User login
October 2016: Click for Credit
Here are 5 articles in the October issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Autism Follow-up Screening by PCPs Yields High Accuracy
To take the posttest, go to: http://bit.ly/2bTLhFS
Expires August 19, 2017
VITALS
Key clinical point:
Primary care providers can conduct the M-CHAT/F following a positive M-CHAT screening for autism spectrum disorders.
Major finding:
Primary care providers and trained interviewers agreed 86.6% of the time on the screening results of the M-CHAT/F for ASDs.
Data source:
A cohort study of 5,071 children, mean age 23 months, screened with the M-CHAT, and a subsequent 197 children screened with the M-CHAT/F in 22 Maryland primary care practices.
Disclosures:
The National Institutes of Mental Health funded the research. Dr. Sturner is director of Total Child Health (TCH), a for-profit subsidiary of the Center for Promotion of Child Development through Primary Care, which conducted the study. Barbara Howard, MD, is president of TCH. Tanya Morrel, PhD, is an employee of and stockholder in TCH, and Paul Bergmann has consulted for the company. The remaining authors had no relevant disclosures.
2. Gallstone Disease Boosts Heart Risk
To take the posttest, go to: http://bit.ly/2c7TP7D
Expires August 18, 2017
VITALS
Key clinical point:
Gallstone disease is associated with an increased risk for coronary heart disease; preventing the former can help mitigate chances of developing the latter.
Major finding:
A meta-analysis revealed a 23% increased chance of CHD in gallstone disease patients.
Data source:
A meta-analysis of seven studies involving 842,553 subjects, and a prospective cohort study of 269,142 participants in three separate studies that took place from 1980 to 2011.
Disclosures:
Funding provided by NIH, Boston Obesity Nutrition Research Center, and United States-Israel Binational Science Foundation. The authors had no relevant financial disclosures.
3. New HER2-testing Guidelines Result in More Women Eligible for Directed Treatment
To take the posttest, go to: http://bit.ly/2cd9llO
Expires July 25, 2017
VITALS
Key clinical point:
New IHC and FISH pathology guidelines categorize more breast cancers as "equivocal" regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive.
Major finding:
By using 2013 guidelines, 358 additional tumors were interpreted as positive, compared with the 2007 guidelines and 298 additional tumors were considered positive, compared with the FDA criteria.
Data source:
A cohort study involving 2,851 breast cancer samples analyzed according to three different pathology guidelines during a 1-year period.
Disclosures:
This study was supported by the Mayo Clinic. Dr. Shah reported having no relevant financial disclosures; his associates reported ties to Merck, Hospira, Ariad Pharmaceuticals, Abbott Molecular, and Genome Diagnostics.
4. Extreme Alcohol Use Worsens HIV Disease
To take the posttest, go to: http://bit.ly/2coIzG3
Expires August 14, 2017
VITALS
Key clinical point:
A pattern of heavy alcohol use over time in HIV-infected patients was associated with accelerated HIV disease progression.
Major finding:
Long-term heavy alcohol use by middle-aged, HIV-infected military veterans was associated with a 1.83-fold increased likelihood of also being in the highest-risk group for accelerated progression of HIV disease.
Data source:
This study included 3,539 U.S. military veterans receiving care for HIV infection at eight VA centers. The impact of their long-term pattern of alcohol use on HIV disease progression was assessed over an 8-year period by annual assessments using validated instruments.
Disclosures:
The presenter reported having no financial conflicts of interest regarding the study, funded by the National Institute on Alcohol Abuse and Alcoholism and the National Institute of Allergy and Infectious Diseases.
5. Weight Loss Boosts TNFis' Psoriatic Arthritis Efficacy
To take the posttest, go to: http://bit.ly/2chD4M1
Expires July 23, 2017
Here are 5 articles in the October issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Autism Follow-up Screening by PCPs Yields High Accuracy
To take the posttest, go to: http://bit.ly/2bTLhFS
Expires August 19, 2017
VITALS
Key clinical point:
Primary care providers can conduct the M-CHAT/F following a positive M-CHAT screening for autism spectrum disorders.
Major finding:
Primary care providers and trained interviewers agreed 86.6% of the time on the screening results of the M-CHAT/F for ASDs.
Data source:
A cohort study of 5,071 children, mean age 23 months, screened with the M-CHAT, and a subsequent 197 children screened with the M-CHAT/F in 22 Maryland primary care practices.
Disclosures:
The National Institutes of Mental Health funded the research. Dr. Sturner is director of Total Child Health (TCH), a for-profit subsidiary of the Center for Promotion of Child Development through Primary Care, which conducted the study. Barbara Howard, MD, is president of TCH. Tanya Morrel, PhD, is an employee of and stockholder in TCH, and Paul Bergmann has consulted for the company. The remaining authors had no relevant disclosures.
2. Gallstone Disease Boosts Heart Risk
To take the posttest, go to: http://bit.ly/2c7TP7D
Expires August 18, 2017
VITALS
Key clinical point:
Gallstone disease is associated with an increased risk for coronary heart disease; preventing the former can help mitigate chances of developing the latter.
Major finding:
A meta-analysis revealed a 23% increased chance of CHD in gallstone disease patients.
Data source:
A meta-analysis of seven studies involving 842,553 subjects, and a prospective cohort study of 269,142 participants in three separate studies that took place from 1980 to 2011.
Disclosures:
Funding provided by NIH, Boston Obesity Nutrition Research Center, and United States-Israel Binational Science Foundation. The authors had no relevant financial disclosures.
3. New HER2-testing Guidelines Result in More Women Eligible for Directed Treatment
To take the posttest, go to: http://bit.ly/2cd9llO
Expires July 25, 2017
VITALS
Key clinical point:
New IHC and FISH pathology guidelines categorize more breast cancers as "equivocal" regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive.
Major finding:
By using 2013 guidelines, 358 additional tumors were interpreted as positive, compared with the 2007 guidelines and 298 additional tumors were considered positive, compared with the FDA criteria.
Data source:
A cohort study involving 2,851 breast cancer samples analyzed according to three different pathology guidelines during a 1-year period.
Disclosures:
This study was supported by the Mayo Clinic. Dr. Shah reported having no relevant financial disclosures; his associates reported ties to Merck, Hospira, Ariad Pharmaceuticals, Abbott Molecular, and Genome Diagnostics.
4. Extreme Alcohol Use Worsens HIV Disease
To take the posttest, go to: http://bit.ly/2coIzG3
Expires August 14, 2017
VITALS
Key clinical point:
A pattern of heavy alcohol use over time in HIV-infected patients was associated with accelerated HIV disease progression.
Major finding:
Long-term heavy alcohol use by middle-aged, HIV-infected military veterans was associated with a 1.83-fold increased likelihood of also being in the highest-risk group for accelerated progression of HIV disease.
Data source:
This study included 3,539 U.S. military veterans receiving care for HIV infection at eight VA centers. The impact of their long-term pattern of alcohol use on HIV disease progression was assessed over an 8-year period by annual assessments using validated instruments.
Disclosures:
The presenter reported having no financial conflicts of interest regarding the study, funded by the National Institute on Alcohol Abuse and Alcoholism and the National Institute of Allergy and Infectious Diseases.
5. Weight Loss Boosts TNFis' Psoriatic Arthritis Efficacy
To take the posttest, go to: http://bit.ly/2chD4M1
Expires July 23, 2017
Here are 5 articles in the October issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Autism Follow-up Screening by PCPs Yields High Accuracy
To take the posttest, go to: http://bit.ly/2bTLhFS
Expires August 19, 2017
VITALS
Key clinical point:
Primary care providers can conduct the M-CHAT/F following a positive M-CHAT screening for autism spectrum disorders.
Major finding:
Primary care providers and trained interviewers agreed 86.6% of the time on the screening results of the M-CHAT/F for ASDs.
Data source:
A cohort study of 5,071 children, mean age 23 months, screened with the M-CHAT, and a subsequent 197 children screened with the M-CHAT/F in 22 Maryland primary care practices.
Disclosures:
The National Institutes of Mental Health funded the research. Dr. Sturner is director of Total Child Health (TCH), a for-profit subsidiary of the Center for Promotion of Child Development through Primary Care, which conducted the study. Barbara Howard, MD, is president of TCH. Tanya Morrel, PhD, is an employee of and stockholder in TCH, and Paul Bergmann has consulted for the company. The remaining authors had no relevant disclosures.
2. Gallstone Disease Boosts Heart Risk
To take the posttest, go to: http://bit.ly/2c7TP7D
Expires August 18, 2017
VITALS
Key clinical point:
Gallstone disease is associated with an increased risk for coronary heart disease; preventing the former can help mitigate chances of developing the latter.
Major finding:
A meta-analysis revealed a 23% increased chance of CHD in gallstone disease patients.
Data source:
A meta-analysis of seven studies involving 842,553 subjects, and a prospective cohort study of 269,142 participants in three separate studies that took place from 1980 to 2011.
