User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Human gene editing consensus study underway
A consensus study of the scientific underpinnings of human gene editing technologies is underway, and the committee of experts behind the effort will independently review potential applications for those technologies, as well as the clinical, ethical, legal, and social implications of their use.
The multidisciplinary committee met Feb. 11 to receive input from select stakeholders as it launches its review, the results of which will represent the official views of the National Academy of Sciences and the National Academy of Medicine.

Among those stakeholders were representatives from several companies commercializing gene editing, a representative from the National Institutes of Health, and patient advocacy groups.
With some caveats, participants lobbied to maintain the existing regulatory framework related to gene therapy.
Michael Werner, cofounder and executive director of the Alliance for Regenerative Medicine, which advocates globally for regenerative medicine and advanced therapies, said his organization believes “the existing regulatory framework overall works for these technologies.”
“We don’t believe the [Food and Drug Administration], for example, needs to create a whole separate oversight process in addition to the process we already have now for gene therapy,” he said, adding that “the ultimate goal here is not to have regulatory action or legislative action that will hinder or delay the development of these technologies.”
The consensus study follows an International Summit on Human Gene Editing held in December, and is the next component of the Human Gene Editing Initiative. The committee will study the potential for gene editing in biomedical research and medicine – including human germline editing – although representatives from each of the companies represented at the meeting noted that they are not currently focused on germline applications.
Rather, the commercial focus is on other areas, such as correcting genes in somatic cells.
“We start with medical need. We want to work on things where there is not currently a therapy that addresses adequately the medical need, and we need the ability to generate a differentiated product,” said Vic Myer, Ph.D., of Editas Medicine in Cambridge, Mass.
The company has projects underway for opthalmologic applications, sickle cell anemia, beta-thalassemia, Duchenne muscular dystrophy, cystic fibrosis, alpha1-antitrypsin deficiency in the liver, and others.
“We are working on a number of different types of edits in a number of different tissues with a number of delivery modalities,” Dr. Myer said, noting that some programs will move quickly, while others will not.
Similarly, Intellia Therapeutics, also of Cambridge, Mass., is “focusing very much on what we hope will be curative products for somatic gene-based disorders,” said Dr. John Leonard, the company’s chief medical officer.
“We limit our work to somatic cells. We thought very carefully about that and that is what we do,” he added, noting that a recently launched division of Intellia is focused on autoimmune oncology opportunities (ex vivo), and on liver disease (in vivo).
The committee of experts conducting the consensus study, which began its information-gathering process in December at the International Summit on Human Gene Editing, will take these and other views expressed at the meeting into consideration during its work over the next year. The study will include a literature review and data gathering via meetings in the United States and abroad. The committee will continue to seek input from researchers, clinicians, policy makers, and the public.
“The committee will also monitor in real time the latest scientific achievements of importance in this rapidly developing field,” according to information from the National Academies.
The field has enormous potential, according to Mr. Werner, who explained that combined, the various types of gene editing technology available are “pretty powerful” in terms of an approach for targeting and changing DNA sequences in human cells.
“We’re talking about the potential to durably treat and potentially even cure diseases that currently represent unmet medical needs,” he said. “We could, in theory, be talking about millions of patients worldwide.”
A consensus study of the scientific underpinnings of human gene editing technologies is underway, and the committee of experts behind the effort will independently review potential applications for those technologies, as well as the clinical, ethical, legal, and social implications of their use.
The multidisciplinary committee met Feb. 11 to receive input from select stakeholders as it launches its review, the results of which will represent the official views of the National Academy of Sciences and the National Academy of Medicine.
Among those stakeholders were representatives from several companies commercializing gene editing, a representative from the National Institutes of Health, and patient advocacy groups.
With some caveats, participants lobbied to maintain the existing regulatory framework related to gene therapy.
Michael Werner, cofounder and executive director of the Alliance for Regenerative Medicine, which advocates globally for regenerative medicine and advanced therapies, said his organization believes “the existing regulatory framework overall works for these technologies.”
“We don’t believe the [Food and Drug Administration], for example, needs to create a whole separate oversight process in addition to the process we already have now for gene therapy,” he said, adding that “the ultimate goal here is not to have regulatory action or legislative action that will hinder or delay the development of these technologies.”
The consensus study follows an International Summit on Human Gene Editing held in December, and is the next component of the Human Gene Editing Initiative. The committee will study the potential for gene editing in biomedical research and medicine – including human germline editing – although representatives from each of the companies represented at the meeting noted that they are not currently focused on germline applications.
Rather, the commercial focus is on other areas, such as correcting genes in somatic cells.
“We start with medical need. We want to work on things where there is not currently a therapy that addresses adequately the medical need, and we need the ability to generate a differentiated product,” said Vic Myer, Ph.D., of Editas Medicine in Cambridge, Mass.
The company has projects underway for opthalmologic applications, sickle cell anemia, beta-thalassemia, Duchenne muscular dystrophy, cystic fibrosis, alpha1-antitrypsin deficiency in the liver, and others.
“We are working on a number of different types of edits in a number of different tissues with a number of delivery modalities,” Dr. Myer said, noting that some programs will move quickly, while others will not.
Similarly, Intellia Therapeutics, also of Cambridge, Mass., is “focusing very much on what we hope will be curative products for somatic gene-based disorders,” said Dr. John Leonard, the company’s chief medical officer.
“We limit our work to somatic cells. We thought very carefully about that and that is what we do,” he added, noting that a recently launched division of Intellia is focused on autoimmune oncology opportunities (ex vivo), and on liver disease (in vivo).
The committee of experts conducting the consensus study, which began its information-gathering process in December at the International Summit on Human Gene Editing, will take these and other views expressed at the meeting into consideration during its work over the next year. The study will include a literature review and data gathering via meetings in the United States and abroad. The committee will continue to seek input from researchers, clinicians, policy makers, and the public.
“The committee will also monitor in real time the latest scientific achievements of importance in this rapidly developing field,” according to information from the National Academies.
The field has enormous potential, according to Mr. Werner, who explained that combined, the various types of gene editing technology available are “pretty powerful” in terms of an approach for targeting and changing DNA sequences in human cells.
“We’re talking about the potential to durably treat and potentially even cure diseases that currently represent unmet medical needs,” he said. “We could, in theory, be talking about millions of patients worldwide.”
A consensus study of the scientific underpinnings of human gene editing technologies is underway, and the committee of experts behind the effort will independently review potential applications for those technologies, as well as the clinical, ethical, legal, and social implications of their use.
The multidisciplinary committee met Feb. 11 to receive input from select stakeholders as it launches its review, the results of which will represent the official views of the National Academy of Sciences and the National Academy of Medicine.
Among those stakeholders were representatives from several companies commercializing gene editing, a representative from the National Institutes of Health, and patient advocacy groups.
With some caveats, participants lobbied to maintain the existing regulatory framework related to gene therapy.
Michael Werner, cofounder and executive director of the Alliance for Regenerative Medicine, which advocates globally for regenerative medicine and advanced therapies, said his organization believes “the existing regulatory framework overall works for these technologies.”
“We don’t believe the [Food and Drug Administration], for example, needs to create a whole separate oversight process in addition to the process we already have now for gene therapy,” he said, adding that “the ultimate goal here is not to have regulatory action or legislative action that will hinder or delay the development of these technologies.”
The consensus study follows an International Summit on Human Gene Editing held in December, and is the next component of the Human Gene Editing Initiative. The committee will study the potential for gene editing in biomedical research and medicine – including human germline editing – although representatives from each of the companies represented at the meeting noted that they are not currently focused on germline applications.
Rather, the commercial focus is on other areas, such as correcting genes in somatic cells.
“We start with medical need. We want to work on things where there is not currently a therapy that addresses adequately the medical need, and we need the ability to generate a differentiated product,” said Vic Myer, Ph.D., of Editas Medicine in Cambridge, Mass.
The company has projects underway for opthalmologic applications, sickle cell anemia, beta-thalassemia, Duchenne muscular dystrophy, cystic fibrosis, alpha1-antitrypsin deficiency in the liver, and others.
“We are working on a number of different types of edits in a number of different tissues with a number of delivery modalities,” Dr. Myer said, noting that some programs will move quickly, while others will not.
Similarly, Intellia Therapeutics, also of Cambridge, Mass., is “focusing very much on what we hope will be curative products for somatic gene-based disorders,” said Dr. John Leonard, the company’s chief medical officer.
“We limit our work to somatic cells. We thought very carefully about that and that is what we do,” he added, noting that a recently launched division of Intellia is focused on autoimmune oncology opportunities (ex vivo), and on liver disease (in vivo).
The committee of experts conducting the consensus study, which began its information-gathering process in December at the International Summit on Human Gene Editing, will take these and other views expressed at the meeting into consideration during its work over the next year. The study will include a literature review and data gathering via meetings in the United States and abroad. The committee will continue to seek input from researchers, clinicians, policy makers, and the public.
“The committee will also monitor in real time the latest scientific achievements of importance in this rapidly developing field,” according to information from the National Academies.
The field has enormous potential, according to Mr. Werner, who explained that combined, the various types of gene editing technology available are “pretty powerful” in terms of an approach for targeting and changing DNA sequences in human cells.
“We’re talking about the potential to durably treat and potentially even cure diseases that currently represent unmet medical needs,” he said. “We could, in theory, be talking about millions of patients worldwide.”
Evidence-based bundles reduced shoulder dystocia rates
ATLANTA – Implementation of evidence-based practice bundles was associated with significant reductions in shoulder dystocia, brachial plexus injury, and operative vaginal delivery in a large multicenter hospital system.
From the 18 months prior to implementation of the bundles – which included a planned vaginal delivery tool to assess for shoulder dystocia risk – to the 36 months after implementation, the rate of shoulder dystocia decreased from 1.7 to 1.4 per 100 births, Dr. Laura Sienas reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.

“This is a 17.6% reduction in the rate of shoulder dystocia. There was a statistically significant association with increasing bundle compliance of both bundles with a decrease in shoulder dystocia,” said Dr. Sienas, a 3rd-year resident at the University of California, Davis.
Additionally, the rate of brachial plexus injury decreased significantly from 2.1 to 1.5 per 1,000 births (a 29% reduction), and the rate of operative vaginal deliveries also decreased significantly, from 6.1 to 5.0 per 100 births (an 18% reduction).
At the same time, there was no significant change in the primary and total Cesarean section rates: 16.5 per 100 births and 30.1 per 100 births, respectively, she noted.
Key elements of the evidence-based practice bundles included an admission risk assessment, and a review and timeout prior to operative vaginal delivery. Low-fidelity shoulder dystocia drills were also introduced for nurses and physicians. While the drills improved teamwork and communication, they did not result in decreased brachial plexus injury rates, Dr. Sienas noted.
Future research should consider whether high-fidelity drills would lower the rate of brachial plexus injury, she added.
Data for this study was collected from 29 maternal centers, with size ranging from small and rural with fewer than 200 deliveries each year, to large urban hospitals with about 5,000 annual births. Baseline data included all singleton vertex births over 34 weeks’ gestation – about 169,000 total births. After all participating centers attained 90% compliance with the evidence-based practice bundles, about 103,000 deliveries occurred. Compliance with the bundles was scored as all or none.
The 29 hospitals in the health system where this study took place have average delivery volumes between 150 and 5,000 births per year, suggesting that the current findings would be applicable to nearly all delivery units in the United States, she said.
Dr. Sienas reported having no financial disclosures.
