User login
A multidisciplinary approach to diaphragmatic endometriosis
Endometriosis affects approximately 11% of women; the disease can be categorized as pelvic endometriosis and extrapelvic endometriosis, based on anatomic presentation. It is estimated that about 12% of extrapelvic disease involves the diaphragm or thoracic cavity.
While diaphragmatic endometriosis often is asymptomatic, patients who are symptomatic can experience progressive and incapacitating pain. because of a traditional focus on the lower pelvic region. Some cases are misdiagnosed as other conditions involving the gastrointestinal tract or of cardiothoracic origin, because of the propensity of diaphragmatic disease to occur posteriorly and hide behind the liver. The variable appearance of endometriotic lesions and the lack of reliable diagnostic or imaging tests also can contribute to delayed diagnosis.

Symptoms usually occur cyclically with the onset of menses, but sometimes are unrelated to menses. Most diaphragmatic lesions occur on the abdominal side and right hemidiaphragm, which may offer evidence for the theory that retrograde menstruation drives the development of endometriosis because of the clockwise flow of peritoneal fluid. However, lesions have been found on all parts of the diaphragm, including the left side only, the thoracic and visceral sides of the diaphragm, and the phrenic nerve. There is no correlation between the size/number of lesions and either pneumothorax or hemothorax, nor pain.
The best diagnostic method is thorough surveillance intraoperatively. In our practice, we routinely inspect the diaphragm for endometriosis at the time of video laparoscopy.
In women who have symptoms, it is important to ensure the best exposure of the diaphragm by properly considering the patient’s positioning and port placement, and by using an atraumatic liver retractor or grasping forceps to gently push the liver down and away from the visual/operative field. Posterior diaphragm viewing can also be enhanced by utilizing a 30-degree laparoscope angled toward the back. At times, it is helpful to cut the falciform ligament near the liver to expose the right side of the diaphragm completely while the patient is in steep reverse Trendelenburg position.
Most lesions in symptomatic patients can be successfully removed with hydrodissection and vaporization or excision. For asymptomatic patients with an incidental finding of diaphragmatic endometriosis, the suggestion is not to treat lesions in order to avoid the potential risk of injury to the diaphragm, phrenic nerve, lungs, or heart – especially when an adequate multidisciplinary team is not available.
Pathophysiology
In addition to retrograde menstruation, there are two other common theories regarding the pathophysiology of thoracic endometriosis. First, high prostaglandin F2-alpha at ovulation may result in vasospasm and ischemia of the lungs (resulting, in turn, in alveolar rupture and subsequent pneumothorax). Second, the loss of a mucus plug during menses may result in communication between the environment and peritoneal cavity.
What is clear is that patients who have symptoms consistent with pelvic endometriosis and chest complaints should be evaluated for both diaphragmatic and pelvic endometriosis. It’s also increasing clear that a multidisciplinary approach utilizing combined laparoscopy and thoracoscopy is a safe and effective method for addressing pelvic, diaphragmatic, and other thoracic endometriosis when other treatments have failed.
A multidisciplinary approach
Since the introduction of video laparoscopy and ease of evaluation of the upper abdomen, more extrapelvic endometriosis – including disease in the upper abdomen and diaphragm – is being diagnosed. The thoracic and visceral diaphragm are the most commonly described sites of thoracic endometriosis, and disease is often right sided, with parenchymal involvement less commonly reported.

Abdominopelvic and visceral diaphragmatic endometriosis are treated endoscopically with hydrodissection followed by excision or ablation. Superficial lesions away from the central diaphragm can be coagulated using bipolar current.
Thoracoscopic treatment varies, involving ablation or excision of smaller diaphragmatic lesions, pulmonary wedge resection of deep parenchymal nodules (using a stapling device), diaphragm resection of deep diaphragmatic lesions using a stapling device, or by excision and manual suturing.
Endoscopic diagnosis and treatment begins by introducing a 10-mm port at the umbilicus and placing three additional ports in the upper quadrant (right or left, depending on implant location). The arrangement (similar to that of a laparoscopic cholecystectomy or splenectomy) allows for examination of the posterior portion of the right hemidiaphragm and almost the entire left hemidiaphragm in addition to routine abdominopelvic exploration.
For better laparoscopic visualization, the patient is repositioned in steep reverse Trendelenburg, and the liver is gently pushed caudally to view the adjacent diaphragm. The upper abdominal walls and the liver also may be evaluated while in this position.
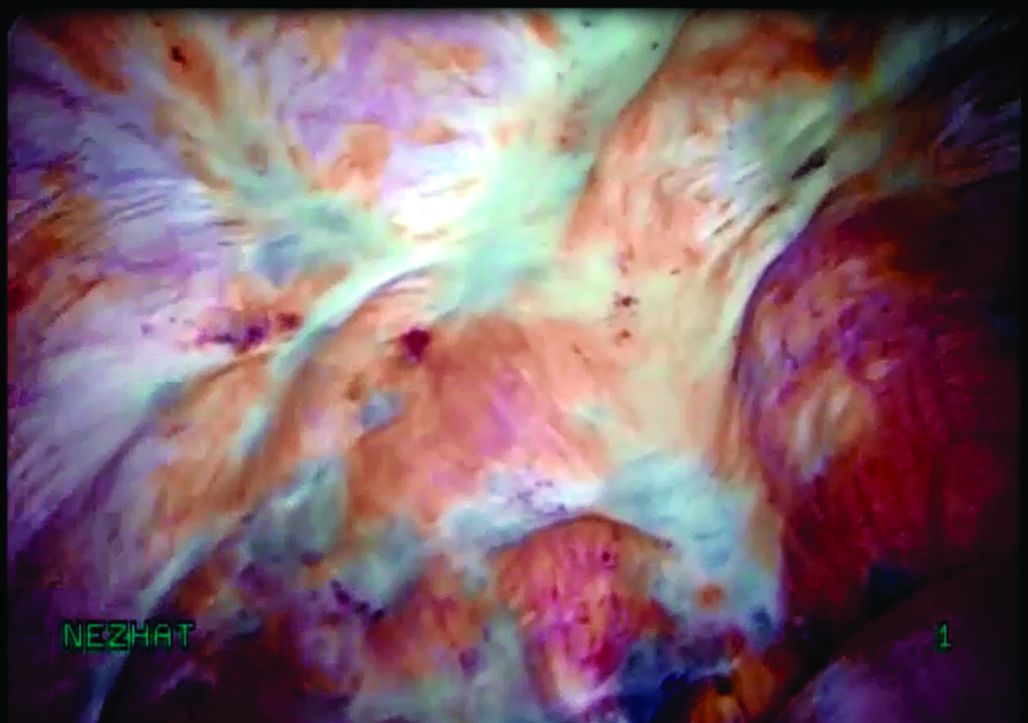
Bluish pigmented lesions are the most commonly reported form of diaphragmatic endometriosis, followed by lesions with a reddish-purple appearance. However, lesions can present with various colors and morphologic appearances, such as fibrotic white lesions or adhesions to the liver.
In our practice, we recommend using the CO2 laser (set at 20-25 watts) with hydrodissection for superficial lesions. The CO2 laser is much more precise and has a smaller depth of penetration and less thermal spread, compared with electrocautery. The CO2 laser beam also reaches otherwise hard-to-access areas behind the liver and has proven to be safe for vaporizing and/or excising many types of diaphragmatic lesions. We have successfully treated diaphragmatic endometriosis in the vicinity of the phrenic nerve and directly in line with the left ventricle.
Watch a video from Dr. Ceana Nezhat demonstrating a step wise vaporization and excision of diaphragmatic endometriosis utilizing different techniques.
(Courtesy Dr. Ceana Nezhat)
Plasma jet energy and ultrasonic energy are good alternatives when a CO2 laser is not available and are preferable to the use of cold scissors because of subsequent bleeding, which requires bipolar hemostasis.
Monopolar electrocautery is not as good a choice for treating diaphragmatic endometriosis because of higher depth of penetration, which may cause tissue necrosis and subsequent delayed diaphragmatic fenestrations. It also may cause unpredictable diaphragmatic muscular contractions and electrical conduction transmitted to the heart, inducing arrhythmia.
For patients treated via combined VALS and VATS procedures, endometriotic lesions involving the entire thickness of the diaphragm should be completely resected, and the defect can be repaired with either sutures or staples.
In all cases, special anesthesia considerations must be made given the inability to completely ventilate the lung. In our practice, we use a double-lumen endotracheal tube for single lung ventilation, if needed. A bronchial blocker is used to isolate the lung when the double-lumen endotracheal tube cannot be inserted.
It is important to note that we do not recommend VATS with VALS in all suspicious cases. We reserve VATS only for patients with catamenial pneumothorax, catamenial hemothorax, hemoptysis, and pulmonary nodules, defined as Thoracic Endometriosis Syndrome. We usually start with medical management first, then proceed to VALS, and finally, VATS, with the intention to treat if the patient fails nonsurgical treatments. It is better to avoid VATS, if possible, because it is associated with longer recovery and more pain; it should be done if all else fails.
