User login
Cutting-edge DNA technology could boost cystic fibrosis screening for newborns
Stanford University scientists say they’ve devised a more accurate and comprehensive DNA test to screen newborns for cystic fibrosis.
Every state screens newborns for cystic fibrosis, but the current sequence of tests can miss cases. The new method, presented in a study published Feb. 1 in the Journal of Molecular Diagnostics, promises to be more efficient and cost effective, researchers said. It may also improve screening for nonwhite babies, for whom cystic fibrosis is rarer and harder to diagnose.
The test “offers the promise of potentially eliminating the false negative results that lead to miss ed cases,” said Dr. Philip Farrell, a former dean of the University of Wisconsin School of Medicine and Public Health, Madison.
Cystic fibrosis is caused by a defect in the CFTR gene. Current genetic screens look for 40 of the most common mutations of the CFTR gene in newborns. Yet, any of the more than 2,000 known mutations in that gene could play a role in the disease, and there are likely others that have not yet been discovered.
The new test uses “next generation” DNA sequencing that can quickly and more cheaply look at the entire CFTR gene, not just selected mutations. It does not require an extra blood sample. Rather, it uses the tiny amount of blood drawn from the common newborn heel stick test that’s already used to screen for a number of diseases, including cystic fibrosis.
The researchers say this advance can enable testing labs to review many newborn samples at a time and reduce costs, allowing a technology previously used to diagnose only individual cases to be applied to a large population.
“Next generation” DNA sequencing has been used in recent years to diagnose disease, but is only now becoming cheap and fast enough to even be considered for large-scale population screening. Scientists from Stanford, the California Department of Public Health, and the University of Texas at Austin conducted the research. Other U.S. scientists have been working on similar newborn screening approaches using next-generation DNA sequencing.
The test is not only quicker and cheaper, but also “very accurate,” said Dr. Iris Schrijver, a Stanford University Medical School pathology professor who is one of the study’s authors. “We can look at the entire gene and assess … all kinds of mutations in this single test,” possibly in half the time of a current DNA test.
A spokesman for the California Department of Public Health, which oversees newborn screenings, said the current cost, including DNA testing, is approximately $113 per newborn, which is typically covered by insurers.
The department declined to make one of its scientists, a coauthor of the study, available for an interview. It also declined to respond directly to questions about the cost of these new tests or whether it might adopt them.
In general, the spokesman noted, the agency’s newborn screening program evaluates potential new testing methods for effectiveness and cost.
“Historically, changes to existing testing methods have been rare, so the department cannot speculate on a timeline for this process,” the spokesman wrote in an email.
However, a Stanford spokeswoman said its laboratory is currently running side-by-side comparisons of the new test and the current one, and its lab physicians expect to meet with public state health officials within the year to discuss next steps.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
Stanford University scientists say they’ve devised a more accurate and comprehensive DNA test to screen newborns for cystic fibrosis.
Every state screens newborns for cystic fibrosis, but the current sequence of tests can miss cases. The new method, presented in a study published Feb. 1 in the Journal of Molecular Diagnostics, promises to be more efficient and cost effective, researchers said. It may also improve screening for nonwhite babies, for whom cystic fibrosis is rarer and harder to diagnose.
The test “offers the promise of potentially eliminating the false negative results that lead to miss ed cases,” said Dr. Philip Farrell, a former dean of the University of Wisconsin School of Medicine and Public Health, Madison.
Cystic fibrosis is caused by a defect in the CFTR gene. Current genetic screens look for 40 of the most common mutations of the CFTR gene in newborns. Yet, any of the more than 2,000 known mutations in that gene could play a role in the disease, and there are likely others that have not yet been discovered.
The new test uses “next generation” DNA sequencing that can quickly and more cheaply look at the entire CFTR gene, not just selected mutations. It does not require an extra blood sample. Rather, it uses the tiny amount of blood drawn from the common newborn heel stick test that’s already used to screen for a number of diseases, including cystic fibrosis.
The researchers say this advance can enable testing labs to review many newborn samples at a time and reduce costs, allowing a technology previously used to diagnose only individual cases to be applied to a large population.
“Next generation” DNA sequencing has been used in recent years to diagnose disease, but is only now becoming cheap and fast enough to even be considered for large-scale population screening. Scientists from Stanford, the California Department of Public Health, and the University of Texas at Austin conducted the research. Other U.S. scientists have been working on similar newborn screening approaches using next-generation DNA sequencing.
The test is not only quicker and cheaper, but also “very accurate,” said Dr. Iris Schrijver, a Stanford University Medical School pathology professor who is one of the study’s authors. “We can look at the entire gene and assess … all kinds of mutations in this single test,” possibly in half the time of a current DNA test.
A spokesman for the California Department of Public Health, which oversees newborn screenings, said the current cost, including DNA testing, is approximately $113 per newborn, which is typically covered by insurers.
The department declined to make one of its scientists, a coauthor of the study, available for an interview. It also declined to respond directly to questions about the cost of these new tests or whether it might adopt them.
In general, the spokesman noted, the agency’s newborn screening program evaluates potential new testing methods for effectiveness and cost.
“Historically, changes to existing testing methods have been rare, so the department cannot speculate on a timeline for this process,” the spokesman wrote in an email.
However, a Stanford spokeswoman said its laboratory is currently running side-by-side comparisons of the new test and the current one, and its lab physicians expect to meet with public state health officials within the year to discuss next steps.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
Stanford University scientists say they’ve devised a more accurate and comprehensive DNA test to screen newborns for cystic fibrosis.
Every state screens newborns for cystic fibrosis, but the current sequence of tests can miss cases. The new method, presented in a study published Feb. 1 in the Journal of Molecular Diagnostics, promises to be more efficient and cost effective, researchers said. It may also improve screening for nonwhite babies, for whom cystic fibrosis is rarer and harder to diagnose.
The test “offers the promise of potentially eliminating the false negative results that lead to miss ed cases,” said Dr. Philip Farrell, a former dean of the University of Wisconsin School of Medicine and Public Health, Madison.
Cystic fibrosis is caused by a defect in the CFTR gene. Current genetic screens look for 40 of the most common mutations of the CFTR gene in newborns. Yet, any of the more than 2,000 known mutations in that gene could play a role in the disease, and there are likely others that have not yet been discovered.
The new test uses “next generation” DNA sequencing that can quickly and more cheaply look at the entire CFTR gene, not just selected mutations. It does not require an extra blood sample. Rather, it uses the tiny amount of blood drawn from the common newborn heel stick test that’s already used to screen for a number of diseases, including cystic fibrosis.
The researchers say this advance can enable testing labs to review many newborn samples at a time and reduce costs, allowing a technology previously used to diagnose only individual cases to be applied to a large population.
“Next generation” DNA sequencing has been used in recent years to diagnose disease, but is only now becoming cheap and fast enough to even be considered for large-scale population screening. Scientists from Stanford, the California Department of Public Health, and the University of Texas at Austin conducted the research. Other U.S. scientists have been working on similar newborn screening approaches using next-generation DNA sequencing.
The test is not only quicker and cheaper, but also “very accurate,” said Dr. Iris Schrijver, a Stanford University Medical School pathology professor who is one of the study’s authors. “We can look at the entire gene and assess … all kinds of mutations in this single test,” possibly in half the time of a current DNA test.
A spokesman for the California Department of Public Health, which oversees newborn screenings, said the current cost, including DNA testing, is approximately $113 per newborn, which is typically covered by insurers.
The department declined to make one of its scientists, a coauthor of the study, available for an interview. It also declined to respond directly to questions about the cost of these new tests or whether it might adopt them.
In general, the spokesman noted, the agency’s newborn screening program evaluates potential new testing methods for effectiveness and cost.
“Historically, changes to existing testing methods have been rare, so the department cannot speculate on a timeline for this process,” the spokesman wrote in an email.
However, a Stanford spokeswoman said its laboratory is currently running side-by-side comparisons of the new test and the current one, and its lab physicians expect to meet with public state health officials within the year to discuss next steps.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
Erythematous Eruption on the Left Leg
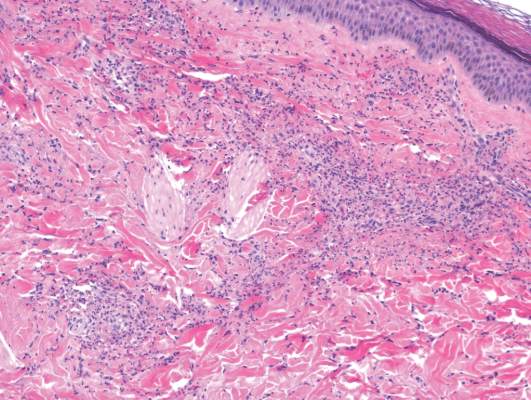
The Diagnosis: Bullous Henoch-Schönlein Purpura
Laboratory tests in this patient showed no abnormalities for complete blood cell count, immunoglobulins, anti–double-stranded DNA, antinuclear antibody, p–antineutrophil cytoplasmic antibodies, lupus anticoagulant, Sjögren antibodies, liver enzymes, and erythrocyte sedimentation rate. Urinalysis was normal. Punch biopsies were obtained and a histologic examination showed an intense inflammatory infiltrate of neutrophils around blood vessels within the dermis (Figure). These blood vessels showed swollen endothelium and narrowing of the vessel lumina with leukocytoclasia. Direct immunofluorescence revealed granular IgA, C3, fibrin, and weak IgM deposits in blood vessels in the papillary dermis consistent with Henoch-Schönlein purpura (HSP).
Henoch-Schönlein purpura is the most common vasculitis in children.1-6 However, its bullous variant is rare, with few pediatric cases reported. Bullous HSP affects arterioles through an IgA-mediated pathway.1-6 It is believed that the bullae are formed secondary to neutrophilic release of matrix metalloproteinase 9 (MMP-9), which degrades extracellular collagen.2 Additionally, bullous fluid from HSP has been noted to have markedly elevated levels of soluble CD23, a form of the CD23 B-cell surface receptor used in antibody feedback regulation and B-cell recruitment, which also has been found to be elevated in the fluid of bullous pemphigoid, suggesting a similar pathogenesis of exaggerated humoral immunity.3
The most common sign of HSP is palpable purpura; however, other cutaneous findings can be present including targetoid plaques, macules, papules, petechiae, and bullae that may become hemorrhagic, ulcerated, necrotic, or scarred.1-6 Bullae appear in the most dependent parts of the body, such as the feet and lower legs. Hydrostatic pressure may play a role in the pathogenesis of this phenomenon.1 When other classic signs of HSP are absent, the presence of bullae clouds the diagnosis and creates controversy regarding treatment, as there is a dearth of literature on proper therapy for severe cutaneous manifestations of HSP.6
Our patient was treated with morphine for pain management along with topical mupirocin and nonadherent dressings for wound care. She also received pulse intravenous methylprednisolone 2 mg/kg daily for 3 days and then was transitioned to oral prednisone 1 mg/kg daily, which was tapered over 3 weeks after discharge. This regimen resulted in resolution of symptoms with rapid regression of bullae and subsequent postinflammatory hyperpigmentation. Prior reports have noted that the presence of bullae does not alter the prognosis or predict probability of renal involvement of this self-limited disease, leading to controversy in determining if treatment offers more favorable outcomes.1,3 One study suggested that steroids only improve symptoms, arthralgia, and abdominal pain, but they do not aid in the resolution of cutaneous lesions or prevent the progression of renal disease.3 Contrarily, others have suggested that the presence of bullae and renal disease is an indication to start treatment.6 This claim is based on the mechanistic finding that immunosuppression with corticosteroids decreases inflammation by inhibiting activator protein 1, a transcription factor for MMP-9, thereby reducing MMP-9 activity and the formation of bullae.4 Clinical anecdotes, including our own, that demonstrate dramatic improvement of hemorrhagic bullae with the administration of corticosteroids substantiate this mechanism. Through the inhibition of neutrophil interactions and IgA production, other anti-inflammatory and immunosuppressive medications such as colchicine, dapsone, and azathioprine also have been reported to aid in resolution of the cutaneous lesions.1,5,6 Although there is a clear drawback to the lack of controlled trials and prospective studies regarding the treatment of bullous HSP, it is nearly impossible to expect such studies to be carried out given the rare and unpredictable nature of the disease. For now, claims derived from case series and case reports guide our understanding of treatment efficacy.
