Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
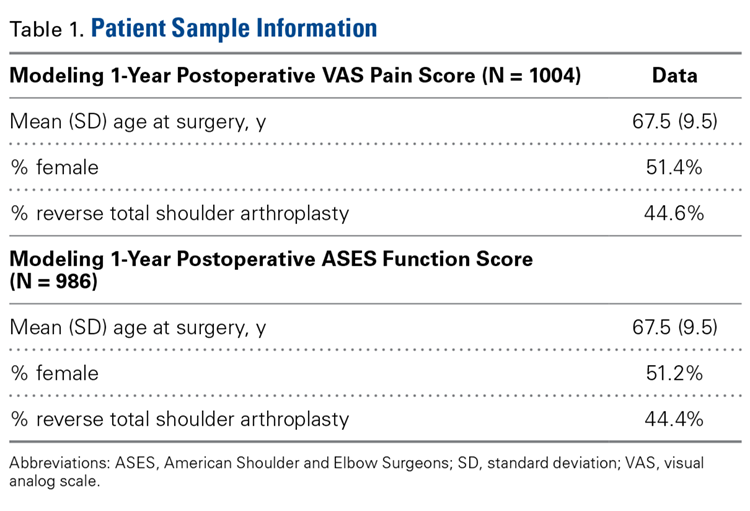
Table 1 lists summary statistics for the population used in these models.
Table 1.
Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
Table 2.
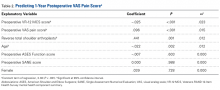
Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
Table 3.
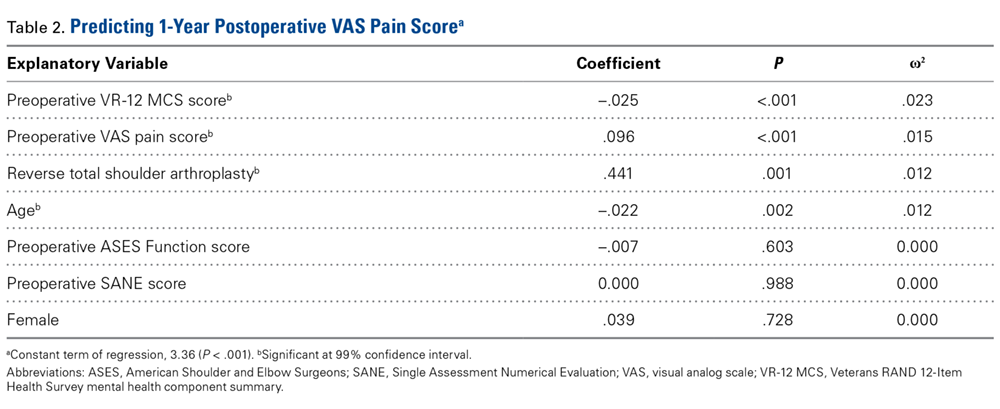
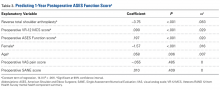
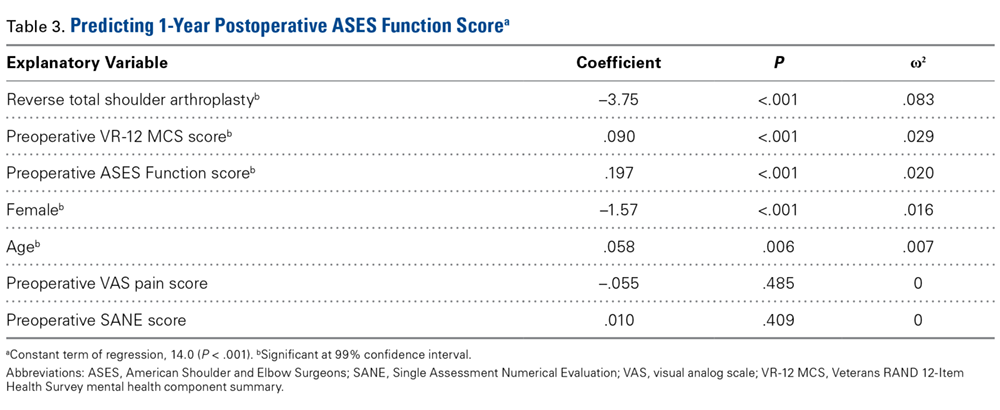
Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
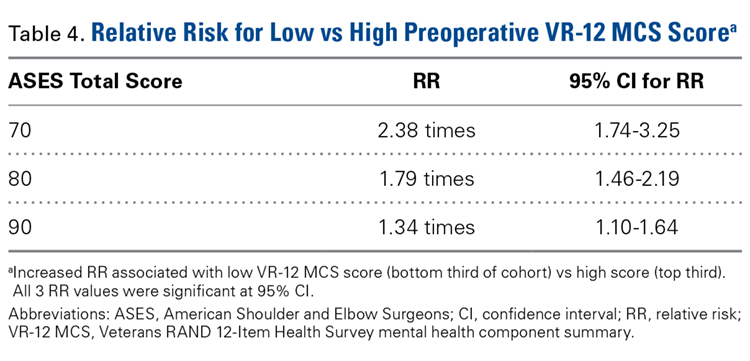
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
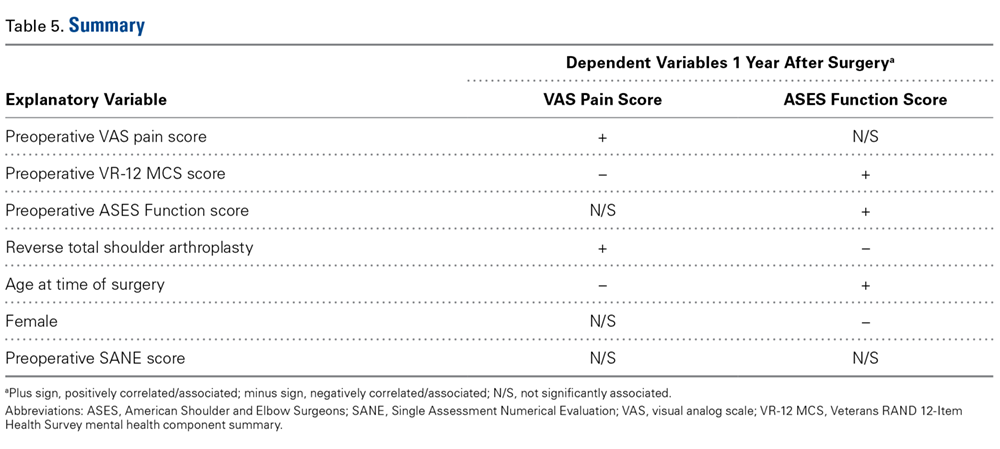
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
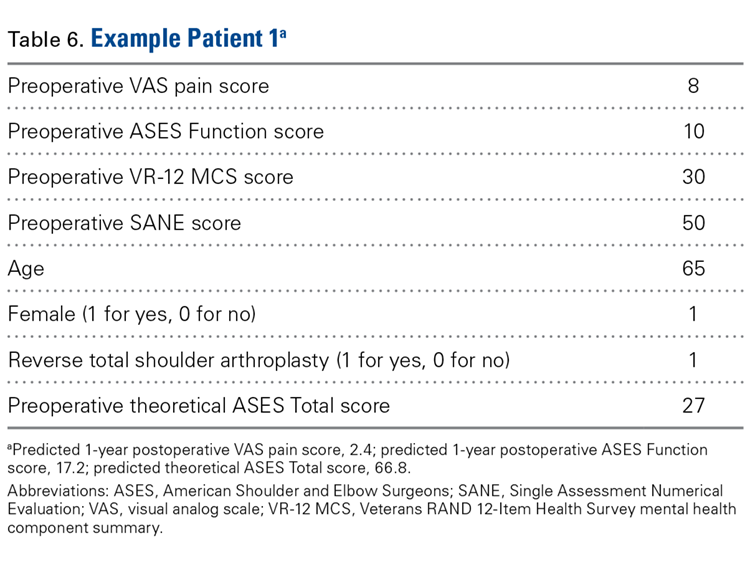
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.
Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
Table 1 lists summary statistics for the population used in these models.
Table 1.
Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
Table 2.
Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
Table 3.
Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
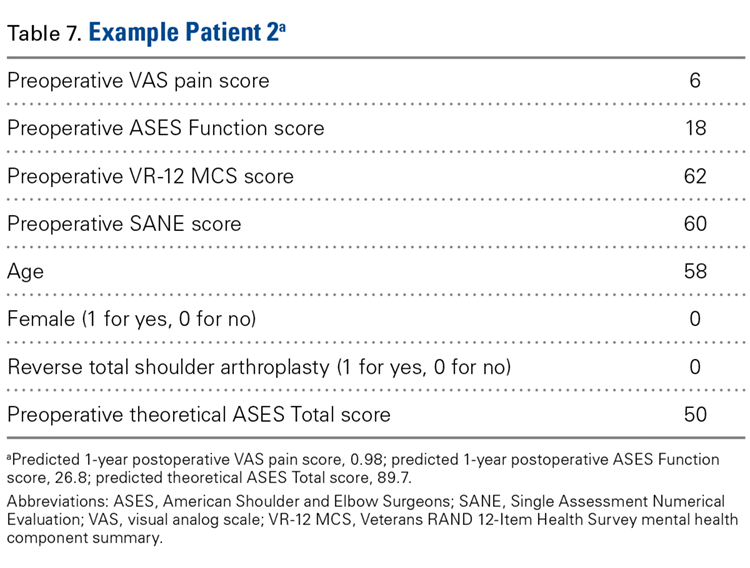
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
Take-Home Points
Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
Table 1 lists summary statistics for the population used in these models.
Table 1.
Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
Table 2.
Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
Table 3.
Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
Measuring observable markers of HVC at the bedside
Measuring observable markers of HVC at the bedside
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
A new tool can help where hospitalists need it most: at the bedside.
The focus on providing high-value care (HVC) continues to grow and expand in health care today. Still, most education around HVC currently happens in a formalized setting – lectures, modules, and so on, says Carolyn D. Sy, MD, interim director of the Hospital Medicine Service at the University of Washington, Seattle, and coauthor of a recent abstract about a new tool to address this shortcoming. “There are no instruments for measuring HVC discussions or practices at the bedside, confounding efforts to assess behavior changes associated with curricular interventions,” she said.
So she and other doctors undertook a study to identify 10 HVC topics in three domains (quality, cost, patient values), then measured their reliability with the goal of designing an HVC Rounding Tool and showing that it is an effective tool to measure observable markers of HVC at the bedside. “This is critical as it addresses an important educational gap in translating HVC from theoretical knowledge to bedside practice,” Dr. Sy said.
The tool is designed to capture multidisciplinary participation, she says, including involvement from not only faculty, fellows, or trainees, but also nursing, pharmacists, families, and other members of the health care team. The tool can be used as a peer feedback instrument to help physicians integrate HVC topics during bedside rounds or as a metric to assess the educational efficacy of future curriculum.
“The HVC Rounding Tool provides an opportunity for faculty development through peer observation and feedback on the integration and role modeling of HVC at the bedside,” Dr. Sy said. “It also is an instrument to help assess the educational efficacy of formal HVC curriculum and translation into bedside practice. Lastly, it is a tool that could be used to measure the relationship between HVC behaviors and actual patient outcomes such as length of stay, readmissions, cost of hospitalization – a feature with increasing importance given our move toward value-based health care.”
SAN DIEGO – A new study offers a double message about the potential impact of obesity on systemic lupus erythematosus (SLE) in women: Excess pounds are linked to a higher risk of patient-reported outcomes such as pain and fatigue, and body mass index may be an appropriate tool to study weight issues in this population.
Researchers found “a strong relationship between body composition and worse outcomes,” Sarah Patterson, MD, a fellow in rheumatology at the University of California, San Francisco, and the lead study author, said at the annual meeting of the American College of Rheumatology.
wildpixel/Thinkstock
While researchers have linked excess weight to worsening outcomes in a variety of rheumatic disorders, there have been few studies examining obesity in SLE. Small studies in 2005 and 2012 linked obesity to less functional capacity, and the later study also linked it to decreased quality of life (Arthritis Rheum. 2005 Nov;52[11]:3651-9/ Int J Rheum Dis. 2012 Jun;15[3]:261-7).
For the new study, Dr. Patterson and her colleagues analyzed findings from surveys of 148 participants in the Arthritis Body Composition and Disability study. All participants were women with a verified SLE diagnosis.
About two-thirds of the sample were white, 14% were Asian, and 13% were African American. The average age was 48 years, the average disease duration was 16 years, and 45% took glucocorticoids.
Researchers used two measurements of obesity: BMI of 30 kg/m2 or greater and fat mass index (FMI) of 13 kg/m2 or greater.
They calculated FMI with data collected via whole dual x-ray absorptiometry. Of the participants, 32% and 30% met criteria for obesity under FMI and BMI definitions, respectively.