ATLANTA – Implementation of evidence-based practice bundles was associated with significant reductions in shoulder dystocia, brachial plexus injury, and operative vaginal delivery in a large multicenter hospital system.
From the 18 months prior to implementation of the bundles – which included a planned vaginal delivery tool to assess for shoulder dystocia risk – to the 36 months after implementation, the rate of shoulder dystocia decreased from 1.7 to 1.4 per 100 births, Dr. Laura Sienas reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
“This is a 17.6% reduction in the rate of shoulder dystocia. There was a statistically significant association with increasing bundle compliance of both bundles with a decrease in shoulder dystocia,” said Dr. Sienas, a 3rd-year resident at the University of California, Davis.
Additionally, the rate of brachial plexus injury decreased significantly from 2.1 to 1.5 per 1,000 births (a 29% reduction), and the rate of operative vaginal deliveries also decreased significantly, from 6.1 to 5.0 per 100 births (an 18% reduction).
At the same time, there was no significant change in the primary and total Cesarean section rates: 16.5 per 100 births and 30.1 per 100 births, respectively, she noted.
Key elements of the evidence-based practice bundles included an admission risk assessment, and a review and timeout prior to operative vaginal delivery. Low-fidelity shoulder dystocia drills were also introduced for nurses and physicians. While the drills improved teamwork and communication, they did not result in decreased brachial plexus injury rates, Dr. Sienas noted.
Future research should consider whether high-fidelity drills would lower the rate of brachial plexus injury, she added.
Data for this study was collected from 29 maternal centers, with size ranging from small and rural with fewer than 200 deliveries each year, to large urban hospitals with about 5,000 annual births. Baseline data included all singleton vertex births over 34 weeks’ gestation – about 169,000 total births. After all participating centers attained 90% compliance with the evidence-based practice bundles, about 103,000 deliveries occurred. Compliance with the bundles was scored as all or none.
The 29 hospitals in the health system where this study took place have average delivery volumes between 150 and 5,000 births per year, suggesting that the current findings would be applicable to nearly all delivery units in the United States, she said.
Dr. Sienas reported having no financial disclosures.
ATLANTA – Implementation of evidence-based practice bundles was associated with significant reductions in shoulder dystocia, brachial plexus injury, and operative vaginal delivery in a large multicenter hospital system.
From the 18 months prior to implementation of the bundles – which included a planned vaginal delivery tool to assess for shoulder dystocia risk – to the 36 months after implementation, the rate of shoulder dystocia decreased from 1.7 to 1.4 per 100 births, Dr. Laura Sienas reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
“This is a 17.6% reduction in the rate of shoulder dystocia. There was a statistically significant association with increasing bundle compliance of both bundles with a decrease in shoulder dystocia,” said Dr. Sienas, a 3rd-year resident at the University of California, Davis.
Additionally, the rate of brachial plexus injury decreased significantly from 2.1 to 1.5 per 1,000 births (a 29% reduction), and the rate of operative vaginal deliveries also decreased significantly, from 6.1 to 5.0 per 100 births (an 18% reduction).
At the same time, there was no significant change in the primary and total Cesarean section rates: 16.5 per 100 births and 30.1 per 100 births, respectively, she noted.
Key elements of the evidence-based practice bundles included an admission risk assessment, and a review and timeout prior to operative vaginal delivery. Low-fidelity shoulder dystocia drills were also introduced for nurses and physicians. While the drills improved teamwork and communication, they did not result in decreased brachial plexus injury rates, Dr. Sienas noted.
Future research should consider whether high-fidelity drills would lower the rate of brachial plexus injury, she added.
Data for this study was collected from 29 maternal centers, with size ranging from small and rural with fewer than 200 deliveries each year, to large urban hospitals with about 5,000 annual births. Baseline data included all singleton vertex births over 34 weeks’ gestation – about 169,000 total births. After all participating centers attained 90% compliance with the evidence-based practice bundles, about 103,000 deliveries occurred. Compliance with the bundles was scored as all or none.
The 29 hospitals in the health system where this study took place have average delivery volumes between 150 and 5,000 births per year, suggesting that the current findings would be applicable to nearly all delivery units in the United States, she said.
Dr. Sienas reported having no financial disclosures.
AT THE PREGNANCY MEETING
Key clinical point: Use of evidence-based practice bundles helped reduce rates of shoulder dystocia, brachial plexus injury, and operative vaginal delivery.
Major finding: Shoulder dystocia rates dropped by 17.6% and brachial plexus injuries by 29% with implementation of the bundles.
Data source: A multicenter prospective study of more than 100,000 births.
Disclosures: Dr. Sienas reported having no financial disclosures.

VIDEO: SMFM panelist addresses Zika virus testing
ATLANTA – Information about managing pregnant patients who have potential exposure to the Zika virus is evolving rapidly, and in light of new recommendations on sexual transmission of the infection, officials from the Society for Maternal-Fetal Medicine convened an expert panel to address the matter.
Leaders from the society joined officials from the Centers for Disease Control and Prevention to discuss the updated guidance – particularly a new recommendation for initially conducting serologic testing in pregnant women who have traveled to endemic areas.
Panel members advised physicians to keep a log of patients with possible Zika virus exposure, so those women can be managed properly in the event of future changes to the guidelines.
In an interview at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, panelist Dr. Brenna Hughes of Brown University, Providence, R.I., stressed the need to work with state health officials to develop local guidelines and testing mechanisms. “It will take a little time to build up the infrastructure for that kind of testing,” she said, adding that it is important to avoid delays.
Dr. Hughes reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ATLANTA – Information about managing pregnant patients who have potential exposure to the Zika virus is evolving rapidly, and in light of new recommendations on sexual transmission of the infection, officials from the Society for Maternal-Fetal Medicine convened an expert panel to address the matter.
Leaders from the society joined officials from the Centers for Disease Control and Prevention to discuss the updated guidance – particularly a new recommendation for initially conducting serologic testing in pregnant women who have traveled to endemic areas.
Panel members advised physicians to keep a log of patients with possible Zika virus exposure, so those women can be managed properly in the event of future changes to the guidelines.
In an interview at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, panelist Dr. Brenna Hughes of Brown University, Providence, R.I., stressed the need to work with state health officials to develop local guidelines and testing mechanisms. “It will take a little time to build up the infrastructure for that kind of testing,” she said, adding that it is important to avoid delays.
Dr. Hughes reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ATLANTA – Information about managing pregnant patients who have potential exposure to the Zika virus is evolving rapidly, and in light of new recommendations on sexual transmission of the infection, officials from the Society for Maternal-Fetal Medicine convened an expert panel to address the matter.
Leaders from the society joined officials from the Centers for Disease Control and Prevention to discuss the updated guidance – particularly a new recommendation for initially conducting serologic testing in pregnant women who have traveled to endemic areas.
Panel members advised physicians to keep a log of patients with possible Zika virus exposure, so those women can be managed properly in the event of future changes to the guidelines.
In an interview at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, panelist Dr. Brenna Hughes of Brown University, Providence, R.I., stressed the need to work with state health officials to develop local guidelines and testing mechanisms. “It will take a little time to build up the infrastructure for that kind of testing,” she said, adding that it is important to avoid delays.
Dr. Hughes reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE PREGNANCY MEETING

OPPTIMUM Trial: No benefit found for vaginal progesterone in preterm birth prevention
ATLANTA – Vaginal progesterone confers no obstetrical or neonatal benefit, and no long-term benefit with respect to cognitive and neurosensory outcomes in children when used to prevent preterm birth, according to findings from the randomized, controlled, double-blind OPPTIMUM trial.
The findings from OPPTIMUM – the largest trial to date looking at progesterone for the prevention of preterm birth – have important implications for current practice. Vaginal progesterone is not currently approved for the prevention of preterm birth in the United States, but is commonly used off label for this purpose.

Prior studies have demonstrated a benefit with respect to progesterone for the prevention of preterm birth, particularly in women with a short cervix, but no studies have looked at long-term outcomes, Dr. Jane E. Norman of the University of Edinburgh reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
In OPPTIMUM, the rate of the primary obstetric outcome of preterm birth or fetal death before 34 weeks’ gestation did not differ significantly for 618 women at risk for preterm birth who were randomized to receive 200 mg of vaginal progesterone daily starting at 22-24 weeks and continuing to 34 weeks’ gestation, compared with 600 women who received placebo (16% vs. 18%; odds ratio, 0.86), Dr. Norman said.
The rate of the primary neonatal composite outcome of death or major morbidity (brain injury or bronchopulmonary dysplasia) also did not differ significantly between the progesterone and placebo groups after a prespecified multiple comparisons procedure (6% vs. 10%; odds ratio, 0.62).
A secondary analysis looking at the individual components of the composite neonatal outcomes showed that progesterone reduced the risk of brain injury and neonatal death, but not bronchopulmonary dysplasia, she said.
Further, no difference was seen in Bayley III cognitive scores (with values imputed for deaths) at 2 years of age in 439 and 430 children born to mothers in the progesterone and placebo groups, respectively (average scores, 97.7 and 97.3; odds ratio, 0.48).
On secondary analyses, some safety signals were noted with respect to neurodevelopmental outcomes.
“We were really surprised that we didn’t show that progesterone prevented preterm birth, and we became concerned that perhaps our cutoff of 34 weeks was just the wrong time to choose a cutoff,” Dr. Norman said, noting that a post hoc survival curve analysis was performed to look at the trajectory to delivery, and a “very marginal benefit” was seen with progesterone, but the difference was not statistically significant.
In addition, subgroup analyses showed no significant benefit of progesterone on obstetrical, neonatal, or childhood outcomes. For example, in women with a short cervix, no evidence was seen that progesterone was more or less effective than in women with a longer cervix. Other subgroups studied included fibronectin-positive and fibronectin-negative women and women with a history of preterm birth. Progesterone was no more or less effective in any of the subgroups, Dr. Norman said.
OPPTIMUM study subjects were women at risk of preterm birth because of a positive fetal fibronectin test result, a history of spontaneous preterm birth at or before 34 weeks’ gestation, or a short cervix (25 mm or less).
All outcomes were adjusted for a previous pregnancy of 14 weeks’ gestation or greater, with study center as a random effect.
“OPPTIMUM is the largest trial of progesterone to prevent preterm birth, and after adjusting for multiple comparisons as we planned, we did not disprove the null hypothesis that progesterone doesn’t prevent preterm birth, it doesn’t reduce adverse neonatal outcomes, and it doesn’t have a beneficial effect on childhood outcomes,” Dr. Norman said, concluding that “there is a remaining unmet need for a safe and effective agent to prevent preterm birth.”
Asked about the safety of progesterone given the findings from secondary analyses in OPPTIMUM, she said, “I would not advise my daughter to take progesterone if she’s pregnant.”
The study drug and placebo were donated by Besins, but the company was not involved in study design or analysis. Funding was provided by the Medical Research Council. Dr. Norman reported having no relevant financial disclosures.
ATLANTA – Vaginal progesterone confers no obstetrical or neonatal benefit, and no long-term benefit with respect to cognitive and neurosensory outcomes in children when used to prevent preterm birth, according to findings from the randomized, controlled, double-blind OPPTIMUM trial.
The findings from OPPTIMUM – the largest trial to date looking at progesterone for the prevention of preterm birth – have important implications for current practice. Vaginal progesterone is not currently approved for the prevention of preterm birth in the United States, but is commonly used off label for this purpose.