Acknowledgment—Quiz photograph courtesy of Steve Taylor, BS, Phoenix, Arizona.
- Trapani S, Mariotti P, Resti M, et al. Severe hemorrhagic bullous lesions in Henoch Schönlein purpura: three pediatric cases and review of the literature [published online July 16, 2009]. Rheumatol Int. 2010;30:1355-1359. doi:10.1007/s00296-009-1055-8.
- Kobayashi T, Sakuraoka K, Iwamoto M, et al. A case of anaphylactoid purpura with multiple blister formation: possible pathophysiologic role of gelatinate (MMP-9). Dermatology. 1990;197:62-64.
- Bansal AS, Dwivedi N, Adsett M. Serum and blister fluid cytokines and complement proteins in a patient with Henoch Schönlein purpura associated with a bullous skin rash. Australas J Dermatol. 1997;38:190-192.
- Aljada A, Ghanim H, Mohanty P, et al. Hydrocortisone suppresses intranuclear activator-protein-1 (AP-1) binding activity in mononuclear cells and plasma matrix metalloproteinase 2 and 9 (MMP-2 and MMP-9). J Clin Endocrinol Metab. 2001;86:5988-5991.
- Iqbal H, Evans A. Dapsone therapy for Henoch-Schönlein purpura: a case series. Arch Dis Child. 2005;90:985-986.
- den Boer SL, Pasmans SG, Wulffraat NM, et al. Bullous lesions in Henoch Schönlein purpura as indication to start systemic prednisone [published online January 5, 2009]. Acta Paediatr. 2010;99:781-783. doi:10.1111/j.1651-2227.2009.01650.x.
The Diagnosis: Bullous Henoch-Schönlein Purpura
Laboratory tests in this patient showed no abnormalities for complete blood cell count, immunoglobulins, anti–double-stranded DNA, antinuclear antibody, p–antineutrophil cytoplasmic antibodies, lupus anticoagulant, Sjögren antibodies, liver enzymes, and erythrocyte sedimentation rate. Urinalysis was normal. Punch biopsies were obtained and a histologic examination showed an intense inflammatory infiltrate of neutrophils around blood vessels within the dermis (Figure). These blood vessels showed swollen endothelium and narrowing of the vessel lumina with leukocytoclasia. Direct immunofluorescence revealed granular IgA, C3, fibrin, and weak IgM deposits in blood vessels in the papillary dermis consistent with Henoch-Schönlein purpura (HSP).
Henoch-Schönlein purpura is the most common vasculitis in children.1-6 However, its bullous variant is rare, with few pediatric cases reported. Bullous HSP affects arterioles through an IgA-mediated pathway.1-6 It is believed that the bullae are formed secondary to neutrophilic release of matrix metalloproteinase 9 (MMP-9), which degrades extracellular collagen.2 Additionally, bullous fluid from HSP has been noted to have markedly elevated levels of soluble CD23, a form of the CD23 B-cell surface receptor used in antibody feedback regulation and B-cell recruitment, which also has been found to be elevated in the fluid of bullous pemphigoid, suggesting a similar pathogenesis of exaggerated humoral immunity.3
The most common sign of HSP is palpable purpura; however, other cutaneous findings can be present including targetoid plaques, macules, papules, petechiae, and bullae that may become hemorrhagic, ulcerated, necrotic, or scarred.1-6 Bullae appear in the most dependent parts of the body, such as the feet and lower legs. Hydrostatic pressure may play a role in the pathogenesis of this phenomenon.1 When other classic signs of HSP are absent, the presence of bullae clouds the diagnosis and creates controversy regarding treatment, as there is a dearth of literature on proper therapy for severe cutaneous manifestations of HSP.6
Our patient was treated with morphine for pain management along with topical mupirocin and nonadherent dressings for wound care. She also received pulse intravenous methylprednisolone 2 mg/kg daily for 3 days and then was transitioned to oral prednisone 1 mg/kg daily, which was tapered over 3 weeks after discharge. This regimen resulted in resolution of symptoms with rapid regression of bullae and subsequent postinflammatory hyperpigmentation. Prior reports have noted that the presence of bullae does not alter the prognosis or predict probability of renal involvement of this self-limited disease, leading to controversy in determining if treatment offers more favorable outcomes.1,3 One study suggested that steroids only improve symptoms, arthralgia, and abdominal pain, but they do not aid in the resolution of cutaneous lesions or prevent the progression of renal disease.3 Contrarily, others have suggested that the presence of bullae and renal disease is an indication to start treatment.6 This claim is based on the mechanistic finding that immunosuppression with corticosteroids decreases inflammation by inhibiting activator protein 1, a transcription factor for MMP-9, thereby reducing MMP-9 activity and the formation of bullae.4 Clinical anecdotes, including our own, that demonstrate dramatic improvement of hemorrhagic bullae with the administration of corticosteroids substantiate this mechanism. Through the inhibition of neutrophil interactions and IgA production, other anti-inflammatory and immunosuppressive medications such as colchicine, dapsone, and azathioprine also have been reported to aid in resolution of the cutaneous lesions.1,5,6 Although there is a clear drawback to the lack of controlled trials and prospective studies regarding the treatment of bullous HSP, it is nearly impossible to expect such studies to be carried out given the rare and unpredictable nature of the disease. For now, claims derived from case series and case reports guide our understanding of treatment efficacy.
Acknowledgment—Quiz photograph courtesy of Steve Taylor, BS, Phoenix, Arizona.
The Diagnosis: Bullous Henoch-Schönlein Purpura
Laboratory tests in this patient showed no abnormalities for complete blood cell count, immunoglobulins, anti–double-stranded DNA, antinuclear antibody, p–antineutrophil cytoplasmic antibodies, lupus anticoagulant, Sjögren antibodies, liver enzymes, and erythrocyte sedimentation rate. Urinalysis was normal. Punch biopsies were obtained and a histologic examination showed an intense inflammatory infiltrate of neutrophils around blood vessels within the dermis (Figure). These blood vessels showed swollen endothelium and narrowing of the vessel lumina with leukocytoclasia. Direct immunofluorescence revealed granular IgA, C3, fibrin, and weak IgM deposits in blood vessels in the papillary dermis consistent with Henoch-Schönlein purpura (HSP).
Henoch-Schönlein purpura is the most common vasculitis in children.1-6 However, its bullous variant is rare, with few pediatric cases reported. Bullous HSP affects arterioles through an IgA-mediated pathway.1-6 It is believed that the bullae are formed secondary to neutrophilic release of matrix metalloproteinase 9 (MMP-9), which degrades extracellular collagen.2 Additionally, bullous fluid from HSP has been noted to have markedly elevated levels of soluble CD23, a form of the CD23 B-cell surface receptor used in antibody feedback regulation and B-cell recruitment, which also has been found to be elevated in the fluid of bullous pemphigoid, suggesting a similar pathogenesis of exaggerated humoral immunity.3
The most common sign of HSP is palpable purpura; however, other cutaneous findings can be present including targetoid plaques, macules, papules, petechiae, and bullae that may become hemorrhagic, ulcerated, necrotic, or scarred.1-6 Bullae appear in the most dependent parts of the body, such as the feet and lower legs. Hydrostatic pressure may play a role in the pathogenesis of this phenomenon.1 When other classic signs of HSP are absent, the presence of bullae clouds the diagnosis and creates controversy regarding treatment, as there is a dearth of literature on proper therapy for severe cutaneous manifestations of HSP.6
Our patient was treated with morphine for pain management along with topical mupirocin and nonadherent dressings for wound care. She also received pulse intravenous methylprednisolone 2 mg/kg daily for 3 days and then was transitioned to oral prednisone 1 mg/kg daily, which was tapered over 3 weeks after discharge. This regimen resulted in resolution of symptoms with rapid regression of bullae and subsequent postinflammatory hyperpigmentation. Prior reports have noted that the presence of bullae does not alter the prognosis or predict probability of renal involvement of this self-limited disease, leading to controversy in determining if treatment offers more favorable outcomes.1,3 One study suggested that steroids only improve symptoms, arthralgia, and abdominal pain, but they do not aid in the resolution of cutaneous lesions or prevent the progression of renal disease.3 Contrarily, others have suggested that the presence of bullae and renal disease is an indication to start treatment.6 This claim is based on the mechanistic finding that immunosuppression with corticosteroids decreases inflammation by inhibiting activator protein 1, a transcription factor for MMP-9, thereby reducing MMP-9 activity and the formation of bullae.4 Clinical anecdotes, including our own, that demonstrate dramatic improvement of hemorrhagic bullae with the administration of corticosteroids substantiate this mechanism. Through the inhibition of neutrophil interactions and IgA production, other anti-inflammatory and immunosuppressive medications such as colchicine, dapsone, and azathioprine also have been reported to aid in resolution of the cutaneous lesions.1,5,6 Although there is a clear drawback to the lack of controlled trials and prospective studies regarding the treatment of bullous HSP, it is nearly impossible to expect such studies to be carried out given the rare and unpredictable nature of the disease. For now, claims derived from case series and case reports guide our understanding of treatment efficacy.
Acknowledgment—Quiz photograph courtesy of Steve Taylor, BS, Phoenix, Arizona.
- Trapani S, Mariotti P, Resti M, et al. Severe hemorrhagic bullous lesions in Henoch Schönlein purpura: three pediatric cases and review of the literature [published online July 16, 2009]. Rheumatol Int. 2010;30:1355-1359. doi:10.1007/s00296-009-1055-8.
- Kobayashi T, Sakuraoka K, Iwamoto M, et al. A case of anaphylactoid purpura with multiple blister formation: possible pathophysiologic role of gelatinate (MMP-9). Dermatology. 1990;197:62-64.
- Bansal AS, Dwivedi N, Adsett M. Serum and blister fluid cytokines and complement proteins in a patient with Henoch Schönlein purpura associated with a bullous skin rash. Australas J Dermatol. 1997;38:190-192.
- Aljada A, Ghanim H, Mohanty P, et al. Hydrocortisone suppresses intranuclear activator-protein-1 (AP-1) binding activity in mononuclear cells and plasma matrix metalloproteinase 2 and 9 (MMP-2 and MMP-9). J Clin Endocrinol Metab. 2001;86:5988-5991.
- Iqbal H, Evans A. Dapsone therapy for Henoch-Schönlein purpura: a case series. Arch Dis Child. 2005;90:985-986.
- den Boer SL, Pasmans SG, Wulffraat NM, et al. Bullous lesions in Henoch Schönlein purpura as indication to start systemic prednisone [published online January 5, 2009]. Acta Paediatr. 2010;99:781-783. doi:10.1111/j.1651-2227.2009.01650.x.
- Trapani S, Mariotti P, Resti M, et al. Severe hemorrhagic bullous lesions in Henoch Schönlein purpura: three pediatric cases and review of the literature [published online July 16, 2009]. Rheumatol Int. 2010;30:1355-1359. doi:10.1007/s00296-009-1055-8.
- Kobayashi T, Sakuraoka K, Iwamoto M, et al. A case of anaphylactoid purpura with multiple blister formation: possible pathophysiologic role of gelatinate (MMP-9). Dermatology. 1990;197:62-64.
- Bansal AS, Dwivedi N, Adsett M. Serum and blister fluid cytokines and complement proteins in a patient with Henoch Schönlein purpura associated with a bullous skin rash. Australas J Dermatol. 1997;38:190-192.
- Aljada A, Ghanim H, Mohanty P, et al. Hydrocortisone suppresses intranuclear activator-protein-1 (AP-1) binding activity in mononuclear cells and plasma matrix metalloproteinase 2 and 9 (MMP-2 and MMP-9). J Clin Endocrinol Metab. 2001;86:5988-5991.
