User login
Drug prices a key focus of Senate HELP examination of Azar nomination
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.

Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.
Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.
Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
AT A SENATE HELP COMMITTEE HEARING
HealthCare.gov seeing more action this fall
Four weeks into the open enrollment for 2018, the number of health insurance plans selected through HealthCare.gov is up by 30% over the first 4 weeks of the 2017 sign-up period, according to data from the Centers for Medicare & Medicaid Services.
From Nov. 1 to Nov. 25 of this year, 2.78 million plans for 2018 were selected on the 39 state marketplaces that use the HealthCare.gov platform, the CMS reported Nov. 29, compared with the 2.14 million plans for 2017 selected from Nov. 1 to Nov. 26 of last year.
Last year, the enrollment numbers were released only every 2 weeks, so direct week-to-week comparisons are not possible. Looking at 2-week periods, however, shows that, despite a drop in the number of selections from the first to the second biweekly period this year, weeks 3 and 4 were still up considerably over last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” the CMS noted. Also, “the weekly snapshot only reports new plan selections and active plan renewals and does not report the number of consumers who have paid premiums to effectuate their enrollment.”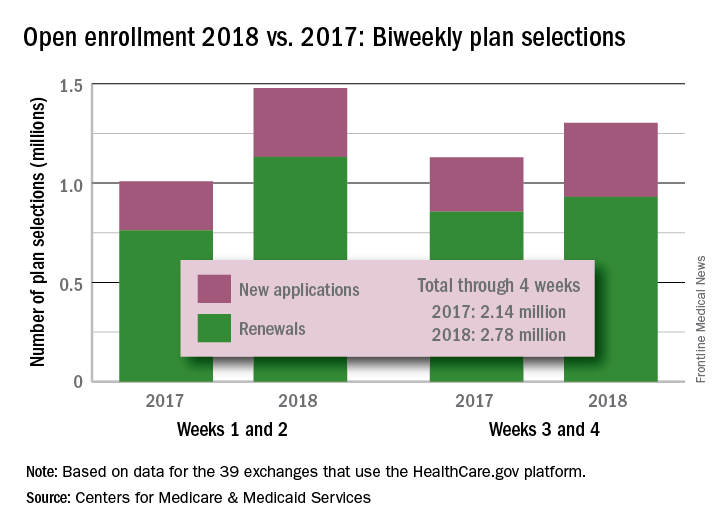
Four weeks into the open enrollment for 2018, the number of health insurance plans selected through HealthCare.gov is up by 30% over the first 4 weeks of the 2017 sign-up period, according to data from the Centers for Medicare & Medicaid Services.
From Nov. 1 to Nov. 25 of this year, 2.78 million plans for 2018 were selected on the 39 state marketplaces that use the HealthCare.gov platform, the CMS reported Nov. 29, compared with the 2.14 million plans for 2017 selected from Nov. 1 to Nov. 26 of last year.
Last year, the enrollment numbers were released only every 2 weeks, so direct week-to-week comparisons are not possible. Looking at 2-week periods, however, shows that, despite a drop in the number of selections from the first to the second biweekly period this year, weeks 3 and 4 were still up considerably over last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” the CMS noted. Also, “the weekly snapshot only reports new plan selections and active plan renewals and does not report the number of consumers who have paid premiums to effectuate their enrollment.”
Four weeks into the open enrollment for 2018, the number of health insurance plans selected through HealthCare.gov is up by 30% over the first 4 weeks of the 2017 sign-up period, according to data from the Centers for Medicare & Medicaid Services.
From Nov. 1 to Nov. 25 of this year, 2.78 million plans for 2018 were selected on the 39 state marketplaces that use the HealthCare.gov platform, the CMS reported Nov. 29, compared with the 2.14 million plans for 2017 selected from Nov. 1 to Nov. 26 of last year.
Last year, the enrollment numbers were released only every 2 weeks, so direct week-to-week comparisons are not possible. Looking at 2-week periods, however, shows that, despite a drop in the number of selections from the first to the second biweekly period this year, weeks 3 and 4 were still up considerably over last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” the CMS noted. Also, “the weekly snapshot only reports new plan selections and active plan renewals and does not report the number of consumers who have paid premiums to effectuate their enrollment.”
VIDEO: Team approach boosts effective blood pressure control
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
Empagliflozin’s heart failure benefits linked to volume drop
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.

“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.
“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.
“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: About according to post hoc analysis of the EMPA-REG OUTCOME study.
Major finding: About half of the observed heart failure benefit was tied to a roughly 3% rise in average hematocrit level.
Data source: Post hoc analysis of data from the 7,028 patients enrolled in the EMPA-REG OUTCOME trial.
Disclosures: The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, the two companies that market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
Fremanezumab may reduce chronic migraine frequency
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.

“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.
“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.
“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The average number of headache days was reduced by 4.3 and 4.6 for fremanezumab quarterly and monthly, respectively, compared with 2.5 for placebo (P less than .001 for both comparisons of fremanezumab to placebo).
Data source: A randomized, double-blind, placebo-controlled, parallel-group study of 1,130 patients with chronic migraine who received 12 weeks of treatment.
Disclosures: Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Vasopressin stimulates red blood cell production
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
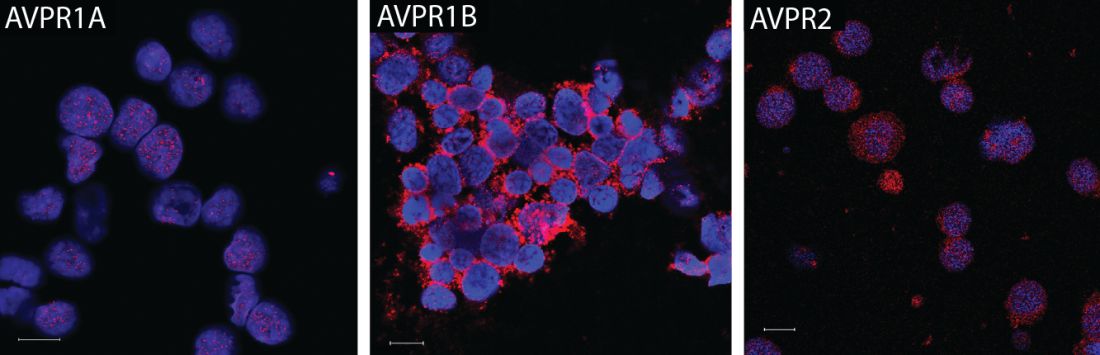
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: In anemic mice, treatment with a vasopressin or a vasopressin receptor agonist significantly increased hematocrit and reticulocyte number vs. controls.
Data source: A series of in vitro and in vivo experiments, plus a retrospective review of anemia incidence data in patients with central diabetes insipidus.
Disclosures: The research was supported by the National Institutes of Health. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
Revised McDonald Criteria Allow Substitution for Dissemination in Time
PARIS—Recommended revisions to the 2010 McDonald diagnostic criteria for multiple sclerosis (MS) include changes that are intended to enable neurologists to diagnose MS sooner in patients with a high likelihood of the disease. One addition allows the use of CSF-specific oligoclonal bands in lieu of demonstration of dissemination in time to make a diagnosis of MS in patients with a clinically isolated syndrome and demonstration of dissemination in space clinically or by MRI. Symptomatic and cortical lesions also may satisfy diagnostic criteria, according to the recommendations. In addition, the revised criteria include guidance to reduce the risk of misdiagnosing MS.

Jeffrey A. Cohen, MD, a neurologist with the Cleveland Clinic’s Mellen Center for MS Treatment and Research, presented the 2017 proposed revisions at the Seventh Joint ECTRIMS–ACTRIMS Meeting.
Dr. Cohen and Alan J. Thompson, MD, consultant neurologist at the National Hospital for Neurology and Neurosurgery in London, cochaired the International Panel on Diagnosis of MS, which drafted the new recommendations. The panel convened in November 2016 and May 2017. The meetings were organized under the International Advisory Committee on Clinical Trials in MS and supported by the US National MS Society and the European Committee for Treatment and Research in MS (ECTRIMS). The panel’s recommendations have been submitted for publication and are in the late stages of revision, Dr. Cohen said.
Facilitate Diagnosis
New data regarding the utility of MRI, CSF, and other tests in the diagnostic process motivated neurologists to reconvene the panel. In addition, “there has been increasing recognition of the continued frequency and potential consequences of misdiagnosis of MS,” Dr. Cohen said.
“We felt that the 2010 McDonald criteria overall performed well,” he said. “We did not anticipate making major changes to the criteria. But we sought to simplify and clarify some of the components of the 2010 criteria. We wanted to facilitate the ability to make the diagnosis of MS in patients who had a high likelihood of the disease but were not currently diagnosable by the 2010 criteria. We wanted to preserve the specificity of the 2010 criteria but promote their appropriate application … to reduce the risk of misdiagnosis.” Finally, the panel “wanted to ensure that any proposed changes did not weaken the existing criteria and were supported by reasonable evidence,” he said. Dr. Cohen highlighted five of the panel’s key revisions.
Recommended Changes
First and probably most controversially, “we propose that in a patient with a typical clinically isolated syndrome, and with fulfillment by either clinical or MRI criteria for dissemination in space, that the presence of CSF-specific oligoclonal bands now allows for diagnosis of MS,” Dr. Cohen said. “It does not represent demonstration of dissemination in time per se, but it allows substitution for demonstration of dissemination in time.”
