User login
Cancer groups offer guidance on musculoskeletal adverse events related to checkpoint inhibitors
Recently released guidelines from two major cancer organizations have provided some of the most comprehensive guidance to date on management of musculoskeletal side effects associated with cancer immunotherapy.
The guidelines, published in February, are a “sorely needed” reference point for the rheumatology community and others who will be encountering patients who experience immune-related adverse events (irAEs), according to Leonard H. Calabrese, DO, the R.J. Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio.
“They’re a good first start, given the fact that up until 4 or 5 months ago, there were no endorsed guidelines that included oncologists and rheumatologists,” Dr. Calabrese said of the guidelines, which were collaboratively developed and recently released by both the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN).
Rheumatologists can add value
“We talk a lot about rheumatologists being aware of these diseases, but it’s been pointed out by some oncologists that unless they’re really knowledgeable and can add considerably to the management, it doesn’t do any good just to be aware of it,” Dr. Calabrese explained. “You need to actually have some procedural knowledge.”

ASCO guidelines also describe a polymyalgia-like syndrome seen in some patients on immune checkpoint inhibitors that according to the guideline authors is characterized by pain, but not true muscle weakness.
In general, the guidelines endorse a stepwise approach, in which milder irAEs can be managed with conservative treatments and without the need to stop the immune checkpoint inhibitor therapy. In contrast, more serious side effects may require more intensive management and either temporary or permanent discontinuation of cancer immunotherapy.
One good example is NCCN’s take on managing inflammatory arthritis.
Mild cases of inflammatory arthritis can be treated with NSAIDs, low-dose prednisone, or intra-articular steroids with no need to stop immune checkpoint inhibitor treatment, according to NCCN guideline authors.
Moderate cases, by contrast, may require holding immunotherapy and treating with prednisone. A rheumatology consult by week 4 is “strongly recommended” if the immune arthritis doesn’t improve, the authors added.
Severe cases may warrant permanent discontinuation of immunotherapy and treatment with methylprednisolone/prednisone, infliximab, or tocilizumab, they added. If the irAE doesn’t improve after 2 weeks, a rheumatology consult should be considered for additional disease-modifying antirheumatic drugs, including methotrexate, leflunomide, or sulfasalazine.
irAEs on the rise
These guidelines are particularly useful for rheumatologists to familiarize themselves with the six Food and Drug Administration–approved immune checkpoint inhibitors, their spectrum of side effects, and how oncologists use the severity of presentation to guide therapy, according to Laura Cappelli, MD.

Understanding irAEs will be increasingly important for rheumatologist as the use of immune checkpoint inhibitors continues to increase, said Dr. Cappelli, who has started a research program at Johns Hopkins to evaluate the rheumatologic adverse effects of these therapies.
Dr. Cappelli said her division sees at least one suspected irAE case per week, most commonly the immune arthritis associated with checkpoint inhibitor therapy.
Likewise, Dr. Calabrese said he is already seeing approximately two new referrals per week for adverse events related to these relatively new therapies.
“It’s far outstripped our notion of what we thought we would be doing,” he said in an interview.
Systems have been set up to encourage interprofessional collaborations, he added, including a “virtual referral clinic” where advanced practitioners working with oncologists communicate with advanced practitioners in each of the specialty areas that are most frequently consulted in order to help facilitate care and triage patients.
In addition, a monthly irAE tumor board was set up to include only cases that have manifest autoimmune or autoinflammatory complications.
“We have a growing group of people who come to this from each area involved, whether it be nephrology, neurology, ophthalmology, gastroenterology, rheumatology, or something else,” Dr. Calabrese said. “That’s been a great learning experience for all of us to talk about these adverse events in real time.”
Critical need for guidance
These guidelines meet a growing need to help practicing clinicians identify and best manage immune-related adverse events, according to Bryan J. Schneider, MD, of the University of Michigan Comprehensive Cancer Center, and vice chair of the NCCN Panel on Management of Immunotherapy-Related Toxicities.

“We’re experienced with chemotherapy, and we are very comfortable with the side effects,” he said. “The immunotherapy story is just an entirely different world because, as I tell patients, the therapies aren’t directly damaging cancer cells like chemotherapy. Instead, they are helping the immune system to identify the cancer cells as abnormal and mount an assault. Proteins on cancer cells may suppress the immune response and these therapies effectively ‘release these brakes’ so the immune system can attack.”
Rheumatologists and those with particular expertise in rheumatologic side effects participated in the development of the ASCO and NCCN guidelines. They include Maria E. Suarez-Almazor, MD, PhD, chief of rheumatology and clinical immunology at the University of Texas MD Anderson Cancer Center, Houston, who served on the ASCO expert panel; Jarushka Naidoo, MBBCh, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, provided expertise in the rheumatologic side effects that were considered by the NCCN panel, according to Dr. Schneider.
Rheumatologist input also informed another set of recommendations on immune checkpoint inhibitor toxicities published several months before the ASCO and NCCN guidelines. The working group for the September 2017 guidelines from the Society for Immunotherapy of Cancer (doi: 10.1186/s40425-017-0300-z) included Dr. Suarez-Almazor, as well as Clifton O. Bingham III, MD, director of the Johns Hopkins Arthritis Center.
Vigilance required
Checkpoint inhibitors have been approved by the FDA to treat a variety of cancers, including melanoma, lung cancer, and Hodgkin lymphoma, as well as lung, liver, kidney, and bladder cancers.
Clinicians managing patients on checkpoint inhibitors should always be vigilant because irAE symptoms can be subtle, according to Julie Brahmer, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins in Baltimore.
“Everyone has to work as a team, which includes being educated on possible side effects to immunotherapy prior to prescribing it,” said Dr. Brahmer, chair of the ASCO panel and vice chair of the NCCN panel that developed the guidelines.
The guidelines were published Feb. 14 in two documents that are similar in content, but different in format. The ASCO guideline was published in the Journal of Clinical Oncology (doi: 10.1200/JCO.2017.77.6385) and the NCCN Clinical Practice Guidelines in Oncology were posted on the NCCN website.
While the first edition of the guidelines focus specifically on immune checkpoint inhibitors, an update anticipated for 2019 will include guidance on chimeric antigen receptor (CAR) T cell therapy, which is associated with several important side effects, notably cytokine release syndrome.
Recently released guidelines from two major cancer organizations have provided some of the most comprehensive guidance to date on management of musculoskeletal side effects associated with cancer immunotherapy.
The guidelines, published in February, are a “sorely needed” reference point for the rheumatology community and others who will be encountering patients who experience immune-related adverse events (irAEs), according to Leonard H. Calabrese, DO, the R.J. Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio.
“They’re a good first start, given the fact that up until 4 or 5 months ago, there were no endorsed guidelines that included oncologists and rheumatologists,” Dr. Calabrese said of the guidelines, which were collaboratively developed and recently released by both the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN).
Rheumatologists can add value
“We talk a lot about rheumatologists being aware of these diseases, but it’s been pointed out by some oncologists that unless they’re really knowledgeable and can add considerably to the management, it doesn’t do any good just to be aware of it,” Dr. Calabrese explained. “You need to actually have some procedural knowledge.”
ASCO guidelines also describe a polymyalgia-like syndrome seen in some patients on immune checkpoint inhibitors that according to the guideline authors is characterized by pain, but not true muscle weakness.
In general, the guidelines endorse a stepwise approach, in which milder irAEs can be managed with conservative treatments and without the need to stop the immune checkpoint inhibitor therapy. In contrast, more serious side effects may require more intensive management and either temporary or permanent discontinuation of cancer immunotherapy.
One good example is NCCN’s take on managing inflammatory arthritis.
Mild cases of inflammatory arthritis can be treated with NSAIDs, low-dose prednisone, or intra-articular steroids with no need to stop immune checkpoint inhibitor treatment, according to NCCN guideline authors.
Moderate cases, by contrast, may require holding immunotherapy and treating with prednisone. A rheumatology consult by week 4 is “strongly recommended” if the immune arthritis doesn’t improve, the authors added.
Severe cases may warrant permanent discontinuation of immunotherapy and treatment with methylprednisolone/prednisone, infliximab, or tocilizumab, they added. If the irAE doesn’t improve after 2 weeks, a rheumatology consult should be considered for additional disease-modifying antirheumatic drugs, including methotrexate, leflunomide, or sulfasalazine.
irAEs on the rise
These guidelines are particularly useful for rheumatologists to familiarize themselves with the six Food and Drug Administration–approved immune checkpoint inhibitors, their spectrum of side effects, and how oncologists use the severity of presentation to guide therapy, according to Laura Cappelli, MD.
Understanding irAEs will be increasingly important for rheumatologist as the use of immune checkpoint inhibitors continues to increase, said Dr. Cappelli, who has started a research program at Johns Hopkins to evaluate the rheumatologic adverse effects of these therapies.
Dr. Cappelli said her division sees at least one suspected irAE case per week, most commonly the immune arthritis associated with checkpoint inhibitor therapy.
Likewise, Dr. Calabrese said he is already seeing approximately two new referrals per week for adverse events related to these relatively new therapies.
“It’s far outstripped our notion of what we thought we would be doing,” he said in an interview.
Systems have been set up to encourage interprofessional collaborations, he added, including a “virtual referral clinic” where advanced practitioners working with oncologists communicate with advanced practitioners in each of the specialty areas that are most frequently consulted in order to help facilitate care and triage patients.
In addition, a monthly irAE tumor board was set up to include only cases that have manifest autoimmune or autoinflammatory complications.
“We have a growing group of people who come to this from each area involved, whether it be nephrology, neurology, ophthalmology, gastroenterology, rheumatology, or something else,” Dr. Calabrese said. “That’s been a great learning experience for all of us to talk about these adverse events in real time.”
Critical need for guidance
These guidelines meet a growing need to help practicing clinicians identify and best manage immune-related adverse events, according to Bryan J. Schneider, MD, of the University of Michigan Comprehensive Cancer Center, and vice chair of the NCCN Panel on Management of Immunotherapy-Related Toxicities.
“We’re experienced with chemotherapy, and we are very comfortable with the side effects,” he said. “The immunotherapy story is just an entirely different world because, as I tell patients, the therapies aren’t directly damaging cancer cells like chemotherapy. Instead, they are helping the immune system to identify the cancer cells as abnormal and mount an assault. Proteins on cancer cells may suppress the immune response and these therapies effectively ‘release these brakes’ so the immune system can attack.”
Rheumatologists and those with particular expertise in rheumatologic side effects participated in the development of the ASCO and NCCN guidelines. They include Maria E. Suarez-Almazor, MD, PhD, chief of rheumatology and clinical immunology at the University of Texas MD Anderson Cancer Center, Houston, who served on the ASCO expert panel; Jarushka Naidoo, MBBCh, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, provided expertise in the rheumatologic side effects that were considered by the NCCN panel, according to Dr. Schneider.
Rheumatologist input also informed another set of recommendations on immune checkpoint inhibitor toxicities published several months before the ASCO and NCCN guidelines. The working group for the September 2017 guidelines from the Society for Immunotherapy of Cancer (doi: 10.1186/s40425-017-0300-z) included Dr. Suarez-Almazor, as well as Clifton O. Bingham III, MD, director of the Johns Hopkins Arthritis Center.
Vigilance required
Checkpoint inhibitors have been approved by the FDA to treat a variety of cancers, including melanoma, lung cancer, and Hodgkin lymphoma, as well as lung, liver, kidney, and bladder cancers.
Clinicians managing patients on checkpoint inhibitors should always be vigilant because irAE symptoms can be subtle, according to Julie Brahmer, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins in Baltimore.
“Everyone has to work as a team, which includes being educated on possible side effects to immunotherapy prior to prescribing it,” said Dr. Brahmer, chair of the ASCO panel and vice chair of the NCCN panel that developed the guidelines.
The guidelines were published Feb. 14 in two documents that are similar in content, but different in format. The ASCO guideline was published in the Journal of Clinical Oncology (doi: 10.1200/JCO.2017.77.6385) and the NCCN Clinical Practice Guidelines in Oncology were posted on the NCCN website.
While the first edition of the guidelines focus specifically on immune checkpoint inhibitors, an update anticipated for 2019 will include guidance on chimeric antigen receptor (CAR) T cell therapy, which is associated with several important side effects, notably cytokine release syndrome.
Recently released guidelines from two major cancer organizations have provided some of the most comprehensive guidance to date on management of musculoskeletal side effects associated with cancer immunotherapy.
The guidelines, published in February, are a “sorely needed” reference point for the rheumatology community and others who will be encountering patients who experience immune-related adverse events (irAEs), according to Leonard H. Calabrese, DO, the R.J. Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio.
“They’re a good first start, given the fact that up until 4 or 5 months ago, there were no endorsed guidelines that included oncologists and rheumatologists,” Dr. Calabrese said of the guidelines, which were collaboratively developed and recently released by both the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN).
Rheumatologists can add value
“We talk a lot about rheumatologists being aware of these diseases, but it’s been pointed out by some oncologists that unless they’re really knowledgeable and can add considerably to the management, it doesn’t do any good just to be aware of it,” Dr. Calabrese explained. “You need to actually have some procedural knowledge.”
ASCO guidelines also describe a polymyalgia-like syndrome seen in some patients on immune checkpoint inhibitors that according to the guideline authors is characterized by pain, but not true muscle weakness.
In general, the guidelines endorse a stepwise approach, in which milder irAEs can be managed with conservative treatments and without the need to stop the immune checkpoint inhibitor therapy. In contrast, more serious side effects may require more intensive management and either temporary or permanent discontinuation of cancer immunotherapy.
One good example is NCCN’s take on managing inflammatory arthritis.
Mild cases of inflammatory arthritis can be treated with NSAIDs, low-dose prednisone, or intra-articular steroids with no need to stop immune checkpoint inhibitor treatment, according to NCCN guideline authors.
Moderate cases, by contrast, may require holding immunotherapy and treating with prednisone. A rheumatology consult by week 4 is “strongly recommended” if the immune arthritis doesn’t improve, the authors added.
Severe cases may warrant permanent discontinuation of immunotherapy and treatment with methylprednisolone/prednisone, infliximab, or tocilizumab, they added. If the irAE doesn’t improve after 2 weeks, a rheumatology consult should be considered for additional disease-modifying antirheumatic drugs, including methotrexate, leflunomide, or sulfasalazine.
irAEs on the rise
These guidelines are particularly useful for rheumatologists to familiarize themselves with the six Food and Drug Administration–approved immune checkpoint inhibitors, their spectrum of side effects, and how oncologists use the severity of presentation to guide therapy, according to Laura Cappelli, MD.
Understanding irAEs will be increasingly important for rheumatologist as the use of immune checkpoint inhibitors continues to increase, said Dr. Cappelli, who has started a research program at Johns Hopkins to evaluate the rheumatologic adverse effects of these therapies.
Dr. Cappelli said her division sees at least one suspected irAE case per week, most commonly the immune arthritis associated with checkpoint inhibitor therapy.
Likewise, Dr. Calabrese said he is already seeing approximately two new referrals per week for adverse events related to these relatively new therapies.
“It’s far outstripped our notion of what we thought we would be doing,” he said in an interview.
Systems have been set up to encourage interprofessional collaborations, he added, including a “virtual referral clinic” where advanced practitioners working with oncologists communicate with advanced practitioners in each of the specialty areas that are most frequently consulted in order to help facilitate care and triage patients.
