing conclusions on the overall efficacy of NAC in the prevention of CIN. One recent study including NAC trials published before June 2006 concluded there has been “significant publication bias throughout the life cycle of this clinical question … further amplified by meta-analyses.”3 It has been estimated a single trial enrolling 1,800 patients (about 10 times larger than most completed trials) would be needed to definitively answer this question.4 The latest meta-analysis includes at least one large RCT of NAC not included in prior meta-analyses and concludes that NAC is effective in the prevention of CIN.5 The pooled relative risk for CIN was 0.62 (95% C.I. 0.44-0.88). These investigators concluded there was no significant publication bias.
Taken together, the primary literature and secondary meta-analyses suggest that NAC is probably effective in the prevention of CIN, although there may be some publication bias. Practically speaking, NAC is essentially without side effects, and the likelihood that it affords some degree of protection suggests it should be used routinely, unless or until larger studies demonstrate otherwise. A NAC dose of 1,200 mg twice daily beginning the day prior and continuing through the day of contrast administration was part of the successful protocol published by Brigouri, et al., in 2007.
Intravenous Crystalloids Trials
A landmark trial published in 1994 showed half-normal saline in 5% dextrose given 12 hours before and 12 hours after administering a radiocontrast agent was superior to half-normal saline plus mannitol or half-normal saline plus furosemide in preventing CIN.6 This regimen remained the standard of care until 2002, when a large RCT compared half- normal saline in 5% dextrose to isotonic normal saline in 1,620 patients undergoing coronary angioplasty.7 About 20% of the patients had underlying renal dysfunction and about 15% were diabetic. The rate of CIN decreased from 2% (14/698) to 0.7% (5/685), a modest-but-statistically-significant difference. After this study, practice generally shifted to using normal saline at 1 mL/kg/hr 12 hours before and 12 hours after contrast procedures. One notable review article published in 2006 concluded that isotonic saline was the best-proven strategy for the prevention of CIN.8
How does intravenous sodium chloride reduce the rate of CIN? The mechanism is unclear, but it may work simply by treating subclinical states of volume depletion. But as free radical oxidation has been implicated in the pathophysiology of CIN, investigators hypothesized that alkalinizing the urine (reducing free radical formation) with isotonic sodium bicarbonate might better protect patients from CIN than saline. In 2004, the first trial demonstrating the efficacy of bicarbonate was stopped early after the rate of CIN had decreased from 13.6% (8/59) in the saline arm to 1.7% (1/60) in the bicarbonate arm.9 The editorial accompanying this small trial cautioned “prospective confirmation should be required before accepting new therapies into routine clinical practice.”
In 2007, four prospective trials comparing various hydration regimens were published; each concluding that bicarbonate is superior to saline. The largest of these studies was the REMEDIAL trial.10 Patients were referred for coronary angiography and had a baseline serum creatinine of 2.0 mg/dl or higher or an estimated GFR below 40 mL/minute/1.73 m2 (or both). In double-blind fashion, patients were randomized to one of three preventative strategies: normal saline plus NAC (n=111), sodium bicarbonate plus NAC (n=108), or normal saline plus NAC plus ascorbic acid (n=107). The primary endpoint was defined as a 25% or higher increase in serum creatinine at 48 hours. This occurred in 9.9% (11/111) of the normal saline plus NAC group, 1.9% (2/108) of the sodium bicarbonate plus NAC group, and 10.3% (11/107) of the normal saline plus NAC plus ascorbic acid group (p=0.019 for sodium bicarbonate plus NAC versus normal saline plus NAC).
The sodium bicarbonate regimen was the same as that reported by Merten in 2004—namely, 154 mEq/L of sodium bicarbonate in 5% dextrose solution, given at 3 mL/kg/hr for one hour before contrast administration and 1 mL/kg/hr for six hours afterward. The saline regimen (154 mEq/L) was the same as that reported by Mueller in 2002—1 mL/kg/hr for 12 hours before contrast administration and 12 hours afterward. All patients received NAC at a dose of 1,200 mg twice daily the day before and the day of contrast administration. It is not possible to conclude from this trial whether sodium bicarbonate without NAC would have been as effective as the regimen studied. Ascorbic acid was included in this trial as another antioxidant to compare with NAC. The three other RCTs published in 2007 are summarized in Table 3 (see p. 21).11,12,13
Recently, two large RCTs of saline versus bicarbonate concluded there was no difference between the two.14,15 These trials were the largest to date, each of them single center and unblinded, and using slightly different methods than the REMEDIAL trial. CIN also was defined more broadly as a 0.5mg/dL or 25% change in creatinine within five days after contrast. Follow-up was only 88% in one trial. Nevertheless, these two new trials reach quite different conclusions than those before. Table 3 (see p. 21) summarizes seven RCTs of saline versus bicarbonate in the prevention of CIN. Differences in design and methods, definitions of CIN, completeness of follow-up, and severity of renal dysfunction among patients studied, make direct comparisons among these trials difficult. But as five of the seven RCTs of saline versus bicarbonate have concluded that bicarbonate is superior, and none have concluded saline is superior, this author recommends that at the present time intravenous sodium bicarbonate be used according to the Merten protocol when providing IVF for the prevention of CIN.
Back to the Case
The patient in the vignette has an estimated GFR of about 32 mL/min by the MDRD equation. With this level of renal dysfunction, the presence of diabetes mellitus, mellitus and assuming at least a 100 cc contrast bolus with the angiography, her risk for CIN is about 14% (eight points on the Mehran scale illustrated in Table 21). Alternatives to coronary angiography are limited in this example, and pharmacologic and IVF measures to prevent CIN are indicated. Borrowing from the regimen used in the REMEDIAL trial, she should ideally receive NAC 1200 mg orally BID for two days, starting one day prior to the procedure (in this case, would begin as soon as the risk for CIN is appreciated and continue for four doses). More importantly, she should receive sodium bicarbonate 154mEq/L at a rate of 3 mL/kg/hr one hour prior to contrast and 1 mL/kg/hr during and for six hours following the contrast procedure.
Bottom Line
Contrast nephropathy risk varies inversely with GFR and can be estimated according to a validated tool. Patients at risk for CIN should be identified early and offered NAC and sodium bicarbonate, if there are no alternatives to administering intravenous contrast. Intravenous saline also is effective, but may not be as effective as bicarbonate. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado Denver and the associate chief, Medical Service, at the Denver VA Medical Center.
References
1. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393-1399.
2. Tepel M, van der Giet M, Schwarzfeld C, et al. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med. 2000;343:180-184.
3. Vaitkus PT and Brar C. N-Acetylcysteine in the prevention of contrast-induced nephropathy: publication bias perpetuated by meta-analyses. Am Heart J. 2007;153:275-280.
4. Bagshaw SM, McAlister FA, Manns BJ, Ghali WA. Acetylcysteine in the prevention of contrast-induced nephropathy: a case study of the pitfalls in the evolution of evidence. Arch Intern Med. 2006;166:161-166.
5. Kelly AM, Dwamena B, Cronin P, Bernstein SJ and Carlos RC. Meta-analysis: effectiveness of drugs for preventing contrast-induced nephropathy. Ann Intern Med. 2008;148:284-294.
6. Solomon R, Werner C, Mann D, et al. Effects of saline, mannitol, and furosemide on acute decreases in renal function induced by radiocontrast agents. N Engl J Med. 1994;331:14-16.
7. Mueller C, Buerkle G, Buettner HJ, et al. Prevention of contrast-media associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Arch Intern Med. 2002;162:329-336.
8. Barrett BJ and Parfrey PS. Preventing nephropathy induced by contrast medium. N Engl J Med. 2006;354:379-386.
9. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with bicarbonate: a randomized controlled trial. JAMA. 2004;291:2328-2334.
10. Brigouri C, Airoldi F, D.Andrea, et al. Renal insufficiency following contrast media administration trial (remedial): a randomized comparison of 3 preventive strategies. Circulation. 2007;115:1211-1217.
11. Masuda M, Yamada T, Mine T, et al. Comparison of usefulness of sodium bicarbonate versus sodium chloride to prevent contrast-induced nephropathy in patients undergoing an emergent coronary procedure. Am J Cardiol. 2007;100:781-786.
12. Recio-Mayoral A, Chaparro M, Prado B, et al. The reno-protective effect of hydration with sodium bicarbonate plus n-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the reno study. J Am Coll Cardiol. 2007;49:1283-1288.
13. Ozcan EE, Guneri S, Akdeniz B, et al. Sodium bicarbonate, n-acetylcysteine, and saline for the prevention of radiocontrast-induced nephropathy. a comparison of 3 regimens for protecting contrast-induced nephropathy (sic) in patients undergoing coronary procedures. a single center prospective controlled trial. Am Heart J. 2007;154:539-544.
14. Maioli M, Toso A, Leoncini M, et al. Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. J Am Coll Cardiol. 2008;52:599-604.
15. Brar SS, Shen AYJ, Jorgensen MB, et al. Sodium bicarbonate vs. sodium chloride for the prevention of contrast medium-induced nephropathy in patients undergoing coronary angiography: a randomized trial. JAMA. 2008;300:1038-1046.
A Truly Different World
(Maj) Heather Cereste, MD, chair of the Bioethics Committee at Wilford Hall Medical Center at Lackland Air Force Base near San Antonio, Texas, and a member of Team Hospitalist, is the only geriatric-trained internist in the U.S. Air Force. From January through May 2007, she served as the attending primary care physician at Balad Trauma Hospital in Balad, Iraq. She recently spoke with The Hospitalist about her experience as a wartime physician.
Q: What motivated you to join the Air Force?
A: I talked to the Air Force near end of third year in residency. A number of things played into my decision. I was in Manhattan during 9/11 and got caught up in the surge of patriotism. I had thought about the military before, and was at a point when I was about to enter geriatrics and wasn’t sure if wanted to go into the traditional workforce or explore something else. I joined the reserves in 2004 and went active in 2006. To be honest with you, I never thought I would be deployed to a combat zone.
—Heather Cereste, MD
Q: What type of training did you receive before going to Iraq?
A: I was just undergoing the credentialing process when I was asked by my commander [to] deploy with her in a few months. I was a little shocked and taken aback, and didn’t feel at all prepared. So I inquired about further training and was referred to the shock trauma group in Baltimore, Md. It was the closest I could get to warfare type of injuries because it’s an urban warfare they fight in Baltimore. There, I was able to gain confidence in doing some procedures, including chest tubes, and refreshing myself about central lines and the acuity of care.
Q: What was it like working in Iraq?



A: Our team worked seven days a week in the intensive care unit. We were on call every fifth night, overnight. We took care of the critically ill patients who came in through ER or who were directed to us. For the most part, we interacted with the coalition people for only 24–48 hours before they were transported out. The American and British people often went to Germany for more definitive care.
Q: What medical conditions did you see?
A: Over five months we managed about 528 critically ill people. There were certainly a lot of postoperative cases. We took care of burns and head wounds, which were increasing in number, a lot of limb amputations, as well as blast injuries and gunshot wounds. Civilians would present at our gates and we could triage them, if we had enough room.
Q: Did you feel like you were in a war zone?
A: It was very surreal. I was one of the last rotations to go when it was a tent hospital, so when we had rain and weather, we’d have to deal with floods, etc. It was a very rustic environment; there was dust was everywhere. The helicopters would come in and land right outside our tents.
Our hospital was right next to the wire–that’s a barbed wire fence that separated our base from the outside of the base–so we heard machine guns constantly while we were doing our rounds. We also got mortared frequently. Disgruntled people on the other side would set up across the river. They had some Russian mortars that they would throw over to our side. Whenever we could identify that the mortars were coming over the wall, sirens would go off and we’d have to dive for cover.
You’re constantly reminded of war, if not by the sounds, than certainly with the injuries. And people were carrying their guns all the time. It was strange to be a physician carrying a gun.
Q: How did your background in geriatrics come into play?
A: Believe it or not, many of the Iraqi civilians we treated were not chronically aged, but were physiology aged. We saw a lot of geriatric syndromes, even in 45-year-olds. Diet and access to care were common issues.
Q: Did you have enough resources?
A: As far as combat hospitals go, in my limited experience, I think we had excellent resources. But sometimes, if patients required extended intensive care and if we didn’t have the dialysis or the level of burn care, we just couldn’t treat them. It was a challenge every day to deal with certain patients who we knew under normal circumstances we could take care of, but because of the circumstance we had to stop care. That made it really hard.
Q: Is there one case that stands out as an example of what can be done in a combat zone?
A: There was one young baby who was a medical case. He was 28 days old when he first presented. He came to the gate with his parents with an infected arm. He had been seen at an outside facility and was treated for some kind of infection.
We thought from an initial admitting diagnosis that he had pericardial infusion. He had a long, protracted course where he required intubation. He was quite the enigma, and required a lot of attention and care and resources. Everyone at the hospital, from the nursing staff, to the medical technicians, to chaplains, would stop by say hello to the baby. We all did our best to keep him alive. He ended up getting discharged; the last we heard he was doing all right. My hope is that he would grow very strong.
It was nice to have a child around. It was also great because the family had entrusted us to take care of him. They seemed grateful when they were finally able to take him home.
Q: Would you go back?
A: Definitely. It was probably the most amazing experience in my life, professional and personally. It’s a wonderful place to do medicine because you’re forced to practice outside your comfort zone. You also feel that your efforts are playing a positive role. You get out of that whole humdrum, “beaten-by-the-system” feeling that I think people may feel here. I got to meet interesting people and be a part of history. And I survived, so that was good. TH
(Maj) Heather Cereste, MD, chair of the Bioethics Committee at Wilford Hall Medical Center at Lackland Air Force Base near San Antonio, Texas, and a member of Team Hospitalist, is the only geriatric-trained internist in the U.S. Air Force. From January through May 2007, she served as the attending primary care physician at Balad Trauma Hospital in Balad, Iraq. She recently spoke with The Hospitalist about her experience as a wartime physician.
Q: What motivated you to join the Air Force?
A: I talked to the Air Force near end of third year in residency. A number of things played into my decision. I was in Manhattan during 9/11 and got caught up in the surge of patriotism. I had thought about the military before, and was at a point when I was about to enter geriatrics and wasn’t sure if wanted to go into the traditional workforce or explore something else. I joined the reserves in 2004 and went active in 2006. To be honest with you, I never thought I would be deployed to a combat zone.
—Heather Cereste, MD
Q: What type of training did you receive before going to Iraq?
A: I was just undergoing the credentialing process when I was asked by my commander [to] deploy with her in a few months. I was a little shocked and taken aback, and didn’t feel at all prepared. So I inquired about further training and was referred to the shock trauma group in Baltimore, Md. It was the closest I could get to warfare type of injuries because it’s an urban warfare they fight in Baltimore. There, I was able to gain confidence in doing some procedures, including chest tubes, and refreshing myself about central lines and the acuity of care.
Q: What was it like working in Iraq?
A: Our team worked seven days a week in the intensive care unit. We were on call every fifth night, overnight. We took care of the critically ill patients who came in through ER or who were directed to us. For the most part, we interacted with the coalition people for only 24–48 hours before they were transported out. The American and British people often went to Germany for more definitive care.
Q: What medical conditions did you see?
A: Over five months we managed about 528 critically ill people. There were certainly a lot of postoperative cases. We took care of burns and head wounds, which were increasing in number, a lot of limb amputations, as well as blast injuries and gunshot wounds. Civilians would present at our gates and we could triage them, if we had enough room.
Q: Did you feel like you were in a war zone?
A: It was very surreal. I was one of the last rotations to go when it was a tent hospital, so when we had rain and weather, we’d have to deal with floods, etc. It was a very rustic environment; there was dust was everywhere. The helicopters would come in and land right outside our tents.
Our hospital was right next to the wire–that’s a barbed wire fence that separated our base from the outside of the base–so we heard machine guns constantly while we were doing our rounds. We also got mortared frequently. Disgruntled people on the other side would set up across the river. They had some Russian mortars that they would throw over to our side. Whenever we could identify that the mortars were coming over the wall, sirens would go off and we’d have to dive for cover.
You’re constantly reminded of war, if not by the sounds, than certainly with the injuries. And people were carrying their guns all the time. It was strange to be a physician carrying a gun.
Q: How did your background in geriatrics come into play?
A: Believe it or not, many of the Iraqi civilians we treated were not chronically aged, but were physiology aged. We saw a lot of geriatric syndromes, even in 45-year-olds. Diet and access to care were common issues.
Q: Did you have enough resources?
A: As far as combat hospitals go, in my limited experience, I think we had excellent resources. But sometimes, if patients required extended intensive care and if we didn’t have the dialysis or the level of burn care, we just couldn’t treat them. It was a challenge every day to deal with certain patients who we knew under normal circumstances we could take care of, but because of the circumstance we had to stop care. That made it really hard.
Q: Is there one case that stands out as an example of what can be done in a combat zone?
A: There was one young baby who was a medical case. He was 28 days old when he first presented. He came to the gate with his parents with an infected arm. He had been seen at an outside facility and was treated for some kind of infection.
We thought from an initial admitting diagnosis that he had pericardial infusion. He had a long, protracted course where he required intubation. He was quite the enigma, and required a lot of attention and care and resources. Everyone at the hospital, from the nursing staff, to the medical technicians, to chaplains, would stop by say hello to the baby. We all did our best to keep him alive. He ended up getting discharged; the last we heard he was doing all right. My hope is that he would grow very strong.
It was nice to have a child around. It was also great because the family had entrusted us to take care of him. They seemed grateful when they were finally able to take him home.
Q: Would you go back?
A: Definitely. It was probably the most amazing experience in my life, professional and personally. It’s a wonderful place to do medicine because you’re forced to practice outside your comfort zone. You also feel that your efforts are playing a positive role. You get out of that whole humdrum, “beaten-by-the-system” feeling that I think people may feel here. I got to meet interesting people and be a part of history. And I survived, so that was good. TH
(Maj) Heather Cereste, MD, chair of the Bioethics Committee at Wilford Hall Medical Center at Lackland Air Force Base near San Antonio, Texas, and a member of Team Hospitalist, is the only geriatric-trained internist in the U.S. Air Force. From January through May 2007, she served as the attending primary care physician at Balad Trauma Hospital in Balad, Iraq. She recently spoke with The Hospitalist about her experience as a wartime physician.
Q: What motivated you to join the Air Force?
A: I talked to the Air Force near end of third year in residency. A number of things played into my decision. I was in Manhattan during 9/11 and got caught up in the surge of patriotism. I had thought about the military before, and was at a point when I was about to enter geriatrics and wasn’t sure if wanted to go into the traditional workforce or explore something else. I joined the reserves in 2004 and went active in 2006. To be honest with you, I never thought I would be deployed to a combat zone.
—Heather Cereste, MD
Q: What type of training did you receive before going to Iraq?
A: I was just undergoing the credentialing process when I was asked by my commander [to] deploy with her in a few months. I was a little shocked and taken aback, and didn’t feel at all prepared. So I inquired about further training and was referred to the shock trauma group in Baltimore, Md. It was the closest I could get to warfare type of injuries because it’s an urban warfare they fight in Baltimore. There, I was able to gain confidence in doing some procedures, including chest tubes, and refreshing myself about central lines and the acuity of care.
Q: What was it like working in Iraq?
A: Our team worked seven days a week in the intensive care unit. We were on call every fifth night, overnight. We took care of the critically ill patients who came in through ER or who were directed to us. For the most part, we interacted with the coalition people for only 24–48 hours before they were transported out. The American and British people often went to Germany for more definitive care.
Q: What medical conditions did you see?
A: Over five months we managed about 528 critically ill people. There were certainly a lot of postoperative cases. We took care of burns and head wounds, which were increasing in number, a lot of limb amputations, as well as blast injuries and gunshot wounds. Civilians would present at our gates and we could triage them, if we had enough room.
Q: Did you feel like you were in a war zone?
A: It was very surreal. I was one of the last rotations to go when it was a tent hospital, so when we had rain and weather, we’d have to deal with floods, etc. It was a very rustic environment; there was dust was everywhere. The helicopters would come in and land right outside our tents.
Our hospital was right next to the wire–that’s a barbed wire fence that separated our base from the outside of the base–so we heard machine guns constantly while we were doing our rounds. We also got mortared frequently. Disgruntled people on the other side would set up across the river. They had some Russian mortars that they would throw over to our side. Whenever we could identify that the mortars were coming over the wall, sirens would go off and we’d have to dive for cover.
You’re constantly reminded of war, if not by the sounds, than certainly with the injuries. And people were carrying their guns all the time. It was strange to be a physician carrying a gun.
Q: How did your background in geriatrics come into play?
A: Believe it or not, many of the Iraqi civilians we treated were not chronically aged, but were physiology aged. We saw a lot of geriatric syndromes, even in 45-year-olds. Diet and access to care were common issues.
Q: Did you have enough resources?
A: As far as combat hospitals go, in my limited experience, I think we had excellent resources. But sometimes, if patients required extended intensive care and if we didn’t have the dialysis or the level of burn care, we just couldn’t treat them. It was a challenge every day to deal with certain patients who we knew under normal circumstances we could take care of, but because of the circumstance we had to stop care. That made it really hard.
Q: Is there one case that stands out as an example of what can be done in a combat zone?
A: There was one young baby who was a medical case. He was 28 days old when he first presented. He came to the gate with his parents with an infected arm. He had been seen at an outside facility and was treated for some kind of infection.
