User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
Cardiopathy no basis for choosing anticoagulation in ESUS
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.

The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.
The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
MUNICH, GERMANY – suggest findings from the ARCADIA trial.
The trial, which was halted early, randomized more than 1,000 ESUS patients with atrial cardiomyopathy to apixaban or placebo. Results showed that apixaban did not improve rates of recurrent stroke of any kind nor safety outcomes such as major hemorrhage and all-cause mortality.
The results were presented at the annual meeting of the European Stroke Organisation Conference.
“We found no benefit of apixaban over aspirin in patients with ESUS who had evidence of atrial cardiopathy, at least based on the criteria in our trial,” said study presenter Hooman Kamel, MD, MS, vice chair for research and chief of neurocritical care in the department of neurology, Weill Cornell Medicine, New York.
“It could be that this concept of thrombogenic atrial cardiopathy really isn’t present unless there is also atrial fibrillation,” he continued, suggesting alternatively that results may be caused by the “incorrect choice of atrial cardiopathy biomarkers or thresholds.”
“We chose these because they were clinically scalable and usable in a multicenter design,” Dr. Kamel explained, adding that there are a number of different proposed biomarkers that could be used in a future study.
The team will now perform secondary analyses over the coming months to “try to help sort out some of these potential explanations.”
Dr. Kamel concluded, however, that, “as of now, no strategy of anticoagulation has been found to be better than antiplatelet therapy for secondary stroke prevention after ESUS.”
Similar results
Approached for comment, session cochair Robin Lemmens, MD, PhD, a neurologist in the department of neurosciences, UZ Leuven (Belgium), noted that this is the third ESUS trial, after the NAVIGATE and RE-SPECT trials, and they have all showed “similar results.”
He said, however, that there “could be various reasons for that, and it’s good that they mentioned looking into the subgroups,” as has been done for those other studies.
“Most of these trials were initiated under the concept that most of these patients would have had underlying atrial fibrillation, and then of course there would have been a benefit for anticoagulation.”
“It turns out that that’s not the case,” Dr. Lemmens said, “probably because there’s a lot of heterogeneity in these patients,” with different reasons for developing stroke, “not just only potentially underlying atrial fibrillation.”
Session cochair Arthur Liesz, MD, PhD, Institute for Stroke and Dementia Research, University Hospital, LMU Munich, added that it is important to consider the definition of atrial cardiopathy in this context.
If this was limited only to structural cardiopathy, then this “was a rather small subpopulation in this study,” he said in an interview.
Dr. Liesz said that it could instead have been conducted with “more stringent cutoffs,” and could have considered blood biomarkers, “which then would have delivered more overlap with structural cardiopathy,” and allowed those patients to be analyzed separately.
Heterogeneous etiologies?
Dr. Kamel began by noting that the failure of NAVIGATE and RESPECT to show a benefit from anticoagulation in the prevention of recurrent stroke in patients with ESUS led to the hypothesis that this is “perhaps due to heterogeneous underlying etiologies.”
Moreover, these etiologies “may require different types of antithrombotic therapy to best prevent recurrence, and one such underlying etiology may be atrial cardiopathy.”
He explained that several observational studies have found, in the absence of atrial fibrillation, associations between stroke and different markers of atrial cardiopathy and, “given the proven benefit of anticoagulation in preventing strokes in patients with atrial fibrillation, it seems plausible” that they may also benefit.
To investigate further, the team conducted ARCADIA, an investigator-initiated, multicenter, randomized trial involving patients aged 45 years and older from 185 sites in the United States and Canada with a clinical diagnosis of stroke that met the consensus criteria for ESUS.
They also were required to have undergone brain imaging to rule out hemorrhagic stroke, and to have a modified Rankin Scale score of 4 or less, indicating up to a moderately severe degree of disability.
They also had atrial cardiopathy, as determined by P-wave terminal force in V1 greater than 5,000mcV*ms on electrocardiography, serum N-terminal prohormone of brain natriuretic peptide levels greater than 250 pg/mL, or a left atrium diameter of at least 3 cm/m2.
The patients were randomly assigned to apixaban 5 mg or 2.5 mg twice daily plus aspirin placebo, or apixaban placebo plus aspirin 81 mg daily. Those diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at physician discretion.
Dr. Kamel reported that, in 2022, after enrollment of 1015 patients with a mean follow-up of 1.8 years, the trial was halted at the planned interim efficacy/futility analysis, adding that there were “no safety concerns.”
The apixaban and aspirin groups were well balanced in terms of their baseline characteristics. The mean age was 68 years, and 54% were female. Three-quarters of the participants were White; 21.1% were Black.
Prior stroke was reported in 19% of patients. Hypertension was common, in about 77%, and type 2 diabetes was seen in 31%. There were relatively few cases of ischemic heart disease, heart failure, and peripheral arterial disease.
The primary efficacy outcome of recurrent stroke of any type occurred in 4.4% of both patients treated with apixaban and those given aspirin, at a hazard ratio of 1.00 (95% confidence interval, 0.64-1.55). Similar findings were seen when looking individually at ischemic and hemorrhagic stroke, and stroke of undetermined type.
There was also no significant difference in the secondary outcomes of recurrent ischemic stroke or systemic embolism, at 4.1% versus 4.4% (HR, 0.92; 95% CI, 0.59-1.44), and recurrent stroke of any type or death from any cause, at 7.3% versus 6.8% (HR, 1.08; 95% CI, 0.76-1.52).
In terms of safety, rates of major hemorrhage were low and almost identical between the groups, at 0.7% with apixaban and 0.8% for aspirin (HR, 1.02; 95% CI, 0.29-3.51), and were similar for all-cause mortality, at 1.8% versus 1.2% (HR, 1.53; 95% CI, 0.63-3.74).
Proportionately more patients treated with aspirin experienced symptomatic intracranial hemorrhage, at 1.1% versus 0%.
The trial results generated a flurry of interest on Twitter.
Thomas Ford, MD, a vascular neurology fellow from Boston Medical Center, described the results as “disappointing,” although he was “curious to see if there was any signal of benefit in subgroup analyses.”
Shadi Yaghi, codirector of the Comprehensive Stroke Center at Brown University, Providence, R.I., added that the trial “begs the question [as to] whether all device-detected atrial fibrillation warrants anticoagulation.”
Replying, Mitchell Elkind, MD, MPhil, professor of neurology and epidemiology at Columbia University Irving Medical Center, New York, said that he agrees with this interpretation.
“Maybe the issue is not with the concept of atrial cardiopathy but with the need to [anticoagulate] all patients with low [atrial fibrillation] burden or incidental [atrial fibrillation] after stroke.”
The study was funded by the National Institutes of Health and the National Institute of Neurological Disorders and Stroke. The study drug was provided in kind by BMS-Pfizer, and ancillary funding for the NTproBNP assays was provided by Roche. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
No added benefit from revascularization in low-risk CAS
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
MUNICH – , suggests a planned interim analysis of ECST-2.
Almost 430 patients with symptomatic and asymptomatic atherosclerotic carotid stenosis greater than or equal to 50% and a Carotid Artery Risk (CAR) score less than 20% were randomly assigned to OMT alone or OMT plus revascularization with carotid endarterectomy (CEA) or carotid artery stenting.
The study, which was presented at the annual European Stroke Organisation Conference, was stopped early because of slow recruitment.
Nevertheless, the current results showed that there was no significant difference at 2 years between the treatment groups in the rate of a composite endpoint, as well as the occurrence of any stroke, myocardial infarction, and periprocedural death.
In other words, “there was no evidence of benefit at 2 years from additional carotid revascularization” in patients with carotid stenosis who had a low to intermediate predicted stroke risk, said study presenter Paul Nederkoorn, MD, PhD, department of neurology, Amsterdam UMC, University of Amsterdam.
He added, however, that the complete 2 years will include additional analyses, including an analysis of silent infarcts on MRI, which may affect the results, and that longer clinical follow-up is required.
Future work will include the design and validation of a novel stroke risk prediction tool that will include MRI plaque imaging and will allow individualized patient selection for revascularization, as well as a cost-effectiveness analysis, he noted.
Conclusions ‘difficult’
Session co-chair Peter Kelly, MD, professor of neurology at Mater University Hospital/University College Dublin, and president-elect of the European Stroke Association, described the findings as “interesting” and that it was “great to see them.”
“I’m sure we’ll be discussing these results for a while,” he added.
But co-chair Else Charlotte Sandset, MD, PhD, a consultant neurologist in the Stroke Unit, department of neurology, Oslo University Hospital, said that it’s “difficult to draw firm conclusions from the trial.”
The patients were highly selected, recruitment was “perhaps a bit too slow,” and the study was probably conducted over too many sites, she said in an interview.
Dr. Sandset also noted that the options available for OMT have changed over the course of the study, as well as the overall approach to management.
“We are more aware of how we should treat” these patients, and “we’re probably a bit more aggressive,” which will have shifted the outcomes in the comparator arm as the study progressed.
“That is the challenge of doing these trials that take many years to run – our practice changes.”
‘Old evidence’
In his presentation, Dr. Nederkoorn pointed out that, while the current guidelines for CEA are “robust,” they are based on “old evidence” from trials conducted 20-30 years ago.
During that time, he said, medical treatment has improved significantly, and the risk for stroke has approximately halved. Yet the decision to perform CEA is still largely based on the degree of stenosis and the patient’s symptom status.
Dr. Nederkoorn suggested, however, that factors such as plaque ulceration and patient characteristics and comorbidities might influence the risk-benefit ratio for revascularization.
The current trial was therefore established to test the hypothesis that patients with carotid stenosis greater than or equal to 50% and a low to intermediate risk of stroke will not benefit from additional carotid revascularization on top of optimized medical therapy.
The team conducted a prospective, multicenter, open clinical trial in which patients with both symptomatic and asymptomatic atherosclerotic carotid stenosis were randomly assigned to revascularization plus OMT or OMT alone.
Dr. Nederkoorn explained that a low to intermediate 5-year risk for stroke was established using the CAR score less than 20%.
This is based on a range of parameters, including the sex and age of the patient, degree of stenosis, the type of and time since the event, and the presence of comorbidities, among other factors.
He said that the data was originally derived from the NASCET trial, which was published in 1998, and the first ECST trial, published in the same year.
Since then, the risk of ipsilateral stroke has “strongly declined,” Dr. Nederkoorn said, and so the CAR score was recalibrated to reflect the likely benefit of current OMT.
For the trial, OMT included antihypertensive and cholesterol-lowering medications, and dietary changes, alongside antiplatelet agents and anticoagulation, if indicated, to achieve predefined, guideline-led lipid and blood pressure targets.
Revascularization included CEA and coronary artery stenting in selected patients and was recommended to be performed within 2 weeks of randomization in symptomatic patients and within 4 weeks in asymptomatic patients.
When the trial started in 2012, the intention was to recruit 2,000 patients, with a planned interim analysis after enrollment of 320 patients.
However, recruitment was suspended in 2019, with 429 patients having been enrolled, as it was clear that achieving a cohort of 2,000 patients was “not practical without a change in the trial design” to include MRI plaque imaging and without further funding.
Dr. Nederkoorn showed that the baseline characteristics of the OMT and revascularization plus OMT groups were comparable. The average age of the patients in the groups was 71-72 years, and 31% were female.
Symptomatic disease was present in about 40% of patients, and about 76% had hypertension. Type 2 diabetes was reported in roughly one-quarter of the patients.
There was no difference in the time from randomization to the revascularization procedure between patients with asymptomatic and symptomatic disease.
Moving to the primary outcome, which was a composite of periprocedural death within 90 days of randomization and clinically manifest stroke or myocardial infarction at 2 years, Dr. Nederkoorn showed that there was no significant difference between the treatment groups.
Despite a suggestion that patients undergoing revascularization experienced “more harm” in the initial follow-up period, particularly in patients with a CAR score greater than 10%, the event curves met at around 18 months.
Overall, the hazard ratio between revascularization plus OMT versus OMT alone was 0.96 (95% confidence interval, 0.53-1.76, P = .90).
Breaking down the composite endpoint, there was a numerically lower rate of any stroke with OMT alone, compared with revascularization plus OMT over the study period, but again the difference was not significant at 2 years, at a hazard ratio of 0.68 (95% CI, 0.32-1.42, P = .30).
There was only one case of periprocedural death, in the revascularization arm. Although myocardial infarction was numerically twice as likely with OMT alone, compared with the combined intervention arm, the difference was not significant, at a hazard ratio of 2.00 (95% CI, 0.68-5.84, P = .21).
The study was funded by the National Institute for Health and Care Research, the Swiss National Science Foundation, The Netherlands Organisation of Scientific Research, and the Leeds Neurology Foundation. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
Researchers discover brain abnormalities in babies who had SIDS
For decades, researchers have been trying to understand why some otherwise healthy babies under 1 year old mysteriously die during their sleep. SIDS is the leading cause of infant death in the U.S., affecting 103 out of every 100,000 babies.
The new study found that babies who died of SIDS had abnormalities in certain brain receptors responsible for waking and restoring breathing. The scientists decided to look at the babies’ brains at the molecular level because previous research showed that the same kind of brain receptors in rodents are responsible for protective breathing functions during sleep.
The study was published in the Journal of Neuropathology & Experimental Neurology. The researchers compared brain stems from 70 babies, some of whom died of SIDS and some who died of other causes.
Despite discovering the differences in the babies’ brains, the lead author of the paper said more study is needed.
Robin Haynes, PhD, who studies SIDS at Boston Children’s Hospital, said in a statement that “the relationship between the abnormalities and cause of death remains unknown.”
She said there is no way to identify babies with the brain abnormalities, and “thus, adherence to safe-sleep practices remains critical.”
The American Academy of Pediatrics recommends numerous steps for creating a safe sleeping environment for babies, including placing babies on their backs on a firm surface. Education campaigns targeting parents and caregivers in the 1990s are largely considered successful, but SIDS rates have remained steady since the practices became widely used.
A version of this article first appeared on WebMD.com.
For decades, researchers have been trying to understand why some otherwise healthy babies under 1 year old mysteriously die during their sleep. SIDS is the leading cause of infant death in the U.S., affecting 103 out of every 100,000 babies.
The new study found that babies who died of SIDS had abnormalities in certain brain receptors responsible for waking and restoring breathing. The scientists decided to look at the babies’ brains at the molecular level because previous research showed that the same kind of brain receptors in rodents are responsible for protective breathing functions during sleep.
The study was published in the Journal of Neuropathology & Experimental Neurology. The researchers compared brain stems from 70 babies, some of whom died of SIDS and some who died of other causes.
Despite discovering the differences in the babies’ brains, the lead author of the paper said more study is needed.
Robin Haynes, PhD, who studies SIDS at Boston Children’s Hospital, said in a statement that “the relationship between the abnormalities and cause of death remains unknown.”
She said there is no way to identify babies with the brain abnormalities, and “thus, adherence to safe-sleep practices remains critical.”
The American Academy of Pediatrics recommends numerous steps for creating a safe sleeping environment for babies, including placing babies on their backs on a firm surface. Education campaigns targeting parents and caregivers in the 1990s are largely considered successful, but SIDS rates have remained steady since the practices became widely used.
A version of this article first appeared on WebMD.com.
For decades, researchers have been trying to understand why some otherwise healthy babies under 1 year old mysteriously die during their sleep. SIDS is the leading cause of infant death in the U.S., affecting 103 out of every 100,000 babies.
The new study found that babies who died of SIDS had abnormalities in certain brain receptors responsible for waking and restoring breathing. The scientists decided to look at the babies’ brains at the molecular level because previous research showed that the same kind of brain receptors in rodents are responsible for protective breathing functions during sleep.
The study was published in the Journal of Neuropathology & Experimental Neurology. The researchers compared brain stems from 70 babies, some of whom died of SIDS and some who died of other causes.
Despite discovering the differences in the babies’ brains, the lead author of the paper said more study is needed.
Robin Haynes, PhD, who studies SIDS at Boston Children’s Hospital, said in a statement that “the relationship between the abnormalities and cause of death remains unknown.”
She said there is no way to identify babies with the brain abnormalities, and “thus, adherence to safe-sleep practices remains critical.”
The American Academy of Pediatrics recommends numerous steps for creating a safe sleeping environment for babies, including placing babies on their backs on a firm surface. Education campaigns targeting parents and caregivers in the 1990s are largely considered successful, but SIDS rates have remained steady since the practices became widely used.
