User login
Smartphone app simultaneously improves multiple chronic disease risk behaviors
ORLANDO – A 12-week intervention involving a smartphone app and weekly coaching by telephone resulted in sustained, clinically meaningful improvement in multiple unhealthy diet and activity behaviors in the randomized, controlled Make Better Choices 2 study.
“It’s far more possible than I would have believed to produce sustained, large-magnitude changes in cardiovascular risk behaviors without using large financial incentives through the use of technologic support and a scalable approach to coaching,” principal investigator Bonnie J. Spring, Ph.D., said at the American Heart Association scientific sessions.

This is an example of what preventive medicine experts term “primordial prevention.” It’s intervention further upstream than primary prevention, which addresses the standard modifiable cardiovascular risk factors before a cardiovascular event has occurred. Primordial prevention addresses the unhealthy behaviors that eventually lead to the standard risk factors.
Make Better Choices 2 included 212 adults, all of whom had four unhealthy behaviors of interest: low fruit and vegetable intake, high consumption of saturated fat, low levels of moderate to vigorous physical activity, and excessive sedentary leisure TV and computer screen time.
The smartphone app was used for self-monitoring on the journey toward goal attainment. The data were uploaded regularly to the remote coach, who provided individualized instruction weekly for 3 months, then every 2 weeks during the next 3 months, and monthly for the final 3 months, explained Dr. Spring, professor of preventive medicine and director of the Center for Behavior and Health at Northwestern University, Chicago.
The study expanded upon the success of the earlier 204-subject Make Better Choices 1 study, which showed that targeting two of the four unhealthy behaviors resulted in efficiently synergistic improvement in all four (Arch Intern Med. 2012 May 28;172[10]:789-96). However, in the earlier trial, participants were paid $175 if they reached their goals. In Make Better Choices 2, Dr. Spring and her coworkers wanted to see if behavioral change could be achieved without a large financial incentive.
Make Better Choices 2 participants were randomized to one of three study arms: simultaneous targeting of fruit and vegetable intake, sedentary screen time, and low moderate to vigorous physical activity; sequential targeting of fruit/vegetables and screen time followed by the physical activity intervention; or a control group that received instruction on reducing stress and improving sleep.
The simultaneous and sequential interventions proved equally effective. And as in Make Better Choices 1, a carryover effect was seen: At 9 months, not only was fruit and vegetable consumption increased by 5.9 servings per day, compared with baseline and leisure screen time reduced by 2 hours and 7 minutes per day, but participants reduced their saturated fat intake by an absolute 3.7% of total calories consumed daily, even though saturated fat wasn’t targeted.
“We think the improvement in saturated fat intake was due mostly to cutting down on hand to mouth snacking behavior by decreasing TV time,” she explained.
Moderate to vigorous physical activity time was increased by an average of 16 minutes per day in the two active treatment arms, compared with controls at 6 months. However, at 9 months, there was no significant difference among the three groups.
“The hardest behavior change for us to initiate and maintain is moderate to vigorous physical activity. I think that warrants more research,” according to Dr. Spring.
Adherence was good, with roughly an 18% dropout rate through 9 months in each study arm.

Session moderator Dr. Sidney C. Smith of the University of North Carolina, Chapel Hill, noted that only about 25% of participants in the trial were men. He’s observed a similarly skewed ratio in other behavioral studies, and he wondered why, given that men have their acute MIs an average of 10 years earlier than women.
“This is a classic challenge in behavior intervention trials. It’s very difficult to get men to enroll,” Dr. Spring replied. “There’s starting to be a body of work trying to address this challenge.”
She added that she believes for some men it’s an issue of control. They want to do things their way, and they confuse support with control.
“This is one of the hopes of having technology available: If you’re a do-it-yourselfer, here are tools to help you do it yourself,” Dr. Spring said.
Once men get on board, however, a consistent finding in behavioral intervention studies is that the strategies work as well in men as in women, she observed.
Make Better Choices 2 was funded by Northwestern University and the National Institutes of Health. Dr. Spring reported having no financial conflicts of interest.
ORLANDO – A 12-week intervention involving a smartphone app and weekly coaching by telephone resulted in sustained, clinically meaningful improvement in multiple unhealthy diet and activity behaviors in the randomized, controlled Make Better Choices 2 study.
“It’s far more possible than I would have believed to produce sustained, large-magnitude changes in cardiovascular risk behaviors without using large financial incentives through the use of technologic support and a scalable approach to coaching,” principal investigator Bonnie J. Spring, Ph.D., said at the American Heart Association scientific sessions.
This is an example of what preventive medicine experts term “primordial prevention.” It’s intervention further upstream than primary prevention, which addresses the standard modifiable cardiovascular risk factors before a cardiovascular event has occurred. Primordial prevention addresses the unhealthy behaviors that eventually lead to the standard risk factors.
Make Better Choices 2 included 212 adults, all of whom had four unhealthy behaviors of interest: low fruit and vegetable intake, high consumption of saturated fat, low levels of moderate to vigorous physical activity, and excessive sedentary leisure TV and computer screen time.
The smartphone app was used for self-monitoring on the journey toward goal attainment. The data were uploaded regularly to the remote coach, who provided individualized instruction weekly for 3 months, then every 2 weeks during the next 3 months, and monthly for the final 3 months, explained Dr. Spring, professor of preventive medicine and director of the Center for Behavior and Health at Northwestern University, Chicago.
The study expanded upon the success of the earlier 204-subject Make Better Choices 1 study, which showed that targeting two of the four unhealthy behaviors resulted in efficiently synergistic improvement in all four (Arch Intern Med. 2012 May 28;172[10]:789-96). However, in the earlier trial, participants were paid $175 if they reached their goals. In Make Better Choices 2, Dr. Spring and her coworkers wanted to see if behavioral change could be achieved without a large financial incentive.
Make Better Choices 2 participants were randomized to one of three study arms: simultaneous targeting of fruit and vegetable intake, sedentary screen time, and low moderate to vigorous physical activity; sequential targeting of fruit/vegetables and screen time followed by the physical activity intervention; or a control group that received instruction on reducing stress and improving sleep.
The simultaneous and sequential interventions proved equally effective. And as in Make Better Choices 1, a carryover effect was seen: At 9 months, not only was fruit and vegetable consumption increased by 5.9 servings per day, compared with baseline and leisure screen time reduced by 2 hours and 7 minutes per day, but participants reduced their saturated fat intake by an absolute 3.7% of total calories consumed daily, even though saturated fat wasn’t targeted.
“We think the improvement in saturated fat intake was due mostly to cutting down on hand to mouth snacking behavior by decreasing TV time,” she explained.
Moderate to vigorous physical activity time was increased by an average of 16 minutes per day in the two active treatment arms, compared with controls at 6 months. However, at 9 months, there was no significant difference among the three groups.
“The hardest behavior change for us to initiate and maintain is moderate to vigorous physical activity. I think that warrants more research,” according to Dr. Spring.
Adherence was good, with roughly an 18% dropout rate through 9 months in each study arm.
Session moderator Dr. Sidney C. Smith of the University of North Carolina, Chapel Hill, noted that only about 25% of participants in the trial were men. He’s observed a similarly skewed ratio in other behavioral studies, and he wondered why, given that men have their acute MIs an average of 10 years earlier than women.
“This is a classic challenge in behavior intervention trials. It’s very difficult to get men to enroll,” Dr. Spring replied. “There’s starting to be a body of work trying to address this challenge.”
She added that she believes for some men it’s an issue of control. They want to do things their way, and they confuse support with control.
“This is one of the hopes of having technology available: If you’re a do-it-yourselfer, here are tools to help you do it yourself,” Dr. Spring said.
Once men get on board, however, a consistent finding in behavioral intervention studies is that the strategies work as well in men as in women, she observed.
Make Better Choices 2 was funded by Northwestern University and the National Institutes of Health. Dr. Spring reported having no financial conflicts of interest.
ORLANDO – A 12-week intervention involving a smartphone app and weekly coaching by telephone resulted in sustained, clinically meaningful improvement in multiple unhealthy diet and activity behaviors in the randomized, controlled Make Better Choices 2 study.
“It’s far more possible than I would have believed to produce sustained, large-magnitude changes in cardiovascular risk behaviors without using large financial incentives through the use of technologic support and a scalable approach to coaching,” principal investigator Bonnie J. Spring, Ph.D., said at the American Heart Association scientific sessions.
This is an example of what preventive medicine experts term “primordial prevention.” It’s intervention further upstream than primary prevention, which addresses the standard modifiable cardiovascular risk factors before a cardiovascular event has occurred. Primordial prevention addresses the unhealthy behaviors that eventually lead to the standard risk factors.
Make Better Choices 2 included 212 adults, all of whom had four unhealthy behaviors of interest: low fruit and vegetable intake, high consumption of saturated fat, low levels of moderate to vigorous physical activity, and excessive sedentary leisure TV and computer screen time.
The smartphone app was used for self-monitoring on the journey toward goal attainment. The data were uploaded regularly to the remote coach, who provided individualized instruction weekly for 3 months, then every 2 weeks during the next 3 months, and monthly for the final 3 months, explained Dr. Spring, professor of preventive medicine and director of the Center for Behavior and Health at Northwestern University, Chicago.
The study expanded upon the success of the earlier 204-subject Make Better Choices 1 study, which showed that targeting two of the four unhealthy behaviors resulted in efficiently synergistic improvement in all four (Arch Intern Med. 2012 May 28;172[10]:789-96). However, in the earlier trial, participants were paid $175 if they reached their goals. In Make Better Choices 2, Dr. Spring and her coworkers wanted to see if behavioral change could be achieved without a large financial incentive.
Make Better Choices 2 participants were randomized to one of three study arms: simultaneous targeting of fruit and vegetable intake, sedentary screen time, and low moderate to vigorous physical activity; sequential targeting of fruit/vegetables and screen time followed by the physical activity intervention; or a control group that received instruction on reducing stress and improving sleep.
The simultaneous and sequential interventions proved equally effective. And as in Make Better Choices 1, a carryover effect was seen: At 9 months, not only was fruit and vegetable consumption increased by 5.9 servings per day, compared with baseline and leisure screen time reduced by 2 hours and 7 minutes per day, but participants reduced their saturated fat intake by an absolute 3.7% of total calories consumed daily, even though saturated fat wasn’t targeted.
“We think the improvement in saturated fat intake was due mostly to cutting down on hand to mouth snacking behavior by decreasing TV time,” she explained.
Moderate to vigorous physical activity time was increased by an average of 16 minutes per day in the two active treatment arms, compared with controls at 6 months. However, at 9 months, there was no significant difference among the three groups.
“The hardest behavior change for us to initiate and maintain is moderate to vigorous physical activity. I think that warrants more research,” according to Dr. Spring.
Adherence was good, with roughly an 18% dropout rate through 9 months in each study arm.
Session moderator Dr. Sidney C. Smith of the University of North Carolina, Chapel Hill, noted that only about 25% of participants in the trial were men. He’s observed a similarly skewed ratio in other behavioral studies, and he wondered why, given that men have their acute MIs an average of 10 years earlier than women.
“This is a classic challenge in behavior intervention trials. It’s very difficult to get men to enroll,” Dr. Spring replied. “There’s starting to be a body of work trying to address this challenge.”
She added that she believes for some men it’s an issue of control. They want to do things their way, and they confuse support with control.
“This is one of the hopes of having technology available: If you’re a do-it-yourselfer, here are tools to help you do it yourself,” Dr. Spring said.
Once men get on board, however, a consistent finding in behavioral intervention studies is that the strategies work as well in men as in women, she observed.
Make Better Choices 2 was funded by Northwestern University and the National Institutes of Health. Dr. Spring reported having no financial conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Remote coaching supported by a smartphone app can simultaneously improve multiple unhealthy lifestyle behaviors.
Major finding: A 12-week intervention incorporating smartphone technology and weekly coaching by telephone produced sustained improvements in multiple unhealthy diet and physical activity behaviors without resorting to financial incentives.
Data source: Make Better Choices 2 was a multicenter trial in which 212 adults with four specific unhealthy behaviors were randomized to a mobile behavioral health intervention or a control group.
Disclosures: The study was funded by Northwestern University and the National Institutes of Health. Dr. Spring reported having no financial conflicts of interest.