We thought from an initial admitting diagnosis that he had pericardial infusion. He had a long, protracted course where he required intubation. He was quite the enigma, and required a lot of attention and care and resources. Everyone at the hospital, from the nursing staff, to the medical technicians, to chaplains, would stop by say hello to the baby. We all did our best to keep him alive. He ended up getting discharged; the last we heard he was doing all right. My hope is that he would grow very strong.
It was nice to have a child around. It was also great because the family had entrusted us to take care of him. They seemed grateful when they were finally able to take him home.
Q: Would you go back?
A: Definitely. It was probably the most amazing experience in my life, professional and personally. It’s a wonderful place to do medicine because you’re forced to practice outside your comfort zone. You also feel that your efforts are playing a positive role. You get out of that whole humdrum, “beaten-by-the-system” feeling that I think people may feel here. I got to meet interesting people and be a part of history. And I survived, so that was good. TH
Reimbursement Rights
Recent changes in healthcare have forced academic medical centers to seek additional resources in the delivery of quality care. In response to internal and external pressures to minimize length of stay, adhere to limitations on the maximum number of admitted patients, focus on evidence-based care, and improve outcomes of care, hospitalists have incorporated non-physician providers (NPPs), such as acute care nurse practitioners (ACNPs), into their group practices.1
Whereas traditional nurse practitioners focus on the promotion of health and management of chronic illness, ACNPs focus on the care of acutely ill patients. Hospitalists utilize NPPs to expand medical service capacity and improve the efficiency and quality of patient care.2
Research indicates physician/nurse practitioner collaboration in the multidisciplinary management of hospitalized medical patients reduces length of stay and improves hospital profit without altering readmissions or mortality.3 Billing and documentation standards for NPP services must comply with current state and federal regulations. Hospitalist groups should become familiar with these guidelines prior to billing for NPP services involved in this patient care model.
The following highlights inpatient services provided by nurse practitioners (NPs) and physician assistants (PAs).
Covered Services
Medicare pays for services considered reasonable and necessary and not otherwise excluded from coverage. NPPs may provide any service permitted by the state scope of practice and performed in conjunction with the appropriate level of supervision or collaboration, as outlined in licensure or billing requirements. Being only limited by state and/or facility regulations, NPP services comprise visits or procedures typically rendered by ancillary staff or considered a physician service (a doctor of medicine, MD, or osteopathy, DO). Additionally, NPPs must meet the insurer-specified qualifications.
Independent Billing
Since 1998, designated NPPs are allowed to submit Medicare Part B claims for services, including procedures, provided in any inpatient or outpatient setting. For billing purposes, these “independent” services do not require physician involvement (e.g. physician initiation of care plan, physician-patient encounter, or physician presence on patient floor/unit) unless otherwise specified by state legislation or facility standards of practice. NPPs do not need to be employed by the physician group. The entity employing the physician group also may employ the NPP.
Claim requirements mandate the use of a national provider identifier (NPI) on all claims, therefore, all NPPs receive an NPI for claim submission. However, not all NPPs may directly bill Medicare or receive direct payment (e.g., physician assistant).1 In this situation, the NPP employer (i.e., physician or group), reports the service with the physician or group provider number and the NPP’s NPI included for identification of who actually provided the service.
Medicare Part B processes NPP claims reported under the independent billing option. Duplicate payments from any other Medicare Part A or Part B source is strictly prohibited and may result in refunds, fines and penalties. Generally, Medicare payment for NPP services is limited to 85% of the allowable physician rate. Financial impact of the 15% rate reduction is typically offset by the increase in physician time. Physicians may use this time to provide more comprehensive or complex services (admissions or consultations), potentially generating more revenue. Consistent with all provider documentation, NPP documentation must support the reported service.
Shared/Split Billing
The shared/split billing option first appeared in 2002 to address facility-based services provided to a single patient by an NPP and physician from the same group practice on the same calendar day. This option only applies to evaluation and management services provided in an emergency department, outpatient or inpatient hospital. It excludes consultations and critical care services. Unlike the independent billing option, the shared/split billing option only involves service provided by nurse practitioners, physician assistants, clinical nurse specialists, and certified nurse-midwives.
In order to qualify as a shared/split service, the NPP and the physician each must have a face-to-face encounter with the patient, although the extent of each provider’s involvement is left to provider discretion and/or local Medicare contractor requirements. The timing of each provider’s visit is irrelevant, as long as the two services are performed on the same date. For example, the NPP may see a hospital inpatient in the morning with a follow-up visit by the physician later in the day.4 When documenting, both the NPP and the physician should identify the name of the individual with whom the service is shared/split. This will allow for appropriate service capture, and ensure that the correct notes are sent to the payer in the event of claim denial and subsequent appeal. Each provider must document their portion of the rendered service and select the visit level supported by the cumulative encounter. The physician need not duplicate the elements performed and documented by the NPP, but merely perform and record the physician-determined critical or key portions. Do not confuse this billing option with teaching physician regulations. Physician and the specified NPPs cannot share or split a service with any other provider type (e.g., residents, medical or nursing students).
Only one claim may be submitted for a shared/split service. The physician may choose to report the service under his own name or under the NPP name. Reimbursement is dependent upon this selection. The physician name secures 100% of the Medicare allowable rate; the NPP name earns 85% of the allowable physician rate.
While the physician has the opportunity to report the service under his own name for the full service rate, the shared/split billing option requires the efforts of two individuals and may be an impractical approach for some physician groups.
“Incident-to”
Hospitalists, or their staff, may have encountered the term “incident-to” and wondered how this billing option applies to hospitalist services. “Incident-to” guidelines only apply to procedures and services performed in a private physician office. In this setting, the patient establishes care with the physician and the physician develops a patient-specific plan of care. Subsequent services may be provided to the established patient by the NPP, yet reported under the physician’s name for 100% of the allowable physician rate. “Incident-to” services cannot be reported by a hospitalist, since hospitalist services only take place in facility-based locations.
Summary
NPPs currently are involved in an extensive number of services within the hospital, and Medicare has two billing options for NPP services provided on behalf of or in conjunction with hospitalists. Each option involves specific rules and regulations with which NPPs and physician groups must comply.
Successful reporting requires understanding of and adherence to federal, state, and facility guidelines. It is important to identify NPP employment relationships, the NPP’s role in the provision of services, the state supervisory or collaborative rules, and local payer interpretations to prevent misrepresentation, misunderstanding, or erroneous reporting. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare benefit policy manual. www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed September 12, 2008.
2. Howie J, Erickson M. Acute care nurse practitioners: creating and implementing a model of care for an inpatient general medical service. Am J of Critical Care. 2002;11:448-458.
3. Cowan M, Shapiro M, et al.. The effect of a multidisciplinary hospitalist/physician and advanced practice nurse collaboration on hospital costs. J Nursing Admin. 2006;36:79-85.
4. CMS. Medicare claims processing manual: Chapter 12, Section 30.6.1B. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed September 14, 2008.
5. Pohlig C. Nonphysician providers in your practice. In: coding for chest medicine 2008. Northbrook, IL: Am Coll Chest Phy. 2008;249-254.
Recent changes in healthcare have forced academic medical centers to seek additional resources in the delivery of quality care. In response to internal and external pressures to minimize length of stay, adhere to limitations on the maximum number of admitted patients, focus on evidence-based care, and improve outcomes of care, hospitalists have incorporated non-physician providers (NPPs), such as acute care nurse practitioners (ACNPs), into their group practices.1
Whereas traditional nurse practitioners focus on the promotion of health and management of chronic illness, ACNPs focus on the care of acutely ill patients. Hospitalists utilize NPPs to expand medical service capacity and improve the efficiency and quality of patient care.2
Research indicates physician/nurse practitioner collaboration in the multidisciplinary management of hospitalized medical patients reduces length of stay and improves hospital profit without altering readmissions or mortality.3 Billing and documentation standards for NPP services must comply with current state and federal regulations. Hospitalist groups should become familiar with these guidelines prior to billing for NPP services involved in this patient care model.
The following highlights inpatient services provided by nurse practitioners (NPs) and physician assistants (PAs).
Covered Services
Medicare pays for services considered reasonable and necessary and not otherwise excluded from coverage. NPPs may provide any service permitted by the state scope of practice and performed in conjunction with the appropriate level of supervision or collaboration, as outlined in licensure or billing requirements. Being only limited by state and/or facility regulations, NPP services comprise visits or procedures typically rendered by ancillary staff or considered a physician service (a doctor of medicine, MD, or osteopathy, DO). Additionally, NPPs must meet the insurer-specified qualifications.
Independent Billing
Since 1998, designated NPPs are allowed to submit Medicare Part B claims for services, including procedures, provided in any inpatient or outpatient setting. For billing purposes, these “independent” services do not require physician involvement (e.g. physician initiation of care plan, physician-patient encounter, or physician presence on patient floor/unit) unless otherwise specified by state legislation or facility standards of practice. NPPs do not need to be employed by the physician group. The entity employing the physician group also may employ the NPP.
Claim requirements mandate the use of a national provider identifier (NPI) on all claims, therefore, all NPPs receive an NPI for claim submission. However, not all NPPs may directly bill Medicare or receive direct payment (e.g., physician assistant).1 In this situation, the NPP employer (i.e., physician or group), reports the service with the physician or group provider number and the NPP’s NPI included for identification of who actually provided the service.
Medicare Part B processes NPP claims reported under the independent billing option. Duplicate payments from any other Medicare Part A or Part B source is strictly prohibited and may result in refunds, fines and penalties. Generally, Medicare payment for NPP services is limited to 85% of the allowable physician rate. Financial impact of the 15% rate reduction is typically offset by the increase in physician time. Physicians may use this time to provide more comprehensive or complex services (admissions or consultations), potentially generating more revenue. Consistent with all provider documentation, NPP documentation must support the reported service.
Shared/Split Billing
The shared/split billing option first appeared in 2002 to address facility-based services provided to a single patient by an NPP and physician from the same group practice on the same calendar day. This option only applies to evaluation and management services provided in an emergency department, outpatient or inpatient hospital. It excludes consultations and critical care services. Unlike the independent billing option, the shared/split billing option only involves service provided by nurse practitioners, physician assistants, clinical nurse specialists, and certified nurse-midwives.
In order to qualify as a shared/split service, the NPP and the physician each must have a face-to-face encounter with the patient, although the extent of each provider’s involvement is left to provider discretion and/or local Medicare contractor requirements. The timing of each provider’s visit is irrelevant, as long as the two services are performed on the same date. For example, the NPP may see a hospital inpatient in the morning with a follow-up visit by the physician later in the day.4 When documenting, both the NPP and the physician should identify the name of the individual with whom the service is shared/split. This will allow for appropriate service capture, and ensure that the correct notes are sent to the payer in the event of claim denial and subsequent appeal. Each provider must document their portion of the rendered service and select the visit level supported by the cumulative encounter. The physician need not duplicate the elements performed and documented by the NPP, but merely perform and record the physician-determined critical or key portions. Do not confuse this billing option with teaching physician regulations. Physician and the specified NPPs cannot share or split a service with any other provider type (e.g., residents, medical or nursing students).
Only one claim may be submitted for a shared/split service. The physician may choose to report the service under his own name or under the NPP name. Reimbursement is dependent upon this selection. The physician name secures 100% of the Medicare allowable rate; the NPP name earns 85% of the allowable physician rate.
While the physician has the opportunity to report the service under his own name for the full service rate, the shared/split billing option requires the efforts of two individuals and may be an impractical approach for some physician groups.
“Incident-to”
Hospitalists, or their staff, may have encountered the term “incident-to” and wondered how this billing option applies to hospitalist services. “Incident-to” guidelines only apply to procedures and services performed in a private physician office. In this setting, the patient establishes care with the physician and the physician develops a patient-specific plan of care. Subsequent services may be provided to the established patient by the NPP, yet reported under the physician’s name for 100% of the allowable physician rate. “Incident-to” services cannot be reported by a hospitalist, since hospitalist services only take place in facility-based locations.
Summary
NPPs currently are involved in an extensive number of services within the hospital, and Medicare has two billing options for NPP services provided on behalf of or in conjunction with hospitalists. Each option involves specific rules and regulations with which NPPs and physician groups must comply.
Successful reporting requires understanding of and adherence to federal, state, and facility guidelines. It is important to identify NPP employment relationships, the NPP’s role in the provision of services, the state supervisory or collaborative rules, and local payer interpretations to prevent misrepresentation, misunderstanding, or erroneous reporting. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare benefit policy manual. www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed September 12, 2008.
2. Howie J, Erickson M. Acute care nurse practitioners: creating and implementing a model of care for an inpatient general medical service. Am J of Critical Care. 2002;11:448-458.
3. Cowan M, Shapiro M, et al.. The effect of a multidisciplinary hospitalist/physician and advanced practice nurse collaboration on hospital costs. J Nursing Admin. 2006;36:79-85.
4. CMS. Medicare claims processing manual: Chapter 12, Section 30.6.1B. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed September 14, 2008.
5. Pohlig C. Nonphysician providers in your practice. In: coding for chest medicine 2008. Northbrook, IL: Am Coll Chest Phy. 2008;249-254.
Recent changes in healthcare have forced academic medical centers to seek additional resources in the delivery of quality care. In response to internal and external pressures to minimize length of stay, adhere to limitations on the maximum number of admitted patients, focus on evidence-based care, and improve outcomes of care, hospitalists have incorporated non-physician providers (NPPs), such as acute care nurse practitioners (ACNPs), into their group practices.1
Whereas traditional nurse practitioners focus on the promotion of health and management of chronic illness, ACNPs focus on the care of acutely ill patients. Hospitalists utilize NPPs to expand medical service capacity and improve the efficiency and quality of patient care.2
Research indicates physician/nurse practitioner collaboration in the multidisciplinary management of hospitalized medical patients reduces length of stay and improves hospital profit without altering readmissions or mortality.3 Billing and documentation standards for NPP services must comply with current state and federal regulations. Hospitalist groups should become familiar with these guidelines prior to billing for NPP services involved in this patient care model.
The following highlights inpatient services provided by nurse practitioners (NPs) and physician assistants (PAs).
Covered Services
Medicare pays for services considered reasonable and necessary and not otherwise excluded from coverage. NPPs may provide any service permitted by the state scope of practice and performed in conjunction with the appropriate level of supervision or collaboration, as outlined in licensure or billing requirements. Being only limited by state and/or facility regulations, NPP services comprise visits or procedures typically rendered by ancillary staff or considered a physician service (a doctor of medicine, MD, or osteopathy, DO). Additionally, NPPs must meet the insurer-specified qualifications.
Independent Billing
Since 1998, designated NPPs are allowed to submit Medicare Part B claims for services, including procedures, provided in any inpatient or outpatient setting. For billing purposes, these “independent” services do not require physician involvement (e.g. physician initiation of care plan, physician-patient encounter, or physician presence on patient floor/unit) unless otherwise specified by state legislation or facility standards of practice. NPPs do not need to be employed by the physician group. The entity employing the physician group also may employ the NPP.
Claim requirements mandate the use of a national provider identifier (NPI) on all claims, therefore, all NPPs receive an NPI for claim submission. However, not all NPPs may directly bill Medicare or receive direct payment (e.g., physician assistant).1 In this situation, the NPP employer (i.e., physician or group), reports the service with the physician or group provider number and the NPP’s NPI included for identification of who actually provided the service.
Medicare Part B processes NPP claims reported under the independent billing option. Duplicate payments from any other Medicare Part A or Part B source is strictly prohibited and may result in refunds, fines and penalties. Generally, Medicare payment for NPP services is limited to 85% of the allowable physician rate. Financial impact of the 15% rate reduction is typically offset by the increase in physician time. Physicians may use this time to provide more comprehensive or complex services (admissions or consultations), potentially generating more revenue. Consistent with all provider documentation, NPP documentation must support the reported service.
Shared/Split Billing
The shared/split billing option first appeared in 2002 to address facility-based services provided to a single patient by an NPP and physician from the same group practice on the same calendar day. This option only applies to evaluation and management services provided in an emergency department, outpatient or inpatient hospital. It excludes consultations and critical care services. Unlike the independent billing option, the shared/split billing option only involves service provided by nurse practitioners, physician assistants, clinical nurse specialists, and certified nurse-midwives.
In order to qualify as a shared/split service, the NPP and the physician each must have a face-to-face encounter with the patient, although the extent of each provider’s involvement is left to provider discretion and/or local Medicare contractor requirements. The timing of each provider’s visit is irrelevant, as long as the two services are performed on the same date. For example, the NPP may see a hospital inpatient in the morning with a follow-up visit by the physician later in the day.4 When documenting, both the NPP and the physician should identify the name of the individual with whom the service is shared/split. This will allow for appropriate service capture, and ensure that the correct notes are sent to the payer in the event of claim denial and subsequent appeal. Each provider must document their portion of the rendered service and select the visit level supported by the cumulative encounter. The physician need not duplicate the elements performed and documented by the NPP, but merely perform and record the physician-determined critical or key portions. Do not confuse this billing option with teaching physician regulations. Physician and the specified NPPs cannot share or split a service with any other provider type (e.g., residents, medical or nursing students).
Only one claim may be submitted for a shared/split service. The physician may choose to report the service under his own name or under the NPP name. Reimbursement is dependent upon this selection. The physician name secures 100% of the Medicare allowable rate; the NPP name earns 85% of the allowable physician rate.
While the physician has the opportunity to report the service under his own name for the full service rate, the shared/split billing option requires the efforts of two individuals and may be an impractical approach for some physician groups.
“Incident-to”
Hospitalists, or their staff, may have encountered the term “incident-to” and wondered how this billing option applies to hospitalist services. “Incident-to” guidelines only apply to procedures and services performed in a private physician office. In this setting, the patient establishes care with the physician and the physician develops a patient-specific plan of care. Subsequent services may be provided to the established patient by the NPP, yet reported under the physician’s name for 100% of the allowable physician rate. “Incident-to” services cannot be reported by a hospitalist, since hospitalist services only take place in facility-based locations.
Summary
NPPs currently are involved in an extensive number of services within the hospital, and Medicare has two billing options for NPP services provided on behalf of or in conjunction with hospitalists. Each option involves specific rules and regulations with which NPPs and physician groups must comply.
Successful reporting requires understanding of and adherence to federal, state, and facility guidelines. It is important to identify NPP employment relationships, the NPP’s role in the provision of services, the state supervisory or collaborative rules, and local payer interpretations to prevent misrepresentation, misunderstanding, or erroneous reporting. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare benefit policy manual. www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed September 12, 2008.
2. Howie J, Erickson M. Acute care nurse practitioners: creating and implementing a model of care for an inpatient general medical service. Am J of Critical Care. 2002;11:448-458.
3. Cowan M, Shapiro M, et al.. The effect of a multidisciplinary hospitalist/physician and advanced practice nurse collaboration on hospital costs. J Nursing Admin. 2006;36:79-85.
4. CMS. Medicare claims processing manual: Chapter 12, Section 30.6.1B. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed September 14, 2008.
5. Pohlig C. Nonphysician providers in your practice. In: coding for chest medicine 2008. Northbrook, IL: Am Coll Chest Phy. 2008;249-254.
Enough Is Enough, I’m Calling a Lawyer
Physicians are no strangers to specialized careers. In narrowing the scope of their practice, specialists develop the expertise and experience to benefit patients and colleagues alike.
Specialization is common in the legal profession, as well, and some legal issues present the need to obtain specialized legal assistance. Just as a patient needing an appendectomy shouldn’t visit a psychiatrist, a medical malpractice client shouldn’t visit a tax attorney.
Before working with an attorney, pose the following questions:
- How many times have you represented clients with my particular legal problem?
- How many of those cases have gone to trial?
- Have you received any specialized training in the area of my legal problem?
- Have you written any articles or taught any courses in the area of my legal problem?
- And, most importantly, what is your philosophy towards handling legal matters?
Some legal issues will require an aggressive attorney; others may need a softer touch, an attorney who will work toward resolving a matter amicably. You should feel comfortable your attorney has the experience to handle the claim and the right philosophy toward litigation. If you want confirmation, feel free to ask for the name of a prior client.
Here are some brief descriptions of the different types of specialized legal services available. Choosing the right attorney will save you time, money and should maximize the possibility that you will have a successful outcome.
Medical Malpractice Defense Counsel
In the unfortunate event you are sued for medical malpractice, you want to make sure your insurance company assigns you an attorney who has substantial experience in defending medical malpractice. These lawsuits are very complex and require defense attorneys to understand not only the legal requirements of the claim, but also the medical conditions and interventions undertaken on the patients’ behalf.
Professional Licensure Defense Counsel
Some attorneys focus on defending health care professionals before licensing agencies, such as the Board of Medical Examiners or the Drug Enforcement Agency. These proceedings often involve issues that are non-medical in nature, such as fraud, sexual misconduct and substance abuse. Attorneys specialized in representing clients before licensing agencies will have a better understanding of how the agency views the issues and will be able to recommend prospective courses of action, such as peer assistance or continuing education programs, making formal disciplinary proceedings less likely.
Labor and Employment Litigator
There are numerous laws governing the workplace, so when an employment issue surfaces, it’s important to work with an experienced labor and employment attorney. Most attorneys further specialize and represent plaintiffs or defendants, so make sure that you consult with an attorney on the right side of your issue.
Personal Injury Litigator
Some personal injury attorneys work on a volume basis and defer much of the process to paralegals and staff members. Other counselors take on a smaller volume of cases and give each case more individual attention. If you are injured in the workplace and need to find a personal injury attorney, you might want to ask a medical malpractice defense lawyer or your insurance company for a referral.