- Iqbal H, Evans A. Dapsone therapy for Henoch-Schönlein purpura: a case series. Arch Dis Child. 2005;90:985-986.
- den Boer SL, Pasmans SG, Wulffraat NM, et al. Bullous lesions in Henoch Schönlein purpura as indication to start systemic prednisone [published online January 5, 2009]. Acta Paediatr. 2010;99:781-783. doi:10.1111/j.1651-2227.2009.01650.x.

A 12-year-old girl presented with an erythematous eruption that had started on the left leg approximately 1 week prior with subsequent spread to the abdomen and arms. She had associated knee pain, myalgia, abdominal pain, nausea, and nonbloody and nonbilious emesis. Her medical history was notable for methicillin-resistant Staphylococcus aureus abscesses, the most recent of which was treated with trimethoprim-sulfamethoxazole; treatment was completed 5 days before the onset of the rash. Family history was notable for her paternal aunt who died of systemic lupus erythematosus. Physical examination showed erythematous macules and purpuric papules with central vesiculation extending up the thighs and lower abdomen associated with edema of the lower extremities and pain after palpation. Tense bullae also were present.

Majority of children aged 6-23 months are not vaccinated for flu
Less than half of children aged 6-23 months are vaccinated for influenza in the United States, according to an analysis of data obtained via the 2003-2013 National Immunization Survey.
The researchers analyzed providers’ reports of influenza vaccinations, received as one or two doses by children aged 6-23 months. The age group studied is at highest risk of influenza-related complications and was the first group of children for which the Advisory Committee on Immunization Practices recommended influenza vaccination, regardless of an individual’s medical condition.

A child’s age was defined by his or her age on Nov. 1 of each influenza season under study. Two full calendar years of data files were combined to enable analysis of full influenza seasons, which cover parts of 2 consecutive calendar years. The percentages of children requiring two doses to be considered fully vaccinated were based on the dosage recommendations for each flu season.
Overall, flu vaccination coverage increased, reaching 45% in the 2011-2012 flu season, up from 5% during the 2002-2003 flu season. Within each racial/ethnic group examined, influenza vaccination coverage also grew; however, lower percentages of non-Hispanic black children and Hispanic children were vaccinated than of non-Hispanic white children during all 10 of the flu seasons studied. Coverage ranged from 24% in Mississippi to 72% in Massachusetts.
“Despite the increase, the majority of children 6-23 months in the United States were not fully vaccinated against influenza,” said Tammy A. Santibanez, Ph.D., of the Centers for Disease Control and Prevention, and her colleagues.
Among other findings consistent throughout each flu season examined was that full influenza vaccination coverage was higher among children requiring only one dose of a flu vaccine, compared with those requiring two doses of a flu vaccine.
“Prevention of influenza among infants and young children is a public health priority because of their high risk for influenza-related complications,” wrote Dr. Santibanez and her colleagues. “Appropriate implementation of evidence-based strategies is needed to increase the percentage of children who are fully vaccinated.”
Read the study in Pediatrics (doi: 10.1542/peds.2015.3280).
Less than half of children aged 6-23 months are vaccinated for influenza in the United States, according to an analysis of data obtained via the 2003-2013 National Immunization Survey.
The researchers analyzed providers’ reports of influenza vaccinations, received as one or two doses by children aged 6-23 months. The age group studied is at highest risk of influenza-related complications and was the first group of children for which the Advisory Committee on Immunization Practices recommended influenza vaccination, regardless of an individual’s medical condition.
A child’s age was defined by his or her age on Nov. 1 of each influenza season under study. Two full calendar years of data files were combined to enable analysis of full influenza seasons, which cover parts of 2 consecutive calendar years. The percentages of children requiring two doses to be considered fully vaccinated were based on the dosage recommendations for each flu season.
Overall, flu vaccination coverage increased, reaching 45% in the 2011-2012 flu season, up from 5% during the 2002-2003 flu season. Within each racial/ethnic group examined, influenza vaccination coverage also grew; however, lower percentages of non-Hispanic black children and Hispanic children were vaccinated than of non-Hispanic white children during all 10 of the flu seasons studied. Coverage ranged from 24% in Mississippi to 72% in Massachusetts.
“Despite the increase, the majority of children 6-23 months in the United States were not fully vaccinated against influenza,” said Tammy A. Santibanez, Ph.D., of the Centers for Disease Control and Prevention, and her colleagues.
Among other findings consistent throughout each flu season examined was that full influenza vaccination coverage was higher among children requiring only one dose of a flu vaccine, compared with those requiring two doses of a flu vaccine.
“Prevention of influenza among infants and young children is a public health priority because of their high risk for influenza-related complications,” wrote Dr. Santibanez and her colleagues. “Appropriate implementation of evidence-based strategies is needed to increase the percentage of children who are fully vaccinated.”
Read the study in Pediatrics (doi: 10.1542/peds.2015.3280).
Less than half of children aged 6-23 months are vaccinated for influenza in the United States, according to an analysis of data obtained via the 2003-2013 National Immunization Survey.
The researchers analyzed providers’ reports of influenza vaccinations, received as one or two doses by children aged 6-23 months. The age group studied is at highest risk of influenza-related complications and was the first group of children for which the Advisory Committee on Immunization Practices recommended influenza vaccination, regardless of an individual’s medical condition.
A child’s age was defined by his or her age on Nov. 1 of each influenza season under study. Two full calendar years of data files were combined to enable analysis of full influenza seasons, which cover parts of 2 consecutive calendar years. The percentages of children requiring two doses to be considered fully vaccinated were based on the dosage recommendations for each flu season.
Overall, flu vaccination coverage increased, reaching 45% in the 2011-2012 flu season, up from 5% during the 2002-2003 flu season. Within each racial/ethnic group examined, influenza vaccination coverage also grew; however, lower percentages of non-Hispanic black children and Hispanic children were vaccinated than of non-Hispanic white children during all 10 of the flu seasons studied. Coverage ranged from 24% in Mississippi to 72% in Massachusetts.
“Despite the increase, the majority of children 6-23 months in the United States were not fully vaccinated against influenza,” said Tammy A. Santibanez, Ph.D., of the Centers for Disease Control and Prevention, and her colleagues.
Among other findings consistent throughout each flu season examined was that full influenza vaccination coverage was higher among children requiring only one dose of a flu vaccine, compared with those requiring two doses of a flu vaccine.
“Prevention of influenza among infants and young children is a public health priority because of their high risk for influenza-related complications,” wrote Dr. Santibanez and her colleagues. “Appropriate implementation of evidence-based strategies is needed to increase the percentage of children who are fully vaccinated.”
Read the study in Pediatrics (doi: 10.1542/peds.2015.3280).
FROM PEDIATRICS

Generic imatinib launched with savings program

Photo by Rhoda Baer
Sun Pharma has announced the US launch of imatinib mesylate tablets, which are a generic version of Novartis’s Gleevec, for indications approved by the US Food and Drug Administration (FDA).
As part of this launch, Sun Pharma has rolled out a savings card program. The goal is to provide greater access to imatinib mesylate tablets for patients who have commercial insurance, but their out-of-pocket cost may exceed an affordable amount.
Sun Pharma’s Imatinib Mesylate Savings Card will reduce patient’s co-payment to $10. The card will also offer patients an additional savings benefit of up to $700 for a 30-day fill to offset any additional out-of-pocket cost should they be required to meet their deductible or co-insurance.
Participating pharmacies across the US can use the patient’s card as part of this program.
Eligible patients can participate in Sun Pharma’s Imatinib Mesylate Savings Card program by registering at www.imatinibrx.com or by requesting a savings card from their oncologist. Sun Pharma will be supplying its Imatinib Mesylate Savings Cards to more than 4500 oncologists.
Sun Pharma has established a Hub service so patients can call and speak with a trained healthcare professional about imatinib mesylate. The number is 1-844-502-5950.
In addition, qualifying patients can receive Sun Pharma’s imatinib mesylate at no cost. Based on qualifications for applying and including a doctor’s prescription, the Hub service will determine if a patient is qualified to receive imatinib mesylate for free. Upon acceptance, the prescription will be processed and delivered to the qualifying patient at no cost.
Sun Pharma’s imatinib mesylate was approved by the FDA in December 2015 and was granted 180 days of marketing exclusivity from the time of its launch. The drug is available in 100 mg and 400 mg tablets.
It is approved to treat:
- Newly diagnosed adult and pediatric patients with Philadelphia-chromosome-positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with Ph+ CML in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adults with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adults with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia, including those who have the FIP1L1-PDGFRα fusion kinase
- Adult patients with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Sun Pharma’s imatinib mesylate is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors. ![]()
Photo by Rhoda Baer
Sun Pharma has announced the US launch of imatinib mesylate tablets, which are a generic version of Novartis’s Gleevec, for indications approved by the US Food and Drug Administration (FDA).
As part of this launch, Sun Pharma has rolled out a savings card program. The goal is to provide greater access to imatinib mesylate tablets for patients who have commercial insurance, but their out-of-pocket cost may exceed an affordable amount.
Sun Pharma’s Imatinib Mesylate Savings Card will reduce patient’s co-payment to $10. The card will also offer patients an additional savings benefit of up to $700 for a 30-day fill to offset any additional out-of-pocket cost should they be required to meet their deductible or co-insurance.
Participating pharmacies across the US can use the patient’s card as part of this program.
Eligible patients can participate in Sun Pharma’s Imatinib Mesylate Savings Card program by registering at www.imatinibrx.com or by requesting a savings card from their oncologist. Sun Pharma will be supplying its Imatinib Mesylate Savings Cards to more than 4500 oncologists.
Sun Pharma has established a Hub service so patients can call and speak with a trained healthcare professional about imatinib mesylate. The number is 1-844-502-5950.
In addition, qualifying patients can receive Sun Pharma’s imatinib mesylate at no cost. Based on qualifications for applying and including a doctor’s prescription, the Hub service will determine if a patient is qualified to receive imatinib mesylate for free. Upon acceptance, the prescription will be processed and delivered to the qualifying patient at no cost.
Sun Pharma’s imatinib mesylate was approved by the FDA in December 2015 and was granted 180 days of marketing exclusivity from the time of its launch. The drug is available in 100 mg and 400 mg tablets.
It is approved to treat:
- Newly diagnosed adult and pediatric patients with Philadelphia-chromosome-positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with Ph+ CML in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adults with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adults with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia, including those who have the FIP1L1-PDGFRα fusion kinase
- Adult patients with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Sun Pharma’s imatinib mesylate is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors. ![]()
Photo by Rhoda Baer
Sun Pharma has announced the US launch of imatinib mesylate tablets, which are a generic version of Novartis’s Gleevec, for indications approved by the US Food and Drug Administration (FDA).
As part of this launch, Sun Pharma has rolled out a savings card program. The goal is to provide greater access to imatinib mesylate tablets for patients who have commercial insurance, but their out-of-pocket cost may exceed an affordable amount.
Sun Pharma’s Imatinib Mesylate Savings Card will reduce patient’s co-payment to $10. The card will also offer patients an additional savings benefit of up to $700 for a 30-day fill to offset any additional out-of-pocket cost should they be required to meet their deductible or co-insurance.
Participating pharmacies across the US can use the patient’s card as part of this program.
Eligible patients can participate in Sun Pharma’s Imatinib Mesylate Savings Card program by registering at www.imatinibrx.com or by requesting a savings card from their oncologist. Sun Pharma will be supplying its Imatinib Mesylate Savings Cards to more than 4500 oncologists.
Sun Pharma has established a Hub service so patients can call and speak with a trained healthcare professional about imatinib mesylate. The number is 1-844-502-5950.
In addition, qualifying patients can receive Sun Pharma’s imatinib mesylate at no cost. Based on qualifications for applying and including a doctor’s prescription, the Hub service will determine if a patient is qualified to receive imatinib mesylate for free. Upon acceptance, the prescription will be processed and delivered to the qualifying patient at no cost.
