User login
Type 2 diabetes in youth needs new treatment options
NEW ORLEANS – For adolescents and children with type 2 diabetes, there aren’t a lot of therapeutic options other than insulin and metformin. And the situation isn’t likely to change without extraordinary collaboration, Kristen J. Nadeau, MD, research director of the department of pediatric endocrinology at Children’s Hospital Colorado, Colorado Springs, said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth appears to differ not only from pediatric type 1 diabetes, but also from adult type 2 diabetes, and current treatment options are limited,” Dr. Nadeau said. The estimated number of type 2 diabetes cases in the United States per year stands at 1,469,000 cases (12.3 per 100) in adults, compared with 5,100 (0.5 per 100) in youth. In adults there is a slight male predominance, whereas in kids girls are almost twice as likely as boys to be affected. Moreover, beta cell function declines faster in youth with type 2 diabetes.

The majority of insulins used by adults with type 2 diabetes are also approved for use in children and adolescents, but the only non-insulin medication approved for youth is metformin. According to Dr. Nadeau, 11 clinical safety and efficacy studies and 3 pharmacokinetic studies are ongoing for four DPP-4 inhibitors, two GLP-1 analogs, three SGLT2 inhibitors, colesevelam, bromocriptine, and insulins. A total of 5,000 youth are needed to complete current and planned trials, which “would require 100% participation from every child diagnosed in the next year, which is not feasible,” she said.
The required safety and efficacy studies are too difficult “because of the combination of unique challenges of the target population, study design concerns, and a lack of collaboration between agencies,” Dr. Nadeau said during a session that focused on the conclusions of the American Diabetes Association’s consensus conference on youth with type 2 diabetes, which took place on Oct. 20, 2015 in Alexandria, Va.
The consensus report was published online in Diabetes Care, and addresses the current status of type 2 diabetes in youth, the challenges of treatment, and priorities for research. Dr. Nadeau co-chaired the effort along with Dr. Philip Zeitler, section head of pediatric endocrinology at Children’s Hospital Colorado and medical director of the Children’s Hospital Colorado Clinical and Translational Research Center, Denver. Collaborators included the American Academy of Pediatrics, the International Society for Pediatric and Adolescent Diabetes, and the Pediatric Endocrine Society.
One example of the research challenges is evident in data from the Today trial, which found that only about 39% of kids with type 2 diabetes live with both parents (J Clin Endocrinol Metab. 2011 Jan; 96[1]:159-67). “Whenever you have only one parent in the home, there are difficulties with transportation by definition, so it’s a lot harder for these kids to participate in studies,” Dr. Nadeau said. “In addition, only 17% of their parents had a college or advanced education and 41% had a household income of less than $25,000 per year.”
The social environment is critical, she continued, because the lifestyle factors associated with type 2 diabetes often result in poor outcomes. “It’s very hard to make lifestyle changes if there is a socioeconomic challenge,” she said. “We can’t make change without understanding the community and culture that these youth live in. It’s also critical that we have participation of minorities and other research participants with diverse backgrounds in order for [clinical] trials to be effective for the population that this disease is affecting.”
Another issue keeping drug trials of youth with type 2 diabetes from being completed is the entry criteria. Some studies require youth to be drug naive and have a hemoglobin A1c greater than 7%. “This is difficult, because many youth that are referred to our diabetes center already come in on metformin, leaving only about 7% of subjects available for this criteria,” Dr. Nadeau explained. Another common study entry criterion is being on metformin and having a hemoglobin A1c of about 7%, “so basically being a metformin failure,” she said. “This is difficult to meet because metformin is relatively effective in the early stages of diabetes.”
“We need clear strategies for research, prevention, and treatment. Clarifying unique pathophysiology, complications, and psychosocial impact will enable industry, academia, funding agencies, advocacy groups, and regulators to collectively evaluate the best approaches to research, treatment, and prevention,” Dr. Nadeau said.
The consensus conference participants recommended the following objectives: clarify the biology of type 2 diabetes in youth, obtain new pediatric information on drugs, encourage the use of appropriate medications, and inform clinical decision-making. “We have a desperate need to understand the actions of drugs in type 2 diabetes youth,” Dr. Nadeau said. “Our current approach is not working. Potential solutions include considering efficacy outcomes besides A1c, potentially looking at improvement in insulin sensitivity, preservation of beta-cell function, trying to prevent the A1c increase instead of looking for an A1c reduction, and trying to extrapolate from effects in adults, if we can understand enough to do that.”
The conference participants also called for infrastructure changes, such as creating a resource for patients with type 2 diabetes in the model of the Type 1 Diabetes Exchange. “We need to have collaborations internationally,” she said. “We also need support for teams and clinical groups to work together to be able to accomplish these collaboratively.”
Dr. Nadeau reported having no financial disclosures.
NEW ORLEANS – For adolescents and children with type 2 diabetes, there aren’t a lot of therapeutic options other than insulin and metformin. And the situation isn’t likely to change without extraordinary collaboration, Kristen J. Nadeau, MD, research director of the department of pediatric endocrinology at Children’s Hospital Colorado, Colorado Springs, said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth appears to differ not only from pediatric type 1 diabetes, but also from adult type 2 diabetes, and current treatment options are limited,” Dr. Nadeau said. The estimated number of type 2 diabetes cases in the United States per year stands at 1,469,000 cases (12.3 per 100) in adults, compared with 5,100 (0.5 per 100) in youth. In adults there is a slight male predominance, whereas in kids girls are almost twice as likely as boys to be affected. Moreover, beta cell function declines faster in youth with type 2 diabetes.
The majority of insulins used by adults with type 2 diabetes are also approved for use in children and adolescents, but the only non-insulin medication approved for youth is metformin. According to Dr. Nadeau, 11 clinical safety and efficacy studies and 3 pharmacokinetic studies are ongoing for four DPP-4 inhibitors, two GLP-1 analogs, three SGLT2 inhibitors, colesevelam, bromocriptine, and insulins. A total of 5,000 youth are needed to complete current and planned trials, which “would require 100% participation from every child diagnosed in the next year, which is not feasible,” she said.
The required safety and efficacy studies are too difficult “because of the combination of unique challenges of the target population, study design concerns, and a lack of collaboration between agencies,” Dr. Nadeau said during a session that focused on the conclusions of the American Diabetes Association’s consensus conference on youth with type 2 diabetes, which took place on Oct. 20, 2015 in Alexandria, Va.
The consensus report was published online in Diabetes Care, and addresses the current status of type 2 diabetes in youth, the challenges of treatment, and priorities for research. Dr. Nadeau co-chaired the effort along with Dr. Philip Zeitler, section head of pediatric endocrinology at Children’s Hospital Colorado and medical director of the Children’s Hospital Colorado Clinical and Translational Research Center, Denver. Collaborators included the American Academy of Pediatrics, the International Society for Pediatric and Adolescent Diabetes, and the Pediatric Endocrine Society.
One example of the research challenges is evident in data from the Today trial, which found that only about 39% of kids with type 2 diabetes live with both parents (J Clin Endocrinol Metab. 2011 Jan; 96[1]:159-67). “Whenever you have only one parent in the home, there are difficulties with transportation by definition, so it’s a lot harder for these kids to participate in studies,” Dr. Nadeau said. “In addition, only 17% of their parents had a college or advanced education and 41% had a household income of less than $25,000 per year.”
The social environment is critical, she continued, because the lifestyle factors associated with type 2 diabetes often result in poor outcomes. “It’s very hard to make lifestyle changes if there is a socioeconomic challenge,” she said. “We can’t make change without understanding the community and culture that these youth live in. It’s also critical that we have participation of minorities and other research participants with diverse backgrounds in order for [clinical] trials to be effective for the population that this disease is affecting.”
Another issue keeping drug trials of youth with type 2 diabetes from being completed is the entry criteria. Some studies require youth to be drug naive and have a hemoglobin A1c greater than 7%. “This is difficult, because many youth that are referred to our diabetes center already come in on metformin, leaving only about 7% of subjects available for this criteria,” Dr. Nadeau explained. Another common study entry criterion is being on metformin and having a hemoglobin A1c of about 7%, “so basically being a metformin failure,” she said. “This is difficult to meet because metformin is relatively effective in the early stages of diabetes.”
“We need clear strategies for research, prevention, and treatment. Clarifying unique pathophysiology, complications, and psychosocial impact will enable industry, academia, funding agencies, advocacy groups, and regulators to collectively evaluate the best approaches to research, treatment, and prevention,” Dr. Nadeau said.
The consensus conference participants recommended the following objectives: clarify the biology of type 2 diabetes in youth, obtain new pediatric information on drugs, encourage the use of appropriate medications, and inform clinical decision-making. “We have a desperate need to understand the actions of drugs in type 2 diabetes youth,” Dr. Nadeau said. “Our current approach is not working. Potential solutions include considering efficacy outcomes besides A1c, potentially looking at improvement in insulin sensitivity, preservation of beta-cell function, trying to prevent the A1c increase instead of looking for an A1c reduction, and trying to extrapolate from effects in adults, if we can understand enough to do that.”
The conference participants also called for infrastructure changes, such as creating a resource for patients with type 2 diabetes in the model of the Type 1 Diabetes Exchange. “We need to have collaborations internationally,” she said. “We also need support for teams and clinical groups to work together to be able to accomplish these collaboratively.”
Dr. Nadeau reported having no financial disclosures.
NEW ORLEANS – For adolescents and children with type 2 diabetes, there aren’t a lot of therapeutic options other than insulin and metformin. And the situation isn’t likely to change without extraordinary collaboration, Kristen J. Nadeau, MD, research director of the department of pediatric endocrinology at Children’s Hospital Colorado, Colorado Springs, said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth appears to differ not only from pediatric type 1 diabetes, but also from adult type 2 diabetes, and current treatment options are limited,” Dr. Nadeau said. The estimated number of type 2 diabetes cases in the United States per year stands at 1,469,000 cases (12.3 per 100) in adults, compared with 5,100 (0.5 per 100) in youth. In adults there is a slight male predominance, whereas in kids girls are almost twice as likely as boys to be affected. Moreover, beta cell function declines faster in youth with type 2 diabetes.
The majority of insulins used by adults with type 2 diabetes are also approved for use in children and adolescents, but the only non-insulin medication approved for youth is metformin. According to Dr. Nadeau, 11 clinical safety and efficacy studies and 3 pharmacokinetic studies are ongoing for four DPP-4 inhibitors, two GLP-1 analogs, three SGLT2 inhibitors, colesevelam, bromocriptine, and insulins. A total of 5,000 youth are needed to complete current and planned trials, which “would require 100% participation from every child diagnosed in the next year, which is not feasible,” she said.
The required safety and efficacy studies are too difficult “because of the combination of unique challenges of the target population, study design concerns, and a lack of collaboration between agencies,” Dr. Nadeau said during a session that focused on the conclusions of the American Diabetes Association’s consensus conference on youth with type 2 diabetes, which took place on Oct. 20, 2015 in Alexandria, Va.
The consensus report was published online in Diabetes Care, and addresses the current status of type 2 diabetes in youth, the challenges of treatment, and priorities for research. Dr. Nadeau co-chaired the effort along with Dr. Philip Zeitler, section head of pediatric endocrinology at Children’s Hospital Colorado and medical director of the Children’s Hospital Colorado Clinical and Translational Research Center, Denver. Collaborators included the American Academy of Pediatrics, the International Society for Pediatric and Adolescent Diabetes, and the Pediatric Endocrine Society.
One example of the research challenges is evident in data from the Today trial, which found that only about 39% of kids with type 2 diabetes live with both parents (J Clin Endocrinol Metab. 2011 Jan; 96[1]:159-67). “Whenever you have only one parent in the home, there are difficulties with transportation by definition, so it’s a lot harder for these kids to participate in studies,” Dr. Nadeau said. “In addition, only 17% of their parents had a college or advanced education and 41% had a household income of less than $25,000 per year.”
The social environment is critical, she continued, because the lifestyle factors associated with type 2 diabetes often result in poor outcomes. “It’s very hard to make lifestyle changes if there is a socioeconomic challenge,” she said. “We can’t make change without understanding the community and culture that these youth live in. It’s also critical that we have participation of minorities and other research participants with diverse backgrounds in order for [clinical] trials to be effective for the population that this disease is affecting.”
