User login
A Novel Technique for Preparing an Allograft Fibula for Use as a Transsacral Graft as Treatment for High-grade Spondylolisthesis
Dermatologic Manifestations of Musicians: A Case Report and Review of Skin Conditions in Musicians
What's Eating You? Triatome Reduviids
The mysterious foreign accent
CASE: Disruptive and withdrawn
Police bring Ms. D, age 33, to our psychiatric facility because of violent behavior at her group home. When confronted for allegedly stealing, she became upset, fought with a housemate, and spat. Six months before coming to our facility she was admitted to a private hospital for psychotic disorder, not otherwise specified (NOS) where she was mute, refused all food and medications, lay in her room, and covered her face with a sheet when someone tried to talk to her.
Ms. D denies having depressive symptoms, sleep disturbance, racing thoughts, thoughts of hurting herself or others, or auditory or visual hallucinations. She complains of poor appetite. Ms. D denies a history of mental illness and says she is not taking any medication. She is upset about being hospitalized and says she will not cooperate with treatment. We cannot obtain her complete psychiatric history but available records indicate that she has 1 previous psychiatric hospitalization for psychotic disorder NOS, and has received trials of haloperidol, lorazepam, diphenhydramine, escitalopram, ziprasidone, and benztropine. Her records do not indicate the dosages of these medications or how she responded to pharmacotherapy.
During her mental status exam, Ms. D is well dressed, covers her hair with a scarf, has no unusual body movements, and responds to questions appropriately. She describes her mood as “okay” but appears upset and anxious about being in the hospital. She exhibits no overt psychotic symptoms and does not appear to be responding to auditory hallucinations or having delusional thoughts. Her cognitive function is intact and her intelligence is judged to be average with impaired insight and judgment. However, she speaks with a distinct accent that sounds Jamaican; otherwise, her speech is articulate with normal rate and tone. When we ask about her accent, Ms. D, who is African American, does not disclose her ethnicity and seems to be unaware of her accent. We did not question the authenticity of her accent until after we obtained collateral information from her family.
The authors’ observations
Based on the available information, we make a provisional diagnosis of psychotic disorder NOS and Ms. D is admitted involuntarily because of concerns about her safety. She is reluctant to accept any treatment and receives an involuntary probate commitment for 90 days. At admission, Ms. D is evasive, guarded, secretive, and at times hostile. Her physical examination reveals no signs or symptoms of focal neurologic deficits. Laboratory testing, including urine toxicology, is unremarkable. She refuses an MRI. Later testing reveals a critical ammonia level of 143 μg/dL, warranting an axis III diagnosis of asymptomatic hyperammonemia.
HISTORY: Paranoia and delusions
Ms. D says she was born and raised in a southern state. She reports that she was born to an Egyptian mother who died during childbirth; her father, who is white, was an ambassador stationed abroad. Ms. D attended school until the 11thgrade and was married at age 19 to a Secret Service agent. She says she has a son who was kidnapped by her husband’s enemies, rescued by paying ransom, and currently lives with his grandfather. Ms. D is paranoid and fears that her life is in danger. She also believes that she has gluten sensitivity that could discolor and damage her hair, which is why she always keeps a scarf on her head for protection.
Through an Internet search, we find articles about Ms. D’s son’s kidnapping. The 7-year-old had been missing for weeks when police found him with his mother in safe condition in another state, after Ms. D called her mother to ask for money and a place to stay. The child was taken from Ms. D’s custody because of concerns for his safety. We also find Ms. D’s mother. Although Ms. D insists her mother is deceased, after some persuasion, she signs a release allowing us to talk to her.
Ms. D’s mother reports that her daughter’s psychiatric problems began when she was pregnant. At the time Ms. D did not have a foreign accent. She had started to “talk funny” when her psychiatric symptoms emerged after she married and became pregnant.
Foreign accent syndrome
A foreign accent can be acquired by normal phenomena, such as being immersed in a foreign language, or a pathological process,1 which can include psychiatric (functional) or neurologic illness (organic causes). Foreign accent syndrome (FAS) is a rare speech disorder characterized by the appearance of a new accent, different from the speaker’s native language, that is perceived as foreign by the listener and in most cases also by the speaker.2 Usually an FAS patient has had no exposure to the accent, although in some cases an old accent has re-emerged.3,4
FAS can result from lesions in brain areas involved in speech production, including precentral gyrus, premotor mid-frontal gyrus, left subcortical prerolandic gyrus, postrolandic gyri, and left parietal area.4 Most FAS cases are secondary to a structural lesion in the brain caused by stroke, traumatic brain injury, cerebral hemorrhage, or multiple sclerosis.2 There are a few cases in the literature of acquired foreign accent with psychogenic etiology in patients with schizophrenia and bipolar disorder with psychotic features.5
TREATMENT: Combination therapy
Based on Ms. D’s unstable mood, irritability, delusional beliefs, and paranoid ideas, we start divalproex, 500 mg/d titrated to 1, 750 mg/d, and risperidone, 3 mg in the morning and 4 mg at bedtime.
The unit psychologist evaluates Ms. D and provides individual psychotherapy, which is mainly supportive and psychoeducational. Ms. D gradually becomes cooperative and friendly. She is not willing to talk about her accent or its origin; however, as her psychiatric symptoms improve, her accent gradually diminishes. The accent never completely resolves, but reduces until it is barely noticeable.
The authors’ observations
Ms. D’s foreign accent was more prominent when she displayed positive psychotic symptoms, such as delusions and disorganized thinking, and gradually disappeared as her psychotic symptoms improved. Ms. D’s case was peculiar because her accent was 1 of the first symptoms before her psychosis fully manifested.
How are FAS and psychosis linked?
Language dysfunction in schizophrenia is common and characterized by derailment and disorganization. Severity of language dysfunction in schizophrenia is directly proportional to overall disease severity.6,7 Various hypotheses have suggested the origin of FAS. In patients with FAS secondary to a neurologic disorder, a lesion usually is found in the dominant brain hemisphere, but the cause is not clear in patients with psychosis who have normal MRI findings. One hypothesis by Reeves et al links development of FAS to the functional disconnection between the left dorsolateral prefrontal cortex (DLPFC) and the superior temporal gyrus (STG) during active psychosis.5 In normal speech production, electric impulses originate in the DLPFC and are transmitted to STG in Wernicke’s area. From there, information goes to Broca’s area, which activates the primary motor cortex to pronounce words. In healthy individuals, word generation activates the DLPFC and causes deactivation of the bilateral STG.8 In schizophrenia, the left STG fails to deactivate in the presence of activation of the left DLPFC.9 Interestingly, STG dysfunction is seen only during active phase of psychosis. Its absence in asymptomatic patients with schizophrenia and bipolar disorder10,11 suggest that a foreign accent-like syndrome may be linked to the functional disconnection between the left DLPFC and left STG dysfunction in patients with active psychosis.5
Performing functional neuroimaging, including positron-emission tomography, functional MRI, and single-photon emission computed tomography, of patients with FAS could shed more light on the possible link between FAS and psychosis. In a case report of a patient with bipolar disorder who developed FAS, MRI initially showed no structural lesion but a later functional imaging scan revealed a cerebral infarct in the left insular and anterior temporal cortex.2
One of the limitations in Ms. D’s case is the lack of neuroimaging studies. For the first few weeks of her hospitalization, it was difficult to communicate with Ms. D. She did not acknowledge her illness and would not cooperate with treatment. She was withdrawn and seemed to experience hysterical mutism, which she perceived as caused by extreme food allergies. Later, as her symptoms continued to improve with pharmacologic and psychotherapeutic interventions, neuroimaging was no longer clinically necessary.
OUTCOME: Accent disappears
As Ms. D improves, psychotherapy evolves to gently and carefully challenging her delusions and providing insight-oriented interventions and trauma therapy. As her delusions gradually start to loosen, Ms. D reveals she had been physically and emotionally abused by her husband.
At discharge after 90 days in the hospital, Ms. D’s symptoms are well managed and she no longer shows signs of a thought disorder. Her thinking is clear, rational, and logical. She demonstrates incredible insight and appreciation that she needs to stay in treatment and continue to take divalproex and risperidone. Her delusions appear to be completely resolved and she is focused on reuniting with her son. Many of her previous delusions appear to be related to trauma and partly dissociative.
Ms. D contacts the psychologist several months later to report she is doing well in the community, staying in treatment, and working on legal means to reunite with her son. No trace of any foreign accent is detectable in her voice.
Related Resources
- Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? Journal of Neurolinguistics. 2006; 19: 385-409.
- Tsuruga K, Kobayashi T, Hirai N, et al. Foreign accent syndrome in a case of dissociative (conversion) disorder. Seishin Shinkeigaku Zasshi. 2008; 110(2): 79-87.
Drug Brand Names
- Benztropine • Cogentin
- Diphenhydramine • Benadryl
- Divalproex • Depakote
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? J Neurolinguistics. 2006;19(5):385-409.
2. Poulin S, Macoir J, Paquet N, et al. Psychogenic or neurogenic origin of agrammatism and foreign accent syndrome in a bipolar patient: a case report. Ann Gen Psychiatry. 2007;6:1.-
3. Takayama Y, Sugishita M, Kido T, et al. A case of foreign accent syndrome without aphasia caused by a lesion of the left precentral gyrus. Neurology. 1993;43:1361-1363.
4. Roth EJ, Fink K, Cherney LR, et al. Reversion to a previously learned foreign accent after stroke. Arch Phys Med Rehabil. 1997;78:550-552.
5. Reeves RR, Burke RS, Parker JD. Characteristics of psychotic patients with foreign accent syndrome. J Neuropsychiatry Clin Neurosci. 2007;19:70-76.
6. Ceccherini-Nelli A, Crow TJ. Disintegration of the components of language as the path to a revision of Bleuler’s and Schneider’s concepts of schizophrenia: linguistic disturbances compared with first-rank symptoms in acute psychosis. Br J Psychiatry. 2003;182:233-240.
7. Harrow M, O’Connell EM, Herbener ES, et al. Disordered verbalizations in schizophrenia: a speech disturbance or thought disorder? Compr Psychiatry. 2003;44:353-359.
8. Friston KJ, Frith CD, Liddle PF, et al. Investigating a network of word generation with positron emission tomography. Proc R Soc Lond B Biol Sci. 1991;244:101-106.
9. Frith CD, Friston K, Herold S, et al. Regional brain activity in chronic schizophrenic patients during the performance of a verbal fluency task. Br J Psychiatry. 1995;167:343-349.
10. Spence SA, Liddle PF, Stefan MD, et al. Functional anatomy of verbal fluency in people with schizophrenia and those at genetic risk. Focal dysfunction and distributed disconnectivity reappraised. Br J Psychiatry. 2011;176:52-60.
11. Dye SM, Spence SA, Bench CJ, et al. No evidence for left superior temporal dysfunction in asymptomatic schizophrenia and bipolar disorder. PET study of verbal fluency. Br J Psychiatry. 1999;175:367-374.
CASE: Disruptive and withdrawn
Police bring Ms. D, age 33, to our psychiatric facility because of violent behavior at her group home. When confronted for allegedly stealing, she became upset, fought with a housemate, and spat. Six months before coming to our facility she was admitted to a private hospital for psychotic disorder, not otherwise specified (NOS) where she was mute, refused all food and medications, lay in her room, and covered her face with a sheet when someone tried to talk to her.
Ms. D denies having depressive symptoms, sleep disturbance, racing thoughts, thoughts of hurting herself or others, or auditory or visual hallucinations. She complains of poor appetite. Ms. D denies a history of mental illness and says she is not taking any medication. She is upset about being hospitalized and says she will not cooperate with treatment. We cannot obtain her complete psychiatric history but available records indicate that she has 1 previous psychiatric hospitalization for psychotic disorder NOS, and has received trials of haloperidol, lorazepam, diphenhydramine, escitalopram, ziprasidone, and benztropine. Her records do not indicate the dosages of these medications or how she responded to pharmacotherapy.
During her mental status exam, Ms. D is well dressed, covers her hair with a scarf, has no unusual body movements, and responds to questions appropriately. She describes her mood as “okay” but appears upset and anxious about being in the hospital. She exhibits no overt psychotic symptoms and does not appear to be responding to auditory hallucinations or having delusional thoughts. Her cognitive function is intact and her intelligence is judged to be average with impaired insight and judgment. However, she speaks with a distinct accent that sounds Jamaican; otherwise, her speech is articulate with normal rate and tone. When we ask about her accent, Ms. D, who is African American, does not disclose her ethnicity and seems to be unaware of her accent. We did not question the authenticity of her accent until after we obtained collateral information from her family.
The authors’ observations
Based on the available information, we make a provisional diagnosis of psychotic disorder NOS and Ms. D is admitted involuntarily because of concerns about her safety. She is reluctant to accept any treatment and receives an involuntary probate commitment for 90 days. At admission, Ms. D is evasive, guarded, secretive, and at times hostile. Her physical examination reveals no signs or symptoms of focal neurologic deficits. Laboratory testing, including urine toxicology, is unremarkable. She refuses an MRI. Later testing reveals a critical ammonia level of 143 μg/dL, warranting an axis III diagnosis of asymptomatic hyperammonemia.
HISTORY: Paranoia and delusions
Ms. D says she was born and raised in a southern state. She reports that she was born to an Egyptian mother who died during childbirth; her father, who is white, was an ambassador stationed abroad. Ms. D attended school until the 11thgrade and was married at age 19 to a Secret Service agent. She says she has a son who was kidnapped by her husband’s enemies, rescued by paying ransom, and currently lives with his grandfather. Ms. D is paranoid and fears that her life is in danger. She also believes that she has gluten sensitivity that could discolor and damage her hair, which is why she always keeps a scarf on her head for protection.
Through an Internet search, we find articles about Ms. D’s son’s kidnapping. The 7-year-old had been missing for weeks when police found him with his mother in safe condition in another state, after Ms. D called her mother to ask for money and a place to stay. The child was taken from Ms. D’s custody because of concerns for his safety. We also find Ms. D’s mother. Although Ms. D insists her mother is deceased, after some persuasion, she signs a release allowing us to talk to her.
Ms. D’s mother reports that her daughter’s psychiatric problems began when she was pregnant. At the time Ms. D did not have a foreign accent. She had started to “talk funny” when her psychiatric symptoms emerged after she married and became pregnant.
Foreign accent syndrome
A foreign accent can be acquired by normal phenomena, such as being immersed in a foreign language, or a pathological process,1 which can include psychiatric (functional) or neurologic illness (organic causes). Foreign accent syndrome (FAS) is a rare speech disorder characterized by the appearance of a new accent, different from the speaker’s native language, that is perceived as foreign by the listener and in most cases also by the speaker.2 Usually an FAS patient has had no exposure to the accent, although in some cases an old accent has re-emerged.3,4
FAS can result from lesions in brain areas involved in speech production, including precentral gyrus, premotor mid-frontal gyrus, left subcortical prerolandic gyrus, postrolandic gyri, and left parietal area.4 Most FAS cases are secondary to a structural lesion in the brain caused by stroke, traumatic brain injury, cerebral hemorrhage, or multiple sclerosis.2 There are a few cases in the literature of acquired foreign accent with psychogenic etiology in patients with schizophrenia and bipolar disorder with psychotic features.5
TREATMENT: Combination therapy
Based on Ms. D’s unstable mood, irritability, delusional beliefs, and paranoid ideas, we start divalproex, 500 mg/d titrated to 1, 750 mg/d, and risperidone, 3 mg in the morning and 4 mg at bedtime.
The unit psychologist evaluates Ms. D and provides individual psychotherapy, which is mainly supportive and psychoeducational. Ms. D gradually becomes cooperative and friendly. She is not willing to talk about her accent or its origin; however, as her psychiatric symptoms improve, her accent gradually diminishes. The accent never completely resolves, but reduces until it is barely noticeable.
The authors’ observations
Ms. D’s foreign accent was more prominent when she displayed positive psychotic symptoms, such as delusions and disorganized thinking, and gradually disappeared as her psychotic symptoms improved. Ms. D’s case was peculiar because her accent was 1 of the first symptoms before her psychosis fully manifested.
How are FAS and psychosis linked?
Language dysfunction in schizophrenia is common and characterized by derailment and disorganization. Severity of language dysfunction in schizophrenia is directly proportional to overall disease severity.6,7 Various hypotheses have suggested the origin of FAS. In patients with FAS secondary to a neurologic disorder, a lesion usually is found in the dominant brain hemisphere, but the cause is not clear in patients with psychosis who have normal MRI findings. One hypothesis by Reeves et al links development of FAS to the functional disconnection between the left dorsolateral prefrontal cortex (DLPFC) and the superior temporal gyrus (STG) during active psychosis.5 In normal speech production, electric impulses originate in the DLPFC and are transmitted to STG in Wernicke’s area. From there, information goes to Broca’s area, which activates the primary motor cortex to pronounce words. In healthy individuals, word generation activates the DLPFC and causes deactivation of the bilateral STG.8 In schizophrenia, the left STG fails to deactivate in the presence of activation of the left DLPFC.9 Interestingly, STG dysfunction is seen only during active phase of psychosis. Its absence in asymptomatic patients with schizophrenia and bipolar disorder10,11 suggest that a foreign accent-like syndrome may be linked to the functional disconnection between the left DLPFC and left STG dysfunction in patients with active psychosis.5
Performing functional neuroimaging, including positron-emission tomography, functional MRI, and single-photon emission computed tomography, of patients with FAS could shed more light on the possible link between FAS and psychosis. In a case report of a patient with bipolar disorder who developed FAS, MRI initially showed no structural lesion but a later functional imaging scan revealed a cerebral infarct in the left insular and anterior temporal cortex.2
One of the limitations in Ms. D’s case is the lack of neuroimaging studies. For the first few weeks of her hospitalization, it was difficult to communicate with Ms. D. She did not acknowledge her illness and would not cooperate with treatment. She was withdrawn and seemed to experience hysterical mutism, which she perceived as caused by extreme food allergies. Later, as her symptoms continued to improve with pharmacologic and psychotherapeutic interventions, neuroimaging was no longer clinically necessary.