Disclosures:
Funding provided by NIH, Boston Obesity Nutrition Research Center, and United States-Israel Binational Science Foundation. The authors had no relevant financial disclosures.
3. New HER2-testing Guidelines Result in More Women Eligible for Directed Treatment
To take the posttest, go to: http://bit.ly/2cd9llO
Expires July 25, 2017
VITALS
Key clinical point:
New IHC and FISH pathology guidelines categorize more breast cancers as "equivocal" regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive.
Major finding:
By using 2013 guidelines, 358 additional tumors were interpreted as positive, compared with the 2007 guidelines and 298 additional tumors were considered positive, compared with the FDA criteria.
Data source:
A cohort study involving 2,851 breast cancer samples analyzed according to three different pathology guidelines during a 1-year period.
Disclosures:
This study was supported by the Mayo Clinic. Dr. Shah reported having no relevant financial disclosures; his associates reported ties to Merck, Hospira, Ariad Pharmaceuticals, Abbott Molecular, and Genome Diagnostics.
4. Extreme Alcohol Use Worsens HIV Disease
To take the posttest, go to: http://bit.ly/2coIzG3
Expires August 14, 2017
VITALS
Key clinical point:
A pattern of heavy alcohol use over time in HIV-infected patients was associated with accelerated HIV disease progression.
Major finding:
Long-term heavy alcohol use by middle-aged, HIV-infected military veterans was associated with a 1.83-fold increased likelihood of also being in the highest-risk group for accelerated progression of HIV disease.
Data source:
This study included 3,539 U.S. military veterans receiving care for HIV infection at eight VA centers. The impact of their long-term pattern of alcohol use on HIV disease progression was assessed over an 8-year period by annual assessments using validated instruments.
Disclosures:
The presenter reported having no financial conflicts of interest regarding the study, funded by the National Institute on Alcohol Abuse and Alcoholism and the National Institute of Allergy and Infectious Diseases.
5. Weight Loss Boosts TNFis' Psoriatic Arthritis Efficacy
To take the posttest, go to: http://bit.ly/2chD4M1
Expires July 23, 2017
Postnatally acquired Zika infection in children usually mild
The clinical course of postnatally acquired Zika virus disease in children younger than 18 years is mild and rarely results in severe illness or death, reported Alyson Goodman, MD, and her associates at the Centers for Disease Control and Prevention (CDC), Atlanta.
There were a total of 158 confirmed or probable postnatally acquired Zika virus disease cases among children younger than 18 years reported to the CDC in the United States between January 2015 and July 2016, wrote researchers in a case series that described the epidemiology, clinical findings, and outcomes of the cases (MMWR. 2016 Sep 30;65:1-4).
The cases were reported in 30 d ifferent states, and the states with the highest numbers of reported cases were Florida (23%), New York (11%), and California (9%). All patients acquired Zika virus infections during travel to a location where mosquito-borne transmission had been documented, according to researchers.
The median patient age was 14 years, the majority of the patients were female (56%), and five patients were pregnant.
Of Zika’s four primary clinical signs and symptoms, 82% of the pediatric population had a rash, 55% had a fever, 29% had conjunctivitis, and 28% had arthralgia, with 70% of the children presenting with two or more of these symptoms.
Only two children were hospitalized because of their infections. No children were reported to have meningitis, encephalitis, or Guillain-Barré syndrome, and no patients with Zika virus infection died, researchers reported.
This data “corroborates previously published reports suggesting that the clinical course of Zika virus disease is typically mild in children, as it is in adults,” Dr. Goodman and her associates wrote.
Severe disease and death in children with postnatally acquired Zika virus infection are rare, the researchers pointed out, but they encouraged physicians to consider a Zika virus disease diagnosis for children with the four common symptoms and who reside in or traveled to an area with active Zika virus transmission. All Zika virus disease cases should be reported to state health departments.
On Twitter @jessnicolecraig
The clinical course of postnatally acquired Zika virus disease in children younger than 18 years is mild and rarely results in severe illness or death, reported Alyson Goodman, MD, and her associates at the Centers for Disease Control and Prevention (CDC), Atlanta.
There were a total of 158 confirmed or probable postnatally acquired Zika virus disease cases among children younger than 18 years reported to the CDC in the United States between January 2015 and July 2016, wrote researchers in a case series that described the epidemiology, clinical findings, and outcomes of the cases (MMWR. 2016 Sep 30;65:1-4).
The cases were reported in 30 d ifferent states, and the states with the highest numbers of reported cases were Florida (23%), New York (11%), and California (9%). All patients acquired Zika virus infections during travel to a location where mosquito-borne transmission had been documented, according to researchers.
The median patient age was 14 years, the majority of the patients were female (56%), and five patients were pregnant.
Of Zika’s four primary clinical signs and symptoms, 82% of the pediatric population had a rash, 55% had a fever, 29% had conjunctivitis, and 28% had arthralgia, with 70% of the children presenting with two or more of these symptoms.
Only two children were hospitalized because of their infections. No children were reported to have meningitis, encephalitis, or Guillain-Barré syndrome, and no patients with Zika virus infection died, researchers reported.
This data “corroborates previously published reports suggesting that the clinical course of Zika virus disease is typically mild in children, as it is in adults,” Dr. Goodman and her associates wrote.
Severe disease and death in children with postnatally acquired Zika virus infection are rare, the researchers pointed out, but they encouraged physicians to consider a Zika virus disease diagnosis for children with the four common symptoms and who reside in or traveled to an area with active Zika virus transmission. All Zika virus disease cases should be reported to state health departments.
On Twitter @jessnicolecraig
The clinical course of postnatally acquired Zika virus disease in children younger than 18 years is mild and rarely results in severe illness or death, reported Alyson Goodman, MD, and her associates at the Centers for Disease Control and Prevention (CDC), Atlanta.
There were a total of 158 confirmed or probable postnatally acquired Zika virus disease cases among children younger than 18 years reported to the CDC in the United States between January 2015 and July 2016, wrote researchers in a case series that described the epidemiology, clinical findings, and outcomes of the cases (MMWR. 2016 Sep 30;65:1-4).
The cases were reported in 30 d ifferent states, and the states with the highest numbers of reported cases were Florida (23%), New York (11%), and California (9%). All patients acquired Zika virus infections during travel to a location where mosquito-borne transmission had been documented, according to researchers.
The median patient age was 14 years, the majority of the patients were female (56%), and five patients were pregnant.
Of Zika’s four primary clinical signs and symptoms, 82% of the pediatric population had a rash, 55% had a fever, 29% had conjunctivitis, and 28% had arthralgia, with 70% of the children presenting with two or more of these symptoms.
Only two children were hospitalized because of their infections. No children were reported to have meningitis, encephalitis, or Guillain-Barré syndrome, and no patients with Zika virus infection died, researchers reported.
This data “corroborates previously published reports suggesting that the clinical course of Zika virus disease is typically mild in children, as it is in adults,” Dr. Goodman and her associates wrote.
Severe disease and death in children with postnatally acquired Zika virus infection are rare, the researchers pointed out, but they encouraged physicians to consider a Zika virus disease diagnosis for children with the four common symptoms and who reside in or traveled to an area with active Zika virus transmission. All Zika virus disease cases should be reported to state health departments.
On Twitter @jessnicolecraig
FROM MMWR
Key clinical point: Postnatally acquired Zika virus disease in children younger than 18 years is mild and rarely results in severe illness or death.
Major finding: Only two children were hospitalized because of their infections, and no children died.
Data source: Case series of 158 confirmed or probable postnatally acquired Zika virus disease cases among children.
Disclosures: The study was funded by the CDC. Author disclosures were not reported.
A different Thanksgiving
Thanksgiving is at least one time when families sit down and focus on the meal. While the turkey may be the centerpiece, at least in our family we are presented with a variety of vegetables, salads, baked goods, and desserts. Some of the dishes remain on the traditional menu because “Aunt Martha always brings her molded salad,” although if the truth be known, she had fallen out of love with making it years ago. Other selections survive as memorials to long-departed family members: “Remember how much Grampy Stevens loved that pickled watermelon rind” that no one has touched since he died 10 years ago?
And although Thanksgiving may be all about the food, it’s really about sitting down together and celebrating each other over a meal. It should really be a happy meal but not one that comes in a box with a plastic toy. But for the parents of a picky eater, Thanksgiving is often destined to be another stressful dining experience. They know that despite the bountiful spread of food, there isn’t going to be anything on the table their child is going to eat.

They can cope with the situation in one of two ways. They can bring something they know he will eat, such as a can of corn or a microwaveable macaroni and cheese so he won’t “starve.” Or they can cast a pall on the festivities by attempting to badger, coax, and coerce him to eat something, as they do every night at home.
Parents may be assisted in their efforts by other family members who will bring something from the picky eater’s “might eat list.” Or, more likely, they will join in a chorus of old favorites such as “Don’t you want to grow up to be big and strong?” Or “You won’t be able to have any of Grandma’s cookies if you don’t eat some dinner.”
