User login
Cultivating competencies for value-based care
It is my privilege this month to assume responsibility for the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology. I am honored to join an impressive board of editors led by Dr Fasiha Kanwal, and anchored by global leaders in the field of gastroenterology and hepatology. This board of editors promises to continue the high level of excellence that has propelled the journal to its preeminent position among clinical journals. I am confident that the practice management section will uphold that tradition and continue to meet the expectation of our readers. I would like to mark this transition by acknowledging the history of the practice management section of Clinical Gastroenterology and Hepatology and outlining a vision for the future.
The section was introduced in 2010 under the leadership of Dr. Joel V. Brill. The section, titled “Practice Management: Opportunities and Challenges,” aimed to help practices navigate the disparate issues facing the field. Some of these issues included use of capnography in endoscopy, the importance of registries for quality reporting, and the burdens of meaningful use on physician practices. Dr Brill introduced this section in a video in May 2010 (https://www.youtube.com/watch?v=8FMsc2Wl5E8). Dr. Brill’s reference to these “interesting and challenging times” in gastroenterology resonates even more loudly today.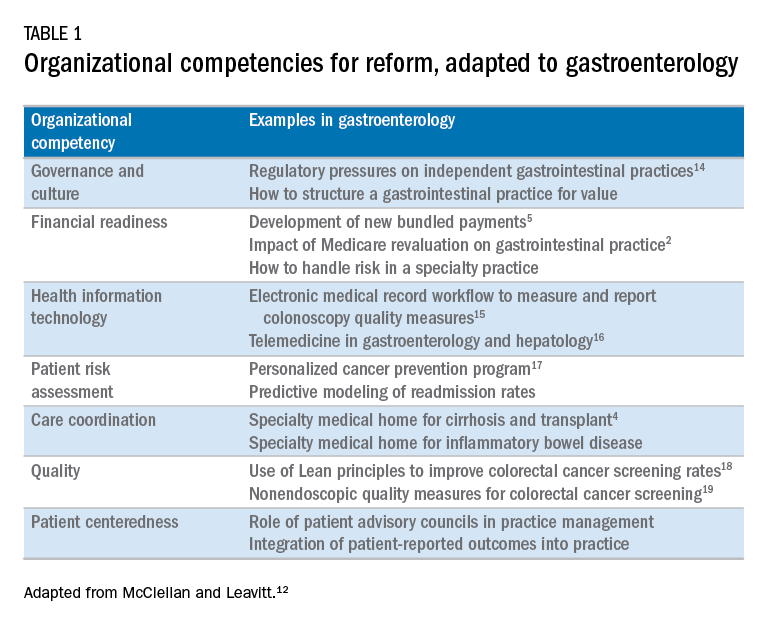
Over the next 5 years, the Road Ahead section will continue and strengthen its focus on the current and emerging issues facing gastroenterology and hepatology practices. I believe that high-value care will continue to be a high priority for patients and payers alike. Early results with payment reform around value have been mixed, in large part because of challenges in health systems and practices developing the competencies required for such reform.12 These competencies include governance and culture, financial readiness, health information technology, patient risk assessment, care coordination, quality, and patient centeredness. I will use this conceptual framework of organizational competencies, and their application in gastroenterology and hepatology, to help curate the Road Ahead section (Table 1). Key themes will include the following:
- • Governance and culture: The structure of health delivery systems, as conceptualized by Donabedian,13 is a key determinant of quality. Structural attributes include regulatory requirements on gastrointestinal practices, such as the rules governing use of anesthesia providers in ambulatory surgical settings; role of allied health professionals in clinical settings; and the impact of financial incentives in driving provider behavior.
- • Financial readiness: Value-based reimbursement, accountable care, medical homes, reference pricing, and physician tiering are some of the new terms in this era of value-based medicine. It is important for practices to assess patient costs longitudinally and manage financial risks. The Road Ahead section will continue to include papers that describe the impact of these reforms on gastroenterology and hepatology practices while providing guidance on implementation of these new models of care. Some examples include papers on the effect of payment policy on specialty practices, the development of a medical home in inflammatory bowel disease, and the physician experience with episode-based payments for colonoscopy.
- • Health information technology: All of the organizational competencies required for reform rely on a robust information technology platform that collects meaningful data and harnesses that data for analytic purposes. These platforms can be enterprise systems deployed by large health delivery systems or smaller, more nimble platforms, created by innovative start-up companies. The Road Ahead will include papers that share best practices in the use of these platforms to provide high-quality and cost-efficient care. In addition, the Road Ahead will continue to explore the use of health information technology to expand the reach of clinicians beyond brick and mortar clinics.
- • Patient risk assessment: Tailoring interventions to high-risk patients is necessary to deploy limited resources in a cost-effective manner. Risk assessment is also needed to more accurately and effectively personalize care for patients with chronic conditions. The Road Ahead will include papers that evaluate risk assessment tools and/or describe real-life implementation of these tools in different contexts.
- • Care coordination: The ability to provide team-based longitudinal care across the continuum of care will be integral to providing high value health care. The Road Ahead will serve as a means to disseminate best practices and innovative methods to care for increasingly complex patients, especially those with chronic diseases, such as cirrhosis and inflammatory bowel disease. For example, papers will explore the implementation of specialty medical homes, patient navigators, community-based care services, and involvement of patients in their own care.
- • Quality improvement: Providing high-value care by definition will require clinicians to accurately measure the quality of care provided to patients and use data to guide process improvement. The Road Ahead will continue to serve as an educational resource for clinicians with papers that discuss challenges and opportunities in quality measurement and improvement. Similarly, this section will present data on novel or impactful quality-improvement initiatives.
- • Patient centeredness: Patient experience measures and patient-reported outcomes are becoming increasingly important as meaningful indicators of quality. These measures are designed to ensure that patient perspectives are incorporated into the governance, design, and delivery of health care. The Road Ahead will serve as a dissemination mechanism for sharing best practices in developing, validating, implementing, and tracking patient-reported outcomes.

I consider Dr. Brill and Dr. Allen as mentors who have taught me tremendously about the business of medicine and the importance of physician leadership. I had the opportunity to coauthor several papers and book chapters with them. More recently, I have had the privilege to work closely with them in my role as the Chair of the American Gastroenterological Association Quality Measures Committee. It is an honor to now join their league as the editor for the Road Ahead section of Clinical Gastroenterology and Hepatology. These are indeed big shoes to fill. The section will retain the “Road Ahead” title in an acknowledgement of the continued importance of the issues outlined by Dr Allen. We will build on this theme to focus on not just the destination, but also the bumps in the road, the unexpected curves, the rest areas, beautiful vistas, and the indulgent road food. Hopefully no accidents along the way!
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Dorn, S.D., Vesy, C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2017;14:924-8.
3. Dorn, S.D. The road ahead 3.0: changing payments, changing practice. Clin Gastroenterol Hepatol. 2016;14:785-9.
4. Meier, S.K., Shah, N.D., Talwalkar, J.A. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
5. Mehta, S.J. Bundled payment for gastrointestinal hemorrhage. Clin Gastroenterol Hepatol. 2016;14:1681-4.
6. Weizman, A.V., Mosko, J., Bollegala, N., et al. Quality improvement primer series: launching a quality improvement initiative. Clin Gastroenterol Hepatol. 2017;14:1067-71.
7. Bernstein, M., Hou, J.K., Weizman, A.V., et al. Quality improvement primer series: how to sustain a quality improvement effort. Clin Gastroenterol Hepatol. 2017;14:1371-5.
8. Bollegala, N., Patel, K., Mosko, J.D., et al. Quality improvement primer series: the plan-do-study-act cycle and data display. Clin Gastroenterol Hepatol. 2016;14:1230-3.
9. Adams, M.A. Covert recording by patients of encounters with gastroenterology providers: path to empowerment or breach of trust?. Clin Gastroenterol Hepatol. 2017;15:13-6.
10. Oza, V.M., El-Dika, S., and Adams, M.A. Reaching safe harbor: legal implications of clinical practice guidelines. Clin Gastroenterol Hepatol. 2016;14:172-4.
11. Lin, M., Pappas, S.C., Sellin, J., et al. Curbside consultations: the good, the bad, and the ugly. Clin Gastroenterol Hepatol. 2016;14:2-4.
12. McClellan, M.B., Leavitt, M.O. Competencies and tools to shift payments from volume to value. JAMA. 2016; 316: 1655–1656
13. Donabedian, A. Evaluating the quality of medical care. Milbank Q. 1966;44:166-203.
14. Rosenberg, F.B., Kim, L.S., Ketover, S.R. Challenges facing independent integrated gastroenterology. Clin Gastroenterol Hepatol. 2017;15:335-8.
15. Leiman, D.A., Metz, D.C., Ginsberg, G.G., et al. A novel electronic medical record-based workflow to measure and report colonoscopy quality measures. Clin Gastroenterol Hepatol. 2016;14:333-7.
16. Cross, R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology Practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
17. Llor, X. Building a cancer genetics and prevention program. Clin Gastroenterol Hepatol. 2016;14:1516-20.
18. Patel, K.K., Cummings, S., Sellin, J., et al. Applying Lean design principles to a gastrointestinal endoscopy program for uninsured patients improves health care utilization. Clin Gastroenterol Hepatol. 2015;13:1556-9.
