User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
People still want their medical intelligence in human form
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.

And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”

This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.

Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.
And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”
This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.
Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.
And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”
This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.
Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Which interventions could lessen the burden of dementia?
Using a microsimulation algorithm that accounts for the effect on mortality, a team from Marseille, France, has shown that interventions targeting the three main vascular risk factors for dementia – hypertension, diabetes, and physical inactivity – could significantly reduce the burden of dementia by 2040.
Although these modeling results could appear too optimistic, since total disappearance of the risk factors was assumed, the authors say the results do show that targeted interventions for these factors could be effective in reducing the future burden of dementia.
Increasing prevalence
According to the World Alzheimer Report 2018, 50 million people around the world were living with dementia; a population roughly around the size of South Korea or Spain. That community is likely to rise to about 152 million people by 2050, which is similar to the size of Russia or Bangladesh, the result of an aging population.
Among modifiable risk factors, many studies support a deleterious effect of hypertension, diabetes, and physical inactivity on the risk of dementia. However, since the distribution of these risk factors could have a direct impact on mortality, reducing it should increase life expectancy and the number of cases of dementia.
The team, headed by Hélène Jacqmin-Gadda, PhD, research director at the University of Bordeaux (France), has developed a microsimulation model capable of predicting the burden of dementia while accounting for the impact on mortality. The team used this approach to assess the impact of interventions targeting these three main risk factors on the burden of dementia in France by 2040.
Removing risk factors
The researchers estimated the incidence of dementia for men and women using data from the 2020 PAQUID cohort, and these data were combined with the projections forecast by the French National Institute of Statistics and Economic Studies to account for mortality with and without dementia.
Without intervention, the prevalence rate of dementia in 2040 would be 9.6% among men and 14% among women older than 65 years.
These figures would decrease to 6.4% (−33%) and 10.4% (−26%), respectively, under the intervention scenario whereby the three modifiable vascular risk factors (hypertension, diabetes, and physical inactivity) would be removed simultaneously beginning in 2020. The prevalence rates are significantly reduced for men and women from age 75 years. In this scenario, life expectancy without dementia would increase by 3.4 years in men and 2.6 years in women, the result of men being more exposed to these three risk factors.
Other scenarios have estimated dementia prevalence with the disappearance of just one of these risk factors. For example, the disappearance of hypertension alone from 2020 could decrease dementia prevalence by 21% in men and 16% in women (because this risk factor is less common in women than in men) by 2040. This reduction would be associated with a decrease in the lifelong probability of dementia among men and women and a gain in life expectancy without dementia of 2 years in men and 1.4 years in women.
Among the three factors, hypertension has the largest impact on dementia burden in the French population, since this is, by far, the most prevalent (69% in men and 49% in women), while intervention targeting only diabetes or physical inactivity would lead to a reduction in dementia prevalence of only 4%-7%.
The authors reported no conflicts of interest.
This article was translated from Univadis France. A version appeared on Medscape.com.
Using a microsimulation algorithm that accounts for the effect on mortality, a team from Marseille, France, has shown that interventions targeting the three main vascular risk factors for dementia – hypertension, diabetes, and physical inactivity – could significantly reduce the burden of dementia by 2040.
Although these modeling results could appear too optimistic, since total disappearance of the risk factors was assumed, the authors say the results do show that targeted interventions for these factors could be effective in reducing the future burden of dementia.
Increasing prevalence
According to the World Alzheimer Report 2018, 50 million people around the world were living with dementia; a population roughly around the size of South Korea or Spain. That community is likely to rise to about 152 million people by 2050, which is similar to the size of Russia or Bangladesh, the result of an aging population.
Among modifiable risk factors, many studies support a deleterious effect of hypertension, diabetes, and physical inactivity on the risk of dementia. However, since the distribution of these risk factors could have a direct impact on mortality, reducing it should increase life expectancy and the number of cases of dementia.
The team, headed by Hélène Jacqmin-Gadda, PhD, research director at the University of Bordeaux (France), has developed a microsimulation model capable of predicting the burden of dementia while accounting for the impact on mortality. The team used this approach to assess the impact of interventions targeting these three main risk factors on the burden of dementia in France by 2040.
Removing risk factors
The researchers estimated the incidence of dementia for men and women using data from the 2020 PAQUID cohort, and these data were combined with the projections forecast by the French National Institute of Statistics and Economic Studies to account for mortality with and without dementia.
Without intervention, the prevalence rate of dementia in 2040 would be 9.6% among men and 14% among women older than 65 years.
These figures would decrease to 6.4% (−33%) and 10.4% (−26%), respectively, under the intervention scenario whereby the three modifiable vascular risk factors (hypertension, diabetes, and physical inactivity) would be removed simultaneously beginning in 2020. The prevalence rates are significantly reduced for men and women from age 75 years. In this scenario, life expectancy without dementia would increase by 3.4 years in men and 2.6 years in women, the result of men being more exposed to these three risk factors.
Other scenarios have estimated dementia prevalence with the disappearance of just one of these risk factors. For example, the disappearance of hypertension alone from 2020 could decrease dementia prevalence by 21% in men and 16% in women (because this risk factor is less common in women than in men) by 2040. This reduction would be associated with a decrease in the lifelong probability of dementia among men and women and a gain in life expectancy without dementia of 2 years in men and 1.4 years in women.
Among the three factors, hypertension has the largest impact on dementia burden in the French population, since this is, by far, the most prevalent (69% in men and 49% in women), while intervention targeting only diabetes or physical inactivity would lead to a reduction in dementia prevalence of only 4%-7%.
The authors reported no conflicts of interest.
This article was translated from Univadis France. A version appeared on Medscape.com.
Using a microsimulation algorithm that accounts for the effect on mortality, a team from Marseille, France, has shown that interventions targeting the three main vascular risk factors for dementia – hypertension, diabetes, and physical inactivity – could significantly reduce the burden of dementia by 2040.
Although these modeling results could appear too optimistic, since total disappearance of the risk factors was assumed, the authors say the results do show that targeted interventions for these factors could be effective in reducing the future burden of dementia.
Increasing prevalence
According to the World Alzheimer Report 2018, 50 million people around the world were living with dementia; a population roughly around the size of South Korea or Spain. That community is likely to rise to about 152 million people by 2050, which is similar to the size of Russia or Bangladesh, the result of an aging population.
Among modifiable risk factors, many studies support a deleterious effect of hypertension, diabetes, and physical inactivity on the risk of dementia. However, since the distribution of these risk factors could have a direct impact on mortality, reducing it should increase life expectancy and the number of cases of dementia.
The team, headed by Hélène Jacqmin-Gadda, PhD, research director at the University of Bordeaux (France), has developed a microsimulation model capable of predicting the burden of dementia while accounting for the impact on mortality. The team used this approach to assess the impact of interventions targeting these three main risk factors on the burden of dementia in France by 2040.
Removing risk factors
The researchers estimated the incidence of dementia for men and women using data from the 2020 PAQUID cohort, and these data were combined with the projections forecast by the French National Institute of Statistics and Economic Studies to account for mortality with and without dementia.
Without intervention, the prevalence rate of dementia in 2040 would be 9.6% among men and 14% among women older than 65 years.
These figures would decrease to 6.4% (−33%) and 10.4% (−26%), respectively, under the intervention scenario whereby the three modifiable vascular risk factors (hypertension, diabetes, and physical inactivity) would be removed simultaneously beginning in 2020. The prevalence rates are significantly reduced for men and women from age 75 years. In this scenario, life expectancy without dementia would increase by 3.4 years in men and 2.6 years in women, the result of men being more exposed to these three risk factors.