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF NEUROPATHY & EXPERIMENTAL NEUROLOGY
Standard measure may underestimate OSA in Black patients
Measurement error may be the culprit in underdiagnosing obstructive sleep apnea in Black patients, compared with White patients, based on data from nearly 2,000 individuals.
, according to Ali Azarbarzin, PhD, of Harvard Medical School, Boston.
“We wanted to examine the implications for obstructive sleep apnea,” which is often caused by a reduction in air flow, Dr. Azarbarzin said in an interview.
In a study presented at the American Thoracic Society’s international conference, Dr. Azarbarzin and colleagues examined data from 1,955 adults who were enrolled in the Multi-Ethnic Study of Atherosclerosis (MESA) Exam 5. The study participants underwent unattended 15-channel polysomnography that included a finger pulse oximeter. The mean age of the participants was 68.3 years, and 53.7% were women. A total of 12.1%, 23.7%, 27.7%, and 36.5% of the participants were Asian, Hispanic, Black, and White, respectively.
Apnea hypopnea index (AHI3P) was similar between Black and White patients, at approximately 19 events per hour. Black participants had higher wake SpO2, higher current smoking rates, and higher body mass index, compared with White participants, but these differences were not significant.
Severity of obstructive sleep apnea (OSA) was based on the hypoxic burden, which was defined as the total area under the respiratory curve. The total ventilatory burden was defined as the event-specific area under the ventilation signal and identified by amplitude changes in the nasal pressure signal. The researchers then calculated desaturation sensitivity (the primary outcome) as hypoxic burden divided by ventilatory burden.
In an unadjusted analysis, desaturation sensitivity was significantly lower in Black patients and Asian patients, compared with White patients (P < .001 and P < .02, respectively). After adjusting for age, sex, body mass index, and time spent in a supine position, desaturation sensitivity was lower only in Black patients, compared with White patients, and this difference persisted in both men and women.
The difference in desaturation sensitivity by race could be caused by differences in physiology or in measurement error, Dr. Azarbarzin told this news organization. If measurement error is the culprit, “we may be underestimating OSA severity in [Black people],” especially in Black women, he said.
However, more research is needed to understand the potential impact of both physiology and device accuracy on differences in oxygen saturation across ethnicities and to effectively identify and treat OSA in all patients, Dr. Azarbarzin said.
The MESA Study was supported by the National Institutes of Health and the National Institute on Aging. Data from MESA were obtained through support from the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences. Dr. Azarbarzin disclosed funding from the National Institutes of Health, the American Health Association, and the American Academy of Sleep Medicine.
A version of this article first appeared on Medscape.com.
Measurement error may be the culprit in underdiagnosing obstructive sleep apnea in Black patients, compared with White patients, based on data from nearly 2,000 individuals.
, according to Ali Azarbarzin, PhD, of Harvard Medical School, Boston.
“We wanted to examine the implications for obstructive sleep apnea,” which is often caused by a reduction in air flow, Dr. Azarbarzin said in an interview.
In a study presented at the American Thoracic Society’s international conference, Dr. Azarbarzin and colleagues examined data from 1,955 adults who were enrolled in the Multi-Ethnic Study of Atherosclerosis (MESA) Exam 5. The study participants underwent unattended 15-channel polysomnography that included a finger pulse oximeter. The mean age of the participants was 68.3 years, and 53.7% were women. A total of 12.1%, 23.7%, 27.7%, and 36.5% of the participants were Asian, Hispanic, Black, and White, respectively.
Apnea hypopnea index (AHI3P) was similar between Black and White patients, at approximately 19 events per hour. Black participants had higher wake SpO2, higher current smoking rates, and higher body mass index, compared with White participants, but these differences were not significant.
Severity of obstructive sleep apnea (OSA) was based on the hypoxic burden, which was defined as the total area under the respiratory curve. The total ventilatory burden was defined as the event-specific area under the ventilation signal and identified by amplitude changes in the nasal pressure signal. The researchers then calculated desaturation sensitivity (the primary outcome) as hypoxic burden divided by ventilatory burden.
In an unadjusted analysis, desaturation sensitivity was significantly lower in Black patients and Asian patients, compared with White patients (P < .001 and P < .02, respectively). After adjusting for age, sex, body mass index, and time spent in a supine position, desaturation sensitivity was lower only in Black patients, compared with White patients, and this difference persisted in both men and women.
The difference in desaturation sensitivity by race could be caused by differences in physiology or in measurement error, Dr. Azarbarzin told this news organization. If measurement error is the culprit, “we may be underestimating OSA severity in [Black people],” especially in Black women, he said.
However, more research is needed to understand the potential impact of both physiology and device accuracy on differences in oxygen saturation across ethnicities and to effectively identify and treat OSA in all patients, Dr. Azarbarzin said.
The MESA Study was supported by the National Institutes of Health and the National Institute on Aging. Data from MESA were obtained through support from the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences. Dr. Azarbarzin disclosed funding from the National Institutes of Health, the American Health Association, and the American Academy of Sleep Medicine.
A version of this article first appeared on Medscape.com.
Measurement error may be the culprit in underdiagnosing obstructive sleep apnea in Black patients, compared with White patients, based on data from nearly 2,000 individuals.
, according to Ali Azarbarzin, PhD, of Harvard Medical School, Boston.
“We wanted to examine the implications for obstructive sleep apnea,” which is often caused by a reduction in air flow, Dr. Azarbarzin said in an interview.
In a study presented at the American Thoracic Society’s international conference, Dr. Azarbarzin and colleagues examined data from 1,955 adults who were enrolled in the Multi-Ethnic Study of Atherosclerosis (MESA) Exam 5. The study participants underwent unattended 15-channel polysomnography that included a finger pulse oximeter. The mean age of the participants was 68.3 years, and 53.7% were women. A total of 12.1%, 23.7%, 27.7%, and 36.5% of the participants were Asian, Hispanic, Black, and White, respectively.
Apnea hypopnea index (AHI3P) was similar between Black and White patients, at approximately 19 events per hour. Black participants had higher wake SpO2, higher current smoking rates, and higher body mass index, compared with White participants, but these differences were not significant.
Severity of obstructive sleep apnea (OSA) was based on the hypoxic burden, which was defined as the total area under the respiratory curve. The total ventilatory burden was defined as the event-specific area under the ventilation signal and identified by amplitude changes in the nasal pressure signal. The researchers then calculated desaturation sensitivity (the primary outcome) as hypoxic burden divided by ventilatory burden.
In an unadjusted analysis, desaturation sensitivity was significantly lower in Black patients and Asian patients, compared with White patients (P < .001 and P < .02, respectively). After adjusting for age, sex, body mass index, and time spent in a supine position, desaturation sensitivity was lower only in Black patients, compared with White patients, and this difference persisted in both men and women.
The difference in desaturation sensitivity by race could be caused by differences in physiology or in measurement error, Dr. Azarbarzin told this news organization. If measurement error is the culprit, “we may be underestimating OSA severity in [Black people],” especially in Black women, he said.
However, more research is needed to understand the potential impact of both physiology and device accuracy on differences in oxygen saturation across ethnicities and to effectively identify and treat OSA in all patients, Dr. Azarbarzin said.
The MESA Study was supported by the National Institutes of Health and the National Institute on Aging. Data from MESA were obtained through support from the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences. Dr. Azarbarzin disclosed funding from the National Institutes of Health, the American Health Association, and the American Academy of Sleep Medicine.
A version of this article first appeared on Medscape.com.
FROM ATS 2023
States move to curb insurers’ prior authorization requirements as federal reforms lag
Amid growing criticism of health insurers’ onerous prior authorization practices, lawmakers in 30 states have introduced bills this year that aim to rein in insurer gatekeeping and improve patient care.
“This is something that goes on in every doctor’s office every day; the frustrations, the delays, and the use of office staff time are just unbelievable,” said Steven Orland, MD, a board-certified urologist and president of the Medical Society of New Jersey.
The bills, which cover private health plans and insurers that states regulate, may provide some relief for physicians as federal efforts to streamline prior authorization for some Medicare patients have lagged.
Last year, Congress failed to pass the Improving Seniors’ Timely Access to Care Act of 2021, despite 326 co-sponsors. The bill would have compelled insurers covering Medicare Advantage enrollees to speed up prior authorizations, make the process more transparent, and remove obstacles such as requiring fax machine submissions.
Last month, however, the Centers for Medicare & Medicaid Services issued a final rule that will improve some aspects of prior authorizations in Medicare Advantage insurance plans and ensure that enrollees have the same access to necessary care as traditional Medicare enrollees.
The insurance industry has long defended prior authorization requirements and opposed legislation that would limit them.
America’s Health Insurance Plans (AHIP) and the Blue Cross Blue Shield Association said in a 2019 letter to a congressional committee when the federal legislation was first introduced, “Prior authorizations enforce best practices and guidelines for care management and help physicians identify and avoid care techniques that would harm patient outcomes, such as designating prescriptions that could feed into an opioid addiction.” AHIP didn’t respond to repeated requests for comment.
But some major insurers now appear willing to compromise and voluntarily reduce the volume of prior authorizations they require. Days before the federal final rule was released, three major insurers – United HealthCare, Cigna, and Aetna CVS Health – announced they plan to drop some prior authorization requirements and automate processes.
United HealthCare said it will eliminate almost 20% of its prior authorizations for some nonurgent surgeries and procedures starting this summer. It also will create a national Gold Card program in 2024 for physicians who meet its eligibility requirements, which would eliminate prior authorization requirements for most procedures. Both initiatives will apply to commercial, Medicare Advantage, and Medicaid businesses, said the insurer in a statement.
However, United HealthCare also announced that in June it will start requiring prior authorization for diagnostic (not screening) gastrointestinal endoscopies for its nearly 27 million privately insured patients, citing data it says shows potentially harmful overuse of scopes. Physician groups have publicly criticized the move, saying it could delay lifesaving treatment, and have asked the insurer to reconsider.
Cigna and Aetna also have moved to pare back prior authorization processes. Scott Josephs, national medical officer for Cigna, told Healthcare Dive that Cigna has removed prior authorization reviews from nearly 500 services since 2020.
An Aetna spokesperson told Healthcare Dive that the CVS-owned payer has implemented a gold card program and rolled back prior authorization requirements on cataract surgeries, video EEGs, and home infusion for some drugs, according to Healthcare Dive.
Cigna has faced increased scrutiny from some state regulators since a ProPublica/The Capitol Forum article revealed in March that its doctors were denying claims without opening patients’ files, contrary to what insurance laws and regulations require in many states.
Over a period of 2 months last year, Cigna doctors denied over 300,000 requests for payments using this method, spending an average of 1.2 seconds on each case, the investigation found. In a written response, Cigna said the reporting by ProPublica and The Capitol Forum was “biased and incomplete.”
States aim to reduce prior authorization volume
The American Medical Association said it has been tracking nearly 90 prior authorization reform bills in 30 states. More than a dozen bills are still being considered in this legislative session, including in Arkansas, California, New Jersey, North Carolina, Maryland, and Washington, D.C.
“The groundswell of activity in the states reflects how big a problem this is,” said an AMA legislative expert. “The issue used to be ‘how can we automate and streamline processes’; now the issue is focused on reducing the volume of prior authorizations and the harm that can cause patients.”
The state bills use different strategies to reduce excessive prior authorization requirements. Maryland’s proposed bill, for example, would require just one prior authorization to stay on a prescription drug, if the insurer has previously approved the drug and the patient continues to successfully be treated by the drug.
Washington, D.C. and New Jersey have introduced comprehensive reform bills that include a “grace period” of 60 days, to ensure continuity of care when a patient switches health plans. They also would eliminate repeat authorizations for chronic and long-term conditions, set explicit timelines for insurers to respond to prior authorization requests and appeals, and require that practicing physicians review denials that are appealed.
Many state bills also would require insurers to be more transparent by posting information on their websites about which services and drugs require prior authorization and what their approval rates are for them, said AMA’s legislative expert.
“There’s a black hole of information that insurers have access to. We would really like to know how many prior authorization requests are denied, the time it takes to deny them, and the reasons for denial,” said Josh Bengal, JD, the director of government relations for the Medical Society of New Jersey.
The legislation in New Jersey and other states faces stiff opposition from the insurance lobby, especially state associations of health plans affiliated with AHIP. The California Association of Health Plans, for example, opposes a “gold card” bill (SB 598), introduced in February, that would allow a select group of high-performing doctors to skip prior authorizations for 1 year.
The CAHP states, “Californians deserve safe, high quality, high-value health care. Yet SB 598 will derail the progress we have made in our health care system by lowering the value and safety that Californians should expect from their health care providers,” according to a fact sheet.
The fact-sheet defines “low-value care” as medical services for which there is little to no benefit and poses potential physical or financial harm to patients, such as unnecessary CT scans or MRIs for uncomplicated conditions.
California is one of about a dozen states that have introduced gold card legislation this year. If enacted, they would join five states with gold card laws: West Virginia, Texas, Vermont, Michigan, and Louisiana.
How do gold cards work?
Physicians who achieve a high approval rate of prior authorizations from insurers for 1 year are eligible to be exempted from obtaining prior authorizations the following year.
The approval rate is at least 90% for a certain number of eligible health services, but the number of prior authorizations required to qualify can range from 5 to 30, depending on the state law.
Gold card legislation typically also gives the treating physician the right to have an appeal of a prior authorization denial by a physician peer of the same or similar specialty.
California’s bill would also apply to all covered health services, which is broader than what United HealthCare has proposed for its gold card exemption. The bill would also require a plan or insurer to annually monitor rates of prior authorization approval, modification, appeal, and denial, and to discontinue services, items, and supplies that are approved 95% of the time.
“These are important reforms that will help ensure that patients can receive the care they need, when they need it,” said CMA president Donaldo Hernandez, MD.
However, it’s not clear how many physicians will meet “gold card” status based on Texas’ recent experience with its own “gold card” law.
The Texas Department of Insurance estimated that only 3.3% of licensed physicians in the state have met “gold card” status since the bill became law in 2021, said Zeke Silva, MD, an interventional radiologist who serves on the Council of Legislation for the Texas Medical Association.
He noted that the legislation has had a limited effect for several reasons. Commercial health plans only make up only about 20% of all health plans in Texas. Also, the final regulations didn’t go into effect until last May and physicians are evaluated by health plans for “gold card” status every 6 months, said Dr. Silva.
In addition, physicians must have at least five prior authorizations approved for the same health service, which the law left up to the health plans to define, said Dr. Silva.
Now, the Texas Medical Association is lobbying for legislative improvements. “We want to reduce the number of eligible services that health plans require for prior authorizations and have more oversight of prior authorization denials by the Texas Department of Insurance and the Texas Medical Board,” said Dr. Silva.
He’s optimistic that if the bill becomes law, the number of physicians eligible for gold cards may increase.
Meanwhile, the AMA’s legislative expert, who declined to be identified because of organization policy, acknowledged the possibility that some prior authorization bills will die in state legislatures this year.
“We remain hopeful, but it’s an uphill battle. The state medical associations face a lot of opposition from health plans who don’t want to see these reforms become law.”
A version of this article originally appeared on Medscape.com.
Amid growing criticism of health insurers’ onerous prior authorization practices, lawmakers in 30 states have introduced bills this year that aim to rein in insurer gatekeeping and improve patient care.
“This is something that goes on in every doctor’s office every day; the frustrations, the delays, and the use of office staff time are just unbelievable,” said Steven Orland, MD, a board-certified urologist and president of the Medical Society of New Jersey.
The bills, which cover private health plans and insurers that states regulate, may provide some relief for physicians as federal efforts to streamline prior authorization for some Medicare patients have lagged.
Last year, Congress failed to pass the Improving Seniors’ Timely Access to Care Act of 2021, despite 326 co-sponsors. The bill would have compelled insurers covering Medicare Advantage enrollees to speed up prior authorizations, make the process more transparent, and remove obstacles such as requiring fax machine submissions.
Last month, however, the Centers for Medicare & Medicaid Services issued a final rule that will improve some aspects of prior authorizations in Medicare Advantage insurance plans and ensure that enrollees have the same access to necessary care as traditional Medicare enrollees.
The insurance industry has long defended prior authorization requirements and opposed legislation that would limit them.