Matrimonial
One of the most common reasons a physician needs to hire counsel is the dissolution of a marriage. These cases raise intense, personal issues dealing with the division of assets, sale of property, and the allocation of parental responsibilities. Many of these issues are the subject of state laws, which attempt to compel an equitable determination. Working with an experienced matrimonial attorney will keep the focus on the legal merits of the case.
Tax Counsel
Tax law is one of the areas in which law schools offer an advanced degree, known as an LLM. It is the equivalent of a post-doctoral training program. These professionals have tremendous experience in representing individuals and businesses in the formation of business entities and in dealing with federal and state taxing authorities.
Medical Entity Formation
Depending on the state you live in, you may have a choice of business entities for your practice, such as corporations, partnerships, limited liability partnerships (LLP), and professional corporations. In choosing and structuring a business entity, you should consult with an attorney who has experience in representing health care professionals. State and federal regulations may affect your choice of an entity. A good attorney also can help clients anticipate and avoid potential dissolution issues, such as disputes over non-compete provisions, distribution of accounts receivable, and transfer of patient files.
Real Property
When attorneys refer to “real property,” they are describing the purchase and development of land, which can raise complex legal issues related to zoning, easements, assessments, restrictive covenants, and leasing.
Intellectual Property
When lawyers refer to “intellectual property,” they are describing the protections provided to a person’s creative efforts, such as copyright, trademarks and patents. Attorneys can earn a formal advanced degree in this area through an LLM program. If you develop an invention or write a book, intellectual property attorneys are best suited to make sure you receive the benefits of your creative efforts.
Trust and Estate
When people die, they leave an estate, which can be the subject of extensive probate proceedings to determine the heirs’ rights. Even if there are no disputes between heirs, there can be probate proceedings to determine the value of the estate and the taxes that might be assessed against it. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
Physicians are no strangers to specialized careers. In narrowing the scope of their practice, specialists develop the expertise and experience to benefit patients and colleagues alike.
Specialization is common in the legal profession, as well, and some legal issues present the need to obtain specialized legal assistance. Just as a patient needing an appendectomy shouldn’t visit a psychiatrist, a medical malpractice client shouldn’t visit a tax attorney.
Before working with an attorney, pose the following questions:
- How many times have you represented clients with my particular legal problem?
- How many of those cases have gone to trial?
- Have you received any specialized training in the area of my legal problem?
- Have you written any articles or taught any courses in the area of my legal problem?
- And, most importantly, what is your philosophy towards handling legal matters?
Some legal issues will require an aggressive attorney; others may need a softer touch, an attorney who will work toward resolving a matter amicably. You should feel comfortable your attorney has the experience to handle the claim and the right philosophy toward litigation. If you want confirmation, feel free to ask for the name of a prior client.
Here are some brief descriptions of the different types of specialized legal services available. Choosing the right attorney will save you time, money and should maximize the possibility that you will have a successful outcome.
Medical Malpractice Defense Counsel
In the unfortunate event you are sued for medical malpractice, you want to make sure your insurance company assigns you an attorney who has substantial experience in defending medical malpractice. These lawsuits are very complex and require defense attorneys to understand not only the legal requirements of the claim, but also the medical conditions and interventions undertaken on the patients’ behalf.
Professional Licensure Defense Counsel
Some attorneys focus on defending health care professionals before licensing agencies, such as the Board of Medical Examiners or the Drug Enforcement Agency. These proceedings often involve issues that are non-medical in nature, such as fraud, sexual misconduct and substance abuse. Attorneys specialized in representing clients before licensing agencies will have a better understanding of how the agency views the issues and will be able to recommend prospective courses of action, such as peer assistance or continuing education programs, making formal disciplinary proceedings less likely.
Labor and Employment Litigator
There are numerous laws governing the workplace, so when an employment issue surfaces, it’s important to work with an experienced labor and employment attorney. Most attorneys further specialize and represent plaintiffs or defendants, so make sure that you consult with an attorney on the right side of your issue.
Personal Injury Litigator
Some personal injury attorneys work on a volume basis and defer much of the process to paralegals and staff members. Other counselors take on a smaller volume of cases and give each case more individual attention. If you are injured in the workplace and need to find a personal injury attorney, you might want to ask a medical malpractice defense lawyer or your insurance company for a referral.
Matrimonial
One of the most common reasons a physician needs to hire counsel is the dissolution of a marriage. These cases raise intense, personal issues dealing with the division of assets, sale of property, and the allocation of parental responsibilities. Many of these issues are the subject of state laws, which attempt to compel an equitable determination. Working with an experienced matrimonial attorney will keep the focus on the legal merits of the case.
Tax Counsel
Tax law is one of the areas in which law schools offer an advanced degree, known as an LLM. It is the equivalent of a post-doctoral training program. These professionals have tremendous experience in representing individuals and businesses in the formation of business entities and in dealing with federal and state taxing authorities.
Medical Entity Formation
Depending on the state you live in, you may have a choice of business entities for your practice, such as corporations, partnerships, limited liability partnerships (LLP), and professional corporations. In choosing and structuring a business entity, you should consult with an attorney who has experience in representing health care professionals. State and federal regulations may affect your choice of an entity. A good attorney also can help clients anticipate and avoid potential dissolution issues, such as disputes over non-compete provisions, distribution of accounts receivable, and transfer of patient files.
Real Property
When attorneys refer to “real property,” they are describing the purchase and development of land, which can raise complex legal issues related to zoning, easements, assessments, restrictive covenants, and leasing.
Intellectual Property
When lawyers refer to “intellectual property,” they are describing the protections provided to a person’s creative efforts, such as copyright, trademarks and patents. Attorneys can earn a formal advanced degree in this area through an LLM program. If you develop an invention or write a book, intellectual property attorneys are best suited to make sure you receive the benefits of your creative efforts.
Trust and Estate
When people die, they leave an estate, which can be the subject of extensive probate proceedings to determine the heirs’ rights. Even if there are no disputes between heirs, there can be probate proceedings to determine the value of the estate and the taxes that might be assessed against it. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
Physicians are no strangers to specialized careers. In narrowing the scope of their practice, specialists develop the expertise and experience to benefit patients and colleagues alike.
Specialization is common in the legal profession, as well, and some legal issues present the need to obtain specialized legal assistance. Just as a patient needing an appendectomy shouldn’t visit a psychiatrist, a medical malpractice client shouldn’t visit a tax attorney.
Before working with an attorney, pose the following questions:
- How many times have you represented clients with my particular legal problem?
- How many of those cases have gone to trial?
- Have you received any specialized training in the area of my legal problem?
- Have you written any articles or taught any courses in the area of my legal problem?
- And, most importantly, what is your philosophy towards handling legal matters?
Some legal issues will require an aggressive attorney; others may need a softer touch, an attorney who will work toward resolving a matter amicably. You should feel comfortable your attorney has the experience to handle the claim and the right philosophy toward litigation. If you want confirmation, feel free to ask for the name of a prior client.
Here are some brief descriptions of the different types of specialized legal services available. Choosing the right attorney will save you time, money and should maximize the possibility that you will have a successful outcome.
Medical Malpractice Defense Counsel
In the unfortunate event you are sued for medical malpractice, you want to make sure your insurance company assigns you an attorney who has substantial experience in defending medical malpractice. These lawsuits are very complex and require defense attorneys to understand not only the legal requirements of the claim, but also the medical conditions and interventions undertaken on the patients’ behalf.
Professional Licensure Defense Counsel
Some attorneys focus on defending health care professionals before licensing agencies, such as the Board of Medical Examiners or the Drug Enforcement Agency. These proceedings often involve issues that are non-medical in nature, such as fraud, sexual misconduct and substance abuse. Attorneys specialized in representing clients before licensing agencies will have a better understanding of how the agency views the issues and will be able to recommend prospective courses of action, such as peer assistance or continuing education programs, making formal disciplinary proceedings less likely.
Labor and Employment Litigator
There are numerous laws governing the workplace, so when an employment issue surfaces, it’s important to work with an experienced labor and employment attorney. Most attorneys further specialize and represent plaintiffs or defendants, so make sure that you consult with an attorney on the right side of your issue.
Personal Injury Litigator
Some personal injury attorneys work on a volume basis and defer much of the process to paralegals and staff members. Other counselors take on a smaller volume of cases and give each case more individual attention. If you are injured in the workplace and need to find a personal injury attorney, you might want to ask a medical malpractice defense lawyer or your insurance company for a referral.
Matrimonial
One of the most common reasons a physician needs to hire counsel is the dissolution of a marriage. These cases raise intense, personal issues dealing with the division of assets, sale of property, and the allocation of parental responsibilities. Many of these issues are the subject of state laws, which attempt to compel an equitable determination. Working with an experienced matrimonial attorney will keep the focus on the legal merits of the case.
Tax Counsel
Tax law is one of the areas in which law schools offer an advanced degree, known as an LLM. It is the equivalent of a post-doctoral training program. These professionals have tremendous experience in representing individuals and businesses in the formation of business entities and in dealing with federal and state taxing authorities.
Medical Entity Formation
Depending on the state you live in, you may have a choice of business entities for your practice, such as corporations, partnerships, limited liability partnerships (LLP), and professional corporations. In choosing and structuring a business entity, you should consult with an attorney who has experience in representing health care professionals. State and federal regulations may affect your choice of an entity. A good attorney also can help clients anticipate and avoid potential dissolution issues, such as disputes over non-compete provisions, distribution of accounts receivable, and transfer of patient files.
Real Property
When attorneys refer to “real property,” they are describing the purchase and development of land, which can raise complex legal issues related to zoning, easements, assessments, restrictive covenants, and leasing.
Intellectual Property
When lawyers refer to “intellectual property,” they are describing the protections provided to a person’s creative efforts, such as copyright, trademarks and patents. Attorneys can earn a formal advanced degree in this area through an LLM program. If you develop an invention or write a book, intellectual property attorneys are best suited to make sure you receive the benefits of your creative efforts.
Trust and Estate
When people die, they leave an estate, which can be the subject of extensive probate proceedings to determine the heirs’ rights. Even if there are no disputes between heirs, there can be probate proceedings to determine the value of the estate and the taxes that might be assessed against it. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
Mind Your Manners
Beginning January 1, 2009, your on-the-job behavior—and that of other healthcare providers—will be held to a new standard. New Joint Commission standards include a requirement for healthcare organizations to create a code of conduct outlining acceptable and unacceptable behaviors for healthcare professionals, and to implement a process for managing problematic behavior. The reason for this unusual step is the belief that disruptive or intimidating behavior by physicians, nurses, and other healthcare workers has a negative impact on the quality of care.
“I think the standard shows that the Joint Commission is interested in behaviors within hospitals and other healthcare organizations, and how that affects quality of care, safety and the patient experience,” says Russell L. Holman, MD, immediate past president of SHM and chief operating officer for Cogent Healthcare, Nashville, Tenn. “By highlighting this as an area to be included in reviews and standards, it causes organizations to look for their own policies on disruptive behaviors.”
Here is a closer look at the new standard and how it might impact hospital medicine.
Not Physicians Only
The Joint Commission standard addresses “the problem of behaviors that threaten the performance of the healthcare team,” mentioning unprofessional behavior, specifically “intimidating and disruptive behaviors.” To many, this seems to target physicians. “In a hospital, there is an unwritten hierarchy, with physicians at the top,” Dr. Holman points out. “As such, some feel that different standards are applied to physician behaviors. For example, if a nurse or a pharmacist uses obscene language, they may be terminated. If a physician does this, they may receive feedback that the language was inappropriate.”
However, the Sentinel Event Alert released by the Joint Commission in July states, “While most formal research centers on intimidating and disruptive behaviors among physicians and nurses, there is evidence that these behaviors occur among other healthcare professionals, such as pharmacists, therapists, and support staff, as well as among administrators.” The alert does not single out physicians or any other healthcare profession regarding bad behaviors.
“I think the Joint Commission has been very clear in its intent that the standard applies equally to physicians and non-physicians,” Dr. Holman says.
When Hospitalists Cross the Line
How will this code of conduct standard affect hospitalists? Because of the nature of their work, they will be held to the standards of any hospital they work in. In the case of hospitalists who are directly employed by a hospital, the response should be straightforward. However, independent hospital medicine groups will have to work with their hospitals on behavior issues. First, these groups will need to decide whether they should have their own policies and procedures for code of conduct. “Hospital medicine groups need appropriate systems of identifying disruptive behavior, monitoring it, and taking any necessary actions to make sure the behavior is not continued,” Dr. Holman stresses.
Second, independent groups must communicate closely with the hospital when a behavior issue arises. “If you have a hospitalist who is not directly employed by the hospital, there is a dual responsibility for managing their disruptive behavior,” Dr. Holman says. “The hospital has medical staff standards, which are reflected in the medical staff bylaws and rules and regulations. These documents need to include policy and procedures around the incidence of disruptive physician behavior.”
But just because procedures are in place doesn’t mean the hospital will address a problem hospitalist. “This is where in practice, things can get a little fuzzy,” Dr. Holman admits. “The hospital may defer the responsibility for managing the physician to the employer. This is the scenario that has come up in hospital medicine.” He adds, “In my personal opinion, there is a dual responsibility. The hospital needs to apply its standard to all medical staff, regardless of specialty, tenure or employment status.” At the same time, the hospital medicine group/employer should have—and should implement—an approach to managing disruptive behavior.
“Different employers will have different capabilities,” Dr. Holman says. “For example, large, multi-specialty medical groups may have an infrastructure, including human resources professionals, risk managers and depth of medical and operational management, in place for dealing with disruptive behavior. … Small practices won’t have this. They may rely more heavily on the hospital’s infrastructure.”
—Russell L. Holman, MD, COO, Cogent Healthcare, Nashville, Tenn.
Regardless of the hospital medicine group’s size and capabilities, it should promote two-way communication with the hospital regarding problems with individual hospitalists. “If an incident occurs in the hospital, the employer needs to know the details so they can follow up,” Dr. Holman says. “They have to be careful about sharing appropriate information, and protect all privacies. And they have to balance this communication with the fact that it doesn’t absolve one or the other from acting. There must be follow through from both parties, including disciplinary or corrective action as necessary.”
Defining “Disruptive”
One concern healthcare leaders—and the people they lead—may have is deciding the standard used in crafting a policy that specifies what types of behavior are unprofessional. “The challenge is defining disruptive behavior,” Dr. Holman says. “Of course, it can be very clear sometimes. But a surgeon throwing instruments in the operating room is different than someone who is a little bit outspoken.” Consider a hospitalist or other physician who’s in the habit of questioning authority; could this requirement lead to efforts to shut them down?
“Naturally, there is a degree of concern amongst physicians that this is a physician-directed standard, and that there may be a tough time distinguishing between the good faith criticisms of outspoken physicians and those who demonstrate physically threatening behavior,” Dr. Holman says.
The best way for hospitals, hospital medicine groups and other healthcare organizations to avoid this is to find established policies on this subject that are fair, carefully phrased and comprehensive, then customize one or more to their own specifications and distribute to all affected employees.
“I think these policies are nice to include in new physician orientations or training programs, so that physicians are aware of them,” Dr. Holman suggests.
For more information on the code of conduct standard, visit www.jointcommis-sion.org/SentinelEvents/SentinelEventAlert/sea_40.htm. TH
Jane Jerrard is a medical writer based in Chicago.
Beginning January 1, 2009, your on-the-job behavior—and that of other healthcare providers—will be held to a new standard. New Joint Commission standards include a requirement for healthcare organizations to create a code of conduct outlining acceptable and unacceptable behaviors for healthcare professionals, and to implement a process for managing problematic behavior. The reason for this unusual step is the belief that disruptive or intimidating behavior by physicians, nurses, and other healthcare workers has a negative impact on the quality of care.
“I think the standard shows that the Joint Commission is interested in behaviors within hospitals and other healthcare organizations, and how that affects quality of care, safety and the patient experience,” says Russell L. Holman, MD, immediate past president of SHM and chief operating officer for Cogent Healthcare, Nashville, Tenn. “By highlighting this as an area to be included in reviews and standards, it causes organizations to look for their own policies on disruptive behaviors.”
Here is a closer look at the new standard and how it might impact hospital medicine.
Not Physicians Only
The Joint Commission standard addresses “the problem of behaviors that threaten the performance of the healthcare team,” mentioning unprofessional behavior, specifically “intimidating and disruptive behaviors.” To many, this seems to target physicians. “In a hospital, there is an unwritten hierarchy, with physicians at the top,” Dr. Holman points out. “As such, some feel that different standards are applied to physician behaviors. For example, if a nurse or a pharmacist uses obscene language, they may be terminated. If a physician does this, they may receive feedback that the language was inappropriate.”
However, the Sentinel Event Alert released by the Joint Commission in July states, “While most formal research centers on intimidating and disruptive behaviors among physicians and nurses, there is evidence that these behaviors occur among other healthcare professionals, such as pharmacists, therapists, and support staff, as well as among administrators.” The alert does not single out physicians or any other healthcare profession regarding bad behaviors.
“I think the Joint Commission has been very clear in its intent that the standard applies equally to physicians and non-physicians,” Dr. Holman says.
When Hospitalists Cross the Line
How will this code of conduct standard affect hospitalists? Because of the nature of their work, they will be held to the standards of any hospital they work in. In the case of hospitalists who are directly employed by a hospital, the response should be straightforward. However, independent hospital medicine groups will have to work with their hospitals on behavior issues. First, these groups will need to decide whether they should have their own policies and procedures for code of conduct. “Hospital medicine groups need appropriate systems of identifying disruptive behavior, monitoring it, and taking any necessary actions to make sure the behavior is not continued,” Dr. Holman stresses.
Second, independent groups must communicate closely with the hospital when a behavior issue arises. “If you have a hospitalist who is not directly employed by the hospital, there is a dual responsibility for managing their disruptive behavior,” Dr. Holman says. “The hospital has medical staff standards, which are reflected in the medical staff bylaws and rules and regulations. These documents need to include policy and procedures around the incidence of disruptive physician behavior.”
But just because procedures are in place doesn’t mean the hospital will address a problem hospitalist. “This is where in practice, things can get a little fuzzy,” Dr. Holman admits. “The hospital may defer the responsibility for managing the physician to the employer. This is the scenario that has come up in hospital medicine.” He adds, “In my personal opinion, there is a dual responsibility. The hospital needs to apply its standard to all medical staff, regardless of specialty, tenure or employment status.” At the same time, the hospital medicine group/employer should have—and should implement—an approach to managing disruptive behavior.
“Different employers will have different capabilities,” Dr. Holman says. “For example, large, multi-specialty medical groups may have an infrastructure, including human resources professionals, risk managers and depth of medical and operational management, in place for dealing with disruptive behavior. … Small practices won’t have this. They may rely more heavily on the hospital’s infrastructure.”
—Russell L. Holman, MD, COO, Cogent Healthcare, Nashville, Tenn.
Regardless of the hospital medicine group’s size and capabilities, it should promote two-way communication with the hospital regarding problems with individual hospitalists. “If an incident occurs in the hospital, the employer needs to know the details so they can follow up,” Dr. Holman says. “They have to be careful about sharing appropriate information, and protect all privacies. And they have to balance this communication with the fact that it doesn’t absolve one or the other from acting. There must be follow through from both parties, including disciplinary or corrective action as necessary.”
Defining “Disruptive”
One concern healthcare leaders—and the people they lead—may have is deciding the standard used in crafting a policy that specifies what types of behavior are unprofessional. “The challenge is defining disruptive behavior,” Dr. Holman says. “Of course, it can be very clear sometimes. But a surgeon throwing instruments in the operating room is different than someone who is a little bit outspoken.” Consider a hospitalist or other physician who’s in the habit of questioning authority; could this requirement lead to efforts to shut them down?
“Naturally, there is a degree of concern amongst physicians that this is a physician-directed standard, and that there may be a tough time distinguishing between the good faith criticisms of outspoken physicians and those who demonstrate physically threatening behavior,” Dr. Holman says.
The best way for hospitals, hospital medicine groups and other healthcare organizations to avoid this is to find established policies on this subject that are fair, carefully phrased and comprehensive, then customize one or more to their own specifications and distribute to all affected employees.
“I think these policies are nice to include in new physician orientations or training programs, so that physicians are aware of them,” Dr. Holman suggests.
For more information on the code of conduct standard, visit www.jointcommis-sion.org/SentinelEvents/SentinelEventAlert/sea_40.htm. TH
Jane Jerrard is a medical writer based in Chicago.
Beginning January 1, 2009, your on-the-job behavior—and that of other healthcare providers—will be held to a new standard. New Joint Commission standards include a requirement for healthcare organizations to create a code of conduct outlining acceptable and unacceptable behaviors for healthcare professionals, and to implement a process for managing problematic behavior. The reason for this unusual step is the belief that disruptive or intimidating behavior by physicians, nurses, and other healthcare workers has a negative impact on the quality of care.
“I think the standard shows that the Joint Commission is interested in behaviors within hospitals and other healthcare organizations, and how that affects quality of care, safety and the patient experience,” says Russell L. Holman, MD, immediate past president of SHM and chief operating officer for Cogent Healthcare, Nashville, Tenn. “By highlighting this as an area to be included in reviews and standards, it causes organizations to look for their own policies on disruptive behaviors.”
Here is a closer look at the new standard and how it might impact hospital medicine.
Not Physicians Only
The Joint Commission standard addresses “the problem of behaviors that threaten the performance of the healthcare team,” mentioning unprofessional behavior, specifically “intimidating and disruptive behaviors.” To many, this seems to target physicians. “In a hospital, there is an unwritten hierarchy, with physicians at the top,” Dr. Holman points out. “As such, some feel that different standards are applied to physician behaviors. For example, if a nurse or a pharmacist uses obscene language, they may be terminated. If a physician does this, they may receive feedback that the language was inappropriate.”