19. Saini, S.D., Adams, M.A., Brill, J.V., et al. Colorectal cancer screening quality measures: beyond colonoscopy. Clin Gastroenterol Hepatol. 2016;14:644-7.
Dr. Gellad is an associate professor of medicine in the division of gastroenterology at Durham VA Medical Center, Durham, N.C.; and Duke Clinical Research Institute, Durham, N.C. He reports a consulting relationship with Merck & Co. and he is also a cofounder and equity holder in Higgs Boson, LLC. He is funded by Veterans Affairs Health Services Research and Development Career Development Award (CDA 14-158 ).
It is my privilege this month to assume responsibility for the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology. I am honored to join an impressive board of editors led by Dr Fasiha Kanwal, and anchored by global leaders in the field of gastroenterology and hepatology. This board of editors promises to continue the high level of excellence that has propelled the journal to its preeminent position among clinical journals. I am confident that the practice management section will uphold that tradition and continue to meet the expectation of our readers. I would like to mark this transition by acknowledging the history of the practice management section of Clinical Gastroenterology and Hepatology and outlining a vision for the future.
The section was introduced in 2010 under the leadership of Dr. Joel V. Brill. The section, titled “Practice Management: Opportunities and Challenges,” aimed to help practices navigate the disparate issues facing the field. Some of these issues included use of capnography in endoscopy, the importance of registries for quality reporting, and the burdens of meaningful use on physician practices. Dr Brill introduced this section in a video in May 2010 (https://www.youtube.com/watch?v=8FMsc2Wl5E8). Dr. Brill’s reference to these “interesting and challenging times” in gastroenterology resonates even more loudly today.
Over the next 5 years, the Road Ahead section will continue and strengthen its focus on the current and emerging issues facing gastroenterology and hepatology practices. I believe that high-value care will continue to be a high priority for patients and payers alike. Early results with payment reform around value have been mixed, in large part because of challenges in health systems and practices developing the competencies required for such reform.12 These competencies include governance and culture, financial readiness, health information technology, patient risk assessment, care coordination, quality, and patient centeredness. I will use this conceptual framework of organizational competencies, and their application in gastroenterology and hepatology, to help curate the Road Ahead section (Table 1). Key themes will include the following:
- • Governance and culture: The structure of health delivery systems, as conceptualized by Donabedian,13 is a key determinant of quality. Structural attributes include regulatory requirements on gastrointestinal practices, such as the rules governing use of anesthesia providers in ambulatory surgical settings; role of allied health professionals in clinical settings; and the impact of financial incentives in driving provider behavior.
- • Financial readiness: Value-based reimbursement, accountable care, medical homes, reference pricing, and physician tiering are some of the new terms in this era of value-based medicine. It is important for practices to assess patient costs longitudinally and manage financial risks. The Road Ahead section will continue to include papers that describe the impact of these reforms on gastroenterology and hepatology practices while providing guidance on implementation of these new models of care. Some examples include papers on the effect of payment policy on specialty practices, the development of a medical home in inflammatory bowel disease, and the physician experience with episode-based payments for colonoscopy.
- • Health information technology: All of the organizational competencies required for reform rely on a robust information technology platform that collects meaningful data and harnesses that data for analytic purposes. These platforms can be enterprise systems deployed by large health delivery systems or smaller, more nimble platforms, created by innovative start-up companies. The Road Ahead will include papers that share best practices in the use of these platforms to provide high-quality and cost-efficient care. In addition, the Road Ahead will continue to explore the use of health information technology to expand the reach of clinicians beyond brick and mortar clinics.
- • Patient risk assessment: Tailoring interventions to high-risk patients is necessary to deploy limited resources in a cost-effective manner. Risk assessment is also needed to more accurately and effectively personalize care for patients with chronic conditions. The Road Ahead will include papers that evaluate risk assessment tools and/or describe real-life implementation of these tools in different contexts.
- • Care coordination: The ability to provide team-based longitudinal care across the continuum of care will be integral to providing high value health care. The Road Ahead will serve as a means to disseminate best practices and innovative methods to care for increasingly complex patients, especially those with chronic diseases, such as cirrhosis and inflammatory bowel disease. For example, papers will explore the implementation of specialty medical homes, patient navigators, community-based care services, and involvement of patients in their own care.
- • Quality improvement: Providing high-value care by definition will require clinicians to accurately measure the quality of care provided to patients and use data to guide process improvement. The Road Ahead will continue to serve as an educational resource for clinicians with papers that discuss challenges and opportunities in quality measurement and improvement. Similarly, this section will present data on novel or impactful quality-improvement initiatives.
- • Patient centeredness: Patient experience measures and patient-reported outcomes are becoming increasingly important as meaningful indicators of quality. These measures are designed to ensure that patient perspectives are incorporated into the governance, design, and delivery of health care. The Road Ahead will serve as a dissemination mechanism for sharing best practices in developing, validating, implementing, and tracking patient-reported outcomes.
I consider Dr. Brill and Dr. Allen as mentors who have taught me tremendously about the business of medicine and the importance of physician leadership. I had the opportunity to coauthor several papers and book chapters with them. More recently, I have had the privilege to work closely with them in my role as the Chair of the American Gastroenterological Association Quality Measures Committee. It is an honor to now join their league as the editor for the Road Ahead section of Clinical Gastroenterology and Hepatology. These are indeed big shoes to fill. The section will retain the “Road Ahead” title in an acknowledgement of the continued importance of the issues outlined by Dr Allen. We will build on this theme to focus on not just the destination, but also the bumps in the road, the unexpected curves, the rest areas, beautiful vistas, and the indulgent road food. Hopefully no accidents along the way!
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Dorn, S.D., Vesy, C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2017;14:924-8.
3. Dorn, S.D. The road ahead 3.0: changing payments, changing practice. Clin Gastroenterol Hepatol. 2016;14:785-9.
4. Meier, S.K., Shah, N.D., Talwalkar, J.A. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
5. Mehta, S.J. Bundled payment for gastrointestinal hemorrhage. Clin Gastroenterol Hepatol. 2016;14:1681-4.
6. Weizman, A.V., Mosko, J., Bollegala, N., et al. Quality improvement primer series: launching a quality improvement initiative. Clin Gastroenterol Hepatol. 2017;14:1067-71.
7. Bernstein, M., Hou, J.K., Weizman, A.V., et al. Quality improvement primer series: how to sustain a quality improvement effort. Clin Gastroenterol Hepatol. 2017;14:1371-5.
8. Bollegala, N., Patel, K., Mosko, J.D., et al. Quality improvement primer series: the plan-do-study-act cycle and data display. Clin Gastroenterol Hepatol. 2016;14:1230-3.
9. Adams, M.A. Covert recording by patients of encounters with gastroenterology providers: path to empowerment or breach of trust?. Clin Gastroenterol Hepatol. 2017;15:13-6.
10. Oza, V.M., El-Dika, S., and Adams, M.A. Reaching safe harbor: legal implications of clinical practice guidelines. Clin Gastroenterol Hepatol. 2016;14:172-4.
11. Lin, M., Pappas, S.C., Sellin, J., et al. Curbside consultations: the good, the bad, and the ugly. Clin Gastroenterol Hepatol. 2016;14:2-4.
12. McClellan, M.B., Leavitt, M.O. Competencies and tools to shift payments from volume to value. JAMA. 2016; 316: 1655–1656
13. Donabedian, A. Evaluating the quality of medical care. Milbank Q. 1966;44:166-203.
14. Rosenberg, F.B., Kim, L.S., Ketover, S.R. Challenges facing independent integrated gastroenterology. Clin Gastroenterol Hepatol. 2017;15:335-8.
15. Leiman, D.A., Metz, D.C., Ginsberg, G.G., et al. A novel electronic medical record-based workflow to measure and report colonoscopy quality measures. Clin Gastroenterol Hepatol. 2016;14:333-7.
16. Cross, R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology Practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
17. Llor, X. Building a cancer genetics and prevention program. Clin Gastroenterol Hepatol. 2016;14:1516-20.
18. Patel, K.K., Cummings, S., Sellin, J., et al. Applying Lean design principles to a gastrointestinal endoscopy program for uninsured patients improves health care utilization. Clin Gastroenterol Hepatol. 2015;13:1556-9.
19. Saini, S.D., Adams, M.A., Brill, J.V., et al. Colorectal cancer screening quality measures: beyond colonoscopy. Clin Gastroenterol Hepatol. 2016;14:644-7.
Dr. Gellad is an associate professor of medicine in the division of gastroenterology at Durham VA Medical Center, Durham, N.C.; and Duke Clinical Research Institute, Durham, N.C. He reports a consulting relationship with Merck & Co. and he is also a cofounder and equity holder in Higgs Boson, LLC. He is funded by Veterans Affairs Health Services Research and Development Career Development Award (CDA 14-158 ).
It is my privilege this month to assume responsibility for the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology. I am honored to join an impressive board of editors led by Dr Fasiha Kanwal, and anchored by global leaders in the field of gastroenterology and hepatology. This board of editors promises to continue the high level of excellence that has propelled the journal to its preeminent position among clinical journals. I am confident that the practice management section will uphold that tradition and continue to meet the expectation of our readers. I would like to mark this transition by acknowledging the history of the practice management section of Clinical Gastroenterology and Hepatology and outlining a vision for the future.