Medicare fumbles penalties for excess heart failure readmissions
ORLANDO – When the Centers for Medicare & Medicaid Services imposes financial penalties on hospitals because of excess readmissions for heart failure, the agency gets it wrong nearly 30% of the time, Hung-Mo Lin, Sc.D. asserted at the American Heart Association scientific sessions.
The problem, she said, is that the agency’s 2012 Inpatient Prospective Payment System Final Rule relies on a formula for estimating the risk-standardized excess readmission ratio that doesn’t take into account the uncertainties surrounding the measurements.

This has serious consequences in terms of the resultant substantial probability of hospital misclassification errors, according to Dr. Lin of the Icahn School of Medicine at Mount Sinai, New York.
How substantial is this error rate? To find out, Dr. Lin and her coworkers retroactively applied the CMS formula to roughly 1.5 million heart failure admissions at nearly 5,000 U.S. hospitals during 2005-2008, then developed confidence intervals for the individual hospitals’ excess readmission ratios and ran the numbers again, this time using the updated formula. They determined that the false-penalty rate was 27.5% for the 2,381 hospitals with an elevated excess admission ratio as defined by the current CMS formula.
Conversely, among the 2,549 hospitals that would have been labeled as good performers using the CMS formula and hence not subject to a punitive payment adjustment, 28.8% actually turned out to be poor performers with excessive heart failure readmissions. Those hospitals would have wrongly escaped penalties, she explained.
Hospital volume mattered. When the investigators stratified their results by hospital volume, they found that the probability of hospital misclassification was twice as great for small hospitals – that is, those in the two bottom quintiles for patient volume – compared to hospitals in the top quintile.
Dr. Lin reported having no financial conflicts regarding this health policy study.
ORLANDO – When the Centers for Medicare & Medicaid Services imposes financial penalties on hospitals because of excess readmissions for heart failure, the agency gets it wrong nearly 30% of the time, Hung-Mo Lin, Sc.D. asserted at the American Heart Association scientific sessions.
The problem, she said, is that the agency’s 2012 Inpatient Prospective Payment System Final Rule relies on a formula for estimating the risk-standardized excess readmission ratio that doesn’t take into account the uncertainties surrounding the measurements.
This has serious consequences in terms of the resultant substantial probability of hospital misclassification errors, according to Dr. Lin of the Icahn School of Medicine at Mount Sinai, New York.
How substantial is this error rate? To find out, Dr. Lin and her coworkers retroactively applied the CMS formula to roughly 1.5 million heart failure admissions at nearly 5,000 U.S. hospitals during 2005-2008, then developed confidence intervals for the individual hospitals’ excess readmission ratios and ran the numbers again, this time using the updated formula. They determined that the false-penalty rate was 27.5% for the 2,381 hospitals with an elevated excess admission ratio as defined by the current CMS formula.
Conversely, among the 2,549 hospitals that would have been labeled as good performers using the CMS formula and hence not subject to a punitive payment adjustment, 28.8% actually turned out to be poor performers with excessive heart failure readmissions. Those hospitals would have wrongly escaped penalties, she explained.
Hospital volume mattered. When the investigators stratified their results by hospital volume, they found that the probability of hospital misclassification was twice as great for small hospitals – that is, those in the two bottom quintiles for patient volume – compared to hospitals in the top quintile.
Dr. Lin reported having no financial conflicts regarding this health policy study.
ORLANDO – When the Centers for Medicare & Medicaid Services imposes financial penalties on hospitals because of excess readmissions for heart failure, the agency gets it wrong nearly 30% of the time, Hung-Mo Lin, Sc.D. asserted at the American Heart Association scientific sessions.
The problem, she said, is that the agency’s 2012 Inpatient Prospective Payment System Final Rule relies on a formula for estimating the risk-standardized excess readmission ratio that doesn’t take into account the uncertainties surrounding the measurements.
This has serious consequences in terms of the resultant substantial probability of hospital misclassification errors, according to Dr. Lin of the Icahn School of Medicine at Mount Sinai, New York.
How substantial is this error rate? To find out, Dr. Lin and her coworkers retroactively applied the CMS formula to roughly 1.5 million heart failure admissions at nearly 5,000 U.S. hospitals during 2005-2008, then developed confidence intervals for the individual hospitals’ excess readmission ratios and ran the numbers again, this time using the updated formula. They determined that the false-penalty rate was 27.5% for the 2,381 hospitals with an elevated excess admission ratio as defined by the current CMS formula.
Conversely, among the 2,549 hospitals that would have been labeled as good performers using the CMS formula and hence not subject to a punitive payment adjustment, 28.8% actually turned out to be poor performers with excessive heart failure readmissions. Those hospitals would have wrongly escaped penalties, she explained.
Hospital volume mattered. When the investigators stratified their results by hospital volume, they found that the probability of hospital misclassification was twice as great for small hospitals – that is, those in the two bottom quintiles for patient volume – compared to hospitals in the top quintile.
Dr. Lin reported having no financial conflicts regarding this health policy study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Nearly 30% of hospitals penalized by Medicare for excess heart failure readmissions are misclassified as such, and a roughly equal percentage of hospitals are wrongly categorized as good performers.
Major finding: The formula Medicare uses to calculate risk-standardized excess heart failure readmission ratios is flawed in that it ignores the uncertainty of the measurements, leading to erroneous imposition of financial penalties.
Data source: This study entailed calculating the level of uncertainty in the Medicare formula, then retroactively applying the formula to nearly 1.5 million heart failure admissions at almost 5,000 U.S. hospitals.
Disclosures: The presenter reported having no financial conflicts regarding this health policy study.