Another issue keeping drug trials of youth with type 2 diabetes from being completed is the entry criteria. Some studies require youth to be drug naive and have a hemoglobin A1c greater than 7%. “This is difficult, because many youth that are referred to our diabetes center already come in on metformin, leaving only about 7% of subjects available for this criteria,” Dr. Nadeau explained. Another common study entry criterion is being on metformin and having a hemoglobin A1c of about 7%, “so basically being a metformin failure,” she said. “This is difficult to meet because metformin is relatively effective in the early stages of diabetes.”
“We need clear strategies for research, prevention, and treatment. Clarifying unique pathophysiology, complications, and psychosocial impact will enable industry, academia, funding agencies, advocacy groups, and regulators to collectively evaluate the best approaches to research, treatment, and prevention,” Dr. Nadeau said.
The consensus conference participants recommended the following objectives: clarify the biology of type 2 diabetes in youth, obtain new pediatric information on drugs, encourage the use of appropriate medications, and inform clinical decision-making. “We have a desperate need to understand the actions of drugs in type 2 diabetes youth,” Dr. Nadeau said. “Our current approach is not working. Potential solutions include considering efficacy outcomes besides A1c, potentially looking at improvement in insulin sensitivity, preservation of beta-cell function, trying to prevent the A1c increase instead of looking for an A1c reduction, and trying to extrapolate from effects in adults, if we can understand enough to do that.”
The conference participants also called for infrastructure changes, such as creating a resource for patients with type 2 diabetes in the model of the Type 1 Diabetes Exchange. “We need to have collaborations internationally,” she said. “We also need support for teams and clinical groups to work together to be able to accomplish these collaboratively.”
Dr. Nadeau reported having no financial disclosures.
Strongly recommend HPV vaccine to increase uptake
To convince parents to get their kids vaccinated against human papillomavirus (HPV), tell them “I strongly believe in the importance of this cancer-preventing vaccine for [their child’s name],” researchers concluded after an online survey of 1,504 parents of children aged 11-17 years.
Sixty-five percent of parents agreed it was a persuasive argument, the highest percentage among 15 statements in favor of vaccination; 69% of 776 surveyed physicians said they’d use it in practice, also the highest physician endorsement for the various arguments (Cancer Epidemiol Biomarkers Prev. 2016 Sep 30. doi: 10.1158/1055-9965.EPI-16-0224).
In general, parents disinclined to vaccinate were most receptive to messages about HPV infection being common, cancers caused by HPV, and HPV vaccine effectiveness.
Other persuasive arguments included “[child’s name] can get anal/cervical cancer as an adult, but you can stop that right now;” and “there will be many things in [child’s name]’s life that you can’t control. But you can control whether [he/she] gets some dangerous kinds of HPV.” 
Both “placed the onus of protection on the parent and emphasized the control they possess over their child’s health. This finding is aligned with the tenets of various theories of fear appeals, which posit that fear messages inspire action if the receiver believes he or she has some control over the situation. Parents without prior intentions to vaccinate their child may be particularly receptive to messages that arouse fear while fostering a sense of efficacy,” said Teri Malo, PhD, of the University of North Carolina, Chapel Hill, and associates.
Although almost 60% of parents said they’d pay attention if told they could control if their child gets HPV cancer, only 37% of physicians said they’d use the argument. It’s not clear why, but the team said the finding was “concerning ... given that it was one of the top messages that would persuade parents without prior intentions to vaccinate their child.”
At present, 40% of girls and 22% of boys aged 13-17 years receive all three HPV shots. The goal of the study was to help doctors increase those numbers with persuasive arguments. “Physician communication about human papillomavirus vaccine is a key determinant of uptake,” but not all physicians strongly recommend the vaccine, especially if they anticipate parent resistance. “We sought to identify messages that would motivate HPV vaccination,” the researchers said.
Argument by analogy was the weakest approach. Only 5% of parents found “would you wait until [child’s name] is in a car accident before you tell [him/her] to wear a seatbelt?” persuasive, and only 9% of physicians said they’d use it, which made it the least endorsed statement in the study.
The same arguments seemed to work regardless of parents’ race, education, or income, or their child’s age or sex, which led the team to suggest the messages will work across demographic subgroups.
Slightly more moms than dads filled out the survey, and most were white, with about 9% of parents black and 14% Hispanic. Most parents lived in metropolitan areas, nearly two-thirds had at least some college, and almost half reported an annual household income of at least $75,000. For simplicity, parents limited their responses to their child with the most recent birthday. About half of children were boys, and just over half hadn’t been vaccinated against HPV.
About two-thirds of the physicians were men. Over half had practiced for at least 20 years, just over half were pediatricians, and the rest were family practitioners.
The work was funded by an unrestricted educational grant from Pfizer to senior investigator Noel Brewer, PhD. Dr. Brewer receives commercial research grants from Merck, maker of the HPV vaccine Gardasil, and Pfizer. He is also a Merck consultant and advisory board member. Coauthor Melissa B. Gilkey, PhD, and Dr. Malo were supported by other grants. The report noted that “the costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with” U.S. law.
To convince parents to get their kids vaccinated against human papillomavirus (HPV), tell them “I strongly believe in the importance of this cancer-preventing vaccine for [their child’s name],” researchers concluded after an online survey of 1,504 parents of children aged 11-17 years.
Sixty-five percent of parents agreed it was a persuasive argument, the highest percentage among 15 statements in favor of vaccination; 69% of 776 surveyed physicians said they’d use it in practice, also the highest physician endorsement for the various arguments (Cancer Epidemiol Biomarkers Prev. 2016 Sep 30. doi: 10.1158/1055-9965.EPI-16-0224).
In general, parents disinclined to vaccinate were most receptive to messages about HPV infection being common, cancers caused by HPV, and HPV vaccine effectiveness.
Other persuasive arguments included “[child’s name] can get anal/cervical cancer as an adult, but you can stop that right now;” and “there will be many things in [child’s name]’s life that you can’t control. But you can control whether [he/she] gets some dangerous kinds of HPV.”
Both “placed the onus of protection on the parent and emphasized the control they possess over their child’s health. This finding is aligned with the tenets of various theories of fear appeals, which posit that fear messages inspire action if the receiver believes he or she has some control over the situation. Parents without prior intentions to vaccinate their child may be particularly receptive to messages that arouse fear while fostering a sense of efficacy,” said Teri Malo, PhD, of the University of North Carolina, Chapel Hill, and associates.
Although almost 60% of parents said they’d pay attention if told they could control if their child gets HPV cancer, only 37% of physicians said they’d use the argument. It’s not clear why, but the team said the finding was “concerning ... given that it was one of the top messages that would persuade parents without prior intentions to vaccinate their child.”
At present, 40% of girls and 22% of boys aged 13-17 years receive all three HPV shots. The goal of the study was to help doctors increase those numbers with persuasive arguments. “Physician communication about human papillomavirus vaccine is a key determinant of uptake,” but not all physicians strongly recommend the vaccine, especially if they anticipate parent resistance. “We sought to identify messages that would motivate HPV vaccination,” the researchers said.
Argument by analogy was the weakest approach. Only 5% of parents found “would you wait until [child’s name] is in a car accident before you tell [him/her] to wear a seatbelt?” persuasive, and only 9% of physicians said they’d use it, which made it the least endorsed statement in the study.
The same arguments seemed to work regardless of parents’ race, education, or income, or their child’s age or sex, which led the team to suggest the messages will work across demographic subgroups.
Slightly more moms than dads filled out the survey, and most were white, with about 9% of parents black and 14% Hispanic. Most parents lived in metropolitan areas, nearly two-thirds had at least some college, and almost half reported an annual household income of at least $75,000. For simplicity, parents limited their responses to their child with the most recent birthday. About half of children were boys, and just over half hadn’t been vaccinated against HPV.
About two-thirds of the physicians were men. Over half had practiced for at least 20 years, just over half were pediatricians, and the rest were family practitioners.
The work was funded by an unrestricted educational grant from Pfizer to senior investigator Noel Brewer, PhD. Dr. Brewer receives commercial research grants from Merck, maker of the HPV vaccine Gardasil, and Pfizer. He is also a Merck consultant and advisory board member. Coauthor Melissa B. Gilkey, PhD, and Dr. Malo were supported by other grants. The report noted that “the costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with” U.S. law.
To convince parents to get their kids vaccinated against human papillomavirus (HPV), tell them “I strongly believe in the importance of this cancer-preventing vaccine for [their child’s name],” researchers concluded after an online survey of 1,504 parents of children aged 11-17 years.
Sixty-five percent of parents agreed it was a persuasive argument, the highest percentage among 15 statements in favor of vaccination; 69% of 776 surveyed physicians said they’d use it in practice, also the highest physician endorsement for the various arguments (Cancer Epidemiol Biomarkers Prev. 2016 Sep 30. doi: 10.1158/1055-9965.EPI-16-0224).
In general, parents disinclined to vaccinate were most receptive to messages about HPV infection being common, cancers caused by HPV, and HPV vaccine effectiveness.
Other persuasive arguments included “[child’s name] can get anal/cervical cancer as an adult, but you can stop that right now;” and “there will be many things in [child’s name]’s life that you can’t control. But you can control whether [he/she] gets some dangerous kinds of HPV.”
Both “placed the onus of protection on the parent and emphasized the control they possess over their child’s health. This finding is aligned with the tenets of various theories of fear appeals, which posit that fear messages inspire action if the receiver believes he or she has some control over the situation. Parents without prior intentions to vaccinate their child may be particularly receptive to messages that arouse fear while fostering a sense of efficacy,” said Teri Malo, PhD, of the University of North Carolina, Chapel Hill, and associates.
Although almost 60% of parents said they’d pay attention if told they could control if their child gets HPV cancer, only 37% of physicians said they’d use the argument. It’s not clear why, but the team said the finding was “concerning ... given that it was one of the top messages that would persuade parents without prior intentions to vaccinate their child.”
At present, 40% of girls and 22% of boys aged 13-17 years receive all three HPV shots. The goal of the study was to help doctors increase those numbers with persuasive arguments. “Physician communication about human papillomavirus vaccine is a key determinant of uptake,” but not all physicians strongly recommend the vaccine, especially if they anticipate parent resistance. “We sought to identify messages that would motivate HPV vaccination,” the researchers said.
Argument by analogy was the weakest approach. Only 5% of parents found “would you wait until [child’s name] is in a car accident before you tell [him/her] to wear a seatbelt?” persuasive, and only 9% of physicians said they’d use it, which made it the least endorsed statement in the study.
The same arguments seemed to work regardless of parents’ race, education, or income, or their child’s age or sex, which led the team to suggest the messages will work across demographic subgroups.
Slightly more moms than dads filled out the survey, and most were white, with about 9% of parents black and 14% Hispanic. Most parents lived in metropolitan areas, nearly two-thirds had at least some college, and almost half reported an annual household income of at least $75,000. For simplicity, parents limited their responses to their child with the most recent birthday. About half of children were boys, and just over half hadn’t been vaccinated against HPV.
About two-thirds of the physicians were men. Over half had practiced for at least 20 years, just over half were pediatricians, and the rest were family practitioners.
The work was funded by an unrestricted educational grant from Pfizer to senior investigator Noel Brewer, PhD. Dr. Brewer receives commercial research grants from Merck, maker of the HPV vaccine Gardasil, and Pfizer. He is also a Merck consultant and advisory board member. Coauthor Melissa B. Gilkey, PhD, and Dr. Malo were supported by other grants. The report noted that “the costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with” U.S. law.
Key clinical point:
Major finding: Sixty-five percent of parents agreed it was a persuasive argument, the highest percentage among 15 statements in favor of vaccination; 69% of 776 surveyed physicians said they’d use it in practice.
Data source: Online survey of 1,504 parents of children aged 11-17 years old, and 776 physicians.
Disclosures: The work was funded by an unrestricted educational grant from Pfizer to senior investigator Noel Brewer, PhD. Dr. Brewer receives commercial research grants from Merck, maker of the HPV vaccine Gardasil, and Pfizer. He is also a Merck consultant and advisory board member. Coauthor Melissa B. Gilkey, PhD, and Dr. Malo were supported by other grants. The report noted that “the costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with” U.S. law.
