User login
No Impact of Race on Cardiovascular Risk Calculations
TOPLINE:
Removing race and incorporating social determinants of health (SDOH) into the pooled cohort risk equations (PCEs) for predicting atherosclerotic cardiovascular disease (ASCVD) outcomes made no difference to patients’ risk scores.
METHODOLOGY:
- Primary prevention guidelines recommend using risk prediction algorithms to assess the 10-year ASCVD risk, with the currently recommended PCEs including race.
- Researchers evaluated the incremental value of revised risk prediction equations excluding race and introducing SDOH in 11,638 participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort.
- Participants were aged between 45 and 79 years, had no history of ASCVD, and were not taking statins.
- Participants were followed up to 10 years for incident ASCVD, including myocardial infarction, coronary heart disease death, and fatal and nonfatal stroke.
TAKEAWAY:
- Risk prediction equations performed similarly in race- and sex-stratified PCEs (C-statistic [95% CI])
- Black female: 0.71 (0.68-0.75); Black male: 0.68 (0.64-0.73); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
- Race-free sex-specific PCEs yielded similar discrimination as race- and sex-stratified PCEs (C-statistic [95% CI]):
- Black female: 0.71 (0.67-0.75); Black male: 0.68 (0.63-0.72); White female: 0.76 (0.73-0.80); White male: 0.68 (0.65-0.71)
- The addition of SDOH to race-free sex-specific PCEs did not improve model performance (C-statistic [95% CI]):
- Black female: 0.72 (0.68-0.76); Black male: 0.68 (0.64-0.72); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
IN PRACTICE:
“The major takeaway is we need to rethink the idea of race in cardiovascular risk prediction,” lead author Arnab Ghosh, MD, assistant professor of medicine at Weill Cornell Medical College and a hospitalist at New York-Presbyterian/Weill Cornell Medical Center, said in a press release.
“It’s essential for clinicians and scientists to consider how to appropriately address the health effects of race as a social construct, which has contributed to health disparities in cardiovascular outcomes,” Dr. Ghosh added.
SOURCE:
The study led by Dr. Ghosh was published online on December 6, 2023, in JAMA Cardiology with an Editor’s Note.
LIMITATIONS:
The study required informed consent for inclusion, which may have led to selection bias.
The REGARDS cohort’s SDOH may not have captured all social and socioeconomic influences on ASCVD outcomes.
DISCLOSURES:
The research was funded by the National Institute of Neurological Disorders and Stroke and the National Institute on Aging of the National Institutes of Health, Department of Health and Human Services, and others. Some authors declared receiving funding, grants, or personal fees from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Removing race and incorporating social determinants of health (SDOH) into the pooled cohort risk equations (PCEs) for predicting atherosclerotic cardiovascular disease (ASCVD) outcomes made no difference to patients’ risk scores.
METHODOLOGY:
- Primary prevention guidelines recommend using risk prediction algorithms to assess the 10-year ASCVD risk, with the currently recommended PCEs including race.
- Researchers evaluated the incremental value of revised risk prediction equations excluding race and introducing SDOH in 11,638 participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort.
- Participants were aged between 45 and 79 years, had no history of ASCVD, and were not taking statins.
- Participants were followed up to 10 years for incident ASCVD, including myocardial infarction, coronary heart disease death, and fatal and nonfatal stroke.
TAKEAWAY:
- Risk prediction equations performed similarly in race- and sex-stratified PCEs (C-statistic [95% CI])
- Black female: 0.71 (0.68-0.75); Black male: 0.68 (0.64-0.73); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
- Race-free sex-specific PCEs yielded similar discrimination as race- and sex-stratified PCEs (C-statistic [95% CI]):
- Black female: 0.71 (0.67-0.75); Black male: 0.68 (0.63-0.72); White female: 0.76 (0.73-0.80); White male: 0.68 (0.65-0.71)
- The addition of SDOH to race-free sex-specific PCEs did not improve model performance (C-statistic [95% CI]):
- Black female: 0.72 (0.68-0.76); Black male: 0.68 (0.64-0.72); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
IN PRACTICE:
“The major takeaway is we need to rethink the idea of race in cardiovascular risk prediction,” lead author Arnab Ghosh, MD, assistant professor of medicine at Weill Cornell Medical College and a hospitalist at New York-Presbyterian/Weill Cornell Medical Center, said in a press release.
“It’s essential for clinicians and scientists to consider how to appropriately address the health effects of race as a social construct, which has contributed to health disparities in cardiovascular outcomes,” Dr. Ghosh added.
SOURCE:
The study led by Dr. Ghosh was published online on December 6, 2023, in JAMA Cardiology with an Editor’s Note.
LIMITATIONS:
The study required informed consent for inclusion, which may have led to selection bias.
The REGARDS cohort’s SDOH may not have captured all social and socioeconomic influences on ASCVD outcomes.
DISCLOSURES:
The research was funded by the National Institute of Neurological Disorders and Stroke and the National Institute on Aging of the National Institutes of Health, Department of Health and Human Services, and others. Some authors declared receiving funding, grants, or personal fees from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Removing race and incorporating social determinants of health (SDOH) into the pooled cohort risk equations (PCEs) for predicting atherosclerotic cardiovascular disease (ASCVD) outcomes made no difference to patients’ risk scores.
METHODOLOGY:
- Primary prevention guidelines recommend using risk prediction algorithms to assess the 10-year ASCVD risk, with the currently recommended PCEs including race.
- Researchers evaluated the incremental value of revised risk prediction equations excluding race and introducing SDOH in 11,638 participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort.
- Participants were aged between 45 and 79 years, had no history of ASCVD, and were not taking statins.
- Participants were followed up to 10 years for incident ASCVD, including myocardial infarction, coronary heart disease death, and fatal and nonfatal stroke.
TAKEAWAY:
- Risk prediction equations performed similarly in race- and sex-stratified PCEs (C-statistic [95% CI])
- Black female: 0.71 (0.68-0.75); Black male: 0.68 (0.64-0.73); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
- Race-free sex-specific PCEs yielded similar discrimination as race- and sex-stratified PCEs (C-statistic [95% CI]):
- Black female: 0.71 (0.67-0.75); Black male: 0.68 (0.63-0.72); White female: 0.76 (0.73-0.80); White male: 0.68 (0.65-0.71)
- The addition of SDOH to race-free sex-specific PCEs did not improve model performance (C-statistic [95% CI]):
- Black female: 0.72 (0.68-0.76); Black male: 0.68 (0.64-0.72); White female: 0.77 (0.74-0.80); White male: 0.68 (0.65-0.71)
IN PRACTICE:
“The major takeaway is we need to rethink the idea of race in cardiovascular risk prediction,” lead author Arnab Ghosh, MD, assistant professor of medicine at Weill Cornell Medical College and a hospitalist at New York-Presbyterian/Weill Cornell Medical Center, said in a press release.
“It’s essential for clinicians and scientists to consider how to appropriately address the health effects of race as a social construct, which has contributed to health disparities in cardiovascular outcomes,” Dr. Ghosh added.
SOURCE:
The study led by Dr. Ghosh was published online on December 6, 2023, in JAMA Cardiology with an Editor’s Note.
LIMITATIONS:
The study required informed consent for inclusion, which may have led to selection bias.
The REGARDS cohort’s SDOH may not have captured all social and socioeconomic influences on ASCVD outcomes.
DISCLOSURES:
The research was funded by the National Institute of Neurological Disorders and Stroke and the National Institute on Aging of the National Institutes of Health, Department of Health and Human Services, and others. Some authors declared receiving funding, grants, or personal fees from various sources.
A version of this article appeared on Medscape.com.
Exercise plan cost-effective in post-stroke cognitive rehab
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
PFO closure may reduce migraine days and prevent stroke
, according to a discussion at the 2023 Scottsdale Headache Symposium.
In two clinical trials evaluating whether PFO closure reduces migraine risk, the primary endpoints were not met, but a signal of benefit on secondary endpoints and the association between PFO, migraine, and stroke are among the reasons that PFO closure should be reevaluated, according to Andrew Charles MD, Director of the Goldberg Migraine Program, University of California, Los Angeles.

Other right-to-left shunt defects have also been associated with both migraine and stroke, leading Dr. Charles to suggest these defects are more a common denominator.
“Stroke during a migraine is, in fact, very uncommon,” Dr. Charles said. “This raises the possibility that it is not the migraine causing the stroke but rather there is a shared risk factor for stroke and migraine,” said Dr. Charles, referring to PFO as well as other right-to-left shunt defects, such as hereditary hemorrhaging telangiectasia in the lungs.
One Intervention, Two Potential Benefits
Fixing these defects is therefore at least theoretically attractive for preventing both migraine and stroke, but Dr. Charles said the opportunity for preventing both migraine and stroke is most attractive in migraine patients who have additional stroke risk factors.
Use of oral contraceptives, which produce a hypercoagulable state, is an example.
“Are these the people we should really be thinking about if they have PFO and migraine, particularly migraine with aura?” Dr. Charles asked.
The association between right-to-left shunts and migraine is strong. Although PFO is common, presenting in 20%-25% of the adult population, it has been found in up to 50% of individuals who have migraine with aura. In patients with migraine but no aura, the prevalence of PFO has been estimated to be approximately 35% or still somewhat elevated relative to the general population.
Primary Endpoint Missed in Clinical Trials
The question of whether risk of migraine can be reduced with repair of PFO or other right-to-left shunts remains unresolved. In two high-quality randomized trials undertaken in PFO repair, neither met its primary endpoint. In one of these, called PRIMA, which was terminated early for slow enrollment, the reduction in mean headache attacks was not significant relative to medical therapy.
In the second, called PREMIUM, device closure of PFO also failed to significantly reduce migraine attacks over sham procedure although it was associated with complete migraine remission (10% vs 1%).
A pooled analysis of these two studies that was conducted subsequently concluded that PFO closure reduces mean monthly migraine days (-3.1 vs. -1.9 days; P = -.02) and increases the likelihood of complete migraine cessation (9% vs. 0.7%; P < .001), but Dr. Charles pointed out the primary endpoint was migraine attacks not migraine days, so other analyses can only be considered hypothesis-generating.
There are several reasons to relook at the relationship between migraine and PFO but the potential to prevent both migraine and stroke with PFO closure could be one of the most important.
Several years ago, Dr. Charles and his coinvestigators from UCLA evaluated more than 700 ischemic strokes. Of these, 127 strokes were characterized as cryptogenic because of lack of another identifiable etiology. While 59% of these patients had PFO, which is several times higher than the general population, the prevalence of PFO in patients with a cryptogenic stroke and a history of migraine was 79% in this published study.
“So, in this group of patients who did not have any other clear cause for a stroke, a diagnosis of PFO was very much overrepresented,” Dr. Charles said.
Migraine Days Might Be a Better Endpoint
For patients with migraine who have risk factors for stroke, this makes PFO closure an attractive intervention, but a positive randomized trial is needed. Several are underway. Importantly, the trials now enrolling are using migraine days, which was significantly reduced in both PREMIUM and PRIMA, rather than migraine attacks as the primary endpoint.
“Migraine days is now accepted by the Food and Drug Administration as a criterion of benefit,” reported Jonathan Tobis, MD, Research Director, Interventional Cardiology, UCLA David Geffen School of Medicine, Los Angeles.
He explained that the FDA insisted on migraine attacks as the endpoint for the PREMIUM trial, but this was a far more challenging endpoint on which to show a statistical benefit. He emphasized that a new set of trials will now test efficacy on the basis of migraine days.
One of these trials, called RELIEF, which is randomizing patients to device closure of PFO or a sham procedure. Both groups are receiving clopidogrel or prasugrel based on a previous observation that patients who respond to these drugs are also more likely to respond to PFO closure.
Another trial, called COMPETE-2, is comparing PFO closure with a device to aspirin plus a sham closure. This trial is ongoing in China.
Stroke is not being evaluated as an endpoint in either trial, but Dr. Charles suggested that this does warrant attention.
“I would also just put it out there that, apart from simply migraine, this is a therapeutic approach that we might actually think about in terms of helping to prevent stroke in our migraine patients,” he said.
Senior author of a recent meta-analysis of trials evaluating PFO closure and control of migraine, Ling Liu, MD, Department of Neurology, University of Sichuan, Chengdu, China, agreed that PFO closure for the treatment of migraine deserves “a reevaluation.”
In his meta-analysis of three randomized trials, one pooled study, and eight retrospective case series with 1,165 patients, PFO closure was associated with a nearly 75% reduction (odds ratio [OR], 0.259; P = .0048) reduction in migraine days and 50% increase in resolution of migraine in patients with a history of migraine with aura (OR, 1.586; P = .227).
The incidence of stroke was not evaluated in this meta-analysis, but Dr. Liu believes that the evidence of reducing the burden of migraine with PFO closure is compelling. Given the evidence from this meta-analysis that PFO closure is safe, Dr. Liu maintained that a definitive trial is needed “especially for migraine with frequent aura.”
As an interventional cardiologist, Dr. Tobis said that when PFO closures is performed for prevention of stroke in patients with migraine, it often leads to reduced migraine activity and, in some cases, elimination of migraine. Like others, he believes new analyses should be conducted.