Prior studies have demonstrated a benefit with respect to progesterone for the prevention of preterm birth, particularly in women with a short cervix, but no studies have looked at long-term outcomes, Dr. Jane E. Norman of the University of Edinburgh reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
In OPPTIMUM, the rate of the primary obstetric outcome of preterm birth or fetal death before 34 weeks’ gestation did not differ significantly for 618 women at risk for preterm birth who were randomized to receive 200 mg of vaginal progesterone daily starting at 22-24 weeks and continuing to 34 weeks’ gestation, compared with 600 women who received placebo (16% vs. 18%; odds ratio, 0.86), Dr. Norman said.
The rate of the primary neonatal composite outcome of death or major morbidity (brain injury or bronchopulmonary dysplasia) also did not differ significantly between the progesterone and placebo groups after a prespecified multiple comparisons procedure (6% vs. 10%; odds ratio, 0.62).
A secondary analysis looking at the individual components of the composite neonatal outcomes showed that progesterone reduced the risk of brain injury and neonatal death, but not bronchopulmonary dysplasia, she said.
Further, no difference was seen in Bayley III cognitive scores (with values imputed for deaths) at 2 years of age in 439 and 430 children born to mothers in the progesterone and placebo groups, respectively (average scores, 97.7 and 97.3; odds ratio, 0.48).
On secondary analyses, some safety signals were noted with respect to neurodevelopmental outcomes.
“We were really surprised that we didn’t show that progesterone prevented preterm birth, and we became concerned that perhaps our cutoff of 34 weeks was just the wrong time to choose a cutoff,” Dr. Norman said, noting that a post hoc survival curve analysis was performed to look at the trajectory to delivery, and a “very marginal benefit” was seen with progesterone, but the difference was not statistically significant.
In addition, subgroup analyses showed no significant benefit of progesterone on obstetrical, neonatal, or childhood outcomes. For example, in women with a short cervix, no evidence was seen that progesterone was more or less effective than in women with a longer cervix. Other subgroups studied included fibronectin-positive and fibronectin-negative women and women with a history of preterm birth. Progesterone was no more or less effective in any of the subgroups, Dr. Norman said.
OPPTIMUM study subjects were women at risk of preterm birth because of a positive fetal fibronectin test result, a history of spontaneous preterm birth at or before 34 weeks’ gestation, or a short cervix (25 mm or less).
All outcomes were adjusted for a previous pregnancy of 14 weeks’ gestation or greater, with study center as a random effect.
“OPPTIMUM is the largest trial of progesterone to prevent preterm birth, and after adjusting for multiple comparisons as we planned, we did not disprove the null hypothesis that progesterone doesn’t prevent preterm birth, it doesn’t reduce adverse neonatal outcomes, and it doesn’t have a beneficial effect on childhood outcomes,” Dr. Norman said, concluding that “there is a remaining unmet need for a safe and effective agent to prevent preterm birth.”
Asked about the safety of progesterone given the findings from secondary analyses in OPPTIMUM, she said, “I would not advise my daughter to take progesterone if she’s pregnant.”
The study drug and placebo were donated by Besins, but the company was not involved in study design or analysis. Funding was provided by the Medical Research Council. Dr. Norman reported having no relevant financial disclosures.
ATLANTA – Vaginal progesterone confers no obstetrical or neonatal benefit, and no long-term benefit with respect to cognitive and neurosensory outcomes in children when used to prevent preterm birth, according to findings from the randomized, controlled, double-blind OPPTIMUM trial.
The findings from OPPTIMUM – the largest trial to date looking at progesterone for the prevention of preterm birth – have important implications for current practice. Vaginal progesterone is not currently approved for the prevention of preterm birth in the United States, but is commonly used off label for this purpose.
Prior studies have demonstrated a benefit with respect to progesterone for the prevention of preterm birth, particularly in women with a short cervix, but no studies have looked at long-term outcomes, Dr. Jane E. Norman of the University of Edinburgh reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
In OPPTIMUM, the rate of the primary obstetric outcome of preterm birth or fetal death before 34 weeks’ gestation did not differ significantly for 618 women at risk for preterm birth who were randomized to receive 200 mg of vaginal progesterone daily starting at 22-24 weeks and continuing to 34 weeks’ gestation, compared with 600 women who received placebo (16% vs. 18%; odds ratio, 0.86), Dr. Norman said.
The rate of the primary neonatal composite outcome of death or major morbidity (brain injury or bronchopulmonary dysplasia) also did not differ significantly between the progesterone and placebo groups after a prespecified multiple comparisons procedure (6% vs. 10%; odds ratio, 0.62).
A secondary analysis looking at the individual components of the composite neonatal outcomes showed that progesterone reduced the risk of brain injury and neonatal death, but not bronchopulmonary dysplasia, she said.
Further, no difference was seen in Bayley III cognitive scores (with values imputed for deaths) at 2 years of age in 439 and 430 children born to mothers in the progesterone and placebo groups, respectively (average scores, 97.7 and 97.3; odds ratio, 0.48).
On secondary analyses, some safety signals were noted with respect to neurodevelopmental outcomes.
“We were really surprised that we didn’t show that progesterone prevented preterm birth, and we became concerned that perhaps our cutoff of 34 weeks was just the wrong time to choose a cutoff,” Dr. Norman said, noting that a post hoc survival curve analysis was performed to look at the trajectory to delivery, and a “very marginal benefit” was seen with progesterone, but the difference was not statistically significant.
In addition, subgroup analyses showed no significant benefit of progesterone on obstetrical, neonatal, or childhood outcomes. For example, in women with a short cervix, no evidence was seen that progesterone was more or less effective than in women with a longer cervix. Other subgroups studied included fibronectin-positive and fibronectin-negative women and women with a history of preterm birth. Progesterone was no more or less effective in any of the subgroups, Dr. Norman said.
OPPTIMUM study subjects were women at risk of preterm birth because of a positive fetal fibronectin test result, a history of spontaneous preterm birth at or before 34 weeks’ gestation, or a short cervix (25 mm or less).
All outcomes were adjusted for a previous pregnancy of 14 weeks’ gestation or greater, with study center as a random effect.
“OPPTIMUM is the largest trial of progesterone to prevent preterm birth, and after adjusting for multiple comparisons as we planned, we did not disprove the null hypothesis that progesterone doesn’t prevent preterm birth, it doesn’t reduce adverse neonatal outcomes, and it doesn’t have a beneficial effect on childhood outcomes,” Dr. Norman said, concluding that “there is a remaining unmet need for a safe and effective agent to prevent preterm birth.”
Asked about the safety of progesterone given the findings from secondary analyses in OPPTIMUM, she said, “I would not advise my daughter to take progesterone if she’s pregnant.”
The study drug and placebo were donated by Besins, but the company was not involved in study design or analysis. Funding was provided by the Medical Research Council. Dr. Norman reported having no relevant financial disclosures.
AT THE PREGNANCY MEETING
Key clinical point: Vaginal progesterone had no obstetrical or neonatal benefit when used to prevent preterm birth.
Major finding: The rate of preterm birth or fetal death before 34 weeks’ gestation did not differ significantly in women treated with vaginal progesterone and those who received placebo (16% vs. 18%; odds ratio, 0.86).
Data source: The randomized, double-blind, placebo-controlled multicenter OPPTIMUM trial.
Disclosures: The study drug and placebo were donated by Besins, but the company was not involved in study design or analysis. Funding was provided by the Medical Research Council. Dr. Norman reported having no relevant financial disclosures.

Congo Red Dot Point-of-care Test Detects Preeclampsia
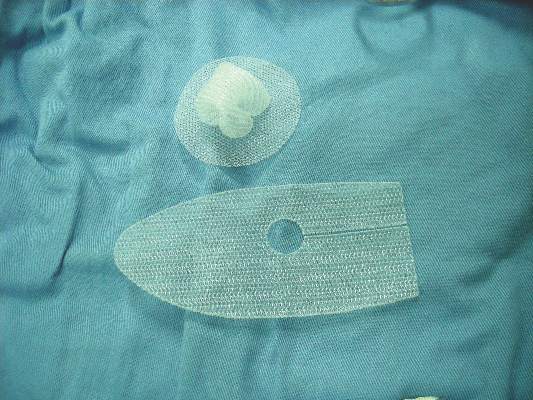
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.

The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.
The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.
The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
AT THE PREGNANCY MEETING
Congo Red Dot point-of-care test detects preeclampsia
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.

Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.

The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.
The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
ATLANTA – A novel, noninvasive, “red dye on paper” diagnostic test allows for rapid screening and identification of preeclampsia at the point of care, according to findings from a prospective clinical study.
Of 343 women enrolled consecutively from a labor and delivery triage unit, 112 had a clinical diagnosis of preeclampsia. The diagnostic test – the Congo Red Dot (CRD) paper test – had an 86% rate of accuracy for detecting preeclampsia, which was superior to several other biochemical tests that were also evaluated, Dr. Kara Rood reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Among the comparator tests, which were conducted using stored urine samples to strengthen the final diagnosis, were the laboratory “gold standard” CRD nitrocellulose test, as well as Protein/Creatinine ratio, and urine and serum placental growth factor (PlGF), sFlt-1, and urine sFlt-1/PlGF (uFP) ratio. Accuracy rates ranged from 60% to 83%, said Dr. Rood, a maternal-fetal medicine fellow at the Ohio State University Wexner Medical Center, Columbus.
The CRD point-of-care test was developed by researchers at Ohio State and Nationwide Children’s Hospital, also in Columbus, in an effort to reduce morbidity among expecting mothers and their unborn children. The current study is the first to test the affordable tool, and the findings promise to have an important impact on the health of women and children, she said.
Study subjects were consecutive women evaluated for preeclampsia at Wexner Medical Center. The CRD test was performed using 0.45 cc of fresh crude urine, and results were scored by trained clinical nurses at the bedside.
The average latency period between a positive paper-based CRD test and delivery was 14 days, which was significantly shorter than the interval for those who tested negative, Dr. Rood said.
The CRD test was developed based on previous findings by Dr. Irina A. Buhimschi of the Center for Perinatal Research in the the Research Institute at Nationwide Children’s Hospital and her colleagues, who discovered that preeclampsia may result from a collection of misfolded proteins that are identifiable in the urine of pregnant women. Congo Red is a dye used by pathologists to identify amyloid plaques in the brains of patients with Alzheimer’s disease, and it was found to bind and incorporate into the abnormally folded proteins in the urine of pregnant women with preeclampsia. The initial CRD test for preeclampsia had an 89% accuracy rate, according to preliminary findings published in 2014.
“This new point-of-care test is a more user-friendly version than the one in the [2014] publication, and can help identify preeclampsia even before clinical symptoms appear,” Dr. Buhimschi said in a press statement, which also noted that the research team is “currently investigating how each misfolded protein collection affects pregnant women. The answer might assist with developing an effective treatment or even preventing preeclampsia.”
Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
AT THE PREGNANCY MEETING
Key clinical point: A noninvasive, “red dye on paper” diagnostic test was effective for rapid screening of preeclampsia.
Major finding: The Congo Red Dot (CRD) paper test had an 86% rate of accuracy for detecting preeclampsia.
Data source: A prospective clinical study of 343 women.
Disclosures: Dr. Rood disclosed that concepts outlined during her presentation are the subject of patents and patent applications filed by Yale University and licensed to private entities for development and commercialization. Some of the study authors are named as inventors of the Congo Red Dot test.
Venetoclax shows promise for relapsed CLL, SLL
Daily oral treatment with venetoclax induced substantial responses with manageable adverse effects in patients with relapsed chronic lymphocytic leukemia or small lymphocytic lymphoma in a first-in-human phase I dose-escalation study.