Researchers also collected survey data regarding measurements of disease activity, depressive symptoms, pain and fatigue.
The study authors controlled their results to account for factors such as age, race, and prednisone use. They found that those defined as obese via FMI had more disease activity and depression than did nonobese women: 14.8 versus 11.5, P = .010, on the Systemic Lupus Activity Questionnaire scale, and 19.8 versus 13.1, P = .004, on the Center for Epidemiologic Studies Depression scale.
On two other scales of pain and fatigue, obese patients scored lower – a sign of worse status – compared with nonobese women: 38.7 versus 44.2, P = .004, on the Short Form 36 (SF-36) Health Survey pain subscale and 39.6 versus 45.2, P = .010, on the SF-36 vitality subscale. The researchers reported similar findings when using BMI to assess obesity.
It’s not clear why obesity and lupus may be linked, Dr. Patterson said, though she noted that inflammation is a shared factor. “People with lupus have arthritis and chronic pain, so there may be this vicious feedback cycle with hindrances to be able to live healthy lifestyles,” she added.
The study has limitations, including that the sample is largely white, while lupus is more common among minority women. In addition, the study does not include underweight patients or track patients over time. “It will be important to look at obesity and patient-reported outcomes to determine whether weight loss results in better outcomes,” Dr. Patterson said.
The study does provide an extra benefit by suggesting that BMI is not an inferior tool to measure the effects of obesity in the SLE population, Dr. Patterson said. BMI has been criticized as a misleading measurement of obesity. But the BMI and FMI measures produced similar results in this study. “That’s really good news in a way for the practicalities of using this information,” she said.
But FMI may still be a better measurement of obesity in the general population, where BMI may be more likely to be thrown off by high muscle mass.
It may seem obvious that obesity is linked to worse lupus outcomes, but rheumatologist Bryant England, MD, of the University of Nebraska, Omaha, said that this research is noteworthy because it highlights the importance of focusing on obesity in the clinic.
Rheumatologists shouldn’t leave obesity to primary care physicians but instead confront it themselves, said Dr. England, who moderated a discussion of new research at an ACR annual meeting press conference. But he cautioned that prudence is especially important when talking about obesity with lupus patients because they may be sensitive about medication-related weight gain.
Dr. Patterson and the other study authors reported having no relevant disclosures. Dr. England also reported no relevant disclosures. The study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
SAN DIEGO – A new study offers a double message about the potential impact of obesity on systemic lupus erythematosus (SLE) in women: Excess pounds are linked to a higher risk of patient-reported outcomes such as pain and fatigue, and body mass index may be an appropriate tool to study weight issues in this population.
Researchers found “a strong relationship between body composition and worse outcomes,” Sarah Patterson, MD, a fellow in rheumatology at the University of California, San Francisco, and the lead study author, said at the annual meeting of the American College of Rheumatology.
wildpixel/Thinkstock
While researchers have linked excess weight to worsening outcomes in a variety of rheumatic disorders, there have been few studies examining obesity in SLE. Small studies in 2005 and 2012 linked obesity to less functional capacity, and the later study also linked it to decreased quality of life (Arthritis Rheum. 2005 Nov;52[11]:3651-9/ Int J Rheum Dis. 2012 Jun;15[3]:261-7).
For the new study, Dr. Patterson and her colleagues analyzed findings from surveys of 148 participants in the Arthritis Body Composition and Disability study. All participants were women with a verified SLE diagnosis.
About two-thirds of the sample were white, 14% were Asian, and 13% were African American. The average age was 48 years, the average disease duration was 16 years, and 45% took glucocorticoids.
Researchers used two measurements of obesity: BMI of 30 kg/m2 or greater and fat mass index (FMI) of 13 kg/m2 or greater.
They calculated FMI with data collected via whole dual x-ray absorptiometry. Of the participants, 32% and 30% met criteria for obesity under FMI and BMI definitions, respectively.
Researchers also collected survey data regarding measurements of disease activity, depressive symptoms, pain and fatigue.
The study authors controlled their results to account for factors such as age, race, and prednisone use. They found that those defined as obese via FMI had more disease activity and depression than did nonobese women: 14.8 versus 11.5, P = .010, on the Systemic Lupus Activity Questionnaire scale, and 19.8 versus 13.1, P = .004, on the Center for Epidemiologic Studies Depression scale.
On two other scales of pain and fatigue, obese patients scored lower – a sign of worse status – compared with nonobese women: 38.7 versus 44.2, P = .004, on the Short Form 36 (SF-36) Health Survey pain subscale and 39.6 versus 45.2, P = .010, on the SF-36 vitality subscale. The researchers reported similar findings when using BMI to assess obesity.
It’s not clear why obesity and lupus may be linked, Dr. Patterson said, though she noted that inflammation is a shared factor. “People with lupus have arthritis and chronic pain, so there may be this vicious feedback cycle with hindrances to be able to live healthy lifestyles,” she added.
The study has limitations, including that the sample is largely white, while lupus is more common among minority women. In addition, the study does not include underweight patients or track patients over time. “It will be important to look at obesity and patient-reported outcomes to determine whether weight loss results in better outcomes,” Dr. Patterson said.
The study does provide an extra benefit by suggesting that BMI is not an inferior tool to measure the effects of obesity in the SLE population, Dr. Patterson said. BMI has been criticized as a misleading measurement of obesity. But the BMI and FMI measures produced similar results in this study. “That’s really good news in a way for the practicalities of using this information,” she said.
But FMI may still be a better measurement of obesity in the general population, where BMI may be more likely to be thrown off by high muscle mass.
It may seem obvious that obesity is linked to worse lupus outcomes, but rheumatologist Bryant England, MD, of the University of Nebraska, Omaha, said that this research is noteworthy because it highlights the importance of focusing on obesity in the clinic.
Rheumatologists shouldn’t leave obesity to primary care physicians but instead confront it themselves, said Dr. England, who moderated a discussion of new research at an ACR annual meeting press conference. But he cautioned that prudence is especially important when talking about obesity with lupus patients because they may be sensitive about medication-related weight gain.
Dr. Patterson and the other study authors reported having no relevant disclosures. Dr. England also reported no relevant disclosures. The study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
SAN DIEGO – A new study offers a double message about the potential impact of obesity on systemic lupus erythematosus (SLE) in women: Excess pounds are linked to a higher risk of patient-reported outcomes such as pain and fatigue, and body mass index may be an appropriate tool to study weight issues in this population.