“Everyone involved in this field believes there is something there,” Dr. Tobis said. The missing link is a clinical trial to confirm it.
Dr. Charles and Dr. Liu report no potential conflicts of interest. Dr. Tobis reports a financial relationship with Holistick Medical.
, according to a discussion at the 2023 Scottsdale Headache Symposium.
In two clinical trials evaluating whether PFO closure reduces migraine risk, the primary endpoints were not met, but a signal of benefit on secondary endpoints and the association between PFO, migraine, and stroke are among the reasons that PFO closure should be reevaluated, according to Andrew Charles MD, Director of the Goldberg Migraine Program, University of California, Los Angeles.
Other right-to-left shunt defects have also been associated with both migraine and stroke, leading Dr. Charles to suggest these defects are more a common denominator.
“Stroke during a migraine is, in fact, very uncommon,” Dr. Charles said. “This raises the possibility that it is not the migraine causing the stroke but rather there is a shared risk factor for stroke and migraine,” said Dr. Charles, referring to PFO as well as other right-to-left shunt defects, such as hereditary hemorrhaging telangiectasia in the lungs.
One Intervention, Two Potential Benefits
Fixing these defects is therefore at least theoretically attractive for preventing both migraine and stroke, but Dr. Charles said the opportunity for preventing both migraine and stroke is most attractive in migraine patients who have additional stroke risk factors.
Use of oral contraceptives, which produce a hypercoagulable state, is an example.
“Are these the people we should really be thinking about if they have PFO and migraine, particularly migraine with aura?” Dr. Charles asked.
The association between right-to-left shunts and migraine is strong. Although PFO is common, presenting in 20%-25% of the adult population, it has been found in up to 50% of individuals who have migraine with aura. In patients with migraine but no aura, the prevalence of PFO has been estimated to be approximately 35% or still somewhat elevated relative to the general population.
Primary Endpoint Missed in Clinical Trials
The question of whether risk of migraine can be reduced with repair of PFO or other right-to-left shunts remains unresolved. In two high-quality randomized trials undertaken in PFO repair, neither met its primary endpoint. In one of these, called PRIMA, which was terminated early for slow enrollment, the reduction in mean headache attacks was not significant relative to medical therapy.
In the second, called PREMIUM, device closure of PFO also failed to significantly reduce migraine attacks over sham procedure although it was associated with complete migraine remission (10% vs 1%).
A pooled analysis of these two studies that was conducted subsequently concluded that PFO closure reduces mean monthly migraine days (-3.1 vs. -1.9 days; P = -.02) and increases the likelihood of complete migraine cessation (9% vs. 0.7%; P < .001), but Dr. Charles pointed out the primary endpoint was migraine attacks not migraine days, so other analyses can only be considered hypothesis-generating.
There are several reasons to relook at the relationship between migraine and PFO but the potential to prevent both migraine and stroke with PFO closure could be one of the most important.
Several years ago, Dr. Charles and his coinvestigators from UCLA evaluated more than 700 ischemic strokes. Of these, 127 strokes were characterized as cryptogenic because of lack of another identifiable etiology. While 59% of these patients had PFO, which is several times higher than the general population, the prevalence of PFO in patients with a cryptogenic stroke and a history of migraine was 79% in this published study.
“So, in this group of patients who did not have any other clear cause for a stroke, a diagnosis of PFO was very much overrepresented,” Dr. Charles said.
Migraine Days Might Be a Better Endpoint
For patients with migraine who have risk factors for stroke, this makes PFO closure an attractive intervention, but a positive randomized trial is needed. Several are underway. Importantly, the trials now enrolling are using migraine days, which was significantly reduced in both PREMIUM and PRIMA, rather than migraine attacks as the primary endpoint.
“Migraine days is now accepted by the Food and Drug Administration as a criterion of benefit,” reported Jonathan Tobis, MD, Research Director, Interventional Cardiology, UCLA David Geffen School of Medicine, Los Angeles.
He explained that the FDA insisted on migraine attacks as the endpoint for the PREMIUM trial, but this was a far more challenging endpoint on which to show a statistical benefit. He emphasized that a new set of trials will now test efficacy on the basis of migraine days.
One of these trials, called RELIEF, which is randomizing patients to device closure of PFO or a sham procedure. Both groups are receiving clopidogrel or prasugrel based on a previous observation that patients who respond to these drugs are also more likely to respond to PFO closure.
Another trial, called COMPETE-2, is comparing PFO closure with a device to aspirin plus a sham closure. This trial is ongoing in China.
Stroke is not being evaluated as an endpoint in either trial, but Dr. Charles suggested that this does warrant attention.
“I would also just put it out there that, apart from simply migraine, this is a therapeutic approach that we might actually think about in terms of helping to prevent stroke in our migraine patients,” he said.
Senior author of a recent meta-analysis of trials evaluating PFO closure and control of migraine, Ling Liu, MD, Department of Neurology, University of Sichuan, Chengdu, China, agreed that PFO closure for the treatment of migraine deserves “a reevaluation.”
In his meta-analysis of three randomized trials, one pooled study, and eight retrospective case series with 1,165 patients, PFO closure was associated with a nearly 75% reduction (odds ratio [OR], 0.259; P = .0048) reduction in migraine days and 50% increase in resolution of migraine in patients with a history of migraine with aura (OR, 1.586; P = .227).
The incidence of stroke was not evaluated in this meta-analysis, but Dr. Liu believes that the evidence of reducing the burden of migraine with PFO closure is compelling. Given the evidence from this meta-analysis that PFO closure is safe, Dr. Liu maintained that a definitive trial is needed “especially for migraine with frequent aura.”
As an interventional cardiologist, Dr. Tobis said that when PFO closures is performed for prevention of stroke in patients with migraine, it often leads to reduced migraine activity and, in some cases, elimination of migraine. Like others, he believes new analyses should be conducted.
“Everyone involved in this field believes there is something there,” Dr. Tobis said. The missing link is a clinical trial to confirm it.
Dr. Charles and Dr. Liu report no potential conflicts of interest. Dr. Tobis reports a financial relationship with Holistick Medical.
, according to a discussion at the 2023 Scottsdale Headache Symposium.
In two clinical trials evaluating whether PFO closure reduces migraine risk, the primary endpoints were not met, but a signal of benefit on secondary endpoints and the association between PFO, migraine, and stroke are among the reasons that PFO closure should be reevaluated, according to Andrew Charles MD, Director of the Goldberg Migraine Program, University of California, Los Angeles.
Other right-to-left shunt defects have also been associated with both migraine and stroke, leading Dr. Charles to suggest these defects are more a common denominator.
“Stroke during a migraine is, in fact, very uncommon,” Dr. Charles said. “This raises the possibility that it is not the migraine causing the stroke but rather there is a shared risk factor for stroke and migraine,” said Dr. Charles, referring to PFO as well as other right-to-left shunt defects, such as hereditary hemorrhaging telangiectasia in the lungs.
One Intervention, Two Potential Benefits
Fixing these defects is therefore at least theoretically attractive for preventing both migraine and stroke, but Dr. Charles said the opportunity for preventing both migraine and stroke is most attractive in migraine patients who have additional stroke risk factors.
Use of oral contraceptives, which produce a hypercoagulable state, is an example.
“Are these the people we should really be thinking about if they have PFO and migraine, particularly migraine with aura?” Dr. Charles asked.
The association between right-to-left shunts and migraine is strong. Although PFO is common, presenting in 20%-25% of the adult population, it has been found in up to 50% of individuals who have migraine with aura. In patients with migraine but no aura, the prevalence of PFO has been estimated to be approximately 35% or still somewhat elevated relative to the general population.
Primary Endpoint Missed in Clinical Trials
The question of whether risk of migraine can be reduced with repair of PFO or other right-to-left shunts remains unresolved. In two high-quality randomized trials undertaken in PFO repair, neither met its primary endpoint. In one of these, called PRIMA, which was terminated early for slow enrollment, the reduction in mean headache attacks was not significant relative to medical therapy.
In the second, called PREMIUM, device closure of PFO also failed to significantly reduce migraine attacks over sham procedure although it was associated with complete migraine remission (10% vs 1%).
A pooled analysis of these two studies that was conducted subsequently concluded that PFO closure reduces mean monthly migraine days (-3.1 vs. -1.9 days; P = -.02) and increases the likelihood of complete migraine cessation (9% vs. 0.7%; P < .001), but Dr. Charles pointed out the primary endpoint was migraine attacks not migraine days, so other analyses can only be considered hypothesis-generating.
There are several reasons to relook at the relationship between migraine and PFO but the potential to prevent both migraine and stroke with PFO closure could be one of the most important.
Several years ago, Dr. Charles and his coinvestigators from UCLA evaluated more than 700 ischemic strokes. Of these, 127 strokes were characterized as cryptogenic because of lack of another identifiable etiology. While 59% of these patients had PFO, which is several times higher than the general population, the prevalence of PFO in patients with a cryptogenic stroke and a history of migraine was 79% in this published study.
“So, in this group of patients who did not have any other clear cause for a stroke, a diagnosis of PFO was very much overrepresented,” Dr. Charles said.
Migraine Days Might Be a Better Endpoint
For patients with migraine who have risk factors for stroke, this makes PFO closure an attractive intervention, but a positive randomized trial is needed. Several are underway. Importantly, the trials now enrolling are using migraine days, which was significantly reduced in both PREMIUM and PRIMA, rather than migraine attacks as the primary endpoint.
“Migraine days is now accepted by the Food and Drug Administration as a criterion of benefit,” reported Jonathan Tobis, MD, Research Director, Interventional Cardiology, UCLA David Geffen School of Medicine, Los Angeles.
He explained that the FDA insisted on migraine attacks as the endpoint for the PREMIUM trial, but this was a far more challenging endpoint on which to show a statistical benefit. He emphasized that a new set of trials will now test efficacy on the basis of migraine days.
One of these trials, called RELIEF, which is randomizing patients to device closure of PFO or a sham procedure. Both groups are receiving clopidogrel or prasugrel based on a previous observation that patients who respond to these drugs are also more likely to respond to PFO closure.
Another trial, called COMPETE-2, is comparing PFO closure with a device to aspirin plus a sham closure. This trial is ongoing in China.
Stroke is not being evaluated as an endpoint in either trial, but Dr. Charles suggested that this does warrant attention.
“I would also just put it out there that, apart from simply migraine, this is a therapeutic approach that we might actually think about in terms of helping to prevent stroke in our migraine patients,” he said.
Senior author of a recent meta-analysis of trials evaluating PFO closure and control of migraine, Ling Liu, MD, Department of Neurology, University of Sichuan, Chengdu, China, agreed that PFO closure for the treatment of migraine deserves “a reevaluation.”
In his meta-analysis of three randomized trials, one pooled study, and eight retrospective case series with 1,165 patients, PFO closure was associated with a nearly 75% reduction (odds ratio [OR], 0.259; P = .0048) reduction in migraine days and 50% increase in resolution of migraine in patients with a history of migraine with aura (OR, 1.586; P = .227).
The incidence of stroke was not evaluated in this meta-analysis, but Dr. Liu believes that the evidence of reducing the burden of migraine with PFO closure is compelling. Given the evidence from this meta-analysis that PFO closure is safe, Dr. Liu maintained that a definitive trial is needed “especially for migraine with frequent aura.”
As an interventional cardiologist, Dr. Tobis said that when PFO closures is performed for prevention of stroke in patients with migraine, it often leads to reduced migraine activity and, in some cases, elimination of migraine. Like others, he believes new analyses should be conducted.
“Everyone involved in this field believes there is something there,” Dr. Tobis said. The missing link is a clinical trial to confirm it.
Dr. Charles and Dr. Liu report no potential conflicts of interest. Dr. Tobis reports a financial relationship with Holistick Medical.
FROM THE 2023 SCOTTSDALE HEADACHE SYMPOSIUM
Less severe strokes with LAA closure vs. DOAC in AFib?
TOPLINE:
Left atrial appendage closure was associated with about half as many disabling or fatal strokes and lower mortality after a stroke, compared with dual oral anticoagulant therapy in patients with atrial fibrillation (AFib), new observational research shows.
METHODOLOGY:
- The retrospective registry analysis included 447 adult patients with nonvalvular AFib, mean age 74 years, who were hospitalized with an ischemic stroke, 322 of whom were receiving direct oral anticoagulant (DOAC) therapy, mostly (84%) apixaban or rivaroxaban, and 125 were treated with left atrial appendage closure (LAAC), almost all (97%) with Watchman or Watchman-FLX devices.
- All patients received standard stroke care, monitoring, and treatment as well as physical therapy/rehabilitation.
- For the primary outcome, researchers used the modified Rankin Scale (mRS) to determine disabling (mRS score of 3-5) and fatal (mRS score of 6) strokes at discharge and at 3 months.
- The study adjusted for age, smoking, paroxysmal AFib, prior major bleeding, prior hemorrhagic stroke, medication adherence, and other risk factors.
TAKEAWAY:
- (38.3% vs. 70.3%; P < .001) and at 3 months (33.3% vs. 56.2%; P < .001), even though the LAAC group had more baseline comorbidity, for example, older age, more smokers, and more prior major bleeding.