If the patient has completed childbearing or passed reproductive age, bilateral salpingectomy, or hysterectomy with or without bilateral salpingo-oophorectomy, may be considered as the first step prior to more aggressive excisional procedures. This is especially true for widespread lesions, as branches of the phrenic nerve are difficult to see and injury could result in paralysis of the diaphragm. It’s important to appreciate that if estrogen stimulation to the diaphragmatic lesions is to cease for the long term, hormonal suppression or surgical treatment including bilateral oophorectomy should be utilized.
My colleagues and I have reported on our experience with a multidisciplinary approach in the treatment of diaphragmatic endometriosis in 25 patients. All had both pelvic and thoracic symptoms, and the majority had endometrial implants on both the thoracic and visceral sides of the diaphragm.
There were two postoperative complications: a diaphragmatic hernia and a vaginal cuff hematoma. Over a follow-up period of 3-18 months, all 25 patients had significant improvement or resolution of their chest complaints, and most remained asymptomatic for more than 6 months (JSLS. 2014 Jul-Sep;18[3]. pii: e2014.00312. doi: 10.4293/JSLS.2014.00312).
Dr. Ceana Nezhat is the fellowship director of Nezhat Medical Center, the medical director of training and education at Northside Hospital, and an adjunct clinical professor of gynecology and obstetrics at Emory University, all in Atlanta. He is president of SRS (Society of Reproductive Surgeons) and past president of AAGL (American Association of Gynecologic Laparoscopists). Dr. Nezhat is a consultant for Novuson Surgical, Karl Storz Endoscopy, Lumenis, and AbbVie; a medical advisor for Plasma Surgical, and a member of the scientific advisory board for SurgiQuest.
Suggested readings
1. Nezhat C, Nezhat F, Nezhat C. Nezhat’s Operative Gynecologic Laparoscopy with Hysteroscopy. Fourth Edition. Cambridge University Press. 2013.
2. Am J Med. 1996 Feb;100(2):164-70.
3. Fertil Steril. 1998 Jun;69(6):1048-55.
4. Clin Obstet Gynecol. 1999 Sep;42(3):699-711.
5. JSLS. 2012 Jan-Mar; 16(1):140-2.
Endometriosis affects approximately 11% of women; the disease can be categorized as pelvic endometriosis and extrapelvic endometriosis, based on anatomic presentation. It is estimated that about 12% of extrapelvic disease involves the diaphragm or thoracic cavity.
While diaphragmatic endometriosis often is asymptomatic, patients who are symptomatic can experience progressive and incapacitating pain. because of a traditional focus on the lower pelvic region. Some cases are misdiagnosed as other conditions involving the gastrointestinal tract or of cardiothoracic origin, because of the propensity of diaphragmatic disease to occur posteriorly and hide behind the liver. The variable appearance of endometriotic lesions and the lack of reliable diagnostic or imaging tests also can contribute to delayed diagnosis.
Symptoms usually occur cyclically with the onset of menses, but sometimes are unrelated to menses. Most diaphragmatic lesions occur on the abdominal side and right hemidiaphragm, which may offer evidence for the theory that retrograde menstruation drives the development of endometriosis because of the clockwise flow of peritoneal fluid. However, lesions have been found on all parts of the diaphragm, including the left side only, the thoracic and visceral sides of the diaphragm, and the phrenic nerve. There is no correlation between the size/number of lesions and either pneumothorax or hemothorax, nor pain.
The best diagnostic method is thorough surveillance intraoperatively. In our practice, we routinely inspect the diaphragm for endometriosis at the time of video laparoscopy.
In women who have symptoms, it is important to ensure the best exposure of the diaphragm by properly considering the patient’s positioning and port placement, and by using an atraumatic liver retractor or grasping forceps to gently push the liver down and away from the visual/operative field. Posterior diaphragm viewing can also be enhanced by utilizing a 30-degree laparoscope angled toward the back. At times, it is helpful to cut the falciform ligament near the liver to expose the right side of the diaphragm completely while the patient is in steep reverse Trendelenburg position.
Most lesions in symptomatic patients can be successfully removed with hydrodissection and vaporization or excision. For asymptomatic patients with an incidental finding of diaphragmatic endometriosis, the suggestion is not to treat lesions in order to avoid the potential risk of injury to the diaphragm, phrenic nerve, lungs, or heart – especially when an adequate multidisciplinary team is not available.
Pathophysiology
In addition to retrograde menstruation, there are two other common theories regarding the pathophysiology of thoracic endometriosis. First, high prostaglandin F2-alpha at ovulation may result in vasospasm and ischemia of the lungs (resulting, in turn, in alveolar rupture and subsequent pneumothorax). Second, the loss of a mucus plug during menses may result in communication between the environment and peritoneal cavity.
What is clear is that patients who have symptoms consistent with pelvic endometriosis and chest complaints should be evaluated for both diaphragmatic and pelvic endometriosis. It’s also increasing clear that a multidisciplinary approach utilizing combined laparoscopy and thoracoscopy is a safe and effective method for addressing pelvic, diaphragmatic, and other thoracic endometriosis when other treatments have failed.
A multidisciplinary approach
Since the introduction of video laparoscopy and ease of evaluation of the upper abdomen, more extrapelvic endometriosis – including disease in the upper abdomen and diaphragm – is being diagnosed. The thoracic and visceral diaphragm are the most commonly described sites of thoracic endometriosis, and disease is often right sided, with parenchymal involvement less commonly reported.
Abdominopelvic and visceral diaphragmatic endometriosis are treated endoscopically with hydrodissection followed by excision or ablation. Superficial lesions away from the central diaphragm can be coagulated using bipolar current.
Thoracoscopic treatment varies, involving ablation or excision of smaller diaphragmatic lesions, pulmonary wedge resection of deep parenchymal nodules (using a stapling device), diaphragm resection of deep diaphragmatic lesions using a stapling device, or by excision and manual suturing.
Endoscopic diagnosis and treatment begins by introducing a 10-mm port at the umbilicus and placing three additional ports in the upper quadrant (right or left, depending on implant location). The arrangement (similar to that of a laparoscopic cholecystectomy or splenectomy) allows for examination of the posterior portion of the right hemidiaphragm and almost the entire left hemidiaphragm in addition to routine abdominopelvic exploration.
For better laparoscopic visualization, the patient is repositioned in steep reverse Trendelenburg, and the liver is gently pushed caudally to view the adjacent diaphragm. The upper abdominal walls and the liver also may be evaluated while in this position.
Bluish pigmented lesions are the most commonly reported form of diaphragmatic endometriosis, followed by lesions with a reddish-purple appearance. However, lesions can present with various colors and morphologic appearances, such as fibrotic white lesions or adhesions to the liver.
In our practice, we recommend using the CO2 laser (set at 20-25 watts) with hydrodissection for superficial lesions. The CO2 laser is much more precise and has a smaller depth of penetration and less thermal spread, compared with electrocautery. The CO2 laser beam also reaches otherwise hard-to-access areas behind the liver and has proven to be safe for vaporizing and/or excising many types of diaphragmatic lesions. We have successfully treated diaphragmatic endometriosis in the vicinity of the phrenic nerve and directly in line with the left ventricle.
Watch a video from Dr. Ceana Nezhat demonstrating a step wise vaporization and excision of diaphragmatic endometriosis utilizing different techniques.
(Courtesy Dr. Ceana Nezhat)
Plasma jet energy and ultrasonic energy are good alternatives when a CO2 laser is not available and are preferable to the use of cold scissors because of subsequent bleeding, which requires bipolar hemostasis.
Monopolar electrocautery is not as good a choice for treating diaphragmatic endometriosis because of higher depth of penetration, which may cause tissue necrosis and subsequent delayed diaphragmatic fenestrations. It also may cause unpredictable diaphragmatic muscular contractions and electrical conduction transmitted to the heart, inducing arrhythmia.
For patients treated via combined VALS and VATS procedures, endometriotic lesions involving the entire thickness of the diaphragm should be completely resected, and the defect can be repaired with either sutures or staples.
In all cases, special anesthesia considerations must be made given the inability to completely ventilate the lung. In our practice, we use a double-lumen endotracheal tube for single lung ventilation, if needed. A bronchial blocker is used to isolate the lung when the double-lumen endotracheal tube cannot be inserted.
It is important to note that we do not recommend VATS with VALS in all suspicious cases. We reserve VATS only for patients with catamenial pneumothorax, catamenial hemothorax, hemoptysis, and pulmonary nodules, defined as Thoracic Endometriosis Syndrome. We usually start with medical management first, then proceed to VALS, and finally, VATS, with the intention to treat if the patient fails nonsurgical treatments. It is better to avoid VATS, if possible, because it is associated with longer recovery and more pain; it should be done if all else fails.