In addition, a monthly irAE tumor board was set up to include only cases that have manifest autoimmune or autoinflammatory complications.
“We have a growing group of people who come to this from each area involved, whether it be nephrology, neurology, ophthalmology, gastroenterology, rheumatology, or something else,” Dr. Calabrese said. “That’s been a great learning experience for all of us to talk about these adverse events in real time.”
Critical need for guidance
These guidelines meet a growing need to help practicing clinicians identify and best manage immune-related adverse events, according to Bryan J. Schneider, MD, of the University of Michigan Comprehensive Cancer Center, and vice chair of the NCCN Panel on Management of Immunotherapy-Related Toxicities.
“We’re experienced with chemotherapy, and we are very comfortable with the side effects,” he said. “The immunotherapy story is just an entirely different world because, as I tell patients, the therapies aren’t directly damaging cancer cells like chemotherapy. Instead, they are helping the immune system to identify the cancer cells as abnormal and mount an assault. Proteins on cancer cells may suppress the immune response and these therapies effectively ‘release these brakes’ so the immune system can attack.”
Rheumatologists and those with particular expertise in rheumatologic side effects participated in the development of the ASCO and NCCN guidelines. They include Maria E. Suarez-Almazor, MD, PhD, chief of rheumatology and clinical immunology at the University of Texas MD Anderson Cancer Center, Houston, who served on the ASCO expert panel; Jarushka Naidoo, MBBCh, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, provided expertise in the rheumatologic side effects that were considered by the NCCN panel, according to Dr. Schneider.
Rheumatologist input also informed another set of recommendations on immune checkpoint inhibitor toxicities published several months before the ASCO and NCCN guidelines. The working group for the September 2017 guidelines from the Society for Immunotherapy of Cancer (doi: 10.1186/s40425-017-0300-z) included Dr. Suarez-Almazor, as well as Clifton O. Bingham III, MD, director of the Johns Hopkins Arthritis Center.
Vigilance required
Checkpoint inhibitors have been approved by the FDA to treat a variety of cancers, including melanoma, lung cancer, and Hodgkin lymphoma, as well as lung, liver, kidney, and bladder cancers.
Clinicians managing patients on checkpoint inhibitors should always be vigilant because irAE symptoms can be subtle, according to Julie Brahmer, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins in Baltimore.
“Everyone has to work as a team, which includes being educated on possible side effects to immunotherapy prior to prescribing it,” said Dr. Brahmer, chair of the ASCO panel and vice chair of the NCCN panel that developed the guidelines.
The guidelines were published Feb. 14 in two documents that are similar in content, but different in format. The ASCO guideline was published in the Journal of Clinical Oncology (doi: 10.1200/JCO.2017.77.6385) and the NCCN Clinical Practice Guidelines in Oncology were posted on the NCCN website.
While the first edition of the guidelines focus specifically on immune checkpoint inhibitors, an update anticipated for 2019 will include guidance on chimeric antigen receptor (CAR) T cell therapy, which is associated with several important side effects, notably cytokine release syndrome.
TB in 2017: Good news and bad news
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.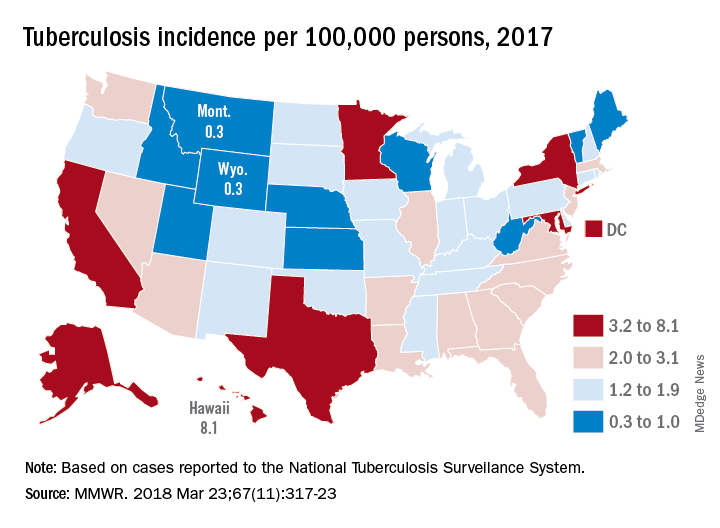
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
FROM MMWR
FDA approves certolizumab label update for pregnancy, breastfeeding
The manufacturer of certolizumab pegol, UCB, announced March 22 that the Food and Drug Administration approved a label update to the biologic that includes pharmacokinetic data showing negligible to low transfer of the biologic through the placenta and minimal mother-to-infant transfer from breast milk.

In the CRIB study, certolizumab levels were below the lower limit of quantification (defined as 0.032 mcg/mL) in 13 out of 15 infant blood samples at birth and in all samples at weeks 4 and 8. No anticertolizumab antibodies were detected in mothers, umbilical cords, or infants.
In the CRADLE study, 56% of 137 breast milk samples from 17 mothers had no measurable certolizumab, and the remaining samples showed minimal levels of the biologic. No serious adverse reactions were noted in the 17 infants in the study.
“It is well recognized that women with chronic inflammatory disease face uncertainty during motherhood given the lack of information on treatment during pregnancy and breastfeeding. Many women with chronic inflammatory disease discontinue their biologic treatment during pregnancy, often when they need disease control the most,” said CRADLE lead study author Megan E. B. Clowse, MD, of Duke University, Durham, N.C., in a press release issued by UCB. “These data for Cimzia provide important information to empower women and healthcare providers making decisions about treatment during pregnancy and breastfeeding.”
UCB said that limited data from an ongoing pregnancy registry regarding the use of certolizumab in pregnant women are not sufficient to inform a risk of major birth defects or other adverse pregnancy outcomes.
The manufacturer of certolizumab pegol, UCB, announced March 22 that the Food and Drug Administration approved a label update to the biologic that includes pharmacokinetic data showing negligible to low transfer of the biologic through the placenta and minimal mother-to-infant transfer from breast milk.
In the CRIB study, certolizumab levels were below the lower limit of quantification (defined as 0.032 mcg/mL) in 13 out of 15 infant blood samples at birth and in all samples at weeks 4 and 8. No anticertolizumab antibodies were detected in mothers, umbilical cords, or infants.
In the CRADLE study, 56% of 137 breast milk samples from 17 mothers had no measurable certolizumab, and the remaining samples showed minimal levels of the biologic. No serious adverse reactions were noted in the 17 infants in the study.
“It is well recognized that women with chronic inflammatory disease face uncertainty during motherhood given the lack of information on treatment during pregnancy and breastfeeding. Many women with chronic inflammatory disease discontinue their biologic treatment during pregnancy, often when they need disease control the most,” said CRADLE lead study author Megan E. B. Clowse, MD, of Duke University, Durham, N.C., in a press release issued by UCB. “These data for Cimzia provide important information to empower women and healthcare providers making decisions about treatment during pregnancy and breastfeeding.”
UCB said that limited data from an ongoing pregnancy registry regarding the use of certolizumab in pregnant women are not sufficient to inform a risk of major birth defects or other adverse pregnancy outcomes.
The manufacturer of certolizumab pegol, UCB, announced March 22 that the Food and Drug Administration approved a label update to the biologic that includes pharmacokinetic data showing negligible to low transfer of the biologic through the placenta and minimal mother-to-infant transfer from breast milk.
In the CRIB study, certolizumab levels were below the lower limit of quantification (defined as 0.032 mcg/mL) in 13 out of 15 infant blood samples at birth and in all samples at weeks 4 and 8. No anticertolizumab antibodies were detected in mothers, umbilical cords, or infants.
In the CRADLE study, 56% of 137 breast milk samples from 17 mothers had no measurable certolizumab, and the remaining samples showed minimal levels of the biologic. No serious adverse reactions were noted in the 17 infants in the study.
“It is well recognized that women with chronic inflammatory disease face uncertainty during motherhood given the lack of information on treatment during pregnancy and breastfeeding. Many women with chronic inflammatory disease discontinue their biologic treatment during pregnancy, often when they need disease control the most,” said CRADLE lead study author Megan E. B. Clowse, MD, of Duke University, Durham, N.C., in a press release issued by UCB. “These data for Cimzia provide important information to empower women and healthcare providers making decisions about treatment during pregnancy and breastfeeding.”
UCB said that limited data from an ongoing pregnancy registry regarding the use of certolizumab in pregnant women are not sufficient to inform a risk of major birth defects or other adverse pregnancy outcomes.
Study links RA flares after joint replacement to disease activity, not medications
Patients with the most severe cases of rheumatoid arthritis are more likely to suffer flares after knee or hip replacement surgery, a new study finds, and it doesn’t seem to matter whether they stop taking biologics before their operation.
“We found that the majority of patients had active disease at the time of surgery, contrary to prior statements that RA patients have inactive disease at the time they go for hip or knee replacement. In fact, the majority – 65% of the patients – reported a flare of RA within 6 weeks of surgery,” lead author Susan M. Goodman, MD, of Cornell University and the Hospital for Special Surgery, New York, said in an interview. “Surprisingly, although more of the flaring patients were taking potent biologics that had been withheld preoperatively, the major risk factor for flares was their baseline disease activity.”

According to Dr. Goodman, the researchers launched the study to better understand how medical decisions prior to joint replacement surgery affect the progress of RA afterward.
In terms of continuing RA drug treatment, she said, “the decision really hinges on the risk of infection versus the risk of flare, and we didn’t know the usual course of events for these patients.”
In addition, she said, “many doctors incorrectly think that the majority of patients with RA have ‘burnt-out’ or inactive disease at the time of hip or knee replacement surgery.”
For the study, the researchers prospectively followed 120 patients who were to undergo joint replacement surgery. (The researchers initially approached 354 patients, of whom 169 declined to participate. Another 65 were dropped from the study for various reasons, including 42 who did not sufficiently fill out questionnaires and were deleted from the final analysis.)
The researchers tracked the patients before surgery and for 6 weeks after surgery. A majority of the patients were female (83%) and white (81%), with a mean age of 62 and a median RA symptom duration of 15 years. A total of 44% underwent hip replacement surgery while the rest underwent knee replacement surgery. Just over half of the patients were taking biologics, which were stopped prior to surgery, while glucocorticoids and methotrexate were usually continued.
Just under two-thirds of the patients flared within the first 6 weeks after surgery. The researchers didn’t find any connection between the flares and stopping biologics or using methotrexate. They did, however, link higher baseline RA activity to postsurgery flaring (odds ratio, 2.11; P = .015).
Dr. Goodman said that she and her colleagues continue to collect data to better understand flares and the link to disease severity. “The long-term implications of this are not yet known. We would like to know the effect on long-term functional outcome and complication rate.”
The National Institutes of Health, the Weill Cornell Clinical Translational Science Center, and the Block Family Foundation supported the study. Dr. Goodman disclosed receiving research funding from Novartis and Roche.
SOURCE: Goodman S et al. J Rheumatol. 2018 Mar 15. doi: 10.3899/jrheum.170366
Patients with the most severe cases of rheumatoid arthritis are more likely to suffer flares after knee or hip replacement surgery, a new study finds, and it doesn’t seem to matter whether they stop taking biologics before their operation.
“We found that the majority of patients had active disease at the time of surgery, contrary to prior statements that RA patients have inactive disease at the time they go for hip or knee replacement. In fact, the majority – 65% of the patients – reported a flare of RA within 6 weeks of surgery,” lead author Susan M. Goodman, MD, of Cornell University and the Hospital for Special Surgery, New York, said in an interview. “Surprisingly, although more of the flaring patients were taking potent biologics that had been withheld preoperatively, the major risk factor for flares was their baseline disease activity.”
According to Dr. Goodman, the researchers launched the study to better understand how medical decisions prior to joint replacement surgery affect the progress of RA afterward.
In terms of continuing RA drug treatment, she said, “the decision really hinges on the risk of infection versus the risk of flare, and we didn’t know the usual course of events for these patients.”
In addition, she said, “many doctors incorrectly think that the majority of patients with RA have ‘burnt-out’ or inactive disease at the time of hip or knee replacement surgery.”
For the study, the researchers prospectively followed 120 patients who were to undergo joint replacement surgery. (The researchers initially approached 354 patients, of whom 169 declined to participate. Another 65 were dropped from the study for various reasons, including 42 who did not sufficiently fill out questionnaires and were deleted from the final analysis.)
The researchers tracked the patients before surgery and for 6 weeks after surgery. A majority of the patients were female (83%) and white (81%), with a mean age of 62 and a median RA symptom duration of 15 years. A total of 44% underwent hip replacement surgery while the rest underwent knee replacement surgery. Just over half of the patients were taking biologics, which were stopped prior to surgery, while glucocorticoids and methotrexate were usually continued.
Just under two-thirds of the patients flared within the first 6 weeks after surgery. The researchers didn’t find any connection between the flares and stopping biologics or using methotrexate. They did, however, link higher baseline RA activity to postsurgery flaring (odds ratio, 2.11; P = .015).
Dr. Goodman said that she and her colleagues continue to collect data to better understand flares and the link to disease severity. “The long-term implications of this are not yet known. We would like to know the effect on long-term functional outcome and complication rate.”
The National Institutes of Health, the Weill Cornell Clinical Translational Science Center, and the Block Family Foundation supported the study. Dr. Goodman disclosed receiving research funding from Novartis and Roche.
SOURCE: Goodman S et al. J Rheumatol. 2018 Mar 15. doi: 10.3899/jrheum.170366
Patients with the most severe cases of rheumatoid arthritis are more likely to suffer flares after knee or hip replacement surgery, a new study finds, and it doesn’t seem to matter whether they stop taking biologics before their operation.
“We found that the majority of patients had active disease at the time of surgery, contrary to prior statements that RA patients have inactive disease at the time they go for hip or knee replacement. In fact, the majority – 65% of the patients – reported a flare of RA within 6 weeks of surgery,” lead author Susan M. Goodman, MD, of Cornell University and the Hospital for Special Surgery, New York, said in an interview. “Surprisingly, although more of the flaring patients were taking potent biologics that had been withheld preoperatively, the major risk factor for flares was their baseline disease activity.”
According to Dr. Goodman, the researchers launched the study to better understand how medical decisions prior to joint replacement surgery affect the progress of RA afterward.
In terms of continuing RA drug treatment, she said, “the decision really hinges on the risk of infection versus the risk of flare, and we didn’t know the usual course of events for these patients.”
In addition, she said, “many doctors incorrectly think that the majority of patients with RA have ‘burnt-out’ or inactive disease at the time of hip or knee replacement surgery.”
For the study, the researchers prospectively followed 120 patients who were to undergo joint replacement surgery. (The researchers initially approached 354 patients, of whom 169 declined to participate. Another 65 were dropped from the study for various reasons, including 42 who did not sufficiently fill out questionnaires and were deleted from the final analysis.)
The researchers tracked the patients before surgery and for 6 weeks after surgery. A majority of the patients were female (83%) and white (81%), with a mean age of 62 and a median RA symptom duration of 15 years. A total of 44% underwent hip replacement surgery while the rest underwent knee replacement surgery. Just over half of the patients were taking biologics, which were stopped prior to surgery, while glucocorticoids and methotrexate were usually continued.
