User login
How Are Doctors Using Tirzepatide vs Semaglutide? A Q&A
When prescribing glucagon-like peptide 1 (GLP-1) medications, many physicians prefer tirzepatide over the more well-known semaglutide due to its superior efficacy in weight loss and A1c reduction. Studies indicated that tirzepatide can lead to greater weight loss than semaglutide.
Factors like insurance coverage, drug availability, and side effects also influence physicians’ choices, with some patients benefiting from the broader dosing options that tirzepatide offers.
In this Q&A, Medscape Medical News explored how physicians can make the best decisions with their patients when choosing between GLP-1 medications tirzepatide and semaglutide for the treatment for type 2 diabetes and obesity.
We spoke to physicians who specialize in medical weight loss on things to consider when choosing between these two medications, such as patient profiles, drug access and availability, and financial considerations. We also discussed the side effect profiles of the medications based on current data in the literature.
Medscape Medical News: How are you deciding which of the two drugs to prescribe?
Caroline Messer, MD, endocrinologist at Lenox Hill Hospital, Northwell, New York City: To some degree, it’s based on insurance. But in general, I’m pushing most patients toward tirzepatide just because the data show that there’s more weight loss and more A1c reduction on tirzepatide. But the research shows that there are more side effects. But I think every practicing clinician who uses these medications knows that there are actually fewer side effects despite what the trial showed.
Sue Decotiis, MD, weight loss doctor, New York City: I think that many doctors that are prescribing these drugs are not really weight loss specialists. It’s just like one of many drugs that they prescribe. And semaglutide (Ozempic) is more well known. I think it’s because they don’t really know that it’s not as good as the other drugs. There are still massive shortages of these drugs. So that’s another reason why a doctor may choose one drug over another. Also, if a patient’s reliant on insurance to cover it, they may go with whatever the insurance company is willing to cover.
Kathleen Dungan, MD, professor of internal medicine, Division of Endocrinology, Diabetes and Metabolism, The Ohio State University Wexner Medical Center and College of Medicine: Some patients may have preferences with the delivery device. In the past year, in particular, availability of these drugs was limited and varied from time to time and geographically, and therefore, patients needed to substitute one drug for another in order to maintain treatment.
Maria Teresa Anton, MD, endocrinologist and educator, Pritikin Longevity Center, Miami: While I do not prescribe these medications, I do focus on integrating them into a comprehensive lifestyle program that empowers patients to make sustainable changes. By fostering an environment of education and support, we enhance their well-being and promote long-term health outcomes. In my practice, I’ve found that the most successful outcomes occur when these medications are combined with a comprehensive approach, including dietary changes, physical activity, and behavioral support.
Medscape Medical News: How do you make the decision of tirzepatide vs semaglutide?
Messer: There’s no guideline per se. Sometimes when I don’t want a patient to lose too much weight, I might consider Ozempic or Wegovy if you know they only have 5 lb to lose. If diabetes, then I might go for the Ozempic instead, just because the weight loss is so drastic with tirzepatide with any kind of appetite.
Decotiis: If somebody has a lot of weight to lose and they’re highly insulin resistant, as most people are when they start these drugs, I really prefer tirzepatide ... because I think patients are going to lose more weight, they’re going to lose more fat. I also see that patients have less side effects because before tirzepatide came out, I was prescribing mostly semaglutide, and there were a lot of side effects. But semaglutide is fine. I mean, it’s a good drug. Maybe it’s better for people that don’t have as much weight to lose. So I don’t have to worry about them hitting that wall after a certain period of time. But it’s a good drug. I mean, I certainly still use it.
Medscape Medical News: What of the data and the literature on the differences in the outcomes and the side effect profile?
Messer: In terms of outcomes, the weight loss is almost double [with tirzepatide]. It depends what trial you’re looking at, but we tend to see like about 15% of your body weight you lose with the semaglutide and 25%-30% with the tirzepatide. The big difference, I suppose…is semaglutide now has a cardiovascular indication and the tirzepatide doesn’t, but I’m very confident that tirzepatide is going to get the same indication.
Decotiis: When that first Lilly study came out in June of 2022, it really blew everybody away. I mean, some patients lost up to 25% of their weight on tirzepatide, whereas on Ozempic, it was really like 15%. Now, in my practice, I really monitor everyone with a body composition scale. I’m not just looking at somebody’s weight or body mass index, I am looking at how much body fat they have, how much muscle mass they have, how much water they have, and how much bone they have.
The golden rule here is make sure the patient loses fat, and you want to make sure they’re not losing muscle or too much water. The patient really needs to be adequately hydrated. So what I’m saying is a lot of people who have lost weight have not reached the promised land because they haven’t lost enough body fat to get them into that healthy zone. But once they reduce the body fat to a certain percentage, let’s say for a woman about 20%, or a man in the low teens, they’re less likely to regain that weight because they haven’t really lost fat. And that’s how we gain health.
A version of this article first appeared on Medscape.com.
When prescribing glucagon-like peptide 1 (GLP-1) medications, many physicians prefer tirzepatide over the more well-known semaglutide due to its superior efficacy in weight loss and A1c reduction. Studies indicated that tirzepatide can lead to greater weight loss than semaglutide.
Factors like insurance coverage, drug availability, and side effects also influence physicians’ choices, with some patients benefiting from the broader dosing options that tirzepatide offers.
In this Q&A, Medscape Medical News explored how physicians can make the best decisions with their patients when choosing between GLP-1 medications tirzepatide and semaglutide for the treatment for type 2 diabetes and obesity.
We spoke to physicians who specialize in medical weight loss on things to consider when choosing between these two medications, such as patient profiles, drug access and availability, and financial considerations. We also discussed the side effect profiles of the medications based on current data in the literature.
Medscape Medical News: How are you deciding which of the two drugs to prescribe?
Caroline Messer, MD, endocrinologist at Lenox Hill Hospital, Northwell, New York City: To some degree, it’s based on insurance. But in general, I’m pushing most patients toward tirzepatide just because the data show that there’s more weight loss and more A1c reduction on tirzepatide. But the research shows that there are more side effects. But I think every practicing clinician who uses these medications knows that there are actually fewer side effects despite what the trial showed.
Sue Decotiis, MD, weight loss doctor, New York City: I think that many doctors that are prescribing these drugs are not really weight loss specialists. It’s just like one of many drugs that they prescribe. And semaglutide (Ozempic) is more well known. I think it’s because they don’t really know that it’s not as good as the other drugs. There are still massive shortages of these drugs. So that’s another reason why a doctor may choose one drug over another. Also, if a patient’s reliant on insurance to cover it, they may go with whatever the insurance company is willing to cover.
Kathleen Dungan, MD, professor of internal medicine, Division of Endocrinology, Diabetes and Metabolism, The Ohio State University Wexner Medical Center and College of Medicine: Some patients may have preferences with the delivery device. In the past year, in particular, availability of these drugs was limited and varied from time to time and geographically, and therefore, patients needed to substitute one drug for another in order to maintain treatment.
Maria Teresa Anton, MD, endocrinologist and educator, Pritikin Longevity Center, Miami: While I do not prescribe these medications, I do focus on integrating them into a comprehensive lifestyle program that empowers patients to make sustainable changes. By fostering an environment of education and support, we enhance their well-being and promote long-term health outcomes. In my practice, I’ve found that the most successful outcomes occur when these medications are combined with a comprehensive approach, including dietary changes, physical activity, and behavioral support.
Medscape Medical News: How do you make the decision of tirzepatide vs semaglutide?
Messer: There’s no guideline per se. Sometimes when I don’t want a patient to lose too much weight, I might consider Ozempic or Wegovy if you know they only have 5 lb to lose. If diabetes, then I might go for the Ozempic instead, just because the weight loss is so drastic with tirzepatide with any kind of appetite.
Decotiis: If somebody has a lot of weight to lose and they’re highly insulin resistant, as most people are when they start these drugs, I really prefer tirzepatide ... because I think patients are going to lose more weight, they’re going to lose more fat. I also see that patients have less side effects because before tirzepatide came out, I was prescribing mostly semaglutide, and there were a lot of side effects. But semaglutide is fine. I mean, it’s a good drug. Maybe it’s better for people that don’t have as much weight to lose. So I don’t have to worry about them hitting that wall after a certain period of time. But it’s a good drug. I mean, I certainly still use it.
Medscape Medical News: What of the data and the literature on the differences in the outcomes and the side effect profile?
Messer: In terms of outcomes, the weight loss is almost double [with tirzepatide]. It depends what trial you’re looking at, but we tend to see like about 15% of your body weight you lose with the semaglutide and 25%-30% with the tirzepatide. The big difference, I suppose…is semaglutide now has a cardiovascular indication and the tirzepatide doesn’t, but I’m very confident that tirzepatide is going to get the same indication.
Decotiis: When that first Lilly study came out in June of 2022, it really blew everybody away. I mean, some patients lost up to 25% of their weight on tirzepatide, whereas on Ozempic, it was really like 15%. Now, in my practice, I really monitor everyone with a body composition scale. I’m not just looking at somebody’s weight or body mass index, I am looking at how much body fat they have, how much muscle mass they have, how much water they have, and how much bone they have.
The golden rule here is make sure the patient loses fat, and you want to make sure they’re not losing muscle or too much water. The patient really needs to be adequately hydrated. So what I’m saying is a lot of people who have lost weight have not reached the promised land because they haven’t lost enough body fat to get them into that healthy zone. But once they reduce the body fat to a certain percentage, let’s say for a woman about 20%, or a man in the low teens, they’re less likely to regain that weight because they haven’t really lost fat. And that’s how we gain health.
A version of this article first appeared on Medscape.com.
When prescribing glucagon-like peptide 1 (GLP-1) medications, many physicians prefer tirzepatide over the more well-known semaglutide due to its superior efficacy in weight loss and A1c reduction. Studies indicated that tirzepatide can lead to greater weight loss than semaglutide.
Factors like insurance coverage, drug availability, and side effects also influence physicians’ choices, with some patients benefiting from the broader dosing options that tirzepatide offers.
In this Q&A, Medscape Medical News explored how physicians can make the best decisions with their patients when choosing between GLP-1 medications tirzepatide and semaglutide for the treatment for type 2 diabetes and obesity.
We spoke to physicians who specialize in medical weight loss on things to consider when choosing between these two medications, such as patient profiles, drug access and availability, and financial considerations. We also discussed the side effect profiles of the medications based on current data in the literature.
Medscape Medical News: How are you deciding which of the two drugs to prescribe?