Researchers found “a strong relationship between body composition and worse outcomes,” Sarah Patterson, MD, a fellow in rheumatology at the University of California, San Francisco, and the lead study author, said at the annual meeting of the American College of Rheumatology.
wildpixel/Thinkstock
While researchers have linked excess weight to worsening outcomes in a variety of rheumatic disorders, there have been few studies examining obesity in SLE. Small studies in 2005 and 2012 linked obesity to less functional capacity, and the later study also linked it to decreased quality of life (Arthritis Rheum. 2005 Nov;52[11]:3651-9/ Int J Rheum Dis. 2012 Jun;15[3]:261-7).
For the new study, Dr. Patterson and her colleagues analyzed findings from surveys of 148 participants in the Arthritis Body Composition and Disability study. All participants were women with a verified SLE diagnosis.
About two-thirds of the sample were white, 14% were Asian, and 13% were African American. The average age was 48 years, the average disease duration was 16 years, and 45% took glucocorticoids.
Researchers used two measurements of obesity: BMI of 30 kg/m2 or greater and fat mass index (FMI) of 13 kg/m2 or greater.
They calculated FMI with data collected via whole dual x-ray absorptiometry. Of the participants, 32% and 30% met criteria for obesity under FMI and BMI definitions, respectively.
Researchers also collected survey data regarding measurements of disease activity, depressive symptoms, pain and fatigue.
The study authors controlled their results to account for factors such as age, race, and prednisone use. They found that those defined as obese via FMI had more disease activity and depression than did nonobese women: 14.8 versus 11.5, P = .010, on the Systemic Lupus Activity Questionnaire scale, and 19.8 versus 13.1, P = .004, on the Center for Epidemiologic Studies Depression scale.
On two other scales of pain and fatigue, obese patients scored lower – a sign of worse status – compared with nonobese women: 38.7 versus 44.2, P = .004, on the Short Form 36 (SF-36) Health Survey pain subscale and 39.6 versus 45.2, P = .010, on the SF-36 vitality subscale. The researchers reported similar findings when using BMI to assess obesity.
It’s not clear why obesity and lupus may be linked, Dr. Patterson said, though she noted that inflammation is a shared factor. “People with lupus have arthritis and chronic pain, so there may be this vicious feedback cycle with hindrances to be able to live healthy lifestyles,” she added.
The study has limitations, including that the sample is largely white, while lupus is more common among minority women. In addition, the study does not include underweight patients or track patients over time. “It will be important to look at obesity and patient-reported outcomes to determine whether weight loss results in better outcomes,” Dr. Patterson said.
The study does provide an extra benefit by suggesting that BMI is not an inferior tool to measure the effects of obesity in the SLE population, Dr. Patterson said. BMI has been criticized as a misleading measurement of obesity. But the BMI and FMI measures produced similar results in this study. “That’s really good news in a way for the practicalities of using this information,” she said.
But FMI may still be a better measurement of obesity in the general population, where BMI may be more likely to be thrown off by high muscle mass.
It may seem obvious that obesity is linked to worse lupus outcomes, but rheumatologist Bryant England, MD, of the University of Nebraska, Omaha, said that this research is noteworthy because it highlights the importance of focusing on obesity in the clinic.
Rheumatologists shouldn’t leave obesity to primary care physicians but instead confront it themselves, said Dr. England, who moderated a discussion of new research at an ACR annual meeting press conference. But he cautioned that prudence is especially important when talking about obesity with lupus patients because they may be sensitive about medication-related weight gain.
Dr. Patterson and the other study authors reported having no relevant disclosures. Dr. England also reported no relevant disclosures. The study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Key clinical point: Obesity is associated with pain and fatigue in systemic lupus erythematosus (SLE).
Major finding: Obese women with SLE had more disease activity than did nonobese women (14.8 versus 11.5, P = .010).
Data source: An analysis of 148 SLE patients (65% white, mean age 48, about 31% obese) with obesity measured by body mass index or fat mass index.
Disclosures: The study authors reported having no relevant disclosures. The National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the study.
SAN DIEGO – The incidence of gout is strongly linked to patients’ concentration of serum uric acid over time, but even so, less than half of patients with levels of 10 mg/dL or above develop the condition by 15 years, according to the largest individual person-level analysis to examine the relationship.
The incidence of gout rose from about 1% after 15 years in patients with a serum uric acid (sUA) level of less than 6 mg/dL to almost 49% in those with 10 mg/dL or higher in the study, which implies “a long period of hyperuricemia preceding the onset of clinical gout” and also “supports a role for additional factors in the pathogenesis of gout,” Nicola Dalbeth, MD, said in her presentation of the results at the annual meeting of the American College of Rheumatology.
jarun011/Thinkstock
The cumulative incidence of gout in the study across 15 years of follow-up at 1-mg/dL intervals of sUA from less than 6 mg/dL to 10 mg/dL or more provides “estimates to guide discussion with hyperuricemic individuals about their risk of developing gout over time,” according to Dr. Dalbeth of the University of Auckland (New Zealand), and her colleagues.
Dr. Dalbeth and her associates found four studies in a search of PubMed and the Database of Genotype and Phenotype from Jan. 1, 1980, to June 11, 2016, that met the inclusion criteria of containing publicly available participant level data, recorded incident gout (via classification criteria, doctor’s diagnosis, or self report of disease), and had a minimum of 3 years of follow-up. The four studies were the Atherosclerosis Risk in Communities study, the Coronary Artery Risk Development in Young Adults study, the original cohort of the Framingham Heart Study, and the offspring cohort of the Framingham Heart Study, comprising 18,889 individuals who were gout free at the beginning of follow-up, which lasted a mean of 11.2 years.
In all studies combined, the incidence of gout at an sUA level of less than 6 mg/dL steadily increased from 0.21% at 3 years of follow-up to 1.12% at 15 years. In contrast, sUA at 10 mg/dL or higher led to gout in 10.00% at 3 years and in 48.57% at 15 years.
The same general pattern held for the incidence of gout in both men and women, although men had a higher incidence across nearly all sUA concentration ranges.
Female sex provided a 30% reduced risk of gout, and European ethnicity nearly halved the risk for gout, compared with non-Europeans, The risk for gout rose across decades of age, starting at 40-49 years, and also increased significantly for each 1-mg/dL interval of sUA starting at 6 mg/dL.
The study’s conclusions are limited by the use of variable definitions of gout and how it was ascertained. In addition, the study did not analyze other endpoints that are associated with hyperuricemia and may be relevant to discuss in counseling people with elevated sUA levels, such as hypertension, chronic kidney disease, and cardiovascular disease, Dr. Dalbeth said.