If the patient has completed childbearing or passed reproductive age, bilateral salpingectomy, or hysterectomy with or without bilateral salpingo-oophorectomy, may be considered as the first step prior to more aggressive excisional procedures. This is especially true for widespread lesions, as branches of the phrenic nerve are difficult to see and injury could result in paralysis of the diaphragm. It’s important to appreciate that if estrogen stimulation to the diaphragmatic lesions is to cease for the long term, hormonal suppression or surgical treatment including bilateral oophorectomy should be utilized.
My colleagues and I have reported on our experience with a multidisciplinary approach in the treatment of diaphragmatic endometriosis in 25 patients. All had both pelvic and thoracic symptoms, and the majority had endometrial implants on both the thoracic and visceral sides of the diaphragm.
There were two postoperative complications: a diaphragmatic hernia and a vaginal cuff hematoma. Over a follow-up period of 3-18 months, all 25 patients had significant improvement or resolution of their chest complaints, and most remained asymptomatic for more than 6 months (JSLS. 2014 Jul-Sep;18[3]. pii: e2014.00312. doi: 10.4293/JSLS.2014.00312).
Dr. Ceana Nezhat is the fellowship director of Nezhat Medical Center, the medical director of training and education at Northside Hospital, and an adjunct clinical professor of gynecology and obstetrics at Emory University, all in Atlanta. He is president of SRS (Society of Reproductive Surgeons) and past president of AAGL (American Association of Gynecologic Laparoscopists). Dr. Nezhat is a consultant for Novuson Surgical, Karl Storz Endoscopy, Lumenis, and AbbVie; a medical advisor for Plasma Surgical, and a member of the scientific advisory board for SurgiQuest.
Suggested readings
1. Nezhat C, Nezhat F, Nezhat C. Nezhat’s Operative Gynecologic Laparoscopy with Hysteroscopy. Fourth Edition. Cambridge University Press. 2013.
2. Am J Med. 1996 Feb;100(2):164-70.
3. Fertil Steril. 1998 Jun;69(6):1048-55.
4. Clin Obstet Gynecol. 1999 Sep;42(3):699-711.
5. JSLS. 2012 Jan-Mar; 16(1):140-2.
Endometriosis affects approximately 11% of women; the disease can be categorized as pelvic endometriosis and extrapelvic endometriosis, based on anatomic presentation. It is estimated that about 12% of extrapelvic disease involves the diaphragm or thoracic cavity.
While diaphragmatic endometriosis often is asymptomatic, patients who are symptomatic can experience progressive and incapacitating pain. because of a traditional focus on the lower pelvic region. Some cases are misdiagnosed as other conditions involving the gastrointestinal tract or of cardiothoracic origin, because of the propensity of diaphragmatic disease to occur posteriorly and hide behind the liver. The variable appearance of endometriotic lesions and the lack of reliable diagnostic or imaging tests also can contribute to delayed diagnosis.
Symptoms usually occur cyclically with the onset of menses, but sometimes are unrelated to menses. Most diaphragmatic lesions occur on the abdominal side and right hemidiaphragm, which may offer evidence for the theory that retrograde menstruation drives the development of endometriosis because of the clockwise flow of peritoneal fluid. However, lesions have been found on all parts of the diaphragm, including the left side only, the thoracic and visceral sides of the diaphragm, and the phrenic nerve. There is no correlation between the size/number of lesions and either pneumothorax or hemothorax, nor pain.
The best diagnostic method is thorough surveillance intraoperatively. In our practice, we routinely inspect the diaphragm for endometriosis at the time of video laparoscopy.
In women who have symptoms, it is important to ensure the best exposure of the diaphragm by properly considering the patient’s positioning and port placement, and by using an atraumatic liver retractor or grasping forceps to gently push the liver down and away from the visual/operative field. Posterior diaphragm viewing can also be enhanced by utilizing a 30-degree laparoscope angled toward the back. At times, it is helpful to cut the falciform ligament near the liver to expose the right side of the diaphragm completely while the patient is in steep reverse Trendelenburg position.
Most lesions in symptomatic patients can be successfully removed with hydrodissection and vaporization or excision. For asymptomatic patients with an incidental finding of diaphragmatic endometriosis, the suggestion is not to treat lesions in order to avoid the potential risk of injury to the diaphragm, phrenic nerve, lungs, or heart – especially when an adequate multidisciplinary team is not available.
Pathophysiology
In addition to retrograde menstruation, there are two other common theories regarding the pathophysiology of thoracic endometriosis. First, high prostaglandin F2-alpha at ovulation may result in vasospasm and ischemia of the lungs (resulting, in turn, in alveolar rupture and subsequent pneumothorax). Second, the loss of a mucus plug during menses may result in communication between the environment and peritoneal cavity.
What is clear is that patients who have symptoms consistent with pelvic endometriosis and chest complaints should be evaluated for both diaphragmatic and pelvic endometriosis. It’s also increasing clear that a multidisciplinary approach utilizing combined laparoscopy and thoracoscopy is a safe and effective method for addressing pelvic, diaphragmatic, and other thoracic endometriosis when other treatments have failed.
A multidisciplinary approach
Since the introduction of video laparoscopy and ease of evaluation of the upper abdomen, more extrapelvic endometriosis – including disease in the upper abdomen and diaphragm – is being diagnosed. The thoracic and visceral diaphragm are the most commonly described sites of thoracic endometriosis, and disease is often right sided, with parenchymal involvement less commonly reported.
Abdominopelvic and visceral diaphragmatic endometriosis are treated endoscopically with hydrodissection followed by excision or ablation. Superficial lesions away from the central diaphragm can be coagulated using bipolar current.
Thoracoscopic treatment varies, involving ablation or excision of smaller diaphragmatic lesions, pulmonary wedge resection of deep parenchymal nodules (using a stapling device), diaphragm resection of deep diaphragmatic lesions using a stapling device, or by excision and manual suturing.
Endoscopic diagnosis and treatment begins by introducing a 10-mm port at the umbilicus and placing three additional ports in the upper quadrant (right or left, depending on implant location). The arrangement (similar to that of a laparoscopic cholecystectomy or splenectomy) allows for examination of the posterior portion of the right hemidiaphragm and almost the entire left hemidiaphragm in addition to routine abdominopelvic exploration.
For better laparoscopic visualization, the patient is repositioned in steep reverse Trendelenburg, and the liver is gently pushed caudally to view the adjacent diaphragm. The upper abdominal walls and the liver also may be evaluated while in this position.
Bluish pigmented lesions are the most commonly reported form of diaphragmatic endometriosis, followed by lesions with a reddish-purple appearance. However, lesions can present with various colors and morphologic appearances, such as fibrotic white lesions or adhesions to the liver.
In our practice, we recommend using the CO2 laser (set at 20-25 watts) with hydrodissection for superficial lesions. The CO2 laser is much more precise and has a smaller depth of penetration and less thermal spread, compared with electrocautery. The CO2 laser beam also reaches otherwise hard-to-access areas behind the liver and has proven to be safe for vaporizing and/or excising many types of diaphragmatic lesions. We have successfully treated diaphragmatic endometriosis in the vicinity of the phrenic nerve and directly in line with the left ventricle.
Watch a video from Dr. Ceana Nezhat demonstrating a step wise vaporization and excision of diaphragmatic endometriosis utilizing different techniques.
(Courtesy Dr. Ceana Nezhat)
Plasma jet energy and ultrasonic energy are good alternatives when a CO2 laser is not available and are preferable to the use of cold scissors because of subsequent bleeding, which requires bipolar hemostasis.
Monopolar electrocautery is not as good a choice for treating diaphragmatic endometriosis because of higher depth of penetration, which may cause tissue necrosis and subsequent delayed diaphragmatic fenestrations. It also may cause unpredictable diaphragmatic muscular contractions and electrical conduction transmitted to the heart, inducing arrhythmia.
For patients treated via combined VALS and VATS procedures, endometriotic lesions involving the entire thickness of the diaphragm should be completely resected, and the defect can be repaired with either sutures or staples.
In all cases, special anesthesia considerations must be made given the inability to completely ventilate the lung. In our practice, we use a double-lumen endotracheal tube for single lung ventilation, if needed. A bronchial blocker is used to isolate the lung when the double-lumen endotracheal tube cannot be inserted.
It is important to note that we do not recommend VATS with VALS in all suspicious cases. We reserve VATS only for patients with catamenial pneumothorax, catamenial hemothorax, hemoptysis, and pulmonary nodules, defined as Thoracic Endometriosis Syndrome. We usually start with medical management first, then proceed to VALS, and finally, VATS, with the intention to treat if the patient fails nonsurgical treatments. It is better to avoid VATS, if possible, because it is associated with longer recovery and more pain; it should be done if all else fails.