Caroline Messer, MD, endocrinologist at Lenox Hill Hospital, Northwell, New York City: To some degree, it’s based on insurance. But in general, I’m pushing most patients toward tirzepatide just because the data show that there’s more weight loss and more A1c reduction on tirzepatide. But the research shows that there are more side effects. But I think every practicing clinician who uses these medications knows that there are actually fewer side effects despite what the trial showed.
Sue Decotiis, MD, weight loss doctor, New York City: I think that many doctors that are prescribing these drugs are not really weight loss specialists. It’s just like one of many drugs that they prescribe. And semaglutide (Ozempic) is more well known. I think it’s because they don’t really know that it’s not as good as the other drugs. There are still massive shortages of these drugs. So that’s another reason why a doctor may choose one drug over another. Also, if a patient’s reliant on insurance to cover it, they may go with whatever the insurance company is willing to cover.
Kathleen Dungan, MD, professor of internal medicine, Division of Endocrinology, Diabetes and Metabolism, The Ohio State University Wexner Medical Center and College of Medicine: Some patients may have preferences with the delivery device. In the past year, in particular, availability of these drugs was limited and varied from time to time and geographically, and therefore, patients needed to substitute one drug for another in order to maintain treatment.
Maria Teresa Anton, MD, endocrinologist and educator, Pritikin Longevity Center, Miami: While I do not prescribe these medications, I do focus on integrating them into a comprehensive lifestyle program that empowers patients to make sustainable changes. By fostering an environment of education and support, we enhance their well-being and promote long-term health outcomes. In my practice, I’ve found that the most successful outcomes occur when these medications are combined with a comprehensive approach, including dietary changes, physical activity, and behavioral support.
Medscape Medical News: How do you make the decision of tirzepatide vs semaglutide?
Messer: There’s no guideline per se. Sometimes when I don’t want a patient to lose too much weight, I might consider Ozempic or Wegovy if you know they only have 5 lb to lose. If diabetes, then I might go for the Ozempic instead, just because the weight loss is so drastic with tirzepatide with any kind of appetite.
Decotiis: If somebody has a lot of weight to lose and they’re highly insulin resistant, as most people are when they start these drugs, I really prefer tirzepatide ... because I think patients are going to lose more weight, they’re going to lose more fat. I also see that patients have less side effects because before tirzepatide came out, I was prescribing mostly semaglutide, and there were a lot of side effects. But semaglutide is fine. I mean, it’s a good drug. Maybe it’s better for people that don’t have as much weight to lose. So I don’t have to worry about them hitting that wall after a certain period of time. But it’s a good drug. I mean, I certainly still use it.
Medscape Medical News: What of the data and the literature on the differences in the outcomes and the side effect profile?
Messer: In terms of outcomes, the weight loss is almost double [with tirzepatide]. It depends what trial you’re looking at, but we tend to see like about 15% of your body weight you lose with the semaglutide and 25%-30% with the tirzepatide. The big difference, I suppose…is semaglutide now has a cardiovascular indication and the tirzepatide doesn’t, but I’m very confident that tirzepatide is going to get the same indication.
Decotiis: When that first Lilly study came out in June of 2022, it really blew everybody away. I mean, some patients lost up to 25% of their weight on tirzepatide, whereas on Ozempic, it was really like 15%. Now, in my practice, I really monitor everyone with a body composition scale. I’m not just looking at somebody’s weight or body mass index, I am looking at how much body fat they have, how much muscle mass they have, how much water they have, and how much bone they have.
The golden rule here is make sure the patient loses fat, and you want to make sure they’re not losing muscle or too much water. The patient really needs to be adequately hydrated. So what I’m saying is a lot of people who have lost weight have not reached the promised land because they haven’t lost enough body fat to get them into that healthy zone. But once they reduce the body fat to a certain percentage, let’s say for a woman about 20%, or a man in the low teens, they’re less likely to regain that weight because they haven’t really lost fat. And that’s how we gain health.
A version of this article first appeared on Medscape.com.
Sex After Pregnancy: Why It Matters and How to Start the Conversation
Sarah, a new mom who’s thrilled about her 3-month-old baby, is struggling with her sex life. Her once vibrant physical relationship with her partner has dwindled, and she’s dealing with painful intercourse and a notable drop in desire.
Pregnancy and childbirth are transformative experiences that affect every facet of a person’s life, including their sexual well-being. Despite this fact, clinicians frequently ignore sexual well-being, beyond contraception, in prenatal and postpartum care. In peripartum care, anticipatory guidance is recognized to be crucial to the well-being of new parents and their babies. Why should sexual well-being get the shaft?
Why Talk About Sex?
Sex is a fundamental aspect of many people’s lives and relationships and can significantly affect overall well-being. Despite cultural narratives that often exclude the sexual function and pleasure aspect of sexual health from peripartum discussions, many new parents face sexual challenges that can worsen their physical and emotional health.
While up to 88% of new parents report problems with sexual well-being, less than 30% report receiving anticipatory guidance about sexual function changes. One study found only 15% of postpartum women reported discussing sexual concerns with their medical providers. And, when new parents receive more information about sexual health, they tend to report improved sexual well-being. Clearly, a gap needs bridging.
Sexual health doesn’t just affect individual well-being; it intertwines with relationship satisfaction. Attending to satisfaction in one’s relationship may be an important component of child health as well.
Declines in the frequency of sexual engagement and desire are common after childbirth. Changes in arousal, orgasm, and sexual pleasure, often accompanied by pain, are also reported by many women. Some birthing parents report changes to the sensation of their genitals that are thought to be related to stretch of the pudendal nerve during parturition. Most experience resolution of these concerns within the first year after childbirth, although some women report persistent problems, including up to 33% with persistent sexual pain.
Many factors can contribute to postpartum sexual issues, including hormonal changes, body image concerns, and mental health conditions. Breastfeeding, for instance, can lead to vaginal dryness and reduced sexual arousal due to hormonal shifts. Body image issues and mood disorders like depression and anxiety can also adversely affect sexual function. Women with postpartum depression are more likely to experience sexual concerns, and the relationship between sexual difficulties and depression can be bidirectional.
Empowerment and Expectations
One commonly cited recommendation is to wait until 6 weeks postpartum before resuming penetrative intercourse after a normal vaginal delivery. However, this guideline lacks robust scientific backing. Many people might feel ready for sexual intercourse much sooner or, conversely, might not feel comfortable at the 6-week mark. As clinicians, we must empower our patients to trust their own bodies and make decisions based on their comfort and readiness.
The 6-week advice can sometimes unintentionally convey to women that they are not experts on their own bodies, or that any kind of sex is risky. Acknowledging the recovery timeline for every person is unique and various forms of sexual expression are safe can help foster a healthier approach to resuming sexual activities. In one study of postpartum sexual behavior, in the first 6 weeks after delivery, the most common kinds of sexual play included giving oral sex to a partner and solo sex. Between 80% and 90% have resumed vaginal-receiving sexual play (including intercourse) by 3 months.
While recognizing that changes to sexual experience occur, we need to reinforce that gradual recovery is expected. And if women express distress about a sexual change, or if those changes persist, primary care providers should be prepared to help them with their concerns.
Parents need to know experiencing pain is not something they should “just deal with” or ignore. Attempting to repeatedly endure sexual pain can cause new issues, such as high-tone dysfunction of the pelvic floor or an understandable decrease in willingness or receptiveness to sexual play of any kind. Encouraging open communication about these issues can help couples navigate these changes more smoothly.
Partners, especially new fathers, also experience sexual and emotional challenges. They can feel blindsided by the changes in their relationship and might struggle with feelings of jealousy or inadequacy. Understanding partners also face difficulties can help in providing a more comprehensive approach to sexual health care.
Starting the Conversation
So, how can we initiate these important conversations with new parents? Start by providing permission. As healthcare providers, we need to create an environment where discussing sexual health is normalized and welcomed. Simple, nonjudgmental statements can open the door to these discussions. For example, saying, “Many people notice changes in their sexual desire or pleasure after childbirth. Has anything like this happened to you or your partner?” can encourage patients to share their concerns.
Assessing the importance to patients of sexual problems can help direct the need for intervention. Follow up on these concerns and offer support, whether through counseling, pelvic floor physical therapy, or a referral to a sexual medicine specialist, a sex therapist, or other appropriate resource.
Let’s return to Sarah. In the ideal world, at 3 months postpartum she will already have had a handful of clinical conversations about her sexual well-being with her healthcare team — at prenatal visits, at well-baby visits, and at her postpartum checkups. Several of these conversations included her partner. They both understand the transition to parenthood could be rocky for their sex lives. They’ve set aside time to connect and stay physically close. She’s listened to her body and only engaged in sexual play for which she feels ready. Now, noting that some aspects of sexual play are persistently uncomfortable, she knows it’s time to follow up. Without shame or anxiety, she books an appointment with you, knowing that you understand how important this issue is for her, her partner, and her baby.
If you’re working with new parents, remember: Open dialogue about sexual health is not just beneficial — it’s essential. Let’s bridge the gap in care by embracing these conversations and offering the support new parents truly need.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester Medical Center, Rochester, New York, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sarah, a new mom who’s thrilled about her 3-month-old baby, is struggling with her sex life. Her once vibrant physical relationship with her partner has dwindled, and she’s dealing with painful intercourse and a notable drop in desire.
Pregnancy and childbirth are transformative experiences that affect every facet of a person’s life, including their sexual well-being. Despite this fact, clinicians frequently ignore sexual well-being, beyond contraception, in prenatal and postpartum care. In peripartum care, anticipatory guidance is recognized to be crucial to the well-being of new parents and their babies. Why should sexual well-being get the shaft?
Why Talk About Sex?
Sex is a fundamental aspect of many people’s lives and relationships and can significantly affect overall well-being. Despite cultural narratives that often exclude the sexual function and pleasure aspect of sexual health from peripartum discussions, many new parents face sexual challenges that can worsen their physical and emotional health.
While up to 88% of new parents report problems with sexual well-being, less than 30% report receiving anticipatory guidance about sexual function changes. One study found only 15% of postpartum women reported discussing sexual concerns with their medical providers. And, when new parents receive more information about sexual health, they tend to report improved sexual well-being. Clearly, a gap needs bridging.
Sexual health doesn’t just affect individual well-being; it intertwines with relationship satisfaction. Attending to satisfaction in one’s relationship may be an important component of child health as well.
Declines in the frequency of sexual engagement and desire are common after childbirth. Changes in arousal, orgasm, and sexual pleasure, often accompanied by pain, are also reported by many women. Some birthing parents report changes to the sensation of their genitals that are thought to be related to stretch of the pudendal nerve during parturition. Most experience resolution of these concerns within the first year after childbirth, although some women report persistent problems, including up to 33% with persistent sexual pain.
