User login
AGA members meet with Rep. Gene Green at Baylor College
In-district meetings with congressional representatives provide a great opportunity for AGA members to establish working relationships with legislators, and help make the voices of our profession and our patients heard.

Members of the Baylor College of Medicine gastroenterology division – Avi Ketwaroo, MD; Richa Shukla, MD; Yamini Natarajan, MD; and Jordan Shapiro, MD – had the opportunity to meet with U.S. Rep. Gene Green, a Democrat from Texas’ 29th Congressional District, as part of AGA’s efforts to link constituents with local representatives. The group discussed the importance of supporting increases in NIH funding to maintain similar levels based on biomedical research inflation, the importance of screening colonoscopy, and improving access to care by opposing the repeal of the Affordable Care Act.
Watch an AGA webinar, available in the AGA Community resource library for AGA members only (community.gastro.org) to learn more about how to set up congressional meetings in your district or contact Navneet Buttar, AGA government and political affairs manager, at nbuttar@gastro.org or 240-482-3221.
ginews@gastro.org
In-district meetings with congressional representatives provide a great opportunity for AGA members to establish working relationships with legislators, and help make the voices of our profession and our patients heard.
Members of the Baylor College of Medicine gastroenterology division – Avi Ketwaroo, MD; Richa Shukla, MD; Yamini Natarajan, MD; and Jordan Shapiro, MD – had the opportunity to meet with U.S. Rep. Gene Green, a Democrat from Texas’ 29th Congressional District, as part of AGA’s efforts to link constituents with local representatives. The group discussed the importance of supporting increases in NIH funding to maintain similar levels based on biomedical research inflation, the importance of screening colonoscopy, and improving access to care by opposing the repeal of the Affordable Care Act.
Watch an AGA webinar, available in the AGA Community resource library for AGA members only (community.gastro.org) to learn more about how to set up congressional meetings in your district or contact Navneet Buttar, AGA government and political affairs manager, at nbuttar@gastro.org or 240-482-3221.
ginews@gastro.org
In-district meetings with congressional representatives provide a great opportunity for AGA members to establish working relationships with legislators, and help make the voices of our profession and our patients heard.
Members of the Baylor College of Medicine gastroenterology division – Avi Ketwaroo, MD; Richa Shukla, MD; Yamini Natarajan, MD; and Jordan Shapiro, MD – had the opportunity to meet with U.S. Rep. Gene Green, a Democrat from Texas’ 29th Congressional District, as part of AGA’s efforts to link constituents with local representatives. The group discussed the importance of supporting increases in NIH funding to maintain similar levels based on biomedical research inflation, the importance of screening colonoscopy, and improving access to care by opposing the repeal of the Affordable Care Act.
Watch an AGA webinar, available in the AGA Community resource library for AGA members only (community.gastro.org) to learn more about how to set up congressional meetings in your district or contact Navneet Buttar, AGA government and political affairs manager, at nbuttar@gastro.org or 240-482-3221.
ginews@gastro.org
AGA comments on Quality Payment proposed rule
AGA provided comments on a proposed rule describing potential changes to the Quality Payment Program (QPP) established under the Medicare Access and CHIP Reauthorization Act (MACRA) for the 2018 performance year. AGA thanks the many members who also submitted comments to CMS to tell the agency how proposed changes will impact you.
For year two, CMS proposed many policies that increase flexibility and incentives under the QPP. However, many proposals target solo practitioners, small practices, and other eligible clinicians with special circumstances. While we support these proposals, AGA’s comments to CMS also ask for changes that are needed to make the QPP work for all gastroenterologists, such as reducing the number of points needed to avoid a payment penalty.
CMS will finalize changes to the QPP during the fall of 2017. Final changes will take effect with the performance period that begins on Jan. 1, 2018. Performance during 2018 will impact payment for services in 2020. AGA members will be notified as soon as the rule is made available by CMS.
Still unsure how to participate in year one?
Make sure your practice is prepared for the 2017 performance year. If you are eligible to participate in 2017, but choose not to, your rates will decrease by 4% in 2019. AGA’s MACRA resource center provides customized advice based on your practice situation to get you on track. It’s not too late to start, but if you wait until Oct. 2, 2017, the deadline to start submitting claims, it will be. Get started now, http://www.gastro.org/macra.
AGA provided comments on a proposed rule describing potential changes to the Quality Payment Program (QPP) established under the Medicare Access and CHIP Reauthorization Act (MACRA) for the 2018 performance year. AGA thanks the many members who also submitted comments to CMS to tell the agency how proposed changes will impact you.
For year two, CMS proposed many policies that increase flexibility and incentives under the QPP. However, many proposals target solo practitioners, small practices, and other eligible clinicians with special circumstances. While we support these proposals, AGA’s comments to CMS also ask for changes that are needed to make the QPP work for all gastroenterologists, such as reducing the number of points needed to avoid a payment penalty.
CMS will finalize changes to the QPP during the fall of 2017. Final changes will take effect with the performance period that begins on Jan. 1, 2018. Performance during 2018 will impact payment for services in 2020. AGA members will be notified as soon as the rule is made available by CMS.
Still unsure how to participate in year one?
Make sure your practice is prepared for the 2017 performance year. If you are eligible to participate in 2017, but choose not to, your rates will decrease by 4% in 2019. AGA’s MACRA resource center provides customized advice based on your practice situation to get you on track. It’s not too late to start, but if you wait until Oct. 2, 2017, the deadline to start submitting claims, it will be. Get started now, http://www.gastro.org/macra.
AGA provided comments on a proposed rule describing potential changes to the Quality Payment Program (QPP) established under the Medicare Access and CHIP Reauthorization Act (MACRA) for the 2018 performance year. AGA thanks the many members who also submitted comments to CMS to tell the agency how proposed changes will impact you.
For year two, CMS proposed many policies that increase flexibility and incentives under the QPP. However, many proposals target solo practitioners, small practices, and other eligible clinicians with special circumstances. While we support these proposals, AGA’s comments to CMS also ask for changes that are needed to make the QPP work for all gastroenterologists, such as reducing the number of points needed to avoid a payment penalty.
CMS will finalize changes to the QPP during the fall of 2017. Final changes will take effect with the performance period that begins on Jan. 1, 2018. Performance during 2018 will impact payment for services in 2020. AGA members will be notified as soon as the rule is made available by CMS.
Still unsure how to participate in year one?
Make sure your practice is prepared for the 2017 performance year. If you are eligible to participate in 2017, but choose not to, your rates will decrease by 4% in 2019. AGA’s MACRA resource center provides customized advice based on your practice situation to get you on track. It’s not too late to start, but if you wait until Oct. 2, 2017, the deadline to start submitting claims, it will be. Get started now, http://www.gastro.org/macra.
How to manage bleeding in patients taking direct oral anticoagulants (DOACs)
Case
A 72-year-old man with a history of nonvalvular atrial fibrillation (AF) and hypertension presents to the ER after an episode of hematochezia. He is prescribed dabigatran 150 mg twice daily for his AF and took his evening dose 2 hours prior to presentation. His initial exam reveals vital signs of BP 120/55, HR 105, RR 14 and bright red stool on rectal exam. His hemoglobin is 8.1 g/dL, down from 12.0 g/dL one month ago. He has normal renal function. How should you manage his gastrointestinal bleeding?
Background
Direct oral anticoagulants (DOACs) consist of two classes of drugs: oral factor Xa inhibitors (apixaban, edoxaban, and rivaroxaban) and direct thrombin inhibitors (dabigatran). They have gained substantial popularity since their commercial introduction in 2010, and are now Food and Drug Administration approved for the treatment of atrial fibrillation (AF) and venous thromboembolism (VTE) in noncancer patients. DOAC use will likely increase given favorable safety profiles, reliable pharmacokinetics, and recent guidelines recommending their use over vitamin K antagonists (VKAs) for treatment of VTE in noncancer patients.1
A primary concern about the routine use of DOACs has been the lack of commercially available direct reversal agents. Unlike warfarin, which has an effective rapid antidote, no direct reversal agent is available for Xa inhibitors, and only recently has there been FDA approval for idarucizumab, a direct thrombin inhibitor reversal drug. Therefore, clinicians are often left wondering how to manage bleeding episodes in patients receiving DOACs.
Literature review
What is the risk of bleeding for patients taking DOACs?
DOACs carry a low but significant risk of bleeding, including life-threatening bleeding. There is now robust data from over 100,000 patients in randomized clinical trials of nonvalvular AF and VTE comparing the risk of major and fatal bleeding between DOACs and VKAs.2 These trials reveal an annual major bleeding rate of 2%-4% in patients with AF and 1%-2% in patients with VTE taking DOACs.
Importantly, DOACs were found to carry a statistically lower risk of major and fatal bleeding than VKAs. Patients taking DOACs have a relative risk of major bleeding of 0.72, compared with VKAs, and a RR of fatal bleeding of 0.53. Additionally, the case fatality rate for major bleeding episodes was 7.6% for DOACs versus 11.0% for warfarin, despite not having an available antidote for DOACs in these trials.3 Although there is an increased risk of bleeding from DOACs, the rates of major bleeding and of serious complications from bleeding are lower than with warfarin.
How long does the effect of a DOAC last?
A significant advantage of DOACs over VKAs in the setting of bleeding is their shorter half-lives, which range from a low estimate of 5 hours for rivaroxaban to a high estimate of 17 hours for dabigatran4-8 (Table 1). Given that it takes 4-5 half-lives for a drug to be functionally eliminated, coagulation typically normalizes in patients taking DOACs within 1-3 days, compared with 3-5 days for warfarin. All DOACs have significant renal clearance, and renal failure will prolong the duration of anticoagulation. For patients who are taking DOACs and present with bleeding, it is important to assess their renal function.
Are coagulation tests helpful when assessing the effect of DOACs?
Prothrombin time (PT/INR) and activated partial thromboplastin time (aPTT) should be measured in all patients presenting with significant bleeding, whether or not the patient is taking a DOAC. PT and aPTT are commonly elevated for patients taking direct thrombin inhibitors and Xa inhibitors. Although a prolonged PT and/or aPTT can be useful in determining if the anticoagulant effect from DOACs is still present, normal values of these tests do not rule out an anticoagulant effect in patients taking DOACs.9,10 Thrombin Time (TT) is a widely available test with quick results, and a normal value rules out the therapeutic effect of dabigatran. Finally, the anti–factor Xa assay is a sensitive test for Xa inhibitors, but requires calibration to the DOAC of interest in order to be reliable. Clinicians should consult with their institution’s laboratory prior to using an anti–factor Xa level to test the anticoagulant effect of a specific DOAC. Repeat coagulation testing may be useful in some clinical circumstances, especially if a patient has renal impairment.
Are there reversal agents for DOACs?
In October 2015, the FDA approved idarucizumab, a monoclonal antibody fragment that binds dabigatran with much greater affinity than thrombin, thus quickly reversing the effect of the direct thrombin inhibitor. FDA approval came in response to an interim analysis of an ongoing open-label trial, RE-VERSE AD.11 This study enrolled 90 adults with major bleeding or need for an emergency procedure taking dabigatran to receive idarucizumab (2.5 g in 50 mL rapid infusion dose given twice less than 15 minutes apart for a total of 5 g). Idarucizumab immediately reversed the effect of dabigatran on clotting tests in 88%-98% of the patients. For patients with major bleeding, the median time for bleeding cessation was 11.4 hours. One thrombotic event was reported within 72 hours of drug administration. Therefore, in patients taking dabigatran with an elevated TT, idarucizumab may be used if the bleeding is life threatening and refractory to initial supportive measures.
There are no FDA-approved antidotes for the factor Xa inhibitors. One promising agent is andexanet-alfa, an inactivated form of factor Xa that irreversibly binds Xa inhibitors. The ongoing, open-label ANNEXA-4 trial12 reported a decrease in anti–factor Xa activity of ~90% after bolus administration of the drug followed by 2-hour infusion in 67 patients with life-threatening bleeding, with clinical hemostasis achieved in 79% in patients by 12 hours. However, thrombotic events occurred in 18% of the patients at 1 month. Additional safety and efficacy data, along with plans for postmarket surveillance, will be needed prior to approval for clinical use.
Are there other options to obtain hemostasis?
Clotting factor products, specifically fresh frozen plasma (FFP) and prothrombin complex concentrates (PCCs), are often used to attempt to reverse anticoagulation from DOACs. While FFP alone has no evidence to support its use in reversing the effect of DOACs, PCCs might reverse anticoagulation for both Xa inhibitors and direct thrombin inhibitors.13 Some experts recommend unactivated PCC over activated PCC because of a theoretically increased thrombotic risk of activated PCC.14 For patients taking Xa inhibitors or dabigatran (if idarucizumab is unavailable) with life-threatening bleeding, PCC should be used in an attempt to reverse the bleeding.
Another strategy to promote hemostasis in bleeding patients taking DOACs is to use antifibrinolytics. Effective for control of bleeding in trauma and surgical patients, tranexamic acid has not been widely studied in nonsurgical bleeding, much less DOAC-related nonsurgical bleeding. A 2014 Cochrane review of a small number of trials suggested a possible mortality benefit from its use in upper GI bleeding, but the quality of included trials was poor.15 The ongoing HALT-IT trial, enrolling 8,000 patients with gastrointestinal bleeding, aims to clarify the mortality benefit of tranexamic acid.16 Despite effectively promoting hemostasis in many populations of bleeding patients, tranexamic acid carries no discernible thrombotic risk.17,18 By preventing clot degradation through a downstream mechanism at low cost and risk, antifibrinolytics are a practical adjunctive therapy to control major bleeding in patients on DOACs.
Can charcoal or dialysis reduce the systemic concentration of DOACs?
In addition to discontinuing the DOAC, both charcoal and dialysis can reduce the systemic concentration of DOACs. If the ingestion was recent, oral activated charcoal can reduce the systemic absorption of DOACs. To date there are no data on the efficacy of charcoal in bleeding patients taking DOACs. However, in two recent trials, administration of a single dose of charcoal in healthy patients led to significantly decreased area under concentration-time curves (AUC) when given at 6 and 8 hours after ingestion of a therapeutic dose of apixaban and rivaroxaban, respectively.19,20 While further studies are needed to confirm its clinical benefit, charcoal is recommended for major bleeding when given within 2 hours of ingestion of a DOAC and may be useful within 8 hours.