The section was introduced in 2010 under the leadership of Dr. Joel V. Brill. The section, titled “Practice Management: Opportunities and Challenges,” aimed to help practices navigate the disparate issues facing the field. Some of these issues included use of capnography in endoscopy, the importance of registries for quality reporting, and the burdens of meaningful use on physician practices. Dr Brill introduced this section in a video in May 2010 (https://www.youtube.com/watch?v=8FMsc2Wl5E8). Dr. Brill’s reference to these “interesting and challenging times” in gastroenterology resonates even more loudly today.
Over the next 5 years, the Road Ahead section will continue and strengthen its focus on the current and emerging issues facing gastroenterology and hepatology practices. I believe that high-value care will continue to be a high priority for patients and payers alike. Early results with payment reform around value have been mixed, in large part because of challenges in health systems and practices developing the competencies required for such reform.12 These competencies include governance and culture, financial readiness, health information technology, patient risk assessment, care coordination, quality, and patient centeredness. I will use this conceptual framework of organizational competencies, and their application in gastroenterology and hepatology, to help curate the Road Ahead section (Table 1). Key themes will include the following:
- • Governance and culture: The structure of health delivery systems, as conceptualized by Donabedian,13 is a key determinant of quality. Structural attributes include regulatory requirements on gastrointestinal practices, such as the rules governing use of anesthesia providers in ambulatory surgical settings; role of allied health professionals in clinical settings; and the impact of financial incentives in driving provider behavior.
- • Financial readiness: Value-based reimbursement, accountable care, medical homes, reference pricing, and physician tiering are some of the new terms in this era of value-based medicine. It is important for practices to assess patient costs longitudinally and manage financial risks. The Road Ahead section will continue to include papers that describe the impact of these reforms on gastroenterology and hepatology practices while providing guidance on implementation of these new models of care. Some examples include papers on the effect of payment policy on specialty practices, the development of a medical home in inflammatory bowel disease, and the physician experience with episode-based payments for colonoscopy.
- • Health information technology: All of the organizational competencies required for reform rely on a robust information technology platform that collects meaningful data and harnesses that data for analytic purposes. These platforms can be enterprise systems deployed by large health delivery systems or smaller, more nimble platforms, created by innovative start-up companies. The Road Ahead will include papers that share best practices in the use of these platforms to provide high-quality and cost-efficient care. In addition, the Road Ahead will continue to explore the use of health information technology to expand the reach of clinicians beyond brick and mortar clinics.
- • Patient risk assessment: Tailoring interventions to high-risk patients is necessary to deploy limited resources in a cost-effective manner. Risk assessment is also needed to more accurately and effectively personalize care for patients with chronic conditions. The Road Ahead will include papers that evaluate risk assessment tools and/or describe real-life implementation of these tools in different contexts.
- • Care coordination: The ability to provide team-based longitudinal care across the continuum of care will be integral to providing high value health care. The Road Ahead will serve as a means to disseminate best practices and innovative methods to care for increasingly complex patients, especially those with chronic diseases, such as cirrhosis and inflammatory bowel disease. For example, papers will explore the implementation of specialty medical homes, patient navigators, community-based care services, and involvement of patients in their own care.
- • Quality improvement: Providing high-value care by definition will require clinicians to accurately measure the quality of care provided to patients and use data to guide process improvement. The Road Ahead will continue to serve as an educational resource for clinicians with papers that discuss challenges and opportunities in quality measurement and improvement. Similarly, this section will present data on novel or impactful quality-improvement initiatives.
- • Patient centeredness: Patient experience measures and patient-reported outcomes are becoming increasingly important as meaningful indicators of quality. These measures are designed to ensure that patient perspectives are incorporated into the governance, design, and delivery of health care. The Road Ahead will serve as a dissemination mechanism for sharing best practices in developing, validating, implementing, and tracking patient-reported outcomes.
I consider Dr. Brill and Dr. Allen as mentors who have taught me tremendously about the business of medicine and the importance of physician leadership. I had the opportunity to coauthor several papers and book chapters with them. More recently, I have had the privilege to work closely with them in my role as the Chair of the American Gastroenterological Association Quality Measures Committee. It is an honor to now join their league as the editor for the Road Ahead section of Clinical Gastroenterology and Hepatology. These are indeed big shoes to fill. The section will retain the “Road Ahead” title in an acknowledgement of the continued importance of the issues outlined by Dr Allen. We will build on this theme to focus on not just the destination, but also the bumps in the road, the unexpected curves, the rest areas, beautiful vistas, and the indulgent road food. Hopefully no accidents along the way!
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Dorn, S.D., Vesy, C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2017;14:924-8.
3. Dorn, S.D. The road ahead 3.0: changing payments, changing practice. Clin Gastroenterol Hepatol. 2016;14:785-9.
4. Meier, S.K., Shah, N.D., Talwalkar, J.A. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
5. Mehta, S.J. Bundled payment for gastrointestinal hemorrhage. Clin Gastroenterol Hepatol. 2016;14:1681-4.
6. Weizman, A.V., Mosko, J., Bollegala, N., et al. Quality improvement primer series: launching a quality improvement initiative. Clin Gastroenterol Hepatol. 2017;14:1067-71.
7. Bernstein, M., Hou, J.K., Weizman, A.V., et al. Quality improvement primer series: how to sustain a quality improvement effort. Clin Gastroenterol Hepatol. 2017;14:1371-5.
8. Bollegala, N., Patel, K., Mosko, J.D., et al. Quality improvement primer series: the plan-do-study-act cycle and data display. Clin Gastroenterol Hepatol. 2016;14:1230-3.
9. Adams, M.A. Covert recording by patients of encounters with gastroenterology providers: path to empowerment or breach of trust?. Clin Gastroenterol Hepatol. 2017;15:13-6.
10. Oza, V.M., El-Dika, S., and Adams, M.A. Reaching safe harbor: legal implications of clinical practice guidelines. Clin Gastroenterol Hepatol. 2016;14:172-4.
11. Lin, M., Pappas, S.C., Sellin, J., et al. Curbside consultations: the good, the bad, and the ugly. Clin Gastroenterol Hepatol. 2016;14:2-4.
12. McClellan, M.B., Leavitt, M.O. Competencies and tools to shift payments from volume to value. JAMA. 2016; 316: 1655–1656
13. Donabedian, A. Evaluating the quality of medical care. Milbank Q. 1966;44:166-203.
14. Rosenberg, F.B., Kim, L.S., Ketover, S.R. Challenges facing independent integrated gastroenterology. Clin Gastroenterol Hepatol. 2017;15:335-8.
15. Leiman, D.A., Metz, D.C., Ginsberg, G.G., et al. A novel electronic medical record-based workflow to measure and report colonoscopy quality measures. Clin Gastroenterol Hepatol. 2016;14:333-7.
16. Cross, R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology Practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
17. Llor, X. Building a cancer genetics and prevention program. Clin Gastroenterol Hepatol. 2016;14:1516-20.
18. Patel, K.K., Cummings, S., Sellin, J., et al. Applying Lean design principles to a gastrointestinal endoscopy program for uninsured patients improves health care utilization. Clin Gastroenterol Hepatol. 2015;13:1556-9.
19. Saini, S.D., Adams, M.A., Brill, J.V., et al. Colorectal cancer screening quality measures: beyond colonoscopy. Clin Gastroenterol Hepatol. 2016;14:644-7.
Dr. Gellad is an associate professor of medicine in the division of gastroenterology at Durham VA Medical Center, Durham, N.C.; and Duke Clinical Research Institute, Durham, N.C. He reports a consulting relationship with Merck & Co. and he is also a cofounder and equity holder in Higgs Boson, LLC. He is funded by Veterans Affairs Health Services Research and Development Career Development Award (CDA 14-158 ).
Salmonella infections: The source may be as close as your patient’s backyard
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates

Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates
Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
I recently received a group text from a friend voicing her frustration that her neighbor had acquired chickens, and she shared a photo of some roaming freely in the front yard. Naturally, my response was related to the potential infectious disease exposure and infections. Another friend chimed in “fresh eggs, and these are free range chickens. They don’t get sick. ... Many people in my area have chickens.” Unbeknownst to my friends, they had helped me select the ID Consult topic for this month.
Nontyphoidal Salmonella bacteria are associated with a wide spectrum of infections which range from asymptomatic gastrointestinal carriage to bacteremia, meningitis, osteomyelitis, and focal infections. Invasive disease is seen most often in children younger than 5 years of age, persons aged 65 years or older, and individuals with hemoglobinopathies including sickle cell disease and those with immunodeficiencies. Annually, the Centers for Disease Control and Prevention estimates that nontyphoidal salmonellosis is responsible for 1.2 million illnesses, 23,000 hospitalizations, and 450 deaths in the United States. Gastroenteritis is the most common manifestation of the disease and is characterized by abdominal cramps, diarrhea, and fever that develops 12-72 hours after exposure. It is usually self-limited. As previously reported in this column (June, 2017), Salmonella is one of the top two foodborne pathogens in the United States, and most outbreaks have been associated with consumption of contaminated food. But wait, contaminated food is not the only cause of some of our most recent outbreaks.