Either approach will be another step toward solidifying the child’s reputation in the family as a picky eater. Rachel is the cousin who plays the piano, and everyone knows that Brandon is going to be a great soccer player. Bobby is the one who won’t eat anything but mac and cheese.
A few years ago I had the thought that instead of allowing Thanksgiving to become an event that highlights and perpetuates the picky eater’s unfortunate habits, why not use the holiday as an opportunity to turn the page and begin a more sensible approach to selective eating?
So for some parents of picky eaters, I have begun to recommend the following: Tell everyone who will be coming to Thanksgiving that the pediatrician says everyone should agree that the event will be all about having a good time and not about who eats or doesn’t eat what’s on the table. And there will be no discussion about the picky eater’s habits – positive or negative.
It might be nice to include on the menu a dish or dessert that the picky eater has eaten in the past. But this is done without ceremony, comment, or preconditions such as “You have to eat some of this to get that.” This silent gesture of kindness also may reassure nervous grandparents who are worried that the child will starve if he doesn’t eat anything for a day despite your reassurance to them that the pediatrician said it was okay.
While I admit that one Thanksgiving with these new rules is unlikely to convert a 6-year-old picky eater into a voracious omnivore, it can be a first step toward helping a family adopt a sensible approach to the child’s eating habits. At least it won’t make things worse and is likely to turn unhappy meals at home into mini feasts that celebrate togetherness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
Thanksgiving is at least one time when families sit down and focus on the meal. While the turkey may be the centerpiece, at least in our family we are presented with a variety of vegetables, salads, baked goods, and desserts. Some of the dishes remain on the traditional menu because “Aunt Martha always brings her molded salad,” although if the truth be known, she had fallen out of love with making it years ago. Other selections survive as memorials to long-departed family members: “Remember how much Grampy Stevens loved that pickled watermelon rind” that no one has touched since he died 10 years ago?
And although Thanksgiving may be all about the food, it’s really about sitting down together and celebrating each other over a meal. It should really be a happy meal but not one that comes in a box with a plastic toy. But for the parents of a picky eater, Thanksgiving is often destined to be another stressful dining experience. They know that despite the bountiful spread of food, there isn’t going to be anything on the table their child is going to eat.
They can cope with the situation in one of two ways. They can bring something they know he will eat, such as a can of corn or a microwaveable macaroni and cheese so he won’t “starve.” Or they can cast a pall on the festivities by attempting to badger, coax, and coerce him to eat something, as they do every night at home.
Parents may be assisted in their efforts by other family members who will bring something from the picky eater’s “might eat list.” Or, more likely, they will join in a chorus of old favorites such as “Don’t you want to grow up to be big and strong?” Or “You won’t be able to have any of Grandma’s cookies if you don’t eat some dinner.”
Either approach will be another step toward solidifying the child’s reputation in the family as a picky eater. Rachel is the cousin who plays the piano, and everyone knows that Brandon is going to be a great soccer player. Bobby is the one who won’t eat anything but mac and cheese.
A few years ago I had the thought that instead of allowing Thanksgiving to become an event that highlights and perpetuates the picky eater’s unfortunate habits, why not use the holiday as an opportunity to turn the page and begin a more sensible approach to selective eating?
So for some parents of picky eaters, I have begun to recommend the following: Tell everyone who will be coming to Thanksgiving that the pediatrician says everyone should agree that the event will be all about having a good time and not about who eats or doesn’t eat what’s on the table. And there will be no discussion about the picky eater’s habits – positive or negative.
It might be nice to include on the menu a dish or dessert that the picky eater has eaten in the past. But this is done without ceremony, comment, or preconditions such as “You have to eat some of this to get that.” This silent gesture of kindness also may reassure nervous grandparents who are worried that the child will starve if he doesn’t eat anything for a day despite your reassurance to them that the pediatrician said it was okay.
While I admit that one Thanksgiving with these new rules is unlikely to convert a 6-year-old picky eater into a voracious omnivore, it can be a first step toward helping a family adopt a sensible approach to the child’s eating habits. At least it won’t make things worse and is likely to turn unhappy meals at home into mini feasts that celebrate togetherness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
Thanksgiving is at least one time when families sit down and focus on the meal. While the turkey may be the centerpiece, at least in our family we are presented with a variety of vegetables, salads, baked goods, and desserts. Some of the dishes remain on the traditional menu because “Aunt Martha always brings her molded salad,” although if the truth be known, she had fallen out of love with making it years ago. Other selections survive as memorials to long-departed family members: “Remember how much Grampy Stevens loved that pickled watermelon rind” that no one has touched since he died 10 years ago?
And although Thanksgiving may be all about the food, it’s really about sitting down together and celebrating each other over a meal. It should really be a happy meal but not one that comes in a box with a plastic toy. But for the parents of a picky eater, Thanksgiving is often destined to be another stressful dining experience. They know that despite the bountiful spread of food, there isn’t going to be anything on the table their child is going to eat.
They can cope with the situation in one of two ways. They can bring something they know he will eat, such as a can of corn or a microwaveable macaroni and cheese so he won’t “starve.” Or they can cast a pall on the festivities by attempting to badger, coax, and coerce him to eat something, as they do every night at home.
Parents may be assisted in their efforts by other family members who will bring something from the picky eater’s “might eat list.” Or, more likely, they will join in a chorus of old favorites such as “Don’t you want to grow up to be big and strong?” Or “You won’t be able to have any of Grandma’s cookies if you don’t eat some dinner.”
Either approach will be another step toward solidifying the child’s reputation in the family as a picky eater. Rachel is the cousin who plays the piano, and everyone knows that Brandon is going to be a great soccer player. Bobby is the one who won’t eat anything but mac and cheese.
A few years ago I had the thought that instead of allowing Thanksgiving to become an event that highlights and perpetuates the picky eater’s unfortunate habits, why not use the holiday as an opportunity to turn the page and begin a more sensible approach to selective eating?
So for some parents of picky eaters, I have begun to recommend the following: Tell everyone who will be coming to Thanksgiving that the pediatrician says everyone should agree that the event will be all about having a good time and not about who eats or doesn’t eat what’s on the table. And there will be no discussion about the picky eater’s habits – positive or negative.
It might be nice to include on the menu a dish or dessert that the picky eater has eaten in the past. But this is done without ceremony, comment, or preconditions such as “You have to eat some of this to get that.” This silent gesture of kindness also may reassure nervous grandparents who are worried that the child will starve if he doesn’t eat anything for a day despite your reassurance to them that the pediatrician said it was okay.
While I admit that one Thanksgiving with these new rules is unlikely to convert a 6-year-old picky eater into a voracious omnivore, it can be a first step toward helping a family adopt a sensible approach to the child’s eating habits. At least it won’t make things worse and is likely to turn unhappy meals at home into mini feasts that celebrate togetherness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

Hair loss on scalp

The FP noted patchy alopecia with scaling of the scalp and made the presumptive diagnosis of tinea capitis. A woods lamp examination did not demonstrate fluorescence. The child was very cooperative and the doctor was able to perform a potassium hydroxide (KOH) preparation by scraping the areas of alopecia with the edge of one glass slide while catching the scale on another slide. Microscopic examination revealed branching hyphae and some broken hairs with fungal elements within the hair shaft. (See video on how to perform a KOH preparation.) This microscopic picture was consistent with Trichophyton tonsurans, the most common cause of tinea capitis in the United States. The reason that the infected area did not fluoresce was that the dermatophyte was within the hair shaft (endothrix) rather than external to the hair (exothrix).
Topical antifungal therapy is not adequate for tinea capitis; oral treatment is needed. Oral antifungal choices include griseofulvin, terbinafine, and fluconazole. Griseofulvin comes in an oral suspension making it a desirable option for children who can’t swallow pills. However, at least 6 to 8 weeks of treatment (20 mg/kg/d) is required. Oral terbinafine tablets are less expensive and shorter courses of therapy may be used. Tablets of 250 mg terbinafine (most affordable of all the choices) can be broken in half for younger children and the dose should always be calculated based on weight. Fluconazole comes in various tablets, strengths, and liquid formulations and can be prescribed for 3 to 6 weeks, as needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Yao C. Tinea capitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:782-787.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP noted patchy alopecia with scaling of the scalp and made the presumptive diagnosis of tinea capitis. A woods lamp examination did not demonstrate fluorescence. The child was very cooperative and the doctor was able to perform a potassium hydroxide (KOH) preparation by scraping the areas of alopecia with the edge of one glass slide while catching the scale on another slide. Microscopic examination revealed branching hyphae and some broken hairs with fungal elements within the hair shaft. (See video on how to perform a KOH preparation.) This microscopic picture was consistent with Trichophyton tonsurans, the most common cause of tinea capitis in the United States. The reason that the infected area did not fluoresce was that the dermatophyte was within the hair shaft (endothrix) rather than external to the hair (exothrix).