Epidermodysplasia Verruciformis and the Risk for Malignancy
To the Editor:
Epidermodysplasia verruciformis (EV) is a rare autosomal-recessive genodermatosis characterized by widespread infection with specific strains of human papillomavirus (HPV). Patients with EV have a unique susceptibility to acquire HPV due to defects in cellular immunity to the presenting antigens.1 These defects may be related to mutations of the EVER genes or due to acquisition of an immunosuppressive condition.2,3 Infections with HPV-3 and HPV-10 do not lead to the development of malignancies. However, infection with HPV-5, HPV-8, and HPV-14 can lead to the development of nonmelanoma skin cancers, usually squamous cell carcinomas (SCCs), in approximately 60% of patients.3,4 This viral condition lasts throughout the patient’s lifetime and presents as tinea versicolor–like macules and patches. These lesions may be confused with seborrheic keratosis or verruca plana.5 Lesions typically are hypopigmented but occasionally may be hyperpigmented or erythematous. They often are found on the trunk, but lesions on the face, arms, palms, legs, and soles have been reported.5 Mucous membranes are always spared. Epidermodysplasia verruciformis often presents in childhood, except in cases related to acquired immunosuppression. The condition has no sex or racial predilection and no geographical preference.5
A 7-year-old boy (Fitzpatrick skin type V) presented with an asymptomatic rash on the trunk (Figure 1), dorsal aspect of the hands, and forehead. The lesions first appeared 5 years prior on the upper back and upper chest and had recently spread to the forehead and frontal aspect of the scalp. The patient had a history of myelomeningocele, which was corrected at birth with surgical placement of a ventriculoperitoneal shunt. The patient was otherwise healthy and met all appropriate developmental milestones for his age group. Family history revealed consanguinity of the patient’s paternal grandparents who were first cousins. The patient’s mother denied any other family member having similar rashes or lesions.

The patient had been treated for pityriasis versicolor on and off for 2 years by another dermatologist. His mother reported faithfully applying ketoconazole cream twice daily for several months with no improvement. She also reported using topical steroids, which did not provide any benefit. The patient and mother denied any associated pruritus, bleeding, burning, or physical discomfort.
Skin examination revealed diffuse, flat, polymorphous, hypopigmented and salmon-colored hyperkeratotic macules and patches with mild scaling on the upper region of the anterior aspect of the chest and upper back (Figure 2A). Additionally, the patient had an extensive number of lesions on the forehead and frontal aspect of the scalp (Figure 2B).

A shave biopsy demonstrated a thick basket weave stratum corneum, koilocytes, and large pale keratinocytes with characteristic blue cytoplasm. These findings were characteristic for EV.
At the patient’s 3-month follow-up visit, he again denied any symptoms associated with the lesions and reported that the appearance was diminishing in severity. On examination there was no evidence of SCC. The mother was advised to discontinue all topical treatments for the patient and return to the office every 3 to 6 months for regular skin surveillance. The mother was further advised to protect the patient from UV radiation with sunscreen and sun-protective clothing.
Epidermodysplasia verruciformis was first reported by Lewandowsky and Lutz6 in 1922. This rare condition often presents in childhood and is characterized by a persistent HPV infection and an autosomal-recessive inheritance pattern. Reports in the literature frequently involve kindreds. Often, patients with EV have a family history of first-degree or second-degree consanguinity.7
The clinical presentation of EV often resembles a pityriasis versicolor–like eruption. However, pityriasis versicolor is less commonly seen in childhood and is more prevalent in patients aged 21 to 30 years, likely due to increased sebum production and changing hormone levels. Furthermore, it is unusual to see pityriasis versicolor affect the face and scalp.8 Lesions of EV vary from hypopigmented and pinkish red macules to confluent patches and hyperkeratotic verrucalike lesions.3 Clinical characteristics also may include dyschromic patches; lesions that resemble flat warts on the trunk, face, and distal arms; and/or lesions that appear similar to seborrheic keratoses on the dorsal aspect of the hands.9,10
Mutations of the EVER gene downregulate a cell’s ability to adequately attack the HPV antigens.11 Although some patients with EV are found to have mutations of the EVER1 and EVER2 genes, a notable portion of patients with EV lack these mutations. Three other causes of EV include acquisition of immunosuppressive conditions including lymphoma, solid organ transplant, and human immunodeficiency virus. If one suspects autosomal-recessive inheritance of EV, genetic testing such as polymerase chain reaction DNA fragment analysis can be performed to determine if there are mutations on the EVER1 or EVER2 genes.12
The inability of patients with EV to mount an immune response to multiple types of HPV increases the risk for developing cutaneous malignancies.7 Additionally, it is known that UV radiation diminishes skin cell immunity, and the combination of EV and UV radiation further increases the risk for developing SCCs.11 The development of nonmelanoma skin cancers usually occurs on sun-exposed skin 20 to 30 years after the onset of lesions, with the highest occurrence of SCCs presenting in the fourth decade of life.1
Protection from UV light exposure is critical to reduce the risk for malignancy. Treatment options for EV lesions have included topical imiquimod 5%, 5-fluorouracil, oral isotretinoin, and intralesional interferon alfa, but patients are often refractory to these interventions. Curettage, surgical excision, electrosurgery, and laser ablation can be effective for individual lesions but carry a greater risk for scarring.1 Photodynamic therapy with aminolevulinic acid and blue light represents a promising option that deserves further study.
Epidermodysplasia verruciformis should be considered as a differential diagnosis in all patients presenting with disseminated lesions resembling pityriasis versicolor that are unresponsive to treatment. A biopsy will help to establish the diagnosis. Patients should minimize sun exposure and report any skin lesions that are changing in appearance.
- Hoffner MV, Camacho FM. Surgical treatment of epidermodysplasia verruciformis. Dermatol Surg. 2010;36:363-367.
- McDermott D, Gammon B, Snijders P. Autosomal dominant epidermodysplasia verruciformis lacking a known EVER1 or EVER2 mutation. Pediatr Dermatol. 2009;26:306-310.
- Patel T, Morrison K, Rady P, et al. Epidermodysplasia verruciformis and susceptibility to HPV. Dis Markers. 2010;29:199-206.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:308-311.
- Oliveira W, Netu C, Rady P, et al. Clinical aspects of epidermodysplasia verruciformis. J Eur Acad Dermatol Venereol. 2003;17:394-398.
- Lewandowsky F, Lutz W. Ein Fall einer bisher nicht beschriebenen Hauterkrankung (epidermodysplasia verruciformis). Arch Dermatol Syphilol. 1922;141:193-203.
- Prystowsky S, Herndon J, Freeman R, et al. Epidermodysplasia verruciformis. Am J Dis Child. 1976;130:437-440.
- Kyriakis KP, Terzoudi S, Palamaras I, et al. Pityriasis versicolor prevalence by age and gender. Mycoses. 2006;49:517-518.
- Nuovo G, Ishag M. The histologic spectrum of epidermodysplasia verruciformis. Am J Surg Pathol. 2000;24:1400-1406.
- Jacobelli S, Laude H, Carlotti A, et al. Epidermodysplasia verruciformis in human immunodeficiency virus-infected patients: a marker of human papillomavirus-related disorders not affected by antiretroviral therapy. Arch Dermatol. 2011;147:590-596.
- Rogers HD, MacGregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:316-320.
- Gober MD, Rady PL, He Q, et al. Novel homozygous frameshift mutation of EVER1 gene in an epidermodysplasia verruciformis patient. J Invest Dermatol. 2007;127:817-820.
To the Editor:
Epidermodysplasia verruciformis (EV) is a rare autosomal-recessive genodermatosis characterized by widespread infection with specific strains of human papillomavirus (HPV). Patients with EV have a unique susceptibility to acquire HPV due to defects in cellular immunity to the presenting antigens.1 These defects may be related to mutations of the EVER genes or due to acquisition of an immunosuppressive condition.2,3 Infections with HPV-3 and HPV-10 do not lead to the development of malignancies. However, infection with HPV-5, HPV-8, and HPV-14 can lead to the development of nonmelanoma skin cancers, usually squamous cell carcinomas (SCCs), in approximately 60% of patients.3,4 This viral condition lasts throughout the patient’s lifetime and presents as tinea versicolor–like macules and patches. These lesions may be confused with seborrheic keratosis or verruca plana.5 Lesions typically are hypopigmented but occasionally may be hyperpigmented or erythematous. They often are found on the trunk, but lesions on the face, arms, palms, legs, and soles have been reported.5 Mucous membranes are always spared. Epidermodysplasia verruciformis often presents in childhood, except in cases related to acquired immunosuppression. The condition has no sex or racial predilection and no geographical preference.5
A 7-year-old boy (Fitzpatrick skin type V) presented with an asymptomatic rash on the trunk (Figure 1), dorsal aspect of the hands, and forehead. The lesions first appeared 5 years prior on the upper back and upper chest and had recently spread to the forehead and frontal aspect of the scalp. The patient had a history of myelomeningocele, which was corrected at birth with surgical placement of a ventriculoperitoneal shunt. The patient was otherwise healthy and met all appropriate developmental milestones for his age group. Family history revealed consanguinity of the patient’s paternal grandparents who were first cousins. The patient’s mother denied any other family member having similar rashes or lesions.
The patient had been treated for pityriasis versicolor on and off for 2 years by another dermatologist. His mother reported faithfully applying ketoconazole cream twice daily for several months with no improvement. She also reported using topical steroids, which did not provide any benefit. The patient and mother denied any associated pruritus, bleeding, burning, or physical discomfort.
Skin examination revealed diffuse, flat, polymorphous, hypopigmented and salmon-colored hyperkeratotic macules and patches with mild scaling on the upper region of the anterior aspect of the chest and upper back (Figure 2A). Additionally, the patient had an extensive number of lesions on the forehead and frontal aspect of the scalp (Figure 2B).
A shave biopsy demonstrated a thick basket weave stratum corneum, koilocytes, and large pale keratinocytes with characteristic blue cytoplasm. These findings were characteristic for EV.
At the patient’s 3-month follow-up visit, he again denied any symptoms associated with the lesions and reported that the appearance was diminishing in severity. On examination there was no evidence of SCC. The mother was advised to discontinue all topical treatments for the patient and return to the office every 3 to 6 months for regular skin surveillance. The mother was further advised to protect the patient from UV radiation with sunscreen and sun-protective clothing.
Epidermodysplasia verruciformis was first reported by Lewandowsky and Lutz6 in 1922. This rare condition often presents in childhood and is characterized by a persistent HPV infection and an autosomal-recessive inheritance pattern. Reports in the literature frequently involve kindreds. Often, patients with EV have a family history of first-degree or second-degree consanguinity.7
The clinical presentation of EV often resembles a pityriasis versicolor–like eruption. However, pityriasis versicolor is less commonly seen in childhood and is more prevalent in patients aged 21 to 30 years, likely due to increased sebum production and changing hormone levels. Furthermore, it is unusual to see pityriasis versicolor affect the face and scalp.8 Lesions of EV vary from hypopigmented and pinkish red macules to confluent patches and hyperkeratotic verrucalike lesions.3 Clinical characteristics also may include dyschromic patches; lesions that resemble flat warts on the trunk, face, and distal arms; and/or lesions that appear similar to seborrheic keratoses on the dorsal aspect of the hands.9,10
Mutations of the EVER gene downregulate a cell’s ability to adequately attack the HPV antigens.11 Although some patients with EV are found to have mutations of the EVER1 and EVER2 genes, a notable portion of patients with EV lack these mutations. Three other causes of EV include acquisition of immunosuppressive conditions including lymphoma, solid organ transplant, and human immunodeficiency virus. If one suspects autosomal-recessive inheritance of EV, genetic testing such as polymerase chain reaction DNA fragment analysis can be performed to determine if there are mutations on the EVER1 or EVER2 genes.12
The inability of patients with EV to mount an immune response to multiple types of HPV increases the risk for developing cutaneous malignancies.7 Additionally, it is known that UV radiation diminishes skin cell immunity, and the combination of EV and UV radiation further increases the risk for developing SCCs.11 The development of nonmelanoma skin cancers usually occurs on sun-exposed skin 20 to 30 years after the onset of lesions, with the highest occurrence of SCCs presenting in the fourth decade of life.1
Protection from UV light exposure is critical to reduce the risk for malignancy. Treatment options for EV lesions have included topical imiquimod 5%, 5-fluorouracil, oral isotretinoin, and intralesional interferon alfa, but patients are often refractory to these interventions. Curettage, surgical excision, electrosurgery, and laser ablation can be effective for individual lesions but carry a greater risk for scarring.1 Photodynamic therapy with aminolevulinic acid and blue light represents a promising option that deserves further study.
Epidermodysplasia verruciformis should be considered as a differential diagnosis in all patients presenting with disseminated lesions resembling pityriasis versicolor that are unresponsive to treatment. A biopsy will help to establish the diagnosis. Patients should minimize sun exposure and report any skin lesions that are changing in appearance.