Vegetarianism may protect against heart failure
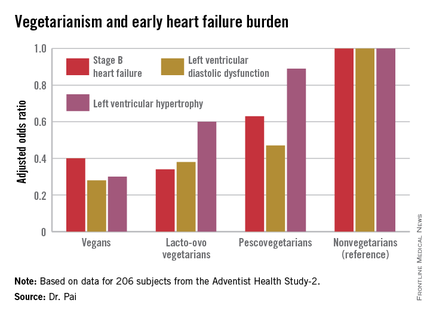
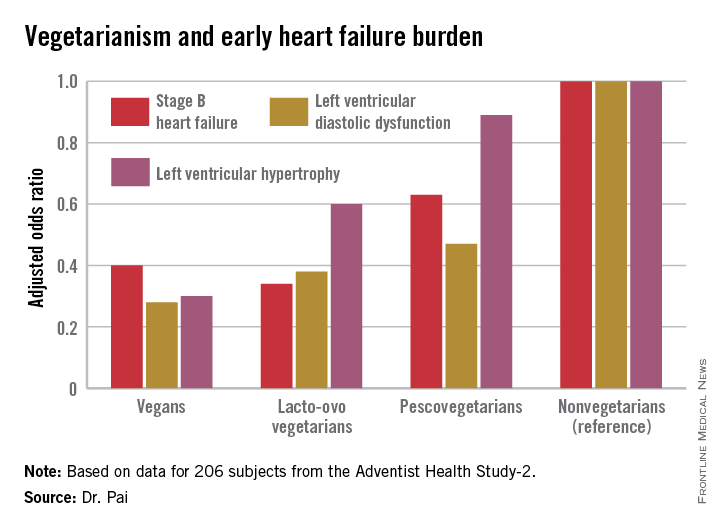
ORLANDO – Elderly individuals who consumed a vegan diet – no meat, fish, dairy, or eggs – were at an adjusted 72% lower risk of prevalent left ventricular diastolic dysfunction as well as 70% lower risk of left ventricular hypertrophy than were nonvegetarians in the Adventist Health Study-2.
The landmark Adventist Health Study-2 (AHS-2) is an ongoing observational epidemiologic study that includes 96,000 subjects. In previously reported findings from AHS-2, a vegetarian diet was associated with reduced risks of diabetes, hypertension, metabolic syndrome, overweight/obesity, all-cause mortality, and some cancers, compared with a nonvegetarian diet of similar caloric intake (Am J Clin Nutr. 2014 Jul;100[suppl 1]:353s-8s).
Because heart failure is a massive and growing problem, affecting 6 million Americans at a direct health care cost of $40 billion annually, AHS-2 investigators decided to look at the relationship between diet and heart failure, Dr. Ramdas G. Pai explained at the American Heart Association scientific sessions.
He and his coinvestigators at Loma Linda (Calif.) University brought in a random sample of 206 AHS-2 participants for a clinic visit which included a full echocardiographic assessment. The cohort had a mean age of 74 years. Echocardiography revealed that left ventricular diastolic dysfunction was present in 60% of subjects, left ventricular hypertrophy in 10%, and an increased left atrial volume index in 45%.
The study population consisted of roughly equal numbers of vegans, lacto-ovo vegetarians as defined by consumption of meat or fish less than once per month and dairy and/or eggs more than once weekly, pescovegetarians who eat fish more than once per month, and meat-eating nonvegetarians.
In a multivariate analysis adjusted for age, race, gender, body surface area, diabetes, hypertension, and history of coronary heart disease, a stepwise increase was seen in the prevalence of early stage B heart failure and its echocardiographic risk factors with increasing nonvegetarianism.
The implication is that a population shift toward a more vegetarian-oriented diet might reduce the overall burden of heart failure in the community, according to Dr. Pai.
He reported having no financial conflicts of interest regarding the AHS-2 analysis.
ORLANDO – Elderly individuals who consumed a vegan diet – no meat, fish, dairy, or eggs – were at an adjusted 72% lower risk of prevalent left ventricular diastolic dysfunction as well as 70% lower risk of left ventricular hypertrophy than were nonvegetarians in the Adventist Health Study-2.
The landmark Adventist Health Study-2 (AHS-2) is an ongoing observational epidemiologic study that includes 96,000 subjects. In previously reported findings from AHS-2, a vegetarian diet was associated with reduced risks of diabetes, hypertension, metabolic syndrome, overweight/obesity, all-cause mortality, and some cancers, compared with a nonvegetarian diet of similar caloric intake (Am J Clin Nutr. 2014 Jul;100[suppl 1]:353s-8s).
Because heart failure is a massive and growing problem, affecting 6 million Americans at a direct health care cost of $40 billion annually, AHS-2 investigators decided to look at the relationship between diet and heart failure, Dr. Ramdas G. Pai explained at the American Heart Association scientific sessions.
He and his coinvestigators at Loma Linda (Calif.) University brought in a random sample of 206 AHS-2 participants for a clinic visit which included a full echocardiographic assessment. The cohort had a mean age of 74 years. Echocardiography revealed that left ventricular diastolic dysfunction was present in 60% of subjects, left ventricular hypertrophy in 10%, and an increased left atrial volume index in 45%.
The study population consisted of roughly equal numbers of vegans, lacto-ovo vegetarians as defined by consumption of meat or fish less than once per month and dairy and/or eggs more than once weekly, pescovegetarians who eat fish more than once per month, and meat-eating nonvegetarians.
In a multivariate analysis adjusted for age, race, gender, body surface area, diabetes, hypertension, and history of coronary heart disease, a stepwise increase was seen in the prevalence of early stage B heart failure and its echocardiographic risk factors with increasing nonvegetarianism.
The implication is that a population shift toward a more vegetarian-oriented diet might reduce the overall burden of heart failure in the community, according to Dr. Pai.
He reported having no financial conflicts of interest regarding the AHS-2 analysis.
ORLANDO – Elderly individuals who consumed a vegan diet – no meat, fish, dairy, or eggs – were at an adjusted 72% lower risk of prevalent left ventricular diastolic dysfunction as well as 70% lower risk of left ventricular hypertrophy than were nonvegetarians in the Adventist Health Study-2.
The landmark Adventist Health Study-2 (AHS-2) is an ongoing observational epidemiologic study that includes 96,000 subjects. In previously reported findings from AHS-2, a vegetarian diet was associated with reduced risks of diabetes, hypertension, metabolic syndrome, overweight/obesity, all-cause mortality, and some cancers, compared with a nonvegetarian diet of similar caloric intake (Am J Clin Nutr. 2014 Jul;100[suppl 1]:353s-8s).
Because heart failure is a massive and growing problem, affecting 6 million Americans at a direct health care cost of $40 billion annually, AHS-2 investigators decided to look at the relationship between diet and heart failure, Dr. Ramdas G. Pai explained at the American Heart Association scientific sessions.
He and his coinvestigators at Loma Linda (Calif.) University brought in a random sample of 206 AHS-2 participants for a clinic visit which included a full echocardiographic assessment. The cohort had a mean age of 74 years. Echocardiography revealed that left ventricular diastolic dysfunction was present in 60% of subjects, left ventricular hypertrophy in 10%, and an increased left atrial volume index in 45%.
The study population consisted of roughly equal numbers of vegans, lacto-ovo vegetarians as defined by consumption of meat or fish less than once per month and dairy and/or eggs more than once weekly, pescovegetarians who eat fish more than once per month, and meat-eating nonvegetarians.
In a multivariate analysis adjusted for age, race, gender, body surface area, diabetes, hypertension, and history of coronary heart disease, a stepwise increase was seen in the prevalence of early stage B heart failure and its echocardiographic risk factors with increasing nonvegetarianism.
The implication is that a population shift toward a more vegetarian-oriented diet might reduce the overall burden of heart failure in the community, according to Dr. Pai.
He reported having no financial conflicts of interest regarding the AHS-2 analysis.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: The closer one gets to a vegan diet, the less likely are echocardiographic risk factors for early heart failure.
Major finding: Vegans were 60% less likely to have stage B heart failure than were nonvegetarians.
Data source: This study examined echocardiographic findings associated with early heart failure in 206 participants in the observational Adventist Health Study-2.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study.
Cold Weather Linked to Increase in Strokes, MI
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.