Just under two-thirds of the patients flared within the first 6 weeks after surgery. The researchers didn’t find any connection between the flares and stopping biologics or using methotrexate. They did, however, link higher baseline RA activity to postsurgery flaring (odds ratio, 2.11; P = .015).
Dr. Goodman said that she and her colleagues continue to collect data to better understand flares and the link to disease severity. “The long-term implications of this are not yet known. We would like to know the effect on long-term functional outcome and complication rate.”
The National Institutes of Health, the Weill Cornell Clinical Translational Science Center, and the Block Family Foundation supported the study. Dr. Goodman disclosed receiving research funding from Novartis and Roche.
SOURCE: Goodman S et al. J Rheumatol. 2018 Mar 15. doi: 10.3899/jrheum.170366
FROM JOURNAL OF RHEUMATOLOGY
Key clinical point:
Major finding: Sixty-five percent of RA patients developed flares after joint replacement surgery, and it was more common in those with higher baseline RA activity (odds ratio, 2.11; P = .015).
Study details: Prospective study of 120 patients with RA who underwent hip replacement (44%) or knee replacement (56%).
Disclosures: The National Institutes of Health, the Weill Cornell Clinical Translational Science Center, and the Block Family Foundation supported the study. The lead author disclosed receiving research funding from Novartis and Roche.
Source: Goodman S et al. J Rheumatol. 2018 Mar 15. doi: 10.3899/jrheum.170366.
Arthritis limits physical activity the most in the South
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
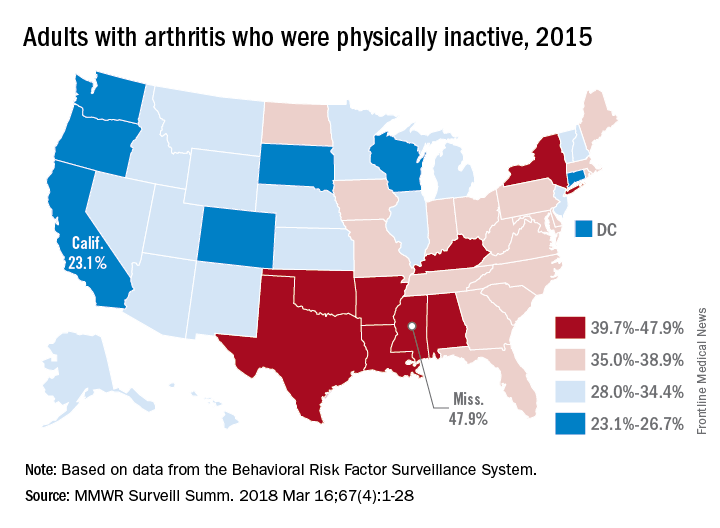
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
FROM MMWR SURVEILLANCE SUMMARIES
Xeljanz: FDA panel recommends ulcerative colitis indication
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study, two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2), a 53-week, phase 3 maintenance trial (OCTAVE Sustain), and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.*
Patients who did not achieve remission, but showed some clinical response (decrease in Mayo score of at least 3 points), were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5 mg and 10 mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior TNF-blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients as part of an open-label extension study who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection (HZ), “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair and vice chair Jean-Pierre Raufman, MD, and Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
*This article was updated on March 12, 2018.
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study, two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2), a 53-week, phase 3 maintenance trial (OCTAVE Sustain), and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.*
Patients who did not achieve remission, but showed some clinical response (decrease in Mayo score of at least 3 points), were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5 mg and 10 mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior TNF-blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients as part of an open-label extension study who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection (HZ), “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair and vice chair Jean-Pierre Raufman, MD, and Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
*This article was updated on March 12, 2018.
SILVER SPRING, MD. – Federal advisors to the Food and Drug Administration on March 8 voted unanimously to recommend approval of an additional indication for tofacitinib (Xeljanz), this time for ulcerative colitis.
Members of the Gastrointestinal Drugs Advisory Committee unanimously voted to recommend two different dosing regimens: 10 mg twice daily for 16 weeks in patients who have not experienced a therapeutic benefit after 8 weeks of treatment, as well as 10 mg twice daily for patients who have an inadequate or loss of response to TNF-blocker therapy, based on the results of several phase 3 clinical trials.
The recommended ulcerative colitis (UC) indication was based on the OCTAVE trials (N Engl J Med 2017;376:1723-36), including a phase 2 study, two identical phase 3 induction trials (OCTAVE Induction 1 and OCTAVE Induction 2), a 53-week, phase 3 maintenance trial (OCTAVE Sustain), and an open-label extension study.
The induction trials enrolled a total of 1,139 patients with moderate to severe UC. Patients in both studies were administered tofacitinib 10 mg twice daily or placebo and were assessed after 8 weeks to judge clinical response. Patients in both studies displayed notable remission rates (18.5% and 16.6%), compared with placebo, according to Eric Maller, MD, executive director of the UC development program at Pfizer.*
Patients who did not achieve remission, but showed some clinical response (decrease in Mayo score of at least 3 points), were then enrolled in the 53-week OCTAVE Sustain, where they were randomized to receive tofacitinib 10 mg twice daily, 5 mg twice daily, or placebo.
During maintenance treatment, both 5 mg and 10 mg doses demonstrated substantial treatment benefits, with 32.4% and 41.0% of patients achieving remission, an increase of 22.0% and 30.7%, compared with placebo, respectively.
As part of the maintenance study, Pfizer analyzed patients with or without prior TNF-blocker failure. This analysis revealed that patients who had previously failed TNF-blocker therapy experienced a greater treatment benefit than those who had not. While the benefit was noticeable in both dosage groups, patients taking the 10-mg dose experienced the greatest benefit, with 70% increase in remission rates, 39% increase in mucosal healing, and 75% increase in steroid-free remission among baseline remitters, compared with patients in the 5-mg group, Dr. Maller said.
Researchers also looked at a subgroup of 295 patients as part of an open-label extension study who had no clinical response to tofacitinib 10 mg twice daily after 8 weeks and subsequently treated them for an additional 8 weeks. After the additional 8 weeks of treatment, over half (51.2%) displayed clinical responses and 8.6% were in remission.
“This is a desperate patient population. These are impressive results,” stated Darrell Pardi, MD, vice chair of the advisory committee and professor of medicine at the Mayo Clinic, Rochester, Minn.
Serious adverse events were seen in 4% of tofacitinib-treated patients in the induction trials, compared with 6% of placebo-treated, according to Lesley Hanes, MD, medical officer with the FDA Center for Drug Evaluation and Research.
Adverse events appeared to be dose dependent, with risk of deaths and malignancies (excluding nonmelanoma skin cancer), opportunistic infections, herpes zoster infection (HZ), “possible” drug-induced liver injury, and cardiovascular and thromboembolic events more common with the 10-mg dose, Dr. Hanes said.
“I think the safety concerns, though, they are dose dependent, the difference between the 5 [mg] and 10 [mg] were not large,” according to Dr. Pardi. “Several of these are mitigatable by dermatologic exam or, hopefully, a vaccine.”
Several of the advisory committee members submitted conflict of interest waivers. Chair and vice chair Jean-Pierre Raufman, MD, and Darrell Pardi, MD, disclosed funding from competing pharmaceutical manufacturers.
*This article was updated on March 12, 2018.
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING
Treat to target in RA: Finding the right path forward
It makes intuitive sense: Setting a specific goal and working quickly and systematically toward it should bring better results than slowly floundering toward an amorphous endpoint.
That’s the basic idea behind treat-to-target (TTT) strategies in rheumatoid arthritis, and since 2010, data seem to support it: Rheumatologists who pick a therapeutic goal and a related disease activity measure and work in partnership with cooperative patients to achieve it, get better clinical responses.
So important has this concept become that it’s now being tied to reimbursement. Rheumatologists who submit proof that they record disease activity measures in their patients will get points toward fulfilling quality reporting requirements for the Merit-Based Incentive Payment System (MIPS) option in the Quality Payment Program established by the Medicare Access and CHIP Reauthorization Act of 2015. Those points go toward achieving a bonus in Medicare reimbursement; those who can’t show it will edge toward a financial ding.
But despite the twin carrots of better patient outcomes and bonus payments from the Centers for Medicare & Medicaid Services and the stick of a 4%-9% Medicare payment penalty during the years 2019-2022 (and 9% thereafter) for quality outcome measures reported in 2017 and beyond, studies show that up to 60% of U.S. rheumatologists don’t regularly incorporate TTT strategies into how they treat their RA patients.

“There are patient reasons. There are doctor reasons. And there are extrinsic reasons. But I would say the number one reason it’s had limited adoption is that it simply hasn’t been made easy enough.”
The ABCs of TTT
In 2010, Austrian rheumatologist Josef Smolen, MD, leading an international task force, proposed 10 recommendations for improving the care of patients with RA. These were based on the concept that choosing a therapeutic target – low disease activity or remission – and aggressively pursuing it with frequent medication changes accompanied by frequent disease activity measurements would result in improved short- and long-term outcomes.
Disease activity measures (DAMs) were crucial to the concept. In order to treat to a target, one must not only choose a target but also have a validated means to regularly measure progress. The task force didn’t say which DAM would be most appropriate, and research since then suggests that the tool used to measure progress doesn’t matter nearly as much as the target itself.
Shared decision making is also a core tenet of the technique. Physicians work with patients to identify the best treatment target for each individual and decide together how to reach it.
It is not a new concept, Dr. Smolen and his colleagues explained in their landmark paper (Ann Rheum Dis. 2010 Apr;69[4]:631-7). “In many other areas of medicine, treatment targets have been defined to improve outcomes, leading to a reduction in the risk of organ damage. In the care of patients with diabetes, hyperlipidemia, and hypertension, these aspects have been adopted widely in practice; doctors order laboratory tests for cholesterol and triglycerides, blood glucose and HbA1c [hemoglobin A1c] levels, check blood pressure, and adapt therapy accordingly, and patients know these values and are aware of the treatment targets.”
Yet rheumatologists had not adopted a similar paradigm, despite the surge in availability of effective disease-modifying antirheumatic drugs (DMARDs). Although clinical studies of these new drugs clearly showed that remission was possible for many patients and that achieving remission quickly could prevent irreversible joint damage, few patients were getting those drugs even if they had long-standing disease.
The task force suggested setting a treatment aim of remission or low disease activity, seeing patients every 1-3 months, and switching therapy as often as necessary to reach that goal. Tracking improvement required consistent measurements and recording of a DAM. The recommendations, which were updated in 2014, didn’t specify a certain DAM, saying that the patient’s individual clinical picture should guide that choice (Ann Rheum Dis. 2016 Jan;75[1]:3-15). Shared decision making between the patient and rheumatologist was at the foundation of this concept.
Fast-forward to 2015. As TTT was increasingly embraced in Europe, data began to emerge supporting its clinical validity. A study presented at the American College of Rheumatology (ACR) annual meeting in San Francisco that year showed that treating RA patients toward a target of remission or low disease activity worked immediately and resulted in higher remission rates.
Sofia Ramiro, MD, of Leiden (Netherlands) University Medical Center found that employing a TTT strategy increased the likelihood that a patient would achieve remission by 52%. She also found that TTT strategies lowered disease activity and even improved remission rates for patients who had never received DMARDs.
But in 2017, a meta-analysis found conflicting results among the 16 published randomized, controlled trials comparing TTT against usual care (Health Technol Assess 2017. doi: 10.3310/hta21710). The authors concluded that TTT was more effective for newly diagnosed patients, in whom it increased the chance of remission by about 50%. For those with longstanding disease, TTT was not significantly different from usual care.
Despite limited, and somewhat contradictory, clinical evidence, TTT is becoming increasingly accepted, especially in Europe. In 2016, the European League Against Rheumatism updated its recommendations for RA management (Ann Rheum Dis. 2017 Jun;76[6]:960-77). The document contained a recommendation to use low disease activity or sustained remission as the treatment target for every patient, to monitor disease activity with a validated measure every 1-3 months, and to change therapy as often as every 3 months in the case of no improvement or by 6 months if the target hasn’t been reached.
In its most recent 2015 RA treatment guidelines, the ACR also endorsed the strategy, though somewhat obliquely, and did not require rheumatologists to conform to it (Arthritis Care Res. 2016 Jan;68[1]:1-25).
The concept of TTT, if not the explicit demand to practice it, now appears in the list of quality indicators rheumatologists can choose from in order to fulfill quality performance reporting requirements in Merit-Based Incentive Payment System. Periodic assessment of disease activity in RA patients with a validated DAM is one of the acceptable quality measures for rheumatology. It’s not designated as a high-priority measure, but there it is, item No. 177, tying clinicians at least indirectly to a TTT approach for their Medicare patients: The percentage of patients aged 18 years and older with a diagnosis of RA who have an assessment and classification of disease activity within 12 months.
Slow on the uptake
Despite the data and the dictum, however, TTT remains an outlier in the United States. The most recent studies suggest that most U.S. rheumatologists do not employ it.
Dr. Curtis is the primary author on one of the newest studies, which employed a 26-question survey about the use of a quantitative measurement in RA patients and attitudes about using it (J Rheumatol. 2018 Jan;45[1]:40-4). The survey went out to almost 2,000 rheumatologists; 439 returned it.
Overall, just 44% said they “always practice in a treat-to-target manner, regularly using a scoring metric.” Younger physicians, those in group practices, and those who made regular use of TNF inhibitors were more likely to practice this way. A total of 35% said they never used a quantitative metric for their RA patients.
“The No. 1 reason given about not using them is that it’s too time-consuming and not easy enough,” Dr. Curtis said in an interview. “Logistics is a key barrier.” Busy clinicians don’t want to spend time entering data into an electronic medical record, and there aren’t easy ways to merge a specific DAM with a practice’s chosen EHR. “There’s a hassle factor, for sure.”
The age gap was interesting but not unexpected, he said. “Older rheumatologists say they like to go by their gut, by a clinical gestalt,” Dr. Curtis said, while younger physicians without decades of experience are more comfortable with such clinical tools. For some, age contributes to a kind of clinical inertia. “Doctors trained in an earlier era might be more tolerant of patients not doing as well. I’m a younger physician, and I have never known the era of not having biologics. They lived and practiced in that era, so their spectrum of what’s ‘normal’ and acceptable for patient progress may be wider.”

He and his colleagues investigated whether a 9-month group-based learning collaborative could improve TTT numbers among 46 rheumatologists at 11 practices. The endpoint was a combination of four TTT principles: recording a disease target, recording a disease activity measure, engaging in shared decision-making, and changing treatment if disease target hasn’t been reached.
At baseline, 64% of visits to these rheumatologists had none of the TTT components present, 33% had one component, and 2.3% had two components; just 3% of the visits included all of the components (Arthritis Care Res. 2017 Aug 22. doi: 10.1002/acr.23343).
The project consisted of nine sessions, most conducted by webinar. The entire practice team took part, learning the principles and practices of TTT, identifying their unique barriers to implementing it, and coming up with their unique way of integrating TTT into their practice. It was fairly successful, Dr. Solomon said in an interview. After the intervention, 57% of the exposed practices had incorporated TTT.
In January, Dr. Solomon published a follow-up study of the stability of those changes (Arthritis Care Res. 2018 Jan 5. doi: 10.1002/acr.23508). He was impressed with the results. Most sites from the first cohort had sustained the improvement during the second training period (52%).