OUTCOME: Accent disappears
As Ms. D improves, psychotherapy evolves to gently and carefully challenging her delusions and providing insight-oriented interventions and trauma therapy. As her delusions gradually start to loosen, Ms. D reveals she had been physically and emotionally abused by her husband.
At discharge after 90 days in the hospital, Ms. D’s symptoms are well managed and she no longer shows signs of a thought disorder. Her thinking is clear, rational, and logical. She demonstrates incredible insight and appreciation that she needs to stay in treatment and continue to take divalproex and risperidone. Her delusions appear to be completely resolved and she is focused on reuniting with her son. Many of her previous delusions appear to be related to trauma and partly dissociative.
Ms. D contacts the psychologist several months later to report she is doing well in the community, staying in treatment, and working on legal means to reunite with her son. No trace of any foreign accent is detectable in her voice.
Related Resources
- Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? Journal of Neurolinguistics. 2006; 19: 385-409.
- Tsuruga K, Kobayashi T, Hirai N, et al. Foreign accent syndrome in a case of dissociative (conversion) disorder. Seishin Shinkeigaku Zasshi. 2008; 110(2): 79-87.
Drug Brand Names
- Benztropine • Cogentin
- Diphenhydramine • Benadryl
- Divalproex • Depakote
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Disruptive and withdrawn
Police bring Ms. D, age 33, to our psychiatric facility because of violent behavior at her group home. When confronted for allegedly stealing, she became upset, fought with a housemate, and spat. Six months before coming to our facility she was admitted to a private hospital for psychotic disorder, not otherwise specified (NOS) where she was mute, refused all food and medications, lay in her room, and covered her face with a sheet when someone tried to talk to her.
Ms. D denies having depressive symptoms, sleep disturbance, racing thoughts, thoughts of hurting herself or others, or auditory or visual hallucinations. She complains of poor appetite. Ms. D denies a history of mental illness and says she is not taking any medication. She is upset about being hospitalized and says she will not cooperate with treatment. We cannot obtain her complete psychiatric history but available records indicate that she has 1 previous psychiatric hospitalization for psychotic disorder NOS, and has received trials of haloperidol, lorazepam, diphenhydramine, escitalopram, ziprasidone, and benztropine. Her records do not indicate the dosages of these medications or how she responded to pharmacotherapy.
During her mental status exam, Ms. D is well dressed, covers her hair with a scarf, has no unusual body movements, and responds to questions appropriately. She describes her mood as “okay” but appears upset and anxious about being in the hospital. She exhibits no overt psychotic symptoms and does not appear to be responding to auditory hallucinations or having delusional thoughts. Her cognitive function is intact and her intelligence is judged to be average with impaired insight and judgment. However, she speaks with a distinct accent that sounds Jamaican; otherwise, her speech is articulate with normal rate and tone. When we ask about her accent, Ms. D, who is African American, does not disclose her ethnicity and seems to be unaware of her accent. We did not question the authenticity of her accent until after we obtained collateral information from her family.
The authors’ observations
Based on the available information, we make a provisional diagnosis of psychotic disorder NOS and Ms. D is admitted involuntarily because of concerns about her safety. She is reluctant to accept any treatment and receives an involuntary probate commitment for 90 days. At admission, Ms. D is evasive, guarded, secretive, and at times hostile. Her physical examination reveals no signs or symptoms of focal neurologic deficits. Laboratory testing, including urine toxicology, is unremarkable. She refuses an MRI. Later testing reveals a critical ammonia level of 143 μg/dL, warranting an axis III diagnosis of asymptomatic hyperammonemia.
HISTORY: Paranoia and delusions
Ms. D says she was born and raised in a southern state. She reports that she was born to an Egyptian mother who died during childbirth; her father, who is white, was an ambassador stationed abroad. Ms. D attended school until the 11thgrade and was married at age 19 to a Secret Service agent. She says she has a son who was kidnapped by her husband’s enemies, rescued by paying ransom, and currently lives with his grandfather. Ms. D is paranoid and fears that her life is in danger. She also believes that she has gluten sensitivity that could discolor and damage her hair, which is why she always keeps a scarf on her head for protection.
Through an Internet search, we find articles about Ms. D’s son’s kidnapping. The 7-year-old had been missing for weeks when police found him with his mother in safe condition in another state, after Ms. D called her mother to ask for money and a place to stay. The child was taken from Ms. D’s custody because of concerns for his safety. We also find Ms. D’s mother. Although Ms. D insists her mother is deceased, after some persuasion, she signs a release allowing us to talk to her.
Ms. D’s mother reports that her daughter’s psychiatric problems began when she was pregnant. At the time Ms. D did not have a foreign accent. She had started to “talk funny” when her psychiatric symptoms emerged after she married and became pregnant.
Foreign accent syndrome
A foreign accent can be acquired by normal phenomena, such as being immersed in a foreign language, or a pathological process,1 which can include psychiatric (functional) or neurologic illness (organic causes). Foreign accent syndrome (FAS) is a rare speech disorder characterized by the appearance of a new accent, different from the speaker’s native language, that is perceived as foreign by the listener and in most cases also by the speaker.2 Usually an FAS patient has had no exposure to the accent, although in some cases an old accent has re-emerged.3,4
FAS can result from lesions in brain areas involved in speech production, including precentral gyrus, premotor mid-frontal gyrus, left subcortical prerolandic gyrus, postrolandic gyri, and left parietal area.4 Most FAS cases are secondary to a structural lesion in the brain caused by stroke, traumatic brain injury, cerebral hemorrhage, or multiple sclerosis.2 There are a few cases in the literature of acquired foreign accent with psychogenic etiology in patients with schizophrenia and bipolar disorder with psychotic features.5
TREATMENT: Combination therapy
Based on Ms. D’s unstable mood, irritability, delusional beliefs, and paranoid ideas, we start divalproex, 500 mg/d titrated to 1, 750 mg/d, and risperidone, 3 mg in the morning and 4 mg at bedtime.
The unit psychologist evaluates Ms. D and provides individual psychotherapy, which is mainly supportive and psychoeducational. Ms. D gradually becomes cooperative and friendly. She is not willing to talk about her accent or its origin; however, as her psychiatric symptoms improve, her accent gradually diminishes. The accent never completely resolves, but reduces until it is barely noticeable.
The authors’ observations
Ms. D’s foreign accent was more prominent when she displayed positive psychotic symptoms, such as delusions and disorganized thinking, and gradually disappeared as her psychotic symptoms improved. Ms. D’s case was peculiar because her accent was 1 of the first symptoms before her psychosis fully manifested.
How are FAS and psychosis linked?
Language dysfunction in schizophrenia is common and characterized by derailment and disorganization. Severity of language dysfunction in schizophrenia is directly proportional to overall disease severity.6,7 Various hypotheses have suggested the origin of FAS. In patients with FAS secondary to a neurologic disorder, a lesion usually is found in the dominant brain hemisphere, but the cause is not clear in patients with psychosis who have normal MRI findings. One hypothesis by Reeves et al links development of FAS to the functional disconnection between the left dorsolateral prefrontal cortex (DLPFC) and the superior temporal gyrus (STG) during active psychosis.5 In normal speech production, electric impulses originate in the DLPFC and are transmitted to STG in Wernicke’s area. From there, information goes to Broca’s area, which activates the primary motor cortex to pronounce words. In healthy individuals, word generation activates the DLPFC and causes deactivation of the bilateral STG.8 In schizophrenia, the left STG fails to deactivate in the presence of activation of the left DLPFC.9 Interestingly, STG dysfunction is seen only during active phase of psychosis. Its absence in asymptomatic patients with schizophrenia and bipolar disorder10,11 suggest that a foreign accent-like syndrome may be linked to the functional disconnection between the left DLPFC and left STG dysfunction in patients with active psychosis.5
Performing functional neuroimaging, including positron-emission tomography, functional MRI, and single-photon emission computed tomography, of patients with FAS could shed more light on the possible link between FAS and psychosis. In a case report of a patient with bipolar disorder who developed FAS, MRI initially showed no structural lesion but a later functional imaging scan revealed a cerebral infarct in the left insular and anterior temporal cortex.2
One of the limitations in Ms. D’s case is the lack of neuroimaging studies. For the first few weeks of her hospitalization, it was difficult to communicate with Ms. D. She did not acknowledge her illness and would not cooperate with treatment. She was withdrawn and seemed to experience hysterical mutism, which she perceived as caused by extreme food allergies. Later, as her symptoms continued to improve with pharmacologic and psychotherapeutic interventions, neuroimaging was no longer clinically necessary.
OUTCOME: Accent disappears
As Ms. D improves, psychotherapy evolves to gently and carefully challenging her delusions and providing insight-oriented interventions and trauma therapy. As her delusions gradually start to loosen, Ms. D reveals she had been physically and emotionally abused by her husband.
At discharge after 90 days in the hospital, Ms. D’s symptoms are well managed and she no longer shows signs of a thought disorder. Her thinking is clear, rational, and logical. She demonstrates incredible insight and appreciation that she needs to stay in treatment and continue to take divalproex and risperidone. Her delusions appear to be completely resolved and she is focused on reuniting with her son. Many of her previous delusions appear to be related to trauma and partly dissociative.
Ms. D contacts the psychologist several months later to report she is doing well in the community, staying in treatment, and working on legal means to reunite with her son. No trace of any foreign accent is detectable in her voice.
Related Resources
- Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? Journal of Neurolinguistics. 2006; 19: 385-409.
- Tsuruga K, Kobayashi T, Hirai N, et al. Foreign accent syndrome in a case of dissociative (conversion) disorder. Seishin Shinkeigaku Zasshi. 2008; 110(2): 79-87.
Drug Brand Names
- Benztropine • Cogentin
- Diphenhydramine • Benadryl
- Divalproex • Depakote
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? J Neurolinguistics. 2006;19(5):385-409.
2. Poulin S, Macoir J, Paquet N, et al. Psychogenic or neurogenic origin of agrammatism and foreign accent syndrome in a bipolar patient: a case report. Ann Gen Psychiatry. 2007;6:1.-
3. Takayama Y, Sugishita M, Kido T, et al. A case of foreign accent syndrome without aphasia caused by a lesion of the left precentral gyrus. Neurology. 1993;43:1361-1363.
4. Roth EJ, Fink K, Cherney LR, et al. Reversion to a previously learned foreign accent after stroke. Arch Phys Med Rehabil. 1997;78:550-552.
5. Reeves RR, Burke RS, Parker JD. Characteristics of psychotic patients with foreign accent syndrome. J Neuropsychiatry Clin Neurosci. 2007;19:70-76.
6. Ceccherini-Nelli A, Crow TJ. Disintegration of the components of language as the path to a revision of Bleuler’s and Schneider’s concepts of schizophrenia: linguistic disturbances compared with first-rank symptoms in acute psychosis. Br J Psychiatry. 2003;182:233-240.
7. Harrow M, O’Connell EM, Herbener ES, et al. Disordered verbalizations in schizophrenia: a speech disturbance or thought disorder? Compr Psychiatry. 2003;44:353-359.
8. Friston KJ, Frith CD, Liddle PF, et al. Investigating a network of word generation with positron emission tomography. Proc R Soc Lond B Biol Sci. 1991;244:101-106.
9. Frith CD, Friston K, Herold S, et al. Regional brain activity in chronic schizophrenic patients during the performance of a verbal fluency task. Br J Psychiatry. 1995;167:343-349.
10. Spence SA, Liddle PF, Stefan MD, et al. Functional anatomy of verbal fluency in people with schizophrenia and those at genetic risk. Focal dysfunction and distributed disconnectivity reappraised. Br J Psychiatry. 2011;176:52-60.
11. Dye SM, Spence SA, Bench CJ, et al. No evidence for left superior temporal dysfunction in asymptomatic schizophrenia and bipolar disorder. PET study of verbal fluency. Br J Psychiatry. 1999;175:367-374.
1. Miller N, Lowit A, O’Sullivan H. What makes acquired foreign accent syndrome foreign? J Neurolinguistics. 2006;19(5):385-409.
2. Poulin S, Macoir J, Paquet N, et al. Psychogenic or neurogenic origin of agrammatism and foreign accent syndrome in a bipolar patient: a case report. Ann Gen Psychiatry. 2007;6:1.-
3. Takayama Y, Sugishita M, Kido T, et al. A case of foreign accent syndrome without aphasia caused by a lesion of the left precentral gyrus. Neurology. 1993;43:1361-1363.
4. Roth EJ, Fink K, Cherney LR, et al. Reversion to a previously learned foreign accent after stroke. Arch Phys Med Rehabil. 1997;78:550-552.
5. Reeves RR, Burke RS, Parker JD. Characteristics of psychotic patients with foreign accent syndrome. J Neuropsychiatry Clin Neurosci. 2007;19:70-76.
6. Ceccherini-Nelli A, Crow TJ. Disintegration of the components of language as the path to a revision of Bleuler’s and Schneider’s concepts of schizophrenia: linguistic disturbances compared with first-rank symptoms in acute psychosis. Br J Psychiatry. 2003;182:233-240.
7. Harrow M, O’Connell EM, Herbener ES, et al. Disordered verbalizations in schizophrenia: a speech disturbance or thought disorder? Compr Psychiatry. 2003;44:353-359.
8. Friston KJ, Frith CD, Liddle PF, et al. Investigating a network of word generation with positron emission tomography. Proc R Soc Lond B Biol Sci. 1991;244:101-106.
9. Frith CD, Friston K, Herold S, et al. Regional brain activity in chronic schizophrenic patients during the performance of a verbal fluency task. Br J Psychiatry. 1995;167:343-349.
10. Spence SA, Liddle PF, Stefan MD, et al. Functional anatomy of verbal fluency in people with schizophrenia and those at genetic risk. Focal dysfunction and distributed disconnectivity reappraised. Br J Psychiatry. 2011;176:52-60.
11. Dye SM, Spence SA, Bench CJ, et al. No evidence for left superior temporal dysfunction in asymptomatic schizophrenia and bipolar disorder. PET study of verbal fluency. Br J Psychiatry. 1999;175:367-374.
CT scan wasn’t ordered, diagnosis was delayed...Stroke symptoms blamed on food poisoning...
CT scan wasn’t ordered, diagnosis was delayed
A 9-YEAR-OLD BOY fell and hit the left side of his head on a coffee table while playing at a friend’s house. His father, who was present, applied ice to the child’s head and took him home. The child subsequently vomited and complained that his jaw hurt. He was given ibuprofen and taken to the emergency department (ED).
The ED physician determined that he needed stitches in his left ear. After the ear was sutured, the child was discharged, even though he had vomited in the examination room.
The child vomited again around midnight, then awoke around 2:30 am and went back to sleep. Around 5:00 am he vomited again and was gasping for air and breathing with difficulty. A call to 911 resulted in the child being airlifted to a trauma center, where a computed tomography (CT) scan revealed a massive hematoma. The brain was herniated and protruding from the bottom of the skull.
After undergoing emergency surgery, the patient spent 3 days in the ICU, some of that time on a ventilator, and several weeks in the hospital. After discharge, he underwent intensive therapy to relearn how to eat and talk. He suffered cognitive losses, emotional difficulties, left-sided weakness, and hemiparesis.
PLAINTIFF’S CLAIM The ED physician should have ordered a CT scan, which would have revealed the hematoma and prompted emergency surgery to relieve the pressure. The physician didn’t tell the parents how to observe the child for a head injury.
THE DEFENSE A CT scan wasn’t necessary. The patient appeared fine in the ED and was neurologically intact with a perfect Glasgow coma score of 15. Hematoma was a low possibility. The parents were told to watch the child and received head injury instructions.
VERDICT $2.4 million Ohio verdict.
COMMENT A variety of decision support tools would suggest CT in the face of vomiting 2 or more times, even with a Glasgow coma score of 15 (see the discussion of the Canadian CT Head Rule and New Orleans Criteria at http://guidelines.gov/content.aspx?id=136&search=neuroimaging+children+head+trauma). Clinical judgment alone may be insufficient to detect potentially catastrophic injury—particularly in younger children.
Stroke symptoms blamed on food poisoning
AN ISCHEMIC, LEFT-SIDED STROKE with left inferior frontoparietal lobe, occipital lobe, and cerebellar infarcts left a 33-year-old man with unclear speech, difficulty walking, major headache, and other stroke symptoms. He was taken by ambulance to a hospital within 1 hour of the onset of symptoms.
Hospital staff diagnosed food poisoning and discharged the man even though he couldn’t walk or speak coherently. The patient suffered brain damage resulting in cognitive impairment with memory loss and confusion.
PLAINTIFF’S CLAIM A proper neurologic work-up wasn’t done; hospital staff should have consulted a neurologist. The patient should have received tissue plasminogen activator (t-PA).