Live poultry-associated salmonellosis (LPAS)
LPAS was first reported in the 1950s. More recent epidemiologic data was published by C. Basler et al. (Emerging Infect Dis. 2016;22[10]:1705-11). LPAS was defined as two or more culture confirmed human Salmonella infections with a combination of epidemiologic, laboratory, or traceback evidence linking illnesses to contact with live poultry. The median outbreak size involved 26 cases (range, 4-363) and 77% (41 of 53) were multistate. The median age of the patients was 9 years (range, less than 1 to 92 years), and 31% were aged 5 years or younger. Exposure to chicks and ducklings was reported in 85% and 38%, respectively. High-risk practices included keeping poultry inside of the home (46%), snuggling baby birds (49%), and kissing baby birds (13%). The median time from purchase of poultry to onset of illness was 17 days (range, 1-672), and 66% reported onset of illness less than 30 days after purchase. Almost 52% reported owning poultry for less than 1 year.
The number of outbreaks continued to increase. From 1990 to 2005, there were a total of 17 outbreaks, compared with 36 between 2006 and 2014. Historically, outbreaks occurred in children around Easter when brightly colored dyed chicks were purchased. In the above review, 80% of outbreaks began in February, March, or April with an average duration of 4.9 months (range, 1-12).
Salmonella isolates
Backyard flocks and LPAS
More recently outbreaks have been associated with backyard flocks occurring year round and affecting both adults and children in contrast to seasonal peaks. The first multistate backyard flock outbreak was documented in 2007. Currently, the CDC is investigating 10 separate multistate outbreaks that began on Jan. 4, 2017. It involves 48 states, 961 infected individuals, 215 hospitalizations, and 1 death. At least 5 salmonella serotypes have been isolated.
What about the hatcheries?
It’s estimated that 50 million live poultry are sold annually. Birds are shipped within 24 hours after hatching via the U.S. Postal Service in boxes containing up to 100 chicks. Delivery occurs within 72 hours of hatching. Approximately 20 mail order hatcheries provide the majority of poultry sold to the general public. The National Poultry Improvement Plan (NPIP) is a voluntary state and federal testing and certification program whose goal is to eliminate poultry disease from breeder flocks to prevent egg-transmitted and hatchery-disseminated diseases. All hatcheries may participate. They also may participate in the voluntary Salmonella monitoring program. Note participation is not mandatory.
Preventing future outbreaks: patient/parental education is mandatory
1. Make sure your parents know about the association of Salmonella and live poultry. Reinforce these are farm animals, not pets. Purchase birds from hatcheries that participate in NPIP and the Salmonella monitoring programs.
2. Chicks, ducklings, or other live poultry should not be taken to schools, day care facilities, or nursing homes. Poultry should not be allowed in the home or in areas where food or drink is being prepared or consumed.
3. Poultry should not be snuggled, kissed, or allowed to touch one’s mouth. Hand washing with soap and water should occur after touching live poultry or any object touched in areas where they live or roam.
4. Contact with live poultry should be avoided in those at risk for developing serious infections including persons aged 5 years or younger, 65 years or older, immunocompromised individuals, and those with hemoglobinopathies.
5. All equipment used to care for live birds should be washed outdoors. Owners should have designated shoes when caring for poultry which should never be worn inside the home.
Hopefully, the next time you see a patient with fever and diarrhea you will recall this topic and ask about their contact with live poultry.
Additional resources to facilitate discussions can be found at www.cdc.gov/salmonella.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Research mentors an invaluable resource to students
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As a medical student, the summer is an excellent time to pursue extracurricular activities. While some people take these weeks to learn new skills in basic science laboratories or travel abroad for international electives, many will assume the role of a student researcher. But, with only 10 weeks of dedicated research time in the summer it can be challenging to see a project from start to finish.
The greatest challenge, however, is not in identifying a project that is possible to complete in 10 weeks. Instead, it has to do with the fact that as students we are inexperienced researchers, and such a short timeline leaves little room to troubleshoot problems when they inevitably arise. This, among other reasons, is why research mentors are an invaluable resource to students.
While my research mentor has helped tremendously in logistical tasks, such as helping me write a research proposal and navigate the IRB process, it’s his experience and knowledge of the research process that I’ve found to be most critical during this 10 week period. During the planning of the project he helped me identify pitfalls and weaknesses in our methods, which has helped me avoid major setbacks during the execution of the project. As a result, the project has been running smoothly and I have yet to run into any significant problems.
Reflecting on this fact has reminded me of the importance of planning ahead. We started outlining and planning this project about 6 months before my research period officially began, when we could both mull over the details without the pressure of time. Though unforeseen problems may still arise, I think this strategy has made all the difference and it’s a lesson I will take with me for future projects.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As a medical student, the summer is an excellent time to pursue extracurricular activities. While some people take these weeks to learn new skills in basic science laboratories or travel abroad for international electives, many will assume the role of a student researcher. But, with only 10 weeks of dedicated research time in the summer it can be challenging to see a project from start to finish.
The greatest challenge, however, is not in identifying a project that is possible to complete in 10 weeks. Instead, it has to do with the fact that as students we are inexperienced researchers, and such a short timeline leaves little room to troubleshoot problems when they inevitably arise. This, among other reasons, is why research mentors are an invaluable resource to students.
While my research mentor has helped tremendously in logistical tasks, such as helping me write a research proposal and navigate the IRB process, it’s his experience and knowledge of the research process that I’ve found to be most critical during this 10 week period. During the planning of the project he helped me identify pitfalls and weaknesses in our methods, which has helped me avoid major setbacks during the execution of the project. As a result, the project has been running smoothly and I have yet to run into any significant problems.
Reflecting on this fact has reminded me of the importance of planning ahead. We started outlining and planning this project about 6 months before my research period officially began, when we could both mull over the details without the pressure of time. Though unforeseen problems may still arise, I think this strategy has made all the difference and it’s a lesson I will take with me for future projects.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their 1st, 2nd, and 3rd years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As a medical student, the summer is an excellent time to pursue extracurricular activities. While some people take these weeks to learn new skills in basic science laboratories or travel abroad for international electives, many will assume the role of a student researcher. But, with only 10 weeks of dedicated research time in the summer it can be challenging to see a project from start to finish.
The greatest challenge, however, is not in identifying a project that is possible to complete in 10 weeks. Instead, it has to do with the fact that as students we are inexperienced researchers, and such a short timeline leaves little room to troubleshoot problems when they inevitably arise. This, among other reasons, is why research mentors are an invaluable resource to students.
While my research mentor has helped tremendously in logistical tasks, such as helping me write a research proposal and navigate the IRB process, it’s his experience and knowledge of the research process that I’ve found to be most critical during this 10 week period. During the planning of the project he helped me identify pitfalls and weaknesses in our methods, which has helped me avoid major setbacks during the execution of the project. As a result, the project has been running smoothly and I have yet to run into any significant problems.
Reflecting on this fact has reminded me of the importance of planning ahead. We started outlining and planning this project about 6 months before my research period officially began, when we could both mull over the details without the pressure of time. Though unforeseen problems may still arise, I think this strategy has made all the difference and it’s a lesson I will take with me for future projects.
Cole Hirschfeld is originally from Phoenix. He received undergraduate degrees in finance and entrepreneurship from the University of Arizona and went on to work in the finance industry for 2 years before deciding to change careers and attend medical school. He is now a 4th year medical student at Cornell University, New York, and plans to apply for residency in internal medicine.
Gods and Monsters
For the first time in history, four generations of physicians work side by side in the U.S. health care system. An expanding population, longer life expectancies, and later retirement ages all contribute to this phenomenon. Each of these generations has made significant contributions to modern surgery and how we practice it. For better and for worse.
Traditionalists, or the Greatest Generation, were true surgical pioneers. DeBakey, Cooley, Fogarty, their names now adorn everything from instruments to medical centers. They truly founded the modern system of surgery. Born between 1900 and 1945, Traditionalists were forged in the crucibles of the Great War and the Great Depression. Their core values were hard work, discipline, and sacrifice. A large number were combat veterans who valued conformity and adherence to the rules. Traditionalists set up our current hierarchical departments of surgery. Mirroring their values, they employed a military chain of command approach. Many traditionalists rose to positions of absolute power, and some were corrupted by this power. Gods became monsters. Abuse, both verbal and physical, came to be commonplace and accepted in the surgical work environment.
Born between 1946 and 1964, Baby Boomers were raised in the aftermath of a war none of them saw. More optimistic and idealistic than the Traditionalists, the Boomers valued success. Their goals became more individualistic. Chasing money, titles, and recognition, Boomers wanted to build a stellar career. Fifty-hour work weeks became 70, 80, or 90. Ambition led to wealth, dramatic successes, and remarkable careers. Their choices also led to divorce, drug abuse, and suicide. While burnout has become a modern concern, its roots are clearly tied to this era. Now serving as our deans and department chairs, the Boomers also made several notable contributions. Specific to our field, Boomers oversaw the development of vascular surgery as an independent specialty and the expansion of fellowship training programs. Coming of age in the 1960s, Boomers also led the integration of our field with the acceptance of both minorities and women.