A second recommendation is that symptomatic and asymptomatic MRI lesions can be considered in the determination of dissemination in space and time. In the 2010 criteria, a symptomatic lesion in a patient with a brainstem or spinal cord syndrome could not be included as MRI evidence of dissemination in time and space.
Third, in addition to juxtacortical lesions, cortical lesions can demonstrate dissemination in space. Neurologists’ ability to detect purely cortical MRI
Fourth, the criteria for primary progressive MS now allow the inclusion of symptomatic and cortical lesions as evidence of the disease. These criteria otherwise have not changed.
Finally, the panel recommends that neurologists determine a provisional disease course, as specified by Lublin et al, at the time of diagnosis and then periodically reevaluate the provisional course based on accumulated evidence.
Avoiding Misdiagnosis
“Much of our discussion started with the issue of misdiagnosis and differential diagnosis in MS,” Dr. Cohen said. “The potential differential diagnosis of MS is quite broad, and misdiagnosis remains an issue even today with advancements in MRI and other testing.” Solomon et al found that neuromyelitis optica spectrum disorders (NMOSDs) were the disorders most commonly misdiagnosed as MS. Physicians also misdiagnosed common conditions like migraine as MS. “Misdiagnosis may have harmful consequences, including inappropriate institution of disease therapy,” Dr. Cohen said.
Neurologists now recognize that aquaporin 4–related NMOSD is a distinct disorder from MS. “However, if you think back to the time that the 2010 criteria were developed, the relationship between NMOSD and MS was not quite as clear. Substantial data have been published since that time,” Dr. Cohen said. “We agreed that the McDonald criteria and the formal criteria for NMOSD largely distinguish the two diseases. However, there may be cases in which there is some uncertainty. Our recommendation is that … the possibility of NMOSD should be considered in all patients being evaluated for MS,” and any patient with features suggesting NMOSD should undergo aquaporin 4 testing.
In general, neurologists should recognize that the McDonald criteria originally were developed to make the diagnosis of MS in patients who have a high likelihood of the disease, not to differentiate MS from other disorders, he said. “Historical events being taken to represent a prior attack should be interpreted with caution if there is no corroborating objective evidence,” Dr. Cohen said. “In cases in which the diagnosis of MS is uncertain, further testing should be pursued. And in some cases, a clinician may want to postpone making a diagnosis pending the accumulation of sufficient data.” CSF testing and spinal MRI are not required to make the diagnosis of MS, but there should be a low threshold for obtaining them.
While data generally support the validity of the 2010 McDonald criteria in geographically diverse populations, children, and older individuals, neurologists should address potentially relevant alternative diagnoses that may be more common in these and other populations (eg, patients with comorbidities), such as infections and nutritional deficiencies.
MAGNIMS Proposal
Several proposals generated discussion during the panel meetings but were not adopted, primarily because the evidence did not justify changing the current criteria. For instance, the 2016 MAGNIMS MRI criteria propose that the number of acquired periventricular lesions be increased from one to three to provide additional specificity. “We reviewed those data … and felt that the modest increase in specificity did not justify making the change,” Dr. Cohen said. The panel also discussed incorporating optic nerve involvement into the criteria, but this proposal was not included in the update.
“The 2017 revisions further refine the well-established McDonald criteria,” Dr. Cohen said. “The appropriate application of the criteria is critical to avoid misdiagnosis. Fundamentally, MS remains a clinical diagnosis. … It requires rigorous synthesis of clinical, imaging, and laboratory data by a clinician with expertise in MS.”
Making a Diagnosis Sooner
Neurologists have been diagnosing MS in patients sooner. At the same time, misdiagnosing other conditions as MS can have profound consequences, including the potentially serious side effects of disease-modifying therapy, said Jeremy Chataway, PhD, consultant neurologist at the National Hospital for Neurology and Neurosurgery, London, in a lecture about the application of the proposed criteria. He described cases in which the 2017 proposed criteria—by allowing the inclusion of a symptomatic spinal cord lesion, or by substituting CSF-specific oligoclonal bands in place of dissemination in time—would have allowed neurologists to diagnose MS sooner. In one case, a patient might have received a diagnosis of MS about two years earlier.
Sometimes a diagnosis of MS “is obvious,” Dr. Chataway said. “Sometimes it is hard, even with advanced MRI. You can see the gradation that is required … to get us to the correct diagnosis.”
—Jake Remaly
Suggested Reading
Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278-286.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69(2):292-302.
Solomon AJ, Bourdette DN, Cross AH, et al. The contemporary spectrum of multiple sclerosis misdiagnosis: A multicenter study. Neurology. 2016;87(13):1393-1399.
PARIS—Recommended revisions to the 2010 McDonald diagnostic criteria for multiple sclerosis (MS) include changes that are intended to enable neurologists to diagnose MS sooner in patients with a high likelihood of the disease. One addition allows the use of CSF-specific oligoclonal bands in lieu of demonstration of dissemination in time to make a diagnosis of MS in patients with a clinically isolated syndrome and demonstration of dissemination in space clinically or by MRI. Symptomatic and cortical lesions also may satisfy diagnostic criteria, according to the recommendations. In addition, the revised criteria include guidance to reduce the risk of misdiagnosing MS.
Jeffrey A. Cohen, MD, a neurologist with the Cleveland Clinic’s Mellen Center for MS Treatment and Research, presented the 2017 proposed revisions at the Seventh Joint ECTRIMS–ACTRIMS Meeting.
Dr. Cohen and Alan J. Thompson, MD, consultant neurologist at the National Hospital for Neurology and Neurosurgery in London, cochaired the International Panel on Diagnosis of MS, which drafted the new recommendations. The panel convened in November 2016 and May 2017. The meetings were organized under the International Advisory Committee on Clinical Trials in MS and supported by the US National MS Society and the European Committee for Treatment and Research in MS (ECTRIMS). The panel’s recommendations have been submitted for publication and are in the late stages of revision, Dr. Cohen said.
Facilitate Diagnosis
New data regarding the utility of MRI, CSF, and other tests in the diagnostic process motivated neurologists to reconvene the panel. In addition, “there has been increasing recognition of the continued frequency and potential consequences of misdiagnosis of MS,” Dr. Cohen said.
“We felt that the 2010 McDonald criteria overall performed well,” he said. “We did not anticipate making major changes to the criteria. But we sought to simplify and clarify some of the components of the 2010 criteria. We wanted to facilitate the ability to make the diagnosis of MS in patients who had a high likelihood of the disease but were not currently diagnosable by the 2010 criteria. We wanted to preserve the specificity of the 2010 criteria but promote their appropriate application … to reduce the risk of misdiagnosis.” Finally, the panel “wanted to ensure that any proposed changes did not weaken the existing criteria and were supported by reasonable evidence,” he said. Dr. Cohen highlighted five of the panel’s key revisions.
Recommended Changes
First and probably most controversially, “we propose that in a patient with a typical clinically isolated syndrome, and with fulfillment by either clinical or MRI criteria for dissemination in space, that the presence of CSF-specific oligoclonal bands now allows for diagnosis of MS,” Dr. Cohen said. “It does not represent demonstration of dissemination in time per se, but it allows substitution for demonstration of dissemination in time.”
A second recommendation is that symptomatic and asymptomatic MRI lesions can be considered in the determination of dissemination in space and time. In the 2010 criteria, a symptomatic lesion in a patient with a brainstem or spinal cord syndrome could not be included as MRI evidence of dissemination in time and space.
Third, in addition to juxtacortical lesions, cortical lesions can demonstrate dissemination in space. Neurologists’ ability to detect purely cortical MRI
Fourth, the criteria for primary progressive MS now allow the inclusion of symptomatic and cortical lesions as evidence of the disease. These criteria otherwise have not changed.
Finally, the panel recommends that neurologists determine a provisional disease course, as specified by Lublin et al, at the time of diagnosis and then periodically reevaluate the provisional course based on accumulated evidence.
Avoiding Misdiagnosis
“Much of our discussion started with the issue of misdiagnosis and differential diagnosis in MS,” Dr. Cohen said. “The potential differential diagnosis of MS is quite broad, and misdiagnosis remains an issue even today with advancements in MRI and other testing.” Solomon et al found that neuromyelitis optica spectrum disorders (NMOSDs) were the disorders most commonly misdiagnosed as MS. Physicians also misdiagnosed common conditions like migraine as MS. “Misdiagnosis may have harmful consequences, including inappropriate institution of disease therapy,” Dr. Cohen said.
Neurologists now recognize that aquaporin 4–related NMOSD is a distinct disorder from MS. “However, if you think back to the time that the 2010 criteria were developed, the relationship between NMOSD and MS was not quite as clear. Substantial data have been published since that time,” Dr. Cohen said. “We agreed that the McDonald criteria and the formal criteria for NMOSD largely distinguish the two diseases. However, there may be cases in which there is some uncertainty. Our recommendation is that … the possibility of NMOSD should be considered in all patients being evaluated for MS,” and any patient with features suggesting NMOSD should undergo aquaporin 4 testing.