Topical antifungal therapy is not adequate for tinea capitis; oral treatment is needed. Oral antifungal choices include griseofulvin, terbinafine, and fluconazole. Griseofulvin comes in an oral suspension making it a desirable option for children who can’t swallow pills. However, at least 6 to 8 weeks of treatment (20 mg/kg/d) is required. Oral terbinafine tablets are less expensive and shorter courses of therapy may be used. Tablets of 250 mg terbinafine (most affordable of all the choices) can be broken in half for younger children and the dose should always be calculated based on weight. Fluconazole comes in various tablets, strengths, and liquid formulations and can be prescribed for 3 to 6 weeks, as needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Yao C. Tinea capitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:782-787.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP noted patchy alopecia with scaling of the scalp and made the presumptive diagnosis of tinea capitis. A woods lamp examination did not demonstrate fluorescence. The child was very cooperative and the doctor was able to perform a potassium hydroxide (KOH) preparation by scraping the areas of alopecia with the edge of one glass slide while catching the scale on another slide. Microscopic examination revealed branching hyphae and some broken hairs with fungal elements within the hair shaft. (See video on how to perform a KOH preparation.) This microscopic picture was consistent with Trichophyton tonsurans, the most common cause of tinea capitis in the United States. The reason that the infected area did not fluoresce was that the dermatophyte was within the hair shaft (endothrix) rather than external to the hair (exothrix).
Topical antifungal therapy is not adequate for tinea capitis; oral treatment is needed. Oral antifungal choices include griseofulvin, terbinafine, and fluconazole. Griseofulvin comes in an oral suspension making it a desirable option for children who can’t swallow pills. However, at least 6 to 8 weeks of treatment (20 mg/kg/d) is required. Oral terbinafine tablets are less expensive and shorter courses of therapy may be used. Tablets of 250 mg terbinafine (most affordable of all the choices) can be broken in half for younger children and the dose should always be calculated based on weight. Fluconazole comes in various tablets, strengths, and liquid formulations and can be prescribed for 3 to 6 weeks, as needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Yao C. Tinea capitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:782-787.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

HPV vaccine and adolescents: What we say really does matter
It has been almost 10 years since the Advisory Committee on Immunization Practices (ACIP) recommended administration of human papillomavirus (HPV) vaccine for 11- to 12-year-old girls and young women up to 26 years of age. Routine administration in preteen boys and young adult males up to 21 years of age was recommended in 2011. An HPV series should be completed by 13 years. So how well are we protecting our patients?
Vaccine coverage
The National Immunization Survey–Teen (NIS-Teen) monitors vaccine coverage annually among adolescents 13-17 years. Data are obtained from individuals from the 50 states, the District of Columbia, the U.S. Virgin Islands, and six major urban areas (MMWR. 2016 Aug 26;65[33]:850-8).

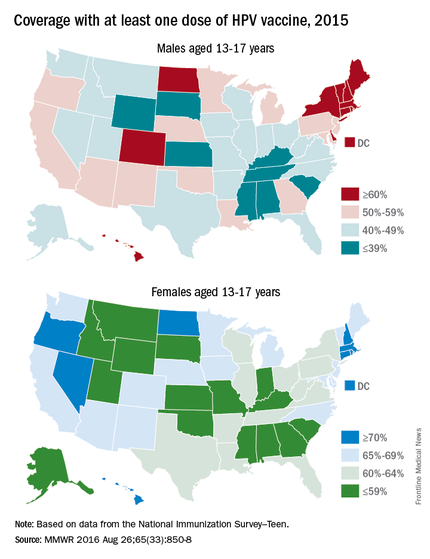
HPV vaccination continues to lag behind Tdap and the meningococcal conjugate vaccine (MCV), although each one is recommended to be administered at the 11- to 12-year visit. In 2015, coverage for receiving at least one dose of HPV vaccine among females was almost 62.8 % and for at least three doses was 41.9%; among males, coverage with at least one dose was 49.8% and for at least three doses was 28.1%. Compared with 2014, coverage for at least one dose of HPV vaccine increased 2.8% in females and 8.1% in males. Males also had a 7.6% for receipt of at least two doses of HPV vaccine, compared with 2014. HPV vaccine coverage in females aged 13 and younger also was lower than for those aged 15 and older. Coverage did not differ for males based on age.
HPV vaccination coverage also differed by state. In 2015, 28 states reported increased coverage in males, but only 7 states had increased coverage in females. Among all adolescents, coverage with at least one dose of HPV vaccine was 56.1%, at least two doses was 45.4%, and at least three doses was 34.9%. In contrast, 86.4% of all adolescents received at least one dose of Tdap, and 81.3% received at least one dose of MCV.
HPV-associated cancers
HPV is the most common sexually transmitted infection in both men and women. It is estimated that 79 million Americans are infected and 14 million new infections occur annually, usually in teens and young adults. Although most infections are asymptomatic and clear spontaneously, persistent infection with oncogenic types can progress to cancer. Cervical and oropharyngeal cancer were the most common HPV-associated cancers in women and men, respectively, in 2008-2012 (MMWR 2016;65:661-6).
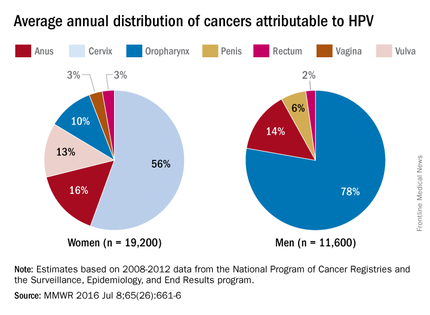
All three HPV vaccines protect against HPV types 16 and 18. These types are estimated to account for the majority of cervical and oropharyngeal cancers, 66% and 62%, respectively. The additional types in the 9-valent HPV will protect against HPV types that cause approximately 15% of cervical cancers.
The association between HPV and cancer is clear. So why isn’t this vaccine being embraced? HPV vaccine is all about cancer prevention. Isn’t it? What are the barriers to HPV vaccination? Are parental concerns the only barrier? Are we recommending this vaccine as strongly as others?
Vaccine safety and efficacy
Safety has been a concern voiced by some parents. Collectively, HPV vaccines were studied in more than 95,000 individuals prior to licensure. Almost 90 million doses of vaccine have been distributed in the United States and more than 183 million, worldwide. The federal government utilizes three systems to monitor vaccine safety once a vaccine is licensed: The Vaccine Adverse Event Reporting System (VAERS), the Vaccine Safety Datalink (VSD), and the Clinical Immunization Safety Assessment (CISA) Network. Ongoing safety studies also are conducted by vaccine manufacturers. Since licensure, no serious safety concerns have been identified. Postvaccination syncope, first identified in the VAERS database in 2006, has declined since observation post injection was recommended by ACIP. Multiple studies in the United States and abroad have not demonstrated a causal association with HPV vaccine and any autoimmune and/or neurologic condition or increased risk for thromboembolism.
Mélanie Drolet, PhD, and her colleagues reviewed 20 studies in nine countries with at least 50% coverage in female adolescents aged 13-19 years. There was a 68% reduction in the prevalence of HPV types 16 and 18 and a 61% reduction in anal warts in the postvaccine era (Lancet Infect Dis. 2015 May;15[5]:565-80). Studies also indicate there is no indication of waning immunity.
Parental perceptions
Some parents feel the vaccine is not necessary because their child is not sexually active and/or is not at risk for acquiring a sexually transmitted infection. Others opt to delay initiation. NHANES (National Health and Nutrition Examination Survey) data from 2011 to 2014 revealed that among females aged 14-26 years whose age was known at the time of their first dose of HPV vaccine, 43% had reported having sex before or in the same year that they received their first dose.
One consistent reason parents indicate for not vaccinating is the lack of recommendation from their child’s health provider. Differences in age and sex recommendations also are reported. NIS-Teen 2013 demonstrated that parents of girls were more likely than parents of boys to receive a provider recommendation (65% vs.42%.) Only 29% of female parents indicated they’d received a provider recommendation to have their child vaccinated with HPV by ages 11-12 years.
Mandy A. Allison, MD, and her colleagues reviewed primary care physician perspectives about HPV vaccine in a national survey among 364 pediatricians and 218 family physicians (FPs). Although 84% of pediatricians and 75% of FPs indicated they always discuss HPV vaccination, only 60% of pediatricians and 59% of FPs strongly recommend HPV vaccine for 11- to 12-year-old girls; for boys it was 52% and 41%. More than half reported parental deferral. For pediatricians who almost never discussed the topic, the reasons included that the patient was not sexually active (54%), the child was young (38%), and the patient was already receiving other vaccines (35%) (Pediatrics. 2016 Feb;137[2]:e20152488).
Providers can be influenced by their perceptions of what value parents place on vaccines. In one study, parents were asked to put a value on specific vaccines. Providers were then asked to estimate how parents ranked the vaccines on a scale of 0-10. Providers underestimated the value placed on HPV vaccine (9.3 vs 5.2) (Vaccine 2014;32:579-84).