If the patient has completed childbearing or passed reproductive age, bilateral salpingectomy, or hysterectomy with or without bilateral salpingo-oophorectomy, may be considered as the first step prior to more aggressive excisional procedures. This is especially true for widespread lesions, as branches of the phrenic nerve are difficult to see and injury could result in paralysis of the diaphragm. It’s important to appreciate that if estrogen stimulation to the diaphragmatic lesions is to cease for the long term, hormonal suppression or surgical treatment including bilateral oophorectomy should be utilized.
My colleagues and I have reported on our experience with a multidisciplinary approach in the treatment of diaphragmatic endometriosis in 25 patients. All had both pelvic and thoracic symptoms, and the majority had endometrial implants on both the thoracic and visceral sides of the diaphragm.
There were two postoperative complications: a diaphragmatic hernia and a vaginal cuff hematoma. Over a follow-up period of 3-18 months, all 25 patients had significant improvement or resolution of their chest complaints, and most remained asymptomatic for more than 6 months (JSLS. 2014 Jul-Sep;18[3]. pii: e2014.00312. doi: 10.4293/JSLS.2014.00312).
Dr. Ceana Nezhat is the fellowship director of Nezhat Medical Center, the medical director of training and education at Northside Hospital, and an adjunct clinical professor of gynecology and obstetrics at Emory University, all in Atlanta. He is president of SRS (Society of Reproductive Surgeons) and past president of AAGL (American Association of Gynecologic Laparoscopists). Dr. Nezhat is a consultant for Novuson Surgical, Karl Storz Endoscopy, Lumenis, and AbbVie; a medical advisor for Plasma Surgical, and a member of the scientific advisory board for SurgiQuest.
Suggested readings
1. Nezhat C, Nezhat F, Nezhat C. Nezhat’s Operative Gynecologic Laparoscopy with Hysteroscopy. Fourth Edition. Cambridge University Press. 2013.
2. Am J Med. 1996 Feb;100(2):164-70.
3. Fertil Steril. 1998 Jun;69(6):1048-55.
4. Clin Obstet Gynecol. 1999 Sep;42(3):699-711.
5. JSLS. 2012 Jan-Mar; 16(1):140-2.

Diaphragmatic and thoracic endometriosis
The first case of diaphragmatic endometriosis was reported by Alan Brews in 19541. Unfortunately, no guidelines exist to enhance the recognition and treatment.
Diaphragmatic and thoracic endometriosis often is overlooked by the gynecologist, not only because of lack of appreciation of the symptoms but also because of the failure to properly work-up the patient and evaluate the diaphragm at time of surgery. In a retrospective review of 3,008 patients with pelvic endometriosis published in Surgical Endoscopy in 2013, Marcello Ceccaroni, MD, PhD, and his colleagues found 46 cases (1.53%) with the intraoperative diagnosis of diaphragmatic endometriosis, six with liver involvement. Multiple diaphragmatic endometriosis lesions were seen in 70% of patients and, the vast majority being right-sided lesions (87%), with 11% of cases having bilateral lesions.2 While in the study, superficial lesions were generally vaporized using the argon beam coagulator, deep lesions were removed by sharp dissection, highlighting the need to have adequately trained minimally invasive surgeons treating diaphragmatic lesions via incision. If a pneumothorax occurred, and reabsorbable suture was placed after adequate expansion of the lung via positive pressure ventilation and progressive air suctioning with complete evacuation of the pneumothorax prior to the final closure (i.e., a purse string around the suction device), then the integrity of the closure could be proven using a bubble test with 500cc of saline placed at the diaphragm.

As the gynecologic surgeon studies Dr. Nezhat’s thorough discourse, it is obvious that, at times, a multidisciplinary team must be involved. Although possible, it would appear that risk of diaphragm paralysis secondary to injury of the phrenic nerve is indeed rare. This likely is because of the greater incidence of right-sided disease, rather than involving the central tendon, and lower likelihood that the lesion penetrates deeply. Nevertheless, a prudent multidisciplinary approach and knowledge of the anatomy will inevitably further reduce this rare complication.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago; director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column. He reported having no financial disclosures related to this column.
References
1. Proc R Soc Med. 1954 Jun; 47(6):461-8.
2. Surg Endosc. 2013 Feb;27(2):625-32.
The first case of diaphragmatic endometriosis was reported by Alan Brews in 19541. Unfortunately, no guidelines exist to enhance the recognition and treatment.
Diaphragmatic and thoracic endometriosis often is overlooked by the gynecologist, not only because of lack of appreciation of the symptoms but also because of the failure to properly work-up the patient and evaluate the diaphragm at time of surgery. In a retrospective review of 3,008 patients with pelvic endometriosis published in Surgical Endoscopy in 2013, Marcello Ceccaroni, MD, PhD, and his colleagues found 46 cases (1.53%) with the intraoperative diagnosis of diaphragmatic endometriosis, six with liver involvement. Multiple diaphragmatic endometriosis lesions were seen in 70% of patients and, the vast majority being right-sided lesions (87%), with 11% of cases having bilateral lesions.2 While in the study, superficial lesions were generally vaporized using the argon beam coagulator, deep lesions were removed by sharp dissection, highlighting the need to have adequately trained minimally invasive surgeons treating diaphragmatic lesions via incision. If a pneumothorax occurred, and reabsorbable suture was placed after adequate expansion of the lung via positive pressure ventilation and progressive air suctioning with complete evacuation of the pneumothorax prior to the final closure (i.e., a purse string around the suction device), then the integrity of the closure could be proven using a bubble test with 500cc of saline placed at the diaphragm.
As the gynecologic surgeon studies Dr. Nezhat’s thorough discourse, it is obvious that, at times, a multidisciplinary team must be involved. Although possible, it would appear that risk of diaphragm paralysis secondary to injury of the phrenic nerve is indeed rare. This likely is because of the greater incidence of right-sided disease, rather than involving the central tendon, and lower likelihood that the lesion penetrates deeply. Nevertheless, a prudent multidisciplinary approach and knowledge of the anatomy will inevitably further reduce this rare complication.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago; director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column. He reported having no financial disclosures related to this column.
References
1. Proc R Soc Med. 1954 Jun; 47(6):461-8.
2. Surg Endosc. 2013 Feb;27(2):625-32.
The first case of diaphragmatic endometriosis was reported by Alan Brews in 19541. Unfortunately, no guidelines exist to enhance the recognition and treatment.
Diaphragmatic and thoracic endometriosis often is overlooked by the gynecologist, not only because of lack of appreciation of the symptoms but also because of the failure to properly work-up the patient and evaluate the diaphragm at time of surgery. In a retrospective review of 3,008 patients with pelvic endometriosis published in Surgical Endoscopy in 2013, Marcello Ceccaroni, MD, PhD, and his colleagues found 46 cases (1.53%) with the intraoperative diagnosis of diaphragmatic endometriosis, six with liver involvement. Multiple diaphragmatic endometriosis lesions were seen in 70% of patients and, the vast majority being right-sided lesions (87%), with 11% of cases having bilateral lesions.2 While in the study, superficial lesions were generally vaporized using the argon beam coagulator, deep lesions were removed by sharp dissection, highlighting the need to have adequately trained minimally invasive surgeons treating diaphragmatic lesions via incision. If a pneumothorax occurred, and reabsorbable suture was placed after adequate expansion of the lung via positive pressure ventilation and progressive air suctioning with complete evacuation of the pneumothorax prior to the final closure (i.e., a purse string around the suction device), then the integrity of the closure could be proven using a bubble test with 500cc of saline placed at the diaphragm.
As the gynecologic surgeon studies Dr. Nezhat’s thorough discourse, it is obvious that, at times, a multidisciplinary team must be involved. Although possible, it would appear that risk of diaphragm paralysis secondary to injury of the phrenic nerve is indeed rare. This likely is because of the greater incidence of right-sided disease, rather than involving the central tendon, and lower likelihood that the lesion penetrates deeply. Nevertheless, a prudent multidisciplinary approach and knowledge of the anatomy will inevitably further reduce this rare complication.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago and past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in metropolitan Chicago; director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column. He reported having no financial disclosures related to this column.
References
1. Proc R Soc Med. 1954 Jun; 47(6):461-8.
2. Surg Endosc. 2013 Feb;27(2):625-32.

Improving our approach to discharge planning
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Since finishing up the initial planning phase of our project, my mentors and I have continued with even more planning as we head into the fall. Coming up with a good plan is the first step in making sure everything goes smoothly later on in a project. The same goes for coming up with a well-thought-out discharge plan when sending a patient to the next level of care.

Getting a patient out of the hospital and into their next destination – whether it’s a long-term acute care facility, skilled nursing facility, inpatient rehabilitation, home, or elsewhere – can approach the same level of complexity as the medical care received in the hospital. Getting a patient to any post-acute care facility can be time-consuming because it involves the coordination of two health care entities and their employees.