The promising effects of the highly selective investigational inhibitor of BCL2 – a protein central to the survival of CLL cells – were noted even in patients with poor prognostic features, who comprised 89% of the cohort, reported Dr. Andrew W. Roberts of Royal Melbourne Hospital, Australia, and his colleagues. The study was published online Jan. 28 in The New England Journal of Medicine.
In the dose escalation phase of the study, 56 patients received active treatment at doses raging from 150 to 1,200 mg daily, and 60 additional patients received weekly stepwise ramp-up with doses beginning at 20 mg daily with weekly increases to 50 mg, 100 mg, and 200 mg daily up to the target dose of 400 mg daily. The patients had received a median of 3 previous therapies (range, 1-11).
Of 116 treated patients, 92 (79%) had a response, and 20% achieved complete remission, including 5% with no minimal residual disease on flow cytometry, the investigators said (N Engl J Med. 2016;374:311-22).
Venetoclax was active at all doses used in the study, and no maximum tolerated dose was identified.
Tumor lysis syndrome occurred in 10 patients, but clinically important sequelae occurred in only 3 of those patients, 2 of whom had severe sequelae. After adjustments were made to dosing schedule, no further cases occurred.
Other side effects included mild diarrhea, upper respiratory tract infection, nausea, and grade 3 or 4 neutropenia, which occurred in 41%-52% of patients. Serious adverse events included febrile neutropenia in 6% of patients, pneumonia in 4%, upper respiratory tract infection in 3%, and immune thrombocytopenia in 3%.
Among the patients with an adverse prognosis, treatment response rates ranged from 71% to 79%, depending on the subgroup. For example, the response rate was 79% in 70 patients with resistance to fludarabine, and 71% in 31 patients with chromosome 17p deletions.
New treatments, including ibrutinib monotherapy and idelalisib in combination with rituximab, have improved outcomes for patients with relapsed CLL, but despite these advances, complete remissions remain uncommon, the authors said.
“This first trial of venetoclax showed the potential of BCL2 antagonism as an additional therapeutic avenue for patients with relapsed CLL,” they wrote, adding that the 79% overall response rate in this study – including deep responses and complete responses without minimal residual disease in patients up to age 86 years and patients with poor prognostic factors – “provides support for further development of venetoclax as a treatment option for patients with heavily pretreated relapsed or refractory CLL or SLL.”
Of note, the Food and Drug Administration on Jan. 28 – the date this study was released – granted venetoclax Breakthrough Therapy Designation for use in combination with hypomethylating agents for the treatment of acute myeloid leukemia patients who aren’t eligible for standard induction chemotherapy. The designation – the third for the agent – is supported by data from a single study of untreated patients aged 65 years or older with AML. Prior venetoclax Breakthrough Therapy Designations were granted in April 2015 for its use as monotherapy in patients with refractory CLL who have the 17p deletion genetic mutation, and in January for its use with rituximab for the treatment of relapsed/refractory CLL.
AbbVie and Genentech supported the study. Dr. Roberts reported receiving grant support and study drugs form AbbVie, serving as an investigator in trials sponsored by Genentech, AbbVie, Janssen, and Beigene, and receiving institutional research funding from Genentech for the development of venetoclax. His coauthors reported ties to various pharmaceutical companies.
Targeted therapies have fundamentally changed the management and outcomes of patients with CLL in recent years, and new findings for second-generation drugs offer even more promise, according to Dr. Wyndham H. Wilson.
Taken together with the recent finding that acalabrutinib has a high degree of Bruton’s tyrosine kinase (BTK) inhibition with lower toxicity than ibrutinib, the findings of Roberts et al. with respect to venetoclax suggest a possible new avenue for combination treatment, Dr. Wilson wrote in an editorial (N Engl J Med. 2016;374;4:386-8).
“The transformative characteristics of acalabrutinib and venetoclax arise from effective targeting of important survival pathways in CLL. Indeed, BTK inhibition produces durable responses, improves survival, and selects for mutations in the BTK-binding domain,” Dr. Wilson said, adding that BCL2 also plays an important role in CLL survival, as indicated by the activity of venetoclax.
While neither venetoclax nor acalabrutinib regularly induce complete remission, in vitro findings show that venetoclax and BTK inhibitors are synergistic, which suggests that combining the two might “further transform the targeted treatment of CLL,” he explained.
Dr. Wilson is with the National Cancer Institute, Bethesda, Md.
Targeted therapies have fundamentally changed the management and outcomes of patients with CLL in recent years, and new findings for second-generation drugs offer even more promise, according to Dr. Wyndham H. Wilson.
Taken together with the recent finding that acalabrutinib has a high degree of Bruton’s tyrosine kinase (BTK) inhibition with lower toxicity than ibrutinib, the findings of Roberts et al. with respect to venetoclax suggest a possible new avenue for combination treatment, Dr. Wilson wrote in an editorial (N Engl J Med. 2016;374;4:386-8).
“The transformative characteristics of acalabrutinib and venetoclax arise from effective targeting of important survival pathways in CLL. Indeed, BTK inhibition produces durable responses, improves survival, and selects for mutations in the BTK-binding domain,” Dr. Wilson said, adding that BCL2 also plays an important role in CLL survival, as indicated by the activity of venetoclax.
While neither venetoclax nor acalabrutinib regularly induce complete remission, in vitro findings show that venetoclax and BTK inhibitors are synergistic, which suggests that combining the two might “further transform the targeted treatment of CLL,” he explained.
Dr. Wilson is with the National Cancer Institute, Bethesda, Md.
Targeted therapies have fundamentally changed the management and outcomes of patients with CLL in recent years, and new findings for second-generation drugs offer even more promise, according to Dr. Wyndham H. Wilson.
Taken together with the recent finding that acalabrutinib has a high degree of Bruton’s tyrosine kinase (BTK) inhibition with lower toxicity than ibrutinib, the findings of Roberts et al. with respect to venetoclax suggest a possible new avenue for combination treatment, Dr. Wilson wrote in an editorial (N Engl J Med. 2016;374;4:386-8).
“The transformative characteristics of acalabrutinib and venetoclax arise from effective targeting of important survival pathways in CLL. Indeed, BTK inhibition produces durable responses, improves survival, and selects for mutations in the BTK-binding domain,” Dr. Wilson said, adding that BCL2 also plays an important role in CLL survival, as indicated by the activity of venetoclax.
While neither venetoclax nor acalabrutinib regularly induce complete remission, in vitro findings show that venetoclax and BTK inhibitors are synergistic, which suggests that combining the two might “further transform the targeted treatment of CLL,” he explained.
Dr. Wilson is with the National Cancer Institute, Bethesda, Md.
Daily oral treatment with venetoclax induced substantial responses with manageable adverse effects in patients with relapsed chronic lymphocytic leukemia or small lymphocytic lymphoma in a first-in-human phase I dose-escalation study.
The promising effects of the highly selective investigational inhibitor of BCL2 – a protein central to the survival of CLL cells – were noted even in patients with poor prognostic features, who comprised 89% of the cohort, reported Dr. Andrew W. Roberts of Royal Melbourne Hospital, Australia, and his colleagues. The study was published online Jan. 28 in The New England Journal of Medicine.
In the dose escalation phase of the study, 56 patients received active treatment at doses raging from 150 to 1,200 mg daily, and 60 additional patients received weekly stepwise ramp-up with doses beginning at 20 mg daily with weekly increases to 50 mg, 100 mg, and 200 mg daily up to the target dose of 400 mg daily. The patients had received a median of 3 previous therapies (range, 1-11).
Of 116 treated patients, 92 (79%) had a response, and 20% achieved complete remission, including 5% with no minimal residual disease on flow cytometry, the investigators said (N Engl J Med. 2016;374:311-22).
Venetoclax was active at all doses used in the study, and no maximum tolerated dose was identified.
Tumor lysis syndrome occurred in 10 patients, but clinically important sequelae occurred in only 3 of those patients, 2 of whom had severe sequelae. After adjustments were made to dosing schedule, no further cases occurred.
Other side effects included mild diarrhea, upper respiratory tract infection, nausea, and grade 3 or 4 neutropenia, which occurred in 41%-52% of patients. Serious adverse events included febrile neutropenia in 6% of patients, pneumonia in 4%, upper respiratory tract infection in 3%, and immune thrombocytopenia in 3%.
Among the patients with an adverse prognosis, treatment response rates ranged from 71% to 79%, depending on the subgroup. For example, the response rate was 79% in 70 patients with resistance to fludarabine, and 71% in 31 patients with chromosome 17p deletions.
New treatments, including ibrutinib monotherapy and idelalisib in combination with rituximab, have improved outcomes for patients with relapsed CLL, but despite these advances, complete remissions remain uncommon, the authors said.
“This first trial of venetoclax showed the potential of BCL2 antagonism as an additional therapeutic avenue for patients with relapsed CLL,” they wrote, adding that the 79% overall response rate in this study – including deep responses and complete responses without minimal residual disease in patients up to age 86 years and patients with poor prognostic factors – “provides support for further development of venetoclax as a treatment option for patients with heavily pretreated relapsed or refractory CLL or SLL.”
Of note, the Food and Drug Administration on Jan. 28 – the date this study was released – granted venetoclax Breakthrough Therapy Designation for use in combination with hypomethylating agents for the treatment of acute myeloid leukemia patients who aren’t eligible for standard induction chemotherapy. The designation – the third for the agent – is supported by data from a single study of untreated patients aged 65 years or older with AML. Prior venetoclax Breakthrough Therapy Designations were granted in April 2015 for its use as monotherapy in patients with refractory CLL who have the 17p deletion genetic mutation, and in January for its use with rituximab for the treatment of relapsed/refractory CLL.
AbbVie and Genentech supported the study. Dr. Roberts reported receiving grant support and study drugs form AbbVie, serving as an investigator in trials sponsored by Genentech, AbbVie, Janssen, and Beigene, and receiving institutional research funding from Genentech for the development of venetoclax. His coauthors reported ties to various pharmaceutical companies.
Daily oral treatment with venetoclax induced substantial responses with manageable adverse effects in patients with relapsed chronic lymphocytic leukemia or small lymphocytic lymphoma in a first-in-human phase I dose-escalation study.
The promising effects of the highly selective investigational inhibitor of BCL2 – a protein central to the survival of CLL cells – were noted even in patients with poor prognostic features, who comprised 89% of the cohort, reported Dr. Andrew W. Roberts of Royal Melbourne Hospital, Australia, and his colleagues. The study was published online Jan. 28 in The New England Journal of Medicine.
In the dose escalation phase of the study, 56 patients received active treatment at doses raging from 150 to 1,200 mg daily, and 60 additional patients received weekly stepwise ramp-up with doses beginning at 20 mg daily with weekly increases to 50 mg, 100 mg, and 200 mg daily up to the target dose of 400 mg daily. The patients had received a median of 3 previous therapies (range, 1-11).
Of 116 treated patients, 92 (79%) had a response, and 20% achieved complete remission, including 5% with no minimal residual disease on flow cytometry, the investigators said (N Engl J Med. 2016;374:311-22).
Venetoclax was active at all doses used in the study, and no maximum tolerated dose was identified.
Tumor lysis syndrome occurred in 10 patients, but clinically important sequelae occurred in only 3 of those patients, 2 of whom had severe sequelae. After adjustments were made to dosing schedule, no further cases occurred.
Other side effects included mild diarrhea, upper respiratory tract infection, nausea, and grade 3 or 4 neutropenia, which occurred in 41%-52% of patients. Serious adverse events included febrile neutropenia in 6% of patients, pneumonia in 4%, upper respiratory tract infection in 3%, and immune thrombocytopenia in 3%.