- There was no significant difference in mortality between groups during hospitalization, but at 3 months, mortality was lower in the LAAC group (14.7% vs. 32.1%; P = .002).
- Multivariate linear regression analysis showed LAAC independently predicted more favorable mRS at discharge (2.8) and 3 months (1.4) (both P < .001) and was associated with less all-cause death at 3 months (odds ratio, 0.28; 95% confidence interval, 0.12-0.64; P = .002).
- Including those that excluded the 14.4% of LAAC patients who also received DOAC therapy, sensitivity analyses patients who got reduced dose DOACs and nonadherent patients yielded nearly identical outcomes to the full cohort analysis.
IN PRACTICE:
“Despite a higher baseline risk profile, patients treated with LAAC who developed IS had better outcomes than those receiving DOAC prophylaxis,” the authors conclude, adding that several ongoing prospective trials could, “shed light on the mechanism(s) responsible for differences in stroke severity.”
SOURCE:
The study was conducted by Mohit K. Turagam, MD, Icahn School of Medicine at Mount Sinai, New York, and colleagues. It was published online in JACC: Clinical Electrophysiology.
LIMITATIONS:
Despite sensitivity analyses and adjustment for risk factors, selection bias, missing data, and other confounding factors could have affected outcomes. The study didn’t evaluate recurrent IS or type and intensity of rehabilitation on outcomes. Lack of imaging data comparing stroke infarct size and volume limits understanding of exact mechanism driving higher stroke severity with DOACs. Because patients who died before reaching hospital weren’t captured in the registry, the actual mortality may be higher than reported.
DISCLOSURES:
Dr. Turagam has served as a consultant for Biosense Webster and Sanofi.
A version of this article first appeared on Medscape.com.
TOPLINE:
Left atrial appendage closure was associated with about half as many disabling or fatal strokes and lower mortality after a stroke, compared with dual oral anticoagulant therapy in patients with atrial fibrillation (AFib), new observational research shows.
METHODOLOGY:
- The retrospective registry analysis included 447 adult patients with nonvalvular AFib, mean age 74 years, who were hospitalized with an ischemic stroke, 322 of whom were receiving direct oral anticoagulant (DOAC) therapy, mostly (84%) apixaban or rivaroxaban, and 125 were treated with left atrial appendage closure (LAAC), almost all (97%) with Watchman or Watchman-FLX devices.
- All patients received standard stroke care, monitoring, and treatment as well as physical therapy/rehabilitation.
- For the primary outcome, researchers used the modified Rankin Scale (mRS) to determine disabling (mRS score of 3-5) and fatal (mRS score of 6) strokes at discharge and at 3 months.
- The study adjusted for age, smoking, paroxysmal AFib, prior major bleeding, prior hemorrhagic stroke, medication adherence, and other risk factors.
TAKEAWAY:
- (38.3% vs. 70.3%; P < .001) and at 3 months (33.3% vs. 56.2%; P < .001), even though the LAAC group had more baseline comorbidity, for example, older age, more smokers, and more prior major bleeding.
- There was no significant difference in mortality between groups during hospitalization, but at 3 months, mortality was lower in the LAAC group (14.7% vs. 32.1%; P = .002).
- Multivariate linear regression analysis showed LAAC independently predicted more favorable mRS at discharge (2.8) and 3 months (1.4) (both P < .001) and was associated with less all-cause death at 3 months (odds ratio, 0.28; 95% confidence interval, 0.12-0.64; P = .002).
- Including those that excluded the 14.4% of LAAC patients who also received DOAC therapy, sensitivity analyses patients who got reduced dose DOACs and nonadherent patients yielded nearly identical outcomes to the full cohort analysis.
IN PRACTICE:
“Despite a higher baseline risk profile, patients treated with LAAC who developed IS had better outcomes than those receiving DOAC prophylaxis,” the authors conclude, adding that several ongoing prospective trials could, “shed light on the mechanism(s) responsible for differences in stroke severity.”
SOURCE:
The study was conducted by Mohit K. Turagam, MD, Icahn School of Medicine at Mount Sinai, New York, and colleagues. It was published online in JACC: Clinical Electrophysiology.
LIMITATIONS:
Despite sensitivity analyses and adjustment for risk factors, selection bias, missing data, and other confounding factors could have affected outcomes. The study didn’t evaluate recurrent IS or type and intensity of rehabilitation on outcomes. Lack of imaging data comparing stroke infarct size and volume limits understanding of exact mechanism driving higher stroke severity with DOACs. Because patients who died before reaching hospital weren’t captured in the registry, the actual mortality may be higher than reported.
DISCLOSURES:
Dr. Turagam has served as a consultant for Biosense Webster and Sanofi.
A version of this article first appeared on Medscape.com.
TOPLINE:
Left atrial appendage closure was associated with about half as many disabling or fatal strokes and lower mortality after a stroke, compared with dual oral anticoagulant therapy in patients with atrial fibrillation (AFib), new observational research shows.
METHODOLOGY:
- The retrospective registry analysis included 447 adult patients with nonvalvular AFib, mean age 74 years, who were hospitalized with an ischemic stroke, 322 of whom were receiving direct oral anticoagulant (DOAC) therapy, mostly (84%) apixaban or rivaroxaban, and 125 were treated with left atrial appendage closure (LAAC), almost all (97%) with Watchman or Watchman-FLX devices.
- All patients received standard stroke care, monitoring, and treatment as well as physical therapy/rehabilitation.
- For the primary outcome, researchers used the modified Rankin Scale (mRS) to determine disabling (mRS score of 3-5) and fatal (mRS score of 6) strokes at discharge and at 3 months.
- The study adjusted for age, smoking, paroxysmal AFib, prior major bleeding, prior hemorrhagic stroke, medication adherence, and other risk factors.
TAKEAWAY:
- (38.3% vs. 70.3%; P < .001) and at 3 months (33.3% vs. 56.2%; P < .001), even though the LAAC group had more baseline comorbidity, for example, older age, more smokers, and more prior major bleeding.
- There was no significant difference in mortality between groups during hospitalization, but at 3 months, mortality was lower in the LAAC group (14.7% vs. 32.1%; P = .002).
- Multivariate linear regression analysis showed LAAC independently predicted more favorable mRS at discharge (2.8) and 3 months (1.4) (both P < .001) and was associated with less all-cause death at 3 months (odds ratio, 0.28; 95% confidence interval, 0.12-0.64; P = .002).
- Including those that excluded the 14.4% of LAAC patients who also received DOAC therapy, sensitivity analyses patients who got reduced dose DOACs and nonadherent patients yielded nearly identical outcomes to the full cohort analysis.
IN PRACTICE:
“Despite a higher baseline risk profile, patients treated with LAAC who developed IS had better outcomes than those receiving DOAC prophylaxis,” the authors conclude, adding that several ongoing prospective trials could, “shed light on the mechanism(s) responsible for differences in stroke severity.”
SOURCE:
The study was conducted by Mohit K. Turagam, MD, Icahn School of Medicine at Mount Sinai, New York, and colleagues. It was published online in JACC: Clinical Electrophysiology.
LIMITATIONS:
Despite sensitivity analyses and adjustment for risk factors, selection bias, missing data, and other confounding factors could have affected outcomes. The study didn’t evaluate recurrent IS or type and intensity of rehabilitation on outcomes. Lack of imaging data comparing stroke infarct size and volume limits understanding of exact mechanism driving higher stroke severity with DOACs. Because patients who died before reaching hospital weren’t captured in the registry, the actual mortality may be higher than reported.
DISCLOSURES:
Dr. Turagam has served as a consultant for Biosense Webster and Sanofi.
A version of this article first appeared on Medscape.com.
PREVENT: AHA’s new risk calculator incorporates CKM health
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Hourly air pollution exposure: A risk factor for stroke
TOPLINE:
METHODOLOGY:
- Limited studies have investigated the association between hourly exposure to air pollutants and specific stroke subtypes, especially in regions with moderate to high levels of air pollution.
- The multicenter case-crossover study evaluated the association between hourly exposure to air pollution and stroke among 86,635 emergency admissions for stroke across 10 hospitals in 3 cities.
- Of 86,635 admissions, 79,478 were admitted for ischemic stroke, 3,122 for hemorrhagic stroke, and 4,035 for undetermined type of stroke.
- Hourly levels of fine particulate matter (PM2.5), respirable PM (PM10), nitrogen dioxide (NO2), and sulfur dioxide (SO2) were collected from the China National Environmental Monitoring Center.
TAKEAWAY:
- Exposure to NO2 and SO2 increased the risk for emergency admission for stroke shortly after exposure by 3.34% (95% confidence interval, 1.41%-5.31%) and 2.81% (95% CI, 1.15%-4.51%), respectively.
- Among men, exposure to PM2.5 and PM10 increased the risk for emergency admission for stroke by 3.40% (95% CI, 1.21%-5.64%) and 4.33% (95% CI, 2.18%-6.53%), respectively.
- Among patients aged less than 65 years, exposure to PM10 and NO2 increased the risk for emergency admissions for stroke shortly after exposure by 4.88% (95% CI, 2.29%-7.54%) and 5.59% (95% CI, 2.34%-8.93%), respectively.
IN PRACTICE:
“These variations in susceptibility highlight the importance of implementing effective health protection measures to reduce exposure to air pollution and mitigate the risk of stroke in younger and male populations,” wrote the authors.
SOURCE:
The study was led by Xin Lv, MD, department of epidemiology and biostatistics, School of Public Health, Capital Medical University, Beijing. It was published online in the journal Stroke.
LIMITATIONS:
- Using data from the nearest monitoring site to the hospital address may lead to localized variations in pollution concentrations when assessing exposure.
- There may be a possibility of residual confounding resulting from time-varying lifestyle-related factors.
DISCLOSURES:
This study was supported by the Zhejiang Provincial Project for Medical Research and Health Sciences. No disclosures were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Limited studies have investigated the association between hourly exposure to air pollutants and specific stroke subtypes, especially in regions with moderate to high levels of air pollution.
- The multicenter case-crossover study evaluated the association between hourly exposure to air pollution and stroke among 86,635 emergency admissions for stroke across 10 hospitals in 3 cities.
- Of 86,635 admissions, 79,478 were admitted for ischemic stroke, 3,122 for hemorrhagic stroke, and 4,035 for undetermined type of stroke.
- Hourly levels of fine particulate matter (PM2.5), respirable PM (PM10), nitrogen dioxide (NO2), and sulfur dioxide (SO2) were collected from the China National Environmental Monitoring Center.
TAKEAWAY:
- Exposure to NO2 and SO2 increased the risk for emergency admission for stroke shortly after exposure by 3.34% (95% confidence interval, 1.41%-5.31%) and 2.81% (95% CI, 1.15%-4.51%), respectively.
- Among men, exposure to PM2.5 and PM10 increased the risk for emergency admission for stroke by 3.40% (95% CI, 1.21%-5.64%) and 4.33% (95% CI, 2.18%-6.53%), respectively.
- Among patients aged less than 65 years, exposure to PM10 and NO2 increased the risk for emergency admissions for stroke shortly after exposure by 4.88% (95% CI, 2.29%-7.54%) and 5.59% (95% CI, 2.34%-8.93%), respectively.
IN PRACTICE:
“These variations in susceptibility highlight the importance of implementing effective health protection measures to reduce exposure to air pollution and mitigate the risk of stroke in younger and male populations,” wrote the authors.
SOURCE:
The study was led by Xin Lv, MD, department of epidemiology and biostatistics, School of Public Health, Capital Medical University, Beijing. It was published online in the journal Stroke.
LIMITATIONS:
- Using data from the nearest monitoring site to the hospital address may lead to localized variations in pollution concentrations when assessing exposure.
- There may be a possibility of residual confounding resulting from time-varying lifestyle-related factors.
DISCLOSURES:
This study was supported by the Zhejiang Provincial Project for Medical Research and Health Sciences. No disclosures were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Limited studies have investigated the association between hourly exposure to air pollutants and specific stroke subtypes, especially in regions with moderate to high levels of air pollution.
- The multicenter case-crossover study evaluated the association between hourly exposure to air pollution and stroke among 86,635 emergency admissions for stroke across 10 hospitals in 3 cities.
- Of 86,635 admissions, 79,478 were admitted for ischemic stroke, 3,122 for hemorrhagic stroke, and 4,035 for undetermined type of stroke.
- Hourly levels of fine particulate matter (PM2.5), respirable PM (PM10), nitrogen dioxide (NO2), and sulfur dioxide (SO2) were collected from the China National Environmental Monitoring Center.
TAKEAWAY:
- Exposure to NO2 and SO2 increased the risk for emergency admission for stroke shortly after exposure by 3.34% (95% confidence interval, 1.41%-5.31%) and 2.81% (95% CI, 1.15%-4.51%), respectively.
- Among men, exposure to PM2.5 and PM10 increased the risk for emergency admission for stroke by 3.40% (95% CI, 1.21%-5.64%) and 4.33% (95% CI, 2.18%-6.53%), respectively.
- Among patients aged less than 65 years, exposure to PM10 and NO2 increased the risk for emergency admissions for stroke shortly after exposure by 4.88% (95% CI, 2.29%-7.54%) and 5.59% (95% CI, 2.34%-8.93%), respectively.