Many factors can contribute to postpartum sexual issues, including hormonal changes, body image concerns, and mental health conditions. Breastfeeding, for instance, can lead to vaginal dryness and reduced sexual arousal due to hormonal shifts. Body image issues and mood disorders like depression and anxiety can also adversely affect sexual function. Women with postpartum depression are more likely to experience sexual concerns, and the relationship between sexual difficulties and depression can be bidirectional.
Empowerment and Expectations
One commonly cited recommendation is to wait until 6 weeks postpartum before resuming penetrative intercourse after a normal vaginal delivery. However, this guideline lacks robust scientific backing. Many people might feel ready for sexual intercourse much sooner or, conversely, might not feel comfortable at the 6-week mark. As clinicians, we must empower our patients to trust their own bodies and make decisions based on their comfort and readiness.
The 6-week advice can sometimes unintentionally convey to women that they are not experts on their own bodies, or that any kind of sex is risky. Acknowledging the recovery timeline for every person is unique and various forms of sexual expression are safe can help foster a healthier approach to resuming sexual activities. In one study of postpartum sexual behavior, in the first 6 weeks after delivery, the most common kinds of sexual play included giving oral sex to a partner and solo sex. Between 80% and 90% have resumed vaginal-receiving sexual play (including intercourse) by 3 months.
While recognizing that changes to sexual experience occur, we need to reinforce that gradual recovery is expected. And if women express distress about a sexual change, or if those changes persist, primary care providers should be prepared to help them with their concerns.
Parents need to know experiencing pain is not something they should “just deal with” or ignore. Attempting to repeatedly endure sexual pain can cause new issues, such as high-tone dysfunction of the pelvic floor or an understandable decrease in willingness or receptiveness to sexual play of any kind. Encouraging open communication about these issues can help couples navigate these changes more smoothly.
Partners, especially new fathers, also experience sexual and emotional challenges. They can feel blindsided by the changes in their relationship and might struggle with feelings of jealousy or inadequacy. Understanding partners also face difficulties can help in providing a more comprehensive approach to sexual health care.
Starting the Conversation
So, how can we initiate these important conversations with new parents? Start by providing permission. As healthcare providers, we need to create an environment where discussing sexual health is normalized and welcomed. Simple, nonjudgmental statements can open the door to these discussions. For example, saying, “Many people notice changes in their sexual desire or pleasure after childbirth. Has anything like this happened to you or your partner?” can encourage patients to share their concerns.
Assessing the importance to patients of sexual problems can help direct the need for intervention. Follow up on these concerns and offer support, whether through counseling, pelvic floor physical therapy, or a referral to a sexual medicine specialist, a sex therapist, or other appropriate resource.
Let’s return to Sarah. In the ideal world, at 3 months postpartum she will already have had a handful of clinical conversations about her sexual well-being with her healthcare team — at prenatal visits, at well-baby visits, and at her postpartum checkups. Several of these conversations included her partner. They both understand the transition to parenthood could be rocky for their sex lives. They’ve set aside time to connect and stay physically close. She’s listened to her body and only engaged in sexual play for which she feels ready. Now, noting that some aspects of sexual play are persistently uncomfortable, she knows it’s time to follow up. Without shame or anxiety, she books an appointment with you, knowing that you understand how important this issue is for her, her partner, and her baby.
If you’re working with new parents, remember: Open dialogue about sexual health is not just beneficial — it’s essential. Let’s bridge the gap in care by embracing these conversations and offering the support new parents truly need.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester Medical Center, Rochester, New York, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sarah, a new mom who’s thrilled about her 3-month-old baby, is struggling with her sex life. Her once vibrant physical relationship with her partner has dwindled, and she’s dealing with painful intercourse and a notable drop in desire.
Pregnancy and childbirth are transformative experiences that affect every facet of a person’s life, including their sexual well-being. Despite this fact, clinicians frequently ignore sexual well-being, beyond contraception, in prenatal and postpartum care. In peripartum care, anticipatory guidance is recognized to be crucial to the well-being of new parents and their babies. Why should sexual well-being get the shaft?
Why Talk About Sex?
Sex is a fundamental aspect of many people’s lives and relationships and can significantly affect overall well-being. Despite cultural narratives that often exclude the sexual function and pleasure aspect of sexual health from peripartum discussions, many new parents face sexual challenges that can worsen their physical and emotional health.
While up to 88% of new parents report problems with sexual well-being, less than 30% report receiving anticipatory guidance about sexual function changes. One study found only 15% of postpartum women reported discussing sexual concerns with their medical providers. And, when new parents receive more information about sexual health, they tend to report improved sexual well-being. Clearly, a gap needs bridging.
Sexual health doesn’t just affect individual well-being; it intertwines with relationship satisfaction. Attending to satisfaction in one’s relationship may be an important component of child health as well.
Declines in the frequency of sexual engagement and desire are common after childbirth. Changes in arousal, orgasm, and sexual pleasure, often accompanied by pain, are also reported by many women. Some birthing parents report changes to the sensation of their genitals that are thought to be related to stretch of the pudendal nerve during parturition. Most experience resolution of these concerns within the first year after childbirth, although some women report persistent problems, including up to 33% with persistent sexual pain.
Many factors can contribute to postpartum sexual issues, including hormonal changes, body image concerns, and mental health conditions. Breastfeeding, for instance, can lead to vaginal dryness and reduced sexual arousal due to hormonal shifts. Body image issues and mood disorders like depression and anxiety can also adversely affect sexual function. Women with postpartum depression are more likely to experience sexual concerns, and the relationship between sexual difficulties and depression can be bidirectional.
Empowerment and Expectations
One commonly cited recommendation is to wait until 6 weeks postpartum before resuming penetrative intercourse after a normal vaginal delivery. However, this guideline lacks robust scientific backing. Many people might feel ready for sexual intercourse much sooner or, conversely, might not feel comfortable at the 6-week mark. As clinicians, we must empower our patients to trust their own bodies and make decisions based on their comfort and readiness.
The 6-week advice can sometimes unintentionally convey to women that they are not experts on their own bodies, or that any kind of sex is risky. Acknowledging the recovery timeline for every person is unique and various forms of sexual expression are safe can help foster a healthier approach to resuming sexual activities. In one study of postpartum sexual behavior, in the first 6 weeks after delivery, the most common kinds of sexual play included giving oral sex to a partner and solo sex. Between 80% and 90% have resumed vaginal-receiving sexual play (including intercourse) by 3 months.
While recognizing that changes to sexual experience occur, we need to reinforce that gradual recovery is expected. And if women express distress about a sexual change, or if those changes persist, primary care providers should be prepared to help them with their concerns.
Parents need to know experiencing pain is not something they should “just deal with” or ignore. Attempting to repeatedly endure sexual pain can cause new issues, such as high-tone dysfunction of the pelvic floor or an understandable decrease in willingness or receptiveness to sexual play of any kind. Encouraging open communication about these issues can help couples navigate these changes more smoothly.
Partners, especially new fathers, also experience sexual and emotional challenges. They can feel blindsided by the changes in their relationship and might struggle with feelings of jealousy or inadequacy. Understanding partners also face difficulties can help in providing a more comprehensive approach to sexual health care.
Starting the Conversation
So, how can we initiate these important conversations with new parents? Start by providing permission. As healthcare providers, we need to create an environment where discussing sexual health is normalized and welcomed. Simple, nonjudgmental statements can open the door to these discussions. For example, saying, “Many people notice changes in their sexual desire or pleasure after childbirth. Has anything like this happened to you or your partner?” can encourage patients to share their concerns.
Assessing the importance to patients of sexual problems can help direct the need for intervention. Follow up on these concerns and offer support, whether through counseling, pelvic floor physical therapy, or a referral to a sexual medicine specialist, a sex therapist, or other appropriate resource.
Let’s return to Sarah. In the ideal world, at 3 months postpartum she will already have had a handful of clinical conversations about her sexual well-being with her healthcare team — at prenatal visits, at well-baby visits, and at her postpartum checkups. Several of these conversations included her partner. They both understand the transition to parenthood could be rocky for their sex lives. They’ve set aside time to connect and stay physically close. She’s listened to her body and only engaged in sexual play for which she feels ready. Now, noting that some aspects of sexual play are persistently uncomfortable, she knows it’s time to follow up. Without shame or anxiety, she books an appointment with you, knowing that you understand how important this issue is for her, her partner, and her baby.
If you’re working with new parents, remember: Open dialogue about sexual health is not just beneficial — it’s essential. Let’s bridge the gap in care by embracing these conversations and offering the support new parents truly need.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester Medical Center, Rochester, New York, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Genitals Are a Window Into Health: Sex as a Vital Sign
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
How Much Does Long COVID Cost Society? New Data Shed Light
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
FROM NATURE
Beware the Manchineel: A Case of Irritant Contact Dermatitis
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated
Case Report
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.




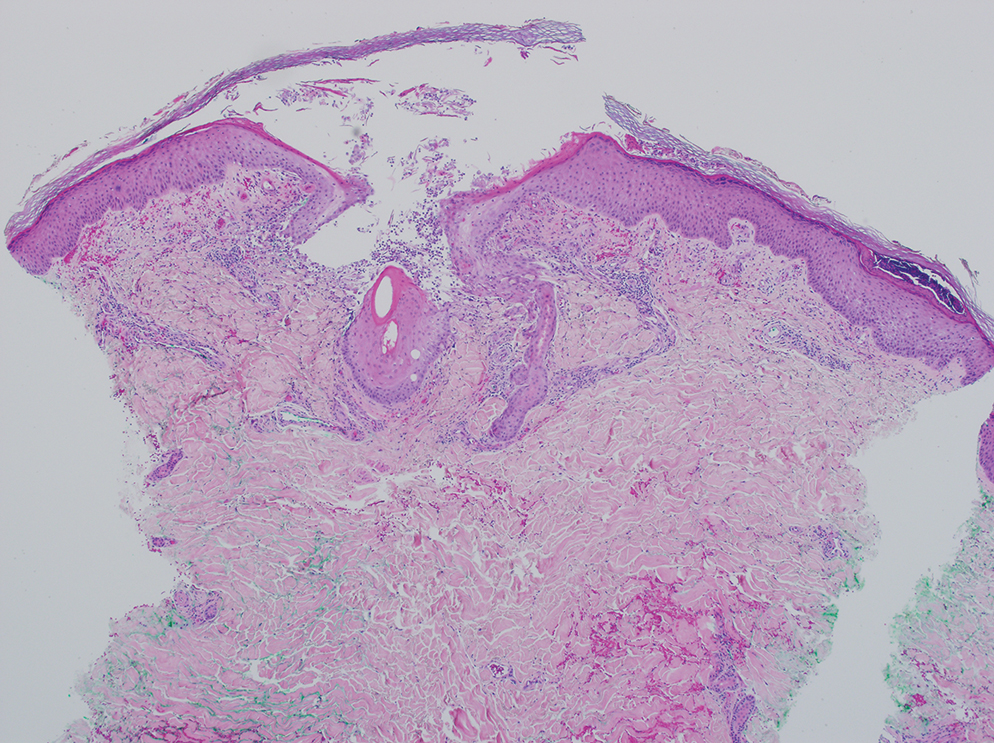
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).

Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
- Most dangerous tree. Guinness World Records. Accessed October 14, 2024. https://www.guinnessworldrecords.com/world-records/most-dangerous-tree
- Naked and Afraid: Garden of Evil (S4E9). Discovery Channel. June 21, 2015. Accessed October 14, 2024. https://go.discovery.com/video/naked-and-afraid-discovery/garden-of-evil
- Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
- Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
- Pitts JF, Barker NH, Gibbons DC, et al. Manchineel keratoconjunctivitis. Br J Ophthalmol. 1993;77:284-288. doi:10.1136/bjo.77.5.284
- Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
- Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
- Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
- Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
- Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
- Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
- Rao KV. Toxic principles of Hippomane mancinella. Planta Med. 1974;25:166-171. doi:10.1055/s-0028-1097927
- Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
- Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated
Case Report
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).
Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated
Case Report
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).
Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
- Most dangerous tree. Guinness World Records. Accessed October 14, 2024. https://www.guinnessworldrecords.com/world-records/most-dangerous-tree
- Naked and Afraid: Garden of Evil (S4E9). Discovery Channel. June 21, 2015. Accessed October 14, 2024. https://go.discovery.com/video/naked-and-afraid-discovery/garden-of-evil
- Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
- Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
- Pitts JF, Barker NH, Gibbons DC, et al. Manchineel keratoconjunctivitis. Br J Ophthalmol. 1993;77:284-288. doi:10.1136/bjo.77.5.284
- Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
- Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
- Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
- Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
- Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
- Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
- Rao KV. Toxic principles of Hippomane mancinella. Planta Med. 1974;25:166-171. doi:10.1055/s-0028-1097927
- Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
- Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
- Most dangerous tree. Guinness World Records. Accessed October 14, 2024. https://www.guinnessworldrecords.com/world-records/most-dangerous-tree
- Naked and Afraid: Garden of Evil (S4E9). Discovery Channel. June 21, 2015. Accessed October 14, 2024. https://go.discovery.com/video/naked-and-afraid-discovery/garden-of-evil
- Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
- Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
- Pitts JF, Barker NH, Gibbons DC, et al. Manchineel keratoconjunctivitis. Br J Ophthalmol. 1993;77:284-288. doi:10.1136/bjo.77.5.284
- Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
- Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
- Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
- Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
- Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
- Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
- Rao KV. Toxic principles of Hippomane mancinella. Planta Med. 1974;25:166-171. doi:10.1055/s-0028-1097927
- Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
- Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
PRACTICE POINTS
- Sap from the manchineel tree—found on the coasts of Caribbean islands, the Atlantic coastline of Central and northern South America, and parts of southernmost Florida—can cause severe dermatologic and ophthalmologic injuries. Eating its fruit can lead to oropharyngeal pain and diarrhea.
- Histopathology of manchineel dermatitis reveals a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which is consistent with irritant contact dermatitis.
- There is no specific treatment for manchineel dermatitis. Case reports advocate a thorough cleansing, application of wet compresses, and observation.

Groups With Highest Unmet Need for PrEP Highlighted in Analysis
LOS ANGELES — Use of preexposure prophylaxis (PrEP) to prevent HIV is increasing overall, but both the rate of increase for starting PrEP and the rate of unmet need differ widely by demographic group, according to new data from a large study.
An analysis by Li Tao, MD, MS, PhD, director of real-world evidence at Gilead Sciences, and colleagues looked at statistical trends from 2019 to 2023 and found that Black, Hispanic, and Medicaid-insured populations continue to lack equitable access to PrEP.
Among the findings were that most new PrEP users were men with HIV risk factors who are commercially insured and live in predominantly non-Hispanic White areas (53% in 2019 and 43% in 2023). For comparison, men living in predominantly Black or Hispanic neighborhoods, or who are insured by Medicaid, saw lower proportions of PrEP use (16% in 2019 and 17% in 2023) despite higher annual increases in PrEP use (11% per year) and higher unmet needs.
Half a Million Real-World Participants
Tao presented her team’s findings at the Infectious Disease Week (IDWeek) 2024 Annual Meeting. The study included “more than half a million real-world PrEP users over the past 5 years,” she said.
The group with the lowest growth in initiation of PrEP in the study period (an annual percentage increase of 2%) and the lowest unmet need included men with HIV risk factors, who were using commercial insurance and living in White-dominant neighborhoods.
HIV risk factors included diagnosis of any sexually transmitted disease, contact with and exposure to communicable diseases, high-risk sexual behavior, contact with a hypodermic needle, long-term prophylaxis, HIV prevention counseling, and HIV screening.
Other men with HIV risk factors (those who were commercially insured, living in Black/Hispanic neighborhoods, or those on Medicaid across all neighborhoods) had a moderate increase in PrEP initiation (an annual percentage increase of 11%-16%) and higher unmet needs.
Researchers gathered data on PrEP prescriptions and new HIV diagnoses (from 2019 to 2023) through the IQVIA pharmacy claims database. PrEP-to-need ratio (PNR) is the number of individuals using PrEP in a year divided by new HIV diagnoses in the previous year. It was calculated for subgroups defined by five PNR-associated factors: Sex, insurance, recorded HIV risk factors (identified by diagnosis or procedure codes), “Ending the HIV Epidemic” jurisdictions, and neighborhood race/ethnicity mix.
Disparities Persist
While PrEP use improved across all the groups studied in the 5 years, “disparities still persist and the need remains very significant,” Tao said. “It’s very crucial for guiding the future HIV prevention options.”
“Long-acting PrEP options may help to address some social determinants structural factors in HIV acquisition,” she added.
What Programs Are Helping?
Some guidelines and programs are helping increase uptake, Tao said.
The United States Preventive Services Task Force (USPSTF) guidelines “reinforce more accessible PrEP programs to individuals like zero-cost sharing or same-day dispensing,” Tao said in a press briefing. “Those kinds of policies are really effective. We can see that after the implementation of the USPSTF guidelines, the copay sharing is really decreasing and is coinciding with the HIV rates declining.”
The Medicaid coverage expansion in 40 states “has been really effective” in PrEP uptake, she added.
Colleen Kelley, MD, MPH, with the Division of Infectious Diseases at the Rollins School of Public Health, Emory University, in Atlanta, who was not part of the research, said there has been a slow but improving uptake of PrEP across the board in the United States, “but the issue is that the uptake has been inequitable.”
Large Study With Recent Data
“This is an extremely large study with very recent data,” Kelley said. “Additionally, they were able to couple (the uptake) with unmet need. People who are at higher risk of acquiring HIV or who live in high-risk areas for HIV should have greater access to PrEP. They have a greater need for PrEP. What we really need to do from an equity perspective is match the PrEP use with the PrEP need and we have not been successful in doing that.”
Kelley added that the finding that the group that had the highest unmet need for PrEP in the study also had no recorded HIV risk factors. “It’s an interesting time to start thinking about beyond risk factor coverage for PrEP,” she said.
Another issue, Kelley said, is that “people are using (PrEP) but they’re also stopping it. People will need to take PrEP many years for protection, but about half discontinue in the first 6-12 months.
“We need to look at how people will persist on PrEP over the long term. That’s the next frontier,” she said. “We hope the long-acting injectables will help overcome some of the PrEP fatigue. But some may just tire of taking medication repeatedly for an infection they don’t have,” she said.
The study was funded by Gilead Sciences. Tao is employed by and is a shareholder of Gilead Sciences. All relevant financial disclosures have been mitigated, according to the paper. Kelley has research grants to her institution from Gilead, Moderna, Novavax, ViiV, and Humanigen.
A version of this article first appeared on Medscape.com.
LOS ANGELES — Use of preexposure prophylaxis (PrEP) to prevent HIV is increasing overall, but both the rate of increase for starting PrEP and the rate of unmet need differ widely by demographic group, according to new data from a large study.
An analysis by Li Tao, MD, MS, PhD, director of real-world evidence at Gilead Sciences, and colleagues looked at statistical trends from 2019 to 2023 and found that Black, Hispanic, and Medicaid-insured populations continue to lack equitable access to PrEP.
Among the findings were that most new PrEP users were men with HIV risk factors who are commercially insured and live in predominantly non-Hispanic White areas (53% in 2019 and 43% in 2023). For comparison, men living in predominantly Black or Hispanic neighborhoods, or who are insured by Medicaid, saw lower proportions of PrEP use (16% in 2019 and 17% in 2023) despite higher annual increases in PrEP use (11% per year) and higher unmet needs.
Half a Million Real-World Participants
Tao presented her team’s findings at the Infectious Disease Week (IDWeek) 2024 Annual Meeting. The study included “more than half a million real-world PrEP users over the past 5 years,” she said.
The group with the lowest growth in initiation of PrEP in the study period (an annual percentage increase of 2%) and the lowest unmet need included men with HIV risk factors, who were using commercial insurance and living in White-dominant neighborhoods.
HIV risk factors included diagnosis of any sexually transmitted disease, contact with and exposure to communicable diseases, high-risk sexual behavior, contact with a hypodermic needle, long-term prophylaxis, HIV prevention counseling, and HIV screening.
Other men with HIV risk factors (those who were commercially insured, living in Black/Hispanic neighborhoods, or those on Medicaid across all neighborhoods) had a moderate increase in PrEP initiation (an annual percentage increase of 11%-16%) and higher unmet needs.
Researchers gathered data on PrEP prescriptions and new HIV diagnoses (from 2019 to 2023) through the IQVIA pharmacy claims database. PrEP-to-need ratio (PNR) is the number of individuals using PrEP in a year divided by new HIV diagnoses in the previous year. It was calculated for subgroups defined by five PNR-associated factors: Sex, insurance, recorded HIV risk factors (identified by diagnosis or procedure codes), “Ending the HIV Epidemic” jurisdictions, and neighborhood race/ethnicity mix.
Disparities Persist
While PrEP use improved across all the groups studied in the 5 years, “disparities still persist and the need remains very significant,” Tao said. “It’s very crucial for guiding the future HIV prevention options.”
“Long-acting PrEP options may help to address some social determinants structural factors in HIV acquisition,” she added.
What Programs Are Helping?
Some guidelines and programs are helping increase uptake, Tao said.