Other scenarios have estimated dementia prevalence with the disappearance of just one of these risk factors. For example, the disappearance of hypertension alone from 2020 could decrease dementia prevalence by 21% in men and 16% in women (because this risk factor is less common in women than in men) by 2040. This reduction would be associated with a decrease in the lifelong probability of dementia among men and women and a gain in life expectancy without dementia of 2 years in men and 1.4 years in women.
Among the three factors, hypertension has the largest impact on dementia burden in the French population, since this is, by far, the most prevalent (69% in men and 49% in women), while intervention targeting only diabetes or physical inactivity would lead to a reduction in dementia prevalence of only 4%-7%.
The authors reported no conflicts of interest.
This article was translated from Univadis France. A version appeared on Medscape.com.
FROM THE EUROPEAN JOURNAL OF EPIDEMIOLOGY
What would you do if ... ?
A few weeks ago we went to Phoenix Theater’s production of “A Chorus Line.” As with all their shows, it was excellent.
The penultimate scene is where one of the auditioning dancers suffers a career-ending injury, forcing the others to consider what they’d do if they couldn’t dance anymore, and facing the fact that sooner or later it will happen to all of them.

Let’s flip it onto us: What if tomorrow you couldn’t practice medicine anymore? To keep it from getting too depressing, let’s say it was because of paperwork. Your medical license expired and you weren’t warned in advance, and because of some legal glitch you can’t ever renew it now.
It’s a good question. I mean, I’ve wanted to be doctor as long as I can remember. (Actually I wanted to be Batman, then a scientist, then a doctor. Though I’d still rather be Batman. I’m even the same age as he was in The Dark Knight Returns.)
For all the paperwork and insurance fights and aggravations the job brings, I still love doing it. I get up on weekday mornings and feel good about going to the office. I generally feel good about what I’ve done to help people (or at least did my best to try) at the end of the day.
During my first year of residency (30 years ago) I remember telling my parents that, if even if I were phenomenally wealthy, I’d still do this job for free. Well, I’m not phenomenally wealthy, but I still enjoy the job.
If I couldn’t do it anymore, I’d be pretty sad. I mean, it’s not like I couldn’t find something else – consulting, research, writing, joining my daughter at her bakery – but I doubt I’d like it as much. Even if money weren’t an issue, there’s only so many jigsaw puzzles to do and books to read.
What about you?
Realistically, most of us won’t do this for the rest of our lives. Our expiration date may be longer than that of a professional dancer, but we still have one. Even if the mind stays sharp, sooner or later we all reach a point where it’s time to move on and leave the field in the capable hands of the next generation, just as a prior group of physicians left it to us. As the line in the song states, “the gift was ours to borrow.” And yes, I still see being able to do this for a living as a privilege and gift. But inevitably we all have to pass it on to the next ones, as will they someday.
But I’ll miss it. An oncologist I know was retired for a few months before he signed up for a nonmedical volunteer job at his old hospital, helping people find the rooms and departments they need to go to. He’s happy with it.
But when you do, you need to do your best to do it without regret. After all, you got to do something that many only dream of. Helping others and (I hope) having a job you enjoy.
I have dancers, and retired dancers, in my practice. The retired ones still miss it, but very few of them leave. They do volunteer teaching at community theaters, or just keep dancing on their own in groups of like-minded friends, as best they can. While medicine has made us one of the longer-lived mammals, it doesn’t stop the years.
When it’s time to walk away and point to tomorrow, do it without regrets, and remember that, even with the sweetness and the sorrow, it was what you did for love.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A few weeks ago we went to Phoenix Theater’s production of “A Chorus Line.” As with all their shows, it was excellent.
The penultimate scene is where one of the auditioning dancers suffers a career-ending injury, forcing the others to consider what they’d do if they couldn’t dance anymore, and facing the fact that sooner or later it will happen to all of them.
Let’s flip it onto us: What if tomorrow you couldn’t practice medicine anymore? To keep it from getting too depressing, let’s say it was because of paperwork. Your medical license expired and you weren’t warned in advance, and because of some legal glitch you can’t ever renew it now.
It’s a good question. I mean, I’ve wanted to be doctor as long as I can remember. (Actually I wanted to be Batman, then a scientist, then a doctor. Though I’d still rather be Batman. I’m even the same age as he was in The Dark Knight Returns.)
For all the paperwork and insurance fights and aggravations the job brings, I still love doing it. I get up on weekday mornings and feel good about going to the office. I generally feel good about what I’ve done to help people (or at least did my best to try) at the end of the day.
During my first year of residency (30 years ago) I remember telling my parents that, if even if I were phenomenally wealthy, I’d still do this job for free. Well, I’m not phenomenally wealthy, but I still enjoy the job.
If I couldn’t do it anymore, I’d be pretty sad. I mean, it’s not like I couldn’t find something else – consulting, research, writing, joining my daughter at her bakery – but I doubt I’d like it as much. Even if money weren’t an issue, there’s only so many jigsaw puzzles to do and books to read.
What about you?
Realistically, most of us won’t do this for the rest of our lives. Our expiration date may be longer than that of a professional dancer, but we still have one. Even if the mind stays sharp, sooner or later we all reach a point where it’s time to move on and leave the field in the capable hands of the next generation, just as a prior group of physicians left it to us. As the line in the song states, “the gift was ours to borrow.” And yes, I still see being able to do this for a living as a privilege and gift. But inevitably we all have to pass it on to the next ones, as will they someday.
But I’ll miss it. An oncologist I know was retired for a few months before he signed up for a nonmedical volunteer job at his old hospital, helping people find the rooms and departments they need to go to. He’s happy with it.
But when you do, you need to do your best to do it without regret. After all, you got to do something that many only dream of. Helping others and (I hope) having a job you enjoy.
I have dancers, and retired dancers, in my practice. The retired ones still miss it, but very few of them leave. They do volunteer teaching at community theaters, or just keep dancing on their own in groups of like-minded friends, as best they can. While medicine has made us one of the longer-lived mammals, it doesn’t stop the years.
When it’s time to walk away and point to tomorrow, do it without regrets, and remember that, even with the sweetness and the sorrow, it was what you did for love.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A few weeks ago we went to Phoenix Theater’s production of “A Chorus Line.” As with all their shows, it was excellent.
The penultimate scene is where one of the auditioning dancers suffers a career-ending injury, forcing the others to consider what they’d do if they couldn’t dance anymore, and facing the fact that sooner or later it will happen to all of them.
Let’s flip it onto us: What if tomorrow you couldn’t practice medicine anymore? To keep it from getting too depressing, let’s say it was because of paperwork. Your medical license expired and you weren’t warned in advance, and because of some legal glitch you can’t ever renew it now.
It’s a good question. I mean, I’ve wanted to be doctor as long as I can remember. (Actually I wanted to be Batman, then a scientist, then a doctor. Though I’d still rather be Batman. I’m even the same age as he was in The Dark Knight Returns.)
For all the paperwork and insurance fights and aggravations the job brings, I still love doing it. I get up on weekday mornings and feel good about going to the office. I generally feel good about what I’ve done to help people (or at least did my best to try) at the end of the day.
During my first year of residency (30 years ago) I remember telling my parents that, if even if I were phenomenally wealthy, I’d still do this job for free. Well, I’m not phenomenally wealthy, but I still enjoy the job.
If I couldn’t do it anymore, I’d be pretty sad. I mean, it’s not like I couldn’t find something else – consulting, research, writing, joining my daughter at her bakery – but I doubt I’d like it as much. Even if money weren’t an issue, there’s only so many jigsaw puzzles to do and books to read.
What about you?