In general, neurologists should recognize that the McDonald criteria originally were developed to make the diagnosis of MS in patients who have a high likelihood of the disease, not to differentiate MS from other disorders, he said. “Historical events being taken to represent a prior attack should be interpreted with caution if there is no corroborating objective evidence,” Dr. Cohen said. “In cases in which the diagnosis of MS is uncertain, further testing should be pursued. And in some cases, a clinician may want to postpone making a diagnosis pending the accumulation of sufficient data.” CSF testing and spinal MRI are not required to make the diagnosis of MS, but there should be a low threshold for obtaining them.
While data generally support the validity of the 2010 McDonald criteria in geographically diverse populations, children, and older individuals, neurologists should address potentially relevant alternative diagnoses that may be more common in these and other populations (eg, patients with comorbidities), such as infections and nutritional deficiencies.
MAGNIMS Proposal
Several proposals generated discussion during the panel meetings but were not adopted, primarily because the evidence did not justify changing the current criteria. For instance, the 2016 MAGNIMS MRI criteria propose that the number of acquired periventricular lesions be increased from one to three to provide additional specificity. “We reviewed those data … and felt that the modest increase in specificity did not justify making the change,” Dr. Cohen said. The panel also discussed incorporating optic nerve involvement into the criteria, but this proposal was not included in the update.
“The 2017 revisions further refine the well-established McDonald criteria,” Dr. Cohen said. “The appropriate application of the criteria is critical to avoid misdiagnosis. Fundamentally, MS remains a clinical diagnosis. … It requires rigorous synthesis of clinical, imaging, and laboratory data by a clinician with expertise in MS.”
Making a Diagnosis Sooner
Neurologists have been diagnosing MS in patients sooner. At the same time, misdiagnosing other conditions as MS can have profound consequences, including the potentially serious side effects of disease-modifying therapy, said Jeremy Chataway, PhD, consultant neurologist at the National Hospital for Neurology and Neurosurgery, London, in a lecture about the application of the proposed criteria. He described cases in which the 2017 proposed criteria—by allowing the inclusion of a symptomatic spinal cord lesion, or by substituting CSF-specific oligoclonal bands in place of dissemination in time—would have allowed neurologists to diagnose MS sooner. In one case, a patient might have received a diagnosis of MS about two years earlier.
Sometimes a diagnosis of MS “is obvious,” Dr. Chataway said. “Sometimes it is hard, even with advanced MRI. You can see the gradation that is required … to get us to the correct diagnosis.”
—Jake Remaly
Suggested Reading
Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278-286.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69(2):292-302.
Solomon AJ, Bourdette DN, Cross AH, et al. The contemporary spectrum of multiple sclerosis misdiagnosis: A multicenter study. Neurology. 2016;87(13):1393-1399.
PARIS—Recommended revisions to the 2010 McDonald diagnostic criteria for multiple sclerosis (MS) include changes that are intended to enable neurologists to diagnose MS sooner in patients with a high likelihood of the disease. One addition allows the use of CSF-specific oligoclonal bands in lieu of demonstration of dissemination in time to make a diagnosis of MS in patients with a clinically isolated syndrome and demonstration of dissemination in space clinically or by MRI. Symptomatic and cortical lesions also may satisfy diagnostic criteria, according to the recommendations. In addition, the revised criteria include guidance to reduce the risk of misdiagnosing MS.
Jeffrey A. Cohen, MD, a neurologist with the Cleveland Clinic’s Mellen Center for MS Treatment and Research, presented the 2017 proposed revisions at the Seventh Joint ECTRIMS–ACTRIMS Meeting.
Dr. Cohen and Alan J. Thompson, MD, consultant neurologist at the National Hospital for Neurology and Neurosurgery in London, cochaired the International Panel on Diagnosis of MS, which drafted the new recommendations. The panel convened in November 2016 and May 2017. The meetings were organized under the International Advisory Committee on Clinical Trials in MS and supported by the US National MS Society and the European Committee for Treatment and Research in MS (ECTRIMS). The panel’s recommendations have been submitted for publication and are in the late stages of revision, Dr. Cohen said.
Facilitate Diagnosis
New data regarding the utility of MRI, CSF, and other tests in the diagnostic process motivated neurologists to reconvene the panel. In addition, “there has been increasing recognition of the continued frequency and potential consequences of misdiagnosis of MS,” Dr. Cohen said.
“We felt that the 2010 McDonald criteria overall performed well,” he said. “We did not anticipate making major changes to the criteria. But we sought to simplify and clarify some of the components of the 2010 criteria. We wanted to facilitate the ability to make the diagnosis of MS in patients who had a high likelihood of the disease but were not currently diagnosable by the 2010 criteria. We wanted to preserve the specificity of the 2010 criteria but promote their appropriate application … to reduce the risk of misdiagnosis.” Finally, the panel “wanted to ensure that any proposed changes did not weaken the existing criteria and were supported by reasonable evidence,” he said. Dr. Cohen highlighted five of the panel’s key revisions.
Recommended Changes
First and probably most controversially, “we propose that in a patient with a typical clinically isolated syndrome, and with fulfillment by either clinical or MRI criteria for dissemination in space, that the presence of CSF-specific oligoclonal bands now allows for diagnosis of MS,” Dr. Cohen said. “It does not represent demonstration of dissemination in time per se, but it allows substitution for demonstration of dissemination in time.”
A second recommendation is that symptomatic and asymptomatic MRI lesions can be considered in the determination of dissemination in space and time. In the 2010 criteria, a symptomatic lesion in a patient with a brainstem or spinal cord syndrome could not be included as MRI evidence of dissemination in time and space.
Third, in addition to juxtacortical lesions, cortical lesions can demonstrate dissemination in space. Neurologists’ ability to detect purely cortical MRI
Fourth, the criteria for primary progressive MS now allow the inclusion of symptomatic and cortical lesions as evidence of the disease. These criteria otherwise have not changed.
Finally, the panel recommends that neurologists determine a provisional disease course, as specified by Lublin et al, at the time of diagnosis and then periodically reevaluate the provisional course based on accumulated evidence.
Avoiding Misdiagnosis
“Much of our discussion started with the issue of misdiagnosis and differential diagnosis in MS,” Dr. Cohen said. “The potential differential diagnosis of MS is quite broad, and misdiagnosis remains an issue even today with advancements in MRI and other testing.” Solomon et al found that neuromyelitis optica spectrum disorders (NMOSDs) were the disorders most commonly misdiagnosed as MS. Physicians also misdiagnosed common conditions like migraine as MS. “Misdiagnosis may have harmful consequences, including inappropriate institution of disease therapy,” Dr. Cohen said.
Neurologists now recognize that aquaporin 4–related NMOSD is a distinct disorder from MS. “However, if you think back to the time that the 2010 criteria were developed, the relationship between NMOSD and MS was not quite as clear. Substantial data have been published since that time,” Dr. Cohen said. “We agreed that the McDonald criteria and the formal criteria for NMOSD largely distinguish the two diseases. However, there may be cases in which there is some uncertainty. Our recommendation is that … the possibility of NMOSD should be considered in all patients being evaluated for MS,” and any patient with features suggesting NMOSD should undergo aquaporin 4 testing.
In general, neurologists should recognize that the McDonald criteria originally were developed to make the diagnosis of MS in patients who have a high likelihood of the disease, not to differentiate MS from other disorders, he said. “Historical events being taken to represent a prior attack should be interpreted with caution if there is no corroborating objective evidence,” Dr. Cohen said. “In cases in which the diagnosis of MS is uncertain, further testing should be pursued. And in some cases, a clinician may want to postpone making a diagnosis pending the accumulation of sufficient data.” CSF testing and spinal MRI are not required to make the diagnosis of MS, but there should be a low threshold for obtaining them.
While data generally support the validity of the 2010 McDonald criteria in geographically diverse populations, children, and older individuals, neurologists should address potentially relevant alternative diagnoses that may be more common in these and other populations (eg, patients with comorbidities), such as infections and nutritional deficiencies.
MAGNIMS Proposal
Several proposals generated discussion during the panel meetings but were not adopted, primarily because the evidence did not justify changing the current criteria. For instance, the 2016 MAGNIMS MRI criteria propose that the number of acquired periventricular lesions be increased from one to three to provide additional specificity. “We reviewed those data … and felt that the modest increase in specificity did not justify making the change,” Dr. Cohen said. The panel also discussed incorporating optic nerve involvement into the criteria, but this proposal was not included in the update.
“The 2017 revisions further refine the well-established McDonald criteria,” Dr. Cohen said. “The appropriate application of the criteria is critical to avoid misdiagnosis. Fundamentally, MS remains a clinical diagnosis. … It requires rigorous synthesis of clinical, imaging, and laboratory data by a clinician with expertise in MS.”
Making a Diagnosis Sooner
Neurologists have been diagnosing MS in patients sooner. At the same time, misdiagnosing other conditions as MS can have profound consequences, including the potentially serious side effects of disease-modifying therapy, said Jeremy Chataway, PhD, consultant neurologist at the National Hospital for Neurology and Neurosurgery, London, in a lecture about the application of the proposed criteria. He described cases in which the 2017 proposed criteria—by allowing the inclusion of a symptomatic spinal cord lesion, or by substituting CSF-specific oligoclonal bands in place of dissemination in time—would have allowed neurologists to diagnose MS sooner. In one case, a patient might have received a diagnosis of MS about two years earlier.