However, the Sentinel Event Alert released by the Joint Commission in July states, “While most formal research centers on intimidating and disruptive behaviors among physicians and nurses, there is evidence that these behaviors occur among other healthcare professionals, such as pharmacists, therapists, and support staff, as well as among administrators.” The alert does not single out physicians or any other healthcare profession regarding bad behaviors.
“I think the Joint Commission has been very clear in its intent that the standard applies equally to physicians and non-physicians,” Dr. Holman says.
When Hospitalists Cross the Line
How will this code of conduct standard affect hospitalists? Because of the nature of their work, they will be held to the standards of any hospital they work in. In the case of hospitalists who are directly employed by a hospital, the response should be straightforward. However, independent hospital medicine groups will have to work with their hospitals on behavior issues. First, these groups will need to decide whether they should have their own policies and procedures for code of conduct. “Hospital medicine groups need appropriate systems of identifying disruptive behavior, monitoring it, and taking any necessary actions to make sure the behavior is not continued,” Dr. Holman stresses.
Second, independent groups must communicate closely with the hospital when a behavior issue arises. “If you have a hospitalist who is not directly employed by the hospital, there is a dual responsibility for managing their disruptive behavior,” Dr. Holman says. “The hospital has medical staff standards, which are reflected in the medical staff bylaws and rules and regulations. These documents need to include policy and procedures around the incidence of disruptive physician behavior.”
But just because procedures are in place doesn’t mean the hospital will address a problem hospitalist. “This is where in practice, things can get a little fuzzy,” Dr. Holman admits. “The hospital may defer the responsibility for managing the physician to the employer. This is the scenario that has come up in hospital medicine.” He adds, “In my personal opinion, there is a dual responsibility. The hospital needs to apply its standard to all medical staff, regardless of specialty, tenure or employment status.” At the same time, the hospital medicine group/employer should have—and should implement—an approach to managing disruptive behavior.
“Different employers will have different capabilities,” Dr. Holman says. “For example, large, multi-specialty medical groups may have an infrastructure, including human resources professionals, risk managers and depth of medical and operational management, in place for dealing with disruptive behavior. … Small practices won’t have this. They may rely more heavily on the hospital’s infrastructure.”
—Russell L. Holman, MD, COO, Cogent Healthcare, Nashville, Tenn.
Regardless of the hospital medicine group’s size and capabilities, it should promote two-way communication with the hospital regarding problems with individual hospitalists. “If an incident occurs in the hospital, the employer needs to know the details so they can follow up,” Dr. Holman says. “They have to be careful about sharing appropriate information, and protect all privacies. And they have to balance this communication with the fact that it doesn’t absolve one or the other from acting. There must be follow through from both parties, including disciplinary or corrective action as necessary.”
Defining “Disruptive”
One concern healthcare leaders—and the people they lead—may have is deciding the standard used in crafting a policy that specifies what types of behavior are unprofessional. “The challenge is defining disruptive behavior,” Dr. Holman says. “Of course, it can be very clear sometimes. But a surgeon throwing instruments in the operating room is different than someone who is a little bit outspoken.” Consider a hospitalist or other physician who’s in the habit of questioning authority; could this requirement lead to efforts to shut them down?
“Naturally, there is a degree of concern amongst physicians that this is a physician-directed standard, and that there may be a tough time distinguishing between the good faith criticisms of outspoken physicians and those who demonstrate physically threatening behavior,” Dr. Holman says.
The best way for hospitals, hospital medicine groups and other healthcare organizations to avoid this is to find established policies on this subject that are fair, carefully phrased and comprehensive, then customize one or more to their own specifications and distribute to all affected employees.
“I think these policies are nice to include in new physician orientations or training programs, so that physicians are aware of them,” Dr. Holman suggests.
For more information on the code of conduct standard, visit www.jointcommis-sion.org/SentinelEvents/SentinelEventAlert/sea_40.htm. TH
Jane Jerrard is a medical writer based in Chicago.
First Paycheck Equals Investment Decisions
Hospitalists setting out on their careers are used to life as struggling students. Once they start earning a sizeable salary, they’re hit with some tough choices: How fast should they pay off medical school loans? Can they afford to give in to the temptation of an expensive reward? How much savings do they really need?
“It is a bit of a shock to start your first job as an attending physician,” says Margaret C. Fang, MD, MPH, assistant adjunct professor of medicine at the University of California Hospital Medicine Group. “Your bank account seems to grow so much faster!” No matter how big that account may seem, it can dwindle away every month if you don’t practice good money management skills.
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, is faculty advisor to a medical student interest group at his university called Money and Medicine. “It’s all about delayed gratification,” he says of the effect a physician’s salary has on a new hospitalist. “I say, just wait one year in your new job to see what your expenses are before you buy that big house or that expensive convertible.”
Do Your Research
Residents and early career hospitalists—and anyone who is having trouble saving some salary—would do well to tackle the subject of money management as if it were a clinical course. “What you do with your money deserves a lot of attention,” Dr. Fang says. “Vigilance about finances is important, but many physicians are not as prepared to deal with money management as they are to care for patients.”
When you’re about to start a job, find out the financial options before you’re faced with a mountain of forms and a heap of decisions. “When I started here, I had all this paperwork: I had to sign up for health insurance, disability, long-term disability, 401(k) and 403(b) plans, and more. It’s really daunting,” Dr. Fang says. “A little upfront research is important, so you can make good decisions about these things.”
When it comes to figuring out how much to contribute to retirement accounts, savings accounts and investments, consider enlisting some outside help. “Many institutions that hire young hospitalists offer financial counseling,” Dr. Fang points out. “I’ve done a lot of independent reading. But if your finances are more challenging—say you’re carrying a lot of debt—it’s reasonable to work with a financial consultant.”
Deal with Debt
Before you start investing your money, take a look at your debt. What to do with it—for instance, should you pay off all of your loans and bills—will be one of the most important decisions a new hospitalist will make.
“The first thing you should do is clear any credit card debt, because it carries such high interest rates,” Dr. Badlani advises. “Do this before investing in a Roth IRA or anything.”
As for student loans, “I recommend taking your time paying off fixed APR loans and federally subsidized loans,” Dr. Badlani says “These typically carry low interest and they are tax deductible. You’re better off investing your money in indexed mutual funds because the stock market averages an 8% to 10% return (long-term), versus loans that are maybe 6% interest, or 4% when you calculate the tax deduction.”
However, if your student loan comes from a private bank, it may carry a higher interest rate and variable APRs. In this case, says Dr. Badlani, “you need to pay off those loans first” or look into consolidating or refinancing high-interest student loans.
Build Your Savings
Once you’ve cleared or reduced any high-interest debt, it’s time to focus on saving some money—no matter how much you’re making. “Residents say they have no money to save,” Dr. Badlani says. “But you need to look at your lifestyle and look for what is called ‘the latte factor.’ If you work hard, you may feel you deserve a treat, so you buy a $4 latte every day—maybe two a day. If you work 27 days a month, this adds up to $200 a month or nearly $3,000 a year. If you put that money in your Roth IRA every year of your residency and your fellowship, that adds up to a cool $150,000—based on 8% to 9% annual return, compounded annually for 30 years and adjusted for investment fees.”
—Sameer Badlani, MD
Starting a money market account or putting money in a certificate of deposit (CD) will keep it liquid. “You should have three to six months’ expenses, in case you lose your job or get sick,” Dr. Badlani says. “But be sure to put this ‘cushion money’ in a money market account, which these days are typically returning 3.5% APR versus regular checking accounts that offer a measly .25%, to offset inflation eating into your savings.”
Invest Early for Retirement
Residents and low-income hospitalists are in an excellent position to start investing for retirement. “While you’re a resident or intern, you most likely qualify for a Roth IRA,” Dr. Badlani explains. “This is the only time you’ll be able to invest in this. It’s a good choice for people with potential for increasing their income. Roth contributions are made after taxes and the account grows tax-free; you never have to pay tax on that money in retirement. For 2008, you’re eligible to contribute to a Roth IRA if you’re single or file as head of household with a modified adjusted gross income of below $114,000, or if you file jointly with income below $166,000.”
Another smart retirement investment for just about any hospitalist is employer-matched contributions. “If your employer will match your [retirement] contribution, that’s free money,” Dr. Badlani points out. “If you’re not taking advantage of that, you’re making a big mistake. Institutions will typically match up to about 5% of an employee’s contribution to a 401(k) or 403(b). Plus, by putting money in a retirement account, you’re reducing your tax burden.”
Online calculators can help you figure out how much to save—including matching funds—for a comfortable retirement. “The $1 million retirement has been the American dream for a long time, but that’s increased now to $1.5 to $1.8 million,” Dr. Badlani says. “But for a comfortable lifestyle and accounting for spiraling healthcare costs, I would recommend aiming for $5 million. That takes a lot of discipline over a long stretch of time.” He recommends the online calculator at www.dinkytown.net, which shows that a 29-year-old earning an annual income of $150,000 can retire at 65 with $5,868,264—if he or she contributes 15% to a 403(b) retirement account with a 5% employer match. “But you have to stick to this every month for the next 36 years,” Dr. Badlani warns. “That takes discipline.”
Regardless of how old you are or how much income you currently have, it’s wise to start practicing smart habits with spending, saving and investing your money. As Dr. Badlani says, “Good money habits last forever.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Hospitalists setting out on their careers are used to life as struggling students. Once they start earning a sizeable salary, they’re hit with some tough choices: How fast should they pay off medical school loans? Can they afford to give in to the temptation of an expensive reward? How much savings do they really need?
“It is a bit of a shock to start your first job as an attending physician,” says Margaret C. Fang, MD, MPH, assistant adjunct professor of medicine at the University of California Hospital Medicine Group. “Your bank account seems to grow so much faster!” No matter how big that account may seem, it can dwindle away every month if you don’t practice good money management skills.
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, is faculty advisor to a medical student interest group at his university called Money and Medicine. “It’s all about delayed gratification,” he says of the effect a physician’s salary has on a new hospitalist. “I say, just wait one year in your new job to see what your expenses are before you buy that big house or that expensive convertible.”
Do Your Research
Residents and early career hospitalists—and anyone who is having trouble saving some salary—would do well to tackle the subject of money management as if it were a clinical course. “What you do with your money deserves a lot of attention,” Dr. Fang says. “Vigilance about finances is important, but many physicians are not as prepared to deal with money management as they are to care for patients.”
When you’re about to start a job, find out the financial options before you’re faced with a mountain of forms and a heap of decisions. “When I started here, I had all this paperwork: I had to sign up for health insurance, disability, long-term disability, 401(k) and 403(b) plans, and more. It’s really daunting,” Dr. Fang says. “A little upfront research is important, so you can make good decisions about these things.”
When it comes to figuring out how much to contribute to retirement accounts, savings accounts and investments, consider enlisting some outside help. “Many institutions that hire young hospitalists offer financial counseling,” Dr. Fang points out. “I’ve done a lot of independent reading. But if your finances are more challenging—say you’re carrying a lot of debt—it’s reasonable to work with a financial consultant.”
Deal with Debt
Before you start investing your money, take a look at your debt. What to do with it—for instance, should you pay off all of your loans and bills—will be one of the most important decisions a new hospitalist will make.
“The first thing you should do is clear any credit card debt, because it carries such high interest rates,” Dr. Badlani advises. “Do this before investing in a Roth IRA or anything.”
As for student loans, “I recommend taking your time paying off fixed APR loans and federally subsidized loans,” Dr. Badlani says “These typically carry low interest and they are tax deductible. You’re better off investing your money in indexed mutual funds because the stock market averages an 8% to 10% return (long-term), versus loans that are maybe 6% interest, or 4% when you calculate the tax deduction.”
However, if your student loan comes from a private bank, it may carry a higher interest rate and variable APRs. In this case, says Dr. Badlani, “you need to pay off those loans first” or look into consolidating or refinancing high-interest student loans.
Build Your Savings
Once you’ve cleared or reduced any high-interest debt, it’s time to focus on saving some money—no matter how much you’re making. “Residents say they have no money to save,” Dr. Badlani says. “But you need to look at your lifestyle and look for what is called ‘the latte factor.’ If you work hard, you may feel you deserve a treat, so you buy a $4 latte every day—maybe two a day. If you work 27 days a month, this adds up to $200 a month or nearly $3,000 a year. If you put that money in your Roth IRA every year of your residency and your fellowship, that adds up to a cool $150,000—based on 8% to 9% annual return, compounded annually for 30 years and adjusted for investment fees.”
—Sameer Badlani, MD
Starting a money market account or putting money in a certificate of deposit (CD) will keep it liquid. “You should have three to six months’ expenses, in case you lose your job or get sick,” Dr. Badlani says. “But be sure to put this ‘cushion money’ in a money market account, which these days are typically returning 3.5% APR versus regular checking accounts that offer a measly .25%, to offset inflation eating into your savings.”
Invest Early for Retirement
Residents and low-income hospitalists are in an excellent position to start investing for retirement. “While you’re a resident or intern, you most likely qualify for a Roth IRA,” Dr. Badlani explains. “This is the only time you’ll be able to invest in this. It’s a good choice for people with potential for increasing their income. Roth contributions are made after taxes and the account grows tax-free; you never have to pay tax on that money in retirement. For 2008, you’re eligible to contribute to a Roth IRA if you’re single or file as head of household with a modified adjusted gross income of below $114,000, or if you file jointly with income below $166,000.”
Another smart retirement investment for just about any hospitalist is employer-matched contributions. “If your employer will match your [retirement] contribution, that’s free money,” Dr. Badlani points out. “If you’re not taking advantage of that, you’re making a big mistake. Institutions will typically match up to about 5% of an employee’s contribution to a 401(k) or 403(b). Plus, by putting money in a retirement account, you’re reducing your tax burden.”
Online calculators can help you figure out how much to save—including matching funds—for a comfortable retirement. “The $1 million retirement has been the American dream for a long time, but that’s increased now to $1.5 to $1.8 million,” Dr. Badlani says. “But for a comfortable lifestyle and accounting for spiraling healthcare costs, I would recommend aiming for $5 million. That takes a lot of discipline over a long stretch of time.” He recommends the online calculator at www.dinkytown.net, which shows that a 29-year-old earning an annual income of $150,000 can retire at 65 with $5,868,264—if he or she contributes 15% to a 403(b) retirement account with a 5% employer match. “But you have to stick to this every month for the next 36 years,” Dr. Badlani warns. “That takes discipline.”
Regardless of how old you are or how much income you currently have, it’s wise to start practicing smart habits with spending, saving and investing your money. As Dr. Badlani says, “Good money habits last forever.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Hospitalists setting out on their careers are used to life as struggling students. Once they start earning a sizeable salary, they’re hit with some tough choices: How fast should they pay off medical school loans? Can they afford to give in to the temptation of an expensive reward? How much savings do they really need?
“It is a bit of a shock to start your first job as an attending physician,” says Margaret C. Fang, MD, MPH, assistant adjunct professor of medicine at the University of California Hospital Medicine Group. “Your bank account seems to grow so much faster!” No matter how big that account may seem, it can dwindle away every month if you don’t practice good money management skills.
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, is faculty advisor to a medical student interest group at his university called Money and Medicine. “It’s all about delayed gratification,” he says of the effect a physician’s salary has on a new hospitalist. “I say, just wait one year in your new job to see what your expenses are before you buy that big house or that expensive convertible.”
Do Your Research
Residents and early career hospitalists—and anyone who is having trouble saving some salary—would do well to tackle the subject of money management as if it were a clinical course. “What you do with your money deserves a lot of attention,” Dr. Fang says. “Vigilance about finances is important, but many physicians are not as prepared to deal with money management as they are to care for patients.”
When you’re about to start a job, find out the financial options before you’re faced with a mountain of forms and a heap of decisions. “When I started here, I had all this paperwork: I had to sign up for health insurance, disability, long-term disability, 401(k) and 403(b) plans, and more. It’s really daunting,” Dr. Fang says. “A little upfront research is important, so you can make good decisions about these things.”
When it comes to figuring out how much to contribute to retirement accounts, savings accounts and investments, consider enlisting some outside help. “Many institutions that hire young hospitalists offer financial counseling,” Dr. Fang points out. “I’ve done a lot of independent reading. But if your finances are more challenging—say you’re carrying a lot of debt—it’s reasonable to work with a financial consultant.”
Deal with Debt
Before you start investing your money, take a look at your debt. What to do with it—for instance, should you pay off all of your loans and bills—will be one of the most important decisions a new hospitalist will make.
“The first thing you should do is clear any credit card debt, because it carries such high interest rates,” Dr. Badlani advises. “Do this before investing in a Roth IRA or anything.”
As for student loans, “I recommend taking your time paying off fixed APR loans and federally subsidized loans,” Dr. Badlani says “These typically carry low interest and they are tax deductible. You’re better off investing your money in indexed mutual funds because the stock market averages an 8% to 10% return (long-term), versus loans that are maybe 6% interest, or 4% when you calculate the tax deduction.”
However, if your student loan comes from a private bank, it may carry a higher interest rate and variable APRs. In this case, says Dr. Badlani, “you need to pay off those loans first” or look into consolidating or refinancing high-interest student loans.
Build Your Savings
Once you’ve cleared or reduced any high-interest debt, it’s time to focus on saving some money—no matter how much you’re making. “Residents say they have no money to save,” Dr. Badlani says. “But you need to look at your lifestyle and look for what is called ‘the latte factor.’ If you work hard, you may feel you deserve a treat, so you buy a $4 latte every day—maybe two a day. If you work 27 days a month, this adds up to $200 a month or nearly $3,000 a year. If you put that money in your Roth IRA every year of your residency and your fellowship, that adds up to a cool $150,000—based on 8% to 9% annual return, compounded annually for 30 years and adjusted for investment fees.”
—Sameer Badlani, MD
Starting a money market account or putting money in a certificate of deposit (CD) will keep it liquid. “You should have three to six months’ expenses, in case you lose your job or get sick,” Dr. Badlani says. “But be sure to put this ‘cushion money’ in a money market account, which these days are typically returning 3.5% APR versus regular checking accounts that offer a measly .25%, to offset inflation eating into your savings.”
Invest Early for Retirement
Residents and low-income hospitalists are in an excellent position to start investing for retirement. “While you’re a resident or intern, you most likely qualify for a Roth IRA,” Dr. Badlani explains. “This is the only time you’ll be able to invest in this. It’s a good choice for people with potential for increasing their income. Roth contributions are made after taxes and the account grows tax-free; you never have to pay tax on that money in retirement. For 2008, you’re eligible to contribute to a Roth IRA if you’re single or file as head of household with a modified adjusted gross income of below $114,000, or if you file jointly with income below $166,000.”
Another smart retirement investment for just about any hospitalist is employer-matched contributions. “If your employer will match your [retirement] contribution, that’s free money,” Dr. Badlani points out. “If you’re not taking advantage of that, you’re making a big mistake. Institutions will typically match up to about 5% of an employee’s contribution to a 401(k) or 403(b). Plus, by putting money in a retirement account, you’re reducing your tax burden.”
Online calculators can help you figure out how much to save—including matching funds—for a comfortable retirement. “The $1 million retirement has been the American dream for a long time, but that’s increased now to $1.5 to $1.8 million,” Dr. Badlani says. “But for a comfortable lifestyle and accounting for spiraling healthcare costs, I would recommend aiming for $5 million. That takes a lot of discipline over a long stretch of time.” He recommends the online calculator at www.dinkytown.net, which shows that a 29-year-old earning an annual income of $150,000 can retire at 65 with $5,868,264—if he or she contributes 15% to a 403(b) retirement account with a 5% employer match. “But you have to stick to this every month for the next 36 years,” Dr. Badlani warns. “That takes discipline.”
Regardless of how old you are or how much income you currently have, it’s wise to start practicing smart habits with spending, saving and investing your money. As Dr. Badlani says, “Good money habits last forever.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Alternative Medications
Complementary and alterative medicine (CAM) is defined as any product, including herbal remedies/foods/teas, vitamins, minerals, and natural products, that can be purchased without a prescription at a health food store, supermarket, from a magazine/newspaper or online, for self-treatment.1
Taylor et al. evaluated CAM perceptions of emergency department patients in Australia. They determined 44% of patients felt that by using CAM they were “drug free,” with 29% of patients agreeing (or strongly agreeing) CAM use is always safe to take with prescription medications. In an earlier study, Eisenberg et al. evaluated CAM use perceptions in the United States and found 79% of patients felt that, combined with prescription drugs, CAM was superior to either modality alone.2 They also found 63% to 72% of CAM-using patients that had seen a medical doctor in the prior year did not disclose the therapy.
The two most common reasons cited by patients were “they felt it wasn’t important for the doctor to know (61%)” and “the doctor didn’t ask (60%).” Overall, national CAM-use surveys have revealed that about 80% of adults typically do not disclose CAM use to medical doctors.
It is, therefore, imperative that physicians ask patients about their CAM use. It also is important to remember there are more foods and beverages that contain some of these “natural” ingredients, and patients need to be queried about the use of these products. CAM products can complicate traditional patient management, either when used alone or in combination with prescription drugs.