Realistically, most of us won’t do this for the rest of our lives. Our expiration date may be longer than that of a professional dancer, but we still have one. Even if the mind stays sharp, sooner or later we all reach a point where it’s time to move on and leave the field in the capable hands of the next generation, just as a prior group of physicians left it to us. As the line in the song states, “the gift was ours to borrow.” And yes, I still see being able to do this for a living as a privilege and gift. But inevitably we all have to pass it on to the next ones, as will they someday.
But I’ll miss it. An oncologist I know was retired for a few months before he signed up for a nonmedical volunteer job at his old hospital, helping people find the rooms and departments they need to go to. He’s happy with it.
But when you do, you need to do your best to do it without regret. After all, you got to do something that many only dream of. Helping others and (I hope) having a job you enjoy.
I have dancers, and retired dancers, in my practice. The retired ones still miss it, but very few of them leave. They do volunteer teaching at community theaters, or just keep dancing on their own in groups of like-minded friends, as best they can. While medicine has made us one of the longer-lived mammals, it doesn’t stop the years.
When it’s time to walk away and point to tomorrow, do it without regrets, and remember that, even with the sweetness and the sorrow, it was what you did for love.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
New guidance on neurological complications of long COVID
also known as postacute sequelae of SARS-CoV-2 infection (PASC).
The new recommendations, which were published online in Physical Medicine & Rehabilitation, are the result of a collaboration between experts from a variety of medical specialties at 41 long COVID clinics across the United States.
Because physical medicine specialists treat individuals with disability and functional impairments, the AAPM&R was among the first organizations to initiate guidance for the assessment and treatment of long COVID and issued its first consensus statement that addressed long COVID–related fatigue in 2021.
Even though the number of COVID cases and hospitalizations has declined from the peak, long COVID continues to be a major public health issue, Steven R. Flanagan, MD, AAPM&R president-elect and Howard A. Rusk Professor of Rehabilitation Medicine at NYU Langone Health, New York, told reporters attending a press briefing.
“There is some evidence that some of the antivirals may actually help reduce the incidence but not everybody gets them,” said Dr. Flanagan. “In our own clinic here, we continue to see many, many people with problems associated with long COVID,” he added.
According to the consensus guidelines, about 80% of patients hospitalized with acute COVID-19 have neurological symptoms. But these symptoms are not just limited to people who had severe illness, said Leslie Rydberg, MD, coauthor of the neurology long COVID guidance statement.
“What we know is that many people with mild or moderate COVID infection end up with neurologic sequelae that last longer than 4 weeks,” said Dr. Rydberg, the Henry and Monika Betts Medical Student Education Chair and assistant residency program director at Shirley Ryan AbilityLab, Chicago.
Dr. Rydberg added that patients who have symptoms for longer than a month after the initial infection should be evaluated. Although the definition of what constitutes PASC is evolving, the guidance states that the literature indicates that it should be defined as the persistence of symptoms 4 weeks beyond the initial infection.
The most common neurological symptoms are headache, weakness, muscular pain, nerve pain, tremors, peripheral nerve issues, sleep issues, and cognitive effects, Dr. Rydberg told reporters.
She added that “identifying patients with progressive or ominous ‘red flag’ neurological symptoms is essential for emergent triaging.”
Among the red flags are sudden or progressive weakness or sudden or progressive sensory changes, because those could indicate an acute neurologic condition – either due to long COVID or other illnesses – such as a stroke or a problem with the spinal cord, Guillain-Barré syndrome, or myopathy.
While those signs and symptoms would likely be flagged by most clinicians, some of the emergent or urgent signs – such as upper motor neuron changes on physical exam – are more subtle, said Dr. Rydberg.
The new guidance spells out steps for initial evaluation, including identification of red flag symptoms, and also provides treatment recommendations.
Experts also recommend clinicians do the following:
- Treat underlying medical conditions such as pain, psychiatric, cardiovascular, respiratory, and other conditions that may be contributing to neurologic symptoms.
- Consider polypharmacy reduction, looking especially closely at medications with a known impact on neurologic symptoms.
- Urge patients to get regular physical activity, as tolerated, while avoiding overuse syndrome.
- Work with physical, occupational, and speech therapists to increase function and independence.
- Refer patients to counseling and community resources for risk factor modification.
The treatment recommendations are more in-depth for specific long-COVID conditions including headache, cranial neuropathies, sleep disturbances, and neuropathies.
The guidance includes a special statement on the importance of ensuring equitable access to care. Underserved, marginalized, and socioeconomically disadvantaged communities had notably higher rates of infection, hospitalization, and death with less access to rehabilitation services before the pandemic, said Monica Verduzco-Gutierrez, MD, chair of the department of rehabilitation medicine at Long School of Medicine, UT Health San Antonio, and a guideline coauthor.
“We know that these communities have been historically underserved, that there’s already access issues, and that they’re disproportionately impacted by the pandemic,” said Dr. Verduzco-Gutierrez. “This continues as patients develop PASC, or long COVID,” she said, adding that these individuals are still less likely to receive rehabilitation services. “This can lead to poorer outcomes and widened disparities.”
The AAPM&R PASC Multi-Disciplinary Collaborative has previously issued consensus guidance on fatigue, breathing discomfort and respiratory distress, cognitive symptoms, cardiovascular complications, pediatrics, and autonomic dysfunction, and will be publishing guidance on mental health soon.
The collaborative is also putting together a compilation of all the guidance – “a ‘greatest hits’ if you like,” said Dr. Verduzco-Gutierrez.
For clinicians who are unaccustomed to caring for patients with long COVID, the hope is that this new guidance will help them manage the condition, Dr. Rydberg said.
The guidance was written with the support of the AAPM&R. Dr. Verduzco-Gutierrez and two coauthors have disclosed grants, contracts, or honoraria from various funding sources, some paid to their institutions and some personal reimbursement for activities related to PASC and broader areas of research and expertise. However, none of the authors have any conflicts relative to the work on the guidance.
A version of this article originally appeared on Medscape.com.
also known as postacute sequelae of SARS-CoV-2 infection (PASC).
The new recommendations, which were published online in Physical Medicine & Rehabilitation, are the result of a collaboration between experts from a variety of medical specialties at 41 long COVID clinics across the United States.
Because physical medicine specialists treat individuals with disability and functional impairments, the AAPM&R was among the first organizations to initiate guidance for the assessment and treatment of long COVID and issued its first consensus statement that addressed long COVID–related fatigue in 2021.
Even though the number of COVID cases and hospitalizations has declined from the peak, long COVID continues to be a major public health issue, Steven R. Flanagan, MD, AAPM&R president-elect and Howard A. Rusk Professor of Rehabilitation Medicine at NYU Langone Health, New York, told reporters attending a press briefing.
“There is some evidence that some of the antivirals may actually help reduce the incidence but not everybody gets them,” said Dr. Flanagan. “In our own clinic here, we continue to see many, many people with problems associated with long COVID,” he added.
According to the consensus guidelines, about 80% of patients hospitalized with acute COVID-19 have neurological symptoms. But these symptoms are not just limited to people who had severe illness, said Leslie Rydberg, MD, coauthor of the neurology long COVID guidance statement.
“What we know is that many people with mild or moderate COVID infection end up with neurologic sequelae that last longer than 4 weeks,” said Dr. Rydberg, the Henry and Monika Betts Medical Student Education Chair and assistant residency program director at Shirley Ryan AbilityLab, Chicago.
Dr. Rydberg added that patients who have symptoms for longer than a month after the initial infection should be evaluated. Although the definition of what constitutes PASC is evolving, the guidance states that the literature indicates that it should be defined as the persistence of symptoms 4 weeks beyond the initial infection.
The most common neurological symptoms are headache, weakness, muscular pain, nerve pain, tremors, peripheral nerve issues, sleep issues, and cognitive effects, Dr. Rydberg told reporters.