Sometimes a diagnosis of MS “is obvious,” Dr. Chataway said. “Sometimes it is hard, even with advanced MRI. You can see the gradation that is required … to get us to the correct diagnosis.”
—Jake Remaly
Suggested Reading
Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278-286.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69(2):292-302.
Solomon AJ, Bourdette DN, Cross AH, et al. The contemporary spectrum of multiple sclerosis misdiagnosis: A multicenter study. Neurology. 2016;87(13):1393-1399.
‘Tea with Freud’: Engaging, authentic, but nonanalytic
If I traveled back in time to meet with a 60-year-old Sigmund Freud, the first thing I would say to him is: “Stop smoking, and get out of Austria!”
That was my thought as I read “Tea with Freud: An Imaginary Conversation about How Psychotherapy Really Works” (Dog Ear Publishing, 2016), in which the author, psychiatrist Steven B. Sandler, MD, holds a series of imaginary meetings with Freud to discuss the evolution of psychoanalysis into Sandler’s preferred mode of short-term dynamic psychotherapy (STDP) and to present case material for Freud’s supervision.
The chapters in “Tea with Freud” alternate between the imagined meetings with Freud and Sandler’s clinical work, presented from what I assume are transcripts of videotaped sessions with some disguises and composites to protect patients’ privacy. These clinical vignettes bring the reader into the nitty-gritty of the treatment room, which may be highly instructive for a lay person – particularly one who has never been in therapy.
At the same time, the book has the potential to be quite misleading. This would not be the case if Sandler were simply trying to introduce the reader to STDP. Instead, he attempts to convince the reader, and apparently himself, that the therapy he practices is a modern rendition of psychoanalysis because it tries to access the patient’s unacceptable, unconscious feelings; encourages her to “remember with emotion” or “experience” her feelings; and leads to some sort of cathartic resolution and improvement in symptoms and outlook.
While, “Aha!” moments and cathartic abreaction were characteristic of very early analyses, modern psychoanalysis is about slow but permanent change in character structure. The unwritten message in the book is that Freud’s true heirs practice psychotherapy as Sandler does. He does not seem to consider the significance of the many psychoanalysts, myself included, practicing psychoanalysis today.
Sandler uses a (mercifully) attenuated Davanloo technique to provoke patients into dramatic enactments. He is highly directive, with statements like, “We don’t solve any particular problem if we jump around all over.” I wonder how he can possibly learn about his patients when he begins with a foregone conclusion about where they should be headed.
His treatments are very brief. During his first session with a patient named Carla, he deduces that she is suffering from unresolved anger related to childhood trauma and manifesting it in chronic anxiety with angry outbursts. He then proceeds to “cure” her in five sessions.
Sandler wonders why some of his patients relapse and decides it is because they have not explored their “positive memories” in treatment, as though memories were univalent.
And he talks way too much.
All of this is decidedly un-analytic, which, again, would not matter if he were only trying to demonstrate STDP in action. Nonanalytic psychotherapies are entitled to be nonanalytic. Sandler has Freud point out precisely these analytic errors, so he must be aware that he is making them. And, yet, he stubbornly maintains his position that his work is analytic. What a waste of time travel it would be to meet with Freud only to reinforce one’s own opinions.
“Tea with Freud” is a way for Sandler to promote STDP and his theories about “positive memories” using an established authority, Freud, to validate them. This makes the book disappointing, but fortunately, there is something more to it. I kept wondering why it was so important to the author to seek out Freud’s – that is, his father’s – approval for his work. The book never answers that question. But in his attempts to understand his motives, Sandler, who is very adept at describing his own thoughts and feelings, becomes a model for the awareness of internal states and the effects of unconscious processes. Perhaps this is the most important lesson in “Tea with Freud.”

Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York.
If I traveled back in time to meet with a 60-year-old Sigmund Freud, the first thing I would say to him is: “Stop smoking, and get out of Austria!”
That was my thought as I read “Tea with Freud: An Imaginary Conversation about How Psychotherapy Really Works” (Dog Ear Publishing, 2016), in which the author, psychiatrist Steven B. Sandler, MD, holds a series of imaginary meetings with Freud to discuss the evolution of psychoanalysis into Sandler’s preferred mode of short-term dynamic psychotherapy (STDP) and to present case material for Freud’s supervision.
The chapters in “Tea with Freud” alternate between the imagined meetings with Freud and Sandler’s clinical work, presented from what I assume are transcripts of videotaped sessions with some disguises and composites to protect patients’ privacy. These clinical vignettes bring the reader into the nitty-gritty of the treatment room, which may be highly instructive for a lay person – particularly one who has never been in therapy.
At the same time, the book has the potential to be quite misleading. This would not be the case if Sandler were simply trying to introduce the reader to STDP. Instead, he attempts to convince the reader, and apparently himself, that the therapy he practices is a modern rendition of psychoanalysis because it tries to access the patient’s unacceptable, unconscious feelings; encourages her to “remember with emotion” or “experience” her feelings; and leads to some sort of cathartic resolution and improvement in symptoms and outlook.
While, “Aha!” moments and cathartic abreaction were characteristic of very early analyses, modern psychoanalysis is about slow but permanent change in character structure. The unwritten message in the book is that Freud’s true heirs practice psychotherapy as Sandler does. He does not seem to consider the significance of the many psychoanalysts, myself included, practicing psychoanalysis today.
Sandler uses a (mercifully) attenuated Davanloo technique to provoke patients into dramatic enactments. He is highly directive, with statements like, “We don’t solve any particular problem if we jump around all over.” I wonder how he can possibly learn about his patients when he begins with a foregone conclusion about where they should be headed.
His treatments are very brief. During his first session with a patient named Carla, he deduces that she is suffering from unresolved anger related to childhood trauma and manifesting it in chronic anxiety with angry outbursts. He then proceeds to “cure” her in five sessions.
Sandler wonders why some of his patients relapse and decides it is because they have not explored their “positive memories” in treatment, as though memories were univalent.
And he talks way too much.
All of this is decidedly un-analytic, which, again, would not matter if he were only trying to demonstrate STDP in action. Nonanalytic psychotherapies are entitled to be nonanalytic. Sandler has Freud point out precisely these analytic errors, so he must be aware that he is making them. And, yet, he stubbornly maintains his position that his work is analytic. What a waste of time travel it would be to meet with Freud only to reinforce one’s own opinions.
“Tea with Freud” is a way for Sandler to promote STDP and his theories about “positive memories” using an established authority, Freud, to validate them. This makes the book disappointing, but fortunately, there is something more to it. I kept wondering why it was so important to the author to seek out Freud’s – that is, his father’s – approval for his work. The book never answers that question. But in his attempts to understand his motives, Sandler, who is very adept at describing his own thoughts and feelings, becomes a model for the awareness of internal states and the effects of unconscious processes. Perhaps this is the most important lesson in “Tea with Freud.”
Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York.
If I traveled back in time to meet with a 60-year-old Sigmund Freud, the first thing I would say to him is: “Stop smoking, and get out of Austria!”
That was my thought as I read “Tea with Freud: An Imaginary Conversation about How Psychotherapy Really Works” (Dog Ear Publishing, 2016), in which the author, psychiatrist Steven B. Sandler, MD, holds a series of imaginary meetings with Freud to discuss the evolution of psychoanalysis into Sandler’s preferred mode of short-term dynamic psychotherapy (STDP) and to present case material for Freud’s supervision.
The chapters in “Tea with Freud” alternate between the imagined meetings with Freud and Sandler’s clinical work, presented from what I assume are transcripts of videotaped sessions with some disguises and composites to protect patients’ privacy. These clinical vignettes bring the reader into the nitty-gritty of the treatment room, which may be highly instructive for a lay person – particularly one who has never been in therapy.
At the same time, the book has the potential to be quite misleading. This would not be the case if Sandler were simply trying to introduce the reader to STDP. Instead, he attempts to convince the reader, and apparently himself, that the therapy he practices is a modern rendition of psychoanalysis because it tries to access the patient’s unacceptable, unconscious feelings; encourages her to “remember with emotion” or “experience” her feelings; and leads to some sort of cathartic resolution and improvement in symptoms and outlook.
While, “Aha!” moments and cathartic abreaction were characteristic of very early analyses, modern psychoanalysis is about slow but permanent change in character structure. The unwritten message in the book is that Freud’s true heirs practice psychotherapy as Sandler does. He does not seem to consider the significance of the many psychoanalysts, myself included, practicing psychoanalysis today.
Sandler uses a (mercifully) attenuated Davanloo technique to provoke patients into dramatic enactments. He is highly directive, with statements like, “We don’t solve any particular problem if we jump around all over.” I wonder how he can possibly learn about his patients when he begins with a foregone conclusion about where they should be headed.
His treatments are very brief. During his first session with a patient named Carla, he deduces that she is suffering from unresolved anger related to childhood trauma and manifesting it in chronic anxiety with angry outbursts. He then proceeds to “cure” her in five sessions.
Sandler wonders why some of his patients relapse and decides it is because they have not explored their “positive memories” in treatment, as though memories were univalent.
And he talks way too much.