When I first heard the term “Generation X” I thought “Dumb name, won’t last.” Not my best prediction. Born between 1965 and 1980, Generation X grew up during the home computer revolution. Quick to adopt new technologies, Gen Xers were far more adaptive to change than previous generations. Labeled as having short attention spans, most Gen Xers were task/goal oriented. While these attributes helped drive the endovascular revolution, they also may be the reason we have approximately 983 FDA-approved devices to treat SFA disease. Generation X entered surgical training eager to please the more senior Traditionalists and Boomers. This wouldn’t last. Children of divorce and latch-key kids, Generation Xers are eclectic, resourceful, and self-reliant. Most of all they value freedom. Watching their predecessors work themselves and others to near death, Generation X revolted. Uncapped duty hours, limitless call, and pyramidal residencies were all institutions in the 1980s, and they all fell. Generation X were portrayed as nihilistic slackers, but their true motivation was often distrust of institutions. Watching the Boomers descend into burnout, Xers tried to achieve a more reasonable work-life balance. Though they successfully fought for lessening the abuses of surgical training, few Gen Xers actually reaped the benefits. I vividly recall watching slack-jawed as an intern scrubbed out of a case to go home because he was post call. A Martian landing in the OR and offering to assist with the anastomosis would have brought no less amazement.
With their careers spanning the endovascular revolution, Generation X has seen perhaps the greatest era of transformation in our profession. Our competition is no longer general or cardiac surgery, but rather interventional radiology and interventional cardiology. Gen X is also the first generation to earn less than its predecessors. Throw in their obscene tuition payments and one can see how Gen Xers fell well short of the financial heights of the Traditionalists and Boomers. The Gen Xers are the masters of the work hard/play hard ethos. You will see them at VEITH entertaining their European colleagues at 3 a.m. and then running the 6 a.m. breakfast sessions. While the Boomers often seemed old by 40, Xers appear desperate to salvage their lost youth.
Born between 1981 and 2006, Millennials are already the most populous generation. Their chief attributes are confidence, sociability, and a realistic outlook. Knowing they can’t please everyone, they rarely try. They want work to be meaningful in and of itself. They also value teamwork over individual approaches. Millennials are civic minded and have a strong sense of volunteerism. Their parents often tried to shelter them from the evils of the world, and they were the first generation of children with schedules. Because of their upbringing, Millennials are far more likely to seek guidance than the independent-minded Gen Xers. Raised to believe their voice mattered, they are now often reviled for it. It is with some degree of awe that I watch our Millennial students brazenly march into the dean’s and chancellor’s office to discuss their “careers.” As a medical student I first saw my dean at graduation, and I certainly didn’t even know what a chancellor was. Generation X is often baffled by the self-interest Millennials exude. But we shouldn’t be, we have seen it before. Raised by Baby Boomers (The Me Generation), Millennials inherited their self-driven outlook. This is also the reason Boomers and Millennials struggle to work together. They are too alike. Boomers see Millennials as “snowflakes” who are scared of work and selfie obsessed. Millennials bristle at the authoritarian nature of Boomers.
For vascular surgery to advance as a field, we need to recruit, train, and mentor this new generation. If only there was some guide: “The Proper Care and Feeding of Millennials." As senior attendings, program directors, and section chiefs, Generation X must now serve as a bridge between two larger forces, the Boomers and their offspring, the Millennials. Of course, whatever generation you are from is the best, but we must confront our biases. It is easy to seek out the same personalities to be your trainees and partners. Don’t. This pool will shrink every year. Millennials are more self-aware of their capabilities and therefore of their limitations. We may become flustered by their need for hand-holding, but what if it is appropriate? Was all of the autonomy you were granted during training truly good for the patients? Graduated responsibility and roles that push their limits help Millennials grow. I know they don’t value punctuality or dress codes, but they are better team players and openly motivated by learning. I formed our integrated vascular residency with two positions per year specifically to foster the team building Millennials crave. Yes, this is the generation that got 8th-place trophies so you must constantly award progress. Fortunately, now that surgery is unencumbered by such things as massive salaries and status, Millennials enter our workforce with purer intentions.

We may want to make Millennials match our values, traits, and behaviors, but each generation has departed radically from the ethos of their predecessors. Let’s see what the kids can do.
Dr. Sheahan is a professor of surgery and Program Director, Vascular Surgery Residency and Fellowship Programs, Louisiana State University Health Sciences Center, School of Medicine, New Orleans. He is also the Deputy Medical Editor of Vascular Specialist.
For the first time in history, four generations of physicians work side by side in the U.S. health care system. An expanding population, longer life expectancies, and later retirement ages all contribute to this phenomenon. Each of these generations has made significant contributions to modern surgery and how we practice it. For better and for worse.
Traditionalists, or the Greatest Generation, were true surgical pioneers. DeBakey, Cooley, Fogarty, their names now adorn everything from instruments to medical centers. They truly founded the modern system of surgery. Born between 1900 and 1945, Traditionalists were forged in the crucibles of the Great War and the Great Depression. Their core values were hard work, discipline, and sacrifice. A large number were combat veterans who valued conformity and adherence to the rules. Traditionalists set up our current hierarchical departments of surgery. Mirroring their values, they employed a military chain of command approach. Many traditionalists rose to positions of absolute power, and some were corrupted by this power. Gods became monsters. Abuse, both verbal and physical, came to be commonplace and accepted in the surgical work environment.
Born between 1946 and 1964, Baby Boomers were raised in the aftermath of a war none of them saw. More optimistic and idealistic than the Traditionalists, the Boomers valued success. Their goals became more individualistic. Chasing money, titles, and recognition, Boomers wanted to build a stellar career. Fifty-hour work weeks became 70, 80, or 90. Ambition led to wealth, dramatic successes, and remarkable careers. Their choices also led to divorce, drug abuse, and suicide. While burnout has become a modern concern, its roots are clearly tied to this era. Now serving as our deans and department chairs, the Boomers also made several notable contributions. Specific to our field, Boomers oversaw the development of vascular surgery as an independent specialty and the expansion of fellowship training programs. Coming of age in the 1960s, Boomers also led the integration of our field with the acceptance of both minorities and women.
When I first heard the term “Generation X” I thought “Dumb name, won’t last.” Not my best prediction. Born between 1965 and 1980, Generation X grew up during the home computer revolution. Quick to adopt new technologies, Gen Xers were far more adaptive to change than previous generations. Labeled as having short attention spans, most Gen Xers were task/goal oriented. While these attributes helped drive the endovascular revolution, they also may be the reason we have approximately 983 FDA-approved devices to treat SFA disease. Generation X entered surgical training eager to please the more senior Traditionalists and Boomers. This wouldn’t last. Children of divorce and latch-key kids, Generation Xers are eclectic, resourceful, and self-reliant. Most of all they value freedom. Watching their predecessors work themselves and others to near death, Generation X revolted. Uncapped duty hours, limitless call, and pyramidal residencies were all institutions in the 1980s, and they all fell. Generation X were portrayed as nihilistic slackers, but their true motivation was often distrust of institutions. Watching the Boomers descend into burnout, Xers tried to achieve a more reasonable work-life balance. Though they successfully fought for lessening the abuses of surgical training, few Gen Xers actually reaped the benefits. I vividly recall watching slack-jawed as an intern scrubbed out of a case to go home because he was post call. A Martian landing in the OR and offering to assist with the anastomosis would have brought no less amazement.
With their careers spanning the endovascular revolution, Generation X has seen perhaps the greatest era of transformation in our profession. Our competition is no longer general or cardiac surgery, but rather interventional radiology and interventional cardiology. Gen X is also the first generation to earn less than its predecessors. Throw in their obscene tuition payments and one can see how Gen Xers fell well short of the financial heights of the Traditionalists and Boomers. The Gen Xers are the masters of the work hard/play hard ethos. You will see them at VEITH entertaining their European colleagues at 3 a.m. and then running the 6 a.m. breakfast sessions. While the Boomers often seemed old by 40, Xers appear desperate to salvage their lost youth.
Born between 1981 and 2006, Millennials are already the most populous generation. Their chief attributes are confidence, sociability, and a realistic outlook. Knowing they can’t please everyone, they rarely try. They want work to be meaningful in and of itself. They also value teamwork over individual approaches. Millennials are civic minded and have a strong sense of volunteerism. Their parents often tried to shelter them from the evils of the world, and they were the first generation of children with schedules. Because of their upbringing, Millennials are far more likely to seek guidance than the independent-minded Gen Xers. Raised to believe their voice mattered, they are now often reviled for it. It is with some degree of awe that I watch our Millennial students brazenly march into the dean’s and chancellor’s office to discuss their “careers.” As a medical student I first saw my dean at graduation, and I certainly didn’t even know what a chancellor was. Generation X is often baffled by the self-interest Millennials exude. But we shouldn’t be, we have seen it before. Raised by Baby Boomers (The Me Generation), Millennials inherited their self-driven outlook. This is also the reason Boomers and Millennials struggle to work together. They are too alike. Boomers see Millennials as “snowflakes” who are scared of work and selfie obsessed. Millennials bristle at the authoritarian nature of Boomers.