Improving HPV coverage: Preventing future HPV-related cancers
HPV vaccine should be recommended with as much conviction as Tdap and MCV at the 11- to 12-year visit for both girls and boys. Administration of all three should occur on the same day. Clinician recommendation is the No. 1 reason parents decide to vaccinate. The mantra “same way, same day” should become synonymous with the 11- to 12-year visit. All who have contact with the patient, beginning with the front desk staff, should know the importance of HPV vaccine, and when and why it is recommended. Often, families spend more time with support staff and have discussions prior to interacting with you.
Anticipate questions about HPV. Why give the vaccine when the child is so young and not sexually active? Is my child really at risk? Is it safe? I read on the Internet. … Questions should be interpreted as a need for additional information and reassurance from you.
Remember to emphasize that HPV vaccine is important because it prevents cancer and it is most effective prior to exposure to HPV.
Additional resources to facilitate your discussions about HPV can be found at www.cdc.gov/hpv.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
It has been almost 10 years since the Advisory Committee on Immunization Practices (ACIP) recommended administration of human papillomavirus (HPV) vaccine for 11- to 12-year-old girls and young women up to 26 years of age. Routine administration in preteen boys and young adult males up to 21 years of age was recommended in 2011. An HPV series should be completed by 13 years. So how well are we protecting our patients?
Vaccine coverage
The National Immunization Survey–Teen (NIS-Teen) monitors vaccine coverage annually among adolescents 13-17 years. Data are obtained from individuals from the 50 states, the District of Columbia, the U.S. Virgin Islands, and six major urban areas (MMWR. 2016 Aug 26;65[33]:850-8).
HPV vaccination continues to lag behind Tdap and the meningococcal conjugate vaccine (MCV), although each one is recommended to be administered at the 11- to 12-year visit. In 2015, coverage for receiving at least one dose of HPV vaccine among females was almost 62.8 % and for at least three doses was 41.9%; among males, coverage with at least one dose was 49.8% and for at least three doses was 28.1%. Compared with 2014, coverage for at least one dose of HPV vaccine increased 2.8% in females and 8.1% in males. Males also had a 7.6% for receipt of at least two doses of HPV vaccine, compared with 2014. HPV vaccine coverage in females aged 13 and younger also was lower than for those aged 15 and older. Coverage did not differ for males based on age.
HPV vaccination coverage also differed by state. In 2015, 28 states reported increased coverage in males, but only 7 states had increased coverage in females. Among all adolescents, coverage with at least one dose of HPV vaccine was 56.1%, at least two doses was 45.4%, and at least three doses was 34.9%. In contrast, 86.4% of all adolescents received at least one dose of Tdap, and 81.3% received at least one dose of MCV.
HPV-associated cancers
HPV is the most common sexually transmitted infection in both men and women. It is estimated that 79 million Americans are infected and 14 million new infections occur annually, usually in teens and young adults. Although most infections are asymptomatic and clear spontaneously, persistent infection with oncogenic types can progress to cancer. Cervical and oropharyngeal cancer were the most common HPV-associated cancers in women and men, respectively, in 2008-2012 (MMWR 2016;65:661-6).
All three HPV vaccines protect against HPV types 16 and 18. These types are estimated to account for the majority of cervical and oropharyngeal cancers, 66% and 62%, respectively. The additional types in the 9-valent HPV will protect against HPV types that cause approximately 15% of cervical cancers.
The association between HPV and cancer is clear. So why isn’t this vaccine being embraced? HPV vaccine is all about cancer prevention. Isn’t it? What are the barriers to HPV vaccination? Are parental concerns the only barrier? Are we recommending this vaccine as strongly as others?
Vaccine safety and efficacy
Safety has been a concern voiced by some parents. Collectively, HPV vaccines were studied in more than 95,000 individuals prior to licensure. Almost 90 million doses of vaccine have been distributed in the United States and more than 183 million, worldwide. The federal government utilizes three systems to monitor vaccine safety once a vaccine is licensed: The Vaccine Adverse Event Reporting System (VAERS), the Vaccine Safety Datalink (VSD), and the Clinical Immunization Safety Assessment (CISA) Network. Ongoing safety studies also are conducted by vaccine manufacturers. Since licensure, no serious safety concerns have been identified. Postvaccination syncope, first identified in the VAERS database in 2006, has declined since observation post injection was recommended by ACIP. Multiple studies in the United States and abroad have not demonstrated a causal association with HPV vaccine and any autoimmune and/or neurologic condition or increased risk for thromboembolism.
Mélanie Drolet, PhD, and her colleagues reviewed 20 studies in nine countries with at least 50% coverage in female adolescents aged 13-19 years. There was a 68% reduction in the prevalence of HPV types 16 and 18 and a 61% reduction in anal warts in the postvaccine era (Lancet Infect Dis. 2015 May;15[5]:565-80). Studies also indicate there is no indication of waning immunity.
Parental perceptions
Some parents feel the vaccine is not necessary because their child is not sexually active and/or is not at risk for acquiring a sexually transmitted infection. Others opt to delay initiation. NHANES (National Health and Nutrition Examination Survey) data from 2011 to 2014 revealed that among females aged 14-26 years whose age was known at the time of their first dose of HPV vaccine, 43% had reported having sex before or in the same year that they received their first dose.
One consistent reason parents indicate for not vaccinating is the lack of recommendation from their child’s health provider. Differences in age and sex recommendations also are reported. NIS-Teen 2013 demonstrated that parents of girls were more likely than parents of boys to receive a provider recommendation (65% vs.42%.) Only 29% of female parents indicated they’d received a provider recommendation to have their child vaccinated with HPV by ages 11-12 years.
Mandy A. Allison, MD, and her colleagues reviewed primary care physician perspectives about HPV vaccine in a national survey among 364 pediatricians and 218 family physicians (FPs). Although 84% of pediatricians and 75% of FPs indicated they always discuss HPV vaccination, only 60% of pediatricians and 59% of FPs strongly recommend HPV vaccine for 11- to 12-year-old girls; for boys it was 52% and 41%. More than half reported parental deferral. For pediatricians who almost never discussed the topic, the reasons included that the patient was not sexually active (54%), the child was young (38%), and the patient was already receiving other vaccines (35%) (Pediatrics. 2016 Feb;137[2]:e20152488).
Providers can be influenced by their perceptions of what value parents place on vaccines. In one study, parents were asked to put a value on specific vaccines. Providers were then asked to estimate how parents ranked the vaccines on a scale of 0-10. Providers underestimated the value placed on HPV vaccine (9.3 vs 5.2) (Vaccine 2014;32:579-84).
Improving HPV coverage: Preventing future HPV-related cancers
HPV vaccine should be recommended with as much conviction as Tdap and MCV at the 11- to 12-year visit for both girls and boys. Administration of all three should occur on the same day. Clinician recommendation is the No. 1 reason parents decide to vaccinate. The mantra “same way, same day” should become synonymous with the 11- to 12-year visit. All who have contact with the patient, beginning with the front desk staff, should know the importance of HPV vaccine, and when and why it is recommended. Often, families spend more time with support staff and have discussions prior to interacting with you.
Anticipate questions about HPV. Why give the vaccine when the child is so young and not sexually active? Is my child really at risk? Is it safe? I read on the Internet. … Questions should be interpreted as a need for additional information and reassurance from you.
Remember to emphasize that HPV vaccine is important because it prevents cancer and it is most effective prior to exposure to HPV.
Additional resources to facilitate your discussions about HPV can be found at www.cdc.gov/hpv.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
It has been almost 10 years since the Advisory Committee on Immunization Practices (ACIP) recommended administration of human papillomavirus (HPV) vaccine for 11- to 12-year-old girls and young women up to 26 years of age. Routine administration in preteen boys and young adult males up to 21 years of age was recommended in 2011. An HPV series should be completed by 13 years. So how well are we protecting our patients?
Vaccine coverage
The National Immunization Survey–Teen (NIS-Teen) monitors vaccine coverage annually among adolescents 13-17 years. Data are obtained from individuals from the 50 states, the District of Columbia, the U.S. Virgin Islands, and six major urban areas (MMWR. 2016 Aug 26;65[33]:850-8).
HPV vaccination continues to lag behind Tdap and the meningococcal conjugate vaccine (MCV), although each one is recommended to be administered at the 11- to 12-year visit. In 2015, coverage for receiving at least one dose of HPV vaccine among females was almost 62.8 % and for at least three doses was 41.9%; among males, coverage with at least one dose was 49.8% and for at least three doses was 28.1%. Compared with 2014, coverage for at least one dose of HPV vaccine increased 2.8% in females and 8.1% in males. Males also had a 7.6% for receipt of at least two doses of HPV vaccine, compared with 2014. HPV vaccine coverage in females aged 13 and younger also was lower than for those aged 15 and older. Coverage did not differ for males based on age.
HPV vaccination coverage also differed by state. In 2015, 28 states reported increased coverage in males, but only 7 states had increased coverage in females. Among all adolescents, coverage with at least one dose of HPV vaccine was 56.1%, at least two doses was 45.4%, and at least three doses was 34.9%. In contrast, 86.4% of all adolescents received at least one dose of Tdap, and 81.3% received at least one dose of MCV.