Discharge planning for post-acute care placement can take many forms and involve many resources. Some studies have shown that certain discharge planning interventions can reduce costs and 30-day readmissions. Many physicians think that discharge planning would help improve outcomes in most groups, but so far the aggregate data do not show that discharge planning account for much improvement in any of these outcomes. Targeting certain groups of hospitalized patients, however, could improve the effect that discharge planning has on these outcomes because more of these scarce resources might be devoted to the right patients earlier in their hospital stays.
A post-acute care placement prediction tool would help hospitalists determine how to allocate their discharge planning resources, including social work, case management, pharmacies, physical therapy, and occupational therapy. While we are working towards integrating this kind of tool in our own institution’s practice, we are also hopeful that we can create a generalizable tool that assists in helping care teams decide how to link patients to the right resources elsewhere.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Since finishing up the initial planning phase of our project, my mentors and I have continued with even more planning as we head into the fall. Coming up with a good plan is the first step in making sure everything goes smoothly later on in a project. The same goes for coming up with a well-thought-out discharge plan when sending a patient to the next level of care.
Getting a patient out of the hospital and into their next destination – whether it’s a long-term acute care facility, skilled nursing facility, inpatient rehabilitation, home, or elsewhere – can approach the same level of complexity as the medical care received in the hospital. Getting a patient to any post-acute care facility can be time-consuming because it involves the coordination of two health care entities and their employees.
Discharge planning for post-acute care placement can take many forms and involve many resources. Some studies have shown that certain discharge planning interventions can reduce costs and 30-day readmissions. Many physicians think that discharge planning would help improve outcomes in most groups, but so far the aggregate data do not show that discharge planning account for much improvement in any of these outcomes. Targeting certain groups of hospitalized patients, however, could improve the effect that discharge planning has on these outcomes because more of these scarce resources might be devoted to the right patients earlier in their hospital stays.
A post-acute care placement prediction tool would help hospitalists determine how to allocate their discharge planning resources, including social work, case management, pharmacies, physical therapy, and occupational therapy. While we are working towards integrating this kind of tool in our own institution’s practice, we are also hopeful that we can create a generalizable tool that assists in helping care teams decide how to link patients to the right resources elsewhere.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
Since finishing up the initial planning phase of our project, my mentors and I have continued with even more planning as we head into the fall. Coming up with a good plan is the first step in making sure everything goes smoothly later on in a project. The same goes for coming up with a well-thought-out discharge plan when sending a patient to the next level of care.
Getting a patient out of the hospital and into their next destination – whether it’s a long-term acute care facility, skilled nursing facility, inpatient rehabilitation, home, or elsewhere – can approach the same level of complexity as the medical care received in the hospital. Getting a patient to any post-acute care facility can be time-consuming because it involves the coordination of two health care entities and their employees.
Discharge planning for post-acute care placement can take many forms and involve many resources. Some studies have shown that certain discharge planning interventions can reduce costs and 30-day readmissions. Many physicians think that discharge planning would help improve outcomes in most groups, but so far the aggregate data do not show that discharge planning account for much improvement in any of these outcomes. Targeting certain groups of hospitalized patients, however, could improve the effect that discharge planning has on these outcomes because more of these scarce resources might be devoted to the right patients earlier in their hospital stays.
A post-acute care placement prediction tool would help hospitalists determine how to allocate their discharge planning resources, including social work, case management, pharmacies, physical therapy, and occupational therapy. While we are working towards integrating this kind of tool in our own institution’s practice, we are also hopeful that we can create a generalizable tool that assists in helping care teams decide how to link patients to the right resources elsewhere.
Monisha Bhatia, a native of Nashville, Tenn., is a fourth-year medical student at Vanderbilt University in Nashville. She is hoping to pursue either a residency in internal medicine or a combined internal medicine/emergency medicine program. Prior to medical school, she completed a JD/MPH program at Boston University, and she hopes to use her legal training in working with regulatory authorities to improve access to health care for all Americans.
Letter from an associate editor: Hurricane Harvey’s wrath
It seemed appropriate this month for me to step aside for the Editor’s commentary and provide a forum for one of our associate editors to talk about his experience during Hurricane Harvey.
John I. Allen, MD, MBA, AGAF
Editor in Chief
We knew that a powerful storm was coming, but very few anticipated the widespread destruction Hurricane Harvey would bring. Houston is no stranger to floods, but the amount of water that Harvey unleashed was record-breaking. Areas that had never flooded were underwater, evacuations were commonplace; the devastation was heart-breaking. In the midst of significant personal tragedy, Houston came together. Neighbors took in flooded colleagues, personal boats were used for rescues, and many braved impassable roads to donate clothes, food, labor and medical aid. Shelters across the city were assisted by volunteers; community groups collected and coordinated distribution of supplies. Medical teams were mobilized to treat chronically ill patients who evacuated without their medications or those injured while escaping the floods.
At one of the largest medical centers in the world, floodgates constructed after Tropical Storm Allison kept the waters at bay. And physicians, nurses, janitors, and other employees slept in hospitals for days to provide care to our patients during the worst of the floods. Those who relieved them worked long hours to see the many patients rescheduled in the aftermath of the storm. After-work crews of neighbors continue to go from house to house removing flooded floor boards and ripping out drywall. Houston came together.

Dr. Ketwaroo is an assistant professor in the division of gastroenterology and hepatology at Baylor College of Medicine, Houston, and an advanced endoscopist at the Michael E. Debakey VA Medical Center in Houston. He is an associate editor for GI & Hepatology News.
It seemed appropriate this month for me to step aside for the Editor’s commentary and provide a forum for one of our associate editors to talk about his experience during Hurricane Harvey.
John I. Allen, MD, MBA, AGAF
Editor in Chief
We knew that a powerful storm was coming, but very few anticipated the widespread destruction Hurricane Harvey would bring. Houston is no stranger to floods, but the amount of water that Harvey unleashed was record-breaking. Areas that had never flooded were underwater, evacuations were commonplace; the devastation was heart-breaking. In the midst of significant personal tragedy, Houston came together. Neighbors took in flooded colleagues, personal boats were used for rescues, and many braved impassable roads to donate clothes, food, labor and medical aid. Shelters across the city were assisted by volunteers; community groups collected and coordinated distribution of supplies. Medical teams were mobilized to treat chronically ill patients who evacuated without their medications or those injured while escaping the floods.
At one of the largest medical centers in the world, floodgates constructed after Tropical Storm Allison kept the waters at bay. And physicians, nurses, janitors, and other employees slept in hospitals for days to provide care to our patients during the worst of the floods. Those who relieved them worked long hours to see the many patients rescheduled in the aftermath of the storm. After-work crews of neighbors continue to go from house to house removing flooded floor boards and ripping out drywall. Houston came together.
Dr. Ketwaroo is an assistant professor in the division of gastroenterology and hepatology at Baylor College of Medicine, Houston, and an advanced endoscopist at the Michael E. Debakey VA Medical Center in Houston. He is an associate editor for GI & Hepatology News.
It seemed appropriate this month for me to step aside for the Editor’s commentary and provide a forum for one of our associate editors to talk about his experience during Hurricane Harvey.
John I. Allen, MD, MBA, AGAF
Editor in Chief
We knew that a powerful storm was coming, but very few anticipated the widespread destruction Hurricane Harvey would bring. Houston is no stranger to floods, but the amount of water that Harvey unleashed was record-breaking. Areas that had never flooded were underwater, evacuations were commonplace; the devastation was heart-breaking. In the midst of significant personal tragedy, Houston came together. Neighbors took in flooded colleagues, personal boats were used for rescues, and many braved impassable roads to donate clothes, food, labor and medical aid. Shelters across the city were assisted by volunteers; community groups collected and coordinated distribution of supplies. Medical teams were mobilized to treat chronically ill patients who evacuated without their medications or those injured while escaping the floods.
At one of the largest medical centers in the world, floodgates constructed after Tropical Storm Allison kept the waters at bay. And physicians, nurses, janitors, and other employees slept in hospitals for days to provide care to our patients during the worst of the floods. Those who relieved them worked long hours to see the many patients rescheduled in the aftermath of the storm. After-work crews of neighbors continue to go from house to house removing flooded floor boards and ripping out drywall. Houston came together.
Dr. Ketwaroo is an assistant professor in the division of gastroenterology and hepatology at Baylor College of Medicine, Houston, and an advanced endoscopist at the Michael E. Debakey VA Medical Center in Houston. He is an associate editor for GI & Hepatology News.

The AHRQ Toolbox: Tools for negotiating shared decision making
This is the second in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Shared decision making means the decision takes into account evidence-based information about available options, the provider’s knowledge and experience, and the patient’s values and preferences. More and more patients and providers want to participate in shared decision making, but the “how” often is neglected in standard medical and graduate medical education. AHRQ provides two resources to assist in your practice’s use of shared decision making.