Sun Pharma’s imatinib mesylate was approved by the FDA in December 2015 and was granted 180 days of marketing exclusivity from the time of its launch. The drug is available in 100 mg and 400 mg tablets.
It is approved to treat:
- Newly diagnosed adult and pediatric patients with Philadelphia-chromosome-positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with Ph+ CML in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adults with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adults with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia, including those who have the FIP1L1-PDGFRα fusion kinase
- Adult patients with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Sun Pharma’s imatinib mesylate is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors. ![]()
Psychotropics low on list of therapies for autism
NEW YORK – Some of the behavioral and psychiatric problems observed in children with autism spectrum disorder (ASD) may improve on atypical antipsychotics, but these drugs do not improve core symptoms and should be used sparingly in this population, according to an expert’s analysis at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Most children with ASD either do not need or will not benefit from available psychotropic medications,” reported Dr. Jeremy M. Veenstra-VanderWeele of the Center for Autism and the Developing Brain, Columbia University, New York.
In a review of the evidence, he suggested that psychopharmacologic treatments for children with ASD, when indicated at all, are only relevant to behavioral issues and psychiatric comorbidities. On an evidence basis, behavioral modification and psychosocial support for the patient and family should come first or at least accompany psychotropic agents.
“These families are desperate and, oftentimes, they cannot get the services that would actually make things better for their child on a behavioral level,” Dr. Veenstra-VanderWeele said. He said that the “pressure to prescribe,” along with a desire to help, drive many clinicians to offer medications, “but we just should be honest and recognize that our evidence does not suggest that we are able to help the majority.”
Most children with ASD do receive one or more prescriptions for psychotropic agents, according to Dr. Veenstra-VanderWeele’s experience. In fact, he reported that he often is asked to consult on a child who has been prescribed two or three medications when it is unclear which, if any, are offering benefit. While he also finds that these agents often are prescribed at low doses, a better approach would be to use an evidence-based therapy at an adequate dose after carefully evaluating the risk-to-benefit ratio.
“I find that a lot of the kids I see in consultation have had, in desperation, more than one medicine started within the time window of response, and that’s really problematic. That is how kids end up on three or four medicines without a clear sense of what led to improvement,” Dr. Veenstra-VanderWeele noted. He suggested that the more appropriate strategy is to attempt to maximize benefit on one therapy, including behavioral therapies, before initiating another.
In his review of psychotropic medicines for ASD comorbidities, he suggested the evidence is “high” that the atypical antipsychotics risperidone and aripiprazole are effective in at least some children for irritability and agitation. He also reported that the evidence of lack of benefit from secretin also should now be labeled as high.
The evidence for benefit from long-acting stimulants for behavioral improvement was labeled as “moderate,” particularly when considered in the context of adverse events. Atomoxetine, a selective norepinephrine reuptake inhibitor also used for attention-deficit/hyperactivity disorder, is another drug placed by Dr. Veenstra-VanderWeele in the category for “moderate” evidence. Two controlled studies have demonstrated activity, but the overall response in each was relatively modest.
In a third group, labeled “insufficient evidence,” he placed both guanfacine, particularly for irritability, and selective serotonin reuptake inhibitors.
Although the strongest evidence for pharmacotherapy to control comorbidities in ASD is related to atypical antipsychotics, he emphasized that these are accompanied with adverse events. Some, such as weight gain, can be difficult to reverse after long-term therapy.
“Particularly in this population, I talk about stopping the medicine at the time that I start the medicine,” Dr. Veenstra-VanderWeele reported. Citing the frequency of rapid weight gain in patients on some atypical antipsychotics, he said that it is important to warn patients that a switch in therapy may be necessary.
“It is often hard to say we are going to switch when everyone feels that the patient is much better. You have to lay it out in advance and write it down, so the family knows what to expect,” Dr. Veenstra-VanderWeele said.
Management of pediatric ASD typically involves multiple coexisting clinical issues. Because “there is always something else going on” in the ASD patient, he emphasized the need for a systematic approach in which medical and behavioral issues and psychiatric comorbidities are addressed in the context of clear goals for each targeted symptom.
Dr. Veenstra-VanderWeele reported financial relationships with Forest Laboratories, Hoffmann-La Roche, Novartis, Seaside Therapeutics, Sunovion Pharmaceuticals, and SynapDx.
NEW YORK – Some of the behavioral and psychiatric problems observed in children with autism spectrum disorder (ASD) may improve on atypical antipsychotics, but these drugs do not improve core symptoms and should be used sparingly in this population, according to an expert’s analysis at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Most children with ASD either do not need or will not benefit from available psychotropic medications,” reported Dr. Jeremy M. Veenstra-VanderWeele of the Center for Autism and the Developing Brain, Columbia University, New York.
In a review of the evidence, he suggested that psychopharmacologic treatments for children with ASD, when indicated at all, are only relevant to behavioral issues and psychiatric comorbidities. On an evidence basis, behavioral modification and psychosocial support for the patient and family should come first or at least accompany psychotropic agents.
“These families are desperate and, oftentimes, they cannot get the services that would actually make things better for their child on a behavioral level,” Dr. Veenstra-VanderWeele said. He said that the “pressure to prescribe,” along with a desire to help, drive many clinicians to offer medications, “but we just should be honest and recognize that our evidence does not suggest that we are able to help the majority.”
Most children with ASD do receive one or more prescriptions for psychotropic agents, according to Dr. Veenstra-VanderWeele’s experience. In fact, he reported that he often is asked to consult on a child who has been prescribed two or three medications when it is unclear which, if any, are offering benefit. While he also finds that these agents often are prescribed at low doses, a better approach would be to use an evidence-based therapy at an adequate dose after carefully evaluating the risk-to-benefit ratio.
“I find that a lot of the kids I see in consultation have had, in desperation, more than one medicine started within the time window of response, and that’s really problematic. That is how kids end up on three or four medicines without a clear sense of what led to improvement,” Dr. Veenstra-VanderWeele noted. He suggested that the more appropriate strategy is to attempt to maximize benefit on one therapy, including behavioral therapies, before initiating another.
In his review of psychotropic medicines for ASD comorbidities, he suggested the evidence is “high” that the atypical antipsychotics risperidone and aripiprazole are effective in at least some children for irritability and agitation. He also reported that the evidence of lack of benefit from secretin also should now be labeled as high.
The evidence for benefit from long-acting stimulants for behavioral improvement was labeled as “moderate,” particularly when considered in the context of adverse events. Atomoxetine, a selective norepinephrine reuptake inhibitor also used for attention-deficit/hyperactivity disorder, is another drug placed by Dr. Veenstra-VanderWeele in the category for “moderate” evidence. Two controlled studies have demonstrated activity, but the overall response in each was relatively modest.
In a third group, labeled “insufficient evidence,” he placed both guanfacine, particularly for irritability, and selective serotonin reuptake inhibitors.
Although the strongest evidence for pharmacotherapy to control comorbidities in ASD is related to atypical antipsychotics, he emphasized that these are accompanied with adverse events. Some, such as weight gain, can be difficult to reverse after long-term therapy.
“Particularly in this population, I talk about stopping the medicine at the time that I start the medicine,” Dr. Veenstra-VanderWeele reported. Citing the frequency of rapid weight gain in patients on some atypical antipsychotics, he said that it is important to warn patients that a switch in therapy may be necessary.
“It is often hard to say we are going to switch when everyone feels that the patient is much better. You have to lay it out in advance and write it down, so the family knows what to expect,” Dr. Veenstra-VanderWeele said.
Management of pediatric ASD typically involves multiple coexisting clinical issues. Because “there is always something else going on” in the ASD patient, he emphasized the need for a systematic approach in which medical and behavioral issues and psychiatric comorbidities are addressed in the context of clear goals for each targeted symptom.
Dr. Veenstra-VanderWeele reported financial relationships with Forest Laboratories, Hoffmann-La Roche, Novartis, Seaside Therapeutics, Sunovion Pharmaceuticals, and SynapDx.
NEW YORK – Some of the behavioral and psychiatric problems observed in children with autism spectrum disorder (ASD) may improve on atypical antipsychotics, but these drugs do not improve core symptoms and should be used sparingly in this population, according to an expert’s analysis at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Most children with ASD either do not need or will not benefit from available psychotropic medications,” reported Dr. Jeremy M. Veenstra-VanderWeele of the Center for Autism and the Developing Brain, Columbia University, New York.
In a review of the evidence, he suggested that psychopharmacologic treatments for children with ASD, when indicated at all, are only relevant to behavioral issues and psychiatric comorbidities. On an evidence basis, behavioral modification and psychosocial support for the patient and family should come first or at least accompany psychotropic agents.
“These families are desperate and, oftentimes, they cannot get the services that would actually make things better for their child on a behavioral level,” Dr. Veenstra-VanderWeele said. He said that the “pressure to prescribe,” along with a desire to help, drive many clinicians to offer medications, “but we just should be honest and recognize that our evidence does not suggest that we are able to help the majority.”
Most children with ASD do receive one or more prescriptions for psychotropic agents, according to Dr. Veenstra-VanderWeele’s experience. In fact, he reported that he often is asked to consult on a child who has been prescribed two or three medications when it is unclear which, if any, are offering benefit. While he also finds that these agents often are prescribed at low doses, a better approach would be to use an evidence-based therapy at an adequate dose after carefully evaluating the risk-to-benefit ratio.
“I find that a lot of the kids I see in consultation have had, in desperation, more than one medicine started within the time window of response, and that’s really problematic. That is how kids end up on three or four medicines without a clear sense of what led to improvement,” Dr. Veenstra-VanderWeele noted. He suggested that the more appropriate strategy is to attempt to maximize benefit on one therapy, including behavioral therapies, before initiating another.
In his review of psychotropic medicines for ASD comorbidities, he suggested the evidence is “high” that the atypical antipsychotics risperidone and aripiprazole are effective in at least some children for irritability and agitation. He also reported that the evidence of lack of benefit from secretin also should now be labeled as high.
The evidence for benefit from long-acting stimulants for behavioral improvement was labeled as “moderate,” particularly when considered in the context of adverse events. Atomoxetine, a selective norepinephrine reuptake inhibitor also used for attention-deficit/hyperactivity disorder, is another drug placed by Dr. Veenstra-VanderWeele in the category for “moderate” evidence. Two controlled studies have demonstrated activity, but the overall response in each was relatively modest.
In a third group, labeled “insufficient evidence,” he placed both guanfacine, particularly for irritability, and selective serotonin reuptake inhibitors.
Although the strongest evidence for pharmacotherapy to control comorbidities in ASD is related to atypical antipsychotics, he emphasized that these are accompanied with adverse events. Some, such as weight gain, can be difficult to reverse after long-term therapy.
“Particularly in this population, I talk about stopping the medicine at the time that I start the medicine,” Dr. Veenstra-VanderWeele reported. Citing the frequency of rapid weight gain in patients on some atypical antipsychotics, he said that it is important to warn patients that a switch in therapy may be necessary.
“It is often hard to say we are going to switch when everyone feels that the patient is much better. You have to lay it out in advance and write it down, so the family knows what to expect,” Dr. Veenstra-VanderWeele said.
Management of pediatric ASD typically involves multiple coexisting clinical issues. Because “there is always something else going on” in the ASD patient, he emphasized the need for a systematic approach in which medical and behavioral issues and psychiatric comorbidities are addressed in the context of clear goals for each targeted symptom.
Dr. Veenstra-VanderWeele reported financial relationships with Forest Laboratories, Hoffmann-La Roche, Novartis, Seaside Therapeutics, Sunovion Pharmaceuticals, and SynapDx.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Try behavioral therapies first, then melatonin for pediatric insomnia
NEW YORK – In children with insomnia, melatonin is the appropriate first-line drug therapy, but pharmacologic treatments come after behavioral interventions, according to an evidence-based summary presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Medication should rarely be our first choice. We should always be trying to combine it with behavioral therapies, because they work just as well and last longer,” reported Dr. Jess P. Shatkin, a professor in the department of child and adolescent psychiatry, New York University.