A clinically significant drug interaction that bears its own warning is that of warfarin and chondroitin/glucosamine. Patients might not tell you that they are taking chondroitin/glucosamine, so you have to ask. Functional foods and beverages that include “natural” ingredients, such as glucosamine and chondroitin, and other CAM abound. Examples include Joint Juice (1,500 mg glucosamine), Vitamin Water, and others.3
Two case reports, and a report from the World Health Organization (WHO) Collaborating Center for International Drug Monitoring, and the MedWatch database point to a potentially serious drug interaction between glucosamine and warfarin.4-7 Although not FDA approved for joint supplementation, the usual daily dose should generally not exceed 1.5 grams of glucosamine and 1.2 grams of chondroitin. Chondroitin may have anti-coagulant activity, which would explain the increase in International Normalized Ratio (INR) seen in patients using it in combination with warfarin. The WHO database identified at least 34 cases of concomitant use, with most cases of increased INR resolving upon glucosamine discontinuation. Nine cases required physician intervention, and in one case a positive rechallenge was documented. In June 2007, there were 81 cases of a possible interaction from the MedWatch database, of these, 61 cases had potential alternate etiologies. Of the 20 possibly-related cases, five led to patient hospitalization due to bleeding complications; the median patient age was 62 years and there were no deaths reported.
Ramsay et al. reported from a United Kingdom survey that 92% of patients admitted to taking herbal medicines while receiving warfarin, noting that significant numbers of patients are in need of close monitoring. They also note that other CAM can interact with warfarin to increase bleeding time or act as anti-platelet agents (e.g., high dose vitamin E [> 400 IU], fish oils, garlic, St. John’s Wort, etc.) They particularly note that all patients receiving warfarin or that will be commencing warfarin be specifically asked about their use of CAM. The mechanism for this interaction still is unclear, but may be due to the inhibition of warfarin metabolism by the CYP2C9 or CYP3A4 enzymes, or a pharmacodynamic interaction between glucosamine and warfarin.
It is critical all patients, particularly those taking warfarin, have a full drug history at all hospitalizations. Make sure you inquire about vitamins and other supplements/CAM. If someone else is doing the intake medication history, make sure they get this information. A nurse might not think to ask. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
1. Taylor DM, Walsham N, Taylor SE, Wong LF. Complementary and alternative medicines versus prescription drugs: perceptions of emergency department patients. Emerg Med J. 2006;23:266-268.
2. Eisenberg DM, Kessler RC, Van Rompay MI, et al.. Perceptions about complementary therapies relative to conventional therapies among adults how use both: results from a national survey. Ann Intern Med. 2001;135:344-351.
3. What is Joint Juice? Joint Juice, Inc. www.jointjuice.com/jointjuice.php. Published 1997. Accessed August 1, 2008.
4. Rozenfeld V, Crain JL, Callahan AK. Possible augmentation of warfarin effect by glucosamine-chondroitin. Am J Health-Syst Pharm. 2004;61:306-307.
5. Knudsen JF, Sokol GH. Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and medwatch database. Pharmacother. 2008;28(4):540-548.
6. Ramsay NA, Kenny MW, Davies G, Patel JP. Complimentary and alternative medicine use among patients starting warfarin. Br J Haematology. 2005;130:777-780.
7. Yue Q-Y, Strandell J, Myrberg O. Concomitant use of glucosamine may potentiate the effect of warfarin. The Uppsalla Monitoring Centre Web site. www.who-umc.org/graphics/9722.pdf; Accessed August 1, 2008.
Complementary and alterative medicine (CAM) is defined as any product, including herbal remedies/foods/teas, vitamins, minerals, and natural products, that can be purchased without a prescription at a health food store, supermarket, from a magazine/newspaper or online, for self-treatment.1
Taylor et al. evaluated CAM perceptions of emergency department patients in Australia. They determined 44% of patients felt that by using CAM they were “drug free,” with 29% of patients agreeing (or strongly agreeing) CAM use is always safe to take with prescription medications. In an earlier study, Eisenberg et al. evaluated CAM use perceptions in the United States and found 79% of patients felt that, combined with prescription drugs, CAM was superior to either modality alone.2 They also found 63% to 72% of CAM-using patients that had seen a medical doctor in the prior year did not disclose the therapy.
The two most common reasons cited by patients were “they felt it wasn’t important for the doctor to know (61%)” and “the doctor didn’t ask (60%).” Overall, national CAM-use surveys have revealed that about 80% of adults typically do not disclose CAM use to medical doctors.
It is, therefore, imperative that physicians ask patients about their CAM use. It also is important to remember there are more foods and beverages that contain some of these “natural” ingredients, and patients need to be queried about the use of these products. CAM products can complicate traditional patient management, either when used alone or in combination with prescription drugs.
A clinically significant drug interaction that bears its own warning is that of warfarin and chondroitin/glucosamine. Patients might not tell you that they are taking chondroitin/glucosamine, so you have to ask. Functional foods and beverages that include “natural” ingredients, such as glucosamine and chondroitin, and other CAM abound. Examples include Joint Juice (1,500 mg glucosamine), Vitamin Water, and others.3
Two case reports, and a report from the World Health Organization (WHO) Collaborating Center for International Drug Monitoring, and the MedWatch database point to a potentially serious drug interaction between glucosamine and warfarin.4-7 Although not FDA approved for joint supplementation, the usual daily dose should generally not exceed 1.5 grams of glucosamine and 1.2 grams of chondroitin. Chondroitin may have anti-coagulant activity, which would explain the increase in International Normalized Ratio (INR) seen in patients using it in combination with warfarin. The WHO database identified at least 34 cases of concomitant use, with most cases of increased INR resolving upon glucosamine discontinuation. Nine cases required physician intervention, and in one case a positive rechallenge was documented. In June 2007, there were 81 cases of a possible interaction from the MedWatch database, of these, 61 cases had potential alternate etiologies. Of the 20 possibly-related cases, five led to patient hospitalization due to bleeding complications; the median patient age was 62 years and there were no deaths reported.
Ramsay et al. reported from a United Kingdom survey that 92% of patients admitted to taking herbal medicines while receiving warfarin, noting that significant numbers of patients are in need of close monitoring. They also note that other CAM can interact with warfarin to increase bleeding time or act as anti-platelet agents (e.g., high dose vitamin E [> 400 IU], fish oils, garlic, St. John’s Wort, etc.) They particularly note that all patients receiving warfarin or that will be commencing warfarin be specifically asked about their use of CAM. The mechanism for this interaction still is unclear, but may be due to the inhibition of warfarin metabolism by the CYP2C9 or CYP3A4 enzymes, or a pharmacodynamic interaction between glucosamine and warfarin.
It is critical all patients, particularly those taking warfarin, have a full drug history at all hospitalizations. Make sure you inquire about vitamins and other supplements/CAM. If someone else is doing the intake medication history, make sure they get this information. A nurse might not think to ask. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
1. Taylor DM, Walsham N, Taylor SE, Wong LF. Complementary and alternative medicines versus prescription drugs: perceptions of emergency department patients. Emerg Med J. 2006;23:266-268.
2. Eisenberg DM, Kessler RC, Van Rompay MI, et al.. Perceptions about complementary therapies relative to conventional therapies among adults how use both: results from a national survey. Ann Intern Med. 2001;135:344-351.
3. What is Joint Juice? Joint Juice, Inc. www.jointjuice.com/jointjuice.php. Published 1997. Accessed August 1, 2008.
4. Rozenfeld V, Crain JL, Callahan AK. Possible augmentation of warfarin effect by glucosamine-chondroitin. Am J Health-Syst Pharm. 2004;61:306-307.
5. Knudsen JF, Sokol GH. Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and medwatch database. Pharmacother. 2008;28(4):540-548.
6. Ramsay NA, Kenny MW, Davies G, Patel JP. Complimentary and alternative medicine use among patients starting warfarin. Br J Haematology. 2005;130:777-780.
7. Yue Q-Y, Strandell J, Myrberg O. Concomitant use of glucosamine may potentiate the effect of warfarin. The Uppsalla Monitoring Centre Web site. www.who-umc.org/graphics/9722.pdf; Accessed August 1, 2008.
Complementary and alterative medicine (CAM) is defined as any product, including herbal remedies/foods/teas, vitamins, minerals, and natural products, that can be purchased without a prescription at a health food store, supermarket, from a magazine/newspaper or online, for self-treatment.1
Taylor et al. evaluated CAM perceptions of emergency department patients in Australia. They determined 44% of patients felt that by using CAM they were “drug free,” with 29% of patients agreeing (or strongly agreeing) CAM use is always safe to take with prescription medications. In an earlier study, Eisenberg et al. evaluated CAM use perceptions in the United States and found 79% of patients felt that, combined with prescription drugs, CAM was superior to either modality alone.2 They also found 63% to 72% of CAM-using patients that had seen a medical doctor in the prior year did not disclose the therapy.
The two most common reasons cited by patients were “they felt it wasn’t important for the doctor to know (61%)” and “the doctor didn’t ask (60%).” Overall, national CAM-use surveys have revealed that about 80% of adults typically do not disclose CAM use to medical doctors.
It is, therefore, imperative that physicians ask patients about their CAM use. It also is important to remember there are more foods and beverages that contain some of these “natural” ingredients, and patients need to be queried about the use of these products. CAM products can complicate traditional patient management, either when used alone or in combination with prescription drugs.
A clinically significant drug interaction that bears its own warning is that of warfarin and chondroitin/glucosamine. Patients might not tell you that they are taking chondroitin/glucosamine, so you have to ask. Functional foods and beverages that include “natural” ingredients, such as glucosamine and chondroitin, and other CAM abound. Examples include Joint Juice (1,500 mg glucosamine), Vitamin Water, and others.3
Two case reports, and a report from the World Health Organization (WHO) Collaborating Center for International Drug Monitoring, and the MedWatch database point to a potentially serious drug interaction between glucosamine and warfarin.4-7 Although not FDA approved for joint supplementation, the usual daily dose should generally not exceed 1.5 grams of glucosamine and 1.2 grams of chondroitin. Chondroitin may have anti-coagulant activity, which would explain the increase in International Normalized Ratio (INR) seen in patients using it in combination with warfarin. The WHO database identified at least 34 cases of concomitant use, with most cases of increased INR resolving upon glucosamine discontinuation. Nine cases required physician intervention, and in one case a positive rechallenge was documented. In June 2007, there were 81 cases of a possible interaction from the MedWatch database, of these, 61 cases had potential alternate etiologies. Of the 20 possibly-related cases, five led to patient hospitalization due to bleeding complications; the median patient age was 62 years and there were no deaths reported.
Ramsay et al. reported from a United Kingdom survey that 92% of patients admitted to taking herbal medicines while receiving warfarin, noting that significant numbers of patients are in need of close monitoring. They also note that other CAM can interact with warfarin to increase bleeding time or act as anti-platelet agents (e.g., high dose vitamin E [> 400 IU], fish oils, garlic, St. John’s Wort, etc.) They particularly note that all patients receiving warfarin or that will be commencing warfarin be specifically asked about their use of CAM. The mechanism for this interaction still is unclear, but may be due to the inhibition of warfarin metabolism by the CYP2C9 or CYP3A4 enzymes, or a pharmacodynamic interaction between glucosamine and warfarin.
It is critical all patients, particularly those taking warfarin, have a full drug history at all hospitalizations. Make sure you inquire about vitamins and other supplements/CAM. If someone else is doing the intake medication history, make sure they get this information. A nurse might not think to ask. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
1. Taylor DM, Walsham N, Taylor SE, Wong LF. Complementary and alternative medicines versus prescription drugs: perceptions of emergency department patients. Emerg Med J. 2006;23:266-268.
2. Eisenberg DM, Kessler RC, Van Rompay MI, et al.. Perceptions about complementary therapies relative to conventional therapies among adults how use both: results from a national survey. Ann Intern Med. 2001;135:344-351.
3. What is Joint Juice? Joint Juice, Inc. www.jointjuice.com/jointjuice.php. Published 1997. Accessed August 1, 2008.
4. Rozenfeld V, Crain JL, Callahan AK. Possible augmentation of warfarin effect by glucosamine-chondroitin. Am J Health-Syst Pharm. 2004;61:306-307.
5. Knudsen JF, Sokol GH. Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and medwatch database. Pharmacother. 2008;28(4):540-548.
6. Ramsay NA, Kenny MW, Davies G, Patel JP. Complimentary and alternative medicine use among patients starting warfarin. Br J Haematology. 2005;130:777-780.
7. Yue Q-Y, Strandell J, Myrberg O. Concomitant use of glucosamine may potentiate the effect of warfarin. The Uppsalla Monitoring Centre Web site. www.who-umc.org/graphics/9722.pdf; Accessed August 1, 2008.
In the Literature
Literature at a Glance
- Postoperative prophylactic LMWH should be considered for arthroscopic knee surgery patients.
- Individualized therapy is required for DVT prophylaxis in the neurosurgical patient.
- SMART-COP is a reasonable screening tool for ICU admission.
- Mediterranean and low-carb diets are safe and effective alternatives to low-fat diets.
- Admissions for ACS in both smokers and non-smokers decrease after implementation of smoking ban.
- Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
- Non-invasive ventilation improved dyspnea, but did not improve short-term mortality rates in patients with acute cardiogenic pulmonary edema.
- COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
LMWH after Arthroscopic Knee Surgery May Prevent VTE Compared to Graduated Compression Stockings
Clinical question: Does low molecular weight heparin (LMWH) prevent venous thromboembolism (VTE) compared to compression stockings without increasing bleeding complications in arthroscopic knee surgery?
Background: Knee arthroscopy is a common orthopedic surgery and postoperative venous thromboprophylaxis is not routinely recommended.
Study design: Randomized, controlled trial with blinding of the investigators.
Setting: Single orthopedic clinic in Italy, with followup at a university hospital.
Synopsis: 1,761 consecutive patients undergoing knee arthroscopy were randomly assigned to full-length graduated compression stockings (CS) for seven days postoperatively, subcutaneous LMWH (nadoparin 3800 units daily) for seven or 14 days postoperatively. The primary outcome of asymptomatic proximal deep venous thrombosis (DVT), symptomatic VTE, and all-cause mortality within three months of surgery was higher with CS (3.2%) than with LMWH for seven or 14 days (0.9% in each group) (P=0.005). There was no significant difference in bleeding events between groups.
The study was underpowered to detect differences in bleeding risk. Furthermore, almost half the events making up the primary outcome were distal DVTs of uncertain clinical significance. Notably, the 14-day LMWH group was discontinued early because of unspecified safety concerns related to longer exposure to LMWH.
Bottom line: Postoperative prophylactic LMWH for seven days may prevent some thromboses after knee surgery and should be considered in higher-risk patients.
Citation: Camporese G, Bernardi E, Prandoni P, et al. Low-molecular-weight heparin versus compression stockings for thrombophylaxis after knee arthroscopy. Ann Intern Med. 2008;14(9):73-82.
Heparins and Compression Devices are Effective in Preventing VTE in a Mixed Neurosurgical Population
Clinical question: What is the efficacy and safety of LMWH, unfractionated heparin, and mechanical devices in preventing VTE in neurosurgical patients?
Background: Neurosurgical patients are at high risk for VTE, but concerns remain regarding the risk of bleeding complications with the use of LMWH or unfractionated heparin (UFH).
Study design: Meta-analysis of 18 randomized trials and 12 cohort studies.
Setting: Patients undergoing spinal surgery or craniotomy.
Synopsis: Among all patients, the pooled DVT rate was 15.5/100. Use of sequential compression devices (SCD) significantly reduced the risk of DVT compared with placebo (relative risk [RR] 0.41, 95% confidence interval [CI] 0.21-0.78). Subcutaneous LMWH was associated with a significantly reduced risk of DVT compared with CS (RR 0.60, 95% CI 0.44-0.81). No other head-to-head comparisons were associated with significant reductions in VTE risk. After adjusting for potential risk factors for DVT and study design, use of heparins or SCDs was associated with a lower risk of DVT. Intracranial hemorrhage (ICH), minor bleeding, major bleeding, or death was not statistically different between any of the groups, although, after adjustment, LMWH was associated with a slightly increased risk of ICH.
The quality of included studies varied considerably and inter-rater agreement on study quality was low, raising the possibility of study selection bias. Potential publication bias was not addressed. Bleeding complications were rare, so the estimates of risk may be imprecise.
Bottom line: Individualized therapy is required for DVT prophylaxis in the neurosurgical patient; SCDs reduce VTE risk and both pharmacologic and mechanical prophylaxis may be indicated in patients with increased VTE risk.
Citation: Collen JF, Jackson JL, Shorr AF, Moores LK. Prevention of venous thromboembolism in neurosurgery: A metaanalysis. Chest. 2008;13(4):237-249.
SMART-COP Predicts Need for ICU Care in CAP
Clinical question: Can a clinical tool predict the need for critical care in community acquired pneumonia (CAP)?
Background: Clinical tools predicting 30-day mortality in community acquired pneumonia (CAP) exist, but do not accurately identify who will require intensive care unit-level care, such as intensive respiratory or vasosuppressor support (IRVS).
Study design: Prospective multi-center observational study.
Setting: Six hospitals in Australia participating in the Australian Community Acquired Pneumonia Study (ACAPS).
Synopsis: Multivariate analysis of a dataset of 882 episodes of CAP identified eight factors that were associated with the need for IRVS, summarized by the mnemonic “SMART-COP” (Systolic blood pressure, Multilobar chest radiography involvement, low Albumin level, high Respiratory rate, Tachycardia, Confusion, poor Oxygenation, and low arterial pH). Assigning one point for five factors and two points for three factors (systolic blood pressure, poor oxygenation, and low arterial pH) a SMART-COP score >3 identified 92.3% (95% CI 84.8-96.9%) of patients who required IRVS, including 84% who did not initially require ICU care. Specificity was 62.3% (CI 58.8-65.7%). Test characteristics for predicting IRVS were superior to existing prediction rules (PSI and CURB-65).
Most patients were drawn from large, urban teaching hospitals in Australia, so the results may not be generalizable. The authors also presented a modification of SMART-COP, using pulse oximetry rather than blood gas results; this may be even more useful in the pre-hospital setting.
Bottom line: SMART-COP is a reasonable screening tool for predicting need for ICU-level care in patients admitted with CAP.
Citation: Charles PGP, Wolfe, R, Whitby, M, et. al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47(3):375-384.
Mediterranean and Low-Carbohydrate Diets are Effective for Weight Loss
Clinical question: Are dietary intervention with low-fat, Mediterranean or low-carbohydrate diets effective?
Background: Obesity is a growing, worldwide problem. Past trials comparing the effectiveness and safety of various dietary interventions have been limited by short follow up and high dropout rates.
Study design: Prospective randomized trial.
Setting: Employees of a research center in Israel.
Synopsis: 322 subjects (average BMI 31) were randomized to a low-fat/restricted-calorie, Mediterranean/ restricted-calorie, or a low-carbohydrate/non-restricted calorie diet. Diet adherence was 84.6% at two years and all groups lost significant amounts of weight. The Mediterranean and low-carbohydrate diets showed similar aver∆age weight loss of 4.4 kg and 4.7 kg, respectively. The low-fat diet group on average lost 2.9 kg. Diabetic patients had improved glycemic control and lower insulin levels with the Mediterranean diet. Subjects assigned to the low-carbohydrate diet had the greatest improvement in lipid profile (20% relative decrease of total cholesterol to HDL ratio).
The trial took place at a single site (a scientific research center in Israel) and included only 14% women, so its generalization is uncertain. The study was based on self-reported dietary intake and may be subject to reporting bias.
Bottom line: Mediterranean and low-carbohydrate diets are safe and effective alternatives to low-fat diets with favorable effects on glycemic control in diabetics and lipid metabolism, respectively.
Citation: Shai I, Schwarz-fuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. NEJM. 2008;359(3):229-241.
Admissions for Acute Coronary Syndrome Decreased after Implementation of Smoke-free Legislation
Clinical question: Is there a reduction in admissions for acute coronary syndrome (ACS) after enactment of smoke-free legislation?
Background: Multiple, small, retrospective studies have shown a decrease in ACS after implementation of smoke-free legislation.
Study design: Prospective observational multi-center cohort study.
Setting: Nine hospitals in Scotland.
Synopsis: Data was collected on all patients admitted with ACS 10 months before and after implementation of smoke-free legislation, which prohibited smoking in all enclosed public and work places in Scotland. After the smoking ban, the number of ACS admissions fell by 17% (95% CI 16-18) in Scotland as a whole, compared with a 4% reduction in England during the same period (England does not have similar smoke-free legislation). Among smokers, former smokers and non-smokers, the number of ACS admissions decreased by 14% (95% CI 12-16), 19% (95% CI 17-21), and 21% (95% CI 18-24), respectively. Among non-smokers, self-reported exposure to second-hand smoke decreased significantly; these reductions were confirmed by measured reductions in serum cotinine levels, even among those who never smoked.
Results were limited by the observational nature of the study, although the authors did attempt to carefully match comparison cohorts by season and geography. Also, secular trends other than legislation may have reduced prevalent smoking in Scotland during the study period.
Bottom line: Admissions for ACS for both smokers and non-smokers decreased after implementation of smoke-free legislation.
Citation: Pell JP, Haw S, Cobbe S, et al. Smoke-free legislation and hospitalizations for acute coronary syndrome. NEJM. 2008;359(5):482-491.
Continuation of Beta-blockers in Patients Hospitalized for Heart Failure Improves Mortality
Clinical question: Does the withdrawal or continuation of beta-blockers in patients hospitalized with decompensated heart failure have any effect on clinical outcomes?
Background: Previous clinical trials have demonstrated mortality benefit with the use of beta-blockers in patients with symptomatic chronic heart failure and left ventricular systolic dysfunction (LVSD), however, controversy exists whether to continue these medications in acute decompensated heart failure.
Study design: Prospective cohort analysis from the OPTIMIZE-HF registry (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure).