America’s Health Insurance Plans (AHIP) and the Blue Cross Blue Shield Association said in a 2019 letter to a congressional committee when the federal legislation was first introduced, “Prior authorizations enforce best practices and guidelines for care management and help physicians identify and avoid care techniques that would harm patient outcomes, such as designating prescriptions that could feed into an opioid addiction.” AHIP didn’t respond to repeated requests for comment.
But some major insurers now appear willing to compromise and voluntarily reduce the volume of prior authorizations they require. Days before the federal final rule was released, three major insurers – United HealthCare, Cigna, and Aetna CVS Health – announced they plan to drop some prior authorization requirements and automate processes.
United HealthCare said it will eliminate almost 20% of its prior authorizations for some nonurgent surgeries and procedures starting this summer. It also will create a national Gold Card program in 2024 for physicians who meet its eligibility requirements, which would eliminate prior authorization requirements for most procedures. Both initiatives will apply to commercial, Medicare Advantage, and Medicaid businesses, said the insurer in a statement.
However, United HealthCare also announced that in June it will start requiring prior authorization for diagnostic (not screening) gastrointestinal endoscopies for its nearly 27 million privately insured patients, citing data it says shows potentially harmful overuse of scopes. Physician groups have publicly criticized the move, saying it could delay lifesaving treatment, and have asked the insurer to reconsider.
Cigna and Aetna also have moved to pare back prior authorization processes. Scott Josephs, national medical officer for Cigna, told Healthcare Dive that Cigna has removed prior authorization reviews from nearly 500 services since 2020.
An Aetna spokesperson told Healthcare Dive that the CVS-owned payer has implemented a gold card program and rolled back prior authorization requirements on cataract surgeries, video EEGs, and home infusion for some drugs, according to Healthcare Dive.
Cigna has faced increased scrutiny from some state regulators since a ProPublica/The Capitol Forum article revealed in March that its doctors were denying claims without opening patients’ files, contrary to what insurance laws and regulations require in many states.
Over a period of 2 months last year, Cigna doctors denied over 300,000 requests for payments using this method, spending an average of 1.2 seconds on each case, the investigation found. In a written response, Cigna said the reporting by ProPublica and The Capitol Forum was “biased and incomplete.”
States aim to reduce prior authorization volume
The American Medical Association said it has been tracking nearly 90 prior authorization reform bills in 30 states. More than a dozen bills are still being considered in this legislative session, including in Arkansas, California, New Jersey, North Carolina, Maryland, and Washington, D.C.
“The groundswell of activity in the states reflects how big a problem this is,” said an AMA legislative expert. “The issue used to be ‘how can we automate and streamline processes’; now the issue is focused on reducing the volume of prior authorizations and the harm that can cause patients.”
The state bills use different strategies to reduce excessive prior authorization requirements. Maryland’s proposed bill, for example, would require just one prior authorization to stay on a prescription drug, if the insurer has previously approved the drug and the patient continues to successfully be treated by the drug.
Washington, D.C. and New Jersey have introduced comprehensive reform bills that include a “grace period” of 60 days, to ensure continuity of care when a patient switches health plans. They also would eliminate repeat authorizations for chronic and long-term conditions, set explicit timelines for insurers to respond to prior authorization requests and appeals, and require that practicing physicians review denials that are appealed.
Many state bills also would require insurers to be more transparent by posting information on their websites about which services and drugs require prior authorization and what their approval rates are for them, said AMA’s legislative expert.
“There’s a black hole of information that insurers have access to. We would really like to know how many prior authorization requests are denied, the time it takes to deny them, and the reasons for denial,” said Josh Bengal, JD, the director of government relations for the Medical Society of New Jersey.
The legislation in New Jersey and other states faces stiff opposition from the insurance lobby, especially state associations of health plans affiliated with AHIP. The California Association of Health Plans, for example, opposes a “gold card” bill (SB 598), introduced in February, that would allow a select group of high-performing doctors to skip prior authorizations for 1 year.
The CAHP states, “Californians deserve safe, high quality, high-value health care. Yet SB 598 will derail the progress we have made in our health care system by lowering the value and safety that Californians should expect from their health care providers,” according to a fact sheet.
The fact-sheet defines “low-value care” as medical services for which there is little to no benefit and poses potential physical or financial harm to patients, such as unnecessary CT scans or MRIs for uncomplicated conditions.
California is one of about a dozen states that have introduced gold card legislation this year. If enacted, they would join five states with gold card laws: West Virginia, Texas, Vermont, Michigan, and Louisiana.
How do gold cards work?
Physicians who achieve a high approval rate of prior authorizations from insurers for 1 year are eligible to be exempted from obtaining prior authorizations the following year.
The approval rate is at least 90% for a certain number of eligible health services, but the number of prior authorizations required to qualify can range from 5 to 30, depending on the state law.
Gold card legislation typically also gives the treating physician the right to have an appeal of a prior authorization denial by a physician peer of the same or similar specialty.
California’s bill would also apply to all covered health services, which is broader than what United HealthCare has proposed for its gold card exemption. The bill would also require a plan or insurer to annually monitor rates of prior authorization approval, modification, appeal, and denial, and to discontinue services, items, and supplies that are approved 95% of the time.
“These are important reforms that will help ensure that patients can receive the care they need, when they need it,” said CMA president Donaldo Hernandez, MD.
However, it’s not clear how many physicians will meet “gold card” status based on Texas’ recent experience with its own “gold card” law.
The Texas Department of Insurance estimated that only 3.3% of licensed physicians in the state have met “gold card” status since the bill became law in 2021, said Zeke Silva, MD, an interventional radiologist who serves on the Council of Legislation for the Texas Medical Association.
He noted that the legislation has had a limited effect for several reasons. Commercial health plans only make up only about 20% of all health plans in Texas. Also, the final regulations didn’t go into effect until last May and physicians are evaluated by health plans for “gold card” status every 6 months, said Dr. Silva.
In addition, physicians must have at least five prior authorizations approved for the same health service, which the law left up to the health plans to define, said Dr. Silva.
Now, the Texas Medical Association is lobbying for legislative improvements. “We want to reduce the number of eligible services that health plans require for prior authorizations and have more oversight of prior authorization denials by the Texas Department of Insurance and the Texas Medical Board,” said Dr. Silva.
He’s optimistic that if the bill becomes law, the number of physicians eligible for gold cards may increase.
Meanwhile, the AMA’s legislative expert, who declined to be identified because of organization policy, acknowledged the possibility that some prior authorization bills will die in state legislatures this year.
“We remain hopeful, but it’s an uphill battle. The state medical associations face a lot of opposition from health plans who don’t want to see these reforms become law.”
A version of this article originally appeared on Medscape.com.
Amid growing criticism of health insurers’ onerous prior authorization practices, lawmakers in 30 states have introduced bills this year that aim to rein in insurer gatekeeping and improve patient care.
“This is something that goes on in every doctor’s office every day; the frustrations, the delays, and the use of office staff time are just unbelievable,” said Steven Orland, MD, a board-certified urologist and president of the Medical Society of New Jersey.
The bills, which cover private health plans and insurers that states regulate, may provide some relief for physicians as federal efforts to streamline prior authorization for some Medicare patients have lagged.
Last year, Congress failed to pass the Improving Seniors’ Timely Access to Care Act of 2021, despite 326 co-sponsors. The bill would have compelled insurers covering Medicare Advantage enrollees to speed up prior authorizations, make the process more transparent, and remove obstacles such as requiring fax machine submissions.
Last month, however, the Centers for Medicare & Medicaid Services issued a final rule that will improve some aspects of prior authorizations in Medicare Advantage insurance plans and ensure that enrollees have the same access to necessary care as traditional Medicare enrollees.
The insurance industry has long defended prior authorization requirements and opposed legislation that would limit them.
America’s Health Insurance Plans (AHIP) and the Blue Cross Blue Shield Association said in a 2019 letter to a congressional committee when the federal legislation was first introduced, “Prior authorizations enforce best practices and guidelines for care management and help physicians identify and avoid care techniques that would harm patient outcomes, such as designating prescriptions that could feed into an opioid addiction.” AHIP didn’t respond to repeated requests for comment.
But some major insurers now appear willing to compromise and voluntarily reduce the volume of prior authorizations they require. Days before the federal final rule was released, three major insurers – United HealthCare, Cigna, and Aetna CVS Health – announced they plan to drop some prior authorization requirements and automate processes.
United HealthCare said it will eliminate almost 20% of its prior authorizations for some nonurgent surgeries and procedures starting this summer. It also will create a national Gold Card program in 2024 for physicians who meet its eligibility requirements, which would eliminate prior authorization requirements for most procedures. Both initiatives will apply to commercial, Medicare Advantage, and Medicaid businesses, said the insurer in a statement.
However, United HealthCare also announced that in June it will start requiring prior authorization for diagnostic (not screening) gastrointestinal endoscopies for its nearly 27 million privately insured patients, citing data it says shows potentially harmful overuse of scopes. Physician groups have publicly criticized the move, saying it could delay lifesaving treatment, and have asked the insurer to reconsider.
Cigna and Aetna also have moved to pare back prior authorization processes. Scott Josephs, national medical officer for Cigna, told Healthcare Dive that Cigna has removed prior authorization reviews from nearly 500 services since 2020.
An Aetna spokesperson told Healthcare Dive that the CVS-owned payer has implemented a gold card program and rolled back prior authorization requirements on cataract surgeries, video EEGs, and home infusion for some drugs, according to Healthcare Dive.
Cigna has faced increased scrutiny from some state regulators since a ProPublica/The Capitol Forum article revealed in March that its doctors were denying claims without opening patients’ files, contrary to what insurance laws and regulations require in many states.
Over a period of 2 months last year, Cigna doctors denied over 300,000 requests for payments using this method, spending an average of 1.2 seconds on each case, the investigation found. In a written response, Cigna said the reporting by ProPublica and The Capitol Forum was “biased and incomplete.”
States aim to reduce prior authorization volume
The American Medical Association said it has been tracking nearly 90 prior authorization reform bills in 30 states. More than a dozen bills are still being considered in this legislative session, including in Arkansas, California, New Jersey, North Carolina, Maryland, and Washington, D.C.
“The groundswell of activity in the states reflects how big a problem this is,” said an AMA legislative expert. “The issue used to be ‘how can we automate and streamline processes’; now the issue is focused on reducing the volume of prior authorizations and the harm that can cause patients.”
The state bills use different strategies to reduce excessive prior authorization requirements. Maryland’s proposed bill, for example, would require just one prior authorization to stay on a prescription drug, if the insurer has previously approved the drug and the patient continues to successfully be treated by the drug.
Washington, D.C. and New Jersey have introduced comprehensive reform bills that include a “grace period” of 60 days, to ensure continuity of care when a patient switches health plans. They also would eliminate repeat authorizations for chronic and long-term conditions, set explicit timelines for insurers to respond to prior authorization requests and appeals, and require that practicing physicians review denials that are appealed.
Many state bills also would require insurers to be more transparent by posting information on their websites about which services and drugs require prior authorization and what their approval rates are for them, said AMA’s legislative expert.
“There’s a black hole of information that insurers have access to. We would really like to know how many prior authorization requests are denied, the time it takes to deny them, and the reasons for denial,” said Josh Bengal, JD, the director of government relations for the Medical Society of New Jersey.
The legislation in New Jersey and other states faces stiff opposition from the insurance lobby, especially state associations of health plans affiliated with AHIP. The California Association of Health Plans, for example, opposes a “gold card” bill (SB 598), introduced in February, that would allow a select group of high-performing doctors to skip prior authorizations for 1 year.
The CAHP states, “Californians deserve safe, high quality, high-value health care. Yet SB 598 will derail the progress we have made in our health care system by lowering the value and safety that Californians should expect from their health care providers,” according to a fact sheet.
The fact-sheet defines “low-value care” as medical services for which there is little to no benefit and poses potential physical or financial harm to patients, such as unnecessary CT scans or MRIs for uncomplicated conditions.
California is one of about a dozen states that have introduced gold card legislation this year. If enacted, they would join five states with gold card laws: West Virginia, Texas, Vermont, Michigan, and Louisiana.
How do gold cards work?
Physicians who achieve a high approval rate of prior authorizations from insurers for 1 year are eligible to be exempted from obtaining prior authorizations the following year.
The approval rate is at least 90% for a certain number of eligible health services, but the number of prior authorizations required to qualify can range from 5 to 30, depending on the state law.
Gold card legislation typically also gives the treating physician the right to have an appeal of a prior authorization denial by a physician peer of the same or similar specialty.
California’s bill would also apply to all covered health services, which is broader than what United HealthCare has proposed for its gold card exemption. The bill would also require a plan or insurer to annually monitor rates of prior authorization approval, modification, appeal, and denial, and to discontinue services, items, and supplies that are approved 95% of the time.
“These are important reforms that will help ensure that patients can receive the care they need, when they need it,” said CMA president Donaldo Hernandez, MD.
However, it’s not clear how many physicians will meet “gold card” status based on Texas’ recent experience with its own “gold card” law.
The Texas Department of Insurance estimated that only 3.3% of licensed physicians in the state have met “gold card” status since the bill became law in 2021, said Zeke Silva, MD, an interventional radiologist who serves on the Council of Legislation for the Texas Medical Association.
He noted that the legislation has had a limited effect for several reasons. Commercial health plans only make up only about 20% of all health plans in Texas. Also, the final regulations didn’t go into effect until last May and physicians are evaluated by health plans for “gold card” status every 6 months, said Dr. Silva.
In addition, physicians must have at least five prior authorizations approved for the same health service, which the law left up to the health plans to define, said Dr. Silva.
Now, the Texas Medical Association is lobbying for legislative improvements. “We want to reduce the number of eligible services that health plans require for prior authorizations and have more oversight of prior authorization denials by the Texas Department of Insurance and the Texas Medical Board,” said Dr. Silva.
He’s optimistic that if the bill becomes law, the number of physicians eligible for gold cards may increase.
Meanwhile, the AMA’s legislative expert, who declined to be identified because of organization policy, acknowledged the possibility that some prior authorization bills will die in state legislatures this year.
“We remain hopeful, but it’s an uphill battle. The state medical associations face a lot of opposition from health plans who don’t want to see these reforms become law.”
A version of this article originally appeared on Medscape.com.
Researchers locate signals in brain related to chronic pain
a new study in Nature Neuroscience concluded.
The researchers used the devices on four patients who had felt endless nerve pain for more than a year. The devices recorded several times a day, which could pave “the way for implanted devices to one day predict pain signals or even short-circuit them,” The New York Times reported.
The study says the pain “was associated with electrical fluctuations in the orbitofrontal cortex, an area involved in emotion regulation, self-evaluation, and decision-making,” The Times reported. “The research suggests that such patterns of brain activity could serve as biomarkers to guide diagnosis and treatment for millions of people with shooting or burning chronic pain linked to a damaged nervous system.”
Ajay Wasan, MD, and a pain specialist at the University of Pittsburgh who was not involved in the study praised it to the Times.
“The study really advances a whole generation of research that has shown that the functioning of the brain is really important to processing and perceiving pain,” he said.
Chronic pain is defined as persistent or recurring and lasting more than three months. The Centers for Disease Control and Prevention says about 20% of Americans experience it. It has been linked with depression, Alzheimer’s disease and other dementias, suicide, and substance use.
Yet, the study’s authors noted, “pain severity is often measured through subjective report, while objective biomarkers that may guide diagnosis and treatment are lacking.”
Medtronic provided devices for the study. The study authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
a new study in Nature Neuroscience concluded.
The researchers used the devices on four patients who had felt endless nerve pain for more than a year. The devices recorded several times a day, which could pave “the way for implanted devices to one day predict pain signals or even short-circuit them,” The New York Times reported.
The study says the pain “was associated with electrical fluctuations in the orbitofrontal cortex, an area involved in emotion regulation, self-evaluation, and decision-making,” The Times reported. “The research suggests that such patterns of brain activity could serve as biomarkers to guide diagnosis and treatment for millions of people with shooting or burning chronic pain linked to a damaged nervous system.”
Ajay Wasan, MD, and a pain specialist at the University of Pittsburgh who was not involved in the study praised it to the Times.
“The study really advances a whole generation of research that has shown that the functioning of the brain is really important to processing and perceiving pain,” he said.