IN PRACTICE:
“These variations in susceptibility highlight the importance of implementing effective health protection measures to reduce exposure to air pollution and mitigate the risk of stroke in younger and male populations,” wrote the authors.
SOURCE:
The study was led by Xin Lv, MD, department of epidemiology and biostatistics, School of Public Health, Capital Medical University, Beijing. It was published online in the journal Stroke.
LIMITATIONS:
- Using data from the nearest monitoring site to the hospital address may lead to localized variations in pollution concentrations when assessing exposure.
- There may be a possibility of residual confounding resulting from time-varying lifestyle-related factors.
DISCLOSURES:
This study was supported by the Zhejiang Provincial Project for Medical Research and Health Sciences. No disclosures were reported.
A version of this article first appeared on Medscape.com.
Study takes fine-grained look at MACE risk with glucocorticoids in RA
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.

“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.

“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
AT ACR 2023
Apixaban cuts stroke but ups bleeding in subclinical AFib: ARTESIA
in the ARTESIA study.
The results appear to contrast somewhat with the recently reported NOAH-AFNET 6 trial, which failed to show a reduction in stroke with the anticoagulant edoxaban versus placebo in a similar patient group, but that trial was stopped early and so was underpowered.
However, the lead investigators of both trials say the studies actually show consistent results – both found a lower rate of stroke than expected in this population, but the confidence intervals for stroke reduction with anticoagulation overlap, suggesting there is likely some effect, albeit less than that in clinical AFib.
The big question is whether the reduction in stroke with anticoagulation outweighs the increase in major bleeding.
A new meta-analysis of the two trials showed that “oral anticoagulation with edoxaban or apixaban reduces the risk of ischemic stroke by approximately one-third and increases major bleeding by roughly double.”
In absolute numbers, there were three fewer ischemic strokes per 1,000 patient-years with anticoagulation in the two trials combined, at the cost of seven more major bleeds.
The lead investigators of the two trials have somewhat different opinions on how these findings may translate into clinical practice.
Jeff Healey, MD, Population Health Research Institute, McMaster University, Hamilton, Ont., lead investigator of the ARTESIA trial, believes that the risks and benefits need to be assessed in individual patients, but there should be some patient groups that will benefit from anticoagulation treatment.
“In patients with pacemakers or implantable loop recorders with continuous monitoring, subclinical AF[ib] is detected in about one third of patients, so this is extremely common,” he said in an interview. “The question is whether this is just a normal feature of getting older or is this like AF[ib] that we see in the clinic which increases stroke risk, and I think we can conclude from ARTESIA that this subclinical AF[ib] is associated with an increased risk of stroke, although that is lower than the risk with clinical AF[ib], and that it can be reduced by anticoagulation.”
Until recently it hasn’t been possible to quantify the risk associated with subclinical AFib, he noted. “But now we have a rich dataset to use to see if we can tease out some specifics on this. Future analyses of this dataset will help define patients where the benefits outweigh the risks of bleeding. For now, I think we can look at the data in a qualitative way and consider the totality of risk factors in each patient – their bleeding risk, stroke risk, how much AF[ib] they have, and make a decision as to whether to give anticoagulation or not.”
But Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), lead investigator of the NOAH-AFNET 6 trial said: “Both trials showed the stroke rate is low in these patients – about 1% per year – and that anticoagulation can reduce it a bit further at the expense of increasing major bleeding. I don’t believe the AF[ib] episodes picked up on these devices constitute a sufficient stroke risk to warrant anticoagulation, given the bleeding risk.”
Dr. Kirchhof suggests an alternate approach of performing further traditional AFib monitoring on these patients.
“I think going forward in my practice, when we come across this device-detected AF[ib], we will do further investigations with an established method for detecting AF[ib] involving surface ECG monitoring – maybe a 3-day or 7-day Holter. If that shows AF[ib], then we will be on firm ground to start anticoagulation. If that doesn’t show AF[ib], we will probably not use anticoagulation.”
The ARTESIA trial and the meta-analysis of the two trials were both presented at the annual scientific sessions of the American Heart Association. Both studies were also simultaneously published online – ARTESIA in the New England Journal of Medicine and the meta-analysis in Circulation.
ARTESIA
For the ARTESIA study, 4012 patients with device-detected AFib and other clinical risk factors for stroke were randomly assigned to treatment with apixaban (5 mg twice daily) or aspirin (81 mg daily).
After a mean follow-up of 3.5 years, the primary endpoint – stroke or systemic embolism – occurred in 55 patients in the apixaban group (0.78% per patient-year), compared with 86 patients in the aspirin group (1.24% per patient-year), giving a hazard ratio of 0.63 (95% confidence interval, 0.45-0.88; P = .007).
“The risk of stroke or systemic embolism was lower by 37% with apixaban than with aspirin, and the risk of disabling or fatal stroke was lower by 49%,” Dr. Healey reported.
In the “on-treatment” population, the rate of major bleeding was 1.71% per patient-year in the apixaban group and 0.94% per patient-year in the aspirin group (HR, 1.80; 95% CI, 1.26-2.57; P = .001).
Fatal bleeding occurred in five patients in the apixaban group and eight patients in the aspirin group. Symptomatic intracranial hemorrhage occurred in 12 patients with apixaban and 15 patients with aspirin.
One of the main findings of the trial is the lower-than-expected risk of ischemic stroke in this population – about 1% per year in the aspirin group, which was reduced to 0.64% per year in the apixaban group.
The authors noted that “simply counting strokes as compared with bleeding events might suggest a neutral overall effect. With apixaban as compared with aspirin, 31 fewer cases of stroke or systemic embolism were seen in the intention-to-treat analysis, as compared with 39 more major bleeding events in the on-treatment analysis.”
However, they pointed out that strokes involve permanent loss of brain tissue, whereas major bleeding is usually reversible, with most patients having complete recovery, which was the case in this study.
“Thus, on the basis of the considerably greater severity of the stroke events prevented than the bleeding events caused, we believe that these findings favor consideration of the use of oral anticoagulation for patients with risk factors for stroke in whom subclinical atrial fibrillation develops,” they concluded.
First well-powered trial addressing this question
Discussing the ARTESIA trial at an AHA press conference, Christine Albert, MD, Cedars-Sinai Medical Center, Los Angeles, said: “I want to emphasize how important this trial is.”
She explained that current guidelines do not recommend any treatment for patients with device-detected AFib that is not shown on ECG, even though it is known this confers some excess risk of stroke.
“ARTESIA is the first well-powered, long-term trial looking at this question,” she said. “It found a clear reduction in the risk of stroke/systemic embolism with apixaban vs aspirin, but there was also a significant amount of bleeding – about an 80% increase. The question is whether the benefit on stroke is worth it given the bleeding risk.”
Dr. Albert highlighted the low absolute risk of stroke in this study population of around 1.2%, pointing out that even with the 37% relative reduction with anticoagulation, stroke is only reduced in absolute terms by 0.4%.
“We are going to have to take this back to committees and guidelines and look at the balance between the benefit on stroke and the increase in bleeding,” she concluded.
Noting that observational studies have shown that the duration of AFib impacts the risk of stroke, Dr. Albert suggested that patients with longer-duration AFib may benefit from anticoagulation to a greater extent; and given that the bleeding seen in ARTESIA was mainly GI bleeding, it might be possible to screen out patients at high risk of GI bleeding.
She also pointed out that a lot of patients discontinued anticoagulation treatment in both ARTESIA and NOAH-AFNET 6, showing that this is not an easy strategy for elderly patients.
In an editorial accompanying publication of the ARTESIA trial, Emma Svennberg, MD, Karolinska Institute, Stockholm, also concluded that, “going forward, we must balance the increased bleeding risks with the risk for disabling strokes,” and that “future substudies and meta-analyses may provide further insights regarding treatment benefits in specific subgroups.”
NOAH-AFNET 6: New subgroup analysis
The previously reported NOAH-AFNET 6 study randomly assigned 2,538 patients with subclinical AFib and additional risk factors for stroke to anticoagulation with edoxaban or placebo. The trial was stopped early, so it was underpowered – but it found no difference between groups in the incidence of the composite endpoint of stroke, systemic embolism, or death from cardiovascular causes or in the incidence of stroke, although there was higher risk of major bleeding.
Again, there was a low rate of stroke in this trial with just 49 strokes in total in the whole study. The NOAH-AFNET-6 investigators concluded that these patients should not receive anticoagulation because the risk of bleeding outweighed any potential benefits.
A new subanalysis of the 259 patients who had durations of subclinical AFib of 24 hours or longer in the NOAH-AFNET 6 trial was presented at the AHA meeting, and simultaneously published online in the European Heart Journal.
This showed that the rate of stroke also appeared low in patients with these long durations of subclinical AFib, and that there was no interaction between the duration of subclinical AFib and the efficacy and safety of oral anticoagulation.
But with such a low number of events in the study as a whole and in the long duration subclinical AFib subgroup (in which there were just two strokes in each treatment group), this analysis was unlikely to show a difference, Dr. Kirchhof commented.
The subgroup analysis did, however, show that patients experiencing subclinical AFib durations of 24 hours or more were more likely to develop clinical AFib over time than those with shorter durations, suggesting the need for regular ECGs in these patients.
Dr. Kirchhof said better methods are needed to detect patients with subclinical AFib at high risk of stroke. “I don’t think our clinical stroke risk factor scores such as CHA2DS2-VASc are sufficient to detect high-risk patients. Patients in both NOAH-AFNET 6 and ARTESIA had a median CHA2DS2-VASc score of 4, but they had a stroke rate of just 1% per year,” he noted.
The meta-analysis of the two trials showed that the results from both are consistent, with an overall reduction in ischemic stroke with oral anticoagulation (relative risk, 0.68). Oral anticoagulation also reduced a composite of cardiovascular death, all-cause stroke, peripheral arterial embolism, myocardial infarction, or pulmonary embolism (RR, 0.85).
There was no significant difference in cardiovascular death (RR, 0.95) or all-cause mortality (RR, 1.08), but anticoagulation significantly increased major bleeding (RR, 1.62).
Aspirin use complicates results
Dr. Healey said further analyses of the ARTESIA data will try to tease out the effect of concomitant aspirin use in the trial.
He explained that patients in this trial were allowed to take a single antiplatelet agent on top of study therapy.
“It is difficult to work out the exact use of antiplatelet therapy as it changed throughout the study,” he said. “About two-thirds were taking antiplatelet agents at the time of enrollment into the trial, but this decreased throughout the study. Many clinicians stopped open-label antiplatelet therapy during the trial when new evidence came out to suggest that there was no added benefit of adding aspirin on top of anticoagulants.
“We need to look carefully as to what impact that may have had,” Dr. Healey added. “We know from other studies that adding an antiplatelet on top of an anticoagulant doesn’t do much to thromboembolic events, but it approximately doubles the risk of major bleeding.”
In contrast, the NOAH-AFNET trial did not allow aspirin use in the anticoagulation group and aspirin was taken by around half the patients in the placebo group who had an indication for its use.
The authors of the meta-analysis pointed out that the omission of aspirin in nearly half of the control patients in NOAH-AFNET 6 and the early termination of the trial may have led to a slightly higher estimate for excess major bleeding with anticoagulation.
The ARTESIA study was supported by the Canadian Institutes for Health Research, the Bristol Myers Squibb-Pfizer Alliance, the Heart and Stroke Foundation of Canada, the Canadian Stroke Prevention Intervention Network, Hamilton Health Sciences, the Advancing Clinical Trials Network and the Population Health Research Institute. Dr. Healey reported research grants and speaking fees from BMS/Pfizer Alliance, Servier, Novartis, Boston Scientific, Medtronic; and acts as a consultant to Bayer, Servier and Boston Scientific. The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
in the ARTESIA study.
The results appear to contrast somewhat with the recently reported NOAH-AFNET 6 trial, which failed to show a reduction in stroke with the anticoagulant edoxaban versus placebo in a similar patient group, but that trial was stopped early and so was underpowered.
However, the lead investigators of both trials say the studies actually show consistent results – both found a lower rate of stroke than expected in this population, but the confidence intervals for stroke reduction with anticoagulation overlap, suggesting there is likely some effect, albeit less than that in clinical AFib.
The big question is whether the reduction in stroke with anticoagulation outweighs the increase in major bleeding.
A new meta-analysis of the two trials showed that “oral anticoagulation with edoxaban or apixaban reduces the risk of ischemic stroke by approximately one-third and increases major bleeding by roughly double.”
In absolute numbers, there were three fewer ischemic strokes per 1,000 patient-years with anticoagulation in the two trials combined, at the cost of seven more major bleeds.
The lead investigators of the two trials have somewhat different opinions on how these findings may translate into clinical practice.
Jeff Healey, MD, Population Health Research Institute, McMaster University, Hamilton, Ont., lead investigator of the ARTESIA trial, believes that the risks and benefits need to be assessed in individual patients, but there should be some patient groups that will benefit from anticoagulation treatment.
“In patients with pacemakers or implantable loop recorders with continuous monitoring, subclinical AF[ib] is detected in about one third of patients, so this is extremely common,” he said in an interview. “The question is whether this is just a normal feature of getting older or is this like AF[ib] that we see in the clinic which increases stroke risk, and I think we can conclude from ARTESIA that this subclinical AF[ib] is associated with an increased risk of stroke, although that is lower than the risk with clinical AF[ib], and that it can be reduced by anticoagulation.”