Setting: 91 academic and community hospitals in the United States.
Synopsis: Data was analyzed on 2,373 registry patients with documented LVSD (EF <40) eligible for beta-blocker therapy. During hospitalization, 1,350 patients were continued on beta-blockers, 79 had therapy withdrawn, 303 were not started, and 632 had beta-blockade initiated. Compared with no beta-blocker treatment, adjusted hazard ratio (HR) for death at 60 and 90 days following discharge was lower in patients who were continued on beta-blockade (HR 0.60, 95% CI 0.37–0.99). Compared with continuation of beta-blockade, withdrawal of beta-blockade increased the risk of death (HR 2.3, 95% CI 1.2–4.6).
Results were limited by the observational nature of the study and short follow up. The reason for discontinuation or not starting beta-blockade was not captured in the database, so it is possible sicker patients had beta-blockers discontinued during hospitalization (although the authors attempted to control for this).
Bottom line: Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
Citation: Fonarow GC, Abraham WT, Albert NM, et al. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure. J Am Coll Cardiol. 2008;52(3):190-199.
Non-invasive Ventilation Does Not Improve Short-term Mortality in Acute Cardiogenic Pulmonary Edema
Clinical question: Does non-invasive ventilation reduce mortality in patients with acute cardiogenic pulmonary edema and are there differences in outcome between use of continuous positive airway pressure (CPAP) or non-invasive positive pressure ventilation (NIPPV)?
Background: In patients with acute cardiogenic pulmonary edema, noninvasive ventilation improves physiologic variables and symptoms, decreases rates of invasive ventilation, and may improve mortality.
Study design: Randomized multi center controlled trial.
Setting: 26 district and regional hospitals in the United Kingdom.
Synopsis: 1,156 patients admitted with acute cardiogenic pulmonary edema between July 2003 and April 2007 were randomized to standard oxygen therapy, versus CPAP or NIPPV. There were no significant differences in seven- or 30-day mortality rates between the standard oxygen therapy versus noninvasive ventilation. Mortality at seven days was 9.8% in the standard oxygen group versus 9.5% in the noninvasive ventilation group (P=0.87); 30-day mortality was 16% in the standard oxygen group and 15% in the non-invasive ventilation group (P=0.64). There were no major differences in treatment outcome with NIPPV compared to CPAP.
Although mortality was not decreased, non-invasive ventilation did improve dyspnea and tachycardia within one hour of therapy.
Bottom line: In patients admitted with acute cardiogenic pulmonary edema, noninvasive ventilation improved dyspnea and some physiological parameters, but did not improve short-term mortality rates.
Citation: Gray A, Goodacre S, Newby D, Masson M, Sampson F, Nicholl J. Noninvasive ventilation in acute cardiogenic pulmonary edema. NEJM. 2008;359(2):142-151.
Cyclooxygenase 2 Inhibitors May Increase the Risk of Ischemic Stroke
Clinical question: Do NSAIDs and COX-2 inhibitors increase the risk of ischemic or hemorrhagic stroke?
Background: Selected cyclooxygenase 2 (COX-2) inhibitors have been shown to increase cardiovascular morbidity in a dose-dependent manner and are now used with caution in patients at risk for cardiovascular disease. Little is known about the safety of these medications and non-aspirin, non-steroidal anti-inflammatory drugs (NSAIDS) in those at risk for cerebrovascular disease.
Study design: Retrospective observational cohort study.
Setting: Tennessee Medicaid Program enrollees.
Synopsis: Data was collected from the medical records of 336,906 subjects. Non-users had a baseline stroke rate of 4.51 strokes/1000 person-years. The rate increased to 5.15/1,000 person-years and 5.95/1,000 person-years for rofecoxib and valdecoxib, respectively. Celecoxib and other NSAIDs did not significantly increase the risk of stroke. Analysis of new users of rofexocib and valdecoxib yielded a similarly increased risk of stroke. Most strokes were ischemic.
Limitations include the ready availability of NSAIDs raising the possibility that some patients classified as non-users were actually users of NSAIDs. Other potential confounders may not have been measured and, therefore, not available for analysis.
Bottom line: COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
Citation: Roumie CL, Mitchel EF, Kaltenback L, Arbogast PG, Gideon P Griffen MR. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke. 2008;39:1037-2045.
Literature at a Glance
- Postoperative prophylactic LMWH should be considered for arthroscopic knee surgery patients.
- Individualized therapy is required for DVT prophylaxis in the neurosurgical patient.
- SMART-COP is a reasonable screening tool for ICU admission.
- Mediterranean and low-carb diets are safe and effective alternatives to low-fat diets.
- Admissions for ACS in both smokers and non-smokers decrease after implementation of smoking ban.
- Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
- Non-invasive ventilation improved dyspnea, but did not improve short-term mortality rates in patients with acute cardiogenic pulmonary edema.
- COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
LMWH after Arthroscopic Knee Surgery May Prevent VTE Compared to Graduated Compression Stockings
Clinical question: Does low molecular weight heparin (LMWH) prevent venous thromboembolism (VTE) compared to compression stockings without increasing bleeding complications in arthroscopic knee surgery?
Background: Knee arthroscopy is a common orthopedic surgery and postoperative venous thromboprophylaxis is not routinely recommended.
Study design: Randomized, controlled trial with blinding of the investigators.
Setting: Single orthopedic clinic in Italy, with followup at a university hospital.
Synopsis: 1,761 consecutive patients undergoing knee arthroscopy were randomly assigned to full-length graduated compression stockings (CS) for seven days postoperatively, subcutaneous LMWH (nadoparin 3800 units daily) for seven or 14 days postoperatively. The primary outcome of asymptomatic proximal deep venous thrombosis (DVT), symptomatic VTE, and all-cause mortality within three months of surgery was higher with CS (3.2%) than with LMWH for seven or 14 days (0.9% in each group) (P=0.005). There was no significant difference in bleeding events between groups.
The study was underpowered to detect differences in bleeding risk. Furthermore, almost half the events making up the primary outcome were distal DVTs of uncertain clinical significance. Notably, the 14-day LMWH group was discontinued early because of unspecified safety concerns related to longer exposure to LMWH.
Bottom line: Postoperative prophylactic LMWH for seven days may prevent some thromboses after knee surgery and should be considered in higher-risk patients.
Citation: Camporese G, Bernardi E, Prandoni P, et al. Low-molecular-weight heparin versus compression stockings for thrombophylaxis after knee arthroscopy. Ann Intern Med. 2008;14(9):73-82.
Heparins and Compression Devices are Effective in Preventing VTE in a Mixed Neurosurgical Population
Clinical question: What is the efficacy and safety of LMWH, unfractionated heparin, and mechanical devices in preventing VTE in neurosurgical patients?
Background: Neurosurgical patients are at high risk for VTE, but concerns remain regarding the risk of bleeding complications with the use of LMWH or unfractionated heparin (UFH).
Study design: Meta-analysis of 18 randomized trials and 12 cohort studies.
Setting: Patients undergoing spinal surgery or craniotomy.
Synopsis: Among all patients, the pooled DVT rate was 15.5/100. Use of sequential compression devices (SCD) significantly reduced the risk of DVT compared with placebo (relative risk [RR] 0.41, 95% confidence interval [CI] 0.21-0.78). Subcutaneous LMWH was associated with a significantly reduced risk of DVT compared with CS (RR 0.60, 95% CI 0.44-0.81). No other head-to-head comparisons were associated with significant reductions in VTE risk. After adjusting for potential risk factors for DVT and study design, use of heparins or SCDs was associated with a lower risk of DVT. Intracranial hemorrhage (ICH), minor bleeding, major bleeding, or death was not statistically different between any of the groups, although, after adjustment, LMWH was associated with a slightly increased risk of ICH.
The quality of included studies varied considerably and inter-rater agreement on study quality was low, raising the possibility of study selection bias. Potential publication bias was not addressed. Bleeding complications were rare, so the estimates of risk may be imprecise.
Bottom line: Individualized therapy is required for DVT prophylaxis in the neurosurgical patient; SCDs reduce VTE risk and both pharmacologic and mechanical prophylaxis may be indicated in patients with increased VTE risk.
Citation: Collen JF, Jackson JL, Shorr AF, Moores LK. Prevention of venous thromboembolism in neurosurgery: A metaanalysis. Chest. 2008;13(4):237-249.
SMART-COP Predicts Need for ICU Care in CAP
Clinical question: Can a clinical tool predict the need for critical care in community acquired pneumonia (CAP)?
Background: Clinical tools predicting 30-day mortality in community acquired pneumonia (CAP) exist, but do not accurately identify who will require intensive care unit-level care, such as intensive respiratory or vasosuppressor support (IRVS).
Study design: Prospective multi-center observational study.
Setting: Six hospitals in Australia participating in the Australian Community Acquired Pneumonia Study (ACAPS).
Synopsis: Multivariate analysis of a dataset of 882 episodes of CAP identified eight factors that were associated with the need for IRVS, summarized by the mnemonic “SMART-COP” (Systolic blood pressure, Multilobar chest radiography involvement, low Albumin level, high Respiratory rate, Tachycardia, Confusion, poor Oxygenation, and low arterial pH). Assigning one point for five factors and two points for three factors (systolic blood pressure, poor oxygenation, and low arterial pH) a SMART-COP score >3 identified 92.3% (95% CI 84.8-96.9%) of patients who required IRVS, including 84% who did not initially require ICU care. Specificity was 62.3% (CI 58.8-65.7%). Test characteristics for predicting IRVS were superior to existing prediction rules (PSI and CURB-65).
Most patients were drawn from large, urban teaching hospitals in Australia, so the results may not be generalizable. The authors also presented a modification of SMART-COP, using pulse oximetry rather than blood gas results; this may be even more useful in the pre-hospital setting.
Bottom line: SMART-COP is a reasonable screening tool for predicting need for ICU-level care in patients admitted with CAP.
Citation: Charles PGP, Wolfe, R, Whitby, M, et. al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47(3):375-384.
Mediterranean and Low-Carbohydrate Diets are Effective for Weight Loss
Clinical question: Are dietary intervention with low-fat, Mediterranean or low-carbohydrate diets effective?
Background: Obesity is a growing, worldwide problem. Past trials comparing the effectiveness and safety of various dietary interventions have been limited by short follow up and high dropout rates.
Study design: Prospective randomized trial.
Setting: Employees of a research center in Israel.
Synopsis: 322 subjects (average BMI 31) were randomized to a low-fat/restricted-calorie, Mediterranean/ restricted-calorie, or a low-carbohydrate/non-restricted calorie diet. Diet adherence was 84.6% at two years and all groups lost significant amounts of weight. The Mediterranean and low-carbohydrate diets showed similar aver∆age weight loss of 4.4 kg and 4.7 kg, respectively. The low-fat diet group on average lost 2.9 kg. Diabetic patients had improved glycemic control and lower insulin levels with the Mediterranean diet. Subjects assigned to the low-carbohydrate diet had the greatest improvement in lipid profile (20% relative decrease of total cholesterol to HDL ratio).
The trial took place at a single site (a scientific research center in Israel) and included only 14% women, so its generalization is uncertain. The study was based on self-reported dietary intake and may be subject to reporting bias.
Bottom line: Mediterranean and low-carbohydrate diets are safe and effective alternatives to low-fat diets with favorable effects on glycemic control in diabetics and lipid metabolism, respectively.
Citation: Shai I, Schwarz-fuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. NEJM. 2008;359(3):229-241.
Admissions for Acute Coronary Syndrome Decreased after Implementation of Smoke-free Legislation
Clinical question: Is there a reduction in admissions for acute coronary syndrome (ACS) after enactment of smoke-free legislation?
Background: Multiple, small, retrospective studies have shown a decrease in ACS after implementation of smoke-free legislation.
Study design: Prospective observational multi-center cohort study.
Setting: Nine hospitals in Scotland.
Synopsis: Data was collected on all patients admitted with ACS 10 months before and after implementation of smoke-free legislation, which prohibited smoking in all enclosed public and work places in Scotland. After the smoking ban, the number of ACS admissions fell by 17% (95% CI 16-18) in Scotland as a whole, compared with a 4% reduction in England during the same period (England does not have similar smoke-free legislation). Among smokers, former smokers and non-smokers, the number of ACS admissions decreased by 14% (95% CI 12-16), 19% (95% CI 17-21), and 21% (95% CI 18-24), respectively. Among non-smokers, self-reported exposure to second-hand smoke decreased significantly; these reductions were confirmed by measured reductions in serum cotinine levels, even among those who never smoked.
Results were limited by the observational nature of the study, although the authors did attempt to carefully match comparison cohorts by season and geography. Also, secular trends other than legislation may have reduced prevalent smoking in Scotland during the study period.
Bottom line: Admissions for ACS for both smokers and non-smokers decreased after implementation of smoke-free legislation.
Citation: Pell JP, Haw S, Cobbe S, et al. Smoke-free legislation and hospitalizations for acute coronary syndrome. NEJM. 2008;359(5):482-491.
Continuation of Beta-blockers in Patients Hospitalized for Heart Failure Improves Mortality
Clinical question: Does the withdrawal or continuation of beta-blockers in patients hospitalized with decompensated heart failure have any effect on clinical outcomes?
Background: Previous clinical trials have demonstrated mortality benefit with the use of beta-blockers in patients with symptomatic chronic heart failure and left ventricular systolic dysfunction (LVSD), however, controversy exists whether to continue these medications in acute decompensated heart failure.
Study design: Prospective cohort analysis from the OPTIMIZE-HF registry (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure).
Setting: 91 academic and community hospitals in the United States.
Synopsis: Data was analyzed on 2,373 registry patients with documented LVSD (EF <40) eligible for beta-blocker therapy. During hospitalization, 1,350 patients were continued on beta-blockers, 79 had therapy withdrawn, 303 were not started, and 632 had beta-blockade initiated. Compared with no beta-blocker treatment, adjusted hazard ratio (HR) for death at 60 and 90 days following discharge was lower in patients who were continued on beta-blockade (HR 0.60, 95% CI 0.37–0.99). Compared with continuation of beta-blockade, withdrawal of beta-blockade increased the risk of death (HR 2.3, 95% CI 1.2–4.6).
Results were limited by the observational nature of the study and short follow up. The reason for discontinuation or not starting beta-blockade was not captured in the database, so it is possible sicker patients had beta-blockers discontinued during hospitalization (although the authors attempted to control for this).
Bottom line: Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
Citation: Fonarow GC, Abraham WT, Albert NM, et al. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure. J Am Coll Cardiol. 2008;52(3):190-199.
Non-invasive Ventilation Does Not Improve Short-term Mortality in Acute Cardiogenic Pulmonary Edema
Clinical question: Does non-invasive ventilation reduce mortality in patients with acute cardiogenic pulmonary edema and are there differences in outcome between use of continuous positive airway pressure (CPAP) or non-invasive positive pressure ventilation (NIPPV)?
Background: In patients with acute cardiogenic pulmonary edema, noninvasive ventilation improves physiologic variables and symptoms, decreases rates of invasive ventilation, and may improve mortality.
Study design: Randomized multi center controlled trial.
Setting: 26 district and regional hospitals in the United Kingdom.
Synopsis: 1,156 patients admitted with acute cardiogenic pulmonary edema between July 2003 and April 2007 were randomized to standard oxygen therapy, versus CPAP or NIPPV. There were no significant differences in seven- or 30-day mortality rates between the standard oxygen therapy versus noninvasive ventilation. Mortality at seven days was 9.8% in the standard oxygen group versus 9.5% in the noninvasive ventilation group (P=0.87); 30-day mortality was 16% in the standard oxygen group and 15% in the non-invasive ventilation group (P=0.64). There were no major differences in treatment outcome with NIPPV compared to CPAP.
Although mortality was not decreased, non-invasive ventilation did improve dyspnea and tachycardia within one hour of therapy.
Bottom line: In patients admitted with acute cardiogenic pulmonary edema, noninvasive ventilation improved dyspnea and some physiological parameters, but did not improve short-term mortality rates.
Citation: Gray A, Goodacre S, Newby D, Masson M, Sampson F, Nicholl J. Noninvasive ventilation in acute cardiogenic pulmonary edema. NEJM. 2008;359(2):142-151.
Cyclooxygenase 2 Inhibitors May Increase the Risk of Ischemic Stroke
Clinical question: Do NSAIDs and COX-2 inhibitors increase the risk of ischemic or hemorrhagic stroke?
Background: Selected cyclooxygenase 2 (COX-2) inhibitors have been shown to increase cardiovascular morbidity in a dose-dependent manner and are now used with caution in patients at risk for cardiovascular disease. Little is known about the safety of these medications and non-aspirin, non-steroidal anti-inflammatory drugs (NSAIDS) in those at risk for cerebrovascular disease.
Study design: Retrospective observational cohort study.
Setting: Tennessee Medicaid Program enrollees.
Synopsis: Data was collected from the medical records of 336,906 subjects. Non-users had a baseline stroke rate of 4.51 strokes/1000 person-years. The rate increased to 5.15/1,000 person-years and 5.95/1,000 person-years for rofecoxib and valdecoxib, respectively. Celecoxib and other NSAIDs did not significantly increase the risk of stroke. Analysis of new users of rofexocib and valdecoxib yielded a similarly increased risk of stroke. Most strokes were ischemic.
Limitations include the ready availability of NSAIDs raising the possibility that some patients classified as non-users were actually users of NSAIDs. Other potential confounders may not have been measured and, therefore, not available for analysis.
Bottom line: COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
Citation: Roumie CL, Mitchel EF, Kaltenback L, Arbogast PG, Gideon P Griffen MR. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke. 2008;39:1037-2045.
Literature at a Glance
- Postoperative prophylactic LMWH should be considered for arthroscopic knee surgery patients.
- Individualized therapy is required for DVT prophylaxis in the neurosurgical patient.
- SMART-COP is a reasonable screening tool for ICU admission.
- Mediterranean and low-carb diets are safe and effective alternatives to low-fat diets.
- Admissions for ACS in both smokers and non-smokers decrease after implementation of smoking ban.
- Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
- Non-invasive ventilation improved dyspnea, but did not improve short-term mortality rates in patients with acute cardiogenic pulmonary edema.
- COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
LMWH after Arthroscopic Knee Surgery May Prevent VTE Compared to Graduated Compression Stockings
Clinical question: Does low molecular weight heparin (LMWH) prevent venous thromboembolism (VTE) compared to compression stockings without increasing bleeding complications in arthroscopic knee surgery?
Background: Knee arthroscopy is a common orthopedic surgery and postoperative venous thromboprophylaxis is not routinely recommended.
Study design: Randomized, controlled trial with blinding of the investigators.
Setting: Single orthopedic clinic in Italy, with followup at a university hospital.
Synopsis: 1,761 consecutive patients undergoing knee arthroscopy were randomly assigned to full-length graduated compression stockings (CS) for seven days postoperatively, subcutaneous LMWH (nadoparin 3800 units daily) for seven or 14 days postoperatively. The primary outcome of asymptomatic proximal deep venous thrombosis (DVT), symptomatic VTE, and all-cause mortality within three months of surgery was higher with CS (3.2%) than with LMWH for seven or 14 days (0.9% in each group) (P=0.005). There was no significant difference in bleeding events between groups.
The study was underpowered to detect differences in bleeding risk. Furthermore, almost half the events making up the primary outcome were distal DVTs of uncertain clinical significance. Notably, the 14-day LMWH group was discontinued early because of unspecified safety concerns related to longer exposure to LMWH.
Bottom line: Postoperative prophylactic LMWH for seven days may prevent some thromboses after knee surgery and should be considered in higher-risk patients.
Citation: Camporese G, Bernardi E, Prandoni P, et al. Low-molecular-weight heparin versus compression stockings for thrombophylaxis after knee arthroscopy. Ann Intern Med. 2008;14(9):73-82.
Heparins and Compression Devices are Effective in Preventing VTE in a Mixed Neurosurgical Population
Clinical question: What is the efficacy and safety of LMWH, unfractionated heparin, and mechanical devices in preventing VTE in neurosurgical patients?
Background: Neurosurgical patients are at high risk for VTE, but concerns remain regarding the risk of bleeding complications with the use of LMWH or unfractionated heparin (UFH).
Study design: Meta-analysis of 18 randomized trials and 12 cohort studies.
Setting: Patients undergoing spinal surgery or craniotomy.
Synopsis: Among all patients, the pooled DVT rate was 15.5/100. Use of sequential compression devices (SCD) significantly reduced the risk of DVT compared with placebo (relative risk [RR] 0.41, 95% confidence interval [CI] 0.21-0.78). Subcutaneous LMWH was associated with a significantly reduced risk of DVT compared with CS (RR 0.60, 95% CI 0.44-0.81). No other head-to-head comparisons were associated with significant reductions in VTE risk. After adjusting for potential risk factors for DVT and study design, use of heparins or SCDs was associated with a lower risk of DVT. Intracranial hemorrhage (ICH), minor bleeding, major bleeding, or death was not statistically different between any of the groups, although, after adjustment, LMWH was associated with a slightly increased risk of ICH.
The quality of included studies varied considerably and inter-rater agreement on study quality was low, raising the possibility of study selection bias. Potential publication bias was not addressed. Bleeding complications were rare, so the estimates of risk may be imprecise.
Bottom line: Individualized therapy is required for DVT prophylaxis in the neurosurgical patient; SCDs reduce VTE risk and both pharmacologic and mechanical prophylaxis may be indicated in patients with increased VTE risk.
Citation: Collen JF, Jackson JL, Shorr AF, Moores LK. Prevention of venous thromboembolism in neurosurgery: A metaanalysis. Chest. 2008;13(4):237-249.