He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.
He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.
He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
AT THE AHA SCIENTIFIC SESSIONS

Cold weather linked to increase in strokes, MI
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.

He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.
He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
ORLANDO – Cold temperature days were associated with a 28% increase in the risk of MI and a 15% increase in stroke over an 18-year period in Ontario, Hong Chen, Ph.D., reported at the American Heart Association scientific sessions.
The relationship between air temperature and cardiovascular events mapped out as a U-shaped pattern, with the lowest-risk trough occurring on days when the temperature averaged 54º F. However, the U-shape was skewed such that the increased risk achieved significance on the cold but not hot days, according to Dr. Chen of Public Health Ontario and the University of Toronto.
He and his coinvestigators looked at the relationship between daily temperature and cardiovascular risk because the epidemiologic data in this area was sparse even though there are intriguing animal studies suggesting that extreme cold weather can induce a prothrombotic inflammatory reaction and hypercoagulable state.
The investigators matched daily temperature and cardiovascular hospital admission data for all 14 health districts in the sprawling province of Ontario for the period 1996-2013. During the study period, there were 443,447 hospitalizations for acute MI, 355,837 for stroke, 237,979 for ischemic stroke, and 1.4 million admissions coded as ischemic heart disease.
In a multivariate analysis controlling for influenza activity, air pollution levels, relative humidity, and day of the week, the adjusted rate of admissions for MI was 28% greater on the coldest 1% of days than on days where the temperature averaged the optimal 54º F. The coldest days were also associated with a 12% increase in the risk of admission for ischemic heart disease, a 15% increase in stroke, and a 19% increase in ischemic stroke.
Dr. Chen and his coworkers also examined their mountain of data to see how selected comorbid conditions might affect temperature-related risk. They found that the risk of admission for ischemic heart disease on cold days was greatest among individuals with a history of conduction disorders, while the risk of cold-related stroke was highest in Ontarians with preexisting arrhythmias.
Dr. Chen reported having no financial conflicts of interest regarding this public health study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Expect noticeably more hospital admissions for stroke and ischemic heart disease on cold weather days.
Major finding: Cold weather brought a 15% increase in the risk of hospital admission for stroke and a 28% rise in admissions for acute MI in Ontario, compared with days when the average temperature was 54º F.
Data source: This retrospective study looked at the association between daily temperature and the risk of hospital admission for acute MI, stroke, and other cardiovascular events over an 18-year period across Ontario.
Disclosures: The presenter reported having no financial conflicts of interest regarding this public health study.

67% of teens have substantial cardiometabolic risk burden, blood donor survey shows
ORLANDO – Fully two-thirds of nearly 25,000 Dallas-area volunteer blood donors ages 16-19 had elevated or borderline total cholesterol, blood pressure, and/or hemoglobin A1c, Dr. Merlyn H. Sayers reported at the American Heart Association scientific sessions.
“It is startling that such a significant percentage of these young, ostensibly healthy volunteers have abnormal cardiometabolic health metrics,” observed Dr. Sayers, president and chief executive officer of Carter BloodCare of Bedford, Tex., a nonprofit organization that is the largest blood bank in the state.
After all, he noted, longitudinal studies have clearly shown that cardiometabolic risk factors present in adolescence will persist into adulthood and are associated with increased risks of cardiovascular disease and diabetes. Moreover, it’s troubling, albeit not really surprising, that for the most part these adolescents don’t seem to care about their cardiometabolic risk, the hematologist-oncologist added.