Unlike charcoal, which can be used for patients on Xa inhibitors or dabigatran, hemodialysis is only effective for reducing serum concentrations of dabigatran because of its low plasma protein binding (~35%). A review of 35 patients (10 with normal renal function) with severe bleeding showed significant reductions in coagulation tests (aPTT, PT, TT) and dabigatran levels after hemodialysis.21 For severe bleeding episodes particularly in patients with impaired renal function, providers should consider the use of continuous renal replacement therapy until clinical hemostasis is achieved.
What is the expert’s opinion?
We asked one of our hematologists with expertise in DOACs for his opinion on this topic. Most patients with DOAC-associated bleeding can be managed with supportive care because of the short half-life of these agents in patients with reasonably preserved renal function. The main scenario for escalating therapy to PCC or idarucizumab is life-threatening bleeding, such as intracranial hemorrhage and gastrointestinal hemorrhage with hemodynamic instability. The threshold for use of idarucizumab for patients taking dabigatran with bleeding should be lower than PCCs because there is better evidence for clinical benefit with less risk.
Developing reversal agents continues to be costly, requiring extensive preclinical work and clinical trials that are difficult to do. Assuming that reversal agents become more affordable in the longer term, and safety profiles are better established, clinicians may eventually have a lower threshold for their use in a wider variety of bleeding episodes. Lastly, adverse outcomes often occur, not during the acute bleeding episode, but several weeks later in patients whose providers delay restarting anticoagulation. Thus, it is important to resume anticoagulant therapy as soon as it is safe to do so.
Back to the case
Our patient was given a 50-g suspension of oral activated charcoal, along with two doses of 1 g intravenous tranexamic acid 8 hours apart. He was typed and crossed for blood, and ultimately received 1 unit of packed red blood cells before stabilizing without other measures. His colonoscopy subsequently revealed a diverticular bleed with a visible vessel that was coagulated. He was discharged 2 days later after remaining clinically stable after colonoscopy.
Bottom line
For the majority of bleeding patients on DOACs, supportive care with transfusions and local hemostatic interventions to control bleeding will likely be sufficient. Because of the short half-lives of DOACs, most patients do not require additional therapy (Table 2), and these patients actually have better outcomes from major bleeding episodes than patients taking VKAs. Antifibrinolytics should be a first-line prohemostatic therapy in major bleeding. Oral activated charcoal may be effective within 2-8 hours after ingestion for reduction of serum DOAC concentrations. Finally, in cases of life-threatening bleeding, idarucizumab can be used to reverse anticoagulation for patients taking dabigatran. When idarucizumab is unavailable, or for patients taking Xa inhibitors, PCC can be used.
Dr. Hagan is chief medical resident at the University of Washington Medical Center in Seattle. Dr. Albert is clinical instructor of medicine at UWMC. Dr. Garcia is professor of medicine and associate medical director of antithrombotic therapy at UWMC. Dr. Huang is an attending with the UWMC Medicine Consult Service and assistant clinical professor in the division of general internal medicine at UW.
Key Points
• The risk of major bleeding, and the case fatality rate of major bleeding, is significantly lower in patients taking DOACs versus VKAs
• For the majority of patients with bleeding on DOACs, withholding anticoagulation and supportive care is sufficient
• Idarucizumab is a novel and effective antidote to dabigatran, but should be reserved for patients with life-threatening bleeding
• Patients with DOAC-associated bleeding should be restarted on anticoagulation as soon as it is safe to do so
Additional Reading
Management of bleeding in patients receiving direct oral anticoagulants. UpToDate 2016.
How do I treat target-specific oral anticoagulant-associated bleeding? Blood 2014.
References
1. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
2. Chai-adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-specific oral anticoagulants: a systematic review and meta-analysis. Blood. 2014;124(15):2450-8.
3. Chai-adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. J Thromb Haemost. 2015;13(11):2012-20.
4. Savaysa (edoxaban) [package insert]. Daiichi Sankyo, Inc, Tokyo, Japan; 2015. www.accessdata.fda.gov/drugsatfda_docs/label/2015/206316lbl.pdf. Accessed January 8th, 2016.
5. Xarelto (rivaroxaban) [package insert]. Janssen Pharmaceuticals, Inc. Titusville, NJ; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/202439s001lbl.pdf. Accessed January 8th, 2016.
6. Pradaxa (dabigatran) [package insert]. Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/022512s007lbl.pdf. Accessed January 8th, 2016.
7. Eliquis (apixaban) [package insert]. Bristol-Myers Squibb Company, Princeton, NJ; 2012. www.accessdata.fda.gov/drugsatfda_docs/label/2012/202155s000lbl.pdf. Accessed January 8th, 2016.
8. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82.
9. Tripodi A. The laboratory and the direct oral anticoagulants. Blood.
2013;121(20):4032-5.
10. Samuelson BT, Cuker A, Siegal DM, Crowther M, Garcia DA. Laboratory Assessment of the Anticoagulant Activity of Direct Oral Anticoagulants (DOACs): A Systematic Review. Chest. 2016;
11. Pollack CV, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015;373(6):511-20.
12. Connolly SJ, Milling TJ, Eikelboom JW, et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors. N Engl J Med. 2016.
13. Dickneite G, Hoffman M. Reversing the new oral anticoagulants with prothrombin complex concentrates (PCCs): what is the evidence?. Thromb Haemost. 2014;111(2):189-98.
14. Sørensen B, Spahn DR, Innerhofer P, Spannagl M, Rossaint R. Clinical review: Prothrombin complex concentrates--evaluation of safety and thrombogenicity. Crit Care. 2011;15(1):201.
15. Bennett C, Klingenberg S, Langholz E, Gluud L. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database of Systematic Reviews 2014, Issue 11. Art. No.: CD006640.
16. Roberts I, Coats T, Edwards P, et al. HALT-IT – tranexamic acid for the treatment of gastrointestinal bleeding: study protocol for a randomised controlled trial. Trials. 2014 Nov 19;15:450.
17. Dyba J, Chan F, Lau K, Chan A, Chan H. Tranexamic Acid is a Weak Provoking Factor for Thromboembolic Events: A Systematic Review of the Literature. Blood. 2013; 122(21): 3629.
18. Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N Engl J Med. 2016; 376(2):136-148.
19. Wang X, Mondal S, Wang J, et al. Effect of Activated Charcoal on Apixaban Pharmacokinetics in Healthy Subjects. American Journal of Cardiovascular Drugs. 2014;14(2):147-154.
20. Ollier E, Hodin S, Lanoiselée J, et al. Effect of Activated Charcoal on Rivaroxaban Complex Absorption. Clin Pharmacokinet. 2016 Dec 2.
21. Chai-adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-8.
22. Schulman S, Kearon C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-4.
23. UW Anticoagulation Services. UW Medicine Pharmacy Services Web site. 2014. Available at https://depts.washington.edu/anticoag, Accessed March 8, 2017.
________________________________________________________________________
Table 1: Pharmacologic Profiles of Xa and Direct Thrombin Inhibitors4-8, 23
tmax t1/2, CrCl 50-80 t1/2 CrCl < 30 Dialyzable?
Apixaban 3-4 h 15 h 17 h No
Dabigatran 1-3 h 17 h 28 h Yes
Edoxaban 1-2 h 10-14 h no data No
Rivaroxaban 2-4 h 9 h 10 h No
tmax = time to peak serum concentration after ingestion, t1/2= serum half-life, CrCl= creatinine clearance in mL/min
*Average values assuming normal hepatic function. Aside from dabigatran, which has minimal hepatic clearance, all other DOACs can have prolonged half-lives in hepatic impairment.
Table 2: Management of Bleeding Patients Taking DOACs
Direct Thrombin Inhibitors (dabigatran)
Xa inhibitors (apixaban, edoxaban, rivaroxaban)Minor Bleeding
• Withhold DOAC
• Local hemostatic measures
Major Bleeding*
All of the above, AND
• Antifibrinolytic if bleeding persists
• Restore physiologic perfusion
• Charcoal if last dose within 2-8 hours
• Transfusion indications:
o Red blood cells: anemia
o Platelets: antiplatelet agents or thrombocytopenia
o Plasma: coagulopathy (dilution, DIC, liver failure), not for DOAC reversal
Life-threatening Bleeding**
All of the above, AND:
• Idarucizumab (confirm anticoagulant effect with thrombin time first)
• If idarucizumab is unavailable, use PCC
• Consider hemodialysis until hemostasis achieved, especially if patient in renal failure
All of the above, AND:
• Unactivated PCC (if available and calibrated to specific Xa inhibitor, confirm anticoagulant effect with anti-Xa level)
* Adapted from the International Society on Thrombosis and Hemostasis: bleeding with a fall in hemoglobin level ≥ 2 g/dL, OR bleeding leading to ≥ 2 units of PRBC transfused.21 Clinicians should perform risk stratification of bleeding episodes using vital signs, laboratory results, the area of bleeding, and patient comorbidities.
**Uncontrolled bleeding, OR symptomatic bleeding in a critical area or organ (such as intracranial, intraocular, intraspinal, retroperitoneal, pericardial, or intramuscular with compartment syndrome).
Case
A 72-year-old man with a history of nonvalvular atrial fibrillation (AF) and hypertension presents to the ER after an episode of hematochezia. He is prescribed dabigatran 150 mg twice daily for his AF and took his evening dose 2 hours prior to presentation. His initial exam reveals vital signs of BP 120/55, HR 105, RR 14 and bright red stool on rectal exam. His hemoglobin is 8.1 g/dL, down from 12.0 g/dL one month ago. He has normal renal function. How should you manage his gastrointestinal bleeding?
Background
Direct oral anticoagulants (DOACs) consist of two classes of drugs: oral factor Xa inhibitors (apixaban, edoxaban, and rivaroxaban) and direct thrombin inhibitors (dabigatran). They have gained substantial popularity since their commercial introduction in 2010, and are now Food and Drug Administration approved for the treatment of atrial fibrillation (AF) and venous thromboembolism (VTE) in noncancer patients. DOAC use will likely increase given favorable safety profiles, reliable pharmacokinetics, and recent guidelines recommending their use over vitamin K antagonists (VKAs) for treatment of VTE in noncancer patients.1
A primary concern about the routine use of DOACs has been the lack of commercially available direct reversal agents. Unlike warfarin, which has an effective rapid antidote, no direct reversal agent is available for Xa inhibitors, and only recently has there been FDA approval for idarucizumab, a direct thrombin inhibitor reversal drug. Therefore, clinicians are often left wondering how to manage bleeding episodes in patients receiving DOACs.
Literature review
What is the risk of bleeding for patients taking DOACs?
DOACs carry a low but significant risk of bleeding, including life-threatening bleeding. There is now robust data from over 100,000 patients in randomized clinical trials of nonvalvular AF and VTE comparing the risk of major and fatal bleeding between DOACs and VKAs.2 These trials reveal an annual major bleeding rate of 2%-4% in patients with AF and 1%-2% in patients with VTE taking DOACs.
Importantly, DOACs were found to carry a statistically lower risk of major and fatal bleeding than VKAs. Patients taking DOACs have a relative risk of major bleeding of 0.72, compared with VKAs, and a RR of fatal bleeding of 0.53. Additionally, the case fatality rate for major bleeding episodes was 7.6% for DOACs versus 11.0% for warfarin, despite not having an available antidote for DOACs in these trials.3 Although there is an increased risk of bleeding from DOACs, the rates of major bleeding and of serious complications from bleeding are lower than with warfarin.
How long does the effect of a DOAC last?
A significant advantage of DOACs over VKAs in the setting of bleeding is their shorter half-lives, which range from a low estimate of 5 hours for rivaroxaban to a high estimate of 17 hours for dabigatran4-8 (Table 1). Given that it takes 4-5 half-lives for a drug to be functionally eliminated, coagulation typically normalizes in patients taking DOACs within 1-3 days, compared with 3-5 days for warfarin. All DOACs have significant renal clearance, and renal failure will prolong the duration of anticoagulation. For patients who are taking DOACs and present with bleeding, it is important to assess their renal function.
Are coagulation tests helpful when assessing the effect of DOACs?
Prothrombin time (PT/INR) and activated partial thromboplastin time (aPTT) should be measured in all patients presenting with significant bleeding, whether or not the patient is taking a DOAC. PT and aPTT are commonly elevated for patients taking direct thrombin inhibitors and Xa inhibitors. Although a prolonged PT and/or aPTT can be useful in determining if the anticoagulant effect from DOACs is still present, normal values of these tests do not rule out an anticoagulant effect in patients taking DOACs.9,10 Thrombin Time (TT) is a widely available test with quick results, and a normal value rules out the therapeutic effect of dabigatran. Finally, the anti–factor Xa assay is a sensitive test for Xa inhibitors, but requires calibration to the DOAC of interest in order to be reliable. Clinicians should consult with their institution’s laboratory prior to using an anti–factor Xa level to test the anticoagulant effect of a specific DOAC. Repeat coagulation testing may be useful in some clinical circumstances, especially if a patient has renal impairment.
Are there reversal agents for DOACs?
In October 2015, the FDA approved idarucizumab, a monoclonal antibody fragment that binds dabigatran with much greater affinity than thrombin, thus quickly reversing the effect of the direct thrombin inhibitor. FDA approval came in response to an interim analysis of an ongoing open-label trial, RE-VERSE AD.11 This study enrolled 90 adults with major bleeding or need for an emergency procedure taking dabigatran to receive idarucizumab (2.5 g in 50 mL rapid infusion dose given twice less than 15 minutes apart for a total of 5 g). Idarucizumab immediately reversed the effect of dabigatran on clotting tests in 88%-98% of the patients. For patients with major bleeding, the median time for bleeding cessation was 11.4 hours. One thrombotic event was reported within 72 hours of drug administration. Therefore, in patients taking dabigatran with an elevated TT, idarucizumab may be used if the bleeding is life threatening and refractory to initial supportive measures.