The number of randomized trials for sleep medications in children is limited, and there is no pharmacotherapy approved by the Food and Drug Administration for this indication, Dr. Shatkin said. Clinicians often extrapolate from adult studies, but Dr. Shatkin said these data are not necessarily transferable. He noted, for example, that a study of zolpidem in children, which is approved for adults, was negative.
The antihistamine diphenhydramine also has been studied in children, and results were mixed. In one of two double-blind, placebo-controlled pediatric studies, parents reported improvement in getting children to sleep. In the other, conducted in children aged 6 months to 15 months, no significant advantage was found for this agent over placebo.
“[Diphenhydramine] Benadryl may make your kids sleep, it may make your patients sleep, it may make you sleep, which is fine, but the data do not convince us that [diphenhydramine] Benadryl is a great treatment for sleep in children,” Dr. Shatkin reported.
Rather, the best data are with melatonin, an endogenous hormone produced on a circadian rhythm correlating with the end-of-day phenomenon known as dim-light melatonin onset (DLMO). In one study conducted in otherwise healthy children aged 6 to 12 years with chronic sleep-onset insomnia, the administration of exogenous melatonin decreased sleep-onset latency by 35 minutes as measured with actigraphy, according to Dr. Shatkin. Similar benefit has been observed in studies conducted in children with attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorders (ASD).
“Melatonin is efficacious in typically developing children and those with neurodevelopmental disorders. It imposes minimal effects on sleep architecture, it is associated with a low risk of side effects, the cost is low, and it is widely available,” Dr. Shatkin said. However, he advised against using this drug in children younger than 6 months old.
“The timing of the dosing is critical and should be based on DLMO,” Dr. Shatkin said. Specifically, he recommended a starting dose of 0.2 to 0.5 mg administered 2-3 hours before sleep time. The dose can be increased as needed by 0.2-0.5 mg per week to a maximum of 3.0 mg. Dr. Shatkin reported that there is “little evidence” to support extended-release formulations, but he did warn that over-the-counter preparations may vary in quality.
As an alternative, clonidine was listed as a second choice for treating insomnia in children. Although this therapy is not supported by controlled data, several open-label studies and chart reviews suggest benefit, and this therapy is less likely than diphenhydramine to produce next-day drowsiness.
Yet, he reiterated that the best evidence-based treatment of sleep problems in children is cognitive-behavioral therapy. He called the techniques – such as regular bedtimes, avoidance of stimuli, and creating a relaxing bedtime ritual – as easy to learn and teach to parents. Obvious problems in the sleep routine, such as irregular bedtimes, typically can be identified with a sleep history. There are numerous strategies to wean children from requiring the presence of a parent to fall asleep, such as “graduated extinction,” which involves incrementally distancing the parent from the child’s bedside.
Empathetic to the frequency of sleep disturbances in children, Dr. Shatkin cited data suggesting that 50% of preschool children, 30% of school-age children, and 40% of adolescents report sleep problems. A survey of child psychiatrists found that most acknowledged prescribing a sleep medication within the past month for pediatric insomnia, but Dr. Shatkin emphasized that behavioral therapies often may produce a longer-lasting result.
For treating pediatric sleep disturbances, “our educational and behavioral efforts really should trump our medications,” Dr. Shatkin said. “We should be using any medication sparingly.”
Dr. Shatkin reported financial relationships with Assurex Health, Edgemont Pharmaceuticals, Eli Lilly, Forest Laboratories, and Lundbeck.
NEW YORK – In children with insomnia, melatonin is the appropriate first-line drug therapy, but pharmacologic treatments come after behavioral interventions, according to an evidence-based summary presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Medication should rarely be our first choice. We should always be trying to combine it with behavioral therapies, because they work just as well and last longer,” reported Dr. Jess P. Shatkin, a professor in the department of child and adolescent psychiatry, New York University.
The number of randomized trials for sleep medications in children is limited, and there is no pharmacotherapy approved by the Food and Drug Administration for this indication, Dr. Shatkin said. Clinicians often extrapolate from adult studies, but Dr. Shatkin said these data are not necessarily transferable. He noted, for example, that a study of zolpidem in children, which is approved for adults, was negative.
The antihistamine diphenhydramine also has been studied in children, and results were mixed. In one of two double-blind, placebo-controlled pediatric studies, parents reported improvement in getting children to sleep. In the other, conducted in children aged 6 months to 15 months, no significant advantage was found for this agent over placebo.
“[Diphenhydramine] Benadryl may make your kids sleep, it may make your patients sleep, it may make you sleep, which is fine, but the data do not convince us that [diphenhydramine] Benadryl is a great treatment for sleep in children,” Dr. Shatkin reported.
Rather, the best data are with melatonin, an endogenous hormone produced on a circadian rhythm correlating with the end-of-day phenomenon known as dim-light melatonin onset (DLMO). In one study conducted in otherwise healthy children aged 6 to 12 years with chronic sleep-onset insomnia, the administration of exogenous melatonin decreased sleep-onset latency by 35 minutes as measured with actigraphy, according to Dr. Shatkin. Similar benefit has been observed in studies conducted in children with attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorders (ASD).
“Melatonin is efficacious in typically developing children and those with neurodevelopmental disorders. It imposes minimal effects on sleep architecture, it is associated with a low risk of side effects, the cost is low, and it is widely available,” Dr. Shatkin said. However, he advised against using this drug in children younger than 6 months old.
“The timing of the dosing is critical and should be based on DLMO,” Dr. Shatkin said. Specifically, he recommended a starting dose of 0.2 to 0.5 mg administered 2-3 hours before sleep time. The dose can be increased as needed by 0.2-0.5 mg per week to a maximum of 3.0 mg. Dr. Shatkin reported that there is “little evidence” to support extended-release formulations, but he did warn that over-the-counter preparations may vary in quality.
As an alternative, clonidine was listed as a second choice for treating insomnia in children. Although this therapy is not supported by controlled data, several open-label studies and chart reviews suggest benefit, and this therapy is less likely than diphenhydramine to produce next-day drowsiness.
Yet, he reiterated that the best evidence-based treatment of sleep problems in children is cognitive-behavioral therapy. He called the techniques – such as regular bedtimes, avoidance of stimuli, and creating a relaxing bedtime ritual – as easy to learn and teach to parents. Obvious problems in the sleep routine, such as irregular bedtimes, typically can be identified with a sleep history. There are numerous strategies to wean children from requiring the presence of a parent to fall asleep, such as “graduated extinction,” which involves incrementally distancing the parent from the child’s bedside.
Empathetic to the frequency of sleep disturbances in children, Dr. Shatkin cited data suggesting that 50% of preschool children, 30% of school-age children, and 40% of adolescents report sleep problems. A survey of child psychiatrists found that most acknowledged prescribing a sleep medication within the past month for pediatric insomnia, but Dr. Shatkin emphasized that behavioral therapies often may produce a longer-lasting result.
For treating pediatric sleep disturbances, “our educational and behavioral efforts really should trump our medications,” Dr. Shatkin said. “We should be using any medication sparingly.”
Dr. Shatkin reported financial relationships with Assurex Health, Edgemont Pharmaceuticals, Eli Lilly, Forest Laboratories, and Lundbeck.
NEW YORK – In children with insomnia, melatonin is the appropriate first-line drug therapy, but pharmacologic treatments come after behavioral interventions, according to an evidence-based summary presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Medication should rarely be our first choice. We should always be trying to combine it with behavioral therapies, because they work just as well and last longer,” reported Dr. Jess P. Shatkin, a professor in the department of child and adolescent psychiatry, New York University.
The number of randomized trials for sleep medications in children is limited, and there is no pharmacotherapy approved by the Food and Drug Administration for this indication, Dr. Shatkin said. Clinicians often extrapolate from adult studies, but Dr. Shatkin said these data are not necessarily transferable. He noted, for example, that a study of zolpidem in children, which is approved for adults, was negative.
The antihistamine diphenhydramine also has been studied in children, and results were mixed. In one of two double-blind, placebo-controlled pediatric studies, parents reported improvement in getting children to sleep. In the other, conducted in children aged 6 months to 15 months, no significant advantage was found for this agent over placebo.
“[Diphenhydramine] Benadryl may make your kids sleep, it may make your patients sleep, it may make you sleep, which is fine, but the data do not convince us that [diphenhydramine] Benadryl is a great treatment for sleep in children,” Dr. Shatkin reported.
Rather, the best data are with melatonin, an endogenous hormone produced on a circadian rhythm correlating with the end-of-day phenomenon known as dim-light melatonin onset (DLMO). In one study conducted in otherwise healthy children aged 6 to 12 years with chronic sleep-onset insomnia, the administration of exogenous melatonin decreased sleep-onset latency by 35 minutes as measured with actigraphy, according to Dr. Shatkin. Similar benefit has been observed in studies conducted in children with attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorders (ASD).
“Melatonin is efficacious in typically developing children and those with neurodevelopmental disorders. It imposes minimal effects on sleep architecture, it is associated with a low risk of side effects, the cost is low, and it is widely available,” Dr. Shatkin said. However, he advised against using this drug in children younger than 6 months old.
“The timing of the dosing is critical and should be based on DLMO,” Dr. Shatkin said. Specifically, he recommended a starting dose of 0.2 to 0.5 mg administered 2-3 hours before sleep time. The dose can be increased as needed by 0.2-0.5 mg per week to a maximum of 3.0 mg. Dr. Shatkin reported that there is “little evidence” to support extended-release formulations, but he did warn that over-the-counter preparations may vary in quality.
As an alternative, clonidine was listed as a second choice for treating insomnia in children. Although this therapy is not supported by controlled data, several open-label studies and chart reviews suggest benefit, and this therapy is less likely than diphenhydramine to produce next-day drowsiness.
Yet, he reiterated that the best evidence-based treatment of sleep problems in children is cognitive-behavioral therapy. He called the techniques – such as regular bedtimes, avoidance of stimuli, and creating a relaxing bedtime ritual – as easy to learn and teach to parents. Obvious problems in the sleep routine, such as irregular bedtimes, typically can be identified with a sleep history. There are numerous strategies to wean children from requiring the presence of a parent to fall asleep, such as “graduated extinction,” which involves incrementally distancing the parent from the child’s bedside.
Empathetic to the frequency of sleep disturbances in children, Dr. Shatkin cited data suggesting that 50% of preschool children, 30% of school-age children, and 40% of adolescents report sleep problems. A survey of child psychiatrists found that most acknowledged prescribing a sleep medication within the past month for pediatric insomnia, but Dr. Shatkin emphasized that behavioral therapies often may produce a longer-lasting result.
For treating pediatric sleep disturbances, “our educational and behavioral efforts really should trump our medications,” Dr. Shatkin said. “We should be using any medication sparingly.”
Dr. Shatkin reported financial relationships with Assurex Health, Edgemont Pharmaceuticals, Eli Lilly, Forest Laboratories, and Lundbeck.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

Anxiety is poorly recognized, treated in children
NEW YORK – Of psychiatric issues affecting child development, generalized anxiety is not getting the attention it deserves and is frequently mistaken for attention-deficit/hyperactivity disorder (ADHD), according to a review of key diagnostic signs and evidence-based therapies presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Pediatricians have an ASD [autism spectrum disorder] toolkit, they have an ADHD toolkit, and they now have a postpartum depression toolkit for moms, but they do not have an anxiety tool kit,” reported Dr. John T. Walkup, director of the division of child and adolescent psychiatry, Cornell University, New York. “So if a kid is 7 or 8 and is inattentive, they have two choices: Either he has ASD or he has ADHD.”

Confusion with ASD is less likely, because there is less symptom crossover, but the differential diagnosis with ADHD is more challenging. For anxiety, symptoms typically peak between the ages of 6 and 12 years. Although the onset of ADHD symptoms, like symptoms of ASD, generally occurs earlier, children with anxiety and ADHD often are brought to the attention of a physician within the same general window of time.