“We found that people could implement it effectively when we gave them the tools to do it,” he said. “It’s definitely achievable, but it takes some commitment and guidance, and the realization that everyone can contribute to success in a collaborative manner.”
Technology, or the lack of it
Many rheumatologists view TTT and the consistent measuring it involves as just one more headache-inducing time suck, said John Cush, MD.

But at the same time, he freely admits that the time spent ticking boxes on a paper form or a computer, and being forced to report those to a federal agency, could be the camel-breaking straw for many.
“It’s going down the path of what makes medicine sucky,” he said in an interview. “Bean counters telling me how to practice medicine, who think they can use this TTT to manage what I do. I don’t need more people trying to regulate my life.”
Dr. Cush has conducted surveys on physician burnout and depression. “Administrative tasks and electronic records are a large part why 24% of people are burning out in medicine.”
Right now, there’s no easy way for many rheumatologists to incorporate regular DAM measures into their EHR system. The extra steps needed to get them there impede physician compliance with the strategy, he and Dr. Curtis agreed. But, Dr. Curtis said, there’s an app for that.
He is the developer of the Rheumatic Disease Activity (READY) measure. The iPad/iPhone app, which is free to download in the app store, is an electronic measurement tool that efficiently captures patient-reported outcomes in RA and other rheumatic conditions.
“This tool really makes it much easier to collect DAM from patients,” Dr. Curtis said. “It is designed for the doc who says, ‘I would take data from patients, just make it easy for me to do that.’ It takes 5-10 minutes to complete, and you get information about pain, fatigue, anxiety, and social interactions and, he said, can be easily integrated into work flow.
On a practice-provided device, the patient answers questions validated on the National Institutes of Health Patient-Reported Outcomes Measurement Information System. It includes a number of electronically scored and validated DAMs and provides trend charts to visualize longitudinal score data and track patient health status over multiple encounters. There are also places to record data about current and past medications.
“The docs input no data, which is the usual deal-killer. All they have to do is figure out how to integrate it into the work flow.”

“ACR has been communicating with the major EMR providers out there to make this easier. We are seeing some tools for iPads and smartphones, as well as paper tools.”
The ACR RISE Registry is another option, said Evan Leibowitz, MD, a rheumatologist in Midland Park, N.J.
“RISE is open to all rheumatologists in this country, and ACR has tried to make it as easy as possible. It can interface with most EMRs. All the physician does is collect the data, and it gets transferred to a HIPAA-protected database where it’s analyzed and presented back to the doctors so they can look at all their metrics. It’s currently the least painful way to get involved in a registry, I think.”
But just as techies are rolling out ways to interface DAMs and EHRs, medicine is marching forward. A new blood test called VECTRA DA measures 12 inflammatory biomarkers and may provide all the information needed to make treatment escalation decisions, Dr. Leibowitz said.
“The least painful option will probably be the VECTRA DA score. It’s a single blood test, which we can do easily since we already draw blood. Rather than filling out a RAPID3 [Routine Assessment of Patient Index Data 3] or a CDAI [Clinical Disease Activity Index], we draw the blood, send it to the company, [and] they return us a score that indicates low, moderate, or high disease activity.”
Studies have found that not only is the VECTRA DA score a good clinical management tool, predicting responses, it can also predict impending relapse.
TTT challenges patients, too
Rheumatologists are not the only ones reluctant to embrace TTT. It challenges patients as well, in a number of ways.
“Patients have to be willing to change treatments as often as you need them to, and that can be every 3-6 months, or even more quickly,” Dr. Curtis said. “The cost can be a factor. And a lot of patients are risk averse. They feel there may be more of a downside to switching than a benefit to be gained, especially if they’ve had RA for a while. Maybe they’re feeling a lot better than they were; their disease is still active, but they don’t feel bad enough to want to change medications.”
Researchers have explored these questions.
Last year, Dr. Michaud published a survey of 48 RA patients who were interviewed about their experiences with DMARDs and the feelings that would prompt them to comply with a treatment regimen – or resist one (Arthritis Care Res. 2017 June 2. doi: 10.1002/acr.23301).
“For patients’ motivations to accept treatment regimens, two themes emerged,” said Dr. Michaud, who is also codirector of the National Data Bank for Rheumatic Diseases. “One, the desire to return to a ‘normal’ life and, two, the fear of future disability due to RA. For motivations to resist treatment regimens, five themes emerged: fear of medications, maintaining control over health, denial of sick identity, disappointment with treatment, and feeling overwhelmed by the cognitive burden of deciding.”
The findings confirm one of TTT’s core tenets: involving patients in treatment decisions, Dr. Michaud said in an interview. “A lot of patients in my studies have reached a place of ‘OK-ness’ with their RA. The don’t want to change what they feel is working. They’re afraid of getting worse because they’ve been there and know what that can be.”
Rapid change-ups to new medications are especially intimidating to long-term patients, he said. “This is a very important aspect of resistance to change. The side effects of these medications, both major and minor, are not something that people want to experience.”

“As a physician, I’m worried about the rare and extremely rare adverse events – things that are really dreaded, that can be fatal. However, these happen in only a couple out of tens of thousands of patients. On the other hand, there are common side effects that occur in up to 20% of our patients. They’re not a serious threat to health, but they impact quality of life every day with nausea, dizziness, diarrhea, headache, and brain fog. As rheumatologists, we really undervalue these, and guess what? When we ask patients, it turns out that nausea and dizziness and diarrhea are not things that they want in their daily lives.”
Dr. Fraenkel of Yale University, New Haven, Conn., explored this topic in a recently published survey of 1,273 RA patients that sought their concerns about taking triple therapy, biologics, and Janus kinase inhibitors (Ann Rheum Dis. 2017 Dec 15. doi: 10.1136/annrheumdis-2017-212407). The survey included seven medication attributes – administration, onset, bothersome side effects, serious infection, very rare side effects, amount of information, and cost – and sought to determine the relative effect of each attribute on patient preference for different treatment options.
“We found five distinct clusters” of patients, Dr. Fraenkel said in an interview. “I will admit I was surprised when I saw the largest group (38%) was most concerned about the cost of their medications. Our assumption is always that the rare and dreaded side effects are the most concerning, but for these patients, cost was the dominant issue. It’s the No. 1 reason patients are noncompliant with their initial treatment recommendations. And with the cost of our biologics, it is a very big deal.”
Her reaction pinpoints an important obstacle in shared decision making: physician bias. “I’d say the vast majority of us argue that the benefit of TTT outweighs the harms. We minimize inflammation, so patients will live longer with less disease impact. But how we get there should be up to the patient. My biases shouldn’t come into play. The decision to intensify is different than the decision about how to intensify. This is where the back-and-forth comes in, making sure the patient understands the pros and cons of escalating or not. If she decided no, she doesn’t incur the risk of a new medication, but she does incur the risk of progressing. The bottom line is that physicians should not bring their biases to the table but describe the facts, the importance of which will be different to different patients who have different goals.”
A patient’s story: Overcoming fear and self-image
Prisha Acharya, PhD, knows a thing or two about rheumatoid arthritis.
As an RA researcher in New York, Dr. Acharya has a vast store of knowledge at her fingertips – everything from long-term treatment outcomes to medication side effects.
But when she was diagnosed with RA last year, at age 38 years, she was overwhelmed. And when she connected with a rheumatologist who wanted to aggressively treat her to a target of low disease activity or even remission, she balked. She became the patient who refuses a treat-to-target strategy.
“He was very clear in communicating the urgency of needing to get the disease under control, and I agreed that was a good thing. But even with all this experience in research, I still felt this resistance. I knew I needed to go aggressive. But I was also worried – worried about the side effects, the long-term effects, the costs. Committing to it was going to make my diagnosis real. I wasn’t ready to do it.”
“Prisha Acharya” is not this patient’s real name. She spoke in an interview on the condition of anonymity because she hasn’t yet discussed her diagnosis with some of her family and friends. In fact, she’s still coming to grips with it herself.
The story of Dr. Acharya’s journey to an RA clinic is one she hears every day in her work. About a year ago, she had some aching and stiffness in her knee, and it spread to her wrists and fingers. Digestive issues arose. She shuffled from doctor to doctor, had knee surgery, visited a gastroenterologist, went on a fibromyalgia medication. She finally broached the topic of a possible autoimmune disorder. By the time she received an RA diagnosis, she could only think of one thing: feeling better.
Her rheumatologist got that. But he also let her know at the first visit that he wanted more for her.
“He said, ‘We’re going to get you feeling better, reduce your pain, and make it so you can get out of bed in the morning,’ but our very first conversation was also about a goal of low disease activity and remission. He explained that we had a brief window of opportunity to make a difference in preventing long-term joint damage and that we had to go for it.”
She was on board with the goal, intellectually at least. However, her gut said something different, especially when they discussed methotrexate.
“There was an association in my head between methotrexate and chemotherapy. I knew it could cause fatigue, nausea, and hair thinning. And the idea of an injection, like I was getting chemo for cancer ... it felt very scary.”
As a compromise, she started hydroxychloroquine and shortly after, added sulfasalazine. She was feeling better, but her disease activity scores were still elevated. “My inflammation scores were climbing, and all this time he was saying ‘You have to start methotrexate. You’re going against my advice,’ but I was not emotionally ready. Despite my experience with RA research, I wouldn’t start it.”
With every visit, her rheumatologist patiently built his case for treatment. With every visit, her relationship and trust of him grew.
“Finally, just recently, I did start methotrexate, first with the pill and now the self-injector. I’m on that and the sulfasalazine, but we are reassessing again soon because I still have pain and my disease still isn’t under control. Now we’re going to talk about increasing the methotrexate and adding a new therapy.”
Dr. Acharya’s experience points to the dichotomy between what patients and physicians see as the most important goals and provides a good lesson about how trust and communication can bring those into clinical alignment.
Her rheumatologist set a very clear goal at the beginning of her treatment – one that came with a price tag she wasn’t yet willing to pay. But he also heard and accepted her goal: She wanted to feel better and give herself time to adjust to a new way of life and a new understanding of who she was.
“His language really helped,” Dr. Archaya said. “He acknowledged what I needed – to get the pain and stiffness under control. And as we built our relationship, I was able to hear his side about the urgency of treatment much better. When I was willing to go aggressive, I was also willing to say ‘I have RA.’ It takes a while to get there.”
She had some words of advice to help rheumatologists bridge the gap between what they want for a patient and what that patient wants for herself.
“An open dialogue is really going to help. When patients are voicing their fears, the rheumatologist can reassure them that, if this medicine doesn’t help or if it gives you terrible side effects, we can work together to find another option. Also, it’s so important for the patient to understand the treat-to-target framework from the very beginning. Everything indicates that the earlier we start treatment and set a goal, the better we can control our disease and the better the rest of our life can be.”
The second thing, Dr. Acharya said, is shared decision making. “I want him to tell me the options but also to work with me at arriving at the decision I eventually make.”
Finally, she said, patients need other resources, and rheumatologists can help direct them to find those.
“It’s so important to connect with like-minded patients in patient advocacy groups. The tips that they have given me about medications and dealing with my disease, no doctor could ever give me because patients are the ones that know those things inside-out.”
It makes intuitive sense: Setting a specific goal and working quickly and systematically toward it should bring better results than slowly floundering toward an amorphous endpoint.
That’s the basic idea behind treat-to-target (TTT) strategies in rheumatoid arthritis, and since 2010, data seem to support it: Rheumatologists who pick a therapeutic goal and a related disease activity measure and work in partnership with cooperative patients to achieve it, get better clinical responses.
So important has this concept become that it’s now being tied to reimbursement. Rheumatologists who submit proof that they record disease activity measures in their patients will get points toward fulfilling quality reporting requirements for the Merit-Based Incentive Payment System (MIPS) option in the Quality Payment Program established by the Medicare Access and CHIP Reauthorization Act of 2015. Those points go toward achieving a bonus in Medicare reimbursement; those who can’t show it will edge toward a financial ding.
But despite the twin carrots of better patient outcomes and bonus payments from the Centers for Medicare & Medicaid Services and the stick of a 4%-9% Medicare payment penalty during the years 2019-2022 (and 9% thereafter) for quality outcome measures reported in 2017 and beyond, studies show that up to 60% of U.S. rheumatologists don’t regularly incorporate TTT strategies into how they treat their RA patients.
“There are patient reasons. There are doctor reasons. And there are extrinsic reasons. But I would say the number one reason it’s had limited adoption is that it simply hasn’t been made easy enough.”
The ABCs of TTT
In 2010, Austrian rheumatologist Josef Smolen, MD, leading an international task force, proposed 10 recommendations for improving the care of patients with RA. These were based on the concept that choosing a therapeutic target – low disease activity or remission – and aggressively pursuing it with frequent medication changes accompanied by frequent disease activity measurements would result in improved short- and long-term outcomes.
Disease activity measures (DAMs) were crucial to the concept. In order to treat to a target, one must not only choose a target but also have a validated means to regularly measure progress. The task force didn’t say which DAM would be most appropriate, and research since then suggests that the tool used to measure progress doesn’t matter nearly as much as the target itself.
Shared decision making is also a core tenet of the technique. Physicians work with patients to identify the best treatment target for each individual and decide together how to reach it.
It is not a new concept, Dr. Smolen and his colleagues explained in their landmark paper (Ann Rheum Dis. 2010 Apr;69[4]:631-7). “In many other areas of medicine, treatment targets have been defined to improve outcomes, leading to a reduction in the risk of organ damage. In the care of patients with diabetes, hyperlipidemia, and hypertension, these aspects have been adopted widely in practice; doctors order laboratory tests for cholesterol and triglycerides, blood glucose and HbA1c [hemoglobin A1c] levels, check blood pressure, and adapt therapy accordingly, and patients know these values and are aware of the treatment targets.”
Yet rheumatologists had not adopted a similar paradigm, despite the surge in availability of effective disease-modifying antirheumatic drugs (DMARDs). Although clinical studies of these new drugs clearly showed that remission was possible for many patients and that achieving remission quickly could prevent irreversible joint damage, few patients were getting those drugs even if they had long-standing disease.
The task force suggested setting a treatment aim of remission or low disease activity, seeing patients every 1-3 months, and switching therapy as often as necessary to reach that goal. Tracking improvement required consistent measurements and recording of a DAM. The recommendations, which were updated in 2014, didn’t specify a certain DAM, saying that the patient’s individual clinical picture should guide that choice (Ann Rheum Dis. 2016 Jan;75[1]:3-15). Shared decision making between the patient and rheumatologist was at the foundation of this concept.
Fast-forward to 2015. As TTT was increasingly embraced in Europe, data began to emerge supporting its clinical validity. A study presented at the American College of Rheumatology (ACR) annual meeting in San Francisco that year showed that treating RA patients toward a target of remission or low disease activity worked immediately and resulted in higher remission rates.
Sofia Ramiro, MD, of Leiden (Netherlands) University Medical Center found that employing a TTT strategy increased the likelihood that a patient would achieve remission by 52%. She also found that TTT strategies lowered disease activity and even improved remission rates for patients who had never received DMARDs.