Chronic pain is defined as persistent or recurring and lasting more than three months. The Centers for Disease Control and Prevention says about 20% of Americans experience it. It has been linked with depression, Alzheimer’s disease and other dementias, suicide, and substance use.
Yet, the study’s authors noted, “pain severity is often measured through subjective report, while objective biomarkers that may guide diagnosis and treatment are lacking.”
Medtronic provided devices for the study. The study authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
a new study in Nature Neuroscience concluded.
The researchers used the devices on four patients who had felt endless nerve pain for more than a year. The devices recorded several times a day, which could pave “the way for implanted devices to one day predict pain signals or even short-circuit them,” The New York Times reported.
The study says the pain “was associated with electrical fluctuations in the orbitofrontal cortex, an area involved in emotion regulation, self-evaluation, and decision-making,” The Times reported. “The research suggests that such patterns of brain activity could serve as biomarkers to guide diagnosis and treatment for millions of people with shooting or burning chronic pain linked to a damaged nervous system.”
Ajay Wasan, MD, and a pain specialist at the University of Pittsburgh who was not involved in the study praised it to the Times.
“The study really advances a whole generation of research that has shown that the functioning of the brain is really important to processing and perceiving pain,” he said.
Chronic pain is defined as persistent or recurring and lasting more than three months. The Centers for Disease Control and Prevention says about 20% of Americans experience it. It has been linked with depression, Alzheimer’s disease and other dementias, suicide, and substance use.
Yet, the study’s authors noted, “pain severity is often measured through subjective report, while objective biomarkers that may guide diagnosis and treatment are lacking.”
Medtronic provided devices for the study. The study authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
FROM NATURE NEUROSCIENCE
The weird world of hydrogels: How they’ll change health care
Imagine a day when a simple injection prompts a broken bone to heal. When tiny, ingestible devices linger in the body, unnoticed, tracking our health or delivering life-saving medications. When brain and heart implants mesh with flesh so seamlessly that the body thinks they’ve been there all along.
These are the dreams of materials scientists who have toiled for decades to mimic the complex architecture of the human body in hopes of replacing broken parts or treating disease.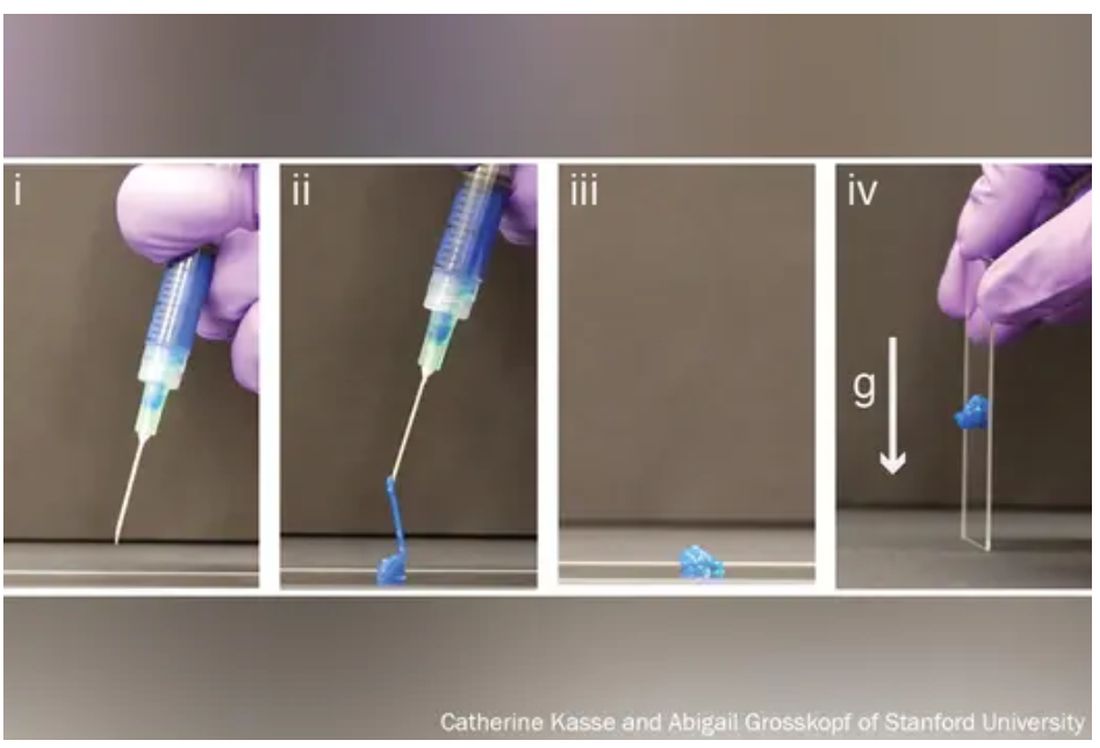
The problem, say bioengineers, is that most replacement and corrective parts – from prosthetics to pacemakers – are made of hard, dry, lifeless materials, like metal or plastic, while biological tissue is soft, wet, and living.
The body knows the difference and tends to reject imitations.
Enter hydrogels, three-dimensional networks of molecules swollen with – by definition – water.
First described in 1960 by creators of soft contact lenses, these weird, shape-shifting substances are able to morph from liquid to solid to a squishy in-between. (Early, simple uses include hair gel or Jell-O.). Slow to gain attention, growing to just 1,000 studies published by 1982, they’ve become the subject of intense study recently, with 100,000 papers published by 2020, and 3,800 already this year alone.
As chemists, biologists, and engineers begin to work more with one another and with medical doctors,
“We are, essentially, hydrogels,” said Benjamin Wiley, PhD, a chemistry professor at Duke University in Durham, N.C. “As people develop new hydrogels that more closely match the tissues in our body, we’ll be able to treat a whole host of ailments we couldn’t treat before.”
From contact lenses to brain implants
Put simply, a hydrogel is like a mesh bag of water.
The mesh is made of polymers, or spaghetti-like strands of molecules, stitched together in a repeating pattern and swollen with H2O, much like the way 3D matrixes in our body surround, support, and give structure to our cells and tissues.
“Imagine a soccer net, with all of these long fibers woven together to create the net,” said Eric Appel, PhD, associate professor of materials science and engineering at Stanford (Calif.) University.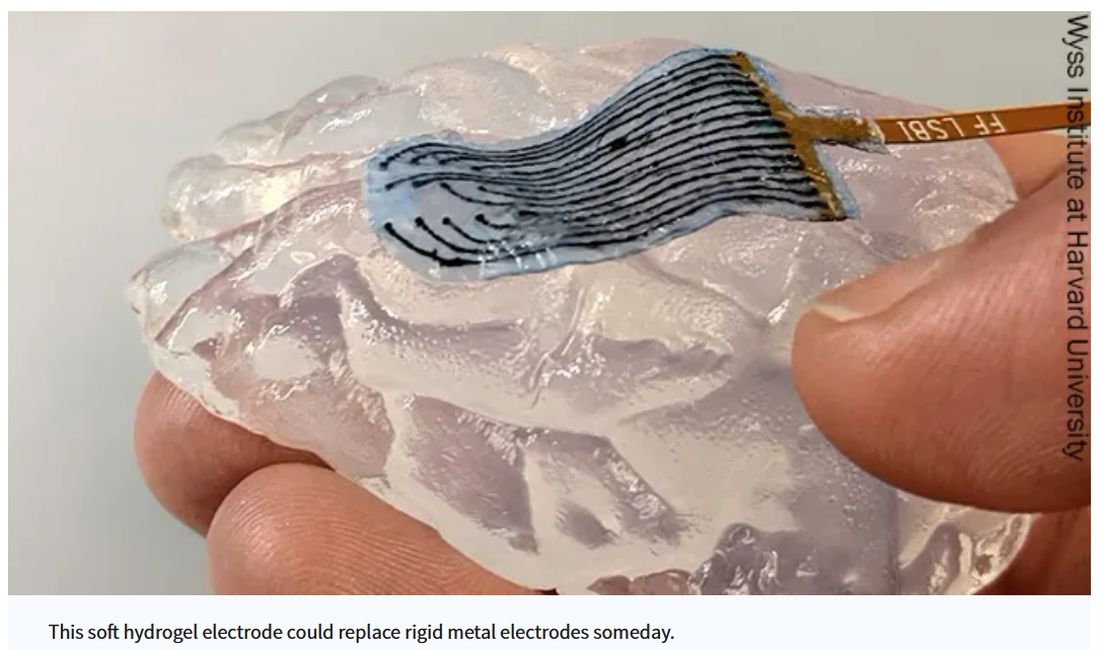
While the broader category of “gels” could be filled with anything, including chemical solvents, water is the key ingredient that sets hydrogels apart, making them ideal for, as some scientists put it, “merging humans and machines.”
Human bones are about 25% water, while muscles hover around 70% and the brain is 85%. The precious liquid plays a host of critical roles, from shuttling nutrients in and waste out to helping cells talk to each other.
Lab-made hydrogels can be loaded with cargo (like a ball in the net), including cells or drugs that help mimic some of those functions.
Hydrogels are soft and pliable like flesh. So, if used in implants, they may be less likely to damage surrounding tissue.
“Think about a metal spoon in your bowl of pudding. As you’re shaking the bowl, the spoon doesn’t stay in place, and you get scarring around the spoon,” said Christina Tringides, PhD, a materials scientist who studies neural engineering. That, she says, is exactly what happens to brain implants when patients breathe or move. “It’s a mechanical mismatch. But with hydrogels, you could get perfect mechanical matching.”
Hydrogels also tend to be nontoxic, so the immune system may be less likely to attack them as foreign bodies.
All this has made hydrogels the new darling of the bioengineering world.
“There has been an absolute explosion of interest in these materials,” Dr. Appel said.
Smarter drug delivery and ingestible electronics
Early versions of hydrogels were thick and gooey, making it hard to get them inside the body.
“Think of a block of Jell-O. You couldn’t inject something like that,” Dr. Appel said.
But Dr. Appel, whose lab develops new drug delivery systems, has been tinkering with gel formulas for years in hopes that these high-tech globs could someday ferry timed-release drugs to just the right spot in the body.
His new hydrogels start as fully formed gels (which help preserve the drug contents) inside a syringe. But once the plunger is pushed, they magically shape-shift to a liquid thin enough to flow easily through a standard needle. Upon exit, they immediately reform into gels, protecting the inherent cargo from degrading.
This could be a game changer at a time when many cutting-edge drugs – think Humira for arthritis or Ozempic for type 2 diabetes – are made of quickly degrading proteins too large and complex to simply jam into a pill. Instead, they must be injected, often frequently.
“Because the gel takes months to dissolve, it slowly delivers the drug over time,” Dr. Appel said. “You could conceivably go from a shot once a week to once every 4 months.”
Such slow-release hydrogels could make vaccines last longer, in turn teaching the body to better resist emerging virus variants, and deliver tumor-busting therapies more precisely, said Dr. Appel, who has formed a startup and hopes to fast-track the first hydrogel drug delivery system to clinical trials within a few years.
Meanwhile, another team at the Massachusetts Institute of Technology has taken a different approach, developing a standard-sized ingestible hydrogel pill that swells up like a puffer fish in the stomach, lasting a month and slowly releasing drugs all the while. To remove the pill, a patient simply drinks a salt-based solution that shrivels the ping-pong ball–sized device so it can be passed out of the body.
In a paper in Nature Communications, the scientists showed the puffer fish pill could also be loaded with tiny cameras or monitors to track conditions like ulcers or cancer.
“The dream is to have a Jell-O-like smart pill that, once swallowed, stays in the stomach and monitors the patient’s health,” said Xuanhe Zhao, PhD, a researcher on the project and associate professor of mechanical engineering at MIT.
Building joints and regrowing bones
Since the 1970s, researchers have mulled using hydrogels to replace human cartilage, a remarkably strong and flexible tissue made of about 90% water but able to withstand the weight of a car on an area about the size of a coin.
Until recently, those efforts have largely failed. Meaning when knee cartilage wears down, things like cartilage transplants, drilling holes to stimulate new growth, or total joint replacements – all of which require lengthy rehab – are the only options.
But that may be about to change.
Dr. Wiley and his colleagues at Duke recently reported that they’d developed the first gel-based cartilage substitute even stronger and more durable than the real thing.
By attaching their hydrogel to a titanium backing to help stick it in place, they hope to repair damaged cartilage “much like a dentist fills a cavity” long before surgery is necessary.
They too have partnered with industry to bring their hydrogel to market – starting with knees.
“Ultimately, the goal is to do any joint – hips, ankles, fingers, and toes,” Dr. Wiley said.
At the University of Toronto, chemist Karina Carneiro, PhD, and dentist Christopher McCulloch, DDS, are also thinking big.
In a recent paper in Proceedings of the National Academy of Sciences, they describe a hydrogel, designed by Dr. Carneiro and made of DNA, that can be injected, migrate to a defect in bone – an irreparable break, hole from surgery, or jawbone withered by age – and fill in the gap like putty. But not only does it patch the hole, it prompts the bone to regenerate.
In rats with holes in their skulls due to surgery, they found that the treatment did not work as well as the existing gold standard for repairing holes in bone – grafting bone from elsewhere in the body. But it did work.
“These are very early days for DNA hydrogels,” cautioned Dr. McCulloch, a study coauthor and professor in the Faculty of Dentistry, noting that it will likely be a decade or more before such technology could be available to patients. “But there is the potential that DNA hydrogel could someday grow bone without having to have highly invasive surgical procedures. That’s a significant advancement.”
A sci-fi future
Perhaps the wildest, and weirdest, potential applications of hydrogels come in the realm of human-machine interaction.
Numerous companies are already dabbling in neural prosthetic or brain computer interfaces that might someday, for instance, let someone who is paralyzed and can’t speak write on a laptop using their thoughts.
The spoon-in-the-Jell-O problem has been a major stumbling block.
But Dr. Tringides, who recently earned her PhD in biophysics from Harvard, is working on it.
She and her team have developed a seaweed-based hydrogel loaded with tiny flecks of nanomaterials that can not only meld nicely into squishy brain tissue but also conduct electricity.
Within a decade, she says, this could replace the clunky platinum metal discs used for electrocorticography – recording electrical activity in the brain to identify where seizures start or doing precise brain surgery.
In 30 to 50 years? Let your imagination run wild.
“I’m a skeptic. I like to take research step by step,” she said. “But things are definitely progressing in an interesting direction.”
A version of this article first appeared on WebMD.com.
Imagine a day when a simple injection prompts a broken bone to heal. When tiny, ingestible devices linger in the body, unnoticed, tracking our health or delivering life-saving medications. When brain and heart implants mesh with flesh so seamlessly that the body thinks they’ve been there all along.
These are the dreams of materials scientists who have toiled for decades to mimic the complex architecture of the human body in hopes of replacing broken parts or treating disease.
The problem, say bioengineers, is that most replacement and corrective parts – from prosthetics to pacemakers – are made of hard, dry, lifeless materials, like metal or plastic, while biological tissue is soft, wet, and living.
The body knows the difference and tends to reject imitations.
Enter hydrogels, three-dimensional networks of molecules swollen with – by definition – water.
First described in 1960 by creators of soft contact lenses, these weird, shape-shifting substances are able to morph from liquid to solid to a squishy in-between. (Early, simple uses include hair gel or Jell-O.). Slow to gain attention, growing to just 1,000 studies published by 1982, they’ve become the subject of intense study recently, with 100,000 papers published by 2020, and 3,800 already this year alone.
As chemists, biologists, and engineers begin to work more with one another and with medical doctors,
“We are, essentially, hydrogels,” said Benjamin Wiley, PhD, a chemistry professor at Duke University in Durham, N.C. “As people develop new hydrogels that more closely match the tissues in our body, we’ll be able to treat a whole host of ailments we couldn’t treat before.”
From contact lenses to brain implants
Put simply, a hydrogel is like a mesh bag of water.
The mesh is made of polymers, or spaghetti-like strands of molecules, stitched together in a repeating pattern and swollen with H2O, much like the way 3D matrixes in our body surround, support, and give structure to our cells and tissues.
“Imagine a soccer net, with all of these long fibers woven together to create the net,” said Eric Appel, PhD, associate professor of materials science and engineering at Stanford (Calif.) University.