THE DEFENSE The history provided at the hospital mentioned that the patient had eaten chocolate cake before the onset of symptoms; the symptoms weren’t significant enough to consider stroke in the differential diagnosis. The plaintiff couldn’t prove that his condition would have been significantly better even if he’d received t-PA.
VERDICT $2.1 million California arbitration award.
COMMENT This story is difficult to believe—food poisoning causing trouble speaking, difficulty walking, and a headache?! One can only wonder whether better documentation of medical decision making would have produced a more understandable response.
CT scan wasn’t ordered, diagnosis was delayed
A 9-YEAR-OLD BOY fell and hit the left side of his head on a coffee table while playing at a friend’s house. His father, who was present, applied ice to the child’s head and took him home. The child subsequently vomited and complained that his jaw hurt. He was given ibuprofen and taken to the emergency department (ED).
The ED physician determined that he needed stitches in his left ear. After the ear was sutured, the child was discharged, even though he had vomited in the examination room.
The child vomited again around midnight, then awoke around 2:30 am and went back to sleep. Around 5:00 am he vomited again and was gasping for air and breathing with difficulty. A call to 911 resulted in the child being airlifted to a trauma center, where a computed tomography (CT) scan revealed a massive hematoma. The brain was herniated and protruding from the bottom of the skull.
After undergoing emergency surgery, the patient spent 3 days in the ICU, some of that time on a ventilator, and several weeks in the hospital. After discharge, he underwent intensive therapy to relearn how to eat and talk. He suffered cognitive losses, emotional difficulties, left-sided weakness, and hemiparesis.
PLAINTIFF’S CLAIM The ED physician should have ordered a CT scan, which would have revealed the hematoma and prompted emergency surgery to relieve the pressure. The physician didn’t tell the parents how to observe the child for a head injury.
THE DEFENSE A CT scan wasn’t necessary. The patient appeared fine in the ED and was neurologically intact with a perfect Glasgow coma score of 15. Hematoma was a low possibility. The parents were told to watch the child and received head injury instructions.
VERDICT $2.4 million Ohio verdict.
COMMENT A variety of decision support tools would suggest CT in the face of vomiting 2 or more times, even with a Glasgow coma score of 15 (see the discussion of the Canadian CT Head Rule and New Orleans Criteria at http://guidelines.gov/content.aspx?id=136&search=neuroimaging+children+head+trauma). Clinical judgment alone may be insufficient to detect potentially catastrophic injury—particularly in younger children.
Stroke symptoms blamed on food poisoning
AN ISCHEMIC, LEFT-SIDED STROKE with left inferior frontoparietal lobe, occipital lobe, and cerebellar infarcts left a 33-year-old man with unclear speech, difficulty walking, major headache, and other stroke symptoms. He was taken by ambulance to a hospital within 1 hour of the onset of symptoms.
Hospital staff diagnosed food poisoning and discharged the man even though he couldn’t walk or speak coherently. The patient suffered brain damage resulting in cognitive impairment with memory loss and confusion.
PLAINTIFF’S CLAIM A proper neurologic work-up wasn’t done; hospital staff should have consulted a neurologist. The patient should have received tissue plasminogen activator (t-PA).
THE DEFENSE The history provided at the hospital mentioned that the patient had eaten chocolate cake before the onset of symptoms; the symptoms weren’t significant enough to consider stroke in the differential diagnosis. The plaintiff couldn’t prove that his condition would have been significantly better even if he’d received t-PA.
VERDICT $2.1 million California arbitration award.
COMMENT This story is difficult to believe—food poisoning causing trouble speaking, difficulty walking, and a headache?! One can only wonder whether better documentation of medical decision making would have produced a more understandable response.
CT scan wasn’t ordered, diagnosis was delayed
A 9-YEAR-OLD BOY fell and hit the left side of his head on a coffee table while playing at a friend’s house. His father, who was present, applied ice to the child’s head and took him home. The child subsequently vomited and complained that his jaw hurt. He was given ibuprofen and taken to the emergency department (ED).
The ED physician determined that he needed stitches in his left ear. After the ear was sutured, the child was discharged, even though he had vomited in the examination room.
The child vomited again around midnight, then awoke around 2:30 am and went back to sleep. Around 5:00 am he vomited again and was gasping for air and breathing with difficulty. A call to 911 resulted in the child being airlifted to a trauma center, where a computed tomography (CT) scan revealed a massive hematoma. The brain was herniated and protruding from the bottom of the skull.
After undergoing emergency surgery, the patient spent 3 days in the ICU, some of that time on a ventilator, and several weeks in the hospital. After discharge, he underwent intensive therapy to relearn how to eat and talk. He suffered cognitive losses, emotional difficulties, left-sided weakness, and hemiparesis.
PLAINTIFF’S CLAIM The ED physician should have ordered a CT scan, which would have revealed the hematoma and prompted emergency surgery to relieve the pressure. The physician didn’t tell the parents how to observe the child for a head injury.
THE DEFENSE A CT scan wasn’t necessary. The patient appeared fine in the ED and was neurologically intact with a perfect Glasgow coma score of 15. Hematoma was a low possibility. The parents were told to watch the child and received head injury instructions.
VERDICT $2.4 million Ohio verdict.
COMMENT A variety of decision support tools would suggest CT in the face of vomiting 2 or more times, even with a Glasgow coma score of 15 (see the discussion of the Canadian CT Head Rule and New Orleans Criteria at http://guidelines.gov/content.aspx?id=136&search=neuroimaging+children+head+trauma). Clinical judgment alone may be insufficient to detect potentially catastrophic injury—particularly in younger children.
Stroke symptoms blamed on food poisoning
AN ISCHEMIC, LEFT-SIDED STROKE with left inferior frontoparietal lobe, occipital lobe, and cerebellar infarcts left a 33-year-old man with unclear speech, difficulty walking, major headache, and other stroke symptoms. He was taken by ambulance to a hospital within 1 hour of the onset of symptoms.
Hospital staff diagnosed food poisoning and discharged the man even though he couldn’t walk or speak coherently. The patient suffered brain damage resulting in cognitive impairment with memory loss and confusion.
PLAINTIFF’S CLAIM A proper neurologic work-up wasn’t done; hospital staff should have consulted a neurologist. The patient should have received tissue plasminogen activator (t-PA).
THE DEFENSE The history provided at the hospital mentioned that the patient had eaten chocolate cake before the onset of symptoms; the symptoms weren’t significant enough to consider stroke in the differential diagnosis. The plaintiff couldn’t prove that his condition would have been significantly better even if he’d received t-PA.
VERDICT $2.1 million California arbitration award.
COMMENT This story is difficult to believe—food poisoning causing trouble speaking, difficulty walking, and a headache?! One can only wonder whether better documentation of medical decision making would have produced a more understandable response.
CDC update: Guidelines for treating STDs
In 2010, the CDC released an update of its Sexually Transmitted Diseases (STD) Treatment Guidelines,1 which were last updated in 2006. The guidelines are widely viewed as the most authoritative source of information on the diagnosis, treatment, and follow-up of STDs, and they are the standard for publicly and privately funded clinics focusing on sexual health.
What’s new
Some of the notable changes made since the last update in 2006 appear in TABLE 1.1,2
Uncomplicated gonorrhea. Cephalosporins are the only class of antibiotic recommended as first-line treatment for gonorrhea. (In a 2007 recommendation revision, the CDC opted to no longer recommend quinolone antibiotics for the treatment of gonorrhea, because of widespread bacterial resistance.3) Preference is now given to ceftriaxone because of its proven effectiveness against pharyngeal infection, which is often asymptomatic, difficult to detect, and difficult to eradicate. Additionally, the 2010 update has increased the recommended dose of ceftriazone from 125 to 250 mg intramuscularly. The larger dose is more effective against pharyngeal infection; it is also a safeguard against decreased bacterial susceptibility to cephalosporins, which, although still very low, has been reported in more cases recently.
The guidelines still recommend that azithromycin, 1 g orally in a single dose, be given with ceftriaxone because of the relatively high rate of co-infection with Chlamydia trachomatis and the potential for azithromycin to assist with eradicating any gonorrhea with decreased susceptibility to ceftriaxone.
Pelvic inflammatory disease. Quinolones have also been removed from the list of options for outpatient treatment of pelvic inflammatory disease. All recommended regimens now specify a parenteral cephalosporin as a single injection with doxycycline 100 mg PO twice a day for 14 days, with or without metronidazole 500 mg PO twice a day for 14 days.
Bacterial vaginosis. Tinidazole, 2 g orally once a day for 2 days or 1 g orally once a day for 5 days, is now an alternative agent for bacterial vaginosis. However, preferred treatments remain metronidazole 500 mg orally twice a day for 7 days, metronidazole gel intravaginally once a day for 5 days, or clindamycin cream intravaginally at bedtime for 7 days.
Newborn gonococcal eye infection. A relatively minor change is the elimination of tetracycline as prophylaxis for newborn gonococcal eye infections, leaving only erythromycin ointment to prevent the condition.
TABLE 1
2010 vs 2006: How have the CDC recommendations for STD treatment changed?1,2
Uncomplicated gonococcal infections of the cervix, urethra, rectum, and pharynx
|
| Pelvic inflammatory disease Parenteral regimens
|
Bacterial vaginosis
|
Prophylaxis for gonococcal eye infection in a newborn
|
Single-dose therapy preferred among equivalent options
Single-dose therapy (TABLE 2), while often more expensive than other options, increases compliance and helps ensure treatment completion. Single-dose therapy administered in your office is essentially directly observed treatment, an intervention that has become the standard of care for other diseases such as tuberculosis. If the single-dose agent is as effective as alternative medications, directly observed on-site administration is the preferred option for treating STDs.
TABLE 2
Single-dose therapies for specific STDs1
| Infection or condition | Single-dose therapy |
|---|---|
| Candida | Miconazole 1200 mg vaginal suppository or Tioconazole 6.5% ointment 5 g intravaginally or Butoconazole 2% cream 5 g intravaginally or Fluconazole 150 mg PO |
| Cervicitis | Azithromycin 1 g PO |
| Chancroid | Azithromycin 1 g PO or Ceftriaxone 250 mg IM |
| Chlamydia urogenital infection | Azithromycin 1 g PO |
| Gonorrhea: conjunctivitis | Ceftriaxone 1 g IM |
| Gonorrhea: uncomplicated infection of the cervix, urethra, rectum | Ceftriaxone 250 mg IM (preferred) or Cefixime 400 mg PO or Single-dose injectable cephalosporin plus Azithromycin 1 g PO |
| Gonorrhea: uncomplicated infection of the pharynx | Ceftriaxone 250 mg IM plus Azithromycin 1 g PO |
| Nongonococcal urethritis | Azithromycin 1 g PO |
| Post-sexual assault prophylaxis | Ceftriaxone 250 mg IM or Cefixime 400 mg PO plus Metronidazole 2 g PO plus Azithromycin 1 g PO |
| Recurrent, persistent nongonococcal urethritis | Metronidazole 2 g PO or Tinidazole 2 g PO plus Azithromycin 1 g PO (if not used for initial episode) |
| Syphilis: primary, secondary, and early latent | Benzathine penicillin G 2.4 million units IM |
| Trichomoniasis | Metronidazole 2 g PO or Tinidazole 2 g PO |
Other guideline recommendations
The CDC’s STD treatment guidelines contain a wealth of useful information beyond treatment advice: recommended methods of confirming diagnoses, analyses of the usefulness of various diagnostic tests, recommendations on how to manage sex partners of those infected, guidance on STD prevention counseling, and considerations for special populations and circumstances.
Additionally, there is a section on screening for STDs reflecting recommendations of the US Preventive Services Task Force (USPSTF); it also includes recommendations from the American College of Obstetricians and Gynecologists. In at least one instance, though, the USPSTF recommendation on screening for HIV infection contradicts other CDC sources.4,5 Also included is guidance on using vaccines to prevent hepatitis A, hepatitis B, and human papillomavirus (HPV), which follows the recommendations of the Advisory Committee on Immunization Practices. When to use DNA testing to detect HPV is described briefly.
A shortcoming of the CDC guidelines
Although the CDC’s STD guidelines remain the most authoritative source of information on the diagnosis and treatment of STDs, they do not seem to use a consistent method for assessing and describing the strength of the evidence behind the recommendations, which family physicians have come to expect. (However, it is sometimes possible to discern the type and strength of evidence for a particular recommendation from the written discussion.)
The new guidelines state that a series of papers to be published in Clinical Infectious Diseases will describe more fully the evidence behind some of the recommendations and include evidence tables. However, in future guideline updates, it would be helpful if the CDC were to include a brief description of the quantity and strength of evidence alongside each recommended treatment option in the tables.
How best to keep up to date
Although the new guidelines summarize the current status of recommendations on the diagnosis, treatment, and prevention of STDs and are a useful resource for family physicians, we cannot stay current simply by referring to them alone over the next 4 to 5 years until a new edition is published. As new evidence develops, changes in recommendations will be published in the Morbidity and Mortality Weekly Report.
Case in point: new interim HIV recommendations. Interim recommendations were recently released on pre-exposure prophylaxis for men who have sex with men.6 (For more on these recommendations, check out this month’s audiocast at jfponline.com.) Final recommendations are expected later this year. Recommendations for post-exposure prophylaxis to prevent HIV infection are also expected soon.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Centers for Disease Control and Prevention, Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55(RR-11):1-94.
3. Campos-Outcalt D. Practice alert: CDC no longer recommends quinolones for treatment of gonorrhea. J Fam Pract. 2007;56:554-558.
4. Branson BM, Handsfield HH, Lampe MA, et al. for the Centers for Disease Control and Prevention (CDC). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17.
5. Campos-Outcalt D. Time to revise your HIV testing routine. J Fam Pract. 2007;56:283-284.
6. Centers for Disease Control and Prevention (CDC). Interim guidance: preexposure prophylaxis for the prevention of HIV infection in men who have sex with men. MMWR Morb Mortal Wkly Rep. 2011;60:65-68.
| New CDC guidance on pre-exposure HIV prophylaxis for men who have sex with men Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
dougco@u.arizona.edu
| New CDC guidance on pre-exposure HIV prophylaxis for men who have sex with men Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
dougco@u.arizona.edu
| New CDC guidance on pre-exposure HIV prophylaxis for men who have sex with men Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
dougco@u.arizona.edu
In 2010, the CDC released an update of its Sexually Transmitted Diseases (STD) Treatment Guidelines,1 which were last updated in 2006. The guidelines are widely viewed as the most authoritative source of information on the diagnosis, treatment, and follow-up of STDs, and they are the standard for publicly and privately funded clinics focusing on sexual health.
What’s new
Some of the notable changes made since the last update in 2006 appear in TABLE 1.1,2
Uncomplicated gonorrhea. Cephalosporins are the only class of antibiotic recommended as first-line treatment for gonorrhea. (In a 2007 recommendation revision, the CDC opted to no longer recommend quinolone antibiotics for the treatment of gonorrhea, because of widespread bacterial resistance.3) Preference is now given to ceftriaxone because of its proven effectiveness against pharyngeal infection, which is often asymptomatic, difficult to detect, and difficult to eradicate. Additionally, the 2010 update has increased the recommended dose of ceftriazone from 125 to 250 mg intramuscularly. The larger dose is more effective against pharyngeal infection; it is also a safeguard against decreased bacterial susceptibility to cephalosporins, which, although still very low, has been reported in more cases recently.
The guidelines still recommend that azithromycin, 1 g orally in a single dose, be given with ceftriaxone because of the relatively high rate of co-infection with Chlamydia trachomatis and the potential for azithromycin to assist with eradicating any gonorrhea with decreased susceptibility to ceftriaxone.
Pelvic inflammatory disease. Quinolones have also been removed from the list of options for outpatient treatment of pelvic inflammatory disease. All recommended regimens now specify a parenteral cephalosporin as a single injection with doxycycline 100 mg PO twice a day for 14 days, with or without metronidazole 500 mg PO twice a day for 14 days.
Bacterial vaginosis. Tinidazole, 2 g orally once a day for 2 days or 1 g orally once a day for 5 days, is now an alternative agent for bacterial vaginosis. However, preferred treatments remain metronidazole 500 mg orally twice a day for 7 days, metronidazole gel intravaginally once a day for 5 days, or clindamycin cream intravaginally at bedtime for 7 days.
Newborn gonococcal eye infection. A relatively minor change is the elimination of tetracycline as prophylaxis for newborn gonococcal eye infections, leaving only erythromycin ointment to prevent the condition.
TABLE 1
2010 vs 2006: How have the CDC recommendations for STD treatment changed?1,2
Uncomplicated gonococcal infections of the cervix, urethra, rectum, and pharynx
|
| Pelvic inflammatory disease Parenteral regimens
|
Bacterial vaginosis
|
Prophylaxis for gonococcal eye infection in a newborn
|
Single-dose therapy preferred among equivalent options
Single-dose therapy (TABLE 2), while often more expensive than other options, increases compliance and helps ensure treatment completion. Single-dose therapy administered in your office is essentially directly observed treatment, an intervention that has become the standard of care for other diseases such as tuberculosis. If the single-dose agent is as effective as alternative medications, directly observed on-site administration is the preferred option for treating STDs.