Among the patients with an adverse prognosis, treatment response rates ranged from 71% to 79%, depending on the subgroup. For example, the response rate was 79% in 70 patients with resistance to fludarabine, and 71% in 31 patients with chromosome 17p deletions.
New treatments, including ibrutinib monotherapy and idelalisib in combination with rituximab, have improved outcomes for patients with relapsed CLL, but despite these advances, complete remissions remain uncommon, the authors said.
“This first trial of venetoclax showed the potential of BCL2 antagonism as an additional therapeutic avenue for patients with relapsed CLL,” they wrote, adding that the 79% overall response rate in this study – including deep responses and complete responses without minimal residual disease in patients up to age 86 years and patients with poor prognostic factors – “provides support for further development of venetoclax as a treatment option for patients with heavily pretreated relapsed or refractory CLL or SLL.”
Of note, the Food and Drug Administration on Jan. 28 – the date this study was released – granted venetoclax Breakthrough Therapy Designation for use in combination with hypomethylating agents for the treatment of acute myeloid leukemia patients who aren’t eligible for standard induction chemotherapy. The designation – the third for the agent – is supported by data from a single study of untreated patients aged 65 years or older with AML. Prior venetoclax Breakthrough Therapy Designations were granted in April 2015 for its use as monotherapy in patients with refractory CLL who have the 17p deletion genetic mutation, and in January for its use with rituximab for the treatment of relapsed/refractory CLL.
AbbVie and Genentech supported the study. Dr. Roberts reported receiving grant support and study drugs form AbbVie, serving as an investigator in trials sponsored by Genentech, AbbVie, Janssen, and Beigene, and receiving institutional research funding from Genentech for the development of venetoclax. His coauthors reported ties to various pharmaceutical companies.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Daily oral treatment with venetoclax induced substantial responses with manageable adverse effects in patients with relapsed chronic lymphocytic leukemia or small lymphocytic lymphoma in a first-in-human phase I dose-escalation study.
Major finding: Of 116 treated patients, 92 (79%) had a response, and 20% achieved complete remission, including 5% with no minimal residual disease on flow cytometry.
Data source: A phase I dose-escalation study involving 116 patients.
Disclosures: AbbVie and Genentech supported the study. Dr. Roberts reported receiving grant support and study drugs form AbbVie, serving as an investigator in trials sponsored by Genentech, AbbVie, Janssen, and Beigene, and receiving institutional research funding from Genentech for the development of venetoclax. His coauthors reported ties to various pharmaceutical companies.
Dabrafenib may be useful in patients who discontinue vemurafenib
Treatment with vemurafenib may result in severe skin toxicity, and dabrafenib appears to be useful in patients who discontinue vemurafenib due to such toxicity, according to a retrospective analysis of the cohort.
About a quarter (26%) of 131 melanoma patients treated in real life conditions with the BRAF inhibitor vemurafenib developed grade 3-4 skin toxicity, and 44% (34) of those patients permanently discontinued treatment, corresponding to 11% of the overall cohort, Dr. Lucie Peuvrel of Nantes (France) University Hospital and colleagues reported in Journal of the European Academy of Dermatology and Venereology.

Discontinuations were mainly due to rash and classic adverse skin reactions, including Stevens-Johnson syndrome, drug reaction with eosinophilia, and systemic symptoms, whereas reactions involving only photosensitivity or cutaneous carcinomas rarely resulted in treatment adjustment; 14 of the remaining 19 patients with grade 3-4 toxicity who continued treatment had no dose adjustment, and 5 had a dose reduction.
Clinical or biological abnormalities occurred in 94% of those with grade 3-4 rashes, the investigators noted (J Eur Acad Dermatol Venereol. 2016 Feb;30[2]:250-7).
Study subjects were patients with a mean age of 60 years who were treated with vemurafenib for melanoma between November 2010 and December 2014. Grade 3-4 skin toxicity that emerged within the first 4-8 weeks of treatment was significantly associated with prolonged overall survival; severe skin rashes also were associated with prolonged median overall survival. Of seven patients who switched to dabrafenib due to their skin reaction, only one experienced recurrence of the reaction.
Vemurafenib, which is approved for the treatment of unresectable stage III-IV BRAF mutant melanoma, is commonly associated with skin toxicity, with severe cases occurring only rarely; the impact of severe forms of toxicity on treatment and patient outcomes was unknown, the investigators said.
The current findings reaffirm that vemurafenib is commonly associated with skin toxicity, but rarely with severe cases. Severe skin adverse reactions permanently preclude use of vemurafenib, but dabrafenib – the only other BRAF inhibitor with market authorization for unresectable stage III-IV BRAF mutant melanoma – “seems to be beneficial in case of vemurafenib-induced skin intolerance,” they noted, adding that for other skin toxicities, including photosensitivity and cutaneous carcinoma, treatment adjustment is generally not required, and that treatment resumption at a reduced dose should be considered after skin improvement in patients with rashes.
The finding of increased survival in cases involving severe skin toxicity that emerges within 4-8 weeks of treatment initiation should be confirmed in other studies, Dr. Peuvrel and associates said.
The authors reported having no conflicts of interest.
Treatment with vemurafenib may result in severe skin toxicity, and dabrafenib appears to be useful in patients who discontinue vemurafenib due to such toxicity, according to a retrospective analysis of the cohort.
About a quarter (26%) of 131 melanoma patients treated in real life conditions with the BRAF inhibitor vemurafenib developed grade 3-4 skin toxicity, and 44% (34) of those patients permanently discontinued treatment, corresponding to 11% of the overall cohort, Dr. Lucie Peuvrel of Nantes (France) University Hospital and colleagues reported in Journal of the European Academy of Dermatology and Venereology.
Discontinuations were mainly due to rash and classic adverse skin reactions, including Stevens-Johnson syndrome, drug reaction with eosinophilia, and systemic symptoms, whereas reactions involving only photosensitivity or cutaneous carcinomas rarely resulted in treatment adjustment; 14 of the remaining 19 patients with grade 3-4 toxicity who continued treatment had no dose adjustment, and 5 had a dose reduction.
Clinical or biological abnormalities occurred in 94% of those with grade 3-4 rashes, the investigators noted (J Eur Acad Dermatol Venereol. 2016 Feb;30[2]:250-7).
Study subjects were patients with a mean age of 60 years who were treated with vemurafenib for melanoma between November 2010 and December 2014. Grade 3-4 skin toxicity that emerged within the first 4-8 weeks of treatment was significantly associated with prolonged overall survival; severe skin rashes also were associated with prolonged median overall survival. Of seven patients who switched to dabrafenib due to their skin reaction, only one experienced recurrence of the reaction.
Vemurafenib, which is approved for the treatment of unresectable stage III-IV BRAF mutant melanoma, is commonly associated with skin toxicity, with severe cases occurring only rarely; the impact of severe forms of toxicity on treatment and patient outcomes was unknown, the investigators said.
The current findings reaffirm that vemurafenib is commonly associated with skin toxicity, but rarely with severe cases. Severe skin adverse reactions permanently preclude use of vemurafenib, but dabrafenib – the only other BRAF inhibitor with market authorization for unresectable stage III-IV BRAF mutant melanoma – “seems to be beneficial in case of vemurafenib-induced skin intolerance,” they noted, adding that for other skin toxicities, including photosensitivity and cutaneous carcinoma, treatment adjustment is generally not required, and that treatment resumption at a reduced dose should be considered after skin improvement in patients with rashes.
The finding of increased survival in cases involving severe skin toxicity that emerges within 4-8 weeks of treatment initiation should be confirmed in other studies, Dr. Peuvrel and associates said.
The authors reported having no conflicts of interest.
Treatment with vemurafenib may result in severe skin toxicity, and dabrafenib appears to be useful in patients who discontinue vemurafenib due to such toxicity, according to a retrospective analysis of the cohort.
About a quarter (26%) of 131 melanoma patients treated in real life conditions with the BRAF inhibitor vemurafenib developed grade 3-4 skin toxicity, and 44% (34) of those patients permanently discontinued treatment, corresponding to 11% of the overall cohort, Dr. Lucie Peuvrel of Nantes (France) University Hospital and colleagues reported in Journal of the European Academy of Dermatology and Venereology.
Discontinuations were mainly due to rash and classic adverse skin reactions, including Stevens-Johnson syndrome, drug reaction with eosinophilia, and systemic symptoms, whereas reactions involving only photosensitivity or cutaneous carcinomas rarely resulted in treatment adjustment; 14 of the remaining 19 patients with grade 3-4 toxicity who continued treatment had no dose adjustment, and 5 had a dose reduction.
Clinical or biological abnormalities occurred in 94% of those with grade 3-4 rashes, the investigators noted (J Eur Acad Dermatol Venereol. 2016 Feb;30[2]:250-7).
Study subjects were patients with a mean age of 60 years who were treated with vemurafenib for melanoma between November 2010 and December 2014. Grade 3-4 skin toxicity that emerged within the first 4-8 weeks of treatment was significantly associated with prolonged overall survival; severe skin rashes also were associated with prolonged median overall survival. Of seven patients who switched to dabrafenib due to their skin reaction, only one experienced recurrence of the reaction.
Vemurafenib, which is approved for the treatment of unresectable stage III-IV BRAF mutant melanoma, is commonly associated with skin toxicity, with severe cases occurring only rarely; the impact of severe forms of toxicity on treatment and patient outcomes was unknown, the investigators said.
The current findings reaffirm that vemurafenib is commonly associated with skin toxicity, but rarely with severe cases. Severe skin adverse reactions permanently preclude use of vemurafenib, but dabrafenib – the only other BRAF inhibitor with market authorization for unresectable stage III-IV BRAF mutant melanoma – “seems to be beneficial in case of vemurafenib-induced skin intolerance,” they noted, adding that for other skin toxicities, including photosensitivity and cutaneous carcinoma, treatment adjustment is generally not required, and that treatment resumption at a reduced dose should be considered after skin improvement in patients with rashes.
The finding of increased survival in cases involving severe skin toxicity that emerges within 4-8 weeks of treatment initiation should be confirmed in other studies, Dr. Peuvrel and associates said.
The authors reported having no conflicts of interest.
FROM JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Key clinical point: Treatment with vemurafenib may result in severe skin toxicity, and dabrafenib appears to be useful in patients who discontinue vemurafenib due to such toxicity.
Major finding: 26% of patients developed grade 3-4 skin toxicity, and 44% of those permanently discontinued treatment with vemurafenib.
Data source: A retrospective cohort study of 131 patients.
Disclosures: The authors reported having no conflicts of interest.

Physicians’ odds of beating addiction higher
Physicians appear to have much greater odds of substance abuse and dependence disorders related to alcohol, opiates, and sedatives than their nonphysician counterparts, some estimates showed.
The good news is that physicians with substance abuse and addiction respond particularly well to treatment – so much so that experts have recommended that the treatment methods employed in specialized programs for impaired health professionals be disseminated and used in programs for the general public.
“In a nutshell, for a physician with addiction who goes to an appropriate program that has expertise working with physicians and then follows up with 5-year monitoring, the average rate of abstinence of about 80% is the polar opposite of that in the general population, Dr. Daniel H. Angres of Northwestern University in Chicago said in an interview.
At best, the abstinence rate after treatment is about 20% for the general population, said Dr. Angres, an addiction psychiatrist and medical director of the Positive Sobriety Institute in Chicago, who has spent more than 3 decades working with physicians and other health care professionals struggling with drug abuse and dependence.