All of this is decidedly un-analytic, which, again, would not matter if he were only trying to demonstrate STDP in action. Nonanalytic psychotherapies are entitled to be nonanalytic. Sandler has Freud point out precisely these analytic errors, so he must be aware that he is making them. And, yet, he stubbornly maintains his position that his work is analytic. What a waste of time travel it would be to meet with Freud only to reinforce one’s own opinions.
“Tea with Freud” is a way for Sandler to promote STDP and his theories about “positive memories” using an established authority, Freud, to validate them. This makes the book disappointing, but fortunately, there is something more to it. I kept wondering why it was so important to the author to seek out Freud’s – that is, his father’s – approval for his work. The book never answers that question. But in his attempts to understand his motives, Sandler, who is very adept at describing his own thoughts and feelings, becomes a model for the awareness of internal states and the effects of unconscious processes. Perhaps this is the most important lesson in “Tea with Freud.”
Dr. Twersky-Kengmana is a psychiatrist and psychoanalyst in private practice in New York.
Accounting 101: Basics you need to know
Physicians practice medicine and communicate within the world of medical language, yet there is a lack of awareness and understanding by many health care professionals of the universal language of business, which is accounting. Just as Latin provides the basic framework for medically related terminology, accounting is the standard language used to convey financial information to both internal and external stakeholders.
Accounting principles are important to physicians at any level. Whether you are starting out in private practice, running a clinical department, or working as an executive in a health care system, most decisions are based on the interpretation of financial data using accounting principles. Accounting standards in the United States are developed by the Financial Accounting Standard Board (FASB) and established as a set of principles and guidelines called Generally Accepted Accounting Principles (GAAP).1–3
Accrual- vs cash-based accounting
There are 2 approaches to recording financial transactions: accrual- and cash-based accounting methods. The main difference between them is in the timing of the recorded financial transactions (when revenue and expenses are recognized on the accounting books). Under GAAP, the matching principle, which is one of the most basic and utilized guidelines of accounting, specifies that accrual accounting be used. In the United States, most businesses (publically traded companies and moderate- to large-sized companies) use accrual accounting, while some individual and smaller businesses, including health care services such as physician practices, use the cash method.1–4
Accrual-based accounting
Accrual-based accounting specifies that revenues are recorded when they are earned, and expenses are recorded when they occur. A health care business may earn revenue for services on one day, but the cash may not be received or recorded on the accounting books for several weeks or months and at an amount less than billed.
Accrual-based accounting provides a more accurate representation of a business’ financial performance, since it uses the principle in which expenses are matched to revenues in the same time period. This enables a more precise representation of true financial performance during a given time frame.1–4
Cash-based accounting
Cash-based accounting is the easiest method to understand and implement because financial transactions are recorded in the accounting books when money is received or spent without the need for complex accounting techniques or integration of accounts receivable or payable.
Despite the ease of use and simplicity in tracking cash flow, this method can be deceiving because revenue may be received or expenses may need to be paid at times that are not consistent with when the revenue has been earned or expenses incurred. This can result in misleading information on the business’ health and the accuracy of tracking financial performance over time, since revenue and expenses for a particular transaction may occur at different times.1–4
Which accounting process to choose?
Even though accrual-based accounting may provide a more accurate financial representation of a business’ performance, many smaller businesses, including physician practices, prefer to use cash-based accounting. In addition, many health care businesses are eligible to use cash-based accounting per Internal Revenue Service (IRS) rules by qualifying for the Gross Receipts Test and being a qualified Personal Service Corporation (PSC):
- The Gross Receipts Test states that if the average annual gross receipts of the business are less than $5 million, the business can use the cash-based accounting method.
- If at least 95% of a business activity involves performing health care services, and at least 95% of the business is owned by employees performing health care services, then the business qualifies as a PSC that may use the cash-based accounting method.
Many physician practices qualify to use cash-based accounting, which reduces the complexity of following accrual-based accounting rules and simplifies overall cash-flow management.5
Read about insurance, capital equipment depreciation, more
CASE New practice opens
Practice A opens its practice on January 1. The practice borrows $20,000 from the bank to purchase hysteroscopic equipment for office-based tubal sterilizations and an additional $50,000 for an ultrasound machine. Both loans have a 5% annual interest rate amortized over 5 years. The practice leases office space and pays rent 2 months in advance at $8,000 ($4,000 per month). On January 1, the practice pays a $1,200 premium for annual property and liability insurance and $12,500 for the first quarter payment for professional liability insurance ($50,000 annually, paid quarterly). Other costs the practice pays in January include: utilities, $400; EHR licensing, $300; technical support, $200; and salaries, $10,000.
The practice purchases 4 sets of sterilization spring devices at $1,500 each ($6,000) to have in stock. One hysteroscopic sterilization procedure is performed on a patient in January using 1 device. The practice is reimbursed $2,500 for the procedure.
In January, the practice bills $150,000 in charges, but after insurance contractual adjustments, January’s revenue is $50,000. Actual cash payments from billings received are $10,000 in January, $30,000 in February, and $10,000 in March.
At first glance, there is a noticeable difference on the sales or recognition of revenues based on the type of accounting (TABLE). With the accrual method, because the billing charges are submitted in January when the services were provided (minus the insurance contractual adjustments), the $50,000 revenue is immediately counted and recognized, even though the practice only received $10,000 cash for those billings during January. While the benefit to accrual accounting is the timely recognition of the revenue when the service was provided, the downside is that much of those billings might actually be paid over 90 days, and some of those billings may go unpaid by the insurance company or the patients, which would require adjustments in later months.
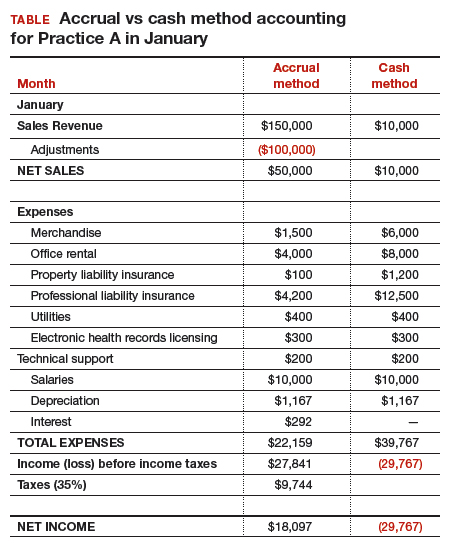
The cash-based method is simpler to understand because the cash received for the month is recognized as the revenue, regardless of the amount charged that month.
Merchandise. In the accrual method, the cost of merchandise sold (the hysteroscopic sterilization implants) is recognized as an expense when the revenue is generated from its sale. In this case, the date that the patient has the hysteroscopic in-office sterilization procedure is when the revenue and the expense of the implant are recognized.
In a cash-based accounting method, the $6,000 cost of the implants is recognized at the time of purchase in January.
Lease. In this scenario, even though 2 months of lease for the office were paid, the accrual method only recognizes the January payment; the second payment is recognized in February. In the cash method, because both months were paid in January, the total expense of $8,000 is recognized in January.
Property liability insurance. The property liability insurance payment is required at the start of the year. In accrual accounting, this expense is divided over 12 months, while in the cash method, the expense is counted at the time the payment is made.
Professional liability insurance. The professional liability insurance expense of $50,000 per year is made in quarterly payments, so for the accrual method, the annual amount would be distributed over 12 months at $4,200 per month. With the cash method, it would be paid—and recognized as an expense—quarterly at $12,500, starting in January.
Capital equipment depreciation. Capital medical equipment (hysteroscopy and ultrasound) can be depreciated using a straight-line 5-year depreciation. A total $70,000 worth of equipment divided by 5 years is $14,000 per year, depreciated over 5 years. One-twelfth of $14,000 equals $1,167, which is recorded as a January depreciation expense. Because the Internal Revenue Code requires capital assets to be depreciated, even for cash-basis taxpayers, the common practice is to record depreciation expense for both cash- and accrual-basis income accounting.6
Interest on loans. A loan’s principal payment will not be included on the income statement. The principal payment, a reduction of a liability (loans payable), is reported on the balance sheet. Only the interest portion of a loan payment is reported on the income statement (interest expense). In accrual accounting, the accrued interest on the loan payment for the year is $3,500 ($292 for January). For the cash-basis method, because the interest is paid annually at year-end, interest will not be expensed until December.
Taxes. The IRS states that, “Individuals, including sole proprietors, partners, and S corporation shareholders, generally have to make estimated tax payments if they expect to owe tax of $1,000 or more when their return is filed. Corporations generally have to make estimated tax payments if they expect to owe tax of $500 or more when their return is filed.”7
Assuming 35% tax liability, the accrual method would create a tax liability of $9,744 on a profit of $27,841. With the cash method, there would be no tax liability because there was no net profit.
Other expenses. The utilities, EHR licensing, tech support, and salaries are expensed the same way for both methods.
Net income. The resulting final net income is vastly different for the month of January depending on the accounting method utilized. The accrual method results in a net income of $18,097, while the cash-basis method results in a net loss of $29,767. Over the course of the year, these imbalances are likely to even out.
Related article:
Business law critical to your practice
Choosing an accounting method
Depending on the accounting method, a practice’s performance and profit will seem very different. The type of accounting method chosen will depend on what goals the owners want to achieve.