Until recently it hasn’t been possible to quantify the risk associated with subclinical AFib, he noted. “But now we have a rich dataset to use to see if we can tease out some specifics on this. Future analyses of this dataset will help define patients where the benefits outweigh the risks of bleeding. For now, I think we can look at the data in a qualitative way and consider the totality of risk factors in each patient – their bleeding risk, stroke risk, how much AF[ib] they have, and make a decision as to whether to give anticoagulation or not.”
But Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), lead investigator of the NOAH-AFNET 6 trial said: “Both trials showed the stroke rate is low in these patients – about 1% per year – and that anticoagulation can reduce it a bit further at the expense of increasing major bleeding. I don’t believe the AF[ib] episodes picked up on these devices constitute a sufficient stroke risk to warrant anticoagulation, given the bleeding risk.”
Dr. Kirchhof suggests an alternate approach of performing further traditional AFib monitoring on these patients.
“I think going forward in my practice, when we come across this device-detected AF[ib], we will do further investigations with an established method for detecting AF[ib] involving surface ECG monitoring – maybe a 3-day or 7-day Holter. If that shows AF[ib], then we will be on firm ground to start anticoagulation. If that doesn’t show AF[ib], we will probably not use anticoagulation.”
The ARTESIA trial and the meta-analysis of the two trials were both presented at the annual scientific sessions of the American Heart Association. Both studies were also simultaneously published online – ARTESIA in the New England Journal of Medicine and the meta-analysis in Circulation.
ARTESIA
For the ARTESIA study, 4012 patients with device-detected AFib and other clinical risk factors for stroke were randomly assigned to treatment with apixaban (5 mg twice daily) or aspirin (81 mg daily).
After a mean follow-up of 3.5 years, the primary endpoint – stroke or systemic embolism – occurred in 55 patients in the apixaban group (0.78% per patient-year), compared with 86 patients in the aspirin group (1.24% per patient-year), giving a hazard ratio of 0.63 (95% confidence interval, 0.45-0.88; P = .007).
“The risk of stroke or systemic embolism was lower by 37% with apixaban than with aspirin, and the risk of disabling or fatal stroke was lower by 49%,” Dr. Healey reported.
In the “on-treatment” population, the rate of major bleeding was 1.71% per patient-year in the apixaban group and 0.94% per patient-year in the aspirin group (HR, 1.80; 95% CI, 1.26-2.57; P = .001).
Fatal bleeding occurred in five patients in the apixaban group and eight patients in the aspirin group. Symptomatic intracranial hemorrhage occurred in 12 patients with apixaban and 15 patients with aspirin.
One of the main findings of the trial is the lower-than-expected risk of ischemic stroke in this population – about 1% per year in the aspirin group, which was reduced to 0.64% per year in the apixaban group.
The authors noted that “simply counting strokes as compared with bleeding events might suggest a neutral overall effect. With apixaban as compared with aspirin, 31 fewer cases of stroke or systemic embolism were seen in the intention-to-treat analysis, as compared with 39 more major bleeding events in the on-treatment analysis.”
However, they pointed out that strokes involve permanent loss of brain tissue, whereas major bleeding is usually reversible, with most patients having complete recovery, which was the case in this study.
“Thus, on the basis of the considerably greater severity of the stroke events prevented than the bleeding events caused, we believe that these findings favor consideration of the use of oral anticoagulation for patients with risk factors for stroke in whom subclinical atrial fibrillation develops,” they concluded.
First well-powered trial addressing this question
Discussing the ARTESIA trial at an AHA press conference, Christine Albert, MD, Cedars-Sinai Medical Center, Los Angeles, said: “I want to emphasize how important this trial is.”
She explained that current guidelines do not recommend any treatment for patients with device-detected AFib that is not shown on ECG, even though it is known this confers some excess risk of stroke.
“ARTESIA is the first well-powered, long-term trial looking at this question,” she said. “It found a clear reduction in the risk of stroke/systemic embolism with apixaban vs aspirin, but there was also a significant amount of bleeding – about an 80% increase. The question is whether the benefit on stroke is worth it given the bleeding risk.”
Dr. Albert highlighted the low absolute risk of stroke in this study population of around 1.2%, pointing out that even with the 37% relative reduction with anticoagulation, stroke is only reduced in absolute terms by 0.4%.
“We are going to have to take this back to committees and guidelines and look at the balance between the benefit on stroke and the increase in bleeding,” she concluded.
Noting that observational studies have shown that the duration of AFib impacts the risk of stroke, Dr. Albert suggested that patients with longer-duration AFib may benefit from anticoagulation to a greater extent; and given that the bleeding seen in ARTESIA was mainly GI bleeding, it might be possible to screen out patients at high risk of GI bleeding.
She also pointed out that a lot of patients discontinued anticoagulation treatment in both ARTESIA and NOAH-AFNET 6, showing that this is not an easy strategy for elderly patients.
In an editorial accompanying publication of the ARTESIA trial, Emma Svennberg, MD, Karolinska Institute, Stockholm, also concluded that, “going forward, we must balance the increased bleeding risks with the risk for disabling strokes,” and that “future substudies and meta-analyses may provide further insights regarding treatment benefits in specific subgroups.”
NOAH-AFNET 6: New subgroup analysis
The previously reported NOAH-AFNET 6 study randomly assigned 2,538 patients with subclinical AFib and additional risk factors for stroke to anticoagulation with edoxaban or placebo. The trial was stopped early, so it was underpowered – but it found no difference between groups in the incidence of the composite endpoint of stroke, systemic embolism, or death from cardiovascular causes or in the incidence of stroke, although there was higher risk of major bleeding.
Again, there was a low rate of stroke in this trial with just 49 strokes in total in the whole study. The NOAH-AFNET-6 investigators concluded that these patients should not receive anticoagulation because the risk of bleeding outweighed any potential benefits.
A new subanalysis of the 259 patients who had durations of subclinical AFib of 24 hours or longer in the NOAH-AFNET 6 trial was presented at the AHA meeting, and simultaneously published online in the European Heart Journal.
This showed that the rate of stroke also appeared low in patients with these long durations of subclinical AFib, and that there was no interaction between the duration of subclinical AFib and the efficacy and safety of oral anticoagulation.
But with such a low number of events in the study as a whole and in the long duration subclinical AFib subgroup (in which there were just two strokes in each treatment group), this analysis was unlikely to show a difference, Dr. Kirchhof commented.
The subgroup analysis did, however, show that patients experiencing subclinical AFib durations of 24 hours or more were more likely to develop clinical AFib over time than those with shorter durations, suggesting the need for regular ECGs in these patients.
Dr. Kirchhof said better methods are needed to detect patients with subclinical AFib at high risk of stroke. “I don’t think our clinical stroke risk factor scores such as CHA2DS2-VASc are sufficient to detect high-risk patients. Patients in both NOAH-AFNET 6 and ARTESIA had a median CHA2DS2-VASc score of 4, but they had a stroke rate of just 1% per year,” he noted.
The meta-analysis of the two trials showed that the results from both are consistent, with an overall reduction in ischemic stroke with oral anticoagulation (relative risk, 0.68). Oral anticoagulation also reduced a composite of cardiovascular death, all-cause stroke, peripheral arterial embolism, myocardial infarction, or pulmonary embolism (RR, 0.85).
There was no significant difference in cardiovascular death (RR, 0.95) or all-cause mortality (RR, 1.08), but anticoagulation significantly increased major bleeding (RR, 1.62).
Aspirin use complicates results
Dr. Healey said further analyses of the ARTESIA data will try to tease out the effect of concomitant aspirin use in the trial.
He explained that patients in this trial were allowed to take a single antiplatelet agent on top of study therapy.
“It is difficult to work out the exact use of antiplatelet therapy as it changed throughout the study,” he said. “About two-thirds were taking antiplatelet agents at the time of enrollment into the trial, but this decreased throughout the study. Many clinicians stopped open-label antiplatelet therapy during the trial when new evidence came out to suggest that there was no added benefit of adding aspirin on top of anticoagulants.
“We need to look carefully as to what impact that may have had,” Dr. Healey added. “We know from other studies that adding an antiplatelet on top of an anticoagulant doesn’t do much to thromboembolic events, but it approximately doubles the risk of major bleeding.”
In contrast, the NOAH-AFNET trial did not allow aspirin use in the anticoagulation group and aspirin was taken by around half the patients in the placebo group who had an indication for its use.
The authors of the meta-analysis pointed out that the omission of aspirin in nearly half of the control patients in NOAH-AFNET 6 and the early termination of the trial may have led to a slightly higher estimate for excess major bleeding with anticoagulation.
The ARTESIA study was supported by the Canadian Institutes for Health Research, the Bristol Myers Squibb-Pfizer Alliance, the Heart and Stroke Foundation of Canada, the Canadian Stroke Prevention Intervention Network, Hamilton Health Sciences, the Advancing Clinical Trials Network and the Population Health Research Institute. Dr. Healey reported research grants and speaking fees from BMS/Pfizer Alliance, Servier, Novartis, Boston Scientific, Medtronic; and acts as a consultant to Bayer, Servier and Boston Scientific. The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
in the ARTESIA study.
The results appear to contrast somewhat with the recently reported NOAH-AFNET 6 trial, which failed to show a reduction in stroke with the anticoagulant edoxaban versus placebo in a similar patient group, but that trial was stopped early and so was underpowered.
However, the lead investigators of both trials say the studies actually show consistent results – both found a lower rate of stroke than expected in this population, but the confidence intervals for stroke reduction with anticoagulation overlap, suggesting there is likely some effect, albeit less than that in clinical AFib.
The big question is whether the reduction in stroke with anticoagulation outweighs the increase in major bleeding.
A new meta-analysis of the two trials showed that “oral anticoagulation with edoxaban or apixaban reduces the risk of ischemic stroke by approximately one-third and increases major bleeding by roughly double.”
In absolute numbers, there were three fewer ischemic strokes per 1,000 patient-years with anticoagulation in the two trials combined, at the cost of seven more major bleeds.
The lead investigators of the two trials have somewhat different opinions on how these findings may translate into clinical practice.
Jeff Healey, MD, Population Health Research Institute, McMaster University, Hamilton, Ont., lead investigator of the ARTESIA trial, believes that the risks and benefits need to be assessed in individual patients, but there should be some patient groups that will benefit from anticoagulation treatment.
“In patients with pacemakers or implantable loop recorders with continuous monitoring, subclinical AF[ib] is detected in about one third of patients, so this is extremely common,” he said in an interview. “The question is whether this is just a normal feature of getting older or is this like AF[ib] that we see in the clinic which increases stroke risk, and I think we can conclude from ARTESIA that this subclinical AF[ib] is associated with an increased risk of stroke, although that is lower than the risk with clinical AF[ib], and that it can be reduced by anticoagulation.”
Until recently it hasn’t been possible to quantify the risk associated with subclinical AFib, he noted. “But now we have a rich dataset to use to see if we can tease out some specifics on this. Future analyses of this dataset will help define patients where the benefits outweigh the risks of bleeding. For now, I think we can look at the data in a qualitative way and consider the totality of risk factors in each patient – their bleeding risk, stroke risk, how much AF[ib] they have, and make a decision as to whether to give anticoagulation or not.”
But Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), lead investigator of the NOAH-AFNET 6 trial said: “Both trials showed the stroke rate is low in these patients – about 1% per year – and that anticoagulation can reduce it a bit further at the expense of increasing major bleeding. I don’t believe the AF[ib] episodes picked up on these devices constitute a sufficient stroke risk to warrant anticoagulation, given the bleeding risk.”
Dr. Kirchhof suggests an alternate approach of performing further traditional AFib monitoring on these patients.
“I think going forward in my practice, when we come across this device-detected AF[ib], we will do further investigations with an established method for detecting AF[ib] involving surface ECG monitoring – maybe a 3-day or 7-day Holter. If that shows AF[ib], then we will be on firm ground to start anticoagulation. If that doesn’t show AF[ib], we will probably not use anticoagulation.”
The ARTESIA trial and the meta-analysis of the two trials were both presented at the annual scientific sessions of the American Heart Association. Both studies were also simultaneously published online – ARTESIA in the New England Journal of Medicine and the meta-analysis in Circulation.
ARTESIA
For the ARTESIA study, 4012 patients with device-detected AFib and other clinical risk factors for stroke were randomly assigned to treatment with apixaban (5 mg twice daily) or aspirin (81 mg daily).
After a mean follow-up of 3.5 years, the primary endpoint – stroke or systemic embolism – occurred in 55 patients in the apixaban group (0.78% per patient-year), compared with 86 patients in the aspirin group (1.24% per patient-year), giving a hazard ratio of 0.63 (95% confidence interval, 0.45-0.88; P = .007).
“The risk of stroke or systemic embolism was lower by 37% with apixaban than with aspirin, and the risk of disabling or fatal stroke was lower by 49%,” Dr. Healey reported.
In the “on-treatment” population, the rate of major bleeding was 1.71% per patient-year in the apixaban group and 0.94% per patient-year in the aspirin group (HR, 1.80; 95% CI, 1.26-2.57; P = .001).