She added that “identifying patients with progressive or ominous ‘red flag’ neurological symptoms is essential for emergent triaging.”
Among the red flags are sudden or progressive weakness or sudden or progressive sensory changes, because those could indicate an acute neurologic condition – either due to long COVID or other illnesses – such as a stroke or a problem with the spinal cord, Guillain-Barré syndrome, or myopathy.
While those signs and symptoms would likely be flagged by most clinicians, some of the emergent or urgent signs – such as upper motor neuron changes on physical exam – are more subtle, said Dr. Rydberg.
The new guidance spells out steps for initial evaluation, including identification of red flag symptoms, and also provides treatment recommendations.
Experts also recommend clinicians do the following:
- Treat underlying medical conditions such as pain, psychiatric, cardiovascular, respiratory, and other conditions that may be contributing to neurologic symptoms.
- Consider polypharmacy reduction, looking especially closely at medications with a known impact on neurologic symptoms.
- Urge patients to get regular physical activity, as tolerated, while avoiding overuse syndrome.
- Work with physical, occupational, and speech therapists to increase function and independence.
- Refer patients to counseling and community resources for risk factor modification.
The treatment recommendations are more in-depth for specific long-COVID conditions including headache, cranial neuropathies, sleep disturbances, and neuropathies.
The guidance includes a special statement on the importance of ensuring equitable access to care. Underserved, marginalized, and socioeconomically disadvantaged communities had notably higher rates of infection, hospitalization, and death with less access to rehabilitation services before the pandemic, said Monica Verduzco-Gutierrez, MD, chair of the department of rehabilitation medicine at Long School of Medicine, UT Health San Antonio, and a guideline coauthor.
“We know that these communities have been historically underserved, that there’s already access issues, and that they’re disproportionately impacted by the pandemic,” said Dr. Verduzco-Gutierrez. “This continues as patients develop PASC, or long COVID,” she said, adding that these individuals are still less likely to receive rehabilitation services. “This can lead to poorer outcomes and widened disparities.”
The AAPM&R PASC Multi-Disciplinary Collaborative has previously issued consensus guidance on fatigue, breathing discomfort and respiratory distress, cognitive symptoms, cardiovascular complications, pediatrics, and autonomic dysfunction, and will be publishing guidance on mental health soon.
The collaborative is also putting together a compilation of all the guidance – “a ‘greatest hits’ if you like,” said Dr. Verduzco-Gutierrez.
For clinicians who are unaccustomed to caring for patients with long COVID, the hope is that this new guidance will help them manage the condition, Dr. Rydberg said.
The guidance was written with the support of the AAPM&R. Dr. Verduzco-Gutierrez and two coauthors have disclosed grants, contracts, or honoraria from various funding sources, some paid to their institutions and some personal reimbursement for activities related to PASC and broader areas of research and expertise. However, none of the authors have any conflicts relative to the work on the guidance.
A version of this article originally appeared on Medscape.com.
also known as postacute sequelae of SARS-CoV-2 infection (PASC).
The new recommendations, which were published online in Physical Medicine & Rehabilitation, are the result of a collaboration between experts from a variety of medical specialties at 41 long COVID clinics across the United States.
Because physical medicine specialists treat individuals with disability and functional impairments, the AAPM&R was among the first organizations to initiate guidance for the assessment and treatment of long COVID and issued its first consensus statement that addressed long COVID–related fatigue in 2021.
Even though the number of COVID cases and hospitalizations has declined from the peak, long COVID continues to be a major public health issue, Steven R. Flanagan, MD, AAPM&R president-elect and Howard A. Rusk Professor of Rehabilitation Medicine at NYU Langone Health, New York, told reporters attending a press briefing.
“There is some evidence that some of the antivirals may actually help reduce the incidence but not everybody gets them,” said Dr. Flanagan. “In our own clinic here, we continue to see many, many people with problems associated with long COVID,” he added.
According to the consensus guidelines, about 80% of patients hospitalized with acute COVID-19 have neurological symptoms. But these symptoms are not just limited to people who had severe illness, said Leslie Rydberg, MD, coauthor of the neurology long COVID guidance statement.
“What we know is that many people with mild or moderate COVID infection end up with neurologic sequelae that last longer than 4 weeks,” said Dr. Rydberg, the Henry and Monika Betts Medical Student Education Chair and assistant residency program director at Shirley Ryan AbilityLab, Chicago.
Dr. Rydberg added that patients who have symptoms for longer than a month after the initial infection should be evaluated. Although the definition of what constitutes PASC is evolving, the guidance states that the literature indicates that it should be defined as the persistence of symptoms 4 weeks beyond the initial infection.
The most common neurological symptoms are headache, weakness, muscular pain, nerve pain, tremors, peripheral nerve issues, sleep issues, and cognitive effects, Dr. Rydberg told reporters.
She added that “identifying patients with progressive or ominous ‘red flag’ neurological symptoms is essential for emergent triaging.”
Among the red flags are sudden or progressive weakness or sudden or progressive sensory changes, because those could indicate an acute neurologic condition – either due to long COVID or other illnesses – such as a stroke or a problem with the spinal cord, Guillain-Barré syndrome, or myopathy.
While those signs and symptoms would likely be flagged by most clinicians, some of the emergent or urgent signs – such as upper motor neuron changes on physical exam – are more subtle, said Dr. Rydberg.
The new guidance spells out steps for initial evaluation, including identification of red flag symptoms, and also provides treatment recommendations.
Experts also recommend clinicians do the following:
- Treat underlying medical conditions such as pain, psychiatric, cardiovascular, respiratory, and other conditions that may be contributing to neurologic symptoms.
- Consider polypharmacy reduction, looking especially closely at medications with a known impact on neurologic symptoms.
- Urge patients to get regular physical activity, as tolerated, while avoiding overuse syndrome.
- Work with physical, occupational, and speech therapists to increase function and independence.
- Refer patients to counseling and community resources for risk factor modification.
The treatment recommendations are more in-depth for specific long-COVID conditions including headache, cranial neuropathies, sleep disturbances, and neuropathies.
The guidance includes a special statement on the importance of ensuring equitable access to care. Underserved, marginalized, and socioeconomically disadvantaged communities had notably higher rates of infection, hospitalization, and death with less access to rehabilitation services before the pandemic, said Monica Verduzco-Gutierrez, MD, chair of the department of rehabilitation medicine at Long School of Medicine, UT Health San Antonio, and a guideline coauthor.
“We know that these communities have been historically underserved, that there’s already access issues, and that they’re disproportionately impacted by the pandemic,” said Dr. Verduzco-Gutierrez. “This continues as patients develop PASC, or long COVID,” she said, adding that these individuals are still less likely to receive rehabilitation services. “This can lead to poorer outcomes and widened disparities.”
The AAPM&R PASC Multi-Disciplinary Collaborative has previously issued consensus guidance on fatigue, breathing discomfort and respiratory distress, cognitive symptoms, cardiovascular complications, pediatrics, and autonomic dysfunction, and will be publishing guidance on mental health soon.
The collaborative is also putting together a compilation of all the guidance – “a ‘greatest hits’ if you like,” said Dr. Verduzco-Gutierrez.
For clinicians who are unaccustomed to caring for patients with long COVID, the hope is that this new guidance will help them manage the condition, Dr. Rydberg said.
The guidance was written with the support of the AAPM&R. Dr. Verduzco-Gutierrez and two coauthors have disclosed grants, contracts, or honoraria from various funding sources, some paid to their institutions and some personal reimbursement for activities related to PASC and broader areas of research and expertise. However, none of the authors have any conflicts relative to the work on the guidance.
A version of this article originally appeared on Medscape.com.