From the point of view of the complaints that initiated an evaluation, “generalized anxiety disorder and the inattentive subtype of ADHD are almost indistinguishable,” Dr. Walkup asserted. He suggested that children who are anxious have difficulty concentrating in class because their minds are “full of ideas, worries, and concerns.” Children with ADHD have difficulty concentrating in class because their minds are “susceptible to distraction,” but the result is the same.
Some children, even those who are only 7 or 8 years old, “can really describe to you that difference,” Dr. Walkup observed, although he said other features can be useful for distinguishing anxiety from other psychiatric disorders, including depression. In taking the history of a child with potential anxiety, key signs include difficulty coping with novel situations, excessive sensitivity to perceived threats, and shyness. These features are less likely to be in children with ADHD or depression.
Once children reach adolescence, social insecurity is more ubiquitous, making this complaint less useful for identifying a child with pathologic anxiety, but here there is also room for confusion without a careful history.
“We see a lot of kids who have social anxiety who get mislabeled as depressed. Socially anxious kids become demoralized, but they do not become anhedonic,” Dr. Walkup reported. In patients who are inhibited with their peers but who do not otherwise report disturbances in mood, generalized anxiety rather than depression may be driving the psychopathology, according to Dr. Walkup, who said this set of circumstances is common.
Once the diagnosis of anxiety is made, both SSRIs and cognitive-behavioral therapy are effective, with response rates of about 55%-60%, Dr. Walkup said. The response rates can climb as high as 80% when the two are combined, particularly when CBT is performed at experienced centers.
With SSRIs, one of the biggest concerns is activation, an adverse event that occurs in up to 10% of patients, Dr. Walkup said. If activation occurs, he advised switching patients to a nonactivating antidepressant, such as duloxetine, nefazodone, or a tricyclic agent, rather than rechallenging them with another SSRI. In his experience, activation on one agent predicts activation on another, but he cautioned against confusing activation with SSRI-induced mania.
“We do see so many kids who get activated on an SSRI and never see another antidepressant again, simply because the doc is afraid of precipitating mania,” Dr. Walkup said. He said mania is a very uncommon adverse event not typically observed, like activation, relatively quickly after initiating therapy. Because of the efficacy of SSRIs for pediatric anxiety, Dr. Walkup advised being slow in abandoning this drug class.
“Antidepressants work extremely well, and SSRIs are the medications of choice,” emphasized Dr. Walkup, who identified atypical antidepressants as a second-line choice in children and benzodiazepines, for which pediatric data are “limited,” as an option further down the list.
However, therapy first requires a diagnosis.
“Identifying anxiety is key,” Dr. Walkup said. “With evidence-based treatments available, there is a need to enhance public awareness and advocacy.”
Dr. Walkup reported no financial relationships.
NEW YORK – Of psychiatric issues affecting child development, generalized anxiety is not getting the attention it deserves and is frequently mistaken for attention-deficit/hyperactivity disorder (ADHD), according to a review of key diagnostic signs and evidence-based therapies presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Pediatricians have an ASD [autism spectrum disorder] toolkit, they have an ADHD toolkit, and they now have a postpartum depression toolkit for moms, but they do not have an anxiety tool kit,” reported Dr. John T. Walkup, director of the division of child and adolescent psychiatry, Cornell University, New York. “So if a kid is 7 or 8 and is inattentive, they have two choices: Either he has ASD or he has ADHD.”
Confusion with ASD is less likely, because there is less symptom crossover, but the differential diagnosis with ADHD is more challenging. For anxiety, symptoms typically peak between the ages of 6 and 12 years. Although the onset of ADHD symptoms, like symptoms of ASD, generally occurs earlier, children with anxiety and ADHD often are brought to the attention of a physician within the same general window of time.
From the point of view of the complaints that initiated an evaluation, “generalized anxiety disorder and the inattentive subtype of ADHD are almost indistinguishable,” Dr. Walkup asserted. He suggested that children who are anxious have difficulty concentrating in class because their minds are “full of ideas, worries, and concerns.” Children with ADHD have difficulty concentrating in class because their minds are “susceptible to distraction,” but the result is the same.
Some children, even those who are only 7 or 8 years old, “can really describe to you that difference,” Dr. Walkup observed, although he said other features can be useful for distinguishing anxiety from other psychiatric disorders, including depression. In taking the history of a child with potential anxiety, key signs include difficulty coping with novel situations, excessive sensitivity to perceived threats, and shyness. These features are less likely to be in children with ADHD or depression.
Once children reach adolescence, social insecurity is more ubiquitous, making this complaint less useful for identifying a child with pathologic anxiety, but here there is also room for confusion without a careful history.
“We see a lot of kids who have social anxiety who get mislabeled as depressed. Socially anxious kids become demoralized, but they do not become anhedonic,” Dr. Walkup reported. In patients who are inhibited with their peers but who do not otherwise report disturbances in mood, generalized anxiety rather than depression may be driving the psychopathology, according to Dr. Walkup, who said this set of circumstances is common.
Once the diagnosis of anxiety is made, both SSRIs and cognitive-behavioral therapy are effective, with response rates of about 55%-60%, Dr. Walkup said. The response rates can climb as high as 80% when the two are combined, particularly when CBT is performed at experienced centers.
With SSRIs, one of the biggest concerns is activation, an adverse event that occurs in up to 10% of patients, Dr. Walkup said. If activation occurs, he advised switching patients to a nonactivating antidepressant, such as duloxetine, nefazodone, or a tricyclic agent, rather than rechallenging them with another SSRI. In his experience, activation on one agent predicts activation on another, but he cautioned against confusing activation with SSRI-induced mania.
“We do see so many kids who get activated on an SSRI and never see another antidepressant again, simply because the doc is afraid of precipitating mania,” Dr. Walkup said. He said mania is a very uncommon adverse event not typically observed, like activation, relatively quickly after initiating therapy. Because of the efficacy of SSRIs for pediatric anxiety, Dr. Walkup advised being slow in abandoning this drug class.
“Antidepressants work extremely well, and SSRIs are the medications of choice,” emphasized Dr. Walkup, who identified atypical antidepressants as a second-line choice in children and benzodiazepines, for which pediatric data are “limited,” as an option further down the list.
However, therapy first requires a diagnosis.
“Identifying anxiety is key,” Dr. Walkup said. “With evidence-based treatments available, there is a need to enhance public awareness and advocacy.”
Dr. Walkup reported no financial relationships.
NEW YORK – Of psychiatric issues affecting child development, generalized anxiety is not getting the attention it deserves and is frequently mistaken for attention-deficit/hyperactivity disorder (ADHD), according to a review of key diagnostic signs and evidence-based therapies presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Pediatricians have an ASD [autism spectrum disorder] toolkit, they have an ADHD toolkit, and they now have a postpartum depression toolkit for moms, but they do not have an anxiety tool kit,” reported Dr. John T. Walkup, director of the division of child and adolescent psychiatry, Cornell University, New York. “So if a kid is 7 or 8 and is inattentive, they have two choices: Either he has ASD or he has ADHD.”
Confusion with ASD is less likely, because there is less symptom crossover, but the differential diagnosis with ADHD is more challenging. For anxiety, symptoms typically peak between the ages of 6 and 12 years. Although the onset of ADHD symptoms, like symptoms of ASD, generally occurs earlier, children with anxiety and ADHD often are brought to the attention of a physician within the same general window of time.
From the point of view of the complaints that initiated an evaluation, “generalized anxiety disorder and the inattentive subtype of ADHD are almost indistinguishable,” Dr. Walkup asserted. He suggested that children who are anxious have difficulty concentrating in class because their minds are “full of ideas, worries, and concerns.” Children with ADHD have difficulty concentrating in class because their minds are “susceptible to distraction,” but the result is the same.
Some children, even those who are only 7 or 8 years old, “can really describe to you that difference,” Dr. Walkup observed, although he said other features can be useful for distinguishing anxiety from other psychiatric disorders, including depression. In taking the history of a child with potential anxiety, key signs include difficulty coping with novel situations, excessive sensitivity to perceived threats, and shyness. These features are less likely to be in children with ADHD or depression.
Once children reach adolescence, social insecurity is more ubiquitous, making this complaint less useful for identifying a child with pathologic anxiety, but here there is also room for confusion without a careful history.
“We see a lot of kids who have social anxiety who get mislabeled as depressed. Socially anxious kids become demoralized, but they do not become anhedonic,” Dr. Walkup reported. In patients who are inhibited with their peers but who do not otherwise report disturbances in mood, generalized anxiety rather than depression may be driving the psychopathology, according to Dr. Walkup, who said this set of circumstances is common.
Once the diagnosis of anxiety is made, both SSRIs and cognitive-behavioral therapy are effective, with response rates of about 55%-60%, Dr. Walkup said. The response rates can climb as high as 80% when the two are combined, particularly when CBT is performed at experienced centers.
With SSRIs, one of the biggest concerns is activation, an adverse event that occurs in up to 10% of patients, Dr. Walkup said. If activation occurs, he advised switching patients to a nonactivating antidepressant, such as duloxetine, nefazodone, or a tricyclic agent, rather than rechallenging them with another SSRI. In his experience, activation on one agent predicts activation on another, but he cautioned against confusing activation with SSRI-induced mania.
“We do see so many kids who get activated on an SSRI and never see another antidepressant again, simply because the doc is afraid of precipitating mania,” Dr. Walkup said. He said mania is a very uncommon adverse event not typically observed, like activation, relatively quickly after initiating therapy. Because of the efficacy of SSRIs for pediatric anxiety, Dr. Walkup advised being slow in abandoning this drug class.
“Antidepressants work extremely well, and SSRIs are the medications of choice,” emphasized Dr. Walkup, who identified atypical antidepressants as a second-line choice in children and benzodiazepines, for which pediatric data are “limited,” as an option further down the list.
However, therapy first requires a diagnosis.
“Identifying anxiety is key,” Dr. Walkup said. “With evidence-based treatments available, there is a need to enhance public awareness and advocacy.”
Dr. Walkup reported no financial relationships.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

EHA creates ‘roadmap’ for hematology research

Photo by Daniel Sone
The European Hematology Association (EHA) has created a “roadmap” for hematology research in Europe.
This guidance document summarizes the current status of basic, translational, and clinical hematology research and identifies areas of unmet scientific and medical need in Europe.
It is intended to help European and national policy makers, funding agencies, charities, research institutes, and researchers make decisions on initiating, funding, or developing research.
The guidance, “The European Hematology Association Roadmap for European Hematology Research: A Consensus Document,” is published in this month’s issue of haematologica.
“For the first time, hematologists in Europe came together to develop a roadmap to guide hematology research in Europe” said Andreas Engert, MD, chair of the EHA Research Roadmap Task Force.
“Hematology in Europe has achieved a lot, but the discipline must focus and collaborate to be efficient and remain successful in improving patient outcomes. The roadmap does just that and will determine the research agenda in Europe in the coming years.”
Roughly 300 experts from more than 20 countries—including clinicians, basic researchers, and patients—contributed to the roadmap. Stakeholders such as national hematology societies, patient organizations, hematology trial groups, and other European organizations were consulted to comment on the final draft version.
The final roadmap has 9 sections: normal hematopoiesis, malignant lymphoid and myeloid diseases, anemias and related diseases, platelet disorders, blood coagulation and hemostatic disorders, transfusion medicine, infections in hematology, and hematopoietic stem cell transplantation.
The roadmap lists priorities and needs in these areas, including the need for targeted therapies based on genomic profiling and chemical biology, the need to eradicate minimal residual disease, and the need for treatments that are better tolerated by elderly patients.
“Now’s the time for Europe to pay attention,” said Ulrich Jäger, MD, chair of the EHA European Affairs Committee.
“With an aging population, the slow recovery from the financial and Euro crises, costly medical breakthroughs and innovations—quite a few of which involve hematology researchers—Europe faces increased health expenditures while budgets are limited.”