The United States Preventive Services Task Force (USPSTF) guidelines “reinforce more accessible PrEP programs to individuals like zero-cost sharing or same-day dispensing,” Tao said in a press briefing. “Those kinds of policies are really effective. We can see that after the implementation of the USPSTF guidelines, the copay sharing is really decreasing and is coinciding with the HIV rates declining.”
The Medicaid coverage expansion in 40 states “has been really effective” in PrEP uptake, she added.
Colleen Kelley, MD, MPH, with the Division of Infectious Diseases at the Rollins School of Public Health, Emory University, in Atlanta, who was not part of the research, said there has been a slow but improving uptake of PrEP across the board in the United States, “but the issue is that the uptake has been inequitable.”
Large Study With Recent Data
“This is an extremely large study with very recent data,” Kelley said. “Additionally, they were able to couple (the uptake) with unmet need. People who are at higher risk of acquiring HIV or who live in high-risk areas for HIV should have greater access to PrEP. They have a greater need for PrEP. What we really need to do from an equity perspective is match the PrEP use with the PrEP need and we have not been successful in doing that.”
Kelley added that the finding that the group that had the highest unmet need for PrEP in the study also had no recorded HIV risk factors. “It’s an interesting time to start thinking about beyond risk factor coverage for PrEP,” she said.
Another issue, Kelley said, is that “people are using (PrEP) but they’re also stopping it. People will need to take PrEP many years for protection, but about half discontinue in the first 6-12 months.
“We need to look at how people will persist on PrEP over the long term. That’s the next frontier,” she said. “We hope the long-acting injectables will help overcome some of the PrEP fatigue. But some may just tire of taking medication repeatedly for an infection they don’t have,” she said.
The study was funded by Gilead Sciences. Tao is employed by and is a shareholder of Gilead Sciences. All relevant financial disclosures have been mitigated, according to the paper. Kelley has research grants to her institution from Gilead, Moderna, Novavax, ViiV, and Humanigen.
A version of this article first appeared on Medscape.com.
LOS ANGELES — Use of preexposure prophylaxis (PrEP) to prevent HIV is increasing overall, but both the rate of increase for starting PrEP and the rate of unmet need differ widely by demographic group, according to new data from a large study.
An analysis by Li Tao, MD, MS, PhD, director of real-world evidence at Gilead Sciences, and colleagues looked at statistical trends from 2019 to 2023 and found that Black, Hispanic, and Medicaid-insured populations continue to lack equitable access to PrEP.
Among the findings were that most new PrEP users were men with HIV risk factors who are commercially insured and live in predominantly non-Hispanic White areas (53% in 2019 and 43% in 2023). For comparison, men living in predominantly Black or Hispanic neighborhoods, or who are insured by Medicaid, saw lower proportions of PrEP use (16% in 2019 and 17% in 2023) despite higher annual increases in PrEP use (11% per year) and higher unmet needs.
Half a Million Real-World Participants
Tao presented her team’s findings at the Infectious Disease Week (IDWeek) 2024 Annual Meeting. The study included “more than half a million real-world PrEP users over the past 5 years,” she said.
The group with the lowest growth in initiation of PrEP in the study period (an annual percentage increase of 2%) and the lowest unmet need included men with HIV risk factors, who were using commercial insurance and living in White-dominant neighborhoods.
HIV risk factors included diagnosis of any sexually transmitted disease, contact with and exposure to communicable diseases, high-risk sexual behavior, contact with a hypodermic needle, long-term prophylaxis, HIV prevention counseling, and HIV screening.
Other men with HIV risk factors (those who were commercially insured, living in Black/Hispanic neighborhoods, or those on Medicaid across all neighborhoods) had a moderate increase in PrEP initiation (an annual percentage increase of 11%-16%) and higher unmet needs.
Researchers gathered data on PrEP prescriptions and new HIV diagnoses (from 2019 to 2023) through the IQVIA pharmacy claims database. PrEP-to-need ratio (PNR) is the number of individuals using PrEP in a year divided by new HIV diagnoses in the previous year. It was calculated for subgroups defined by five PNR-associated factors: Sex, insurance, recorded HIV risk factors (identified by diagnosis or procedure codes), “Ending the HIV Epidemic” jurisdictions, and neighborhood race/ethnicity mix.
Disparities Persist
While PrEP use improved across all the groups studied in the 5 years, “disparities still persist and the need remains very significant,” Tao said. “It’s very crucial for guiding the future HIV prevention options.”
“Long-acting PrEP options may help to address some social determinants structural factors in HIV acquisition,” she added.
What Programs Are Helping?
Some guidelines and programs are helping increase uptake, Tao said.
The United States Preventive Services Task Force (USPSTF) guidelines “reinforce more accessible PrEP programs to individuals like zero-cost sharing or same-day dispensing,” Tao said in a press briefing. “Those kinds of policies are really effective. We can see that after the implementation of the USPSTF guidelines, the copay sharing is really decreasing and is coinciding with the HIV rates declining.”
The Medicaid coverage expansion in 40 states “has been really effective” in PrEP uptake, she added.
Colleen Kelley, MD, MPH, with the Division of Infectious Diseases at the Rollins School of Public Health, Emory University, in Atlanta, who was not part of the research, said there has been a slow but improving uptake of PrEP across the board in the United States, “but the issue is that the uptake has been inequitable.”
Large Study With Recent Data
“This is an extremely large study with very recent data,” Kelley said. “Additionally, they were able to couple (the uptake) with unmet need. People who are at higher risk of acquiring HIV or who live in high-risk areas for HIV should have greater access to PrEP. They have a greater need for PrEP. What we really need to do from an equity perspective is match the PrEP use with the PrEP need and we have not been successful in doing that.”
Kelley added that the finding that the group that had the highest unmet need for PrEP in the study also had no recorded HIV risk factors. “It’s an interesting time to start thinking about beyond risk factor coverage for PrEP,” she said.
Another issue, Kelley said, is that “people are using (PrEP) but they’re also stopping it. People will need to take PrEP many years for protection, but about half discontinue in the first 6-12 months.
“We need to look at how people will persist on PrEP over the long term. That’s the next frontier,” she said. “We hope the long-acting injectables will help overcome some of the PrEP fatigue. But some may just tire of taking medication repeatedly for an infection they don’t have,” she said.
The study was funded by Gilead Sciences. Tao is employed by and is a shareholder of Gilead Sciences. All relevant financial disclosures have been mitigated, according to the paper. Kelley has research grants to her institution from Gilead, Moderna, Novavax, ViiV, and Humanigen.
A version of this article first appeared on Medscape.com.
FROM IDWEEK 2024
Pediatric Myasthenia Gravis: Don’t Treat Children Like Adults
SAVANNAH, GEORGIA — At a pathophysiological level, juvenile myasthenia gravis (MG) seems to be identical to the adult form, neuromuscular specialists learned. But there are still important differences between children and their elders that affect pediatric care.
For example, “we have to think a little bit differently about the side effect profiles of the medications and their toxicity because children may react to medications differently,” said Matthew Ginsberg, MD, a pediatric neurologist based in Akron, Ohio, in a presentation at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
And then there’s the matter of adherence. “It’s hard to get adults to take medication, but a teenager is sometimes an exceptional challenge,” Ginsberg said.
Case In Point: A 13-Year-Old With MG
Pediatric MG is rare. Cases in children are estimated to account for 10% of MG cases diagnosed each year. According to a 2020 report, “the majority will present with ptosis and a variable degree of ophthalmoplegia [paralysis of eye muscles].”
Ginsberg highlighted a case of a 13-year-old girl who’d been healthy but developed fatigable ptosis and mild restriction of extraocular movements. The patient’s acetylcholine receptor antibodies were very elevated, but she didn’t have MuSK antibodies.
“This isn’t a diagnostic conundrum. She has autoimmune myasthenia gravis with ocular manifestations,” Ginsberg said. “For someone like this, whether it’s an adult or a child, many people would start symptomatic treatment with an acetylcholinesterase inhibitor like pyridostigmine.”
The use of the drug in children is similar to that in adults, he said, although weight-based dosing is used. “Usually it’s around 3-7 mg/kg/d, but it’s still very individualized based on patient response.” The timing of symptoms can affect the distribution of doses throughout the day, he said.
“There are extended-release formulations of the medication, and I think some people use them more than I do,” he said. “The side effects are basically similar to adults. Most of the patients I have on it tolerate it really well and don’t have a lot of the muscarinic side effects that you would expect.”
Consider Prescription Eye Drops for Ptosis
Alpha-1A agonists oxymetazoline and apraclonidine in the form of topical eye drops can help with ptosis. “They potentially avoid some of the systemic toxicity of the other medications,” Ginsberg said. “So they might be an option if you’re really just trying to target ptosis as a symptom.”
However, it can be difficult to get insurers to cover these medications, he said.
The 13-year-old patient initially improved but developed difficulty walking. “Her hands began to feel heavy, and she had difficulty chewing and nasal regurgitation. On her exam, she still had fatigable ptosis plus hypernasal speech and generalized weakness. At this point, we’re starting to see that she has generalized myasthenia gravis that may be an impending crisis.”
The Young Patient Worsens. Now What?
The patient was admitted and given intravenous immunoglobulin at 2 g/kg over a couple days. But her symptoms worsened following initial improvement.
Glucocorticoids can play a larger role in treatment at this stage, and the patient was initially on prednisone. But there are reasons for caution, including effects on bone growth and interference with live vaccines.
However, live vaccines aren’t common in children, with the exception of the MMRV vaccine, he said. “It’s worth noting that you can give that second dose as early as 3 months after the initial one, so most patients really should be able to complete a course before they start on immunosuppression,” he said.
Another option is immunotherapy. “There’s a really large menu of options for immunotherapy in myasthenia gravis right now,” Ginsberg said. “It’s great that we have all these options, but it adds to the complexity.”
Rituximab may be considered based on early data, he said. And thymectomy — removal of the thymus gland — should be considered early.
Don’t Neglect Supportive Care
Ginsberg urged colleagues to consider supportive care measures. Advocacy groups such as the Myasthenia Gravis Foundation of America can help with weight management and diet/exercise counseling, especially in patients taking glucocorticoids.
He added that “school accommodations are very important in this age group. They might need a plan, for example, to have modified gym class or an excuse not to carry a book bag between classes.”
How did the 13-year-old do? She underwent thymectomy, and her disease remained stable after 6 months. “Her rituximab was discontinued,” Ginsberg said. “She considered participating in a clinical trial but then started seeing improvements. About a year after the thymectomy, she just stopped her steroids on her own, and she was fine.”
Ginsberg had no disclosures.
A version of this article appeared on Medscape.com.
SAVANNAH, GEORGIA — At a pathophysiological level, juvenile myasthenia gravis (MG) seems to be identical to the adult form, neuromuscular specialists learned. But there are still important differences between children and their elders that affect pediatric care.