“We give all these youngsters an opportunity to go to the Carter BloodCare website and confidentially retrieve their values. But despite all manner of urging on our part that these results are important, at best only about 20% of the individuals actually do so, and that rate varies substantially by race and ethnicity,” according to Dr. Sayers. “Where appropriate, we need to find ways to impose behavior modification on a group that is relatively resistant to guidance and intervention. Even the best kids, as teenagers, really don’t take this sort of advice about their health risk very seriously. They regard themselves as immortal during their teenage years.”
Noting that behavioral change is not a core strength among transfusion medicine specialists, Dr. Sayers appealed to his audience of cardiologists for suggestions as to how to encourage lifestyle modification in this youthful group without browbeating them to the point that they’re driven off from becoming serial blood donors.
It’s not widely appreciated that across the U.S. during the school year, 20% of all unpaid blood donors are high school students. These high school blood drives provide an as-yet untapped opportunity to screen adolescents for cardiometabolic risk at low cost and minimal inconvenience to participants, said Dr. Sayers of the University of Texas, Dallas.
“We need allies to help us to ensure we get the kids’ attention better,” he explained. “I want to leave you with the sense that perhaps you will see these blood drives as an opportunity to find interventions that might address primordial prevention of cardiometabolic risk.”
He presented a study of 24,925 youths aged 16-19 who donated blood to Carter BloodCare during 2011-2012. Since blood is drawn for obligatory infectious diseases screening at each donation, Dr. Sayers and coinvestigators were able to measure nonfasting total cholesterol and HbA1c in every teen donor. Blood pressure is also measured at every donation.
The investigators used widely accepted definitions of elevated blood pressure, cholesterol, and HbA1c: namely, at least 140/80 mm Hg, 200 mg/dL, and 6.5%, respectively.
While the percentage of teen blood donors with borderline or elevated levels of all three cardiometabolic risk factors was in the low single figures, 21% of boys and 15% of girls were positive for two out of the three.
The prevalence of cardiometabolic risk factors varied by ethnicity. Sixteen percent of white adolescents had elevated or borderline levels of two risk factors. So did 24% of African Americans, 22% of Asian Americans, and 18% of Hispanics.
“These are really staggering results,” commented session chair Dr. Seth S. Martin of Johns Hopkins University, Baltimore. “This is a call to action now that you’ve identified all these kids who are on a trajectory that doesn’t look good.”
As to how physicians can help to favorably alter that trajectory, however, audience members admitted to being stumped, especially since many young people stop going to a primary care physician for preventive care during their teenage years.
“The big problem here is how to use this information to initiate lifestyle change,” observed Dr. Lewis H. Kuller, professor and past chair of epidemiology at the University of Pittsburgh.
Dr. Sayers reported having no financial conflicts regarding his study.
ORLANDO – Fully two-thirds of nearly 25,000 Dallas-area volunteer blood donors ages 16-19 had elevated or borderline total cholesterol, blood pressure, and/or hemoglobin A1c, Dr. Merlyn H. Sayers reported at the American Heart Association scientific sessions.
“It is startling that such a significant percentage of these young, ostensibly healthy volunteers have abnormal cardiometabolic health metrics,” observed Dr. Sayers, president and chief executive officer of Carter BloodCare of Bedford, Tex., a nonprofit organization that is the largest blood bank in the state.
After all, he noted, longitudinal studies have clearly shown that cardiometabolic risk factors present in adolescence will persist into adulthood and are associated with increased risks of cardiovascular disease and diabetes. Moreover, it’s troubling, albeit not really surprising, that for the most part these adolescents don’t seem to care about their cardiometabolic risk, the hematologist-oncologist added.
“We give all these youngsters an opportunity to go to the Carter BloodCare website and confidentially retrieve their values. But despite all manner of urging on our part that these results are important, at best only about 20% of the individuals actually do so, and that rate varies substantially by race and ethnicity,” according to Dr. Sayers. “Where appropriate, we need to find ways to impose behavior modification on a group that is relatively resistant to guidance and intervention. Even the best kids, as teenagers, really don’t take this sort of advice about their health risk very seriously. They regard themselves as immortal during their teenage years.”
Noting that behavioral change is not a core strength among transfusion medicine specialists, Dr. Sayers appealed to his audience of cardiologists for suggestions as to how to encourage lifestyle modification in this youthful group without browbeating them to the point that they’re driven off from becoming serial blood donors.
It’s not widely appreciated that across the U.S. during the school year, 20% of all unpaid blood donors are high school students. These high school blood drives provide an as-yet untapped opportunity to screen adolescents for cardiometabolic risk at low cost and minimal inconvenience to participants, said Dr. Sayers of the University of Texas, Dallas.
“We need allies to help us to ensure we get the kids’ attention better,” he explained. “I want to leave you with the sense that perhaps you will see these blood drives as an opportunity to find interventions that might address primordial prevention of cardiometabolic risk.”
He presented a study of 24,925 youths aged 16-19 who donated blood to Carter BloodCare during 2011-2012. Since blood is drawn for obligatory infectious diseases screening at each donation, Dr. Sayers and coinvestigators were able to measure nonfasting total cholesterol and HbA1c in every teen donor. Blood pressure is also measured at every donation.
The investigators used widely accepted definitions of elevated blood pressure, cholesterol, and HbA1c: namely, at least 140/80 mm Hg, 200 mg/dL, and 6.5%, respectively.
While the percentage of teen blood donors with borderline or elevated levels of all three cardiometabolic risk factors was in the low single figures, 21% of boys and 15% of girls were positive for two out of the three.
The prevalence of cardiometabolic risk factors varied by ethnicity. Sixteen percent of white adolescents had elevated or borderline levels of two risk factors. So did 24% of African Americans, 22% of Asian Americans, and 18% of Hispanics.
“These are really staggering results,” commented session chair Dr. Seth S. Martin of Johns Hopkins University, Baltimore. “This is a call to action now that you’ve identified all these kids who are on a trajectory that doesn’t look good.”
As to how physicians can help to favorably alter that trajectory, however, audience members admitted to being stumped, especially since many young people stop going to a primary care physician for preventive care during their teenage years.
“The big problem here is how to use this information to initiate lifestyle change,” observed Dr. Lewis H. Kuller, professor and past chair of epidemiology at the University of Pittsburgh.
Dr. Sayers reported having no financial conflicts regarding his study.
ORLANDO – Fully two-thirds of nearly 25,000 Dallas-area volunteer blood donors ages 16-19 had elevated or borderline total cholesterol, blood pressure, and/or hemoglobin A1c, Dr. Merlyn H. Sayers reported at the American Heart Association scientific sessions.
“It is startling that such a significant percentage of these young, ostensibly healthy volunteers have abnormal cardiometabolic health metrics,” observed Dr. Sayers, president and chief executive officer of Carter BloodCare of Bedford, Tex., a nonprofit organization that is the largest blood bank in the state.
After all, he noted, longitudinal studies have clearly shown that cardiometabolic risk factors present in adolescence will persist into adulthood and are associated with increased risks of cardiovascular disease and diabetes. Moreover, it’s troubling, albeit not really surprising, that for the most part these adolescents don’t seem to care about their cardiometabolic risk, the hematologist-oncologist added.
“We give all these youngsters an opportunity to go to the Carter BloodCare website and confidentially retrieve their values. But despite all manner of urging on our part that these results are important, at best only about 20% of the individuals actually do so, and that rate varies substantially by race and ethnicity,” according to Dr. Sayers. “Where appropriate, we need to find ways to impose behavior modification on a group that is relatively resistant to guidance and intervention. Even the best kids, as teenagers, really don’t take this sort of advice about their health risk very seriously. They regard themselves as immortal during their teenage years.”
Noting that behavioral change is not a core strength among transfusion medicine specialists, Dr. Sayers appealed to his audience of cardiologists for suggestions as to how to encourage lifestyle modification in this youthful group without browbeating them to the point that they’re driven off from becoming serial blood donors.
It’s not widely appreciated that across the U.S. during the school year, 20% of all unpaid blood donors are high school students. These high school blood drives provide an as-yet untapped opportunity to screen adolescents for cardiometabolic risk at low cost and minimal inconvenience to participants, said Dr. Sayers of the University of Texas, Dallas.
“We need allies to help us to ensure we get the kids’ attention better,” he explained. “I want to leave you with the sense that perhaps you will see these blood drives as an opportunity to find interventions that might address primordial prevention of cardiometabolic risk.”
He presented a study of 24,925 youths aged 16-19 who donated blood to Carter BloodCare during 2011-2012. Since blood is drawn for obligatory infectious diseases screening at each donation, Dr. Sayers and coinvestigators were able to measure nonfasting total cholesterol and HbA1c in every teen donor. Blood pressure is also measured at every donation.
The investigators used widely accepted definitions of elevated blood pressure, cholesterol, and HbA1c: namely, at least 140/80 mm Hg, 200 mg/dL, and 6.5%, respectively.
While the percentage of teen blood donors with borderline or elevated levels of all three cardiometabolic risk factors was in the low single figures, 21% of boys and 15% of girls were positive for two out of the three.
The prevalence of cardiometabolic risk factors varied by ethnicity. Sixteen percent of white adolescents had elevated or borderline levels of two risk factors. So did 24% of African Americans, 22% of Asian Americans, and 18% of Hispanics.
“These are really staggering results,” commented session chair Dr. Seth S. Martin of Johns Hopkins University, Baltimore. “This is a call to action now that you’ve identified all these kids who are on a trajectory that doesn’t look good.”
As to how physicians can help to favorably alter that trajectory, however, audience members admitted to being stumped, especially since many young people stop going to a primary care physician for preventive care during their teenage years.
“The big problem here is how to use this information to initiate lifestyle change,” observed Dr. Lewis H. Kuller, professor and past chair of epidemiology at the University of Pittsburgh.
Dr. Sayers reported having no financial conflicts regarding his study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Two-thirds of 16- to 19-year-olds have borderline or frank hypertension, hypercholesterolemia, and/or high blood glucose.
Major finding: Of a very large group of 16- to 19-year-old blood donors, 67% had borderline or elevated total cholesterol, blood pressure, and/or hemoglobin A1c levels.
Data source: A retrospective analysis of total cholesterol, blood pressure, and HbA1c levels in 24,925 Dallas-area blood donors aged 16-19.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study.
‘Fear and ignorance’ drive rise in bilateral mastectomy
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.

In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.

He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.
In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.
He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.
In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.
He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
EXPERT ANALYSIS FROM SABCS 2015

Final follow-up of BCIRG-006 shows important cardiac safety differences
SAN ANTONIO – Final 10-year analysis of the landmark BCIRG-006 trial underscores the safety advantages of a nonanthracycline, trastuzumab-based adjunctive treatment regimen in early-stage HER2-positive breast cancer.
At a median 10.3 years of follow-up in the phase III randomized trial of 3,222 patients, a substantial reduction in the risk of cardiac toxicity was evident in the women assigned to six cycles of docetaxel (Taxotere) and carboplatin plus 1 year of trastuzumab (the TCH arm), compared with the two anthracycline-containing study arms, Dr. Dennis J. Slamon reported at the San Antonio Breast Cancer Symposium.