To the Editor:
Epidermodysplasia verruciformis (EV) is a rare autosomal-recessive genodermatosis characterized by widespread infection with specific strains of human papillomavirus (HPV). Patients with EV have a unique susceptibility to acquire HPV due to defects in cellular immunity to the presenting antigens.1 These defects may be related to mutations of the EVER genes or due to acquisition of an immunosuppressive condition.2,3 Infections with HPV-3 and HPV-10 do not lead to the development of malignancies. However, infection with HPV-5, HPV-8, and HPV-14 can lead to the development of nonmelanoma skin cancers, usually squamous cell carcinomas (SCCs), in approximately 60% of patients.3,4 This viral condition lasts throughout the patient’s lifetime and presents as tinea versicolor–like macules and patches. These lesions may be confused with seborrheic keratosis or verruca plana.5 Lesions typically are hypopigmented but occasionally may be hyperpigmented or erythematous. They often are found on the trunk, but lesions on the face, arms, palms, legs, and soles have been reported.5 Mucous membranes are always spared. Epidermodysplasia verruciformis often presents in childhood, except in cases related to acquired immunosuppression. The condition has no sex or racial predilection and no geographical preference.5
A 7-year-old boy (Fitzpatrick skin type V) presented with an asymptomatic rash on the trunk (Figure 1), dorsal aspect of the hands, and forehead. The lesions first appeared 5 years prior on the upper back and upper chest and had recently spread to the forehead and frontal aspect of the scalp. The patient had a history of myelomeningocele, which was corrected at birth with surgical placement of a ventriculoperitoneal shunt. The patient was otherwise healthy and met all appropriate developmental milestones for his age group. Family history revealed consanguinity of the patient’s paternal grandparents who were first cousins. The patient’s mother denied any other family member having similar rashes or lesions.
The patient had been treated for pityriasis versicolor on and off for 2 years by another dermatologist. His mother reported faithfully applying ketoconazole cream twice daily for several months with no improvement. She also reported using topical steroids, which did not provide any benefit. The patient and mother denied any associated pruritus, bleeding, burning, or physical discomfort.
Skin examination revealed diffuse, flat, polymorphous, hypopigmented and salmon-colored hyperkeratotic macules and patches with mild scaling on the upper region of the anterior aspect of the chest and upper back (Figure 2A). Additionally, the patient had an extensive number of lesions on the forehead and frontal aspect of the scalp (Figure 2B).
A shave biopsy demonstrated a thick basket weave stratum corneum, koilocytes, and large pale keratinocytes with characteristic blue cytoplasm. These findings were characteristic for EV.
At the patient’s 3-month follow-up visit, he again denied any symptoms associated with the lesions and reported that the appearance was diminishing in severity. On examination there was no evidence of SCC. The mother was advised to discontinue all topical treatments for the patient and return to the office every 3 to 6 months for regular skin surveillance. The mother was further advised to protect the patient from UV radiation with sunscreen and sun-protective clothing.
Epidermodysplasia verruciformis was first reported by Lewandowsky and Lutz6 in 1922. This rare condition often presents in childhood and is characterized by a persistent HPV infection and an autosomal-recessive inheritance pattern. Reports in the literature frequently involve kindreds. Often, patients with EV have a family history of first-degree or second-degree consanguinity.7
The clinical presentation of EV often resembles a pityriasis versicolor–like eruption. However, pityriasis versicolor is less commonly seen in childhood and is more prevalent in patients aged 21 to 30 years, likely due to increased sebum production and changing hormone levels. Furthermore, it is unusual to see pityriasis versicolor affect the face and scalp.8 Lesions of EV vary from hypopigmented and pinkish red macules to confluent patches and hyperkeratotic verrucalike lesions.3 Clinical characteristics also may include dyschromic patches; lesions that resemble flat warts on the trunk, face, and distal arms; and/or lesions that appear similar to seborrheic keratoses on the dorsal aspect of the hands.9,10
Mutations of the EVER gene downregulate a cell’s ability to adequately attack the HPV antigens.11 Although some patients with EV are found to have mutations of the EVER1 and EVER2 genes, a notable portion of patients with EV lack these mutations. Three other causes of EV include acquisition of immunosuppressive conditions including lymphoma, solid organ transplant, and human immunodeficiency virus. If one suspects autosomal-recessive inheritance of EV, genetic testing such as polymerase chain reaction DNA fragment analysis can be performed to determine if there are mutations on the EVER1 or EVER2 genes.12
The inability of patients with EV to mount an immune response to multiple types of HPV increases the risk for developing cutaneous malignancies.7 Additionally, it is known that UV radiation diminishes skin cell immunity, and the combination of EV and UV radiation further increases the risk for developing SCCs.11 The development of nonmelanoma skin cancers usually occurs on sun-exposed skin 20 to 30 years after the onset of lesions, with the highest occurrence of SCCs presenting in the fourth decade of life.1
Protection from UV light exposure is critical to reduce the risk for malignancy. Treatment options for EV lesions have included topical imiquimod 5%, 5-fluorouracil, oral isotretinoin, and intralesional interferon alfa, but patients are often refractory to these interventions. Curettage, surgical excision, electrosurgery, and laser ablation can be effective for individual lesions but carry a greater risk for scarring.1 Photodynamic therapy with aminolevulinic acid and blue light represents a promising option that deserves further study.
Epidermodysplasia verruciformis should be considered as a differential diagnosis in all patients presenting with disseminated lesions resembling pityriasis versicolor that are unresponsive to treatment. A biopsy will help to establish the diagnosis. Patients should minimize sun exposure and report any skin lesions that are changing in appearance.
- Hoffner MV, Camacho FM. Surgical treatment of epidermodysplasia verruciformis. Dermatol Surg. 2010;36:363-367.
- McDermott D, Gammon B, Snijders P. Autosomal dominant epidermodysplasia verruciformis lacking a known EVER1 or EVER2 mutation. Pediatr Dermatol. 2009;26:306-310.
- Patel T, Morrison K, Rady P, et al. Epidermodysplasia verruciformis and susceptibility to HPV. Dis Markers. 2010;29:199-206.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:308-311.
- Oliveira W, Netu C, Rady P, et al. Clinical aspects of epidermodysplasia verruciformis. J Eur Acad Dermatol Venereol. 2003;17:394-398.
- Lewandowsky F, Lutz W. Ein Fall einer bisher nicht beschriebenen Hauterkrankung (epidermodysplasia verruciformis). Arch Dermatol Syphilol. 1922;141:193-203.
- Prystowsky S, Herndon J, Freeman R, et al. Epidermodysplasia verruciformis. Am J Dis Child. 1976;130:437-440.
- Kyriakis KP, Terzoudi S, Palamaras I, et al. Pityriasis versicolor prevalence by age and gender. Mycoses. 2006;49:517-518.
- Nuovo G, Ishag M. The histologic spectrum of epidermodysplasia verruciformis. Am J Surg Pathol. 2000;24:1400-1406.
- Jacobelli S, Laude H, Carlotti A, et al. Epidermodysplasia verruciformis in human immunodeficiency virus-infected patients: a marker of human papillomavirus-related disorders not affected by antiretroviral therapy. Arch Dermatol. 2011;147:590-596.
- Rogers HD, MacGregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:316-320.
- Gober MD, Rady PL, He Q, et al. Novel homozygous frameshift mutation of EVER1 gene in an epidermodysplasia verruciformis patient. J Invest Dermatol. 2007;127:817-820.
- Hoffner MV, Camacho FM. Surgical treatment of epidermodysplasia verruciformis. Dermatol Surg. 2010;36:363-367.
- McDermott D, Gammon B, Snijders P. Autosomal dominant epidermodysplasia verruciformis lacking a known EVER1 or EVER2 mutation. Pediatr Dermatol. 2009;26:306-310.
- Patel T, Morrison K, Rady P, et al. Epidermodysplasia verruciformis and susceptibility to HPV. Dis Markers. 2010;29:199-206.
- Hultgren TL, Srinivasan SK, DiMaio DJ. Epidermodysplasia verruciformis occurring in a patient with human immunodeficiency virus: a case report. Cutis. 2007;79:308-311.
- Oliveira W, Netu C, Rady P, et al. Clinical aspects of epidermodysplasia verruciformis. J Eur Acad Dermatol Venereol. 2003;17:394-398.
- Lewandowsky F, Lutz W. Ein Fall einer bisher nicht beschriebenen Hauterkrankung (epidermodysplasia verruciformis). Arch Dermatol Syphilol. 1922;141:193-203.
- Prystowsky S, Herndon J, Freeman R, et al. Epidermodysplasia verruciformis. Am J Dis Child. 1976;130:437-440.
- Kyriakis KP, Terzoudi S, Palamaras I, et al. Pityriasis versicolor prevalence by age and gender. Mycoses. 2006;49:517-518.
- Nuovo G, Ishag M. The histologic spectrum of epidermodysplasia verruciformis. Am J Surg Pathol. 2000;24:1400-1406.
- Jacobelli S, Laude H, Carlotti A, et al. Epidermodysplasia verruciformis in human immunodeficiency virus-infected patients: a marker of human papillomavirus-related disorders not affected by antiretroviral therapy. Arch Dermatol. 2011;147:590-596.
- Rogers HD, MacGregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:316-320.
- Gober MD, Rady PL, He Q, et al. Novel homozygous frameshift mutation of EVER1 gene in an epidermodysplasia verruciformis patient. J Invest Dermatol. 2007;127:817-820.
Practice Points
- Epidermodysplasia verruciformis (EV) is a rare genodermatosis that usually presents in early childhood and presents as verrucous papules and plaques most commonly on the skin of the head, neck, and upper extremities. It often is misdiagnosed at pityriasis versicolor.
- Mutations of the EVER1 and EVER2 genes have been identified as a source for developing EV.
- Epidermodysplasia verruciformis produces wartlike lesions in individuals who have a unique susceptibility to acquiring the human papillomavirus and early onset of nonmelanoma skin cancers, most commonly squamous cell carcinomas related to viral oncogenesis.
- Avoidance and protection from UV exposure is a critical component of treatment plans for patients with EV.

Limit primary site radiation, but not craniospinal dose in medulloblastoma
BOSTON – For children with average-risk medulloblastoma, it is safe to limit the radiation boost to the posterior fossa, but reducing doses to the craniospinal axis results in worse outcomes among younger children, and is not advisable, according to results from the largest trial conducted in this population.
There were no significant differences in either 5-year event-free survival (EFS) or overall survival (OS) between children who received an involved field radiation therapy boost (boost to the tumor bed only) or a standard volume boost (to the whole posterior fossa) in a phase III randomized trial, reported lead author Jeff M. Michalski, MD, MBA, FASTRO, professor of radiation oncology at Washington University, St. Louis.
“We conclude that the survival rates and event-free survival rates following reduced boost volumes were comparable to standard radiation treatment volumes for the primary tumor site. This is the first trial to state definitively that there is no survival difference between these two approaches,” he said at a briefing following his presentation of the data in an oral abstract session at the annual meeting of the American Society for Radiation Oncology.
“However, the reduced craniospinal axis irradiation was associated with a higher event rate and worse survival. We believe that physicians can adopt smaller boost volumes to the posterior fossa in children with average-risk medulloblastoma, average risk being no evidence of spread at the time of diagnosis and near-complete or complete resection. But for all children, the standard of 23.4 Gy remains necessary to retain high-level tumor control,” he added.
Aggressive malignancy
Medulloblastoma, an aggressive tumor with the propensity to spread from the lower brain to the upper brain and spine, is the most common brain malignancy in children. The current standard of care for children with average-risk disease is surgical resection followed by systemic chemotherapy followed by irradiation to both the posterior fossa and to the craniospinal axis.
“Unfortunately, this strategy has significant negative consequences for the patients’ neurocognitive abilities, endocrine function, and hearing,” Dr. Michalski said.
The Children’s Oncology Group ACNS0331 trial was designed to determine whether reducing the volume of the boost from the whole posterior to the tumor bed only would compromise EFS and OS, and whether reducing the dose to the craniospinal axis from the current 23.4 Gy to 18 Gy in children aged 3-7 years would compromise survival measures.
The trial had two randomizations, both at the time of study enrollment. In the first, children from the ages of 3 to 7 years were randomly assigned to either low-dose craniospinal irradiation (18 Gy, 116 children) or to the standard dose (23.4 Gy, 110 children). All children aged 8 and older were assigned to receive the standard dose.
For the second randomization, all children were randomly allocated to either involved field RT boost or to standard volume boost to the whole posterior fossa.
Following radiation, all children were assigned to nine cycles of maintenance chemotherapy.