For example, “we have to think a little bit differently about the side effect profiles of the medications and their toxicity because children may react to medications differently,” said Matthew Ginsberg, MD, a pediatric neurologist based in Akron, Ohio, in a presentation at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
And then there’s the matter of adherence. “It’s hard to get adults to take medication, but a teenager is sometimes an exceptional challenge,” Ginsberg said.
Case In Point: A 13-Year-Old With MG
Pediatric MG is rare. Cases in children are estimated to account for 10% of MG cases diagnosed each year. According to a 2020 report, “the majority will present with ptosis and a variable degree of ophthalmoplegia [paralysis of eye muscles].”
Ginsberg highlighted a case of a 13-year-old girl who’d been healthy but developed fatigable ptosis and mild restriction of extraocular movements. The patient’s acetylcholine receptor antibodies were very elevated, but she didn’t have MuSK antibodies.
“This isn’t a diagnostic conundrum. She has autoimmune myasthenia gravis with ocular manifestations,” Ginsberg said. “For someone like this, whether it’s an adult or a child, many people would start symptomatic treatment with an acetylcholinesterase inhibitor like pyridostigmine.”
The use of the drug in children is similar to that in adults, he said, although weight-based dosing is used. “Usually it’s around 3-7 mg/kg/d, but it’s still very individualized based on patient response.” The timing of symptoms can affect the distribution of doses throughout the day, he said.
“There are extended-release formulations of the medication, and I think some people use them more than I do,” he said. “The side effects are basically similar to adults. Most of the patients I have on it tolerate it really well and don’t have a lot of the muscarinic side effects that you would expect.”
Consider Prescription Eye Drops for Ptosis
Alpha-1A agonists oxymetazoline and apraclonidine in the form of topical eye drops can help with ptosis. “They potentially avoid some of the systemic toxicity of the other medications,” Ginsberg said. “So they might be an option if you’re really just trying to target ptosis as a symptom.”
However, it can be difficult to get insurers to cover these medications, he said.
The 13-year-old patient initially improved but developed difficulty walking. “Her hands began to feel heavy, and she had difficulty chewing and nasal regurgitation. On her exam, she still had fatigable ptosis plus hypernasal speech and generalized weakness. At this point, we’re starting to see that she has generalized myasthenia gravis that may be an impending crisis.”
The Young Patient Worsens. Now What?
The patient was admitted and given intravenous immunoglobulin at 2 g/kg over a couple days. But her symptoms worsened following initial improvement.
Glucocorticoids can play a larger role in treatment at this stage, and the patient was initially on prednisone. But there are reasons for caution, including effects on bone growth and interference with live vaccines.
However, live vaccines aren’t common in children, with the exception of the MMRV vaccine, he said. “It’s worth noting that you can give that second dose as early as 3 months after the initial one, so most patients really should be able to complete a course before they start on immunosuppression,” he said.
Another option is immunotherapy. “There’s a really large menu of options for immunotherapy in myasthenia gravis right now,” Ginsberg said. “It’s great that we have all these options, but it adds to the complexity.”
Rituximab may be considered based on early data, he said. And thymectomy — removal of the thymus gland — should be considered early.
Don’t Neglect Supportive Care
Ginsberg urged colleagues to consider supportive care measures. Advocacy groups such as the Myasthenia Gravis Foundation of America can help with weight management and diet/exercise counseling, especially in patients taking glucocorticoids.
He added that “school accommodations are very important in this age group. They might need a plan, for example, to have modified gym class or an excuse not to carry a book bag between classes.”
How did the 13-year-old do? She underwent thymectomy, and her disease remained stable after 6 months. “Her rituximab was discontinued,” Ginsberg said. “She considered participating in a clinical trial but then started seeing improvements. About a year after the thymectomy, she just stopped her steroids on her own, and she was fine.”
Ginsberg had no disclosures.
A version of this article appeared on Medscape.com.
SAVANNAH, GEORGIA — At a pathophysiological level, juvenile myasthenia gravis (MG) seems to be identical to the adult form, neuromuscular specialists learned. But there are still important differences between children and their elders that affect pediatric care.
For example, “we have to think a little bit differently about the side effect profiles of the medications and their toxicity because children may react to medications differently,” said Matthew Ginsberg, MD, a pediatric neurologist based in Akron, Ohio, in a presentation at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
And then there’s the matter of adherence. “It’s hard to get adults to take medication, but a teenager is sometimes an exceptional challenge,” Ginsberg said.
Case In Point: A 13-Year-Old With MG
Pediatric MG is rare. Cases in children are estimated to account for 10% of MG cases diagnosed each year. According to a 2020 report, “the majority will present with ptosis and a variable degree of ophthalmoplegia [paralysis of eye muscles].”
Ginsberg highlighted a case of a 13-year-old girl who’d been healthy but developed fatigable ptosis and mild restriction of extraocular movements. The patient’s acetylcholine receptor antibodies were very elevated, but she didn’t have MuSK antibodies.
“This isn’t a diagnostic conundrum. She has autoimmune myasthenia gravis with ocular manifestations,” Ginsberg said. “For someone like this, whether it’s an adult or a child, many people would start symptomatic treatment with an acetylcholinesterase inhibitor like pyridostigmine.”
The use of the drug in children is similar to that in adults, he said, although weight-based dosing is used. “Usually it’s around 3-7 mg/kg/d, but it’s still very individualized based on patient response.” The timing of symptoms can affect the distribution of doses throughout the day, he said.
“There are extended-release formulations of the medication, and I think some people use them more than I do,” he said. “The side effects are basically similar to adults. Most of the patients I have on it tolerate it really well and don’t have a lot of the muscarinic side effects that you would expect.”
Consider Prescription Eye Drops for Ptosis
Alpha-1A agonists oxymetazoline and apraclonidine in the form of topical eye drops can help with ptosis. “They potentially avoid some of the systemic toxicity of the other medications,” Ginsberg said. “So they might be an option if you’re really just trying to target ptosis as a symptom.”
However, it can be difficult to get insurers to cover these medications, he said.
The 13-year-old patient initially improved but developed difficulty walking. “Her hands began to feel heavy, and she had difficulty chewing and nasal regurgitation. On her exam, she still had fatigable ptosis plus hypernasal speech and generalized weakness. At this point, we’re starting to see that she has generalized myasthenia gravis that may be an impending crisis.”
The Young Patient Worsens. Now What?
The patient was admitted and given intravenous immunoglobulin at 2 g/kg over a couple days. But her symptoms worsened following initial improvement.
Glucocorticoids can play a larger role in treatment at this stage, and the patient was initially on prednisone. But there are reasons for caution, including effects on bone growth and interference with live vaccines.
However, live vaccines aren’t common in children, with the exception of the MMRV vaccine, he said. “It’s worth noting that you can give that second dose as early as 3 months after the initial one, so most patients really should be able to complete a course before they start on immunosuppression,” he said.
Another option is immunotherapy. “There’s a really large menu of options for immunotherapy in myasthenia gravis right now,” Ginsberg said. “It’s great that we have all these options, but it adds to the complexity.”
Rituximab may be considered based on early data, he said. And thymectomy — removal of the thymus gland — should be considered early.
Don’t Neglect Supportive Care
Ginsberg urged colleagues to consider supportive care measures. Advocacy groups such as the Myasthenia Gravis Foundation of America can help with weight management and diet/exercise counseling, especially in patients taking glucocorticoids.
He added that “school accommodations are very important in this age group. They might need a plan, for example, to have modified gym class or an excuse not to carry a book bag between classes.”
How did the 13-year-old do? She underwent thymectomy, and her disease remained stable after 6 months. “Her rituximab was discontinued,” Ginsberg said. “She considered participating in a clinical trial but then started seeing improvements. About a year after the thymectomy, she just stopped her steroids on her own, and she was fine.”
Ginsberg had no disclosures.
A version of this article appeared on Medscape.com.
FROM AANEM 2024
FDA OKs Novel Levodopa-Based Continuous Sub-Q Regimen for Parkinson’s Disease
Due to the progressive nature of Parkinson’s disease, “oral medications are eventually no longer as effective at motor symptom control and surgical treatment may be required. This new, non-surgical regimen provides continuous delivery of levodopa morning, day, and night,” Robert A. Hauser, MD, MBA, director of the Parkinson’s and Movement Disorder Center at the University of South Florida, Tampa, said in a news release.
The FDA approval was supported by results of a 12-week, phase 3 study evaluating the efficacy of continuous subcutaneous infusion foscarbidopa/foslevodopa in adults with advanced Parkinson’s disease compared with oral immediate-release carbidopa/levodopa.
The study showed that patients treated with foscarbidopa/foslevodopa had superior improvement in motor fluctuations, with increased “on” time without troublesome dyskinesia and decreased “off” time, compared with peers receiving oral immediate-release carbidopa/levodopa.
At week 12, the increase in “on” time without troublesome dyskinesia was 2.72 hours for foscarbidopa/foslevodopa continuous infusion versus 0.97 hours for carbidopa/levodopa (P =.0083).
Improvements in “on” time were observed as early as the first week and persisted throughout the 12 weeks.
The approval of foscarbidopa/foslevodopa for advanced Parkinson’s disease was also supported by a 52-week, open-label study which evaluated the long-term safety and efficacy of the drug.
Most adverse reactions with foscarbidopa/foslevodopa were non-serious and mild or moderate in severity. The most frequent adverse reactions were infusion site events, hallucinations, and dyskinesia.
Full prescribing information is available online.
AbbVie said coverage for Medicare patients is expected in the second half of 2025.
A version of this article appeared on Medscape.com.
Due to the progressive nature of Parkinson’s disease, “oral medications are eventually no longer as effective at motor symptom control and surgical treatment may be required. This new, non-surgical regimen provides continuous delivery of levodopa morning, day, and night,” Robert A. Hauser, MD, MBA, director of the Parkinson’s and Movement Disorder Center at the University of South Florida, Tampa, said in a news release.
The FDA approval was supported by results of a 12-week, phase 3 study evaluating the efficacy of continuous subcutaneous infusion foscarbidopa/foslevodopa in adults with advanced Parkinson’s disease compared with oral immediate-release carbidopa/levodopa.
The study showed that patients treated with foscarbidopa/foslevodopa had superior improvement in motor fluctuations, with increased “on” time without troublesome dyskinesia and decreased “off” time, compared with peers receiving oral immediate-release carbidopa/levodopa.
At week 12, the increase in “on” time without troublesome dyskinesia was 2.72 hours for foscarbidopa/foslevodopa continuous infusion versus 0.97 hours for carbidopa/levodopa (P =.0083).