Fatal bleeding occurred in five patients in the apixaban group and eight patients in the aspirin group. Symptomatic intracranial hemorrhage occurred in 12 patients with apixaban and 15 patients with aspirin.
One of the main findings of the trial is the lower-than-expected risk of ischemic stroke in this population – about 1% per year in the aspirin group, which was reduced to 0.64% per year in the apixaban group.
The authors noted that “simply counting strokes as compared with bleeding events might suggest a neutral overall effect. With apixaban as compared with aspirin, 31 fewer cases of stroke or systemic embolism were seen in the intention-to-treat analysis, as compared with 39 more major bleeding events in the on-treatment analysis.”
However, they pointed out that strokes involve permanent loss of brain tissue, whereas major bleeding is usually reversible, with most patients having complete recovery, which was the case in this study.
“Thus, on the basis of the considerably greater severity of the stroke events prevented than the bleeding events caused, we believe that these findings favor consideration of the use of oral anticoagulation for patients with risk factors for stroke in whom subclinical atrial fibrillation develops,” they concluded.
First well-powered trial addressing this question
Discussing the ARTESIA trial at an AHA press conference, Christine Albert, MD, Cedars-Sinai Medical Center, Los Angeles, said: “I want to emphasize how important this trial is.”
She explained that current guidelines do not recommend any treatment for patients with device-detected AFib that is not shown on ECG, even though it is known this confers some excess risk of stroke.
“ARTESIA is the first well-powered, long-term trial looking at this question,” she said. “It found a clear reduction in the risk of stroke/systemic embolism with apixaban vs aspirin, but there was also a significant amount of bleeding – about an 80% increase. The question is whether the benefit on stroke is worth it given the bleeding risk.”
Dr. Albert highlighted the low absolute risk of stroke in this study population of around 1.2%, pointing out that even with the 37% relative reduction with anticoagulation, stroke is only reduced in absolute terms by 0.4%.
“We are going to have to take this back to committees and guidelines and look at the balance between the benefit on stroke and the increase in bleeding,” she concluded.
Noting that observational studies have shown that the duration of AFib impacts the risk of stroke, Dr. Albert suggested that patients with longer-duration AFib may benefit from anticoagulation to a greater extent; and given that the bleeding seen in ARTESIA was mainly GI bleeding, it might be possible to screen out patients at high risk of GI bleeding.
She also pointed out that a lot of patients discontinued anticoagulation treatment in both ARTESIA and NOAH-AFNET 6, showing that this is not an easy strategy for elderly patients.
In an editorial accompanying publication of the ARTESIA trial, Emma Svennberg, MD, Karolinska Institute, Stockholm, also concluded that, “going forward, we must balance the increased bleeding risks with the risk for disabling strokes,” and that “future substudies and meta-analyses may provide further insights regarding treatment benefits in specific subgroups.”
NOAH-AFNET 6: New subgroup analysis
The previously reported NOAH-AFNET 6 study randomly assigned 2,538 patients with subclinical AFib and additional risk factors for stroke to anticoagulation with edoxaban or placebo. The trial was stopped early, so it was underpowered – but it found no difference between groups in the incidence of the composite endpoint of stroke, systemic embolism, or death from cardiovascular causes or in the incidence of stroke, although there was higher risk of major bleeding.
Again, there was a low rate of stroke in this trial with just 49 strokes in total in the whole study. The NOAH-AFNET-6 investigators concluded that these patients should not receive anticoagulation because the risk of bleeding outweighed any potential benefits.
A new subanalysis of the 259 patients who had durations of subclinical AFib of 24 hours or longer in the NOAH-AFNET 6 trial was presented at the AHA meeting, and simultaneously published online in the European Heart Journal.
This showed that the rate of stroke also appeared low in patients with these long durations of subclinical AFib, and that there was no interaction between the duration of subclinical AFib and the efficacy and safety of oral anticoagulation.
But with such a low number of events in the study as a whole and in the long duration subclinical AFib subgroup (in which there were just two strokes in each treatment group), this analysis was unlikely to show a difference, Dr. Kirchhof commented.
The subgroup analysis did, however, show that patients experiencing subclinical AFib durations of 24 hours or more were more likely to develop clinical AFib over time than those with shorter durations, suggesting the need for regular ECGs in these patients.
Dr. Kirchhof said better methods are needed to detect patients with subclinical AFib at high risk of stroke. “I don’t think our clinical stroke risk factor scores such as CHA2DS2-VASc are sufficient to detect high-risk patients. Patients in both NOAH-AFNET 6 and ARTESIA had a median CHA2DS2-VASc score of 4, but they had a stroke rate of just 1% per year,” he noted.
The meta-analysis of the two trials showed that the results from both are consistent, with an overall reduction in ischemic stroke with oral anticoagulation (relative risk, 0.68). Oral anticoagulation also reduced a composite of cardiovascular death, all-cause stroke, peripheral arterial embolism, myocardial infarction, or pulmonary embolism (RR, 0.85).
There was no significant difference in cardiovascular death (RR, 0.95) or all-cause mortality (RR, 1.08), but anticoagulation significantly increased major bleeding (RR, 1.62).
Aspirin use complicates results
Dr. Healey said further analyses of the ARTESIA data will try to tease out the effect of concomitant aspirin use in the trial.
He explained that patients in this trial were allowed to take a single antiplatelet agent on top of study therapy.
“It is difficult to work out the exact use of antiplatelet therapy as it changed throughout the study,” he said. “About two-thirds were taking antiplatelet agents at the time of enrollment into the trial, but this decreased throughout the study. Many clinicians stopped open-label antiplatelet therapy during the trial when new evidence came out to suggest that there was no added benefit of adding aspirin on top of anticoagulants.
“We need to look carefully as to what impact that may have had,” Dr. Healey added. “We know from other studies that adding an antiplatelet on top of an anticoagulant doesn’t do much to thromboembolic events, but it approximately doubles the risk of major bleeding.”
In contrast, the NOAH-AFNET trial did not allow aspirin use in the anticoagulation group and aspirin was taken by around half the patients in the placebo group who had an indication for its use.
The authors of the meta-analysis pointed out that the omission of aspirin in nearly half of the control patients in NOAH-AFNET 6 and the early termination of the trial may have led to a slightly higher estimate for excess major bleeding with anticoagulation.
The ARTESIA study was supported by the Canadian Institutes for Health Research, the Bristol Myers Squibb-Pfizer Alliance, the Heart and Stroke Foundation of Canada, the Canadian Stroke Prevention Intervention Network, Hamilton Health Sciences, the Advancing Clinical Trials Network and the Population Health Research Institute. Dr. Healey reported research grants and speaking fees from BMS/Pfizer Alliance, Servier, Novartis, Boston Scientific, Medtronic; and acts as a consultant to Bayer, Servier and Boston Scientific. The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
FROM AHA 2023
Artificial intelligence presents opportunities, challenges in neurologic practice
PHOENIX – and it presents opportunities for increased production and automation of some tasks. However, it is prone to error and ‘hallucinations’ despite an authoritative tone, so its conclusions must be verified.
Those were some of the messages from a talk by John Morren, MD, an associate professor of neurology at Case Western Reserve University, Cleveland, who spoke about AI at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
He encouraged attendees to get involved in the conversation of AI, because it is here to stay and will have a big impact on health care. “If we’re not around the table making decisions, decisions will be made for us in our absence and won’t be in our favor,” said Dr. Morren.
He started out his talk by asking if anyone in the room had used AI. After about half raised their hands, he countered that nearly everyone likely had. Voice assistants like SIRI and Alexa, social media with curated feeds, online shopping tools that provide product suggestions, and content recommendations from streaming services like Netflix all rely on AI technology.
Within medicine, AI is already playing a role in various fields, including medical imaging, disease diagnosis, drug discovery and development, predictive analytics, personalized medicine, telemedicine, and health care management.
It also has potential to be used on the job. For example, ChatGPT can generate and refine conversations towards a specific length, format, style, and level of detail. Alternatives include Bing AI from Microsoft, Bard AI from Google, Writesonic, Copy.ai, SpinBot, HIX.AI, and Chatsonic.
Specific to medicine, Consensus is a search engine that uses AI to search for, summarize, and synthesize studies from peer-reviewed literature.
Trust, but verify
Dr. Morren presented some specific use cases, including patient education and responses to patient inquiries, as well as generating letters to insurance companies appealing denial of coverage claims. He also showed an example where he asked Bing AI to explain to a patient, at a sixth- to seventh-grade reading level, the red-flag symptoms of myasthenic crisis.
AI can generate summaries of clinical evidence of previous studies. Asked by this reporter how to trust the accuracies of the summaries if the user hasn’t thoroughly read the papers, he acknowledged the imperfection of AI. “I would say that if you’re going to make a decision that you would not have made normally based on the summary that it’s giving, if you can find the fact that you’re anchoring the decision on, go into the article yourself and make sure that it’s well vetted. The AI is just good to tap you on your shoulder and say, ‘hey, just consider this.’ That’s all it is. You should always trust, but verify. If the AI is forcing you to say something new that you would not say, maybe don’t do it – or at least research it to know that it’s the truth and then you elevate yourself and get yourself to the next level.”
Limitations
The need to verify can create its own burden, according to one attendee. “I often find I end up spending more time verifying [what ChatGPT has provided]. This seems to take more time than a traditional way of going to PubMed or UpToDate or any of the other human generated consensus way,” he said.
Dr. Morren replied that he wouldn’t recommend using ChatGPT to query medical literature. Instead he recommended Consensus, which only searches the peer-reviewed medical literature.
Another key limitation is that most AI programs are date limited: For example, ChatGPT doesn’t include information after September 2021, though this may change with paid subscriptions. He also starkly warned the audience to never enter sensitive information, including patient identifiers.
There are legal and ethical considerations to AI. Dr. Morren warned against overreliance on AI, as this could undermine compassion and lead to erosion of trust, which makes it important to disclose any use of AI-generated content.
Another attendee raised concerns that AI may be generating research content, including slides for presentations, abstracts, titles, or article text. Dr. Morren said that some organizations, such as the International Committee of Medical Journal Editors, have incorporated AI in their recommendations, stating that authors should disclose any contributions of AI to their publications. However, there is little that can be done to identify AI-generated content, leaving it up to the honor code.
Asked to make predictions about how AI will evolve in the clinic over the next 2-3 years, Dr. Morren suggested that it will likely be embedded in electronic medical records. He anticipated that it will save physicians time so that they can spend more time interacting directly with patients. He quoted Eric Topol, MD, professor of medicine at Scripps Research Translational Institute, La Jolla, Calif., as saying that AI could save 20% of a physician’s time, which could be spent with patients. Dr. Morren saw it differently. “I know where that 20% of time liberated is going to go. I’m going to see 20% more patients. I’m a realist,” he said, to audience laughter.
He also predicted that AI will be found in wearables and devices, allowing health care to expand into the patient’s home in real time. “A lot of what we’re wearing is going to be an extension of the doctor’s office,” he said.
For those hoping for more guidance, Dr. Morren noted that he is the chairman of the professional practice committee of AANEM, and the group will be putting out a position statement within the next couple of months. “It will be a little bit of a blueprint for the path going forward. There are specific things that need to be done. In research, for example, you have to ensure that datasets are diverse enough. To do that we need to have inter-institutional collaboration. We have to ensure patient privacy. Consent for this needs to be a little more explicit because this is a novel area. Those are things that need to be stipulated and ratified through a task force.”
Dr. Morren has no relevant financial disclosures.
PHOENIX – and it presents opportunities for increased production and automation of some tasks. However, it is prone to error and ‘hallucinations’ despite an authoritative tone, so its conclusions must be verified.
Those were some of the messages from a talk by John Morren, MD, an associate professor of neurology at Case Western Reserve University, Cleveland, who spoke about AI at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
He encouraged attendees to get involved in the conversation of AI, because it is here to stay and will have a big impact on health care. “If we’re not around the table making decisions, decisions will be made for us in our absence and won’t be in our favor,” said Dr. Morren.
He started out his talk by asking if anyone in the room had used AI. After about half raised their hands, he countered that nearly everyone likely had. Voice assistants like SIRI and Alexa, social media with curated feeds, online shopping tools that provide product suggestions, and content recommendations from streaming services like Netflix all rely on AI technology.
Within medicine, AI is already playing a role in various fields, including medical imaging, disease diagnosis, drug discovery and development, predictive analytics, personalized medicine, telemedicine, and health care management.
It also has potential to be used on the job. For example, ChatGPT can generate and refine conversations towards a specific length, format, style, and level of detail. Alternatives include Bing AI from Microsoft, Bard AI from Google, Writesonic, Copy.ai, SpinBot, HIX.AI, and Chatsonic.
Specific to medicine, Consensus is a search engine that uses AI to search for, summarize, and synthesize studies from peer-reviewed literature.
Trust, but verify
Dr. Morren presented some specific use cases, including patient education and responses to patient inquiries, as well as generating letters to insurance companies appealing denial of coverage claims. He also showed an example where he asked Bing AI to explain to a patient, at a sixth- to seventh-grade reading level, the red-flag symptoms of myasthenic crisis.