There are no FDA-approved antidotes for the factor Xa inhibitors. One promising agent is andexanet-alfa, an inactivated form of factor Xa that irreversibly binds Xa inhibitors. The ongoing, open-label ANNEXA-4 trial12 reported a decrease in anti–factor Xa activity of ~90% after bolus administration of the drug followed by 2-hour infusion in 67 patients with life-threatening bleeding, with clinical hemostasis achieved in 79% in patients by 12 hours. However, thrombotic events occurred in 18% of the patients at 1 month. Additional safety and efficacy data, along with plans for postmarket surveillance, will be needed prior to approval for clinical use.
Are there other options to obtain hemostasis?
Clotting factor products, specifically fresh frozen plasma (FFP) and prothrombin complex concentrates (PCCs), are often used to attempt to reverse anticoagulation from DOACs. While FFP alone has no evidence to support its use in reversing the effect of DOACs, PCCs might reverse anticoagulation for both Xa inhibitors and direct thrombin inhibitors.13 Some experts recommend unactivated PCC over activated PCC because of a theoretically increased thrombotic risk of activated PCC.14 For patients taking Xa inhibitors or dabigatran (if idarucizumab is unavailable) with life-threatening bleeding, PCC should be used in an attempt to reverse the bleeding.
Another strategy to promote hemostasis in bleeding patients taking DOACs is to use antifibrinolytics. Effective for control of bleeding in trauma and surgical patients, tranexamic acid has not been widely studied in nonsurgical bleeding, much less DOAC-related nonsurgical bleeding. A 2014 Cochrane review of a small number of trials suggested a possible mortality benefit from its use in upper GI bleeding, but the quality of included trials was poor.15 The ongoing HALT-IT trial, enrolling 8,000 patients with gastrointestinal bleeding, aims to clarify the mortality benefit of tranexamic acid.16 Despite effectively promoting hemostasis in many populations of bleeding patients, tranexamic acid carries no discernible thrombotic risk.17,18 By preventing clot degradation through a downstream mechanism at low cost and risk, antifibrinolytics are a practical adjunctive therapy to control major bleeding in patients on DOACs.
Can charcoal or dialysis reduce the systemic concentration of DOACs?
In addition to discontinuing the DOAC, both charcoal and dialysis can reduce the systemic concentration of DOACs. If the ingestion was recent, oral activated charcoal can reduce the systemic absorption of DOACs. To date there are no data on the efficacy of charcoal in bleeding patients taking DOACs. However, in two recent trials, administration of a single dose of charcoal in healthy patients led to significantly decreased area under concentration-time curves (AUC) when given at 6 and 8 hours after ingestion of a therapeutic dose of apixaban and rivaroxaban, respectively.19,20 While further studies are needed to confirm its clinical benefit, charcoal is recommended for major bleeding when given within 2 hours of ingestion of a DOAC and may be useful within 8 hours.
Unlike charcoal, which can be used for patients on Xa inhibitors or dabigatran, hemodialysis is only effective for reducing serum concentrations of dabigatran because of its low plasma protein binding (~35%). A review of 35 patients (10 with normal renal function) with severe bleeding showed significant reductions in coagulation tests (aPTT, PT, TT) and dabigatran levels after hemodialysis.21 For severe bleeding episodes particularly in patients with impaired renal function, providers should consider the use of continuous renal replacement therapy until clinical hemostasis is achieved.
What is the expert’s opinion?
We asked one of our hematologists with expertise in DOACs for his opinion on this topic. Most patients with DOAC-associated bleeding can be managed with supportive care because of the short half-life of these agents in patients with reasonably preserved renal function. The main scenario for escalating therapy to PCC or idarucizumab is life-threatening bleeding, such as intracranial hemorrhage and gastrointestinal hemorrhage with hemodynamic instability. The threshold for use of idarucizumab for patients taking dabigatran with bleeding should be lower than PCCs because there is better evidence for clinical benefit with less risk.
Developing reversal agents continues to be costly, requiring extensive preclinical work and clinical trials that are difficult to do. Assuming that reversal agents become more affordable in the longer term, and safety profiles are better established, clinicians may eventually have a lower threshold for their use in a wider variety of bleeding episodes. Lastly, adverse outcomes often occur, not during the acute bleeding episode, but several weeks later in patients whose providers delay restarting anticoagulation. Thus, it is important to resume anticoagulant therapy as soon as it is safe to do so.
Back to the case
Our patient was given a 50-g suspension of oral activated charcoal, along with two doses of 1 g intravenous tranexamic acid 8 hours apart. He was typed and crossed for blood, and ultimately received 1 unit of packed red blood cells before stabilizing without other measures. His colonoscopy subsequently revealed a diverticular bleed with a visible vessel that was coagulated. He was discharged 2 days later after remaining clinically stable after colonoscopy.
Bottom line
For the majority of bleeding patients on DOACs, supportive care with transfusions and local hemostatic interventions to control bleeding will likely be sufficient. Because of the short half-lives of DOACs, most patients do not require additional therapy (Table 2), and these patients actually have better outcomes from major bleeding episodes than patients taking VKAs. Antifibrinolytics should be a first-line prohemostatic therapy in major bleeding. Oral activated charcoal may be effective within 2-8 hours after ingestion for reduction of serum DOAC concentrations. Finally, in cases of life-threatening bleeding, idarucizumab can be used to reverse anticoagulation for patients taking dabigatran. When idarucizumab is unavailable, or for patients taking Xa inhibitors, PCC can be used.
Dr. Hagan is chief medical resident at the University of Washington Medical Center in Seattle. Dr. Albert is clinical instructor of medicine at UWMC. Dr. Garcia is professor of medicine and associate medical director of antithrombotic therapy at UWMC. Dr. Huang is an attending with the UWMC Medicine Consult Service and assistant clinical professor in the division of general internal medicine at UW.
Key Points
• The risk of major bleeding, and the case fatality rate of major bleeding, is significantly lower in patients taking DOACs versus VKAs
• For the majority of patients with bleeding on DOACs, withholding anticoagulation and supportive care is sufficient
• Idarucizumab is a novel and effective antidote to dabigatran, but should be reserved for patients with life-threatening bleeding
• Patients with DOAC-associated bleeding should be restarted on anticoagulation as soon as it is safe to do so
Additional Reading
Management of bleeding in patients receiving direct oral anticoagulants. UpToDate 2016.
How do I treat target-specific oral anticoagulant-associated bleeding? Blood 2014.
References
1. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
2. Chai-adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-specific oral anticoagulants: a systematic review and meta-analysis. Blood. 2014;124(15):2450-8.
3. Chai-adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. J Thromb Haemost. 2015;13(11):2012-20.
4. Savaysa (edoxaban) [package insert]. Daiichi Sankyo, Inc, Tokyo, Japan; 2015. www.accessdata.fda.gov/drugsatfda_docs/label/2015/206316lbl.pdf. Accessed January 8th, 2016.
5. Xarelto (rivaroxaban) [package insert]. Janssen Pharmaceuticals, Inc. Titusville, NJ; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/202439s001lbl.pdf. Accessed January 8th, 2016.
6. Pradaxa (dabigatran) [package insert]. Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/022512s007lbl.pdf. Accessed January 8th, 2016.
7. Eliquis (apixaban) [package insert]. Bristol-Myers Squibb Company, Princeton, NJ; 2012. www.accessdata.fda.gov/drugsatfda_docs/label/2012/202155s000lbl.pdf. Accessed January 8th, 2016.
8. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82.
9. Tripodi A. The laboratory and the direct oral anticoagulants. Blood.
2013;121(20):4032-5.
10. Samuelson BT, Cuker A, Siegal DM, Crowther M, Garcia DA. Laboratory Assessment of the Anticoagulant Activity of Direct Oral Anticoagulants (DOACs): A Systematic Review. Chest. 2016;
11. Pollack CV, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015;373(6):511-20.
12. Connolly SJ, Milling TJ, Eikelboom JW, et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors. N Engl J Med. 2016.
13. Dickneite G, Hoffman M. Reversing the new oral anticoagulants with prothrombin complex concentrates (PCCs): what is the evidence?. Thromb Haemost. 2014;111(2):189-98.
14. Sørensen B, Spahn DR, Innerhofer P, Spannagl M, Rossaint R. Clinical review: Prothrombin complex concentrates--evaluation of safety and thrombogenicity. Crit Care. 2011;15(1):201.
15. Bennett C, Klingenberg S, Langholz E, Gluud L. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database of Systematic Reviews 2014, Issue 11. Art. No.: CD006640.
16. Roberts I, Coats T, Edwards P, et al. HALT-IT – tranexamic acid for the treatment of gastrointestinal bleeding: study protocol for a randomised controlled trial. Trials. 2014 Nov 19;15:450.
17. Dyba J, Chan F, Lau K, Chan A, Chan H. Tranexamic Acid is a Weak Provoking Factor for Thromboembolic Events: A Systematic Review of the Literature. Blood. 2013; 122(21): 3629.
18. Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N Engl J Med. 2016; 376(2):136-148.
19. Wang X, Mondal S, Wang J, et al. Effect of Activated Charcoal on Apixaban Pharmacokinetics in Healthy Subjects. American Journal of Cardiovascular Drugs. 2014;14(2):147-154.
20. Ollier E, Hodin S, Lanoiselée J, et al. Effect of Activated Charcoal on Rivaroxaban Complex Absorption. Clin Pharmacokinet. 2016 Dec 2.
21. Chai-adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-8.
22. Schulman S, Kearon C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-4.
23. UW Anticoagulation Services. UW Medicine Pharmacy Services Web site. 2014. Available at https://depts.washington.edu/anticoag, Accessed March 8, 2017.
________________________________________________________________________
Table 1: Pharmacologic Profiles of Xa and Direct Thrombin Inhibitors4-8, 23
tmax t1/2, CrCl 50-80 t1/2 CrCl < 30 Dialyzable?
Apixaban 3-4 h 15 h 17 h No
Dabigatran 1-3 h 17 h 28 h Yes
Edoxaban 1-2 h 10-14 h no data No
Rivaroxaban 2-4 h 9 h 10 h No
tmax = time to peak serum concentration after ingestion, t1/2= serum half-life, CrCl= creatinine clearance in mL/min
*Average values assuming normal hepatic function. Aside from dabigatran, which has minimal hepatic clearance, all other DOACs can have prolonged half-lives in hepatic impairment.
Table 2: Management of Bleeding Patients Taking DOACs
Direct Thrombin Inhibitors (dabigatran)
Xa inhibitors (apixaban, edoxaban, rivaroxaban)Minor Bleeding
• Withhold DOAC
• Local hemostatic measures
Major Bleeding*
All of the above, AND
• Antifibrinolytic if bleeding persists
• Restore physiologic perfusion
• Charcoal if last dose within 2-8 hours
• Transfusion indications:
o Red blood cells: anemia
o Platelets: antiplatelet agents or thrombocytopenia
o Plasma: coagulopathy (dilution, DIC, liver failure), not for DOAC reversal
Life-threatening Bleeding**
All of the above, AND:
• Idarucizumab (confirm anticoagulant effect with thrombin time first)
• If idarucizumab is unavailable, use PCC
• Consider hemodialysis until hemostasis achieved, especially if patient in renal failure
All of the above, AND:
• Unactivated PCC (if available and calibrated to specific Xa inhibitor, confirm anticoagulant effect with anti-Xa level)
* Adapted from the International Society on Thrombosis and Hemostasis: bleeding with a fall in hemoglobin level ≥ 2 g/dL, OR bleeding leading to ≥ 2 units of PRBC transfused.21 Clinicians should perform risk stratification of bleeding episodes using vital signs, laboratory results, the area of bleeding, and patient comorbidities.
**Uncontrolled bleeding, OR symptomatic bleeding in a critical area or organ (such as intracranial, intraocular, intraspinal, retroperitoneal, pericardial, or intramuscular with compartment syndrome).
Case
A 72-year-old man with a history of nonvalvular atrial fibrillation (AF) and hypertension presents to the ER after an episode of hematochezia. He is prescribed dabigatran 150 mg twice daily for his AF and took his evening dose 2 hours prior to presentation. His initial exam reveals vital signs of BP 120/55, HR 105, RR 14 and bright red stool on rectal exam. His hemoglobin is 8.1 g/dL, down from 12.0 g/dL one month ago. He has normal renal function. How should you manage his gastrointestinal bleeding?
Background
Direct oral anticoagulants (DOACs) consist of two classes of drugs: oral factor Xa inhibitors (apixaban, edoxaban, and rivaroxaban) and direct thrombin inhibitors (dabigatran). They have gained substantial popularity since their commercial introduction in 2010, and are now Food and Drug Administration approved for the treatment of atrial fibrillation (AF) and venous thromboembolism (VTE) in noncancer patients. DOAC use will likely increase given favorable safety profiles, reliable pharmacokinetics, and recent guidelines recommending their use over vitamin K antagonists (VKAs) for treatment of VTE in noncancer patients.1
A primary concern about the routine use of DOACs has been the lack of commercially available direct reversal agents. Unlike warfarin, which has an effective rapid antidote, no direct reversal agent is available for Xa inhibitors, and only recently has there been FDA approval for idarucizumab, a direct thrombin inhibitor reversal drug. Therefore, clinicians are often left wondering how to manage bleeding episodes in patients receiving DOACs.
Literature review
What is the risk of bleeding for patients taking DOACs?
DOACs carry a low but significant risk of bleeding, including life-threatening bleeding. There is now robust data from over 100,000 patients in randomized clinical trials of nonvalvular AF and VTE comparing the risk of major and fatal bleeding between DOACs and VKAs.2 These trials reveal an annual major bleeding rate of 2%-4% in patients with AF and 1%-2% in patients with VTE taking DOACs.
Importantly, DOACs were found to carry a statistically lower risk of major and fatal bleeding than VKAs. Patients taking DOACs have a relative risk of major bleeding of 0.72, compared with VKAs, and a RR of fatal bleeding of 0.53. Additionally, the case fatality rate for major bleeding episodes was 7.6% for DOACs versus 11.0% for warfarin, despite not having an available antidote for DOACs in these trials.3 Although there is an increased risk of bleeding from DOACs, the rates of major bleeding and of serious complications from bleeding are lower than with warfarin.