Improvements in “on” time were observed as early as the first week and persisted throughout the 12 weeks.
The approval of foscarbidopa/foslevodopa for advanced Parkinson’s disease was also supported by a 52-week, open-label study which evaluated the long-term safety and efficacy of the drug.
Most adverse reactions with foscarbidopa/foslevodopa were non-serious and mild or moderate in severity. The most frequent adverse reactions were infusion site events, hallucinations, and dyskinesia.
Full prescribing information is available online.
AbbVie said coverage for Medicare patients is expected in the second half of 2025.
A version of this article appeared on Medscape.com.
Due to the progressive nature of Parkinson’s disease, “oral medications are eventually no longer as effective at motor symptom control and surgical treatment may be required. This new, non-surgical regimen provides continuous delivery of levodopa morning, day, and night,” Robert A. Hauser, MD, MBA, director of the Parkinson’s and Movement Disorder Center at the University of South Florida, Tampa, said in a news release.
The FDA approval was supported by results of a 12-week, phase 3 study evaluating the efficacy of continuous subcutaneous infusion foscarbidopa/foslevodopa in adults with advanced Parkinson’s disease compared with oral immediate-release carbidopa/levodopa.
The study showed that patients treated with foscarbidopa/foslevodopa had superior improvement in motor fluctuations, with increased “on” time without troublesome dyskinesia and decreased “off” time, compared with peers receiving oral immediate-release carbidopa/levodopa.
At week 12, the increase in “on” time without troublesome dyskinesia was 2.72 hours for foscarbidopa/foslevodopa continuous infusion versus 0.97 hours for carbidopa/levodopa (P =.0083).
Improvements in “on” time were observed as early as the first week and persisted throughout the 12 weeks.
The approval of foscarbidopa/foslevodopa for advanced Parkinson’s disease was also supported by a 52-week, open-label study which evaluated the long-term safety and efficacy of the drug.
Most adverse reactions with foscarbidopa/foslevodopa were non-serious and mild or moderate in severity. The most frequent adverse reactions were infusion site events, hallucinations, and dyskinesia.
Full prescribing information is available online.
AbbVie said coverage for Medicare patients is expected in the second half of 2025.
A version of this article appeared on Medscape.com.
Wrinkles, Dyspigmentation Improve with PDT, in Small Study
.
“Our study helps capture and quantify a phenomenon that clinicians who use PDT in their practice have already noticed: Patients experience a visible improvement across several cosmetically important metrics including but not limited to fine lines, wrinkles, and skin tightness following PDT,” one of the study authors, Luke Horton, MD, a fourth-year dermatology resident at the University of California, Irvine, said in an interview following the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session.

For the study, 11 patients underwent a 120-minute incubation period with 17% 5-aminolevulinic acid over the face, followed by visible blue light PDT exposure for 16 minutes, to reduce rhytides. The researchers used a Vectra imaging system to capture three-dimensional images of the patients before the procedure and during the follow-up. Three dermatologists analyzed the pre-procedure and post-procedure images and used a validated five-point Merz wrinkle severity scale to grade various regions of the face including the forehead, glabella, lateral canthal rhytides, melolabial folds, nasolabial folds, and perioral rhytides.
They also used a five-point solar lentigines scale to evaluate the change in degree of pigmentation and quantity of age spots as well as the change in rhytid severity before and after PDT and the change in the seven-point Global Aesthetic Improvement Scale (GAIS) to gauge overall improvement of fine lines and wrinkles.
After a mean follow-up of 4.25 months, rhytid severity among the 11 patients was reduced by an average of 0.65 points on the Merz scale, with an SD of 0.20. Broken down by region, rhytid severity scores decreased by 0.2 points (SD, 0.42) for the forehead, 0.7 points (SD, 0.48) for the glabella and lateral canthal rhytides, 0.88 points (SD, 0.35) for the melolabial folds and perioral rhytides, and 0.8 points (SD, 0.42) for the nasolabial folds. (The researchers excluded ratings for the melolabial folds and perioral rhytides in two patients with beards.)
In other findings, solar lentigines grading showed an average reduction of 1 point (SD, 0.45), while the GAIS score improved by 1 or more for every patient, with an average of score of 1.45 (SD, 0.52), showing that some degree of improvement in facial rhytides was noted for all patients following PDT.
“The degree of improvement as measured by our independent physician graders was impressive and not far off from those reported with CO2 ablative laser,” Horton said. “Further, the effect was not isolated to actinic keratoses but extended to improved appearance of fine lines, some deep lines, and lentigines. Although we are not implying that PDT is superior to and should replace lasers or other energy-based devices, it does provide a real, measurable cosmetic benefit.”
Clinicians, he added, can use these findings “to counsel their patients when discussing field cancerization treatment options, especially for patients who may be hesitant to undergo PDT as it can be a painful therapy with a considerable downtime for some.”
Lawrence J. Green, MD, clinical professor of dermatology, The George Washington University, Washington, DC, who was asked to comment on the study results, said that the findings “shine more light on the long-standing off-label use of PDT for lessening signs of photoaging. Like studies done before it, I think this adds an additional benefit to discuss for those who are considering PDT treatment for their actinic keratoses.”
Horton acknowledged certain limitations of the study including its small sample size and the fact that physician graders were not blinded to which images were pre- and post-treatment, “which could introduce an element of bias in the data,” he said. “But this being an unfunded project born out of clinical observation, we hope to later expand its size. Furthermore, we invite other physicians to join us to better study these effects and to design protocols that minimize adverse effects and maximize clinical outcomes.”
His co-authors were Milan Hirpara; Sarah Choe; Joel Cohen, MD; and Natasha A. Mesinkovska, MD, PhD.
No relevant disclosures were reported. Green had no relevant disclosures.
A version of this article appeared on Medscape.com.
.
“Our study helps capture and quantify a phenomenon that clinicians who use PDT in their practice have already noticed: Patients experience a visible improvement across several cosmetically important metrics including but not limited to fine lines, wrinkles, and skin tightness following PDT,” one of the study authors, Luke Horton, MD, a fourth-year dermatology resident at the University of California, Irvine, said in an interview following the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session.
For the study, 11 patients underwent a 120-minute incubation period with 17% 5-aminolevulinic acid over the face, followed by visible blue light PDT exposure for 16 minutes, to reduce rhytides. The researchers used a Vectra imaging system to capture three-dimensional images of the patients before the procedure and during the follow-up. Three dermatologists analyzed the pre-procedure and post-procedure images and used a validated five-point Merz wrinkle severity scale to grade various regions of the face including the forehead, glabella, lateral canthal rhytides, melolabial folds, nasolabial folds, and perioral rhytides.
They also used a five-point solar lentigines scale to evaluate the change in degree of pigmentation and quantity of age spots as well as the change in rhytid severity before and after PDT and the change in the seven-point Global Aesthetic Improvement Scale (GAIS) to gauge overall improvement of fine lines and wrinkles.
After a mean follow-up of 4.25 months, rhytid severity among the 11 patients was reduced by an average of 0.65 points on the Merz scale, with an SD of 0.20. Broken down by region, rhytid severity scores decreased by 0.2 points (SD, 0.42) for the forehead, 0.7 points (SD, 0.48) for the glabella and lateral canthal rhytides, 0.88 points (SD, 0.35) for the melolabial folds and perioral rhytides, and 0.8 points (SD, 0.42) for the nasolabial folds. (The researchers excluded ratings for the melolabial folds and perioral rhytides in two patients with beards.)
In other findings, solar lentigines grading showed an average reduction of 1 point (SD, 0.45), while the GAIS score improved by 1 or more for every patient, with an average of score of 1.45 (SD, 0.52), showing that some degree of improvement in facial rhytides was noted for all patients following PDT.
“The degree of improvement as measured by our independent physician graders was impressive and not far off from those reported with CO2 ablative laser,” Horton said. “Further, the effect was not isolated to actinic keratoses but extended to improved appearance of fine lines, some deep lines, and lentigines. Although we are not implying that PDT is superior to and should replace lasers or other energy-based devices, it does provide a real, measurable cosmetic benefit.”
Clinicians, he added, can use these findings “to counsel their patients when discussing field cancerization treatment options, especially for patients who may be hesitant to undergo PDT as it can be a painful therapy with a considerable downtime for some.”
Lawrence J. Green, MD, clinical professor of dermatology, The George Washington University, Washington, DC, who was asked to comment on the study results, said that the findings “shine more light on the long-standing off-label use of PDT for lessening signs of photoaging. Like studies done before it, I think this adds an additional benefit to discuss for those who are considering PDT treatment for their actinic keratoses.”
Horton acknowledged certain limitations of the study including its small sample size and the fact that physician graders were not blinded to which images were pre- and post-treatment, “which could introduce an element of bias in the data,” he said. “But this being an unfunded project born out of clinical observation, we hope to later expand its size. Furthermore, we invite other physicians to join us to better study these effects and to design protocols that minimize adverse effects and maximize clinical outcomes.”
His co-authors were Milan Hirpara; Sarah Choe; Joel Cohen, MD; and Natasha A. Mesinkovska, MD, PhD.
No relevant disclosures were reported. Green had no relevant disclosures.
A version of this article appeared on Medscape.com.
.
“Our study helps capture and quantify a phenomenon that clinicians who use PDT in their practice have already noticed: Patients experience a visible improvement across several cosmetically important metrics including but not limited to fine lines, wrinkles, and skin tightness following PDT,” one of the study authors, Luke Horton, MD, a fourth-year dermatology resident at the University of California, Irvine, said in an interview following the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session.
For the study, 11 patients underwent a 120-minute incubation period with 17% 5-aminolevulinic acid over the face, followed by visible blue light PDT exposure for 16 minutes, to reduce rhytides. The researchers used a Vectra imaging system to capture three-dimensional images of the patients before the procedure and during the follow-up. Three dermatologists analyzed the pre-procedure and post-procedure images and used a validated five-point Merz wrinkle severity scale to grade various regions of the face including the forehead, glabella, lateral canthal rhytides, melolabial folds, nasolabial folds, and perioral rhytides.
They also used a five-point solar lentigines scale to evaluate the change in degree of pigmentation and quantity of age spots as well as the change in rhytid severity before and after PDT and the change in the seven-point Global Aesthetic Improvement Scale (GAIS) to gauge overall improvement of fine lines and wrinkles.
After a mean follow-up of 4.25 months, rhytid severity among the 11 patients was reduced by an average of 0.65 points on the Merz scale, with an SD of 0.20. Broken down by region, rhytid severity scores decreased by 0.2 points (SD, 0.42) for the forehead, 0.7 points (SD, 0.48) for the glabella and lateral canthal rhytides, 0.88 points (SD, 0.35) for the melolabial folds and perioral rhytides, and 0.8 points (SD, 0.42) for the nasolabial folds. (The researchers excluded ratings for the melolabial folds and perioral rhytides in two patients with beards.)