While the broader category of “gels” could be filled with anything, including chemical solvents, water is the key ingredient that sets hydrogels apart, making them ideal for, as some scientists put it, “merging humans and machines.”
Human bones are about 25% water, while muscles hover around 70% and the brain is 85%. The precious liquid plays a host of critical roles, from shuttling nutrients in and waste out to helping cells talk to each other.
Lab-made hydrogels can be loaded with cargo (like a ball in the net), including cells or drugs that help mimic some of those functions.
Hydrogels are soft and pliable like flesh. So, if used in implants, they may be less likely to damage surrounding tissue.
“Think about a metal spoon in your bowl of pudding. As you’re shaking the bowl, the spoon doesn’t stay in place, and you get scarring around the spoon,” said Christina Tringides, PhD, a materials scientist who studies neural engineering. That, she says, is exactly what happens to brain implants when patients breathe or move. “It’s a mechanical mismatch. But with hydrogels, you could get perfect mechanical matching.”
Hydrogels also tend to be nontoxic, so the immune system may be less likely to attack them as foreign bodies.
All this has made hydrogels the new darling of the bioengineering world.
“There has been an absolute explosion of interest in these materials,” Dr. Appel said.
Smarter drug delivery and ingestible electronics
Early versions of hydrogels were thick and gooey, making it hard to get them inside the body.
“Think of a block of Jell-O. You couldn’t inject something like that,” Dr. Appel said.
But Dr. Appel, whose lab develops new drug delivery systems, has been tinkering with gel formulas for years in hopes that these high-tech globs could someday ferry timed-release drugs to just the right spot in the body.
His new hydrogels start as fully formed gels (which help preserve the drug contents) inside a syringe. But once the plunger is pushed, they magically shape-shift to a liquid thin enough to flow easily through a standard needle. Upon exit, they immediately reform into gels, protecting the inherent cargo from degrading.
This could be a game changer at a time when many cutting-edge drugs – think Humira for arthritis or Ozempic for type 2 diabetes – are made of quickly degrading proteins too large and complex to simply jam into a pill. Instead, they must be injected, often frequently.
“Because the gel takes months to dissolve, it slowly delivers the drug over time,” Dr. Appel said. “You could conceivably go from a shot once a week to once every 4 months.”
Such slow-release hydrogels could make vaccines last longer, in turn teaching the body to better resist emerging virus variants, and deliver tumor-busting therapies more precisely, said Dr. Appel, who has formed a startup and hopes to fast-track the first hydrogel drug delivery system to clinical trials within a few years.
Meanwhile, another team at the Massachusetts Institute of Technology has taken a different approach, developing a standard-sized ingestible hydrogel pill that swells up like a puffer fish in the stomach, lasting a month and slowly releasing drugs all the while. To remove the pill, a patient simply drinks a salt-based solution that shrivels the ping-pong ball–sized device so it can be passed out of the body.
In a paper in Nature Communications, the scientists showed the puffer fish pill could also be loaded with tiny cameras or monitors to track conditions like ulcers or cancer.
“The dream is to have a Jell-O-like smart pill that, once swallowed, stays in the stomach and monitors the patient’s health,” said Xuanhe Zhao, PhD, a researcher on the project and associate professor of mechanical engineering at MIT.
Building joints and regrowing bones
Since the 1970s, researchers have mulled using hydrogels to replace human cartilage, a remarkably strong and flexible tissue made of about 90% water but able to withstand the weight of a car on an area about the size of a coin.
Until recently, those efforts have largely failed. Meaning when knee cartilage wears down, things like cartilage transplants, drilling holes to stimulate new growth, or total joint replacements – all of which require lengthy rehab – are the only options.
But that may be about to change.
Dr. Wiley and his colleagues at Duke recently reported that they’d developed the first gel-based cartilage substitute even stronger and more durable than the real thing.
By attaching their hydrogel to a titanium backing to help stick it in place, they hope to repair damaged cartilage “much like a dentist fills a cavity” long before surgery is necessary.
They too have partnered with industry to bring their hydrogel to market – starting with knees.
“Ultimately, the goal is to do any joint – hips, ankles, fingers, and toes,” Dr. Wiley said.
At the University of Toronto, chemist Karina Carneiro, PhD, and dentist Christopher McCulloch, DDS, are also thinking big.
In a recent paper in Proceedings of the National Academy of Sciences, they describe a hydrogel, designed by Dr. Carneiro and made of DNA, that can be injected, migrate to a defect in bone – an irreparable break, hole from surgery, or jawbone withered by age – and fill in the gap like putty. But not only does it patch the hole, it prompts the bone to regenerate.
In rats with holes in their skulls due to surgery, they found that the treatment did not work as well as the existing gold standard for repairing holes in bone – grafting bone from elsewhere in the body. But it did work.
“These are very early days for DNA hydrogels,” cautioned Dr. McCulloch, a study coauthor and professor in the Faculty of Dentistry, noting that it will likely be a decade or more before such technology could be available to patients. “But there is the potential that DNA hydrogel could someday grow bone without having to have highly invasive surgical procedures. That’s a significant advancement.”
A sci-fi future
Perhaps the wildest, and weirdest, potential applications of hydrogels come in the realm of human-machine interaction.
Numerous companies are already dabbling in neural prosthetic or brain computer interfaces that might someday, for instance, let someone who is paralyzed and can’t speak write on a laptop using their thoughts.
The spoon-in-the-Jell-O problem has been a major stumbling block.
But Dr. Tringides, who recently earned her PhD in biophysics from Harvard, is working on it.
She and her team have developed a seaweed-based hydrogel loaded with tiny flecks of nanomaterials that can not only meld nicely into squishy brain tissue but also conduct electricity.
Within a decade, she says, this could replace the clunky platinum metal discs used for electrocorticography – recording electrical activity in the brain to identify where seizures start or doing precise brain surgery.
In 30 to 50 years? Let your imagination run wild.
“I’m a skeptic. I like to take research step by step,” she said. “But things are definitely progressing in an interesting direction.”
A version of this article first appeared on WebMD.com.
Imagine a day when a simple injection prompts a broken bone to heal. When tiny, ingestible devices linger in the body, unnoticed, tracking our health or delivering life-saving medications. When brain and heart implants mesh with flesh so seamlessly that the body thinks they’ve been there all along.
These are the dreams of materials scientists who have toiled for decades to mimic the complex architecture of the human body in hopes of replacing broken parts or treating disease.
The problem, say bioengineers, is that most replacement and corrective parts – from prosthetics to pacemakers – are made of hard, dry, lifeless materials, like metal or plastic, while biological tissue is soft, wet, and living.
The body knows the difference and tends to reject imitations.
Enter hydrogels, three-dimensional networks of molecules swollen with – by definition – water.
First described in 1960 by creators of soft contact lenses, these weird, shape-shifting substances are able to morph from liquid to solid to a squishy in-between. (Early, simple uses include hair gel or Jell-O.). Slow to gain attention, growing to just 1,000 studies published by 1982, they’ve become the subject of intense study recently, with 100,000 papers published by 2020, and 3,800 already this year alone.
As chemists, biologists, and engineers begin to work more with one another and with medical doctors,
“We are, essentially, hydrogels,” said Benjamin Wiley, PhD, a chemistry professor at Duke University in Durham, N.C. “As people develop new hydrogels that more closely match the tissues in our body, we’ll be able to treat a whole host of ailments we couldn’t treat before.”
From contact lenses to brain implants
Put simply, a hydrogel is like a mesh bag of water.
The mesh is made of polymers, or spaghetti-like strands of molecules, stitched together in a repeating pattern and swollen with H2O, much like the way 3D matrixes in our body surround, support, and give structure to our cells and tissues.
“Imagine a soccer net, with all of these long fibers woven together to create the net,” said Eric Appel, PhD, associate professor of materials science and engineering at Stanford (Calif.) University.
While the broader category of “gels” could be filled with anything, including chemical solvents, water is the key ingredient that sets hydrogels apart, making them ideal for, as some scientists put it, “merging humans and machines.”
Human bones are about 25% water, while muscles hover around 70% and the brain is 85%. The precious liquid plays a host of critical roles, from shuttling nutrients in and waste out to helping cells talk to each other.
Lab-made hydrogels can be loaded with cargo (like a ball in the net), including cells or drugs that help mimic some of those functions.
Hydrogels are soft and pliable like flesh. So, if used in implants, they may be less likely to damage surrounding tissue.
“Think about a metal spoon in your bowl of pudding. As you’re shaking the bowl, the spoon doesn’t stay in place, and you get scarring around the spoon,” said Christina Tringides, PhD, a materials scientist who studies neural engineering. That, she says, is exactly what happens to brain implants when patients breathe or move. “It’s a mechanical mismatch. But with hydrogels, you could get perfect mechanical matching.”
Hydrogels also tend to be nontoxic, so the immune system may be less likely to attack them as foreign bodies.
All this has made hydrogels the new darling of the bioengineering world.
“There has been an absolute explosion of interest in these materials,” Dr. Appel said.
Smarter drug delivery and ingestible electronics
Early versions of hydrogels were thick and gooey, making it hard to get them inside the body.
“Think of a block of Jell-O. You couldn’t inject something like that,” Dr. Appel said.
But Dr. Appel, whose lab develops new drug delivery systems, has been tinkering with gel formulas for years in hopes that these high-tech globs could someday ferry timed-release drugs to just the right spot in the body.
His new hydrogels start as fully formed gels (which help preserve the drug contents) inside a syringe. But once the plunger is pushed, they magically shape-shift to a liquid thin enough to flow easily through a standard needle. Upon exit, they immediately reform into gels, protecting the inherent cargo from degrading.
This could be a game changer at a time when many cutting-edge drugs – think Humira for arthritis or Ozempic for type 2 diabetes – are made of quickly degrading proteins too large and complex to simply jam into a pill. Instead, they must be injected, often frequently.
“Because the gel takes months to dissolve, it slowly delivers the drug over time,” Dr. Appel said. “You could conceivably go from a shot once a week to once every 4 months.”
Such slow-release hydrogels could make vaccines last longer, in turn teaching the body to better resist emerging virus variants, and deliver tumor-busting therapies more precisely, said Dr. Appel, who has formed a startup and hopes to fast-track the first hydrogel drug delivery system to clinical trials within a few years.
Meanwhile, another team at the Massachusetts Institute of Technology has taken a different approach, developing a standard-sized ingestible hydrogel pill that swells up like a puffer fish in the stomach, lasting a month and slowly releasing drugs all the while. To remove the pill, a patient simply drinks a salt-based solution that shrivels the ping-pong ball–sized device so it can be passed out of the body.
In a paper in Nature Communications, the scientists showed the puffer fish pill could also be loaded with tiny cameras or monitors to track conditions like ulcers or cancer.
“The dream is to have a Jell-O-like smart pill that, once swallowed, stays in the stomach and monitors the patient’s health,” said Xuanhe Zhao, PhD, a researcher on the project and associate professor of mechanical engineering at MIT.
Building joints and regrowing bones
Since the 1970s, researchers have mulled using hydrogels to replace human cartilage, a remarkably strong and flexible tissue made of about 90% water but able to withstand the weight of a car on an area about the size of a coin.
Until recently, those efforts have largely failed. Meaning when knee cartilage wears down, things like cartilage transplants, drilling holes to stimulate new growth, or total joint replacements – all of which require lengthy rehab – are the only options.
But that may be about to change.
Dr. Wiley and his colleagues at Duke recently reported that they’d developed the first gel-based cartilage substitute even stronger and more durable than the real thing.
By attaching their hydrogel to a titanium backing to help stick it in place, they hope to repair damaged cartilage “much like a dentist fills a cavity” long before surgery is necessary.
They too have partnered with industry to bring their hydrogel to market – starting with knees.
“Ultimately, the goal is to do any joint – hips, ankles, fingers, and toes,” Dr. Wiley said.
At the University of Toronto, chemist Karina Carneiro, PhD, and dentist Christopher McCulloch, DDS, are also thinking big.
In a recent paper in Proceedings of the National Academy of Sciences, they describe a hydrogel, designed by Dr. Carneiro and made of DNA, that can be injected, migrate to a defect in bone – an irreparable break, hole from surgery, or jawbone withered by age – and fill in the gap like putty. But not only does it patch the hole, it prompts the bone to regenerate.
In rats with holes in their skulls due to surgery, they found that the treatment did not work as well as the existing gold standard for repairing holes in bone – grafting bone from elsewhere in the body. But it did work.
“These are very early days for DNA hydrogels,” cautioned Dr. McCulloch, a study coauthor and professor in the Faculty of Dentistry, noting that it will likely be a decade or more before such technology could be available to patients. “But there is the potential that DNA hydrogel could someday grow bone without having to have highly invasive surgical procedures. That’s a significant advancement.”
A sci-fi future
Perhaps the wildest, and weirdest, potential applications of hydrogels come in the realm of human-machine interaction.
Numerous companies are already dabbling in neural prosthetic or brain computer interfaces that might someday, for instance, let someone who is paralyzed and can’t speak write on a laptop using their thoughts.
The spoon-in-the-Jell-O problem has been a major stumbling block.
But Dr. Tringides, who recently earned her PhD in biophysics from Harvard, is working on it.
She and her team have developed a seaweed-based hydrogel loaded with tiny flecks of nanomaterials that can not only meld nicely into squishy brain tissue but also conduct electricity.
Within a decade, she says, this could replace the clunky platinum metal discs used for electrocorticography – recording electrical activity in the brain to identify where seizures start or doing precise brain surgery.
In 30 to 50 years? Let your imagination run wild.
“I’m a skeptic. I like to take research step by step,” she said. “But things are definitely progressing in an interesting direction.”
A version of this article first appeared on WebMD.com.
Care bundle improves outcome in ICH: INTERACT3
The INTERACT3 study showed that timely administration of a care bundle that included early intensive lowering of systolic blood pressure, strict glucose control, treatment of fever, and rapid reversal of abnormal anticoagulation led to less disability, lower rates of death, and better overall quality of life.
“This is a groundbreaking result. It is the first-ever published trial in ICH patients to show a clear benefit on functional outcomes and on mortality,” lead investigator Craig Anderson, MD, director of global brain health at the George Institute for Global Health, Sydney, said in an interview.
“These results show that, if we can organize care and focus on optimal management of these four aspects of the health of the patient, they do better,” Dr. Anderson said.
‘Game changer’
“This is a game changer because now we have level A evidence showing something is definitely beneficial for these patients,” Dr. Anderson added. “That means hospitals have the imperative to organize their systems to do these things and maximize care. We have never had that before.”
Dr. Anderson noted that, while some previous studies have suggested benefit from various interventions, such as early lowering of blood pressure, the results have not been conclusive.
“This means the intervention has not always been implemented, leading to large variations in clinical practice. But now we have a package that is proven to work; this should become a guideline-recommended practice,” he commented.
The INTERACT-3 results were presented at the European Stroke Organisation conference in Munich. They were also simultaneously published online in The Lancet.
Dr. Anderson explained that, until now, there haven’t been any proven treatments for ICH. “There has been a lot of energy and research put into the field, but this has resulted in several interventions that are ‘probably useful’ or which have a level B recommendation,” he said. “No therapy has been shown to be beneficial in a totally conclusive way, so we are still not entirely sure exactly whether the treatments we use actually make a difference.”
The INTERACT3 researchers therefore decided to evaluate a care package consisting of a bundle of several treatments in the hope that they may have additive or synergistic effects.
The study involved 7,036 patients with imaging-confirmed spontaneous ICH who presented within 6 hours of symptom onset to one of 121 hospitals in 10 mainly low- and middle-income countries: Brazil, China, India, Mexico, Nigeria, Pakistan, Peru, Sri Lanka, Vietnam, and Chile.
Using a cluster design, all hospitals started with usual care as a control and then at some point during the study started using the care bundle intervention.
The care-bundle protocol included the early intensive lowering of systolic blood pressure (target, < 140 mm Hg), strict glucose control (target, 6.1-7.8 mmol/L in those without diabetes and 7.8-10.0 mmol/L in those with diabetes), antipyrexia treatment (target body temperature, ≤ 37.5° C), and rapid reversal of warfarin-related anticoagulation (target international normalized ratio, 1.5) in patients for whom these variables were abnormal.
Overall, the modified intention-to-treat population included 3,221 patients who were assigned to the care-bundle group and 3,815 who were assigned to the usual-care group. Primary outcome data were available for 2,892 patients in the care-bundle group and 3,363 patients in the usual-care group.