The accrual method provides a more accurate picture of business flow and performance and will be less subject to monthly variations due to large purchases or variations in expenses. If the practice chooses this method using an income statement, it should also employ a cash-flow statement.
The cash method of accounting will give a convenient and practical summary of the practice’s cash flow.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- About the FASB. Financial Accounting Standards Board website. http://www.fasb.org/jsp/FASB/PageSectionPage&cid=1176154526495. Accessed November 7, 2017.
- What is the difference between accrual accounting and cash accounting? Investopedia. https://www.investopedia.com/ask/answers/121514/what-difference-between-accrual-accounting-and-cash-accounting.asp. Accessed November 7, 2017.
- Accounting Basics (Explanation). Part 2: Income Statement. Accounting Coach. https://www.accountingcoach.com/accounting-basics/explanation/2. Accessed November 7, 2017.
- Stickney C, Weil R. Financial Accounting: An Introduction to Concepts, Methods, and Uses. 11th ed. Nashville, TN: Southwestern College Publishing Group; 2006:97-110.
- Internal Revenue Service. Publication 538 (12/2016), Accounting Periods and Methods. https://www.irs.gov/publications/p538#en_US_201612_publink1000270634. Revised December 2016. Accessed November 7, 2017.
- Klinefelter D, McCorkle D, Klose S. Financial Management: Cash vs. Accrual Accounting. Risk Management. AgriLife Extension. Texas A&M System. http://agrilife.org/agecoext/files/2013/10/rm5-16.pdf. Published 2013. Accessed November 7, 2017.
- Internal Revenue Service. Small Business and Self-Employed Tax Center: Estimated Taxes. https://www.irs.gov/businesses/small-businesses-self-employed/estimated-taxes. Updated November 2, 2017. Accessed November 7, 2017.

Dr. Hart is Senior Director, Global Medical Affairs, Surgical Innovations at Medtronic, and Voluntary Faculty, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, University of South Florida Morsani College of Medicine, Tampa.

Dr. Kim is Associate Clinical Professor, Department of Obstetrics and Gynecology, Cedars-Sinai Medical Center, Los Angeles, California, and Associate Clinical Professor, David Geffen School of Medicine, University of California-Los Angeles.
Dr. Hart reports that he is a full-time employee of Medtronic. Dr. Kim reports no financial relationships relevant to this article.
Dr. Hart is Senior Director, Global Medical Affairs, Surgical Innovations at Medtronic, and Voluntary Faculty, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, University of South Florida Morsani College of Medicine, Tampa.
Dr. Kim is Associate Clinical Professor, Department of Obstetrics and Gynecology, Cedars-Sinai Medical Center, Los Angeles, California, and Associate Clinical Professor, David Geffen School of Medicine, University of California-Los Angeles.
Dr. Hart reports that he is a full-time employee of Medtronic. Dr. Kim reports no financial relationships relevant to this article.
Dr. Hart is Senior Director, Global Medical Affairs, Surgical Innovations at Medtronic, and Voluntary Faculty, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, University of South Florida Morsani College of Medicine, Tampa.
Dr. Kim is Associate Clinical Professor, Department of Obstetrics and Gynecology, Cedars-Sinai Medical Center, Los Angeles, California, and Associate Clinical Professor, David Geffen School of Medicine, University of California-Los Angeles.
Dr. Hart reports that he is a full-time employee of Medtronic. Dr. Kim reports no financial relationships relevant to this article.
Physicians practice medicine and communicate within the world of medical language, yet there is a lack of awareness and understanding by many health care professionals of the universal language of business, which is accounting. Just as Latin provides the basic framework for medically related terminology, accounting is the standard language used to convey financial information to both internal and external stakeholders.
Accounting principles are important to physicians at any level. Whether you are starting out in private practice, running a clinical department, or working as an executive in a health care system, most decisions are based on the interpretation of financial data using accounting principles. Accounting standards in the United States are developed by the Financial Accounting Standard Board (FASB) and established as a set of principles and guidelines called Generally Accepted Accounting Principles (GAAP).1–3
Accrual- vs cash-based accounting
There are 2 approaches to recording financial transactions: accrual- and cash-based accounting methods. The main difference between them is in the timing of the recorded financial transactions (when revenue and expenses are recognized on the accounting books). Under GAAP, the matching principle, which is one of the most basic and utilized guidelines of accounting, specifies that accrual accounting be used. In the United States, most businesses (publically traded companies and moderate- to large-sized companies) use accrual accounting, while some individual and smaller businesses, including health care services such as physician practices, use the cash method.1–4
Accrual-based accounting
Accrual-based accounting specifies that revenues are recorded when they are earned, and expenses are recorded when they occur. A health care business may earn revenue for services on one day, but the cash may not be received or recorded on the accounting books for several weeks or months and at an amount less than billed.
Accrual-based accounting provides a more accurate representation of a business’ financial performance, since it uses the principle in which expenses are matched to revenues in the same time period. This enables a more precise representation of true financial performance during a given time frame.1–4
Cash-based accounting
Cash-based accounting is the easiest method to understand and implement because financial transactions are recorded in the accounting books when money is received or spent without the need for complex accounting techniques or integration of accounts receivable or payable.
Despite the ease of use and simplicity in tracking cash flow, this method can be deceiving because revenue may be received or expenses may need to be paid at times that are not consistent with when the revenue has been earned or expenses incurred. This can result in misleading information on the business’ health and the accuracy of tracking financial performance over time, since revenue and expenses for a particular transaction may occur at different times.1–4
Which accounting process to choose?
Even though accrual-based accounting may provide a more accurate financial representation of a business’ performance, many smaller businesses, including physician practices, prefer to use cash-based accounting. In addition, many health care businesses are eligible to use cash-based accounting per Internal Revenue Service (IRS) rules by qualifying for the Gross Receipts Test and being a qualified Personal Service Corporation (PSC):
- The Gross Receipts Test states that if the average annual gross receipts of the business are less than $5 million, the business can use the cash-based accounting method.
- If at least 95% of a business activity involves performing health care services, and at least 95% of the business is owned by employees performing health care services, then the business qualifies as a PSC that may use the cash-based accounting method.
Many physician practices qualify to use cash-based accounting, which reduces the complexity of following accrual-based accounting rules and simplifies overall cash-flow management.5
Read about insurance, capital equipment depreciation, more
CASE New practice opens
Practice A opens its practice on January 1. The practice borrows $20,000 from the bank to purchase hysteroscopic equipment for office-based tubal sterilizations and an additional $50,000 for an ultrasound machine. Both loans have a 5% annual interest rate amortized over 5 years. The practice leases office space and pays rent 2 months in advance at $8,000 ($4,000 per month). On January 1, the practice pays a $1,200 premium for annual property and liability insurance and $12,500 for the first quarter payment for professional liability insurance ($50,000 annually, paid quarterly). Other costs the practice pays in January include: utilities, $400; EHR licensing, $300; technical support, $200; and salaries, $10,000.
The practice purchases 4 sets of sterilization spring devices at $1,500 each ($6,000) to have in stock. One hysteroscopic sterilization procedure is performed on a patient in January using 1 device. The practice is reimbursed $2,500 for the procedure.
In January, the practice bills $150,000 in charges, but after insurance contractual adjustments, January’s revenue is $50,000. Actual cash payments from billings received are $10,000 in January, $30,000 in February, and $10,000 in March.
At first glance, there is a noticeable difference on the sales or recognition of revenues based on the type of accounting (TABLE). With the accrual method, because the billing charges are submitted in January when the services were provided (minus the insurance contractual adjustments), the $50,000 revenue is immediately counted and recognized, even though the practice only received $10,000 cash for those billings during January. While the benefit to accrual accounting is the timely recognition of the revenue when the service was provided, the downside is that much of those billings might actually be paid over 90 days, and some of those billings may go unpaid by the insurance company or the patients, which would require adjustments in later months.
The cash-based method is simpler to understand because the cash received for the month is recognized as the revenue, regardless of the amount charged that month.
Merchandise. In the accrual method, the cost of merchandise sold (the hysteroscopic sterilization implants) is recognized as an expense when the revenue is generated from its sale. In this case, the date that the patient has the hysteroscopic in-office sterilization procedure is when the revenue and the expense of the implant are recognized.
In a cash-based accounting method, the $6,000 cost of the implants is recognized at the time of purchase in January.
Lease. In this scenario, even though 2 months of lease for the office were paid, the accrual method only recognizes the January payment; the second payment is recognized in February. In the cash method, because both months were paid in January, the total expense of $8,000 is recognized in January.
Property liability insurance. The property liability insurance payment is required at the start of the year. In accrual accounting, this expense is divided over 12 months, while in the cash method, the expense is counted at the time the payment is made.
Professional liability insurance. The professional liability insurance expense of $50,000 per year is made in quarterly payments, so for the accrual method, the annual amount would be distributed over 12 months at $4,200 per month. With the cash method, it would be paid—and recognized as an expense—quarterly at $12,500, starting in January.