TABLE 2
Single-dose therapies for specific STDs1
| Infection or condition | Single-dose therapy |
|---|---|
| Candida | Miconazole 1200 mg vaginal suppository or Tioconazole 6.5% ointment 5 g intravaginally or Butoconazole 2% cream 5 g intravaginally or Fluconazole 150 mg PO |
| Cervicitis | Azithromycin 1 g PO |
| Chancroid | Azithromycin 1 g PO or Ceftriaxone 250 mg IM |
| Chlamydia urogenital infection | Azithromycin 1 g PO |
| Gonorrhea: conjunctivitis | Ceftriaxone 1 g IM |
| Gonorrhea: uncomplicated infection of the cervix, urethra, rectum | Ceftriaxone 250 mg IM (preferred) or Cefixime 400 mg PO or Single-dose injectable cephalosporin plus Azithromycin 1 g PO |
| Gonorrhea: uncomplicated infection of the pharynx | Ceftriaxone 250 mg IM plus Azithromycin 1 g PO |
| Nongonococcal urethritis | Azithromycin 1 g PO |
| Post-sexual assault prophylaxis | Ceftriaxone 250 mg IM or Cefixime 400 mg PO plus Metronidazole 2 g PO plus Azithromycin 1 g PO |
| Recurrent, persistent nongonococcal urethritis | Metronidazole 2 g PO or Tinidazole 2 g PO plus Azithromycin 1 g PO (if not used for initial episode) |
| Syphilis: primary, secondary, and early latent | Benzathine penicillin G 2.4 million units IM |
| Trichomoniasis | Metronidazole 2 g PO or Tinidazole 2 g PO |
Other guideline recommendations
The CDC’s STD treatment guidelines contain a wealth of useful information beyond treatment advice: recommended methods of confirming diagnoses, analyses of the usefulness of various diagnostic tests, recommendations on how to manage sex partners of those infected, guidance on STD prevention counseling, and considerations for special populations and circumstances.
Additionally, there is a section on screening for STDs reflecting recommendations of the US Preventive Services Task Force (USPSTF); it also includes recommendations from the American College of Obstetricians and Gynecologists. In at least one instance, though, the USPSTF recommendation on screening for HIV infection contradicts other CDC sources.4,5 Also included is guidance on using vaccines to prevent hepatitis A, hepatitis B, and human papillomavirus (HPV), which follows the recommendations of the Advisory Committee on Immunization Practices. When to use DNA testing to detect HPV is described briefly.
A shortcoming of the CDC guidelines
Although the CDC’s STD guidelines remain the most authoritative source of information on the diagnosis and treatment of STDs, they do not seem to use a consistent method for assessing and describing the strength of the evidence behind the recommendations, which family physicians have come to expect. (However, it is sometimes possible to discern the type and strength of evidence for a particular recommendation from the written discussion.)
The new guidelines state that a series of papers to be published in Clinical Infectious Diseases will describe more fully the evidence behind some of the recommendations and include evidence tables. However, in future guideline updates, it would be helpful if the CDC were to include a brief description of the quantity and strength of evidence alongside each recommended treatment option in the tables.
How best to keep up to date
Although the new guidelines summarize the current status of recommendations on the diagnosis, treatment, and prevention of STDs and are a useful resource for family physicians, we cannot stay current simply by referring to them alone over the next 4 to 5 years until a new edition is published. As new evidence develops, changes in recommendations will be published in the Morbidity and Mortality Weekly Report.
Case in point: new interim HIV recommendations. Interim recommendations were recently released on pre-exposure prophylaxis for men who have sex with men.6 (For more on these recommendations, check out this month’s audiocast at jfponline.com.) Final recommendations are expected later this year. Recommendations for post-exposure prophylaxis to prevent HIV infection are also expected soon.
In 2010, the CDC released an update of its Sexually Transmitted Diseases (STD) Treatment Guidelines,1 which were last updated in 2006. The guidelines are widely viewed as the most authoritative source of information on the diagnosis, treatment, and follow-up of STDs, and they are the standard for publicly and privately funded clinics focusing on sexual health.
What’s new
Some of the notable changes made since the last update in 2006 appear in TABLE 1.1,2
Uncomplicated gonorrhea. Cephalosporins are the only class of antibiotic recommended as first-line treatment for gonorrhea. (In a 2007 recommendation revision, the CDC opted to no longer recommend quinolone antibiotics for the treatment of gonorrhea, because of widespread bacterial resistance.3) Preference is now given to ceftriaxone because of its proven effectiveness against pharyngeal infection, which is often asymptomatic, difficult to detect, and difficult to eradicate. Additionally, the 2010 update has increased the recommended dose of ceftriazone from 125 to 250 mg intramuscularly. The larger dose is more effective against pharyngeal infection; it is also a safeguard against decreased bacterial susceptibility to cephalosporins, which, although still very low, has been reported in more cases recently.
The guidelines still recommend that azithromycin, 1 g orally in a single dose, be given with ceftriaxone because of the relatively high rate of co-infection with Chlamydia trachomatis and the potential for azithromycin to assist with eradicating any gonorrhea with decreased susceptibility to ceftriaxone.
Pelvic inflammatory disease. Quinolones have also been removed from the list of options for outpatient treatment of pelvic inflammatory disease. All recommended regimens now specify a parenteral cephalosporin as a single injection with doxycycline 100 mg PO twice a day for 14 days, with or without metronidazole 500 mg PO twice a day for 14 days.
Bacterial vaginosis. Tinidazole, 2 g orally once a day for 2 days or 1 g orally once a day for 5 days, is now an alternative agent for bacterial vaginosis. However, preferred treatments remain metronidazole 500 mg orally twice a day for 7 days, metronidazole gel intravaginally once a day for 5 days, or clindamycin cream intravaginally at bedtime for 7 days.
Newborn gonococcal eye infection. A relatively minor change is the elimination of tetracycline as prophylaxis for newborn gonococcal eye infections, leaving only erythromycin ointment to prevent the condition.
TABLE 1
2010 vs 2006: How have the CDC recommendations for STD treatment changed?1,2
Uncomplicated gonococcal infections of the cervix, urethra, rectum, and pharynx
|
| Pelvic inflammatory disease Parenteral regimens
|
Bacterial vaginosis
|
Prophylaxis for gonococcal eye infection in a newborn
|
Single-dose therapy preferred among equivalent options
Single-dose therapy (TABLE 2), while often more expensive than other options, increases compliance and helps ensure treatment completion. Single-dose therapy administered in your office is essentially directly observed treatment, an intervention that has become the standard of care for other diseases such as tuberculosis. If the single-dose agent is as effective as alternative medications, directly observed on-site administration is the preferred option for treating STDs.
TABLE 2
Single-dose therapies for specific STDs1
| Infection or condition | Single-dose therapy |
|---|---|
| Candida | Miconazole 1200 mg vaginal suppository or Tioconazole 6.5% ointment 5 g intravaginally or Butoconazole 2% cream 5 g intravaginally or Fluconazole 150 mg PO |
| Cervicitis | Azithromycin 1 g PO |
| Chancroid | Azithromycin 1 g PO or Ceftriaxone 250 mg IM |
| Chlamydia urogenital infection | Azithromycin 1 g PO |
| Gonorrhea: conjunctivitis | Ceftriaxone 1 g IM |
| Gonorrhea: uncomplicated infection of the cervix, urethra, rectum | Ceftriaxone 250 mg IM (preferred) or Cefixime 400 mg PO or Single-dose injectable cephalosporin plus Azithromycin 1 g PO |
| Gonorrhea: uncomplicated infection of the pharynx | Ceftriaxone 250 mg IM plus Azithromycin 1 g PO |
| Nongonococcal urethritis | Azithromycin 1 g PO |
| Post-sexual assault prophylaxis | Ceftriaxone 250 mg IM or Cefixime 400 mg PO plus Metronidazole 2 g PO plus Azithromycin 1 g PO |
| Recurrent, persistent nongonococcal urethritis | Metronidazole 2 g PO or Tinidazole 2 g PO plus Azithromycin 1 g PO (if not used for initial episode) |
| Syphilis: primary, secondary, and early latent | Benzathine penicillin G 2.4 million units IM |
| Trichomoniasis | Metronidazole 2 g PO or Tinidazole 2 g PO |
Other guideline recommendations
The CDC’s STD treatment guidelines contain a wealth of useful information beyond treatment advice: recommended methods of confirming diagnoses, analyses of the usefulness of various diagnostic tests, recommendations on how to manage sex partners of those infected, guidance on STD prevention counseling, and considerations for special populations and circumstances.
Additionally, there is a section on screening for STDs reflecting recommendations of the US Preventive Services Task Force (USPSTF); it also includes recommendations from the American College of Obstetricians and Gynecologists. In at least one instance, though, the USPSTF recommendation on screening for HIV infection contradicts other CDC sources.4,5 Also included is guidance on using vaccines to prevent hepatitis A, hepatitis B, and human papillomavirus (HPV), which follows the recommendations of the Advisory Committee on Immunization Practices. When to use DNA testing to detect HPV is described briefly.
A shortcoming of the CDC guidelines
Although the CDC’s STD guidelines remain the most authoritative source of information on the diagnosis and treatment of STDs, they do not seem to use a consistent method for assessing and describing the strength of the evidence behind the recommendations, which family physicians have come to expect. (However, it is sometimes possible to discern the type and strength of evidence for a particular recommendation from the written discussion.)
The new guidelines state that a series of papers to be published in Clinical Infectious Diseases will describe more fully the evidence behind some of the recommendations and include evidence tables. However, in future guideline updates, it would be helpful if the CDC were to include a brief description of the quantity and strength of evidence alongside each recommended treatment option in the tables.
How best to keep up to date
Although the new guidelines summarize the current status of recommendations on the diagnosis, treatment, and prevention of STDs and are a useful resource for family physicians, we cannot stay current simply by referring to them alone over the next 4 to 5 years until a new edition is published. As new evidence develops, changes in recommendations will be published in the Morbidity and Mortality Weekly Report.
Case in point: new interim HIV recommendations. Interim recommendations were recently released on pre-exposure prophylaxis for men who have sex with men.6 (For more on these recommendations, check out this month’s audiocast at jfponline.com.) Final recommendations are expected later this year. Recommendations for post-exposure prophylaxis to prevent HIV infection are also expected soon.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Centers for Disease Control and Prevention, Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55(RR-11):1-94.
3. Campos-Outcalt D. Practice alert: CDC no longer recommends quinolones for treatment of gonorrhea. J Fam Pract. 2007;56:554-558.
4. Branson BM, Handsfield HH, Lampe MA, et al. for the Centers for Disease Control and Prevention (CDC). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17.
5. Campos-Outcalt D. Time to revise your HIV testing routine. J Fam Pract. 2007;56:283-284.
6. Centers for Disease Control and Prevention (CDC). Interim guidance: preexposure prophylaxis for the prevention of HIV infection in men who have sex with men. MMWR Morb Mortal Wkly Rep. 2011;60:65-68.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Centers for Disease Control and Prevention, Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55(RR-11):1-94.
3. Campos-Outcalt D. Practice alert: CDC no longer recommends quinolones for treatment of gonorrhea. J Fam Pract. 2007;56:554-558.
4. Branson BM, Handsfield HH, Lampe MA, et al. for the Centers for Disease Control and Prevention (CDC). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17.
5. Campos-Outcalt D. Time to revise your HIV testing routine. J Fam Pract. 2007;56:283-284.
6. Centers for Disease Control and Prevention (CDC). Interim guidance: preexposure prophylaxis for the prevention of HIV infection in men who have sex with men. MMWR Morb Mortal Wkly Rep. 2011;60:65-68.
Urine drug testing: An unproven risk management tool?
As a member of the editorial board of the Journal of Pain & Palliative Care Pharmacotherapy, an author of numerous scholarly articles about chronic pain (some of which are cited here), and a person who lives with chronic pain, I would like to comment on “Is it time to drug test your chronic pain patient?” (J Fam Pract. 2010;59:628-633). Drs. McBane and Weigle recommend the use of pain agreements and drug testing for every patient with noncancer chronic pain, but fail to mention that there is insufficient evidence of the efficacy of both adherence monitoring tools.1 In addition, a recent article in The American Journal of Bioethics recommends against the “universal application of pain agreements” and suggests that they can harm the patient/physician relationship.2 Consent for drug testing often comes from the pain contract3—agreements that have been called “unconscionable adhesion contracts” and may be unenforceable.4
The authors also suggest that urine drug testing is noninvasive. Nothing could be further from the truth. Drug testing of people with pain may be considered a suspicionless and warrantless search of bodily fluids and in certain cases may be unconstitutional.5 There is no question that drug misuse, abuse, addiction, and overdose are devastating to individuals, families, and society. However, using unproven risk management tools that may cause greater harm than good is just bad medicine.
Mark Collen
Sacramento, Calif
1. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
2. Payne R, Anderson E, Arnold R, et al. A rose by any other name: pain contracts/agreements. Am J Bioeth. 2010;10:5-12.
3. Collen M. Analysis of controlled substance agreements from private practice physicians. J Pain Palliat Care Pharmacother. 2009;23:357-364.
4. Collen M. Opioid contracts and random drug testing for people with chronic pain—think twice. J Law Med Ethics. 2009;37:841-845.
5. Collen M. The Fourth Amendment and random drug testing of people with chronic pain. J Pain Palliat Care Pharmacother. 2011;25:in press.
As a member of the editorial board of the Journal of Pain & Palliative Care Pharmacotherapy, an author of numerous scholarly articles about chronic pain (some of which are cited here), and a person who lives with chronic pain, I would like to comment on “Is it time to drug test your chronic pain patient?” (J Fam Pract. 2010;59:628-633). Drs. McBane and Weigle recommend the use of pain agreements and drug testing for every patient with noncancer chronic pain, but fail to mention that there is insufficient evidence of the efficacy of both adherence monitoring tools.1 In addition, a recent article in The American Journal of Bioethics recommends against the “universal application of pain agreements” and suggests that they can harm the patient/physician relationship.2 Consent for drug testing often comes from the pain contract3—agreements that have been called “unconscionable adhesion contracts” and may be unenforceable.4
The authors also suggest that urine drug testing is noninvasive. Nothing could be further from the truth. Drug testing of people with pain may be considered a suspicionless and warrantless search of bodily fluids and in certain cases may be unconstitutional.5 There is no question that drug misuse, abuse, addiction, and overdose are devastating to individuals, families, and society. However, using unproven risk management tools that may cause greater harm than good is just bad medicine.
Mark Collen
Sacramento, Calif
As a member of the editorial board of the Journal of Pain & Palliative Care Pharmacotherapy, an author of numerous scholarly articles about chronic pain (some of which are cited here), and a person who lives with chronic pain, I would like to comment on “Is it time to drug test your chronic pain patient?” (J Fam Pract. 2010;59:628-633). Drs. McBane and Weigle recommend the use of pain agreements and drug testing for every patient with noncancer chronic pain, but fail to mention that there is insufficient evidence of the efficacy of both adherence monitoring tools.1 In addition, a recent article in The American Journal of Bioethics recommends against the “universal application of pain agreements” and suggests that they can harm the patient/physician relationship.2 Consent for drug testing often comes from the pain contract3—agreements that have been called “unconscionable adhesion contracts” and may be unenforceable.4
The authors also suggest that urine drug testing is noninvasive. Nothing could be further from the truth. Drug testing of people with pain may be considered a suspicionless and warrantless search of bodily fluids and in certain cases may be unconstitutional.5 There is no question that drug misuse, abuse, addiction, and overdose are devastating to individuals, families, and society. However, using unproven risk management tools that may cause greater harm than good is just bad medicine.
Mark Collen
Sacramento, Calif
1. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
2. Payne R, Anderson E, Arnold R, et al. A rose by any other name: pain contracts/agreements. Am J Bioeth. 2010;10:5-12.
3. Collen M. Analysis of controlled substance agreements from private practice physicians. J Pain Palliat Care Pharmacother. 2009;23:357-364.
4. Collen M. Opioid contracts and random drug testing for people with chronic pain—think twice. J Law Med Ethics. 2009;37:841-845.
5. Collen M. The Fourth Amendment and random drug testing of people with chronic pain. J Pain Palliat Care Pharmacother. 2011;25:in press.
1. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
2. Payne R, Anderson E, Arnold R, et al. A rose by any other name: pain contracts/agreements. Am J Bioeth. 2010;10:5-12.
3. Collen M. Analysis of controlled substance agreements from private practice physicians. J Pain Palliat Care Pharmacother. 2009;23:357-364.
4. Collen M. Opioid contracts and random drug testing for people with chronic pain—think twice. J Law Med Ethics. 2009;37:841-845.
5. Collen M. The Fourth Amendment and random drug testing of people with chronic pain. J Pain Palliat Care Pharmacother. 2011;25:in press.
Diffuse abdominal pain, vomiting
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission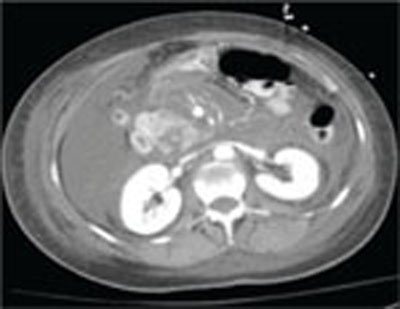
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
How best to diagnose asthma in infants and toddlers?