FROM PHYSICIAN MEDICINE & REHABILITATION
‘Robust evidence’ that exercise cuts Parkinson’s risk in women
Investigators found that among almost 99,000 women participating in the ongoing E3N study, those who exercised the most frequently had up to a 25% lower risk for PD than their less-active counterparts.
The results highlight the importance of exercising early in mid-life to prevent PD later on, study investigator Alexis Elbaz, MD, PhD, research director, French Institute of Health and Medical Research (Inserm), Paris, said in an interview.
This is especially critical since there is no cure nor disease-modifying treatments. The medications that are available are aimed at symptom reduction.
“Finding ways to prevent or delay the onset of Parkinson’s is really important, and physical activity seems to be one of the possible strategies to reduce the risk,” Dr. Elbaz said.
The study was published online in Neurology.
Direct protective effect?
Results from previous research examining the relationship physical activity and PD has been inconsistent. One meta-analysis showed a statistically significant association among men but a nonsignificant link in women.
The investigators noted that some of the findings from previous studies may have been affected by reverse causation. As nonmotor symptoms such as constipation and subtle motor signs such as tremor and balance issues can present years before a PD diagnosis, patients may reduce their physical activity because of such symptoms.
To address this potential confounder, the researchers used “lag” analyses, where data on physical activity levels in the years close to a PD diagnosis are omitted.
The study relied on data from the E3N, an ongoing cohort study of 98,995 women, born between 1925 and 1950 and recruited in 1990, who were affiliated with a French national health insurance plan that primarily covers teachers. Participants completed a questionnaire on lifestyle and medical history at baseline and follow-up questionnaires every 2-3 years.
In six of the questionnaires, participants provided details about various recreational, sports, and household activities – for example, walking, climbing stairs, gardening, and cleaning. The authors attributed metabolic equivalent of task (MET) values to each activity and multiplied METs by their frequency and duration to obtain a physical activity score.
Definite and probable PD cases were determined through self-reported physician diagnoses, anti-parkinsonian drug claims, and medical records, with diagnoses verified by an expert panel.
Researchers investigated the relationship between physical activity and PD onset in a nested-case control study that included 25,075 women (1,196 PD cases and 23,879 controls) with a mean age of 71.9 years. They found physical activity was significantly lower in cases than in controls throughout follow-up.
The difference between cases and controls began to increase at 10 years before diagnosis (P-interaction = .003). “When we looked at the trajectories of physical activity in PD patients and in controls, we saw that in the 10 years before the diagnosis, physical activity declined at a steeper rate in controls. We think this is because those subtle prodromal symptoms cause people to exercise less,” said Dr. Elbaz.
In the main analysis, which had a 10-year lag, 1,074 women developed incident PD during a mean follow-up of 17.2 years. Those in the highest quartile of physical activity had a 25% lower risk for PD vs. those in the lowest quartile (adjusted hazard ratio [HR], 0.75, 95% confidence interval [CI], 0.63-0.89).
The risk for PD decreased with increasing levels of physical activity in a linear fashion, noted Dr. Elbaz. “So doing even a little bit of physical activity is better than doing nothing at all.”
Analyses that included 15-year and 20-year lag times had similar findings.
Sensitivity analyses that adjusted for the Mediterranean diet and caffeine and dairy intake also yielded comparable results. This was also true for analyses that adjusted for comorbidities such as body mass index, hypertension, hypercholesterolemia, diabetes, and cardiovascular disease, all of which can affect PD risk.
“This gives weight to the idea that diabetes or cardiovascular diseases do not explain the relationship between physical activity and PD, which means the most likely hypothesis is that physical activity has a direct protective effect on the brain,” said Dr. Elbaz.
Studies have shown that physical activity affects brain plasticity and can reduce oxidative stress in the brain – a key mechanism involved in PD, he added.
Physical activity is a low-risk, inexpensive, and accessible intervention. But the study was not designed to determine the types of physical activity that are most protective against PD.
The study’s main limitation is that it used self-reported physical activity rather than objective measures such as accelerometers. In addition, the participants were not necessarily representative of the general population.
Robust evidence
In an accompanying editorial, Lana M. Chahine, MD, associate professor in the department of neurology at the University of Pittsburgh, and Sirwan K. L. Darweesh, MD, PhD, Radboud University Medical Center, Donders Institute for Brain, Cognition and Behaviour, Center of Expertise for Parkinson and Movement Disorders, Nijmegen, the Netherlands, said the study “provides robust evidence” that physical activity reduces risk for PD in women.
“These results show that the field is moving in the right direction and provide a clear rationale for exercise trials to prevent or delay the onset of manifest PD in at-risk individuals” they wrote.
The study highlights “gaps” in knowledge that merit closer attention and that “further insight is warranted on how much the effects on PD vary by type, intensity, frequency, and duration of physical activity,” the editorialists noted.
Another gap is how the accuracy of assessment of physical activity can be improved beyond self-report. “Wearable sensor technology now offers the potential to assess physical activity remotely and objectively in prevention trials,” they added.
Other areas that need exploring relate to mechanisms by which physical activity reduces PD risk, and to what extent effects of physical activity vary between individuals, Dr. Chahine and Dr. Darweesh noted.
Commenting for this article, Michael S. Okun, MD, executive director of the Fixel Institute for Neurological Diseases at University of Florida Health, and medical adviser for the Parkinson’s Foundation, said the findings are “significant and important.”
Based on only a handful of previous studies, it was assumed that physical activity was associated with reduced Parkinson’s diagnosis only in men, said Dr. Okun. “The current dataset was larger and included longer-term outcomes, and it informs the field that exercise may be important for reducing the risk of Parkinson’s disease in men as well as in women.”
The investigators, the editorialists, and Dr. Okun reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators found that among almost 99,000 women participating in the ongoing E3N study, those who exercised the most frequently had up to a 25% lower risk for PD than their less-active counterparts.
The results highlight the importance of exercising early in mid-life to prevent PD later on, study investigator Alexis Elbaz, MD, PhD, research director, French Institute of Health and Medical Research (Inserm), Paris, said in an interview.
This is especially critical since there is no cure nor disease-modifying treatments. The medications that are available are aimed at symptom reduction.
“Finding ways to prevent or delay the onset of Parkinson’s is really important, and physical activity seems to be one of the possible strategies to reduce the risk,” Dr. Elbaz said.
The study was published online in Neurology.
Direct protective effect?
Results from previous research examining the relationship physical activity and PD has been inconsistent. One meta-analysis showed a statistically significant association among men but a nonsignificant link in women.
The investigators noted that some of the findings from previous studies may have been affected by reverse causation. As nonmotor symptoms such as constipation and subtle motor signs such as tremor and balance issues can present years before a PD diagnosis, patients may reduce their physical activity because of such symptoms.
To address this potential confounder, the researchers used “lag” analyses, where data on physical activity levels in the years close to a PD diagnosis are omitted.
The study relied on data from the E3N, an ongoing cohort study of 98,995 women, born between 1925 and 1950 and recruited in 1990, who were affiliated with a French national health insurance plan that primarily covers teachers. Participants completed a questionnaire on lifestyle and medical history at baseline and follow-up questionnaires every 2-3 years.
In six of the questionnaires, participants provided details about various recreational, sports, and household activities – for example, walking, climbing stairs, gardening, and cleaning. The authors attributed metabolic equivalent of task (MET) values to each activity and multiplied METs by their frequency and duration to obtain a physical activity score.
Definite and probable PD cases were determined through self-reported physician diagnoses, anti-parkinsonian drug claims, and medical records, with diagnoses verified by an expert panel.
Researchers investigated the relationship between physical activity and PD onset in a nested-case control study that included 25,075 women (1,196 PD cases and 23,879 controls) with a mean age of 71.9 years. They found physical activity was significantly lower in cases than in controls throughout follow-up.