Audience member Daniel H. Solomon, MD, of Brigham and Women’s Hospital, Boston, said after the presentation that it is possible that age might not be independent of sUA level because it’s unknown when patients first had hyperuricemia, and so it could just serve as a marker of the duration of the effect of hyperuricemia. “You showed us that the longer you wait for people who have higher [sUA] levels, the more likely you are to observe gout. So it’s probably some mixture of duration [of hyperuricemia] and age,” he said.
Dr. Dalbeth agreed, saying that it could also help to explain why the incidence of gout is lower at younger ages in women but then subsequently becomes higher.
The Health Research Council of New Zealand supported the research. Dr. Dalbeth reported receiving consulting fees, grants, or speaking fees from Takeda, Horizon, Menarini, AstraZeneca, Ardea Biosciences, Pfizer, and Cymabay, but none are related to this study. Two other authors also had several financial disclosures, but none of the others did.
SAN DIEGO – The incidence of gout is strongly linked to patients’ concentration of serum uric acid over time, but even so, less than half of patients with levels of 10 mg/dL or above develop the condition by 15 years, according to the largest individual person-level analysis to examine the relationship.
The incidence of gout rose from about 1% after 15 years in patients with a serum uric acid (sUA) level of less than 6 mg/dL to almost 49% in those with 10 mg/dL or higher in the study, which implies “a long period of hyperuricemia preceding the onset of clinical gout” and also “supports a role for additional factors in the pathogenesis of gout,” Nicola Dalbeth, MD, said in her presentation of the results at the annual meeting of the American College of Rheumatology.
jarun011/Thinkstock
The cumulative incidence of gout in the study across 15 years of follow-up at 1-mg/dL intervals of sUA from less than 6 mg/dL to 10 mg/dL or more provides “estimates to guide discussion with hyperuricemic individuals about their risk of developing gout over time,” according to Dr. Dalbeth of the University of Auckland (New Zealand), and her colleagues.
Dr. Dalbeth and her associates found four studies in a search of PubMed and the Database of Genotype and Phenotype from Jan. 1, 1980, to June 11, 2016, that met the inclusion criteria of containing publicly available participant level data, recorded incident gout (via classification criteria, doctor’s diagnosis, or self report of disease), and had a minimum of 3 years of follow-up. The four studies were the Atherosclerosis Risk in Communities study, the Coronary Artery Risk Development in Young Adults study, the original cohort of the Framingham Heart Study, and the offspring cohort of the Framingham Heart Study, comprising 18,889 individuals who were gout free at the beginning of follow-up, which lasted a mean of 11.2 years.
In all studies combined, the incidence of gout at an sUA level of less than 6 mg/dL steadily increased from 0.21% at 3 years of follow-up to 1.12% at 15 years. In contrast, sUA at 10 mg/dL or higher led to gout in 10.00% at 3 years and in 48.57% at 15 years.
The same general pattern held for the incidence of gout in both men and women, although men had a higher incidence across nearly all sUA concentration ranges.
Female sex provided a 30% reduced risk of gout, and European ethnicity nearly halved the risk for gout, compared with non-Europeans, The risk for gout rose across decades of age, starting at 40-49 years, and also increased significantly for each 1-mg/dL interval of sUA starting at 6 mg/dL.
The study’s conclusions are limited by the use of variable definitions of gout and how it was ascertained. In addition, the study did not analyze other endpoints that are associated with hyperuricemia and may be relevant to discuss in counseling people with elevated sUA levels, such as hypertension, chronic kidney disease, and cardiovascular disease, Dr. Dalbeth said.
Audience member Daniel H. Solomon, MD, of Brigham and Women’s Hospital, Boston, said after the presentation that it is possible that age might not be independent of sUA level because it’s unknown when patients first had hyperuricemia, and so it could just serve as a marker of the duration of the effect of hyperuricemia. “You showed us that the longer you wait for people who have higher [sUA] levels, the more likely you are to observe gout. So it’s probably some mixture of duration [of hyperuricemia] and age,” he said.
Dr. Dalbeth agreed, saying that it could also help to explain why the incidence of gout is lower at younger ages in women but then subsequently becomes higher.
The Health Research Council of New Zealand supported the research. Dr. Dalbeth reported receiving consulting fees, grants, or speaking fees from Takeda, Horizon, Menarini, AstraZeneca, Ardea Biosciences, Pfizer, and Cymabay, but none are related to this study. Two other authors also had several financial disclosures, but none of the others did.
SAN DIEGO – The incidence of gout is strongly linked to patients’ concentration of serum uric acid over time, but even so, less than half of patients with levels of 10 mg/dL or above develop the condition by 15 years, according to the largest individual person-level analysis to examine the relationship.
The incidence of gout rose from about 1% after 15 years in patients with a serum uric acid (sUA) level of less than 6 mg/dL to almost 49% in those with 10 mg/dL or higher in the study, which implies “a long period of hyperuricemia preceding the onset of clinical gout” and also “supports a role for additional factors in the pathogenesis of gout,” Nicola Dalbeth, MD, said in her presentation of the results at the annual meeting of the American College of Rheumatology.
jarun011/Thinkstock
The cumulative incidence of gout in the study across 15 years of follow-up at 1-mg/dL intervals of sUA from less than 6 mg/dL to 10 mg/dL or more provides “estimates to guide discussion with hyperuricemic individuals about their risk of developing gout over time,” according to Dr. Dalbeth of the University of Auckland (New Zealand), and her colleagues.
Dr. Dalbeth and her associates found four studies in a search of PubMed and the Database of Genotype and Phenotype from Jan. 1, 1980, to June 11, 2016, that met the inclusion criteria of containing publicly available participant level data, recorded incident gout (via classification criteria, doctor’s diagnosis, or self report of disease), and had a minimum of 3 years of follow-up. The four studies were the Atherosclerosis Risk in Communities study, the Coronary Artery Risk Development in Young Adults study, the original cohort of the Framingham Heart Study, and the offspring cohort of the Framingham Heart Study, comprising 18,889 individuals who were gout free at the beginning of follow-up, which lasted a mean of 11.2 years.
In all studies combined, the incidence of gout at an sUA level of less than 6 mg/dL steadily increased from 0.21% at 3 years of follow-up to 1.12% at 15 years. In contrast, sUA at 10 mg/dL or higher led to gout in 10.00% at 3 years and in 48.57% at 15 years.
The same general pattern held for the incidence of gout in both men and women, although men had a higher incidence across nearly all sUA concentration ranges.