How long does the effect of a DOAC last?
A significant advantage of DOACs over VKAs in the setting of bleeding is their shorter half-lives, which range from a low estimate of 5 hours for rivaroxaban to a high estimate of 17 hours for dabigatran4-8 (Table 1). Given that it takes 4-5 half-lives for a drug to be functionally eliminated, coagulation typically normalizes in patients taking DOACs within 1-3 days, compared with 3-5 days for warfarin. All DOACs have significant renal clearance, and renal failure will prolong the duration of anticoagulation. For patients who are taking DOACs and present with bleeding, it is important to assess their renal function.
Are coagulation tests helpful when assessing the effect of DOACs?
Prothrombin time (PT/INR) and activated partial thromboplastin time (aPTT) should be measured in all patients presenting with significant bleeding, whether or not the patient is taking a DOAC. PT and aPTT are commonly elevated for patients taking direct thrombin inhibitors and Xa inhibitors. Although a prolonged PT and/or aPTT can be useful in determining if the anticoagulant effect from DOACs is still present, normal values of these tests do not rule out an anticoagulant effect in patients taking DOACs.9,10 Thrombin Time (TT) is a widely available test with quick results, and a normal value rules out the therapeutic effect of dabigatran. Finally, the anti–factor Xa assay is a sensitive test for Xa inhibitors, but requires calibration to the DOAC of interest in order to be reliable. Clinicians should consult with their institution’s laboratory prior to using an anti–factor Xa level to test the anticoagulant effect of a specific DOAC. Repeat coagulation testing may be useful in some clinical circumstances, especially if a patient has renal impairment.
Are there reversal agents for DOACs?
In October 2015, the FDA approved idarucizumab, a monoclonal antibody fragment that binds dabigatran with much greater affinity than thrombin, thus quickly reversing the effect of the direct thrombin inhibitor. FDA approval came in response to an interim analysis of an ongoing open-label trial, RE-VERSE AD.11 This study enrolled 90 adults with major bleeding or need for an emergency procedure taking dabigatran to receive idarucizumab (2.5 g in 50 mL rapid infusion dose given twice less than 15 minutes apart for a total of 5 g). Idarucizumab immediately reversed the effect of dabigatran on clotting tests in 88%-98% of the patients. For patients with major bleeding, the median time for bleeding cessation was 11.4 hours. One thrombotic event was reported within 72 hours of drug administration. Therefore, in patients taking dabigatran with an elevated TT, idarucizumab may be used if the bleeding is life threatening and refractory to initial supportive measures.
There are no FDA-approved antidotes for the factor Xa inhibitors. One promising agent is andexanet-alfa, an inactivated form of factor Xa that irreversibly binds Xa inhibitors. The ongoing, open-label ANNEXA-4 trial12 reported a decrease in anti–factor Xa activity of ~90% after bolus administration of the drug followed by 2-hour infusion in 67 patients with life-threatening bleeding, with clinical hemostasis achieved in 79% in patients by 12 hours. However, thrombotic events occurred in 18% of the patients at 1 month. Additional safety and efficacy data, along with plans for postmarket surveillance, will be needed prior to approval for clinical use.
Are there other options to obtain hemostasis?
Clotting factor products, specifically fresh frozen plasma (FFP) and prothrombin complex concentrates (PCCs), are often used to attempt to reverse anticoagulation from DOACs. While FFP alone has no evidence to support its use in reversing the effect of DOACs, PCCs might reverse anticoagulation for both Xa inhibitors and direct thrombin inhibitors.13 Some experts recommend unactivated PCC over activated PCC because of a theoretically increased thrombotic risk of activated PCC.14 For patients taking Xa inhibitors or dabigatran (if idarucizumab is unavailable) with life-threatening bleeding, PCC should be used in an attempt to reverse the bleeding.
Another strategy to promote hemostasis in bleeding patients taking DOACs is to use antifibrinolytics. Effective for control of bleeding in trauma and surgical patients, tranexamic acid has not been widely studied in nonsurgical bleeding, much less DOAC-related nonsurgical bleeding. A 2014 Cochrane review of a small number of trials suggested a possible mortality benefit from its use in upper GI bleeding, but the quality of included trials was poor.15 The ongoing HALT-IT trial, enrolling 8,000 patients with gastrointestinal bleeding, aims to clarify the mortality benefit of tranexamic acid.16 Despite effectively promoting hemostasis in many populations of bleeding patients, tranexamic acid carries no discernible thrombotic risk.17,18 By preventing clot degradation through a downstream mechanism at low cost and risk, antifibrinolytics are a practical adjunctive therapy to control major bleeding in patients on DOACs.
Can charcoal or dialysis reduce the systemic concentration of DOACs?
In addition to discontinuing the DOAC, both charcoal and dialysis can reduce the systemic concentration of DOACs. If the ingestion was recent, oral activated charcoal can reduce the systemic absorption of DOACs. To date there are no data on the efficacy of charcoal in bleeding patients taking DOACs. However, in two recent trials, administration of a single dose of charcoal in healthy patients led to significantly decreased area under concentration-time curves (AUC) when given at 6 and 8 hours after ingestion of a therapeutic dose of apixaban and rivaroxaban, respectively.19,20 While further studies are needed to confirm its clinical benefit, charcoal is recommended for major bleeding when given within 2 hours of ingestion of a DOAC and may be useful within 8 hours.
Unlike charcoal, which can be used for patients on Xa inhibitors or dabigatran, hemodialysis is only effective for reducing serum concentrations of dabigatran because of its low plasma protein binding (~35%). A review of 35 patients (10 with normal renal function) with severe bleeding showed significant reductions in coagulation tests (aPTT, PT, TT) and dabigatran levels after hemodialysis.21 For severe bleeding episodes particularly in patients with impaired renal function, providers should consider the use of continuous renal replacement therapy until clinical hemostasis is achieved.
What is the expert’s opinion?
We asked one of our hematologists with expertise in DOACs for his opinion on this topic. Most patients with DOAC-associated bleeding can be managed with supportive care because of the short half-life of these agents in patients with reasonably preserved renal function. The main scenario for escalating therapy to PCC or idarucizumab is life-threatening bleeding, such as intracranial hemorrhage and gastrointestinal hemorrhage with hemodynamic instability. The threshold for use of idarucizumab for patients taking dabigatran with bleeding should be lower than PCCs because there is better evidence for clinical benefit with less risk.
Developing reversal agents continues to be costly, requiring extensive preclinical work and clinical trials that are difficult to do. Assuming that reversal agents become more affordable in the longer term, and safety profiles are better established, clinicians may eventually have a lower threshold for their use in a wider variety of bleeding episodes. Lastly, adverse outcomes often occur, not during the acute bleeding episode, but several weeks later in patients whose providers delay restarting anticoagulation. Thus, it is important to resume anticoagulant therapy as soon as it is safe to do so.
Back to the case
Our patient was given a 50-g suspension of oral activated charcoal, along with two doses of 1 g intravenous tranexamic acid 8 hours apart. He was typed and crossed for blood, and ultimately received 1 unit of packed red blood cells before stabilizing without other measures. His colonoscopy subsequently revealed a diverticular bleed with a visible vessel that was coagulated. He was discharged 2 days later after remaining clinically stable after colonoscopy.
Bottom line
For the majority of bleeding patients on DOACs, supportive care with transfusions and local hemostatic interventions to control bleeding will likely be sufficient. Because of the short half-lives of DOACs, most patients do not require additional therapy (Table 2), and these patients actually have better outcomes from major bleeding episodes than patients taking VKAs. Antifibrinolytics should be a first-line prohemostatic therapy in major bleeding. Oral activated charcoal may be effective within 2-8 hours after ingestion for reduction of serum DOAC concentrations. Finally, in cases of life-threatening bleeding, idarucizumab can be used to reverse anticoagulation for patients taking dabigatran. When idarucizumab is unavailable, or for patients taking Xa inhibitors, PCC can be used.
Dr. Hagan is chief medical resident at the University of Washington Medical Center in Seattle. Dr. Albert is clinical instructor of medicine at UWMC. Dr. Garcia is professor of medicine and associate medical director of antithrombotic therapy at UWMC. Dr. Huang is an attending with the UWMC Medicine Consult Service and assistant clinical professor in the division of general internal medicine at UW.
Key Points
• The risk of major bleeding, and the case fatality rate of major bleeding, is significantly lower in patients taking DOACs versus VKAs
• For the majority of patients with bleeding on DOACs, withholding anticoagulation and supportive care is sufficient
• Idarucizumab is a novel and effective antidote to dabigatran, but should be reserved for patients with life-threatening bleeding
• Patients with DOAC-associated bleeding should be restarted on anticoagulation as soon as it is safe to do so
Additional Reading
Management of bleeding in patients receiving direct oral anticoagulants. UpToDate 2016.
How do I treat target-specific oral anticoagulant-associated bleeding? Blood 2014.
References
1. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
2. Chai-adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-specific oral anticoagulants: a systematic review and meta-analysis. Blood. 2014;124(15):2450-8.
3. Chai-adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. J Thromb Haemost. 2015;13(11):2012-20.
4. Savaysa (edoxaban) [package insert]. Daiichi Sankyo, Inc, Tokyo, Japan; 2015. www.accessdata.fda.gov/drugsatfda_docs/label/2015/206316lbl.pdf. Accessed January 8th, 2016.
5. Xarelto (rivaroxaban) [package insert]. Janssen Pharmaceuticals, Inc. Titusville, NJ; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/202439s001lbl.pdf. Accessed January 8th, 2016.
6. Pradaxa (dabigatran) [package insert]. Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT; 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/022512s007lbl.pdf. Accessed January 8th, 2016.
7. Eliquis (apixaban) [package insert]. Bristol-Myers Squibb Company, Princeton, NJ; 2012. www.accessdata.fda.gov/drugsatfda_docs/label/2012/202155s000lbl.pdf. Accessed January 8th, 2016.
8. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82.
9. Tripodi A. The laboratory and the direct oral anticoagulants. Blood.
2013;121(20):4032-5.
10. Samuelson BT, Cuker A, Siegal DM, Crowther M, Garcia DA. Laboratory Assessment of the Anticoagulant Activity of Direct Oral Anticoagulants (DOACs): A Systematic Review. Chest. 2016;
11. Pollack CV, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015;373(6):511-20.
12. Connolly SJ, Milling TJ, Eikelboom JW, et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors. N Engl J Med. 2016.
13. Dickneite G, Hoffman M. Reversing the new oral anticoagulants with prothrombin complex concentrates (PCCs): what is the evidence?. Thromb Haemost. 2014;111(2):189-98.
14. Sørensen B, Spahn DR, Innerhofer P, Spannagl M, Rossaint R. Clinical review: Prothrombin complex concentrates--evaluation of safety and thrombogenicity. Crit Care. 2011;15(1):201.
15. Bennett C, Klingenberg S, Langholz E, Gluud L. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database of Systematic Reviews 2014, Issue 11. Art. No.: CD006640.
16. Roberts I, Coats T, Edwards P, et al. HALT-IT – tranexamic acid for the treatment of gastrointestinal bleeding: study protocol for a randomised controlled trial. Trials. 2014 Nov 19;15:450.
17. Dyba J, Chan F, Lau K, Chan A, Chan H. Tranexamic Acid is a Weak Provoking Factor for Thromboembolic Events: A Systematic Review of the Literature. Blood. 2013; 122(21): 3629.
18. Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N Engl J Med. 2016; 376(2):136-148.
19. Wang X, Mondal S, Wang J, et al. Effect of Activated Charcoal on Apixaban Pharmacokinetics in Healthy Subjects. American Journal of Cardiovascular Drugs. 2014;14(2):147-154.
20. Ollier E, Hodin S, Lanoiselée J, et al. Effect of Activated Charcoal on Rivaroxaban Complex Absorption. Clin Pharmacokinet. 2016 Dec 2.
21. Chai-adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-8.
22. Schulman S, Kearon C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-4.
23. UW Anticoagulation Services. UW Medicine Pharmacy Services Web site. 2014. Available at https://depts.washington.edu/anticoag, Accessed March 8, 2017.
________________________________________________________________________
Table 1: Pharmacologic Profiles of Xa and Direct Thrombin Inhibitors4-8, 23
tmax t1/2, CrCl 50-80 t1/2 CrCl < 30 Dialyzable?
Apixaban 3-4 h 15 h 17 h No
Dabigatran 1-3 h 17 h 28 h Yes
Edoxaban 1-2 h 10-14 h no data No
Rivaroxaban 2-4 h 9 h 10 h No
tmax = time to peak serum concentration after ingestion, t1/2= serum half-life, CrCl= creatinine clearance in mL/min
*Average values assuming normal hepatic function. Aside from dabigatran, which has minimal hepatic clearance, all other DOACs can have prolonged half-lives in hepatic impairment.
Table 2: Management of Bleeding Patients Taking DOACs
Direct Thrombin Inhibitors (dabigatran)
Xa inhibitors (apixaban, edoxaban, rivaroxaban)Minor Bleeding
• Withhold DOAC
• Local hemostatic measures
Major Bleeding*
All of the above, AND
• Antifibrinolytic if bleeding persists
• Restore physiologic perfusion
• Charcoal if last dose within 2-8 hours
• Transfusion indications:
o Red blood cells: anemia
o Platelets: antiplatelet agents or thrombocytopenia
o Plasma: coagulopathy (dilution, DIC, liver failure), not for DOAC reversal
Life-threatening Bleeding**
All of the above, AND:
• Idarucizumab (confirm anticoagulant effect with thrombin time first)
• If idarucizumab is unavailable, use PCC
• Consider hemodialysis until hemostasis achieved, especially if patient in renal failure
All of the above, AND:
• Unactivated PCC (if available and calibrated to specific Xa inhibitor, confirm anticoagulant effect with anti-Xa level)
* Adapted from the International Society on Thrombosis and Hemostasis: bleeding with a fall in hemoglobin level ≥ 2 g/dL, OR bleeding leading to ≥ 2 units of PRBC transfused.21 Clinicians should perform risk stratification of bleeding episodes using vital signs, laboratory results, the area of bleeding, and patient comorbidities.