In other findings, solar lentigines grading showed an average reduction of 1 point (SD, 0.45), while the GAIS score improved by 1 or more for every patient, with an average of score of 1.45 (SD, 0.52), showing that some degree of improvement in facial rhytides was noted for all patients following PDT.
“The degree of improvement as measured by our independent physician graders was impressive and not far off from those reported with CO2 ablative laser,” Horton said. “Further, the effect was not isolated to actinic keratoses but extended to improved appearance of fine lines, some deep lines, and lentigines. Although we are not implying that PDT is superior to and should replace lasers or other energy-based devices, it does provide a real, measurable cosmetic benefit.”
Clinicians, he added, can use these findings “to counsel their patients when discussing field cancerization treatment options, especially for patients who may be hesitant to undergo PDT as it can be a painful therapy with a considerable downtime for some.”
Lawrence J. Green, MD, clinical professor of dermatology, The George Washington University, Washington, DC, who was asked to comment on the study results, said that the findings “shine more light on the long-standing off-label use of PDT for lessening signs of photoaging. Like studies done before it, I think this adds an additional benefit to discuss for those who are considering PDT treatment for their actinic keratoses.”
Horton acknowledged certain limitations of the study including its small sample size and the fact that physician graders were not blinded to which images were pre- and post-treatment, “which could introduce an element of bias in the data,” he said. “But this being an unfunded project born out of clinical observation, we hope to later expand its size. Furthermore, we invite other physicians to join us to better study these effects and to design protocols that minimize adverse effects and maximize clinical outcomes.”
His co-authors were Milan Hirpara; Sarah Choe; Joel Cohen, MD; and Natasha A. Mesinkovska, MD, PhD.
No relevant disclosures were reported. Green had no relevant disclosures.
A version of this article appeared on Medscape.com.
Adjuvant Chemo Beneficial in TNBC With High Immune Infiltration
TOPLINE:
These “immune-hot” patients had a 5-year DFS rate of 96.9% compared with 79.4% in the control group.
METHODOLOGY:
- In some studies, adding extended capecitabine to standard adjuvant chemotherapy has been shown to improve DFS in patients with early-stage TNBC, and one subset analysis suggested improved outcomes were most strongly associated with high immune infiltration.
- Researchers conducted a retrospective analysis of CBCSG010, a randomized phase 3 clinical trial, to identify the specific population that benefited from adjuvant capecitabine by analyzing the immune infiltration status of the tumors.
- The CBCSGO10 study of 585 patients originally found adjuvant capecitabine improved 5-year survival in patients with TNBC by 5.9%.
- This analysis included 207 patients (capecitabine arm, n = 104; control arm, n = 103) with serial formalin-fixed, paraffin-embedded tumor specimens, of which RNA sequencing data were available from 36 patients (capecitabine, n = 24; control, n = 12).
- Transcriptome data on the tumor microenvironment were validated with immunohistochemical staining of two markers, programmed death-ligand 1 (PD-L1) and CD8, as well as stromal tumor-infiltrating lymphocytes (sTILs); patients with high PD-L1, CD8, and sTIL expression levels were defined as “immune hot.”
TAKEAWAY:
- Patients with TNBC and high immune infiltration treated with capecitabine had a 5-year DFS rate of 96.9% compared with 79.4% in the control group (hazard ratio [HR], 0.13; 95% CI, 0.03-0.52; P = .049).
- In the capecitabine group, the immune-hot patients had a higher 5-year DFS rate (96.9%) compared with immune-cold patients (76.4%; HR, 0.11; 95% CI, 0.04-0.29; P = .028).
- Gene ontology analysis showed greater enrichment of immune-related pathways in patients without recurrence in the capecitabine group, as well as higher expression of TYMP, a key liver enzyme in the metabolism of capecitabine.
- High expression levels of immune biomarkers PD-L1, CD8, and sTILs were associated with significantly improved DFS in the capecitabine group.
IN PRACTICE:
“Our study suggested that immune-hot patients with TNBC are more likely to benefit from adjuvant capecitabine and that combining immunotherapy with chemotherapy may be expected to be more effective in immune-hot patients,” wrote the study authors.
SOURCE:
The study was led by Wenya Wu, MMed, and Yunsong Yang, MD, at the Department of Breast Surgery, Fudan University Shanghai Cancer Center in Shanghai, People’s Republic of China. It was published online October 2024 in JNCCN — Journal of the National Comprehensive Cancer Network.
LIMITATIONS:
The retrospective nature of the sample collection limited the availability of RNA sequencing data. External verification was challenging due to limited accessibility of transcriptome data from patients treated with additional adjuvant capecitabine or standard chemotherapy alone. The criteria for identifying immune-hot tumors require further exploration and determination.
DISCLOSURES:
This study was funded by the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Shanghai Science and Technology Development Foundation. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
These “immune-hot” patients had a 5-year DFS rate of 96.9% compared with 79.4% in the control group.
METHODOLOGY:
- In some studies, adding extended capecitabine to standard adjuvant chemotherapy has been shown to improve DFS in patients with early-stage TNBC, and one subset analysis suggested improved outcomes were most strongly associated with high immune infiltration.
- Researchers conducted a retrospective analysis of CBCSG010, a randomized phase 3 clinical trial, to identify the specific population that benefited from adjuvant capecitabine by analyzing the immune infiltration status of the tumors.
- The CBCSGO10 study of 585 patients originally found adjuvant capecitabine improved 5-year survival in patients with TNBC by 5.9%.
- This analysis included 207 patients (capecitabine arm, n = 104; control arm, n = 103) with serial formalin-fixed, paraffin-embedded tumor specimens, of which RNA sequencing data were available from 36 patients (capecitabine, n = 24; control, n = 12).
- Transcriptome data on the tumor microenvironment were validated with immunohistochemical staining of two markers, programmed death-ligand 1 (PD-L1) and CD8, as well as stromal tumor-infiltrating lymphocytes (sTILs); patients with high PD-L1, CD8, and sTIL expression levels were defined as “immune hot.”
TAKEAWAY:
- Patients with TNBC and high immune infiltration treated with capecitabine had a 5-year DFS rate of 96.9% compared with 79.4% in the control group (hazard ratio [HR], 0.13; 95% CI, 0.03-0.52; P = .049).
- In the capecitabine group, the immune-hot patients had a higher 5-year DFS rate (96.9%) compared with immune-cold patients (76.4%; HR, 0.11; 95% CI, 0.04-0.29; P = .028).
- Gene ontology analysis showed greater enrichment of immune-related pathways in patients without recurrence in the capecitabine group, as well as higher expression of TYMP, a key liver enzyme in the metabolism of capecitabine.
- High expression levels of immune biomarkers PD-L1, CD8, and sTILs were associated with significantly improved DFS in the capecitabine group.
IN PRACTICE:
“Our study suggested that immune-hot patients with TNBC are more likely to benefit from adjuvant capecitabine and that combining immunotherapy with chemotherapy may be expected to be more effective in immune-hot patients,” wrote the study authors.
SOURCE:
The study was led by Wenya Wu, MMed, and Yunsong Yang, MD, at the Department of Breast Surgery, Fudan University Shanghai Cancer Center in Shanghai, People’s Republic of China. It was published online October 2024 in JNCCN — Journal of the National Comprehensive Cancer Network.
LIMITATIONS:
The retrospective nature of the sample collection limited the availability of RNA sequencing data. External verification was challenging due to limited accessibility of transcriptome data from patients treated with additional adjuvant capecitabine or standard chemotherapy alone. The criteria for identifying immune-hot tumors require further exploration and determination.
DISCLOSURES:
This study was funded by the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Shanghai Science and Technology Development Foundation. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
These “immune-hot” patients had a 5-year DFS rate of 96.9% compared with 79.4% in the control group.
METHODOLOGY:
- In some studies, adding extended capecitabine to standard adjuvant chemotherapy has been shown to improve DFS in patients with early-stage TNBC, and one subset analysis suggested improved outcomes were most strongly associated with high immune infiltration.
- Researchers conducted a retrospective analysis of CBCSG010, a randomized phase 3 clinical trial, to identify the specific population that benefited from adjuvant capecitabine by analyzing the immune infiltration status of the tumors.
- The CBCSGO10 study of 585 patients originally found adjuvant capecitabine improved 5-year survival in patients with TNBC by 5.9%.
- This analysis included 207 patients (capecitabine arm, n = 104; control arm, n = 103) with serial formalin-fixed, paraffin-embedded tumor specimens, of which RNA sequencing data were available from 36 patients (capecitabine, n = 24; control, n = 12).
- Transcriptome data on the tumor microenvironment were validated with immunohistochemical staining of two markers, programmed death-ligand 1 (PD-L1) and CD8, as well as stromal tumor-infiltrating lymphocytes (sTILs); patients with high PD-L1, CD8, and sTIL expression levels were defined as “immune hot.”
TAKEAWAY:
- Patients with TNBC and high immune infiltration treated with capecitabine had a 5-year DFS rate of 96.9% compared with 79.4% in the control group (hazard ratio [HR], 0.13; 95% CI, 0.03-0.52; P = .049).
- In the capecitabine group, the immune-hot patients had a higher 5-year DFS rate (96.9%) compared with immune-cold patients (76.4%; HR, 0.11; 95% CI, 0.04-0.29; P = .028).
- Gene ontology analysis showed greater enrichment of immune-related pathways in patients without recurrence in the capecitabine group, as well as higher expression of TYMP, a key liver enzyme in the metabolism of capecitabine.
- High expression levels of immune biomarkers PD-L1, CD8, and sTILs were associated with significantly improved DFS in the capecitabine group.
IN PRACTICE:
“Our study suggested that immune-hot patients with TNBC are more likely to benefit from adjuvant capecitabine and that combining immunotherapy with chemotherapy may be expected to be more effective in immune-hot patients,” wrote the study authors.
SOURCE:
The study was led by Wenya Wu, MMed, and Yunsong Yang, MD, at the Department of Breast Surgery, Fudan University Shanghai Cancer Center in Shanghai, People’s Republic of China. It was published online October 2024 in JNCCN — Journal of the National Comprehensive Cancer Network.
LIMITATIONS:
The retrospective nature of the sample collection limited the availability of RNA sequencing data. External verification was challenging due to limited accessibility of transcriptome data from patients treated with additional adjuvant capecitabine or standard chemotherapy alone. The criteria for identifying immune-hot tumors require further exploration and determination.
DISCLOSURES:
This study was funded by the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Shanghai Science and Technology Development Foundation. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.