AI can generate summaries of clinical evidence of previous studies. Asked by this reporter how to trust the accuracies of the summaries if the user hasn’t thoroughly read the papers, he acknowledged the imperfection of AI. “I would say that if you’re going to make a decision that you would not have made normally based on the summary that it’s giving, if you can find the fact that you’re anchoring the decision on, go into the article yourself and make sure that it’s well vetted. The AI is just good to tap you on your shoulder and say, ‘hey, just consider this.’ That’s all it is. You should always trust, but verify. If the AI is forcing you to say something new that you would not say, maybe don’t do it – or at least research it to know that it’s the truth and then you elevate yourself and get yourself to the next level.”
Limitations
The need to verify can create its own burden, according to one attendee. “I often find I end up spending more time verifying [what ChatGPT has provided]. This seems to take more time than a traditional way of going to PubMed or UpToDate or any of the other human generated consensus way,” he said.
Dr. Morren replied that he wouldn’t recommend using ChatGPT to query medical literature. Instead he recommended Consensus, which only searches the peer-reviewed medical literature.
Another key limitation is that most AI programs are date limited: For example, ChatGPT doesn’t include information after September 2021, though this may change with paid subscriptions. He also starkly warned the audience to never enter sensitive information, including patient identifiers.
There are legal and ethical considerations to AI. Dr. Morren warned against overreliance on AI, as this could undermine compassion and lead to erosion of trust, which makes it important to disclose any use of AI-generated content.
Another attendee raised concerns that AI may be generating research content, including slides for presentations, abstracts, titles, or article text. Dr. Morren said that some organizations, such as the International Committee of Medical Journal Editors, have incorporated AI in their recommendations, stating that authors should disclose any contributions of AI to their publications. However, there is little that can be done to identify AI-generated content, leaving it up to the honor code.
Asked to make predictions about how AI will evolve in the clinic over the next 2-3 years, Dr. Morren suggested that it will likely be embedded in electronic medical records. He anticipated that it will save physicians time so that they can spend more time interacting directly with patients. He quoted Eric Topol, MD, professor of medicine at Scripps Research Translational Institute, La Jolla, Calif., as saying that AI could save 20% of a physician’s time, which could be spent with patients. Dr. Morren saw it differently. “I know where that 20% of time liberated is going to go. I’m going to see 20% more patients. I’m a realist,” he said, to audience laughter.
He also predicted that AI will be found in wearables and devices, allowing health care to expand into the patient’s home in real time. “A lot of what we’re wearing is going to be an extension of the doctor’s office,” he said.
For those hoping for more guidance, Dr. Morren noted that he is the chairman of the professional practice committee of AANEM, and the group will be putting out a position statement within the next couple of months. “It will be a little bit of a blueprint for the path going forward. There are specific things that need to be done. In research, for example, you have to ensure that datasets are diverse enough. To do that we need to have inter-institutional collaboration. We have to ensure patient privacy. Consent for this needs to be a little more explicit because this is a novel area. Those are things that need to be stipulated and ratified through a task force.”
Dr. Morren has no relevant financial disclosures.
PHOENIX – and it presents opportunities for increased production and automation of some tasks. However, it is prone to error and ‘hallucinations’ despite an authoritative tone, so its conclusions must be verified.
Those were some of the messages from a talk by John Morren, MD, an associate professor of neurology at Case Western Reserve University, Cleveland, who spoke about AI at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
He encouraged attendees to get involved in the conversation of AI, because it is here to stay and will have a big impact on health care. “If we’re not around the table making decisions, decisions will be made for us in our absence and won’t be in our favor,” said Dr. Morren.
He started out his talk by asking if anyone in the room had used AI. After about half raised their hands, he countered that nearly everyone likely had. Voice assistants like SIRI and Alexa, social media with curated feeds, online shopping tools that provide product suggestions, and content recommendations from streaming services like Netflix all rely on AI technology.
Within medicine, AI is already playing a role in various fields, including medical imaging, disease diagnosis, drug discovery and development, predictive analytics, personalized medicine, telemedicine, and health care management.
It also has potential to be used on the job. For example, ChatGPT can generate and refine conversations towards a specific length, format, style, and level of detail. Alternatives include Bing AI from Microsoft, Bard AI from Google, Writesonic, Copy.ai, SpinBot, HIX.AI, and Chatsonic.
Specific to medicine, Consensus is a search engine that uses AI to search for, summarize, and synthesize studies from peer-reviewed literature.
Trust, but verify
Dr. Morren presented some specific use cases, including patient education and responses to patient inquiries, as well as generating letters to insurance companies appealing denial of coverage claims. He also showed an example where he asked Bing AI to explain to a patient, at a sixth- to seventh-grade reading level, the red-flag symptoms of myasthenic crisis.
AI can generate summaries of clinical evidence of previous studies. Asked by this reporter how to trust the accuracies of the summaries if the user hasn’t thoroughly read the papers, he acknowledged the imperfection of AI. “I would say that if you’re going to make a decision that you would not have made normally based on the summary that it’s giving, if you can find the fact that you’re anchoring the decision on, go into the article yourself and make sure that it’s well vetted. The AI is just good to tap you on your shoulder and say, ‘hey, just consider this.’ That’s all it is. You should always trust, but verify. If the AI is forcing you to say something new that you would not say, maybe don’t do it – or at least research it to know that it’s the truth and then you elevate yourself and get yourself to the next level.”
Limitations
The need to verify can create its own burden, according to one attendee. “I often find I end up spending more time verifying [what ChatGPT has provided]. This seems to take more time than a traditional way of going to PubMed or UpToDate or any of the other human generated consensus way,” he said.
Dr. Morren replied that he wouldn’t recommend using ChatGPT to query medical literature. Instead he recommended Consensus, which only searches the peer-reviewed medical literature.
Another key limitation is that most AI programs are date limited: For example, ChatGPT doesn’t include information after September 2021, though this may change with paid subscriptions. He also starkly warned the audience to never enter sensitive information, including patient identifiers.
There are legal and ethical considerations to AI. Dr. Morren warned against overreliance on AI, as this could undermine compassion and lead to erosion of trust, which makes it important to disclose any use of AI-generated content.
Another attendee raised concerns that AI may be generating research content, including slides for presentations, abstracts, titles, or article text. Dr. Morren said that some organizations, such as the International Committee of Medical Journal Editors, have incorporated AI in their recommendations, stating that authors should disclose any contributions of AI to their publications. However, there is little that can be done to identify AI-generated content, leaving it up to the honor code.
Asked to make predictions about how AI will evolve in the clinic over the next 2-3 years, Dr. Morren suggested that it will likely be embedded in electronic medical records. He anticipated that it will save physicians time so that they can spend more time interacting directly with patients. He quoted Eric Topol, MD, professor of medicine at Scripps Research Translational Institute, La Jolla, Calif., as saying that AI could save 20% of a physician’s time, which could be spent with patients. Dr. Morren saw it differently. “I know where that 20% of time liberated is going to go. I’m going to see 20% more patients. I’m a realist,” he said, to audience laughter.
He also predicted that AI will be found in wearables and devices, allowing health care to expand into the patient’s home in real time. “A lot of what we’re wearing is going to be an extension of the doctor’s office,” he said.
For those hoping for more guidance, Dr. Morren noted that he is the chairman of the professional practice committee of AANEM, and the group will be putting out a position statement within the next couple of months. “It will be a little bit of a blueprint for the path going forward. There are specific things that need to be done. In research, for example, you have to ensure that datasets are diverse enough. To do that we need to have inter-institutional collaboration. We have to ensure patient privacy. Consent for this needs to be a little more explicit because this is a novel area. Those are things that need to be stipulated and ratified through a task force.”
Dr. Morren has no relevant financial disclosures.
AT AANEM 2023
Pregnancy in rheumatic disease quadruples risk of cardiovascular events
SAN DIEGO – Pregnant individuals with autoimmune rheumatic diseases (ARDs) are at least four times more likely to experience an acute cardiovascular event (CVE) than are pregnant individuals without these conditions, according to new research presented at the annual meeting of the American College of Rheumatology. Pregnant individuals with primary antiphospholipid syndrome (APS) had a 15-fold increase in CVE risk.
Patients who experienced CVEs were also more likely to experience preterm birth and other adverse pregnancy outcomes (APOs).
Rashmi Dhital, MD, a rheumatology fellow at the University of California, San Diego, and colleagues examined the medical records of pregnant individuals in California who had delivered singleton live-born infants from 2005 to 2020. Using data from the Study of Outcomes in Mothers and Infants (SOMI) database, an administrative population-based birth cohort in California, they identified more than 7 million individuals, 19,340 with ARDs and 7,758 with APS.
They then analyzed how many patients experienced an acute CVE during pregnancy and up to 6 weeks after giving birth.
CVEs occurred in 2.0% of patients with ARDs, 6.9% of individuals with APS, and 0.4% of women without these conditions. CVE risk was four times higher in the ARDs group (adjusted relative risk, 4.1; 95% confidence interval, 3.7-4.5) and nearly 15 times higher in the APS group (aRR, 14.7; 95% CI, 13.5-16.0) than in the comparison group. Patients with systemic lupus erythematosus (SLE) had a sixfold higher risk of CVE, which was further exacerbated by concomitant APS (18-fold higher risk) or lupus nephritis (15-fold higher risk).
Dr. Dhital also classified CVEs as either venous thromboembolism and non-VTE events. Pregnant patients with APS had a high risk for VTE-only CVE (40-fold greater) and a 3.7-fold higher risk of non-VTE events, compared with pregnant patients without these conditions. Patients with SLE along with lupus nephritis had a 20-fold increased risk of VTE-only CVE and an 11-fold higher risk of non-VTE CVE.
Although the study grouped rheumatic diseases together, “lupus is generally driving these results,” Sharon Kolasinski, MD, of the University of Pennsylvania, Philadelphia, noted in an interview. She moderated the plenary session where the research was presented. “If you take out lupus, then what is the risk? That would be an interesting question.”
Between 25% and 30% of all CVEs occurred in the postpartum period, highlighting the importance of close monitoring of cardiovascular risks and events in women with ARDs or APS both during pregnancy and postpartum, Dr. Dhital noted.
Recognizing these risks “can sometimes be challenging due to a lower suspicion of CVE in younger patients, and also symptoms overlap with normal pregnancy,” Dr. Dhital said during her plenary presentation. Working with other clinical teams could help physicians detect these risks in patients.
“It’s important for us to remember that there’s increased risk of cardiovascular events in pregnancy in our patients. It’s uncommon, but it’s not zero,” added Dr. Kolasinski, and this study highlighted when physicians should be more focused about that risk.
Dr. Dhital noted there were some limitations to the study that are inherent in using administrative databases for research that relies on ICD codes, including “the availability of information on disease activity, medications, and labs, which may restrict clinical interpretation.”
SOMI data reinforced by National Inpatient Sample study
The findings were complemented by a study using the National Inpatient Sample database to explore CVE risk in pregnant individuals with various rheumatic diseases. Lead author Karun Shrestha, MD, a resident physician at St. Barnabas Hospital in New York, and colleagues identified delivery hospitalizations from 2016 to 2019 for individuals with SLE, RA, and systemic vasculitis and looked for CVEs including preeclampsia, peripartum cardiomyopathy (PPCM), heart failure, stroke, cardiac arrhythmias, and VTE.
Out of over 3.4 million delivery hospitalizations, researchers identified 5,900 individuals with SLE, 4,895 with RA, and 325 with vasculitis. After adjusting for confounding factors such as race, age, insurance, and other comorbidities, SLE was identified as an independent risk factor for preeclampsia (odds ratio, 1.5; 95% CI, 1.1-2.1), arrhythmia (OR, 3.17; 95% CI, 1.73-5.79), and venous thrombosis (OR, 8.4; 95% CI, 2.9-22.1). Vasculitis was tied to increased risk for preeclampsia (OR, 4.7; 95% CI, 2-11.3), stroke (OR, 513.3; 95% CI, 114-2,284), heart failure (OR, 24.17; 95% CI, 4.68-124.6), and PPCM (OR, 66.7; 95% CI, 8.7-509.4). RA was tied to an increased risk for preeclampsia (OR, 1.5; 95% CI, 1.05-2.1).
Patients with SLE or vasculitis had longer, more costly hospital stays, compared with those without these conditions, and they experienced higher rates of in-hospital mortality. While previous research has demonstrated that patients with SLE have higher risk of cardiac events, there is less literature on CVE risk in pregnancies for vasculitis, Dr. Shrestha said in an interview.
“It’s something to work on,” he said.
Adverse pregnancy outcomes higher with ARDs, APS
In a second abstract also led by Dr. Dhital using SOMI data, researchers found that pregnant individuals with ARDs or APS had a higher risk of experiencing an APO – preterm birth or small-for-gestational age – than individuals without these conditions. CVEs exacerbated that risk, regardless of underlying chronic health conditions.