**Uncontrolled bleeding, OR symptomatic bleeding in a critical area or organ (such as intracranial, intraocular, intraspinal, retroperitoneal, pericardial, or intramuscular with compartment syndrome).
Statin use reduces death and decompensation in cirrhosis patients
Statin use in cirrhosis patients lowers the risk of death, Dr. Ulrich Bang and his associates reported in a retrospective case-cohort analysis.
After applying selection criteria, the investigators identified 5,417 patients with alcoholic cirrhosis from the Danish National Patient Registry based on the International Classification of Diseases, 10th revision, Danish National Prescription Registry based on the Anatomical Therapeutic Chemical, Danish Register of Causes of Death, and the Danish Civil Registration System from 1995 through 2014.
To conduct statistical analysis, the 5,417 were split into two groups – the first being an unmatched cohort. The unmatched cohort, which included all 5,417 patients, was not statistically balanced between statin vs. nonstatin users. Of the 5,417 patients, 744 were selected into a matched cohort using propensity scores (PS). This group was statistically balanced with one patient using statins being compared with two nonstatin users.
The unmatched group of 5,417 patients had 794 members (15%) who had used statins at least twice in a 30-day time period between first reported use and last reported use.
“In the unmatched cohort, we found mortality rates of 96 (86-106) per 1,000 [patient-years] for patients in therapy with statins and 121 (117-125) for the nonstatin patients and a [hazard ratio] of 0.66 (0.59-0.75) for statins vs. no statins,” the researchers wrote.
The PS-matched group’s “mortality rates were 88 (73-105) and 127 (114-142) for statin vs. nonstatin patients, respectively, and the HR was 0.57 (0.45-0.71)” (Aliment Pharmacol Ther. 2017 Oct;46[7]:673-80).
When analyzing decompensation, the rate of decompensation was 135 (114-160) per 1,000 person-years in those who had used statins for treatment. Among patients who had not undergone statin treatment, the rate was 361 (348-375) per 1,000 person-years. These results corresponded to an HR rate of 0.29 in an adjusted analysis. This varied from the PS-matched group, which experienced decompensation rates of 133 (104-170) for statin users and 234 (202-272) for nonstatin users.
In a subcohort analysis of 387 patients suffering from cirrhosis who had received consistent doses of statins, they had a reduced risk of death compared to an unmatched group of 4,975 patients who had not used statins. Patients receiving consistent doses of statins were said to be in a “stable” state. Ultimately, it was found for each 25% increase in stable state statin dosing, the risk of death decreased by 16%.
“The use of statins was associated with a reduced risk of decompensation and death in patients with alcoholic cirrhosis and the association between use of statins and death was more pronounced in patients with cirrhosis compared with noncirrhotic controls,” the investigators noted. “No convincing dose-response association was found but patients with a more constant exposure to statins may benefit more from the treatment.”
One coauthor had previously served as an adviser to Ferring Pharmaceuticals and as a speaker for Norgine Danmark. There were no other financial disclosures to report.
Statin use in cirrhosis patients lowers the risk of death, Dr. Ulrich Bang and his associates reported in a retrospective case-cohort analysis.
After applying selection criteria, the investigators identified 5,417 patients with alcoholic cirrhosis from the Danish National Patient Registry based on the International Classification of Diseases, 10th revision, Danish National Prescription Registry based on the Anatomical Therapeutic Chemical, Danish Register of Causes of Death, and the Danish Civil Registration System from 1995 through 2014.
To conduct statistical analysis, the 5,417 were split into two groups – the first being an unmatched cohort. The unmatched cohort, which included all 5,417 patients, was not statistically balanced between statin vs. nonstatin users. Of the 5,417 patients, 744 were selected into a matched cohort using propensity scores (PS). This group was statistically balanced with one patient using statins being compared with two nonstatin users.
The unmatched group of 5,417 patients had 794 members (15%) who had used statins at least twice in a 30-day time period between first reported use and last reported use.
“In the unmatched cohort, we found mortality rates of 96 (86-106) per 1,000 [patient-years] for patients in therapy with statins and 121 (117-125) for the nonstatin patients and a [hazard ratio] of 0.66 (0.59-0.75) for statins vs. no statins,” the researchers wrote.
The PS-matched group’s “mortality rates were 88 (73-105) and 127 (114-142) for statin vs. nonstatin patients, respectively, and the HR was 0.57 (0.45-0.71)” (Aliment Pharmacol Ther. 2017 Oct;46[7]:673-80).
When analyzing decompensation, the rate of decompensation was 135 (114-160) per 1,000 person-years in those who had used statins for treatment. Among patients who had not undergone statin treatment, the rate was 361 (348-375) per 1,000 person-years. These results corresponded to an HR rate of 0.29 in an adjusted analysis. This varied from the PS-matched group, which experienced decompensation rates of 133 (104-170) for statin users and 234 (202-272) for nonstatin users.
In a subcohort analysis of 387 patients suffering from cirrhosis who had received consistent doses of statins, they had a reduced risk of death compared to an unmatched group of 4,975 patients who had not used statins. Patients receiving consistent doses of statins were said to be in a “stable” state. Ultimately, it was found for each 25% increase in stable state statin dosing, the risk of death decreased by 16%.
“The use of statins was associated with a reduced risk of decompensation and death in patients with alcoholic cirrhosis and the association between use of statins and death was more pronounced in patients with cirrhosis compared with noncirrhotic controls,” the investigators noted. “No convincing dose-response association was found but patients with a more constant exposure to statins may benefit more from the treatment.”
One coauthor had previously served as an adviser to Ferring Pharmaceuticals and as a speaker for Norgine Danmark. There were no other financial disclosures to report.
Statin use in cirrhosis patients lowers the risk of death, Dr. Ulrich Bang and his associates reported in a retrospective case-cohort analysis.
After applying selection criteria, the investigators identified 5,417 patients with alcoholic cirrhosis from the Danish National Patient Registry based on the International Classification of Diseases, 10th revision, Danish National Prescription Registry based on the Anatomical Therapeutic Chemical, Danish Register of Causes of Death, and the Danish Civil Registration System from 1995 through 2014.
To conduct statistical analysis, the 5,417 were split into two groups – the first being an unmatched cohort. The unmatched cohort, which included all 5,417 patients, was not statistically balanced between statin vs. nonstatin users. Of the 5,417 patients, 744 were selected into a matched cohort using propensity scores (PS). This group was statistically balanced with one patient using statins being compared with two nonstatin users.
The unmatched group of 5,417 patients had 794 members (15%) who had used statins at least twice in a 30-day time period between first reported use and last reported use.
“In the unmatched cohort, we found mortality rates of 96 (86-106) per 1,000 [patient-years] for patients in therapy with statins and 121 (117-125) for the nonstatin patients and a [hazard ratio] of 0.66 (0.59-0.75) for statins vs. no statins,” the researchers wrote.
The PS-matched group’s “mortality rates were 88 (73-105) and 127 (114-142) for statin vs. nonstatin patients, respectively, and the HR was 0.57 (0.45-0.71)” (Aliment Pharmacol Ther. 2017 Oct;46[7]:673-80).
When analyzing decompensation, the rate of decompensation was 135 (114-160) per 1,000 person-years in those who had used statins for treatment. Among patients who had not undergone statin treatment, the rate was 361 (348-375) per 1,000 person-years. These results corresponded to an HR rate of 0.29 in an adjusted analysis. This varied from the PS-matched group, which experienced decompensation rates of 133 (104-170) for statin users and 234 (202-272) for nonstatin users.
In a subcohort analysis of 387 patients suffering from cirrhosis who had received consistent doses of statins, they had a reduced risk of death compared to an unmatched group of 4,975 patients who had not used statins. Patients receiving consistent doses of statins were said to be in a “stable” state. Ultimately, it was found for each 25% increase in stable state statin dosing, the risk of death decreased by 16%.
“The use of statins was associated with a reduced risk of decompensation and death in patients with alcoholic cirrhosis and the association between use of statins and death was more pronounced in patients with cirrhosis compared with noncirrhotic controls,” the investigators noted. “No convincing dose-response association was found but patients with a more constant exposure to statins may benefit more from the treatment.”
One coauthor had previously served as an adviser to Ferring Pharmaceuticals and as a speaker for Norgine Danmark. There were no other financial disclosures to report.
FROM ALIMENTARY PHARMACOLOGY & THERAPEUTICS
Key clinical point:
Major finding: As likelihood of stable state increases by 25% with statin dose, death risk decreases by 16%.
Data source: A retrospective case-cohort analysis of information obtained from registrants in the Danish National Patient Registry based on International Classification of Diseases, 10th revision (ICD-10), Danish National Prescription Registry based on the Anatomical Therapeutic Chemical (ATC), Danish Register of Causes of Death, and the Danish Civil Registration System between the years 1995 and 2014.
Disclosures: One coauthor had previously served as an adviser to Ferring Pharmaceuticals and as a speaker for Norgine Danmark. There were no other financial disclosures to report.
QI enthusiast to QI leader: Jonathan Bae, MD, SFHM
Editor’s Note: This SHM series highlights the professional pathways of quality improvement leaders. This month features the story of Jonathan Bae, MD, SFHM, associate chief medical officer for patient and clinical quality at Duke University Health System, Durham, N.C.
With a father and two sisters in medicine, Jonathan Bae was destined to become a physician – or something completely different, as he explains.
“Either outcome is common when you have a parent who is a doctor,” said Dr. Bae, who has two siblings who chose a different career path. But while Dr. Bae’s desire to be a clinician was set at an early age, his interest in quality improvement work came much later.
Twelve years ago, Dr. Bae matched in Duke’s Medicine-Pediatrics residency program because he wanted to be well equipped to treat patients across the age spectrum. Completing residency in 2009, Dr. Bae enjoyed providing clinical care as a hospitalist, but discovered that he also enjoyed teaching. To enhance his skills as a clinician educator, Dr. Bae enrolled in the Academic Hospitalist Academy, where the curriculum introduced him to quality improvement and patient safety, and some aspects of hospital administration. “Jeff Glasheen’s talk on the drivers of medicine, and how to find your unique voice and identity … brought together my interest in education and quality work,” Dr. Bae recalled.
“I left the meeting energized with new information, and then the opportunity came up to lead a QI initiative here,” he said. The project focused on improving improve care delivery to diabetic patients, specifically the completion of foot exams. “We saw our rates of screening go from less than 50% to greater than 80%,” Dr. Bae said. “I found it to be extremely gratifying to be involved in implementing changes that could lead to care improvement for patients.”
Once Dr. Bae made his interests in QI work known to colleagues and administrators, the projects came readily. Following his chief residency year, Dr. Bae remained with Duke Medicine Residency Program as an associate program director for QI, “which was a great platform for doing project work that aligned my interests in teaching and doing QI work,” he said. In addition to developing a residency curriculum in QI, Dr. Bae initiated a program to incentivize GME trainees across the health system in performance metrics such as readmissions, patient satisfaction, hand hygiene, and safety event reporting. The outcomes, Dr. Bae said, “have had an improved quality and safety impact on our organization.”
From there, Dr. Bae initiated multiple projects focused on reducing readmissions and mortality. Currently, he is standardizing the mortality review process across three hospitals in Duke’s health system. Consistent methodology and language will allow for more accurate analysis and comparison of factors contributing to patient mortality in the system, Dr. Bae said, adding, “We have already learned a lot about care delivery and operations, and measures that can be taken to reduce gaps in care delivery and keep patients safe.”
Looking back on the days when he only thought about providing care, Dr. Bae said, “my world view has changed but my desire to change the world hasn’t. I now do more quality work because I find it so gratifying. In the QI space, I’m affecting not one, but many people at a time.”
He encourages hospitalists with similar interests to seek out colleagues and leaders – internal and external to their institutions – that will help them initiate and implement projects that feed their passions. Getting to know the QI basics is the simple part, Dr. Bae said.
“There’s no magic behind PDSA cycles or models of improvement,” he said. “It’s the team and people you pull together that makes a project successful.”
His current work centers on understanding and building health care provider resiliency at Duke. “I feel this … is going to make a tremendous difference for our organization,” Dr. Bae said. “The system should be designed to promote well-being, not just prevent burnout.”
Claudia Stahl is content manager at the Society of Hospital Medicine.
Editor’s Note: This SHM series highlights the professional pathways of quality improvement leaders. This month features the story of Jonathan Bae, MD, SFHM, associate chief medical officer for patient and clinical quality at Duke University Health System, Durham, N.C.
With a father and two sisters in medicine, Jonathan Bae was destined to become a physician – or something completely different, as he explains.
“Either outcome is common when you have a parent who is a doctor,” said Dr. Bae, who has two siblings who chose a different career path. But while Dr. Bae’s desire to be a clinician was set at an early age, his interest in quality improvement work came much later.
Twelve years ago, Dr. Bae matched in Duke’s Medicine-Pediatrics residency program because he wanted to be well equipped to treat patients across the age spectrum. Completing residency in 2009, Dr. Bae enjoyed providing clinical care as a hospitalist, but discovered that he also enjoyed teaching. To enhance his skills as a clinician educator, Dr. Bae enrolled in the Academic Hospitalist Academy, where the curriculum introduced him to quality improvement and patient safety, and some aspects of hospital administration. “Jeff Glasheen’s talk on the drivers of medicine, and how to find your unique voice and identity … brought together my interest in education and quality work,” Dr. Bae recalled.
“I left the meeting energized with new information, and then the opportunity came up to lead a QI initiative here,” he said. The project focused on improving improve care delivery to diabetic patients, specifically the completion of foot exams. “We saw our rates of screening go from less than 50% to greater than 80%,” Dr. Bae said. “I found it to be extremely gratifying to be involved in implementing changes that could lead to care improvement for patients.”