“Policy makers are rightfully cautious when spending the taxpayers’ money. So it is our responsibility to provide the policy makers with the information and evidence they need to decide where their support impacts knowledge and health most efficiently, to the benefit of patients and society. The Research Roadmap delivers on that. Now, it is up to the policy makers in the EU to deliver too.” ![]()
Photo by Daniel Sone
The European Hematology Association (EHA) has created a “roadmap” for hematology research in Europe.
This guidance document summarizes the current status of basic, translational, and clinical hematology research and identifies areas of unmet scientific and medical need in Europe.
It is intended to help European and national policy makers, funding agencies, charities, research institutes, and researchers make decisions on initiating, funding, or developing research.
The guidance, “The European Hematology Association Roadmap for European Hematology Research: A Consensus Document,” is published in this month’s issue of haematologica.
“For the first time, hematologists in Europe came together to develop a roadmap to guide hematology research in Europe” said Andreas Engert, MD, chair of the EHA Research Roadmap Task Force.
“Hematology in Europe has achieved a lot, but the discipline must focus and collaborate to be efficient and remain successful in improving patient outcomes. The roadmap does just that and will determine the research agenda in Europe in the coming years.”
Roughly 300 experts from more than 20 countries—including clinicians, basic researchers, and patients—contributed to the roadmap. Stakeholders such as national hematology societies, patient organizations, hematology trial groups, and other European organizations were consulted to comment on the final draft version.
The final roadmap has 9 sections: normal hematopoiesis, malignant lymphoid and myeloid diseases, anemias and related diseases, platelet disorders, blood coagulation and hemostatic disorders, transfusion medicine, infections in hematology, and hematopoietic stem cell transplantation.
The roadmap lists priorities and needs in these areas, including the need for targeted therapies based on genomic profiling and chemical biology, the need to eradicate minimal residual disease, and the need for treatments that are better tolerated by elderly patients.
“Now’s the time for Europe to pay attention,” said Ulrich Jäger, MD, chair of the EHA European Affairs Committee.
“With an aging population, the slow recovery from the financial and Euro crises, costly medical breakthroughs and innovations—quite a few of which involve hematology researchers—Europe faces increased health expenditures while budgets are limited.”
“Policy makers are rightfully cautious when spending the taxpayers’ money. So it is our responsibility to provide the policy makers with the information and evidence they need to decide where their support impacts knowledge and health most efficiently, to the benefit of patients and society. The Research Roadmap delivers on that. Now, it is up to the policy makers in the EU to deliver too.” ![]()
Photo by Daniel Sone
The European Hematology Association (EHA) has created a “roadmap” for hematology research in Europe.
This guidance document summarizes the current status of basic, translational, and clinical hematology research and identifies areas of unmet scientific and medical need in Europe.
It is intended to help European and national policy makers, funding agencies, charities, research institutes, and researchers make decisions on initiating, funding, or developing research.
The guidance, “The European Hematology Association Roadmap for European Hematology Research: A Consensus Document,” is published in this month’s issue of haematologica.
“For the first time, hematologists in Europe came together to develop a roadmap to guide hematology research in Europe” said Andreas Engert, MD, chair of the EHA Research Roadmap Task Force.
“Hematology in Europe has achieved a lot, but the discipline must focus and collaborate to be efficient and remain successful in improving patient outcomes. The roadmap does just that and will determine the research agenda in Europe in the coming years.”
Roughly 300 experts from more than 20 countries—including clinicians, basic researchers, and patients—contributed to the roadmap. Stakeholders such as national hematology societies, patient organizations, hematology trial groups, and other European organizations were consulted to comment on the final draft version.
The final roadmap has 9 sections: normal hematopoiesis, malignant lymphoid and myeloid diseases, anemias and related diseases, platelet disorders, blood coagulation and hemostatic disorders, transfusion medicine, infections in hematology, and hematopoietic stem cell transplantation.
The roadmap lists priorities and needs in these areas, including the need for targeted therapies based on genomic profiling and chemical biology, the need to eradicate minimal residual disease, and the need for treatments that are better tolerated by elderly patients.
“Now’s the time for Europe to pay attention,” said Ulrich Jäger, MD, chair of the EHA European Affairs Committee.
“With an aging population, the slow recovery from the financial and Euro crises, costly medical breakthroughs and innovations—quite a few of which involve hematology researchers—Europe faces increased health expenditures while budgets are limited.”
“Policy makers are rightfully cautious when spending the taxpayers’ money. So it is our responsibility to provide the policy makers with the information and evidence they need to decide where their support impacts knowledge and health most efficiently, to the benefit of patients and society. The Research Roadmap delivers on that. Now, it is up to the policy makers in the EU to deliver too.” ![]()
HPV vaccinations get a boost from MOC requirements
Pediatricians saw an increase in the human papillomavirus vaccines administered after participating in a maintenance of certification Part IV program focused on improving vaccine rates.
Researchers “found that participation in the MOC Part IV by primary care pediatricians was associated with a significant increase in captured opportunities for HPV vaccine initiation at prevention visits and for doses 1 and 2 at acute visits,” wrote Dr. Alexander Fiks of The Children’s Hospital of Philadelphia and colleagues. The article was published online in Pediatrics (2016 Feb. 3 [doi: 10.1542/peds.2015-0675]).

For the project, vaccination captured opportunity was defined as a visit at which an eligible patient saw a pediatrician or nurse practitioner and received a dose of the HPV vaccine. A baseline period was established in calendar year 2012 and the intervention period was between Jan. 1 and Nov. 30, 2013, and looked both at captured opportunities during preventive and acute visits. Providers received quarterly performance feedback reports, which included individual results as well as information on how others in the program were doing.
Twenty-seven primary care pediatricians volunteered to participate in the program. They identified barriers in literature and group discussion and viewed an educational webinar that, among other things, included strategies to overcoming barriers to vaccination. They also took part in quarterly calls to review performance and decide on areas of improvement for the next quarter.
During preventive visits, dose 1 captured opportunities captured by MOC participants rose from the baseline period of 27.9% to 37.9% in the MOC period. Dose 2 captured opportunities rose from 87.7% to 93.3% and dose 3 from 94.1% to 94.5%. During acute visits, captured opportunities for dose 1 rose from 2% to 2.9%, from 28.2% to 34.2% for dose 2, and 24.5% to 32.2% for dose 3.
For the 200 other providers in the network, who were also tracked during the same baseline period and MOC period, for preventive visits, captured opportunities rose from 25.2% to 29.4% for dose 1, 85.7% to 88.1% for dose 2, and 89.4% to 92.2% for dose 3. During acute visits, captured opportunities rose from 1.2% to 1.4% for dose 1, 20% to 20.5% for dose 2, and 20% to 22.3% for dose 3.
“Although the magnitude of improvement for HPV dose 1 at acute visits was small given clinician difficulty in engaging in lengthy conversations regarding vaccination at these visits, capture opportunities rose significantly for dose 1 for all visits,” the authors noted. “Vaccination increased for HPV dose 2 at acute visits to a much greater extent than for dose 1, likely because families had already agreed to accept the vaccine and were receptive to clinician recommendation, which was supported by all the MOC activities.”
Dr. Fiks and colleagues added that the lack of improvement for HPV doses 2 and 3 at preventive visits “likely reflected the high baseline vaccination rates, representing a ceiling effect.”
The authors noted that despite improvements, several barriers remained to further improve the rate of captured opportunities, including many pediatricians resisting vaccinating younger adolescents “under the sometimes mistaken assumption that they can determine who is and who will become sexually active. ... In addition, clinicians are known to perceive a higher level of parental resistance among parents of younger adolescents, indicating a need to further support improved communications with specific messaging strategies.”
They also added that because of the way the study was designed, with a focus on the effect of MOC on the individual provider absent an overall organizational push, it may have constrained the ability to improve vaccination rates more broadly.
In South Carolina, we’ve used MOC extensively to engage pediatricians in quality improvement [with the first goal of moving] new policy into practice ... Engaging these practices and doing this quality improvement work, the MOC requirement is a huge carrot for us to put out there to engage practices in doing this kind of work. [The second goal] is basically just looking at outcomes of kids and could your outcomes be better and if they are not good, what kinds of resources can help them be better.

|
Dr. Francis E. Rushton Jr. |
The other role the MOC Part IV credit plays is that when we do this quality improvement work, we embed a quality improvement team in each of our participating practices and that team would include a chief clinician, a nurse, and front office manager or somebody who works with administrative staff. Often, you get some excitement and some engagement with the chief clinician, but it’s hard to spread that excitement and engagement among the other clinicians in the practice until some of them realize, “hey I’ve got to pay attention to this because this is the only way I am going to be able to maintain my board certification, that this process is going to give me Part IV MOC credit.”
Dr. Francis E. Rushton Jr., a pediatrician in Beaufort, S.C., made these comments in an interview.
In South Carolina, we’ve used MOC extensively to engage pediatricians in quality improvement [with the first goal of moving] new policy into practice ... Engaging these practices and doing this quality improvement work, the MOC requirement is a huge carrot for us to put out there to engage practices in doing this kind of work. [The second goal] is basically just looking at outcomes of kids and could your outcomes be better and if they are not good, what kinds of resources can help them be better.
|
|
Dr. Francis E. Rushton Jr. |
The other role the MOC Part IV credit plays is that when we do this quality improvement work, we embed a quality improvement team in each of our participating practices and that team would include a chief clinician, a nurse, and front office manager or somebody who works with administrative staff. Often, you get some excitement and some engagement with the chief clinician, but it’s hard to spread that excitement and engagement among the other clinicians in the practice until some of them realize, “hey I’ve got to pay attention to this because this is the only way I am going to be able to maintain my board certification, that this process is going to give me Part IV MOC credit.”
Dr. Francis E. Rushton Jr., a pediatrician in Beaufort, S.C., made these comments in an interview.
In South Carolina, we’ve used MOC extensively to engage pediatricians in quality improvement [with the first goal of moving] new policy into practice ... Engaging these practices and doing this quality improvement work, the MOC requirement is a huge carrot for us to put out there to engage practices in doing this kind of work. [The second goal] is basically just looking at outcomes of kids and could your outcomes be better and if they are not good, what kinds of resources can help them be better.
|
|
Dr. Francis E. Rushton Jr. |
The other role the MOC Part IV credit plays is that when we do this quality improvement work, we embed a quality improvement team in each of our participating practices and that team would include a chief clinician, a nurse, and front office manager or somebody who works with administrative staff. Often, you get some excitement and some engagement with the chief clinician, but it’s hard to spread that excitement and engagement among the other clinicians in the practice until some of them realize, “hey I’ve got to pay attention to this because this is the only way I am going to be able to maintain my board certification, that this process is going to give me Part IV MOC credit.”
Dr. Francis E. Rushton Jr., a pediatrician in Beaufort, S.C., made these comments in an interview.
Pediatricians saw an increase in the human papillomavirus vaccines administered after participating in a maintenance of certification Part IV program focused on improving vaccine rates.
Researchers “found that participation in the MOC Part IV by primary care pediatricians was associated with a significant increase in captured opportunities for HPV vaccine initiation at prevention visits and for doses 1 and 2 at acute visits,” wrote Dr. Alexander Fiks of The Children’s Hospital of Philadelphia and colleagues. The article was published online in Pediatrics (2016 Feb. 3 [doi: 10.1542/peds.2015-0675]).
For the project, vaccination captured opportunity was defined as a visit at which an eligible patient saw a pediatrician or nurse practitioner and received a dose of the HPV vaccine. A baseline period was established in calendar year 2012 and the intervention period was between Jan. 1 and Nov. 30, 2013, and looked both at captured opportunities during preventive and acute visits. Providers received quarterly performance feedback reports, which included individual results as well as information on how others in the program were doing.
Twenty-seven primary care pediatricians volunteered to participate in the program. They identified barriers in literature and group discussion and viewed an educational webinar that, among other things, included strategies to overcoming barriers to vaccination. They also took part in quarterly calls to review performance and decide on areas of improvement for the next quarter.