But in 2017, a meta-analysis found conflicting results among the 16 published randomized, controlled trials comparing TTT against usual care (Health Technol Assess 2017. doi: 10.3310/hta21710). The authors concluded that TTT was more effective for newly diagnosed patients, in whom it increased the chance of remission by about 50%. For those with longstanding disease, TTT was not significantly different from usual care.
Despite limited, and somewhat contradictory, clinical evidence, TTT is becoming increasingly accepted, especially in Europe. In 2016, the European League Against Rheumatism updated its recommendations for RA management (Ann Rheum Dis. 2017 Jun;76[6]:960-77). The document contained a recommendation to use low disease activity or sustained remission as the treatment target for every patient, to monitor disease activity with a validated measure every 1-3 months, and to change therapy as often as every 3 months in the case of no improvement or by 6 months if the target hasn’t been reached.
In its most recent 2015 RA treatment guidelines, the ACR also endorsed the strategy, though somewhat obliquely, and did not require rheumatologists to conform to it (Arthritis Care Res. 2016 Jan;68[1]:1-25).
The concept of TTT, if not the explicit demand to practice it, now appears in the list of quality indicators rheumatologists can choose from in order to fulfill quality performance reporting requirements in Merit-Based Incentive Payment System. Periodic assessment of disease activity in RA patients with a validated DAM is one of the acceptable quality measures for rheumatology. It’s not designated as a high-priority measure, but there it is, item No. 177, tying clinicians at least indirectly to a TTT approach for their Medicare patients: The percentage of patients aged 18 years and older with a diagnosis of RA who have an assessment and classification of disease activity within 12 months.
Slow on the uptake
Despite the data and the dictum, however, TTT remains an outlier in the United States. The most recent studies suggest that most U.S. rheumatologists do not employ it.
Dr. Curtis is the primary author on one of the newest studies, which employed a 26-question survey about the use of a quantitative measurement in RA patients and attitudes about using it (J Rheumatol. 2018 Jan;45[1]:40-4). The survey went out to almost 2,000 rheumatologists; 439 returned it.
Overall, just 44% said they “always practice in a treat-to-target manner, regularly using a scoring metric.” Younger physicians, those in group practices, and those who made regular use of TNF inhibitors were more likely to practice this way. A total of 35% said they never used a quantitative metric for their RA patients.
“The No. 1 reason given about not using them is that it’s too time-consuming and not easy enough,” Dr. Curtis said in an interview. “Logistics is a key barrier.” Busy clinicians don’t want to spend time entering data into an electronic medical record, and there aren’t easy ways to merge a specific DAM with a practice’s chosen EHR. “There’s a hassle factor, for sure.”
The age gap was interesting but not unexpected, he said. “Older rheumatologists say they like to go by their gut, by a clinical gestalt,” Dr. Curtis said, while younger physicians without decades of experience are more comfortable with such clinical tools. For some, age contributes to a kind of clinical inertia. “Doctors trained in an earlier era might be more tolerant of patients not doing as well. I’m a younger physician, and I have never known the era of not having biologics. They lived and practiced in that era, so their spectrum of what’s ‘normal’ and acceptable for patient progress may be wider.”
He and his colleagues investigated whether a 9-month group-based learning collaborative could improve TTT numbers among 46 rheumatologists at 11 practices. The endpoint was a combination of four TTT principles: recording a disease target, recording a disease activity measure, engaging in shared decision-making, and changing treatment if disease target hasn’t been reached.
At baseline, 64% of visits to these rheumatologists had none of the TTT components present, 33% had one component, and 2.3% had two components; just 3% of the visits included all of the components (Arthritis Care Res. 2017 Aug 22. doi: 10.1002/acr.23343).
The project consisted of nine sessions, most conducted by webinar. The entire practice team took part, learning the principles and practices of TTT, identifying their unique barriers to implementing it, and coming up with their unique way of integrating TTT into their practice. It was fairly successful, Dr. Solomon said in an interview. After the intervention, 57% of the exposed practices had incorporated TTT.
In January, Dr. Solomon published a follow-up study of the stability of those changes (Arthritis Care Res. 2018 Jan 5. doi: 10.1002/acr.23508). He was impressed with the results. Most sites from the first cohort had sustained the improvement during the second training period (52%).
“We found that people could implement it effectively when we gave them the tools to do it,” he said. “It’s definitely achievable, but it takes some commitment and guidance, and the realization that everyone can contribute to success in a collaborative manner.”
Technology, or the lack of it
Many rheumatologists view TTT and the consistent measuring it involves as just one more headache-inducing time suck, said John Cush, MD.
But at the same time, he freely admits that the time spent ticking boxes on a paper form or a computer, and being forced to report those to a federal agency, could be the camel-breaking straw for many.
“It’s going down the path of what makes medicine sucky,” he said in an interview. “Bean counters telling me how to practice medicine, who think they can use this TTT to manage what I do. I don’t need more people trying to regulate my life.”
Dr. Cush has conducted surveys on physician burnout and depression. “Administrative tasks and electronic records are a large part why 24% of people are burning out in medicine.”
Right now, there’s no easy way for many rheumatologists to incorporate regular DAM measures into their EHR system. The extra steps needed to get them there impede physician compliance with the strategy, he and Dr. Curtis agreed. But, Dr. Curtis said, there’s an app for that.
He is the developer of the Rheumatic Disease Activity (READY) measure. The iPad/iPhone app, which is free to download in the app store, is an electronic measurement tool that efficiently captures patient-reported outcomes in RA and other rheumatic conditions.
“This tool really makes it much easier to collect DAM from patients,” Dr. Curtis said. “It is designed for the doc who says, ‘I would take data from patients, just make it easy for me to do that.’ It takes 5-10 minutes to complete, and you get information about pain, fatigue, anxiety, and social interactions and, he said, can be easily integrated into work flow.
On a practice-provided device, the patient answers questions validated on the National Institutes of Health Patient-Reported Outcomes Measurement Information System. It includes a number of electronically scored and validated DAMs and provides trend charts to visualize longitudinal score data and track patient health status over multiple encounters. There are also places to record data about current and past medications.
“The docs input no data, which is the usual deal-killer. All they have to do is figure out how to integrate it into the work flow.”
“ACR has been communicating with the major EMR providers out there to make this easier. We are seeing some tools for iPads and smartphones, as well as paper tools.”
The ACR RISE Registry is another option, said Evan Leibowitz, MD, a rheumatologist in Midland Park, N.J.
“RISE is open to all rheumatologists in this country, and ACR has tried to make it as easy as possible. It can interface with most EMRs. All the physician does is collect the data, and it gets transferred to a HIPAA-protected database where it’s analyzed and presented back to the doctors so they can look at all their metrics. It’s currently the least painful way to get involved in a registry, I think.”
But just as techies are rolling out ways to interface DAMs and EHRs, medicine is marching forward. A new blood test called VECTRA DA measures 12 inflammatory biomarkers and may provide all the information needed to make treatment escalation decisions, Dr. Leibowitz said.
“The least painful option will probably be the VECTRA DA score. It’s a single blood test, which we can do easily since we already draw blood. Rather than filling out a RAPID3 [Routine Assessment of Patient Index Data 3] or a CDAI [Clinical Disease Activity Index], we draw the blood, send it to the company, [and] they return us a score that indicates low, moderate, or high disease activity.”
Studies have found that not only is the VECTRA DA score a good clinical management tool, predicting responses, it can also predict impending relapse.
TTT challenges patients, too
Rheumatologists are not the only ones reluctant to embrace TTT. It challenges patients as well, in a number of ways.
“Patients have to be willing to change treatments as often as you need them to, and that can be every 3-6 months, or even more quickly,” Dr. Curtis said. “The cost can be a factor. And a lot of patients are risk averse. They feel there may be more of a downside to switching than a benefit to be gained, especially if they’ve had RA for a while. Maybe they’re feeling a lot better than they were; their disease is still active, but they don’t feel bad enough to want to change medications.”
Researchers have explored these questions.
Last year, Dr. Michaud published a survey of 48 RA patients who were interviewed about their experiences with DMARDs and the feelings that would prompt them to comply with a treatment regimen – or resist one (Arthritis Care Res. 2017 June 2. doi: 10.1002/acr.23301).
“For patients’ motivations to accept treatment regimens, two themes emerged,” said Dr. Michaud, who is also codirector of the National Data Bank for Rheumatic Diseases. “One, the desire to return to a ‘normal’ life and, two, the fear of future disability due to RA. For motivations to resist treatment regimens, five themes emerged: fear of medications, maintaining control over health, denial of sick identity, disappointment with treatment, and feeling overwhelmed by the cognitive burden of deciding.”
The findings confirm one of TTT’s core tenets: involving patients in treatment decisions, Dr. Michaud said in an interview. “A lot of patients in my studies have reached a place of ‘OK-ness’ with their RA. The don’t want to change what they feel is working. They’re afraid of getting worse because they’ve been there and know what that can be.”
Rapid change-ups to new medications are especially intimidating to long-term patients, he said. “This is a very important aspect of resistance to change. The side effects of these medications, both major and minor, are not something that people want to experience.”
“As a physician, I’m worried about the rare and extremely rare adverse events – things that are really dreaded, that can be fatal. However, these happen in only a couple out of tens of thousands of patients. On the other hand, there are common side effects that occur in up to 20% of our patients. They’re not a serious threat to health, but they impact quality of life every day with nausea, dizziness, diarrhea, headache, and brain fog. As rheumatologists, we really undervalue these, and guess what? When we ask patients, it turns out that nausea and dizziness and diarrhea are not things that they want in their daily lives.”
Dr. Fraenkel of Yale University, New Haven, Conn., explored this topic in a recently published survey of 1,273 RA patients that sought their concerns about taking triple therapy, biologics, and Janus kinase inhibitors (Ann Rheum Dis. 2017 Dec 15. doi: 10.1136/annrheumdis-2017-212407). The survey included seven medication attributes – administration, onset, bothersome side effects, serious infection, very rare side effects, amount of information, and cost – and sought to determine the relative effect of each attribute on patient preference for different treatment options.
“We found five distinct clusters” of patients, Dr. Fraenkel said in an interview. “I will admit I was surprised when I saw the largest group (38%) was most concerned about the cost of their medications. Our assumption is always that the rare and dreaded side effects are the most concerning, but for these patients, cost was the dominant issue. It’s the No. 1 reason patients are noncompliant with their initial treatment recommendations. And with the cost of our biologics, it is a very big deal.”
Her reaction pinpoints an important obstacle in shared decision making: physician bias. “I’d say the vast majority of us argue that the benefit of TTT outweighs the harms. We minimize inflammation, so patients will live longer with less disease impact. But how we get there should be up to the patient. My biases shouldn’t come into play. The decision to intensify is different than the decision about how to intensify. This is where the back-and-forth comes in, making sure the patient understands the pros and cons of escalating or not. If she decided no, she doesn’t incur the risk of a new medication, but she does incur the risk of progressing. The bottom line is that physicians should not bring their biases to the table but describe the facts, the importance of which will be different to different patients who have different goals.”
A patient’s story: Overcoming fear and self-image
Prisha Acharya, PhD, knows a thing or two about rheumatoid arthritis.
As an RA researcher in New York, Dr. Acharya has a vast store of knowledge at her fingertips – everything from long-term treatment outcomes to medication side effects.
But when she was diagnosed with RA last year, at age 38 years, she was overwhelmed. And when she connected with a rheumatologist who wanted to aggressively treat her to a target of low disease activity or even remission, she balked. She became the patient who refuses a treat-to-target strategy.
“He was very clear in communicating the urgency of needing to get the disease under control, and I agreed that was a good thing. But even with all this experience in research, I still felt this resistance. I knew I needed to go aggressive. But I was also worried – worried about the side effects, the long-term effects, the costs. Committing to it was going to make my diagnosis real. I wasn’t ready to do it.”
“Prisha Acharya” is not this patient’s real name. She spoke in an interview on the condition of anonymity because she hasn’t yet discussed her diagnosis with some of her family and friends. In fact, she’s still coming to grips with it herself.
The story of Dr. Acharya’s journey to an RA clinic is one she hears every day in her work. About a year ago, she had some aching and stiffness in her knee, and it spread to her wrists and fingers. Digestive issues arose. She shuffled from doctor to doctor, had knee surgery, visited a gastroenterologist, went on a fibromyalgia medication. She finally broached the topic of a possible autoimmune disorder. By the time she received an RA diagnosis, she could only think of one thing: feeling better.
Her rheumatologist got that. But he also let her know at the first visit that he wanted more for her.
“He said, ‘We’re going to get you feeling better, reduce your pain, and make it so you can get out of bed in the morning,’ but our very first conversation was also about a goal of low disease activity and remission. He explained that we had a brief window of opportunity to make a difference in preventing long-term joint damage and that we had to go for it.”
She was on board with the goal, intellectually at least. However, her gut said something different, especially when they discussed methotrexate.
“There was an association in my head between methotrexate and chemotherapy. I knew it could cause fatigue, nausea, and hair thinning. And the idea of an injection, like I was getting chemo for cancer ... it felt very scary.”
As a compromise, she started hydroxychloroquine and shortly after, added sulfasalazine. She was feeling better, but her disease activity scores were still elevated. “My inflammation scores were climbing, and all this time he was saying ‘You have to start methotrexate. You’re going against my advice,’ but I was not emotionally ready. Despite my experience with RA research, I wouldn’t start it.”
With every visit, her rheumatologist patiently built his case for treatment. With every visit, her relationship and trust of him grew.
“Finally, just recently, I did start methotrexate, first with the pill and now the self-injector. I’m on that and the sulfasalazine, but we are reassessing again soon because I still have pain and my disease still isn’t under control. Now we’re going to talk about increasing the methotrexate and adding a new therapy.”
Dr. Acharya’s experience points to the dichotomy between what patients and physicians see as the most important goals and provides a good lesson about how trust and communication can bring those into clinical alignment.
Her rheumatologist set a very clear goal at the beginning of her treatment – one that came with a price tag she wasn’t yet willing to pay. But he also heard and accepted her goal: She wanted to feel better and give herself time to adjust to a new way of life and a new understanding of who she was.
“His language really helped,” Dr. Archaya said. “He acknowledged what I needed – to get the pain and stiffness under control. And as we built our relationship, I was able to hear his side about the urgency of treatment much better. When I was willing to go aggressive, I was also willing to say ‘I have RA.’ It takes a while to get there.”
She had some words of advice to help rheumatologists bridge the gap between what they want for a patient and what that patient wants for herself.
“An open dialogue is really going to help. When patients are voicing their fears, the rheumatologist can reassure them that, if this medicine doesn’t help or if it gives you terrible side effects, we can work together to find another option. Also, it’s so important for the patient to understand the treat-to-target framework from the very beginning. Everything indicates that the earlier we start treatment and set a goal, the better we can control our disease and the better the rest of our life can be.”
The second thing, Dr. Acharya said, is shared decision making. “I want him to tell me the options but also to work with me at arriving at the decision I eventually make.”
Finally, she said, patients need other resources, and rheumatologists can help direct them to find those.
“It’s so important to connect with like-minded patients in patient advocacy groups. The tips that they have given me about medications and dealing with my disease, no doctor could ever give me because patients are the ones that know those things inside-out.”
It makes intuitive sense: Setting a specific goal and working quickly and systematically toward it should bring better results than slowly floundering toward an amorphous endpoint.