The primary outcome was functional recovery, measured with the Modified Rankin Scale at 6 months. Results show that the likelihood of a poor functional outcome was lower in the care-bundle group (common odds ratio, 0.86; P = .015).
Patients who received the interventional care bundle also had a significantly lower rate of serious adverse events (16.0% vs. 20.1%) and mortality (14.1% vs. 17.0%).
NNT of 35 to save one life free of disability
“The number needed to treat (NNT) is just 35 to save a life free of disability,” Dr. Anderson commented. “That’s pretty good. We estimate that this care bundle would save tens of thousands of lives a year if universally adopted.”
The intervention group also spent less time in hospital and had improved health-related quality of life.
Dr. Anderson pointed out that the interventions included in the care bundle were all relatively easy to perform.
“They just require a bit more nursing time and the use of a few inexpensive medicines and maybe infusion pumps, but we’re not talking about the need for skilled surgery or a new therapy costing hundreds of thousands of dollars, so this care bundle should be very straightforward to implement. While we haven’t done a formal cost-effectiveness analysis, I would say it will definitely be good value for money.”
Dr. Anderson believes the rapid lowering of blood pressure is a very important part of the care bundle. He noted that target levels were achieved, on average, in 2.3 hours, compared with 4.0 hours in the control group. But he stressed that this was not just a trial of blood pressure reduction and that the whole package is important.
He gave a couple of possible reasons why this trial was successful whereas previous trials did not show a clear benefit of blood pressure lowering in ICH.
“Firstly, it was a very large trial with more than 7,000 patients – that is more than three times larger than any other trial in ICH. And secondly, the package of care means there are several different interventions that together show a real benefit,” he said. “It’s like the polypill, or a rehabilitation program – if you put several different things together, the whole package can show really positive results.”
Dr. Anderson also pointed out that the study included a wide spectrum of ICH patients, and the benefit of the care bundle was seen across all groups and all stroke severities.
“There were a lot of patients with a large ICH, and if anything, they showed an even larger benefit with the bundle of care,” he said.
The researchers note that the burden of ICH is greatest in low- and middle-income countries. In 2019, 30% of all stroke cases in these countries were ICH, almost double the proportion seen in high-income countries (16%). This is in part attributable to high rates of hypertension and limited resources for primary prevention, including identification and management of stroke risk factors by health care services.
‘Outstanding example’ of less therapeutic negativity
Lili Song, MD, PhD, joint lead author and head of the Stroke Program at the George Institute China, Beijing, said, “A lack of proven treatments for ICH has led to a pessimistic view that not much can be done for these patients.
“However, with INTERACT3, we demonstrate on a large scale how readily available treatments can be used to improve outcomes in resource-limited settings,” she said. “We hope this evidence will inform clinical practice guidelines across the globe and help save many lives.”
In a comment that accompanied the article, Wendy Ziai, MD, Matthew Bower, MD, and Daniel Hanley, MD, Johns Hopkins University, Baltimore, say the INTERACT3 study shows that “an intracerebral hemorrhage care bundle focused on physiological control interventions, whether synergistic or not, might promote better outcomes in hospitals where care has not previously optimized sustained interventions.”
Pointing out that the care bundle has minimal risks of cost and coordination and a high public health effect, they conclude: “This effort is an outstanding example of why less therapeutic negativity, and more intervention might benefit survivors of intracerebral hemorrhage.”
The INTERACT3 study was funded by the Department of Health and Social Care, the Foreign, Commonwealth and Development Office, the Medical Research Council, and the Wellcome Trust (all in the United Kingdom), the West China Hospital Outstanding Discipline Development 1–3-5 Programme, the National Health and Medical Research Council of Australia, Sichuan Credit Pharmaceutical, and Takeda (China).
A version of this article first appeared on Medscape.com.
The INTERACT3 study showed that timely administration of a care bundle that included early intensive lowering of systolic blood pressure, strict glucose control, treatment of fever, and rapid reversal of abnormal anticoagulation led to less disability, lower rates of death, and better overall quality of life.
“This is a groundbreaking result. It is the first-ever published trial in ICH patients to show a clear benefit on functional outcomes and on mortality,” lead investigator Craig Anderson, MD, director of global brain health at the George Institute for Global Health, Sydney, said in an interview.
“These results show that, if we can organize care and focus on optimal management of these four aspects of the health of the patient, they do better,” Dr. Anderson said.
‘Game changer’
“This is a game changer because now we have level A evidence showing something is definitely beneficial for these patients,” Dr. Anderson added. “That means hospitals have the imperative to organize their systems to do these things and maximize care. We have never had that before.”
Dr. Anderson noted that, while some previous studies have suggested benefit from various interventions, such as early lowering of blood pressure, the results have not been conclusive.
“This means the intervention has not always been implemented, leading to large variations in clinical practice. But now we have a package that is proven to work; this should become a guideline-recommended practice,” he commented.
The INTERACT-3 results were presented at the European Stroke Organisation conference in Munich. They were also simultaneously published online in The Lancet.
Dr. Anderson explained that, until now, there haven’t been any proven treatments for ICH. “There has been a lot of energy and research put into the field, but this has resulted in several interventions that are ‘probably useful’ or which have a level B recommendation,” he said. “No therapy has been shown to be beneficial in a totally conclusive way, so we are still not entirely sure exactly whether the treatments we use actually make a difference.”
The INTERACT3 researchers therefore decided to evaluate a care package consisting of a bundle of several treatments in the hope that they may have additive or synergistic effects.
The study involved 7,036 patients with imaging-confirmed spontaneous ICH who presented within 6 hours of symptom onset to one of 121 hospitals in 10 mainly low- and middle-income countries: Brazil, China, India, Mexico, Nigeria, Pakistan, Peru, Sri Lanka, Vietnam, and Chile.
Using a cluster design, all hospitals started with usual care as a control and then at some point during the study started using the care bundle intervention.
The care-bundle protocol included the early intensive lowering of systolic blood pressure (target, < 140 mm Hg), strict glucose control (target, 6.1-7.8 mmol/L in those without diabetes and 7.8-10.0 mmol/L in those with diabetes), antipyrexia treatment (target body temperature, ≤ 37.5° C), and rapid reversal of warfarin-related anticoagulation (target international normalized ratio, 1.5) in patients for whom these variables were abnormal.
Overall, the modified intention-to-treat population included 3,221 patients who were assigned to the care-bundle group and 3,815 who were assigned to the usual-care group. Primary outcome data were available for 2,892 patients in the care-bundle group and 3,363 patients in the usual-care group.
The primary outcome was functional recovery, measured with the Modified Rankin Scale at 6 months. Results show that the likelihood of a poor functional outcome was lower in the care-bundle group (common odds ratio, 0.86; P = .015).
Patients who received the interventional care bundle also had a significantly lower rate of serious adverse events (16.0% vs. 20.1%) and mortality (14.1% vs. 17.0%).
NNT of 35 to save one life free of disability
“The number needed to treat (NNT) is just 35 to save a life free of disability,” Dr. Anderson commented. “That’s pretty good. We estimate that this care bundle would save tens of thousands of lives a year if universally adopted.”
The intervention group also spent less time in hospital and had improved health-related quality of life.
Dr. Anderson pointed out that the interventions included in the care bundle were all relatively easy to perform.
“They just require a bit more nursing time and the use of a few inexpensive medicines and maybe infusion pumps, but we’re not talking about the need for skilled surgery or a new therapy costing hundreds of thousands of dollars, so this care bundle should be very straightforward to implement. While we haven’t done a formal cost-effectiveness analysis, I would say it will definitely be good value for money.”
Dr. Anderson believes the rapid lowering of blood pressure is a very important part of the care bundle. He noted that target levels were achieved, on average, in 2.3 hours, compared with 4.0 hours in the control group. But he stressed that this was not just a trial of blood pressure reduction and that the whole package is important.
He gave a couple of possible reasons why this trial was successful whereas previous trials did not show a clear benefit of blood pressure lowering in ICH.
“Firstly, it was a very large trial with more than 7,000 patients – that is more than three times larger than any other trial in ICH. And secondly, the package of care means there are several different interventions that together show a real benefit,” he said. “It’s like the polypill, or a rehabilitation program – if you put several different things together, the whole package can show really positive results.”
Dr. Anderson also pointed out that the study included a wide spectrum of ICH patients, and the benefit of the care bundle was seen across all groups and all stroke severities.
“There were a lot of patients with a large ICH, and if anything, they showed an even larger benefit with the bundle of care,” he said.
The researchers note that the burden of ICH is greatest in low- and middle-income countries. In 2019, 30% of all stroke cases in these countries were ICH, almost double the proportion seen in high-income countries (16%). This is in part attributable to high rates of hypertension and limited resources for primary prevention, including identification and management of stroke risk factors by health care services.
‘Outstanding example’ of less therapeutic negativity
Lili Song, MD, PhD, joint lead author and head of the Stroke Program at the George Institute China, Beijing, said, “A lack of proven treatments for ICH has led to a pessimistic view that not much can be done for these patients.
“However, with INTERACT3, we demonstrate on a large scale how readily available treatments can be used to improve outcomes in resource-limited settings,” she said. “We hope this evidence will inform clinical practice guidelines across the globe and help save many lives.”
In a comment that accompanied the article, Wendy Ziai, MD, Matthew Bower, MD, and Daniel Hanley, MD, Johns Hopkins University, Baltimore, say the INTERACT3 study shows that “an intracerebral hemorrhage care bundle focused on physiological control interventions, whether synergistic or not, might promote better outcomes in hospitals where care has not previously optimized sustained interventions.”
Pointing out that the care bundle has minimal risks of cost and coordination and a high public health effect, they conclude: “This effort is an outstanding example of why less therapeutic negativity, and more intervention might benefit survivors of intracerebral hemorrhage.”
The INTERACT3 study was funded by the Department of Health and Social Care, the Foreign, Commonwealth and Development Office, the Medical Research Council, and the Wellcome Trust (all in the United Kingdom), the West China Hospital Outstanding Discipline Development 1–3-5 Programme, the National Health and Medical Research Council of Australia, Sichuan Credit Pharmaceutical, and Takeda (China).
A version of this article first appeared on Medscape.com.
The INTERACT3 study showed that timely administration of a care bundle that included early intensive lowering of systolic blood pressure, strict glucose control, treatment of fever, and rapid reversal of abnormal anticoagulation led to less disability, lower rates of death, and better overall quality of life.
“This is a groundbreaking result. It is the first-ever published trial in ICH patients to show a clear benefit on functional outcomes and on mortality,” lead investigator Craig Anderson, MD, director of global brain health at the George Institute for Global Health, Sydney, said in an interview.
“These results show that, if we can organize care and focus on optimal management of these four aspects of the health of the patient, they do better,” Dr. Anderson said.
‘Game changer’
“This is a game changer because now we have level A evidence showing something is definitely beneficial for these patients,” Dr. Anderson added. “That means hospitals have the imperative to organize their systems to do these things and maximize care. We have never had that before.”
Dr. Anderson noted that, while some previous studies have suggested benefit from various interventions, such as early lowering of blood pressure, the results have not been conclusive.
“This means the intervention has not always been implemented, leading to large variations in clinical practice. But now we have a package that is proven to work; this should become a guideline-recommended practice,” he commented.
The INTERACT-3 results were presented at the European Stroke Organisation conference in Munich. They were also simultaneously published online in The Lancet.
Dr. Anderson explained that, until now, there haven’t been any proven treatments for ICH. “There has been a lot of energy and research put into the field, but this has resulted in several interventions that are ‘probably useful’ or which have a level B recommendation,” he said. “No therapy has been shown to be beneficial in a totally conclusive way, so we are still not entirely sure exactly whether the treatments we use actually make a difference.”
The INTERACT3 researchers therefore decided to evaluate a care package consisting of a bundle of several treatments in the hope that they may have additive or synergistic effects.
The study involved 7,036 patients with imaging-confirmed spontaneous ICH who presented within 6 hours of symptom onset to one of 121 hospitals in 10 mainly low- and middle-income countries: Brazil, China, India, Mexico, Nigeria, Pakistan, Peru, Sri Lanka, Vietnam, and Chile.
Using a cluster design, all hospitals started with usual care as a control and then at some point during the study started using the care bundle intervention.
The care-bundle protocol included the early intensive lowering of systolic blood pressure (target, < 140 mm Hg), strict glucose control (target, 6.1-7.8 mmol/L in those without diabetes and 7.8-10.0 mmol/L in those with diabetes), antipyrexia treatment (target body temperature, ≤ 37.5° C), and rapid reversal of warfarin-related anticoagulation (target international normalized ratio, 1.5) in patients for whom these variables were abnormal.
Overall, the modified intention-to-treat population included 3,221 patients who were assigned to the care-bundle group and 3,815 who were assigned to the usual-care group. Primary outcome data were available for 2,892 patients in the care-bundle group and 3,363 patients in the usual-care group.
The primary outcome was functional recovery, measured with the Modified Rankin Scale at 6 months. Results show that the likelihood of a poor functional outcome was lower in the care-bundle group (common odds ratio, 0.86; P = .015).
Patients who received the interventional care bundle also had a significantly lower rate of serious adverse events (16.0% vs. 20.1%) and mortality (14.1% vs. 17.0%).
NNT of 35 to save one life free of disability
“The number needed to treat (NNT) is just 35 to save a life free of disability,” Dr. Anderson commented. “That’s pretty good. We estimate that this care bundle would save tens of thousands of lives a year if universally adopted.”
The intervention group also spent less time in hospital and had improved health-related quality of life.
Dr. Anderson pointed out that the interventions included in the care bundle were all relatively easy to perform.
“They just require a bit more nursing time and the use of a few inexpensive medicines and maybe infusion pumps, but we’re not talking about the need for skilled surgery or a new therapy costing hundreds of thousands of dollars, so this care bundle should be very straightforward to implement. While we haven’t done a formal cost-effectiveness analysis, I would say it will definitely be good value for money.”
Dr. Anderson believes the rapid lowering of blood pressure is a very important part of the care bundle. He noted that target levels were achieved, on average, in 2.3 hours, compared with 4.0 hours in the control group. But he stressed that this was not just a trial of blood pressure reduction and that the whole package is important.
He gave a couple of possible reasons why this trial was successful whereas previous trials did not show a clear benefit of blood pressure lowering in ICH.
“Firstly, it was a very large trial with more than 7,000 patients – that is more than three times larger than any other trial in ICH. And secondly, the package of care means there are several different interventions that together show a real benefit,” he said. “It’s like the polypill, or a rehabilitation program – if you put several different things together, the whole package can show really positive results.”
Dr. Anderson also pointed out that the study included a wide spectrum of ICH patients, and the benefit of the care bundle was seen across all groups and all stroke severities.
“There were a lot of patients with a large ICH, and if anything, they showed an even larger benefit with the bundle of care,” he said.
The researchers note that the burden of ICH is greatest in low- and middle-income countries. In 2019, 30% of all stroke cases in these countries were ICH, almost double the proportion seen in high-income countries (16%). This is in part attributable to high rates of hypertension and limited resources for primary prevention, including identification and management of stroke risk factors by health care services.
‘Outstanding example’ of less therapeutic negativity
Lili Song, MD, PhD, joint lead author and head of the Stroke Program at the George Institute China, Beijing, said, “A lack of proven treatments for ICH has led to a pessimistic view that not much can be done for these patients.
“However, with INTERACT3, we demonstrate on a large scale how readily available treatments can be used to improve outcomes in resource-limited settings,” she said. “We hope this evidence will inform clinical practice guidelines across the globe and help save many lives.”
In a comment that accompanied the article, Wendy Ziai, MD, Matthew Bower, MD, and Daniel Hanley, MD, Johns Hopkins University, Baltimore, say the INTERACT3 study shows that “an intracerebral hemorrhage care bundle focused on physiological control interventions, whether synergistic or not, might promote better outcomes in hospitals where care has not previously optimized sustained interventions.”
Pointing out that the care bundle has minimal risks of cost and coordination and a high public health effect, they conclude: “This effort is an outstanding example of why less therapeutic negativity, and more intervention might benefit survivors of intracerebral hemorrhage.”