HPV-associated cancers
HPV is the most common sexually transmitted infection in both men and women. It is estimated that 79 million Americans are infected and 14 million new infections occur annually, usually in teens and young adults. Although most infections are asymptomatic and clear spontaneously, persistent infection with oncogenic types can progress to cancer. Cervical and oropharyngeal cancer were the most common HPV-associated cancers in women and men, respectively, in 2008-2012 (MMWR 2016;65:661-6).
All three HPV vaccines protect against HPV types 16 and 18. These types are estimated to account for the majority of cervical and oropharyngeal cancers, 66% and 62%, respectively. The additional types in the 9-valent HPV will protect against HPV types that cause approximately 15% of cervical cancers.
The association between HPV and cancer is clear. So why isn’t this vaccine being embraced? HPV vaccine is all about cancer prevention. Isn’t it? What are the barriers to HPV vaccination? Are parental concerns the only barrier? Are we recommending this vaccine as strongly as others?
Vaccine safety and efficacy
Safety has been a concern voiced by some parents. Collectively, HPV vaccines were studied in more than 95,000 individuals prior to licensure. Almost 90 million doses of vaccine have been distributed in the United States and more than 183 million, worldwide. The federal government utilizes three systems to monitor vaccine safety once a vaccine is licensed: The Vaccine Adverse Event Reporting System (VAERS), the Vaccine Safety Datalink (VSD), and the Clinical Immunization Safety Assessment (CISA) Network. Ongoing safety studies also are conducted by vaccine manufacturers. Since licensure, no serious safety concerns have been identified. Postvaccination syncope, first identified in the VAERS database in 2006, has declined since observation post injection was recommended by ACIP. Multiple studies in the United States and abroad have not demonstrated a causal association with HPV vaccine and any autoimmune and/or neurologic condition or increased risk for thromboembolism.
Mélanie Drolet, PhD, and her colleagues reviewed 20 studies in nine countries with at least 50% coverage in female adolescents aged 13-19 years. There was a 68% reduction in the prevalence of HPV types 16 and 18 and a 61% reduction in anal warts in the postvaccine era (Lancet Infect Dis. 2015 May;15[5]:565-80). Studies also indicate there is no indication of waning immunity.
Parental perceptions
Some parents feel the vaccine is not necessary because their child is not sexually active and/or is not at risk for acquiring a sexually transmitted infection. Others opt to delay initiation. NHANES (National Health and Nutrition Examination Survey) data from 2011 to 2014 revealed that among females aged 14-26 years whose age was known at the time of their first dose of HPV vaccine, 43% had reported having sex before or in the same year that they received their first dose.
One consistent reason parents indicate for not vaccinating is the lack of recommendation from their child’s health provider. Differences in age and sex recommendations also are reported. NIS-Teen 2013 demonstrated that parents of girls were more likely than parents of boys to receive a provider recommendation (65% vs.42%.) Only 29% of female parents indicated they’d received a provider recommendation to have their child vaccinated with HPV by ages 11-12 years.
Mandy A. Allison, MD, and her colleagues reviewed primary care physician perspectives about HPV vaccine in a national survey among 364 pediatricians and 218 family physicians (FPs). Although 84% of pediatricians and 75% of FPs indicated they always discuss HPV vaccination, only 60% of pediatricians and 59% of FPs strongly recommend HPV vaccine for 11- to 12-year-old girls; for boys it was 52% and 41%. More than half reported parental deferral. For pediatricians who almost never discussed the topic, the reasons included that the patient was not sexually active (54%), the child was young (38%), and the patient was already receiving other vaccines (35%) (Pediatrics. 2016 Feb;137[2]:e20152488).
Providers can be influenced by their perceptions of what value parents place on vaccines. In one study, parents were asked to put a value on specific vaccines. Providers were then asked to estimate how parents ranked the vaccines on a scale of 0-10. Providers underestimated the value placed on HPV vaccine (9.3 vs 5.2) (Vaccine 2014;32:579-84).
Improving HPV coverage: Preventing future HPV-related cancers
HPV vaccine should be recommended with as much conviction as Tdap and MCV at the 11- to 12-year visit for both girls and boys. Administration of all three should occur on the same day. Clinician recommendation is the No. 1 reason parents decide to vaccinate. The mantra “same way, same day” should become synonymous with the 11- to 12-year visit. All who have contact with the patient, beginning with the front desk staff, should know the importance of HPV vaccine, and when and why it is recommended. Often, families spend more time with support staff and have discussions prior to interacting with you.
Anticipate questions about HPV. Why give the vaccine when the child is so young and not sexually active? Is my child really at risk? Is it safe? I read on the Internet. … Questions should be interpreted as a need for additional information and reassurance from you.
Remember to emphasize that HPV vaccine is important because it prevents cancer and it is most effective prior to exposure to HPV.
Additional resources to facilitate your discussions about HPV can be found at www.cdc.gov/hpv.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.

Early epilepsy increases risk of later comorbid ADHD in autism
VIENNA – Early-onset idiopathic epilepsy occurring before age 7 years nearly doubles the likelihood that a child with autism spectrum disorder will later develop comorbid attention-deficit/hyperactivity disorder, Johnny Downs, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Comorbid ADHD is common in the setting of autism spectrum disorder (ASD). In a search for risk factors for the comorbid condition, he and his coinvestigators reviewed the physical health records prior to age 7 years of 3,032 patients with ASD referred at ages 3-17 years to child and adolescent mental health services clinics serving South London.

“That’s information that often doesn’t make it into the clinical psychiatric record,” noted Dr. Downs, a child psychiatrist at King’s College London.
Half of the 3,032 subjects were diagnosed with ASD at age 6-12 years and another 39% at age 13-17. During 5 years of prospective follow-up after being diagnosed with ASD in this longitudinal observational study, 25.5% of patients were diagnosed with comorbid ADHD. Looking back through the early physical health records, 114 (3.76%) of study participants had experienced early-onset epilepsy before age 7 years.
This large sample size allowed for robust multivariate adjustment for potential confounders. In a multivariate analysis, ASD patients with a history of early-onset epilepsy were at a significant 1.75-fold increased risk for subsequent comorbid ADHD. The analysis was adjusted for family history of epilepsy, sociodemographic factors, intellectual disability, previous head injury, perinatal complications, central nervous system tumors, early meningitis, and other confounders.
“The take-home message would be if you’ve got social and communication difficulties in a young child appearing at the age of 5, 6, or 7 [years], and there’s a history of seizures, we are seeing from observational data that the child is at increased risk of ADHD over the age of 7,” Dr. Downs said in an interview.
Compared with white subjects with ASD, the risk of developing comorbid ADHD was reduced by 37% in black and by 52% in Asian patients with ASD.
He plans further studies aimed at determining whether conventional ADHD management strategies have the same risk/benefit ratios in children with ASD and comorbid ADHD as in those with ADHD alone.
Dr. Downs reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
VIENNA – Early-onset idiopathic epilepsy occurring before age 7 years nearly doubles the likelihood that a child with autism spectrum disorder will later develop comorbid attention-deficit/hyperactivity disorder, Johnny Downs, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Comorbid ADHD is common in the setting of autism spectrum disorder (ASD). In a search for risk factors for the comorbid condition, he and his coinvestigators reviewed the physical health records prior to age 7 years of 3,032 patients with ASD referred at ages 3-17 years to child and adolescent mental health services clinics serving South London.
“That’s information that often doesn’t make it into the clinical psychiatric record,” noted Dr. Downs, a child psychiatrist at King’s College London.
Half of the 3,032 subjects were diagnosed with ASD at age 6-12 years and another 39% at age 13-17. During 5 years of prospective follow-up after being diagnosed with ASD in this longitudinal observational study, 25.5% of patients were diagnosed with comorbid ADHD. Looking back through the early physical health records, 114 (3.76%) of study participants had experienced early-onset epilepsy before age 7 years.
This large sample size allowed for robust multivariate adjustment for potential confounders. In a multivariate analysis, ASD patients with a history of early-onset epilepsy were at a significant 1.75-fold increased risk for subsequent comorbid ADHD. The analysis was adjusted for family history of epilepsy, sociodemographic factors, intellectual disability, previous head injury, perinatal complications, central nervous system tumors, early meningitis, and other confounders.
“The take-home message would be if you’ve got social and communication difficulties in a young child appearing at the age of 5, 6, or 7 [years], and there’s a history of seizures, we are seeing from observational data that the child is at increased risk of ADHD over the age of 7,” Dr. Downs said in an interview.
Compared with white subjects with ASD, the risk of developing comorbid ADHD was reduced by 37% in black and by 52% in Asian patients with ASD.
He plans further studies aimed at determining whether conventional ADHD management strategies have the same risk/benefit ratios in children with ASD and comorbid ADHD as in those with ADHD alone.