For vascular surgery to advance as a field, we need to recruit, train, and mentor this new generation. If only there was some guide: “The Proper Care and Feeding of Millennials." As senior attendings, program directors, and section chiefs, Generation X must now serve as a bridge between two larger forces, the Boomers and their offspring, the Millennials. Of course, whatever generation you are from is the best, but we must confront our biases. It is easy to seek out the same personalities to be your trainees and partners. Don’t. This pool will shrink every year. Millennials are more self-aware of their capabilities and therefore of their limitations. We may become flustered by their need for hand-holding, but what if it is appropriate? Was all of the autonomy you were granted during training truly good for the patients? Graduated responsibility and roles that push their limits help Millennials grow. I know they don’t value punctuality or dress codes, but they are better team players and openly motivated by learning. I formed our integrated vascular residency with two positions per year specifically to foster the team building Millennials crave. Yes, this is the generation that got 8th-place trophies so you must constantly award progress. Fortunately, now that surgery is unencumbered by such things as massive salaries and status, Millennials enter our workforce with purer intentions.
We may want to make Millennials match our values, traits, and behaviors, but each generation has departed radically from the ethos of their predecessors. Let’s see what the kids can do.
Dr. Sheahan is a professor of surgery and Program Director, Vascular Surgery Residency and Fellowship Programs, Louisiana State University Health Sciences Center, School of Medicine, New Orleans. He is also the Deputy Medical Editor of Vascular Specialist.
For the first time in history, four generations of physicians work side by side in the U.S. health care system. An expanding population, longer life expectancies, and later retirement ages all contribute to this phenomenon. Each of these generations has made significant contributions to modern surgery and how we practice it. For better and for worse.
Traditionalists, or the Greatest Generation, were true surgical pioneers. DeBakey, Cooley, Fogarty, their names now adorn everything from instruments to medical centers. They truly founded the modern system of surgery. Born between 1900 and 1945, Traditionalists were forged in the crucibles of the Great War and the Great Depression. Their core values were hard work, discipline, and sacrifice. A large number were combat veterans who valued conformity and adherence to the rules. Traditionalists set up our current hierarchical departments of surgery. Mirroring their values, they employed a military chain of command approach. Many traditionalists rose to positions of absolute power, and some were corrupted by this power. Gods became monsters. Abuse, both verbal and physical, came to be commonplace and accepted in the surgical work environment.
Born between 1946 and 1964, Baby Boomers were raised in the aftermath of a war none of them saw. More optimistic and idealistic than the Traditionalists, the Boomers valued success. Their goals became more individualistic. Chasing money, titles, and recognition, Boomers wanted to build a stellar career. Fifty-hour work weeks became 70, 80, or 90. Ambition led to wealth, dramatic successes, and remarkable careers. Their choices also led to divorce, drug abuse, and suicide. While burnout has become a modern concern, its roots are clearly tied to this era. Now serving as our deans and department chairs, the Boomers also made several notable contributions. Specific to our field, Boomers oversaw the development of vascular surgery as an independent specialty and the expansion of fellowship training programs. Coming of age in the 1960s, Boomers also led the integration of our field with the acceptance of both minorities and women.
When I first heard the term “Generation X” I thought “Dumb name, won’t last.” Not my best prediction. Born between 1965 and 1980, Generation X grew up during the home computer revolution. Quick to adopt new technologies, Gen Xers were far more adaptive to change than previous generations. Labeled as having short attention spans, most Gen Xers were task/goal oriented. While these attributes helped drive the endovascular revolution, they also may be the reason we have approximately 983 FDA-approved devices to treat SFA disease. Generation X entered surgical training eager to please the more senior Traditionalists and Boomers. This wouldn’t last. Children of divorce and latch-key kids, Generation Xers are eclectic, resourceful, and self-reliant. Most of all they value freedom. Watching their predecessors work themselves and others to near death, Generation X revolted. Uncapped duty hours, limitless call, and pyramidal residencies were all institutions in the 1980s, and they all fell. Generation X were portrayed as nihilistic slackers, but their true motivation was often distrust of institutions. Watching the Boomers descend into burnout, Xers tried to achieve a more reasonable work-life balance. Though they successfully fought for lessening the abuses of surgical training, few Gen Xers actually reaped the benefits. I vividly recall watching slack-jawed as an intern scrubbed out of a case to go home because he was post call. A Martian landing in the OR and offering to assist with the anastomosis would have brought no less amazement.
With their careers spanning the endovascular revolution, Generation X has seen perhaps the greatest era of transformation in our profession. Our competition is no longer general or cardiac surgery, but rather interventional radiology and interventional cardiology. Gen X is also the first generation to earn less than its predecessors. Throw in their obscene tuition payments and one can see how Gen Xers fell well short of the financial heights of the Traditionalists and Boomers. The Gen Xers are the masters of the work hard/play hard ethos. You will see them at VEITH entertaining their European colleagues at 3 a.m. and then running the 6 a.m. breakfast sessions. While the Boomers often seemed old by 40, Xers appear desperate to salvage their lost youth.
Born between 1981 and 2006, Millennials are already the most populous generation. Their chief attributes are confidence, sociability, and a realistic outlook. Knowing they can’t please everyone, they rarely try. They want work to be meaningful in and of itself. They also value teamwork over individual approaches. Millennials are civic minded and have a strong sense of volunteerism. Their parents often tried to shelter them from the evils of the world, and they were the first generation of children with schedules. Because of their upbringing, Millennials are far more likely to seek guidance than the independent-minded Gen Xers. Raised to believe their voice mattered, they are now often reviled for it. It is with some degree of awe that I watch our Millennial students brazenly march into the dean’s and chancellor’s office to discuss their “careers.” As a medical student I first saw my dean at graduation, and I certainly didn’t even know what a chancellor was. Generation X is often baffled by the self-interest Millennials exude. But we shouldn’t be, we have seen it before. Raised by Baby Boomers (The Me Generation), Millennials inherited their self-driven outlook. This is also the reason Boomers and Millennials struggle to work together. They are too alike. Boomers see Millennials as “snowflakes” who are scared of work and selfie obsessed. Millennials bristle at the authoritarian nature of Boomers.
For vascular surgery to advance as a field, we need to recruit, train, and mentor this new generation. If only there was some guide: “The Proper Care and Feeding of Millennials." As senior attendings, program directors, and section chiefs, Generation X must now serve as a bridge between two larger forces, the Boomers and their offspring, the Millennials. Of course, whatever generation you are from is the best, but we must confront our biases. It is easy to seek out the same personalities to be your trainees and partners. Don’t. This pool will shrink every year. Millennials are more self-aware of their capabilities and therefore of their limitations. We may become flustered by their need for hand-holding, but what if it is appropriate? Was all of the autonomy you were granted during training truly good for the patients? Graduated responsibility and roles that push their limits help Millennials grow. I know they don’t value punctuality or dress codes, but they are better team players and openly motivated by learning. I formed our integrated vascular residency with two positions per year specifically to foster the team building Millennials crave. Yes, this is the generation that got 8th-place trophies so you must constantly award progress. Fortunately, now that surgery is unencumbered by such things as massive salaries and status, Millennials enter our workforce with purer intentions.
We may want to make Millennials match our values, traits, and behaviors, but each generation has departed radically from the ethos of their predecessors. Let’s see what the kids can do.
Dr. Sheahan is a professor of surgery and Program Director, Vascular Surgery Residency and Fellowship Programs, Louisiana State University Health Sciences Center, School of Medicine, New Orleans. He is also the Deputy Medical Editor of Vascular Specialist.
Alternative therapies
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.

Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.

Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.
Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
Alternative therapies, from vitamins and supplements to meditation and acupuncture, have become increasingly popular treatments in the United States for many medical problems in the past few decades. In 2008, the National Institutes of Health reported that nearly 40% of adults and 12% of children had used “complementary or alternative medicine” (CAM) in the preceding year. Other surveys have suggested that closer to 30% of general pediatric patients and as many as 75% of adolescent patients have used CAM at least once. These treatments are especially popular for chronic conditions that are managed but not usually cured with current evidence-based treatments. Psychiatric conditions in childhood sometimes have a long course, and have effective but controversial treatments, as with stimulants for ADHD. Parents sometimes feel guilty about their child’s problem and want to use “natural” methods or deny the accepted understanding of their child’s illness. So it is not surprising that families may investigate alternative treatments, and such treatments have multiplied.
While there is evidence that parents and patients rarely discuss these treatments with their physicians, it is critical that you know what therapies your patients are using. You should focus on tolerance in the context of protecting the child from harm and improving the child’s functioning. If you have ever recommended chicken soup for a cold, then you have prescribed complementary medicine, so it is not a stretch for you to offer some input about the other alternative therapies your patients may be considering.
It is important to note that rigorous, case-controlled studies of efficacy of most alternative therapies are few in number and usually small in size (so any evidence of efficacy is weaker), and that the products themselves are not regulated by the Food and Drug Administration or other public body. This means that the family (and you) will have to do some homework to ensure that the therapy they purchase comes from a reputable source and is what it purports to be.