The INTERACT3 study was funded by the Department of Health and Social Care, the Foreign, Commonwealth and Development Office, the Medical Research Council, and the Wellcome Trust (all in the United Kingdom), the West China Hospital Outstanding Discipline Development 1–3-5 Programme, the National Health and Medical Research Council of Australia, Sichuan Credit Pharmaceutical, and Takeda (China).
A version of this article first appeared on Medscape.com.
FROM ESO 2023
Younger age of type 2 diabetes onset linked to dementia risk
, new findings suggest.
Moreover, the new data from the prospective Atherosclerosis Risk in Communities (ARIC) cohort also suggest that the previously identified increased risk for dementia among people with prediabetes appears to be entirely explained by the subset who go on to develop type 2 diabetes.
“Our findings suggest that preventing prediabetes progression, especially in younger individuals, may be an important way to reduce the dementia burden,” wrote PhD student Jiaqi Hu of Johns Hopkins University, Baltimore, and colleagues. Their article was published online in Diabetologia.
The result builds on previous findings linking dysglycemia and cognitive decline, the study’s lead author, Elizabeth Selvin, PhD, of the Bloomberg School of Public Health at Johns Hopkins, said in an interview.
“Our prior work in the ARIC study suggests that improving glucose control could help prevent dementia in later life,” she said.

Other studies have also linked higher A1c levels and diabetes in midlife to increased rates of cognitive decline. In addition, Dr. Selvin noted, “There is growing evidence that focusing on vascular health, especially focusing on diabetes and blood pressure, in midlife can stave off dementia in later life.”
This new study is the first to examine the effect of diabetes in the relationship between prediabetes and dementia, as well as the age of diabetes onset on subsequent dementia.
Prediabetes linked to dementia via diabetes development
Of the 11,656 ARIC participants without diabetes at baseline during 1990-1992 (age 46-70 years), 20.0% had prediabetes (defined as A1c 5.7%-6.4% or 39-46 mmol/mol). During a median follow-up of 15.9 years, 3,143 participants developed diabetes. The proportions of patients who developed diabetes were 44.6% among those with prediabetes at baseline versus 22.5% of those without.
Dementia developed in 2,247 participants over a median follow-up of 24.7 years. The cumulative incidence of dementia was 23.9% among those who developed diabetes versus 20.5% among those who did not.
After adjustment for demographics and for the Alzheimer’s disease–linked apolipoprotein E (APOE) gene, prediabetes was significantly associated with incident dementia (hazard ratio [HR], 1.19). However, significance disappeared after adjustment for incident diabetes (HR, 1.09), the researchers reported.
Younger age at diabetes diagnosis raises dementia risk
Age at diabetes diagnosis made a difference in dementia risk. With adjustments for lifestyle, demographic, and clinical factors, those diagnosed with diabetes before age 60 years had a nearly threefold increased risk for dementia compared with those who never developed diabetes (HR, 2.92; P < .001).
The dementia risk was also significantly increased, although to a lesser degree, among those aged 60-69 years at diabetes diagnosis (HR, 1.73; P < .001) and age 70-79 years at diabetes diagnosis (HR, 1.23; P < .001). The relationship was not significant for those aged 80 years and older (HR, 1.13).
“Prevention efforts in people with diabetes diagnosed younger than 65 years should be a high priority,” the authors urged.
Taken together, the data suggest that prolonged exposure to hyperglycemia plays a major role in dementia development.
“Putative mechanisms include acute and chronic hyperglycemia, glucose toxicity, insulin resistance, and microvascular dysfunction of the central nervous system. ... Glucose toxicity and microvascular dysfunction are associated with increased inflammatory and oxidative stress, leading to increased blood–brain permeability,” the researchers wrote.
Dr. Selvin said that her group is pursuing further work in this area using continuous glucose monitoring. “We plan to look at ... how glycemic control and different patterns of glucose in older adults may be linked to cognitive decline and other neurocognitive outcomes.”
The researchers reported no relevant financial relationships. Dr. Selvin has reported being on the advisory board for Diabetologia; she had no role in peer review of the manuscript.
A version of this article first appeared on Medscape.com.
, new findings suggest.
Moreover, the new data from the prospective Atherosclerosis Risk in Communities (ARIC) cohort also suggest that the previously identified increased risk for dementia among people with prediabetes appears to be entirely explained by the subset who go on to develop type 2 diabetes.
“Our findings suggest that preventing prediabetes progression, especially in younger individuals, may be an important way to reduce the dementia burden,” wrote PhD student Jiaqi Hu of Johns Hopkins University, Baltimore, and colleagues. Their article was published online in Diabetologia.
The result builds on previous findings linking dysglycemia and cognitive decline, the study’s lead author, Elizabeth Selvin, PhD, of the Bloomberg School of Public Health at Johns Hopkins, said in an interview.
“Our prior work in the ARIC study suggests that improving glucose control could help prevent dementia in later life,” she said.
Other studies have also linked higher A1c levels and diabetes in midlife to increased rates of cognitive decline. In addition, Dr. Selvin noted, “There is growing evidence that focusing on vascular health, especially focusing on diabetes and blood pressure, in midlife can stave off dementia in later life.”
This new study is the first to examine the effect of diabetes in the relationship between prediabetes and dementia, as well as the age of diabetes onset on subsequent dementia.
Prediabetes linked to dementia via diabetes development
Of the 11,656 ARIC participants without diabetes at baseline during 1990-1992 (age 46-70 years), 20.0% had prediabetes (defined as A1c 5.7%-6.4% or 39-46 mmol/mol). During a median follow-up of 15.9 years, 3,143 participants developed diabetes. The proportions of patients who developed diabetes were 44.6% among those with prediabetes at baseline versus 22.5% of those without.
Dementia developed in 2,247 participants over a median follow-up of 24.7 years. The cumulative incidence of dementia was 23.9% among those who developed diabetes versus 20.5% among those who did not.
After adjustment for demographics and for the Alzheimer’s disease–linked apolipoprotein E (APOE) gene, prediabetes was significantly associated with incident dementia (hazard ratio [HR], 1.19). However, significance disappeared after adjustment for incident diabetes (HR, 1.09), the researchers reported.
Younger age at diabetes diagnosis raises dementia risk
Age at diabetes diagnosis made a difference in dementia risk. With adjustments for lifestyle, demographic, and clinical factors, those diagnosed with diabetes before age 60 years had a nearly threefold increased risk for dementia compared with those who never developed diabetes (HR, 2.92; P < .001).
The dementia risk was also significantly increased, although to a lesser degree, among those aged 60-69 years at diabetes diagnosis (HR, 1.73; P < .001) and age 70-79 years at diabetes diagnosis (HR, 1.23; P < .001). The relationship was not significant for those aged 80 years and older (HR, 1.13).
“Prevention efforts in people with diabetes diagnosed younger than 65 years should be a high priority,” the authors urged.
Taken together, the data suggest that prolonged exposure to hyperglycemia plays a major role in dementia development.
“Putative mechanisms include acute and chronic hyperglycemia, glucose toxicity, insulin resistance, and microvascular dysfunction of the central nervous system. ... Glucose toxicity and microvascular dysfunction are associated with increased inflammatory and oxidative stress, leading to increased blood–brain permeability,” the researchers wrote.
Dr. Selvin said that her group is pursuing further work in this area using continuous glucose monitoring. “We plan to look at ... how glycemic control and different patterns of glucose in older adults may be linked to cognitive decline and other neurocognitive outcomes.”
The researchers reported no relevant financial relationships. Dr. Selvin has reported being on the advisory board for Diabetologia; she had no role in peer review of the manuscript.
A version of this article first appeared on Medscape.com.
, new findings suggest.
Moreover, the new data from the prospective Atherosclerosis Risk in Communities (ARIC) cohort also suggest that the previously identified increased risk for dementia among people with prediabetes appears to be entirely explained by the subset who go on to develop type 2 diabetes.
“Our findings suggest that preventing prediabetes progression, especially in younger individuals, may be an important way to reduce the dementia burden,” wrote PhD student Jiaqi Hu of Johns Hopkins University, Baltimore, and colleagues. Their article was published online in Diabetologia.
The result builds on previous findings linking dysglycemia and cognitive decline, the study’s lead author, Elizabeth Selvin, PhD, of the Bloomberg School of Public Health at Johns Hopkins, said in an interview.
“Our prior work in the ARIC study suggests that improving glucose control could help prevent dementia in later life,” she said.
Other studies have also linked higher A1c levels and diabetes in midlife to increased rates of cognitive decline. In addition, Dr. Selvin noted, “There is growing evidence that focusing on vascular health, especially focusing on diabetes and blood pressure, in midlife can stave off dementia in later life.”
This new study is the first to examine the effect of diabetes in the relationship between prediabetes and dementia, as well as the age of diabetes onset on subsequent dementia.
Prediabetes linked to dementia via diabetes development
Of the 11,656 ARIC participants without diabetes at baseline during 1990-1992 (age 46-70 years), 20.0% had prediabetes (defined as A1c 5.7%-6.4% or 39-46 mmol/mol). During a median follow-up of 15.9 years, 3,143 participants developed diabetes. The proportions of patients who developed diabetes were 44.6% among those with prediabetes at baseline versus 22.5% of those without.
Dementia developed in 2,247 participants over a median follow-up of 24.7 years. The cumulative incidence of dementia was 23.9% among those who developed diabetes versus 20.5% among those who did not.
After adjustment for demographics and for the Alzheimer’s disease–linked apolipoprotein E (APOE) gene, prediabetes was significantly associated with incident dementia (hazard ratio [HR], 1.19). However, significance disappeared after adjustment for incident diabetes (HR, 1.09), the researchers reported.
Younger age at diabetes diagnosis raises dementia risk
Age at diabetes diagnosis made a difference in dementia risk. With adjustments for lifestyle, demographic, and clinical factors, those diagnosed with diabetes before age 60 years had a nearly threefold increased risk for dementia compared with those who never developed diabetes (HR, 2.92; P < .001).
The dementia risk was also significantly increased, although to a lesser degree, among those aged 60-69 years at diabetes diagnosis (HR, 1.73; P < .001) and age 70-79 years at diabetes diagnosis (HR, 1.23; P < .001). The relationship was not significant for those aged 80 years and older (HR, 1.13).
“Prevention efforts in people with diabetes diagnosed younger than 65 years should be a high priority,” the authors urged.
Taken together, the data suggest that prolonged exposure to hyperglycemia plays a major role in dementia development.
“Putative mechanisms include acute and chronic hyperglycemia, glucose toxicity, insulin resistance, and microvascular dysfunction of the central nervous system. ... Glucose toxicity and microvascular dysfunction are associated with increased inflammatory and oxidative stress, leading to increased blood–brain permeability,” the researchers wrote.
Dr. Selvin said that her group is pursuing further work in this area using continuous glucose monitoring. “We plan to look at ... how glycemic control and different patterns of glucose in older adults may be linked to cognitive decline and other neurocognitive outcomes.”
The researchers reported no relevant financial relationships. Dr. Selvin has reported being on the advisory board for Diabetologia; she had no role in peer review of the manuscript.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
Earlier anticoagulation safe in stroke with AFib: ELAN
, a new study suggests.
The ELAN trial found that starting DOAC treatment earlier was not associated with an increased risk for intracranial hemorrhage (ICH) but rather was linked to a lower rate of ischemic events.
“We conclude that there is no reason to delay DOAC treatment in these patients. Our results suggest that early DOAC treatment is reasonable; it is unlikely to cause harm, and it is probably better at reducing ischemic events,” lead investigator of the study, Urs Fischer, MD, professor of neurology at University Hospital Basel (Switzerland), commented in an interview.
“This trial will change clinical practice in that we can feel much more reassured that starting DOAC treatment early in these patients will not cause harm,” he said.
Senior investigator Jesse Dawson, MD, professor of stroke medicine at Queen Elizabeth University Hospital, Glasgow, added: “This issue of timing of DOAC treatment causes a lot of anxiety in our daily workload. Clinicians are scared of causing an ICH, so they tend to wait. These results will ease a lot of that anxiety.”

Dr. Fischer presented the results of the ELAN trial at the European Stroke Organisation Conference (ESOC) in Munich. The trial was also simultaneously published online in The New England Journal of Medicine.
He explained that patients presenting with acute ischemic stroke who are found to have atrial fibrillation need to be started on anticoagulation to reduce the risk for a recurrent stroke. But there are no clear guidelines on when to start anticoagulation in these patients at present, with concerns that starting very early may increase the risk for hemorrhagic transformation and ICH.
Based on observations that patients with larger strokes have a higher risk for ICH in the early post-stroke period, some guidelines advise different times for starting anticoagulation for different stroke severities: 1 day for a transient ischemic attack, 3 days for a minor stroke, 6 days for a moderate stroke, and 12 days for a severe stroke – known as the 1-, 3-, 6-, 12-day rule.
“But this is not based on evidence – just on expert opinion,” Dr. Fischer noted. “The ELAN trial was conducted to obtain more solid information on optimal timing for starting anticoagulation and whether we can safely start a DOAC earlier than these guidelines currently advise.”
For the trial, which was conducted in 15 countries, 2,013 patients with an acute ischemic stroke and found to have AFib were randomly selected to start DOAC treatment earlier or later.
The later-treatment strategy followed the current approach of starting treatment at day 3 or 4 after a minor stroke, day 6 or 7 after a moderate stroke, or day 12, 13, or 14 after a major stroke, whereas the earlier-treatment group started DOAC treatment within 48 hours after a minor or moderate stroke or on day 6 or 7 after a major stroke.
In terms of stroke severity, which was defined on imaging-based criteria, 37% of patients had a minor stroke, 40% had a moderate stroke, and 23% had a major stroke.
The primary outcome was a composite of recurrent ischemic stroke, systemic embolism, major extracranial bleeding, symptomatic intracranial hemorrhage, or vascular death within 30 days after randomization.
Results showed that this occurred in 2.9% in the early-treatment group and 4.1% in the later-treatment group (risk difference, –1.18 percentage points; 95% confidence interval, –2.84-0.47) by 30 days.
Recurrent ischemic stroke occurred in 1.4% in the early-treatment group and 2.5% in the later-treatment group (odds ratio, 0.57; 95% CI, 0.29-1.07). Symptomatic intracranial hemorrhage occurred in two participants (0.2%) in both groups by 30 days.
The rates of the outcomes increased only slightly more at 90 days than at 30 days, “findings that suggest there was not an excessive risk associated with early anticoagulation through that period,” the researchers report in the NEJM paper.
“Early treatment initiation can therefore be supported if indicated or if desired,” they conclude.
“The most important finding was that among 2,000 patients randomized, there was a very low rate of bleeding complications and no increase in any bleeding complication in the early DOAC group. This has been a major worry about starting anticoagulation early,” Dr. Fischer commented.
“These are very practical findings in that we can keep things simple,” Dr. Dawson added. “If the patient has a big stroke, anticoagulation with a DOAC can now be started at 6 days. For everyone else, we can start DOAC treatment as soon as possible without fear of causing harm. So, we can now confidently give patients with a minor or moderate stroke, as defined by imaging, a beneficial treatment as soon as we establish they are having an ischemic stroke and have AFib.”
Dr. Dawson pointed out that about 25% of patients with ischemic stroke are found to have AFib on admission ECG, and in another 4%-5%, AFib is found in the first 48 hours. “These are the patients we are targeting in this study.”
The researchers note that the trial did not have a statistical superiority or noninferiority design but rather aimed to estimate the treatment effects of early initiation versus later initiation of DOACs.
“This trial was slightly different in that we weren’t testing a strict statistical hypothesis because we didn’t have any data with which to formulate what sort of effect size to aim for, so we performed a qualitative trial to look at what the event rates were with the two approaches,” Dr. Fischer explained. “Our main findings are that ICH rates were not increased with early DOAC treatment and that ischemic event rates were numerically reduced, but because we didn’t have strict statistical limits, we can only say this is a high probability but not a certainty.”
Dr. Dawson added: “We can say from these results that there is a high level of probability that early DOAC treatment does not cause harm and a reasonable probability that it reduces risks of a recurrent stroke or other ischemic event.”
The researchers give an estimate of the effect size for the primary composite endpoint, which combines the major ischemic and bleeding events, ranging from a 2.8% lower risk to a 0.5% higher risk with early DOAC treatment.
“So, it is very likely that the composite endpoint would be lower,” Dr. Dawson said.