At baseline the three treatment groups were well balanced in terms of cardiovascular risk factors. Yet over the course of the study only 4 women in the TCH arm developed clinical heart failure, compared with 21 patients who received four cycles of doxorubicin (Adriamycin) and cyclophosphamide (Cytoxan) followed by four cycles of docetaxel and 1 year of trastuzumab (AC-TH), and 8 patients in the control arm who got four cycles of doxorubicin and cyclophosphamide followed by four cycles of docetaxel (AC-T).
Thus, adding docetaxel to 1 year of trastuzumab (Herceptin) conferred a fivefold increase in this major cardiac complication, compared with trastuzumab alone, noted Dr. Slamon, professor of medicine and chief of the division of hematology-oncology at the University of California, Los Angeles.
His presentation of the final analysis also provided important new information on the issue of treatment-related subclinical reductions in cardiac reserve as manifest by decreased left ventricular ejection fraction (LVEF).
A greater than 10% reduction in LVEF occurred in 9.4% of the TCH group, 19.2% of the AC-TH group, and 11.8% of the AC-T control group. In 2009 when Dr. Slamon presented the 5-year follow-up of BCIRG-006 at the San Antonio Breast Cancer Symposium, he was able to report that during the first year post treatment the no-anthracycline TCH group showed a recovery of LVEF to near baseline while in the AC-TH and AC-T groups the LVEF did not bounce back through the 5-year mark. The question raised at that point was how long would their LVEF remain diminished.
“With the 10-year data, with LVEFs measured annually after the end of treatment, this loss is real and is maintained. The question now is, what will become of these patients when they acquire their long-term age-related cardiac risk factors after we’ve already compromised their LVEF to some degree?” he said.
The primary endpoint in BCIRG-006 was disease-free survival (DFS). At final follow-up, with a total of 876 such events, the DFS rate was 74.6% in the AC-TH group and statistically similar at 73% in the TCH group, both of which were superior to the 67.9% figure in the AC-T control arm. Only 10 DFS events separated the TCH and AC-TH groups at 10 years. Overall survival rates in the two trastuzumab arms weren’t significantly different either.
To answer the question of whether patients with higher-risk HER2-positive early breast cancer require anthracycline-based adjunctive therapy in order to maximize benefit, the investigators did a subanalysis restricted to the roughly 400 women with four or more positive lymph nodes. The DFS rate was 62.9% with TCH and a near-identical 62.8% with AC-TH, both superior to the 53.6% DFS rate in the AC-T group.
All eight cases of acute leukemia occurred in the AC-TH and AC-T study arms.
The study was sponsored by Sanofi with additional support from Genentech. The presenter reported serving on advisory boards for BioMarin, Genentech/Roche, Pfizer, and Novartis.
SAN ANTONIO – Final 10-year analysis of the landmark BCIRG-006 trial underscores the safety advantages of a nonanthracycline, trastuzumab-based adjunctive treatment regimen in early-stage HER2-positive breast cancer.
At a median 10.3 years of follow-up in the phase III randomized trial of 3,222 patients, a substantial reduction in the risk of cardiac toxicity was evident in the women assigned to six cycles of docetaxel (Taxotere) and carboplatin plus 1 year of trastuzumab (the TCH arm), compared with the two anthracycline-containing study arms, Dr. Dennis J. Slamon reported at the San Antonio Breast Cancer Symposium.
At baseline the three treatment groups were well balanced in terms of cardiovascular risk factors. Yet over the course of the study only 4 women in the TCH arm developed clinical heart failure, compared with 21 patients who received four cycles of doxorubicin (Adriamycin) and cyclophosphamide (Cytoxan) followed by four cycles of docetaxel and 1 year of trastuzumab (AC-TH), and 8 patients in the control arm who got four cycles of doxorubicin and cyclophosphamide followed by four cycles of docetaxel (AC-T).
Thus, adding docetaxel to 1 year of trastuzumab (Herceptin) conferred a fivefold increase in this major cardiac complication, compared with trastuzumab alone, noted Dr. Slamon, professor of medicine and chief of the division of hematology-oncology at the University of California, Los Angeles.
His presentation of the final analysis also provided important new information on the issue of treatment-related subclinical reductions in cardiac reserve as manifest by decreased left ventricular ejection fraction (LVEF).
A greater than 10% reduction in LVEF occurred in 9.4% of the TCH group, 19.2% of the AC-TH group, and 11.8% of the AC-T control group. In 2009 when Dr. Slamon presented the 5-year follow-up of BCIRG-006 at the San Antonio Breast Cancer Symposium, he was able to report that during the first year post treatment the no-anthracycline TCH group showed a recovery of LVEF to near baseline while in the AC-TH and AC-T groups the LVEF did not bounce back through the 5-year mark. The question raised at that point was how long would their LVEF remain diminished.
“With the 10-year data, with LVEFs measured annually after the end of treatment, this loss is real and is maintained. The question now is, what will become of these patients when they acquire their long-term age-related cardiac risk factors after we’ve already compromised their LVEF to some degree?” he said.
The primary endpoint in BCIRG-006 was disease-free survival (DFS). At final follow-up, with a total of 876 such events, the DFS rate was 74.6% in the AC-TH group and statistically similar at 73% in the TCH group, both of which were superior to the 67.9% figure in the AC-T control arm. Only 10 DFS events separated the TCH and AC-TH groups at 10 years. Overall survival rates in the two trastuzumab arms weren’t significantly different either.
To answer the question of whether patients with higher-risk HER2-positive early breast cancer require anthracycline-based adjunctive therapy in order to maximize benefit, the investigators did a subanalysis restricted to the roughly 400 women with four or more positive lymph nodes. The DFS rate was 62.9% with TCH and a near-identical 62.8% with AC-TH, both superior to the 53.6% DFS rate in the AC-T group.
All eight cases of acute leukemia occurred in the AC-TH and AC-T study arms.
The study was sponsored by Sanofi with additional support from Genentech. The presenter reported serving on advisory boards for BioMarin, Genentech/Roche, Pfizer, and Novartis.
SAN ANTONIO – Final 10-year analysis of the landmark BCIRG-006 trial underscores the safety advantages of a nonanthracycline, trastuzumab-based adjunctive treatment regimen in early-stage HER2-positive breast cancer.
At a median 10.3 years of follow-up in the phase III randomized trial of 3,222 patients, a substantial reduction in the risk of cardiac toxicity was evident in the women assigned to six cycles of docetaxel (Taxotere) and carboplatin plus 1 year of trastuzumab (the TCH arm), compared with the two anthracycline-containing study arms, Dr. Dennis J. Slamon reported at the San Antonio Breast Cancer Symposium.
At baseline the three treatment groups were well balanced in terms of cardiovascular risk factors. Yet over the course of the study only 4 women in the TCH arm developed clinical heart failure, compared with 21 patients who received four cycles of doxorubicin (Adriamycin) and cyclophosphamide (Cytoxan) followed by four cycles of docetaxel and 1 year of trastuzumab (AC-TH), and 8 patients in the control arm who got four cycles of doxorubicin and cyclophosphamide followed by four cycles of docetaxel (AC-T).
Thus, adding docetaxel to 1 year of trastuzumab (Herceptin) conferred a fivefold increase in this major cardiac complication, compared with trastuzumab alone, noted Dr. Slamon, professor of medicine and chief of the division of hematology-oncology at the University of California, Los Angeles.
His presentation of the final analysis also provided important new information on the issue of treatment-related subclinical reductions in cardiac reserve as manifest by decreased left ventricular ejection fraction (LVEF).
A greater than 10% reduction in LVEF occurred in 9.4% of the TCH group, 19.2% of the AC-TH group, and 11.8% of the AC-T control group. In 2009 when Dr. Slamon presented the 5-year follow-up of BCIRG-006 at the San Antonio Breast Cancer Symposium, he was able to report that during the first year post treatment the no-anthracycline TCH group showed a recovery of LVEF to near baseline while in the AC-TH and AC-T groups the LVEF did not bounce back through the 5-year mark. The question raised at that point was how long would their LVEF remain diminished.
“With the 10-year data, with LVEFs measured annually after the end of treatment, this loss is real and is maintained. The question now is, what will become of these patients when they acquire their long-term age-related cardiac risk factors after we’ve already compromised their LVEF to some degree?” he said.
The primary endpoint in BCIRG-006 was disease-free survival (DFS). At final follow-up, with a total of 876 such events, the DFS rate was 74.6% in the AC-TH group and statistically similar at 73% in the TCH group, both of which were superior to the 67.9% figure in the AC-T control arm. Only 10 DFS events separated the TCH and AC-TH groups at 10 years. Overall survival rates in the two trastuzumab arms weren’t significantly different either.
To answer the question of whether patients with higher-risk HER2-positive early breast cancer require anthracycline-based adjunctive therapy in order to maximize benefit, the investigators did a subanalysis restricted to the roughly 400 women with four or more positive lymph nodes. The DFS rate was 62.9% with TCH and a near-identical 62.8% with AC-TH, both superior to the 53.6% DFS rate in the AC-T group.
All eight cases of acute leukemia occurred in the AC-TH and AC-T study arms.
The study was sponsored by Sanofi with additional support from Genentech. The presenter reported serving on advisory boards for BioMarin, Genentech/Roche, Pfizer, and Novartis.
AT SABCS 2015
Key clinical point: An adjuvant trastuzumab-based, nonanthracycline regimen for early HER2-positive breast cancer offers important cardiac safety benefits over the alternatives.
Major finding: Women with early HER2-positive breast cancer experienced less risk of long-term cardiac toxicity and acute leukemia if their adjuvant therapy consisted of six cycles of docetaxel plus carboplatin and 1 year of trastuzumab than if they received trastuzumab plus an anthracycline.
Data source: This was a phase III, 3,222-patient, three-armed clinical trial with a median 10.3 years of follow-up.
Disclosures: The study was sponsored by Sanofi with additional support from Genentech. The presenter reported serving on advisory boards for BioMarin, Genentech/Roche, Pfizer, and Novartis.