Many of the alternative therapies patients are investigating will be herbs or supplements. Omega-3 fatty acids are critical to multiple essential body functions, and are taken in primarily via certain foods, primarily fish and certain seeds and nuts. A deficiency in certain omega-3 fatty acids can cause problems in infant neurological development and put one at risk for heart disease, rheumatologic illness, and depression. Supplementation with Omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], specifically) has a solid evidence base as an effective adjunctive treatment for depression and bipolar disorder in adults. In addition, randomized, placebo-controlled, double-blind studies have demonstrated efficacy in treatment of children with mild to moderate ADHD at doses of 1,200 mg/day. There are some studies that have demonstrated improvement in hyperactivity in children with autism with supplementation at similar doses. These supplements have very low risk of side effects. They are a reasonable recommendation to your patients whose children have mild to moderate ADHD, and they want to manage it without stimulants.
Families also may be considering physical or mechanical treatments. Acupuncture has demonstrated efficacy in the treatment of fatigue and pain, migraines, and addiction, although there are very few studies in children and adolescents. There is some evidence for its efficacy in treatment of mild to moderate depression and anxiety in adults, but again no research has been done in youth. Hypnotherapy has shown modest efficacy in treatment of anticipatory anxiety symptoms, headache, chronic pain, nausea and vomiting, migraines, hair-pulling and skin picking as well as compulsive eating and smoking cessation in adults. There is some clinical evidence for its efficacy in children and adolescents, and its safety is well established. Massage therapy has shown value in improving mood and behavior in children with ADHD, but not efficacy as a first-line treatment for ADHD symptoms. Chiropractic care, which is among the most commonly used alternative therapies, claims to be effective for the treatment of anxiety, depression, ADHD, behavioral problems of autism and even schizophrenia and bipolar disorder, but there is no significant scientific evidence to support these claims. And neurofeedback, which is a variant of biofeedback in which patients practice calming themselves or improving focus while watching an EEG has shown modest efficacy in the treatment of ADHD in children in early studies. It is worth noting that all of these therapies may be costly and not covered by insurance.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
Additional readings
1. Child Adolesc Psychiatr Clin N Am. 2013 Jul;22(3):375-80.
2. J Am Acad Child Adolesc Psychiatry. 2008;47(4):364-8.
3. J Am Acad Child Adolesc Psychiatry. 2011;50(10):991-1000.
4. J Am Acad Child Adolesc Psychiatry. 2014 Jun; 53(6):658-66.
5. J Am Acad Child Adolesc Psychiatry. 2016 Oct;55(10):S168-9.
Swiss freedom, hidden witnesses, and beer
Most of medical practice is mundane. Just a few interesting cases pass through now and then to break up the clinical routine, a rhythm that’s fine with me.
More often, patients expand my vistas by telling me about places I’ve never been and things I didn’t know and couldn’t imagine. Sometimes these tales are even more riveting than atopic dermatitis or mildly dysplastic nevi. Learning about them leaves me smiling and scratching my head. What will they tell me about next?

“I always come to Boston around this time,” she said. “But today I actually am celebrating Swiss National Day.”
“No kidding,” I said. “What is Swiss National Day?”
“We commemorate the founding of Switzerland in 1291,” she said.
“And how do you celebrate it?” I asked.
“Well, we are Swiss,” she said, “so we work all day. Then we have a party in the evening.
“That is how it used to be anyway,” she said. “About 40 years ago, the parties on the left and right made a deal and established two holidays: Labor Day on May 1st and the National Holiday on August 1st. Now we get those whole days off.”
“Which was the end of Swiss civilization as we know it,” I suggested.
“That’s exactly what my father said when it happened,” said Valentina, with a restrained, Swiss smile. “But somehow life goes on for us, even with 2 days a year off.”

* * * * * * * * * * * * * * * * * * * * * * *
When I picked up his chart, I saw that my patient’s last name suggested that he hailed from one of the countries left after the breakup of Yugoslavia. We’ll call him Magovcevic.
As soon as I walked in, however, it was clear that wherever he came from was nowhere near Serbia. His features and accent were Brazilian.
“I come from Minas Gerais,” he said, “in the South, not far from Rio.”
“So how come you have a Slavic name?” I asked him.
“My parents had a different last name,” he said.
“Then how did you come to be called Magovcevic?” I asked.
“I’m in the witness protection program,” he said.
I had to hold onto the sink to stay upright. Of all the possible responses he could have made, that one was not on my list.
“Did you pick the name yourself?” I asked. I don’t think I’d ever given a thought to how family names are chosen for people in witness protection.
“No, they gave it to me,” he said. “I was still a minor.”
At that point I stopped asking questions. Whatever it was that he witnessed as a minor that landed him in witness protection I didn’t want to know about.
* * * * * * * * * * * * * * * * * * * * * * *
Myrna was very happy to tell me that her son was doing well in college and had a good summer job.
“He works in a beer garden downtown,” she said. “The tips are great.”
“What is he studying in school?” I asked.
“Fermentation studies,” she replied.
After she’d said he was moonlighting in a beer garden, I thought she was pulling my leg. I know college students have keg parties after class, but I didn’t know they studied what goes into the kegs during class.
But Myrna was serious. “He’s interested in biochemistry,” she explained. “He wants to focus on developing better beers.”
A younger colleague whom I told about this chuckled at my perplexity. “Sure,” she said, “fermentation studies is the hot new field. Lots of people are getting into it.”
I have long since resigned myself to being clueless about what younger people are into, especially social media. But I found myself bemused at how it just never occurred to me that bright young biochemists might burn with ambition to bring the world better craft beers.
I have since learned that fermentation studies have other applications too. Like wine. And wine, like cosmetics, has been around a lot longer than dermatology.
* * * * * * * * * * * * * * * * * * * * * * *
Skin is interesting, but the people inside it are often even more so. Who knows what I’ll run into tomorrow? I won’t even try to guess.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com.
Most of medical practice is mundane. Just a few interesting cases pass through now and then to break up the clinical routine, a rhythm that’s fine with me.
More often, patients expand my vistas by telling me about places I’ve never been and things I didn’t know and couldn’t imagine. Sometimes these tales are even more riveting than atopic dermatitis or mildly dysplastic nevi. Learning about them leaves me smiling and scratching my head. What will they tell me about next?
“I always come to Boston around this time,” she said. “But today I actually am celebrating Swiss National Day.”
“No kidding,” I said. “What is Swiss National Day?”
“We commemorate the founding of Switzerland in 1291,” she said.
“And how do you celebrate it?” I asked.
“Well, we are Swiss,” she said, “so we work all day. Then we have a party in the evening.
“That is how it used to be anyway,” she said. “About 40 years ago, the parties on the left and right made a deal and established two holidays: Labor Day on May 1st and the National Holiday on August 1st. Now we get those whole days off.”
“Which was the end of Swiss civilization as we know it,” I suggested.
“That’s exactly what my father said when it happened,” said Valentina, with a restrained, Swiss smile. “But somehow life goes on for us, even with 2 days a year off.”
* * * * * * * * * * * * * * * * * * * * * * *
When I picked up his chart, I saw that my patient’s last name suggested that he hailed from one of the countries left after the breakup of Yugoslavia. We’ll call him Magovcevic.
As soon as I walked in, however, it was clear that wherever he came from was nowhere near Serbia. His features and accent were Brazilian.
“I come from Minas Gerais,” he said, “in the South, not far from Rio.”
“So how come you have a Slavic name?” I asked him.
“My parents had a different last name,” he said.
“Then how did you come to be called Magovcevic?” I asked.
“I’m in the witness protection program,” he said.
I had to hold onto the sink to stay upright. Of all the possible responses he could have made, that one was not on my list.
“Did you pick the name yourself?” I asked. I don’t think I’d ever given a thought to how family names are chosen for people in witness protection.
“No, they gave it to me,” he said. “I was still a minor.”
At that point I stopped asking questions. Whatever it was that he witnessed as a minor that landed him in witness protection I didn’t want to know about.
* * * * * * * * * * * * * * * * * * * * * * *
Myrna was very happy to tell me that her son was doing well in college and had a good summer job.
“He works in a beer garden downtown,” she said. “The tips are great.”
“What is he studying in school?” I asked.
“Fermentation studies,” she replied.
After she’d said he was moonlighting in a beer garden, I thought she was pulling my leg. I know college students have keg parties after class, but I didn’t know they studied what goes into the kegs during class.
But Myrna was serious. “He’s interested in biochemistry,” she explained. “He wants to focus on developing better beers.”
A younger colleague whom I told about this chuckled at my perplexity. “Sure,” she said, “fermentation studies is the hot new field. Lots of people are getting into it.”
I have long since resigned myself to being clueless about what younger people are into, especially social media. But I found myself bemused at how it just never occurred to me that bright young biochemists might burn with ambition to bring the world better craft beers.
I have since learned that fermentation studies have other applications too. Like wine. And wine, like cosmetics, has been around a lot longer than dermatology.
* * * * * * * * * * * * * * * * * * * * * * *
Skin is interesting, but the people inside it are often even more so. Who knows what I’ll run into tomorrow? I won’t even try to guess.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com.
Most of medical practice is mundane. Just a few interesting cases pass through now and then to break up the clinical routine, a rhythm that’s fine with me.
More often, patients expand my vistas by telling me about places I’ve never been and things I didn’t know and couldn’t imagine. Sometimes these tales are even more riveting than atopic dermatitis or mildly dysplastic nevi. Learning about them leaves me smiling and scratching my head. What will they tell me about next?