At a median follow-up of 6.6 years, 5-year EFS estimates for the primary site irradiation endpoint were 82.2% for 227 patients who received the involved-field radiation, compared with 80.8% for 237 patients who received whole posterior fossa irradiation.
Respective 5-year OS estimates were 84.1% and 85.2%. The upper limit of the hazard ratio confidence interval (CI) for the involved field therapy was lower than the prespecified limit, indicating that involved-field radiation was noninferior.
For the endpoint of low- vs. standard-dose craniospinal irradiation, the 5-year EFS estimates were 72.1% and 82.6%, respectively. The upper limit of the hazard ratio CI exceeded the prespecified limit, indicating that EFS was worse with the low-dose strategy.
Similarly, respective 5-year OS estimates were 78.1% and 85.9%, with the upper limit of the CI also higher than the prespecified upper limit.
When the investigators looked at the patterns of failure among the children in the two randomizations, they saw that there was no significant difference in the rate of isolated local failure between the involved-field or whole posterior fossa groups, or between the low-dose or high-dose craniospinal irradiation groups.
The finding that radiation volume to the primary site can be reduced is likely to be practice changing, said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
However, the worse survival with the low-dose craniospinal radiation “leaves the COG investigators with the challenge to explore other avenues for reducing toxicity of craniospinal irradiation,” she said.
BOSTON – For children with average-risk medulloblastoma, it is safe to limit the radiation boost to the posterior fossa, but reducing doses to the craniospinal axis results in worse outcomes among younger children, and is not advisable, according to results from the largest trial conducted in this population.
There were no significant differences in either 5-year event-free survival (EFS) or overall survival (OS) between children who received an involved field radiation therapy boost (boost to the tumor bed only) or a standard volume boost (to the whole posterior fossa) in a phase III randomized trial, reported lead author Jeff M. Michalski, MD, MBA, FASTRO, professor of radiation oncology at Washington University, St. Louis.
“We conclude that the survival rates and event-free survival rates following reduced boost volumes were comparable to standard radiation treatment volumes for the primary tumor site. This is the first trial to state definitively that there is no survival difference between these two approaches,” he said at a briefing following his presentation of the data in an oral abstract session at the annual meeting of the American Society for Radiation Oncology.
“However, the reduced craniospinal axis irradiation was associated with a higher event rate and worse survival. We believe that physicians can adopt smaller boost volumes to the posterior fossa in children with average-risk medulloblastoma, average risk being no evidence of spread at the time of diagnosis and near-complete or complete resection. But for all children, the standard of 23.4 Gy remains necessary to retain high-level tumor control,” he added.
Aggressive malignancy
Medulloblastoma, an aggressive tumor with the propensity to spread from the lower brain to the upper brain and spine, is the most common brain malignancy in children. The current standard of care for children with average-risk disease is surgical resection followed by systemic chemotherapy followed by irradiation to both the posterior fossa and to the craniospinal axis.
“Unfortunately, this strategy has significant negative consequences for the patients’ neurocognitive abilities, endocrine function, and hearing,” Dr. Michalski said.
The Children’s Oncology Group ACNS0331 trial was designed to determine whether reducing the volume of the boost from the whole posterior to the tumor bed only would compromise EFS and OS, and whether reducing the dose to the craniospinal axis from the current 23.4 Gy to 18 Gy in children aged 3-7 years would compromise survival measures.
The trial had two randomizations, both at the time of study enrollment. In the first, children from the ages of 3 to 7 years were randomly assigned to either low-dose craniospinal irradiation (18 Gy, 116 children) or to the standard dose (23.4 Gy, 110 children). All children aged 8 and older were assigned to receive the standard dose.
For the second randomization, all children were randomly allocated to either involved field RT boost or to standard volume boost to the whole posterior fossa.
Following radiation, all children were assigned to nine cycles of maintenance chemotherapy.
At a median follow-up of 6.6 years, 5-year EFS estimates for the primary site irradiation endpoint were 82.2% for 227 patients who received the involved-field radiation, compared with 80.8% for 237 patients who received whole posterior fossa irradiation.
Respective 5-year OS estimates were 84.1% and 85.2%. The upper limit of the hazard ratio confidence interval (CI) for the involved field therapy was lower than the prespecified limit, indicating that involved-field radiation was noninferior.
For the endpoint of low- vs. standard-dose craniospinal irradiation, the 5-year EFS estimates were 72.1% and 82.6%, respectively. The upper limit of the hazard ratio CI exceeded the prespecified limit, indicating that EFS was worse with the low-dose strategy.
Similarly, respective 5-year OS estimates were 78.1% and 85.9%, with the upper limit of the CI also higher than the prespecified upper limit.
When the investigators looked at the patterns of failure among the children in the two randomizations, they saw that there was no significant difference in the rate of isolated local failure between the involved-field or whole posterior fossa groups, or between the low-dose or high-dose craniospinal irradiation groups.
The finding that radiation volume to the primary site can be reduced is likely to be practice changing, said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
However, the worse survival with the low-dose craniospinal radiation “leaves the COG investigators with the challenge to explore other avenues for reducing toxicity of craniospinal irradiation,” she said.
BOSTON – For children with average-risk medulloblastoma, it is safe to limit the radiation boost to the posterior fossa, but reducing doses to the craniospinal axis results in worse outcomes among younger children, and is not advisable, according to results from the largest trial conducted in this population.
There were no significant differences in either 5-year event-free survival (EFS) or overall survival (OS) between children who received an involved field radiation therapy boost (boost to the tumor bed only) or a standard volume boost (to the whole posterior fossa) in a phase III randomized trial, reported lead author Jeff M. Michalski, MD, MBA, FASTRO, professor of radiation oncology at Washington University, St. Louis.
“We conclude that the survival rates and event-free survival rates following reduced boost volumes were comparable to standard radiation treatment volumes for the primary tumor site. This is the first trial to state definitively that there is no survival difference between these two approaches,” he said at a briefing following his presentation of the data in an oral abstract session at the annual meeting of the American Society for Radiation Oncology.
“However, the reduced craniospinal axis irradiation was associated with a higher event rate and worse survival. We believe that physicians can adopt smaller boost volumes to the posterior fossa in children with average-risk medulloblastoma, average risk being no evidence of spread at the time of diagnosis and near-complete or complete resection. But for all children, the standard of 23.4 Gy remains necessary to retain high-level tumor control,” he added.
Aggressive malignancy
Medulloblastoma, an aggressive tumor with the propensity to spread from the lower brain to the upper brain and spine, is the most common brain malignancy in children. The current standard of care for children with average-risk disease is surgical resection followed by systemic chemotherapy followed by irradiation to both the posterior fossa and to the craniospinal axis.
“Unfortunately, this strategy has significant negative consequences for the patients’ neurocognitive abilities, endocrine function, and hearing,” Dr. Michalski said.
The Children’s Oncology Group ACNS0331 trial was designed to determine whether reducing the volume of the boost from the whole posterior to the tumor bed only would compromise EFS and OS, and whether reducing the dose to the craniospinal axis from the current 23.4 Gy to 18 Gy in children aged 3-7 years would compromise survival measures.
The trial had two randomizations, both at the time of study enrollment. In the first, children from the ages of 3 to 7 years were randomly assigned to either low-dose craniospinal irradiation (18 Gy, 116 children) or to the standard dose (23.4 Gy, 110 children). All children aged 8 and older were assigned to receive the standard dose.
For the second randomization, all children were randomly allocated to either involved field RT boost or to standard volume boost to the whole posterior fossa.
Following radiation, all children were assigned to nine cycles of maintenance chemotherapy.
At a median follow-up of 6.6 years, 5-year EFS estimates for the primary site irradiation endpoint were 82.2% for 227 patients who received the involved-field radiation, compared with 80.8% for 237 patients who received whole posterior fossa irradiation.
Respective 5-year OS estimates were 84.1% and 85.2%. The upper limit of the hazard ratio confidence interval (CI) for the involved field therapy was lower than the prespecified limit, indicating that involved-field radiation was noninferior.
For the endpoint of low- vs. standard-dose craniospinal irradiation, the 5-year EFS estimates were 72.1% and 82.6%, respectively. The upper limit of the hazard ratio CI exceeded the prespecified limit, indicating that EFS was worse with the low-dose strategy.
Similarly, respective 5-year OS estimates were 78.1% and 85.9%, with the upper limit of the CI also higher than the prespecified upper limit.
When the investigators looked at the patterns of failure among the children in the two randomizations, they saw that there was no significant difference in the rate of isolated local failure between the involved-field or whole posterior fossa groups, or between the low-dose or high-dose craniospinal irradiation groups.
The finding that radiation volume to the primary site can be reduced is likely to be practice changing, said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
However, the worse survival with the low-dose craniospinal radiation “leaves the COG investigators with the challenge to explore other avenues for reducing toxicity of craniospinal irradiation,” she said.
Key clinical point: Primary site irradiation in children with medulloblastoma can be limited to the tumor bed rather than the whole posterior fossa.
Major finding: There were no differences in EFS or OS when radiation was limited to the tumor bed, but reduced dose to the craniospinal axis was associated with worse survival.
Data source: Randomized phase III trial of 690 children with average-risk medulloblastoma.
Disclosures: The National Cancer Institute funded the study. Dr. Michalski and Dr. Jacobson reported no relevant conflicts of interest.
Teen birth rates continue to decline in the United States
The teen birth rate of 22.3/1,000 females aged 15-19 years for 2015 was down by almost 8% from the year before and marks the seventh consecutive year of historic lows. Since 1991, when 61.8/1,000 teens aged 15-19 gave birth, the rate has fallen 64%, the NCHS reported.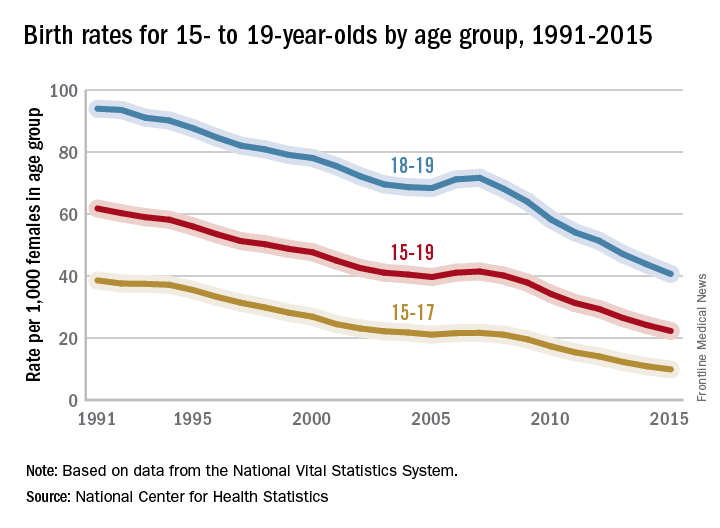
For teens aged 15-19 years, the birth rate declined for each race/ethnicity: dropping 8% for non-Hispanic whites and Hispanics, 9% for non-Hispanic blacks, 10% for Asians or Pacific Islanders, and 6% for American Indians or Alaska Natives. All rates for 2015 were historically low.
The teen birth rate of 22.3/1,000 females aged 15-19 years for 2015 was down by almost 8% from the year before and marks the seventh consecutive year of historic lows. Since 1991, when 61.8/1,000 teens aged 15-19 gave birth, the rate has fallen 64%, the NCHS reported.
For teens aged 15-19 years, the birth rate declined for each race/ethnicity: dropping 8% for non-Hispanic whites and Hispanics, 9% for non-Hispanic blacks, 10% for Asians or Pacific Islanders, and 6% for American Indians or Alaska Natives. All rates for 2015 were historically low.
The teen birth rate of 22.3/1,000 females aged 15-19 years for 2015 was down by almost 8% from the year before and marks the seventh consecutive year of historic lows. Since 1991, when 61.8/1,000 teens aged 15-19 gave birth, the rate has fallen 64%, the NCHS reported.
For teens aged 15-19 years, the birth rate declined for each race/ethnicity: dropping 8% for non-Hispanic whites and Hispanics, 9% for non-Hispanic blacks, 10% for Asians or Pacific Islanders, and 6% for American Indians or Alaska Natives. All rates for 2015 were historically low.
Registry, multisite care, bundled vaccines improve HPV vaccination rate among teens
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
FROM PEDIATRICS
Key clinical point:
Major finding: In 2014, the national average of adolescents receiving three or more doses of the HPV vaccine was 40% for girls and 22% for boys. At Denver Health, those rates were 67% and 60%, respectively.
Data source: A retrospective study of 11,463 adolescent patients.