The key is proper treatment in a setting with other health professionals and long-term monitoring; without both, the outcomes won’t be as good, he stressed. But Dr. Angres added that there is more to it than that. Often, the very factors that drive a person to become a physician and help that person succeed in the endeavor are the factors that can improve the odds of beating addiction, he explained.
Scope of the problem
Substance abuse and dependence in general are on the rise. This is true among physicians as well as the general public. Opioid use has been a particular problem. A 2008 review by Dr. Mark S. Gold, former chair of the psychiatry department at the University of Florida, Gainesville, and Lisa J. Merlo, Ph.D., also of the university, noted that 12%-23% of physicians admit to prescription opioid use, compared with 1%-4% of nonphysicians (Harv Rev Psychiatry. 2008;16[3]:181-94).

However, Dr. Angres said there are few data to suggest that physicians are at substantially increased risk of addiction.
“The rule of thumb is that addiction affects probably 1 in 10 people. We can comfortably say about 10% will have an addiction problem at some point in their lives,” he said.
But addiction is a disease with genetic underpinnings, and while there was a time when it was thought that perhaps physicians had greater risk because they had greater access, the playing field with respect to access has been leveled over time. There are no good data to suggest that more than 15% of physicians are affected, Dr. Angres noted.
That’s not to say certain specialties aren’t overrepresented among addicts, he added.

Anesthesiologists, for example, have been shown to have a greater risk of addiction – perhaps as a result of their having access to, and/or excess exposure to, drugs like fentanyl and propofol. In fact, the review by Dr. Gold and Dr. Merlo also noted an increasing trend for abuse of sublingual and intravenously administered analgesics among health care professionals. Not far behind anesthesiologists are surgeons, pain doctors, and emergency physicians, Dr. Gold said in an interview. “We have proposed a number of theories to explain this, from self-selection bias to selecting anesthesia because of student drug use to second- and third-hand occupational exposure risks.”
Meanwhile, another 2008 study by Dr. Gold, Dr. Merlo, and their colleagues demonstrated that chronic secondhand exposure to low doses of drugs such as fentanyl and propofol among health care professionals in the operating room might sensitize vulnerable individuals to the “rewarding effects of these drugs, placing them at higher risk for developing an addiction.” The authors concluded that the findings, while they served only as “preliminary support for an unproven hypothesis,” suggest a need for workplace protections (J Addict Dis. 2008;27[3]:67-75).
Dr. Gold also led a more recent study comparing psychiatric and substance use disorders among physicians in a state Physician’s Health Program (PHP) with those in a general treatment population. He and his colleagues found that 99 physicians referred to the PHP for suspected impairment had similar lifetime use of alcohol, opiates, and sedatives as a group of age, sex, and education status–matched persons in a general treatment population.
However, the physicians had significantly higher odds of meeting DSM-IV criteria for abuse/dependence disorders related to alcohol (odds ratio, 2.56), opiates (OR, 86.58), and sedatives (OR, 54.76), the authors reported (J Addic Med. 2013 Mar-Apr;7[2]:108-12).
Further, the physicians had significantly lower odds of lifetime use, but higher odds of lifetime abuse/dependence, for cocaine/crack cocaine and cannabis vs. the comparison group, as well as lower lifetime amphetamine use (OR, 0.21) with no difference in abuse/dependence vs. the comparison group, and lower odds of psychiatric disorders, including obsessive-compulsive disorder, major depression, and specific phobias.
While Dr. Gold and his colleagues concluded that more research is needed to understand psychiatric morbidity in physicians, and while physicians in certain specialties may have an increased likelihood of addiction in relation to exposure to drugs in the operating room setting, most physicians “get addicted in ways that are similar to others in the population,” Dr. Angres said: They have a pain problem, they get a drug like hydrocodone or other narcotic, they have a particular kind of experience that “goes above and beyond the pain management” (some individuals have a paradoxical effect in which they feel connected and energized, for example), and they become addicted.
The main drug of choice, even among physicians, is alcohol, he noted, explaining that stress is another common precipitating factor.
There is a definite relationship between stress and addiction; alcohol may be used to cope with stress, and those who are vulnerable to addiction can become dependent.
“Physicians are more stressed today than ever. The whole landscape of medicine, the economics of medicine means physicians have to see more patients and spend less time with patients,” Dr. Angres said, adding that factors like electronic medical records requirements and concerns about malpractice all contribute to increasing stress levels and are likely also increasing the rate of addiction and other forms of physician impairment or distress, including cognitive difficulties, depression, and anxiety.
Affected physicians, sometimes referred to as “disruptive physicians,” are increasingly a focus of programs and protocols to promote physician wellness.*
Northwestern and other high-level academic centers are “gearing up” for the problem. It is becoming more common for physicians to undergo screening when they are hired, and to undergo random screening to make sure they aren’t under the influence, he explained.
“And I also think that the medical community is much more attuned to detecting this and helping people gain access to proper assessment, rehabilitation, and reentry,” he added.
Treatment and outcomes
Treatment for physicians is often provided through state PHPs, some of which are under the umbrella of a licensing board or are part of a diversion program involving an autonomous entity.
“PHPs are really critical,” Dr. Angres said, explaining that they provide education, conduct research to help reduce malpractice claims, and ensure proper assessment of physicians, and they do long-term monitoring involving wellness checks.
While there is some controversy about the role of PHPs – some physicians have resented the monitoring, say they have felt coerced into participating, and have demanded more choice regarding treatment options – these programs are highly successful and data driven, Dr. Angres said.
“When the outcomes are clearly very good with a certain kind of protocol, you want to stick with that, particularly if public safety is involved,” he said, adding that these programs work because they are more supportive than punitive, they treat affected physicians for their disease, and they help physicians do what they need to do to safely reenter the practice of medicine.
Punitive programs would drive substance abuse/dependence problems underground, making them more dangerous, he said.
There is a great deal of debate about the appropriate duration of treatment, but most importantly, physicians should be with other physicians.
“What gets people sober is really being with other people who are sober,” he said, adding that a peer group of others with similar experiences and a similar life path is critical.
Twelve-step programs, which employ this principle as part of treatment and aftercare, result in better outcomes, and it is also crucial that physicians be treated by personnel who are experienced and conversant with working with physicians, because there are important factors necessary for successful reentry and engagement in the workplace.
Medications also are an important part of care, in many cases.
Dr. Gold’s research has long focused on the evaluation and treatment of impaired health professionals.
“After the discovery of the antiopiate withdrawal efficacy of clonidine, we tried an experimental medication – naltrexone – as a treatment for impaired health professional opiate addicts. … Naltrexone was both safe and effective. Injectable naltrexone is now widely recognized as a safe and effective treatment to prevent opiate relapse,” he said in an interview.
Naltrexone is particularly important for the treatment of addicted anesthesiologists, as they are at high risk of relapse when they return to work; their relapses are often overdoses after detoxification, he said.
Five-year outcomes studies suggest that with appropriate treatment, outcomes are indeed excellent among physicians, compared with their peers. Two such studies, led by researchers from the Institute of Behavior and Health in Rockville, Md., respectively showed that 102 anesthesiologists treated and monitored under PHP supervision had excellent outcomes similar to those of other impaired physicians (Anesth Analg. 2009;109[3]:891-6), and that 144 surgeons treated under PHP supervision had positive outcomes similar to those of nonsurgeons (Arch Surg. 2011;146[11]:1286-91).
In their review article, Dr. Gold and Dr. Merlo concluded that for physicians overall, “appropriate intervention (e.g., typically in with the state PHP), methods of evaluation and treatment for addicted physicians are extremely effective. The combination of medical, psychosocial, and support group interventions, combined with extensive posttreatment monitoring and drug testing, generally results in sustained recovery among the physicians who attend specialized treatment programs. These outcomes are typically obtained even when physicians did not enter treatment voluntarily. Thus, it is likely that impaired professional programs represent the best treatment available for opioid use disorders, and nonphysician addicts would likely experience a similar benefit from participating in such a program.”
Dr. Angres agreed that physicians in general are “a good outcome group.”
“If treated and monitored appropriately, these are some of the best outcomes we see in addiction treatment,” he said.
Many factors are involved in the superior results among physicians vs. their nonphysician counterparts, he said, explaining that physicians tend to be particularly conscientious, hard-working individuals with good support systems and personality variables that allow them to persevere under difficult circumstances. They also have a great deal riding on recovery in terms of reentering the practice of medicine.
“So motivation is a big issue. ... All of these things come together,” he said.
Changing trends
In addition to the stress-related factors that appear to be contributing to increased substance abuse and dependence, concerning cultural trends are emerging.
“We have an epidemic among young adults,” Dr. Angres said.
Heroin, prescription opiates, psychostimulants, binge drinking – all are occurring in epidemic proportions throughout our culture, including among the new generation of medical students and young physicians, he added.
“We are seeing for the first time, even in the last year or so, medical students, residents, and young adults who are addicted to drugs like heroin because it is so ubiquitous. So this is a new phenomenon. This is just a new reality. It’s not a massive problem [in medicine], but it is something that we’re seeing that we didn’t see before. ... These are emerging issues that are disconcerting,” he said.
Dr. Gold also noted the changing trends, explaining that over the course of his career, substance misuse and dependence have emerged and changed.
“In the ’70s and ’80s, medical students rarely presented in need of treatment, but when they did, they had alcohol, tobacco, and benzodiazepine problems. Residents ... had problems with prescription opiates, and many programs reported overdoses. More recently, medical students no longer smoke cigarettes. ... Now it is marijuana,” he said, adding that binge drinking, club drugs, and psychostimulant abuse also are on the rise.
Students now are more like their peers and unlike their mentors with respect to drug misuse, use, and dependence, and there is an emerging concern that the most heavily involved students in terms of drug abuse and addiction will select one specialty or another based on drug access, said Dr. Gold, now professor (adjunct) at the University of Southern California, Los Angeles, and at Washington University in St. Louis.
“They often are surprised that the college of medicine, their patients, and professors do not accept as appropriate behavior the taking of another person’s [attention-deficit/hyperactivity disorder] medication, or smoking cannabis, or taking drugs for their mentees,” he said.
As for treatment in this new era of substance abuse and dependence, the approach remains much the same, Dr. Angres said, noting that medication-assisted treatment may be necessary for heroin addiction. A concern, however, is that the relapse rate may be higher.
“We don’t know what that will mean,” he said. “It will be years before we can see how it plays out with physicians with [heroin], but you do the same things, with perhaps some extra support above and beyond [the standard approach].”
Dr. Angres disclosed that he is part owner of the Positive Sobriety Institute, which treats addicted professionals, including physicians. Dr. Gold reported having no relevant financial disclosures.
*Correction, 03/09/2016: An earlier version of this story misstated the term sometimes used to describe physicians with addictive behaviors
Physicians appear to have much greater odds of substance abuse and dependence disorders related to alcohol, opiates, and sedatives than their nonphysician counterparts, some estimates showed.
The good news is that physicians with substance abuse and addiction respond particularly well to treatment – so much so that experts have recommended that the treatment methods employed in specialized programs for impaired health professionals be disseminated and used in programs for the general public.
“In a nutshell, for a physician with addiction who goes to an appropriate program that has expertise working with physicians and then follows up with 5-year monitoring, the average rate of abstinence of about 80% is the polar opposite of that in the general population, Dr. Daniel H. Angres of Northwestern University in Chicago said in an interview.