Dr. Downs reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
VIENNA – Early-onset idiopathic epilepsy occurring before age 7 years nearly doubles the likelihood that a child with autism spectrum disorder will later develop comorbid attention-deficit/hyperactivity disorder, Johnny Downs, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Comorbid ADHD is common in the setting of autism spectrum disorder (ASD). In a search for risk factors for the comorbid condition, he and his coinvestigators reviewed the physical health records prior to age 7 years of 3,032 patients with ASD referred at ages 3-17 years to child and adolescent mental health services clinics serving South London.
“That’s information that often doesn’t make it into the clinical psychiatric record,” noted Dr. Downs, a child psychiatrist at King’s College London.
Half of the 3,032 subjects were diagnosed with ASD at age 6-12 years and another 39% at age 13-17. During 5 years of prospective follow-up after being diagnosed with ASD in this longitudinal observational study, 25.5% of patients were diagnosed with comorbid ADHD. Looking back through the early physical health records, 114 (3.76%) of study participants had experienced early-onset epilepsy before age 7 years.
This large sample size allowed for robust multivariate adjustment for potential confounders. In a multivariate analysis, ASD patients with a history of early-onset epilepsy were at a significant 1.75-fold increased risk for subsequent comorbid ADHD. The analysis was adjusted for family history of epilepsy, sociodemographic factors, intellectual disability, previous head injury, perinatal complications, central nervous system tumors, early meningitis, and other confounders.
“The take-home message would be if you’ve got social and communication difficulties in a young child appearing at the age of 5, 6, or 7 [years], and there’s a history of seizures, we are seeing from observational data that the child is at increased risk of ADHD over the age of 7,” Dr. Downs said in an interview.
Compared with white subjects with ASD, the risk of developing comorbid ADHD was reduced by 37% in black and by 52% in Asian patients with ASD.
He plans further studies aimed at determining whether conventional ADHD management strategies have the same risk/benefit ratios in children with ASD and comorbid ADHD as in those with ADHD alone.
Dr. Downs reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
AT THE ECNP CONGRESS
Key clinical point: Youths with autism spectrum disorder and a history of early-onset epilepsy before age 7 years are at an increased risk of subsequent comorbid ADHD.
Major finding: Youths with autism spectrum disorder who have a history of early-onset epilepsy before age 7 years are at 1.75-fold increased likelihood of subsequently developing comorbid ADHD.
Data source: This longitudinal study included 3,032 children and adolescents with autism spectrum disorder, 26% of whom developed ADHD during 5 years of prospective follow-up.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study, which was conducted free of commercial support.

Planning, education smooth transition to longer-acting clotting factors
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.

Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.
Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.
Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
EXPERT ANALYSIS AT WFH 2016 WORLD CONGRESS
Key clinical point: Transitioning patients to extended half-life clotting factor concentrates requires tailoring treatment to individual patients.
Major finding: Many patients can transition from on-demand dosing with factor IX to prophylaxis infusions once every 2 weeks.
Data source: Review of a hemophilia treatment center experience transitioning patients to extended half-life products.
Disclosures: Jennifer Maahs, RN-BC, disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.

Do as I say, not as I do! A futile plea
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.

Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.
Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
I am constantly amazed when parents come in complaining about their child’s nail biting or irritable attitude “no matter how many times I tell her” as they do these same things in front of me!
We have not evolved that far from our nonverbal ancestors to expect that words will speak louder than actions. Looking closely, you can see even very young infants gazing closely at their parents, then mirroring their facial expressions a few minutes later (because of slower processing). Mirroring is probably the correct word for this as the mirror neuron system of the brain has as its primary and crucial function allowing humans to copy what they see in others.
Children look to model, especially those who are slightly older and more adept than they are. Older siblings bask in this adoration at times and squeal in frustration at other times that their younger sister is “mocking” them by copying their speech and actions. When children are picking up serious negative behaviors from siblings or peers, particularly in adolescence, we need to coach parents to take action.
But watching parents is the most powerful or “salient” stimulus for learning. Some theorize that the long period of childhood evolved to allow children to learn the incredible amount of information necessary to live independently in our complex culture. This learning begins very early and requires close contact and careful observation of the minute details of how the parent survives every day.
Eating is a great primitive example of why children must model their parents. How do animals know which plants are poisonous? By watching others eat and spit, choke, or vomit. Entire families have nonpreferred foods passed on by modeling refusal as well as lack of exposure on the table. Conversely, picky eaters need to observe others, preferably admired peers and parents, eating those vegetables. (Tasting is also necessary, but that’s a topic for another day!) It is worth asking about family meals, without the distraction of a TV, as they are key moments to model nutritious eating for their lifetime.
In “underdeveloped” countries, infants are naturally carried everywhere and observing constantly. In our “developed” country, many infants spend hours each day at day care, modeling their caregivers or watching media examples of people interacting, which may not be the models parents would consciously choose. Parents often ask us about childcare, anxious about the extremely rare threat of abduction, when we should instead be advising them about what models they want for their children during this critical learning period.
Emotion cueing is a crucial component of modeling and an untaught constant of typical parent-child interaction. Crawling infants placed on a clear surface over a “visual cliff” that appeared to be a sudden precipice look to the parent’s affect to decide how to act. The mother was instructed to show fear or joy when her baby reached the apparent danger and looked up for a warning. When fear was shown, the infants backed off and cried. When joy was shown, the baby crawled gaily across the “cliff.” For parents who do not come by signaling confidence naturally but want to model this for their children, I advise they “fake it until you make it!”
Parents are instructing their progeny in how to feel and act in every situation, whether they know it or not. Confident parents model bravery; kind parents model compassion; flexible parents model resilience; patient parents model tolerance; anxious parents model caution; angry parents model aggression. Ignoring parents (think: on their cellphone, distracted, depressed, inebriated, or high) leave their children to feel confused and insecure. An adaptive child of an ignoring parent may demand information by crying, clinging, fighting with siblings, or hitting the parent. They are desperate for the parental attention to teach them and keep them safe. A more passive child may become increasingly inhibited in their exploration of the world. We need to consider possible modeling failures when such child reaction patterns are the complaint, and remember that the adverse model may not be in the room, requiring us to ask, “What other adult models does he see?”
Studies have shown that infants learn resilience when experiencing “mistakes” in parent-infant interaction; learning how to tolerate and repair an interaction that is not perfect. This is really good news for parents who feel that they must be perfect models for their children! For parents of anxious or obsessive children, I sometimes prescribe making mistakes and saying “Oh well,” as well as rewarding the child when they can say “Oh well” themselves. No child is too old to benefit from observing a parent apologize sincerely for a mistake.
Language is modeled, right down to accent. But when parents complain about their child cussing, raising their voice in anger, having an “attitude,” or “talking back,” it is worth asking (parent and child) “Where do you think they/you have heard talk like that?” It may be childcare providers, peers, TV, video games or online media (all of which may warrant a change), but it also may reflect interactions at home.
Children make stronger memories when emotions are high as these may signal danger, making recall more salient to survival. This salience helps explain the lasting detriments to learning and health of growing up with psychological abuse, marital discord, partner violence, mental illness, or criminal behavior (among the Adverse Childhood Experiences). Such experiences cause stress and a sense of the world as a dangerous place, but also become models for the child’s own later relationships as adults. While unavoidable, they can be buffered by parents’ explaining them and providing alternative positive modeling.
Watching the parent conduct their craft, a key component of apprenticeship and family businesses in the past, has been replaced by YouTube and avatars for learning physical skills. But “modeling the process” of pride in craftsmanship, persistence in a task, and recovering and starting over when things go awry are omitted from training videos. These are good reasons to assure that parents do chores, crafts, cooking, or camping with their children as some things will surely go wrong, giving parents the chance to model resilience and problem solving!
Although teens may protest conversations and activities, they are watching their parents for how to be a spouse, a neighbor, a friend, a leader, a citizen. Parents, who may be cutting their teens loose, need to continue to expect/require participation in family meals and outings. Those are opportunities to model adult-level interactions with each other and with the community as well as to talk about their activities at work, in volunteering, in charity, and in religious practice. The moral development of the adolescent is shaped by what they see to the degree that when parents state one moral code but violate it themselves (for example, cheating on taxes, running red lights), the teen is less likely to follow the principles long term that the parents have verbalized.
Parents often relate to us as though we were their own parents. While this “projection” can interfere with disclosure on touchy subjects, it is also an opportunity for us to model ways of relating and reacting from sympathizing with the 4-year-old screaming about vaccines to asking an 8-year-old why he thinks his parents are getting a divorce.
Parenting (and being a pediatrician) is an opportunity to enjoy reliving your youth or to get a “do over” of parts you would like to have different for your child. Playfulness and silliness model joy for the child that can last a lifetime.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.

Americas are declared measles free by PAHO
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.

In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.
In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
The Americas are measles free.
The region is the first in the world to have eradicated the disease, according to Pan-American Health Organization officials who spoke during a media briefing.
“Bye-bye measles,” said PAHO director Carissa F. Etienne, MD, during the briefing.