That’s the basic idea behind treat-to-target (TTT) strategies in rheumatoid arthritis, and since 2010, data seem to support it: Rheumatologists who pick a therapeutic goal and a related disease activity measure and work in partnership with cooperative patients to achieve it, get better clinical responses.
So important has this concept become that it’s now being tied to reimbursement. Rheumatologists who submit proof that they record disease activity measures in their patients will get points toward fulfilling quality reporting requirements for the Merit-Based Incentive Payment System (MIPS) option in the Quality Payment Program established by the Medicare Access and CHIP Reauthorization Act of 2015. Those points go toward achieving a bonus in Medicare reimbursement; those who can’t show it will edge toward a financial ding.
But despite the twin carrots of better patient outcomes and bonus payments from the Centers for Medicare & Medicaid Services and the stick of a 4%-9% Medicare payment penalty during the years 2019-2022 (and 9% thereafter) for quality outcome measures reported in 2017 and beyond, studies show that up to 60% of U.S. rheumatologists don’t regularly incorporate TTT strategies into how they treat their RA patients.
“There are patient reasons. There are doctor reasons. And there are extrinsic reasons. But I would say the number one reason it’s had limited adoption is that it simply hasn’t been made easy enough.”
The ABCs of TTT
In 2010, Austrian rheumatologist Josef Smolen, MD, leading an international task force, proposed 10 recommendations for improving the care of patients with RA. These were based on the concept that choosing a therapeutic target – low disease activity or remission – and aggressively pursuing it with frequent medication changes accompanied by frequent disease activity measurements would result in improved short- and long-term outcomes.
Disease activity measures (DAMs) were crucial to the concept. In order to treat to a target, one must not only choose a target but also have a validated means to regularly measure progress. The task force didn’t say which DAM would be most appropriate, and research since then suggests that the tool used to measure progress doesn’t matter nearly as much as the target itself.
Shared decision making is also a core tenet of the technique. Physicians work with patients to identify the best treatment target for each individual and decide together how to reach it.
It is not a new concept, Dr. Smolen and his colleagues explained in their landmark paper (Ann Rheum Dis. 2010 Apr;69[4]:631-7). “In many other areas of medicine, treatment targets have been defined to improve outcomes, leading to a reduction in the risk of organ damage. In the care of patients with diabetes, hyperlipidemia, and hypertension, these aspects have been adopted widely in practice; doctors order laboratory tests for cholesterol and triglycerides, blood glucose and HbA1c [hemoglobin A1c] levels, check blood pressure, and adapt therapy accordingly, and patients know these values and are aware of the treatment targets.”
Yet rheumatologists had not adopted a similar paradigm, despite the surge in availability of effective disease-modifying antirheumatic drugs (DMARDs). Although clinical studies of these new drugs clearly showed that remission was possible for many patients and that achieving remission quickly could prevent irreversible joint damage, few patients were getting those drugs even if they had long-standing disease.
The task force suggested setting a treatment aim of remission or low disease activity, seeing patients every 1-3 months, and switching therapy as often as necessary to reach that goal. Tracking improvement required consistent measurements and recording of a DAM. The recommendations, which were updated in 2014, didn’t specify a certain DAM, saying that the patient’s individual clinical picture should guide that choice (Ann Rheum Dis. 2016 Jan;75[1]:3-15). Shared decision making between the patient and rheumatologist was at the foundation of this concept.
Fast-forward to 2015. As TTT was increasingly embraced in Europe, data began to emerge supporting its clinical validity. A study presented at the American College of Rheumatology (ACR) annual meeting in San Francisco that year showed that treating RA patients toward a target of remission or low disease activity worked immediately and resulted in higher remission rates.
Sofia Ramiro, MD, of Leiden (Netherlands) University Medical Center found that employing a TTT strategy increased the likelihood that a patient would achieve remission by 52%. She also found that TTT strategies lowered disease activity and even improved remission rates for patients who had never received DMARDs.
But in 2017, a meta-analysis found conflicting results among the 16 published randomized, controlled trials comparing TTT against usual care (Health Technol Assess 2017. doi: 10.3310/hta21710). The authors concluded that TTT was more effective for newly diagnosed patients, in whom it increased the chance of remission by about 50%. For those with longstanding disease, TTT was not significantly different from usual care.
Despite limited, and somewhat contradictory, clinical evidence, TTT is becoming increasingly accepted, especially in Europe. In 2016, the European League Against Rheumatism updated its recommendations for RA management (Ann Rheum Dis. 2017 Jun;76[6]:960-77). The document contained a recommendation to use low disease activity or sustained remission as the treatment target for every patient, to monitor disease activity with a validated measure every 1-3 months, and to change therapy as often as every 3 months in the case of no improvement or by 6 months if the target hasn’t been reached.
In its most recent 2015 RA treatment guidelines, the ACR also endorsed the strategy, though somewhat obliquely, and did not require rheumatologists to conform to it (Arthritis Care Res. 2016 Jan;68[1]:1-25).
The concept of TTT, if not the explicit demand to practice it, now appears in the list of quality indicators rheumatologists can choose from in order to fulfill quality performance reporting requirements in Merit-Based Incentive Payment System. Periodic assessment of disease activity in RA patients with a validated DAM is one of the acceptable quality measures for rheumatology. It’s not designated as a high-priority measure, but there it is, item No. 177, tying clinicians at least indirectly to a TTT approach for their Medicare patients: The percentage of patients aged 18 years and older with a diagnosis of RA who have an assessment and classification of disease activity within 12 months.
Slow on the uptake
Despite the data and the dictum, however, TTT remains an outlier in the United States. The most recent studies suggest that most U.S. rheumatologists do not employ it.
Dr. Curtis is the primary author on one of the newest studies, which employed a 26-question survey about the use of a quantitative measurement in RA patients and attitudes about using it (J Rheumatol. 2018 Jan;45[1]:40-4). The survey went out to almost 2,000 rheumatologists; 439 returned it.
Overall, just 44% said they “always practice in a treat-to-target manner, regularly using a scoring metric.” Younger physicians, those in group practices, and those who made regular use of TNF inhibitors were more likely to practice this way. A total of 35% said they never used a quantitative metric for their RA patients.
“The No. 1 reason given about not using them is that it’s too time-consuming and not easy enough,” Dr. Curtis said in an interview. “Logistics is a key barrier.” Busy clinicians don’t want to spend time entering data into an electronic medical record, and there aren’t easy ways to merge a specific DAM with a practice’s chosen EHR. “There’s a hassle factor, for sure.”
The age gap was interesting but not unexpected, he said. “Older rheumatologists say they like to go by their gut, by a clinical gestalt,” Dr. Curtis said, while younger physicians without decades of experience are more comfortable with such clinical tools. For some, age contributes to a kind of clinical inertia. “Doctors trained in an earlier era might be more tolerant of patients not doing as well. I’m a younger physician, and I have never known the era of not having biologics. They lived and practiced in that era, so their spectrum of what’s ‘normal’ and acceptable for patient progress may be wider.”
He and his colleagues investigated whether a 9-month group-based learning collaborative could improve TTT numbers among 46 rheumatologists at 11 practices. The endpoint was a combination of four TTT principles: recording a disease target, recording a disease activity measure, engaging in shared decision-making, and changing treatment if disease target hasn’t been reached.
At baseline, 64% of visits to these rheumatologists had none of the TTT components present, 33% had one component, and 2.3% had two components; just 3% of the visits included all of the components (Arthritis Care Res. 2017 Aug 22. doi: 10.1002/acr.23343).
The project consisted of nine sessions, most conducted by webinar. The entire practice team took part, learning the principles and practices of TTT, identifying their unique barriers to implementing it, and coming up with their unique way of integrating TTT into their practice. It was fairly successful, Dr. Solomon said in an interview. After the intervention, 57% of the exposed practices had incorporated TTT.
In January, Dr. Solomon published a follow-up study of the stability of those changes (Arthritis Care Res. 2018 Jan 5. doi: 10.1002/acr.23508). He was impressed with the results. Most sites from the first cohort had sustained the improvement during the second training period (52%).
“We found that people could implement it effectively when we gave them the tools to do it,” he said. “It’s definitely achievable, but it takes some commitment and guidance, and the realization that everyone can contribute to success in a collaborative manner.”
Technology, or the lack of it
Many rheumatologists view TTT and the consistent measuring it involves as just one more headache-inducing time suck, said John Cush, MD.
But at the same time, he freely admits that the time spent ticking boxes on a paper form or a computer, and being forced to report those to a federal agency, could be the camel-breaking straw for many.
“It’s going down the path of what makes medicine sucky,” he said in an interview. “Bean counters telling me how to practice medicine, who think they can use this TTT to manage what I do. I don’t need more people trying to regulate my life.”
Dr. Cush has conducted surveys on physician burnout and depression. “Administrative tasks and electronic records are a large part why 24% of people are burning out in medicine.”
Right now, there’s no easy way for many rheumatologists to incorporate regular DAM measures into their EHR system. The extra steps needed to get them there impede physician compliance with the strategy, he and Dr. Curtis agreed. But, Dr. Curtis said, there’s an app for that.
He is the developer of the Rheumatic Disease Activity (READY) measure. The iPad/iPhone app, which is free to download in the app store, is an electronic measurement tool that efficiently captures patient-reported outcomes in RA and other rheumatic conditions.
“This tool really makes it much easier to collect DAM from patients,” Dr. Curtis said. “It is designed for the doc who says, ‘I would take data from patients, just make it easy for me to do that.’ It takes 5-10 minutes to complete, and you get information about pain, fatigue, anxiety, and social interactions and, he said, can be easily integrated into work flow.
On a practice-provided device, the patient answers questions validated on the National Institutes of Health Patient-Reported Outcomes Measurement Information System. It includes a number of electronically scored and validated DAMs and provides trend charts to visualize longitudinal score data and track patient health status over multiple encounters. There are also places to record data about current and past medications.
“The docs input no data, which is the usual deal-killer. All they have to do is figure out how to integrate it into the work flow.”
“ACR has been communicating with the major EMR providers out there to make this easier. We are seeing some tools for iPads and smartphones, as well as paper tools.”
The ACR RISE Registry is another option, said Evan Leibowitz, MD, a rheumatologist in Midland Park, N.J.
“RISE is open to all rheumatologists in this country, and ACR has tried to make it as easy as possible. It can interface with most EMRs. All the physician does is collect the data, and it gets transferred to a HIPAA-protected database where it’s analyzed and presented back to the doctors so they can look at all their metrics. It’s currently the least painful way to get involved in a registry, I think.”
But just as techies are rolling out ways to interface DAMs and EHRs, medicine is marching forward. A new blood test called VECTRA DA measures 12 inflammatory biomarkers and may provide all the information needed to make treatment escalation decisions, Dr. Leibowitz said.
“The least painful option will probably be the VECTRA DA score. It’s a single blood test, which we can do easily since we already draw blood. Rather than filling out a RAPID3 [Routine Assessment of Patient Index Data 3] or a CDAI [Clinical Disease Activity Index], we draw the blood, send it to the company, [and] they return us a score that indicates low, moderate, or high disease activity.”
Studies have found that not only is the VECTRA DA score a good clinical management tool, predicting responses, it can also predict impending relapse.
TTT challenges patients, too
Rheumatologists are not the only ones reluctant to embrace TTT. It challenges patients as well, in a number of ways.
“Patients have to be willing to change treatments as often as you need them to, and that can be every 3-6 months, or even more quickly,” Dr. Curtis said. “The cost can be a factor. And a lot of patients are risk averse. They feel there may be more of a downside to switching than a benefit to be gained, especially if they’ve had RA for a while. Maybe they’re feeling a lot better than they were; their disease is still active, but they don’t feel bad enough to want to change medications.”
Researchers have explored these questions.
Last year, Dr. Michaud published a survey of 48 RA patients who were interviewed about their experiences with DMARDs and the feelings that would prompt them to comply with a treatment regimen – or resist one (Arthritis Care Res. 2017 June 2. doi: 10.1002/acr.23301).
“For patients’ motivations to accept treatment regimens, two themes emerged,” said Dr. Michaud, who is also codirector of the National Data Bank for Rheumatic Diseases. “One, the desire to return to a ‘normal’ life and, two, the fear of future disability due to RA. For motivations to resist treatment regimens, five themes emerged: fear of medications, maintaining control over health, denial of sick identity, disappointment with treatment, and feeling overwhelmed by the cognitive burden of deciding.”
The findings confirm one of TTT’s core tenets: involving patients in treatment decisions, Dr. Michaud said in an interview. “A lot of patients in my studies have reached a place of ‘OK-ness’ with their RA. The don’t want to change what they feel is working. They’re afraid of getting worse because they’ve been there and know what that can be.”
Rapid change-ups to new medications are especially intimidating to long-term patients, he said. “This is a very important aspect of resistance to change. The side effects of these medications, both major and minor, are not something that people want to experience.”
“As a physician, I’m worried about the rare and extremely rare adverse events – things that are really dreaded, that can be fatal. However, these happen in only a couple out of tens of thousands of patients. On the other hand, there are common side effects that occur in up to 20% of our patients. They’re not a serious threat to health, but they impact quality of life every day with nausea, dizziness, diarrhea, headache, and brain fog. As rheumatologists, we really undervalue these, and guess what? When we ask patients, it turns out that nausea and dizziness and diarrhea are not things that they want in their daily lives.”
Dr. Fraenkel of Yale University, New Haven, Conn., explored this topic in a recently published survey of 1,273 RA patients that sought their concerns about taking triple therapy, biologics, and Janus kinase inhibitors (Ann Rheum Dis. 2017 Dec 15. doi: 10.1136/annrheumdis-2017-212407). The survey included seven medication attributes – administration, onset, bothersome side effects, serious infection, very rare side effects, amount of information, and cost – and sought to determine the relative effect of each attribute on patient preference for different treatment options.
“We found five distinct clusters” of patients, Dr. Fraenkel said in an interview. “I will admit I was surprised when I saw the largest group (38%) was most concerned about the cost of their medications. Our assumption is always that the rare and dreaded side effects are the most concerning, but for these patients, cost was the dominant issue. It’s the No. 1 reason patients are noncompliant with their initial treatment recommendations. And with the cost of our biologics, it is a very big deal.”
Her reaction pinpoints an important obstacle in shared decision making: physician bias. “I’d say the vast majority of us argue that the benefit of TTT outweighs the harms. We minimize inflammation, so patients will live longer with less disease impact. But how we get there should be up to the patient. My biases shouldn’t come into play. The decision to intensify is different than the decision about how to intensify. This is where the back-and-forth comes in, making sure the patient understands the pros and cons of escalating or not. If she decided no, she doesn’t incur the risk of a new medication, but she does incur the risk of progressing. The bottom line is that physicians should not bring their biases to the table but describe the facts, the importance of which will be different to different patients who have different goals.”
A patient’s story: Overcoming fear and self-image
Prisha Acharya, PhD, knows a thing or two about rheumatoid arthritis.
As an RA researcher in New York, Dr. Acharya has a vast store of knowledge at her fingertips – everything from long-term treatment outcomes to medication side effects.
But when she was diagnosed with RA last year, at age 38 years, she was overwhelmed. And when she connected with a rheumatologist who wanted to aggressively treat her to a target of low disease activity or even remission, she balked. She became the patient who refuses a treat-to-target strategy.