Capital equipment depreciation. Capital medical equipment (hysteroscopy and ultrasound) can be depreciated using a straight-line 5-year depreciation. A total $70,000 worth of equipment divided by 5 years is $14,000 per year, depreciated over 5 years. One-twelfth of $14,000 equals $1,167, which is recorded as a January depreciation expense. Because the Internal Revenue Code requires capital assets to be depreciated, even for cash-basis taxpayers, the common practice is to record depreciation expense for both cash- and accrual-basis income accounting.6
Interest on loans. A loan’s principal payment will not be included on the income statement. The principal payment, a reduction of a liability (loans payable), is reported on the balance sheet. Only the interest portion of a loan payment is reported on the income statement (interest expense). In accrual accounting, the accrued interest on the loan payment for the year is $3,500 ($292 for January). For the cash-basis method, because the interest is paid annually at year-end, interest will not be expensed until December.
Taxes. The IRS states that, “Individuals, including sole proprietors, partners, and S corporation shareholders, generally have to make estimated tax payments if they expect to owe tax of $1,000 or more when their return is filed. Corporations generally have to make estimated tax payments if they expect to owe tax of $500 or more when their return is filed.”7
Assuming 35% tax liability, the accrual method would create a tax liability of $9,744 on a profit of $27,841. With the cash method, there would be no tax liability because there was no net profit.
Other expenses. The utilities, EHR licensing, tech support, and salaries are expensed the same way for both methods.
Net income. The resulting final net income is vastly different for the month of January depending on the accounting method utilized. The accrual method results in a net income of $18,097, while the cash-basis method results in a net loss of $29,767. Over the course of the year, these imbalances are likely to even out.
Related article:
Business law critical to your practice
Choosing an accounting method
Depending on the accounting method, a practice’s performance and profit will seem very different. The type of accounting method chosen will depend on what goals the owners want to achieve.
The accrual method provides a more accurate picture of business flow and performance and will be less subject to monthly variations due to large purchases or variations in expenses. If the practice chooses this method using an income statement, it should also employ a cash-flow statement.
The cash method of accounting will give a convenient and practical summary of the practice’s cash flow.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Physicians practice medicine and communicate within the world of medical language, yet there is a lack of awareness and understanding by many health care professionals of the universal language of business, which is accounting. Just as Latin provides the basic framework for medically related terminology, accounting is the standard language used to convey financial information to both internal and external stakeholders.
Accounting principles are important to physicians at any level. Whether you are starting out in private practice, running a clinical department, or working as an executive in a health care system, most decisions are based on the interpretation of financial data using accounting principles. Accounting standards in the United States are developed by the Financial Accounting Standard Board (FASB) and established as a set of principles and guidelines called Generally Accepted Accounting Principles (GAAP).1–3
Accrual- vs cash-based accounting
There are 2 approaches to recording financial transactions: accrual- and cash-based accounting methods. The main difference between them is in the timing of the recorded financial transactions (when revenue and expenses are recognized on the accounting books). Under GAAP, the matching principle, which is one of the most basic and utilized guidelines of accounting, specifies that accrual accounting be used. In the United States, most businesses (publically traded companies and moderate- to large-sized companies) use accrual accounting, while some individual and smaller businesses, including health care services such as physician practices, use the cash method.1–4
Accrual-based accounting
Accrual-based accounting specifies that revenues are recorded when they are earned, and expenses are recorded when they occur. A health care business may earn revenue for services on one day, but the cash may not be received or recorded on the accounting books for several weeks or months and at an amount less than billed.
Accrual-based accounting provides a more accurate representation of a business’ financial performance, since it uses the principle in which expenses are matched to revenues in the same time period. This enables a more precise representation of true financial performance during a given time frame.1–4
Cash-based accounting
Cash-based accounting is the easiest method to understand and implement because financial transactions are recorded in the accounting books when money is received or spent without the need for complex accounting techniques or integration of accounts receivable or payable.
Despite the ease of use and simplicity in tracking cash flow, this method can be deceiving because revenue may be received or expenses may need to be paid at times that are not consistent with when the revenue has been earned or expenses incurred. This can result in misleading information on the business’ health and the accuracy of tracking financial performance over time, since revenue and expenses for a particular transaction may occur at different times.1–4
Which accounting process to choose?
Even though accrual-based accounting may provide a more accurate financial representation of a business’ performance, many smaller businesses, including physician practices, prefer to use cash-based accounting. In addition, many health care businesses are eligible to use cash-based accounting per Internal Revenue Service (IRS) rules by qualifying for the Gross Receipts Test and being a qualified Personal Service Corporation (PSC):
- The Gross Receipts Test states that if the average annual gross receipts of the business are less than $5 million, the business can use the cash-based accounting method.
- If at least 95% of a business activity involves performing health care services, and at least 95% of the business is owned by employees performing health care services, then the business qualifies as a PSC that may use the cash-based accounting method.
Many physician practices qualify to use cash-based accounting, which reduces the complexity of following accrual-based accounting rules and simplifies overall cash-flow management.5
Read about insurance, capital equipment depreciation, more
CASE New practice opens
Practice A opens its practice on January 1. The practice borrows $20,000 from the bank to purchase hysteroscopic equipment for office-based tubal sterilizations and an additional $50,000 for an ultrasound machine. Both loans have a 5% annual interest rate amortized over 5 years. The practice leases office space and pays rent 2 months in advance at $8,000 ($4,000 per month). On January 1, the practice pays a $1,200 premium for annual property and liability insurance and $12,500 for the first quarter payment for professional liability insurance ($50,000 annually, paid quarterly). Other costs the practice pays in January include: utilities, $400; EHR licensing, $300; technical support, $200; and salaries, $10,000.
The practice purchases 4 sets of sterilization spring devices at $1,500 each ($6,000) to have in stock. One hysteroscopic sterilization procedure is performed on a patient in January using 1 device. The practice is reimbursed $2,500 for the procedure.
In January, the practice bills $150,000 in charges, but after insurance contractual adjustments, January’s revenue is $50,000. Actual cash payments from billings received are $10,000 in January, $30,000 in February, and $10,000 in March.
At first glance, there is a noticeable difference on the sales or recognition of revenues based on the type of accounting (TABLE). With the accrual method, because the billing charges are submitted in January when the services were provided (minus the insurance contractual adjustments), the $50,000 revenue is immediately counted and recognized, even though the practice only received $10,000 cash for those billings during January. While the benefit to accrual accounting is the timely recognition of the revenue when the service was provided, the downside is that much of those billings might actually be paid over 90 days, and some of those billings may go unpaid by the insurance company or the patients, which would require adjustments in later months.
The cash-based method is simpler to understand because the cash received for the month is recognized as the revenue, regardless of the amount charged that month.
Merchandise. In the accrual method, the cost of merchandise sold (the hysteroscopic sterilization implants) is recognized as an expense when the revenue is generated from its sale. In this case, the date that the patient has the hysteroscopic in-office sterilization procedure is when the revenue and the expense of the implant are recognized.
In a cash-based accounting method, the $6,000 cost of the implants is recognized at the time of purchase in January.
Lease. In this scenario, even though 2 months of lease for the office were paid, the accrual method only recognizes the January payment; the second payment is recognized in February. In the cash method, because both months were paid in January, the total expense of $8,000 is recognized in January.
Property liability insurance. The property liability insurance payment is required at the start of the year. In accrual accounting, this expense is divided over 12 months, while in the cash method, the expense is counted at the time the payment is made.
Professional liability insurance. The professional liability insurance expense of $50,000 per year is made in quarterly payments, so for the accrual method, the annual amount would be distributed over 12 months at $4,200 per month. With the cash method, it would be paid—and recognized as an expense—quarterly at $12,500, starting in January.
Capital equipment depreciation. Capital medical equipment (hysteroscopy and ultrasound) can be depreciated using a straight-line 5-year depreciation. A total $70,000 worth of equipment divided by 5 years is $14,000 per year, depreciated over 5 years. One-twelfth of $14,000 equals $1,167, which is recorded as a January depreciation expense. Because the Internal Revenue Code requires capital assets to be depreciated, even for cash-basis taxpayers, the common practice is to record depreciation expense for both cash- and accrual-basis income accounting.6
Interest on loans. A loan’s principal payment will not be included on the income statement. The principal payment, a reduction of a liability (loans payable), is reported on the balance sheet. Only the interest portion of a loan payment is reported on the income statement (interest expense). In accrual accounting, the accrued interest on the loan payment for the year is $3,500 ($292 for January). For the cash-basis method, because the interest is paid annually at year-end, interest will not be expensed until December.
Taxes. The IRS states that, “Individuals, including sole proprietors, partners, and S corporation shareholders, generally have to make estimated tax payments if they expect to owe tax of $1,000 or more when their return is filed. Corporations generally have to make estimated tax payments if they expect to owe tax of $500 or more when their return is filed.”7
Assuming 35% tax liability, the accrual method would create a tax liability of $9,744 on a profit of $27,841. With the cash method, there would be no tax liability because there was no net profit.
Other expenses. The utilities, EHR licensing, tech support, and salaries are expensed the same way for both methods.
Net income. The resulting final net income is vastly different for the month of January depending on the accounting method utilized. The accrual method results in a net income of $18,097, while the cash-basis method results in a net loss of $29,767. Over the course of the year, these imbalances are likely to even out.
Related article:
Business law critical to your practice
Choosing an accounting method
Depending on the accounting method, a practice’s performance and profit will seem very different. The type of accounting method chosen will depend on what goals the owners want to achieve.