In 1994, countries across the Americas collectively declared their determination to rid the region of endemic measles transmission by 2000, agreeing to implement PAHO-recommended surveillance and immunization strategies, including the introduction and expanded use of the triple viral vaccine (MMR) against measles, mumps, and rubella.
In 2007, an expert international committee began verifying absence of the disease regionally. Although the disease was largely thought to have been wiped out in the Americas by 2002, officials postponed making an announcement until elimination of both measles and rubella could be declared jointly. An outbreak of measles in 2013 thwarted this plan, with the last confirmed case of reported endemic measles in the Americas not occurring until July 2015 in Brazil. In all, five vaccine-preventable diseases have been eliminated in the region, according to PAHO: smallpox in 1971, polio in 1994, and rubella and congenital rubella syndrome in 2015.
“The tasks of verification was not without its challenges, and countries overcame a number of geopolitical difficulties, including [maintaining] high vaccination coverage for very mobile populations, limited – and often no – access to deprived areas, and the presence of conflict situations,” Merceline Dahl-Regis, MD, the Bahamas’ chief medical officer and chair of PAHO’s elimination verification committee, said during the media briefing. She credited the expansion of national immunization programs, the “stellar work” conducted by various national commissions, and excellent communication between the nations’ respective governments, local and federal, as critical to the success of the effort. Also credited by other officials is PAHO’s revolving vaccine fund, which provides five-dose vials of MMR for about 1 dollar each.
Globally, since use of the MMR vaccine began, there has been a 95% drop in cases over a 35-year period, from 4.5 million cases in 1980 to approximately 244,700 in 2015. At the time the initiative to eradicate the disease was announced, measles was among the top five most common killers of children under the age of 5 years worldwide. The vaccine-preventable disease took the lives of 114,900 children globally in 2014, according to the World Health Organization. Worldwide, about 85% of children are vaccinated against measles by their first birthday, up from 73% in 2000.
Keeping vaccination rates high and immediately reporting any imported cases of the disease are essential to maintaining this milestone, according to PAHO officials.
“Importation of measles from other parts of the world into the Americas will continue, and we must be ready to detect and respond quickly, but today, let us celebrate,” Capt. Mary Agocs, MD, a Red Cross senior adviser to the elimination initiative, said during the briefing.
On Twitter @whitneymcknight
FROM A PAHO MEDIA BRIEFING

FDA approves biosimilar adalimumab
There are “no clinically meaningful differences” between Amgen’s biosimilar adalimumab (Amjevita) and AbbVie’s branded product Humira, the Food and Drug Administration noted it its Sept. 23 announcement of Amjevita’s approval.
Although Amjevita (adalimumab-atto) is expected to cost less than Humira, Amgen has not released price information or a launch date pending ongoing litigation with AbbVie over intellectual property rights, an Amgen spokeswoman said.
The products carry an identical black box warning of tuberculosis and other serious infections, as well as lymphoma and other malignancies “reported in children and adolescent patients treated with [tumor necrosis factor] blockers including adalimumab.” As with Humira, “the most common expected adverse reactions with Amjevita are infections and injection site reactions,” the FDA said. Both products are approved in 20 mg/0.4 mL and 40 mg/0.8 mL prefilled injections, but Humira also has a 10 mg/0.2 mL option.
Amjevita was unanimously recommended for approval by an FDA review panel in July. Although “the biosimilar pathway is still a new frontier,” it’s likely to “enhance access to treatment for patients with serious medical conditions,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in the agency statement.
The approval follows the FDA’s approval of biosimilar infliximab (Inflectra) in April 2016 and biosimilar etanercept (Erelzi) in August 2016. Inflectra has not hit the U.S. market yet, but the European experience with biosimilar infliximab – generally positive – may give an indication of how Amjevita will fare in the United States. It’s perhaps a third or more less expensive than the original product (Remicade) and often used for new starts. There is uncertainty, however, about switching patients already established on Remicade, especially when it’s forced by cost issues.
Interchangeability is a concern in the United States as well. The FDA is working on the issue but has not yet released guidance, and the agency was careful to note in its statement that Amjevita was “approved as a biosimilar, not as an interchangeable product.” Biosimilar adalimumab, meanwhile, is under review in Europe, according to an Amgen statement.
The FDA approved Amjevita after reviewing structural and functional characteristics, pharmacokinetics and pharmacodynamics data, clinical immunogenicity data, and other clinical safety and effectiveness data that demonstrated similarity to Humira, including two phase III trials for plaque psoriasis and rheumatoid arthritis.
An AbbVie spokesperson said the company “anticipated Amgen’s product would be approved,” but noted the ongoing litigation.
There are “no clinically meaningful differences” between Amgen’s biosimilar adalimumab (Amjevita) and AbbVie’s branded product Humira, the Food and Drug Administration noted it its Sept. 23 announcement of Amjevita’s approval.
Although Amjevita (adalimumab-atto) is expected to cost less than Humira, Amgen has not released price information or a launch date pending ongoing litigation with AbbVie over intellectual property rights, an Amgen spokeswoman said.
The products carry an identical black box warning of tuberculosis and other serious infections, as well as lymphoma and other malignancies “reported in children and adolescent patients treated with [tumor necrosis factor] blockers including adalimumab.” As with Humira, “the most common expected adverse reactions with Amjevita are infections and injection site reactions,” the FDA said. Both products are approved in 20 mg/0.4 mL and 40 mg/0.8 mL prefilled injections, but Humira also has a 10 mg/0.2 mL option.
Amjevita was unanimously recommended for approval by an FDA review panel in July. Although “the biosimilar pathway is still a new frontier,” it’s likely to “enhance access to treatment for patients with serious medical conditions,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in the agency statement.
The approval follows the FDA’s approval of biosimilar infliximab (Inflectra) in April 2016 and biosimilar etanercept (Erelzi) in August 2016. Inflectra has not hit the U.S. market yet, but the European experience with biosimilar infliximab – generally positive – may give an indication of how Amjevita will fare in the United States. It’s perhaps a third or more less expensive than the original product (Remicade) and often used for new starts. There is uncertainty, however, about switching patients already established on Remicade, especially when it’s forced by cost issues.
Interchangeability is a concern in the United States as well. The FDA is working on the issue but has not yet released guidance, and the agency was careful to note in its statement that Amjevita was “approved as a biosimilar, not as an interchangeable product.” Biosimilar adalimumab, meanwhile, is under review in Europe, according to an Amgen statement.
The FDA approved Amjevita after reviewing structural and functional characteristics, pharmacokinetics and pharmacodynamics data, clinical immunogenicity data, and other clinical safety and effectiveness data that demonstrated similarity to Humira, including two phase III trials for plaque psoriasis and rheumatoid arthritis.
An AbbVie spokesperson said the company “anticipated Amgen’s product would be approved,” but noted the ongoing litigation.
There are “no clinically meaningful differences” between Amgen’s biosimilar adalimumab (Amjevita) and AbbVie’s branded product Humira, the Food and Drug Administration noted it its Sept. 23 announcement of Amjevita’s approval.
Although Amjevita (adalimumab-atto) is expected to cost less than Humira, Amgen has not released price information or a launch date pending ongoing litigation with AbbVie over intellectual property rights, an Amgen spokeswoman said.
The products carry an identical black box warning of tuberculosis and other serious infections, as well as lymphoma and other malignancies “reported in children and adolescent patients treated with [tumor necrosis factor] blockers including adalimumab.” As with Humira, “the most common expected adverse reactions with Amjevita are infections and injection site reactions,” the FDA said. Both products are approved in 20 mg/0.4 mL and 40 mg/0.8 mL prefilled injections, but Humira also has a 10 mg/0.2 mL option.
Amjevita was unanimously recommended for approval by an FDA review panel in July. Although “the biosimilar pathway is still a new frontier,” it’s likely to “enhance access to treatment for patients with serious medical conditions,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in the agency statement.
The approval follows the FDA’s approval of biosimilar infliximab (Inflectra) in April 2016 and biosimilar etanercept (Erelzi) in August 2016. Inflectra has not hit the U.S. market yet, but the European experience with biosimilar infliximab – generally positive – may give an indication of how Amjevita will fare in the United States. It’s perhaps a third or more less expensive than the original product (Remicade) and often used for new starts. There is uncertainty, however, about switching patients already established on Remicade, especially when it’s forced by cost issues.
Interchangeability is a concern in the United States as well. The FDA is working on the issue but has not yet released guidance, and the agency was careful to note in its statement that Amjevita was “approved as a biosimilar, not as an interchangeable product.” Biosimilar adalimumab, meanwhile, is under review in Europe, according to an Amgen statement.
The FDA approved Amjevita after reviewing structural and functional characteristics, pharmacokinetics and pharmacodynamics data, clinical immunogenicity data, and other clinical safety and effectiveness data that demonstrated similarity to Humira, including two phase III trials for plaque psoriasis and rheumatoid arthritis.
An AbbVie spokesperson said the company “anticipated Amgen’s product would be approved,” but noted the ongoing litigation.