“He was very clear in communicating the urgency of needing to get the disease under control, and I agreed that was a good thing. But even with all this experience in research, I still felt this resistance. I knew I needed to go aggressive. But I was also worried – worried about the side effects, the long-term effects, the costs. Committing to it was going to make my diagnosis real. I wasn’t ready to do it.”
“Prisha Acharya” is not this patient’s real name. She spoke in an interview on the condition of anonymity because she hasn’t yet discussed her diagnosis with some of her family and friends. In fact, she’s still coming to grips with it herself.
The story of Dr. Acharya’s journey to an RA clinic is one she hears every day in her work. About a year ago, she had some aching and stiffness in her knee, and it spread to her wrists and fingers. Digestive issues arose. She shuffled from doctor to doctor, had knee surgery, visited a gastroenterologist, went on a fibromyalgia medication. She finally broached the topic of a possible autoimmune disorder. By the time she received an RA diagnosis, she could only think of one thing: feeling better.
Her rheumatologist got that. But he also let her know at the first visit that he wanted more for her.
“He said, ‘We’re going to get you feeling better, reduce your pain, and make it so you can get out of bed in the morning,’ but our very first conversation was also about a goal of low disease activity and remission. He explained that we had a brief window of opportunity to make a difference in preventing long-term joint damage and that we had to go for it.”
She was on board with the goal, intellectually at least. However, her gut said something different, especially when they discussed methotrexate.
“There was an association in my head between methotrexate and chemotherapy. I knew it could cause fatigue, nausea, and hair thinning. And the idea of an injection, like I was getting chemo for cancer ... it felt very scary.”
As a compromise, she started hydroxychloroquine and shortly after, added sulfasalazine. She was feeling better, but her disease activity scores were still elevated. “My inflammation scores were climbing, and all this time he was saying ‘You have to start methotrexate. You’re going against my advice,’ but I was not emotionally ready. Despite my experience with RA research, I wouldn’t start it.”
With every visit, her rheumatologist patiently built his case for treatment. With every visit, her relationship and trust of him grew.
“Finally, just recently, I did start methotrexate, first with the pill and now the self-injector. I’m on that and the sulfasalazine, but we are reassessing again soon because I still have pain and my disease still isn’t under control. Now we’re going to talk about increasing the methotrexate and adding a new therapy.”
Dr. Acharya’s experience points to the dichotomy between what patients and physicians see as the most important goals and provides a good lesson about how trust and communication can bring those into clinical alignment.
Her rheumatologist set a very clear goal at the beginning of her treatment – one that came with a price tag she wasn’t yet willing to pay. But he also heard and accepted her goal: She wanted to feel better and give herself time to adjust to a new way of life and a new understanding of who she was.
“His language really helped,” Dr. Archaya said. “He acknowledged what I needed – to get the pain and stiffness under control. And as we built our relationship, I was able to hear his side about the urgency of treatment much better. When I was willing to go aggressive, I was also willing to say ‘I have RA.’ It takes a while to get there.”
She had some words of advice to help rheumatologists bridge the gap between what they want for a patient and what that patient wants for herself.
“An open dialogue is really going to help. When patients are voicing their fears, the rheumatologist can reassure them that, if this medicine doesn’t help or if it gives you terrible side effects, we can work together to find another option. Also, it’s so important for the patient to understand the treat-to-target framework from the very beginning. Everything indicates that the earlier we start treatment and set a goal, the better we can control our disease and the better the rest of our life can be.”
The second thing, Dr. Acharya said, is shared decision making. “I want him to tell me the options but also to work with me at arriving at the decision I eventually make.”
Finally, she said, patients need other resources, and rheumatologists can help direct them to find those.
“It’s so important to connect with like-minded patients in patient advocacy groups. The tips that they have given me about medications and dealing with my disease, no doctor could ever give me because patients are the ones that know those things inside-out.”
Immunotherapy regimen influences inflammatory arthritis presentation
Variations in the clinical presentation of immunotherapy-induced inflammatory arthritis is partly explained by which treatment regimen was used to treat the cancer, a single-center study suggests.
While immune checkpoint inhibitors (ICI) have revolutionized the field of oncology, their use for an ever-widening range of indications had created an increasing population of patients referred to rheumatologists for the management of immune-related adverse events (IrAEs), according to Laura C. Cappelli, MD, and her colleagues at John Hopkins University, Baltimore.
Well-established guidelines exist for managing adverse events such as colitis and pneumonitis, but there are only preliminary guidelines for evaluating and treating immunotherapy-induced inflammatory arthritis (IA). “This may stem from a lack of consistent reporting of rheumatologic IrAEs in clinical trials, the non–life threatening nature of [inflammatory arthritis], or lack of recognition of musculoskeletal symptoms by treating providers,” they wrote in Seminars in Arthritis and Rheumatism.
Clinical trials have reported ranges of arthralgia in 1%-43% of patients treated with ICIs, but no accurate estimate of the incidence of IA exists.
The researchers noted that treating patients with ICI-induced IA is complicated by a history of active or recently treated cancer and concerns over using immunosuppression in the context of ICI therapy.
They set out to evaluate the clinical presentations of 30 patients seen in their clinic with ICI-induced IA. Patients were a median of 59 years old and 12 (40%) were female. Tumor types included metastatic melanoma, non–small cell lung cancer, small cell lung cancer, colorectal cancer, Hodgkin lymphoma, cutaneous lymphoma, renal cell carcinoma, duodenal carcinoma, Merkel cell carcinoma, cutaneous basal cell carcinoma, and cutaneous squamous cell carcinoma.
Sixteen patients were treated with anti–programmed cell death protein 1 (PD-1)/programmed death ligand 1 monotherapy, and 14 were treated with combination anti–CTLA-4/PD-1 therapy.
Patients on combination therapy were significantly younger (7.5 years, P = 0.01) and were more likely to have metastatic melanoma as their underlying cancer.
Patients who received combination therapy were more likely to present first with knee IA (n = 10) and none had small joint involvement. In contrast, initial small joint involvement was more common in the monotherapy group (n = 6).
C-reactive protein levels were significantly higher in the combination therapy group (4mg/dL vs. 0.5mg/dL, P = 0.03). Only monotherapy patients were positive for anti–citrullinated peptide antibodies, rheumatoid factor, or antinuclear antibodies.
Most of the patients in the study had an additional IrAE, with colitis being the most common (n=10), followed by thyroid disease, pneumonitis, and rash. Patients on PD-1 or programmed death ligand 1 monotherapy were more likely to have IA as their first IrAE.
The research team noted that the median time to symptom onset was 5 months after ICI initiation.
Diagnosis of IA following patient-reported symptoms was an average of 5.2 months, with a significant difference in lag time to diagnosis depending on initial joint presentation. For example, patients with initial small joint involvement had a 10 month longer lag time to IA diagnosis than those with knees as the initial joint involved.
In terms of treatment, 24 patients were treated with systemic corticosteroids and 10 required additional immunosuppression. The need for corticosteroids did not differ by ICI treatment regimen, but those treated with combination therapy were more likely to require additional immunosuppression (P = 0.02).
Tumor necrosis factor inhibitors with or without methotrexate were prescribed for seven patients. All of the patients had a clinical improvement in their arthritis symptoms. Four had a complete tumor response at the time of tumor necrosis factor inhibitor initiation with none having tumor progression.
The three patients treated with methotrexate monotherapy had a complete or sustained partial tumor response to ICI therapy and their cancer did not develop during IA management follow-up.
The authors went on to look at the persistence of IA after cessation of therapy in a subset of 21 patients. They found that 18 of these patients still had IA symptoms months after stopping treatment. They suggested that the delay in diagnosis and treatment seen in their study might explain the finding.
The study provides “critical information, not just for rheumatologists as they try to recognize subgroups in ICI-induced IA and diagnose patients with this new entity, but also for oncology providers who are usually first to encounter patients with ICI-induced IA and subsequently refer patients to rheumatology,” Dr. Cappelli and colleagues wrote.
The experience so far with using immunosuppression in ICI-induced IA “has been reassuring in terms of cancer outcomes, but more studies are needed to confirm this finding,” they concluded.
SOURCE: Cappelli LC et al. Semin Arthritis Rheum. doi: 10.1016/j.semarthrit. 2018.02.011.
Variations in the clinical presentation of immunotherapy-induced inflammatory arthritis is partly explained by which treatment regimen was used to treat the cancer, a single-center study suggests.
While immune checkpoint inhibitors (ICI) have revolutionized the field of oncology, their use for an ever-widening range of indications had created an increasing population of patients referred to rheumatologists for the management of immune-related adverse events (IrAEs), according to Laura C. Cappelli, MD, and her colleagues at John Hopkins University, Baltimore.
Well-established guidelines exist for managing adverse events such as colitis and pneumonitis, but there are only preliminary guidelines for evaluating and treating immunotherapy-induced inflammatory arthritis (IA). “This may stem from a lack of consistent reporting of rheumatologic IrAEs in clinical trials, the non–life threatening nature of [inflammatory arthritis], or lack of recognition of musculoskeletal symptoms by treating providers,” they wrote in Seminars in Arthritis and Rheumatism.
Clinical trials have reported ranges of arthralgia in 1%-43% of patients treated with ICIs, but no accurate estimate of the incidence of IA exists.
The researchers noted that treating patients with ICI-induced IA is complicated by a history of active or recently treated cancer and concerns over using immunosuppression in the context of ICI therapy.
They set out to evaluate the clinical presentations of 30 patients seen in their clinic with ICI-induced IA. Patients were a median of 59 years old and 12 (40%) were female. Tumor types included metastatic melanoma, non–small cell lung cancer, small cell lung cancer, colorectal cancer, Hodgkin lymphoma, cutaneous lymphoma, renal cell carcinoma, duodenal carcinoma, Merkel cell carcinoma, cutaneous basal cell carcinoma, and cutaneous squamous cell carcinoma.
Sixteen patients were treated with anti–programmed cell death protein 1 (PD-1)/programmed death ligand 1 monotherapy, and 14 were treated with combination anti–CTLA-4/PD-1 therapy.
Patients on combination therapy were significantly younger (7.5 years, P = 0.01) and were more likely to have metastatic melanoma as their underlying cancer.
Patients who received combination therapy were more likely to present first with knee IA (n = 10) and none had small joint involvement. In contrast, initial small joint involvement was more common in the monotherapy group (n = 6).
C-reactive protein levels were significantly higher in the combination therapy group (4mg/dL vs. 0.5mg/dL, P = 0.03). Only monotherapy patients were positive for anti–citrullinated peptide antibodies, rheumatoid factor, or antinuclear antibodies.
Most of the patients in the study had an additional IrAE, with colitis being the most common (n=10), followed by thyroid disease, pneumonitis, and rash. Patients on PD-1 or programmed death ligand 1 monotherapy were more likely to have IA as their first IrAE.
The research team noted that the median time to symptom onset was 5 months after ICI initiation.
Diagnosis of IA following patient-reported symptoms was an average of 5.2 months, with a significant difference in lag time to diagnosis depending on initial joint presentation. For example, patients with initial small joint involvement had a 10 month longer lag time to IA diagnosis than those with knees as the initial joint involved.
In terms of treatment, 24 patients were treated with systemic corticosteroids and 10 required additional immunosuppression. The need for corticosteroids did not differ by ICI treatment regimen, but those treated with combination therapy were more likely to require additional immunosuppression (P = 0.02).
Tumor necrosis factor inhibitors with or without methotrexate were prescribed for seven patients. All of the patients had a clinical improvement in their arthritis symptoms. Four had a complete tumor response at the time of tumor necrosis factor inhibitor initiation with none having tumor progression.
The three patients treated with methotrexate monotherapy had a complete or sustained partial tumor response to ICI therapy and their cancer did not develop during IA management follow-up.
The authors went on to look at the persistence of IA after cessation of therapy in a subset of 21 patients. They found that 18 of these patients still had IA symptoms months after stopping treatment. They suggested that the delay in diagnosis and treatment seen in their study might explain the finding.
The study provides “critical information, not just for rheumatologists as they try to recognize subgroups in ICI-induced IA and diagnose patients with this new entity, but also for oncology providers who are usually first to encounter patients with ICI-induced IA and subsequently refer patients to rheumatology,” Dr. Cappelli and colleagues wrote.
The experience so far with using immunosuppression in ICI-induced IA “has been reassuring in terms of cancer outcomes, but more studies are needed to confirm this finding,” they concluded.
SOURCE: Cappelli LC et al. Semin Arthritis Rheum. doi: 10.1016/j.semarthrit. 2018.02.011.
Variations in the clinical presentation of immunotherapy-induced inflammatory arthritis is partly explained by which treatment regimen was used to treat the cancer, a single-center study suggests.
While immune checkpoint inhibitors (ICI) have revolutionized the field of oncology, their use for an ever-widening range of indications had created an increasing population of patients referred to rheumatologists for the management of immune-related adverse events (IrAEs), according to Laura C. Cappelli, MD, and her colleagues at John Hopkins University, Baltimore.
Well-established guidelines exist for managing adverse events such as colitis and pneumonitis, but there are only preliminary guidelines for evaluating and treating immunotherapy-induced inflammatory arthritis (IA). “This may stem from a lack of consistent reporting of rheumatologic IrAEs in clinical trials, the non–life threatening nature of [inflammatory arthritis], or lack of recognition of musculoskeletal symptoms by treating providers,” they wrote in Seminars in Arthritis and Rheumatism.
Clinical trials have reported ranges of arthralgia in 1%-43% of patients treated with ICIs, but no accurate estimate of the incidence of IA exists.
The researchers noted that treating patients with ICI-induced IA is complicated by a history of active or recently treated cancer and concerns over using immunosuppression in the context of ICI therapy.
They set out to evaluate the clinical presentations of 30 patients seen in their clinic with ICI-induced IA. Patients were a median of 59 years old and 12 (40%) were female. Tumor types included metastatic melanoma, non–small cell lung cancer, small cell lung cancer, colorectal cancer, Hodgkin lymphoma, cutaneous lymphoma, renal cell carcinoma, duodenal carcinoma, Merkel cell carcinoma, cutaneous basal cell carcinoma, and cutaneous squamous cell carcinoma.
Sixteen patients were treated with anti–programmed cell death protein 1 (PD-1)/programmed death ligand 1 monotherapy, and 14 were treated with combination anti–CTLA-4/PD-1 therapy.
Patients on combination therapy were significantly younger (7.5 years, P = 0.01) and were more likely to have metastatic melanoma as their underlying cancer.
Patients who received combination therapy were more likely to present first with knee IA (n = 10) and none had small joint involvement. In contrast, initial small joint involvement was more common in the monotherapy group (n = 6).
C-reactive protein levels were significantly higher in the combination therapy group (4mg/dL vs. 0.5mg/dL, P = 0.03). Only monotherapy patients were positive for anti–citrullinated peptide antibodies, rheumatoid factor, or antinuclear antibodies.
Most of the patients in the study had an additional IrAE, with colitis being the most common (n=10), followed by thyroid disease, pneumonitis, and rash. Patients on PD-1 or programmed death ligand 1 monotherapy were more likely to have IA as their first IrAE.
The research team noted that the median time to symptom onset was 5 months after ICI initiation.