EADV: Oral nicotinamide reduces transepidermal water loss
COPENHAGEN – Oral nicotinamide markedly reduces transepidermal water loss (TEWL), raising the prospect that it could be effective in the treatment of atopic dermatitis, Dr. Andrew C. Chen reported at the annual congress of the European Academy of Dermatology and Venereology.
“Nicotinamide is safe, accessible over the counter as a vitamin supplement, and inexpensive. It may be a new systemic therapy for conditions with impaired skin barrier function,” according to Dr. Chen of Royal Alfred Hospital in Sydney.
While nicotinic acid, also known as niacin, famously causes vasodilatory side effects including pronounced flushing and headache, nicotinamide is something else altogether: an amide form of vitamin B3 with a well-established safety profile and no vasodilatory side effects, he explained.
Dr. Chen presented a substudy of the phase III double-blind, multicenter, placebo-controlled Oral Nicotinamide to Reduce Actinic Cancer trial (ONTRAC), in which 386 patients with at least two nonmelanoma skin cancers in the previous 5 years were randomized to oral nicotinamide at 500 mg twice daily or placebo for 12 months. This landmark study showed that nicotinamide did indeed reduce the incidence of nonmelanoma skin cancer (N Engl J Med 2015;373:1618-26).
A secondary endpoint in ONTRAC was oral nicotinamide’s effect on skin barrier function as measured by TEWL. Among the 292 ONTRAC participants with standardized TEWL measurements obtained at the forehead, left forearm, and left leg at baseline and every 3 months thereafter, nicotinamide resulted in significantly less TEWL than placebo at every time point after baseline. At the midforehead, for example, TEWL was 5% less than with placebo at 3 months and 6 months, 6% less at 9 months, and 6% less at the 12-month mark. At the forearm and midleg, the difference was 7% at 12 months. Side effects were similar to placebo.
During the course of the 12-month study, TEWL was 15% greater in controls during the Australian winter as compared with summer. Oral nicotinamide essentially reduced TEWL by a magnitude equivalent to roughly half the variation between the extremes of summer and winter, Dr. Chen noted.
The ONTRAC trial was supported by the Australian National Health and Medical Research Council. Dr. Chen reported having no financial conflicts regarding the study.
COPENHAGEN – Oral nicotinamide markedly reduces transepidermal water loss (TEWL), raising the prospect that it could be effective in the treatment of atopic dermatitis, Dr. Andrew C. Chen reported at the annual congress of the European Academy of Dermatology and Venereology.
“Nicotinamide is safe, accessible over the counter as a vitamin supplement, and inexpensive. It may be a new systemic therapy for conditions with impaired skin barrier function,” according to Dr. Chen of Royal Alfred Hospital in Sydney.
While nicotinic acid, also known as niacin, famously causes vasodilatory side effects including pronounced flushing and headache, nicotinamide is something else altogether: an amide form of vitamin B3 with a well-established safety profile and no vasodilatory side effects, he explained.
Dr. Chen presented a substudy of the phase III double-blind, multicenter, placebo-controlled Oral Nicotinamide to Reduce Actinic Cancer trial (ONTRAC), in which 386 patients with at least two nonmelanoma skin cancers in the previous 5 years were randomized to oral nicotinamide at 500 mg twice daily or placebo for 12 months. This landmark study showed that nicotinamide did indeed reduce the incidence of nonmelanoma skin cancer (N Engl J Med 2015;373:1618-26).
A secondary endpoint in ONTRAC was oral nicotinamide’s effect on skin barrier function as measured by TEWL. Among the 292 ONTRAC participants with standardized TEWL measurements obtained at the forehead, left forearm, and left leg at baseline and every 3 months thereafter, nicotinamide resulted in significantly less TEWL than placebo at every time point after baseline. At the midforehead, for example, TEWL was 5% less than with placebo at 3 months and 6 months, 6% less at 9 months, and 6% less at the 12-month mark. At the forearm and midleg, the difference was 7% at 12 months. Side effects were similar to placebo.
During the course of the 12-month study, TEWL was 15% greater in controls during the Australian winter as compared with summer. Oral nicotinamide essentially reduced TEWL by a magnitude equivalent to roughly half the variation between the extremes of summer and winter, Dr. Chen noted.
The ONTRAC trial was supported by the Australian National Health and Medical Research Council. Dr. Chen reported having no financial conflicts regarding the study.
COPENHAGEN – Oral nicotinamide markedly reduces transepidermal water loss (TEWL), raising the prospect that it could be effective in the treatment of atopic dermatitis, Dr. Andrew C. Chen reported at the annual congress of the European Academy of Dermatology and Venereology.
“Nicotinamide is safe, accessible over the counter as a vitamin supplement, and inexpensive. It may be a new systemic therapy for conditions with impaired skin barrier function,” according to Dr. Chen of Royal Alfred Hospital in Sydney.
While nicotinic acid, also known as niacin, famously causes vasodilatory side effects including pronounced flushing and headache, nicotinamide is something else altogether: an amide form of vitamin B3 with a well-established safety profile and no vasodilatory side effects, he explained.
Dr. Chen presented a substudy of the phase III double-blind, multicenter, placebo-controlled Oral Nicotinamide to Reduce Actinic Cancer trial (ONTRAC), in which 386 patients with at least two nonmelanoma skin cancers in the previous 5 years were randomized to oral nicotinamide at 500 mg twice daily or placebo for 12 months. This landmark study showed that nicotinamide did indeed reduce the incidence of nonmelanoma skin cancer (N Engl J Med 2015;373:1618-26).
A secondary endpoint in ONTRAC was oral nicotinamide’s effect on skin barrier function as measured by TEWL. Among the 292 ONTRAC participants with standardized TEWL measurements obtained at the forehead, left forearm, and left leg at baseline and every 3 months thereafter, nicotinamide resulted in significantly less TEWL than placebo at every time point after baseline. At the midforehead, for example, TEWL was 5% less than with placebo at 3 months and 6 months, 6% less at 9 months, and 6% less at the 12-month mark. At the forearm and midleg, the difference was 7% at 12 months. Side effects were similar to placebo.
During the course of the 12-month study, TEWL was 15% greater in controls during the Australian winter as compared with summer. Oral nicotinamide essentially reduced TEWL by a magnitude equivalent to roughly half the variation between the extremes of summer and winter, Dr. Chen noted.
The ONTRAC trial was supported by the Australian National Health and Medical Research Council. Dr. Chen reported having no financial conflicts regarding the study.
AT THE EADV CONGRESS
Key clinical point: Oral nicotinamide is a safe, inexpensive vitamin, which may be of value in patients with disorders of skin barrier function, such as atopic dermatitis.
Major finding: Transepidermal water loss was essentially cut in half with oral nicotinamide at 500 mg twice daily, compared with placebo.
Data source: This double-blind, randomized trial of oral nicotinamide versus placebo included 292 subjects with transepidermal water loss measurements obtained at multiple body sites every 3 months for 1 year.
Disclosures: The ONTRAC trial was supported by the Australian National Health and Medical Research Council. The presenter reported having no financial conflicts regarding the study.
EADV: Fresolimumab shows early promise in scleroderma
COPENHAGEN – The recent success of fresolimumab in treating early diffuse cutaneous systemic sclerosis in a proof-of-concept study signals better days ahead in the treatment of scleroderma, Dr. Thomas Krieg predicted at the annual congress of the European Academy of Dermatology and Venereology.
“There will be new and better treatments based upon our improved understanding of the pathophysiology of this complex multifaceted disease. New targeted therapies are likely,” according to Dr. Krieg, chairman of the department of dermatology and venereology and dean of the medical faculty at the University of Cologne (Germany).