NO RELIABLE WAY EXISTS TO DIAGNOSE ASTHMA IN INFANTS AND TODDLERS. Recurrent wheezing, especially apart from colds, combined with physician-diagnosed eczema or atopic dermatitis, eosinophilia, and a parental history of asthma, increase the probability of a subsequent asthma diagnosis in the absence of other causes (strength of recommendation: B, 2 good-quality cohort studies).
Evidence summary
Wheezing in children is common and the differential diagnosis is broad. The many potential causes include upper respiratory infection, asthma, cystic fibrosis, foreign body aspiration, vascular ring, tracheomalacia, primary immunodeficiency, and congenital heart disease.1
Outpatient primary care cohort studies estimate that about half of children wheeze before they reach school age. Only one-third of children who wheeze during the first 3 years of life, however, continue to wheeze into later childhood and young adulthood.2-4
These findings have led some experts to suggest that not all wheezing in children is asthma and that asthma exists in variant forms.5-7 Variant wheezing patterns include transient early wheezing, which seems to be most prevalent in the first 3 years of life; wheezing without atopy, which occurs most often at 3 to 6 years of age; and wheezing with immunoglobulin E-associated atopy, which gradually increases in prevalence from birth and dominates in the over-6 age group. It is children in this last group whom we generally consider to have asthma.
Objective measures of lung function are challenging to perform in young children. Clinical signs and symptoms thus suggest the diagnosis of asthma.
Atopy, rhinitis, and eczema most often accompany persistent wheezing
Primary care cohort studies provide the best available evidence on which findings in infants and toddlers most likely predict persistent airway disease in childhood. A whole-population cohort study followed nearly all children born on the Isle of Wight from January 1989 through February 1990 to evaluate the natural history of childhood wheezing and to study associated risk factors.8 Children were seen at birth and at 1, 2, 4, and 10 years of age.
Findings most associated with current wheezing (within the last year) in 10-year-olds were atopy (odds ratio [OR]=4.38; 95% confidence interval [CI], 3.07-6.25), rhinitis (OR=3.72; 95% CI, 2.21-6.27), and eczema (OR=3.04; 95% CI, 2.05-4.51).8
An index to predict asthma
Since 1980, the Tucson Children’s Respiratory Study has followed 1246 healthy newborns seen by pediatricians affiliated with a large HMO in Tucson, Arizona. Questionnaires about parental asthma history and prenatal smoking history were obtained at enrollment. Childhood wheezing and its frequency, as well as physician-diagnosed allergies or asthma, were assessed at ages 2 and 3. If the child had wheezed in the past year, then the child was considered to be an “early wheezer.” If the frequency was 3 or more on a 5-point scale, then the child was considered to be an “early frequent wheezer.” Questionnaires were re-administered at ages 6, 8, 11, and 13. Three episodes of wheezing within the past year or a physician diagnosis of asthma with symptoms in the past year was considered “active asthma.” Blood specimens for eosinophils were obtained at age 10.
Using these data, the researchers developed stringent and loose criteria (TABLE 1) and odds ratios (TABLES 2 and 3) for childhood factors most predictive of an asthma diagnosis at an older age. The findings of the study may help clinicians care for wheezing infants and toddlers.9
TABLE 1
A clinical index of asthma risk9*
| Major criteria | Minor criteria |
|---|---|
| Parental asthma (history of physician diagnosis of asthma in a parent) | Allergic rhinitis (physician diagnosis of allergic rhinitis as reported in questionnaires at ages 2 or 3 y) |
| Eczema (physician diagnosis of atopic dermatitis as reported in questionnaires at ages 2 or 3 y) | Wheezing apart from colds |
| Eosinophilia (≥4%) | |
| *Stringent index for predicting asthma: Child has early, frequent wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. Loose index for predicting asthma: Child has early wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. | |
TABLE 2
Likelihood of active asthma predicted by stringent index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 9.8 (5.6-17.2) | 27.5 (24.6-30.4) | 96.3 (95.1-97.5) | 47.5 (44.3-50.7) | 91.6 (89.8-93.4) |
| At 8 y | 5.8 (2.9-11.2) | 16.3 (13.7-18.9) | 96.7 (95.4-98.0) | 43.6 (40.1-47.1) | 88.2 (85.9-90.5) |
| At 11 y | 4.3 (2.4-7.8) | 15 (12.6-17.4) | 96.1 (94.8-97.4) | 42.0 (38.7-45.3) | 85.6 (83.3-87.9) |
| At 13 y | 5.7 (2.8-11.6) | 14.8 (12.1-17.5) | 97.0 (95.7-98.3) | 51.5 (47.7-55.3) | 84.2 (81.4-87.0) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
TABLE 3
Likelihood of active asthma predicted by loose index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 5.5 (3.5-8.4) | 56.6 (53.3-59.9) | 80.8 (78.3-83.3) | 26.2 (23.4-29.0) | 93.9 (92.4-95.4) |
| At 8 y | 4.4 (2.8-6.8) | 50.5 (47.0-54.0) | 81.1 (78.3-83.9) | 29.4 (26.2-32.6) | 91.3 (89.3-93.3) |
| At 11 y | 2.6 (1.8-3.8) | 40.1 (36.8-43.4) | 79.6 (76.9-82.3) | 27.1 (24.1-30.1) | 87.5 (85.3-89.7) |
| At 13 y | 3.0 (1.9-4.6) | 39.3 (35.5-43.1) | 82.1 (79.1-85.1) | 31.7 (28.1-35.3) | 86.5 (83.9-89.1) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
Recommendations
A European and United States expert panel guide to the diagnosis and treatment of asthma in childhood, PRACTALL, states that “asthma should be suspected in any infant with recurrent wheezing and cough episodes. Frequently, diagnosis is possible only through long-term follow-up, consideration of the extensive differential diagnoses, and by observing the child’s response to bronchodilator and/or anti-inflammatory treatment.”10
The National Asthma Education and Prevention Program’s Expert Panel Report 3 (EPR-3) notes that diagnostic evaluation for asthma in children 0 to 4 years of age should include history, symptoms, physical examination, and assessment of quality of life.1
1. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma. NIH publication 07-4051. Bethesda, Md: National Heart, Lung, and Blood Institute; 2007. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed June 20, 2008.
2. Martinez FD, Wright AL, Taussig LM, et al. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med. 1995;332:133-138.
3. Sears MR, Greene JM, Willan AR, et al. A longitudinal, population-based cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414-1422.
4. Jenkins MA, Hopper JL, Bowes G, et al. Factors in childhood as predictors of asthma in adult life. BMJ. 1994;309:90-93.
5. Rusconi F, Galassi C, Corbo GM, et al. Risk factors for early, persistent, and late-onset wheezing in young children. SIDRIA Collaborative Group. Am J Respir Crit Care Med. 1999;167:1617-1622.
6. Stein RT, Martinez FD. Asthma phenotypes in childhood: lessons from an epidemiologic approach. Paediatr Respir Rev. 2004;5:155-161.
7. Stein RT, Holberg CJ, Morgan WJ, et al. Peak flow variability, methacholine responsiveness and atopy as markers for detecting different wheezing phenotypes in childhood. Thorax. 1997;52:946-952.
8. Arshad SH, Kurukulaaratchy RJ, Fenn M, et al. Early life risk factors for current wheeze, asthma, and bronchial hyper-responsiveness at 10 years of age. Chest. 2005;127:502-508.
9. Castro-Rodriguez JA, Holberg CJ, Wright AL, et al. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162:1403-1406.
10. Bacharier LB, Boner A, Carlsen KH, et al. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63:5-34.
NO RELIABLE WAY EXISTS TO DIAGNOSE ASTHMA IN INFANTS AND TODDLERS. Recurrent wheezing, especially apart from colds, combined with physician-diagnosed eczema or atopic dermatitis, eosinophilia, and a parental history of asthma, increase the probability of a subsequent asthma diagnosis in the absence of other causes (strength of recommendation: B, 2 good-quality cohort studies).
Evidence summary
Wheezing in children is common and the differential diagnosis is broad. The many potential causes include upper respiratory infection, asthma, cystic fibrosis, foreign body aspiration, vascular ring, tracheomalacia, primary immunodeficiency, and congenital heart disease.1
Outpatient primary care cohort studies estimate that about half of children wheeze before they reach school age. Only one-third of children who wheeze during the first 3 years of life, however, continue to wheeze into later childhood and young adulthood.2-4
These findings have led some experts to suggest that not all wheezing in children is asthma and that asthma exists in variant forms.5-7 Variant wheezing patterns include transient early wheezing, which seems to be most prevalent in the first 3 years of life; wheezing without atopy, which occurs most often at 3 to 6 years of age; and wheezing with immunoglobulin E-associated atopy, which gradually increases in prevalence from birth and dominates in the over-6 age group. It is children in this last group whom we generally consider to have asthma.
Objective measures of lung function are challenging to perform in young children. Clinical signs and symptoms thus suggest the diagnosis of asthma.
Atopy, rhinitis, and eczema most often accompany persistent wheezing
Primary care cohort studies provide the best available evidence on which findings in infants and toddlers most likely predict persistent airway disease in childhood. A whole-population cohort study followed nearly all children born on the Isle of Wight from January 1989 through February 1990 to evaluate the natural history of childhood wheezing and to study associated risk factors.8 Children were seen at birth and at 1, 2, 4, and 10 years of age.
Findings most associated with current wheezing (within the last year) in 10-year-olds were atopy (odds ratio [OR]=4.38; 95% confidence interval [CI], 3.07-6.25), rhinitis (OR=3.72; 95% CI, 2.21-6.27), and eczema (OR=3.04; 95% CI, 2.05-4.51).8
An index to predict asthma
Since 1980, the Tucson Children’s Respiratory Study has followed 1246 healthy newborns seen by pediatricians affiliated with a large HMO in Tucson, Arizona. Questionnaires about parental asthma history and prenatal smoking history were obtained at enrollment. Childhood wheezing and its frequency, as well as physician-diagnosed allergies or asthma, were assessed at ages 2 and 3. If the child had wheezed in the past year, then the child was considered to be an “early wheezer.” If the frequency was 3 or more on a 5-point scale, then the child was considered to be an “early frequent wheezer.” Questionnaires were re-administered at ages 6, 8, 11, and 13. Three episodes of wheezing within the past year or a physician diagnosis of asthma with symptoms in the past year was considered “active asthma.” Blood specimens for eosinophils were obtained at age 10.
Using these data, the researchers developed stringent and loose criteria (TABLE 1) and odds ratios (TABLES 2 and 3) for childhood factors most predictive of an asthma diagnosis at an older age. The findings of the study may help clinicians care for wheezing infants and toddlers.9
TABLE 1
A clinical index of asthma risk9*
| Major criteria | Minor criteria |
|---|---|
| Parental asthma (history of physician diagnosis of asthma in a parent) | Allergic rhinitis (physician diagnosis of allergic rhinitis as reported in questionnaires at ages 2 or 3 y) |
| Eczema (physician diagnosis of atopic dermatitis as reported in questionnaires at ages 2 or 3 y) | Wheezing apart from colds |
| Eosinophilia (≥4%) | |
| *Stringent index for predicting asthma: Child has early, frequent wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. Loose index for predicting asthma: Child has early wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. | |
TABLE 2
Likelihood of active asthma predicted by stringent index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 9.8 (5.6-17.2) | 27.5 (24.6-30.4) | 96.3 (95.1-97.5) | 47.5 (44.3-50.7) | 91.6 (89.8-93.4) |
| At 8 y | 5.8 (2.9-11.2) | 16.3 (13.7-18.9) | 96.7 (95.4-98.0) | 43.6 (40.1-47.1) | 88.2 (85.9-90.5) |
| At 11 y | 4.3 (2.4-7.8) | 15 (12.6-17.4) | 96.1 (94.8-97.4) | 42.0 (38.7-45.3) | 85.6 (83.3-87.9) |
| At 13 y | 5.7 (2.8-11.6) | 14.8 (12.1-17.5) | 97.0 (95.7-98.3) | 51.5 (47.7-55.3) | 84.2 (81.4-87.0) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
TABLE 3
Likelihood of active asthma predicted by loose index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 5.5 (3.5-8.4) | 56.6 (53.3-59.9) | 80.8 (78.3-83.3) | 26.2 (23.4-29.0) | 93.9 (92.4-95.4) |
| At 8 y | 4.4 (2.8-6.8) | 50.5 (47.0-54.0) | 81.1 (78.3-83.9) | 29.4 (26.2-32.6) | 91.3 (89.3-93.3) |
| At 11 y | 2.6 (1.8-3.8) | 40.1 (36.8-43.4) | 79.6 (76.9-82.3) | 27.1 (24.1-30.1) | 87.5 (85.3-89.7) |
| At 13 y | 3.0 (1.9-4.6) | 39.3 (35.5-43.1) | 82.1 (79.1-85.1) | 31.7 (28.1-35.3) | 86.5 (83.9-89.1) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
Recommendations
A European and United States expert panel guide to the diagnosis and treatment of asthma in childhood, PRACTALL, states that “asthma should be suspected in any infant with recurrent wheezing and cough episodes. Frequently, diagnosis is possible only through long-term follow-up, consideration of the extensive differential diagnoses, and by observing the child’s response to bronchodilator and/or anti-inflammatory treatment.”10
The National Asthma Education and Prevention Program’s Expert Panel Report 3 (EPR-3) notes that diagnostic evaluation for asthma in children 0 to 4 years of age should include history, symptoms, physical examination, and assessment of quality of life.1
NO RELIABLE WAY EXISTS TO DIAGNOSE ASTHMA IN INFANTS AND TODDLERS. Recurrent wheezing, especially apart from colds, combined with physician-diagnosed eczema or atopic dermatitis, eosinophilia, and a parental history of asthma, increase the probability of a subsequent asthma diagnosis in the absence of other causes (strength of recommendation: B, 2 good-quality cohort studies).
Evidence summary
Wheezing in children is common and the differential diagnosis is broad. The many potential causes include upper respiratory infection, asthma, cystic fibrosis, foreign body aspiration, vascular ring, tracheomalacia, primary immunodeficiency, and congenital heart disease.1
Outpatient primary care cohort studies estimate that about half of children wheeze before they reach school age. Only one-third of children who wheeze during the first 3 years of life, however, continue to wheeze into later childhood and young adulthood.2-4
These findings have led some experts to suggest that not all wheezing in children is asthma and that asthma exists in variant forms.5-7 Variant wheezing patterns include transient early wheezing, which seems to be most prevalent in the first 3 years of life; wheezing without atopy, which occurs most often at 3 to 6 years of age; and wheezing with immunoglobulin E-associated atopy, which gradually increases in prevalence from birth and dominates in the over-6 age group. It is children in this last group whom we generally consider to have asthma.
Objective measures of lung function are challenging to perform in young children. Clinical signs and symptoms thus suggest the diagnosis of asthma.
Atopy, rhinitis, and eczema most often accompany persistent wheezing
Primary care cohort studies provide the best available evidence on which findings in infants and toddlers most likely predict persistent airway disease in childhood. A whole-population cohort study followed nearly all children born on the Isle of Wight from January 1989 through February 1990 to evaluate the natural history of childhood wheezing and to study associated risk factors.8 Children were seen at birth and at 1, 2, 4, and 10 years of age.
Findings most associated with current wheezing (within the last year) in 10-year-olds were atopy (odds ratio [OR]=4.38; 95% confidence interval [CI], 3.07-6.25), rhinitis (OR=3.72; 95% CI, 2.21-6.27), and eczema (OR=3.04; 95% CI, 2.05-4.51).8
An index to predict asthma
Since 1980, the Tucson Children’s Respiratory Study has followed 1246 healthy newborns seen by pediatricians affiliated with a large HMO in Tucson, Arizona. Questionnaires about parental asthma history and prenatal smoking history were obtained at enrollment. Childhood wheezing and its frequency, as well as physician-diagnosed allergies or asthma, were assessed at ages 2 and 3. If the child had wheezed in the past year, then the child was considered to be an “early wheezer.” If the frequency was 3 or more on a 5-point scale, then the child was considered to be an “early frequent wheezer.” Questionnaires were re-administered at ages 6, 8, 11, and 13. Three episodes of wheezing within the past year or a physician diagnosis of asthma with symptoms in the past year was considered “active asthma.” Blood specimens for eosinophils were obtained at age 10.