Disclosures: This study received no external funding, and the researchers had no relevant disclosures to report.
Most children with JIA get different diagnosis as adults
Two-thirds of children diagnosed with juvenile idiopathic arthritis are classified later as having a different form of arthritis as adults, with 72% of them requiring disease-modifying medication and 13% forced into retirement, according to a cross-sectional analysis of a registry database.
But among patients with inactive disease, more than one-third are off medication, and the majority have either no or very mild disabilities, reported Filipa Oliveira-Ramos, MD, of Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Lisbon, and her colleagues (RMD Open 2016;2:e000304. doi: 10.1136/rmdopen-2016-000304).
The team used data from the Rheumatic Diseases Portuguese Register database to discern how rheumatic disease classifications evolve as people with JIA grow into adulthood. The analysis comprised 426 patients and examined fulfillment of adult classification criteria, function as assessed by the Health Assessment Questionnaire (HAQ), clinical disease characteristics as assessed by the Juvenile Arthritis Damage Index–articular (JADI-A) and Juvenile Arthritis Damage Index–extra-articular (JADI-E), and disease activity.
The patients were a mean of 34 years old at the time of the last visit entered into the database. The patients’ mean disease duration was 22.5 years, including 80% with at least 10 years and 24% with more than 30 years.
All had been diagnosed with JIA, at a mean age of about 10 years. Disease categories were persistent oligoarthritis (19%), extended oligoarthritis (14%), rheumatoid factor–positive polyarthritis (17%), rheumatoid factor–negative polyarthritis (18%), systemic disease (10%), enthesitis-related arthritis (19%), psoriatic arthritis (3%), and undifferentiated arthritis (1%).
A total of 72% of patients were still employed, although 13% had retired because of disease-related disability. Most (67%) still had active disease, and 72% were taking a disease-modifying antirheumatic drug.
JIA had evolved into numerous new diagnoses, the team observed. Most patients with systemic-onset JIA (92%) were classified as having adult Still’s disease – more than half (58%) with persistent systemic features and about 42% with predominately polyarticular involvement.
The majority of patients with RF-positive polyarthritis (96%) and of those with RF-negative polyarthritis as children (57%) fulfilled the adult criteria for rheumatoid arthritis.
Patients who had persistent oligoarthritis as children were, as adults, most likely be classified with spondyloarthritis (35%), although 59% remained unclassifiable.
Most of the patients with extended oligoarthritis as children were later classified as having either rheumatoid arthritis (39%) or spondyloarthritis (26%). Most patients with juvenile enthesitis-related arthritis were also reclassified as having spondyloarthritis (95%).
All of those with childhood psoriatic arthritis retained that classification as adults.
A smaller portion of patients (21%) were unclassified as adults, the investigators said. Most of these patients had RF-negative polyarticular or oligoarticular classifications as children.
In a series of multivariate analyses, the team found a number of significant associations with adult outcomes. After adjustment for International League of Associations for Rheumatology (ILAR) category, inactive adult disease was associated with shorter disease duration, less delay in diagnosis, a lower HAQ score, and less exposure to corticosteroids. A higher HAQ score was associated with a longer disease duration and exposure to biologics, while a lower HAQ was associated with the persistence of systemic disease features.
Higher JADI-A scores were associated with disability-related retirement, longer disease duration, and past or current use of biologics.
Another series of multivariate models assessed outcomes associated with inactive disease. Patients who were older at disease onset were more likely to have inactive disease as adults. A positive test for anticitrullinated protein antibodies decreased the likelihood of disease inactivity by 93%.
Finally, the investigators evaluated associations with function and clinical characteristics. Younger age at disease onset was associated with higher HAQ and JADI scores in adulthood. Patients with RF-positive polyarthritis and systemic-onset JIA were more likely to have worse JADI-A and JADI-E scores, compared with patients who had persistent oligoarthritis. Corticosteroid exposure was also predictive of worse extra-articular scores on the JADI.
“Understanding the way these juvenile diseases progress could add useful information for the ongoing discussion of a new classification capable of better unifying the language between pediatric and adult care,” the authors concluded.
None of the authors had financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
This is an important article in that it highlights one of the fundamental flaws of the juvenile idiopathic arthritis classification.
The manifestations of the rheumatic diseases often evolve over time. There may be psoriasis before arthritis, but there also may be arthritis before psoriasis. Similarly, children with an ultimate diagnosis of Crohn’s disease may first present to the rheumatologist with arthritis.
The definition of JIA requires only the onset of arthritis lasting more than 3 weeks before 16 years of age with the exclusion of other obvious cause. A careful reading of the subclassification criteria quickly reveals that many children are “unclassifiable” because of family history or other factors.
The present study makes it clear that by the time they reach adulthood, a significant number of individuals who were told they had JIA will, in fact, meet criteria for a different classification. This would be of only casual interest were it not for the fact that these children will have previously been entered into databases about the natural history of JIA with erroneous classifications.
More worrisome is that fact that some will have been included in therapeutic trials with erroneous classifications as well. The pediatric rheumatology community would do well to recognize the urgent need for a reassessment of the classification criteria and nomenclature to better reflect the diversity of causes of childhood arthritis.
Thomas Lehman, MD, is chief of pediatric rheumatology at the Hospital for Special Surgery, New York. He has no relevant disclosures.
This is an important article in that it highlights one of the fundamental flaws of the juvenile idiopathic arthritis classification.
The manifestations of the rheumatic diseases often evolve over time. There may be psoriasis before arthritis, but there also may be arthritis before psoriasis. Similarly, children with an ultimate diagnosis of Crohn’s disease may first present to the rheumatologist with arthritis.
The definition of JIA requires only the onset of arthritis lasting more than 3 weeks before 16 years of age with the exclusion of other obvious cause. A careful reading of the subclassification criteria quickly reveals that many children are “unclassifiable” because of family history or other factors.
The present study makes it clear that by the time they reach adulthood, a significant number of individuals who were told they had JIA will, in fact, meet criteria for a different classification. This would be of only casual interest were it not for the fact that these children will have previously been entered into databases about the natural history of JIA with erroneous classifications.
More worrisome is that fact that some will have been included in therapeutic trials with erroneous classifications as well. The pediatric rheumatology community would do well to recognize the urgent need for a reassessment of the classification criteria and nomenclature to better reflect the diversity of causes of childhood arthritis.
Thomas Lehman, MD, is chief of pediatric rheumatology at the Hospital for Special Surgery, New York. He has no relevant disclosures.
This is an important article in that it highlights one of the fundamental flaws of the juvenile idiopathic arthritis classification.
The manifestations of the rheumatic diseases often evolve over time. There may be psoriasis before arthritis, but there also may be arthritis before psoriasis. Similarly, children with an ultimate diagnosis of Crohn’s disease may first present to the rheumatologist with arthritis.
The definition of JIA requires only the onset of arthritis lasting more than 3 weeks before 16 years of age with the exclusion of other obvious cause. A careful reading of the subclassification criteria quickly reveals that many children are “unclassifiable” because of family history or other factors.
The present study makes it clear that by the time they reach adulthood, a significant number of individuals who were told they had JIA will, in fact, meet criteria for a different classification. This would be of only casual interest were it not for the fact that these children will have previously been entered into databases about the natural history of JIA with erroneous classifications.
More worrisome is that fact that some will have been included in therapeutic trials with erroneous classifications as well. The pediatric rheumatology community would do well to recognize the urgent need for a reassessment of the classification criteria and nomenclature to better reflect the diversity of causes of childhood arthritis.
Thomas Lehman, MD, is chief of pediatric rheumatology at the Hospital for Special Surgery, New York. He has no relevant disclosures.
Two-thirds of children diagnosed with juvenile idiopathic arthritis are classified later as having a different form of arthritis as adults, with 72% of them requiring disease-modifying medication and 13% forced into retirement, according to a cross-sectional analysis of a registry database.
But among patients with inactive disease, more than one-third are off medication, and the majority have either no or very mild disabilities, reported Filipa Oliveira-Ramos, MD, of Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Lisbon, and her colleagues (RMD Open 2016;2:e000304. doi: 10.1136/rmdopen-2016-000304).
The team used data from the Rheumatic Diseases Portuguese Register database to discern how rheumatic disease classifications evolve as people with JIA grow into adulthood. The analysis comprised 426 patients and examined fulfillment of adult classification criteria, function as assessed by the Health Assessment Questionnaire (HAQ), clinical disease characteristics as assessed by the Juvenile Arthritis Damage Index–articular (JADI-A) and Juvenile Arthritis Damage Index–extra-articular (JADI-E), and disease activity.
The patients were a mean of 34 years old at the time of the last visit entered into the database. The patients’ mean disease duration was 22.5 years, including 80% with at least 10 years and 24% with more than 30 years.
All had been diagnosed with JIA, at a mean age of about 10 years. Disease categories were persistent oligoarthritis (19%), extended oligoarthritis (14%), rheumatoid factor–positive polyarthritis (17%), rheumatoid factor–negative polyarthritis (18%), systemic disease (10%), enthesitis-related arthritis (19%), psoriatic arthritis (3%), and undifferentiated arthritis (1%).
A total of 72% of patients were still employed, although 13% had retired because of disease-related disability. Most (67%) still had active disease, and 72% were taking a disease-modifying antirheumatic drug.
JIA had evolved into numerous new diagnoses, the team observed. Most patients with systemic-onset JIA (92%) were classified as having adult Still’s disease – more than half (58%) with persistent systemic features and about 42% with predominately polyarticular involvement.
The majority of patients with RF-positive polyarthritis (96%) and of those with RF-negative polyarthritis as children (57%) fulfilled the adult criteria for rheumatoid arthritis.
Patients who had persistent oligoarthritis as children were, as adults, most likely be classified with spondyloarthritis (35%), although 59% remained unclassifiable.
Most of the patients with extended oligoarthritis as children were later classified as having either rheumatoid arthritis (39%) or spondyloarthritis (26%). Most patients with juvenile enthesitis-related arthritis were also reclassified as having spondyloarthritis (95%).
All of those with childhood psoriatic arthritis retained that classification as adults.
A smaller portion of patients (21%) were unclassified as adults, the investigators said. Most of these patients had RF-negative polyarticular or oligoarticular classifications as children.
In a series of multivariate analyses, the team found a number of significant associations with adult outcomes. After adjustment for International League of Associations for Rheumatology (ILAR) category, inactive adult disease was associated with shorter disease duration, less delay in diagnosis, a lower HAQ score, and less exposure to corticosteroids. A higher HAQ score was associated with a longer disease duration and exposure to biologics, while a lower HAQ was associated with the persistence of systemic disease features.
Higher JADI-A scores were associated with disability-related retirement, longer disease duration, and past or current use of biologics.
Another series of multivariate models assessed outcomes associated with inactive disease. Patients who were older at disease onset were more likely to have inactive disease as adults. A positive test for anticitrullinated protein antibodies decreased the likelihood of disease inactivity by 93%.
Finally, the investigators evaluated associations with function and clinical characteristics. Younger age at disease onset was associated with higher HAQ and JADI scores in adulthood. Patients with RF-positive polyarthritis and systemic-onset JIA were more likely to have worse JADI-A and JADI-E scores, compared with patients who had persistent oligoarthritis. Corticosteroid exposure was also predictive of worse extra-articular scores on the JADI.
“Understanding the way these juvenile diseases progress could add useful information for the ongoing discussion of a new classification capable of better unifying the language between pediatric and adult care,” the authors concluded.
None of the authors had financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
Two-thirds of children diagnosed with juvenile idiopathic arthritis are classified later as having a different form of arthritis as adults, with 72% of them requiring disease-modifying medication and 13% forced into retirement, according to a cross-sectional analysis of a registry database.
But among patients with inactive disease, more than one-third are off medication, and the majority have either no or very mild disabilities, reported Filipa Oliveira-Ramos, MD, of Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Lisbon, and her colleagues (RMD Open 2016;2:e000304. doi: 10.1136/rmdopen-2016-000304).
The team used data from the Rheumatic Diseases Portuguese Register database to discern how rheumatic disease classifications evolve as people with JIA grow into adulthood. The analysis comprised 426 patients and examined fulfillment of adult classification criteria, function as assessed by the Health Assessment Questionnaire (HAQ), clinical disease characteristics as assessed by the Juvenile Arthritis Damage Index–articular (JADI-A) and Juvenile Arthritis Damage Index–extra-articular (JADI-E), and disease activity.
The patients were a mean of 34 years old at the time of the last visit entered into the database. The patients’ mean disease duration was 22.5 years, including 80% with at least 10 years and 24% with more than 30 years.