Female sex provided a 30% reduced risk of gout, and European ethnicity nearly halved the risk for gout, compared with non-Europeans, The risk for gout rose across decades of age, starting at 40-49 years, and also increased significantly for each 1-mg/dL interval of sUA starting at 6 mg/dL.
The study’s conclusions are limited by the use of variable definitions of gout and how it was ascertained. In addition, the study did not analyze other endpoints that are associated with hyperuricemia and may be relevant to discuss in counseling people with elevated sUA levels, such as hypertension, chronic kidney disease, and cardiovascular disease, Dr. Dalbeth said.
Audience member Daniel H. Solomon, MD, of Brigham and Women’s Hospital, Boston, said after the presentation that it is possible that age might not be independent of sUA level because it’s unknown when patients first had hyperuricemia, and so it could just serve as a marker of the duration of the effect of hyperuricemia. “You showed us that the longer you wait for people who have higher [sUA] levels, the more likely you are to observe gout. So it’s probably some mixture of duration [of hyperuricemia] and age,” he said.
Dr. Dalbeth agreed, saying that it could also help to explain why the incidence of gout is lower at younger ages in women but then subsequently becomes higher.
The Health Research Council of New Zealand supported the research. Dr. Dalbeth reported receiving consulting fees, grants, or speaking fees from Takeda, Horizon, Menarini, AstraZeneca, Ardea Biosciences, Pfizer, and Cymabay, but none are related to this study. Two other authors also had several financial disclosures, but none of the others did.
Key clinical point: After 15 years of serum uric acid at 10 mg/dL or more, about half of people develop gout, likely leaving additional factors that contribute to its pathogenesis.
Major finding: The incidence of gout rose to about 1% after 15 years in patients with a serum uric acid (sUA) level of less than 6 mg/dL to almost 49% in those with 10 mg/dL or higher.
Data source: An analysis of 18,889 participants in four longitudinal observational cohort studies for whom baseline serum uric acid levels were available.
Disclosures: The Health Research Council of New Zealand supported the research. Dr. Dalbeth reported receiving consulting fees, grants, or speaking fees from Takeda, Horizon, Menarini, AstraZeneca, Ardea Biosciences, Pfizer, and Cymabay, but none are related to this study. Two other authors also had several financial disclosures, but none of the others did.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
ACOG, along with the American Urogynecologic Society (AUGS), issued an interim update to an April 2017 practice bulletin on pelvic organ prolapse (POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
ACOG, along with the American Urogynecologic Society (AUGS), issued an interim update to an April 2017 practice bulletin on pelvic organ prolapse (POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
ACOG, along with the American Urogynecologic Society (AUGS), issued an interim update to an April 2017 practice bulletin on pelvic organ prolapse (POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
The use of topical timolol maleate as a treatment for chronic diabetic and chronic venous ulcers showed increased wound healing compared with controls, according to the results of a prospective observational study of 60 patients.
In the treatment group, 30 patients with chronic leg ulcer (15 diabetic ulcers; 15 venous) received topical application of 0.5% timolol maleate (a beta-blocker) plus conventional antibiotic and wound dressing therapy. In the control group, 30 patients (identical split between diabetic and venous ulcers) were treated with conventional therapy alone, according to a report published in the November issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Elsevier Inc.
Venous and diabetic leg ulcer healing rates were significantly better at 4, 8, and 12 weeks in the 30 timolol-treated patients than in the 30 patients who received conventional treatment alone, according to Bindhiya Thomas, MS, and colleagues at the Government Medical College, Kottayam, Kerala, India.
The researchers found no significant difference in healing rates due to sex, between smokers and nonsmokers, or alcohol consumers vs. nonconsumers and they saw no major adverse effects due to timolol application (J Vasc Surg: Venous and Lym Dis 2017;5:844-50).
They reported that the limitations of their study included the lack of randomization and a formal power assessment.
“Topical application of timolol maleate is an effective therapeutic option for the treatment of chronic diabetic ulcer and chronic venous ulcer patients to improve ulcer healing by promoting keratinocyte migration,” the researchers concluded.
The use of topical timolol maleate as a treatment for chronic diabetic and chronic venous ulcers showed increased wound healing compared with controls, according to the results of a prospective observational study of 60 patients.
In the treatment group, 30 patients with chronic leg ulcer (15 diabetic ulcers; 15 venous) received topical application of 0.5% timolol maleate (a beta-blocker) plus conventional antibiotic and wound dressing therapy. In the control group, 30 patients (identical split between diabetic and venous ulcers) were treated with conventional therapy alone, according to a report published in the November issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Elsevier Inc.
Venous and diabetic leg ulcer healing rates were significantly better at 4, 8, and 12 weeks in the 30 timolol-treated patients than in the 30 patients who received conventional treatment alone, according to Bindhiya Thomas, MS, and colleagues at the Government Medical College, Kottayam, Kerala, India.
The researchers found no significant difference in healing rates due to sex, between smokers and nonsmokers, or alcohol consumers vs. nonconsumers and they saw no major adverse effects due to timolol application (J Vasc Surg: Venous and Lym Dis 2017;5:844-50).
They reported that the limitations of their study included the lack of randomization and a formal power assessment.
“Topical application of timolol maleate is an effective therapeutic option for the treatment of chronic diabetic ulcer and chronic venous ulcer patients to improve ulcer healing by promoting keratinocyte migration,” the researchers concluded.
The use of topical timolol maleate as a treatment for chronic diabetic and chronic venous ulcers showed increased wound healing compared with controls, according to the results of a prospective observational study of 60 patients.
In the treatment group, 30 patients with chronic leg ulcer (15 diabetic ulcers; 15 venous) received topical application of 0.5% timolol maleate (a beta-blocker) plus conventional antibiotic and wound dressing therapy. In the control group, 30 patients (identical split between diabetic and venous ulcers) were treated with conventional therapy alone, according to a report published in the November issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Elsevier Inc.
Venous and diabetic leg ulcer healing rates were significantly better at 4, 8, and 12 weeks in the 30 timolol-treated patients than in the 30 patients who received conventional treatment alone, according to Bindhiya Thomas, MS, and colleagues at the Government Medical College, Kottayam, Kerala, India.
The researchers found no significant difference in healing rates due to sex, between smokers and nonsmokers, or alcohol consumers vs. nonconsumers and they saw no major adverse effects due to timolol application (J Vasc Surg: Venous and Lym Dis 2017;5:844-50).
They reported that the limitations of their study included the lack of randomization and a formal power assessment.