SMART-COP Predicts Need for ICU Care in CAP
Clinical question: Can a clinical tool predict the need for critical care in community acquired pneumonia (CAP)?
Background: Clinical tools predicting 30-day mortality in community acquired pneumonia (CAP) exist, but do not accurately identify who will require intensive care unit-level care, such as intensive respiratory or vasosuppressor support (IRVS).
Study design: Prospective multi-center observational study.
Setting: Six hospitals in Australia participating in the Australian Community Acquired Pneumonia Study (ACAPS).
Synopsis: Multivariate analysis of a dataset of 882 episodes of CAP identified eight factors that were associated with the need for IRVS, summarized by the mnemonic “SMART-COP” (Systolic blood pressure, Multilobar chest radiography involvement, low Albumin level, high Respiratory rate, Tachycardia, Confusion, poor Oxygenation, and low arterial pH). Assigning one point for five factors and two points for three factors (systolic blood pressure, poor oxygenation, and low arterial pH) a SMART-COP score >3 identified 92.3% (95% CI 84.8-96.9%) of patients who required IRVS, including 84% who did not initially require ICU care. Specificity was 62.3% (CI 58.8-65.7%). Test characteristics for predicting IRVS were superior to existing prediction rules (PSI and CURB-65).
Most patients were drawn from large, urban teaching hospitals in Australia, so the results may not be generalizable. The authors also presented a modification of SMART-COP, using pulse oximetry rather than blood gas results; this may be even more useful in the pre-hospital setting.
Bottom line: SMART-COP is a reasonable screening tool for predicting need for ICU-level care in patients admitted with CAP.
Citation: Charles PGP, Wolfe, R, Whitby, M, et. al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47(3):375-384.
Mediterranean and Low-Carbohydrate Diets are Effective for Weight Loss
Clinical question: Are dietary intervention with low-fat, Mediterranean or low-carbohydrate diets effective?
Background: Obesity is a growing, worldwide problem. Past trials comparing the effectiveness and safety of various dietary interventions have been limited by short follow up and high dropout rates.
Study design: Prospective randomized trial.
Setting: Employees of a research center in Israel.
Synopsis: 322 subjects (average BMI 31) were randomized to a low-fat/restricted-calorie, Mediterranean/ restricted-calorie, or a low-carbohydrate/non-restricted calorie diet. Diet adherence was 84.6% at two years and all groups lost significant amounts of weight. The Mediterranean and low-carbohydrate diets showed similar aver∆age weight loss of 4.4 kg and 4.7 kg, respectively. The low-fat diet group on average lost 2.9 kg. Diabetic patients had improved glycemic control and lower insulin levels with the Mediterranean diet. Subjects assigned to the low-carbohydrate diet had the greatest improvement in lipid profile (20% relative decrease of total cholesterol to HDL ratio).
The trial took place at a single site (a scientific research center in Israel) and included only 14% women, so its generalization is uncertain. The study was based on self-reported dietary intake and may be subject to reporting bias.
Bottom line: Mediterranean and low-carbohydrate diets are safe and effective alternatives to low-fat diets with favorable effects on glycemic control in diabetics and lipid metabolism, respectively.
Citation: Shai I, Schwarz-fuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. NEJM. 2008;359(3):229-241.
Admissions for Acute Coronary Syndrome Decreased after Implementation of Smoke-free Legislation
Clinical question: Is there a reduction in admissions for acute coronary syndrome (ACS) after enactment of smoke-free legislation?
Background: Multiple, small, retrospective studies have shown a decrease in ACS after implementation of smoke-free legislation.
Study design: Prospective observational multi-center cohort study.
Setting: Nine hospitals in Scotland.
Synopsis: Data was collected on all patients admitted with ACS 10 months before and after implementation of smoke-free legislation, which prohibited smoking in all enclosed public and work places in Scotland. After the smoking ban, the number of ACS admissions fell by 17% (95% CI 16-18) in Scotland as a whole, compared with a 4% reduction in England during the same period (England does not have similar smoke-free legislation). Among smokers, former smokers and non-smokers, the number of ACS admissions decreased by 14% (95% CI 12-16), 19% (95% CI 17-21), and 21% (95% CI 18-24), respectively. Among non-smokers, self-reported exposure to second-hand smoke decreased significantly; these reductions were confirmed by measured reductions in serum cotinine levels, even among those who never smoked.
Results were limited by the observational nature of the study, although the authors did attempt to carefully match comparison cohorts by season and geography. Also, secular trends other than legislation may have reduced prevalent smoking in Scotland during the study period.
Bottom line: Admissions for ACS for both smokers and non-smokers decreased after implementation of smoke-free legislation.
Citation: Pell JP, Haw S, Cobbe S, et al. Smoke-free legislation and hospitalizations for acute coronary syndrome. NEJM. 2008;359(5):482-491.
Continuation of Beta-blockers in Patients Hospitalized for Heart Failure Improves Mortality
Clinical question: Does the withdrawal or continuation of beta-blockers in patients hospitalized with decompensated heart failure have any effect on clinical outcomes?
Background: Previous clinical trials have demonstrated mortality benefit with the use of beta-blockers in patients with symptomatic chronic heart failure and left ventricular systolic dysfunction (LVSD), however, controversy exists whether to continue these medications in acute decompensated heart failure.
Study design: Prospective cohort analysis from the OPTIMIZE-HF registry (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure).
Setting: 91 academic and community hospitals in the United States.
Synopsis: Data was analyzed on 2,373 registry patients with documented LVSD (EF <40) eligible for beta-blocker therapy. During hospitalization, 1,350 patients were continued on beta-blockers, 79 had therapy withdrawn, 303 were not started, and 632 had beta-blockade initiated. Compared with no beta-blocker treatment, adjusted hazard ratio (HR) for death at 60 and 90 days following discharge was lower in patients who were continued on beta-blockade (HR 0.60, 95% CI 0.37–0.99). Compared with continuation of beta-blockade, withdrawal of beta-blockade increased the risk of death (HR 2.3, 95% CI 1.2–4.6).
Results were limited by the observational nature of the study and short follow up. The reason for discontinuation or not starting beta-blockade was not captured in the database, so it is possible sicker patients had beta-blockers discontinued during hospitalization (although the authors attempted to control for this).
Bottom line: Beta-blockers should be continued whenever possible in patients hospitalized for heart failure with LVSD.
Citation: Fonarow GC, Abraham WT, Albert NM, et al. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure. J Am Coll Cardiol. 2008;52(3):190-199.
Non-invasive Ventilation Does Not Improve Short-term Mortality in Acute Cardiogenic Pulmonary Edema
Clinical question: Does non-invasive ventilation reduce mortality in patients with acute cardiogenic pulmonary edema and are there differences in outcome between use of continuous positive airway pressure (CPAP) or non-invasive positive pressure ventilation (NIPPV)?
Background: In patients with acute cardiogenic pulmonary edema, noninvasive ventilation improves physiologic variables and symptoms, decreases rates of invasive ventilation, and may improve mortality.
Study design: Randomized multi center controlled trial.
Setting: 26 district and regional hospitals in the United Kingdom.
Synopsis: 1,156 patients admitted with acute cardiogenic pulmonary edema between July 2003 and April 2007 were randomized to standard oxygen therapy, versus CPAP or NIPPV. There were no significant differences in seven- or 30-day mortality rates between the standard oxygen therapy versus noninvasive ventilation. Mortality at seven days was 9.8% in the standard oxygen group versus 9.5% in the noninvasive ventilation group (P=0.87); 30-day mortality was 16% in the standard oxygen group and 15% in the non-invasive ventilation group (P=0.64). There were no major differences in treatment outcome with NIPPV compared to CPAP.
Although mortality was not decreased, non-invasive ventilation did improve dyspnea and tachycardia within one hour of therapy.
Bottom line: In patients admitted with acute cardiogenic pulmonary edema, noninvasive ventilation improved dyspnea and some physiological parameters, but did not improve short-term mortality rates.
Citation: Gray A, Goodacre S, Newby D, Masson M, Sampson F, Nicholl J. Noninvasive ventilation in acute cardiogenic pulmonary edema. NEJM. 2008;359(2):142-151.
Cyclooxygenase 2 Inhibitors May Increase the Risk of Ischemic Stroke
Clinical question: Do NSAIDs and COX-2 inhibitors increase the risk of ischemic or hemorrhagic stroke?
Background: Selected cyclooxygenase 2 (COX-2) inhibitors have been shown to increase cardiovascular morbidity in a dose-dependent manner and are now used with caution in patients at risk for cardiovascular disease. Little is known about the safety of these medications and non-aspirin, non-steroidal anti-inflammatory drugs (NSAIDS) in those at risk for cerebrovascular disease.
Study design: Retrospective observational cohort study.
Setting: Tennessee Medicaid Program enrollees.
Synopsis: Data was collected from the medical records of 336,906 subjects. Non-users had a baseline stroke rate of 4.51 strokes/1000 person-years. The rate increased to 5.15/1,000 person-years and 5.95/1,000 person-years for rofecoxib and valdecoxib, respectively. Celecoxib and other NSAIDs did not significantly increase the risk of stroke. Analysis of new users of rofexocib and valdecoxib yielded a similarly increased risk of stroke. Most strokes were ischemic.
Limitations include the ready availability of NSAIDs raising the possibility that some patients classified as non-users were actually users of NSAIDs. Other potential confounders may not have been measured and, therefore, not available for analysis.
Bottom line: COX-2 inhibitors should be used with caution in patients with increased cerebrovascular disease risk.
Citation: Roumie CL, Mitchel EF, Kaltenback L, Arbogast PG, Gideon P Griffen MR. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke. 2008;39:1037-2045.
3 ... 2 ... 1 ... Moving Day

SHM is growing, changing, evolving and advancing. If you have been a member or been engaged with the society for the past few years, this isn’t news to you. Our membership is growing; the products, publications and services we offer are expanding; attendance at our annual meeting is increasing; and we are continuing to create new and valuable online resources. These are tangible signs of growth that many of you see and touch on a regular basis. On a day-to-day basis, I see the same things, but because I work for SHM, I have the opportunity to see the growth and change from within the organization.
When I signed on with SHM more than three years ago, I walked through the door and into a small office, approximately 3,000 square feet in size with about 13 full-time staff members. Since then, we have grown steadily, consistently adding new faces to the SHM team and expanding into new places by breaking through a wall into an adjacent space. Flash forward to the present day. Between April and July 2008, SHM has added 13 new faces to the staff. At the end of September 2008, we broke ground on construction of our new corporate headquarters, a 16,000-square-foot office in downtown Philadelphia.
Since its inception 12 years ago, SHM has called 190 Independence Mall home, but just as the hospital medicine movement has grown, so has SHM and the staff supporting the society. This winter, SHM will be moving our corporate headquarters to the new facility at 1500 Spring Garden. The process to find our new headquarters has been an extensive one. We began the search for a new office approximately one year ago, and as I am writing this, final construction documents have been sent to a list of general contractors.
During the past six months, SHM has been working with projects managers, architects, engineers, and consultants to take our new office from a “blank slate” to a finished and fully operational office before the end of 2008. As you read this article, construction on the new headquarters is fully underway. Workers are putting up drywall, running cables, laying carpet, and installing equipment that will be the supporting foundation for the staff and society for the next decade.
So, by now you are probably asking, “What does this mean to me? I don’t see these people on a daily basis, and I don’t work at SHM headquarters.” At a very basic level it means SHM will have a new address and new phone numbers. Your letters, applications, registrations, and anything addressed to SHM will be routed to our new home. Additionally, as part of our move, SHM will implement a new phone system. Our toll-free, 1-800 number will remain the same, however, all of the people who work for SHM will have new office phone numbers.
It is important you know how to reach SHM in our new home, but even more important is to know that this move is a significant milestone in the evolution of the society and the next step in providing you, our members, with ever-improving and enhanced levels of service and support. In creating a new facility, we are further equipping staff with the tools they need to serve you, creating technical capacities to meet current and future needs, and setting a stage for SHM’s continued growth in support of the growing hospital medicine movement.
During the weeks and months ahead, the SHM team will be preparing for the launch of the new One Day Hospitalist University, opening of the new Fellowship in Hospital Medicine and[Add Another New Program Here. In addition to all of these new and exciting initiatives, we will be organizing files, packing boxes and preparing for our move. As we transition to new desks, new phones, new commutes and a new environment, we would like to take a moment to thank you for your support and understanding while we take another significant step in the history of the Society of Hospital Medicine.
Behind the Scenes
Change is in the air
By Geri Barnes

It’s autumn and there is a bite to the air. Every year around this time, I vacillate between being depressed about the pending winter and energized by the change of season. This year, I definitely am excited and energized.
As weather is one of those environmental dynamics that impacts daily life, so do changes in the healthcare arena impact on SHM and its life. We’ve seen “never events” come into being, an expansion of CMS’ Hospitals Compare, and an increasing focus on pay-for-performance. All of these factors are designed to improve patient care, particularly care of the hospitalized patient. SHM staff needs to be ready to support the hospital medicine community.


SHM long has been focused on defining and providing hospitalists with the education and resources needed for every day practice, as well as for imple- menting cutting-edge quality improvement interventions. To support these focus areas, our staff members were organized in one department, Education and Quality Initiatives. During the last year, we decided our efforts would be better served by creating two departments: Education and Meetings and Quality Initiatives. Last summer, we hired two new staff members to lead the department and move the quality efforts forward. Jane Kelly-Cummings, RN, CPHQ, senior director, Quality Initiatives, has more than 20 years of experience in clinical practice, quality improvement, patient safety, healthcare informatics and quality improvement education. Linda Boclair, MT (ASCP), MEd, MBA, brings to SHM 25 years of management in the healthcare industry and serves as the Quality Initiatives Department director. You will be hearing more about the Quality Initiatives Department in the near future.
I am heading up the newly organized Education and Meetings Department. I am joined by Erica Pearson, director, Meetings; Theresa Jones, education project manager; Meghan Pitzer, meetings coordinator; and Carolyn Brennan, director, Research Program Development. We are charged with managing SHM’s Education Enterprise, which includes meetings and all other educational activities that support our members.
For meetings, we focus on leading our volunteers in the development of relevant program and educational content, ensuring we meet the requirements for continuing medical education (CME) programs. We design and implement meeting logistics with a common goal: the attendees leave the meeting feeling nothing could have been better organized. The Education and Meetings staff has focused their energies on the following meetings:
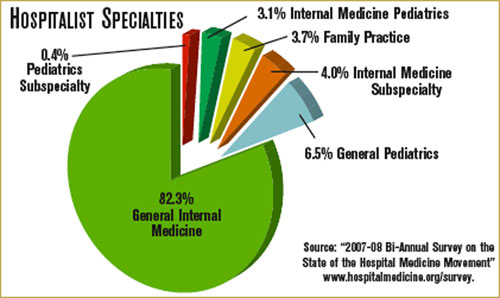
- The cornerstone of our meetings is the SHM annual meeting. Hospital Medicine 2009 will take place May 14-17, 2009, in Chicago at the Hyatt Regency. The planning of the program and logistics began in March 2008, and the organizational effort will continue through the end of the meeting. This comprehensive program includes annual meeting education sessions over the course of two and a half days and another full day of seven concurrent pre-courses.
- An important educational event is SHM’s Leadership Academy. Established in 2005, the Level I Academy has been presented semi-annually, with the eighth event taking place in Los Angeles this past September. Based on a need for the next level of leadership skills, Level II started in 2006 and recently presented for the third time. All events have basically sold out, and their popularity continues to grow.
- SHM instituted the One-Day Hospitalist University (ODHU) series this year, presenting four of our best pre-courses on a regional basis. The goal is to present ODHU in four different locations during the course of the year. The first ODHU takes place this month in Baltimore; the next is Feb. 3-4 in Atlanta.
- Pediatric Hospital Medicine 2009 was held in July in Denver. As the lead sponsor, SHM organized this successful conference, which was co-sponsored by the American Pediatric Association and the American Academy of Pediatrics.
- Expert Training Sessions is a new series of educational events that provide the opportunity to learn quality improvement strategies for glycemic control, VTE prevention, or transitions of care directly from an expert and interact on a personal basis. Presented in Boston and Nashville and planned for St. Louis, this initiative already is proving successful and we are hoping to expand in the near future.
The other major focus area for the Education and Meetings Department lies in meeting the educational needs of the hospital medicine community. Staff, working with the Education Committee, are exploring new and exciting ways to identify needs and define strategies to deliver relevant programming. The efforts, which will lead to a comprehensive education plan that will drive the activities the next few years, are focused on the following:
- Life-long learning has become the standard for physicians in general and hospitalists in particular. SHM is in the early stages of identifying and developing resources that will be readily accessible on the SHM Web site, such as a hospital medicine reading list on clinical and healthcare-systems topics based on the Core Competencies.
- The Education Committee is exploring the possibility of developing an evidence-based medicine (EBM) primer, which can be used to practice and teach EBM. It will be designed for the practicing hospitalist in a community hospital setting and will define how to research, read, and use EBM journal articles.
- SHM is exploring the use of Web 2.0 to continually assess needs, deliver educational programs, and communicate with members and faculty.
- The needs of academic hospitalists are unique and SHM is dedicated to support this important segment of our constituency. Joining with the Society of General Internal Medicine (SGIM), SHM is planning an Academic Boot Camp that will focus on education skills, research, mentoring, and career pathways.
- SHM is developing a comprehensive communication and education program to become the main resource for hospitalists as they engage in Maintenance of Certification.
So, the welcome winds of change blow, bringing the energy and organization needed to accomplish our education and quality goals. We are confident our internal changes will result in moving our agenda forward in ways previously only imagined.
Volunteer Search
Interested in being a part of an SHM Committee or Task Force? Now is your chance! Nominations are open for SHM Committees and Task Forces. This is your opportunity to shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit www.hospitalmedicine.org and click on “About SHM,” then click on “Committees.” Here, you will see a full list of committees, as well as task forces and current members. For each committee you would like to serve on, please submit your name and a one- to two-paragraph statement about why you are qualified and interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitlamedicine.org by Dec. 5. Appointments will be made in February, take affect in May and last one year. TH
SHM is growing, changing, evolving and advancing. If you have been a member or been engaged with the society for the past few years, this isn’t news to you. Our membership is growing; the products, publications and services we offer are expanding; attendance at our annual meeting is increasing; and we are continuing to create new and valuable online resources. These are tangible signs of growth that many of you see and touch on a regular basis. On a day-to-day basis, I see the same things, but because I work for SHM, I have the opportunity to see the growth and change from within the organization.
When I signed on with SHM more than three years ago, I walked through the door and into a small office, approximately 3,000 square feet in size with about 13 full-time staff members. Since then, we have grown steadily, consistently adding new faces to the SHM team and expanding into new places by breaking through a wall into an adjacent space. Flash forward to the present day. Between April and July 2008, SHM has added 13 new faces to the staff. At the end of September 2008, we broke ground on construction of our new corporate headquarters, a 16,000-square-foot office in downtown Philadelphia.
Since its inception 12 years ago, SHM has called 190 Independence Mall home, but just as the hospital medicine movement has grown, so has SHM and the staff supporting the society. This winter, SHM will be moving our corporate headquarters to the new facility at 1500 Spring Garden. The process to find our new headquarters has been an extensive one. We began the search for a new office approximately one year ago, and as I am writing this, final construction documents have been sent to a list of general contractors.
During the past six months, SHM has been working with projects managers, architects, engineers, and consultants to take our new office from a “blank slate” to a finished and fully operational office before the end of 2008. As you read this article, construction on the new headquarters is fully underway. Workers are putting up drywall, running cables, laying carpet, and installing equipment that will be the supporting foundation for the staff and society for the next decade.
So, by now you are probably asking, “What does this mean to me? I don’t see these people on a daily basis, and I don’t work at SHM headquarters.” At a very basic level it means SHM will have a new address and new phone numbers. Your letters, applications, registrations, and anything addressed to SHM will be routed to our new home. Additionally, as part of our move, SHM will implement a new phone system. Our toll-free, 1-800 number will remain the same, however, all of the people who work for SHM will have new office phone numbers.
It is important you know how to reach SHM in our new home, but even more important is to know that this move is a significant milestone in the evolution of the society and the next step in providing you, our members, with ever-improving and enhanced levels of service and support. In creating a new facility, we are further equipping staff with the tools they need to serve you, creating technical capacities to meet current and future needs, and setting a stage for SHM’s continued growth in support of the growing hospital medicine movement.
During the weeks and months ahead, the SHM team will be preparing for the launch of the new One Day Hospitalist University, opening of the new Fellowship in Hospital Medicine and[Add Another New Program Here. In addition to all of these new and exciting initiatives, we will be organizing files, packing boxes and preparing for our move. As we transition to new desks, new phones, new commutes and a new environment, we would like to take a moment to thank you for your support and understanding while we take another significant step in the history of the Society of Hospital Medicine.
Behind the Scenes
Change is in the air
By Geri Barnes
It’s autumn and there is a bite to the air. Every year around this time, I vacillate between being depressed about the pending winter and energized by the change of season. This year, I definitely am excited and energized.
As weather is one of those environmental dynamics that impacts daily life, so do changes in the healthcare arena impact on SHM and its life. We’ve seen “never events” come into being, an expansion of CMS’ Hospitals Compare, and an increasing focus on pay-for-performance. All of these factors are designed to improve patient care, particularly care of the hospitalized patient. SHM staff needs to be ready to support the hospital medicine community.