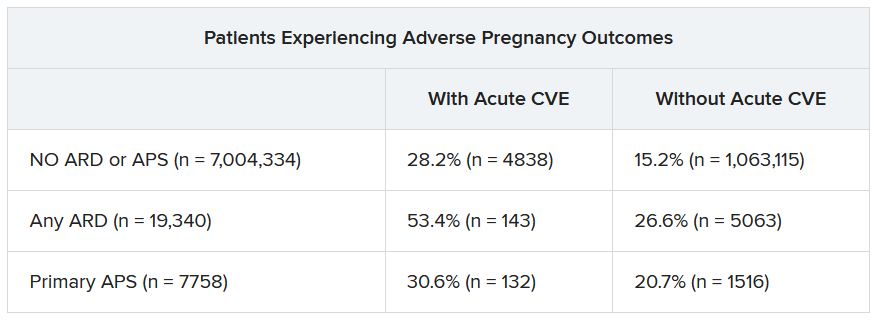
Over half of patients with an ARD and a CVE during pregnancy experienced an APO – most commonly preterm birth. More than one in four pregnant individuals without ARD or APS who experienced a CVE also had an APO.
After differentiating CVEs as either VTE and non-VTE events, patients with ARD and a non-VTE CVE had a fivefold greater risk of early preterm birth (< 32 weeks) and a threefold higher risk of moderate preterm birth (32 to < 34 weeks).
“These findings highlight the need for close monitoring and management of pregnant women, not only for adverse outcomes, but also for cardiovascular risks and events, in order to identify those at the highest risk for adverse outcomes,” the authors wrote. “This need is particularly significant for individuals with ARDs, as 53.4% of our population with an ARD and CVE in pregnancy experienced an APO.”
Dr. Dhital, Dr. Kolasinski, and Dr. Shrestha disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – Pregnant individuals with autoimmune rheumatic diseases (ARDs) are at least four times more likely to experience an acute cardiovascular event (CVE) than are pregnant individuals without these conditions, according to new research presented at the annual meeting of the American College of Rheumatology. Pregnant individuals with primary antiphospholipid syndrome (APS) had a 15-fold increase in CVE risk.
Patients who experienced CVEs were also more likely to experience preterm birth and other adverse pregnancy outcomes (APOs).
Rashmi Dhital, MD, a rheumatology fellow at the University of California, San Diego, and colleagues examined the medical records of pregnant individuals in California who had delivered singleton live-born infants from 2005 to 2020. Using data from the Study of Outcomes in Mothers and Infants (SOMI) database, an administrative population-based birth cohort in California, they identified more than 7 million individuals, 19,340 with ARDs and 7,758 with APS.
They then analyzed how many patients experienced an acute CVE during pregnancy and up to 6 weeks after giving birth.
CVEs occurred in 2.0% of patients with ARDs, 6.9% of individuals with APS, and 0.4% of women without these conditions. CVE risk was four times higher in the ARDs group (adjusted relative risk, 4.1; 95% confidence interval, 3.7-4.5) and nearly 15 times higher in the APS group (aRR, 14.7; 95% CI, 13.5-16.0) than in the comparison group. Patients with systemic lupus erythematosus (SLE) had a sixfold higher risk of CVE, which was further exacerbated by concomitant APS (18-fold higher risk) or lupus nephritis (15-fold higher risk).
Dr. Dhital also classified CVEs as either venous thromboembolism and non-VTE events. Pregnant patients with APS had a high risk for VTE-only CVE (40-fold greater) and a 3.7-fold higher risk of non-VTE events, compared with pregnant patients without these conditions. Patients with SLE along with lupus nephritis had a 20-fold increased risk of VTE-only CVE and an 11-fold higher risk of non-VTE CVE.
Although the study grouped rheumatic diseases together, “lupus is generally driving these results,” Sharon Kolasinski, MD, of the University of Pennsylvania, Philadelphia, noted in an interview. She moderated the plenary session where the research was presented. “If you take out lupus, then what is the risk? That would be an interesting question.”
Between 25% and 30% of all CVEs occurred in the postpartum period, highlighting the importance of close monitoring of cardiovascular risks and events in women with ARDs or APS both during pregnancy and postpartum, Dr. Dhital noted.
Recognizing these risks “can sometimes be challenging due to a lower suspicion of CVE in younger patients, and also symptoms overlap with normal pregnancy,” Dr. Dhital said during her plenary presentation. Working with other clinical teams could help physicians detect these risks in patients.
“It’s important for us to remember that there’s increased risk of cardiovascular events in pregnancy in our patients. It’s uncommon, but it’s not zero,” added Dr. Kolasinski, and this study highlighted when physicians should be more focused about that risk.
Dr. Dhital noted there were some limitations to the study that are inherent in using administrative databases for research that relies on ICD codes, including “the availability of information on disease activity, medications, and labs, which may restrict clinical interpretation.”
SOMI data reinforced by National Inpatient Sample study
The findings were complemented by a study using the National Inpatient Sample database to explore CVE risk in pregnant individuals with various rheumatic diseases. Lead author Karun Shrestha, MD, a resident physician at St. Barnabas Hospital in New York, and colleagues identified delivery hospitalizations from 2016 to 2019 for individuals with SLE, RA, and systemic vasculitis and looked for CVEs including preeclampsia, peripartum cardiomyopathy (PPCM), heart failure, stroke, cardiac arrhythmias, and VTE.
Out of over 3.4 million delivery hospitalizations, researchers identified 5,900 individuals with SLE, 4,895 with RA, and 325 with vasculitis. After adjusting for confounding factors such as race, age, insurance, and other comorbidities, SLE was identified as an independent risk factor for preeclampsia (odds ratio, 1.5; 95% CI, 1.1-2.1), arrhythmia (OR, 3.17; 95% CI, 1.73-5.79), and venous thrombosis (OR, 8.4; 95% CI, 2.9-22.1). Vasculitis was tied to increased risk for preeclampsia (OR, 4.7; 95% CI, 2-11.3), stroke (OR, 513.3; 95% CI, 114-2,284), heart failure (OR, 24.17; 95% CI, 4.68-124.6), and PPCM (OR, 66.7; 95% CI, 8.7-509.4). RA was tied to an increased risk for preeclampsia (OR, 1.5; 95% CI, 1.05-2.1).
Patients with SLE or vasculitis had longer, more costly hospital stays, compared with those without these conditions, and they experienced higher rates of in-hospital mortality. While previous research has demonstrated that patients with SLE have higher risk of cardiac events, there is less literature on CVE risk in pregnancies for vasculitis, Dr. Shrestha said in an interview.
“It’s something to work on,” he said.
Adverse pregnancy outcomes higher with ARDs, APS
In a second abstract also led by Dr. Dhital using SOMI data, researchers found that pregnant individuals with ARDs or APS had a higher risk of experiencing an APO – preterm birth or small-for-gestational age – than individuals without these conditions. CVEs exacerbated that risk, regardless of underlying chronic health conditions.
Over half of patients with an ARD and a CVE during pregnancy experienced an APO – most commonly preterm birth. More than one in four pregnant individuals without ARD or APS who experienced a CVE also had an APO.
After differentiating CVEs as either VTE and non-VTE events, patients with ARD and a non-VTE CVE had a fivefold greater risk of early preterm birth (< 32 weeks) and a threefold higher risk of moderate preterm birth (32 to < 34 weeks).
“These findings highlight the need for close monitoring and management of pregnant women, not only for adverse outcomes, but also for cardiovascular risks and events, in order to identify those at the highest risk for adverse outcomes,” the authors wrote. “This need is particularly significant for individuals with ARDs, as 53.4% of our population with an ARD and CVE in pregnancy experienced an APO.”
Dr. Dhital, Dr. Kolasinski, and Dr. Shrestha disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – Pregnant individuals with autoimmune rheumatic diseases (ARDs) are at least four times more likely to experience an acute cardiovascular event (CVE) than are pregnant individuals without these conditions, according to new research presented at the annual meeting of the American College of Rheumatology. Pregnant individuals with primary antiphospholipid syndrome (APS) had a 15-fold increase in CVE risk.
Patients who experienced CVEs were also more likely to experience preterm birth and other adverse pregnancy outcomes (APOs).
Rashmi Dhital, MD, a rheumatology fellow at the University of California, San Diego, and colleagues examined the medical records of pregnant individuals in California who had delivered singleton live-born infants from 2005 to 2020. Using data from the Study of Outcomes in Mothers and Infants (SOMI) database, an administrative population-based birth cohort in California, they identified more than 7 million individuals, 19,340 with ARDs and 7,758 with APS.
They then analyzed how many patients experienced an acute CVE during pregnancy and up to 6 weeks after giving birth.
CVEs occurred in 2.0% of patients with ARDs, 6.9% of individuals with APS, and 0.4% of women without these conditions. CVE risk was four times higher in the ARDs group (adjusted relative risk, 4.1; 95% confidence interval, 3.7-4.5) and nearly 15 times higher in the APS group (aRR, 14.7; 95% CI, 13.5-16.0) than in the comparison group. Patients with systemic lupus erythematosus (SLE) had a sixfold higher risk of CVE, which was further exacerbated by concomitant APS (18-fold higher risk) or lupus nephritis (15-fold higher risk).
Dr. Dhital also classified CVEs as either venous thromboembolism and non-VTE events. Pregnant patients with APS had a high risk for VTE-only CVE (40-fold greater) and a 3.7-fold higher risk of non-VTE events, compared with pregnant patients without these conditions. Patients with SLE along with lupus nephritis had a 20-fold increased risk of VTE-only CVE and an 11-fold higher risk of non-VTE CVE.
Although the study grouped rheumatic diseases together, “lupus is generally driving these results,” Sharon Kolasinski, MD, of the University of Pennsylvania, Philadelphia, noted in an interview. She moderated the plenary session where the research was presented. “If you take out lupus, then what is the risk? That would be an interesting question.”
Between 25% and 30% of all CVEs occurred in the postpartum period, highlighting the importance of close monitoring of cardiovascular risks and events in women with ARDs or APS both during pregnancy and postpartum, Dr. Dhital noted.
Recognizing these risks “can sometimes be challenging due to a lower suspicion of CVE in younger patients, and also symptoms overlap with normal pregnancy,” Dr. Dhital said during her plenary presentation. Working with other clinical teams could help physicians detect these risks in patients.
“It’s important for us to remember that there’s increased risk of cardiovascular events in pregnancy in our patients. It’s uncommon, but it’s not zero,” added Dr. Kolasinski, and this study highlighted when physicians should be more focused about that risk.
Dr. Dhital noted there were some limitations to the study that are inherent in using administrative databases for research that relies on ICD codes, including “the availability of information on disease activity, medications, and labs, which may restrict clinical interpretation.”
SOMI data reinforced by National Inpatient Sample study
The findings were complemented by a study using the National Inpatient Sample database to explore CVE risk in pregnant individuals with various rheumatic diseases. Lead author Karun Shrestha, MD, a resident physician at St. Barnabas Hospital in New York, and colleagues identified delivery hospitalizations from 2016 to 2019 for individuals with SLE, RA, and systemic vasculitis and looked for CVEs including preeclampsia, peripartum cardiomyopathy (PPCM), heart failure, stroke, cardiac arrhythmias, and VTE.
Out of over 3.4 million delivery hospitalizations, researchers identified 5,900 individuals with SLE, 4,895 with RA, and 325 with vasculitis. After adjusting for confounding factors such as race, age, insurance, and other comorbidities, SLE was identified as an independent risk factor for preeclampsia (odds ratio, 1.5; 95% CI, 1.1-2.1), arrhythmia (OR, 3.17; 95% CI, 1.73-5.79), and venous thrombosis (OR, 8.4; 95% CI, 2.9-22.1). Vasculitis was tied to increased risk for preeclampsia (OR, 4.7; 95% CI, 2-11.3), stroke (OR, 513.3; 95% CI, 114-2,284), heart failure (OR, 24.17; 95% CI, 4.68-124.6), and PPCM (OR, 66.7; 95% CI, 8.7-509.4). RA was tied to an increased risk for preeclampsia (OR, 1.5; 95% CI, 1.05-2.1).
Patients with SLE or vasculitis had longer, more costly hospital stays, compared with those without these conditions, and they experienced higher rates of in-hospital mortality. While previous research has demonstrated that patients with SLE have higher risk of cardiac events, there is less literature on CVE risk in pregnancies for vasculitis, Dr. Shrestha said in an interview.
“It’s something to work on,” he said.
Adverse pregnancy outcomes higher with ARDs, APS
In a second abstract also led by Dr. Dhital using SOMI data, researchers found that pregnant individuals with ARDs or APS had a higher risk of experiencing an APO – preterm birth or small-for-gestational age – than individuals without these conditions. CVEs exacerbated that risk, regardless of underlying chronic health conditions.
Over half of patients with an ARD and a CVE during pregnancy experienced an APO – most commonly preterm birth. More than one in four pregnant individuals without ARD or APS who experienced a CVE also had an APO.
After differentiating CVEs as either VTE and non-VTE events, patients with ARD and a non-VTE CVE had a fivefold greater risk of early preterm birth (< 32 weeks) and a threefold higher risk of moderate preterm birth (32 to < 34 weeks).
“These findings highlight the need for close monitoring and management of pregnant women, not only for adverse outcomes, but also for cardiovascular risks and events, in order to identify those at the highest risk for adverse outcomes,” the authors wrote. “This need is particularly significant for individuals with ARDs, as 53.4% of our population with an ARD and CVE in pregnancy experienced an APO.”
Dr. Dhital, Dr. Kolasinski, and Dr. Shrestha disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ACR 2023