All had been diagnosed with JIA, at a mean age of about 10 years. Disease categories were persistent oligoarthritis (19%), extended oligoarthritis (14%), rheumatoid factor–positive polyarthritis (17%), rheumatoid factor–negative polyarthritis (18%), systemic disease (10%), enthesitis-related arthritis (19%), psoriatic arthritis (3%), and undifferentiated arthritis (1%).
A total of 72% of patients were still employed, although 13% had retired because of disease-related disability. Most (67%) still had active disease, and 72% were taking a disease-modifying antirheumatic drug.
JIA had evolved into numerous new diagnoses, the team observed. Most patients with systemic-onset JIA (92%) were classified as having adult Still’s disease – more than half (58%) with persistent systemic features and about 42% with predominately polyarticular involvement.
The majority of patients with RF-positive polyarthritis (96%) and of those with RF-negative polyarthritis as children (57%) fulfilled the adult criteria for rheumatoid arthritis.
Patients who had persistent oligoarthritis as children were, as adults, most likely be classified with spondyloarthritis (35%), although 59% remained unclassifiable.
Most of the patients with extended oligoarthritis as children were later classified as having either rheumatoid arthritis (39%) or spondyloarthritis (26%). Most patients with juvenile enthesitis-related arthritis were also reclassified as having spondyloarthritis (95%).
All of those with childhood psoriatic arthritis retained that classification as adults.
A smaller portion of patients (21%) were unclassified as adults, the investigators said. Most of these patients had RF-negative polyarticular or oligoarticular classifications as children.
In a series of multivariate analyses, the team found a number of significant associations with adult outcomes. After adjustment for International League of Associations for Rheumatology (ILAR) category, inactive adult disease was associated with shorter disease duration, less delay in diagnosis, a lower HAQ score, and less exposure to corticosteroids. A higher HAQ score was associated with a longer disease duration and exposure to biologics, while a lower HAQ was associated with the persistence of systemic disease features.
Higher JADI-A scores were associated with disability-related retirement, longer disease duration, and past or current use of biologics.
Another series of multivariate models assessed outcomes associated with inactive disease. Patients who were older at disease onset were more likely to have inactive disease as adults. A positive test for anticitrullinated protein antibodies decreased the likelihood of disease inactivity by 93%.
Finally, the investigators evaluated associations with function and clinical characteristics. Younger age at disease onset was associated with higher HAQ and JADI scores in adulthood. Patients with RF-positive polyarthritis and systemic-onset JIA were more likely to have worse JADI-A and JADI-E scores, compared with patients who had persistent oligoarthritis. Corticosteroid exposure was also predictive of worse extra-articular scores on the JADI.
“Understanding the way these juvenile diseases progress could add useful information for the ongoing discussion of a new classification capable of better unifying the language between pediatric and adult care,” the authors concluded.
None of the authors had financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
Key clinical point:
Major finding: The childhood diagnosis of JIA is reclassified to another form of arthritis in two-thirds of patients in adulthood.
Data source: The Rheumatic Diseases Portuguese Register.
Disclosures: None of the authors had financial disclosures.
NIH workshop yields youth suicide prevention road map
The National Institutes of Health has released a 10-year road map for optimizing youth suicide prevention efforts.
The abridged version of the final report from a March 2016 NIH Pathways to Prevention Workshop entitled “Advancing Research to Prevent Youth Suicide,” highlights strategies for guiding the next decade of research on youth suicide prevention, Todd D. Little, PhD, from Texas Tech University, Lubbock, and his colleagues reported online Oct. 3.
The article outlines 29 recommendations aimed at improving data systems, enhancing data collection and analysis, and strengthening the research and practice community, and calls on researchers and practitioners to “unite to stop youth suicide in order to circumvent its associated economic cost and devastating pain and suffering” (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1568).
“Adherence to the recommendations summarized herein provides us with a road map to our ultimate goal – eliminating suicide,” the authors concluded.
In an accompanying evidence review, Holly C. Wilcox, PhD, and her colleagues from Johns Hopkins University, Baltimore, identified studies and potentially linkable external data systems with suicide outcomes and concluded that community data systems should be linked to suicide prevention data for the purpose of evaluating and enhancing prevention efforts.
“By integrating data from health care delivery systems, health insurance systems, and other populationwide data sources ... a national health research data infrastructure could be developed,” they wrote, adding that such a “national resource” could facilitate linkage with suicide prevention data (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1281).
During a press telebriefing on the panel’s findings, Dr. Little, who served as panel and workshop chair, stressed that suicide is the second-leading cause of death among youth aged 10 to 24 years, and in young adults aged 25 to 34 years.
“Although these numbers are disheartening, we feel that suicide prevention is possible. New research strategies that embrace the complex factors involved in suicide can be coordinated and are necessary,” he said, adding that “the complexity of suicide prevention must be embraced in order to forge new research strategies,” and that researchers and practitioners must work together and with the larger “policy, practice, and research communities” to promote data sharing and stop youth suicide.
Dr. Little also noted the importance of destigmatizing suicide attempts and suicidal behavior to remove one of the roadblocks to reporting, which in turn will increase the available data for linkage.
The linkage of data from various sources, such as emergency departments, electronic health records, Medicaid, and Medicare, is particularly important for informing future prevention efforts, said panelist Leslie-Ann Byam, project director for the Families First Project at Evidence-Based Associates in Washington.
Continuing to work in the field and to work with young people without having information that encompasses that kind of data leaves practitioners at a disadvantage in terms of planning, she said.
Panelist Kathleen M. Roche, PhD, of George Washington University in Washington, stressed the importance of obtaining data on subpopulations of youth at very elevated risk of suicide, including transgender youth, Latinas, and Native Americans.
The NIH workshop was cosponsored by the NIH Office of Disease Prevention, the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Center for Complementary and Integrative Health. Individual authors were supported by grants from the National Science Foundation; the NIH; the Penn State Quantitative Social Sciences Initiative; the Institute for Measurement, Methodology, Analysis, and Policy at Texas Tech University; and the National Center for Advancing Translational Sciences. Dr. Little reported receiving fees from Yhat Enterprises outside the submitted work. The evidence review was funded by the Agency for Healthcare Research and Quality. The review authors reported having no disclosures.
The National Institutes of Health has released a 10-year road map for optimizing youth suicide prevention efforts.
The abridged version of the final report from a March 2016 NIH Pathways to Prevention Workshop entitled “Advancing Research to Prevent Youth Suicide,” highlights strategies for guiding the next decade of research on youth suicide prevention, Todd D. Little, PhD, from Texas Tech University, Lubbock, and his colleagues reported online Oct. 3.
The article outlines 29 recommendations aimed at improving data systems, enhancing data collection and analysis, and strengthening the research and practice community, and calls on researchers and practitioners to “unite to stop youth suicide in order to circumvent its associated economic cost and devastating pain and suffering” (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1568).
“Adherence to the recommendations summarized herein provides us with a road map to our ultimate goal – eliminating suicide,” the authors concluded.
In an accompanying evidence review, Holly C. Wilcox, PhD, and her colleagues from Johns Hopkins University, Baltimore, identified studies and potentially linkable external data systems with suicide outcomes and concluded that community data systems should be linked to suicide prevention data for the purpose of evaluating and enhancing prevention efforts.
“By integrating data from health care delivery systems, health insurance systems, and other populationwide data sources ... a national health research data infrastructure could be developed,” they wrote, adding that such a “national resource” could facilitate linkage with suicide prevention data (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1281).
During a press telebriefing on the panel’s findings, Dr. Little, who served as panel and workshop chair, stressed that suicide is the second-leading cause of death among youth aged 10 to 24 years, and in young adults aged 25 to 34 years.
“Although these numbers are disheartening, we feel that suicide prevention is possible. New research strategies that embrace the complex factors involved in suicide can be coordinated and are necessary,” he said, adding that “the complexity of suicide prevention must be embraced in order to forge new research strategies,” and that researchers and practitioners must work together and with the larger “policy, practice, and research communities” to promote data sharing and stop youth suicide.
Dr. Little also noted the importance of destigmatizing suicide attempts and suicidal behavior to remove one of the roadblocks to reporting, which in turn will increase the available data for linkage.
The linkage of data from various sources, such as emergency departments, electronic health records, Medicaid, and Medicare, is particularly important for informing future prevention efforts, said panelist Leslie-Ann Byam, project director for the Families First Project at Evidence-Based Associates in Washington.
Continuing to work in the field and to work with young people without having information that encompasses that kind of data leaves practitioners at a disadvantage in terms of planning, she said.
Panelist Kathleen M. Roche, PhD, of George Washington University in Washington, stressed the importance of obtaining data on subpopulations of youth at very elevated risk of suicide, including transgender youth, Latinas, and Native Americans.
The NIH workshop was cosponsored by the NIH Office of Disease Prevention, the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Center for Complementary and Integrative Health. Individual authors were supported by grants from the National Science Foundation; the NIH; the Penn State Quantitative Social Sciences Initiative; the Institute for Measurement, Methodology, Analysis, and Policy at Texas Tech University; and the National Center for Advancing Translational Sciences. Dr. Little reported receiving fees from Yhat Enterprises outside the submitted work. The evidence review was funded by the Agency for Healthcare Research and Quality. The review authors reported having no disclosures.
The National Institutes of Health has released a 10-year road map for optimizing youth suicide prevention efforts.
The abridged version of the final report from a March 2016 NIH Pathways to Prevention Workshop entitled “Advancing Research to Prevent Youth Suicide,” highlights strategies for guiding the next decade of research on youth suicide prevention, Todd D. Little, PhD, from Texas Tech University, Lubbock, and his colleagues reported online Oct. 3.
The article outlines 29 recommendations aimed at improving data systems, enhancing data collection and analysis, and strengthening the research and practice community, and calls on researchers and practitioners to “unite to stop youth suicide in order to circumvent its associated economic cost and devastating pain and suffering” (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1568).
“Adherence to the recommendations summarized herein provides us with a road map to our ultimate goal – eliminating suicide,” the authors concluded.
In an accompanying evidence review, Holly C. Wilcox, PhD, and her colleagues from Johns Hopkins University, Baltimore, identified studies and potentially linkable external data systems with suicide outcomes and concluded that community data systems should be linked to suicide prevention data for the purpose of evaluating and enhancing prevention efforts.
“By integrating data from health care delivery systems, health insurance systems, and other populationwide data sources ... a national health research data infrastructure could be developed,” they wrote, adding that such a “national resource” could facilitate linkage with suicide prevention data (Ann Intern Med. 2016 Oct 4. doi: 10.7326/M16-1281).
During a press telebriefing on the panel’s findings, Dr. Little, who served as panel and workshop chair, stressed that suicide is the second-leading cause of death among youth aged 10 to 24 years, and in young adults aged 25 to 34 years.
“Although these numbers are disheartening, we feel that suicide prevention is possible. New research strategies that embrace the complex factors involved in suicide can be coordinated and are necessary,” he said, adding that “the complexity of suicide prevention must be embraced in order to forge new research strategies,” and that researchers and practitioners must work together and with the larger “policy, practice, and research communities” to promote data sharing and stop youth suicide.
Dr. Little also noted the importance of destigmatizing suicide attempts and suicidal behavior to remove one of the roadblocks to reporting, which in turn will increase the available data for linkage.
The linkage of data from various sources, such as emergency departments, electronic health records, Medicaid, and Medicare, is particularly important for informing future prevention efforts, said panelist Leslie-Ann Byam, project director for the Families First Project at Evidence-Based Associates in Washington.
Continuing to work in the field and to work with young people without having information that encompasses that kind of data leaves practitioners at a disadvantage in terms of planning, she said.
Panelist Kathleen M. Roche, PhD, of George Washington University in Washington, stressed the importance of obtaining data on subpopulations of youth at very elevated risk of suicide, including transgender youth, Latinas, and Native Americans.
The NIH workshop was cosponsored by the NIH Office of Disease Prevention, the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Center for Complementary and Integrative Health. Individual authors were supported by grants from the National Science Foundation; the NIH; the Penn State Quantitative Social Sciences Initiative; the Institute for Measurement, Methodology, Analysis, and Policy at Texas Tech University; and the National Center for Advancing Translational Sciences. Dr. Little reported receiving fees from Yhat Enterprises outside the submitted work. The evidence review was funded by the Agency for Healthcare Research and Quality. The review authors reported having no disclosures.
Congenital Zika syndrome includes range of neurologic abnormalities
Researchers have proposed the term “congenital Zika syndrome” to cover the range of severe damage and developmental abnormalities – including microcephaly – caused by Zika virus infection.