Dr. Fischer noted that a previous study (TIMING) tried to address the issue of earlier versus later anticoagulation in these patients but was stopped early after 880 patients had been enrolled because of slow recruitment.
“Results from this study failed to show superiority of early versus late DOAC treatment but they did suggest noninferiority, and they also found no increase in major bleeding complications, which is an added reassurance,” he commented.
Another trial looking at early versus late anticoagulation in these patients, OPTIMAS, is ongoing in the United Kingdom and is aiming to randomize 3,500 patients.
Imaging-based assessment of stroke severity
In the ELAN trial, the definition of stroke severity was based on imaging rather than on the National Institutes of Health Stroke Scale (NIHSS).
“We took a cautious approach by using imaging to define stroke severity. So, when using these results in clinical practice, it is important that patients are selected for the timing of DOAC treatment based on the imaging results,” Dr. Dawson explained. “This is very straightforward, as the size of the stroke can be seen clearly on the routine CT imaging that all patients receive up front. This is a very pragmatic and simple protocol. And advanced imaging is not required.”
He noted that though clinicians tend to use the NIHSS clinical symptom score to define mild, moderate, and severe stroke, the imaging approach is actually more accurate when determining the risk for bleeding and ICH. And though imaging results often correlate with NIHSS scores, there can be some exceptions.
Commenting on the ELAN trial results at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that the trial showed that early administration of DOACs in these patients was safe and did not increase the rate of ICH.
“There was a very low ICH rate with only two events in each group. And then there was above a 1% reduction in the composite outcome including ischemic vascular events and bleeding,” he noted.
“This is important because there are many thousands of patients with acute ischemic stroke and AFib, and now we have a large study showing we can treat them with a DOAC early, and this appears to be safe and it appears also be more effective in terms of outcome events,” Dr. Tsivgoulis said.
But he highlighted one important caveat: The majority of patients had mild or moderate stroke.
A version of this article first appeared on Medscape.com.
, a new study suggests.
The ELAN trial found that starting DOAC treatment earlier was not associated with an increased risk for intracranial hemorrhage (ICH) but rather was linked to a lower rate of ischemic events.
“We conclude that there is no reason to delay DOAC treatment in these patients. Our results suggest that early DOAC treatment is reasonable; it is unlikely to cause harm, and it is probably better at reducing ischemic events,” lead investigator of the study, Urs Fischer, MD, professor of neurology at University Hospital Basel (Switzerland), commented in an interview.
“This trial will change clinical practice in that we can feel much more reassured that starting DOAC treatment early in these patients will not cause harm,” he said.
Senior investigator Jesse Dawson, MD, professor of stroke medicine at Queen Elizabeth University Hospital, Glasgow, added: “This issue of timing of DOAC treatment causes a lot of anxiety in our daily workload. Clinicians are scared of causing an ICH, so they tend to wait. These results will ease a lot of that anxiety.”
Dr. Fischer presented the results of the ELAN trial at the European Stroke Organisation Conference (ESOC) in Munich. The trial was also simultaneously published online in The New England Journal of Medicine.
He explained that patients presenting with acute ischemic stroke who are found to have atrial fibrillation need to be started on anticoagulation to reduce the risk for a recurrent stroke. But there are no clear guidelines on when to start anticoagulation in these patients at present, with concerns that starting very early may increase the risk for hemorrhagic transformation and ICH.
Based on observations that patients with larger strokes have a higher risk for ICH in the early post-stroke period, some guidelines advise different times for starting anticoagulation for different stroke severities: 1 day for a transient ischemic attack, 3 days for a minor stroke, 6 days for a moderate stroke, and 12 days for a severe stroke – known as the 1-, 3-, 6-, 12-day rule.
“But this is not based on evidence – just on expert opinion,” Dr. Fischer noted. “The ELAN trial was conducted to obtain more solid information on optimal timing for starting anticoagulation and whether we can safely start a DOAC earlier than these guidelines currently advise.”
For the trial, which was conducted in 15 countries, 2,013 patients with an acute ischemic stroke and found to have AFib were randomly selected to start DOAC treatment earlier or later.
The later-treatment strategy followed the current approach of starting treatment at day 3 or 4 after a minor stroke, day 6 or 7 after a moderate stroke, or day 12, 13, or 14 after a major stroke, whereas the earlier-treatment group started DOAC treatment within 48 hours after a minor or moderate stroke or on day 6 or 7 after a major stroke.
In terms of stroke severity, which was defined on imaging-based criteria, 37% of patients had a minor stroke, 40% had a moderate stroke, and 23% had a major stroke.
The primary outcome was a composite of recurrent ischemic stroke, systemic embolism, major extracranial bleeding, symptomatic intracranial hemorrhage, or vascular death within 30 days after randomization.
Results showed that this occurred in 2.9% in the early-treatment group and 4.1% in the later-treatment group (risk difference, –1.18 percentage points; 95% confidence interval, –2.84-0.47) by 30 days.
Recurrent ischemic stroke occurred in 1.4% in the early-treatment group and 2.5% in the later-treatment group (odds ratio, 0.57; 95% CI, 0.29-1.07). Symptomatic intracranial hemorrhage occurred in two participants (0.2%) in both groups by 30 days.
The rates of the outcomes increased only slightly more at 90 days than at 30 days, “findings that suggest there was not an excessive risk associated with early anticoagulation through that period,” the researchers report in the NEJM paper.
“Early treatment initiation can therefore be supported if indicated or if desired,” they conclude.
“The most important finding was that among 2,000 patients randomized, there was a very low rate of bleeding complications and no increase in any bleeding complication in the early DOAC group. This has been a major worry about starting anticoagulation early,” Dr. Fischer commented.
“These are very practical findings in that we can keep things simple,” Dr. Dawson added. “If the patient has a big stroke, anticoagulation with a DOAC can now be started at 6 days. For everyone else, we can start DOAC treatment as soon as possible without fear of causing harm. So, we can now confidently give patients with a minor or moderate stroke, as defined by imaging, a beneficial treatment as soon as we establish they are having an ischemic stroke and have AFib.”
Dr. Dawson pointed out that about 25% of patients with ischemic stroke are found to have AFib on admission ECG, and in another 4%-5%, AFib is found in the first 48 hours. “These are the patients we are targeting in this study.”
The researchers note that the trial did not have a statistical superiority or noninferiority design but rather aimed to estimate the treatment effects of early initiation versus later initiation of DOACs.
“This trial was slightly different in that we weren’t testing a strict statistical hypothesis because we didn’t have any data with which to formulate what sort of effect size to aim for, so we performed a qualitative trial to look at what the event rates were with the two approaches,” Dr. Fischer explained. “Our main findings are that ICH rates were not increased with early DOAC treatment and that ischemic event rates were numerically reduced, but because we didn’t have strict statistical limits, we can only say this is a high probability but not a certainty.”
Dr. Dawson added: “We can say from these results that there is a high level of probability that early DOAC treatment does not cause harm and a reasonable probability that it reduces risks of a recurrent stroke or other ischemic event.”
The researchers give an estimate of the effect size for the primary composite endpoint, which combines the major ischemic and bleeding events, ranging from a 2.8% lower risk to a 0.5% higher risk with early DOAC treatment.
“So, it is very likely that the composite endpoint would be lower,” Dr. Dawson said.
Dr. Fischer noted that a previous study (TIMING) tried to address the issue of earlier versus later anticoagulation in these patients but was stopped early after 880 patients had been enrolled because of slow recruitment.
“Results from this study failed to show superiority of early versus late DOAC treatment but they did suggest noninferiority, and they also found no increase in major bleeding complications, which is an added reassurance,” he commented.
Another trial looking at early versus late anticoagulation in these patients, OPTIMAS, is ongoing in the United Kingdom and is aiming to randomize 3,500 patients.
Imaging-based assessment of stroke severity
In the ELAN trial, the definition of stroke severity was based on imaging rather than on the National Institutes of Health Stroke Scale (NIHSS).
“We took a cautious approach by using imaging to define stroke severity. So, when using these results in clinical practice, it is important that patients are selected for the timing of DOAC treatment based on the imaging results,” Dr. Dawson explained. “This is very straightforward, as the size of the stroke can be seen clearly on the routine CT imaging that all patients receive up front. This is a very pragmatic and simple protocol. And advanced imaging is not required.”
He noted that though clinicians tend to use the NIHSS clinical symptom score to define mild, moderate, and severe stroke, the imaging approach is actually more accurate when determining the risk for bleeding and ICH. And though imaging results often correlate with NIHSS scores, there can be some exceptions.
Commenting on the ELAN trial results at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that the trial showed that early administration of DOACs in these patients was safe and did not increase the rate of ICH.
“There was a very low ICH rate with only two events in each group. And then there was above a 1% reduction in the composite outcome including ischemic vascular events and bleeding,” he noted.
“This is important because there are many thousands of patients with acute ischemic stroke and AFib, and now we have a large study showing we can treat them with a DOAC early, and this appears to be safe and it appears also be more effective in terms of outcome events,” Dr. Tsivgoulis said.
But he highlighted one important caveat: The majority of patients had mild or moderate stroke.
A version of this article first appeared on Medscape.com.
, a new study suggests.
The ELAN trial found that starting DOAC treatment earlier was not associated with an increased risk for intracranial hemorrhage (ICH) but rather was linked to a lower rate of ischemic events.
“We conclude that there is no reason to delay DOAC treatment in these patients. Our results suggest that early DOAC treatment is reasonable; it is unlikely to cause harm, and it is probably better at reducing ischemic events,” lead investigator of the study, Urs Fischer, MD, professor of neurology at University Hospital Basel (Switzerland), commented in an interview.
“This trial will change clinical practice in that we can feel much more reassured that starting DOAC treatment early in these patients will not cause harm,” he said.
Senior investigator Jesse Dawson, MD, professor of stroke medicine at Queen Elizabeth University Hospital, Glasgow, added: “This issue of timing of DOAC treatment causes a lot of anxiety in our daily workload. Clinicians are scared of causing an ICH, so they tend to wait. These results will ease a lot of that anxiety.”
Dr. Fischer presented the results of the ELAN trial at the European Stroke Organisation Conference (ESOC) in Munich. The trial was also simultaneously published online in The New England Journal of Medicine.
He explained that patients presenting with acute ischemic stroke who are found to have atrial fibrillation need to be started on anticoagulation to reduce the risk for a recurrent stroke. But there are no clear guidelines on when to start anticoagulation in these patients at present, with concerns that starting very early may increase the risk for hemorrhagic transformation and ICH.
Based on observations that patients with larger strokes have a higher risk for ICH in the early post-stroke period, some guidelines advise different times for starting anticoagulation for different stroke severities: 1 day for a transient ischemic attack, 3 days for a minor stroke, 6 days for a moderate stroke, and 12 days for a severe stroke – known as the 1-, 3-, 6-, 12-day rule.
“But this is not based on evidence – just on expert opinion,” Dr. Fischer noted. “The ELAN trial was conducted to obtain more solid information on optimal timing for starting anticoagulation and whether we can safely start a DOAC earlier than these guidelines currently advise.”
For the trial, which was conducted in 15 countries, 2,013 patients with an acute ischemic stroke and found to have AFib were randomly selected to start DOAC treatment earlier or later.
The later-treatment strategy followed the current approach of starting treatment at day 3 or 4 after a minor stroke, day 6 or 7 after a moderate stroke, or day 12, 13, or 14 after a major stroke, whereas the earlier-treatment group started DOAC treatment within 48 hours after a minor or moderate stroke or on day 6 or 7 after a major stroke.
In terms of stroke severity, which was defined on imaging-based criteria, 37% of patients had a minor stroke, 40% had a moderate stroke, and 23% had a major stroke.
The primary outcome was a composite of recurrent ischemic stroke, systemic embolism, major extracranial bleeding, symptomatic intracranial hemorrhage, or vascular death within 30 days after randomization.
Results showed that this occurred in 2.9% in the early-treatment group and 4.1% in the later-treatment group (risk difference, –1.18 percentage points; 95% confidence interval, –2.84-0.47) by 30 days.
Recurrent ischemic stroke occurred in 1.4% in the early-treatment group and 2.5% in the later-treatment group (odds ratio, 0.57; 95% CI, 0.29-1.07). Symptomatic intracranial hemorrhage occurred in two participants (0.2%) in both groups by 30 days.
The rates of the outcomes increased only slightly more at 90 days than at 30 days, “findings that suggest there was not an excessive risk associated with early anticoagulation through that period,” the researchers report in the NEJM paper.
“Early treatment initiation can therefore be supported if indicated or if desired,” they conclude.
“The most important finding was that among 2,000 patients randomized, there was a very low rate of bleeding complications and no increase in any bleeding complication in the early DOAC group. This has been a major worry about starting anticoagulation early,” Dr. Fischer commented.
“These are very practical findings in that we can keep things simple,” Dr. Dawson added. “If the patient has a big stroke, anticoagulation with a DOAC can now be started at 6 days. For everyone else, we can start DOAC treatment as soon as possible without fear of causing harm. So, we can now confidently give patients with a minor or moderate stroke, as defined by imaging, a beneficial treatment as soon as we establish they are having an ischemic stroke and have AFib.”
Dr. Dawson pointed out that about 25% of patients with ischemic stroke are found to have AFib on admission ECG, and in another 4%-5%, AFib is found in the first 48 hours. “These are the patients we are targeting in this study.”
The researchers note that the trial did not have a statistical superiority or noninferiority design but rather aimed to estimate the treatment effects of early initiation versus later initiation of DOACs.
“This trial was slightly different in that we weren’t testing a strict statistical hypothesis because we didn’t have any data with which to formulate what sort of effect size to aim for, so we performed a qualitative trial to look at what the event rates were with the two approaches,” Dr. Fischer explained. “Our main findings are that ICH rates were not increased with early DOAC treatment and that ischemic event rates were numerically reduced, but because we didn’t have strict statistical limits, we can only say this is a high probability but not a certainty.”
Dr. Dawson added: “We can say from these results that there is a high level of probability that early DOAC treatment does not cause harm and a reasonable probability that it reduces risks of a recurrent stroke or other ischemic event.”
The researchers give an estimate of the effect size for the primary composite endpoint, which combines the major ischemic and bleeding events, ranging from a 2.8% lower risk to a 0.5% higher risk with early DOAC treatment.
“So, it is very likely that the composite endpoint would be lower,” Dr. Dawson said.
Dr. Fischer noted that a previous study (TIMING) tried to address the issue of earlier versus later anticoagulation in these patients but was stopped early after 880 patients had been enrolled because of slow recruitment.
“Results from this study failed to show superiority of early versus late DOAC treatment but they did suggest noninferiority, and they also found no increase in major bleeding complications, which is an added reassurance,” he commented.
Another trial looking at early versus late anticoagulation in these patients, OPTIMAS, is ongoing in the United Kingdom and is aiming to randomize 3,500 patients.
Imaging-based assessment of stroke severity
In the ELAN trial, the definition of stroke severity was based on imaging rather than on the National Institutes of Health Stroke Scale (NIHSS).
“We took a cautious approach by using imaging to define stroke severity. So, when using these results in clinical practice, it is important that patients are selected for the timing of DOAC treatment based on the imaging results,” Dr. Dawson explained. “This is very straightforward, as the size of the stroke can be seen clearly on the routine CT imaging that all patients receive up front. This is a very pragmatic and simple protocol. And advanced imaging is not required.”
He noted that though clinicians tend to use the NIHSS clinical symptom score to define mild, moderate, and severe stroke, the imaging approach is actually more accurate when determining the risk for bleeding and ICH. And though imaging results often correlate with NIHSS scores, there can be some exceptions.
Commenting on the ELAN trial results at the ESOC meeting, Georgios Tsivgoulis, MD, professor of neurology, University of Athens, said that the trial showed that early administration of DOACs in these patients was safe and did not increase the rate of ICH.
“There was a very low ICH rate with only two events in each group. And then there was above a 1% reduction in the composite outcome including ischemic vascular events and bleeding,” he noted.
“This is important because there are many thousands of patients with acute ischemic stroke and AFib, and now we have a large study showing we can treat them with a DOAC early, and this appears to be safe and it appears also be more effective in terms of outcome events,” Dr. Tsivgoulis said.
But he highlighted one important caveat: The majority of patients had mild or moderate stroke.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023