“Topical application of timolol maleate is an effective therapeutic option for the treatment of chronic diabetic ulcer and chronic venous ulcer patients to improve ulcer healing by promoting keratinocyte migration,” the researchers concluded.
Clozapine, olanzapine, and oral and long-acting injectable formulations of risperidone proved superior on more schizophrenia outcomes that did other second-generation antipsychotics, according to a review of the effectiveness of treatments for adults with the illness. Meanwhile, psychosocial interventions were found to be more effective than “usual care” in “improving two or more outcomes.”
Those were some of the findings of Marian S. McDonagh, PharmD, and her associates in the review of hundreds of studies on the effectiveness of first-generation antipsychotics (FGAs), second-generation antipsychotics (SGAs), and psychosocial treatments in outpatient adults with schizophrenia. The researchers, who are affiliated with the Pacific Northwest Evidence-based Practice Center and worked on behalf of the Agency for Healthcare Research and Quality, asked two key questions: What did head-to-head comparisons show in terms of SGAs vs. SGAs and FGAs vs. SGAs, and what did trials show for usual care, which they defined as “elements of medication treatment ... rehabilitation services, and psychotherapy.” They reported the findings in a recent Comparative Effectiveness Review.
Dr. McDonagh and her associates conducted a literature search of the evidence on antipsychotics and found one systematic review (SR) of 138 trials (n = 47,189); 24 trials (n = 6,672) for SGAs vs. SGAs; one SR of 111 trials (n = 118,503); and five trials (n = 1,055) for FGAs vs. SGAs. For psychosocial interventions, they found 13 SRs of 271 trials (n = 25,050) and looked at 27 trials that were not included in the reviews (n = 6,404).
They found no evidence showing newer SGAs as superior to older SGAs on any outcomes. When FGAs were compared with SGAs, the reviewers found that olanzapine, risperidone, ziprasidone, and aripiprazole were similar to haloperidol “on some outcomes of benefit, and were superior on overall adverse events and withdrawal due to adverse events.”
Most of the findings were consistent with previous reviews that compared SGAs, and SGAs vs. FGAs. However, a new finding is that risperidone long-acting injectables and olanzapine are associated with significantly lower withdrawals tied to adverse events than are “most other SGAs.” In addition, Dr. McDonagh and her associates found that clozapine proved superior to other SGAs in preventing self-harm and suicides. Two SGAs, olanzapine and risperidone, were more likely to lead to improved scores on the Positive and Negative Syndrome Scale than was quetiapine.
When the reviewers looked at psychosocial interventions and compared them with usual care, the researchers found results that were consistent with some previous findings and different from others. For family interventions, they found the strongest evidence for interventions that last 7 to 12 months. The team also found that “the number of sessions was more predictive of relapse than was duration of treatment.” Their findings also showed that supported employment led to better outcomes for work over 2 years, compared with usual care. “More patients either gained employment (competitive or any job), had more hours worked, were employed longer, or earned more money than those receiving usual care,” the authors wrote. Also, patients who received assertive community treatment “were more likely to be living independently and to be employed, and they were less likely to be homeless or to discontinue treatment, compared with patients assigned to usual care.”
Dr. McDonagh and her associates said future review research should evaluate the comparative effectiveness of psychosocial interventions and compare them with one another. They also said future research should evaluate other nonpharmacologic, deviced-based treatments, such as electroconvulsive therapy and transcranial magnetic stimulation.
Clozapine, olanzapine, and oral and long-acting injectable formulations of risperidone proved superior on more schizophrenia outcomes that did other second-generation antipsychotics, according to a review of the effectiveness of treatments for adults with the illness. Meanwhile, psychosocial interventions were found to be more effective than “usual care” in “improving two or more outcomes.”
Those were some of the findings of Marian S. McDonagh, PharmD, and her associates in the review of hundreds of studies on the effectiveness of first-generation antipsychotics (FGAs), second-generation antipsychotics (SGAs), and psychosocial treatments in outpatient adults with schizophrenia. The researchers, who are affiliated with the Pacific Northwest Evidence-based Practice Center and worked on behalf of the Agency for Healthcare Research and Quality, asked two key questions: What did head-to-head comparisons show in terms of SGAs vs. SGAs and FGAs vs. SGAs, and what did trials show for usual care, which they defined as “elements of medication treatment ... rehabilitation services, and psychotherapy.” They reported the findings in a recent Comparative Effectiveness Review.
Dr. McDonagh and her associates conducted a literature search of the evidence on antipsychotics and found one systematic review (SR) of 138 trials (n = 47,189); 24 trials (n = 6,672) for SGAs vs. SGAs; one SR of 111 trials (n = 118,503); and five trials (n = 1,055) for FGAs vs. SGAs. For psychosocial interventions, they found 13 SRs of 271 trials (n = 25,050) and looked at 27 trials that were not included in the reviews (n = 6,404).
They found no evidence showing newer SGAs as superior to older SGAs on any outcomes. When FGAs were compared with SGAs, the reviewers found that olanzapine, risperidone, ziprasidone, and aripiprazole were similar to haloperidol “on some outcomes of benefit, and were superior on overall adverse events and withdrawal due to adverse events.”
Most of the findings were consistent with previous reviews that compared SGAs, and SGAs vs. FGAs. However, a new finding is that risperidone long-acting injectables and olanzapine are associated with significantly lower withdrawals tied to adverse events than are “most other SGAs.” In addition, Dr. McDonagh and her associates found that clozapine proved superior to other SGAs in preventing self-harm and suicides. Two SGAs, olanzapine and risperidone, were more likely to lead to improved scores on the Positive and Negative Syndrome Scale than was quetiapine.
When the reviewers looked at psychosocial interventions and compared them with usual care, the researchers found results that were consistent with some previous findings and different from others. For family interventions, they found the strongest evidence for interventions that last 7 to 12 months. The team also found that “the number of sessions was more predictive of relapse than was duration of treatment.” Their findings also showed that supported employment led to better outcomes for work over 2 years, compared with usual care. “More patients either gained employment (competitive or any job), had more hours worked, were employed longer, or earned more money than those receiving usual care,” the authors wrote. Also, patients who received assertive community treatment “were more likely to be living independently and to be employed, and they were less likely to be homeless or to discontinue treatment, compared with patients assigned to usual care.”
Dr. McDonagh and her associates said future review research should evaluate the comparative effectiveness of psychosocial interventions and compare them with one another. They also said future research should evaluate other nonpharmacologic, deviced-based treatments, such as electroconvulsive therapy and transcranial magnetic stimulation.