The SHARE Approach is a five-step process for shared decision making:
- Seek your patient’s participation.
- Help your patient explore & compare treatment options.
- Assess your patient’s values and preferences.
- Reach a decision with your patient.
- Evaluate your patient’s decision.
AHRQ’s SHARE Approach curriculum provides both a quick overview (for the busy clinician) and an extensive course (complete with slides and a trainer’s module). The website provides the clinician the opportunity to learn the key elements of the SHARE Approach, while providing the educator a full curriculum with slides, handouts, and a video in order to demonstrate the approach. Complementing the SHARE curriculum, AHRQ’s Effective Health Care Program offers excellent, easy-to-read summaries of evidence reports to help clinicians and consumers make informed health care decisions. AHRQ recently released Lung Cancer Screening Tools, including a decision aid, for patients and clinicians to facilitate discussions about lung cancer screening with low-dose computed tomography.
The SHARE Approach and other tools can be found at the NCEPCR website.
Dr. Bierman is the director of the Center for Evidence and Practice Improvement at AHRQ. Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
This is the second in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Shared decision making means the decision takes into account evidence-based information about available options, the provider’s knowledge and experience, and the patient’s values and preferences. More and more patients and providers want to participate in shared decision making, but the “how” often is neglected in standard medical and graduate medical education. AHRQ provides two resources to assist in your practice’s use of shared decision making.
The SHARE Approach is a five-step process for shared decision making:
- Seek your patient’s participation.
- Help your patient explore & compare treatment options.
- Assess your patient’s values and preferences.
- Reach a decision with your patient.
- Evaluate your patient’s decision.
AHRQ’s SHARE Approach curriculum provides both a quick overview (for the busy clinician) and an extensive course (complete with slides and a trainer’s module). The website provides the clinician the opportunity to learn the key elements of the SHARE Approach, while providing the educator a full curriculum with slides, handouts, and a video in order to demonstrate the approach. Complementing the SHARE curriculum, AHRQ’s Effective Health Care Program offers excellent, easy-to-read summaries of evidence reports to help clinicians and consumers make informed health care decisions. AHRQ recently released Lung Cancer Screening Tools, including a decision aid, for patients and clinicians to facilitate discussions about lung cancer screening with low-dose computed tomography.
The SHARE Approach and other tools can be found at the NCEPCR website.
Dr. Bierman is the director of the Center for Evidence and Practice Improvement at AHRQ. Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
This is the second in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Shared decision making means the decision takes into account evidence-based information about available options, the provider’s knowledge and experience, and the patient’s values and preferences. More and more patients and providers want to participate in shared decision making, but the “how” often is neglected in standard medical and graduate medical education. AHRQ provides two resources to assist in your practice’s use of shared decision making.
The SHARE Approach is a five-step process for shared decision making:
- Seek your patient’s participation.
- Help your patient explore & compare treatment options.
- Assess your patient’s values and preferences.
- Reach a decision with your patient.
- Evaluate your patient’s decision.
AHRQ’s SHARE Approach curriculum provides both a quick overview (for the busy clinician) and an extensive course (complete with slides and a trainer’s module). The website provides the clinician the opportunity to learn the key elements of the SHARE Approach, while providing the educator a full curriculum with slides, handouts, and a video in order to demonstrate the approach. Complementing the SHARE curriculum, AHRQ’s Effective Health Care Program offers excellent, easy-to-read summaries of evidence reports to help clinicians and consumers make informed health care decisions. AHRQ recently released Lung Cancer Screening Tools, including a decision aid, for patients and clinicians to facilitate discussions about lung cancer screening with low-dose computed tomography.
The SHARE Approach and other tools can be found at the NCEPCR website.
Dr. Bierman is the director of the Center for Evidence and Practice Improvement at AHRQ. Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
Under our noses
If you graduated from medical school after 1990, you may be surprised to learn that there was a time when the typical general pediatrician could go through an entire day of seeing patients and not write a single prescription for a stimulant medication. In fact, he or she could go for several months without writing for any controlled substance.
ADHD is a modern phenomenon. There always have been children with “ants in their pants” who couldn’t sit still. And there always were “daydreamers” who didn’t pay attention in school. But in the 1970s, the number of children who might now be labeled as having ADHD was nowhere near the 11% often quoted for the prevalence in the current pediatric population.
Could there be some genetic selection process that is favoring the birth and survival of hyperactive and distractible children? In the last decade or two, biologists have discovered evolutionary changes in some animals occurring at pace far faster than had been previously imagined. However, a Darwinian explanation seems unlikely in the case of the emergence of ADHD.
Could it be a diet laced with high fructose sugars or artificial dyes and food coloring? While there continues to be a significant number of parents whose anecdotal observations point to a relationship between diet and behavior, to date controlled studies have not supported a dietary cause for the ADHD phenomenon.
Within a few years of beginning my dual careers as parent and pediatrician, I began to notice that children who were sleep deprived often were distractible and inattentive. Some also were hyperactive, an observation that initially seemed counterintuitive. Over the ensuing four decades, I have become more convinced that a substantial driver of the emergence of the ADHD phenomenon is the fact that the North American lifestyle places sleep so far down on its priority list that a significant percentage of both the pediatric and adult populations are sleep deprived.
I freely admit that my initial anecdotal observations have evolved to the point of an obsession. Of course, I look at the data that show that children are getting less sleep than they did a century ago and suspect that this decline must somehow be reflected in their behavior (“Never enough sleep: A brief history of sleep recommendations for children” by Matricciani et al. Pediatrics. 2012 Mar;129[3]:548-56). And, of course, I wonder whether the success and popularity of stimulant medication to treat ADHD is just chance or whether it simply could be waking up a bunch of children who aren’t getting enough sleep.
At times, it has been a lonely several decades, trying to convince parents and other pediatricians that sleep may be the answer. I can’t point to my own research because I have been too busy doing general pediatrics. I can only point to the observations of others that fit into my construct.
You can imagine the warm glow that swept over me when I came across an article in the Washington Post titled “Could some ADHD be a type of sleep disorder? That would fundamentally change how we treat it” (A.E. Cha, Sep. 20, 2017). The studies referred to in the article are not terribly earth shaking. But it was nice to read some quotes in a national newspaper from scientists who share my suspicions about sleep deprivation as a major contributor to the ADHD phenomenon. I instantly felt less lonely.
Unfortunately, it is still a long way from this token recognition in the Washington Post to convincing parents and pediatricians to do the heavy lifting that will be required to undo decades of our society’s sleep-unfriendly norms. It’s so much easier to pull out a prescription pad and write for a stimulant.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Email him at pdnews@frontlinemedcom.com.
If you graduated from medical school after 1990, you may be surprised to learn that there was a time when the typical general pediatrician could go through an entire day of seeing patients and not write a single prescription for a stimulant medication. In fact, he or she could go for several months without writing for any controlled substance.
ADHD is a modern phenomenon. There always have been children with “ants in their pants” who couldn’t sit still. And there always were “daydreamers” who didn’t pay attention in school. But in the 1970s, the number of children who might now be labeled as having ADHD was nowhere near the 11% often quoted for the prevalence in the current pediatric population.
Could there be some genetic selection process that is favoring the birth and survival of hyperactive and distractible children? In the last decade or two, biologists have discovered evolutionary changes in some animals occurring at pace far faster than had been previously imagined. However, a Darwinian explanation seems unlikely in the case of the emergence of ADHD.
Could it be a diet laced with high fructose sugars or artificial dyes and food coloring? While there continues to be a significant number of parents whose anecdotal observations point to a relationship between diet and behavior, to date controlled studies have not supported a dietary cause for the ADHD phenomenon.
Within a few years of beginning my dual careers as parent and pediatrician, I began to notice that children who were sleep deprived often were distractible and inattentive. Some also were hyperactive, an observation that initially seemed counterintuitive. Over the ensuing four decades, I have become more convinced that a substantial driver of the emergence of the ADHD phenomenon is the fact that the North American lifestyle places sleep so far down on its priority list that a significant percentage of both the pediatric and adult populations are sleep deprived.
I freely admit that my initial anecdotal observations have evolved to the point of an obsession. Of course, I look at the data that show that children are getting less sleep than they did a century ago and suspect that this decline must somehow be reflected in their behavior (“Never enough sleep: A brief history of sleep recommendations for children” by Matricciani et al. Pediatrics. 2012 Mar;129[3]:548-56). And, of course, I wonder whether the success and popularity of stimulant medication to treat ADHD is just chance or whether it simply could be waking up a bunch of children who aren’t getting enough sleep.
At times, it has been a lonely several decades, trying to convince parents and other pediatricians that sleep may be the answer. I can’t point to my own research because I have been too busy doing general pediatrics. I can only point to the observations of others that fit into my construct.