One such therapy is fresolimumab. This high-affinity neutralizing antibody targets all three isoforms of transforming growth factor–beta (TGF-beta), long believed to be a key player in the development of fibrosis. Fibrosis in patients with systemic sclerosis can affect the skin, lungs, heart, kidneys, and GI tract.
The recent U.S. open-label fresolimumab proof-of-concept study led by investigators at Boston University included 15 patients with early diffuse cutaneous systemic sclerosis. Eight patients received a single 5-mg/kg dose, while the other seven got two 1-mg/kg doses. All were then followed for 24 weeks.
The results make a strong case for TGF-beta as playing a pivotal role in the pathogenesis of systemic sclerosis, according to Dr. Krieg, who wasn’t involved in the study. The investigators characterized the rate of decline in clinical skin disease in response to fresolimumab as assessed using the modified Rodnan skin score (mRSS) as “unprecedented.” The subjects averaged mRSS reductions of 5.1 points at week 3 or 4, increasing to 6.3 points at week 7 and 8 points at week 11 (J Clin Invest. 2015;125[7]:2795-807). To put that into context, the median improvement in mRSS scores in seven previous clinical trials of other agents was an anemic 2.9 points at 6 months and 3.4 at 1 year.
Skin biopsies showed that the fresolimumab-induced rapid decline in mRSS was accompanied by a sharp drop in skin biomarkers of TGF-beta activity, including expression of the genes thrombospondin-1, cartilage oligomeric protein, and connective tissue growth factor. In addition, dermal myofibroblast infiltration dropped off.
The logical next steps in the research effort are to go larger and longer in terms of clinical trials of fresolimumab for scleroderma skin disease, and also to assess whether fresolimumab is effective in treating the fibrotic disease involving the internal organs of scleroderma patients.
Fresolimumab was well tolerated in this study. That’s also been true thus far in studies using higher doses and multiple doses for other diseases where fibrosis figures prominently. As the TGF-beta inhibitor’s side-effect profile becomes better characterized, it will be important to compare the adverse events associated with fresolimumab to the known substantial morbidity associated with current therapies.
The current treatments for the fibrotic disease in systemic sclerosis are unsatisfactory: cyclophosphamide is not terribly effective and carries the risk of malignancy, while “the jury is still out” on stem cell transplantation for systemic sclerosis, as ongoing studies attempt to establish the risk-benefit ratio of this intervention, the dermatologist said.
As for corticosteroids, Dr. Krieg believes they’re overused in systemic sclerosis.
“I have to tell you, many patients come to our center on relatively high doses of corticosteroids. Yet if you go through the literature there’s more or less no evidence for a beneficial role for corticosteroids in systemic sclerosis. And there is an increased risk of developing severe renal crisis, especially with higher doses in patients with diffuse systemic sclerosis,” the dermatologist cautioned.
More than a dozen drugs are now in clinical trials for systemic sclerosis. In addition to fresolimumab, tyrosine kinase inhibitors including imatinib (Gleevec) and nilotinib (Tasigna) are being evaluated for their antifibrotic effects. Other investigational agents target the inflammatory and vascular components of the disease.
Fresolimumab is owned by Sanofi. The fresolimumab study was supported by the National Institutes of Health. Dr. Krieg reported having no financial conflicts regarding his presentation.
COPENHAGEN – The recent success of fresolimumab in treating early diffuse cutaneous systemic sclerosis in a proof-of-concept study signals better days ahead in the treatment of scleroderma, Dr. Thomas Krieg predicted at the annual congress of the European Academy of Dermatology and Venereology.
“There will be new and better treatments based upon our improved understanding of the pathophysiology of this complex multifaceted disease. New targeted therapies are likely,” according to Dr. Krieg, chairman of the department of dermatology and venereology and dean of the medical faculty at the University of Cologne (Germany).
One such therapy is fresolimumab. This high-affinity neutralizing antibody targets all three isoforms of transforming growth factor–beta (TGF-beta), long believed to be a key player in the development of fibrosis. Fibrosis in patients with systemic sclerosis can affect the skin, lungs, heart, kidneys, and GI tract.
The recent U.S. open-label fresolimumab proof-of-concept study led by investigators at Boston University included 15 patients with early diffuse cutaneous systemic sclerosis. Eight patients received a single 5-mg/kg dose, while the other seven got two 1-mg/kg doses. All were then followed for 24 weeks.
The results make a strong case for TGF-beta as playing a pivotal role in the pathogenesis of systemic sclerosis, according to Dr. Krieg, who wasn’t involved in the study. The investigators characterized the rate of decline in clinical skin disease in response to fresolimumab as assessed using the modified Rodnan skin score (mRSS) as “unprecedented.” The subjects averaged mRSS reductions of 5.1 points at week 3 or 4, increasing to 6.3 points at week 7 and 8 points at week 11 (J Clin Invest. 2015;125[7]:2795-807). To put that into context, the median improvement in mRSS scores in seven previous clinical trials of other agents was an anemic 2.9 points at 6 months and 3.4 at 1 year.
Skin biopsies showed that the fresolimumab-induced rapid decline in mRSS was accompanied by a sharp drop in skin biomarkers of TGF-beta activity, including expression of the genes thrombospondin-1, cartilage oligomeric protein, and connective tissue growth factor. In addition, dermal myofibroblast infiltration dropped off.
The logical next steps in the research effort are to go larger and longer in terms of clinical trials of fresolimumab for scleroderma skin disease, and also to assess whether fresolimumab is effective in treating the fibrotic disease involving the internal organs of scleroderma patients.
Fresolimumab was well tolerated in this study. That’s also been true thus far in studies using higher doses and multiple doses for other diseases where fibrosis figures prominently. As the TGF-beta inhibitor’s side-effect profile becomes better characterized, it will be important to compare the adverse events associated with fresolimumab to the known substantial morbidity associated with current therapies.
The current treatments for the fibrotic disease in systemic sclerosis are unsatisfactory: cyclophosphamide is not terribly effective and carries the risk of malignancy, while “the jury is still out” on stem cell transplantation for systemic sclerosis, as ongoing studies attempt to establish the risk-benefit ratio of this intervention, the dermatologist said.
As for corticosteroids, Dr. Krieg believes they’re overused in systemic sclerosis.
“I have to tell you, many patients come to our center on relatively high doses of corticosteroids. Yet if you go through the literature there’s more or less no evidence for a beneficial role for corticosteroids in systemic sclerosis. And there is an increased risk of developing severe renal crisis, especially with higher doses in patients with diffuse systemic sclerosis,” the dermatologist cautioned.
More than a dozen drugs are now in clinical trials for systemic sclerosis. In addition to fresolimumab, tyrosine kinase inhibitors including imatinib (Gleevec) and nilotinib (Tasigna) are being evaluated for their antifibrotic effects. Other investigational agents target the inflammatory and vascular components of the disease.
Fresolimumab is owned by Sanofi. The fresolimumab study was supported by the National Institutes of Health. Dr. Krieg reported having no financial conflicts regarding his presentation.
COPENHAGEN – The recent success of fresolimumab in treating early diffuse cutaneous systemic sclerosis in a proof-of-concept study signals better days ahead in the treatment of scleroderma, Dr. Thomas Krieg predicted at the annual congress of the European Academy of Dermatology and Venereology.
“There will be new and better treatments based upon our improved understanding of the pathophysiology of this complex multifaceted disease. New targeted therapies are likely,” according to Dr. Krieg, chairman of the department of dermatology and venereology and dean of the medical faculty at the University of Cologne (Germany).
One such therapy is fresolimumab. This high-affinity neutralizing antibody targets all three isoforms of transforming growth factor–beta (TGF-beta), long believed to be a key player in the development of fibrosis. Fibrosis in patients with systemic sclerosis can affect the skin, lungs, heart, kidneys, and GI tract.
The recent U.S. open-label fresolimumab proof-of-concept study led by investigators at Boston University included 15 patients with early diffuse cutaneous systemic sclerosis. Eight patients received a single 5-mg/kg dose, while the other seven got two 1-mg/kg doses. All were then followed for 24 weeks.
The results make a strong case for TGF-beta as playing a pivotal role in the pathogenesis of systemic sclerosis, according to Dr. Krieg, who wasn’t involved in the study. The investigators characterized the rate of decline in clinical skin disease in response to fresolimumab as assessed using the modified Rodnan skin score (mRSS) as “unprecedented.” The subjects averaged mRSS reductions of 5.1 points at week 3 or 4, increasing to 6.3 points at week 7 and 8 points at week 11 (J Clin Invest. 2015;125[7]:2795-807). To put that into context, the median improvement in mRSS scores in seven previous clinical trials of other agents was an anemic 2.9 points at 6 months and 3.4 at 1 year.
Skin biopsies showed that the fresolimumab-induced rapid decline in mRSS was accompanied by a sharp drop in skin biomarkers of TGF-beta activity, including expression of the genes thrombospondin-1, cartilage oligomeric protein, and connective tissue growth factor. In addition, dermal myofibroblast infiltration dropped off.
The logical next steps in the research effort are to go larger and longer in terms of clinical trials of fresolimumab for scleroderma skin disease, and also to assess whether fresolimumab is effective in treating the fibrotic disease involving the internal organs of scleroderma patients.
Fresolimumab was well tolerated in this study. That’s also been true thus far in studies using higher doses and multiple doses for other diseases where fibrosis figures prominently. As the TGF-beta inhibitor’s side-effect profile becomes better characterized, it will be important to compare the adverse events associated with fresolimumab to the known substantial morbidity associated with current therapies.
The current treatments for the fibrotic disease in systemic sclerosis are unsatisfactory: cyclophosphamide is not terribly effective and carries the risk of malignancy, while “the jury is still out” on stem cell transplantation for systemic sclerosis, as ongoing studies attempt to establish the risk-benefit ratio of this intervention, the dermatologist said.
As for corticosteroids, Dr. Krieg believes they’re overused in systemic sclerosis.
“I have to tell you, many patients come to our center on relatively high doses of corticosteroids. Yet if you go through the literature there’s more or less no evidence for a beneficial role for corticosteroids in systemic sclerosis. And there is an increased risk of developing severe renal crisis, especially with higher doses in patients with diffuse systemic sclerosis,” the dermatologist cautioned.
More than a dozen drugs are now in clinical trials for systemic sclerosis. In addition to fresolimumab, tyrosine kinase inhibitors including imatinib (Gleevec) and nilotinib (Tasigna) are being evaluated for their antifibrotic effects. Other investigational agents target the inflammatory and vascular components of the disease.
Fresolimumab is owned by Sanofi. The fresolimumab study was supported by the National Institutes of Health. Dr. Krieg reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE EADV CONGRESS