Clozapine, olanzapine, and oral and long-acting injectable formulations of risperidone proved superior on more schizophrenia outcomes that did other second-generation antipsychotics, according to a review of the effectiveness of treatments for adults with the illness. Meanwhile, psychosocial interventions were found to be more effective than “usual care” in “improving two or more outcomes.”
Those were some of the findings of Marian S. McDonagh, PharmD, and her associates in the review of hundreds of studies on the effectiveness of first-generation antipsychotics (FGAs), second-generation antipsychotics (SGAs), and psychosocial treatments in outpatient adults with schizophrenia. The researchers, who are affiliated with the Pacific Northwest Evidence-based Practice Center and worked on behalf of the Agency for Healthcare Research and Quality, asked two key questions: What did head-to-head comparisons show in terms of SGAs vs. SGAs and FGAs vs. SGAs, and what did trials show for usual care, which they defined as “elements of medication treatment ... rehabilitation services, and psychotherapy.” They reported the findings in a recent Comparative Effectiveness Review.
Dr. McDonagh and her associates conducted a literature search of the evidence on antipsychotics and found one systematic review (SR) of 138 trials (n = 47,189); 24 trials (n = 6,672) for SGAs vs. SGAs; one SR of 111 trials (n = 118,503); and five trials (n = 1,055) for FGAs vs. SGAs. For psychosocial interventions, they found 13 SRs of 271 trials (n = 25,050) and looked at 27 trials that were not included in the reviews (n = 6,404).
They found no evidence showing newer SGAs as superior to older SGAs on any outcomes. When FGAs were compared with SGAs, the reviewers found that olanzapine, risperidone, ziprasidone, and aripiprazole were similar to haloperidol “on some outcomes of benefit, and were superior on overall adverse events and withdrawal due to adverse events.”
Most of the findings were consistent with previous reviews that compared SGAs, and SGAs vs. FGAs. However, a new finding is that risperidone long-acting injectables and olanzapine are associated with significantly lower withdrawals tied to adverse events than are “most other SGAs.” In addition, Dr. McDonagh and her associates found that clozapine proved superior to other SGAs in preventing self-harm and suicides. Two SGAs, olanzapine and risperidone, were more likely to lead to improved scores on the Positive and Negative Syndrome Scale than was quetiapine.
When the reviewers looked at psychosocial interventions and compared them with usual care, the researchers found results that were consistent with some previous findings and different from others. For family interventions, they found the strongest evidence for interventions that last 7 to 12 months. The team also found that “the number of sessions was more predictive of relapse than was duration of treatment.” Their findings also showed that supported employment led to better outcomes for work over 2 years, compared with usual care. “More patients either gained employment (competitive or any job), had more hours worked, were employed longer, or earned more money than those receiving usual care,” the authors wrote. Also, patients who received assertive community treatment “were more likely to be living independently and to be employed, and they were less likely to be homeless or to discontinue treatment, compared with patients assigned to usual care.”
Dr. McDonagh and her associates said future review research should evaluate the comparative effectiveness of psychosocial interventions and compare them with one another. They also said future research should evaluate other nonpharmacologic, deviced-based treatments, such as electroconvulsive therapy and transcranial magnetic stimulation.
Key clinical point: Clozapine appears superior to other second-generation antipsychotics in preventing self-harm.
Major finding: “Olanzapine, risperidone, ziprasidone, and aripiprazole were similar to haloperidol on some outcomes of benefit.”
Data source: One systematic review (SR) of 138 trials (n = 47,189) and 24 trials (n = 6,672) for SGAs vs. SGAs; one SR of 111 trials (n = 118,503) and 5 trials (n = 1,055) for first-generation antipsychotics (FGAs) vs. SGAs; 13 SRs of 271 trials (n = 25,050); and 27 trials (n = 6,404) for psychosocial interventions.
Disclosures: Dr. McDonagh is affiliated with the Pacific Northwest Evidence-based Practice Center, and worked on behalf of the Agency for Healthcare Research and Quality.
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores
In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores
In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
Cardiac testing of Emergency Department patients with chest pain leads to increased revascularization without reduction in admissions for acute MI
Retrospective cohort study of ED patients presenting with chest pain but without evidence of ischemia, shows that non-invasive cardiac testing of these patients lead to more coronary angiograms (92.1 per 1,000 patients) within 30 days, but no significant reduction of admissions for acute MI at 1 year (remained 7.8 per 1,000 patients tested).
Citation: Sandhu AT, Heidenreich PA, Bhattacharya J, Bundorf MK. Cardiovascular Testing and Clinical Outcomes in Emergency Department Patients With Chest Pain. JAMA Intern Med. Published online 2017 June 26. doi: 10.1001/jamainternmed.2017.2432.
Facebook star ratings and “likes” correlate with patient satisfaction scores
In a cross-sectional analysis of 136 New York State hospitals, the study found increased Facebook star ratings correlated (P less than .003) with overall increased HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score (21/23 HCAHPS). HCAHPS measures also positively correlated (P less than .05) with adjusted number of “likes” on Facebook but to a lesser degree (3/21 HCAHPS). Neither star ratings nor number of “likes” correlate with Medicare spending or 30-day all-cause readmission rate.
Citation: Campbell L, Yue L. Are Facebook user ratings associated with hospital cost, quality, and patient satisfaction? BMJ Qual Saf. 2017 July 19. doi:10.1136/bmjqs-2016-006291.
Candida auris remains an ongoing health care facility transmission risk
Multidrug-resistant fungus Candida auris is an emerging pathogen and a transmission risk across health care facilities. From June 2016 through May 2017, 77 cases of clinical infection have been reported to the Centers for Disease Control and Prevention from seven states, though most (90%) cases are clustered in the New York City metropolitan area. Most patients had multiple medical conditions and extensive health care facility exposure. The CDC recommends contact precautions, private rooming, daily and terminal cleaning with disinfectant active against Clostridium difficile spores, and notification to receiving health care facilities about C. auris colonization or infection on transfer to help reduce the spread of C. auris throughout the United States.
Citation: Tsay S, Welsh RM, Adams EH, et al. Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities – United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep. 2017;66:51415.
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, the risks associated with unplanned pregnancy will generally be higher than risks associated with contraceptive use.”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
Robert Boston/Washington University
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, the risks associated with unplanned pregnancy will generally be higher than risks associated with contraceptive use.”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
Robert Boston/Washington University
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, the risks associated with unplanned pregnancy will generally be higher than risks associated with contraceptive use.”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
Robert Boston/Washington University
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.