Once Dr. Bae made his interests in QI work known to colleagues and administrators, the projects came readily. Following his chief residency year, Dr. Bae remained with Duke Medicine Residency Program as an associate program director for QI, “which was a great platform for doing project work that aligned my interests in teaching and doing QI work,” he said. In addition to developing a residency curriculum in QI, Dr. Bae initiated a program to incentivize GME trainees across the health system in performance metrics such as readmissions, patient satisfaction, hand hygiene, and safety event reporting. The outcomes, Dr. Bae said, “have had an improved quality and safety impact on our organization.”
From there, Dr. Bae initiated multiple projects focused on reducing readmissions and mortality. Currently, he is standardizing the mortality review process across three hospitals in Duke’s health system. Consistent methodology and language will allow for more accurate analysis and comparison of factors contributing to patient mortality in the system, Dr. Bae said, adding, “We have already learned a lot about care delivery and operations, and measures that can be taken to reduce gaps in care delivery and keep patients safe.”
Looking back on the days when he only thought about providing care, Dr. Bae said, “my world view has changed but my desire to change the world hasn’t. I now do more quality work because I find it so gratifying. In the QI space, I’m affecting not one, but many people at a time.”
He encourages hospitalists with similar interests to seek out colleagues and leaders – internal and external to their institutions – that will help them initiate and implement projects that feed their passions. Getting to know the QI basics is the simple part, Dr. Bae said.
“There’s no magic behind PDSA cycles or models of improvement,” he said. “It’s the team and people you pull together that makes a project successful.”
His current work centers on understanding and building health care provider resiliency at Duke. “I feel this … is going to make a tremendous difference for our organization,” Dr. Bae said. “The system should be designed to promote well-being, not just prevent burnout.”
Claudia Stahl is content manager at the Society of Hospital Medicine.
Editor’s Note: This SHM series highlights the professional pathways of quality improvement leaders. This month features the story of Jonathan Bae, MD, SFHM, associate chief medical officer for patient and clinical quality at Duke University Health System, Durham, N.C.
With a father and two sisters in medicine, Jonathan Bae was destined to become a physician – or something completely different, as he explains.
“Either outcome is common when you have a parent who is a doctor,” said Dr. Bae, who has two siblings who chose a different career path. But while Dr. Bae’s desire to be a clinician was set at an early age, his interest in quality improvement work came much later.
Twelve years ago, Dr. Bae matched in Duke’s Medicine-Pediatrics residency program because he wanted to be well equipped to treat patients across the age spectrum. Completing residency in 2009, Dr. Bae enjoyed providing clinical care as a hospitalist, but discovered that he also enjoyed teaching. To enhance his skills as a clinician educator, Dr. Bae enrolled in the Academic Hospitalist Academy, where the curriculum introduced him to quality improvement and patient safety, and some aspects of hospital administration. “Jeff Glasheen’s talk on the drivers of medicine, and how to find your unique voice and identity … brought together my interest in education and quality work,” Dr. Bae recalled.
“I left the meeting energized with new information, and then the opportunity came up to lead a QI initiative here,” he said. The project focused on improving improve care delivery to diabetic patients, specifically the completion of foot exams. “We saw our rates of screening go from less than 50% to greater than 80%,” Dr. Bae said. “I found it to be extremely gratifying to be involved in implementing changes that could lead to care improvement for patients.”
Once Dr. Bae made his interests in QI work known to colleagues and administrators, the projects came readily. Following his chief residency year, Dr. Bae remained with Duke Medicine Residency Program as an associate program director for QI, “which was a great platform for doing project work that aligned my interests in teaching and doing QI work,” he said. In addition to developing a residency curriculum in QI, Dr. Bae initiated a program to incentivize GME trainees across the health system in performance metrics such as readmissions, patient satisfaction, hand hygiene, and safety event reporting. The outcomes, Dr. Bae said, “have had an improved quality and safety impact on our organization.”
From there, Dr. Bae initiated multiple projects focused on reducing readmissions and mortality. Currently, he is standardizing the mortality review process across three hospitals in Duke’s health system. Consistent methodology and language will allow for more accurate analysis and comparison of factors contributing to patient mortality in the system, Dr. Bae said, adding, “We have already learned a lot about care delivery and operations, and measures that can be taken to reduce gaps in care delivery and keep patients safe.”
Looking back on the days when he only thought about providing care, Dr. Bae said, “my world view has changed but my desire to change the world hasn’t. I now do more quality work because I find it so gratifying. In the QI space, I’m affecting not one, but many people at a time.”
He encourages hospitalists with similar interests to seek out colleagues and leaders – internal and external to their institutions – that will help them initiate and implement projects that feed their passions. Getting to know the QI basics is the simple part, Dr. Bae said.
“There’s no magic behind PDSA cycles or models of improvement,” he said. “It’s the team and people you pull together that makes a project successful.”
His current work centers on understanding and building health care provider resiliency at Duke. “I feel this … is going to make a tremendous difference for our organization,” Dr. Bae said. “The system should be designed to promote well-being, not just prevent burnout.”
Claudia Stahl is content manager at the Society of Hospital Medicine.
RANGE: Small PFS edge in urothelial cancer with VEGFR-2 inhibitor
MADRID – For patients with advanced or metastatic urothelial cancer that progressed on platinum-based chemotherapy, a combination of the vascular endothelial growth factor receptor (VEGFR)-2 inhibitor ramucirumab and docetaxel offered a small but significant improvement in progression-free survival (PFS) compared with docetaxel alone.
Among 437 patients treated in the phase 3 RANGE trial, investigator-assessed PFS, the primary endpoint, was 4.07 months for patients randomized to ramucirumab and docetaxel, compared with 2.76 months for patients assigned to docetaxel and placebo, translating into a hazard ratio (HR) for ramucirumab of 0.757 (P = .0118).
“RANGE is the first phase 3 study to demonstrate a progression-free survival advantage over chemotherapy alone in platinum-refractory advanced or metastatic urothelial carcinoma,” lead author Daniel P. Petrylak, MD of Yale University, New Haven, Conn., said at a briefing at the European Society for Medical Oncology Congress.
But Richard Cathomas, Dr.med, of Kantonsspital Graubünden, in Chur, Switzerland, who was not involved in the study, said it “is too early for these results alone to change the standard of care second-line treatment, which is immune checkpoint inhibition.”
He noted that the magnitude of the benefit with ramucirumab was just 1.3 months, “and, while statistically significant, it raises the question of whether it is clinically relevant.”
He acknowledged that the improvement in response rates seen with ramucirumab in RANGE indicates a potential role for angiogenesis inhibitors in the treatment of urothelial cancers.
In the RANGE trial, results of which were published in The Lancet, investigators at 124 sites in 23 countries enrolled 530 patients with advanced or metastatic urothelial carcinoma who experienced progression during or after platinum-based chemotherapy.
Patients were randomly assigned to receive intravenous docetaxel 75 mg/m2 plus intravenous ramucirumab 10 mg/kg or matching placebo on day 1 of each repeating 21-day cycle until disease progression or discontinuation of treatment for other reasons. The primary endpoint was assessed in an intention-to-treat analysis in the first 437 patients randomized.
As noted, at a median follow-up in the ITT analysis of 5.0 months, investigator-assessed PFS favored the addition of ramucirumab, as did a blinded central review of outcomes, which determined a median PFS of 4.04 months with ramucirumab plus docetaxel compared with 2.46 months for docetaxel alone (HR 0.672, P = .0005).
Ramucirumab/docetaxel was also associated with an improvement in the objective response rate, at 24.5% compared with 14.0% for placebo/docetaxel.
Treatment toxicities were similar between the study arms, although patients in the ramucirumab arm experienced slightly less anemia compared with those in the placebo arm.
In all, 209 of 263 patients assigned to ramucirumab/docetaxel, and 229 of 267 patients assigned to placebo/docetaxel had their treatments discontinued, primarily because they experienced disease progression.
There were no significant changes in quality of life measures during the trial, and there were no differences in quality of life between the treatment arms, Dr. Petrylak reported.

Ultimately, the combination of ramucirumab and docetaxel may be best suited for use as a third-line treatment for patients with platinum-resistant metastatic urothelial cancer that has progressed after second-line therapy with an immune checkpoint inhibitor, said Yohann Loriot, MD, of Gustave-Roussy Cancer Institute in Villejuif, France, the invited discussant at the presidential symposium where the RANGE data were presented.
However, for patients who have a short response to first-line platinum-based chemotherapy, have no visceral metastases, or are ineligible to receive immunotherapy, ramucirumab plus docetaxel could be a suitable second-line option, he said.
The RANGE trial was funded by Eli Lilly. Dr. Petrylak disclosed research funding from the company. Dr. Cathomas and Dr. Loriot disclosed consulting or advisory roles with companies other than Lilly.
MADRID – For patients with advanced or metastatic urothelial cancer that progressed on platinum-based chemotherapy, a combination of the vascular endothelial growth factor receptor (VEGFR)-2 inhibitor ramucirumab and docetaxel offered a small but significant improvement in progression-free survival (PFS) compared with docetaxel alone.
Among 437 patients treated in the phase 3 RANGE trial, investigator-assessed PFS, the primary endpoint, was 4.07 months for patients randomized to ramucirumab and docetaxel, compared with 2.76 months for patients assigned to docetaxel and placebo, translating into a hazard ratio (HR) for ramucirumab of 0.757 (P = .0118).
“RANGE is the first phase 3 study to demonstrate a progression-free survival advantage over chemotherapy alone in platinum-refractory advanced or metastatic urothelial carcinoma,” lead author Daniel P. Petrylak, MD of Yale University, New Haven, Conn., said at a briefing at the European Society for Medical Oncology Congress.
But Richard Cathomas, Dr.med, of Kantonsspital Graubünden, in Chur, Switzerland, who was not involved in the study, said it “is too early for these results alone to change the standard of care second-line treatment, which is immune checkpoint inhibition.”
He noted that the magnitude of the benefit with ramucirumab was just 1.3 months, “and, while statistically significant, it raises the question of whether it is clinically relevant.”
He acknowledged that the improvement in response rates seen with ramucirumab in RANGE indicates a potential role for angiogenesis inhibitors in the treatment of urothelial cancers.
In the RANGE trial, results of which were published in The Lancet, investigators at 124 sites in 23 countries enrolled 530 patients with advanced or metastatic urothelial carcinoma who experienced progression during or after platinum-based chemotherapy.
Patients were randomly assigned to receive intravenous docetaxel 75 mg/m2 plus intravenous ramucirumab 10 mg/kg or matching placebo on day 1 of each repeating 21-day cycle until disease progression or discontinuation of treatment for other reasons. The primary endpoint was assessed in an intention-to-treat analysis in the first 437 patients randomized.
As noted, at a median follow-up in the ITT analysis of 5.0 months, investigator-assessed PFS favored the addition of ramucirumab, as did a blinded central review of outcomes, which determined a median PFS of 4.04 months with ramucirumab plus docetaxel compared with 2.46 months for docetaxel alone (HR 0.672, P = .0005).
Ramucirumab/docetaxel was also associated with an improvement in the objective response rate, at 24.5% compared with 14.0% for placebo/docetaxel.
Treatment toxicities were similar between the study arms, although patients in the ramucirumab arm experienced slightly less anemia compared with those in the placebo arm.
In all, 209 of 263 patients assigned to ramucirumab/docetaxel, and 229 of 267 patients assigned to placebo/docetaxel had their treatments discontinued, primarily because they experienced disease progression.
There were no significant changes in quality of life measures during the trial, and there were no differences in quality of life between the treatment arms, Dr. Petrylak reported.
Ultimately, the combination of ramucirumab and docetaxel may be best suited for use as a third-line treatment for patients with platinum-resistant metastatic urothelial cancer that has progressed after second-line therapy with an immune checkpoint inhibitor, said Yohann Loriot, MD, of Gustave-Roussy Cancer Institute in Villejuif, France, the invited discussant at the presidential symposium where the RANGE data were presented.
However, for patients who have a short response to first-line platinum-based chemotherapy, have no visceral metastases, or are ineligible to receive immunotherapy, ramucirumab plus docetaxel could be a suitable second-line option, he said.
The RANGE trial was funded by Eli Lilly. Dr. Petrylak disclosed research funding from the company. Dr. Cathomas and Dr. Loriot disclosed consulting or advisory roles with companies other than Lilly.
MADRID – For patients with advanced or metastatic urothelial cancer that progressed on platinum-based chemotherapy, a combination of the vascular endothelial growth factor receptor (VEGFR)-2 inhibitor ramucirumab and docetaxel offered a small but significant improvement in progression-free survival (PFS) compared with docetaxel alone.
Among 437 patients treated in the phase 3 RANGE trial, investigator-assessed PFS, the primary endpoint, was 4.07 months for patients randomized to ramucirumab and docetaxel, compared with 2.76 months for patients assigned to docetaxel and placebo, translating into a hazard ratio (HR) for ramucirumab of 0.757 (P = .0118).
“RANGE is the first phase 3 study to demonstrate a progression-free survival advantage over chemotherapy alone in platinum-refractory advanced or metastatic urothelial carcinoma,” lead author Daniel P. Petrylak, MD of Yale University, New Haven, Conn., said at a briefing at the European Society for Medical Oncology Congress.
But Richard Cathomas, Dr.med, of Kantonsspital Graubünden, in Chur, Switzerland, who was not involved in the study, said it “is too early for these results alone to change the standard of care second-line treatment, which is immune checkpoint inhibition.”
He noted that the magnitude of the benefit with ramucirumab was just 1.3 months, “and, while statistically significant, it raises the question of whether it is clinically relevant.”
He acknowledged that the improvement in response rates seen with ramucirumab in RANGE indicates a potential role for angiogenesis inhibitors in the treatment of urothelial cancers.
In the RANGE trial, results of which were published in The Lancet, investigators at 124 sites in 23 countries enrolled 530 patients with advanced or metastatic urothelial carcinoma who experienced progression during or after platinum-based chemotherapy.
Patients were randomly assigned to receive intravenous docetaxel 75 mg/m2 plus intravenous ramucirumab 10 mg/kg or matching placebo on day 1 of each repeating 21-day cycle until disease progression or discontinuation of treatment for other reasons. The primary endpoint was assessed in an intention-to-treat analysis in the first 437 patients randomized.