The difference between cases and controls began to increase at 10 years before diagnosis (P-interaction = .003). “When we looked at the trajectories of physical activity in PD patients and in controls, we saw that in the 10 years before the diagnosis, physical activity declined at a steeper rate in controls. We think this is because those subtle prodromal symptoms cause people to exercise less,” said Dr. Elbaz.
In the main analysis, which had a 10-year lag, 1,074 women developed incident PD during a mean follow-up of 17.2 years. Those in the highest quartile of physical activity had a 25% lower risk for PD vs. those in the lowest quartile (adjusted hazard ratio [HR], 0.75, 95% confidence interval [CI], 0.63-0.89).
The risk for PD decreased with increasing levels of physical activity in a linear fashion, noted Dr. Elbaz. “So doing even a little bit of physical activity is better than doing nothing at all.”
Analyses that included 15-year and 20-year lag times had similar findings.
Sensitivity analyses that adjusted for the Mediterranean diet and caffeine and dairy intake also yielded comparable results. This was also true for analyses that adjusted for comorbidities such as body mass index, hypertension, hypercholesterolemia, diabetes, and cardiovascular disease, all of which can affect PD risk.
“This gives weight to the idea that diabetes or cardiovascular diseases do not explain the relationship between physical activity and PD, which means the most likely hypothesis is that physical activity has a direct protective effect on the brain,” said Dr. Elbaz.
Studies have shown that physical activity affects brain plasticity and can reduce oxidative stress in the brain – a key mechanism involved in PD, he added.
Physical activity is a low-risk, inexpensive, and accessible intervention. But the study was not designed to determine the types of physical activity that are most protective against PD.
The study’s main limitation is that it used self-reported physical activity rather than objective measures such as accelerometers. In addition, the participants were not necessarily representative of the general population.
Robust evidence
In an accompanying editorial, Lana M. Chahine, MD, associate professor in the department of neurology at the University of Pittsburgh, and Sirwan K. L. Darweesh, MD, PhD, Radboud University Medical Center, Donders Institute for Brain, Cognition and Behaviour, Center of Expertise for Parkinson and Movement Disorders, Nijmegen, the Netherlands, said the study “provides robust evidence” that physical activity reduces risk for PD in women.
“These results show that the field is moving in the right direction and provide a clear rationale for exercise trials to prevent or delay the onset of manifest PD in at-risk individuals” they wrote.
The study highlights “gaps” in knowledge that merit closer attention and that “further insight is warranted on how much the effects on PD vary by type, intensity, frequency, and duration of physical activity,” the editorialists noted.
Another gap is how the accuracy of assessment of physical activity can be improved beyond self-report. “Wearable sensor technology now offers the potential to assess physical activity remotely and objectively in prevention trials,” they added.
Other areas that need exploring relate to mechanisms by which physical activity reduces PD risk, and to what extent effects of physical activity vary between individuals, Dr. Chahine and Dr. Darweesh noted.
Commenting for this article, Michael S. Okun, MD, executive director of the Fixel Institute for Neurological Diseases at University of Florida Health, and medical adviser for the Parkinson’s Foundation, said the findings are “significant and important.”
Based on only a handful of previous studies, it was assumed that physical activity was associated with reduced Parkinson’s diagnosis only in men, said Dr. Okun. “The current dataset was larger and included longer-term outcomes, and it informs the field that exercise may be important for reducing the risk of Parkinson’s disease in men as well as in women.”
The investigators, the editorialists, and Dr. Okun reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators found that among almost 99,000 women participating in the ongoing E3N study, those who exercised the most frequently had up to a 25% lower risk for PD than their less-active counterparts.
The results highlight the importance of exercising early in mid-life to prevent PD later on, study investigator Alexis Elbaz, MD, PhD, research director, French Institute of Health and Medical Research (Inserm), Paris, said in an interview.
This is especially critical since there is no cure nor disease-modifying treatments. The medications that are available are aimed at symptom reduction.
“Finding ways to prevent or delay the onset of Parkinson’s is really important, and physical activity seems to be one of the possible strategies to reduce the risk,” Dr. Elbaz said.
The study was published online in Neurology.
Direct protective effect?
Results from previous research examining the relationship physical activity and PD has been inconsistent. One meta-analysis showed a statistically significant association among men but a nonsignificant link in women.
The investigators noted that some of the findings from previous studies may have been affected by reverse causation. As nonmotor symptoms such as constipation and subtle motor signs such as tremor and balance issues can present years before a PD diagnosis, patients may reduce their physical activity because of such symptoms.
To address this potential confounder, the researchers used “lag” analyses, where data on physical activity levels in the years close to a PD diagnosis are omitted.
The study relied on data from the E3N, an ongoing cohort study of 98,995 women, born between 1925 and 1950 and recruited in 1990, who were affiliated with a French national health insurance plan that primarily covers teachers. Participants completed a questionnaire on lifestyle and medical history at baseline and follow-up questionnaires every 2-3 years.
In six of the questionnaires, participants provided details about various recreational, sports, and household activities – for example, walking, climbing stairs, gardening, and cleaning. The authors attributed metabolic equivalent of task (MET) values to each activity and multiplied METs by their frequency and duration to obtain a physical activity score.
Definite and probable PD cases were determined through self-reported physician diagnoses, anti-parkinsonian drug claims, and medical records, with diagnoses verified by an expert panel.
Researchers investigated the relationship between physical activity and PD onset in a nested-case control study that included 25,075 women (1,196 PD cases and 23,879 controls) with a mean age of 71.9 years. They found physical activity was significantly lower in cases than in controls throughout follow-up.
The difference between cases and controls began to increase at 10 years before diagnosis (P-interaction = .003). “When we looked at the trajectories of physical activity in PD patients and in controls, we saw that in the 10 years before the diagnosis, physical activity declined at a steeper rate in controls. We think this is because those subtle prodromal symptoms cause people to exercise less,” said Dr. Elbaz.
In the main analysis, which had a 10-year lag, 1,074 women developed incident PD during a mean follow-up of 17.2 years. Those in the highest quartile of physical activity had a 25% lower risk for PD vs. those in the lowest quartile (adjusted hazard ratio [HR], 0.75, 95% confidence interval [CI], 0.63-0.89).
The risk for PD decreased with increasing levels of physical activity in a linear fashion, noted Dr. Elbaz. “So doing even a little bit of physical activity is better than doing nothing at all.”
Analyses that included 15-year and 20-year lag times had similar findings.
Sensitivity analyses that adjusted for the Mediterranean diet and caffeine and dairy intake also yielded comparable results. This was also true for analyses that adjusted for comorbidities such as body mass index, hypertension, hypercholesterolemia, diabetes, and cardiovascular disease, all of which can affect PD risk.
“This gives weight to the idea that diabetes or cardiovascular diseases do not explain the relationship between physical activity and PD, which means the most likely hypothesis is that physical activity has a direct protective effect on the brain,” said Dr. Elbaz.
Studies have shown that physical activity affects brain plasticity and can reduce oxidative stress in the brain – a key mechanism involved in PD, he added.
Physical activity is a low-risk, inexpensive, and accessible intervention. But the study was not designed to determine the types of physical activity that are most protective against PD.
The study’s main limitation is that it used self-reported physical activity rather than objective measures such as accelerometers. In addition, the participants were not necessarily representative of the general population.
Robust evidence
In an accompanying editorial, Lana M. Chahine, MD, associate professor in the department of neurology at the University of Pittsburgh, and Sirwan K. L. Darweesh, MD, PhD, Radboud University Medical Center, Donders Institute for Brain, Cognition and Behaviour, Center of Expertise for Parkinson and Movement Disorders, Nijmegen, the Netherlands, said the study “provides robust evidence” that physical activity reduces risk for PD in women.