You can imagine the warm glow that swept over me when I came across an article in the Washington Post titled “Could some ADHD be a type of sleep disorder? That would fundamentally change how we treat it” (A.E. Cha, Sep. 20, 2017). The studies referred to in the article are not terribly earth shaking. But it was nice to read some quotes in a national newspaper from scientists who share my suspicions about sleep deprivation as a major contributor to the ADHD phenomenon. I instantly felt less lonely.
Unfortunately, it is still a long way from this token recognition in the Washington Post to convincing parents and pediatricians to do the heavy lifting that will be required to undo decades of our society’s sleep-unfriendly norms. It’s so much easier to pull out a prescription pad and write for a stimulant.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Email him at pdnews@frontlinemedcom.com.
If you graduated from medical school after 1990, you may be surprised to learn that there was a time when the typical general pediatrician could go through an entire day of seeing patients and not write a single prescription for a stimulant medication. In fact, he or she could go for several months without writing for any controlled substance.
ADHD is a modern phenomenon. There always have been children with “ants in their pants” who couldn’t sit still. And there always were “daydreamers” who didn’t pay attention in school. But in the 1970s, the number of children who might now be labeled as having ADHD was nowhere near the 11% often quoted for the prevalence in the current pediatric population.
Could there be some genetic selection process that is favoring the birth and survival of hyperactive and distractible children? In the last decade or two, biologists have discovered evolutionary changes in some animals occurring at pace far faster than had been previously imagined. However, a Darwinian explanation seems unlikely in the case of the emergence of ADHD.
Could it be a diet laced with high fructose sugars or artificial dyes and food coloring? While there continues to be a significant number of parents whose anecdotal observations point to a relationship between diet and behavior, to date controlled studies have not supported a dietary cause for the ADHD phenomenon.
Within a few years of beginning my dual careers as parent and pediatrician, I began to notice that children who were sleep deprived often were distractible and inattentive. Some also were hyperactive, an observation that initially seemed counterintuitive. Over the ensuing four decades, I have become more convinced that a substantial driver of the emergence of the ADHD phenomenon is the fact that the North American lifestyle places sleep so far down on its priority list that a significant percentage of both the pediatric and adult populations are sleep deprived.
I freely admit that my initial anecdotal observations have evolved to the point of an obsession. Of course, I look at the data that show that children are getting less sleep than they did a century ago and suspect that this decline must somehow be reflected in their behavior (“Never enough sleep: A brief history of sleep recommendations for children” by Matricciani et al. Pediatrics. 2012 Mar;129[3]:548-56). And, of course, I wonder whether the success and popularity of stimulant medication to treat ADHD is just chance or whether it simply could be waking up a bunch of children who aren’t getting enough sleep.
At times, it has been a lonely several decades, trying to convince parents and other pediatricians that sleep may be the answer. I can’t point to my own research because I have been too busy doing general pediatrics. I can only point to the observations of others that fit into my construct.
You can imagine the warm glow that swept over me when I came across an article in the Washington Post titled “Could some ADHD be a type of sleep disorder? That would fundamentally change how we treat it” (A.E. Cha, Sep. 20, 2017). The studies referred to in the article are not terribly earth shaking. But it was nice to read some quotes in a national newspaper from scientists who share my suspicions about sleep deprivation as a major contributor to the ADHD phenomenon. I instantly felt less lonely.
Unfortunately, it is still a long way from this token recognition in the Washington Post to convincing parents and pediatricians to do the heavy lifting that will be required to undo decades of our society’s sleep-unfriendly norms. It’s so much easier to pull out a prescription pad and write for a stimulant.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Email him at pdnews@frontlinemedcom.com.
‘Without clinical prodrome’
For the most part pediatricians are insulated from death. Our little patients are surprisingly resilient. Once past that anxiety-provoking transition from placental dependence to air breathing, children will thrive in an environment that includes immunizations, potable water, and adequate nutrition. But pediatric deaths do occur infrequently in North America, and they are particularly unsettling to us because we are so unaccustomed to processing the emotions that swirl around the end of life. Did I miss something at the last health maintenance visit? Should I have taken more seriously that call last week about what sounded like a simple viral prodrome? Should I have asked that mother to make an appointment?

Their approach, which has been labeled the Robert’s Program, is particularly appealing because it is careful to address the families’ concerns about their surviving and future children. I found the inclusion of the dead child’s pediatrician and the office of the chief medical examiner in the summation of the investigation especially appealing.
However, I have trouble envisioning how this novel approach, funded by several philanthropic organizations, could be rolled out on a larger scale. Here in Maine and in many other smaller cash-strapped communities, the medical examiner’s office is overburdened with opioid overdoses and traumatic deaths. The police and sheriffs’ departments may lack sufficient training and experience to do careful scene investigations.
In reviewing the summary of the 17 deaths included in the article, I was struck by the inclusion of 3 cases in which the final cause of death was meningitis or encephalitis “without clinical prodrome.”
While a thorough investigation did eventually unearth the cause of death in these three cases, it is in that devilish prodrome that the seeds of guilt can continue to germinate. Parents and physicians will continue to wonder whether someone else with more sensitive antennae might have picked up those early signs of impending disaster. The answer is that there probably wasn’t anyone with better antennae, but there may have been someone with better luck.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
For the most part pediatricians are insulated from death. Our little patients are surprisingly resilient. Once past that anxiety-provoking transition from placental dependence to air breathing, children will thrive in an environment that includes immunizations, potable water, and adequate nutrition. But pediatric deaths do occur infrequently in North America, and they are particularly unsettling to us because we are so unaccustomed to processing the emotions that swirl around the end of life. Did I miss something at the last health maintenance visit? Should I have taken more seriously that call last week about what sounded like a simple viral prodrome? Should I have asked that mother to make an appointment?
Their approach, which has been labeled the Robert’s Program, is particularly appealing because it is careful to address the families’ concerns about their surviving and future children. I found the inclusion of the dead child’s pediatrician and the office of the chief medical examiner in the summation of the investigation especially appealing.
However, I have trouble envisioning how this novel approach, funded by several philanthropic organizations, could be rolled out on a larger scale. Here in Maine and in many other smaller cash-strapped communities, the medical examiner’s office is overburdened with opioid overdoses and traumatic deaths. The police and sheriffs’ departments may lack sufficient training and experience to do careful scene investigations.
In reviewing the summary of the 17 deaths included in the article, I was struck by the inclusion of 3 cases in which the final cause of death was meningitis or encephalitis “without clinical prodrome.”
While a thorough investigation did eventually unearth the cause of death in these three cases, it is in that devilish prodrome that the seeds of guilt can continue to germinate. Parents and physicians will continue to wonder whether someone else with more sensitive antennae might have picked up those early signs of impending disaster. The answer is that there probably wasn’t anyone with better antennae, but there may have been someone with better luck.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
For the most part pediatricians are insulated from death. Our little patients are surprisingly resilient. Once past that anxiety-provoking transition from placental dependence to air breathing, children will thrive in an environment that includes immunizations, potable water, and adequate nutrition. But pediatric deaths do occur infrequently in North America, and they are particularly unsettling to us because we are so unaccustomed to processing the emotions that swirl around the end of life. Did I miss something at the last health maintenance visit? Should I have taken more seriously that call last week about what sounded like a simple viral prodrome? Should I have asked that mother to make an appointment?
Their approach, which has been labeled the Robert’s Program, is particularly appealing because it is careful to address the families’ concerns about their surviving and future children. I found the inclusion of the dead child’s pediatrician and the office of the chief medical examiner in the summation of the investigation especially appealing.
However, I have trouble envisioning how this novel approach, funded by several philanthropic organizations, could be rolled out on a larger scale. Here in Maine and in many other smaller cash-strapped communities, the medical examiner’s office is overburdened with opioid overdoses and traumatic deaths. The police and sheriffs’ departments may lack sufficient training and experience to do careful scene investigations.
In reviewing the summary of the 17 deaths included in the article, I was struck by the inclusion of 3 cases in which the final cause of death was meningitis or encephalitis “without clinical prodrome.”
While a thorough investigation did eventually unearth the cause of death in these three cases, it is in that devilish prodrome that the seeds of guilt can continue to germinate. Parents and physicians will continue to wonder whether someone else with more sensitive antennae might have picked up those early signs of impending disaster. The answer is that there probably wasn’t anyone with better antennae, but there may have been someone with better luck.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
The cost of leadership
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.
Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.
Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Do you practice as a team member? How is your team defined? Is it made up solely of physicians? Does it include mid-level providers? Does it extend to mental health and social service providers in your office? Do you consider nonproviders such as receptionists as team members? Do you consider the whole office “your team”? Or, is it a smaller team with just yourself and one or two other physicians along with a mid-level provider or two?