As noted, at a median follow-up in the ITT analysis of 5.0 months, investigator-assessed PFS favored the addition of ramucirumab, as did a blinded central review of outcomes, which determined a median PFS of 4.04 months with ramucirumab plus docetaxel compared with 2.46 months for docetaxel alone (HR 0.672, P = .0005).
Ramucirumab/docetaxel was also associated with an improvement in the objective response rate, at 24.5% compared with 14.0% for placebo/docetaxel.
Treatment toxicities were similar between the study arms, although patients in the ramucirumab arm experienced slightly less anemia compared with those in the placebo arm.
In all, 209 of 263 patients assigned to ramucirumab/docetaxel, and 229 of 267 patients assigned to placebo/docetaxel had their treatments discontinued, primarily because they experienced disease progression.
There were no significant changes in quality of life measures during the trial, and there were no differences in quality of life between the treatment arms, Dr. Petrylak reported.
Ultimately, the combination of ramucirumab and docetaxel may be best suited for use as a third-line treatment for patients with platinum-resistant metastatic urothelial cancer that has progressed after second-line therapy with an immune checkpoint inhibitor, said Yohann Loriot, MD, of Gustave-Roussy Cancer Institute in Villejuif, France, the invited discussant at the presidential symposium where the RANGE data were presented.
However, for patients who have a short response to first-line platinum-based chemotherapy, have no visceral metastases, or are ineligible to receive immunotherapy, ramucirumab plus docetaxel could be a suitable second-line option, he said.
The RANGE trial was funded by Eli Lilly. Dr. Petrylak disclosed research funding from the company. Dr. Cathomas and Dr. Loriot disclosed consulting or advisory roles with companies other than Lilly.
AT ESMO 2017
Key clinical point: Adding the VEGFR-2 inhibitor ramucirumab to docetaxel slightly improved progression-free survival of advanced/metastatic urothelial carcinoma.
Major finding: Investigator-assessed PFS was 4.07 months for patients randomized to ramucirumab and docetaxel, vs. 2.76 months for docetaxel/placebo.
Data source: Randomized phase 3 trial of 530 patients with urothelial carcinoma that progressed during or after platinum-based chemotherapy.
Disclosures: The RANGE trial was funded by Eli Lilly. Dr. Petrylak disclosed research funding from the company. Dr. Cathomas and Dr. Loriot disclosed consulting or advisory roles with companies other than Lilly.
Do not withhold opioid addiction drugs from patients taking benzodiazepines
The opioid addiction medications buprenorphine and methadone should not be withheld from patients who are taking benzodiazepines or other drugs that depress the central nervous system, the Food and Drug Administration advised in a safety alert posted Sept. 20.
The combined use of these medication-assisted treatment (MAT) drugs and central nervous system (CNS) depressants can lead to serious side effects. But the harm associated with opioid addiction that remains untreated usually outweighs those risks, the agency said. After reviewing this issue, the FDA said, it is requiring that this information be added to the drug labels of buprenorphine and methadone in addition to “recommendations for minimizing the use of [MAT] drugs and benzodiazepines together.”
Discontinuing MAT drugs is a goal, but patients might need medication-assisted treatment indefinitely. “Use should continue for as long as patients are benefiting and their use contributes to the intended treatment goals,” the alert said.
The opioid addiction medications buprenorphine and methadone should not be withheld from patients who are taking benzodiazepines or other drugs that depress the central nervous system, the Food and Drug Administration advised in a safety alert posted Sept. 20.
The combined use of these medication-assisted treatment (MAT) drugs and central nervous system (CNS) depressants can lead to serious side effects. But the harm associated with opioid addiction that remains untreated usually outweighs those risks, the agency said. After reviewing this issue, the FDA said, it is requiring that this information be added to the drug labels of buprenorphine and methadone in addition to “recommendations for minimizing the use of [MAT] drugs and benzodiazepines together.”
Discontinuing MAT drugs is a goal, but patients might need medication-assisted treatment indefinitely. “Use should continue for as long as patients are benefiting and their use contributes to the intended treatment goals,” the alert said.
The opioid addiction medications buprenorphine and methadone should not be withheld from patients who are taking benzodiazepines or other drugs that depress the central nervous system, the Food and Drug Administration advised in a safety alert posted Sept. 20.
The combined use of these medication-assisted treatment (MAT) drugs and central nervous system (CNS) depressants can lead to serious side effects. But the harm associated with opioid addiction that remains untreated usually outweighs those risks, the agency said. After reviewing this issue, the FDA said, it is requiring that this information be added to the drug labels of buprenorphine and methadone in addition to “recommendations for minimizing the use of [MAT] drugs and benzodiazepines together.”
Discontinuing MAT drugs is a goal, but patients might need medication-assisted treatment indefinitely. “Use should continue for as long as patients are benefiting and their use contributes to the intended treatment goals,” the alert said.
Preferred osteoporosis treatment order with teriparatide, denosumab reaffirmed
DENVER – A treatment regimen for postmenopausal women with osteoporosis that started with teriparatide (TPTD) for 2 years and switched to denosumab (DMAB) improved their spine trabecular microarchitecture – a predictor of fracture risk independent of areal bone mineral density – in a new analysis of the DATA trial and its extension study, DATA-Switch.
On the other hand, the converse strategy of switching from denosumab to teriparatide resulted in a temporary decline in bone mineral density. “The observed transient decrease in bone density corresponds to extremely elevated bone formation and resorptions markers, suggesting that high bone turnover is a cause of the transient loss,” Joy Tsai, MD, an instructor in medicine at Massachusetts General Hospital, Boston, said in an interview at a poster session of the annual meeting of the American Society for Bone and Mineral Research.

“Our take-home is that for patients who are at extremely high risk of fracture, combination strategy is a treatment strategy to be considered,” said Dr. Tsai, who presented the results of the study at the meeting.
The findings also reinforce the general strategy of treating with anabolic therapy followed by an antiresorptive agent, rather than the other way around.
Specifically, “we would caution against the use of teriparatide immediately following denosumab because of this transient decrease in bone density that correlates with high bone turnover,” Dr. Tsai said.
The DATA and DATA-Switch studies randomized 94 postmenopausal women with osteoporosis to 2 years of TPTD (20 mcg/day), DMAB (60 mg every 6 months), or both drugs for 2 years. In DATA-Switch, women who received TPTD in the first 2 years were switched to DMAB, and those receiving DMAB were switched to TPTD. Women in the combination group were switched to DMAB only.
The researchers used dual-energy x-ray absorptiometry (DXA) spine scans to assess spine trabecular microarchitecture by calculating trabecular bone score (TBS) at 0, 12, 24, 30, 36, and 48 months.
After 2 years, TPTD alone was associated with a 2.7% increase in TBS over baseline (P = .009), while DMAB alone was associated with a 1.8% increase (P = .118 vs. baseline). Combination treatment led to a 4.5% increase (P = .017 vs. baseline).
In the 6 months after the treatment switch at year 2, the researchers noted increases in TBS in the combination-to-DMAB group (2.1%) and the TPTD-to-DMAB group (2.0%), but the DMAB-to-TPTD group experienced a decrease of 1.1% over months 24-30 (P less than .05 compared with other groups).
The decrease in TBS was temporary: At 48 months, all groups had an overall increase in TBS (TPTD-to-DMAB group, 5.1%; DMAB-to-TPTD group, 3.6%; combination-to-DMAB group, 6.1%). There were no significant differences between the groups.
From baseline to month 48, the percentage of patients considered to be at high risk of fracture based on TBS score (1.23 or less) dropped from 24% to 8% in the TPTD-to-DMAB group, from 18% to 14% in the DMAB-to-TPTD group, and from 39% to 11% in the combination-to-DMAB group.
“Ultimately, at the 4-year mark all three groups increased trabecular bone scores, so it also supports our rationale to consider the use of these treatment strategies, specifically the ones when you’re switching to or continuing denosumab,” Dr. Tsai said.
Amgen and Eli Lilly funded the study. Dr. Tsai reported having no financial disclosures.
DENVER – A treatment regimen for postmenopausal women with osteoporosis that started with teriparatide (TPTD) for 2 years and switched to denosumab (DMAB) improved their spine trabecular microarchitecture – a predictor of fracture risk independent of areal bone mineral density – in a new analysis of the DATA trial and its extension study, DATA-Switch.
On the other hand, the converse strategy of switching from denosumab to teriparatide resulted in a temporary decline in bone mineral density. “The observed transient decrease in bone density corresponds to extremely elevated bone formation and resorptions markers, suggesting that high bone turnover is a cause of the transient loss,” Joy Tsai, MD, an instructor in medicine at Massachusetts General Hospital, Boston, said in an interview at a poster session of the annual meeting of the American Society for Bone and Mineral Research.
“Our take-home is that for patients who are at extremely high risk of fracture, combination strategy is a treatment strategy to be considered,” said Dr. Tsai, who presented the results of the study at the meeting.
The findings also reinforce the general strategy of treating with anabolic therapy followed by an antiresorptive agent, rather than the other way around.
Specifically, “we would caution against the use of teriparatide immediately following denosumab because of this transient decrease in bone density that correlates with high bone turnover,” Dr. Tsai said.
The DATA and DATA-Switch studies randomized 94 postmenopausal women with osteoporosis to 2 years of TPTD (20 mcg/day), DMAB (60 mg every 6 months), or both drugs for 2 years. In DATA-Switch, women who received TPTD in the first 2 years were switched to DMAB, and those receiving DMAB were switched to TPTD. Women in the combination group were switched to DMAB only.
The researchers used dual-energy x-ray absorptiometry (DXA) spine scans to assess spine trabecular microarchitecture by calculating trabecular bone score (TBS) at 0, 12, 24, 30, 36, and 48 months.
After 2 years, TPTD alone was associated with a 2.7% increase in TBS over baseline (P = .009), while DMAB alone was associated with a 1.8% increase (P = .118 vs. baseline). Combination treatment led to a 4.5% increase (P = .017 vs. baseline).
In the 6 months after the treatment switch at year 2, the researchers noted increases in TBS in the combination-to-DMAB group (2.1%) and the TPTD-to-DMAB group (2.0%), but the DMAB-to-TPTD group experienced a decrease of 1.1% over months 24-30 (P less than .05 compared with other groups).
The decrease in TBS was temporary: At 48 months, all groups had an overall increase in TBS (TPTD-to-DMAB group, 5.1%; DMAB-to-TPTD group, 3.6%; combination-to-DMAB group, 6.1%). There were no significant differences between the groups.
From baseline to month 48, the percentage of patients considered to be at high risk of fracture based on TBS score (1.23 or less) dropped from 24% to 8% in the TPTD-to-DMAB group, from 18% to 14% in the DMAB-to-TPTD group, and from 39% to 11% in the combination-to-DMAB group.
“Ultimately, at the 4-year mark all three groups increased trabecular bone scores, so it also supports our rationale to consider the use of these treatment strategies, specifically the ones when you’re switching to or continuing denosumab,” Dr. Tsai said.
Amgen and Eli Lilly funded the study. Dr. Tsai reported having no financial disclosures.
DENVER – A treatment regimen for postmenopausal women with osteoporosis that started with teriparatide (TPTD) for 2 years and switched to denosumab (DMAB) improved their spine trabecular microarchitecture – a predictor of fracture risk independent of areal bone mineral density – in a new analysis of the DATA trial and its extension study, DATA-Switch.
On the other hand, the converse strategy of switching from denosumab to teriparatide resulted in a temporary decline in bone mineral density. “The observed transient decrease in bone density corresponds to extremely elevated bone formation and resorptions markers, suggesting that high bone turnover is a cause of the transient loss,” Joy Tsai, MD, an instructor in medicine at Massachusetts General Hospital, Boston, said in an interview at a poster session of the annual meeting of the American Society for Bone and Mineral Research.
“Our take-home is that for patients who are at extremely high risk of fracture, combination strategy is a treatment strategy to be considered,” said Dr. Tsai, who presented the results of the study at the meeting.
The findings also reinforce the general strategy of treating with anabolic therapy followed by an antiresorptive agent, rather than the other way around.
Specifically, “we would caution against the use of teriparatide immediately following denosumab because of this transient decrease in bone density that correlates with high bone turnover,” Dr. Tsai said.
The DATA and DATA-Switch studies randomized 94 postmenopausal women with osteoporosis to 2 years of TPTD (20 mcg/day), DMAB (60 mg every 6 months), or both drugs for 2 years. In DATA-Switch, women who received TPTD in the first 2 years were switched to DMAB, and those receiving DMAB were switched to TPTD. Women in the combination group were switched to DMAB only.
The researchers used dual-energy x-ray absorptiometry (DXA) spine scans to assess spine trabecular microarchitecture by calculating trabecular bone score (TBS) at 0, 12, 24, 30, 36, and 48 months.
After 2 years, TPTD alone was associated with a 2.7% increase in TBS over baseline (P = .009), while DMAB alone was associated with a 1.8% increase (P = .118 vs. baseline). Combination treatment led to a 4.5% increase (P = .017 vs. baseline).
In the 6 months after the treatment switch at year 2, the researchers noted increases in TBS in the combination-to-DMAB group (2.1%) and the TPTD-to-DMAB group (2.0%), but the DMAB-to-TPTD group experienced a decrease of 1.1% over months 24-30 (P less than .05 compared with other groups).
The decrease in TBS was temporary: At 48 months, all groups had an overall increase in TBS (TPTD-to-DMAB group, 5.1%; DMAB-to-TPTD group, 3.6%; combination-to-DMAB group, 6.1%). There were no significant differences between the groups.
From baseline to month 48, the percentage of patients considered to be at high risk of fracture based on TBS score (1.23 or less) dropped from 24% to 8% in the TPTD-to-DMAB group, from 18% to 14% in the DMAB-to-TPTD group, and from 39% to 11% in the combination-to-DMAB group.