Using these data, the researchers developed stringent and loose criteria (TABLE 1) and odds ratios (TABLES 2 and 3) for childhood factors most predictive of an asthma diagnosis at an older age. The findings of the study may help clinicians care for wheezing infants and toddlers.9
TABLE 1
A clinical index of asthma risk9*
| Major criteria | Minor criteria |
|---|---|
| Parental asthma (history of physician diagnosis of asthma in a parent) | Allergic rhinitis (physician diagnosis of allergic rhinitis as reported in questionnaires at ages 2 or 3 y) |
| Eczema (physician diagnosis of atopic dermatitis as reported in questionnaires at ages 2 or 3 y) | Wheezing apart from colds |
| Eosinophilia (≥4%) | |
| *Stringent index for predicting asthma: Child has early, frequent wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. Loose index for predicting asthma: Child has early wheezing plus at least 1 of the 2 major criteria or 2 of the 3 minor criteria. | |
TABLE 2
Likelihood of active asthma predicted by stringent index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 9.8 (5.6-17.2) | 27.5 (24.6-30.4) | 96.3 (95.1-97.5) | 47.5 (44.3-50.7) | 91.6 (89.8-93.4) |
| At 8 y | 5.8 (2.9-11.2) | 16.3 (13.7-18.9) | 96.7 (95.4-98.0) | 43.6 (40.1-47.1) | 88.2 (85.9-90.5) |
| At 11 y | 4.3 (2.4-7.8) | 15 (12.6-17.4) | 96.1 (94.8-97.4) | 42.0 (38.7-45.3) | 85.6 (83.3-87.9) |
| At 13 y | 5.7 (2.8-11.6) | 14.8 (12.1-17.5) | 97.0 (95.7-98.3) | 51.5 (47.7-55.3) | 84.2 (81.4-87.0) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
TABLE 3
Likelihood of active asthma predicted by loose index9
| Active asthma | OR (95% CI) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|
| At 6 y | 5.5 (3.5-8.4) | 56.6 (53.3-59.9) | 80.8 (78.3-83.3) | 26.2 (23.4-29.0) | 93.9 (92.4-95.4) |
| At 8 y | 4.4 (2.8-6.8) | 50.5 (47.0-54.0) | 81.1 (78.3-83.9) | 29.4 (26.2-32.6) | 91.3 (89.3-93.3) |
| At 11 y | 2.6 (1.8-3.8) | 40.1 (36.8-43.4) | 79.6 (76.9-82.3) | 27.1 (24.1-30.1) | 87.5 (85.3-89.7) |
| At 13 y | 3.0 (1.9-4.6) | 39.3 (35.5-43.1) | 82.1 (79.1-85.1) | 31.7 (28.1-35.3) | 86.5 (83.9-89.1) |
| CI, confidence interval; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value. | |||||
Recommendations
A European and United States expert panel guide to the diagnosis and treatment of asthma in childhood, PRACTALL, states that “asthma should be suspected in any infant with recurrent wheezing and cough episodes. Frequently, diagnosis is possible only through long-term follow-up, consideration of the extensive differential diagnoses, and by observing the child’s response to bronchodilator and/or anti-inflammatory treatment.”10
The National Asthma Education and Prevention Program’s Expert Panel Report 3 (EPR-3) notes that diagnostic evaluation for asthma in children 0 to 4 years of age should include history, symptoms, physical examination, and assessment of quality of life.1
1. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma. NIH publication 07-4051. Bethesda, Md: National Heart, Lung, and Blood Institute; 2007. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed June 20, 2008.
2. Martinez FD, Wright AL, Taussig LM, et al. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med. 1995;332:133-138.
3. Sears MR, Greene JM, Willan AR, et al. A longitudinal, population-based cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414-1422.
4. Jenkins MA, Hopper JL, Bowes G, et al. Factors in childhood as predictors of asthma in adult life. BMJ. 1994;309:90-93.
5. Rusconi F, Galassi C, Corbo GM, et al. Risk factors for early, persistent, and late-onset wheezing in young children. SIDRIA Collaborative Group. Am J Respir Crit Care Med. 1999;167:1617-1622.
6. Stein RT, Martinez FD. Asthma phenotypes in childhood: lessons from an epidemiologic approach. Paediatr Respir Rev. 2004;5:155-161.
7. Stein RT, Holberg CJ, Morgan WJ, et al. Peak flow variability, methacholine responsiveness and atopy as markers for detecting different wheezing phenotypes in childhood. Thorax. 1997;52:946-952.
8. Arshad SH, Kurukulaaratchy RJ, Fenn M, et al. Early life risk factors for current wheeze, asthma, and bronchial hyper-responsiveness at 10 years of age. Chest. 2005;127:502-508.
9. Castro-Rodriguez JA, Holberg CJ, Wright AL, et al. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162:1403-1406.
10. Bacharier LB, Boner A, Carlsen KH, et al. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63:5-34.
1. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma. NIH publication 07-4051. Bethesda, Md: National Heart, Lung, and Blood Institute; 2007. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed June 20, 2008.
2. Martinez FD, Wright AL, Taussig LM, et al. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med. 1995;332:133-138.
3. Sears MR, Greene JM, Willan AR, et al. A longitudinal, population-based cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414-1422.
4. Jenkins MA, Hopper JL, Bowes G, et al. Factors in childhood as predictors of asthma in adult life. BMJ. 1994;309:90-93.
5. Rusconi F, Galassi C, Corbo GM, et al. Risk factors for early, persistent, and late-onset wheezing in young children. SIDRIA Collaborative Group. Am J Respir Crit Care Med. 1999;167:1617-1622.
6. Stein RT, Martinez FD. Asthma phenotypes in childhood: lessons from an epidemiologic approach. Paediatr Respir Rev. 2004;5:155-161.
7. Stein RT, Holberg CJ, Morgan WJ, et al. Peak flow variability, methacholine responsiveness and atopy as markers for detecting different wheezing phenotypes in childhood. Thorax. 1997;52:946-952.
8. Arshad SH, Kurukulaaratchy RJ, Fenn M, et al. Early life risk factors for current wheeze, asthma, and bronchial hyper-responsiveness at 10 years of age. Chest. 2005;127:502-508.
9. Castro-Rodriguez JA, Holberg CJ, Wright AL, et al. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162:1403-1406.
10. Bacharier LB, Boner A, Carlsen KH, et al. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63:5-34.
Evidence-based answers from the Family Physicians Inquiries Network
Is C difficile to blame for your patient’s diarrhea?
• A C difficile diagnosis should be made by one of several widely available testing protocols, including a 2-step method using the common antigen assay to determine whether C difficile is present, followed by an enzyme immunoassay for toxins A and B to improve specificity. B
• Oral metronidazole should be used for initial treatment of mild to moderate C difficile infection, and oral vancomycin and possibly intravenous metronidazole for severe cases. A
• Metronidazole should not be used after an initial recurrence or for long-term therapy because of the risk of neurotoxicity. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Mary S, an 82-year-old patient you recently treated for bronchitis with a 3-day course of levofloxacin, calls your office complaining of diarrhea and abdominal cramps. She describes the diarrhea as nonbloody and particularly foul smelling and asks if she can take loperamide for her symptoms.
If Mary S were your patient, what would you tell her?
The incidence of Clostridium difficile infection (CDI) has been on the rise since 2000, when a common epidemic strain began circulating in North America.1 Although hospitalization or residency in a long-term care facility remains a classic risk factor for CDI, physicians in out-patient settings are increasingly likely to see patients with community-acquired CDI.
Recently updated guidelines from the Society for Health-care Epidemiology of America (SHEA) and the Infectious Diseases Society of America define CDI as the presence of diarrhea (≥3 unformed stools in 24 hours) and either a positive stool test for toxigenic C difficile or its toxins or colonoscopic or histopathologic findings demonstrating pseudomembranous colitis.2 That said, the clinical features of CDI are nonspecific and many patients do not fit the classic profile. So diagnosing CDI requires a high index of suspicion.
The text and tables that follow detail some surprising things about who is likely to develop CDI and which treatment options to employ (and, in some cases, avoid).
Is it CDI? Looking beyond the obvious
Antibiotic use and advanced age, like hospitalization, are classic risk factors for CDI.3 Diarrhea typically begins during or shortly after a course of antibiotics, but may develop as long as 8 weeks after treatment is completed. While any antibiotic, including metronidazole, can precipitate CDI, clindamycin, cephalosporins, extended-spectrum penicillins, and quinolones are most frequently implicated.4 Epidemiologic studies have suggested an association between gastric acid-reducing agents—primarily proton-pump inhibitors—and CDI.4-7 But this link remains controversial, as other investigations have not found a clear relationship.8
In addition to diarrhea, approximately 28% of patients with CDI develop a fever (as high as 104°F); 50% develop leukocytosis (up to 50,000 cells/mcL); and 22% develop abdominal pain, usually localized to the lower quadrants.9 These symptoms, however, are not specific to C difficile, and could be due to a different enteric pathogen, intra-abdominal sepsis, inflammatory bowel disease, or adverse effects of medication, among other causes.9
Markers for severe CDI include age >70 years, leukocyte count >20,000 cells/mcL, albumin level <2.5 g/dL, small-bowel obstruction or ileus, and a computed tomography (CT) scan showing colorectal inflammation.10 Severe CDI can lead to toxic megacolon, bowel perforation, sepsis, and even death.
In addition to considering CDI in patients with nonspecific symptoms, it is important to include it in the differential diagnosis of patients who do not fit the classic profile. In a recent study of patients with CDI at 4 Veterans Affairs facilities, almost half (49%) of those studied had no exposure to antimicrobial drugs. The researchers further found that the median age of patients with CDI was 61 years—younger than that found in previous studies—and that 20% of the cases were community-acquired.11
Consider CDI in children, too. Risk factors for CDI in pediatric patients include disruption of the normal microflora of the gastrointestinal tract, compromised immune status, poor diet, underlying health conditions, concurrent infections, and cancer.12
Diagnostic testing: Consider a 2-step assay
Patients with symptoms suggestive of CDI should undergo laboratory testing to confirm the diagnosis. TABLE 1 lists the tests that are widely available in the United States.3 Only liquid stools should be tested and just one sample should be sent to the lab, as multiple samples do not increase the diagnostic yield.13 In addition, tests should be used only for diagnosis, and not as a “test of cure.” This is because patients can shed C difficile toxin and spores for several weeks after completing treatment, and there are wide variations in the sensitivity of toxin assays.
Infants <1 year old have high rates of asymptomatic toxigenic strains of C difficile, and until 2008, recommendations from SHEA discouraged testing the stools of such young patients. Because of the difficulty in differentiating incidental colonization from true CDI in this patient population, the authors of a recent review suggested using more than one diagnostic approach when testing children <1 year of age.14
We advocate a 2-step assay—that is, testing for both glutamate dehydrogenase (GDH)—an antigen common to all strains of C difficile—and C difficile toxins A and B. The common antigen test is sensitive, but may detect carriers who do not have active disease. The enzyme immunoassay (EIA) for toxins A and B helps to improve specificity. Therefore, positive results of both tests would be considered a positive finding, negative results of both tests would be considered a negative finding, and one positive result with one negative result would require another test for toxin detection.3
The reverse-transcriptase polymerase chain reaction (RT-PCR) assay, which detects the toxin B gene of C difficile, is the newest test for CDI. The RT-PCR assay detects only toxigenic strains of C difficile, and all toxigenic strains produce toxin B, making it more specific than testing for the common antigen. The RT-PCR assay also has better sensitivity than the cytotoxin assay, which also tests for toxin B. The major limitation of the RT-PCR assay is the frequency of false-positive results in hospitalized patients with a high incidence of C difficile colonization.3
Routine laboratory studies, including a complete blood count with differential and a complete metabolic panel, are often useful to ascertain the presence and degree of leukocytosis, dehydration, and other metabolic abnormalities and to test for hypoalbuminemia. Fecal leukocytes can be seen in colitis and may be useful in select cases.
Imaging studies such as radiography, CT, and endoscopy have largely been superseded by lab testing for CDI. Plain radiographs are usually normal in patients with CDI, unless the patient has an ileus or toxic megacolon. CT is useful, however, in suspected cases of fulminant CDI or toxic megacolon, and may reveal colonic-wall thickening, pericolonic stranding, or ascites.9 Colonoscopy is preferred over sigmoidoscopy because up to one-third of patients with pseudomembranous colitis will have involvement of the right colon only.9 However, this test carries the risk of perforation in patients with fulminant colitis.
TABLE 1
Lab tests for C difficile infection
| Test | Substance detected | Time needed | Sensitivity | Specificity |
|---|---|---|---|---|
| Cytotoxin | Toxin B | 1-3 d | 95% | 90%-95% |
| Toxin culture | Toxigenic C difficile† | 3-5 d | >95% | 80%-90% |
| EIA toxin A or A/B | Toxin A or A/B | Hours | 75%-80% | 97%-98% |
| EIA GDH* | C difficile | Hours | 95%-100% | 70%-80% |
| EIA GDH* and toxin A/B | C difficile and C difficile toxin | Hours | 95%-100% | 97%-98% |
| RT-PCR | Toxigenic C difficile† | Hours | >98% | 80%-99% |
| *GDH is the common C difficile antigen. †All toxigenic strains produce toxin B. EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; RT-PCR, reverse-transcriptase polymerase chain reaction. Adapted from: Bartlett JG. Infect Control Hosp Epidemiol. 2010.3 | ||||
Treatment: What to consider, what to avoid
Of the 2 antibiotics most commonly used to treat CDI—metronidazole and vancomycin—only the latter has been approved by the US Food and Drug Administration for this indication. Nevertheless, metronidazole is generally recommended as first-line therapy and has the advantage of being much less expensive than vancomycin. However, an RCT found that oral vancomycin was superior to metronidazole in patients with severe disease.15 The time to resolution of diarrhea may be shorter with oral vancomycin than with metronidazole, as well.16
Recent guidelines suggest that clinicians consider 3 factors in deciding how to treat a first episode of CDI: the patient’s age, peak white blood cell count, and peak serum creatinine level.2 TABLE 2 presents an overview of treatment recommendations for both an initial episode of CDI and recurrences.
Treat severe CDI without delay. For patients with suspected severe CDI, treatment should be started empirically, without waiting for test results. Avoid antiperistaltic agents, which can obscure symptoms and precipitate toxic megacolon.2 Discontinue an antibiotic, if the patient is taking one, as soon as possible after the original infection has been adequately treated. If other infections need to be treated concurrently, we recommend that the course of treatment for CDI be extended until after the other antibiotic regimens have been stopped.
Avoid probiotics in this group. The use of probiotics, both for prevention and to help restore normal bowel flora in patients with CDI, has been advocated for many years. One RCT showed that a yogurt drink containing Lactobacillus and other bacteria reduced the risk of CDI in individuals ≥50 years of age who were taking antibiotics,17 but the guideline development panel recommended against using probiotics until larger trials have been completed.2
Probiotics are not without risk, and several cases of bacteremia have been reported.18,19 Immunocompromised patients appear to be at comparably higher risk, and probiotics should be avoided in this group. Numerous adjunctive agents, including intraluminal toxin binders, biotherapeutic agents, monoclonal antibodies, and a C difficile vaccine, are in various stages of development.2
How to handle recurrences
Relapse rates for CDI range from 6% to 25%,2 and affect patients who receive either vancomycin or metronidazole for the initial treatment. The mechanism relates to either relapse of the original infection or reinfection of susceptible patients with a new strain of C difficile.
Risk of relapse. Elderly patients treated with metronidazole seem to be particularly susceptible to CDI relapse.20 Other risk factors include the administration of non-C difficile antibiotics during or after treatment of CDI, a defective immune response against toxin A, glucocorticoid use, prior stroke, and concurrent use of a proton-pump inhibitor.21-25
TABLE 2 lists tapering and/or pulsed dosing of oral vancomycin as treatment for patients with a second recurrence. We often prescribe the following 6-week regimen, telling patients to take 125 mg vancomycin:
- 4 times a day for one week,
- then 2 times a day for one week,
- then once a day for one week,
- then every other day for one week, and
- finally, every 72 hours for 2 weeks.
Oral metronidazole should not be used beyond the first recurrence or for long-term therapy because of cumulative neurotoxicity, which can be irreversible.2
Management of patients whose CDI recurs after a long course of vancomycin is challenging. Oral rifaximin therapy (400 mg twice a day for 14 days), started immediately at the end of the oral vancomycin course, was shown to cure 7 of 8 patients with multiple relapses.26 Other potential treatment options are oral nitazoxanide, IV tigecycline, or IV immunoglobulin.
CASE You explain to Mary S that diagnostic tests are needed before you can determine whether she can safely take loperamide. When she comes in later that day, you collect a stool sample for C difficile antigen and toxin testing, and order a complete blood count and electrolyte panel.
The patient’s C difficile tests come back positive, her white blood cell count is <15,000 cells/mcL, and her creatinine level is ≤1.5 times her baseline, so you start her on oral metronidazole 500 mg every 8 hours for 14 days. (If the antigen assay had been positive and the toxin negative, you would have either repeated the test or treated Mary S empirically with metronidazole. If the initial antigen assay had been negative, you would have advised her to take the loperamide.)
You schedule a follow-up visit a day or 2 after starting therapy. If the patient is dehydrated or her symptoms have not improved by then, hospitalization may be required.
TABLE 2
Treatment recommendations for C difficile infection
| Clinical description | Clinical evidence | Recommended treatment |
|---|---|---|
| Initial episode (mild or moderate) | Leukocytosis with a white cell count <15,000 cells/mcL and creatinine <1.5 times premorbid level | Metronidazole (oral) 500 mg TID for 10-14 d |
| Initial episode (severe) | Leukocytosis with a white cell count ≥15,000 cells/mcL or creatinine ≥1.5 times premorbid level | Vancomycin (oral) 125 mg QID for 10-14 d |
| Initial episode (severe, complicated) | Hypotension or shock, ileus, megacolon | Vancomycin 500 mg QID (oral or by NG tube) plus metronidazole 500 mg (IV). If complete ileus, consider adding rectal instillation of vancomycin |
| First recurrence | Same as initial episode | |
| Second recurrence | Vancomycin in a tapered and/or pulsed regimen | |
| NG, nasogastric. Adapted from: Cohen SH, et al. Infect Control Hosp Epidemiol. 2010.2 | ||
CORRESPONDENCE
Richard R. Watkins, MD, MS, Division of Infectious Diseases, Akron General Medical Center, 224 West Exchange Street, Suite 290, Akron, OH 44302; rwatkins@agmc.org
1. Gerding DN. Global epidemiology of Clostridium difficile infection in 2010. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S32-S34.
2. Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431-455.
3. Bartlett JG. Detection of Clostridium difficile infection. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S35-S37.
4. Dial S, Alrasadi K, Manoukian C, et al. Risk of Clostridium difficile diarrhea among hospital inpatients prescribed proton pump inhibitors: cohort and case-control studies. CMAJ. 2004;171:33-38.
5. Dial S, Delaney JA, Barkun AN, et al. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294:2989-2995.
6. Cunningham R, Dale B, Undy B, et al. Proton pump inhibitors as a risk factor for Clostridium difficile diarrhoea. J Hosp Infect. 2003;54:243-245.
7. Howell MD, Novack V, Grgurich P, et al. Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection. Arch Intern Med. 2010;170:784-790.
8. Shah S, Lewis A, Leopold D, et al. Gastric acid suppression does not promote clostridial diarrhoea in the elderly. QJM. 2000;93:175-181.
9. Bartlett JG, Gerding DN. Clinical recognition and diagnosis of Clostridium difficile infection. Clin Infect Dis. 2008;46(suppl 1):S12-S18.
10. Henrich TJ, Krakower D, Bitton A, et al. Clinical risk factors for severe Clostridium difficile-associated disease. Emerg Infect Dis. 2009;15:415-422.
11. Kutty PK, Woods CW, Sena AC, et al. Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA. Emerg Infect Dis. 2010;16:197-204.
12. Pituch H. Clostridium difficile is no longer just a nosocomial infection or an infection of adults. Int J Antimicrob Agents. 2009;33(suppl 1):S42-S45.
13. Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006;119:356.e7-e8.
14. Bryant K, McDonald LC. Clostridium difficile infections in children. Pediatr Infect Dis J. 2009;28:145-146.
15. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
16. Belmares J, Gerding DN, Parada JP, et al. Outcome of metronidazole therapy for Clostridium difficile disease and correlation with a scoring system. J Infect. 2007;55:495-501.
17. Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ. 2007;335:80.-
18. Ledoux D, Labombardi VJ, Karter D. Lactobacillus acidophilus bacteraemia after use of a probiotic in a patient with AIDS and Hodgkin’s disease. Int J STD AIDS. 2006;17:280-282.
19. Hammerman C, Bin-Nun A, Kaplan M. Safety of probiotics: comparison of two popular strains. BMJ. 2006;333:1006-1008.
20. Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
21. Nair S, Yadav D, Corpuz M, et al. Clostridium difficile colitis: factors influencing treatment failure and relapse—a prospective evaluation. Am J Gastroenterol. 1998;93:1873-1876.
22. Garey KW, Sethi S, Yadav Y, et al. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect. 2008;70:298-304.
23. Das R, Feuerstadt P, Brandt LJ. Glucocorticoids are associated with increased risk of short-term mortality in hospitalized patients with Clostridium difficile-associated disease. Am J Gastroenterol. 2010;105:2040-2049.
24. Cadena J, Thompson GR, 3rd, Patterson JE, et al. Clinical predictors and risk factors for relapsing Clostridium difficile infection. Am J Med Sci. 2010;339:350-355.
25. Linsky A, Gupta K, Lawler EV, et al. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med. 2010;170:772-778.
26. Johnson S, Schriever C, Galang M, et al. Interruption of recurrent Clostridium difficile-associated diarrhea episodes by serial therapy with vancomycin and rifaximin. Clin Infect Dis. 2007;44:846-848.
• A C difficile diagnosis should be made by one of several widely available testing protocols, including a 2-step method using the common antigen assay to determine whether C difficile is present, followed by an enzyme immunoassay for toxins A and B to improve specificity. B
• Oral metronidazole should be used for initial treatment of mild to moderate C difficile infection, and oral vancomycin and possibly intravenous metronidazole for severe cases. A
• Metronidazole should not be used after an initial recurrence or for long-term therapy because of the risk of neurotoxicity. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Mary S, an 82-year-old patient you recently treated for bronchitis with a 3-day course of levofloxacin, calls your office complaining of diarrhea and abdominal cramps. She describes the diarrhea as nonbloody and particularly foul smelling and asks if she can take loperamide for her symptoms.
If Mary S were your patient, what would you tell her?
The incidence of Clostridium difficile infection (CDI) has been on the rise since 2000, when a common epidemic strain began circulating in North America.1 Although hospitalization or residency in a long-term care facility remains a classic risk factor for CDI, physicians in out-patient settings are increasingly likely to see patients with community-acquired CDI.
Recently updated guidelines from the Society for Health-care Epidemiology of America (SHEA) and the Infectious Diseases Society of America define CDI as the presence of diarrhea (≥3 unformed stools in 24 hours) and either a positive stool test for toxigenic C difficile or its toxins or colonoscopic or histopathologic findings demonstrating pseudomembranous colitis.2 That said, the clinical features of CDI are nonspecific and many patients do not fit the classic profile. So diagnosing CDI requires a high index of suspicion.
The text and tables that follow detail some surprising things about who is likely to develop CDI and which treatment options to employ (and, in some cases, avoid).
Is it CDI? Looking beyond the obvious
Antibiotic use and advanced age, like hospitalization, are classic risk factors for CDI.3 Diarrhea typically begins during or shortly after a course of antibiotics, but may develop as long as 8 weeks after treatment is completed. While any antibiotic, including metronidazole, can precipitate CDI, clindamycin, cephalosporins, extended-spectrum penicillins, and quinolones are most frequently implicated.4 Epidemiologic studies have suggested an association between gastric acid-reducing agents—primarily proton-pump inhibitors—and CDI.4-7 But this link remains controversial, as other investigations have not found a clear relationship.8
In addition to diarrhea, approximately 28% of patients with CDI develop a fever (as high as 104°F); 50% develop leukocytosis (up to 50,000 cells/mcL); and 22% develop abdominal pain, usually localized to the lower quadrants.9 These symptoms, however, are not specific to C difficile, and could be due to a different enteric pathogen, intra-abdominal sepsis, inflammatory bowel disease, or adverse effects of medication, among other causes.9
Markers for severe CDI include age >70 years, leukocyte count >20,000 cells/mcL, albumin level <2.5 g/dL, small-bowel obstruction or ileus, and a computed tomography (CT) scan showing colorectal inflammation.10 Severe CDI can lead to toxic megacolon, bowel perforation, sepsis, and even death.
In addition to considering CDI in patients with nonspecific symptoms, it is important to include it in the differential diagnosis of patients who do not fit the classic profile. In a recent study of patients with CDI at 4 Veterans Affairs facilities, almost half (49%) of those studied had no exposure to antimicrobial drugs. The researchers further found that the median age of patients with CDI was 61 years—younger than that found in previous studies—and that 20% of the cases were community-acquired.11
Consider CDI in children, too. Risk factors for CDI in pediatric patients include disruption of the normal microflora of the gastrointestinal tract, compromised immune status, poor diet, underlying health conditions, concurrent infections, and cancer.12
Diagnostic testing: Consider a 2-step assay
Patients with symptoms suggestive of CDI should undergo laboratory testing to confirm the diagnosis. TABLE 1 lists the tests that are widely available in the United States.3 Only liquid stools should be tested and just one sample should be sent to the lab, as multiple samples do not increase the diagnostic yield.13 In addition, tests should be used only for diagnosis, and not as a “test of cure.” This is because patients can shed C difficile toxin and spores for several weeks after completing treatment, and there are wide variations in the sensitivity of toxin assays.
Infants <1 year old have high rates of asymptomatic toxigenic strains of C difficile, and until 2008, recommendations from SHEA discouraged testing the stools of such young patients. Because of the difficulty in differentiating incidental colonization from true CDI in this patient population, the authors of a recent review suggested using more than one diagnostic approach when testing children <1 year of age.14
We advocate a 2-step assay—that is, testing for both glutamate dehydrogenase (GDH)—an antigen common to all strains of C difficile—and C difficile toxins A and B. The common antigen test is sensitive, but may detect carriers who do not have active disease. The enzyme immunoassay (EIA) for toxins A and B helps to improve specificity. Therefore, positive results of both tests would be considered a positive finding, negative results of both tests would be considered a negative finding, and one positive result with one negative result would require another test for toxin detection.3
The reverse-transcriptase polymerase chain reaction (RT-PCR) assay, which detects the toxin B gene of C difficile, is the newest test for CDI. The RT-PCR assay detects only toxigenic strains of C difficile, and all toxigenic strains produce toxin B, making it more specific than testing for the common antigen. The RT-PCR assay also has better sensitivity than the cytotoxin assay, which also tests for toxin B. The major limitation of the RT-PCR assay is the frequency of false-positive results in hospitalized patients with a high incidence of C difficile colonization.3
Routine laboratory studies, including a complete blood count with differential and a complete metabolic panel, are often useful to ascertain the presence and degree of leukocytosis, dehydration, and other metabolic abnormalities and to test for hypoalbuminemia. Fecal leukocytes can be seen in colitis and may be useful in select cases.
Imaging studies such as radiography, CT, and endoscopy have largely been superseded by lab testing for CDI. Plain radiographs are usually normal in patients with CDI, unless the patient has an ileus or toxic megacolon. CT is useful, however, in suspected cases of fulminant CDI or toxic megacolon, and may reveal colonic-wall thickening, pericolonic stranding, or ascites.9 Colonoscopy is preferred over sigmoidoscopy because up to one-third of patients with pseudomembranous colitis will have involvement of the right colon only.9 However, this test carries the risk of perforation in patients with fulminant colitis.
TABLE 1
Lab tests for C difficile infection
| Test | Substance detected | Time needed | Sensitivity | Specificity |
|---|---|---|---|---|
| Cytotoxin | Toxin B | 1-3 d | 95% | 90%-95% |
| Toxin culture | Toxigenic C difficile† | 3-5 d | >95% | 80%-90% |
| EIA toxin A or A/B | Toxin A or A/B | Hours | 75%-80% | 97%-98% |
| EIA GDH* | C difficile | Hours | 95%-100% | 70%-80% |
| EIA GDH* and toxin A/B | C difficile and C difficile toxin | Hours | 95%-100% | 97%-98% |
| RT-PCR | Toxigenic C difficile† | Hours | >98% | 80%-99% |
| *GDH is the common C difficile antigen. †All toxigenic strains produce toxin B. EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; RT-PCR, reverse-transcriptase polymerase chain reaction. Adapted from: Bartlett JG. Infect Control Hosp Epidemiol. 2010.3 | ||||
Treatment: What to consider, what to avoid
Of the 2 antibiotics most commonly used to treat CDI—metronidazole and vancomycin—only the latter has been approved by the US Food and Drug Administration for this indication. Nevertheless, metronidazole is generally recommended as first-line therapy and has the advantage of being much less expensive than vancomycin. However, an RCT found that oral vancomycin was superior to metronidazole in patients with severe disease.15 The time to resolution of diarrhea may be shorter with oral vancomycin than with metronidazole, as well.16
Recent guidelines suggest that clinicians consider 3 factors in deciding how to treat a first episode of CDI: the patient’s age, peak white blood cell count, and peak serum creatinine level.2 TABLE 2 presents an overview of treatment recommendations for both an initial episode of CDI and recurrences.
Treat severe CDI without delay. For patients with suspected severe CDI, treatment should be started empirically, without waiting for test results. Avoid antiperistaltic agents, which can obscure symptoms and precipitate toxic megacolon.2 Discontinue an antibiotic, if the patient is taking one, as soon as possible after the original infection has been adequately treated. If other infections need to be treated concurrently, we recommend that the course of treatment for CDI be extended until after the other antibiotic regimens have been stopped.
Avoid probiotics in this group. The use of probiotics, both for prevention and to help restore normal bowel flora in patients with CDI, has been advocated for many years. One RCT showed that a yogurt drink containing Lactobacillus and other bacteria reduced the risk of CDI in individuals ≥50 years of age who were taking antibiotics,17 but the guideline development panel recommended against using probiotics until larger trials have been completed.2
Probiotics are not without risk, and several cases of bacteremia have been reported.18,19 Immunocompromised patients appear to be at comparably higher risk, and probiotics should be avoided in this group. Numerous adjunctive agents, including intraluminal toxin binders, biotherapeutic agents, monoclonal antibodies, and a C difficile vaccine, are in various stages of development.2
How to handle recurrences
Relapse rates for CDI range from 6% to 25%,2 and affect patients who receive either vancomycin or metronidazole for the initial treatment. The mechanism relates to either relapse of the original infection or reinfection of susceptible patients with a new strain of C difficile.
Risk of relapse. Elderly patients treated with metronidazole seem to be particularly susceptible to CDI relapse.20 Other risk factors include the administration of non-C difficile antibiotics during or after treatment of CDI, a defective immune response against toxin A, glucocorticoid use, prior stroke, and concurrent use of a proton-pump inhibitor.21-25
TABLE 2 lists tapering and/or pulsed dosing of oral vancomycin as treatment for patients with a second recurrence. We often prescribe the following 6-week regimen, telling patients to take 125 mg vancomycin:
- 4 times a day for one week,
- then 2 times a day for one week,
- then once a day for one week,
- then every other day for one week, and
- finally, every 72 hours for 2 weeks.
Oral metronidazole should not be used beyond the first recurrence or for long-term therapy because of cumulative neurotoxicity, which can be irreversible.2
Management of patients whose CDI recurs after a long course of vancomycin is challenging. Oral rifaximin therapy (400 mg twice a day for 14 days), started immediately at the end of the oral vancomycin course, was shown to cure 7 of 8 patients with multiple relapses.26 Other potential treatment options are oral nitazoxanide, IV tigecycline, or IV immunoglobulin.
CASE You explain to Mary S that diagnostic tests are needed before you can determine whether she can safely take loperamide. When she comes in later that day, you collect a stool sample for C difficile antigen and toxin testing, and order a complete blood count and electrolyte panel.
The patient’s C difficile tests come back positive, her white blood cell count is <15,000 cells/mcL, and her creatinine level is ≤1.5 times her baseline, so you start her on oral metronidazole 500 mg every 8 hours for 14 days. (If the antigen assay had been positive and the toxin negative, you would have either repeated the test or treated Mary S empirically with metronidazole. If the initial antigen assay had been negative, you would have advised her to take the loperamide.)
You schedule a follow-up visit a day or 2 after starting therapy. If the patient is dehydrated or her symptoms have not improved by then, hospitalization may be required.
TABLE 2
Treatment recommendations for C difficile infection
| Clinical description | Clinical evidence | Recommended treatment |
|---|---|---|
| Initial episode (mild or moderate) | Leukocytosis with a white cell count <15,000 cells/mcL and creatinine <1.5 times premorbid level | Metronidazole (oral) 500 mg TID for 10-14 d |
| Initial episode (severe) | Leukocytosis with a white cell count ≥15,000 cells/mcL or creatinine ≥1.5 times premorbid level | Vancomycin (oral) 125 mg QID for 10-14 d |
| Initial episode (severe, complicated) | Hypotension or shock, ileus, megacolon | Vancomycin 500 mg QID (oral or by NG tube) plus metronidazole 500 mg (IV). If complete ileus, consider adding rectal instillation of vancomycin |
| First recurrence | Same as initial episode | |
| Second recurrence | Vancomycin in a tapered and/or pulsed regimen | |
| NG, nasogastric. Adapted from: Cohen SH, et al. Infect Control Hosp Epidemiol. 2010.2 | ||
CORRESPONDENCE
Richard R. Watkins, MD, MS, Division of Infectious Diseases, Akron General Medical Center, 224 West Exchange Street, Suite 290, Akron, OH 44302; rwatkins@agmc.org
• A C difficile diagnosis should be made by one of several widely available testing protocols, including a 2-step method using the common antigen assay to determine whether C difficile is present, followed by an enzyme immunoassay for toxins A and B to improve specificity. B
• Oral metronidazole should be used for initial treatment of mild to moderate C difficile infection, and oral vancomycin and possibly intravenous metronidazole for severe cases. A
• Metronidazole should not be used after an initial recurrence or for long-term therapy because of the risk of neurotoxicity. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Mary S, an 82-year-old patient you recently treated for bronchitis with a 3-day course of levofloxacin, calls your office complaining of diarrhea and abdominal cramps. She describes the diarrhea as nonbloody and particularly foul smelling and asks if she can take loperamide for her symptoms.
If Mary S were your patient, what would you tell her?
The incidence of Clostridium difficile infection (CDI) has been on the rise since 2000, when a common epidemic strain began circulating in North America.1 Although hospitalization or residency in a long-term care facility remains a classic risk factor for CDI, physicians in out-patient settings are increasingly likely to see patients with community-acquired CDI.
Recently updated guidelines from the Society for Health-care Epidemiology of America (SHEA) and the Infectious Diseases Society of America define CDI as the presence of diarrhea (≥3 unformed stools in 24 hours) and either a positive stool test for toxigenic C difficile or its toxins or colonoscopic or histopathologic findings demonstrating pseudomembranous colitis.2 That said, the clinical features of CDI are nonspecific and many patients do not fit the classic profile. So diagnosing CDI requires a high index of suspicion.
The text and tables that follow detail some surprising things about who is likely to develop CDI and which treatment options to employ (and, in some cases, avoid).