There has been a lot written about primary care teams as a natural consequence of the medical home model. In an article in AAP News, Gonzalo J. Paz-Soldán, MD, a member of the American Academy of Pediatrics Council on Community Pediatrics and regional executive medical director, pediatrics, at Reliant Medical Group, Worcester, Mass., suggests that pediatricians should be taking on leadership roles in directing these teams. He claims that in addition to improving the “quality, value, patient experience,” our leadership also will benefit “provider and staff wellness and engagement.” In other words, taking charge will return the joy of pediatrics, and make us more resilient in the face of burnout.
It’s hard to argue with the notion that having more control improves our chances of satisfaction. Most of us who owned and ran our own small practices will tell you that when we were captains of the ship, those were our most rewarding and productive years.
However, assuming a leadership in a large multilevel team of providers and support staff is another story. As Dr. Paz-Soldán observes, most of us were not trained for leadership roles. I would add that the path to medical school does not select for those skills or interest. In addition to requiring a certain set of skill and aptitudes that we may not have, leadership demands a substantial time commitment.
Leading means attending what are often poorly conceived meetings (the topic for a future Letters from Maine), and receiving and writing emails – none of which involve actually taking care of patients. Like it or not, the ugly truth is that seeing patients is what generates our bottom lines. Time spent going to meetings and communicating with your teams members cannot be considered “billable hours.”
So here is our dilemma: Do we abandon the solo and small group practice model, sell out to large entities, lose control of our professional destiny, and spend our time grousing about it? Or
There are a few saintly and gifted physicians who have the skills, energy, and commitment to become leaders and still spend enough time seeing patients to satisfy both their emotional and financial professional needs. However, in my experience, when physicians move into leadership roles, the additional responsibilities cannibalize their commitment to patient care and the skills that made them talented physicians.
Given my aversion to meetings and my disinterest in organization on a large scale, I think if I were a college student considering a career taking care of children, I would take a hard look at becoming a nurse practitioner or physician’s assistant. I might not make as much money, nor would my parents be able to introduce me as their “son the doctor.” But I would be content spending more time doing what I enjoyed.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Everything We Say And Do: The physician patient
Editor’s note: “Everything We Say and Do” provides readers with thoughtful and actionable communication tactics that can positively impact patients’ experience of care. In the next series of columns, physicians will share how their experiences as patients have shaped their professional approach.
In May 2007, I received my acceptance letter for medical school. One month later, I was diagnosed with cancer.
The clinic visit was only supposed to be a routine postoperative follow-up after a simple cyst resection. I really hoped that my doctor was mistaken as he walked me through what to expect, and when he was finished, the desperate look in my eyes demanded answers.

After I fully absorbed the initial shock of the grave news, I eventually found the strength to analyze the situation at hand. Ultimately, I adopted a more positive outlook and fought cancer head on. Contending with cancer while tackling the rigors of medical school was tedious, but despite the hardships, my experience catalyzed my determination and molded my personality as a physician.
What I say and do
I employ active listening and practice patience, especially when it comes to family members.
As both a cancer survivor and a physician, I am able to integrate empathy and diligence by putting myself in my patients’ shoes. My experience in a hospital bed during medical school granted me an extremely intriguing perspective towards medicine.
Why I do it
When I was a patient, the most crucial thing to my family was information. Most physicians did not take the time to explain my course of care, which elevated my family’s angst and anxiety. The experience taught me the importance of patience and communication.
But there were good examples. I still remember the physician who comforted my mother and assuaged her concerns. She held my mother’s hand and showed empathy. When my mother cried, she cried. That physician taught me that it was acceptable for physicians to express emotions.
When my surgeon rounded on me in the morning after my procedure, she was not wearing a white coat, which made her appear relatable. Her contagious confidence and humble demeanor were endorsement enough for her capabilities, showing me that a physician’s persona supersedes the conventional coat.
How I do it
I try to put myself in my patients’ shoes. I rejoice with them. I mourn with them. My uninhibited display of emotions affirms empathy. I dissolve all barriers by not wearing a white coat and ask my patients for a partnership. After all, I once walked miles in those shoes.
Dr. Sharma is a chief hospitalist for Sound Physicians at the Sierra Campus of The Hospitals of Providence, El Paso, Texas. She is a columnist for the El Paso Times and the medical contributor for KVIA Channel 7 ABC News. Her work has appeared on kevinmd.com, Thrive Global, and in El Paso magazine.
Editor’s note: “Everything We Say and Do” provides readers with thoughtful and actionable communication tactics that can positively impact patients’ experience of care. In the next series of columns, physicians will share how their experiences as patients have shaped their professional approach.
In May 2007, I received my acceptance letter for medical school. One month later, I was diagnosed with cancer.
The clinic visit was only supposed to be a routine postoperative follow-up after a simple cyst resection. I really hoped that my doctor was mistaken as he walked me through what to expect, and when he was finished, the desperate look in my eyes demanded answers.
After I fully absorbed the initial shock of the grave news, I eventually found the strength to analyze the situation at hand. Ultimately, I adopted a more positive outlook and fought cancer head on. Contending with cancer while tackling the rigors of medical school was tedious, but despite the hardships, my experience catalyzed my determination and molded my personality as a physician.
What I say and do
I employ active listening and practice patience, especially when it comes to family members.
As both a cancer survivor and a physician, I am able to integrate empathy and diligence by putting myself in my patients’ shoes. My experience in a hospital bed during medical school granted me an extremely intriguing perspective towards medicine.
Why I do it
When I was a patient, the most crucial thing to my family was information. Most physicians did not take the time to explain my course of care, which elevated my family’s angst and anxiety. The experience taught me the importance of patience and communication.
But there were good examples. I still remember the physician who comforted my mother and assuaged her concerns. She held my mother’s hand and showed empathy. When my mother cried, she cried. That physician taught me that it was acceptable for physicians to express emotions.
When my surgeon rounded on me in the morning after my procedure, she was not wearing a white coat, which made her appear relatable. Her contagious confidence and humble demeanor were endorsement enough for her capabilities, showing me that a physician’s persona supersedes the conventional coat.
How I do it
I try to put myself in my patients’ shoes. I rejoice with them. I mourn with them. My uninhibited display of emotions affirms empathy. I dissolve all barriers by not wearing a white coat and ask my patients for a partnership. After all, I once walked miles in those shoes.
Dr. Sharma is a chief hospitalist for Sound Physicians at the Sierra Campus of The Hospitals of Providence, El Paso, Texas. She is a columnist for the El Paso Times and the medical contributor for KVIA Channel 7 ABC News. Her work has appeared on kevinmd.com, Thrive Global, and in El Paso magazine.
Editor’s note: “Everything We Say and Do” provides readers with thoughtful and actionable communication tactics that can positively impact patients’ experience of care. In the next series of columns, physicians will share how their experiences as patients have shaped their professional approach.
In May 2007, I received my acceptance letter for medical school. One month later, I was diagnosed with cancer.
The clinic visit was only supposed to be a routine postoperative follow-up after a simple cyst resection. I really hoped that my doctor was mistaken as he walked me through what to expect, and when he was finished, the desperate look in my eyes demanded answers.
After I fully absorbed the initial shock of the grave news, I eventually found the strength to analyze the situation at hand. Ultimately, I adopted a more positive outlook and fought cancer head on. Contending with cancer while tackling the rigors of medical school was tedious, but despite the hardships, my experience catalyzed my determination and molded my personality as a physician.
What I say and do
I employ active listening and practice patience, especially when it comes to family members.
As both a cancer survivor and a physician, I am able to integrate empathy and diligence by putting myself in my patients’ shoes. My experience in a hospital bed during medical school granted me an extremely intriguing perspective towards medicine.
Why I do it
When I was a patient, the most crucial thing to my family was information. Most physicians did not take the time to explain my course of care, which elevated my family’s angst and anxiety. The experience taught me the importance of patience and communication.
But there were good examples. I still remember the physician who comforted my mother and assuaged her concerns. She held my mother’s hand and showed empathy. When my mother cried, she cried. That physician taught me that it was acceptable for physicians to express emotions.
When my surgeon rounded on me in the morning after my procedure, she was not wearing a white coat, which made her appear relatable. Her contagious confidence and humble demeanor were endorsement enough for her capabilities, showing me that a physician’s persona supersedes the conventional coat.
How I do it
I try to put myself in my patients’ shoes. I rejoice with them. I mourn with them. My uninhibited display of emotions affirms empathy. I dissolve all barriers by not wearing a white coat and ask my patients for a partnership. After all, I once walked miles in those shoes.
Dr. Sharma is a chief hospitalist for Sound Physicians at the Sierra Campus of The Hospitals of Providence, El Paso, Texas. She is a columnist for the El Paso Times and the medical contributor for KVIA Channel 7 ABC News. Her work has appeared on kevinmd.com, Thrive Global, and in El Paso magazine.
Inclusive sexual health counseling and care
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.

Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.

Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).