During preventive visits, dose 1 captured opportunities captured by MOC participants rose from the baseline period of 27.9% to 37.9% in the MOC period. Dose 2 captured opportunities rose from 87.7% to 93.3% and dose 3 from 94.1% to 94.5%. During acute visits, captured opportunities for dose 1 rose from 2% to 2.9%, from 28.2% to 34.2% for dose 2, and 24.5% to 32.2% for dose 3.
For the 200 other providers in the network, who were also tracked during the same baseline period and MOC period, for preventive visits, captured opportunities rose from 25.2% to 29.4% for dose 1, 85.7% to 88.1% for dose 2, and 89.4% to 92.2% for dose 3. During acute visits, captured opportunities rose from 1.2% to 1.4% for dose 1, 20% to 20.5% for dose 2, and 20% to 22.3% for dose 3.
“Although the magnitude of improvement for HPV dose 1 at acute visits was small given clinician difficulty in engaging in lengthy conversations regarding vaccination at these visits, capture opportunities rose significantly for dose 1 for all visits,” the authors noted. “Vaccination increased for HPV dose 2 at acute visits to a much greater extent than for dose 1, likely because families had already agreed to accept the vaccine and were receptive to clinician recommendation, which was supported by all the MOC activities.”
Dr. Fiks and colleagues added that the lack of improvement for HPV doses 2 and 3 at preventive visits “likely reflected the high baseline vaccination rates, representing a ceiling effect.”
The authors noted that despite improvements, several barriers remained to further improve the rate of captured opportunities, including many pediatricians resisting vaccinating younger adolescents “under the sometimes mistaken assumption that they can determine who is and who will become sexually active. ... In addition, clinicians are known to perceive a higher level of parental resistance among parents of younger adolescents, indicating a need to further support improved communications with specific messaging strategies.”
They also added that because of the way the study was designed, with a focus on the effect of MOC on the individual provider absent an overall organizational push, it may have constrained the ability to improve vaccination rates more broadly.
Pediatricians saw an increase in the human papillomavirus vaccines administered after participating in a maintenance of certification Part IV program focused on improving vaccine rates.
Researchers “found that participation in the MOC Part IV by primary care pediatricians was associated with a significant increase in captured opportunities for HPV vaccine initiation at prevention visits and for doses 1 and 2 at acute visits,” wrote Dr. Alexander Fiks of The Children’s Hospital of Philadelphia and colleagues. The article was published online in Pediatrics (2016 Feb. 3 [doi: 10.1542/peds.2015-0675]).
For the project, vaccination captured opportunity was defined as a visit at which an eligible patient saw a pediatrician or nurse practitioner and received a dose of the HPV vaccine. A baseline period was established in calendar year 2012 and the intervention period was between Jan. 1 and Nov. 30, 2013, and looked both at captured opportunities during preventive and acute visits. Providers received quarterly performance feedback reports, which included individual results as well as information on how others in the program were doing.
Twenty-seven primary care pediatricians volunteered to participate in the program. They identified barriers in literature and group discussion and viewed an educational webinar that, among other things, included strategies to overcoming barriers to vaccination. They also took part in quarterly calls to review performance and decide on areas of improvement for the next quarter.
During preventive visits, dose 1 captured opportunities captured by MOC participants rose from the baseline period of 27.9% to 37.9% in the MOC period. Dose 2 captured opportunities rose from 87.7% to 93.3% and dose 3 from 94.1% to 94.5%. During acute visits, captured opportunities for dose 1 rose from 2% to 2.9%, from 28.2% to 34.2% for dose 2, and 24.5% to 32.2% for dose 3.
For the 200 other providers in the network, who were also tracked during the same baseline period and MOC period, for preventive visits, captured opportunities rose from 25.2% to 29.4% for dose 1, 85.7% to 88.1% for dose 2, and 89.4% to 92.2% for dose 3. During acute visits, captured opportunities rose from 1.2% to 1.4% for dose 1, 20% to 20.5% for dose 2, and 20% to 22.3% for dose 3.
“Although the magnitude of improvement for HPV dose 1 at acute visits was small given clinician difficulty in engaging in lengthy conversations regarding vaccination at these visits, capture opportunities rose significantly for dose 1 for all visits,” the authors noted. “Vaccination increased for HPV dose 2 at acute visits to a much greater extent than for dose 1, likely because families had already agreed to accept the vaccine and were receptive to clinician recommendation, which was supported by all the MOC activities.”
Dr. Fiks and colleagues added that the lack of improvement for HPV doses 2 and 3 at preventive visits “likely reflected the high baseline vaccination rates, representing a ceiling effect.”
The authors noted that despite improvements, several barriers remained to further improve the rate of captured opportunities, including many pediatricians resisting vaccinating younger adolescents “under the sometimes mistaken assumption that they can determine who is and who will become sexually active. ... In addition, clinicians are known to perceive a higher level of parental resistance among parents of younger adolescents, indicating a need to further support improved communications with specific messaging strategies.”
They also added that because of the way the study was designed, with a focus on the effect of MOC on the individual provider absent an overall organizational push, it may have constrained the ability to improve vaccination rates more broadly.
FROM PEDIATRICS
Key clinical point: Incorporating HPV vaccine outcomes in maintenance of certification requirements boosted captured opportunities for vaccine initiation.
Major finding: MOC participants significantly increase captured opportunities relative to nonparticipants by 5.7% for HPV dose 1 at preventive visits.
Data source: Twenty-seven primary care pediatricians from 11 practices in The Children’s Hospital of Philadelphia primary care network voluntarily chose to participate in the project with no incentives provided other than receiving MOC Part IV credit.
Disclosures: Study authors reported no potential conflicts of interest.

Meningococcal B vaccine added to 2016 immunization schedule
The new 2016 recommended immunization schedule for children and adolescents reflects the addition of meningococcal B vaccine and various other changes.
Each year, a new immunization schedule is approved and published by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, and the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Obstetricians and Gynecologists.
The addition of meningococcal B vaccine is shown by a blue bar indicating vaccination at 10 years for children at increased risk. Non–high-risk persons aged 16-18 years may be considered for vaccination, as indicated by a purple bar. The footnotes indicate that the two MenB vaccines “are not interchangeable; the same vaccine product must be used for all doses.” Also, Bexsero requires a two-dose series administered at least 1 month apart. Trumenba requires a three-dose series, with the second dose at least 2 months after the first and the third dose at least 6 months after the first.

Trumenba (Wyeth Pharmaceuticals) was licensed by the Food and Drug Administration in October 2014 and Bexsero (Novartis) was licensed in January 2015.
The human papillomavirus (HPV) vaccine is now referred to as 9vHPV, to reflect the availability of Merck’s Gardasil 9, which was licensed in December 2014 to replace the prior 4-valent version. A purple bar has been added to the HPV row for ages 9-10 years to indicate that children with a history of sexual abuse are at increased risk of HPV infection and should be vaccinated.
Other changes to the 2016 schedule and footnotes include:
• A change in the order of the vaccines to group vaccines according to the recommended ages of administration, as well as to the order of the footnotes
• The addition of a purple bar for Haemophilus influenzae type b (Hib) vaccine for children aged 5-18 years; this reflects a recommendation to vaccinate certain high-risk children in this age group who have not been immunized.
• A revision to the footnote for the hepatitis B vaccine to clarify the timing as well as the new CDC-recommended interval for postvaccination serologic testing of infants born to hepatitis B surface antigen (HBsAg)-positive mothers.
• A revision to the footnote for the DTaP vaccine to clarify recommendations to be taken after an inadvertently early administration of the fourth dose of that vaccine.
• An update to the footnote for the inactivated polio vaccine offering guidance on the vaccination of children who have received all doses of oral-only polio vaccine before age 4 years.
To see the immunization schedule, go to www.cdc.gov/vaccines.
The new 2016 recommended immunization schedule for children and adolescents reflects the addition of meningococcal B vaccine and various other changes.
Each year, a new immunization schedule is approved and published by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, and the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Obstetricians and Gynecologists.
The addition of meningococcal B vaccine is shown by a blue bar indicating vaccination at 10 years for children at increased risk. Non–high-risk persons aged 16-18 years may be considered for vaccination, as indicated by a purple bar. The footnotes indicate that the two MenB vaccines “are not interchangeable; the same vaccine product must be used for all doses.” Also, Bexsero requires a two-dose series administered at least 1 month apart. Trumenba requires a three-dose series, with the second dose at least 2 months after the first and the third dose at least 6 months after the first.
Trumenba (Wyeth Pharmaceuticals) was licensed by the Food and Drug Administration in October 2014 and Bexsero (Novartis) was licensed in January 2015.
The human papillomavirus (HPV) vaccine is now referred to as 9vHPV, to reflect the availability of Merck’s Gardasil 9, which was licensed in December 2014 to replace the prior 4-valent version. A purple bar has been added to the HPV row for ages 9-10 years to indicate that children with a history of sexual abuse are at increased risk of HPV infection and should be vaccinated.
Other changes to the 2016 schedule and footnotes include:
• A change in the order of the vaccines to group vaccines according to the recommended ages of administration, as well as to the order of the footnotes
• The addition of a purple bar for Haemophilus influenzae type b (Hib) vaccine for children aged 5-18 years; this reflects a recommendation to vaccinate certain high-risk children in this age group who have not been immunized.
• A revision to the footnote for the hepatitis B vaccine to clarify the timing as well as the new CDC-recommended interval for postvaccination serologic testing of infants born to hepatitis B surface antigen (HBsAg)-positive mothers.
• A revision to the footnote for the DTaP vaccine to clarify recommendations to be taken after an inadvertently early administration of the fourth dose of that vaccine.
• An update to the footnote for the inactivated polio vaccine offering guidance on the vaccination of children who have received all doses of oral-only polio vaccine before age 4 years.
To see the immunization schedule, go to www.cdc.gov/vaccines.
The new 2016 recommended immunization schedule for children and adolescents reflects the addition of meningococcal B vaccine and various other changes.
Each year, a new immunization schedule is approved and published by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, and the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Obstetricians and Gynecologists.
The addition of meningococcal B vaccine is shown by a blue bar indicating vaccination at 10 years for children at increased risk. Non–high-risk persons aged 16-18 years may be considered for vaccination, as indicated by a purple bar. The footnotes indicate that the two MenB vaccines “are not interchangeable; the same vaccine product must be used for all doses.” Also, Bexsero requires a two-dose series administered at least 1 month apart. Trumenba requires a three-dose series, with the second dose at least 2 months after the first and the third dose at least 6 months after the first.
Trumenba (Wyeth Pharmaceuticals) was licensed by the Food and Drug Administration in October 2014 and Bexsero (Novartis) was licensed in January 2015.
The human papillomavirus (HPV) vaccine is now referred to as 9vHPV, to reflect the availability of Merck’s Gardasil 9, which was licensed in December 2014 to replace the prior 4-valent version. A purple bar has been added to the HPV row for ages 9-10 years to indicate that children with a history of sexual abuse are at increased risk of HPV infection and should be vaccinated.
Other changes to the 2016 schedule and footnotes include:
• A change in the order of the vaccines to group vaccines according to the recommended ages of administration, as well as to the order of the footnotes
• The addition of a purple bar for Haemophilus influenzae type b (Hib) vaccine for children aged 5-18 years; this reflects a recommendation to vaccinate certain high-risk children in this age group who have not been immunized.
• A revision to the footnote for the hepatitis B vaccine to clarify the timing as well as the new CDC-recommended interval for postvaccination serologic testing of infants born to hepatitis B surface antigen (HBsAg)-positive mothers.
• A revision to the footnote for the DTaP vaccine to clarify recommendations to be taken after an inadvertently early administration of the fourth dose of that vaccine.
• An update to the footnote for the inactivated polio vaccine offering guidance on the vaccination of children who have received all doses of oral-only polio vaccine before age 4 years.
To see the immunization schedule, go to www.cdc.gov/vaccines.