In the Oct. 3 online edition of JAMA Neurology, Adriana Suely de Oliveira Melo, MD, PhD, of the Instituto de Pesquisa Professor Amorim Neto in Campina Grande, Brazil, and her coauthors report on 11 babies with congenital Zika virus infection who were followed from gestation to 6 months of age.
Researchers observed hypoplasia of the cerebellar vermis and cerebellum in nine patients, while MRI and CT imaging also found that all patients showed callosal hypoplasia, reduced cerebral volume, abnormal cortical development, and subcortical calcifications.
Four of the infants showed gyral disorganization, five showed evidence of pachygyria, and two had lissencephaly (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3720).
“Although there was variable damage resulting from brain lesions associated with [Zika virus] congenital infection, a common pattern of brain atrophy and changes associated with disturbances in neuronal migration were observed,” the authors wrote. “Some patients presented with mild brain atrophy and calcifications, and others presented with more severe malformations, such as the absence of the thalamus and lissencephaly.”
Three of the infants died after delivery, representing a fatality rate of 27.3%. All three were found to have akinesia deformation sequence or arthrogryposis. One of the three pregnancies also involved polyhydramnios, and the infant was delivered at 36 weeks because of severe maternal respiratory distress.
All but one of the pregnant women had reported a skin rash at a median of 9.5 weeks in the pregnancy, suggesting Zika virus infection was acquired early.
Postmortem tissue analysis of two of the infants who died found Zika virus genome in the brain, cerebellum, spinal cord, and lung; a higher viral load in the tissue of one of the infants was associated with more severe brain damage.
Overall, nine patients tested positive for Zika virus using real-time reverse-transcription polymerase chain
reactions during gestation and/or after birth, while two patients only had serologic evidence of infection.
“It was interesting to note that the viral sequences amplified from patients 1 and 7 after birth gained a new substitution, V23I, which is located in the envelope domain I and may be implicated in viral tropism to different tissues.”
The study was supported by Consellho Nacional de Desenvolvimento e Pesquisa, Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, and Prefeitura Municipal de Campina Grande. No conflicts of interest were declared.
Many unanswered questions remain about Zika virus: How frequently does asymptomatic infection or second- and third-trimester infection lead to CNS disease? What are the long-term sequelae of intrauterine Zika virus infection? What is the reason for the substantial size, severity, and unexpected complications of the recent Zika virus outbreak in the Americas, compared with what has been seen with this virus in the past? And a broader question: How many CNS birth defects presently of unclear cause will be found to be virus induced?
It would be valuable to have adult and pediatric neurologists network with the U.S. Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus–induced Guillain-Barré syndrome and CNS disease. This would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiological studies.
Dr. Raymond P. Roos is with the Department of Neurology at the University of Chicago. These comments are adapted from an accompanying editorial (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3677). No conflicts of interest were declared.
Many unanswered questions remain about Zika virus: How frequently does asymptomatic infection or second- and third-trimester infection lead to CNS disease? What are the long-term sequelae of intrauterine Zika virus infection? What is the reason for the substantial size, severity, and unexpected complications of the recent Zika virus outbreak in the Americas, compared with what has been seen with this virus in the past? And a broader question: How many CNS birth defects presently of unclear cause will be found to be virus induced?
It would be valuable to have adult and pediatric neurologists network with the U.S. Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus–induced Guillain-Barré syndrome and CNS disease. This would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiological studies.
Dr. Raymond P. Roos is with the Department of Neurology at the University of Chicago. These comments are adapted from an accompanying editorial (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3677). No conflicts of interest were declared.
Many unanswered questions remain about Zika virus: How frequently does asymptomatic infection or second- and third-trimester infection lead to CNS disease? What are the long-term sequelae of intrauterine Zika virus infection? What is the reason for the substantial size, severity, and unexpected complications of the recent Zika virus outbreak in the Americas, compared with what has been seen with this virus in the past? And a broader question: How many CNS birth defects presently of unclear cause will be found to be virus induced?
It would be valuable to have adult and pediatric neurologists network with the U.S. Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus–induced Guillain-Barré syndrome and CNS disease. This would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiological studies.
Dr. Raymond P. Roos is with the Department of Neurology at the University of Chicago. These comments are adapted from an accompanying editorial (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3677). No conflicts of interest were declared.
Researchers have proposed the term “congenital Zika syndrome” to cover the range of severe damage and developmental abnormalities – including microcephaly – caused by Zika virus infection.
In the Oct. 3 online edition of JAMA Neurology, Adriana Suely de Oliveira Melo, MD, PhD, of the Instituto de Pesquisa Professor Amorim Neto in Campina Grande, Brazil, and her coauthors report on 11 babies with congenital Zika virus infection who were followed from gestation to 6 months of age.
Researchers observed hypoplasia of the cerebellar vermis and cerebellum in nine patients, while MRI and CT imaging also found that all patients showed callosal hypoplasia, reduced cerebral volume, abnormal cortical development, and subcortical calcifications.
Four of the infants showed gyral disorganization, five showed evidence of pachygyria, and two had lissencephaly (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3720).
“Although there was variable damage resulting from brain lesions associated with [Zika virus] congenital infection, a common pattern of brain atrophy and changes associated with disturbances in neuronal migration were observed,” the authors wrote. “Some patients presented with mild brain atrophy and calcifications, and others presented with more severe malformations, such as the absence of the thalamus and lissencephaly.”
Three of the infants died after delivery, representing a fatality rate of 27.3%. All three were found to have akinesia deformation sequence or arthrogryposis. One of the three pregnancies also involved polyhydramnios, and the infant was delivered at 36 weeks because of severe maternal respiratory distress.
All but one of the pregnant women had reported a skin rash at a median of 9.5 weeks in the pregnancy, suggesting Zika virus infection was acquired early.
Postmortem tissue analysis of two of the infants who died found Zika virus genome in the brain, cerebellum, spinal cord, and lung; a higher viral load in the tissue of one of the infants was associated with more severe brain damage.
Overall, nine patients tested positive for Zika virus using real-time reverse-transcription polymerase chain
reactions during gestation and/or after birth, while two patients only had serologic evidence of infection.
“It was interesting to note that the viral sequences amplified from patients 1 and 7 after birth gained a new substitution, V23I, which is located in the envelope domain I and may be implicated in viral tropism to different tissues.”
The study was supported by Consellho Nacional de Desenvolvimento e Pesquisa, Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, and Prefeitura Municipal de Campina Grande. No conflicts of interest were declared.
Researchers have proposed the term “congenital Zika syndrome” to cover the range of severe damage and developmental abnormalities – including microcephaly – caused by Zika virus infection.
In the Oct. 3 online edition of JAMA Neurology, Adriana Suely de Oliveira Melo, MD, PhD, of the Instituto de Pesquisa Professor Amorim Neto in Campina Grande, Brazil, and her coauthors report on 11 babies with congenital Zika virus infection who were followed from gestation to 6 months of age.
Researchers observed hypoplasia of the cerebellar vermis and cerebellum in nine patients, while MRI and CT imaging also found that all patients showed callosal hypoplasia, reduced cerebral volume, abnormal cortical development, and subcortical calcifications.
Four of the infants showed gyral disorganization, five showed evidence of pachygyria, and two had lissencephaly (JAMA Neurol. 2016 Oct 3. doi: 10.1001/jamaneurol.2016.3720).
“Although there was variable damage resulting from brain lesions associated with [Zika virus] congenital infection, a common pattern of brain atrophy and changes associated with disturbances in neuronal migration were observed,” the authors wrote. “Some patients presented with mild brain atrophy and calcifications, and others presented with more severe malformations, such as the absence of the thalamus and lissencephaly.”
Three of the infants died after delivery, representing a fatality rate of 27.3%. All three were found to have akinesia deformation sequence or arthrogryposis. One of the three pregnancies also involved polyhydramnios, and the infant was delivered at 36 weeks because of severe maternal respiratory distress.
All but one of the pregnant women had reported a skin rash at a median of 9.5 weeks in the pregnancy, suggesting Zika virus infection was acquired early.
Postmortem tissue analysis of two of the infants who died found Zika virus genome in the brain, cerebellum, spinal cord, and lung; a higher viral load in the tissue of one of the infants was associated with more severe brain damage.
Overall, nine patients tested positive for Zika virus using real-time reverse-transcription polymerase chain
reactions during gestation and/or after birth, while two patients only had serologic evidence of infection.
“It was interesting to note that the viral sequences amplified from patients 1 and 7 after birth gained a new substitution, V23I, which is located in the envelope domain I and may be implicated in viral tropism to different tissues.”
The study was supported by Consellho Nacional de Desenvolvimento e Pesquisa, Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, and Prefeitura Municipal de Campina Grande. No conflicts of interest were declared.
Key clinical point:
Major finding: Congenital Zika syndrome is associated with microcephaly, reduced cerebral volume, cerebellar hypoplasia, lissencephaly with hydrocephalus, and fetal akinesia deformation sequence.
Data source: Prospective study of 11 Zika-affected infants followed from gestation to 6 months of age.
Disclosures: The study was supported by Consellho Nacional de Desenvolvimento e Pesquisa, Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, and Prefeitura Municipal de Campina Grande. No conflicts of interest were declared.
Complementary medicine impedes children’s flu vaccination
Children treated with complementary and alternative medicine (CAM) therapies were significantly less likely to receive the annual influenza vaccine than those who didn’t use alternative medicine, based on data from 9,000 children aged 4-17 years in the Child Complementary and Alternative Medicine File of the 2012 National Health Interview Survey.
“CAM has been implicated as lending support to antivaccine/vaccine-hesitant viewpoints via criticism of vaccination, public health, and conventional medicine from adults using CAM, as well as from CAM practitioners and practitioners-in-training,” wrote William K. Bleser, Ph.D., and his colleagues at Pennsylvania State University, University Park.
No significant differences in vaccination rates were noted for children who had used three other categories of nonconventional care: biologically based therapies (such as herbal supplements), mind-body therapies (such as yoga), and multivitamins.
“There is an opportunity for U.S. public health, policy, and conventional medical professionals and educators to improve vaccine uptake and child health by better engaging both CAM and conventional medicine practitioners-in-training, parents of children using particular domains of CAM, and the CAM practitioners advising them,” the researchers said.
Find the full article in Pediatrics (2016. doi: 10.1542/peds.2015-4664).
Children treated with complementary and alternative medicine (CAM) therapies were significantly less likely to receive the annual influenza vaccine than those who didn’t use alternative medicine, based on data from 9,000 children aged 4-17 years in the Child Complementary and Alternative Medicine File of the 2012 National Health Interview Survey.
“CAM has been implicated as lending support to antivaccine/vaccine-hesitant viewpoints via criticism of vaccination, public health, and conventional medicine from adults using CAM, as well as from CAM practitioners and practitioners-in-training,” wrote William K. Bleser, Ph.D., and his colleagues at Pennsylvania State University, University Park.
No significant differences in vaccination rates were noted for children who had used three other categories of nonconventional care: biologically based therapies (such as herbal supplements), mind-body therapies (such as yoga), and multivitamins.
“There is an opportunity for U.S. public health, policy, and conventional medical professionals and educators to improve vaccine uptake and child health by better engaging both CAM and conventional medicine practitioners-in-training, parents of children using particular domains of CAM, and the CAM practitioners advising them,” the researchers said.
Find the full article in Pediatrics (2016. doi: 10.1542/peds.2015-4664).
Children treated with complementary and alternative medicine (CAM) therapies were significantly less likely to receive the annual influenza vaccine than those who didn’t use alternative medicine, based on data from 9,000 children aged 4-17 years in the Child Complementary and Alternative Medicine File of the 2012 National Health Interview Survey.
“CAM has been implicated as lending support to antivaccine/vaccine-hesitant viewpoints via criticism of vaccination, public health, and conventional medicine from adults using CAM, as well as from CAM practitioners and practitioners-in-training,” wrote William K. Bleser, Ph.D., and his colleagues at Pennsylvania State University, University Park.
No significant differences in vaccination rates were noted for children who had used three other categories of nonconventional care: biologically based therapies (such as herbal supplements), mind-body therapies (such as yoga), and multivitamins.
“There is an opportunity for U.S. public health, policy, and conventional medical professionals and educators to improve vaccine uptake and child health by better engaging both CAM and conventional medicine practitioners-in-training, parents of children using particular domains of CAM, and the CAM practitioners advising them,” the researchers said.
Find the full article in Pediatrics (2016. doi: 10.1542/peds.2015-4664).