“These results show that the field is moving in the right direction and provide a clear rationale for exercise trials to prevent or delay the onset of manifest PD in at-risk individuals” they wrote.
The study highlights “gaps” in knowledge that merit closer attention and that “further insight is warranted on how much the effects on PD vary by type, intensity, frequency, and duration of physical activity,” the editorialists noted.
Another gap is how the accuracy of assessment of physical activity can be improved beyond self-report. “Wearable sensor technology now offers the potential to assess physical activity remotely and objectively in prevention trials,” they added.
Other areas that need exploring relate to mechanisms by which physical activity reduces PD risk, and to what extent effects of physical activity vary between individuals, Dr. Chahine and Dr. Darweesh noted.
Commenting for this article, Michael S. Okun, MD, executive director of the Fixel Institute for Neurological Diseases at University of Florida Health, and medical adviser for the Parkinson’s Foundation, said the findings are “significant and important.”
Based on only a handful of previous studies, it was assumed that physical activity was associated with reduced Parkinson’s diagnosis only in men, said Dr. Okun. “The current dataset was larger and included longer-term outcomes, and it informs the field that exercise may be important for reducing the risk of Parkinson’s disease in men as well as in women.”
The investigators, the editorialists, and Dr. Okun reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM NEUROLOGY
Internet use a modifiable dementia risk factor in older adults?
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN GERIATRICS SOCIETY
What to expect in the new concussion guidelines
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
The antimicrobial peptide that even Pharma can love
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.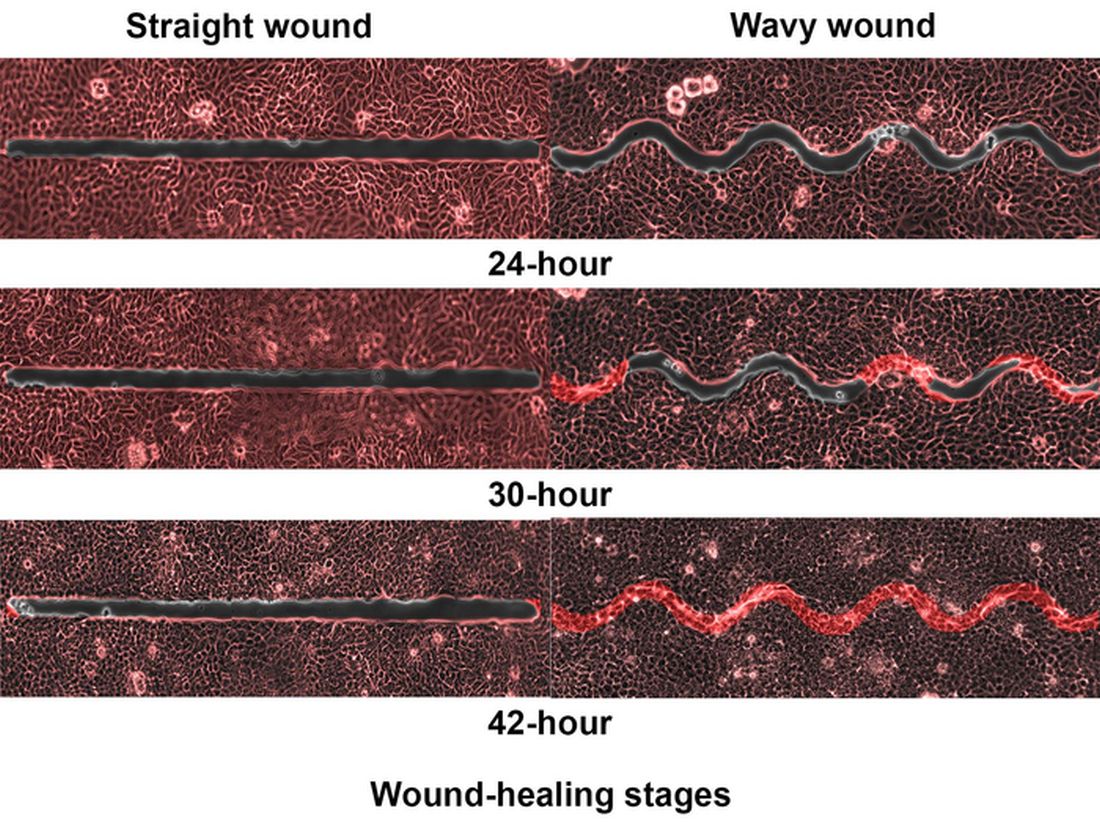
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
AHA urges action against racial inequities in stroke care
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
FROM STROKE
Deep sleep may mitigate the impact of Alzheimer’s pathology
Investigators found that deep sleep, also known as non-REM (NREM) slow-wave sleep, can protect memory function in cognitively normal adults with a high beta-amyloid burden.
“Think of deep sleep almost like a life raft that keeps memory afloat, rather than memory getting dragged down by the weight of Alzheimer’s disease pathology,” senior investigator Matthew Walker, PhD, professor of neuroscience and psychology, University of California, Berkeley, said in a news release.
The study was published online in BMC Medicine.
Resilience factor
Studying resilience to existing brain pathology is “an exciting new research direction,” lead author Zsófia Zavecz, PhD, with the Center for Human Sleep Science at the University of California, Berkeley, said in an interview.
“That is, what factors explain the individual differences in cognitive function despite the same level of brain pathology, and how do some people with significant pathology have largely preserved memory?” she added.
The study included 62 cognitively normal older adults from the Berkeley Aging Cohort Study.
Sleep EEG recordings were obtained over 2 nights in a sleep lab and PET scans were used to quantify beta-amyloid. Half of the participants had high beta-amyloid burden and half were beta-amyloid negative.
After the sleep studies, all participants completed a memory task involving matching names to faces.
The results suggest that deep NREM slow-wave sleep significantly moderates the effect of beta-amyloid status on memory function.
Specifically, NREM slow-wave activity selectively supported superior memory function in adults with high beta-amyloid burden, who are most in need of cognitive reserve (B = 2.694, P = .019), the researchers report.
In contrast, adults without significant beta-amyloid pathological burden – and thus without the same need for cognitive reserve – did not similarly benefit from NREM slow-wave activity (B = –0.115, P = .876).
The findings remained significant after adjusting for age, sex, body mass index, gray matter atrophy, and previously identified cognitive reserve factors, such as education and physical activity.
Dr. Zavecz said there are several potential reasons why deep sleep may support cognitive reserve.
One is that during deep sleep specifically, memories are replayed in the brain, and this results in a “neural reorganization” that helps stabilize the memory and make it more permanent.
“Other explanations include deep sleep’s role in maintaining homeostasis in the brain’s capacity to form new neural connections and providing an optimal brain state for the clearance of toxins interfering with healthy brain functioning,” she noted.
“The extent to which sleep could offer a protective buffer against severe cognitive impairment remains to be tested. However, this study is the first step in hopefully a series of new research that will investigate sleep as a cognitive reserve factor,” said Dr. Zavecz.
Encouraging data
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said although the study sample is small, the results are “encouraging because sleep is a modifiable factor and can therefore be targeted.”
“More work is needed in a larger population before we can fully leverage this stage of sleep to reduce the risk of developing cognitive decline,” Dr. Griffin said.
Also weighing in on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the study is “exciting on two fronts – we may have an additional marker for the development of Alzheimer’s disease to predict risk and track disease, but also targets for early intervention with sleep architecture–enhancing therapies, be they drug, device, or digital.”
“For the sake of our brain health, we all must get very familiar with the concept of cognitive or brain reserve,” said Dr. Lakhan, who was not involved in the study.