Diagnosis of IA following patient-reported symptoms was an average of 5.2 months, with a significant difference in lag time to diagnosis depending on initial joint presentation. For example, patients with initial small joint involvement had a 10 month longer lag time to IA diagnosis than those with knees as the initial joint involved.
In terms of treatment, 24 patients were treated with systemic corticosteroids and 10 required additional immunosuppression. The need for corticosteroids did not differ by ICI treatment regimen, but those treated with combination therapy were more likely to require additional immunosuppression (P = 0.02).
Tumor necrosis factor inhibitors with or without methotrexate were prescribed for seven patients. All of the patients had a clinical improvement in their arthritis symptoms. Four had a complete tumor response at the time of tumor necrosis factor inhibitor initiation with none having tumor progression.
The three patients treated with methotrexate monotherapy had a complete or sustained partial tumor response to ICI therapy and their cancer did not develop during IA management follow-up.
The authors went on to look at the persistence of IA after cessation of therapy in a subset of 21 patients. They found that 18 of these patients still had IA symptoms months after stopping treatment. They suggested that the delay in diagnosis and treatment seen in their study might explain the finding.
The study provides “critical information, not just for rheumatologists as they try to recognize subgroups in ICI-induced IA and diagnose patients with this new entity, but also for oncology providers who are usually first to encounter patients with ICI-induced IA and subsequently refer patients to rheumatology,” Dr. Cappelli and colleagues wrote.
The experience so far with using immunosuppression in ICI-induced IA “has been reassuring in terms of cancer outcomes, but more studies are needed to confirm this finding,” they concluded.
SOURCE: Cappelli LC et al. Semin Arthritis Rheum. doi: 10.1016/j.semarthrit. 2018.02.011.
FROM SEMINARS IN ARTHRITIS AND RHEUMATISM
Key clinical point: The clinical features of patients with immunotherapy-induced inflammatory arthritis differ according to the treatment regimen used.
Major findings: Combination immune checkpoint inhibitor therapy was associated with higher C-reactive protein levels and a higher likelihood of having a large joint affected first.
Study details: A single-center, retrospective cohort study of 30 patients with rheumatologist-confirmed inflammatory arthritis after receiving immune checkpoint inhibitor therapy.
Disclosures: The study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Disease and the Jerome L. Greene Foundation.
Source: Cappelli LC et al. Semin Arthritis Rheum. doi: 10.1016/j.semarthrit. 2018.02.011.
Mast cell synovitis: potential target in RA?
MAUI, HAWAII – Could mast cell-rich synovitis become a novel target in patients with early rheumatoid arthritis?
Investigators at the University of London believe so. In a small but provocative study presented at the 2017 annual meeting of the American College of Rheumatology, they demonstrated that these mast cells are not an innocent bystander in joint inflammation; rather, they play an active albeit still incompletely understood role in the synovial inflammatory infiltrate and in disease progression, Orrin M. Troum, MD, said at the 2018 Rheumatology Winter Clinical Symposium.
Treatment with synthetic DMARDs was partially effective, both clinically and at the cellular level. Mean mast cell density fell from 14.2/mm2 at baseline to 8.2/mm2 at 6 months. But synovial mast cells were still present at 6 months in 9 of 20 patients. Those nine patients had significantly higher DAS28 scores – a mean of 4.08 versus 2.41 in the synovial mast cell–negative group – as well as higher synovitis scores. Disease remission as defined by a DAS28 score below 2.6 was achieved in only 2 of 9 patients with persistent mast cell-rich synovitis, as compared with 8 of 11 mast cell-negative patients.
Moreover, four of the nine patients with persistent mast cell-rich synovitis after 6 months of synthetic DMARDs had synovial lymphoid aggregates of CD20-positive B cells and/or CD138-positive plasma cells; in contrast, none of the 11 synovial mast cell-negative patients did, noted Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, who is in private practice in Santa Monica, Calif.
In theory, if a baseline synovial tissue immune cell profile could be identified that’s predictive of high-level responsiveness to synthetic DMARDs or, conversely, nonresponsiveness, tissue specimens could be used to stratify patients with early RA to different initial treatment strategies. The problem with that is few rheumatologists in the United States – and indeed worldwide – are proficient at performing ultrasound-guided synovial biopsies, according to Dr. Troum.
His description of the London study prompted a question as to whether any of the biologics used in rheumatology can inhibit mast cells. Arthur Kavanaugh, MD, symposium director, said the only agent that comes to mind is imatinib (Gleevec), a tyrosine kinase inhibitor used in the treatment of aggressive systemic mastocytosis as well as for certain leukemias.
“It has a ton of toxicity, though,” said Dr. Kavanaugh, professor of medicine and director of the Center for Innovative Therapy in the division of rheumatology, allergy, and immunology at the University of California, San Diego.
Dr. Troum reported having no financial conflicts regarding his presentation.
MAUI, HAWAII – Could mast cell-rich synovitis become a novel target in patients with early rheumatoid arthritis?
Investigators at the University of London believe so. In a small but provocative study presented at the 2017 annual meeting of the American College of Rheumatology, they demonstrated that these mast cells are not an innocent bystander in joint inflammation; rather, they play an active albeit still incompletely understood role in the synovial inflammatory infiltrate and in disease progression, Orrin M. Troum, MD, said at the 2018 Rheumatology Winter Clinical Symposium.
Treatment with synthetic DMARDs was partially effective, both clinically and at the cellular level. Mean mast cell density fell from 14.2/mm2 at baseline to 8.2/mm2 at 6 months. But synovial mast cells were still present at 6 months in 9 of 20 patients. Those nine patients had significantly higher DAS28 scores – a mean of 4.08 versus 2.41 in the synovial mast cell–negative group – as well as higher synovitis scores. Disease remission as defined by a DAS28 score below 2.6 was achieved in only 2 of 9 patients with persistent mast cell-rich synovitis, as compared with 8 of 11 mast cell-negative patients.
Moreover, four of the nine patients with persistent mast cell-rich synovitis after 6 months of synthetic DMARDs had synovial lymphoid aggregates of CD20-positive B cells and/or CD138-positive plasma cells; in contrast, none of the 11 synovial mast cell-negative patients did, noted Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, who is in private practice in Santa Monica, Calif.
In theory, if a baseline synovial tissue immune cell profile could be identified that’s predictive of high-level responsiveness to synthetic DMARDs or, conversely, nonresponsiveness, tissue specimens could be used to stratify patients with early RA to different initial treatment strategies. The problem with that is few rheumatologists in the United States – and indeed worldwide – are proficient at performing ultrasound-guided synovial biopsies, according to Dr. Troum.
His description of the London study prompted a question as to whether any of the biologics used in rheumatology can inhibit mast cells. Arthur Kavanaugh, MD, symposium director, said the only agent that comes to mind is imatinib (Gleevec), a tyrosine kinase inhibitor used in the treatment of aggressive systemic mastocytosis as well as for certain leukemias.
“It has a ton of toxicity, though,” said Dr. Kavanaugh, professor of medicine and director of the Center for Innovative Therapy in the division of rheumatology, allergy, and immunology at the University of California, San Diego.
Dr. Troum reported having no financial conflicts regarding his presentation.
MAUI, HAWAII – Could mast cell-rich synovitis become a novel target in patients with early rheumatoid arthritis?
Investigators at the University of London believe so. In a small but provocative study presented at the 2017 annual meeting of the American College of Rheumatology, they demonstrated that these mast cells are not an innocent bystander in joint inflammation; rather, they play an active albeit still incompletely understood role in the synovial inflammatory infiltrate and in disease progression, Orrin M. Troum, MD, said at the 2018 Rheumatology Winter Clinical Symposium.
Treatment with synthetic DMARDs was partially effective, both clinically and at the cellular level. Mean mast cell density fell from 14.2/mm2 at baseline to 8.2/mm2 at 6 months. But synovial mast cells were still present at 6 months in 9 of 20 patients. Those nine patients had significantly higher DAS28 scores – a mean of 4.08 versus 2.41 in the synovial mast cell–negative group – as well as higher synovitis scores. Disease remission as defined by a DAS28 score below 2.6 was achieved in only 2 of 9 patients with persistent mast cell-rich synovitis, as compared with 8 of 11 mast cell-negative patients.
Moreover, four of the nine patients with persistent mast cell-rich synovitis after 6 months of synthetic DMARDs had synovial lymphoid aggregates of CD20-positive B cells and/or CD138-positive plasma cells; in contrast, none of the 11 synovial mast cell-negative patients did, noted Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, who is in private practice in Santa Monica, Calif.
In theory, if a baseline synovial tissue immune cell profile could be identified that’s predictive of high-level responsiveness to synthetic DMARDs or, conversely, nonresponsiveness, tissue specimens could be used to stratify patients with early RA to different initial treatment strategies. The problem with that is few rheumatologists in the United States – and indeed worldwide – are proficient at performing ultrasound-guided synovial biopsies, according to Dr. Troum.
His description of the London study prompted a question as to whether any of the biologics used in rheumatology can inhibit mast cells. Arthur Kavanaugh, MD, symposium director, said the only agent that comes to mind is imatinib (Gleevec), a tyrosine kinase inhibitor used in the treatment of aggressive systemic mastocytosis as well as for certain leukemias.
“It has a ton of toxicity, though,” said Dr. Kavanaugh, professor of medicine and director of the Center for Innovative Therapy in the division of rheumatology, allergy, and immunology at the University of California, San Diego.
Dr. Troum reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM RWCS 2018
NIAID proposes 3-pronged plan for universal influenza vaccine
Three specific research areas were proposed by the National Institute of Allergy and Infectious Diseases (NIAID) in its development plan for a universal influenza vaccine, as detailed in a report published online in the Journal of Infectious Diseases.
Anthony S. Fauci, MD, director of the NIAID, spoke with Frontline Medical News in an interview regarding the plan and noted that he and his colleagues felt that it was important to accelerate the effort for a universal vaccine.
“The strategic plan also includes a description of research resources essential to advancing these three research areas that [the] NIAID will develop, support, and provide for the scientific community,” wrote Dr. Erbelding and her coauthors.
The development plan comes 8 months after scientists from academia, industry, and government convened for the NIAID Pathway to a Universal Influenza Vaccine workshop to address knowledge gaps and strategy, which was summarized last year in the journal Immunity (2017;47: 599-603). The scientists at the workshop developed criteria that would define a universal vaccine and decided that a universal vaccine for influenza should do three things: be at least 75% effective against symptomatic influenza infection; protect against group I and II influenza A viruses; and have durable protections that lasts at least 1 year and preferably through multiple seasons.
“Clearly, a vaccine that would cover most or all seasonal strains of influenza and also provide protection during a pandemic is highly desirable,” wrote Catharine I. Paules, MD, of the University of Maryland, Baltimore, and her coauthors in the workshop summary.
Dr. Fauci told Frontline Medical News how “experts from all over the country addressed their thoughts and concerns with us last year [at the workshop], and now we have a development plan,” he said. “But the next step will be doing the research and finding more resources. ... The work is yet to be done.”
The development plan was published amid an ongoing historic flu season.
Dr. Fauci noted that this season had particular circumstances that made it worse than normal. “I don’t think that, had we had this plan in place a year ago, it would have had an impact on this flu season,” he said.
The authors reported no relevant financial conflicts and that the National Institutes of Health produced this plan.
SOURCE: Erbelding E et al. J Infect Dis. 2018 Feb 28. doi: 10.1093/infdis/jiy103.
Three specific research areas were proposed by the National Institute of Allergy and Infectious Diseases (NIAID) in its development plan for a universal influenza vaccine, as detailed in a report published online in the Journal of Infectious Diseases.
Anthony S. Fauci, MD, director of the NIAID, spoke with Frontline Medical News in an interview regarding the plan and noted that he and his colleagues felt that it was important to accelerate the effort for a universal vaccine.
“The strategic plan also includes a description of research resources essential to advancing these three research areas that [the] NIAID will develop, support, and provide for the scientific community,” wrote Dr. Erbelding and her coauthors.
The development plan comes 8 months after scientists from academia, industry, and government convened for the NIAID Pathway to a Universal Influenza Vaccine workshop to address knowledge gaps and strategy, which was summarized last year in the journal Immunity (2017;47: 599-603). The scientists at the workshop developed criteria that would define a universal vaccine and decided that a universal vaccine for influenza should do three things: be at least 75% effective against symptomatic influenza infection; protect against group I and II influenza A viruses; and have durable protections that lasts at least 1 year and preferably through multiple seasons.
“Clearly, a vaccine that would cover most or all seasonal strains of influenza and also provide protection during a pandemic is highly desirable,” wrote Catharine I. Paules, MD, of the University of Maryland, Baltimore, and her coauthors in the workshop summary.
Dr. Fauci told Frontline Medical News how “experts from all over the country addressed their thoughts and concerns with us last year [at the workshop], and now we have a development plan,” he said. “But the next step will be doing the research and finding more resources. ... The work is yet to be done.”
The development plan was published amid an ongoing historic flu season.
Dr. Fauci noted that this season had particular circumstances that made it worse than normal. “I don’t think that, had we had this plan in place a year ago, it would have had an impact on this flu season,” he said.
The authors reported no relevant financial conflicts and that the National Institutes of Health produced this plan.
SOURCE: Erbelding E et al. J Infect Dis. 2018 Feb 28. doi: 10.1093/infdis/jiy103.
Three specific research areas were proposed by the National Institute of Allergy and Infectious Diseases (NIAID) in its development plan for a universal influenza vaccine, as detailed in a report published online in the Journal of Infectious Diseases.
Anthony S. Fauci, MD, director of the NIAID, spoke with Frontline Medical News in an interview regarding the plan and noted that he and his colleagues felt that it was important to accelerate the effort for a universal vaccine.
“The strategic plan also includes a description of research resources essential to advancing these three research areas that [the] NIAID will develop, support, and provide for the scientific community,” wrote Dr. Erbelding and her coauthors.
The development plan comes 8 months after scientists from academia, industry, and government convened for the NIAID Pathway to a Universal Influenza Vaccine workshop to address knowledge gaps and strategy, which was summarized last year in the journal Immunity (2017;47: 599-603). The scientists at the workshop developed criteria that would define a universal vaccine and decided that a universal vaccine for influenza should do three things: be at least 75% effective against symptomatic influenza infection; protect against group I and II influenza A viruses; and have durable protections that lasts at least 1 year and preferably through multiple seasons.
“Clearly, a vaccine that would cover most or all seasonal strains of influenza and also provide protection during a pandemic is highly desirable,” wrote Catharine I. Paules, MD, of the University of Maryland, Baltimore, and her coauthors in the workshop summary.
Dr. Fauci told Frontline Medical News how “experts from all over the country addressed their thoughts and concerns with us last year [at the workshop], and now we have a development plan,” he said. “But the next step will be doing the research and finding more resources. ... The work is yet to be done.”
The development plan was published amid an ongoing historic flu season.
Dr. Fauci noted that this season had particular circumstances that made it worse than normal. “I don’t think that, had we had this plan in place a year ago, it would have had an impact on this flu season,” he said.
The authors reported no relevant financial conflicts and that the National Institutes of Health produced this plan.
SOURCE: Erbelding E et al. J Infect Dis. 2018 Feb 28. doi: 10.1093/infdis/jiy103.
FROM THE JOURNAL OF INFECTIOUS DISEASES