“I always come to Boston around this time,” she said. “But today I actually am celebrating Swiss National Day.”
“No kidding,” I said. “What is Swiss National Day?”
“We commemorate the founding of Switzerland in 1291,” she said.
“And how do you celebrate it?” I asked.
“Well, we are Swiss,” she said, “so we work all day. Then we have a party in the evening.
“That is how it used to be anyway,” she said. “About 40 years ago, the parties on the left and right made a deal and established two holidays: Labor Day on May 1st and the National Holiday on August 1st. Now we get those whole days off.”
“Which was the end of Swiss civilization as we know it,” I suggested.
“That’s exactly what my father said when it happened,” said Valentina, with a restrained, Swiss smile. “But somehow life goes on for us, even with 2 days a year off.”
* * * * * * * * * * * * * * * * * * * * * * *
When I picked up his chart, I saw that my patient’s last name suggested that he hailed from one of the countries left after the breakup of Yugoslavia. We’ll call him Magovcevic.
As soon as I walked in, however, it was clear that wherever he came from was nowhere near Serbia. His features and accent were Brazilian.
“I come from Minas Gerais,” he said, “in the South, not far from Rio.”
“So how come you have a Slavic name?” I asked him.
“My parents had a different last name,” he said.
“Then how did you come to be called Magovcevic?” I asked.
“I’m in the witness protection program,” he said.
I had to hold onto the sink to stay upright. Of all the possible responses he could have made, that one was not on my list.
“Did you pick the name yourself?” I asked. I don’t think I’d ever given a thought to how family names are chosen for people in witness protection.
“No, they gave it to me,” he said. “I was still a minor.”
At that point I stopped asking questions. Whatever it was that he witnessed as a minor that landed him in witness protection I didn’t want to know about.
* * * * * * * * * * * * * * * * * * * * * * *
Myrna was very happy to tell me that her son was doing well in college and had a good summer job.
“He works in a beer garden downtown,” she said. “The tips are great.”
“What is he studying in school?” I asked.
“Fermentation studies,” she replied.
After she’d said he was moonlighting in a beer garden, I thought she was pulling my leg. I know college students have keg parties after class, but I didn’t know they studied what goes into the kegs during class.
But Myrna was serious. “He’s interested in biochemistry,” she explained. “He wants to focus on developing better beers.”
A younger colleague whom I told about this chuckled at my perplexity. “Sure,” she said, “fermentation studies is the hot new field. Lots of people are getting into it.”
I have long since resigned myself to being clueless about what younger people are into, especially social media. But I found myself bemused at how it just never occurred to me that bright young biochemists might burn with ambition to bring the world better craft beers.
I have since learned that fermentation studies have other applications too. Like wine. And wine, like cosmetics, has been around a lot longer than dermatology.
* * * * * * * * * * * * * * * * * * * * * * *
Skin is interesting, but the people inside it are often even more so. Who knows what I’ll run into tomorrow? I won’t even try to guess.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com.
Nature versus nurture: 50 years of a popular debate
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7

In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7
In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
This basic question has been debated at settings ranging from scientific conferences to dinner tables for many decades. The media also has covered it in forms ranging from documentaries to the popular comedy movie “Trading Places” (1983). Yet, despite so much attention and so much research devoted to resolving this timeless debate, the arguments continue to this day.
A lack of a clear answer, however, by no means implies that we have not made major advances in our understanding. This short review takes a look at the progression of this seemingly eternal question by categorizing the development of the nature versus nurture question into three main stages. While such a partitioning is somewhat oversimplified with regard to what the various positions on this issue have been at different times, it does illustrate the way that the debate has gradually evolved.
Part 1: Nature versus nurture
The origins of the nature versus nurture debate date back far beyond the past 50 years. The ancient Greek philosopher Galen postulated that personality traits were driven by the relative concentrations of four bodily fluids or “humours.” In 1874, Sir Francis Galton published “English Men of Science: Their Nature and Nurture,” in which he advanced his ideas about the dominance of hereditary factors in intelligence and character at the beginning of the eugenics movement.1 These ideas were in stark opposition to the perspective of earlier scholars, such as the philosopher John Locke, who popularized the theory that children are born a “blank slate” and from there develop their traits and intellectual abilities through their environment and experiences.
The other primary school of thought in the mid-1960s was psychoanalysis, which was based on the ideas of Sigmund Freud, MD. Psychoanalysis maintains that the way that unconscious sexual and aggressive drives were channeled through various defense mechanisms was of primary importance to the understanding of both psychopathology and typical human behavior.
While these two perspectives were often very much in opposition to each other, they shared in common the view that the environment and a person’s individual experiences, i.e. nurture, were the prevailing forces in development. In the background, more biologically oriented research and clinical work was slowly beginning to work its way into the field, especially at certain institutions, such as Washington University in St. Louis. Several medications of various types were then available, including chlorpromazine, imipramine, and diazepam.
Overall, however, it is probably fair to say that, 50 years ago, it was the nurture perspective that held the most sway since psychodynamic treatment and behaviorist research dominated, while the emerging fields of genetics and neuroscience were only beginning to take hold.
Part 2: Nature and nurture
From the 1970s to the end of the 20th century, a noticeable shift occurred as knowledge of the brain and genetics – supported by remarkable advances in research techniques – began to swing the pendulum back toward an increased appreciation of nature as a critical influence on a person’s thoughts, feelings, and behavior.
Researchers Stella Chess, MD, and Alexander Thomas, MD, for example, conducted the New York Longitudinal Study, in which they closely observed a group of young children over many years. Their studies compelled them to argue for the significance of more innate temperament traits as critical aspects of a youth’s overall adjustment.2 The Human Genome Project was launched in 1990, and the entire decade was designated as the “Decade of the Brain.” During this time, neuroscience research exploded as techniques, such as MRI and PET, allowed scientists to view the living brain like never before.
The type of research investigation that perhaps was most directly relevant to the nature-nurture debate and that became quite popular during this time was the twin study. By comparing the relative similarities among monozygotic and dizygotic twins raised in the same household, it became possible to calculate directly the degree to which a variable of interest (intelligence, height, aggressive behavior) could be attributed to genetic versus environmental factors. When it came to behavioral variables, a repeated finding that emerged was that both genetic and environmental influences are important, often at close to a 50/50 split in terms of magnitude.3,4 These studies were complemented by molecular genetic studies, which were beginning to be able to identify specific genes that conveyed usually small amounts of risk for a wide range of psychiatric disorders.
Yet, while twin studies and many other lines of research made it increasingly difficult to argue for the overwhelming supremacy of either nature or nurture, the two domains generally were treated as being independent of each other. Specific traits or symptoms in an individual often were thought of as being the result of either psychological (nurture) or biological (nature) causes. Terms such as “endogenous depression,” for example, were used to distinguish those who had symptoms that were thought generally to be out of reach for “psychological” treatments, such as psychotherapy. Looking back, it might be fair to say that one of the principle flaws in this perspective was the commonly held belief that, if something was brain based or biological, then it therefore implied a kind of automatic “wiring” of the brain that was generally driven by genes and beyond the influence of environmental factors.
Part 3: Nature is nurture (and vice versa)
As the science progressed, it became increasingly clear that the nature and nurture domains were hopelessly intertwined with one another. From early PET-scan studies showing that both medications and psychotherapy not only changed the brain but also did so in ways similar to behavioral-genetic studies showing how genetically influenced behaviors actually cause certain environmental events to be more likely to occur, research continued to demonstrate the bidirectional influences of genetic and environmental factors on development.5,6 This appreciation rose to even greater heights with advances in the field of epigenetics, which was able to document some of the specific mechanisms through which environmental factors cause genes involved in regulating the plasticity of the brain to turn on and off.7
In thinking through some of this complexity, however, it is important to remember the hopeful message that is contained in this rich understanding. All of these complicated, interacting genetic and environmental factors give us many avenues for positive intervention. Now we understand that not only might a medication help strengthen some of the brain connections needed to reduce and cope with that child’s anxiety, but so could mindfulness, exercise, and addressing his parents’ symptoms. When the families ask me whether their child’s struggles are behavioral or psychological, the answer I tend to give them is “yes.”
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington.
Email him at pdnews@frontlinemedcom.com. Follow him on Twitter @pedipsych.
References
1. “English Men of Science: Their Nature and Nurture” (London: MacMillan & Co., 1874)
2. “Temperament: Theory and Practice” (New York: Brunner/Mazel, 1996)
3. “Nature and Nurture during Infancy and Early Childhood” (New York: Cambridge University Press, 1988)
4. Nat Genet. 2015;47(7):702-9.
5. Arch Gen Psychiatry. 1992;49(9):681-9.
6. Dev Psychopathol. 1997 Spring;9(2):335-64.
7. JAMA Psychiatry. 2017;74(6):551-2.
New hospitalist unit has stellar patient satisfaction scores
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at john.nelson@nelsonflores.com
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at john.nelson@nelsonflores.com
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at john.nelson@nelsonflores.com
From the Editors: Hanging up the scalpel
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.

Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.
Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.
Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
From the Washington Office: Receiving an increase in Medicare payment and avoiding a penalty
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.

One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: quality@facs.org.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.
One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: quality@facs.org.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.
One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: quality@facs.org.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.