“Ultimately, at the 4-year mark all three groups increased trabecular bone scores, so it also supports our rationale to consider the use of these treatment strategies, specifically the ones when you’re switching to or continuing denosumab,” Dr. Tsai said.
Amgen and Eli Lilly funded the study. Dr. Tsai reported having no financial disclosures.
AT ASBMR
Key clinical point:
Major finding: After 24 months, teriparatide alone increased trabecular bone score (TBS) by 2.7%, denosumab (DMAB) alone by 1.8%, and the combination by 4.5%.
Data source: A new analysis of data from 94 postmenopausal women with osteoporosis who participated in the DATA trial and its extension study, DATA-Switch.
Disclosures: Amgen and Eli Lilly funded the study. Dr. Tsai reported having no financial disclosures.
Flotetuzumab for AML passes phase 1 test
MADRID – Flotetuzumab, a novel bispecific monoclonal antibody that employs a proprietary technology to redirect T lymphocytes to kill CD123-expressing cells, was safe and demonstrated efficacy in patients with acute myeloid leukemia in a phase 1 trial, based on data presented at the European Society for Medical Oncology (ESMO) Congress.
Flotetuzumab combines a portion of antibody recognizing CD3, which is an activating molecule expressed by T cells, and an arm that recognizes CD123 on the cancer cell, explained Norbert Vey, MD, PhD, Head, Leukemia Treatment Unit, Institut Paoli-Calmettes, Marseille, France. This bispecific quality, produced through a proprietary technology called Dual-Affinity ReTargeting, is considered promising because CD123 is expressed by more than 90% of AML cells and is highly expressed on stem cells involved in initiating myelodysplastic syndrome (MDS).
In this dose-ranging study (NCT02152956), 42 patients with AML and 5 patients with MDS were treated in the first cycle with infusions of flotetuzumab on either a continuous 7-day or a 4-days-on, 3-days-off schedule. For subsequent cycles, patients received the 4-days-on, 3-days-off schedule. Continuous infusion is employed due to the short half-life of flotetuzumab.
The most common adverse events were infusion-related reactions, which were observed in 76.6% of patients. Pyrexia, a potential sign of cytokine release syndrome (CRS), was observed in 23.4% of patients, who were given tocilizumab at the earliest sign of CRS. Two patients had grade 3 CRS, and one discontinued therapy. There was also one case of grade 3 myalgia. Dr. Vey characterized the overall level of adverse events as “acceptable.”
In addition to its relative safety, flotetuzumab was associated with “encouraging antileukemic activity,” Dr. Vey said. Six of 14 patients receiving doses that exceeded 500 ng/kg per day had objective responses and two of these patients had complete responses. Again, toxicity at these dose levels was considered manageable.
“This rate of clinical response is exciting,” commented Tim Somervaille, MD, Senior Group Leader, Leukemia Biology Laboratory, Cancer Research UK Institute, Manchester (England). An ESMO-invited discussant on this paper, Dr. Somervaille expressed enthusiasm in general about a growing role for bispecific T-cell engagers. Blinatumomab, the first of these agents, received regulatory approval for refractory AML in 2014.
“There are a number of these bispecific T cell antibodies that are in early-phase trials,” said Dr. Somervaille, citing several that also target CD123 within the context of a different partner antigen than that employed by flotetuzumab. He also mentioned ongoing efforts to develop bispecific natural killer cell engagers that target malignant cells through immune activation.
As for flotetuzumab, the phase 1 trial provided adequate data to encourage further development.
“A cohort expansion is now ongoing and enrolling patients at 11 sites in the United States and Europe,” Dr. Vey reported. “A clinical update on these results is expected by the end of the year.”
Dr. Vey reported financial relationships with Bristol-Myers Squibb, Novartis, and Servier.
MacroGenics retains full development and commercialization rights to flotetuzumab in the United States, Canada, Mexico, Japan, South Korea, and India. Servier participates in the development and has rights to flotetuzumab in all other countries. The U.S. Food and Drug Administration has granted orphan drug designation to flotetuzumab for the investigational treatment of AML, according to a press release from MacroGenics.
MADRID – Flotetuzumab, a novel bispecific monoclonal antibody that employs a proprietary technology to redirect T lymphocytes to kill CD123-expressing cells, was safe and demonstrated efficacy in patients with acute myeloid leukemia in a phase 1 trial, based on data presented at the European Society for Medical Oncology (ESMO) Congress.
Flotetuzumab combines a portion of antibody recognizing CD3, which is an activating molecule expressed by T cells, and an arm that recognizes CD123 on the cancer cell, explained Norbert Vey, MD, PhD, Head, Leukemia Treatment Unit, Institut Paoli-Calmettes, Marseille, France. This bispecific quality, produced through a proprietary technology called Dual-Affinity ReTargeting, is considered promising because CD123 is expressed by more than 90% of AML cells and is highly expressed on stem cells involved in initiating myelodysplastic syndrome (MDS).
In this dose-ranging study (NCT02152956), 42 patients with AML and 5 patients with MDS were treated in the first cycle with infusions of flotetuzumab on either a continuous 7-day or a 4-days-on, 3-days-off schedule. For subsequent cycles, patients received the 4-days-on, 3-days-off schedule. Continuous infusion is employed due to the short half-life of flotetuzumab.
The most common adverse events were infusion-related reactions, which were observed in 76.6% of patients. Pyrexia, a potential sign of cytokine release syndrome (CRS), was observed in 23.4% of patients, who were given tocilizumab at the earliest sign of CRS. Two patients had grade 3 CRS, and one discontinued therapy. There was also one case of grade 3 myalgia. Dr. Vey characterized the overall level of adverse events as “acceptable.”
In addition to its relative safety, flotetuzumab was associated with “encouraging antileukemic activity,” Dr. Vey said. Six of 14 patients receiving doses that exceeded 500 ng/kg per day had objective responses and two of these patients had complete responses. Again, toxicity at these dose levels was considered manageable.
“This rate of clinical response is exciting,” commented Tim Somervaille, MD, Senior Group Leader, Leukemia Biology Laboratory, Cancer Research UK Institute, Manchester (England). An ESMO-invited discussant on this paper, Dr. Somervaille expressed enthusiasm in general about a growing role for bispecific T-cell engagers. Blinatumomab, the first of these agents, received regulatory approval for refractory AML in 2014.
“There are a number of these bispecific T cell antibodies that are in early-phase trials,” said Dr. Somervaille, citing several that also target CD123 within the context of a different partner antigen than that employed by flotetuzumab. He also mentioned ongoing efforts to develop bispecific natural killer cell engagers that target malignant cells through immune activation.
As for flotetuzumab, the phase 1 trial provided adequate data to encourage further development.
“A cohort expansion is now ongoing and enrolling patients at 11 sites in the United States and Europe,” Dr. Vey reported. “A clinical update on these results is expected by the end of the year.”
Dr. Vey reported financial relationships with Bristol-Myers Squibb, Novartis, and Servier.
MacroGenics retains full development and commercialization rights to flotetuzumab in the United States, Canada, Mexico, Japan, South Korea, and India. Servier participates in the development and has rights to flotetuzumab in all other countries. The U.S. Food and Drug Administration has granted orphan drug designation to flotetuzumab for the investigational treatment of AML, according to a press release from MacroGenics.
MADRID – Flotetuzumab, a novel bispecific monoclonal antibody that employs a proprietary technology to redirect T lymphocytes to kill CD123-expressing cells, was safe and demonstrated efficacy in patients with acute myeloid leukemia in a phase 1 trial, based on data presented at the European Society for Medical Oncology (ESMO) Congress.
Flotetuzumab combines a portion of antibody recognizing CD3, which is an activating molecule expressed by T cells, and an arm that recognizes CD123 on the cancer cell, explained Norbert Vey, MD, PhD, Head, Leukemia Treatment Unit, Institut Paoli-Calmettes, Marseille, France. This bispecific quality, produced through a proprietary technology called Dual-Affinity ReTargeting, is considered promising because CD123 is expressed by more than 90% of AML cells and is highly expressed on stem cells involved in initiating myelodysplastic syndrome (MDS).
In this dose-ranging study (NCT02152956), 42 patients with AML and 5 patients with MDS were treated in the first cycle with infusions of flotetuzumab on either a continuous 7-day or a 4-days-on, 3-days-off schedule. For subsequent cycles, patients received the 4-days-on, 3-days-off schedule. Continuous infusion is employed due to the short half-life of flotetuzumab.
The most common adverse events were infusion-related reactions, which were observed in 76.6% of patients. Pyrexia, a potential sign of cytokine release syndrome (CRS), was observed in 23.4% of patients, who were given tocilizumab at the earliest sign of CRS. Two patients had grade 3 CRS, and one discontinued therapy. There was also one case of grade 3 myalgia. Dr. Vey characterized the overall level of adverse events as “acceptable.”
In addition to its relative safety, flotetuzumab was associated with “encouraging antileukemic activity,” Dr. Vey said. Six of 14 patients receiving doses that exceeded 500 ng/kg per day had objective responses and two of these patients had complete responses. Again, toxicity at these dose levels was considered manageable.
“This rate of clinical response is exciting,” commented Tim Somervaille, MD, Senior Group Leader, Leukemia Biology Laboratory, Cancer Research UK Institute, Manchester (England). An ESMO-invited discussant on this paper, Dr. Somervaille expressed enthusiasm in general about a growing role for bispecific T-cell engagers. Blinatumomab, the first of these agents, received regulatory approval for refractory AML in 2014.
“There are a number of these bispecific T cell antibodies that are in early-phase trials,” said Dr. Somervaille, citing several that also target CD123 within the context of a different partner antigen than that employed by flotetuzumab. He also mentioned ongoing efforts to develop bispecific natural killer cell engagers that target malignant cells through immune activation.
As for flotetuzumab, the phase 1 trial provided adequate data to encourage further development.
“A cohort expansion is now ongoing and enrolling patients at 11 sites in the United States and Europe,” Dr. Vey reported. “A clinical update on these results is expected by the end of the year.”
Dr. Vey reported financial relationships with Bristol-Myers Squibb, Novartis, and Servier.
MacroGenics retains full development and commercialization rights to flotetuzumab in the United States, Canada, Mexico, Japan, South Korea, and India. Servier participates in the development and has rights to flotetuzumab in all other countries. The U.S. Food and Drug Administration has granted orphan drug designation to flotetuzumab for the investigational treatment of AML, according to a press release from MacroGenics.
AT ESMO 2017
Key clinical point: The phase 1 trial provided adequate data to encourage further development of flotetuzumab for patients with acute myeloid leukemia.
Major finding: Six of 14 patients receiving doses that exceeded 500 ng/kg per day had objective responses and two of these patients had complete responses.
Data source: Phase 1 dose-escalation study in 42 patients with AML and 5 patients with MDS.
Disclosures: Dr. Vey reported financial relationships with Bristol-Myers Squibb, Novartis, and Servier.
AGA releases new clinical guideline on therapeutic drug monitoring in IBD
AGA has issued a new clinical guideline on the role of therapeutic drug monitoring (TDM) in the management of IBD, published in the September 2017 issue of Gastroenterology. The guideline focuses on the application of TDM for biologic therapy, specifically anti–tumor necrosis factor-alpha (TNF) agents and thiopurines, and addresses questions about the risks and benefits of reactive TDM, routine proactive TDM, or no TDM in guiding treatment changes. AGA’s recommendations include:
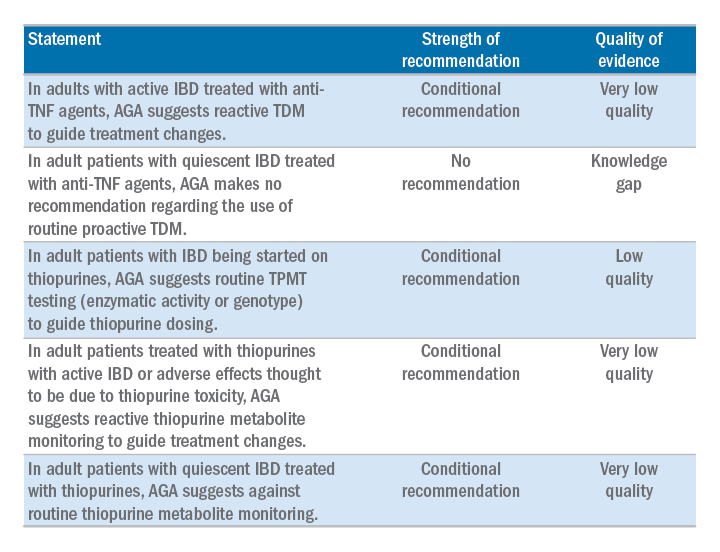
The guideline is accompanied by a technical review, Clinical Decision Support Tool, and patient companion, which provides key points and important information directly to patients about this approach, written at an appropriate reading level. Access the patient companion in the Patient Info Center, www.gastro.org/IBD.
AGA has issued a new clinical guideline on the role of therapeutic drug monitoring (TDM) in the management of IBD, published in the September 2017 issue of Gastroenterology. The guideline focuses on the application of TDM for biologic therapy, specifically anti–tumor necrosis factor-alpha (TNF) agents and thiopurines, and addresses questions about the risks and benefits of reactive TDM, routine proactive TDM, or no TDM in guiding treatment changes. AGA’s recommendations include:
The guideline is accompanied by a technical review, Clinical Decision Support Tool, and patient companion, which provides key points and important information directly to patients about this approach, written at an appropriate reading level. Access the patient companion in the Patient Info Center, www.gastro.org/IBD.
AGA has issued a new clinical guideline on the role of therapeutic drug monitoring (TDM) in the management of IBD, published in the September 2017 issue of Gastroenterology. The guideline focuses on the application of TDM for biologic therapy, specifically anti–tumor necrosis factor-alpha (TNF) agents and thiopurines, and addresses questions about the risks and benefits of reactive TDM, routine proactive TDM, or no TDM in guiding treatment changes. AGA’s recommendations include:
The guideline is accompanied by a technical review, Clinical Decision Support Tool, and patient companion, which provides key points and important information directly to patients about this approach, written at an appropriate reading level. Access the patient companion in the Patient Info Center, www.gastro.org/IBD.