“Brain reserve refers to our ability to buttress against the threat of dementia and classically it’s been associated with ongoing brain stimulation (i.e., higher education, cognitively demanding job),” he noted.
“This line of research now opens the door that optimal sleep health – especially deep NREM slow wave sleep – correlates with greater brain reserve against Alzheimer’s disease,” Dr. Lakhan said.
The study was supported by the National Institutes of Health and the University of California, Berkeley. Dr. Walker serves as an advisor to and has equity interest in Bryte, Shuni, Oura, and StimScience. Dr. Zavecz and Dr. Lakhan report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators found that deep sleep, also known as non-REM (NREM) slow-wave sleep, can protect memory function in cognitively normal adults with a high beta-amyloid burden.
“Think of deep sleep almost like a life raft that keeps memory afloat, rather than memory getting dragged down by the weight of Alzheimer’s disease pathology,” senior investigator Matthew Walker, PhD, professor of neuroscience and psychology, University of California, Berkeley, said in a news release.
The study was published online in BMC Medicine.
Resilience factor
Studying resilience to existing brain pathology is “an exciting new research direction,” lead author Zsófia Zavecz, PhD, with the Center for Human Sleep Science at the University of California, Berkeley, said in an interview.
“That is, what factors explain the individual differences in cognitive function despite the same level of brain pathology, and how do some people with significant pathology have largely preserved memory?” she added.
The study included 62 cognitively normal older adults from the Berkeley Aging Cohort Study.
Sleep EEG recordings were obtained over 2 nights in a sleep lab and PET scans were used to quantify beta-amyloid. Half of the participants had high beta-amyloid burden and half were beta-amyloid negative.
After the sleep studies, all participants completed a memory task involving matching names to faces.
The results suggest that deep NREM slow-wave sleep significantly moderates the effect of beta-amyloid status on memory function.
Specifically, NREM slow-wave activity selectively supported superior memory function in adults with high beta-amyloid burden, who are most in need of cognitive reserve (B = 2.694, P = .019), the researchers report.
In contrast, adults without significant beta-amyloid pathological burden – and thus without the same need for cognitive reserve – did not similarly benefit from NREM slow-wave activity (B = –0.115, P = .876).
The findings remained significant after adjusting for age, sex, body mass index, gray matter atrophy, and previously identified cognitive reserve factors, such as education and physical activity.
Dr. Zavecz said there are several potential reasons why deep sleep may support cognitive reserve.
One is that during deep sleep specifically, memories are replayed in the brain, and this results in a “neural reorganization” that helps stabilize the memory and make it more permanent.
“Other explanations include deep sleep’s role in maintaining homeostasis in the brain’s capacity to form new neural connections and providing an optimal brain state for the clearance of toxins interfering with healthy brain functioning,” she noted.
“The extent to which sleep could offer a protective buffer against severe cognitive impairment remains to be tested. However, this study is the first step in hopefully a series of new research that will investigate sleep as a cognitive reserve factor,” said Dr. Zavecz.
Encouraging data
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said although the study sample is small, the results are “encouraging because sleep is a modifiable factor and can therefore be targeted.”
“More work is needed in a larger population before we can fully leverage this stage of sleep to reduce the risk of developing cognitive decline,” Dr. Griffin said.
Also weighing in on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the study is “exciting on two fronts – we may have an additional marker for the development of Alzheimer’s disease to predict risk and track disease, but also targets for early intervention with sleep architecture–enhancing therapies, be they drug, device, or digital.”
“For the sake of our brain health, we all must get very familiar with the concept of cognitive or brain reserve,” said Dr. Lakhan, who was not involved in the study.
“Brain reserve refers to our ability to buttress against the threat of dementia and classically it’s been associated with ongoing brain stimulation (i.e., higher education, cognitively demanding job),” he noted.
“This line of research now opens the door that optimal sleep health – especially deep NREM slow wave sleep – correlates with greater brain reserve against Alzheimer’s disease,” Dr. Lakhan said.
The study was supported by the National Institutes of Health and the University of California, Berkeley. Dr. Walker serves as an advisor to and has equity interest in Bryte, Shuni, Oura, and StimScience. Dr. Zavecz and Dr. Lakhan report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators found that deep sleep, also known as non-REM (NREM) slow-wave sleep, can protect memory function in cognitively normal adults with a high beta-amyloid burden.
“Think of deep sleep almost like a life raft that keeps memory afloat, rather than memory getting dragged down by the weight of Alzheimer’s disease pathology,” senior investigator Matthew Walker, PhD, professor of neuroscience and psychology, University of California, Berkeley, said in a news release.
The study was published online in BMC Medicine.
Resilience factor
Studying resilience to existing brain pathology is “an exciting new research direction,” lead author Zsófia Zavecz, PhD, with the Center for Human Sleep Science at the University of California, Berkeley, said in an interview.
“That is, what factors explain the individual differences in cognitive function despite the same level of brain pathology, and how do some people with significant pathology have largely preserved memory?” she added.
The study included 62 cognitively normal older adults from the Berkeley Aging Cohort Study.
Sleep EEG recordings were obtained over 2 nights in a sleep lab and PET scans were used to quantify beta-amyloid. Half of the participants had high beta-amyloid burden and half were beta-amyloid negative.
After the sleep studies, all participants completed a memory task involving matching names to faces.
The results suggest that deep NREM slow-wave sleep significantly moderates the effect of beta-amyloid status on memory function.
Specifically, NREM slow-wave activity selectively supported superior memory function in adults with high beta-amyloid burden, who are most in need of cognitive reserve (B = 2.694, P = .019), the researchers report.
In contrast, adults without significant beta-amyloid pathological burden – and thus without the same need for cognitive reserve – did not similarly benefit from NREM slow-wave activity (B = –0.115, P = .876).
The findings remained significant after adjusting for age, sex, body mass index, gray matter atrophy, and previously identified cognitive reserve factors, such as education and physical activity.
Dr. Zavecz said there are several potential reasons why deep sleep may support cognitive reserve.
One is that during deep sleep specifically, memories are replayed in the brain, and this results in a “neural reorganization” that helps stabilize the memory and make it more permanent.
“Other explanations include deep sleep’s role in maintaining homeostasis in the brain’s capacity to form new neural connections and providing an optimal brain state for the clearance of toxins interfering with healthy brain functioning,” she noted.
“The extent to which sleep could offer a protective buffer against severe cognitive impairment remains to be tested. However, this study is the first step in hopefully a series of new research that will investigate sleep as a cognitive reserve factor,” said Dr. Zavecz.
Encouraging data
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said although the study sample is small, the results are “encouraging because sleep is a modifiable factor and can therefore be targeted.”
“More work is needed in a larger population before we can fully leverage this stage of sleep to reduce the risk of developing cognitive decline,” Dr. Griffin said.
Also weighing in on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the study is “exciting on two fronts – we may have an additional marker for the development of Alzheimer’s disease to predict risk and track disease, but also targets for early intervention with sleep architecture–enhancing therapies, be they drug, device, or digital.”
“For the sake of our brain health, we all must get very familiar with the concept of cognitive or brain reserve,” said Dr. Lakhan, who was not involved in the study.
“Brain reserve refers to our ability to buttress against the threat of dementia and classically it’s been associated with ongoing brain stimulation (i.e., higher education, cognitively demanding job),” he noted.
“This line of research now opens the door that optimal sleep health – especially deep NREM slow wave sleep – correlates with greater brain reserve against Alzheimer’s disease,” Dr. Lakhan said.
The study was supported by the National Institutes of Health and the University of California, Berkeley. Dr. Walker serves as an advisor to and has equity interest in Bryte, Shuni, Oura, and StimScience. Dr. Zavecz and Dr. Lakhan report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM BMC MEDICINE