At best, the abstinence rate after treatment is about 20% for the general population, said Dr. Angres, an addiction psychiatrist and medical director of the Positive Sobriety Institute in Chicago, who has spent more than 3 decades working with physicians and other health care professionals struggling with drug abuse and dependence.
The key is proper treatment in a setting with other health professionals and long-term monitoring; without both, the outcomes won’t be as good, he stressed. But Dr. Angres added that there is more to it than that. Often, the very factors that drive a person to become a physician and help that person succeed in the endeavor are the factors that can improve the odds of beating addiction, he explained.
Scope of the problem
Substance abuse and dependence in general are on the rise. This is true among physicians as well as the general public. Opioid use has been a particular problem. A 2008 review by Dr. Mark S. Gold, former chair of the psychiatry department at the University of Florida, Gainesville, and Lisa J. Merlo, Ph.D., also of the university, noted that 12%-23% of physicians admit to prescription opioid use, compared with 1%-4% of nonphysicians (Harv Rev Psychiatry. 2008;16[3]:181-94).
However, Dr. Angres said there are few data to suggest that physicians are at substantially increased risk of addiction.
“The rule of thumb is that addiction affects probably 1 in 10 people. We can comfortably say about 10% will have an addiction problem at some point in their lives,” he said.
But addiction is a disease with genetic underpinnings, and while there was a time when it was thought that perhaps physicians had greater risk because they had greater access, the playing field with respect to access has been leveled over time. There are no good data to suggest that more than 15% of physicians are affected, Dr. Angres noted.
That’s not to say certain specialties aren’t overrepresented among addicts, he added.
Anesthesiologists, for example, have been shown to have a greater risk of addiction – perhaps as a result of their having access to, and/or excess exposure to, drugs like fentanyl and propofol. In fact, the review by Dr. Gold and Dr. Merlo also noted an increasing trend for abuse of sublingual and intravenously administered analgesics among health care professionals. Not far behind anesthesiologists are surgeons, pain doctors, and emergency physicians, Dr. Gold said in an interview. “We have proposed a number of theories to explain this, from self-selection bias to selecting anesthesia because of student drug use to second- and third-hand occupational exposure risks.”
Meanwhile, another 2008 study by Dr. Gold, Dr. Merlo, and their colleagues demonstrated that chronic secondhand exposure to low doses of drugs such as fentanyl and propofol among health care professionals in the operating room might sensitize vulnerable individuals to the “rewarding effects of these drugs, placing them at higher risk for developing an addiction.” The authors concluded that the findings, while they served only as “preliminary support for an unproven hypothesis,” suggest a need for workplace protections (J Addict Dis. 2008;27[3]:67-75).
Dr. Gold also led a more recent study comparing psychiatric and substance use disorders among physicians in a state Physician’s Health Program (PHP) with those in a general treatment population. He and his colleagues found that 99 physicians referred to the PHP for suspected impairment had similar lifetime use of alcohol, opiates, and sedatives as a group of age, sex, and education status–matched persons in a general treatment population.
However, the physicians had significantly higher odds of meeting DSM-IV criteria for abuse/dependence disorders related to alcohol (odds ratio, 2.56), opiates (OR, 86.58), and sedatives (OR, 54.76), the authors reported (J Addic Med. 2013 Mar-Apr;7[2]:108-12).
Further, the physicians had significantly lower odds of lifetime use, but higher odds of lifetime abuse/dependence, for cocaine/crack cocaine and cannabis vs. the comparison group, as well as lower lifetime amphetamine use (OR, 0.21) with no difference in abuse/dependence vs. the comparison group, and lower odds of psychiatric disorders, including obsessive-compulsive disorder, major depression, and specific phobias.
While Dr. Gold and his colleagues concluded that more research is needed to understand psychiatric morbidity in physicians, and while physicians in certain specialties may have an increased likelihood of addiction in relation to exposure to drugs in the operating room setting, most physicians “get addicted in ways that are similar to others in the population,” Dr. Angres said: They have a pain problem, they get a drug like hydrocodone or other narcotic, they have a particular kind of experience that “goes above and beyond the pain management” (some individuals have a paradoxical effect in which they feel connected and energized, for example), and they become addicted.
The main drug of choice, even among physicians, is alcohol, he noted, explaining that stress is another common precipitating factor.
There is a definite relationship between stress and addiction; alcohol may be used to cope with stress, and those who are vulnerable to addiction can become dependent.
“Physicians are more stressed today than ever. The whole landscape of medicine, the economics of medicine means physicians have to see more patients and spend less time with patients,” Dr. Angres said, adding that factors like electronic medical records requirements and concerns about malpractice all contribute to increasing stress levels and are likely also increasing the rate of addiction and other forms of physician impairment or distress, including cognitive difficulties, depression, and anxiety.
Affected physicians, sometimes referred to as “disruptive physicians,” are increasingly a focus of programs and protocols to promote physician wellness.*
Northwestern and other high-level academic centers are “gearing up” for the problem. It is becoming more common for physicians to undergo screening when they are hired, and to undergo random screening to make sure they aren’t under the influence, he explained.
“And I also think that the medical community is much more attuned to detecting this and helping people gain access to proper assessment, rehabilitation, and reentry,” he added.
Treatment and outcomes
Treatment for physicians is often provided through state PHPs, some of which are under the umbrella of a licensing board or are part of a diversion program involving an autonomous entity.
“PHPs are really critical,” Dr. Angres said, explaining that they provide education, conduct research to help reduce malpractice claims, and ensure proper assessment of physicians, and they do long-term monitoring involving wellness checks.
While there is some controversy about the role of PHPs – some physicians have resented the monitoring, say they have felt coerced into participating, and have demanded more choice regarding treatment options – these programs are highly successful and data driven, Dr. Angres said.
“When the outcomes are clearly very good with a certain kind of protocol, you want to stick with that, particularly if public safety is involved,” he said, adding that these programs work because they are more supportive than punitive, they treat affected physicians for their disease, and they help physicians do what they need to do to safely reenter the practice of medicine.
Punitive programs would drive substance abuse/dependence problems underground, making them more dangerous, he said.
There is a great deal of debate about the appropriate duration of treatment, but most importantly, physicians should be with other physicians.
“What gets people sober is really being with other people who are sober,” he said, adding that a peer group of others with similar experiences and a similar life path is critical.
Twelve-step programs, which employ this principle as part of treatment and aftercare, result in better outcomes, and it is also crucial that physicians be treated by personnel who are experienced and conversant with working with physicians, because there are important factors necessary for successful reentry and engagement in the workplace.
Medications also are an important part of care, in many cases.
Dr. Gold’s research has long focused on the evaluation and treatment of impaired health professionals.
“After the discovery of the antiopiate withdrawal efficacy of clonidine, we tried an experimental medication – naltrexone – as a treatment for impaired health professional opiate addicts. … Naltrexone was both safe and effective. Injectable naltrexone is now widely recognized as a safe and effective treatment to prevent opiate relapse,” he said in an interview.
Naltrexone is particularly important for the treatment of addicted anesthesiologists, as they are at high risk of relapse when they return to work; their relapses are often overdoses after detoxification, he said.
Five-year outcomes studies suggest that with appropriate treatment, outcomes are indeed excellent among physicians, compared with their peers. Two such studies, led by researchers from the Institute of Behavior and Health in Rockville, Md., respectively showed that 102 anesthesiologists treated and monitored under PHP supervision had excellent outcomes similar to those of other impaired physicians (Anesth Analg. 2009;109[3]:891-6), and that 144 surgeons treated under PHP supervision had positive outcomes similar to those of nonsurgeons (Arch Surg. 2011;146[11]:1286-91).
In their review article, Dr. Gold and Dr. Merlo concluded that for physicians overall, “appropriate intervention (e.g., typically in with the state PHP), methods of evaluation and treatment for addicted physicians are extremely effective. The combination of medical, psychosocial, and support group interventions, combined with extensive posttreatment monitoring and drug testing, generally results in sustained recovery among the physicians who attend specialized treatment programs. These outcomes are typically obtained even when physicians did not enter treatment voluntarily. Thus, it is likely that impaired professional programs represent the best treatment available for opioid use disorders, and nonphysician addicts would likely experience a similar benefit from participating in such a program.”
Dr. Angres agreed that physicians in general are “a good outcome group.”
“If treated and monitored appropriately, these are some of the best outcomes we see in addiction treatment,” he said.
Many factors are involved in the superior results among physicians vs. their nonphysician counterparts, he said, explaining that physicians tend to be particularly conscientious, hard-working individuals with good support systems and personality variables that allow them to persevere under difficult circumstances. They also have a great deal riding on recovery in terms of reentering the practice of medicine.
“So motivation is a big issue. ... All of these things come together,” he said.
Changing trends
In addition to the stress-related factors that appear to be contributing to increased substance abuse and dependence, concerning cultural trends are emerging.
“We have an epidemic among young adults,” Dr. Angres said.
Heroin, prescription opiates, psychostimulants, binge drinking – all are occurring in epidemic proportions throughout our culture, including among the new generation of medical students and young physicians, he added.
“We are seeing for the first time, even in the last year or so, medical students, residents, and young adults who are addicted to drugs like heroin because it is so ubiquitous. So this is a new phenomenon. This is just a new reality. It’s not a massive problem [in medicine], but it is something that we’re seeing that we didn’t see before. ... These are emerging issues that are disconcerting,” he said.
Dr. Gold also noted the changing trends, explaining that over the course of his career, substance misuse and dependence have emerged and changed.
“In the ’70s and ’80s, medical students rarely presented in need of treatment, but when they did, they had alcohol, tobacco, and benzodiazepine problems. Residents ... had problems with prescription opiates, and many programs reported overdoses. More recently, medical students no longer smoke cigarettes. ... Now it is marijuana,” he said, adding that binge drinking, club drugs, and psychostimulant abuse also are on the rise.
Students now are more like their peers and unlike their mentors with respect to drug misuse, use, and dependence, and there is an emerging concern that the most heavily involved students in terms of drug abuse and addiction will select one specialty or another based on drug access, said Dr. Gold, now professor (adjunct) at the University of Southern California, Los Angeles, and at Washington University in St. Louis.
“They often are surprised that the college of medicine, their patients, and professors do not accept as appropriate behavior the taking of another person’s [attention-deficit/hyperactivity disorder] medication, or smoking cannabis, or taking drugs for their mentees,” he said.
As for treatment in this new era of substance abuse and dependence, the approach remains much the same, Dr. Angres said, noting that medication-assisted treatment may be necessary for heroin addiction. A concern, however, is that the relapse rate may be higher.
“We don’t know what that will mean,” he said. “It will be years before we can see how it plays out with physicians with [heroin], but you do the same things, with perhaps some extra support above and beyond [the standard approach].”
Dr. Angres disclosed that he is part owner of the Positive Sobriety Institute, which treats addicted professionals, including physicians. Dr. Gold reported having no relevant financial disclosures.
*Correction, 03/09/2016: An earlier version of this story misstated the term sometimes used to describe physicians with addictive behaviors
Physicians appear to have much greater odds of substance abuse and dependence disorders related to alcohol, opiates, and sedatives than their nonphysician counterparts, some estimates showed.
The good news is that physicians with substance abuse and addiction respond particularly well to treatment – so much so that experts have recommended that the treatment methods employed in specialized programs for impaired health professionals be disseminated and used in programs for the general public.
“In a nutshell, for a physician with addiction who goes to an appropriate program that has expertise working with physicians and then follows up with 5-year monitoring, the average rate of abstinence of about 80% is the polar opposite of that in the general population, Dr. Daniel H. Angres of Northwestern University in Chicago said in an interview.