The accrual method provides a more accurate picture of business flow and performance and will be less subject to monthly variations due to large purchases or variations in expenses. If the practice chooses this method using an income statement, it should also employ a cash-flow statement.
The cash method of accounting will give a convenient and practical summary of the practice’s cash flow.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- About the FASB. Financial Accounting Standards Board website. http://www.fasb.org/jsp/FASB/PageSectionPage&cid=1176154526495. Accessed November 7, 2017.
- What is the difference between accrual accounting and cash accounting? Investopedia. https://www.investopedia.com/ask/answers/121514/what-difference-between-accrual-accounting-and-cash-accounting.asp. Accessed November 7, 2017.
- Accounting Basics (Explanation). Part 2: Income Statement. Accounting Coach. https://www.accountingcoach.com/accounting-basics/explanation/2. Accessed November 7, 2017.
- Stickney C, Weil R. Financial Accounting: An Introduction to Concepts, Methods, and Uses. 11th ed. Nashville, TN: Southwestern College Publishing Group; 2006:97-110.
- Internal Revenue Service. Publication 538 (12/2016), Accounting Periods and Methods. https://www.irs.gov/publications/p538#en_US_201612_publink1000270634. Revised December 2016. Accessed November 7, 2017.
- Klinefelter D, McCorkle D, Klose S. Financial Management: Cash vs. Accrual Accounting. Risk Management. AgriLife Extension. Texas A&M System. http://agrilife.org/agecoext/files/2013/10/rm5-16.pdf. Published 2013. Accessed November 7, 2017.
- Internal Revenue Service. Small Business and Self-Employed Tax Center: Estimated Taxes. https://www.irs.gov/businesses/small-businesses-self-employed/estimated-taxes. Updated November 2, 2017. Accessed November 7, 2017.
- About the FASB. Financial Accounting Standards Board website. http://www.fasb.org/jsp/FASB/PageSectionPage&cid=1176154526495. Accessed November 7, 2017.
- What is the difference between accrual accounting and cash accounting? Investopedia. https://www.investopedia.com/ask/answers/121514/what-difference-between-accrual-accounting-and-cash-accounting.asp. Accessed November 7, 2017.
- Accounting Basics (Explanation). Part 2: Income Statement. Accounting Coach. https://www.accountingcoach.com/accounting-basics/explanation/2. Accessed November 7, 2017.
- Stickney C, Weil R. Financial Accounting: An Introduction to Concepts, Methods, and Uses. 11th ed. Nashville, TN: Southwestern College Publishing Group; 2006:97-110.
- Internal Revenue Service. Publication 538 (12/2016), Accounting Periods and Methods. https://www.irs.gov/publications/p538#en_US_201612_publink1000270634. Revised December 2016. Accessed November 7, 2017.
- Klinefelter D, McCorkle D, Klose S. Financial Management: Cash vs. Accrual Accounting. Risk Management. AgriLife Extension. Texas A&M System. http://agrilife.org/agecoext/files/2013/10/rm5-16.pdf. Published 2013. Accessed November 7, 2017.
- Internal Revenue Service. Small Business and Self-Employed Tax Center: Estimated Taxes. https://www.irs.gov/businesses/small-businesses-self-employed/estimated-taxes. Updated November 2, 2017. Accessed November 7, 2017.

Inhaled loxapine quells agitation in personality disorders
PARIS – The inhaled powder formulation of loxapine appears to be a safe and effective treatment for acute agitation in patients with personality disorders, Diego R. Mendez Mareque, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Inhaled loxapine is approved for the treatment of acute agitation associated with schizophrenia or bipolar I disorder. Its use in patients with borderline personality and other personality disorders is off label. But this inhaled typical antipsychotic shows promise in filling an unmet need for a rapid-acting, minimally invasive treatment for acute agitation in patients with personality disorders, a very common scenario in psychiatric wards and emergency departments, and one that can quickly escalate to aggression and violence, noted Dr. Mendez Mareque of the Galician Health Service in Ferrol, Spain.
He presented a prospective, longitudinal, observational pilot study of 14 patients with personality disorders treated with a single 10-mg dose of inhaled loxapine while experiencing acute agitation in a psychiatric emergency department or psychiatric ward. Their mean baseline score on the Excited Component of the Positive and Negative Syndrome Scale (PANSS-EC) was 20.8 out of a possible 35 points. The scale assesses five domains: excitement, tension, uncooperativeness, hostility, and poor impulse control.
Within 10 minutes after administration of inhaled loxapine by a health care professional, 11 patients showed a significant drop on the PANSS-EC. They were calm, nonsedated, and ready for assessment. Within 20 minutes, their PANSS-EC scores were reduced by roughly half, compared with baseline.
Three patients were nonresponders. They received rescue treatment with oral or injectable antipsychotics and benzodiazepines.
None of the 14 patients had a history of airway disease, and none experienced bronchospasm, a known possible side effect of inhaled loxapine, the psychiatrist noted.
The results of this Spanish observational study confirm the benefits of inhaled loxapine for treating agitation in patients with borderline personality disorder previously described in a German case series (J Clin Psychopharmacol. 2015 Dec;35[6]:741-3).
Dr. Mendez Mareque reported having no financial conflicts of interest regarding his study.
PARIS – The inhaled powder formulation of loxapine appears to be a safe and effective treatment for acute agitation in patients with personality disorders, Diego R. Mendez Mareque, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Inhaled loxapine is approved for the treatment of acute agitation associated with schizophrenia or bipolar I disorder. Its use in patients with borderline personality and other personality disorders is off label. But this inhaled typical antipsychotic shows promise in filling an unmet need for a rapid-acting, minimally invasive treatment for acute agitation in patients with personality disorders, a very common scenario in psychiatric wards and emergency departments, and one that can quickly escalate to aggression and violence, noted Dr. Mendez Mareque of the Galician Health Service in Ferrol, Spain.
He presented a prospective, longitudinal, observational pilot study of 14 patients with personality disorders treated with a single 10-mg dose of inhaled loxapine while experiencing acute agitation in a psychiatric emergency department or psychiatric ward. Their mean baseline score on the Excited Component of the Positive and Negative Syndrome Scale (PANSS-EC) was 20.8 out of a possible 35 points. The scale assesses five domains: excitement, tension, uncooperativeness, hostility, and poor impulse control.
Within 10 minutes after administration of inhaled loxapine by a health care professional, 11 patients showed a significant drop on the PANSS-EC. They were calm, nonsedated, and ready for assessment. Within 20 minutes, their PANSS-EC scores were reduced by roughly half, compared with baseline.
Three patients were nonresponders. They received rescue treatment with oral or injectable antipsychotics and benzodiazepines.
None of the 14 patients had a history of airway disease, and none experienced bronchospasm, a known possible side effect of inhaled loxapine, the psychiatrist noted.
The results of this Spanish observational study confirm the benefits of inhaled loxapine for treating agitation in patients with borderline personality disorder previously described in a German case series (J Clin Psychopharmacol. 2015 Dec;35[6]:741-3).
Dr. Mendez Mareque reported having no financial conflicts of interest regarding his study.
PARIS – The inhaled powder formulation of loxapine appears to be a safe and effective treatment for acute agitation in patients with personality disorders, Diego R. Mendez Mareque, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Inhaled loxapine is approved for the treatment of acute agitation associated with schizophrenia or bipolar I disorder. Its use in patients with borderline personality and other personality disorders is off label. But this inhaled typical antipsychotic shows promise in filling an unmet need for a rapid-acting, minimally invasive treatment for acute agitation in patients with personality disorders, a very common scenario in psychiatric wards and emergency departments, and one that can quickly escalate to aggression and violence, noted Dr. Mendez Mareque of the Galician Health Service in Ferrol, Spain.
He presented a prospective, longitudinal, observational pilot study of 14 patients with personality disorders treated with a single 10-mg dose of inhaled loxapine while experiencing acute agitation in a psychiatric emergency department or psychiatric ward. Their mean baseline score on the Excited Component of the Positive and Negative Syndrome Scale (PANSS-EC) was 20.8 out of a possible 35 points. The scale assesses five domains: excitement, tension, uncooperativeness, hostility, and poor impulse control.
Within 10 minutes after administration of inhaled loxapine by a health care professional, 11 patients showed a significant drop on the PANSS-EC. They were calm, nonsedated, and ready for assessment. Within 20 minutes, their PANSS-EC scores were reduced by roughly half, compared with baseline.
Three patients were nonresponders. They received rescue treatment with oral or injectable antipsychotics and benzodiazepines.
None of the 14 patients had a history of airway disease, and none experienced bronchospasm, a known possible side effect of inhaled loxapine, the psychiatrist noted.
The results of this Spanish observational study confirm the benefits of inhaled loxapine for treating agitation in patients with borderline personality disorder previously described in a German case series (J Clin Psychopharmacol. 2015 Dec;35[6]:741-3).
Dr. Mendez Mareque reported having no financial conflicts of interest regarding his study.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Eleven of 14 acutely agitated patients with various personality disorders were calm, nonsedated, and ready for assessment within 10 minutes after a single dose of inhaled loxapine.
Data source: A prospective observational pilot study of inhaled loxapine in 14 acutely agitated patients with personality disorders.
Disclosures: The study presenter reported having no financial conflicts of interest.