Is it CDI? Looking beyond the obvious
Antibiotic use and advanced age, like hospitalization, are classic risk factors for CDI.3 Diarrhea typically begins during or shortly after a course of antibiotics, but may develop as long as 8 weeks after treatment is completed. While any antibiotic, including metronidazole, can precipitate CDI, clindamycin, cephalosporins, extended-spectrum penicillins, and quinolones are most frequently implicated.4 Epidemiologic studies have suggested an association between gastric acid-reducing agents—primarily proton-pump inhibitors—and CDI.4-7 But this link remains controversial, as other investigations have not found a clear relationship.8
In addition to diarrhea, approximately 28% of patients with CDI develop a fever (as high as 104°F); 50% develop leukocytosis (up to 50,000 cells/mcL); and 22% develop abdominal pain, usually localized to the lower quadrants.9 These symptoms, however, are not specific to C difficile, and could be due to a different enteric pathogen, intra-abdominal sepsis, inflammatory bowel disease, or adverse effects of medication, among other causes.9
Markers for severe CDI include age >70 years, leukocyte count >20,000 cells/mcL, albumin level <2.5 g/dL, small-bowel obstruction or ileus, and a computed tomography (CT) scan showing colorectal inflammation.10 Severe CDI can lead to toxic megacolon, bowel perforation, sepsis, and even death.
In addition to considering CDI in patients with nonspecific symptoms, it is important to include it in the differential diagnosis of patients who do not fit the classic profile. In a recent study of patients with CDI at 4 Veterans Affairs facilities, almost half (49%) of those studied had no exposure to antimicrobial drugs. The researchers further found that the median age of patients with CDI was 61 years—younger than that found in previous studies—and that 20% of the cases were community-acquired.11
Consider CDI in children, too. Risk factors for CDI in pediatric patients include disruption of the normal microflora of the gastrointestinal tract, compromised immune status, poor diet, underlying health conditions, concurrent infections, and cancer.12
Diagnostic testing: Consider a 2-step assay
Patients with symptoms suggestive of CDI should undergo laboratory testing to confirm the diagnosis. TABLE 1 lists the tests that are widely available in the United States.3 Only liquid stools should be tested and just one sample should be sent to the lab, as multiple samples do not increase the diagnostic yield.13 In addition, tests should be used only for diagnosis, and not as a “test of cure.” This is because patients can shed C difficile toxin and spores for several weeks after completing treatment, and there are wide variations in the sensitivity of toxin assays.
Infants <1 year old have high rates of asymptomatic toxigenic strains of C difficile, and until 2008, recommendations from SHEA discouraged testing the stools of such young patients. Because of the difficulty in differentiating incidental colonization from true CDI in this patient population, the authors of a recent review suggested using more than one diagnostic approach when testing children <1 year of age.14
We advocate a 2-step assay—that is, testing for both glutamate dehydrogenase (GDH)—an antigen common to all strains of C difficile—and C difficile toxins A and B. The common antigen test is sensitive, but may detect carriers who do not have active disease. The enzyme immunoassay (EIA) for toxins A and B helps to improve specificity. Therefore, positive results of both tests would be considered a positive finding, negative results of both tests would be considered a negative finding, and one positive result with one negative result would require another test for toxin detection.3
The reverse-transcriptase polymerase chain reaction (RT-PCR) assay, which detects the toxin B gene of C difficile, is the newest test for CDI. The RT-PCR assay detects only toxigenic strains of C difficile, and all toxigenic strains produce toxin B, making it more specific than testing for the common antigen. The RT-PCR assay also has better sensitivity than the cytotoxin assay, which also tests for toxin B. The major limitation of the RT-PCR assay is the frequency of false-positive results in hospitalized patients with a high incidence of C difficile colonization.3
Routine laboratory studies, including a complete blood count with differential and a complete metabolic panel, are often useful to ascertain the presence and degree of leukocytosis, dehydration, and other metabolic abnormalities and to test for hypoalbuminemia. Fecal leukocytes can be seen in colitis and may be useful in select cases.
Imaging studies such as radiography, CT, and endoscopy have largely been superseded by lab testing for CDI. Plain radiographs are usually normal in patients with CDI, unless the patient has an ileus or toxic megacolon. CT is useful, however, in suspected cases of fulminant CDI or toxic megacolon, and may reveal colonic-wall thickening, pericolonic stranding, or ascites.9 Colonoscopy is preferred over sigmoidoscopy because up to one-third of patients with pseudomembranous colitis will have involvement of the right colon only.9 However, this test carries the risk of perforation in patients with fulminant colitis.
TABLE 1
Lab tests for C difficile infection
| Test | Substance detected | Time needed | Sensitivity | Specificity |
|---|---|---|---|---|
| Cytotoxin | Toxin B | 1-3 d | 95% | 90%-95% |
| Toxin culture | Toxigenic C difficile† | 3-5 d | >95% | 80%-90% |
| EIA toxin A or A/B | Toxin A or A/B | Hours | 75%-80% | 97%-98% |
| EIA GDH* | C difficile | Hours | 95%-100% | 70%-80% |
| EIA GDH* and toxin A/B | C difficile and C difficile toxin | Hours | 95%-100% | 97%-98% |
| RT-PCR | Toxigenic C difficile† | Hours | >98% | 80%-99% |
| *GDH is the common C difficile antigen. †All toxigenic strains produce toxin B. EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; RT-PCR, reverse-transcriptase polymerase chain reaction. Adapted from: Bartlett JG. Infect Control Hosp Epidemiol. 2010.3 | ||||
Treatment: What to consider, what to avoid
Of the 2 antibiotics most commonly used to treat CDI—metronidazole and vancomycin—only the latter has been approved by the US Food and Drug Administration for this indication. Nevertheless, metronidazole is generally recommended as first-line therapy and has the advantage of being much less expensive than vancomycin. However, an RCT found that oral vancomycin was superior to metronidazole in patients with severe disease.15 The time to resolution of diarrhea may be shorter with oral vancomycin than with metronidazole, as well.16
Recent guidelines suggest that clinicians consider 3 factors in deciding how to treat a first episode of CDI: the patient’s age, peak white blood cell count, and peak serum creatinine level.2 TABLE 2 presents an overview of treatment recommendations for both an initial episode of CDI and recurrences.
Treat severe CDI without delay. For patients with suspected severe CDI, treatment should be started empirically, without waiting for test results. Avoid antiperistaltic agents, which can obscure symptoms and precipitate toxic megacolon.2 Discontinue an antibiotic, if the patient is taking one, as soon as possible after the original infection has been adequately treated. If other infections need to be treated concurrently, we recommend that the course of treatment for CDI be extended until after the other antibiotic regimens have been stopped.
Avoid probiotics in this group. The use of probiotics, both for prevention and to help restore normal bowel flora in patients with CDI, has been advocated for many years. One RCT showed that a yogurt drink containing Lactobacillus and other bacteria reduced the risk of CDI in individuals ≥50 years of age who were taking antibiotics,17 but the guideline development panel recommended against using probiotics until larger trials have been completed.2
Probiotics are not without risk, and several cases of bacteremia have been reported.18,19 Immunocompromised patients appear to be at comparably higher risk, and probiotics should be avoided in this group. Numerous adjunctive agents, including intraluminal toxin binders, biotherapeutic agents, monoclonal antibodies, and a C difficile vaccine, are in various stages of development.2
How to handle recurrences
Relapse rates for CDI range from 6% to 25%,2 and affect patients who receive either vancomycin or metronidazole for the initial treatment. The mechanism relates to either relapse of the original infection or reinfection of susceptible patients with a new strain of C difficile.
Risk of relapse. Elderly patients treated with metronidazole seem to be particularly susceptible to CDI relapse.20 Other risk factors include the administration of non-C difficile antibiotics during or after treatment of CDI, a defective immune response against toxin A, glucocorticoid use, prior stroke, and concurrent use of a proton-pump inhibitor.21-25
TABLE 2 lists tapering and/or pulsed dosing of oral vancomycin as treatment for patients with a second recurrence. We often prescribe the following 6-week regimen, telling patients to take 125 mg vancomycin:
- 4 times a day for one week,
- then 2 times a day for one week,
- then once a day for one week,
- then every other day for one week, and
- finally, every 72 hours for 2 weeks.
Oral metronidazole should not be used beyond the first recurrence or for long-term therapy because of cumulative neurotoxicity, which can be irreversible.2
Management of patients whose CDI recurs after a long course of vancomycin is challenging. Oral rifaximin therapy (400 mg twice a day for 14 days), started immediately at the end of the oral vancomycin course, was shown to cure 7 of 8 patients with multiple relapses.26 Other potential treatment options are oral nitazoxanide, IV tigecycline, or IV immunoglobulin.
CASE You explain to Mary S that diagnostic tests are needed before you can determine whether she can safely take loperamide. When she comes in later that day, you collect a stool sample for C difficile antigen and toxin testing, and order a complete blood count and electrolyte panel.
The patient’s C difficile tests come back positive, her white blood cell count is <15,000 cells/mcL, and her creatinine level is ≤1.5 times her baseline, so you start her on oral metronidazole 500 mg every 8 hours for 14 days. (If the antigen assay had been positive and the toxin negative, you would have either repeated the test or treated Mary S empirically with metronidazole. If the initial antigen assay had been negative, you would have advised her to take the loperamide.)
You schedule a follow-up visit a day or 2 after starting therapy. If the patient is dehydrated or her symptoms have not improved by then, hospitalization may be required.
TABLE 2
Treatment recommendations for C difficile infection
| Clinical description | Clinical evidence | Recommended treatment |
|---|---|---|
| Initial episode (mild or moderate) | Leukocytosis with a white cell count <15,000 cells/mcL and creatinine <1.5 times premorbid level | Metronidazole (oral) 500 mg TID for 10-14 d |
| Initial episode (severe) | Leukocytosis with a white cell count ≥15,000 cells/mcL or creatinine ≥1.5 times premorbid level | Vancomycin (oral) 125 mg QID for 10-14 d |
| Initial episode (severe, complicated) | Hypotension or shock, ileus, megacolon | Vancomycin 500 mg QID (oral or by NG tube) plus metronidazole 500 mg (IV). If complete ileus, consider adding rectal instillation of vancomycin |
| First recurrence | Same as initial episode | |
| Second recurrence | Vancomycin in a tapered and/or pulsed regimen | |
| NG, nasogastric. Adapted from: Cohen SH, et al. Infect Control Hosp Epidemiol. 2010.2 | ||
CORRESPONDENCE
Richard R. Watkins, MD, MS, Division of Infectious Diseases, Akron General Medical Center, 224 West Exchange Street, Suite 290, Akron, OH 44302; rwatkins@agmc.org
1. Gerding DN. Global epidemiology of Clostridium difficile infection in 2010. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S32-S34.
2. Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431-455.
3. Bartlett JG. Detection of Clostridium difficile infection. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S35-S37.
4. Dial S, Alrasadi K, Manoukian C, et al. Risk of Clostridium difficile diarrhea among hospital inpatients prescribed proton pump inhibitors: cohort and case-control studies. CMAJ. 2004;171:33-38.
5. Dial S, Delaney JA, Barkun AN, et al. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294:2989-2995.
6. Cunningham R, Dale B, Undy B, et al. Proton pump inhibitors as a risk factor for Clostridium difficile diarrhoea. J Hosp Infect. 2003;54:243-245.
7. Howell MD, Novack V, Grgurich P, et al. Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection. Arch Intern Med. 2010;170:784-790.
8. Shah S, Lewis A, Leopold D, et al. Gastric acid suppression does not promote clostridial diarrhoea in the elderly. QJM. 2000;93:175-181.
9. Bartlett JG, Gerding DN. Clinical recognition and diagnosis of Clostridium difficile infection. Clin Infect Dis. 2008;46(suppl 1):S12-S18.
10. Henrich TJ, Krakower D, Bitton A, et al. Clinical risk factors for severe Clostridium difficile-associated disease. Emerg Infect Dis. 2009;15:415-422.
11. Kutty PK, Woods CW, Sena AC, et al. Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA. Emerg Infect Dis. 2010;16:197-204.
12. Pituch H. Clostridium difficile is no longer just a nosocomial infection or an infection of adults. Int J Antimicrob Agents. 2009;33(suppl 1):S42-S45.
13. Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006;119:356.e7-e8.
14. Bryant K, McDonald LC. Clostridium difficile infections in children. Pediatr Infect Dis J. 2009;28:145-146.
15. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
16. Belmares J, Gerding DN, Parada JP, et al. Outcome of metronidazole therapy for Clostridium difficile disease and correlation with a scoring system. J Infect. 2007;55:495-501.
17. Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ. 2007;335:80.-
18. Ledoux D, Labombardi VJ, Karter D. Lactobacillus acidophilus bacteraemia after use of a probiotic in a patient with AIDS and Hodgkin’s disease. Int J STD AIDS. 2006;17:280-282.
19. Hammerman C, Bin-Nun A, Kaplan M. Safety of probiotics: comparison of two popular strains. BMJ. 2006;333:1006-1008.
20. Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
21. Nair S, Yadav D, Corpuz M, et al. Clostridium difficile colitis: factors influencing treatment failure and relapse—a prospective evaluation. Am J Gastroenterol. 1998;93:1873-1876.
22. Garey KW, Sethi S, Yadav Y, et al. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect. 2008;70:298-304.
23. Das R, Feuerstadt P, Brandt LJ. Glucocorticoids are associated with increased risk of short-term mortality in hospitalized patients with Clostridium difficile-associated disease. Am J Gastroenterol. 2010;105:2040-2049.
24. Cadena J, Thompson GR, 3rd, Patterson JE, et al. Clinical predictors and risk factors for relapsing Clostridium difficile infection. Am J Med Sci. 2010;339:350-355.
25. Linsky A, Gupta K, Lawler EV, et al. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med. 2010;170:772-778.
26. Johnson S, Schriever C, Galang M, et al. Interruption of recurrent Clostridium difficile-associated diarrhea episodes by serial therapy with vancomycin and rifaximin. Clin Infect Dis. 2007;44:846-848.
1. Gerding DN. Global epidemiology of Clostridium difficile infection in 2010. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S32-S34.
2. Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431-455.
3. Bartlett JG. Detection of Clostridium difficile infection. Infect Control Hosp Epidemiol. 2010;31(suppl 1):S35-S37.
4. Dial S, Alrasadi K, Manoukian C, et al. Risk of Clostridium difficile diarrhea among hospital inpatients prescribed proton pump inhibitors: cohort and case-control studies. CMAJ. 2004;171:33-38.
5. Dial S, Delaney JA, Barkun AN, et al. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294:2989-2995.
6. Cunningham R, Dale B, Undy B, et al. Proton pump inhibitors as a risk factor for Clostridium difficile diarrhoea. J Hosp Infect. 2003;54:243-245.
7. Howell MD, Novack V, Grgurich P, et al. Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection. Arch Intern Med. 2010;170:784-790.
8. Shah S, Lewis A, Leopold D, et al. Gastric acid suppression does not promote clostridial diarrhoea in the elderly. QJM. 2000;93:175-181.
9. Bartlett JG, Gerding DN. Clinical recognition and diagnosis of Clostridium difficile infection. Clin Infect Dis. 2008;46(suppl 1):S12-S18.
10. Henrich TJ, Krakower D, Bitton A, et al. Clinical risk factors for severe Clostridium difficile-associated disease. Emerg Infect Dis. 2009;15:415-422.
11. Kutty PK, Woods CW, Sena AC, et al. Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA. Emerg Infect Dis. 2010;16:197-204.
12. Pituch H. Clostridium difficile is no longer just a nosocomial infection or an infection of adults. Int J Antimicrob Agents. 2009;33(suppl 1):S42-S45.
13. Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006;119:356.e7-e8.
14. Bryant K, McDonald LC. Clostridium difficile infections in children. Pediatr Infect Dis J. 2009;28:145-146.
15. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
16. Belmares J, Gerding DN, Parada JP, et al. Outcome of metronidazole therapy for Clostridium difficile disease and correlation with a scoring system. J Infect. 2007;55:495-501.
17. Hickson M, D’Souza AL, Muthu N, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ. 2007;335:80.-
18. Ledoux D, Labombardi VJ, Karter D. Lactobacillus acidophilus bacteraemia after use of a probiotic in a patient with AIDS and Hodgkin’s disease. Int J STD AIDS. 2006;17:280-282.
19. Hammerman C, Bin-Nun A, Kaplan M. Safety of probiotics: comparison of two popular strains. BMJ. 2006;333:1006-1008.
20. Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
21. Nair S, Yadav D, Corpuz M, et al. Clostridium difficile colitis: factors influencing treatment failure and relapse—a prospective evaluation. Am J Gastroenterol. 1998;93:1873-1876.
22. Garey KW, Sethi S, Yadav Y, et al. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect. 2008;70:298-304.
23. Das R, Feuerstadt P, Brandt LJ. Glucocorticoids are associated with increased risk of short-term mortality in hospitalized patients with Clostridium difficile-associated disease. Am J Gastroenterol. 2010;105:2040-2049.
24. Cadena J, Thompson GR, 3rd, Patterson JE, et al. Clinical predictors and risk factors for relapsing Clostridium difficile infection. Am J Med Sci. 2010;339:350-355.
25. Linsky A, Gupta K, Lawler EV, et al. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med. 2010;170:772-778.
26. Johnson S, Schriever C, Galang M, et al. Interruption of recurrent Clostridium difficile-associated diarrhea episodes by serial therapy with vancomycin and rifaximin. Clin Infect Dis. 2007;44:846-848.