At best, the abstinence rate after treatment is about 20% for the general population, said Dr. Angres, an addiction psychiatrist and medical director of the Positive Sobriety Institute in Chicago, who has spent more than 3 decades working with physicians and other health care professionals struggling with drug abuse and dependence.
The key is proper treatment in a setting with other health professionals and long-term monitoring; without both, the outcomes won’t be as good, he stressed. But Dr. Angres added that there is more to it than that. Often, the very factors that drive a person to become a physician and help that person succeed in the endeavor are the factors that can improve the odds of beating addiction, he explained.
Scope of the problem
Substance abuse and dependence in general are on the rise. This is true among physicians as well as the general public. Opioid use has been a particular problem. A 2008 review by Dr. Mark S. Gold, former chair of the psychiatry department at the University of Florida, Gainesville, and Lisa J. Merlo, Ph.D., also of the university, noted that 12%-23% of physicians admit to prescription opioid use, compared with 1%-4% of nonphysicians (Harv Rev Psychiatry. 2008;16[3]:181-94).
However, Dr. Angres said there are few data to suggest that physicians are at substantially increased risk of addiction.
“The rule of thumb is that addiction affects probably 1 in 10 people. We can comfortably say about 10% will have an addiction problem at some point in their lives,” he said.
But addiction is a disease with genetic underpinnings, and while there was a time when it was thought that perhaps physicians had greater risk because they had greater access, the playing field with respect to access has been leveled over time. There are no good data to suggest that more than 15% of physicians are affected, Dr. Angres noted.
That’s not to say certain specialties aren’t overrepresented among addicts, he added.
Anesthesiologists, for example, have been shown to have a greater risk of addiction – perhaps as a result of their having access to, and/or excess exposure to, drugs like fentanyl and propofol. In fact, the review by Dr. Gold and Dr. Merlo also noted an increasing trend for abuse of sublingual and intravenously administered analgesics among health care professionals. Not far behind anesthesiologists are surgeons, pain doctors, and emergency physicians, Dr. Gold said in an interview. “We have proposed a number of theories to explain this, from self-selection bias to selecting anesthesia because of student drug use to second- and third-hand occupational exposure risks.”
Meanwhile, another 2008 study by Dr. Gold, Dr. Merlo, and their colleagues demonstrated that chronic secondhand exposure to low doses of drugs such as fentanyl and propofol among health care professionals in the operating room might sensitize vulnerable individuals to the “rewarding effects of these drugs, placing them at higher risk for developing an addiction.” The authors concluded that the findings, while they served only as “preliminary support for an unproven hypothesis,” suggest a need for workplace protections (J Addict Dis. 2008;27[3]:67-75).
Dr. Gold also led a more recent study comparing psychiatric and substance use disorders among physicians in a state Physician’s Health Program (PHP) with those in a general treatment population. He and his colleagues found that 99 physicians referred to the PHP for suspected impairment had similar lifetime use of alcohol, opiates, and sedatives as a group of age, sex, and education status–matched persons in a general treatment population.
However, the physicians had significantly higher odds of meeting DSM-IV criteria for abuse/dependence disorders related to alcohol (odds ratio, 2.56), opiates (OR, 86.58), and sedatives (OR, 54.76), the authors reported (J Addic Med. 2013 Mar-Apr;7[2]:108-12).
Further, the physicians had significantly lower odds of lifetime use, but higher odds of lifetime abuse/dependence, for cocaine/crack cocaine and cannabis vs. the comparison group, as well as lower lifetime amphetamine use (OR, 0.21) with no difference in abuse/dependence vs. the comparison group, and lower odds of psychiatric disorders, including obsessive-compulsive disorder, major depression, and specific phobias.
While Dr. Gold and his colleagues concluded that more research is needed to understand psychiatric morbidity in physicians, and while physicians in certain specialties may have an increased likelihood of addiction in relation to exposure to drugs in the operating room setting, most physicians “get addicted in ways that are similar to others in the population,” Dr. Angres said: They have a pain problem, they get a drug like hydrocodone or other narcotic, they have a particular kind of experience that “goes above and beyond the pain management” (some individuals have a paradoxical effect in which they feel connected and energized, for example), and they become addicted.
The main drug of choice, even among physicians, is alcohol, he noted, explaining that stress is another common precipitating factor.
There is a definite relationship between stress and addiction; alcohol may be used to cope with stress, and those who are vulnerable to addiction can become dependent.
“Physicians are more stressed today than ever. The whole landscape of medicine, the economics of medicine means physicians have to see more patients and spend less time with patients,” Dr. Angres said, adding that factors like electronic medical records requirements and concerns about malpractice all contribute to increasing stress levels and are likely also increasing the rate of addiction and other forms of physician impairment or distress, including cognitive difficulties, depression, and anxiety.
Affected physicians, sometimes referred to as “disruptive physicians,” are increasingly a focus of programs and protocols to promote physician wellness.*
Northwestern and other high-level academic centers are “gearing up” for the problem. It is becoming more common for physicians to undergo screening when they are hired, and to undergo random screening to make sure they aren’t under the influence, he explained.
“And I also think that the medical community is much more attuned to detecting this and helping people gain access to proper assessment, rehabilitation, and reentry,” he added.
Treatment and outcomes
Treatment for physicians is often provided through state PHPs, some of which are under the umbrella of a licensing board or are part of a diversion program involving an autonomous entity.
“PHPs are really critical,” Dr. Angres said, explaining that they provide education, conduct research to help reduce malpractice claims, and ensure proper assessment of physicians, and they do long-term monitoring involving wellness checks.
While there is some controversy about the role of PHPs – some physicians have resented the monitoring, say they have felt coerced into participating, and have demanded more choice regarding treatment options – these programs are highly successful and data driven, Dr. Angres said.
“When the outcomes are clearly very good with a certain kind of protocol, you want to stick with that, particularly if public safety is involved,” he said, adding that these programs work because they are more supportive than punitive, they treat affected physicians for their disease, and they help physicians do what they need to do to safely reenter the practice of medicine.
Punitive programs would drive substance abuse/dependence problems underground, making them more dangerous, he said.
There is a great deal of debate about the appropriate duration of treatment, but most importantly, physicians should be with other physicians.
“What gets people sober is really being with other people who are sober,” he said, adding that a peer group of others with similar experiences and a similar life path is critical.
Twelve-step programs, which employ this principle as part of treatment and aftercare, result in better outcomes, and it is also crucial that physicians be treated by personnel who are experienced and conversant with working with physicians, because there are important factors necessary for successful reentry and engagement in the workplace.
Medications also are an important part of care, in many cases.
Dr. Gold’s research has long focused on the evaluation and treatment of impaired health professionals.
“After the discovery of the antiopiate withdrawal efficacy of clonidine, we tried an experimental medication – naltrexone – as a treatment for impaired health professional opiate addicts. … Naltrexone was both safe and effective. Injectable naltrexone is now widely recognized as a safe and effective treatment to prevent opiate relapse,” he said in an interview.
Naltrexone is particularly important for the treatment of addicted anesthesiologists, as they are at high risk of relapse when they return to work; their relapses are often overdoses after detoxification, he said.
Five-year outcomes studies suggest that with appropriate treatment, outcomes are indeed excellent among physicians, compared with their peers. Two such studies, led by researchers from the Institute of Behavior and Health in Rockville, Md., respectively showed that 102 anesthesiologists treated and monitored under PHP supervision had excellent outcomes similar to those of other impaired physicians (Anesth Analg. 2009;109[3]:891-6), and that 144 surgeons treated under PHP supervision had positive outcomes similar to those of nonsurgeons (Arch Surg. 2011;146[11]:1286-91).
In their review article, Dr. Gold and Dr. Merlo concluded that for physicians overall, “appropriate intervention (e.g., typically in with the state PHP), methods of evaluation and treatment for addicted physicians are extremely effective. The combination of medical, psychosocial, and support group interventions, combined with extensive posttreatment monitoring and drug testing, generally results in sustained recovery among the physicians who attend specialized treatment programs. These outcomes are typically obtained even when physicians did not enter treatment voluntarily. Thus, it is likely that impaired professional programs represent the best treatment available for opioid use disorders, and nonphysician addicts would likely experience a similar benefit from participating in such a program.”
Dr. Angres agreed that physicians in general are “a good outcome group.”
“If treated and monitored appropriately, these are some of the best outcomes we see in addiction treatment,” he said.
Many factors are involved in the superior results among physicians vs. their nonphysician counterparts, he said, explaining that physicians tend to be particularly conscientious, hard-working individuals with good support systems and personality variables that allow them to persevere under difficult circumstances. They also have a great deal riding on recovery in terms of reentering the practice of medicine.
“So motivation is a big issue. ... All of these things come together,” he said.
Changing trends
In addition to the stress-related factors that appear to be contributing to increased substance abuse and dependence, concerning cultural trends are emerging.
“We have an epidemic among young adults,” Dr. Angres said.
Heroin, prescription opiates, psychostimulants, binge drinking – all are occurring in epidemic proportions throughout our culture, including among the new generation of medical students and young physicians, he added.
“We are seeing for the first time, even in the last year or so, medical students, residents, and young adults who are addicted to drugs like heroin because it is so ubiquitous. So this is a new phenomenon. This is just a new reality. It’s not a massive problem [in medicine], but it is something that we’re seeing that we didn’t see before. ... These are emerging issues that are disconcerting,” he said.
Dr. Gold also noted the changing trends, explaining that over the course of his career, substance misuse and dependence have emerged and changed.
“In the ’70s and ’80s, medical students rarely presented in need of treatment, but when they did, they had alcohol, tobacco, and benzodiazepine problems. Residents ... had problems with prescription opiates, and many programs reported overdoses. More recently, medical students no longer smoke cigarettes. ... Now it is marijuana,” he said, adding that binge drinking, club drugs, and psychostimulant abuse also are on the rise.
Students now are more like their peers and unlike their mentors with respect to drug misuse, use, and dependence, and there is an emerging concern that the most heavily involved students in terms of drug abuse and addiction will select one specialty or another based on drug access, said Dr. Gold, now professor (adjunct) at the University of Southern California, Los Angeles, and at Washington University in St. Louis.
“They often are surprised that the college of medicine, their patients, and professors do not accept as appropriate behavior the taking of another person’s [attention-deficit/hyperactivity disorder] medication, or smoking cannabis, or taking drugs for their mentees,” he said.
As for treatment in this new era of substance abuse and dependence, the approach remains much the same, Dr. Angres said, noting that medication-assisted treatment may be necessary for heroin addiction. A concern, however, is that the relapse rate may be higher.
“We don’t know what that will mean,” he said. “It will be years before we can see how it plays out with physicians with [heroin], but you do the same things, with perhaps some extra support above and beyond [the standard approach].”
Dr. Angres disclosed that he is part owner of the Positive Sobriety Institute, which treats addicted professionals, including physicians. Dr. Gold reported having no relevant financial disclosures.
*Correction, 03/09/2016: An earlier version of this story misstated the term sometimes used to describe physicians with addictive behaviors

Hernia repair: Studies don’t support use of higher-cost biological mesh
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point: The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, and the expense associated with their use cannot be justified at this time, a systematic review of the literature suggested.
Major finding: Available evidence remains insufficient to determine whether cost and clinical benefits exist with the use of biological mesh for abdominal wall hernia repair.
Data source: A systematic review of the literature, yielding 20 eligible studies.
Disclosures: This study was supported by the Hudson-Penn Endowment fund at University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.