SHM long has been focused on defining and providing hospitalists with the education and resources needed for every day practice, as well as for imple- menting cutting-edge quality improvement interventions. To support these focus areas, our staff members were organized in one department, Education and Quality Initiatives. During the last year, we decided our efforts would be better served by creating two departments: Education and Meetings and Quality Initiatives. Last summer, we hired two new staff members to lead the department and move the quality efforts forward. Jane Kelly-Cummings, RN, CPHQ, senior director, Quality Initiatives, has more than 20 years of experience in clinical practice, quality improvement, patient safety, healthcare informatics and quality improvement education. Linda Boclair, MT (ASCP), MEd, MBA, brings to SHM 25 years of management in the healthcare industry and serves as the Quality Initiatives Department director. You will be hearing more about the Quality Initiatives Department in the near future.
I am heading up the newly organized Education and Meetings Department. I am joined by Erica Pearson, director, Meetings; Theresa Jones, education project manager; Meghan Pitzer, meetings coordinator; and Carolyn Brennan, director, Research Program Development. We are charged with managing SHM’s Education Enterprise, which includes meetings and all other educational activities that support our members.
For meetings, we focus on leading our volunteers in the development of relevant program and educational content, ensuring we meet the requirements for continuing medical education (CME) programs. We design and implement meeting logistics with a common goal: the attendees leave the meeting feeling nothing could have been better organized. The Education and Meetings staff has focused their energies on the following meetings:
- The cornerstone of our meetings is the SHM annual meeting. Hospital Medicine 2009 will take place May 14-17, 2009, in Chicago at the Hyatt Regency. The planning of the program and logistics began in March 2008, and the organizational effort will continue through the end of the meeting. This comprehensive program includes annual meeting education sessions over the course of two and a half days and another full day of seven concurrent pre-courses.
- An important educational event is SHM’s Leadership Academy. Established in 2005, the Level I Academy has been presented semi-annually, with the eighth event taking place in Los Angeles this past September. Based on a need for the next level of leadership skills, Level II started in 2006 and recently presented for the third time. All events have basically sold out, and their popularity continues to grow.
- SHM instituted the One-Day Hospitalist University (ODHU) series this year, presenting four of our best pre-courses on a regional basis. The goal is to present ODHU in four different locations during the course of the year. The first ODHU takes place this month in Baltimore; the next is Feb. 3-4 in Atlanta.
- Pediatric Hospital Medicine 2009 was held in July in Denver. As the lead sponsor, SHM organized this successful conference, which was co-sponsored by the American Pediatric Association and the American Academy of Pediatrics.
- Expert Training Sessions is a new series of educational events that provide the opportunity to learn quality improvement strategies for glycemic control, VTE prevention, or transitions of care directly from an expert and interact on a personal basis. Presented in Boston and Nashville and planned for St. Louis, this initiative already is proving successful and we are hoping to expand in the near future.
The other major focus area for the Education and Meetings Department lies in meeting the educational needs of the hospital medicine community. Staff, working with the Education Committee, are exploring new and exciting ways to identify needs and define strategies to deliver relevant programming. The efforts, which will lead to a comprehensive education plan that will drive the activities the next few years, are focused on the following:
- Life-long learning has become the standard for physicians in general and hospitalists in particular. SHM is in the early stages of identifying and developing resources that will be readily accessible on the SHM Web site, such as a hospital medicine reading list on clinical and healthcare-systems topics based on the Core Competencies.
- The Education Committee is exploring the possibility of developing an evidence-based medicine (EBM) primer, which can be used to practice and teach EBM. It will be designed for the practicing hospitalist in a community hospital setting and will define how to research, read, and use EBM journal articles.
- SHM is exploring the use of Web 2.0 to continually assess needs, deliver educational programs, and communicate with members and faculty.
- The needs of academic hospitalists are unique and SHM is dedicated to support this important segment of our constituency. Joining with the Society of General Internal Medicine (SGIM), SHM is planning an Academic Boot Camp that will focus on education skills, research, mentoring, and career pathways.
- SHM is developing a comprehensive communication and education program to become the main resource for hospitalists as they engage in Maintenance of Certification.
So, the welcome winds of change blow, bringing the energy and organization needed to accomplish our education and quality goals. We are confident our internal changes will result in moving our agenda forward in ways previously only imagined.
Volunteer Search
Interested in being a part of an SHM Committee or Task Force? Now is your chance! Nominations are open for SHM Committees and Task Forces. This is your opportunity to shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit www.hospitalmedicine.org and click on “About SHM,” then click on “Committees.” Here, you will see a full list of committees, as well as task forces and current members. For each committee you would like to serve on, please submit your name and a one- to two-paragraph statement about why you are qualified and interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitlamedicine.org by Dec. 5. Appointments will be made in February, take affect in May and last one year. TH
SHM is growing, changing, evolving and advancing. If you have been a member or been engaged with the society for the past few years, this isn’t news to you. Our membership is growing; the products, publications and services we offer are expanding; attendance at our annual meeting is increasing; and we are continuing to create new and valuable online resources. These are tangible signs of growth that many of you see and touch on a regular basis. On a day-to-day basis, I see the same things, but because I work for SHM, I have the opportunity to see the growth and change from within the organization.
When I signed on with SHM more than three years ago, I walked through the door and into a small office, approximately 3,000 square feet in size with about 13 full-time staff members. Since then, we have grown steadily, consistently adding new faces to the SHM team and expanding into new places by breaking through a wall into an adjacent space. Flash forward to the present day. Between April and July 2008, SHM has added 13 new faces to the staff. At the end of September 2008, we broke ground on construction of our new corporate headquarters, a 16,000-square-foot office in downtown Philadelphia.
Since its inception 12 years ago, SHM has called 190 Independence Mall home, but just as the hospital medicine movement has grown, so has SHM and the staff supporting the society. This winter, SHM will be moving our corporate headquarters to the new facility at 1500 Spring Garden. The process to find our new headquarters has been an extensive one. We began the search for a new office approximately one year ago, and as I am writing this, final construction documents have been sent to a list of general contractors.
During the past six months, SHM has been working with projects managers, architects, engineers, and consultants to take our new office from a “blank slate” to a finished and fully operational office before the end of 2008. As you read this article, construction on the new headquarters is fully underway. Workers are putting up drywall, running cables, laying carpet, and installing equipment that will be the supporting foundation for the staff and society for the next decade.
So, by now you are probably asking, “What does this mean to me? I don’t see these people on a daily basis, and I don’t work at SHM headquarters.” At a very basic level it means SHM will have a new address and new phone numbers. Your letters, applications, registrations, and anything addressed to SHM will be routed to our new home. Additionally, as part of our move, SHM will implement a new phone system. Our toll-free, 1-800 number will remain the same, however, all of the people who work for SHM will have new office phone numbers.
It is important you know how to reach SHM in our new home, but even more important is to know that this move is a significant milestone in the evolution of the society and the next step in providing you, our members, with ever-improving and enhanced levels of service and support. In creating a new facility, we are further equipping staff with the tools they need to serve you, creating technical capacities to meet current and future needs, and setting a stage for SHM’s continued growth in support of the growing hospital medicine movement.
During the weeks and months ahead, the SHM team will be preparing for the launch of the new One Day Hospitalist University, opening of the new Fellowship in Hospital Medicine and[Add Another New Program Here. In addition to all of these new and exciting initiatives, we will be organizing files, packing boxes and preparing for our move. As we transition to new desks, new phones, new commutes and a new environment, we would like to take a moment to thank you for your support and understanding while we take another significant step in the history of the Society of Hospital Medicine.
Behind the Scenes
Change is in the air
By Geri Barnes
It’s autumn and there is a bite to the air. Every year around this time, I vacillate between being depressed about the pending winter and energized by the change of season. This year, I definitely am excited and energized.
As weather is one of those environmental dynamics that impacts daily life, so do changes in the healthcare arena impact on SHM and its life. We’ve seen “never events” come into being, an expansion of CMS’ Hospitals Compare, and an increasing focus on pay-for-performance. All of these factors are designed to improve patient care, particularly care of the hospitalized patient. SHM staff needs to be ready to support the hospital medicine community.
SHM long has been focused on defining and providing hospitalists with the education and resources needed for every day practice, as well as for imple- menting cutting-edge quality improvement interventions. To support these focus areas, our staff members were organized in one department, Education and Quality Initiatives. During the last year, we decided our efforts would be better served by creating two departments: Education and Meetings and Quality Initiatives. Last summer, we hired two new staff members to lead the department and move the quality efforts forward. Jane Kelly-Cummings, RN, CPHQ, senior director, Quality Initiatives, has more than 20 years of experience in clinical practice, quality improvement, patient safety, healthcare informatics and quality improvement education. Linda Boclair, MT (ASCP), MEd, MBA, brings to SHM 25 years of management in the healthcare industry and serves as the Quality Initiatives Department director. You will be hearing more about the Quality Initiatives Department in the near future.
I am heading up the newly organized Education and Meetings Department. I am joined by Erica Pearson, director, Meetings; Theresa Jones, education project manager; Meghan Pitzer, meetings coordinator; and Carolyn Brennan, director, Research Program Development. We are charged with managing SHM’s Education Enterprise, which includes meetings and all other educational activities that support our members.
For meetings, we focus on leading our volunteers in the development of relevant program and educational content, ensuring we meet the requirements for continuing medical education (CME) programs. We design and implement meeting logistics with a common goal: the attendees leave the meeting feeling nothing could have been better organized. The Education and Meetings staff has focused their energies on the following meetings:
- The cornerstone of our meetings is the SHM annual meeting. Hospital Medicine 2009 will take place May 14-17, 2009, in Chicago at the Hyatt Regency. The planning of the program and logistics began in March 2008, and the organizational effort will continue through the end of the meeting. This comprehensive program includes annual meeting education sessions over the course of two and a half days and another full day of seven concurrent pre-courses.
- An important educational event is SHM’s Leadership Academy. Established in 2005, the Level I Academy has been presented semi-annually, with the eighth event taking place in Los Angeles this past September. Based on a need for the next level of leadership skills, Level II started in 2006 and recently presented for the third time. All events have basically sold out, and their popularity continues to grow.
- SHM instituted the One-Day Hospitalist University (ODHU) series this year, presenting four of our best pre-courses on a regional basis. The goal is to present ODHU in four different locations during the course of the year. The first ODHU takes place this month in Baltimore; the next is Feb. 3-4 in Atlanta.
- Pediatric Hospital Medicine 2009 was held in July in Denver. As the lead sponsor, SHM organized this successful conference, which was co-sponsored by the American Pediatric Association and the American Academy of Pediatrics.
- Expert Training Sessions is a new series of educational events that provide the opportunity to learn quality improvement strategies for glycemic control, VTE prevention, or transitions of care directly from an expert and interact on a personal basis. Presented in Boston and Nashville and planned for St. Louis, this initiative already is proving successful and we are hoping to expand in the near future.
The other major focus area for the Education and Meetings Department lies in meeting the educational needs of the hospital medicine community. Staff, working with the Education Committee, are exploring new and exciting ways to identify needs and define strategies to deliver relevant programming. The efforts, which will lead to a comprehensive education plan that will drive the activities the next few years, are focused on the following:
- Life-long learning has become the standard for physicians in general and hospitalists in particular. SHM is in the early stages of identifying and developing resources that will be readily accessible on the SHM Web site, such as a hospital medicine reading list on clinical and healthcare-systems topics based on the Core Competencies.
- The Education Committee is exploring the possibility of developing an evidence-based medicine (EBM) primer, which can be used to practice and teach EBM. It will be designed for the practicing hospitalist in a community hospital setting and will define how to research, read, and use EBM journal articles.
- SHM is exploring the use of Web 2.0 to continually assess needs, deliver educational programs, and communicate with members and faculty.
- The needs of academic hospitalists are unique and SHM is dedicated to support this important segment of our constituency. Joining with the Society of General Internal Medicine (SGIM), SHM is planning an Academic Boot Camp that will focus on education skills, research, mentoring, and career pathways.
- SHM is developing a comprehensive communication and education program to become the main resource for hospitalists as they engage in Maintenance of Certification.
So, the welcome winds of change blow, bringing the energy and organization needed to accomplish our education and quality goals. We are confident our internal changes will result in moving our agenda forward in ways previously only imagined.
Volunteer Search
Interested in being a part of an SHM Committee or Task Force? Now is your chance! Nominations are open for SHM Committees and Task Forces. This is your opportunity to shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit www.hospitalmedicine.org and click on “About SHM,” then click on “Committees.” Here, you will see a full list of committees, as well as task forces and current members. For each committee you would like to serve on, please submit your name and a one- to two-paragraph statement about why you are qualified and interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitlamedicine.org by Dec. 5. Appointments will be made in February, take affect in May and last one year. TH
Changing of the Guard

Starting a new job—any new job—brings with it trepidations. What’s the boss going to be like? Is there a strict dress code? Am I in over my head? When is payday? Did I make the right choice in taking it?
The nervous energy can be overwhelming. Only the strong survive the first day of human resources training, the endless line of personal questions from new co-workers, and the information technology grunts explaining your computer will be ready in a few days.
Fortunately, I made it through the first day, the second day, and the first week as the new editor of The Hospitalist. Whew! With newbie formalities out of the way, my attention is focused on settling into a routine and learning how best to lead the editorial charge for this news magazine. To that end, I want to say I’m excited to be on board!
Let’s start with a little background about me: I’ve been a writer, copy editor, and section editor for nearly two decades. The majority of my professional experience has been in the newspaper industry where I’ve worked in news, sports, and business departments at papers big and small.
To clear this up right away: I am not a doctor and—admittedly—not an expert in hospital medicine. In fact, except for the births of my two sons, I have spent very little time in or around hospitals the past 20 years. I do know, however, hospital medicine is a growing field, and I am thrilled to jump on this train as it leaves the station.
Some of you may believe a solid knowledge of medicine is a pre-requisite to edit a hospital medicine-focused magazine. For me, though, news is news. An editor may not understand every nuance of the subject matter, but he sure knows a good story when he sees one. My expertise is in developing a story, from concept through research and writing, all the way to presentation and publication. I hope my lack of medical background, in some ways, actually will allow me to bring a fresh set of eyes and editing to the content.
All of this said, my best asset in this new role is my editorial partner: Physician Editor Jeffrey Glasheen, MD. As a practicing hospitalist and leader of a hospital medicine group, Dr. Glasheen is on the front lines of hospital medicine, possesses a strong knowledge of all things SHM, and deals directly with the issues facing all of you dear readers. His passion for his role as physician editor inspires me. No doubt I will lean on him as I learn the ins and outs of hospital medicine.
Others I will look to for guidance include Editorial Director Lisa Dionne here at Wiley-Blackwell; the staff at SHM; and members of Team Hospitalist. Finally, I look to you for ideas and feedback. Who better to inform The Hospitalist pages? This magazine has a narrow focus (hospital medicine), but its readership is diverse and the trends are plentiful.
Because this is the November issue of an election year, I would like to commit to a non-partisan platform of fairness in reporting. I also believe in accurate, straightforward writing, and will maintain high standards at all levels when editing the magazine.
Now, for my first big announcement as editor: In addition to receiving the monthly magazine, you now receive our recently launched weekly electronic publication: the TH eWire. In the eWire, Associate Editor Stephanie Cajigal and I take the “pulse” of hospital medicine and offer up critical news and information we think you will value.
Once again, I am thrilled to be here and eager to make contact with as many hospitalists as possible in the coming months. I encourage you to share your opinions, offer up a story idea, or impart constructive criticism about anything and everything you see in The Hospitalist.
Regardless of the reason, I look forward to hearing from you. TH
Jason Carris is editor of The Hospitalist magazine. Send questions and comments to jcarris@wiley.com.
Starting a new job—any new job—brings with it trepidations. What’s the boss going to be like? Is there a strict dress code? Am I in over my head? When is payday? Did I make the right choice in taking it?
The nervous energy can be overwhelming. Only the strong survive the first day of human resources training, the endless line of personal questions from new co-workers, and the information technology grunts explaining your computer will be ready in a few days.
Fortunately, I made it through the first day, the second day, and the first week as the new editor of The Hospitalist. Whew! With newbie formalities out of the way, my attention is focused on settling into a routine and learning how best to lead the editorial charge for this news magazine. To that end, I want to say I’m excited to be on board!
Let’s start with a little background about me: I’ve been a writer, copy editor, and section editor for nearly two decades. The majority of my professional experience has been in the newspaper industry where I’ve worked in news, sports, and business departments at papers big and small.
To clear this up right away: I am not a doctor and—admittedly—not an expert in hospital medicine. In fact, except for the births of my two sons, I have spent very little time in or around hospitals the past 20 years. I do know, however, hospital medicine is a growing field, and I am thrilled to jump on this train as it leaves the station.
Some of you may believe a solid knowledge of medicine is a pre-requisite to edit a hospital medicine-focused magazine. For me, though, news is news. An editor may not understand every nuance of the subject matter, but he sure knows a good story when he sees one. My expertise is in developing a story, from concept through research and writing, all the way to presentation and publication. I hope my lack of medical background, in some ways, actually will allow me to bring a fresh set of eyes and editing to the content.
All of this said, my best asset in this new role is my editorial partner: Physician Editor Jeffrey Glasheen, MD. As a practicing hospitalist and leader of a hospital medicine group, Dr. Glasheen is on the front lines of hospital medicine, possesses a strong knowledge of all things SHM, and deals directly with the issues facing all of you dear readers. His passion for his role as physician editor inspires me. No doubt I will lean on him as I learn the ins and outs of hospital medicine.
Others I will look to for guidance include Editorial Director Lisa Dionne here at Wiley-Blackwell; the staff at SHM; and members of Team Hospitalist. Finally, I look to you for ideas and feedback. Who better to inform The Hospitalist pages? This magazine has a narrow focus (hospital medicine), but its readership is diverse and the trends are plentiful.
Because this is the November issue of an election year, I would like to commit to a non-partisan platform of fairness in reporting. I also believe in accurate, straightforward writing, and will maintain high standards at all levels when editing the magazine.
Now, for my first big announcement as editor: In addition to receiving the monthly magazine, you now receive our recently launched weekly electronic publication: the TH eWire. In the eWire, Associate Editor Stephanie Cajigal and I take the “pulse” of hospital medicine and offer up critical news and information we think you will value.
Once again, I am thrilled to be here and eager to make contact with as many hospitalists as possible in the coming months. I encourage you to share your opinions, offer up a story idea, or impart constructive criticism about anything and everything you see in The Hospitalist.
Regardless of the reason, I look forward to hearing from you. TH
Jason Carris is editor of The Hospitalist magazine. Send questions and comments to jcarris@wiley.com.
Starting a new job—any new job—brings with it trepidations. What’s the boss going to be like? Is there a strict dress code? Am I in over my head? When is payday? Did I make the right choice in taking it?
The nervous energy can be overwhelming. Only the strong survive the first day of human resources training, the endless line of personal questions from new co-workers, and the information technology grunts explaining your computer will be ready in a few days.
Fortunately, I made it through the first day, the second day, and the first week as the new editor of The Hospitalist. Whew! With newbie formalities out of the way, my attention is focused on settling into a routine and learning how best to lead the editorial charge for this news magazine. To that end, I want to say I’m excited to be on board!
Let’s start with a little background about me: I’ve been a writer, copy editor, and section editor for nearly two decades. The majority of my professional experience has been in the newspaper industry where I’ve worked in news, sports, and business departments at papers big and small.
To clear this up right away: I am not a doctor and—admittedly—not an expert in hospital medicine. In fact, except for the births of my two sons, I have spent very little time in or around hospitals the past 20 years. I do know, however, hospital medicine is a growing field, and I am thrilled to jump on this train as it leaves the station.
Some of you may believe a solid knowledge of medicine is a pre-requisite to edit a hospital medicine-focused magazine. For me, though, news is news. An editor may not understand every nuance of the subject matter, but he sure knows a good story when he sees one. My expertise is in developing a story, from concept through research and writing, all the way to presentation and publication. I hope my lack of medical background, in some ways, actually will allow me to bring a fresh set of eyes and editing to the content.
All of this said, my best asset in this new role is my editorial partner: Physician Editor Jeffrey Glasheen, MD. As a practicing hospitalist and leader of a hospital medicine group, Dr. Glasheen is on the front lines of hospital medicine, possesses a strong knowledge of all things SHM, and deals directly with the issues facing all of you dear readers. His passion for his role as physician editor inspires me. No doubt I will lean on him as I learn the ins and outs of hospital medicine.
Others I will look to for guidance include Editorial Director Lisa Dionne here at Wiley-Blackwell; the staff at SHM; and members of Team Hospitalist. Finally, I look to you for ideas and feedback. Who better to inform The Hospitalist pages? This magazine has a narrow focus (hospital medicine), but its readership is diverse and the trends are plentiful.
Because this is the November issue of an election year, I would like to commit to a non-partisan platform of fairness in reporting. I also believe in accurate, straightforward writing, and will maintain high standards at all levels when editing the magazine.
Now, for my first big announcement as editor: In addition to receiving the monthly magazine, you now receive our recently launched weekly electronic publication: the TH eWire. In the eWire, Associate Editor Stephanie Cajigal and I take the “pulse” of hospital medicine and offer up critical news and information we think you will value.
Once again, I am thrilled to be here and eager to make contact with as many hospitalists as possible in the coming months. I encourage you to share your opinions, offer up a story idea, or impart constructive criticism about anything and everything you see in The Hospitalist.
Regardless of the reason, I look forward to hearing from you. TH
Jason Carris is editor of The Hospitalist magazine. Send questions and comments to jcarris@wiley.com.